19 minute read
On the Front Lines: An Informal Survey


Scott Campbell, MD
How do emergency physicians and other frontline clinicians feel about their work these days?The leaders of the San Francisco Emergency Physicians Association (SFEPA), a 30+-year old group dedicated to improving emergency medical services, conducted a quick online survey of members and others, eliciting about 90 responses, 80% of them emergency physicians. This nonscientific survey was intended to get a glimpse of impressions and opinions of those working in various emergency settings, and some select results follow. –Editors
Advertisement

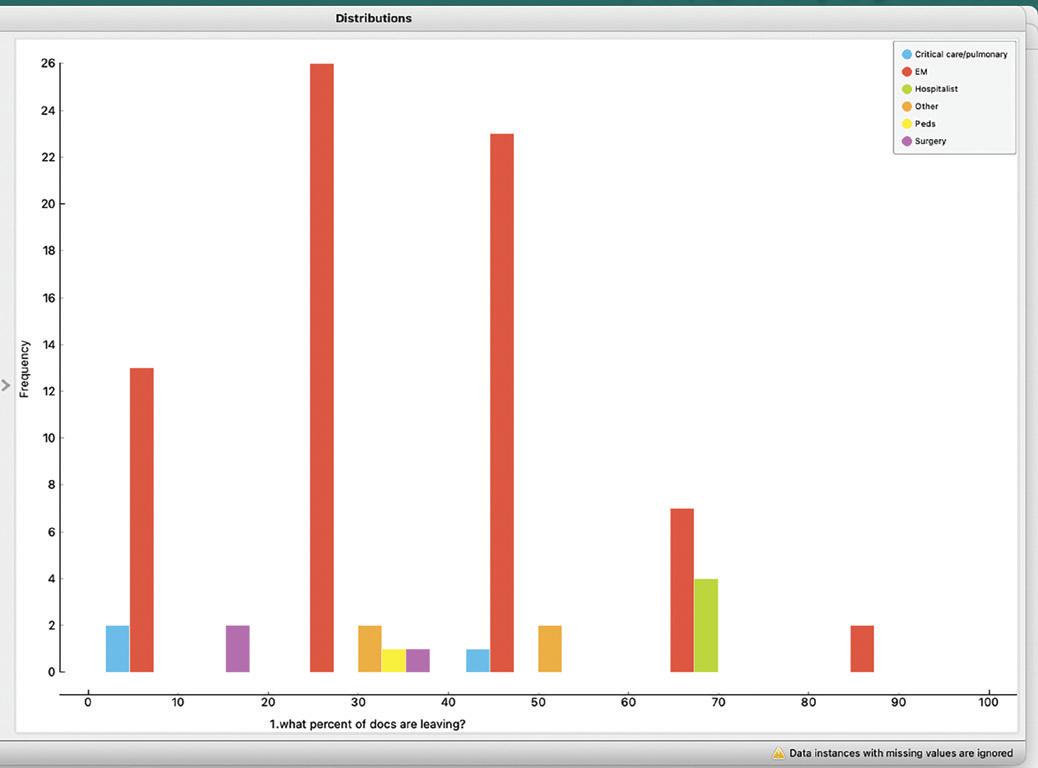
