• Biomechanical implications for post-traumatic knee osteoarthritis in young adults - the underloading paradox: are we protecting or harming?
• Gut gains: Exploring the role of heavier food to train the gut
• Acetabular labral tears: an overview of diagnosis and management
Contents
REGULARS
02
From the Chair
Dr Kay Copeland shares SMA’s 2025 outlook, including the ASICS SMA Conference at the forefront.
03
From the CEO
Jamie Crain talks about exciting new milestones for 2025 starting with a new Student Management System.
Opinions expressed throughout the magazine are the contributors’ own and do not necessarily reflect the views or policy of Sports Medicine Australia (SMA). Members and readers are advised that SMA cannot be held responsible for the accuracy of statements made in advertisements nor the quality of goods or services advertised. All materials copyright. On acceptance of an article for publication, copyright passes to the publisher.
FEATURES
04
Acetabular labral tears: an overview of diagnosis and management
Dr Joshua Heerey explores current research and clinical trends to improve the understanding and management of acetabular labral pathology.
18
Accelerating the early rehabilitation pathway and reducing the patient burden after proximal hamstring tendon repair
Dr Jay Ebert examines how to enhance early rehabilitation following proximal hamstring tendon repair to speed up recovery and lessen the burden on patients.
Publisher Sports Medicine Australia State Netball and Hockey Centre - Parkville 10 Brens Drive, Parkville VIC 3052 sma.org.au ISSN No. 2205-1244 PP No. 226480/00028
Copy Editors
Archie Veera and Sarah Djemal
Marketing and Member
Engagement Manager
Sarah Hope
Design/Typesetting
Perry Watson Design
Cover photograph
Getty Images / jacoblund
Content photographs
Author supplied; www.gettyimages.com.au
10
Healing of acute ACL rupture managed with the Cross Bracing Protocol –study insights Meike van Haeringen shares learnings from the Cross Bracing Protocol for acute ACL rupture, examining its impact on healing, stability, and long-term knee health.
24
Gut Gains: Exploring the Role of Heavier Food to Train the Gut
Isabel Martinez investigates the impact of increased food consumption on gut health in endurance athletes and its potential effects on performance.
30
Biomechanical implications for post-traumatic knee osteoarthritis in young adults – the underloading paradox: are we protecting or harming?
Matthew Savage explores whether underloading after ACL injuries accelerates post-traumatic knee osteoarthritis and raises costs in young adults.
29
Tackling concussion: SMA’s national campaign to support safer sport
INTERVIEWS
36
People who Shaped SMA: Professor Anthony Leicht
40
5 Mins With: Associate Professor Kathryn Mills & Associate Professor Ryan Timmins
42
Sports Medicine Around the World: Europe
46
Sports Trainer Spotlight: Maithree Wijayasekara
FROM THE CHAIR
Building a safer sporting future through SMA’s 2025 initiatives
AS WE STEP INTO 2025, SMA REMAINS COMMITTED TO EDUCATING AND SUPPORTING THE SPORTING COMMUNITY ACROSS AUSTRALIA. OUR FOCUS IS ON ENSURING THAT SPORTS MEDICINE AND SPORTS SCIENCE PROFESSIONALS, ATHLETES, COACHES, AND CLUBS HAVE ACCESS TO THE LATEST EVIDENCEBASED INFORMATION TO PROMOTE SAFER SPORT AT ALL LEVELS.
One of the key initiatives this year is the national distribution of our concussion management poster to over 40,000 clubs, schools and sports medicine professionals. This follows the release of the Guidelines for Concussion in Youth and Community Sport a year ago and reinforces SMA’s role in ensuring that best-practice concussion education reaches every level of the sporting community. Awareness and education are critical in managing concussion, and we are proud to play a leading role in delivering these vital resources.
We are also pleased to announce the launch of abstracts and registrations for the 2025 ASICS SMA Conference, to be held in Hobart this October. With an impressive line-up of keynote presenters and a diverse program, this year’s conference will bring together leaders from the sports medicine and sports science communities for collaboration, knowledge sharing, and networking. We look forward to welcoming delegates to what promises to be another outstanding event.
In 2025, the SMA Board is reviewing our Constitution to ensure it remains
In 2025, the SMA Board is reviewing our Constitution to ensure it remains fit for purpose and reflects modern governance practices.
fit for purpose and reflects modern governance practices. As SMA continues to grow, it is essential that our structure supports a strong and sustainable future. Over the coming months, members will have the opportunity to provide feedback on proposed changes, with any revisions to be presented for approval at the AGM in November.
Looking ahead, we are also exploring opportunities to expand SMA’s international presence. By partnering with sports medicine associations in other countries, we aim to extend our reach and
provide access to our professional development events on a global scale. Strengthening these connections will help SMA grow its influence and share expertise more broadly.
Closer to home, our Safer Sports team has been actively working on several initiatives to enhance education and training. A key milestone was the launch of our new learning platform, aXcelerate, that has improved the experience for our Safer Sport Program course participants. Additionally, we are identifying new ways to educate Australia’s clubs and community sporting organisations, ensuring that they have the knowledge and tools to build a safer and more resilient sporting environment.
SMA remains dedicated to advancing sports medicine and supporting the broader sporting community. We look forward to another year of collaboration, innovation, and meaningful impact.
Dr Kay Copeland Chair, Sports Medicine Australia
FROM THE CEO
Kicking off the New Year as we elevate education and expand our reach
IT’S BEEN A PRODUCTIVE START TO 2025 AT SMA, WITH A FOCUS ON READINESS FOR OUR UPCOMING PEAK SEASON WITHIN SMA EDUCATION AND TRAINING.
Amajor milestone has been the launch of our new Student Management System, which completely modernises how we deliver training. This major upgrade enhances the user experience, offering a more intuitive enrolment interface, improved accessibility, and streamlined course management. It’s a major step in strengthening our Safer Sports Program and ensuring sports trainers and volunteers have access to high-quality education.
We will soon release an updated version of our Sports Trainer Manual, the primary resource for our Level 1 and 2 Sports Trainer courses. This revision, led by our Scientific Advisory Committee and subject matter experts, ensures alignment with the latest sports medicine research. Thank you to all who have contributed to this important work.
Our Scientific Advisory Committee is also revising many of our Injury Fact Sheets, some of our most popular free resources for clubs, parents, and community sport volunteers. Keeping these materials up to date ensures they remain a trusted tool for grassroots sport.
In this issue, you’ll find our Concussion Guidelines poster offering practical guidance on recognising and managing concussion.
In February, we delivered our first Level 1 Sports Trainer course in Colombo, Sri Lanka, in partnership with Elite Akademy Sports Medicine. This program engaged passionate learners and represents SMA’s growing international reach which includes Singapore and the Pacific. We look forward to expanding our training footprint globally.
You’ll find our Concussion Guidelines poster in this issue of Sport Health Distributed in hard copy to 40,000 clubs and schools, it provides practical guidance on recognising and managing concussion. A year after the release of the Guidelines for Concussion in Youth and Community Sport, SMA
remains committed to concussion education. Thank you to our campaign partners — ASICS, Elastoplast, and Gallagher — and Government Partners — VicSport, Sport West, the Tasmanian Government, and the Northern Territory Government — for their support. We also appreciate the efforts of our members, clubs, clinics, sporting organisations and individuals who have shared these resources within their networks, helping to spread this critical message.
This issue’s feature articles include Dr Joshua Heerey’s review of current research and clinical trends in acetabular labral pathology, Dr Jay Ebert’s work on optimising early rehabilitation for proximal hamstring tendon repair, and Isabel Martinez’s exploration of how heavier food intake affects gut health and performance in endurance athletes. Matt Savage investigates whether underloading after ACL injuries worsens posttraumatic knee osteoarthritis and its economic burden, while Meike van Haeringen examines the Cross Bracing Protocol for acute ACL rupture and its impact on healing, stability, and long-term knee health.
We hope you enjoy this edition of Sport Health.
Jamie Crain CEO, Sports Medicine Australia
An overview of diagnosis and management Acetabular labral tears
DR JOSHUA HEEREY, La Trobe Sport and Exercise Medicine Research Centre (2024 SMA & ACSEP Conference – Early Career Researcher – Ken Maguire Award for Best Paper in Clinical Sports Medicine)
Acetabular labral tears are now recognized as a source of pain (hip-related pain) in active people. The advancement of imaging and surgical techniques has improved our understanding of the acetabular labrum and its role in hip-related pain and osteoarthritis (OA) development. This review article will summarise contemporary research and trends in clinical practice to improve your understanding and management of acetabular labral pathology.
The acetabular labrum is an intraarticular fibrocartilaginous triangle that traverses the anterior and posterior bony acetabular rim, joining with the transverse acetabular ligament inferiorly to create a continuous ring. The labrum enhances joint stability,
distributes contact stress, delivers proprioceptive feedback, and maintains negative intra-articular pressure. It has been suggested that only the outer 1/3 of the labrum has a blood supply, which may affect its ability to heal after injury. Nociceptive free nerve endings are primarily located within the superior and anterior portions of the labrum, indicating that it can generate pain in some people.
Most labral tears have a complex aetiology. Risk factors for labral tears include, history of joint trauma, childhood hip conditions (e.g., hip dysplasia, Perthes’ disease), capsular laxity and alterations in bony hip morphology present in conditions such as femoroacetabular impingement syndrome.
Diagnosis of labral tears
The diagnosis of labral tears can be challenging, due to the proximity of bony, articular and musculotendinous structures and overlap in symptoms between different conditions (e.g., adductor-related groin pain).
A thorough examination that includes evaluation of a triad of symptoms, clinical signs, and imaging findings is recommended.
Symptoms
Common symptoms may include groin pain with associated mechanical symptoms, such as clicking or locking. However, mechanical symptoms can also result from extra-articular conditions (e.g. snapping hip syndrome) and often have an imprecise relationship with imaging confirmed labral tears.
Clinical signs
Hip impingement tests such as the flexion-adduction-internal-rotation (FADIR) test and flexion-internalrotation (FIR) test are commonly used clinical tests for labral tears; however, their clinical utility is limited by high sensitivity and low specificity. When test sensitivity is high, a negative test will rule out the disorder (e.g., labral
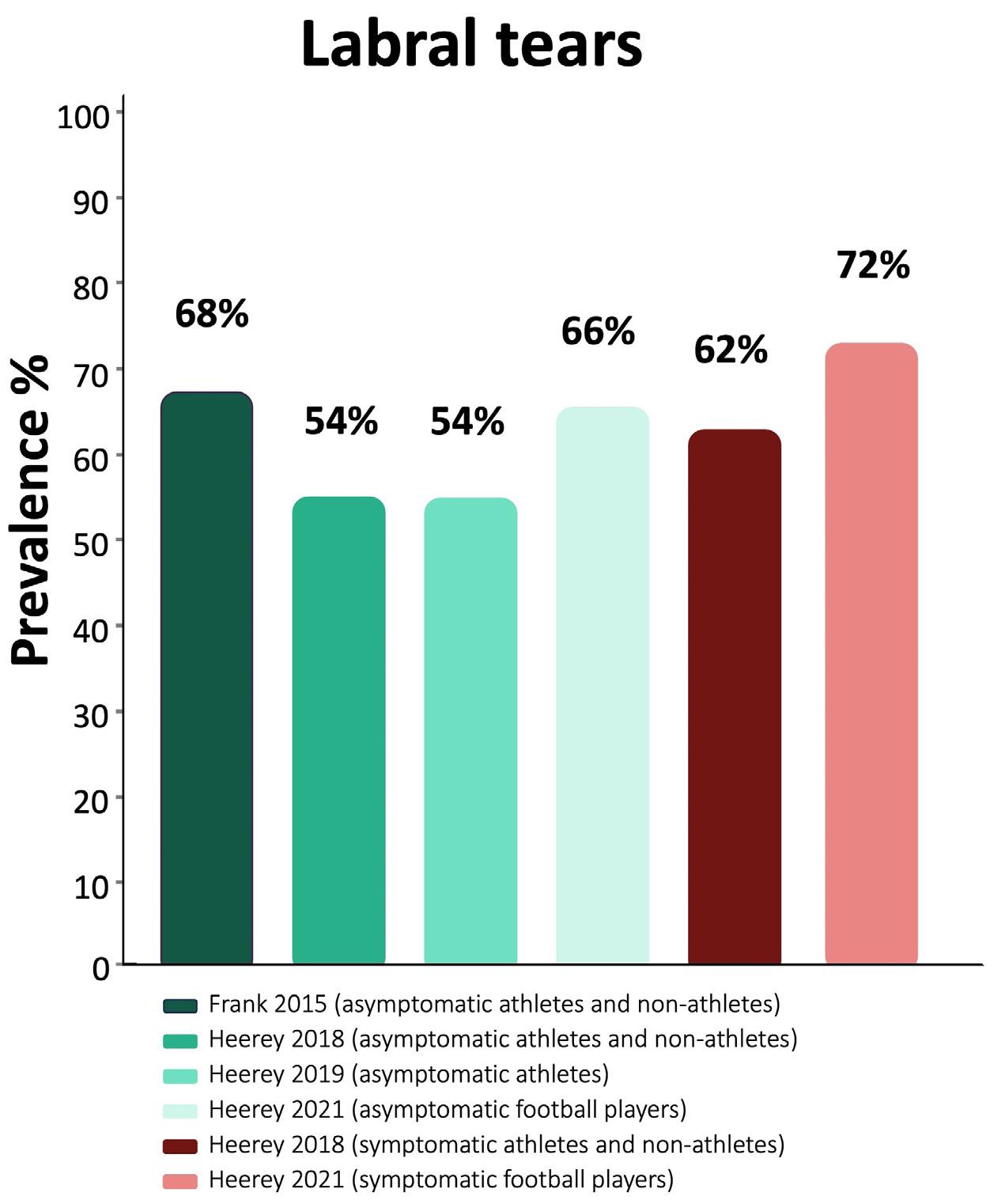
Recent evidence suggests that a high and similar prevalence of labral tears are seen in people with (62%) and without pain (54%).
tear). If test specificity is high, a positive test will rule in the disorder. Therefore, hip impingement tests may be positive in people with and without a labral tear. In clinical settings, the FADIR (Figure 1) and FIR tests may assist in excluding labral conditions. The Thomas test (Figure 2) may be a useful clinical test as it has been shown to increase the probability of a
Figure 1. Flexion-adduction-internal-rotation (FADIR) test
Figure 2. Thomas test
Photo: Yuri Arcurs/ Getty Images
Acetabular labral tears
An overview of diagnosis and management
labral tear being present when positive (i.e. reproduction of familiar hip and/or groin pain and/or painful mechanical symptoms).
