Free Education from the Education Universe and the ACG Annual Scientific Meeting that keeps you current on treatment, therapy and management of key GI conditions and disorders
Free subscriptions to The American Journal of Gastroenterology, Clinical and Translational Gastroenterology, EvidenceBased GI: An ACG Publication and the unique ACG Case Reports Journal
Practice management tools that help you improve efficiency and increase profitability in your practice
Prior Authorization Letter Generator gives members access to custom letters with relevant data and research that payors are requesting
Leadership Training offers members Leadership YOU a weekend that brings together a community of established and emerging leaders to cultivate core competencies that drive effectiveness and impact
FEATURED CONTENTS
TRAINEE HUB
Guidance from the Mayo Clinic on implementing upstander training for GI fellows to support colleagues and patients
PAGE 17
KINDNESS-INFLUENCED TRUST AND HEALING IN HEALTH CARE
GETTING IT RIGHT
What gastroenterologists should know about the evolving "gray market" landscape for drugs and supplements and its regulation by the FDA
Leonard Berry, PhD, MBA, on the dimensions of kindness and their importance in medicine, from the Emily Couric Memorial Lecture at ACG 2024 in Philadelphia. PAGE 25
PAGE 21
PHOENIX, ARIZONA | OCTOBER 24–29, 2025
CONTENTS
“When you combine kindness-influenced trust with competence-influenced trust, it has stronger effects on healing.”
—Leonard L. Berry, PhD, MBA, "Kindness-Influenced
6
//
MESSAGE FROM THE PRESIDENT
Dr. Amy Oxentenko on the new Workforce of the Future Task Force to address workforce challenges and take a proactive approach
7
//
NOVEL & NOTEWORTHY
Recent member accomplishments and awards, a recap from ACG 2024 in Philadelphia, the new ACG Strategic Plan & more
8
// GI EYE
Dr. Galen Leung shares a snapshot of a thermal spring at Yellowstone National Park
17 // TRAINEE HUB
Guidance on implementing upstander training for GI fellows from the Mayo Clinic
21 // GETTING IT RIGHT
Navigating the "gray market" landscape for drugs and supplements
25
//
COVER STORY
KINDNESS-INFLUENCED TRUST AND HEALING IN HEALTH CARE
Dr. Leonard Berry on the dimensions of kindness and their importance in medicine
29 // ACG PERSPECTIVES
29 CULINARY CONNECTIONS
Members of the ACG staff share their recipes, stories of family, and spirit of collaboration
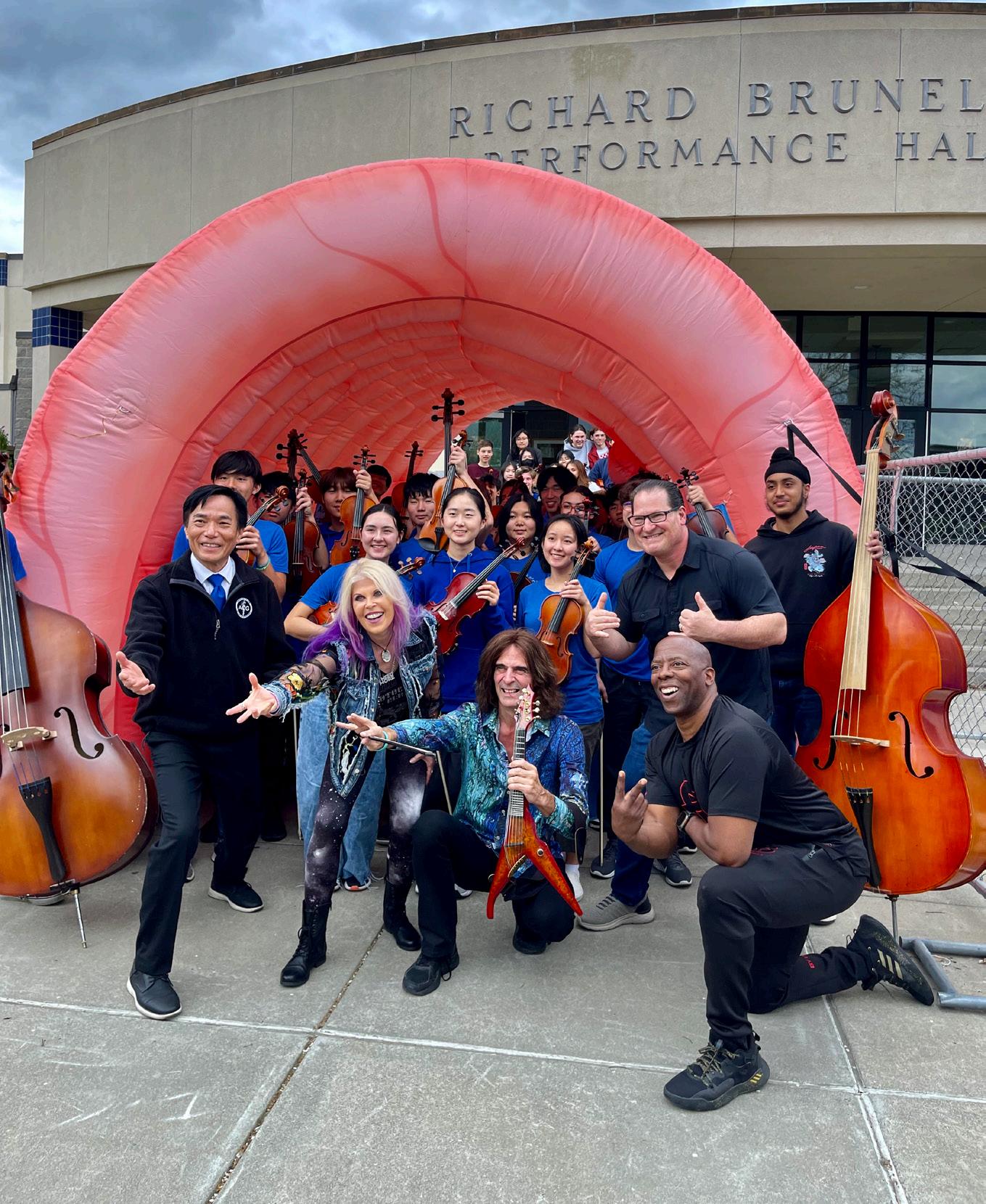
33 BRIDGING MEDICINE AND MUSIC
Dr. Ronald Hsu advances CRC awareness through the power of music
35 NORTH AMERICAN GI TRAINING GRANT
Dr. Partha Pal shares his experience training in advanced endoscopy at Allegheny Health Network
37 PATIENT PERSPECTIVE
A GI patient offers her colonoscopy experience to highlight how trauma-informed care made a difference
39 // INSIDE THE JOURNALS
40 AJG
A new ACG Guideline and podcast on H. pylori Infection by Chey, et al., & Natural History of Indeterminate Liver Nodules in Patients with Advanced Liver Disease by Singal, et al
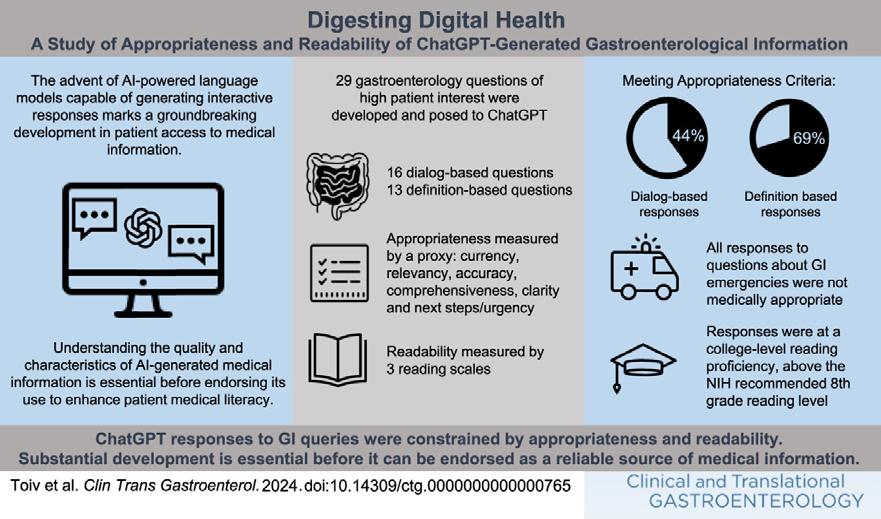
40 CTG
Digesting Digital Health: A Study of Appropriateness and Readability of ChatGPT-Generated Gastroenterological Information by Toiv, et al
40 ACGCRJ
Introducing the 2024-2025 ACGCRJ Editorial Board and a case by Hussain, et al., with an accompanying podcast
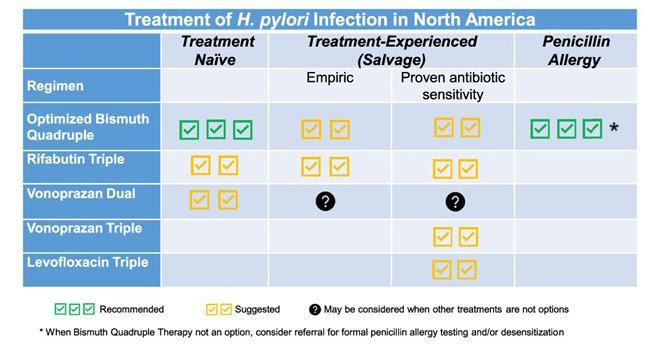
42 ACG GUIDELINE HIGHLIGHTS: HELICOBACTER PYLORI
A visual summary of ACG's 2024 Clinical Guideline on H. pylori by Chey, et al
44 // REACHING THE CECUM
PATIENT HANDOUT: FOCAL LIVER LESIONS
Information for patients to understand growths found on the liver during imaging
ACG MAGAZINE
MAGAZINE STAFF
Executive Director Bradley C. Stillman, JD
Editor in Chief; Vice President, Communications Anne-Louise B. Oliphant
Senior Manager, Communications Becky Abel
Art Director Emily Garel
Senior Graphic Designer Antonella Iseas
BOARD OF TRUSTEES
President: Amy S. Oxentenko, MD, FACG
President-Elect: William D. Chey, MD, FACG
Vice President: Costas H. Kefalas, MD, MMM, FACG
Secretary: Neil H. Stollman, MD, FACG
Treasurer: Nicholas J. Shaheen, MD, MPH, MACG
Immediate Past President: Jonathan A. Leighton, MD, FACG
Past President: Daniel J. Pambianco, MD, FACG
Director, ACG Institute: Neena S. Abraham, MD, MSc, MACG
Co-Editors, The American Journal of Gastroenterology:
Jasmohan S. Bajaj, MD, MS, FACG
Millie D. Long, MD, MPH, FACG
Chair, Board of Governors: Sita S. Chokhavatia, MD, MACG
Vice Chair, Board of Governors: Harish K. Gagneja, MD, MACG
Trustee for Administrative Affairs: Irving M. Pike, MD, FACG
TRUSTEES
Brooks D. Cash, MD, FACG
Dayna S. Early, MD, FACG
Jill K. J. Gaidos, MD, FACG
Seth A. Gross, MD, FACG
David J. Hass, MD, FACG
James C. Hobley, MD, MSc, FACG
Vonda G. Reeves, MD, MBA, FACG
Aasma Shaukat, MD, MPH, FACG
Jay N. Yepuri, MD, MS, FACG
Patrick E. Young, MD, FACG
CONNECT WITH ACG
youtube.com/ACGastroenterology
facebook.com/AmCollegeGastro
x.com/amcollegegastro
@amcollegegastro.bsky.social
bit.ly/ACG-Linked-In
CONTACT
IDEAS & FEEDBACK
We'd love to hear from you. Send us your ideas, stories and comments. ACGMag@gi.org
CONTACT ACG
American College of Gastroenterology 11333 Woodglen Drive, Suite 100 North Bethesda, MD 20852 (301) 263-9000 | gi.org
DIGITAL EDITIONS
GI.ORG/ACGMAGAZINE
American College of Gastroenterology is an organization with an international membership of over 19,000 individuals from 86 countries. The College's vision is to be the preeminent organization supporting health care professionals who provide compassionate, equitable, high-quality, state-of-the-art, and personalized care to promote digestive health. The mission of the College is to provide tools, services, and accelerate advances in patient care, education, research, advocacy, practice management, professional development and clinician wellness, enabling our members to improve patients’ digestive health and to build personally fulfilling careers that foster wellbeing, meaning and purpose.
CONTRIBUTING WRITERS
George Abdelsayed, MD, FACG
Dr. Abdelsayed is Associate Professor of Medicine at Robert Wood Johnson Medical School, Director of Ambulatory Hepatology, and Chief Quality Officer at Rutgers Health. He is a past member of the ACG FDA Related Matters Committee.
Becky Abel, M.Ed.
Becky is ACG’s Senior Communications Manager and has been with the College since 2019. Prior to joining ACG, she was a communications contractor for NIDDK and the NIH Office of Research on Women’s Health. To fuel her creativity, she enjoys cooking, crafting, listening to podcasts, and doting on her cats.
Leonard L. Berry, PhD, MBA
Dr. Berry is the University Distinguished Professor of Marketing and Regents Professor, M.B. Zale Chair in Retailing and Marketing Leadership, Presidential Professor for Teaching Excellence at the Texas A&M University Mays Business School, and Senior Fellow, Institute for Healthcare Improvement.
Khushboo Gala, MBBS
Dr. Gala is an Advanced Endoscopy Fellow and prior Chief GI Fellow at Mayo Clinic Rochester. She served as co-Editor-in-Chief of ACG Case Reports Journal from 2023-2024.
Emily Garel
Emily is ACG’s Art Director and has been crafting exceptional designs for the College since 2015. In addition to her many creative endeavors, she also enjoys climbing, playing Dungeons & Dragons, and cuddling her hairless cats.
Ronald K. Hsu, MD, FACG
Dr. Hsu is Clinical Professor of Medicine at UC Davis and currently serves as ACG Governor for Northern California and on several ACG committees.
Neen LeMaster
Neen is the Assistant Managing Editor of ACG Scholarly Publications. Their culinary curiosity led them to prior stints as a cheesemonger and confectioner, and currently fuels them as they work on a project to hike in all 50 U.S. states.
Galen Leung, MD
Dr. Leung is Assistant Professor of Clinical Medicine at the Perelman School of Medicine at the University of Pennsylvania. He is a member of the ACG Educational Affairs and Research Committees, as well as the ACG Institute Early Career Leadership Program 2023-2024 cohort.
