The not-for-profit hospital clash between mission and revenue
12 Regional round-up Female patients at increased risk from adverse outcomes after ALI
23 Venous disease VenoValve impact assessed by CEAP grade
www.vascularspecialistonline.com
Endoscopic vein harvest under the microscope
By Bryan Kay
STUDY DETAILS ASPECTS OF EARLY CARE IMPROVEMENTS AFTER PUBLICATION OF SVS APPROPRIATE USE CRITERIA FOR CLAUDICATION
AN OBSERVATIONAL STUDY of intermittent claudication (IC) practice patterns before and after publication of the Society for Vascular Surgery (SVS) appropriate use criteria (AUC) for IC management points to a series of areas where care has improved, alongside aspects still in need of attention, according to the authors.
The researchers noted improvements in optimal medical therapy (OMT), particularly in the postoperative setting, and patient selection, as well as a decrease in complex aortoiliac and infrapopliteal peripheral vascular interventions (PVIs). However, they reported no changes in medical optimization or bypass practices, and an increase in endovascular common femoral artery (CFA) and infrapopliteal disease interventions, “suggesting that there may be further improvement in this area.”
The data, drawn from the Vascular Quality Initiative (VQI), were presented during the 2024 Eastern Vascular Society annual meeting in Charleston, South Carolina (Sept. 19–22) by Andrea Alonso, MD, a general surgery resident at Boston Medical Center, on behalf of a research team led by Jeffrey
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors
Bernadette Aulivola, MD | O. William Brown, MD | Elliot L. Chaikof, MD, PhD
| Carlo Dall’Olmo, MD | Alan M. Dietzek MD, RPVI, FACS | John F. Eidt, MD | Robert Fitridge, MD | Dennis R. Gable, MD | Linda Harris, MD | Krishna Jain, MD | Larry Kraiss, MD | Joann Lohr, MD
| James McKinsey, MD | Joseph Mills, MD | Erica L. Mitchell, MD, MEd, FACS | Leila Mureebe, MD | Frank Pomposelli, MD | David Rigberg, MD | Clifford Sales, MD | Bhagwan Satiani, MD | Larry Scher, MD | Marc Schermerhorn, MD | Murray L. Shames, MD | Niten Singh, MD | Frank J. Veith, MD | Robert Eugene Zierler, MD
Resident/Fellow Editor
Saranya Sundaram, MD
Executive Director SVS
Kenneth M. Slaw, PhD
Senior Director for Public Affairs and Advocacy
Megan Marcinko, MPS
Manager of Marketing
Kristin Spencer
Communications Specialist
Marlén Gomez
SVS Consultant
Beth Bales
Published by BIBA News, which is a subsidiary of BIBA Medical Ltd.
Publisher Stephen Greenhalgh
Content Director Urmila Kerslake
Global Sales Director Sean Langer
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution Jocelyn Hudson, Jamie Bell, Éva Malpass and George Barker
Design Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe
526 Fulham Road, London SW6 5NR, United Kingdom
BIBA Medical, North America
155 North Wacker Drive – Suite 4250, Chicago, IL 60606, USA
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of healthcare policy. Content for Vascular Specialist is provided by BIBA News. Content for the news from SVS is provided by the Society for Vascular Surgery. | The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and BIBA News will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services, or the quality or endorsement of advertised products or services, mentioned herein. | The Society for Vascular Surgery headquarters is located at 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. | POSTMASTER: Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. | RECIPIENT: To change your address, e-mail subscriptions@bibamedical.com | For missing issue claims, e-mail subscriptions@bibamedical. com. Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by BIBA News. Printed by Ironmark
In his address at the 2024 Vascular Annual Meeting (VAM), Society for Vascular Surgery Immediate
Hospital Bitcoin
Solidarity in vascular surgery
Frontal assault on reimbursements
Past President Joseph Mills, MD, eloquently stated—and please excuse the paraphrase Dr. Mills—that we as a specialty need to come together and become cohesive, as opposed to divided. Give three vascular surgeons a clinical problem and it is assured you will receive five opinions. Over the last few years, we have seen very public mudslinging directed at vascular surgeons who have chosen private practice careers. The falsehood projected that our private practice colleagues are avaricious and not patient-focused is simply a distortion of reality. There are unscrupulous people everywhere, even in our ivory towers! Curren cy in private practice is hard cash, while, in our precious hospitals, it’s simply called work relative value units (wRVUs), or hospital Bitcoin. We don’t really know its value, hospitals can’t explain it to us, and in our everchanging field, there are some procedures without wRVUs assigned to them.
Administrative harm
Overcoming divisive issues
Former Polish president Lech Walesa spurred the concept of Solidarnos´´c, or solidarity, through the trade union of the same name. Although we’re not necessarily suggesting that we unionize and incite a national strike, the reality is we would benefit from a little more solidarity in our specialty. We are in the ballpark of 3,000 vascular surgeons in the U.S., for a population of nearly 350 million. Although we lack the prowess of Einstein, the math simply doesn’t make sense. There is simply no way we could manage all who need vascular care in this country. Then why are we so preoccupied with the noise of what the interventional cardiologist, nephrologist and radiologist are doing? Were we appointed to police vascular care? The reality is that there are plenty of those interventionalists who do respectable work, so why not embrace that? We need to be the strongest we can be, and that entails leading vascular care from all perspectives. Let us be the standard bearer and fight for things that really matter.
Administrative harm is defined as the adverse consequences of administrative decisions within a healthcare enterprise that affect patient care, professional practice and organizational efficiencies.1 Colloquially stated, these are the things that hospital decision-makers decree
that make our patients’ lives and our lives incredibly difficult: operating room (OR) time cuts, equipment and device decisions, compensation changes, etc. Any of us who practice within the walls of a large conglomerate, even part-time, are affected dramatically by administrative harm. We should all address this as a unifying challenge. Most of our current hot-button topics are just different ways to look at a problem, depending on how your lens is tinted. We feel administrative harm is not like these other issues. Administrative decisions affect us all, usually unfavorably. When was the last time you heard the administration say: “Dr. Bismuth, we feel you are working too hard. You need a pay raise and an extra two weeks’ vacation, and we won’t take no for an answer”? Are we really training our residents and fellows for the realities of vascular practice in the U.S.? Do they understand administrative harm? Is there an understanding that the more hospital Bitcoin we are asked to mine, the more that places a premium on time and can affect education? Do they realize that there is a national push to “defund vascular surgery”? The truth is that the Centers for Medicare & Medicaid Services (CMS) has slowly been mounting a frontal assault on reimbursements, and we are naïve to think that this doesn’t impact those of us salaried in hospital-based systems. Our specialty depends not only on the academicians—rapidly becoming an enigma who seem to now just produce confounding Vascular Quality Initiative (VQI) analyses— but also on our private and community practitioners, who are delivering the lion’s share of vascular care nationwide, and doing it well.
However, in the face of these local and national administrative harms, our small and highly skilled specialty has chosen instead to debate issues that, by their very nature, are divisive among our own ranks. Atherectomy, office-based lab (OBL) use, cardiology, the concept of an independent board, the list goes on. So, who is harming who? Are the threats facing our
Were we appointed to police vascular care? The reality is there are plenty of those interventionalists who do respectable work, so why not embrace that?
continued on page 7
Jean Bismuth
Jonathan Cardella
FROM THE COVER
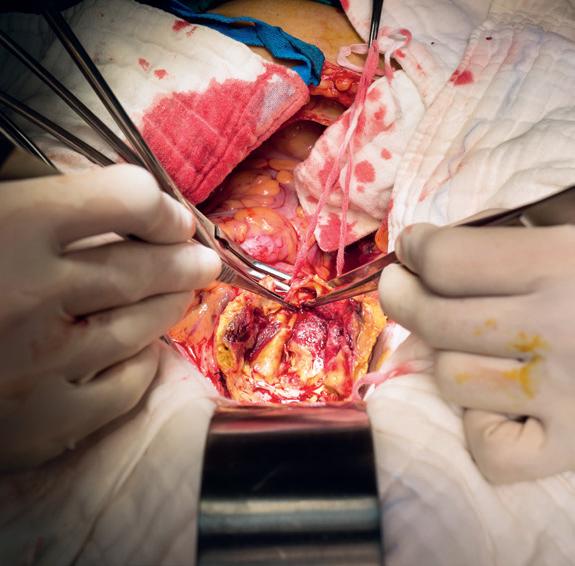
Two separate analyses that looked at the impact made by the method used to harvest great saphenous vein (GSV) on the long-term patency of lower extremity arterial bypasses demonstrated markedly different results over the issue of whether open harvest was superior to the endoscopic approach.
One, a collaborative effort between the University of Iowa in Iowa City and Henry Ford Hospital in Detroit, was drawn from Vascular Quality Initiative (VQI) data and showed that a lower postoperative wound complication rate when performing endoscopic harvest of GSV over the open approach came at the expense of worse long-term patency outcomes. The other, from a research team at Wayne State University in Dayton, Ohio, probed an institutional experience, reporting no significant difference in patency rates between the two techniques. Both sets of results were delivered at the 2024 Midwestern Vascular Surgical Society (MVSS) annual meeting in Chicago (Sept. 12–14).
The former, delivered by Mohamad Chahrour, MD, a vascular surgery resident at the University of Iowa and previously a general surgery resident at Henry Ford, won the John R. Pfeifer Best Venous Paper Award.
The use of endoscopic vein harvest for lower extremity bypass remains a contentious issue in vascular surgery over possible damage caused to the harvested GSV, with open harvest the preferred method in the absence of robust evidence favoring either technique.
Superiority of open approach?
Amid this ongoing debate, Chahrour and colleagues sought to compare outcomes between the two approaches and determine whether there has been any improvement in endoscopic harvest outcomes over time.
They plumbed VQI lower extremity infrainguinal bypass registry data from 2011–2023, propensity matching 7,929 open harvest patients to 2,643 subjects who underwent endoscopic harvest.
Short-term outcome data revealed open harvest was associated with an increased rate of surgical site infection and higher length of stay, procedure time and estimated blood loss.
However, Chahrour told MVSS 2024, open harvest was superior in terms of both primary and secondary patency: At one-year follow-up, the primary patency rate was 71% for open vs. 65% for endoscopic harvest; secondary patency 90% vs. 85%; and major adverse limb events (MALE) 25% vs. 30%.
became equivalent in the second half. We started with a 13% difference in patency in 2011 and, in 2020, we saw a difference of 3%, which was non-statistically significant. However, it is important to note that this comparison is between unmatched and unadjusted samples and that those findings should be analyzed with caution.”
Concluding, Chahrour said the study demonstrated endoscopic harvest’s association with improved short-term outcomes but “open vein harvest was associated with improved long-term outcomes, both with increased patency and increased limb salvage,” he said, adding: “Endoscopic vein harvest is improving with new technologies and more experience. We believe a repeat outcomes analysis will be needed to reflect those advances in the future.”
Conversely,
no significant differences?
The analysis of Wayne State University’s institutional experience, meanwhile, showed conflicting results. Presenting the data, Justin Robbins, MD, Wayne State University’s chief general surgery resident, pointed toward endoscopic GSV harvesting’s mid1990s roots and now widespread use in coronary artery bypass grafting (CABG).
ence in need for amputation. “However, there was a significant difference in incision breakdown, 12% [for endoscopic harvest] vs. 21%; surgical site infection, 25% vs. 71%; and procedure duration, which was shorter by half an hour at least for endoscopic harvest.”
When looking at patency rates, Robbins said there was no difference between open and endoscopic harvest for primary, primary-assisted or secondary patency.
“We feel that, with experienced providers, endoscopic harvest can be a safe option for great saphenous vein harvest for lower extremity arterial bypass,” Robbins concluded. “However, it is unrealistic to believe that every vascular program can hire someone with 20 years endoscopic harvest experience.
“ We feel that, with experienced providers, endoscopic harvest can be a safe option for great saphenous vein harvest for lower extremity arterial bypass”
JUSTIN ROBBINS
Studies exploring its applicability in lower extremity bypass grafting have so far produced mixed results, with some showing decreased patency and others reporting no change, Robbins said.
He highlighted a 2021 Journal of Vascular Surgery meta-analysis—which contained 12 comparative studies—that found “a significant decrease” in patency rates with endoscopic harvest.
“ Open vein harvest was associated with improved long-term outcomes, both with increased patency and increased limb salvage”
MOHAMAD CHAHROUR
“We performed a subgroup analysis in which we looked at the outcomes based on the outflow target,” Chahrour said. “Endoscopic harvest was again associated with worse outcomes regardless of the target vessel, with almost 25–50% increased odds of loss of primary patency at one year.”
On the other hand, the analysis revealed that endoscopic harvest outcomes improved over time. Primary patency went from 59% in 2011, gradually increasing to reach 70% in 2020. “This could be due to advanced technologies in the new endoscopes or due to experience accumulated by the vein harvesters,” Chahrour said.
“When we compared outcomes based on technique by years, we saw that open was superior in the first half and
“Of note, the last study that was conducted was in 2019, from a single center, and they found no difference in patency rates among the two groups [open and endoscopic], and they attributed this significantly to provider experience with endoscopic harvest,” Robbins said.
The Wayne State University researchers sought to catalogue their institutional experience with endoscopic harvest and its impact on patency in light of their retention of a highly experienced vein harvester as part of their vascular surgery team.
The retrospective study encompassed 340 chronic limb-threatening ischemia [CLTI] patients undergoing infrainguinal bypass with GSV from 2013–2023—111 through open harvesting of the vein and 229 endoscopically. The experienced harvester, a physician assistant (PA) who spent two decades in cardiothoracic (CT) surgery, where the PA performed endoscopic harvesting for coronary bypasses, has been a part of the Wayne State vascular team for seven years.
Robbins and colleagues found no difference in need for arterial surgery within one or five years, as well as no differ-
“It’s important to collaborate with CT surgery groups in your institutions if this is something you want to do, because those providers are going to need the experience with short-segment harvest, where they can make those errors. With some of the previous CT surgery studies, they have shown that less experienced providers more likely injure at the junction of the ostium when they’re doing endoscopic harvest. In our group, we saw no effect on patency up to five years and decreased wound complications.”
Contradictory findings come under scrutiny
Jill Colglazier, MD, program director of the vascular surgery integrated residency at the Mayo Clinic in Rochester, Minnesota, who was a moderator of the MVSS session in which the Wayne State paper was presented, asked Robbins if he was able to explain the apparent contradictions between the two studies.
Robbins said he had noted during Chahrour’s presentation the previous day that, “when [the University of Iowa-Henry Ford group] looked at [the VQI registry] patency rates, they also noted, as the years went on, that patency rate difference decreased, and they feel that could have been a possible correlation.”
At Wayne State, on the other hand, the vascular surgery group used the same provider for each of their cases of endoscopic vein harvest for lower extremity bypass.
Alexander D. Shepard, MD, one of the University of Iowa-Henry Ford paper authors and a Henry Ford Health vascular surgeon, opined that the Wayne State study was “a good example of what happens with increased operator experience,” but said he maintained a skepticism of endoscopic harvest. “I think it’s getting better and better, but my concern is with the marginal vein,” he added.
For his part, under questioning after presenting the VQI data, Chahrour tackled the issue of a vein harvester’s experience level. “Because the VQI doesn’t allow for that variable, how do you think you can mitigate that bias, since I think that is probably the number one determinant of the outcome?” he was asked by one attendee.
“For CABGs, there were two trials in the New England Journal of Medicine [NEJM] around 2009 that showed superior outcomes with open [harvest]; the only difference was in the REGROUP trial [looking at open vein harvesting for CABG] of 2019 [in which] they only allowed the experienced harvesters,” answered Chahrour. “So, the first take-home message from that was, if we are going to adopt an endoscopic vein harvest method, then we have to get the PAs to harvest the veins because they are more experienced.”
The Shockwave E8 experience: Featuring the new Shockwave peripheral IVL workhorse
Paul J. Foley III, MD, a vascular surgeon and director of the non-invasive vascular lab at Doylestown Hospital in Doylestown, Pennsylvania, and adjunct associate professor of surgery at the University of Pennsylvania in Philadelphia, discusses the virtues of the new Shockwave E8 IVL catheter.
