Business Development Manager: Andrew Jackson Ph: 0400 604 646 ajackson@wfmedia.com.au
PUBLISHED BY Westwick-Farrow Media
A.B.N. 22 152 305 336 www.wfmedia.com.au
Head Office Unit 5, 6-8 Byfield Street, North Ryde Locked Bag 2226 North Ryde BC NSW 1670 AUSTRALIA ph: +61 2 9168 2500
If you have any queries regarding our privacy policy please email privacy@wfmedia.com.au
Subscriptions for unregistered readersprice on application
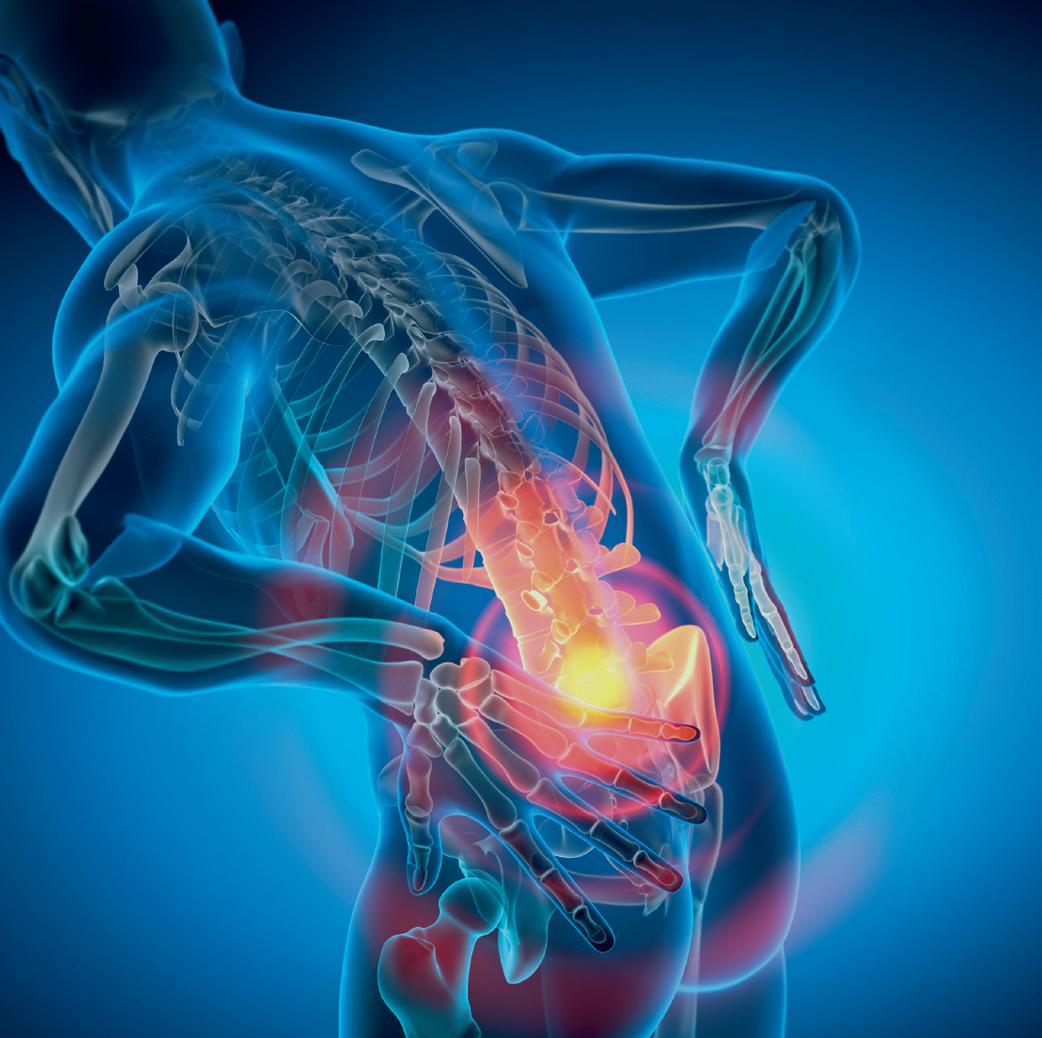
A new way to conceptualise pain
The idea that a patient’s pain is always trying to tell us something is an increasingly outdated notion.
These days, pain researchers — and much of the medical community — accept that pain can be a disease in its own right; and is not always justified by something physical.
As multi-award winning clinical consultant pharmacist and pain management educator Joyce McSwan puts it, “Pain is meant to serve a function — to alert us to keep away from its trigger. But sometimes our pain response can become dysregulated and out of proportion.
“The communication pathways in our body can become overprotective and tell us that a stimulus is harmful when it may not be,” she said.
In fact, McSwan — who is also the founder of PainWise — estimates that this misfiring of the body’s pain response accounts for around 40–50% of chronic pain cases.
She says events, like moving furniture, can cause a severe pain reaction in people living with chronic lower back pain, even if an injury did not occur.
“It can be debilitating and the patient can be convinced they have torn something — but nothing is coming up in imaging, and there are no other physical red flags, like signs of numbness or weakness of legs.
“In this case, it is likely due to musculoskeletal or nerve sensitivity that has caused the pain flare-up. It could also be a limbic response — a psychological trigger or somatic memory of a former injury or combination of both,” she said.
McSwan also says that pain is complex, meaning it can be challenging for healthcare workers to distinguish between pain with a physical cause, and a dysregulated sensitised pain response. Especially when the two can co-occur.
“The lines can become blurred and it is challenging for both clinician and patient to decipher what is going on,” she said.
“Likewise, you could have someone with a chronic disease like arthritis, who has also gained weight and become more sedentary, with mental health implications. Even the slightest of movement can set off a severe pain response in this individual — and that response can be disproportionate to the arthritic pain they previously lived with.” >
Develop multidisciplinary pain expertise
To handle pain cases appropriately, McSwan says clinicians need to understand pain as an area of study “really well”.
“If you aren’t confident doing differential diagnosis for pain, you can easily go down the wrong rabbit hole and offer patients the wrong advice and treatment.
“Understanding the relationship between pain and lifestyle factors like smoking, weight gain and even a person’s gait keeps it holistic,” she said.
Next, the clinician should get to know the patient’s history intimately, she recommended.
“Once upon a time, they may have had an acute fall. Then, other insidious episodes might have made it more sensitive.
“Now, the patient avoids moving because it hurts too much. They are unable to work and their mental health has been affected.
“At this point, the flare-up is starting to sound like a pain syndrome. So, unless there are obvious red flags, there is little gained in doing an MRI,” she said.
Calm down the dysregulation
Assuming the patient has a chronic pain syndrome, and not an acute injury, McSwan says a few simple techniques can work.
“To handle pain cases appropriately, McSwan says clinicians need to understand pain as an area of study “really well”.”
“In place of opioids, patients with severe low back pain could be given low intensity heat wrap therapy for a prolonged period, prompted to walk regularly within their pain threshold and simple analgesia only if appropriate.
“Giving patients a plan is reassuring and will help them to self-monitor and only return to ED if they deteriorate or have red flag symptoms.”
Managing patient expectations
Even though this approach has been shown to work in ED settings, McSwan warns that denying people medication could cause distress.
“Most patients with severe pain expect medication, so it can be really hard to use a different approach,” she said.
Likewise, telling someone an MRI is unnecessary could be invalidating, she warned.
“It might come across as though you are not taking the pain seriously — or that you think it’s all in the patient’s head.
“No-one with a suspected slipped disk or torn ligament wants to hear that their agony is just pain syndrome or a limbic response.”
With this in mind, McSwan said good communication is essential, as is talking through the rationale for your diagnosis.