Imaging findings
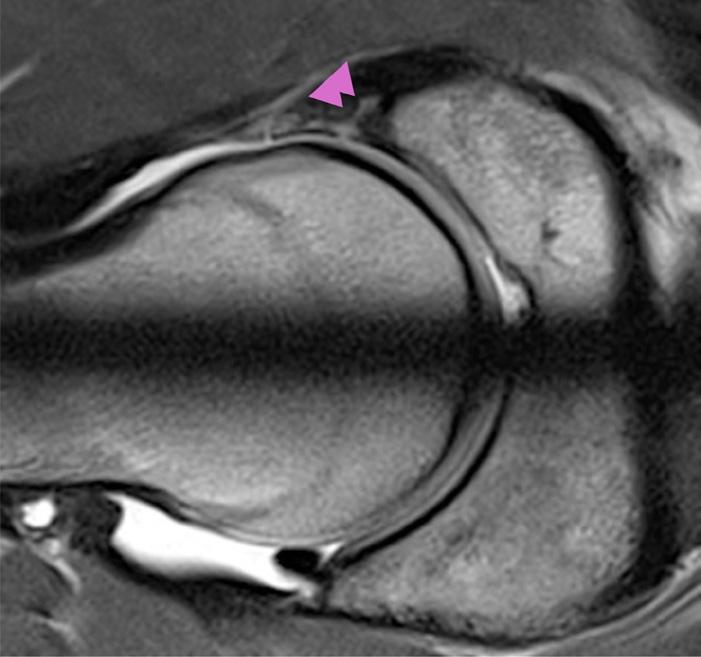
Magnetic resonance imaging (MRI) is the preferred imaging technique for labral tears, as it provides excellent softtissue contrast (Figure 3). Other less common imaging techniques for labral conditions include contrast-enhanced CT and ultrasound. While MRI has improved our understanding of labral tears, it may have led to an over-reliance on imaging findings. Imaging can be
helpful to exclude serious pathology (i.e., red flags), but is increasingly used to identify structural hip conditions that are assumed to be related to pain and to inform treatment decisions.
Recent evidence suggests that a high and similar prevalence of labral tears are seen in people with (62%) and without pain (54%) (Figure 4) Interestingly, the severity of labral tears also appear similar in those with and without symptoms. Therefore, hip joint imaging findings should be considered alongside injury history (acute vs chronic), patient characteristics (e.g., age, sex, activity level), clinical examination, and wider physiological, psychological, and social
Figure 3. MRI appearance of a labral tear (double pink arrow)
Figure 4. Prevalence of labral tears in symptomatic and asymptomatic individuals
Photo: Biserka Stojanovicperlb /Getty Images
factors to avoid misdiagnosis. Hip joint imaging findings that exist alongside symptoms and clinical findings may be relevant and influence treatment decisions. A diagnostic intra-articular injection should be considered if there is uncertainty about the relevance of a labral tear observed on imaging.
Labral tears and development of hip osteoarthritis
Labral pathology is thought to expediate the development of cartilage loss and hip OA development. Our world-first longitudinal study of young adult athletes with hip pain confirmed the important role of the acetabular labrum in maintenance of cartilage health. In this large-scale study of 143 football (soccer or AFL) we identified that those with labral tears of greater severity (macerated labral tears and paralabral cysts) had greater cartilage loss over a period of 2 years. Further work is now needed to identify the best treatment to prevent cartilage loss and hip OA development in young adults with labral tears.
Treatment of labral tears
People with a labral tear can often get better (reduction in hip pain and improvement in function) with a comprehensive rehabilitation program. A rehabilitation program should be at least three months in duration and include education, exercise therapy and physical activity. Education is critical to enable the individual to engage in exercise therapy and physical activity with confidence. Conceptualising hip-related pain solely through a pathoanatomical lens may lead people to only seek interventions that “cure” structural joint damage, such as hip surgery. Therefore, when communicating hip joint imaging findings, clinicians should use the CLEAR principle: Consistent L anguage: The terminology used by clinicians to describe
In this large-scale study of 143 football (soccer or AFL) we identified that those with labral tears of greater severity had greater cartilage loss over a period of 2 years.
imaging can affect an individual’s thoughts and actions. Clinicians should avoid using threatening language. For example, “labral tear” denotes something that is damaged and requires fixing, where “labral changes or alterations” may reduce pain-related behaviour and anxiety.
Epidemiological information: It is important to provide age, sex and activity matched imaging findings of asymptomatic populations as this will assist to provide context and enable discussion about relevance (see figure 4)
A ssessment of Relevance: Clinicians should be honest about the relevance of imaging findings. This discussion
Photo: Ross Helen / Getty Images
Acetabular labral tears
An overview of diagnosis and management
should address the limitations and strengths of different imaging techniques, the imprecise relationship with pain, limitations of clinical examination findings to identify tissuebased pathology, and the prognostic ability of imaging features if known.
Exercise therapy should focus on improving the strength, endurance and neuromuscular control of hip muscles, as this combined approach is thought to help reduce symptoms and improve function. Trunk muscles should also be a key focus of exercise therapy. If symptoms allow, physical activity should be implemented alongside the other aspects of rehabilitation. There is a role for intra-articular injections when hip pain is stopping the individual from undertaking rehabilitation. It is important to remember that not all people with a labral tear will benefit from rehabilitation. Hip arthroscopy is an effective treatment for labral tears and can provide pain reduction and improvement in function.
Key tips
ٚ Labral tears can be a source of hiprelated pain in young active adults.
ٚ A triad of symptoms, clinical findings, and diagnostic imaging is needed to diagnose labral tears.
ٚ The prevalence of imaging-defined labral tears appears similar in those with and without hip pain.
ٚ A rehabilitation program should be at least three months in duration and include education, exercise therapy and physical activity.
ٚ Hip arthroscopy can be an effective treatment for labral tears in those who do not benefit from rehabilitation.
For article references, please email info@sma.org.au
It has been suggested that only the outer 1/3 of the labrum has a blood supply, which may affect its ability to heal after injury.
About the Author
Dr Joshua Heerey is an APA Sport and Exercise Physiotherapist at Lifecare Prahran Sports Medicine and Research Fellow at La Trobe Sport and Exercise Medicine Research Centre. His research has involved exploring the relationship between imaging findings of the hip and groin region and pain and identifying risk factors for early hip osteoarthritis (OA). Dr Heerey has a clinical interest in the management of hip and groin conditions, including athletic groin pain, femoroacetabular impingement syndrome, labral tears, and hip OA.
Photo: VORONA / Getty Images
Healing of acute ACL rupture
managed with the Cross Bracing Protocol
– study insights
MEIKE VAN HAERINGEN, University of Amsterdam (2024 SMA & ACSEP Conference – ASICS Best Poster in Clinical Sports Medicine)
What do we know about ACL healing?
An acute complete anterior cruciate ligament (ACL) rupture is a devastating injury and often accompanied with concomitant injuries such as meniscus lesions, articular cartilage damage, subchondral bone impaction and collateral ligament injuries. Moreover, ACL rupture has potentially devastating long-term consequences such as tibiofemoral instability, decreased activity participation, an increased risk of developing knee osteoarthritis, and impaired long-term knee-related Quality of Life (QOL).
Current treatment strategies are surgical reconstruction of the ACL followed by rehabilitation or rehabilitation alone which are based on the assumption that a ruptured ACL has limited healing capacity. However, studies have shown that the ACL has a rich blood supply, and that ruptured ACLs undergo the typical phases of the healing process after injury similar to the medial collateral ligament (MCL), albeit at a slower healing rate.
The KANON trial has demonstrated spontaneous ACL healing on MRI in about one-third of patients managed with rehabilitation alone. In addition, those with a healed ACL reported better patient reported outcomes compared to the non-healed and ACL and ACL surgery groups at 2 years follow up. In view of these findings the novel Cross Bracing Protocol (CBP) has been developed by Dr Mervyn Cross and Dr Tom Cross and utilizes the orthopaedic principles of “anatomical reduction” and “immobilisation” of injured ACL tissue to facilitate ACL healing. Previous research has shown that the ACL is shortest at 90°-135° of knee flexion and that the gap distance between the torn ligament ends is a critical barrier to healing. Based on this, the CBP recommends immobilising the knee at 90° knee flexion approximating the ruptured
ACL epi-ligamentous tissues, reducing the gap distance in an attempt to support the healing process across the ligament.
Findings from the first 80 patients with ACL rupture managed with the novel CBP showed promising outcomes, with 90% of people achieving a continuous ACL (signs of healing) 3 months after injury. In addition, a spectrum of ACL healing was observed on 3-month MRI and patients with higher volume and better aligned ACL healing (a taut and thick ligament) reported better clinical outcomes than those with less optimal ACL healing (a thin and/or elongated ligament) or no ACL healing. However, this study was limited by its small sample size, highlighting the need for further investigation in a larger cohort to continue exploring the potential for ACL healing with this novel non-surgical treatment strategy.
Furthermore, these promising findings raise new questions, such as: Who is most suitable for the CBP? And do certain “patient” and “MRI factors” – including the nature of the ACL rupture – play a role in the quality of ACL healing? Currently, we do not know the answers to the above intriguing questions for ACL rupture and ACL healing. Addressing these knowledge gaps through further research could inform future prognostic studies and ultimately help identify which patients would benefit most from the CBP.
Having considered all of the above, our two study aims were to:
1. Investigate ACL healing (in terms of continuity and thickness) on 3-month MRI in 235 people treated with the CBP.
2. Identify patient and MRI characteristics associated with the quality of ACL healing on 3-month MRI (continuous and thick vs. continuous and thin).
Photo: Ilona Shorokhova / Getty Images
Healing of acute ACL rupture
managed with the Cross Bracing Protocol – study insights
How did we go about this?
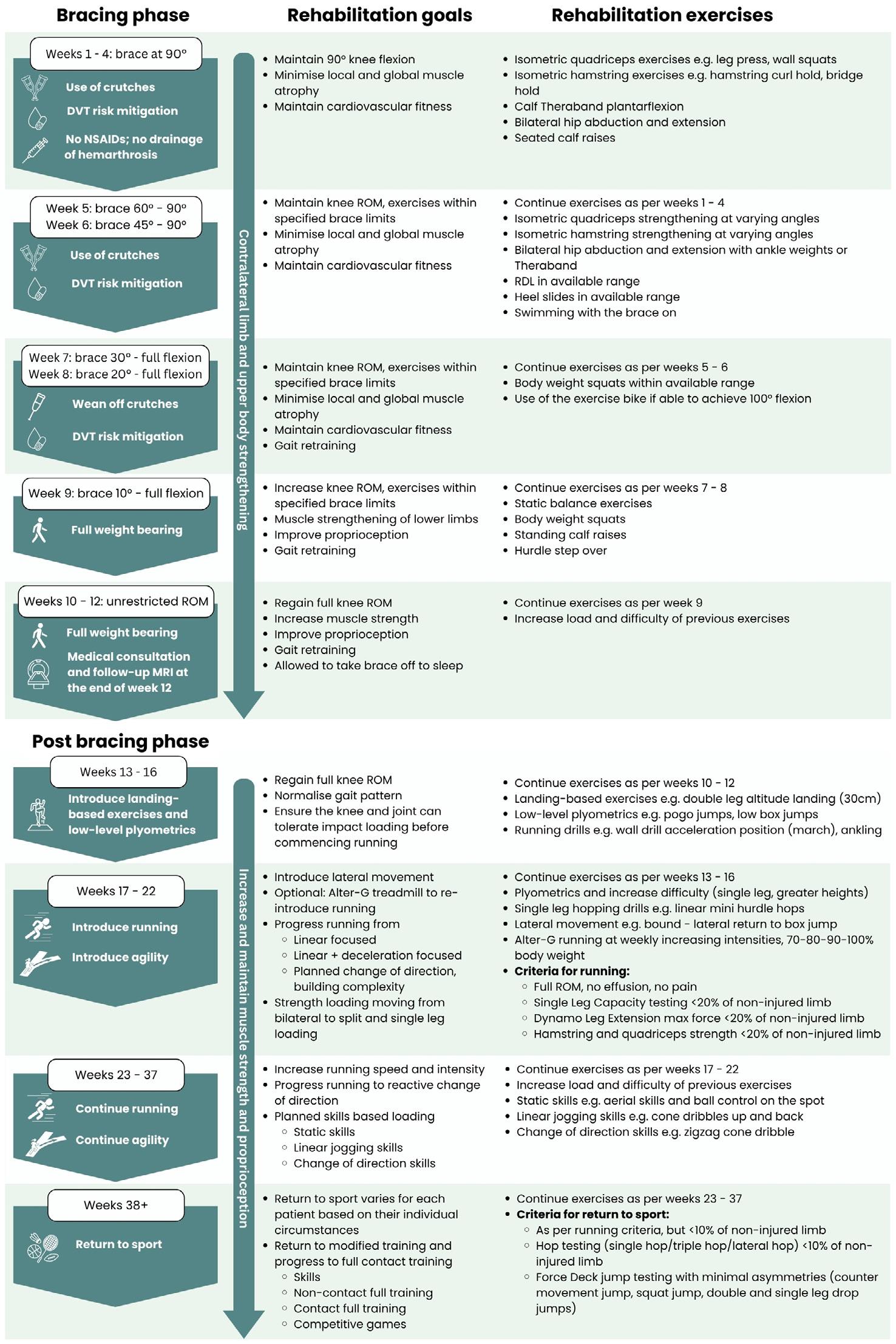
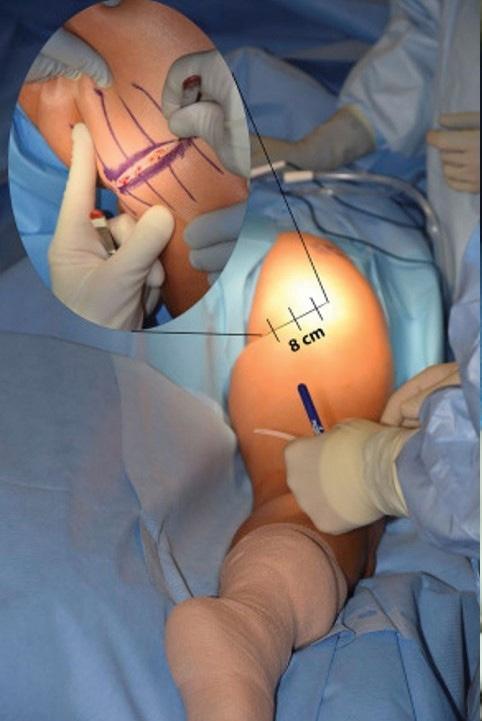
The CBP is summarised in Figure 1
We identified patients of all ages with an MRI confirmed ACL rupture, managed with the CBP between March 2016 and June 2023. Patients were considered eligible for the CBP if they presented with an MRI confirmed complete rupture of the ACL within one month of injury, and were functionally independent and capable of managing a period of knee immobilisation.
ACL healing was assessed on 3-month MRI by two radiologists after treatment with the CBP. We defined ACL healing as the presence of ACL continuity, further differentiated as either a thickened continuous ACL or a thinned continuous ACL based on the validated and published ACLOAS scoring system.
