11 minute read
Seven ways to achieve brighter teeth


By Emeritus Professor Laurence J. Walsh AO

Improving the appearance of teeth is a common request from patients. Intrinsic tooth colour varies between individuals and changes over the lifespan, with greater saturation in the yellow range in the later years of life.1-3 Yellow teeth are considered less popular because a yellow tooth colour adds to a perception of advanced age and reduced vitality.4
Common contributors to external stains are tannins and polyphenols from beverages (such as tea, coffee and red wine), coloured molecules from beverages (such as cola drinks) and pigments from foods (such as berries and soy sauce). Mouth rinses that contain active ingredients which are positively charged (chlorhexidine and quaternary ammonium compounds) will also bind to the negatively charged enamel surface and pellicle, causing discolouration.5,6
This article describes seven methods which can create variations in tooth colour to reduce the fundamental progression towards yellowing, other than traditional in office or at home bleaching methods, or the use of veneers.
1. Micropolishing toothpastes
The stain removal capabilities of conventional toothpastes depends on their abrasiveness, as measured by their relative dentine abrasivity (RDA) value.7 If one rates various abrasives used in toothpastes according to their abrasivity, sodium bicarbonate and dicalcium phosphate dihydrate (also known as brushite) are considered soft; hydrated silica and calcium pyrophosphate are medium; and alumina and perlite are hard. The most widely used abrasive particle in toothpastes is particulate hydrated silica. Typically, the particles of hydrated silica are roughly polyhedral with sharp edges.8
There are international regulatory restrictions on the maximum abrasion levels permitted in a toothpaste and hence there are limits to how far the idea of using abrasive technologies alone to improve the appearance of teeth can be pushed.9-11
In micropolishing toothpastes, the abrasive particles are reduced in size by processes such as micronising or ball milling. These methods can be used with all common abrasive particles found in toothpastes including silica, calcium car- bonate and naturally occurring minerals. Using smaller particles is more effective for removing extrinsic stains, provided that the bristles of the tooth brush can reach the area to properly apply the micronised particles in a slurry. In practical terms, this means that micropolishing toothpastes are very effective for removing stain on labial surfaces, but not interdentally. For patients who have a regular daily intake of tea and coffee, such toothpastes can be particularly good for reducing the buildup of tannins and polyphenols.12-14
For patients whose lifestyle does not contain foods or drinks that cause extrinsic staining, there is no value in using micropolishing toothpastes on a regular basis. On the other hand, for patients who are regular drinkers of tea or coffee, micronised particles can reduce the inevitable accumulation of external stains on their labial tooth surfaces.
2. Nano hydroxyapatite
One particular agent which is attracting current interest is nano hydroxyapatite. These nanoparticles are considered to have medium abrasivity.15 The enormous surface area of these nanoparticles means that there is sufficient saturation of apatite species into the water phase that they can contribute to remineralisation.16,17 While traditional abrasive particles used in commercial toothpastes are designed to help remove plaque and stains while causing only negligible levels of damage to tooth surfaces or gingival tissues, from a chemical perspective, most abrasive particle types other than nano hydroxyapatite are unable to contribute to remineralisation.18,19
Recent analyses indicate that regular use of oral care products containing nano hydroxyapatite exerts a whitening action on teeth.20 There are multiple reasons for this. Since hydroxyapatite nanoparticles are white and opaque, if they are deposited onto the surface of teeth they can mask the yellow appearance of teeth, as well as acting as an abrasive to remove extrinsic stains.21,22 There is some suggestion that a layer of white particles not only masks the underlying yellow colour of teeth, but may also block reflection of light from the dentine core of the tooth, not allowing this to pass through the tooth and back to any observers.23 Lastly, the nanoparticles may also fill in microcracks and defects in the enamel surface and enhance its reflectivity.24 As could be predicted, there is a dose-response relationship between the concentration of nano hydroxyapatite in toothpastes and its whitening effects on teeth.25,26

3. Decolourising surface stains
In this approach, the extrinsic stains which accumulate remain on the tooth surface, but are chemically altered by oxidation, so that they no longer absorb light and make the tooth surface appear dull. By its very nature, such an approach must be used periodically to “touch up” the appearance of the surface. Several methods that can be used to decolourise surface stains including an oxidising agent (such as hydrogen peroxide) in a regular toothpaste;27 adding an oxidising agent (such as a powder containing PAP+ and nano hydroxyapatite) to an existing toothpaste; using a low concentration (0.5%) hydrogen peroxide mouthwash; applying whitening strips; applying paint-on gels; and using peroxide and non-peroxide whitening strips.
