
COMMON SENSE VOICE OF THE AMERICAN ACADEMY OF EMERGENCY MEDICINE VOLUME 31, ISSUE 2 MARCH/APRIL 2024 Thank You and Farewell We Are Family (Physicians) Transitioning into Your Role as a Medical Educator Stitches in Time: The 10 Commandments of Laceration Repair for Trainees President’s Message 2 5 Editor’s Message 58 Young Physicians Section 61 AAEM/RSA Editor's Message: 60 AAEM/RSA President's Message Closing Time Preview of the 2024 AAEM Scientific Assembly Pg 28
Officers
President
Jonathan S. Jones, MD FAAEM
President-Elect
Robert Frolichstein, MD FAAEM
Secretary-Treasurer
L.E. Gomez, MD MBA FAAEM
Immediate Past President
Lisa A. Moreno, MD MS MSCR FAAEM FIFEM
Past Presidents Council Representative
Tom Scaletta, MD MAAEM FAAEM
Board of Directors
Heidi Best, MD FAAEM
Laura J. Bontempo, MD MEd FAAEM
Kimberly M. Brown, MD MPH FAAEM
Phillip A. Dixon, MD MBA MPH FAAEM CHCQMPHYADV
Robert P. Lam, MD FAAEM
Bruce Lo, MD MBA RDMS FAAEM
Vicki Norton, MD FAAEM
Kraftin Schreyer, MD MBA FAAEM
YPS Director
Fred E. Kency, Jr., MD FAAEM
AAEM/RSA President
Leah Colucci, MD MS
CEO, AAEM-PG
Ex-Officio Board Member
Mark Reiter, MD MBA MAAEM FAAEM
Editor, JEM
Ex-Officio Board Member
Stephen R. Hayden, MD FAAEM
Editor, Common Sense
Ex-Officio Board Member
Edwin Leap II, MD FAAEM
Executive Director
Missy Zagroba, CAE
Executive Director Emeritus
Kay Whalen, MBA CAE
Common Sense Editors
Mel Ebeling, MS3, Resident Editor
Stephanie Burmeister, MLIS, Managing Editor
Articles appearing in Common Sense are intended for the individual use of AAEM members. Opinions expressed are those of the authors and do not necessarily represent the official views of AAEM or AAEM/RSA. Articles may not be duplicated or distributed without the explicit permission of AAEM. Permission is granted in some instances in the interest of public education. Requests for reprints should be directed to AAEM, 555 East Wells Street, Suite 1100, Milwaukee, WI 53202, Tel: (800)
The photographs included in Dr. Christo Philip’s article “Do
plan, we invite all readers of Common Sense to report any
publication or activity which may restrain trade or limit competition. You may confidentially file a report at info@aaem.org or by calling 800-884-aaem.
Mission Statement
The American Academy of Emergency Medicine (AAEM) is the specialty society of emergency medicine. AAEM is a democratic organization committed to the following principles:
1. Every individual, regardless of race, ethnicity, sexual identity or orientation, religion, age, socioeconomic or immigration status, physical or mental disability must have unencumbered access to quality emergency care.
2. The practice of emergency medicine is best conducted by a physician who is board certified or eligible by either the American Board of Emergency Medicine (ABEM) or the American Osteopathic Board of Emergency Medicine (AOBEM).
3. The Academy is committed to the personal and professional well-being of every emergency physician which must include fair and equitable practice environments and due process.
4. The Academy supports residency programs and graduate medical education free of harassment or discrimination, which are essential to the continued enrichment of emergency medicine, and to ensure a high quality of care for the patient.
5. The Academy is committed to providing affordable high quality continuing medical education in emergency medicine for its members.
6. The Academy supports the establishment and recognition of emergency medicine internationally as an independent specialty and is committed to its role in the advancement of emergency medicine worldwide.
Membership Information
Fellow and Full Voting Member (FAAEM): $525* (Must be ABEM or AOBEM certified, or have recertified for 25 years or more in EM or Pediatric EM)
Associate: $150 (Limited to graduates of an ACGME or AOA approved emergency medicine program within their first year out of residency) or $250 (Limited to graduates of an ACGME or AOA approved emergency medicine program more than one year out of residency)
Fellow-in-Training Member: $75 (Must be graduates of an ACGME or AOA approved emergency medicine program and be enrolled in a fellowship)
Emeritus Member: $250 (Please visit www.aaem.org for special eligibility criteria)
International Member: $150 (Non-voting status)
Resident Member: $60 (voting in AAEM/RSA elections only)
Transitional Member: $60 (voting in AAEM/RSA elections only)
International Resident Member: $30 (voting in AAEM/RSA elections only)
Student Member: $40 (voting in AAEM/RSA elections only)
International Student Member: $30 (voting in AAEM/RSA elections only)
Pay dues online at www.aaem.org or send check or money order
COMMONSENSE TM
Table of Contents
to: AAEM,
East Wells Street, Suite 1100, Milwaukee, WI 53202 Tel: (800) 884-2236, Fax: (414) 276-3349, Email:
555
info@aaem.org
884-2236, Fax: (414) 276-3349, Email: info@aaem.org AAEM is a non-profit, professional organization. Our mailing list is private. AAEM ANTITRUST COMPLIANCE PLAN:
part of AAEM's antitrust
As
compliance
AAEM
All Those Kids Belong to You?” (January/February 2024) were pixelated and blurry. We apologize for this error. AAEM-0224-522 COMMON SENSE MARCH/APRIL 2024 Foundation Contributions 8 PAC Contributions ....................................................................................................................... 8 LEAD-EM Contributions 9 Upcoming Events 9 Financial Wellness: TINA “There Is No Alternative” Or is There? 23 The Whole Physician: Breaking Free from Work Dread 25 Wellness Committee: Wellness and Resilience: Nurturing a Healthy Emergency Medicine Community at AAEM24 34 Government and National Affairs Committee: Is It Time for a Flexner Report 2.0? 39 Operations Management Section: Risk Management in the ED 42 Locum Tenens Section: Venture into the Unknown because the Status Quo is Unsatisfying .... 49 Aging Well in Emergency Medicine Interest Group: Choosing Emergency Medicine............. 53 Academic Affairs Committee: Why Should I Continue to be an Emergency Physician? 55 The Lost Art of Listening: A Case for Narrative Medicine 56 AAEM/RSA President’s Message: Closing Time 60 AAEM/RSA Editor’s Message: Stitches in Time: The 10 Commandments of Laceration Repair for Trainees 61 Announcing The Joint Commission Reform Task Force 63 AAEM/RSA Resident Journal Review: Steroid Use in Community-Acquired Pneumonia 67 AAEM Job Bank 71
COMMONSENSE
Featured Articles
2
President’s Message: Thank You and Farewell

In his last President’s Message, Dr. Jones reflects on his tenure as AAEM President during the past two years of uncertainty and change. He argues that the next few years will be crucial for emergency medicine and while he does have fears for the future of U.S. healthcare, he also has hope. Dr. Jones closes his last President’s Message with the transcript of his testimony to the FTC where he discusses these fears…and his hope for the future of emergency medicine.
5
Editor’s Message: We Are Family (Physicians)
10
AAEM Board of Directors Election: Candidate Platform Statements
Voting for the AAEM Board of Directions Election is open now. Please review the candidate statements then exercise your democratic right to vote and make your voice heard.
28
AAEM24: Preview of the 2024 AAEM Scientific Assembly

Join AAEM for the 30th annual Scientific Assembly from April 27-May 1, 2024, in Austin, TX.
36 Adventures in New Zealand

In his Editor’s Message, Dr. Leap reflects on the versatility of emergency physicians and how we play the role of family physician for our family and neighbors. Even our pets benefit from our role as an EM doctor. And Dr. Leap’s response? “I think you’ll be fine.”

AAEM member Dr. Jack Perkins and his family have spent nearly the past year living and working in New Zealand. In this article, Dr. Perkins shares what he loves about EM in New Zealand, what he realizes he now appreciates about the U.S. healthcare system, and more than a few quirks about his temporary home.
46
Social EM & Population Health Committee: Street Medicine: Uncheck Your Biases
In this interview, Dr. Victor Cisneros shares his experiences working in street medicine, delivering medical services directly to an unhoused patient population by physically reaching them wherever they are in need. Dr. Cisneros stresses that while the surroundings may be different from a typical EM setting, the need to be an advocate for these patients remains constant.
44
Pain and Addiction Committee: A Rose by Any Other Name: Tertiary Prevention for Opioid Use Disorder
Harm reduction refers to tertiary prevention: preventing complications of a disease once it is already present. Dr. Moore states that we commonly embrace this practice in medicine but because of reasons rooted in stigma and misunderstanding, tertiary prevention for opioid use disorder is often viewed in a different light. But, says Dr. Moore, it works.
58
Young Physicians Section: Transitioning into Your Role as a Medical Educator

There were certainly teaching opportunities in residency, but was there ever formal instruction in how to teach? In this article, Dr. McGowan provides a few tips on how to reframe your perspective as an educator.
VOICE OF THE AMERICAN ACADEMY OF EMERGENCY MEDICINE VOLUME 31, ISSUE 2 MARCH/APRIL 2024
COMMON SENSE MARCH/APRIL 2024 1
Thank You and Farewell
Jonathan S. Jones, MD FAAEM

This will be my last President’s Message. At the AAEM Scientific Assembly this April in Austin, Texas, I will be proud to turn the Presidency over to Bob Frolichstein who will do an amazing job. Bob is astute, patient, compassionate, and dedicated. He lives the Academy’s Mission every day. Every aspect of his long involvement with the Academy has helped further our goals and improve our specialty. (He does drink IPAs though, so maybe it’ll be a complete disaster.)
There is good in medicine, there is bad, and then there is dangerous. Quite simply, private equity is dangerous.
These next few years will be crucial for our specialty. Thanks to the work of countless leaders within our Academy, the scourge of private equity, lack of due process, and the
corporate practice of medicine are finally being discussed not only by physicians, but by politicians, policy makers, the media, and most importantly, our patients.
We are at a crucial point. Emergency medicine, and medicine in general, is in crisis. And while talk and knowledge about this crisis is important, it won’t matter if there is no action. I am supremely confident that our Academy is poised to put the words into action. While I am certainly happy to see changes in other professional societies within the house of medicine to finally realize the threat of CPOM, I am honored to have been entrusted with leading the only organization which has never wavered in our stance.
create the most powerful messaging and so I was asked to relay an example of how private equity and the corporate practice of medicine are endangering our patients as well as us as physicians. I will close this President’s Message with a transcript of my testimony. But before that, I would like to share just a few brief thoughts.
While it’s not our mission, the way I’ve explained AAEM to others at times is that we believe that in conjunction with the patient, rigorously trained emergency medicine specialists should make every single decision regarding patient care in the emergency department. That’s it. Sure, I need to explain it to some non-physicians or even to some ivory tower physicians out of touch with what is actually happening in the community, but it’s really that simple.
Our passion, logic, perseverance, and unwavering ethics are paying off. On March 5 of this year, the Federal Trade Commission (FTC) held a workshop titled, “Private Capital, Public Impact: An FTC Workshop on Private Equity in Healthcare.” The American Academy of Emergency Medicine was the only emergency medicine society invited and I, as President, was the only physician participant on the panel.

Politicians and policy makers need stories as well as data to
First, I was not invited because I am special. I was invited because you have made this Academy special. AAEM is not the largest or richest specialty society in medicine or even within our specialty. But that doesn’t matter. What matters is that we speak the truth. We are respected where it matters, in this case, in Washington, D.C.
Second, the exact details of the story I shared was unique to me, but I know that many of you have frightening similar stories which could have been shared. And they should be shared. During the session, it was announced that a joint investigation by the Federal Trade Commission, Department of Justice, and Department of Health and Human Services will be launching an inquiry into the impact of corporate ownership in healthcare. I strongly encourage you to submit your stories and comments and have provided the link and QR codes at the end of my message.
Third, simply, I love what emergency medicine was, somewhat is, and certainly can be. We are given opportunities to help people when
AAEM PRESIDENT’S MESSAGE
>> COMMON SENSE MARCH/APRIL 2024 2
I am scared for the future of U.S. healthcare…But my recent experiences have also given me hope. We can make healthcare healthy again. We can bring the care back to it.
they feel their worst, when they are sick, injured, suffering, and at times dying. We help them. We comfort them. We are there for them in their time of greatest need. I can think of no more honorable profession. It is a great responsibility and I embrace it. I hope you feel the same way.
Forth and finally, I am truly humbled to have been entrusted with the leadership of this Academy. I have tried as best as I could. I have made many mistakes and hopefully a few successes. If I have failed you in any way, then I am sorry. If I have helped you in any way, well, that was my job and I am honored that I could. Every single accomplishment of this Academy is not because of me, the officers, or the board. It is because of you. Thank you.
Here is my testimony to the FTC as given on March 5, 2024.
Hi. I am Dr. Jonathan Jones. I am an emergency physician in Jackson, MS, and have been in practice for over a decade. I am the President of the American Academy of Emergency Medicine and strive to live by our mission which is to ensure that every single patient who comes to an emergency department receives expert and compassionate care.
I’ve worked at multiple hospitals and under multiple employment models and I can definitively say that working under a private equity backed management group has been the worst experience of my professional life. It was also the worst possible experience for my patients.
Until about a year ago I worked at a community hospital whose emergency department staffing had changed to a PE controlled contract management group.
patients at one time. Instead of managing up to 8 to 10 patients at a time, I was responsible for up to 18 at a time. This is far outside what is considered safe by any of the emergency medicine specialty societies.
Additionally, this change was not made in consultation with the physicians or the medical director which would typically be the case. Instead, these changes were simply dictated to us and despite having discussions with the firm that this would create an unsafe environment, the changes were made.

This was a fairly large hospital with multiple specialties and we received referrals from the rural parts of the state. After the PE group took over the contract for ER physician services, changes began immediately.
The first change was a reduction in staffing levels, as there were fewer doctors in the ED at any one time. The overall number of patients in the ED changed little. The result was that each physician was now responsible for more
I am truly humbled to have been entrusted with the leadership of this Academy…If I have failed you in any way, then I am sorry. If I have helped you in any way, well, that was my job and I am honored that I could. Every single accomplishment of this Academy is not because of me, the officers, or the board. It is because of you. Thank you.
Very soon after the coverage was decreased, the PE backed contract group in conjunction with the hospital placed an even greater emphasis on accepting as many patients in transfer from other hospitals as possible. This was done regardless of the availability of inpatient beds. When we doctors again questioned this, we were frankly told that the transferred patients had better insurance.
I and the other doctors were told multiple times that we had to accept patients even if the hospital and ED was full. This resulted in more patients despite no increase in nurse staffing and an actual decrease in physician staffing. Patients routinely completed their entire hospital stay without ever leaving the emergency department.
At times, patients transferred to us with the promise of an inpatient bed and of seeing a specialist, instead were placed overnight in the hallway of the emergency department. I and the other doctors communicated the unsafe
>> COMMON SENSE MARCH/APRIL 2024 3 AAEM PRESIDENT’S MESSAGE

nature of this and were routinely told this was non-negotiable and that we could either stop complaining or be terminated.
I’d like to briefly share one example which left an impact on me and ultimately led me to look for a new hospital and group. A patient was transferred to us from a small rural hospital after having an acute stroke. This was on an evening shift and we didn’t even have a neurologist on call that day. But since we would the next day, we were told that that was good enough.
In regards to stroke care, time is of the essence. I knew we did not have anything to offer this patient during the acute phase of his stroke. Other nearby hospitals did. However, despite my objections, the patient arrived and spent the entire night on a stretcher in our hallway. I cared for him as best as I could, but he effectively received no treatment for his stroke.
He could have received timely evaluation by a neurologist and potential treatment had he gone to multiple nearby hospitals. I will never know if he suffered irreversible harm from this experience, but I do know that he did not receive the expected care for an acute stroke. I
know that I was disgusted and disappointed. I believe I did the best I could for him, but I also felt ashamed that I participated in this case.
This is but one example of the complete disregard for patient health in exchange for profit which happened once the PE group took over the physician contract. Emphasis was solely on profits, not patients. The health of the patients, the work environment for doctors and nurses, the entire patient experience—none of this seemed to matter anymore. Only short-term profits mattered.

I studied and trained to be a doctor to help patients not to extract every dollar out of the experience. When I realized that helping patients was clearly not the top priority under this contract and that this would never change, I left. Given that this same PE backed group staffed four other local emergency departments and had a commanding share of the market I had to leave my city as well.
I travelled over two hours away to a small, rural hospital in the northern part of the state. PE had no involvement at this hospital. While it was small and lacked resources of a large medical center, the experience couldn’t have been more different. I was not only allowed but encouraged to ethically treat patients.
That PE backed group went bankrupt last year. While I shed no tears for the firm, I also realized that they were no longer covering my or any of the other doctor’s malpractice insurance despite that we paid for it and the promises they had made. The gross violation of their contract with us perfectly exemplified their approach to healthcare in general.
I now work at a large tertiary center back in Jackson, MS. This emergency department is busy and there is no private equity involvement. Yes, there are often long waits and at times patients still stay too long in the ED when the hospital is full. But the level of care these patients receive is completely different than at the PE controlled site. Extra nurses are called in. And when it was clear that the hospital was getting busier, physician staffing levels were increased.
Yes, the emergency department can still be a busy and stressful place. This is where patients are most vulnerable. This means we have an even higher ethical obligation to our patients in the ED than anywhere else. It is refreshing to work with a group and at a hospital which understands and embraces this.
There is good in medicine, there is bad, and then there is dangerous. Quite simply, private equity is dangerous. Dangerous for patients and for their doctors and nurses. PE is a threat to the health of this country.
To be completely honest, I am scared for the future of U.S. healthcare. I also know that I would be scared to be treated at a PE backed hospital or physician staffing group. But my recent experiences have also given me hope. We can make healthcare healthy again. We can bring the care back to it.
There are innumerable good people working in every emergency department right now. I, as well as thousands of other doctors and nurses care about you. Removing the scourge of private equity would free us to be able to actually provide that care that we want to.
Thank you.
Private Capital, Public Impact: An FTC Workshop on Private Equity in Health Care –Video (Dr. Jones at 1:22:00) Justice Department, Federal Trade Commission, and Department of Health and Human Services Issue Request for Public Input as Part of Inquiry into Impacts of Corporate Ownership Trend in Health Care COMMON SENSE MARCH/APRIL 2024 4 AAEM PRESIDENT’S MESSAGE
Edwin Leap II, MD FAAEM

Whether we like it or not, we are all family physicians in the end. Because for so many of the people we love, we are the first stop for any health issue, the most trusted resource when questions arise, the urgent care for injury and illness and often, the translator of information they receive from others.
I was reminded of this in an odd manner last week. We have two outside cats, Frodo the big half Manx orange tabby and his litter-mate, the grey tabby Leo. (Who actually has a stubby, crooked tail.)

But on some level, I was Leo’s family veterinarian. I assessed him, made a provisional diagnosis and later, simply consoled him with the best thing a cat can get on a bad day. A cold hot-dog cut into pieces.
Leo has long sported an upturned lip which looks like a scowl. We originally thought it as a little off-putting, as if he were annoyed all the time. It may be congenital or due to some old unknown injury. Turns out that, like every cat, Leo loves to have his face rubbed and is just your standard farm cat who digs his life outside.
So as I mentioned, last week I noticed that he seemed a little weary. He was sleeping a lot and was lazier than his normal feline nature dictated. Then I saw the large, soft mass on his right shoulder. “Uh oh,” I thought. At about 14, I figured Leo was on his way out from some strange cat tumor. This is the cycle of things for farm cats, so I was a little sad but not surprised. Our forest is a necropolis of expired pets anyway. I thought I could see his future, unless perchance it was a benign lipoma. But that didn’t explain his lassitude. I felt his nose to see if he were febrile. He was not.
However, a day later he uncharacteristically walked in the front door, meowing and complaining. He jumped onto the kitchen counter (a thing he hasn’t done for a decade since moving outside). He kept complaining until I gave him something to eat. And I noticed the big, wet patch on his shoulder and the mass gone. Apparently something ruptured and drained and he was none the worse for the wear.
Who knows what it was or if it will recur. (Frankly, it’s a small miracle that he and his brother have evaded coyotes and hawks so far, so every day is a gift I suppose.)
But on some level, I was Leo’s family veterinarian. I assessed him, made a provisional diagnosis and later, simply consoled him with the best thing a cat can get on a bad day. A cold hot-dog cut into pieces. (My version of the turkey sandwich we dispense so commonly.)
Although of course, I am neither vet nor pediatrician, neither family doc or internist, I have functioned in many of these rolls. I have sutured my children and their friends at home. I have reassured them that no, their stomach pain was not likely to be cancer and their cold was simply that. I have called in prescriptions for their ear infections and vomiting (and I do it without a hint of anxiety or professional concern). When the children were small, my wife once remarked that she had no idea how mothers without physicians at home managed—sick kids are scary!
Over the years many friends and family have called me to go through lab, CT, or MRI reports because just having the report available on MyChart doesn’t help allay any of the anxiety
associated with reading it. 87% lymphocytes, low sodium of 129, Adenopathy, likely cyst, nodule, follow up CT, inflammation, all of these have meaning to us but less clarity to our patients. Medicalease is a dark and terrifying language not unlike the speech of Mordor, and it requires careful translation. The clarity we bring, along with consolation (or guidance) goes a long way and it is one of the gifts that medical education gives to us, and that we give to others.
When my wife had a terrible bout with cancer many years ago, my ability to watch her, to care for her at home, to speak with her physicians and to be diligent over her condition all combined to made our journey slightly less terrifying.
When my father-in-law became ill, and then ended up on the ventilator with COVID, my understanding of what was happening, along with that of his ICU nurse son, helped us to make proper decisions about his care. (And my wife’s dedication to her father helped him rehab afterward.)
And more recently, when my mother-in-law became critical ill after a brief respiratory
>>
EDITOR’S MESSAGE We Are Family (Physicians)
COMMON SENSE MARCH/APRIL 2024 5

Our jobs may begin behind the ED doors. But they extend far beyond to the people we know and love all around us.
illness, I was able to speak to her physicians and advocate for her, as well as help translate her daily results for the family. Sadly, she finally passed away, but I was able to be the family’s physician during her final dark days.
We often wonder if we could do other things as emergency physicians. There’s urgent care and palliative care, sports medicine and toxicology and a host of other options. But it’s important that we remember that we are already so much more to those who know us, love us and trust us. We are physicians not only for family but friends, not only for neighbors and colleagues but fellow parishioners in church or in other
organizations.
We bring a lot to the table. Sometimes it’s CPR by the playing field. Other times it’s the quick evaluation of a friend that says, “that looks badly infected, I’m taking you to the hospital.” And more often than all the rest, it’s “I think you’ll be fine. But call me if you have any concerns and I’ll come over again.”
Our jobs may begin behind the ED doors. But they extend far beyond to the people we know and love all around us.
EDITOR’S MESSAGE
COMMON SENSE MARCH/APRIL 2024 6










Penn State Health Emergency Medicine
About Us:
Penn State Health is a multi-hospital health system serving patients and communities across central Pennsylvania. We are the only medical facility in Pennsylvania to be accredited as a Level I pediatric trauma center and Level I adult trauma center. The system includes Penn State Health Milton S. Hershey Medical Center, Penn State Health Children’s Hospital and Penn State Cancer Institute based in Hershey, Pa.; Penn State Health Hampden Medical Center in Enola, Pa.; Penn State Health Holy Spirit Medical Center in Camp Hill, Pa.; Penn State Health Lancaster Medical Center in Lancaster, Pa.; Penn State Health St. Joseph Medical Center in Reading, Pa.; Pennsylvania Psychiatric Institute, a specialty provider of inpatient and outpatient behavioral health services, in Harrisburg, Pa.; and 2,450+ physicians and direct care providers at 225 outpatient practices. Additionally, the system jointly operates various healthcare providers, including Penn State Health Rehabilitation Hospital, Hershey Outpatient Surgery Center and Hershey Endoscopy Center.
We foster a collaborative environment rich with diversity, share a passion for patient care, and have a space for those who share our spark of innovative research interests. Our health system is expanding and we have opportunities in both academic hospital as well community hospital settings. Benefit highlights include:

• Competitive salary with sign-on bonus
• Comprehensive benefits and retirement package
• Relocation assistance & CME allowance
• Attractive neighborhoods in scenic central Pa.


Heather Peffley, PHR CPRP - Penn State Health Lead Physician Recruiter hpeffley@pennstatehealth.psu.edu
Penn State Health is fundamentally committed to the diversity of our faculty and staff. We believe diversity is unapologetically expressing itself through every person’s perspectives and lived experiences. We are an equal opportunity and affirmative action employer. All qualified applicants will receive consideration for employment without regard to age, color, disability, gender identity or expression, marital status, national or ethnic origin, political affiliation, race, religion, sex (including pregnancy), sexual orientation, veteran status, and family medical or genetic information. FOR MORE INFORMATION PLEASE CONTACT:
JOIN OUR TEAM EMERGENCY MEDICINE OPPORTUNITIES AVAILABLE COMMON SENSE MARCH/APRIL 2024 7
AAEM Foundation Contributors – Thank You!
AAEM established its Foundation for the purposes of (1) studying and providing education relating to the access and availability of emergency medical care and (2) defending the rights of patients to receive such care and emergency physicians to provide such care. The latter purpose may include providing financial support for litigation to further these objectives. The Foundation will limit financial support to cases involving physician practice rights and cases involving a broad public interest. Contributions to the Foundation are tax deductible.
Levels of recognition to those who donate to the AAEM Foundation have been established. The information below includes a list of the different levels of contributions. The Foundation would like to thank the individuals below who contributed from 12/1/2023 to 3/1/2024.
Contributions $1000 and above
Bruce M. Lo, MD MBA RDMS FAAEM
Fred Earl Kency, Jr., MD FAAEM FACEP
Jonathan S. Jones, MD FAAEM
Kimberly M. Brown, MD MPH FAAEM
Kraftin E. Schreyer, MD MBA FAAEM
Mark Reiter, MD MBA MAAEM FAAEM
Megan Long, MD FAAEM
Peter G. Anderson, MD FAAEM
Tom Scaletta, MD MAAEM FAAEM
Contributions $500-$999
Mark S. Penner, DO FAAEM
Nate T. Rudman, MD FAAEM
William E. Franklin, DO MBA FAAEM
Contributions $250-$499
Brian D. Barbas, MD FAAEM
Chris M. Paschall, MD FAAEM
Daniel F. Danzl, MD MAAEM
Eric W. Brader, MD FAAEM
Kay Whalen, MBA CAE
Kevin Allen, MD FAAEM
Larry A. Nathanson, MD FAAEM
Oscar A. Marcilla, MD FAAEM
Scott P. Marquis, MD FAAEM
Teresa M. Ross, MD FAAEM
Travis J. Maiers, MD FAAEM
Contributions $100-$249
Alexander Tsukerman, MD FAAEM
Ann Loudermilk, MD FAAEM
Antonios D. Katsetos, DO FAAEM
Ben Harris, MD FAAEM
Bradley K. Gerberich, MD FAAEM
Brian Gacioch, FAAEM
Brian R. Potts, MD MBA FAAEM
Chaiya Laoteppitaks, MD FAAEM
Charles E. Cady, MD FAAEM FAEMS
David C. Crutchfield, MD FAAEM
Don L. Snyder, MD FAAEM
Erem Emmanuel Bobrakov, MD FAAEM
Eric J. Muehlbauer, MJ CAE
Eric S. Kenley, MD FAAEM
Gary M. Gaddis, MD PhD MAAEM
FAAEM FIFEM
H. Edward Seibert, MD FAAEM
Jeffrey A. Rey MD, MD FAAEM
Joseph T. Bleier, MD FAAEM
Katrina Kissman, MD FAAEM
Kevin C. Reed, MD FAAEM
Leonardo L. Alonso, DO FAAEM
Marianne Haughey, MD FAAEM
Mark D. Thompson, MD FAAEM
Mark E. Zeitzer, MD FAAEM
Mary Jane Brown, MD FAAEM
Paul M. Clayton, MD FAAEM
Paul W. Gabriel, MD FAAEM
Robert A. Frolichstein, MD FAAEM
Robert Boyd Tober, MD FAAEM
Robert E. Gruner, MD
Robert J. Feldman, MD FAAEM
Robert R. Westermeyer, II, MD FAAEM
Sarah B. Dubbs, MD FAAEM
AAEM PAC Contributors – Thank You!
Contributions $500-$999
Fred Earl Kency, Jr., MD FAAEM FACEP
Mark S. Penner, DO FAAEM
Contributions $250-$499
Daniel D’Souza, DO FAAEM
Eric W. Brader, MD FAAEM
Travis J. Maiers, MD FAAEM
Contributions $100-$249
Alexander Tsukerman, MD FAAEM
Brian R. Potts, MD MBA FAAEM
Stuart M. Gaynes, MD FAAEM
William T. Freeman, MD FAAEM
Contributions up to $99
Ameer Sharifzadeh, MD FAAEM
Andrew M. Flanagan, DO FAAEM
Eric M. Ketcham, MD MBA FAAEM FASAM
Everett T. Fuller, MD FAAEM
Jessica Bates, MD FAAEM
Jonathan W. Graff, DO FAAEM
Justin L. Berkowitz, DO FAAEM
Katherine Ryan, MD FAAEM
Linda Sanders, MD FAAEM
Neal Handly, MD
Patrick W. Daly, MD FAAEM
Peter H. Hibberd, MD FACEP FAAEM
Rian Pillitteri, MD FAAEM
Ryan Horton, MD FAAEM
Stephanie Eden, MD FAAEM
William Peter Kehr, MD
AAEM PAC is the political action committee of the American Academy of Emergency Medicine. Through AAEM PAC, the Academy is able to support legislation and effect change on behalf of its members and with consideration to their unique concerns. Our dedicated efforts will help to improve the overall quality of health care in our country and to improve the lot of all emergency physicians.
All contributions are voluntary and the suggested amount of contribution is only a suggestion. The amount given by the contributor, or the refusal to give, will not benefit or disadvantage the person being solicited.
Levels of recognition to those who donate to the AAEM PAC have been established. The information below includes a list of the different levels of contributions. The PAC would like to thank the individuals below who contributed from 12/1/2023 to 3/1/2024.
Chaiya Laoteppitaks, MD FAAEM
Derek L. Marcantel, MD FAAEM
Gary M. Gaddis, MD PhD MAAEM
FAAEM FIFEM
Jeffrey A. Rey MD, MD FAAEM
Katrina Kissman, MD FAAEM
Mark D. Thompson, MD FAAEM
Megan Long, MD FAAEM
Paul M. Clayton, MD FAAEM
Peter G. Anderson, MD FAAEM
Robert A. Frolichstein, MD FAAEM
Scott P. Marquis, MD FAAEM
Stuart M. Gaynes, MD FAAEM
William T. Freeman, MD FAAEM
Contributions up to $99
Alex Kaplan, MD FAAEM
Ameer Sharifzadeh, MD FAAEM
Elizabeth Lojewski, DO FAAEM
Joseph T. Bleier, MD FAAEM
Kevin C. Reed, MD FAAEM
Marc D. Squillante, DO FAAEM
Patricia Phan, MD FAAEM
Peter H. Hibberd, MD FACEP FAAEM
Peter M.C. DeBlieux, MD FAAEM
Ryan Horton, MD FAAEM
COMMON SENSE MARCH/APRIL 2024 8
LEAD-EM Contributors – Thank You!
The AAEM Institute for Leadership, Education & Advancement in the Development of Emergency Medicine, Inc. (LEAD-EM) was established after the tragic and unexpected death of AAEM president, Dr. Kevin G. Rodgers.
The Kevin G. Rodgers Fund and the Institute will LEAD-EM just like Dr. Rodgers did. The funds will support important projects such as development of leadership qualities, and clinical and operational knowledge of emergency physicians with a view toward improving and advancing the quality of medical care in emergency medicine, and public health, safety and well-being overall. LEAD-EM would like to thank the individuals below who contributed from 12/1/2023 to 3/1/2024.
Contributions $500-$999
Fred Earl Kency, Jr., MD FAAEM FACEP
Mark S. Penner, DO FAAEM
Contributions $250-$499
Daniel D’Souza, DO FAAEM
Eric W. Brader, MD FAAEM
Travis J. Maiers, MD FAAEM
Contributions $100-$249
Alexander Tsukerman, MD FAAEM
Brian R. Potts, MD MBA FAAEM
Chaiya Laoteppitaks, MD FAAEM
Derek L. Marcantel, MD FAAEM
Gary M. Gaddis, MD PhD MAAEM FAAEM FIFEM
Jeffrey A. Rey MD, MD FAAEM
Katrina Kissman, MD FAAEM
Mark D. Thompson, MD FAAEM
Megan Long, MD FAAEM
Paul M. Clayton, MD FAAEM
Peter G. Anderson, MD FAAEM
Robert A. Frolichstein, MD FAAEM
Scott P. Marquis, MD FAAEM
Stuart M. Gaynes, MD FAAEM
William T. Freeman, MD FAAEM
Contributions up to $99
Alex Kaplan, MD FAAEM
Ameer Sharifzadeh, MD FAAEM
Elizabeth Lojewski, DO FAAEM
Joseph T. Bleier, MD FAAEM
Kevin C. Reed, MD FAAEM
Marc D. Squillante, DO FAAEM
Patricia Phan, MD FAAEM
Peter H. Hibberd, MD FACEP FAAEM
Peter M.C. DeBlieux, MD FAAEM
Ryan Horton, MD FAAEM
Upcoming Events: AAEM Directly, Jointly Provided, & Recommended
AAEM is featuring the following upcoming conferences and activities for your consideration. For a complete listing of upcoming conferences and other meetings, please visit: aaem.org/education/events
AAEM Events
2024 Oral Board Review Courses
Dates Announced aaem.org/education/oral-boards/
April 27-May 1, 2024
30th Annual Scientific Assembly (Austin, TX) www.aaem.org/aaem24
May 31-June 1, 2024
12th Annual FLAAEM Scientific Assembly (Miami, FL) www.aaem.org/get-involved/chapter-divisions/flaaem/
Jointly Provided
Re-Occurring Monthly Spanish Education Series*
Jointly provided by the AAEM International Committee https://www.aaem.org/committees/international/spanish-education-series/ (CME not provided)
June 25-29, 2024
UC Davis Emergency Medicine Summer Conference: InformED
Jointly provided by UC Davis Health https://na.eventscloud.com/ereg/index.php?eventid=784125&
July 24-26, 2024
Coalition for Physician Well-Being Joy & Wholeness Summit
Jointly provided by the Coalition for Physician Well-Being
https://www.forphysicianwellbeing.org/annual-national-conference
October 21-25, 2024
19th Annual Emergency Medicine Update: Hot Topics 2024
Jointly provided by UC Davis Health
Recommended
2024 ACMT Annual Scientific Meeting & Symposia
April 10-14, 2024 (Washington, DC)
https://www.acmt.net/annualmeeting/
The Difficult Airway Course: EmergencyTM
May 3-5, 2024 (Boston, MA) | May 31-June 2, 2024 (Las Vegas, NV)
September 6-8, 2024 (San Diego, CA) November 8-10, 2024 (Orlando, FL) theairwaysite.com/a-course/the-difficult-airway-course-emergency/
Online CME
Recognizing Life-Threatening Emergencies in People with VEDSthesullivangroup.com/TSG_UG/VEDSAAEM/
COMMON SENSE MARCH/APRIL 2024 9
PLATFORM STATEMENTS
Dear AAEM Member,
Enclosed are the candidate statements for the 2024 AAEM Board of Directors Election.
As you are aware, the call for nominations was sent to all voting members. Those AAEM members who appear on the enclosed ballot have indicated their willingness to serve on the AAEM board.
Statements from each of the candidates full listing of previous board service and awards as well as AAEM activities dating back five years (2019 and on) are on the following pages. Please review the enclosed information, then exercise your democratic right to vote for the representatives you would like to see serve as AAEM’s leaders. Remember, we have a one member, one vote system, so your voice counts. Please follow these instructions for casting your ballot in the 2024 election.
If You Will Attend the Scientific Assembly:
• We recommend that you do not complete your official ballot at this time. There will be a Candidates’ Forum held during the Scientific Assembly on Monday, April 29, 2024, 5:30pm-6:30pm CT, where you can hear the candidates respond to direct questions from the voting membership. You will be asked to submit your ballot online at the conclusion of the Forum.
• If certain of your choices or unsure if you will attend the Forum, you may vote online at aaem.org/about-us/ leadership/election. Voting will remain open until April 29, 2024 at 11:59pm CT.
If You Are Unable to Attend the Scientific Assembly:
• You may complete your official ballot online at aaem.org/about-us/leadership/elections. Online voting will remain open until April 29, 2024 at 11:59pm CT.
Balloting Procedure for 2024:
• Voting ballots will only be available online. Please visit aaem.org/about-us/leadership/elections to cast your vote electronically.
Thank you for your continued support of AAEM. Please call (800) 884-2236 with any questions you may have regarding the election procedure.
Sincerely,
 Missy Zagroba, CAE Executive Director
Missy Zagroba, CAE Executive Director
COMMON SENSE MARCH/APRIL 2024 10