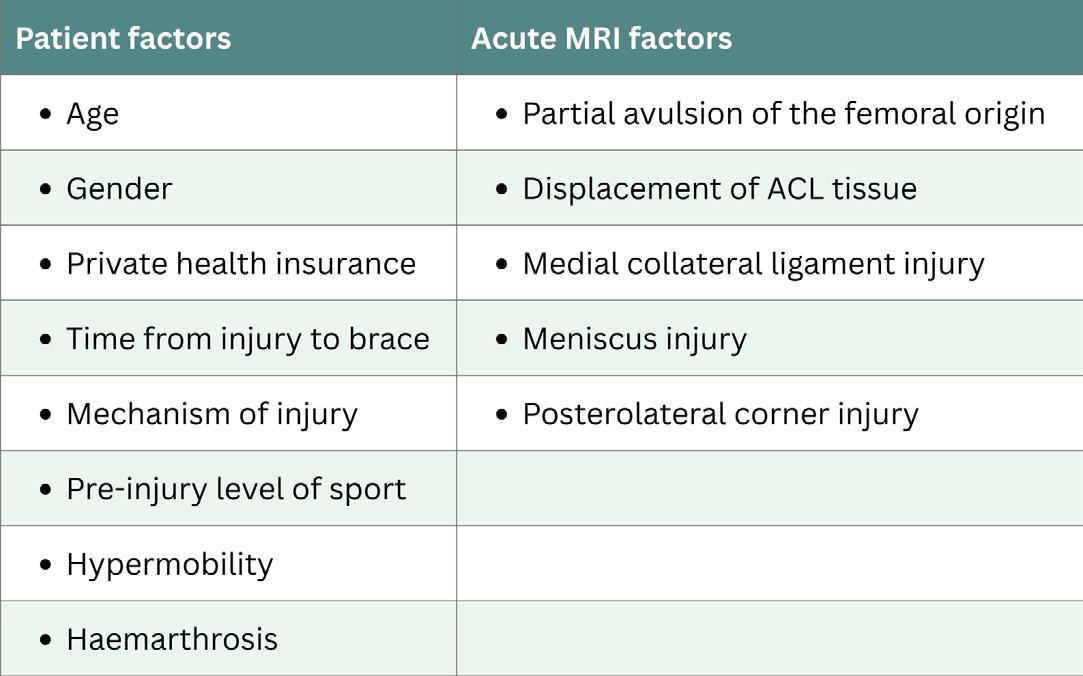
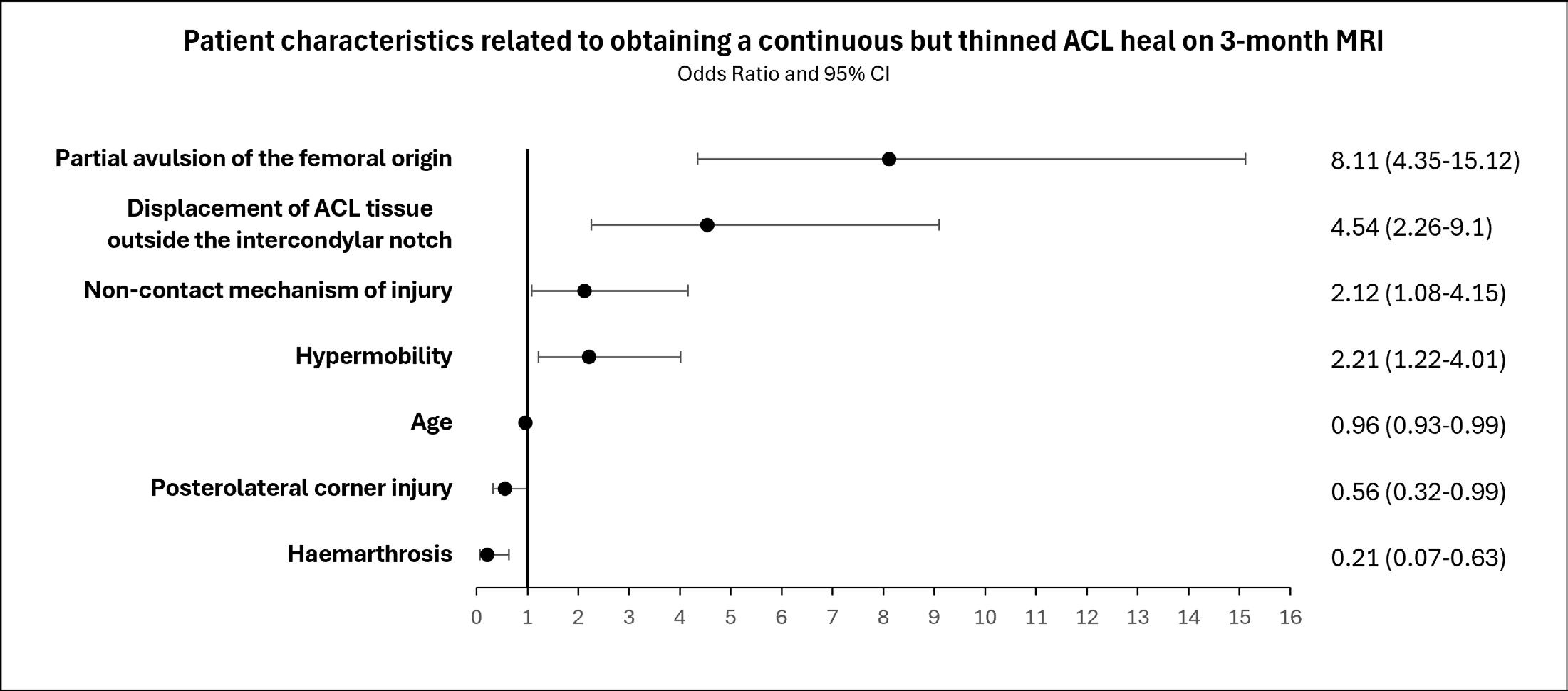
For our second aim, we chose patient and MRI characteristics based on hypothesised relationships and clinical relevance and are shown in Figure 2 . We used univariable logistic regression analyses to assess the association between patient characteristics and acute MRI characteristics and the quality of ACL healing on 3-month MRI (continuous and thick versus continuous and thin).
The KANON trial has demonstrated spontaneous ACL healing on MRI in about one-third of patients managed with rehabilitation alone.
Figure 1. Summary of the Cross Bracing Protocol.
Photo of me on day 1 of the CBP for my ACL injured knee.
Figure 2 . Baseline patient and MRI characteristics included in the univariable logistic regression analyses.
WHAT DID WE FIND?
ACL healing
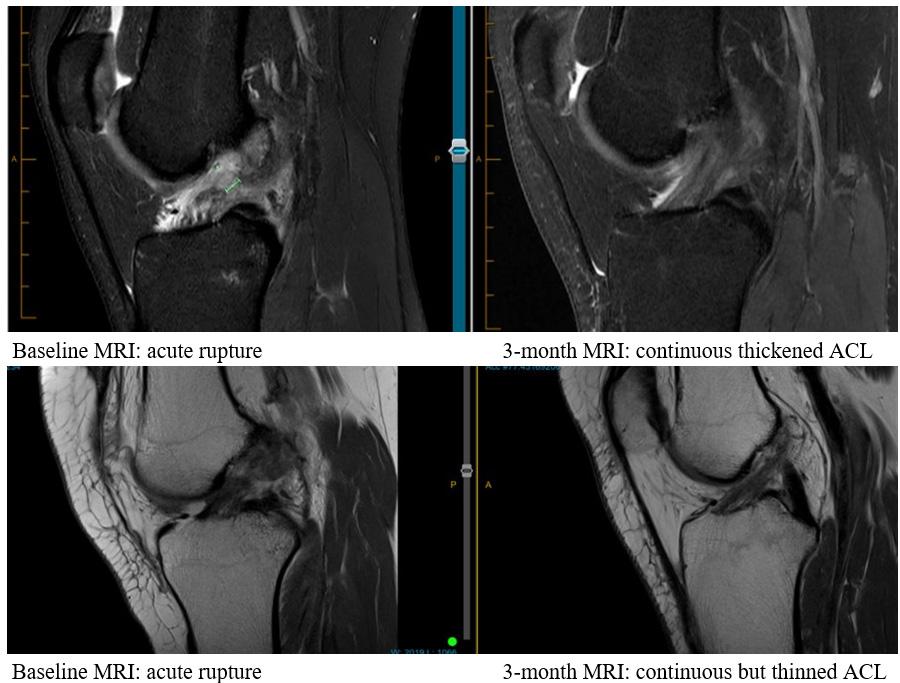
We invited 275 eligible patients of which 235 patients provided consent for participation in this study. We found signs of ACL healing (ACL-continuity) on 3-month MRI in 95% of the patients. Looking at the quality of ACL healing, we found that 63% had a thickened continuous ACL, 33% a thinned continuous ACL, and 5% a discontinuous or non-anatomical heal. Figure 3 shows MRI examples of two patients with a continuous and thickened ACL heal and a continuous but thinned ACL heal after management with the CBP.
Associated factors with the quality of ACL healing
We identified factors associated with the quality of ACL healing at 3-months after management with the CBP which
Figure 3. MRI images of two patients after following the Cross Bracing Protocol.
Baseline MRI: acute rupture
Baseline MRI: acute rupture
3-month MRI: continuous but thinned ACL
3-month MRI: continuous thickened ACL
Healing of acute ACL rupture
managed with the Cross Bracing Protocol – study insights
are shown in Figure 4. We found that patients with a partial avulsion of the femoral origin, displacement of ACL tissue outside the intercondylar notch, non-contact mechanism of injury, and hypermobility were associated with achieving less optimal ACL healing (continuous and thin ACL) on 3-month MRI. On the other hand, patients who were older, with a posterolateral corner injury, and haemarthrosis were associated with achieving more ACL healing (continuous and thick ACL) on 3-month MRI.
What does this mean?
Our high healing rates provide further evidence that the ACL has the potential to heal non-surgically. Moreover, it indicates that the CBP may facilitate ACL healing, although clinical trials are needed to compare outcomes with other treatment strategies.
Findings from the first 80 patients managed with the CBP showed that those with more ACL healing on 3-month MRI had better knee function and QOL compared to those with less
We found signs of ACL healing (ACL-continuity) on 3-month MRI in 95% of the patients.
or no ACL healing. However, we did not assess important long-term outcomes, including knee function, survivorship of the healed ACL, return-to-sport rates, prevalence of osteoarthritis, and long term QOL in this study. This is an interesting area for further exploration, requiring longitudinal studies to inform clinical practice.
Research on patient or MRI factors that influence ACL healing is sparse. Previous studies investigating factors affecting ACL healing included patients
with partial ACL ruptures, which may have a greater healing potential due to the ACL fibres that remain in continuity acting as a construct to enable healing of the partially torn ACL elements. The CBP is the first bracing method to utilize a 90° knee flexion block to attempt to address the gap distance between ruptured ligament ends. This “reduction and immobilisation” of the ruptured ACL is what makes the CBP so novel and pioneering. Locking the knee at 90° flexion, approximates the ACL, in attempt to enable ACL tissue to bridge the gap between ligament remnants aiding ACL healing.
As shown in Figure 4, we found that patients with a partial avulsion of the femoral origin or displacement of ACL tissue outside the intercondylar notch were most strongly associated with less optimal ACL healing (a continuous and thin ACL) on 3-month MRI. Perhaps this is due to the anatomical challenge faced by the ACL tissue having to reattach to the femoral origin, or the displaced tissue having to reduce back into the intercondylar notch
Figure 4. Forest plot demonstrating
resulting in less tissue contributing to the healing process and thus the chance of obtaining a thinner “lower volume” heal. Alternatively, the avulsed and/or displaced tissue might attach to surrounding structures, such as the posterior cruciate ligament (PCL) or lateral wall (LW). Such nonanatomic ACL healing is analogous to a mal-united displaced fracture that is not anatomically reduced by an adequate closed reduction.
Our findings provide valuable preliminary insights into baseline factors related to ACL healing on 3-month MRI. However, it is important to note that our analysis assessed each “patient” and “MRI” factor independently. Future studies should explore possible interactions between these factors and the “spectrum of ACL healing,” whilst adjusting for potential confounders. This could help inform prognostic studies and improve our understanding of which patients are most suitable for the CBP.
For article references, please email info@sma.org.au
Take home messages
ٚ Traditionally, management strategies have been based on the assumption that the ACL has limited ability to heal.
ٚ This study provides further evidence that ACL ruptures can heal non-surgically.
ٚ The CBP might be a valuable non-surgical treatment option with potential to aid ACL healing, but clinical trials are needed to compare outcomes with other treatments.
ٚ This study identified factors associated with ACL healing quality at 3-months after CBP management, for exploration in further studies.
ٚ In the future, clinicians may advise on patients’ healing potential based on their characteristics and the nature of their ACL injury. This may help inform treatment decisions between surgical and non-surgical management for acute ACL rupture.
About the Authors
Meike van Haeringen is a 4th year medical student at the University of Amsterdam in the Netherlands. She is an elite athlete with a history of ACL injuries. In 2023 she completed her research thesis on ACL healing and the Cross Bracing Protocol as a part of her Master’s degree through an exchange at The Centre for Health Exercise and Sports Medicine at the University of Melbourne.
Dr Tom Cross is a specialist who has practised sports medicine for the past 28 years. Over that period, he completed 5 years of specialist post-graduate training in sport & exercise medicine and gained fellowship to the Australasian College of Sport & Exercise Physicians (ACSEP). He has worked with many professional sport teams including as head doctor to the Sydney Swans for 5 years. He pioneered the Cross Bracing Protocol alongside his father Dr Mervyn Cross.
A/Prof Steph Filbay is an NHMRC Emerging Leadership Fellow, Dame Kate Campbell Fellow, and Principal Research Fellow at the University of Melbourne. She leads a research team focused on improving outcomes for people with ACL injury and post-traumatic knee osteoarthritis. She has presented her research over 100 times across 10 countries. She has received numerous awards and grants, including a recent NHMRC Investigator Grant to fund 5 years of research aimed at improving outcomes for people with ACL injury and post-traumatic knee osteoarthritis.
Photo: Productimagepro / Getty Images
Journal of Science and Medicine in Sport and sister journal JSAMS Plus
Official journals of Sports Medicine Australia
JSAMS – most cited article in 2024
How can outdoor sports protect themselves against climate change-related health risks? – A prevention model based on an expert Delphi Study
Sven Schneider, Marlen Niederberger, Luke Kurowski, Luisa Bade
Exercise in the Management of Polycystic Ovary Syndrome: A Position Statement from Exercise and Sport Science Australia
Angelo Sabag, Rhiannon K. Patten, Alba Moreno-Asso, Giorgia E. Colombo, Xela Dafauce Bouzo, Lisa J. Moran, Cheryce Harrison, Maryam Kazemi, Aya Mousa, Chau Tien Tay, Angelica Lindén Hirschberg, Leanne M. Redman, Helena J. Teede
JSAMS Plus – most cited article in 2024
Head injury assessment in youth men’s rugby league players: An evaluation of game play characteristics and video review of potential concussion signs
Andrew J. Gardner, Martin A. Lang, Suzi Edwards, Ben Jones, Grant L. Iverson, Douglas P. Terry
JSAMS Plus – most downloaded article in 2024
The Ultra Mentality – Foundations for maximising athletic mental performance
Andrew J. Gardner, Robert Gilbert
Ask the JSAMS Authors
Video Interviews exploring Editor’s
Choice Articles with Key Authors
A Note From the JSAMS Editor-In-Chief
The Journal of Science and Medicine in Sport (JSAMS) is an Australia-based scientific journal with international reach, published by Elsevier on behalf of SMA. JSAMS covers a broad spectrum of sport-related research, organised into five key areas:
1. Sport and Exercise Medicine (Prof Toomas Timpka, Linköping University, Sweden)
2. Sport Injury (Prof Fiona Wilson, Trinity College, Ireland)
3. Exercise Therapy (Prof Dennis Taaffe, Edith Cowan University, Australia)
4. Sport Science (A/Prof Jason Siegler, Arizona State University, USA)
5. Physical Activity and Public Health (Prof Jo Salmon, Deakin University, Australia)
Each section is led by a Deputy Editor with specialised expertise, supported by dedicated Associate Editors to ensure rigorous peer review and issue development. This comprehensive editorial structure upholds JSAMS’s
commitment to publishing highquality, clinically relevant research. For this purpose, JSAMS publishes a diverse range of article categories, including:
ٚ Original Research
ٚ Review Articles (systematic/scoping reviews, and meta-analyses only)
ٚ Consensus Statements and Clinical Practice Guidelines
ٚ Brief Reports and Case Reports
ٚ Letters to the Editor
ٚ Viewpoints
ٚ Registered Reports
The following article types are considered by invitation only:
ٚ Cornerstone Reviews (proposal required)
ٚ Counterpoints to a Viewpoint
ٚ Editorials
ٚ Special Issues (proposal required)
JSAMS remains committed to strengthening the AUS-NZ research community, as reflected in our Editorial Board membership and the support of SMA. At the same time, we welcome skilled and
dedicated scientists interested in contributing to our Editorial Board.
