20 minute read
What Is Preventing the Industry from Providing Electronic Product Information?

from IPI Winter 2020
by Senglobal

Abstract In 2017, the European Commission published a report regarding the possible improvements for product information texts used for human medicinal products. The improvements aim to facilitate safe and effective use of medicinal products and, as a result of the report, the European Medicines Agency (EMA) and the national heads of medicines agencies (HMA) agreed on a project to implement structured electronic ePI.
Several national electronic patient information (ePI) projects have already demonstrated the potential of a triple-win situation: • Patients: Effective provisioning of information to patients, elevating their “user experience” and improving the overall compliance; • Industry: Optimising internal processes and improved compliance for managing documents containing patient information; • Agency: Facilitating improved work processes between industry and agencies, streamlining the review process and improving analytics capabilities.
It is the intent of the ePI project to harmonise the national initiatives to achieve a common solution related to the identification medicinal product (IDMP) master data, including the controlled vocabularies provided by SPOR.
This paper looks at what is preventing us from providing electronic product information as well as how industry can support the wider ePI project. Background In 2004, the requirement “the package leaflet shall reflect the results of consultations with target patient groups to ensure that it is legible, clear and easy to use” was added to Article 59, Directive 2004/27/EC of the European Parliament and of the Council of 31 March 2004. And in 2017, the long-awaited report providing an overview of patient target group experiences was finally published.
Before the 2017 report was published, two studies were published, each initiated by the European Commission: The first one was on the package leaflet (PL) and the summary of product characteristics of medicinal products (SmPC) for human use (so called PIL-S study)1. The second report gave more insight into feasibility and value of a possible “key information section” in PLs and SmPCs for human use (PILs-BOX study)2. The general result concluded that readability (comprehension and layout) still needs to be improved for PLs rather than for SmPCs. It was recommended to consider revising the existing guidelines (e.g. readability, content and layout-related issues), to allow more flexibility among different medicines in the QRD template (in the framework of the existing legislation) and to introduce guidance on translations. In parallel, the input from patients should be improved and a more iterative assessment process may be introduced without delaying the authorisation process.
The final report from the Commission on the SmPC and PL for medicinal products for human use was adopted by the European Parliament and the Council on March 22, 2017 3. It concluded that the use of electronic formats brings new opportunities for these documents and recommended exploring the use of electronic media to provide information included in these documents to the patient in the future. However, the report does not recommend the removal of the paper leaflet from the box, which some may consider unfortunate, as removing the need for the paper leaflet could bring benefits to the patient. Continuing to provide paper in the box and give the patient the option to view the ePI could cause confusion if the electronic version differs (because it reflects recent updates) from the paper. Removing the need for a paper leaflet in the box and having the electronic version as the legal requirement would take away this potential confusion and ensure patients always have access to the most recent version. Action Plan EMA took the leadership in generating an action plan on how to achieve the abovementioned objectives4. The starting point was a publicly broadcasted workshop that took place on November 28, 2018, in London at EMA. Representatives of all national competent authorities (NCA), EMA including European Commission, several pharmaceutical industry associations, patients and consumers’ organisations, healthcare professionals’ organisations and academia, health technology assessment bodies (HTAs) and payers took part in the information exchange. EMA presented an outline of potential future use cases and international standards to be employed in the event of an electronic PL being generated5 .
Representatives from several Member States as well as from pharmaceutical industry projects on electronic developments presented and ran a live demonstration on what an ePI could look like and what the advantages would be. Up to now, a broad range of similar, deviating proposals and developments are underway in many NCAs6. However, for European purposes a harmonised and standardised approach is essential as marketing authorisation holders and regulatory agencies will not be able to assess each electronic publication on a national or company specific solution. In addition, the publication process needs to be automated based on the authorisation issued by the competent authority. In addition to several technical requirements, the features of an application presenting an electronic product information need to be evaluated against patients’ requirements, whether they can and will use them and whether this approach supports the required improvement of comprehension and better readability of PLs7,8 and thereby the better use of medicines by patients and consumers.