Endovascular interventions for chronic limb-threatening ischemia (CLTI) are technically demanding endeavors. Multi-level arterial disease, long-length lesions and other complex plaque characteristics are frequently encountered when treating these patients.1,2 Calcium modification with intravascular lithotripsy (IVL) has emerged as a useful tool to combat the challenges of calcified lesions with the goal of maximizing luminal gain to achieve improved endovascular outcomes, both radiographically and clinically.3 Balanced lithotripsy pulse delivery across longer-length lesions, as well as effectively treating calcified disease across multiple arterial beds, can be laborious considering the number of available pulses and the length of the IVL catheter relative to the extent of disease.
but no intervention was performed. The patient’s son, who lives in the U.S., brought him to the office for vascular surgery evaluation. The patient’s past medical history is notable for hypertension, hypercholesterolemia and a heavy smoking history. On physical examination, he had a palpable left femoral pulse but non-palpable pedal pulses in the left foot. Preoperative ankle brachial index (ABI) of the left lower extremity was severely reduced at 0.31 and the left toe pressure was zero. He was taken to the operating room for a left lower extremity arteriogram and endovascular intervention.
Arteriogram, left lower extremity
To address this, the Shockwave IVL peripheral portfolio has now been enhanced with the addition of the Shockwave E8 catheter. The Shockwave E8 contains eight emitters across an 80mm-length balloon platform with treatment diameters ranging from 2.5–6mm and the ability to deliver up to 400 pulses. A working length of 150cm now provides an extended reach for more distal disease. The Shockwave E8 catheter allows for expanded application of IVL in treating a wide range of infrainguinal disease. Longer-length lesions involving the superficial femoral (SFA) and popliteal arteries or disease involving multiple tibial arteries that may have previously required a very selective pulse delivery approach can now be more broadly treated with the Shockwave E8.
Case report
The following case highlights the versatility of the Shockwave E8 IVL catheter to treat long-length lesions in two tibial arteries.
History
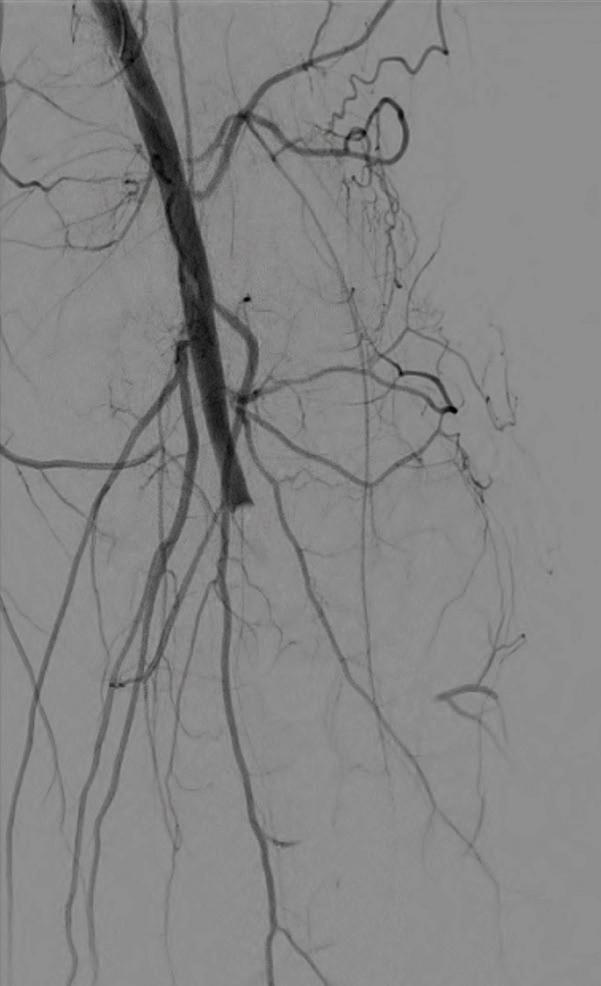
A 78-year-old man who resides in Uzbekistan presented to the office with CLTI of the left lower extremity manifested by a non-healing gangrenous left toe ulcer and associated rest pain (Figure 1). He was initially evaluated by providers in his home country and had a recent arteriogram in Uzbekistan demonstrating severe multi-level arterial disease in the left lower extremity,
An arteriogram of the left lower extremity was performed via antegrade left common femoral artery access based on preoperative review of the lower extremity arteriogram from Uzbekistan. Scattered non-calcified plaque with moderate to high-grade stenoses were identified in the proximal and mid superficial femoral artery. Diffuse severe calcified tibial artery disease was identified. There was a long segment stenosis of the proximal and mid posterior tibial artery coupled with a more distal occlusion. The proximal peroneal artery was calcified and occluded with distal reconstitution identified. There was complete occlusion of the anterior tibial artery (Figure 2).
Shockwave E8 3mm x 80mm to the posterior tibial artery
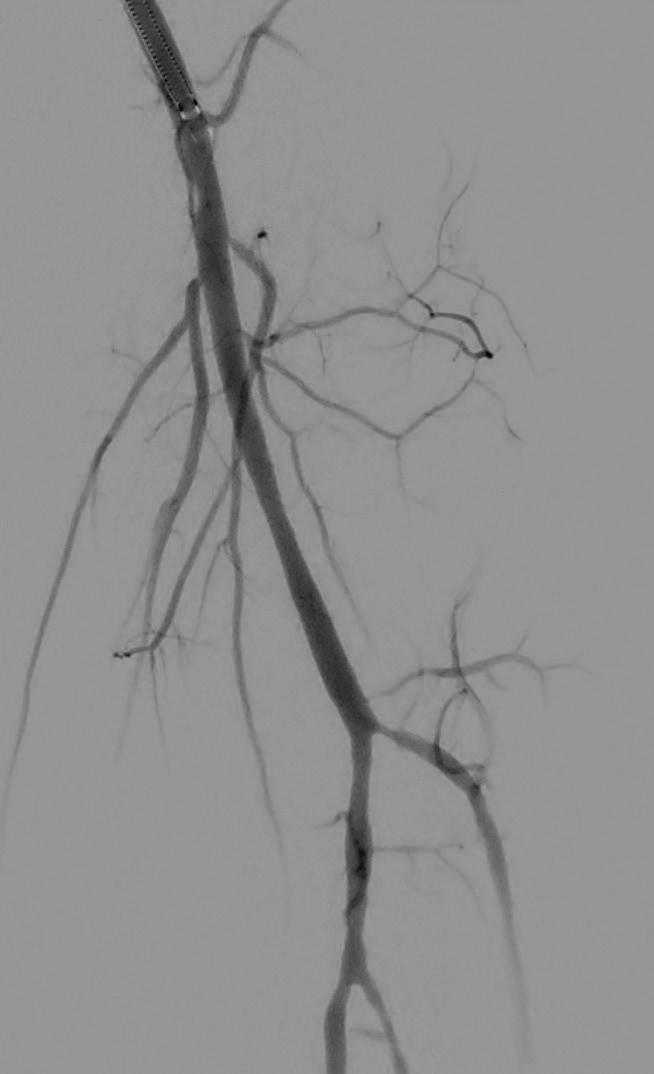
The posterior tibial artery was successfully crossed first. The long-length posterior tibial artery disease was treated with a Shockwave E8 3.0mm x 80mm IVL catheter, with no pre-dilatation required. A total of 200 pulses were delivered along the length of the posterior tibial artery (Figure 3).
Shockwave E8 3mm x 80mm to the peroneal artery
Following this, the peroneal artery occlusion was successfully crossed. The longlength peroneal artery disease was treated with the same Shockwave E8 3mm x 80mm IVL catheter also with no pre-dilatation required. The remaining 200 pulses were
delivered across the length of the peroneal artery disease (Figure 3).
Left SFA intervention
To ensure adequate inline blood flow to the tibial vessels, the SFA disease was treated with drug-coated balloon angioplasty, followed by self-expanding stent placement.
Post-intervention arteriogram
An excellent technical result was achieved. The SFA was widely patent with no significant residual stenosis. The posterior tibial and peroneal arteries were widely patent with brisk flow and no residual stenosis. Significantly improved flow was identified to the foot (Figure 4).
Post-intervention follow-up
The patient had an uneventful postoperative recovery. His post-intervention lower extremity arterial studies demonstrated a significant improvement in both the ABI and toe-brachial index (TBI). At his onemonth postoperative visit, he had completely healed the toe ulcer without any further intervention (Figure 5).
References
1. Fitzgerald PJ et al. Contribution of localized calcium deposits to dissection after angioplasty. An observational study
using intravascular ultrasound. Circulation, 1992
2. Rocha-Singh KJ et al. Peripheral arterial calcification: Prevalence, mechanism, detection, and clinical implications. Catheter Cardiovasc Interv, 2014
3. Armstrong E. VIVA Late Breaking Clinical Trial, 2022
PAUL J. FOLEY III is a paid consultant of Shockwave Medical.
Peripheral Important Safety Information
In the United States: Rx only.
Indications for Use—The Shockwave Medical Intravascular
Lithotripsy (IVL) System is intended for lithotripsy-enhanced balloon dilatation of lesions, including calcified lesions, in the peripheral vasculature, including the iliac, femoral, ilio-femoral, popliteal, infra-popliteal, and renal arteries. Not for use in the coronary, carotid or cerebral vasculature
Contraindications—Do not use if unable to pass 0.014” (M5, M5+, S4, E8 or 0.018” (L6) guidewire across the lesion-Not intended for treatment of in-stent restenosis or in coronary, carotid, or cerebrovascular arteries. Warnings—Only to be used by physicians who are familiar with interventional vascular procedures—Physicians must be trained prior to use of the device— Use the generator in accordance with recommended settings as stated in the Operator’s Manual. Precautions—use only the recommended balloon inflation medium—Appropriate anticoagulant therapy should be administered by the physician—Decision regarding use of distal protection should be made based on physician assessment of treatment lesion morphology.
Adverse effects—Possible adverse effects consistent with standard angioplasty include—Access site complications— Allergy to contrast or blood thinner. Arterial bypass surgery—Bleeding complications—Death— Fracture of guidewire or device—Hypertension/Hypotension— Infection/sepsis—Placement of a stent—renal failure—Shock/ pulmonary edema—target vessel stenosis or occlusion— Vascular complications. Risks unique to the device and its use—Allergy to catheter material(s)—Device malfunction or failure—Excess heat at target site.
Prior to use, please reference the Instructions for Use for more information on indications, contraindications, warnings, precautions and adverse events. www.shockwavemedical. com/IFU. SPL-73151 Rev. A
Paul J. Foley III
COMMENT& ANALYSIS
Invisible ties: The unique journey that landed one medical student on vascular surgery rotation CORNER STITCH
Medical student Bailey Richardson recounts the deeply personal life events that led to her unique journey into vascular surgery.
DESPITE REQUESTING TRANSPLANT FOR MY third-year surgery rotation as a medical student, I got placed on vascular surgery. I remember sitting with my mama, debating if I should try to switch. Ultimately, I left it alone, letting fate decide. Fast forward to my second week on service, I heard the residents discuss a patient in the emergency department with a ruptured abdominal aortic aneurysm (AAA). Quickly, one of the MS4s and I searched the board, trying to figure out who it could be, in the hopes of get-
ting to follow the case into the operating room (OR). When I saw my mentor’s name on the screen, my heart stopped; I felt empty. I rushed to the bay, only to find him in his neatly pressed blue-and-white stripped pajamas, smiling, and telling me that he was going to be “alright.” Despite developing a non-intervenable endoleak weeks after his life-saving operation, I will forever cherish the extra time I spent with him and his family prior to sending him home in his last days.
Meanwhile, in the midst of my mentor’s hospital stay, my grandmother was admitted for surgical treatment of her symptomatic AAA. Though her initial fenestrated endovascular aneurysm repair (FEVAR) was successful, her course was riddled with postoperative pseudoaneurysms requiring multiple take-backs. Frequent intubations, combined with her severe cardiopulmonary disease (COPD) and other comorbidities, ultimately resulted in a two-month stay in the cardiovascular intensive care unit (CVICU).
Those days were long, and, honestly, my own personal hell. I knew just enough in medicine at the time to understand her poor prognosis. Deep down, I knew that this was not the vascular team’s fault in any way, shape or form. Her outcomes were a perfect storm of poor overall health and, frankly, bad luck. She was the first person I watched die.
For a long time after losing both my
THE CLASH BETWEEN MISSION AND REVENUE FOR NOT-FOR-PROFIT, TAX-EXEMPT HOSPITALS
By Bhagwan Satiani, MD
Hospitals represent one of the largest industries in the U.S., with revenues greater than $1.4 trillion. The American Hospital Association reports that there are 5,200 nonfederal, short-term general, and other special hospitals in the country, of which 3,000 are non-for-profits (NFPs), 1,300 for-profits (FPs), and about 1,000 state and local government organizations. About 60% of community hospitals are NFP entities and managed by a community board.
People use 501(c)(3) and NFP terms interchangeably, which they are not. The former are recognized by the Internal Revenue Service (IRS), a federal agency, as being tax-exempt because of their charitable programs under the tax code. Section 501(c)(3) of the code authorizes tax exemption for NFP organizations pursuing charitable, religious, educational or scientific missions. An NFP is usually organized as a corporation and designated as such by the state. NFP status does not automatically confer tax exemption.
Though not that many NFPs do not do so, but FPs must run lean, efficient organizations since they are also focused on providing a return on investment. Because they are tax-exempt, NFPs pay no tax on net income, state and local corporate income taxes, local property taxes, and sales tax on their purchases. These are taxable events for FPs. NFPs do not have shareholders and do not pay dividends, whereas FPs may do so. NFPs contend that they do generate taxable revenue through the likes of payroll taxes and taxes from non-patient care.
IRS
There are regulations common to all hospitals, but some apply only to 501(c)(3) and NFP hospitals. The IRS requires hospitals to report and describe “community benefits” as a percentage of hospital expenses. The tax benefits for NFPs in relation to providing community benefits hinge on an “open medical staff
mentor and grandmother, on a service that had piqued my interest, I was terrified to go near the team. I didn’t want to be looked at as the “poor medical student” who was involved with two recent deaths. Things improved as time went on, and my heart slowly shifted. I stopped looking at what I had lost and focused on what I had gained: insight and perspective. It wasn’t until my fourth year, on vascular surgery again, that I realized the invisible ties that had been there all along, pulling me to the field where I belong.
The patient population in vascular surgery is very special. They often have multiple comorbidities, requiring physicians to be technically advanced in both surgery and medicine. Growing up in a two-redlight town in rural South Carolina, I can easily relate to the stubborn and misunderstood population.
By pursuing
this
field, I will fulfill deep-rooted goals that I had not realized until my fourth year of medical school
and ER [emergency room], regardless of ability to pay; community board of directors; caring for all patients covered by Medicare and Medicaid or ability to pay; and using surplus funds to maintain facilities, equipment and patient care, [and] advance medical training, research and education.”1
The IRS also requires all hospitals to file Schedule H of Form 990 and, though not required, to self-report compliance with “community benefits” activities every three years. However, there are no specific rules or definition of community benefit activities.
Should NFPs be required to provide community benefits in proportion to their tax-exemption benefits? This view recently gained favor after a study concluded that NFP hospitals do not provide more free care than other types of hospitals, and sometimes even less care than FP or government hospitals.2
How much benefit to hospitals is there?
A recent report suggested that 2,927 U.S. NFP hospitals received $37.4 billion in total tax benefits in 2021. These included “federal income tax ($11.5 billion; 31%), sales tax ($9.1 billion; 24%), property tax ($7.8 billion; 21%), state income tax ($3.7
By pursuing this field, I will fulfill deep-rooted goals that I had not realized until my fourth year of medical school: patient continuity, medical complexity and innovation. I am blessed that, one day, I will get to see aspects of both my mentor and grandmother in my patients, thus reminding me of the magnitude of my duty as a future vascular surgeon.
BAILEY RICHARDSON is a fourth-year medical student at the Medical University of South Carolina in Charleston.
billion; 10%), charitable contributions ($3.2 billion; 8%), bond financing ($2.1 billion; 6%), and federal unemployment tax ($200 million; <1%).”3 In 2020, a Senate committee reported that benefits averaged $9.4 million per hospital. Although some of the numbers may be flawed, the committee concluded that many of the largest NFP hospitals spend less than 2% of their total revenue on charity care. The Lown Institute Hospitals Index reported that 80% of NFP hospitals spent less on “financial assistance and community investment than the estimated value of their tax breaks.”4
The American Hospital Association declared that hospitals spent 15.5% of their total annual expenses in 2020 as benefits to the community, of which 6.9% was due to financial assistance and unreimbursed Medicaid and other programs.