Hydrogen peroxide-containing polyethylene strips have been used for many years, with the concept being that the adhesive provides a sustained exposure of the tooth surface to the hydrogen peroxide bleaching agent.28-30 Bleaching strips are also available that use alternative oxidants such as PAP. This has the advantage of avoiding gingival soft tissue irritation, which will otherwise cause sensitivity (Figure 1).
If a paint-on material is being used, removing saliva from the surfaces of the teeth to be treated will improve the results that are obtained, because saliva contains lactoperoxidase and catalase that will inactivate hydrogen peroxide by converting it into water and oxygen.
4. Repelling surface stains
Sodium hexametaphosphate is an ingredient found in some toothpastes (such as in the Oral-B Pro-Health series). This has the ability to bind strongly to pellicle and enamel because of the strong charge of the polyphosphate component.
As a result, when the polyphosphate has bound to pellicle on a freshly brushed tooth, the coating prevents the accumulation of stains from the diet. A second effect is that the existing stains do not bind as strongly to pellicle as the hexametaphosphate and so they will be dislodged and displaced.31
Numerous randomised controlled trials of stain removal and the rate of deposition of stains by sodium hexametaphosphate have been undertaken, testing the effects on external stains in patients with diverse backgrounds and lifestyles. Reductions in external stain of up to 90% have been seen with regular use of such toothpastes twice-daily over six weeks.32,33
5. Professional prophylaxis
Prophylaxis using a rubber cup or an abrasive particle beam device is a highly efficient way of removing external stains from all aspects of teeth. Methods that rely upon the patient will inevitably fail to reach interdental areas,34 whereas professional prophylaxis deals with all erupted surfaces of teeth. As well as removing extrinsic stains, calculus and dental plaque, depending on the type of abrasive that is used in the prophylaxis paste, a micro polishing effect of the tooth surface can also be achieved. Likewise, graded abrasive disks can rapidly polish a tooth surface (Figure 2). Normal enamel is not microscopically smooth. Small irregularities on the enamel surface at the micron scale readily scatter light, particularly light of the shorter wavelengths in the visible spectrum. When such small irregularities are removed by polishing, more specular mirrorlike reflections occur from labial surfaces, making these appear brighter.
6. Tooth surface lightening
In this approach, a remineralising treatment is undertaken using optimal conditions to ensure that a surface layer of regularly formed perfectly crystalline fluorapatite is formed on the tooth surface.35,36 To achieve this, enamel micro abrasion is performed (using phosphoric acid and pumice) and the patient then uses a topical crème containing CPP-ACP (GC Tooth Mousse™) or CPP-ACP and 900 ppm fluoride (GC Tooth Mousse Plus™) over the following four weeks, each night before retiring (Figure 3).
The timing of night time use is designed to ensure that there is optimal availability of the rate-limiting ingredient of calcium ions during the overnight period when the resting salivary flow and intraoral pH will drop. Such products are able to drive remineralisation reactions under acidic pH conditions (down to pH 4 in the case of Tooth Mousse Plus). This is possible because of the release of stabilised calcium and phosphate and fluoride at the ideal atomic stoichiometric ratios to form fluorapatite. The perfectly formed mineral crystals on the surface are better able to reflect short wavelengths of visible light, particularly those in the blue and violet range, making the tooth appear less yellow. The yellow to blue tooth colour shift that is achieved produces an overall improvement in the perception of tooth shade and the effect is permanent.
7. Shade reversion agents
T his concept relies on the application of a single dye, such as blue covarine, or a mixture of dyes, onto the tooth surface (Figure 4). The dyes can be applied as part of a toothpaste, or applied directly in a mixture that contains a binding agent, so that they are retained on the tooth surface for several hours. These light blue and purple dyes reflect violet and blue light, making the tooth appear less yellow for as long as there is a sufficient amount of retained dye on the surface of the tooth.
Figure 3. Tooth lightening. A: 10% CPP-ACP topical crème with 900 ppm fluoride. B: Baseline appearance. The incisal edges were smoothed with a disk and then enamel microabrasion undertaken. C: Appearance after 4 weeks of daily use of GC Tooth Mousse Plus™. Note the reduction in yellow.
