
COMMON SENSE Purpose VOICE OF THE AMERICAN ACADEMY OF EMERGENCY MEDICINE VOLUME 29, ISSUE 5 SEPTEMBER/OCTOBER 2022 Editor’s Message: 7 Financial Wellness: 12 Young Physicians Section: 34 AAEM/RSA President’s Message: 39 AAEM/RSA Editor’s Message: 40 What’s in a Name?A Physician by Any Other Name Would Not Smell as Sweet Breaking Bad News: Practical Applications in the Emergency Department Thanks for Saving My Life. Sorry I was an A--hole Minimize the Cost of Your Student Loans Page 3
TM
Table of Contents COMMONSENSE
Regular Features
President’s Message: Purpose
Officers
President
Jonathan S. Jones, MD FAAEM
President-Elect
Robert Frolichstein, MD FAAEM
Secretary-Treasurer
L.E. Gomez, MD MBA FAAEM
Immediate Past President
Lisa A. Moreno, MD MS MSCR FAAEM FIFEM
Past Presidents Council Representative
William T. Durkin, Jr., MD MBA MAAEM FAAEM
Board of Directors
Kimberly M. Brown, MD MPH FAAEM
Phillip A. Dixon, MD MBA MPH FAAEM CHCQMPHYADV
Al O. Giwa, LLB MD MBA MBE FAAEM
Robert P. Lam, MD FAAEM
Bruce Lo, MD MBA RDMS FAAEM
Vicki Norton, MD FAAEM
Carol Pak-Teng, MD FAAEM
Kraftin Schreyer, MD MBA FAAEM
YPS Director
Fred E. Kency, Jr., MD FAAEM
AAEM/RSA President
Leah Colucci, MD MS
Editor, JEM
Ex-Officio Board Member
Stephen R. Hayden, MD FAAEM
Editor, Common Sense
Ex-Officio Board Member
Andy Mayer, MD FAAEM
Executive Director
Missy Zagroba, CAE
Executive Director Emeritus
Kay Whalen, MBA CAE
AAEM/RSA Executive Director
Madeleine Hanan, MSM
Common Sense Editors
Mehruba Anwar Parris, MD, Assistant Editor
Alessandra Della Porta, MD, Resident Editor
Stephanie Burmeister, MLIS, Managing Editor
Articles appearing in Common Sense are intended for the individual use of AAEM members. Opinions expressed are those of the authors and do not necessarily represent the official views of AAEM or AAEM/RSA. Articles may not be duplicated or distributed without the explicit permission of AAEM. Permission is granted in some instances in the interest of public education. Requests for reprints should be directed to AAEM, 555 East Wells Street, Suite 1100, Milwaukee, WI 53202, Tel: (800) 884-2236, Fax: (414) 276-3349, Email: info@aaem.org
AAEM is a non-profit, professional organization. Our mailing list is private.
3
Editor’s Message: Thanks for Saving My Life. Sorry I was an A--hole 7
Financial Wellness: A 5-part Series on Managing Money Wisely: Minimize the Cost of Your Student Loans 12
Heart of a Doctor: This is What I Trained For: How the Science of Medicine Begets the Art 14
Young Physicians Section: Breaking Bad News: Practical Applications in the Emergency Department 34
AAEM/RSA President’s Message: A Physician by Any Other Name Would Not Smell as Sweet 39
AAEM/RSA Editor’s Message: What’s in a Name? 40
Foundation Contributions 9
PAC Contributions 10
LEAD-EM Contributions 11
Upcoming Conferences 11
AAEM Job Bank .............................................................................................................................53
Featured Articles
Rural Medicine Interest Group: Critical Access ............................................................................16
Government and National Affairs Committee: Navigating the Impact of Overturning Roe v. Wade on EM Physicians 19
Operations Management Committee: Pediatric Emergency Department Operations: Are We Pediatric Ready? 21
Toxic Individuality Syndrome Fosters Public Health COVID-19 Inequities in the United States 23
Women in Emergency Medicine Section: Abortion is Health Care 25
Wellness Committee: We Are At Risk 26
Government and National Affairs Committee: OSHA must renew its COVID-19 Emergency Temporary Standard Regarding Airborne Pathogens 27
Academic Affairs Committee: Advice for Young Academic Faculty ..............................................30
Efficiency in the Emergency Department: A Solutions-based Approach .....................................32
Opinion: Enemy Combatants in Our COVID War ...........................................................................36
Weapons Screening in the ED: Take the Survey! .........................................................................42
Opinion: The Long Game!!!! 43
Emergency Ultrasound Section: Ultrasound Guided Peripheral Intravenous Access Correlation with Emergency Department Holds 44
Critical Care Medicine Section: In Praise of the Ultrasound-Guided Peripheral Intravenous Catheter 46
Emergency Ultrasound Section: Use of Point of Care Ultrasound During Distal Extremity Reduction in an Emergency Department Setting: A Pilot Study 47
AAEM/RSA Resident Journal Review: Is There a Potential Role for Methylene Blue in Septic Shock?
......................................................................................................................................50
Mission Statement
The American Academy of Emergency Medicine (AAEM) is the specialty society of emergency medicine. AAEM is a democratic organization committed to the following principles:
1. Every individual, regardless of race, ethnicity, sexual identity or orientation, religion, age, socioeconomic or immigration status, physical or mental disability must have unencumbered access to quality emergency care.
2. The practice of emergency medicine is best conducted by a physician who is board certified or eligible by either the American Board of Emergency Medicine (ABEM) or the American Osteopathic Board of Emergency Medicine (AOBEM).
3. The Academy is committed to the personal and professional well-being of every emergency physician which must include fair and equitable practice environments and due process.
4. The Academy supports residency programs and graduate medical education free of harassment or discrimination, which are essential to the continued enrichment of emergency medicine, and to ensure a high quality of care for the patient.
5. The Academy is committed to providing affordable high quality continuing medical education in emergency medicine for its members.
6. The Academy supports the establishment and recognition of emergency medicine internationally as an independent specialty and is committed to its role in the advancement of emergency medicine worldwide.
Membership Information
Fellow and Full Voting Member (FAAEM): $525* (Must be ABEM or AOBEM certified, or have recertified for 25 years or more in EM or Pediatric EM)
Associate: $150 (Limited to graduates of an ACGME or AOA approved emergency medicine program within their first year out of residency) or $250 (Limited to graduates of an ACGME or AOA approved emergency medicine program more than one year out of residency)
Fellow-in-Training Member: $75 (Must be graduates of an ACGME or AOA approved emergency medicine program and be enrolled in a fellowship)
Emeritus Member: $250 (Please visit www.aaem.org for special eligibility criteria)
International Member: $150 (Non-voting status)
Resident Member: $60 (voting in AAEM/RSA elections only)
Transitional Member: $60 (voting in AAEM/RSA elections only)
International Resident Member: $30 (voting in AAEM/RSA elections only)
Student Member: $40 (voting in AAEM/RSA elections only)
International Student Member: $30 (voting in AAEM/RSA elections only)
Pay dues online at www.aaem.org or send check or money order to:
AAEM, 555 East Wells Street, Suite 1100, Milwaukee, WI 53202 Tel: (800) 884-2236, Fax: (414) 276-3349, Email: info@aaem.org
AAEM-0822-164
.......................................................................................................
COMMON SENSE SEPTEMBER/OCTOBER 20222
Purpose
Jonathan S. Jones, MD FAAEM

hat is the pur pose of a specialty soci ety or association? Or, perhaps, more specifically for us, what is the purpose of an academy? I think we all know what our mission statement is, maybe not verbatim, but we know the gist. As should be the case, some of us identify with or hold in high esteem one part of our mission more than another. However, what I believe is that all of us agree with the mission in general, otherwise, we would not be members. While I think about our mission statement every day and I read it prior to every AAEM meeting, recently, I’ve been thinking more broadly about societies, associations, and academies.
One thing I always emphasized when teaching students and residents is that if you don’t know the answer to something, look it up. I wasn’t en tirely sure I knew what these words specifically meant, so I looked them up. Edited slightly from Merriam-Webster:
Society: a voluntary association of individuals for common ends; an enduring and cooperating social group whose members have developed organized patterns of relationships through interaction with one another; a community, nation, or broad grouping of people having common traditions, institutions, and collective actives and interests
College: an organized body of persons en gages in a common pursuit or having common interests or duties
Association: an organization of persons having a common interest
Academy: a society of learned persons orga nized to advance art, science, or literature
After a bit of reflection, the first thing I decided is that, while all of these words apply to what we do, I am glad that we are an Academy. And after seeing that the definition of academy included the word society, which itself included the word association, I felt a little better about the fact that I couldn’t really tell the difference between all these words. I really contemplated
Weach part of these definitions trying to under stand if the American Academy of Emergency Medicine is living up to it’s potential.
First, we are a “voluntary association.” While this seems obvious on the surface, I think there are different degrees of “voluntary.” Many orga nizations which are ostensibly voluntary really are not. Physicians are often pressured into joining organizations either from their employer or from belief that membership is “required” in order to keep or advance their career. I am proud that AAEM is truly voluntary. While I want our Academy to grow, I don’t want to grow if even one single member feels coerced into joining.
Next, we associate with “common interests” and “for common ends.” Our common interests are the practice of emer gency medicine and our common ends are described in our mis sion statement. Simple enough.
And we’re a society of “learned persons.” I like that. Next time you’re having a bad day, just remember that you are indeed a learned person. And we aim to advance art, science, or literature. And when AAEM operates to its full potential, I think we can easily change that “or” to “and.”
I have been reflecting and writing about specific words and definitions, not because I plan to take the MCAT again, but because I am con cerned that many organizations, ours included, don’t always act in ways consistent with their purpose. The Andy’s (an affectionate term for the current and most recent Common Sense editor) will not like this, but I think a cliché may help: You can’t be everything to everyone.
What started this entire thought experiment for me? Simple, several recent actions the Academy has taken have been somewhat divisive with our own members. I have received feedback, written and verbal. I have received praise and concern for our actions. While I won’t bore you with another cliché about pleas ing everyone, I do know this is impossible as well. However, I would be derelict in my duties as president if I didn’t consider possible causes and solutions to member disengagement. So, I have, and the prior few paragraphs describe how I started.
And my plans moving forward can be explained with two somewhat different words: Focus and Specialization.
Focus
The general focus of the Academy will be to stay tightly bound to our mission statement. I will encourage us to focus on our core values and issues. I’ll paraphrase our mission statement a bit, but to me, our core issues are: unencumbered access to expert physi cian-led care for all patients; the importance of our specialty, residency training, and board
[R]egardless of your individual priorities, opinions, and other organizational involvement, if you belive in our mission, then you belong. And more than this, you need to feel that you belong.”
>> AAEM PRESIDENT’S MESSAGE
COMMON SENSE SEPTEMBER/OCTOBER 2022 3
certification; the personal and professional health of EM physicians; and the development and propagation of EM knowledge.
These are truly the common ends which should unite us all. And that is what I want to focus on—what unites us. In my last Common Sense message, I stated that I wanted the Academy to be a “safe space” for all of us. What this means is that regardless of your individual priorities, opinions, and other organizational involvement, if you believe in our mission, then you belong. And more than this, you need to feel that you belong. One member recently wrote to me stating that he is led “to believe that there is no room” for someone like him in the Academy. This affected me deeply.
highly trained physicians of practice rights? Do you replace said physicians with lower trained alternatives? Do you withhold the best possible care to any patient for any reason? If so, then I’m sorry to inform you but we’re currently full and there is no room for you. It’s really that simple.
(my undergraduate degree is in physics, so apologies for the analogy). Special or specific work of the Academy is that which is obviously related to emergency medicine, but which does not directly or not consistently affect each and every member.
If you endeavor to provide the best possible care to every patient in your ED, then there is room for you. If you despise the undue influ ence of the corporate practice of medicine and its detrimental effects on patient care as well as physician well-being, then there is room for you. If you want to educate yourself on the newest advances in the field and help propagate this knowledge, then there is room for you.
In fact, it’s simpler for me to think of people who we actually don’t have room for. Do you sign sham agreements with hospitals to deprive
I will focus general Academy business, resourc es, statements, and effort on initiatives which unite us, on initiatives core to our mission. Another way I think about this is how I work recruiting new members. They ask, why should I join? And, what does the Academy stand for? Our answer should be simple and clear. It should be something that no ethical EM physi cian can disagree with. The hard part should be convincing the potential member that the cost of joining is worth it, not that our work is noble and good. That should be obvious.
Specialization
You may note that I used the word “general” several times above. This is on purpose and not out of laziness. The general work of the Academy needs to be as above. However, that does not exclude specific work of the Academy. Just as physicists can have a general and special theory of relativity, so can the Academy have a general and also a special purpose
Depending on your practice setting, sub-spe cialization, or simply just your interests, the specific aspects of EM may be more important to you than the general aspects. What should we do for people with passion in specialized areas? Well, first of all we need to make sure that we have “room” for these members too. But I don’t simply want to make room for mem bers with specialized interests and expertise. I want to ensure the Academy has opportunities to allow these interests to develop while at the same time ensuring that one single sub-spe cialized interest or area does not overtake others or the Academy in general.
This is why we have Sections. And thanks to the foresight of my predecessor, Dr. Lisa Moreno, AAEM now has more Sections than ever. This is wonderful. Sections are different than committees, task forces, and interest groups. Sections already have a degree of in ternal autonomy which sets them apart. Section leaders are directly elected from Section mem bers. Sections have semi-independent finances and structure. And while all Sections and mem bers are obviously part of the Academy and all support the Academy’s mission, their specific areas of emphasis differ. The final distinction of Sections is that while membership is restricted to Academy members, individual membership is completely voluntary.
While above I mentioned that I will work to focus general Academy business on initiatives core to our mission, I must add to that. In order for this Academy of learned persons to reach its full potential, I must also work to provide effective opportunities for our members’ spe cialized interests and skills. And so, I will con tinue to work to provide Sections with an even greater level of autonomy within the Academy. Specifically, discussions are underway to fa cilitate more timely and independent action by each Section.
In the end, and possibly after a heated debate, we need to always remember one thing—AAEM’s mission. We support patients, we support true emergency medicine specialists, we support each other’s health and wellbeing, we support robust research and education.”
>> AAEM PRESIDENT’S MESSAGE
COMMON SENSE SEPTEMBER/OCTOBER 20224
This may sound odd at first, but I view it as a strength when members of one Section disagree with members of another or with members who are not in any Section. This is diversity of thought and this is good. Indeed, I welcome robust and difficult discussions on areas of importance to EMS, Women, JEDI, Ultrasound, Critical Care, or Young Physicians. Agree or disagree with initiatives of which these Sections view as vitally important, as long as we offer respectful advice, consistent support, and a welcoming hand, then it doesn’t matter. In the end, and possibly after a heated debate, we need to always remember one thing—AAEM’s mission. We support patients, we support true emergency medicine specialists, we support each other’s health and well-being, we support robust research and education.
Combining Focus and Specialization for the Betterment of the Academy
I’m not suggesting that we do anything new, novel, or untested. Strength in diversity is not a new idea. Working together for a common
end is not a new strategy. Just reach into your pocket and pull out any coin (but maybe not if you’re in Malta this September for the MEMC).
E pluribus unum. Out of many, one. This motto first appeared on a US coin in 1795 and has by law been included on every coin since 1873.
While I suppose the pessimist could say this was an early case of government propaganda, I don’t think so. I think someone realized that what this early country was trying to do was hard, that it was important, and that it may fail.
I also feel it is not a coincidence that the motto became more prominent shortly after ratifica tion of the 13th amendment. It is also important to remember that this motto is not a statement of fact, rather is a stated aspirational goal. We may make it happen, we may not, but we must try (sorry Yoda). And while we are not fighting for the survival of our country, we are fighting for the survival of our specialty.
That is my vision for the Academy. I foresee an Academy with a laser focus on practice rights, corporate practice of emergency medicine, and physician autonomy and well-being. Within this

Academy, I envision groups of learned people coalescing to focus on specialized areas within this field. It may seem contradictory or even counterproductive, but it can work. The United States of America has shown that it can work. This model will need consistent evaluation and adjustment, but it will work.
That is my plan. But I want yours as well. I want feedback. I need to know why you joined, why you pay dues, and why you volunteer. Also remember the governing structure of the Academy (which I am proud is the most directly responsive to members of any medical organization of which I belong). The president can lead but the true work is done by the fif teen member democratically elected board of directors, which has final approval of nearly everything. And the call for elections will come soon. Be on the lookout and consider running or nominating another. Reach out to me or any board member. But always remember the aspi rational goal from over two hundred years ago: E pluribus unum.
AAEM PRESIDENT’S MESSAGE
Build confidence with each case encounter! scan for more information Oral Board Review Course 2022 Dates: Nov 30 and Dec 1 www.aaem.org/education/events/oral-boards COMMON SENSE SEPTEMBER/OCTOBER 2022 5
How can you help?
Join your colleagues and make a gift or a pledge today.
Gifts at all levels can be paid in one year or pledged over two to five years. We encourage individuals, physician groups, and companies to help support the fight!
The AAEM Foundation
AAEM was established in 1993 to promote fair and equitable practice environments necessary to allow emergency physicians to deliver the highest quality of patient care. AAEM later established the AAEM Foundation to defend the rights of such care and the emergency physicians who provide it.
Recently, AAEM-Physician Group, a subsidiary of the American Academy of Emergency Medicine (AAEM), filed suit in the Superior Court of California against Envision Healthcare Corporation to avoid a takeover of an emergency department contract that was held by and independent group. Issues at stake include lay influence over the patient-physician relationship, control of the fees charged, prohibited remuneration for referrals, and unfair restraint of the practice of a profession.
Our specialty is in crisis. We cannot let these practices continue here and across the country.
AAEM is the only EM organization that speaks and acts against the harmful influences of the corporate practice of medicine.
in Honor and Gifts in
at all levels can be given In Honor Of or In Memory Of a program director, mentor, and/or colleague.
of gifts made In Honor or In Memory will be sent to the honoree or their family and listed in our Annual Report.
ACMS-0718-026
$50,000+ Champion Circle $25,000 - $49,999 President’s Club $10,000 - $24,999 Advocate $5,000 - $9,999 Steward $2,500 - $4,999 Ambassador $1,000 - $2,499 Supporter Up to $1,000 Friend Our Goal: $2.5 million by 2025 Gifts
Memory Gifts
Notification
Ways to Give • Donate Online • Scan QR Code • Employer Matching Gift • Return the Donation/Pledge Form • Planned Giving The AAEM Foundation gratefully accepts IRA distributions, contributions through donor-advised funds, planned gifts and bequests. https://www.aaem.org/donate/aaem-foundation The AAEM Foundation is a 501(c)(3) non-profit organization. EIN: 20-2080841 American Academy of Emergency Medicine Foundation 555 East Wells Street, Suite 1100, Milwaukee, WI 53202 (414) 276-7390 • (800) 884-2236 • Fax: (414) 276-7390 25% 50% 75% Donate Now COMMON SENSE SEPTEMBER/OCTOBER 20226
Thanks for Saving My Life. Sorry I was an A--hole
Andrew Mayer, MD FAAEM

ecently, I have had some time to reflect on emergency medicine and my 30 plus year career. I have to admit that this last winter was hard. Taking care of Covid patient after Covid patient and listening to every opinion about vac cines and treatment led me to my worst level of burnout of my career. It is hard really to say why Omicron in particular was hard on me. Of course, my hospital was overwhelmed with cases of Covid but it was not anything like the original wave or Delta. Like everyone else we had huge amounts of boarding and swarms of agency nurses. I think the issue for me was that everyone including myself was just tired. I saw members of my group and the hospital staff have moments when a small obstacle seemed to be their tipping point causing an outburst or atypical reaction to the specific stressor. These reactions were easily recognizable as a product of the chronic stress of working through Covid. This all caused me to look back and think about why I went into emergency medicine and what still makes it the career I would still choose if I had to do over again.
Remember that as an emergency physician you get to do cool stuff. No matter where you work or what the administrative, pay, or nursing situ ation is right now you still get to do really won derful things. Many cases which are run of the mill for us would quickly overwhelm many other physicians. Our skill set is impressive and was not gained easily. You need to remember this fact before you walk into the room of the next 90-year-old weak old lady with the 70-year-old daughter who wants you to make her better. You
Rmay not expect much in the way of career satisfaction from this case but there are so many opportunities to make a difference in any emergency department. We just need to remem ber to look for them and reflect and cherish them when they do come along. This will help make the weak and dizzy cases more bearable.
What is your favorite case? Think of the case which makes you smile. My personal favorite case in all of medicine is the Nursemaid’s elbow. This case to me brings bedside clin ical medicine to a level of perfection. There is nothing more satisfying to me than this simple case. Remember the times you have walked into that room with the crying toddler being held by the very concerned mother who is sure that their child’s arm is broken. The mother looks at you with alarm when their child whimpers more loudly when you reduce the subluxation feeling that very grat ifying pop. You can use your best self-assured doctor lines that everything will be fine and that the child will be playing in minutes as if nothing happened. The look of disbelief from the mother that quickly turns to gratitude when five minutes later she comes out the room stating that “yes, my baby is playing with the car keys just like you said” is priceless to me. No tests or no prolonged anything except fixing a problem that needed fixing. That mother will always remember that interaction.
Your best case ever could be a complex trauma resuscitation, quickly defibrillating the patient whose eyes rolled back in front of you, fixing that complex lip laceration, or whatever. Be honest with yourself when considering this idea. Each of us has a procedure we love to do or a diagnosis we love to make. Please just think about what that case is for you and remember the joy you feel when your training, skills, and experience makes a difference in another human being’s life and the satisfaction you feel from it.
These feelings of satisfaction can come from less obvious situations. Connecting with a family of a dying patient and talking them through the DNR process can change the way a family remembers their loved one. You’re helping to create a situation where your patient

“No matter where you work or what the administrative, pay, or nursing situation is right now you still get to do really wonderful things.”
>> EDITOR’S MESSAGE
COMMON SENSE SEPTEMBER/OCTOBER 2022 7
can die peacefully with their family standing and praying around them instead of the horrible memory of a prolonged and difficult death in an ICU has real meaning. Take the win whenever and wherever you can and realize that the things you do actually matter more often than you may think. Don’t focus on the chronic pain patient or the violent patient that tried to suck part of your soul right from your body. Try and fight back by focusing on the good which you do and not the difficult or problematic patients which can get you down if you do not fight back.
What do you do on your way home from a shift? We often become side tracked with life and the phone calls and plans we need to focus on when we walk out of the back door of the hospital. Maybe you should just take a minute to run through the cases you had on that shift and look for the gems that you did not notice or appreciate at the time. These may not be obvi ous to us as emergency physicians. Remember
that several of the patients and their families will remember their “ER” visit you had with them that day for the rest of their lives. Johnny will re member the day he broke his arm as a teenag er and hopefully the nice doctor who comforted them while reducing and splinting their wrist. A middle-aged wife will remember that you were thorough and decided to take another look and to go a bit further to find the PE, MI, or whatev er the diagnosis. Your skill and professionalism changed that family’s history forever. Do not discount this when you are reflecting on your day. It may have been a totally ordinary day for you on that shift but think of the dramatic and life changing events for some of your patients and their families which were among your ordi nary list of emergency department patients for that day. That particular day was not ordinary to them and your intelligence, training and kind ness changed their lives.
Often, we all know that our patients do not appreciate our efforts or skill. Few overdoses

awaken after the narcan and politely thank the physician and nurse who literally just saved their life. We must accept this part of emergen cy medicine while knowing that it did and will continue to matter. A recent act of contrition by one of my hospital’s emergency department patients brought this all into focus for me. A floral bouquet arrived with a simple note stat ing “Thank you for saving my life. Sorry I was an--hole.” Our patients are often not nice or appreciative of our work but sometimes even the most difficult of them appreciate what you did for them. Most of the time, it is really okay when you are not thanked or feel appreciated for your efforts. You probably did not go into emergency medicine for the appreciation expressed by your patients but instead to save lives and help people. We can easily get bogged down by the negative but remember that what you do does matter. Try and own that fact and it will help.

EDITOR’S MESSAGE
Go Green! Did you know you can read the full issue of Common Sense online even before the print copy hits your mailbox? It’s true! To go paperless, please visit aaem.org/resources/publications/common-sense (or scan the QR code) and click on “Electronic Issue Only” to update your preferences.
COMMON SENSE SEPTEMBER/OCTOBER 20228
AAEM Foundation Contributors – Thank You!
AAEM established its Foundation for the purposes of (1) studying and providing education relating to the access and availability of emergency medical care and (2) defending the rights of patients to receive such care and emergency physicians to provide such care. The latter purpose may include providing financial support for litigation to further these objectives. The Foundation will limit financial support to cases involving physician practice rights and cases involving a broad public interest. Contributions to the Foundation are tax deductible.

