EXPLORING THE STAFFING CRISES THROUGH NEW MODELS OF CARE
Recruitment and Retention Tactics

texasnurses.org
MAGAZINE TNA: Empowering Texas Nurses to advance the profession | Issue 2, 2023
TEXASNURSING
ISSUE 2, 2023
Volume 97, Number 2
EDITOR IN CHIEF: Serena Bumpus
MANAGING EDITOR: Lisa Maxwell
COPY EDITORS: Gabi Nintunze, Natalie Hill
4807 Spicewood Springs Rd., Bldg 3, Suite 100, Austin, TX 78759-8444
P: 800.TNA.2022 or 512.452.0645; F: 512.452.0648
tna@texasnurses.org | texasnurses.org
MISSION
Empowering Texas Nurses to advance the profession
VISION
Nurses transforming health
TEXAS NURSING (ISSN 0095-36X) is published quarterly—
Winter, Spring, Summer, Fall—by the Texas Nurses Association, 4807 Spicewood Springs Rd., Bldg. 3, Suite 100, Austin, TX 78759-8444
Periodical postage is paid in Austin, Texas.
One-year subscriptions: $30 (nursing schools, libraries, hospitals, non-nurses, out-of-state nurses), foreign $35; single copy $3.00. Subscription is not available to non-member Texas nurses. Some back issues may be viewed online at texasnurses.org
PUBLISHING PARTNER
Monarch Media & Consulting, Inc.
P: 512.680.3989 or 512.293.9277; F: 866.328.7199 monarchmediainc.com | chellie@monarchmediainc.com
Advertising inquiries: call Chellie Thompson at 512.293.9277.
TEXAS NURSING is indexed in The Cumulative Index to Nursing and Allied Health Literature and in the International Nursing Index. 16mm, 35mm microfilm, 105mm microfiche, article copies available from University Microfilms International: 1.800.521.3044. Statements of fact and opinion are made on the responsibility of the authors alone and do not imply an opinion on the part of the officers or the membership of TNA.
POSTMASTER
Send address changes to TEXAS NURSING , 4807 Spicewood Springs Rd., Bldg. 3, Suite 100, Austin, TX 78759-8444.
ARE YOU MOVING?
Need to change your address? If so, provide it quickly and easily in the Members Only section of the TNA website, texasnurses.org Or mail your new address—at least six weeks prior to your move— to Texas Nurses Association headquarters. We’ll make sure your TEXAS NURSING makes the move with you.
FEEDBACK EMAIL OR LETTER GUIDELINES
TEXAS NURSING will select emails/letters on the basis of readership interest and relevance to current nursing/health care events. TEXAS NURSING reserves the right to edit all letters. Guide: Limit to 200 words; focus on single issue; include writer’s name, mailing address, and daytime phone. Send to: editor@texasnurses.org
Copyright 2023 © Texas Nurses Association
BOARD OF DIRECTORS
OFFICERS:
Joyce Batcheller DNP, RN, NEA-BC, FAONL, FAAN, President jbatcheller7@yahoo.com
Colleen Marzilli, PhD, DNP, RN, CNE, NEA-BC, Secretary cmarzilli@uttyler.edu
Gloria Lorea, DNP, RN, NEA-BC, Treasurer glorialoeradnp@gmail.com
Tamara “Tammy” Eades, DNP, MSN, RN, Past President eades@uta.edu
DIRECTORS:
Patricia Freier, MSN, RN-BC, CPHQ patricia.freier@sbcglobal.net
Lucindra Campbell-Law, PhD, ANP, APRN, PMHNP, BC campbel1@stthom.edu
Edtrina Moss, PhD, RN-BC edtrina@comcast.net
Brandon “Kit” Bredimus, DNP, RN, CEN, CPEN, CNML, NE-BC, CENP, NEA-BC kit.bredimus@midlandhealth.org
Mary Vitullo, MBA, MSN, RN-BC, PCCN, NE-BC, CLSBB vitullo.mary@yahoo.com
CHIEF EXECUTIVE OFFICER: Serena Bumpus, DNP, RN, NEA-BC, sbumpus@texasnurses.org
TNA DISTRICT PRESIDENTS
Dist. 1: Jackeline Biddle Richard, DNP, JD, RN, CNE, jackie.richard1@icloud.com
Dist. 3: Christopher Rougeux, MSN, RN, crougeux99@gmail.com; District office: Jamie R. Rivera, JamieRivera@texashealth.org
Dist. 4: Robert Castillo, MSN, RN, CCRN, NE-BC, 817-229-6478, robert.castillo@utsouthwestern.edu; tnad4.nursingnetwork.com; District Secretary Lori Batchelor, batchelorb@prodigy.net
Dist. 5: Bonnie Clipper, DNP, MA, MBA, RN, CENP, FACHE, FAAN, bclipper1@gmail.com, tna5.org
Dist. 7: Connie Barker, APRN. PhD. FNP-C, crbarker1@yahoo.com, tnadistrict7@gmail.com
Dist. 8: Donna R. Wallis, MBA, MSN, RN, 210-486-3089 dwallis3@alamo.edu, tna8.org
Dist. 9: Nancy Yuill, PhD, RN, nyuill@yahoo.com
District office: Melanie Truong, RN, Executive Secretary, tna9@tnadistrict9.com, tnadistrict9.com
Dist. 17: Mari Cuellar, NEA-BC, MSN, RN, mari.cuellar@christushealth.org
Dist. 18: Belinda Gallegos, belinda.gallegos@ttuhsc.edu
Dist. 19: Dixie R. Rose, RN, dixiegtc@gmail.com
Dist. 35: Karen Koerber-Timmons, PhD, RN, CLNC, CNE, NEA-BC, CCRN, RN-BC mkkoerbertimmons@gmail.com
At-Large: Contact TNA, 800-862-2022, ext. 129, brichey@texasnurses.org
TEXAS NURSING MAGAZINE | ISSUE 2, 2023 PAGE 2



Virtual Nursing Keeping Pace with a Race Horse PAGE 3 ISSUE 2, 2023 | TEXAS NURSING MAGAZINE 5 PRESIDENT’S NOTES TNA Listening Tours 6 TNA MEMBER NEWS Kudos Contents IN EVERY ISSUE ARTICLES AND FEATURES 18 HEALTH AND HEALING IN HARMONY A New Model of Care 8 OUTSTANDING 25 TEXAS NURSES 2023 Congratulations! 20 THE STOPLIGHT HUDDLE Supporting a Culture of Teamwork and Quality Patient Care 23 THE TNA MENTOR PROGRAM Grow Your Career Share Your Insight The Candidate-Centric Recruitment Model Putting Nurses First NURSE STAFFING in 10 14 16
10% of people in Texas have a substance use disorder.
Welcome to Be Well Texas. We’re Glad You’re Here.
Be Well Texas is working to transform how people living with SUD and non-severe mental illness throughout Texas are cared for and treated. Our mission is to provide access to high-quality, low-barrier, evidence-based treatment statewide.

Be Well Texas is accepting new referrals. Refer a patient today.
• Virtual visits, anywhere in Texas.