L.E. Gomez, MD MBA MPH FAAEM
CANDIDATE FOR PRESIDENT-ELECT
Current Leadership Role/Employer: Healthcare Analyst & Consultant, University of Maryland
Clinical EM Practice Employment Type: Attending Emergency Physician for the University of Maryland Hospitals mentoring residents and peers. Analyst and consultant for GLG Network, working directly with clients at top corporations, investment firms, management consultancies, and non-profits to improve efficiencies, understand markets, and propose solutions to meet organizational goals.
Clinical Hours in the ED per Month: 36
Additional Leadership Roles: Physician Leader and Consultant for Health & Welfare Committee, NAACP, Anne Arundel County, Committee on Public Health and Consumer Affairs, Physician Consultant to Physical and Mental Health Sub Committee, Caucus of African American Leaders
Nominated/Endorsed by: Lisa. A Moreno, MD MS MSCR FAAEM FIFEM; Amin Antoine Kazzi, MD MAAEM FAAEM; Gary M. Gaddis,
MD PhD MAAEM FAAEM FIFEM
Membership: 2006-2024
Disclosure: Nothing to disclose.
Attendance Record for AAEM BOD Meetings: 100%
AAEM Activities (past five years)
AAEM Board of Directors-Secretary-Treasurer
AAEM Board of Directors-At-Large Board Member
Executive Committee-Secretary/Treasurer
AAEM Physician Group Board of Directors-Director
AAEM Physician Group Board of Directors-Member
Chapter Division Committee-Member
Capital Region Chapter Board of Directors-Secretary/Treasurer
Justice, Equity Diversity & Inclusion Committee-Chair
Justice, Equity Diversity & Inclusion Committee-Board Liaison
Ethics Committee-Board Liaison
Ethics Committee-Member
Candidate Statement for President-Elect
Government and National Affairs Committee, Member
Latin American Health & Education Committee-Board Liaison
Oral Board Review Course Work Group-Board Liaison
Social EM and Population Health Committee-Board Liaison
Social EM and Population Health Committee-Member
Scientific Assembly-Moderator
Mediterranean Emergency Medicine Congress (MEMC)-Track Chair
MEMC-Speaker
MEMC-Poster Judge
Common Sense Author
I am asking for your vote, as candidate for President-Elect of AAEM because I believe it’s time to fully live up to our stated goals with a renewed commitment to growth, openness and inclusion of all emergency physicians and protect the highest aspirations of our specialty: not just how we practice but why we chose to practice emergency medicine. I have gained the qualifications, experience, and passion to lead AAEM into this new future of fully living up to our mission because during my several years in various leadership roles at AAEM, including our BOD, I have equally fought for the principles of unencumbered access to quality of care for our patients and for boarded EM Specialist. This includes the equitable protection and well-being of our peers, to ensure fair and equitable practice environments and due process. I advocated for these principles as a past Chair of the Justice, Equity, Diversity and Inclusion Section, liaison to our Ethics Committee and Social EM and Population Health Committee. As your current SecretaryTreasurer, I have also served as a member of our Executive Committee in conferences and meetings to guide our organizational course at the highest level of our organization. I have co-signed our checks in a timely manner and ensured, together with our staff, that budgets, audits, and treasurer reports are comprehensible, transparent, and accessible to all board members and our organization. I have fought to protect equity in our lobbying to ensure representation of our entire membership not solely the interest of one political view over another.
As a board member of our AAEM Practice Group, I have helped champion fair and equitable practice environments that include our lawsuit against Envision to protect the takeover of our practices and prevent lay ownership and corporate abuses and ensure ethical business practices prevail.
PLATFORM STATEMENTS Continued on page 21 >>
COMMON SENSE MARCH/APRIL 2024 11

Vicki Norton, MD FAAEM
CANDIDATE FOR PRESIDENT-ELECT
Current Employer: EMED LLP
Clinical EM Practice Employment Type: I am a partner in a Democratic Physician Group at a Community Teaching Hospital with a Medical School Affiliation.
Clinical Hours in the ED per Month: 132
Additional Leadership Roles: Vice President for Palm Beach County Medical Society
Nominated/Endorsed by: Jonathan S. Jones, MD FAAEM; Robert A. Frolichstein, MD FAAEM; Robert M. McNamara, MD MAAEM FAAEM
Membership: 2007-2024
Disclosure: Nothing to disclose.
Attendance Record for AAEM BOD Meetings: 100%
AAEM Activities (past five years)
AAEM Board of Directors-At-Large Board Member
James Keaney Award Winner
Chapter Division Committee Board Liaison
California Chapter Board of Directors-Board Liaison
Capital Region Chapter Board of Directors-Board Liaison
Delaware Valley Board of Directors-Board Liaison
Florida Chapter Board of Directors-President
Florida Chapter Board of Directors-Board Liaison
Great Lakes Chapter Board of Directors-Board Liaison
India Chapter Board of Directors-Board Liaison
Lebanon Chapter Board of Directors-Board Liaison
Louisiana Chapter Board of Directors-Board Liaison
Mediterranean Chapter Board of Directors-Board Liaison
Missouri Chapter Board of Directors-Board Liaison
Candidate Statement for President-Elect
New York Chapter Board of Directors-Board Liaison
Texas Chapter Board of Directors-Board Liaison
Tennessee Chapter Board of Directors-Board Liaison
Uniformed Services Chapter Board of Directors-Board Liaison
Justice, Equity, Diversity & Inclusion Committee-Member Emergency Medicine Workforce Committee-Board Liaison
AAEM Membership Committee-Member Lobbyist Task Force-Chair
Women in Emergency Medicine Council-Immediate Past Chair
Women in Emergency Medicine Council-Board Liaison
Leadership Academy-Mentor Scientific Assembly-Moderator
Health Policy in Emergency Medicine (HPEM)-Speaker Common Sense Author
As a member of AAEM for the last 17 years, I am honored to be nominated for President-Elect. I am thankful for having had the opportunity to serve on the Board the past 4 years, and I continue to be as passionate as ever about the ideals and values of our organization. I have shown initiative, determination, diligence, and innovation as an At-Large Director. I will continue to fight the outside interests that threaten our specialty: the corporate practice of medicine and private equity control, the lack of due process for physicians, and the interference in the doctor-patient relationship.
I have been an advocate for emergency medicine, inside and outside of AAEM, and will continue to do so in the future. I previously served as the President of the Florida Chapter of AAEM and as the chair of the Women in Emergency Medicine committee. I served as a county delegate to the annual Florida Medical Association (FMA) meeting, a Florida Delegate to the AMA, and as Vice President of my county medical society. I wrote a resolution to support a corporate practice of medicine prohibition that was passed by the FMA House of Delegates. Due to my work, a corporate practice of medicine prohibition bill was introduced in the Florida legislature this last session. On a national level, I have fought for American Medical Association support for a national corporate practice of medicine prohibition through introducing a resolution to the AMA House of Delegates and debating the issue on the house floor. I have met with legislators at a state and national level to bring awareness to the issue of the corporate practice of medicine and garner support for more stringent legislation. I am also involved in the Advisory Board of Take Medicine Back, a multi-specialty advocacy group fighting the private equity infiltration of healthcare.
Additionally, as an At-Large Director of the AAEM Board, I spearheaded a way for AAEM members to stay on top of new legislation and to communicate directly with lawmakers. With the launch of our Grassroots Action Center using a software called Quorum, members can act with just the click of Continued on page 21 >>
PLATFORM
STATEMENTS
COMMON SENSE MARCH/APRIL 2024 12

Mark A. Shank, DO FAAEM
CANDIDATE FOR PRESIDENT-ELECT
Current Employer: Sarasota Emergency Associates
Clinical EM Practice Employment Type: We are a small democratic group in Southwest Florida with strong ties to the hospital. We have a strong EM residency that takes nine residents per year. We have an established relationship with Florida State University and see their medical students rotating regularly.
Clinical Hours in the ED per Month: 130-150
Additional Leadership Roles: N/A
Nominated/Endorsed by: Sagar C. Galwankar, MD FAAEM
Membership: 2018-2024
Disclosure: Nothing to disclose.
AAEM Activities (past five years)
Florida Chapter Division-Member
Emergency Medical Services Section-Member
Women in Emergency Medicine Section-Member
Oral Board Review Course-Examiner
Candidate Statement for President-Elect
Thank you for the opportunity to participate in the selection of the President-Elect for the American Academy of Emergency Medicine. I have been a member for several years now and have been proud to support those that have stepped up to take this group to the next level and to protect our specialty. I have donated my time in the past with the AAEM board review team. Seeing all that is going on in the world and knowing how much emergency medicine has changed and been challenged recently has brought me a new found vigor and passion to step up and contribute not only financially but with my personal time and experience. My fledgling EM career was built on a desire to help others, not just patients but my peers. I first started out in emergency medicine as an RN in a busy level 3 trauma center in Grand Rapids. It was here that I developed the desire to move on from the role of nursing to my current role as an EM physician. As a natural leader, I ascended to the position of assistant medical director my second year out of residency. This was followed by medical director after only a short period of time. While in this role I was able to attend both phase one and two of the ED directors academy as well as the Harvard negotiation conference and the Estes Park Leadership training conference. I have utilize these skills to help educate the residents as well as my colleagues as we care for our patients in the Emergency department. In 2022 I was selected to the board of Global Billing Inc. in Sarasota. I am currently in the running for the vice CEO of my group. I have ample leadership experience and training as well as board experience. I am excited to participate and take a more active role in the leadership of AAEM as it continues to defend our specialty.
PLATFORM STATEMENTS
COMMON SENSE MARCH/APRIL 2024 13

Phillip A. Dixon, MD MBA MPH FAAEM CHCQM-PHYADV
CANDIDATE FOR SECRETARY-TREASURER
Current Leadership Role/Employer: Medical Director, Utilization Management, Department Of Emergency Medicine at The Ohio State University Wexner Medical Center
Clinical EM Practice Employment Type: My clinical EM practice is mostly at a major academic hospital, although we have smaller clinical sites that all faculty also work at 2-3 times per month.
Clinical Hours in the ED per Month: 20
Additional Leadership Roles: Fellowship Director, Administration, UH Emergency Department OSUWMC
Nominated/Endorsed by: Jonathan S. Jones, MD; Robert A. Frolichstein, MD FAAEM
Membership: 2013-2024
Disclosure: Nothing to disclose.
Attendance Record for AAEM BOD Meetings: 100%
AAEM Activities (past five years)
AAEM Board of Directors-YPS Director
AAEM Board of Directors-At-Large Board Member
Academic Affairs Committee-Board Liaison
Education Committee-Board Liaison
Ethics Committee-Board Liaison
Government and National Affairs Committee-Member
Government and National Affairs Committee-Vice Chair
Government and National Affairs Committee-Co-Chair
Government and National Affairs Committee-Board Liaison
Candidate Statement for Secretary-Treasurer
To the Membership of AAEM,
Great Lake Chapter Division-Member
AAEM/RSA – Legacy Assembly-Member
Social Media Committee-Board Liaison
Young Physicians Section Council-Board Liaison
Scientific Assembly-Speaker
Scientific Assembly-Poster Judge
Mediterranean Emergency Medicine Congress (MEMC)-Poster Judge
MEMC-Abstract Moderator
I would first like to thank you, the AAEM membership, for the opportunity for serving on the AAEM board for the past 4 years as the YPS director and subsequently an At-Large board member. I am now running to be your secretary-treasurer. It has been my honor to have represented this organization and to bring a unique perspective to AAEM. I am asking for the opportunity to continue to serve on the board for AAEM. I am so proud to have been able to represent this amazing and wonderful organization, as I truly believe this is THE organization that represents both the patients and emergency physicians and their best interests. Patients receive better care when the emergency physician is treated with dignity and respect. I am excited of the prospect to continue to participate in the board’s collaborative approach and effective communication in order to achieve the best outcome for the members of AAEM.
It is my goal to continue to serve this great organization and continue to bring additional knowledge and unique skill set to the AAEM board. Among these unique skills are a business background obtained through a MBA degree, as well as previous experience in advocacy leadership. In the past, I have helped developed AAEM’s business and investment plans and would like to continue to improve’ AAEM’s financial operations. As SecretaryTreasurer, I will work with the rest of the board to make sure all of our financial decisions are in the best interest of the membership. I am also enthusiastic about continuing involvement in board initiatives that will propel the AAEM mission and vision forward, including advocating for our specialty on Capitol Hill. In terms of advocacy, I am the board liaison to the Government Affairs Committee and continue to advocate for passage of Due Process protections for our specialty from CMGs. I have worked with our lobbying firms on passage on a due process bill, and would like to see this get re-introduced as legislation this year among other legislative priorities. As shown by our Envision lawsuit, we must fight the Corporate Practice of Medicine. We must also fight the continued threat of Scope of Practice of NPPs.
Continued on page 22 >>
PLATFORM STATEMENTS
COMMON SENSE MARCH/APRIL 2024 14

Frank L. Christopher, MD FAAEM
CANDIDATE FOR AT-LARGE BOARD MEMBER
Current Leadership Role/Employer: President, Lugnut Medical Services, PLLC
Clinical EM Practice Employment Type: Provide Locums Emergency Medicine services at a variety at small facilities and Critical Access Hospitals in rural North Carolina
Clinical Hours in the ED per Month: 72
Additional Leadership Roles: N/A
Nominated/Endorsed by: Robert A. Frolichstein, MD FAAEM; Robert M. McNamara, MD MAAEM FAAEM; Vicki Norton, MD FAAEM
Membership: 1999-2024
Disclosure: Nothing to disclose.
AAEM Activities (past five years)
Joe Lex Educator of the Year Award Winner
Mitchell Goldman Service Award Winner (4x)
Membership Committee-Vice Chair
Oral Board Review Course National Course Director
Oral Board Review Course National Advisor
Oral Board Review Course Vice Chair
Candidate Statement for At-Large Board Member Champion of the Emergency Physician.
Oral Board Review Course Regional Course Director (Orlando)
Oral Board Review Course Examiner/Course Director
Education Committee-Member
Scientific Assembly-Moderator
Leadership Academy-Participant Common Sense Author
When the Academy re-branded several years ago, those words were chosen by the Academy Leadership to summarize why the Academy was formed and encapsulate how it has evolved. As demonstrated recently, the Academy has proven itself to be just that the Champion of the Emergency Physician. Not the Champion of a Membership Number. Not the Champion of the Largest Corporate Donor. The Academy represents all Emergency Physicians. (Even if they are not members!)
I am running for an At-Large position on the Board because I see the tremendous continued potential of the Academy. I see it in our current and future colleagues who are now entering the workforce having navigated the gauntlet of medical school, matching, and EM residency, having done so during a global pandemic and despite overwhelming changes in academia.
The future strength of the Academy is our colleagues. Those who are now becoming eligible to join our ranks as board-certified Emergency Physicians (and Fellows of the Academy) chose to enter this demanding specialty in the face of the global threat of COVID. They have watched, perhaps tangentially, the uncertainty over the future of the specialty, supply and demand mismatches, reimbursement changes, and evolving administrative structures.
They are smart. They are resilient. They have proven themselves. And they are the future of the Academy and the specialty we love. I believe it is the Academy’s job to continue to be their Champion, for they have earned it. This academy exists to ensure they have the continuing medical education, the economic know-how, an understanding of the workforce challenges, and an ability to navigate the constantly evolving landscape of the market forces in play.
I am inspired by our newest colleagues, and it is for them that I am seeking a position on the Board to continue to shape the Academy to share our message, drive necessary change, and shape the priorities of work to benefit our membership, our specialty, and our patients.
I’ve had the privilege of teaching, and later leading, the Oral Board Review Course for several years, and have been fortunate to be able to use that platform to talk to our new colleagues about the educational, legislative, policy, and personal growth and leadership opportunities the Academy provides to its members. I was inspired to get involved by Academy leaders such as Bob McNamara and Kevin Rodgers, each of whom reached out directly to me. I hope to help identify and develop the next generation of Academy leadership through a term on your Board.
PLATFORM STATEMENTS Continued on page 22 >>
COMMON SENSE MARCH/APRIL 2024 15

Fred E. Kency, Jr., MD FAAEM
CANDIDATE FOR AT-LARGE BOARD MEMBER
Current Employer: Baptist Medical Center
Clinical EM Practice Employment Type: Academic and Community
Clinical Hours in the ED per Month: 160+
Additional Leadership Roles: ACEP Coucilor
Nominated/Endorsed by: Robert A. Frolichstein, MD FAAEM; Vicki Norton, MD FAAEM; William T. Durkin, Jr. MD
MBA MAAEM FAAEM
Membership: 2015-2024
Disclosure: Nothing to disclose.
Attendance Record for AAEM BOD Meetings: 100%
AAEM Activities (past five years)
AAEM Board of Directors-YPS Director
Clinical Practice Committee-Board Liaison
Justice, Equity, Diversity & Inclusion Committee-Member
Justice, Equity, Diversity & Inclusion Section-Member
Women in Emergency Medicine Section-Member
Simulation Interest Group-Board Liaison
Membership Committee-Board Liaison
Section Leadership Committee-Board Liaison
Oral Board Review Course-Examiner
Candidate Statement for At-Large Board Member
Young Physicians Section Council-Member
Young Physicians Section Council-YPS Director
Young Physicians Section Council-Board Liaison
Leadership Academy-Mentor
Scientific Assembly-Poster Judge
Scientific Assembly-Abstract Reviewer
Mediterranean Emergency Medicine Congress (MEMC)-Poster Judge
Common Sense Author
Fred Earl Kency Jr, MD, FAAEM FACEP is a board-certified emergency physician and a native of Jackson, Mississippi. He received his Bachelors of Science in Biology from Alcorn State University and his Doctorate of Medicine from the University of South Alabama College of Medicine in Mobile, Alabama. Dr. Kency proudly served in the United States Navy for four years, and was deployed to Africa and Europe, prior to his honorable discharge. He returned home to Jackson, MS to complete his emergency medicine residency at the University of Mississippi Medical Center. Dr. Kency currently works in community medicine as well as academic emergency medicine working mostly with medical students at the University of Mississippi Medical Center.
Dr. Kency has been a member of AAEM since 2015. He has served in many leadership roles to include AAEM’s Resident and Student Association (AAEM/RSA) Board of Directors, AAEM’s Young physician Section (YPS-AAEM) council member, and most recently elected as AAEM YPS Director for three terms. As an AAEM board member, Dr. Kency has never missed a single board meeting, solidifying his dedication to the role his peers elected him too. He has also served on a host of committees within AAEM/RSA, YPS-AAEM, and AAEM.
Dr. Kency wants to continue his leadership in AAEM serving his first term as an At-Large board member. Dr. Kency’s passions include helping physicians with leadership training, financial awareness training, and continuing to be an advocate for Justice, Equity, Diversity, and Inclusion. Dr. Kency prides himself on successfully contributing to strategic decisions that positively impact the organization’s direction and long-term goals.
I humbly request your vote and support. Together we can continue to bring about positive change and work towards a brighter future for all Emergency Physicians. Let me continue to be your AAEM Champion and make a difference for us all. Thank you for your consideration.
PLATFORM
STATEMENTS
COMMON SENSE MARCH/APRIL 2024 16

Robert P. Lam, MD FAAEM
CANDIDATE FOR AT-LARGE BOARD MEMBER
Current Leadership Role/Employer: Director of Medical Education, Emergency Medicine Specialists PC
Clinical EM Practice Employment Type: Community practice with independent democratic group
Clinical Hours in the ED per Month: 140
Additional Leadership Roles: University of Colorado Health Southern Region Director of Physician Wellness
Nominated/Endorsed by: Jonathan S. Jones, MD FAAEM; Loice A. Swisher, MD MAAEM FAAEM; Robert A. Frolichstein, MD FAAEM
Membership: 2002-2024
Disclosure: Nothing to disclose.
Attendance Record for AAEM BOD Meetings: 89%
AAEM Activities (past five years)
AAEM Board of Directors-At-Large Board Member
AAEM Foundation-At Large Director
AAEM LEAD-EM-At Large Director
James Keaney Award Winner
Wellness Committee-Board Liaison
Palliative Care Committee-Board Liaison
Rural Medicine Interest Group-Board Liaison
Justice, Equity, Diversity & Inclusion Section-Member
Missouri Chapter Division-Member
Leadership Academy Task Force-Co-Chair
Candidate Statement for At-Large Board Member
Leadership Academy-Speaker
Medical Student Ambassador-Mentor
AAEM Health Advocacy Day-Participant
AAEM Residency Visit Speaker
Common Sense Author
Scientific Assembly-Speaker
Scientific Assembly-Moderator
Mediterranean Emergency Medicine Congress (MEMC)-Speaker
MEMC-Abstract Poster Judge
MEMC-Abstract Reviewer
It has been an honor to serve as a member of the board of directors for the past three years. Serving on the board of directors has allowed me to see how AAEM has embraced its role as the champion and conscience of emergency medicine. I have come to witness that AAEM is truly the advocate for the personal and professional well-being of the individual emergency physician.
I am very proud of the work that the AAEM Board continues to do for our members. We continue to speak out against workforce issues, support our committees and sections towards greater autonomy and develop the next generation of leaders. I’m most proud of how we are the only professional society in emergency medicine that is not afraid to fight the corporate practice of medicine with our lawsuit against Envision. We are making a difference as an academy and I am confident that history will reflect, as it has time and time again, that emergency medicine is a better specialty because of AAEM.
As your advocate on the board, I will continue to fight against the constant threat of the corporate practice of medicine, lack of due process and the non-physician scope of practice. I will advocate for EM to be a leader as the specialty that promotes physician well-being and inclusivity. I will continue to advocate for fair and equitable practice settings with structures and tactics that evolve with our changing workforce. I will continue to ensure that our academy is true to our mission as the champion of the emergency physician.
About Me:
I am a burnout survivor who transformed mid-career burnout into a passion for advocacy for physician well-being. I started my path in wellness with AAEM, having founded the AAEM wellness committee and currently serve at the board liaison. I currently serve as Director of Physician Wellness for the southern region of University of Colorado Health. I bring my passion, program development skills and experience as a physician leader to the board.
I practice as part of an independent democratic group Emergency Medicine Specialists PC in Colorado Springs, Colorado. Having been directly affected by contract management groups at many points in my career, working for and advocating for a fair and equitable practice continues to be a central
Continued on page 22 >>
PLATFORM STATEMENTS
COMMON SENSE MARCH/APRIL 2024 17
PLATFORM STATEMENTS
Kevin C. Reed, MD FAAEM
CANDIDATE FOR AT-LARGE BOARD MEMBER
Current Leader Roles/Employers: Vice Chief, Department of Emergency Medicine MedStar Georgetown University Hospital; Assistant Professor of Emergency Medicine, MedStar Georgetown University Hospital & MedStar Washington Hospital Center
Clinical EM Practice Employment Type: Primarily academic, tertiary care, high acuity urban hospital with 3 year Emergency Medicine Residency program with 30 residents and multiple Fellowships.
Clinical Hours in the ED per Month: 80
Additional Leadership Roles: MedStar System Co-Chair Cord Compression Oversight Committee
Nominated/Endorsed by: William T. Durkin, Jr., MD MBA MAAEM FAAEM; Laura J. Bontempo, MD Med; Joanne Williams, MD MAAEM FAAEM
Membership: 2002-2024
Disclosure: Nothing to disclose.
AAEM Activities (past five years)
Capital Region Chapter Board of Directors-President Operations Management Section-Member Education Committee-Member Education Committee-Co-Chair
Candidate Statement for At-Large Board Member
Scientific Assembly Planning Work Group-Ex-Officio Speaker Development Subcommittee-Chair Speaker Development Subcommittee-Member Common Sense Author
I joined the Academy in 2002, shortly after completing Emergency Medicine residency at the University of Maryland Medical System, excited to become part of an organization that tirelessly supports the careers and well-being of emergency medicine physicians. In 2004, I was honored to become a Fellow of the Academy.
For nearly 20 years, it has been my privilege to work with truly outstanding educators across the country as a member of the Education Committee. In addition to helping plan many of AAEM’s incredible educational offerings, my particular focus has been on programming for the annual Scientific Assembly and helping to create the one-of-a-kind Speaker Development Group. I have enjoyed the opportunity to serve as both Vice-Chair and then Chair of the Education Committee. I was truly honored to be selected for the AAEM Joe Lex Educator of the Year Award in 2017. Looking to further support our local members, I am very excited to have recently been elected President for the DC Capitol Region AAEM Chapter in December, 2023. Working with the newly elected board members we are excited about increasing local engagement to assist with AAEM legislative efforts and advocacy with members of Congress and the House of Representatives. We need to continue to fight for our rights and our specialty.
In my day job, I have worked as an emergency medicine attending since 2001 at both urban and community sites as well as 2 tertiary care hospitals, including the main teaching site for our great EM residency program at MedStar Georgetown University Hospital. Over the past 10 years, I have been fortunate to have served in multiple leadership roles within MedStar Emergency Physicians, including positions of Vice-Chair and Chair at 3 very busy, high acuity Emergency Departments. These roles have provided me with the opportunity to better understand the multi-faceted challenges facing emergency medicine physicians each day. With a rapidly changing work-force environment, increasing pressures on equitable reimbursement and a shortage of qualified clinical support staff, the challenges our specialty faces have never been greater.
I believe in the academy’s commitment to its members and to promoting an environment in which we, as emergency medicine physicians, can provide the highest quality care for our patients. I hope to apply a unique perspective gathered from over 20 years of clinical, educational, and administrative experience to help serve you, our members and most vital asset. If elected, I promise to work tirelessly with the AAEM Board to further advance our shared vision and goals. I will continue to advocate for the personal and professional well-being of every member, support increased diversity within our Academy and specialty, work to enhance our outstanding CME offerings and continue to support international EM programs and societies.
I appreciate your consideration and look forward to speaking with many of you at the upcoming Candidates’ Forum at the Scientific Assembly in Austin.
COMMON SENSE MARCH/APRIL 2024 18
Robert E. Suter, DO MHA FAAEM
CANDIDATE FOR AT-LARGE BOARD MEMBER
Current Leadership Role/Employer: Clinician and Consultant, Managing Partner, Texas Emergency Physicians, P.A.
Clinical EM Practice Employment Type: Have practiced in essentially every conceivable practice setting- urban, suburban, rural, international, academic, community, government, for-profit, and not for profit hospitals in independent contractor, democratic group partner, and employee status. Medical Director and Regional Medical Director/COO. Recently retired Brigadier General in the U.S. Army Reserve who served as CMO for DoD COVID assistance and other emergency responses.
Clinical Hours in the ED per Month: 36
Additional Leadership Roles: Past President of ACEP, ACOEP, IFEM, EMRA, and have served in important roles at AMA, AOA, Texas Osteopathic Medical Association, and Texas Medical Association. Recently retired combat veteran, Brigadier General in the U.S. Army Reserve who commanded medical forces in the Middle East including Iraq and Afghanistan.
Nominated/Endorsed by: William T. Durkin, Jr., MD MBA MAAEM FAAEM; Amin Antoine Kazzi, MD MAAEM FAAEM; Lisa. A. Moreno, MD MS MSCR FAAEM FIFEM
Membership: 2010-2024
Disclosure: Nothing to disclose.
AAEM Activities (past five years)
MEMC-Track Chair
International Committee-Member
Texas Chapter Division-Member
Uniformed Services Chapter Division-Member
Mediterranean Emergency Medicine Congress (MEMC)-Speaker
Candidate Statement for At-Large Board Member
Emergency physicians are under attack from multiple directions. We feel it every day. Moral injury from hospitals, insurers, groups, and worse, even from the patients we are trying to help. The perverse consequences of EMTALA that were never anticipated when it became law almost 40 years ago. It is exhausting. We need to find better paths to support our patients and each other. As an experienced strategic leader who still works in “the pit” I am passionately committed to working with our diverse Board to accomplish these goals. Yes, I have served on the AAEM Board and contributed in many other key roles at the national and international level over the past 20 years and I am humbled to have received the James Keaney Leadership Award in recognition of these AAEM accomplishments. Why is this important? By your membership in AAEM, you have demonstrated your commitment to supporting the very highest ideals that must guide our beloved specialty, and AAEM must deliver by representing these ideals forcefully and effectively. What you need now are experienced proven Warriors, like me, to work together to represent you in the battles we face in this decade and beyond. To do this I need your vote. With your vote, as a Board Member I will work collaboratively to advance the AAEM ideals and agenda that are most important to you, your patients, and our specialty. Thank you for your support.
PLATFORM STATEMENTS
COMMON SENSE MARCH/APRIL 2024 19

