12358 Negative biopsy histolog y in men with PI-RADS score 5: Is it useful PSMA PET/CT evaluation?
Pietro Pepe, Ludovica Pepe, Michele Pennisi
12449 Does intravesical Bacillus Calmette-Guérin for bladder cancer protect from COVID-19?
Anastasia MacDonald, Lexia Bao, Vahid Mehrnoush, Asmaa Ismail, Livio Di Matteo, Ahmed Zakaria, Hazem Elmansy, Peter Black, Ahmed Kotb
12703 Management of urinar y stones: State of the art and future perspectives by Experts in Stone Disease
Athanasios Papatsoris, Alberto Budia Alba, Juan Antonio Galán Llopis, Murtadha Al Musafer, Mohammed Alameedee, Hammad Ather, Juan Pablo Caballero-Romeu, Antònia Costa-Bauzá, Athanasios Dellis, Mohamed El Howairis, Giovanni Gambaro, Bogdan Geavlete, Adam Halinski, Bernhard Hess, Syed Jaffry, Dirk Kok, Hichem Kouicem, Luis Llanes, Juan M Lopez Martinez, Elenko Popov, Allen Rodgers, Federico Soria, Kyriaki Stamatelou, Alberto Trinchieri, Christian Tuerk
12382 Factors associated to hemoglobin decrease after percutaneous nephrolithotomy: A retrospective study
Syarif, Abdul Azis, Saidah Rahmat A , Ahmad Taufik Fadillah Zainal, Ade Nusraya
12369 Comparison of two percutaneous nephrolithotomy methods for the treatment of pediatric kidney stones: Mini-percutaneous nephrolithotomy and standard percutaneous nephrolithotomy
Kadir Karkin, Mubariz Aydamirov, Bug ra Aksay, Eyu ˝ p Kaplan, Gu˝c lu˝Gu ˝ rlen, Adem Altunkol, Ferhat Ortaog lu, O ̈ mer Faruk Akgu
n, Ediz Vurus kan, Zafer Go
khan Gu
12393 Dynamic renal scans as a modality for follow-up of flexible ureteroscopy
Murad Asali, Osman Hallak
12523 Exploring the potential of combined B-mode features and color Doppler ultrasound in the diagnosis of ureteric stone as an alter native to ionizing radiation exposure by computed tomography
Ahmed M Abdel Gawad, Bahaa-Eldin A Moustafa, Tamer A Abouelgreed, Esam A Elnady, Saed Khater, Mohamed Rehan, Mohamed F Elebiary, Basem A Fathy, Ahmed Shaalan, Nasser Ramadan, Mohamed Hindawy, Salma F Abdelkader
12367 Role of urine glycosaminoglycan levels in the diagnosis and follow-up in men with lower urinar y tract symptoms
Hasan Riza Aydin, Cagri Akin Sekerci, Huseyin Kocakgol, Banu Isbilen Basok, Fevzi Bedir, Ahmet Ozgur Guctas, Firat Akdeniz, Hamit Zafer Aksoy, Mehmet Akif Ramazanoglu, Yiloren Tanidir
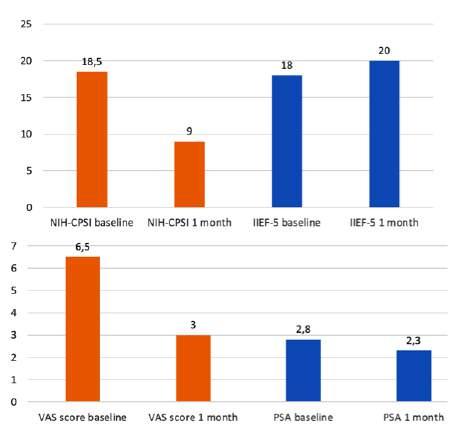
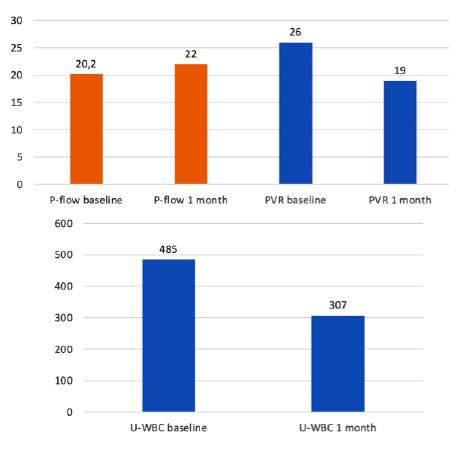
12582 Efficacy of Palmitoylethanolamide, Epilobium and Calendula suppositories for the treatment of patients with chronic prostatitis/chronic pelvic pain syndrome type III
Giuseppe Morgia, Arturo Lo Giudice, Maurizio Carrino, Salvatore Voce, Andrea Cocci, Giulio Reale, Andrea Minervini, Sebastiano Cimino, Giorgio Ivan Russo, Francesca Zingone
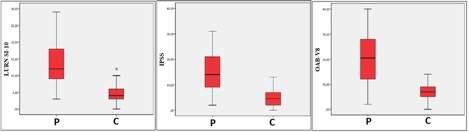
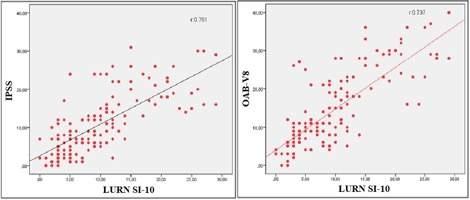
12415 Reliability and validity analysis of Turkish version of the Symptoms of Lower Urinar y Tract Dysfunction Research Network Symptom Index-10 questionnaire
Serkan Akan, Hasan Huseyin Tavukcu, Meftun Culpan, David Cella
