Speech/Language Therapy
Historically, it has proven difficult to use speech therapy alone to improve the basic processing abilities of phonological memory, working memory, and speed of processing found to be deficient in C/APD. Speech therapy techniques often require years of intervention before substantial improvement is seen, resulting in unacceptably long periods during which the individual experiences difficulty with daily living skills, academics, and socialization (Ross et al., 2011) Speech therapy usually consists of accommodative strategies to help children function despite the existence of C/APD. Fey et al. (2011) stated that there is a lack of direction as to interventions that providers working with children with APD should use. They further concluded that they did not find any compelling evidence that existing auditory interventions had a significant impact on auditory and language disorder, or on academic outcomes of school-age children with APD Choudhury and Chavira (2017) agreed, stating short-term intervention studies fail to show evidence of improvement in auditory function in school-age children as current approaches manage APD using simple deficit-specific treatment approaches.
Occupational Therapy
Occupational therapists work with children to help alleviate or find accommodations for difficulty with sensory processing. As APD is an aspect of sensory processing, occupational therapists help find accommodative techniques to help a child function despite the underlying cause of the problem. They use the same devices as audiologists, speech pathologists, and other professionals who work with this diagnosis (Reynolds et al., 2016)
Auditory Programs
Auditory training (AT) programs have been developed to provide remediation for auditory perception and related learning deficits (Gillam et al., 2001). According to Weihing et
5
al. (2015), although traditional auditory training approaches used for remediating C/APD show transfer of learning occurs, the magnitude of the transfer effect is larger for tasks that are more like the trained tasks. Traditional methods follow a behavioral model to teach a particular task, which improves a particular skill related to that task. According to Burgoyne et al. (2012), skills directly taught in this manner had the greatest gains, however there was little evidence of generalization to skills not directly taught in the intervention.
Frequency Modulation Systems
Frequency modulation (FM) systems are devices that use radio waves to send speech and other signals to hearing aids. They use the same type of signal as an FM radio, however the frequency band used in these systems is designated for personal use. These systems have two components: a microphone, which in a classroom would be used by the teacher, and a receiver, which is either hooked to hearing aids or a set of headphones used by a student. FM systems have been shown to increase the understanding of students of what is being said by their teacher (Anderson & Goldstein, 2004). However, as Nguyen and Bentler (2011) pointed out, children seem to be reluctant to use them and therefore they may not have a great deal of impact. They further concluded that although the use of FM systems enhances reading skills, increase s attention span, and reduces distractibility, current evidence shows that unless the functioning of these devices is frequently verified, some advantages may be lost.
The Tomatis® Method
The Tomatis® Method was developed to address the shortcomings of traditional therapies and, as such, aims to rebuild vestibular and auditory functions using a developmentally based passive program to retract and rebuild both listening and vestibular functions (Sollier 2005) by stimulating the rich interconnections between the ear and the nervous system (Thompson &
6
Andrews, 2000) Because the Tomatis® Method is not task-specific but is aimed at directly remediating dysfunctional neural auditory pathways, it may have a broader impact.
The specific equipment used to administer the program houses four aspects tha t are important to Dr. Tomatis’ theories of how the ear perceives sound, which is transferred to the brain for processing. According to Thompson and Andrews (2000 ), these four aspects are
1. Filters , which regulate sound so that the information is altered or modified to focus evenly on the specific frequency band range of a good functioning ear to suppress distortion.
2. An electronic gating mechanism enables the ear to attune itself automatically and spontaneously for listening.
3. Provides a control to vary the balance of sound between the right and left ears.
4. The timing delay of sound reception between the bone and air conduction can be changed to slow down the processing of information internally and to awaken the individual to attend to incoming information (Thompson & Andrews, 2000).
Existing research on the Tomatis® Method is scant and has often yielded mixed results. The use of this method in clinical practice is varied covering several diagnose s and symptoms and has thus proven difficult to research. Most of the research does not contain a control group, usually has a small number of participants, is retrospective in nature, and the majority are case studies. These studies are often not well defined and thus are not re-duplicatable. However, overall, existing research on the Tomatis® Method suggests that it may be effective in directly remediating auditory processing. Currently, according to Gilmore (1999), the existing research on the Tomatis® Method consists mainly of case studies and the impact of the method on individuals, but generally these
7
have not included control groups, or have failed to follow guidelines of what constitutes a control group. Bernard-Bonnin (2002) agreed that there is a lack of controlled research studies of C/APD interventions, where existing research on commercial auditory training programs, including the Tomatis® Method are most often case studies on C/APD rather than more rigorous investigations. Additionally, previous studies have been too broad and vague to be reduplicated (Bernard-Bonnin, 2002). Corbett et al. (2008) were critical of the available Tomatis® Method research and the findings therein.
Most of the research is nonexperimental consisting of individual case studies. For example, Ross-Swain’s retrospective study suggests that the Tomatis® Method can be effective as an intervention strategy for APD as all subjects in her study demonstrated improvement in skills required for adequate auditory processing. Ross-Swain (2007) reviewed the pre- and posttreatment assessment results of 41 randomly selected participants (18 female and 23 male) ranging in age from 4.3 years to 19.8 years with a mean age of 12.1 years who received 90 hours of Tomatis sound stimulation. All participants demonstrated weakness in auditory processing skills and were not receiving any other form of therapy during the treatment period . Pre and post assessment using the Test of Auditory Perceptual Skills (TAPS) showed that on average the participants’ scores fell below average before the sound stimulation and that this average increased to fall within typical limits on the post test. Gerritsen (2010) used a retrospective design to reanalyze results of a previous study by Corbett et al. (2008), which Gerritsen maintains was erroneously analyzed as a cross-over design She stated that the number of participants in the group (11) was too small to yield significance and that the group was too heterogeneous to be analyzed as a group. She therefore reanalyzed the study as 11 case studies and included analyses on the Vineland Adaptive Behavior Scales-Interview Edition (VABS;
8
Sparrow, 1984), the Behavior Assessment System for Children (BASC; Reynold & Kamphaus, 1999), and the Short Sensory Profile (SSP; Dunn, 1999) where data had been collected but not reported by Corbett et al. These additional results were not included here as they are irrelevant to the current study. There was significant change found in receptive vocabulary measured by the Peabody Picture Vocabulary Test – Third Edition (PPVT-III; L.M. Dunn & Dunn, 1997), and expressive vocabulary measured by the Expressive One-Word Picture Vocabulary Test – Third Edition (EOWPVT, 3 rd Ed., Brownell, 2000) in 6 of the 11 subjects using raw scores vs. standard scores Pertinent scores on the PPVT and EOWPVT were only reported on 10/11 participants. Three participants showed significant change in raw scores on the PPVT and 3 participants showed changes in EOWPVT, where one showed change in both. Similarly, in two case studies
Tatum et al. (2004) reported observational findings of a 14-year-old non-verbal female diagnosed with autism who began to speak after the Tomatis® Method was introduced to her regular prescribed therapies. She had reportedly received eight extensive courses of speech therapy including oral motor therapy since the age of 4 and could only make three sounds when she started the Tomatis® Method. No standardized tests were used in this case study. In a second case study Tatum et al. (2004) reported that a 9-year-old boy diagnosed with attention deficit hyperactive disorder (ADHD) and auditory processing disorder (APD) was assessed pre- and post-using the Lindamood Auditory Conceptualization Test (LAC). He received a combination program of the Tomatis® Method and the Lindamood ® Phoneme Sequencing Program (LiPS). His pre-test score equated to a grade equivalent of the middle of second grade for phonemic/phonological awareness and improved to above his grade level at the beginning of fifth grade after 60 hours of training (Tatum et al., 2004).
9
To date there are only two experimental studies, which found somewhat mixed results Sacarin (2013) found statistically significant improvement in processing speed, auditory attention, phonological awareness, and phonemic decoding efficiency while engaged in reading activities in the experimental group who received the Tomatis® Method. She investigated the early effects of the Tomatis® Method on 25 participants aged between 7 and 13 with attention deficit disorder (ADD) Fifteen participants received the first phase of the Tomatis® Method, while the remaining 10 served as a control and were stabilized on ADD medication 3 months prior to and throughout the study. The Tomatis group showed significant improvements in processing speed, phonological awareness, phonemic decoding efficiency when reading, as well as behavior and auditory attention. This study was done on a small portion of the Tomatis® Method. Corbett et al. (2008) performed a cross-over study with 11 heterogeneous participants. They sought to show improvements in receptive and expressive language in children with autism. They used two groups: Placebo/Tomatis group and a Tomatis/Placebo group. The reported benefits varied widely from subject to subject. These included transitions from nonverbal to verbal, ability to imitate words, increased receptive and expressive vocabulary, improvements in skills of daily living, motor skills, social skills, communication skills, attention and decreases in hyperactivity, and atypical behaviors. According to Gerritsen (2010), the experiment had several flaws, which led her to reanalyze the results by doing a retrospective study where she looked at each participant as a case study as stated previously. Certified Tomatis consultants are trained to design individualized programs based on the proprietary Tomatis Listening Test, an in-depth history, and profile of the individual they are treating. This has been used to argue against the efficacy of the treatment in past research regarding the Tomatis® Method. Opponents state that the method is only as efficacious as the
10
therapist using it and the rapport they have with the client and family. This would arguably fit any therapeutic intervention, and thus, to address this opposition I chose to use a generic program.
The Gap My Research Can F ill
In addition to the shortcomings of previous research mentioned above, there are several other general criticisms of previous research on the Tomatis® Method. One is that the outcome of treatment, being that it is individualized, depends directly on the ability of the practitioner and their training. A second is that the research was done by a practitioner who had a therapeutic alliance with the individual and or family and directly impacted the outcomes (Gerritsen, 2009). A third is that the listening test proprietary to the Tomatis® Method is not standardized and does not assess functional outcomes.
Several previous studies have however suggested that the Tomatis® Method may work as a treatment; therefore, this study seeks to fill that gap by exploring whether controlled studies of the Tomatis® Method can be performed and to examine resulting outcomes in children with C/APD who go through this protocol. This study was designed to be replicable and used standardized assessments to make quantifiable conclusions that will be comparable to future studies of this kind.
Research Intentions
As stated earlier, my research study had a three-fold intent. On the one hand, it was a pilot study to determine the feasibility of the study design. To that end, I examined potential recruitment efforts, ability to implement and complete testing and treatment protocols (i.e., pertinent standardized instruments), and the best number of instruments to use based on testing times and relevance to C/APD and its possible functional impacts. I additionally looked at
11
retention and treatment fidelity. On the other hand, I examine d the feasibility of conducting more rigorous research studies on the Tomatis® Method. This pilot study was designed to be replicable and used standardized assessments to make quantifiable conclusions that will be comparable to future studies of this kind. I included various other related measures in this study because as explained earlier, we know that C/APD affects various other functions such as communication and attention. To that end, I assessed trends in between -group changes following treatment using pre-post outcomes of several measures of importance to measure possible changes in C/APD. These were Staggered Spondaic Word (SSW) test, SCAN-3:C Tests for Auditory Processing Disorders for Children (SCAN-3:C), and CTOPP-2: Comprehensive Test of Phonological Processing–Second Edition (CTOPP-2). Possible functional changes achieved due to improvements in C/APD were measured using IVA-2 CPT (Integrated Visual & Auditory 2 Continuous Performance Test), Woodcock Johnson IV test (WJ-IV), and Interactive Metronome Long Form test (IM). The outcomes of these measures were used to determine whether the resulting trends showed improvements in C/APD, auditory and visual attention, neurotiming, learning capabilities, and speech and language capacities that warranted further investigation.
Following in the next chapter is a review of the literature related to C/APD and the Tomatis® Method, including research that was completed and the practices that have emerged from that research. The literature review covers multiple areas of function shown to be impacted by deficits in auditory processing, as these could potentially also be remediated using the Tomatis® Method.
12
CHAPTER TWO REVIEW OF THE LITERATURE
Background and Statement of the Problem
C/APD is the focus of my study because it impacts so many different aspects of daily living for children diagnosed with this condition. The Tomatis® Method was chosen as the treatment method to study because it may remediate the symptoms associated with C/APD and possibly change the functional outcomes in children with this diagnosis The study therefore examined potential recruitment efforts, ability to implement and complete testing and treatment protocols, retention and treatment fidelity, as well as the feasibility of conducting more rigorous research studies on the Tomatis® Method.
In addition, co -morbid factors may also be positively impacted by the Tomatis® Method.
C/APD may coexist with intellectual disability, autism spectrum disorder (ASD), attention deficit hyperactive disorder (ADHD), and d yslexia; however, there is no indication that one causes the other. According to Billiet and Bellis (2011), “present findings investigating the relationship between dyslexia and central auditory processing suggest that some children with dyslexia may exhibit a C/APD that is a contributing or co-morbid factor to their reading deficits”
(p. 230). Ferre (2015) stated that during an assessment, attention deficit, sensory dysregulation, executive dysfunction, anxiety, and depression should be differentiated from impaired auditory integration.
Currently, parents pay for various therapies out of pocket as these are not deemed approved by insurance companies. Some of these programs can be of great value in improving skills; however, due to being intensive, they require a large output of funds all at one time. Many parents are unable to come up with the funds. While these therapies are not extraordinarily
13
expensive therapies, due to lack of insurance payment and due to the intensive mode of treatment of several hours over a short period of time, these therapies may become a burden on parents.
The Tomatis® Method may be a foundational program that is crucial to accelerating the results one gets from speech/language therapy, occupational therapy, physical therapy, and educational therapies.
The Tomatis® Method was created and perfected by Dr. Alfred A. Tomatis, a French earnose-throat doctor who specialized in oto-rhino-laryngology (www.tomatis.com). He won a gold medal for scientific research at the Brussels International Exposition in 1958. Dr. Tomatis created the Tomatis® Method as a “sound stimulation and educational intervention that improves listening” (Tomatis, 1996, p.197). He devoted a significant part of his professional life to studying the relationship between the ear and the voice, and by extension, between listening, communication, and learning.
To date, the research that is available on the Tomatis® Method is mostly in the form of case studies and anecdotal accounts of individuals' personal experiences with the method. A limited number of controlled research studies that examine commercial auditory training programs, including the Tomatis® Method, exist. The studies that are about this subject most often consist of case studies on C/APD rather than more rigorous investigations (BernardBonnin, 2002). Therefore, a gap exists in knowledge about the effectiveness and efficacy of the Tomatis® Method; such a gap, if filled, could provide a better understanding of how to most efficiently work with children who have C/APD.
Central Auditory Processing Disorder: A Complex Diagnosis
The Tomatis® Method is designed to address several critical aspects of C/APD, which is but one part of a more complicated overarching circuit called sensory processing disorder (SPD;
14
APA, 2013) by which humans navigate and understand their environment (Bellis, 1997).
Sensory processing (SP) is the neurological process that organizes sensations from one’s own body and from the environment and makes it possible to use the body effectively within the environment (Ayres, 1979). In this literature review, I am therefore presenting research regarding SPD that has relevance to this study, because positive findings of change in auditory processing could be related to changes in the entire sensory processing neurological complex within an individual. This would have implications for follow-up research, which may look at the possibility of the Tomatis® Method having an impact on the entire sensory processing complex. SP allows for the effective use of one’s body within its environment (Ayres, 1979). In the 1960s, Ayres theorized that impaired sensory processing might result in various functional problems, which she later labeled sensory integration dysfunction (Ayres, 1979). Sensory “processing” rather than sensory “integration” is commonly used to distinguish the disorder from both the theory and the intervention (Miller, Anzalone, et al., 2007). SPD has been further grouped into three patterns of sensory processing that include sensory modulation disorder (SMD), sensory-based motor disorder (SBMD), and sensory discrimination disorder (SDD; Miller et al., 2012; Ayres, 1989). They further stated that SDD in the visual and auditory systems can lead to a learning and/or language disability (Miller, Shenoy, et al., 2007).
Dunn’s (1997) model of SP is based on knowledge from neuroscience and behavioral science. This model of sensory processing hypothesizes that interaction between neurological thresholds and behavioral responses exists. Dunn (1999) used the intersection of two continuums to describe four sensory processing patterns (i.e., registration, seeking, sensitivity, and avoiding).
The interaction of neurological thresholds and behavioral responses provides a method for explaining how children process sensory information and guidance for intervention planning
15
(Dunn, 1999). Additionally, interesting to note here is the finding by Kayser et al. (2005) that in the macaque monkey, integration of touch and sound stimulation occurs at the second stage of the auditory cortex.
SMD subtypes include sensory over-responsivity, sensory under-responsivity, and sensory seeking/craving. Individuals diagnosed with sensory processing difficulties are additionally often difficult to understand because they do not process incoming auditory information correctly, given their difficulties in auditory processing (Bellis, 1997). Moreover, preliminary research in mice shows that the dysfunction of the ear (stopping sensory processing) results in attention deficit and hyperactivity (ADH; Antoine et al., 2013). Sensory processing deficits also have been found to be correlated with higher levels of stereotypic, rigid, and repetitive behaviors common to ASD symptoms (Foss-Feig et al., 2012). Given these symptoms, the DSM-V (American Psychiatric Association, 2013) has included sensory challenges as one of the diagnostic criteria for ASD.
Central Auditory Processing Disorder
C/APD is a condition in which patients are experiencing listening difficulties in the absence of clearly identifiable peripheral auditory deficit (Mülder et al., 2007). Additionally, C/APD is the inability to attend to and discriminate or understand auditory input correctly.
Patients with C/APD typically have normal pure tone thresholds but experience difficulties in various auditory tasks, including mainly sound localization or speech comprehension in noisy environments (Mülder et al., 2007) The National Institute on Deafness and other Communication Disorders (NIDCD) in the United States described children with auditory processing disorders as typically having normal hearing and normal intelligence (NIDCD, 2001).
The clinical criteria for C/APD are not identified in the Diagnostic and Statistical Manual of
16
Mental Disorders Fifth Edition (DSM-V, American Psychiatric Association, 2013); however, clinical criteria for evidence can be found in the research and articles presented by the American Speech-Language Hearing Association (ASHA, 2005). The American Speech-Language-Hearing Association Consensus Committee (2005) defined auditory processing as difficulties in the processing of auditory information in the central nervous system (CNS) as demonstrated by poor performance in one or more of the following skills: sound localization and lateralization; auditory discrimination; auditory pattern recognition; temporal aspects of audition, including temporal integration, temporal discrimination (e.g., temporal gap detection), temporal ordering, and temporal masking; auditory performance in competing for acoustic signals (including dichotic listening); and auditory performance with degraded acoustic signals.
The C/APD research available on ASHA shows that there are no unique sets of clinical characteristics or any pattern of deficits on test batteries that clearly define the behaviors and difficulties that are possessed by individuals affected by C/APD (ASHA, 2005). Silman et al. (2000) reported the p revalence of C/APD in children to be between 3 – 5%. Chermak and Musiek (1997) estimated that the prevalence of C/APD in the school-aged population is approximately 2% to 3%, and the estimated prevalence of C/APD in the older adult population above the age of 75 is nearly 70% (Stach et al., 1990). Many adult populations may also experience C/APD. Adults who have aphasia have been shown to have a high incidence of central auditory nervous system involvement, as have individuals who have certain neurological diseases (Purdy et al., 2016) such as multiple sclerosis and Parkinson’s disease. Individuals who have received closed-head trauma often have central and/or peripheral auditory involvement (Purdy et al., 2016).
17
Central Auditory Processing Disorder: Possible Symptoms
C/APD students are diagnosed as having ADHD due to the similarity of attentive, processing, and behavioral problems they exhibit (i.e., poor listening skills and difficulty remembering verbal information). Although these symptoms may be similar, the actual neural processing of auditory input in the central nervous system is intact for individuals diagnosed with ADHD, whereas the auditory input in the central nervous system is not intact for individuals diagnosed with C/APD (ASHA, 2005). Results from studies indicated lower central auditory processing ability, and significant correlations between reading and ADHD symptoms and reading and central auditory processing ability in the ADHD with learning disability (LD) group, suggesting that central auditory processing deficits are more likely to be associated with LD than ADHD (Gomez & Condon, 1999).
Central Auditory Processing Disorder: Possible Causes
While C/APD is most commonly identified in individuals with normal hearing, individuals with sensorineural (nerve-related) hearing loss can also experience C/APD and related cognitive, academic, and social difficulties (Culbertson & Gilbert, 1986). An individual who does poorly on auditory tests, even with amplification, may have a central component to their disability. Significant word-discrimination difficulty, when serious pathology has been ruled out, may also signal a processing deficit. The commonly held belief is that a C/APD is caused by a lesion at some point along the central auditory pathway, including the peripheral system (i.e., person’s hearing ability), which results in the brain’s inability to adequately process the auditory input (Bellis, 2011). Other possible causes include tumors of the c entral auditory nervous system (CANS), premature birth/low birth weight, extrinsic brain damage, metabolic disorders, cardiovascular disorders, and epilepsy (Bellis, 2011).
18
Sound undergoes complex processing by intricate neural mechanisms and ne ural networks. These mechanisms and networks are composed of structures located in the brainstem, subcortex, primary and association areas of the auditory cortex, and the corpus callosum. These structures are responsible for transmitting, enhancing, or inhibiting, reshaping, refining, and assigning recognition and meaning to the once airborne vibrations. Much of the auditory processing is a preconscious event. However, the result is an auditory perceptual event (ASHA, 1996).
Auditory processing is the decomposition of acoustic signals into frequency components (Fletcher, 1940). This transformation from the time domain to appropriate time -frequency representations depends on the mechanical properties and the anatomical organization of the cochlea, where each frequency element leads to the vibration of the basilar membrane only at specific locations, due to resonance effects. Therefore, each mechanosensory hair cell on the membrane responds only to a limited range of frequencies or the frequency bandwidth and such frequency analysis leads to the tonotopical organization of the cochlea as manifested in the tuning curve properties of the ascending auditory nerve fibers (Kiang et al., 1967; Kiang & Moxon, 1974).
Cochlear nucleus is the first “relay station” that receives inputs mainly from the ipsilateral auditory nerve fibers and sends outputs to both ipsilateral and contralateral superior olivary nuclei (Kandel et al., 2000). The tonotopical organization is preserved in the cochlear nucleus, and neurons in the cochlear nucleus can be classified into several types based on their morphological features and their response maps, showing areas of excitation and inhibition plotted on the sound-level vs. frequency coordinates. In addition, spiking patterns can also be classified into several categories based on the shape of pre-stimulus time histograms (Kiang,
19
1984
). Spectro-temporal sound levels and some other forms of coding schemes are already employed at this level (Oertel, 1991), but it remains to be seen what kind of computations the cochlear nuclei perform.
Binaural inputs first meet each other at the superior olivary nuclei, a group of nuclei in the pons, which receive inputs from (anterior ventral) cochlea nuclei bilaterally and send outputs to four inferior colliculi through lateral lemniscus (Kandel et al., 2000; Konishi, 2003). The superior olivary nuclei thus play a very important role in sound localization by exploiting binaural cues and is, in fact, one of the best characterized auditory stations from functional viewpoints. The lateral superior olive exploits the interaural level differences (ILD) a major cue in localizing high-frequency sounds where some cells are excited by ipsilateral sounds and inhibited by contralateral sounds (E-I cells), leading to faithfully encoding the intensity differences as small as 10 dB SPL. Other cells are responsive to similar variations in the sound intensities at both ears (E-E cells; Caird & Klinke, 1983). The superior medial olive is involved in detecting the interaural time differences (ITD), which is particularly useful for locating lowfrequency sounds. The superior medial olive is believed to be the site of the coincidence detection originally proposed by Jeffress (1948), where a spatial array of cells receives inputs from both ipsilateral and contralateral sides but with different “wire length” from the two sides. The differing wire lengths cause a certain internal delay for signals to reach, and thus the convergence of the signals from the two ears coincides only when the difference in these latencies matches exactly to the arrival time difference of the sounds between the two ears (Joris et al., 1998; Palmer, 2004).
The primary auditory cortex is the first cortical station that receives inputs from the auditory thalamus and further processes the acoustic signals to make sense of them (King &
20
Schnupp, 2007). Auditory cortical neurons have a wide variety of receptive field sizes and show highly heterogeneous response patterns, and it is currently unclear as to what acoustic features these neurons respond to, or what stimulus would be optimal for exciting auditory neurons. However, no consensus on the definition of the auditory cortex has been reached because many functional subregions seem to exist. Among many areas more than ten divisions in cats as well as in monkeys seem involved in the auditory signal processing, several primary areas have a tonotopic map (the primary auditory cortex, the anterior auditory field, and the posterior, ventral, and anteroposterior auditory areas), suggesting their roles in spectro-tempora l and binaural analysis based on the information directly inherited from subcortical areas (Miller & Cowen, 2001). In contrast, some non-tonotopic areas (the secondary auditory cortex and the supraSylvian fringe) typically have broader tuning curves and longer durations. These are thought to be involved in processing communication signals and non-spectral stimuli (Rauschecker & Tian, 2000).
Central Auditory Processing Disorder: Possible Effects
According to Ross-Swain (2007), “to learn, a child must be able to attend to, listen to, and separate important speech from all of the other noises at school and home. When auditory skills are weak, the child may experience information overload” (p.141). C/APD is a deficit in processing auditory information, which can further be negatively impacted by environmental conditions, such as excessive noise, unfavorable acoustics in a room, and other such factors. Individuals diagnosed with C/APD usually have IQs within normal range and also have hearing sensitivity thresholds within the normal range. C/APD may also be defined as a difficulty for children with normal hearing to listen selectively in the presence of noise, to combine information from two ears properly, to process speech when it is slightly degraded, and to
21
integrate auditory information when it is delivered faster than the individual with C/APD can process (Moore, 2006). Tallal (2008) further stated that children with C/APD could be characterized by severe deficits in higher-order auditory processing, specifically rapid temporal integration of acoustically varying signals and serial memory. These children may also have difficulty in discrimination and sequencing rapidly presented auditory information, especially when the stimuli are short tones, short vowels, or short transition consonants in combination with brief interstimulus intervals (Tallal, 2008)
Perceiving speech in an acoustically noisy environment requires intelligent use of redundant multi-dimensional cues spread over wide-ranging time scales. The majority of psychoacoustic and speech perception research has focused on spectral cues (from roughly 4008000 Hz) that are available through an auditory critical band filtering mechanism (Glasbe rg & Moore, 1990), and on nearly logarithmic loudness growth (Delgutte, 1996). Human perception allows for nearly independent processing, focusing on the position and motion of vocal tract resonances in spectral regions with good signal to noise ratios. Moreover, human perception has a context-dependence that can last for hundreds of milliseconds (Allen, 1994).
