
Intravascular QUARTERLY Global Disclaimer: The views and opinions expressed in the Intervascular Quarterly Newsletter are those of the authors and do not necessarily reflect the official policies or positions of the Association for Vascular Access (AVA) or any of its leaders, volunteers, employees, committees, networks or other groups associated with AVA. For information on this publication, please email info@avainfo.org.



3 AUGUST 2022 | VOLUME XII | ISSUE 3 THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS A GLIMPSE AT THE FUTURE OF POST-ACUTE CARE .................... 05 INITIATION OF A ROBUST CLABSI BUNDLE: ONE NICU’S JOURNEY TO ZERO HARM ........................................................................ 08 WELCOME TO OUR NEWEST MEMBERS ............................................. 10 2023 AVA BOARD OF DIRECTORS ........................................................... 12 A DECADE OF SECURITY: DATA-DRIVEN PRACTICE CHANGE 14 ULTIMATE GUIDE TO PICCS FOR PATIENTS AND CAREGIVERS: AVA AND MIGHTY WELL COLLABORATE TO EMPOWER PATIENTS LIVING WITH PICCS ................................................................. 17 2022 AWARD WINNERS .............................................................................. 18 ISAVE THAT PODCAST SEASON 5 ........................................................... 21 SELF-ADVOCACY SAVED MY LIFE ........................................................ 22 SAFER TOGETHER: A NATIONAL ACTION PLAN TO ADVANCE PATIENT SAFETY .............................................................................................. 26 IMPACT CASE STUDY: HENRY FORD HOSPITAL’S HEMATOLOGYONCOLOGY UNIT USES AHRQ SAFETY PROGRAM TO LOWER BLOODSTREAM INFECTIONS .................................................................... 28 NETWORK NEWS ............................................................................................. 31 THANK YOU INDUSTRY PARTNERS ...................................................... 36 IQ CONTENT


REFERENCES 1.Doraiswamy S, Abraham A, Mamtani R, Cheema S. Use of telehealth during the COVID-19 pandemic: scoping review. Journal of medical internet research. 2020;22(12):e24087. 2.Banksdoi:10.2196/24087MA.The Growing Case for Health System Pharmacies. Specialty Pharmacy Continuum. Published July 8, 2022. Accessed July 14, 2022. System-Specialty-Pharmacies/67462specialtypharmacycontinuum.com/Online-First/Article/07-22/The-Growing-Case-For-Health-https://www.
If the COVID-19 Pandemic has taught us anything, it is that care delivery models are rapidly evolving in healthcare. Now more than ever patients are receiving care outside of the acute care setting through telehealth, outpatient clinics, and in-home therapies with the aim of reducing unnecessary hospital admissions and emergency department visits.1 Another vital goal of this transition is the reduction of cost amongst healthcare systems. One such example is that the cost associated of Intravenous Gamma Globulin therapy (IVIG) administration in the home setting is 62% lower than in a medical office and 87% lower than the hospital outpatient setting.2 To answer this need, home infusion and outpatient ambulatory care facilities are developing models that facilitate the shift of patients to a clinic or home-based care.
VA-BC™ AVA Clinical
VA-BC™, LN Chair-Elect BACSIG
There have been great strides in this area, but there is still work to be done to provide more services in patient homes, medical offices, and outpatient Asclinics.novel
J.Blake Hotchkiss BSN, CCRN, Education Specialist
The Beyond Acute Care Special Interest Group (BACSIG) has been working diligently over the past year to increase its membership with the goal to embark on developing new educational opportunities designed to improve vascular access care across the continuum of patient care. This includes tapping into the experience and knowledge of a diversified group comprised of patients, families, caregivers, nurses, respiratory therapists, vascular access specialists, discharge planners, skilled nursing and rehab facilities, infusion centers, home infusion organizations, home care agencies, mobile vascular access services, outpatient clinics, and their respective professional membership societies and associations. So far we have identified interested members who practice in one or more of these many settings and subsequently appointed new people the BACSIG Executive Leadership Committee. In the near future, we will be calling on our SIG members to join us as we move forward and put our vision into action.
A CAREPOST-ACUTEFUTUREATGLIMPSETHEOF
5 AUGUST 2022 | VOLUME XII | ISSUE 3
solutions to key problems in these practice settings are being developed, one gap that still exists is the variance in practice driven by the lack of consistent education of clinicians around safe vascular access care and maintenance. Despite our best efforts, patients and their caregivers still have a limited number of resources and education available to them regarding vascular access devices.
Erik Samarpan RN,
In 2018, the Center for Medicare Medicaid Services reported that there were 11,869 home health agencies registered in the U.S. alone. According to The Fortune Business Insights in their 2022 forecast report, the home infusion therapy market size was 34.54 billion in 2021.2 They forecast that the size will increase by 6.8% from 2021 through 2028.2 With the post-acute care market continuing to expand at a brisk pace, clinicians need resources to help educate and inform patients.
RN,

6 INTRAVASCULAR QUARTERLY THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS © 2021 Care+Wear. All rights reserved. Using PICC line covers can save healthcare systems 1 billion dollars by reducing PICC line migration © 2022 Care+Wear. All rights reserved.
7 AUGUST 2022 | VOLUME XII | ISSUE 3 © 2021 Care+Wear. All rights reserved. Care+Wear PICC line cover improves patient and physician overall experience while reducing costs © 2022 Care+Wear. All rights reserved.
INITIATION OF A ROBUST CLABSI BUNDLE: ONE NICU’S JOURNEY TO ZERO HARM 8 INTRAVASCULAR QUARTERLY THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS
INTRODUCTION
CHG (Chlorhexidine gluconate) bathing is performed on older babies to help decrease the risk of infections. ON NEXT PAGE
CONTINUED
Angela A. Alderman RNC-NIC, BSN, VA-BCTM
The Neonatal Intensive Care Unit (NICU) consists of one of the most vulnerable patient populations within the healthcare system. For patients with extremely low birthweights and immature immune systems, preventioninfectioncontinues to be a challenge for those care providers even with the best of intentions in mind. Like most institutions, the prevention of central line associated blood stream infections (CLABSI) has become a priority from a cost and patient safety perspective. Preterm or sick infants depend on central lines to provide nutrition and medication for several weeks and sometimes months after birth. Umbilical catheters and peripherally inserted central catheters (PICC) are widely utilized in this population and require special care. Antiseptic solutions, adhesive use, and venous depletion have become problematic in small babies creating chemical burns, adhesive trauma, and disruptions in skin integrity. The utilization of small catheters has led to an increased risk of thrombus formation and line occlusions. With all the forementioned complications, a zero CLABSI rate seems daunting and incredibly challenging. Just like any other journey, creating a CLABSI bundle has twists, turns, unexpected paths, and inevitably you reach the destination to zero. So, you must ask the question, “What’s the secret to a successful trip?”
WHAT IS IN YOUR CLABSI BUNDLE? Many institutions assess the need for robust bundle solutions based on data. We ask ourselves, “do we really have a problem?” or state, “we have a low CLABSI rate.” Shifting the focus to prevention of harm is imperative. One of the bestkept secrets is this pivot of culture. This culture shift ensures everyone is responsible for the line no matter the role they play on the healthcare team. In our institution, we succeeded in obtaining a ZERO CLABSI rate in the NICU for more than a year. This did not come without challenges. We started with low hanging fruit. Designated line carts were stocked with supplies for changing fluids and dressings. Custom preassembled IV sets were created to avoid piecing fluid tubing together for uncomplicated fluid changes. A custom dressing change kit was also created. Each intervention aims to avoid the risk of touch contamination. We standardized our dressing change and insertion process and created a PICC team within the NICU comprised of a specific group of neonatal nurses and nurse practitioners. This team inserts lines, changes dressings, discontinues lines, and handles all line and dressing complications. Research shows that having a specialized team is one strategy to decrease the risk of line infections and complications. All insertions, tubing changes, and dressing changes are observed and audited. This process is the new normal and has been cultivated by our culture of safety. Nursing leadership rounds on every central line several times a week utilizing bedside K-cards. During each shift, bedside team rounds discuss line necessity and line entries.
New products incorporated in our bundle elements were the use of tissue adhesive at insertion sites of all vascular access devices, CHG pledgets instead of alcohol for scrubbing needleless connectors prior to line entries, and alcohol-based port protecting caps. Having these pieces stocked and readily available to staff made them more likely to be used appropriately.
We developed and utilized educational pamphlets to partner with parents and caregivers of babies with central lines. The focus for this education is on infection prevention, comfort, hand hygiene, and complications. In our journey we joined the Solutions for Patient Safety which gave us valuable resources and connections with other institutions. Assessing our feeding protocols and making changes to advance feedings in a timely manner meant fewer line days for most of our patients.
The creation of a CLABSI roadmap with all bundle elements was implemented and then incorporated in an electronic format for easier data collection. Bedside nursing staff are responsible for attesting these elements each shift. Our accountability equals reliability in CLABSI prevention.
Although we made significant improvements to the bundle, we revisited the most basic elements of any infection prevention strategy. We implemented UV light boxes for sanitizing cell phones, badges, pens, and watches for all staff and visitors. We re-educated staff on the importance of hand hygiene and placed important signs near sinks to help visitors and other staff maintain compliance.
THE SECRET TO A SUCCESSFUL JOURNEY
INITIATION OF A ROBUST CLABSI BUNDLE, CONTINUED FROM PREVIOUS PAGE
A change in culture with a focus on safety and harm prevention continues to be the key to our success as each intervention builds upon the next. Deep diving into central line infection cases and learning from each one must be a priority. Holding staff accountable with processes and procedures creates this culture shift. Remembering to pivot from “we can’t” to “how can we, despite our circumstances” opens the door to a multitude of possibilities. We have a motto in our children’s hospital, “Keeping 1 child safe means you’re a hero, keeping 100s of children safe means you’re a hero at Carilion Children’s.”
9 AUGUST 2022 | VOLUME XII | ISSUE 3

THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS Welcome to our Newest Members (Joined May 1, 2022 - August 1, 2022) Isabel MaeYvetteSidneeMeredithSujanaNigelAdreaGessnerAlexisKeithRichardAdetolaJoshuaLaurenTaraAnnaDaphneMelissaTamaraItohanGabrielleAriaBryanBrittanyCarliDaciaJessicaDavidsethJessicaEricaKathrynMonicapilarKristineFranAndresMaggieMorganAndreiaTekimbriaCindyImaniLauraJadaAddysenDianColleenRhiannonTannerLaRinaPaulCaitlinJanelyHannahAndreaNatalieKoryAllisonMitchelleJennaVictoriaAnievasFowlkesBobrickMwangiWrightEvensonHoffmannHiroskyRaymondBonilla-MendozaHaugheyLapreWinsteadGrazierSundstromHanniganWalkerWalkerLambJonesDavisChambersBartlettAllenCaldwellDeSpainTurnerMaresVillicanaCampbellLewisLawrenceMartinezSchmitzSharverMercadoTaylorTerranoLeavittGrahamBarnhartHsuTanisMochaCasonNavarreDarkoWilsonWrightStirnDukeAdedejiDoughertyBairdBakerPantleyKelleyRuseRupakhetiVogelPowellMezaJoyJarata Sarah LindseyGracePaulErinRebeccaTonyaRaeannMariaLindseyNeelBarbaraDarleneElmerLacyJon-EnRupMichelleMollySarahMariaPatriciaDarleneRhiannonKathleenArleneKellyAllanJenniferColleenBryanBenjaminFeliciaAmberBarbaraRoxannaRafaelCathyShaunAprilMadisonBeckyErinYoungSarahSarahJenniferEdeechelseaAmyKimberlyLoriCarrieNicoleAlejandroBradleyErinSadieMichaelMicheleAnabelHendricksHernandez-JohnsonRundall-AemmerChanWilcoxMullisMorganBeanesMitchellGrabruckLafleurGurnettWalthierlangWhitakerIveyNguyenDonahueHeeKimMeyersElliottIvanoffWinborneMcFerrenWillsBokowEstesTanisCheekAsherWiechmanKitchenKellyWujecCatalanStewartTurtonPrattGoudreauYuenPerezVargasMauriWrightBarnesMalchowAmatyaYeungBurdetteJaldinGarnerBarrettPatelSheldonTeresaRecondoWolfMinnsPierceNelsonMooreHillardUndis Eric White Kari BrookeMichaelAnnaChelseaChelseaBryanDerekSarahKaityShannonSarahEdwardDanaKevinNorelleMargaritaMaxineTamaTanyaRupBusayoMariaKangSantoshNancyJessicaElviraMubinShingMarie-GraceCarolynSarahRowenaLeighElizaLynetteReginaldMicheleBrendaNancyMichaelTaraMattJenniferMichaelPamelaMeganCatherineGretchenWhitneyHeatherKathrynMichelleGaajGeenaLeslieMichaelBrandonMorganEatonColungaGoldenArackalMeyerJohnsonRobinsonDombroskyHaleMelbyKaneSchellingGilzingerMathisonWiederholtMisleyMcConnPhanWardenMorrisonBoyce-ObenchainRamirezJoyRomanovitchDuatinChynowethTorralbaCookThomasMarcheseSheungYousufCastroMeyerSloanTelangShenCruzGbadeboShahAcharyaLlanqueCarlinFearringtonMurilloMitchellTownsellMartinEstanteGatesPenningtonKirbyBivensFoxMcDonaldYoungHendersonClouserMcCuenSnyder Marissa Ziniti Leslie LeandroSearfossRojas Arias Murielle Laime Sasha ElizabethKerieJohnTylerColetteAmyShelbiBridgetteTrishaMatthewLindseyKaylaMatthewXuStringfellowSheilaChristineBrianaMelissaWhitneyToniStacyMargretJonathanEvelynJaimeTheresaAllisonChrisHammamStephanieAmandaDavidTedCandiceKarenMindiluTylerRonaldKristinaFrancesMelyshaRebeccaAndreaAnneKerriAngieDawnKariDebraSilviaTaraMaryCherylDonnaHarrisCampionWestmorelandCarboneMelvinMargalejoRaffinPowellCampbellRedmondMyersIrwinMcCloskeyPruittPruittShirnHearnRossTayagWoehlerMunteanMayGeiger-DowneyHobbsFehlKussowBroglenDurhamAhmedNickelGilbertMercadoCamachoDuronTeagueDistonAtkinsMcGiboneyDahmThorneBittermanClaxtonQuintiliani-XuemeiVarnumForshawTownsendGeorgeCakanicWoodcockKlopfensteinSarverKittGentryHallLopezUng Danielle AshleyLisaPhilippaManpreetCrallKaurSumlinFergusonHancock Hancock Sean M Tai Chieh kan Danielle Vilela Whitney CherylChrisDouglasAnastasiaLaurenTimMaimunaSteveShannonMariaVangieKeziaJenniferMichaelChrisVincentRhondaJoanCirliaBenjaminElizabethAlexaNicholasVictoriaSamanthaAnnaSethKarenJerryLaurenAdenikeRachaelKendallRebeccaGracieNicoleKyleyAlyssaMitchChantalLaceeOliviaMariaJuwanHannahDanicaKristaCynthiaHaleyMiaChristopherPageTurnerMartinezEmerickMaloyFrasierLaumanKolliegboMaloCuapingMcCloudAdamsVigbedorQuinaLeBartsKettenhofenCollinsRomanKleinWickstromShomakerPetersenAbelTidwellLindellRodriguezHullettBakerRoachStonehillBarkettRogersFaggionatoAlvarezBartelloBentleyBottiDavisFerraraFinlaysonFitzgeraldAmanGervaisDelMarGomezHillyerJacksonJallowKellyLussierThillMironovaShookBaconVaughns ®


Michelle DeVries will step into the President-Elect role, Staci Harrison will step into the Secretary role, and Nael Mhaissen will serve another term as Director-at-Large.
They will be joined by continuing Board Members
It is with great pleasure and honor that we inform you the slate of candidates for the 2023 AVA Board of Directors recommended by the AVA Board of Development Commission (BDC), has been accepted by the membership. Thank you to everyone who participated and cast their vote!
Tonya Heim, President, MHA, MSN, RN, NEA-BC; Tonja Stevens, AGACNP, RN, BSN, VA-BC™, Presidential Advisor, and; Directors-at-Large Karen Laforet, RN, MCISc-AHCP, CCHNⒸ, CVAAⒸ, VABC™, Chaitenya Razdan, MBA, and Nieltje Gedney, BA.
2023 SECRETARY: STACI HARRISON, DNP, RN Staci Harrison is an innovative leader with more than 25 years of experience in nursing. Currently, she serves as the Southern California Regional Director of Medical-Surgical and Critical Care for Kaiser Permanente, where she leads the vascular access workgroup. Staci has proven success in leadership roles where she has collaborated with groups to achieve excellent patient care outcomes. She has been instrumental in fostering the collaborative efforts across the Kaiser Healthcare system while leading the vascular access workgroup. After earning her Doctor of Nursing Practice in 2017, she lends her knowledge at various universities as an instructor in their online curriculum. As a member of the board, she will utilize her collaborative and leadership skills to transport the mission and vision of AVA.
The individuals who will join the returning AVA Board Members on January 1st, 2023 are Mark Rowe, Lynn Deutsch, and Warren McGlauflin.
2023 TREASURER: MARK ROWE, MNSC, RNP, VA-BC TM Mark is a graduate of the University of Arkansas for Medical Sciences (UAMS) with both a bachelor’s and master’s in nursing science. His initial eight years in the art of nursing were in the specialty of burns/trauma but for the past 30 years, he has focused on Vascular Access as a clinical/education specialty. As a Senior Vascular Access Specialist, along with a great nursing team, assist by hosting the Vascular Access Residency program. He retired from beside service in December of 2021 but remain active in the education of the specialty. He was honored to serve as 2014-2015 Board President of the Association for Vascular Access (AVA) after serving as Director at Large for four years and past Scientific Meeting Chairperson.
2023 PRESIDENT-ELECT: MICHELLE DEVRIES, MPH, CIC, VA-BC TM, FAPIC
12 INTRAVASCULAR QUARTERLY THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS
INCOMING 2023 AVA BOARD MEMBERS
Chellie DeVries has been involved in Infection Control for more than 25 years, with a focus in vascular access. With a background in Hospital and Molecular Epidemiology her interest is in improving safety and outcomes associated with all types of vascular access devices. She has published and taught internationally and throughout the United States on topics at the intersection of vascular access, patient safety and Infection Prevention and previously served on the Vascular Access Certification Corporation (VACC) Board of Directors. She is currently serving as co-president of her local network (HoosierVAN) and is thrilled to join her colleagues as part of the National AVA board.