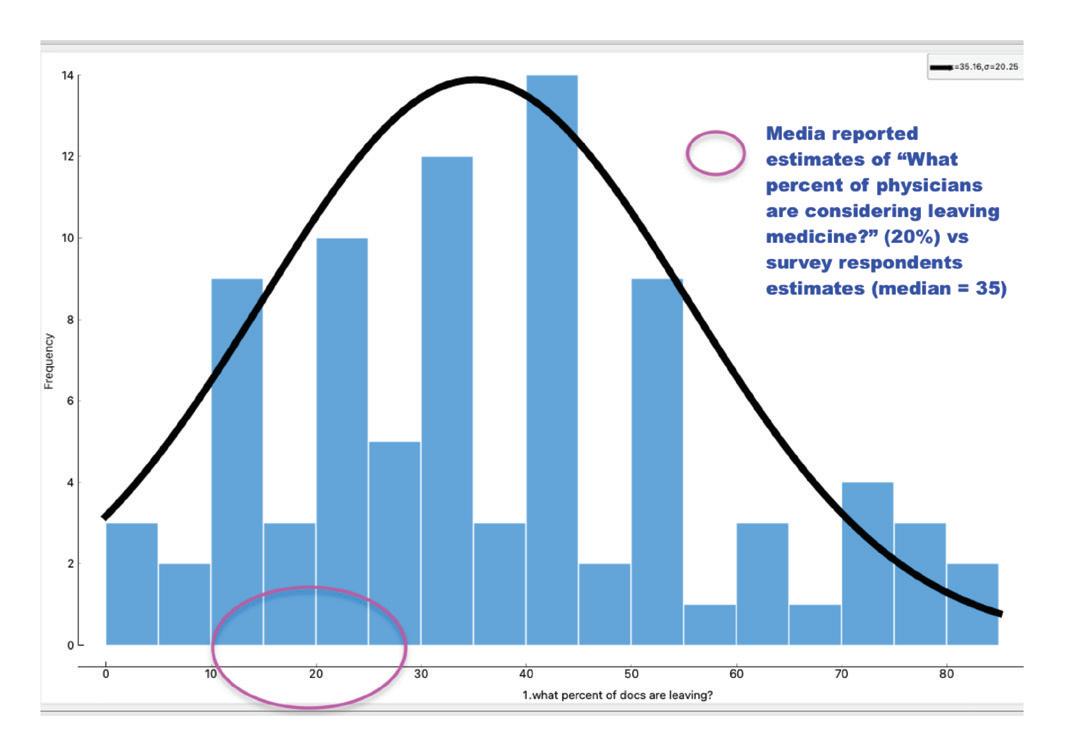
Mental health—no surprise was big here as were wait times, nursing staffing and legal repercussions. It was surprising how high the estimates were for "What percent of docs do you think are leaving medicine?" (majority thought 35 to 45%!)
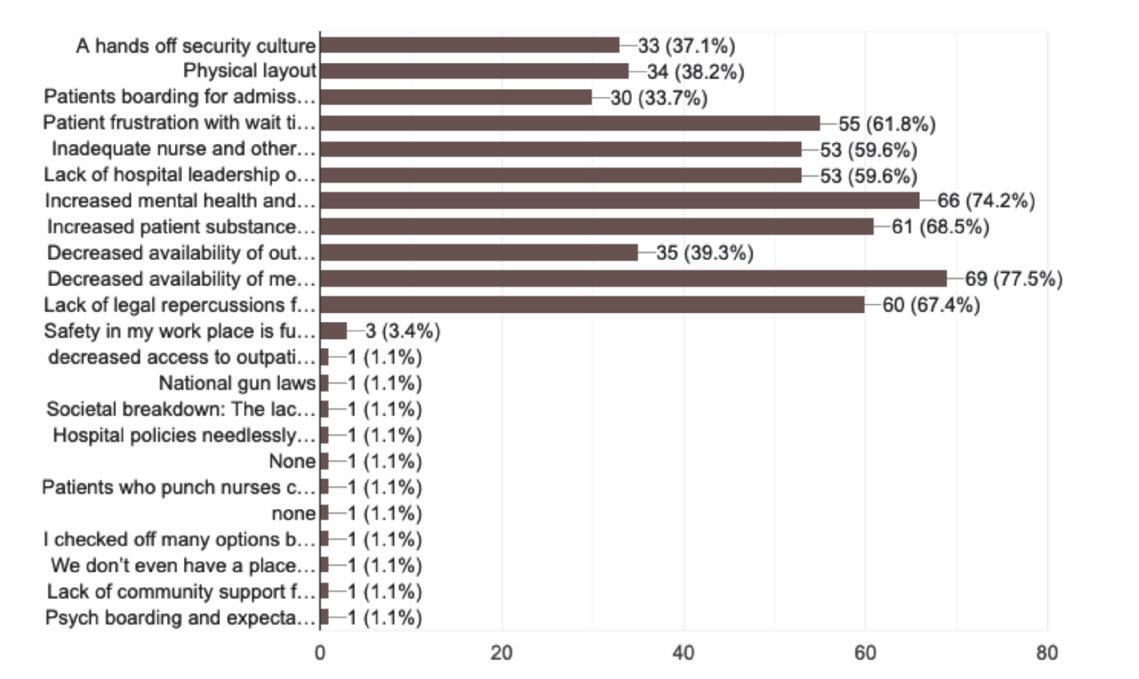
"What are the potential contributors to patient violence?"


Solutions: The top thing respondents wanted was less annoying tasks, particularly administrative:

A National Hospital Based Physician Burnout Survey
San Francisco Emergency Physicians Association
Hello and thanks for responding last month.