• Comprehensive medication and behavioral services for substance use disorder, including alcohol and opioid.
• Insurance not required for patients who qualify. If qualified, all services, medication and labs are covered.
• Bilingual services available.
REFER A PATIENT, 24/7.
We’re Glad You’re Here
Call 888-85-BeWell or visit BeWellTexas.org
President’s Notes
Joyce Batcheller DNP, RN, NEA-BC, FAONL, FAAN

TNA LISTENING TOURS Reframing Challenges Into Possibilities
NURSING WORKFORCE ISSUES are the consistent top message from across the state. You may recall that TNA’s CEO, Serena Bumpus, DNP, RN, NEA-BC, Director of Government Affairs, Jack Frazee and I have traveled to four cities so far; and the message is the same: all are experiencing some level of difficulty in hiring, retaining, and engaging their workforce. And everything is interdependent and magnified. For example, the faculty shortages lead to limiting qualified applicants’ entry into schools, which limits the numbers of graduates produced; hospitals are increasing the number of LVNs they hire which causes bed closures in skilled facilities and nursing homes; ambulatory settings and clinics cannot compete with sign on bonuses and salaries that are being offered by other settings which creates shortages in those settings; and new jobs are being created as care is being redesigned by companies such as CVS, Walmart, and Amazon.
Healthcare organizations are experiencing major financial losses due to loss of funding available during the pandemic and nurse leaders are being told to eliminate the use of travelers and premium pay plans despite high patient volumes. As a result, we see staffing challenges, high levels of stress/mental health concerns increasing, high levels of RN turnover, and continued or increased violence in the workplace.
Additionally, Texas is continuing to grow, and new hospitals and additional bed capacity are being planned.
ARE WE SURPRISED?
No. I believe the concerns we are hearing will be addressed in the new TNA strategic plan and goals. The TNA board, CEO and staff held a formal strategic planning session in March. Once it is finalized, we will share it with you, and I will invite your feedback about what is planned. We need some very practical, immediate activities and some long-range, audacious ideas to address the issues before us. While not a surprise—it was great to learn that many organizations are developing different models of care and incorporating different kinds of technology. For example, the implementation of virtual nursing care and telehealth services to support bedside nurses in providing in-person care is popular in many settings. Some organizations are doing virtual admissions and discharges and using virtual sitters and low camera capabilities to enable night-time monitoring. Universities are implementing virtual reality along with simulation to enhance competency development for students.
WHAT ELSE SHOULD WE BE DOING?
I am including a citation to a recent article that I believe you will find helpful—and overwhelming. We have so many reports
EQUITY PAUSE: A structured time to pause, reflect and remind us of our shared goals and discuss what we may be able to do to better.
Example Ideas:
Start a meeting by allowing 30 seconds to review the goal of the committee or the purpose of the specific meeting as the framework for “why am I here?”
What is the connection between racial equity and items on the agenda we plan to discuss?
Start a change-of-shift report with a 30-second equity pause to remind ourselves we are here for continuity and to provide high-quality care.
Did we support each other to feel empowered to speak up during our discussions so everyone could be heard?
and suggestions for issues to address to move us ahead while we are trying to keep on top of the day-to-day issues.
We need to reframe/flip challenges into possibilities and be creative in designing the work environments for the future. Can you imagine the possibilities we could develop if the topic of innovation were on every meeting agenda? Ask yourself, what will it take to fall in love with being a nurse and contributing to the profession again? Should we commit to an Equity Pause (see below) in different forums to assess how well we are doing? We can add this practice at the beginning of meetings to reframe our thinking for the future. Everyone can commit to the Equity Pause!
We need to share best practices/new models of care and other innovations with each other across the districts and state. We could speed patient care improvements by “stealing shamelessly from each other”. To begin to support this, TNA will be hosting poster presentations for the first time at the upcoming TNA conference in June in Houston. Innovative practices will be shared through Nurse Talks and other communication tools. Please join me by continuing to be engaged in the important work TNA is leading. Be willing to share a best practice or innovation you've learned. Also encourage other colleagues to join TNA to strengthen the voice of nurses in Texas and to let their voices be heard. i
REFERENCES
Yoder-Wise, P. , Batcheller, J. and Sullivan, L. Issues of Concern: What Nurse Leaders Say and Need to Consider. Nurse Leader. Published Feb. 17, 2023. Accessed: www. nurseleader.com/article/S1541-4612(23)00041-1/fulltext
Virginia Mason institute. Equity Pause Toolkit (2020) Accessed: www.virginiamasoninstitute.org/equitypause-toolkit/
PAGE 5 ISSUE 2, 2023 | TEXAS NURSING MAGAZINE
TNA MEMBER NEWS
SPOTLIGHT ON YOU
KUDOS
The following organizations received ANCC’s Magnet designation: Baylor Scott & White Health –College Station Region, Memorial Hermann Katy, Christus Mother Frances Tyler

Dr. Cynthia Weston, DNP, APRN, FNP-BC, CHSE was selected as a fellow of the American Association of Nurse Practitioners. The University of North Texas Health Science Center at Fort Worth also named Cindy as the founding dean of its new College of Nursing.
Catherine Robichaux, PhD, RN, Alumna CCRN was appointed editor of the ethics column for The Online Journal of Issues in Nursing and as a member of the panel to revise the Code of Ethics with Interpretive Statements to be released in 2025.


Tracey Ramsey Abbott, DNP, MPAff, RN, CAIP, CNAMB was accepted into the Healing Politics Campaign School.


Chris Rougeux , MSN, RN, HCA Healthcare/ Medical City Healthcare was elected TNA District 3 President.


Megan Flores, RN, BSN, QMHP-CS, Nurse Manager, Crisis Mental Health Services, My Health My Resources of Tarrant County was elected TNA District 3 Vice President (President Elect).
Brandi Rougeux, Nursing Director, Behavioral Health, Texas Health HEB was elected TNA District 3 Director.




Jennelle Scroggins, MSN, RN, CCRN-K, CPHQ, Director of Clinical Operations, Medical City Fort Worth was elected TNA District 3 Treasurer.
Delores Mack , MPH, BSN, BS, RN, City of Arlington was elected TNA District 3 Leadership Succession Chair.

Congratulations to the following hospitals for receiving the prestigious Pathway to Excellence designation: Baylor Scott & White Medical Center Lake Pointe in Rowlett, Texas, Texas Health Center for Diagnostics and Surgery in Plano, Texas, Texas Health Harris Methodist Hospital Stephenville in Stephenville, Texas.

Jamie K. RoneyHernandez , DNP, RN, NPD-BC, CCRN-K, has joined TNA staff as the new Director of Nursing Professional Development.

Anna Gore, MSN, RN, has been promoted to serve as chief nursing officer for Christus Santa Rosa Hospital in San Marcos, Texas. Most recently, Ms. Gore was the administrative director for the hospital’s intensive care and progressive care units.
Christine Martinez , MSN, R.N., was appointed chief nursing officer of Laredo Medical Center.
Kit Bredimus, DNP, RN, CEN, CPEN, CNML, NE-BC, CENP, NEA-BC achieved AONL Fellowship designation.
Colleen Marzilli, PhD, DNP, MBA, RN-BC, CCM, PHNA-BC, CNE, NEA- BC has been promoted to Professor at University of Texas at Tyler



Missam Merchant, MBA, BSN, RN, CENP, CCRN, PCCN, CV-BC, GERO-BC, MEDSURG-BC, NE-BC is sending a team to East Africa to train 35 nurses for free in peri-operative nursing.
Sharon Cannon, Ed.D, RN, ANEF received the AONL Foundation Friend of the Year Award, a national award for active commitment to the Foundation. i
TEXAS NURSING MAGAZINE | ISSUE 2, 2023 PAGE 6
Meet the Team
We’ve created the next generation of aromatherapy tools to calm and comfort patients at every stage of care, letting our team, help yours.


No drowsiness, no IVs, no prescriptions, no drug interactions.

TALK TO OUR TEAM SOOTHINGSCENTS.COM/CONSULTATIONS
Queasiness Anxiousness Breathe Easy Energize & Uplift Morning Sickness
