Factors Involved in Auditory Processing
The ear houses both the vestibular and cochlear systems and are involved in 90% of all the sensory information that stimulates the brain (Tomatis & Thompson, 1991). The brain receives sound stimulation not only through the ear canal but also through the bone that surrounds it. Even when the ear is functioning within typical limits, there is no guarantee that an individual is actually listening, as the brain can choose to tune things out (Tomatis & Thompson, 1991; Gitomer, 2016; Perreau et al., 2017). The ears transmit, and the brain processes both the
22
acoustic and vestibular sensory messages received by the ears, which may show farther reaching benefits of the Tomatis® Method to include other sensory systems.
Diagnosis of Central Auditor Processing Disorders
According to the British Society of Audiology (2011), “C/APD impacts on everyday life through disordered listening and consequent reduction in the ability to act on what is heard” (Para #3)
Diagnosis of C/APD is presently complicated by three factors (Jerger & Musiek, 2000):
1. Other types of childhood disorders may exhibit similar behaviors. Examples are attention-deficit/hyperactivity disorder (ADHD), language impairment, reading disability (dyslexia), learning disability, autistic spectrum disorders, and reduced intellectual functioning.
2. Some of the audiological procedures presently used to evaluate children suspected of C/APD fail to differentiate them adequately from children with other problems.
3. In assessing children suspected of having a C/APD, other processes and functions are likely to be encountered that affect the interpretation of test results. Examples are a lack of motivation, lack of sustained attention, lack of cooperation, and lack of understanding. These confounding factors are vital to consider in order to ensure that they do not lead to the erroneous diagnosis of an auditory problem. Because of these potential confounding factors, the differential diagnosis of C/APD requires the systematic acquisition of information sufficient to identify an auditory-specific deficit.
Bellis and Ferre (1999) described a method of profiling C/APD. Each profile is related to its underlying neurophysiologic region of dysfunction in the brain as well as to its higher-level
23
language and learning implications and sequels. Their model may be described as both neurophysiologic and neuropsychological, in which profiles are derived that encompass the whole of the audition, from underlying auditory mechanisms to language, learning, and other high-level, complex behaviors. The Bellis/Ferre model includes three primary profiles a nd two secondary profiles. The three primary profiles represent auditory and related dysfunction in the primary auditory cortex (usually left hemisphere); non-primary auditory cortex (usually right hemisphere); corpus callosum (interhemispheric dysfunction). Secondary profiles represent dysfunction and associated sequels that may be considered to represent higher-level language, attention, and/or executive function and, therefore, some may argue against their inc lusion under the umbrella of C/APD. Finally, even if the “central” compound of C/APD is certainly a major characteristic of these disorders and might well be a critical aspect of most of its forms, more recent observations on the perceptual consequences of cochlear hearing loss (Moore, 2006) raise the issue of potential peripheral influences on degraded auditory performances not reflected in audiometric measurements (Moore, 2006). The same observations have been made for the role of the olivocochlear efferent system regulation on outer hair cell functions (Suga et al., 2000), and therefore, the term C/APD was preferred in the later years to APD or even (C)APD for (central) auditory processing disorders, which may well prove to be anatomically imprecise. As long as available detailed knowledge on the close relationship between peripheral and central auditory processing will not be significantly increased, the more general and cautious term of C/APD is certainly more adequate, even if this term increases the likelihood of seeing more pathologies fall under the already wide scope of APD.
Based on central auditory test findings, clinicians should be able to determine the presence or absence of a disorder. Bellis (2003) recommended that the identification of C/APD
24
be based on abnormal findings on one or more test tools, combined with significant educational and behavioral findings. In addition to identifying the presence of the disorder, all attempts should be made to identify the underlying process or processes that are dysfunctional. Considerations should allow for the development of a multidisciplinary, deficit-specific management plan addressing each child’s individual needs (Mülder et al., 2007).
Despite the increase in referrals for C/APD evaluation from professionals like teachers, psychologists, and speech-language pathologists along with a demand from parents who hear about this on the Internet and various other sources, audiologists are reluctant to include C/APD assessment in their clinical practices (Kraus & Anderson, 2016). According to Kraus and Anderson (2016), there are several factors that contribute to this reluctance; specifically, there is disagreement as to the existence of C/APD separately from deficits in attention, memory, and cognitive functions (Cacace & McFarland 1998; Moore et al., 2010). This reluctance exists d ue to the findings that C/APD is often comorbid with language learning difficulties, dyslexia, memory, and attention deficit disorder, which complicates findings of the test results (Sharma et al., 2009). Audiologists have disagreements on the very definition of C/APD and on test battery criteria. Wilson and Arnott (2013) assessed 150 school-aged children using nine different diagnostic criteria to determine the rate of C/APD and found that the rates of diagnosis varied between 7.3 and 96.0%. According to Wilson et al. (2012), clinicians are not confident about the efficacy of treatments that are purported to improve auditory processing as the existing studies used differing methodologies, and thus comparing studies is difficult.
No general consensus among clinicians and researchers has been reached on the test battery selection, assessment procedures, and diagnostic criteria for C/APDs (Ferguson et al. 2011). In addition, to test selection and assessment procedures, no consensus has been achieved
25
about which cutoff scores classify a child as pass or fail on C/APD assessments. Cutoff criteria recommended by the American Academy of Audiology and ASHA are different from the cutoff criteria recommended by the Central Test Battery (CTB) developed by Katz (1992). The inclusion of non-speech tests in the diagnosis of C/APD may reduce the confounding influence of language on an individual’s performance (Moore, 2006). Individuals with language impairment perform poorly on speech tests and perform well on non-speech tests (Moore, 2006); therefore, the use of non-speech tests would help to differentiate receptive language impairments from C/APD (McArthur, 2009).
In a survey of auditory processing diagnostic practices in the United States, Emanuel (2002) reported the most popular questionnaires used in American clinics were the Children's Auditory Performance Scale (CHAPS ; Smoski et al., 1998), Fisher’s Auditory Problems
Checklist (FAPC; Fisher, 1976), and the Screening Identification for Targeting Educational Risk (SIFTER; Anderson, 1989). CHAPS was developed as a tool for collecting and systematizing data on a wide range of observed listening behaviors displayed by children with C/APD as well as children with other hearing difficulties who were mainstreamed into a regular classroom. CHAPS may be completed by schoolteachers, parents, caregivers, or any other persons who can provide hearing information on a child’s performance in different social environments (Smoski et al., 1998). As a result, it is convenient for clinicians to obtain and compare children’s auditory performance in different auditory environments and to make appropriate recommendations for follow-up management and intervention. SIFTER is utilized to provide a method, by which children with hearing problems can be identified in an educa tional environment. Similar to CHAPS, SIFTER is also formatted as a rating scale, with 1 to 5 representing a degree of performance from good to not satisfactory. Performance is rated in the areas of academics,
26
attention, communication, class participation, and school behavior. SIFTER is designed for classroom teachers to complete, and evaluation is focused on children’s educational problems (Anderson, 1989).
A broad consensus exists among audiology specialists and researchers that a C/APD diagnostic battery is not comprehensive if it does not include electrophysiological measures (Bellis, 2003). In recent years, more and more investigators have paid attention to the application of electrophysiological procedures for assessing central auditory nervous system (CANS) function. These procedures include the auditory brainstem response (ABR), middle latency response (MLR), and auditory late evoked response. An obvious advantage of auditory electrophysiological assessment is its objectivity. In addition, electrophysiological tests can be performed regardless of a child’s age. These tests can also be used when the physical or cognitive disability of adults or children makes it impossible to use behavioral tests to assess central auditory function. Auditory electrophysiological tests do not need active cooperation or behavioral response, they carry less linguistic load, and therefore the test results are less affected by cognitive factors in addition to specific auditory abilities (Bellis, 2003). Auditory evoked potentials are classified according to when in time they occur. The ABR is a short latency response (less than 10 msec post-stimulus onsets), which provides objective evidence of the integrity of the auditory brainstem. The MLR and the late latency response recordings, including the P300 and mismatch negativity (MMN), provide information about the cortical and subcortical areas of the auditory pathway and will not be included in this review.
Jerger and Musiek (2000) stated that the diagnosis of C/APD, while having a primary auditory deficit, is complicated by the similarity of the behaviors of children with C/APD and those of ADHD, language, reading, and learning disorders, and autistic spectrum disorders, along
27
with children who have lower intelligence. I have therefore added several sections to the literature review as there are possible correlations, and the results of this study could potentially impact several other diagnoses as well. My thought is that this may additionally serve as a basis to study the impacts of the intervention on other diagnoses. This is demonstrated with a literature that is replete with references to similarities between the presenting symptoms of C/APD, ADHD, specific language impairment (SLI), dyslexia, and autistic spectrum disorder (ASD), particularly in children.
Central Auditory Processing Disorder and Associated Challenges
In looking at clinical findings of children who have undergone treatment with the Tomatis® Method, one notices the presence of language difficulties in those who have a diagnosis of C/APD. As a speech/language pathologist, I am interested in finding out whether the Tomatis® Method has an impact on functional outcomes in communication as a byproduct of changes within the central auditory processing circuit. As speech/language outcomes are generally believed to be linked to cognition, it is further interesting to me to assess for any cognitive changes. According to Krüger et al. (2001), C/APD often present with language disorders, sensory integration dysfunction, and learning disabilities (LD). They further noted that the majority of children presented with deficits involving both the visual and auditory modalities, as well as problems with motor abilities and concentration skills. Within this majority group, further subgroups of problem areas were found to occur together. The results suggest that a multimodal perceptual approach is useful for enhancing the diagnosis of and choosing interventions for these children (Krüger et al., 2001). This indicates that should the Tomatis® Method prove efficacious in treating C/APD, there may be implications for its use in other diagnosis that are frequently treated using speech and language pathology approaches.
28
Central Auditory Processing Disorder and Specific Language Impairment
Ferguson et al. (2011) studied 22 children clinically diagnosed with specific language impairment (SLI) and 19 with ADP, who were otherwise normal hearing children. The parents were asked to complete questionnaires regarding communication, listening, and behavior. Ferguson et al. (2011) found that despite varying diagnoses of SLI or C/APD, both groups of children had similar profiles. They, therefore, concluded that it was probably the route of differential diagnosis versus actual differences in behaviors that resulted in different names for the diagnosis. A further finding was that the children diagnosed with SLI or C/APD had similar performance on a broad range of assessments, including communication, listening, behavior, and cognitive. However, both groups were consistently outperformed by mainstream schoolchildren (Ferguson et al., 2011).
Archibald and Gathercole (2006) measured short-term and working memory as well as phonological awareness of 20 children aged 7 – 11 diagnosed with SLI. To be able to find the prevalence of short-term and working memory profiles of the SLI group in the normally developing population, the performance of the SLI group was compared with the 636 children of the standardization sample of the Working Memory Test Battery for Children (WMTB-C). Ninety-five percent of the participants scored in the deficit range on the working memory composite. This was higher than for any other of the language measures except for the Reca lling Sentences subtest, which is highly dependent on memory as well. Seventy percent scored in the deficit range on the verbal short-term memory measure, 50% scored in the deficit range on the visuospatial composite, and 38% on the phonological awareness measure. Interestingly the finding that less than half of the SLI group presented with deficits of phonological awareness
29
contradicted previous reports that children with a diagnosis of SLI present with impaired phonological awareness skills.
Cumming et al. (2015) measured auditory processing of 45 children with SLI who, on average, were 9 years old and compared the results with 50 age-matched controls. They found a relationship between the severity of auditory impairments and the severity of language impairments. In their sample of children, auditory processing was impaired when compared to age-matched controls. They found strong associations between poor auditory processing and poor written and spoken language.
Central Auditory Processing Disorder and Oral and Written Language Deficits
Hulme and Snowling (2014) found that a close association exists between different aspects of oral language and reading impairment. According to Sollier (2005), the Tomatis® Method, along with improving listening , which consists of attending to and then processing speech also improves speech and processing language one reads. Further, Sharma et al. (2009) concluded that language impairment and reading disorder commonly cooccur with C/APD I, therefore, found it necessary to include assessments relating to oral language in the pilot study and therefore present the existing research that looks at possible connections between the two.
Lallier et al. (2013) compared 17 dyslexic children to an identical numbe r of control children and found evidence that a processing disorder of both visual and audition happened simultaneously in some dyslexic individuals. Another study on 36 children diagnosed with developmental dyslexia by their local education authority showed severe literary and phonological deficits in the test battery performed by the researchers. Cutini et al. (2016) found that there is probably “functionally-atypical right-lateralized processing of slower temporal modulations in children with developmental dyslexia” (p. 47). Christmann et al. (2015) assessed
30
the auditory processing of German vowel center stimuli. They did this while using the same task for linguistic and nonlinguistic conditions. They also systematically varied those temporal and spectral parameters that are part of the German vowel system. Results showed that most of the dyslexic participants also had auditory deficits. These were found in both speech and nonspeech stimuli, which “support the existence of a general auditory processing impairment in developmental dyslexia” (Christmann et al., 2015, p. 107).
In addition, the early findings of Tallal and Piercy (1973) led to the proposal that phonological deficits associated with learning language impairments (LLI) result from rapidly changing sensory inputs. Their research showed that children with LLI were unable to identify rapid changes in formant transitions (e.g., /ba/and /da/) and that by extending the same differences between transitions, the LLI children were better able to identify these differences. According to this temporal hypothesis theory, poor auditory temporal perception causes poor speech (phonological) perception, which then impacts on language acquisition and reading (Tallal & Piercy, 1973). Moreover, Wright et al. (1997) supported these claims by reporting that language problems were a result of auditory perceptual deficits in both temporal and spectral domains. A series of tone in masking noise tasks (backward, simultaneous onset and delay, and forward) were performed in children with SLI (n -8) and a TD group (n =8). There was no difference between the two groups in the detection of a long 300 ms tone -in-quiet. However, the SLI children had significantly higher (poorer) detection thresholds in noise for short 20ms tone for all tasks compared to the TD group, particularly for the backward masking task. The same pattern of results was shown for three out of four conditions when the marker included a spectral notch; thus, the SLI children were unable to take advantage of the notched condition. Together these data showed that the children with SLI had both a temporal deficit, which was particularly
31
marked for backward masking and a spectral deficit (Wright et al., 1997). Children with SLI performed significantly worse than the control group on frequency discrimination tasks (Nickisch & Massinger, 2009).
Central Auditory Processing Disorder and Learning Deficits
The findings explained in the previous paragraph extend to learning difficulties more generally, with suggestions that phonological processing deficits are central to both C/APD and learning deficits. Sharma et al. (2009) argued that there is a correlation between C/APD and learning difficulties. The researchers assessed a group of 68 children with suspected C/APD based on reports from parents, teachers, or healthcare professionals, such as audiologists, speech and language pathologists, and educational psychologists. The children underwent a large battery of tests to assess auditory processing, including dichotic digits (DDT), frequency pattern test (FPT), random gap detection test, compressed consonant-vowel-consonant words and masking level differences, reasoning ability, language, reading, phonology, auditory memory, and sustained auditory and visual attention. The authors showed that 72% of children had C/APD, 76% had language impairment (LI), and 73% had reading disorder (RD). Further 10% had C/APD + RD, 10% had C/APD + LI, 12% had RD + LI, and 47% had all three (C/APD + RD + LI). Only 4% had only C/APD. Thus, they concluded that LI and RD commonly co-occurred with C/APD, with more children showing symptoms of two or more disorders than only one (Sharma et al., 2009). Further, Murphy and Schochat (2011) a nalyzed the effect of nonverbal auditory training using two experiments. The first consisted of 12 dyslexic children between the ages of 7 to 14 who were compared to a group of 18 untrained dyslexic children. The second experiment consisted of 18 dyslexic children whose performance was evaluated at three points in time, 2 months prior to the beginning of and at the end of the training. This was carried out over
32
a period of 2 months using a computer program that trained discrimination skills. The results of the first experiment showed significant improvements not only in the nonverbal auditory skills that were trained but also in phonological awareness tasks. In the second experiment, results showed significant improvement in phonemic and text reading tasks. This clearly suggests a link between verbal tasks and nonverbal auditory processing skills (Murphy & Schochat, 2011).
An intimate relationship exists between language, attention, and auditory skills. Auditory processing disorders often coexist with learning disabilities, language disorders, attention-deficit disorders, and dyslexia (Cacace & MacFarland, 1998; Chermak & Musiek, 1997). These disorders are heterogeneous in nature. For example, children with language -based learning problems often exhibit deficits in auditory perception, and the neural encoding of speech sounds at both cortical and brainstem levels (Cunningham et al., 2000), especially when background noise is introduced (Bradlow et al., 2003). Depending on the severity of the C/APD, children will have difficulty not only with perceiving and discriminating sound, attending to sound, and localizing sound, but also show difficulties with other auditory skills that make up the hierarchy of auditory processing skills, such as phonological awareness, auditory association, and auditory feedback (Bellis, 1996).
Miller and Wagstaff (2011) also looked at the relationship between C/APD and learning difficulties. The researchers recruited 64 children who had either received a clinical diagnosis of C/APD from audiologists or were receiving services for language impairment. They also included 20 typically developing (TD) children. All the children underwent a large battery of tests, including auditory processing. They did not find any group with means differences between the two groups. However, they did find that reading fluency was deficient in the C/APD group. As reading fluency is directly connected to C/APD, Amitay et al. (2002) suggest
33
that a large portion of disabled readers suffer from diverse difficulties in auditory processing. This is not to say that all impaired readers have a C/APD. Still, for the purposes of this study, we can hypothesize that remediating the C/APD will have the added benefit of remediating to some extent, the language and reading deficits within this population.
Central Auditory Processing Disorder and Psychosocial Difficulties
Reports suggest untreated C/APD commonly leads to reduced communication function, which in turn can have psychosocial impacts such as loneliness, social anxiety, depression, anger, and fear (Crandell, 1998). It is therefore not unreasonable to expect that should the Tomatis® Method be efficacious in remediating C/APD, it would also help certain psychosocial diagnoses, as mentioned in this section. Communication difficulties have been shown to lead to reductions in physical health and psychosocial health status as well as the overall quality of life (Bess et al., 1998; Crandell, 1998 ). Davis et al. (1986) examined the psychosocial function of children with mild to moderate sensorineural hearing loss. Their findings suggest that children with hearing loss are more likely to exhibit aggressive behaviors and to express corporal complaints than their peers with normal hearing. On the Child Behavior Checklist (CBC), a parental rating scale, participants with hearing loss produced patterns of greater impulsivity and aggressive behaviors, as well as more social isolation and academic difficulties, compared to the instrument’s normative data set.
C/APD in children undermines social interaction. Children with C/APD find keeping up with conversations difficult; by the time they hear and process what someone says on the playground, others will have responded, and the conversation will have moved on. The lag in processing conversations tends to lead children to refrain from participating in group conversations. Hovering around quietly or alternatively, due to the frustrations of not keeping
34
up, just preferring one’s own company may become a child’s preferred response to C/APD Making friends, especially in group settings, is simply too hard. The C/APD combined with the avoidance behaviors can become a vicious cycle as the lack of social interaction leads to less than normal conversation and language stimulation, the main ways auditory processing skills gradually improve (Nixon, 2015).
While the difficulties C/APD children have with background sounds in typically noisy classrooms are well known, less understood are the humiliations and disappointments experienced daily (Nixon, 2015). During the school day, a child will get called on to participate in one way or another. Generally, this participation is preceded by a question or request that requires an immediate response. For children with auditory processing problems, immediate responses are no easy feat and often impossible. Children with C/APD need a few seconds to process questions or requests, while the rest of the class looks on and waits, and then, they need to decide on a response (ASHA, 2005).
Central Auditory Processing Disorder and Cognition
Keller et al. (2006) also showed an association between auditory processing and cognition. They investigated auditory processing abilities using a range of 39 speech tests (SSW, phonemic synthesis test, speech-in-noise) in a group of children who had been diagnosed with a nonverbal learning disability (NVLD) by clinical psychologists. The diagnosis of C/APD was made in just under two-thirds of the NVLD sample (61%). These children had significantly poorer results on language and memory tests (digit span, sentence mem ory) than the NVLD children who were not diagnosed as having C/APD. The authors proposed that C/APD may be less prevalent in children with higher intelligence, although they also suggested that intelligence may act as a buffer in the identification of C/APD (Keller e t al., 2006).
35
Central Auditory Processing Disorder and Comorbid Conditions
As mentioned earlier, auditory disorders are widely accepted as often being a coexisting diagnosis with ASD, I thought it important to add the following research here. Should the intervention studied show a positive impact on C/APD, it is not unreasonable to assume that it may possibly also help certain symptoms associated with ASD and will, therefore, be relevant to future research. The results from behavioral and electrophysiologic testing showed that children with ASD have abnormalities in auditory processing (Steinschneider & Dunn, 2002; Wetherby et al., 1981). For example, children with ASD have been found to have difficulty recognizing speech in the presence of background noise (Alcantara et al., 2004) and a diminished ability to attend to specific sounds in environments with multiple complex sound sources (Teder-Salejarvi et al., 2005). Although auditory processing deficits are not fully understood in ASD, a variety of auditory treatments and listening therapies with little empirical evidence are marketed to parents to reduce or eliminate abnormal behavioral responses to sound in children with ASD (Corbett et al., 2008; Neysmith-Roy, 2001). Specific atypical behaviors due to an overall hyperresponsiveness in the ASD group resulted in hypersensitivity to sound, sensory defensiveness to tactile stimulation, sensory modulation dysfunction, aversion, and/or lack of habituation to sensory stimuli (Baranek et al., 1997). Ashburner et al. (2008) investigated the sensory processing abilities and educational outcomes in a sample of children with ASD. A pattern of auditory filtering difficulties, sensory under-responsiveness, and sensory seeking were associated with academic underachievement in children with ASD. Difficulty understanding the teacher in the presence of background noise was found to be a strong predictor of poor academic performance. Teder-Salejarvi et al. (2005) found similar results for performance in noisy
36
environments and recommended that children with ASD may benefit from an acoustically simplified setting.
Behavioral Treatments for Central Auditory Processing Disorder
Current standard practice in therapy for C/APD consists of finding accommodative and compensatory strategies to help an individual function despite the underlying difficulty (Cacace & McFarland, 1998) and was reiterated by Bellis (2007) where he stated that treatment usually focuses on changing the environment and teaching compensatory strategies. Bellis further stated that it is the individual therapist who decides on the number of hours, which in turn are dependent on payers and strategies given to an individual, all of which are dependent on the therapist’s preferences and style.
Speech/Language Therapy
The extent of the ability to process auditory information can directly impact how well a child communicates in language and/or speech. As described throughout the paper, children with C/APD appear to be prime subjects for the Tomatis® Method. I therefore found it important to incorporate research on speech therapy as there are various research projects that studied the effects of the Tomatis® Method on auditory processing and learning done in Europe and Canada. Gilmore (1999) studied the efficacy of the Tomatis® Method for children with learning and communication disorders. He reported that the Tomatis® Method resulted in positive changes in the domains of auditory processing, psychomotor, cognitive, linguistic, and personal/social adjustment. He additionally reported that his findings were consistent with clinicians’ reports of beneficial effects. Other investigators also demonstrated that the Tomatis® Method has proven to be effective in the areas of learning, communication, and social pragmatics (Kershner et al., 1986; Gilmore, 1999).
37
Improving basic processing abilities found to be deficient in C/APD like phonological memory, working memory, and speed of processing through speech therapy alone whereby AP is addressed using accommodations and modifications have proven to be difficult (Cacace & McFarland, 1998). Speech therapy techniques often require years of intervention before substantial improvement is seen, resulting in the individual having difficulty with daily living skills, academics, and socialization. Speech therapy usually consists of accommodative strategies to help children function despite the existence of C/APD, and thus, commercial auditory training programs have been developed to provide remediation for auditory perception and related learning deficits (Gillam et al., 2001).
Moncrieff and Wertz (2008), as well as Bellis and Anzalone (2008), tested dichotic listening intervention as a possible effective bottom-up treatment intervention for individuals diagnosed with C/APD. Dichotic listening intervention has been used in research related to language, reading disorders, and the clinical diagnosis of auditory processing disorders. Dichotic listening is when two different auditory stimuli are presented simultaneously to the listener. In the Moncrieff and Wertz (2008) study, children with dichotic left ear deficits received intensive training in two-phased clinical trials that were designed to establish the efficacy of directly training dichotic listening. They further stated that since dichotic listening presents more information than can be easily identified, it can also be sensitive to non-auditory factors, including intelligence, attention, working memory, language, and motivation.
Occupational Therapy
Occupational therapists use body work to help children. They work on creating integration of auditory, ocular, and vestibular movement. They use materials and activities that use balance and sensory integration to help build appropriate neural networks in the brain. They
38
work with specific movement exercises to integrate the body bilaterally to allow for higher functions. They may also use therapies such as interactive metronome (IM). Additional commercial programs used are those also used by SLPs such as PACE = Processing and Cognitive Enhancement, the Lindamood Phonemic Sequencing TM (LiPS), and Earobics to name a few. They also work to find accommodations to help an individual function regardless of the underlying cause. Currently o ccupational therapists use strategies to compensate for lacking skills by teaching attribution and cognitive strategies, adapting environments, and suggesting meaningful activities to be incorporated throughout the day (Dourn, 2010).