Trisha M.
Trisha is a writer and GI patient who reached out to the College to share her colonoscopy experience anonymously, aiming to highlight trauma-informed care.
Anne-Louise Bateman Oliphant, MPP
Anne-Louise is ACG's Vice President of Communications. A member of the College’s staff since 1995, she has been Editor-in-Chief of ACG MAGAZINE since its inception in 2017. An artist and painter, Anne-Louise also enjoys expressing her creativity in the kitchen using colorful ingredients.
Amy S. Oxentenko, MD, FACG
ACG President Dr. Amy Oxentenko is Professor of Medicine at Mayo Clinic in Rochester, MN, and is the Vice Dean of Mayo Clinic Practice. Her clinical interests include proximal bowel luminal diseases.
Partha Pal, MD, DNB, FASGE, MRCP (UK)
Dr. Pal is a Consultant Gastroenterologist at the Asian Institute of Gastroenterology in Hyderabad, India. He is the recipient of a 2023 ACG International Training Grant and trained at Allegheny Health Network in Pittsburgh, PA.
Douglas A. Simonetto, MD
Dr. Simonetto is GI Program Director and Associate Professor of Medicine at Mayo Clinic Rochester.
Madhu Mathew Vennikandam, MD
Dr. Vennikandam is an attending physician at Northwestern Medicine and a member of the ACG FDA Related Matters Committee.
Elida Voth, MD
Dr. Voth is a GI and hepatology fellow at Mayo Clinic Rochester.
Xiao Jing “Iris” Wang, MD
Dr. Wang is Associate GI Program Director and Assistant Professor at Mayo Clinic Rochester. She currently serves on ACG’s Educational Affairs and Training Committees.
ENVISIONING THE GI WORKFORCE OF THE FUTURE
Amy S. Oxentenko, MD, FACG
REFLECTING ON THE 2024 ACG ANNUAL SCIENTIFIC MEETING in Philadelphia, one word captures the atmosphere perfectly: ‘alive!’ In the past four years, we have navigated numerous post-pandemic changes. However, this year stood out with record attendance, remarkable clinical advances, and a palpable passion for innovation.
While it might be tempting to rest on our laurels, now is the time to lean in and plan for the future. Significant workforce challenges impact daily practices. This was evident in our member survey fielded last fall, Board of Governors’ meetings, and conversations with colleagues nationwide, regardless of practice type, size, or location. Challenges include staffing shortages, retention difficulties, reduced full-time equivalents due to burnout, and an exodus from medicine. Additionally, reliance on external specialties for anesthetizing procedures has strained our capabilities. Staffing shortfalls across all roles have impacted practice efficiency and patient care availability. While optimizing the current workforce is crucial, we must plant the seeds of transformation to build the workforce of the future.
Addressing the workforce of the future in gastroenterology involves embracing technological advancements, fostering continuous education, and promoting a diverse, inclusive, and flexible work environment. By integrating innovative technologies such as artificial intelligence, robotics, and telemedicine, the field of gastroenterology can enhance diagnostic accuracy, streamline procedures, and improve patient outcomes. This proactive approach not only keeps the field at the forefront of medical innovation but also ensures that care teams are well-equipped to oversee the evolving landscape of healthcare.
To tackle these challenges, we are forming a Workforce of the Future Task Force, divided into three workgroups. Each workgroup will focus on three domains: Recruit, Train, and Retain. By addressing these areas, we aim to optimize the current workforce and transform it for the future.
“Addressing the workforce of the future in gastroenterology involves embracing technological advancements, fostering continuous education, and promoting a diverse, inclusive, and flexible work environment.”
The first workgroup, led by Dr. Neil Stollman, will address physician workforce needs, exploring questions like: How many gastroenterologists should we train annually? Should training duration change? What role does locum tenens play? What are the actual needs and locations of those needs? How can we reengage those who left the workforce? What will future GI patient care look like? How do we incorporate new training modalities in an era of automation and artificial intelligence?
The second workgroup, led by Dr. Dayna Early, will focus on anesthesia support for endoscopic procedures, addressing questions like: Do we have sufficient guidance on appropriate sedation? Is propofol overused? Are we adequately training in conscious sedation during GI fellowship? If future needs require more propofol-based sedation, can GI ensure safe administration? How should our training paradigms evolve to meet changing anesthetic needs?
The third workgroup, led by Dr. Tauseef Ali, will examine other essential roles within the GI care team, including endoscopy technicians, nursing support, and advanced practice providers. They will explore questions like: How do we attract more individuals to these roles? How can we offer career advancement opportunities to reduce turnover? Do care team members have the necessary skills for what they are asked to do? What role can our society play in advancing the entire care team through skill acquisition, advancement, and automation?
Investing in the training and professional development of those within the field of gastroenterology is crucial. Encouraging lifelong learning and providing opportunities for skill enhancement will help all care team members to stay updated with the latest research, techniques, and best practices. Additionally, promoting diversity and inclusion within the workforce can lead to a more holistic understanding of patient needs and foster a collaborative environment where different perspectives drive innovation. By addressing these key areas, gastroenterology can remain ahead of its time, delivering superior care and adapting to future challenges with agility and expertise.
Now we must get to work! BOOM!
—Amy
Note wor thy Note wor thy
NOVEL & NOTEWORTHY TEEMS WITH CONGRATULATIONS!
Kudos to those recognized with ACG’s highest honors in 2024: Irving M. Pike, MD, MACG (Samuel S. Weiss Award) and Mark B. Pochapin, MD, FACG (Berk/Fise Clinical Achievement Award). Congratulations to the ACG 2024 GI Jeopardy winners, Chelsea M. Forbes, MD, and Robert E. Spiller, DO, from the National Capital Consortium/Walter Reed National Military Medical Center.
N&N also honors winners of ACG’s Tenth Annual SCOPY Awards, Social Media Acumen Awards, the Healio-ACG Clinical Innovation Award, as well as the 2024 Sherman Prize winners.
For more College honors and a special “year in review” summary, follow the link to explore the 2023-2024 Awards & Leadership Booklet: bit.ly/ acg-2024-awards-leadership.
GROUNDED REFLECTION SAPPHIRE POOL AT BISCUIT BASIN IN YELLOWSTONE NATIONAL PARK
Galen Leung, MD
The Sapphire Pool at Biscuit Basin in Yellowstone National Park is a stunningly clear, blue thermal spring, and one of the many breathtaking natural wonders that the park offers. Yellowstone’s vast landscape is not only filled with vibrant geothermal features but is also home to a diverse array of iconic wildlife.
Equipment:
Sony Alpha 7C Full-Frame Mirrorless Camera
Sony FE 24-105mm F4 G OSS Standard Zoom Lens
Captured at: 25mm, F/11, 1/30th second, ISO 3200
Post-processed in Adobe Photoshop
What captured my attention:
Every day as a doctor, I bear witness to human perseverance, hope, and often, the unexpected beauty that emerges from disaster. A couple of years ago, after completing my final fellowship, I took a trip with my father to Yellowstone National Park. I wandered through the park's vast landscapes, camera hanging from my neck, determined to capture the perfect shot. After passing by many awe-inspiring sights, one in particular held my attention: the Yellowstone Sapphire Pool. It wasn’t just the pool’s striking beauty that captivated me—after all, the entire day had been filled with remarkable scenes.
What truly drew me in was the story that I learned about this vibrant thermal pool. The Sapphire Pool was not always the place of serenity that I saw when I visited. Historically, it was an active geyser and, at another point, would erupt scorching mud. Now the hot spring’s peaceful environment is maintained by a balanced circulation of deeper hot water that is cooled by surface temperature.
It was this perfect equilibrium between opposing forces—heat and cold, chaos and calm—that had transformed the once turbulent geyser into a place of serene beauty, a reminder that true transformation often comes from finding harmony in change. To me, the Sapphire Pool is nature’s little way of teaching perseverance and how beauty often emerges not from stillness, but from the dance between turmoil and tranquility – reminding us that even in the heart of chaos, grace can be found.
Technical Challenges
This trip was full of unexpected challenges. A few days earlier, I had accidentally dropped my mirrorless camera into the lake at Schwabacher Landing in Grand Teton National Park and had to rent a replacement from a nearby shop as I was determined to capture the perfect shot of Yellowstone’s golden sunset. That evening, I found myself trudging through a mosquito-infested field filled with bison dung, my focus locked on the sun hovering just above the horizon. After too many shots that didn’t feel quite right, I realized I was so obsessed with the idea of a perfect picture that I had missed the beauty right in front of me. It was my dad who called me back, pointing out a visitor-friendly hot spring with the ideal view – a place I had completely overlooked in my narrow pursuit of perfection.
Personal Significance of Photography
Through photography, moments, feelings, and perspectives become immortal – point and click, and a memory is transformed into light, frozen in time. That’s what first drew me to photography; it was a way to capture life’s fleeting moments, a simple yet profound act of preservation. However, as I delved deeper into the craft, I discovered that photographs do more than just hold memories still. They reveal how I see the world, how I feel it. Photography, for me, has become an autobiographical lens – a way to shape and relive memories not just as they were, but as I experienced them
If I recall a dark-blue night as vivid and full of life, photography lets me recreate that vibrant energy by layering exposures, drawing out the hidden spectrum of light and color that filled the air. If a person or object stands out in my memory, sharp and
distinct, the aperture function allows me to bring it into focus, blurring the rest – capturing my exact perspective at that time. Photography allows me not just to freeze a moment, but to unveil the vision behind it – to give shape to the story my memory holds.
About
Galen Leung, MD, is Assistant Professor of Clinical Medicine at the Perelman School of Medicine at the University of Pennsylvania. He is a member of the ACG Educational Affairs Committee, the ACG Research Committee, and the ACG Institute Early Career Leadership Program 2023-2024 cohort.
[ACG 2024 HIGHLIGHTS]
ACG AWARDS & LEADERSHIP BOOKLET
Explore all the 2024 award winners in this annual compendium that includes the “Year in Review,” featured lecturers, College committee updates, news from the journals, and College achievements.
READ: bit.ly/acg-2024-awards-leadership
SCOPY AWARDS
An impressive group of 26 winners were honored with ACG’s Service Award for Colorectal Cancer Outreach, Prevention & Year-round Excellence. The SCOPY Awards recognize community education and public awareness efforts to advance colorectal cancer screening and prevention by ACG members and their staffs. See all 2024 winners: bit.ly/scopy-awards-24
GI JEOPARDY
The smart, strategic, and stalwart team of Chelsea M. Forbes, MD, and Robert E. Spiller, DO, from the National Capital Consortium/Walter Reed National Military Medical Center in Bethesda, MD, won the 2024 GI Jeopardy trophy! Dr. Spiller of the United States Army joined forces with Dr. Forbes of the United States Navy to emerge as champions of land and sea after an intense live competition at ACG 2024. Congratulations!
[DISRUPTORS]
HEALIO DISRUPTIVE INNOVATORS AWARDS at ACG 2024 –Now in its seventh year, the Healio Disruptive Innovators Awards celebrate the achievements of exemplary leaders in gastroenterology and hepatology. Winners were selected by readers of Healio Gastroenterology who cast more than 3,000 votes to decide who was truly disrupting the field among an impressive list of nominees. The ceremony is held each year in conjunction with the ACG Annual Scientific Meeting. The College and Healio together sponsor the Clinical Innovation Award, which this year went to Lin Chang, MD, FACG, of UCLA.
[#DIVERSITYINGI
PHILLY FUN RUNS]
Early bird runners gathered as champions of #DiversityinGI in Philadelphia during ACG 2024. Dedicated co-leaders rallied the groups and led the charge up the Rocky Steps at the Philadelphia Museum of Art. Thank you to Ironwood Pharmaceuticals for generously sponsoring this event each year since 2020! The #DiversityinGI virtual 5K and fun runs benefit the ACG DEI Committee’s Summer Scholars Program.
[REMEMBERING PROFESSOR WARREN]
J. ROBIN WARREN, MBBS, the Australian pathologist who, with Barry J. Marshall, MBBS, FACG, shared a Nobel Prize in Medicine for the discovery that Helicobacter pylori caused most stomach ulcers, died in July 2024 at age 87. Professor Warren and Professor Marshall published a paradigm-shifting paper about their findings in The Lancet in 1984. Professor Marshall’s account of their work was the cover story of ACG MAGAZINE Fall 2021, “Curiosity-Driven Discovery.”
Read: bit.ly/acg-magazine-fall-2021
Clockwise from top left: The SCOPY Awards turned 10 at ACG 2024. Jason A. Dominitz, MD, MHS, FACG, and Douglas J. Robertson, MD, MPH, of the Veterans Health Administration National Colorectal Cancer Screening Program won the 2024 “Grand SCOPY” for work above and beyond; Pooja Singhal, MD, FACG, (“Lakeside Goes Blue” CRC Awareness Event); David A. Greenwald, MD, FACG, and Mikhalya Brown, Icahn School of Medicine at Mount Sinai (“Passport to Your Health” Mount Sinai “Get Your Rear in the Clear” CRC Awareness Month Events).
Some of the Social Media Ambassadors for Evidence-Based GI pictured with their 2024 SCOPY Award for creativity of their “EBGI vs. CRC” Colorectal Cancer Awareness Campaign
Chelsea M. Forbes, MD, and Robert E. Spiller, DO, bring the coveted GI Jeopardy trophy home to the National Capital Consortium.
Saturday, October 26th co-leaders Dr. Aasma Shaukat and Dr. Sara Goff on either side of ACG 2023-2024 President Dr. Jonathan Leighton (center with sign)
Sunday, October 27th co-Leaders Dr. Sophie Balzora (with sign) and Dr. Patrick Young (center).
[IBD
HONOREES]
The Bruce and Cynthia Sherman Charitable Foundation established the Sherman Prize in 2016 to provide national recognition and financial prizes to pioneering IBD professionals who exemplify excellence in Crohn’s disease and ulcerative colitis. ACG collaborates to promote this prize and share news of the winners with the GI community.
Visit ShermanPrize.org to view the Honor Roll of past Sherman Prize recipients, watch inspiring short tribute films, and sign up to receive notification of the 2025 nomination cycle.
