
FEATURING
• Sport and society still haven’t found the middle ground on clean air
• Implications of jet lag and Olympic performance
• Low back pain in athletes: What do we know and what do we need to know

• Sport and society still haven’t found the middle ground on clean air
• Implications of jet lag and Olympic performance
• Low back pain in athletes: What do we know and what do we need to know
02
From the Chair
SMA Board Chair, Dr Kay Copeland, introduces the SMA Sports Doctors special interest group and other education initiatives planned this year.

03
From the CEO
Jamie Crain highlights the 2024 Member Survey results and and summarises this issue’s feature articles.

Opinions expressed throughout the magazine are the contributors’ own and do not necessarily reflect the views or policy of Sports Medicine Australia (SMA). Members and readers are advised that SMA cannot be held responsible for the accuracy of statements made in advertisements nor the quality of goods or services advertised. All materials copyright. On acceptance of an article for publication, copyright passes to the publisher.
04
Low back pain in athletes – What do we know and what do we need to know?
Dr Larissa Trease explores the experiences of elite athletes with low back pain (LBP) and factors associated with and predictive of recovery.


11
Returning to our roots
SMA’s major partner, ASICS, shares its development and innovation in the basketball space since the 1950s.
Publisher Sports Medicine Australia State Netball and Hockey Centre – Parkville 10 Brens Drive, Parkville VIC 3052 sma.org.au
ISSN No. 2205-1244 PP No. 226480/00028
Copy Editors
08
SMA 2024 Membership Survey Highlights
A summary of the survey results and our response to Member feedback.

Archie Veera and Anelia du Plessis
Marketing and Member
Engagement Manager
Sarah Hope
Design/Typesetting
Perry Watson Design
Cover photograph
ImageSource/gettyimages/ master1305
Content photographs
Author supplied; www.gettyimages.com.au
13
Implications of jet lag and Olympic performance
Dr Stephen Jasper correlates jet lag with an elite athlete’s performance, in the lead up to Paris 2024.

21
Injury Epidemiology in Police Force Recruits
Vanessa Sutton sheds light on the complex relationship between pain, injury history and persistent disability in Police Force Recruits.


18
2024 SMA & ACSEP Conference –Meet your keynote speakers
Introducing an exceptional line-up of internationally and nationally acclaimed speakers who are joining us this year to take on cutting edge science.

25
Sport and society still haven’t found the middle ground on clean air
Dr John Orchard provides an interesting take on the new definition of “clean air” and how it affects elite athletes.
30
Modifiable risk factors of paediatric Anterior Cruciate Ligament injuries: Insights from a systematic review
Theresa Heering examines ACL injuries in children aged 5-14 years and the injury risk reduction strategies that should be implemented.

35
5 Mins With: Associate Professor Clare Minahan

39
People Who Shaped SMA: Professor Evert Verhagen

42
Sports Medicine Around the World: Singapore

47
Sports Trainer Highlight: Robert Ferguson


DR KAY COPELAND, SMA BOARD CHAIR, ANNOUNCES AN EXCITING NEW SPECIAL INTEREST GROUP LED BY OUR SPORTS DOCTOR MEMBERS.
Welcome to the latest edition of Sport Health.
In April, the SMA Board of Directors met to review SMA’s Strategic Plan. The new Strategic Plan for 2024-2027 is currently in development and takes into account the diverse voices and opinions of our multi-disciplinary membership base. We look forward to launching the new Strategic Plan to members in July.
We’re excited to introduce SMA Sports Doctors, a dynamic new special interest group led by a team of dedicated sports doctor members. Among the exciting initiatives underway is the launch of our revamped website in early July, featuring the popular ‘Find a Sports Doctor’ tool. This user-friendly search engine enables the public to easily locate sports doctors in their area. Additionally, the group is developing specialised courses tailored to support the continuous professional growth of our Sports Doctor members.
With concussion an everpresent concern, we have a consistent schedule of Concussion Management online courses for our members and associates
It is wonderful to partner with ACSEP for the 2024 SMA and ACSEP Conference. The joint conference will be this year’s premier occasion for sports medicine in Australia. We have an exciting line-up of speakers organised and are thrilled to be welcoming Associate Professor Clare Minahan as this year’s Refshauge Lecturer. To find out more about her and what her presentation will encompass, be sure to read her ‘5 Mins With’ interview featured in this edition of Sport Health.
With concussion an ever-present concern, we have a consistent schedule of Concussion Management online courses planned over the next few months. This course is targeted towards medical practitioners, coaches, athletes, parents, and officials to enhance understanding of how best to support player well-being in competition and return to play.
Applications for ASMF Fellowship are now open, and I encourage anyone who is contemplating their submission to apply. The new ASMF Fellows will be announced at the Fellow’s Dinner during the Conference. I look forward to joining these celebrations with all our ASMF Fellows, both new and old.

Dr Kay Copeland

Welcome to the second issue of Sport Health in 2024.
The results of our recent Member Survey are in, and we are delighted to see some excellent feedback from members which will directly inform our Strategic Plan for FY25-FY27. Of note is the consensus amongst members that SMA’s greatest point of difference is our multidisciplinary nature, demonstrated through our comprehensive professional development program of events. With this in mind, the SMA team will continue to develop new opportunities for quality learning and connection amongst our broad membership base that are focused on ease of access, value for money, and a convenient format. We will also increase the number of events for career development, and with the help of our State Councils arrange additional networking opportunities.
It was pleasing to note that over 83% of members believed SMA is in a better place than just 12 months ago. With recent investments made in new membership systems we intend to build on this progress to ensure our program of activities and communications remains as relevant
SMA’s greatest point of difference is our multidisciplinary nature, demonstrated through our comprehensive professional development program of events
as possible. To assist with this, we encourage all members to log into the member portal to check that their details and preferences are up to date.
In a first for SMA, we are excited to announce the creation of the SMA Student Network. This special interest group will be led by members of the former Executive Committee of SEMSA, who has joined forces with SMA, to help build relevant career-focused networking and educational events for our Student Associates from all disciplines, throughout their degree years.
For our accredited Sports Trainer Associates, we are excited to
announce the forthcoming launch of our new sports trainer coverage booking system, Sports Trainer Connect. This new platform allows parties to advertise coverage opportunities on a dedicated part of SMA’s website, and SMA-accredited sports trainers will be able to review and pitch their services directly.
We are also delighted to share that SMA will once again be the exclusive provider of sports trainers at the 2024 UniSport Nationals in Canberra. Expressions of interest are now being sought and we encourage all interested sports trainers to take part.
In this issue, we have topical research presented across multiple streams of sports medicine. Dr Lari Trease focusses on low back pain presentations for clinicians working in sport, while Theresa Heering discusses the importance of paediatric ACL injuries. Dr John Orchard refines the concept of “clean air” for athletes post the COVID pandemic, and Vanessa Sutton shares injury history and key performance metrics in Police Force Recruits. Lastly, Dr Steve Jasper outlines the affect jet lag and time zones have on an Olympic athlete’s performance, as we gear up for the Paris 2024 Summer Olympic Games.
We hope you enjoy reading this edition of Sport Health.

Jamie Crain
LOW BACK PAIN IS A COMMON PRESENTATION TO ALL CLINICIANS WORKING IN SPORT, AND THOSE WORKING IN PRIVATE PRACTICE WITH ACTIVE MEMBERS OF THE COMMUNITY. UP TO 90% OF OLYMPIANS WILL EXPERIENCE AN EPISODE OF LBP IN THEIR CAREER, WITH EFFECTS WHICH CAN LAST BEYOND THEIR SPORTING ENDEAVOURS.
DR LARISSA TREASE, 2022 SMA Conference – Ken Maguire Award for Best Paper in Clinical Sports Medicine

More than three quarters of Australians will experience LBP in their lifetime. While most community LBP is benign and selflimiting, Australia spends $4.8 billion per year on LBP management.
Athletes experience rates of low back pain (LBP) exceeding that of the general population. Up to a third of Olympic athletes report ongoing post-career pain and functional limitation attributed to injuries, including low back pain, sustained during their athletic careers.
Depending on the sport that an athlete is participating in, the 12-month prevalence of LBP ranges between 1% (runners) to 82% (cyclists), with sports commonly reporting a high prevalence of LBP including gymnastics, rowing and cricket. Established risk factors for athlete LBP include high or changing training volume, increased length of sporting career, and older age. Once athletes’ experience back pain, their risk for future episodes increases. Risk factors for LBP in athletes are dramatically different from those in the community, where risk factors for LBP include smoking, obesity, low
physical activity, low socio-economic status, and reduced general health.
Optimal management of athletic low back pain is poorly researched, with few randomised control trials evaluating the effectiveness of commonly used treatments for LBP in athletes. Exercise has been demonstrated to reduce pain and improve function in different athletic groups. However, the clinical applicability of this research is limited by the lack of comparison of exercise types, the use of only a single intervention when clinical practice often involves multiple concurrent

therapies to optimise recovery, and the failure to document the impact of any intervention on return to sport or performance outcomes, which are important measures for athletes and their clinicians.
Looking at all sports participants, a 2021 systematic review, published by Thornton and colleagues, on the management of LBP in athletes highlighted that the current clinical and research approach had a strong biomedical focus. This research identified that there was a paucity of research examining interventions
Depending on the sport that an athlete is participating in, the 12-month prevalence of LBP ranges between 1% (runners) to 82% (cyclists), with sports commonly reporting a high prevalence of LBP including gymnastics, rowing and cricket.
for LBP in the areas of athlete psychological or social well-being. This is despite well-established knowledge of the impact of psychosocial factors on the recovery of community members from LBP.
Specifically focussed on the sport of rowing, a Delphi study, published by Wilkie and colleagues, of experienced and expert clinicians recommended a four-phase approach to management of LBP. Key factors in the initial presentation and acute care phases