 Aaron Salinas, DNP, APRN, FNP-BC, PMHNP-BC, NRP UT Health Rio Grande Valley
Allison Wojcik, BSN, RN, AMB-BC Baylor Scott & White, Round Rock
Amanda Williams, BSN, RN, OCN, ONN-CG Baylor Scott & White, Round Rock
Amy Boothe, DNP, RN, CHSE Texas Tech HSC School of Nursing, Lubbock
Autumn McNiel, MSN, RN, NEA-BC Baylor Scott & White, Marble Falls
Elisabeth Frost, RN-BSN, IBCLC Baylor Scott & White, Round Rock
Hollis Franco, Ph.D., RN, MEDSURG-BC Texas Tech HSC School of Nursing, Lubbock
Janna Berg, BSN, RN, CPN Children’s Medical Center, Dallas
Jill Sarro, MSN, RN, CPHON Texas Children’s Hospital, Houston
Keira Brown, RN, BSN, RN-BC Baylor Scott & White, Irving
Kelly C. Mullis, MBA, BSN, RN, CNOR, NEA-BC Baylor Scott & White, Marble Falls
Krystal Rae McClung, BSN, RN Baylor Scott & White, Round Rock
Linda Venzke, MSN, RN UTMB, Galveston
Lori Spies, Ph.D., APRN, FNP-C, FAANP Baylor Louise Herrington School of Nursing
Madalyn Penland, BSN, RN Baylor Scott & White, Round Rock
Marie Kelly Lindley, Ph.D., RN, CNE Baylor Louise Herrington School of Nursing
Meaghen Pleasants, MSNEd, RN, CMSRN Baylor University Medical Center, Dallas
Melonie Ankerholz, RN, MSN-MHA Baylor Scott & White, Marble Falls
Michelle Rhea, RN, MS, NE-BC Memorial Hermann Southwest Hospital, Houston
Rhonda Manor-Coombes, BSN, RN, TCRN Baylor Scott & White, Lakeway
Sally A. Gillam, DNP, MAHS, RN, NEA-BC Baylor Scott & White, Hutto
Scott M. Williams, DNP, RN, NE-BC Baylor Scott & White, Irving
TaCharra Laury, DNP, APRN, ACNP-BC, AOCNP University of Texas MD Anderson Cancer Center
Tera Holland, BSN, RN, CPN Children’s Health, Children’s Medical Center, Dallas
Yasmin La-arni S. Horlador, RN, BSN Baylor Scott & White, Lakeway
Aaron Salinas, DNP, APRN, FNP-BC, PMHNP-BC, NRP UT Health Rio Grande Valley
Allison Wojcik, BSN, RN, AMB-BC Baylor Scott & White, Round Rock
Amanda Williams, BSN, RN, OCN, ONN-CG Baylor Scott & White, Round Rock
Amy Boothe, DNP, RN, CHSE Texas Tech HSC School of Nursing, Lubbock
Autumn McNiel, MSN, RN, NEA-BC Baylor Scott & White, Marble Falls
Elisabeth Frost, RN-BSN, IBCLC Baylor Scott & White, Round Rock
Hollis Franco, Ph.D., RN, MEDSURG-BC Texas Tech HSC School of Nursing, Lubbock
Janna Berg, BSN, RN, CPN Children’s Medical Center, Dallas
Jill Sarro, MSN, RN, CPHON Texas Children’s Hospital, Houston
Keira Brown, RN, BSN, RN-BC Baylor Scott & White, Irving
Kelly C. Mullis, MBA, BSN, RN, CNOR, NEA-BC Baylor Scott & White, Marble Falls
Krystal Rae McClung, BSN, RN Baylor Scott & White, Round Rock
Linda Venzke, MSN, RN UTMB, Galveston
Lori Spies, Ph.D., APRN, FNP-C, FAANP Baylor Louise Herrington School of Nursing
Madalyn Penland, BSN, RN Baylor Scott & White, Round Rock
Marie Kelly Lindley, Ph.D., RN, CNE Baylor Louise Herrington School of Nursing
Meaghen Pleasants, MSNEd, RN, CMSRN Baylor University Medical Center, Dallas
Melonie Ankerholz, RN, MSN-MHA Baylor Scott & White, Marble Falls
Michelle Rhea, RN, MS, NE-BC Memorial Hermann Southwest Hospital, Houston
Rhonda Manor-Coombes, BSN, RN, TCRN Baylor Scott & White, Lakeway
Sally A. Gillam, DNP, MAHS, RN, NEA-BC Baylor Scott & White, Hutto
Scott M. Williams, DNP, RN, NE-BC Baylor Scott & White, Irving
TaCharra Laury, DNP, APRN, ACNP-BC, AOCNP University of Texas MD Anderson Cancer Center
Tera Holland, BSN, RN, CPN Children’s Health, Children’s Medical Center, Dallas
Yasmin La-arni S. Horlador, RN, BSN Baylor Scott & White, Lakeway
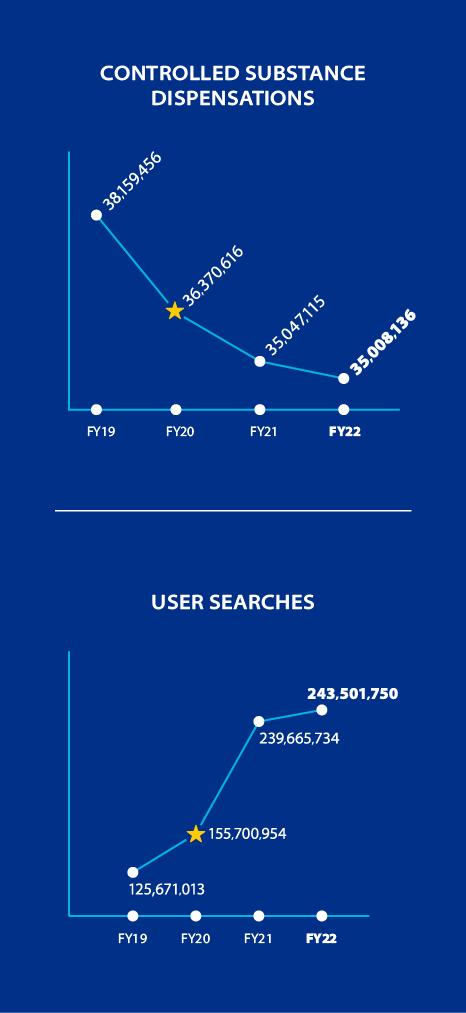
PMP Data Show Progress and Opportunity to Address Opioid Epidemic
It has been nearly three years since the Texas Legislature mandated that prescribers and pharmacists check the Texas Prescription Monitoring Program (PMP) before prescribing or dispensing opioids, benzodiazepines, barbiturates and carisoprodol. Since the mandate took effect on March 1, 2020, there has been a steady decrease in the number of controlled substances dispensed and an increase in user registrations and searches of the PMP database.
Dispensation data from the Texas State Board of Pharmacy show a 3.6 percent decrease in controlled substance dispensations, from 36.3 million in fiscal year (FY) 2020 to just over 35 million in FY 2022. During the same period, user searches increased by nearly 57 percent, from 155.7 million to 243.5 million.
The importance of using the PMP as a patient care tool is greater than ever as opioid overdose deaths continue to rise nationwide. In Texas, predicted opioid overdose death data from the Centers for Disease Control and Prevention (CDC) increased from 1,520 in the 12 months ending in March 2020 to 2,756 in August 2022. While most of those deaths occurred due to synthetic opioids such as fentanyl, more than 21 percent were attributed to natural and semisynthetic opioids, including hydrocodone – the most commonly prescribed controlled substance in Texas.
Checking the PMP for every patient every time helps prevent opioid misuse and overdose in your community. Please visit txpmp.org for more data reports and resources for effectively communicating with patients about the risks associated with opioid misuse.
Sources:
Ahmad, F.B., Cisewski, J.A., Rossen, L.M., and Sutton, P. (2023). Provisional drug overdose death counts. Centers for Disease Controls and Prevention, National Center for Health Statistics. Retrieved from, https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm.
Texas State Board of Pharmacy. (2022). Fiscal Year 2022 PMP Data Annual Summary. Retrieved from, https://txpmp.org/assets/images/PMP_FY-22-Annual-Summary_Data-Reports.pdf.
Check the Texas PMP at the txpmp.org Every patient. Every time.
ADVERTORIAL
ADVERTORIAL
Virtual Nursing
Keeping Pace with a Race Horse