12294 Differences in bladder neck angles between female patients with overactive bladders and healthy peers
Mehmet Yoldas, Mehmet Zeynel Keskin
12395 The use of urodynamic to assess the mechanism of incontinence in patients with Yang-Monti based catheterizable cutaneous stomas
M Abdelwadood, Eman H Ibrahim, Tamer A Abouelgreed, Yasser M Haggag, Mohamed M Yassin, Mohamed A Elhelaly, El-Sayed I El-Agamy, Basem Fathi, Salma F Abdelkader, Sameh S Ali, Naglaa M Aboelsoud, Nasser Ramadan, Mohamed Sobhy, Tarek Gharib
continued on page III
Prevenzione della calcolosi renale con l’acqua Lauretana, la più leggera d’Europa
La prevalenza della calcolosi renale è in aumento in tutto il mondo e si stima che il tasso di recidiva sia del 50% (1).
Un ridotto volume urinario dovuto a un’insufficiente assunzione di liquidi o a una loro eccessiva perdita rappresenta uno dei più cruciali fattori di rischio (2).
Una meta-analisi sul ruolo dell’assunzione di liquidi nella prevenzione secondaria dell’urolitiasi ha concluso che un’elevata assunzione totale di liquidi per ottenere un volume di urina superiore a 2,0 a 2,5 L/giorno riduce il rischio di recidiva di calcoli (3).
In definitiva, un’adeguata assunzione di liquidi rappresenta la più importante misura nutrizionale per prevenire la recidiva di calcoli, indipendentemente dalla loro composizione (2).
Da sottolineare che nel corso di una colica renale non è da forzare l’idratazione orale che deve essere mantenuta normale (4).
L’acqua deve essere preferibilmente a basso residuo fisso e sono da evitare le acque ricche di sodio (5).
Le acque minerali, in base al contenuto totale di Sali in milligrammi dopo l’evaporazione di 1 litro di acqua minerale essiccata a 180°C (residui secchi) possono essere classificate come (6):
• acque a bassissimo contenuto minerale,
• acque a basso contenuto minerale,
• acque a medio contenuto minerale,
• acque fortemente mineralizzate.
L’acqua minerale Lauretana delle Prealpi Biellesi, è leggerissima, con poco sodio e un pH leggermente acido, inoltre la ricerca di insetticidi, erbicidi, fungicidi, nematocidi, acaricidi, alghicidi, rodenticidi ha dato esito negativo (7).
L’acqua minerale Lauretana, in quanto povera di sodio, non ha controindicazioni nei soggetti affetti da ipertensione arteriosa (8), e trova, inoltre, una precisa indicazione nei casi in cui sia necessario un adeguato e corretto apporto idrico per la prevenzione della calcolosi urinaria, in particolare nei soggetti metabolicamente predisposti e nella prevenzione delle recidive dopo trattamento (9).
Bibliografia
1. Siener R. Nutrition and Kidney Stone Disease. Nutrients. 2021 Jun 3;13(6):1917.
2. Siener, R.; Hesse, A. Fluid intake and epidemiology of urolithiasis. Eur. J. Clin. Nutr. 2003, 57, S47–S51.
3. Fink HA, Akornor JW, Garimella PS, et al. Diet, fluid, or supplements for secondary prevention of nephrolithiasis: a systematic review and meta-analysis of randomized trials. Eur Urol. 2009; 56: 72-80.