included: early identification of red and yellow flags, prompt control of pain, continued physical loading in the form of cross training, the targeted regaining of rowing-specific movement patterns, while concurrently undertaking education and empowerment of both the athlete and coach. The subacute rehabilitation and return to sport phases emphasised the need for progressively increasing on-water training volume and intensity, with concomitant reduction in crosstraining, the importance of interdisciplinary involvement in return to sport planning and the focus on ensuing any modifiable risk factors for rowing related LBP were addressed as part of secondary LBP prevention. While this was a study of clinicians with a specialist interest in the sport of rowing, both the phased approach to LBP management and the broad principles of each phase could be applied by sports clinicians to athletes participating in other sports.
Qualitative work examining rowers with LBP, published by Wilson and colleagues in 2020, highlighted that the culture and environment in which the athlete trains can be impactful on their recovery. This group identified two cultures reported by athletes: one of openness, where the coach modifies training load, the medical staff provide treatment, and the teammates provide support. This environment resulted in inclusion of the injured rower with improved self-esteem and self-efficacy and, as a result a more positive experience of LBP. Contrasting this was those rowers who reported a culture of concealment, resulting in a delay to, or failure to obtain treatment, minimal modification of training with subsequent reduced performance and a feeling of isolation, all leading to a negative LBP experience. Again, these principles can be applied by sports clinicians working with athletes in different sports and those working with active community members.
What do we know and what do we need to know?
Adolescent athletes from different sporting backgrounds who were involved in a qualitative study published in 2023 (Wall et.al.) described three themes that impacted their LBP experience: 1) the culture of normalising LBP, which the authors reported negated the safeguarding efforts that should be in place to protect adolescent athletes against pain and injury in sport, 2) the experience of LBP changed how athletes perceive themselves with increasing awareness by the adolescent of their own limits and for their need for self-advocacy and 3) the ability of an episode of LBP to impact across the other domains of a young athletes life, such as their participation at school, their daily function and their emotional health. Clinicians treating adolescent athletes in clinic and sporting environments should consider and explore these themes to optimise their patient’s recovery journey.
There is minimal research on the primary or secondary prevention of LBP in any athletic group. Perich and
Clinicians treating adolescent athletes in clinic and sporting environments should consider and explore the themes of the sporting culture, self perception and the impact on school, daily function and emotional health.
colleagues, from Perth WA, published a study focussed on adolescent female rowers (2011) which demonstrated that the prevalence of LBP at midand end-of-season can be positively influenced by screening, education, and exercise prescription across the season. This study provides clinicians with implementable tools which could help to prevent LBP in athletes.
Our recent research (presented at the 2022 SMA Conference) asked clinicians and coaches working in elite sport and elite athletes who had experienced LBP what factors they perceived were important in athletes’ LBP recovery. This group of experts identified six clusters of factors, which mapped to the well-known domains of biological, psychological and social influences of LBP recovery, a paradigm which is well established in community LBP management.
Factors in the biological domain grouped to three clusters: (i) the athlete rehabilitation journey; (ii) the athletes’ physical factors; and (iii) non-modifiable risk factors that an athlete may present with. Key recovery factors for clinicians to explore and ensure in this domain included early identification of red flags and the prompt management of serious pathologies, such as inflammatory arthropathies. Rehabilitation and return to sport planning needed to include graded exposure to optimal loading, alongside individualised plans that had measurable goals, considered the whole athlete, and addressed biomechanical contributors.
Factors in the psychological cluster including the statement rated as most important to recovery, which was “buy in from the athlete”. This cluster also included the importance of athlete
honesty about their symptoms, identifying any fear they may have about their LBP experience and their past LBP recovery experience, both positive and negative. The athletes’ mindset was perceived to be important to recovery with factors such as optimism, motivation, catastrophisation, and anxiety being highlighted by participants.
Finally, the social factors of the athlete included the two clusters ranked most important for recovery. The first was the athlete’s coach and clinical relationships, which could result in athlete empowerment. The second was the inter-disciplinary team surrounding the athlete and how this group communicated, used unifying and consistent messaging, and explained and discussed treatment options. An athlete-centred shared decisionmaking approach by this group was perceived as contributing to recovery.
The combined learnings from current research in athlete LBP highlights the importance of the environment, culture and relationships of an athlete in their recovery journey. As recommended in the systematic review on athlete LBP management (Thornton, 2022), clinicians should adopt a biopsychosocial approach when caring for athletes who present with LBP. This could involve exploring the current sport environment, stressors, and sense of agency that the athlete has, along with evaluating their mental health and supports that they can access, both clinical and social in nature.
The effectiveness of the biopsychosocial approach in helping an athlete become pain free and return to their sport is yet to be established, and Sport Health readers can contribute to our efforts to increase the research-based knowledge in this area by encouraging athletes that they work with to consider participating our ongoing research.
While most community LBP is benign and self-limiting, Australia spends $4.8 billion per year on LBP management.
We are currently recruiting participants into a prospective longitudinal cohort study: eligible athletes are aged 16 to 35, competing at the National level (national league or championships) or representing Australia in Olympic, Paralympic or Commonwealth Games sports. Athletes need to have acute LBP (<6 weeks duration) and be recruited to the study no more than 14 days following their first consultation with a health care provider. Further information for clinicians and athletes is available on our website www.athletelowbackpain.com.
For article references, please email info@sma.org.au.

Dr Larissa Trease is a Canberra based, Specialist Sport and Exercise Physician with more than 15 years’ experience in elite sport. Lari has been a team Doctor for Australian Summer (2016) and Winter (2014) Olympic, Paralympic (2008) and Youth Olympic (2012) Teams. She has had many roles within the Australian High Performance Sporting system, including providing leadership, medical care, and policy advice across three institutes of sport, and five National sporting organisations. She currently consults part-time at the Australian Institute of Sport, is the Team Doctor for the Australian Cross-Country Ski Team and a member of the World Rowing Sports Medicine Commission.
Larissa has a career-long interest in optimising medical care for elite athletes through research. She is a PhD Candidate at La Trobe Sport and Exercise Medicine Research Centre (LASEM), La Trobe University, where her research focuses on predicting the recovery of elite athletes from low back pain. She is a National Health and Medical Research Council (NHMRC) PhD scholarship recipient. Lari’s research aims to assist clinicians, coaches and athletes in elite sport to better understand the recovery trajectory and important recovery factors in athletes with LBP.
IN MARCH WE CONDUCTED OUR ANNUAL MEMBER SURVEY. ALL MEMBERS AND ASSOCIATES WERE INVITED TO PARTICIPATE, AND REPRESENTATION OF EACH DISCIPLINE WAS GENERALLY PROPORTIONAL TO MEMBERSHIP ACROSS ALL STATES AND TERRITORIES AND REFLECTIVE OF SMA’S MULTIDISCIPLINARY PROFILE.
Thank you to those members who took the time to respond. The feedback was comprehensive, and demonstrates that members have a strong connection to, and vested interest in the future of SMA.
The results have provided us with an understanding of our members’ needs, priorities, and satisfaction levels.
We’re pleased to report that 93% of the respondents are satisfied with the overall value of their membership. Nearly 30% were extremely satisfied, underscoring the real value of the professional development, content, discounts and services we offer.
An even more encouraging outcome is that over 83% of members stated that they believe SMA is performing better now than this time last year.

Members identified several services as the most valuable to their professional growth, including:
ٚ Opportunities for continued learning and skill enhancement through professional development.
ٚ Connections and professional relationships among members through networking.
ٚ Access to the latest research and industry insights through highquality journals and publications.
ٚ SMA’s Professional indemnity insurance for Sports Trainers.
Ongoing professional development remains a priority across all membership categories. Members have placed an emphasis on accessibility and convenience: more online events, including webinars, virtual workshops, and online training sessions. Additionally, there is a strong interest in high-quality, in-person events that offer valuable networking and hands-on learning opportunities.
Over 83% of members stated that they believe SMA is performing better now than this time last year.
The SMA annual Conference remains a key professional development experience, offering significant value through sessions, workshops, and networking opportunities.
Nearly 90% of respondents are satisfied with the frequency and relevance of our communications. Our weekly update emails are central to our communication strategy, as is informing and building engagement through our social channels. We will further finesse our communications to make it even more relevant to members going forward.
Members have told us that they wish to see further investment in professional development opportunities, including CPD tracking, and in-person symposia. Other member priorities include:
ٚ Enhancing ways to connect members with each other including
I joined SMA for some different perspectives fairly late in my career and have been very pleased with what I’ve learned.
- SMA Member
improved opportunities for learning, mentoring, and networking.
ٚ Advancing research and research advocacy, with better support for research initiatives, and a stronger voice in advocating for the sports medicine industry.
ٚ Establishing a clear and distinct position within the industry, especially in relation to other
associations which our members may also be members of. By clarifying our unique value proposition, we can strengthen our professional identity and better serve our members.
Sports Trainer Associates highlighted those needs critical to their professional development. They have asked for more courses that cater specifically to their career growth. Ensuring broader access to training, particularly in remote and rural areas, is essential for their continued growth and capability.

In the few months since the survey, SMA has already taken action. We have identified new projects for inclusion within our Strategic Plan, as well as several new initiatives which will boost our capabilities:
ٚ The Board has endorsed a major project to transform our Safer Sports Program delivery. This project’s outcome will deliver a more consistent and modern experience for course participants and improve our internal efficiency.
ٚ We will be launching our online ‘Find a Sports Doctor’ tool, allowing the public to locate SMA Sports Doctors within their local area. This new tool is part of a
re-launch of SMA Sports Doctors (formerly SDrA), a special interest group for medical professionals with an active interest in sports injury management and professional development.
ٚ Certificates of membership have been reinstated, with distribution to all members and associates, which will be reissued upon renewal.
ٚ Sports Trainer Connect – A new online booking system that will allow outside organisations and entities to advertise and connect with SMA Sports Trainer Associates.
Other projects we’re launching over the coming months include CPD tracking for members, and the launch of an SMA student network which will provide networking and PD growth opportunities tailored specifically to the needs of our Student and PhD Student Associates.
These are just a handful of the initiatives we have in the pipeline, all of which will enhance the overall member experience and support the ongoing professional growth of our multidisciplinary community.
We look forward to providing even more for our members in the coming months and meeting many of you at our upcoming events.









ASICS IS A LEADING PERFORMANCE SPORTS BRAND, CONTINUOUSLY DELIVERING HIGH-QUALITY, HIGHLY FUNCTIONAL FOOTWEAR FOR ENTHUSIASTS AND PROFESSIONAL ATHLETES ALIKE. THE BRAND HAS BEEN INNOVATING IN SPORTS PERFORMANCE TECHNOLOGY SINCE 1949, IN HOPES OF INSPIRING PEOPLE TO BE HEALTHY AND HAPPY THROUGH MOVEMENT.
Beyond the running arena, ASICS also produces quality sports footwear for track and field, tennis, football, netball, cricket, hockey and basketball.
The first sports athletic shoe produced by ASICS (or ONITSUKA Co. Ltd as it was known at the time) was a basketball shoe. At the time, basketball shoes were thought to be the most difficult athletic shoe to manufacture, but product was repeatedly tested and refined, until the first model was released in the spring of 1950.
Since this time, ASICS has continued to develop and innovate in the basketball space, with the brand leading the basketball footwear category in Japan.
Basketball participation rates for both adults and children continue to grow in Australia. The latest AusPlay data indicates that there is an estimate 1.11 million adults (15yrs+) and 476,000 children (0-14yrs) playing basketball. This is an increase of 1.3% in participation rates from the previous financial year and approximately 1.7% increase from prior to COVID-19.*

While participation numbers vary by age and gender, it is apparent that more and more young people in Australia are choosing basketball as their sport or physical activity of choice.
In February 2024, ASICS Oceania introduced the first ASICS Basketball shoes into the range here in Australia with the release of the Nova Surge 2 and the Gel-Burst. Additional models will be introduced in the coming seasons including the Nova Surge Low.
The Nova Surge Low basketball shoe provides energized cushioning for the aerial player and lateral stability to promote responsive transitions, while delivering excellent comfort.
The FLYTEFOAM™ Propel midsole foam provides responsive cushioning underfoot, while the lateral support in the midsole is improved through the expanded gauge at the lateral forefoot with an added PU material for side-to-side stability.
The synthetic leather in the upper is reinforced with PU material on the lateral side providing a secure hold on the foot.
To better understand the performance of ASICS basketball product in reference to popular product in the basketball market, ASICS Oceania partnered with Dr Chris Bishop PhD and his team at The Biomechanics Lab (TBL) to complete testing of ASICS products. Dr Bishop comments, “Despite the high lower limb injury rates in Basketball, the sales strategy for this footwear product category has traditionally been driven by marketing and player representation. From a biomechanical standpoint, considering the speed, high impact and change of direction demands of the sport, the players we see demand protection, without compromising agility and performance. In our opinion, that unique synergy of performance hasn’t really existed in the market to date. So, when we engaged with the consumer, irrespective of gender, the overwhelming feedback was players want a shoe that allows them to perform at their best. What that

shoe was, or its required design or features, was unknown to the player. They lacked advice. What they were dead fast on however was the shoe had to be comfortable. Comfort on court meant better performance.”
“At TBL, and in collaboration with UniSA, we have been exploring the phenomenon of footwear comfort for the best part of 10 years across a range of sports. This was our first foray into basketball. What really surprised me was the overwhelming feedback on the on-court comfort of


the range. Blinded, the Nova Surge Low consistently ranked as the most preferred shoe on comfort, agility and on-court performance compared to industry comparators. The big differentiating factor amongst player feedback, as well as in biomechanical testing, was how the shoe seemed to optimise the perception of stability and reduce the lateral thrust of force when landing and changing direction. Where 10 years ago the market felt they needed high-top designs to feel stable, intuitive geometric design seems to have leveraged and optimised the heel collar system and midsole design to provide enhanced stability to the foot, without compromising increased weight from extra shoe upper material.”
* (2023, October 1). AUSPLAY
National Sport and Physical Activity Participation Report October 2023. Clearinghouse for Sport. Retrieved May 20, 2024, from https://www. clearinghouseforsport.gov.au/research/ ausplay/results/participation-report
DR STEPHEN JASPER, The Jet Lag Guy