THE VIRTUAL NURSING LANDSCAPE and even the terminology has created a curious and inspiring buzz among the nursing community and the healthcare industry as a whole. Wherever your place in the industry—integrated delivery system, ambulatory health, providers and payers, advocacy, healthcare technology solutions or service delivery you are likely hearing and seeking to understand what Virtual Nursing means and its potential to impact health outcomes and the health of the nursing profession. This article aims to share a summary of industry activity in virtual nursing services and the impacts this vision and strategy can have on our calling in nursing. Virtual nursing has been defined and evolved over time with attempts from all players in the industry. The common theme among most definitions is that virtual nursing is a model of care that leverages technology to integrate an experienced nurse into the acute care setting to provide agreed-upon services to the patient and bedside team. The experienced nurse, in this model, is working from a remote location. Schuelke, Aurit, Connot, & Denney (2019) define the work activity of virtual nursing in six core roles: patient education, staff mentoring/education, real-time quality/
By Patches Pace Seely, MBA, RN
The work activity of virtual nursing falls into six core roles: patient education, staff mentoring/education, real-time quality/patient safety surveillance, physician rounding, admission activities, and discharge activities.
patient safety surveillance, physician rounding, admission activities, and discharge activities. Terri Hinkley, EdD, MBA, BSN, CEO of the Medical-Surgical Nursing Certification Board states “the certification being built notes an important distinction between virtual nursing and telehealth nursing in that virtual nursing provides support to the acute/hospitalbased patient in partnership with the bedside care team as opposed to a nurse caring for a patient remotely in a post-acute or less acute setting” (T. Hinkley, personal communication, April 21, 2023). As definitions continue to evolve, that distinction is breaking through as a theme in defining virtual nursing versus telehealth nursing.
BENEFITS OF VIRTUAL NURSING
I do not believe it’s a bold statement to say the development of modernized care delivery models, enabled by technology, is an industry imperative. Virtual nursing models, including programs architected by hospitals, partnerships
with industry service providers to provide virtual nursing services or some hybrid of the two will continue to refine the programs to answer the call to adapt to the current and forecasted state of healthcare.
There are several studied benefits to virtual nursing programs.
RETENTION
Retaining nurses and stabilizing the workforce is fundamental to the profession, the industry and is a priority for the United States, as the impending shortage is a risk to public health. The NSCBN 2023 Environmental Scan: Nursing at a Crossroads—An Opportunity for Action cites a McKinsey survey conducted in November 2021 stating that “32% of RNs indicated a likelihood to leave their current position involving direct patient care, up from 22% in February 2021”. The November 2021 survey indicated that 39% of those intending to leave would be leaving to retire, return to school or leave the profession. Primary reasons
TEXAS NURSING MAGAZINE | ISSUE 2, 2023 PAGE 10
were due to insufficient staffing levels, desire for higher pay, not feeling listened to or supported at work, and the emotional toll of the job. Virtual nursing, given its less-physical demands offers a great respite to nurses nearing retirement age who have deep expertise and still desire to transfer knowledge and mentor less-experienced nurses. Additionally, with staffing levels continuing to need to adapt to shortages, the virtual model serves as an augmentation to the inpatient care team thereby offsetting critical tasks to care like admission histories, high quality medication list acquisition and discharge teaching. Rotating nurses through bedside care delivery and a virtual role is an impactful way for organizations to send the message that nurses who remain at the bedside are valuable and that flexible scheduling through new care delivery models is possible. Increasing retention has an immediate return on investment for hospital systems recovering from volume, payer, CMI and LOS instability.
MENTORSHIP
Virtual nursing programs expand a unit’s capability to mentor and educate new graduate nurses. The state of readiness to practice for our nursing graduates who answered the call to join the nursing profession has been slowly declining. In research conducted using Performance-Based Development Systems (PBDS) in the last decade, studying more than 10,000 new graduate nurses there has been a year over year decline in initial competency. Specifically in 2015, 23% of new graduate nurses scored as “acceptable” to practice compared to 8% “acceptable” to practice in 2020 (Kavanaugh & Sharpnack, 2021). This research does not account for the impacts of a global pandemic nor the rising complexity of patients entering the inpatient setting. The knowledge transfer and contextual learning opportunity between a new graduate nurse and an experienced virtual nurse can fortify the safety of the new graduate nurse as they enter practice. The “mentor” role of the virtual nurse has the potential to
impact the closure of the experienceto-complexity gap we face in nursing today. Academia is poised to impact the gap as well, using virtual capabilities. Academia and care delivery systems forming partnerships to advance our education models will be yet another intervention needed to support our new graduate nurses and their journey to practice effectively.
AVOIDING MISSED CARE
From hospital-based virtual nursing programs to vendors providing virtual nursing services to a hospital system, there are common products offered with fairly consistent claims. Some programs survey the native EHR for signs of missed care or signs a patient may be declining. There is an advancing body of research evaluating the impact of missed care. Missed care is defined as any aspect of care that is omitted (in part or whole) or
delayed, including clinical, emotional or administrative care. The framework of missed care assumes environmental factors impacting the nurse’s capacity to complete these care interventions. Impacts like staffing and resource elements, team and skill mix dynamics and how those impact what value is placed on which care behavior is needed most (Shuelke & Connot, 2020). Virtual nurses can assist in identifying and prioritizing tasks for less-experienced nurses working in the hospital environment. When the virtual nursing prioritization is aligned with nurse sensitive indicator objectives, prioritization of missed care items becomes grounded in clinical safety and quality.
RETURN ON INVESTMENT
Whether you are an organization looking to start a virtual nursing program or an organization seeking to purchase this service from a vendor, understanding how the operational metrics for the virtual nursing team are collected, monitored and used for performance improvement are foundational. To show return on investment, virtual nursing must

PAGE 11 ISSUE 2, 2023 | TEXAS NURSING MAGAZINE
Virtual nursing, given its less-physical demands offers a great respite to nurses nearing retirement age who have deep expertise and still desire to transfer knowledge and mentor less-experienced nurses.
measure and perfect both operational and clinical impact for the organization. Making a virtual model CFO-proof will ensure sustainability of the model and support the narrative for spread and scale. Without operational metrics around how the virtual nurse can impact the productivity of the bedside nurse, building a business case will be challenged. There are measurable impacts to lengths of stay and speed to initiation of care seen in virtual nursing programs. Attribution of these outcomes to reduction in length of stay or other operationally valuable metrics is difficult to account for. Ashley VonNida, DNP, MBA, MSN, CNO of Equum Medical shared that purchased virtual nursing programs
can in some cases be neutral to budget as nursing units are operating at a high vacancy rate already (A. VonNida, personal conversation, April 17, 2023). As we look to innovate care delivery models, finance and productivity models will need aligned modifications to ensure financial outcomes of virtual nursing are sustainable.
VIRTUAL NURSING COMPETENCIES
Working in a virtual environment creates an unique and evolving skill set requiring the profession of nursing to define competencies for virtual nurses. The Academy of Medical-Surgical Nurses, in collaboration with virtual nursing thought
A Reputation for Excellence!
Educating nurses since 1890, UTMB SON offers undergraduate, graduate and doctoral degree tracks, designed to meet the unique needs of each nursing professional. Our graduates are skilled in providing patient-centered care and are developed to become leaders in health care.

UTMB SON’s teaching innovations have resulted in consistently high national rankings and alumni who have distinguished themselves as leaders throughout Texas and the United States. Today, informed by tradition, our vision continues to be our mission—to be the best in nursing education, research and practice in order to improve health for people around the world.
Programs Offered
BACHELOR OF SCIENCE IN NURSING
• BSN Traditional (on-campus)
• RN-BSN (online)
MASTER OF SCIENCE IN NURSING (ONLINE)
• Family Nurse Practitioner
• Adult-Gerontology Acute Care Nurse Practitioner
• Adult-Gerontology Primary Care Nurse Practitioner
• Neonatal Nurse Practitioner
• Clinical Nurse Leader
• Executive Nurse Leader
• Nurse Educator
CERTIFICATE (ONLINE)
• Post MSN - Adult-Gerontology Acute Care Nurse Practitioner
• Post BSN/MSN - Nurse Educator
• Post Bachelors - Rural Telehealth (any health science)
DOCTOR OF NURSING PRACTICE (ONLINE)
• BSN to DNP
▪ Family Nurse Practitioner
▪ Adult-Gerontology Acute Care Nurse Practitioner
▪ Dual Family Nurse Practitioner/ Adult-Gerontology Acute Care Nurse Practitioner
• MSN to DNP DOCTOR OF PHILOSOPHY IN NURSING (ONLINE)
• BSN to PhD
• MSN to PhD
leaders is working methodically on a virtual nursing certification. This certification further legitimizes the role of the virtual nurse and elevates this care model in the profession. The scope of the certification is virtual nursing, (virtual nursing services being provided in the acute care/hospital setting in partnership with a bedside clinical team) not telehealth nursing. There are key domains of expertise the certification think tank has developed. Quality and safety, patient and family education, communication, teamwork and interprofessional collaboration, coaching and mentoring, leadership and informatics and technology are the seven domains. Like most certification exams, each domain is weighted differently. AMSN continues to move through the process of achieving the virtual nursing certification with the underlying assumption there will be more virtual nurses to validate the domains, weights and questions as time passes.
SUMMARY
Whether you are starting your journey to create a virtual nursing program in your organization, purchase a service from a vendor, considering a career in virtual nursing or just beginning your research you are poised to impact this maturing care delivery model. Virtual nursing is not a passing fad but an evolution that demands more research, scrutiny, dialogue, commitment and celebration. There are impacts to be made in retention, mentorship, reduced missed care and improved cost of care. The virtual nurses in practice or leading virtual programs have developed a knowledge base being further legitimized by a developing certification. As they say in Texas, the horse is out of the barn and now we are called to improve the performance of the horse, the ground and the barn! i
Patches Seely, MBA, RN, patches.pace76@gmail.com
REFERENCES
Kavanagh, J. & Sharpnack, P.A., (January 31, 2021) “Crisis in competency: a defining moment in nursing education. OJIN: The Online Journal of Issues in Nursing Vol. 26, No. 1, Manuscript 2.
Shuelke, S., Aunit, S., Connor, N. & Denney, S. (October 2019) “Virtual nursing: the reality in quality care. Nursing Administration Quarterly 2019 Oct./ Dec.; 43(4): 322-328.
To learn more about our programs, visit: https://nursing.utmb.edu
National Council of State Boards of Nursing (January 2023). “NCSBN 2023 environmental scan: nursing at a crossroads - an opportunity for action”. Journal of Nursing Regulation Vol. 13 Suppl. S1-S48.
TEXAS NURSING MAGAZINE | ISSUE 2, 2023 PAGE 12
THE UNIVERSITY OF TEXAS MEDICAL BRANCH