DIRECTOR2023-2024ATLARGE: LYNN DEUTSCH, MSN, RN, CRNI, VA-BC TM Lynn has been a nurse for 42 years and has worked as a vascular access nurse since 2000. She has an ADN, BSN, and MSN in nursing. She was CRNI of the Year in 2015. She has been certified in infusion therapy since 1997 and VA-BC since 2015. She has worked in a variety of settings including home infusion and ambulatory infusion. She currently works as an adjunct professor of nursing in the clinical setting in addition to her full-time vascular access position. She brings clinical expertise as a vascular access nurse and educator. She believes AVA is a multidisciplinary organization whose goal is to provide the best vascular access care to all patients. She believes in collaboration among other professional organizations to improve patient care. She looks forward to having the opportunity to serve this organization.
DIRECTOR2023-2024ATLARGE: WARREN MCGLAUFLIN, RN, BS, VA-BC TM Warren became involved in vascular access in 2008 when he joined radiology at Central Maine Medical Center. In 2010 he joined MEVAN (Maine Vascular Access Network) and AVA – it was at this time he attended his first AVA scientific meeting. This started his journey to learn all there was regarding the most current vascular access research and evidence-based practice. In 2015 he became a Nurse Leader covering the new revenue-based cost center for the vascular access team. This helped them develop into a more independent team working within the scope of practice of the members. Since the inception of the VAST he has sat on the CLABSI reduction committee and helped brings rates down to 0, as well as root cause committees, blood draw complication reduction committees, and policy writing for vascular access. He has remained committed to AVA remaining a member and having attended multiple scientific meetings as well as sitting on the D-Team (becoming chair for the 2022 scientific meeting) for 4 years.
Nael Mhaissen is a pediatric infectious disease physician at Valley Children’s Healthcare in Madera, California, where he has been serving in different leadership roles including: the medical director of the infectious disease division, the medical director of infection prevention and control, and the chair of the health information management committee. He also chairs the committee of vascular access safety, which is a collaborative workgroup he created joining the efforts and expertise of the vascular access and the infection prevention teams and shifting the paradigm from focusing on preventing CLABSIs to focusing on preventing ALL vascular access related safety issues.
Dr. Mhaissen believes that improving the quality of care and ensuring patient safety require a comprehensive and multidisciplinary approach that breaks the boundaries between the different disciplines and brings everyone’s expertise and goals together rather than focusing on the individual problems in silo.
13 AUGUST 2022 | VOLUME XII | ISSUE 3
DIRECTOR2023-2024ATLARGE: NAEL MHAISSEN, MD



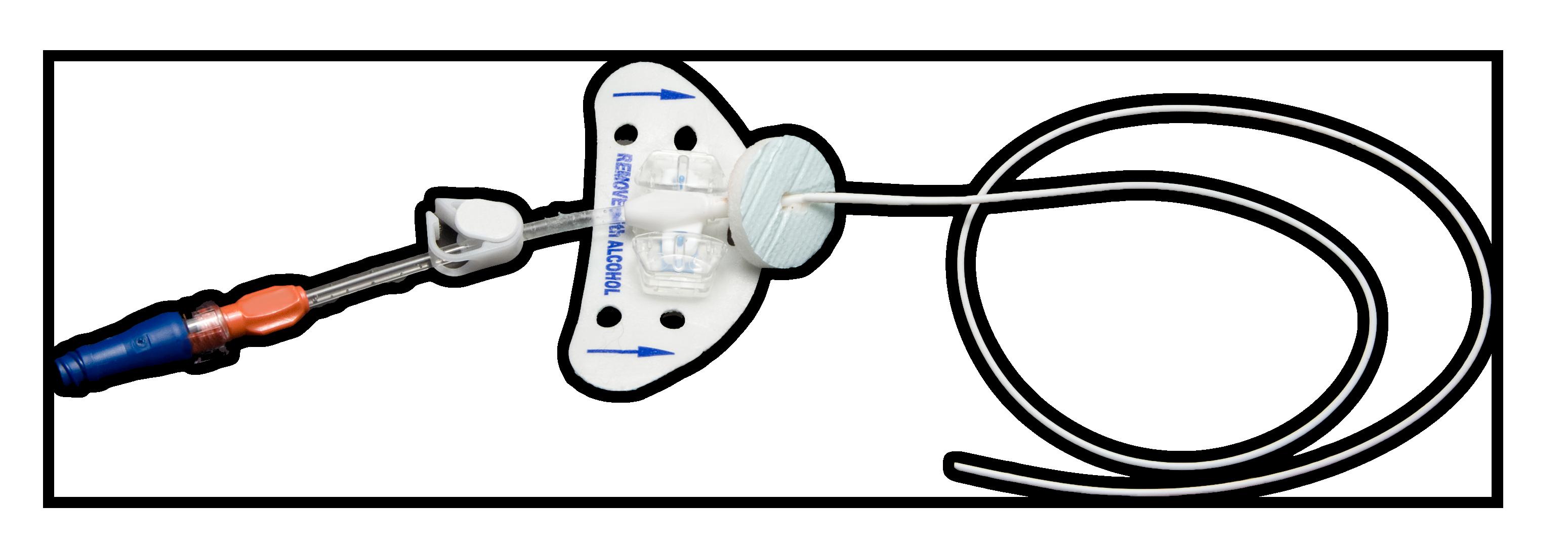
In my practice at The Clatterbridge Cancer Centre NHS Foundation Trust, Liverpool – a specialised cancer treatment centre based within the Merseyside and Cheshire region, England – many of our cancer patients may have a peripherally inserted central catheter (PICC) placed to receive various forms of intravenous therapies including chemotherapy and immunotherapies in addition to being able to retrieve atraumatic blood samples. The PICC must remain securely in place until the end of the patient’s need for the catheter. The end of need (EON) for this patient population may include stopping or completing therapy, moving to an implanted venous access device (IVAD, i.e., port, porta-cath), or through the end of life.
In 2007, I commenced the role of the Intraveous and Interventional Clinical Nurse Specialist prior to developing a larger vascular access team (VAT) as capacity and demand grew. One of the primary tasks of the role was to place PICCs, among other vascular access devices, for our large oncology population. As I believe data is vital to assess success or areas for improvement, I began tracking every patient from implant to explant of their PICC. From 2007 to 2011, various adhesive securement devices (ASD) were employed to ensure the PICC would stay in place through activities of daily living.1,2 Simultaneously, the VAT increased successful placements and continued to track results. The problem of catheter replacements secondary to migration and dislodgement became apparent. The below table shows the increased number of PICCs placed by our small team and the number of PICCs that reached the end of need during my first years in charge of the PatientsVAT.dealing with a cancer diagnosis, multiple infusions, blood specimens, side effects, and other life events should not be subject to catheter replacement and delays in treatment because a catheter was not secured. In 2012, the VAT explored options to decrease securement failures and came upon a completely different approach to securing catheters. A subcutaneous anchored securement system (SASS) deploys atraumatic nitinol feet under the skin while the patient is still numb from the lidocaine used during the insertion procedure. As the name implies, the device anchors the catheter and remains with the PICC until the end of need.3,4 With chemotherapy medications our patients receive, it is critical that we dwell the tip of the PICC in the lower one-third of the superior vena cava (SVC) near the cavalatrial junction.5 Hemodilution at this optimal position decreases the probability of vessel damage and thrombus formation. For a VAT member placing a PICC, 40cm to 50cm of the small catheter must be navigated past upper arm valves and vessel branches to reside in the target area. Securing the tip in this location depends on the clinician’s choice of engineered securement device (ESD) to safeguard the catheter in the optimal position.7
A DECADE OF SECURITY: DATA-DRIVEN PRACTICE CHANGE Carol McCormick, RN, BSc Hons, MSc CONTINUED ON NEXT PAGE YEAR OFNUMBERPICCSPLACED NUMBERRECORDEDREMOVALWITHDATA DWELLMEANTIME(DAYS) REACHINGNUMBERENDOFNEED REACHINGPERCENTENDOFNEED 2007 16 2 Not reported 0 0% 2008 26 4 109 3 75% 2009 119 59 88 34 59% 2010 193 193 105 147 76% 2011 313 313 103 258 82% Cumulative 667 571 101 442 77%
14 INTRAVASCULAR QUARTERLY THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS
Based on the repeated need for catheter replacement from 2007 to 2011 and the substantial increase in the VAT’s PICC placement requests, it became necessary to avoid catheter replacement, minimize additional patient trauma, and ensure appointments are available for new patients. Therefore, in 2012, after trying a couple of
YEAR SECUREMENTADHESIVEDEVICE ASD DWELLMEANTIME(DAYS) SUBCUTANEOUSANCHORSECUREMENTSYSTEM SASS DWELLMEANTIME(DAYS) 2009 58% 88 Unavailable NA 2010 76% 105 Unavailable NA 2011 82% 103 Unavailable NA 2012 77% 110 92% 132 2013 ND NA 93% 118 2014 ND NA 95% 111 2015 83% 140 96% 154 2016 92% 127 96% 141 2017 ND NA 96% 139 2018 ND NA 99% 128 2019 ND NA 100% 137 2020 ND NA 99% 163 This table shows results from 2009 through 2020. ND = Not enough data or < 30 subjects | NA = Not applicable YEAR SECUREMENTADHESIVEDEVICE SECUREDOFNUMBERPICCSWITHASD SUBCUTANEOUSANCHORSECUREMENTSYSTEM NUMBER OF WITHSECUREDPICCSSASS 2009 20% 59 NA 0 2010 12% 193 NA 0 2011 11% 313 NA 0 2012 14% 224 < 1% (0.4%) 231 2013 0% 5 < 1% (0.5%) 576 2014 17% 12 < 1% (0.5%) 800 2015 12% 42 < 1% (0.3%) 936 2016 5% 62 < 1% (0.6%) 1114 2017 7% 15 < 1% (0.003%) 1269 2018 0% 9 < 1% (0.003%) 1062 2019 0% 9 0% 1159 2020 0% 1 < 1% (0.003%) 1166 NA = Not available until 2012 CONTINUED ON NEXT PAGE
15 different adhesive securement devices (ASD), we discovered a subcutaneous anchor securement system (SASS) that was new to the Asmarket.4theSASS was first introduced, we trialed it on 30 patients and carefully tracked the results. The SASS is an entirely different method of securement from the ASD but did not take long to convince the VAT and the patients that it improved the likelihood of reaching the EON with one PICC. Interestingly, patients who, at the time of the trial period, had experienced a PICC failure when secured with an ASD and required a replacement, felt more confidence with the securement of their line and reported increased satisfaction with the service. As our team saw the improvement in the securement of the PICCs, we quickly decreased our use of ASDs. Significantly limiting the need for replacement for any reason, including; infection, skin issues, migration, and dislodgement, among others, was an important outcome for our patients and our Focusingteam. on the main reason for securing a catheter, our