“After collecting their history, you might want to provide the evidence that explains the pain syndrome. At the same time, you should still acknowledge that their pain is very real and affecting them.
“Just because there isn’t a mechanical reason for it, it doesn’t make the pain any more tolerable. It just necessitates a different treatment approach,” she concluded.
Joyce McSwan
Building awareness around deprescribing and sustainability
Kristin Michaels, Chief Executive of Advanced Pharmacy Australia (AdPha)
Awareness of medicines safety is important in every care conversation.
In 2023, Advanced Pharmacy Australia (AdPha), then known as SHPA, launched MedsAware: Deprescribing Action Week — a campaign to encourage care conversations around the risks associated with ‘polypharmacy’ and the benefits that can come from ‘deprescribing’.
As a professional body representing medicines experts in this age of patientcentred care, we saw this wonderful opportunity to build awareness for a process which ultimately should be a collaboration between patient and provider. Our overarching aim through MedsAware was to embed deprescribing as a central principle of health care, to reduce polypharmacy and ensure more people stay out of hospital. Indeed, the first use of ‘deprescribing’ in medical literature was published in our flagship journal — the Journal of Pharmacy Practice and Research (JPPR) — in 2003.
In only two years, MedsAware has reached a cumulative Australian audience greater than 11 million, grown its social media footprint by 30%, enlisted seven partners representing medical, pharmacy and aged care stakeholders and has received government support from Australian senators and MPs. Deprescribing 101
The need to broaden understanding around deprescribing is urgent.
In Australia, 250,000 people are admitted to hospital each year due to medicatedrelated issues.
Numerous studies show that much of this can be attributed to polypharmacy and inappropriate use of medicines.
For example, research suggests that onequarter of people on multiple medicines have adverse effects directly attributable to the additive effects of those medicines.
And the problem only looms larger in vulnerable cohorts of patients, with evidence showing that psychotropic medicines are being overused to control challenging behaviours in older people and people with disability.
As our population ages, we can’t ignore the impacts that unchecked polypharmacy will have on our health system.
And it’s not just our health system that suffers, the effects can be felt all around us.
Globally health systems account for 4.4% of all greenhouse gas emissions and sadly for us in Australia this number sits even higher at 7%. Hospitals and medicines have a significant carbon footprint, accounting for two thirds of Australia’s healthcare emissions. This makes Australia one of the highest emitters of greenhouse gases related to healthcare in the world.
For patient and planet
As health professionals we have a responsibility to be thinking about sustainability in everything we do. For we are not just health professionals, but also global citizens.
Building ‘planetary consciousness’ in healthcare practice, policy, research, and education is critical; we cannot ignore the fact that climate change is the biggest health threat of this century. Reducing the impact of medicines on the natural environment is indeed a fundamental principle of Australia’s National Medicines Policy and a key objective of both the Health Technology Assessment (HTA) Policy and Methods Review and the Australia’s National Health and Climate Strategy.
So this year, MedsAware will seek to empower both safe and sustainable use of medicine. By taking small, conscious steps, beginning with
a simple conversation between patient and health provider, we can all help reduce the environmental impact of medicines.
A core tenet of Advanced Pharmacy Australia is collaboration, and MedsAware has enabled us to collaborate with numerous health and medical groups with a shared goal to keep Australians out of hospital by improving medicines use. These stakeholders extend from medicine, general practice to aged care. This year we are particularly proud to take this important message internationally with the support of the European Association of Hospital Pharmacists (EAHP) as well as our ongoing partner, the International Pharmaceutical Federation (FIP).
Through the support of our many partners, our hope for MedsAware 2025 is to show that deprescribing affords us the opportunity to not only improve medicines safety and patient care directly, but to contribute to a more sustainable and healthier planet.
To find out more, visit https://adpha.au/newsadvocacy/MedsAware.
Kristin Michaels, Chief Executive of Advanced Pharmacy Australia (AdPha)
Predicting chronic pain within three days of injury
After only one to three days of a whiplash injury, scientists can predict which patients will develop chronic pain based on the extent of ‘cross-talk’ between two regions of the brain, and the person’s anxiety level after the injury, according to a new Northwestern Medicine study.
The study showed the more the hippocampus, the brain’s memory centre, talked to the cortex — involved in long-term memory storage — the more likely the person is to develop chronic pain.
In addition, the higher a person’s anxiety immediately after the car accident, the more precisely scientists could predict the chronic pain people reported one year after the accident.
Heightened activity, a risk factor
The communication between the hippocampus and the cortex is thought to be indexing the formation of new memories related to the subject’s accident and pain, said first author Paulo Branco, assistant professor of anaesthesiology and pain medicine at Northwestern University Feinberg School of Medicine.
“The hippocampus is responsible for consolidating new memories into long-lasting ones,” he said.
While the researchers don’t know why this heightened connectivity is a risk factor for chronic pain, they hypothesise that the brain of these individuals has encoded a strong memory associating a head and neck movement with pain.
“This creates expectations and associations,” Branco said.
“If the memory has high emotional significance, then it makes these patients associate this movement with pain. When the brain receives these signals, it pays more attention to them based on the painful memories that were formed by the accident.
“While we commonly think of pain as relating only to an injury, it is the brain that actually makes up the pain experience,” he said. “The brain makes the decision about whether a movement should be painful or not, and we think this may rely on previous experiences stored in memory.”
Timing of pain and prevention strategies
“Now that we know there is this critical time period when this happens, we can focus our treatment efforts at this early stage to prevent
chronic pain rather than try to cure it, which is much more difficult,” said corresponding author Apkar V Apkarian, Director of the Center for Translational Pain Research and a professor of neuroscience at Feinberg.
“Since anxiety plays an important role for the brain changes, targeting the anxiety immediately after the injury may be able to halt these changes, possibly through anti-anxiety drugs or other medications,” Apkarian said. “Future novel treatments targeting hippocampal activity and connectivity through pharmacology or through neuromodulation techniques also are possible.”
The Apkarian lab has shown in previously published research that, beyond injury parameters, the brain plays a critical role in the development and maintenance of chronic pain. But until now the mechanisms of that remained poorly understood. How and why
does the brain predispose patients to develop chronic pain? And is there a critical period during which brain changes occur that place patients at risk for chronic pain? The new study answers those questions.
Current treatments for chronic pain remain minimal and unacceptable, researchers said, and as a result a large proportion of patients use opioids, contributing to the ongoing national opioid epidemic.
Identifying early predictors
This large-scale longitudinal study was conducted through a collaboration between the Technion-Israel Institute of Technology, Northwestern University and McGill University.
Researchers collected the largest longitudinal brain-imaging dataset to date with more than 200 whiplash patients recruited, 177 of whom completed magnetic resonance imaging testing. The goal of the study was to identify
early predictors of the transition from acute to chronic pain.
This patient population provided a unique opportunity to study early brain changes after injury, as the onset of pain can be traced back to the time of the accident. The data was collected from March 2016 until December 2021.
Patients underwent functional magnetic resonance imaging within three days of injury, allowing investigators to examine brain activity in regions implicated in learning and memory at this critical timepoint. These patients were then followed over the next 12 months to assess pain levels and track which individuals developed chronic pain and which ones recovered. Participants also performed a large array of psychological and psychophysical tests, which investigators used to complement brain-imaging findings.
What’s next?
In the short term, the investigators plan to further study the underlying mechanisms behind the hippocampal response to injury, by assessing which additional physiological (cortisol, inflammation) and psychological (trauma and stress-related disorders, fear of movement) factors may further drive these brain mechanisms.
They also aim to test whether these findings are generalisable across other chronic pain conditions. In the long term, the goal is to target these maladaptive responses early after injury to test their causal role in the development of chronic pain. This could involve the use of pharmacological treatments, cognitive-behavioural therapy or transcranial magnetic stimulation.