Clearly, NFP and tax-exempt hospitals provide valuable and necessary services to the public, including funding critical research and revenue-losing inpatient programs such as behavioral health, nephrology, burns, pulmonology, and infectious diseases—often in inner city or rural communities where FP hospitals may not exist. Operating margins for NFPs have hovered between 1 and 3%.
Bailey Richardson
continued from page 6
Although hospital margins have been hit over the past few years, management consultants Kaufman Hall reported that, for the previous 12 months, hospital operating margins increased significantly. In April 2024, they went from <1% to 4.3% the previous month. This was primarily due to increasing volumes but also higher prices.
Compensation
Besides proportional community benefits, excessive compensation provided to senior NFP hospital executives is a major source of criticism. This is because the public accepts large sums for FP companies beholden to investors and shareholders, while the expectation for NFPs is the opposite.
On average, NFP hospital CEOs earn about $700,000, exceeding by $300,000 the salaries of university presidents. The Senate report stated that “in 2021, the most recent year for which data is available for all of the 16 hospital chains, those companies’ CEOs averaged more than $8 million in compensation and collectively made over $140 million.”
Excessive compensation for NFP hospital board members is also a concern. As an ex-officio board member at a large health system for four years in the early 1990s, little or no compensation was offered, even though we dedicated many
hours before, during and after each board or sub-committee meeting. Most board members are productive citizens and own important businesses or have often highpaying jobs. Compensation for NFP board members has now become commonplace. The percentage of hospital boards offering cash compensation has doubled from 13% in 2018 to 27% in 2022, compared to only a 3% increase from 2014 to 2018. However, trustee compensation has sometimes been negatively associated with NFP hospital charity care provision. Even though board members, trustees and other insiders have a fiduciary responsibility towards the NFP entity, and are not permitted to benefit themselves or other insiders, my own experience is that, in many ways, they benefit from their presence and contacts.5
For-profit activities
Health systems are always looking for new revenue to subsidize losing service lines, new construction, ambulatory centers, administrative hiring, modern technology, litigation and the cost of new regulations. However, analysis of IRS data by Kaiser Health Network showed that NFP health systems “held more than $283 billion in stocks, hedge funds, private equity, venture funds and other investment assets in 2019.” Only 7% of their total investments were principally related to
GUEST EDITORIAL WHO HARMED WHO?
continued from page 2
specialty existential, or are they internal? Have we leveraged ourselves in such a way that reveals our true value to hospitals? A specialty that fills the coffers of healthcare systems while enabling complex surgery in other realms: we are the proverbial “firefighters,” always available to help sick patients and keep colleagues out of medicolegal peril. In the words of Navy SEAL Jocko Willink, it is indispensable that we take “extreme ownership” of our destiny. This means taking responsibility for everything that impacts our mission, including mistakes, failures, successes and challenges that will affect our abilities to perform the mission in the current and future environment. We should embrace sisu, the extraordinary and indomitable Finnish spirit to never quit and go beyond all limitations, especially in the face of extreme adversity.
Where do we go from here? With a specialty as small as ours, is this time for a unionized approach? Is there a minimum pay we should all receive for the multitude of hats we wear in a health system? SVS President-elect Keith Calligaro, MD, and others have attempted to lend transparency to this via the Pharify compensation survey, but is this enough? Even salary may be a hot-button
their nonprofit missions. The biggest concern is the substantial mergers and acquisitions of hospitals and physician groups by health systems and private equity investors.
Suggestions
There are several common-sense suggestions advanced by healthcare and legal experts. Congress needs to define exactly what constitutes community benefits to justify a hospital claiming NFP status. The Affordable Care Act required NFP hospitals to conduct community health needs assessments in their geographic area, which included seeking input from low-income, underserved areas. However, Congress did not take the next step and require hospitals to address these concerns. In addition, there are no precise and reasonable standards for what constitutes financial assistance to qualify under community benefits.
The IRS Form 990 listing filed by NFP hospitals lists, among other details, the community benefits they provide. This form is confusing and unclear, leading to partial and inexact data. For instance, hospitals often classify unreimbursed care for some patients as a bad debt expense, because many poor patients do not complete hospitals’ financial assistance processes. This form needs to be revised based on clarification of community benefits and standards for financial assistance. Form 990 could also report forgone federal, state and local taxes,
topic, as it can create a have-and-have-not scenario. Instead, we should address the administrative harm happening locally, regionally and nationally. This is our biggest threat. We could call 20 vascular surgeons around the country at any hour for clinical advice, and they would happily answer the phone. It’s time for us to lean on each other in our non-clinical struggles. To share our experiences and triumphs and display solidarity in an effort to unite us. Perhaps eliminating our greatest existential threat will bring us back on the same page. We have a rare opportunity and obligation to unify and protect our specialty, for ourselves and those who follow. It seems there is more to digest here than breakfast at Denny’s, so let’s break it down. Clinically, educationally and administratively, we all face significant challenges. We have had great victories and even failures in these realms. Somewhere in this country, someone is fixing your endoleak or maybe re-opening your bypass, but there is also someone enjoying time with loved ones having survived a ruptured aneurysm. We share in these victories and defeats, yet our righteous indignation regarding many of the topics outlined above only fulfills our need for a zero-sum game, where there are winners
as well as savings associated with using tax-exempt bonds, in the interests of complete transparency.
NFP hospitals are vital to healthcare delivery in the U.S. Tightening some regulations, clarification by Congress, and the recruitment of board members with a diversity of views and backgrounds6 will result in increased transparency and provide assurance to taxpayers that their hard-earned taxes are being used for the benefit of their communities.
References
1. https://www.gao.gov/products/gao-23106777
2. Bai G, Zare H, Eisenberg MD, Polsky D, Anderson GF. Analysis suggests government and nonprofit hospitals’ charity care is not aligned with their favorable tax treatment. Health Aff (Millwood). 2021;40(4):629–636
3. Plummer E, Socal MP, Bai G. Estimation of tax benefit of US nonprofit hospitals. JAMA. Published online September 26, 2024. doi:10.1001/jama.2024.13413
6. Satiani B, Prakash S. It is time for more physician and nursing representation on hospital boards in the US. https://hospitalmedical-management.imedpub.com/ it-is-time-for-more-physician-and-nursingrepresentation-on-hospital-boards-in-theus.php?aid=9753.
BHAGWAN SATIANI is an associate editor for Vascular Specialist. He is not an attorney.
and losers. This only harms us. This division has made us more susceptible to the one threat we all share: administrative harm. The more divided we become, the easier we are to ignore. So, the next time you post, comment, malign or fall on the proverbial sword, ask yourself who harmed who? Let our next headline in the New York Times be “Vascular surgery, a David and Goliath story defining the standard for vascular care among all providers.” Instead of a haughty quest for a nebulous vascular superiority (that may not exist), we call for unity. Together we need to fight our common battles while attracting more candidates to join our ranks.
Reference 1. Burden M, Astik G, Auerbach A, et al. Identifying and measuring administrative harms experienced by hospitalists and administrative leaders. JAMA Intern Med 2024 Sep 1;184(9):1014–1023
JONATHAN CARDELLA is an associate professor of surgery at Yale School of Medicine in New Haven, Connecticut. JEAN BISMUTH is chief of vascular surgery at University of South Florida (USF) Health/Tampa General Hospital in Tampa.
Bhagwan Satiani
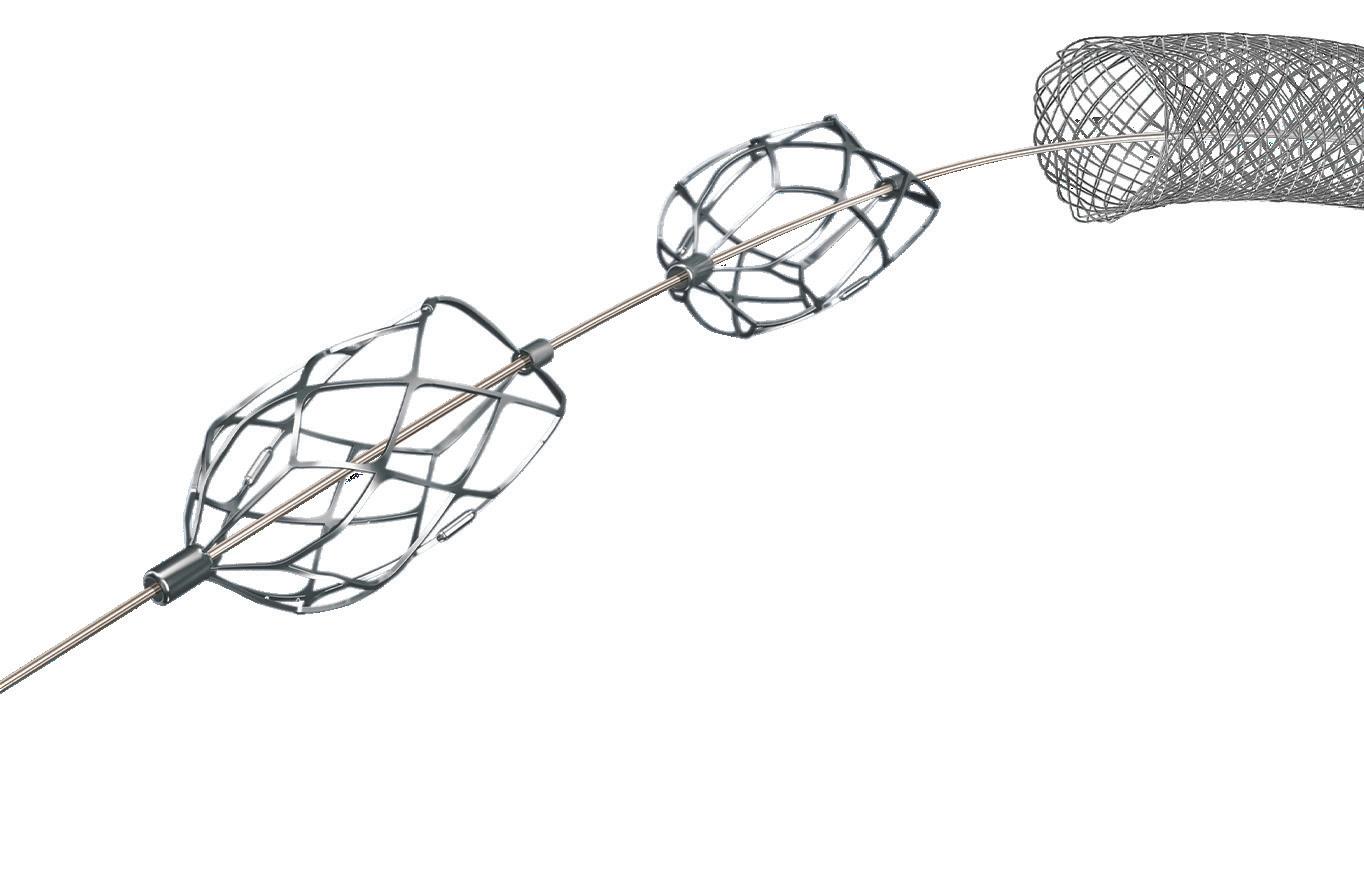
Pounce Thrombectomy
Platform use in acute limb ischemia: Vascular surgeons weigh in
Interventions for acute limb ischemia (ALI) represent up to 16% of the case volume for vascular surgeons and cost healthcare systems $26,000–$29,000 per patient in hospitalization costs.1 While revascularization may be achieved via open or endovascular approaches, guidelines recommend selection of the technique that will provide the most rapid restoration of arterial flow with the least risk to the patient.2
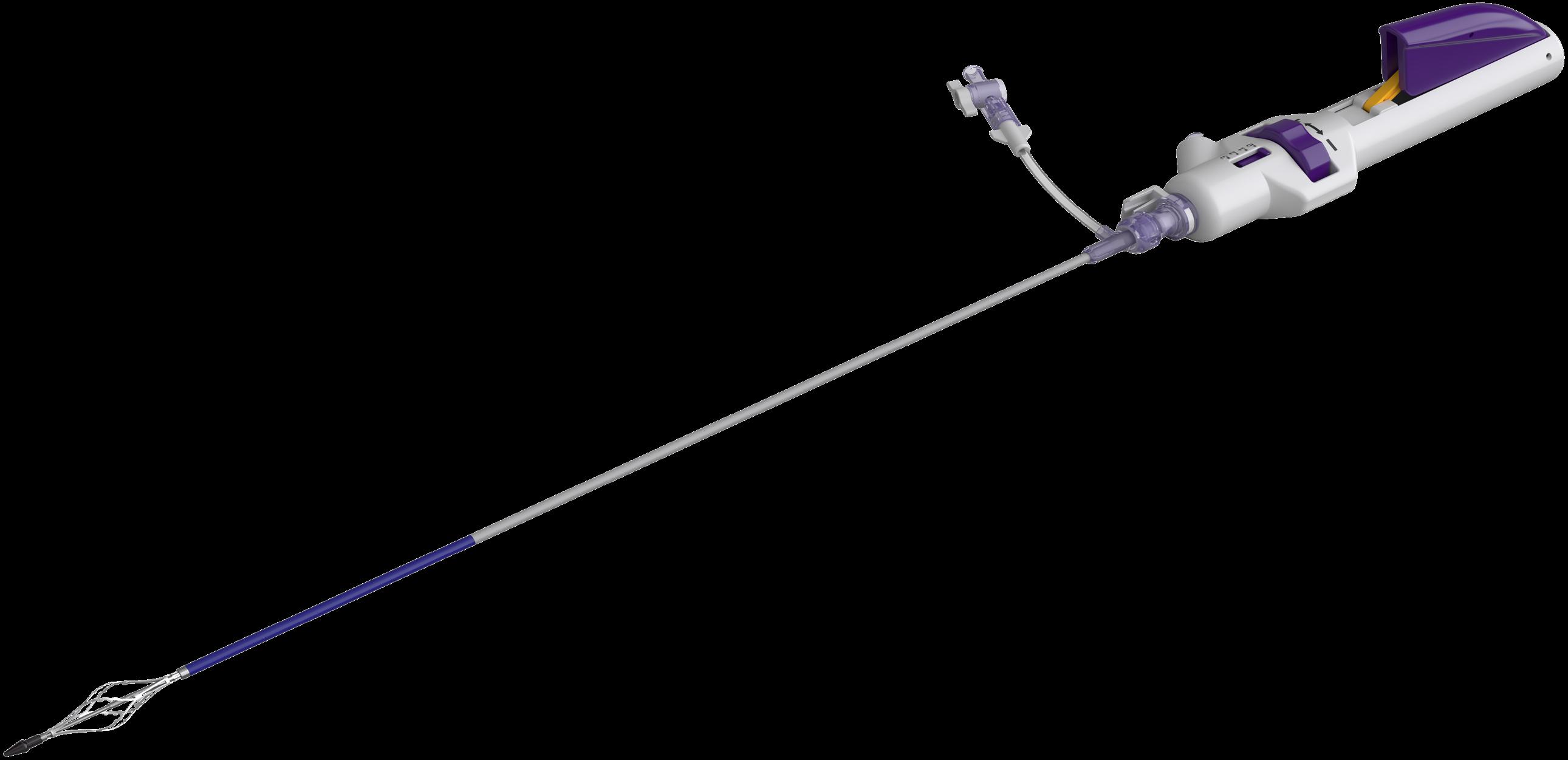
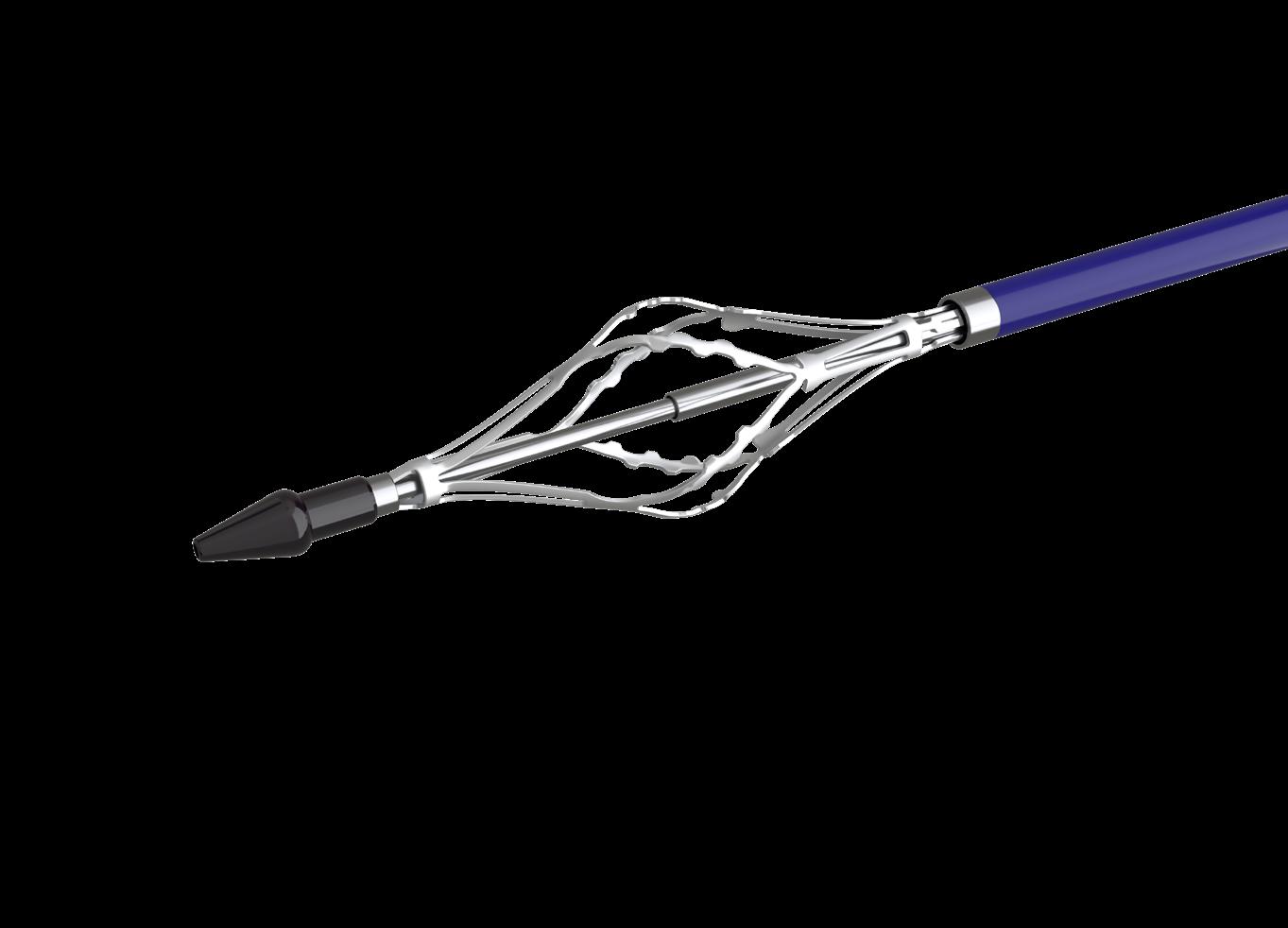
Endovascular treatment to remove clots and restore blood flow is now a common alternative to surgery for revascularization in ALI. 3 In recent years, percutaneous thrombectomy has become a viable option for vascular surgeons seeking single-session revascularization without the risks associated with thrombolytics4 or the need for costly intensive care unit (ICU) or hospital admissions. Until recently, the mainstays of percutaneous thrombectomy for ALI have been pharmacomechanical or aspiration devices. In 2021, Surmodics introduced the PounceTM Thrombectomy System, a purely mechanical solution that relies on a dual-basket technology to capture and remove chronic or acute emboli or thrombi without aspiration, lytics or capital equipment.