Accommodations and Compensatory Strategies
Compensatory Strategies
Compensatory strategies help patients to live with the residual effects of their disorders, and to succeed in spite of them. Compensatory strategy training includes the strengthening of active listening techniques and linguistic, metalinguistic, and metacognitive abilities.
Strengthening metacognitive and metalinguistic skills enables the child to recognize conditions that interfere with learning. They also allow the use of executive control strategies and linguistic resources, enabling the child to improve listening outcomes for him or herself (Chermak & Musiek, 1997). Students learn to use compensatory and metacognitive strategies to increase their access to auditory instruction at the universal, targeted, and intensive levels. Since all students are expected to listen in the classroom, these are skills that the regular classroom teacher or other professionals can model and teach. Organization, active listening, and self-advocacy are skills that all students need. As students’ needs become more significant, specialized instruction is critical (Chermak & Musiek, 1997).
39
Practitioners use two different approaches, top-down and bottom-up. The top-down approach is teacher-centered and focuses on language and cognition. According to Friel- Patti (1999), speech-language pathologists support the top-down approach, commonly referred to as the network model. The network model “emphasizes the distributed nature of information processing within the nervous system… the integration of sound, meaning, and intention involves more than the auditory neural pathway” (p. 347). Alternately, the bottom -up theory is supported by audiologists. This student-centered approach focuses on signal quality and environmental modifications. The bottom-up theory is commonly referred to as the pathway model. Friel- Patti (1999) stated that audiologists support the pathway model, “which is based on the auditory nervous system and the centers along the pathway that processes auditory information. The focus is on the specification of the stimuli and the level of the auditory nervous system being evaluated” (p. 347).
According to Patrusky’s (2013) meta-analysis, a significant difference in post-treatment intervention sessions existed when a combination of bottom-up and top-down treatment approaches was employed. Based on these eight bottom-up intervention treatments, the treatment approaches that appeared to consistently yield significant positive results were the following: (a )
auditory discrimination including following directions, listening and speaking, classroom modifications designed to reduce the effects of noise, increasing visual cues and specific remedial and compensatory strategies; (b) improving ability to process, recall, and execute multistep directions; (c) personal assistive listening devices such as FM or hearing aid; (d )
dichotic auditory training (testing that involved the presentation of the same stimulus to both ears simultaneously); (e) speech-sound discrimination; and (f) Earobics, a program that integrates cognitive and language skills in the development of children’s auditory skills in phonemic
40
awareness, auditory processing, and phonics. Based on seven top-down intervention treatments, the interventions that appeared to consistently yield significant positive results were the following: (a) Fast ForWord computer-assisted training; (b) Lindamood phonemic sequencing;
(c) distinguishing phonemic sound changes; (d ) identifying, detecting, producing, or deleting specific phonemes, reinforcing memory, and reasoning skills within nonsense syllables that differ by a single phoneme; (e) teaching listening comprehension; and (f) teaching higher language skills. Most of the investigated C/APD case studies employed a combination of both bottom-up and top-down treatments in the intervention. Additionally, according to Patrusky’s (2013) meta-analysis, the 16 intervention studies that were included in the meta-analysis met the criteria for effective intervention according to ASHA technical report (2005).
Frequency Modulation Systems
Frequency modulation (FM) systems are devices that use radio waves to send speech and other signals to hearing aids. They use the same type of signal as an FM radio; however, the frequency band used in these systems is designated for personal use. These systems have two components: a microphone, which in a classroom would be used by the teacher, and a receiver, which is either hooked to hearing aids or a set of headphones used by a student. FM systems have been shown to increase the understanding of students of what is being said by their teacher (Anderson & Goldstein, 2004).
According to Reynolds et al. (2016), a systematic review of the published research related to the effectiveness of FM systems indicated moderate support for the use of these to improve children’s ability to listen and attend in a classroom. However, as Nguyen and Bentler (2011) point out, children seem to be reluctant to use them and therefore they may not have a great deal of impact. They further concluded that although the use of FM systems enhances
41
reading skills, increases attention span, and reduces distractibility, current evidence shows that unless the functioning of these devices is frequently verified, some advantages may be lost.
According to Keith et al. (2019), despite evidence of efficacy of FM systems, children discontinued use on an average after 2 years and 9 months. The y found that the range of use varied widely from 4 months to 6 years and 1 month. Fifty percent of children stopped using these systems in Grade 6 at around 10 – 11 years of age. Keith et al. (2019) found that the children did not stop using the systems because they did not need these anymore, but rather overwhelmingly because they were self-conscious. Other reasons stated included coping better, the aids were uncomfortable, lack of school support, teachers’ reluctance to use the mic, mic being transferred to several teachers, lost aids, sound was too distracting, medication was more suitable in cases of ADHD, and the child started alternate therapy (Keith et al., 2019).
Auditory Programs
Auditory training has been shown to alter the neural responses to sound at the cortical level in humans (Hayes et al., 2003). When the input is processed correctly, language acquisition is possible. The study was undertaken to find out if auditory training targeted to remediate perceptually based learning difficulties would improve the neural brainstem encoding in the children suffering from the learning difficulties. Nine participants with learning difficulties such as dyslexia followed an auditory perceptual training computer-based program and were compared to 10 controls pre-post using brainstem response testing to the syllable /da/ in quiet and in background noise. Transient and sustained brainstem responses were evaluated. There was no significant change between the two groups for the primary pathway afferent volley, which is neural events occurring earlier than 11ms after stimulus onset. However, there was a significant increase in the experimental group over the control group for quiet-to-noise
42
inter-response correlations of the sustained response, which falls between 11 – 50 ms after the onset of the stimulus. Their conclusion was that auditory training could alter the preconscious neural encoding of complex sounds in the auditory brainstem by improving its neural synchrony.
Pre-post testing also showed brainstem response timing related to changes in cortical physiology, perceptual, academic, and cognitive measures (Hayes et al., 2003 ; Chermak & Musiek, 2002).
The Tomatis® Method
Dr. Tomatis’ discoveries were made in the Sorbonne’s physiology laboratory and were then presented to the Academy of the Sciences and the Academy of Medicine in Paris in 1957 and 1960 (www.tomatis.com). His discoveries were named the “Tomatis® Laws” and are
• The voice only contains what the ear can hear.
• If hearing is modified, the voice is immediately and unconsciously modified.
• It is possible to transform phonation permanently by means of auditory stimulation undertaken over a certain time (the law of remanence).
The Tomatis® Method intervention is based on the theory that due to human neurophysiology, the auditory/vestibular systems housed in the ear have important connections with the entire body (Tomatis, 1974). Tomatis (1974) state d that these connections include cortical and sub-cortical structures that are stimulated and balanced when auditory/vestibular input is perceived correctly. He further stated that on the flip side, if the input is perceived incorrectly, these very connections tire and create erroneous connections (Tomatis, 1974).
Sollier (2005) stated that the Tomatis® Method intervention provides auditory/vestibular stimulation, re-educating listening as well as vestibular functions, and, therefore the processing of what is heard, as well as that which is received by the vestibular system. Sollier continued to say that the developmental steps of listening and of the vestibular functions are retraced and
43
rebuilt correctly. Sollier stated that this method is a sound stimulation program administered through both air and bone conduction using specially designed headphones. The sound transmitted by these headphones is filtered and otherwise manipulated through patented programs using electronic devices specifically designed for this purpose (Sollier, 2005).
The child listens to filtered sounds of Mozart music and Gregorian chants, which are believed to be physically relaxing and stimulating (Sollier, 2005) and similar to the earliest experiences of sound, heard prenatally and in early life (DeCaspar et al., 1994). Dr. Tomatis proposed, and Horowitz (2012) concurred, that high-frequency sound is an important source of stimulation to the brain. High-frequency sounds are important because 80% of the hair cells in the cochlea respond to sounds of 1000 Hz and higher. The stimulation from the Tomatis ® Method extends to 20,000 Hz. The expected outcome of the Tomatis® Method is that the ear will transmit sound more optimally, resulting in the improved function of the brain as all the systems will start working in improved harmony (Tomatis, 1974).
Previous Studies on Tomatis® Method
The Tomatis® Method was developed to address the shortcomings of traditional therapies that focus on providing compensatory and accommodative strategies to individuals and is designed to remediate the underlying source of the problems (Sollier 200 5). He further stated that the method aims to rebuild the vestibular and auditory functions by accessing these using both air and bone conduction through the ear, which houses both the cochlear and vestibular systems and is thus ideal as it is designed to specifically stimulate the rich interconnections between the ear and the nervous system (Sollier, 2005). Thompson and Andrews (2000 ) agreed with Sollier stating that changes brought about by the program are not task-specific and directly remediate the dysfunction, resulting in broader impacts.
44
MacDonald and Nicoloff (2008) applied the Tomatis® Method in two case studies one of a 6-year-old female, and the other of a 51-year-old male. Both were tested pre- and postadministration of the Tomatis® Method using the Listening Test, which is much like an audiometric hearing test, but specific to the Tomatis® Method, and only used by practitioners who are certified in using the method. The audiometer was set to different parameters from those that are used by audiologists, and the test included 25 frequencies (where a typical audiometric screening may contain five to ten frequencies). All of the frequencies were tested via bone and air conduction, and selectivity and laterality were also tested. Each of the subjects received one complete program of the Tomatis® Method and no other therapy. The Tomatis® Method consisted of 90 hours in total. These hours were divided over three separate sessions, each consisting of 15 hours. The 15 hours were administered in increments of two hours/day, Monday through Friday for 3 consecutive weeks. A break of 4 weeks was taken between each of the three sessions. The post-test revealed more balanced ears, and the clients reported being happier and more energetic, as well as having improved musical ability and found it easier to understand and produce speech.
Tatum et al. (2004) used the Tomatis® Method therapy, along with speech therapy in two case studies. The first was a 14- year-old female on the autistic spectrum who had no speech despite speech therapy, and who, according to post-testing, showed a gain of the functional use of 34 words and 17 sounds. She also showed improvements in social interactions. The second case study was of a 9-year-old male with ADHD and auditory processing disorder who, per posttesting, showed an increase in phonemic awareness from a mid-second-grade level in the pre-test to a beginning fifth-grade level at post-testing in a period of just 4 months.
45
Ross-Swain (2007) summarized findings in a retrospective study on the Tomatis® Method. The study included 41 randomly selected clients, including 18 females and 23 males ranging in age from 4.3 to 19.8 years of age. The Tomatis® Method was used with all 41 clients; pre- and post-testing was completed using the Test of Auditory Perceptual Skills (Psychological and Educational Publications, Inc. 1996) and the Token Test for Children (Pro-Ed, 2007). Posttesting showed statistically significant improvements in immediate auditory memory, auditory sequencing, interpretation of directions, auditory discrimination, and auditory cohe sion. In addition, post-testing showed a reduction in auditory latency when compared to the clients’ pretests.
Bonthuys and Botha (2016) also conducted a systematic review, that sought to determine the evidence on how the Tomatis® Method compared to other self-regulation interventions with tertiary students. A total of 35 articles met their inclusion criteria. The evidence was thematically analyzed using narrative analysis. Findings suggested the Tomatis® Method is superior to alternative self-regulation approaches in decreasing psychosocial and emotional stressors, as well as enhancing the well-being of students. The Tomatis® Method was as effective as alternative approaches in promoting self-awareness and self-monitoring. Alternative methods were more effective than the Tomatis® Method in aspects of critical thinking; however, they appeared to compare well with other interventions for the promotion of self-regulation among tertiary students (Bonthuy & Botha, 2016).
Stillitano et al. (2014) studied the effectiveness of the Tomatis® Method in patients with tinnitus. A young male patient who had chronic tinnitus since the age of 6 was selected. The patient was assessed with Tinnitus Handicap Inventory (THI), Tinnitus Sample Case History (TSCH), psychological questionnaires, pure tone audiometry, pitch and loudness of tinnitus, and
46
loudness discomfort level. THI gave a result of 34 (Grade 2). He additionally had a diagnosis of bipolar disorder. His hearing was normal, and the tinnitus was prevalent in the left ear with the pitch at 3000 Hz and the loudness at 30 dB HL. The treatment consisted of listening to Mozart music and Gregorian chants with a headphone and bone vibrator. The music frequencies were filtered using different intensities of stimulation and delays between air and bone conduction. After 70 hours of the Tomatis® Method treatment, THI decreased to 6 (Grade 1), and the tinnitus loudness decreased to 18 dB HL. After 105 hours of treatment, THI was reduced to 2 (Grade 1), and the tinnitus loudness decreased to 13 dB HL.
Stillitano et al. (2016) investigated the Tomatis® Method on the artistic voice, testing the stabilization or the improvement of some vocal parameters, as well as the effect on the formants of voice. A group of N = 19 subjects, of singers and actors, were assessed by complete clinical ENT evaluations, including fibrolaryngoscopy, otoscopy, and clinical audiometry. The voice analysis was carried out with the Multi-Dimensional Voice Program (MDVP) and with the Praat software. The results demonstrate that after the treatment there is an increase in the mean of energy density on the third formant of voice (F3). An improvement in the ability to maintain a constant intensity of the vocal emission resulted from MDVP analysis with a reduction in the standard deviation of the voice amplitude. The improvement in auditory perception, particularly for 3 kHz, determined better intelligibility and articulation of the words. The improved auditory perception in the zone of 3 kHz reduced the phenomenon of nasalization and gave expressive power to the artistic voice. The decrease of Peak-Amplitude Variation (vAm) led to a stable voice emission with better control.
47
Research Gaps
As there appears to be limited research that examines the Tomatis® Method, the remainder of this chapter will explain several factors pertinent to my study. As explained earlier, due to similarities in symptoms of various diagnoses, the literature covers several possible diagnoses as these may also be studied using the Tomatis® Method in the future. Furthermore, there are clinical anecdotes and client testimonials vis a vis improvement experienced after the Tomatis® Method that was not experienced while using other therapies or medications. Practitioners of this method look at it as an integrative method that integrates the senses and therefore changes pathways in the brain to help development. As learning and development is directly related to the senses developing typically, I have addressed various subjects related to this as they are directly dependent on typical C/APD and thus could be positively impacted by the Tomatis® Method and thus would pertain to future studies on the subject. Some of these areas are auditory processing (AP), central auditory processing (CAP) and sensory processing (SP), auditory processing disorders, C/APD and learning difficulties, C/APD and ASD, the psychological impact of C/APD, diagnosis and assessment of C/APD, and t he Tomatis® Method.
To date, the research that is available on the Tomatis® Method is mostly in the form of case studies and anecdotal accounts of individuals’ personal experiences with the method. A limited number of controlled research studies that examine commercial auditory training programs, including the Tomatis® Method exists (Gilmore, 1999; Bernard-Bonnin, 2002). The studies that exist on the subject of remediation of C/APD using the Tomatis ® Method consist of case studies rather than more rigorous investigations (Bernard-Bonnin, 2002).
Based on my review of the literature, a gap in knowledge about the effectiveness and efficacy of the Tomatis® Method appears to exist. As my research proposes, if this gap is filled,
48
evidence may be developed to demonstrate that the Tomatis® Method can provide a better understanding of how to most efficiently work with children who have C/APD. Given that C/APD is a comorbid diagnosis in many different cases, should the Tomatis® Method be shown to be successful in the treatment of C/APD, it would follow that the method may also be efficacious in treating several related diagnoses.
Summary
Hearing is one of our most important senses as it gives us access to spoken language, necessary for the development of speech, language, and communication in general. The identification, diagnosis, and treatment of C/APD in children is important for several reasons, including co-morbidity and confusion with language impairment, d yslexia and other reading problems, behavioral problems, attention deficit disorders, and academic underachievement or failure. Untreated C/APD commonly leads to reduced communication function, which in turn can have psychosocial impacts such as loneliness, social anxiety, depression, anger, and fear (Crandell, 1998). However, no general consensus has been reached among clinicians and researchers on the test battery selection, assessment procedures, and diagnostic criteria for C/APD (Ferguson et al., 2011). According to Moncrieff (2007), in addition to test selection and assessment procedures, no consensus about which cutoff scores classify a child as pass or fail on C/APD tests has been established. Current standards in the diagnosis and treatment of C/APD do not meet changing evidence-based practice (EBP) principles. Moncrieff further stated that EBP has evolved to include patient perspectives and the opinions of authorities that are considered against a background of high-quality peer-reviewed research. Establishing the reliability and validity of the diagnostic battery of test choices used for diagnosing C/APD as well as the most effective evidence-based interventions has yet to be accomplished (Moncrieff, 2007).
49
One method that has risen to the attention of clinicians, such as Bernard-Bonnin (2002) is the Tomatis® Method. According to Sollier (2005), the Tomatis® Method remediates the problems associated with C/APD rather than being an accommodation as in the case of frequency modulation (FM) systems that use radio waves to send speech and other signals to hearing aids, and augmentative and alternative communication (AAC) devices (http://www.tomatis.com) The Tomatis® Method intervention provides auditory/vestibular stimulation, re-educating listening as well as vestibular functions, and, therefore the processing of what is heard, as well as what is received by the vestibular system (Sollier, 2005).
50
Table 1
Definition of Terms
Term Definition
Auditory Processing Disorder (APD): A condition, in which patients are experiencing listening difficulties in the absence of clearly identifiable peripheral auditory deficit (National Institute on Deafness and other Communication Disorders, 2001).
Abnormal Tonal Patterning: When a tone is misinterpreted either in timing or perceived pitch, it is named abnormal tonal patterning; this results in an auditory processing disorder (Bellis, 1997).
Auditory Decoding Deficit: Information is processed inaccurately and slowly, and words may be misheard or confused; furthermore, rules for grammar and tense are poorly remembered. Many children with this deficit are often wrongly described as having a hearing deficiency (Bellis, 1997).
Auditory Processing: The decomposition of acoustic signals into frequency components (Fletcher, 1940).
Autism Spectrum Disorder (ASD): The name for a group of developmental disorders, which includes a wide range of symptoms, skills, and levels of disability, including social problems and difficulties communicating (The National Institute of Mental Health, 2016).
Central Auditory Processing Disorder (C/APD):
The inability to attend to and discriminate or understand auditory input correctly (ASHA, 2005).
Sensory Processing (SP): The neurological process that organizes sensations from one’s own body and from the environment and makes it possible to use the body effectively within the environment (Ayres, 1979).
Sensory Processing Disorder (SPD): A condition, in which the brain has trouble receiving and responding to information that comes in through the senses (Ayres, 1979).
Sensory Modulation Disorder (SMD): A specific type of sensory processing disorder (SPD). This refers specifically to the brain’s ability to respond appropriately to the sensory environment and to remain at the appropriate level of arousal or alertness (Ayres, 1979).
Sensory-Based Motor Disorder (SBMD):
Sensory Discrimination Disorder (SDD):
Difficulty with balance, motor coordination, and the performance of skilled, non-habitual and/or habitual motor tasks (Ayres, 1979).
Difficulty interpreting subtle qualities of objects, places, people, or other environments (Ayres, 1979).
51
Total Communication (TC): An educational philosophy that was introduced to the field of deaf education in the 1960s (Schow & Nerbonne, 2017). TC utilizes all modalities of communication (spoken, signed, and written) as well as lip-reading, and gestures in the education of deaf children.
Auditory Brainstem Response (ABR): An electrical signal evoked from the brainstem in response to a presented sound. This is event-related (i.e., evoked by the onset of the stimulus; i.e., 1 –20msec.) (Staecker & Thompson, 2013).
Middle Latency Response (MLR): An electrical signal evoked from the brainstem in response to a presented sound. This is event-related (i.e., evoked by the onset of the stimulus; i.e., 10
50msec.) (Staecker & Thompson, 2013).
Auditory Late Potentials: An electrical signal evoked from the brainstem in response to a presented sound. This is event-related (i.e., evoked by the onset of the stimulus; i.e., 50 –1000msec.) (Staecker & Thompson, 2013).
Corpus callosum: The transverse band of nerve fibers that connects the right and left cerebral hemispheres (The American Heritage® Science Dictionary)
Auditory Decoding: Matching letter sounds to their written symbols and the ability to discriminate the various sounds heard (Paige et al., 2018)
Tonotopical: The anatomic organization , by which specific sound frequencies are received by specific receptors in the inner ear with nerve impulses traveling along selected pathways to specific sites in the brain. (Merriam-Webster Medical Dictionary)
Prosody: The rhythm and intonational aspect of language. (Merriam-Webster Medical Dictionary)
Top -down : Controlled, directed, or instituted from the top level. Proceeding by breaking large general aspects into smaller, more detailed constituents. (MerriamWebster Medical Dictionary) In this paper relating to cortical structures to lower brain areas
Bottom-up : Starting at sensory input, moving up to the cortical level of the brain. (Merriam- Webster Medical Dictionary)
52
–
Research Questions
The research questions pertaining to the primary aim of the study were
Q1. Will the Tomatis® Method training be successfully implemented in the clinical setting, where all the required study components, including participant recruiting, pre and post-testing, and implementation of the method over 6 months is completed?
My first hypothesis was that the Tomatis® Method training will be successfully implemented in the clinical setting, with all the study components, including participant recruiting, pre- and post-testing, and implementation of the method over 6 months.
Q2. Will the participants perceive they have benefited from the Tomatis® Method?
My second hypothesis was that participants will perceive they have benefited from the Tomatis® Method
Q3. Will the types of instruments used to assess the participants' pre and post-treatment yield the desired information to ascertain the efficacy of the intervention?
My third hypothesis was that the types of instruments used to assess the participants' pre- and post-treatment will yield information that confirms the efficacy of the intervention.
Based on the literature review, there appear to be no large-scale published studies on the efficacy of the Tomatis® Method in remediating C/APD in children aged 5 – 12 years. The current study, therefore, also aimed to cover this gap by pilot testing a small group of children aged 5
12. Given the small sample size, it became the study’s secondary aim to assess the hypothesis that participants would show an improvement in C/APD and related functions such as
53
–
language. To that end the specific research questions pertaining to the secondary aim of the study (i.e., the treatment outcomes) were
Q4. Will participants (aged 5 to 12 years), show improvements in auditory processing abilities as measured by the auditory processing tests after completing the Tomatis® Method?
My fourth hypothesis was that participants identified with auditory processing disorders (APD) will show improvements in auditory processing abilities as measured by the auditory processing tests listed below after completing the Tomatis® Method.
Auditory Processing Disorder Battery
- Temporal Processing i.e., Time Compressed Speech (SCAN-3C) and Pitch Patterns
- Lexical (word) integration i.e., Competing words and Sentences (SCAN-3C) and SSW test
- Organization i.e., Staggered Spondaic Words (SSW) Test reversals The SSW Test for right and left ear has indicators for each of the CAP categories (Katz, 1992).
- Lexical extraction i.e., Staggered Spondaic Words (SSW) Test and sentence measures
- Auditory Memory i.e., Staggered Spondaic Words (SSW) order effect as well as measures that use digit memory or word memory.
Q5 Will participants (aged 5 to 12 years), show improvements in cognition and oral comprehension, as measured by the Woodcock Johnson IV Test (WJ-IV) after completing the Tomatis® Method.
54
My fifth hypothesis, therefore, was that participants identified with auditory processing disorders (APD) will show improvements in oral language, as measured by the Woodcock Johnson IV Test (WJ-IV) after completing the Tomatis® Method.
Selected Tests
- Listening comprehension cluster from the Test of Oral Language (WJ-IV) i.e., Oral comprehension and ii. Understanding directions
- Visual processing cluster from the Cognitive Test (WJ-IV) i.e., Visualization-Spatial Relations and ii. Visualization-Block Rotation and Visual-Auditory Learning
Q6 Will participants (aged 5 to 12 years), show improvements in their ability for phonological awareness as measured by the Comprehensive Test of Phonological Processing 2nd Edition (CTOPP-2), after completing the Tomatis® Method?
My sixth hypothesis, therefore, was that participants identified with auditory processing disorders (APD) will show improvements in their ability to show phonological awareness based on the results of the Comprehensive Test of Phonological Processing 2 nd Edition (CTOPP -2), after completing the Tomatis® Method.
Selected Composites
- Phonological Awareness (CTOPP-2), i.e., Elis ion, Blending Words and Sound matching
- Phonological Memory (CTOPP-2), i.e. , Memory for Digits and Nonword Repetition
- Rapid Naming (CTOPP -2), i.e., Rapid Digit Naming and Rapid Letter Naming.
55
Q7 Will participants (aged 5 to 12 years), show improvements in Full Scale Attention, as measured by the IVA-2 CPT (Integrated Visual & Auditory 2 Continuous Performance Test), after completing the Tomatis® Method?
My seventh hypothesis, therefore, was that participants identified with auditory processing disorders (APD) will show improvements in Full Scale Attention, as measured by the IVA-2 CPT (Integrated Visual & Auditory 2 Continuous Performance Test), after completing the Tomatis® Method
Q8 Will participants (aged 5 to 12 years), show improvements in Neurotiming, as measured by the Interactive Metronome® (IM), after completing the Tomatis® Method?
My eighth hypothesis, therefore, was that participants identified with auditory processing disorders (APD) will show improvements in Neurotiming, as measured by the Interactive Metronome® (IM), after completing the Tomatis® Method
What follows is a description of the research performed and the findings thereof
56
CHAPTER THREE METHODS
The intention of this study was three-fold. The study examined potential recruitment efforts, ability to implement and complete testing and treatment protocols, retention and treatment fidelity, as well as the feasibility of conducting more rigorous reasearch studies on the Tomatis® Method Pilot studies are a crucial component of study design when planning studies of novel interventions. Per Van Teijlingen and Hundley (2001), pilot studies assess the feasibility of a treatment and a bigger study design. The smaller-scale study precedes a largescale clinical trial. It serves to determine needed resources, recruitment strategies, and to collect preliminary data and provide support for the rationale of funding for the large main study. Researchers may identify fundamental problems with all aspects of a study and thus may choose to rethink various aspects of the trial rather than moving on to full trial (O’Cathain et al., 2015).