2024 SHERMAN PRIZES
Millie D. Long, MD, MPH, FACG, Interim Division Chief; Professor of Medicine; Director of the Fellowship Program in the Division of Gastroenterology and Hepatology, University of North Carolina School of Medicine, Chapel Hill, NC
2024
Dermot P.B. McGovern, MBBS, D. Phil (Oxon), FRCP (Lon), FACG, Director of Translational Medicine at the F. Widjaja Inflammatory Bowel Disease Institute; Director of the Precision Medicine Initiative; Professor of Medicine and Biomedical Sciences; Joshua L. and Lisa Z. Greer Endowed Chair in IBD Genetics at Cedars-Sinai, Los Angeles, CA
EMERGING LEADER PRIZE
[IBD 101]
Jordan E. Axelrad, MD, MPH, FACG, Associate Professor in the Department of Medicine at the NYU Grossman School of Medicine; Co-Director, Inflammatory Bowel Disease Center at NYU Langone Health, New York, NY
Together Sunanda V. Kane, MD, MSPH, MACG; Lisa B. Malter, MD, FACG; David P. Hudesman, MD, FACG; and David T. Rubin, MD, FACG, directed an introductory IBD course for first-year fellows as a one-day live course in collaboration with NYU Langone Health in September. In addition to a powerhouse faculty, the “secret sauce” of IBD 101 is the use of GroupObserved Structured Clinical Examination (GOSCE) simulation rotations.
[GUIDELINES GURUS]
The second volume of the ACG Guide to the Guidelines series by Brennan M. R. Spiegel, MD, MSHS, FACG, and Hetal A. Karsan, MD, FACG, launched at ACG 2024 in Philadelphia. Each chapter includes carefully selected vignettes designed to illustrate key concepts from guidelines, followed by a conversationstyle discussion and a multiple-choice quiz. Dr. Spiegel and Dr. Karsan also co-directed a wellattended and highly engaging evening course covering topics in both Volume 1 and Volume 2.
Purchase: members.gi.org/store
SHERMAN
Monday, October 28th co-leader Dr. Reezwana Chowdhury (with sign) next to co-leader Dr. Dana Lukin and Dr. Leighton
Tuesday, October 29th co-leaders Dr. Baha Moshiree (with sign) and Dr. Grant Hutchins (second from left)
Barry J. Marshall, MBBS, FACG and J. Robin Warren, MBBS
Photo left: 2024 "IBD 101" faculty. Photo right: ACG 2023-2024 President Jonathan A. Leighton, MD, FACG, was one of the IBD 101 faculty in September.
Co-authors Brennan M. R. Spiegel, MD, MSHS, FACG, and Hetal A. Karsan, MD, FACG, with Volume 2 of their “ACG Guide to the Guidelines” series
[SOCIAL MEDIA STARS]
ACG’s Social Media Acumen Awards celebrate those in the GI world who are passionate about using social media for good – for connection, education, and storytelling, for advancing the GI profession, and for educating patients. At ACG 2024 in Philadelphia, the Public Relations Committee Chair, Reezwana Chowdhury, MD, FACG, presented 27 awards honoring individuals for their sharp wit, good judgment, and significant impact on the GI community via social media. Additionally, 35 special awards recognized the Social Media Ambassadors for the ACG publication Evidence-Based GI
See all the 2024 Social Media Acumen winners: bit.ly/acg2024-sm-acumen
The launch of the College’s updated Strategic Plan at the ACG 2024 meeting in Philadelphia was marked by a 37-foot display at the Pennsylvania Convention Center entitled, “A History of Commitment, Collegiality, Connection & Clinical Excellence…and a Bold Vision for the Future.” Key elements included a timeline of major milestones offering a glimpse back at the College’s history with archival photos, a showcase of today’s vibrant programs and publications, and a celebration of ACG’s members. ACG Past President Jonathan A. Leighton, MD, FACG, and current President Amy S. Oxentenko, MD, FACG, commissioned the update, which was envisioned and accomplished by a work group co-chaired by Aasma Shaukat, MD, MPH, FACG, and Costas H. Kefalas, MD, MMM, FACG.
View the display: bit.ly/acg-strategic-plan-display-2024
ACG members attended the 16th Annual Meeting of the Society of Gastroenterology and Hepatology in Nigeria (Jos, Nigeria, in July 2024). Of those pictured, three are recipients of ACG’s International Training Grant: Akwi W. Asombang, MD, MPH, FACG (2014); Evaristus S. Chukwudike, MD (2021); and Stella-Maris Chinma Egboh, MD (2022). Also pictured, Chair of ACG’s International Relations Committee Kenechukwu ChudyOnwugaje, MD, FACG.
L to R: Evaristus S. Chukwudike, MD; Kenechukwu Chudy-Onwugaje, MD, FACG (Chair, ACG International Relations Committee); Stella-Maris Chinma Egboh, MD; Akwi Asombang, MD, MPH, FACG
ACG’s delegates to the American Medical Association, R. Bruce Cameron, MD, MACG, and March Seabrook, MD, FACG, represented the College at AMA's 2024 Interim Meeting in Lake Buena Vista, Florida, in November.
(Photo left) 2023-2024 Co-Editors in Chief, ACG Case Reports Journal, Vibhu Chittajallu, MD, and Khushboo Gala, MBBS, receive an ACG Social Media Acumen Award. (Photo right) A group shot at the ACG SCOPY Awards and Social Media Acumen Awards hosted by ACG’s Public Relations Committee at ACG 2024 in Philadelphia.
[A BOLD VISION]
[ACG MEMBERS IN NIGERIA]
[AMA REPS]
R. Bruce Cameron, MD, MACG and March E. Seabrook, MD, FACG
[VISITING PROFESSORS]
The Edgar Achkar Visiting Professorship (EAVP) is a signature offering of the ACG Institute for Clinical Research & Education. Since 2014, EAVP has provided GI training programs with visiting professors for lectures, small group discussions, panel discussions, and one-on-one visits with trainees and faculty. A source of inspiration, mentoring, and clinical education, almost every GI training program in the United States has hosted an EAVP visit. Starting in 2021, the program offers a Visiting Scholar in Equity, Diversity & Ethical Care under the auspices of the ACG Institute’s Center for Leadership, Ethics & Equity (LE&E Center).
and Ethical Care
The ACG MAGAZINE celebrates the creativity and contributions of the co-editors of the “Culinary Connections” feature, Christina A. Tennyson, MD; Alexander Perelman, DO; and Vani Paleti, MD (also known as the #ACGFoodies). For ACG 2024, they championed a new “Gut Master” apron for sale at the ACG Store that benefited the Share Food Program, a local Philadelphia non-profit whose mission is eradicating food insecurity among children, families, and seniors in the region. The three also published Volume 3 of the Culinary Connections Collection with gut healthy recipes and personal reflections from ACG members.
Explore the latest recipes: bit.ly/acg-foodies-3
Tyler M. Berzin, MD, MS, FACG, Harvard Medical School/Beth Israel Deaconess Medical Center Visit to University of Illinois – Chicago, May 28-29
David T. Rubin, MD, FACG, University of Chicago Medicine Visit to Augusta University, August 9
*Linda Anh B. Nguyen, MD, FACG, Stanford Digestive Health Center Visit to Cedars-Sinai Medical Center, September 5
John E. Pandolfino, MD, MSCI, FACG, Northwestern Medicine Visit to Oregon Health Sciences University and Oregon Gut Club, October 11 – 12, 2024
* ACG Visiting Scholar in Equity, Diversity,
[GUT MASTERS]
The ACG Foodies: Christina A. Tennyson, MD; Alexander Perelman, DO; and Vani Paleti, MD, editors of the “Culinary Connections” feature in ACG MAGAZINE.
[SAMUEL WEISS AWARD]
2024 SAMUEL S. WEISS AWARD: IRVING M. PIKE, MD, MACG Highest Honor for Unwavering Dedication and Exceptional Commitment to ACG
For his steadfast dedication to the ACG, its mission, and its future; his commitment as a leader and educator; and his pioneering contributions to quality and endoscopic practices across the nation, Irving M. Pike, MD, MACG, is the 2024 recipient of the prestigious ACG Samuel S. Weiss Award. This award in commemoration of ACG’s founding father, Dr. Samuel Weiss, is presented periodically, and not necessarily annually, to a Fellow of the College in recognition of outstanding career service to ACG.
Recognized for his tremendous positive impact on gastroenterology, patient care, and the direction of the ACG, Dr. Pike transformed the future of endoscopy care across the United States in his role as the driving force and visionary leader behind the establishment of the Gastroenterology Quality Improvement Consortium, Ltd., (GIQuIC), for which he served as the Founding Director and President from 2009 to 2017. Today, the GIQuIC is the largest national clinical data registry for gastroenterology and approximately one-third of all gastroenterologists in the country participate.
Dr. Pike has served on the ACG’s Practice Management Committee, Archives Committee, Credentials Committee, Finance and Budget Committee, and Nominating Committee. He was Chair of the Practice Management Committee, Finance and Budget Committee, and Nominating Committee. He served as Co-Chair of the 2005 ACG/ASGE Task Force for the Development of Quality Indicators for Gastrointestinal Endoscopy and again as Co-Chair of the Task Force in 2015 for the update of these indicators.
Named an ACG Trustee in 2006, Dr. Pike’s dedicated service to the College included the ACG Presidency from 2017-2018. After his tenure as Past President, Dr. Pike remained on the Board in 2020 as Trustee for Administrative Affairs. This appointment continues over a five-year tenure, reflecting his vibrant and ongoing commitment to the College and the Board of Trustees’ respect and admiration for his abilities and achievements.
Dr. Pike is widely heralded as “a man of genuine empathy and kindness,” a tribute noted by one of his nominators. Another wrote, “I often tap Irving for advice and have found his integrity to be impeccable, his wisdom to be invaluable, and his loyalty and dedication to the ACG to be unwavering.”
About Dr. Pike
Dr. Pike started his career in private GI practice in Virginia Beach, VA, and helped establish Gastrointestinal and Liver Specialists of Tidewater, PLLC, a practice of over 40 physicians and providers. He served as a community faculty member for the Eastern Virginia Medical School. Dr. Pike served as Chief of Staff of Sentara Bayside Hospital and President of the Virginia Beach Medical Society. In 2012, Dr. Pike moved to Alamo, CA, to accept the role of John Muir Health’s first Senior Vice President and Chief Medical Officer. Dr. Pike retired from this role in the summer of 2021. He currently is Co-Director of the University of California San Francisco Network Physician Leadership Academy.
[BERK/FISE AWARD]
2024 BERK/FISE AWARD TO MARK B. POCHAPIN, MD,
FACG
A Superb Clinical Gastroenterologist, Educator, and Innovative Servant Leader
For his excellence in patient care, research, teaching, and mentoring, along with his singular achievement of leading the College with skill, empathy, and vision during the worst days of the COVID-19 pandemic, the 2024 Berk/Fise Clinical Achievement Awardee is Mark B. Pochapin, MD, FACG. Dr. Pochapin is an astute clinician, inspiring teacher, and respected colleague who is a staunch champion of colorectal cancer screening, colonoscopy, reducing disparities, and promoting a diverse workforce. Dr. Pochapin’s distinguished career fully embodies the attributes of the Berk/Fise Clinical Achievement Award, which recognizes not only clinical excellence, but also contributions in patient care, clinical science, clinical education, technological innovation, and public and community service.
During his tenure as ACG President during the COVID-19 pandemic in 2020, Dr. Pochapin was exemplary for his steady and reassuring servant leadership, and his commitment to supporting ACG members during that unprecedented era. He led his own GI division and institution on the front line of the pandemic outbreak in New York City and was able to translate this experience into effective leadership of the broader community of gastroenterologists.
One nominator wrote of Dr. Pochapin’s time as President, “I am not sure there was anyone in our history of great leadership of the College who would have had the personality, interpersonal skills, organizational skills, tolerance, and integrative skills to lead us all through some of the darkest times we have had in medicine. He was instrumental in making sure the members all had the best information, much less a resilient and brilliant broad plan of approach to provide education and information to GI practitioners at all levels.”
His leadership of the College during those uncertain days was nothing short of inspirational. One nominator described how during his ACG presidency Dr. Pochapin “coined the term ‘beacon’ related to what to he thought the College should be for others but, appropriately, we immediately recognized that Mark's shining example of leadership and eternal optimism most represented that symbol.”
Noted by his nominators for his relentless energy, ambition, creativity, and innovative nature, Dr. Pochapin is described as “a wonderful communicator who exudes honesty and sincerity.” He is recognized as a leader who “inspires and motivates all in his presence,” and who has a “dedicated interest in developing and coaching people to help them become the best versions of themselves.”
About Dr. Pochapin
Dr. Pochapin is the Sholtz-Leeds Professor of Gastroenterology; Director of the Division of Gastroenterology and Hepatology; and Vice Chair of Clinical Affairs in the Department of Medicine at NYU Grossman School of Medicine/NYU Langone Health. Dr. Pochapin served as ACG President from 2019-2020 and played a key role in the development and launch of the ACG Institute's Young Physician Leadership Scholars Program. For his service as President during the COVID-19 pandemic, the College presented him with the “Beacon Award for Outstanding Leadership in Extraordinary Times.”
Learn About
TRAINEE HUB
Implementing Upstander Training in Gastroenterology Fellowship
WOMEN AND UNDERREPRESENTED MINORITIES (URM) IN MEDICINE CONTINUE TO FACE CHALLENGES IN THE FORM OF MICROAGGRESSIONS (i.e., microinvalidations, microinsults, and microassaults) despite growing acknowledgment and increased awareness of the importance of diversity, equity, and inclusion (DEI) in the workplace. These incidents adversely affect professional identity development, cause emotional distress, and are associated with a decline of women and URM in leadership roles and procedural-heavy subspecialties such as gastroenterology (GI). A call to action is needed for effective and comprehensive allyship, in addition to coaching, mentorship, and sponsorship.
Elida Voth, MD; Khushboo Gala, MBBS; Douglas A. Simonetto, MD; Xiao Jing “Iris” Wang, MD, Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, MN
“The bystander effect, or bystander apathy, is a social psychological theory that demonstrates individuals are less likely to offer help to a victim when there are other people present.”
What is the “Bystander Effect”?
The bystander effect, or bystander apathy, is a social psychological theory that demonstrates individuals are less likely to offer help to a victim when there are other people present. When you are in a larger crowd, you may be less likely to receive assistance if targeted by aggression or harassment in any form. The bystander effect suggests people often fail to respond when witnessing microaggressions and bias due to fear of confrontation, lack of confidence in their skills, and the belief that others are better equipped to respond. If the chance to call out inappropriate behavior or harassment in support of the victim is missed, rumination may occur with a negative impact on mental health or perceptions of safety in the workplace for both the victim and the bystander.