4. Hernhard Hess. Renal colic. In The Stone Hand Book. Edizioni Scripta Manent, Milano 2013.
5. Zanasi A. Guida all’uso ragionato delle acque minerali. Giugno 1999.
6. Decreto Legislativo numero 105 del 25 gennaio 1992.
7. Claudio Medana, Dipartimento Di Biotecnologie Molecolari e Scienze per la Salute - Università di Torino. 12.12. 2023.
8. Prof. Dott. Giancarlo Levra. Scuola di specializzazione in Idrologia Medica -Università degli Studi di Pisa.
9. Dott. Marco Laudi Direttore U.O. di Urologia Ospedale Mauriziano Umberto I Torino.
EDITORIAL BOARD
EDITOR IN CHIEF
Alberto Trinchieri (Milan, Italy)
ASSOCIATE EDITORS
Emanuele Montanari, Department of Urology, IRCCS Foundation Ca’ Granda Ospedale Maggiore Policlinico, University of Milan, Italy – Gianpaolo Perletti, Department of Biotechnology and Life Sciences, Section of Medical and Surgical Sciences, University of Insubria, Varese, Italy; Department of Human Structure and Repair, Ghent University, Ghent, Belgium - Angelo Porreca, Robotic Urology and Mini Invasive Urologic Surgery Unit, Abano Terme Hospital, Abano Terme, Italy
EXECUTIVE EDITORIAL BOARD
Alessandro Antonelli, Department of Urology, Azienda Ospedaliera Universitaria Integrata (A O U I ), Verona, Italy - Antonio Celia, Department of Urology, San Bassiano Hospital, Bassano del Grappa, Italy - Luca Cindolo, Department of Urology, Villa Stuart Hospital, Rome, Italy - Andrea Minervini, Department of Urology, University of Florence, Unit of Oncologic Minimally-Invasive Urology and Andrology, Careggi Hospital, Florence, Italy - Bernardo Rocco, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy - Riccardo Schiavina, Department of Urology, University of Bologna, Bologna, Italy
ADVISORY EDITORIAL BOARD
Pier Francesco Bassi, Urology Unit, A Gemelli Hospital, Catholic University of Rome, Italy – Francesca Boccafoschi, Health Sciences Department, University of Piemonte Orientale in Novara, Italy – Alberto Bossi, Department of Radiotherapy, Gustave Roussy Institute, Villejuif, France –Tommaso Cai, S Chiara Hospital, Trento, Italy –Paolo Caione, Department of Nephrology-Urology, Bambino Gesù Pediatric Hospital, Rome, Italy – Luca Carmignani, Urology Unit, San Donato Hospital, Milan, Italy –Liang Cheng, Department of Urology, Indiana University School of Medicine, Indianapolis, IN; Department of Pathology and Laboratory Medicine, Indiana University School of Medicine, Indianapolis, IN – Giovanni Colpi, Retired Andrologist, Milan, Italy – Giovanni Corona, Department of Urology, University of Florence, Careggi Hospital, Florence, Italy – Antonella Giannantoni, Department of Surgical and Biomedical Sciences, University of Perugia, Italy – Paolo Gontero, Department of Surgical Sciences, Molinette Hospital, Turin, Italy – Steven Joniau, Organ Systems, Department of Development and Regeneration, KU Leuven, Belgium – Frank Keeley, Bristol Urological Institute, Southmead Hospital, Bristol UK – Laurence Klotz, Division of Urology, Department of Surgery, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, Ontario, Canada – Börje Ljungberg, Urology and Andrology Unit, Department of Surgical and Perioperative Sciences, Umeå University, Umeå, Sweden –Nicola Mondaini, Uro-Andrology Unit, Santa Maria Annunziata Hospital, Florence, Italy – Gordon Muir, Department of Urology, King's College Hospital, London, UK –Giovanni Muto, Urology Unit, Bio-Medical Campus University, Turin, Italy – Anup Patel, Department of Urology, St Mary's Hospital, Imperial Healthcare NHS Trust, London, UK – Glenn Preminger, Division of Urologic Surgery, Duke University Medical Center, Durham, NC, USA – David Ralph, St. Peter's Andrology Centre and Institute of Urology, London, UK – Allen Rodgers, Department of Chemistry, University of Cape Town, Cape Town, South Africa – Francisco Sampaio, Urogenital Research Unit, State University of Rio de Janeiro, Rio de Janeiro, RJ, Brazil – Kemal Sarica, Department of Urology, Kafkas University Medical School, Kars, Turkey – Luigi Schips, Department of Urology, San Pio da Pietrelcina Hospital, Vasto, Italy – Hartwig Schwaibold, Bristol Urological Institute, Southmead Hospital, Bristol, UK – Alchiede Simonato, Department of Urology, University of Verona, Azienda Ospedaliera Universitaria Integrata, Verona, Italy – Carlo Terrone, Department of Urology, IRCCS S Martino University Hospital, Genova, Italy – Anthony Timoney, Bristol Urological Institute, Southmead Hospital, Bristol, UK – Andrea Tubaro, Urology Unit, Sant’Andrea Hospital, “La Sapienza” University, Rome, Italy – Richard Zigeuner, Department of Urology, Medical University of Graz, Graz, Austria
