
N e w s
a p r i l | 2 0 2 4
FROM THE FOUNDATION WORKING TO END MELANOMA
Articles
01
From the Desk of Sam Guild, President AIM at Melanoma Foundation
02
03
Celebrating a Milestone: 20 Years of the Dallas Steps Against Melanoma Walk
By Mara Klecker
In Plain English: Tumor-Infiltrating Lymphocyte (“TIL”) Therapy for Advanced Melanoma
By Kim Margolin, M.D., FACP, FASCO
04
May is Brain Tumor Awareness Month
05
The FDA Approval of TIL Therapy and What it Means for Advanced Melanoma: An Interview with Dr. Allison Betof Warner, MD, PhD


FROM THE DESK OF Sam Guild
PRESIDENT | AIM AT MELANOMA FOUNDATION
Happy Spring!
Spring is a season of things new and renewed, and this newsletter fits that theme.
On the “new” front is the FDA’s approval in February of Amtagvi (lifileucel), the TILs therapy for the treatment of metastatic melanoma (read about all FDA approved treatments for melanoma here). We have two articles in this newsletter to help you understand the treatment and approval. The first is a newly updated version of an In Plain English article by Dr. Kim Margolin that we ran a few years ago explaining how TILs therapy works and who can receive it. The second is a print version of a TILs therapy Q&A with Dr. Allison Betof-Warner based on the webinar that she did with me a few weeks ago (watch the webinar here). Both doctors endeavor to explain the treatment in a way that is accessible to all of us.
In the “renewed” category is an article on our oldest Steps Against Melanoma walk, which is in Dallas and was coordinated both this year and last year by Julie Frampton, a melanoma survivor and AIM volunteer extraordinaire. Due to a severe rain, thunder, and lightning storm, the walk, scheduled for last weekend, was cancelled. Despite the cancellation, we want all of you to know that the walk in Dallas is celebrating its 20th anniversary. That’s 20 years of community, 20 years of fundraising for research, and 20 years of hope. Thank you to all who have walked, donated, and volunteered in Dallas over the years—and in every Steps Against Melanoma walk across the country You are all making a difference in the fight against melanoma and the search for the cure!
AIM continues to celebrate our 20th anniversary this year, which really means continuing to fulfill our mission. I’m printing our mission here because it’s what leads us every day:
Founded in 2004, AIM at Melanoma is a global foundation dedicated to finding more effective treatments and, ultimately, the cure for melanoma.
By directing and funding paradigm-shifting research initiatives; educating patients, healthcare professionals, and the public; and advocating for survivors and their families, AIM at Melanoma’s goal is to end this disease in our lifetime while improving the lives of those it affects.
You might remember that AIM was founded—and our mission was defined—by my mother, Valerie Guild, after the death of my sister, Charlie, at age 26 from melanoma. I’m proud to carry on her mission. (Read about the founding of AIM here.)
Most important, we can’t fulfill our mission without your support, so thank you for all you do.
SamGuild
1
Celebrating a Milestone:
20 Years of the Dallas Steps Against Melanoma Walk
by Mara Klecker
On April 20th, melanoma survivors, their families, and supporters were set to gather in Dallas for the annual AIM at Melanoma Steps Against Melanoma walk. Unfortunately, rain, thunderstorms, and lightning caused the cancellation of the walk but not the celebration! This year marks two decades of the Dallas walk, with each walk drawing hundreds of participants and serving as a fundraiser for melanoma research The goal for this year’s Dallas walk is $30,000. But those who’ve attended over the last 20 years say the event’s impact goes far beyond the dollars that are fundraised
“The 20th anniversary represents 20 years of hope to me,” said Julie Frampton, the coordinator of this year’s Dallas Steps Against Melanoma walk and a melanoma survivor herself. “No matter how advanced AIM at Melanoma becomes or where it branches off to, there’s still this grassroots community ”

That community feel is what keeps people coming back year after year, even if they’ve moved out of Texas or never lived there at all Frampton said many of this year’s participants live all over the U.S. They make a point to travel to AIM walks to be alongside other survivors with whom they’ve connected over the years.