This research was supported by the Department of Defense, National Institute on Drug Abuse and the National Institutes of Health.
Progress on new hypertension and lipid guidelines
Lipid and hypertension related health issues affect millions of Australians — around 4.5 million Australian adults have high blood pressure and 8.5 million have abnormal blood lipid levels. Each is a major risk factor for cardiovascular disease and stroke.
In a bid to improve outcomes, the Heart Foundation and the Stroke Foundation have joined forces to progress the development of two bespoke sets of guidelines: one for managing and treating hypertension (high blood pressure) and another for managing and treating lipids (such as cholesterol).
The development will be progressed by both foundations in collaboration with Hypertension Australia, clinical and disease prevention communities, and those working primary health care, with whom collaboration is essential for achieving a new standard of best practice.
The foundations will conduct a systematic review of existing literature later this year, with key stakeholders invited to participate. It is anticipated that the two new guidelines will be finalised and ready for implementation early next year (2025).
The work will support the Roadmap of the Hypertension Taskforce.
Heart Foundation CEO David Lloyd said, “There have been significant advances in medications
and treatments for these conditions in recent years. These advancements make the current guidelines outdated.
“The Heart and Stroke Foundations are very much looking forward to working with key stakeholders from the clinical and disease prevention communities to design new guidelines that ensure patients receive the most up-to-date and evidence-backed advice for their health care.”
While the lipid guideline is completely new, the hypertension guideline is an update of the 2017 Heart Foundation/High Blood Pressure Council of Australia Guideline and should be smaller in scale.
There have been significant advances in medications and treatments for lipids and hypertension in recent years, making new guidelines and an update necessary, according to the Heart and Stroke Foundations.
Lipids and hypertension have been covered in part in the 2023 Heart Foundation/Australian Chronic Disease Association Risk Prediction Guideline and the forthcoming Heart Foundation/Cardiac Society of Australian and New Zealand Acute Coronary Syndromes Guideline. However, this will be a more comprehensive review. Implemented together, these four guidelines will complement each
other and help reduce the chronic disease burden in the Australian community.
Stroke and heart attacks are largely preventable through best-practice management of risk factors such as cholesterol and hypertension, reminded Stroke Foundation CEO Lisa Murphy.
“The Australian clinical and disease prevention sectors have an exciting opportunity to help us progress the review and redesign of a global gold standard in clinical guidelines for helping people improve the management of their cholesterol and blood pressure,” Murphy said.
“Health professionals, particularly in primary care, are seeking guidance on new therapies that have become available since the previous guidelines were released, recent evidence on thresholds and targets for treatment, and new diagnostic technologies,” the foundations said in a statement.
New guidelines are essential for ensuring that patients receive the most current and evidence-based treatments, the statement said.
The Australian Atherosclerosis Society is also supporting the initiatives of the Heart and Stroke Foundations to update current guidelines.
Your chemical dosing options for on-premise laundry
Operators of on-premise laundry facilities in hospitals, care homes and other healthcare settings are now faced with a comprehensive choice of chemical dosing solutions. With so many options available, dosing systems expert SEKO looks at the various units available in the market today.
Peristaltic
A peristaltic pump is a motor-driven system that rotates in order to turn rollers (normally two or three) which have flexible peristaltic tubing passing between them. The rotation of the rollers compresses the peristaltic tubing, forcing the chemical to be pumped through to the next phase of the process.
Peristaltic pumps can inject chemical in accurate, consistent increments and offer a low maintenance requirement, with only the tubing to be replaced over time.
SEKO’s peristaltic laundry range includes WashMulti Peri, which offers precise automated chemical injection for as many as 16 washers and is designed to serve machines handling up to 100 kg — ideal for larger sites processing heavy volumes of bed linen, towels and uniforms.
Solenoid
Solenoid-driven dosing pumps generate a magnetic field that pulls or pushes a plunger or piston to regulate the flow of chemical. Thanks to their precise flow control, low power consumption and minimal maintenance, solenoid dosing systems are
a popular choice for on-premise laundries where high wash standards must be achieved in the face of budgetary constraints.
WashMulti Solenoid is among SEKO’s most popular on-premise laundry solutions, favoured across the healthcare sector for its vast array of dosing options. The system can inject as many as eight chemicals and stores up 100 formulas, all accessible via an intuitive user interface.
Pneumatic
Air-driven chemical dosing systems help operators reduce maintenance requirement and costs thanks to the absence of consumable parts such as peristaltic tubing. Pneumatic systems offer precise, consistent detergent injection and can be modified depending on the viscosity of the chemical being pumped.
SEKO’s leading air-driven laundry product is WashMulti Air, which offers multiple flow rates up to 360 litres per hour and features a Proof of Dosing flowmeter to guarantee dosing accuracy.
The system’s flush sequence before and after dosing avoids contamination and reduces chemical contact time, meaning healthcare managers can rely on their laundry dosing system to perform every time.
Venturi
Venturi-based dosing products use only water power to draw chemical and because of the absence of moving parts are an excellent
choice for operators looking to reduce maintenance costs and downtime.
SEKO’s award-winning LS100 is a leading venturi-powered dosing system, injecting up to 10 chemicals in as many as four washers, making it perfect for healthcare on-premise laundries of every size. Plus, its modularity means operators can easily add additional units as their laundries grow.
As well as delivering hundreds of thousands of doses before users even need to think about venturi cartridge replacement, the intelligent system includes an intuitive touchscreen display and ergonomic formula selector for ease of use and error reduction.
IoT-enabled
The development of the Internet of Things (IoT) has seen on-premise laundry dosing system manufacturers begin to include the technology in their equipment in recent years. By connecting products to PCs, laptops and smart devices, users are able to access process data such as chemical consumption at their convenience, providing invaluable insight into their laundry’s cost while highlighting opportunities for savings.
SEKO is at the heart of this revolution, with its unique SekoWeb and SekoBlue apps which offer 24/7 remote access to laundry equipment. Operators can check system status and adjust programming in an instant for immediate improvements while reducing unnecessary travel as part of a sustainable operation.
Surrounded by pristine bushland and bringing together a unique blend of nature, architecture and medicine, Wyvern Private Hospital in the Sydney suburb of Terrey Hills is designed to meet the Gold WELL Building Standard, which recognises buildings that foster a culture of health, wellbeing and quality of life indoors.
Construction of the hospital began in April 2022 and was accompanied by a comprehensive biodiversity management and environmental stewardship plan that included the planting of 250 banksia trees, installation of 39 nestboxes and clearing of litter to protect local wildlife.
The $100 million-plus private surgical and rehabilitation hospital services Sydney’s Northern Beaches community, an aging catchment forecast to see a 23% rise in retiree-aged residents by 2031.
With the launch of the hospital, more residents in the Northern Beaches are now able to access private surgical and rehabilitation services closer to home, and experience what is perhaps the state’s most natural and tranquil clinical setting, said Dr William Sears, founder and Chairman of Wyvern Health. >
Images courtesy of Wyvern Private Hospital.
The philosophy to build a hospital ‘by the doctors for the patients’ has guided Wyvern Health since inception — this includes the choice of site, hospital design, surgeon and other staffing decisions. The hospital’s vision and mission to provide ‘care without compromise’ informs its approach to every aspect of care for patients, staff, community and the environment.
The hospital’s facilities include eight operating theatres including a hybrid theatre and cardiac cath lab, 76 surgical and inpatient beds, nine ICU beds and clinical support units including medical imaging, pathology, rehabilitation, hydrotherapy pool and pharmacy. Owned by the $3.6 billion Australian Unity Healthcare Property Trust
(AUHPT), the hospital is leased for 30 years to Wyvern Health, which operates under a doctor-owned model.