- a problem of the past: Cross-sectional and health-economic comparison of adhesive and subcutaneous engineered stabilization devices for securing PICCs,” Journal of Vascular Access, 20(1), pp. NP6–NP7. Available at: https://www.embase.com/
5. Gorski, L.A. et al. (2021) “Infusion Therapy Standards of Practice, 8th Edition,” Journal of Infusion Nursing, 44(1S), pp. S1–S224. doi:10.1097/NAN.0000000000000396.
1. TIDI Products, L. (2020) Grip-Lok ® OEM Bulk Package. Neenah, WI.
2. Medcomp Components, Inc. (2019) STATLOCK ® PICC PLUS INSTRUCTIONS FOR USE. Harleysville, PA.
3. Macmillan, T. et al. (2018) “SecurAcath for Securing Peripherally Inserted Central Catheters: A NICE Medical Technology Guidance,” Applied Health Economics and Health Policy, 16(6), pp. doi:10.1007/s40258-018-0427-1.779–791.
6. Balsorano, P. et al. (2020) “Peripherally inserted central catheter–related thrombosis rate in modern vascular access era—when insertion technique matters: A systematic review and meta-analysis,” Journal of Vascular Access, 21(1), pp. 7.doi:10.1177/1129729819852203.45–54.McParlan,D.(2019)“PICCmigration
16 INTRAVASCULAR QUARTERLY THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS replacements caused by migration or dislodgement dropped to nearly zero as the number of PICCs placed increased significantly over a decade. The table below compares the removals related to migration and dislodgement and the clear increase in demand for our services. Improving patient outcomes does not take place if the problem is not identified. Inputting data into an Excel spreadsheet and ignoring what that data is telling us is an act of futility. As professionals specializing in vascular access, I believe we must continually assess our current practices, stay up to date on new technology, and thoroughly analyze the data to improve outcomes. For example, securement issues begin with the facts or the data and, in this case, ends with our patients needing only one PICC to finish their care. REFERENCES
4. Interrad Medical Inc. (2020) SecurAcathInternational IFU. Hannover, Germany.
search/ &id=L625831420&from=export.results?subaction=viewrecord A DECADE OF SECURITY: DATA-DRIVEN PRACTICE CHANGE, CONTINUED FROM PREVIOUS PAGE AVAjustdiscountSpecialfor AVA10 The code entitles you to a 10% discount on designer scrubs as well as all Care+Wear products including PICC Line Covers, port access tops, and outfits for premature infants who are being cared for in the NICU. Remember to use AVA10 to receive your discount. Learn more here. AVA has partnered with Care+Wear to launch a joint discount program DESIGNER SCRUBS FOR HEALTHCARE PROFESSIONALS AND SPECIALIZED GARMENTS DESIGNED FOR PATIENTS WITH SPECIFIC MAINTENANCE NEEDS FOR THEIR VASCULAR ACCESS.




In order to treat her neurological tick-borne illness, she required daily vascular access, including three different PICCs over the course of 18 months, followed by a port for another 3.5 years. Adapting to daily life with a medical device raised many questions and concerns for her and Mighty Well’s community members. With a social reach of over 600,000 users, Mighty Well has compiled the most common questions and concerns regarding vascular access with the goal of providing patients with the information they need.
“So what exactly is a PICC, and how do I care for it?”the Mighty Well team gets this question every single day from patients all across the world. Emily Levy, Mighty Well’s Co-Founder, also wondered the same thing.
Written by Mighty Well’s clinical nurse educator with input from their patient community -- and reviewed by the AVA -- the Ultimate Guide to PICCs can be shared digitally and in printed form, and it includes topics such as:
• PICC Care: Complications to watch out for These free resources provide caregivers and clinicians with the answers needed to empower patients and, ultimately, save lines! Discover the Ultimate Guide to PICCs for yourself and your patients here and the first episode of the eLearning video series below.
ULTIMATE GUIDE TO PICCS FOR PATIENTS CAREGIVERS:AND AVA WITHPATIENTSTOCOLLABORATEMIGHTYANDWELLEMPOWERLIVINGPICCS EMILY 24 HOURS SECONDAFTERPICCPLACEMENT AVAILABLE ON MOBILE AND DESKTOP
In April 2022, Mighty Well partnered with the Association of Vascular Access to amplify its impact by producing the Ultimate Guide to PICCs for Patients and Caregivers and an accompanying eLearning video series. These patient-friendly resources explain medical terminology in easily digestible language and empower users to care for their PICC at home or on the go.
17 AUGUST 2022 | VOLUME XII | ISSUE 3
• PICC placement: How to prepare
• What is a PICC: Who needs one?



CONGRATULATIONS
DAVID M. MARKLE JR., RN, VA-BC™, EMT-B contributions. She has shared her research and practice innovations through numerous national and virtual presentations. Her nursing and professional achievements have been recognized through scholarships and awards including being named a Corridor Business Journal Forty under 40 Honoree.
The Association for Vascular Access (AVA) created the Dr. Janet Pettit Scholar recognition to honor and commemorate outstanding contributions to the art and science of neonatal and pediatric vascular access. Dr. Pettit epitomized the mission and values of our organization.
WE’RE PROUD TO ANNOUNCE THE 2022 AVA IMPACT AWARD WINNERS!
As a former PediNeoSIG Chair, PediNeoSIG Liaison for the AVA D-Team, current PediNeoSIG Chair Advisor, and engaged PedNeoSIG member for 14 years, Ms. Davis has provided visionary leadership for pediatric and neonatal clinicians in the area of vascular access with an extraordinary heart for collaboration and mentorship. In honor of the life work of Dr. Janet Pettit, please join AVA and the PediNeoSIG as we congratulate Ms. Mary Beth Davis as the 2022 Dr. Janet Pettit Scholar.
THE18 E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS
KRISTIN K. JACOBS, DNP, MBA, RN, VA-BC™ , NEA-BC
MARY BETH HOVDA DAVIS, MSN, RN, VA-BC™
TARA LYNN SHEVLIN FAIN, BS, RN, VA-BC™
TO OUR 2022 JANET PETTIT SCHOLAR!
This year AVA and the Pediatric Neonatal Special Interest Group (PediNeoSIG) recognizes Mary Beth Hovda Davis, as the 2022 Dr. Janet Pettit Scholar. Ms. Davis is a Nursing Practice Leader for the Pediatric Vascular Access service at The University of Iowa Stead Family Children’s Hospital in Iowa City, Iowa, where she has practiced for 15 years. From the national and global perspectives, Ms. Davis has led the cutting edge of pediatric vascular access education and practice with pacesetting publications. As the lead author on the position paper for minimum education and training for pediatric and neonatal intravenous insertion, she provided the foundation for AVA to develop a foundational eLearning course, a first in this specialty. She has collaborated globally to explore vascular access practice in children and changed practice to reduce patient harm through her distinct scholarly
Thank you for your exceptional leadership within your organization and your contributions to vascular access in your community.




















































Stephanie has been an active member of AVA since 2008, and served on the board of directors from 2018-19. She is also a member of GulfVAN, serving as their president from 2009-2013. Most notably, she helped to develop AVA’s Pediatric Special Interest Group (SIG) and served as the SIG president from 20132016. Dr. Pitts has also presented at every AVA consecutively since 2010.
The highest honor bestowed by AVA, the Herbst Award is granted annually to a member exemplifying AVA’s mission, including being a recognized expert in vascular access, for making significant contributions to the art and science of vascular access, and for positively affecting patient outcomes in vascular Throughoutaccess.her career, Dr. Stephanie Pitts has been a leading innovator in Pediatric Vascular Access, designing products and programs aimed at improving knowledge and efficacy in the field of vascular access. Stephanie developed and implemented the Vascular Access program at St Joseph’s Children’s Hospital, contributing to improved quality of care. As an industry leader, Stephanie has enhanced clinical vascular access expertise in medical device sales through the development of evidence-based clinical education and support programs at two international medical device companies. Finally, Dr. Pitts has been a leader in collaboration, connecting industry and clinical leaders to develop evidence-based vascular access education aimed at improving outcomes. Dr. Pitts has published within the Journal of the Association for Vascular Access (JAVA) on pediatric ethanol locking and pediatric vascular access program best practices, as well as two AVA position papers. Additionally, Stephanie contributed to the miniMAGIC study on appropriate pediatric device selection in collaboration with the AVATAR group. Most recently, she co-developed the minimum competency guidelines for pediatric PIVC insertion and care. Her DNP project was a continuation of this work, developing these guidelines into online modules. This will change the way we educate and provide pediatric vascular access care.
JOIN US IN STEPHANIECONGRATULATINGPITTSFORBEING THIS YEAR’S HERBST AWARD WINNER
STEPHANIE PITTS, DNP, RN, CPN, VA-BC™ , NEA-BC
19 AUGUST 2022 | VOLUME XII | ISSUE 3
The Association for Vascular Access (AVA) congratulates Stephanie Pitts, DNP, RN, CPN, VA-BC, NEA-BC on being the 2022 recipient of the Suzanne LaVerre Herbst Award for Excellence in Vascular Access.