Haig Aintablian, MD FAAEM
CANDIDATE FOR YPS DIRECTOR
Current Leadership Role/Employer: Fellowship Director, Space Medicine, UCLA Health
Clinical EM Practice Employment Type: Faculty Physician, UCLA Health Department of Emergency Medicine
Fellowship Director, UCLA Space Medicine Director, UCLA Space Medicine Center Flight Surgeon
Clinical Hours in the ED per Month: 40
Additional Leadership Roles: Founder & Councilmember, Space Medicine Fellowship Council Space Medicine Task Force, ABEM
Nominated/Endorsed by: Self-nomination
Membership: 2016-2024
Disclosure: Nothing to disclose.
AAEM Activities (past five years)
Resident of the Year Award Winner
AAEM Board of Directors-AAEM/RSA Representative
California Chapter Board of Directors-Resident Representative
California Chapter Board of Directors-Director
Critical Care Medicine Section-Member
Emergency Medical Services Section-Member
Emergency Medicine Workforce Committee-Member
AAEM/RSA Advocacy Committee-Board Liaison
Candidate Statement for YPS Director
AAEM/RSA Board of Directors-Member
AAEM/RSA-President
AAEM/RSA Board of Directors-Immediate Past President Awards Committee-Member
Young Physicians Section Council-Member
Scientific Assembly-Speaker
Common Sense Author
Joining the American Academy of Emergency Medicine (AAEM) Board of Directors is a prospect I approach with both humility and excitement. My journey in emergency medicine has been both enriching and challenging, and it’s these experiences that fuel my desire to contribute more broadly to our field through AAEM.
As President of the AAEM Resident and Student Association (AAEM/RSA), I had the privilege of navigating complex issues that impacted our profession. We addressed vital concerns such as the training differences between residents and non-physician practitioners, the CMG expansion of EM residency programs, and the importance of resident advocacy. These topics weren’t just policy matters; they were about ensuring the best care for our patients and supporting the integrity of our profession. The weight of these responsibilities was not lost on me, and I carried them with the utmost seriousness and dedication throughout my training and early attending-hood.
Beyond AAEM/RSA, being selected as one of the three residents for the inaugural American Board of Emergency Medicine (ABEM) Resident Advisory Panel was extremely valuable. This role wasn’t just about representing residents or understanding the importance of board certification; it was a testament to my commitment to our collective voice in shaping the future of emergency medicine.
My work in developing Space Medicine as a new subspecialty symbolizes my belief in the endless possibilities of our field. This endeavor has been more than just an academic pursuit; it’s been about pushing the boundaries of what emergency medicine can be, especially as we venture into new frontiers like space.
Seeking a position on the AAEM Board of Directors is a natural extension of my passion for emergency medicine. I don’t just see this as a leadership role; I view it as an opportunity to serve our community, bringing forth the insights and experiences I have gained to help navigate the challenges and opportunities ahead.
In this role, I hope to foster an environment where innovation, education, and patient care are at the forefront. It’s about collaborating, listening, and leading with empathy and understanding. I am eager to work with the board, our members, and the broader medical community to ensure that emergency medicine continues to be a field marked by excellence, compassion, and progress with AAEM as our representative organization.
PLATFORM STATEMENTS
COMMON SENSE MARCH/APRIL 2024 20
PLATFORM STATEMENTS
Continued from page 11

L.E. Gomez, MD MBA MPH FAAEM
CANDIDATE FOR PRESIDENT-ELECT
Together with our Ethics and Social EM Committee leadership, I helped create and host a podcast series to ensure we educate everyone interested in research that supports the value of living up to our vision and mission as the premier organization in emergency medicine.
My clinical practice and teaching roles with residents in emergency medicine at the University of Maryland and associate professor at Howard University and my fortunate opportunity to be educated at some of the best schools in the country: Cornell, Mt. Sinai, BU, University of Chicago and MBA and MPH at the Hopkins and experiences as medical director in my nearly thirty years in emergency medicine practice and now consultant for business performance, have enhanced my skills and dedication to advocacy. My roles in Government and National Affairs and advocacy on The Hill included a Fellowship in Congress and authorship of an AAEM Policy Statement calling for greater accountability by EMS, Law Enforcement, and our judicial system.
Help me continue our dedication to the foundational ideals of AAEM, and bring our message abroad as we grow internationally. Your vote ensures we continue this work to lead us into a brighter future of collaboration over divisiveness.
Continued from page 12
 Vicki Norton, MD FAAEM CANDIDATE FOR PRESIDENT-ELECT
Vicki Norton, MD FAAEM CANDIDATE FOR PRESIDENT-ELECT
a button to email, call, or tweet at legislators. Emergency physicians are amazing patient and community advocates and that should not cease when they go home after a shift.
As President-Elect, I will restore due process for emergency physicians. I and numerous other AAEM leaders have spoken to federal legislators about this issue many times and encouraged their support of a national due process bill. A bipartisan, bicameral bill is soon to be introduced.
Our duty as physicians is to help our patients: to be their advocates, to be their safety net when they need it most. However, physicians need a champion too. I will be that champion for Emergency Medicine physicians everywhere. I ask that you vote for me for President-Elect so that I may to continue to serve AAEM and our members. Thank you for this opportunity.
>> COMMON SENSE MARCH/APRIL 2024 21
PLATFORM STATEMENTS
Continued from page 14

Phillip A. Dixon, MD MBA MPH FAAEM CHCQM-PHYADV CANDIDATE FOR SECRETARY-TREASURER
Just for some additional personal background, I have been involved with AAEM since my second year of residency. I was on the executive board of AAEM/RSA as a resident and YPS-AAEM board after residency. I believe in AAEM’s mission and values above all else. AAEM has a unique perspective on physician advocacy and fair practice, which speak to me as a clinician. AAEM is the premier EM physician organization and I am so proud to
be a member of such a strong and dedicated organization. I will continue to be an active member in AAEM as long as I am an emergency physician. I am deeply grateful for the trust and support extended by the AAEM membership and the organization as a whole. The impact AAEM has had on me both as a person and a leader in emergency medicine is immeasurable. As I seek the opportunity to continue serving on the AAEM board, I am excited about the possibility of contributing to the future growth and enduring impact of our organization. Thank you for considering my candidacy, and I look forward to the opportunity to serve you as Secretary-Treasurer.
Thank you.
Sincerely,
Phillip A. Dixon MD MBA MPHÂ FAAEM
CHCQM-PHYADV
Continued from page 15
 Frank
Frank
L.
Christopher,
MD FAAEM CANDIDATE FOR AT-LARGE BOARD MEMBER
During my twenty years of active service in the Army, I was charged to develop future leaders. Promotions, it’s said, are about potential, not performance. I am proud to say that several of the then-junior officers under my charge as a senior leader have gone on to be excellent leaders and role models on their own.
I hope to do the same as a member of the Board and thank you for your support!
Continued from page 17

Robert P. Lam, MD FAAEM CANDIDATE FOR AT-LARGE BOARD MEMBER
priority. I bring the experience of having my career turned upside down by CMGs as a central motivating experience against the corporate practice of medicine to my service on the board.
I am on the faculty for the University of Colorado School of Medicine working directly in medical education. I bring my passion for medical education, mentorship, and professional development to my service on the board. I was co-chair for our Leadership Academy Task Force which has reorganized Leadership Academy into a direct mentorship and leadership development program for the future leaders of our academy.
COMMON SENSE MARCH/APRIL 2024 22
TINA “There Is No Alternative” … Or is There?
Chris McNeil, MD
TINA (There Is No Alternative) is a term that has been frequently used in financial circles for the last decade. It refers to the lack of alternatives to investing your money outside of equities (stocks) since the great financial crisis. In response to the 2008-2009 great financial crisis, the Federal Reserve made a policy to drastically lower interest rates in addition to quantitative easing (the Federal Reserve purchases bonds to support the market i.e., “money printing”) to provide support for economic recovery from that recession. Over the decade since, policymakers have intermittently attempted to raise interest rates and slow the pace of quantitative easing without success. Investors and markets have grown accustomed to a low interest rate environment, and they throw a tantrum every time the Federal Reserve attempts to tighten financial conditions.
“ The average return for the stock market over the long run is 8-9%. If you can safely get 5% in a money market or short-term bond investment, that is almost two-thirds of the expected return of the stock market with little to no risk.

ing in fixed-income, the recent rate hiking experiment of the Federal Reserve to combat inflation over the last couple of years has resulted in the worst two-year performance of bonds in nearly a century.
More recently, in response to the shutdown of the economy during COVID, policymakers once again slashed rates and flooded the market with stimulus to “protect” the economy. Thanks guys! The result of supply chain disruptions, along with this extra government stimulus, resulted in horrific inflation that they are currently working on taming.
Until recently, the extremely low interest rate environment and low yields on bonds and other fixed-income investments have been unattractive additions to a portfolio. Fixed-income investments typically offer a fixed payment in the form of interest and low volatility. Historically, these have provided a balance to portfolios and a safe haven during market volatility. They have been a more significant component of investment portfolios for short-term goals, conservative investors, and retirees. However, due to the low interest rate environment since the great financial crisis, these investments have not kept up with the pace of inflation. Hence the term TINA.
Conservative investors and retirees have had to venture farther out on the risk curve to meet their return needs and keep their savings on pace with inflation. These investors have been forced to allocate more money to equities and alternative investments. Even worse for them if they have
Until recently, TINA has led many investors (rightly so) to ignore fixed-income investments and chase returns in the stock market instead. However, now that interest rates have risen substantially over the last two years, the concept of TINA may be dead for the foreseeable future, as fixed-income investments are now looking more enticing.
For the first time in over a decade, bonds, CDs, and money markets are providing an attractive yield. The average return for the stock market over the long run is 8-9%. If you can safely get 5% in a money market or short-term bond investment, that is almost two-thirds of the expected return of the stock market with little to no risk. Conservative and fixed-income investors have not had this opportunity in many years. Fixedincome investments come in many flavors, but we’ll review the three most common.
y A bank Certificate of Deposit (CD) is a financial product offered by banks in which customers deposit a fixed sum of money for a predetermined period, typically ranging from a few months to several years, in exchange for a fixed interest rate. These investments now have attractive rates for short-term money. However, the money invested is locked up for the term of the CD.
FINANCIAL WELLNESS
>> COMMON SENSE MARCH/APRIL 2024 23
y A money market fund is a mutual fund that invests in short-term, high-quality securities such as government bonds, CDs, and commercial paper. These funds aim to provide investors with a low-risk option for preserving capital while generating modest returns and maintaining liquidity. You can withdraw your money at any time from a money market fund.
y A bond is a debt instrument that governments, municipalities, or companies issue to raise capital. When you purchase a bond, you lend the money to the issuer in exchange for periodic interest payments and the return of the principal amount at maturity. Bonds come with various terms, interest rates, and levels of risk. Municipal bonds also offer an exemption from federal income tax on the interest earned. Bond prices are inversely correlated to the bond yield. As rates go up, the bond’s current value decreases and vice versa. In a declining interest rate environment, bonds are attractive investments as the bond will continue to pay the stated interest rate and it will appreciate in value as interest rates fall. Purchasing bonds in a high interest rate environment is a way to capitalize on the interest paid and potential value growth should rates drop in the future. Investors must know the current interest rate environment to determine if a bond investment
fits their goals and needs. The current environment, in which rates have risen dramatically over the last couple of years, has allowed many investors to consider bonds as a viable way to grow their investments, with lower risk than the volatile stock market.
For the first time in over a decade, conservative investors and retirees have options for reasonable, safe returns in fixed-income investments that can keep pace with inflation and offer portfolio growth. Suppose you are a moderate or conservative investor or someone in retirement. In that case, I highly recommend taking a look at fixed-income investments for your portfolio or speaking with your financial professional to help determine if this investment finally has a place in your portfolio.
The concept of TINA may be dead for the foreseeable future.
Dr. Chris McNeil, the author of this article, is an emergency physician and former emergency medicine residency program director who transitioned his career to finance. He owns a registered investment advisory firm, VitalStone Financial, LLC, and specializes in financial planning for physicians.

FINANCIAL WELLNESS
COMMON SENSE MARCH/APRIL 2024 24
Breaking Free from Work Dread
Amanda Dinsmore, MD, Kendra Morrison, DO, and Laura Cazier, MD



Arecent conference in Ottawa revealed the poll results of over 750 hospital workers.1 It found that 41% dread going to work. Some of the symptoms described were exhaustion, difficulty sleeping, and anxiety about working.2 Since the reasons cited were due to staffing shortages and staff turnover, it seems likely a lot of us in the U.S. feel similarly. Certainly, in speaking with our emergency medicine colleagues, a lot of us experience work dread.
In “The Epidemic of Work Dread,” Michael Hersh, MD describes several familiar dread symptoms like getting a feeling in the pit of our stomachs when trying to enjoy time with family.3 We might sit as long as possible in the parking lot, hesitating to go in to work. Dread can look like doomscrolling on our phones or daydreaming about early retirement.
So let’s talk about dread.
Definition
In Brene Brown’s Atlas of the Heart, she explores the 87 common human emotions and experiences.4 Dread is grouped with other emotions experienced when things are uncertain or too much. “Dread occurs frequently in response to high-probability negative events; its magnitude increases as the dreaded event draws nearer.” Emergency physicians work in challenging, quite literally life-and-death circumstances. It makes sense that we have a predilection for work dread. Let’s have compassion for ourselves for that.
Brown clarifies that anxiety and dread are perceived threats in the future. This is different from fear, which is a threat in the present.
Benefits
Dread can serve us if we’re taking action to prepare in some way. “The purpose of dread is to help prepare you,” psychologist Ali Mattu suggests. “It’s to help you think about what might happen. It’s to help you take actions that you can right now.”5 For example, if you dread doing certain workups (dizziness comes to mind) or procedures, maybe it’s time to sign up for a refresher course on that topic. If you dread running into a particular colleague, maybe a difficult conversation needs to happen. Those could be useful responses to dread.
Drawbacks
On the other hand, spending too much time experiencing dread has negative consequences. There’s only so much preparation that we can reasonably do. Beyond that, it’s not serving a beneficial purpose. And, frankly, many of us stay in dread with no intention of doing anything useful about it in the first place.
Brene Brown explains that dread can make an anticipated negative event even worse. We can convince ourselves that work will be such a dumpster fire that we escalate ourselves into what she calls a “dread-frenzy.” That’s particularly problematic because even if our shift goes okay, we’re so “dread-exhausted” that we can’t appreciate it. When we are spending our time in dread, we’re bringing what might be into our present moment. And we’re feeling it when it hasn’t even happened yet. Have you felt tension in your neck and shoulders or clenched your jaw when thinking of working your next shift? Your body is physically experiencing a version of the very thing you’re trying to avoid. It doesn’t know the difference between imagining it and the real thing. And we do it to ourselves over and over.

When we are spending our time in dread, we’re bringing what might be into our present moment. And we’re feeling it when it hasn’t even happened yet.
THE WHOLE PHYSICIAN
>>
COMMON SENSE MARCH/APRIL 2024 25
What would serve us so much more is recharging in our time off work, rather than pre-living the stress. No wonder we’re exhausted!
Breaking Free
There is an important concept called metacognition. It’s awareness and understanding of your thought processes. You’re not your thoughts—you are the watcher of your thoughts. Just because your brain offers certain thoughts up for consideration, you don’t have to take the bait and engage. You can notice a particular thought (you can even say something like, “Oh hello there again”) and allow it to pass without judgment (“I see you, but this time I’m going to pick something else to think about”). This is mindfulness.
“ You’re not your thoughts—you are the watcher of your thoughts. Just because your brain offers certain thoughts up for consideration, you don’t have to take the bait and engage.

This is liberating because when you realize you are allowed to curate your thoughts, you realize:
y work can’t force you to obsess about it (take that dumpster fire!!).
y that jerk consultant, ex, in-law, or horrible political figure can’t hijack any more time from your precious life than they already have—unless you decide to think about him/her.
The goal is to stay in this moment. Enjoy it. It’s the only thing that is real. The past is over except when you bring it into your present by thinking about it. The future is yet to be determined. If you’re having trouble getting out of your head and back into your body, try questions like these:
y What noises can you hear?
y Can you feel any textures on your skin?
y Who is with you?
y Are there any smells?
y Is there anything you haven’t noticed before in your field of vision?

When motivational speaker, author, and former lawyer Mel Robbins is on edge, she puts her hand on her heart and repeats, “I’m okay, I’m safe, I’m loved” as many times as needed to come back to the present moment.6 In this particular moment, all of those things are true.
Mel Robbins also asks the question, “What is the harm in thinking, ‘What if it all works out?’” If you aren’t doing anything useful with your dread, this possibility feels so much better. And who is to say that it’s not going to work out better than expected? You’ll find out soon enough.
One thought that can serve us well is, “I’m a freaking EM Doc (a BAFERD, if you will). If the feces hits the fan at work, I can trust myself that I’ll do what needs to be done to deal with it then.” Until then, though, we can make a deal with ourselves that we only need to live it once. Preliving what you dread multiple times only distracts us from everything in our lives that we love.
Remember, our work dread can serve a purpose if it prompts us to prepare, have a difficult conversation, or meet a challenge head-on. But outside of that, the pre-stressing over a future yet to be determined keeps us from recharging and experiencing all the goodness of what exists in this moment. Trust yourself to handle garbage when the time comes. But until then, go do something that lights you up inside and enjoy every moment.
thewholephysician.com
References
1. https://www.businesswire.com/news/home/20240102067721/en/41Per-Cent-of-Ontario’s-Hospital-Workers-Dread-Going-Into-Work-NewPoll-Suggests-Staffing-Crisis-to-Worsen-Without-Course-Correction-bythe-Ford-Government
2. https://www.sudbury.com/local-news/poll-58-of-northern-hospital-workersdread-going-to-work-due-to-staffing-8071397
3. https://www.kevinmd.com/2022/06/the-epidemic-of-work-dread.html
4. Brown, Brené, Atlas of the Heart: Mapping Meaningful Connection and the Language of Human Experience. New York, Random House, 2021.
5. https://www.npr.org/2022/11/22/1138759124/transform-the-way-you-dealwith-dread
6. Robbins, Mel, The High 5 Habit: Take Control of Your Life with this One Simple Habit. Carlsbad, CA, Hay House, 2021.
THE WHOLE PHYSICIAN
COMMON SENSE MARCH/APRIL 2024 26
WELCOME TO AUSTIN!
On behalf of the Scientific Planning Work Group of the American Academy of Emergency Medicine Education Committee, we are looking forward to welcoming you to AAEM24 Scientific Assembly and to Austin, Texas. This event is one of the most anticipated academic conferences of the year, with a focus on cutting edge clinical medicine as well as practical application to patient care. Networking opportunities are plentiful as well as open invitations to attend any committee, section, or interest group meetings.
AAEM’s Scientific Assembly will take an innovative and practical look at various topics within emergency medicine that shape our field of practice. We are excited to expand the conversation on the topics of toxicology, cardiology, critical care, infectious disease, and many more. By combining discussion from leading scholars with innovative medical nuances, we hope to provide a resource to enhance the understanding of our beloved specialty.
AAEM continues to feature several learning styles: 20-minute track talks; seven-minute, “short and sweet” Breve Dulce lectures; 45-minute plenaries; hands-on Small Group Clinics; and add-on courses (formerly known as pre-conference courses). The Meeting of the Minds literature review panels are back by popular demand. The competitions at Scientific Assembly continue to grow: listen to oral abstract presentations, watch up-and-coming speakers at Open Mic, and browse the poster gallery for research posters and baffling case encounters in the Photo Competition. Many AAEM groups are planning social events to supplement your educational time with opportunities to meet new colleagues as well as socialize with cherished friends.
The planning work group has invested significant time and thought to ensure that every participant has an educational, enjoyable, and safe experience in Austin. We look forward to sharing these amazing topics and engaging presenters with you.
We look forward to seeing you in Austin!

EIGHT EM DOCS WALK INTO A SHIFT SHOW
Sunday, April 28 | 4:00pm – 5:20pm




BREVE DULCE
These ever-popular “short and sweet” sessions are seven-minute overviews and 25 slides packed full of information! Plan to catch a variety of Breve Dulce topics at AAEM24 to round out your educational experience. The “Stacked Session” in Breve Dulce II on Tuesday, April 30 will feature back-to-back lectures on similar topics: ThoracicRespiratory, Cardiology, Critical Care, Cardiology, Ultrasound, Pediatrics, and Trauma.
“Eight Docs” is a collaborative effort by the eight AAEM Sections providing a fun, fresh take on a traditional lecture. Follow Dr. Calhoun as she works her way through a traumatic shift, taking care of a psychiatric patient, aided by her specialist colleagues. Each section will provide a “breakout” lecture meant to help Dr. Calhoun (and you) take better care of the patient at hand, from pre-hospital care to final disposition and beyond.


BOOST YOUR CME BY SIGNING UP FOR AN ADD-ON COURSE (FORMERLY KNOWN AS A PRE-CONFERENCE COURSE) BEFORE OR AFTER AAEM24.
April 27-May 1, 2024 Austin, TX #AAEM24 aaem.org/aaem24
CO-LEAD
Christopher Colbert, DO FAAEM
CO-LEAD Molly K. Estes, MD FAAEM FACEP
CO-VICE LEAD Zachary Repanshek, MD FAAEM
CO-VICE LEAD Julie Vieth, MD FAAEM
>> COMMON SENSE MARCH/APRIL 2024 28
30th Annual SCIENTIFIC ASSEMBLY

COMPETITIONS
MEETING OF THE MINDS
Watch as prominent EM practitioners debate the pros and cons of the latest practicechanging articles on transfusion practices in trauma. Bring your questions for an audience Q&A with the experts.
SECURE YOUR SPOT AT AAEM24 TODAY AND BECOME AN ACTIVE PART OF A COMMUNITY SHAPING THE FUTURE OF EMERGENCY CARE.
Plan to browse the poster displays or attend abstract presentations at AAEM24. The following competitions will be taking place during the conference.
y AAEM and Journal of Emergency Medicine Resident and Student Research Competition
y AAEM/RSA & Western Journal of Emergency Medicine Population Health Research Competition
y Photo Competition
y AAEM Young Physicians Section (YPS) Research Competition
y AAEM/RSA Resident Breve Dulce Competition
y CCMS-AAEM Breveloquent Competition
y Sim Sono Sleuthing Case Challenge
y Open Mic Competition – Onsite sign-ups available!

RELAX & RECHARGE WITH WELLNESS EVENTS
SMALL GROUP CLINIC
SCAN THE QR CODE to learn more about competitions



These sessions provide personal and handson education. At AAEM24, 25 slots will be filled with advanced registration and five slots will be available on a first-come, first served-basis.
Not only does AAEM24 offer enriching education, it is also a motivational retreat where you leave feeling a renewed passion for emergency medicine. Throughout the Assembly, stop by the Wellness Room for a sanctuary from the conference bustle. The AAEM Wellness Committee has also planned the following events to participate in: Lost in Austin – Walk with the Wellness Committee, Smash Your Stress Away, Airway at AAEM, Wellness Paint’N’Sip, Wellness New Attendee Reception, Mental Health Action Plan Workshop, and the Wellness Committee with Women in Emergency Medicine Coffee Meet-Up. Some events require pre-registration.



COLLABORATE AND NETWORK WITH COLLEAGUES FROM AROUND THE WORLD.

SCAN
>>
COMMON SENSE MARCH/APRIL 2024 29
THE QR CODE to learn more about wellness events
#AAEM24
AAEM/RSA RESIDENT TRACK AT AAEM24
April 30, 2024 | 8:55am – 5:50pm
The AAEM/RSA Resident Track programming is selected by residents, for residents. The goal of the track is to prepare residents for their careers in emergency medicine by concentrating on clinical topics and lectures on career success. The session concludes with the AAEM/RSA Breve Dulce Competition, featuring resident presentations on the theme of Learning While Teaching: gaining a new perspective while teaching that furthered your own learning, or improved on the way you were taught.

NETWORK AT SOCIAL EVENTS
TAKE TIME TO CELEBRATE AND RECHARGE AT SOCIALS FROM JEDI-AAEM, WIEM-AAEM, AND WELLNESS THROUGHOUT AAEM24.
Join AAEM for networking and other fun activities throughout the Assembly. Kick off AAEM24 at our Opening Reception. Enjoy light hors d’oeurves and drinks while networking with colleagues and exhibitors. Spend time with the Women in EM Section at their Networking Lunch. Explore opportunities to get involved in AAEM with the engagEM!
Social. Attend Airway at AAEM for an evening which promises to showcase the great range of human experience—to enlighten minds, expose vulnerabilities, and quietly suggest ways to overcome the challenges we all face each day.
KEYNOTE SPEAKER

SCAN THE QR CODE to learn more about social events



DOCTORS AND LITIGATION: TIME FOR A NEW PARADIGM
Tuesday, April 30, 2024 | 8:00am - 8:45am
Gita Pensa, MD FAAEM
PLENARY SPEAKERS
EMERGENCY CARDIOLOGY 2024: THE ARTICLES YOU’VE GOT TO KNOW!
Sunday, April 28, 2024 | 1:45pm - 2:30pm

Amal Mattu, MD FAAEM
RECENT RESUSCITATION AND CRITICAL CARE ARTICLES YOU’VE GOT TO KNOW!
Sunday, April 28, 2024 | 2:40pm - 3:25pm

Michael Winters, MD, MBA, FAAEM

Skyler Lentz, MD FAAEM FACEP
April 27-May 1, 2024 Austin, TX
aaem.org/aaem24
>>
COMMON SENSE MARCH/APRIL 2024 30
PLENARY SPEAKERS, CONTINUED
PEM LITERATURE UPDATE
Monday, April 29, 2024 | 8:00am - 8:45am

Ilene Claudius, MD FAAEM

Mimi Lu, MD FAAEM
MINI LAW SCHOOL FOR PHYSICIANS
Monday, April 29, 2024 | 8:55am - 9:40am

Melanie Heniff, MD JD MHA FAAEM FAAP

Malia J. Moore, MD FAAEM

Joseph P. Wood, MD JD FAAEM
EMERGENCY MEDICINE UNIONS: RESTORING THE POWER OF WORKING PHYSICIANS
Monday, April 29, 2024 | 3:15pm - 4:00pm

Leon C. Adelman, MD, MBA, FAAEM

Sean Codier, DO FAAEM

David Levin, DO, FAAEM

Bryce Pulliam, MD FAAEM
30th Annual SCIENTIFIC ASSEMBLY
WHEN MINUTES COUNT - UPDATES IN EMERGENCY NEUROLOGY
Tuesday, April 30, 2024 | 1:30pm - 2:15pm
Wan-Tsu W. Chang, MD FAAEM
ADVOCACY IN EMERGENCY MEDICINE
Wednesday, May 1, 2024 | 8:10am - 8:55am

Vicki Norton, MD FAAEM

Mercy M. Hylton, MD MBA FAAEM

Deborah Fletcher, MD FAAEM
TRANSFUSION PRACTICES IN TRAUMA: HOW CONTEMPORARY LITERATURE CAN AND SHOULD CHANGE WHAT WE DO!
Wednesday, May 1, 2024 | 10:00am – 10:45am

Harman Singh Gill, MD FAAEM

Luke J. Duncan, MD FAAEM

Michael Dittillo, DO
VISIT THE AAEM24 WEBSITE FOR FULL EDUCATIONAL DETAILS INCLUDING THE SCIENTIFIC PROGRAM, HOTEL AND TRAVEL INFORMATION, AND MORE! AAEM.ORG/AAEM24 >> COMMON SENSE MARCH/APRIL 2024 31
AAEM24 SPEAKERS
Leon C. Adelman, MD MBA FAAEM
Jason Adler, MD
Miguel F. Agrait Gonzalez, MD FAAEM
FACEP CAQ-SM
Leen Alblaihed, MBBS MHA FAAEM
Hala Ashraf, DO
Amil Badoolah, DO
Keith Baker, MD
Jerome Balbin, MD FAAEM
Algis Baliunas, MD FAAEM
Isabel Barata, MS MD MBA FAAP
FACEP FAAEM
Alex Barbuto, MD FAAEM
Stacey Barnes, DO FAAEM
Rahul G. Bhat, MD
Neha Bhatnagar, MD
Eliot H. Blum, MD FACEP
Michael Bond, MD FAAEM FACEP
Laura J. Bontempo, MD MEd FAAEM
Joelle C. Borhart, MD FAAEM
Matthew Borloz, MD FAAEM FACEP
Joseph Bove, DO FAAEM
Vonzella A. Bryant, MD FAAEM
Katharine Burns, MD FAAEM
Christine Butts, MD FAAEM
Lindsey Caley, MD
Elisabeth Calhoun, MD MPH FAAEM
Brian Cameron, MD FAAEM
David J. Carlberg, MD FAAEM
Jennifer Carnell, MD FAAEM
Matthew Carvey, MD
John Casey, DO MA FACEP
FACOEP-D
Wan-Tsu W. Chang, MD FAAEM
Yash Chavda, DO MBA FAAEM
Eric Chin, MD MBA FAAEM
Matt Christensen, MD
Kene Chukwuanu, MD FAAEM
Ilene Claudius, MD
Sean Codier, DO FAAEM
William Cooper, MD
Juliet Corcillo, MD
Neil K. Dasgupta, MD FAAEM
Blake Davidson, MD
Joshua J. Davis, MD FAAEM
Peter DeBlieux, MD FAAEM
Michael Dittillo, DO
Christopher Doty, MD MAAEM FAAEM
FACEP
Luke J. Duncan, MD
Sean B. Eden, PA-C
Alyssa Eily, MD
Molly K. Estes, MD FAAEM FACEP
Cheyenne Falat, MD
Cayla Fappiano, MD
Frederick Fiesseler, DO FAAEM
Deborah Fletcher, MD FAAEM
Lauren Friend, MD
Brian Q. Gacioch, MD
Manish Garg, MD FAAEM
Sean P. Geary, MD FAAEM FACEP
Harman Singh S. Gill, MD FAAEM
Alexander Giuliano, MD
David H Gordon, MD FAAEM
June Gordon, MD
Michael Gottlieb, MD FAAEM
Matthew Graber, MD PhD FAAEM
Annette Grajny, MD MS
John C. Greenwood, MD FAAEM
Marianne Haughey, MD FAAEM
Brian T. Hawkins, Md
Arya Hawkins-Zafarnia, MD MA
Megan Healy, MD FAAEM
Melanie Heniff, MD JD MHA FAAEM FAAP
Jason Hine, MD FAAEM
Max Hockstein, MD FAAEM
Kami M. Hu Windsor, MD FAAEM
FACEP
Maite Huis in ‘t Veld, MD FAAEM
Mercy M. Hylton, MD MBA FAAEM
Anne K. Ickes, DO
Alexander Iteen, MD
Paul S. Jansson, MD MS FAAEM
Gregory N. Jasani, MD FAAEM
Naomi Jean-Baptiste, MD
Kristine Jeffers, MD FAAEM
Prianka K. Kandhal, MD FAAEM FAAP
Ryan Kelly, MD MSc
Danya Khoujah, MBBS MEHP FAAEM
Patrick G. Kishi, MD FAAEM
Alex Y. Koo, MD FAAEM FACEP
Venkat Kotamraju, MBBS MRCS
PGDipMedTox MAcadMed CMQ
CPPS RCPathME FEBEM FRCEM
Alyssa Krepela, MD
Rebecca Kreston, MD MSPH
Beth J. Kushner, DO FAAEM
Ochan Kwon, MD
Diana Ladkany, MD FAAEM
Jonathan Lee, MD FAAEM
Skyler Lentz, MD FAAEM FACEP
Nathaniel T. Leu, MD MS FAAEM
David Levin, DO FAAEM
Bruce M. Lo, MD MBA FAAEM
Bobbi-Jo Lowie, MD
Mimi Lu, MD
Phillip D. Magidson, MD MPH FAAEM
Amy Marks, MD
Amal Mattu, MD FAAEM
Lisa Maurer, MD
Nicole S. McCoin, MD FAAEM FACEP
Gabriella Miller, MD
Ferdinando L. Mirarchi, DO
Sara Misthal, MD FAAEM
Siamak Moayedi, MD FAAEM
Robert Mohr, MD
Joel Moll, MD
Malia J. Moore, MD FAAEM
Jessica Moore, MD
Melissa Myers, MD FAAEM
Robert K. Needleman, MD FAAEM
Nirajan Nepal, MD
Vicki Norton, MD FAAEM
James O’Brien, MD
OluMide (Lu) Ojeifo, MD
Ava Omidvar, MD MPH FP-C
Brian Parker, MD MS FAAEM
Casey Patrick, MD FAEMS
Jessica Pelletier, DO
Gita Pensa, MD FAAEM
Andrew Phillips, MD
Valerie A. Pierre, MD FAAEM
Elizabeth Pontius, MD FAAEM
Bryce Pulliam, MD FAAEM
Steven A. Radloff, MD
Mark Ramzy, DO
Rebecca Raven, MD
Ralph J. Riviello, MD MS FAAEM
Andrew Rizzo, DO FAAEM
Robert Rodriguez, MD
Michelle Romeo, MD FAAEM
Lauren S. Rosenblatt, MD
Shana EN Ross, DO MSc FAAEM FACEP
Jonathan Rowland, MD
Amanda Russo, DO
Novneet Sahu, MD
Alexis Salerno, MD FPD-AEMUS
Evelyn Schraft, MD
Kraftin E. Schreyer, MD MBA FAAEM
Shawn Sethi, DO FAAEM
Andrew W. Shannon, MD MPH FAAEM
Joseph Shiber, MD FAAEM FCCM FNCS
Richard D. Shih, MD
Ninad Shroff, MD FAAEM FAWM
Matthew S. Siket, MD
Michael M. Silverman, MD MBA FAAEM FACEP
Branden Skarpiak, MD DTM&H FAAEM
Tierra Smith, MD
Ryan Spangler, MD
Eric Steinberg, DO MEHP FAAEM
Kathleen Stephanos, MD FAAEM
Joshua Stierwalt, MD MPH MA
Sawali Sudarshan, MD PhD FAAEM
Tina W. Sundaram, MD MS FAAEM
Rebecca G. Theophanous, MD MHSc FAAEM FACEP
Arleigh R. Trainor, MD FAAEM FACEP
Joseph R. Twanmoh, MD MBA FAAEM
Mary Unanyan, DO
Stefani A. Vande Lune, MD JD
Jordan Vaughn, MD
Julie T. Vieth, MD FAAEM FACEP
Christian Wade, MD
Elias E. Wan, MD FAAEM
Tyler Webb, MD
Jim Webley, MD FAAEM
Benjamin White, MD FAAEM
Anne Whitehead, MD FAAEM FACEP
Joanne Williams, MD MAAEM FAAEM
George Willis, MD FACEP FAAEM
Rachel Wiltjer, DO
Mike Winters, MD MBA FAAEM
Carmen Wolfe, MD
Joseph P Wood, MD JD MAAEM FAAEM
Gregory Wu, MD FAAEM FACEP
Katy Wyszynski, MS OMS-IV
Nicole A. Yuzuk, DO
Bassam Zahid, MD FAAEM
Mitchell Zekhtser, DO
Bob Zemple, MD MBA FAAEM FACEP
Tony Zitek, MD FAAEM
Matthew Zuckerman, MD
Jaryd Zummer, MD
April 27-May 1, 2024 Austin, TX
aaem.org/aaem24
#AAEM24
THANK YOU TO ALL AAEM24 SPEAKERS FOR YOUR INVALUABLE CONTRIBUTIONS, ENRICHING OUR CONFERENCE WITH KNOWLEDGE, INNOVATION, AND INSPIRATION. YOUR EXPERTISE HAS TRULY MADE A DIFFERENCE. >> COMMON SENSE MARCH/APRIL 2024 32
30th Annual SCIENTIFIC ASSEMBLY
THANKS TO OUR 2024 INDUSTRY PARTNERS
AAEM extends its thanks and appreciation to the following industry partners who have funded activities at the 2024 AAEM Scientific Assembly.
GOLD SPONSOR – $20,000-$49,999 SUPPORT LEVEL
y Abbott
y Ambience
SILVER SPONSOR – $5,000-$19,000 SUPPORT LEVEL
y LogixHealth


AAEM24 EXHIBITORS – THANK YOU
Plan your visit to the exhibit hall in Austin to network with these exhibitors:
y Alleviate, LLC
y American Board of Emergency Medicine (ABEM)
y ApolloMD
y AstraZeneca
y Auburn University – Physicians Executive MBA Program
y Bennett Pharmaceuticals of America
y Brault Practice Solutions
y BRC
y CardioVision Care
y Concord Medical Group
y Corevant Health Partners
y CSL Behring
y Emergency Care Partners
y EMrecruits by R1
y ER Doc Finance
y Federation of State Medical Boards
y Fujifilm Sonosite
y GBR Medical
y Hamilton Medical
y Inari Medical Inc.
y Indian Health Service
y Indiana University – Kelley School of Business
y IntuiTap Medical, Inc.
y Island Health
y Kansas Emergency Physicians
y Kosmos by EchoNous
y LogixHealth
y Luminos Pro
y Marlab Inc.
y MeMed
y Mindray
y Moonstone Nutrition
y OHK Medical Devices
y Penn State Health
y PEPID

y Physician Wealth Advisors
y Praxi Management
y Quest Healthcare Solutions
y Resolv Healthcare
y Rosh Review, A Blueprint Test Prep Company
y Siemens Healthineers
y SimKit
y The Dental Box
y The Permanente Medical Group
y The Whole Physician
y United States Air Force
y Victoria Emergency Associates
y Ventra Health
y Vituity
y Washington Emergency Care Physicians
y WestJEM
y Zerowet, Inc.