Seeing the same faces year after year is also a testament to the progress made in melanoma research over the last two decades, said Sam Guild, president of AIM at Melanoma Thanks to advancements in available treatments for melanoma, survivorship looks much different than it did when the first group of people walked in support of melanoma research in Dallas back in 2004.
“Every year, we see more and more familiar faces, which is evidence that the work we’re doing is making a difference,” Guild said “And we’ll receive messages and donations from people who can’t attend because they have moved away or are just busy living their lives, and that, too, is evidence of the progress we’ve made. But we are vividly reminded that there is still much work to be done when we acknowledge the people who are no longer with us at the ‘roll call’ ”
2

The “roll call” at the Dallas walk is an annual tradition to honor those lost to the disease Participants gather to hear each name, the year they died, and a detail that their surviving family wants to share about their loved one Each year, the list of names grows longer.
“What started off as a list of maybe three or four names has now grown to well over 50,” Julie said. “We always take a moment of silence to honor them ”
Even with this important and sobering tribute, the event always has a fun and celebratory mood because so many survivors are gathered

Additionally, a DJ will be playing music, and the warm-up before the walk can be a form of energy-boosting jazzercise The kids who are attending can get their faces painted and a photo booth will be set up with artwork celebrating 20 years of walking to end melanoma. This year, Frampton had wrangled some high school and college students to volunteer, which doubles as a way to spread awareness and educate young people about skin cancer and get them an onsite skin check
“It’s super important to me to bridge that gap and bring awareness,” Frampton said.
Scott Murray has emceed the walk since its start. He’s a melanoma survivor himself and said after decades of emceeing various fundraisers for a variety of organizations, he’s still struck by the stories from the families who’ve lost loved ones to melanoma.
“There’s this fellowship there – but it’s a fellowship with a mission,” said Scott. “It’s this mission of coming together to eradicate this insidious disease.”
Scott said it’s the “loving, caring group of people” that has drawn him back for two decades.
Chris White, the honoree at this year’s Dallas walk, attended the event for the first time last year. He wasn’t surprised by the level of support and love he felt, he said – it’s similar to the camaraderie he’s felt from connecting with other survivors online But connecting in person is even more powerful

Click here to donate to the Dallas Steps Against Melanoma walk and to get any updates since the cancellation
3
He credits that support for encouraging him to continue sharing his own melanoma story Chris was diagnosed with anorectal mucosal melanoma (a rare type of melanoma) in 2018 and found out it had metastasized to his lymph nodes, lungs, liver, kidneys and eventually his brain Over 18 months, he underwent multiple surgeries, bouts of immunotherapy, chemotherapy and radiation and a clinical trial for tumor-infiltrating lymphocytes. By 2021, Chris had no evidence of disease
Chris is now a self-published author with his most recent book, “Killing Cancer with TILs.” He also serves as a key opinion leader on the patient experience in autologous cell therapy clinical trials and travels as a keynote inspirational speaker.
“I’ve found meaning and reason in everything I’ve been through, and I hope to have an impact in sharing my story,” Chris said



"Being surrounded by people who understand the melanoma story offers "the same underlying current that you feel when you ' re with family "
Julie Frampton, 2024 Dallas Steps Against Melanoma Walk Coordinator & Melanoma Survivor
For Frampton, being surrounded by people who understand the melanoma story offers “the same underlying current that you feel when you’re with family.” She credits AIM at Melanoma and its programs for helping to connect and build that family of people who understand the melanoma journey
Gathering each year in Dallas – even if it means traveling across the country to do so – is about “togetherness and hope and love,” she said “It’s this blanketed warmth you can only get from these people who are walking this walk with you.”
4



HAPPY20THANNIVERSARYDALLAS!
We are deeply grateful for all you do!