20 INTRAVASCULAR QUARTERLY THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS We look forward to welcoming every one to the 2022 AVA Annual Scientific Meeting, September 30 - October 3, 2022 at the outstanding Minneapolis Conference Center. Pre-Meeting Workshops will be held immediately prior to AVASM2022 on September 29. REGISTRATION IS OPEN Join us in –Minneapolis in-person ! Annual Scientificwww.avainfo.org/annualMeeting




The guests discuss the state of PIV insertion and the use of visualization technologies; chiefly Near Infrared (NIR).
Judy is joined by Dr. Steve Bedwell, Keynote Speaker at AVA’s Annual Scientific Meeting 2022.
HAVE YOU BEEN
ISAVE That Podcast Season 5
SEASON 5, EPISODE 5
DR. STEVE BEDWELL, AVASM2022 KEYNOTE SPEAKER
21 AUGUST 2022 | VOLUME XII | ISSUE 3 WWW.AVAINFO.ORG/PODCASTSUBSCRIBENOWONTHEFOLLOWINGPLATFORMS:
Thank you to AccuVein for sponsoring this episode of iSaveThat Podcast!
AVA would like to thank Adhezion Biomedical LLC for sponsoring this episode.
PIV INSERTION & VISUALIZATION TECHNOLOGIES Guests include Dr. Tom Hopkins, Tom Sutton, Cheryl Wozniak, Blake Hotchkiss and Judy Thompson.
A NEW STANDARD OF CARE ... A NEW LAYER OF PROTECTION Sarah Capalla joins the podcast to discuss the implementation tissue adhesive hospital-wide. The what, why, and how of a house strategy to improve the patient experience and the cost savings in both staff time and material costs.
In this episode
LISTENING?
Dr. Lorelle Wuerz discusses various aspects of catheter patency and offers a sneak peek into her webinar on Sept 9th. She and Judy talk about staff shortages and the return of the New York ‘vibe’. In the second segment, Judy and Blake discuss emerging diseases and hospital onset bacteremias with epidemiologists, Michelle DeVries and DJ Shannon.
In “How to Screw Up, Stress Out & Get Nothing Done!” attendees will learn how to handle the tsunami of major adversity, and also the day-to-day hiccups and lesser turmoils that are part of our daily lives. Effective, sciencesmart tactics explained in simple terms so that you can put them to work immediately; powerful and time- efficient.
Thank you to Genentech for sponsoring this episode!











LIFE –THE DREADED
SAVED
CLOT
Living with a terminal disease as a young adult is sort of like trying to fight off a lion.
Kezia Fitzgerald, CIO, Co-Founder, CareAline
22 INTRAVASCULAR QUARTERLY THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS
SELF-ADVOCACY MY SVC
Imagine having to fend off the attacks of a lion all-day, every day. You don’t know a thing about lions, so you seek out the best lion tamer around. You find a lion tamer to help make the beast leave you alone, and you trust the professional to do their job. You follow the lion tamer’s instructions, but the lion isn’t backing off. In fact, it’s getting more aggressive, and you feel that at any moment the lion is going to decide you are a great meal and gobble you up. The lion tamer insists that the lion is not as aggressive as you think, stating that you are tired from working to make it go away, and brushes off the things you are observing. You seek out information on how to tell if a lion is becoming more dangerous and find that you are indeed correct in your experience – and that this lion is very close to eating you for dinner. You rush to find another lion tamer who listens to your observations and gives you the tools you need to survive the increased danger and finally get away from the lion for good.
As a two-time cancer survivor and bereaved cancer mom, I lived through this type of scenario, in a few different ways.
When you have two family members going through cancer treatment, you quickly learn how to live with central lines. I was terrified of getting a port at first, but once I did, it was one of my favorite tools for managing my medical care. Managing a PICC line and a central line in a toddler, on the other hand, was a bigger challenge – one that I had to solve so that we wouldn’t have any delays in treatment or extra challenges on our plate. After my Hodgkin’s Lymphoma was in remission, and Saoirse had died of neuroblastoma, I embarked on a mission to make the line securement devices I developed for our family available to hospitals and patients alike who needed them. Running a company focused on vascular access care from a patient perspective led to connections and friendships that allowed me to have knowledge about my access needs and wants when my Hodgkin’s relapsed just two years later.
CONTINUED ON NEXT PAGE

After two years of living with stable disease, and another two years of multiple failed immunotherapies, I had to start chemo again – and I refused to start without a new port. I knew my veins well enough to know I needed central access to avoid major discomfort and complications. Of course, any line comes with risks, and I would need the potential for multiple access points, so my doctor ordered a double lumen port. I needed a double power injectable port for my imaging and treatment, so I chose that option. The new treatment helped some, but after a few months, it was clearly not going to finish off the “lion.” I sought out another doctor’s opinion and learned about a few newer treatments, and one that had the potential to work. After nearly 6 months, I convinced my primary team to give it a try. It banished that pesky “lion” in two treatments. Eight months, two additional triple lumen CVCs and an ASCT later, I was at last free from working hard daily to evict my “lion.” My reliable port was still working, and it was nice to not have to get a PIV every time I needed labs. I no longer needed it two years after placement, but the COVID pandemic meant I didn’t want to brave the hospital just to have it out – especially with the immune system of a “newborn” posttransplant. A year later, I was in the middle of a big move and decided that I would deal with it sometime, just not right then. It wasn’t giving me problems, so I figured I would get around to it, eventually.
A few months later, in the middle of a cross country road trip, I started to notice my face was puffy. It honestly felt like moon face from steroids. I asked all my clinical teams if there was something that could be causing the swelling and fluid retention in my face. I wondered if it was the hormone replacement therapy I was on. I wondered if it was potentially a post treatment cardiac issue. No one had an answer (except to say that it could be my weight gain).
One day I woke up and couldn’t swallow my food. I won’t lie, it terrified me. I felt like my neck and face were swollen more than they had been the day before. I flashed back to my “lion,” and the first thought was my cancer was back (my neck nodes were always a problem). Quickly I wondered if I had a blood clot in my port lumen. I reached out to my doctors, told them what my symptoms were, my suspicion of a possible clot, and asked if it would be safe for me to fly home to have an in-person appointment. After asking a lot of questions, and having lab work done, my doctors didn’t believe it was a clot, and ok’d me to fly and check in when I got there. With an adjustment to my hormone prescription, the throat swelling seemed to taper off some between then and my flight home a month later, but I was still puffy. My appointment was uneventful – they flushed and drew labs from my port without much trouble – and I was referred to a nutritionist to talk about my post treatment weight gain. Still, no one investigated my suspicion of a clot. After 10 years of cancer treatment, I can recognize the difference between weight gain and third
(To learn more about Fitzgerald’s cancer story, the safety devices she innovated, and her company CareAline, visit CareAline.com)
BACSIG
23 AUGUST 2022 | VOLUME XII | ISSUE 3 CONTINUED ON NEXT PAGE







spacing. The feeling in my face wasn’t weight gain, but I thought maybe it was a reaction to being on the hormones. Because my dosage had recently been changed, I figured I would give my body time to adjust. I thought maybe this was just some of the long-term side effects that I would have to manage my life around post-transplant. And my port had drawn blood – how could it be clotted off?
About two weeks later, after flying back to our RV on the west coast, my whole family came down with covid. We were vaccinated and boosted, so luckily had very mild cases, and were feeling better in a few days with lots of fluids and rest. About 5 days after testing positive I was feeling well enough to take a short walk on the beach and get some fresh air.
THE24 E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS
The following morning, I woke up and couldn’t walk across our camper without stopping to catch my breath. My heart was racing. My face, neck and even chest were swollen and full of fluid. Then my husband saw my ears – any amount of movement, and he watched them turn purple. I knew something was horribly wrong. I started searching and realized I had been right about the clot – and now I knew where it was. I had a clot in my SVC – right where the tip of my port catheter sat. We were traveling from the central Oregon coast to Portland that day, so we drove – about 3 hours – and my husband dropped me off at the closest ED to our campground; a satellite facility. I told them what I suspected, and my extensive medical history, and they took my case seriously and got me in quickly. They did a workup – labs, cultures, heart monitor, etc. – and sent me for a CT scan. It confirmed I had a clot in my SVC. They consulted with their vascular surgery team by phone and put me on oral anticoagulants and sent me home.
The next day I woke up with more swelling than the day before. My neck was bigger, I still couldn’t walk far, and my arms were heavy. I called the on-call nurse from the ED and asked what to do. She suggested I go back as the increased symptoms were very concerning. Assuming if I went back to the same ED, they would escalate my case faster, I returned. After trying to advocate for myself for hours with the “middleman” hospitalist who was taking direction from the vascular surgery team over the phone, I was again sent home without additional intervention. Exhausted, frustrated, uncomfortable and scared, I hoped that I would be at least a little better in the morning. I was worse. I could barely lift my arms, and my neck was even larger than the day before. I needed someone to take down the “lion” before I became its dinner. After phone calls to the team who had suggested I go home, I decided I needed a new team to take me seriously. My husband drove me into Portland to OHSU – where interventional radiology was developed. I knew I was in the right place. I was immediately taken in and rotated through doctors, nurses, techs, and specialists. They sent bloodwork, checked monitors, and ordered a more detailed CT. It showed occlusive thrombus of the SVC extending from the inferior right brachiocephalic, left brachiocephalic and left subclavian veins – as well as a network of collateral veins that had been growing to try and compensate for the fact
SELF ADVOCACY, CONTINUED FROM PREVIOUS PAGE CONTINUED ON NEXT PAGE

