News From the Foundation Working to End Melanoma | Fall 2024
From the Desk of Sam Guild, President AIM at Melanoma Foundation
An Insider’s View of Medical Issues Facing Patients with Melanoma
Nailing Down on the Ultraviolet Exposure Occurring During the Curing and Drying of a Manicure by Mandi Murph, PhD, MBA, Director of Medical Education
New Specialty Manages Skin Concerns and Keeps Patients on Therapy by Mandi Murph, PhD, MBA, Director of Medical Education
Side Effect Central: Colitis by Mandi Murph, PhD, MBA, Director of Medical Education
Times Have Changed for Melanoma Survival by Mandi Murph, PhD, MBA, Director of Medical Education
In Plain English: Update on Melanoma Vaccines, 2024 by Kim Margolin, M.D., FACP, FASCO
FROM THE DESK OF Sam Guild
PRESIDENT | AIM AT MELANOMA FOUNDATION
Dear
Friends and Supporters,
As we transition into fall, I wanted to take a moment to share some highlights from this busy spring and summer, particularly my experience at the European Society for Medical Oncology’s (ESMO) annual meeting in beautiful Barcelona
One of the key themes at ESMO this year was a status check on immunotherapies, marking a decade since the groundbreaking approval of combination nivolumab (Opdivo) plus ipilimumab (Yervoy) and pembrolizumab (Keytruda) alone. The data presented was a powerful reminder of the impact these therapies have had on patients with metastatic melanoma. Remarkably, we learned that approximately 43% of patients treated with combination nivolumab plus ipilimumab and 34% of patients treated with pembrolizumab achieved a sustained, long-term survival, a testament to the advancements we've made in this field However, it was equally clear that there is still much work to be done in the pursuit of better treatments for all
Included this newsletter is our most recent installment of In Plain English Dr Kim Margolin gives an update and explanation on the latest in vaccines for cancer and melanoma specifically
We also highlight a Dutch study suggesting that patients with advanced melanoma now survive longer than their predecessors and achieve outcomes once thought to occur only in clinical trials According to the study, patients in the Netherlands who respond to immune checkpoint inhibitors are likely to achieve long-term survival, further emphasizing the progress being made in melanoma treatment
Additionally, we’re excited to introduce a new series for our newsletter titled Side Effect Central This series of articles is designed to help patients with melanoma and their caregivers understand the side effects that typically accompany melanoma treatments Our goal is to explain what side effects to expect during treatment and to encourage open communication with your medical team about these experiences
We also have an interesting article about a new medical specialty called oncodermatology This specialty focuses on managing skin concerns and allowing patients to stay on their treatment regimen
As if that’s not enough, we've covered an important topic: Nailing Down on the Ultraviolet Exposure Occurring During the Curing and Drying of a Manicure This article discusses the potential risks associated with UV exposure during nail treatments, which is especially relevant for those concerned about skin health.
Finally, we have a Q&A with Dr. Lynn Schuchter, who served as the President of the American Society of Clinical Oncology (ASCO) from June 2023 – June 2024. She is currently the Chair of the ASCO Board of Directors and sits on the organization’s government relations committee. Dr. Schuchter is also a Medical Oncologist at Penn Medicine, chief of the Division of HematologyOncology at the Abramson Cancer Center at the University of Pennsylvania, and the Director of the Tara Miller Melanoma Center
Thank you for your ongoing support and commitment to our mission Together, we can continue to push for progress in melanoma research and treatment
Dr. Lynn Schuchter served as the President of the American Society of Clinical Oncology (ASCO) from June 2023 – June 2024. She is currently the Chair of the ASCO Board of Directors and sits on the organization’s government relations committee. Dr. Schuchter is also a Medical Oncologist at Penn Medicine, chief of the Division of HematologyOncology at the Abramson Cancer Center at the University of Pennsylvania, and the Director of the Tara Miller Melanoma Center. She has been routinely recognized by America’s Top Doctors and Best Doctors in America For seventeen years, Philadelphia magazinerecognizedherasa“TopDoc.”Sheisatthe forefrontofissuesthatfacepatientswithmelanoma.
What advocacy issues are important for patients with cancer?
A number of advocacy issues are important to patients diagnosed with melanoma and other types of cancer. These include telemedicine, prior authorizations, copays and drug shortages. There is also a big shift in cancer treatment towards survivorship care, including long-term comfort care. Lastly, scientific advances are still needed, and research fundingisimportanttofacilitatethat.
Whatcanyoutellusabouttheissueoftelemedicine?
During the pandemic, clinics discovered telemedicine is a great way to deliver care Patients with melanoma and other cancers benefitted from and enjoy telemedicine because they could attend doctor’s visits in the comfortoftheirhomeswithoutthehassleoftraveling
The problem is that Congress has to re-authorize our ability to continue telemedicine. The authorization for telemedicine ends at the end of December 2024. We all need Congress to act on this – the ability to provide telemedicine care to our patients, not just cancer patients, but allpatients.
Telemedicine is also effective for dermatology and primary care visits. Using these new technologies, a dermatologist can see a patient’s skin lesion We want patients to push Congress to act on legislation in this way
Whatissuedelaystreatmentadministrationtopatients?
Another big problem is the issue of prior authorization. When clinicians try to order treatments for patients, there is much scrutiny from insurance companies. They are the ones approving the scans and the treatments that patients need. These prior authorizations from the insurance companies often delay access to treatment Sometimes, there are additional delays unrelated to prior authorizations, which magnifiesthechallengesthatcancoincidewithpriorauthorizations
What can you tell us about treatment copays?
At ASCO and other professional organizations, a concern for patients is treatment copays It seems unreasonable that patients have insurance and then have this extra financial burden of copays for medications We are looking at what we can do for copays for therapies that are benefitting patients with cancer.
You’ve heard the stories Some patients are not taking medications or are choosing a different medication because they are unable to figure out how to pay for their treatment of choice They also have rent, electric bills, and food
The way patients pay for medications in this country is far from ideal. Many insurance plans distinguish between medications that are given by a healthcare provider and those that are taken orally or are self-injected at home. The former are typically covered by a health plan’s medical benefits, with minimal to moderate copays However, the latter can sometimes have high copays, resulting in the patient paying in the thousands or hundreds of thousands of dollars to receive their treatment
Medicare provides coverage for some of the new immunotherapies for intravenous treatment. If you do not have other insurance, then you will pay a 20% copay
The big goal is universal coverage, especially for patients with cancer. We should continue to push for universal coverage or reform of the current payment structure at every opportunity Access to medications is also really important. We need to ensure that patients get the treatments that really work
Is there a problem impacting clinical treatment that has gone unresolved for some time?
Drug shortages are an old problem. Although drug shortages have been a big problem for more than a decade, this past year or two has brought about a worsening crisis in drug availability.