A 2023 retrospective study5 of 44 consecutive patients treated for lower extremity limb ischemia with suspected thrombus using the Pounce system demonstrated 83% technical success, defined in the study as effective removal of thrombus from the peripheral arterial segments where the system was used.
Notably, unlike previous studies of percutaneous thrombectomy devices in ALI, the study population included patients with subacute (15–30 days of symptoms; 16% of patients) and chronic (>30 days; 43% of patients) limb ischemia in addition to ALI (≤14 days; 41% of patients). In just one of 44 cases, thrombolysis was used to resolve thrombus secondary to treatment with the Pounce system. Procedural success, defined in the study as restoration of pulsatile flow to the foot and resolution of ischemic pain, was 95%.
Moving on from aspiration
Vascular surgeon Vince Weaver, MD (consultant to Surmodics), from the Vascular Specialty Center in Baton Rouge, Louisiana, uses percutaneous thrombectomy for most of his ALI cases. Today, the Pounce system is his go-to device.
“I’ve had access to just about all the arterial thrombectomy devices and have whittled them down,” he says. “Our practice
still has the Angiojet pharmacomechanical system [Boston Scientific], but I really don’t use it anymore due to the use of tPA [tissue plasminogen activator] and [the] device’s systemic effects [e.g., renal impairment].”6
As for aspiration, Weaver used the Indigo aspiration system (Penumbra) and QuickClear thrombectomy system (Philips) as his primary percutaneous devices until about two years ago, when he started using the Pounce system. “The limitation I found with suction thrombectomy is that you could go in and take out a lot of fresh clot, but when you take your post-thrombectomy angiograms, you see that there’s a lot of residual thrombus and organized stuff remaining. With the Pounce system, after one, maybe
fresh thrombus, but thrombus is usually not homogeneous.”
Efficiency and time management
Ferrer Cardona finds it efficient to be able to treat a range of heterogeneous clots with the PounceTM platform.
“For us, time management is critical. Elective procedures are 60% to 80% of our practice. We schedule these weeks in advance,” he says. “But patients with ALI or ALI and CLI [critical limb ischemia] can’t wait. They present at all times, and you have to treat them in a very time-sensitive manner because the outcomes are worse with delays. So, those two realities have to somehow coexist. That requires time management and efficiency.”
It takes him about 45 minutes to “treat what I’m going to treat with the Pounce system,” he says. “Let’s say I have an emergent patient come with rest pain; if, based
Pounce LP system very quickly, without major setup. You just open the package, get out the embolus, and a major problem is often resolved within minutes without surgical cutdown or another procedure with tPA.” Leville believes the Pounce platform’s mechanism of action is particularly suited for this application. “What I like about the Pounce platform is that it behaves more like a Fogarty balloon,” he says. “You start distal to the thrombus and withdraw back, just as you would with a Fogarty. In situations where you’re concerned about distal embolization, it can make more sense to use a Pounce platform. We do Fogarty procedures without wire access all the time—you just thread the catheter down the leg, inflate the balloon, and withdraw the clot. The Pounce platform behaves very much like that. That’s why I use it. The last thing I want to do is to have to convert a case from percutaneous to open surgical or overnight tPA in the intensive care unit if that’s not what we had planned. The Pounce platform gives me a third option.”
References
1. Gupta R, Siada SS, Bronsert M, Al-Musawi MH, Nehler MR, Jeniann AY. High rates of recurrent revascularization in acute limb ischemia–a national surgical quality improvement program study. Ann Vasc Surg. 2022;87:334–342
on my experience, I feel confident I can get that patient in and out in a timely manner
“ The most significant benefit of the Pounce system over aspiration is that it’s effective in treating both acute and chronic clot”
LUCAS FERRER CARDONA
two passes, I’ve been able to remove, if not all, at least a significant amount of that more organized thrombus. I’ve been getting much more robust thrombectomy with the device, and my success rate has been much higher for the right patient.”
Lucas Ferrer Cardona, MD (consultant to Surmodics), a vascular surgeon with the Dell Seton Medical Center at the University of Texas Hospital in Austin, has gravitated toward use of the Pounce system for similar reasons.
“The most significant benefit of the Pounce system over aspiration is that it’s effective in treating both acute and chronic clot,” he says. “Aspiration works great for
and my staff knows that and my cath lab manager knows that—then my flexibility to treat all patients and not have to put some things off and triage some patients increases significantly. Whatever makes that easier, more effective, and more predictable is going to benefit patients and the hospital. You’re using less human capital, you’re using less space, you’re using less time that can be used for treating additional patients.”
A new option for distal embolization
Vascular surgeons have also found significant benefit in using the Pounce platform as a bailout device for distal embolization during planned percutaneous lower-limb interventions. The PounceTM LP (Low-Profile ) Thrombectomy System, introduced in 2024, is intended for use in 2–4mm peripheral arteries, making it suitable for tibial occlusions. The original Pounce system is intended for use in 3.5–6mm arteries.
“Embolizing plaque is terrible, and we really have had limited options to get that embolus out,” says Christopher Leville, MD (consultant to Surmodics), a vascular surgeon with the CentraCare-St. Cloud Hospital in St. Cloud, Minnesota. “We used to try to use Export catheters [Medtronic] or other devices, or even a SpiderFX filter [Medtronic] or other devices, but everything was suboptimal. In these situations, you can use the
2. Gerhard-Herman MD, Gornik HL, Barrett C, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2017;69(11):e71–126
3. Lind B, Morcos O, Ferral H, et al Endovascular strategies in the management of acute limb ischemia. Vasc Specialist Int. 2019;35(1):4
4. Ebben HP, Jongkind V, Wisselink W, Hoksbergen AW, Yeung KK. Catheter directed thrombolysis protocols for peripheral arterial occlusions: a systematic review. Eur J Vasc Endovasc Surg 2019;57(5):667–675
5. Gray BH, Wheibe E, Dicks AB, Low ML, Tingen JS. Pounce thrombectomy system to treat acute and chronic peripheral arterial occlusions. Ann Vasc Surg 2023;96:104-114
6. Acosta S, Karonen E, Eek F, Butt T. Shortterm complications and outcomes in Pharmaco-mechanical thrombolysis first and catheter-directed thrombolysis first in patients with acute lower limb ischemia. Ann Vasc Surg. 2023;94:253–262
A version of this article first appeared in Endovascular Today.
Caution: Federal (U.S.) law restricts the Pounce™ Thrombectomy System and Pounce™ LP Thrombectomy System to sale by or on the order of a physician. Please refer to each product’s Instructions for Use for indications, contraindications, warnings and precautions. SURMODICS, POUNCE, and SURMODICS and POUNCE logos are trademarks of Surmodics, Inc., and/or its affiliates. Third-party trademarks are the property of their respective owners.
CASE REPORTS
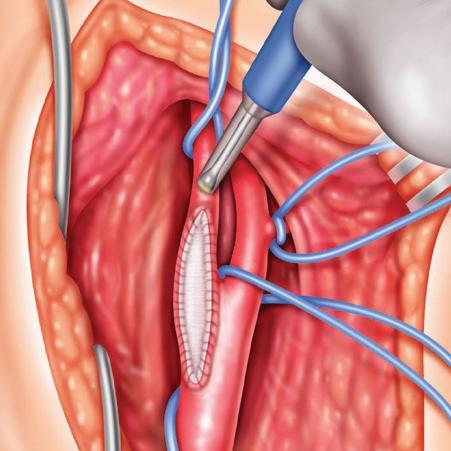
Removal of acute and organized SFA thrombus
VINCE WEAVER highlights a case in which the thrombus in the left superficial femoral artery (SFA) is tackled.
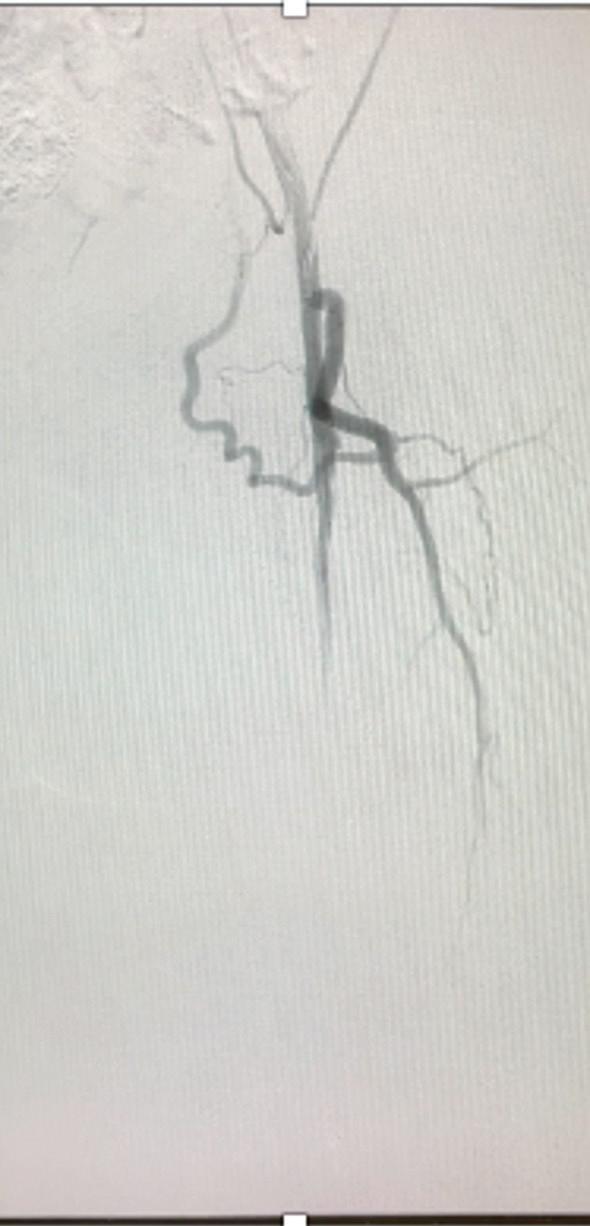
■ Patient presentation and diagnostics
A 45-year-old man with a history of embolic and thrombotic events presented with left leg pain of one-week duration. The initial angiogram (Figure 1) showed new arterial thrombus in the mid to distal left SFA.
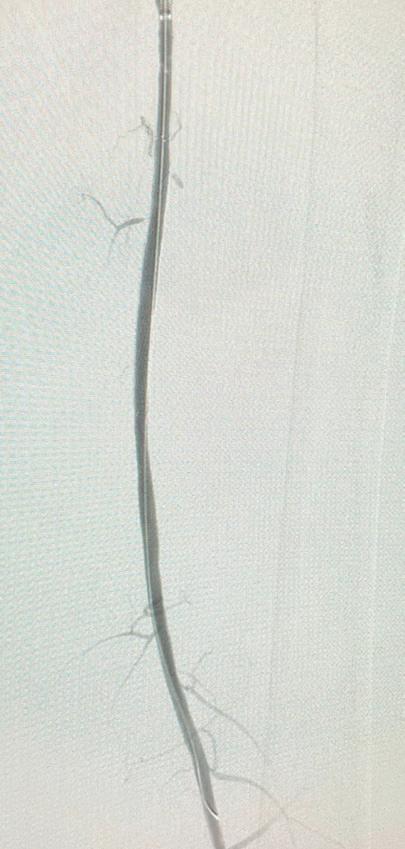
■ Thrombectomy
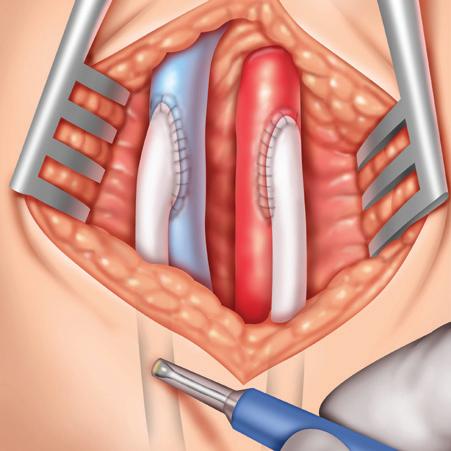
The Pounce system basket wire was deployed distal to the thrombus and the funnel catheter deployed proximal to the thrombus. The baskets were withdrawn into the funnel catheter and the system was removed, completing the first device pass. Balloon angioplasty was also performed to clear residual disease. The final angiogram showed full restoration of SFA flow (Figure 2)
■ Post-procedure outcome
The patient was discharged the next day. The Pounce system aided in the removal of acute and organized thrombus in one pass.
Removal of organized infrapopliteal arterial thrombus
LUCAS FERRER CARDONA presents a case of complete thrombus in below-the-knee arteries.