We aim to place greater emphasis on the emerging field of Exercise Therapy, the expanded scope of Physical Activity and Public Health, and the growing importance of qualitative research and mixed-methods studies, including those addressing environmental issues in sport.
As a journal with a clear position in ongoing scientific debates, JSAMS strives to align its editorial processes with its values. Our policies reflect this commitment. Original research submissions must justify the exclusion of either sex with explicit, convincing reasoning. Preprint policies define clear guidelines for manuscripts previously published on preprint servers. Systematic review evaluation criteria ensure rigorous assessment, addressing concerns over the increasing volume of such studies. These principles are upheld through transparent editorial policies, online documents, and editorial commentaries.
JSAMS serves a broad audience of professionals in sports medicine, physiotherapy, and sport science, encompassing related disciplines such as podiatry, biomechanics, exercise physiology, motor control and learning, sport and exercise psychology, sports nutrition, public health, and rehabilitation.
Each year, we present the Paper of the Year award at the SMA Conference. In 2022, the award was given to Dr Jaroslaw Krzywanski for his paper Vaccine versus infection – COVID-19related loss of training time in elite athletes, while in 2023, it was awarded to Dr Kathryn Dane for her paper “It’s always the bare minimum” - A qualitative study of players’ experiences of tackle coaching in women’s rugby union. The evaluation process for the 2024 award is currently underway.
With such a wide range of opportunities, isn’t it time to find the perfect space for your research within JSAMS?
PROFESSOR TIM MEYER MD PHD
Accelerating the early rehabilitation pathway and reducing the patient burden after proximal hamstring tendon repair
DR JAY EBERT, University of Western Australia (2024 SMA & ACSEP Conference
– Senior Career Researcher – ASICS Best Paper in Clinical Sports Medicine)
Photo:
Proximal
Hamstring Injury Epidemiology, Injury Mechanism and Common Presentation
Hamstring injuries are commonly encountered during recreational and sporting activities, accounting for about 30% of all lower extremity pathologies. It has been reported that proximal hamstring tendon ruptures make up about 10% of all hamstring injuries. These may be isolated to a single tendon (or two tendons), or may result in avulsion of the biceps femoris, semimembranosus and semitendinosus tendons from the ischial tuberosity. Most often (albeit not always) these tendon avulsion injuries occur when the hamstring muscles are eccentrically contracting in a position of simultaneous hip flexion and knee extension. At this time, the hamstring muscles are being loaded forcefully in a position of maximal stretch. Common injury mechanisms therefore are varied though can include a slip of the foot forward during a trivial daily or occupational setting, or during running/sprinting or being pushed forcefully from behind in a recreational or sporting environment.
Clinically, patient presentation following injury can also be varied. Often patients may report a sharp pain at time of injury located around the buttock or posterior thigh, which may also be accompanied by an audible crack or pop. Immediate weight-bearing ability may be compromised, while sitting
Hamstring injuries are commonly encountered during recreational and sporting activities, accounting for about 30% of all lower extremity pathologies.
(due to compression over the injury site), postures/movements that require increased hip flexion (such as putting on shoes and socks) and activities that require hamstring activation (such as squatting and stair ascent) can be challenging. Bruising and swelling can often be encountered given the traumatic nature of such injuries. Nonetheless, regardless of the injury mechanism, the end result can be painful and functionally limiting, with a persistent and significant level of disability if missed or misdiagnosed.
Post-injury Treatment Pathways
Following proximal hamstring tendon injury, the best treatment pathway will be dictated by the severity and/or nature (partial or complete avulsion) of the injury, the number of tendons involved, the chronicity of the injury and the degree of tendon retraction. Non-operative treatment may present
a viable option for low function patients and/or those with proximal tendinopathy, partial, single or two tendon tears (also depending on the degree of retraction). This may involve an immediate period of relative rest and/or activity modification, with a progressive therapy program then important in improving function and permitting an eventual graduated return of the patient back to their daily, recreational and/or sporting activities. Other concomitant treatments also reported include non-steroidal anti-inflammatory medications and injection therapies.
For patients with a more significant proximal hamstring tendon injury, a persistent significant strength and functional deficit can remain, while these patients may have a higher risk of sciatic nerve pathology due to tethering by the retracted tendons. Therefore, for patients that have had two tendon injuries with a higher degree of tendon retraction, or complete three tendon injuries, especially seeking a return to an otherwise active lifestyle, surgical repair is often indicated. Several systematic reviews have now demonstrated the benefit of surgical repair specifically in these patients with encouraging functional restoration and return to sport (RTS) rates, and superior outcomes from surgery versus a nonoperative management pathway.
Accelerating the early rehabilitation pathway and
reducing the patient burden after proximal hamstring tendon repair
Post-operative Surgical Management
Despite an increasing number of published post-operative rehabilitation protocols and studies reporting outcomes in patients undergoing proximal hamstring tendon repair in the context of tendon avulsions, there is a lack of consensus on postoperative rehabilitation regimes. A wide array of (and extensive variation in) immobilization techniques, weight-bearing restrictions and active rehabilitation regimens have been used, with many centers prescribing knee braces, hip braces or hip-kneeankle orthoses in the post-operative care of these patients, despite their perceived limitations. Historically, these have been employed to reduce tension from the early surgical repair. Interestingly, a more recent review of published post-operative protocols suggested 71% of postoperative protocols included the use of a brace/orthosis to restrict or fix range of motion of either the hip or knee. Furthermore, the majority of protocols insist on immediate nonweightbearing or toe-touch weightbearing, with a mean return to full weight-bearing of approximately 7 weeks which is likely conservative and certainly a burden on patients.
Accelerated post-operative rehabilitation pathways have now been well established following many orthopedic surgical interventions and, with respect to the pathway for patients following proximal hamstring tendon repair surgery, may provide benefits such as improved blood flow to accelerate biological healing, early longitudinal strain inducing organized collagen formation, prevention (or at least limiting) postoperative muscle atrophy, the early return of neuromuscular control and return to trivial daily and occupational activities, and psychosocial benefits.
Of course, the development of accelerated pathways must be undertaken in a well-supervised and controlled manner. To date, no study has been conducted to compare a historically conservative versus more accelerated early rehabilitation pathway in patients following surgical repair of acute proximal hamstring tendon avulsions.
Participants and Study Design
We sought to embark on a randomized controlled trial (RCT), investigating the role of an accelerated early postoperative regimen after proximal hamstring tendon repair, named the
PHARRLAP trial (Proximal Hamstring Avulsion Rehabilitation Regimes: Longitudinal versus Accelerated Protocol). For the current study, 57 patients were recruited, subsequently undergoing proximal hamstring tendon repair followed by either a traditional braced, partial weightbearing rehabilitation regime (‘conservative’ protocol, n=30) or an accelerated, unbraced regime, that permitted full weight-bearing as tolerated (‘accelerated’ protocol, n=27).
Recruited patients were a communitylevel cohort, experiencing their proximal hamstring tendon avulsion injury during either sport or recreational activities (n=33), or work tasks or activities of daily living (n=24). Importantly, the two recruited and randomized groups were well balanced for pertinent demographics (sex, age, body mass index) and injury history (mechanism or injury and time from injury to surgery), with all avulsions complete 3-tendon ruptures and all repairs acute and undertaken within 42 days (6 weeks) of the injury.
The rehabilitation programs undertaken by patients were developed based on a combination of existing published protocols and
A recent review found that 71% of post-operative protocols recommend a brace or orthosis to limit hip or knee motion.
recommendations, and the research team’s clinical experience, while further input was gathered from university and other private therapy groups actively engaged in the treatment of patients undergoing proximal hamstring repair. While patients progressed through a guided program that initially consisted of early hip/knee mobility, isometric muscular contractions and ambulatory guidance, followed by varied closed and open kinetic chain exercises, and then more functional and plyometric activities as deemed relevant, this progression was largely similar between groups. The primary difference between groups was the full weightbearing as tolerated and no use of a brace in the accelerated group, versus six weeks of brace use and a restricted early weightbearing pathway followed by the conservative group, along with some variation in early exercises due to the weightbearing (and bracing) restrictions.
We sought to evaluate the recovery of patients following proximal hamstring tendon repair and the experimental early post-operative rehabilitation protocols, via a range of outcomes including patient-reported outcome measures (PROMs) relevant to proximal hamstring issues, lower extremity function and disability, general health and overall patient satisfaction. Furthermore, the recovery of peak isokinetic hamstring (and quadriceps) strength was assessed, as was the recovery of single limb hop performance. Of the recruited cohort, while two recruited patients were omitted immediately at the time of surgery due to surgical complications (conservative group, n=2), and a further two patients were withdrawn between 6-12 weeks post-surgery due to early re-injuries requiring further surgery (conservative group, n=2), all other patients were retained and assessed at 6- and-12 months post-surgery.
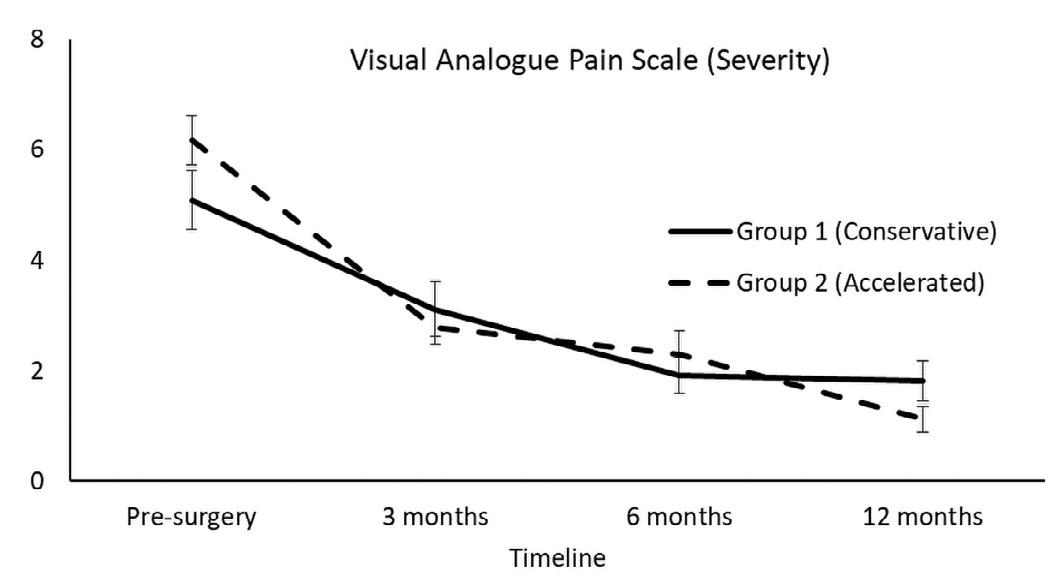
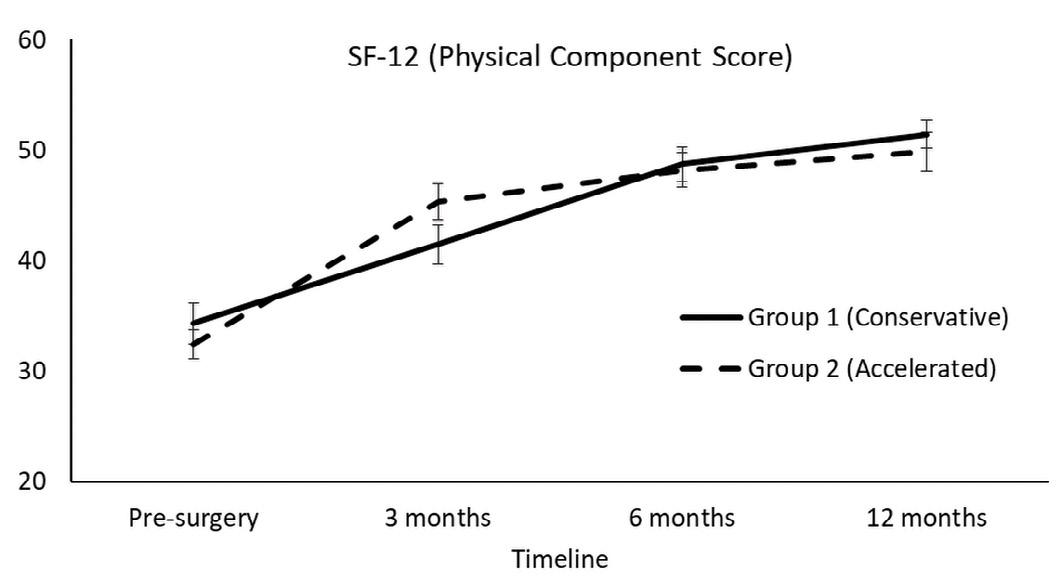
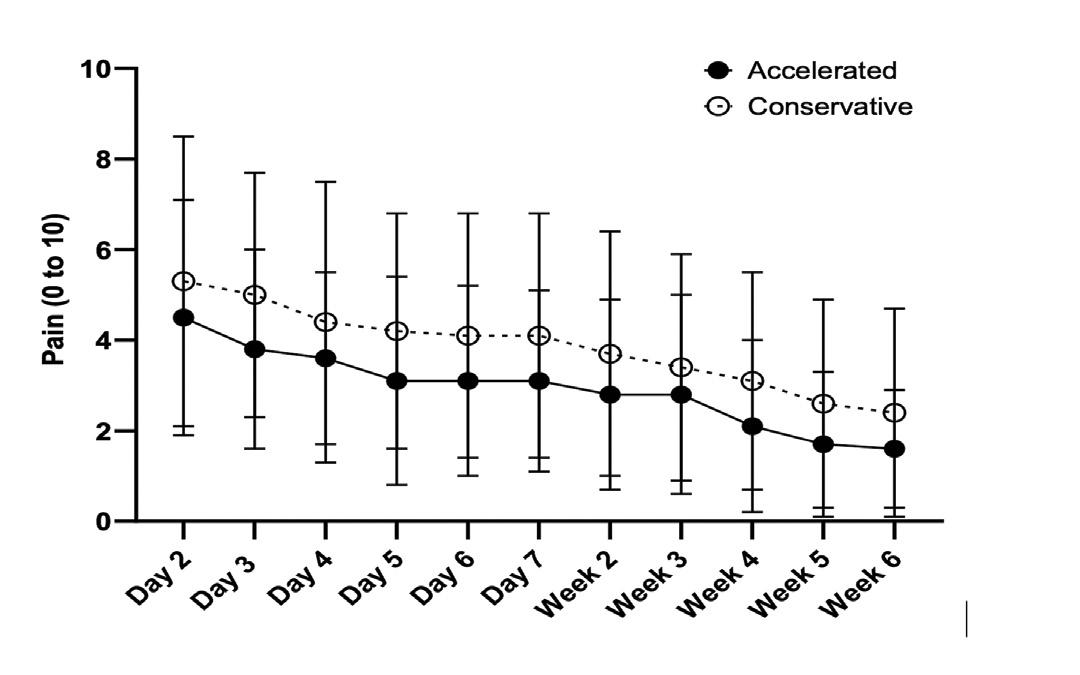
Primary Study Findings
Firstly, the evaluation of hamstringrelated pain over the first 6 weeks demonstrated consistently lower (albeit not statistically significant) hamstring pain in the accelerated (versus conservative) rehabilitation group. All other PROMs improved and, while the accelerated group reported a better Physical Component Score for the 12-item Short Form Health survey at 3 months, as well as a lower severity of hamstring pain at 12 months, there were no other group differences. The 12-month reported satisfaction rates were relatively high, with 89% and 96% of the ‘conservative’ and ‘accelerated’ rehabilitation groups, respectively, being satisfied with their overall postoperative outcome. Of interest, while a higher limb symmetry index (LSI) was observed in the accelerated group at 6 months post-surgery, no other postoperative differences were observed between groups in strength or single
Accelerating the early rehabilitation pathway
and reducing the patient burden after proximal hamstring tendon repair
limb hop performance outcomes. Importantly, there were no significant complications or re-injuries within the first 12 postoperative months as a result of the early accelerated protocol.