Introduction
With the Olympic Games in Paris (officially the Games of the XXXIII Olympiad) only weeks away, there’s a great deal of interest in maximising the performance of athletes who are competing in the games. It’s a long way from Australia to Paris, and athletes travelling there from Australia will be flying a long way, crossing multiple time zones. The difference between winning a gold medal and coming home with a silver medal is often down to fractions of a second –milliseconds – and it’s vital that they are able to perform at their peak.
Background
The Olympic Games are truly global, with host cities having been all around the world in Europe, North America, South America, and of course, twice in Australia. Often the participating athletes travel long distances across multiple time zones, and like other travellers are at risk of experiencing jet lag.
My own international travel in my previous career informed my
Jet lag tools such as Re-timer glasses or Sunnex lamps use bluegreen light to offset the effects of jet lag, while light at the red end of the spectrum has no effect on the circadian rhythm.
research, as I was employed in the pharmaceutical industry in clinical research and travelling the world. I conducted research for my PhD in jet lag and executive performance in the international business space. Typically, there is no thought of preparation for business travellers, and no or very limited support available. Yet it is vitally important that these
workers perform at their peak to facilitate international business, and simple measures can absolutely transform the effect of jet lag.
Olympic medal research
I took on the project of analysing the Olympic Games medal tallies and the effect of jet lag on performance. I began my analysis with the 1960 Olympic Games in Rome and finished with the then most recent games in Rio de Janeiro in 2016. The reason I began my analysis in 1960 was that until then, international jet travel was uncommon, and most people still travelled internationally by boat. There’s no such thing as boat lag – in order to experience jet lag, people need to travel rapidly across multiple time zones.
Analysing the data for the Olympic Games proved to be challenging, to say the least. Firstly, they are only held every four years, unlike most other tournaments that are annual. This means that for the same time period, you would only have a quarter of the data compared with, for example, the NBA.
A bigger problem is the appearance and disappearance of key nations, disqualifying a lot of the data. The Soviet Union was a behemoth in terms of Olympic medal counts until its dissolution in 1991, becoming no less than 15 separate republic that competed at subsequent Games individually. Nor was there any longer a separate East Germany and West Germany, but a single Germany after 1990.
Small countries competing at the Olympic Games would typically have volatile results – for example, the nation with the highest number of Olympic medals per capita is the tiny state of San Marino in Southern Europe, while the island nation of Tonga also punches well above its weight.
During the time period of data analysis China underwent massive cultural change, from being a non-participant in the early games to a powerhouse that hosted the 2008 Games in Beijing.
Many countries such as Australia, the USA, Russia and Canada have multiple time zones, and a decision about which time zone would be used had to be made as the starting point (in all cases, the most populous one).
Finally, there was a massive change in the number of gold medals awarded per Olympic Games, rising from 152 gold medals at Rome in 1960, to more than double with 306 at Rio in 2016. All of these factors made analysing the medal counts and jet lag challenging.
Let’s start by looking at what jet lag isn’t.
Imagine that you’re living in Sydney or Melbourne, and you’re going to travel the full length of the Trans-Siberian railway, from Vladivostok to Moscow, a journey of seven days. (I realise that now is not the time to be travelling to Russia, but let’s use this analogy.) You

board a plane in Sydney or Melbourne to fly overnight to Tokyo, a flight time of about 10 hours. Arriving early in the morning at the airport, you take a train into central Tokyo. One you arrive, you need to get to the town of Sakaiminato – half a day’s travelling and three trains away from Tokyo. You get to the ferry terminal for the boat ride to Vladivostok. Arriving at Vladivostok after 44 hours on the ferry, you clear customs and get in a taxi to your hotel. Finally – finally! – you check into your grim Soviet-era hotel. You are exhausted. You just want to jump into the shower, grab a bite to eat, and get into bed. You have a severe case of travel exhaustion.
But you are not jetlagged.
Vladivostok is in the same time zone as the east coast of Australia. While it is arduous travelling for such a long time, the time zone hasn’t changed, so there’s no disturbance to the circadian rhythm.
Now let’s contrast a second scenario – a supersonic flight from Sydney to London. The flight, which is the
If you think back to how well Australia performed at the Beijing and Tokyo Olympics (14 and 17 gold medals respectively) versus our medal tally at London and Rio de Janeiro (in both cases, 8 gold medals), you can see that our gold medal tally is approximately halved when our athletes fly long distances across multiple time zones to compete.

latest technology, only takes three hours from take-off to landing. You have a comfortable seat that you can recline in easily (first class, of course), with healthy meals and a chauffeur in London to take you to your hotel. You arrive at your London hotel refreshed after a pleasant journey.
But the jet lag will be brutal.
What has happened in the second scenario that didn’t happen in the first was a massive disruption in time zones. Our bodies run on a clock called the circadian rhythm, which is why we’re most awake during the daytime and most asleep at night, and why we don’t typically eat a large meal at three o’clock in the morning. The circadian rhythm is a biological phenomenon, involving such variables as core body temperature, metabolic rate, cortisol and melatonin levels.
To regulate the circadian rhythm, we have special receptors in the eyes in the intrinsically photosensitive retinal ganglion cells of the retina that detect light but have no input into vision.
These cells send a signal to a part of the brain called the suprachiasmatic nucleus, which regulates the circadian rhythm by releasing the hormone melatonin when it is dark. The word melatonin is derived from the Greek word melas meaning “black” or “dark”, which is also where we get the word for melanin, the dark pigment in the skin. The existence of these cells that detect daylght explains why many blind people know when it’s daylight, even if they can’t see it.
These cells are most sensitive to light in the blue-green part of the spectrum. Jet lag tools such as Re-timer glasses or Sunnex lamps use blue-green light to offset the effects of jet lag, while light at the red end of the spectrum has no effect on the circadian rhythm.
Having discussed the circadian rhythm, let’s now add the concept of chronotypes – because not everyone’s circadian rhythm runs the same. We talk about some people being morning people – people who naturally wake up early and have done half a day’s work before breakfast. Don’t expect these people to be the life of the party
in the evening though; they’re likely to want to be in bed well before 9 pm. Other people are what we refer to as night owls – they like to be up at the crack of noon, and don’t even think of speaking to them until their first cup of coffee. But in the evening, they absolutely come alive. This diversity in circadian rhythms is referred to as chronotypes, where people peak at different times of the day.
Age is one of the key factors that affects chronotypes, as any parent of small children will be only too aware. When you have small children, sleepins are a thing of the past. On the other hand, teenagers will make those same parents ask themselves what happened, as they struggle to get their teenage children out of bed in the morning, and their children stay up until all hours at night. There’s a general trend for people: infants and toddlers are morning people, switching to being evening people as teenagers peaking at age 17-18 years, then drifting back to being a morning person in later life.
Sex is only a minor factor, with males on average being slightly more inclined to being an evening person and peaking

in their teenage night owl behaviour slightly stronger and slightly later in life.
There is, however, a strong genetic basis for chronotype. While there are several genes that regulate the circadian rhythm, one specific gene (the PER3 gene on chromosome 1) appears to have an impact. People with a deletion in this gene are typically night owls – and there’s nothing that can be done to alter that.
Chronotype has a direct impact on jet lag because it interacts with the direction of flight, which I’ll now discuss.
The direction of flight has a significant impact on jet lag, and for most people, “east is a beast, west is best”. This makes sense when you think about it: if you fly west, the day seems to stretch out, so westbound travellers need to stay up late and sleep in the next day, which most of us find is
easy. If you fly east, however, travellers need to go to bed early (when they’re not yet tired) and wake up early (when they’re still tired), and for most of us this is much harder. This is why you often hear of people going from Australia to Europe for a holiday and experiencing little jet lag when they get to Europe, only to be hideously jetlagged when they return to Australia.
There are two completely different mechanisms to adjust to different time zones, called phase advance (for flying east) and phase delay (for flying west). To illustrate the difference between these two mechanisms, an animal study was conducted where the active ingredient in Viagra (sildenafil) was injected into hamsters in a jet lag simulation. The treatment was effective, but only for the eastbound simulation. Sadly, no human data are available.
Examining the Olympic medal counts over several decades, a couple of patterns emerged: firstly, there were
fewer gold medals for athletes as they crossed more time zones. If you think back to how well Australia performed at the Beijing and Tokyo Olympics (14 and 17 gold medals respectively) versus our medal tally at London and Rio de Janeiro (in both cases, 8 gold medals) and you can see that our gold medal tally is approximately halved when our athletes fly long distances across multiple time zones to compete.
The surprising result when I did the analysis was that the average number of silver medals increased when crossing multiple time zones. What this points to is that athletes who would otherwise have won a gold medal miss out by a small fraction, and instead come home with a silver medal.
Often the difference between a gold medal and a silver one is measured in milliseconds – so an athlete and their coach may not notice any impairment due to jet lag, until that final result.
How do you manage jet lag? There are four key cost-effective

and drug-free strategies that can reduce the deficit in performance due to jet lag:
1. Know thyself. You’ll typically know whether you’re a morning person, a night owl, or in between, and if you don’t, you can ask your nearest and dearest. Being a night owl isn’t a matter of being lazy – it’s age-related and there are genetic factors that determine your chronotype. There are some free online quizzes that clarify this, such as the Morningness Eveningness Questionnaire.
2. Direction of flight. Now that you know your chronotype, look at the direction of the flight. For most people, “east is a beast, west is best”, but if you’re very much a morning person, you’ll be the other way around, with eastbound flights being less stressful than westbound flights.
3. Scheduling. Adjust your current schedule to the new time zone as much as possible in advance. This could include arriving to your destination as early as possible. if flying west, wake up and go to bed later than usual, and if flying east, earlier. If you can give yourself a full week to scheduling before you leave, it will make adjusting to the new time zone so much easier.
4. Sunlight. As I mentioned earlier, our circadian rhythm is calibrated to sunlight, so a simple strategy of getting outdoors as much as possible will help reset your body clock. If you are scheduling to the new time zone and there’s no sunlight when you want to be awake (or you’re travelling to somewhere dark), then consider the use of artificial light sources that mimic sunlight such as Re-timer glasses or Sunnex lamp that have the frequency of light calibrated to have maximum impact on jet lag.
Clearly, there are benefits of managing jet lag for athletes who travel internationally. The number of gold medals typically gets cut in half when competitors fly across the world to compete, and these simple adjustments can make a huge difference in total gold medal count.
It is absolutely vital that athletes’ jet lag is managed comprehensively in order for them to perform at their best and potentially win gold medals. The simple, low-cost, drugfree strategies that I have outlined here could have a substantial impact on performance and abilities at the upcoming Paris Olympic Games, and I would urge athletes and coaches to do everything possible to offset the effect of crossing multiple time zones to compete. These adjustments, while only slight, can make the difference
between coming home with a gold medal versus a silver one.
I’d highly encourage you to read my detailed paper titled
“Travel across time zones and the implications for human performance post pandemic: Insights from elite sport”
Published in Frontiers in December 2022. Scan the QR code to access the article.


Dr Stephen Jasper is the director of The Jet Lag Guy, an organisation dedicated to supporting international business travellers manage and maintain their health and cognitive function. After completing a PhD examining jet lag and executive performance, he published an academic article on the effect of jet lag on Olympic medal counts.
His mission is to transform the conversation around jet lag. He has gained national and international media attention as a subject matter expert on the effect of jet lag on Olympic medal counts, with interviews with The Australian, 3AW, ABC Radio Brisbane, ABC Radio Melbourne Drive and Canberra Drive, and BBC Breakfast Radio Gloucestershire.
IN OCTOBER 2024, SMA IS CO-CONVENING OUR CONFERENCE WITH THE AUSTRALASIAN COLLEGE OF SPORT AND EXERCISE PHYSICIANS (ACSEP) AT THE ICONIC MCG. A HALLMARK OF SMA’S ANNUAL CONFERENCE IS THE HIGH CALIBRE OF KEYNOTE SPEAKERS, AND THIS YEAR IS NO DIFFERENT.