5
IN PLAIN ENGLISH
TUMOR-INFILTRATING LYMPHOCYTE (“TIL”) THERAPY FOR ADVANCED MELANOMA
Background
Immunotherapyof Melanoma
The explosion of immunotherapy over the past decade has revolutionized the treatment of melanoma and nearly every other adult type of cancer As a reminder, this form of treatment stimulates the body’s immune system to find, attack and kill tumor cells Of all cancers, melanoma has benefited the most from immunotherapy, in large part because the mutations caused by extensive sun damage lead to changes in the genetic material of the malignant cells that can be recognized by cells of the immune system, which are further stimulated by a variety of forms of immunotherapy Additionally, because melanoma is so resistant to chemotherapy and radiation, the relative benefits of immunotherapy are greater in patients with melanoma, who have few other choices for effective treatments
What are TIL cells? What is TIL therapy?
TIL cells are tumor-infiltrating lymphocytes and are composed of CD8 and CD4 cells, the so-called killers and helpers of our immune system that are critically important in the immunologic fight against cancer as well as certain kinds of infections.
Note: We are rerunning an update on this TIL therapy article that originally ran in our newsletter and on our website in November of 2022 because of the February 2024 FDA accelerated approval of lifileucel (Amtagvi). Lifileucel is the cell therapy product, and the overall regimen is detailed below.
BY KIM MARGOLIN, M.D., FACP, FASCO
TIL therapy refers to a treatment that involves extracting T lymphocytes from a patient’s tumor and growing them in special liquid containing lymphocyte growth factors This liquid expands the numbers, enhances the activity of T lymphocytes, and leaves the tumor cells to die off. TIL cells are then given back to the patient via intravenous (in the vein through a needle) infusion In successful treatments, these TIL cells will find, attack, and kill tumor cells The factors that determine whether a patient will go into remission from TIL therapy are not well understood, but the number of cells that can be given may be an important factor, so the goal of laboratory expansion of TIL cells is usually several billion cells.
The TIL cell approach for advanced melanoma has been under investigation for nearly 35 years, starting in the mid1980s in the laboratories at the National Cancer Institute’s Surgery Branch There, Dr Steve Rosenberg worked tirelessly and trained dozens of investigators (surgeons, medical oncologists, and laboratory scientists) to develop and improve on methods and outcomes of TIL therapy.
6
While much of this research has been preclinical (in animals, where the conditions can be manipulated and the outcomes measured in much shorter timeframes than in people), an extensive series of clinical trials testing the new therapy in people with cancer has provided new insights These insights include the best ways to obtain the tumor that the cells are taken from, cultivate the TIL cells, select the best cells to give back to the patient, and treat the patient with additional immune system-directed medications to optimize the anti-tumor effects of the TIL cell therapy.
Who can get TIL? How does the treatment work?
If the patient’s tumor tested positive for the BRAF mutation, patients must also have had exposure to one of the three pairs of oral medications that target malignant cells with this mutation. Some patients have also received interleukin-2 (IL-2), the T cell growth and activation factor that is used in small amounts in laboratory preparation of TIL. In high doses, IL-2 causes T lymphocytes in the blood and tumor to multiply and become activated and provides a modest chance of remission when given alone to patients with melanoma However, high doses of IL-2 can also cause a lot of (reversible) side effects and dangers to the patient The TIL regimen also includes a few doses of high-dose IL-2, as detailed below, but IL-2 is stopped if there are dangerous effects, so this component of the regimen is not likely to pose serious risks or discomforts to melanoma patients undergoing TIL therapy. The FDA approval for lifileucel is restricted to patients who have already received one or more of the standard treatments noted above, including targeted therapy for those with a BRAF-mutated melanoma