We sent the survey to approximately 500 physicians and got about 100 responses. (Primarily EM physicians). It’s not incredibly scientific of course but does offer some insight; happy to answer any burning questions.
Thanks, again
Scott
Scott J. Campbell MD, MPH San Francisco Emergency Physicians Association Scampbell@zhourmed.com
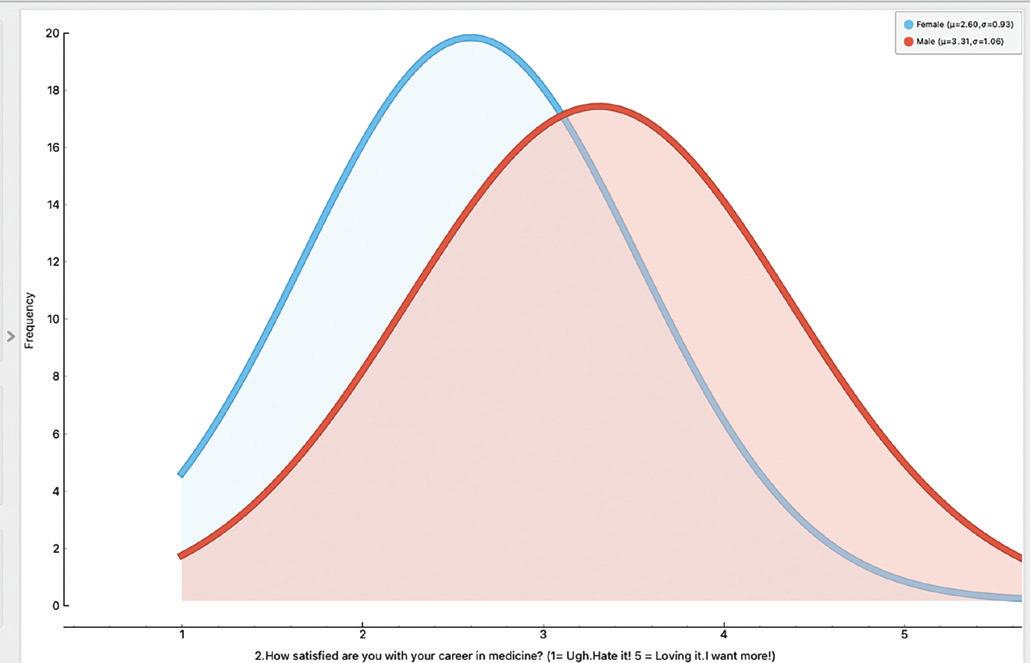
Media are (likely) significantly underestimating the % of physicians looking to leave medicine (“20%”). Unfortunately, looks to be closer to 35 to 40% How satisfied are you with your career in medicine? (by specialty and sex). It’s concerning regarding female vs male and career satisfaction disparities, especially in emergency medicine.


Top 5 reasons physicians would leave? 1. Support for less annoying, non-clinical tasks 2. Less admin burden 3. Safer working environment 4. Higher compensation 5. More time off

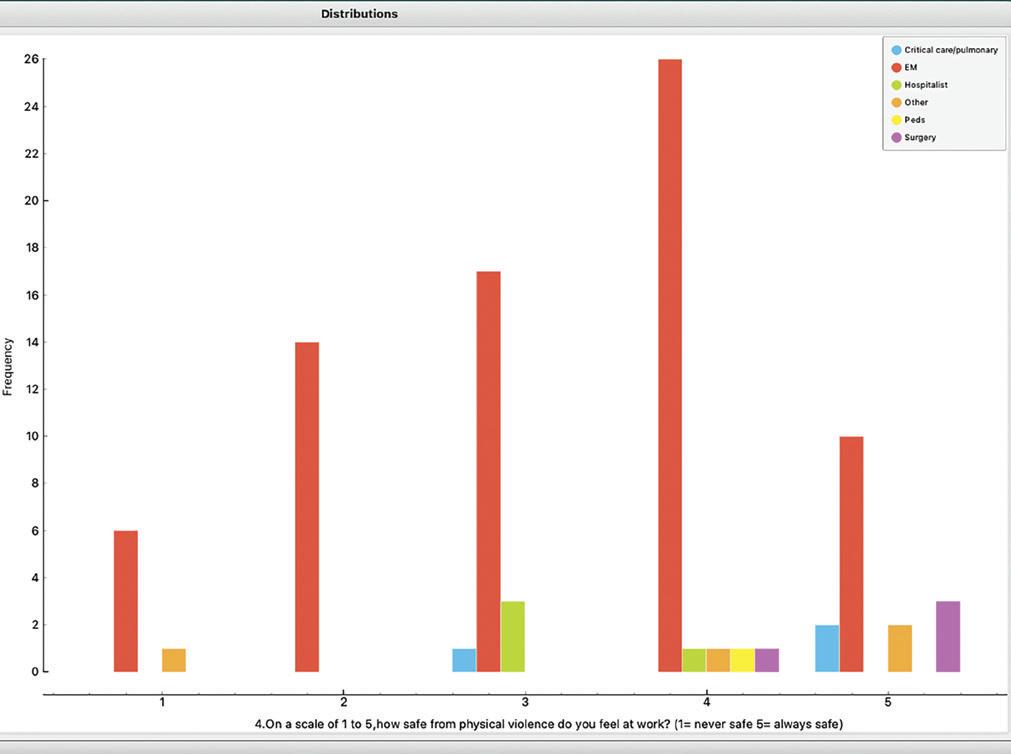
On a scale of 1-5, how safe from violence at work do you feel? (never =1 to always 5) (by specialty and sex). Women in emergency medicine do not feel at all safe at work vs men.
ON THE FRONT LINES: AN INFORMAL SURVEY
continued from page 15
What are the top 5 drivers of possible increased patient violence in the hospital? 1. Decrease mental health service availability combined
with increased mental, behavioral, and substance abuse issues in patients
2.Lack of legal repercussions when HCW assaulted 3.Patient frustration with wait times 4.Inadequate nurse and other staff levels 5.Lack of ownership by hospital leadership of truly owning
HCW safety