Studies have demonstrated that microaggressions are frequent occurrences during medical training and have been associated with positive depression screen and decreased medical school satisfaction in U.S. medical students. Commonly, these microaggressions occur during patient encounters, perhaps even with a large multidisciplinary team on rounds; however, similarly impactful situations can arise after interactions with peers, allied health staff, and faculty. For many trainees, it may be difficult to recognize these experiences and empathize with others if they have not been personally affected.
Upstander Training: How We Did It
Upstander training teaches the ability to recognize and respond to microaggressions and bias in support of a victim, and is currently lacking in graduate medical education. We implemented upstander training as part of the core curriculum for our
GI fellowship program in the form of a workshop as part of our program’s DEI curriculum.
Mayo Upstander Training Curriculum
Our aim of this educational initiative was to develop an interactive curriculum relevant to our general and 4th year GI fellowship programs as outlined here:
• Describe the concept and discuss the relevance/importance of upstander training
• Illustrate 6 steps to take when confronted with discrimination, harassment, or hate speech
1. Self-Talk Yourself Into Action Self-doubt and self-talk often leads to inaction.
2. Focus on the Target/Victim (Not the Aggressor)
The idea is to make the victim feel included and provide them the support they need.
3. Use Body Language and Positioning to Shift the Power Dynamic
The goal is to diminish the power dynamic of the aggressor. The way we stand influences our self-confidence and the impression that we give to others.
4. De-escalate Through Tone & Volume
The way we speak (tone, word choice, and volume) should be calculated to create a sense of calm.
5. Engage the Crowd in Helping There is safety in numbers; try to engage those around to help diffuse the situation.
6. Continue to Support the Target/ Victim
Let the victim be heard and give them a sense of belonging. Focus on helping them feel accepted and emphasize that they are a valuable part of the group.
• Help the audience implement these steps during an interactive session with three case examples
We specifically geared our cases towards clinical encounters faced by GI fellows, including one example in the general GI clinic and two in the inpatient setting. These were conducted in an open forum style, with the session leaders (our chief fellows) soliciting responses and opinions to these case-based situations from the audience.
The Impact of Our Experience
A pre- and post-survey was given to fellows participating in the session to understand their previous experiences with upstander training and feedback for the curriculum. Among our cohort, 6 out of 7 (85.7%) women reported facing discrimination and 6 out of 8 (75.0%) of those identifying with a racial minority had personally experienced discrimination during their medical training, with even more reporting witnessing discrimination. However, few participants had a thorough understanding of the bystander effect and upstander training, despite many previously participating in anti-discrimination training. After our upstander training session, participants were more confident in their ability to respond in these situations. In general, upstander training was well-received, and the majority agreed that it should be continued in a longitudinal fashion and found the session to be educationally beneficial.
Lessons Learned and Tips for Implementation
We found that, given the potentially sensitive nature of the discussion and the cases, it is of utmost importance to create an optimal learning environment for these discussions, which includes a closed room of peers/program leadership, acknowledging the potentially emotional aspect of these experiences, and emphasis of support from peers, training program, and divisional leadership. In order to “break the ice,” each chief fellow shared a personal experience they had encountered during medical training where they wished they
would have had the courage to stand up for a colleague, or where they were personally targeted and wished others helped. We also found it helpful to have tangible resources, such as employee assistance programs, wellbeing resources, and where to report misconduct at our institution, should trainees experience or witness these events.
Our upstander training program included a didactic session to introduce the concepts of upstander training, and discussed case-based examples as a large group. For programs which may wish to replicate this training, we recommend simulated practice in real time with small groups that can be repeated on a longitudinal basis to optimize the experience. Additionally, we advise budgeting for an adequate amount of time to debrief after the exercise, as this allows trainees the opportunity to share personal experiences and reflect on the impact of these interactions on their medical training experience with the support of their program. The support and engagement from faculty and/or division leadership cannot be understated.
In future sessions, we plan on an interactive, simulation-based session to mimic a real-life situation with active use of phrases and body language to practice the skills of an effective upstander. Ultimately, the prevalence of microaggressions toward URM and women in medicine requires institutional support and ongoing efforts to address systemic inequities in medicine, as they are associated with increased physician burnout, rates of depression, decreased performance, and poor job satisfaction. Additionally, in order to increase diversity in the leaky pipeline of academic medicine, we must focus efforts on retaining our women and
“Upstander training teaches the ability to recognize and respond to microaggressions and bias in support of a victim, and is currently lacking in graduate medical education.”
URM physicians. The effective utilization of upstander training is an important tool to empower physician trainees in becoming an ally when microaggressions occur, in an effort to promote a flourishing and diverse workplace.
About
Khushboo Gala, MBBS
Dr. Gala is an Advanced Endoscopy Fellow and prior Chief GI Fellow at Mayo Clinic Rochester. She served as co-Editor-inChief of ACG Case Reports Journal from 2023-2024.
Douglas A. Simonetto, MD
Dr. Simonetto is GI Program Director and Associate Professor of Medicine at Mayo Clinic Rochester.
Elida Voth, MD
Dr. Voth is a GI and hepatology fellow at Mayo Clinic Rochester.
Xiao Jing “Iris” Wang, MD
Dr. Wang is Associate GI Program Director and Assistant Professor at Mayo Clinic Rochester. She currently serves on ACG’s Educational Affairs and Training Committees and is co-chair of the ACG GI Circle online community.
“For programs who may wish to replicate this training, we recommend simulated practice in real time with small groups that can be repeated on a longitudinal basis to optimize the experience.”
SUBMIT YOUR APPLICATION for the ACG 2025 International GI Training Grant Awards
The International Relations Commi ee of the American College of Gastroenterology is now accepting applications for the 2025 International GI Training Grants. Each training grant will award one fellowship, with a maximum of $10,000, during 2025. Grants are to be used for travel to and from the training center and to the ACG Annual Meeting, as well as for incidental expenses related to the training. The training must take place between July 1, 2025, and June 30, 2026.
INTERNATIONAL GI TRAINING GRANT
This grant provides partial financial support to physicians outside the United States and Canada to receive clinical or clinical research training or education in Gastroenterology and Hepatology in selected medical training centers in North America.
WHO IS ELIGIBLE? Physicians who are not citizens or residents of the United States or Canada, and who are working in gastroenterology or related areas, are eligible to apply together with their training institution.
SUBMISSION DEADLINE March 31, 2025 APPLY HERE traininggrant.gi.org
This grant provides partial financial support to United States and Canadian GI Fellows in training, or GI Physicians who have completed their training within the last five years, to receive clinical or clinical research training or education in Gastroenterology and Hepatology outside of North America.
WHO IS ELIGIBLE? GI Fellows in training who are enrolled in an accredited gastroenterology fellowship program, or GI Physicians who completed their training within the last five years, and are citizens of the United States or Canada, or have a U.S. green card, are eligible to apply together with their training institution.
SUBMISSION DEADLINE March 31, 2025 APPLY HERE traininggrant.gi.org
GETTING IT
Navigating the Gray Market
Gastroenterologists’ Insights on the Gray Market, Herbals, and Their Regulation by the FDA
By George Abdelsayed, MD, FACG and Madhu Mathew Vennikandam, MD; Members of the 2023-2024 FDA Related Matters Committee
AS GASTROENTEROLOGISTS PLAY
A VITAL ROLE in understanding and addressing the complexities of digestive health in patients, there is an emerging concern about the growing influence of the gray market on herbal supplements. The evolution of the gray market has added a layer of complexity, particularly concerning herbal products and their regulation by the U.S. Food and Drug Administration (FDA). It is important for gastroenterologists to be aware of patients seeking alternative remedies through these channels, as the efficacy and safety of such products can be questionable. This article explores what gastroenterologists should know about this evolving landscape and their regulation by the FDA.
OVERVIEW
Herbal supplements are frequently used by individuals seeking relief from digestive issues. However, the lack of standardization in herbal products poses challenges for gastroenterologists, as variations in composition and potency can impact treatment outcomes.
With the increased popularity of Complementary and Alternative Medicine (CAM), the public continues to seek alternative remedies for various diseases to improve their quality of life and longevity. CAM is widely employed in the treatment of Irritable Bowel Syndrome and up to 50 percent of patients declared that they used some form of CAM for their gastrointestinal symptoms, ranging from biologically active compounds to mind–body interventions.1
Studies indicate a rising trend in patients seeking herbal alternatives for gastrointestinal issues. A survey published in The Journal of Gastroenterology and Hepatology found that 41 percent of patients with digestive concerns had used herbal supplements in the past year.2 Commonly used herbs include ginger, peppermint, and chamomile, with reported benefits in alleviating symptoms such as bloating and indigestion.
Various challenges, including supply and demand imbalances, difficulties with obtaining prior authorization for medications, and increased cost of medications, among others, have led some manufacturers to capitalize on this situation by providing alternative routes for patients seeking to obtain remedies of interest.
The so-called “gray market” (sometimes referred to as the parallel or diversion market) describes distribution channels not authorized by drug manufacturers to distribute legitimate medications to the public. These medications are diverted from a legitimate supply chain in response to price point differentials or availability gaps in different areas of the country.3
In the context of herbal supplements, this often involves the sale of products that claim health
benefits without the rigorous scrutiny applied by regulatory bodies. The World Health Organization (WHO) estimated that the world market for herbal medicines and herbal products is worth $62 billion and would hit $5 trillion by 2050.4 Retailers of such products generally do not comply or are not familiar with the requirements of governmental agencies, including the FDA. This is an issue that impacts public safety and our nation's economy.
Victims of the gray market span a wide range of ages and statuses in our population. Among the more vulnerable victims may be teenagers, who may find prescription pills and dietary supplements easier to obtain through this market. Regrettably, physicians are frequently cited as among the most common sources of gray market supplements (whether wittingly or unwittingly), further contributing to the drug abuse crisis in the United States. It is difficult to quantify and investigate the true extent of this problem. The gray market for pharmaceutical products has existed for many years. Unfortunately, with prescription drugs, the diversion process which gray marketers use may involve both routine prescription drugs as well as controlled substances, and even counterfeit drugs. This underscores the need for gastroenterologists to be vigilant about products that may not undergo the rigorous regulatory scrutiny required by official channels.
Although the counterfeiting of many medicines in the gray market has been documented, the counterfeiting of gastroenterology medications, particularly herbal medications and some dietary supplements, has been poorly identified. One explanation for this may be that many dietary supplements and other products, including herbal medications, generally undergo significantly less scrutiny by the FDA and the scrutiny process may not start until the product is well into the marketplace.
Conditions for which herbal remedies are used include abdominal pain, acid reflux or heartburn, food allergies, nausea or vomiting, peptic ulcer disease, and chronic liver disease, including fatty liver disease and cirrhosis. The obesity epidemic has prompted many patients to seek “quick fix” remedies. This is why many of the currently available
medications for obesity, such as the GLP-1 agonists, have a prohibitively long waiting period and are generally prioritized to diabetic patients.
REGULATORY OVERSIGHT OF DIETARY SUPPLEMENTS & HERBAL PRODUCTS
The FDA regulates dietary supplements, including herbal products, under the Dietary Supplement Health and Education Act (DSHEA).5 The DSHEA was further enhanced by the Dietary Supplement and Nonprescription Drug Consumer Protection Act, enacted in 1996, which requires manufacturers to notify the FDA about deaths, life-threatening injuries, hospitalizations, disability, birth defects, and requirements for medical intervention for the prevention of any of these problems. In June 2007, the FDA also published comprehensive regulations for Current Good Manufacturing Practices for those who manufacture, package, or hold dietary supplement products. These regulations focus on practices that ensure the identity, purity, quality, strength, and composition of dietary supplements. The regulatory framework for herbals is less stringent compared to prescription medications. However, data from the Government Accountability Office (GAO) reveal that the FDA faces challenges in fully overseeing the dietary supplement market.
With several thousands of different products on the market and limited resources, the agency struggles to monitor the safety and efficacy of each product. Datadriven decision-making is imperative for gastroenterologists facing the complexities of the herbal supplement landscape. Keeping abreast of FDA recalls and warnings related to specific products is vital for patient safety. The data underscore the importance of collaboration with pharmacists, dietitians, and other healthcare professionals to share insights and enhance the collective understanding of herbals in the context of digestive health.
In the dynamic landscape of digestive health, gastroenterologists must navigate the complexities of the gray market and herbal supplements. Staying informed, fostering open communication with patients, and collaborating with other healthcare professionals are crucial steps to ensure comprehensive and effective care in an era when patients increasingly seek alternative remedies.
Gastroenterologists face the challenge of communicating effectively with patients about herbal supplements. Many patients may not disclose their use of herbal products, assuming they are natural and, therefore, safe. Creating an open dialogue with patients is crucial for understanding their full health profile and ensuring safe and effective treatment plans. Given the data on patient preferences for herbal remedies, gastroenterologists must be proactive in addressing herbal supplement use during patient consultations. A study in The American Journal of Gastroenterology emphasized that open communication between healthcare providers and patients is crucial in understanding the reasons behind herbal supplement usage and potential interactions with prescribed medications.
In the face of a growing gray market and increased patient reliance on herbal supplements, gastroenterologists must leverage data to navigate this complex terrain. Staying informed about FDA regulations, actively engaging with patients regarding herbal supplement use, and fostering interdisciplinary collaboration are essential strategies for ensuring patient safety and promoting optimal digestive health.
RECOMMENDATIONS FOR GASTROENTEROLOGISTS ON HERBAL SUPPLEMENTS
1. Stay Informed: Stay up to date on the latest research and FDA regulations regarding herbal supplements.
2. Educate Patients: Encourage open communication with patients about their use of herbal products, emphasizing the importance of disclosure for comprehensive healthcare.
3. Collaborate with Pharmacists: Working closely with pharmacists can provide valuable insights into potential herb-drug interactions and ensure patients receive accurate information.
4. Stay Connected: Connect with your local, state, and national medical societies.
REFERENCES
1. Larussa T, Rossi M, Suraci E, Marasco R, Imeneo M, Abenavoli L, Luzza F. Use of Complementary and Alternative Medicine by Patients with Irritable Bowel Syndrome According to the Roma IV Criteria: A Single-Center Italian Survey. Medicina (Kaunas). 2019 Feb 13;55(2):46. doi: 10.3390/medicina55020046. PMID: 30781771; PMCID: PMC6409648.