Levels of recognition to those who donate to the AAEM Foundation have been established. The information below includes a list of the different levels of contributions. The Foundation would like to thank the individuals below who contributed from 1-1-22 to 8-25-22
Contributions $1000 and above
Anisha Malhotra, MD
John V. Murray, MD FAAEM
Jonathan S. Jones, MD FAAEM
Megan Long, MD FAAEM
Nathan J. McNeil, MD FAAEM
Peter G. Anderson, MD FAAEM
Timothy E. Korber, MD FAAEM
William A. Berk, MD FAAEM
Contributions $500-$999
Bret M. Birrer, MD FAAEM
David A. Farcy, MD MAAEM FAAEM
FCCM
David E. Ramos, MD FAAEM
Kathleen P. Kelly, MD FAAEM
Lillian Oshva, MD FAAEM
Mark Reiter, MD MBA MAAEM FAAEM
Philip Beattie, MD FAAEM
Vladana Aleman
Contributions $250-$499
Alex Flaxman, MD MSE
Algis J. Baliunas, MD FAAEM
Allison Zanaboni, MD FAAEM
Azalea Saemi, MD FAAEM
Benjamin J. Ricke, MD FAAEM
Bradley Judson, MD FAAEM
Bruce E. Lohman, MD FAAEM
Bryan K. Miksanek, MD FAAEM
Charles Chris Mickelson, MD FAAEM
Daniel F. Danzl, MD MAAEM
David Thomas Williams, MD FAAEM
Deborah D. Fletcher, MD FAAEM
Domenic F. Coletta Jr., MD FAAEM
Douglas W. McFarland, MD FAAEM
Eric D. Lucas, MD FAAEM
Eric W. Brader, MD FAAEM
Frosso Adamakos, MD FACEP FAAEM
James W. Small, MD FAAEM
Jamie Kuo, MD FAAEM
Jason Reaves, MD FAAEM
John H. Kelsey, MD FAAEM
John R. Matjucha, MD FAAEM
Joseph W. Raziano, MD FAAEM
Justin Barrett Williams, MD FAAEM
Larry D. Weiss, MD JD MAAEM FAAEM
Michael Luszczak, DO FAAEM
Peter B. Mishky, MD FAAEM
Phillip L. Rice Jr., MD FAAEM
Robert Hanrahan, MD
Ron Koury, DO FAAEM
Sahibzadah M. Ihsanullah, MD FAAEM
Contributions $100-$249
Allen L. Roberts, MD FAAEM
Allie Min, MD FAAEM
Andy Walker, MD MAAEM
Ann Loudermilk, MD FAAEM
Anthony J. Callisto, MD FAAEM
Anthony R. Rosania III, MD FAAEM
Arjun Banerjee, MD
Brent R. King, MD FAAEM FACEP FAAP
Brian R. Potts, MD MBA FAAEM
Bryan Beaver, MD FAAEM
Bunmi Olarewaju, DO FAAEM
Carlos F. Garcia-Gubern, MD FAAEM
Catherine V. Perry, MD FAAEM
Chaiya Laoteppitaks, MD FAAEM
Christopher F. Tana, FAAEM
Clayton J. Overton III, MD MPH MSPH FAAEM
Clayton Ludlow, DO FAAEM
Dan M. Mayer, MD FAAEM
Daniel S. Medina, DO
Darin E. Neven, MD FAAEM
David W. Kelton, MD FAAEM
David W. Lawhorn, MD MAAEM
Donald L. Slack, MD FAAEM
Elizabeth C. Ritz, MD FAAEM
Eric J. Muehlbauer, MJ, CAE
Eric S. Kenley, MD FAAEM
Floyd W. Hartsell, MD FAAEM
Fred Earl Kency Jr., MD FAAEM FACEP
Gary M. Gaddis, MD PhD FAAEM FIFEM
Gayle Galletta, MD FAAEM
Heather M. Mezzadra, MD FAAEM
Holly A. Gardner, MD FAAEM
Ian R. Symons, MD FAAEM
Isaac A. Odudu, MD FAAEM
James A. Pfaff, MD FAAEM
James G. Sowards, MD FAAEM
James R. Gill, MD MBA FAAEM
James Webley, MD FAAEM
Jamie J. Adamski, DO FAAEM
Jeffrey A. Rey, MD FAAEM
Jeffrey John Glinski, MD FAAEM
Jorge L. Infante, MD FAAEM
Joshua A. Pruitt, MD FAAEM CMTE
Julia D. Whiting, MD FAAEM
Julianne Wysocki Broadwater, DO FAAEM
Justin P. Anderson, MD FAAEM
Karl A. Nibbelink, MD FAAEM
Kathleen Hayward, MD FAAEM
Kathryn Getzewich, MD FAAEM
Kathryn Kirsch, MD, FAAEM
Kevin S. Barlotta, MD FAAEM
Kraftin E. Schreyer, MD MBA FAAEM
Laura J. Bontempo, MD MEd FAAEM
Leon Adelman, MD MBA FAAEM
Marco Anshien, MD
Marilyn R. Geninatti, MD FACC FAAEM
CWSP
Mark E. Zeitzer, MD FAAEM
Mary Ann H. Trephan, MD FAAEM
Mary Jane Brown, MD FAAEM
Matthew B. Underwood, MD FAAEM
Megan Algeo, MD FAAEM
Merlin T. Curry, MD FAAEM
Mike Lesniak
Nancy Conroy, MD FAAEM
Nathaniel Johnson, FAAEM
Nicholas G. Ross, MD FAAEM
Pamela A. Ross, MD FAAEM
Patrick A. Aguilera, MD FAAEM
Paul W. Gabriel, MD FAAEM
Ramon J. Pabalan, MD FAAEM
Robert Bruce Genzel, MD FAAEM
Robert P. Lam, MD FAAEM
Rose Valentine Goncalves, MD FAAEM
Sabrina J. Schmitz, MD FAAEM
Scott Plasner, DO FAAEM
Shanna M. Calero, MD FAAEM
Steven Schmidt
Sundeep J. Ekbote, MD FAAEM
Tara Shapiro, DO FAAEM
Teresa M. Ross, MD FAAEM
Terrence M. Mulligan, DO MPH FAAEM
FACOEP FIFEM FACEP FNVSHA
FFSEM HPF
Valerie Hoerster, MD
William B. Halacoglu, DO FAAEM
William K. Clegg, MD FAAEM
William T. Freeman, MD FAAEM
Contributions up to $99
Alec C. Robitaille
Alex Kaplan, MD FAAEM
Andrea C. Santoyo
Andrew DeVries
Chris Hummel, MD FAAEM
Erin M. Khouri, DO FAAEM
Evan T. Burdette, MS
Ivan Novikov
James Cirone, DO
Jason D. May, MD FAAEM
Jason Hine, MD FAAEM
Jennifer A. Martin, MD FAAEM
Jessica Moore, MD
Joanne Williams, MD MAAEM FAAEM
Julia Alegria Astudillo
Kasey Gore
Kennadie P. Campbell
Peter M.C. DeBlieux, MD FAAEM
Richard Scott Johnson, FAAEM
Ron S. Fuerst, MD FAAEM
Ruth P. Crider, MD FAAEM
Sameer M. Alhamid Jr., MD FRCPC
FACEP FAAEM
Sierra Cloud
Sumintra Wood, MD
Theodore B. Olson II, DO
Trecia Henriques, FAAEM
What stood out to you from this issue of Common Sense? Have a question, idea, or opinion? Andy Mayer, MD FAAEM, editor of Common Sense, welcomes your comments and suggestions. Submit a letter to the editor and continue the conversation. Submit a Letter to the Editor Submit a Letter to the Editor at: www.aaem.org/resources/publications/common-sense/letters-to-the-editor COMMON SENSE SEPTEMBER/OCTOBER 2022 9
PAC Contributors –
AAEM PAC is the political action committee of the American Academy of Emergency Medicine. Through AAEM PAC, the Academy is able to support legislation and effect change on behalf of its members and with consideration to their unique concerns. Our dedicated efforts will help to improve the overall quality of health care in our country and to improve the lot of all emergency physicians.

All contributions are voluntary and the suggested amount of contribution is only a suggestion. The amount given by the contributor, or the refusal to give, will not benefit or disadvantage the person being solicited.
Levels of recognition to those who donate to the AAEM PAC have been established. The information below includes a list of the differ ent levels of contributions. The PAC would like to thank the individuals below who contributed from 1-1-22 to 8-25-22
Contributions $1000 and above
William T. Durkin Jr., MD MBA MAAEM FAAEM
Contributions $500-$999
Andrew P. Mayer, MD FAAEM
Damian Liebhardt, DO FAAEM FAWM
David A. Farcy, MD MAAEM FAAEM FCCM
Jonathan S. Jones, MD FAAEM
Lisa A. Moreno, MD MS MSCR FAAEM FIFEM
Robert A. Frolichstein, MD FAAEM
S. Eliza Dunn, MD
Scott K. Rineer, MD MPH FAAEM
Contributions $250-$499
Allison Zanaboni, MD FAAEM
Brian J. Cutcliffe, MD FAAEM
Bruce E. Lohman, MD FAAEM
Charles Chris Mickelson, MD FAAEM
Eric D. Lucas, MD FAAEM
Eric W. Brader, MD FAAEM
Garrett Sterling, MD FAAEM
John R. Matjucha, MD FAAEM
Joseph T. Bleier, MD FAAEM
Kevin Allen, MD FAAEM
Lisandro Irizarry, MD FAAEM
Marianne Haughey, MD FAAEM
Mark D. Thompson, MD FAAEM
Alberto R. Rivera, MD FACEP FAAEM
Alex You, MD FAAEM
Allen L. Roberts, MD FAAEM
Andrew Wilson
Anthony J. Callisto, MD FAAEM
Anthony R. Rosania III, MD FAAEM
Benson Yeh, MD FAAEM
Brett Bechtel, MD FAAEM
Brian Charity, DO FAAEM
Brian D. Stogner Jr., FAAEM
Brian R. Potts, MD MBA FAAEM
Bryan K. Miksanek, MD FAAEM
Catherine V. Perry, MD FAAEM
Chaiya Laoteppitaks, MD FAAEM
David Touchstone, MD FAAEM
David W. Kelton, MD FAAEM
Don L. Snyder, MD FAAEM
Donald L. Slack, MD FAAEM
Elizabeth Edwards, FAAEM
Eric S. Kenley, MD FAAEM
Evan A. English, MD FAAEM
Felipe H. Grimaldo Jr., MD FAAEM
Floyd W. Hartsell, MD FAAEM
Gary W. Fausone, MD FAAEM
Ian R. Symons, MD FAAEM
J. David Gatz, MD FAAEM FACEP
James W. Small, MD FAAEM
Jason Reaves, MD FAAEM
Jeffrey A. Rey, MD FAAEM
Justin P. Anderson, MD FAAEM
Karl A. Nibbelink, MD FAAEM
Kathryn Getzewich, MD FAAEM
Kristen A. Weibel, MBA MD
Lauren P. Sokolsky, MD FAAEM
Lawrence A. Melniker, MD MS MBA FAAEM
Leah B. Colucci, MD MS

Leonardo L. Alonso, DO FAAEM
Lillian Oshva, MD FAAEM
Mark A. Antonacci, MD FAAEM
Mark A. Newberry, DO FAAEM FACEP
Matthew B. Underwood, MD FAAEM
Matthew C. Bombard, DO FAAEM
Matthew W. Turney, MD FAAEM
Megan Long, MD FAAEM
Michael R. Magoon, MD FAAEM
Nate T. Rudman, MD FAAEM
Owen T. Traynor, MD FAAEM
Patrick O’Toole III
Paul E. Stromberg, MD FAAEM
Penelope Goode, MD FAAEM
Peter M.C. DeBlieux, MD FAAEM
Philip Beattie, MD FAAEM
Phillip L. Rice Jr., MD FAAEM
Rebecca K. Carney-Calisch, MD FAAEM
Rebecca N. Mills, MD FAAEM
Rhett W. Silver, MD FAAEM
Robert Boyd Tober, MD FAAEM
Robert Bruce Genzel, MD FAAEM
Robert E. Stambaugh, MD FAAEM
Robert P. Lam, MD FAAEM
Ryan L. Tenzer, MD FAAEM
Sam S. Torbati, MD FAAEM
Sameer D. Mistry, MD CPE FAAEM
Scott P. Marquis, MD FAAEM
Sean M. Abraham, DO FAAEM
Shane R. Sergent, DO FAAEM
Shireen Khan, MD

Sundeep J. Ekbote, MD FAAEM
Thomas B. Ramirez, MD FAAEM
Thomas Heniff, MD FAAEM
Timothy J. Schaefer, MD FAAEM
Tina F. Edwards, FAAEM
Tracy R. Rahall, MD FAAEM
Trisha Anest, MD FAAEM
Ugo E. Gallo, MD FAAEM
William T. Freeman, MD FAAEM
Contributions up to $99
Ahmed Mahmood, MD FAAEM
Ann Loudermilk, MD FAAEM
Anne M. LaHue
Charles Spencer III, MD FAAEM
Chelsea Rodenberg, FAAEM
Chris Hummel, MD FAAEM
D. Shannon Waters, MD FAAEM
Eric J. Zoog, MD FAAEM
Erin M. Khouri, DO FAAEM
Ernest H. Leber Jr., MD FAAEM
Hilary McManus
James P. Alva, MD FAAEM
Jose I. Ruiz-Quinones, MD FAAEM
Kevin Robert Brown, MD FAAEM
Marc D. Squillante, DO FAAEM
McKaila Allcorn, DO FAAEM
Peter Stueve, DO
Richard Burke Neville, MD FAAEM
Richard Scott Johnson, FAAEM
Robert E. Gruner, MD
Ruth P. Crider, MD FAAEM
Stephen J. Lowery, FAAEM
Stuart M. Gaynes, MD FAAEM
Walter M. D’Alonzo, MD FAAEM
William J. Taylor, MD
AAEM
Thank You! Providing You With Top-Tier Emergency Physicians Learn More: aaemlocumgroup.com AAEM-LG facilitates fair and transparent relationships between high-quality, board-certified emergency physicians and hospitals and independent emergency medicine staffing groups. in Partnership With: COMMON SENSE SEPTEMBER/OCTOBER 202210
LEAD-EM Contributors – Thank You!
The AAEM Institute for Leadership, Education & Advancement in the Development of Emergency Medicine, Inc. (LEAD-EM) was estab lished after the tragic and unexpected death of AAEM president, Dr. Kevin G. Rodgers.
The Kevin G. Rodgers Fund and the Institute will LEAD-EM just like Dr. Rodgers did. The funds will support important projects such as development of leadership qualities, and clinical and operational knowledge of emergency physicians with a view toward improving and advancing the quality of medical care in emergency medicine, and public health, safety and well-being overall. LEAD-EM would like to thank the individuals below who contributed from 1-1-22 to 8-25-22
Contributions $1000 and above
Jonathan S. Jones, MD FAAEM
Mercy M. Hylton, MD FAAEM
Timothy E. Korber, MD FAAEM
Contributions $500-$999
Daniel F. Danzl, MD MAAEM
Mark Reiter, MD MBA MAAEM FAAEM
Contributions $250-$499
Anthony J. Callisto, MD FAAEM
Domenic F. Coletta Jr., MD FAAEM
Eric D. Lucas, MD FAAEM
Eric W. Brader, MD FAAEM
Fred Earl Kency Jr., MD FAAEM FACEP
Jason Reaves, MD FAAEM
Jason T. Schaffer, MD FAAEM
Joseph T. Bleier, MD FAAEM
Kathleen Hayward, MD FAAEM
Michael R. Burton, MD FAAEM
Sahibzadah M. Ihsanullah, MD FAAEM
William E. Hauter, MD FAAEM
Zachary Worley, DO FAAEM
Contributions $100-$249
Ann Loudermilk, MD FAAEM
Bobby Kapur, MD MPH CPE FAAEM
Brian R. Potts, MD MBA FAAEM
Carol Pak-Teng, MD FAAEM
Christopher Kang, MD FAAEM
Clayton Ludlow, DO FAAEM
Cory Duncan, MD FAAEM FACEP
Daniel Elliott, MD FAAEM
David W. Kelton, MD FAAEM
David W. Lawhorn, MD MAAEM
Deborah Dean, MD FAAEM
Elizabeth Weinstein, MD FAAEM FAAP
Eric S. Kenley, MD FAAEM
Floyd W. Hartsell, MD FAAEM
Frank L. Christopher, MD FAAEM
Gary M. Gaddis, MD PhD FAAEM FIFEM
Ian R. Symons, MD FAAEM
Jason Hine, MD FAAEM
Jeffery M. Pinnow, MD FAAEM FACEP
John R. Matjucha, MD FAAEM
Joshua A. Pruitt, MD FAAEM CMTE
Lillian Oshva, MD FAAEM
Lisandro Irizarry, MD FAAEM
Marc D. Squillante, DO FAAEM
Mark A. Foppe, DO FAAEM FACOEP
Mark E. Zeitzer, MD FAAEM
Megan Healy, MD FAAEM
Melanie S. Heniff, MD JD FAAEM FAAP
Melissa Ann Barton, MD FAAEM
Michael C. Bond, MD FAAEM FACEP
Nate T. Rudman, MD FAAEM
Nathaniel Johnson, FAAEM
Nimish Mehta, MD FAAEM
Paul W. Gabriel, MD FAAEM
Phillip L. Rice Jr., MD FAAEM
Sabrina J. Schmitz, MD FAAEM
Sarah B. Dubbs, MD FAAEM
Thomas R. Tobin, MD MBA FAAEM
William T. Freeman, MD FAAEM
Contributions up to $99
Ana Maria Navio Serrano Sr., MD PhD
Gerald E. Maloney Jr., DO FAAEM
Jason D. May, MD FAAEM
Jennifer A. Martin, MD FAAEM
Marianne Haughey, MD FAAEM
McKaila Allcorn, DO FAAEM
Nancy Conroy, MD FAAEM
Peter N. Shitebongnju
Peter Stueve, DO
Robert W. Bankov, MD FAAEM FACEP
Ruth P. Crider, MD FAAEM
Stephanee J. Evers, MD FAAEM
Upcoming Conferences: AAEM Directly, Jointly Provided, & Recommended
AAEM is featuring the following upcoming conferences and activities for your consideration. For a complete listing of upcoming conferences and other meetings, please visit: aaem.org/education/events
AAEM Events
October 6, 2022
GLAAEM Educational Symposium
https://www.aaem.org/get-involved/chapter-divisions/glaaem/ educational-symposium
November 30 and December 1, 2022
Virtual Oral Board Review Courses aaem.org/education/events/oral-boards
April 21-25, 2023
29th Annual Scientific Assembly (New Orleans, LA) www.aaem.org/aaem23
Jointly Provided
Re-Occurring Monthly
Unmute Your Probe: Virtual Ultrasound Webinar Series
Jointly provided by EUS-AAEM aaem.org/eus
Re-Occurring Monthly
Spanish Education Series*
Jointly provided by the AAEM International Committee https://www.aaem.org/get-involved/committees/committee-groups/ international/spanish-education-series
September 21, 2022
WiEM Osteopathic Webinar Series: Rock Your Aways/How to Shine on Rotations*
Jointly provided by the Women in Emergency Medicine Section (WiEM)
September 27, 2022
EMS Section Webinar Series-Future of EMS Physicians*
Jointly provided by the Emergency Medical Services Section
October 10, 2022
WiEM IMG Student Webinar Series: Preparing for Interview Season* Jointly provided by the Women in Emergency Medicine Section (WiEM) October 26, 2022
AAEMLa Educational Symposium & Annual Meeting https://www.aaem.org/get-involved/chapter-divisions/aaemla/symposium
November 2-6, 2022
Emergency Medicine Update: Hot Topics (Waimea, HI)
Jointly provided by UC Davis ces.ucdavis.edu/emh2022
Recommended
September 23-25, 2022
The Difficult Airway Course: EmergencyTM (Minneapolis, MN) theairwaysite.com
November 11-13, 2022
The Difficult Airway Course: EmergencyTM (San Diego, CA) theairwaysite.com
*CME not available
COMMON SENSE SEPTEMBER/OCTOBER 2022 11
Minimize the Cost of Your Student Loans
 James M. Dahle, MD FAAEM FACEP
James M. Dahle, MD FAAEM FACEP

One of the most significant differences between the finances of a physician and that of most Americans is that the average doctor comes out of medical school owing between $200,000 and $300,000 in student loans. Recent medical school exit surveys show that more than 10% owe more than $300,000 and 2% owe more than $400,000. These students typically have little in the way of assets, and thus start their careers with a very negative net worth. Managing these loans properly and getting “back to broke” quickly is an important part of overall physician financial management.
The average resident cannot afford to make significant payments on such large student loans. Thus, the first aspect of proper student loan management is ensuring low payments during residency. This feature is built into federal loans via the Income Driven Repayment (IDR) pro grams. With these programs, most commonly Pay As You Earn (PAYE) and Revised Pay As You Earn (REPAYE), your payment is based only on your family size and income. The monthly payments have no relationship to your total loan burden or your loan interest rates. For a typical resi dent, the IDR payment on even a $400,000+ student loan burden will be just a few hundred dollars. Most residents will want to enroll in REPAYE, as it subsidizes your interest rate by forgiving one half of unpaid interest every month. However, there are a few unique situations where married residents may wish to enroll in PAYE.
Federal student loans should almost never be put into deferment or for bearance. In fact, consolidating loans to enable you to skip the six month grace period and starting payments right away is probably a smarter move for most. With private student loans, deferment (if allowed) may be a more reasonable option, but an even better one is to refinance those loans every time you can get a lower interest rate. Several private stu dent loan companies will offer residents payments limited to just $100 a month, serving the same function as the federal IDR programs.
Federal student loans are eligible for three types of forgiveness pro grams. The first, best, and most reliable is the Public Service Loan Forgiveness (PSLF). The program is designed to allow government and non-profit employees working full-time to have their federal student loans forgiven, completely tax-free, after just 10 years of payments. Practically speaking, this means that almost all academic, Veterans Administration (VA), military, and non-profit employee doctors should qualify to have most of their federal student loans completely forgiven within just a few years of leaving training. Since most residencies and fellowships are government entities or non-profits, all of those small IDR payments count toward the 120 required monthly on-time payments. Thus, after a threeyear residency and a one-year fellowship, an academician needs make
the minimum payment for only 6 years (one of which will have very low payments because payments will still be based on the fellow salary), before having the rest forgiven.
The second type of forgiveness program is through the IDR programs themselves. After 20 (PAYE) or 25 (REPAYE) years of payments, the remainder of your federal student loans will be forgiven. However, this forgiveness will be taxable in the year you receive it, making it a much worse deal than PSLF. Besides, unless you have a high debt to income ratio, you will likely have your loans paid off before receiving IDR forgive ness. Nevertheless, it is an option for those in private practice with large student loans.
The final type of forgiveness is a potential “mass forgiveness” program favored by many left-leaning politicians. So far this forgiveness has only been offered to selected groups of people such as those who have been identified as having attended institutions considered predatory. While some politicians have advocated for as much as $50,000 forgiven, a more likely amount is just $10,000, and even that may be means-tested, eliminating the benefit for most attending physicians. This type of forgive ness can be safely ignored by most physicians as it is not a large enough percentage of their loan burden to “move the needle.” If you get it, you get it, but do not let the possibility affect your overall student loan plan.
If you do not expect to receive forgiveness, the best way to get rid of student loans is to refinance them early and often, and then make large payments on them until they are gone. This technique, often called “Live Like a Resident”, involves maintaining a similar lifestyle to the one you could afford as a resident while earning as an attending and sending the
>> FINANCIAL WELLNESS: A 5-PART SERIES ON MANAGING MONEY WISELY COMMON SENSE SEPTEMBER/OCTOBER 202212
difference to the lender. Payments of $10,000 a month or more are pos sible, and will eliminate even large student loan burdens within 2-5 years of leaving training. Rapid payment of student loans is the best trial run for achieving financial independence. If you have the financial discipline to pay off your student loans within five years, you have the discipline to make work optional by mid-career.
The student loan holiday during the pandemic is likely now nearing the end. For more than two years, no payments have been due on federal student loans and no interest has accumulated. While 0% is a better rate than these doctors could have received refinancing, with the rapid rise in interest rates in 2022, doctors refinancing now will not qualify for as low of rates as they would have had they refinanced before 2022. However, all of those “non-payments” will count toward PSLF. Thus a physician who finished a long period of training in 2019 could theoretically now qualify for PSLF without ever making a four-figure student loan payment.
Doctors with complicated student loan situations should seek profes sional advice from a student loan specialist. Paying a flat fee of a few hundred dollars may be worth tens of thousands of dollars in interest savings or even hundreds of thousands of dollars in additional forgive ness. Managing student loans properly can help you to minimize the cost

of your education, reduce the financial stress in your life, build wealth faster, and most importantly, be able to worry less, be less burned out, and concentrate better on your education and patient care.
James M. Dahle, MD FAAEM FACEP, is a practicing emergency physician and the founder of “The White Coat Investor,” the most widely-read physician specific financial website in the world, a best-selling author,



“Managing student loans properly can help you to minimize the cost of your education, reduce the financial stress in your life, build wealth faster, and most importantly, be able to worry less, be less burned out, and concentrate better on your education and patient care.”
FINANCIAL WELLNESS: A 5-PART SERIES ON MANAGING MONEY WISELY
MEDICAL STUDENT SCHOLARSHIP Apply by October 28, 2022 COMMON SENSE SEPTEMBER/OCTOBER 2022 13
This is What I Trained For: How the Science of Medicine Begets the Art
 Pavitra Parimala Krishnamani, MD MS
Pavitra Parimala Krishnamani, MD MS
“I’m not stupid, I just want to make it to Christmas so I can be with my boys. That would mean a lot to them,” she said.
My heart broke. Ms. Bernstein was a kind mid dle-aged woman I saw with an aggressive form of cancer in her abdo men. When I met her, she was swollen…everywhere. The skin on her legs was taut, her abdomen was so filled with fluid that it seemed to have little room to go before popping. She was short of breath as she strug gled to sit down on the stretcher and raise her legs up.
“Has it ever felt like this in the past when you’ve struggled with a lot of fluid building up in your belly or legs?” I asked.
“I mean, it’s never swollen up this bad. I’m generally pretty healthy, except for this doozy of course,” she said referring to the cancer, “I’ve become one and a half times my weight in just two weeks! I can’t hardly walk or sit or even lift my legs onto the bed on my own. My legs are so swollen it’s hard to even bend my knees.” Her husband, who had just joined us in the room nodded.
“Is there anything I can do for you, sweet pea,” he asked, gently touching her arm.
“No, I think I’m alright for now,” she said to him. She turned her attention back to me. “Honestly, I don’t have much experience being sick,” she said. Looking through her medical history, it was apparent she really didn’t: she hadn’t struggled with any chronic conditions other than the abdominal cancer she had recently been diagnosed with. She didn’t drink alcohol, didn’t smoke cigarettes, ate healthy, and dedicated a good por tion of her time to raising her family.
“Tell me more about your diagnosis,” I prompted.
“Well, I was doing just fine until really a few months ago, when they diagnosed me with this cancer and since then, I’ve needed to have liquid drained from my belly twice, but I’ve never been this swollen,” she said struggling to get some breaths in between her words. “Draining the liquid helps with the symptoms, but I’m not stupid, I know that it doesn’t take the cancer away.”
Her husband flinched when he heard her put into words what both of them knew. Her cancer was far along and her therapy was meant to pro long life, with a slim chance of cure. After a quick examination, I stepped out of the room and placed some orders, including a diuretic to help make Ms. Bernstein more comfortable. I kept a broad set of medical con ditions in mind as I thought through her current condition, making sure I evaluated for heart failure, kidney failure, lymphatic involvement, and potential new clots as I tried to explain her symptoms.
Shortly thereafter, I checked back in to see how Ms. Bernstein was doing and let the couple know we would be admitting her to the hospital. Mr. Bernstein was at Ms. Bernstein’s bedside holding her hand.
“How are you folks doing?” I asked.
“Oh, so much better, doc!” Ms. Bernstein exclaimed, “Now that my knees can bend more, that’s all they seem to want to do,” she grinned widely while demonstrating the mobility she had gained with just one dose of the diuretic.
“I was so surprised,” Mr. Bernstein said, “When the nurse came in and pressed on her legs just a short while ago, she was actually able to find some give in her legs. Before, they were all hard…”
“…Like a drum,” Ms. Bernstein finished her husband’s sentence. The way they looked at each other was beautiful. Mr. Bernstein’s eyebrows furrowed in concern and compassion as he looked down at her legs, pressing down on her pale skin. Her calves were soft after releasing all the fluid they had been holding on to for the past few weeks. “You’ve had to go through so much,” he said softly while gently pressing on Ms. Bernstein’s feet.
“I know, honey, but we’ll get through it together,” Ms. Bernstein comforted him.
“You’re strong.” Mr. Bernstein’s tone was definitive, and his voice was filled with admiration for his wife’s determination in her battle with cancer. Though Ms. Bernstein knew that her condition would deteriorate from the
The reality he lived in was one where his soulmate—this woman who he saw as strong and unshakeable—would never turn weak and frail.”
HEART OF A DOCTOR
>> COMMON SENSE SEPTEMBER/OCTOBER 202214
cancer, Mr. Bernstein hadn’t been able to see or accept that reality yet. The reality he lived in was one where his soulmate—this woman who he saw as strong and unshakeable—would never turn weak and frail.
After all, that was the reality he had planned for. He didn’t expect to lose the love of his life before they had a chance to retire together. He didn’t expect to miss out on those golden years that his friends and parents had told him would be a new renaissance in his relationship.
As they locked fingers and eyes, Ms. Bernstein’s expression of strength was her ability to look into the future, know it may be bleak, and yet be willing to march onwards in order to share in more moments with her husband and children.
“Thank you,” I said. I couldn’t help but express my gratitude for Ms. Bernstein for allowing me to be a part of such a private and powerful moment in her life. “Thank you for letting me be a part of your care here today.”
Ms. Bernstein and her husband looked up at me. “Of course, doc. Thank you for getting me all situated down here and getting us admitted to the right place. We appreciate your patience; I know we’re just full of questions!”
“Well, I’m here to answer them,” I smiled and nodded before stepping out so as to not further intrude in their privacy. As I left and glanced back at the two of them in the exam room, fingers intertwined, I was reminded about why I chose to take care of people with cancer. The job
is emotionally challenging, but couples like the Bernsteins show me how valuable it is to have a trained physician available during moments of vulnerability.
Medicine is an art and a science, and an understanding of the science of medicine allows me to practice the art of medicine. It allows me to serve as a guide for my patients and their loved ones as they search for strength during moments of fear and anxiety. It allows me to relieve my patients and their families of the stressors associated with uncertainty, giving them the time and space to just be together in the moment and search for meaning in one another’s presence.
Imagining Ms. Bernstein’s future is challenging and sometimes heart breaking, but the opportunity to allow her and her husband just a sliver of peace to be there for each other in the present is priceless. The feeling I had as I left my shift that day is difficult to describe; I just couldn’t help thinking to myself, this is what I trained for.
Medicine is an art and a science, and an understanding of the science of medicine allows me to practice the art of medicine.”
HEART OF A DOCTOR WWW.YPSAAEM.ORG INFO@YPSAAEM.ORG Young Physicians Section (YPS) AAEM FREE Personalized resources for your first 5 years out of residency! GET PUBLISHED IN COMMON SENSE MENTORING PROGRAM RULES OF THE ROAD FOR YOUNG EMERGENCY PHYSICIANS eBOOK CV REVIEW SERVICE NETWORKING
COMMON SENSE SEPTEMBER/OCTOBER 2022 15
RURAL MEDICINE INTEREST GROUP
Critical Access
Robyn Hitchcock, MD FAAEM, Rural Medicine Interest Group Chair

AAEM recent ly started the “Rural Medicine Interest Group.”
A case I had recently re minds me why this is an important forum.
I am working at a new Locums job on the Oregon coast. When people that live in the northwest have a hankering to see the ocean, this is typically where they go. The Washington coast for the most part is unapproachable and rocky, but the Oregon coast has many areas of approach and a plethora of sandy beaches and little seaside towns. Somehow, despite the fact that I’ve lived in the “Upper Left” for nearly 20 years, I have never made it to the Oregon coast. So this is a great opportunity for me to finally go, explore a little, and get paid to be here. I think it’s a win-win.