A/Prof Clare Minahan

A/Prof Clare Minahan is delivering SMA’s prestigious Sir William Refshauge Lecture.
Clare is an applied Sports Scientist with interests in the advancement of human performance and a key focus on the determinants of performance in female athletes. She applies her knowledge of female athletes to lead the development, implementation, and delivery of ‘GAPS’; an inclusive sports pathway program for emerging and parasport athletes in developing countries of the Pacific. GAPS is now formally recognised and supported by the Commonwealth Games Federation as their flagship sports development initiative for women in developing countries of the Commonwealth.
Clare’s Conference presentation focuses on the advancement of athletic performance in women and understanding their potential. There is plenty of investment in injury prevention strategies and sport participation programs for women, however sport performance research is largely ignored – only 3% of all sport performance research is performed exclusively in women. Clare will divulge how she aims to unlock new dimensions of athletic excellence and redefine our understanding of human potential, with her research in this area.
2024 VINCE HIGGINS
Dr Dinesh Palipana OAM
Dr Dinesh Palipana OAM is delivering ACSEP’s distinguished Vince Higgins Lecture.
Dinesh is a doctor, lawyer, disability advocate and researcher, and was the first quadriplegic medical intern in Queensland. He is an ambassador to the Human Rights Commission’s Includability program, a founding member of Doctors with Disabilities Australia, and an advisory board member to HealthyLife. He was awarded the Medal of the Order of Australia in 2019. His autobiography, Stronger, was published by Pan Macmillan in 2022.
Dinesh co-leads the BioSpine project, which combines the most promising advances in spinal cord injury recovery, founded at centres like EPFL, UCLA and Duke University. BioSpine aims to reverse paralysis in people with spinal cord injury using thought-controlled rehabilitation, electrical stimulation, virtual reality and drug therapy.
Dinesh’s dream is to see a future where people who sustain paralysis through spinal cord injury can recover. The project is on the verge of publishing results on an initial study of five people, with a larger sample study in the works over the next couple years.

A/Prof Brent Edwards
Brent is an Associate Professor and UCalgary Research Excellence Chair within the Faculty of Kinesiology at the University of Calgary. Brent’s keynote investigates lower-extremity bone strain during locomotion and the relationship between stress fracture risk and practical alterations in training intensity, training volume, and spatial-temporal kinematics. His research may benefit runners of all levels, athletes and military personnel that participate in running activity.

A/Prof Prue Cormie
Prue is an accredited exercise physiologist whose research and clinical work focuses on the role of exercise in the management of cancer. Prue will explore how cancer patients who take exercise medicine – who perform quality exercise regularly – experience fewer and less severe treatment-related side effects, have a lower relative risk of some types of cancer recurrence, and a lower relative risk of dying from some types of cancer.

Prof Lauren Ball
Lauren has earned an international reputation for improving health of communities by creating knowledge, translating it into real life scenarios and evaluating improvements for people, health care providers and funders. Lauren will discuss the work of her research centre in Springfield QLD, with a focus on creating solutions to complex needs across diverse areas including physical activity, healthy eating, health services, domestic violence, financial wellbeing plus more.

Prof Martin Hägglund
Martin is professor of physiotherapy at the Department of Medical and Health Sciences at Linköping University in Sweden. He’s also a senior researcher in the Football Research Group (FRG) that has led a large-scale injury surveillance study in professional football in collaboration with UEFA, known as the UEFA Elite Club Injury Study. Martin’s focal research includes sports injury epidemiology, injury prevention and implementation, and return to sport protocols.

Dr Andrew Massey
Andrew joined FIFA in 2020 as Medical Director and is involved in preparing the medical infrastructure for FIFA from World Cups to grassroots football. He began his career in the game as a professional footballer and combined this with his studies in Physiotherapy. Prior to joining FIFA, Andrew was Head of Medical Services at Liverpool F.C. responsible for the medical, physiotherapy and sport science departments.

Dr Ruth Chimenti, DPT, PhD
Ruth is an Assistant Professor in the Department of Physical Therapy and Rehabilitation Science at the University of Iowa. She has clinical experience in orthopaedic physical therapy and research training in biomechanics and ultrasound imaging. Ruth’s work focuses on the evaluation of underlying mechanisms that contribute to pain and disability in foot and ankle musculoskeletal conditions and development of their treatment strategies to optimise clinical outcomes.





In occupational training, the rigorous demands placed on recruits, particularly within specialised sectors such as law enforcement, often serve as a crucible, testing physical and psychological resilience. My recent cross-sectional cohort study conducted on incoming Police Force recruits from January 2022 to October 2022 offers invaluable insights into the complex relationship between injury history, persistent disability, and physical performance. My research also adds to the minimal data available on law enforcement injury, pain, and performance data worldwide.
Law enforcement agencies around the globe have contended with the challenge of optimising recruit training and physical capabilities testing. Challenges include the practices and procedures of physical examinations to ensure a balance of both efficacy and safety amongst recruits. Despite stringent entry standards, the prevalence of injuries, particularly those affecting the lower limbs, continues
to be an immense problem for law enforcement agencies. Such injuries can impose individual hardship on the recruit and incur substantial costs to the government and society, considering the considerable financial investment in training a single recruit.
During Police Force training, a recruit can expect to be instructed in a diverse program of modules, spanning crucial aspects of theory to practical skills. The training regimen for many Police Force academies around the globe incorporates physical fitness sessions that involve obstacle training as well as occupational safety training, covering essential skills such as arrest and restraint techniques. Beyond the physical domain, recruits are instructed in theoretical studies, including basic fundamentals of investigative scenarios and in-depth immersion into legal studies. Driving skills for general operations and in
emergency settings, weapons training and specialised skills dependent on the location of the policing organisation, rounds out the basic skills imparted to police recruits as they are introduced to their new careers.
To ensure the capability, robustness, and resilience of Police Force recruits, rigorous tests are applied to ensure the recruits are up for the challenges that lie ahead. A commonly applied test in assessing cardiorespiratory baseline fitness is the beep-test. In this test, performance is graded, with a higher level achieved indicating better cardiorespiratory ability. Police Forces worldwide use the beep-test as well as other police-specific functional testing. While not formally validated, the policespecific functional test used in this study has been employed for over ten years. It involves a timed sprint around a track, transitioning to a second lap filled with various obstacles – balance beams, fences, walls, sand pits, hurdles, window climbs, fence scaling and
various weighted carries (e.g., kettlebell farmers walk). The faster a recruit finishes the course, the better their occupation-specific functional capacity is perceived. This approach ensures recruits are not just fit, but wellprepared for the physical demands they will face in their policing careers ahead. This component is then retested upon completion of basic Police Force training to assess their progress.
My study was conducted at an Australian Police Force Academy, where we invited recruits embarking on an extensive 28-week training program to complete a comprehensive online survey that included patientrecorded outcome measures, and we received responses from 121 recruits. Physical performance data from participating recruits were captured by physical training staff at the Police Force Academy. Key metrics evaluated included injury history within the preceding 12

months, persistent disability levels, cardiorespiratory fitness assessed via a multi-stage fitness test (commonly known as the beep-test), and occupation-specific functional capacity gauged by a Police Force specific Physical Performance Evaluation.
injury prevalence
In my study, I wanted to ascertain whether recruits had injuries or pain prior to undergoing the rigorous tests and training required to become a qualified police officer. We found that 1-in-2 recruits reported at least one
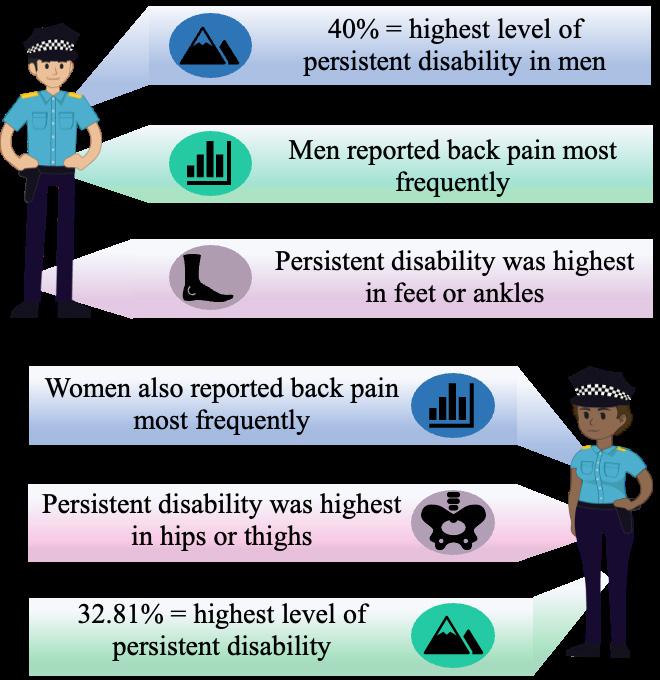
injury with varying degrees of pain or physical limitations experienced within 12 months of joining the Police Force. Further, 1-in-5 of recruits experienced more than one injury region in the preceding 12 months. Recruits who had a prior injury indicated a level of persistent disability that ranged from 0% to 40%. I also found that preacademy injuries were most frequently reported in the lower back and knees. These findings differ slightly from what is experienced during training as Police Force recruits mainly experience lower-limb and not lowerback pain during their training. This data highlights the need to expand pre-screening processes to assess how these injuries may affect performance and potentially latent vulnerabilities going into training and beyond.
The most pertinent discovery of my research for the Police Force was that a significant relationship between persistent disability resulting from pre-academy injuries and impaired physical performance in occupationalspecific tasks exists. Recruits exhibiting higher levels of persistent disability demonstrated worse outcomes in the physical performance evaluation, which is designed to encompass a range of physical challenges mirroring
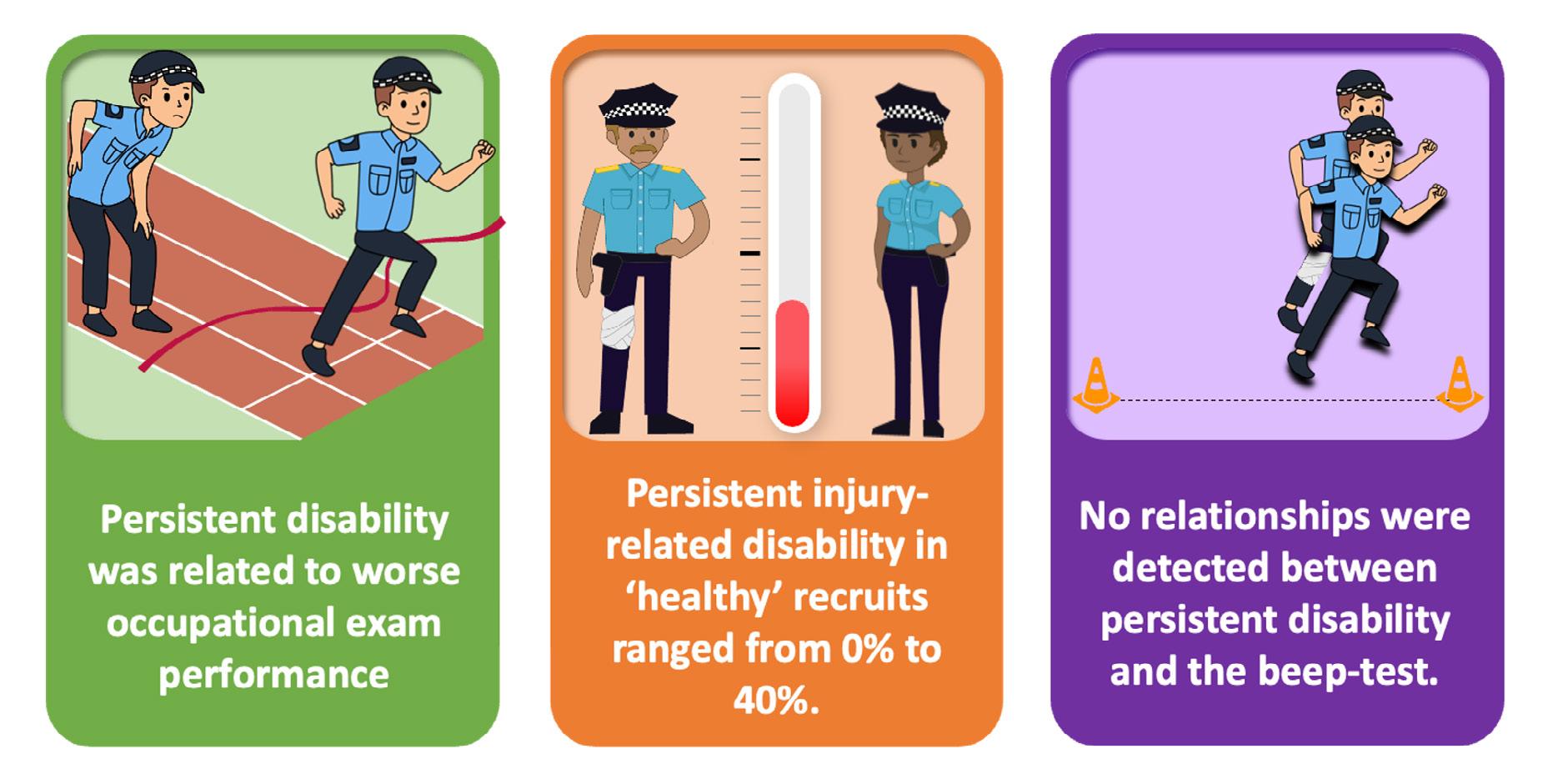
real-world obstacles and physical challenges faced by those in policing and law enforcement. Interestingly, whilst persistent disability emerged as a significant determinant of timeto-completion in functional testing, its impact on cardiorespiratory fitness test levels appeared negligible.
My study’s findings convey implications for Australian Police Force training programs and overarching policy frameworks governing police force recruitment. Due to globally recognised recruitment challenges in the current employment climate for tactical-related professions (including military recruits), most Police Force entry standards around the world have been reduced to facilitate increased recruitment. However, it goes without saying it is vital that the standard of graduating Police Force officers is maintained. Thus, implementing strategies to better screen for injury history and persistent disability, with interventions designed to address this persistent disability, may improve occupational skill standards, irrespective of entrance standards.
Finally, my study’s findings underscore the necessity of revisiting existing screening protocols to incorporate more nuanced assessments capable of capturing latent vulnerabilities that might predispose recruits to injury or functional limitations. This more detailed approach would not only safeguard the well-being of the individual who is about to undertake physically arduous occupational training but also enable increased chances of operational readiness of a recruit throughout their training and onwards to maintaining public safety as a graduated Police Officer.
My study identified recruits’ persistent injury related disability before the commencement of Police Force recruit training. Thus, it is imperative to understand how persistent
disability and performance metrics influence future performance throughout academy training and academy attrition. Future studies will address these issues
Figure 3. Quantification of the performance and persistent-disability relationship