>> VISIT THE EXHIBIT HALL TO MAKE NEW CONNECTIONS – EXHIBITING AND SPONSORSHIP OPPORTUNITIES ARE STILL AVAILABLE. SCAN THE QR CODE for the most up-to-date sponsor and exhibitor list COMMON SENSE MARCH/APRIL 2024 33
#AAEM24
Wellness and Resilience: Nurturing a Healthy Emergency Medicine Community at AAEM24
Al’ai Alvarez, MD,* Neha Bhatnagar, MD, † and Jennifer Kanapicki-Comer, MD §



Emergency medicine faces a critical issue of burnout. Leigh et al. found that 71.4% of urban and 85.7% of rural emergency medicine physicians experience burnout.1 Since the onset of the COVID-19 pandemic, Nguyen et al. reported a burnout rate of 74.7% among emergency medicine physicians, attributing this to emotional strain and increased workload.2
Institutions must prioritize practice efficiency and cultivate a wellness culture. Institutions can:
y Create supportive work environments
y Implement wellness programs and retreats to alleviate stress and foster camaraderie
y Strive for healthy work-life harmony3
y Provide and seek mental health resources and support
y Encourage open discussions about stress and burnout
However, individual actions also play a crucial role in personal and colleague well-being. We as individuals can:
y Practice self-compassion and mindfulness
y Establish clear professional boundaries4,5
y Prioritize physical and mental health and wellness
y Cultivate a positive work environment and relationships
y Seek professional support when needed
A crucial component of these interventions is fostering a sense of community. In the post-pandemic era, a feeling of interpersonal distance has emerged, particularly where virtual events have become the norm. These events include department meetings, interviews, individual Zoom meetings, and online conferences. While convenient, this shift towards virtual interactions often leads to a sense of social disconnection. Gathering in person, building relationships, networking actively, and participating in shared wellness activities are vital for combating burnout and nurturing awellness-oriented culture.
On behalf of AAEM, the Wellness Committee acknowledges the significance of tackling these challenges, and we welcome you to join us in person at the following events we will be spearheading during the AAEM Scientific Assembly 2024 in Austin, TX.
Wellness Room: A free space dedicated to relaxation and rejuvenation, prayer and meditation, creativity and comfort (open daily during the conference, starting Saturday, April 27, 2024, at 8am and ending Wednesday, May 1, at 12pm).
Wellness Committee Meeting: Meet and mingle with Wellness Committee leaders and colleagues, discuss our initiatives, and brainstorm ideas for our future endeavors (Sunday, April 28, 4-5pm).
Smash Your Stress Away!: A fun and engaging stress-relief activity (Sunday, April 28, 7-8pm). This is an offsite event at Breaking Point Austin where you can safely smash objects, splatter paint, throw axes, or solve an escape room for the sake of Wellness! Registration required. Transportation is not included but it will be coordinated with other registrants.
“Lost in Austin” Walk: A social and physical wellness walk (Sunday, April 28, 7:15-9:30pm). During this leisurely walking tour, discover the charm of Austin, TX. Connect with colleagues, explore the city’s hidden gems, and refresh your mind and body. Lace up for a unique blend of wellness and exploration.
New Attendee Reception: Networking and community-building (Monday, April 29, 6-7pm). Join AAEM leaders from the AAEM Board of Directors, AAEM/RSA Board of Directors, Chapter Divisions, Committees, Interest Groups, and Sections over drinks and hors d’oeuvres. Representatives will welcome first-time attendees to the Scientific Assembly and connect them to fellow AAEM members based on their interests.
Airways Event: Back by popular demand! An ever-entertaining, engaging, and educational session (Monday, April 29, 7-10pm). We all have stories to tell. Sometimes, they are funny or uncomfortable; sometimes, they are heartbreaking and full of life lessons. Other times, they affirm our decision to become physicians in the first place. Come to an evening event that promises to showcase a fantastic range of human experiences, enlighten minds, expose vulnerabilities, commiserate, and suggest ways to overcome the challenges we all face each day.
April 27-May 1, 2024 Austin, TX
aaem.org/aaem24
>> COMMON SENSE MARCH/APRIL 2024 34
Mental Health Action Plan Activity: Building strategies for mental well-being (Tuesday, April 30, 6-7pm). Create your own Mental Health Action Plan: a helpful visual tool for caring for your mental health on good, average, or tough days!

References
*AAEM Wellness Committee Co-Chair, @alvarezzzy †Wellness Committee Co-Chair, @nbhatnagar_md §Wellness Committee Vice-Chair, @kanapicki
1. Leigh R, Van Aarsen K, Foxcroft L, Lim R. P012: Does physician burnout differ between urban and rural emergency medicine physicians? A comparison using the Maslach Burnout Inventory tool. CJEM. 2020;22(S1):S68-S69. doi:10.1017/cem.2020.220
2. Nguyen, J., Liu, A., Mckenney, M., Liu, H., Ang, D., & Elkbuli, A. (2021). Impacts and challenges of the COVID-19 pandemic on emergency medicine physicians in the United States. The American Journal of Emergency Medicine, 48, 38–47. https://doi.org/10.1016/j. ajem.2021.03.088.
3. Wilding M. How to Stop Taking Work So Personally. Harv Bus Rev [Internet] 2023 [cited 2024 Jan 24]; Available from: https://hbr.org/2023/10/ how-to-stop-taking-work-so-personally
Paint ‘n Sip: Create your own souvenir and meet fellow art lovers (Tuesday, April 30, 7-9pm). Join the Wellness Committee for a creative, relaxing evening of painting and sipping beverages! All art supplies will be provided—registration is required.
Wellness Committee and Women in EM Joint Coffee Meetup: An early morning opportunity for wellness discussion and networking (Wednesday, May 1, 7-8am). Join the Wellness Committee and WiEM for our combined coffee meet-up. Grab a coffee and meet other members in an informal setting.
The Wellness Committee at AAEM invites you to the Scientific Assembly 2024 in Austin, TX, to engage in activities designed to promote well-being and resilience in our community. Join us for a unique experience that combines wellness, connection, and personal growth. Visit the AAEM24 webpage for more details and to participate in our wellness journey.
4. Jennings RE, Gabriel AS, Lanaj K. Want to Be a Better Leader? Stop Thinking About Work After Hours. Harv Bus Rev [Internet] 2024 [cited 2024 Jan 24]; Available from: https://hbr.org/2024/01/want-to-be-a-betterleader-stop-thinking-about-work-after-hours
5. Kohli SJ. How to Set Boundaries When You’ve Never Been Taught How [Internet]. Gt. Good. [cited 2024 Jan 24]; Available from: https:// greatergood.berkeley.edu/article/item/how_to_set_boundaries_when_ youve_never_been_taught_how
6. AAEM SA24 Networking Events site: https://aaem24.eventscribe.net/ agenda.asp?BCFO=&pfp=NetworkingEvents&fa=&fb=&fc=&fd= 7. &all=1&mode=
30th Annual SCIENTIFIC ASSEMBLY
COMMON SENSE MARCH/APRIL 2024 35
Adventures in New Zealand
Jack Perkins, MD FAAEM

Editor’s Note: Jack Perkins, MD FAAEM, and his family have spent nearly a year living and working in New Zealand. Over the holidays, Dr. Perkins shared his thoughts about the country and practicing emergency medicine in New Zealand and has graciously agreed to share his thoughts with the entire Academy. A follow-up article written by Dr. Perkins will appear in the next issue of Common Sense and will entail information and tips that he learned while planning this adventure.
New Zealand Quirks
y Mullets are highly fashionable for young boys.
y When Kiwis end a conversation that involves a plan, they may use the phrase “Sweet As.” This caught me off guard and resulted in a confused look the first time I heard this.
y Kiwis go barefoot everywhere, yet I have not seen a “foot versus glass” injury.
y Kiwis of all ages curse during regular conversation in any setting (including teachers at school and patients even when not angry).
y There is no security screening when flying within New Zealand (NZ).
y Mince pie is left out for Santa here as I presume they want to give him GI upset.
Things I Love about Emergency Medicine Here
y While it is possible to be sued, it is much less likely and the difference in practice style is apparent in terms of streamlining care to what is needed for the patient (now whether that need can be met is a separate discussion point).
y In seven months, only two patients have yelled at me and both were “drug seeking.” One called me a “wanker” for not prescribing albuterol and the other was addicted to nitrous oxide we use for reductions.
y The “ACC” system for injuries is incredible as it removes lawyers from injury claims. It covers anyone (Kiwi or tourist) for any injury and related expenses for that injury anywhere in NZ. So, if you go to an amusement park or go skiing, there is minimal to no liability paperwork as there is no need to sue—your medical care is covered.1
Kiwis go barefoot everywhere, yet I have not seen a “foot versus glass” injury.

y Work/life balance is a priority in New Zealand. EM physicians in my group receive 30% FTE “buy down” to engage in wellness, QI, research, education, or some other activity that benefits the hospital or healthcare system. For part of my 30% I have begun a weekly case series for the residents and my colleagues.
y Any consultant (anywhere in New Zealand) will pick up the phone (direct connection) and provide advice and look at images without any concern about “relationship to the patient” or medico legal issues. Since they centralize specialty services (such as neurosurgery) to large cities, this is an essential element to prevent unnecessary transfers. Neurosurgery will only fly (everything goes by helicopter) head bleeds that are likely to need intervention. Really good for patients and the system.
y On nights when the waiting room is packed, we have had different services begin picking up patients waiting to be seen. The pediatrics residents do this frequently and simply verbally run the case by one of the ED attendings (much like ACPs in the U.S., we have to discuss but not see each patient presented to us).
y EM attendings do not work overnight in my hospital (Taranaki Base Hospital, New Plymouth), we sign out to the EM Resident at 1am and are available by phone until 7:00am when the next attending comes in. The resident can call and ask you to come in but this is rare, so I live six minutes from the hospital and sleep in my own bed while “on call.”
y EM attendings are NZ government employees and thus we belong to a union (yes, there was a strike while I was here but I did not participate in picketing) which means the contracts are largely standardized—but so are benefits. All EM attendings receive two weeks of paid CME per 12 months and when you are at a CME conference, that time is counted as hours worked meaning you have less shifts when you return.
Mount Taranaki from the Tasman Sea a few miles from New Plymouth (city in which we are residing).
>> COMMON SENSE MARCH/APRIL 2024 36
y I can’t say that I have encountered a single patient who has been upset when the resources that patients should receive (formal echo, admission, cath, etc) is not attainable due to health system limitations. The lack of “entitlement” is I believe a byproduct of Kiwis understanding the limitations of a national healthcare system and that they truly accept the concept that “it is what it is for better or worse.”
y We perform a shift handover as a group at 4:00pm daily and always begin by reciting a Māori Karakia (prayer) together. It is a wonderful way to remind ourselves that New Zealand is a bicultural country and Māori patients have numerous barriers to achieving equitable healthcare resources and outcomes.2
Things that are Different here in Emergency Medicine
y They use a lot of Tramadol, Codeine, and Bactrim for adults of any age.
y EM physicians at my hospital do not see acute CVAs! Patients come to the Resus bay and are seen by the Medicine Resident with Tele Neurology (we intubate if needed) to consider lytics and flight to Auckland for thrombectomy.
y EM attendings do not have admitting privileges (Medicine Residents can say no).

y Radiologists are gatekeepers of CT imaging, and they decline a lot of requests (but they go home at 4:00pm and then it is much easier to obtain CTs).
y Not every patient presenting to the ED is seen by EM physicians, some patients are direct referrals to Peds, Gen Surg, Ortho, Medicine, Psych.
y Healthcare and social inequities largely affect only one population (indigenous Māori which is 20% of NZ population) and unfortunately the inequities stretch across education, healthcare literacy, healthcare access, healthcare outcomes, and persistent racism (from some Kiwis of European descent).
It’s been amazing to be immersed somewhere with a different approach to life (work, work, work and wait until retirement to enjoy life is the antithesis of Kiwi culture).
Things I Appreciate about the U.S. Healthcare System in Comparison to New Zealand
y Primary care access represents a challenge in the U.S., however in NZ it is a colossal issue and undermines a principal focus of nationalized health care.
y It is easier to see specialists of any type in the U.S. either in the ED or in follow up (wait times for a stress test here can exceed a year).
y While mental health care is far from adequate in the US, it is worse here both in the ED (resources) and in the community. One notable exception is the phenomenal “Taranaki Retreat” and their free holistic approach to mental health care for the community.3
y U.S. patients are much sicker, and care of the critically ill patient is a routine part of EM care. Critically ill patients are far less common here and I work here at a teaching hospital (level two trauma equivalent) that has a catchment area of 100k.
y The electronic health record system here is archaic and much less than ideal for patient care.
y It is very tough to see more than one patient per hour as all charting must be done prior to discharge.
y I really miss our peer counselors and addiction medicine services as although opioid addiction disorder is rare, I have insufficient resources for patients with alcohol use disorder.
y Dentists are like unicorns in NZ, wait times can exceed two years for routine dental care and some children simply do not get dental care at all.
What I Would Recommend to Anyone Contemplating a Similar Adventure
y This has been the best year of our life together as a family (Karen and I both agree on this) and we have only been here seven months.
y Kiwis prioritize work/life balance in every industry and are quite active when not working. It’s been amazing to be immersed somewhere with a different approach to life (work, work, work and wait until retirement to enjoy life is the antithesis of Kiwi culture).
y At the top of the list of benefits is the extra time with our kids (10, 12, 14), whether simply having dinner together, exploring Taranaki, or enjoying the exceptional natural beauty of NZ.
ADVENTURES IN NEW ZEALAND (EM INCLUDED)
Lake Mangamahoue near New Plymouth
>> COMMON SENSE MARCH/APRIL 2024 37
y Mid-career is the ideal time for this adventure as it is a tremendous, unexpected benefit to work in a different healthcare system and achieve a frame of reference for our U.S. healthcare system. I viewed the U.S. system as completely dysfunctional after COVID and the past few years of nursing and bed shortages. I just needed to step away and see something else to appreciate what works well for patients in the U.S.
y The school system here is a wonderful contrast for our kids as my youngest is in a Māori immersion program that highlights the country’s attempts to blend together Māori and European heritage into one Kiwi culture. My oldest is in an all-girls high school here and loves their approach to education. She states, “At New Plymouth Girls High, the teachers teach the content without opinions from themselves, principals, or government. As students we get to generate our own point of view.”
y While it is unusual to hit the pause button mid-career, if you could create an ideal “retirement” year but spend that with your kids, the effort to create the opportunity may seem less daunting.
New Zealand is as advertised—incredible.
I welcome any questions and offer my assistance in helping any fellow physician explore what could be the best decision of your life.4 For anyone who is interested in this amazing country we have a specific Facebook page with more photos.5 We live in New Plymouth, NZ (North Island) which has a very temperate climate (like San Diego) and locals can ski and surf on the same day. Mount Taranaki is the dominant local landmark.6 While I will be returning to Virginia next summer, our family had a really tough time with that decision, and it came down to grandparents in the U.S. New Zealand is as advertised—incredible.
References
1. https://www.acc.co.nz/about-us/who-we-are/what-we-do/
2. “Traditional Karakia” Link to text and audio file: https://www.otago.ac.nz/ maori/world/te-reo-maori/karakia-prayers
3. https://taranakiretreat.org.nz/
4. If you are interested in contacting Dr. Perkins, please let us know at cseditor@aaem.org
5. https://www.facebook.com/profile. php?id=100094513364265&mibextid=LQQJ4d
6. https://www.newzealand.com/int/new-plymouth/




ADVENTURES IN NEW ZEALAND (EM INCLUDED)
Mount Maunganui overlooking the city of Tauranga (North Island)
Mount Taranaki from the trail of one of dozens of local hiking routes.
Mount Taranaki behind us as we hiked to the Pouakai Tarns reflecting pools.
View overlooking Tasman Sea from Oakura Winery and Bistro (15 minutes from our house).
COMMON SENSE MARCH/APRIL 2024 38
Is It Time for a Flexner Report 2.0?
Deborah Fletcher, MD and Gregory Jasani, MD


The year was 1904 and a mom in rural Louisiana had a sick child with high fever and abdominal pain. She wanted to call the doctor but was worried. This mom had no idea if this person was a doctor, what his training was, and if he could help. But he was all she had and had to trust him. The child worsened overnight, and the doctor was called to the home. He said the young girl had appendicitis and he needed to operate right away. He had ether in his bag and prepared her for surgery on the family dining table. He removed her appendix and left the tube to drain into a pan under the table. She did well and lived well over 100, and loved telling me this story when I was a new attending ED physician. She was lucky to have had one of the well-trained physicians who took care of her in her youth.
Around that time the American Medical Association (AMA) had heard many complaints about “quack” physicians and the poor educational quality of medical schools. The AMA had been founded in 1847 with the mission “to promote the art and science of medicine and the betterment of public health.” They wanted to improve public trust in medicine and knew to do that meant having quality training with improved standards of medical education. They organized a Committee on Medical Education (CME) to review the current medical schools and make recommendations on quality improvement for reform. In walks Abraham Flexner. He was hired by the Carnegie Foundation for the Advancement of Teaching to do just that. He visited all the medical schools in North America at that time—155 in total—and found some astounding things. During this process, he chose Johns Hopkins as his “gold standard” for medical education to which he held the other schools to for review. He knew that their education plan included two years of intense coursework followed by two years of clinical training. He also knew of the rigorous training for physicians in Europe, which helped him model some of his ideas.
Flexner set out on the mission—visiting and reviewing all 155 medical schools in North America. Imagine what he saw—a huge variety in quality! Across the country, there were no standards but vast differences in admission criteria, graduation criteria, curricula, teachers/ professors, and assessments. He went to rural schools, urban schools, all of them, and documented their standards. Many of the schools were “for profit”—a doctor or group of doctors would get together and open a school to make money. Sadly, the quality of education was not at the forefront of many of these places. They did not follow the same rules or learn the same things across the country—some had shortened degrees of two years, some did not require dissection or research. Some did not even have a full-time teaching physician on staff. Some
Flexner set out on the mission—visiting and reviewing all 155 medical schools in North America. Imagine what he saw.
Abraham Flexner, circa 1910
only allowed the students to observe but not participate. He had criticism of many institutions, large and small. However, he came away from this process with a great understanding of the medical education system and saw positives and negatives and was in a great position to make recommendations.
In an excerpt from his 1910 Flexner Report, he states:
The striking and significant facts which are here brought out are of enormous consequence not only to the medical practitioner, but to every citizen of the United States and Canada; for it is a singular fact that the organization of medical education in this country has hitherto been such as not only to commercialize the process of education itself, but also to obscure in the minds of the public any discrimination between the well trained physician and the physician who has had no adequate training whatsoever. As a rule, Americans, when they avail themselves of the services of a physician, make only the slightest inquiry as to what his previous training and preparation have been. One of the problems of the future is to educate the public itself to appreciate the fact that very seldom, under existing conditions, does a patient receive the best aid which is possible to give him in
GOVERNMENT AND NATIONAL AFFAIRS COMMITTEE
>>
COMMON SENSE MARCH/APRIL 2024 39
the present state of medicine, and that this is due mainly to the fact that a vast army of men is admitted to the practice of medicine who are untrained in sciences fundamental to the profession and quite without a sufficient experience with disease. A right education of public opinion is one of the problems of future medical education… For twenty-five years there has been an enormous over-production of uneducated and ill trained medical practitioners. This has been in absolute disregard to the public welfare and without any serious thought of the interests of the public.
This report helped create change quickly. The AMA finally had the data they needed to effect sweeping change. This national report helped state medical boards to quantify quality and create rules at the state level. Schools closed across the country because they could not meet the recommendations for quality education. Many merged with university programs where there were better teachers and laboratories. Within 25 years of the implementation of these changes, there were only 66 medical schools left out of the initial 155. (Of note, Flexner was also responsible for advocating for closure of five out of seven historically black medical schools because they did not meet his standards. This is still considered a negative consequence of his report.)
Following the Flexner report and with the improvement in physician education, the public trust and respect of physicians improved greatly. There were great advances in science and medicine—just think, penicillin was discovered in 1928, then finally there was enough mass produced for military use in 1943. Research and treatment of cancer has saved many lives.
Trauma systems coordinate to help victims during the “golden hour.” Medicine was advancing, and being a physician was an honorable and respected profession. Patients and families could finally feel confident that their physician was well educated and trained.
However, this is a changing landscape now. For many years, doctors have worked side by side with nurses and encouraged nurses to have more education so that they could assist physicians better. The nurse practitioner field of study was meant to do just that—help the physician in the care of patients. The first NP certificate program was created in 1965 by Dr. Henry Silver to supervise his nurse Loretta Ford. It was not intended to be an independent, unsupervised
practice. However, in the past ten years there has been an explosion of nurse practitioner programs, most of which are completely online, to help registered nurses advance their degrees. These programs are a booming business for educators—there are many nurses who see becoming an NP to practice “healthcare.” There are very few who actually go help care for patients in rural areas. The AMA has been following this trend and has geographical maps to prove this point.
Let’s think about all of these “for profit” NP programs that seem to be everywhere now. Admission requirements? Varied. Some programs do not require a nursing degree previously, in some cases, not even nursing experience. There are even programs with 100% admission rates. Graduation requirements? Varied. Curriculum? The depth of education just isn’t preparing for independent unsupervised practice. There are classes in the curriculum for “The Role of the Nurse Practitioner,” and NP advocacy. Also, the students often have to find their own clinical classes and preceptors—it is not standardized by the program so their education is all over the board. Teachers? Again, varied and unstructured. The program can just accept any physician (or NP) preceptor to sign off as “teaching” their student—because they mainly are not organizing these clinical rotations for them. NP programs are collecting tuition money from students to “provide” the education, but the programs are often not the ones “providing” the clinical teaching. Does any of this sound familiar? It does look like medical education pre-1910—the “anything goes” time of profit and poor-quality education. You can almost take Flexner’s statement above and apply it now to NP education (repeated for emphasis):
It is time again to revisit the education system of those who are taking care of our patients.
The striking and significant facts which are here brought out are of enormous consequence not only to the medical practitioner, but to every citizen of the United States and Canada; for it is a singular fact that the organization of medical education in this country has hitherto been such as not only to commercialize the process of education itself, but also to obscure in the minds of the public any discrimination between the well trained physician and the physician who has had no adequate training whatsoever. As a rule, Americans, when they avail themselves of the services of a physician, make only the slightest inquiry as to what his previous training and
GOVERNMENT AND NATIONAL AFFAIRS COMMITTEE >>
COMMON SENSE MARCH/APRIL 2024 40
preparation have been. One of the problems of the future is to educate the public itself to appreciate the fact that very seldom, under existing conditions, does a patient receive the best aid which is possible to give him in the present state of medicine, and that this is due mainly to the fact that a vast army of men is admitted to the practice of medicine who are untrained in sciences fundamental to the profession and quite without a sufficient experience with disease. A right education of public opinion is one of the problems of future medical education…For twenty-five years there has been an enormous over-production of uneducated and ill trained medical practitioners. This has been in absolute disregard to the public welfare and without any serious thought of the interests of the public.
It is time again to revisit the education system of those who are taking care of our patients. NPs have entered medicine and are influencing many state legislators that they are qualified to perform independent patient care. Unfortunately, as physicians, we often see bad outcomes for patients: poor workups, increased cost/utilization of services when one does things they are not fully trained to do. NP education has changed from seasoned nurses going to brick and mortar school to quick online programs and degree mills. NP educators are now recommending against the independent practice of NPs in the emergency department due to the wide variety of their education. There are some great nurse practitioners, who are well-educated, and want to work as a team to have the best patient outcomes. We need to find them and support best practice collaboration.
In the interest of the public, it is time for an unbiased outside agency report on nurse practitioner programs (like the Flexner Report as was done on medical schools). In summary:
y Medical school education had a significant proliferation of schools in the early 1900s.
y Medical education was not nationally standardized, which led to the decrease in quality of physicians and confidence patients had for physicians.
y The AMA created the Council on Medical Education in 1904, which contracted with an outside agency, the Carnegie Foundation for the Advancement of Teaching, which chose an unbiased surveyor Abraham Flexner to evaluate all medical schools and provide recommendations for medical school reform.
y The Flexner Report recommended that American medical schools enact higher admission and graduation standards.
y The Flexner Report recommendations helped standardize medical school education for the United States, and over time improved the quality of medical education and patient care.
y Nurse Practitioner education has had a significant proliferation of schools, including online programs.
y Nurse Practitioner programs do not have national standards for admissions, education, or graduation.
y Nurse Practitioner programs do not have national standards for clinical education, clinical preceptors, and clinical locations.
There should now be an outside agency to do an unbiased survey of nurse practitioner programs to provide recommendations for NP education reform. The AMA ordered one for medical schools years ago and took the recommendations to improve the care of patients. Hopefully, there will be something similar for nurse practitioner programs. It should all be about transparency, safety, and the interests of the public we serve.
GOVERNMENT AND NATIONAL AFFAIRS COMMITTEE
COMMON SENSE MARCH/APRIL 2024 41
Risk Management in the ED
Kraftin E. Schreyer, MD MBA FAAEM

Risk is inherent to emergency medicine (EM). Emergency departments (EDs) are full of undifferentiated patients, many of whom present acutely ill and without additional clinical context or information. Management must be done expeditiously in a constrained time frame in a chaotic environment. Furthermore, the threat of malpractice is always looming. In addition to the inherent risk within our field, additional risks can develop from variation in care delivery. The lack of standardized processes, equipment, transitions of care, and interactions with consultant or ancillary services can all contribute to increased risk within EM. As such, every ED would benefit from recognition of risk and consideration of a risk management strategy.
Risk management, in and of itself, is a well-established process often undertaken within a silo of a hospital’s risk management department. Many times, decisions regarding risk, while well-intended to improve patient care, are made by administration, without frontline physician input. As operational leaders, it behooves us to be a part of risk management on behalf of our departments. To be a full participant in risk mitigation efforts, though, one must understand the process behind risk management. Risk must first be identified, then quantified and prioritized. Key risk events, including sentinel events, should be further investigated. Steps should be taken to learn from risk events, and ultimately, risk control measures should be enacted.
When risks are identified, they are often categorized for further stratification. Risks are often looked at in terms of the chance of loss or gain, diversifiability, subjectivity, and responsiveness to external factors. Key risk
indicators can also be used to identify risks and can be defined before or after a risk event. Within EM, risks can be categorized in other ways, such as situational, conditional or personnel related risks. Situational risks might include transitions of care, interactions with consultants or ancillary services, procedures, equipment, documentation, or disposition. Conditional risks might include high risk or time-sensitive diagnoses, or those diagnoses requiring transfer for a higher level of care. Personnel risks might include insufficient familiarity with a system (e.g., for new hires), or insufficient fund of knowledge (e.g., for trainees).
Risk quantification and prioritization is often reflected in an organization’s risk attitude, which translates to a degree of risk tolerance. Policies and goals are established in accordance with an organization’s appetite for, or aversion to, risk. Risks can further be quantified and prioritized using a framework known an enterprise risk management (ERM). Within ERM, risks are categorized into hazard risks, operational risks, financial risks, and strategic risks. Hazard risks are threats to either property (damage/ theft) or personnel (employee injury). Operational risks can be external or internal to the organization. External operational risks might include problems with supply chain, whereas internal risks include technology, security, quality control, and training of employees. For EM, financial risks might include the billing and revenue cycle, insurance audits, malpractice, and litigation.
The investigation and reporting of risks events if often done by the risk management team, centralized throughout a hospital or health system. Individual people and departments should be encouraged to report risks through established internal reporting systems, so that they may be escalated by the risk management department if needed.
Many times, decisions regarding risk, while well-intended to improve patient care, are made by administration, without frontline physician input

Risk management strategies may be instituted system wide but may also be employed on a local level. Generally, there are four strategic approaches to risk management. Risks can be retained, that is, accepted as an essential piece of departmental operations. Conversely, risks can be avoided and removed entirely from the departmental milieu. The transfer of risk to a third party, such as an insurance company, is another strategy. Finally, risk reduction or mitigation involves taking actions to limit the occurrence, impact, or both, of a risk.
A key tool for risk management is a risk map (Figure 1). Risk maps plot risks based on the likelihood of occurrence of the risk and the severity of the risk. As such, the maps are sectored into four quadrants—one low risk, one high risk, and two medium risk quadrants.
OPERATIONS MANAGEMENT SECTION
>>
COMMON SENSE MARCH/APRIL 2024 42
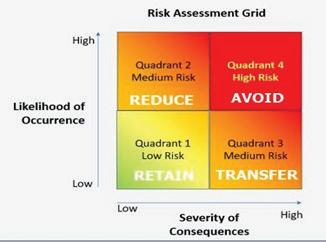
Risk management strategies are then targeted towards each quadrant. For those risks that are both low severity and low frequency, retention is the strategy of choice. Since they are low impact overall, the department is willing to internally assume those risks. Conversely, the highest risks, that are both likely to occur and have severe consequences when they do, should be avoided entirely. The approach to medium risks depends
on if they are more likely to occur or have more severe consequences. For those risks that are more likely to occur, reduction is the risk management strategy of choice. For those that have more severe consequences, the ideal reduction methodology is to transfer the risk outside of the department, possibly to a third party (e.g., insurance). There is inherent risk in EM, both on a departmental level and individual levels, particularly with regard to patient diagnostics, care, and communication. As departmental leaders, we should constantly be asking ourselves how we can minimize risk within our department. We should be involved in the risk management process alongside hospital administration. Establishing a risk management committee, or including risk management as a subset of a patient safety or quality committee may be a preliminary step to take to ensure risk management is a regular focus of your ED. A standardized approach to risk, using a risk map or other risk management tools, may allow your team to consistently identify, categorize, prioritize, and manage risk in an effective manner.
References
• Content adapted from RMI 5105, Fox School of Business
• https://catalyst.nejm.org/doi/full/10.1056/CAT.18.0197
• https://www.sciencedirect.com/science/article/pii/S0733862720300079
• https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7061389/
OPERATIONS MANAGEMENT SECTION
Figure 1. Example of a Risk Map
COMMON SENSE MARCH/APRIL 2024 43
A Rose by Any Other Name: Tertiary Prevention for Opioid Use Disorder
Jessica Moore, MD FAAEM