As shown in the diagram, the TIL cell regimen begins with patient assessment, making sure that candidates for this therapy have a safely accessible tumor one that can be partially or fully removed with a small surgical procedure Patients with tumors in the brain, the spinal cord, bones, and other less safely accessible locations would not qualify for TIL therapy Patients must also be in generally good medical and physical condition, which means they are judged by their doctor to be healthy enough to get through all phases of the regimen, including several days of chemotherapy and a one to two week period of low blood counts that necessitate supportive care with antibiotics, blood transfusions, and potentially intravenous feeding
The next step after tumor excision is chopping up the tissue into small fragments, placing them in an incubator at body temperature in growth medium for up to three weeks, and checking the cells for viability (must be alive) and freedom from contamination
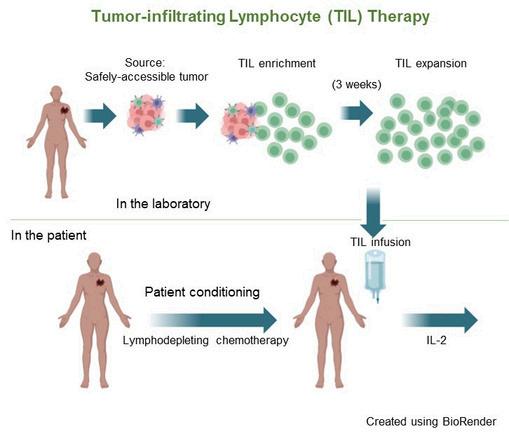
7
Meanwhile, the patient is first prepared by the administration of two chemotherapy drugs over five to seven days These drugs do not kill melanoma cells but lower the patient’s blood lymphocyte count dramatically (along with other cells originating in the bone marrow, which causes all blood cells to be reduced). The body’s reaction to this lymphocyte reduction (termed “lymphodepletion”) is to produce growth factors that stimulate its production of new lymphocytes The infused TIL cells are also further expanded and stimulated It is likely that in the near future, we will have purified and safely administered forms of these lymphocyte growth factors that can be given instead of chemotherapy and possibly also replace the IL-2 that is given after TIL infusion
Because of the risks involved with very low blood counts for one to two weeks, patients must be hospitalized for the supportive measures detailed above and for close nursing and physician supervision during this time and during the two days of high-dose IL-2 that follow TIL infusion. Thereafter, patients are discharged from the hospital and monitored in the clinic
What are the most current results of TIL cell therapy?
Most of the published results of TIL cell therapy for melanoma have come from the National Cancer Institute Surgery Branch mentioned above; additional data are from a small number of cancer centers, mostly in the U.S but also in other countries, where different research approaches have been taken to the optimization of this and related forms of cell therapy for cancer On the average, about 1/3 of patients receiving TIL therapy go into remission However, many of those patients still relapse subsequently, so it is clear that we need to find better approaches and better ways to select the best regimen and its timing for each patient
The first trial ever to randomize TIL therapy against standard immunotherapy for advanced melanoma patients in first relapse following single-agent PD-1 blockade was reported by Haanen et al. at the 2022 annual meeting of the European Society of Medical Oncology.
In this study, 168 patients with similar characteristics whose melanoma was not controlled with PD-1 antibodies were randomly assigned to receive either ipilimumab or undergo TIL therapy The results strongly favored TIL therapy, with over twice (49%) the response rate of ipilimumab (21%) Average time without relapse or death were also over twice as long in patients who received TIL therapy. Of note is that patients who were randomized to ipilimumab did not have the opportunity to “cross over” to receive TIL therapy if they relapsed, so it is not possible to know from this study whether early use of TIL is better than later use of TIL Now that we also have data showing about a 30% rate of remission for patients in relapse after single-agent PD-1 blockade with pembrolizumab or nivolumab who go on to receive ipilimumab plus nivolumab, we need to design trials to demonstrate whether TIL therapy is truly superior to other available options and discover the optimal timing Perhaps all or nearly all patients with advanced melanoma should have a TIL product harvested from a resected tumor metastasis and stored frozen in a laboratory to be used later if the patient relapses following non-TIL therapy.
These exciting results for TIL cell therapy as an option and a hope for patients who do not achieve long term benefit from standard immunotherapy supported the February, 2024 accelerated FDA approval, which is based on smaller patient numbers than full approval, does not require randomization, and is judged to fulfill a critical unmet need But it will still be necessary to perform the post-marketing, randomized trial needed for full FDA approval of TIL therapy for advanced melanoma Further studies are ongoing to improve TIL therapy with other technical adjustments, patient selection, and optimization of the timing and sequence, as we have covered in other issues of In Plain English.
There remain many questions and potential obstacles to the approved and now-available form of TIL therapy for advanced melanoma, including cost, time requirements, and access issues The practical ones concern the exorbitant cost of cell therapy but considering that cell therapy is a “one and done” strategy, it may not prove to be more expensive than sequences of less complex treatments punctuated by relapses. The length of time required to prepare the TIL cell product has also been reduced as laboratory advances are made currently to only about three weeks
8
Access to centers with experience that can safely administer this therapy may be challenging, but many of the principles follow those of other forms of high-dose therapy, like bone marrow transplantation (but without the need for a donor), which is now widely available, safe and effective
Taken together, the pooled results of TIL cell therapy from a number of US and ex-US centers as well as the industry-sponsored studies are remarkably good, considering that these studies most often enrolled patients who had exhausted all other therapies with known benefit
But we must not lose sight of the fact that the rising tide also lifts all boats, so that while TIL cell and related strategies are being worked on to improve their outcomes, safety, lower costs and enhance accessibility, other treatments for melanoma and other cancers are also in the works Competition is good, as it brings out the creativity of scientists and the enthusiasm of clinical investigators. It is possible that sometime in the near or distant future, TIL cell therapy will have become not only commonplace but maybe even obsolete, moving aside in favor of treatments that are even more effective, safe, well-tolerated and affordable. Look for those advances in coming issues of In Plain English.
KIM MARGOLIN, M.D., FACP, FASCO


