3 minute read
Oral Hygiene Abstracts 2023


By Emer. Prof. Laurence Walsh AO
Filtration on wheels: When natural ventilation is inadequate
As the COVIID-19 pandemic has proceeded, ventilation has been recognised increasingly as an important tool in infection control in health workplaces with poor air management. Many hospitals in Ireland and the UK do not have mechanical ventilation systems such as airconditioning and instead depend on natural ventilation. Poorly ventilated spaces harbouring infectious persons, such as hospital wards, can pose a considerable threat to both patients and healthcare workers, with nosocomial COVID-19 outbreaks reported in the literature. The effectiveness of natural ventilation varies with atmospheric conditions and building design. In a challenge test of a legacy design ward, portable high-efficiency particulate air (HEPA) filtration units were used. Such units have previously been shown to remove SARS-CoV-2 RNA from air samples taken in COVID-19-surge hospital units. This study reports the effects of a portable air filtration unit (AFU) in clearing a common hospital air pollutant (nebulized Ventolin (salbutamol)) from a ward bay under renovation. Such fugitive drug aerosols of respirable size are common in hospitals and are useful proxies for persistence and circulation of infectious particles of respiratory origin. There was no heating, ventilation or air conditioning system for air handling in the ward. Laser light scattering was used to measure the concentration (μg/m3) of nebulised airborne particles in the size range of 0.3–2.5 μm. Mean peak particle count over background was lowest in the “windows open, AFU on” condition and particle clearance was fastest. The “windows alone” condition was unable to reduce concentrations back to baseline levels without aid of the AFU. Overall, the portable AFU successfully augmented natural ventilation in airborne particle clearance from a legacy design hospital ward by increasing the clearance rate of particles. The combination of AFU and natural ventilation may be synergistic, possibly because secondary air movement from the AFU increases currents through the windows.
Fennelly M, et al. Portable HEPA filtration successfully augments natural-ventilation-mediated airborne particle clearance in a legacy design hospital ward. J Hosp Infect. 2023;131:54-57
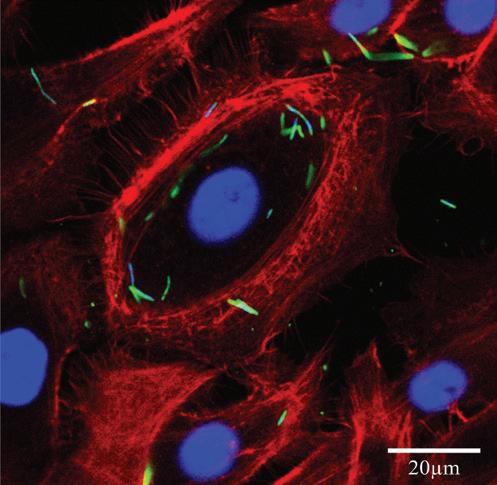
Gingival epithelial cell infection by SARS-CoV-2 is unlikely
SARS-CoV-2, the causative agent of COVID-19, is mainly transmitted by first infecting nasal and lung epithelial cells. Host cell entry by SARS-CoV-2 is mediated by the binding of the spike protein, a transmembrane class I fusion protein that is exposed on the viral surface, with the angiotensin converting enzyme 2 (ACE2) receptor on the host cell. In addition to ACE2, other host cell factors including transmembrane serine protease 2 (TMPRSS2) and Furin are required for viral entry, however alternative receptors including CD147 have been proposed. The mouth is also believed to be a viral portal site since certain types of oral epithelial cells were shown to express the ACE2 receptor. The oral cavity structures, keratinized and non-keratinized mucosa and salivary glands’ epithelia express SARS-CoV-2 entry and transmission factors, especially ACE2 and TMPRSS2. However, it is unclear whether oral epithelial cells are directly infected by SARS-CoV-2. In this study, we examined epithelial cells of oral gingiva. We found that KRT5+ and KRT18+ gingival epithelial cells do not express ACE2, but highly express TMPRSS2 and Furin as well as CD147, which was proposed to be an alternative receptor for SARS-CoV-2. However, using SARS-CoV-2 pseudoviruses containing the spike protein, it was observed that gingival epithelial cells were not susceptible to infection due to their lack of ACE2 expression and the inability of CD147 to mediate viral entry. These results strongly suggest that epithelial cells from the gingiva are not susceptible to SARSCoV-2 and CD147 is not a receptor for the SARS-CoV-2 virus. The susceptibility of oral cells from other oral structures under healthy and pathological conditions still needs to be confirmed to better understand the role of the oral cavity in COVID-19 infection and transmission. In this study, we found that previously detected ACE2 RNA expressed in gingival epithelial cells did not equate to expression of the ACE2 receptor on cell-surface. The use of cell-surface staining and in vitro/in vivo infection models with SARSCoV-2 pseudovirus or live virus is needed to confirm ACE2 expression and infection susceptibility of epithelial and non-epithelial cells in various oral tissues. An important question remains as to the source of virus found in the saliva of people infected with COVID-19 if the virus in saliva did not originate from oral epithelial cells. It can be argued that in such cases the infected lung and nasal epithelial cells are the source of virus in the saliva. More studies are still needed to confirm the susceptibility of different cell types found in various oral tissues and susceptibility to SARS-CoV-2 and the many variants under healthy and pathologic conditions to better understand the role of the oral cavity in COVID-19 infection and transmission. Bontempo A, et al. Assessment of SARS-CoV-2 entry in gingival epithelial cells expressing CD147. Eur J Oral Sci. 2023;131:e12906