I was working my first full shift after orienta tion. Within minutes of taking sign outs in the morning, half a dozen people checked in. That’s quite a few in a single coverage critical access facility. So I was chugging through the list, trying to get all my workups and evalua tions started. A 39-year-old woman presented with a chief complaint of vomiting blood, so I focused on her chart. This unfortunate young lady was now sober, but already had severe liver damage from alcoholism and carried a di agnosis of alcoholic cirrhosis. She had no prior history of GI bleeds. But the high volume of blood she described vomiting is typically from esophageal varices in somebody with cirrhosis. She was tachycardic to 126 but normotensive, kind of gray looking and jaundiced. She had not vomited since that one episode that nearly filled her bedside garbage at home.
I started of course with standard labs and some volume resuscitation with saline. Her hemoglobin came back at 9.3, her INR was 1.9, and she was not on blood thinners. I reached out to the general surgeon on call who does endoscopy at this facility. Unfortunately, they typically can’t manage esophageal varices
because they don’t have the right specialty equipment or training. He was performing a colonoscopy so I had to wait for him to finish, but he confirmed that he was unable to care for this patient.
Then I think I made a decision that saved this young lady’s life. At least I like to think so. She was less tachycardic but still had an elevated heart rate around 110. I had already ordered vitamin K to try and bump up her clotting func tion. I knew I was going to have to transfer her and wanted to do everything I could to stabilize her. So despite the fact that she was not bleed ing in the ED, I ordered TXA which helps blood clot better and decided to continue her volume resuscitation with FFP to avoid further dilution of clotting factors (as a critical access place of course, we do not have platelets or cryo on hand).
Just as the TXA was hanging and the FFP was almost ready she started vomiting blood again. About 500 ml of clotting blood into the emesis bag. She continued to vomit off and on over the next hour. But since I already had the clotting factors hanging, the total amount she threw up was only about 750 ml. By the end of the hour she was just dry heaving bilious saliva. We got
her under control.
Of course I was busy during this hour. I wasn’t just sitting there watching her throw up. I called the nearby (60 miles away) hospital and spoke with gastroenterology. We added rocephin, reglan, and octreotide. I ordered a repeat hemoglobin and made sure I got her type and crossed with several units of packed red blood cells. We pulled out our oral tube which can help tamponade these bleeds through pressure in the esophagus. I haven’t done one since res idency so the nurse and I reviewed the instruc tions together in case we had to go there. And of course all this time I’m desperately hunting for a bed.
The closest hospital is an hour away and although GI accepted, they had no ICU beds. I tried to do an ED to ED transfer, but got re fused. I tried to pull the EMTALA card, but the ED said they can’t do a scope in the emergency department; it has to be an ICU bed. So they didn’t have the capacity to care for her, I had to keep looking. The transfer center called all up and down the coast and inland and we finally found a bed in Portland, 3 ½ hours away by ground. The Oregon coast is often foggy and
When people live in a small town they’re making health care choices they don’t realize they’re making.”
>> COMMON SENSE SEPTEMBER/OCTOBER 202216
overcast but luck was with me that day because the helicopter was flying. The helicopter had been on standby for some time, and now finally had a place to go.
I got on the phone with the intensivist and told her all about the patient. When I updated the vital signs, repeat hemoglobin, blood transfu sion, etc., the young woman who was probably an ICU fellow said to me, “Is it really safe to transfer somebody in that condition?”
“Well, I could keep her here until we run out of blood products and then she dies,” I replied. “That is my only other choice.”
I heard the squeak on the other end of the line. “Oh, ok. We will be waiting for her.”
This is why we need a rural medicine interest group. People at large academic institutions have no idea what it’s like being at a place with limited resources. When people live in a small town they’re making health care choices they don’t realize they’re making. A ruptured aneurysm, massive trauma, or a bad head bleed is going to die before we get them to a facility capable of caring for them. Every. Time. Sometimes we have to ship unstable people. We do our best to stabilize them within the

will die here. The problems we face on a daily basis are seldom addressed in national discus sion. I’m hoping to engage this conversation on a national level for awareness and facilitation both from the emergency medicine community, and the people we care for.


Back to the case...The repeat blood count which should have taken 10 minutes somehow took 40 minutes. The helicopter doesn’t come directly to our facility, our paramedics have to take the patient to a rendezvous point 20 min utes away from the hospital. I made them wait for the blood test, and sure enough her repeat hemoglobin was 6.2. So I got two units of red cells hanging as she headed out the door, and sent a third one with them. The helicopter has a fourth.
As of today I haven’t heard back what hap pened. Typically if she deteriorated en route somebody would have let us know. So I think she made it okay.
I made a lucky or perhaps intuitive decision to start aggressive clotting factors before she started bleeding again. We did not have to go with the pressure tube in the esophagus which has a huge complication rate and a high mor bidity and mortality just placing it. The team of nurses who I had just met did not question my decisions to be proactively aggressive. And I’m pretty sure we saved a life.
A good day at a critical access hospital.
‘Well, I could keep her here until we run out of blood products and then she dies,’ I replied. ‘That is my only
CRITICAL CARE MEDICINE SECTION
2022-2023 AAEM/RSA Board of Directors & Medical Student Council Nominations Opening Soon! COMMON SENSE SEPTEMBER/OCTOBER 2022 17
COMMON SENSE SEPTEMBER/OCTOBER 202218
Navigating the Impact of Overturning Roe v. Wade on EM Physicians
 Kendall I. Moore, MD MBA
Kendall I. Moore, MD MBA

nless you have been living under a rock, you will have heard that the U.S. Supreme Court, in their decision in the case of Dobbs vs. Jackson Women’s Health (Dobbs), reversed precedent on Roe v. Wade, a 1973 decision in which the Court ruled that women had the constitutional right to abortion under the 14th amendment. With the CDC citing abortions being performed over 500,000 times a year, how will this ruling impact emergency medicine (EM) physicians across America? Will there be a noticeable impact, such as patients seeking post abortion care or requesting abortion resources? Will we have to change the discus sions we have with patients or limit resources offered due to fear of legal jeopardy at the state level? The Dobbs decision will certainly impact some emergency medicine physicians more than others based on their state of practice. In some states, a full ban on abortions was au tomatically triggered once the Supreme Court decision was published. EM physicians in these states must face the reality of quickly changing their practice without clear guidance on how to provide care while complying with the law in emergency scenarios. In certain other states, abortion laws remain unchanged and, while the in-state treatment by physicians in such states may remain the same, the influx of out-ofstate patients seeking care in their emergency departments presents a myriad of issues and questions that hospital systems will need to resolve. What follows is an exploration of the potential impacts of the Dobbs decision on the emergency medicine practice. Please note, it is not meant to provide any legal advice for
Uphysicians to follow; it is simply an exploration of what we can expect.
Leaving political views aside, based on data published by the University of California San Francisco (USCF), complications from legal abortions are rare. Less than 1% of legal abor tions lead to emergency department (ED) visits. Likewise, less than 1% of abortion related chief complaints present to the ED.1 As such, if women in abortion-banned states only sought legal out-of-state abortions or abstained from getting abortions altogether, then the USCF data could be reassuring for ED physicians. However, research and history show that the Supreme Court’s decision will not stop women from seeking abortions; rather, patients will look for alternative options and, for those without the economic means to obtain legal out-of-state abortions, the alternatives are dangerous. As is seen in countries with restrictive abortion laws, a prohibition on abortion may contribute to a
higher rate of unsafe abortions and, in turn, abortion complications.5
With the possible increase of patients present ing to the ED due to complications resulting from unsafe and/or illegal abortions, novel questions arise as to what obligations emer gency physicians will have under this new legal paradigm. For those of us who practice in a state where abortion is illegal, could we find ourselves faced with an obligation to report our patients to authorities? If we treat a patient with abortion-related complaints, are we subject to liability as a participating party in the abortion procedure? States where abortions are fully legal may see a large influx of out-of-state patients seeking information on abortions. Will we be able to communicate freely with these out-of-state patients about their care options knowing abortions are illegal in their resident state? Additionally, how do we insure privacy for these patients in the age of interoperability and portable health records? All of these issues are still developing, but we are starting to see bills introduced that protect patients who cross state lines for abortion care, such as the “Ensuring Access to Abortion Act.”3
Recently, Centers for Medicare and Medicaid Service and the U.S. Department of Health and Human Services have released guidelines for physicians in states with abortion bans. These guidelines serve as a reminder of the Emergency Medical Treatment and Labor Act, stating that, as physicians, we have a duty to treat any patient presenting to the ED and pro vide life saving measures when necessary. This
[A]s physicians, we have a duty to treat any patient presenting to the ED and provide life saving measures when necessary…federal law supersedes state law when physicians are administering what the clinician believes are life saving measures.”
GOVERNMENT AND NATIONAL AFFAIRS COMMITTEE
>> COMMON SENSE SEPTEMBER/OCTOBER 2022 19
guidance clarifies and reminds physicians that, regardless of the state in which they practice, federal law supersedes state law when physicians are administering what the clinician believes are life saving measures.4,5 Nonetheless, while the federal law does provide avenues for defense, it does not preclude that lawsuits will be brought forth that will place physi cians’ often time-critical decisions under a microscope.
Emergency medicine physicians practicing in states under an abor tion ban should keep an eye out for future bills related to this issue at both the state and federal level because, while there is a defense and guidance in place by federal organizations, you may still find yourself in the crosshairs at the state level. EM physicians dealing with abortion complications across the country should consult the legal teams at their facilities on best practices and EDs should similarly equip their physicians with the resources needed to provide timely and legal care to their patient populations.
References
1. Ansirh.org. 2022. Safety of abortion in the United States - ANSIRH. [online] Available at: https://www.ansirh.org/sites/default/files/publications/ files/safetybrief12-14.pdf [Accessed 22 July 2022].
2. Cms.gov. 2022. Reinforcement of EMTALA Obligations specific to Patients who are Pregnant or are Experiencing Pregnancy Loss (QSO-2122-HospitalsUPDATED JULY 2022). [online] Available at: https://www.cms. gov/files/document/qso-22-22-hospitals.pdf [Accessed 22 July 2022].
3. Congressman Jamie Raskin. 2022. Reps. Raskin, Fletcher and Strickland Introduce Bill to Protect the Right To Travel for Abortion Services. [online] Available at: https://raskin.house.gov/press-releases?id=46AFA911-CF7743E8-AA9A-C84CA5C004D0 [Accessed 22 July 2022].

4. HHS.gov. 2022. Following President Biden’s Executive Order to Protect Access to Reproductive Health Care, HHS Announces Guidance to Clarify that Emergency Medical Care Includes Abortion Services. [online] Available at: https://www.hhs.gov/about/news/2022/07/11/followingpresident-bidens-executive-order-protect-access-reproductive-health-carehhs-announces-guidance-clarify-that-emergency-medical-care-includesabortion-services.html [Accessed 22 July 2022].
5. Singh, S., Remez, L., Sedgh, G., Kwok, L. and Onda, T., 2017. Abortion Worldwide 2017: Uneven Progress and Unequal Access. [online] Guttmacher.org. Available at: https://www.guttmacher.org/sites/default/ files/report_pdf/abortion-worldwide-2017.pdf [Accessed 22 July 2022].
GOVERNMENT AND NATIONAL AFFAIRS COMMITTEE
COMMON SENSE SEPTEMBER/OCTOBER 202220
Pediatric Emergency Department Operations: Are We Pediatric Ready?

Children have unique physical, psycho-social, and medical needs that differ from adults when seeking care in the emer gency department (ED). In the National Hospital Ambulatory Medical Care data from 2014, approximately 20% of ED visits were for children younger than 15 years old.1 Children have unique challenges associated with ED visits and it is imperative that EDs are ready to address these problems. Having an ED ready to take care of an adult patient does not necessarily make it prepared to provide care for a child.
In 2018, the American Academy of Pediatrics (AAP) published guidelines to ensure pediatric readiness in emergency departments.1 In their policy statement, specific steps and resources for pediatric readiness were published. Despite the recognition of the numerous unique chal lenges facing pediatric operations, there are few resources which exist within national and international organizations that address this topic or specifically target those issues. While there is a robust focus on clinical management of children, attention to the specific operational needs is lacking. In review of the published literature, ED operations articles that address specific pediatric operations are few and far between.

One of the most significant operational chal lenges that pediatric EDs face is the difference and variability in pharmaceutical dosing as well as stocking of pediatric supplies. In contrast to adult EDs where stocking a medication at a standard dose or having a standard size for
equipment supplies is sufficient, pediatric EDs require meticulous preparation to stock and sample age and weight specific supplies. As a result, this resource requirement involves more personnel and resource allocation. Inadequately addressing this need poses a risk for having an inadequate supply or age-inap propriate items, leading to an increased risks for errors, confusion, provider frustration, and increased personnel use. Furthermore, ED pharmacists, stock personnel, and technicians are not always available, and pediatric care can be challenging enough without the delays associated with obtaining appropriately sized equipment or pediatric dosed medication. At this time, there are no minimal requirements set by pediatric organizations or even the local departments for the staffing of ED personnel in pediatric ED. As compared to the adult population, the care of children in a pediatric ED is resource heavy with regards to person nel use. The AAP has recommended a dyad management model, combining both physician coordinators and nursing coordinators to effectively manage a pediatric ED.1 However, most pediatric EDs are not staffed with either of these roles, let alone both. Operational committees should consider this when planning adequate staffing or mobilizing resources for pediatric care.
Among the operational challenges seen in pe diatrics, none may be more ubiquitous than the management of parents. Parents of children are often themselves in significant distress, even when their child is not at serious risk,
and most EDs are inadequately prepared to address the distressed parent. Previous stud ies have shown that parent presence during pediatric resuscitations and complex medical care could greatly reduce risk of negative outcomes.2 However, most EDs poorly accom modate these needs due to shortage of space, staff, personnel, or even child-life resources. Increasing awareness of this specific need and including this in pediatric operational discus sions and planning can improve the overall flow and outcomes in the ED, as well as both parent and patient experience.
In addition to the unique medical challenges posed by pediatric patients, there are numerous other factors such as anxiety, inconsolability, stranger anxiety, previous adverse effects, and the foreign ED setting which can make pediatric patients even more difficult to manage. Factors such as experienced staff, adequate staffing numbers, and a calm and supportive environ ment can help greatly reduce the adverse psy chological effects that children may experience while in the ED.
 Virteeka Sinha, MD, Akiva Dym, MD, Anthony Rosania, MD MHA FAAEM
Virteeka Sinha, MD, Akiva Dym, MD, Anthony Rosania, MD MHA FAAEM
HAVING AN ED READY TO TAKE CARE OF AN ADULT PATIENT DOES NOT NECESSARILY MAKE IT PREPARED TO PROVIDE CARE FOR A CHILD.”
OPERATIONS MANAGEMENT COMMITTEE
>> COMMON SENSE SEPTEMBER/OCTOBER 2022 21
There is growing evidence that supports the use of technology and other forms of distrac tion in order to help reduce stress for pediatric patients and improve outcomes. Active distrac tion techniques have been shown to reduce pain, fear, and anxiety during procedures and interventions in the ED.3 Despite this, many EDs do not consider this in their operational costs and staffing when designing or planning for pediatric readiness. Financial constraints, security concerns, safety, and lack of child proofing in the ED are common hindrances to the use of technology in pediatric care in the ED. Child-life staff or other personnel with pediatric training should be included in conver sations related to pediatric operations.
Furthermore, the saying “children are not simply young adults,” applies to their tolerance of waits and periods of uncertainty. In addition, their episodes of acute illness may be far more dynamic than in adults. Guidelines that are child (and parent) friendly and safe should be incorporated into ED care plans. This means in creased sensitivity to turnaround times for labs and studies. The fact that more of their visits end in discharges can lead to more discharges per hour, and more variability in lengths of stay than we see in the adult population. This creates additional challenges associated with staffing and resources. Most pediatric EDs need to entertain this unique characteristic while dis cussing pediatric operations. This enhances the need for more organizational leadership and establishment of working committees towards this goal.

Pediatric vital signs are age specific and affect length of stay and disposition times. Pediatric vital signs often require more attention as com pared to adult patients, and repeating vitals in the ED prior to disposition is common practice for the pediatric population. Adequate vital sign remeasurements occur more frequently in the pediatric ED than in most adult or general EDs. In contrast with the adult patient population, the presence of unexplained tachycardia at discharge in children has been associated with return visits and need for subsequent admission.4 Targeted quality improvement in this area has been associated with complete documentation of vital signs without increasing LOS. This means that repeat measurements of these vital signs, as well as adequate training and staffing of support staff and ED technicians must be considered.
Anticipatory guidance is essential across the spectrum of all patients seen in the ED but is of most significance in pediatric patients. A wide variety of pediatric care focuses on preventative and anticipatory guidance: child proofing, road safety, helmet use, and social and psychological support. Given the potential impact of anticipatory guidance, these actions remain important even in the acute setting of the emergency department. More than simply reducing repeat visits, such interventions can have a significant impact of overall pediatric morbidity and mortality. Speaking with children and parents is thus essential, however quite challenging in the dynamic milieu of the emer gency department. In order to facilitate this process, pediatric ED operational leadership
should include budgeting, hiring, and retention of patient care navigators, patient educators, and child-life personnel to help optimize the ability to provide anticipatory guidance to all patients and family members. In addition, informational booklets, educational videos, and websites should be available to provide to families to help reduce the hurdles to patient education in the ED setting.
As described, pediatric ED operations pose many specific and unique challenges which are not normally encountered in the adult ED. As such, it is critical that adequate planning be taken to ensure measures are in place to help address these challenges and address the needs of a pediatric ED. Organizations must devote specific workgroups and committees to focus on pediatric operational readiness and identify ways to manage many of these unique issues. Differences in patient flow, metrics, staffing, and other resource utilization must be identified and properly planned for. In ad dition, additional research must be performed to assess and improve pediatric patient flow, pediatric outcomes, specific pediatric resource needs, and reducing parent and patient anxiety within the ED setting. Lastly, separate pediatric clinical and operational guidelines must be established in every ED to adequately prepare for and address the unique needs required by a pediatric patient population.
References
1. Remick, K., Gausche-Hill, M., Joseph, M. M., Brown, K., Snow, S. K., Wright, J. L. Pediatric Readiness in the Emergency Department. Annals of Emergency Medicine, 72(6), e123–e136.
2. Bekkering, H. J., Woodgate, R. L. The Parental Experience of Unexpectedly Losing a Child in the Pediatric Emergency Department. Omega, 84(1), 28–50.
3. Arıkan, A., Esenay, F. I. Active and Passive Distraction Interventions in a Pediatric Emergency Department to Reduce the Pain and Anxiety During Venous Blood Sampling: A Randomized Clinical Trial. Journal of Emergency Nursing, 46(6), 779–790.
4. Vukovic, A. A., Berry, C., Johnson, D. P. (2019). A Discharge Vital Sign Documentation Improvement Initiative in the Pediatric Emergency Department. Pediatrics, 144(3), e20190436.
THERE IS GROWING EVIDENCE THAT SUPPORTS THE USE OF TECHNOLOGY AND OTHER FORMS OF DISTRACTION IN ORDER TO HELP REDUCE STRESS FOR PEDIATRIC PATIENTS AND IMPROVE OUTCOMES.”
COMMON SENSE SEPTEMBER/OCTOBER 202222
Toxic Individuality Syndrome Fosters Public Health COVID-19 Inequities in the United States
Tai Donovan,* Salma Yusuf, MD, † and William Mundo, MD MPH
Introduction
COVID-19 barely qualified as a distant memory before Omicron and a multitude of variants fought for their time on the global stage. The world had just grasped a small glimpse of normalcy since the virus first made its debut appearance in December 2019 before monkeypox decided to step in and take the spotlight. The United States and many countries globally are still finding their footing from the social and economic devas tation that accompanied the virus along with the loss of millions of lives. The pandemic wreaked havoc on our food systems, global enterprise, employment, public health, and created multiple crises amongst societ ies’ most vulnerable and not so vulnerable. No country or person was exempt from the effects of the virus, and yet, the United States, which only accounts for 4% of the world’s population, suffered worse outcomes compared to other countries and accounted for one-fifth of the world’s COVID-19 deaths. According to Our World in Data, to date, the U.S. has had 373.76 million confirmed cases with 1.2 million of those being con firmed deaths.1
So how is it possible that a country predicted to be the most prepared for a pandemic by the Johns Hopkins Center for Global Health Security just two months shy of COVID-19’s first appearance, eventually landed itself in one of the top spots for having the worst outcomes?2 Despite the resources, preparation, and expertise that all seemed in place, there were still many factors that contributed to the country’s poor response to the pandemic. Increased rates of morbidities amongst its aging popula tion and a fractured health system further impacted by partisan politics were just some of the determinants that the country had to work against. While the COVID-19 pandemic shook the world to its core and had profound economic, social, and medical implications for everyone, it has not impacted everyone the same way. In terms of the pandemic’s dispro portionate global pattern, nothing explains this disparity better than the negative influence of a pervasive culture of toxic individualism common within America.
Amongst Americans, a historical entitlement has existed that often contradicts the collective utilitarian benefit, especially as it pertains to en acting public health measures. Individuality and freedom are the corner stones of what defines American culture. The United States is a country that has had a historically treacherous journey in balancing the rights of the individual and collective good. More than 100 years ago, Jacobson v. Massachusetts was the case that highlighted the vital clash between respect for individual liberty and preserving the health of the public when the state required vaccination against smallpox during a major smallpox epidemic in the United States.3 How could it be that people are still trying to solve the same problems we have been having for years when it comes to enacting public health measures? It should be that during times of public health crises and emergencies, such as with the ongo ing COVID pandemic, that there should not be limitations on authority to impose mandatory restrictions on personal liberty for public health purposes for the collective benefit.4,5 While there is an understanding that during crises, governmental authorities delegate decisions that bal ance public health protections and civil liberties, many U.S. citizens will choose their own self-interest in lieu of their civic responsibility towards others.6 Nothing has made this more evident than the unavoidable melt down you would see on any given day with just five little words, “you must wear a mask.”
The current COVID pandemic has highlighted how, in times of public health distress, individualism can have deadly consequences, especially as it pertains to our nation's most vulnerable communities. Across the US, COVID-19 has claimed more than 200,000 lives.7 As a result, while the U.S. has only 5% of the world’s population, it carries 20% of the world’s COVID-19 burden of disease (number of cases and deaths).8 The economic and social implications of COVID will continue to have substantial implications for the next generations and may potentially exacerbate underlying social inequities. Many in the U.S. responded with a culture of toxic freedom and individualism, resisting public health regulations and exacerbated by the lack of political leadership and misinformation.
What is Toxic Individuality Syndrome?
Toxic individuality syndrome is a constellation of signs that include selfishness, lack of empathy for others, acting out of freedom without considering consequences, and disregard for anything that does not impact the individual directly.9 Individualism and personal liberty are a concept of self-re liance, personal freedom, and responsibility. It becomes toxic when it becomes an egocentric pursuit that does not