Study Conclusions and Clinical Implications
The current study has shown that after proximal hamstring repair surgery, post-operative outcomes following an accelerated rehabilitation regimen were largely comparable to a traditionally conservative rehabilitation pathway, albeit demonstrating better early physical health-related quality of life scores. Importantly, the accelerated regimen did not adversely affect outcomes or jeopardize the integrity of the repair, which is a primary reason why many protocols and clinicians still advocate a conservative post-operative process.
At present, a conservative period of lengthy brace use and assisted weight bearing with crutches is often employed in patients following proximal hamstring tendon repair. While not justified, it is largely a result of the lack of research in the area, also highlighted by the variation reported in current published post-operative protocols. Nonetheless, it remains a significant burden for patients early post-operatively in undertaking many trivial activities of daily living and also the re-introduction to the workplace. The early outcomes of the PHARRLAP trial have shown that an accelerated early rehabilitation regimen is safe and efficacious after proximal hamstring tendon repair.
Acknowledgements
The authors would like to acknowledge the collaborative contribution of the clinical, academic and research partners involved, including the University of Western Australia, the HFRC Rehabilitation Clinic, Coastal Orthopaedics, the Perth Orthopaedic and Sports Medicine Centre and the Fiona Stanley Fremantle Hospitals Group.
For article references, please email info@sma.org.au
About the Author
Dr Jay Ebert is a Senior Lecturer in musculoskeletal rehabilitation at the School of Human Sciences (Exercise and Sport Science), at the University of Western Australia, as well as the Director of Research at the Perth Orthopaedic and Sports Medicine Research Institute,and a Director of the Orthopaedic Research Foundation of Western Australia. Clinically, he is a Director and practicing Accredited Exercise Physiologist at the HFRC Rehabilitation Clinic in Perth, Western Australia. He completed his PhD in 2008 in the field of cartilage repair, biomechanics and exercise rehabilitation, and has extensive experience working with patients of all musculoskeletal conditions, with a particular focus on lower limb injury and post-operative rehabilitation following orthopaedic surgery.
“I’ve worked in a wide range of settings and been fortunate to teach health professionals and to learn from the best. Despite all that experience, I still find Clinical Sports Medicine It makes me, and my athletes, better.”
–Mario Bizzini, PT, PhD, Former Executive Board Member, International Federation of Sports Physical Therapy (IFSPT)
Now in its sixth edition, the world-leading series Brukner & Khan’s Clinical Sports Medicine is a practical guide to physiotherapy and musculoskeletal medicine. Written for students and those early in their careers, this first book in the collection, Clinical Practice, a great patient-focused clinician. It lays out the clinical sciences that underpin our field and details the principles of assessment and multidisciplinary treatment.
Key features
■ 87 practice pearls that turn years of clinical experience into expert advice
■ 380 figures, 280 of which are new to this edition
■ 74 feature boxes to highlight advanced clinical issues
■ 69 QR codes with hours of additional content
What’s new
■ Chapter outline, learning objectives and key points for every chapter
■ 16 new chapters covering how to be a better clinician, how to interpret clinical sciences, and the principles that underpin quality clinical practice
■ All chapters reworked from scratch by 90 world-leading experts
Gut Gains
Exploring the Role of Heavier Food to Train the Gut
IF THERE ARE 10 ENDURANCE RUNNERS TOEING THE LINE OF A RACE, HOW MANY DO YOU THINK WILL EXPERIENCE GUT SYMPTOMS DURING THE EVENT?
Around nine out of ten of these athletes will likely get gut symptoms during exercise, especially in events lasting more than 3 hours. While minor symptoms like belching and flatulence can be inconvenient, severe symptoms such as nausea, vomiting, and diarrhoea can turn a well-prepared race into a desperate crawl to the finish line or a dreaded “DNF”.
Athletes train their muscles and mind to be stronger but often forget a key player – the gut. The gastrointestinal tract’s ability to digest and absorb food during exercise determines how much fuel is available for working muscles. However, strenuous exercise causes the gut to shut down, making athletes more prone to gut issues. In endurance and ultra-endurance events, nutrition during exercise is crucial to support prolonged effort, but a balance between fuelling needs and feeding tolerance is more important to prevent worsening of gut symptoms. Just like muscles, the gut can be trained to become better at simultaneously eating and exercising, rather than its usual “rest and digest”.
Training the Gut
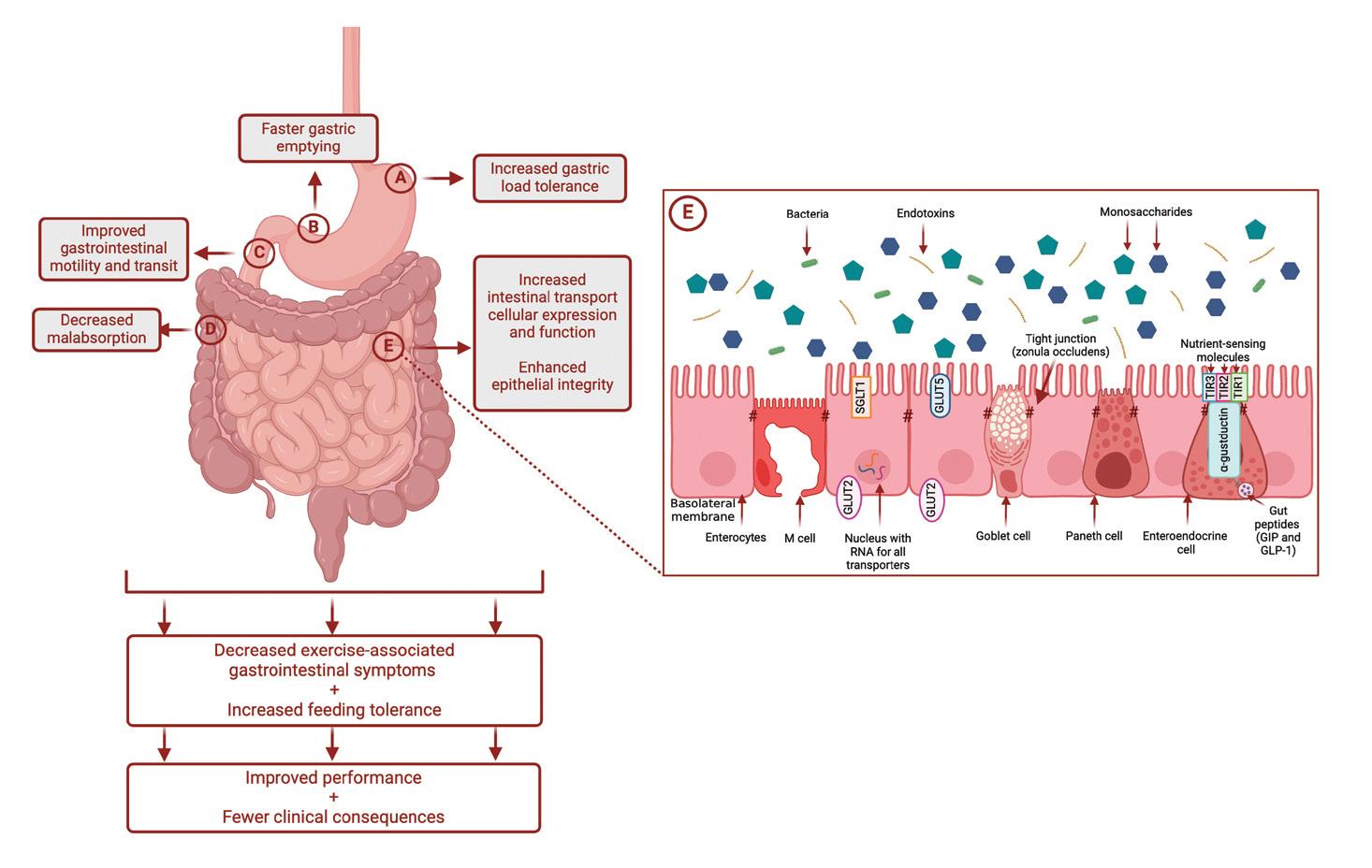
The gut’s tolerance to food and fluid during exercise can be gradually developed through repeated exposures, a strategy known as “gut-training”. This approach can lead to various adaptations within the gastrointestinal tract such as faster gastric emptying, increased gastric load tolerance, and improved gastrointestinal motility and absorption (Figure 1), helping reduce the risk of gut symptoms during exercise. While these benefits may sound promising, supporting evidence in athletes is limited.
Several ways of training the gut have been proposed though most are anecdotal. A common feature is challenging the gut with large amounts of food or fluid in a structured and repeated manner during training, prior to a key race. Examples include training with large volumes of fluid, training with a full stomach, practicing the raceday nutrition plan, training with high carbohydrate intake during exercise, and increasing daily carbohydrate intake. Based on a recent systematic literature review, only three of these
ISABEL G. MARTINEZ, Monash University (2024 SMA & ACSEP Conference – ASICS Best Poster in Sports
and Exercise Science)
Athletes train their muscles and mind to be stronger but often forget a key player – the gut. Just like muscles, the gut can be trained to become better at simultaneously eating and exercising, rather than its usual “rest and digest”
Photo: michelangeloop / Getty Images
Figure 1. Schematic illustration of the potential mechanisms by which ‘gut-training’ or repetitive ‘feeding-challenge’ may provide beneficial outcomes in gastrointestinal integrity, function, systemic responses, and exercise-associated gastrointestinal symptoms (Ex-GIS). Reprinted from “The Effect of Gut-training and Feeding-challenge on Markers of Gastrointestinal Status in Response to Endurance Exercise: A Systematic Literature Review”, by Martinez, et. al., 2023, Sports Medicine, 53(6):1175-1200. doi: 10.1007/s40279-023-01841-0.
protocols (training with large volumes of fluid, training with high carbohydrate intake during exercise, and increasing daily carbohydrate intake) have been scientifically investigated and showed positive results.
Most of the evidence supporting the benefits of gut-training focuses on challenging the gut with a high carbohydrate intake during exercise over repeated and consecutive days, known as a repetitive feedingchallenge. This approach has been shown to benefit recreational endurance athletes, by reducing the severity of gut symptoms and carbohydrate malabsorption following a two-week protocol of
Gut Gains
Exploring the Role of Heavier Food to Train the Gut
1 h moderate intensity run with 90 g/h of carbohydrate from glucose and fructose. However, when a similar protocol was tested among elite athletes, these effects were not observed, suggesting that training level and usual carbohydrate intakes play a role.
A key limitation of the two-week repetitive feeding-challenge protocol is its feasibility. Participants in these studies reported symptomatic improvements within 1 week but found it challenging to follow the protocol for two weeks. This highlights the need to investigate a more
practical approach that aligns with an athlete’s usual training program.
Exploring the role of nutrient density
Training the gut with carbohydrates during exercise improves intestinal absorption and gut symptoms, but could consuming nutritionally dense food during exercise offer additional benefits? Our most recent study aimed to answer this question. Like how lifting heavier weights builds stronger muscles, we hypothesised that further challenging the gut with harder to digest nutrients (i.e., fat and protein) would enhance the gut-training adaptations. For
example, a higher gastric load from nutrient-dense food would be a greater stimulus in improving gastric accommodation (how well the stomach expands and adapts to food without causing discomfort) and/or gastric emptying (how quickly the contents of the stomach leave and enter the intestine). This could reduce the severity of upper-gastrointestinal symptoms such as upper abdominal fullness or pain, belching, or regurgitation, leading to better tolerance of feeding during exercise.