Putting Nurses First
An Innovative Candidate-Centric Recruitment Model
 By
By
HEALTHCARE IS EXPERIENCING A NURSING SHORTAGE. During the COVID-19 pandemic, healthcare facilities experienced an increase in nursing turnover while the need for nurses is anticipated to grow by 6% by 2031 (NSI Solutions, 2022; U.S. Bureau Labor Statistics, 2022). Securing top talent to fill nursing positions can be challenging. It has been estimated to take an average of 87 days to recruit an experienced registered nurse (RN) (U.S. Bureau Labor Statistics, 2022; Woodward & Willgerdot, 2022). On average, the turnover cost for an RN is $46,100 with the average hospital having a turnover cost between $5.2 million and $9 million (NSI Solutions, 2022).
One large healthcare system with hospitals located throughout Central and North Texas, including a nursing workforce of
more than 12,000, used innovative recruitment practices with a candidate-centric approach to improve the experience of a nurse interested in a position. The healthcare system was experiencing a higher-than-normal vacancy rate, which, at its highest was 20.9%. Additionally, the healthcare system recruitment data revealed that fewer than 20% of qualified, experienced RN applicants were being offered positions or accepting offers for employment. A team made up of members of the recruitment department along with nursing leaders across the system, explored the reasons that 80% of qualified, experienced candidates were not being offered or accepting positions, or were withdrawing their application prior to being offered a position. Part of the reason qualified nurses were not being offered
TEXAS NURSING MAGAZINE | ISSUE 2, 2023 PAGE 14
Alaina Tellson, PhD, RN, NPD-BC, NE-BC (corresponding author)
Cindy Murray, MBA, MHA, BSN, RN, CENP
Carrie Boysen
Jamie Dodd, BSN, RN, NE-BC
Lauren Maldonado
Christine Mohl, MSN, BBA, RN, CNML
Janice Walker, DHA, MBA-HCM, BSN, RN, NEA-BC
positions was due to the candidate not having the amount of specialty experience the hiring manager was looking for in a candidate, or another candidate was selected for the position. Once a candidate was not selected for a position, the process ended. Candidates were not considered for other open positions within the organization unless they reapplied. Candidates withdrawing their application and/or declining offers reported that it was due to lengthy delays in the recruiting and interview processes. There was the potential that a candidate would have to have multiple interviews on different days to allow for peer interviewing in addition to leadership interviews. This often led to candidates losing interest or accepting positions elsewhere. The focus was shifted from filling a position to a more efficient and candidate-centric model of recruitment.
The candidate-centric model places the candidate at the center of the recruitment process and improves efficiencies. This model was designed with the candidate’s needs in mind rather than focusing on the recruiters’ and hiring managers’ needs during the process, such as timing of interviews. Rather than focusing on one open position per candidate, this new model focuses on identifying where in the organization the candidate would be a best fit considering all the qualifications and interview outcomes. This model was developed with three themes in mind:
streamlining the process from application to hire,
focusing on the candidate’s potential and competencies, and
finding a position for a qualified, competent candidate within the organization.
The goal was for the process to not exceed seven business days if possible (see table below).
An escalation process is in place in the event there are any issues for a candidate during the hiring process. The escalation protocols allow recruiters to elevate when the hiring team
RECRUITMENT / HIRING STEPS TIMELINE TASKS
needs additional support to manage the hiring decision or when a candidate declines due to compensation offered, meaning compensation negotiation is needed. Candidates who are not made an offer are quicky reviewed by the recruitment manager and the chief nursing officer of the facility to determine if there are other positions available within the facility which the candidate is qualified for and interested in.
Moving the recruitment focus for filling a position to a candidate-centric model based on the candidate’s desires and competencies allows the healthcare system to place candidates in a position in which they will be successful. This shift of focus led to a decrease in RN vacancy rate from a high of 20.9% in July 2021 to 5.6% in March 2023 nearing the goal of 5%. The number of candidates meeting job requirements increased by 25%, turnover reduced from 24.1% to 21.6% and labor costs decreased by 48% with the decrease in contracted nurse labor usage.
Nursing leaders and recruitment departments should develop and implement recruitment efforts to address the nursing shortage by focusing on the candidate. Nursing leaders and recruiters must overcome the nursing shortage that was exacerbated by the pandemic by focusing not on what they cannot change, but rather by seeking opportunities for creative solutions. Showing nurses that an organization cares about them prior to hiring them creates a culture of inclusion and satisfaction. i
Alaina Tellson, PhD, RN, NPD-BC, NE-BC, alaina.tellson@bswhealth.org
REFERENCES
NSI Nursing Solutions, Inc. (2022). 2022 NSI National Health Care Retention & RN Staffing Report. www.nsinursingsolutions.com accessed October 1, 2022.
U.S. Bureau Labor (2022). Registered nurses: Occupational Outlook Handbook. U.S. Bureau Labor statistics. www.bls.gov/ooh/healthcare/registered-nurses.htm
Published September 8, 2022. accessed October 26, 2022.
Woodward, K.F. & Willgerdot, M.A. (2022). A systematic review of registered nurse turnover and retention in the United States. Nursing Outlook, 70(4), 664-678.doi: 10.1016/j.outlook.2022.04.005.
Candidate applies online
System screens for basic qualifications and nicotine use
Application
Days 1 and 2
Recruiter Phone Screen Day 3
Hiring Manager Virtual Interview Day 4
Offer Day 5
Pre-hire Onboarding
Activities
Days 6 and 7
Candidate receives email notification of receipt
Within two business days:
Recruiter reviews application and sends and invite to meet
Candidate has a phone screen with the recruiter
Recruiter verifies candidate’s experience, skills and interests, discusses openings
Candidate interviews virtually with the nurse manager and peers
Hiring manager interviews for fit with the positions, department and facility assessing the candidate across all openings
Within one business day:
Offer decision is communicated to the recruiter
Recruiter prepares the offer, secures approvals and communicates the offer to the candidate
Candidate accepts offer and receives an email with clear directions on next steps to complete the hire
Onboarding specialist, hiring manager and recruiter remain in contact with the candidate providing updates
Withing two business days:
Appointment scheduled with employee health
Background checks begin
PAGE 15 ISSUE 2, 2023 | TEXAS NURSING MAGAZINE
NURSE STAFFING in
By Jack Frazee, JD
Is your hospital following the Nurse Staffing Statute Requirements? Is your organization's nurse staffing committee meeting to develop and evaluate a nurse staffing plan?
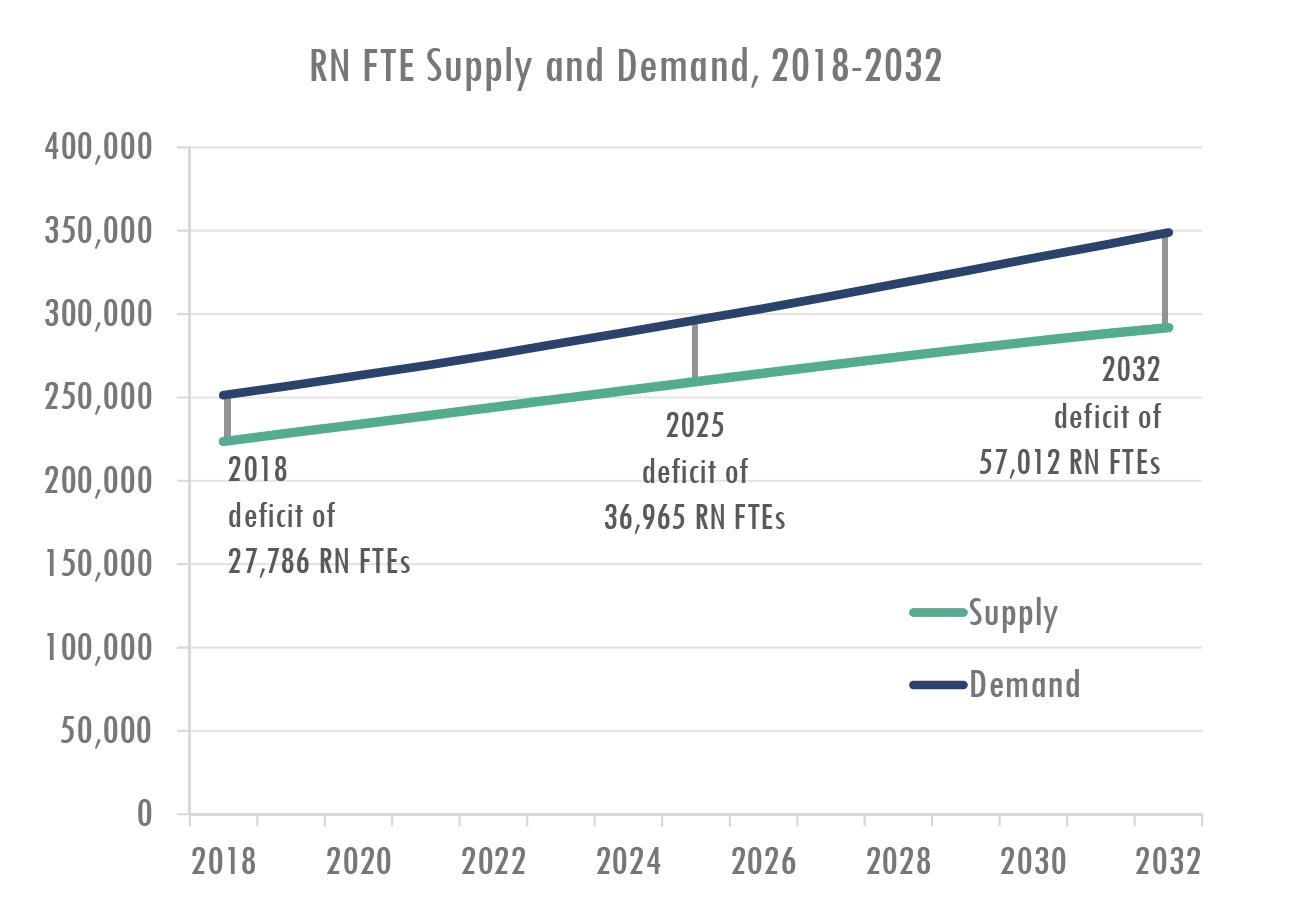
AT TNA, THE NUMBER ONE ISSUE we hear about from Texas nurses is insufficient staffing. In any given facility, it seems there are too many patients, and not enough nurses to treat them.
One source of the problem is that we do not have enough nurses in the workforce generally to keep pace with demand. Research from the Texas Center for Nursing Workforce Studies shows the number of licensed nurses simply is not keeping pace with demand for their services. Notably, this data was collected in 2018, then updated in 2020, and does not