How long do you plan to practice medicine? (by sex and specialty). Many EM physicians want out now or in the next five years, particularly women. What things interest you outside of your current clinical medicine? Lots of interest in more teaching, lecturing (50%); International health; Lifestyle medicine; Volunteerism, and medical device

Finally, what concerns you most about the current state of hospital-based medicine?


Scott Campbell MD, is a retired San Francisco emergency physician and former president of the San Francisco Emergency Physicians Association.
UNEDITED ANSWERS TO OPEN MIC PRIOR QUESTION:
• Poor access to outpatient clinics and mental health has caused explosion of patients coming to ED, as well as increased annoyance and frustration by patients and staff, and resulting decrease quality interactions, decreased quality of care, decreased empathy, increased burnout. Boarders (including pts waiting for psych, SNF placements, memory care etc) has led to overflow and hallway medicine (which is also linked to worse outcomes, worse satisfaction, inhumane care, staff moral injury). • Decreasing compensation while hospital administrator comp skyrockets. • Boarders, boarders, boarders! This leads to obstipation and downstream queues. Also poor outpatient access, leading to more nonemergent visits. • Like a primary care axis, emergency departments not used for actual emergency medicine, homeless/social issues, difficult that everything gets dumped on the ED in the end, limited flexibility for office/outpatient specialties, 40-hour workweek expectation for full-time at KP. • Everyone else quitting and those of us left having to work more. • I worry that emergency medicine takes on too much work that others fail to do.
• Inability to say 'no' in the ER.