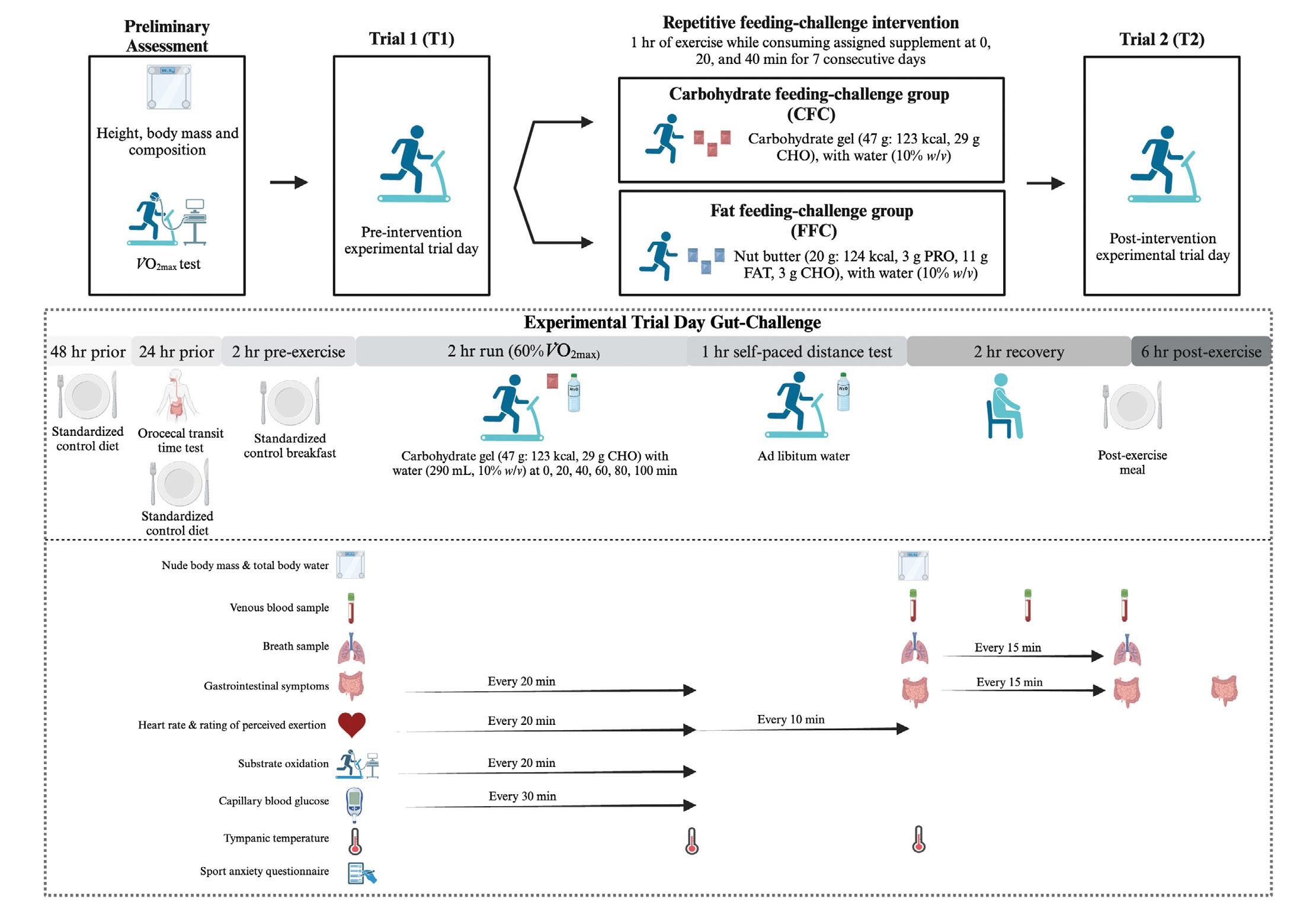
Our recent study aimed to investigate the effects of a 7-day repetitive feeding-
Figure 2 . Schematic illustration of the study design. V̇O2max : maximal oxygen consumption, PRO: protein, CHO: carbohydrate, kcal: calories, w/v: weight per volume, h: hours, min: minutes, %: percentage). Reprinted from “Repetitive Feeding-Challenge With Different Nutritional Densities on Markers of Gastrointestinal Function, Substrate Oxidation, and Endurance Exercise Performance”, by Martinez, et. al., 2025, International Journal of Sport Nutrition and Exercise Metabolism, (Ahead of Print). doi: 10.1123/ijsnem.2024-0145
challenge using a high-fat versus a high-carbohydrate supplement on markers of gastrointestinal function, glucose availability, substrate oxidation, and subsequent performance when consuming a high carbohydrate intake (87 g/h) during endurance exercise. (Figure 2)
How did we do it?
ٚ Forty-four endurance athletes (i.e., runners, triathletes) participated in the study.
ٚ A pre-intervention gut-challenge trial was completed by the athletes which consisted of a 2 h steadystate run while taking an inhouse developed low-fructose carbohydrate gel (3.8 g/100 g glucose, 0.2 g/100 g fructose, 10.2 g/100 g sucrose, 6.3 g/100 g maltose, and 29.4 g/100 g total maltooligosaccharide) every 20 min, followed by 1 h self-paced distance test with as much water as desired.
ٚ Athletes were randomly assigned to either a fat (20 g nut butter: 124 kcal, 11 g fat, 3 g protein, 3 g carbohydrates) or carbohydrate feeding-challenge group (47 g carbohydrate gel: 123 kcal, 29 g carbohydrates) which they consumed every 20 min during 1 h of moderate intensity running or cycling (running for majority of the sessions) for seven consecutive days.
ٚ A follow-up post-intervention gut-challenge trial was then completed by athletes.
ٚ The following outcomes were assessed during the trials:
– Resting orocaecal transit time (time it takes for food to move through the gut at rest)
– Feeding tolerance (how well athletes could tolerate food/ fluid during exercise)
– Carbohydrate malabsorption (how much carbohydrate is not absorbed in the intestine)
– Gut symptoms (how prevalent and severe the gut symptoms are during and after exercise)
– Blood glucose availability (how much glucose is in the blood during exercise)
– Whole-body fat and carbohydrate oxidation (how much fat or carbohydrate is used as fuel during exercise on a whole-body level)
Exposure of the gut to the volume and/or type of food that will be ingested during a race, needs to be done repetitively during training – so far, daily for at least 1 week appears to work.
Photo: GlobalStock / Getty Images
Gut Gains
Exploring the Role of Heavier Food to Train the Gut
What did we find out?
ٚ The repetitive feeding-challenge for 7 days with fat did not differ to the repetitive feeding-challenge with carbohydrate in terms of orocaecal transit time at rest, feeding tolerance, glucose availability, and whole-body fat and carbohydrate oxidation rates, in response to a subsequent gut-challenge trial.
ٚ The repetitive feeding-challenge with fat improved the severity of total- and upper-gut symptoms during exercise to a similar extent as the repetitive feedingchallenge with carbohydrate.
ٚ No difference in exercise performance during the 1 h selfpaced distance test was observed between groups in both trials.
Overall, the repetitive feedingchallenge with fat did not enhance nor worsen gastrointestinal function, substrate oxidation, endurance exercise performance, and gut symptoms when compared with a carbohydrate repetitive feeding-challenge.
On
the road or trail
Should athletes start training with nut butters? The answer is “it depends”. The findings from this recent study along with previous evidence underlines that the supplement to be used during guttraining should be race-specific. Using nutritionally dense food could be an option for those who will be running ultras (i.e. >4 h and at a relatively lower intensity), wherein solid foods with protein and fat are commonly ingested. The key takeaway is that exposure of the gut to the volume and/ or type of food that will be ingested during a race, needs to be done repetitively during training – so far, daily for at least 1 week appears to work. How this can be modified to fit within the usual design of a training program
(i.e., consisting of sessions of varying intensity and duration) or whether the same effects would be observed if guttraining is done on non-consecutive days, warrants further investigation.
Read more about the study here!
If you’re an athlete who experiences gut issues during exercise, consider working with a qualified sports dietitian to help tailor the gut-training approach specific to your needs and goals.
For article references, please email info@sma.org.au
About the Author
Isabel G. Martinez, MSc, RD, PhD (cand.)
Isabel is a nutrition scientist and sports dietitian who specializes in gastrointestinal issues in endurance and ultra-endurance athletes.
Aside from her dietetic credentials both in the Philippines and USA, she holds a Master of Science in Exercise Physiology from the University of Illinois and a Diploma in Sports Nutrition from the International Olympic Committee as the program’s scholarship recipient. Isabel is currently a doctoral candidate at Monash University in Australia investigating management strategies for exercise-associated gastrointestinal symptoms. She is involved in various consultancy roles which include nutrition & exercise testing services and sports nutrition product development. When not in the lab, you will likely find her outside running or windsurfing down at the bay.
Photo:
Drazen Zigic / Getty Images
Tackling concussion
SMA’s national campaign to support safer sport
Concussion remains a significant concern in Australian sport, with an estimated 100,000 sportrelated concussions occurring each year—95% of them in community and school settings. To address this, SMA launched a national campaign aimed at improving concussion awareness and management across all levels of sport.
A key element of the campaign is the distribution of SMA’s concussion management poster to more than 38,000 schools and community sports clubs nationwide. Developed by SMA, the poster simplifies the graded return-to-play framework outlined in the AIS Concussion Guidelines for Youth and Community Sport into four clear steps. It provides essential guidance on recognising and managing concussion, helping ensure a safe return to play.
Raising awareness at the community level is crucial to improving concussion management. While elite athletes have access to dedicated medical teams, most concussions occur in local sporting environments, where coaches, parents, teachers, and sports trainers play a key role in ensuring player safety.
SMA continues to advocate for a government-backed, multi-platform national awareness campaign to further educate the sporting community and reinforce bestpractice concussion management.
The campaign has been made possible with the support of SMA’s Elite Partner,
ASICS, a long-standing advocate for community sport safety and wellbeing. SMA also acknowledges the valuable contributions of its Community Partners, Elastoplast and Gallagher, and Government Partners, VicSport, Sport West, the Northern Territory Government, and the Tasmanian Government.
For more information and access to the poster, scan the QR code.
Biomechanical
implications
for post-traumatic knee osteoarthritis in young adults
– the underloading paradox: are we protecting or harming?
Photo: SeventyFour / Getty Images
MATTHEW SAVAGE, La Trobe University Sport and Exercise Medicine Research Centre (2024 SMA & ACSEP Conference – People’s Choice Award for Best Poster)
The problem: posttraumatic osteoarthritis
With an ever-increasing rate of traumatic knee injuries, such as anterior cruciate ligament (ACL) ruptures, the longer-term effects of these injuries will continue to grow. One of the most common and burdensome consequences of ACL injuries is the accelerated development of knee osteoarthritis (OA), termed post-traumatic OA. Posttraumatic OA affects an estimated one in two people within a decade of traumatic knee injury, leading to persistent symptoms, impaired quality of life, reduced psychological wellbeing and work-related problems. Given that traumatic knee injuries typically occur during adolescence and young adulthood, individuals are developing OA at a much earlier age and thus living longer with these problems than older individuals with non-traumatic OA. Indeed, the economic burden of post-traumatic OA exceeds $600 million annually in direct hospital costs alone, and early workforce departures due to OA in younger individuals are estimated to cost over $7 billion per year.
Previous research has identified effective treatments for OA in older adults, such as exercise and weight management. Current recommendations suggest applying these treatments to young adults with, or at risk of, post-traumatic knee OA, with little evidence available to support this notion. Treatment strategies that may work for older adults don’t necessarily apply to younger adults with post-traumatic OA, where the underlying causes, risk factors, and pathophysiology differ. In those with post-traumatic OA, structural changes such as osteophyte growth (bony spurs) and joint space
narrowing are more likely in the lateral compartments, as opposed to predominantly occurring in the medial compartment in those with non-traumatic OA. Despite the fact that most research in this space has focused on structural outcomes, it is symptoms (e.g., pain) that drive the burden of OA, and motivate patients to seek treatment. Fortunately, individuals at risk of post-traumatic OA are easily identifiable, as they will typically seek healthcare at the time of injury. The problem, however, is that we don’t understand why some people go on to develop OA, and others do not.
Could
altered biomechanics be part of the problem?
The economic burden of post-traumatic OA exceeds $600 million annually in direct hospital costs alone
Changes in biomechanics following a traumatic injury may influence the likelihood of someone developing OA later in life. Altered biomechanics (e.g., how the knee joint moves during walking) are consistently associated with the onset and progression of OA in older adults, but the relationship with post-traumatic OA is less clear. Indeed, research has suggested that biomechanical risk factors for the onset and progression of OA differ
Photo:
Biomechanical implications for post-traumatic knee osteoarthritis in young adults
– the underloading paradox: are we protecting or harming?
between traumatic and non-traumatic populations. Following traumatic knee injuries, altered biomechanics are prevalent and often persist even after surgical intervention (e.g., ACL reconstruction (ACLR)) Our recent systematic review sheds new light on how altered knee biomechanics might contribute to the onset and progression of post-traumatic knee OA in younger adults. These findings are important to not only guide future prevention and management strategies, but could also inform current clinical practice, helping clinicians educate patients and improve long-term outcomes.
What did we do?
We searched five electronic databases for studies investigating the relationship between knee biomechanics and future joint structure (imaging) or future symptoms (patientreported outcomes) in individuals with a history of surgery for a traumatic knee injury. We included 18 studies in total, 17 of which were following ACLR. 14 studies investigated walking; the others assessed drop landings and a forward hop. Where possible, we
pooled the results of these studies in a meta-analysis, but due to the diversity and variety (heterogeneity) of the included studies, we were unable to combine them all. For this reason, the remaining studies were summarised narratively. To best describe and aid clinical interpretation of our results, we defined joint loading as a term encompassing any kinetic measure (e.g., joint contact force, joint moments, ground reaction forces).
What did we find?
Underloading of the patellofemoral joint – a potential risk factor for post-traumatic OA?
We found that lower patellofemoral contact forces (the patella and femur pushing against each other during dynamic tasks) post-ACLR were associated with worsening future trochlear cartilage health. This contrasts with what we typically see with older adults with OA, where greater magnitudes of joint loading are associated with the progression of both structural changes (e.g., joint space narrowing) and patient symptoms. This is perhaps unsurprising when you consider the nature of articular cartilage, which relies on appropriate stimulus and joint loads for health. Articular cartilage responds favourably to mechanical load, and this is important for maintaining structure and function. However, damage to knee cartilage is common following a traumatic injury, and the early postinjury and early post-operative period often involves rest, or unloading, which prevents the cartilage from receiving necessary stimuli. This combination of insufficient loading (or ‘underloading’) on already damaged
We included 18 studies in total, 17 of which were following ACLR. 14 studies investigated walking; the others assessed drop landings and a forward hop
cartilage may provide the perfect storm contributing to the accelerated onset of post-traumatic OA.
The relationship between joint loading and tibiofemoral OA is more inconsistent
We found inconsistent evidence for the relationship between joint loading and tibiofemoral joint structure over time. This may be explained by study heterogeneity (e.g., different study populations, sample sizes, imaging methods, structural outcomes). Nonetheless, our results reinforce previous findings that biomechanical risk factors for OA differ between traumatic and non-traumatic populations. We cannot adopt a onesize-fits-all approach when treating both traumatic and non-traumatic OA.
What about the relationship between joint loading and future symptoms?
Due to the limited number of studies in this area, and heterogeneity between
them, we were unable to pool these studies statistically in meta-analyses. As such, these findings should be interpreted with caution. We found that lower measures of medial tibiofemoral joint compartment load were associated with better symptoms over time. Interestingly, this is similar to findings in non-traumatic OA.
However, when examining vertical loading alone, we found that lower loading six-months post-ACLR may be associated with worse future symptoms over time. However, lower loading at two-years post-surgery may actually be linked to better future symptoms, indicating that time post-surgery may influence the relationship between joint loading and future symptoms.
What does this mean for clinical practice?
The patellofemoral compartment is commonly affected by post-traumatic OA Optimising patellofemoral loads post-operatively and addressing altered biomechanics may present potential preventive or treatment strategies for post-traumatic patellofemoral OA. The use of force plates in clinical and sports settings is booming, as they have been shown to be easy to use, valid, and reliable for assessing ground reaction forces, a crude overall measure of lower-limb mechanical loading. Clinicians can use force plates to evaluate mechanical loading during various tasks post-surgery and use this information to guide conversations around long-term prognosis. Force plates can also be used to identify individual asymmetries or deficits in loading patterns, which can be
Biomechanical implications for post-traumatic knee osteoarthritis in young adults
– the underloading paradox: are we protecting or harming?
targeted with specific interventions. Options such as strength training, gait re-education and biofeedback, and treatment adjuncts such as knee braces, footwear, and insoles have been shown to influence joint loading. However, future clinical trials are required to confirm the effectiveness of these approaches in preventing or slowing post-traumatic OA.
If we identify that someone is underloading, however, it is also important to consider the chicken and egg question. Are these individuals experiencing pain because they are underloading their joint? Or are they underloading BECAUSE they are trying to offload a persistently painful limb? Or in the absence of pain, is it due to other factors, such as muscle strength, impaired proprioception, or psychosocial factors such as fear avoidance? As always, exploring potential reasons through thorough and individualised assessments is crucial.