The Nurse Staffing Statute empowers nurses to create staffing policies and plans for hospitals via a nurse staffing committee. Each hospital is required to have a nurse staffing committee as a standing committee of the hospital and are required to meet at least quarterly. The hospital is required to compensate nurses for committee time.
reflect the impact of the COVID-19 pandemic on the Texas nursing workforce. However, we know that safe staffing is about more than the whole number of licensed nurses in Texas. Safe staffing also depends upon the policies of individual facilities.
This is where a law passed by the Texas Legislature in 2009 comes into play— Chapter 257 of the Health and Safety Code, also known as the Nurse Staffing statute. This law empowers nurses to create staffing policies and plans for hospitals via a nurse staffing committee. Each hospital is required to have a nurse staffing committee as a standing committee of the hospital. The committee must include the chief nursing officer as a voting member of the committee, and at least 60 percent of the committee is required to be made up of nurses who provide direct patient care at least 50 percent of their work time and are selected by their peers who provide direct patient care during at least 50 percent of their work time. These committees are required to meet at least quarterly, and the hospital is required to compensate nurses for the time spent working on the committee. Importantly, nurse staffing committees are tasked with developing and recom -
The statute explicitly makes this reported information public information. That means we can request the data from the state and see which hospitals are compliant and which are not.
mending to the hospital’s governing body a nurse staffing plan. Nurse staffing plans are meant to follow nurse-sensitive outcome measures to evaluate the effectiveness of the plan, and the committee should, at least semiannually, evaluate the effectiveness of the staffing plan and variations between the plan and the actual staffing. This data and information should be submitted to the hospital’s governing body in a report that details nurse staffing and patient care outcomes, including an evaluation of the effectiveness of the staffing plan and variations from the plan. The statute requires the committee to consider patient needs, nursing-sensitive quality indicators, nurse satisfaction measures collected by the hospital, and evidence-based nurse staffing standards. This work does not simply happen in the vacuum of one hospital—the statute
TEXAS NURSING MAGAZINE | ISSUE 2, 2023 PAGE 16
also requires hospitals to report staffing information to the Texas Department of State Health Services. Each hospital is required to report:
Whether the hospital’s governing body has adopted a nurse staffing policy as required by the statute;
Whether the hospital has estab lished a nurse staffing committee that meets the membership require ments of the statute;
Whether the nurse staffing commit tee has evaluated the hospital’s nurse staffing plan and has reported the results of the evaluation to the hospital’s governing body; and
What nurse-sensitive outcome measures the committee adopted for use in evaluating the hospital’s nurse staffing plan.

The statute explicitly makes this reported information public information. That means we can request the data from the state and see which hospitals are compliant and which are not.
TNA has requested this information and learned that not every hospital in Texas is compliant with this law. We are working to increase compliance with the statute, educate hospital management about the importance of this law, and are gath ering evidence of compliance issues. If you are a Texas nurse working in the hos pital setting, you can assist our work.
CALL TO ACTION
Does your hospital have a nurse staffing committee?

Is your committee meeting the requirements of the nurse staffing statute?
We would love to hear your feedback about how this law is working in practice as the public health emergency declaration expires and we return to the normal rules of business in healthcare. Your input is valuable to our research into this law, its performance in Texas over the past 14 years, and whether compliance issues need to be addressed. Contact TNA's Government Affairs department to share your perspective: governmentalaffairs@ texasnurses.org
ISSUE 2, 2023 | TEXAS NURSING MAGAZINE
TRAIN TODAY. LEAD TOMORROW. SERVE ALWAYS. @tamunursing nursing.tamu.edu BECOME AN AGGIE NURSE.
Courtesy Texas Center for Nursing Workforce Studies
ANEWMODEL
By Teresa Walding BSN, RN, NC-BC
ACHIEVING OPTIMAL HEALTH AND HEALING requires a holistic approach that recognizes the inherent health within individuals and the crucial role of the mind-body connection. The Inside-Out Harmony Model of Care is based on aligning our thinking with the principles of innate health to facilitate a state of balance and improved patient outcomes. In this article, we will explore how recognizing innate health, understanding the mind-body connection, and aligning with the principles of innate health can promote healing and well-being, leading to harmony in health and improved health outcomes.
THE INSIDE-OUT MODEL OF CARE
As humans, we are complex beings with interconnected systems of mind, body, and spirit. As a result, our thoughts, beliefs, and emotions play a significant role in shaping our health and well-being. Yet, in the traditional healthcare model, the focus has primarily been on external factors such as symptoms, diagnoses, and treatments. However, a paradigm shift is taking place, recognizing the power of thought in healthcare and embracing an inside-out model of care.
In this model of care, individuals are encouraged to realize that their thoughts and beliefs are not just abstract concepts but have a tangible impact on their physical health. Furthermore, it is understood that our thinking is not just limited to our cognitive processes. Still, it also affects our physiological responses, including stress levels, immune system function, and overall health outcomes.