‡
Nothing has made this more evident than the unavoidable meltdown you would see on any given day with just five little words, ‘you must wear a mask.’” >> COMMON SENSE SEPTEMBER/OCTOBER 2022 23
serve the person's best interests and leads to an increasing number of people becoming more willing to violate the social contract. Toxic indi viduality and freedom stem from the origins of our country's abiding allegiance to individualism. The belief that for the greater good for everyone is where individuals are left free to pursue their behaviors and own satisfaction independently of its impacts on others. In this setting, we promote a culture of toxic freedom, which means freedom at the expense of the known consequences it has on others. As a country, we firmly believe that emphasizing individual achievement, self-fulfillment, and allowing people to achieve personal liberty, does not implicate the rights of others to do the same. When this way of thinking only goes in one direction, it inadvertently limits another's ability to do the same, which in turn denies others' of the same freedom, leading to toxic freedom.
Public Health Equity: How can individualism be toxic?
Toxic individuality can become a danger to public health when an individual holds on tightly to a myopic, false sense of entitlement to freedom that eventually leads to a lack of willingness to learn and becomes the ideology that fuels them making uninformed decisions that affect others around them. The danger comes when an individual’s decisions per petuate a cycle of harm that contributes to the consequences that they do not have to experience. This whole idea takes consequences and reasoning out of the equation, and without being well-informed, a person can think their ignorance is just as good as one's expertise. Similarly, to how we have things now with how COVID proliferated through a lack of safe public health practices that disproportionately hurt minorities and those of lower SES.10 The COVID pandemic has forced the United States to see the flaws that exist in our public health system. By not taking a public health approach to COVID, we are missing out on the public goods and community resources that we have (since they remain closed in many places)—many of which can serve as a healthy coping mech anism, including public gatherings or festivals, theaters, schools, and libraries. As a result, creating a cycle between worsening health mental health outcomes and physical outcomes. COVID will continue to present unique challenges on top of the current challenges we face every day. Our children and grandchildren inherit a sicker and less safe world with the increase of fires and other “natural” disasters, rising sea levels, and extinction of species. With COVID in the mix of the other public health challenges we face, toxic individuality will continue to widen the gap for our society's sickest and marginalized members.
Toxic individuality, what is the remedy?
There are many ways we can move forward to combat toxic individual ism. First, we can learn from collectivist thinking and values from com munities/cultures within our society (solidarity and interdependence) and teach them in schools. Second, we can teach public health/population health perspectives—begin with the health curriculum in early education. Third, we can learn from other parts of the world that are doing well in re sponding to COVID—what have they done? What can we incorporate in our approach? Lastly, we must redesign our health approach and adopt a family and community-centered approach instead of focusing just on the individual level.
Success should equal collaboration and interdisciplinary actions. Any one person's experiences are shaped by the results of others' actions as much as their own decisions/behaviors. Overall, the state of health is just as much a product of one's own decisions ansd behaviors as it is due to the milieu that a person lives and experiences. The action of a few can determine the factors that determine the health of anyone controlled. We ignore this at our peril at the expense of future success. Not much more than half of the U.S. population complies with, and values/understands the importance of wearing a mask. COVID is persisting and proliferat ing here more than in other countries because of this, combined with American individualism's abiding allegiance. Our society is overdue to rethink its worship of civil liberties over civic responsibilities. In the wake of another public health crisis declared with monkeypox, the delayed response of the U.S., will we see a repeat of where the country was with COVID? In a society where leaders are divided on pandemic politics, one has to question why one of the richest countries in the world with so many tools at its disposal is struggling to contain the outbreaks. As we have seen people's reaction towards COVID-19 toxic individualism is heavily present in society and if we don't stop it, it will continue to go into the current monkeypox outbreak.
With COVID in the mix of the other public health challenges we face, toxic individuality will continue to widen the gap for our society's sickest and marginalized members.”
TOXIC INDIVIDUALITY SYNDROME FOSTERS PUBLIC HEALTH COVID-19 INEQUITIES IN THE UNITED STATES Continued on page 29 >> COMMON SENSE SEPTEMBER/OCTOBER 202224
Abortion is Health Care
Liz Calhoun, MD FAAEM

Abortion is health care.
Why are we making a statement on a political issue? Because this is not one. Bodily autonomy is not a political issue; it is a basic human right that has been turned into a political issue.
Abortion care is an essential part of our scope of practice. Bodily auton omy is an issue that affects every physician, regardless of specialty. As physicians, we all took an oath the day we were conferred our degree. Though the wording may vary, the sentiment behind each is the same.
“I will respect the autonomy and dignity of my patient...I will not use my medical knowledge to violate human rights and civil liberties, even under threat.”1
If we stand by and do nothing, if we do not raise our voices now, we are complicit in stripping away the autonomy and dignity of our patients. If we stand by and do not take the appropriate medical response, for fear of legal action, we have doubly betrayed our patients: first with protecting our own self-interest, and secondly with the risk to their health and lives.
If you believe that there will be exceptions made for the life and health of the mother, think again. There are politicians who believe there should be no exceptions.2 The Tennessee trigger law, set to go into effect on August 25, 2022, does not require the burden of proof that an abortion was medically necessary to be on the prosecutor. The law allows for physicians to be charged with a felony and then provide an affirmative defense that the abortion was medically necessary.3, 4

“Every individual… must have unencumbered access to quality emer gency care.”5
“A physician’s primary duty is to the patient. The integrity of this doc tor-patient relationship requires that emergency physicians control their own practices free of outside interference.”6
If we stand by and be told we are not allowed to practice medicine as we see fit, we are denying our core values as a society. Each day, we provide care to women with complications from spontaneous abortions, induced abortions, and ectopic pregnancies. We give medication to end non-via ble pregnancies and protect the body of the person carrying the embryo/ fetus. We perform perimortem c-sections. We resuscitate hemorrhaging patients. We give antibiotics for septic abortions. We provide comfort to those who are given bad news about their pregnancy, regardless of whether it was desired.
Can you stand by and watch when each of these patients comes into your ED? Can you tell these patients that they do not get to choose if they live or die—and you don’t either? Can you tell them that you value avoiding an arrest over their life? Can you look them in the eye and tell them that they do not have the rights to their own body?
If you think this doesn’t involve us, think again.
References
1. World Medical Association. “WMA Declaration of Geneva”. WMA. Retrieved 28 June 2022.
2. https://www.inquirer.com/politics/election/abortion-pennsylvaniacandidates-2022-midterm-governor-mastriano-fetterman-shapirooz-20220624.html
3. 3https://www.tennessean.com/story/news/2022/07/26/tennessee-abortiontrigger-law-ban-2022-expected-august/10061093002/
4. https://www.capitol.tn.gov/Bills/111/Bill/SB1257.pdf
5. https://www.aaem.org/about-us/our-values
6. https://www.aaem.org/about-us/our-values/vision-statement
WOMEN IN EMERGENCY MEDICINE
Can you tell these patients that they do not get to choose if they live or die—and you don’t either?” COMMON SENSE SEPTEMBER/OCTOBER 2022 25
We Are At Risk
Loice Swisher, MD MAAEM FAAEM
SURGEON GENERAL’S WARNING: Entering the medical profession may seriously impact your health. Physicians may be affected by burnout, compassion fatigue, depression, and sui cidal ideation. SURGEON GENERAL’S WARNING: During medical edu cation trainees likely will develop capacity for suicide through knowledge acquisition and availability of lethal means.
The life’s journey of a physician does not carry a surgeon general’s warn ing; however, there are those who argue that it should. In a November 2016 blog post, Dr. Pamela Wible called for a surgeon general’s warning and/or informed consent when entering the medical school as to “be informed of the health hazards inherent in the medical profession.”1
Featuring two medical students who killed themselves, Dr. Wible high lighted the risk of suicide in trainees.
In 2018, the first National Physician Suicide Awareness Day was brought into being through CORD to “shine a light and speak its name” on phy sician suicide. There has been increased awareness, however that in creased awareness was not enough to prevent Dr. Lorna Breen’s death in 2020. Her family has worked tirelessly to pass legislation through congress to support the mental health of first responders. The Lorna Breen Act was passed in March 2022. Yet that was not enough to prevent another emergency medicine physician from dying by suicide this June—again rocking our community.

Awareness and talking about suicide are not enough. I believe we need to intentionally address ways to mitigate each of the three fac tors in Joiner’s Theory. I call for each of us to have a plan for when crisis comes. Probably each of us has mentally rehearsed perimortem C-section and many of us fortunately will never experience that trauma.
Although there are limited statistics on physician suicide, the risk is much greater for attending physicians long after training. As with the general population, the middle-aged white male is the largest demographic. Women physicians compared to women in the general population die by their own hand more than twice of general population of women.
Really is this surprising? Physicians learn about death. We overcome fear. We are given access to lethal means. When one looks a Joiner’s Theory of Suicide, physicians acquire one factor which will always be there—the capacity to die by suicide.
We are at risk. Because of our education and profession, we are at risk for suicide. And this is not a new thing. Physicians have been killing themselves more than the average person for more than 150 years. The new thing is that we are talking about this.
However, it is virtually certain that at some point in our lives there will be a rough road because of our job.
I propose that each of us should develop our own crisis management plan creating the “Red Shield” by focusing on developing connections, remembering our calling (meaning), and practicing self-compassion.
If you or someone you know is experiencing suicidal thoughts or a crisis, please call or text 988 to reach the Suicide & Crisis Lifeline.
References
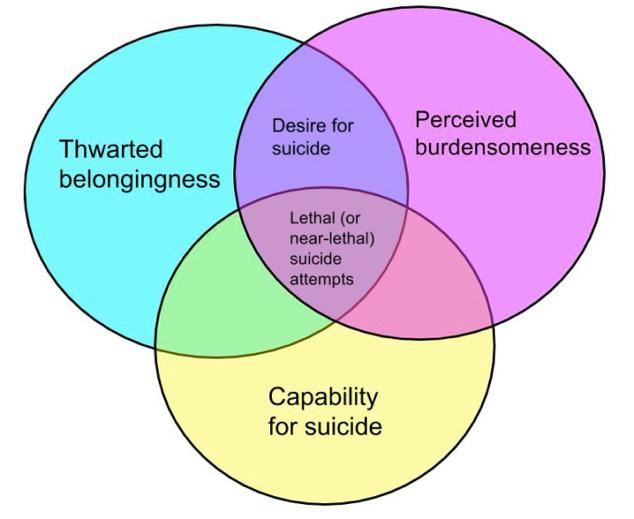
1. Surgeon General Warning: Medical school may kill your child. https://www. idealmedicalcare.org/surgeon-generals-warning-medical-school-may-killyour-child/
2. Is your resident at risk for suicide? https://cordemblog.com/2017/02/21/ is-your-resident-at-risk-of-suicide/
WELLNESS COMMITTEE
COMMON SENSE SEPTEMBER/OCTOBER 202226
OSHA must renew its COVID-19 Emergency Temporary Standard Regarding Airborne Pathogens
Gregory Jasani, MD and Gary Gaddis, MD PhD MAAEM FAAEM FIFEM
Recently, the Occupational Safety and Health Administration (OSHA) permitted expiration of its “COVID-19 Emergency Temporary Standard (ETS),” concerning man datory workplace protections from “airborne pathogens” such as the SARS-CoV-2 virus. This ETS was issued on June 28, 2021. Its expiration should be of concern to all health care workers, and it deserves to be reversed. As we will explain, the protections provided by the ETS deserve to be made permanent.
This ETS specified new, enforceable regulatory protections for health care workers. Institutions not in compliance could be fined. Before its issuance, federal guidance regarding “airborne pathogens” as issued by the Centers for Disease Control, were non-enforceable suggestions, not enforceable mandates.
Of course, the ETS as its name implies, was not issued with the clear intent that it became permanent. As an ETS, it was set to “automatically” expire no later than 12 months after it was introduced. OSHA had the power to make this ETS permanent, but failed to do so. We lament this wasted opportunity. The ETS that OSHA put out was sorely needed given the new realities that COVID has forced upon the health care system. We believe that OSHA must revisit this issue and produce a permanent standard for airborne pathogens, not just to protect us during this pan demic but for the next one as well.
Working in health care institutions during the COVID-19 pandemic came with significant risk. Health care workers were three times more likely to be infected with COVID-19 compared to the general public.1 This high infectivity rate was likely exacerbated by PPE shortages during the initial phases of the pandemic. In the early days of the pan demic, there were even alarming news stories of hospitals and other health care organizations that actually forbade their employees from wearing masks and other PPE.2
Obviously, PPE shortages and restrictions were unsafe and unaccept able for those working in health care. For instance, these shortages spurred the development of movements such as “Get Us PPE.”3 Hospitals and other health care organizations mobilized quickly, in most cases, to implement new voluntary standards and practices. With remarkable speed, wearing masks, eye protection, and gowns became ubiquitous in the health care field.
The Centers for Disease Control (CDC) developed COVID-19 rec ommendations for health care providers, which stated that providers “should wear well-fitting source control,” undoubtedly helped spur this

change.4 However, one important aspect lacking in the CDC’s recom mendations was enforcement. The CDC can give recommendations, but its recommendations are not enforceable. Further, those recommenda tions did not carry any penalties for employers who do not follow them. To properly protect health care workers, the federal government needed to do more.
Therefore, President Joe Biden, within one day of assuming the Presidency, issued Executive Order 13999, regarding Protecting Worker Health and Safety. Stating that “ensuring the health and safety of workers is a national priority and moral imperative,” the executive order required the federal government to “take swift action to reduce the risk that workers may contract COVID-19 in the workplace.”5 It spelled out actions for various federal agencies to take, including tasking OSHA with determining if an ETS for COVID-19 was indicated.
OSHA determined that an ETS was indeed necessary and officially in troduced it on June 28, 2021. The ETS placed several requirements on health care employers. It specified multiple requirements that it deemed health care employers must fulfill to best protect their employees against COVID-19. These included the development of a written COVID-19 plan to address steps the workplace will take to combat COVID-19, following
The COVID-19 pandemic, for all of the suffering it has caused, has helped advance our understanding of best practices for airborne contagion prevention.”
GOVERNMENT AND NATIONAL AFFAIRS COMMITTEE
>> COMMON SENSE SEPTEMBER/OCTOBER 2022 27
CDC guidance on cleaning and disinfection, physical distancing of em ployees when appropriate, and screening and removing COVID positive employees. Most importantly, however, the ETS mandated health care employers to provide facemask and other forms of PPE to their em ployees. Additionally, employers were forbidden from retaliating against employees for adhering to this standard.6
The importance of codifying these protections as employer obligations, and not simply suggestions, cannot be overstated. Adequate PPE is ab solutely necessary to protect health care workers from airborne infection. OSHA’s ETS was an important step to ensure that the PPE shortages and re strictions on mask wearing we witnessed during this pandemic never happen again. The CDC issues recommendations, but the ETS has consequences including loss of certification and significant fines. The ETS not only codified best practices for prevention and protection, it also placed the onus on hospitals and other health care employers to ensure that they are adequately protecting their employees.
Although OSHA’s ETS may seem unpar alleled to some younger physicians, there is precedent for OSHA to produce, imple ment, and enforce workplace standards in response to a significant health event. In the early 1990s, consequent to the AIDS epidemic, OSHA created the Bloodborne Pathogens Standard. This standard laid out requirements for employers “to protect workers who are occupationally exposed to blood or other potentially infectious organisms.” Among other things, it required that gloves be provided to employees, that disposable needles be used, and that post-exposure prophylaxis be made available to any employee who was potentially ex posed to a bloodborne organism 7
These practices were not only effective against workplace HIV transmis sion. They also were effective against other occupationally-acquired dis eases. In 1987, there were 8,700 cases of Hepatitis B acquired among health care workers. By 1995, four years after the Bloodborne Pathogen Standard was published, only 800 occupationally-acquired cases were reported.8 These practices that this standard introduced are now known as “universal precautions,” meaning that they are used for all patients. Most physicians cannot imagine practicing medicine without them. Yet, if it were not for this OSHA standard, these basic protective measures might not have become universal. OSHA’s actions ensured that all em ployees would enjoy this level of protection.
OSHA did not permit its Bloodborne Pathogen Standards to lapse after they were issued, and they should not have permitted the Airborne Pathogen ETS to lapse, either. The protections conferred by the ETS clearly work and they undoubtedly saved lives.
However, in addition to making a permanent standard based upon the ETS, we would also encourage OSHA to expand it. The ETS only ap plied to COVID-19. While this is understandable given recent events, the final standard should be more far-reaching. COVID-19 is one of the worst airborne pathogens that our nation has faced but it will likely not be the last. The lessons learned during this pan demic about the importance of PPE will continue to be applicable regardless of what organism is responsible. Developing an Airborne Pathogen Standard, similar to the Bloodborne Pathogen Standard, would codify these life saving measures for future generations of health care workers.
OSHA should be applauded for introduc ing the ETS; it codified best practices for keeping health care workers safe during one of the worst public health crises of a generation. The COVID-19 pandemic, for all of the suffering it has caused, has helped advance our understanding of best practices for airborne contagion preven tion. It has also shown us how vulnerable we are to these pathogens when basic, protective measures are lacking. It is unlikely that COVID-19 is the last, or even the worst, airborne pathogen our nation will face.
As the human population of the globe increases, we will encroach upon more “wild places” and acquire zoonoses such as COVID-19 that were previously unknown to human medicine. We should all fear a future air borne pathogen with the infectivity of emerging SARS-CoV-2 variants, the transmissibility before a patient is symptomatic that characterizes SARS-CoV-2 (but did not characterize the SARS outbreak that began in February of 2003 or the MERS outbreak that began in April of 2012), and the case-fatality rate of 15% for the prior SARS outbreak and of 34% for the prior MERS outbreak.
When the next airborne pathogen surfaces, health care workers deserve the best protection, both medically and legally, possible. This mandates extension of the “airborne pathogen” ETS into a permanent measure.
As those bringing this warning to our community, we alone are not em powered to advocate effectively for change. However, our professional colleges and associations have that power.
We believe that OSHA must revisit this issue and produce a permanent standard for airborne pathogens, not just to protect us during this pandemic but for the next one as well.”
GOVERNMENT AND NATIONAL AFFAIRS COMMITTEE >> COMMON SENSE SEPTEMBER/OCTOBER 202228
We call on the leadership of the American Academy of Emergency Medicine, as well as the leaders of the American College of Emergency Physicians, the Society for Academic Emergency Medicine, the National Association of Emergency Medical Services Physicians, the Emergency Nurses Association, and others to join in a movement designed to result in updating and permanent enforcement of a useful airborne pathogen standard.
Further, advocacy need not be limited to emergency medicine or nursing organizations. It is logical that all organizations devoted to the care of patients “have a dog in this fight.” Let’s build a coalition designed to gain permanent protections that the COVID-19 pandemic has taught us to value!
References
1. Nguyen LH, Drew DA, Graham MS, Joshi AD, Guo CG, Ma W, Mehta RS, Warner ET, Sikavi DR, Lo CH, Kwon S, Song M, Mucci LA, Stampfer MJ, Willett WC, Eliassen AH, Hart JE, Chavarro JE, Rich-Edwards JW, Davies R, Capdevila J, Lee KA, Lochlainn MN, Varsavsky T, Sudre CH, Cardoso MJ, Wolf J, Spector TD, Ourselin S, Steves CJ, Chan AT; COronavirus Pandemic Epidemiology Consortium. Risk of COVID-19 among front-line health-care workers and the general community: a prospective cohort study. Lancet Public Health. 2020 Sep;5(9):e475-e483.
2. Fadel L. Doctors Say Hospitals Are Stopping Them From Wearing Masks. NPR. April 2, 2020.
3. Get Us PPE. https://getusppe.org/
4. Interim Infection Prevention and Control Recommendations for Healthcare Personnel During the Coronavirus Disease 2019 (COVID-19) Pandemic. CDC. Updated Feb 2, 2022. https://www.cdc.gov/coronavirus/2019-ncov/ hcp/infection-control-recommendations.html#anchor_1604360748519
5. Executive Order on Protecting Worker Health and Safety. The White House. January 21, 2021. https://www.whitehouse.gov/briefing-room/ presidential-actions/2021/01/21/executive-order-protecting-worker-healthand-safety/
6. Statement on the Status of the OSHA COVID-19 Healthcare ETS. OSHA. December 27, 2021. https://www.osha.gov/coronavirus/ ETS#:~:text=OSHA%20COVID%2D19%20Healthcare%20 ETS&text=On%20June%2021%2C%202021%2C%20 OSHA,healthcare%20or%20healthcare%20support%20services
7. OSHA’s Bloodborne Pathogen Standard. OSHA. https://www.osha.gov/ sites/default/files/publications/bbfact01.pdf
8. Statement of Charles N Jeffress Assistant Secretary Occupational Health and Safety Administration U.S. Department of Labor Before The Subcommittee on Workforce Protections House Education and Workforce Committee. OSHA. June 22, 2000. https://www.osha.gov/news/ testimonies/06222000
Continued from page 24
References
*Windsor University School of Medicine, St. Kitts, West Indies
†Windsor University School of Medicine, St. Kitts, West Indies
‡University of Colorado, School of Medicine, Anschutz Medical Center, Denver
1. Our World in Data, n.d.
2. Ellerbeck & Cunningham, 2021
3. Gostin LO. Jacobson v Massachusetts at 100 years: police power and civil liberties in tension. Am J Public Health. 2005;95(4):576-581.
4. Gostin LO, Friedman EA, Wetter SA. Responding to Covid-19: How to Navigate a Public Health Emergency Legally and Ethically. Hastings Cent Rep. 2020;50(2):8-12.
5. Gostin LO, Hodge JG, Jr. US Emergency Legal Responses to Novel Coronavirus: Balancing Public Health and Civil Liberties. Jama. 2020;323(12):1131-1132.
6. Wang ML, Behrman P, Dulin A, et al. Addressing inequities in COVID-19 morbidity and mortality: research and policy recommendations. Transl Behav Med. 2020;10(3):516-519.
7. CDC. Excess Deaths Associated with COVID-19: Provisional Death Counts for Coronavirus Disease (COVID-19). National Center for Health Statistics. 2020.
8. Shadmi E, Chen Y, Dourado I, et al. Health equity and COVID-19: global perspectives. Int J Equity Health. 2020;19(1):104.
9. Abedi V, Olulana O, Avula V, et al. Racial, Economic, and Health Inequality and COVID-19 Infection in the United States. J Racial Ethn Health Disparities. 2020:1-11.
10. Winkel J. Climate Change and Social Inequality. United Nations, Department of Economics, and Social Affairs. 2017(152).
TOXIC INDIVIDUALITY SYNDROME FOSTERS PUBLIC HEALTH COVID-19 INEQUITIES IN THE UNITED STATES
GOVERNMENT AND NATIONAL AFFAIRS COMMITTEE
Tell Us Your Opinion! The editors of Common Sense want to hear from you! What articles did you like or which ones, not so much? Submissions are open for future issues. Please visit aaem.org/resources/publications/common-sense or contact cseditor@aaem.org for more information. This is where your voice can be heard! COMMON SENSE SEPTEMBER/OCTOBER 2022 29
Advice for Young Academic Faculty
Mary Claire O’Brien, MD FAAEM

You get a lot of advice in life and in emergen cy medicine, much of it not worth having. Here’s some good advice from an old academician.
“If you don’t toot your own horn, nobody will.”
My mother gave me this advice when I was 16. We had driven to Arthur Treacher’s, a fast food store that was opening on Second Street Pike in Southampton, Pennsylvania, a few doors down from the McDonalds. There were signs in the window: “Coming Soon! North Atlantic Whitefish!” The sign that interested me said, “Help Wanted.”
I was in high school saving for college and needed a job for nights and weekends. My mother sat outside in the car chain-smoking while I filled out an application. When I got back, her ashtray was piled with Marlboro stubs, Brick Red lipstick on the tips.
“Did you do it?” she asked.
“Yes,” I mumbled.
“Good,” she said. “Good.”
She looked over. I did not look back.
“Did you put down you are an ‘A’ student?” she said. “That you are in the Honor Society?”
“Mom!” I said. “They don’t care about that. This is Arthur Treacher’s. It’s a job wiping tables and serving fish.”
“If you don’t toot your own horn, nobody will,” she said. “Get back in there.”
I have quoted my mother many times when telling junior faculty how to keep track of their work performance: everything you do, count it! Toot your own horn, because both academic and corporate medicine are all about “deliverables.”

Examples:
• You and a colleague are asked to write up protocols for APP’s to see children in a newly built urgent care. You meet a few times to do the work. Not only do you count the protocols themselves as a “deliverable,” you also count the cooperative effort. Perhaps it wasn’t an official “committee,” depending on the size of the project and the number of individuals involved. But it was at the very least a “working group.” A larger working group is a “task force.” Put it on your CV!
• Every single time someone else toots a horn for you—every text message, every thank-you email, every handwritten note—whether it is from a nurse, a consultant, a patient, a family member—scan these into PDF’s and put them on your hard drive under a folder called “Thank You.” Accumulate them. Use them when it is time to go up for promotion to reflect your excellent patient care. Read them when you are discouraged. Keep those notes!
“Don’t sweat the Hotdogs.”
I was working in the ED one steamy day in 1985—a typical Philadelphia broiler when the back of your neck drips and even the windows sweat. I was an intern.
My patient was asthmatic, gasping, bug-eyed, her neck muscles sucking in with every breath. She looked bad. I put her on oxygen and told the nurse to give her sub-Q epinephrine. I started an IV and pushed some corticosteroids. We hung an aminophylline drip, one of the recommend ed treatments back then. The respiratory therapist set up a nebulizer treatment.
We watched.
The second year resident wandered over. He was broad-shouldered and self-confident—a Brooks Brothers model in rumpled scrubs. Curious and eager to criticize.
He was a Grade-A Hotdog.
He glanced at the aminophylline bag—calculating the patient’s weight in his mind, asking the nurse about the bolus dose, squinting. The patient was weeping with anxiety. I was nervous. The attending walked over, Dr. David Wagner.
But external presentations, committee membership, student and resident interviews, workshops, enrolling patients in clinical trials, developing clinical guidelines, quality improvement reviews, mentoring students and residents, participating in faculty development, and writing manuscripts—these things are all ‘your job’ too.”
ACADEMIC AFFAIRS COMMITTEE
>> COMMON SENSE SEPTEMBER/OCTOBER 202230
“Isn’t there evidence to suggest that aminophylline’s primary effect is diuretic?” the resident said, addressing Dr. Wagner and ignoring me. He was very full of himself. “Increasingly, I see support for continuous beta agonists—and not for intravenous aminophylline.”
Dr. Wagner smiled. He was kindhearted and soft spoken. “Well,” he said. “That might be.”
The resident harrumphed. “I read an important article about this just last week,” he said to Dr. Wagner, before walking back to his own patients.
I nearly passed out.
Dr. Wagner was the Chair of the Department and a full professor. He is one of the founding fathers of emergency medicine. We might have called him “Daddy Wags” behind this back, but that was pure affection. We admired him even if we didn’t fear him.
“Dr. Wagner,” I whispered. “Doesn’t it upset you when your residents correct you?”
He grinned. “I expect my residents to out-book me,” he said. “The day they can out-doctor me, I’ll hang up my stethoscope.”
Young faculty, you will meet residents (both your own and consultants) and faculty (ditto) who are Hotdogs. Do not engage emotionally with Hotdogs—neither their attitudes nor their expertise. They might be right!
Listen to them and don’t take umbrage. You are a faculty member. You are ABEM-boarded or soon to be. Do not sweat the Hotdogs. Be open-minded and willing to listen
“Don’t burn your bridges.”
At the end of my fellowship year in 1989, I was worn to pieces. After three years of residency (pre- 80-hour work week), another tough year as an EMS fellow/new attending, and big personal demands at home—a spouse who was a full-time physician and an infant daughter—I was be leaguered. Burnt out. Ok, I was angry.
While I never said anything out loud that was unkind or derogatory about my training or my co-workers, it must have been obvious to the people who cared about me that I was at the end of my rope. One of them was Dr. Steve Davidson, my fellowship director at the Medical College of Pennsylvania (MCP). He offered some unsolicited but very important advice: “Don’t burn your bridges.”
In life, and in medicine, you never know where your path is going to lead. I didn’t want to follow Dr. Davidson’s advice, but boy am I glad I did!
A few years later, I was asked to start an emergency residency pro gram in NJ. In those days, aspiring programs had to write their own curricula from scratch—there was no standard national curriculum. Pre-internet, this meant combing through every textbook you owned or could borrow—hard copies of Tintinalli, Roberts and Hedges, Schwartz’s Surgery, Fleisher and Ludwig’s Pediatrics, Merrill’s Radiology, Harrison’s
and Cecil’s Internal Medicine. Old journals. Old conference schedules. Anything you could find in the library on microfilm (old school). If you were well connected with your emergency medicine colleagues, you looked at examples of curricula from other programs. If I had let my temper and fatigue get the better of my professional relationships at my old program, I would have had no one to rely on in my hour of need. The generosity and encouragement of my MCP friend Dr. Bob McNamara saved me. He opened his intellectual coffers and shared everything, which helped me both write a new curriculum and navigate the RRC successfully.
Don’t burn your bridges!
Say “Yes.”
When you are a new faculty member, your department and your insti tution expect a certain amount of “citizenship” from you. Yes, your pri mary job is seeing patients in the emergency department and bedside teaching. But external presentations, committee membership, student and resident interviews, workshops, enrolling patients in clinical trials, developing clinical guidelines, quality improvement reviews, mentoring students and residents, participating in faculty development, and writing manuscripts—these things are all “your job” too. It is confusing to new faculty who know they want to do academic medicine but aren’t always sure what that means. My advice: in the beginning of your career, to the extent you are able, you should say “yes” as professional opportunities present themselves. It is very unusual for a new faculty member to know exactly which direction their career path will lead. I have been a residen cy program director, an EMS county medical director, an oral examiner, a vice-chair for faculty affairs, a public health researcher, an internation al public policy advocate, and a senior associate dean. I could not have imagined any of this as a new faculty member. My academic career has been interesting and fruitful because when unexpected opportunities presented themselves, I said “yes.”
Say “No.”
Academic medicine has three missions—clinical care, education, and research. There is an expectation that a faculty member will do all three. But the key to sustainability in academics is balancing these activities so that you maintain personal wellness. How much you can say “yes” is a direct function of your health, your outside responsibilities, and your professional experience. After you learn to say “yes,” you have to learn to say “no.” Only then will your academic career be both successful and sustainable.
You will know when your plate starts to feel full. Before it overflows, practice saying, “Wow, that sounds like a wonderful opportunity. I wish I could say yes. I really don’t have the bandwidth right now to give that all the attention it deserves. Thank you so much for considering me.” I am not joking: say it exactly that way, and repeat if necessary. Your family will thank you for it!
ACADEMIC AFFAIRS COMMITTEE COMMON SENSE SEPTEMBER/OCTOBER 2022 31
Efficiency in the Emergency Department: A Solutionsbased Approach
 James Gill, MD MBA FAAEM
James Gill, MD MBA FAAEM