The bigger picture
While altered biomechanics are likely to form just one piece of a large and complex puzzle in preventing and treating post-traumatic OA, other factors must also be considered. These include concomitant injuries to articular cartilage and subchondral bone, persistent haematoma and inflammation, body weight, and muscle strength deficits. Additionally, we know little about the role of socio-gendered factors in post-traumatic OA. Women experience worse self-reported and activity-related outcomes, face higher injury risks than men, and demonstrate distinct biomechanical differences. Despite this, no studies reported results stratified by sex, so we were unable to draw conclusions about the impact of potential biomechanical differences. However, while high-quality randomised controlled trial evidence is
still needed, addressing underloading and optimising knee biomechanics could be a promising approach for clinicians to proactively support longterm joint health and hopefully improve long term outcomes for individuals following traumatic knee injuries.
For article references, please email info@sma.org.au
Our results confirm that biomechanical OA risk factors differ between traumatic and nontraumatic groups.
About the Author
Matt Savage, La Trobe University Sport and Exercise Medicine Research Centre
Matt.Savage@latrobe.edu.au
Matt is a musculoskeletal physiotherapist and PhD student at the La Trobe University Sport and Exercise Medicine Research Centre. Matt has worked both in the NHS and in sport in the UK, as well as in private practice here in Australia. His research focuses on knee biomechanics as a potential risk factor for post-traumatic osteoarthritis and explores the use of slim-fit knee braces as a potential treatment option for individuals at risk of post-traumatic osteoarthritis.
Photo:
For elite performance
People who Shaped SMA Professor Anthony Leicht
Can you tell us about your journey into academia and what inspired your career in exercise science and sports medicine?
I originally pursued an undergraduate degree in biology, which put me on an unconventional path. Towards the end of my degree, I had the opportunity to conduct research with Professor Graham Allen, a physical education expert and exercise physiologist trained in the US. His mentorship led me to
an undergraduate Honours program, where I focused on diet, exercise, and recovery - specifically, how the body responds to these factors.
This sparked my interest in exercise physiology, and I continued my research with Prof Allen, who later served as SMA’s president from 1997 to 1999. I went on to complete a PhD studying exercise training and heart rate variability, exploring
how the heart responds to exercise and its potential health benefits.
During my PhD, I developed a strong passion for research and discovered my love for teaching. At the same time, I maintained a deep involvement in basketball. Initially a player, I soon realised my strengths lay elsewhere, leading me to become a referee. I officiated at the state, national, and international levels throughout my PhD and into my academic career.
Ultimately, my combined interests in basketball, exercise science, and research guided me into academia, where I continue to explore the intersections of sport, health, and education.
As a result, I was offered a position at James Cook University at the end of my PhD to teach and conduct research in sport and exercise. What started as a six-month contract has turned into 26 years - something I never expected!
Part of what kept me here was the lifestyle, but more importantly, I truly enjoyed teaching and researching at a regional university. The smaller class sizes and close-knit community allowed me to connect more deeply with students and engage with them on a personal level.
What drew you to focus on cardiovascular and Exercise Physiology across a range of populations, from elite athletes and to patients with chronic diseases? My interest in exercise and human performance stems from my deep
involvement in basketball. As a referee, I worked closely with elite athletes - players and referees. This exposure, along with my academic role, connected me with local sports teams and medical professionals, including surgeons and doctors who were eager to explore how exercise could benefit their patients’ health. This combination of influences allowed me to bridge the gap between sports performance and medical research.
A major turning point in my journey was meeting my PhD supervisor at the University of Southern Queensland. He had trained in a prestigious exercise physiology laboratory in Washington State during the 1970s, a time when Australian exercise scientists often had to go overseas for advanced training. Hearing his stories and learning from his experiences sparked my passion for research and broadened my perspective on exercise science.
My research has since evolved to focus on cardiovascular function and human performance. I was always interested in medicine growing up and initially considered becoming a doctor, but
ultimately, I found a way to combine my interests in cardiovascular health, exercise, and sport to explore their broader benefits. Over the years, my work has spanned both elite sports and clinical applications.
Much of my research has focused on patients with peripheral vascular disease, i.e., individuals who struggle to walk due to restricted blood flow in their legs. Our studies have explored how exercise can improve their mobility, independence, and overall quality of life. At the same time, I’ve maintained my involvement in elite sport, working with FIBA (the International Basketball Federation) personnel to study the training and performance of referees who perform at major competitions like the Olympics and World Championships.
More recently, I’ve expanded my research into occupational athletes - military personnel, emergency responders, and other professionals who require both high physical fitness and sharp cognitive abilities under stress. We’ve been investigating how exercise can enhance their
performance, particularly in demanding environments that involve physical, cognitive, and environmental stressors, such as extreme heat.
While exercise is widely recognised for its benefits, our research also examines its potential drawbacks, particularly in cardiovascular health. Understanding both the advantages and limitations of exercise helps us refine training programs for athletes, patients, and occupational professionals alike. Ultimately, my goal is to use exercise science to enhance mobility, performance, and quality of life across a broad spectrum of individuals - from elite athletes to those managing chronic diseases.
Your research often involves exercise and human performance. What sparked your interest in this area and why is it significant?
My interest in exercise science and human performance was sparked by an unexpected encounter with a supervisor at my university - someone I hadn’t even known was there. When I came across his work and heard his stories, I realised he had studied alongside some of the biggest names in the field, people I had only seen in research papers. Yet, here he was, quietly teaching and conducting research in a small corner of the university. He was a great mentor, and he really helped me understand the focus of exercise science and human performance. While we knew a lot about things like different fuel sources and muscle groups, there was still so much to learn, especially about the mechanisms behind why exercise works so well and what types of exercise provide the most benefit. That curiosity really got me hooked.
At the same time, my basketball career fuelled my interest in performance. I wanted to be faster, stronger, and able to perform better in games. This personal drive, combined with my growing research interests, made exercise science a natural fit. As I
People who shaped SMA
Professor Anthony Leicht
dove deeper into the field, I started looking at it in a broader context.
Today, we often associate exercise science with elite athletes, whether it’s rugby league, AFL, or any other professional sport. But the benefits of exercise extend far beyond elite competition. Exercise plays a crucial role in improving the lives of people with chronic diseases like diabetes and heart disease, enhancing the well-being of the general community, and optimising the performance of occupational athletes who need to maintain peak physical and cognitive performance, often under extreme stress.
Stress comes in many forms - physical, mental, and environmental. Living in this region, we’ve developed a particular interest in how heat and climate-related stress affect performance and health. Understanding how people react to these challenges and how exercise can help has been an interest.
Ultimately, exercise is essential for maintaining independence, mobility, and overall quality of life. The more active you are, the greater the longterm benefits. However, we’re also uncovering some potential downsides to exercise, particularly in its effects on cardiovascular function. Our research has explored these aspects - not to discourage physical activity, but to better understand how different types of exercise can impact the body in both positive and negative ways. While exercise has its pros and cons, in the big picture, its longterm benefits are undeniable.
What areas of exercise science do you think require more attention or research in the coming years? This is an interesting question. While we’ve learned a lot about exercise
over the past century, there’s still much we don’t fully understand - especially the mechanisms behind why it works so well.
We know exercise affects fuel usage, hormone release, and even gene expression, but the complexity of human response makes it difficult to pinpoint exactly how these factors interact. For example, two people can do the same work out and get vastly different results. Why? Is it due to genetics, body type, fitness level, or something else?
Currently, exercise recommendations, like 30 minutes of walking five days a week, work for the general population, but individuals often need more tailored approaches. Some require more intensity, different types of exercise, or greater frequency to achieve the same benefits. At the elite level, even a 1% improvement in performance can determine whether an athlete wins a gold medal or misses out entirely. Understanding adaptation at this level could revolutionise training strategies.
For me, this is what keeps exercise science fascinating. There’s still so much to discover, and every breakthrough brings us closer to optimising exercise for health, performance, and longevity. The more we learn, the better we can improve lives.
In my opinion, there’s still a lot we don’t fully understand about exercise. It’s not just about telling people to “go and exercise”. We know that certain types of exercise can extend lifespan by a few years, but the real question is: how? What are the underlying mechanisms?
Is it because exercise improves mental well-being, making people happier? Is it driven by hormonal changes,
cardiovascular adaptations, or a combination of multiple factors? We have some insights, but I don’t think we fully grasp the complete picture yet.
This is one of the reasons why I keep doing it, I still don’t know everything. I still have questions. Which is the best mode, duration, frequency, what’s the best for that person or this person? Is it because we’re getting improvements in hormones? Is it chemicals or substances we still don’t know about that are circulating in our body? Is it a genetic activation or is there something else going on? Or it could be a combination of these.
Research in various fields is gradually expanding our understanding of exercise, but we still have a long way to go, which is exciting because it means there’s still so much to discover. The application of this knowledge is crucial, whether in elite sports, community health, or other relevant settings.
However, the pace of advancement seems slower than in the past. Historically, we saw major leaps in understanding despite limited technology, yet now, with all our
advancements, progress feels incremental. This suggests we might not be asking the right questions or looking at the problem from the right angles.
To gain deeper insights, I’ve started collaborating with experts in data science, machine learning, and AI to analyse exercise from a broader perspective. The human body isn’t a simple, linear system where one action leads to one predictable responseit’s an intricate web of interactions across systems. Achieving a universal understanding of these complexities remains a challenge, but ongoing research will continue to refine our knowledge and help future generations push the boundaries even further.
How did you first get involved with SMA and what has been your highlight so far?
As I mentioned earlier, my introduction to SMA came through Prof Graham Allen. He encouraged me to attend an SMA Conference in Brisbane, and I had a great experience. After finishing my PhD, I officially joined SMA and got involved. While I stayed connected over the years, it’s only in more recent times that I’ve become more actively engaged.
As an exercise scientist, I’ve been involved with various professional organisations, but SMA stood out to me because of its multidisciplinary nature. It brings together a diverse range of professionals - physiotherapists, dietitians, sports physicians, podiatrists, and more. That exposure allowed me to expand my knowledge beyond my own field, which was a key reason I became more involved with SMA.
I’ve been a member for over 20 years, though for much of that time, I was more of a passive participant - attending conferences, presenting
SMA plays a crucial role in promoting the importance of sport and exercise in Australia, not just for health, but also as part of our national identity.
research occasionally, and staying in the background. However, in recent years, I’ve taken on a more active role at both the state and national levels, contributing to the organisation and supporting its members. I believe SMA plays a crucial role in promoting the importance of sport and exercise in Australia, not just for health, but also as part of our national identity.
As an international referee, I’ve often noticed how central sport is to Australian culture. When I travelled overseas for games, one of the first things people ask me is, “What sports do you play?” In many countries, a single sport dominates - football in Europe, for example, or basketball and gridiron in the US. But in Australia, we engage with a wide variety of sports. We see it in the news, we read about it in the papers, we play it, we watch it. That deep connection to sport is something unique about SMA. It reflects Australia’s passion for sport and exercise, whether as participants, professionals, or spectators.
That broad engagement is what keeps me interested in SMA today. No matter who I talk to, there’s always a point of connection. If I mention SMA, people often recognise it - whether from the concussion guidelines, training courses, or even discussions around the major
sports doping scandal from years ago. It’s an organisation that reaches across different aspects of Australian society, making it an important platform for conversation, education, and advancement in sports medicine.
Would you recommend SMA to those starting their career in sports medicine? And why?
Yes. For me, the biggest value has been the opportunity to engage with a wide range of professionals. SMA, as a multidisciplinary organisation, provides a broad perspective on sport, exercise, and physical activity.
When I attend a conference, I don’t just focus on exercise science - I explore topics in physical activity, sport, injury management, and beyond. Sport and exercise are deeply embedded in our culture and are influenced by many factors, making SMA’s multidisciplinary nature something I truly appreciate. Every conference or professional development session I attend teaches me something new. Something I can apply in my teaching, research, or to help my students and graduates engage more effectively in the sport, exercise, and health industries.
Very few professionals work in isolation. We constantly collaborate with others, so understanding different perspectives and building connections is invaluable. That’s one of the things I’ve enjoyed most - the engagement and friendships I’ve developed with people I might never have met otherwise.
For new graduates and emerging health professionals, this kind of engagement is crucial. Expanding your horizons, understanding the broader health, sport, and exercise landscape, and building relationships with others in the field will make a huge difference in your career.
5 Minutes With A/Prof Kathryn Mills & A/Prof Ryan Timmins
Congratulations on your new role as Co-Chairs of the Conference Committee! What aspect of this role excites you the most, and why?
Ryan: Seeing how the Conference has evolved over the past 13 years is exciting. The most rewarding part is making sessions more engaging and interactive, creating hands-on learning opportunities for practitioners and researchers worldwide.
Kathryn: I love bringing together early-career researchers and practitioners. The exchange of ideas between science and practice is invaluable and helping to facilitate that collaboration is what excites me the most.
Could you walk us through the abstract review process? How do you plan to ensure it is completed efficiently and on time?
Kathryn: It’s a team effort. Our Conference board is carefully selected, and we rely on impartial, blinded reviewers to ensure fairness. Each reviewer has a manageable workload and a few weeks to complete their assessments. Once reviews are in, Ryan, Chief Judge Evert Verhagen, and I compile scores and finalise presentations.
Ryan: The process is well-established thanks to years of experience. Our job is to streamline it further by organising presentations into common themes to enhance the overall Conference experience.
Based on your experience reviewing abstracts, what key advice would you offer to researchers preparing their submissions?
Ryan: Keep it simple and clear. Not everyone reviewing abstracts will be a content expert, so align your conclusions with your findings. Conferences are for discussion –It’s fine to submit pilot studies or works in progress.
Kathryn: Emphasise the impact and relevance of your research. Many clinicians attend this Conference, so making your work applicable to their practice is crucial.
With world-leading Keynote Speakers at this year’s Conference, how do you plan to leverage their expertise to enhance the event’s impact?
Kathryn: We’ve asked our keynotes to include practical applications of their expertise so attendees can immediately implement their insights into research or clinical practice.
The focus remains on maintaining SMA’s welcoming atmosphere while integrating new presentation formats to enhance accessibility and relevance. The Conference continues to evolve, ensuring it remains engaging, collaborative, and impactful
Ryan: Building on last year’s success at the MCG, we aim to enhance hands-on learning. Bringing in worldleading keynotes will help deliver practical takeaways that attendees can apply as soon as they return to work.
If given the opportunity, is there anything you would modify in the current format of the SMA Conference? Why or why not?
Ryan: I enjoy the traditional in-person format. Networking, spontaneous discussions, and face-toface interactions are hard to replicate virtually. Hobart’s centralised venue should enhance this experience.
Kathryn: The SMA Conference is known for its friendly and approachable atmosphere. While we don’t want to change that, we are considering adding case presentations and rapid-fire sessions to make content more accessible and engaging.
Sports Medicine in Europe
BUT EUROPE ISN’T A COUNTRY! WHILE THIS IS OBVIOUS, EUROPE STANDS OUT AS THE CONTINENT THAT HAS MOST COLLECTIVELY ORGANIZED ITSELF DESPITE ITS MANY INDIVIDUAL NATIONS. THE MAP ON THE NEXT PAGE HIGHLIGHTS THE 50 COUNTRIES THAT MAKE UP EUROPE TODAY.
It is important to note that some countries, such as Russia and Turkey, have territories in both Europe and Asia, but are usually included in lists of European countries due to historical, cultural, and political considerations. Kazakhstan is also sometimes included in some definitions of Europe due to its small portion of territory located west of the Urals.