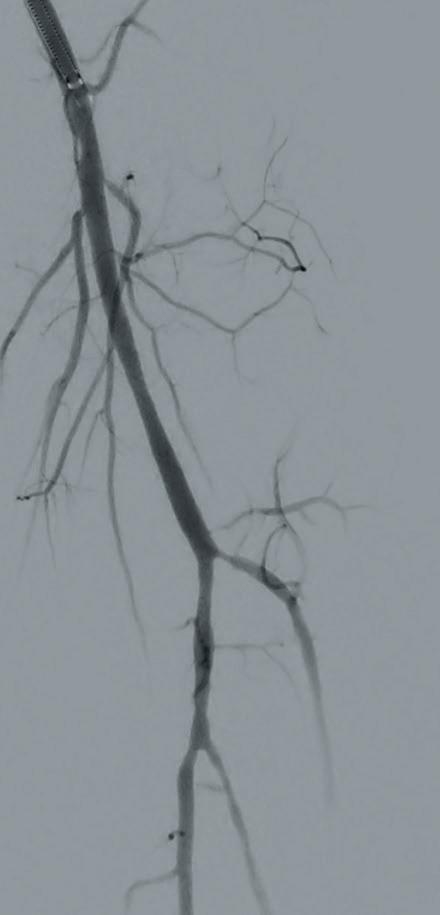
■ Patient presentation and diagnostics
A male patient presented with immediate onset of numbness, pain and decreased function in his lower left leg. The initial angiogram showed complete thrombosis of the left popliteal, tibioperoneal trunk (TPT) and tibial arteries (Figure 1)
■ Thrombectomy
Two Pounce system passes removed organized thrombus from the popliteal artery, but distal flow continued to be hampered by an occlusion in the proximal anterior tibial (AT) artery. One pass with the Pounce LP System resulted in complete removal and resolution of the thrombus burden with improved flow through the AT to the plantar arch (Figure 2)
■ Post-procedure outcome
The patient was discharged after two days. The combination of Pounce and Pounce LP systems allowed for complete removal of organized thrombus from below-the-knee vessels without the need for thrombolytics or surgical intervention.
Removal of brachial and ulnar artery thrombus
CHRISTOPHER LEVILLE demonstrates the use of Pounce LP in the upper extremity.
■ Patient presentation and diagnostics
A man in his late 60s presented with a cold left hand symptomatic for 24 hours. An initial ultrasound showed a partial occlusion of the left ulnar artery (Figure 1) and complete occlusion of the patient’s left brachial artery. The patient was not a candidate for tPA and open surgical thrombectomy was not deemed appropriate.
■ Thrombectomy
Two Pounce system passes in the mid and distal brachial artery, respectively, were followed by one Pounce LP system pass in the ulnar artery. Final angiograms showed complete resolution of the ulnar artery (Figure 2) and a patent brachial artery, with no embolization to the patient’s hand.
■ Post-procedure outcome
The patient was discharged the day after the intervention, with instructions to maintain his warfarin regimen for three months. At one-month follow-up, the patient’s brachial and ulnar arteries continued to show patency and good flow.
FROM THE COVER STUDY DETAILS
ASPECTS OF EARLY CARE IMPROVEMENTS AFTER PUBLICATION OF SVS APPROPRIATE USE CRITERIA FOR CLAUDICATION
continued from page 1
Siracuse, MD, an attending vascular surgeon at Boston Medical Center and professor of surgery and radiology at Boston University.
The SVS AUC, published in the Journal of Vascular Surgery (JVS) in April 2022, came amid a significant increase in the number of interventions for claudication over the past couple of decades, despite medical therapy being the first-line treatment for the less advanced form of peripheral arterial disease (PAD).
The research team defined the preAUC period as January 2018–December 2019, with the period after the AUC’s publication in JVS set as May 2022–December 2023. The period in between was excluded for matters related to the COVID-19 pandemic.
All patients with claudication who underwent an intervention in the VQI PVI, and suprainguinal and infrainguinal bypass registries were included in the analysis.
Alonso informed EVS 2024 that the investigators tried to adhere to as many of the SVS AUC principles as possible, pointing out the exception of exercise therapy, which is not available as part of the VQI.
The team primarily looked at complex aortoiliac and femoropopliteal lesions, as well as isolated infrapopliteal lesions.
“When we looked at PVI demographics, we saw that, post-AUC, there was a significant increase in severe disease as an indication for interventions, and that there was a significant increase in optimal medical therapy [OMT] use following the AUC [publication] in the postoperative period,” Alonso told EVS 2024 attendees. “However, we noted that there was no significant change in current smoking or preoperative medical therapy.”
Among significant comorbidities in
the patient population, Alonso pointed to an increased number of interventions in patients with coronary artery disease (CAD), but a significant decrease in those on dialysis.
Homing in on interventions in specific anatomic segments, Alonso and colleagues saw that there was a significant decrease in the number of endovascular interventions for complex
“An important limitation of this study is that, as it was observational, we were unable to conclude if the changes seen were due to the guidelines or other external factors”
ANDREA ALONSO
aortoiliac and femoropopliteal disease, but a notable increase in endovascular treatment for disease in the CFA and isolated infrapopliteal disease.
“With suprainguinal bypass, we didn’t see any significant changes in the use of extra-anatomic revascularization, and, in the infrainguinal bypass registry, we did not see any changes in bypasses, specifically those using prosthetic conduit,” she said.
“An important limitation of this study is that, as it was observational, we were unable to conclude if the changes seen
were due to the guidelines or other external factors, and we were unable to evaluate exercise therapy.”
The SVS AUC for IC was the work of a multidisciplinary team of experts who evaluated several unique scenarios for disease in the aortoiliac, CFA and femoropopliteal regions, Alonso pointed out. They looked at several variables, including exercise therapy, OMT use, smoking, medical risk, degree of lifestylelimiting disease, walking distance, lesion location, endovascular interventions and the type of bypass used.
“The key principles of the AUC are that the first-line treatment [for patients with claudication] is a combination of exercise therapy, medical therapy and smoking cessation, and that interventions may have a benefit if a patient has undergone conservative management and has severe lifestyle-limiting disease, and more short distance walking,” Alonso observed.
As published in JVS, those key AUC principles for the management of IC—by anatomic segment—are as follows: “invasive interventions for femoropopliteal disease should be reserved for patients with severe lifestyle limitations and a short walking distance; in the CFA, open common femoral endarterectomy will provide greater net benefit than endovascular intervention; in the infrapopliteal segment, invasive intervention is of unclear benefit and could be harmful.”
Additionally, Alonso noted from the AUC that, in the aortoiliac region, patients who may have a benefit from invasive interventions for claudication could undergo endovascular treatment primarily, but also inline bypasses in certain scenarios.
Discussion afterward raised the specter of payment and reimbursement.
Rabih Chaer, MD, chief of vascular surgery at the University of Pittsburgh in Pittsburgh, Pennsylvania, suggested that guidelines themselves “are not going to change practice patterns, unless this perhaps impacts reimbursements and insurance providers.” He asked Alonso whether she thought this scenario would eventually play out. Alonso agreed that changes in practice would have to come through reimbursement channels, adding that, “to a point, AUCs do affect payment.” According to the AUC for IC paper published in JVS, the Centers for Medicare & Medicaid Services and other payors have taken notice of AUC, primarily for their role in reducing overuse.—Bryan Kay
SVS unveils latest round of members to
CEA ‘remains useful and relevant’ in era of improving medical therapy EUROPE
FINDINGS FROM A RETROSPECTIVE analysis delivered at the recent European Society for Vascular Surgery (ESVS) annual meeting (Sept. 24–27) in Kraków, Poland, provide evidence that—for symptomatic carotid artery stenosis patients—endarterectomy “remains a useful and relevant intervention in the era of improving medical therapy.”
Presenter Sashini Iddawela, MBBS, from University College London Hospital NHS Trust in London, England, noted that urgent carotid endarterectomy (CEA) is currently the first-line recommendation for symptomatic, significant carotid stenosis. There is also speculation that symptomatic stenosis could be substantially reduced thanks to today’s advances in optimal medical therapy (OMT) and anti-major cardiovascular event (MACE) medications.
Iddawela and her colleague Daryll Baker, BMBCh, a consultant vascular surgeon at Royal Free London NHS Foundation Trust, undertook a study in an effort to determine whether or not patients undergoing CEA were already on OMT prior to their index admission. They performed a retrospective analysis of 124 patients receiving urgent CEA following development of a stroke or transient ischemic attack between 2021 and 2023. Overall, 36 patients (29%) were on a combination of an antiplatelet, antihypertensive and statin during their index presentation. According to the researchers, there was no significant difference between the proportion of patients on antiplatelets, antihypertensives or statins pre- versus post-CEA. However, patients with ischemic heart disease, diabetes or hypertension were observed as being significantly more likely to be on OMT.
This led to the conclusion that patients undergoing CEA are generally multimorbid and more likely to be on risk-modifying therapy at their index presentation. Thus, the researchers state that CEA should still be considered a useful intervention in these patients.—Jamie Bell
become Distinguished Fellows
The Society for Vascular Surgery (SVS) has welcomed 11 surgeons to its ranks of Distinguished Fellows.
he new fellows have distinguished themselves by making sustained and substantial contributions to the Society, said current SVS President Matthew Eagleton, MD, himself a fellow. “Becoming a Distinguished Fellow is an honor based on longstanding efforts in research, service, and/or education,” Eagleton said. “Applicants typically have broad recognition of their excellence and competence and significant service to the SVS.”
The 2024 group of honorees are listed as follows: Rana Afifi, MD, University of Texas Health Science Center at Houston, Texas; Jayer Chung, MD, Baylor College of Medicine,
Houston; Gert de Borst, MD, University Medical Center, Utrecht, the Netherlands; Chelsea Dorsey, MD, University of Chicago Medical Center; Sukgu Han, MD, University of Southern California in Los Angeles; Karen J. Ho, MD, Northwestern Medicine Feinberg School of Medicine in Chicago; Shang Loh, MD, University of Pennsylvania, Perelman School of Medicine, in Philadelphia; Nicolas Mouawad, MD, McLaren Bay Heart and Vascular in Bay City, Michigan; Elina Quiroga, MD, University of Washington in Seattle; Bjoern Suckow, MD, of Dartmouth Hitchcock Medical Center, Lebanon, New
Matthew Eagleton
Hampshire; and Gabriela Velazquez, MD, Wake Forest University School of Medicine, Winston-Salem, North Car-
Active, International and Senior SVS members may submit applications to become a Distinguished Fellow, denoted as DFSVS after a surgeon’s name, by March 1 of every year.—Beth Bales
The Surgical Doppler You Can
RELIABLE
It’s the next generation of our Trans-Q-taneous Intraoperative (TQI) Doppler System, combining the reliability and cost effectiveness of the original TQI Doppler with new, user-friendly features.
Increased Portability
In addition to its smaller size, the TQI 2.0 Doppler now features an IV pole mount and a handle for easy transport.
Greater Control
The modern design of the TQI 2.0 Doppler allows for a foot pedal for increased control from the surgical field.
Improved Sound
The TQI 2.0 Doppler System is optimized for clear audio signals for both intraoperative and transcutaneous use.
VTI’s single-use surgical Doppler probes provide a higher degree of performance reliability since probe failure due to reprocessing is eliminated. You’ll reach for your Doppler with confidence!
COST-EFFECTIVE
Single-use surgical Doppler probes eliminate reprocessing costs as well as the hidden expenses associated with the malfunctioning of reusable probes such as lost OR time.
Visit our TQI product page on our website.
DISPARITIES
Female patients found to be at increased risk from adverse outcomes after an ALI diagnosis
RESULTS FROM A NEW STUDY HIGHLIGHTING that female patients are at increased risk of adverse outcomes after acute limb ischemia (ALI) lend weight to the possibility of underdiagnosis and management of vascular disease among women, the authors behind the research report.
Investigators from the University of Pittsburgh Medical Center (UPMC) in Pittsburgh, Pennsylvania, found that females who presented with ALI were less likely to have had prior vascular interventions, less frequently on a preoperative statin or antiplatelet agent and more likely to be hypercoagulable. They had a higher rate of mortality after revascularization except when medically optimized, and female patients also had “notably higher amputation rates following endovascular interventions,” the UPMC research team found.
The results were delivered by Mikayla Lowenkamp, MD, a vascular surgery resident at UPMC, during a session dedicated to diversity, equity and inclusion (DEI) at the 2024 Eastern Vascular Society (EVS) annual meeting in Charleston, South Carolina (Sept. 19–22).
Lowenkamp set the scene for the study by pointing to the “underrepresentation of female patients” in key trials and a resultant “lack of sex-based guidelines regarding the evaluation, diagnosis and management” of vascular disease in women. “As a result, recent literature has found a differ-
COMPLEX
AORTIC HYBRID AORTIC
ence in amputation and mortality rates following acute limb ischemia,” she said.
Lowenkamp and colleagues looked to identify sex-specific predictors of major amputation and mortality, as well as sex-specific differences in the presentation, management and outcomes in patients undergoing revascularization for ALI in a retrospective cohort study of cases from a multihospital system. All patients who underwent a revascularization procedure for ALI from 2016–2023 were included, with 548 meeting inclusion criteria. Female patients were older and made up 46% of the cohort. They were less likely to have a history of cardiovascular disease, specifically lower rates of coronary artery disease (CAD), Lowenkamp told EVS 2024.
and multivariable analyses. Increasing age, a cancer history and an advanced Rutherford classification were all predictors of an increased mortality risk, Lowenkamp added.
On subgroup analysis, the association between women and mortality did not differ except in the context of preoperative optimal medical therapy (OMT): “In female patients on optimal medical care, mortality risk after revascularization was equivalent to males,” she said. “In female patients not on OMT, their mortality risk was significantly increased in comparison to males.”
Study data demonstrated that females report earlier after symptom onset and were more likely to go to the operating room within 24 hours in comparison to their male counterparts, despite no differences in Rutherford ALI classification on presentation.
There were no differences in either the initial surgical approach—endovascular vs. open—or in terms of endovascular strategy. But female patients were less likely to undergo thrombolysis or bypass. After intervention, female patients were less frequently discharged on an antiplatelet, and experienced an increased rate of mortality on both univariable
ARCH: ‘WE BELIEVE THERE IS STILL A ROLE FOR A VERSATILE MULTIPLE-BRANCHED ARCH OPTION’
MID-TERM RESULTS FROM AN analysis of a series of hybrid aortic arch reconstructions utilizing overlapping single thoracic branch endoprostheses in a dual-branch configuration showed the technique to be safe and versatile.
Delivered at the 2024 Western Vascular Society (WVS) annual meeting in Colorado Springs, Colorado (Sept. 7–10), the paper was the winner of the WVS Rapid Fire Competition.
Presenter Evan R. Brownie, MD, a vascular surgeon at Intermountain Health in Murray, Utah, characterized use of the procedure following the commercial launch and subsequent widespread use of the Gore Tag thoracic branch endoprosthesis (TBE).
Despite this, Brownie said, “we believe
there is still a role for a versatile multiplebranched arch option.”
Brownie and colleagues performed their first 49 TBE deployments in 44 patients from October 2022 to December 2023, five of which involved the dual-TBE configuration in question. Median followup was six months, and up to 12 months.
“All of these patients had at least one prior sternotomy with an existing ascending aortic stent graft, some sort of systolic heart failure and one of the five patients had a prior recurrent laryngeal nerve injury at the time of their index procedure, henceforth why—even though we do an equal number of zone 0 deployments off a single branch—we are trying to minimize risk for this patient population and the discrepancies that can
Furthermore, there were no differences in overall amputation rates between the sexes on univariable analysis, and sex was not a predictor of amputation on multivariable analysis, Lowenkamp continued. “And the association between females and amputation did not differ among the subgroups, except in patients who received an endovascular-first approach; they were 2.6 times as likely to undergo a major amputation.” Concluding, Lowenkamp emphasized the data showing a higher rate of long-term morality alongside a higher rate of amputation following endovascular intervention, commenting that “one can speculate that may be due to smaller vessel size, differences in chronicity or distribution of the disease.”
Posing a question from the meeting floor, Alan M. Dietzek, MD, the chief of vascular surgery at Nuvance Health in Danbury, Connecticut, said the take-home message from the study results seemed to be women not being on OMT, and asked Lowenkamp whether, given the totality of the data, this prompted a preference for an endovascular or open surgical approach.
Lowenkamp said her takeaway was more centered on a need to ensure that female patients are medically optimized should they require a vascular intervention.
be seen with a single branch perfusing all of the great vessels,” he explained.
Three of the five underwent a dual brachiocephalic configuration with a left carotid-to-subclavian transposition through a left cervical incision, Brownie said. The other two had a left-commoncarotid-to-right-common-carotid transposition, he added, explaining that “we do a separate arteriotomy in the right carotid artery to maintain cerebral perfusion throughout the case.”
For the endovascular portion of the procedure, he continued, “we obtained bilateral percutaneous femoral and bilateral percutaneous arm access. We do a zone 2 thoracic branch stent graft, put
“An appropriate trial design and regulatory application could bridge the gap until we have a dedicated arch graft available”
EVAN R. BROWNIE
in an oversized Viabahn (Gore) stent graft in position, then extend proximally with our zone 0 stent graft and deploy it. So, we are gaining the overlap seal between the devices, as well as the parallel seal zone, just to maintain perfusion to the subclavian limb.”