• The corporatization of medical care, VC backed medical groups. • It is run by folks with MBA, who have never practiced clinically. There is no parallel in any other professional. Academic hospitals are in double jeopardy, as physicians have to deal with hospital and university administrators, each vying to be more incompetent, obnoxious and destructive. • Lack of capacity throughout our system (from unsafe conditions in the ED waiting room, to no capacity in MRI, inpatient and outpatient settings at our center). • I said most of it above. But staffing is a huge problem. It feels like nurses are leaving in droves. From the outpatient side (I do outpt pulmonary too) there needs to be more time with patients in the outpatient world (especially for primary care- if they can do a better job with their patients less will end up in the hospital!) • The health care, mental health care, substance abuse care, homeless resource and elder care systems are completely broken and the Emergency Dept has become the "catch-all" for all. Our hallways are full of homeless people that want a place to sleep, elderly people that are not sick but can't care for themselves. • Because of EMTALA, a physician is required to see everyone that shows up at an Emergency Department. • Cms metrics that don't meaningfully affect patient outcome but affect physician practice by means of reimbursement/penalty and hospital accreditation. • General population lacks respect for healthcare workers. Patients are sources of financial gain. Healthcare is a business. The business is to make money. People, in general, are not very bright. Average intelligence and below average frequent the ED. Intelligent patients want to tell you how to practice. So many efforts are being made to control physician practice. Contract management companies are largely about billing for services rendered. • Our patient population is getting less healthy which means they use the system more. There's not enough access to primary care appointments which leads to more people coming to the ER instead, this causes long ER wait times. The majority of the hospitals in the bay area are overcrowded and at capacity so it makes it difficult and frustrating to get specialist care for the patients that really need it and you can't transfer patients so they just sit in the ER and don't get care. The state of mental health care is sad and frustrating and feels like a revolving door for most of our chronically mentally ill. • Uncompensated work (overtime after shifts, patient calls/emails, charting, lectures). • The emergency department is already the safety net for the entire system and we are cracking under the weight of the pressure. What happens if this breaks too? Already patients aren’t getting the follow up and care they need, so they came back more sick and require even more recourses. • Ever increasing reliance on emergency departments to solve all the ever increasing failures in public health, primary care, and social issues. No recognition or support from hospital leaders when hospital is full yet ED must keep its doors open. Experienced nurses and doctors leaving practice. Nurses with minimal bedside experience.
• Not centralized. Small ICUs and moderate sized hospitals are too many in Japan.
• Staff ratios are already pushing remaining staff to overwork, and will only worsen as more leave the field / new hires come into a worsening field. There needs to be a significant increase in ED staffing and compensation before the whole system collapses. Or at the very least, there needs to be a push for some of the “overcrowding” to be shared with inpatient units, as the number of boarders becomes increasingly unsafe. • Lack of nurse staffing, and inadequate FTE when "fully staffed", lack of urgency by hospital systems about critical overcapacity issues/boarding, behavioral health delays and capacity issues ,terrible transport delays, constant executive leadership turnover, lack of vision in leadership, not listening to front line clinicians but highly compensated consultants instead. • Every shift is miserable and I have to code patients in triage because the ED runs at 50% capacity because there are no nurses to staff beds. • Increasing patient visits, boarders, violence and acuity. Increasing tribalism and physicians taking their stress out on each other (usually the ED). No more compensation nor adjustments in work environment or hospital throughput. • Lack of outpatient resources and the resulting need for the ED to be the safety net for all services. Lack of understanding that nursing needs/deserves better compensation. Too much admin. We don’t need MDs not seeing patients Too much influence of insurance and for profit groups on billing and how it negatively effects care. • Way too much money given to admin and health insurers, not enough basic care provided to patients who need it. • US medicine is all about money. Every issue. I practiced half my career overseas and half here. If you leave the system and see how it is elsewhere, the quest for the almighty dollar in everything we do here becomes even more obvious.
UNEDITED ANSWERS TO OPEN MIC PRIOR QUESTION:
continued from page 17
• Emergency medicine is no more emergency medicine or may be never been emergency medicine in the UK. We call extended triage as emergency medicine. In majority of NHS hospitals EM physicians don't or unable to do any Airway procedures or look after critically unwell patients independently and rely completely on Anesthesia and critical care colleagues. Arrive and call anesthetist - Breathe - Call Critical care - Drama - Exist (Unfortunately this has become the ABCDE of EM in many places).
• Powerlessness.