2. Fifi AC, Axelrod CH, Chakraborty P, Saps M. Herbs and Spices in the Treatment of Functional Gastrointestinal Disorders: A Review of Clinical Trials. Nutrients. 2018 Nov 9;10(11):1715. doi: 10.3390/ nu10111715. PMID: 30423929; PMCID: PMC6266883.
3. Ehrenpreis ED, Kulkarni P, Burke C; FDA-Related Matters Committee of the American College of Gastroenterology. What gastroenterologists should know about the gray market, herbal remedies, and compounded pharmaceuticals and their regulation by the Food and Drug Administration. Am J Gastroenterol. 2013 May;108(5):642-6. doi: 10.1038/ajg.2012.348. PMID: 23644956.
4. Ajazuddin, Saraf S. Legal regulations of complementary and alternative medicines in different countries. Pharmacogn Rev. 2012 Jul;6(12):154-60. doi: 10.4103/0973-7847.99950. PMID: 23055642; PMCID: PMC3459458.
5. https://www.fda.gov/food/dietary-supplements
ABOUT
George Abdelsayed, MD, FACG, is Associate Professor of Medicine at Robert Wood Johnson Medical School, Director of Ambulatory Hepatology, and Chief Quality Officer at Rutgers Health.
Madhu Mathew Vennikandam, MD, is an attending physician at Northwestern Medicine and a member of the ACG FDA Related Matters Committee.
“Many patients may not disclose their use of herbal products, assuming they are natural and, therefore, safe. Creating an open dialogue with patients is crucial for understanding their full health profile and ensuring safe and effective treatment plans.”
Cheers to Food and Gut Health!
and even a
have shared their
Who are the #ACGfoodies? A group of GI physicians, fellows, registered dietitians, and
Who are the #ACGfoodies? A group of GI physicians, fellows, registered dietitians, and even a GI psychologist have shared their culinary journeys along with healthy plant forward recipes in the pages of ACG
plant forward recipes in the
Kindness-Influenced Trust and Healing in Health Care
The 2024 Emily Couric Memorial Lecture
Leonard L. Berry, PhD, MBA
KKINDNESS-INFLUENCED TRUST AND HEALING IN HEALTH CARE.
What an honor to deliver the Emily Couric Lecture. I have read about her, and she was a remarkable leader and person.
I want to start with Alice's story. Alice had a biopsy on a mass in her stomach. Her gastroenterologist was in his car driving home in heavy traffic. At the traffic light, he saw the pathology results pop up in Epic and it was good news. The mass was benign. It was a Friday afternoon before a long holiday weekend. Despite fatigue from the work week, Alice's physician drove back to the hospital to call her with the good news, instantly relieving her of her intense anxiety and bringing her to tears of gratitude.
Alice's doctor could have waited until he was back at work on Tuesday, but he didn't wait. He drove back to the hospital and called Alice – and demonstrating the power of kindness in doing so. Health care is a high-emotion service, especially for seriously ill patients. High-emotion services are those in which even the anticipation of receiving them creates intense anxiety and emotions, especially for seriously ill patients.
I'd like to share with you in my time today an unfancy model. So here I am, an academic, and I have one of the least fancy models that you'll ever see at a medical conference. Here it is: Kindness to patients influences patients’ trust, and patients’ trust, in turn, influences healing of patients and the clinicians who care for them.
So, let's review each part of this unfancy model. Drawing from the definition of Dean and Doty, “Kindness is purposeful, voluntary action undertaken with sensitivity to the needs or desires of another person and actively directed towards fostering their well-being or flourishing.” Based on my research and the research of others, I propose six dimensions of kindness: deep listening, empathy, generous acts, timely care, gentle honesty, and support for family caregivers. I'll talk briefly about each.
Kindness to Patients
AN UNFANCY MODEL
Patients' Trust
FIRST is deep listening. Actively listening to patients conveys respect for their self-knowledge, builds trust, and improves treatment decisions. The failure to listen well is timeinefficient because the odds of making the wrong treatment decision are far greater, impeding what could be effective, efficient – and kind – health care. Deep listening helps clinicians learn not only what is the matter with the patient but also, very importantly, what matters to the patient.
SECOND is empathy, a term with which we are all familiar. Among the many definitions of empathy in the literature, my favorite comes from a nurse, Teresa Wiseman: seeing from the other person’s perspective, avoiding judgment when assessing the situation, recognizing the emotions present, and responding in a caring way. I've done much of my research in oncology, and I've interviewed many cancer clinicians in addition to patients and their family members. In interviewing clinicians, one of the questions I typically ask is, “Is there a certain word or phrase you'll never use with a patient?”
And every single time I've asked that question to someone who works in oncology, they have had “never words” to share. Here are some examples from my research:
“Actively listening to patients conveys respect for their selfknowledge, builds trust, and improves treatment decisions.”
Healing of Patients and Those Who Care for Them
“There is nothing more that we can do for you.” That's a “never” phrase. Curative treatment may no longer be possible, but there's always something more clinicians can do to help their patients, even when curative treatment is no longer indicated.
“Why did you wait so long to come in?” which needlessly creates a feeling of guilt.
“You failed chemo.” The patient didn't fail chemo. Chemo failed the patient.
“You were lucky it is only stage two,” which trivializes a serious condition. The word “lucky” is a poor choice when talking to someone who has stage two cancer.
“Let's not worry about that now.” This is one of the most common “never” phrases. Non-answers to patients who want to know more about their prognosis, who have a right to know, heighten the anxiety that already exists.
"Never" words lack empathy; they create emotional suffering; they are unkind.
I recommend assembling with your colleagues to discuss the "never" words you unintentionally use with patients or with each other. Make a list of them and then commit as a clinical group to banishing those words, to never using them again.
THIRD is generous acts. Generosity is an input to a healthcare organization’s success, not just an output, because generosity wins the hearts of its stakeholders; the patients, of course,
but also the families, employees, vendors, the community. Generosity is embedded in a concept that I call volunteerism, which is discretionary effort.
Discretionary effort is the difference between the actual energy and effort we put into our service to others and the minimum amount of energy and effort required to avoid any kind of adverse consequence as the service provider. Volunteerism, going beyond the minimum standard to provide a greater service to others, is generous and it is kind.
My first major study in healthcare occurred in the 2001-2002 academic year when I took a sabbatical leave to study in residence at the Mayo Clinic. Mayo Clinic is far from perfect; no health system is perfect. But one of Mayo’s greatest strengths is its teamwork culture. Mayo Clinic’s core competency, in my view, is that it is a high volunteerism organization with clinicians pooling their knowledge to serve patients with complex disease. Clinicians, often from different specialties, helping one another with difficult cases, facilitates correct diagnoses and effective treatment.
FOURTH is timely care. Heightened emotions are likely to intensify the need for timely service. Timeliness is often controllable. It's a function of reimagining the service system to improve efficiency, but also empathy and extra effort.
Recall the story I started with, Alice's story. The gastroenterologist, exhausted from a hard week, was almost home for the long weekend. Yet, when he learned that his patient's biopsy was benign, he turned around and drove back to the hospital to call the patient. I started with that story because it collectively illustrates empathy, generosity, and timely care. This one kindness meant so much to that patient.
“Kindness in healthcare must extend beyond the patient to the family and other caregivers, especially in cases of serious illness. Supporting family caregivers in a role they are often ill-prepared to perform, both cognitively and emotionally, bridges kindness and practicality.”
FIFTH is gentle honesty. Asking patients how much they want to know about their illness is informative and it is kind. Most patients want to hear the truth in honest, well-chosen words that convey a sense of partnership and that gives them voice in reaching treatment decisions that are right for them.
In an interview with an oncology nurse, she said something that I'll never forget. She said, “A doctor may say to a patient, ‘we can continue treatment, or we can just do supportive care.’” And then the nurse added, “We have to take the word 'just' out of that sentence.” In this context, the word “just” is a “never” word because the doctor has put a thumb on the scale towards continued curative treatment, when that might not be the most humane way to care for that patient.
SIXTH and last, but not least, is supporting family caregivers. Kindness in healthcare must extend beyond the patient to the family and other caregivers, especially in cases of serious illness. Supporting family caregivers in a role they are often ill-prepared to perform, both cognitively and emotionally, bridges kindness and practicality. Preparing family caregivers to be more effective, to be more prepared, to be more confident in taking care of their loved one benefits all parties.
The kindness dimensions influence patients’ trust. Moorman and coauthors define trust as, “the willingness to rely on an exchange partner with whom one has confidence.” No service requires trust between the provider and receiver of a service more than health care because of
“'Never' words lack empathy; they create emotional suffering; they are unkind”
its intimacy, variability, complexity, and personal importance to the patient.
Trust is the bedrock for establishing genuine relationships with patients. And patients’ trust influences healing. Healing of patients, but also of those of you who care for patients.
The primary missions of health care, in my view, are to offer health (prevention of disease) and healing (physical and mental healing, when possible, and emotional healing as needed). Health and healing are about more than medications, technology, procedures, and cures. They concern furthering a person's well-being. That's the way I, as a student of your profession, view healing. You can heal even when you cannot cure.
The unfancy model that we have discussed leads to this proposition: Kindness-influenced trust, when combined with competence-influenced trust, has stronger effects on healing than competence-influenced trust alone. What this means is when your patient engages with you for the first time, they arrive trusting your competence. They trust that you know what a doctor is supposed to know, that you have the skills that a doctor is supposed to have. They trust your competence unless they learn otherwise. But kindness-influenced trust must be earned through your interactions with patients — through your listening, empathy, generous acts, timeliness, gentle honesty, and concern for the family, as needed. When you combine kindnessinfluenced trust with competenceinfluenced trust, it has stronger effects on healing. Let me show you just how much.
“Trust is the bedrock for establishing genuine relationships with patients. And patients’ trust influences healing. Healing of patients, but also of those of you who care for patients.”
making in which patients are wellinformed, and their voices are heard. It encourages therapeutic alliance in which patients believe their clinician has their best interests at heart. It influences relational strength between patients and their clinicians, contributing to patients’ and clinicians’ sense of psychological safety, enabling more candid communication. It encourages improved patient followthrough with treatment plans, reduced patient anxiety, and less decisional regret. It encourages more humane end of life care. And it encourages greater patient satisfaction and staff morale.
So here are the primary take home points: Kindness is multidimensional. It's powerful. And it's voluntary. We control it. Every one of us. We control how much volunteerism we're going to put in each service act. We control how much kindness we wish to layer on to our competence.
I conclude with the story of Susan. Susan was my student about six or seven years ago in the seminar
“Improving Healthcare Service” that I teach in our business school. I love teaching that course. Most of my students either go to medical school or pursue a non-clinical career in health care. Susan, now healthy, was diagnosed with brain cancer when she was 14 years old. And in the seminar, in one of the papers that she wrote and then presented to her classmates, she told this story:
“When Ava, my nurse, came by before surgery, she looked at me in the eye and she said, ‘Susan, I'm going to braid your hair back so we only shave what we need.’ What Ava did shaped how I viewed myself every time I glanced in the mirror during recovery and whenever I walked into school surrounded by normal girls. Ava probably doesn't remember braiding my hair, but that moment has stuck with me for the last six years.”
The power of kindness.
Thank you for the honor of delivering the Emily Couric Lecture. Thank you so much.
“When you combine kindness-influenced trust with competenceinfluenced trust, it has stronger effects on healing.”
Further Reading
Never-Words: What Not to Say to Patients with Serious Illness. Rana Lee Adawi Awdish, MD; Gillian Grafton, DO; Leonard L. Berry, PhD, MBA. Mayo Clinic Proceedings, Volume 99, Issue 10, 1553 – 1557. DOI: https://doi.org/10.1016/ j.mayocp.2024.05.011
About
Leonard L. Berry, PhD, MBA, is the University Distinguished Professor of Marketing and Regents Professor, M.B. Zale Chair in Retailing and Marketing Leadership, Presidential Professor for Teaching Excellence at the Texas A& M University Mays Business School, and Senior Fellow, Institute for Healthcare Improvement.
Culinary Connections:
ACG Staff Flavors
Editors Vani Paleti, MD; Alexander Perelman, DO & Christina Tennyson, MD
OVER THE YEARS, THE ACG MAGAZINE EDITORIAL TEAM HAS ENJOYED ALL THE MOUTH-WATERING RECIPES contributed by the #ACGfoodies. Now, thanks to an invitation from Culinary Connections section editors Christina Tennyson, MD; Vani Paleti, MD; and Alexander Perelman, DO, the ACG staff have the opportunity to share a few of their own favorite dishes with the ACG family.
A team effort by Anne-Louise Oliphant and Becky Abel resulted in a template for a healing broth made with all the veggies in A-L’s fridge. Emily Garel, ACG’s Art Director who gives ACG MAGAZINE its distinctive look, contributed her favorite recipe for empanadas. Arguably, the most talented and devoted foodie of the entire ACG staff is Neen LeMaster (AKA “The Kitchen Magician”) whose many culinary skills include baking, candy making, and a deft hand constructing elegant displays of cheese and charcuterie. Neen’s Vegetable Tarte Tatin is an exquisite offering from a generous and talented home chef.
Just like so much of the work done by ACG’s staff, this “Staff Flavors” column is a team effort, involving creativity, open communication, deep respect for everyone’s talents, and a willingness to step up and help.
We hope you enjoy!
Anne-Louise, Becky, Emily, and Neen
ANNE-LOUISE OLIPHANT AND BECKY ABEL
When Anne-Louise was under the weather this summer, her ACG MAGAZINE creative collaborator Becky rallied in support of her recovery and collaborated on a recipe for a vegetablebased healing broth. The basics of this particular soup came from clearing out the veggie drawer in A-L’s fridge, but the spirit of this recipe can be recreated using any vegetables and herbs you have on hand to create a soothing brew that may just cure what ails you.
Becky loves soups and remembers fondly that her mom, Donna, also created homemade broths with this same “clean out the fridge” method. As a vegetarian, Becky will often add some TVP crumbles to her soup pot for extra protein.
Starting with a core of aromatics including onions, celery, carrots, shallots, garlic, ginger, and fennel, the flavor builds with the addition of zucchini, jalapeño, and parsley. Becky and A-L were chatting as A-L was making this soup, and Becky had a brainstorm when she recommended a touch of turmeric!