One key aspect of the inside-out model of care is the understanding that our natural healing ability is a built-in capacity that every human being possesses equally. When individuals realize this fact, it removes the burden of constantly searching for external solutions and empowers them to tap into their own inherent healing mechanisms.
O F C A ER
Stress is a well-known contributor to various health issues, and reducing stress levels is crucial for overall well-being. In the traditional model of care, stress is often seen as a byproduct of external circumstances, and efforts are focused on managing those circumstances. However, in the inside-out model of care, stress is recognized as being created by our own thoughts and beliefs about those circumstances. For example, consider a doctor with a patient with chronic foot pain that does not seem to improve despite repeated surgeries. In the traditional model of care, the doctor may continue to search for external causes and cures for the pain. However, in the inside-out model of care, the doc -
TEXAS NURSING MAGAZINE | ISSUE 2, 2023 PAGE 18
tor may realize that the patient’s thoughts and beliefs about the pain and fear of their foot not getting better could contribute to the body’s stress response, which in turn affects the healing process. By addressing the patient’s thought patterns and beliefs, the doctor may be able to help the patient reduce stress and support the body’s natural healing ability.
In this model of care, individuals are encouraged to realize that their thoughts and beliefs are not just abstract concepts but have a tangible impact on their physical health.
Embracing an inside-out model of care also involves shifting from a mindset of focusing on why things happen to asking what we can do next. It encourages individuals to take ownership of their thoughts and beliefs and recognize that they have the power to change their perspective and respond to their circumstances. By developing a deeper understanding of the inside-out nature of our thinking, individuals can learn to manage their thoughts, reduce stress, and improve their overall health and well-being.
Implementing an inside-out model of care requires a paradigm shift in healthcare practices. It involves incorporating the coaching skills of the provider to help people take charge of their health through self-reflection, internal awareness of the thought/feeling connection impacting our health, and education about the role of thought in health into healthcare protocols. Healthcare providers play a crucial role in guiding patients to recognize and manage their thoughts and beliefs in their healthcare journey.
THE POWER OF THOUGHT
In conclusion, the power of thought in healthcare cannot be underestimated. Embracing an inside-out model of care that recognizes the role of thoughts and beliefs in shaping our health and well-being can lead to improved health outcomes, reduced stress, and better overall well-being. By realizing the inherent healing capacity within ourselves and learning to manage our thoughts, we can navigate life’s challenges with resilience and empower ourselves to take charge of our health. It’s time to shift the paradigm, embrace a more holistic approach to healthcare that integrates the mind, body, and spirit, and recognize thought’s power in promoting optimal health and well-being. i
Teresa Walding BSN, RN, NC-BC, teresa@nursecoaching.com
REFERENCES
Blevins, K., Monroe, (2016), The 3PP Diagram Guide. Retrieved from https:// threeprinciplesparadigm.com/courses/the-3pp-diagram-guide-diagrams-audio-mp3/ El-Mokadem, J., DiMarko, K., Kelley, T. M., & Duffeld, L. (2020). Three Principles/Innate Health:The efficacy of a new psycho-spiritual mental health education intervention for people with chronic fatigue syndrome. Spirituality in Clinical Practice, DOI: 10.1037/ scp0000232 Date 13.10.21
Kelly, T.M., PhD. Pettit, W.F., MD Sedgeman. J., PhD, Pransky, J., PhD. 2021 One Generic Mental Illness: A Principle-Based Psycho-Spiritual Explanation of General Factor p and Its Application to Spiritually Informed Clinical Practice. Journal of Spiritual Psychology and Counseling. eISSN: 2458-9675
Kelley, T.M., Pranky, J., & Lambert, E. (2015). Realizing improved mental health through understanding three spiritual principles. Spirituality in Clinical Practice, 2 (4), 267-281. McCright, L. (2019, June). Self-care and the resilience paradigm. AHNA, Beginnings, 39(3), 25.
McCright, L. (2017). The revolution in nursing begins. AHNA Beginnings, 37 (2) 21-22. Pettit, B. (2019). Mind, Brain, Body Connection Course. Why the understanding of mind is vital to our health. Retrieved from https://thedrspettit.com/mbbc-access-fall-2019/ Sapolsky, R. (2004). Why Zebras Don’t Get Ulcers. Henry Holt and Company, LLC. New York, NY
Walding, T. (2019). Releasing Chronic Pain. AHNA Beginnings, 38 (1), 25.
PAGE 19 ISSUE 2, 2023 | TEXAS NURSING MAGAZINE
lives with NurseCoaching.com's self-paced program and live coaching calls. Become a Board-Certified Nurse Coach on your schedule. Apply now. nursecoaching.com
for TPAPN
A PEER SUPPORT PARTNER
Peer Assistance Program for Nurses (TPAPN) peer support partners provide an empathetic listening ear to TPAPN participants. Start advocating today! tpapn.org TEXAS PEER ASSISTANCE PR OGRAM FO R NURSES
Transform
Volunteer
BECOME
Texas
THE
STOPLIGHT HUDDLE
By Lorrie Kirby MSN, RN, CMSRN
A Simple Tactic That Supports a Culture of Teamwork, Promoting Quality Patient Care and Nurse Satisfaction
DEVELOPING A CULTURE THAT SUPPORTS a healthy workplace is imperative in nursing today to achieve quality patient care while promoting nurse satisfaction. Beyond the complex discussions of staffing guidelines and conversations of census and acuity, creative processes, and innovative thinking that support effective teamwork can be game changers
for nursing teams. The Stoplight Huddle is a tactic with the purpose of managing workload among the team. The process is quick and simple, but the outcomes can be dynamic including individual nurse support, teaching critical thinking through priority identification, proactive teamwork, and optimal team readiness and effectiveness all while develop -

ing a culture that supports a healthy workplace. If done well, nursing teams improve patient care, increase their flex-
If done well, nursing teams improve patient care, increase their flexibility to handle throughput, and leave the end of their shift as a team.

TEXAS NURSING MAGAZINE | ISSUE 2, 2023 PAGE 20
ibility to handle throughput, and leave the end of their shift as a team instead of one or two nurses staying late to complete their tasks and finish charting. This intentional huddle proactively leads to a culture of embedded teamwork, the added benefit of good morale, and the potential of less incidental overtime. It is a win in the development of a healthy nursing workforce and an environment of satisfaction.
This intentional huddle proactively leads to a culture of embedded teamwork, the added benefit of good morale, and the potential of less incidental overtime. It is a win in the development of a healthy nursing workforce and an environment of satisfaction.

The Stoplight Huddle takes five minutes or less depending on the number of nursing staff attending. Each nurse and patient care technician should arrive on time at a designated time prepared to articulate their stoplight color of red, yellow, or green and why, meaning their top three priorities or interventions most urgent to complete. Nursing staff have multiple competing priorities at any given time, but the idea is to bring only the top three priorities for quick identification of available assistance. Articulating red indicates being notably behind or drowning as we say in nursing terms, yellow indicates busy but handling the
CARE FOR THE CAREGIVER