To put an end to the wars that regularly bloodied the continent and culminated in the World War II, European politicians began the process of building what we know today as the European Union. It was a step-by-step process, first mainly in the economic field (coal and steel, European Economic Community) and then gradually in politics (1958 European Parliament) with the launch of a common currency, the Euro, in 1999.
In the field of medicine, each EU Member State is responsible for the organisation and provision of health services and medical care in their territory. The role of the EU in the context of health policy therefore complements national policies. In the field of health, the EU adopts legislation and recommendations
to protect the population, for example on health products and patients’ rights. This coordination on public health issues is essential given the free movement of people and goods in the internal market.
Cooperation within the EU on public health issues helps address common health challenges. This is achieved by the number of European medical organisations such as, The European Council of Medical Orders (CEOM), the European Junior Doctors (EJD), the European Union of General Practitioners/Family Physicians (UEMO) or an important one for Sports Medicine, the European Union of Medical Specialists (UEMS), or by medical specialty societies such as the European Society of Medicine, the European Society of Medical Oncology, the European Society of Respirology ERS or the European Medicines Agency EMA among many others.
It was therefore only a matter of time before a continental federation dealing with sports medicine would see the light of day.
THE HISTORY OF EFSMA
From an objective, historical perspective, EFSMA’s origins trace back to 1980 with the establishment of
the North-Western European Chapter (NWEC), a Multinational Regional Group of the Fédération Internationale de Médecine du Sport (FIMS). As the name says, this group put together the national associations of northern Europe, as they were already an organised association in the South since 1956 known as le Groupement Latin de Médecine du Sport GLMS.
At the FIMS World Congress in Amsterdam in 1990, the delegates of the NWEC held a meeting, and discussions began to establish a European Federation as it remained the only continent without one. Lobbying and discussions with the other European Groups (GLMS, Balkan Group and the Central European Countries) started.
In 1994, a meeting was held on December 17 in Brussels, with participants from different European Groups of Sports Medicine. A European Federation of Sports Medicine (EFSM) was formed because of this meeting. The aim of the EFSM was to group together Sports Medicine Associations of the European Countries in a common effort to promote Sports Medicine throughout Europe. In 1995, a first constitutive meeting at the VII European Congress of Sports Medicine in Granada, to discuss the aims, objectives and the draft Statutes of the EFSM. In 1996, a second constitutive meeting at the First Congress of the European College of Sport Science in Nice. Finally, the European Federation of Sports Medicine in 1997 during the IX European Congress of Sports Medicine in Porto.
Spor ts Medicine is a speciality
Spor ts Medicine is a semi-speciality
Spor ts Medicine is not a speciality
Not a member of EFSMA / No information
Par t of the EU
* ISRAEL (not featured on this map) is a member of EFSMA, but Spor ts Medicine is not a specialty
The “historical” founders were Sven Anderson (SWE), Moira O’Brien (IRL), John Wesseling (NED) and Norbert Bachl (AUT). The First Council of Delegates of the EFSM took place at this occasion and the Draft Statutes were approved and the First Executive Committee was elected, composed of Prof Norbert Bachl (AUT) the first EFSMA President; Dr Pierre Berteau (FRA), Vice President; Dr Costas Christodoulakis (CYP), Vice President; Prof Fabio Pigozzi (ITA), Secretary General; Dr John Wesseling (NED), Treasurer; Prof Eva Martos (HUN), Dr Ian Adams (GBR), Dr Cesar Fernandez (ESP), Members; and Dr
André Debruyne (BEL) and Dr Untea Gheorghe (ROM), Substitute Members. In 1998, EFSM was recognised by FIMS as a Multinational Group. In the same year, a relationship with the Council of Europe was established to promote an active participation in this important political organisation.
The first EFSM Congress took place in Innsbruck (AUT) in 1999. The second one followed in 2001 in Oviedo (SPA), and during the Council of Delegates, the name of the Federation was agreed to be changed to EFSMA – European Federation of Sports Medicine Associations. The 3rd EFSMA
Congress of Sports Medicine was held in Hasselt (BEL), in May 2003, and the 4th in Lemesos (CYP), in October 2005.
2005 was a pivotal year, marked by a preliminary meeting between EFSMA Executive Board representatives and the European Union of Medical Specialists (UEMS), including Secretary General, Dr Bernard Maillet, at the UEMS headquarters in Brussels. The meeting aimed to define the process for the EU’s recognition of Sports Medicine as a specialisation. These efforts led to the official recognition of EFSMA as a Multidisciplinary Joint Committee (MJC) within the EU.
Photo:
Fourleaflover
/
Getty
Images Vector modified by SMA
Sports Medicine in Europe
In 2006, the Committee started the process to develop a minimum curriculum for the specialisation of sports medicine for the recognition of this discipline in the EU. In 2007, the 5th European Congress of Sports Medicine was held in Prague (CZE). During the 6th Congress in 2009 in Antalya (TUR) a new President, Joseph Cummiskey from Ireland, was elected.
The 7th Congress took place in Salzburg (AUT) in 2011, the 8th in Strasbourg (FRA) in 2013, where Albert Debruyne (BEL) was elected new President. The 9th Congress took place in Antwerp (BEL) in 2015, the 10th in Estoril (POR) in 2017, and this time, Maurizio Casasco (ITA ) became the new Chairman. The 11th Congress was held in Portoroz (SLO) in 2019. Unfortunately, in 2021, the 12th Congress planned in Budapest was cancelled because of the COVID-19 pandemic.
Therefore, the election of a new Executive Committee took place in Brighton (UK) in May 2022, with Maurizio Casasco from Italy confirmed with Chairmanship. In 2023, the 12th EFSMA Congress
was held in Wroclaw, Poland, and the next one (13th) will take place in September 2025 in Bucharest (ROM).
Since EFSMA’s inception, congresses and general assemblies have been held every two years, while the Executive Committee and the Scientific and Educational Commission typically meet twice a year to manage current affairs and plan activities. This ongoing coordination is no small task and demands a well-structured organisation!
OBJECTIVES OF EFSMA
ٚ To have Sports Medicine recognised as a speciality within the European Union and in all of Europe.
ٚ To develop and harmonise education in Sports Medicine throughout Europe and to get Sports Medicine included in the basic curricula at all medical schools and educational institutions.
ٚ To be a Pan-European forum in Sports Medicine for the improvement of communication among sports medicine organisations in Europe; to
coordinate European Sports Medicine movements and to cooperate with Sport Science disciplines in Europe.
ٚ To increase understanding of the importance of physical activity and sports training for the whole European population and dissemination of knowledge of the principles and methods of Sports Medicine for prevention, treatment and rehabilitation of injuries and diseases.
ٚ To encourage the exchange of scientific results and experiences and engage in common research.
ٚ To establish common strengths and propagate a Sports Medicine Code of Ethics throughout Europe.
SPORTS MEDICINE AS A RECOGNISED MEDICAL SPECIALITY
As underlined in the objectives of EFSMA, the recognition of Sports Medicine as a full medical speciality in all the EU countries was a primary objective of the institution since its creation. As the reality has shown, this was no easy task!
Photo: Emeryk Drozdowski
/Getty Images
Basically, each country regulates its medical system as it sees it, and this also concerns which specialties are recognised or not. As we will see, sports medicine, although widely practiced throughout Europe, is not registered as a “full” specialty in all countries of the continent – (see Map on previous page). In some countries, it is called a subspecialty, in others, it is called interdisciplinary in-depth training, in others still, sports medicine has no official status.
At the continental level, the acceptance of a medical discipline as a specialty is subject to community rules. The first, issued by the political authorities of the European Union, stipulates that the specialty must be officially practiced in 2/5 of the EU countries. In the current context of the 27 EU member states, this means it must be practiced in 11 countries (27 x 2/5). Achieving this goal has been EFSMA’s priority mission since the beginning of this undertaking in 2005.
To achieve this, the organisation approached UEMS, the European Union of Medical Specialists. This is a non-profit organisation that brings together more than 1.6 million medical specialists from all EU countries and their neighbours. This organisation is a link between national medical specialists and the EU. EFSMA set up a committee whose task was to manage to gather all the elements for an official application for recognition to the EU.
It would be unfair not to mention the central role of my colleague Nicolas Christodoulou, from Cyprus, who coordinated all the activities that led to the desired goal – the recognition in March 2024 by the European Commission of the Sports Medicine specialty. It took a tremendous effort to finally get 11 governments – rather than the medical organisations of the nations – to submit the required documents to Brussels!
How many times did we think we had achieved it, only to be met with an unforeseen obstacle? From 2005 to
2024, we had to keep believing, and the work is still ongoing. Under current regulations, EU members without a specialty must address this gap within the next 2 years. Additionally, holders of a sports medicine specialist title from any EU country are now authorised to use this qualification across all EU nations, with or without further specialisation. Given the tight timeline for these changes, some delays are expected, but the direction is clear, and it is promising.
VARIA
For several years, EFSMA was able to publish an official journal.
Unfortunately, this promising initiative could not be sustained. However, following a decision made during the EFSMA Executive Committee Meeting in February 2018, the official journal of the Italian Federation of Sports Medicine became one of EFSMA’s official journals.
Finally, one point worth noting is that EFSMA, as an ambitious organisation, has a permanent headquarters in Lausanne, close to major international sports and Olympic federations. Not bad, right?
CONCLUSION
EFSMA has now existed for almost 30 years, and it is objectively possible to draw a positive assessment of its action during this period. Not only is it able to organise excellent scientific Congresses every 2 years in the different member countries, with quite honourable participation, but it also finds the resources - in particular human - to maintain efficient and proactive committees. And as emphasised, this organisation has successfully maintained pressure on political authorities to have the discipline officially recognised, creating a ripple effect across all 41 member countries to date.
About the Author
Peter Jenoure, MD, is a sports doctor who has been passionate about the discipline for over 50 years. He has had the privilege of living his passion in all its forms, as a team doctor, researcher, teacher, member of national and international commissions (including EFSMA), and many more, and editor of the ‘Sports Medicine Around the World’ feature of this Sport Health magazine for over 10 years now.
This presentation wouldn’t have been possible without the efficient help from Anca Ionescu, Emin Ergen and André Debruyne. Thank you, dear friends!
Maithree Wijayasekara Sports Trainer Spotlight
Can you walk us through your journey from being a doctor in Sri Lanka to your current role as a sports trainer in Australia, and what inspired this transition?
Back in Sri Lanka, I had opportunities to work as a doctor with a rugby union team, especially during the COVID-19 period when we had to follow strict protective measures. I have always been passionate about sports. I was a sprinter and cricketer during my school and university days.
When my wife received a job offer in Sydney as an emergency department doctor, we decided to move to Australia. I did not want the both of us working in hospitals, as it would leave little time for us as a family. I saw this as an opportunity to explore a career in sports, which I love.
Initially, I found it challenging to find a direct pathway into sports medicine in Australia. So, I started from scratch, earning my Certificate III in Fitness. That is when I came across Sports Medicine Australia’s Level 1 and Level 2 Sports Trainer courses. After reviewing the curriculum, I realised this was exactly what I was looking for. I completed my Level 1 course in Sydney, and that was the beginning of my journey here.
What challenges did you face when starting your career in sports medicine in Australia, and how did you overcome them?
The biggest challenge was my medical background. If I had pursued becoming a sports physician in Australia, it would have taken another five to seven years. However, I wanted to be directly involved in on-field action rather than working in hospitals.
Interestingly, my medical degree was often seen as a disadvantage when applying for sports-related roles. Many employers considered me “overqualified” rather than seeing how my background could be an asset. In Australia, specific degrees are required for specific roles, so despite being a doctor, my qualifications did not align with physiotherapy or other recognised sports-related degrees.
Starting from the basics was the best decision. It allowed me to build credibility within the industry and gain practical experience relevant to the Australian system.
When I came across SMA and its programs, I was impressed by what they offered and the impact they had on the sports industry.
What motivated you to pursue the SMA Level 1 and Level 2 Sports Trainer courses, and how have they shaped your career?
My passion for sports drove me to explore this field further. When I came across SMA and its programs, I was impressed by what they offered and the impact they had on the sports industry.
A major influence was Harry Saban, my course instructor in Sydney. He
was incredibly knowledgeable and inspiring. His teaching convinced me to continue pursuing certifications and advancing my career. The courses provided me with practical skills and the confidence to step into this field in Australia.
You are now an instructor with SMA. How has teaching others Impacted your career?
I have always loved teaching. Back in Sri Lanka, I was a Basic Life Support instructor, and I wanted to continue sharing knowledge here in Australia.
For me, teaching is a two-way process. While I educate students, I also learn from their experiences. Life experiences provide invaluable lessons that no textbook can offer. Each student brings unique case scenarios and discussing them enriches everyone’s knowledge.
I am grateful to Mitchell Jarvis from SMA for giving me the opportunity to teach, and I thoroughly enjoy being part of SMA’s training programs.
Maithree Wijayasekara
How has your experience with the Kalamunda Rugby Union Club contributed to your skills in athlete management and injury prevention? Initially, when I mentioned I was a doctor, people hesitated, unsure of how to position me within the team. However, my head trainer, Jimmy Singh, was very welcoming and supportive.
By the time I joined, I had completed my Level 1 Sports Trainer course, so I was prepared. The club’s leadership, including Barry Jordan, the president and director of rugby, recognised the value of having a doctor on their medical team. Working with them has been an amazing experience, the boys and the girls from premier teams to most Junior teams are well disciplined, and the club feels like a family now.
Can you describe a highpressure situation during a sporting event where you had to make a critical decision? One of the most intense situations I faced was last rugby season
when a player suffered a severe concussion. He had convulsions and was unresponsive at times.
I immediately assessed him and signalled my head trainer. We had discussed emergency protocols before the season, so we knew that moving him without proper support could be dangerous. With the help of sports trainers from the opposing team and a nurse who was present, we managed the situation until the ambulance arrived.
The match officials from Rugby WA were very professional and did not pressure us to restart the game, which created a calm environment. The player was hospitalised for further observation but thankfully had no acute complications. However, on-site, his condition was concerning, and quick, informed decision-making was critical.
Looking ahead, what are your long-term career goals in sports medicine and high performance?
My ultimate goal is to work with a state or national-level team. Whether it is rugby, cricket, or even para-athletics, I would love to be part of an elite sports team in Western Australia.
While I have a strong medical background, I am still building experience in high-performance sports. Being part of a state-level team would be the perfect place to refine my skills and gain handson experience with elite athletes.
One of the most intense moments I faced was during last rugby season, when I quickly assessed a player with a severe concussion and signaled my head trainer.
Would you recommend SMA’s Sports Trainer courses to others?
Absolutely! Whenever I meet physiotherapy, chiropractic, Allied health student or anyone who is interested in Sports, First Aid and Sports Medicine I recommend SMA.
I know firsthand what they teach, and the pathways available for those who complete their courses.
I also want to take a moment to thank some of the people who have supported me along the way: Harry Saban from Sydney, Mitch, Samantha, and Kaitlyn from SMA NSW, Zeb and Caitlin from SMA WA, and the Kalamunda Rugby Union Club. Their support has been invaluable in my journey.
Kickstart the season with an SMA Level 1 or Level 2 Sports Trainer certification and boost your resume.