“Is the hospitalist going to admit that 88-year-old weak and dizzy patient?” my colleague asked as I hung up the phone.
“I don’t know.” I responded. His retort was biting, but not sarcastic. He’d had helpful and considerate advice for the short time I’d known him, but never so trite.
He said, “Well, I don’t know either and I’m pretty certain the hospitalist doesn’t know.”
It was a Robert Frost moment. I’d come to the fork in the road.
Do you have a similar story? Most of us do. Efficiency has and continues to require a lot of focused effort. The above prompting from my colleague prompted me to seek a solution. Are you receiving any similar prompts? For me, it has been a rewarding and even refreshing since that initial prompt from my concerned colleague. My response to accept the chal lenge has added longevity and job satisfaction to an otherwise incredibly challenging specialty we share.
There is one approach that encompasses all efficiency issues: maintaining a solutions-based focus. However, losing focus is quite easy. There are countless unproductive matters, situations, etc., that we simply can’t change that redirect our focus toward unproductive problems for which there are not solutions within our sphere of influence. For instance, fo cusing on the line of ambulances that piles up as we go on divert for the fourth time in 24 hours with a waiting room spilling into the administrative offices can be terribly unproductive and only leads to frustration without any hope for a solution. However, if we focus instead on, for example, what one step we can take to clear one bed, we might make some small progress. Each small solution can add to larger solutions.
The 88-year-old patient with weakness and dizziness above has several pieces. My colleague prompted my recognition of poor communication and inadequate information. The solution to my poor communication was to prepare the information with the end point in mind and shaping my words in that direction. I ad dressed inadequate information related to elderly weak and dizzy patient by answering one ques tion: has the patient’s activities of daily living changed. For you, this
may be either a different question or a different set of patients altogether. The point is to look for the question or questions that help streamline your disposition.
If there are several patient symptoms that slow your efficiency or disrupt your flow, choose one symptom, such as low back pain and focus on what can be learned to add to both comfort level and making the patient better. Most recently, the challenge with low back pain was closing the loop in a timely manner. After giving my typical information, I offer addi tional information and encourage the patient to stay, read the information written in a short, consolidated paragraph which repeats what I’ve said. This developed from a problem I noticed frequently occurring. The patient did not understand where they would be going after discharge, why there were no x-rays performed nor what a typical course of radiculopathy would entail. I was able to uncover the answers above by asking what the patients didn’t understand and adjusting the discharge information, so the patient and nurse knew what to expect.
There are still some patients that require more. In those patients, I simply ask the nurse to join me as I discharge the patient so there are no missed points, and we discharge the patient all at the same time. I applied this approach to patients with other symptoms with a particular focus on improving their symptoms. Ultimately, learning how to address the complaints in a manner that was directed toward a combination of understanding what the patient hoped to gain, being forthright and concise about the possibilities allowed disposition discussion is far more seamless when the patient feels better.
The solution to my poor communication was to prepare the information with the end point in mind and shaping my words in that direction.”
>>
COMMON SENSE SEPTEMBER/OCTOBER 202232
Two Unproductive Actions
Reducing multitasking and the number of steps we take can greatly improve efficiency. No one multitasks well. Studies have shown there is a mental reset with each interruption of a few seconds to recall what we were doing and where we were in the task. Reducing interruptions is possibly the most important factor to efficiency and mental well-being. We must acknowledge the tremendous frustration of repeated interrup tions and voice these honestly and in confidence. One of my previous medical directors use to say, “Praise in public. Criticize in private.” For those that repeatedly interrupt with non-emergent issues, it is critical to re-direct in a pleasant manner. There are at least three ways this can be accomplished. First, re-check your pa tients frequently while anticipating the patient’s needs and the timing of those needs. For example, I make a mental note to recheck patients with headache 30-45 minutes after IV medication.
Second, provide alternate avenues and check them frequently. For example, we have two-way radios and a “com ment” box in our computer system that signal an update. Search for ways to help the nurses, technicians, and unit coordinators to save their time and do them consistently. Lastly, and most importantly, focus on reducing the interruptions by addressing the interruptions before they happen. For example, let’s say you are frequently interrupted by nurses to discharge a patient. Focus on printing the discharge information and letting the nurse know where it will be. Personally, I find it easier to get them the informa tion often before they ask while I’m going to see another patient.
Multitasking is a disease with no easy cure. Interruptions drastically increase the risk of multitasking by reducing focus on one task at a time. A walk through the emergency department can illustrate reducing multi tasking and saving steps. Let’s say you walk into the emergency depart ment there are several patients on the board. You recognize your limit is to pick up four at a time, so you do. These are a 65 year with chest pain, an 88-year-old with weakness, a 32-year-old with a headache, and a 28-year-old with back pain. My personal approach is to order labs on the two older patients, go see the two younger, order pain meds, finish both younger patient charts at the same time printing discharge instructions. Many of these patients will not require imaging allowing me to discharge the patient with back pain immediately. I take those the discharge papers

directing to the nurse on my way to see two to four more patients and see the two older patients on my second tour around the emergency department. Your numbers may be different, but the reductions most beneficial to me in this scenario is focusing on finishing a task at a time, saving my steps and that of the nurses while reducing the interruptions. The discharge paperwork printed after seeing the two younger patients remains at my workstation until the patient with headache is rechecked 30 minutes after meds. It is carried on my third pass around the ED in hopes the patient has improved, and can be handed directly to the nurse, limiting an interruption of the nurse informing me of patient improvement and saving the nurse’s steps.
Last, but certainly not least. Be patient with yourself and do not overextend. Find the number of patients that is comfortable and safe. Rome wasn’t built in a day, and no one is asking (or at least they shouldn’t be) you to see 3 ½ sick patients an hour without help. Find the number of people you can carry at once without reducing efficiency. If you find yourself interrupted too often for extended periods, the number of active patients you are carrying at once is probably too high. When you reach that point, find some people to discharge first, admit second. Discharging patients is the absolute most important task for the emergency department. It frees us and the nurse from additional interruptions, allows a patient from the lobby to get a bed, and allows our colleagues to help us work togeth er to get people where they ultimately need to be. Admitting patients also removes tasks from the list, but commonly doesn’t immediately help the nurse who has more work in the short term when the patient is admitted. One exception to the discharge first rule could be admitting critical pa tients. These patients often require enormous resources that we simply don’t have. Our nurses are often caring for four, maybe six patients at a time. They simply cannot spare a moment, much less give the undivided attention critical patients often require. Helping them with a disposition, central line, intubation, EJ IV, etc., is critical, but the most important help is the call to the critical care physician to find a prompt direction.
We have a wonderfully challenging specialty. It remains a privilege to be a part of such a dynamic workplace. Problems are most often opportuni ties if we put our minds and energy toward solutions.
Multitasking is a disease with no easy cure.”
EFFICIENCY IN THE EMERGENCY DEPARTMENT: A SOLUTIONS-BASED APPROACH WOMEN'S WISDOM A Podcast by WiEMS AAEM New Episodes Monthly! Catch Up On Past Episodes COMMON SENSE SEPTEMBER/OCTOBER 2022 33
Breaking Bad News: Practical Applications in the Emergency Department
Reed Wise, MS and Danielle Goodrich, MD FAAEM FACEP


Breaking bad news is one of the most difficult tasks physicians are asked to do. An emotional mine field awaits even the most experienced communicators given that each patient has their own unique set of goals, expectations, and desires that must be considered. Approaching emotionally taxing conver sations without a plan can decrease the efficacy of the conversation and may lead to miscommunication and adverse patient reactions. In this article, we present a model, SPIKES, originally developed to deliver cancer diagnoses, for adaptation to the emergency room setting. The SPIKES model focuses on six critical facets: (1) Setting Up the Interview, (2) Perception, (3) Invitation to the Encounter, (4) Knowledge, (5) Empathy and Emotion, and (6) Summary and Strategy.1 Within this framework, the authors lay out the four primary goals for an interview in which bad news is discussed which include information gathering, collabo rating with the patient on treatment strategies, transmitting medical informa tion, and providing support. Given the nuances and stakes at play, entering the conversation prepared is necessary to create an environment for suc cessful communication with your patients and their families.

S When “Setting Up the Interview,” the physician should take space both physically as well as mentally to privately acknowledge their own feelings and create a plan. Location as well as the involvement of those that the patient wishes to accompany them while they receive their diagnosis are important considerations. Moreover, this may be a life-changing moment for the patient and they will appreciate your full support, so ensuring adequate time is also necessary. Additional considerations also include sitting at the level of the patient and making eye contact to express support through body language.
P Perception. Every patient’s level of understanding of their condition differs so “before you tell, ask” about your patient’s knowledge to assess their basis of knowledge. Politely correct any misin formation once they are done sharing to tailor the conversation to the patient’s needs. Useful open ended questions include: “What do you know about your condition?” or “What are your goals for treatment?” Assess for illness denial, such as omission of difficult details, unrealistic expectations, and wishful thinking.
I In the “Invitation to the Encounter” the physician allows the patient to discuss the topic on their own terms. Every patient receives bad news differently so it can be beneficial to engage the patient on their terms. For example, would the patient prefer to get the news now? Would they prefer someone else to be present? Do they prefer to have someone else receive their news?
K When sharing Knowledge with a patient, the physician should alert the patient before deliv ering the bad news. Consider beginning with a statement like, “I have some heavy news for you, are you ready for me to share it?” or similar prompts to ensure that the patient is indeed ready for the conversation. Employing empathy, eliminating medical jargon, and avoiding extreme bluntness can go a long way toward helping patients digest difficult information. If there is a lot of information to be shared, such as a complex diagnosis or treatment plan, it can be helpful to break up the news with periodic assessments of patient comprehension and goals. Statements such as “Does that make sense?” or “Would you like to discuss some alternatives to my suggested treatment plan?” can be helpful to break up the interview and recenter it on the patient’s goals and level of understanding.
YOUNG PHYSICIANS
Our patients need to know their diagnoses so that we can adequately treat and care for them, but that does not mean that sharing poor prognoses is easy for either the patient or the physician.”
SECTION
>> COMMON SENSE SEPTEMBER/OCTOBER 202234
E Perhaps the most difficult aspect of the model is “Empathy and Emotions.” Both the patient and physician may be feeling intense emotions during the conversation—sadness, denial, silence, and anger are common reactions. Use empathetic communication techniques to help ease the burden of managing emotionally heavy conversations. For example, observe the patient’s or families’ response and identify the emotions using open ended questions. Verbalize the reason for the emo tions and make connecting statements. Remember, catering to emotional responses is just as important as sharing the actual information. But, keep in mind that you are human and have your own feelings, so be sure to acknowledge your own feelings and seek help if needed. Maintaining one’s own mental wellbeing is crucial to taking care of others.
S Summary and Strategy to close the interview. This step is important because a clear plan for the future lessens the anxiety our patients may
feel about their new diagnosis. Make sure to explore treatment options, acknowledge discomfort with the prognosis, and reexamine whether expectations are realistic. Ideally, the treatment plan should be a shared responsibility between patient and provider.
Our patients need to know their diagnoses so that we can adequately treat and care for them, but that does not mean that sharing poor progno ses is easy for either the patient or the physician. The aim of this article and the SPIKES model is to serve as a starting point to more effectively bridge the information between patients and physicians.
References
1. Baile WF, Buckman R, Lenzi, Glober G, Beale EA, Kudelka AP. SPIKESA six-step protocol for delivering bad news: application to the patient with cancer. Oncologist. 2000;5(4):302-11. Doi:10.1634/theoncologist.5-4-302. PMID: 10964998.
Membership Categories
Fellow and Full Voting – FAAEM Dues: $525 Board certified in emergency medicine or pediatric emergency medicine
Associate Dues: $250 Graduate of an ACGME or AOA approved emergency medicine training program and not yet taken or passed your EM board Fellow-in-Training Dues: $75 Graduate of an ACGME or AOA approved emergency medicine training program and currently enrolled in a fellowship

International Member
Dues: $150 Physicians with an interest in emergency medicine who practice outside of the United States or Canada
Emeritus Member
AAEM is the leader within our field in preserving the integrity of the physicianpatient relationship by fighting for a future in which all patients have access to board certified emergency physicians and physician rights are protected.
Member Benefits
Publications
Free subscriptions to the Journal of Emergency Medicine and Common Sense
Education
Dues: $250 Full voting member who has practiced emergency medicine for 30 or more years and has been a full voting member for a minimum of 10 years -or- at least 65 years of age and have been a full voting member for a minimum of 10 years Special circumstances may lead to a request for emeritus membership and will be reviewed on a case-by-case basis. See www.aaem.org/membership for more information.
Learn more and join today at: www.aaem.org/membership
Group Membership
Free registration to the Annual Scientific Assembly with
deposit and discounted registration for other AAEM events
Members-Only Section
Access the AAEM Job Bank, your Advanced Resuscitation Expertise Card (for Full Voting members), and other academic and career-based benefits
Learn more about these and other member benefits at www.aaem.org/membership/benefits
American Academy of Emergency Medicine
555 East Wells Street, Suite 1100, Milwaukee, WI 53202-3823 (800) 884-2236 info@aaem.org www.aaem.org
AAEM offers group memberships to allow hospitals/groups to pay for the memberships of all their EM board certified & board eligible physicians.
100% ED Group Membership
Criteria: All board certified and board eligible physicians at your hospital/group must be members
Discount: 10% discount on membership dues
ED Group Membership
Criteria: Two-thirds of all board certified and board eligible physicians at your hospital/ group must be members
Discount: 5% discount on membership dues
For group memberships, AAEM will invoice the group directly. If you are interested in learning more about the benefits of belonging to an AAEM ED group, please contact us at info@aaem.org or (800) 884-2236.
Join Today! www.aaem.org/membership
YOUNG PHYSICIANS SECTION
refundable
AAEM-0822-164 COMMON SENSE SEPTEMBER/OCTOBER 2022 35
Enemy Combatants in Our COVID War
Gary Gaddis, MD PhD MAAEM FAAEM FIFEM
The COVID-19 pandemic has caused many burdens for all of us in health care, not the least of which is anger. Dr. Mary Claire O’Brien spoke to the burden of her anger in her essay “Standing the Post,” which appeared in the May/June Common Sense. She noted that lately, she has opened her shifts out by saying to herself, “Help me not lose my temper for eight and a half freaking hours.” I share her anger. However, I will close this essay by offering a paradigm that I hope may help enhance sanity and decrease anger, with the intent that if my para digm helps me, perhaps it will help others.
But first, let’s acknowledge that we have lots of reasons for justified anger. Some of us retain anger at those who failed to secure us personal protective equipment (PPE) early in the pandemic. Others retain anger at the ineffective national leadership that characterized the first year of the pandemic. Our former President ignored the briefings of the best and brightest in our foreign intelligence services in February of 2020, and then washed his hands of responsibility for initiating a sensible nationwide response. Instead, he left such matters to the various states.
In my state, not to be outdone, our state’s so-called leadership lateraled much of the responsibility for managing the pandemic to the cities and counties. This led to various states and even smaller units of government bidding against each other for sorely needed and critical supplies such as ventilators and PPE, which ended up costing a lot of extra money, and which enriched profiteers, etc., etc. ARRRGGGHH! It makes me angry just to write this!
However, most of my current anger is at those who have not only de clined immunization, but also are militantly anti-masking, and thus mili tantly anti-science. Most of these people align politically with our former President, whom I call the “Pied Piper of the Pandemic.” He misled his followers with no regard to the consequences of his bellicosity or nihilism. I make no apologies for my core belief that my anger, my white-hot rage against not only our former President, but also these patients, is fully justified.
Dr. O’Brien wrote eloquently, stating, “I am mad because at this point in the pandemic, so much of it seems preventable. I am mad because the vaccines are not keeping health care workers safe. I’m mad because unvaccinated people show up sick as stink with COVID pneumonia and
expect us to fix it. Believe me, we clinicians are all worn out with this. We are mad at the patients. Here is the irony: we are mad at each other!”
I agree with Dr. O’Brien!
The emotions she related seem highly akin to the emotions of the fictional Dr. “Hawkeye” Pierce, in a long-running drama series called “M*A*S*H.” “M*A*S*H” fictionalized the activities of real Mobile Army Surgical Hospital units during the Korean War. Numerous episodes found the character of Dr. Pierce, a general surgeon, enraged at the general stupidity of war, at the needless human toll caused by people senselessly killing each other, at those who caused the toll and stupidity, and at times even against members of his own M*A*S*H unit.
The reference to a M*A*S*H unit are germane, because medical care teams the world over are at war against a recently-emerged microbial enemy, with some bewildering characteristics. For instance, who ever heard of a viral infection that promotes abnormal blood clotting, rather than causing hemorrhage? Just as the fictional Dr. Pierce was often en raged while doing his part in the Korean War, I find myself occasionally enraged as I engage in the COVID war.
M*A*S*H not only provides a military paradigm. It provides a framework that I have been using to deflect my anger and help me focus upon the matter at hand, when confronted by a science-denying COVID patient.
Doctors in forward-deployed military hospitals, such as M*A*S*H units and modern military hospitals, provide care not only to injured combat ants who are members of the American military, and our allies. They also on occasion must provide medical care to enemy combatants. It matters not that the enemy combatant, who is now a patient, may have been lobbing artillery shells or firing bullets at the hospital’s position yesterday. What matters is that a human being, who may or may not have been conscripted into service of an enemy of our nation, now is a vulnerable human being who needs and wants proper medical care.
I find that when I frame the anti-science COVID patient as an enemy combatant in this fashion, it helps me to take better care of that patient, because I mentally channel the ethics, empathy, and professionalism of the military doctors who have been providing care to enemy combatants for centuries. If those military doctors could and can do it, then so can I.
The COVID-19 pandemic has caused many burdens for all of us in health care, not the least of which is anger.”
>> OPINION
COMMON SENSE SEPTEMBER/OCTOBER 202236
That’s my coping mechanism. The voluntarily un-vaccinated, mask-avoid ing, anti-science patient who is now trusting me to provide my best care, to the best of my ability, can know that although I hate their choices and what those choices have done to my nation that I love, I know that I am still treating a scared individual who has chosen to follow some very bad advice perpetrated by the “Pied Piper of the Pandemic.”
Some would ask why I make a special distinction for COVID patients who are so militantly anti-science. They would say that these patients who won’t take anti-COVID measures are no different than others whom





we treat, because they also became ill consequent to their choices. We treat many patients who are ill due at least in part to their personal choices, among these being smokers, alcohol and drug abusers, and patients with the disease of obesity.









However, smokers, the intoxicated, and patients with obesity don’t generally or directly threaten our health. In contrast, people who have acquired COVID and enter our emergency departments coughing a transmissible dose of virus actually have directly threatened our health—es pecially early-on. More than 3000 American health care workers have died of COVID-19 disease.
So, yes, I have a special level of anger at the unvaccinat ed, non-mask-wearing COVID patients whom I am obligat ed to treat, but I can manage the anger by acknowledging it and then proceeding to implement my professionalism, just as military physicians across the centuries have also done when forced to provide care for enemy combatants. When I view these persons, these patients, as an enemy combatant whom I am treating in this COVID war, then it becomes easy to put my emotions on a shelf and then proceed to provide the best possible care that I can deliver.



I hope that my ideas are helpful to others, who know they are angry, but who may be having trouble developing a paradigm to help them put their anger in a box such that they can focus upon the tasks at hand.


What matters is that a human being, who may or may not have been conscripted into service of an enemy of our nation, now is a vulnerable human being who needs and wants proper medical care.”
OPINION
Join or Renew Today! aaemrsa.org/membership COMMON SENSE SEPTEMBER/OCTOBER 2022 37
COMMON SENSE SEPTEMBER/OCTOBER 202238
A Physician by Any Other Name Would Not Smell as Sweet
Leah Colucci, MD MS
The first time I introduced myself to a patient as “Dr. Colucci,” I almost choked on the words. It was so much easier for me to say, “Hi, I am Leah. What can I do for you today?” Calling myself a doctor was one of the toughest transitions I made from being a medical student to becoming an MD. At first it felt like I did not deserve the title. I endured years of hard work and training and yet still I understand the overwhelming amount of knowledge and skill I have yet to obtain. It was also a struggle in social circles. I would tell people I meet, when asked what I do, “I work in the hospital.” Rarely would I convey that I am a resi dent physician. As a female, the majority of the time, it is assumed I am a nurse. One time, I even clarified that I am a physician and was met with the response “oh, like a physician assistant.”
None of this truly bothered me until one day a patient asked me, after hours of time spent together, “When will I see a doctor? I am scared and want to talk to a doctor.” She was concerned and simply a proper intro duction would have provided reassurance. What hit me at that moment was the possibility that I had seen numerous patients who felt as if they never even saw a physician. This was occurring primarily because I was introduced to the patient as the “provider.” It was always the finishing line of the nurse assessment, “the provider will be in to see you soon.”
I could not believe that I, as a patient advocate, who encourages every one I meet to clarify the role of their “provider,” was allowing the use of this meaningless word to further confuse patients as a term to describe myself.
There have been numerous articles written on the harm of using the word “provider” when referring to a physician. Some point out that replacing the respected title with a murky one is an effort to lower the power and nobility of our profession—we do not refer to lawyers as legal provid ers. Some reference that being devalued to a “provider” implies that health care is just a commodity. Our patients deserve better than their health being equated to retail. Overall, it is a term that is originating from insurance sec tors. If we deceive patients enough to make all “providers” interchangeable, then it becomes easy for insurance companies to force patients into feeling like they can and should be seen by any provider, especially those that
come at a lesser cost to the insurer. The only winning in this scenario is the pocketbooks of the corporations that have successfully convinced the nation of a physician shortage, despite the number of unmatched physi cians each year growing.

What I have not seen enough of, is the added harm caused to residents who are already struggling with imposter syndrome. Some studies have cited up to 82% of medical students and residents experience imposter syndrome and this has been demonstrated to be one of the contributing factors for burnout. It is already difficult for us to announce to the room that we are in fact a physician. It is even harder to overcome the word “provider” when we have been introduced as such. It is the responsibility of all of us to introduce each other by our role. As a resident, I will intro duce my co-residents as doctor.
If you are an attending reading this, please advocate for your residents and address them as a physician in patient care settings. So often I have heard senior physicians discuss how they can help residents with im poster syndrome—this is a simple way to become a part of the solution. Our patients deserve to have access to physicians, and they should know when they are being seen by one. A great first step in addressing health care literacy is to teach patients the role of who is treating them. Patients who understand who is on their team—including RNs and techs—will have a better trust in our system and value the care they are receiving. Language is an important tool and I am committed to using it to serve my patients.
If we deceive patients enough to make all ‘providers’ interchangeable, then it becomes easy for insurance companies to force patients into feeling like they can and should be seen by any provider, especially those that come at a lesser cost to the insurer.”
AAEM/RSA PRESIDENT’S MESSAGE
COMMON SENSE SEPTEMBER/OCTOBER 2022 39
What’s in a Name?

What comes to mind when you hear, think, or read the word “abortion”?
For many, and this may have changed given the recent Supreme Court ruling, it provokes feelings of anger, distrust, sadness, and fear. Does it bring to mind recent images of people mourning and celebrating on the steps of the court? Maybe it causes reflection for people capable of becoming pregnant and those that support us, to a time when you were pregnant, considered becoming pregnant, or faced the end of a pregnancy.
But what about as physicians? How does the meaning change? How many different forms of abortion does the American College of Obstetrics and Gynecology (ACOG) define? Spontaneous. Induced. Medical. Procedural. Threatened. Therapeutic. Complete. Inevitable.