Chris Smith, General Manager Healthcare Property at Australian Unity, said both the local community and investors will benefit from the operations of Wyvern Private Hospital.
“Australian Unity is proud to be partnering with Wyvern Health to deliver world-class health infrastructure to meet Sydney’s current and future needs. The hospital is a key asset in our healthcare property portfolio and will deliver long-term income returns for investors whilst providing critical care to the community,” Smith said.
Images courtesy of Wyvern Private Hospital.
A 3D approach to clinical problems
Could anatomically accurate 3D printed models mimic exactly the way body parts feel and move?
Biomedical engineers at UNSW Sydney have ambitious plans to explore ways to make 3D model even more useful for medical professionals, by developing the use of different printing materials that recreate the complex way body parts feel and move.
The plans come after researchers at the Tyree Foundation Institute of Health Engineering (IHealthE) recently designed and created a patient-based anatomical 3D model of a young child’s skull which helped surgeons devise and plan an innovative way of successfully removing a life-threatening tumour.
The team also created an exact replica of a specific patient’s trachea (windpipe) to help clinicians determine whether a certain surgical procedure could be performed safely.
3D printed models
“What we have been doing is making patientspecific 3D printed models so that clinicians can practise specific surgery techniques unique to their patient,” said Dr Keng-Yin Lai, a postdoctoral research fellow at UNSW who helped create the models.
“They are geometrically and anatomically accurate which is really useful. But I think the future in this space is using even more
realistic materials during the 3D printing process and therefore understanding how parts of the body are actually going to bend and flex during surgeries.”
The first bespoke 3D printing project came about when Catherine Banks and Jacob Fairhall from Sydney Children’s Hospital, part of the Randwick Hospitals Campus, approached the team at IHealthE to produce an exact replica of eight-year-old Issac Lee’s skull.
Issac had been diagnosed with a craniopharyngioma, a rare and complex tumour at the base of his brain, and had already undergone two major craniotomy surgeries that required part of his skull being temporarily removed.
Banks and her team proposed a third, but this time less invasive, procedure via Issac’s nose and requested a 3D printed model of his brain and the tumour be created from imaging scans.
The model needed to show the precise size, shape and location of the tumour, but also other critical structures, such as the optic nerves, which had to be taken into consideration to ensure they were not damaged during the operation.
Pushing the envelope
Within 48 hours the IHealthE team were able confirm such a model could be designed and produced, which not only assisted in the surgical planning, but also helped Issac’s family understand the complexity of the procedure.
“I think we have a role as health professionals to constantly try to push the envelope of what we can offer our patients,” said Banks, a specialist ear, nose and throat surgeon.
“The merging of people in the health profession with biomedical engineers and technical experts, such as those at IHealthE, is absolutely vital as we move forward over the next decade.
“These 3D printed anatomical models allow us as surgeons to think about different trajectories for procedures. The models allow us to really plan our angles of attack, and consider all the instrumentation that we will need, so they are invaluable for providing us with more information than we’d get just from MRI or CT scans.”
Lai subsequently helped design and produce a series of 3D printed tracheas for anaesthetist Phil Black, who wanted to determine whether he would be able to safely use a certain type of breathing tube on a young patient during complex spinal surgery planned for early 2025.
Black was presented with four different designs, which allowed him to be confident
that an appropriate tube could be passed through the patient’s trachea, even though it was being significantly restricted due to the abnormal curvature of his spine.
“The primary issue with this patient, a young boy, is scoliosis, which is a quite severe curvature of the spine that is affecting his airway and breathing.
“The operation to fix that is long and difficult, maybe 12 to 16 hours. And he needs what is called an endotracheal tube placed in his airway — so I wanted to know what type and size would fit and where the problem points may be.
“I asked the IHealthE team if they would be able to 3D print this patient’s trachea, because there is nothing like having an accurate model in your hand and actually trying to pass a tube down it to give you reassurance ahead of the procedure.
“We can try to do calculations from a CT scan, but it is quite arduous. In this case it was great to have something simple and straightforward to show my colleagues and utilise their expertise in a very quick way.
“People were able to propose ideas and we could easily test the suggestions, which really streamlined the decision-making process.
“I think 3D printing for specific patients is definitely going to become more widespread in the future, especially as it gets even faster. In the future it may get to the point where a patient comes in, and within an hour or two
the CT scan and subsequent 3D model might be available to help predict and plan the best medical procedure.”
Educating patients
Banks says the 3D printed models are also an important tool to educate patients and their families about the procedure that is being planned, to help them evaluate, give consent and also understand what will be happening.
“Even medical professionals can have some difficulty looking at two-dimensional CT or MRI scans and understanding the threedimensional relationship between critical structures,” she explained.
“So you can imagine how hard it is for someone with no medical knowledge to be shown scans and try to figure out how it all comes together.
“The 3D models are fantastic in demonstrating the spatial relationships between all the vital structures and we can show patients and their family what we are trying to achieve and help them to better understand the procedure and consider the risks before they give consent.”
Despite their limitations as two-dimensional representations, the scans are fundamental to the process of creating the 3D models.
Experts such as Lai are able to use powerful computer programs to convert each of the segments of the scans into a design of an exact 3D replica of the patient’s body.
Sections of the model can be printed in different colours and at different opacity levels to better highlight certain structures, aiding both the surgeons and the patient in terms of better understanding the procedure.
Depending on the complexity of the specific request, it takes Lai around 8–10 days to create the three-dimensional model in the program — in consultation with the clinician to ensure it is accurately representing all the key structures in the best and clearest way.
Once everything is approved, the design is sent to the 3D printer which creates the model in approximately 20–30 hours — again, this varies from model to model.
The 3D models created so far have been produced using a photosensitive resin which is hardened, or cured, via exposure to ultraviolet light.
Bio-mimicking materials
IHealthE researchers are now exploring the possibility of printing with so-called biomimicking materials.
“At the moment with these 3D models they are anatomically accurate and that allows the clinicians and the patients to better visually understand the dynamics of certain structures,” said Gabriel Graterol Nisi, Senior Technical Engineer at IHealthE.
“But in the future I can imagine using a mixture of printing materials that can also mimic the precise texture and hardness and flexibility of the tissues or bone structures.
“The bio-mimicking materials can be created, for example, by depositing the resin in complex patterns that recreate porous bone structures, fibrotic tissues and ligaments.
“Using that would allow us the ability to replicate musculoskeletal models that match bone density characteristics and behave like native bone when force is applied such as discectomy, drilling, reaming or sawing.
“With 3D models using those materials the surgeons would not only be able to plan, but also accurately practise the procedure and really understand the way everything will feel and react.
“That is the next step in future developments and I think it will only enhance even further the possibilities of surgical planning.”
Black agreed that developments in biomimicking materials would be hugely beneficial to medical professionals.
“For a certain select group of patients it could be essential to have 3D models made of materials that accurately mimic the real body part.
“Different patients have bodies with different degrees of flexibility and pliability and tightness. So being able to know exactly how much a piece of tissue will be able to move, or compress, or distend would certainly be beneficial.
“It would definitely be a big advantage compared to just looking at scans on a screen — to be able to physically test how much the tissue moves and in which direction it might move.”
Integrated acute services
The bespoke patient-specific 3D printing service, believed to be unique in Australia, has grown out of the recent relocation of IHealthE to the new UNSW Integrated Acute Services Building (IASB) attached to the Randwick Hospitals Campus as part of the multimillion-dollar Randwick Health & Innovation Precinct project.
Within the new building, UNSW is housing stateof-the-art research, clinical innovation, biomedical and teaching facilities across 10 floors.