Procedures were typically staged, Brownie said, with the transposition performed two days prior to the endovascular repair. Following transposition, there were no strokes, cranial nerve injuries or early thrombosis, he told WVS 2024. Similarly, following endovascular repair, there were no cases of spinal cord, renal or bowel ischemia.
Furthermore, one patient was returned to the operating room for an access site complication, one had a stroke, and there were no type I or II endoleaks, nor gutter leaks. Sixty percent of these patients have already demonstrated sac regression, Brownie added.
“An appropriate trial design and regulatory application could bridge the gap until we have a dedicated arch graft available,” he concluded. “And, of course, this will largely be dependent on compensation and reimbursement for such procedures.”
Mikayla Lowenkamp
WESTERN VASCULAR
THE JAPANESE CONCEPT OF IKIGAI AND HOW MENTORSHIP MIGHT HELP SPECIALTY
AMID CHALLENGES OF VASCULAR SURGERY WORKFORCE SHORTAGE
THE JAPANESE CONCEPT OF IKIGAI, or an individual’s reason for being, underpinned the message behind a fresh call for mentorship in vascular surgery and how mentoring could aid efforts to plug a shortage in the specialty’s workforce.
Roy M. Fujitani, MD, chief of vascular and endovascular surgery at the University of California, Irvine, in Orange, California, made the plea to gathered colleagues in his Western Vascular Society (WVS) presidential address during the 2024 WVS annual meeting in Colorado Springs, Colorado (Sept 7–10).
Integrating the core spheres of ikigai made up of what a person is good at, what they love doing, what the world needs, and what they can be paid for—with mentorship creates a “meaningful framework for personal and professional development,” he told attendees.
Those spheres combine to create passion (a person’s strengths plus love), mission (love plus need), vocation (need plus remuneration) and profession (remuneration plus strengths), he said. If an individual doesn’t combine all four spheres, they may not achieve “full fulfillment,” said Fujitani, who grew up in the rural area of Ahualoa in Hawaii, the grandchild of Japanese immigrants. He laid out the scale of the challenge to vascular surgery from the predicted work-
MIDWESTERN VASCULAR
force shortage through 2030 and beyond: “According to some estimates, the current number of vascular surgeons may not meet the current demand for vascular surgery services over the next decade, with estimates reaching 35–45%.”
Along with the demands of an aging population, the rise of chronic disease, and an aging vascular workforce, Fujitani pointed to training and recruitment concerns: a restricted number of fellowship programs and the breadth of choices available to medical students—some which are perceived as having better work-life balance and financial rewards, he said. “Without intervention, the gap between the supply of vascular surgeons
“Foster strong mentorship with our young mentees, identifying the very brightest, the very best, to safeguard the future of our vascular surgery specialty”
ROY M. FUJITANI
and the demand for services may widen by 2030 and beyond.”
This is where mentorship and the concept of ikigai might have a dual role to play, Fujitani explained. “Early and persistent mentorship is a critical element in the safeguarding of vascular surgery,” he said.
Across the spheres, the experienced surgeon can support and provide advice to mentees as they pursue what they love doing and identify their strengths, and spur skill development by providing opportunity as they discover what they are good at, Fujitani continued. In terms of what the world needs, mentors can help guide purposeful careers that not only fulfill personal ambitions but also contribute to society, as well as support mentees as they navigate career choices that align with their skills and financial and personal fulfillment.
“I fully encourage you to actively participate in first gaining your ikigai yorokobi, activities that bring you intrinsic fulfilment and happiness, and then foster strong mentorship with our young mentees, identifying the very brightest, the very best, to safeguard the future of our vascular surgery specialty.”
EASTERN VASCULAR
Regional societies see presidential changing of the guards LEADERSHIP
BRAJESH K. LAL, MD, ASSUMED THE Eastern Vascular Society (EVS) presidency during the 2024 EVS annual meeting. He took over from Kathleen Ozsvath, MD. Patrick Muck, MD, assumed the reins of the Midwestern Vascular Surgical Society (MVSS) at the conclusion of the 2024 MVSS annual meeting, succeeding Bernadette Aulivola, MD,. Ahmed Abou-Zamzam Jr., MD, has taken over as the 2024–25 president of the Western Vascular Society (WVS) following the conclusion of the society’s 2024 annual meeting. He was passed the presidential gavel by Roy Fujitani, MD.
During the EVS annual meeting, meanwhile, members of the society, staged a successful day of service in the heart of the downtown Charleston community.
Several senior society members and advanced practice providers were joined by representatives of industry partners on the evening of Friday, Sept. 20, at a community center where they performed screenings for peripheral arterial disease (PAD), handed out free compression stockings as part of an effort to address awareness of venous disease, and sought to educate local residents on the signs and symptoms of both venous and arterial conditions.
The event was held in conjunction with the American Venous Forum (AVF) and the Medical University of South Carolina.
‘Investing in the people of vascular surgery’
Outgoing Midwestern Vascular Surgical Society (MVSS) President Bernadette Aulivola, MD, underscored the importance of “investing in the people of vascular surgery—those learning about it and those progressing through their careers,” for the future of the specialty.
At the heart of this effort, she told the 2024 MVSS annual meeting in Chicago (Sept. 12–14), is mentorship and, crucially, performing the role of mentor early on.
“We know if we engage medical students early that medical students have a higher likelihood of applying to surgical residency if they see that [mentorship] early, because the pipeline is super early,” said the division director of vascular surgery and endovascular therapy at Loyola University in Maywood, Illinois.
“One study that took a look at general
surgery residents found that about two thirds of them identified certain qualities within their mentors that made them choose that mentor’s specialty. Those are based on the skills and achievements of that mentor, but also that the mentor talked about what they do passionately. So, we should talk about what we do.”
Aulivola also pointed to research showing the overlapping factors that impact a medical student’s decision: the process experiential learning—or “getting their hands on stuff”—played an important role in addition to mentorship alone, for instance. Another study involving a simulation skills course showed that 90% of participants attributed their interest to the technical portion and 70% linked it to the mentorship happening at the same time, she added.
A TEAM SPORT: A PRESCRIPTION FOR THE FUTURE OF VASCULAR SURGERY
OUTGOING EASTERN VASCULAR SOCIETY (EVS) PRESIDENT KATHLEEN Ozsvath, MD, used her presidential address to tackle the needs of those practicing the specialty moving forward, combining themes of family, collaboration, diversity, equity and inclusion (DEI). Ozsvath, who serves as chief of surgery at Samaritan Hospital in Troy, New York, set the tone by invoking elements of her own story: a family history that includes highly successful immigrants; a feeling early in life of not fitting in; a personal journey into vascular surgery initially discouraged by those who would be mentors.
Titling her address “Vascular surgery: An EVS team sport and family affair combined with finding your superpower,” Ozsvath provided a prescription for change in a specialty increasingly made up of a more diverse workforce and facing a rising tide of vascular disease. The address, which took place during the 2024 EVS annual meeting in Charleston, South Carolina (Sept. 19–22), saw Ozsvath urge the next generation of vascular surgeons—both trainees and medical students—to pursue their dreams and to ignore any naysayers who may be attempting to discourage them.
At the outset of her own journey in medicine, she faced her own version of discouragement: “As a medical student, I was told I couldn’t be a surgeon because I’m a female,” she said. “Of course, I smiled, said, ‘Thank you, sir,’ and went to New York.”
Roy M. Fujitani
VenaCore
Thrombectomy Catheter TM
Designed to Address Challenging Venous Occlusions
Dynamic Control
Quick compress handle lever for element collapse and expansion
Engage. Separate. Remove. Modified off-axis edge design for in-line vessel treatment of venous occlusions
VenaCore device offers long-awaited interventional solution for challenging venous occlusions
Despite the recent growth in mechanical thrombectomy devices for acute deep vein thrombosis (DVT), interventional options for wall adherent venous obstruction are extremely limited. Residual venous obstruction after medical or interventional therapy for the treatment of acute DVT is associated with an increased incidence of post-thrombotic syndrome (PTS).1,2 Managing venous obstruction and the associated symptoms at its initial onset remains a challenge for interventionalists. However, as Steven D. Abramowitz, MD, chair and director of vascular surgery for MedStar Health in Washington, D.C., says, a new technology—the VenaCore™ thrombectomy catheter (Inari Medical)—might be able to “change the care algorithm” for patients burdened by the long-term complications of venous obstruction.
“Arevolutionary technology like VenaCore addresses a previously unmet procedural need and allows operators to remove venous occlusions from within the vein lumen,” he explains. “As an endovascular tool, it has enough engagement with venous obstruction to remove adherent clot from the vein wall, as well as force to grab post-thrombotic scar tissue. The unique design of the device allows for effective treatment of acute and chronic pathology without harming the vein wall. VenaCore is the first FDA [Food and Drug Administration]-approved device that is designed to address challenging venous occlusions in a wide variety of patients.”
The ClotTriever® (Inari) Outcomes (CLOUT) registry demonstrated that mechanical thrombectomy using the ClotTriever system can have similar procedural success regardless of newly diagnosed DVT chronicity.2 However, removing refractory wall-adherent material can still be challenging. Balloon maceration or other adjuvant techniques can be of limited success. When used with the ClotTriever system, VenaCore can target focal treatment areas of underlying venous obstruction that may reduce the severity of associated complications.
tomatic patients who have venous occlusions that are challenging to treat”, says Abramowitz. Many DVT patients are relegated to compression therapy once symptoms begin. For those eligible for iliofemoral stent placement, femoropopliteal inflow disease can limit the likelihood of long-term stent durability and patency.
According to Abramowitz, many PTS patients with poor inflow suffer from poor long-term stent patency outcomes. Balloon venoplasty has therefore represented the most frequent intervention for primaryand secondary-assisted patency, but this approach itself is associated with an incredibly “high rate of recurrence” and “very shortlived results.”
“We were doing these procedures with great frequency, with little or no return,” he recalls. “That’s because, as much as you want to balloon the scar tissue ‘out of the way’ in the femoropopliteal segment, all you’re doing is shifting something that’s solid to the side—and it bounces back. It’s not like arterial disease, which can remodel around a treated segment. Venous disease and post-thrombotic scar do not positively remodel.”
“ VenaCore on its own, and in conjunction with RevCore, truly disrupts all of our current care algorithms when it comes to venous occlusions”
STEVEN D. ABRAMOWITZ
with anticoagulation alone with persistent symptoms; those whose stents failed as a result of poor inflow; and those in whom stents would otherwise have been contraindicated due to poor inflow, which can now be restored to allow for iliofemoral stenting.
Case 1: Material removed (1); IVUS pre- (2) and post-intervention (3). Case 2: venogram pre(4) and postintervention (5); and chronic material (6)
PTS for many years presented to the office with hemosiderosis and atrophic blanche. An ultrasound in the femoral vein showed a post-thrombotic scar related to a prior femoropopliteal DVT. The patient was brought in for intervention with VenaCore and underwent a successful procedure with no complications.
References
1. Iding AFJ et al. Residual venous obstruction as an indicator of clinical outcomes following deep vein thrombosis: A management study. Thromb Haemost 2023 Aug
2. Dexter D et al. Safety and effectiveness of mechanical thrombectomy from the fully enrolled multicenter, prospective CLOUT registry. JSCAI. 2023 March
Residual venous outflow obstruction is not only associated with a higher future risk of DVT and pulmonary embolism (PE), but also has a significant impact on a patient’s Villalta score, as well as their venous disease-related disability and quality-of-life outcomes. The pain associated with PTS can be “pretty severe, and lifestyle-limiting,” Abramowitz states, citing venous claudication, ulceration and trophic skin changes as notable symptoms.
“While I utilize VenaCore to improve outcomes in acutely presenting patients, the other patients who benefit from VenaCore-assisted thrombectomy are symp-
Such a lack of interventional options and physicians’ subsequent inclination towards more conservative management has created a huge array of patients who, historically, have disengaged from their vascular specialists and had minimal contact with healthcare beyond that initial recommendation. In Abramowitz’s view, the situation has created a “really unique physician-patient interaction”—both in terms of treatment opportunities and re-education. The VenaCore device represents a leading solution that may ameliorate things for interventionists treating patients with a history of venous disease. He highlights three distinct patient groups who can now be addressed and for whom the device may open doors: those with prior iliofemoral or femoropopliteal DVT treated
“VenaCore on its own, and in conjunction with RevCore™ [Inari], truly disrupts all of our current care algorithms when it comes to venous occlusions that are difficult to treat,” Abramowitz says, alluding to the disconcerting fact that many providers have historically been reticent to offer intervention, or even follow-up management in the outpatient setting. “It was essentially seeing somebody every three to six months when you had nothing to offer them. VenaCore not only disrupts the interventional algorithm, but also the care algorithm for these patients, revitalizing and reengaging those patients who’ve been told there are no options.”
VenaCore case report 1
A man in his late 40s was diagnosed with an extensive iliofemoral DVT while traveling five months prior to outpatient consultation with severe symptoms, despite anticoagulation therapy. Mechanical thrombectomy with ClotTriever, despite adjuvant manoeuvres, was only partially successful at removing highly-wall adherent thrombus. VenaCore was used to mobilize additional material within the vein for a technically optimal result.
VenaCore case report 2
A woman in her early 60s who has had
Disclosure: Steven D. Abramowitz is a paid consultant of Inari Medical. All views and opinions expressed here by Abramowitz are his own and do not represent those of Inari Medical.
Indications For Use:
The ClotTriever Thrombectomy System in indicated for the (1) non-surgical removal of thrombi and emboli from blood vessels (2) injection, infusion and/or aspiration of contrast media and other fluids into or from a blood vessel. The ClotTriever Thrombectomy System is intended for use in the peripheral vasculature, including deep vein thrombosis (DVT). The VenaCore Thrombectomy Catheter is indicated for (1) The non-surgical removal of thrombi and emboli from blood vessels. (2) Injection, infusion, and/or aspiration of contrast media and other fluids into or from a blood vessel. The VenaCore Thrombectomy Catheter is intended for use in the peripheral vasculature. The RevCore Thrombectomy Catheter is indicated for (1) The non-surgical removal of thrombi and emboli from blood vessels. (2) Injection, infusion, and/or aspiration of contrast media and other fluids into or from a blood vessel. The RevCore Thrombectomy Catheter is intended for use in the peripheral vasculature.
Caution: Federal (USA) law restricts this device to sale by or on the order of a physician.
Refer to Indications for Use for complete Indications for Use, contraindications, warnings and precautions. For Indications for Use of non-Inari products, please refer to the manufacturer. All copyrights and trademarks are property of their respective owners.
Steven D. Abramowitz
REGIONAL ROUND-UP
Compiled by Bryan Kay
CONTINUED FROM PAGE 13
VQI
CAROTID ENDARTERECTOMY: THE IMPORTANCE OF DOCTOR-PATIENT CONVERSATIONS ABOUT QUITTING SMOKING FOR BETTER STROKE OUTCOMES IN SETTING OF ASYMPTOMATIC STENOSIS
A NEW ANALYSIS THAT SHOWS current smokers who undergo carotid endarterectomy (CEA) for asymptomatic carotid stenosis are at increased risk of long-term stroke and death compared to former or never smokers helps reinforce the importance of physicians talking to patients about quitting their smoking habit.
That was one of the key messages from the authors behind study findings showing a stroke rate among current smokers that was nearly twice as great as their former-smoker—defined as those who quit at least 30 days prior to surgery—and never-smoker counterparts. The data were reported at the 2024 Midwestern Vascular Surgical Society (MVSS) annual meeting in Chicago (Sept. 12–14). In an interview with Vascular Specialist, presenting author Hassan Cham-
seddine, MD, a research fellow at Henry Ford Health in Detroit, Michigan, describes the rationale behind digging into the Vascular Quality Initiative (VQI) in order to try to uncover evidence around the benefit from smoking cessation amid questions over CEA use among the patient population at hand.
“Currently, the Society for Vascular Surgery [SVS] recommends an endarterectomy for patients with an asymptomatic carotid stenosis if their stenosis is greater than 70%,” he explains.
“The evidence for the benefit of endarterectomy in this population comes from landmark trials—ACAS and ACST-1—but those trials are very old, and they are currently under increased scrutiny because the medical therapy arm back then does not reflect contemporary medical management. More
recent studies—including the SPACE-2 trial—did not show any difference between CEA and best medical therapy in this population. And, all over the country, there is some doubt over the benefit, or necessity, of endarterectomy in asymptomatic patients.”