BOARD OF REVIEWERS
Maida Bada, Department of Urology, S Pio da Pietrelcina Hospital, ASL 2 Abruzzo, Vasto, Italy - Lorenzo Bianchi, Department of Urology, University of Bologna, Bologna, Italy - Mariangela Cerruto, Department of Urology, Azienda Ospedaliera Universitaria Integrata (A O U I ), Verona, Italy - Francesco Chessa, Department of Urology, University of Bologna, Bologna, Italy - Daniele D’Agostino, Robotic Urology and Mini In-
vasive Urologic Surgery Unit, Abano Terme Hospital, Abano Terme, Italy - Fabrizio Di Maida, Department of Urology, University of Florence, Unit of Oncologic Minimally-Invasive Urology and Andrology, Careggi Hospital, Florence, Italy - Antonio Galfano, Urology Unit, Niguarda Hospital, Milan, Italy - Michele Marchioni, Department of Medical, Oral and Biotechnological Sciences, "G. d'Annunzio" University of Chieti, Laboratory of Biostatistics, Chieti, Italy - Andrea Mari, Department of Urology, University of Florence, Unit of Oncologic Minimally-Invasive Urology and Andrology, Careggi Hospital, Florence, Italy - Luigi Napolitano, Unit of Urology, Department of Neurosciences, Reproductive Sciences, and Odontostomatology University of Naples “Federico II”, Naples, Italy - Antonio Porcaro, Department of Urology, Azienda Ospedaliera Universitaria Integrata (A O U I ), Verona, Italy - Stefano Puliatti, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy - Daniele Romagnoli, Robotic Urology and Mini Invasive Urologic Surgery Unit, Abano Terme Hospital, Abano Terme, Italy - Chiara Sighinolf, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy - Tommaso Silvestri, Urology Clinic, Department of Medical, Surgical and Health Science, University of Trieste, Trieste, Italy - Petros Sountoulides, Aristotle University of Thessaloniki, Department of Urology, Thessaloniki, Greece - Alessandro Tafuri, Department of Urology, Vito Fazzi Hospital, Lecce, Italy
SIEUN EDITOR
Pasquale Martino, Department of Emergency and Organ Transplantation-Urology I, University Aldo Moro, Bari, Italy
SIEUN EDITORIAL BOARD
Emanuele Belgrano, Department of Urology, Trieste University Hospital, Trieste, ItalyFrancesco Micali, Department of Urology, Tor Vergata University Hospital, Rome, ItalyMassimo Porena, Urology Unit, Perugia Hospital, Perugia, Italy – Francesco Paolo Selvaggi, Department of Urology, University of Bari, Italy – Carlo Trombetta, Urology Clinic, Cattinara Hospital, Trieste, Italy – Giuseppe Vespasiani, Department of Urology, Tor Vergata University Hospital, Rome, Italy – Guido Virgili, Department of Urology, Tor Vergata University Hospital, Rome, Italy
UrOP EDITOR
Carmelo Boccafoschi, Department of Urology, Città di Alessandria Clinic, Alessandria, Italy
UrOP EDITORIAL BOARD
Renzo Colombo, Department of Urology, San Raffaele Hospital, Milan, Italy – Roberto Giulianelli, Department of Urology, New Villa Claudia, Rome, Italy – Massimo Lazzeri, Department of Urology, Humanitas Research Hospital, Rozzano (Milano), Italy – Angelo Porreca, Department of Urology, Polyclinic Abano Terme, Abano Terme (Padova), Italy –Marcello Scarcia, Department of Urology, "Francesco Miulli" Regional General Hospital, Acquaviva delle Fonti (Bari), Italy – Nazareno Suardi, Department of Urology, San Raffaele Turro, Milano, Italy
GUN EDITOR
Arrigo Francesco Giuseppe Cicero, Medical and Surgical Sciences Department, Sant’Orsola-Malpighi University Hospital, Bologna, Italy
GUN EDITORIAL BOARD
Gianmaria Busetto, Department of Urology, Sapienza University of Rome, Italy –Tommaso Cai, Department of Urology, Santa Chiara Regional Hospital, Trento, Italy –Elisabetta Costantini, Andrology and Urogynecological Clinic, Santa Maria Hospital of Terni, University of Perugia, Terni, Italy – Angelo Antonio Izzo, Department of Pharmacy, University of Naples, Italy – Vittorio Magri, ASST Nord Milano, Milano, Italy – Salvatore Micali, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy – Gianni Paulis, Andrology Center, Villa Benedetta Clinic, Rome, Italy – Francesco Saverio Robustelli della Cuna, University of Pavia, Italy – Giorgio Ivan Russo, Urology Department, University of Catania, Italy – Konstantinos Stamatiou, Urology Department, Tzaneio Hospital, Piraeus, Greece – Annabella Vitalone, Department of Physiology and Pharmacology, Sapienza University of Rome, Rome, Italy
PARTNER CELEBRATING WITH US
ORIGINAL PAPERS
12431 Robotic-assisted laparoscopic pyeloplasty for the treatment of ureteropelvic junction obstr uction – How should success be deter mined?