The spaces are designed to facilitate partnerships in tech solutions for diagnosis, treatment and prevention of a wide range of conditions, with researchers and clinicians sharing ideas, prototypes and data analyses.
As shown with the success of the patientbased anatomical 3D printed models, such collaborations are already helping to uncover unmet clinical needs and design innovative solutions to improve patient outcomes.
Sandy Wigley, Strategy and Innovation Project Officer at IHealthE, said the 3D printing highlights the strengths of the Institute and showcases the benefits of being based in the IASB in close proximity to clinicians and medical experts.
“The main aim of IHealthE is to pair unmet clinical needs with novel medical technology solutions,” she said.
“It isn’t about us just creating something cool and then trying to find a problem that it can be used for. We are here to hear what problems need to be solved and then creating a technology that can fix it.
“Our innovation team have a wealth of engineering experience and experience with medical technology startups. We have professors of practice with decades of experience working with med-tech, as well as specialist engineers who are able to do rapid prototyping when fast solutions are required.
Patient-specific 3D printed models have been produced using a photosensitive resin which is then cured under UV light.
Image from UNSW/Jake Willis.
A day in the life of Gabby Rowsell
Midwife, Mater Mothers’
Hospital, South Brisbane
5:45 I am a big routine person, so wake up at 5:45 alarm every day. I’ve never been a ‘snoozer’ on my alarm, so once I’m awake, I’m awake.
5:50 After five minutes of mindfulness I head straight to the coffee machine for a flat white while I get ready for work and have a quick scroll on my phone.
6:00 Breakfast varies from day to day, depending on how I feel. I am partial to a smoothie or simple avo on toast. When I get a bit of extra time on the weekends I love cooking a big breakfast.
6:20 I aim to leave the house by 6:20 am. I live very close to the hospital, so I walk to work most days while listening to a podcast. I find this the best way to clear my head before a busy day. My housemate also works at the hospital so we sometimes can walk together and catch up.
7:30 I start every shift by checking all my equipment and making a plan. Sometimes we have students working with us, so it’s important to make sure we’re on the same page and discuss their learning goals. Something that is super important for a midwife is to make a connection with the woman and family quickly. This is obviously a very emotional and heightened time for families, so I do everything I can to reassure them and make sure they feel safe and cared for. Obviously, the stage of labour impacts how much we can connect before the baby arrives.
The role of a midwife is so broad; it is far more than just delivering babies. We provide emotional and physical support to women and their support people, we respond to emergencies, communicate to doctors and other allied health professionals, document, and advocate for our patients.
6:45 Work as a midwife is varied every day. In a clinical setting, the day shift starts now. I am employed at Mater’s Birth Suite and Pregnancy Assessment Centre. We have education every morning with our fantastic clinical facilitators; they keep us up to date on changes in policies, updates in the department and training opportunities.
7:00 We all head to the handover room to find out which room we’re allocated to, and then go and meet the family we’re looking after. You really can be walking into anything at the start of the shift. A woman might be in early labour, or about to have a baby, be on her way to the operating theatre, or even be postnatal. The previous midwife will give a detailed handover about their progress and expectations, and then I start my day.
Midwife Gabby Rowsell shares her day working in the birth suites at South Brisbane’s Mater Mothers’ Hospital.
8:40 Every morning we have a huddle with team leaders, midwives, doctors, administration staff and management to discuss the readiness of Birth Suite and PAC for the day, and to discuss staffing, high-risk patients, learning opportunities, recognition of staff, and hospital-wide notices.
9:15 From here the day can vary. The birth suite is a rolling 24/7 system, so as soon as your patient has her baby, you care for her for a few hours after birth and then transfer her and her baby to the postnatal ward.
If I’m working in the Pregnancy Assessment Centre (PAC), the day looks a little different. This department behaves like an emergency department, open 24/7 to patients with pregnancy-related emergencies. Each staff member in PAC cares for two to four patients at a time, initiating investigations such as blood tests, ultrasounds, fetal monitoring and observations. I love working here, it’s all about diagnosing, reassuring, and crisis management in a timely and stressfree manner.
If I am in my other role as a Research Midwife, I work at the Fetal Growth Clinic within the Maternal Fetal Medicine department at Mater. This is a specialised research-based clinic that was developed to monitor and protect growth-restricted babies from all over Queensland. So, if I am working in that role the next day, I get my fun coloured scrubs out ready to wear in the morning.
I work here two days a week within a team of doctors, midwives and sonographers. This role is so fulfilling in its own way — women with growth-restricted babies are often terrified of potential outcomes and just want their baby safely in their arms. I spend a lot of time talking about the ins and outs of having a little baby, as well as discussing different clinical trials these women are welcome to be a part of.
I take bloods, assess ultrasounds, make delivery plans and provide a safe space for these women to share their concerns.
9:00 Time for coffee number two! Another flat white from the hospital cafe (I try to keep to two coffees a day but sometimes that doesn’t work).
15:00 Depending on who I’m assigned to, I can potentially stay with one woman the entire day or deliver multiple babies in 12 hours! My personal record is five babies in one shift. Birth is beautiful but very unpredictable — it can take minutes or hours or days.
19:30 Depending on the day, sometimes a debrief is required. Whether it’s calling my mum on the walk home, or a formal debrief at work, it is so important for me to wind down from the day.
20:00 Time to relax after a shower, some dinner and sometimes a glass of rosé.
18:45 The majority of midwives in the birth suites do 12-hour shifts, so come 6:45 pm we’re handing over to the night staff and saying goodbye to our patients.
19:15 I’m clocking out and walking home (or trying to convince a colleague to drop me home). If I get an earlier clock-off, I’ll be at reformer Pilates or going on a long walk along the river.
21:00 I’m often in bed reading and setting my alarm for the next day.
A Day in the Life is a regular column opening the door into the life of a person working in their field of health care. If you would like to share a day in your working life, please write to: hh@wfmedia.com.au
Supplied.
Abortion management and hospital stay
Taking the first dose of a pill used in medical abortions at home can reduce the amount of time a patient needs to be hospitalised, researchers say.
An international trial involving 435 women has found that 71% of patients who managed early stages of abortion at home after 12 weeks of pregnancy spent fewer than nine hours in hospital, compared to 46% of patients who took the first step at hospital.
A medical abortion involves taking two types of pills to end a pregnancy: mifepristone, which blocks the hormone progesterone and therefore causes the lining of the uterus to break down, and misoprostol, which makes the womb contract.
In this trial, all patients received the first dose of mifepristone in the clinic as usual, but some patients then took the first dose of misoprostol at home. Previous studies indicate that most
medical abortions after 12 weeks of pregnancy are completed eight to 12 hours after the first misoprostol dose and require an average of two to three misoprostol doses, with some patients needing to stay overnight in hospital.
“Currently, most abortions after 12 weeks of pregnancy take place in hospitals and may require an overnight stay, which some women find stressful and isolating. Our trial results show that taking the first dose of misoprostol at home decreases the average time women spent in hospital, enabling them to leave the hospital within nine hours after admission and without an overnight stay,” said Dr Johanna Rydelius, from the Sahlgrenska Academy at the University of Gothenburg, who was an author of the paper published in The Lancet
“Offering the choice to take the first dose of misoprostol at home provides a safe and effective alternative to taking all misoprostol doses at hospital and enables women to self-manage some of the process, potentially leading to feelings of autonomy during a time where women can feel extremely vulnerable,” Rydelius said.
“Our study found 1% of the women who took misoprostol at home completed the abortion before attending hospital for the next dose. Previous studies suggest a 1% complete abortion rate within two hours after the misoprostol first dose, and women who took misoprostol at home were made aware of this risk when choosing to take part in the trial and provided with a number to call if they had any concerns. It’s extremely important that women who are given the choice to take the first dose of misoprostol at home are clearly informed about the very small risk of the abortion occurring before attending the hospital.”