The research team—led by senior author Loay Kabbani, MD, vice chair of surgery for research and program director of the vascular surgery fellowship at the same institution—looked at all members of the patient population undergoing CEA from 2013–2023 logged in the VQI. Of the 77,664 included, 24% were current, 51% former and 25% never smokers.
The data showed the three groups had similar rates of perioperative complications, but, at 18-month follow-up, former smokers exhibited strokes comparable to never smokers—and both were “significantly lower” than current smokers (0.8%, 0.9% and 1.5%, respectively), Chamseddine points out.
In terms of major adverse cardiac events (MACE)—a combination of stroke, myocardial infarction and death—quitting smoking at least 30 days prior reduced MACE risk among former smokers when compared to current smokers, “but not by
as much as those who never smoked,” adds Chamseddine.
Kabbani says the results help highlight a dual purpose. “Number one, this shows the benefit of smoking cessation for the patient, but [number two] also for the physician: If I’m a physician and I’m seeing a patient with asymptomatic disease that has significant stenosis, and there is a question mark about the benefit of the operation, if we want the patient to have the best long-term outcome, we really need to convince them to stop smoking before the operation. They do better in the long run in multiple settings, including decreased myocardial infarction and death.”
Kabbani underscores the importance of physician efforts around the subject of cessation: “Time and time again, we see that if a physician talks to a patient about quitting smoking, they have twice as much chance of stopping.”
“Time and time again, we see that if a physician talks to a patient about quitting smoking, they have twice as much chance of stopping”
LOAY KABBANI
Smoking:
AN ANALYSIS OF THE BEST-CLI RANDOMIZED controlled trial found that smokers with chronic limbthreatening ischemia (CLTI) should be preferentially treated with open bypass over endovascular intervention. Researchers from the University of California San Diego (UCSD) looked at BEST-CLI patients stratified into two groups related to smoking status—current smokers and non-smokers (a combination of never smokers and former smokers)—and discovered the paradox of the smokers’ effect: current smokers among those who underwent a bypass and those who received an endovascular procedure had better overall survival than non-smokers. However, the UCSD study revealed that current smokers who got a bypass “had this protective effect against major adverse limb events (MALE) and we didn’t see that in the endovascular group,” presenting author Rohini Patel, MD, a general surgery resident at UCSD, tells Vascular Specialist after delivering results from the analysis at the 2024 Western Vascular Society (WVS) annual meeting in
Colorado Springs, Colorado (Sept. 7–10).
Having previously looked at smoking in peripheral arterial disease (PAD) patients through the lens of the Vascular Quality Initiative (VQI) and finding that former smokers and never smokers had similar outcomes to one another, and that current smokers had worse outcomes than former smokers, the research team increasingly leant on the theory that, if they could get smokers to quit their habit, then they could have similar outcomes to people who never smoked.
physician interaction on the topic, remains important, Patel says, but “the reality is that a lot of these patients are going to continue smoking, so, the thought is, knowing that information, what can we do? Is there something we can do that would maybe be better? That’s where our analysis has led us—to an open bypass as maybe a preferential treatment in these patients, if they are still going to continue smoking.”
Looking ahead, Patel says BEST-CLI is laden with more nuanced smoking data than the VQI, suggesting the trial might help yield further evidence around pack years and the extent of former smokers’ habits. Determining the optimal interval for smoking cessation is another potential area of future study, she adds.
“Our theory was that in patients who could have either an endovascular approach or an open approach—which is not every patient, but in the ones who could—that maybe we should really be doing an open approach in them first, because it tends to protect—at least in BEST-CLI—against major adverse limb events,” Patel explains.
The perennial mission to instigate smoking cessation, either though pharmacotherapy, counselling or regular
Andrew Barleben, MD, an associate professor of vascular and endovascular surgery at UCSD and senior author of the analysis, points to the unique vantage point brought to this patient population by vascular surgery.
“This helps us know, a little bit more, that vascular surgery provides a unique capability to do both open or endovascular surgery on these patients,” he says, “and that it emboldens our practitioners who help with care for these patients on the interventional side. To this end, they can hopefully easily get a venous ultrasound to see if there is an available vein for these patients, who may have difficulty quitting smoking or may intermittently quit smoking, and achieve better outcomes than if they just underwent endovascular intervention.”
Hassan Chamseddine
Rohini Patel
PRODUCT ADVANTAGES
Type I and type III bovine collagen extracellular matrix Hemostatic properties
DIVERSITY EDUCATION AND REPRESENTATION AT CORE OF INCLUSIVITY EFFORTS FOR DEI COMMITTEE
By Marlén Gomez
THE SVS DIVERSITY, EQUITY AND INCLUSION (DEI) Committee continues to make strides in advancing inclusivity within the organization, with several projects underway to address both ongoing challenges and new opportunities.
The DEI Committee has seen considerable progress since its inception, following the transition from a task force to a standing committee, says Chair Rana Afifi, MD, who outlined upcoming initiatives, emphasizing the importance of education and representation in fostering an inclusive environment.
Afifi noted that the committee’s work is now informed by a comprehensive report that evaluates SVS progress in DEI efforts. The report highlights positive strides, but also underscores areas where work remains, she said.
One key area of focus is enhancing inclusivity within the committee itself. Afifi explained that certain demographics remain underrepresented.
One of the committee’s upcoming initiatives is an educational campaign designed to broaden understanding of DEI issues, not only in terms of race and ethnicity, but also factors like neurodiversity, ageism, and other social and structural determinants of health. The campaign will feature 20
microlearning modules, based on storytelling and practical, everyday scenarios.
“Education is key,” Afifi emphasized. “A lot of the sensitivity and resistance around DEI comes from misinformation and a lack of understanding.”
The first of these modules is expected to be piloted within the next two months, with full rollout anticipated within the year. Afifi expressed hope that these educational materials will facilitate more open and constructive conversations around DEI, moving away from the tense or sensitive nature that can often surround such discussions.
“The goal is not just to improve awareness but to make DEI an integral part of daily practice and patient care within the vascular surgery community,” Afifi said.
across various organizational efforts. “We are working in collaboration with other committees to ensure that DEI is not just a checklist but has actual impact and results,” Afifi said.
The committee has been actively involved in supporting SVS members who are working on DEI-related projects, offering guidance and assistance in publishing articles and developing educational resources.
Afifi
In addition to educational outreach, the DEI Committee is preparing for its third annual DEI Summit, scheduled for December. Although not yet open to the public, the summit aims to engage a broad range of vascular societies, both regional and international, in a unified effort to address DEI challenges. Afifi emphasized the importance of collaboration, noting that the committee is working closely with other SVS committees—such as the Vascular Annual Meeting (VAM) Committee—to ensure that DEI principles are integrated
“The goal is not just to improve awareness but to make DEI an integral part of daily practice and patient care within the vascular surgery community”
RANA AFIFI
One of the key challenges identified is improving racial and ethnic diversity within SVS membership. While the organization has seen a slight increase in diversity, Afifi acknowledged that this progress is not enough
“We need to be intentional about increasing diversity within the SVS, especially in leadership roles,” said Afifi. The committee has been working closely with the Appointments and Nominations committees to ensure that diverse candidates are considered for leadership positions, but more needs to be done to encourage members from underrepresented groups to apply.
“We can’t improve representation if we don’t have people applying for these roles,” Afifi pointed out. The committee is actively reaching out to affinity societies and exploring ways to remove barriers that may be preventing members from pursuing leadership opportunities.
As chair, Afifi has set several goals for her term, with education and increased representation at the forefront. She hopes that the new educational campaign will help dispel misconceptions about DEI and make it a more approachable topic within the SVS.
“I’m not naive enough to think we can solve everything, but I do hope we can move the needle and make some real progress,” said Afifi.
The committee is also focused on fostering collaboration between the various SVS sections, seeking ways to ensure that all are included in DEI discussions, possibly by appointing permanent liaisons from underrepresented groups.
Rana
VASCULAR SCIENCE
SVS member picks up prestigious American Heart Association accolade for scientific work
A PROMINENT VASCULAR SURGEON-SCIENTIST
and Society for Vascular Surgery (SVS) member is the 2024 recipient of the American Heart Association (AHA) Joseph A. Vita Award, which recognizes published work that has had a transformative impact on basic, translational or clinical cardiovascular research. Through the Gallagher Lab, Katherine Gallagher, MD, and her team of researchers have become a fixture in the translational vascular science space, producing a prodigious output of research and publications.
Her lab, based at the University of Michigan in Ann Arbor, has also produced several SVS Foundation James S.T. Yao Resident Research Award recipients in recent years, including the most recent: University of Michigan integrated vascular surgery resident, Kevin D. Mangum, MD.
Gallagher spoke of her honor at receiving the landmark award, telling Vascular Specialist her interest in translational research was embedded early on.
“I’ve always had an interest in immunology and how immune cells influence the vascular system—both a healthy system and one with disease—and have always been interested in looking at it from a more a translational research standpoint,” says the University of Michigan professor of surgery, microbiology and immunology. In the last 10–12 years, there has been a lot more interest in the immune system and the role that it plays in vascular diseases, as well as the development of various immune therapies. I’ve had an interest in how we can try to manipulate these immune cells, which are very inflammatory in vascular disease, and then try to reverse this inflammation.”
Gallagher arrived at Michigan as a junior scientist 15 years ago, starting her lab with just one other team member. It has since grown to include between 15–20 colleagues, with its research interest morphing from tissue regeneration and metabolic disease to, now, a full spectrum of cardiovascular diseases, including aneurysmal, atherosclerotic and COVID19-related impacts on vascular disease.
She is particularly proud of her lab’s success in shepherding the next generation of vascular surgeonscientists. “We have had lot of success with mentees, getting NIH [National Institutes of Health] grants, SVS Foundation funding, AHA awards, and so on,” Gallagher says. “That’s the part I find most exciting: the next generation and trying to get them thinking about science and translational therapies.”
She highlighted the importance of translational vascular science to the future of vascular surgery. “A lot of the therapies we are going to see coming down the pipeline in the next 20 years are going to be immune and cell-based therapies. Unless vascular surgeons are involved at the forefront of research, then there is less bench-bedside translation, which hurts vascular patients. So, it is really important for vascular surgeons to be involved in translational research in order to allow our patients to benefit from the latest, greatest, innovative treatments.”
To that end, her lab’s focus has now turned toward how immune cells interact with other structural cells in blood vessels and pathological processes, with the aim of developing nanomedicine therapies to target those interactions, she added.—Bryan Kay
VRIC 2025 VASCULAR RESEARCH INITIATIVES CONFERENCE ABSTRACTS DUE
ABSTRACTS FOR THE 2025 VASCULAR Research Initiatives Conference (VRIC) are being accepted through Nov. 20.
VRIC, which is held in Baltimore, Maryland, this year, emphasizes the exchange of basic and translational vascular science that stimulates thoughtful discussion and motivates participants to discover solutions to important problems affecting vascular patients. It brings together vascular surgeons, vascular biologists and physicians with an interest in vascular problems, vascular surgery and research trainees.
The conference will be held on Tuesday, April 22, in conjunction with the American Heart Association’s Vascular Discovery 2025 Scientific Sessions: From Genes to Medicine.
Abstract submissions will be accepted through the Vascular Discovery abstract portal. To submit an abstract to VRIC, individuals will need to create a free account with the American Heart Association, or sign into their previously existing account. There is a non-refundable fee to submit an abstract to VRIC and/or Vascular Discovery. The fee allows researchers to submit one abstract to one or both meetings.
Any trainees who submit an abstract for VRIC will be automatically considered for the 2025 VRIC Trainee Award. Visit vascular.org/VRIC25 to learn more.—Kristin Spencer
Katherine Gallagher
CLASS OF 2024–25: VQI ANNOUNCES THIRD ANNUAL SET OF FELLOWSHIP IN TRAINING PROGRAM AWARDEES
By Beth Bales
The Vascular Quality Initiative (VQI) Patient Safety Organization’s Fellowship in Training (FIT) Program has announced its third class of FIT participants for 2024–25 alongside the new FIT scholars.
VQI FIT began in January 2022 and is designed to introduce residents and fellows in vascular surgery and other cardiovascular-related training programs to the SVS’ Vascular Quality Initiative (VQI). It aims to foster an understanding of quality processes and metrics through mentorship in the VQI, in collaboration with the Association of Program Directors in Vascular Surgery (APDVS), American College of Cardiology (ACC) and Society for Vascular Medicine.
Participants and mentors use clinical performance data from the VQI registries to enable trainees to learn about quality improvement in healthcare. Each trainee works on projects involving either health services and outcomes research or quality improvement, all designed to improve patient health outcomes.
Adam Johnson, MD, chair of the VQI FIT Committee, looks beyond these current projects and into the future. “What really excites me are the people in the program that we’re investing in, giving them skills they need to have a successful next project,” he said. These skills will help “build who they are as innovators and changemakers and help them become the next generation of leaders in vascular surgery.”
The 2024–25 FIT participants, (mentors), centers, and projects are:
Quality Projects
● Lisa Vi (mentor Miranda Witheford), University Health Network, Toronto, Canada; studying the impact of homelessness on vascular surgery
● Chinmayee Pottie, (Matthew Corrierre), The Ohio State University, Columbus; how distance to a high-volume center, insurance and primary care provider affect patients with severe late-stage aortic and peripheral arterial disease
● Lindsey A. Olivere, (Michael Madigan), University of Pittsburgh Medical Center (UPMC); working on an institutional quality improvement project to establish a post-amputation care pathway in order to centralize and improve care delivery to amputees
● Gabrielle Rieth (Matthew Corriere), The Ohio State University; utilizing thromboelastography (TEG) to correct coagu-
lopathy and improve patient outcomes in vascular surgery
● Vinay Bhushan Lakki, (Abhishek Singh), Creighton University Medical Center, Omaha, Nebraska; implementing standardized patient selection criteria for carotid artery stenting
● Ioannis Tsouknidas, (Robert Meisner), Lankenau Medical Center, Wynnewood, Pennsylvania; studying limb preservation, including indications, techniques and results
● Falen Demsas, (Nikolaos Zacharias), Massachusetts General Hospital, Boston; examining how to implement culturally competent surgical care practices to reduce disparities in surgical outcomes among underserved populations
● Brandon Gaston , (Nikolaos Zacharias), Massachusetts General Hospital; performing a retrospective head-to-head comparison of frailty calculators for predicting outcomes, length of stay and post-surgery readmission
Research Projects
ing the correlation between residence in limited food-access or low-income areas and outcomes following revascularization for PAD
● Karan Chawla, (Matthew Blecha), Loyola Medical Center, Maywood, Illinois; examining variation in thoracoabdominal aortic aneurysm repair (TAAA) and carotid interventions across institutions
● Lorela Weise, (Matthew Blecha), Loyola University; examining the thoracic endovascular aortic repair (TEVAR)-complex aortic dataset to determine the efficacy of petticoat placement and its association with 30-day mortality
Angela Danielle Sickels , (Adam Beck), University of Alabama Medical Center, Birmingham; evaluating the optimal threshold diameter in women’s elective AAAs
● Menna Hegazi (Nii-Kabu Kabutey), University of California, Irvine; evaluating the presence and clinical significance of various disparities in dialysis access
● Isaac Naazie (Linda Harris), Buffalo General Medical Center, New York; investigating the comparative effectiveness of treatment modalities, identifying predictors of adverse outcomes in vascular surgery
ment Scholarship Awards to continue research and/or work more closely with VQI/ PSO staff and committees. The scholarship is named for Dr. Jack L. Cronenwett, the VQI registry’s co-founder, vascular surgeon and educator. He is professor of surgery emeritus at Dartmouth-Hitchcock Medical Center, was professor of the Dartmouth Center for Health Care Policy and Clinical Practice for nearly 34 years and is chief medical officer for Fivos, VQI’s data management partner.