The most amazing part was that I hadn’t realized how long I had been feeling terrible until I felt better. I hadn’t been able to walk an incline or up a flight of stairs without being breathless for months. I had such chronic fatigue that I attributed to post-transplant life, until I was able to be active and mobile without fatigue just days after surgery. My face was going back to normal, and I started to look like myself again in the mirror. The symptoms and changes had happened so slowly, I didn’t notice how severe they were becoming. My body had tried to compensate, so I didn’t see the changes clearly. It was only when they were retreating that I saw how much impact the clot had on my everyday life. I learned early that only I know what is happening in my body – I am the only one inside myself feeling exactly what is going on. I have to listen to my intuition and gut and push for answers. I’ve been close to death three times in my life – twice from relapsed cancer fighting past treatments, and once from SVC syndrome. Each time the “lion” crept up slowly, steadily, and then charged at the last moment. I was the first to feel the symptoms but couldn’t always convince others – or even myself – what was really happening. Each time I had to speak up and ask for better options, second opinions, “special” considerations, and sometimes just to be heard. And each time a clinician had to hear me and take Iaction.can’tfully describe the emotional roller coaster that is self-advocacy as a long-term patient. Even during my active treatment for cancer, I was living a full and busy life with motherhood, business ownership, marriage, home repairs, school pickup, and more. Cancer and treatment had to fit into my life – I wasn’t going to change my life to make it fit around cancer. I spent years advocating for myself to make the schedule work, to have treatments that I could drive to and from on my own, to fit appointments in during school hours. The world of cancer treatment isn’t built for an active young adult, but I would have missed 10 years of living if I had let it control my time. Without confidence and a strongwilled personality, I think I would have been taken by a “lion” long ago. For now, I’ve locked him in a cage and shipped him far away, hopefully never to be seen again. It’s time to focus on experiencing life, and helping others gain freedom from their own “lions,” big and small. I hope my experiences can help another person speak up, advocate for, and receive better care. And I hope clinicians will take a moment to step into the mind of their patients and truly hear them when they share their experience with their “lion.” We live with our “lion” daily, so we know him best.
25 AUGUST 2022 | VOLUME XII | ISSUE 3 SELF ADVOCACY, CONTINUED FROM PREVIOUS PAGE that blood flow was constricted for so long. As I had suspected, this clot had been there for a while. I was put on a heparin drip overnight and scheduled for a thrombectomy the next morning.
ABOUT THE AUTHOR Kezia Fitzgerald’s unique view of healthcare and talents for innovation have spurred the creation of new products and designs to improve quality of life for patients and caregivers and meet the needs of ever-changing hospital staff workflows and hospital safety CareAline®protocols.
The IR physician could see that I was a well-informed and involved patient. He talked me through the possible options and listened to my thoughts. We were on the same page. I needed everything removed. It was a two-day procedure. The first to remove as much of the clot as possible, and the port itself. Overnight I had a lysis catheter to drip medication directly into my SVC to try and dissolve the clot they couldn’t remove. The next day they removed the lysis catheter and placed a stent in my scarred and narrowed SVC. The relief was immediate. Fluid was draining quickly, and I finally felt like there was progress toward feeling better. One more night in the ICU, and I was able to go home safely.
Sleeves and Wraps are supported by evidence, FDA registered medical devices, used as part of safety bundles in hospitals, and loved by thousands of patients and caregivers worldwide. Kezia has won multiple awards and was an Alumnus in Residence and a Healthcare Industry Mentor for the 2018 MassChallenge cohort, where she drove CareAline to win a gold award in 2017. Kezia is a developer of the Young Innovators Workshop for iSPI’s Pediatric2040 conferences. When she is not innovating in healthcare, Kezia is first and foremost, a mother of two to her daughter – Saoirse – who died from Neuroblastoma in 2011 at 18-months-old, and son – Lochlan –who is a curious (and healthy!) nineyear-old. Kezia is a two-time young adult cancer survivor, bereaved cancer mom, and is currently in remission from Hodgkin’s Lymphoma.

Safer Together: A National Action Plan to Advance Patient Safety illuminates the collective insights of the 27 member organizations of the National Steering Committee for Patient Safety (NSC), convened in 2018 by the Institute for Healthcare Improvement and committed to achieving safer care and reducing harm to patients and caregivers.
Action Plan includes 17 recommendations to advance patient safety, with a focus on eliminating inequities at the point of care. Supplemented by both a Self-Assessment Tool and an Implementation Resource Guide, the Plan centers on four foundational and interdependent priority areas:
• Culture, Leadership, and Governance: to demonstrate and foster commitments to safety as a core value and promote the development of safety cultures.
26 INTRAVASCULAR QUARTERLY THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS IMPACT CASE STUDY SAFER
• Workforce Safety: to ensure the safety and resiliency of organizations and workforces as a precondition to advancing patient safety with a unified, total systems-based approach to eliminate harm to both patients and the workforce.
• Patient and Family Engagement: to instill the practice of co-designing and co-producing care with patients, families, and care partners to ensure their meaningful partnership in all aspects of care design, delivery, and operations.
• Learning System: to foster networked and continuous learning within and across health care organizations at all levels to encourage widespread sharing, learning, and improvement.
The NSC considers these areas to be foundational because they create the fertile soil that allows broader safety initiatives to take root and be cultivated. They are also interdependent because advancing in one area alone is difficult without advancing in all of them. And they each benefit from widespread collaboration and coordination. The resulting recommendations in these four areas build on the substantial body of experience, evidence, and lessons learned that the NSC has gathered and will test and implement together to allow for future refinements as our understanding, experience, and evidence evolve over time.
TOGETHER: A NATIONAL ACTION PLAN TO ADVANCE PATIENT SAFETY
Though U.S. researchers have identified many evidence-based, effective best practices for harm reduction over the past 20 years, they are seldom shared nationally or implemented effectively across multiple organizations. Reducing preventable harm requires a total systems approach: a coordinated, proactive strategy in which risks are anticipated and systemwide safety processes are applied across the entire healthcare continuum through robust collaboration among all Thestakeholders.National
The NSC is co-chaired by Jeffrey Brady, M.D., M.P.H., Director of AHRQ’s Center for Quality Improvement and Patient Safety, and Tejal K. Gandhi, M.D., M.P.H., CPPS, Senior Fellow, Institute for Healthcare Improvement; Chief Safety and Transformation Officer, Press Ganey Associates.


28 INTRAVASCULAR QUARTERLY THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS IMPACT CASE STUDY - FEBRUARY 2022
CUSP is a method that can help clinical teams make care safer by combining improved teamwork, clinical best practices, and the science of patient safety. The Core CUSP toolkit gives clinical teams the training resources and tools to apply the CUSP method and build their capacity to address patient safety issues.
PROGRAM TO LOWER BLOODSTREAM INFECTIONS
Using AHRQ’s Comprehensive Unit-based Safety Program (CUSP), Henry Ford Hospital in Detroit has reduced the incidence of central line-associated bloodstream infections (CLABSIs) in its hematology-oncology unit by 75 percent, documenting only two between July 2020 and June 2021. The reduction not only prevented patient harm, it also saved an estimated $385,000 in healthcare costs that would have been incurred to treat the infections.
Eager for a solution, unit staff and the PICC team responded positively when surveyed about their willingness to undertake the CUSP protocol training, Hebel said. In 2019, Henry Ford’s leadership had assembled a core team of frontline staff and executive leaders who supported the rollout of CUSP in several units, and the unit staff built on that foundation, according to Swati Verma, M.S., the hospital’s principal management engineer for performance excellence and “Thequality.infrastructure was in place for teams to quickly add patient safety projects through the CUSP methodology,” Verma said.
HENRY FORD HOSPITAL’S HEMATOLOGY-ONCOLOGY UNIT USES AHRQ SAFETY
In 2019, the unit recorded 16 CLABSIs, eight of which were from PICC lines. This was the highest number since the hospital started tracking infection rates, according to Kelsey Hebel, M.S.N., R.N., the unit’s clinical nurse specialist.
Most patients on Henry Ford’s 40-bed hematology-oncology unit need peripherally inserted central catheter (PICC) lines for chemotherapy, blood transfusions, or intravenous nutrition.
As unit staff examined root causes of its CLABSI rates, they found that staff weren’t using a standard protocol for pre-insertion of PICC lines. “Everyone on the unit was doing it differently. Everyone was preparing a patient differently,” Hebel said. The lack of a standardized process affected patients awaiting a PICC line placement, according to Sharron Alejandria, B.S.N., R.N., a unit educator specializing in interventional radiology.
“We didn’t consistently educate our patients about properly maintaining their PICC lines or the importance of their daily baths [with chlorhexidine gluconate] to decrease the potential spread of bacteria,” Alejandria said. Complicating matters, patients weren’t routinely informed of the indications for or benefits of the PICC before the PICC team arrived. In addition, the PICC team encountered delays when patients’ rooms weren’t cleaned beforehand, Alejandria added. “This is a sterile procedure, and the room has to be cleaned before the procedure can begin.”
As they implemented CUSP’s teamwork and communication module, the unit’s nursing staff realized “we had a lack of understanding of what our workflow looked like and what the PICC team’s workflow looked like,” Hebel said.
CONTINUED ON NEXT PAGE
A unit nurse explains the upcoming procedure and the need for a daily chlorhexidine bath to the patient. Those messages are reinforced when the PICC team arrives to perform the procedure, Alejandria said. “This leaves the patient feeling confident that everyone across the disciplines—health provider, nurses, PICC team—has a handle on what’s going on.”
29 AUGUST 2022 | VOLUME XII | ISSUE 3
PICC line inserted by specialized team at Henry Ford Hospital’s hematology-oncology unit, where bloodstream infections have dropped by 75 percent in one year. PICC line inserted by specialized team at Henry Ford Hospital’s hematology-oncology unit, where bloodstream infections have dropped by 75 percent in one year.
With the CUSP protocol fully in place, the process by which PICC lines are ordered, placed, and maintained now is clear and consistent. Once an order is put into a patient’s chart, the PICC team reviews it and contacts the hematology-oncology unit to schedule an appointment for the patient.
With CLABSI rates down dramatically in one year, the hematology-oncology unit has its eyes on eliminating CLABSIs completely and sharing their experience with units that use other types of invasive lines. Henry Ford now is expanding the new process to other patient care
“Ourunits.goal is zero [infections],” said Hebel. “This was kind of a first step. We’re continuing to check our data and see great progress with this.”
Not only have the teams since learned each other’s responsibilities, they’ve come to rely on each other for education and troubleshooting. For example, the PICC team has developed general education for unit staff to address potential issues before they arise, according to Alejandria. In turn, Hebel said, the unit staff has “no problem saying to the PICC team, ‘This isn’t working, can you take a look?’”
INTRAVASCULAR QUARTERLY THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS 2022–2026 STRATEGIC PLAN NATIONAL INSTITUTE OF NURSING RESEARCH MISSION: Lead nursing research to solve pressing health challenges and inform practice and policy—optimizing health and advancing health equity into the future. RESEARCH LENSES Reduce healthattainingdisadvantageandanplaceinequitiesandtheultimatelyandeliminatesystemicstructuralthatsomeatunfair,unjust,avoidableintheirfullpotential. Health Equity DeterminantsSocialofHealth andPopulationCommunityHealth PreventionandHealthPromotion Systems and Models of Care Identify play,live,peopleconditionsbyandimproveapproacheseffectivetohealthqualityoflifeaddressingtheinwhichareborn,learn,work,andage. Address critical health challenges at a macro level that characteristics.peopleaffectpersistentlygroupsofwithshared Prevent disease and thehealthpromotethroughcontinuum tertiary.primordialprevention—fromofto Address modelssystemsthroughpolicyorganizational,clinical,andchallengesnewandofcare.