The addition of this antiinflammatory spice adds depth of flavor and truly elevates the healing properties. Finishing the soup with handfuls of fresh spinach and chopped fresh cilantro just before serving lends vivid green to the dish.
Becky’s advice for anyone who makes A-L’s healing broth, “Don’t spill it on your shirt or it will stain everything!”
NEEN C. LEMASTER
I learned a lot about cooking and the importance of sharing what you have from my family. Leading up to the winter holidays, our dining room table would be lined completely with tins and plates lovingly packed full of my parents’ homemade Italian cookies. They were gifts for everyone from friends and family to my flute teacher and swim coaches. If a friend didn’t have somewhere to be for the holidays, there was always an extra spot at the tables we stretched through two rooms of the house.
When I moved to Boston for college, I met a kindred spirit halfway through
HEALING BROTH
Ingredients:
• 2 Tbsp plain oil
• 2 medium onions, chopped
• 3 stalks celery, diced
• 2 shallots minced
• 4 gloves garlic, chopped
• 1 thumb-sized knob of ginger, peeled and finely minced
• 1 small bulb fresh fennel, diced
• 2 large carrots. peeled and diced
• 1 Tbsp ground turmeric
• 2 tsp sea salt
• 2 tsp freshly ground black pepper
• 1 small zucchini, chopped
• 1 small jalapeno pepper, minced or to taste
• 1 small bunch fresh parsley, chopped
• 10 cups water
• Several large handfuls fresh spinach, chopped (you could use chard, kale, beet greens, etc.)
• 1 small bunch fresh cilantro, chopped
Steps:
1. Chop the veggies, garlic, ginger, greens, and herbs you have on hand. Quantities are just suggestions, tinker with the ingredients and amounts.
2. Sauté the onions, celery, shallots, garlic, ginger, fennel, and carrots in the plain oil until crisp tender.
3. Add turmeric, salt, and pepper and stir to combine.
4. Add chopped zucchini, jalapeno, and chopped parsley and stir as these veggies soften, about a minute.
5. Add the water and bring to a boil, then turn down the heat to medium-low.
6. Simmer for 20 to 25 minutes.
7. Add handfuls of fresh spinach to wilt in the pot.
8. Finish with chopped fresh cilantro at the last minute.
9. Taste for salt and add more as needed, along with another grind of fresh black pepper.
10. Serve and feel better soon!
SAVORY ROOT VEGETABLE TARTE TATIN
Pre-rolled refrigerated pie crust will most certainly work here if you don’t wish to make your own, but I’ve included the pastry crust method I use if you'd like to make it from scratch. The dough can be made a day or two in advance and refrigerated wrapped tightly in plastic wrap.
For the filling, selecting a variety of sizes and colors of vegetables will make for an eye-catching tarte, but choose what you like best. I recommend at least one carrot or parsnip to fill in the small spaces between larger vegetables. The vegetables can be roasted up to four hours before assembling the tart, but keep them at room temperature. You will need a 9- or 9 ½-inch pie pan for this recipe.
Pastry Ingredients:
• 4 oz. unsalted butter, very cold and cut into small cubes
• 1 ¼ cup all-purpose flour
• 1/4 cup water
• 1 Tbsp sugar
• 1/2 tsp salt
Filling Ingredients:
• 5-6 root vegetables (such as carrots, parsnips, rutabaga, beets, sweet potatoes, butternut squash, or yellow/red potatoes), peeled and cut into 1/2 in. thick slices
• 1 red onion, cut into 1/2 in. thick rings
• 3 Tbsp olive oil
• 1/3 cup sugar
• 1 Tbsp red or white wine vinegar
• 4 oz. feta, crumbled
• 1/4 cup mixed fresh herbs (I like rosemary, thyme, and sage here), finely chopped
• Kosher salt and pepper
Make the pastry:
1. For the pastry crust, combine the flour, salt, and sugar in a bowl.
2. Add the butter and use a pastry cutter or two forks to work it into the flour until only pea-size pieces remain. You can also use the pulse function on a food processor for this step.
Make the filling:
1. Preheat the oven to 400°F.
2. Arrange the sliced root vegetables and onion in a single layer on a parchment or foil-lined baking sheet.
3. Add the cold water and mix to moisten just until the pieces will adhere together when pressed. Gather the dough into a ball, flatten into a disc, wrap tightly in plastic wrap, and refrigerate for at least 30 minutes.
7. Remove from the heat, add the wine vinegar, and swirl to combine.
8. Quickly pour this mixture into the pie pan and swirl the pan to coat the bottom in a thin layer of caramel.
3. Drizzle the vegetables with the olive oil, then season with salt and pepper.
4. Roast for 30-35 minutes, until tender and just golden at the edges. Set aside to cool slightly.
5. Combine the sugar with 2 Tbsp of water in a small saucepan over medium-high heat.
6. Once the mixture is simmering, swirl the pan to distribute the heat and cook until the syrup just begins to turn light amber.
Assembly and baking:
1. Remove the chilled pastry dough from the refrigerator and lightly flour a counter.
2. Roll the dough into a 12-inch circle and then drape over the vegetables.
3. Tuck the dough down into the pan around the edges of the vegetables.
4. Prick the surface all over with a fork.
9. Arrange the root vegetables atop the caramel in the pie pan as close together as possible. Use smaller vegetables like carrots and parsnips to fill in the spaces between larger ones. Place the onion rings in an even layer atop the vegetables.
10. Sprinkle on the crumbled feta and half of the chopped herbs.
5. Bake at 400°F for 20 minutes and then lower the oven temp to 350°F and bake for 15-20 minutes more, until the crust is golden brown.
6. Allow the tarte tatin to cool in the pan for 5 minutes, then run a knife around the edge to loosen.
7. Invert onto a large plate for serving and sprinkle with the remaining herbs.
Photo Credit: Platter, Free Form Sea Glass plate from Riverside Design Group (@riversidedesigns)
incredibly talented baker, and eventually we started making dinner for our friends once a week. As I built independent traditions through cooking with and for friends, I felt profoundly connected to my family at home in Pittsburgh. That’s the beautiful thing about sharing a meal—suddenly a dish is so much more than food on the table; it represents connection and becomes a memory.
This savory, vegetarian tarte tatin is a culmination of many shared gifts and memories. I think of Kris teaching me to make pastry crust back in that tiny dormitory kitchen, my aunt making a roasted vegetable and feta dish last Christmas, and the tiny restaurant my partner and I went to in France that served an apple tarte tatin so beautiful I (almost) didn’t want to cut into it.
One of the things I love most about this versatile recipe is that it requires no rushing and has several steps that may be done in advance. So take your time, enjoy
EMILY GAREL
Like my chosen family, I love to connect with people through food, something they instilled in me when they welcomed me into their large and loving clan. Community and belonging are something I cherish, as I did not grow up feeling as if I had either. Kidnapped by my biological dad as a child and faced with a disconnected relationship with my birth mom, I felt as if I didn’t have a support system or a sense of belonging. My family of choice changed all that. Making foods with them, such as empanadas (Peruvian), palacinky (French/ Slovak), lumpia (Filipino), and the ever sugary—and sometimes wonkylooking—Santa cookies connects me to this generous family, their past, and their culture—and gives me a sense of pride, inclusion, and belonging.
Archie would make empanadas with his mom, and now his children make empanadas with him. It’s a family tradition that feels like a rite of passage. We typically make them around the holidays, in larger quantities, because empanadas are made to share with family and friends. It’s not an exaggeration to say that empanadas are my love language. With this family recipe, I hope you enjoy the process of making empanadas and sharing with the people you love as well.
We would like to hear from you if you have personal connections with GI & gastronomy. Contact ACG magazine staff by email at acgmag@gi.org to share your story with the ACG community. You can also tweet using #ACGfoodies to connect with the community.
EMPANADAS (MAKES ABOUT 40)
Ingredients:
• Empanada pastry dough (I prefer La Salteña)
• 2 lbs. ground beef
• 1/2 cup white onion
• 3/4 cup celery
• 1 Tbsp minced garlic
• 3/4 cup raisins
• Paprika
Cooking Meat:
• Oregano
• Cumin
• Bay leaves
• 7–8 boiled eggs
• Egg yolk wash: 5 eggs (can add more if needed)
• Honey
1. In a skillet over medium heat, start to brown the meat.
2. Add in onion, celery, minced garlic, and raisins.
3. Add in paprika, oregano, cumin, bay leaves (all to taste)
4. Once meat is browned, and taste is to your liking, drain liquid. (You don’t want soggy empanadas!)
Empanada Filling:
1. Lay out empanada shells, and using a dinner spoon, scoop meat into the center of the empanada shell.
2. Add a few pieces of boiled egg, and honey to taste.
3. Fold empanada shell over to close and use the tip of a fork to press down the edges. Place on baking tray.
Baking the Empanadas:
1. Preheat oven to 350° F.
2. Bake for 8 minutes, remove from oven, then brush egg wash over top.
3. Put back in oven and bake until golden brown.
BRIDGING MEDICINE AND MUSIC
appreciate the power of music. With the rapidly increasing rates of youngonset colon cancer, reaching out to adults at their screening age is crucial."
Dr. Hsu told the orchestra and audience that every one of us is a bridge and that we have to treasure our lives, including enjoying music and caring for our health: "Every musician is a bridge, and so is every physician in reaching out to their audience or patients. Melodies can resonate with any audience."
The same is true for outreach messages, such as colon cancer prevention. Practicing medicine and playing music transcend gender, age, race, profession, and country. Dr. Hsu says that both disciplines are complementary to keep our physical and mental health strong if we make the best of each.
TAKING THE MESSAGE TO THE CALIFORNIA STATEHOUSE IN 2023
ACG Governor Ronald K. Hsu, MD, FACG Advances Colorectal Awareness Through the Power of Music
By Ronald K. Hsu MD, FACG, and Monica Stark
A violin that has been gutted and reconfigured to fit a skeleton hangs in a cabinet inside Dr. Ronald Hsu's home as a reminder that the violin and the musician are inseparable. Without the instrument's bridge, there is no sound, no voice.
As an endoscopist, the endoscope is Dr. Hsu's instrument that saves lives, and as a violinist, the violin is his instrument to heal souls. Dr. Hsu says every musician and each physician can be a bridge to connect with listeners.
Dissecting the stringed instrument was not in his wheelhouse, but Dr. Hsu knew who to ask: a violin maker in Woodland, CA, whose specialty is instruments from the Renaissance and Baroque periods. Dr. Hsu's son Ryan then made a 3D-printed skeleton that connects to it.
Ryan Hsu, now a medical student, and Dr. Hsu’s daughter Kacey played violin at Davis Senior High School in Davis, CA. Dr. Hsu had been taking lessons from the school's orchestra director, Angelo Moreno, and UC Davis Baroque Ensemble music director Michael Sand.
THE LAUNCH OF “BRIDGING MEDICINE AND MUSIC”
As the relationships developed, the Hsu family and Mr. Moreno shared their passions for music and medicine and, in 2022, created an annual colorectal cancer education program, “Bridging Medicine and Music,” which coincides with Colorectal Cancer Awareness Month each March. In the program's introduction, “Bridging Medicine and Music” is described as an initiative connecting "two powerful disciplines in healing to raise colon cancer awareness, where physicians and musicians join hands to educate our community on the importance of screening to prevent colorectal cancer, the second most common cause of cancer death, and to
In 2023, Dr. Hsu expanded the program to include a special event, “Light the Capitol Blue - Colon Cancer Awareness Rally,” jointly organized by the California Colorectal Cancer Coalition (C4) and the ACG. The event brought the message of colorectal cancer prevention to the legislators at the California State Capitol in Sacramento.
"We let a lot of people who may be unaware of the dangers of colorectal cancer know the importance of screening. I'm not the one who can decide things, but at least I can use my contacts with legislators, clinicians, and health advocates to connect them," said Dr. Hsu.
"That's why I'm passionate to build these bridges."
ELECTRIC VIOLINIST MARK WOOD SHARES HIS MUSIC IN 2024
This year, Mark Wood, the original string master of the Trans-Siberian Orchestra, and his wife, rock singer Laura Kaye, were on board with Dr. Hsu and Angelo Moreno to rock out with Davis High School students for two “Bridging Medicine and Music” shows as part of Wood’s “Electrify Your Symphony's 2023-24 Evolution Tour.”
Playing an electric violin inside a giant inflatable colon just outside Davis High's Richard Brunelle Performance Hall, Wood set the stage for audience
Bridging Medicine and Music 2024 with electric violinist Mark Wood (center)
members as they arrived. The setlist included "Crazy Train" by Ozzy Osbourne, "Thunderstruck" by AC/DC, "Fight Song" a pop song by Rachel Platten, Aerosmith's "Dream On," Led Zeppelin's "Stairway to Heaven," and Santana's "Oye Como Va."
In addition to the in-person program, Dr. Hsu and the team at Davis High School live-streamed the performance to all American College of Gastroenterology members and communities nationwide. Dr. Hsu invited several ACG leaders to make short videos highlighting ACG's commitment and mission in raising CRC awareness to include in the program.
As the current ACG Governor for Northern California, colorectal cancer prevention outreach is important to Dr. Hsu as it's the second highest cancercausing death in the United States.
MUSIC’S POWER TO PROMOTE CONNECTION AND WELL-BEING
"People get to their well-being differently – music and medicine can help us. With science, we have medication and surgery to fix the physical body, and with music, we have an art that can soothe the mind," Dr. Hsu said.
When violinist Wood visited Sutter Hospital's Sophie's Place – the children's center's group music therapy room – he was taken aback by the human-to-human connection as he watched the children smile and tap their feet while playing music with them. "That's everything. The connection is being made," Wood said.
Named after a young singer-songwriter named Sophie Barton — whose mission was to help others through the power of music — Sophie's Place includes a common area for groups, a high-tech recording room, a private session room, and ample storage space for the generously donated instruments. There is space for children to
write and record their music, a place to be loud and connect with others, "and a place encouraging expression, creativity and most of all, healing." according to the Sutter Health website. Music can conduct human emotion faster than any art form. As the poet Henry Wadsworth Longfellow wrote, "Music is the universal language of mankind."
ARTICLE CONTRIBUTORS
Ronald K. Hsu MD, FACG, and Monica Stark, a reporter for The Davis Enterprise where she first heard and wrote about the local “Bridging Medicine and Music” program.