Bowen and colleagues (2009) stated that feasibility testing breaks down into different components such as acceptability, demand, implementation practicality, and limited-efficacy testing. These then serve to determine whether the study design needs changes in any area. The findings then help to determine if a more extensive study is worth being conducted.
This pilot study serves as a preliminary test of the feasibility of the implementation (the extent to which the intervention can be delivered as planned), acceptability (reaction to intertreatment by participants), the success probability of a larger statistically significant study, and whether the intervention yields preliminary data worthy of further research.
57
Description of Research Design
General Design
In order for the design to be of practical use for high-quality trial, this study adopted a randomized control design. The study consisted of two groups: Tomatis and control, each with four participants for a total of eight participants. The eight participants were randomly assigned to one of the two groups. Both groups underwent pre -post testing using standardized testing methods widely accepted in the field of auditory therapy (i.e., occupational, speech, audiology, and psychology) that deal with C/APD. The group on the waitlist for the intervention served as the control. The Tomatis group received the Tomatis® Method, which was the secondary focus of the hypotheses. The primary aim was to determine the feasibility of such a study.
Recruitment
Recruitment targeted children aged 5 to 11 years old. The recruitment efforts were made by contacting various online parent groups, word of mouth, solicitation of various support groups for parents of children with special needs, and contacting several schools that specialize in children with special needs. Children were recruited in the Los Angeles County area using a letter of invitation to participate in the study (Appendix A).
Treatment and Testing
Both groups were tested pre- and post-treatment. Testing consisted of standardized testing methods widely accepted in the fields of auditory therapy (i.e., o ccupational, speech, audiology and psychology) that attempt to remediate C/APD. The independent variable in the study was treatment: the administration of the Tomatis® Method versus a wait-list control. Participants in the experimental group received all three intensives of a generic typical Tomatis Program using their proprietary Tomatis AudioPro TAPS machines. Upon completion of
58
treatment by the treatment group, a second pre-test was administered to the control group as they had not yet received the treatment, and a post-test was administered to the treatment group. The assessments used were chosen because they are well accepted by audiologists and speech/language pathologists as being the gold standard for diagnosing APD. These are all routinely used by audiologists, speech/language pathologists, and occupational therapists in differential diagnosis and goal setting. The following assessments served both as diagnostic to qualify a participant for the study, as well as pre-post analyses and were conducted by myself:
Staggered Spondaic Word (SSW) Test
In the SSW, competing spondaic words (two semantically related word pairs) were presented, one to each ear, with staggered onsets so that the second syllable of the initial stimulus was aligned with the onset of the first syllable of the second stimulus. The subject repeated back both spondees. Verdun et al. (2015) theorized that a uditory processing (AP) impairs the command of spoken language. They used the Staggered Spondaic Words (SSW) test to test their theory that APD correlates to age, gender, and educational level. They were able to show that there was a correlation and that therefore this test is important in the diagnosis of human communication disorders and in identifying children at risk for learning disorders. Thus, it was assumed that should the SSW findings change from below typical to within typical limits post a treatment, there is subsequent remediation of the learning disorder.
Competing Words Test (SCAN -3:C)
The Competing Words test is a dichotic integration task that reflects the development of the auditory system, auditory maturation, and hemispheric specialization for language. Semantically unrelated monosyllable word pairs with simultaneous onset times were presented to both ears. The individual repeated both words giving the right e ar first for the first 15 word pairs,
59
and then the left ear first for the last 15-word pairs. The test enables assessment of ear advantage. Poor performance possibly indicates delay in maturation, underlying neurological disorganization, or damage to auditory pathways (Keith, 2008). Per Keith (2008), abnormalities shown by dichotic word test results are related to a wide range of specific disabilities, including C/APD, language disability, learning disability, and reading disorder.
Competing Sentences Test (SCAN-3:C)
The Competing Sentences test is a dichotic separation speech task that reflects the development of the auditory system, auditory maturation, and hemispheric specialization for language. Semantically unrelated sentences with simultaneous onset times and duration were presented to the two ears. The individual repeated the sentence from one ear only, while ignoring the competing sentence in the opposite ear. The 10 sentences heard in the right ear were repeated first, followed by the 10 sentences in the left ear (Keith, 2008).
Low Redundancy Speech Perception
Auditory Figure Ground (AFG) test +0dB (SCAN-3:C): The Auditory Figure Ground test examines an individual’s ability to understand a series of one -syllable words presented in a speech babble background noise of equal intensity (+0dB S/N ratio). Twenty words were presented to each ear.
Time Compressed Sentences Test (SCAN-3: C)
The Time Compressed Sentences test is a test of degraded speech perception and, to a lesser degree, temporal processing. Sentences were presented at a rapid rate with 60% time compression. The individual repeated 10 sentences from the right ear and then 10 sentences from the left ear (Keith, 2008).
60
IVA-2 CPT (Integrated Visual & Auditory 2 Continuous Performance Test)
IVA-2 is a computerized test where participants were told that they would see or hear the numbers “1” or “2” and that they were to click the mouse when presented with a visual or auditory “1” and not click when presented with a “2”. The task shifted between visual and auditory stimuli. In high demand sections of the test, the “1” is presented frequently and then presented with a “2”, which made it difficult to stop clicking. This condition is counted towards impulsivity. The low demand section was for errors or omission where the opposite occurs.
Woodcock Johnson IV Test (WJ -IV)
WJ-IV (Schrank and Wendling, 2018) is a measure of cognitive, oral language, and achievement. Only the listening comprehension cluster from the Test of Oral Language and the visual processing cluster from the Cognitive Test were used. The Listening comprehension cluster consisted of two subtests. Oral comprehension where the participant says the word that is missing at the end of each dictated sentence or very brief paragraph. In understanding directions, the participant showed the ability to follow complex oral instructions by pointing to different parts of pictures. The visual processing cluster included two subtests. In Visualization -Spatial Relations, the examinee tried to select by sight alone, from many choices, the fragments that can be assembled into a given geometric shape. In Visualization -Block Rotation , the examinee tried to match drawings of three-dimensional block constructions that have been rotated in space.
CTOPP-2: Comprehensive Test of Phonological Processing – Second Edition
The CTOPP-2 (Wagner et al., 2013) is a norm-referenced measure designed to assess phonological processing skills related to reading. This instrument evaluated three categories phonological awareness, phonological memory, and rapid naming. These were assessed using
61
subtests that measured elision, blending, phoneme isolation, short-term memory, rapid naming, and segmentation.
Table 2
Pre and Post Assessments
Assessment Skill Measured
SSW Diagnose Central Auditory Processing Disorder
SCAN-3:C Tests for Auditory Processing Disorders in Children
Scheduled Time Assessor
Prior to random assignment; Post Completion of Randomized Intervention
Post C/APD diagnosis, but prior to random assignment; Post Completion of Randomized Intervention
IVA-2 CPT Visual and Auditory Integration Post C/APD diagnosis, but prior to random assignment; Post Completion of Randomized Intervention
IM Neurotiming Post C/APD diagnosis, but prior to random assignment; Post Completion of Randomized Intervention
WJ-IV Listening Comprehension Cluster and Visual Processing Cluster
CTOPP-2 Phonological processing skills
The Tomatis Listening Test
Listening profile
Post C/APD diagnosis, but prior to random assignment; Post Completion of Randomized Intervention
Post C/APD diagnosis, but prior to random assignment; Post Completion of Randomized Intervention
Post C/APD diagnosis, but prior to random assignment; Post Completion of Randomized Intervention for those who fall in the control group. The treatment group will additionally be assessed at the 2-week mark of each break period
Myself scored by audiologist
Myself
Myself
Myself
Speech/Language Pathologist or Teacher
Speech/Language Pathologist
Myself
62
Outcomes
The dependent variables in the study were the processing parameters: Auditory processing was assessed using the SSW and SCAN-3:C; visualization and visual-auditory skills, oral comprehension, and understanding directions were assessed using the WJ-IV; phonological awareness, phonological memory, and rapid symbolic naming were assessed using the CTOPP2; full scale attention and response control were assessed using IVA-2 CPT; temporal processing was assessed using IM long form.
The possible confounding variables in the study were varying other interventions that certain participants continued receiving during the experiment. These consisted of speech therapy, occupational therapy, behavioral interventions, music lessons, soccer, and other sports training. These were not controllable variables, because it is unethical to demand that the children stop all other programs to be in the experiment.
Note: X = What was done, N/A = Was not done Procedures
Upon recruitment, if a family decided they wanted to participate in the study and contacted me, they were sent the necessary information (i.e., the letter of invitation to participate). The parents were told that in order to participate in the study, they had to agree that their child would be randomly assigned to either the treatment group or the control group The
63
Table 3 Research Design Pre and Post-Testing Sequences Group Pretest 1 1 program of the Tomatis® Method (3 Intensives with 4 weeks break between each) Post-test Pretest 2 Treatment X X X N/A Control X N/A N/A X
parents or guardians consequently gave consent on behalf of the participants who participated in the study. Additionally, assent was solicited but not required from the participants aged 7 to 11 years of age.
All participants were pre-tested with the battery described in Table 3 above. Once identified and tested, the participants were randomly assigned to either the Tomatis® Method or to the waitlisted (control) group to form two equal groups.
Once the final eight participants had been pretested and assigned to a group, the four participants assigned to the treatment group received one full program of the Tomatis® Method The remaining four participants were assigned to the control group and waitlisted. Upon completion of one program of the Tomatis® Method by the treatment group, all participants were tested a second time using the same battery as was performed for the pretest. The second test of the treatment group was classified as a post-test, and the second test of the control group was classified as the second pre-test. The test results were uploaded into SPSS for statistical analyses using a signed-rank test so that trends could be inferentially analyzed. All participants were aware of the group they were assigned to. The study sought to examine whether or not the changes one could expect after exposure to the Tomatis® Method occurred or not. Half the participants received the entire Tomatis® Method procedure, which was uniform across all participants. The other half of the participants were waitlisted and are currently receiving the same program as the treatment group as all participants have been retested, and all data for this dissertation have been collected.
As a speech/language pathologist and Tomatis® Method certified practitioner, I performed a short battery of auditory processing tests that are used in standard practice when
64
diagnosing auditory processing disorder. These tests were scored and interpreted with the help of Dr. Jay R. Lucker, audiologist and scored blind. Additionally, the CTOPP-2: Comprehensive Test of Phonological Processing– Second Edition, requiring approximately 30 minutes as well as the Following Multistep Directions and Visual-Spatial domain subtests of the Woodcock Johnson IV Test (WJ- IV) requiring approximately 20 minutes total and the SCAN-3C were also administered for pre-post comparison of results. A trained technician administered the Listening Test proprietary to the Tomatis® Method to help with initial generic programming purposes only. All the experimental participants’ tests were looked at simultaneously, and similarities and differences noted. These then informed the clinician's judgment in generating a generic program along with the guidance of an expert clinician. The final protocol was pre-written for all three intensives at the same time before beginning the treatment. I found it necessary to mention this as it signifies deviance from the regular programming, which is typically done intensive by intensive and where necessary even changed during any given treatment session or intensive. Programming is usually done before each intensive following changes in the child’s Listening Test, profile as reported by parents, and observations made by the clinician. A Listening Test is ususally performed in between each intensive for the purpose of informing the programing for the next intensive. The occupational therapist within the clinic additionally administered the IVA-2 CPT and IM tests that served as the baseline and posttest for full-scale attention, and neurotiming (a parameter specific to IM therapy), respectively. The respective testing program automatic ally scored these tests.
65
The Tomatis® Method Protocol
The protocol followed in this study consisted of 64 hours of listening in total and spanned approximately nine months including final reruitment and all testing. The first intensive of the Tomatis treatment consisted of 12 days, where the participants came to the clinic for the Tomatis® Method, five times per week (Monday - Friday) for 2 weeks and for the two extra days (Monday and Tuesday of the third week) for 2 hours each day The subsequent two intensives consisted of 10 days each, with 2 hours of treatment per day. Each of the intensives was followed by a break of approximately 4 weeks.
Assessments were done in the 2 months preceding the Monday that the treatment was scheduled to begin on. The participants in the treatment group were assigned a time slot for the treatment that carried through the entire experiment. The participants were re-evaluated approximately one month after the treatment was completed, with families whose schedules permitted it. The control group participants were re-evaluated at their earliest convenience post completion of the treatment by the experimental group. The Listening test was administered per the Tomatis® Method protocol and was only completed during the pre and post-testing so as not to interfere with the pre-planned protocols.
A program for each of the three intensives was written before starting the treatment and was based on prior knowledge of progression by children with APD. The protocols were not individualized as would typically occur in practice by a Tomatis c onsultant. A generic program was used for the sake of uniformity and to keep procedures standardized. The treatment protocol focused specifically on acoustic and vestibular inputs received by the ear because the ears transmit, and the brain processes both the acoustic and vestibular sensory messages received by the ears. As prescribed in the Tomatis® Method, intervention consisted of listening to a variety
66
of music consisting of certain Mozart tracks, waltzes, and Gregorian chants, with the gating effect, precession/delay, and filtration that are all parameters of the Tomatis ® Method On certain days, all participants spent a half-hour repeating words and songs into a microphone while music filtered to certain frequencies was playing softly through the headphones in the background. The mother’s voice component was omitted for the sake of keeping the program generic for all participants.
Using a generic program also addresses claims such as “Finally, the clinical background of the practitioner including his or her ability to form a therapeutic alliance with the individual –and if a child with the family- will be an integral part of the success of the intervention.” (https://www.sacarin.com/scientific-publiations).
The music was delivered using proprietary h eadphones designed for use with the TAPS machines. The headphones use a bone conductor embedded at the midpoint of the headphone band that connects the left and right air conduction cups that sit over the ears. This strategic placement of the bone conductor allows for it to sit on the junction of the anterior fontanelle once it is fused, to propagate the sound equally throughout. These headphones allow for the stimulation through both air and bone conduction at varying speeds and times as controlled by proprietary functions called gating and precession and delay. These headphones, in conjunction with the TAPS, allow for a strategic reduction of the intensity of sound input in the left ear versus the right ear to normalize balance (70% left ear vs. 100% right ear stimulation) in ears undergoing the Tomatis® Method of sound stimulation. Tomatis believed that this was the ideal balance between the ears for voice control, language acquisition, and motor control (Tomatis, 1981).
67
The sound was differentially filtered through the TAPS machine, depending on a predetermined frequency and corresponding amplitude. Depending on the frequency and amplitude specifications, low frequencies are attenuated, and higher frequencies are boosted and vice versa. This brings the brain’s attention to changes in input, presumably resulting in better attention, linguistic and vestibular functions. The TAPS allowed for manipulation of concentrating on any frequency band needed to address stresses in the vestibular, language, and attention frequencies as determined by Dr. Tomatis in his design of the Listening Test parameters.
Upon completion of the post-testing, the data were uploaded to SPSS for statistical analyses. The findings were then descriptively analyzed and reviewed. The trends were then used to make judgments regarding further study of the Tomatis® Method and APD.
68
CHAPTER FOUR RESULTS
The primary purpose of this chapter is to present the findings of the study in the context of the feasibility of such a study and secondarily in presenting data collected and analyses related to the stated treatment hypotheses. Overall, in 13/17 subtests, all participants in the treatment group improved, which was not seen in the control group. Additionally, scores of the treatment group showed greater improvements in the tests, in which there were some improvements in some of the participants in the control group. On 5/17 tests, at least one participant in the treatment group improved vs. no improvement in the control group. I will describe the recruitment, attendance, pre-post assessment results, and other factors pertaining to the feasibility of such a study. Following are the results for each question the study attempted to answer.
Q1. Will the Tomatis® Method training be successfully implemented in the clinical setting, where all the required study components, including participant recruiting, pre and post-testing, and implementation of the method over 6 months are completed?
Recruitment
The target of this study was to recruit 30 participants through an audiologist who specialises in C/APD assessment and treatment. The audiologist was to refer qualified participants who came to her office for assessment. The participants were to complete the rest of the assessments through me and I was to then randomly assign each to either the treatment or control group. This initial plan to recruit children diagnosed with APD from pediatric audiologists specializing in diagnosis and treatment of APD was unsucessful due to the inability of the referring audiologist to absorb the costs associated with administering necessary
69
assessments. Due to a lack of finding other audiologists specializing in the area of APD in children in the Los Angeles area, an alternative recruitment plan, in which I used tests of auditory processig under the guidance and supervision of an audiologist to assess changes in APD rather than to qualify children for the study was more successful. These alternate rec ruiting efforts included contacting and explaining the study and possible benefits to several possible sources such as pediatricians and other therapists such as audiologists, speech-language pathologists, psycholgists, and occupational therapy private practices. This did not yield any results, and thus the recruiting parameters had to be broadened yet again. These included various online parent groups, word of mouth, soliciting various support groups for parents with children with special needs, and using a letter of invitation to participate in the study (Appendix A). Addtionally efforts through direct advertising to parent support groups on the web, word of mouth, as well as directly contacting private tutoring institutions and alternative educational programs, proved much more successful and resulted in a final sample of 22 participants being recruited.
70
Participants
Figure 1
Flow of Participants Though the Experiment
Initial Cohort
N = 22 (6 F; 16 M)
Pre-Screening
Pre-Testing
Post-Testing
Analysed
Recruitment efforts resulted in an initial cohort of 22 participants, of which 7 were recruited through word of mouth, 3 were recruited through referrals from teachers in specialized schools, 4 were recruited through parent groups, and 8 were recruited through advertising on the web and in a parent magazine. The group consisted of 6 females and 16 males. Before pretesting, two children (male), one 12 years old and the other 13 years old, were disqualified as they were older than the cut-off age 11, to not exceed 12 years of age by the end of the
71
Recrutied 7: word of mouth 3: teacher referrals 4: parent groups 8: web and magazine advertizement Moved to next step (N=14) Allocatd o treatment Group and received entire intervention (N= 4) Assessed (N = 3) Lost to follow-up due to being out of country (N = 1) Analysed (N= 3) 1: excluded from analysis (out of country no post-test available) Allocated to Control on standby to receive intervention (N=4) Assessed (N = 4) Analysed (N= 4) Excluded (N=8) 2: age 2: receiving alternate therapy for APD 2: dropped out due to distance 2: wanted the home program Excluded (N=6) 3: qaulified and dropped out due to time constraints 3: disqualified due to ASD
experiment. There were two children (male) already receiving an alternative therapy to address their APD and were therefore disqualified. Two children, 1 (female) and 1 (male), decided not to pursue the study as it was too far for them to commute and were consequently excluded. A family with two children, 1 (female) and 1 (male), dropped out prior to pre-testing as they wanted the therapy done in the home. An additional three children (males) were pre -tested and qualified for the study and dropped out due to time constraints. Additionally, three children, 2 (male) and 1 (female), were disqualified, and pre-testing discontinued due to having a current diagnosis of autism spectrum disorder.
The final count of children who were pre-tested and received one entire program of the Tomatis® Method was 8, of which 5 children were male, and 3 children were female. Of the 8 participants, 2 were aged 5 - 6, 1 was aged 7, 3 were aged 9 – 10, and 2 were aged 11. The participants were Caucasian (n = 4), Hispanic (n = 3), and African American (n = 1). From the final group, 3 participants were receiving various services and extracurricular activities in the community. All participants were (per parent report) not on medications during the study. The children were receiving or had received speech and language therapy, or reading and writing intervention, or were showing signs of severe behaviors. The children were additionally not showing sufficient improvements following interventions geared to remediating these symptom s, and all were suspected of having C/APD.
72
Treatment Delivery
The study spanned approximately nine months, primarily due to scheduling families for pre- and post-testing. The participants came to the clinic for the Tomatis® Method, five times per week (Monday – Friday) for 2 hours each day for 12 days for the first intensive and 10 days each for the second and third intensives. There was a break of 4 weeks between each of the intensives. The first intensive was a little difficult for the youngest two participants due to not being used to complying . They wanted to continually visit the toy room so they could get any toy they wanted. So it was less about not wanting to do the program and more about not having the freedom to do as they wished. They were much more compliant during the next two intensives. Despite being told that they would have fixed times for the entire intensive, we did have to occasionally move times around to accommodate participants due to various reasons and other commitments. However, all four participants completed all three intensives on schedule with occasionally coming in at a different time during the day than per schedule.
Pre- and Post-Testing
The actual assessments went smoothly, with the younger children needing breaks and occasional promises of rewards during the pre-test. The testing was done over 2 days at the parents’ convenience. This would have been better achieved if we had been able to schedule all
73
Characteristics of Participants Participant Characteristics Treatment Group N = 4 Control Group N = 4 Male Female Male Female Number of Participants 3 1 2 2 Mean Age 7.4 11.2 8.8 10.55 Age Range 5.6 – 10.8 11.2 7.5 – 10.11 9.8 – 11.3
Table 4 Demographic
the children at one time and scheduled them out for the duration of the treatment and post-test. This would have given me more control and would have possibly resulted in the analyses of the entire cohort, resulting in the analyses of equal number of participants in each of the groups analyzed. This was not possible as recruiting was still going on while we were testing interested candidates in order to ensure we achieved a minimum participant count to proceed with the study.
Post-testing proved more difficult due to changed schedules with the new school year. One participant in the treatment group completed all three intensives and was unable to come back for post testing as he was out of the country due to a family emergency. This left the final count for the study pre-post-testing with three participants in the treatment group and four in the control group.
Q2. Will the parents of participants perceive their child to have benefited from the Tomatis® Method?
Although there was no formal questionnaire, each participant’s parent was verbally asked if they perceived their child to have benefited from the treatment at the end of the treatment. All parents agreed that their child had benefited from the treatment and were interested in knowing if it was possible to get additional treatment.
Comments of parents included one parent, in particular, mentioning that before the treatment, her child was very disruptive in school and that she was called into school to either stay with her child or to take him home due to disruptive, volatile behaviors. However, he had received the award of the most improved student in behaviors during the end-of-year classroom celebrations. This was after just one session. The gains have continued and are showing in the home and in school, where he no longer requires his mother to be present to behave more calmly,
74
and she is not called into school to control him anymore. She reported, “He is like a different child. He is now able to listen and negotiate. He has patience now, where he can tolerate not getting what he wants immediately.”
A second child was initially described by parents as very slow in her speech and very clumsy. Following the intervention, she was reported as talking much more typically and having fewer accidents. This was reported after just the second session, and the improvements were reported as continuing to improve through to the post-testing.
While the fourth child did not offer any behavioral changes, a third child who was described as having problems with sleeping through the night and having severe tantrums when he did not get what he wanted, was reported to be much calmer and sleeping alone and through the night. The tantrums were described as being both less severe and less frequent.
His mother explained that she did not need to stay in her child’s room for hours as she waited for him to fall asleep. She added that once he was asleep, he stayed asleep or at least in his own room until it was time to get up the next morning. The family do not need to pick up and leave when he gets distraught anymore. She explained that a s he quieted quite easily once distraught, they could stay in the setting and did not have to hurry to their car and go home.
Q3. Will the types of instruments used to assess the participants' pre and post-treatment yield the desired information to ascertain the efficacy of the intervention?
The instruments used yielded the desired information. As shown here below each assessment used yielded important information pertinent to changes that may be expected in auditory processing function as well as in related functional outcomes in the areas assessed by the instruments chosen and used in this study.
75
Descriptive Statistics
Q4 Will participants show improvements in auditory processing abilities as measured by the auditory processing tests after completing the Tomatis® Method?
Auditory Processing Composite
The Auditory Processing Composite score of the SCAN-3:C was used to assess auditory processing. Figure 2 shows the results. All three participants in the treatment group had higher scores on the tests contributing to the composite variable after the tre atment than before, while three participants in the control group had lower posttest than pretest scores, and one had minimal gains across the study period.
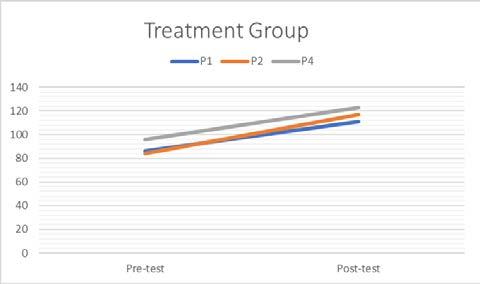
SCAN-3:C Auditory Processing Composite Individual Scores
Figure 3 shows results
the SSW: RNC test where all three participants in the treatment group improved to fall within typical limits, while one participant in the control group improved to fall within typical limits, one improved, and two participants had no change.
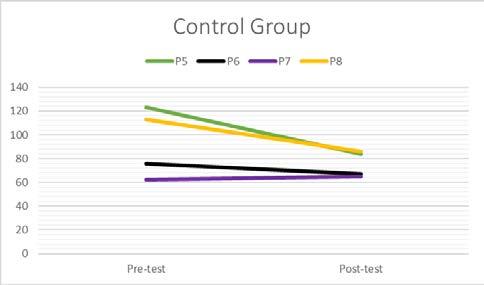
76
Figure 2
of
SSW:RNC Individual Scores
Figure
results
the
LNC test where all three participants in the treatment group improved and two fell within typical limits, while all four participants in the control group improved, and two fell within typical limits .