What’s in a name? Specifically, what is meant by the name “harm reduction”?
Harm reduction refers to tertiary prevention: preventing complications of a disease once it is already present. We commonly embrace this practice in medicine, whether it be prescribing aspirin for patients who have had a stroke or scheduling regular ophthalmologic and podiatric exams for those with diabetes. However, for reasons rooted in stigma and misunderstanding, tertiary prevention for opioid use disorder (OUD) is often viewed in a different light.
What do we know about harm reduction for OUD? Simply put, it works. Evidence shows that many harm reduction measures are not only associated with reduced morbidity and mortality among patients who use opioids, but they also are associated with positive outcomes for communities as a whole. Various harm reduction measures have been associated with decreased rates of violent criminal activity, decreased publicly discarded injection materials, and even decreased needlestick injuries among first responders.1-4
an overdose, those who use opioids are likely to be in contact with others who use opioids, meaning they may be the ones most likely to successfully reverse an opioid overdose and save a life. Naloxone distribution and overdose training is not associated with compensatory substance use in studies.10,11
What do we know about harm reduction for opioid use disorder?
How do we encourage and implement harm reduction from the emergency department (ED)? There are several simple, tangible ways we can promote decreased morbidity and mortality for our ED patients with OUD: Non-stigmatizing language: Utilize non-stigmatizing language in documentation, in communication with patients, and in communication with other healthcare professionals. The National Institute on Drug Abuse (NIDA) has a helpful, easy-to-use webpage describing preferred language when discussing substance use disorders.5 Language is one of the simplest ways we can help to reduce the stigmas that come with substance use disorders, and thus help promote more equitable medical care.6
Simply put, it works.
Initiation of evidence-based treatments: Buprenorphine is an FDA-approved medication for OUD (MOUD) that has clearly proven mortality benefit, as well as well-defined benefits in many patient-centered and public-health related outcomes. Prescribing it no longer requires a DATA-waiver (“X-waiver”), so any practitioner with DEA Schedule III privileges can prescribe it. Think about buprenorphine prescribing especially for patients presenting for nonfatal overdose; just as you would for any other chief complaint, treat the underlying cause. Did you know that according to one study, the three-day mortality for patients presenting to the ED after naloxone administration by EMS is higher than the mortality for those presenting for STEMI treated with PCI for a whole year?12 We would not discharge many patients with such a mortality rate, so it is worth taking a few extra minutes to provide good counseling and initiate evidence-based treatments whenever indicated. ED initiation of buprenorphine is associated with superior outcomes compared to delaying to outpatient initiation.13-16 While some cite buprenorphine diversion as a concern, nonprescribed buprenorphine use has actually been associated with decreased rates of opioid overdose17. In other words, diversion of buprenorphine does not seem to come with the same harms historically associated with diversion of full opioid agonists. Buprenorphine use is associated with positive health outcomes even for those who are continuing to use substances3
Naloxone prescribing and dispensing: Naloxone distribution is associated with decreased fatal opioid overdoses as well as reductions in opioid-related ED visits.7,8 It has also shown to be cost effective.9 Have a low threshold to prescribe it. It is even better if you can provide it directly to the patient in the ED (“naloxone dispensing”), as prescription fill rates have been historically very low for a variety of reasons, including cost and stigma. Counsel patients and families on how to use it. While patients cannot administer naloxone to themselves while experiencing
Controlling pain and withdrawal: Uncontrolled pain and withdrawal are some of the most commonly cited reasons why patients cannot tolerate hospitalization for necessary medical care.18 Even if a patient is not currently taking MOUD, allowing them to continue treatment for their potentially life-threatening medical condition (for example, IV antibiotics for endocarditis) is critical. Remember that patients who use opioids typically have significant opioid tolerance and dependence and will need higher doses of opioids than an opioid-naive patient to achieve control of symptoms.
PAIN AND ADDICTION COMMITTEE
>> COMMON SENSE MARCH/APRIL 2024 44
Counseling patients to use with others: Counsel patients to use substances in the safest conditions possible. This means using with other people, in a familiar place, and with naloxone available. Taking turns allows one person to be available if emergency help is needed.
Counseling on safe injection practices: Encourage patients to utilize only a small sample of substance before using their full dose, in case the supply is stronger than anticipated. Patients should be instructed to adequately sanitize their skin and utilize new, clean materials whenever possible. If possible, injection into the upper extremity is safer than injection into the groin or neck.19
“Never Use Alone” Hotline20: A volunteer on the end of this hotline will stay on the phone with someone while using substances, and call for emergency help if the person stops responding. The patient has the option to remain anonymous. Consider saving the number in your phone to share with patients: (877) 696-1996.
HIV and HCV screening: Interactions with healthcare are an important opportunity to screen for transmissible diseases such as HIV and Hepatitis C. The CDC recommends universal opt-out HIV screening in EDs in areas with a prevalence of >1%.21
Knowing your community resources: Know the resources in your area and encourage patients to use them. Needle exchanges are proven to reduce transmissible diseases such as HIV and HCV.22,23 Evidence shows that those who engage with needle exchanges are actually more likely to enter treatment for OUD in the future.24,25 While there are misconceptions that syringe exchange programs “enable” use, studies have not shown an association with an increase in substance use.24
Compassion: Those who use drugs are often dehumanized and met with irritation when seeking medical care. A simple “I’m glad you came to be evaluated today” creates a very different environment than “Why did you wait so long to come in?” Try utilizing “Thanks for sharing those
References
1. Havnes I, Bukten A, Gossop M, Waal H, Stangeland P, Clausen T. Reductions in convictions for violent crime during opioid maintenance treatment: a longitudinal national cohort study. Drug Alcohol Depend 2012;124(3):307-10. (In eng). DOI: 10.1016/j.drugalcdep.2012.02.005.
2. Wood E, Kerr T, Small W, et al. Changes in public order after the opening of a medically supervised safer injecting facility for illicit injection drug users. Cmaj 2004;171(7):731-4. (In eng). DOI: 10.1503/cmaj.1040774.
3. Gjersing L, Bretteville-Jensen AL. Is opioid substitution treatment beneficial if injecting behaviour continues? Drug Alcohol Depend 2013;133(1):121-6. (In eng). DOI: 10.1016/j.drugalcdep.2013.05.022.
4. Groseclose SL, Weinstein B, Jones TS, Valleroy LA, Fehrs LJ, Kassler WJ. Impact of increased legal access to needles and syringes on practices of injecting-drug users and police officers--Connecticut, 19921993. J Acquir Immune Defic Syndr Hum Retrovirol 1995;10(1):82-9. (In eng).
details with me” instead of “You know drugs are bad for you, right?” Most patients understand the risk of harm from substance use, and they are coming to us for help, not to be shamed for their medical condition. Patients are more likely to come to us for the care they need when they feel they will be met with kindness, respect, and understanding. Remember that addiction is a neurobiological disease, and not a choice of the patient or deficiency of willpower. We must always treat it as such.
Remember that addiction is a neurobiological disease, and not a choice of the patient or deficiency of willpower. We must always treat it as such.
So, what’s in a name? While the term “harm reduction” is unfortunately often politicized and misunderstood, at its root tertiary prevention means improving our patients’ long term health outcomes. As the primary healthcare access point for many patients with substance use disorders, we have an incredible opportunity to reduce harms for our patients: by reducing mortality and related medical complications, but also by engaging in treatment, creating trusting relationships, and meeting patients where they are.
Give it a try. You may even find that you are more satisfied with your encounters when you are able to align more with your patients and provide tangible, evidence-based interventions.
5. National Institutes of Health, National Institute on Drug Abuse. Words Matter - Terms to Use and Avoid When Talking About Addiction. (https:// nida.nih.gov/nidamed-medical-health-professionals/health-professionseducation/words-matter-terms-to-use-avoid-when-talking-about-addiction).
6. Kelly JF, Westerhoff CM. Does it matter how we refer to individuals with substance-related conditions? A randomized study of two commonly used terms. Int J Drug Policy 2010;21(3):202-7. (In eng). DOI: 10.1016/j. drugpo.2009.10.010.
7. Walley AY, Xuan Z, Hackman HH, et al. Opioid overdose rates and implementation of overdose education and nasal naloxone distribution in Massachusetts: interrupted time series analysis. Bmj 2013;346:f174. (In eng). DOI: 10.1136/bmj.f174.
PAIN AND ADDICTION COMMITTEE
Continued
>> COMMON SENSE MARCH/APRIL 2024 45
on page 65
Street Medicine: Uncheck Your Biases
Silvi Spirollari Pomeroy, OMS-IV

The term street medicine is self-defining delivering medical services directly to an unhoused patient population by physically reaching them— whether in encampments, on the streets, wherever they are in need. This represents a groundbreaking form of medicine, recognizing a patient demographic with a healthcare access gap while simultaneously addressing additional social determinants hindering them from receiving proper care.
The statistics are clearcut, unhoused individuals face a significantly reduced average lifespan compared to housed counterparts, while simultaneously having exponentially higher healthcare costs. Despite these stark realities, street medicine remains a much understaffed and unfamiliar to many healthcare practitioners. As a medical student, my initial encounter with the term “street medicine” led me to erroneously connect it with other misunderstood topics from lecture, similar to the Krebs cycle or bilirubin metabolism disorders.
Arriving in the country at the age of two, I witnessed early on the disparities associated with limited healthcare access.
The reality is the field itself is vitally crucial, yet underserved and undersupplied. Focusing on one aspect, unhoused individuals have higher rates of substance use disorders and mental illness, yet many street medicine teams do not have access to full time psychiatric care. Scaling this facet by the intricated complexity of the pathology, both medical and social, prevalent in unhoused population paints a picture of a complex medical field that demands more advocacy champions.
One such champion is Dr. Victor Cisneros, MD MPH CPH, who can speak for the importance of street medicine via his experience leading a mobile unit in Coachella Valley, California, while also serving as the Director of Diversity, Equity, and Inclusion & Community Health Outreach for graduate medical education at Eisenhower Health, embodying the advocacy needed to address the unique healthcare needs of those experiencing homelessness.
Silvi Pomeroy (SP):
Tell us about your interest in Social Emergency Medicine and Street Medicine.
Victor Cisneros (VC):
My interest in these fields stems from personal experiences as an immigrant. Arriving in the country at the age of two, I witnessed early on the disparities associated with limited healthcare access, leading to the use of the emergency department as our primary care due to a lack of insurance. I encountered barriers like language difficulties and food insecurity. My perspective deepened during my MPH studies, providing valuable tools and insights often not covered in medical school, particularly in understanding the impact of social determinants of health. I believe these factors are as crucial, if not more so, than prescribing medication or treating a diagnosis.
Social Emergency Medicine (Social EM) is about integrating these social determinants into acute care settings, like the ED. The aim is not to burden practitioners with additional screening tools, but to optimize and collaborate with colleagues like social workers. Breaking down silos in the emergency department (ED) is vital; understanding that roles, like physician, social worker, and case manager, should not be assumed but rather comprehended collectively. The key lies in understanding the landscape of each other’s roles.
SP: What are modifications that emergency medicine programs nationally can make to be more conscious of the unhoused population?
VC: Recognizing the significance of this issue is the initial step for residency programs. Internal champions are crucial to advocate for the unhoused patient population and emphasize the importance of addressing social determinants of health. Without this awareness, progress can feel like an uphill battle.
The second step involves having individuals, like myself, or other passionate colleagues who are well-versed in understanding and trained to tackle these issues. Investing in the education of the next generation of residents requires Social EM fellowship-trained professionals or those with a keen understanding of public health and health-related social needs.
To effectively educate residents, innovative approaches are essential. However, residency programs must secure institutional buy-in and emphasize the importance of these initiatives. Building a curriculum and
SOCIAL EM & POPULATION HEALTH COMMITTEE
>> COMMON SENSE MARCH/APRIL 2024 46
exposing residents to real-world challenges will help cultivate internal champions within the program. With this foundation, recruitment efforts can flourish, and the pieces will naturally fall into place.
SP: Street Medicine Involves a large role falling on primary care physicians, such as EM, IM, and FM to fill larger gaps and treat complex conditions that may be beyond standard scope of care. How can we expand street medicine to become a more interdisciplinary medical effort?

VC: Expanding street medicine requires tackling the challenge of behavioral health, particularly psychiatry, which is already underserved. Identifying psychiatrist champions willing to serve this patient population, even if it’s not the most financially rewarding, is crucial. Collaborating with residency programs is key, integrating street medicine into their training. At Eisenhower, our upcoming psychiatry program presents an opportunity to incorporate psychiatry into the mobile clinic, complementing our existing partnerships with community therapists who volunteer their time for therapy screenings during medical assessments.
Legal partnerships are equally important. While social workers can identify temporary housing, legal advice becomes essential for contracts or housing-related issues. Patients sometimes need assistance with forms or preventing eviction, making legal support a valuable component.
Street medicine shouldn’t solely burden emergency and primary care physicians—it necessitates a multidisciplinary approach. Achieving this goal is challenging, but the comprehensive nature of primary care aligns well with the street medicine ethos. The diverse skill set of emergency medicine physicians enables us to care for anyone in need, a philosophy synonymous with the unpredictability of street medicine encounters.
Embracing the innovative nature of reaching those in need is essential. The surroundings may change, but the patient remains constant.
An illustrative example from street medicine involves creatively addressing a patient’s potential plantar fasciitis at night. Unable to purchase shoe inserts, we utilized a women’s hygiene pad to provide comfort by wrapping it inside the patient’s existing shoe padding. While seemingly simple for us, it made a world of difference for the patient, highlighting the importance of innovative thinking and resourcefulness in street medicine.”
SP: What advice would you give to the medical community regarding building strong relationships with members of the unhoused community?
VC: Firstly, it’s crucial to shed biases. We must leave preconceived notions at the door, avoiding the assumption that everyone experiencing homelessness is solely due to substance abuse or personal choices. While we may encounter individuals seeking substances, addressing this issue requires a nuanced approach involving addiction medicine and potential therapy, recognizing that addiction can extend beyond substances to other aspects of life.
Understanding the unhoused patient population is paramount. Checking our own biases is the initial step, ensuring they don’t hinder us from treating them with the same dignity and respect as any other patient. Additionally, recognizing the unique conditions they face is vital.
Discharging someone without considering their access to essential resources like pharmacies, blankets, or food is impractical. Some states have implemented a homeless discharge checklist, acknowledging the need for a structured follow-up process. While it may seem burdensome to physicians, it prevents patients from being discharged to the streets without a plan. The checklist includes considerations like medication needs, follow-up arrangements, vaccinations, and screenings, tailored to the distinct living environments of the unhoused population. Understanding and acknowledging these differences are critical. Ignoring them sets the stage for failure when attempting to provide meaningful assistance to this patient population.
SP: What do medical records look like in a street medicine setting?
VC: While approaches vary across programs, I’ll provide an overview of our process at our institution. Currently, our system is paper-based. Collaborating with local community volunteers in medicine, who serve uninsured patients in our community clinic, we document patient encounters in diverse settings—whether it’s a chair, standing up, or within a tent. Basic information is recorded on a paper chart, encompassing history,
SOCIAL EM & POPULATION COMMITTEE
>> COMMON SENSE MARCH/APRIL 2024 47
Checking our own biases is the initial step, ensuring they don’t hinder us from treating them with the same dignity and respect as any other patient.
physical examination, differential diagnosis, developing a plan, and executing it on-site.
At the end of each event, when services are concluded, we transcribe all paper charts into the electronic EMR of our community clinic partner, and the paper documentation is securely shredded. The upcoming mobile clinic aims to streamline this process, hopefully with the incorporation of EPIC, mirroring the efficiency of an ER visit. This transition enables us to track this transient patient population more effectively, monitoring outcomes and identifying revisits across the community. The seamless connection between street medicine and our emergency department allows us to correlate patient history, providing valuable insights for comprehensive and coordinated care.
SP: There are some concerns regarding the lack of structural oversight that can be in place with no legal logarithm or law regarding functionality. How would you address these individuals that are worried about this?
VC: Firstly, there is literature that states the protective Good Samaritan law plays a pivotal role. In my perspective, whether you encounter a patient in a clinic, an ER, or on the streets, the only difference lies in the environment. The patient remains the patient. If you adhere to the standard of care you would provide in any other setting, it remains consistent. For instance, if someone presents with chest pain and raises concerns for care out of the limitation of the environment, I’d promptly call an ambulance, just as I would in an outpatient clinical setting.
Historically, this patient population has been appreciative of our outreach efforts. Their gratitude is evident, considering that this may be the only form of care they receive.
Street medicine is not a novel concept, and precedents already exist for handling such situations. Following established practices and standards of care ensures a seamless and ethical approach to delivering medical services in diverse environments.
SP: Community support is very important, especially from a fundraising perspective. How can we continue to educate the community in general about the importance of street medicine and get our non-medical community involved?
VC: To effect change, community education is pivotal. By highlighting the importance of addressing homelessness and sharing statistics, we paint a picture that transcends individual immunity.
This could be anyone in our community—a neighbor or a family member. Examining healthcare outcomes reinforces the idea that neglecting this vulnerable population results in increased emergency department visits, placing a significant financial burden on the healthcare system. Data supports the notion that a preventative approach is not only humane but also cost effective. Institutions recognize that preventing ER admissions can ultimately save resources and taxpayer dollars, as hospitals often absorb the cost of treating uninsured patients.

Maintaining a standard of care similar to any clinic or emergency department ensures a positive interaction. Understanding your limitations as a physician is crucial—recognizing when the situation exceeds your capabilities and requires additional help. The patient retains the capacity to decide whether to proceed with care, allowing them to decline treatment, akin to an AMA process. We document thoroughly, explaining all associated risks and providing instructions for the patient to call 911 if they change their mind, a procedure consistent with any other patient encounter.
Educating the community on these approaches is crucial, emphasizing the potential for creative solutions without relying solely on tax dollars or government funding. This is an opportunity to cultivate awareness and support for street medicine, fostering champions who advocate for our patients across the social spectrum. Embracing the innovative nature of reaching those in need is essential. The surroundings may change, but the patient remains constant. Let’s educate ourselves, our communities, and champion the transformative potential of street medicine.
SOCIAL EM & POPULATION COMMITTEE
COMMON SENSE MARCH/APRIL 2024 48
Venture into the Unknown because the Status Quo is Unsatisfying
Rob Mohr, MD – Locum Tenens Section Chair-Elect
By the end of this article, I aim to convince you that you can improve the quality of your life by confronting your discomfort and walking into uncertainty, that the old way of looking at employment is outdated, and that the lessons you learned from the previous generation of doctors and your faculty in residency are perpetuating a problem. I will argue that physicians are being gas lit into sacrificing themselves not for the betterment of their patients but for the advancement of parasitic business interests and it is resulting in not only dissatisfaction, but in many cases, existential crisis.
We tell ourselves we are doing the best we can with what we have, but deep in the recesses of our subconscious we know that it could be better
Take a moment and honestly assess how you are delivering care when you go to work. Are you truly delivering care in the way that you dreamed you would when you decided to become a doctor? Think back to when you were a medical student when your perspective on medicine was closer to how a patient thinks rather than how a doctor practices. How many times over the past few years have you walked out of a patient’s room and felt uneasy about the lack of resolution you have brought to that patient? We tell ourselves we are doing the best we can with what we have, but deep in the recesses of our subconscious we know that it could be better. The emergency department is in a dire state not because we lack the resources needed to fix it, but rather because it has been co-opted by parasitic forces that seek primarily to extract profit and offset risky short-sighted business decisions.
Let’s look at what has become a typical work environment today.
You are working for a large multi-specialty group that holds contracts in several states. You arrive for your morning shift and come in to see a full waiting room. People are coughing on each other, one patient is sprawled out on the floor with a blanket they brought from home as several faces look up at you with an expression centered somewhere between hope and disdain. You come in and log into the clunky EMR (read Picis, Medhost, Meditech) and see that there are a dozen patients boarding and at least twice that many waiting to be seen. You see the name of a new APP that you have never met assigned to a few of them. Recognizing the
urgency of the situation (a situation that is unfortunately typical) you dive right in and put your name on five of the most pressing charts.
Over the course of the next 10 hours you do your absolute best to put out the hottest fires, and with 30 minutes left in the shift the next doc comes in ready to pick up where you left off. You spend the next hour and a half charting and make your way home with the sky looking the same way it did when you came in…dark.
You walk out to your car, not with a feeling of a job well done, but more likely a feeling of depletion. On your drive home you think back to what you did today, but give up on the exercise when you realize that you saw 3.1 patients per hour. Again. You make it home, spend some time with your loved ones, and recharge your battery just enough to make going back the next morning an acceptable option, After all the pay is OK and at least it is reliably coming, unlike during the height of COVID.
That night you drift off to sleep quickly, but just like the night before, you find yourself awake at 3:00am with a feeling of uneasiness. The waking thoughts vary from night to night, but they are reliably there, chipping away at your wellbeing.
The next morning you again come into the shift, log in, and slog through the day. On the first chart you pick up you notice that the patient was just here yesterday and saw that new APP. When you go in to see them for the same ankle pain they were here with yesterday you take a look at the splint that the APP fashioned and notice just a single layer of padding around the ankle. Sadly this isn’t the first time this has happened, but every time you get one of the “new APPs” spooled up, they disappear only to have another brand new under-trained “provider” adding to your work by performing their own sub par work. The next patient presents with an elevated Wells score, positive D-Dimer, and you scan him on the cheap antiquated 16 slice scanner your department says is good enough. You know it’s not ideal, but “hey, it’s what we have.” After you suppress that thought yet again, you caffeinate, muddle through the onerous task of placing orders in the crappy cheap EMR that the administrator who hasn’t worked in a department in a decade (if ever) purchased from an office ten states away. It’s there for billing and little else since you really can’t look up old charts in any way that allows you to keep up with patient volume.
You spend some time reviewing the patients in process and realize that the guy in bed three is pretty sick. You start the resuscitation, talk to nursing, and realize that this guy is going to need a higher level of care. Given your department is owned by XYZ you start calling out to your sister XYZ hospitals only to find that they are full and cannot accept at this time. You don’t have a clerk after 5:00pm so you ask your nurse to
LOCUM TENENS SECTION
>> COMMON SENSE MARCH/APRIL 2024 49
help you start making calls to other hospitals. She has six rooms today because admin called off the extra swing shift nurse because the morning was slow, but she says that she will do what she can. Three hours and at least six phone calls later you get the patient accepted and you can finally go home…an hour late.
These issues, my colleagues, are what we call red flags. Any one of these red flags could occur in any department on any given day. However all too often they have become the norm. The gravity of a single one escapes our attention, but in accumulation they wear down our ability to find satisfaction in what should be one of the noblest professions. We worked so hard to be here, and have been taught that this ailing system “just is what it is.” The problem is that it does not have to be this way. We trained as emergency physicians to be pillars of stability serving patients in crisis, yet we find ourselves sacrificing our wellbeing to serve business organizations whose goals are misaligned with the needs of our patients.
Our patients aren’t crazy, they just don’t trust us anymore.
Patients are noticing the dysfunction in our field too. The average patient is more skeptical of the medical system than in years past. There are public facing articles in prestigious publications discussing the expense and dysfunction of the medical system and that patients are turning to alternative medicine in record numbers. Patients are willing to walk away from evidence-based medicine to see people with less training because the qualification that they seek over all else is someone who will sit down with them, have time to listen to them, and are reliably available. This is embarrassing!
Today’s doctors do want to work hard.
The old guard physicians may scoff at this assertion, calling newer generation weak, lazy, or unwilling to sacrifice. However what they fail to understand is the current generation of new physician’s world differs from theirs. Their time was a time when the emergency physician had a vested interest in the success of his practice. In the “old model” hard work and dirty hands were part of building a successful practice. It made sense that you worked long hours, many of which were unpaid because you had franchise. Today’s generation of emergency physicians are disenfranchised. We are essentially being taxed without representation—cuts are made without regard to the interests of doctors or patients in order for corporations to extract a profit and deliver it to investors who are unfamiliar with the practice of medicine. The perpetuation of this old guard paradigm benefits the desires of these malignant companies.
But isn’t reimbursement for physician service decreasing?
The large groups like to pretend that they are doing all they can to pay physicians but their hands are tied due to reductions in CMS and insurance reimbursements. While it is true that reimbursements tied to physician billing are stagnating or going down in many cases, the facility fees are skyrocketing and many hospitals have gone back to subsidizing emergency departments, so in fact the money is there, it’s just how it gets there and the accounting that has changed.
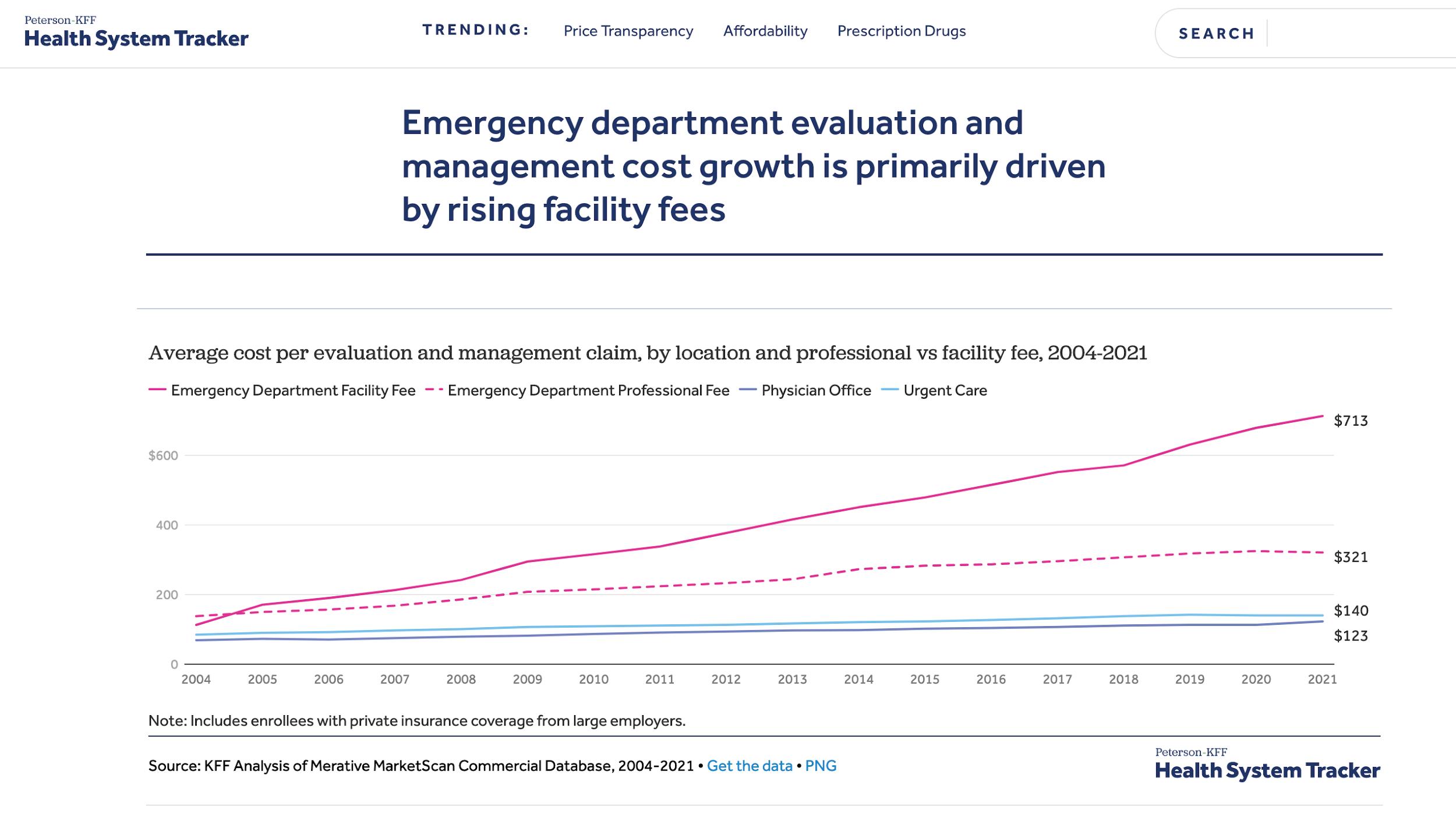
LOCUM TENENS SECTION >> COMMON SENSE MARCH/APRIL 2024 50
Does your understanding of physician employment match the current environment?
The bottom line is the rules have changed and as such your business tactics need to adapt. It is time that we turn the table on these malignant interests. Team Health, American Physician Partners, Sound Physicians, Envision, and others not named for the sake of brevity are bad for our patients. There are now peer reviewed articles in the Journal of the American Medical Association as well as a number of publicly facing articles in The New York Times and many other publications that show that private equity (PE) is harmful to patients and doctors alike. It is time that we use their business models against them and make their harmful ventures unprofitable. Becoming a free agent is a way to do this. The PE staffing model is in crisis. All across the country and in most major cities these management groups are increasingly turning to locum tenens to fill not only their short term staffing needs, but their ongoing needs as well. Opportunity is abundant, accessible, and more lucrative than ever.
We trained as emergency physicians to be pillars of stability serving patients in crisis, yet we find ourselves sacrificing our wellbeing to serve business organizations whose goals are misaligned with the needs of our patients.
difference. Also it allows you to have benefits tailored to your specific needs. If you are young and single, you might prefer to have a high deductible plan, buy into a health share, or fund an HSA. As a free agent physician you get to decide your CME budget and more importantly how to spend it. Want to go on that trip to “Essentials of EM” in Vegas—tax deduction. Annual corporate meeting for your own professional corporation to review your strategy for 2025—tax deduction. W2 or non-free agent 1099 work for malignant companies isn’t the answer, it’s the low hanging fruit that debt ridden residents and young physicians first reach for when they aren’t aware of all the options.
I can’t do locums./ I have a family.
A common objection to working locums is, “I have a family. I need reliable income.” Or, “I have a family I can’t travel.” Looking at locum tenens in this way is an antiquated paradigm. I cannot tell you how many times I have worked a locums shift in my own town or a short drive away and still slept in my own bed at night. In the last five years of working as a locum tenens physician the only time that I was not able to obtain the number of shifts that I desired was for three months back in 2020 at the height of COVID. You might recall that many so-called “employed” docs too found themselves struggling for hours in this situation. Oftentimes a locums doc is sleeping in their own bed and getting the same number of shifts as their “employed” colleagues, but setting their own hours and getting paid 35 to 45 percent or more. Bottom line is the system is in crisis mode because greedy people did dumb things and because of it there is more opportunity today to reliably work as a free agent without the traditional burdens associated with working locum tenens.
But I need the benefits.
Working as a 1099 free agent gives you the ability to tailor your benefits to your needs. As employees of their own professional corporations, free agent physicians are able to contribute dramatically more to retirement through products like Solo 401k than they ever could as W2 employees. Marketplace health insurance may be more expensive, however it may be able to be provided to your “employees” e.g. yourself as an “employee benefit” and as such potentially a tax write off. Given free agent physicians tend to make 30 to 45 percent more than their W2 colleagues, this combined increase in income and tax savings often makes up the
I can’t leave this job I need reliable income. A great emergency physician and practice owner once told me, “No group is ever more than 90 days from a not for cause contract termination.” Past stability does not predict future results. Groups are trading contracts at higher levels than ever. The stability of any one group’s contract has never been more tenuous than it is today. Thinking that you have any more stability as a W2 employee is a delusion that we tell ourselves in order to not acknowledge the fragility of the emergency contract market. Employees of American Physician Partners had no notice before their company folded up shop left them without pay and without tail insurance in some cases. Groups like Schumacher, USACS, Team Health, Envision, and Sound continuously cycle contracts back and forth at hospitals across the country. The companies come in, extract as much value as they can and then shed the contract when their typical practices patterns result in the inevitable crisis. It happens over and over at the same places, no group ever learns because it’s more profitable to make some money up front and then let someone else deal with it when it doesn’t work.
Free agency as a means of learning the business of medicine.
Free agency is a phenomenal way to understand the business of emergency medicine as well. When you work in only one place day in and day out you assume the problems in your shop are the same problems everywhere else. You assume the medications listed as being on a national shortage are short everywhere. You assume that the problems in your shop are just par for the course. You then begin to internalize those problems, they even change the way you practice medicine. However as you see more of the world, you better understand which problems are
LOCUM TENENS SECTION
>> COMMON SENSE MARCH/APRIL 2024 51
local system problems and which aren’t. Strangely enough you notice that medications on “national backorder” in one shop are different from the ones on “national backorder” in your other shop. More importantly you disambiguate your identity as an emergency physician from the place where you are practicing. When you do this the system’s problems do not become your problems. You are able to advocate for yourself but when the system does not or cannot adapt you then have the ability to look inside and decide whether or not you are still able to deliver the ethical standard of care in a way that you desire. As a free agent you get used to reviewing contracts, negotiating pay, and have a much better sense of trends in the market. Yes, you will get it wrong from time to time, but as a free agent you walk in with mental flexibility and that keeps you less tied to the impact of any one decision good or bad.
Free agency as an alternative to unionization. There is a lot of talk around unionization of emergency physicians in America right now. Maybe unionization is a good thing. Maybe it isn’t. However what I do know is doctors are as different as individuals as we are well trained. While I am not against unionization if it brings down the malignant forces in industry by making anticompetitive practices unprofitable, I am skeptical that doctors will be able to get enough cohesiveness of thought to make this a widespread solution in the short term. However as a free agent you can advocate for your patients and yourselves by being loyal to organizations that prioritize ethical care but mobile when they do not. It is imperative for your own wellbeing as well as the care of your patients that you understand what your values are. Really take time and codify how you want to practice. You need to have standards for how you will work and what is important to you. When those standards aren’t met it is your duty as a physician to bring them forward and advocate for your patients, your colleagues, and yourself, but when your standards are not or cannot be met you should not be forced to compromise continuously.
Free agency as a hedge to anticompetitive trends.
The practice of emergency medicine has seen consolidation occurring at record levels since COVID. Entire swaths of the United States are dominated by one or two large multistate practice groups and competition for employment is plummeting. These large companies come in, buy out or force out many of the local or regional groups in the area and then drop rates and hire on cheaper less trained labor. Free agency returns the leverage of the free market to an industry that has been taken over by anticompetitive behavior. It is common for a large contract management group to claim that the low pay rate offered in a given city is market value, but when there is no competition in the market, who is to know? Interestingly enough, what frequently happens in these situations is that the low rates stifle recruitment. This results in burn out of overworked
docs. Eventually this reaches a critical point and the irresponsible companies are forced to bring in locums at 35 to 45 percent higher pay. This then reveals that the true market value lies far north of what had been offered. The contract management companies realize this and exploit the low business acumen of new graduates. They bring in a new grad for a low wage, run him into the ground and then squeeze a few years out of them.
Free agency as another solution in the mental health toolkit.
Locum tenens has itself changed over the past decade. While once seen as a last resort for washouts, money hungry sleaze bags, and social miscreants, locum tenens is now another means for young, intelligent, self-empowered doctors to reclaim autonomy and job craft a good life. In a world where investment banks have co-opted physician’s humanistic values for their benefit it is our chance to push back and show them that we have a voice. It is our opportunity to use the market to better ourselves and our practice of medicine. When properly informed and ethically executed, the free agent can use locum tenens to regain autonomy, increase stability, and stay out from under the thumb of corporate greed in medicine.
This article exists to reassure physicians that all is not lost. I want you to know that you are not crazy for being upset at the status quo. You worked hard to be where you are. Your dissatisfaction with the system is not going to get better by just trying harder and being more understanding. Our system has been co-opted and we will take it back, but until then the solution does not lie in rolling over and capitulating to malignant forces that do not have the interests of you or your patients in mind. There are many solutions and free agency is only one of them. Free agency from the outside appears daunting and full of uncertainty, but I want to reassure you that within uncertainty lies some of the best opportunities in life. Over the past two years I have traveled internationally dozens of times to multiple continents and experienced some of the best moments in my adult life, all while making more money and having more autonomy in the way I practice than I have ever had. There is hope, you don’t have to live with red flags every day, but in order to have this you must question the assertions that you assumed to be true and shed “good enough” then walk into uncertainty in order to touch better.
If you want to learn more about job crafting and the nuts and bolts of locum tenens I recommend you check out the “Guide to Locum Tenens” on the AAEM-Locum Tenens Section website and watch some of the recorded talks on “The Nuts & Bolts of Locum Tenens” also available on the LTS website.1 The Locum Tenens section is growing and we are hungry for leaders who want to disrupt the market to make medicine better.
Continued on page 54 >>
LOCUM TENENS SECTION
COMMON SENSE MARCH/APRIL 2024 52
Choosing Emergency Medicine
Marianne Haughey, MD FAAEM

Emergency medicine is said to suffer one of the highest burnout rates of all medical specialties, and as such, emergency medicine as a specialty could certainly use some added touches of “wellness.” Further, the reputation of emergency medicine as a potentially attractive career choice has suffered, partly due to the matter of burnout and partly due to the perception of an imminent oversupply of emergency physicians. These perceptions may well have caused the growing number of unmatched emergency medicine residency positions in 2022 and 2023. Thus, there have been many discussions and suggestions about how to incorporate wellness into the lives of emergency physicians. As an associate program director, I also have had the opportunity and motive to consider and discuss challenges with the EM match over the last couple of years. As one who has a vested interest in both excellent emergency care as I get older as well as interest in how to keep our lives balanced as physicians I have had some thoughts.