Dr. Margolin is a Medical Director of the SJCI Melanoma Program, St. John’s Cancer Institute. She worked at City of Hope for 30 years and also held faculty positions at the Seattle Cancer Care Alliance/University of Washington and at Stanford University Among her academic achievements were long-term leadership of the Cytokine Working Group, leadership involvement in the Cancer Immunotherapy Trials Network, participation in the Southwest Oncology Group’s Melanoma Committee, and many positions in the American Society of Clinical Oncology and the Society for Immunotherapy of Cancer. Dr. Margolin has reviewed grants for many cancer-related nonprofit organizations and governmental agencies. She has also served as a member of the Oncology Drugs Advisory Committee to the FDA, the American Board of Internal Medicine’s Medical Oncology certification committee, and the Scientific Advisory Committee of the European Organization for the Research and Treatment of Cancer
Dr. Margolin collaborates with AIM at Melanoma to write our In Plain English articles to provide timely updates on new developments for patients, caregivers, and other individuals with an interest in medical advances in melanoma
9

May is Brain Tumor Awareness Month
To help highlight the importance of brain metastases, the American Brain Tumor Association (ABTA), the Melanoma Research Foundation (MRF), and AIM at Melanoma are partnering to raise awareness about the risks and impact of brain metastases
On Thursday, May 9, the ABTA will host a free webinar for patients, caregivers, and survivors entitled “How Metastatic Brain Tumors Affect Your Melanoma Care.” This webinar, in partnership with AIM and the MRF, will provide a deeper dive into the brain metastases experience for melanoma, exploring risks, progression, signs & symptoms, treatment options, and management This webinar will also include a live Q&A with the speakers.
An estimated 7% to 10% of patients with melanoma develop brain metastases.
Are You at Risk for Brain Metastases?

Brain metastases are not unique to melanoma; other cancers like lung, breast, kidney and colon cancer can also spread to the brain. Metastatic brain tumors are the most common type of brain tumor in adults Multiple brain metastases can be common.
Understanding the unique characteristics of metastatic brain tumors can help doctors create effective, individualized treatment
Understanding your risks can help empower you to better advocate for yourself. Knowing what to ask your doctor can be difficult and hard to remember
10

THEFDAAPPROVALOFTIL THERAPYANDWHATITMEANS FORADVANCEDMELANOMA
AnInterviewwithDr.AllisonBetofWarner,MD,PhD
AssistantProfessorintheDepartmentofMedicine, DivisionofMedicalOncology
DirectorofMelanomaMedicalOncology, DirectorofSolidTumorCellularTherapy,andco-DirectorofthePigmentedLesionandMelanomaProgram, StanfordMedicine
11