Whatever improvement of the design and layout of paper PL has been achieved, the flexibility due to the legal framework remains restricted. The access to an electronic version could offer many more benefits to the patient, including: • Improved searching of product information with the potential for tailoring it for personal use of patient, or advanced analytics from regulators;
• Offers options to explain medical terms; • Monitors updates of a patient’s regularly used medicines; • Enlarges the font size on the screen or
‘reads out’ the product information text (for patients with impaired visibility, for example); • Easy access to educational material, informing videos etc.9,10; • Easy automated translation to other languages, in addition to the EU ones (e.g. Arabic, Turkish etc).
In the best case, these developments and their evaluation of usefulness are accompanied by scientific support, analysis and assessment. Key Principles for ePI The key principles of the expectations, requirements and conditions of an electronic version of the PL were published by EMA in January 202011. The EMA’s key principles focuses on six areas:
• Defining what ePI is and the standards to be used to generate it; • Benefits for public health, making information more accessible to all patients; • Efficiency gains within regulatory systems; • Existing legislative framework, confirming that ePI must comply with existing legislation and complement the paper PL; • Processes for reviewing/assessing the ePI and how some NCAs may take a different approach.
The EU context confirms that ePI should support all official EU languages so that patients can read information in their preferred language, but patients would benefit from ePI being automatically translated into other languages outside the EU ones, so that they have access to the information they need in a language they understand.
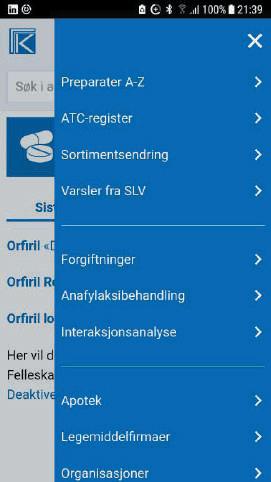
It is important to understand that ePI covers all authorised, statutory product information for medicines (i.e. SmPC, package leaflet and labelling), but not additional information under the responsibility of NCAs such as educational material. However, this additional information may be published electronically via the same application using the common EU electronic standard, which has not yet been agreed. ePI is adapted for electronic handling and allows dissemination via the worldwide web, e-platforms and print. ePI will need to comply with the published key principles. Managing electronic product information could be split into two distinct areas – data management and patient usage: Data Management: Companies will need to have the ability to manage the data content of the PL; traditionally this is managed in Word and PDF in a generally unstructured format. Companies may need to consider how they manage this data within their organisation, potentially using structured authoring tools to ensure the data complies with the requirements, which may be more detailed than the current QRD templates. Data used within the PL will need to be validated and controlled to ensure that it remains compliant throughout the product life-cycle. Patient Usage: Users of the medicinal products will have access to trusted data in a well-regulated format as outlined in the Directive 2013/37/EU12 and the General Data Protection Regulation (Regulation (EU) 2016/679)13. The benefit for users (patients, care givers and healthcare professionals) is the provision of up-to-date information from a trusted source available in several formats to best support the needs of the patient. Overview of Current National ePI Initiatives In several EU Member States, different projects have been initiated by pharmaceutical companies, trade associations or agencies to demonstrate how ePI can be realised and disseminated. In most cases the current QRD Template was the starting point to create an XML structure and the appropriate style sheet transformed the text file into a format that can be presented by browser technology. Norway: The Norwegian Medicines Agency (NOMA) started a collaboration with the Norwegian pharma association (LMI) which publishes a compendium of product information representing about 80% of the market. As the paper version is also available online, this electronic version has been adapted for mobile devices and includes search for medicines, barcode reading, personalised medicines list, “My daily dose” function, photos of tablets/capsules, and instruction videos. PLs are imported from EMA & NOMA as well as real-time alerts from NOMA on important safety issues, shortage situations, etc. For HCP users, additional information is offered: Prescription texts (mainly based on the approved SmPCs, risk management plans (RMP) from NOMA and drug interactions from NOMA’s database.


Sweden: Since 2018 the basic information for approved medicinal products is available on FASS via websites, apps and web integrations including SmPC and PL in XML format for most marketed medicines.