The study took place at six hospitals in Sweden between January 2019 and December 2022. All participants were given mifepristone oral pills at an outpatient clinic and provided with a time to return. Women between 12 and 22 weeks pregnant planning to undergo a medical abortion and who chose to take part in the trial were randomised to either receive their first dose of misoprostol at home or at the hospital.
Women in the home treatment group administered the first dose of misoprostol vaginally at home and returned to hospital two hours later for the remaining treatment. Women in the hospital group selfadministered the first dose of misoprostol upon arrival at the hospital. All participants then took repeated doses of misoprostol under the tongue every three hours until the abortion occurred.
The patients were asked to complete a follow-up survey two to four weeks after
“Our study found 1% of the women who took misoprostol at home completed the abortion before attending hospital for the next dose,” Dr Johanna Rydelius, from the Sahlgrenska Academy at the University of Gothenburg.
the abortion. Five out of six participants in both trial arms (171/200 of those in the home treatment group and 152/188 of those in the hospital treatment group) said they were very satisfied with the care they received.
When asked ‘if you were to choose, where would you prefer to take the first dose of misoprostol?’, 78% of women in the home group and 51% of women in the hospital group said they’d prefer to take the first dose of misoprostol at home.
“Every patient who seeks abortion care must navigate a unique set of personal and medical circumstances. The choice of selfadministering the first dose of misoprostol at home may provide some patients with a sense of autonomy and comfort during what can be a very overwhelming time in their lives. In addition, providing the option of the first dose of misoprostol at home would enable more abortion clinics with no overnight facilities to provide medical abortions for women who are over 12 weeks pregnant, something particularly important for locations where access to abortion care is limited,” said author Professor Kristina Gemzell Danielsson, from Sweden’s Karolinska Institutet.
The authors acknowledge some limitations of the study, including that the researchers were advised by the Data and Safety Monitoring Board to end the trial early due to a lower-than-expected enrolment and slow progress towards the trial’s target of 784 participants. However, trial site feedback suggests the enrolment rate was not due to reluctance to take misoprostol at home but rather due to patients feeling overwhelmed by the overall situation.
Ahead of her time
Laini Bennett*
Dr Beverley Rowbotham AO has achieved remarkable success in her career, opening the doors for other women on boards in the health and medical industry. Recognised with an Order of Australia for distinguished service to medicine, she shares her journey and nine leadership lessons learned.
Lesson 1: Pursue a purposeful career
Choose a career that gives you purpose and meaning. “I decided to do medicine because I wanted to be of use, and medicine seemed to be a good meeting place of science and being human,” Rowbotham explains. Her career choice was influenced by this fundamental desire to contribute positively to society.
Lesson 2: Embrace your background and influences
Growing up in Brisbane, Australia, Rowbotham’s upbringing significantly shaped her career. Her father was a journalist and her mother, a nurse, transitioned to being a stayat-home mum.
Despite societal expectations of that era, her parents encouraged her and her sister to pursue education and supported their ambitions. “My parents couldn’t have done more for my sister and me in terms of getting us launched. They really believed in education and supported us in whatever we wanted to do,” she reflects.
Lesson 3: Invest in help to support the work-life juggle
Juggling a demanding career and a young family was a significant challenge for Rowbotham. With four young boys and a husband who was a neurosurgeon, she made the difficult decision to move away from acute care. “The idea of both of us in cars going to hospitals in the middle of the night was not going to work,” she recalls.
Rowbotham worked part-time while her children were young, enlisting help from family, local student babysitters and nannies. “I gradually built out all the support I needed, including my mother, who drove everybody to cricket,” she says. Her husband still cooks their meals.
This balance allowed her to continue her professional journey while managing family responsibilities. She recommends that women with young families invest in the support they need rather than trying to juggle domestic duties with their jobs “because it’s a long game, and you need to invest in yourself”.
Lesson 4: Learn how to influence at the highest level
Rowbotham’s move from practising medicine to executive roles was a combination of timing and opportunity. After transitioning from bedside care to diagnostics in pathology, she joined the board of a disability charity and the Royal College of Pathologists of Australasia. Sitting on a board offered an ‘aha’ moment as she realised that all the
critical decisions affecting how doctors practised were made in board rooms, from funding to resourcing.
“What I learned was that being on a board required a different language and set of skills, so that if doctors were going to make that leap to get up there with the lawyers and the accountants who typically sit on boards, they would have to learn the lingo and the rules of play, just as we’d learned it for practising medicine,” she explains.
Joining a board can also open the door to additional director roles, including in other sectors. Since becoming a director on the disability charity’s board, Rowbotham has sat on numerous boards, including with aged care provider Bolton Clarke.
“As one of only two women on the 32-member AMA Federal Council, Rowbotham understands the unique challenges and opportunities of being a female leader in a maledominated environment.”
Lesson 5: Make an impact through leadership
Rowbotham’s involvement in leadership roles, such as Chairing the AMA Federal Committee and as a ministerial appointment on four federal government healthcare policy committees, allowed her to advocate for significant advancements in the medical field. One of her proudest achievements was her role in the early days of genomics, where she advocated for the necessary infrastructure and training to support this vital area of health care.
“We were enlisting the health minister at federal and state levels to say genomics is coming, it’s vital to health care, and we’re not ready for it,” she explains.
Lesson 6:
Seek support from mentors and champions
Throughout her career, Rowbotham benefited from having mentors and champions who supported and guided her. One such mentor was John Fahey, the former Premier of New South Wales and President of the World AntiDoping Agency. They had worked together on another board, and when Rowbotham was elected Chair of the prestigious Australian Medical Association (AMA) Federal Council, she sought his advice. “He was more than happy to talk me through how to manage a large group of opinionated people,” she says.
Lesson 7: Female leadership offers different perspectives
As one of only two women on the 32-member AMA Federal Council, Rowbotham understands the unique challenges and opportunities of being a female leader in a male-dominated environment.
“We were the outliers. And I think everybody needs an outlier — somebody who sees the world differently,” she says, explaining that women bring a different tone and perspective to conversations at this level.
Rowbotham was elected as chair of the AMA Federal Council five times. Under her leadership, the Council voted on initiatives to improve healthcare policies and practices, including supporting same-sex marriage (“People who suffer from discrimination, it affects their health”). Another groundbreaking initiative was the establishment of the AMA Equity and Diversity Committee, setting a
target of 50% women on the Council. Not all members were supportive. “That took some advocacy and persuasion,” she says. Today, the target is close to being achieved.
Lesson 8: Establish opportunities for others
Rowbotham wants more medical professionals operating at the board level, where policy decisions influence how doctors practice medicine and what funding they receive. To support this goal, she established two scholarships for final-year medical students, funding training with the Australian Institute of Company Directors’ board directors course. However, she noticed distinct differences in how men and women approached the application process, with rarely more than two women applying annually.
“It was a revelation for me,” she says. “Women do not see themselves as somebody who might benefit from having a set of learnings that prepares them to be head of the radiology department or Royal Brisbane Hospital,” she says. “They just don’t envision this in their career.”
She wants to encourage more women to step into leadership roles and bridge the confidence gap.
Lesson 9: Share your life lessons
For other women seeking leadership roles, Rowbotham draws on her lifetime of experience to recommend the following:
• Find a purpose worth serving: leadership requires courage and effort, and having a strong purpose helps justify the sacrifices and criticisms that come with the role.
• Be attentive to opportunities and changes: be aware of the world around you, including noticing when doors of opportunity open and close in your career.