ofWarner,MD, PhDaboutthenewlyFDAapprovedtreatmentformelanomacalledlifileucel(Amtagvi),TILtherapyor TILs,fortumor-infiltratinglymphocytes.
WhatisTILtherapy(Amtagvi™orlifileucel),andhowdoesitwork?
TILs stands for tumor-infiltrating lymphocytes and is another form of immunotherapy. Immunotherapy in melanoma usually means checkpoint inhibitors, which are drug treatments that activate a patient’s immune cells so they can seek and kill tumor cells. By contrast, TIL therapy is a cellular therapy that administers immune cells to a patient, rather than using a drug to activate immune cells.
The general idea is that some patients will get traditional checkpoint inhibitors and their immune system will become activated. Treatment is successful when enough immune cells are able to find and kill tumor cells. However, sometimes not enough of those immune cells find the tumor TIL therapy approaches this problem a slightly different way. With TIL therapy, a piece of the tumor is removed to extract the immune cells that were able to find and attack the tumor. Those active tumor cells are expanded into the billion-fold range and then returned to the patient.
Patients will have surgery to remove between 1.5 and 4 centimeters of tumor, which is then sent to a company. In the case of TILs for melanoma, the company is Iovance, and they process the tissue and remove the tumor cells Iovance then grows the good T cells and returns them as a frozen product.
Patients will then receive up to seven days of chemotherapy to get rid of the immune cells that do not work. This treatment also gets rid of the cells and suppressive signals that could compete with these new immune cells that we plan to give back to the patient. Then, we provide the patient with their expanded immune cells and a medicine called high-dose IL-2 that helps keep those cells active and alive
12
WhatisIL-2?
IL-2, or interleukin 2, is an older medicine. If you have ever had the flu, a high fever, and shaking chills, your body is making IL-2 to trigger an immune response. IL-2 is a natural molecule that your body makes to turn on your T-cells We give it at higher doses It is a cytokine, a signaling molecule that turns on T-cells in the body
Whatisthelengthoftimethatpatientsareinthehospital forTILtherapyandwhatistherecoverytime?
Every patient is different, and every center does this differently Some centers will admit the patient to the hospital for chemotherapy. Centers that see a lot of patients with cellular therapy or bone marrow transplants will often give chemotherapy as an outpatient treatment. Chemotherapy accounts for five to seven days of the total admission time.
Everyone will get the cells and the IL-2 in the hospital. Cells take one day. IL-2 takes up to three additional days after that. Most patients are hospitalized for 10 to 14 days after cell treatment. The total length of the hospitalization is dependent on how quickly people recover from the chemotherapy and the IL-2. In addition, the rate at which the blood cells return after chemotherapy is essential We can give estimates, but everyone is going to be markedly different
HowlongdoesittaketogrowanadequatenumberofTcellstoputbackintothepatientaftertheoriginal tumorharvest?
In clinical trials, the production time was about 22 days. The actual time between when they come out of a patient and when the clinician gets them back to give the cells to a patient with the approved product is 35 days That difference is because those cells need to undergo a ton of testing to ensure that they are not infected with anything before they are put back into the patient. Then the company (Iovance) makes sure the cells are expanded, healthy, and alive; extra testing makes the total period 35 days.