Marie Lien, Mathias Sørstrand Æsøy, Karin Hjelle, Bjarte Almås, Patrick Juliebø-Jones, Øyvind Ulvik
12389 Pediatric renal transplantation: A single center experience
Shakhawan Hama Amin Said, Saiwan Hayas Agha, Goran Fryad Abdulla, Mzhda Sahib Jaafar, Rawa Bapir, Nali H Hama, Ismaeel Aghaways, Aso Omer Rashid, Berun A Abdalla, Fahmi H Kakamad
12387 Evaluating prognostic indicators for in-Hospital mor tality in Four nier's gangrene: A 7-year study in a ter tiar y Hospital
Soetojo Wirjopranoto, Mohammad Reza Affandi, Faisal Yusuf Ashari, Yufi Aulia Azmi, Kevin Muliawan Soetanto
12335 Effects of antisper m antibodies post vasectomy reversal on pregnancy rates
Tamer A Abouelgreed, Mohamed A Amer, Hassan Mamdouh, Ahmed F El-Sherbiny, Hany Aboelwafa, Omar A Omar, Mohammed Abdelshakour, Mohammad Elesawy, Mohamed Sonbol, Ahmed N Maawad, Elsayed M Zayed, Mostafa T Eldestawy
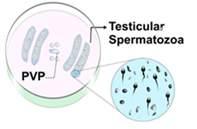
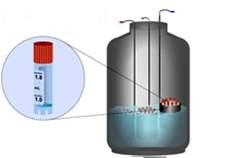
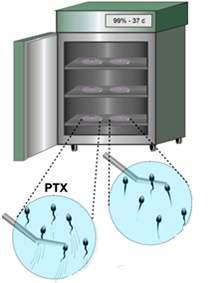
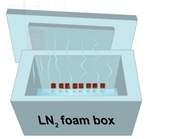
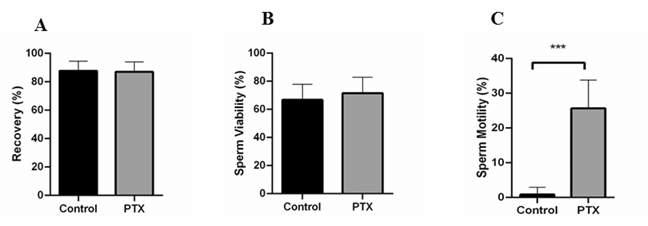
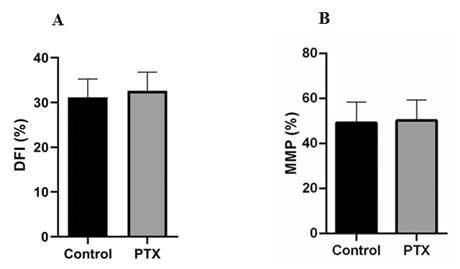
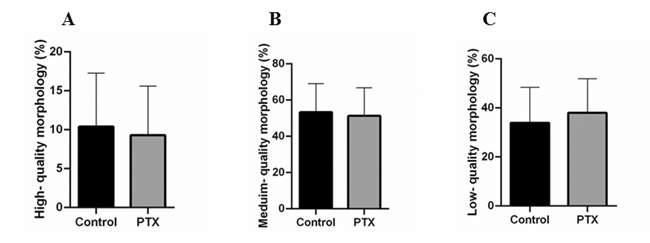
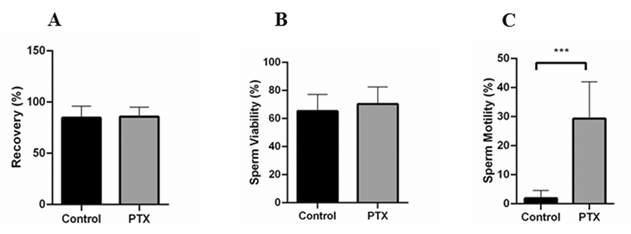
12525 Pentoxifylline treatment as a safe method for selecting viable testicular sper matozoa before cr yopreser vation of a small numbers of sper matozoa in azoosper mia individuals
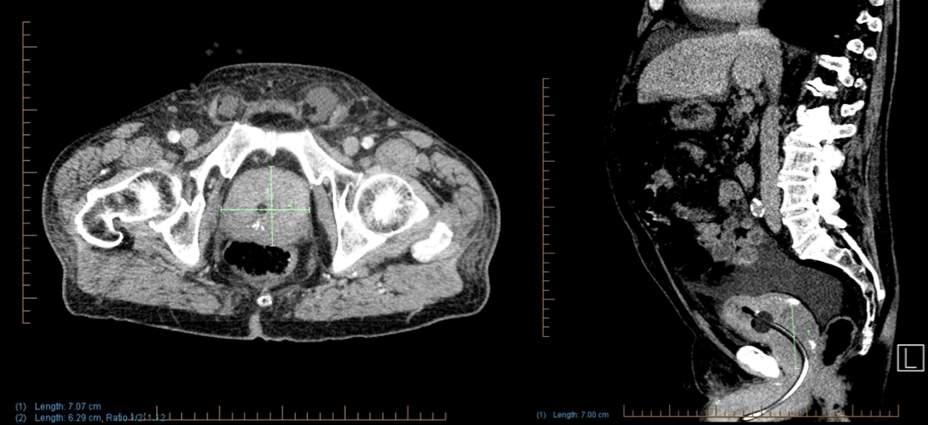
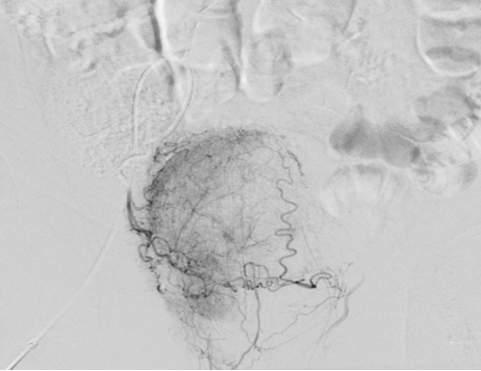
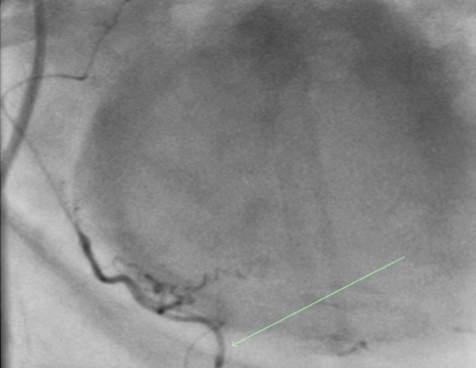
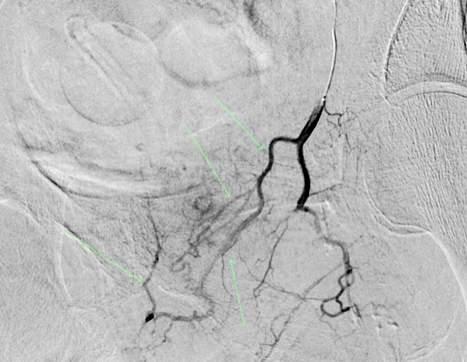
12306 Prostatic ar ter y embolization for intractable hematuria in patients with unregulated coagulation parameters: Three case repor ts Manuel Belmonte, Abdulghani Khogeer, Ghizlane Moussaoui, Rafael Melo, Louis-Martin Boucher, Tatiana Villalpando-Cabrera, Serge Carrier, Mélanie Aubé-Peterkin
CASE REPORTS
12483 An unusual “linitis plastica” like breast cancer bladder metastasis
Riccardo Farci, Simona Tolu, Matilde Trombetta, Alessandro Murgia, Andrea Solinas