For every 1% of persistent disability
A recruit will perform the functional fitness test up to 12.34 seconds slower than an unincumbered counterpart
and further position the relevance of our findings into tangible and usable tools that will improve retention based on health and functional capacity.
My cross-sectional study amongst WA Police Force recruits sought to shed light on the complex relationship between injury history, persistent disability, and physical performance. The findings underscore the imperative of adopting a multifaceted approach, including the early identification of injuries and resulting persistent disability prior to academy commencement and introducing targeted management strategies. This would likely reduce injury risk and optimise the operational readiness of recruits to complete training and be ready to engage in full duties upon completing their training.

Vanessa Sutton, is a final-year Master of Medical and Health Science by research candidate at Edith Cowan University, with a research interest in nutrition, health and injury prevention. Following the attainment of a Bachelor’s degree in Health Science (Maj. Nutritional Bioscience) in 2021 and motivated by her personal experiences and those of her family, who have served for generations in the Western Australia Police Force, Vanessa’s research has achieved international recognition. Vanessa has been awarded both the ASICS Best Early Career Researcher Award for Sports Injury Prevention at the 2023 ASICS Sports Medicine Australia Conference, and she was also awarded the 2022 Australian Epidemiological Association’s top student prize. Vanessa brings a unique perspective to her research, shaped by nearly a decade of service in the Royal Australian Air Force (RAAF) Police. Her active military service is recognised with the Australian Active Service Medal, Iraq Medal and Australian Defence Medal.
DR JOHN ORCHARD AM, Sport & Exercise Physician
Legend has it that John Snow turned off the Broad St Pump in central London (Figure 1) in 1854 during a cholera outbreak to help clean the water supply.[1] Historians agree that he was the leading advocate of cleaning the water supply with his epidemiological study of the cholera outbreak. It is perhaps the most legendary public health action of all time. Until the water had been cleaned no one realised how dirty it was. With social discussion from the 1850s less faithfully recorded, we don’t know how many people complained about the efforts to clean the water; Twitter wasn’t around for anyone to post “my pronouns are prosecute/Snow”, but perhaps the anger and resistance to change would have been there.
Our modern concept of clean air was initially focussed on reducing air pollution (for example from car exhaust), still an important aim. In the 21st Century, we’ve needed to consider clean air from multiple new perspectives. The circulating amount of CO2 is the primary pollutant relating to global warming. Pollution from bushfire smoke became particularly relevant in Australia in 2019.[2] Then in the second year of the
COVID pandemic we appreciated that the virus was airborne and “clean air” developed an additional meaning of “air which was free of circulating respiratory viruses”.
In the modern era we have superb non-fiction writers like Michael Lewis to document the story behind the story. In the sporting world, he is most famous for writing “Moneyball” and “The Blind Side”.[3, 4] His sporting novels are similar to his finance novels (which often focus on arbitrage); Lewis’ obsession is in profiling someone or some group with inspired ideas who found a competitive advantage (a way of beating the traditional market). One exception is his book “The Premonition: A pandemic story”.[5] Whereas he normally writes a story profiling the winners and explaining why they won, The Premonition looks at how the USA (and UK) squandered their advantage in being the most prepared countries for the COVID pandemic (when they had many experts who were almost certain a modern pandemic would eventually come). The winners (namely those who found the competitive advantage) in the 2020 and 2021 years of the pandemic were actually Australia and New Zealand.[6, 7] Part of their advantage and “winningness” included that Michael Lewis wasn’t

allowed to enter either country to interview anyone in 2020 or 2021! The majority of Australians knew how well we were doing at the time (Mark McGowan as a left-wing Premier in a traditionally right-wing state of Western Australia was re-elected with a record 70% of the vote in 2021 for shutting down his state to the rest of country to keep COVID out). Australia was one of the safest countries to live with respect to mortality – in the history of the humankind – from April
Sport and society still haven’t found the middle ground on
2020 to March 2021 as we had hardly any COVID or any other respiratory viruses circulating in the community. [6, 7] [8] A recent review from The Lancet confirms that in almost every country life expectancy dropped in 2020 and 2021 with Australia and NZ being exceptions.[9] This was for a period that both seemed long (at the time) but was quite short historically. Ironically in the years when Australia and NZ were “winning” against COVID [8] it felt to many as if we were losing, because we could appreciate the loss of freedoms more than appreciate the reduction in deaths. In sporting terms though, the pandemic is now “over” in the same way that a football match is “over” if you were leading during the first half, and have now squandered that lead so badly you’ve decided to turn the TV off and no longer watch the match. The virus is now winning and our life expectancy is lower than it was in 2019 (also phrased that we still suffer “excess deaths”).
Professionally, 2020 and 2021 were very stressful years for those of us working in sport.[10, 11] On a personal level, though, I noticed one pleasant side effect. My major chronic health problem – chronic sinus infections – which I’d suffered from for 30 years, sharing them with 10% of the population,[12] disappeared completely. I used to buy sinus washout kits the way other people brought toothbrushes and toothpaste. But in 2020 and 2021 I didn’t get sinus infections, and relative to previous years, neither did many athletes.[13] I’ve noticed a return of sinus complaints in athletes in 2022 and 2023, but so far post “return to normal”, I have managed to hold them at bay with my new understanding of what “clean air” means.
I’m now in the (maybe) 2-5% of people who still wear masks on public transport, on planes and at airports and in other crowded indoor venues (including when listening to lectures at conferences). I carry around an Aranet 4 portable CO2 monitor to work out when I might need to mask up. When I work in the clinic I still mask up and
keep the window open to circulate air (which brings the CO2 readings down from 1500 to 600, Figure 3).
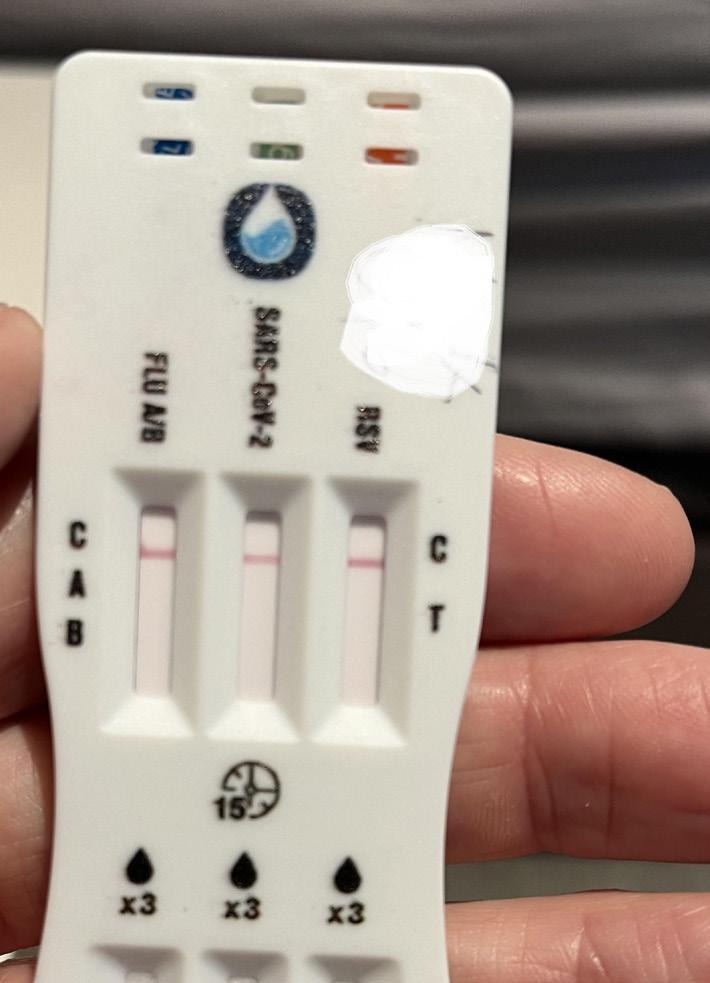
If someone in our house gets a sore throat or runny nose, we still use RATs and we still isolate anyone ill. Other people don’t want to bother and perhaps don’t need to bother, because they weren’t sufferers of chronic sinus problems like I was; and they don’t have cancer, and aren’t immunosuppressed or just elderly. But in the field of Sport & Exercise Medicine, where our athletes are healthy and “over COVID”, there are still reasons we should bother a bit more than we are currently (in 2024, which for those counting is year 5 of the pandemic but a year since the end of the emergency phase was declared).
Sports medicine (and other) conferences
At least two recent Australasian sports medicine conferences since we “opened back up” have turned out to be superspreader events in terms of both COVID-19 and Influenza A. Are sports medicine conferences any different to other mass gatherings
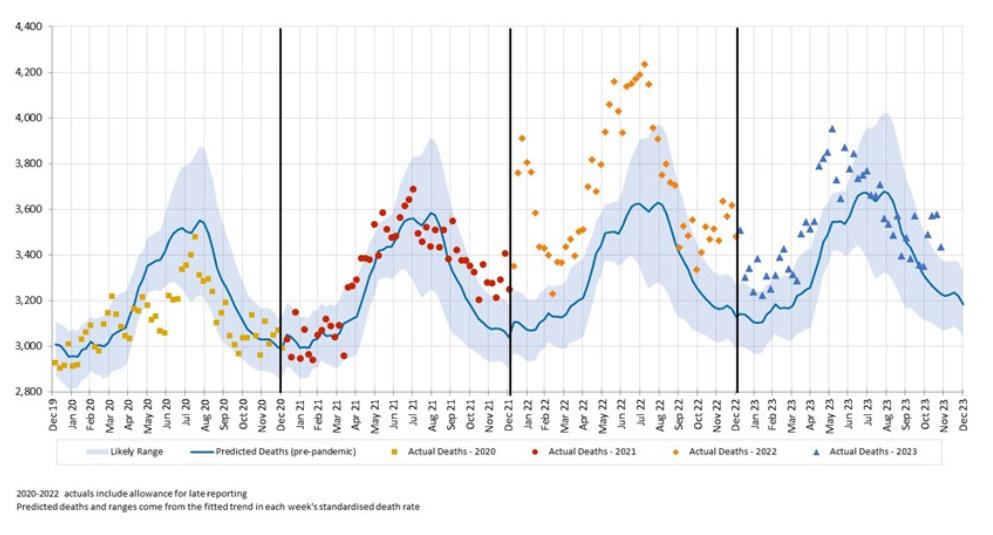
Figure 2: Expected versus actual deaths Australia for 2020, 2021, 2022 and 2023 (reproduced from www.actuaries.digital/2024/03/04/ excess-mortality-for-2023-likely-to-be-about-half-of-2022/)