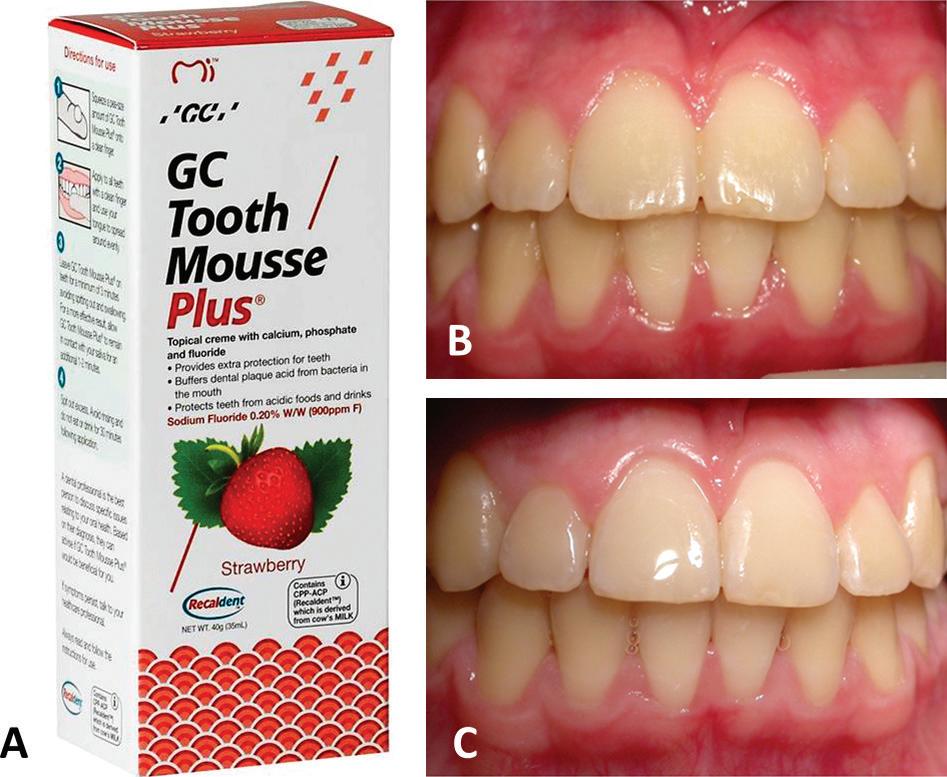
Figure 4. Relevant chemical structures. A: Typical tannins from tea that cause extrinsic staining. B: CI 74160/ copper phthalocyanine/ blue covarine dye used in Oral-B toothpastes. C: CI17200/ D&C Red No. 33 (upper) and CI42090/FD&C Blue No.1 (lower) used in HiSmile V34 colour corrector foam and serum.
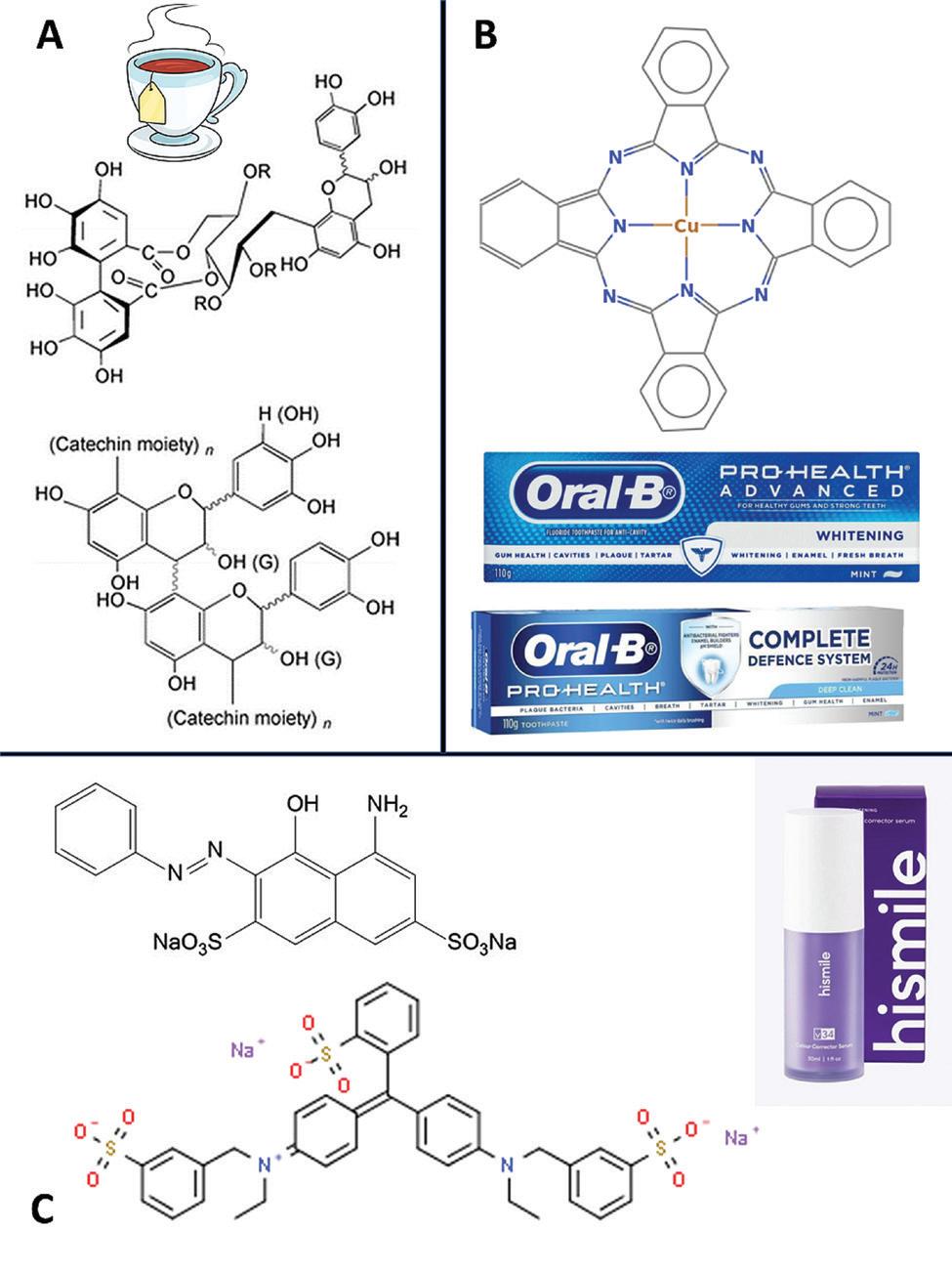
Blue covarine dye (also known as copper phthalocyanine or CI 74160) is used in several Oral-B toothpastes for the specific purpose of changing the optical properties of the teeth to gain a short-term improvement in their appearance.37-40 There are other violet dye mixtures available on the market for gaining an improvement in the shade of the teeth for several hours, e.g. HiSmile™ V34 colour corrector foam or serum, which uses CI 17200/D&C Red No. 33, and CI 42090/ FD&C Blue No.1. These types of products are brushed on to the teeth and left in place.
About the author
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology. Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 390 journal papers, with a citation count of over 18,300 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.
References
1. Joiner A. Tooth colour: a review of the literature. J Dent. 2004;32 (Suppl 1):3-12.
2. Joiner A, et al. A review of tooth color and whiteness. J Dent. 2008;36(Suppl 1):2-7.
3. Gómez Polo C, et al. Correlation of natural tooth colour with aging in the Spanish population. Int Dent J. 2015;65:227-234.