• The overwhelming environment of profit over patients… THIS is the source of today’s moral injury. • Non-profits hoarding cash for endless turbulent times and not investing direct care. • The nurses, who have a different agenda, run the emergency department. The administration continues to have a market driven philosophy vs patient care oriented. Not having enough input into my work environment- I never thought I would be told what to do and how to practice medicine. • Patient entitlement, lack of continuity of providers. • Crowding and lack of staff. There is nowhere to put patients and not enough people to take care of them. The powers that be want to cut corners and make us do more with less, while they earn their millions and cut our salaries. • We feel comfortable pitting ourselves against each other and other medical specialties/professions and are hesitant to address the bigger, truer drivers and profiteers of strained medicine such as pharmacy, insurance, and administration. I believe that fighting for limited resources (such as time, funding) could be improved by dealing with the factors that create the limits in the first place. It also doesn't help that many in our profession feel more comfortable ignoring these issues and that many outside of our profession are not willing to believe a privileged group like ours can suffer. We need a megaphone for these issues, and these problems have to be on the lips of all doctors in hospital medicine, and these issues have to be brought up to lawmakers. • All about patient volume and not quality. Patients have innumerable medical and social needs. They can’t get into see other physicians due to insurance or transport constraints or there just not being any available. They are kicking people out of the inpatient side as fast as they can but inpatient is now the ONLY place where actual tests and care and consultation can be done. You are forced to play chicken with other specialists and providers: everyone says this isn’t their problem to help the patient with and pass the buck and the patient gets left stuck unless someone blinks and goes out of their way to help. And that group is the first to burn out. Also I am ID. And while a lot of lip service is given to the value and knowledge of ID docs, when we are actually called to consult people seem to believe they are calling us to do something beneath them or act like ‘what should I use to treat this and how long’ is an easy curbside question and not literally our whole job and what we trained an extra 2 years to answer. Finally, ID docs make less than even PCPs and actually act as many patients PCPs but they are overlooked in all the talks about resources and the like. • More experienced physicians driven out by overwhelming practice burdens, leaving younger physicians to miss out on benefits of learning from them. • Unhealthy skepticism, anti-vax movement, EMRs, bloated hospital admin, constant fear of litigation, regulatory agencies, stagnant wages in the setting of inflation and overhead costs, sunk cost fallacy, inertia, professional handcuffs, community obligation without a route to escape, etc. • Massive increases in volume, with unrealistic turnaround time expectations. Hopefully not leading to increasing errors. • Shit rolls downhill. Every case that a specialty doesn't think is a quick fix goes to the hospitalist service. These patients have nowhere to go. Nurses have caps but physicians don't so we just have to suck it up. We haven't gotten a raise, cost-of-living or otherwise for 5 years despite handling the pandemic while the administrators got 7 figure bonuses. We're told there's not room in the budget for us to get a raise, so we can’t recruit, so we have less doctors to handle more patients, so patients get less time/care, so they stay longer in the hospital, rinse and repeat.
• Too much admin. Too much "productivity" emphasis.
• See above re: lack of patient responsibility for their behavior; lack of collegiality in many interactions with consultants/other services; the external threats to our medical system by new fangled techbased systems such as Amazon, etc, that may provide an excuse for our leadership to try to squeeze yet more out of us for less, under the pretense of saving the organization. Outpatient providers are leaving, and this places additional stress on clinics, with the overflow of patients invariably ending up in ED. Outpatient providers favoring telehealth for all encounters, where patients prefer to be seen in person and again, end up in ED. Lack of forethought and meaningful planning from leadership to appropriately staff the department, in the face of ever-increasing patient volumes. Lack of real and meaningful acknowledgment of the fact that our schedules, and the lack of any circadian planning, is crippling our health (particularly an issue in ED environment where there’s no pattern or rhyme to our schedules whatsoever). • ER can’t go on zoom, we need buildings space supplies and staff and even though we support the whole medical center they abuse us, steal our nurses and send us patients while they zoom as if we had infinite places to put them. We don’t, they are in our waiting rooms bathroom hallway parking lot and they are angry and uncomfortable and they leave and or bad things happen, people fall, bleed, vomit, the other end, sugar crashes, Blood pressure soars, fib races, Covid spreads etc..: we aren’t urgent care infusion center transfusion center pre op pre admit your extra procedure lab a psych ward or a nursing home except we are right now and we can’t even practice our specialty any more, we have something called a front system I call a system failure, corporate people are making decisions clinicians should, priorities are all wrong, our boss is quitting, our nurses striking, my colleagues futility pinging away our labor dreams on social media when they should actually be marching loudly in the streets and I’ll probably get dinged for not attending enough required wellness because I’ve been too busy with required performance improvement as if admin actually had any commitment to real collaboration and changing anything when the docs are apparently all requesting modules on saving time and dealing with patient complaints – sigh—can’t make this up.