where dozens fly in from multiple different venues? Perhaps it is just that Australian SEM physicians are now so familiar with respiratory diagnosis[10, 11] we are amongst the last remaining groups that could still be bothered to test (even if not bothered enough to mask). In the days before we knew any better, people used to complain about “the air conditioning” in hotel rooms causing blocked noses and
sore throats. Now we realise it is almost certainly a high percentage of conference attendees catching whatever respiratory viruses are circulating (as if you’ve spent thousands of non-refundable dollars to attend, people don’t tend to “stay home when sick”[6]). We are now realising that in the absence of precautions a high percentage of conference attendees will catch COVID (again) as


a cost of attending. So this is a clear challenge as to how we can keep conferencing without the tax of high risk of getting a respiratory illness.
When can elite athletes “afford to get sick”?
Professional athletes bore some of the worst psychological impacts of the lockdown years,[14] with some Australians athletes having to do 14 days of hotel quarantine on 5 or more occasions over 2020-2021. Understandably, as a group they are well and truly “over” what they went through in these years and some are too traumatised to even discuss any ongoing COVID precautions. Yet denial can’t escape anyone from two unarguable facts: (1) That COVID is still circulating and if you live a “normal” life you’ll inevitably catch it again; (2) That even though you are now allowed to compete/play while COVID positive, that it only has one possible effect on your athletic performance and that is to reduce it. It’s a challenging question (for team selectors) as to whether a superstar with COVID will perform better than a fringe player who is
Sport and society still haven’t found the middle ground on
COVID-free. It is a fact, not a question, that the superstar’s performance will only potentially be worse, not better, if competing/playing with COVID. Athletes love to use the cliché of “doing the one percenters” to try to get better, and wearing a mask on a crowded plane, for example, absolutely is a one percenter (in both senses – that it improves your chances of performing well at your destination, and that only about one percent of athletes could be bothered taking this performanceenhancing measure). Doctors arguing with athletes that they should consider masking all the time in crowded venues are not currently going to win very often, but it is worth considering when this argument might be won. On the way to compete in an Olympic Games, for example, where you get one shot every four years. That would make a lot of sense. In the lead up to a Grand Final (where statistically you are doing well if you manage to play in one every fourth year of your career).
A State of Origin match, maybe. Your International or first grade debut match. NASA put its astronauts into quarantine in the lead up to shuttle launches because they “couldn’t afford to have anyone sick” after they had been blasted into space.[15] Athletes need to ask themselves “when can I afford to get sick?” That is the time when you don’t need take precautions. When you can’t afford to get sick, you should be taking some precautions (and if you lived in Australia and New Zealand in 2020-21 you know what they are and which ones can still be done with minimal inconvenience).
The specialty of sport and exercise medicine has been surprised in two different directions in the past few decades. The bad news is that the majority of medical interventions, where investigated, have been shown not to work.[16, 17] The good news is that an exercise-based intervention (the signature treatment of SEM) works not only for treating many presentations,

but has the side-effect of decreasing all-cause mortality (improving longevity). Many SEM physicians have added dietary advice to their exercise advice as our clientele moves towards patients seeking the healthiest possible lifestyle specialist advice. It makes sense for us to consider “clean air” advice for patients, given it is now evident that avoiding respiratory viruses also increases longevity. [6,
The realities that we get more respiratory viruses in winter which explains the higher death rates every winter, along with the fact that Japan – with a mask-wearing and clean-air culture – has higher life expectancy than any other large country tell us that clean-air is a universal good like regular exercise. The differential death rates from Australia in 2020, 2021 compared to 2022 and 2023 should beg the question to everyone interested in health: do you want to be breathing the air that causes you to live longer (virus-free) or causes you to die quicker (containing viruses)?


Can capitalism provide the disruption?
Almost all of the heavy lifting at cleaning the air during 2020-21 was done by governments, usually against the resistance of business. Now that the population has swung from being a clear majority interested in clean air to being a clear majority no longer interested, the governments in Australia and New Zealand are unlikely to legislate to assist with cleaning the air. Are we stuck with dirty air for good? There may be a way out.
Imagine the hypothetical of a highrise hotel that has two sections. To be eligible to stay in a room in the top ‘x’ (“green”) floors, the hotel institutes a rule that you need to submit a negative RAT every day for COVID and Influenza, and if you have any cough or runny nose (despite testing negative) you need to wear a mask when outside your room. In the bottom ‘y’ (“orange”) floors, it is business as usual, so that if you tested positive for COVID or started coughing profusely staying in one of the green floors they’d just refund your money and offer to rebook you into one of the orange floors. In addition, the hotel would apply the same policies to their staff, so that a staff member who tested positive would only work in the orange floors and you’d have a
guarantee on the green floors that all room cleaners, waiters and bartenders were free from respiratory viruses.
The big question is what would happen to a hotel who decided on a mixed policy and how many green floors would there would end up being and how many orange floors would there end up being? A hotel that did some market research would soon find that there might be a market for the green floors for people on business or holiday that were well and “couldn’t afford to get sick”. But in running such a mixed policy, they would be drawing attention to their orange floors being full of customers and staff with COVID and other respiratory diseases. It might sound like a bad idea for a hotel to split
their floors like this until they realised that they might not be under any obligation to provide the orange floors, as that is the service every other hotel currently provides. In other words, in Australia and New Zealand in 2020 and 2021 (due to government legislation), every hotel was a “green” hotel and anyone who wanted an orange hotel couldn’t have one. But from 2022-2024, every hotel is now an orange hotel and no one is servicing whatever market there is for green hotels. Neither is anyone offering green airline flights or green function centres or green cruise ships. The challenge for capitalism is to answer: why not? It isn’t everyone’s cup of tea to go back to doing RATs, but maybe cancer patients, doctors attending a conference and athletes about to play in a Grand Final might be some of the groups who could form the basis for such a market.
The biggest advances of capitalism come from developing a product that the consumers didn’t previously realise that they wanted. The product road testing for green hotels or green airline flights was all done in 2020 and 2021. If there were companies out there brave enough to offer such a product, would anyone want to buy it? The marketing should be obvious: “Can you afford to get sick? If not, stay/fly/eat here”.
For article references, please email info@sma.org.au

John Orchard is a Sydney-based Sport & Exercise Medicine physician. Opinions expressed in this article are personal. The main conflict to declare is having personally been a chronic sinus infection sufferer prior to 2020 but having been remarkably infection-free since pandemic measures were introduced.
THERESA HEERING, 2023
ASICS SMA Conference –ASICS Best Poster in Sports Injury Prevention
Why is it important to research paediatric ACL injuries?
Anterior cruciate ligament (ACL) injuries have severe consequences for the individual (e.g., long rehabilitation phase, risk of less future physical activity participation) and the health care system (e.g., high treatment cost) and are reported at increasing rates in children aged 5-14-years1. In Australia, females aged 5-14-years displayed the highest annual injury growth rates of ACL injuries compared to same aged boys (10.4% girls vs. 7.3% boys) but also older populations aged 15-44 years. 2 Thus, risk reduction approaches considering children’s unique needs are warranted to address the increasing risk of paediatric ACL injuries. 2
What to do we know about paediatric ACL injuries?
We know that most paediatric ACL injuries occur in sport settings during either organised (e.g., team sport, such as soccer) or non-organised, recreational activities (e.g., outdoor play, backyard trampoline). 3 However,

the actual injury mechanism (e.g., body position at time of injury) in this age group is not well understood and assumed to be similar to the injury mechanism observed in adolescents and adults.4 In adolescents and adults, ACL injuries occur most commonly in situations without body-contact, shortly after initial ground contact during landing or running related movements with sudden change in direction (e.g., a side-cutting
movement) or deceleration. An injury occurs when the load on the ACL is too high. When analysing a series of adult ACL injuries, it seemed that ‘axial compression force’ is the primary force responsible for non-contact ACL injury. 5 Additional movement characteristics such as a strong activation of the quadriceps muscle group or a medial displacement of the knee may increase the loading of the ACL and lower the force threshold for ACL injury. 5


How can individuals at risk be identified?
In Australia, females aged 5-14-years displayed the highest annual injury growth rates of ACL injuries compared to same aged boys.
For adolescents and adults, risk identification is based on examining factors that were previously mechanically linked to ACL loading (e.g., quadriceps muscle force). Risk factors are often classified as internal risk factors that are inherent to an individual such as anatomical or biomechanical factors, or external risk factors that are outside the
influence of the individual (e.g., weather, equipment). Of particular interest for effective risk reduction approaches are risk factors that can be modified through interventions –so called modifiable risk factors (e.g., biomechanical factors). To identify such risk factors, a variety of physical screening tasks and movement analysis strategies can be used. However, risk reduction approaches are often designed for adolescents and adults and lack specificity to children’s unique development.
In my PhD research, I wanted to understand modifiable risk factors and their assessment in paediatric populations. I conducted a systematic literature review and aimed firstly, to identify the modifiable factors mechanically linked to an increased risk of paediatric ACL injury and secondly, to determine the physical screening tasks and data collection tools used to examine modifiable risk factors in children aged under 14 years. The results of the systematic literature review were published as academic article (reference provided below) and presented as a poster at the 2023 Asics SMA conference.
What did the systematic literature review reveal?
The majority of the 40 eligible studies examined modifiable risk in regard to ACL injury risk in girls aged 10–13 years. These studies mainly focused on intrinsic risk factors as opposed to extrinsic risk factors. Similar to
Modifiable risk factors of paediatric
assessments in adolescents and adults, paediatric participants performed various physical screening tasks examined primarily with laboratorybased data collection protocols (e.g., marker-based 3D motion capture). Physical screening tasks included muscle strength testing, change in direction (e.g., side-cutting task) and/ or jump-landing tasks. A bilateral drop vertical jump was the most frequently examined physical screening task in the paediatric population. The findings of the systematic review suggest that modifiable risk factors are present in children, boys (e.g., larger medial knee displacement during counter movement jumps) and girls (e.g., larger medial knee displacement during tuck jump performance), aged 6-13 years. Accordingly, risk reduction strategies should be implemented as early as possible, regardless of sex/
AA promising strategy to decrease injury risk in childhood could be the development of a variety of skills considered foundational for sport participation.
gender, to improve body control and good movement techniques during movements that load the ACL and are observed at the time of ACL injury. Considering that most paediatric sport practices occur at the community-
level with few resources, cost-effective in-field assessment could be an important strategy for implementing injury risk screening in paediatric populations. However, in-field measures need further development to be child and ACL injury specific and easy to apply by the wider community.
Suggestions for childhood specific risk reduction strategies
Low proficiency in movement skills considered foundational for sport participation (e.g., jump, throw, bodyweight squat) may be linked to an increased risk of severe sporting injuries such as ACL injuries in paediatric populations. This is the next step in my PhD and if this link can be established, foundational movement skill proficiency, could be used as an easy-to-assess screening indicator for increased risk of injury and additionally


as a readiness-to-train indicator before starting demanding sport participation. Further, a promising strategy to decrease injury risk in childhood could be the development of a variety of athletic skills such as strength, speed, endurance, gross motor coordination and foundational movement skills. Here, participating in multiple sports seems advantageous rather than focusing on a single sport due to a larger exposure to multiple skills and less repetitive movements.
Finally, effective sport injury risk reduction is restricted by limited knowledge of sport injuries and lack of involvement of relevant stakeholders such as sport clubs, coaches, parents/guardians and the athletes themselves. Initiating conversations with coaches and athletes especially at the community-level, to understand their current knowledge, attitudes, and practices related to sports injury prevention could be crucial to overcome potential barriers to implementing prevention strategies.
For safe physical activity participation and the reduction of severe sporting injuries such as ACL injuries it is imperative to develop age-specific risk reduction approaches that are implemented at all levels of sport participation. For instance, a simple and cost-effective risk reduction strategy could be focussing on the development on movement skills considered foundational for sport participation in entry level organised sports and/or school based physical education. To develop targeted risk reduction approaches, important next steps are to better understand the actual injury mechanism and risk factors that are unique to paediatric populations. Additionally, relevant stakeholders should be involved in the development of these approaches to improve implementation and uptake.
Want to know more?
For the open access systematic literature review article see:
Heering, T., Rolley, T. L., Lander, N., Fox, A., Barnett, L. M., & Duncan, M. J. (2023). Identifying modifiable risk factors and screening strategies associated with anterior cruciate ligament injury risk in children aged 6 to 13 years: A systematic review. Journal of sports sciences, 41(14), 1337-1362.
The poster presented at the 2023 ASICS SMA Conference can be accessed by scanning the QR code.