4. Newton JT, et al. The impact of tooth colour on the perceptions of age and social judgements. J Dent. 2021;112:103771.
5. Walsh LJ. Cosmetic dentistry – the discoloured tooth. Brisbane: Knowledge Books and Software, 2002. ISBN: 1875219994.
6. Walsh LJ. Tooth stain removal: a critical appraisal. ADAQ News 2017;637:13-14.
7. González-Cabezas C, et al. Abrasivity testing of dentifrices - Challenges and current state of the art. Monogr Oral Sci. 2013;23:100-107.
8. Joiner A. Whitening toothpastes: A review of the literature. J Dent. 2010;38:e17-e24.
9. International Standards Organisation ISO 11609, Dentistry-Toothpastes. Requirements, Test Methods and Marking, 1995.
10. Goldberg M, et al. Undesirable and adverse effects of tooth-whitening products: A review. Clin Oral Investig. 2010;14:1-10.
11. Wiegand A, Schlueter N. The role of oral hygiene: Does toothbrushing harm? Monogr Oral Sci. 2014;25:215-219.
12. Raoufi S, Birkhed D. Effect of whitening toothpastes on tooth staining using two different colour-measuring devices - a 12-week clinical trial. Int Dent J. 2010; 60:419-423.
13. Schemehorn BR, et al. Abrasion, polishing, and stain removal characteristics of various commercial dentifrices in vitro. J Clin Dent. 2011;22:11-18.
14. Casado BGS, et al. Efficacy of dental bleaching with whitening dentifrices: A systematic review. Int J Dent. 2018;2018:7868531.