Dating back to my time as an emergency medical technician, I remember thinking how strange that the medical vernacular for what the public calls a “miscarriage” is termed an “abortion.” I experienced how difficult it was to explain to patients that the connotation of the word they knew was distinct from the medical denotation, as I described their loss of desired pregnancy with the word “abortion.” Later in medical school, I studied the language of obstetrics as I rotated through labor and delivery and women’s health clinics. I overcame my own discomfort with the word in honor of medical tradition and adaptation of new meaning. More than that, I recognized the importance of standardization. A common, agreed upon language that allowed us to communicate clearly about a condition. I stopped asking myself, nor seeking to understand, the cost of using a word that has only become increasingly emotionally and politically charged.
Last week, I was thinking about a patient who came through the emer gency department with a chief complaint of vaginal bleeding. She was pregnant, but unfortunately (as she was a person who desired pregnancy), her ultrasound showed no embryonic cardiac activity and her cervical os was open. What she was experiencing was a spontaneous abortion, an event I am certain nearly everyone who is a frequent reader of this publication has diagnosed and treated. To call her miscarriage an abor tion, while medically accurate, may carry a psychological burden for the patient, but what of other implications? In the age of open medical re cords and a time when few seek to understand the nuance of what abor tion can mean inside our specialty, I would argue that the repercussions of documentation without context and clarification could be unpredictable and lasting. For example, if this patient were to be discharged home with misoprostol, how do we document to ensure there is clarity that this med ication is being prescribed as the necessary treatment to a spontaneous abortion, and not for induction to end a viable pregnancy?
Currently, 21 states have legalized or protected the right to induced
abortion, leaving 29 states in which residents seeking abortion face com plete bans, gestational bans, or uncertain future surrounding the legality of once constitutional right.1 As providers in the emergency department who will continue to see patients who have had an abortion, how should we document to protect patient privacy and reduce stigma while main taining accuracy and acknowledging risks of the different types of abor tion? Furthermore, as we begin to see the consequences of the near total reductions in access, how do we counsel and treat patients who are seeking or have experienced an abortion that occurred outside the health care setting?
These are far-reaching questions that cannot be fully examined and answered in this article. However, the criticality of initiating these conver sations and writing appropriate guidelines for documentation must not be downplayed as these patients will continue to present to emergency departments nationwide in increasing numbers. To assist with these conversations, ACOG has guidelines referencing how to discuss abortion with patients and common frequently asked questions.2 Relevant to this discussion, they also have recommendations on the preferred language surrounding different types of abortion care which was used as a guide in the word selection for this article.3 Finally, for patients who have addi tional questions beyond our scope, ACOG recommends several resourc es including an abortion finder, links to the National Abortion Federation and Guttmacher Institute, which assists with referrals to providers and
Alessandra Della Porta, MD and Mel Ebeling, BS
“As we learn to navigate new considerations for this patient population and fine-tune our interviewing techniques and documentation standards, we must ensure that empathy is always communicated in our words and actions.”
AAEM/RSA EDITOR’S MESSAGE
>> COMMON SENSE SEPTEMBER/OCTOBER 202240
publishes an overview of state abortion laws, and the National Network of Abortion Funds, which maintains a directory of organizations that can help pay for abortion care.4

As part of the development of best practices, it is also imperative to begin reviewing relevant literature and free open-access medical educa tion resources as they emerge on pertinent history of present illness and treatment options when evaluating patients for complications of abortion. These complications include but are not limited to hemorrhage, retained products of conception, infection, amniotic fluid embolisms, uterine perforation, and vaginal lacerations.5,6 Complications vary greatly if the abortion is performed in the traditional setting or is considered “unsafe,” defined by the World Health Organization as a “procedure for terminating an unintended pregnancy either by individuals without the necessary skills or in an environment that does not conform to minimum medical standards, or both.”7 While the complication rate varies based on com plications type (i.e. rates of bleeding are more common than infection), it is estimated that in developed nations 30 people die for every 100,000 unsafe abortions that are performed.8
As we learn to navigate new considerations for this patient population and fine-tune our interviewing techniques and documentation standards, we must ensure that empathy is always communicated in our words and actions. Finally, it is important to discuss these cases, while protecting patient privacy, with our colleagues, mentors, residents, and attendings, as, similar to gun violence, the preventable morbidity and mortality can be challenging for our personal wellbeing.
Abortion is more than just a name for a medical procedure—its legality has real, lasting impacts on our patients’ health and wellness, as well as our own. It is our responsibility to address these impacts and prepare for our patients’ needs as they present to our departments.
References
1. Kitchener C, Schaul K, Kirkpatrick N, Santamarina D, Tierney L. Abortion is now banned in these states. See where laws have changed. The Washington Post. https://www.washingtonpost.com/politics/2022/06/24/ abortion-state-laws-criminalization-roe/. Published June 24, 2022. Accessed August 4, 2022.
2. How to talk about abortion. American College of Obstetrics and Gynecology . https://www.acog.org/advocacy/abortion-is-essential/comeprepared. Published 2022. Accessed August 4, 2022.
3. ACOG Guide to language and Abortion. American College of Obstetrics and Gynecology. https://www.acog.org/contact/media-center/abortionlanguage-guide. Accessed August 4, 2022.
4. Abortion care. American College of Obstetrics and Gynecology. https:// www.acog.org/womens-health/faqs/induced-abortion#:~:text=Dilation%20 and%20Curettage%20(D%26C)%3A,after%2012%20weeks%20of%20 pregnancy. Published July 2022. Accessed August 4, 2022.

5. Orlowski MH, Soares WE, Kerrigan KA, Zerden ML. Management of Postabortion Complications for the Emergency Medicine Clinician. Ann Emerg Med. 2021;77(2):221-232. doi:10.1016/j. annemergmed.2020.09.008
6. Swaminathan A, Long B. Post Abortion Complications. Emergency Medicine: Reviews and Perspectives. July 2022. https://www.emrap.org/ episode/emrap2022july1/postabortion. Accessed August 4, 2022.

7. Abortion. World Health Organization. https://www.who.int/news-room/factsheets/detail/abortion. Published November 25, 2021. Accessed August 4, 2022.
8. Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2(6):e323-e333. doi:10.1016/S2214-109X(14)70227-X
AAEM/RSA EDITOR’S MESSAGE
Use MyAAEM to collaborate with peers & stay up to date with the latest events and announcements. Login to MyAAEMLogin to MyAAEM Visit: aaem.org/membership/myaaem COMMON SENSE SEPTEMBER/OCTOBER 2022 41
Weapons Screening in the ED: Take the Survey!
Gregory Jasani, MD and Gary Gaddis, MD PhD MAAEM FAAEM FIFEM
hree recent examples of violence against physicians, other health care providers, and family members of patients have underscored the hazards we can risk when we report to work. All three incidents involved the use of a weapon that could have been detected by any metal detection device, before that weapon was turned on the victims.
Many of us were shocked when two physicians, a receptionist, and the husband of a patient were killed, gunned down by an angry patient in Tulsa, Oklahoma on June 1, 2022.1 That tragedy was followed during the same week by a physician and two nurses being stabbed by a patient in an ED in metropolitan Los Angeles, California.2 On July 11, 2022, a para medic and a nurse were stabbed by a patient at SSM DePaul Hospital in St. Louis, Missouri. The paramedic required admission for a tube thoracostomy due to a hemopneumothorax and the nurse suffered stab wounds to the neck.3 Clearly, each assailant had lethal intent.

Violence, both verbally threatened and physically inflicted, is not new to our specialty. Medicine, in general, experiences rates of workplace violence that far surpass just about every other private industry. For us in the ED, our work environment is particularly prone to violence.4 As one of the few places in the hospital that is open to the general public at all times and with a mandate to treat anyone who walks through our doors, we are often the ones who fall victim to violence. Not surprisingly, workplace violence can have detrimental impacts on physician emotional wellbeing, burnout, and even patient care.
Yet, what is being done to curb this violence and are countermeasures being taken? The three recent incidents in Oklahoma, California, and Missouri highlight the vulnerability of health care institutions to individuals with weapons.
We assert that understanding and quantifying current systems of weapons interdiction can lead to the development of “best practices” for weapons screening at EDs as an essential step toward helping keep us safe at work.
TBefore such “best practic es” can be developed, it is first necessary to learn the current state of weapons screening practices in the EDs of our nation. Toward that end, we have developed a short survey seeking to characterize and better un derstand weapons screening and interdiction in our nation, via learning of the practices in your ED.
You can access the survey by scanning the QR code below or by visiting surveymonkey.com/r/8TCBDVL.
Of course, participation is voluntary but we hope you will share your information and experiences with us in this IRB-approved survey. We find it incomprehensible that resistance exists in some quarters against insti tuting weapon screening and interdiction prac tices similar to those adopted at airports more than two decades ago, without widespread objections, to help ensure traveler safety. We thank you for your consideration.
Please visit surveymonkey.com/r/8TCBDVL to take the survey.
References
1. Hanna J, Watts A. Gunman who killed 4 at Oklahoma medical building had been a patient of a victim, police chief says. CNN; June 2, 2022. https://www.cnn.com/2022/06/02/us/tulsa-hospital-shooting-thursday/ index.html Accessed July 29, 2022.
2. Helsel P, Blankstein A. Suspect in custody after stabbing doctor, 2 nurses at Los Angeles hospital, police say. NBC News; June 3, 2022. https://www. msn.com/en-us/news/us/medical-staff-stabbed-at-hospital-in-los-angeles/ ar-AAY3KYO Accessed July 29, 2022.
3. NBC 5 On Your Side. 100% Preventable. Paramedic furious she was attacked at St. Louis Hospital. July 28, 2022. https://www.ksdk.com/article/ news/investigations/prevent-violence-against-health-care-workers/63ab55dc8a-0cf5-4549-b6cb-81e049950580 Accessed July 29, 2022.
4. NBC 5 On Your Side. Underreported, pervasive and getting worse: Health care workers attacked by patients. July 21, 2022. https://www.ksdk.com/ video/news/investigations/under-reported-pervasive-and-getting-worsehealth-care-workers-attacked-by-patients/63-21a46ec9-e56a-4f18-beba393aeeba4970 Accessed July 29, 2022
Violence, both verbally threatened and physically inflicted, is not new to our specialty.” COMMON SENSE SEPTEMBER/OCTOBER 202242
The Long Game!!!!
Raviraj J. Patel, MD FAAEM
Iwas recently reading AAEM’s magazine highlighting the effort and resources being put behind the lawsuit in California aiming to reestablish the laws prohibiting CPOM and I couldn’t think that maybe we are being short sighted.
The best analogy I could think of is how the GOP/Republican party has played the long game to gain power over this country despite not having won the popular vote more than once in a presidential election in over 30 years. Brett Kavanaugh and Amy Coney Barrett were on GWB Jr’s legal team in 2000, 20 years later both now on the Supreme Court. This is how the GOP, the money backing them, and their strategists operate, they are looking at a 25, 50, even 100 year timeline. Karl Rove pushed the grassroots strategy of funding local circuit court judges and ultimately 20 years later the GOP firmly controls SCOTUS and the judiciary system of the U.S. Meanwhile the Democrats keep going after the crown of the presidency not realizing they are losing everywhere else.
Along these lines, it feels like AAEM is going after the crown with this lawsuit. I propose a concurrent but different strategy, one that is steeped in time that is looking at a 25 to 50 year horizon. If we want to take down the corporate practice of medicine, we have to dismantle the corporate medicine behemoth ACEP helped create and that takes time, inge nuity, and persistence. Only then can we have a health care system that is truly equitable, accessible, and affordable.
I propose we start by reaching out to medical students. They are the most impressionable and idealistic, they are our grassroots. We need to capture the hearts and minds of the youth so when they are attendings with resources they will join the fight.
Second, we need to ally with like-minded spe cialty societies that are fighting the same battle. Anesthesia, radiology, hospitalist medicine, and critical care to name a few to collectively join forces.

Third we should identify states where CMG’s and PE backed health care have the least infiltration and fund efforts in those states to en force CPOM laws, back the democratic groups, and ultimately drive them out. This will create our stronghold states by which to launch the next offensive. It will also create a grassroots group of physicians by which to support the next endeavor.
These three ideas are just a starting point and I’m sure the AAEM Board of Directors can devise a much more thorough strategy to take back EM and therefore paving the way to take back all of medicine from the corporate profi teers that have hijacked it.
We have to play the long game!!!
If we want to take down the corporate practice of medicine, we have to dismantle the corporate medicine behemoth ACEP helped create and that takes time, ingenuity, and persistence.”
OPINION COMMON SENSE SEPTEMBER/OCTOBER 2022 43
Ultrasound Guided Peripheral Intravenous Access Correlation with Emergency Department Holds
Morgan Ritz, MD

Abstract
Establishing peripheral intravenous (PIV) access is an essential and rate limiting step in providing patient care in at least one-fourth of Emergency Department (ED) patients and almost all admitted patients.1 Placing a PIV can be particularly challenging in the ED where patients frequently present with hypovolemia, sepsis, combativeness, scarred limbs, or other limiting conditions.3 As patient numbers increase intrahospital, ED patient holds increase as well.4,5 In addition, emergency physicians at sites with out a PIV team perceive that they get requests to place more ultrasound guided peripheral intravenous catheters (USGPIVs) when there are more ED holds. Data was collected at our main teaching hospital, Crozer Chester Medical Center, over a three month period between total number of ED patients, total number of ED patient holds, and total USGPIVs placed. A positive correlation was found to show that as ED patient holds increase, USGPIVs also increase. Further data would need to be gath ered to determine if specially designated PIV teams, nurses, or techs completing this task leads to more physician time being spent managing other aspects of patient care.
Introduction
Establishing peripheral intravenous (PIV) access is an essential and rate limiting step in providing patient care in at least one-fourth of Emergency Department (ED) patients and almost all admitted patients.1 PIV access is essential not only for critical patient medication administration but also in non-critical patients for laboratory testing and med administration. Placing a PIV can be particularly challenging in the ED where patients frequently present with hypovolemia, sepsis, combativeness, scarred limbs or other limiting conditions.3 Patients with difficult IV access can be subjected to painful and repeated access attempts, delays in care, and increased risk of complications such hematomas, bleeding, infection, and thrombosis.2 If peripheral access is especially difficult or cannot be obtained, a patient may receive a central venous catheter or midline cath eter. A midline catheter for access is becoming more popular in admitted patients with difficult IV access, however this line may be placed by nonemergency medicine clinicians, such as Interventional Radiology (IR), during day time hours depending on hospital specific protocols. This may not always be helpful for the ED care teams which run with a constant influx and efflux of patients with frequent care needs.
As patient numbers increase intrahospital, ED patient holds increase as well.4,5 ED patient holds are patients who are placed in the hospital under observation or admission status but are waiting in the ER until an inpatient bed is available. Holding a patient in the ED consumes provider and nursing time and efforts. Holds can lead to decreased time to pain management, increased adverse outcomes, increased wait times as well
as patients who leave without full evaluation.6 In addition, emergency physicians at sites without a PIV team have the impression that they get requests to place more USGPIVs when there are more ED holds. The procedure may take only 10-15 minutes in set up, material gathering, and procedure completion, however this time builds up a burden on ER physicians who are trying to see new patients, admit or discharge current ones, and even triaging or screening the waiting room as patients waiting to be seen increase as the ED patient hold number increases.9
Methods
The primary objective of this study was to determine the number of USGPIV performed compared with the number of ED holds in discreet 24-hour periods. This study did not have a control or comparison group. The secondary objectives were to determine the number of patients requiring central venous access or midline after USGPIV placement by the ED and the maximum number of USGPIVs placed in the same patient. The study is a prospective chart review comparing the number of USGPIV placed by physicians and the number of ED patient holds. Data was obtained from patient charts from August 2021 to October 2021 at Crozer Chester Medical Center Emergency Department (ED). An ED “hold” was defined as a patient who is placed in observation or admitted to the hospital for over four hours, a crisis patient being held in the ER over four hours, or a transfer patient who is being held in the ER for over four hours. Inclusion criteria included any patient seen in the ED. Exclusion criteria included patients in the waiting room or ED patients that have been discharged.
In a 24-hour period the number of total ER patients (excluding waiting room patients), number of ER hold patients, and USGPIVs was collected twice, about twelve hours apart. The numbers were averaged for each 24-hour period and plotted on a scatter plot with the X-axis representing the number of holds in the department and the Y-axis representing the number of USGPIVs recorded.
Results
Data was collected over a three month period at our main hospital lo cation of Crozer Chester Medical Center as this is our largest teaching hospital with 24-hour resident ED coverage. However, certain days were excluded during data collection, including resident physician conference days and journal club days, when the residents are not in the depart ment. These USGPIVs needed to be logged in the chart to be consid ered part of the data set. Data was concluded over three months with a total of 66 days of data at the end of the collection. Figure 1 illustrates the general trend showing USGPIVs compared to total ED patients and ED patient holds over the three months. The correlation coefficient was
EMERGENCY ULTRASOUND SECTION
>> COMMON SENSE SEPTEMBER/OCTOBER 202244
Figure 1: Scatter plot data showing total number of roomed ED patients, total ED patient holds, and recorded USPIVs per day over a three month period
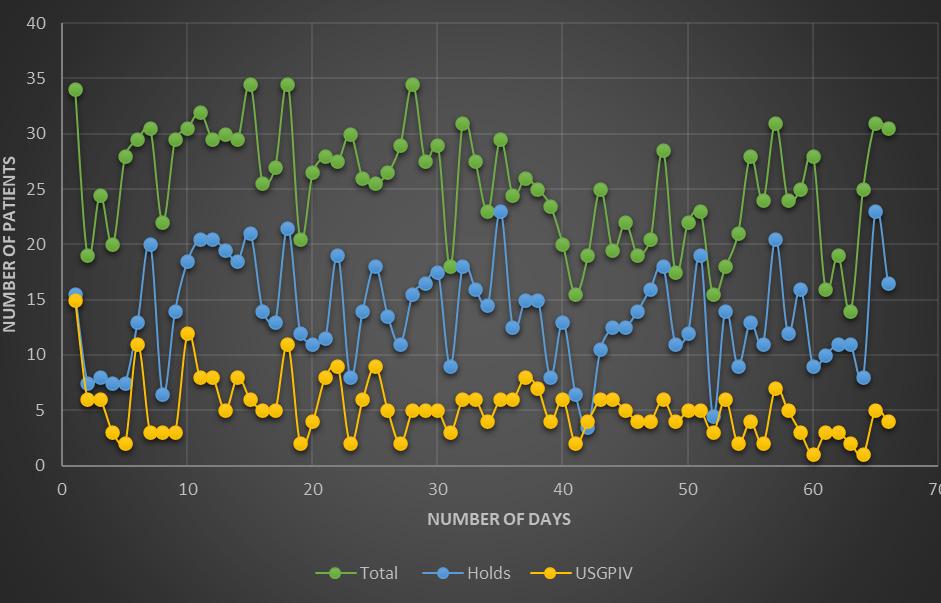
calculated between total number of ED patient holds and total number of USGPIVs placed. A pearson correlation coefficient (r) was calculated at 0.5179 showing that as the number of ED patient holds increase there is a positive correlation with increasing USGPIVs (Figure 2). Data collection was stopped after three months as the hospital system was transitioning between electronic medical records which would have significantly inter fered with data entry and collection. The maximum number of USGPIVs placed in a single patient was three. Four patients over three months requiring USGPIV placement went on to have a central line or midline placed as well.

Discussion
Establishing PIV access is a critical step in patient care in the medical field. This step becomes more challenging in ED patients with significant comorbidities, access limitations, significant dehydration, altered men tation, etc. Staffing limitations and the COVID-19 pandemic has not only increased ED wait times but also ED patient holds due to the lack of inpatient hospital beds. Emergency physicians at sites without a PIV team anecdotally felt that they received more requests to place more USGPIVs when there are more ED holds. Data collected over a three month period showed that there is a positive correlation between the number of USGPIVs placed and the number of ED holds. Many confounders can contribute to this correlation including decreased nurse to patient ratio, influx of newly graduated nurses, staffing shortages, patient isolation requirements, higher acuity, and increased frequency of lab draws. The increased responsibilities and tasks of ED nurses as the number of ED holds increase can cause nurses to defer to USGPIVs quicker in those with difficult IV access or if the patient subjectively says they have been a “hard stick” in the past. Increasing USGPIV requests can increase patient wait times as labs and medications can be delayed pending intravenous access. Other systems can try and compensate for this by employing designated IV teams skilled in placing difficult patient lines or ultrasound educated tech and nursing staff who are skilled at placing USGPIVs in a difficult patient population. Further studies would need to evaluate an ED system prior to and after employment of a PIV team which operates through the ED to limit cofounders and compare patient hold numbers, patient LOS, and USGPIV requests.
Figure 2: Scatter plot representing correlation between number of patient holds versus number of USPIVs recorded over a three month period
References
1. Liu YT, Alsaawi A, Bjornsson HM. Ultrasound-guided peripheral venous access. European Journal of Emergency Medicine. 2013:1. doi:10.1097/ mej.0b013e328363bebc
2. Fields JM, Piela NE, Au AK, Ku BS. Risk factors associated with difficult venous access in adult Ed patients. The American Journal of Emergency Medicine. 2014;32(10):1179-1182. doi:10.1016/j.ajem.2014.07.008
3. Walsh G. Difficult peripheral venous access: Recognizing and managing the patient at risk. Journal of the Association for Vascular Access 2008;13(4):198-203. doi:10.2309/java.13-4-7
4. Morley C, Unwin M, Peterson GM, Stankovich J, Kinsman L. Emergency department crowding: A systematic review of causes, consequences and solutions. PLOS ONE. 2018;13(8). doi:10.1371/journal.pone.0203316
5. Definition of boarded patient. ACEP //. https://www.acep.org/patient-care/ policy-statements/definition-of-boarded-patient/. Accessed October 15, 2021.
6. Public health impact of ed crowding and boarding of inpatients. https:// www.acep.org/globalassets/uploads/uploaded-files/acep/clinical-andpractice-management/policy-statements/information-papers/public-healthimpact-of-ed-crowding-and-boarding-of-inpatients.pdf. Accessed October 15, 2021.
7. Au AK, Rotte MJ, Grzybowski RJ, Ku BS, Fields JM. Decrease in central venous catheter placement due to use of ultrasound guidance for peripheral intravenous catheters. The American Journal of Emergency Medicine. 2012;30(9):1950-1954. doi:10.1016/j.ajem.2012.04.016
8. Dargin JM, Rebholz CM, Lowenstein RA, Mitchell PM, Feldman JA. Ultrasonography-guided peripheral intravenous catheter survival in ED patients with difficult access. The American Journal of Emergency Medicine. 2010;28(1):1-7. doi:10.1016/j.ajem.2008.09.001
9. Witting MD. IV access difficulty: Incidence and delays in an urban emergency department. The Journal of Emergency Medicine 2012;42(4):483-487. doi:10.1016/j.jemermed.2011.07.030
10. Stein J, George B, River G, Hebig A, McDermott D. Ultrasonographically guided peripheral intravenous cannulation in emergency department patients with difficult intravenous access: A randomized trial. Annals of Emergency Medicine. 2009;54(1):33-40. doi:10.1016/j. annemergmed.2008.07.048
11. Moore CL. Ultrasound first, second, and last for Vascular Access. Journal of Ultrasound in Medicine. 2014;33(7):1135-1142. doi:10.7863/ ultra.33.7.1135
EMERGENCY ULTRASOUND SECTION Continued on page 49 >> COMMON SENSE SEPTEMBER/OCTOBER 2022 45
In Praise of the Ultrasound-Guided Peripheral Intravenous Catheter
David Gordon, MD FAAEM,* Alexander Bracey, MD FACEP, † and Neil Dasgupta, MD FAAEM ‡
Excellence at any kind of ultrasound guided vascular access begins with the humble peripheral intravenous catheter (IV). While it can be a hassle, time consuming, and certainly not as exciting or catechol amine-secretion-inducing as a central line, placing peripheral lines will make you a master of ultrasound guided procedures.
Mastery of the ultrasound guided vascular access technique is an essen tial skill for the emergency physician. Ultrasound guided venous cannu lation are more successful, and just as safe. Ultrasound guided central venous access for the internal jugular, subclavian, axillary, and femoral veins is recommended by the European Society of Anesthesiology, and offers several benefits over the landmark or palpation based approach.1,2 Further, ultrasound use for radial arterial lines can result in faster inser tion, in less attempts compared to palpation technique. This remains true for the ultrasound guided peripheral IV (USIV).3 A 2018 meta-anal ysis of 1660 patients from eight studies found that USIVs were more successful (81% vs. 70%), required less attempts, and did not increase complications when compared to the palpation technique. These results suggest the use of US improves successful cannulation in those with difficult IV access. Perhaps most importantly, USIVs lead to better patient satisfaction.4
USIV has all the components to serve as the foundational technique for any ultrasound guided vascular access procedure in that it is common, low risk, and is arguably a more difficult technique than the cannulation of larger vessels that utilize modified Seldinger technique. Every step in the process reinforces key fundamentals: gathering supplies, setting up the room and optimizing positioning, talking your patient through the fear and apprehension, how much pressure you place on the skin, and follow ing your needle tip to a small target. Once you develop the technique for placement of the USIV it translates to any ultrasound guided procedure.
Beyond simply serving as a training tool for the venous cannulation during higher risk procedures, peripheral IVs can and should be used for critical interventions in the early resuscitation phase. Peripheral vasopressors have a very low risk of complications, especially in the setting of a safety protocol.5 Most extravasation can be managed conservatively, and vasopressors can often be restarted at another peripheral site.6 Peripheral IV’s can also be used to rapidly transfuse blood, with short, large-bore peripheral IVs providing flow rates far faster than a triple lumen, and approaching a centrally placed introducer sheath.7 Hypertonic saline (3%) can also be safely administered through
a peripheral IV.8 This is all accomplished without the complications of central lines. However, none of these interventions are possible without dedicated, frequent practice.
USIV’s are a fast, safe, and effective way to obtain IV access in all pa tients, and can be used for critical interventions that prevent morbidity and mortality. The technical skills are transferable to every other IV access and ultrasound guided procedure-excellence with placing an USIV can lead to excellence at central venous lines and arterial lines. Their safety and tolerability allow safe skill acquisition for other high-risk procedures. This skill translates to the Emergency Physician’s expanding vascular access toolbox to include newer techniques, such as midlines, REBOA, and ECMO. The road to mastery of vascular cannulation is paved with ultrasound guided peripheral IVs.
References
* Assistant Professor, Department of Emergency Medicine, University of Florida-Jacksonville
† Assistant Professor, Program Director, Resuscitation and Emergency Critical Care and Assistant Program Director, Emergency Medicine, Albany Medical Center Hospital


‡ Assistant Clinical Professor, Director of Emergency Critical Care, Nassau University Medical Center
1. Lamperti M, Biasucci DG, Disma N, Pittiruti M, Breschan C, Vailati D, Subert M, Traškaitė V, Macas A, Estebe JP, Fuzier R, Boselli E, Hopkins P. European Society of Anaesthesiology guidelines on perioperative use of ultrasound-guided for vascular access (PERSEUS vascular access). Eur J Anaesthesiol. 2020 May;37(5):344-376. doi: 10.1097/EJA.0000000000001180. Erratum in: Eur J Anaesthesiol. 2020 Jul;37(7):623. PMID: 32265391.
2. Saugel B, Scheeren TWL, Teboul JL. Ultrasound-guided central venous catheter placement: a structured review and recommendations for clinical practice. Crit Care. 2017 Aug 28;21(1):225. doi: 10.1186/s13054-0171814-y. PMID: 28844205; PMCID: PMC5572160.
3. Shiver S, Blaivas M, Lyon M. A prospective comparison of ultrasoundguided and blindly placed radial arterial catheters. Acad Emerg Med. 2006 Dec;13(12):1275-9. doi: 10.1197/j.aem.2006.07.015. Epub 2006 Nov 1. PMID: 17079789.
CRITICAL CARE MEDICINE SECTION
Continued on page 52 >> COMMON SENSE SEPTEMBER/OCTOBER 202246
Use of Point of Care Ultrasound During Distal Extremity Reduction in an Emergency Department Setting: A Pilot Study
Morgan Ritz, MD and Maxwell Cooper, MD

Objective
Hand and foot fractures are common injuries which lead to chronic pain and disability with loss of function if not diagnosed and re duced appropriately. Using a physical exam to guide reductions can lead to increased radiation exposure, pain with repeat reduction attempts, and fracture malalignments. Intra-reduction use of ultrasound can improve alignment, without increasing radiation exposure. Our pilot study wanted to evaluate the clinical efficacy of reduction of hand and foot fractures under ultrasound guidance compared to a traditional technique.
Methods
Patients with injuries of the hands and feet completed an x-ray. If the fracture was in need of reduction, including displacement or angulation, the patient would be randomly selected to undergo traditional reduction or reduction with serial ultrasonography followed by a post reduction x-ray. The primary efficacy endpoint was the number of reduction at tempts after post-reduction x-ray. Secondary endpoints were remaining displacement and angulation from anatomic position post-reduction.
Results
A total of nine patients were enrolled for hand fracture reduction, five of which were ultrasound guided. There were no foot fractures. There was no statistical significance between the remaining displacement (p-value 0.06) and angulation (p-value 0.48) between the two groups, however the goal sample size of 20 was not met. Although, ultrasound-guided reduc tions led to closer anatomic position of the fractures in both displacement and angulation.
Conclusion
Ultrasound is a promising tool for hand reductions, however further data will need to be collected before a definitive statement can be made to wards its utility when compared to traditional techniques.