WhoiseligibleforTILtherapy?
TIL therapy is a brand-new and highly complex therapy The patients who are good candidates for TIL therapy are up and active during the day, able to do their work around the house or work full or part time, and maintain their body weight. That’s the kind of patient who will do well with TIL therapy.
A few categories of patients are expressly excluded from receiving TIL therapy. For example, uveal melanoma is not included in the FDA approval. There are ongoing clinical trials for TILs in uveal melanoma, but patients with uveal melanoma are not at this time eligible for the FDA-approved product.
13
Patients need to have good heart and lung function. The function of those organs will be tested as part of the workup. It’s not safe to give TIL therapy if patients do not have good heart, lung, and kidney function. The patients must be well enough to make it through the chemotherapy and the IL-2 therapy, both filtered out by the kidneys.
Patients who are on treatment-dose steroids, whether it is for brain metastasis or if it is because of an immunotherapy side effect, are not eligible for TIL therapy. The reason is because steroids inactivate the T-cells. Patients who have had a history of hypophysitis and are on replacement doses are okay to receive TIL therapy. Patients who are actively being treated on doses of steroids above 10 mg of prednisone are not eligible for TIL therapy until or unless they come off that steroid
The last population of patients for whom TIL therapy is not appropriate includes those who have symptomatic or untreated brain metastases. We do not know whether TIL therapy is safe for these patients. High doses of chemotherapy can increase the risk of bleeding in the brain and is very dangerous. Brain metastases are at a high risk of bleeding and the IL-2 can cause swelling around a brain metastasis, which could be very dangerous. There are ongoing clinical trials looking at TIL therapy for patients with brain metastasis but the commercial product is not intended for the population with untreated metastasis. If brain metastasis is stable for a period of time after radiation therapy, then TIL therapy could be appropriate.
WhichlineoftherapyisTILs?
The approval is second line or later It is not approved for frontline therapy There is a clinical trial going on that combines TILs with pembrolizumab, which could potentially become a frontline therapy. Still, it is a phase 3 trial that is now being enrolled. The FDA approval and most of the clinical trials for TIL therapy are for patients who have progressed on checkpoint inhibitors. If patients have a B-Raf mutation, they must have had, and not tolerated or not responded to, the BRAF/ MEK inhibitor combination therapy. Therefore, TIL therapy is a second- line or later therapy.
Whatkindofoutcomeshaveweseenfromthispatient population?
The biggest trial with lifileucel (Amtagvi), the approved therapy, is the C-144-01 trial (NCT02360579) There were two separate cohorts, but all were patients with melanoma that had progressed on standard checkpoint inhibitor plus a BRAF+ MEK inhibitor, if they had the B-Raf mutation In total, the trial enrolled 153 patients that met these criteria. The response rate was 31.4%, meaning that 31 out of 100 had their tumors shrink or disappear. That is not nearly as high as we would like it to be. Clinical trials are working to improve upon these numbers to bring up efficacy. However, the promise here is that over 40% of the patients whose tumors responded were still responding after 18 months plus. We expect that to be durable. These responding patients are also off all other cancer therapy with ongoing disease control.
A major clinical study that gave TIL therapy as second line after progression on antiPD-L1 therapy showed that those patients do very well. Patients in that trial had a 50% response rate and a 20% complete response rate.
14
WhataboutthesideeffectsofTILtreatment,particularly withIL-2?
The biggest two sources of side effects in the whole process come from the chemotherapy and the IL-2. The TIL cells that are expanded and given back to the patient have very little toxicity.
The chemotherapy is a preparative regimen. Two chemotherapy drugs are given, cyclophosphamide and fludarabine. These are used for most cellular therapies. The main side effects of those agents include nausea and vomiting. We give patients lots of anti-nausea medicines, so these are minimized. Patients will lose their hair from this chemotherapy regimen.
The most significant risk is that the white blood cell counts will decrease That puts patients at a high risk for infection Red blood cells will also go down as a side effect of the treatment Patients often need to be supported with blood transfusions during the process. Platelets go down as they also are part of this effect. Low platelets put patients at risk of bleeding, which is why patients with brain metastasis would be at an increased risk for bleeding. That is a critical issue. Those counts will come back up on their own. Patients’ white blood cell counts are supported with a medicine called G-CSF. The medicine helps those white blood cells return faster to protect patients from infection.
The other side effects come from IL-2, but it has improved from years ago. The way we give IL-2 today is different from the way IL-2 was administered 20 years ago and we have even improved from the C-144-01 study One of the things that we have learned throughout this process is that we can be less aggressive with the IL-2 treatment. However, this is a tough treatment. It is tough for the patients and their doctors. This treatment is very handson and involved. TIL therapy involves a huge team.
In the earliest days of TILs, we thought patients needed to get six or eight doses of IL-2. Some older regimens included more than 15 doses of IL-2. The toxicity of IL-2 is cumulative. Cutting that down helps the patient significantly. Many patients on IL-2 experienced fevers, shaking, chills, and low blood pressure. IL-2 causes capillary leak syndrome, when fluid leaks out of the bloodstream and goes into your hands and feet, which swell. The fluid can also go into the lungs and that causes patients to require oxygen The combination of the blood pressure going down and fluid leaking out can damage the kidneys. Clinicians have learned to be very vigilant about these toxicities.
Recent data came out that changed the way clinicians think about TIL therapy. No data suggests more IL-2 is better for these patients. Some IL-2 is necessary based on previous trials that tried to leave it out and that did not work well. As soon as patients start running into side effects with IL-2, we can stop the treatment and the regimen’s efficacy is the same. Years ago, we were doing everything we could to keep going with patients on more IL-2, including monitoring blood pressure or putting them on blood pressure support medications or even on dialysis Clinicians have learned they do not need to do that anymore
15

The side effects are completely different. With checkpoint inhibitors, like pembrolizumab, the side effects result from auto-immunity, when the immune system turns on itself That is not what we see with TIL therapy With TIL regimens, the side effects stem from chemotherapy and IL-2 treatment. The main differences also include the duration. With TIL therapy, the side effects are mostly limited to the first 14 days, which is the time that the patients are getting chemotherapy and IL-2 and recovering in the hospital under close supervision. There are very few new side effects that appear after that. This can be an intense period, but it is a much more limited period.
With checkpoint inhibitors, the toxicities can last days, weeks or months Sometimes they might even be lifelong.
Ifpreviousimmunotherapy treatmentscausedmultiple adverseevents,willTILtherapy havemore?
We have not seen that. Adverse events mediated by immunotherapy or checkpoint blockade occur when the T- cells get turned on, similar to auto-immune events. As long as those events have been completely resolved before TIL therapy, we have not seen it retrigger the same side effects. The one caveat to that is the eye The eye may experience uveitis TIL therapy can cause uveitis, and it is essential to resolve any prior uveitis before treating a patient with TILs. Any patient who has had uveitis should have had an eye exam before the treatment with TILs to make sure that it has completely resolved.
16