• The fact that everything falls back to the physician when we truly have very little say or power over anything. • So many issues. Low pay, poorly staffed, increasing responsibilities of the ED physician where not enough PCP availability drives patients to ED, expected working hours greater than national ED average. Poor patient care because wait times are so long. Few resources. High burnout. Poor recognition of how hard the ED has worked during the pandemic, where we got pulled into doing ICU, IR, hospitalist work. • Increasing amount of work for inflation depreciated pay, worsening staff safety, lack of recognition and support by other physicians / hospital admin / patients for EM being truly frontline in an increasingly difficult practice environment, a system that is causing worsening patient care. • Decreased availability to primary care leads significant increases in ER visits. We are not protected with patient caps and the fact that we are carrying 15 patients at a time without a full staff or an ER big enough to attend to these patients, does not matter to the patients, the health system, etc. We are still expected to perform at the same level and deliver the same care despite this overwhelming reality. Not to mention each shift is so challenging that it is hard to recover between them. The toll on our well-bring and negative impact on our families and patients is too much to bear. • Capitalist for profit system of US health care not conducive to federal mandate for ER to care for all comers in a decent humanitarian way. We who choose to work in ED become witness to huge amounts of real time chronic suffering (drugs, homeless, mental, uninsured) yet can’t do anything meaningful to help. And it hurts and burns us out, especially with suffering plus after covid because we are part of this broken fucked up system. And the high paid surgeons, specialists, and concierge med folks give zero shits about our 24/7 work, our burnout, our patients. • Everyone is part-time or not interested in partnership- creates less investment in sites and EM in general. Decreasing doc compensation in the face of increasing wages to other positions- makes going to medical school seem like a bad financial decision. • Lack of accountability of violent and aggressive behavior towards our colleagues in the local legal system. • EM-boarding and lack of ability to receive reimbursement for quality care.
• Low pay, high volume, bad consultants.
• The ER has become the dumping ground for all patients who cannot access their physicians or even care to establish a primary care doctor, regardless of how acute their complaints are. Then, patients' expectations in promptness of care and giving out exact diagnoses are distorted to what the emergency departments was designed to do and what they can handle. We are not the urgent care, amazon.com, or McDonald’s. The push to quickly see and dispo patients when there's high volume become dangerous to patient safety and to the mental health of the staff caring for these patients. • For-profit groups, too many residents, decreasing insurance pay -> to decrease pay. • Lack of admin/hospital executive commitment to people/staff over profit, admin's continued effort to do more with less, and the continued talk about likely to recommend/patient satisfaction scores with no desire to spend money to improve staffing and hospital capacity to decrease wait times/improve flow at every level of care. • Money reigns over everything. Out of touch decisionmakers. • Contract metrics from for-profit hospital corporations and CEOs and C-suite executives with no clinical experience. • Lack of adequate administration causing loss in nursing, staffing, loss of trust, poor financial decisions leading to inadequate patient care. Inability to transfer patients for higher level of care due to inadequate staffing nationally. Overuse of ED for nonemergent cases. Overcrowding of entire hospital systems. I fear the US healthcare system is moving towards total collapse.
• Emergency medicine had become the primary source of Healthcare for everyone. It's not intended for that and not staffed for that.
• Administrative burdens and dangerous mid levels. • We need significant reforms. I work in EM, and we have become the dumping ground for all of medicine. Can't get that non-emergent test on a Thursday? Send them to the ER. Chronic issue that's suddenly slightly worse? Send them to the ER. Meanwhile there is increased government oversight hindering my ability to practice while increasing my liability. We have been asked to do more with less for many years, and it's getting worse. It is driving people out of medicine. • Corporate business and insurance business taking over medical practice at all levels. • EM is the safety net of health care and it is breaking. Our system is so dysfunctional and it all rolls down to us. We're expected to do more and more with less and less (staff, rooms, time, etc.) and when the physicians quit in frustration we'll be replaced by PAs and NPs. • ED staffing is terrible, private equity in EM. • CMGs reducing staffing levels for both doctors and nurses to bare minimums, but then increasingly higher rates of malpractice suits, often for system problems out of your control. Being responsible for midlevel mistakes when you don’t even see the patient. system where you’re presumed guilty of malpractice until you prove your innocence. • The for profit system of medicine has failed. The only people who benefit are top hospital admins, insurance companies and pharma. The profit is at the expense of patient care. The inequities are increasing. What used to be possible in the outpatient follow up world no longer is, while what used to be an “acceptable” admission no longer is either. It is now also effecting those with private insurance. Working with inadequate resources puts us in a position where we are part of providing inadequate care and a terrible patient experience. We are bogged down with meaningless clicks in the name of increasing revenue and pressured to take it upon ourselves to correct the metric of the month or improve the patient experience without being given any means to do so. It is demoralizing to be practicing medicine in the current healthcare system yet the needs of the people are many and increasing. • Hospital leadership completely sold out to price centric medicine but call it value driven patient centric.