12363 Management of an elder ly patient with retention of a steel nail in the scrotum: A case repor t Iacopo Meneghetti, Novella Cesta, Luca Mosillo, Simone Belli, Daniele Bianchi, Maurizio De Maria
REVIEWS
12307 The role of immunotherapy in urological cancers
Efe Bosnali, Enes Malik Akdas, Engin Telli, Kerem Teke, Onder Kara
12323 The influence of oral antioxidants on men with infer tility: A systemic review
Tamer A Abouelgreed, Mohamed A Amer, Hassan Mamdouh, Ahmed F El-Sherbiny, Hany Aboelwafa, Sameh F Fahmy, Omar A Omar, Mohammed Abdelshakour, Mohammad Elesawy, Mohamed Sonbol, Ahmed N Maawad, Osama K Elsayed
Edizioni Scripta Manent s.n.c.
Via Melchiorre Gioia 41/A - 20124 Milano, Italy
Tel +39 0270608060
e-mail: scriman@tin.it
web: www edizioniscriptamanent eu
Registrazione: Tribunale di Milano n 289 del 21/05/2001
Direttore Responsabile: Pietro Cazzola
Direzione Marketing e PR: Donatella Tedeschi
Comunicazione e Media: Ruben Cazzola
Grafica e Impaginazione: Stefania Cacciaglia
Affari Legali: Avv Loredana Talia (MI)
Ai sensi della legge 675/96 è possibile in qualsiasi momento opporsi all’invio della rivista comunicando per iscritto la propria decisione a: Edizioni Scripta Manent s n c - Via Melchiorre Gioia, 41/A - 20124 Milano
The Publisher is not liable for the opinion expressed by the Authors of the articles and for images used by them
GENERAL INFORMATION
AIMS AND SCOPE
“Archivio Italiano di Urologia e Andrologia” publishes papers dealing with the urological, nephrological and andrological sciences
Original articles on both clinical and research fields, reviews, editorials, case reports, abstracts from papers published elsewhere, book rewiews, congress proceedings can be published
ORIGINAL PAPER
Negative biopsy histology in men with PI-RADS score 5: Is it useful PSMA PET/CT evaluation?
1 Urology Unit, Cannizzaro Hospital, Catania, Italy;
2 Department of Human Pathology in Adult and Developmental Age "Gaetano Barresi", University of Messina, Italy
Summary
Introduction: To evaluate the accuracy of PSMA PET/CT in men with mpMRI PI-RADS score 5 negative biopsy histology.