The shortages impact drugs critical to curing certain cancers and drugs that increase the survival of other types of cancers. Sometimes, clinics don’t have common chemotherapy drugs like cisplatin and carboplatin
The big goal is universal coverage, especially for patients with cancer. We should continue to push for universal coverage or reform of the current payment structure at every opportunity
It hasn’t affected the immunotherapy drugs commonly used in melanoma because drug shortages focus on generic drugs (i.e. the patent protection has expired, so that others can make generic drugs) Some companies are not as interested in manufacturing generic drugs [because the profit margins are not as high as a patent-protected drug].
This issue of access to regular drugs that we use for our patients is a crisis However, there are also some supportive care medicines that we don’t have access to, including pain medications and intravenous fluids. The medical community should not expect or accept drug shortages as an issue that we all become accustomed to navigating.
ASCO has put forward several legislative solutions to Congress. For example, there could be more authority given to the FDA There are greater incentives that Congress could put together. We want to ensure that at the state and federal levels, people are talking to Congress about what they might be able to do
What is survivorship care for people impacted by advanced or metastatic cancer versus those survivors of early-stage or in-situ disease?
Patients with early-stage cancers, especially in situ, will be cured of their disease In these instances, clinicians are primarily focused on survivorship issues.
The survivorship issues could include managing long-term complications of surgery, or long-term side effects of treatment, but they also mean understanding a patient’s future risk of other types of cancers.
Sometimes melanoma does run in families or runs alongside other types of cancers. Therefore, part of a survivorship plan for patients who had cancer means understanding the family history of cancers, including breast cancer, ovarian cancer, and pancreatic cancer We need to put the right screening programs in place.
During survivorship, the long-term consequences of treatment need to be addressed. Many patients will receive immunotherapy, which can have permanent side effects, especially endocrine issues It’s really important that patients have access to the specialists that they will need in survivorship care after cancer.
For example, after melanoma, surviving patients should continue to see a dermatologist We know that if patients have one primary melanoma, then they are at risk for a second primary melanoma and other types of skin cancer
Survivorship means addressing any long-term consequences of treatment and early detection strategies to diagnose any other types of cancer, including types of skin cancer
What about survivorship care for patients with advanced or metastatic cancer?
Oncologists are thrilled to be incorporating long-term survivorship into care planning For patients with advanced, metastatic melanoma in Stage IV, clinicians used to focus on managing the side effects of treatment and understanding risks of therapy. Medical oncologists were not thinking about survivorship care.
In recent practice, patients with Stage IV melanoma may achieve “no evidence of disease ” Some of those patients that survive metastatic melanoma are already 8-10 years post-cancer They are technically cured of their previous Stage IV disease.
Therefore, the same emphasis on early-stage patients applies to survivors of late-stage disease That means survivors of metastatic melanoma need to have their mammograms, colon cancer screenings, or PSA tests Medical oncologists are now having to think about survivorship care, especially for patients who previously were treated for metastatic melanoma. Patients are moving off of treatment in survivorship.
It is not uncommon for patients to have more than one type of cancer. Clinicians need to make sure that among survivors, cancer screening is in place, risk factors are known, and other health issues are taken care of, such as high blood pressure and cholesterol. Clinicians should frame this as a “Wellness Plan” for Stage IV melanoma survivorship It’s a wonderful new world in treatment issues!
What does medical care need to address in the longterm treatment of patients with melanoma?
Amazing progress has occurred in melanoma many patients may be cured. Unfortunately, many other patients are not benefitting from the treatments Alternatively, there are patients who responded to treatment initially and then it stopped working. In these cases, the melanoma cells became resistant to the treatment
Therefore, we still need to address symptoms that patients may develop as a result of their treatment for metastatic can1cer. That means clinicians must have important conversations about hospice and palliative care with patients and their families Too many patients and their families are caught off guard. Patients are not having those important conversations with their spouses and families earlier in the melanoma journey
Clinicians need to emphasize the importance of communication between physicians or nurse practitioners and their patients They need to be prepared to share prognostic information, which helps patients to plan for the future and allows them to address symptoms around pain management, shortness of breath, and other related symptoms
As much as clinicians address curing the cancer, they also need to address comfort care. Not all patients will benefit from treatment, and some patients with melanoma develop brain metastases That is a devastating consequence of melanoma. These are difficult conversations.
Clinicians want to maintain hope and have seen much progress in the field When treatments are not working, how do physicians communicate that? Clinicians want to understand a patient’s priorities and values so that they can plan
There’s work on how best to communicate this information. Legislative work and inroads are needed to reimburse physicians, nurses, and nurse practitioners for the time it takes to have those difficult conversations in the clinic. Clinicians hope they will not need to focus on supportive, end-of-life, and palliative care Still, it remains an important part of the work
What other medical research issues need to be addressed to benefit patients with melanoma?
There are unmet needs in melanoma Scientists need to be unrelenting in their pursuit of finding new approaches and new treatments for this disease. The field would also be served by a better understanding of which patients need treatments and which do not That is critical because clinicians are overtreating many patients.
We need to continue to press for research funding We are very concerned about the cuts to the National Institutes of Health and the National Cancer Institute. These cuts reduce the investment in research funding for new targets and new approaches The advances in cancer care, treatment of melanoma, and other types of cancer have all happened because of clinical trials, which may be partially or entirely funded through federal research grants. Preserving research funding is, therefore, an important initiative.
Lastly, the holy grail for patients with melanoma and other cancers is to use immunotherapy without its associated side effects. Untangling the benefit derived from the immunotherapy, like ipilimumab, nivolumab, or pembrolizumab, from the immunemediated adverse reactions like colitis, hepatitis, or pneumonitis, is vital.
Nailing Down on the Ultraviolet Exposure Occurring During the Curing and Drying of a Manicure
by Mandi Murph, PhD, MBA, Director of Medical Education
It’s a health risk many may not know exists – nail lamps Nail lamps are a UV light source used during manicures and pedicures to dry polish or to harden/fix artificial nails. The lamps are only used for a few minutes at a time but leave long-lasting effects after repeated exposure.
Beautifully manicured nails symbolize health, vitality, and self-care. Yet ironically the nail lamps used to achieve this look increase the risk of nonmelanoma skin cancer on the hands and feet.