For article references, please email info@sma.org.au

Theresa Heering is a final year cotutelle PhD student at the Centre of Physical Activity, Sport and Exercise Science at Coventry University, UK and School of Health and Social Development at Deakin University, Australia. Her background as graduate of human movement science (Bachelor of Science, University of Münster; Master of Science, Ruhr-Universität Bochum) and engagement as children’s sport coach led to her interest in understanding the increasing prevalence of anterior cruciate ligament injury (ACL) risk in children aged 6-13 years. Theresa’s PhD research aims to present the current knowledge on the characteristics and scenarios and specifically, modifiable risk factors of paediatric ACL injuries and to explore a novel way to identify paediatric ACL injury risk, namely through evaluating children’s movement skill proficiency. Theresa is due to submit her PhD thesis in the first quarter of 2024.

Check out the Cornerstone reviews under Topics
Improving menstrual health literacy in sport.
K. McGawley; D. Sargent; D. Noordhof; C.E. Badenhorst; R. Julian; A.D. Govus
Aligning categories of mental health conditions with intervention types in high-performance sports: A narrative cornerstone review and classification framework
Carolina Lundqvist; David P. Schary; Jenny Jacobsson; Laura Korhonen; Toomas Timpka
What is the most appropriate age for the first cardiac screening of athletes?
Jessica Orchard, Kimberly G. Harmon, Flavio D´Ascenzi, Tim Meyer, Guido E. Pieles JSAMS Plus
Call for papers: Physical Activity for People
Guest editors: Leanne Hassett;

This special Issue accepts articles on research in policy or practice evaluating the broad topic of physical activity for people living with disability across the lifespan.
Submission deadline: 30 September 2024
https://www.sciencedirect.com/journal/jsams-plus/about/call-for-papers# physical-activity-for-people-living-with-disability
• Factors associated with gym-based fitness injuries: a case-control study. L. Noteboom et al
• Disordered eating in elite youth athletes: A scoping review of studies published since 2000. C Walton et al
• Comparison of selected exercise training modalities in the management of PCOS: a systematic review and meta-analysis to inform evidence-based guidelines. A. Sabago et al
• Skier and snowboarder speeds at US Ski Area. L.L Stepan et al
• The effects of weather factors and altitude on physical and technical performance in professional soccer: a systematic review. S Illmer et al

24th International Congress on Snowsports Trauma and SafetyThe biennial meeting of the International Society for Snowsports Safety (ISSS)
Edited by Irving Scher, Jeremy Witchalls, Tracey Dickson
Exercise Oncology Edited by David Mizrahi, Carolina Sandler, Rob Newton Erika Rees-Punia

Can you tell us about your background and what motivated you to pursue a career in sports science?
I had a really active childhood and played multiple sports. I loved playing sport, competing in it, or watching it. I always thought I would be a physio because if I couldn’t be an elite sportsperson, then that would be one way to get involved. Then in year nine, I went to the Victorian Institute of Sport on a school excursion, and I saw a sports scientist delivering a VO2 Max test to an endurance runner. They were wearing a tracksuit and I thought that suits me perfectly. So, on the spot I switched to understanding
what a sports scientist is, what an exercise physiologist an, and from that day on, would pursue that as a career. I love the idea of trying to push boundaries in people who are highly motivated and already so talented.
Can you explain your role with the AIS Female Performance and Health Initiative?
This initiative started with a conversation I had with Swimming Australia where we started to understand that female athletes in Australia actually knew little about female specific health and wellness. We knew we had to do something
about it if we were to support their performance and health going forward. We then approached the Australian Institute of Sport and the timing was good because they were also thinking the same thing. So with the help of the few people there, including Ally Campbell, we began the Female Performance and Health Initiative (FPHI). A couple of years later, we formalised positions of which I am now the Research Lead for the FPHI. I have responsibility around coordinating research projects, cochairing the Women in Sport Congress, and engaging with universities so that we can have a collective message,
5 minutes with
by doing work together rather than replicating things. I chair a Research Reference Group, which includes academics from around Australia, and I also chair a Research Advisory Group, which includes senior individuals around Australia with interest in female athlete performance and health.
As the FPHI Research Lead, what are your goals for the FPHI’s Research and Advisory Groups?
There are multiple goals. Number one is quality research. So, to try and encourage quality research, and to understand where the quality research is out there. What I mean by quality is ‘performed with robust scientific methodology’, but also that there is consensus around the findings of that research. That means not just cherrypicking individual bits of research, but understanding what is out there and where the gaps might be, then trying to communicate that to the Australian sports system, performance support, elite female athletes, pathways athletes, and women athletes in general.
Is there a particular area of female athlete health and performance that you believe is misunderstood?
I think there’s a perception out there that female athletes would know a lot about themselves and that everything they do know about themselves is accurate. So, I think there are a lot of myths that we need to bust. That’s particularly in the health space. And it’s probably misunderstood that they’re well supported right from when they begin their athletic career through to when they retire. So, we’ve got a lot of work to do in the health and wellness space just to bring female athletes onto a platform where they’re healthy, well, and uninjured.
Really, what I think is missing then is the narrative, the resources, and the investment in breaking that ceiling of performance for female athletes. We

In terms of sports performance research, there is only 3% performed exclusively on female athletes.
there is only 3% performed
tend to think that if we improve their health, and wellness, we’ve done our job with female athletes. If we improve participation rates, that will increase performance, and there’s no doubt that it will, but it certainly doesn’t push human potential in terms of breaking that glass ceiling for female athletes. That’s what we hear with male athletes all the time, where the narrative around male athletes is faster, higher, stronger. For female athletes, it’s healthier, more athletes participating, and feeling well, so there’s a really different narrative. What I think is missing is pushing performance, breaking that glass ceiling in terms of performance for female athletes, and really understanding
human potential. In terms of sports performance research, there is only 3% performed exclusively on female athletes. So, how are we supposed to understand what our human potential is, when half the population doesn’t have any research done in it?
You are the Refshauge Lecturer at the 2024 SMA & ACSEP Conference. What are you most looking forward to at this year’s Conference and can you provide us with some insight into your opening presentation? I’d really like to explore this idea of research in the performance of female athletes and where we might go from here. How do we advance female performance rather than repeat what has been done in male athletes? Where are some opportunities there? So really shaping the history of female athletes, looking at what has been done in the past and what is currently being done for female athletes, but also where the opportunities are to advance that performance.
I am really looking forward to this conference. I think the idea of it being a joint conference with Sports Medicine Australia and the Australasian College of Sports and Exercise Physicians will give us a comprehensive picture of where we are in terms of Australia’s research, programs and clinical practice. In particular, I’m interested in female athletes, so it’ll be nice to see if that area has advanced in the last 12 months.
What advice do you have for others starting their career in sports and exercise science?
My advice would be for practitioners. I think treat the human in front of them, regardless of their background, abilities, sex or gender. By all means look at the research, but absolutely treat the individual in front of them. And don’t be afraid to explore other genders, sexes, races, or abilities in your practice, and particularly in your research.
At the AIS FPHI, I coordinate research projects, co-chair the Women in Sport Congress, and engage with universities so that we can form a collective message.



Can you tell us about your educational background? What made you decide on a career as a human movement scientist? I used to be a runner at a national level. I injured my knee when I was 17 and couldn’t run anymore, at that level, at least. I wanted to figure out what happened, why it happened, and what I could do about it. So that was the exact moment I had to decide what to do after high school, and I came across these studies. I thought, “that’s it, that’s what I need”. It helps me explain why my knee got hurt and what I could have done about it. It also helps me to help others to prevent it. That was my background for doing it. So, I started studying that in Amsterdam, far from where I was born. Amsterdam is the Party City so running didn’t really go well anymore. But studying went really well, and I enjoyed it greatly. That’s how I got into this field.
Can you talk about your work regarding the prevention of sports and physical activity related injuries?
Is there a part of your research that you are particularly proud of?
The work I’m most proud of would be every project that has an outcome that is practically helpful, whether it’s a positive outcome or not. We always think in trials, “Okay, we need to prevent injuries, we need to show a percentage of reduction of injuries, or else it fails.” Rather, every project that leads to an outcome teaches us something about practice that we can mould into a message that will help, and I think even if it’s one outcome, we should be proud of that. I’m most proud of, in the past few years, the PhDs and the Masters students I have been able to supervise because I can bring them to a certain level of my knowledge at that very moment, and they bring that further into their own realm. That’s how
Every project that leads to an outcome teaches us something about our practice that we can mould into a helpful message.
How did you first become involved with organisations such as Cirque du Soleil and the Union of European Football Associations?
we shape a research topic or field: by helping each other excel and bringing the collective knowledge to a new level. I think that’s the thing I’m most proud of. It could have been any other field, but luckily, I do it in this one.

All by chance, I guess. Some people say chance doesn’t exist. However, it’s really through random encounters. You can meet someone, or someone introduces you to someone else and you start to talk about things, and you’ll see that there is mutual interest and mutual benefit. Cirque du Soleil, for instance, they were looking for someone who could help them a little bit with their views on injury prevention. I started to talk with them and said maybe this could be an approach, and they thought it was interesting. So, they invited me in and said, why don’t you develop it for us? UEFA was a little bit similar. I was asked to give a second opinion on a project they were running, and they said they wanted to do more research. I said you can always call me if you need some feedback. The day after, they called me and one thing led to another. It is a bit of random encounters, but you need to have the baggage to make them work. There is certainly some luck involved, but there is also hard work and an open mind. I’d say keep an open mindset and be helpful to other people, then from one comes the other.
How and when did you first join SMA? What was your motivation for being an SMA member?
I don’t really know anymore when I became a member. I remember my very first SMA Conference in Port Douglas at least 20 years ago. What I found so positive about SMA is that it’s so different from other conferences, and it’s a real community. There’s been many other conferences where people show up, do a show and tell, look how good I am, look what I have to offer. You can have these ego-centric types of environments, and SMA is the complete opposite. We are here together to solve the problem. I can’t do it alone, you can’t do it alone, so let’s join together. That
brings work on the one hand, but it also brings people together. It’s also a social environment, you feel warm and welcomed. I don’t see that anywhere else. So that was my motivation to become an SMA member.
How has being part of SMA helped you in your career?
The only way to answer that is where would I have been without SMA. I don’t know because SMA has always been part of my career. There are a lot of great projects that came out of collaborations with my Australian colleagues. Surely, being part of SMA helped because it was a ‘green card’ for my university to allow me to go to Australia occasionally and sit down with colleagues and engage with their research. So it definitely has been a great help. Again, that open community is helpful because it’s easy to email or call and say, “Hey, I have a problem or an idea”. I wouldn’t have had these connections if it wasn’t for SMA. I might have had other connections, but I guess they would have been less valuable. That community feel has been a vital part of my SMA experience.
What is the best piece of advice you have received in your career?
Don’t take ‘no’ for granted. That was a piece of advice I received after a paper was rejected. As a young aspiring academic, that is annoying because you believe you wrote the best paper ever. I’ve learned that this advice means a lot for your career because if a grant doesn’t get accepted the first time, the second time, or a third time, you always make new connections by writing it again. There’s always a new idea that finds its way to the surface. The same with papers. If one journal doesn’t want it, take the loss and see why it wasn’t a good fit for that journal, whether you really did something wrong or if it was just not the right outlet. There’s always room for ideas and there’s always room to grow, so don’t take ‘no’ for granted.