I will always remember… one of the attendings in the ED…pouncing upon the meal cart when it arrived, not for himself, but to hand out trays to patients saying, ‘being in the emergency department means always being an advocate for patients!
I have had cause recently to reflect on what led me to the path of emergency medicine. I entered medical school in 1988, and the ED that summer. I chose EM in 1991, matched in 1992. For reference, The TV show “ER” first aired in 1994. My career choice occurred before EM became popular. The emergency department was not glamorous, it was not pretty. Most of those I worked with were not those who were children of doctors (although some were children of nurses), as EM was fairly disreputable. It was most definitely the most blue collar of the possible medical fields. It was recognized that it was hard work and that I would get my hands very dirty if I chose it as my profession.
But the joy! Of all the areas that I worked in the hospital, in the ED I had such direct contact with patients! I heard from them directly and even as a first-year student who had essentially wandered in off the street to shadow, I could help someone in a small way. I will always remember Steve Saef, one of the attendings in the ED early in my wanderings, pouncing upon the meal cart when it arrived, not for himself, but to hand out trays to patients saying, “being in the emergency department means always being an advocate for patients!” I helped him hand out the trays and got multiple shy “thank yous” in reply.
Of course, many patients were beyond responding, or incapable for whatever reason of summoning a verbal thanks. Some were just so ill, but some were so trodden down by society that the ability to give thanks was now beyond them.
The need in these patients was beyond anything I encountered elsewhere in my rotations. Of course, the ability to have a “fresh” patient, to travel the diagnostic and therapeutic paths before any other physicians grew on me as I learned more medicine. Importantly, the devotion to providing care to all comers demonstrated by my role models was an additional, powerful draw.
EM was not the most competitive field when I entered. Of my class of 170 or so, three chose EM. I can’t speak for the others but although I did very well on my clinical rotations, I did not have the highest board scores, nor was I a member of AOA. I also knew my chosen specialty was a difficult one, with hard hours, overnight, holiday, and weekend work for the rest of my career.
AGING WELL IN EMERGENCY MEDICINE INTEREST GROUP
>> COMMON SENSE MARCH/APRIL 2024 53
A few years after I entered, EM became “hot” as a specialty to draw medical students. There was lots of conversation about it becoming a “lifestyle” specialty. That it would be easy, limited. That it would be possible to do “three shifts a week” and then be off the rest of the time. Droves of students, most with better scores and accolades than I had had upon leaving medical school, filled the ranks of the applicants. Thankfully, by that time I had gained a bit of experience under my belt, so I had medicine to teach.
There are emergency physicians now moving on to run hospitals, run for political office, and working on policies to help other humans at least partly because they were face-to-face with societies failures to care appropriately.
Along with the purported “lifestyle” qualities of the specialty came some losses. If you only come in for three shifts a week, then you don’t really serve on hospital or medical school committees. You are isolated from the community of medicine and the hospital. You are less invested in the processes and policies of the hospital and medical school at large. When so isolated, it becomes more and more draining to deal with the definite difficulties of the specialty, and you have less support. It is emotionally and physically draining. Also, if you are only doing three shifts a week it becomes easier to replace you with someone else who also only does three shifts a week perhaps with less value, but also with less cost for whoever is paying the bills.
I think there was a basic error in this shift. EM is never going to be easy. The shifts are hard, true, but more importantly we are the front door to the hospital and the failures of society. We are witnesses to the broken pieces—whether uninsured patients who can’t get their medications filled, those suffering abuse (whether child or adult, sexual or other physical abuse), patients with psychiatric illness not having their needs met
LOCUM TENENS SECTION
Continued from page 52
References
1. AAEM Guide to Locum Tenens: https://www.aaem.org/get-involved/ sections/lt/guide/
2. Turning to Alternative medicine: https://www.nbcnews.com/health/ health-news/americans-really-want-believe-alternative-therapiescancer-n925976#
3. https://www.nih.gov/news-events/news-releases/according-newgovernment-survey-38-percent-adults-12-percent-children-usecomplementary-alternative-medicine
4. https://bmccomplementmedtherapies.biomedcentral.com/articles/10.1186/ s12906-020-03157-2
5. Rate of AMA increasing: https://pubmed.ncbi.nlm.nih.gov/35490566/
6. AMA discharges: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6445898/
by the medical machine, those brought down by the illness of addiction, or even just the elderly trying to live independently, but alone and failing. We are the nexus of medicine meets advocacy—it is right in front of our faces, like it or not. And the beauty is that allowing yourself to advocate—to see the pain of our fellow humans, but to give voice to their need when they cannot do it themselves is not just a job but a mission. And a sense of mission is actually protective against burnout.
So I would suggest to all those speaking to medical students and those interested in medicine shift the conversation from “EM is easy—it is shift work,” to “EM is hard, people are in great need, but I never leave a shift without doing at least one small thing to help another human being” and maybe even “I want to advocate for my fellow humans, and from my position of privilege this is the best way I can learn what the needs are so I can help and raise my voice constructively to help solve issues.” There are emergency physicians now moving on to run hospitals, run for political office, and working on policies to help other humans at least partly because they were face-to-face with societies failures to care appropriately. And there are those now teaching the next generation.
Twenty-eight years in, it still gives me joy to do one at least small thing every shift to help someone. On a good day there are many more good things than that. I welcome those who want to join me in my mission as I advocate for my patients in a tough job. This has kept me “well” during my current 28-year career as an attending.
7. Facility Fees: https://www.healthsystemtracker.org/brief/how-do-facilityfees-contribute-to-rising-emergency-department-costs/
8. PE is dangerous: https://www.nytimes.com/2023/12/26/upshot/hospitalsmedical-errors.html#:~:text=The%20study%2C%20published%20in%20 JAMA,not%20bought%20by%20such%20investors.
9. https://jamanetwork.com/journals/jama/fullarticle/2813379?guestAccessK ey=160722c5-3ed7-4eea-b0b8-e9c669dd2df5&utm_source=twitter&utm_ medium=social_jama&utm_term=12175399851&utm_campaign=news_ alert&linkId=257502349
10. https://www.cnn.com/2023/12/26/health/private-equity-hospitals-riskierhealth-care/index.html
11. https://www.nytimes.com/2023/04/28/opinion/private-equity.html
AGING WELL IN EMERGENCY MEDICINE INTEREST GROUP
COMMON SENSE MARCH/APRIL 2024 54
Why Should I Continue to be an Emergency Physician?
José A. Rubero, MD FAAEM FACEP
Maybe you got to that time where you’re grappling with the challenges of being tired, frustrated, overworked, and underpaid as an emergency medicine physician.
We all (including myself) had, have, or will have the same question after working for some time. The concerns of burnout, how satisfied are you with your work or where you work, financial responsibilities, and various other factors are some of the reasons that we may think to change careers, retire, or “move on.”
There are many articles talking about emergency medicine physicians experiencing some of the highest rates of burnout. Some contributing factors include working on the front line, spending more time documenting/charting instead of taking care of the patient, or using your own unpaid time to document, consistent high intensity and stressful shifts, unpredictability, and irregular circadian rhythm. There’s also a fear of litigation at all times, as well as the patient or family “knowing” more than you because of “web” consulting or their expectations.
The decision to continue to be an emergency medicine physician despite these challenges can be influenced by several factors. Here are a few possible reasons that remind me of why I want to continue to be an emergency physician.
Passion for Helping Others. Many individuals in emergency medicine are driven by a genuine passion for helping people in critical situations. The fulfillment that comes from making a positive impact on someone’s life during a medical emergency can outweigh the challenges of the job. I still remember when I came to one of my shifts and I found my nurses crying tears of happiness. I asked why they were crying and that moment I knew how important our job is. In one of the rooms in the ED there was a birthday cake with a family and their two year old child celebrating his birthday because I saved his life after a drowning accident.
Sense of Purpose. Emergency medicine physicians often find a deep sense of purpose in their work. The ability to save lives and provide immediate care in critical situations can be a powerful motivator. My sense of purpose is also renewed when I see some of my medical students who were interested in other specialties change their minds to become EM physicians.
Adrenaline and Variety. Emergency medicine is known for its fast-paced and unpredictable nature. Some physicians thrive in this environment, enjoying the adrenaline rush and the variety of cases they encounter. Being a medical detective can be part of that unpredictable nature when often we do not know what is wrong with our patients, and it is our job us to find out, good or bad.
Professional Growth. Despite the challenges, working in emergency medicine can offer continuous learning opportunities. The diverse range of cases can contribute to professional growth and development. Every day, when I come to work, I always learn something new. I try to be up-to-date at all times to make sure that I am able to better care my patients.
Commitment to Community Health. Some physicians feel a strong commitment to serving their community’s health needs, especially in emergency situations. This sense of responsibility can drive them to continue working despite the challenges. Being part of a disaster team can be a great example of how you can serve your community or any other community, especially in times of need. Helping victims from a natural disaster or large gathering events exemplifies that commitment.
Financial Stability (Long-Term). While the immediate financial rewards may not be high, some individuals see emergency medicine as a long-term investment. As they gain experience and expertise, there may be opportunities for better compensation or advancement in their careers.
Continued on page 59 >>

The fulfillment that comes from making a positive impact on someone’s life during a medical emergency can outweigh the challenges of the job.
COMMITTEE
ACADEMIC AFFAIRS
COMMON SENSE MARCH/APRIL 2024 55
The Lost Art of Listening: A Case for Narrative Medicine
Suchismita Datta, MD* and Yash Chavda, DO MBA †


Within the history of medical education, there is a tug-of-war between basic science knowledge and clinical practice and vice versa. Which is dominant?1 Over time, medical education often trends towards a constructivist view, that is, the theory that learners construct knowledge rather than passively take in information.
This is as opposed to the post-positivist view that retains that there is an objective truth, but experiences of such truths are imperfect because the experiences are ameliorated by the person’s values and experiences.
critical reflection, reflexivity, dialogue, and narratives.3 Some of the theorists behind this paradigm are Friere and Kincheloe. They are known to be the early founders and proponents of critical pedagogy—which believes that power and cognitive dynamics contextualize teaching and learning and that teachers can empower students through authentic knowledge. Emphasis is placed on the concept of “praxis” which is
with the potential to impact learner attitudes, knowledge, and skills, there is a paucity of studies that look at how this translates to the bedside care of patients.4
Over the last decade and a half there has been an increase in scholarly interest in theorizing narrative medicine, and also formally incorporating it into medical education and subsequently studying and publishing about the process.
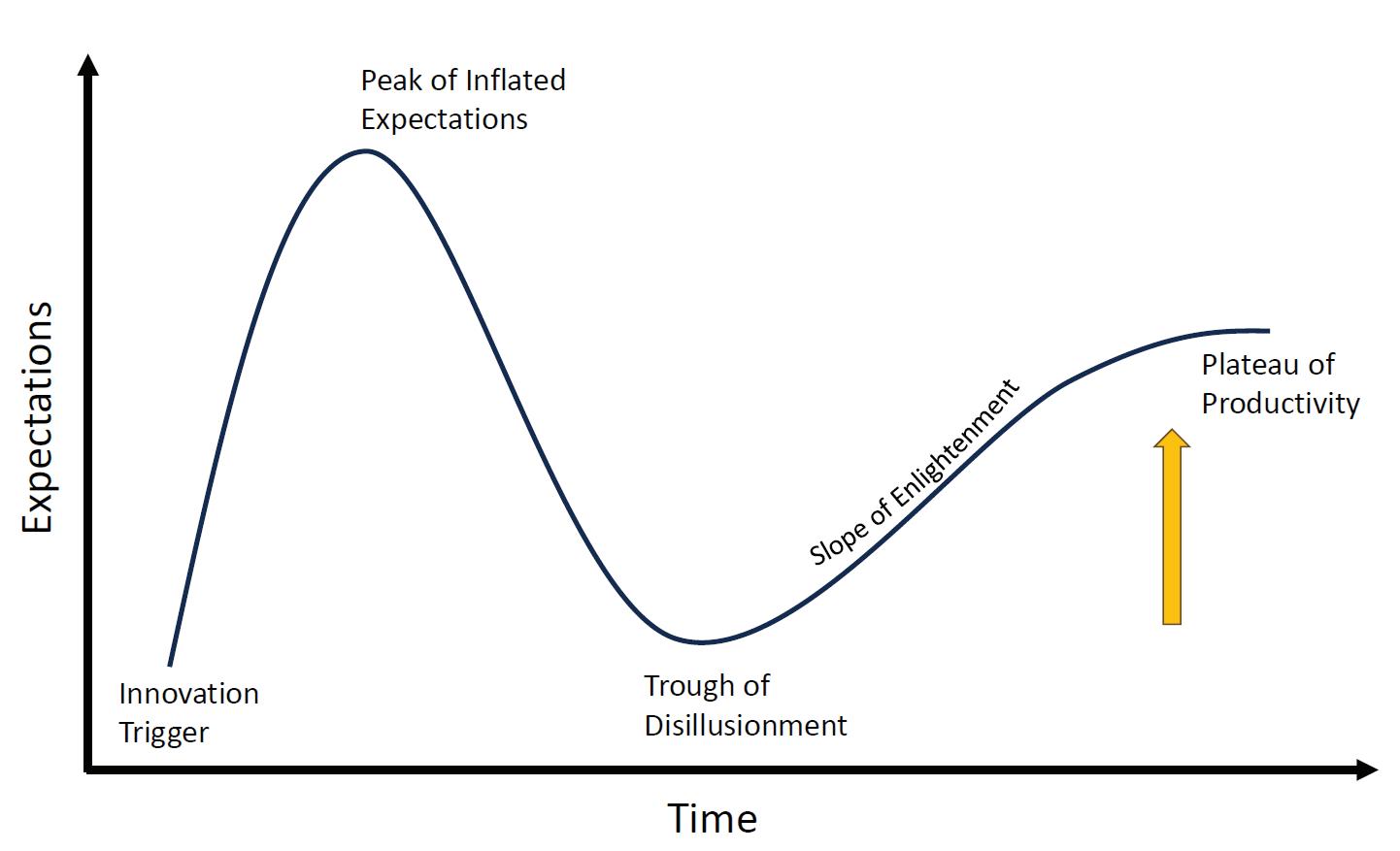
Where does narrative medicine fit into medical education paradigms? Storytelling and listening have always been central to the practice of medicine and medical education. As Sayantani Dasgupta, a pediatrician and established narrative medicine expert, so eloquently puts it in her TedTalk “before diagnostic CAT scans, treatments for blood loss, or cures for tuberculosis—what we had was the ability to show up and to listen; to stand witness to birth, death, illness, suffering, joy, and everything else that life has to offer.” However, this has not been grounded in theory.
In terms of educational theory, narrative medicine most closely aligns with the transformative paradigm,2 in that it aims to positively change student outlook, and employs methods such as
that theory should inform action, reflection should follow action, which should then modify theory and subsequently inform action. While the theory is interesting, there is a question on the practical applications of narrative medicine. Why does it matter? With technology having a steadily increasing impact on the practice of clinical care, the threat of losing the singularity of the patient story becomes more imminent. In many medical specialties, clinicians operate with little information to make high-stakes decisions and reliance on algorithms and heuristics becomes a “necessary evil.” The field of narrative medicine seeks to bridge the gap between pathophysiology and the experiential knowledge contained in the patient story by employing narrative competence.4 Although there is evidence to suggest that narrative medicine is an effective pedagogic tool
The situation of narrative medicine can be evaluated as a trend concerning the Gartner cycle (Figure 1). The Gartner cycle traces the journey of innovations and is increasingly used by scholars across disciplines including health professions education and research. It is characterized by three stages: peak, disappointment, and recovery of expectations.5
Research and development relating to narrative medicine in medical education began with its onset in the early 2000s led by Dr. Rita Charon. Dr. Charon established the first masters of science program in narrative medicine at Columbia University in New York City which can be considered the innovation trigger for the exponential uptick in stage one of the Gartner Cycle.
The years 2013 to 2018 mark the first quick dip and then a relative lull in scholarly interest around narrative medicine, culminating in the trough of disillusionment part of the Gartner Cycle of Hype. There are seldom negative articles published in regards to narrative medicine but one of the few was published in 2013.6 The
>>
COMMON SENSE MARCH/APRIL 2024 56
Figure 1: Gartner’s Hype Cycle
article argues that narrative medicine’s approach to medical humanities is too utilitarian and that medical learners need to be exposed to an environment of pure thought and reflection instead.6
Following this, after 2018, narrative medicine in health professions education trended back upwards towards the slope of enlightenment, and now closer to the plateauing tail of the Gartner cycle. It is difficult to disregard the role of the pandemic in this phenomenon. Physicians and medical learners became masked warriors trying their best to provide medical care under duress and with the lack of required resources. This has led to increased burnout, loss of empathy, and disillusionment. The stressors of the pandemic likely led to the need to humanize healthcare again which drove interest in narrative medicine.
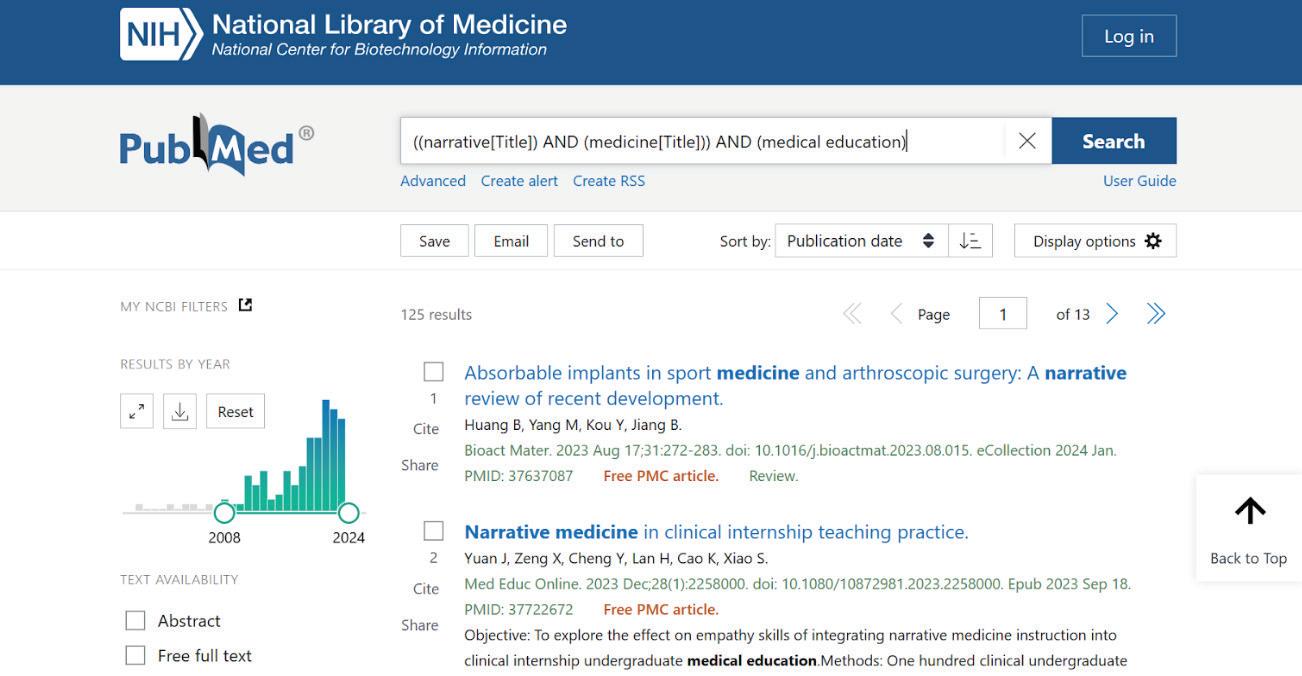
The aforementioned journey of narrative medicine can be seen in the publication trends around it. There is an initial exponential uptick, followed by a fast dip and small lull, and then trending up again (Figure 2).
References
The most recent publications have been exploring different applications of narrative medicine in medical education, including topics such as diversity, equity, and inclusion.7 There are medical specialties that are piloting narrative medicine curricula and publishing-related medical education research. Until recently there have been no formalized narrative medicine programs in the field of emergency medicine. In July 2023, a group of emergency medicine faculty in Boston, United States, published the first emergency medicine-based narrative medicine medical education study.8 Overall, this suggests that the trend is situated on the slope of enlightenment headed toward the plateau of productivity.
*Assistant Professor of Emergency Medicine, Director of Emergency Medicine Research - NYU Long Island Hospital Department of Emergency Medicine
†Clinical Assistant Professor of Emergency Medicine, Director of Emergency Medicine Ultrasound - NYU Long Island Hospital Department of Emergency Medicine
1. Kendall PL, Reader GG. Innovations in Medical Education of the 1950s Contrasted with Those of the 1970s and 1980s. J Health Soc Behav. 1988;29(4):279-293. doi:10.2307/2136863
2. Baker L, Shing LK, Wright S, Mylopoulos M, Kulasegaram K, Ng S. Aligning and Applying the Paradigms and Practices of Education [published correction appears in Acad Med. 2020 Jan;95(1):150]. Acad Med. 2019;94(7):1060. https://doi.org/10.1097/ACM.0000000000002693
3. Mertens, D. M. (2007). Transformative Paradigm: Mixed Methods and Social Justice. Journal of Mixed Methods Research, 1(3), 212-225. https:// doi.org/10.1177/1558689807302811
Narrative medicine aligns with the transformative paradigm. It seeks to positively change student outlook by employing methods such as critical reflection, reflexivity, dialogue, and narratives. With multiple metrics, technologies, increasing patient numbers, and reduced patient encounter times, physicians are at an increased risk of forgetting the art of listening. Narrative medicine theoretically can help bring medicine back to its roots, and by understanding its history and where it is going, one can be a part of that change.
4. Milota MM, van Thiel GJMW, van Delden JJM. Narrative medicine as a medical education tool: A systematic review. Med Teach. 2019;41(7):802810. https://doi.org/10.1080/0142159X.2019.1584274
5. Ozgur Dedehayir, Martin Steinert, The hype cycle model: A review and future directions, Technological Forecasting and Social Change, Volume 108, 2016, Pages 28-41, ISSN 0040-1625, https://doi.org/10.1016/j. techfore.2016.04.005
6. O’Mahony S. Against narrative medicine. Perspect Biol Med. 2013;56(4):611-619. https://doi.org/10.1353/pbm.2013.0032
7. Holdren S, Iwai Y, Lenze NR, Weil AB, Randolph AM. A Novel Narrative Medicine Approach to DEI Training for Medical School Faculty. Teach Learn Med. https://doi.org/10.1080/10401334.2022.2067165
8. Malik Z, Ahn J, Schwartz A, Blackie M. Narrative medicine workshops for emergency medicine residents: Effects on empathy and burnout. AEM Educ Train. 2023;7(4):e10895. Published 2023 Jul 20. https://doi. org/10.1002/aet2.10895
Figure 2: Publications about narrative medicine and medical education
THE LOST ART OF LISTENING: A CASE FOR NARRATIVE MEDICINE
COMMON SENSE MARCH/APRIL 2024 57

Transitioning into Your Role as a Medical Educator
Jennifer McGowan, MD FAAEM FAWM
We spend three to four years of residency learning to become outstanding, competent clinicians. We graduate as newly minted attending emergency physicians, ready to treat patients, lead healthcare teams, and teach the next generation. But when do we learn how to teach effectively? Most of us model the methods by which we learned but have no formal education in what makes an effective educator. There were certainly teaching opportunities in residency, but was there ever formal instruction in how to teach? I hope so, but for many (me included), it was a trial-and-error method of finding your own style. Although medical education fellowships and graduate programs for education are great, many physicians cannot devote the time or resources to do these.
This article is designed to give you a few quick tips to help you reframe your perspective as an educator.

Teaching is not about you. It is not about your knowledge, your skills, or how good of a physician you are. It is about the learner and their growth. This seems obvious, but if you listen to many people teach their residents, students, or ED colleagues, you will hear many declarations of knowledge from the teacher and not much feedback from the learner. Often, those of us in a teaching role look at teaching as a way to impart our knowledge on the captive audience. Instead, we should reframe teaching as an exercise to help our learners connect concepts between their existing knowledge, challenge them to grow their own theories, and actively participate in their learning instead of allowing them to zone out, smiling and nodding politely as we drone on endlessly.
Asking learners questions can be a big part of your teaching. Seems easy, but we all could probably improve on this technique too. When you ask a question, wait and listen for the response. On average, educators only wait 0.7 to 1.5 seconds for a response to a question before giving the answer. Imagine being a learner, trying to retrieve an answer—it will take longer than one second! Let them take longer. Let them struggle to remember—this internal struggle to retrieve the information buried in their brain is when the learning occurs. Waiting just three to five seconds will allow your learners to formulate an answer and make your teaching more engaging. For more complex questions, allowing 10 to 15 seconds may be appropriate. On a busy ED
shift, try asking your learners a complex question, then go see a patient. Give them time to think, or to look things up if needed. Remember point one, it is not about you explaining what you know, it is about helping them remember all the things they know!
Make giving frequent, intentional feedback your homework as an educator. Feedback should be specific and directed, with clear goals of actions to continue or improve upon. Do not comment on personality traits, rather focus on relevant competencies.
If you are having trouble visualizing this, think back to the milestones utilized in residency: patient care, medical knowledge, interpersonal and communication skills, etc. If you are in a role in which you give a written evaluation at the end of a rotation, try to think about feedback on each shift. I like to keep an ongoing notes tab on my phone, making it easy to jot things down in real time that might be forgotten in a few weeks. However, you do not need to wait until the end of the month, rotation, or year to give your feedback—feedback is best given within a short interval. Debrief with your resident after a resuscitation to discuss what went well and what could improve. Discuss with your student how they could have structured their consult more clearly for their consultant after they hang up the phone. Take five minutes at the end of a shift to talk about one to two things your learners did great on, and one to two goals to
There were certainly teaching opportunities in residency, but was there ever formal instruction in how to teach?
YOUNG PHYSICIANS SECTION
>> COMMON SENSE MARCH/APRIL 2024 58
work towards on the next shift. Be sure to focus on both the positives and the areas for improvement with specific examples of each.
Please, take gender out of the feedback process. No stereotypical gender descriptors should make their way onto a professional evaluation or in verbal feedback. Many times, a female learner may be described as “timid and passive” whereas a male colleague with identical behaviors would receive the adjectives of “thoughtful and collected.” Take this a step further and try to be an advocate for your learners (or colleagues!) on shift. The next time you hear someone describe a female learner as “opinionated and bossy,” ask yourself: if this was a male, would the descriptors instead be “confident in their decisions and in control of the room?” Reflect on number three—avoid this language in your own feedback (remember: competencies, not personality traits!), and beware of the bias of others.
The learning environment is more effective when learners feel safe. Again, this seems like common sense, but it is important to keep this in mind when you are interacting with your student or residents. Be non-judgmental and emphasize being open to questions, concerns, and feedback. You can take this a step further by sharing stories of mistakes you have made or lessons you have learned during your own training or patient care. Show the learners how you correct your own knowledge gaps, such as explaining “this is my method of looking things up when I don’t know.” Equally as important is creating an inclusive environment, where learners feel free to express themselves, their thoughts, and their views without fear of shame or reprimanding. It should go without saying that expressing your own social or political views on your learners can create quite an uncomfortable learning environment for your students if their views differ, so please keep these topics and views separate from your role as an educator.
ACADEMIC AFFAIRS COMMITTEE
Continued from page 55
Job Satisfaction. Despite the challenges, some emergency medicine physicians find intrinsic satisfaction in their work. Knowing that they are making a difference in people’s lives can be a powerful motivator. At the same time that you are helping your patients, I also find satisfaction when I see medical students and residents grow to be colleagues and even work side by side in the same ED.
It’s important to evaluate your own motivations and priorities. If the challenges become too overwhelming, seeking support, discussing concerns with colleagues, or exploring ways to achieve a better work-life balance may be beneficial. Additionally, considering potential career changes or
Finally, in this same vein, be accommodating as best you can. Learners desire your approval and are generally trying their best to earn it. If something unexpected arises, your learners are probably stressed about how you will perceive their requests or needs. Try to accommodate schedule changes, be flexible, and be understanding. Life happens—we all expect this understanding from our colleagues, and our learners are very grateful when we can treat them with the same respect and consideration they deserve.
Make small changes. It can be daunting and overwhelming if you believe you need to do a complete overhaul of your teaching strategies or instructional design. No one expects you to redesign an entire residency curriculum overnight, to create an in-service program for an EMS agency, or revamp the small group sessions for the local medical school all on the first day. What you can do today is pick one or two of these points and try to integrate them into your daily routine. It can be as simple as deciding to give dedicated feedback at the end of shift, or by committing to allowing five seconds for learners to answer your questions before providing the answer. Choose one small thing to help your learners, integrate it into your daily routine, then choose another. These small revisions to your teaching strategies can yield big results in your learner’s knowledge gains. There is a wonderful book, “Small Teachings” (Lang, 2016), if you are interested in further strategies to increase your educational impact.
Ultimately, remember learning is supposed to be hard—both for you and your learners. It is ok to struggle to figure out what works for you, what you can incorporate on shift, and keep changing things that do not work. You are learning how to be a more effective educator—it is a process, and it takes work!
seeking additional qualifications could open up new opportunities for personal and professional growth.
Dr. Rubero is the Clerkship Director and Core Faculty for the Emergency Medicine Residency Program at HCA Healthcare/USF Morsani College of Medicine GME, HCA Florida Oak Hill Hospital; Professor of Emergency Medicine at University of Central Florida College of Medicine, Florida State of Florida College of Medicine, NOVA University College of Osteopathic Medicine, and LECOM College of Osteopathic Medicine as well as Associate Professor of Emergency Medicine at USF Morsani College of Medicine.
YOUNG PHYSICIANS SECTION
COMMON SENSE MARCH/APRIL 2024 59
Closing Time
Leah Colucci, MD MS

Tt’s been two years and many Common Sense pieces later, but this is officially the last time I will write to you as AAEM/RSA President. This has been such a wonderful journey, and I am so proud of what our board has accomplished.
Over the last two years we have consistently stood up for resident education and protections for them when midlevels encroach in their teaching environments. We have reminded residencies and fellowships that these terms and positions are protected and preserved for our MD/DO trainees.
We continue to fight against private equity and contract management groups taking advantage of residents. We have supported legislation against the corporate practice of medicine.
This has been such a wonderful journey, and I am so proud of what our board has accomplished.
We have been actively engaged in improving board exams and the study materials that are available. We are working closely with ABEM so that our voice is heard in the Becoming Certified campaign. We also are working with ACGME to support improved residency program requirements.
We hosted a successful Health Policy in Emergency Medicine Symposium and have two more currently being planned (in Austin, Texas, and Washington D.C.). We want to arm our residents and medical students with the resources needed to talk to lobbyists.
We are working on a professional development curriculum to help our residents learn how to budget, contract negotiate, and bill.
We created EMIG toolkits to revamp medical schools that don’t have active ones or need more support.
We created locums education to give our residents a different perspective on job prospects.