Whether used at home or in salons, the UV intensity penetrating the skin from nail lamps is comparable to tanning beds, which are known drivers of melanoma and nonmelanoma skin cancer. Recent research links nail lamp use to cutaneous squamous cell carcinoma (also called squamous cell skin cancer) and other skin cell damage. Nail lamps (sometimes called gel lamps) emit unknown levels of UV-A light and potentially small amounts of UV-B light and therefore expose a manicure client’s hands and fingers to harm
This article gives information about nail lamps, explains differences in ultraviolet (UV) light, and provides data about the risk to those who use them during manicures Finally, this article will provide simple strategies that manicure lovers can employ to keep their skin safe, keep nails decorated, and reduce the risk for skin cancer
There are several different types of manicures While a simple manicure includes trimming, filing, and polish, a more extensive manicure includes the application of artificial nails and the polish or decoration of those nails A simple manicure with nail polish or one that applies acrylic nails might include the use of a nail lamp for drying purposes But manicures that include the application of a type of artificial nail called gel or polygel nails must use a nail lamp as part of the fixing process
Artificial nail enhancements such as acrylic nails, gel nails, polygel nails, and dip powder nails, are trending in the U S and combine for a global artificial nails market that exceeds a billion dollars Additionally, the market for artificial nails is expected to have steady upward growth over the next ten years.[1]
Each type of artificial nail is applied using different chemical methods and techniques. Gel nails and the hybrid product polygel nails use a gel polymer that is crosslinked or fixed under a nail lamp Gel and polygel nails are popular because the product is odorless during application, and once applied, the nails are flexible (so they feel natural), durable, and considered high-quality. Typically, gel nails last two to three weeks before they are removed, refilled, or redone
Placing hands under the nail lamp is necessary to finish this type of manicure Without the fixation step, the gel or polygel nail polymer will not fully cure or harden, and the product will not be set
In addition to being used to affix gel and polygel nails, nail lamps are sometimes used to quickly dry acrylic nails or to dry the polish on a standard manicure. Acrylic nails are artificial enhancements that cover the natural nail with a hard exterior surface to decorate. They are chosen for the product’s strength which prevents chipping, is longerlasting, and is low maintenance compared to natural nails. Acrylic nails can be embossed by trimming to different lengths or shapes, colorfully painted, and decorated with glitter, gems, or other embellishments.
TypesofUltraviolet(UV) LightWavesandNailLamps
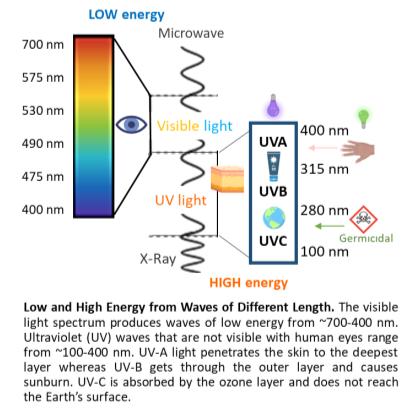
UV light can penetrate the skin and mutate human DNA. When DNA is mutated, cancerous tumors can form. In 2012, the International Agency for Research on Cancer evaluated and classified ultravioletemitting devices (wavelengths 100–400 nanometers [nm], encompassing UV-A, UVB, and UV-C) as carcinogenic to humans These wavelengths are shorter than visible light and cannot be seen by human eyes.
UV light waves come in several forms – UVA (400-315 nm), UV-B (315-280 nm), and UV-C (280-100 nm) UV-C comes from space and is absorbed by the ozone layer protecting Earth. Therefore, this type of UV wave is irrelevant here as it does not apply to nail lamps
In contrast, UV-A and UV-B pass through the ozone layer and reach the Earth’s surface. UV-A causes photoaging and the appearance of lines and wrinkles in the skin, while UV-B causes sunburns Both UV-A and UV-B are linked to the development of skin cancers by causing DNA damage.
Nail lamps use either fluorescent bulbs or lightemitting diode (LED) lamps, and both emit UV light. Fluorescent lamps emit wavelengths of 410300 nm, whereas LED lamps emit wavelengths of 425-375 nm, with peak emissions at 375 nm and 385 nm, respectively.[2] The FDA notes that there is no danger to human skin from these lamps when there is at least 10 inches of distance between the lamps and human skin, such as in a typical room.[3] But hands under nail lamps are extremely close to the light source and UV emission and therefore concerning.
Devices known to emit high, concentrated doses of UV-A include tanning beds, which are known to contribute to the development of skin cancer. A tanning bed is designed to emit a UV index of 12, which is the amount of UV one would experience during midday in the tropics.[4] Studies evaluating tanning beds and nail lamps indicated the UV-A radiation to the skin is similar [5]
Nail lamps require less than ten minutes to achieve their results, highlighting an issue: The UV exposure is concentrated and rapidly reaches an unnaturally high level at each exposure. Further, damage accumulates when exposure to artificial devices becomes routine Indeed, patients have reported receiving blistering sunburns on their hands after salon visits for gel nails.[6]
DoesanAgencyMonitorNail LampsorUVExposure?
In the U.S., no agency evaluates, standardizes, or routinely certifies the UV intensity emitted from nail lamps used in spas and salons. One study tested 17 different nail lamps from 16 salons and observed a wide range of measurements, such as intensity of UVA emitted from the lamps and the number and type of bulbs used in each. In other words, there was a significant lack of consistency among values collected from the salons. The lack of consistency was attributed to different brands of nail lamps, bulb wattages, and the number of bulbs per device However, the researchers found a strong correlation between the amount of UV-A irradiance emitted and a high light bulb wattage.[7]
Among the 17 nail lamps in the research study, the minimum UV-A irradiance was 0.6 mW/cm2, and the maximum was 15.7 mW/cm2, which is an enormous variation Since the average time for exposure during a single visit was 8 minutes, the energy dosage each client might experience could differ dramatically.[7]
For example, for the lowest dose measured, over 200 visits to the salon would be required before a client reached a level sufficient to damage DNA. This damage would increase the risk of cancer but it would still be a relatively low risk over a long period of time However, the highest dose measured in the salon study would require only eight visits by a client to reach a dangerous exposure level At the higher dose, the DNA damage would start accumulating faster, increasing the risk for cancer to develop.[7]
Another study on UV-A lamps may help explain why some salon visits could be more harmful to certain clients than others The researchers observed high UV-A variability from the lamps, and prolonged exposure sufficient to induce DNA damage. More importantly, during prolonged usage, the internal temperature of the lamps increased. The temperature rise magnified the intensity of the UV-A and caused more DNA damage.[8] This observation suggests that a nail lamp that is kept on for multiple clients has the potential to cause far more DNA damage to the later clients.
" …for the lowest dose measured, over 200 visits to the salon would be required before a client reached a level sufficient to damage DNA… the highest dose measured in the salon study would require only eight visits by a client to reach a dangerous exposure level… "
" …decades of exposure are not necessarily required for skin cancer to appear One patient diagnosed with several squamous cell carcinomas on both hands visited a nail salon eight times in one year… "
Research literature has numerous observational studies linking nail lamps to the development of skin cancer.