15. Epple M, et al. A critical review of modern concepts for teeth whitening. Dent J. 2019;7:79.
16. Chen L, et al. Hydroxyapatite in oral care products - a review. Materials 2021;14:4865.
17. O’Hagan-Wong K, et al. The use of hydroxyapatite toothpaste to prevent dental caries. Odontology 2022;110:223-230.
18. Sarembe S, et al. In vitro whitening effect of a hydroxyapatite-based oral care gel. Eur J Dent. 2020;14:335-341.
19. Limeback H, et al. Biomimetic hydroxyapatite and caries prevention: A systematic review and metaanalysis. Can J Dent Hyg. 2021;55:148-159.
20. Limeback H, et al. Tooth whitening with hydroxyapatite: a systematic review. Dent J. 2023;11:50.
21. Niwa M, et al. Polishing and whitening properties of toothpaste containing hydroxyapatite. J. Mater. Sci. Mater. Med. 2001;12:277-281.
22. Dabanoglu A, et al. Whitening effect and morphological evaluation of hydroxyapatite materials. Am J Dent. 2009;22:23-29.
23. Steinert S, et al. Daily application of a toothpaste with biomimetic hydroxyapatite and its subjective impact on dentin hypersensitivity, tooth smoothness, tooth whitening, gum bleeding, and feeling of freshness. Biomimetics 2020;5:17.
24. Fabritius-Vilpoux K, et al. Quantitative affinity parameters of synthetic hydroxyapatite and enamel surfaces in vitro. Bioinspired Biomim Nanobiomater. 2019;8:141-153.
25. Kim BI, et al. Tooth whitening effect of toothpastes containing nanohydroxyapatite. Key Eng Mater. 2006;309:541-544.
26. Shang R, et al. Tooth whitening with an experimental toothpaste containing hydroxyapatite nanoparticles. BMC Oral Health 2022;22:331.
27. Kleber CJ, et al. In vitro tooth whitening by a sodium bicarbonate/peroxide dentifrice. J Clin Dent. 1998;9:16-21.
28. Gerlach RW, et al. A randomized clinical trial comparing a novel 5.3% hydrogen peroxide bleaching strip to 10%, 15% and 20% carbamide peroxide tray-
An important point is that shade reversion agents do not remove extrinsic stains, but provide a temporary brightening effect that reduces the yellow appearance of the teeth. It is good practice to always combine shade reversion agents with a method that removes extrinsic stains.
Conclusions
Each of the seven strategies discussed above can be used in various combinations to achieve worthwhile outcomes. Key considerations are the extent of effort that the patient is prepared to make in using products as part of their self-performed oral care, versus relying on professional interventions undertaken in the dental clinic. It is important to understand the patients’ demands and to have a realistic approach to meeting these, that takes into account practicability as well as cost.
based bleaching systems. Compend Contin Educ Dent. 2000;21:S22-S28.
29. Gerlach RW, et al. Objective and subjective whitening response of two self-directed bleaching systems. Am J Dent. 2002;15:7A-12A.
30. Walsh LJ. New Oral-B 3D White Whitestrips provide a useful adjunct to in-office or at home bleaching treatments. Australas Dent Pract. 2014; 25(1):12-14.
31. Park YD, et al. Research about changes of abrasiveness and whiteness of each dentifrice including nano-hydroxyapatite, sodium metaphosphate. Key Eng Mater. 2006;309:545-548.
32. Gerlach RW, et al. Removal of extrinsic stain using a 7.0% sodium hexametaphosphate dentifrice: a randomized clinical trial. J Clin Dent. 2002;13(1):6-9. 33. Gerlach RW, et al. Extrinsic stain removal with a sodium hexametaphosphate-containing dentifrice: comparisons to marketed controls. J Clin Dent. 2002;13(1):10-14.
34. Walsh LJ. Interdental cleaning – the final frontier for mechanical plaque control. Auxiliary 2016;26(3):18-19.
35. Walsh LJ Tooth lightening: a new concept of maximizing surface aesthetics. Australas Dent Pract. 2008;19(2):48-50.
36. Walsh LJ. Molecular and pharmaceutical aspects of novel methods and materials for the prevention of tooth structure loss. Curr Pharm Biotechnol. 2017;18(1):45-51.
37. Joiner A et al. A novel optical approach to achieving tooth whitening, J Dent. 2008;36:s8-s14.
38. Collins LZ, et al. Instant tooth whitening from a silica toothpaste containing blue covarine. J Dent. 2008;36:s21-s25.
39. Joiner A. A silica toothpaste containing blue covarine: a new technological breakthrough in whitening. Int Dent J. 2009;59(5): 284-288.
40. Tao D, et al. Tooth whitening evaluation of blue covarine containing toothpastes. J Dent. 2017;67: S20-S24.