Top Row L to R: Live performance with Dr. Hsu’s son Ryan, daughter Kacey, and Davis Senior High School Baroque Ensemble conducted by Angelo Moreno in Palestrina, Italy, July 2014. Ronald K. Hsu, MD, FACG, and Musician Mark Wood in 2024. Dr. Hsu and Irving M. Pike, MD, MACG, (ACG Past President) at the “Light the Capitol Blue – Colon Cancer Awareness Rally” at the State Capitol of California, Sacramento, CA, in 2023. Middle Row L to R: Mark Wood performing at Sutter Children’s Center Sophie’s Place in Sacramento, March 2024. The inaugural “Bridging Medicine and Music” Concert Program Directors – Ronald K. Hsu, MD, FACG; Michael Sand; and Angelo Moreno, February 2022. Mark Wood at Sophie’s Place in 2024. Bottom Row L to R: Dr. Hsu with healing instruments: the colonoscope and the violin. Promotional
graphic from the 2022 Bridging Music and Medicine event. Dr. Hsu performs in a concert with student musicians at Davis Senior High School.
A TRANSFORMATIVE OPPORTUNITY: TRAINING IN ENDOSCOPIC MANAGEMENT OF IBD COMPLICATIONS AT AHN
I am deeply grateful for the invaluable opportunity provided by the ACG International Training Award, enabling me to fulfill my dream experience at Allegheny Health Network (AHN) in Pittsburgh during the summer of 2024.
During my training under Dr. Gursimran Kochhar and esteemed interventional endoscopists at AHN's interventional endoscopy unit, I gained extensive experience in advanced techniques such as endoscopic stricturotomy, balloon dilation, and stenting for inflammatory bowel disease (IBD) strictures.
Under Dr. Kochhar's leadership, AHN handles a high volume of such cases, providing me with exposure across various locations, including the ileal pouch. Despite performing these procedures in India previously, I lacked formal training and expert feedback, which I received abundantly during my tenure at AHN. These insights significantly bolstered my confidence and skill set, allowing me to perform five endoscopic stricturotomies shortly
after returning to India, compared to just six cases over the past two years. This underscores the pressing need for such interventions in resource-limited settings.
During my tenure, I systematically reviewed the literature on endoscopic management of strictures, which I submitted as an abstract for the ACG Annual Scientific Meeting.
My time at AHN also led to the publication of the inaugural Indian series on endoscopic stricturotomy in IBD in the Indian Journal of Gastroenterology (doi: 10.1007/s12664-024-01618-x), detailing techniques from standalone stricturotomy to hybrid approaches with balloon dilation and graded stricturotomy at intervals. These techniques were refined following my training at AHN.
Dr. Kochhar and his colleagues fostered a supportive environment where I felt at home and could freely seek guidance on various aspects of my training. The program was meticulously organized well before my arrival, ensuring a seamless learning experience.
In addition to managing IBD complications endoscopically, I benefitted
from exposure to Dr. Kochhar's IBD clinic, where I learned about emerging therapies soon to be available in India. I also observed clinical trials in drug-eluting balloons for endoscopic balloon dilation being conducted at AHN under Dr. Kochhar’s leadership.
Given my interest in advancing minimally invasive IBD therapies, I observed complex procedures such as endoscopic ultrasound-guided anastomosis, cholangioscopy, tissue acquisition, deep enteroscopy, and endoscopic suturing. These observations under expert guidance significantly enhanced my proficiency. I am indebted to advanced endoscopists, including Dr. Abhijit Kulkarni, Dr. Adam Kichler, Dr. Manish Dhawan, GI fellow Dr. Hardik Shah, and all the other faculty and support staff for making my journey a memorable one. I also experienced periodic masterclasses and multidisciplinary meetings at AHN.
Through ward rounds and interactions with Dr. Kochhar and his team, I deepened my
Partha Pal, MD, DNB, FASGE, MRCP (UK), Asian Institute of Gastroenterology, Hyderabad, India, Recipient, ACG International Training Award 2023
understanding and readiness to apply these advanced techniques. Dr. Kochhar's mentorship was instrumental in preparing me for my oral presentation at DDW 2024 on the CACTUS CD trial, comparing imaging techniques in Crohn’s disease. I also gathered essential tips during Dr. Kochhar’s and other experts’ talks at DDW on endoscopic management of IBD complications.
Back in India, I have initiated interventional IBD procedures at one of the few dedicated centers in the country, thereby making a substantial impact on IBD management nationwide. In the future, I intend to form an interventional IBD training center in India to train fellow colleagues across the country, disseminating the knowledge I gained in Pittsburgh.
I extend my heartfelt thanks to ACG for this transformative opportunity, which has profoundly advanced my expertise in the field of endoscopic management of IBD complications.
Photo opposite page: Dr. Gursimran Kochhar and Dr. Pal. Photos this page clockwise from top left: Dr. Pal in front of AHN Allegheny General sign. Dr. Pal and Dr. Gursimran Kochhar. Dr. Hardik Shah and Dr. Pal. Dr. Pal
FROM A PATIENT’S POINT OF VIEW
How, exactly, does trauma-informed care make a difference?
By Trisha M.
Trisha M. approached ACG MAGAZINE as a forum to publish her personal reflection on her experience of colonoscopy. We honored her preference to remain anonymous as the author.
Content Warning: Discussion of past assault and medical procedures
As a patient, I try my best to live a healthy lifestyle and to follow the recommendations of medical science. I exercise, I wear sunscreen, and I attend to my recommended screenings on time, every year. So as my 50th birthday approached, I knew I was due for a colonoscopy. Thankfully, several of my friends had reassured me that "it’s not as bad as you might think,” and I scheduled the initial consultation.
If I could change one thing about that initial conversation with my GI doctor, though, I would’ve told him right away that I am a rape survivor. I was vaguely aware of the term “trauma-informed care,” but I didn’t understand how it could make a difference in the face of a procedure like colonoscopy. (After all, the procedure itself doesn’t change, so what options did I really have?) I remember wrestling with whether or not to broach the topic as I walked to his office; my OB/GYN knew of my trauma
“I was vaguely aware of the term 'traumainformed care,' but I didn’t understand how it could make a difference in the face of a procedure like colonoscopy.”
history, certainly, but was it relevant here, in preparation for a colonoscopy?
My GI doctor was welcoming and patient, and he was enthusiastic about his role in preventing colon cancer. He encouraged my questions. He exuded cheerfulness, professionalism, and candor. I liked him, and I trusted him. We talked through my medical history – such as my history of deep vein thrombosis and ongoing anticoagulation – but I didn’t mention the rape. We set a date for the procedure, and I left the office feeling as well-prepared as any first-timer could be.
Two weeks before the procedure, I had a horrendous nightmare about it. I muscled my way through a slew of panic attacks, I set up an extra counseling session or two, and I sought advice from my GI doctor’s office. But I was too overwhelmed. When I say “nightmare,” I don’t mean just a bad dream about monsters, I mean a full-on PTSD re-living of the rape. And in this nightmare, it all happened again in the imagined context of my upcoming colonoscopy, complete with the detail that sedation kept me utterly unable to respond yet fully aware and feeling everything.
Yes, it was that bad.
In retrospect, maybe I shouldn’t have been surprised by the nightmare’s appearance as my colonoscopy date grew closer. Even though my assault happened over thirty years ago, it is something I carry with me every moment of every day.
In that moment, Fear won. I canceled the colonoscopy.
It took months for me to try again, and to ask about what traumainformed practices might be possible. I requested an additional consultation appointment before rescheduling the procedure itself. For that, my doctor led me to his office—not an exam room— and I confided in him about my history, my beyond-the-pale anxieties, my nightmare—everything. His empathy and patience resonated as he replied, “I’m glad you’re telling me this now. Let’s think about how we can get through this together.”
Trauma-informed care, he said, includes room for slight modification
to “the usual way” of going about a medical procedure—modifications that are non-essential to the procedure being performed but can be essential to the patient.
He told me who would be in the room, he described how my body would be positioned—and covered— and he explained the sequence of events: before the procedure, during, and afterward. And he invited me to think about adjustments that might help me feel more comfortable. (There are many options here, and what worked for me might be horrifically triggering to another survivor. What’s most important is the conversation, and the choice.)
I replied that, most of all, I needed him to be verbally repetitive in reminders of my safety: “I’m with you.” “I see you.” “I’m here to keep you safe.” And, knowing of my tendency to shiver violently when I am upset, I asked for warm blankets. We laughed as we realized how simple these requests were. Simple, but powerful.
I’m not going to sugar-coat how hard it was: On procedure day, I was still terrified. My nurse was wonderful, promising that she’d be with me the whole time. Being hooked up to the various monitors and even getting the IV in place was not upsetting to me, although I know those essential parts are worrisome to patients even without trauma histories. My doctor came to check on me several times, and at each visit he reminded me, “I know how hard this is for you, and I thank you for your trust. I’m going to keep you safe.”
When I woke up, I was indeed covered in warm blankets. It was my husband’s voice that I heard first, softly calling my name. Those two elements, warmth and my husband’s voice, set me on tangibly good footing for this recovery stage. I felt fine, physically— there was no discomfort. It took several minutes for me to become aware of where I was and what had just
“Now, hopefully, I can help other fearful patients talk to their doctors with more candor than they might have otherwise; I hope, too, that my experience can help physicians understand just how critical trauma-informed practices can be.”
happened.
Once that realization dawned, I started to cry, and I didn’t stop for well over an hour. I didn’t want to open my eyes, because seeing that I was in a hospital room would only remind me of what had just happened to my body. At times it was a trickle of tears down my cheeks; at others it was curledup, wracking sobs.
Later that afternoon, after a nap and some food, I sent a message to my doctor in which I asked him to thank our team of nurses, to assure them that I felt their care even though I couldn’t visibly respond in the moment.
Now, writing about this experience, I’ve found a more holistic perspective. Consider, from my point of view, what this procedure required of me: it’s a voluntary procedure, yes, but it’s so strenuously recommended that it feels required. Combined with my history of trauma, that sense of obligation can diminish my feelings of autonomy regarding what happens to my body. Of course, I want to protect my life and my future health, yes! But in order to do so, I had to legally consent to having a probe inserted into my body, where it would fish around and press into every crevice inside me. All while projecting images on a screen for everyone in the room to see. All while I was unconscious. I had to state—verbally and in writing—that I wanted this to happen to me.
That alone is a devastatingly hard fact to reconcile. I likely would not have been able to move beyond it without my doctor’s empathy, patience, and willingness to employ trauma-informed care practices. For me, there were three critical elements. First, even while I was sobbing and, in
“My doctor and nurses allowed the space for me to feel scared: They offered me comfort, and they were brave in the face of my tears.”
truth, unable to be comforted despite everyone’s best efforts, my doctor gave me the space to feel everything I was feeling. No one tried to minimize my experience by saying, “It’s no big deal! You’ll be fine!” and no one said the absurd lie, “There’s nothing to be scared of!” Because, despite the routine nature of this preventive—and critically important—medical procedure, I did have a lot to be scared of. My doctor and nurses allowed the space for me to feel scared: They offered me comfort, and they were brave in the face of my tears.
Second: tangible, sensory comforts. For me, these were the warm blankets I asked my doctor for. At one point I had six warmed blankets covering me. And as I walked out of the hospital, I did not shiver.
Third, and most foundationally, my doctor’s openness to a difficult conversation. It helped me to know in advance what the details of this procedure would entail. He was willing to listen. He reminded me of my safety, yes, but he never, ever minimized my reactions to this day. Instead, he affirmed them. He held my trust as sacred, and he welcomed my insights as a partner in this procedure.
I’m thankful that I don’t have to end this with a statement of, “And that colonoscopy saved my life.” My findings were as relatively normal as can be.
Now, hopefully, I can help other fearful patients talk to their doctors with more candor than they might have otherwise; I hope, too, that my experience can help physicians understand just how critical traumainformed practices can be.
And when I’m due for another colonoscopy, I’ll be there.
My doctor will bring the warm blankets.
Inside the JOURNALS
AN
UPDATE TO ACG’S
CLINICAL
GUIDELINES on Helicobacter pylori infection by Chey, et al., offers substantial changes to earlier recommendations for treatment naïve and treatment experienced patients.
More in the Red Journal: read and listen to a podcast on the risks of hepatocellular carcinoma in cases of indeterminate liver nodules.
In CTG, authors put ChatGPT to the test with questions about symptoms and treatments for gastrointestinal conditions as well as definitionbased queries on prevalent topics in gastroenterology.
ACG Case Reports Journal welcomes its 2024-2025 Editorial Board under the leadership of Prateek Harne, MBBS, MD, and Muhammad Nadeem Yousaf, MD. This journal is edited by GI fellows-intraining.
ACG Clinical Guideline: Treatment of HelicobacterpyloriInfection
William D. Chey, MD, FACG; Colin W. Howden, MD, FACG; Steven F. Moss, MD, FACG; Douglas R. Morgan, MD, MPH, FACG; Katarina B. Greer, MD, MSEpi; Shilpa Grover, MD, MPH; Shailja C. Shah, MD, MPH. The American Journal of Gastroenterology 119(9):1730-1753, September 2024. | DOI: 10.14309/ajg.0000000000002968
An updated clinical practice guideline offers therapy options and recommendations for Helicobacter pylori infection among treatment naïve and treatment experienced patients. The authors provide “substantial changes” to the 2017 guideline and address who to test, the need for universal post-treatment test-of-cure, and antibiotic susceptibility testing.
READ: bit.ly/acg-h-pylori-2024
Most Read in Red: Natural History of Indeterminate Liver Nodules in Patients with Advanced Liver Disease: A Multicenter Retrospective Cohort Study
Amit G. Singal, MD, MS; Neehar D. Parikh, MD, MS; Kirti Shetty, MD; Steven-Huy Han, MD; Cassie Xie, MS; Jing Ning, PhD; Jo Ann Rinaudo, PhD; Ashwini Arvind, MD; Anna S. Lok, MD; Fasiha Kanwal, MD, MSHS; the Translational Liver Cancer Investigators. The American Journal of Gastroenterology 119(11):2251-2258, November 2024. | DOI: 10.14309/ajg.0000000000002827
In this large multicenter cohort study, authors found that the magnitude of hepatocellular carcinoma (HCC) risk is high yet variable in patients with indeterminate liver nodules. HCC risk was 4-fold higher in patients with LI-RADS 4 (LR-4) than those with LI-RADS 3 (LR-3) lesions.