Introduction
Hand and foot fractures encompass about one percent of fractures in our department. They are common injuries which can lead to chronic pain and disability with loss of function if not diagnosed and reduced appropri ately. About 10% of all fractures occur in the bones of the foot along with 18% occurring in the hand. Initial management includes ice, rest, immo bilization, and elevation. Any delay in treatment can increase a patient’s risk for non-union, avascular necrosis, vascular injuries, compartment syndrome, and post-traumatic osteoarthritis.1-3 Common reduction prac tice includes initial diagnostic x-rays with physical exam guided fracture
Abstractreduction and post reduction films. It is up to the physician’s discretion whether a repeat reduction is attempted afterwards if minor malalignment still remains. Some institutions use fluoroscopy for intra-reduction eval uation; however, this leads to additional radiation exposure for both the patient and physician along with increased cost and time until reduction completion. Additionally, fluoroscopy is not available in every emergency department (ED). Physical exam guided reduction may avoid the problem of fluoroscopic radiation however it can still lead to increased radiation exposure with repeat x-rays, pain with repeat reduction attempts after imaging, and can leave the patient with unintended malalignments. Intrareduction use of ultrasound can be used, in a similar manner to fluoros copy, to improve alignment, without increasing radiation exposure.
Materials and Methods
This was a non-blinded prospective randomized controlled trial enrolling a convenience sample of emergency department patients requiring fracture reduction of the hand or foot. This took place at our main campus emergency department as well as our community campus and free-standing suburb emergency department. Our main campus Institutional Review Board approved trial prior to patient recruitment. Randomization ensured physicians were not biased in choosing between ultrasound and standardized physical exam reduction techniques based on severity of fracture displacement or angulation on initial pre-reduction x-rays. Patients were recruited and consented concurrent with procedural consent and randomized in a one-to-one fashion using simple random ization and an open-source available randomizer (www.randomization. com) to reduction guided by serial intra-reduction ultrasounds followed by a post reduction x-ray or physical exam guided reduction with a post reduction x-ray. Once a patient was deemed eligible the ultrasound fellow would place the patient in the open-source randomizer and give the primary team the patient’s treatment arm status, ether ultrasound guided or not. Fracture reduction was performed by the primary patient care team while intra-reduction ultrasound was performed and supervised by the ultrasound team consisting of the primary investigator (Ultrasound Director) or the co-investigator (Ultrasound Fellow), both of whom are trained in ultrasonography. Investigators measured: pre and post bone displacement from anatomic normal (in millimeters), pre and post bone degree of angulation from anatomic normal, number of repeat reduction attempts after post reduction x-ray, time elapsed since initial injury, frac ture anatomical location, and a series of patient identifiers. Excluded pa tients included pregnant women, prisoners, and children under 12 years of age. Those patients 12 to 17 years old required both patient assent and parental consent.
EMERGENCY ULTRASOUND SECTION
>> COMMON SENSE SEPTEMBER/OCTOBER 2022 47
Results
The primary efficacy endpoint was the number of reduction attempts after post-reduction x-ray. Secondary endpoints included remaining dis
PATIENT
26
0
26 Ultrasound 0
48 Ultrasound 0 0.1
29 Ultrasound 0 1.7
ANATOMIC LOCATION
5th proximal phalanx 8640
Due to the limited number of patients, we were unable to hit our goal directed power of 0.8. An unpaired t-test with a 95% confidence interval gives a p-value of 0.06 between the ultrasound and traditional physical exam reduction group of post reduction displacement and p-value 0.48 between ultra sound and traditional physical exam reduction for post reduction angulation. Neither result is statistically significant; however, this insignifi cance is expected in a small pilot study.
0 1st metacarpal 1440
5th meta carpal base 15
5th metacarpal 60
26 Ultrasound 0 0.7 7.6 5th metacarpal 990
24 Physical exam 0 0.6 2 4th phalanx 15
14 Physical exam 0 0.8 21 5th meta carpal base 180
29 Physical exam 0 1.6 15 5th metacarpal 120
29 Physical exam 0 1.2 4.8 5th metacarpal 5760
SINCE
Table 1: Pilot data collected from nine patients. Remaining displacement and angulation measured from normal anatomic location and alignment post reduction using ultrasound.
placement and remaining degree of angulation from anatomic position post-reduction measured using ultrasound (Table 1). An unpaired t-test was used to compare the means between mean displacement and mean angulation post-reduction between ultrasound and standard reduction techniques (Table 2). Sample size was set with a goal of 20 patients, with 10 in each group, to achieve an adequate power of 0.8; however, this was not met secondary to convenience sampling hindered by decreased patient volume associated with the COVID-19 pandemic. The pandemic initially decreased the total number of patients that were seen in the emergency department then later filled the emergency department with boarding inpatient holds so that fewer non-critical patients, such as hand and foot pain or injuries, were seen. The study was concluded after two years before the sample size goal was met due to faculty turnover.
ULTRASOUND GUIDED PHYSICAL EXAM
Mean remaining displacement post-reduction (mm) 0.74 1.05
Mean remaining angulation post- reduction (degrees) 7.12 10.70
Table 2: Secondary endpoints of mean displacement and mean angulation between ultrasound and traditional physical exam reduction groups.
The primary efficacy endpoint was the number of reduction attempts after post-re duction x-ray. This was zero for both the ultrasound and standard reduction groups. Secondary endpoints included the remaining displacement from anatomic position post reduction and remaining degree of angulation post-reduction measured using ultrasound. An ultrasound-guided reduction technique appears to lead to a closer anatomic position of the fracture in both displacement and an gulation. All of the patients in the pilot study were hand fractures, with a majority of fifth metacarpal or boxer’s fractures. The vast majority of patients were found to be in their 20s by age. There were no harms or unintended side effects in either group.
Discussion
Ultrasound has become a versatile tool and imaging modality in emergency departments with applications spanning into prehospital management with portable options. It is a quick, inex pensive, and non-radioactive tool which is becoming more frequently utilized for fracture reductions, especially for long bone fractures, at institutions with and without fluoroscopy. Prior studies have shown “real time” fracture diagnosis and treatment with adequate visualization of the reduction.4 Other pilot studies have shown its promising use in austere environments with its portable options and accurate fracture diagnoses.5,6 Our pilot study was designed to explore the concept of it replacing traditional physical exam guided reduction techniques for hand and foot fractures in the ED, the underlying presumption being that intermittent visualization leads to higher quality fracture reduction as quantified by number of repeat x-rays needed as well as remaining displacement distance and angulation which could facilitate healing and decrease chronic pain, especially in smaller anatomical fracture locations, such as the hand. Although our study fell short of its desired patient total, leading to a non-sta tistically significant data set in only hand
EMERGENCY ULTRASOUND SECTION
GUIDED
AGE (YEARS) TYPE OF REDUCTION NUMBER OF POST REDUCTION REPEAT ATTEMPTS REMAINING DISPLACEMENT POSTREDUCTION (MM) REMAINING ANGULATION POSTREDUCTION (DEGREES)
TIME
INJURY (MIN)
Ultrasound
0.7 4
0.5
8
16
>> COMMON SENSE SEPTEMBER/OCTOBER 202248
fractures, it demonstrated clinical utility with its trends toward improved secondary endpoints.
Most authors recommend nonoperative management for up to 40°-50° of apex dorsal angulation in the fifth finger, 30° at the fourth or ring finger, 20° at the third or middle finger, and 15° at the second or index finger.7,8 It has also been reported that volar angles up to 70° have been tolerat ed with conservative management and no long-term functional deficit, yet more than 30° of dorsal angulation can lead to weakness of grip.9 Metacarpal shaft fractures can be more delicate. Mobility at the carpo metacarpal joint allows the patient to adapt appropriately to 10°-15° of apex dorsal angulation in the fourth and fifth fingers, respectively, without functional impairment.8,10 Conversely, the second and third fingers can tolerate only minimal apex dorsal angulation, and reduction should be attempted with greater than 10° of angulation.
Limitations
During preparation for the pilot study, sample size was set with a goal of 20 patients, with 10 in each group, to achieve an adequate power of 0.8; however, this was not met secondary to convenience sampling by a subset of emergency physicians (limited to the ultrasound team) hindered by decreased patient volume associated with the covid-19 pan demic. The study set out to intervene on hand and foot fractures but all of the patients in the pilot study were hand fractures, with a majority of fifth metacarpal or boxer’s fractures. The foot fractures encountered did not need reduction secondary to lack of displacement or angulation. The vast majority of patients were also found to be in their 20s by age which limits generalizability of the intervention to a more versatile age group.
Conclusions
If ultrasound reductions can minimize post reduction angulation this could decrease chronic pain and discomfort for fractures who received non-operative management and for those patients who never followed up with orthopedic or hand specialists after their ED visit.11 Further studies could complete follow-up calls to both treatment groups to investigate if patients received outpatient surgery and if they experienced any chronic pain or discomfort from their injuries several months out. It was easy to visualize fracture reductions and make reduction adjustments in real time as well as see a changed angulation and displacement pre and post reduction under ultrasound imaging, despite a fracture’s initial injury timeline. Further studies are needed to fully compare ultrasound and tra ditional physical reduction techniques, but in a hospital system with and without fluoroscopy, ultrasound may one day become its replacement.
Ethical Considerations
All human studies have been reviewed by the appropriate ethics committee, our Institutional Review Board (IRB), and have therefore been performed in accordance with the ethical standards laid down in an appropriate version of the Declaration of Helsinki. All persons gave their informed consent prior to their inclusion in the study. IRB study number CKHS 20-006.
Acknowledgements
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Additional thank you to Dr. Michael Shalaby for your inspiration and assistance.
References
1. Van Onselen EB, Karim RB, Hage JJ, Ritt MJ. Prevalence and distribution of hand fractures. J Hand Surg Br 2003; 28:491.
2. Suh N, Ek ET, Wolfe SW. Carpal fractures. J Hand Surg Am 2014; 39:785.
3. Hatch RL, Alsobrook JA, Clugston JR; Diagnosis and management of metatarsal fractures. Am Fam Physician. 2007 Sep 1576(6):817-26
4. Sabzghabaei A, Shojaee M, Arhami Dolatabadi A, Manouchehrifar M, Asadi M. Ultrasound-Guided Reduction of Distal Radius Fractures. Emerg (Tehran). 2016;4(3):132–135.
5. McManus JG, Morton MJ, Crystal CS, et al. Use of ultrasound to assess acute fracture reduction in emergency care settings. Am J Disaster Med 2008;3(4):241-247.
6. McNeil CR, McManus J, Mehta S. The accuracy of portable ultrasonography to diagnose fractures in an austere environment. Prehosp Emerg Care. 2009;13(1):50-52. doi:10.1080/10903120802474513
7. Chin SH, Vedder NB. MOC-PSSM CME article: Metacarpal fractures. Plast Reconstr Surg 2008;121(1 Suppl):1-13. doi:10.1097/01. prs.0000294704.48126.8c
8. Day CS, Stern PJ. Fractures of the Metacarpals and Phalanges. In: Wolf SW, editor. Green’s operative hand surgery. Philadelphia: Elsevier Churchill Livingstone; 2011.
9. Ali A, Hamman J, Mass DP. The biomechanical effects of angulated boxer’s fractures. J Hand Surg Am. 1999;24(4):835-844. doi:10.1053/ jhsu.1999.0835
10. McNemar TB, Howell JW, Chang E. Management of metacarpal fractures. J Hand Ther. 2003;16:143–51. doi: 10.1016/S0894-1130(03)80009-1.
11. Ford DJ, Ali MS, Steel WM. Fractures of the fifth metacarpal neck: is reduction or immobilization necessary?. J Hand Surg Br. 1989;14(2):165167. doi:10.1016/0266-7681(89)90119-8
Continued from page 46
EMERGENCY ULTRASOUND SECTION
12. Schoenfeld E, Boniface K, Shokoohi H. Ed technicians can successfully place ultrasound-guided intravenous catheters in patients with poor vascular access. The American Journal of Emergency Medicine. 2011;29(5):496-501. doi:10.1016/j.ajem.2009.11.021
13. Davis EM, Feinsmith S, Amick AE, et al. Difficult intravenous access in the emergency department: Performance and impact of ultrasound-guided IV insertion performed by nurses. Am J Emerg Med. 2021;46:539-544. doi:10.1016/j.ajem.2020.11.013
EMERGENCY ULTRASOUND SECTION
COMMON SENSE SEPTEMBER/OCTOBER 2022 49
Is There a Potential Role for Methylene Blue in Septic Shock?
Christianna Sim, MD MPH, Taylor M. Douglas, MD, Wesley Chan, MD, and Christopher Kiang, MD Editors: Kami M. Hu, MD FAAEM and Donald Doukas, MD
Clinical Question
What is the utility of methylene blue as adjuvant therapy in treating pa tients with septic shock?
Introduction
Septic shock remains the most common cause of shock and the leading cause of ICU mortality in the United States.1,2 An essential aspect of treatment is the management of hypotension, often with vasopressors, to achieve hemodynamic stability.3 While potentially life-saving, the use of catecholaminergic vasopressors, such as norepinephrine, epinephrine, and dopamine, are not without risk. These agents, especially at high doses, can lead to dysrhythmias, myocardial ischemia, hypercoagulability, immunomodulation, and gastrointestinal hypoperfusion.4 Catecholaminesparing adjuvant agents, such as vasopressin and corticosteroids, are often used in patients with high vasopressor requirements. Some have suggested that methylene blue (MB), traditionally used to treat methemo globinemia, could be an adjuvant therapy in septic shock.
The physiologic basis for this suggestion is MB’s action as an inhibitor of the nitric oxide-cyclic guanosine monophosphate (NO-cGMP) pathway. Increased levels of cGMP result in, amongst other things, increased smooth muscle relaxation and vasodilation, myocardial depression, and increased vascular permeability. Nitric oxide (NO) and soluble guanylyl cyclase (sGC), key factors in the NO-cGMP pathway, both exist in high levels in states of distributive (e.g. septic) shock, and under the influence of circulating endotoxins and inflammatory cytokines, inducible nitric oxide synthetase (iNOS) further increases NO levels and cGMP pro duction. This induction of iNOS and excessive NO synthesis have been implicated as causative agents in the vasodilation and hyporeactivity to vasopressors seen in septic patients.5,6 But while the pathophysiologic basis of the utility of MB in septic shock is promising, there have only been a few clinical studies assessing the benefit it may have in patients with septic shock.
Kwok ES, Howes D. Use of methylene blue in sepsis: a systematic review. J Intensive Care Med. 2006;21(6):359-363.
The pathophysiology and treatment of sepsis is a multifactorial process. Because NO itself has numerous roles, including those in beneficial path ways, inhibition of all NOS subtypes has previously been shown to lead to deleterious effects. This small systematic review investigates the role of MB’s specific inhibition of iNOS in the treatment of sepsis.
This systematic review pooled articles from MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trial database that met their inclusion criteria: human studies with participants at least 16 years old who were treated with MB for sepsis, septic shock, or refractory septic shock. After further vetting by two independent reviewers, 13 articles
were included, two of which were small randomized clinical trials (RCTs), and the rest observational studies. Both RCTs compared isotonic saline to MB administration, one examining patients with septic shock and the other examining patients with severe sepsis. All studies demonstrated a significant increase in systemic vascular resistance, an increase in the mean arterial pressure (MAP), and/or a decrease in pressor require ments in patients who received MB compared to those receiving saline.
This review’s article selection process included the whole spectrum of sepsis severity. Despite this, the major limitation of this review is its small number of studies with only two RCTs. Of the two RCTs, different admin istration methods of MB were used (bolus with stepwise infusions versus slower fixed infusion), further adding to the heterogeneity between the included studies. Additionally, the significance of MB’s influence on he modynamic variables on septic shock mortality needs further investiga tion. Overall, with the limited number of studies available, this systematic review does an excellent job introducing the topic of methylene blue in septic shock and sets the stage for future controlled clinical trials.
Kirov MY, Evgenov OV, Evgenov NV, et al. Infusion of methylene blue in human septic shock: a pilot, randomized, controlled study. Crit Care Med. 2001;29(10):1860-1867.
This small open-label, single-center, single-blinded randomized controlled pilot study in Russia sought to evaluate the effects of continuous infusion MB on the hemodynamics and organ function of patients presenting with septic shock.
Eligible patients fulfilled the following criteria: severe sepsis less than 72 hours, septic shock diagnosed less than 24 hours before randomization, on mechanical ventilation, and had pulmonary artery catheters in place. Twenty patients with severe sepsis and septic shock were enrolled during a two-year span. Patients who were less than 18 years of age, pregnant, or receiving corticosteroids, immunosuppressants, chemotherapy, or those with end-stage neoplasms were excluded from the study.
The patients were randomized 1:1 into groups receiving either MB infu sion or a corresponding volume of isotonic saline. The MB group had an intravenous bolus injection of MB (2 mg/kg for 15 mins) followed two hours later by an infusion at stepwise increasing rates of 0.25, 0.5, 1, and 2 mg/kg/hr that were maintained for one hour each. Patients’ hemo dynamics were monitored using a pulmonary artery catheter and a radial arterial line. Serial hemodynamics and organ function variables were assessed over 24 hours, as well as the survival rate at day 28.
There was no differences between groups in baseline character istics including demographics, amount of organ dysfunction, initial
RESIDENT JOURNAL REVIEW
>> COMMON SENSE SEPTEMBER/OCTOBER 202250
hemodynamics, and laboratory variables. The study population was 55% male with an average age of 50 years. MB was noted to reduce the requirement for norepinephrine, epinephrine, and dopamine by as much as 87%, 81%, and 40%, respectively (p <0.05). MB led to the resolution of shock in seven patients vs. three patients in the control group. There was no difference between groups in the duration of shock and need for vasopressor support.
The authors concluded that in septic shock, MB improves hemodynamic function and reduces the need for adrenergic support. They noted that additional differences may have missed because of the short observation period, noting that to avoid the risk of toxic effects, they did not adminis ter methylene blue beyond six hours and kept the total accumulated dose of MB at 5.75 mg/kg. Though limited by design and size, this study war rants further discussion to explore multiple hypotheses in further studies.
Pasin L, Umbrello M, Greco T, et al. Methylene blue as a vasopressor: a meta-analysis of randomised trials. Crit Care Resusc. 2013;15(1):42-48.
Unfortunately, many studies evaluating methylene blue in patients with shock have been underpowered, potentially underestimating its effects. To address this issue, Pasin et al. performed a meta-analysis of ran domized controlled trials evaluating the effects of MB in hypotensive adult patients, examining the primary endpoint of MAP one hour-post administration.
Of the 82 studies reviewed, only five trials were randomized to receive MB or placebo (86 vs 88 patients, respectively, for a total of 174 pa tients). Two trials examined patients with septic shock admitted to the ICU, one looked at patients receiving liver transplants, and the other two included patients undergoing cardiac surgery. In three of the five studies, MB was administered as a bolus ranging from 1.5-3 mg/kg. It was given as an infusion in the other two studies: as a 0.5 mg/kg/h infusion over six hours in one study and as 1.5 mg/kg over one hour after administra tion of a bolus in the other. All studies reported mortality (a secondary endpoint of the meta-analysis, along with cardiac index), but only four reported MAP.
Overall, the use of MB was associated with a statistically significant increase in MAP with a mean difference of 6.93 mmHg (95% CI 1.6712.18, p=0.01), with four of the five studies reporting significant decreases in vasopressor requirements after MB administration. Only two of the studies reported cardiac index, in which there was no statistically significant improvement with MB. The overall mortality was lower in the MB group, 16.1% (14/88) compared to the placebo group, 23% (20/86), but this difference was not found to be statistically significant. Across all studies, no serious adverse effects were reported.
This meta-analysis provides compelling evidence that MB does increase MAP. The authors argue that despite the lack of standardized dosing or administration, the total dose of MB received in all studies was within a
range of 1.5-3 mg/kg but given the heterogeneity across clinical settings and administration strategies, the appropriate dose warrants further study. All but one study was single-centered, potentially limiting both generalizability and external validity, and with such a small total number of patients, the results may still collectively be underpowered to show a mortality benefit.
Porizka M, Kopecky P, Dvorakova H, et al. Methylene blue administration in patients with refractory distributive shock - a retrospective study. Sci Rep. 2020;10(1):1828. doi:10.1038/ s41598-020-58828-4
This small, single-center, retrospective study completed in the Czech Republic looked at the use of methylene blue (MB) in patients with refractory distributive shock, including patients with and without septic shock. The study included patients on high-dose norepinephrine without cardiogenic shock, more specifically defined as a norepinephrine re quirement of >0.5 mcg/kg/min with a measured cardiac index >2.4 L/min/ m2. Patients were divided based on their response to MB administration: patients who saw a 10% reduction in norepinephrine within two hours of MB dose were deemed “responders,” while those with less of a response were “non-responders.” Investigators then compared data between groups at baseline and points for 12 hours after MB administration, look ing specifically at hemodynamic effect and mortality.
Twenty patients from a span of eight years were identified; all had re ceived a single bolus dose of MB. The study population was comprised primarily of surgical patients with vasoplegia after cardiopulmonary bypass, with only two of the 20 patients having septic shock. Nine patients (45%) were responders. There were no significant differences between groups in baseline demographics or illness severity scores. There was no difference between groups in MB dose, time from onset of refractory shock to intervention, or in use of adjunctive vasopressin or hydrocortisone. Non-responders did have a significantly higher baseline base deficit (12.9 vs 5.5, p=0.001) and lower pH (7.16 vs 7.26, p=0.037) than responders. After MB administration, responders had lower lactates, lower norepinephrine requirements, and lower mortality within 24 hours (0% vs. 45%, p = 0.038) and at 30 days (44% vs 100%, p=0.008) than nonresponders.
A retrospective study with a small n, it remains one of the larger evalu ating the use of MB. While all patients were in severe distributive shock, only two of the 20 were septic, resulting in an inability to draw conclu sions regarding the effectiveness of MB in septic shock. Some of the study population were also receiving inotropic therapy, which may con found the data. While all the patients received the same dosing strategy, the authors admit that there is no clear guideline for what dose of MB is appropriate for distributive shock. They hypothesize, given the more severe baseline acidosis in the nonresponders, that MB administration earlier in the course may lead to improved outcomes, preventing pro found tissue hypoxia and progression into refractory vasoplegia.
RESIDENT JOURNAL REVIEW
>> COMMON SENSE SEPTEMBER/OCTOBER 2022 51
Conclusion
The existing evidence remains woefully limited, but shows that MB is associated with increased MAP and decreased vasopressor require ments, which could help mitigate some of the adverse effects caused by catecholaminergic agents. Data shows that the iNOS activity and sGC upregulation are increased in the first eight hours, suggesting there may be an early therapeutic window in which it may be more effective;7,8 its use in the emergency department could be crucial in this subset of se verely ill patients with refractory septic shock. The lack of mortality bene fit may be attributed to the small sample sizes of current studies and the ideal dosing strategy remains unconfirmed, although some recommend a dose of 1-2 mg/kg as a single bolus, while others have suggested an infusion.9-11 Despite a generally favorable safety profile, MB use it is con traindicated in patients with pulmonary hypertension or acute lung injury due to known vasoconstrictive effects in the pulmonary vasculature, and in patients with G6PD deficiency due to risk of precipitating hemolysis. Although no clear mortality benefit has yet been shown, the potential for MB to decrease vasopressor requirements while posing a minimal risk of adverse effects makes it a viable option for patients in refractory septic shock.
Answer
It is unclear if the use of MB in septic shock has any mortality benefit, but it has been shown to improve hemodynamics and decrease vaso pressor requirements. While it should not replace the standard of care, its use could be considered for those patients with refractory shock who are not responding to standard therapy. Further study is needed to determine an optimal dosing strategy.
References
1. Angus DC, van der Poll T. Severe sepsis and septic shock [published correction appears in N Engl J Med. 2013 Nov 21;369(21):2069]. N Engl J Med. 2013;369(9):840-851. doi:10.1056/NEJMra1208623
2. Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29(7):1303-1310. doi:10.1097/00003246-200107000-00002
3. Scheeren TWL, Bakker J, De Backer D, et al. Current use of vasopressors in septic shock. Ann Intensive Care. 2019;9(1):20. doi:10.1186/s13613-019-0498-7
4. Dünser MW, Hasibeder WR. Sympathetic overstimulation during critical illness: adverse effects of adrenergic stress [published correction appears in J Intensive Care Med. 2016 Sep;31(8):NP1]. J Intensive Care Med. 2009;24(5):293-316. doi:10.1177/0885066609340519
5. Förstermann U, Sessa WC. Nitric oxide synthases: regulation and function. Eur Heart J. 2012;33(7):829-837d. doi:10.1093/eurheartj/ehr304
6. Cauwels A. Nitric oxide in shock. Kidney Int. 2007;72(5):557-565. doi:10.1038/sj.ki.5002340
7. Evora PR, Ribeiro PJ, Vicente WV, et al. Methylene blue for vasoplegic syndrome treatment in heart surgery: fifteen years of questions, answers, doubts and certainties. Rev Bras Cir Cardiovasc. 2009;24(3):279-288. doi:10.1590/s0102-76382009000400005
8. Evora PR. Methylene blue does not have to be considered only as rescue therapy for distributive shock. J Med Toxicol. 2013;9(4):426. doi:10.1007/ s13181-013-0333-8
9. Jang DH, Nelson LS, Hoffman RS. Methylene blue for distributive shock: a potential new use of an old antidote. J Med Toxicol. 2013;9(3):242-249. doi:10.1007/s13181-013-0298-7
10. van Haren FM, Pickkers P, Foudraine N, et al. The effects of methylene blue infusion on gastric tonometry and intestinal fatty acid binding protein levels in septic shock patients. J Crit Care. 2010;25(2):358.e1-358.e3587. doi:10.1016/j.jcrc.2010.02.008
11. Brown G, Frankl D, Phang T. Continuous infusion of methylene blue for septic shock. Postgrad Med J. 1996;72(852):612-614. doi:10.1136/ pgmj.72.852.612
Continued from page 45
CRITICAL CARE MEDICINE SECTION
4. van Loon FHJ, Buise MP, Claassen JJF, Dierick-van Daele ATM, Bouwman ARA. Comparison of ultrasound guidance with palpation and direct visualization for peripheral vein cannulation in adult patients: a systematic review and meta-analysis. The Br J Anaesth. 2018 Aug;121(2):358-366. doi: 10.1016/j.bja.2018.04.047. Epub 2018 Jul 2. PMID: 30032874.
5. Tran QK, Mester G, Bzhilyanskaya V, Afridi LZ, Andhavarapu S, Alam Z, Widjaja A, Andersen B, Matta A, Pourmand A. Complication of vasopressor infusion through peripheral venous catheter: A systematic review and meta-analysis. Am J Emerg Med. 2020 Nov;38(11):2434-2443. doi: 10.1016/j.ajem.2020.09.047. Epub 2020 Sep 28. PMID: 33039229.
6. Lewis T, Merchan C, Altshuler D, Papadopoulos J. Safety of the Peripheral Administration of Vasopressor Agents. Journal of Intensive Care Medicine. 2019;34(1):26-33. doi:10.1177/0885066616686035
7. Traylor S, Bastani A, Butris-Daut N, Christensen M, Marsack P, Rodgers L, Todd B. Are three ports better than one? An evaluation of flow rates using all ports of a triple lumen central venous catheter in volume resuscitation. Am J Emerg Med. 2018 May;36(5):739-740. doi: 10.1016/j. ajem.2017.09.058. Epub 2017 Oct 4. PMID: 29079377.
8. Mesghali E, Fitter S, Bahjri K, Moussavi K. Safety of Peripheral Line Administration of 3% Hypertonic Saline and Mannitol in the Emergency Department. J Emerg Med. 2019 Apr;56(4):431-436. doi: 10.1016/j. jemermed.2018.12.046. Epub 2019 Feb 8. PMID: 30745195.
RESIDENT JOURNAL REVIEW
COMMON SENSE SEPTEMBER/OCTOBER 202252
AAEM Job Bank Service
Promote Your Open Position