For example, one patient with nonmelanoma skin cancer on her hands and feet reported getting manicures and pedicures every 2-3 weeks for a decade. Her routine included UV nail lamp use, and she recalls receiving blistering skin damage from at least one experience at a salon Over time, she developed eight skin tumors on her fingers and 46 precancerous actinic keratoses on her fingers and feet.[9]
Another patient diagnosed with skin cancer squamous cell carcinoma had a 15-year history of twice-monthly nail lamp exposure for acrylic nails. Three stages of Mohs surgery were needed to remove her skin cancer.[10]
Squamous cell carcinomas were also found on the left and right hands of another woman who used UV devices routinely. Over 25 actinic keratoses on her hands were treated with cryotherapy. There were no other skin lesions or suspicious areas on her entire body just her hands This diagnosis came after an 18-year history of UV nail lamp use every three weeks at a salon.[11]
Dr. Julia Curtis, a dermatologist in the Department of Dermatology at the University of Utah only sees the occasional patient with skin cancer possibly associated with manicures or pedicures One patient “had manicures and pedicures for most of their adult life, and they were developing skin cancers on their hands and feet It’s concerning,” she recalled
Further, Dr. Curtis said, “There has certainly been an increase in the amount of people using UV nail lamps recently We don’t have the data yet, but in 10-15 years, we could see a spike in terms of skin cancer around the hands and feet.”
A surprising report suggests that decades of exposure are not necessarily required for skin cancer to appear. One patient diagnosed with several squamous cell carcinomas on both hands visited a nail salon eight times in one year before her cancer appeared.[10]
It is not understood why there is so much variation between the timing of exposure and cancer between the cases, but the level of genetic risk for an individual can be a factor (more on this topic, below). Additional environmental and occupational exposures could also be factors And it cannot be presumed that a case of skin cancer appearing on the hands was caused solely by UV nail lamps.
Further complicating the subject is the fact that some literature has shown the risk of nail lamps to be negligible. It is no wonder the general public reports confusion about this topic.
Not all individuals bear the same risk of developing nonmelanoma skin cancer In addition, any risk for cancer is not a guarantee – it’s a possibility. Even among families with a very strong history of disease, there is likely to be a surviving member who was never afflicted by the disease.
Individuals with a moderate to high risk of developing nonmelanoma skin cancer include those with a family history of skin cancers, individuals with fair complexions, people with photosensitivity disorders, and patients who are immunosuppressed. People at the highest risk have a genetic susceptibility to developing skin cancer
Groups at the highest risk of developing nonmelanoma skin cancer are most at-risk to damage from nail lamps and other UV exposures because of their susceptibility Unexpected or unknown factors, such as medications, could combine to further increase their risk.[12]
Medications that suppress the immune system after an organ transplantation are a known risk factor for developing skin cancer, yet other lesser-known medications may have a similar effect. Some prescribed and over-the-counter drugs can cause a user to become more sensitive to the effects from UV waves.
Some antihypertensive drugs are photosensitizing, which would magnify the intensity of UV exposure. Danish studies, for example, suggest that the risk for squamous cell carcinoma increases with long-term use of the diuretic hydrochlorothiazide, which is prescribed to treat high blood pressure or edema [13,14]
Other drugs such as oral contraceptives that contain estrogen and progestin increase photosensitivity.[15] In addition, prescription antibiotics like tetracyclines, fluoroquinolones, and sulfonamides are photosensitizing. Over-the-counter nonsteroidal anti-inflammatory drugs also belong to this category Acne medications like prescription retinoids and topical creams can also increase light sensitivity or cause photocontact dermatitis. [16]
If someone with a lower risk of skin cancer takes photosensitizing medications before UV light exposure, their natural barriers will be diminished and their risk increases. They become sensitized to the effects of UV light.
RecommendationsforaSaferManicure
A simple recommendation is not to use nail lamps or use them as infrequently as possible. If you get standard manicures or even acrylic nails, tell your manicurist that you’d like your nails to dry naturally.
But if it’s important to you to have routinely manicured gel nails or polygel nails which require use of a nail lamp, consider some additional strategies for long-term healthy skin. You can employ several steps to protect your skin from the UV rays emitted from a nail lamp
Apply a broad-spectrum, water-resistant sunscreen of SPF 30 or higher to the hands and fingertips before a manicure that includes nail lamp use [17,18]
Another option recommended by dermatologists and doctors is to wear UV-A protective gloves, which will act as a barrier to the UV rays [7]
When it comes to at-home manicures, you have the power to minimize UV exposure Choose LED lamps over fluorescent ones for less UV-A exposure.
More importantly, turning off the nail lamp after each use can significantly reduce the increase in UV-A emitted from temperature elevations.[8]
Even if you are convinced that your risk for skin cancer is exceedingly low, UV-A does more than cause indirect DNA damage Repeated exposure causes photoaging in addition to DNA damage. Taking preventative measures can therefore reduce unnatural skin aging
Following these safety measures can help you keep your hands and fingers safe from the UV light emitted by nail lamps. Treat your skin well so that it can last a lifetime.
Be informed, be smart about UV exposure, and follow a simple concept: Bepolishedandprotected.
References
Global Artificial Nails Market Report Coverage. Spherical Insights. 2023. www.sphericalinsights.com /reports/artificial-nails-market. Accessed July 30, 2024. 1
Shihab N and Lim HW. Potential cutaneous carcinogenic risk of exposure to UV nail lamp: A review. Photodermatol Photoimmunol Photomed. 2018;34(6):362-365. doi: 10.1111/phpp.12398. 2 . Federal Drug Administration. Compact Fluorescent Lamps (CFLs) – Fact Sheet. Accessed 8.13.2024. https://www.fda.gov/radiation-emitting-products/home-business-and-entertainmentproducts/compact-fluorescent-lamps-cfls-fact-sheetfaq
4
3 International Agency for Research on Cancer. IARC Monographs on the Identification of Carcinogenic Hazards to Humans. https://monographs.iarc.who.int/list-of-classifications. Accessed August 5, 2024.
6
5 Freeman C, Hull C, Sontheimer R et al. Squamous cell carcinoma of the dorsal hands and feet after repeated exposure to ultraviolet nail lamps. Dermatol Online J 2020;26(3):13030/qt1rd1k82v.
Wilson J and Maraka J. Need for sun cream with your manicure? Dangers of UV nail dryers. J Plast Reconstr Aesthet Surg. 2016;69(6):871. doi: 10.1016/j.bjps.2016.03.011.
Shipp LR, Warner CA, Rueggeberg FA et al. Further investigation into the risk of skin cancer associated with the use of UV nail lamps. JAMA Dermatol. 2014;150(7):775-6. doi: 10.1001/jamadermatol.2013.8740.