Materials and methods: From January 2011 to January 2023, 180 men with PI-RADS score 5 underwent systematic plus mpMRI/TRUS biopsy; 25/180 (13 9%) patients had absence of cancer and six months from biopsy were submitted to: digital rectal examination, PSA and PSA density exams, mpMRI and 68GaPSMA PET/CT evaluation (standardized uptake value “SUVmax” was reported)
Results: In 24/25 (96%) patients PSA and PSA density significantly decreased, moreover, the PI-RADS score was downgraded resulting < 3; in addition, median SUVmax was 7 5 Only 1/25 (4%) man had an increased PSA value (from 10 5 to 31 ng/ml) with a confirmed PI-RADS score 5, SUVmax of 32 and repeated prostate biopsy demonstrating a Gleason score 9/ISUP Grade Group 5 PCa
Conclusions: The strict follow up of men with PI-RADS score 5 and negative histology reduce the risk of missing csPCa especially if PSMA PET/CT evaluation is in agreement with downgrading of mpMRI (PI-RADS score < 3)
Submitted 5 February 2024; Accepted 18 february 2024
INTRODUCTION
Multiparametric magnetic image resonance (mpMRI) is recommended in men with suspicion prostate cancer (PCa) (1), but, still today, systematic prostate biopsies should be always combined with mpMRI/TRUS fusion biopsy due to the false negative rate (2-4) of mpMRI (15-20% of the cases) (5) The aggressiveness of clinically significant (csPCa) is correlated with the mpMRI Prostate Imaging Reporting and Data System (PI-RADS) scores; the detection rate for csPCa of suspicious mpMRI lesions performing targeted biopsy ranges from 65 3 to 83 8% (6) and in the presence of a suspicious area with PI-RADS score 5 ranges from 59 2 to 86% of the cases (7, 8) Therefore, a negative biopsy in men with PI-RADS score 5 need a thorough clinical follow up to avoid missing csPCa diagnosis
In our study, the follow up of men with negative biopsy histology of PI-RADS score 5 lesions has been reported i n c l u d i n g p ro s t a t e - s p e c i f i c m e m b r a n e a n t i g e n ( P S M A ) positron-emission tomography (PET/CT) evaluation
MATERIALS AND METHODS
From January 2011 to January 2023, 2,405 men (median age: 64 years; range: 41-86 years) underwent extended (median 20 cores; range: 16-22) or saturation (SPBx: median 26 cores; range: 22-30) transperineal prostate biopsy for the suspicion of cancer (9-11) Informed consents were obtained from all participants included in the study following institutional ethical committee approval Before biopsy the patients underwent pelvic mpMRI using a 1 5 and 3 0 Tesla scanner (ACHIEVA 3T; Philips Healthcare Best, the Netherlands) equipped with surface 16-channel phased-array coil; multi-planar turbo spinecho T2-weighted, axial diffusion weighted imaging (high b-value - 2000 s/mm2), and axial dynamic contrast enhanced MRI were performed for each patient (12) The systematic biopsy was performed transperineally and mpMRI lesions with PI-RADS score > 3 (1 380/2 405 equal to 57 4% of the cases) were submitted to targeted biopsy (TPBx: four cores performing a transperineal cognitive approach, anterior zone of the gland) or a fusion guided-biopsy (Hitachi 70 Arietta ecograph, Chiba, Japan) (13-15) All the patients were sedated and received a single intraoperative dose of antibiotic prophylaxis The detection rate for csPCa has been evaluated (16); moreover, the Clavien-Dindo grading system for the classification of biopsy complications was used (17)
All the 180 men with PI-RADS score 5 had not dysuria, irritative urinary symptoms or stranguria In 155/180 (86 1%) patients a stage T1c PCa was diagnosed, and 145/155 (93 5%) of them (Table 1) were classified as csPCa (International Society of Urologic Pathology “ISUP Grade Group “GG” > 2); in detail, 85/145 (58 6%), 30/145 (20 7%) and 30/145 (20 7%) csPCa were diagnosed in the peripheric, anterior or both zones of the prostate, respectively The median total PSA was 8 9 ng/ml (range: 2 7-95 ng/ml); moreover, quantitative biopsy histology, PSA density (PSAD), PSA free/total are listed in Table 1 SPBx diagnosed 5/155 (3 2%) csPCa and 8/155 (5 2%) indolent PCa located outside the PI-RADS 5 lesions