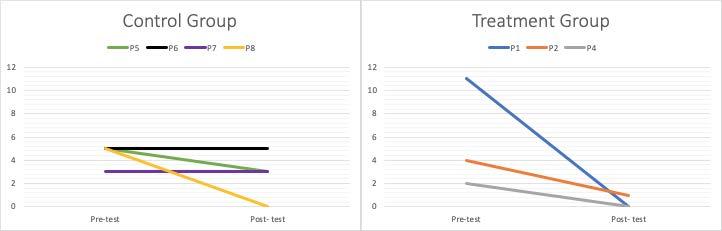
SSW:LNC Individual Scores
Figure
results
the
test where all three participants in the treatment group improved to fall within typical limits, while all four participants in the control group continued to fail in this area where two improved slightly, one decreased, and one showed no change
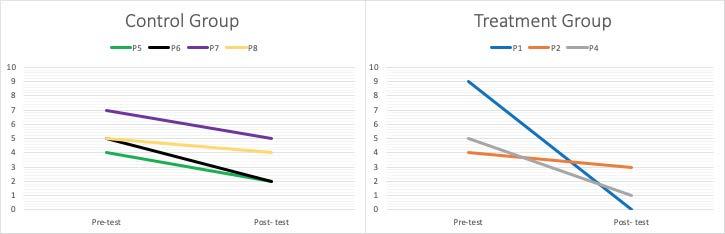
77
Figure 3
4 shows
of
SSW:
Figure 4
5 shows
of
SSW: REV
Q5. Will participants show improvements in cognition and oral comprehension, as measured by the Woodcock Johnson IV Test (WJ-IV) after completing the Tomatis® Method?
Cognitive Abilities and Oral Language Measures
Children’s cognitive abilities and oral language measures on the Woodcock Johnson IV were measured before and after the treatment or control period, and the changes in scores are characterized in Figures 6, 7, 8, and 9 respectively.
Cognitive Abilities
The cognitive abilities of participants were measured using the visualization and visualauditory learning subtests of the WJ-IV. Figure 6 shows the results. In the subtest visualauditory learning, all three participants in the treatment group had higher scores on the tests after the treatment than before. In comparison, one participant in the control group had a higher score, and one participant in the control group had a lower posttest than pretest scores, and two participants had no change in scores after the study period.
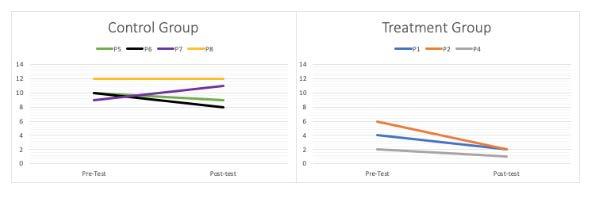
78
5
Figure
SSW:REV Individual Scores
Oral Comprehension
The oral comprehension of participants was measured using the comprehension cluster and subtests of the WJ-IV. Figures 7, 8 , and 9 show the results. For all three variables (the listening comprehension cluster, oral comprehension, and understanding directions), a similar pre-post pattern was seen when comparing the treatment and control groups. All three participants in the treatment group showed improved scores from the beginning and the end of the treatment period. On the other hand, those in the control group were more likely to show some decline or no change in the same skills over the same period.
Figure 7 shows the results in the listening comprehension cluster where all three participants in the treatment group had higher scores on the tests after the treatment than before. In comparison, only one participant in the control group had a higher score, and three participants had lower scores after the control period on the post-test.
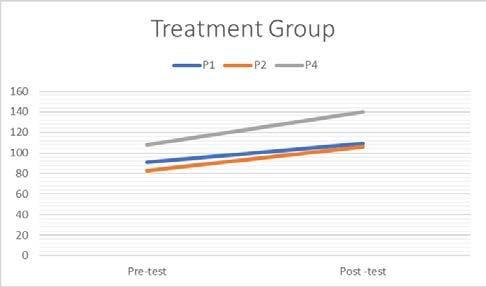
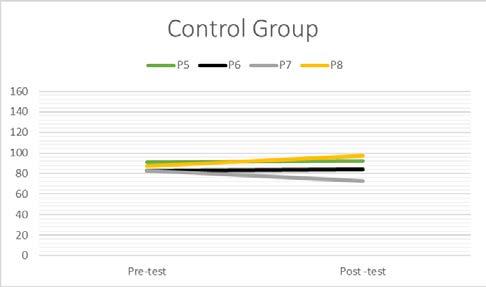
79 Figure 6
WJ-IV: Visual Auditory Learning Individual Scores
WJ-IV: Listening Comprehension Individual Scores
Figure 8 shows the results in the Oral Comprehension test where all three participants in the treatment group had higher scores on the tests after the treatment than before. In comparison, only one participant in the control group had a higher score, two participants had lower scores, and one participant had no change in scores after the control period on the post-test.
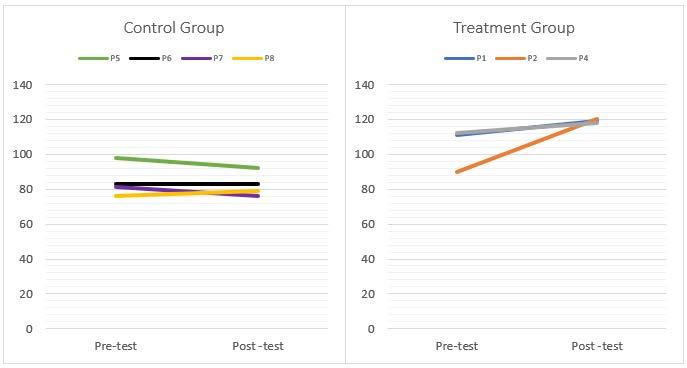
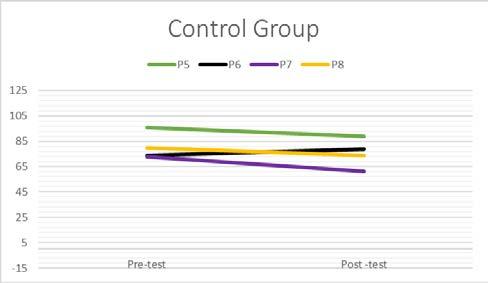
WJ-IV: Oral Comprehension Individual Scores
Figure 9 shows the results in the Understanding Directions test where all three participants in the treatment group had higher scores on the test after treatment than before
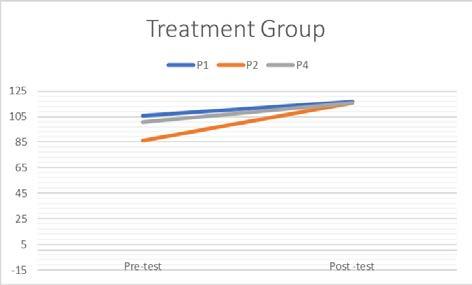
80
Figure 7
Figure 8
treatment. In comparison, only one participant had higher scores, and three participants had lower scores after the control period on the post-test.
Figure 9
WJ-IV: Understanding Directions Individual Scores
Q6. Will participants show improvements in their ability for phonological awareness as measured by the Comprehensive Test of Phonological Processing 2nd Edition (CTOPP-2), after completing the Tomatis® Method training?
Phonological Processing
The Phonological Awareness composite score of the CTOPP-2 consisting of three subtests (Elision, Blending Words, and Phonemic Isolation), the Phonological Memory composite score of the CTOPP-2 consisting of two subtests (Memory for Digits and Nonword Repetition), and the Rapid Symbolic Naming composite score of the CTOPP-2 consisting of two subtests (Rapid Digit Naming and Rapid Letter Naming) were used to assess Phonological processing. Figures 10, 11, and 12 show the results. The phonological awareness of participants was measured using the phonological awareness composite of the Comprehensive Test of Phonological Processing 2 nd Edition (CTOPP-2)
Figure 10 shows the results. For the composite and one of the subtests (Elision), all three participants in the treatment group showed higher scores on the post-treatment tests while three
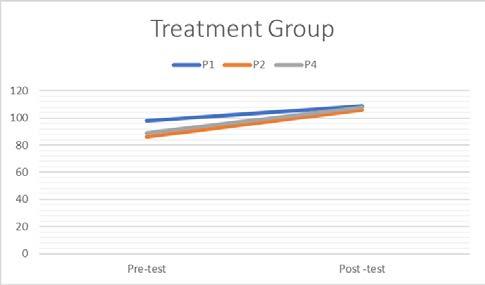
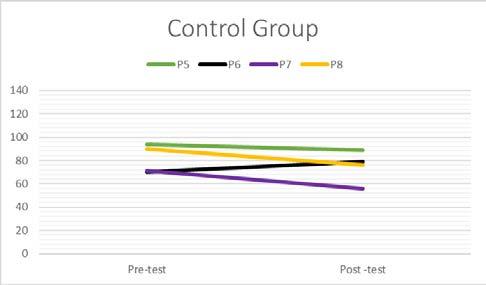
81
participants showed lower scores, and one participant showed no change post the control period on the post-test. In the subtest blending words in the treatment group, two participants showed higher scores, and one participant showed no change in scores post-treatment, while one participant showed higher scores, two participants showed lower scores, and one participant showed no change after the control period posttest. In the subtest phonemic isolation/sound matching, all three participants in the treatment group showed higher scores post-treatment, while in the control group, two participants showed slightly lower scores, and two participants showed no change after the control period posttest.
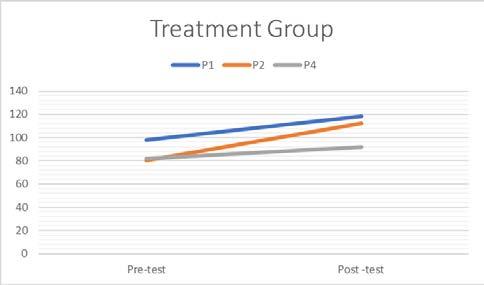
Figure 11 shows the results for the Phonological Memory composite score of the CTOPP – 2 consisting of two subtests (Memory for Digits and Nonword Repetition) used to assess Phonological processing. The treatment group showed an improvement in all participants as compared to the control group in which three participants improved and one declined. Although three participants improved in both groups, the differences in the increase in scores representing the improvement was bigger than 1 SD in the treatment group vs. the three improved participants in the control group.
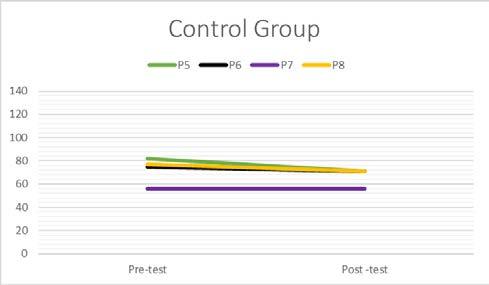
82
Figure 10
CTOPP-2 Composite 1: Phonological Awareness Individual Scores
Figure
shows the results
the Rapid
score
the CTOPP – 2 consisting of two subtests (Rapid Digit Naming and Rapid Letter Naming) used to assess Phonological processing. The treatment group showed one participant improved, one declined, and one showed no change as compared to the control group, where all four participants declined.
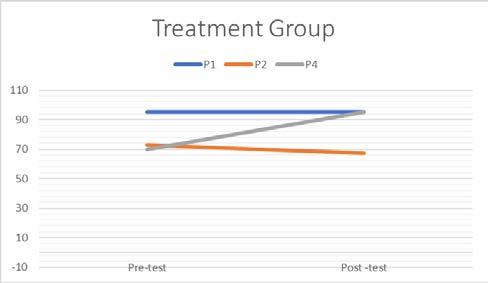
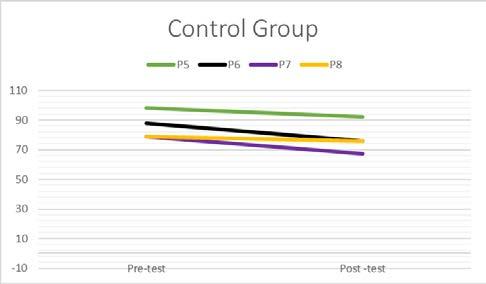
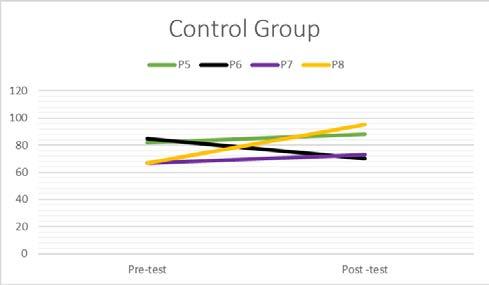
Q7. Participants will show improvements in Full Scale Attention, as measured by the IVA-2 CPT (Integrated Visual & Auditory 2 Continuous Performance Test), after completing Tomatis® Method training.
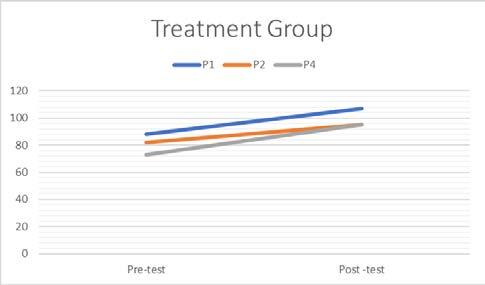
83
Figure 11
CTOPP-2 Composite 2: Phonological Memory Individual Scores
12
for
Symbolic Naming composite
of
Figure 12
CTOPP-2 Composite 3: Rapid Symbolic Naming Individual Scores
Full Scale Attention Quotient
The Full Scale Attention Quotient of the IVA-2 is based on separate Auditory Attention and Visual Attention Quotients scores and was used to assess attention over time. Figure 13 shows the results. The treatment group showed all three participants improved, as compared to the control group, where one participant improved, one declined, one showed no change, and one was unable to complete testing.
Figure 13
IVA-2:
Full Scale Attention Quotient Individual Scores
Full Scale Response Control Quotient
The Full Scale Response Control Quotient of the IVA-2 is based on separate Auditory and Visual Response Control Quotient scores and was used to assess response (initiation or inhibition) over time. Figure 14 shows the results. The treatment group showed all three participants improved, as compared to the control group, where one participant improved, two declined, and one was unable to complete testing.
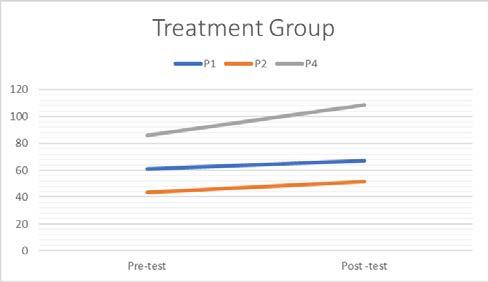
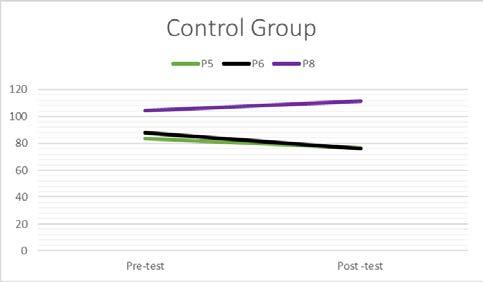
84
Q8. Participants will show improvements in Neurotiming, as measured by the Interactive Metronome® (IM), after completing Tomatis® Method training.
Temporal Processing Measures
The Interactive Metronome® (IM) was used to assess Neurotiming. Figure 15 shows the results. The treatment group showed improvement by way of coming closer to the normal limits and the change in each was by a much larger percentage as compared to the control group, where two participants declined in performance, that is, went further away from the norm expected for age, and the two who improved did so by a smaller percentage
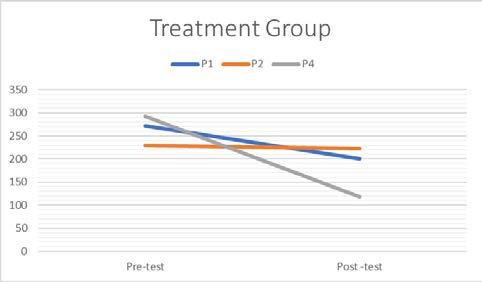
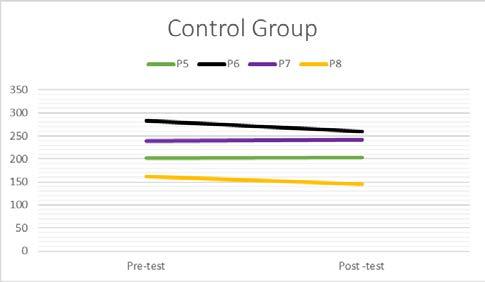
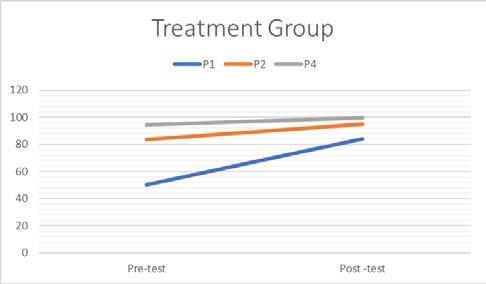
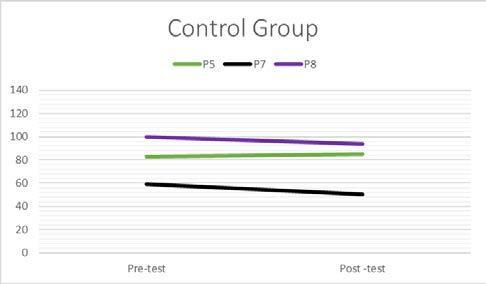
85
Figure 14
IVA-2: Full Scale Response Quotient Individual Scores
Figure 15
IM: Long Form Neurotiming Individual Scores
CHAPTER FIVE DISCUSSION Overview of the Study
The aim of this study was to examine the feasibility of treating a group of children diagnosed with C/APD using the Tomatis® Method. To that end, the study measured feasibility in terms of recruitment effectiveness, implementation and testing ability, and trends in betweengroup changes following treatment. Even though there were some challenges in recruitment, all the components of the intervention, including pre and post-testing, were successfully implemented during the entire p rogram. Participants’ parents perceived their child to have benefited from the program. The implementation of the study, once the intitial recruiting strategy had been changed, was successful.
The target of this study was to recruit 30 participants through an audiologist who specialises in C/APD assessment and treatment. Various difficulties over a number of months in the above stated recruitment method along with a lack of adequate funding and time constraints, prompted me to find alternative modes of recruiting participants. Given these problems, future researchers should consider face-to-face recruiting in pertinent pediatrician offices. Schools may be an additional option for recruiting as well as advertising and public announcements.
Attendance was 100% for both groups until the post-test. At that point, this changed as one of the intervention children was unable to come back for post-testing due to a family emergency that took him outside the country. The attrition for the group was extremely low, given that only one participant did not complete post-testing; however, he completed the entire treatment protocol to the end.
86
The secondary purpose of this experiment was to explore the benefits of the Tomatis® Method (Tomatis, 1996) in children who have difficulties with auditory processing and learning. Of particular interest to me as a speech/language pathologist was the potential improvements in the underlying processes and the possible effects on speech/language and learning. I wanted to find a design that could be easily duplicated if results were found to be fair, unbiased, and informative I hoped this study would show that children with neurological difficulties should be offered the Tomatis® Method of training as a normal part of habilitative services to remediate underlying processes such as auditory processing that negatively impact speech, language, and learning.
Discussion of the Data and Comparison to the Literature Reviewed
Due to the small final sample size (N=7), the achievement of statistical significance was not expected, and thus analyses were done to find trends in the data that were then descriptively analyzed (Fogarty & Wardle, 2015) Thus, patterns in the data for the final seven participants were presented in the descriptive analysis as one of the initial eight participants who started the study in the treatment group and completed the treatment did not return for post-testing. The final sample contained pre-post data from three participants in the treatment group and four participants in the control group. The data on outcome variables were analyzed using the inferential analyses from signed-rank tests for all of the outcome variables that are presented and characterized (Appendices E and F).
The final sample size was eight, where 7/8 (treatment = 3; control = 4) were included in the analyses of the results. In order to address the research questions in a data-based context, the pre- and post-test scores were compared to look at differences between the two groups and described using descriptive statistics. The number of cases in each group is shown as part of a
87
descriptive analysis of the raw data in the form of standardized and normed scores per assessment parameters, which was considered appropriate given the nature of this study.
The pre-post-test results of this pilot study showed overall trends of improvement in the treatment group, which were not present in the control group. Overall, all the participants in the treatment group showed improvements in most of the subtests; the control group had mixed results and in most cases the improvement changes, when present, were not as robust as the improvements shown in the treatment group This pilot study is not powerful enough to show that the Tomatis® Method may play an important part in remediating n eurologically based deficits underlying communication and learning in children; however, it does suggest that further study is warranted.
RQ1. Will participants show improvements in auditory processing abilities as measured by the auditory processing tests after completing the Tomatis® Method?
The results showed a pattern of improvement in the treatment group that was not found in the control group after completing the Tomatis® Method. The results showed consistent trends of improvement in the treatment group that was not seen in the control group. In particular, all three participants in the treatment group moved to the typical limit in three out of the five subtests on the SSW and two out of the three participants fell within typical limits on one of the five subtests with no change in one subtest. However, in the control group one out of the four participants moved to typical limits on one of the subtests, and two of the four participants moved to typical limits on a second subtest; however, all participants remained below typical limits on three out of the five subtests. Although some within the control group increased performance to fall within typical limits on certain subtests, the treatment group appeared to have made greater gains as they started from a point of higher deficit than the control group. The
88
pattern that was seen in all the tests was that the treatment group saw greater gains on all the assessments, and none showed any decrease in any subtests given, while in the control group most participants showed either a decrease in scores, or little to no gain. This pattern of findings demonstrates that the Tomatis® Method may have an impact on auditory processing ability and warrants further study to ascertain whether it may be a useful tool for therapists to use when dealing with children with a diagnosis of C/APD.
These preliminary findings are consistent with previous studies and if they hold true in follow-up studies could support the conclusions of the Ross-Swain (2007) study that found that post-testing showed statistically significant improvements in immediate auditory memory, auditory sequencing, interpretation of directions, auditory discrimination, and auditory cohesion.
Ross-Swain (2007) summarized findings in a retrospective study on the Tomatis® Method, where the study’s post-testing showed significant improvements in immediate auditory memory, auditory sequencing, interpretation of directions, auditory discrimination, and auditory cohesion.
In addition, the post-testing showed a reduction in auditory latency.
RQ2. Will participants show improvements in cognitive abilities and oral language as measured by the Woodcock Johnson IV Test (WJ-IV) after completing the Tomatis® Method?
The preliminary results showed a pattern of improvement in the treatment group that was not found in the control group after completing the Tomatis® Method. Figures 6, 7, 8, and 9, give visuals of the pre-post-tests, which also show it would be worthwhile to research this intervention. There were improvements in the Visual Auditory Learning subtest of the WJ-IV Test of Cognitive Abilities in the treatment group that were not present in the control group.
Although all participants improved o n this assessment the pattern of improvement in the treatment group could be interpreted as being more importantly impacted in the desired direction
89
vs. the control group. These findings, if they hold true in follow-up studies, could support the conclusions drawn by Hayes et al. (2003). They concluded that auditory training could alter the preconscious neural encoding of complex sounds in the auditory brainstem by improving its neural synchrony. Additionally, the pre-post testing in that study also showed brainstem response to timing related to changes in cortical physiology, perceptual, academic, and cognitive measures (Hayes et al., 2003).
The results showed a pattern of improvement in the treatment group that was not found in the control group after completing the Tomatis® Method. The findings uphold my notion that it is worthwhile to research this intervention, as clearly there were improvements in three of the three subtests of the WJ-IV Test of Oral Language tested in the treatment group that was not present in the control group.
The findings on the Oral Language test showed a pattern of improvement in all three tests for all participants in the treatment group versus the control group where one participant improved in each test (Listening Comprehension, Oral Comprehension, and Understanding Directions). Of the participants, three declined in the Listening Comprehension and Understanding directions subtests, and two declined and one showed no change in the Oral Comprehension subtest. These findings, if they hold true in follow-up studies, could support the findings of Tatum et al. (2004) who used the Tomatis® Method therapy along with speech therapy and analyzed the speech of a 14- year-old female who had no speech before the treatment where results showed a gain of the use of 34 words and 17 sounds post-treatment. This warrants further study as it could also support findings by MacDonald and Nicoloff (2008) who applied the Tomatis® Method in two case studies, one of a 6-year-old female, and the other of a
90
51-year-old male. Post testing resulted in improved musical ability and improved ease in understanding and producing speech.
RQ3. Will participants (aged 5 to 12 years) show improvements in their ability for phonological awareness as measured by the Comprehensive Test of Phonological Processing 2nd Edition (CTOPP-2), after completing the Tomatis® Method?
The results showed a pattern of improvement in the treatment group that was not found in the control group after completing the Tomatis® Method. Once again, results appear to justify the need for continued research as there were improvements in these three su btests of the CTOPP -2 in the treatment group that was not present in the control group.
The findings on the Phonological Awareness test showed a pattern of improvement in all three participants in the treatment group versus a decline in three and no change in one participant in the control group. These findings, if they hold true in follow-up studies, could support the conclusions of Tatum et al. (2004). They used the Tomatis® Method therapy along with speech therapy to treat a 9-year-old male with ADHD and auditory processing disorder. The participant showed an increase in phonemic awareness post-treatment. Further, Ross-Swain (2007) summarized findings in a retrospective study on the Tomatis® Method, where post-testing showed statistically significant improvements in immediate auditory memory, auditory sequencing, interpretation of directions, auditory discrimination, and auditory cohesion. Also, post-testing showed a reduction in auditory latency when compared to the clients’ pre -tests. The findings of this study appear to be in agreement with the CTOPP pre -post-testing.
RQ4. Will participants (aged 5 to 12 years) show improvements in Full Scale Attention, as measured by the IVA-2 CPT (Integrated Visual & Auditory 2 Continuous Performance Test), after completing the Tomatis® Method?