7 Finn E, Dussan L, Rosenthal S et al. Temperature Is a Key Factor Governing the Toxic Impact of Ultra-Violet Radiation-Emitting Nail Dryers When Used on Human Skin Cells. Int J Toxicol 2024:10915818241268617. Online ahead of print. doi: 10.1177/10915818241268617.
8 Freeman C, Hull C, Sontheimer R et al. Squamous cell carcinoma of the dorsal hands and feet after repeated exposure to ultraviolet nail lamps. Dermatol Online J. 2020;26(3):13030/qt1rd1k82v.
9 MacFarlane DF and Alonso CA. Occurrence of nonmelanoma skin cancers on the hands after UV nail light exposure. Arch Dermatol. 2009;145(4):447-9. doi: 10.1001/archdermatol.2008.622.
10 Ratycz M, Lender JA and Gottwald LD. Multiple Dorsal Hand Actinic Keratoses and Squamous Cell Carcinomas: A Unique Presentation following Extensive UV Nail Lamp Use. Case Rep Dermatol. 2019;11(3):286-291. doi: 10.1159/000503273.
11 Metko D, Mehta S, Mcmullen E, et al. A systematic review of the risk of cutaneous malignancy associated with ultraviolet nail lamps: what is the price of beauty? Eur J Dermatol 2024;34(1):26-30. doi: 10.1684/ejd.2024.4616.
12 Schmidt SAJ, Schmidt M, Mehnert F et al. Use of antihypertensive drugs and risk of skin cancer. J Eur Acad Dermatol Venereol. 2015;29(8):1545-54. doi: 10.1111/jdv.12921
13 Pedersen SA, Gaist D, Schmidt SAJ et al. Hydrochlorothiazide use and risk of nonmelanoma skin cancer: A nationwide case-control study from Denmark. J Am Acad Dermatol. 2018;78(4):673681.e9. doi: 10.1016/j.jaad.2017.11.042
14 Cooper SM and George S. Photosensitivity reaction associated with use of the combined oral contraceptive. Br J Dermatol. 2001;144(3):641-2. doi: 10.1046/j.1365-2133.2001.04111.x.
15 Moore DE. Drug-induced cutaneous photosensitivity: incidence, mechanism, prevention and management. Drug Saf. 2002;25(5):345-72. doi: 10.2165/00002018-200225050-00004.
16 American Academy of Dermatology Association. Artificial Nails: Dermatologists’ Tips for Reducing Nail Damage. https://www.aad.org/public/everyday-care/nail-caresecrets/basics/pedicures/reduce-artificial-nail-damage. Accessed August 7, 2024.
American Academy of Dermatology Association. Gel Manicures: Tips for Healthy Nails. https://www.aad.org/public/everyday-care/nail-care-secrets/basics/pedicures/gel-manicures. Accessed August 7, 2024.
NEW SPECIALTY MANAGES SKIN CONCERNS AND KEEPS PATIENTS ON THERAPY
by Mandi Murph, PhD, MBA, Director of Medical Education
Cancer treatment including and especially melanoma unfortunately, produces a risk of side effects impacting the feeling and vitality of the skin Changes in the skin’s appearance may cause affected patients to experience severe distress and quality of life issues.
For some, skin concerns could accompany a desire to discontinue their treatment
SA potential solution has emerged for the 75% of patients with cancer who experience dermatologic side effects [1] A new dermatology specialty – oncodermatology –supports patients with cancer who develop unique skin concerns. The specialty is sometimes abbreviated as “SOD” to emphasize the Supportive role of the OncoDermatologists [2]
The goal of oncodermatologists is to manage skin issues, allowing patients with cancer to continue treatment without interruption, dose modification, or discontinuation Oncodermatologists recognize they are not treating the tumor. Instead, by treating the individual’s skin, they are optimizing cancer treatment outcomes and quality-of-life preservation [3]
Treatment discontinuation and dose reduction due to skin concerns became a subject after the first targeted therapies to treat colorectal cancer were approved in 2009 A hallmark side effect of the drugs was a severe, acne-like rash covering the face and chest [4] Some patients’ feelings about their facial appearance caused avoidance of social activities and public-facing errands.
Since then, unwanted dermatologic drug side effects have grown into a massive clinical issue Between 2013 and 2022, there were over three million reports about undesirable drug side effects to the FDA. Included in this data were 10,698 reports of cancer drugs with skin concerns, especially frequent rash and dry skin [1] Immunotherapies and targeted therapies are two of the main causes of dermatologic side effects, and melanoma is treated primarily with immunotherapies and targeted therapies Oncodermatologists can be especially helpful to patients with melanoma who are undergoing treatment
Radiation therapy can also negatively affect skin. For patients who receive radiation therapy, 95% will be affected by acute radiation dermatitis, which causes blistering, peeling, reddening, and pain [5] Oncodermatologists may consult with patients about hygiene, moisturization, sun protection, topical aqueous creams, topical corticosteroids, dressings, and camouflage products.[5,6]
Thus far, supportive oncodermatology has decreased therapy discontinuation and improved outcomes in cancer centers Studies show that many practices with supportive oncodermatologists provided an appointment for consultation within the same day or the next day the patient reported symptoms [2] One institution showed that less than 15% of cases were recommended for drug discontinuation after consultation and treatment by oncodermatology [7] By allowing these patients to remain on therapy, their risk for cancer progression was diminished.
If you are experiencing skin-related side effects from your melanoma treatment, ask your oncologist if there is an oncodermatologist to which s/he can refer you
To learn more, read an interview with a practicing oncodermatologist on our affiliate site, AIM at Skin Cancer, called What is Oncodermatology? –Everything You Need to Know
References
1. Salah S, Kerob D, Laurent CP et al. EVALUATION OF ANTICANCER THERAPY- RELATED DERMATOLOGIC ADVERSE EVENTS: INSIGHTS FROM FDA’S FAERS DATASET. 2024;S0190-9622(24)02532-5. doi: 10.1016/j.jaad.2024.07.1456.
2. Freites-Martinez A, Apalla Z, Fattore D et al. Supportive oncodermatology practices in Europe and the USA. J Eur Acad Dermatol Venereol. 2024;38(5):e440-e443. doi: 10.1111/jdv.19679.
3. Dang T. What is Oncodermatology? – Everything You Need to Know. 2024. https://aimatskincancer.org/interviews-with-leadingdermatologists/what-is-oncodermatology-everything-you-need-to-know/. Accessed August 9, 2024.
4. Pinto C, Barone CA, Girolomoni G et al. Management of skin toxicity associated with cetuximab treatment in combination with chemotherapy or radiotherapy. Oncologist. 2011;16(2):228-38. doi: 10.1634/theoncologist.2010-0298.