We continue to provide education on resident unionization so that each residency program can make the right choice for them.
Our efforts toward improving DEI in our specialty are ongoing as well as our mentorship. We host specific office hours to help URiM applicants match, but also have a Road to Match mentorship for all of our medical students.

This list of what we achieved and created could go on. I am proud of what we have accomplished, but I am excited to see what the new leadership does. I will be staying on the board as AAEM/RSA Past President and hope to watch our organization grow! Thank you for an amazing last two years.


AAEM/RSA PRESIDENT’S MESSAGE
COMMON SENSE MARCH/APRIL 2024 60

Stitches in Time: The 10 Commandments of Laceration Repair for Trainees
Mel Ebeling, BS
Laceration repair is a very common procedure in the emergency department (ED), and if you are a medical student or intern on your emergency medicine rotation, you may be asked to perform laceration repairs with varying levels of oversight. But let’s face it—being given a silicone suture pad and told to practice simple interrupted and mattress sutures does not equate to proficiency in laceration management.
Certainly, technical skills are crucial, but managing a laceration involves a variety of other skills, including irrigation, local anesthesia infiltration, wound dressings, antibiotic and vaccine considerations, patient counseling, and documentation. Are you prepared to manage all aspects of a laceration from start to finish? If yes, can you do so efficiently?
survey. Other times, especially for lower acuity patients whose only chief complaint is a laceration, you may be the one responsible for asking the patient about their vaccination status. Take time to review the Centers for Disease Control and Prevention’s guidance about when and what kind of tetanus prophylaxis should be provided.1
Commandment #3: Thou Shalt Not Be Wasteful.

But let’s face it—being given a silicone suture pad and told to practice simple interrupted and mattress sutures does not equate to proficiency in laceration management.
Commandment #2: Thou Shalt Test the Tendons.
From trainee to trainee, I have compiled several tips and important considerations, the “10 Commandments of Laceration Repair,” designed to guide you towards independently managing lacerations in the ED. Of course, though, this is not medical advice, and you should always refer to your institution’s policies/ procedures and your supervising attending’s guidance when performing laceration repairs on patients.
Commandment #1: Thou Shalt Ask About Tetanus.
Every open wound necessitates questioning about tetanus vaccination status. For multitrauma patients transported to a designated trauma center, nursing or pharmacy staff in the bay may ask about the timing of the last tetanus vaccine as part of the standardized secondary
Lacerations to the distal extremities should raise your suspicion for injury to underlying tendons. For example, lacerations on the volar surface of the hand are at risk of flexor tendon injury, while those on the dorsal surface are at risk of extensor tendon injury. While different institutions and physicians have different comfort levels regarding lacerations complicated by tendon injury, orthopedic or plastic surgery is often consulted to repair injured tendons (especially flexor tendons). However, it is your job in the ED to determine whether injury to the tendon has occurred (or is likely to have occurred) and a consult is needed. For any and every laceration to the hand or foot, you should always test the full range of motion of the injured area. Elson’s test, for example, can be useful in determining whether extensor tendons are injured.2
When it comes to performing laceration repairs (or any procedure, really), being prepared is paramount. Having the wrong supplies is wasteful in two ways: (1) you are wasting valuable time on your shift by having to go back and forth between the supply room, and (2) by opening the wrong supplies, you are wasting materials that add up in cost over time. While you may not personally eat that cost, being mindful about the increasing costs of healthcare and factors that contribute to that is important. Ensure that when you enter the room to manage someone’s laceration that you have all anticipated supplies: laceration repair kit (typically includes your needle drivers, scissors, forceps, and needles for drawing and administering anesthetic); local anesthesia (e.g., vial of lidocaine 1% with epinephrine); plastic basin, bag, or chuck pads (for catching water during the irrigation process); and a container of sterile saline or potable water with a needle and syringe for irrigation (see Commandment #5). You may have noticed that I did not include sterile gloves on that list of supplies to grab. Use of nonsterile gloves (i.e., typical clean nitrile gloves) does not significantly increase risk of infection compared to sterile gloves, and nonsterile gloves are much cheaper.3 This is just another way to combat waste in medicine.
Commandment #4: Thou Shalt Not Break Thine Back.
Ergonomics is everything. Setting yourself up for success starts with ensuring that you can perform laceration repair comfortably. Even lacerations that only require a quick, single suture
AAEM/RSA EDITOR’S MESSAGE
>> COMMON SENSE MARCH/APRIL 2024 61
can place unnecessary strain on your back due to the location of the laceration and/or your positioning for that duration of time. While you may not feel it initially, cumulative poor positioning can lead to chronic pain, and creating an environment where you can perform a procedure comfortably does not take much extra time. Sit down if there is a chair available. If not, raise or lower the patient’s bed as needed so that you do not have to strain your back while standing. Use a side table for your supplies at an appropriate height. Remember, taking care of others first requires that you take care of yourself.
Commandment #5: Thou Shalt Clean Wounds Properly.
Irrigation is a critical part of laceration management, and there are right and wrong ways to perform this technique. Pressure is the name of the game. To remove debris and dilute the bacterial load in the wound below a certain threshold, consistent application of 5-8 psi of pressure is necessary, which can be achieved with an 18-gauge needle attached to a 30- or 60-mL syringe.4 Note that current evidence suggests that using potable water instead of sterile saline does not increase the risk of infection, so either can be used to irrigate wounds, and potable water may be more cost-effective (see Commandment #3).5
Commandment #6: Thou Shalt Choose Thy Suture Wisely.
When deciding what suture material to use, the first decision that must be made is whether to use absorbable or nonabsorbable suture. This is an important decision, as it determines whether the patient will need to follow up for suture removal. Institutions that have better patient return rates and are well-equipped with the infrastructure to offer suture removal care may
lean towards nonabsorbable sutures in indicated scenarios. On the other hand, institutions with patient populations that rarely seek follow up may use absorbable chromic gut whenever possible. Next, you would decide whether to use a braided or monofilament suture. Each type of suture material has its pros, cons, and specific uses. While more detailed discussion of each material is outside the scope of this article, it can be easily researched. Know that if you are in the medical student role specifically, perhaps even in the intern role, it would be important to clarify suture material with your supervising resident or attending before performing the repair to ensure it has the strength and properties to keep the laceration edges approximated while healing occurs.
Commandment #7: Thou Shalt
Beware the Bite!
Human, cat, and dog bites are at increased risk of infection and, as a result, are not always sutured. Thus, try your best to ascertain the mechanism of injury for every laceration to determine the necessity for antibiotic therapy. For an isolated laceration to the knuckle, it may be safest to assume that it was caused by a punch to someone else’s teeth (“fight bite”) and provide antibiotic prophylaxis. Before starting your emergency medicine rotation, read up on current antibiotic guidelines for different types of bites.
Commandment #8: Thou Shalt Write a Procedure Note.
Laceration repair is one of the most common procedures performed in EDs in the United States, but it is also a major source of malpractice claims.6,7 Thorough documentation is essential! For each laceration performed, ensure that you document the characteristics of the laceration repaired (e.g., length/size and
location), how it was irrigated, whether undermining or debridement was performed, which and how much anesthetic was utilized, the type and size of suture used, the number of sutures placed, how the wound was dressed, and what counseling was provided. Documentation is part of laceration management. If you are a medical student and are expected to assist in note-writing, this will significantly help your team and is one way to show that you are taking ownership of your patients.
Commandment #9: Thou Shalt Educate Thy Patient.
Patients should be educated on how to take care of their wounds following discharge, whether they need to return for suture removal as well as when that would occur, and warning signs that should prompt their return for medical evaluation. Some electronic health record systems have great discharge instructions and information sheets that can be printed out for patients; other times, you may be responsible for writing these yourself. In either case, still have a discussion with your patient about these topics and ensure their understanding using the teach-back method.
Commandment #10: Thou Shalt Double-Check with Authority. As with anything in medicine, it is never wrong (and depending on your level and confidence is encouraged or required) to double-check that you have the correct materials and accurate understanding of the procedure technique to be performed with your supervising resident or attending before starting. Recall that laceration repair is a real procedure with risks and benefits, and patient safety is the most important part.
Continued on page 73 >>
[L]aceration repair is a real procedure with risks and benefits, and patient safety is the most important part.
AAEM/RSA EDITOR’S MESSAGE
COMMON SENSE MARCH/APRIL 2024 62
Announcing The Joint Commission Reform Task Force
Gary M. Gaddis, MD PhD FIFEM MAAEM FAAEM

Do you think The Joint Commission for Accreditation of Hospital Organizations (JCHAO) (which is now called “The Joint Commission” or “TJC”) had a huge role in the creation and enabling of the current opiate death epidemic that continues to plague the United States? Would you love to be able to do something about that? Would you like to see TJC publicly rebuked and punished for its arrogance and its misleading pronouncements, which have attempted to place the blame solely upon those of us who are physicians, while ignoring the influence upon the health care system that TJC’s pain standards caused? Would you like to see TJC pay for its creation and continuation of its flawed Pain Standards, which were introduced in February of 2002? Those standards were not officially, fully discontinued for more than 15 years, despite recurrent and strong condemnation of those standards from numerous medical organizations.
Would you also like to see TJC rebuked for failing to set standards or expectations that would force hospital system leaders to finally provide solutions to the matter of emergency department boarding and crowding? Do you feel like TJC has persistently and systematically turned a blind eye toward this issue, as if it is too inconvenient or too complex to be addressed and solved?
If you would like to have TJC be forced to publicly admit and pay for its culpabilities, you are far from alone. You should be interested in knowing that the AAEM Board of Directors has recently approved the creation of a new task force, “the Joint Commission Reform Task Force.” This column will describe the goals for the task force and the rationale for its formation. I am the author of this column because I proposed this task force and will serve as the task force’s initial Chair. I would like to invite you to attend the task force’s organizational meeting during the 2024 AAEM Scientific Assembly (SA) in April in Austin, TX (the time, date, and location of the meeting is to be determined).
In case you are unaware, TJC is by far the largest of the several “third party accreditation” organizations that accredit hospitals as regards the safety of their practices. Hospital organizations must gain and retain “third party” approval, to enable them to receive reimbursement from health insurers, as well as from the Medicare and Medicaid programs. However, hospitals are not forced to utilize TJC for accreditation. Other accreditation organizations also exist.1
Don’t for a minute think that anarchy is a goal of the task force. TJC and the other third-party review/accreditation organizations clearly serve an important and useful function. All large organizations can “normalize deviance,” and hospitals and hospital systems, as large organizations, are no exception. As an example of “normalizing deviance,” consider the way
“If you would like to have TJC be forced to publicly admit and pay for its culpabilities, you are far from alone.
that many hospitals handle workplace violence committed by patients or visitors against their employees. Rather than encouraging the wronged employee to file criminal charges, administrators acting on behalf of their organization often ask the employee/victim how they could have more effectively handled the situation that led to violence, so that violence would have been avoided. In other words, within most hospital organizations, the first inclination has been to blame the victim. Fortunately, TJC has developed new standards regarding the reporting and handling of violent incidents. This is but one example of a “good” that can be accomplished by meaningful third-party review of hospital organizations. Thus, the task force will welcome a more effective function being provided by these third-party review and accreditation bodies.
The principal objectives of the task force will be five-fold:
To hold TJC responsible for creating the environment that facilitated if not caused the current and ongoing opiate death epidemic.
The Task Force will disseminate data that supports this assertion.
The Task Force will then encourage its membership to share this data with the Attorney Generals of the various states, in attempts to persuade them to initiate civil litigation against TJC on behalf of the citizens of their states. This litigation can be patterned after litigation previously filed in the Federal Court for the Southern District of West Virginia by an attorney from Dallas, TX. This attorney has assured me he will be happy to cooperate with the task force. The purpose of this litigation would be to recover some of the considerable expenses that the opiate epidemic has foisted upon our nation.
TJC currently holds assets that markedly exceed its debts by a margin of approximately $330 million (2022 Audit by KPMG). This considerable sum could be removed from TJC by favorable litigation and court verdicts, to provide a small measure of compensation to various states, counties, and cities for the costs they have encountered in dealing with this crisis. It is envisioned that the “Tobacco Settlement” of 1998 may serve as a useful initial model for dissemination of any funds that might be recovered from such litigation.
>> COMMON SENSE MARCH/APRIL 2024 63
To hold TJC responsible for enabling the longcontinuing problem of emergency department boarding and crowding (EDB&C).
The Centers for Medicare and Medicaid Services (CMS) has, since late in the prior decade, required hospitals to collect data for its “ED-2” measure. “ED-2” is defined as the median time each month that elapses between the time of a decision to admit the patient to a specific type of inpatient bed, and the time that the patient leaves the ED. CMS continues to require collection of “ED-2” data. However, CMS has never set a standard for what is an acceptable value for “ED-2.” TJC has also failed to leverage the CMS-required “ED-2” data, toward establishing a reasonable standard to be enforced as a condition of hospital reaccreditation.
Because neither CMS nor TJC have taken the opportunity to create an accreditation standard for “ED-2,” they demonstrate that they really have no interest in ameliorating a safety risk that can be estimated to have caused between 3000 and 35,000 avoidable deaths annually for at least the past decade. The exact number deaths estimated depends upon the
“We in AAEM will have nothing to fear… By acting together, we can be the sleeping giant that finally awakens to force our nation’s leaders to require useful TJC reform.
assumptions utilized to create the estimated avoidable death toll. The details of the estimates will be discussed at the Austin meeting of the task force.
TJC and the other hospital accreditation organizations deserve to be publicly shamed for their continuing ignoring of this ongoing matter, toward encouraging them to create and enforce a useful standard for “ED-2,” to address this problem.
To educate the AAEM membership regarding how TJC revenues are realized.
Many physicians are unaware that the funding for TJC and the other accreditation bodies flows not from any governmental sources, but rather, from the hospitals that TJC and similar organizations accredit. None of the accreditation organizations have ever publicly acknowledged this huge conflict of interest (COI) that this funding mechanism creates. The COI constrains the accrediting body from making findings that would impose significant costs upon the organizations being accredited, such as fixing EDB&C. The task force will educate the membership of the nature of this COI and of the existence of alternative accrediting bodies.
“We may be David to the Joint Commission’s Goliath, but TJC has much culpability. It is time to publicize that culpability, to leverage for useful change.
To force TJC site survey teams to share their findings not only with leaders of the hospital’s administration, as is currently done, but also with committees composed of rank-and-file physicians and hospital employees. Those of us at the patient care interface are much more well-positioned to recognize risky and reversible patient safety issues and other relevant problems, and much more well-positioned to anticipate the unintended consequences of TJC edicts, than administrators. Responsible oversight that rank and file health care workers could provide has never been welcomed, and only upper-level administrators have had the opportunity to review and then possibly appeal TJC’s site surveyors’ findings.
This must change. Committees composed of rank-and-file health care workers also deserve to have the opportunity to review and appeal site survey team findings and edicts. TJC and other accreditation bodies must end their willful blindness against useful input from those of us who can recognize real problems that must be addressed, rather than irrelevant issues such as whether members of the health care team eating or drinking in designated areas near patient care units.
To gain Congressional review of TJC and other accreditation bodies’ activities.
Because of its culpability in causing the opiate crisis, and because of its persistent failure to act to ameliorate EDB&C which causes avoidable deaths, the stretch goal of the task force will be to have TJC’s leaders, as spokespersons for the nation’s largest hospital accreditation body, to be compelled to answer for their organization’s considerable shortcomings to the American people, via being subpoenaed to appear before relevant Congressional or Senate Committees, such as:
y The United States Senate’s Committee on Health, Education, Labor, and Pensions, chaired by Sen. Bernie Sanders (I-VT) and Ranking Member Bill Cassidy (R-LA), or
y The United States Congress’ Subcommittee on Science, Space, and Technology Committee, Chaired by Rep Frank Lucas (R-OK), and Ranking Member Rep. Zoe Lofgren (D-CA).
y Further, there happen to be 17 physicians currently serving as Congressional Representatives and four serving as U.S. Senators. A ready-made audience already exists for airing our grievances before elected representatives who can be expected to be sympathetic to our cause.
ANNOUNCING THE JOINT COMMISSION REFORM TASK FORCE
>> COMMON SENSE MARCH/APRIL 2024 64
The task force has a “stretch goal” of serving as a persuasive tool to promote the increased recruitment of new members to AAEM.
Young physicians should find an idealistic physician organization that aggressively pursues goals useful to all emergency physicians, such as confronting TJC and such as forcing TJC to finally admit its culpability for the opiate death crisis, and such as faulting TJC for turning a blind eye to the matter of EDB&C, to be worthy of their joining.
I know from personal communications with former elected leaders of ACEP that America’s largest emergency physician organization has no interest in pursuing the goals of this task force. They are fearful of angering representatives of TJC. I submit that by acting collectively, we in AAEM will have nothing to fear. We can shine a bright light on TJC’s severe shortcomings once we gain the right audience. By acting together, we can be the sleeping giant that finally awakens to force our nation’s leaders to require useful TJC reform (and also, reform of the other
Continued from page 45
8. Coffin PO, Behar E, Rowe C, et al. Nonrandomized Intervention Study of Naloxone Coprescription for Primary Care Patients Receiving Long-Term Opioid Therapy for Pain. Ann Intern Med 2016;165(4):245-52. (In eng). DOI: 10.7326/m15-2771.
9. Cherrier N, Kearon J, Tetreault R, Garasia S, Guindon E. Community Distribution of Naloxone: A Systematic Review of Economic Evaluations. Pharmacoecon Open 2022;6(3):329-342. (In eng). DOI: 10.1007/s41669021-00309-z.
10. Jones JD, Campbell A, Metz VE, Comer SD. No evidence of compensatory drug use risk behavior among heroin users after receiving take-home naloxone. Addict Behav 2017;71:104-106. (In eng). DOI: 10.1016/j.addbeh.2017.03.008.
11. Colledge-Frisby S, Rathnayake K, Nielsen S, et al. Injection Drug Use Frequency Before and After Take-Home Naloxone Training. JAMA Netw Open 2023;6(8):e2327319. (In eng). DOI: 10.1001/ jamanetworkopen.2023.27319.
12. Weiner Sg MM, Baker O P, Bernson D MPH, Schuur Jd MM. One year mortality of patients treated with naloxone for opioid overdose by emergency medical services. Subst Abus 2022;43(1):99-103. (In eng). DOI: 10.1080/08897077.2020.1748163.
13. Streck JM, Ochalek TA, Badger GJ, Sigmon SC. Interim buprenorphine treatment during delays to comprehensive treatment: Changes in psychiatric symptoms. Exp Clin Psychopharmacol 2018;26(4):403-409. (In eng). DOI: 10.1037/pha0000199.
14. Sigmon SC, Ochalek TA, Meyer AC, et al. Interim Buprenorphine vs. Waiting List for Opioid Dependence. N Engl J Med 2016;375(25):25042505. (In eng). DOI: 10.1056/NEJMc1610047.
15. D’Onofrio G, O’Connor PG, Pantalon MV, et al. Emergency departmentinitiated buprenorphine/naloxone treatment for opioid dependence: a randomized clinical trial. Jama 2015;313(16):1636-44. (In eng). DOI: 10.1001/jama.2015.3474.
16. Shastry S, Counts C, Shegog E, Loo G, Cowan E. Emergency Department Utilization Patterns in Patients with Opioid-Related
hospital accreditation organizations). We as clinicians have power over TJC that we have not yet recognized, let alone seized.
AAEM is known for its fighting spirit, as exemplified by the current Envision lawsuit, and by its prolonged and dogged advocacy for the pit doc. For AAEM to now take on TJC the next logical fight. It is in our genes. We may be David to the Joint Commission’s Goliath, but TJC has much culpability. It is time to publicize that culpability, to leverage for useful change.
I hope to meet many of you in Austin as we form subcommittees to begin to work toward realizing our objectives.
References
1. For more information, see “The Joint Commission: Addressing Some Misconceptions” on page 29 of the January/February 2024 issue of Common Sense.
Emergency Department Visits. Subst Use Misuse 2022;57(6):995-998. (In eng). DOI: 10.1080/10826084.2022.2046098.
17. Carlson RG, Daniulaityte R, Silverstein SM, Nahhas RW, Martins SS. Unintentional drug overdose: Is more frequent use of non-prescribed buprenorphine associated with lower risk of overdose? Int J Drug Policy 2020;79:102722. (In eng). DOI: 10.1016/j.drugpo.2020.102722.
18. Simon R, Snow R, Wakeman S. Understanding why patients with substance use disorders leave the hospital against medical advice: A qualitative study. Subst Abus 2020;41(4):519-525. (In eng). DOI: 10.1080/08897077.2019.1671942.
19. Miller S. The ASAM Principles of Addiction Medicine. 2018.
20. Never Use Alone, Inc. Never Use Alone. 10/1/2023 (https://neverusealone. com/).
21. Centers for Disease Control and Prevention. HIV Screening. 2006. (https://www.cdc.gov/hiv/guidelines/testing.html).
22. Aspinall EJ, Nambiar D, Goldberg DJ, et al. Are needle and syringe programmes associated with a reduction in HIV transmission among people who inject drugs: a systematic review and meta-analysis. Int J Epidemiol 2014;43(1):235-48. (In eng). DOI: 10.1093/ije/dyt243.
23. Hurley SF, Jolley DJ, Kaldor JM. Effectiveness of needle-exchange programmes for prevention of HIV infection. Lancet 1997;349(9068):1797800. (In eng). DOI: 10.1016/s0140-6736(96)11380-5.
24. Hagan H, McGough JP, Thiede H, Hopkins S, Duchin J, Alexander ER. Reduced injection frequency and increased entry and retention in drug treatment associated with needle-exchange participation in Seattle drug injectors. J Subst Abuse Treat 2000;19(3):247-52. (In eng). DOI: 10.1016/ s0740-5472(00)00104-5.
25. Strathdee SA, Ricketts EP, Huettner S, et al. Facilitating entry into drug treatment among injection drug users referred from a needle exchange program: Results from a community-based behavioral intervention trial. Drug Alcohol Depend 2006;83(3):225-32. (In eng). DOI: 10.1016/j. drugalcdep.2005.11.015.
ANNOUNCING THE JOINT COMMISSION REFORM TASK FORCE
YOUNG PHYSICIANS SECTION
COMMON SENSE MARCH/APRIL 2024 65
COMMON SENSE MARCH/APRIL 2024 66
Steroid Use in Community-Acquired Pneumonia
Authors: Victoria Zaccone, MD, Wesley Chan, MD, Christopher Kiang, MD, and Michelle Chen, DO
Editors: Kami M. Hu, MD FAAEM FACEP and Donald Doukas, MD
Clinical question: Does corticosteroid use in patients with community-acquired pneumonia improve mortality?
Introduction
According to the CDC, pneumonia accounted for 1.4 million ER visits in 2021. Despite available vaccinations against several serotypes of S. pneumonia, a common causative agent, pneumonia’s mortality rate remains high1 and accounts for 50% of all episodes of sepsis and septic shock.2 While great efforts have been made to improve sepsis care, important clinical questions persist regarding optimal therapy for community-acquired pneumonia (CAP). Several studies have explored corticosteroid use in CAP, with varying results.
The 2019 American Thoracic Society/Infectious Disease Society of America guidelines for CAP do not recommend the routine use of corticosteroids for non-severe CAP (strong recommendation, high quality of evidence) or severe CAP (conditional recommendation, moderate quality of evidence). However, they do align with the Surviving Sepsis Campaign’s recommendation to use corticosteroids in patients with CAP and refractory septic shock.3 Most recently, the Society of Critical Care Medicine released 2024 guidelines on the use of corticosteroids in CAP and recommends administering corticosteroids to adult patients hospitalized with severe bacterial CAP (strong recommendation, moderate certainty).4 Thus, our review aims to examine the current literature on steroid use in community-acquired pneumonia.
Skinner EH, Lloyd M, Janus E, Ong ML, Karahalios A, Haines TP, Kelly AM, Shackell M, Karunajeewa H. The IMPROVE-GAP Trial aiming to improve evidence-based management of communityacquired pneumonia: study protocol for a stepped-wedge randomised controlled trial. Trials. 2018 Feb 5;19(1):88. doi: 10.1186/s13063017-2407-4.
The Surviving Sepsis Campaign (SSC) was established in 2002, and sepsis treatment bundles were created to reduce mortality. A database study of 49,331 patients showed that a higher in-hospital mortality was reported when the three-hour bundle was completed later than the desired timeframe, especially when the administration of antibiotics was delayed (odds ratio [OR] 1.04 per hour). The IMPROVE-GAP trial evaluated if a bundle of evidence-supported treatments, including adjunctive corticosteroids, would improve outcomes in patients with CAP.
IMPROVE-GAP was a stepped-wedged, cluster-randomized effectiveness trial conducted between August 1, 2016, and October 29, 2017. The trial included all adult patients (aged ≥18) admitted to Western Health GIM (Melbourne, Australia) between this time who met a standardized
CAP case definition, defined as a new infiltrate on chest X-ray and the presence of at least one acute respiratory sign or symptom. Patients were excluded if palliative care was initiated on admission or if they were enrolled in a concurrent inpatient research study (including prior enrollment in IMPROVE-GAP within <90 days). In total, 401 patients were analyzed under the bundled care arm and 415 under the usual care arm. Baseline characteristics were similar between the two groups. The primary outcome was hospital length of stay (LOS). Secondary outcomes were inpatient mortality, 30- and 90-day mortality, the requirement for ICU admission, mechanical ventilation, hospital readmission within 30 and 90 days, protocol adherence, and intervention-related adverse events.
The intervention protocol termed the “CAP Service,” included the following: 1) routine corticosteroid prescription (50 mg of prednisolone acetate or equivalent for seven days) with predefined contraindications;
2) switch from parenteral to oral antibiotics according to predefined rules;
3) early mobilization and progressive mobilization daily with predefined contraindications; and 4) routine screening for malnutrition and targeted nutritional therapy.
No difference in the primary outcome of LOS between the control and intervention groups was observed, even after adjusting for age and sex and with subgroup analyses. However, there was a two-fold increase in new insulin prescriptions in patients with diabetes in the intervention group (unadjusted odds ratio, 1.96; 95% CI, 0.73-5.25). Additionally, the number of gastrointestinal bleeding events, while small, was marginally higher for the intervention group (nine events [2.2%] versus three events [0.7%]; the unadjusted estimated difference in mean proportions, 0.008; 95% CI, 0.005-0.010). Of the nine patients in the intervention group with bleeding events, six had received corticosteroids at the full recommended dose. None of the gastrointestinal bleeding events resulted in death.
IMPROVE-GAP concluded that a bundled approach, including adjunctive corticosteroids for treating patients hospitalized with CAP did not improve the duration of hospitalization or other clinical outcomes. In fact, the CAP service was associated with a small increased incidence of gastrointestinal bleeding and hyperglycemia.
Overall, IMPROVE-GAP was a well-designed trial. However, the bundled nature of this study makes it more challenging to determine the effectiveness or harms of a single intervention, although it seems less likely that early mobilization and targeted nutritional therapy are the culprits for the observed adverse effects. Additionally, even though this study incorporated a broad and representative range of patients and CAP severity, an individualized approach with consideration given to the severity of CAP and individual comorbidities may better guide the utility of corticosteroids in patients hospitalized with CAP.
AAEM/RSA RESIDENT JOURNAL
REVIEW
>> COMMON SENSE MARCH/APRIL 2024 67
Wittermans E, Vestjens SMT, Spoorenberg SMC, Blok WL, Grutters JC, Janssen R, Rijkers GT, Smeenk FWJM, Voorn GP, van de Garde EMW, Bos WJW; Santeon-CAP Study Group; Members of the Santeon-CAP Study Group. Adjunctive treatment with oral dexamethasone in nonICU patients hospitalised with communityacquired pneumonia: a randomised clinical trial. Eur Respir J. 2021 Aug 12;58(2):2002535. doi: 10.1183/13993003.02535-2020.
While the IMPROVE-GAP trial failed to show any benefit for the broad use of steroids in all patients hospitalized with CAP, Wittermans et al. assessed whether oral steroids would impact the length of stay in non-ICU patients hospitalized with CAP.
This double-blind, randomized control study occurred in the Netherlands at four different academic institutions. Patients were stratified based on PSI (Port Severity Index) class, with classes I-III deemed the non-severe CAP subgroup and IV-V as the severe CAP subgroup. Half of each subgroup was randomized to either the dexamethasone or placebo group. The primary outcome was length of stay (LOS); secondary outcomes were ICU upgrades and 30-day all-cause mortality. LOS was determined based on half-day intervals (noon delineated the intervals). All patients needed to be enrolled in the ED within 24 hours and were tracked during their hospital stay until they were medically cleared for discharge, died, transferred, or upgraded to ICU status. Secondary outcomes were based on the intention-to-treat principle. Those who missed one or more doses of the medication, had the diagnosis altered, or were discharged on the day of study entry were excluded from the per-protocol analysis. Subgroup analyses were performed within CAP severity groups, as well as CRP levels and S. pneumoniae urine antigen results. Hospital-free days (HFDs) were also calculated to determine if dexamethasone affected hospital utilization.
The study included adult patients with new opacification on chest radiographs and two pre-defined clinical features of pneumonia. Patients were excluded if they were pregnant, immunocompromised, had received corticosteroids or immunosuppressive medications in the last six weeks, could not tolerate dexamethasone, were admitted to the ICU, or had a known tropical worm infection.
Of the projected 600 patients, only 412 were enrolled, with 156 being severe CAP. The study ended early after the second interim analysis due to a slower-than-anticipated enrollment rate and a shorter LOS than those projected when calculating sample size. The study did not hit target enrollment, and there was no statistically significant difference in 30-day mortality between groups that had originally been anticipated based on prior studies (p=0.033). Despite this, there was still a 0.5-day decrease in median LOS in the intervention group (4.5 days, 95% CI, 4.0-5.0) compared to placebo (5.0 days, 95% CI, 4.6-5.4), even though there was no statistically significant difference between non-severe and severe CAP subgroups. ICU upgrades were also significantly lower in the intervention group (n=5, 3%) when compared to placebo (n=14, 7%) (p=0.030).
While there was no difference seen in 30-day mortality, there was a trend toward higher 30-day readmission rates in the steroid group (n=20, 10%) versus placebo (n=9, 5%), but they were not statistically significant (p=0.051). Additionally, the incidence of hyperglycemia occurred more frequently in the intervention group (n=14, 7%) compared to placebo (n=1, 1%) (p=0.001). Subgroup analysis also showed a decrease in length of stay with patients whose CRP was above the median.
Overall, this study showed decreased LOS in patients with dexamethasone use in CAP. However, the risks and benefits of corticosteroids need to be weighed as there was no 30-day mortality benefit, but there was an increased risk of hyperglycemia and readmission rates. This study did elucidate an area of future research to determine how inflammatory markers can predict clinical response to steroids with CAP.
Meduri GU, Shih MC, Bridges L, Martin TJ, El-Solh A, Seam N, Davis-Karim A, Umberger R, Anzueto A, Sriram P, Lan C, Restrepo MI, Guardiola JJ, Buck T, Johnson DP, Suffredini A, Bell WA, Lin J, Zhao L, Uyeda L, Nielsen L, Huang GD; ESCAPe Study Group. Low-dose methylprednisolone treatment in critically ill patients with severe community-acquired pneumonia. Intensive Care Med. 2022 Aug;48(8):1009-1023. doi: 10.1007/ s00134-022-06684-3.
While the IMROVE-GAP and Wittermans et al. oral dexamethasone studies evaluated corticosteroid use in all CAP severities, the ESCAPe study group assessed whether there was any benefit to an extended steroid treatment regimen for ICU patients suffering from severe CAP. The hypothesis was generated because most hospital deaths occur after the eradication of bacteria from tracheal secretions and the bloodstream, which implies that adequate antibiotic treatment alone may be insufficient in further improving outcomes. The host’s inability to fully down-regulate systemic inflammation and restore tissue homeostasis may be the dominant pathophysiologic processes contributing to acute and chronic adverse outcomes in CAP.5,6 As such, the authors hypothesized that a 20-day low-dose methylprednisolone treatment would reduce 60-day mortality and improve clinical outcomes.
This study was a double-blinded, randomized controlled trial across 42 United States Veterans Affairs (VA) medical centers during a five-year period. Adult patients with a clinical diagnosis of severe CAP were enrolled within 72 to 96 hours of hospital presentation. Inclusion criteria required admission to intensive care and the presence of one major or three minor modified American Thoracic Society/Infectious Disease Society of America criteria for severe pneumonia.
Methylprednisolone or placebo was given in a double-blinded fashion. The treatment course was a 20-day methylprednisone tapering course, starting at 40mg IV infusion. The primary outcome was all-cause mortality at 60 days.
AAEM/RSA RESIDENT JOURNAL REVIEW
>> COMMON SENSE MARCH/APRIL 2024 68
The authors screened 3936 patients and enrolled 485. The study was powered for 1406 patients and was stopped early due to low recruitment.
The mean age was 69; 96% were male, and 93% were white. 33% of the patients were on mechanical ventilation at enrollment.
For the primary outcome, there was no difference in mortality (16% versus 18%, 95% CI -8 to 5%, p=0.61). Mortality was also similar at 180 days. There were no differences in the secondary outcomes, including vasopressor-dependent shock, incidence of ARDS, days of mechanical ventilation, ICU length of stay, or hospital length of stay.
The authors concluded that in patients with severe CAP in the ICU, a 20-day low-dose steroid course did not significantly reduce all-cause 60-day mortality. The authors theorized the difference from some previous studies could have resulted from missed timing for glucocorticoid steroids and inadequate methylprednisolone dosing to achieve optimal anti-inflammatory response. They cite several limitations to the trial, starting with a low target sample size, which results in the analyses being underpowered. In addition, being from the VA hospital system in the United States, the study is almost entirely white males, differing from the general population.
Overall, the ESCAPe trial was a well-designed, high-quality trial. However, the underpowered nature of the study and the specific patient population make it challenging to fully accept the negative result. There could be a phenotype of patients who would benefit from corticosteroid treatment. Future research should be guided to identify adequate dosage and duration of corticosteroid treatment for appropriate patients hospitalized with CAP.
Dequin PF, Meziani F, Quenot JP, Kamel T, Ricard JD, Badie J, Reignier J, Heming N, Plantefève G, Souweine B, Voiriot G, Colin G, Frat JP, Mira JP, Barbarot N, François B, Louis G, Gibot S, Guitton C, Giacardi C, Hraiech S, Vimeux S, L’Her E, Faure H, Herbrecht JE, Bouisse C, Joret A, Terzi N, Gacouin A, Quentin C, Jourdain M, Leclerc M, Coffre C, Bourgoin H, Lengellé C, CailleFénérol C, Giraudeau B, Le Gouge A; CRICSTriGGERSep Network. Hydrocortisone in Severe Community-Acquired Pneumonia. N Engl J Med. 2023 May 25;388(21):1931-1941. doi: 10.1056/ NEJMoa2215145.
Like the ESCAPe Trial, the Community-Acquired Pneumonia: Evaluation of Corticosteroids (CAPE COD) trial evaluated whether adjunctive corticosteroids benefited ICU patients with CAP. In particular, the trial evaluated whether early treatment with steroids was associated with a reduced 28-day mortality
This double-blind RCT included 795 adult patients with severe pneumonia across 31 French intensive care units (ICUs). The authors assigned patients to receive either intravenous steroids (200mg daily of hydrocortisone) or placebo (intravenous saline) in addition to the standard CAP treatment. The primary outcome measured was death at 28 days
Inclusion criteria were met if the patient had been admitted to one of the participating ICUs for severe CAP. Severity of pneumonia was defined by at least one of the four criteria: initiation of mechanical ventilation with positive end-expiratory pressure of at least 5cmH2O; initiation of oxygen through a high-flow nasal cannula with a ratio of partial pressure of arterial oxygen to inspired fraction of oxygen (PaO2:FIO2) of <300, with FIO2 of 50% or more; patients on a non-rebreathing mask with a PaO2: FIO2 >300; or a Pulmonary Severity Index score of >130. Exclusion criteria included do-not-intubate orders, pneumonia caused by influenza, and patients in septic shock
In addition to standard therapy for severe CAP (antibiotics and supportive care), patients in the intervention group received 200mg of hydrocortisone within the first 24 hours of onset of any of the severity criteria described above for four days. If by day four, the medical team determined the clinical condition had not improved (also based on predetermined criteria), hydrocortisone was continued for eight or 14 days, with a predetermined taper. The control group received saline for the same duration and plan as the intervention group. Secondary outcomes were death by day 90; length of ICU stay; escalation of oxygen support to non-invasive ventilation or endotracheal intubation (for those not previously requiring support); escalation to endotracheal intubation (for those not previously intubated); initiation of vasopressors by day 28; the number of ventilator-free days and vasopressor free days by day 28; the change in PaO2:FIO2 by day seven; the change in Sequential Organ Failure Assessment (SOFA); and the quality of life by day 90 (as measured by the 36-Item Short For Health Survey). Several safeties were also in place, including secondary infections or gastrointestinal bleeding by day 28, daily insulin administered by day seven, and weight gain by day seven
The authors of CAPE-COD found that by day 28, death had occurred in significantly fewer patients in the early steroid group, specifically, 25 out of 400 (6.2%; 95% confidence interval [CI], 3.9 to 8.6,) compared with the placebo group 47 out of 395 (11.9%; 95% CI, 8.7 to15.1). This accounted for a statistically significant absolute difference of −5.6 percentage points (95% CI, −9.6 to −1.7; P=0.006)
In the subgroup analysis for secondary outcomes, patients in the hydrocortisone group also fared well. Death by day 90 was significantly lower compared to placebo, as well as reduced escalation of respiratory support (for those previously not intubated), mechanical ventilation, and vasopressor initiation by day 28, and reduced ICU stay. Furthermore, no significant safety issues were observed, although the potential neuromuscular and psychiatric side effects of steroids were not specifically assessed
CAPE COD demonstrated that early steroid use was associated with reduced 28-day mortality for patients with severe CAP. This study is also significant because it excluded patients in refractory shock, eliminating any confounding benefit to steroid administration. The study does have some limitations; most notably, the dosing regimen and administration of
AAEM/RSA RESIDENT JOURNAL REVIEW
>> COMMON SENSE MARCH/APRIL 2024 69
hydrocortisone used were not backed by a high level of evidence, and the control group’s mortality was much lower than expected (possibly due to a less-than-expected severity of illness). Finally, no standardized microbiological investigation was mandated, and most patients did not have a pathogen isolated. It is also worth noting that the population was limited to French ICUs, something worth considering when generalizing the findings to the U.S. population, as well as including ICU level-of-care patients only
Conclusion
The existing literature does not recommend the routine use of corticosteroids in non-severe hospitalized CAP patients. The potential reduction in length of stay likely does not outweigh the risk for adverse outcomes, including increased rates of GI bleed, readmission, and hyperglycemia, as well as potential neurologic and psychiatric sequelae that were not addressed in these studies.
The greatest benefit from steroids seems to be in patients hospitalized with severe CAP. The CAPE-COD study revealed a significantly lower 28-day mortality rate with hydrocortisone compared to placebo (6.2% versus 11.9%, 95% CI, -9.6 to -1.7; P=0.006), with this benefit persisting at 90 days. Although the ESCAPe trial did not demonstrate a mortality benefit from extended low-dose methylprednisolone in severe CAP patients, this likely underscores the importance of selecting the appropriate steroid type, dosage, and duration of treatment.
Clinical question: Does corticosteroid use in patients hospitalized with community-acquired pneumonia improve mortality?
Answer
Recent evidence may indicate a shift in managing community-acquired pneumonia. While the 2019 American Thoracic Society/Infectious Disease Society of America guidelines for CAP support steroid use only in cases of CAP with refractory septic shock, the Society of Critical Care Medicine now recommends steroid use in severe CAP. Like many illnesses, a more tailored treatment strategy is likely the most effective approach for CAP, with severity being an important factor when deciding
on steroid use. Further research is needed to determine the appropriate patient, medication, and duration for corticosteroid administration.
References
1. Curtin, Sally C, et al. “Deaths: Leading Causes for 2020 | National Vital Statistics ...” Deaths: Leading Causes for 2020, CDC National Vital Statistics Reports, 5 Dec. 2023, www.cdc.gov/nchs/data/nvsr/nvsr72/ nvsr72-13.pdf.
2. American Thoracic Society. Top Pneumonia Facts. Available from: https:// www.thoracic.org/patients/patient-resources/resources/top-pneumoniafacts.pdf. Accessed March 24, 2024.
3. Metlay JP, Waterer GW, Long AC, Anzueto A, Brozek J, Crothers K, Cooley LA, Dean NC, Fine MJ, Flanders SA, Griffin MR, Metersky ML, Musher DM, Restrepo MI, Whitney CG. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019 Oct 1;200(7):e45-e67. doi: 10.1164/rccm.201908-1581ST. PMID: 31573350; PMCID: PMC6812437.
4. Bram MD, MSc, FRCPC, FCCM1,2; Balk, Robert A MD, MCCM4; Asehnoune, Karim MD5; Cadena, Rhonda MD, FNCS, FCCM6; Carcillo, Joseph A. MD7; Correa, Ricardo MD8; Drover, Katherine BHSc9; Esper, Annette M. MD, MSc10; Gershengorn, Hayley B. MD, ATSF, FCCM11,12; Hammond, Naomi E. RN, BN, MN, MPH PhD13,14; Jayaprakash, Namita MB, MD, BcH, BAO15,16; Menon, Kusum MD, MSc17,18; Nazer, Lama PharmD, FCCM19; Pitre, Tyler MD1,2; Qasim, Zaffer A. MD20; Russell, James A. MD21; Santos, Ariel P. MD, MPH, FCCM22; Sarwal, Aarti MD, FCCM, FAAN, FNCS RPNI23; Spencer-Segal, Joanna MD, PhD24; Tilouche, Nejla MD25; Annane, Djillali MD, PhD (Chair)26,27,28; Pastores, Stephen M. MD, MACP, FCCP, FCCM (Chair)29. 2024 Focused Update: Guidelines on Use of Corticosteroids in Sepsis, Acute Respiratory Distress Syndrome, and Community-Acquired Pneumonia. Critical Care Medicine ():10.1097/CCM.0000000000006172, January 19, 2024. | DOI: 10.1097/CCM.0000000000006172
5. Musher, Daniel M., Roberto Montoya, and Anna Wanahita. “Diagnostic value of microscopic examination of Gram-stained sputum and sputum cultures in patients with bacteremic pneumococcal pneumonia.” Clinical infectious diseases 39.2 (2004): 165-169.
6. Corrales-Medina, Vicente F., and Daniel M. Musher. “Immunomodulatory agents in the treatment of community-acquired pneumonia: a systematic review.” Journal of Infection 63.3 (2011): 187-199.
AAEM/RSA RESIDENT JOURNAL REVIEW
COMMON SENSE MARCH/APRIL 2024 70