• Learn and move on: not everything you attempt will be successful. Failure is part of the journey. Learn from setbacks and continue to strive towards your goals.
*Laini Bennett interviews successful career women about their leadership lessons learned. Visit lainibennett.com to read more stories about inspiring women.
Rowbotham at the AMA women’s breakfast.
Better care and efficiency
with electronic journey patient boards
The implementation of electronic patient journey boards (EPJBs) at Alfred Health has increased the effectiveness and efficiency of patient care across each of its three Victorian campuses, a report has found.
Researchers from the Health and Social Care Unit in the School of Public Health and Preventive Medicine at Monash University, supported by the Digital Health Cooperative Research Centre (DHCRC), undertook an evaluation to formally review the impact and effectiveness of the Alcidion EPJBs across The Alfred, Caulfield and Sandringham sites in Victoria.
Key findings
• Access to patient information: Real-time integration across multiple systems led to significant improvement in the alignment of patient information between electronic medical records and patient journey boards in wards. As a result, clinicians now have direct access to the most up-to-date patient information to support care journey management.
• Consistent ways of working: Across the footprint of more than 30 inpatient wards the team have aligned on patient flow management, consolidating 30 approaches to 9 variations closely mapped to the clinical workflow, which supports improved availability and consistency of patient information across the service.
• Discharge planning: Implementation of EPJBs led to a significant improvement in estimated discharge date (EDD) compliance, with EDD captured for more than 97% of patients up from 62%, supporting optimised length of stay and better hospital planning.
• Outlier reduction: While admissions increased by 10% during the trial period, outliers at the point of admission — those allocated outside their home ward — saw a reduction of 2%, indicating improved visibility of available beds, supporting improved patient safety and length of stay.
The introduction of the EPJBs played a pivotal role in a range of service improvement initiatives to realise these results.
Alfred Health Chief Digital Health Officer Amy McKimm said as a predominantly digital health service, Alfred Health is committed to improving patient care by ensuring patient-level health data flows across the health service.
“Our goal is to have a process that can oversee patient management and flow across all patient care pathways, identifying areas of concern or constraint. This is regardless of whether the patient is within our hospital walls, in their home or with partnered hospitals/health services,” McKimm said.
The role of patient journey boards
Patient journey boards facilitate the coordination of care across the health service. They are a visual management tool to provide access to critical information about each patient’s progress, to enable health service staff to view and make decisions based on available information.
EPJBs integrate patient information; replace white boards and paper; remove manual bed allocation systems; improve real-time planning of bed capacity to meet demand; assist with future and retrospective bed flow audits; and eliminate risk and inefficiency of data duplication (manual board vs electronic medical record).
Alfred Health recognised the need for improved patient flow and data collection and started the transition from manual patient journey boards to EPJBs in November 2022.
Alcidion CEO Kate Quirke said the research showed not only the impact of EPJBs in practice but also the many ‘ripple effects’ journey boards have along the patient journey.
“The research has highlighted the wide range of benefits delivered through real-time data
integration and intelligent user interface design, supporting clinicians with a digital clinical workflow that releases time to care,” Quirke said. “We often talk about effective patient flow and these findings demonstrate it in practice.”
A cooperative and collaborative partnership
DHCRC CEO Annette Schmiede said the research project reflects the focus of the recently released Digital Health Blueprint and demonstrates the benefits of a cooperative and collaborative partnership; with Alfred Health, Monash University and Alcidion working hand in hand to deliver a robust evaluation of EPJBs in practice.
“The Digital Health Blueprint called for modern foundations to underpin a collaborative, standards-based health system that is safe and secure,” Schmiede said.
“In practice, this requires a commitment from industry, university researchers and health service providers to independently and rigorously assess the effectiveness of new innovations to deliver a health system that is fit for purpose.”
Alfred Health’s Chief Allied Health Information Officer Lauren Solomon and Allied Health Workforce Officer - Digital Health Angie Bezen presented at the Digital Health Festival in 2024, on interoperability in allied health demand management. Visit digitalhealthfest.com.au for more information about this year’s event.
The role of culture and connection in improving Aboriginal health
U NSW Sydney researchers are calling for a rethink of the health system’s approach to closing the gap following their research highlighting the role of culture and connection in improving Aboriginal health outcomes.
Study co-author Dr Aryati Yashadhana, from the School of Population Health at UNSW Medicine & Health, said “Our research shows that when Aboriginal people have the freedom to practise culture on Country, it has a positive impact on their health and wellbeing.”
Around 280 people attended cultural camps or wallays across Yuwaalaraay, Gamilaraay (Northwestern NSW) and Yuin (Far South Coast NSW) in 2022. Of these, about 100 people participated in yarning circles or surveys for the study by the Gaawaadhi Gadudha Research Collaborative (translating to “from saltwater to freshwater”).
The camps were held in ‘cultural landscapes’ minimally impacted by colonisation and
urbanisation, and facilitated by cultural knowledge holders of Country. They provided exposure to sacred teaching sites, sharing of language and cultural knowledge, and participation in cultural practices such as weaving, woodwork and ceremonial dance.
The researchers examined how these camps affected the cultural health and wellbeing of attendees.
“These camps had an overwhelmingly positive impact on indicators of self-rated cultural health. This included an increase in people’s sense of connection to Country, mob and ancestors, pride in Aboriginal identity, and knowledge of cultural stories, foods, and medicines,” Yashadhana said.
“The vast majority of those who attended reported a sense of healing, with the camps helping with stress relief, inter-generational healing, and the journey to overcoming trauma, which in turn had a positive impact on their overall health and wellbeing.”
Study co-author Associate Professor Brett Biles, UNSW’s Pro Vice-Chancellor Indigenous Engagement and Research, said the research underscored the importance of cultural health and the need to integrate Indigenous knowledges into public health strategies and programs. A shift away from the deficitfocused ‘gap’, which measures individual health outcomes against non-Aboriginal counterparts, was also needed.
“Aboriginal peoples have sustained their cultural practices for over 60,000 years, yet we continue to focus on these gaps which inadvertently position Aboriginal people as deficient and also neglect Aboriginal ways of understanding health,” he said.
“While comparative epidemiology remains a useful tool in addressing health inequity, it is not the only way; we should also be focusing on the strengths that have been practised as part of Aboriginal cultures for thousands of years.”
The shift would need to start with policy reforms to ensure Aboriginal knowledge was respected and incorporated into health approaches, Biles said.
“Adopting Aboriginal ways of understanding health is crucial. In Aboriginal knowledge, the health of people, family, Mob, culture and Country are symbiotic. They also involve spiritual, emotional and physical dimensions.”
Acknowledgement and engagement on the importance of supporting cultural health initiatives, like cultural camps, would be a good starting point, Biles added, noting more support would be needed to overcome challenges like limited access to Country and funding.
“We also need further research that explores the largely untapped potential and long-term impacts of cultural engagement on health and wellbeing,” he said.
In Conversation
with Dr Karen Luxford
Amy Sarcevic
After 30 years in the healthcare sector, Dr Karen Luxford has seen many changes to safety and quality standards, but there is one new trend keeping her on her toes — AI.
In the last 50 years, the standards by which healthcare quality is measured by third party accreditors have evolved considerably.
Where hospitals were once assessed solely by clinical metrics, like hand hygiene and medication safety, they must now uphold rigorous standards in all aspects of care — from consumer engagement to patient communication.
“Safe communication is assessed with the same rigour as medication and hygiene protocols,” said Dr Karen Luxford, Group CEO of the Australian Council on Healthcare Standards (ACHS).
“We increasingly recognise that non-clinical metrics can be just as crucial as traditional, clinical ones, when it comes to maintaining quality health care.”