Meagan Capen, CPNP-AC, MSN, VA-BC™
|
Our members gathered for our first in-person meeting post pandemic in March 2022 where Michele Biscossi, ACNP-BC, MS, RN, CNL, VA-BC discussed how to reduce CLABSI rates and occlusions with needle-less connectors Sponsored by BD. We are excited to announce our 2022 FLAVAN AVA Scholarship Winner Austin Green, BSN, RN, VA-BC™. Austin has been practicing vascular access for 3.5 years with the AdventHealth system throughout Central Florida.
ForWinner!more FLAVAN
FLAVAN President David Markle, RN, VA-BC™ FLAVAN Secretary/ DianaTreasurerMelton, MSHA, RN, CRNI, VA-BC™ FLAVAN Presidential Advisor
|
Facebook! NETWORK NEWS
|
FLAVAN has a busy Summer and Fall with four in-person meetings being held throughout Orlando and Jacksonville along with one virtual meeting currently planned. We are hard at work planning our yearly summit which will return in 2023.
31 AUGUST 2022 | VOLUME XII | ISSUE 3 FLAVAN
Austin has demonstrated vascular access leadership within his facilities where he has over 1000 hours precepting new nurses to vascular access and implemented processes to reduce CLABSIs including forming a CLABSI committee which consists of physicians, infection prevention, hospital leadership and vascular access team members. Austin is excited to attend his first AVA conference in OurSeptember.second meeting for the year we welcomed Dr. Jack LeDonne, MD, FACS, VA-BC™ who presented improving quality improvement with dressings Sponsored by Eloquest Healthcare.
FLAVAN members Luz Caicedo, MPH, CPH, CIC, CRCST, VABC™ and David Markle, RN, VA-BC™, EMT-B have been hard at work preparing their poster which will be on display at the 2022 AVA Conference in Minneapolis, Minnesota this September.
FLAVAN is proud to have our very own board member David Markle, RN, VA-BC™, EMT-B as a 2022 AVA Impact Award news and upcoming events please visit our website by clicking the link FLAVAN and don’t forget to like us on







THE32 E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULARDMVVANACCESS DMVVAN (DC/MD/VA Vascular Access Network) held their first in-person meeting in nearly 2 years today, July 24, 2022 as Joe Bunch, RN presented Optimizing the use of Midlines sponsored by Access Vascular, Inc. It was great to have folks together again! NETWORK NEWS





GulfVAN is pleased to announce their scholarship recipients for 2022: The Nina Marie Marino‐Willaims Scholarship was named after our 2017 Manny Matters Person of the Year. Manny Matters is GulfVAN’s community outreach program that encourages nursing students from the Tampa Bay Area to attend our meetings and enhance their knowledge of vascular access before entering the workforce. Nina loved rainbows, and her scholarship logo was created to honor her spirit.
Jenny Bokor from Tampa General Hospital (who cared for Nina in the Jodihospital)Stumpfrom UF Health Leesburg Diane Greene from Cape Coral Hospital Congratulations to all!
Jill Nolte OzarkVAN Scholarship has been awarded to Kay Coulter from Infusion Knowledge. Kay has been instrumental in educating the Tampa Bay Area and beyond in safe vascular access. Congratulations Kay! Jill would be thrilled that you are the first scholarship recipient attending in her name.
The Jill Nolte OzarkVAN Scholarship was created this year to honor the legacy of our friend and colleague, Jill Nolte. Jill founded OzarkVAN in MO and sadly the network is now closing without her leadership. Jill was committed to improving the education of healthcare professionals. She was a fierce advocate for patients and believed they all deserved an excellent vascular access experience. Jill embodied AVA’s mission and vision statements. She wanted to protect patients, improve lives, and provide all patients, worldwide, with safe vascular access. Throughout her nursing career, regardless of nursing unit type or the country she was in, Jill dedicated her time to educating peers, patients, and the community about safe vascular access care. GulfVAN is honored to establish this scholarship in her Ourname.first‐ever
Kristin Jacobs, DNP, MSN, RN, VA-BC™
33 NETWORK NEWS
GULFVAN
NINA MARIE SCHOLARSHIPMARINO‐WILLAIMSRECIPIENTSARE:
Photo credit for Nina: Lesley Marino and Philip Nolte Photo credit for Jill: Philip Nolte


34 INTRAVASCULAR QUARTERLY THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS


35 AUGUST 2022 | VOLUME XII | ISSUE 3 PRESIDENT Tonja Stevens, AGACNP, RN, BSN, VA-BC™ PRESIDENT-ELECT Tonya Heim, MHA, MSN, RN, NEA-BC PRESIDENTIAL ADVISOR Jocelyn Grecia Hill, MN, RN, CVAA(c), VA-BC™ CHIEF OPERATIONS OFFICER Tonya Hutchinson, thutchison@avainfo.orgCAE MARKETING MANAGER & ANALYTICS DIRECTOR Kayce A. kmaisel@avainfo.orgMaisel DIRECTOR OF EDUCATIONCLINICAL Judy jthompson@avainfo.orgMSNEd.,Thompson,RN,VA-BC™ CLINICAL EDUCATION SPECIALIST Blake Hotchkiss, BSN, RN, CCRN, CRNI, bhotchkiss@avainfo.orgVA-BC™ ADMINISTRATIVE ASSISTANT Jennifer jfinlayson@avainfo.orgFinlayson SECRETARY Chellie (Michelle) DeVries, MPH, CIC, VA-BC™ TREASURER Jon Bell, RN, MSN, VA-BC™ DIRECTOR-AT-LARGE Staci Harrison, DNP, RN DIRECTOR-AT-LARGE Swapna Kakani, MPH DIRECTOR-AT-LARGE Karen Laforet, RN, MCISc-AHCP, CCHN, CVAA, VA-BC™ DIRECTOR-AT-LARGE Nael Mhaissen, MD DIRECTOR-AT-LARGE Chaitenya Razdan, MBA 2022 BOARD OF DIRECTORS AVA STAFF AVA CURRENTLY HAS 52 ACTIVEwww.avainfo.org/networksNETWORKS


INTRAVASCULAR QUARTERLY THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS Thank you to our loyal Industry Partners for sharing AVA’s mission. Email partner@avainfo.org to design a program that becomes an indispensable instrument for advancing education, awareness, adoption and expansion. ACADEMY 80 0 .79 2 .9 0 79 EXT. 10 5 | PARTNER@AVAINFO.ORG | WWW.AVAINFO.ORG 2022 STRATEGIC PARTNERS: AccuVein, Inc. • Access Vascular • Ben Guard • Eloquest Healthcare • Parker Laboratories • StatSeal (Biolife, LLC) • SterileCare 2022 ENTERPRISE PARTNERS: 3 M • Adhezion • AngioDynamics B. Braun Medical • BD • Genentech Medline Industries • PDI • PFM Medical ICU Medical •Teleflex ANGEL 2022 ANGEL PARTNERS: GusGear • Lineus Medical • MightyWell • CareAline









AUGUST 2022 | VOLUME XII | ISSUE 3 ForLookingBeenYou’veMarkettoAdvertisethe... space available on AVAinfo.org Insertion, Care, and Maintenance of PERIPHERALLY INSERTED CENTRAL CATHETERS FOR NEONATES AND PEDIATRIC PATIENTS a Vascular Access resource created by the Association for Vascular Access Mastering pediatric and neonatal vascular access device insertion is a technical challenge but a highly rewarding addition to any vascular access team. Developing expertise in pediatric and neonatal PICCs requires knowledge and experience through evidence-based literature, including AVA’s newest educational offering, available now. NEW PEDIATRICAVA & RESOURCENEONATALAVAILABLENOW AVA’s “Insertion, Care, And Maintenance of PICCs For Neonates And Pediatric Patients” is now available as a digital asset, $75 for AVA members / $99 for non-members. Eleven chapters of detailed instruction The editorial team has compiled the latest in PICC instruction for pediatric and neonatal patients, including detailed diagrams, best practices by age group, key clinical components, and so much more! Copyright © 2022 by the Association for Vascular Access. All rights reserved. No portion of this book may be reproduced in any form without written permission.