5. Behroozian T, Goldshtein D, Wolf JR et al. MASCC clinical practice guidelines for the prevention and management of acute radiation dermatitis: part 1) systematic review. Lancet Oncol. 2023;58. doi: 10.1016/S1470-2045(23)00067-0
6. Girnita A, Bjerring P, Kauppi S et al. INDIVIDUAL ARTICLE: NECOM 3: A Practical Algorithm for the Management of Radiation Therapy-Related Acute Radiation Dermatitis. 2023;22(11): SF400354s3.
7. Betancourt NJ, Johnson AN, Clawson RC et al. Electronic consultation in supportive oncodermatology: a single center retrospective cohort. Derm Online J. 2024;30(1). doi: 10.5070/D330163303
sideeffect central Colitis
BY MANDI MURPH, PHD, MBA DIRECTOR OF MEDICAL EDUCATION
Side Effect Central is a new series of articles designed to help patients with melanoma and their caregivers understand the side effects that typically accompany melanoma treatments Our goal is to explain what side effects to expect during treatment and to encourage communication with your medical team about these side effects.
Side effects can range from mild to very serious, and doctors cannot predict who will suffer more side effects than others Serious side effects can cause patients to interrupt or discontinue treatment, so managing them is a critical piece of melanoma treatment.
What should patients know?
What is colitis?
Colitis is an inflammation of the gastrointestinal lining It is among the most common side effects observed in patients receiving immunotherapy or immune checkpoint inhibitors, especially CTLA-4 inhibitors, such as ipilumimab (Yervoy). In fact, 30-45% of patients receiving CTLA-4 inhibitors will experience some level of colitis Colitis is cited as a frequent reason for treatment interruption and discontinuation.
Inflammation in the gastrointestinal lining can cause bloating, cramping, diarrhea, and pain in the abdomen
Excessive watery diarrhea is a symptom of colitis (albeit not definitive, due to multiple other causes of diarrhea) that can indicate when a patient might be developing colitis. Moderate watery diarrhea, increasing to more than five loose bowel movements per day, usually arises five to ten weeks after immunotherapy begins, or after the second to third dose of immunotherapy.
Although colitis can be a serious and potentially life-threatening complication, most patients will not have colitis that develops into a more serious condition requiring immediate intervention Less than 11% of patients treated with single-agent ipilimumab or combination regimens containing ipilimumab will develop severe colitis. Infrequent but possible complications arising from serious colitis include bowel perforation, dehydration, hospitalization, sepsis, and shock Patients should promptly communicate with their health care team and seek treatment when observing any of the symptoms listed below.
Mild to moderate symptoms report to your health care team
Abdominal pain
An increase of 4-6 stools per day
Blood or mucus in stool
Serious symptoms—report to your health care team
An increase of 7 or more stools per day
Decreased appetite
Fever
Rapid change in gastrointestinal function
Severe cramping and persistent abdominal pain
Call 911
Shock, distress, abnormal or unstable blood pressure
Why does colitis occur?
Immunotherapy is designed to supercharge the immune system. Unfortunately, the gastrointestinal tract can become susceptible to an immune system-provoked injury as an unintended consequence Although immunotherapy is created with targeted properties aimed at the tumor’s environment, sometimes it non-specifically activates too much of the immune system throughout the body
Nearly every organ system in the body is at risk for an unprovoked injury by CTLA-4 inhibitors. However, immunotherapy works so well in many patients that the risk of side effects is deemed worthwhile to achieve the possible results Prompt and thorough communication about side effects by patients with their medical team allows for appropriate clinical support, and these two together allow immunotherapy to be used safely and successfully in many patients Individual perspectives about treatment ideals should be discussed with your clinician
What can a clinician do for colitis?
Rapid identification and treatment can reduce the risk of progression from mild colitis Management can avoid drug interruption or discontinuation and allow a patient to remain on therapy. Once a definitive diagnosis is made, supportive hydration, along with drugs such as loperamide, diphenoxylate/atropine, or a slow steroid taper may be given. Severe colitis may require intravenous steroids, such as budesonide, infliximab, or vedolizumab
Bottom line: Patients should communicate regularly with their medical team about any of the signs of colitis noted above. Clinicians can then manage and treat the colitis in order to allow patient to remain on immunotherapy or resume treatment as quickly as possible.
References:
Frey C and Etminan M. Adverse Events of PD-1, PD-L1, CTLA-4, and LAG-3 Immune Checkpoint Inhibitors: An Analysis of the FDA Adverse Events Database. Antibodies (Basel). 2024;13(3):59. doi: 10.3390/antib13030059.
Ho C and Samlowski W. Outcome of an Accelerated Treatment Algorithm for Patients Developing Diarrhea as a Complication of Ipilimumab-Based Cancer Immunotherapy in a Community Practice. Curr Oncol. 2024;31(6):3529-3545. doi: 10.3390/curroncol31060260.
Machado AP, Shaikh AS, Saji A et al. Outcomes of Budesonide as a Treatment Option for Immune Checkpoint Inhibitor-Related Colitis in Patients with Cancer. Cancers (Basel). 2024;16(10):1919. doi: 10.3390/cancers16101919.
Oliveira C, Mainoli B, Duarte GS et al. Immune related serious adverse events with immune checkpoint inhibitors: Systematic review and network meta analysis. Eur J Clin Pharmacol. 2024;80(5):677-684. doi: 10.1007/s00228-024-03647-z.
TIMESHAVECHANGEDFOR MELANOMASURVIVAL
SURVIVAL TIMES AFTER A MELANOMA DIAGNOSIS HAVE PLATEAUED— WHICH IS A GOOD THING. READ ON FOR WHY.
A Dutch study suggests that patients with advanced melanoma survive longer than their predecessors and achieve outcomes thought to occur only in clinical trials According to the study, patients in the Netherlands who respond to immune checkpoint inhibitors will likely achieve long-term survival.
When researchers graphed the patient populations’ outcomes over time, their survival curves leveled off in a straight line, reaching a plateau. A plateau means that the remaining patients are surviving longterm The plateau is good because if the patients’ outcomes continued to decline over time, a steep downward slope or curve would appear In addition, the period where the plateau was observed was between three and five years after treatment for advanced melanoma.
When the researchers looked at melanoma-only survival, which eliminated other cause-of-death factors, the plateau was much straighter for longer. The straight trend line was surprising and wonderful to see on the graph It suggests that if patients with melanoma pass away three to five years after diagnosis, many reasons are unrelated to the cancer.
A steep decline in survival after diagnosis is the kind of data that researchers used to see. Historically, a patient diagnosed with advanced melanoma had a median overall survival time of less than one year. Only 10% of patients would survive five years after diagnosis in the past. Times have changed.