AAEM Job Bank
Promote Your Open Position
To place an ad in the Job Bank:
Equitable positions consistent with the Mission Statement of the American Academy of Emergency Medicine and absent of restrictive covenants, will be published (upon approval). All ads run for a six month period or until canceled and will appear in the AAEM member magazine Common Sense and online. For pricing and more information visit www.aaem.org/membership/benefits/ job-bank.
Complete a Job Bank registration form, along with the Criteria for Advertising Section, and submit payment. If you are an outside recruiting agent, the Job Bank Criteria for Advertising must be downloaded and completed by a representative from the recruiting hospital/group.
Direct all inquiries to: www.aaem.org/membership/benefits/job-bank or email info@aaem.org.
Positions Available
For further information on a particular listing, please use the contact information listed.
Section I: Positions listed in Section I are in compliance with elements AAEM deems essential to advertising in our job bank. Fairness practices include democratic and equitable work environments, due process, no post contractual restrictions, no lay ownership, and no restrictions on residency training and have been given the AAEM Certificate of Workplace Fairness.
Section II: Positions listed in Section II are in compliance with elements AAEM deems essential to advertising in our job bank. Fairness practices include democratic and equitable work environments, due process, no post contractual restrictions, no lay ownership, and no restrictions on residency training but have not been given the AAEM Certificate of Workplace Fairness.
Section III: Positions listed in Section III are hospital, non-profit or medical school employed positions, military/government employed positions, or an independent contractor position and therefore cannot be in complete compliance with AAEM workplace fairness practices.
COLORADO
Southern Colorado Emergency Medical Associates (SCEMA) is hiring full time and part time emergency medicine physicians. Must be BC/BE in emergency medicine. We are looking for hard-working team players to join our group. SCEMA is a rare, democratic group of over 30 years based in Southern Colorado with a 2-year partnership track. Come live and work in the beautiful Front Range of Colorado. We offer a superior financial package including a competitive hourly compensation pre-partnership with initial hiring range of 230K-280K and partnership income based on productivity. Partners average over $370k/yr, plus additional benefits valued over $70k/yr
including 13% profit sharing in a 401k, a SCEMA funded cash balance plan, $6k/yr CME, and productivity bonuses. Full time status only requires approximately 14 shifts/month, 8-10 hours shifts, between two facilities based in Pueblo, CO associated with Parkview Medical Center. Please email Dr. Whitney at mcwhit515@gmail.com for further information. (PA 2011)
Email: mkodonnell7@gmail.com
MISSISSIPPI
Join ER Group LTD on the Mississippi Coast! No buy-in or noncompete. Equal RVU/volume based pay AND group ownership from day one! Local SDG, 100% physician ownership! Seeking to add several partners as we have recently taken over
CALIFORNIA
California Rare Northern California partnership opportunity. We are members of AAEM-PG! We are Mountain Medicine P.C. in Yreka, California. We staff a beautiful ED with everything that you could want as an emergency physician. We are a level 4 trauma center seeing about 12,500 patient per year with APP coverage. Short, transparent partnership track. $275 per hour. Yreka is situated in the Shasta Valley & surrounded by the Klamath Mountains. Small town feel, relaxed lifestyle and one of the most affordable places to live in California. Alpine living with hiking, fishing and camping right outside of your doorstep as well as some of the nation’s best backcountry skiing and mountaineering. Live in nearby Mount Shasta, a spiritual and outdoor recreation mecca, or in Ashland, Oregon, an academic and cultural hub hosting Southern Oregon University and The Oregon Shakespeare Festival. Opportunities abound! Contact: recruitment@ruralpacmed.com (PA 2022) Email: recruitment@ruralpacmed.com
COLORADO
CarePoint Health is seeking Full Time Emergency Physicians to join their team in Denver, Colorado. CarePoint is an independent democratic physician-owned and led practice. We have no outside investors or debt and have over 300 equal physician owners. We staff six busy Denver Metro Emergency Departments and seven Freestanding Emergency Departments. We offer a highly competitive incentive/benefits package, and a three year partnership track. Apply to learn more! (PA 2030)
Email: hduncan@carepointhc.com
Website: https://carepointhc.com/
IDAHO
Full-time opportunity available within the EPIC TVI Division at West Valley Medical Center. West Valley Medical Center is a 27k visit ED with 12-hour single covered shifts and 30 hours of overlapping APP coverage M-F and 20 hours of APP coverage Sat and Sun. West Valley Medical Center is located in Caldwell, Idaho (Boise is 20 minutes away). Annual volume of approximately 27,000. Daily volume averages approximately 74. Admission rate of approximately 13%. Associate rate starts at $200/hour. This is a 2-year partnership position with benefits. (PA 2028)
Email: hduncan@carepointhc.com
Website: https://carepointhc.com/
another ED (from a CMG!). We use Epic EMR/Dragon, 8 and 10 hour shifts. Currently averaging between $250-300/hr gross pay. Most partners live in Ocean Springs, a beautiful small town with great schools and very low crime! If you have any questions or are genuinely interested and feel like our group would be a good fit for you, please reach out! (PA 2048)
Email: jasonleeblack@mac.com
Website: https://sites.google.com/view/ERGroupLTD
KANSAS
CarePoint Health is seeking well-trained emergency physicians to join our practice in Wichita, Kansas. Our team is responsible for covering four Emergency Departments in Wichita, including Wesley Medical Center: A Level I Trauma Center. Completion of an ACGME accredited emergency medicine residency is required. New graduate emergency medicine physicians and Visa applicants are encouraged to apply. The Wall Street Journal just ranked Wichita a top place to live based on its affordable cost of living, excellent housing opportunities, excellent job market, wonderful cultural opportunities, and a strong community spirit. (PA 2029)
Email: hduncan@carepointhc.com
Website: https://carepointhc.com/
SECTION II: POSITIONS RECOGNIZED AS BEING IN FULL COMPLIANCE WITH AAEM’S JOB BANK CRITERIA
SECTION I: POSITIONS RECOGNIZED AS BEING IN FULL COMPLIANCE WITH AAEM’S JOB BANK CRITERIA AND GIVEN THE AAEM CERTIFICATE OF WORKPLACE FAIRNESS
AAEM/RSA RESIDENT JOURNAL REVIEW COMMON SENSE MARCH/APRIL 2024 71
CALIFORNIA
EMERGENCY MEDICINE PHYSICIAN San Francisco Bay
Area Contra Costa Regional Medical Center in Martinez, CA, is currently looking for a CA-licensed, BC/BE Emergency Medicine Physician for a full-time, benefited position or a 1099 contract position. The schedule is a mix of days and nights (always double coverage). Our Safety-Net hospital offers a 23-bed ER (17 monitored and 6 non-monitored) that sees over 35,000 patients per year. This is an exceptional opportunity to join a supportive, close-knit, mission driven group to serve the community by providing quality care in our safety-net system. We offer flexibility in scheduling, a competitive compensation package and a collaborative environment of care. We are conveniently located in the East San Francisco Bay, with easy access to Lake Tahoe, San Francisco, the Napa Valley, the Sierra Foothills and all coastal areas. For more information, email your CV and cover letter to recruit@cchealth.org. EOE (PA 2023) Email: recruit@cchealth.org
COLORADO
The Department of Emergency Medicine of the Denver Health and Hospital Authority is recruiting a passionate and talented Emergency Physician to serve as Clerkship Director and Assistant Residency Program Director for the Denver Health Residency in Emergency Medicine (DHREM). The Clerkship Director will be responsible for the education of emergency medicine bound medical students at both Denver Health and the University of Colorado School of Medicine, ongoing mentorship for EM-bound students as core EM Specialty-Specific Advisor, and oversight of off-service residents/fellows rotating through the Denver Health emergency department. As an Assistant Residency Director, this position will serve as a core member of the Residency Leadership team, focusing on projects related to health equity and pipeline programs, recruitment, and supporting all educational and academic missions of the residency program. The Denver Health Residency in Emergency Medicine is one of the oldest and most highly regarded Emergency Medicine training programs in the country with a longstanding legacy of training future leaders in our specialty. The department educates over 60 local and visiting emergency-medicine-bound students each year, providing an unparalleled clinical experience with students working at both of our core clinical sites, Denver Health and the University of Colorado Hospital. Students are exposed to our breadth of faculty expertise through didactics, mentorship, and unique educational opportunities focusing on Emergency Medical Service (EMS), Social Emergency Medicine, and Ultrasound. With one of the first funded externships for Underrepresented in Medicine (UiM) Emergency Medicine applicants in the country, our department continues to push opportunities to support and diversify our program and our specialty. With more than 12 fellowship programs across our core institutions, the Department of Emergency Medicine has a deep commitment to educational excellence and scholarship and a robust group of hard-working and committed educators. Applicants should submit CV and cover letter to: Aaron Ortiz, Manager Provider Recruitment aaron.ortiz@dhha.org (PA 2015)
Email: aaron.ortiz@dhha.org
Website: https://www.denverhealth.org
COLORADO
The Department of Emergency Medicine at Denver Health Medical Center is recruiting a passionate and talented Emergency Physician to serve as Director of Quality and Safety. This position will serve as a core member on our clinical operations team, focusing on setting strategy, implementing initiatives and tracking outcomes related to the quality and safety of the care provided to our patients. The emergency department at Denver Health includes 57 adult beds, 19 pediatric beds, and a separate 23-bed clinical decision unit. With a combined annual census of more than 100,000 patients from highly diverse cultures and backgrounds, the ED at Denver Health is the second busiest in Colorado. The Ernest E Moore MD Shock Trauma Center at Denver Health is the primary trauma referral center for the Rocky Mountain Region. Additionally, the acuity managed by the adult ED is high, with a 25% admission rate. Staffing in the adult and pediatric EDs is provided by board-certified emergency physicians, emergency medicine residents and subspecialty fellows, and advanced practice providers. Strong and extremely collaborative relationships exist among physicians, advanced practice providers, nursing, and consultative services. Denver Health is a large urban health care center that is proud to serve as a primary Anchor Institution to the Denver metro area, and its diverse community. Denver Health is a major academic affiliate of the University of Colorado School of Medicine, based at the
University of Colorado Anschutz Medical Campus. All faculty ultimately report to the Director of Service for Emergency Medicine at Denver Health, contributing to our mission of excellence in patient care, education, research, and professional development, and have meaningful responsibilities and faculty appointments in the University of Colorado School of Medicine’s academic Department of Emergency Medicine. Applicants should submit CV and cover letter to: Aaron Ortiz, Manager Provider Recruitment aaron.ortiz@dhha.org (PA 2016)
Email: aaron.ortiz@dhha.org
Website: https://www.denverhealth.org
COLORADO
The Department of Emergency Medicine at Denver Health Medical Center is recruiting a passionate and talented senior Emergency Physician to serve as Director of Diversity, Equity, Inclusion and Belonging. This position will serve as a core member on our department’s leadership team, developing, implementing, and monitoring outcomes of strategies to enhance our departmental DEIB efforts, institutional including the recruitment, retention, and support of faculty. The emergency department at Denver Health includes 57 adult beds, 19 pediatric beds, and a separate 23-bed clinical decision unit. With a combined annual census of more than 100,000 patients from highly diverse cultures and backgrounds, the ED at Denver Health is the second busiest in Colorado. The Ernest E Moore MD Shock Trauma Center at Denver Health is the primary trauma referral center for the Rocky Mountain Region. Additionally, the acuity managed by the adult ED is high, with a 25% admission rate. Staffing in the adult and pediatric EDs is provided by board-certified emergency physicians, emergency medicine residents and subspecialty fellows, and advanced practice providers. Strong and extremely collaborative relationships exist among physicians, advanced practice providers, nursing, and consultative services. Denver Health is a large urban health care center that is proud to serve as a primary Anchor Institution to the Denver metro area, and its diverse community. Denver Health is a major academic affiliate of the University of Colorado School of Medicine, based at the University of Colorado Anschutz Medical Campus. All faculty ultimately report to the Director of Service for Emergency Medicine at Denver Health, contributing to our mission of excellence in patient care, education, research, and professional development, and have meaningful responsibilities and faculty appointments in the University of Colorado School of Medicine’s academic Department of Emergency Medicine. Applicants should submit CV and cover letter to: Aaron Ortiz, Manager Provider Recruitment aaron.ortiz@dhha.org (PA 2017)
Email: aaron.ortiz@dhha.org
Website: https://www.denverhealth.org
CONNECTICUT
Trinity Health Of New England seeks BC/BE EM Physicians to join our emergency medicine teams at Mercy Medical Center in Springfield, Massachusetts, Saint Francis Hospital and Medical Center in Hartford, Connecticut and Saint Mary’s Hospital in Waterbury, Connecticut. Our practice model empowers our physicians to work at their highest level, while allowing time for professional development and family life. Whether you are focused on providing outstanding patient-centered care or driven to grow into a leadership role, you will thrive at Trinity Health Of New England. To learn more, visit our provider portal at www. JoinTrinityNE.org (PA 2024)
Email: dhowe@trinityhealthofne.org
Website: https://www.jointrinityne.org/Physicians
DELAWARE
ChristianaCare, a recognized leader in healthcare, is seeking Emergency Medicine Physicians. You will be part of a dynamic team covering four state-of-the-art Emergency Departments in Delaware and Maryland. Why ChristianaCare? • The ED’s at ChristianaCare’s Christiana Hospital, Wilmington Hospital, Union Hospital, and the free-standing emergency department in Middletown, Delaware treat a combined total of more than 225,000 patients each year. • Christiana Hospital ranks in the top 25 in the country for emergency visits and is Delaware’s only Level I trauma center that treats adults and children - the only center of its kind between Philadelphia and Baltimore. (PA 2019)
Email: megan.hopkins@christianacare.org
Website: https://christianacare.org/us/en
LOUISIANA
Ochsner Health is seeking board certified/board eligible physicians to join our Division of Pediatric Emergency Medicine at Ochsner Medical Center and Ochsner Hospital for Children. Our opportunity includes an employed physician group that
offers competitive fair market compensation plus benefits; an in-house pediatric intensivist and hospitalist attendings 24/7 to assist with streamlined pediatric admissions and patient care; all facilities utilizing Epic electronic health records integrating care across the system and facilitating seamless multi-hospital practice; and all specialties available for consultation and easy one-call transfer from our community emergency departments to our main campus. (PA 2033)
Email: courtney.lawhun@ochsner.org
Website: https://ochsner.wd1.myworkdayjobs.com/ OchsnerPhysician/job/New-Orleans---New-Orleans-Region--Louisiana/Pediatric-Emergency-Medicine_REQ_00158668
MASSACHUSETTS
MASS EYE AND EAR and the DEPARTMENT OF EMERGENCY MEDICINE MASSACHUSETTS GENERAL HOSPITAL
Emergency Medicine Positions Mass Eye and Ear, in conjunction with the Department of Emergency Medicine at Massachusetts General Hospital, is seeking BC/BE emergency physicians for FT/ PT academic faculty positions. Candidates must be committed to excellence in clinical care and teaching; both traditional and nocturnist schedules are available. Academic appointment will be at the instructor, assistant professor, or associate professor level at Harvard Medical School. MEE is a world-renowned Harvard teaching hospital focusing on evaluating and treating ocular and otolaryngologic conditions. The ED at MEE treats approximately 30,000 adult and pediatric patients annually and is adding 24/7 emergency medicine coverage for ENT and lower-acuity ocular patients. Ophthalmologists will continue to evaluate and treat higher-acuity ocular patients, and subspecialist ophthalmology and otolaryngology consults will remain available. The ED will also continue to be staffed by ophthalmology and otolaryngology residents and APPs. MEE is connected to MGH, a high volume, high acuity level 1 adult and pediatric trauma and burn center caring for over 120,000 patients annually. Patients can readily be transferred between the hospitals as necessary. Inquiries for these novel positions should be accompanied by a curriculum vitae and may be submitted by email (LNentwich@ mgh. harvard.edu) to: Lauren Nentwich, MD Vice Chair for Clinical Affairs Department of Emergency Medicine Massachusetts General Hospital Boston, Massachusetts 02114 We are an equal opportunity employer, and all qualified applicants will receive consideration for employment without regard to race, color, religion, sex, national origin, disability status, protected veteran status, gender identity, sexual orientation, pregnancy and pregnancy-related conditions, or any other characteristic protected by law. (PA 2049)
Email: LNENTWICH@mgh.harvard.edu
Website: http://www.massgeneral.org || http://www. masseyeandear.org
MICHIGAN
The American Board of Emergency Medicine (ABEM) is seeking their next Executive Director, Professional and Clinical Affairs. Candidates must hold an M.D., or D.O., and be ABEM certified in Emergency Medicine (EM). They will have served at least ten years of full-time work experience as an EM physician with a track record of outstanding mentorship and leadership qualities, strong and successful experience in program building, policy development, external relations and engagement, advancing diversity, equity, and inclusion initiatives, and integration across programs and institutions. Please email ABEM_ExecDirector@ wittkieffer.com for more information. (PA 2040)
Email: ABEM_ExecDirector@wittkieffer.com
Website: https://www.abem.org/public
MINNESOTA
Winona Health is seeking a BC/BE EM Physician to join our Emergency Medicine team located in a Midwest college community along the banks of the Mississippi River. • Full-time and part-time, employed positions joining an established team of Physicians, Physician Assistants, nurses and support staff • Full-time and part-time nights or day/night opportunities • Responsible for the acute care of ER patients • 11,000-12,000 visits annually • Level IV trauma and stroke certified facility • Electronic Medical Record, CPOE, patient tracking, bedside US, Dragon • Progressive team of providers committed to quality; evidence-based care, exceptional patient satisfaction; and integrated technology • Competitive hourly compensation & benefits package including sign-on incentive, paid malpractice with tail coverage, $7,500 annual CME & dues/license, moving expenses, health/life/dental insurance, retirement programs and more (PA 2031)
Email: dholtzclaw@winonahealth.org
Website: http://www.winonahealth.org
SECTION III: POSITIONS NOT RECOGNIZED AS BEING IN FULL COMPLIANCE WITH AAEM’S JOB BANK ADVERTISING CRITERIA
COMMON SENSE MARCH/APRIL 2024 72
NEW YORK
Stony Brook University and the Renaissance School of Medicine seek an accomplished and dynamic academic leader to serve as the Chair, Department of Emergency Medicine. This is an extraordinary opportunity for a new Chair to lead a highperforming group of distinguished faculty and staff to further the advancement of clinical care, education, and research in Emergency Medicine within an exceptional, growing University and academic healthcare system. The Department of Emergency Medicine, recognized as a regional leader for comprehensive care - providing contemporary emergency services, is home to 50 accomplished adult and pediatric faculty, a robust residency program, and five fellowship programs. Emergency Medicine is one of 25 academic departments in the Renaissance School of Medicine at Stony Brook University, conducting research and providing services to a patient population of 1.5 million people in Suffolk County on Long Island in New York. The Renaissance School of Medicine is a public medical school in Stony Brook, New York; it is part of Stony Brook University, a designated flagship institution of the State University of New York (SUNY) system and one of 62 members of the Association of American Universities (AAU) - the invitation-only organization of the best research universities in North America. The School of Medicine educates 500+ medical students, 750+ residents and fellows with 57 ACGME accredited residencies and fellowships in a broad range of specialties. The School of Medicine is one of five health sciences schools within the overarching Stony Brook Medicine organization, which is also home to 628-bed Stony Brook University Hospital and Stony Brook Children’s Hospital, Long Island’s premier academic medical center, two additional community hospitals and multiple outpatient care sites. The successful candidate will bring exceptional leadership and operational skills, the ability to enhance clinical operations in emergency medicine across the system and build upon an exceptional research and educational programs. This leader will provide strategic leadership of adult and pediatric emergency
AAEM/RSA EDITOR’S MESSAGE
Continued from page 62
References
services and shape the advancement of a comprehensive emergency medicine clinical care model. The Chair, in collaboration with senior leadership, will foster innovative care delivery models, viable approaches to enhance patient throughput, length of stay, reduction in cost, and elevate the patient experience. This leader will have demonstrated success leading within a complex academic health system and possess the ability to initiate and lead change through collaboration and inspiration. Applicants must hold an MD or MD/PhD degree (or equivalent degree), current certification by the American Board of Emergency Medicine, must have or be eligible to obtain a New York medical license, and possess academic accomplishments that merit appointment at the rank of associate professor or higher. For confidential nominations or expressions of interest, please contact Aaron Mitra, Linda Komnick, or Kim Smith through the office of Katie Haddock via khaddock@wittkieffer.com. The Stony Brook University Renaissance School of Medicine values diversity and is committed to equal opportunity for all persons regardless of age, color, disability, ethnicity, marital status, national origin, race, religion, sex, sexual orientation, veteran status or any other status protected by law. (PA 2036)
Email: khaddock@wittkieffer.com
Website: http://www.stonybrook.edu/
OHIO
Job Overview: As one of the oldest medical schools in the country, the University of Cincinnati College of Medicine (COM) has a reputation for training best-in-class health care professionals and developing cutting-edge procedures and research that improves the health and clinical care of patients. In partnership with the UC Health academic healthcare system and Cincinnati Children’s Hospital Medical Center, College of Medicine doctors transform the world of medicine. The Department of Emergency Medicine’s world-renowned faculty and staff offer an outstanding research, teaching, and medical practice environment. The University of Cincinnati (UC), College of Medicine (COM) invites
1. Tetanus: For Clinicians. Published January 23, 2020. Accessed January 30, 2024. https://www.cdc.gov/tetanus/clinicians.html#wound-management
2. Lin M. Quick clinical tip: Elson’s test for the finger. ALiEM. Published July 29, 2013. Accessed January 30, 2024. https://www.aliem.com/elsons-test/
3. Rietz A, Barzin A, Jones K, Mounsey A. Sterile or non-sterile gloves for minor skin excisions?. J Fam Pract. 2015;64(11):723-727.
4. Forsch RT. Essentials of skin laceration repair. Am Fam Physician 2008;78(8):945-951.
applications and nominations for the Chair of the Department of Emergency Medicine. Reporting to the Dean of the College of Medicine, the Chair will model next-level leadership empowering faculty and staff, setting a tone of shared purpose with the College and UC Health, and establishing the highest standards in patient care and educational outcomes, research impact, and financial stewardship. Essential Functions: The Chair will be responsible for recruitment, development, and retention of an exceptional and diverse faculty. The Chair will foster opportunities to expand research across divisions and institutions, with a focus on interdisciplinary and collaborative team-based scholarship. The Chair will elevate the department in this moment of true transformation at a systems level and promote partnerships across the College of Medicine, UC Health, community partners and external stakeholders. The applicant must demonstrate a record of educational and scholarly achievement, with recognition at the national level, and a strong commitment to advancing the practice and education of emergency medicine. The successful candidate will be an accomplished leader who understands current trends in healthcare and medical education and values the tripartite mission academic medical institutions promote. It is of the utmost importance that the Chair is a visible, democratic, and collaborative leader who advocates for patients, learners, staff and faculty members within the Department, College of Medicine, University and Health System. Minimum Qualifications: • An outstanding MD, MD/PhD, DO, or equivalent clinician with substantial leadership experience. • Significant academic, clinical, and administrative experience in a University Health Science Center or comparable organization, preferably at the rank of a Professor or Associate Professor academically. • American Board of Emergency Medicine Certified with demonstrated understanding of all elements of health care delivery, including strategy, business planning, operations, and finance. (PA 2039)
Email: adrienne.piontek@uc.edu
Website: https://jobs.uc.edu/job-invite/94816/
5. Forsch RT, Little SH, Williams C. Laceration Repair: A Practical Approach. Am Fam Physician. 2017;95(10):628-636.
6. Singer AJ, Thode HC Jr, Hollander JE. National trends in ED lacerations between 1992 and 2002. Am J Emerg Med. 2006;24(2):183-188. doi:10.1016/j.ajem.2005.08.021
7. Pfaff JA, Moore GP. Reducing risk in emergency department wound management. Emerg Med Clin North Am. 2007;25(1):189-201. doi:10.1016/j.emc.2007.01.009

SECTION III: POSITIONS NOT RECOGNIZED AS BEING IN FULL COMPLIANCE WITH AAEM’S JOB BANK ADVERTISING CRITERIA — continued
COMMON SENSE MARCH/APRIL 2024 73

COMMONSENSE 555 East Wells Street / Suite 1100 Milwaukee, WI 53202-3823 PRSRT STD U.S. POSTAGE PAID MILWAUKEE, WI PERMIT NO. 0188