91
The results showed a pattern of improvement in the treatment group that was not found in the control group after completing the Tomatis® Method. According to the results, continued research of this intervention is warranted, as clearly there were improvements in these subtests of IVA-2 in the treatment group that was not present in the control group. The findings on the Full Scale Attention Quotient test showed a pattern of improvement in all three participants in the treatment group versus an improvement in one participant, a decline in one participant, and no change in one participant where the fourth participant was unable to complete this test in the control group. These findings, if they hold true in follow-up studies, could support the findings of Bon thuys and Botha (2016). They conducted a systematic review that sought to determine the evidence on how the Tomatis® Method compared to other self-regulation interventions with tertiary students. Bonthuys and Botha (2016) suggested the Tomatis® Method is superior to alternative self-regulation approaches in decreasing psychosocial and emotional stressors, as well as enhancing the well-being of tertiary students. The Tomatis® Method was as effective as alternative approaches in promoting self-awareness and selfmonitoring. Furthermore, results on the Full Scale Response Control Quotient showed that all three participants in the treatment group showed improvement. In the control group one participant showed an improvement, two declined, and one participant was unable to complete the test These preliminary findings warrant further stud y
RQ5. Will participants (aged 5 to 12 years) show improvements in Neurotiming, as measured by the Interactive Metronome® (IM), after completing the Tomatis® Method?
The results showed a pattern of improvement in the treatment group that was not found in the control group after completing the Tomatis® Method.
92
The findings on the IM Long Form test showed a pattern of improvement in all three participants in the treatment group versus improvement in two participants and a decline in two participants in the control group. These findings, if they hold true in follow- up studies, could support the findings that auditory training has been found to alter the neural responses to sound at the cortical level in humans. Pre-post testing also showed brainstem response timing related to changes in cortical physiology, perceptual, academic, and cognitive measures (Hayes et al., 2003).
Recommendations for Further Research
The resulting trends found in this p ilot study were encouraging and suggest that further research on this method should be pursued as this could be a useful tool in therapy with children who are diagnosed with C/APD. Practitioners of the Tomatis® Method consider this an integrative program that addresses underlying sensory, vestibular processing and use the program to integrate various aspects of development. There appear to be improvements in the treatment group that outweigh the control group when looking at the preliminary findings on various tests of functional outcomes dependent on typical APD skills. The results warrant further research into how the method affects these skills. Future research should look at finding more robust sources of referrals where a pool of more homogeneous participants may be found, such as schools and tutoring establishments specializing in a specific learning disability. The research should qualify children whose baseline testing results fall within similar limits to ensure better comparison is possible. The research should also take a more focused approach and target one or two pertinent skills necessary for communication and learning. This would be more easily done in a school that specializes in children who have learning disabilities, as this would eliminate many of the obstacles I had to face in recruiting. It would be imperative to have a much more
93
robust sample to perform the treatment and to allow for power and significance in the findings. A school setting would additionally offer better control on fidelity to the program and pre - and post-testing.
I would like to see the Tomatis® Method become a more widely used program should these results hold true in further study. This program, if shown to be efficacious in further study, could result in a net gain of long-term output of funds as, in my experience, it shortens the time needed for other therapies and may sometimes lead to a child no longer needing further intervention.
Recruiting
The research process includes recruitment of participants and can be difficult especially for underfunded projects (Joseph et. al., 2016). These authors propose five strategies, which I believe would be helpful in improving recruitment efforts in a future study. These strategies are leveraging social networks and personal contacts, fostering collaboration with identified community gatekeepers, use recruitment platforms, create materials that clearly describe the study, and build relationships with potential participants that are based on respect and trust (Joseph et al., 2016).
Study Design
An additional suggestion given the population in this study is to perform the study in a school specializing in children with specific learning difficulties related to C/APD, which would not only solve the recruitment difficulties, but additionally make the design of the study more readily feasible. This would additionally help with decreasing any possible attrition issues when using a larger sample.
94
Assumptions
The primary assumption of this study was that the efficacy of the Tomatis® Method could be evaluated and assessed by using a program of 64 hours of listening over a period of 4 months. The secondary assumption was that there would be positive changes in the treatment group as compared to the control group. Thus, the study examined the research design and the efficacy of the Tomatis® Method on children aged 5 – 12 diagnosed with C/APD
According to the studies reviewed in the literature review above, it was reasonable to assume that improving and/or normalizing auditory processing in an individual would result in downstream improvements in oral and written language. In order to further solidify this assumption, I analyzed pre- and post-testing for phonological awareness, following multistep directions and visual-spatial domain. I also assessed working memory, auditory and visual attention, and focus to see if these improved given improvements in auditory processing.
Limitations of the Study
The study was mainly limited due to the small sample size. The study, therefore, lacked the power to conduct tests of statistical significance, and results were thus presented in descriptive trends. Findings may thus not generalize to larger studies and should thus be interpreted with caution. The small size was due to difficulties recruiting a group of participants that were a homogeneous group, within the age range required. The study was therefore conducted on a very small group of participants, which was however, sufficient to show trends and showed the feasibility of a bigger study. There were other factors involved, such as other interventions, which could not be controlled during the study period, due to limited resources. Further, one of the participants completed the pre-test as well as the entire program, reported the
95
positive change, but declined to come back for the post-test, further impacting the size of the study.
A second limitation was that the criteria of acceptance in order to get the eight final participants were rather broad, which resulted in two participants who were diagnosed with ASD as toddlers, and the diagnoses were later removed. Thus, there could be underlying confounding variables that could not be controlled for, such as other senses being impacted, which compounds the stress on the auditory system. The possibility of extracting the extent of the impact of other senses impacting the function of the auditory system was outside the scope of this study.
A third limitation was that all the children were receiving some form of outside treatment, which varied from simple tutoring to formal therapies like speech/language, occupational, music, Orton-Gillingham approach, and Lindamood Bell instruction. These are all methods of training used by instructors and therapists to remediate the impacts of auditory processing difficulties and learning disabilities in children. These can, therefore, be assumed to have had some impact on the results of both the treatment and control groups.
A fourth limitation was that there was no audiological testing to qualify participants for the study. Participants were accepted based upon parent feedback of the participant having a diagnosis of APD or being suspected as having APD. Thus, the sample is less homogeneous than should be used in a future formal study for this treatment, as although tested using the SSW a complete auditory battery of tests and in-depth analyses of auditory processing components present in the participants was not possible at the time of pre -post testing, due to limited resources.
96
Delimitations
The delimitations of this study included boundaries and exclusions in the development of the study design. This study looked at the feasibility of recruiting a treatment group who would receive the therapy and included a control group of like peers. There would be no comparison between other therapies. The study would only include children who were already diagnosed with C/APD, which excluded adults and children who may have an auditory processing disorder but who were not yet diagnosed.
Summary
Results of this pilot study and the literature review point to the fact that such studies can be done, and that there is a need for additional research to be performed before the Tomatis® Method can be unequivocally proclaimed as the gold standard for the treatment of APD in children aged 5 – 12 years. However, the current study, as well as the existing research , all point to the method as a beneficial addition to current treatments used in remediating APD in children aged 5 -12 years. This research adds to the positive findings of previous research on the Tomatis® Method of training, which all show trends of improvements in children diagnosed with learning disabilities, autism spectrum disorder, speech and language, and APD. The current pilot study has clearly shown that research on the efficacy of the Tomatis® Method training in remediating APD is well worth pursuing as there is a marked difference in positive trends in the treatment group versus the control group. In addition, although the sample was small, the overall compliance was excellent and attests to the feasibility of such a study.
Following the design of the pilot study and to ensure power and significance, future researchers should pursue a strong experimental design, which will include power to show significance. These should include well-designed studies of both quantitative and qualitative
97
design to ensure that effective clinically proven interventions such as this are used to help children and are not discarded simply due to claims of lack of research. Such claims could possibly result in a child not improving functionally due to a lack of other researched standard therapies not impacting certain individuals.
Clinical evidence and positive parent reports by thousands of therapists and families around the world should not be ignored, when such a program can only add value to what a therapist can do for a child who has APD, especially when there is a good chance that it will offer a better quality of life for the child and their family all with low risk to benefit. On the flip side, if existing clinical evidence is ignored, it may result in a child being deprived of the only thing that could help him/her due to being an outlier within a specific diagnosed population. A question to ponder is possible negative consequences that may result from not offering the Tomatis® Method to children. Particularly when little risk is associated with the clinically shown potential benefits that the body of existing literature, as well as the current study’s preliminary findings, have revealed. The results of this study showed marked trends in the desired direction, certainly worth further investigation to add to the body of evidence in support of the positive effects of the Tomatis® Method. This finding is important as it minimizes possible negative effects of a method should it not work. These effects include loss of time and money, dealing with the emotions of expectations that were not met, and damage to credibility.
The results of this pilot study show not only the feasibility of such a study but also show encouraging trends showing that the Tomatis® Method may improve auditory processing. The trends in the results further sh ow that the intervention may also positively impact related functions such as visual auditory learning, listening comprehension, oral comprehension, understanding directions, phonological awareness and memory, full scale attention and response,
98
and neurotiming. According to Faulkner (2003), feasibility studies using between 5 – 20 individuals may be reasonable as 80% of problems will be identified using 10 individuals and 90% using 20 individuals. These preliminary findings, therefore, warrant validation in the performance of clinical trials in individuals with a range of sensory, motor, and learning difficulties.
99
References
Alcántara, J. I., Weisblatt, E. J., Moore, B. C., & Bolton, P. F. (2004). Speech‐in‐noise perception in high‐functioning individuals with autism or Asperger's syndrome. Journal of Child Psychology and Psychiatry , 45 (6), 1107-1114.
Allen, J. B. (1994). How do humans process and recognize speech? IEEE Transactions on S peech and Audio Processing , 2 (4), 567-577.
American Academy of Audiology (2010). Practice Guidelines for the Diagnosis, Treatment, and Management of Children and Adults with Central Auditory Processing Disorder (CAPD).
https://audiology-web.s3.amazonaws.com/migrated/CAPD%20Guidelines%208-
2010.pdf_539952af956c79.73897613.pdf
American Psychiatric Association (2013). Diagnostic and statistical manual of mental d isorders (5TH ed.). American Psychiatric Association.
American Speech-Language-Hearing Association Task Force on Central Auditory Processing
Consensus Development (1996). Central auditory processing: current status of research and implications for clinical practice. American Journal of Audiology, 5, 41-54.
American Speech-Language-Hearing Association (2005). Central auditory processing disorders
- Technical statement.
Amitay, S., Ahissar, M., & Nelken, I. (2002). Auditory processing deficits in reading disabled adults. Journal of the Association for Research in Otolaryngology , 3 (3), 302–320.
https://doi.org/10.1007/s101620010093
Anderson, K. L. (1989). SIFTER: Screening Instrument for Targeting Educational Risk in
children identified by h earing screening or who have known h earing loss: User's manual
Interstate Printers & Publishers.
100
Anderson, K. L., & Goldstein, H. (2004). Speech perception benefits of FM and infrared devices to children with hearing aids in a typical classroom. Language, Speech, and Hearing Services in Schools, 35 , 169-184.
Antoine, M. W., Hübner, C. A., Arezzo, J. C., & Hébert, J. M. (2013). A causative link between inner ear defects and long-term striatal dysfunction. Science, 341 (6150), 1120-1123.
Archibald, L. M. D., & Gathercole, S. E. (2006) Short-term and working memory in specific language impairment. International Journal of Language & Communication Disorders, 41, 675–693. https://doi.org/10.1080/13682820500442602
Ashburner, J., Ziviani, J., & Rodger, S. (2008). Sensory processing and classroom emotional, behavioral, and educational outcomes in children with autism spectrum disorder. American Journal of Occupational Therapy , 62 (5), 564-573.
Ayres, A. J. (1979). Sensory integration and the child . Western Psychological Services.
Ayres, A. J. (1989). Sensory integration and praxis tests. Western Psychological Services.
Baranek, G. T., Foster, L. G., & Berkson , G. (1997). Tactile defensiveness and stereotyped behaviors. American Journal of Occupational Therapy, 51, 91–95.
Bellis, T. J. (1996). Central auditory processing disorders. Singular Publishing Group.
Bellis, T. J. (1997). Understanding auditory p rocessing d isorders in children.
http://www.asha.org/public/hearing/disorders/understand-apd -child.htm
Bellis, T. J. (2003). Assessment and management of central auditory processing disorders in the educational setting: From science to practice (2nd ed.). Thomson Learning
101
Bellis, T. J. (2007). Differential diagnosis of (central) auditory processing disorder in older listeners. In F. E. Musiek & G. D. Chermak (Eds.), Handbook of (central) auditory processing disorder: Auditory neuroscience and diagnosis (Vol. 1, pp. 319-346). Plural Publishing.
Bellis, T. J. (2011). Assessment and management of central auditory processing disorders in the educational setting (rev ed.) Singular/Delmar Learning.
Bellis, T. J., & Anzalone, A. M. (2008). Intervention approaches for individuals with (central) auditory processing disorder. Contemporary Issues in Communication Science & Disorders, 35 , 143-153.
Bellis, T. J., & Ferre, J. M. (1999). Multidisciplinary approach to the differential diagnosis of central auditory processing disorders in children. Journal of the American Academy of Audiology , 10 , 319-328.
Bernard-Bonnin, A. (2002). The use of alternative therapies in treating children with attention deficit hyperactivity disorder. Paediatrics & Child Health, 7 (10), 710-718.
Bess, F. H., Dodd-Murphy, J., & Parker, R. A. (1998). Children with minimal sensorineural hearing loss: Prevalence, educational performance, and functional status. Ear and Hearing , 19 (5), 339-354.
Billiet , C R., & Bellis, T. J. (2011). The relationship between brainstem temporal processing and performance on tests of central auditory function in children with reading disorders
Journal of Speech, Language, and Hearing Research , 54 (1), 228–242.
https://doi.org/10.1044/1092-4388(2010/09-0239)
102
Bonthuys, A., & Botha, K. (2016). Tomatis® Method (Tomatis, 1996, p. 197) comparative efficacy in promoting self-regulation in tertiary students: A systematic review. Journal of Psychology in Africa , 26 (1), 92-106.
Bottom-up. (n.d.). Merriam-Webster Dictionary. Retrieved April 18, 2017, from MerriamWebster.com website https://www.merriam-webster.com/dictionary/bottom-up
Bowen, D. J., Kreuter, M., Spring, B., Cofta-Woerpel, L., Linnan, L., Weiner, D., Bakken, S., Kaplan, C. P., Squiers, L., Febrizio, C., & Fernandez, M. (2009). How we design feasibility studies. American Journal of Prev en tive Medicine, 36 (5), 452-457.
Bradlow, A. R., Kraus, N., & Hayes, E. (2003). Speaking clearly for children with learning disabilities: Sentence perception in noise. Journal of Speech Language Hearing Research, 46 (1), 80 – 97.
Brownell, R. (2000). Expressive One -Word Picture Vocabulary Test - Third Edition (EOWPVT, 3 rd Ed.) Technical Manual . Academic Therapy Publications.
British Society of Audiology. (2011). Position statement: Auditory pro cessing disorder (APD)
http://www.thebsa.org.uk/
Burgoyne, K., Duff, F. J., Clarke, P. J., Buckley, S., Snowling, M. J., & Hulme, C. (2012). Efficacy of a reading and language intervention for children with Down syndrome: A randomized controlled trial. Journal of Child Psychology and Psychiatry , 53(10), 1044–1053. https://doi.org/10.1111/j.1469-7610.2012.02557.x
Cacace, A. T. , & McFarland, D. J. (1998). Central auditory processing disorder in school-aged children: A critical review. Journal of Speech Language Hearing Research , 41(2), 355373. https://doi.org/10.1044/jslhr.4102.355
103
Caird, D., & Klinke, R. (1983). Processing of binaural stimuli by cat superior olivary complex neurons. Experimental Brain Research , 52 (3), 385-399.
Chermak, G. D., & Musiek, F. E. (1997). Central auditory processing disorders: New perspectives. Singular Publishing Group .
Chermak, G. D. & Musiek , F. E. (2002). Auditory training: Principles and approaches for remediating and managing auditory processing disorders. Seminars in Hearing, 23 , 297–308.
Choudhury, M., & Chavira, P. (2017). Narrative review of evidence based intervention approaches for auditory processing disorder (APD). Perspectives of the ASHA Special Interest Groups, 2 (2), 152–156. https://doi.org/10.1044/persp2.SIG2.152
Christmann, C. A., Lachmann, T., & Steinbrink, C. (2015). Evidence for a general auditory processing deficit in developmental dyslexia from a discrimination paradigm using speech versus non-speech sounds matched in complexity. Journal of Speech, Language and Hearing Research (Online), 58 (1), 107-121.
doi:http://dx.doi.org.fgul.idm.oclc.org/10.1044/2014JSLHR-L-14-0174
Corbett, B. A., Shickman, K., & Ferrer, E. (2008). Brief report: The effects of Tomatis sound therapy on language in children with autism. Journal of Autism and De velopmental Disorders, 38 (3), 562-566.
Corpus callosum. (n.d.). The American Heritage ® Science Dictionary. Retrieved April 19, 2017 from Dictionary.com website http://www.dictionary.com/browse/corpus-callosum
Crandell, C. C. (1998). Using sound field FM amplification in the educational setting. The Hearing Journa l, 51 (5), 10-19.
104
Culbertson, J. L., & Gilbert, L. E. (1986). Children with unilateral sensorineural he aring loss: Cognitive, academic, and social development. Ear and Hearing , 7 (1), 38-42.
Cumming, R., Wilson, A., & Goswami, U. (2015). Basic auditory processing and sensitivity to prosodic structure in children with specific language impairments: A new look at a perceptual hypothesis. Frontiers in Psychology , 6 .
https://doi.org/10.3389/fpsyg.2015.00972
Cunningham, J., Nicol, T., Zecker, S., & Kraus, N (2000) Speech-evoked neurophysiologic responses in children with learning problems: Development and behavioral correlates of perception. Ear Hear, 21 (6), 554–68.
Cutini, S., Szucs, D., Mead, N., Huss, M., & Goswami, U. (2016). Atypical right hemisphere response to slow temporal modulations in children with developmental dyslexia.
NeuroImage; Amsterdam, 143 , 40–49. https://doi.org/10.1016/j.neuroimage.2016.08.012
Davis, J. M., Elfenbein, J., Schum, R., & Bentler, R. A. (1986). Effects of mild and moderate hearing impairments on language, educational, and psychosocial behavior of children. Journal of S peech and Hearing Disorders, 51 (1), 53-62.
DeCasper, A., Lecanuet, J., Busnel, M., Granier-Deferre, C., & Maugeais, R. (1994). Fetal reactions to recurrent maternal speech. Infant Behavior and Development, 17 , 159– 164.
Delgutte, B. (1996). Physiological models for basic auditory percepts. In H. I. Hawkins, T. A.
McMullen, A. N. Popper, R.R. Fay (Eds.), Auditory computation (pp. 157-220). Springer.
Dourn, R. (2010). The role of occupational therapy with central auditory processing disorder: A systematic literature review [M.S., The College of St. Scholastica]. https://searchproquest-com.fgul.idm.oclc.org/docview/743816416/abstract/DE6BCE820B3F48F0PQ/1
105
Dunn, W. (1997). The impact of sensory processing abilities on the daily lives of young children and their families: a conceptual model. Infants & Young Children , 9 (4), 23-35.
Dunn, W. (1999). The sensory p rofiles. The Psychological Corporation.
Dunn, L. M., & Dunn, L. M. (1997). Peabody picture vocabulary test- III . Circle Pines, MN: American Guidance Service.
Emanuel, D. C. (2002). The auditory processing battery: Survey of common practices. Journal of the American Academy of Audiology , 1 3 (2), 93-117.
Faulkner, L. (2003). Beyond the five-user assumption: Benefits of increased sample sizes in usability testing. Behavior Research M ethods, Instruments, & Computers: A Journal of the Psychonomic Society, Inc, 35 (3), 379–383. https://doi.org/10.3758/bf03195514
Ferguson, M. A., Hall, R. L., Riley, A., & Moore, D. R. (2011). Communication, listening, cognitive and speech perception skills in children with auditory processing disorder (APD) or specific language impairment (SLI). Journal of Speech, Language, and Hearing Research , 54 (1), 211-227.
Ferre, J. M. (2015). Auditory dysfunction beyond the 8th nerve : Understanding central auditory processing disorders. Perspectives on Hearing and Hearing Disorders: Research and Diagnostics, 19 (1), 4–11. https://doi.org/10.1044/hhd19.1.4
Fey, M. E., Richard, G. J., Geffner, D., Kamhi, A. G., Medwetsky, L., Paul, D., Ross - Swain, D., Wallach, G. P., Frymark, T., & Schooling, T. (2011). Auditory processing disorder and Auditory/Language interventions: An evidence-based systematic review. Language, Speech & Hearing Services in Schools (Online), 42 (3), 246-264A.
https://doi.org/10.1044/0161-1461(2010/10-0013)
Fisher, L. (1976). Fisher’s auditory problems checklist. Educational Audiology Association.
106
Fletcher, H. (1940). Auditory patterns. Reviews of M odern Physics, 12 (1), 47.
Fogarty, S., & Wardle, J. (2015). Integrative medicine case series: A clinician’s guide to publication. Advances in Integrative Medicine, 2 (3), 147-151.
Foss-Feig, J. H., Heacock, J. L., & Cascio, C. J. (2012). Tactile responsiveness patterns and their association with core features in autism spectrum disorders. Research in Autism S pectrum Disorders, 6 (1), 337-344.
Friel- Patti, S. (1999). Clinical forum: Treatment for central auditory processing disorders. Clinical decision-making in the assessment and intervention of central auditory processing disorders. Language, Speech & Hearing Services in Schools, 30 (4), 345.
Gerritsen, J. (2009). A review of research done on Tomatis Auditory Stimulation.
Gerritsen, J. (2010). The effect of Tomatis therapy on children with autism: Eleven case studies. International Journal of Listening , 24 (1), 50–6.
https://doi.org/10.1080/10904010903466378
Gillam, R. B., Crofford, J. A., Gale, M. A., & Hoffman, L. M. (2001) Language change following computer-assisted language instruction with Fast ForWord or Laureate Learning Systems software. American Journal of Speech Language Pathology, 10 (3), 231–47.
Gilmore, T. (1999) The efficacy of the Tomatis Method for Children with Learning and Communication Disorders: A meta-analysis International Journal of Listening, 13(1 ), 12-23
Gitomer, J. (2016). I'm sorry, I didn't hear you. Could you repeat that? Grand Rapids Business Journal, 34 (3), 11.
107
Glasberg, B. R., & Moore, B. C. (1990). Derivation of auditory filter shapes from notched-noise data. Hearing Research , 47 (1-2), 103-138.
Gomez, R., & Condon, M. (1999). Central auditory processing ability in children with ADHD with and without learning disabilities. Journal of Learning Disabilities, 32 (2), 150-158.
Hayes, E. A., Warrier, C. M., Nicol, T. G., Zecker, S. G., & Kraus, N. (2003). Neural plasticity following auditory training in children with learning problems. Clinical Neurophysiology: Official Journal of the International Federation of Clinical Neurophysiology, 114 (4), 673–684.
Horowitz, S. S. (2012). The universal sense: How hearing shapes the mind (1st U.S. ed.). Bloomsbury.
Hulme, C., & Snowling, M. J. (2014). The interface between spoken and written language: Developmental disorders. Philosophical Transactions of the Royal Society B: Biological Sciences, 369 (1634), 20120395. https://doi.org/10.1098/rstb.2012.0395
Jeffress, L. A. (1948). A place theory of sound localization. Journal of Comparative and Physiological Psychology, 41 (1), 35 –39. https://doi.org/10.1037/h0061495
Jerger, J., & Musiek, F. (2000). Report of the consensus conference on the diagnosis of auditory processing. Journal of the American Academy o f Audiology , 11 (9), 467-474.
Jones, P. R., Moore, D. R., & Amitay, S. (2015). Development of auditory selective attention: Why children struggle to hear in noisy environments. Developmental Psychology , 51 (3), 353–369. https://doi.org/10.1037/a0038570
Joris, P. X., Smith, P. H., & Yin, T. C. (1998). Coincidence detection in the auditory system: 50 years after Jeffress. Neuron , 21 (6), 1235-1238.
108
Joseph, R. P., Keller, C., & Ainsworth, B. E. (2016). Recruiting participants into pilot trials : Techniques for researchers with shoestring budgets Californian Journal of Health
Promotion , 14 (2), 81–89.
Kandel, E. R. , Schwartz, J. H., & Jessell, T. M. (Eds.) . (2000). Principles of neural science (Vol. 4, pp. 1227-1246). McGraw-Hill.
Karns, C. M., Isbell, E., Giuliano, R. J., & Neville, H. J. (2015). Auditory attention in childhood and adolescence: An event-related potential study of spatial selective attention to one of two simultaneous stories. Developmental Cognitive Neuroscience, 13 , 53–67.
https://doi.org/10.1016/j.dcn.2015.03.001
Katz, J. (1992). Classification of auditory processing disorders. In J. Katz, N. Stecker, & D. Henderson (Eds.), Central a uditory p rocessing: A transdisciplinary view (pp. 81 – 92).
Mosby Yearbook.
Kayser, C., Petkov, C. I., Augath, M., & Logothetis, N. K. (2005). Integration of touch and sound in auditory cortex. Neuron , 48 (2), 373-384.
Keith, R. W. (2008). SCAN-3:C: Test for Auditory Processing Disorders in Children -Revised . Psychological Corporation.
Keith, W., Purdy, S., Baily, M. R., & Kay, F. (2019). New Zealand guidelines on auditory processing disorder, Trans-Tasman Online Conference 2020.
Keller, W. D., Tiller, K. L., & McFarland, D. J. (2006). Auditory processing disorder in children diagnosed with nonverbal learning disability. American Journal of Audiology, 15, 10813.