1. Search functionality. 2. Basic product information. 3. Package leaflet. 4. Summary of product characteristics. 5. Fass-text (version of the SmPC adapted to HCP). 6. Images of tablets and capsules. 7. Information on medication management for capsules and tablets (i.e. whether they are to be swallowed without splitting, swallowed without crushing, may be split in two, etc.). 8. Information on which generic products are classified as interchangeable by the Swedish Medical Products Agency (MPA). 9. Information on whether the company participates in the Swedish
Pharmaceutical Insurance (insurance system for injuries related to medicinal products). 10. DHPC (Direct Healthcare Professional
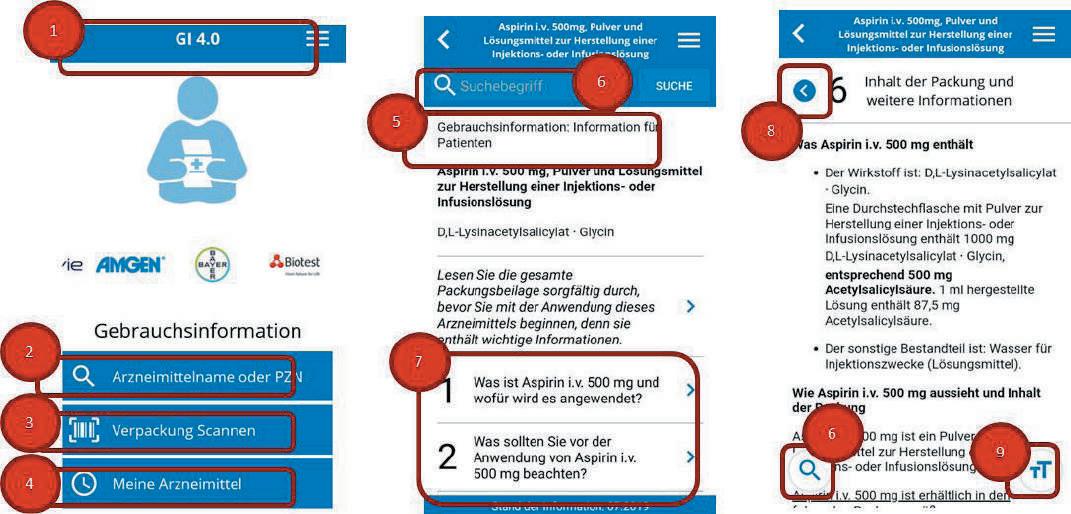
Communications), from the MPA. 11. Contact information to the companies. 12. Pharmacies' inventory status (to check if a specific medication is in stock in a certain pharmacy). 13. Packages and prices within the Swedish reimbursement system, and conditions in the reimbursement. 14. Swedish environmental classification of pharmaceuticals. 15. Text-to-speech, print, print in large text. Alerts on changes of product information. FASS for Mobile Devices 1. Search product or substance. 2. Basic information. 3. Package leaflet. 4. Expand selected text section. 5. Pharmacies' inventory status (to check if a specific medication is in stock in a certain pharmacy). Check for pharmacies nearby. Germany: The scope of the project is to provide up-to-date PLs real time on mobile devices and desktop computers, based on a validated process using authority approved information in a user-friendly electronic format. This includes a reader option to help people with disabilities, a font size enlargement or a print option as well. The screen shots display the functions in more detail: 1. General menu. 2. Search for product name or PZN. 3. Scanning PZN-& FMD-Code. 4. List of individually selected products. 5. Package leaflet of the selected product. 6. Search for a term of interest. 7. Navigation through sections. 8. Back and forth button. 9. Enlarge font size button. Spain: The agency requires the use of a specific application to create a semi-


structured SmPC and PL. The tool allows the import of an existing product information text, editing information snippets (using XML editor functionality) and interactions with the agency to assess and confirm the modifications.