Go on to the next line of therapy, which can include several other options. They may choose to do a clinical trial after TIL. Some will choose to re-try a checkpoint inhibitor. After we have “reset” the immune response with TILs, there have been patients who then responded to checkpoint inhibition, even when they did not previously. We are trying to understand that further. The takeaway message is that TIL therapy is not the last line of defense. We think about it early if it is appropriate for the patient.
IsTILtherapyapprovedformucosalandothertypesofmelanoma?
Acral, mucosal, cutaneous, and melanoma of unknown primary origin are approved These types of melanoma were included in the initial clinical trial and are appropriate for TIL therapy Uveal melanoma was not included in the clinical trial and, therefore, is not part of the FDA indication.
Lookingforwardintothefuture,whereareweheadingwithTILtherapy?
We are working on many things, including making better drugs – more efficacy, a higher response rate, and less toxic or safer for patients. As many patients have pointed out, not everyone is eligible for TIL therapy because of their age, a history of lung issues, a history of heart issues, or kidney problems. One of the biggest challenges here is the IL-2 therapy. If we could find a way to get rid of the IL-2 or minimize that amount people need, then many more patients would be eligible to receive TILs. Several trials and companies are working on that. A phase 1 clinical trial is now trying to eliminate the need for IL-2. That’s where we are going –eliminating the IL-2.
Getting rid of IL-2 in the regimen may also allow us to eventually move this treatment into outpatient treatment, as the IL-2 is the riskiest part of the treatment at this point. I do foresee a future with this being an outpatient treatment. That will be contingent upon what we can do to engineer cells that do not need IL-2 but do not have a lot of added toxicity.
17
TellusaboutthecentersthatcanofferTILtherapy.
To become an authorized TIL treatment center, an arduous process is necessary for patient safety. Depending on the set-up of the center and what resources are already in place, hundreds of hours of work may be needed. Then, there is an evaluation process, and an on-site audit, and the center must have certain clinical teams in place with safety measures and checkpoints. The drugs website lists authorized treatment centers. There are 26 authorized treatment centers in the U.S. right now. We expect that number to expand as more sites make it through this process. You can also find information about approved drugs and centers on the aimatmelanoma.org website.
Whataboutinsurancecoverage?
TIL therapy is covered by Medicare as long as the patient meets all eligibility criteria. Private insurers are paying for this treatment, but the insurance approval process is not well defined yet. We usually have to contact the different companies with CMS and insurance codes. If a patient is appropriate, then insurance should approve the treatment. It may take an authorized treatment center to work on it and it may take some advocacy on the patient’s behalf. This is an exceptionally expensive treatment. The drug alone, just the cells, is $515,000. This does not include the IL-2, the hospitalization, or the chemotherapy. Insurers are trying to figure out how to do this The surgery is not included in that cost The surgery and treatment need to get approved For patients who meet the eligibility criteria, this should be approved, but it may need some work because it’s new. We are teaching the insurers about it.
Watch the Webinar

18
hosted by Sam Guild, President of AIM at Melanoma
Saturday, May 11, 2024
The Angeles Clinic and Research Institute
Los Angeles, California
Virtual & In- Person
IntelligentImmunotherapyInnovationsinInitialTherapy
Mucosal,Acral,UvealFutures–TimetoInvest!
NeoAdjuvant&AdjuvantTherapy:QuestionsGettingAnswered
ClinicalTrialOptions–NewData,FutureTherapies
CellularTherapy:TILTomorrowandFurther
RadiationTherapyinMelanoma,NovelParadigms

registration open upcomingpatient symposiums

REGISTERFOR MAY11TH
19

THEFOUNDATIONWORKINGTO#ENDMELANOMA