IN SINGAPORE, SPORTS MEDICINE STANDS AS A RELATIVELY NEW SUBSPECIALTY. IN 2005, A WORKGROUP WAS APPOINTED BY THE JOINT COMMITTEE ON SPECIALIST TRAINING TO ESTABLISH SPORTS MEDICINE AS A SPECIALTY, AND IN 2007, SINGAPORE’S FIRST SPORTS MEDICINE TRAINEESHIP COMMENCED. PRIOR TO THAT, PRACTITIONERS HAD TO COMPLETE THEIR POST-GRADUATE SPORTS MEDICINE TRAINING ABROAD. SPORTS MEDICINE WAS FINALLY ESTABLISHED IN THE SUB-SPECIALTY REGISTER IN 2011. CURRENTLY, THERE ARE 36 SPORTS PHYSICIANS LISTED IN THE SPORTS MEDICINE REGISTER.
Sports Medicine is a comprehensive field encompassing sport and exercise medicine, along with sports sciences such as exercise physiology, sports biomechanics, strength and conditioning, sports nutrition, and sports psychology.
Sport and Exercise Medicine Physicians must be familiar with a wide variety of sports, and related physical activities, including performing arts medicine and military medicine. The population catered to is diverse, ranging from elite and professional athletes to recreational athletes, children, women, the elderly, as well as individuals with disabilities.
Role of Sport and Exercise Medicine Physician: A Sport and Exercise Medicine
Physician is a doctor, not a surgeon,

specializing in the diagnosis and nonoperative treatment of musculoskeletal injuries. These physicians perform a holistic approach, extending beyond treating injuries; they also work with healthy individuals seeking performance enhancement and clinical populations requiring exercise testing and exercise prescription.
How does one become Sport and Exercise Medicine physician in Singapore?
To become a specialist in Sport and Exercise Medicine in Singapore, one will first need to complete medical school and obtain a base specialty in family medicine, internal medicine, orthopedic surgery, or emergency medicine. These four disciplines are considered relevant foundation training before embarking on the Sports Medicine Sub-Specialty
Training program (SpMed SST).
The SpMed SST program is a structured three-year program and comprises various placements at hospitals, national sports associations, and sports science facilities. The training culminates in a final examination, including OSCE stations, MCQ, and literature review.
The goals of the SpMed SST are to produce Sports Physicians that:
1. Are clinically competent in the diagnosis and management of sports injuries and sportsrelated medical conditions in a tertiary care setting.
2. Are clinically competent in fulfilling the duties of a Team Physician, including pre-participation screening, event medical coverage,
doping control and counseling, early management of sports injuries, and sports-related medical conditions in a primary care setting.
3. Are proficient in exercise testing and prescription in both diseased and disease-free populations.
4. Possess habits of life-long learning to build upon their knowledge and skills
5. Are proficient in applying the principles of Sports Science (i.e. Exercise Physiology, Strength and Conditioning, Sports Nutrition, Sports Biomechanics, Sports Psychology) in the management of competitive and recreational athletes.
6. Are fairly familiar with a wide variety of sports.
7. Foster professional and healthy interactions within the multidisciplinary team supporting the athlete, including coaches, sports administrators, sports scientists, paramedical professionals (e.g. sports physiotherapists, podiatrists, sports trainers), and medical colleagues from other disciplines (e.g. sports orthopedic surgeons).
8. Are proficient in conducting applied research in the fields of Sports and Exercise Science and Medicine.
Many physicians and health professionals with a keen interest in sports medicine belong to the Sports Medicine Association Singapore (SMAS). SMAS is the registered society for Sports Medicine and Sports Science professionals in Singapore. The focus is on the promotion of the specialty and providing education to their members and the community. The members embody the multidisciplinary spirit of the specialty and include doctors, physiotherapists, podiatrists, sports nutritionists and dieticians, exercise physiologists, sports scientists, and sports psychologists.
DUKE-NUS Medical School offers an elective program on exercise medicine and exercise prescription. Medical students on rotation with Orthopaedic Surgery may also be scheduled observerships in the Sport and Exercise Medicine clinic. Unfortunately, Sport and Exercise Medicine is currently not included in the standard curriculum for the three medical universities in Singapore. However, discussions are underway to integrate its content into standard undergraduate curricula which would hopefully inspire budding Sport and Exercise Medicine physicians early in their career.
Despite Sport and Exercise Medicine being a relatively new medical specialty, there has been increased demand and interest in the last decade. To cater to medical doctors in family medicine or other registered specialists who are keen to extend their qualifications in sports medicine, a 1-year part-time Graduate Diploma in Sports Medicine (GDSM) program, developed by Lee Kong Chian School of Medicine in partnership with the Singapore Sport & Exercise Medicine Centre at Changi General Hospital was rolled out in 2018. To date, there are 112 graduates from the program.

The Sport and Exercise Medicine Centre at the Singapore Sports Institute (SSI) is dedicated in providing comprehensive care for Team Singapore athletes, aiming to optimize their performance capabilities. This center constitutes a multi-disciplinary team, which includes sport and exercise medicine physicians, physiotherapists, sports biomechanists, sports nutritionists, sports psychologists, sports physiologists, strength and conditioning coaches, sports masseurs, and podiatrists.
The services include:
ٚ Medical clearance and musculoskeletal screening
ٚ Management of acute and chronic musculoskeletal injuries
ٚ Maximizing athlete’s maximum performance potential and injury prevention
ٚ Planning and execution of major game support
ٚ Coordination of external services, such as specialist consultation and intervention
Exercise is Medicine Singapore (EIMS) is part of a global health initiative supported by the American College of Sports Medicine (ACSM) to make physical activity assessment and promotion a standard in clinical care, connecting health care with evidence-based physical activity resources for people everywhere and of all abilities. Singapore takes the lead in EIM efforts within Southeast Asia, hosting the EIM Southeast Asia Regional Centre within its borders.
ٚ For physical activity to become a vital sign, with healthcare providers routinely discussing it with their patients
ٚ For the physician to either prescribe appropriate physical activity to each patient or refer the patient to a certified health

and fitness professional
ٚ To put in place a framework for allied health and fitness professionals to work with physicians in implementing the exercise plan
ٚ For the public to begin to ask for and expect physicians to discuss physical activity during each consultation/visit
The future for Sport and Exercise Medicine is promising, with increased awareness of the importance of physical activity and sports participation. As more people engage in sports and exercise, there is an increased demand for injury prevention, injury management, and performance optimization.
Furthermore, Sport and Exercise Medicine plays a fundamental role in supporting individuals across diverse age groups, and activity levels, including those with chronic diseases and disabilities. A holistic approach, tailoring treatment, exercise prescriptions, and rehabilitation programs to address the specific needs of each demographic contributes to our populations’ overall health and well-being.

Clin Asst Prof Mandy Zhang
MB BCh BAO (Ireland), MRCS (Edinburgh), M.Med Family Medicine (Singapore), MSpMed (Australia), FAMS (SpMed)
Clin Asst Prof Mandy Zhang is a graduate of Royal College of Surgeons in Ireland (RCSI), with post graduate qualifications in Membership of the Royal College of Surgeons (Edinburgh), Masters of Family Medicine (Singapore), Masters of Sports Medicine (Australia) along with certifications from American College of Sports Medicine (ACSM) Exercise Physiologist (USA), FIFA diploma in football medicine, International Society for Medical Shockwave Treatment (ISMST) in the use of Radial Shockwaves. She is also a Fellow of the Academy of Medicine Singapore. Dr Zhang’s clinical interests include sports injury prevention, musculoskeletal sonography, and performing arts medicine. She was the chief secretariat for Sports Safety Committee Singapore and has provided medical coverage for high-key sporting events such as Southeast Asian (SEA) Games, Singapore FORMULA 1 Grand Prix and ONE Fighting Championship, and the Special Olympics Singapore National Games.






What motivated you to become a sports trainer?
Around about 1987, my children had left home and I wanted to put back a little bit of commitment into the community. I joined the Volunteer Rescue Association (VRA) who go to motor vehicle accidents. At that time, there was a lot of emphasis placed on getting people out of cars at accidents and giving first aid. So, they were the first ones called to motor vehicle accidents and I enjoyed that training. At the same time, I was also studying martial arts and I became an instructor assisting the class in martial arts. As time moved on, around about the 1990s, I also ended up working in the open cut mines in the Hunter Valley. Because of my involvement with the VRA, I was asked if I would like to join the emergency response team in the mines for the Mines Rescue, responding to any emergencies that occurred at the mines. That was very professional. We were trained by paramedics and fire brigade personnel, and no expense was spared training us with lots of first aid and we were trained to the occupational level in first aid.
During that time, there was a lot of talk on injuries in sport. Head injuries had raised its head and litigation, and all of that. In martial arts, the training certificates you receive are not recognised other than in the martial arts arena, as a black belt or an instructor. So, a few of the instructors said we should look around for an Australian recognised accreditation for training personnel. I found

out that the Newcastle Knights, the football team, were running the level one at that time under a chap by the name of Chris Koczynski, better known as Cos, who was the strapper and the conditioner for the Newcastle Knights. So, I went down there, and I did my level one and my level two sports trainer courses. Newcastle at that time they had a very good Second Division football side. At our training sessions we had some great sports trainers and we trained at Marathon Stadium as it was known then. We had the ability to have the Knights doctor, Dr Neil Halpin, come to give lectures when he was treating the Knights players, and that was a really professional, well-designed course. Some of those trainers were massage therapists too. They added value. They went and did remedial massage classes, which I thought was a good idea because it’s always adding to your
knowledge of the human body and illnesses. I then did a remedial massage course too over a couple of years.
So at that time, I was a martial arts instructor, an SMA member, a remedial massage therapist, and I was doing some training all the time, because you’re training every month in the mines in first aid, vehicle rescues, anything to do with injuries and working that out. That was the case until 2010 when I retired and came up to Queensland. I had kept my SMA membership going but in 2015, I let go of my membership because I wasn’t doing that much, and I didn’t think I was going to need it anymore. Then three or four years ago, a friend of mine asked me if I’d be in his corner if he took up Masters boxing. So I said yes, because you’re handling cuts and bruises and all that type of stuff. From there, I had to get in touch


Some of the trainers I worked with were massage therapists too, which I thought was a good idea because it’s adding to your knowledge of the human body and illnesses. I then did a remedial massage course myself.

with SMA and I got reaccredited as a level 2 SMA sports trainer in Brisbane. Now I look after my friend as far as fitness and diet, and I’m in his corner with his Masters boxing.
How long have you been a sports trainer and which sports have you covered?
I’d say since roughly 1995, I’ve been a Level 2 sports trainer. I was mainly a sports trainer for martial arts, self-defence, and now boxing. I was invited to participate at the UniSport Nationals last year, and I looked after the basketball and volleyball there, along with four or five other SMA sports trainers.
What has been a highlight of your sports trainer career so far?
The highlight would be UniSport Nationals on the Gold Coast for the three or four days we were there. With the number of people there,
that was an eye-opener. I’d never looked at basketball very much. It was either rugby league, boxing, or martial arts. It was interesting and eye-opening with different injuries. Rugby league is all bashing, but basketball was more 3 tonnes of ice, and not so many contact injuries which was good and challenging.
How has being part of SMA helped you as a sports trainer? It’s mixing with very knowledgeable people. You talk to very professional people, even on a community level, every sports trainer is very professional. And you’re always learning. The association, the meeting of other sports trainers at events, you’re always learning and always improving. It’s a community of well-trained people. Of the few people who have gone through to their level two’s with SMA, they know what they’re doing, and they know what they’re talking about.
I was invited to participate at the UniSport Nationals last year, and I looked after the basketball and volleyball there, along with four or five other SMA sports trainers.
What is your advice to people thinking about starting sports training?
I would say first aid is a must. Get into as much first aid as you can and as high as you can afford, because it costs money to do not just ordinary first aid, but to climb up and do a little bit further. Try and get as much experience with injuries as you can. And learn from Sports Medicine Australia.