The authorised product information (1 SmPC; 2 PL) is published at https://cima. aemps.es/cima/publico/home.html
The text information is fragmented by sections (not only Word and/or PDF any more) using an XML editor (as mentioned above). The patient and HCP benefits from easy search and navigation. The semistructured version allows personalisation (favourite medicines with alerts whenever a change occurs). Links with other information formats (images, video...) are possible, so is the offer of information for people with disabilities and/or relevant

for subpopulations (children, elderly, by gender, etc…). In addition, it is possible to map data from section 4.1 of the SmPC with diagnostic codes or cross-reference the content section 4.8 of the SmPC with the ADR database. Netherlands: The KIJKsluiter Foundation uses animation videos and accessible software to make information available to patients. KIJKsluiter is available as a web and mobile app containing over 8000 animation videos, which takes the most important information from the PL and explains it in a very easy-to-understand way. The videos are personalised to the patient’s age and gender and to the medicine’s form of administration. They provide targeted information to the patient (omitting details that they do not need to read) and explain why the medication has been prescribed. The videos are available in multiple languages, namely Dutch, English, Turkish and Arabic.

Belgium: In 2018, a 24-month-project was set up to evaluate whether the paper PL and an e-PIL offer similarities regarding safe and effective usage of a medicine. The scope is restricted to a selection of 15 centrally approved medicinal products restricted to hospital use only and marketed in Belgium and/or Luxembourg.
The PL and SmPC is available in Dutch and French language. There is some navigational support, but not as sophisticated as in some of the other national projects. However, the focus of the project is quite specific. The results of the 24-month survey should be available in autumn 2020 and due to very positive feedback so far, the project will be extended for one year and the scope extended to include more products. International Project Overview In February 2018, the EMA survey14 resulted in several international projects to provide product information electronically with a certain degree of structured information15 .
The analysis of all responses was separated into several areas of interest and did predefine the subsections of the Key Principles Document11 .
USFDA and Health Canada (HC) implemented the HL7 Standard on Structured Product Labeling (SPL)16 combining the content of labelling and the data structures from the Common Product Model (CPM), both based on HL7 Version 3. This standard has not been updated since 2016. Nowadays, a more implementer- / user-friendly follow-up was published to allow a more straightforward implementation of software solutions: Fast Healthcare Interoperability Resources (FHIR). According to HL7 “FHIR combines the best features of HL7's v2, HL7 v3 and CDA product lines while leveraging the latest web standards and applying a tight focus on implementability.”17. For the new EU ePI standard it is likely that FHIR will be considered as a re-use of data elements from other IDMP-related implementations. Expectations and Challenges As demonstrated in the overview of national solutions, ePI (mainly PDF format) is already offered by some regulatory agencies via their websites, or in cooperation with pharmaceutical trade associations. In those



cases, the authorised text is generally used, however, the ePI project intends to offer much more, but that doesn’t come without challenges. Paper PL versus ePI “…Implementation of ePI does not imply any change to the legislation currently applicable to the PI. The development of ePI does not change the content of the PI (the information contained within the PI, headings, text or formatting) or create a new legal obligation to use ePI. In addition, this initiative does not change the interpretation of European pharmaceutical legislation...”11
Having both paper PL and an ePI available may result in a patient having access to different versions of the patient information. It takes time for changes to the text to be available in a printed PL, whereas the ePI could be updated (and available to the patient) almost immediately. Since electronic is always more accurate and upto-date, the purpose of the paper version of the PL should be questioned. This does
not mean paper is no longer a prominent medium to convey information on a medicine to a patient, but it could be printed at the site of the dispenser (pharmacy, doctor, shop, etc.) if and when required, rather than always being provided within the box. Rather than being considered an obstacle, this should be seen as a real valueadd opportunity, since access to electronic information becomes ‘the norm’ for most people, and it holds the potential to elevate the patient experience and compliance – with tailored information shared with the patient in a format that suits them best.