Azhar Hussain, MBBS; Vishnu Charan Suresh Kumar, MBBS; Hafiz Muzaffar Akbar Khan, MD. ACG Case
READ: bit.ly/acgcrj-hussain-et-al
BEHIND THE CASE: ACGCRJ Associate Editor Dr. Tina Boortalary is joined by advanced endoscopist and former ACGCRJ Co-Editor-inChief Dr. Nicholas McDonald to discuss this unique case published in the August 2024 issue.
Digesting Digital Health: A Study of Appropriateness and Readability of ChatGPTGenerated Gastroenterological Information
Avi Toiv, MD; Zachary Saleh, MD; Angela Ishak, MD; Eva Alsheik, MD; Deepak Venkat, MD; Neilanjan Nandi, MD, FACG; Tobias E. Zuchelli, MD. Clinical and Translational Gastroenterology 15(11):e00765. November 2024. | DOI: 10.14309/ ctg.0000000000000765
Authors analyzed responses generated by ChatGPT to 16 dialog-based queries assessing symptoms and treatments for gastrointestinal conditions and 13 definition-based queries on prevalent topics in gastroenterology. Three board-certified gastroenterologists evaluated output appropriateness with a 5-point Likert-scale proxy measurement of currency, relevance, accuracy, comprehensiveness, clarity, and urgency/next steps. ChatGPT responses to 44% of the 16 dialog-based and 69% of the 13 definitionbased questions were deemed appropriate, and the proportion of appropriate responses within the two groups of questions was not significantly different (P = 0.17). Notably, none of ChatGPT’s responses to questions related to gastrointestinal emergencies were designated appropriate.
READ: bit.ly/ctg-digesting-digital-health
Meet the 2024–2025 ACGCRJ EDITORIAL BOARD
Prateek Harne, MBBS, MD
Editor-in-Chief
Allegheny Health Network Pittsburgh, PA
Muhammad Nadeem Yousaf, MD
Editor-in-Chief
University of Missouri Columbia, MO
Daniyal Abbas, MD
Associate Editor Harlem Hospital Center New York, NY
Dushyant Dahiya, MD
Associate Editor University of Kansas Kansas City, KS
Daniel Marino, MD, MBA
Associate Editor
NYU Langone
New York, NY
ACGCRJ is a fully open access journal. View all published case reports for free. acgcasereports.com
Thanks to outgoing ACGCRJ Editorial Board members!
We thank the outgoing members of the Editorial Board for their outstanding service to the Journal and wish them continued success in their careers.
Vibhu Chittajallu, MD
Khushboo Gala, MBBS
Smit Deliwala, MD
Banreet Dhindsa, MD
Yue-Sai Jao, MD
Sonya Bhaskar, MD
Associate Editor University of South Florida Tampa, FL
Umer Farooq, MD
Associate Editor St. Louis University St. Louis, MO
Krystal Mills, MD
Associate Editor
Mayo Clinic Rochester Rochester, MN
Tina Boortalary, MD
Associate Editor Thomas Jefferson University Philadelphia, PA
Abel Joseph, MD
Associate Editor Stanford University Stanford, CA
Ahmed Telbany, MD, MPH
Associate Editor
University of New Mexico Albuquerque, NM
Robert J. Pattison, MD, MPH
Nicholas Placone, MD
Shazia Rashid, MD
Achintya Singh, MD
Gianna Stoleru, MD
Vaishnavi Boppana, MD
Associate Editor
University of New Mexico Albuquerque, NM
Rahul Karna, MD
Associate Editor
University of Minnesota Minneapolis, MN
Himesh Zaver, MD
Associate Editor
University of Virginia Charlottesville, VA
ACG GUIDELINE Highlights
ACG GUIDELINE Highlights
Epidemiology
Treatment of Helicobacter pylori Infection
Epidemiology
When to Test for H. pylori
Epidemiology
When to Test for H. pylori
When to Test for H. pylori
Treatment for H. pylori
for
Abx = antibiotic
b.i.d. = twice a day
Treatment of Helicobacter pylori Infection
William D. Chey, MD, FACG; Colin W. Howden, MD, FACG; Steven F. Moss, MD, FACG; Douglas R. Morgan, MD, MPH, FACG; Katarina B. Greer, MD, MSEpi; Shilpa Grover, MD, MPH; Shailja C. Shah, MD, MPH
Concept and Content: Erica Duh, MD | Reviewers: William D. Chey, MD, FACG and Shailja C. Shah, MD, MPH
Treatment of Helicobacter pylori Infection
William D. Chey, MD, FACG; Colin W. Howden, MD, FACG; Steven F. Moss, MD, FACG; Douglas R. Morgan, MD, MPH, FACG; Katarina B. Greer, MD, MSEpi; Shilpa Grover, MD, MPH; Shailja C. Shah, MD, MPH
• H. pylori prevalence in North America is 30%-40%
Typically acquired in childhood
Concept and Content: Erica Duh, MD | Reviewers: William D. Chey, MD, FACG and Shailja C. Shah, MD, MPH
William D. Chey, MD, FACG; Colin W. Howden, MD, FACG; Steven F. Moss, MD, FACG; Douglas R. Morgan, MD, MPH, FACG; Katarina B. Greer, MD, MSEpi; Shilpa Grover, MD, MPH; Shailja C. Shah, MD, MPH
• H. pylori prevalence in North America is 30%-40%
• More prevalent among non-White races or ethnicities, those living in crowded or poor sanitary conditions, and early generation immigrants from endemic regions.
Concept and Content: Erica Duh, MD | Reviewers: William D. Chey, MD, FACG and Shailja C. Shah, MD, MPH
• Typically acquired in childhood
Benign Conditions
• H. pylori prevalence in North America is 30%-40%
Premalignant and Malignant Conditions
• Typically acquired in childhood
• More prevalent among non-White races or ethnicities, those living in crowded or poor sanitary conditions, and early generation immigrants from endemic regions.
Conditions
• Adult household members of H. pylori positive individuals
• High risk gastric premalignant condition
• More prevalent among non-White races or ethnicities, those living in crowded or poor sanitary conditions, and early generation immigrants from endemic regions.
• Dyspepsia if <60 years without alarm features (GI bleeding, vomiting, unexplained weight loss, iron deficiency)
• ITP
Benign Conditions
• Dyspepsia if <50 years with high risk for gastric cancer
• Dyspepsia if <60 years without alarm features (GI bleeding, vomiting, unexplained weight loss, iron deficiency)
• Unexplained IDA
• Current or prior history of PUD
• Adult household members of H. pylori positive individuals
• ITP
• Dyspepsia if <50 years with high risk for gastric cancer
• Dyspepsia if <60 years without alarm features (GI bleeding, vomiting, unexplained weight loss, iron deficiency)
• Endoscopy with biopsies if dyspepsia and alarm features, NSAID use, family history of gastric cancer, immigration from high incidence region
• Dyspepsia if <50 years with high risk for gastric cancer
• Endoscopy with biopsies if dyspepsia and alarm features, NSAID use, family history of gastric cancer, immigration from high incidence region
• PPI b.i.d.
• Endoscopy with biopsies if dyspepsia and alarm features, NSAID use, family history of gastric cancer, immigration from high incidence region
bismuth quadruple
Optimized bismuth quadruple
Rifabutin Triple
Optimized bismuth quadruple
Rifabutin Triple
PCAB Dual
Rifabutin Triple
• Unexplained IDA
- Atrophy, intestinal metaplasia, dysplasia
• High risk gastric premalignant condition
• MALT lymphoma
Premalignant and Malignant Conditions
• MALT lymphoma
Premalignant and Malignant Conditions
- Autoimmune gastritis
• Adult household members of H. pylori positive individuals
• ITP
• Chronically taking NSAID or starting daily aspirin therapies
• Unexplained IDA
• Current or prior history of PUD
• Chronically taking NSAID or starting daily aspirin therapies
• Chronically taking NSAID or starting daily aspirin therapies
• Current or prior history of PUD
• Tetracycline 500 mg q.i.d.
• PPI b.i.d.
• High risk gastric premalignant condition
- Atrophy, intestinal metaplasia, dysplasia
- Family history of gastric cancer
- Autoimmune gastritis
- Foreign born with immigration from high incidence region
- Atrophy, intestinal metaplasia, dysplasia
- Family history of gastric cancer
- High risk race or ethnicity
- Autoimmune gastritis
- Foreign born with immigration from high incidence region
- Family history of gastric cancer
- High risk race or ethnicity
- Foreign born with immigration from high incidence region
William D. Chey, MD, FACG; Colin W. Howden, MD, FACG; Steven F. Moss, MD, FACG; Douglas R. Morgan, MD, MPH, FACG; Katarina B. Greer, MD, MSEpi; Shilpa Grover, MD, MPH; Shailja C. Shah, MD, MPH The American Journal of Gastroenterology 119(9):p 1730-1753, September 2024. | DOI: 10.14309/ ajg.0000000000002968
William D. Chey, MD, FACG; Colin W. Howden, MD, FACG; Steven F. Moss, MD, FACG; Douglas R. Morgan, MD, MPH, FACG; Katarina B. Greer, MD, MSEpi; Shilpa Grover, MD, MPH; Shailja C. Shah, MD, MPH The American Journal of Gastroenterology 119(9):p 1730-1753, September 2024. | DOI: 10.14309/
ajg.0000000000002968
William D. Chey, MD, FACG; Colin W. Howden, MD, FACG; Steven F. Moss, MD, FACG; Douglas R. Morgan, MD, MPH, FACG; Katarina B. Greer, MD, MSEpi; Shilpa Grover, MD, MPH; Shailja C. Shah, MD, MPH The American Journal of Gastroenterology 119(9):p 1730-1753, September 2024. | DOI: 10.14309/ ajg.0000000000002968
= three times a day
Treatment
H. pylori Regimens for H. pylori Treatment
Attend an upcoming
ACG POSTGRADUATE COURSE
ACG POSTGRADUATE COURSE Attend an upcoming
2024
2024 ACG’s Functional GI and Motility Disorders School & Southern Regional Postgraduate Course
ACG Weekly Virtual Grand Rounds
2024
December 6–8, 2024
REGISTER NOW: gi.org/ACGVGR
ACG Weekly Virtual Grand Rounds
Renaissance Nashville Hotel, Nashville, TN
2024 ACG’s Functional GI and Motility Disorders School & Southern Regional Postgraduate Course
2025
December 6–8, 2024
Plus our monthly webinar series focused on career-based topics!
REGISTER NOW: gi.org/ACGVGR
2025 ACG’s NEW Esophagus School & Western Regional Postgraduate Course
Renaissance Nashville Hotel, Nashville, TN
Plus our monthly webinar series focused on career-based topics!
2025
January 24–26, 2025
Mandalay Bay, Las Vegas, NV
2025 ACG’s NEW Esophagus School & Western Regional Postgraduate Course
January 24–26, 2025
2025 ACG’s IBD School & ACG/FGS Annual Spring Symposium
March 7–9, 2025
Mandalay Bay, Las Vegas, NV
Naples Grande Beach Resort, Naples, FL
2025 ACG’s IBD School & ACG/FGS Annual Spring Symposium
2025 ACG/LGS Regional Postgraduate Course & Women Leading with Guts Course
March 7–9, 2025
March 14–16, 2025
Naples Grande Beach Resort, Naples, FL
DoubleTree by Hilton, New Orleans, LA
2025 ACG/LGS Regional Postgraduate Course & Women Leading with Guts Course
March 14–16, 2025
2025 ACG’s Endoscopy School & Eastern Regional Postgraduate Course
June 6–8, 2025
DoubleTree by Hilton, New Orleans, LA
Washington Marriott Metro Center, Washington, DC
2025 ACG’s Endoscopy School & Eastern Regional Postgraduate Course
June 6–8, 2025
2025 ACG’s Functional GI and Motility Disorders School & Midwest Regional Postgraduate Course
August 22–24, 2025
Washington Marriott Metro Center, Washington, DC
Marriott Indianapolis Place, Indianapolis, IN
2025 ACG’s Functional GI and Motility Disorders School & Midwest Regional Postgraduate Course
August 22–24, 2025
2025 ACG’s NEW Esophagus School & ACG/VGS/MASGNA Regional Postgraduate Course
Marriott Indianapolis Place, Indianapolis, IN
September 5–7, 2025
Williamsburg Lodge, Williamsburg, VA
2025 ACG’s NEW Esophagus School & ACG/VGS/MASGNA Regional Postgraduate Course
September 5–7, 2025
Williamsburg Lodge, Williamsburg, VA
FOCAL LIVER LESIONS
Information for Patients, Parents, and Caregivers: Understanding ACG’s Clinical Guideline on Focal Liver Lesions
WHAT ARE FOCAL LIVER LESIONS?
A focal liver lesion is a growth that can be seen on imaging, such as a CT scan or MRI scan. These are usually benign (non-cancerous), but they may require follow-up or more testing to make sure they do not change into cancer. Those at risk for developing focal liver lesions may include individuals with obesity or polycystic ovary syndrome (PCOS) and those using hormonal therapy, including birth control pills or anabolic steroids. These lesions often do not cause any symptoms and can be found in patients who have no history of liver disease.
QUESTIONS FOR YOUR DOCTOR
• What tests do I need to find out if anything needs to be done for this lesion?
• Will this lesion require any treatment, or how should I monitor this lesion?
ACG TREATMENT GUIDELINES
• If a lesion is found, your doctor will ask you some questions about symptoms (such as weight loss), or reasons you may have chronic liver disease (like viral hepatitis), and risks for having cancer.
• A blood sample will check your liver function tests, rule out viral hepatitis, and search for cancer-specific markers.
• Your doctor will also often recommend further liver scans to see the type of lesion you have.
LEARN MORE
Read the 2024 Guideline: bit.ly/ajg-frenette-et-al
• Is there any chance of this lesion becoming cancer?
RISKS AND COMPLICATIONS
• Your doctor may recommend a test to sample the liver lesion, known as a biopsy, if the scan looks abnormal or is growing quickly.
• If cancer is suspected or diagnosed, you may need surgery to remove the lesions.
• Surgery may be more likely if you have large lesions (larger than two inches), are a man, or have a specific marker in your blood called beta-catenin that may increase the risk of cancer.
Find a gastroenterologist near you: gi.org/FindaGI