workload, and green indicates being caught up and ready to help others. Once everyone has stated their stoplight color and top three priorities, the charge nurse can begin to assign task support where staff that are green can help a team member that is red. It is often that staff members begin to offer their help before the charge nurse can even assign the task support. The main goal will be the entire team becoming yellow leading to green within the next thirty minutes creating a flexibility of the team’s readiness to handle admissions and/or a change in condition rapid response clinical event.
The Stoplight Huddle can work for all team sizes, either by the entire team coming together as one team huddle group or by assigning more than one huddle group creating smaller pods among larger teams. To achieve success, the Stoplight Huddle needs to be quick, to the point, and everyone should show up able to state their stoplight color and why by listing their top three priorities. Yes, there are some shifts where the entire team is red, but that is not that often and actually becomes the perfect shift to test the huddle. On a shift that is overwhelming, when everyone on the team is mentally moving at lightning speed, it does help to create a pause that identifies the top three priorities. This step often allows a mental release of less important priorities until after the posthuddle thirty minutes is complete, allowing for a recentering to the real sense of urgency priorities. This is very important because it is often when asking a busy nurse what help is needed, the answer is
stated as; ‘I don’t know, I’m just too busy to even tell you.’ Sometimes, it is not actually getting task assistance that creates the biggest impact but the pause and act of identifying the three most important priorities, therefore trimming the task list in the nurse’s brain from maybe eight items to three. The other five items don’t go away, but they do become prioritized at another time after the post-huddle thirty minutes is over. This mental shift creates as much support as someone taking an actual task off your plate. If a nurse recenters and a task is completed by another team member or the charge nurse, the nurse has the potential to become less overwhelmed quickly. This works really well to support new nurses learning to prioritize.
hardwiring occurs, the team members learn to plan for the huddle just like any other task. However, in the beginning there will be some that say they do not have time to come because they are too busy. It is imperative that everyone is engaged to reap the benefits.
There are three main pitfalls to consider when attempting to roll out the Stoplight Huddle. The team needs to set a designated time and everyone needs to show up at that time. Day and night shifts may need different times designated. If everyone doesn’t show up on time, it wastes the time of everyone that did

PAGE 21 ISSUE 2, 2023 | TEXAS NURSING MAGAZINE
As
Has the Texas Board of Nursing contacted you regarding your nursing license? stephanie.warnocklaw@gmail.com
Let me defend your license against the Board. DFW and Statewide In
Johnson,
for the Caregiver
and
Watch videos, download free resources, and get more information on preparedness, resiliency, and self-care.
Stephanie Warnock Nurse Attorney
disaster situations, nurses must care for others while caring for themselves and their family. Texas Nurses Association and Texas Organization of Nurse Executives, with support from Johnson &
developed Care
to help nurses before, during
after disasters.
[ ]
show up promptly, and that team will need to decide if they continue or wait for the nurse that is stuck in a patient room. As hardwiring occurs, the team members learn to plan for the huddle just like any other task. However, in the
beginning there will be some that say they do not have time to come because they are too busy. It is imperative that everyone is engaged to reap the benefits. The second pitfall is the length of the huddle. This huddle is meant to
SHOW UP. BE PREPARED. BE AMAZED.
PURPOSE
To manage workload among the team. This supports associates by promoting staffing effectiveness to achieve quality patient care and a healthy work environment.
Promotes teamwork with the entire team working at an optimal state so all members experience yellow to green status throughout the shift.
PROCESS (3 - 5 MINUTES)
Arrive at Stoplight huddle on time.
Charge Nurse asks everyone their color and why (top three priorities).
Charge Nurse and team develop quick plan to support each person improving their color to achieve a stable workload over the next 30 minutes.
I'M
VERY BEHIND
What are the most urgent 3 interventions?
EXAMPLE: One patient has high BP needing further assessment. Two patients need medications. One PICC dressing change is due.
I'M PRETTY GOOD
What are the most urgent 3 interventions?
EXAMPLE: I need to chart my last patient assessment, hang one antibiotic, and check blood-sugar results for one patient.
I'M CAUGHT UP! HOW CAN I HELP?
EXAMPLE: I just need to complete my intentional rounding and chart.
PITFALLS
Not showing up on time so it takes longer than 3 - 5 minutes. This wastes everyone's time.
Staff giving a lengthy report instead of sharing the top three priorities with which they need help.
Charge nurse walking to each team member asking "How are you doing?" The team needs to hear the discussion.
be quick. If the team shows up and a nurse starts giving a long list of what is happening in the patient load, similar to giving a report, redirection to listing only the top three priorities is needed. Success is achieved when the team can identify where support needs to be given. Being able to articulate concisely allows others to identify how to offer support. The last pitfall occurs when the team does not gather and the charge nurse walks to each individual team member asking how they are doing. This
is ineffective and doesn’t allow the team to hear the articulation of the priorities, doesn’t allow anyone on the team to offer or be assigned a task to help, and basically increases the workload of the charge nurse.
In closing, the Stoplight Huddle is a creative tactic that proactively addresses workload by encouraging a culture of teamwork and empowering nurses to pause and identify their top three priorities. It is a quick and simple approach that can effectively turn an overwhelming shift into a manageable shift in 30 minutes. If needed, a second Stoplight Huddle can be repeated to achieve workload balance. Nursing is a team sport. This is just another avenue to work as a team to manage the workload of an entire unit by supporting individual team members. As nurses, we have an opportunity to support our peers positively, impacting patient care and nurse satisfaction with a simple, innovative tactic that is nurse driven, adds no cost, and elevates a healthy workforce. i
Lorrie Kirby, MSN, RN, CMSRN, lkirby@ascension.org
TEXAS NURSING MAGAZINE | ISSUE 2, 2023 PAGE 22
Success is achieved when the team can identify where support needs to be given. Being able to articulate concisely allows others to identify how to offer support.
ALTHOUGH I DIDN’T REALIZE IT AT THE TIME, early in my career I had a mentor. This person was available when I needed guidance, asked questions to help me set and achieve goals, and helped me work through issues I encountered at work. Today, many years later, I still think about some of the advice she gave me and how her words of encouragement helped me make choices that would lead me to the career I have today. In modern work environments we recognize how impactful mentoring can be both to help guide nurses early in their career, or inform nurses who may be looking to make a career change. That’s why TNA is launching a mentoring program— to help our members connect with others who can provide growth and development, lend support to navigate challenges, and share insights based on their experiences. Our program is designed to be flexible, convenient and relatively short-term, to minimize the impact on your time.
GROW YOUR CAREER—BE A MENTEE
If you are looking for someone who can objectively help you with challenges you’re facing, talk about options for your next career step, or share more about a specific area of nursing, we hope you’ll sign up to be a mentee. Becoming a mentee gives you the opportunity to ask questions, talk about challenges, and discuss career goals with someone who can share their experiences and help you grow in your career.
SHARE YOUR INSIGHT—BE A MENTOR
If you are interested in having a positive, direct impact on another nurse, we hope you’ll sign up to be a mentor. Becoming a mentor gives you the opportunity to share your knowledge, experience and insights with a nurse who may be facing a challenge you’ve encountered or considering a career move you’ve experienced. You may even learn something from your mentee!


TNA Mentor Program
By Julia Menegay, MBA, TNA COO


Applications are open until July 1, and the Fall mentoring session will begin on August 1. For more information, go to our website (texasnurses.org) and select Mentor Program under “Member Zone.” i
•
PAGE 23 ISSUE 2, 2023 | TEXAS NURSING MAGAZINE
You care. Make it a career. Find an exciting and challenging career in one of 23 HHS Health and Specialty Care System facilities across Texas. Contact a recruiter at healthcareers@hhsc.state.tx.us
offer predictable work schedules, set caseloads and an excellent benefits package, including:
We
Starting this spring, more competitive salaries at
supported living centers
state hospitals and state
• Health and retirement benefits
• Sick leave, paid vacation leave and up to 15 paid holidays a year
23D0255 Hiring at all levels and at every facility
• Shift differential pay
The

4807 Spicewood Springs Rd. Bldg. 3, Suite 100 Austin, TX 78759 KEEP LIVING YOUR WAY. You can, with these benefits and discounts from TNA & AMBA: • Dental & Vision Plans • Long Term Care & Home Health Care Insurance • Medical Air Services Association (MASA) • Cancer, Heart & Stroke, Accident, and Disability Insurances • Medicare Solutions • Final Expenses Whole Life & Guaranteed Acceptance Life Insurance • Annuity • Start Hearing, Inc. • Hospital Stay Coverage • Discounts on Travel, Dining & more LIVE LIFE, UNINTERRUPTED. Learn More: 1-877-556-4582 myambabenefits.info/tna TNA - Texas Nurses Association PEER REVIEW? LETTER OF INVESTIGATION? I CAN HELP! Joyce Stamp Lilly RN JD Registered Nurse and Attorney 713.759.6430 • jslilly@me.com www.nurse-lawyer.com YOUR BOARD COMPLAINT RESOURCE NursingComplaintHelp.com The most affordable and beneficial website to help you develop a plan and respond to Board complaints and Investigations against your license.