The Belgian project may demonstrate that effective and safe use of a medicinal product is not impaired by the availability of just electronic product information (without the paper leaflet). Furthermore, there may be benefits to a patient if they are able to receive alerts about a medicinal product that they use regularly and if they have immediate access to the most up-todate patient information. Often the paper leaflet is discarded and cannot be referred to. Concerns will regularly be raised as the percentage of internet use is still not 100%, especially in the age group above 65, which is why it still may be necessary for printed copies of the patient information to be printed at the point of dispensing: preferred e-platforms. Although many future developments using ePI are outside the scope of this ePI initiative, structured ePI data will enable subsequent development of functionalities such as easier selection of information on medicines of interest, automatic update notifications, and access to authorized or supportive video or audio content or other interactive materials (in line with the appropriate guidance) and online adverse-reaction reporting tools.”11
The overview of current national ePI initiatives (summarised in this document) demonstrates that technically all of this is possible. In most cases, the number of medicinal products in scope is limited, but the processes to present up-to-date information, indicate relevant changes, and link important safety information, usage instruction videos or other important information is working well. Interoperability with other Initiatives Interoperability and the general requirements on how to exchange data from SPOR services and export towards a product information database is fundamental. The existing SPOR API may already provide a sufficient service to consume data. However, the substance database and the product database are still under development. So, the service is not yet complete.

National Initiatives Patients are already benefitting from the national initiatives and can obtain information about their medication in electronic format. However, if national solutions continue to develop independently, challenges will emerge with the willingness of companies to use multiple, different solutions so there is a need for the ePI requirements and solutions to be harmonised, at least across the EU. Structured Data vs PDF “The structured nature of ePI will offer new opportunities to better personalize PI to the needs of individual patients / consumers by enabling more efficient retrieval of information (e.g. in online multi-level searches) and facilitating the use of their
The usage of FHIR offers pre-defined resources, which define the exchangeable content based on data types and common sets of metadata with an integrated human-readable component. Although a built-in extension mechanism to cover remaining content is available, it might be that for the purpose of ePI, additional resources are required or existing resources require modification.
One of the benefits of ePI would be the improvement of data exchange; it is valuable to understand the large amount of dependencies, e.g. in case of dosing management, the intent to avoid medication errors and to support decision management systems in hospitals18 and the basic impact of authorised, statutory product information for medicines19 . Conclusion In summary, the electronic product information (ePI) will provide up-to-date information at any time or location to any user with an ‘easy-to-read’ font size (or read out for people with disabilities); it may include explanation of medical terms; it will allow for access to educational material and instructions for administration, and could indicate major changes for a certain period of time. As such, this initiative could also be considered as a way to facilitate marketing of (newly authorised) medicines in all Member States and redistribution of medicines available in other Member States to countries experiencing shortages or where medicines are not marketed.
On its way to success, some hurdles need to be overcome, which could prevent the success of ePI within the EU – harmonisation and the potential conflict of paper versus electronic. A change of the current legislation by the European Commission is not foreseen in the short term, although ePI can provide significant benefits for patients, agencies, HCPs and the pharmaceutical industry as demonstrated by the national projects (reviewed in this document). It has also been shown that in collaboration between authorities and the pharmaceutical trade associations or dedicated information companies, the patient is already able to access electronic product information (in some countries). However, the missing part here is the agreement on a common technical structure and a proper tool to edit the information.