The impact of AI
Having worked in the sector for more than thirty years — and five years at ACHS — Luxford has witnessed this evolution firsthand.
But while she is no stranger to change, there is one trend keeping her on her toes — and set to alter ACHS’s approach more drastically than any other since its inception.
“We are continually adapting to keep up with artificial intelligence (AI),” Luxford said.
“We are starting to see AI being used in many areas of health care, and, while there are clear benefits of using it, we need to give equal attention to the ways in which it might impact on healthcare quality.”
While this may be true for any new fixture of the healthcare system, Luxford says AI is a different challenge.
“At its current speed of development, AI is outpacing legal frameworks, ethics principles and governance structures,” she said.
“So, we need to continually reassess these structures and ensure we are upholding safety standards in all aspects of health care, including the ever-growing use cases of AI.”
The importance of governance
To this end, ACHS recently sat down with AI experts at an Executive Innovation Forum, which was organised for its hospital and health service members.
“We discussed the safety and quality governance implications of AI, whether we can trust its output, and how we can decide if it is being used appropriately.
“And it all came down to good governance — ensuring you have the right policies and procedures to assess any new AI tool,” Luxford said.
Image: Supplied.
What does good governance look like?
For Luxford, good governance is summarised as “the right processes, the right policies, and the right people” — and that includes everyone along the care continuum.
“It’s not just a matter for the board and executive team — good governance runs throughout an organisation. It should be just as visible to staff on the frontline as it is to those who sit behind desks,” she said.
In an AI context, Luxford also said some governance pillars currently needed more focus than others.
“Training in the AI space is so important,” she said. “We’re still seeing a large portion of healthcare services where staff aren’t properly trained in AI.
“Ideally, we need to upskill people to a level where they fully understand the benefits and risks, as well as implications for areas like patient privacy. If staff only know how to operate the technology and nothing else, that is not sufficient.”
Creating a safety culture is also paramount, she argued.
“You need systems and protocols in place, so that staff can proactively raise concerns and take precautions.”
Next phase of evolution
While adapting to the evolving technology landscape forms a major part of Luxford’s strategic plan this year, it is not the only megatrend she has to contend with.
She says addressing the next phase of evolution in healthcare accreditation will be challenging on multiple fronts.
“As well as technology uncertainty, we are dealing with global challenges, like climate change and workforce shortages.
“We know that hospitals contribute around 8% of the world’s carbon emissions, and that climate change is the WHO’s number one health issue.
“Our focus will be on making sure Australian healthcare providers are addressing this
through their governance processes. All the while managing human resource constraints.”
As a market-leading provider of accreditation, training and healthcare consulting, ACHS is also focused on its own internal governance structures.
“We are always focused on how we can improve governance, internally, to ensure we are promoting and exemplifying the best standards,” she said.
Looking ahead
While the future may be littered with change, Luxford maintains a positive outlook.
While new technology may be the greatest challenge, it will also be a close friend — a tool to help keep healthcare standards as high as possible, she said.
“A key thing for us will be, how do we use all the amazing tools out there at our disposal, to make assessment processes more streamlined for all? And how can we use technology to free up staff for optimal performance,” she concluded.
Collaborating to help Australians meet physical activity recommendations
Luke Snabaitis*
We all know that being physically active is important for our health, but getting people to actually move enough to meet the recommended guidelines can be a challenge. In 2022, only 22% of Australians met the physical activity recommendations, which call for adults to engage in 2.5 to 5 hours of moderate-intensity physical activity each week or 1.25 to 2.5 hours of vigorous-intensity physical activity, along with two musclestrengthening sessions, a week.
For those under 18, it’s 60 minutes a day, and if you’re over 64, add some balance and flexibility exercises. This is where hospital and health professionals, including exercise physiologists, can step in and collaborate to help improve health outcomes.
Exercise physiologists are healthcare professionals who specialise in using exercise as a form of medicine to help patients achieve their health goals. They tailor exercise plans to each individual’s needs, focusing on safety and effectiveness. More importantly, they use behaviour change strategies to help patients follow through with their exercise plans. Have you ever prescribed a treatment, only to find out later that the patient didn’t follow through? That’s where behaviour change techniques come into play. Exercise physiologists use motivational interviewing and other strategies to guide patients towards embracing physical activity.
By working together, health professionals and exercise physiologists can create a more comprehensive approach to patient
care. For instance, during a referral, exercise physiologists can dive deep into a patient’s motivations, beliefs and concerns about exercise, helping them develop a plan that suits their lifestyle and addresses any fears or misconceptions.
Consider a scenario where a physiotherapist refers a patient to an exercise physiologist because the patient isn’t engaging in the prescribed exercises. A 45-minute conversation with the patient can reveal the root of the issue and lead to a personalised plan that resonates with the patient’s values and goals.
Health professionals can start by asking patients simple questions about their physical activity habits. For example:
“How physically active are you?”
“What does being physically active mean to you?”
“What’s your daily routine like?”
These questions open the door to conversations about physical activity and can reveal opportunities for referrals to exercise physiologists. By discussing a patient’s current exercise habits and any challenges they’re facing, we can help them set achievable goals and create a low-barrier plan to incorporate more movement into their routine. Tracking progress can help keep patients motivated and committed to making long-term changes.
It’s essential to look at each patient holistically, considering how physical activity can impact their overall health. While you may
have expertise in a specific area of health, collaborating with exercise physiologists can provide a broader perspective and enhance patient care.
Exercise physiologists can help understand contraindications to exercise for specific health conditions and provide training or support to set up referral pathways. This partnership can strengthen our collective efforts to improve patient outcomes.
Many articles emphasise the importance of physical activity, but they often miss the ‘how’ of getting patients to move more. This is where exercise physiologists excel. They can work with you to help patients overcome barriers and find ways to integrate physical activity into their lives.
So, if you haven’t already, start a conversation with an exercise physiologist. Share what you’ve learned about your patient’s physical activity habits and ask for their input on how to best support them. By working together, we can create a more active, healthier population.
We all know that physical activity is crucial for longevity and quality of life, so let’s make it a central part of our patient care. By collaborating with exercise physiologists and focusing on both the ‘what’ and the ‘how’ of promoting physical activity, we can help our patients lead healthier, more fulfilling lives.
If you’re looking for more resources or want to connect with an exercise physiologist, check your hospital’s intranet page to find someone nearby. Together, we can make a difference in our patients’ lives by encouraging them to move more and live better.
*Luke Snabaitis is an Advanced Exercise Physiologist at Sunshine Coast Health and is a member of Exercise & Sports Science Australia.
3-in-1 Cream Cloths
New look, expanded indications
Same trusted Contiplan formula, refreshed look and feel.
Our 3-in-1 Cream Cloths don’t just cleanse, they protect and help to restore, making them indispensable for effective skin recovery.
3-in-1 Cream Cloths are now suitable for managing all forms of moisture-associated skin damage (MASD), including:
– Incontinence-associated dermatitis (IAD)
– Intertriginous dermatitis (ITD)
Plus, they’re safe to use on broken skin and are suitable for all ages, including neonates.*
Powered by Advanced Barrier Protection (ABP™) Technology, 3-in-1 Cream Cloths help to restore skin integrity and promote healing.
Cleanse
Gently removes dirt and bodily fluids without causing maceration.
Moisturise
Concentrated emollients hydrate and strengthen the skin’s natural barrier.
Protect
Creates a barrier against irritants to aid recovery.
Scan the QR code to request a FREE Clinell Contiplan 3-in-1 Cream Cloths pack†
*As with applications of any liquid to the baby’s skin, tissue viability should be considered for extremely or very low birth weight babies.
†This offer is only available for Australian Healthcare Facilities. While stocks last.