To place an ad in the Job Bank: Equitable positions consistent with the Mission Statement of the American Academy of Emergency Medicine and absent of restrictive covenants, will be published (upon approval). All ads run for a six month period or until canceled and will appear in the AAEM member magazine Common Sense and online. For pricing and more information visit www.aaem.org/membership/benefits/ job-bank.
Complete a Job Bank registration form, along with the Criteria for Advertising Section, and submit payment. If you are an outside recruiting agent, the Job Bank Criteria for Advertising must be downloaded and completed by a repre sentative from the recruiting hospital/group.
Direct all inquiries to: www.aaem.org/membership/benefits/job-bank or email info@aaem.org.
Positions Available
For further information on a particular listing, please use the contact information listed.
Section I: Positions in full compliance with AAEM’s job bank advertising criteria, meaning the practice is wholly-owned by its physicians, with no lay shareholders; the practice is equitable and democratic; due process is guaranteed after a pro bationary period of no more than one year; there are no post-employment restrictive covenants; and board certified emergency physicians are treated equally, whether they achieved ABEM/AOBEM/RCPSC certification via resi dency training or the practice track.
Section II: Positions that cannot be in full compliance with AAEM’s job bank criteria, because they are employee positions with hospitals or medical schools and the practice is not owned by its emergency physicians. Thus there may not be financial transparency or political equity.
Section III: Positions that cannot be in full compliance with AAEM’s job bank criteria, because they are government or military employee positions. The practice is not owned by its emergency physicians, and there may not be financial transparency or political equity.
Section IV: Position listings that are independent contractor positions rather than owner-partner or employee positions.
ARIZONA
Residency Program Director, Emergency Medicine Chandler, Arizona Dignity Health Medical Group – Arizona (DHMG-AZ) seeks an experienced leader and visionary to serve as the Founding Program Director, Emergency Medicine in East Valley Phoenix at Chandler Regional Medical Center and Mercy Gilbert Medical Center. This is an exciting opportunity to help establish, build, and lead a new residency program from the ground up. The ideal candidate will have strong experience in administrative, educational, and clinical services, BC in Emergency Medicine, an unrestricted Arizona medical license, and 3+ years of educational experience. Send CV to providers@dignityhealth. org or call (888) 599-7787. dignityphysiciancareers.org (PA 1917)
Email: providers@dignityhealth.org
Website: https://dignityphysiciancareers.org/ SepOct, NovDec, JanFeb
CALIFORNIA
EMERGENCY MEDICINE PHYSICIAN - San Francisco Bay Area; Contra Costa Regional Medical Center in Martinez, CA, is currently looking for a CA-licensed, BC/BE Emergency Medicine Physician for a full-time, benefited position or a 1099 contract position. The schedule is a mix of days and nights (always double coverage). Our Safety-Net hospital offers a 23-bed ER (17 monitored and 6 non-monitored) that sees over 35,000 patients per year. This an exceptional opportunity to join a supportive, close-knit, mission driven group to serve the community by providing quality care in our safety-net system. We offer flexibility in scheduling, a competitive compensation package and a collaborative environment of care. We are conveniently located in the East San Francisco Bay, with easy access to Lake Tahoe, San Francisco, the Napa Valley, the Sierra Foothills and all coastal areas. Fore more information about this unique opportunity, email your CV and cover letter to recruit@cchealth.org. (PA 1886)
Email: recruit@cchealth.org
Website: https://cchealth.org/medicalcenter/ MayJun, JulAug, SepOct
CALIFORNIA
The Department of Emergency Medicine at Stanford University is seeking a Board-Certified Emergency Medicine physician to join the department in the role of Section Chief of Ultrasound. The position includes a full-time faculty appointment in the Clinician Educator Line. Rank will be determined by the qualifications and experience of the successful candidate. Applicants who meet criteria for the rank of Associate Professor or Professor are preferred. Stanford Emergency Medicine is dedicated to transforming healthcare for all by leading in the advancement of emergency medicine through innovation and scientific discovery. We have a strong focus on precision emergency medicine - the use of information and technology to improve the care of individual patients and their communities. Key areas of focus include optimizing access to care; capitalizing on technology and digital health tools; leveraging human-centered data to individualize treatment decisions; advancing population and global health; and redesigning medical education. Of particular interest are candidates who have experience in health innovation and information technology to advance and optimize the delivery of emergency care. The Section Chief of Ultrasound will serve as our departmental leader in ultrasound, supporting the operational, educational, and administrative missions, as well as interdepartmental point-of-care ultrasound (POCUS) projects, and research and scholarship in ultrasound to facilitate the ongoing academic productivity and success of our ultrasound section. In addition, this position will serve as Co-Director of the Stanford Hospital and Clinics POCUS enterprise initiative. Clinical responsibilities will include patient care in the emergency department at Stanford Hospital, a world-renowned, academic medical center with approximately 90,000 adult Emergency Department visits annually. Our faculty consists of over 100 board-certified emergency physicians with broad scholarly interests and extramural funding. We sponsor 13 fellowship programs, a four-year residency program, required and advanced student clerkships, and several courses available to learners throughout our university. Stanford is an equal employment opportunity and affirmative action employer. All qualified applicants will receive consideration for employment without regard to race, color, religion, sex, sexual orientation, gender identity, national origin, disability, protected veteran status, or any other characteristic protected by law. Stanford welcomes applications from all who would bring additional
dimensions to the University’s research, teaching and clinical missions. The Department of Emergency Medicine, School of Medicine and Stanford University value faculty who are committed to advancing diversity, equity, and inclusion. Candidates may optionally include as part of their application a statement or a brief discussion of how their work will further these ideals. Please submit a letter of interest and curriculum vitae to: Jody Vogel, MD, MSc Vice Chair for Academic Affairs
Email: emedacademicaffairs@stanford.edu (PA 1900)
Email: emedacademicaffairs@stanford.edu Website: http://www.emed.stanford.edu JulAug, SepOct, NovDec
INDIANA
The Indiana University School of Medicine (IUSM) Department of Emergency Medicine is seeking applications for Division Chief of Simulation. We are a statewide network of emergency departments striving to set new standards of training for medical students, residents, fellows, and pre-hospital providers while providing quality care for a diverse patient population. The vision of the department is to improve the health and well-being of every life entrusted to us. The Simulation Division within the Department of Emergency Medicine is in the second year of an ambitious five-year plan with the goal of becoming one of the top five simulation divisions in the United States. The work of the division is completed under the direction of the chief and five additional faculty members. Further, the division has a fellowship program. Fellows can develop expertise in the educational, administrative, and research aspects of simulation and receive the leadership training necessary to direct their own simulation program. Simulation training takes place at the 30,000 square foot Indiana University Health (IUH) Simulation Center at Fairbanks Hall, which is led by a member of the division. The fellowship program ranges from one to two years and accepts up to three fellows per year. While the division’s primary focus is emergency medicine, the team provides consultation and simulation tools for other specialties, such as surgery, pediatrics, anesthesia, and obstetrics, to train health care providers how to respond in high-intensity crisis situations. For the long term, however, the division expects to broaden its scope to any specialty or interprofessional group with an educational goal that is best served by immersive training. As the nation’s largest medical school, IUSM is committed to being an institution that not only reflects the diversity of the learners we teach and the patient
SECTION II: POSITIONS NOT RECOGNIZED AS BEING IN FULL COMPLIANCE WITH AAEM’S JOB BANK ADVERTISING CRITERIA (Below are hospitals, non-profit or medical school employed positions.)
SECTION I: POSITIONS RECOGNIZED AS BEING IN FULL COMPLIANCE WITH AAEM’S JOB BANK CRITERIA
None Available at this time. COMMON SENSE SEPTEMBER/OCTOBER 2022 53
POSITIONS NOT RECOGNIZED AS BEING IN FULL COMPLIANCE WITH AAEM’S JOB BANK ADVERTISING CRITERIA
populations we serve, but also pursues the values of diversity, equity and inclusion that inform academic excellence. We desire candidates who enhance our representational diversity, as well as those whose work contributes to equitable and inclusive learning and working environments for our students, staff, and faculty. IUSM strives to take an anti-racist stance, regularly evaluating and updating its policies, procedures, and practices to confer equitable opportunities for contribution and advancement for all members of our community. We invite individuals who will join us in our mission to advance racial equity to transform health and wellbeing for all throughout the state of Indiana. IUSM provides concierge and dual career services to assist new faculty with their personal or family’s relocation needs. Requirements Doctorate or Terminal Degree Required; Boardcertified MD or DO We are seeking someone who has at least five years of experience post-GME training, is well-established in medical simulation, and would qualify to be hired at the rank of associate or full professor. Individuals can apply to fill the division chief and fellowship director role or conduct a search for a fellowship director upon hire. https://indiana.peopleadmin.com/ postings/12748 (PA 1899)
Email: kimgibso@iu.edu
Website: https://medicine.iu.edu/emergency-medicine JulAug, SepOct, NovDec
INDIANA
The Indiana University School of Medicine (IUSM) Department of Emergency Medicine seeks a strong academic leader to serve as the Program Director for the IUSM Emergency Medicine Residency Program. Our residency program is one of the largest three-year ACGME accredited training programs in the country with 73 residents between the categorical EM and combined EM/Peds training programs. IUSM has long been regarded as one of the premier training programs for emergency medicine and continually seeks to improve the educational experience for our residents through a continuous improvement mindset. Demonstrated leadership ability in medical education is essential. Experience working in a culturally diverse environment is highly preferred. The IUSM EM Residency is led by a collaborative team of faculty to include the Program Director (PD), Associate Program Director and multiple Assistant Program Directors. The PD will represent the department as a leader in graduate medical education. Responsibilities and expectations for the PD include but are not limited to: · Maintain an effective educational environment allowing our residents to be educated across all ACGME competencies · Comply with all ACGME training requirements for all clinical and didactic educational experiences · Educational innovation for curriculum development and implementation · Professional development of the residency leadership team · Demonstrate a commitment to Diversity, Equity and Inclusion with vision to increase the representational diversity in the residency program to improve care for our patient population · Use a scholarly approach in the administration of the residency program and disseminate innovations and outcomes in internal, external and peer-reviewed presentations and publications. · Annual strategic planning and continuous quality improvement · Resident assessment, mentorship and improvement plans · National presence in Emergency Medicine organizations · Accreditation monitoring and preparation. The Program Director reports to the Vice Chair of Education and the Chair in the Department of Emergency Medicine. The Department of Emergency Medicine includes a statewide network of emergency departments striving to set new standards of training for medical students, residents, fellows and pre-hospital providers while providing quality care for a diverse patient population. The Department is ranked in the top 15 for NIH funded research nationally in Emergency Medicine and is home to one of the oldest residency programs in the country. We work in an environment that has rich research infrastructure, including the highest-ranked Clinical and Translational Science Institute (CTSI) in the United States and a nationally ranked medical bio-informatics institution. Candidates must have an MD or DO and be board certified in Emergency Medicine with the ability to obtain a license to practice medicine in Indiana. All candidates must also have educational leadership experience with experience and knowledge of the Electronic Residency Application Service (ERAS) and National Residency Matching Program (NRMP) match process. Doctorate or terminal degree required. Interested candidates should attach a letter of interest addressed to the attention of Peter Pang, MD, MS, FACC FACEP, Rolly McGrath Chair and Professor, Department of Emergency Medicine, Indiana University School of Medicine. (PA 1913)
Email: kimgibso@iu.edu
Website: https://indiana.peopleadmin.com/postings/12938
SepOct, NovDec, JanFeb
MISSOURI
Mercy Clinic is seeking an Emergency Medicine Physician to work in a state-of-the-art emergency department on campus of Mercy Hospital in Washington, MO (near St Louis, MO). Mercy Clinic is a physician-led and professionally managed multi-specialty group. With over 2,500 primary care and specialty physicians, Mercy Clinic is the fourth largest integrated physician organization in the country. The Position Offers: • Competitive hourly rate with productivity bonus • Ability to moonlight at other Mercy Hospitals in St. Louis and surrounding area • Comprehensive benefits including health, dental, vision and CME • Relocation assistance and professional liability coverage • System-wide EPIC EMR
About Mercy Hospital Washington: • 187-bed acute care hospital • Only Level III Trauma Center between St. Louis and Jefferson City • Close to 40,000 Emergency visits annually • Mercy offers an experienced medical staff that is specially trained in trauma care. • Medical Director for eight EMS communities (PA 1919)
Email: emily.feuerstein@mercy.net
Website: https://careers.mercy.net SepOct, NovDec, JanFeb
NORTH CAROLINA
FACULTY LEADER, EMERGENCY MEDICINE DIVERSITY, EQUITY & INCLUSION Wake Forest School of Medicine’s Department of Emergency Medicine has a rare opportunity to join our academic faculty team in a leadership position with a scholarly focus on Emergency Medicine Diversity, Equity & Inclusion. This position will be an integral part of our ongoing EM departmental DEI initiatives and the successful candidate will take over leadership of our active DEI committee. There are additional opportunities to participate and lead new and ongoing initiatives throughout the medical school and health system impacting patient care across our learning healthcare system with Atrium Health. (PA 1889)
Email: michael.ginsberg@wakehealth.edu MayJun, JulAug, SepOct
NORTH CAROLINA
Wake Forest School of Medicine has a rare opportunity to join our academic faculty team as a Clinical Assistant Professor dedicated to clinical teaching and patient care activities during overnight hours. This permanent nocturnist position will be responsible for excellent patient care, bedside teaching of residents and medical students, and participation in the teaching academic mission. A full clinical faculty appointment at the School of Medicine will align this position with opportunities for academic advancement. Our ED features a Level 1 trauma center, an accredited chest pain center, stroke center, a burn center and full subspecialty backup. (PA 1897)
Email: michael.ginsberg@wakehealth.edu Website: https://school.wakehealth.edu/ JulAug, SepOct, NovDec
NORTH CAROLINA
Duke Pediatrics is seeking an innovative physician leader to serve as Division Chief for Pediatric Emergency Medicine. Proven leadership and excellence in clinical care, education, scholarship, and administrative experience are required. Duke Children’s is ranked among the nation’s finest for pediatric care and the department is #1 in NIH funding for pediatric clinical science departments. The Greater Triangle area of Raleigh, Durham, Chapel Hill is culturally diverse, economically resilient and nationally recognized as a great place to live and work. Interested individuals should submit a statement of academic interest and curriculum vitae prior to May 27, 2022 to: http://www. practicematch.com/physicians/job-details.cfm/699090 (PA 1904)
Email: debbie.hackney@duke.edu Website: https://pdc.dukehealth.org/ JulAug, SepOct, NovDec
NORTH CAROLINA
Wake Forest Emergency Providers is currently seeking to add to our team of exceptional patient-centered emergency physicians in the Blue Ridge Mountains due to our continued expansion and growth. We offer a unique employment model inclusive of salary, RVU based incentive, paid malpractice, benefits, CME allowance and relocation. Our physicians have local influence on practice decisions, and a strong provider voice in care delivery. These positions are located in Boone, North Carolina, a beautiful town in the Blue Ridge Mountains with a booming local economy, friendly people, thriving arts and food cultures and a wide variety of indoor and outdoor recreational activities in both the community and on the campus of Appalachian State University. Boone is 84 miles from Asheville, 100 miles to Charlotte and 87 miles to the Piedmont Triad. (PA 1927)
Email: michael.ginsberg@wakehealth.edu Website: http://www.wakehealth.edu SepOct, NovDec, JanFeb
NORTH CAROLINA
Wake Forest Emergency Providers is seeking to add to our team in the Greensboro NC metro region. We are the contracted service provider for Cone Health Emergency Medicine. These full-time (144 hours/month) positions rotate across all of Cone Health’s hospitals, including a 628-bed teaching hospital with a Level 2 Trauma Center and community hospitals of 238 beds, 175 beds and 80 beds. We offer a unique employment model inclusive of salary, RVU based incentive, paid malpractice, benefits, CME allowance and relocation. Our physicians have local influence on practice decisions, and a strong provider voice in care delivery. Greensboro is in North Carolina’s Piedmont Triad region and features a moderate climate with all four seasons and housing costs ˜38% below the national average. Residents enjoy a vibrant restaurant scene, a wide variety of indoor and outdoor recreational opportunities and close proximity to the Appalachian Mountains and Atlantic Coast beaches. (PA 1928)
Email: michael.ginsberg@wakehealth.edu Website: http://wakehealth.edu SepOct, NovDec, JanFeb
ONTARIO
Located in beautiful Windsor, Ontario, Canada, our client, Windsor Regional Hospital (WRH), is situated directly across the border from Detroit, Michigan. WRH is the regional provider of advanced care in complex trauma, renal dialysis, cardiac care, stroke and neurosurgery, and intensive care. WRH is seeking fulltime or part-time Emergency Medicine Physicians to contribute to the top tier care provided in the Department of Emergency Medicine. Pathway licensure is available for US Board Certified Physicians through WRH and the College of Physicians of Ontario. Please forward a CV in confidence to: Robb Callaghan, E-mail: rcallaghan@medfall.com Tel: 289-238-9079 (PA 1921) Email: medfall@medfall.com Website: https://www.medfall.com/ SepOct, NovDec, JanFeb
WASHINGTON
Virginia Mason Franciscan Health is seeking an emergency medicine residency-trained BC BE physician to join our group in beautiful Seattle, Washington. Virginia Mason, established in 1920 in Seattle, WA, is internationally recognized as a preeminent health care organization focused on delivering quality services to our patients. We have a 336-bed hospital in Seattle and multispecialty medical group practice with more than 450 physicians. With a network of primary, specialty, neighborhood clinics and regional medical centers; you will find our culture is the very definition of best practices and a model that is the benchmark for other medical organizations. Join us, and find out how many ways Virginia Mason offers you the chance to focus on what really matters—your patients. Highlights of position 0.5 FTE with opportunities to increase. Competitive compensation and benefits package. Exceptional specialty support. Annual volume 24,000. Shifts 8-10 hours. No night shifts. Admission rate 28%. Comprehensive Stroke Center with onsite Neurohospitalist. Regional hyperbaric medicine referral center. Qualifications ABEM or AOBEM BC/BE Ability to obtain a medical professional license in the State of WA Ability to obtain a DEA with full prescriptive authority needed for specific practice ACLS PALS Diversity, Equity and Inclusion at Virginia Mason We commit to fostering an equitable, diverse and intentionally inclusive environment – we strive for all to feel valued, respected and that they belong. Our unique life experiences and backgrounds make our patient care extraordinary. Our diversity fuels our culture of innovation and transformative health care. Our differences are
SECTION II:
(Below are hospitals, non-profit or medical school employed positions.) COMMON SENSE SEPTEMBER/OCTOBER 202254
SECTION II: POSITIONS NOT RECOGNIZED AS BEING IN FULL COMPLIANCE WITH AAEM’S JOB BANK ADVERTISING CRITERIA, CONTINUED
our strengths and inspire a promising future. About Virginia Mason Franciscan Health Virginia Mason Franciscan Health brings together two award winning health systems in Washington State – CHI Franciscan and Virginia Mason. As one integrated health system with the most patient access points in western Washington our team includes 18,000 staff and nearly 5,000 employed physicians and affiliated providers. At Virginia Mason Franciscan Health you will find the safest and highest quality of care provided by our expert, compassionate medical care team at 11 hospitals and nearly 300 sites throughout the greater Puget Sound region. Our integrated health system has nearly 1,500 hospital beds including Bailey-Boushay House, the first skilled-
nursing and outpatient chronic care management program in the United States designed specifically to meet the needs of people with HIV/AIDS; Benaroya Research Institute, internationally recognized for autoimmune disease research; and Virginia Mason Institute, a teaching organization which coaches health care professionals and others around the world in the Virginia Mason Production System, an innovative lean management method for improving quality and safety. (PA 1930)
Email: stephanie.collins-russell@virginiamason.org
Website: https://www.commonspirit.careers/job/seattle/ emergency-medicine-downtown-seattle/35300/33248729232
SepOct, NovDec, JanFeb
None Available at this time.
(Below are independent contractor positions.)
CALIFORNIA
The Monterey Bay Emergency Physicians are looking a stellar FP physician. We are a great, independent, single-hospital group looking for an intelligent, efficient, and excited provider to join us as we look to increase coverage in our Clinical Decision Unit. This is an exciting opportunity for a motivated provider to join a vibrant team that provides outstanding care. Our department is dedicated to excellence in patient care, supportive teamwork and professional growth. The CDU provider will be responsible for evaluating and treating patients who present to the ER and require short-term observation and care. This position is for scheduled shifts only, there is no on-call requirement. The provider will initiate and interpret diagnostic evaluation(s) as appropriate. Our hospital is truly a gem, perched above the Pacific Ocean. We have 250 beds, a full call panel, and a great nursing staff. Salary is competitive, shifts are equitable and scheduling is fair. (PA 1885)
Email: kavitha.weaver@chomp.org
MayJun, JulAug, SepOct
CALIFORNIA
Pacific Redwood Medical Group of Mendocino County, California is seeking a BC/BE Emergency Medicine Physician to join our stable, independent, democratic group. We currently staff all three emergency departments in our county and are looking for a new physician to join our team. We offer flexibility in scheduling, a competitive compensation package including health insurance, 401k contribution and a business expense reimbursement plan, in a collaborative environment of care. Mendocino County includes endless opportunities for hiking, biking, kayaking, camping, adventuring and more in our redwood forests, beaches and mountains. Come join us in Northern California! (PA 1894)
Email: hr@prmg365.com
MayJun, JulAug, SepOct
CALIFORNIA
Come live the SLO life! Central Coast Emergency Physicians is seeking to hire a full-time BC/BE emergency physician. We are a fully independent ER physician owned group staffing two local community emergency rooms in Paso Robles and San Luis Obispo. We have a healthy call panel, easy access to imaging and ancillary resources, and staff to the mindset of practicing in this speciality is a marathon and not a sprint. We do not staff any mid-levels. A full time position involves at least 100 hours/month and includes full benefits, paid CME and vacation, malpractice and disability coverage, as well as living in one of the state’s most beautiful places! (PA 1896)
Email: bcknox@gmail.com
Website: https://ccepslo.com/ JulAug, SepOct, NovDec
CALIFORNIA
Seeking EM Physician for democratic two-hospital group in Berkeley/Oakland Berkeley Emergency Medical Group (BEMG) is a democratic EM practice serving two Sutter Health hospitals in the San Francisco Bay Area. We are seeking an EM Physician candidate to serve our diverse patient population at Alta Bates Summit Medical Center’s two emergency departments in Berkeley and Oakland. Combined volumes of 85,000/year. BEMG employs 45 Physicians. The group has outstanding staffing, flexible schedules, and paid occurrence malpractice coverage. In addition, we offer competitive compensation and a flexible benefits package. Send CV and cover letter to jobs@ bayem.org . (PA 1924)
Email: admin@bayem.org Website: http://bemg.org/ SepOct, NovDec, JanFeb
COLORADO
SDG in Colorado is hiring a full time EM physician to join our group this fall. We staff Platte Valley Medical Center in Brighton, CO. Both our hospital and community are rapidly expanding and we are hiring to accommodate increasing volumes. We are a close-knit group with very little turnover; this is a rare opportunity for the Denver metro area. Pay and benefits are very competitive for Colorado and our group places high value on work life balance. Please contact candace.harrod@bcephealth.com and ryan.klemt@bcephealth.com for more information, as well as to provide CVs. (PA 1911)
Email: candacemd11@yahoo.com Website: http://bcephealth.com SepOct, NovDec, JanFeb
OREGON
Emergency Specialists of Oregon (ESO) is recruiting both Full Time and Part Time Emergency Medicine (BC) Physicians to join our independent, democratic group. ESO practices at Providence Newberg Medical Center, a community hospital located in Newberg, Oregon (~25 miles SW of Portland). We have approximately 24,000 annual visits, excellent hospitalist and specialist support, and are part of a regional health system, allowing for expedited transfers and consults. We have 32 hours of Physician coverage, augmented with additional hours of APP coverage. ESO offers competitive pay and independent contractor status. Newberg is nestled in Oregon wine country, with easy access to a wide range of outdoor and cultural pursuits. Commuting to the hospital from Portland and its surrounding suburbs is common. Contact: Tom Johnson, MD; esomedicaldirector@gmail.com. Please include CV and interest statement. (PA 1888)
Email: esomedicaldirector@gmail.com MayJun, JulAug, SepOct
WASHINGTON
North Sound Emergency Medicine, a well-established, large democratic provider group in Everett, Washington, is looking for an EM residency-trained BC/BE physician. This is a tremendous opportunity to join an exceptional team of clinicians who are dedicated to excellence, providing evidence-based patient care in a supportive environment, while offering opportunities for professional growth, education, and development. Our practice site has a very stable contract and sees more than 80,000 patients annually in a state-of-the-art 79-bed ED: the largest and busiest ED in the state of Washington and one of the busiest in the nation. One of the most desirable places to live, the greater Seattle area offers an abundance of recreational activities from scuba diving and skiing to backpacking the Pacific Crest Trail, professional sports teams, and a myriad of cultural amenities, ranging from opera and ballet to museums and theater. (PA 1903)
Email: cmgilliland@northsoundem.com Website: http://www.northsoundem.com JulAug, SepOct, NovDec
(Below are hospitals, non-profit or medical school employed positions.)
SECTION III: POSITIONS NOT RECOGNIZED AS BEING IN FULL COMPLIANCE WITH AAEM’S JOB BANK ADVERTISING CRITERIA
(Below are military/government employed positions.)
SECTION IV: POSITIONS NOT RECOGNIZED AS BEING IN FULL COMPLIANCE WITH AAEM’S JOB BANK ADVERTISING CRITERIA
COMMON SENSE SEPTEMBER/OCTOBER 2022 55
Pre-Sorted

WI

COMMONSENSE 555 East Wells Street / Suite 1100 Milwaukee, WI 53202-3823
Standard Mail US Postage PAID Milwaukee,
Permit No. 1310 Submit by Oct. 9, 2022 AAEM23 AAEM23 Competition Competition Abstracts Abstracts aaem.org/aaem23