Finally, the (currently) mandatory printed leaflet needs to be removed from the package and the respective legislation being replaced by more flexible regulation that improves usability and offers an improved experience for most patients with a tailored delivery of the PL information. According to B. Sträter, Article 58 Directive 2001/83/ EU could be interpreted such that the required content of the PL is provided on the outer package via a 2D-matrix code which navigates the user to the ePI21. If this is an accepted interpretation, then a legal change would not be necessary. REFERENCES
1. https://ec.europa.eu/health/sites/health/ files/files/committee/75meeting/pil_s.pdf 2. https://ec.europa.eu/health/sites/health/ files/files/committee/75meeting/pilbx.pdf 3. https://ec.europa.eu/health/sites/health/fles/ fles/documents/2017_03_report_smpc-pl_en.pdf 4. https://www.ema.europa.eu/documents/other/

european-medicines-agency-action-plan-relatedeuropean-commissions-recommendationsproduct_en.pdf 5. https://www.ema.europa.eu/documents/ presentation/presentation-common-electronicstandard-potential-features-use-cases-escanlan_en.pdf 6. https://www.ema.europa.eu/en/events/ european-commission-heads-medicinesagencies-hma-european-medicines-agencyema-workshop-electronic 7. https://ec.europa.eu/health//sites/health/ files/files/eudralex/vol2/c/2009_01_12_ readability_guideline_fnal_en.pdf 8. http://ipimediaworld.com/wp-content/ uploads/2012/05/Pages-from-IPI- Volume-2Issue-2-18.pdf 9. https://www.ema.europa.eu/en/humanregulatory/marketing-authorisation/productinformation-requirements 10. https://www.ema.europa.eu/documents/ presentation/presentation-what- packageleafet-how-review-it-claire-espinasse_en-0.pdf 11. https://www.ema.europa.eu/documents/ regulatory-procedural-guideline/electronicproduct-information-human-medicineseuropean-union-key-principles_en.pdf 12. https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2013:175:0001:0008:EN:PDF 13. https://eur-lex.europa.eu/eli/reg/2016/679/oj 14. https://ec.europa.eu/eusurvey/runner/EPI 15. https://www.ema.europa.eu/documents/ presentation/presentation-overviewinitiatives-ema-hma-mapping-r-gonzalezquevedo_en.pdf 16. https://www.hl7.org/implement/standards/ product_brief.cfm?product_id=440 17. https://www.hl7.org/fhir/index.html 18. Maxwell S, Eichler HG, Bucsics A, Haefeli WE, Gustafsson LL; e-SPC Consortium. e-SPC - delivering drug information in the 21st century: developing new approaches to deliver drug information to prescribers. Br J Clin Pharmacol. 2012;73(1):12-15. doi:10.1111/j.13652125.2011.03981.x 19. Ammenwerth E, Aly AF, Bürkle T, Christ P, Dormann H, Friesdorf W; ...Memorandum on the use of information technology to improve medication safety. Methods of Information in Medicine 53 (05), 336-343; 2014 doi: 10.3414/ ME14-01-0040 20. https://www.ema.europa.eu/en/documents/ other/european-medicines-agencies-networkstrategy-2025-protecting-public-health-time-
Dr. Klaus Menges
Klaus Menges, Regulatory Affairs Senior Expert. Klaus joined the Federal Health Office in 1985. Until September 2018, Klaus represented BfArM in several European working groups and was nominated as Regulatory Chair in the ICH WG M8 on electronic submission Considering the broad regulatory experience he was also highly engaged in solutions for better readable product information texts.
Jennie May
Jennie May, Director Regulatory Informatics and Operations, PharmaLex. Jennie has over 20 years experience in the industry, with a focus on systems and processes to support the regulatory affairs business. She has held roles at Hospira and Allergan but has also worked for software vendors ISI (now DXC Technology) and IQVIA. Jennie has a wealth of experience including RIM System implementation, business process review and improvement, regulatory intelligence and publishing.
rapid-change_en.pdf 21. Sträter B; Pharmakovigilanz-Label-Change II; Pharm.Ind.82(09), 1089-1092, 2020
Stan van Belkum
Stan van Belkum, Deputy Director at Medicines Evaluation Board, The Netherlands. Stan has been Deputy Director of the Medicines Evaluation Board in the Netherlands since 2013. He has a long career in national and international initiatives around electronic regulatory information and information technology. He has also been part of the development of the eCTD with ICH and CESP with the HPRA in Ireland.
Peter Leister
Peter Leister, Executive Consultant, Technology Enabled Smart Services (TESS), PharmaLex. Peter is a pharmacist by education and has over 20 years of experience in the Life Sciences sector, with a track record of successes as an entrepreneur and C-level executive for large global services firms. He has worked with most of the global pharmaceutical companies focussing on strategy, portfolio- and process-optimisation, eClinical-, Safety- and Regulatorytransformations, organi-sational redesign, outsourcing, large-scale change and implementations.