109
Kershner, J., Cummings, R., Clarke, K., Hadfield, A., & Kershner, B. (1986). Evaluation of the Tomatis Listening Training Program with learning disabled children. Canadian Journal of Special Education, 2, 1 -32.
Kiang, N. Y. S. (1984). Stimulus representation in the discharge patterns of auditory neurons . The Nervous System, 3 (2) , 639 -674.
Kiang, N. Y. S., & Moxon, E. C. (1974). Tails of tuning curves of auditory‐nerve fibers. The Journal of the Acoustical Society of America , 55 (3), 620-630.
Kiang, N., Sachs, M. B., & Peake, W. T. (1967). Shapes of tuning curves for single auditory nerve fibers. Journal of the Acoustical Society of America , 42 (6), 1341-1342.
King, A. J., & Schnupp, J. W. (2007). The auditory cortex. Current Biology , 17 (7), R236-R239.
Konishi, M. (2003). Coding of auditory space. Annual Review of Neuroscience, 26 (1), 31-55.
Kraus, N., & Anderson , S. (2016). Chapter 3 Auditory p rocessing disorder: Biological basis and treatment efficacy. In C. LePrell , E. Lobarina, A. N. Popper, & R. R. Fay (E ds.), Translational research in audiology, neurotology, and the hearing sciences . (Springer Handbook of Auditory Research 58 ). Springer International Publishing.
https://doi.org/10.1007/978-3-319-40848-4_3
Krüger, R. J., Krüger, J. J., Hugo, R., & Campbell, N. G. (2001). Relationship patterns between central auditory processing disorders and language disorders, learning disabilities, and sensory integration dysfunction. Communication Disorders Quarterly , 22 (2), 87-98.
Lallier, M., Donnadieu, S., & Valdois, S. (2013). Developmental dyslexia: Exploring how much phonological and visual attention span disorders are linked to simultaneous auditory processing deficits. Annals of Dyslexia; New York , 63 (2), 97–116.
https://doi.org/10.1007/s11881-012 -0074-4
110
MacDonald, K., & Nicoloff, F. (2008. January ). Using the Tomatis Method to help children and adults with central auditory processing disorder unravel the seeming complexities of everyday life: Two case studies. Ricochet, vol. 2 .
McArthur, G. M. (2009). Auditory processing disorders: Can they be treated? Current Opinion in Neurology , 22 (2), 137-143.
Miller, C. A., & Wagstaff, D. A. (2011). Behavioral profiles associated with auditory processing disorder and specific language impairment. Journal of Communication Disorders, 44 (6), 745–763. https://doi.org/10.1016/j.jcomdis.2011.04.001
Miller, E. K., & Cohen, J. D. (2001). An integrative theory of prefrontal cortex function. Annual Review of Neuroscience, 24 (1), 167-202.
Miller, K. J., Shenoy, P., Miller, J. W., Rao, R. P., & Ojemann, J. G. (2007). Real-time functional brain mapping using electrocorticography. Neuroimage, 37 (2), 504-507.
Miller, L. J., Anzalone, M. E., Lane, S. J., Cermak, S. A., & Osten, E. T. (2007). Concept evolution in sensory integration: A proposed nosology for diagnosis. American Journal of Occupational Therapy, 61, 135-140.
Miller, L. J., Nielsen, D. M., & Schoen, S. A. (2012). Attention deficit hyperactivity disorder and sensory modulation disorder: A comparison of behavior and physiology. Research in Developmental Disabilities, 33 (3), 804– 818. https://doi.org/10.1016/j.ridd.2011.12.005
Moncrieff, D. (2007). Evidence-based practice in the diagnosis and treatment of auditory processing disorders Perspectives on Hearing and Hearing Disorders: Research and Diagnostics, 11 (1), 12-15.
111
Moncrieff, D. W., & Wertz, D. (2008). Auditory rehabilitation for interaural asymmetry: Preliminary evidence of improved dichotic listening performance following intensive training. International Journal of Audiology , 47 (2), 84-97.
Moore, D. R. (2006). Auditory processing disorder (APD) Potential contribution of mouse research. Brain Research , 1091 (1), 200-206.
Moore, D. R. (2006) Auditory processing disorder (APD): Definition, diagnosis, neural basis, and intervention. Audiological Medicine, 4 (1), 4-11.
https://doi.org/10.1080/16513860600568573
Moore, D. R. (2018). Editorial: Auditory p rocessing disorder. Ear and Hearing , 39 (4), 617–620.
https://doi.org/10.1097/AUD.0000000000000582
Moore, D. R., Ferguson, M. A., Edmondson-Jones, A. M., Ratib, S., & Riley, A. (2010). Nature of auditory processing disorder in children. Pediatrics, 126 (2), e382–390.
Mülder, H. E., Rogiers, M., & Hoen, M. (2007). Auditory Processing Disorders I: Definition, diagnostic, etiology and management. Speech and Hearing Review, 6 (7), 239-266.
Murphy, C. F. B., & Schochat, E. (2011). Effect of nonlinguistic auditory training on phonological and reading skills. Folia Phoniatrica et Logopaedica; Basel, 63 (3), 147–53.
https://doi.org/10.1159/000316327
Musiek, F. (1983a). Assessment of central auditory dysfunction: The Dichotic Digits Test revisited. Ear and Hearing, 4, 79-83.
Musiek, F. (1983b). Dichotic Digits Test [Audiotape]. Dartmouth-Hitchcock Medical Center
Schow, R. L., & Nerbonne, M. A . (2017). Introduction to audiologic rehabilitation . Pearson.
Neysmith-Roy, J. M. (2001). The Tomatis method with severely autistic boys: Individual case studies of behavioral changes. South African Journal of Psychology , 31 (1), 19-28.
112
Nguyen, H., & Bentler, R. (2011). Optimizing FM Systems. ASHA Leader, 16 (12), 5–6.
https://doi-org/10.1044/leader.FTR6.16122011.5
Nickisch, A., & Massinger, C. (2009). Auditory processing in children with specific language impairments: Are there deficits in frequency discrimination, temporal auditory processing or general auditory processing? Folia Phoniatrica et Logopaedica, 61 (6), 323-8.
https://doi.org/10.1159/000252848
Nixon, G. (2015, July 2) 9 Surprising Consequences of Auditory Processing Disorder Gemm Learning. https://gemmlearning.com/blog/auditory-processing/9-consequences-ofauditory-processing-disorder-in-children/
O’Cathain, A., Hoddinott, P., Lewin, S., Thomas, K. J., Young, B., Adamson, J., Jansen, Y. J., Mills, N., Moore, G., & Donovan, J. L. (2015). Maximising the impact of qualitative research in feasibility studies for randomised controlled trials: Guidance for researchers.
Pilot and Feasibility Studies, 1 (1), 32. https://doi.org/10.1186/s40814-015-0026-y
Oertel, D. (1991). The role of intrinsic neuronal properties in the encoding of auditory information in the cochlear nuclei. Current Opinion in Neurobiology , 1 (2), 221-228.
Paige, D. D., Rupley , W. H., Smith, G. S., Olinger, C., Leslie, M. (2018) Acquisition of letter naming knowledge, phonological awareness, and spelling knowledge of kindergarten children at risk for learning to read. Child Development Research, 2018, 1-10.
https://doi.org/10.1155/2018/2142894
Palmer, A. R. (2004). Reassessing mechanisms of low-frequency sound localisation. Current Opinion in Neurobiology , 14 (4), 457-460.
113
Patrusky, L. H. (2013). Central auditory processing disorder: A literature review on interdisciplinary management, intervention, and implications for educators [Doctoral dissertation, University of Central Florida Orlando, Florida].
Perreau, A. E., Wu, Y. H., Tatge, B., Irwin, D., & Corts, D. (2017). Listening effort measured in adults with normal hearing and cochlear implants. Journal of the American Academy of Audiology , 28 (8), 685–697.
Prosody. (n.d.). Merriam-Webster Dictionary. Retrieved April 18, 2017, from MerriamWebster.com website https://www.merriam-webster.com/dictionary/prosody
Purdy, S. C., Wanigasekara, I., Cañete, O. M., Moore, C., & McCann, C. M. (2016). Aphasia and auditory processing after stroke through an international classification of functioning, disability and health lens. Seminars in Hearing , 37 (3), 233–246.
https://doi.org/10.1055/s-0036-1584408
Rauschecker, J. P., & Tian, B. (2000). Mechanisms and streams for processing of “what” and “where” in auditory cortex. Proceedings of the National Academy of Sciences, 97 (22), 11800-11806.
Reynolds, C.R. & Kamphaus, R.W. (1999). Behavior Assessment System for Children [Assessment instrument]. Bloomington, MN: Pearson.
Reynolds, S., Kuhaneck, H. M., & Pfeiffer, B. (2016). Systematic review of the effectiveness of frequency modulation devices in improving academic outcomes in children with auditory processing difficulties. The American Journal of Occupational Therapy, 70 (1), 1-12.
https://doi.org/10.5014/ajot.2016.016832
114
Ross, S. M., Sheard, M. K., Cheung, A., Elliott, L., & Slavin, R. (2011). Promoting primary pupils’ social-emotional learning and pro-social behaviour: Longitudinal evaluation of the Together 4 All Programme in Northern Ireland. Effective Education , 3 (2), 61–81.
https://doi.org/10.1080/19415532.2012.665773
Ross-Swain, D. (2007). The effects of auditory stimulation on auditory processing disorder: A summary of the findings. International Journal of Listening, 21 (2), 140-155.
Sacarin, L. (2013). Early effects of the Tomatis Listening Method in children with a ttention d eficit [PsyD, Antioch University Seattle]. https://search-proquestcom.fgul.idm.oclc.org/docview/1650715640/abstract/A235AE26CC6B4A3APQ/1
Schrank, F. A., & Wendling, B. J. (2018). The Woodcock– Johnson IV: Tests of cognitive abilities, tests of oral language, tests of achievement. In D. P. Flanagan & E. M. McDonough (Eds.), Contemporary intellectual assessment: Theories, tests, and issues (pp. 383–451). The Guilford Press.
Sharma, M. , Purdy, S. , & Kelly, A. S. (2009). Comorbidity of auditory processing, language a nd reading disorders. Journal of Speech Language and Hearing Research, 52 (3), 706-722.
Sharma, M., Purdy, S., Newall, P., Wheldall, K., Beaman, R., & Dillon, H. (2006). Electrophysiological and behavioral evidence of auditory processing deficits in children with reading disorder. Clinical Neurophysiology , 117 (5), 1130–1144.
Silman, S , Silverman, C A , & Emmer, M B. (2000) Central auditory processing disorders and reduced motivation: Three case studies Journal of the American Academy of Audiology, 11 (2), 57–63.
Smith, T. (2001). Discrete trial training in the treatment of autism. Focus on Autism and Other Developmental Disabilities, 16 , 86-92. https://doi.org/10.1177/108835760101600204
115
Smoski, W. J., Brunt, M. A., & Tannahill, J. C. (1998). CHAPS: Children's Auditory
Performance Scale: Instruction manual
Sollier, P. (2005). Listening for wellness: An introduction to the Tomatis Method. Mozart Center Press.
Sparrow, S. S., Balla, D. A., & Cicchetti, D. V. (1984). The Vineland Adaptive B ehavior
S cales: Interview Edition, Expanded Form (VABS): Technical Manual. Pearson.
Stach, B. A., Spretnjak, M. L., & Jerger, J. (1990). The prevalence of central presbyacusis in a clinical population. Journal of the American Academy of Audiology, 20 (4), 229-238
Staecker, H., & Thompson, J. (2013). Auditory brainstem response. In S. E. Kountakis (Ed.), Encyclopedia of otolaryngology, head and neck surgery (pp. 209–209). Springer Berlin Heidelberg. https://doi.org/10.1007/978-3-642-23499-6_200126
Steinschneider, M., & Dunn, M. (2002). Electrophysiology in developmental neuropsychology. Handbook of neuropsychology , (vol. 8, pt. 1. Pp. 91-146). Elsevier
Stillitano, C., Fioretti, A., Cantagallo, M., & Eibenstein, A. (2014). THE EFFECTS OF THE TOMATIS METHOD ON TINNITUS. International Journal, 4 (2), 2307-2083.
Stillitano, C., Rosati, N., Cisternino, S., Fioretti, A., Iaconelli, S., & Eibenstein, A. (2016). The effects of the Tomatis Method on the artistic voice. International Journal of Listening , 31 (2), 113-120.
Suga, N., Gao, E., Zhang, Y., Ma, X., & Olsen, J. F. (2000). The corticofugal system for hearing: Recent progress. Proceedings of the National Academy of Sciences, 97 (22), 1180711814.
Tallal, P. (2008). Fast ForWord.
http://ies.ed.gov/ncee/wwc/pdf/intervention_reports/wwc_ffw_031913.pdf
116
Tallal, P. , & Piercy, M. (1973). Defects of non-verbal auditory perception in children with developmental aphasia. Nature, 241 , 468-469.
Tatum, J. M., Oelfke, J. K., & McCauley, C. P. (2004). Tomatis-assisted speech therapy. International Journal of Tomatis Method Research, 1 (1), 37 –42.
Teder-Sälejärvi, W. A., Pierce, K. L., Courchesne, E., & Hillyard, S. A. (2005). Auditory spatial localization and attention deficits in autistic adults. Cognitive Brain Research , 23 (2), 221234.
The National Institute of Mental Health (2015). Autism Spectrum Disorder.
https://www.nimh.nih.gov/health/topics/autism-spectrum-disorders-asd/index.shtml
Thompson, B. M., & Andrews, S. R. (2000). An historical commentary on the physiological effects of music: Tomatis, Mozart and neuropsychology. Integrative Physiological and Behavioral Science, 35 (3), 174–188 https://doi.org/10.1007/BF02688778
Tomatis, A. A. (1974). Vers l'écoute humaine, Tome 2: Qu'est-ce que l'oreille humaine? Les Edition E.S.F. Collection "Sciences de l'Education ", 183 pages, ill
Tomatis, A. A. (1981). La Nuit Uterine . Editions Stock, Paris, 256 pages.
Tomatis, A. A. (1996). The ear and language . Moulin.
Tomatis, A., & Thompson, B. (1991). The conscious ear: My life of transformation through listening . Station Hill Press.
http://www.tomatis.com/en/the-group/history-and-development.html
Tonotopical. (n.d.). Merriam-Webster Dictionary. Retrieved April 18, 2017, from MerriamWebster.com website
https://www.merriam-webster.com/dictionary/tonotopical
Top-down. (n.d.). Merriam-Webster Dictionary. Retrieved April 18, 2017, from MerriamWebster.com website
https://www.merriam-webster.com/dictionary/top-down
117
Van Teijlingen, E., & Hundley, V (2001). The importance of pilot studies. Social Research
Updates, 35.
Verdun, N. M., Zwetsch , I. C., Costa-Ferreira, M. I. D. da, Verdun, N. M., Zwetsch, I. C., & Costa-Ferreira, M. I. D. da. (2015). Characterization of types of errors committed in the evaluation of auditory processing through Staggered Spondaic Word test. Revista
CEFAC, 17 (6), 1848–1854. https://doi.org/10.1590/1982-0216201517622714
Wagner, R. K., Torgesen, J. K., Rashotte, C. A., & Pearson, N. A. (2013). Comprehensive Test of Phonological Processing-Second Edition (CTOPP-2)
Weihing, J., Chermak, G. D., & Musiek, F. E. (2015). Auditory training for central auditory processing disorder. Seminars in Hearing , 36 (4), 199–215. https://doi.org/10.1055/s0035-1564458
Wetherby, A. M., Koegel, R. L., & Mendel, M. (1981). Central auditory nervous system dysfunction in echolalic autistic individuals. Journal of Speech, Language, and Hearing Research , 24 (3), 420-429.
Wilson, W. J., & Arnott, W. (2013). Using different criteria to diagnose (central) auditory processing disorder: How big a difference does it make? Journal of Speech, Language, and Hearing Research: JSLHR, 56 (1), 63–70. https://doi.org/10.1044/10924388(2012/11-0352
Wilson, W. J., Arnott, W., & Henning, C. (2012). A systematic review of electrophysiological outcomes following auditory training in school-age children with auditory processing deficits. International Journal of Audiology , 52 (11), 721–730.
118
M. (1997). Deficits in auditory temporal and spectral resolution in language -impaired children . Nature, 387, 176-178.
119
Wright, B. A. Lombardino, L. J., King, W. M., Puranik, C. S., Leonard, C. M., & Merzenich, M.
APPENDIX A
Fielding Graduate University
Letter of Invitation to Participate in Dissertation Study
My name is Sharmila QuenimHerr, M.S. CCC- SLPL/R, Speech-Language Pathologist. I am currently pursuing my PhD. in the Infant and Early Childhood Development program with Fielding Graduate University at 2020 De La Vina St., Santa Barbara, California. As a student, I am completing my dissertation on the efficacy of the Tomatis Method on Learning Difficulties, Reading, and Writing Difficulties, including Dyslexia potentially related to Central Auditory Processing Disorder. Participants should be between 6 – 11 years of age. If mature enough, a child aged as young as five years may qualify. All participants will initially be evaluated to determine the baseline (get Pre-test scores) for the study. If the participant qualifies for the study, he/she will be randomly assigned to one of two groups, either the Tomatis group (intervention group) or the control group (delayed intervention). I would like to invite you to participate in my study that will span ~ 9 months, where the participants who were randomly assigned to the Tomatis group will come to the clinic for the Tomatis® Method 5 times per week (Monday - Friday) for 2 hours, for a duration of 2 weeks. For the first stage, the participants will come to the clinic for two extra days (Monday and Tuesday of the third week). The participants will then take a break from the intervention for four weeks. The participants will return for two additional rounds of therapy for ten days each and will have one additional break of 4 weeks in between the 2nd and 3rd stage. On the other hand, the participants who were randomly assigned to the control group will receive no intervention and will remain on the waitlist for delayed intervention. Evaluations will be done in the month preceding the Monday that therapy is scheduled to begin on, at which time each participant will be assigned a time slot for the
120
intervention that will carry through the entire study if in the treatment group. If you are in the control group, you will remain on a delayed intervention waitlist. The participants will be evaluated again one month after the study is completed. The Listening test will be administered per the Tomatis Protocol to all participants in addition to the speech/language testing to be done by a Speech/Language Pathologist prior to, and at the end of the program, the participant was randomly assigned to. Once post-testing is complete, the groups will be reversed, and the control group will receive the exact same intervention that the intervention group just finished, and the intervention group will receive no intervention, as was the case for the initial control group. All participants will once again be evaluated at the end of the intervention received by the second group, i.e., the initial control group. The entire study will be at no charge to the participants.
The entire study will be done at the address stated below after school hours so that it does not interfere with a student's academic life.
The potential benefits of the program include improvement in sensory processing leading to calmer, more focused, and attentive states of being. Improved communication skills related to improved auditory processing abilities. Enhanced ability to learn in the classroom environment due to better Sensory Processing Capacity. Improved reading and writing ability. Return to Regular Education Classroom without accommodations.
All the information we gather as well as all the results of this study will be kept confidential. All the results will be anonymous as we will not divulge any names in our write up about the study; only age and gender will be made known in any publications or talks given by the researcher.
The address, at which the study will take place is: If you have any questions please call me at:
4455 W. 117 th St. 310-926-8785
4th floor
Or Email: squenim@gmail.com Hawthorne, CA 90250
121
APPENDIX B
Fielding Graduate University
Informed Consent Form
THE EFFICACY OF THE TOMATIS ® METHOD IN REMEDIATING APD IN CHILDREN
Parental Permission Letter
07-20-2018
Dear Parent:
I am a student in the School of Infant and Early Childhood Development at Fielding Graduate University, Santa Barbara, California and I would like to include your child, along with his or her peers, in a research study about the efficacy of Tomatis® Method in remediating Auditory Processing Deficits. This study is supervised by Dr. Susan Stillman . This study is part of my Fielding dissertation.
If you give permission for your child to participate in this study, he or she will Participate in a study, the purpose of which is to determine whether the Tomatis® Method, a sound training program, results in remediating C/APD. Thirty participants will be chosen at random from the total number of participants who are referred for participation in the study and meet the specified criteria to participate. The participants will be randomly divided into two equal groups. Participants will be evaluated pre-treatment with a battery of various standardized evaluations appropriate for Auditory Processing Difficulties and related learning difficulties.
Half the participants will not receive therapy initially and will serve as the control group, while the other half, the treatment group will receive one program of the Tomatis® Method. At the end
122
of the program, all the participants will be tested again, and the second half will start the program. All participants will be retested once again after the second group has finished the program. The Tomatis® Method consists of 64 hours of vestibular and auditory stimulation using the Tomatis® Method proprietary equipment over a period of 4 months. At the end of the 4-month program, all subjects will be re-evaluated with the same assessments. Pre and post-test result comparisons will be made to ascertain whether the scores account for statistically significant differences in Auditory Processing and related learning difficulties, both in the prepost evaluation and in between the two groups. If change is significant between groups, it will show that the Tomatis® Method remediates APD.
How Many Children Will Take Part In The Study?
We will use 30 participants between the ages of 5 and 11, who have auditory processing difficulties and related learning difficulties, absent any other comorbid diagnoses except for ADHD.
What Is Involved In The Study ?
If in the treatment group, your child will stay at school after school is out for the Tomatis ® Method 5 times per week (Monday - Friday) for 2 hours, for a duration of 2 weeks. For the first stage, your child will stay in school once it is out for two extra days (Monday and Tuesday of the third week). Your child will then take a break from the intervention for four weeks and follow his/her regular school schedule. Your child will return for two additional rounds of therapy for ten days each and will have one additional break of 4 weeks in between the 2 nd and 3rd stage. If in the control group, your child will not take part in the Tomatis® Method initially. Evaluations will be done in the month preceding the Monday that therapy is scheduled to begin on, at which
123
time your child will be assigned a time slot for the intervention that will carry through the entire experiment. The children will be evaluated one month again after the intervention is completed. The Listening test will be administered per the Tomatis Protocol. The control group will then receive the Tomatis® Method, while the intervention group will not. All participants will once again be evaluated at the end of the intervention.
How Long Will My Child Be In The Study?
The study for the treatment group involves 32 total days where the child will remain in school once it lets out. This will last approximately 2 hours/day (Monda y – Friday). The total time involved in participation will be approximately 64 hours. The entire study will span over the school year.
I will explain this research activity to your child so that he or she can understand. Your child may only participate if he or she agrees to do so.
Your decision whether or not to allow your child to participate will not affect the services normally provided to students by his/her school.
The information your child provides will be kept strictly confidential. Your permission allows the researcher, supervising faculty, and possibly a confidential Research Assistant to see your child’s data. Your child’s data may also be inspected by representatives of the Fielding Graduate University Institutional Review Board.
124
The results of this research study will be published in my dissertation and possibly published in subsequent journals, books, or presentations. After the study is finished, a summary of the results will be made available to all parents.
Your child is free to decline to participate or to withdraw from this study at any time, either during or after participation. Should your child withdraw, his or her data will be removed from the study and destroyed.
If you have any questions about the study, please tell me Sharmila QuenimHerr or Dr. Susan Stillman before signing this form. If at any time you have questions about your child’s rights as a research participant, contact the Fielding Graduate University IRB by email at: irb@fielding.edu or by telephone at: 805-898-4033.
Please discuss this study with your child and check the appropriate line below. Two copies of this permission letter have been provided. Please sign and date the bottom of this form. Return one copy to the researcher and keep the other copy for your files
Sincerely,
Sharmila QuenimHerr (Researcher)
Email: squenimherr@email.fielding.edu
Dr. Susan Stillman (Faculty Advisor)
Email: sstillman@fielding.edu
125
ITS – Integrated Therapy Solutions Fielding Graduate University 8885 Venice Blvd. Ste. 105 2020 De La Vina Street Los Angeles, CA 90034 Santa Barbara, CA 93105 310-926-8785 805-687-1099 / 800-340 -1099
I have read and understood the information provided and do / do not (circle one) give permission for my child _____________________________ (name of child) to participate in the research project described above. _____________________________________
PARENT’S NAME (please print) _____________________________________
PARENT’S SIGNATURE _____________________________________
Date
126
APPENDIX C
Fielding Graduate University
Assent for Children Ages 7 – 12
THE EFFICACY OF THE TOMATIS ® METHOD IN REMEDIATING APD IN CHILDREN
Dear Participant, I am a student at Fielding Graduate University. I am doing a project to see if the Tomatis® Method, which is the name of a sound training program, will help a child be able to listen to and understand what other people are saying more easily. You are one of the thirty children who were asked to take part in this project because you find it difficult to understand what other people are saying. We will divide the thirty of you into two equal groups. We will do some testing before you start the program and again when you have finished the program to see if the program was able to help you in understanding the other people better than before you did the program. For this project, half of you will do the Tomatis® Method right after you are first tested. The Tomatis® Method will be done in a classroom in your school where you and other children in your group will listen to music and also repeat words and sing for 2 hours every day that you come to the center. You will be playing with the other children and a therapist who will be making sure your music is playing properly and that you are comfortable while listening. You will first stay in school after school ends for 12 days from Monday – Friday, and then you will go home as usual after school for four weeks. You will then stay after school for ten days and then again take a break for four weeks. You will then stay after school one last time for 10 days,
127
and that will be the end of the program. You will then be tested again one month after you finish the program. The second half will do exactly the same, but after the first group has been finished.
While you are listening, you may get a little emotional or uncomfortable. Some children get very tired. If you do get tired or feel upset, please talk to your mum or dad, your teacher, and myself. You can also talk to the therapist who is with you during your listening so we can help you through the program.