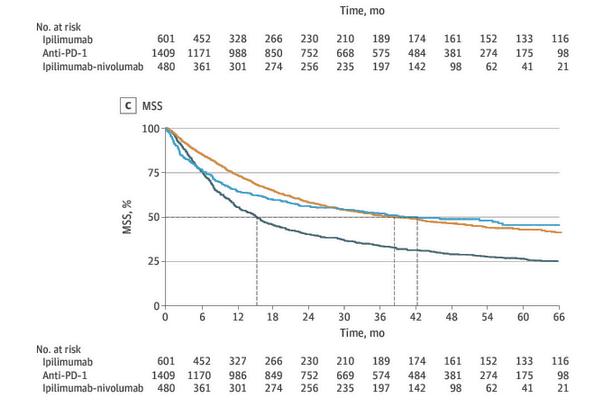
Using 2490 patients included in the Dutch Melanoma Treatment Registry, the 2-year overall survival rate was 50 9%, the 3-year was 44.0%, and the 5-year was 35.9%. Looking into the data further, the researchers noticed that the survival outcomes also depended on the type of immune checkpoint inhibitor therapy the patients received. Not all treatments extend survival for the same amount of time.
For example, patients treated with ipilimumab (Yervoy) alone (601 patients fell in this category, which is expressed as n=601) had an average 5-year survival rate of 24.9%. In other words, approximately ¼ of patients survive five years after diagnosis.
In contrast, patients who received an anti-PD-1 immune checkpoint inhibitor (n=1409) had an average 5-year survival rate of 39.1%. (The specific anti-PD-1 therapy was not provided in the methods of the study, but the drugs that are approved for melanoma as anti-PD-1 immune checkpoint inhibitors are nivolumab [Opdivo] and pembrolizumab [Keytruda], so it would be one of those.) However, if patients received both ipilimumab (Yervoy) and nivolumab (Opdivo) in combination (n=480), the rate of 5-year survival increased to the highest percentage, 41 2%
These survival achievements were unfathomable before 2011 when ipilimumab was approved, which ushered in a new era of immune checkpoint inhibitors In addition, 43 7% of the patients had metastases to more than three organ sites, demonstrating the researchers did not select only the healthiest patients for the study Doing that would likely make the results look far better
When researchers compared these results to patients in clinical trials, they observed that the survival percentages in this study were actually higher. This is more good news because it suggests that current treatment protocols achieve very positive outcomes no matter where they are administered
Outcomes for melanoma are unrelated to whether or not a patient was treated as part of an academic clinical trial Oftentimes, there is a perceived bias that patients in clinical trials receive better care with experimental therapy, versus a clinical practice setting using approved standardof-care This study proves otherwise
Lastly, the study showed that there may be some early signs that the initial therapeutic response hints at survival outcomes for patients with melanoma. Among patients who developed a complete response during their first-line treatment with an immune checkpoint inhibitor, more than 90% survived more than three years, suggesting that the response to treatment lasts for an extended period of time.
All this comes as more good news to patients, caregivers, and survivors.
turnhopeintoACTION
At AIM at Melanoma, we believe in the strength and resilience of our community. Whether you’re a patient, caregiver, or advocate, your journey is filled with hope, knowledge, and the power to make a difference.
YourSupportMatters!
Your gift funds lifesaving research and provides vital information and support to those affected by melanoma. Whether you choose to make a one-time donation, set up a recurring contribution, or honor a loved one with a special gift, your generositycansavelives.
Stay Informed: Access the latest research and treatment options. Connect: Join a community that understands and supports you. Advocate: Help raise awareness and drive change for better
IN PLAIN ENGLISH
RECAP AND BACKGROUND ON TUMOR VACCINES
We last visited the topic of vaccines in September of 2021, and in the three years since then, remarkable progress has been made in the field of cancer immunotherapy, including the development and testing of vaccines that now have great promise in the treatment of cancer. Most cancer prevention vaccines, meanwhile, remain “not ready for prime time.”
At the time of the last review, much of the article was about general principles of vaccine biology, technical aspects of vaccine preparation, and medical applications of a small number of strategies that could be considered tumor vaccines but are highly complex. For example, an immune cell-based vaccine against prostate cancer, sipuleucel-T (Provenge), is produced by exposing patient dendritic cells (a type of white blood cell) to a protein made from attaching a tumor-nonspecific antigen, prostatic acid phosphatase (PAP), to a growth- and immuneenhancing protein, granulocyte-monocyte colony stimulating factor (GM-CSF). When a bag of these cells is infused back into the patient’s vein, a modest immune response against prostate cancer can be detected among the T-lymphocytes—the immune cells that seek to detect and destroy cancer cells. These patients live longer and experience a delay in symptoms related to advanced prostate cancer than those who do not receive this treatment.¹
Many other attempts (with little success) have been made to use this form of tumor vaccine against cancer—taking advantage of the fact that dendritic cells are considered mother nature’s most potent antigenpresenting cells (cells that are required for the body to take up and process foreign invaders like infectious organisms and malignant cells) and are key players in the activation of T cells to perform immune-based killing. Our tissues are simply too efficient at controlling overactive immune responses after they’ve protected us—and thus, we often don’t control necessary immune responses against cancer. Tumor cells have also evolved—exactly as described by Darwin—to escape immunemediated killing by producing factors that are immunosuppressive, causing the T cell response to be ineffective in multiple ways.
Another complex approach to tumor vaccine that has enjoyed greater application and is pertinent to melanoma (detailed in both the intratumoral therapies and vaccines episodes of In Plain English) is the herpes simplex virus-based TVEC (Imlygic). This vaccine consists of a genetically engineered form of herpes simplex (the virus that causes cold sores) as well as the gene for GM-CSF, the same immunestimulating drug mentioned above. (It does not cause a herpes infection.) When injected directly into tumor metastases, TVEC delivers its DNA to tumor cells, which take up the genes and produce GM-CSF in the region of the tumor, thus immunizing the patient against tumor antigens by drawing immune cells into the area.
While the success of this approach is limited to relatively small, easilyinjectable tumors, it is capable of causing regression even at distant, uninjected metastases. Newer vaccines intended for similar direct injection with different engineered genes are being tested both alone and in combination with some of our other highly-active immunotherapy drugs such as nivolumab (Opdivo) or pembrolizumab (Keytruda) and appear very promising in melanoma.
These types of vaccines are called “oncolytic virotherapy” for their ability to cause direct destruction of the injected tumor as a way of introducing tumor antigens to immune cells.²
Introduction to the role of mutated DNA as a basis for tumor vaccine
Possibly the most exciting strategy in the field of tumor vaccine development for advanced cancer has emerged over the last three years and arose out of remarkable success and speed in the development of vaccines against the Covid-19 virus starting in 2020. The company that first announced success in this area—a German company called BioNtech, under the wife-husband research team of the Turkish scientists Ozlem Tureci and Ugur Sahin— had originally been working on a vaccine against cancer but turned those efforts and applied the technology to Covid19 to address the ravages of the worldwide viral pandemic.