38 INTRAVASCULAR QUARTERLY THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS AVA MEMBER PRICE: $99 digital only $129 print only $159 bundle (print and digital) NON AVA MEMBER PRICE: $129 digital only $169 print only $199 bundle (print and digital) Digital Access: • Not a downloadable le. It is not printable and is for view on your device only. The digital access is not shareable with another account. You will receive a redemption key and an access link after purchase. • Corrections and incremental updates to version one will automatically populate your digital copy (no additional charge) AVAILABLE NOW RESOURCE GUIDE FOR VASCULAR ACCESS The 2021 AVA Resource Guide for Vascular Access: AVA's Recommended Study Guide for Vascular Access Board Certi cation provides an overview of basic vascular access knowledge and covers essential elements that clinicians implement on a daily basis. Throughout the Resource Guide, readers have access to high de nition images, videos, illustrations and engaging animations that give them a greater understanding of the concepts. The guide may be used to prepare for the vascular access board certi cation examination (VA-BC™), as well as serve as a resource throughout professional practice. PURCHASE IT ONLINE TODAY! Check out the Resource Guide sneak peak videos on our YouTube channel!



39 AUGUST 2022 | VOLUME XII | ISSUE 3 Educational Offerings from AVA Learn more at www.avainfo.org I Save That Podcast • Streaming on Spotif y, SoundCloud, iTunes, Stitcher, Google Play Music, iHeart Radio, Pandora, Amazon Music Intravascular Quarterly (IQ) • Published quarterly • E-newsletter sent to AVA members AVA Resource Guide for Vascular Access • Prepare for the VA-BC™ exam, as well as ser ve as a resource throughout professional practice AVA Academy • Continuing Education courses ALL available on demand • Procedural courses, webinars, scientific meeting sessions, etc. Journal of the Association for Vascular Access • Published quarterly • Approximately 3,000 subscribers Available anywhere you get your podcasts ACADEMY









your
Always
your
your
your
The information presented in this PDF is free to download and share and made available by The Association for Vascular Access AVA)strictly for educational purposes. This document is meant to provide general information and understanding of Vascular Access devices andprocedures. It is not meant to provide specific medical advice. AVA, it's Board of Directors, staff and members are not liable for outcomesassociated with your care. AVA encourages the use of this document for Vascular Access education, provided is not modified. Please share it with clinicians, patientsand their families and attribute this resource to AVA. You may also include the links to our additional resources (if applicable). AVA'sinformational resources educate these clinicians, patients and their families to ensure they receive safe Vascular Access care. Feel free toprint, post and share this document within your healthcare institution, as well as on social media. If you have questions, please contactava@avainfo.org. For Patients and Families AWAY IF IV SITE HAS ANY OF THE FOLLOWING: to wash hands or use hand sanitizer when going inand out of room. have technology to help us place your IV.If you are not getting IV fluids or medicines, you might not need an IV.Protect IV from accidently getting pulled out. will talk with about IV needs.select the best IV for care.choose the best site for IV.ask for help if cannot get IV after 2 attempts.clean skin before inserting IV.scrub the end of IV every time use it. BASIC RULES: up on the latest at www.avainfo.org/isavethatline out more online.
We will
you
YOUR
we
I NFORM US RIGHT
See
probably
AVA advance its mission, which is Protect the Patient | Educate the Clinician | Save the Line. You can also support the AVA Foundation, which focuses on advancing Education, Research and Innovation in vascular access. Take the pledge, be involved and join AVA in our mission to keep our patients free of infection!
I S A V E
www.avainfo.org A Guide
our
We will
You already know about the ISAVE That Line campaign AVA launched in 2006 to bring crucial principles of vascular access device management directly to the bedside. Putting patients and emphasizes a “back to basics” approach, essential to reducing the risk of infection and improving the management of all vascular access devices. On the centeredclinician-version, ISAVE stands for: On the ISAVEcenteredpatient-version,standsfor:
If you’d like laminated full-size sheet versions of this patient asset already printed, we have those available for sale in the AVA store in packs of 10 for $25. Click here to purchase yours.
your
I S A V E
Remember, purchasing official ISAVE assets directly helps
our
your
your
We
your
We will
veins
We will
S A V E Stay
your
XPECT US TO FOLLOW
Value
We
EE US CHECK YOUR IV OFTEN SK US TO CLEAN OUR HANDS ALUE YOUR VEINS S T O P emperaturewelling Change ainozing Is it working? Is there Swelling, Temperature change, Oozing, Pain?Is your IV dressing clean, dry and not peeling?Is your IV still needed? Expect us
Introducing NEW addition to the ISAVE family that supports this program from the ground level: A patient-friendly version Written and edited by patients and caregivers, this new resource is completely FREE as a downloadable PDF. Please share and distribute this resource in your facilities, with your colleagues, on your social media platforms, with your patients and with your family. simply ask that you not amend it without prior permission from AVA. Implement insertion care and maintenance bundles Scrupulous hand hygiene disinfect every needleless connector Vein EnsurePreservationPatency Inform us right away us check your IV Ask us to clean hands your Expect us to follow basic rules
we
Find
THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS
We will
We
often
our
first, ISAVE encourages


AUGUST 2022 | VOLUME XII | ISSUE 3 • Review course content, outlines and objectives • Purchase courses • Add courses to your personal Course List • Available to Members, Non-members and all site visitors with a Guest Account • If you're not an AVA member, consider Joining AVA or you may create a Guest Account at no charge • Sign in to your personal AVA Academy Account • Launch your courses • Take quizzes • Available to Members and Non-members with a Guest Account • You will need to sign in to the AVA website prior to clicking Launch My Courses above The Association for Vascular Access (AVA), in collaboration with The Clinician Exchange (TCX), launched a new, best-in-class learning management system tailored to aspiring and established vascular access clinicians. Providing cutting edge training, critically-acclaimed presentations from scientific meetings, journal review courses and much more, AVA Academy is a groundbreaking initiative that advances the heart of AVA’s mission – Protect the Patient | Educate the Clinician | Save the Line. Academy curriculum is now available to the public, and to active AVA members at a discount. It's our mission to create greater public awareness of vascular access and to empower our members with significantly more educational resources, networking opportunities, and advocacy tools in support of and dedication to the patients that we are entrusted to serve. ADEMYopen!isAcademyAVAalways View Course Catalog Launch My Courses Learn more at www.avainfo.org/AcademyLaunch Looking to further your education but struggling to find the time amidst a busy work schedule? AVA Academy is always open! AVA Academy is now open to all curious minds Choose and enroll in your classes today!




THE42 E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS CALL FOR MANUSCRIPTS We invite you to submit original manuscripts in the field of Vascular Access. We are interested in receiving manuscripts on clinical practice, education and research related to vascular access including articles on vascular access manufacturing and technology, and vascular access care and maintenance issues in hospitals, home settings, hospice, and alternative care facilities. We also invite submissions to our Patient/Consumer Perspective column where we ask you to share personal stories or “lessons learned” about caring for, living with or having a vascular access device. In about 1000 words and in conversational style, present your story. You can submit on behalf of someone or encourage them to write it themselves. FOR COMPLETE INSTRUCTIONS SEE: Information for Authors at www.avajournal.com Or contact the JAVA Editor at JAVAEditor@avainfo.org Want to make money? JOIN AVA’S SURVEY PANEL Share your expertise, make money, and help AVA -Follow the instructions online to start today www.avainfo.org/SurveyPanel


AUGUST 2022 | VOLUME XII | ISSUE 3 The special enhanced edition of Vessel Health and Preservation: The Right Approach for Vascular Access is now available to purchase. Get yours today for just $9.99! Hours of exclusive audio interviews with the authors discussing their areas of expertise are embedded into this version of the book, as well as animated videography capturing elements from actual vascular access procedures. AVA has also elevated the overall readability, and through Apple, Amazon and Barnes & Noble has added note-taking and flash card functionality for readers. 1,50000

THE E-NEWS PUBLICATION OF THE ASSOCIATION FOR VASCULAR ACCESS

45 AUGUST 2022 | VOLUME XII | ISSUE 3 Copyright 2022 Association for Vascular Access. All rights reserved. www.youtube.com/AssociationForVascularAccessAssociationwww.linkedin.com/company/association-for-vascular-access/Associationwww.instagram.com/i@itwitter.com/ISaveThatLine@ISaveThatLinewww.facebook.com/associationforvascularaccess/savethatlinesavethat-line/ForVascularAccessForVascularAccess Disclaimer: AVA (Association for Vascular Access) is a professional organization of vascular access professionals dedicated to improving vascular access practice and patient outcomes through education and other means. AVA publishes this periodic electronic newsletter for our membership and other interested parties for information purposes only. AVA distributes this electronic newsletter with the understanding that AVA is not engaged in rendering medical or professional service through the distribution of the IQ publication. AVA is not giving advice and does not subscribe to guarantee the accuracy or efficacy of the information provided. Privacy Policy and Unsubscribe Information -AVA maintains strict rules of confidence with regards to your email address and all other personal contact information. We will not, under any circumstances, sell, transfer, or provide your email address to any third party for any reason. Email lists are compiled on an opt-in basis by AVA for the sole purpose of distributing the IQ newsletter. AVA does not condone or participate in the distribution of unsolicited email. If you feel that you have received an email transmission from AVA in error, please contact AVA at info@avainfo.org and ask to be removed from the list. All removal requests are addressed promptly. FOR COMMENTS OR SUGGESTIONS, PLEASE SUBMIT TO AVA@AVAINFO.ORG SUBMISSION DATES ARE: February 1 deadline for submissions for February issue May 1 deadline for submissions for May issue August 1 deadline for submissions for August issue November 1 deadline for submissions for November issue DO YOU LIKE WHAT YOU READ HERE? Would you like to be part of this publication? Do you have something interesting, informative or new going on in your place of practice? Have you cared for a special or interesting patient? Do you or your colleagues have new or innovative ways of doing things? Have you been to or presented to any meetings or conferences? WE INVITE YOU TO SUBMIT FOR PUBLICATION Writing a submission does not mean that you have to write the next great American novel. It is more about presenting pertinent information in a brief, fun and creative way. Please submit to ava@avainfo.org