I am happy to answer all your questions at any time. You can call me at 310-926-8785, or you can ask your mum or dad to help you email me at squenimherr@email.fielding.edu
By signing this form, you are saying that you would like to participate and agree that you will get the therapy either immediately or later after the first group has finished. I a m also asking your parent or guardian to sign a Parental Permission Form, which will give you permission to join one of our groups. Thank you very much,
Sharmila QuenimHerr
128
I have thought about being in this program. If I have any questions, I have asked them and gotten answers.
I agree to be in this study. I know I do not have to agree. I also know that I can change my mind and quit at any time. I know that I can talk to my parents or Sharmila QuenimHerr about not being in this study at any time.
This project is under the supervision of:
Dr. Susan Stillman
Email: sstillman@fielding.edu
Fielding Graduate University
2020 De La Vina Street
Santa Barbara, CA 93105-3814
805-687-1099
129
___________________________ _____________________________ ________ Name Signature Date
APPENDIX D
Fielding Graduate University
Parent Feedback Form
Client Name: ______________________________________
Date: __________________
Form Competed by: ________________________________________________________
Please note overall changes in the following areas:
Key:
-2= Significant negative change
-1 = negative change
0 = no change
1 = positive change
2 = significant positive change
A: Sleep Comments
B: Eating Habits
C: Toileting
D: Responses to sound
E: Responses to touch
130
-1 0 1 2
-2
-1 0 1 2
-2
-1 0 1 2
-2
-1 0 1 2
-2
-1 0 1 2
-2
131
Responses to movement -2 -1 0 1 2 G: Mood/behavior -2 -1 0 1 2 H: Activity Levels -2 -1 0 1 2 I: Attention -2 -1 0 1 2 J: Spatial Awareness -2 -1 0 1 2 K: Gross Motor Coordination Skills -2 -1 0 1 2 L: Fine Motor Coordination Skills -2 -1 0 1 2 M: Play Skills -2 -1 0 1 2
Self Care Skills (feeding, dressing) -2 -1 0 1 2
Listening Skills -2 -1 0 1 2
Communication & Language -2 -1 0 1 2
F:
N:
O:
P:
Further Comments (changes in routine, structure, family situation) and any examples:
Please use these examples as a guide to help you complete the weekly Observation form.
A. Sleep ( i.e., duration, frequency of night waking, sleep patterns, nap schedule, bedtime routine including ease of falling asleep, increased awareness of own needs).
B. Eating (i.e., food/taste preferences, increased oral motor skills, sitting at mealtimes, taste/smell tolerance, reduced or increased mouthing, gagging, biting, increased awareness of own needs).
C. Toileting (i.e., bladder/bowel issues, bed wetting, toilet training status, independence in self toileting).
D. Response to sound (i.e., tolerance for sounds, noticing new sounds in the environment, the speed at identifying sounds, recognition of sounds, reaction to noise, e.g., covering ears; screaming; crying).
E. Response to Touch (i.e., participation in messy play, tolerance of grooming, e.g., hair washing teeth cleaning, the texture of clothes, tolerance of food textures, increased awareness of touch, seeking touch, awareness of temperature/pain, level of force/pressure used in fine motor play).
F. Response to Movement (i.e., tolerance of a variety of movement, e.g., playground equipment, level of avoidance of movement activities, seeking excessive movement, lack of safety awareness, less fear of movement).
G. Mood & Behaviour (i.e., tantrums, tolerance for transitions and/or routine changes, reduced crying, less clingy, reduced aggression, level of anxiety/stress, increase range of moods appropriate to the situation, less self-stimulatory/repetitive behaviors, e.g., rocking; flapping).
132
H. Activity Levels (i.e., over-responsive/hyperactive, under-responsive/low activity levels, energy levels).
I. Attention (i.e., level of alertness appropriate to the activity, distractibility, ability to attain and maintain attention during independent and adult-led tasks, amount of “on-task” behaviors).
J. Spatial Awareness (i .e., tolerance of open or closed spaces, e.g., supermarkets/lifts, awareness of self in relation to others and the environment, need to touch everything in the room to understand the space, improved visual motor skills, improved handwriting).
K. Gross Motor Coordination Skills (i.e., the level of participation in gross motor activity, e.g., P.E.; sports; dance, quality of movement, falling over less, improved ball skills, improved skills, e.g., jumping; hopping).
L. Fine Motor Coordination Skills ( i.e., pencil control, handwriting, use of tools, e.g., scissors; cutlery, buttons/shoelaces).
M. Play & Social Skills (i.e., the expansion of play skills, play alone or with others, use of pretend play less controlling in play, less structured in play).
N. Self-Care Skills ( i.e., development of skills, improved organization, length of routine, improved independence, level of participation, rigidity of hygiene rituals).
O. Listening Skills ( i.e., ability to follow instructions, ability to tune into sounds, ability to tune out background noise).
P. Communication & Language (i.e., eye contact, awareness of others, range of facial expressions, appropriateness of interactions/use of voice, able to verbalize needs, level of peer interaction, use of language/words).
133
* Failure is at -2SD. The number of failures refers to the number of participants that did not achieve a pass rate in the test and, therefore, would require intervention for APD.
134
APPENDIX E
Table E1
Measure Group Test n Mean SD Range Total Number of *Failures RNC Treatment Pre-test 3 5.7 2.8 2 - 11 100 % Post-test 3 0.3 1.9 0 - 1 0% Control Pre-test 4 4.5 1.00 3 - 5 100% Post-test 4 2.75 0.00 3 - 5 75% RC Treatment Pre-test 3 8.67 6 2 - 19 33% Post-test 3 2 6 2 - 4 0% Control Pre-test 4 9.25 0.00 6 - 15 100% Post-test 4 10.5 2.50 6 - 18 100% LC Treatment Pre-test 3 15.3 5.6 8 - 25 67% Post-test 3 6 6 4 - 6 67% Control Pre-test 4 14.5 3.51 11 -18 100% Post-test 4 15.5 3.79 10 - 18 100% LNC Treatment Pre-test 3 6 1.8 4 -9 100% Post-test 3 1.3 1.7 1 - 3 33% Control Pre-test 4 5.25 1.26 4 - 7 100% Post-test 4 3.25 1.50 2 - 5 50% REV Treatment Pre-test 3 4 3.6 2 - 6 67% Post-test 3 1.67 1.7 1 - 3 0% Control Pre-test 4 10.25 1.26 9 - 12 100% Post-test 4 10 1.83 2 - 5 100%
Auditory Processing Speed , The SSW test
Table E2
Assessment Group Test n Mean SD Range Improve Decline No change SCAN-3:C Auditory Processing Composite Treatment Pre-test 3 88.66 6.429 84-96 3 0 0 Post-test 3 117.00 6.000 111-123 Control Pre-test 4 82.25 22.20 65-113 0 4 0 Post-test 4 71.25 11.98 61-86
Auditory Processing Composite , The SCAN-3:C Test
Cognitive Abilities, Woodcock Johnson IV Test (WJ -IV)
135
Table E3
Assessment Group Test n Mean SD Range Improve Decline No Change Visualization Treatment Pre-test 3 94.66 8.14 89-104 3 0 0 Post-test 3 108.67 17.47 94-128 Control Pre-test 4 87.50 6.95 79-96 4 0 0 Post-test 4 98.75 7.18 88-103 VisualAuditory Learning Treatment Pre-test 3 94.00 12.76 83-108 3 0 0 Post-test 3 118.33 18.82 106.140 Control Pre-test 4 86.00 3.829 83-91 3 1 0 Post-test 4 84.75 8.53 73-92
Table E4
CLUSTER/Test Group Test n Mean SD Range Improve Decline No change LISTENING COMPREHENSION Treatment Pretest 3 97.66 10.40 86-106 3 0 0 Posttest 3 116.33 0.57 116-117 Control Pretest 4 80.75 10.62 73-96 1 3 0 Posttest 4 75.75 11.64 61-89 Oral Comprehension Treatment Pretest 3 104.33 12.42 90-112 3 0 0 Posttest 3 119.00 1.00 118-120 Control Pretest 4 84.50 9.469 76-98 1 2 1 Posttest 4 82.50 6.95 76-92 Understanding Directions Treatment Pretest 3 91.00 6.24 86-98 3 0 0 Posttest 3 107.66 1.52 106-109 Control Pretest 4 81.25 12.52 70-94 1 3 0 Posttest 4 75.00 13.83 56-89
Oral Comprehension , Woodcock Johnson IV Test (WJ -IV)
Table E5
Phonological Awareness, The CTOPP-2 Test
136
Assessment Group Test n Mean SD Range Improve Decline No change CTOPP-2 Phonological Awareness Composite Treatment Pretest 3 86.66 9.86 80-98 3 0 0 Posttest 3 107.33 13.61 92-118 Control Pretest 4 72.50 11.387 56-82 0 3 1 Posttest 4 67.25 7.50 56-71 Elision Treatment Pretest 3 7.33 2.30 6-10 3 0 0 Posttest 3 9.66 1.527 8-11 Control Pretest 4 6.00 2.82 4-10 0 3 1 Posttest 4 3.25 1.50 1-4 Blending Words Treatment Pretest 3 9.33 1.15 8-10 2 0 1 Posttest 3 11.66 1.52 10-13 Control Pretest 4 5.50 1.29 4-7 1 2 1 Posttest 4 5.25 0.957 4-6 Phoneme Isolation/Sound Matching Treatment Pretest 3 6.66 2.08 5-9 3 0 0 Posttest 3 11.66 3.21 8-14 Control Pretest 4 5.25 3.50 1-9 2 2 0 Posttest 4 5.75 1.25 4-7
137
Table E6
Composite/subtests Group Test n Mean SD Range Improve Decline No change CTOPP-2 Phonological Memory Treatment Pretest 3 81.00 7.54 73-88 3 0 0 Posttest 3 99.00 6.928 95-107 Control Pretest 4 75.25 9.60 67-85 3 1 0 Posttest 4 81.50 11.958 70-95 Memory for Digits Treatment Pretest 3 7.00 3.46 5-11 3 0 0 Posttest 3 8.00 3.46 6-12 Control Pretest 4 8.25 2.217 6-11 1 3 0 Posttest 4 7.5 2.88 4-11 Nonword Repetition Treatment Pretest 3 6.66 2.08 5-9 3 0 0 Posttest 3 11.33 1.15 10-12 Control Pretest 4 3.5 1.73 2-6 3 1 0 Posttest 4 6.25 2.21 3-8
Phonological Memory
Rapid Symbolic Naming , The CTOPP-2 Test
138
Table E7
Composite/subtests Group Test n Mean SD Range Improve Decline No change CTOPP-2 Rapid Symbolic Naming Treatment Pretest 3 79.33 13.65 70-95 1 1 1 Posttest 3 82.33 14.189 67-95 Control Pretest 4 86.00 9.05 79-98 0 4 0 Posttest 4 77.75 10.40 67-92 Rapid Digit Naming Treatment Pretest 3 7.33 2.08 5-9 1 2 0 Posttest 3 7.0 2.64 4-9 Control Pretest 4 8.0 1.82 6-10 0 2 2 Posttest 4 6.25 2.629 4-10 Rapid Letter Naming Treatment Pretest 3 5.66 4.50 1-10 1 2 0 Posttest 3 8.0 2.64 5-10 Control Pretest 4 7.25 1.258 6-9 0 3 1 Posttest 4 6.25 0.957 5-7
Table E8
Full Scale Attention and Auditory Attention Quotient and Visual Attention Quotient, The IVA-2
139
COMPOSITE/ subtests Group Test n Mean SD Range Improve Decline No change IVA-2 FULL SCALE ATTENTION QUOTIENT Treatment Pretest 3 63.50 21.31 43.686 3 0 0 Posttest 3 82.26 22.74 66.9108.4 Control Pretest 3 72.2 38.99 28.8104.3 1 1 1 Posttest 3 72.33 41.52 28.8111.5 IVA-2 Auditory Attention Quotient Treatment Pretest 3 48.60 33.54 20.085.9 3 0 0 Posttest 3 79.76 24.68 63.8108.2 Control Pretest 3 81.66 23.75 60.4107.3 2 0 1 Posttest 3 81.96 28.13 52.40108.4 IVA-2 Visual Attention Quotient Treatment Pretest 3 59.93 26.04 35.987.6 3 0 0 Posttest 3 87.63 18.78 70.8107.9 Control Pretest 3 66.83 51.42 7.7101.1 1 1 1 Posttest 3 65.50 53.47 7.7113.2
Full Scale Response Control Quotient and Auditory Response Quotient and Visual Response
Quotient, The IVA -2 Test
, IM Long Form Test
140
Table E9
COMPOSITE/ subtest Group Test n Mean SD Range Improve Decline No change IVA-2 FULL SCALE RESPONSE CONTROL QUOTIENT Treatment Pretest 3 76.1 23.10 50.194.3 3 0 0 Posttest 3 92.96 8.04 84.199.8 Control Pretest 3 80.60 20.53 59.1100.0 1 2 0 Posttest 3 76.33 23.11 50.193.7 IVA-2 Auditory Response Quotient Treatment Pretest 3 78.06 15.40 64.394.7 3 0 0 Posttest 3 92.50 10.34 83.3103.7 Control Pretest 3 84.26 30.72 50.7111.0 1 1 1 Posttest 3 85.06 30.858 50.7110.4 IVA-2 Visual Response Quotient Treatment Pretest 3 83.36 23.18 56.798.8 3 0 0 Posttest 3 94.06 13.34 79.9106.4 Control Pretest 3 80.86 7.04 76.789.0 1 2 0 Posttest 3 73.13 18.35 59.594.0
Neurotiming
Assessment Group Test n Mean SD Range Improve Decline No change IM Long Form Treatment Pre-test 3 264.73 31.85 230-292.6 3 0 0 Posttest 3 180.30 55.54 117.5-223.0 Control Pre-test 4 221.45 51.43 162.2-282.7 2 2 0 Posttest 4 212.72 50.469 145.80-259.6
Table E10
APPENDIX F
Changes compared by group scores
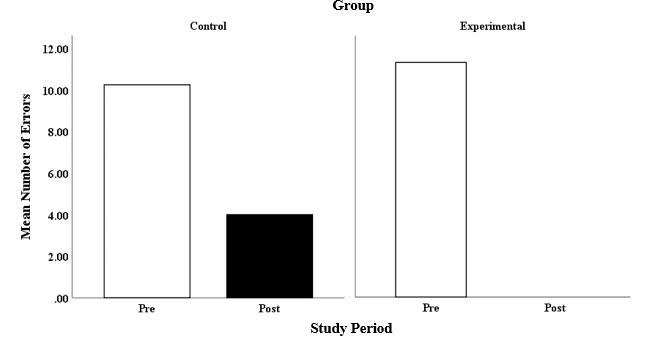
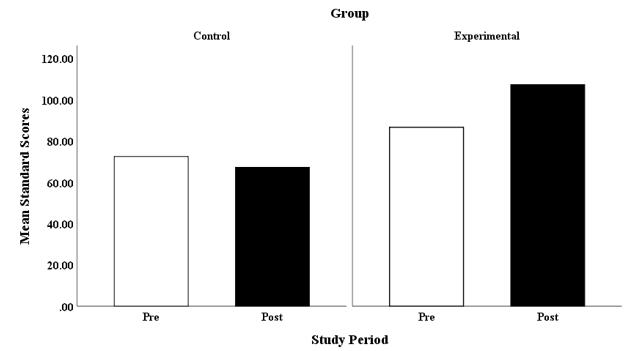
141
Figure F1
SCAN-3:C Auditory Processing Composite Group Scores
Figure F2
SSW:RNC Group Score
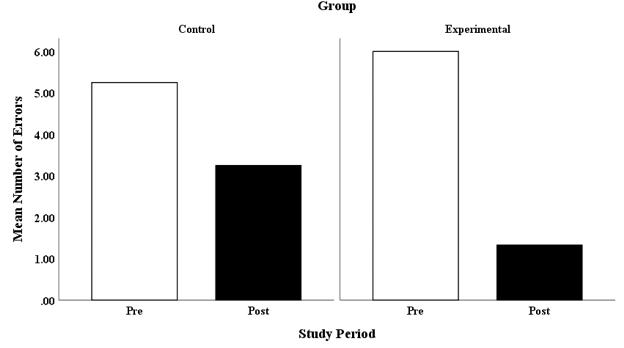
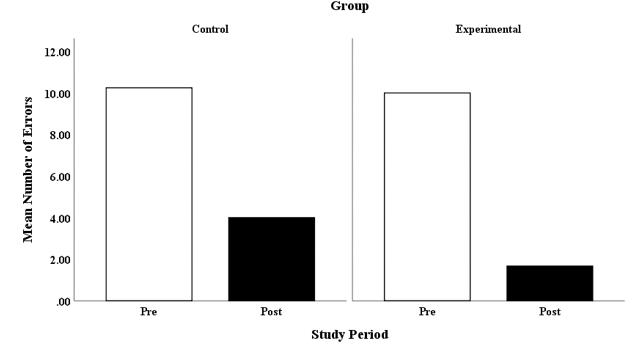
142
Figure F3
SSW:LNC Group Scores
Figure F4
SSW:REV Group Scores
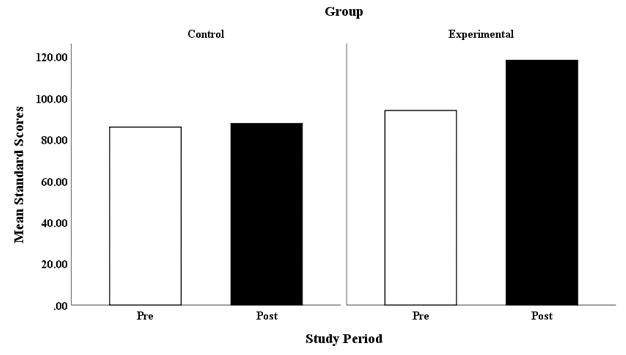
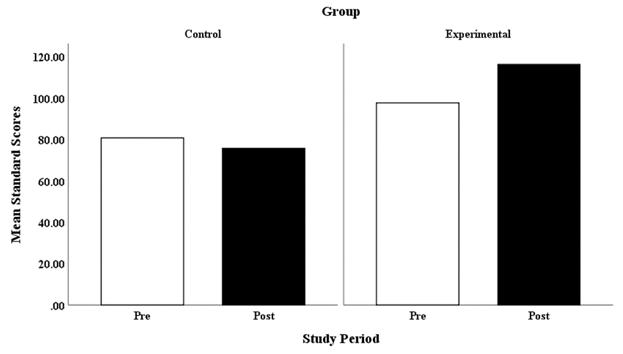
143
Figure F5
WJ-IV: Visual Auditory Learning Group Scores
Figure F6
WJ-IV: Listening Comprehension Group Scores
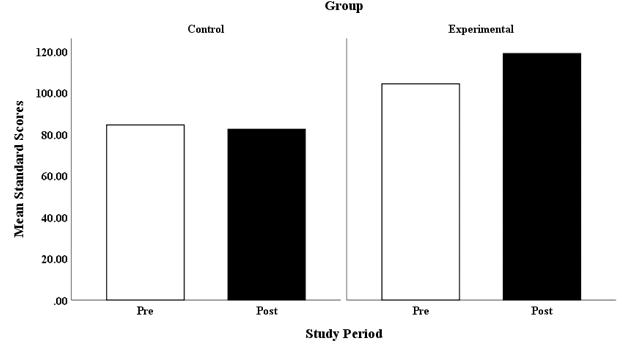
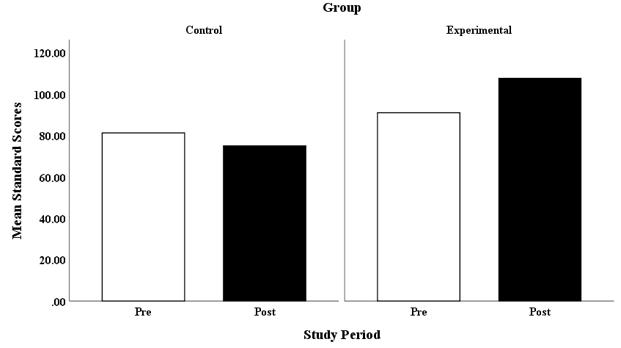
144
Figure F7
WJ-IV: Oral Comprehension Group Scores
Figure F8
WJ-IV: Understanding Directions Group Scores
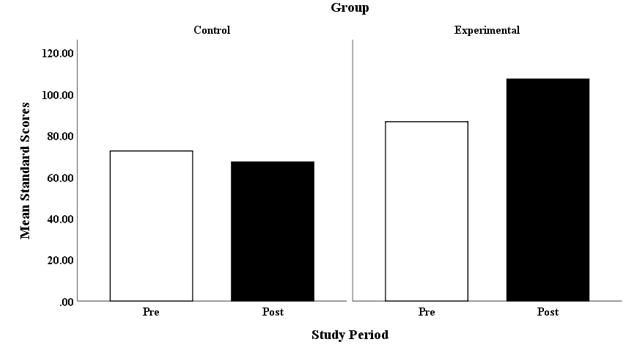
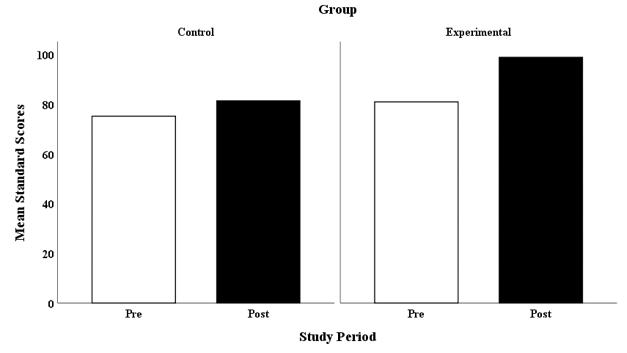
145
Figure F9
CTOPP-2 Composite 1: Phonological Awareness Group Scores
Figure F10
CTOPP-2 Composite 2: Phonological Memory Group Scores
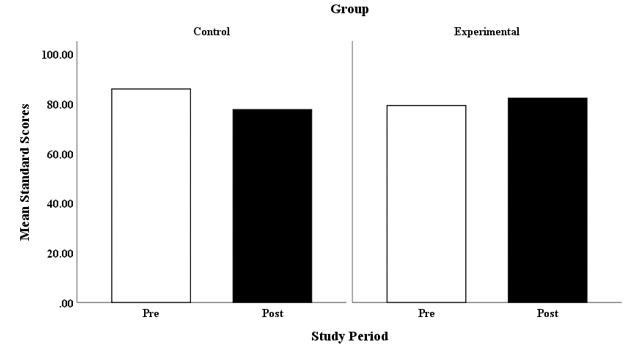
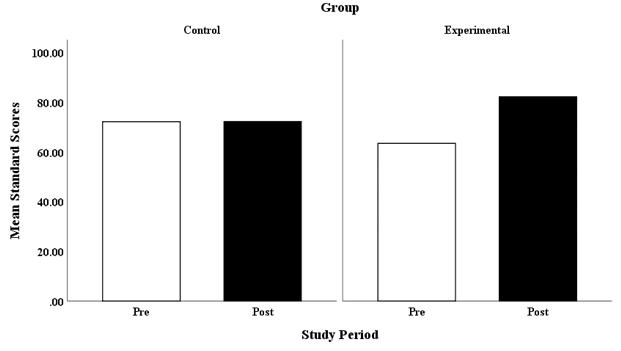
146
Figure F11
CTOPP-2 Composite 3: Rapid Symbolic Naming Group Scores
Figure F12
IVA-2: Full Scale Attention Quotient Group Scores
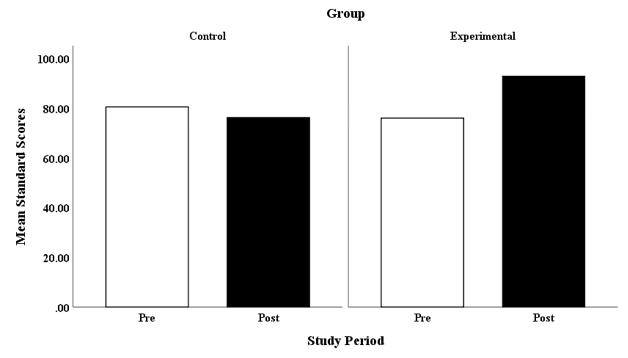
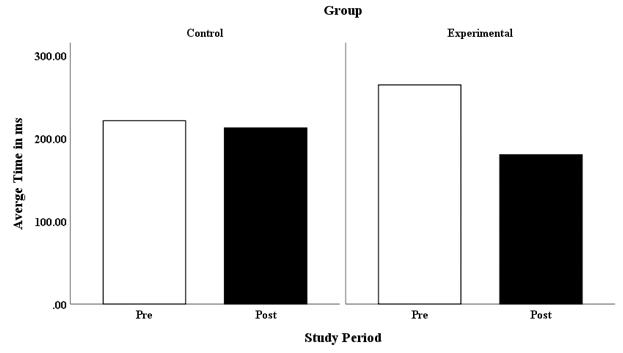
147
Figure F13
IVA-2: Full Scale Response Quotient Group Scores
Figure F14
IM: Long Form Neurotiming Group Scores
ProQuest Number:
28490846
INFORMATION TO ALL USERS
The quality and completeness of this reproduction is dependent on the quality and completeness of the copy made available to ProQuest. Distributed
This work may be used in accordance with the terms of the Creative Commons license or other rights statement, as indicated in the copyright statement or in the metadata associated with this work. Unless otherwise specified in the copyright statement or the metadata, all rights are reserved by the copyright holder.
This work is protected against unauthorized copying under Title 17, United States Code and other applicable copyright laws.
Microform Edition where available © ProQuest LLC. No reproduction or digitization of the Microform Edition is authorized without permission of ProQuest LLC.
ProQuest LLC

789 East Eisenhower Parkway P.O. Box 1346
Ann Arbor, MI 48106 - 1346 USA
by
LLC
). Copyright of the Dissertation is held by the Author unless otherwise noted.
ProQuest
(
2021