Scholars named
Five vascular trainees have been selected as FIT Scholars for 2024–25. The safety program is part of the VQI. They are:
● Christine Kariya (Danny Bertges), University of Connecticut, Farmington; implementing patient-reported outcomes (PRO) for better understanding of outcomes in endovascular treatment of PAD and venous care in women with varicose veins, particularly in underserved populations
● Mitri Khoury (Nikolaos Zacharias), University of Arizona, Tuscon; refining the PSO definition of “medically unfit” using registry information and major adverse outcomes to help determine treatment plans
● Guillermo Polanco Serra, (Pouya Entezami), Henry Ford Health, Detroit; evaluating the effectiveness of novel endovascular treatments to hemodialysis salvage
● Michael Chaney, (Jason Ryan), Western
“[These skills will help] build who they are as innovators and changemakers and help them become the next generation of leaders in vascular surgery”
ADAM JOHNSON
Michigan University, Kalamazoo; evaluating the association between Global Limb Anatomic Staging System (GLASS) scoring, and amputation-free survival and wound healing after isolated proximal endovascular intervention
● Lara Lopes, (Ashley Vavra), Northwestern Memorial Hospital, Chicago; examin-
● Irina Kanzafarova, (Michael Stoner) University of Rochester, New York; studying outcomes of infrainguinal bypass surgery with simultaneous distal outflow endovascular intervention versus standard infrainguinal bypass surgery
● Justin Jay Bader , (Cassius Iyad Ochoa Chaar), Yale New Haven Hospital, Connecticut; using patient databases and known predictive risk factors to design and build a model to predict the risk of post-contrast acute kidney injury depending on volume of contrast given
● Camila Guetter, (Marc Schermerhorn), Beth Israel Deaconess Medical Center, Boston; investigating the relationship between diabetes mellitus and antidiabetic medications with changes in aneurysmal sac size post-endovascular aneurysm repair (EVAR) for AAA
● Guarang Joshi, (Marc Schermerhorn), Thomas Jefferson University, Philadelphia; identifying the ideal off-the-shelf graft for promoting the best outcomes in endovascular repair for ruptured AAA
In addition, past participants also received the Jack. L. Cronenwett Quality Improve-
● Christopher Chow (Arash Bornack), University of Miami, Florida; evaluating outcomes of carotid artery stenting in patients with uncommon conditions such as variant aortic arch anatomy or patients with primary carotid artery dissection
● Mikayla Lowenkamp (Michael Madigan), UPMC; smoking cessation and medical management in vascular diseases, including developing educational materials and integrating tobacco specialists into outpatient clinics
● Saranya Sundaram (Thomas Brothers), Medical University of South Carolina; tracking carotid endarterectomies and outcomes after new quality improvement measures were implemented, including data on the ease of use of the measure at the six- and 12-month marks
● Amanda Filiberto (Adam Beck), University of Alabama at Birmingham; studying data and outcomes to ascertain if the VQI’s definition of acute kidney injury after surgery should be changed to align with the updated national definition
Learn more about the FIT Program and its participants at vqi.org.
Adam Johnson
Brandon Gaston, FIT fellow, Mitri Khoury, FIT scholar, and Nikolaos Zacharias, FIT mentor
SOCIETY BRIEFS
Compiled by Marlén Gomez and Kristin Spencer
SVS launches VascuLEARN
THE SVS HAS DEBUTED ITS RENAMED online learning management system (LMS), now known as SVS VascuLEARN. The platform was formerly called SVS OnDemand. VascuLEARN hosts hours of educational content for vascular surgeons, trainees and allied health professionals. After logging in with SVS credentials, users will see a slew of content that is available to them, including a list of microlearning videos that range in topic, as well as coding and reimbursement resources and past webinars from the SVS.
Additionally, those who attended the Vascular Annual Meeting (VAM), Vascular Quality Initiative (VQI) annual meeting and/ or the Society for Vascular Nursing (SVN) Annual Conference in the years 2022, 2023 and/or 2024 can view session recordings through the LMS.
To access VascuLEARN, visit vascular.org and login using SVS credentials. VascuLEARN is available to all SVS members, with limited content being available to nonmembers as well.
SVN hosts virtual roundtable on PAD awareness
ON TUESDAY, SEPT. 24, THE SOCIETY for Vascular Nursing (SVN), in collaboration with the PAD Collaborative and the American Association of Wound Care (AAWC), presented a virtual roundtable titled “PAD: What is it? Leg Circulation Disease is More Common Than You Know—Are You at Risk?”
The event was moderated by Natalie S. Evans, MD, a vascular medicine specialist at the University Hospitals Harrington Heart and Vascular Institute in Cleveland.
The event for SVN members explored the risks of peripheral arterial disease (PAD), with discussion emphasizing how location impacts risk factors.
SVN virtual roundtables are designed to foster informal, collaborative discussions on important issues within vascular nursing. A recording of the event will be available to SVN members on the society website.
Members can submit future topic requests by emailing svs@svnnet.org
ABS seeks vascular surgeon nominations for council position
The American Board of Surgery (ABS) seeks nominations for vascular surgeons to serve on its council for a six-year term, starting July 1, 2025. The deadline for submissions is Tuesday, Nov. 12, at 4:30 p.m., Eastern Time. To apply, visit vascular.org/ABSnominations
SVS LAUNCHES LEADERSHIP PODCAST SERIES
IN COLLABORATION WITH THE Physician Assistant Section, the SVS Leadership Development Committee, is set to launch a leadership development podcast in partnerhsip with Audible Bleeding
The first episode, scheduled to be recorded this fall, will spotlight the SVS Leadership Development Program (LDP) and feature insights from committee Chair Manuel GarciaToca, MD, and SVS Executive Director Kenneth M. Slaw, PhD.
The podcast series will initially consist
of three episodes per year.
“Leadership in vascular surgery is not just about managing a team; it’s about developing the skills to inspire and elevate everyone involved in patient care. The LDP is designed to provide those essential skills,” said Garcia-Toca.
To learn more, visit vascular.org/LDP.
SVS and APSA convene for quarterly meeting
THE SVS AND THE AMERICAN PEDIATRIC SURGICAL ASSOCIATION (APSA) Pediatric Vascular Surgery Interest Group convened for its quarterly meeting on Tuesday, Oct. 1. The focus of this quarter’s meeting was arterial thrombosis in children.
The panel for the meeting was made up of experts in pediatric surgery, pediatric hematology and vascular surgery: Erica L. Mitchell, MD, Med; Gavin Roach, MD, MS; David H. Rothstein, MD, MS; and Reagan Williams, MD. The speakers covered a brief overview of pathophysiology and delivered case-based presentations covering trauma, catheter-induced arterial injury and compressive syndromes.
Meeting attendees had an opportunity to gain an improved understanding of etiologies of provoked and spontaneous arterial thrombosis in pediatric vascular patients; the treatment strategies for thrombosis, including anticoagulation/lytic therapies, and endovascular approaches and open approaches; and post-treatment management, including anticoagulation, imaging and long-term follow-up.
In 2021, the SVS and APSA joined together to create a collaborative, interdisciplinary task force to address gaps in pediatric vascular care.
Jimenez joins JVS-CIT as DEI editor
THE JOURNAL OF VASCULAR SURGERY-CASES, INNOVATIONS AND Techniques (JVS-CIT) has appointed Juan Carlos Jimenez, MD, as its new associate editor and diversity, equity and inclusion (DEI) officer. Jimenez, who serves as clinical professor of surgery and director of the Gonda Venous Center at the University of California, Los Angeles (UCLA), will oversee about 200 submissions annually in his role as editor, contributing his expertise in vascular surgery and academic publishing. Jimenez is also the vice chair for justice, equity, diversity, and inclusion at UCLA, a role that will inform his work on the JVS-CIT editorial board.
To learn more about the journal, visit jvscit.org.
‘Voices of Vascular’ series celebrates Ochoa for Hispanic History Month
THE SVS FOUNDATION “VOICES of Vascular” series is celebrating Lyssa Ochoa, MD, for this year’s Hispanic History Month.
A Mexican American vascular surgeon, Ochoa is dedicated to serving underserved communities. Raised in Mission, Texas, she founded the San Antonio Vascular and Endovascular (SAVE) Clinic to help address healthcare disparities, particularly in areas with high rates of diabetes-related amputations.
Perioperative care in open aortic vascular surgery: join upcoming webinar
A WEBINAR ON “PERIOPERATIVE Care in Open Aortic Vascular Surgery: Recommendations from ERAS and SVS” was held by the SVS Leadership Development Committee on Oct. 15. Enhanced Recovery After Surgery (ERAS) is a comprehensive perioperative care pathway that utilizes evidence‐based best practices across specialties to promote early recovery for patients undergoing major surgery. Implementing ERAS protocols has been shown to reduce recovery time, complications and readmissions while improving patient and staff satisfaction.
This webinar reviewed the recommendations for perioperative care in open aortic vascular surgery based on the consensus statement developed by the ERAS Society and the SVS in 2022.
Topics covered during the webinar included why ERAS is needed in vascular surgery; the necessary collaboration of surgery and anesthesia in implementation of successful ERAS pathways; current guidelines; as well as a literature review of ERAS open aortic surgery and guidelines in practice.
Visit vascular.org/ERAS for more details on this webinar.
Review with VESAP6
The sixth edition of the Vascular Education and Self-Assessment Program (VESAP6) is available for both members and nonmembers of the SVS to purchase. The electronic review program offers over 600 review questions and includes detailed discussions and references throughout.
To learn more about VESAP6 and to purchase the resource, visit vascular.org/VESAP
Manuel Garcia-Toca
CLINICAL&DEVICENEWS
Compiled by Bryan Kay, Jamie Bell and Éva Malpass
Bioprosthetic venous valve imparts sustained clinical improvement at one year regardless of CEAP category
A NEW PAPER THAT DRILLS INTO THE IMPACT OF a novel bioprosthetic venous valve replacement by CEAP (Clinical, Etiological, Anatomical and Pathophysiological) classification shows sustained clinical improvement regardless of grading, with patients classed as C4b exhibiting greater resolution of symptoms and quicker ulcer healing within the first three months after implantation than those with more advanced disease.
The findings emerged during the 2024 Midwestern Vascular Surgical Society (MVSS) annual meeting in Chicago (Sept. 12–14) in the latest analysis of the SAVVE (Surgical Antireflux Venous Valve Endoprosthesis) multicenter pivotal trial, which assesses the safety and efficacy of the VenoValve (enVVeno Medical) in patients with chronic venous insufficiency.
The fully enrolled trial—made up of 75 patients from 21 sites in the U.S.—measures outcomes from device implant in diseased patients in CEAP categories C4b, C4c, C5 and C6.
The paper presented at MVSS 2024 sought to elucidate how the valve affects disease severity, pain levels, quality
Carotid intervention linked to improved survival versus medical management in symptomatic patients
NEW STUDY DATA SUGGEST THAT THE interventional treatment of symptomatic carotid artery disease may result in an improved rate of age-adjusted overall survival compared to medical management. However, the same study—presented at this year’s European Society for Vascular Surgery (ESVS) annual meeting (Sept. 24–27) in Kraków, Poland—also indicates a relatively low future ipsilateral stroke risk among patients who were not offered carotid intervention, highlighting medical management’s importance as a standalone strategy in patients deemed to be “high risk.”
Findings from the study in question were delivered by Eric T.A. Lim, MBChB, from the Department of Vascular & Endovascular Surgery at Waikato Hospital, Hamilton, New Zealand, on behalf of Manar Khashram, MBChB, from the same institution, and other investigators, in an abstract presentation at ESVS 2024. The prospective, observational study—undertaken in a single center in New Zealand—aimed to assess the outcomes of symptomatic stenosis cases managed non-operatively.
Patients who underwent carotid intervention had a 0.25 (0.17–0.5) hazard ratio of survival compared to patients managed conservatively when adjusted for age. The overall survival rates at one and four years were 88% and 57%, respectively, and corresponding ipsilateral stroke-free survival rates at both one and four years were 97% in the medically managed patient group.
of life and ulcer healing at the point of enrollment out to 12-month follow-up.
C6 patients comprised 50% of the study population. “What was interesting to see here was that 70% of the patients who were enrolled in the study had a nonhealing ulcer for more than a year or so,” Raghu Motaganahalli, MD, a SAVVE trial principal investigator who is chief of vascular surgery and program director at Indiana University in Indianapolis, told MVSS 2024. He reported primary and secondary patency rates for the valve of 87% and 96%, respectively, adding that there were four reinterventions and no procedural-related deaths or devicerelated infections. Benefits from device implantation in terms of venous reflux time were seen after three months, significantly decreasing, he added.
“The C4b category patients had more resolution of their symptoms”
RAGHU MOTAGANAHALLI
In terms of clinical improvement by CEAP classification, Motaganahalli reported gains in revised Venous Clinical Severity Score (rVCSS) across CEAP categories at three- and six-month follow-up. Compared to the baseline, he said there was an overall 9-point gain in rVCSS at 12-month follow-up after valve implantation. Visual Analog Score (VAS) for pain assessment improved by almost 50% at one year, Motaganahalli, continued, and quality of life, as measured by the VEINES-QOL/ Sym instrument, also “significantly improved” across the CEAP spectrum.
Medinol announces first-inhuman implantation of drug-eluting peripheral stent in Australia
MEDINOL HAS ANNOUNCED THE successful first-in-human implantation of the ChampioNIR drug-eluting peripheral stent by Gerard S. Goh, MD, head of interventional radiology, and Thodur Vasudevan, MBBS, a vascular surgeon, both from the Alfred Hospital in Melbourne, Australia.
With a hybrid mechanical design, radial support is provided by the metallic component of the stent, whereas the longitudinal structure is provided by a bioresorbable polymeric mesh providing unsurpassed flexibility and long-term durability in even the most challenging anatomies. Its drug-elution paradigm releases drug from the entire cylindrical area of the stent. “We were impressed with ChampioNIR’s deliverability and its straightforward deployment,” said Goh. “The frictionless deployment mechanism made the precise positioning of the stent very straightforward.”
The CHAMPIONSHIP study of the device will enroll a total of 30 patients across seven sites in Australia and the U.S. Sahil Parikh, MD, an interventional cardiologist at Columbia University Irving Medical Center in New York City and principal investigator, commented: “The ChampioNIR stent represents a breakthrough in treatment for superficial femoral artery [SFA] lesions.”
Motaganahalli also noted a decrease in the use and need for compression stockings in tandem with the increase in patient quality of life.
Meanwhile, ulcer area was reduced from 18.16cm 2 at baseline to 3cm2 “It was also interesting to see that if a patient has an ulcer for less than three months, they have a 100% resolution of the ulceration over time,” Motaganahalli added.
Concluding, he said: “For patients with chronic venous insufficiency, VenoValve was a novel treatment option. It has shown improvement by rVCSS, we have seen a reduction in pain as evidenced by VAS, ulcers heal, limb swelling is improved by the VEINESQOL/Sym score, and all improvements are shown within the first three months of the clinical period.”
During discussion, Motaganahalli highlighted how the paper helps draw attention to the timing of optimal intervention. “By the time you transition from a C4b, or a C4c, to a C6 category, you have a lot of damage in those patients,” he said. “That is exactly the purpose of this paper: to see where to intervene and when to intervene. In fact, the C4b category patients had more resolution of their symptoms. Ulcers heal much more quickly in that group of patients—they were the ones [who tended] to improve within the three-month window—as opposed to much more advanced disease.”
INDICATIONS FOR USE IN THE U.S.: The GORE® VIABAHN® VBX Balloon
Expandable Endoprosthesis is indicated for the treatment of de novo or restenotic lesions found in iliac arteries with reference vessel diameters ranging from 5 mm–13 mm and lesion lengths up to 110 mm, including lesions at the aortic bifurcation. The GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis is also indicated for use with thoracoabdominal and pararenal branched devices indicated with the GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis as a branch component.* CONTRAINDICATIONS: Do not use the GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis in patients with known hypersensitivity to heparin, including those patients who have had a previous incident of Heparin-Induced Thrombocytopenia (HIT) type II. Refer to Instructions for Use at eifu.goremedical.com for a complete description of all applicable indications, warnings, precautions and contraindications for the markets where this product is available.
With a 1 Fr profile reduction on most sizes, the VBX Stent Graft enables you to confidently address complex aortoiliac occlusive disease with greater versatility.
primary patency at 5 years per lesion1
89.5% of patients improved ≥ 1 Rutherford category from baseline at 5 years1 100%
freedom from target lesion revascularization (fTLR) at 5 years per subject1 89.1%
1. Holden A, Takele E, Hill A, et al. Long-term follow-up of subjects with iliac occlusive disease treated with the Viabahn VBX Balloon-Expandable Endoprosthesis. Journal of Endovascular Therapy. In press.
W. L. Gore & Associates, Inc. Flagstaff, Arizona 86004 goremedical.com
Please see accompanying prescribing information in this journal.
Products listed may not be available in all markets.
GORE, Together, improving life, VBX, VIABAHN and designs are trademarks of W. L. Gore & Associates.