From these studies emerged the concept of a tumor mutation burden (TMB), which is a measure of how many abnormal sequences, or mutations, are detected in a specific amount of tumor DNA when compared with the normal tissue of the relevant organ. And from that concept came a remarkable finding: Generally (but not in all tumor types), the higher the tumor mutation burden, the more likely the cancer will respond to immunotherapy. A threshold of about 10 or more mutations among every 1000 of the basic units in DNA has been used to distinguish high from low tumor mutation burden. Melanoma, which almost always features a significant amount of sun-induced DNA damage, usually has a TMB well over 10, except when it arises, in rare cases, from the internal membranes (mucosal melanoma) or the pigmented tissues of the eye (uveal melanoma), which have little to no sun exposure and very few mutations.
In the case of tumors with very low TMB, a potent antitumor immune response may still occur—instead of a large number of mutations adding up to make an adequate immune response, a single strong antigenic stimulus can occur in a few cancers that are known to be caused by viruses.
For example, head and neck cancer and cervical cancer are often caused by a virus called HPV, and the rare skin cancer Merkel cell carcinoma is frequently due to a related virus, the Merkel cell polyoma virus. Virus antigens are more potently recognized by our immune system, in part because they are more threatening to our health, and in part because the immune system has not been exposed to those antigens over a long period and become tolerant to their presence.
How is a tumor neo-antigen vaccine produced and tested?
The field of sequencing and analyzing the mutations in tumor genetic material has grown tremendously with the advent of high-throughput machines and informatics, including machine learning and artificial intelligence applications. These developments have allowed researchers to discover and select the most immunogenic protein fragments used in neo-antigen vaccines and to produce vaccines from the messenger RNA (mRNA is the genetic material based on DNA sequences that provides the pattern for the sequence of all of our body’s proteins). It is relatively easy to produce specific mRNA sequences in the laboratory and to tag these mRNAs with various substances that provide functions such as the uptake of these mRNAs into tumor cells.
Immunologic intelligence is critical here, as there are many checks and balances in the immune response; thus, not only is it important to select the best sequences but it is also necessary to know which ones might compete or even cause immune suppression or exhaustion of immune cells due to overly strong responses to antigens delivered repetitively into the patient.
The strategy taken by the current developers of tumor neo-antigenbased vaccines is to select the best antigenic sequences predictive of an immune response (these predictions are done with AI, and the current protocol is based on the selection of 34 such sequences). The synthetic mRNA is then wrapped in a lipid nanoparticle (a tiny ball of mRNA wrapped up inside of a layer of a fatty substance that facilitates its uptake into antigen-presenting cells as detailed earlier in this issue). There, the mRNA performs its usual function of encoding protein or protein fragments that are then utilized by immune cells to elaborate an immune response and immunize the patient against tumor antigens.
To date, the mRNA/lipid nanoparticle approach has been limited to investigation in the adjuvant setting, where tumor has been removed surgically but based on its stage has a high risk of relapse. Relapses come from the growth of tiny particles of tumor, sometimes only one or a few cells, that escaped from the primary tumor prior to its surgical removal. This is the stage at which most animal experiments have shown the greatest likelihood that a tumor vaccine will work to reduce the chance of relapse and, hopefully, prolong survival. Further, it is likely that the combination of vaccine with our other most powerful immunotherapy, the immune checkpoint blocking antibodies (such as nivolumab or pembrolizumab) will provide a higher likelihood of benefit.
This possibility has already been tested in a randomized study of patients with resected melanoma at high risk of relapse, in which 2/3 or approximately 100 patients received the standard adjuvant immunotherapy (pembrolizumab for one year following surgery) and the remaining patients (just under 50) also received a vaccine based on their own tumor’s neo-antigens, based on the mutations found in the DNA sequences of tissue removed at the time of surgery. Early analysis of this study, which enrolled about 135 patients, has shown a large benefit for the combination, and a confirmatory study is expected to provide sufficient data in a larger number of patients to support approval by the FDA of this vaccine combination for patients with resected melanoma at high risk of relapse.³
IN MEMORIAM
It is largely through the efforts of Dr. Jeffrey Weber and his colleagues that this study and many prior research projects focused on developing melanoma vaccines were possible. We would like to dedicate this issue to and acknowledge the lifelong efforts of Dr. Weber, who devoted his research career to cancer immunotherapy and the development of effective vaccines against melanoma and other cancers. Dr. Weber recently succumbed to pancreatic cancer, a disease for which immunotherapy has failed to move the needle but for which enormous efforts continue, to achieve effective treatment for this devastating malignancy. We thank Dr. Weber and recognize his life’s work on behalf of patients with melanoma and others in the development of highly effective cancer immunotherapy.
References
1. Pre-existing immune status associated with response to combination of sipuleucel-T and ipilimumab in patients with metastatic castration-resistant prostate cancer. Sinha M, Zhang L, Subudhi S, Chen B, Marquez J, Liu EV, Allaire K, Cheung A, Ng S, Nguyen C, Friedlander TW, Aggarwal R, Spitzer M, Allison JP, Small EJ, Sharma P, Fong L.J Immunother Cancer. 2021 May;9(5):e002254. doi: 10.1136/jitc-2020-002254.PMID: 33986125
2. Intratumoral Immunotherapy: Is It Ready for Prime Time? Ghosn M, Tselikas L, Champiat S, Deschamps F, Bonnet B, Carre É, Testan M, Danlos FX, Farhane S, Susini S, Suzzoni S, Ammari S, Marabelle A, De Baere T.Curr Oncol Rep. 2023 Aug;25(8):857-867. doi: 10.1007/s11912-023-01422-4. Epub 2023 May 2.PMID: 37129706 Review.
3. Individualised neoantigen therapy mRNA-4157 (V940) plus pembrolizumab versus pembrolizumab monotherapy in resected melanoma (KEYNOTE-942): a randomised, phase 2b study. Weber JS, Carlino MS, Khattak A, Meniawy T, Ansstas G, Taylor MH, Kim KB, McKean M, Long GV, Sullivan RJ, Faries M, Tran TT, Cowey CL, Pecora A, Shaheen M, Segar J, Medina T, Atkinson V, Gibney GT, Luke JJ, Thomas S, Buchbinder EI, Healy JA, Huang M, Morrissey M, Feldman I, Sehgal V, Robert-Tissot C, Hou P, Zhu L, Brown M, Aanur P, Meehan RS, Zaks T.Lancet. 2024 Feb 17;403(10427):632-644. doi: 10.1016/S0140-6736(23)02268-7. Epub 2024 Jan 18