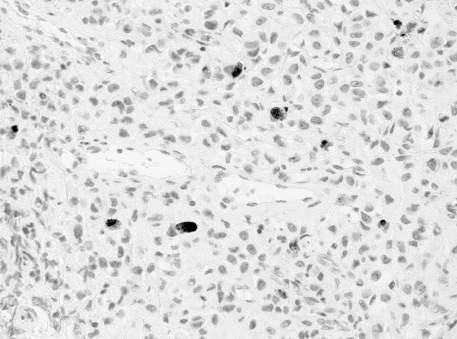
In the remaining 25/180 (13 9%) patients with absence of cancer: 1/25 (4%) had a specific granulomatous prostatitis (Mycobacterium Tubercolosis), 8/25 (32%) an aspecific granulomatous prostatitis, and 16/25 (64%) a normal parenchyma None of the patients had significant complications (only Clavien-Dindo grade I) following prostate
biopsy, requiring hospital admission The men with granulomatous prostatitis underwent specific antibiotic therapy followed by laboratory showing negative culture of urine and semen; moreover, the urine and sperm search for Mycobacterium Tuberculosis test including the semen polymerase chain reaction (PCR) (TB-PCR) were negative The clinical follow up of patients without proven diagnosis of PCa including PSMA PET/CT evaluation has been reported
RESULTS
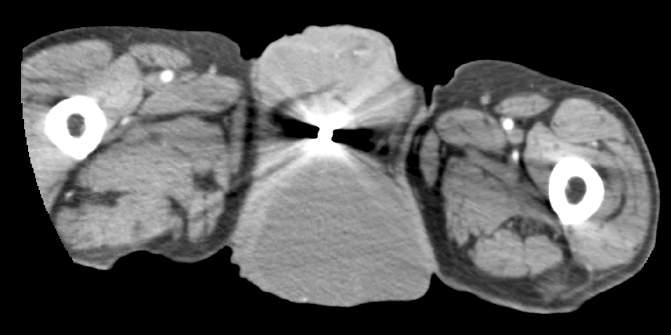
All the 25 men with PI-RADS score 5 and negative histology six months from biopsy underwent: digital rectal examination (DRE), PSA, PSAD, mpMRI and PSMA PET/CT evaluation (Table 2) PET/CT imaging was performed using a CT-integrated PET scanner (Biograph 6; Siemens, Knoxville, TN, USA); 68Ga-PSMA-11 was given to patients via an intravenous bolus; images were processed to obtain PET, CT, and PET-CT fusion sections in the axial, coronal, and sagittal planes with a thickness of approximately 0 5 ~ cm The location of focal uptake on 68Ga-PSMA PET/TC, three-dimensional size, and standardised uptake value (SUVmax) values were reported on a per-lesion basis with a sextant scheme (18, 19) Twenty-four (96%) patients did not underwent repeated prostate biopsy because PSA significantly decreased, moreover, the initial PI-RADS score 5 was significantly downgraded by a repeated mpMRI to PI-RADS score < 3 (Table 2); in addition, median SUVmax was 7 5 (range: 432) Only 1/25 (4%) man, who was submitted 3 years before to transurethral prostate resection for benign prostate enlargement, had an increased PSA value (from 10 5 to 31 ng/ml) with a confirmed PI-RADS score 5 and
Table 1.
Clinical parameters in 155 men with prostate cancer and PI-RADS score 5 submitted to systematic plus fusion targeted biopsy (TPBx)
Quantitative biopsy histolog y PI-RADS score 5
Number of patients (pts) 155 pts
initial biopsy
repeat biopsy
csPCa
70/155 (45%)
85/155 (55%)
145/180 (86 1%)
Median mpMRI index lesion diameter 23 millimeter (range) (16-31)
Detection of csPCa (ISUP GG > 2) 145 pts
Systematic prostate biopsy
137 (94 5%)
TPBx 138 (95 2%)
Median number of positive cores 13
TPBx (range) 3 (2-4)
Systematic biopsy (range) 10 (7-20)
Median GPC 75%
TPBx (range)
Systematic biopsy (range)
80% (60-100%)
75% (50-100%)
PSA density (range) 0.21 (0.16-0.26)
PSA free/total (range) 12% (7-32%)
Median prostate weight (grams) 50 (20-130 grams)
ISUP: Internationa Society of Urologic Patho ogy Grade Groups; mpMRI: Mu t parametr c magnet c resonance image; GPC: Greatest percentage of cancer; PI-RADS: Prostate Imaging Reporting and Data System
Table 2.
Clinical follow up (six months from prostate biopsy) in 25 men with initial PI-RADS score 5 and negative histology for prostate cancer
Biopsy Aspecific *Specific Nor mal csPCa histolog y granulomatous granulomatous parenchyma ISUPGG5 prostatitis prostatitis
Number of patients 8 cases 1 case 15 cases 1 case initial biopsy 6 (75%) 1 (100%) 7 (46 6%) 1 (100%) repeat biopsy 2 (25%) - 8 (63 4%)
DRE: D gita rectal examination; P -RADS: Prostate Imag ng Reporting and Data System; DRE: Digita rectal evaluat on; *Mycobacter um Tubercolosis; GaPSMA PET/CT: Ga l um prostate-specif c membrane ant gen positron-emission tomography; SUVmax: Standardized uptake va ue; ISUP GG: International Soc ety of Uro ogic Patho ogy Grade Groups
intraprostatic SUVmax of 32 and suspicious bone metastases; TPBx and systematic biopsy demonstrated the presence of a Gleason score 9/ISUP GG5 PCa (6/24 positive cores) located in the anterior zone of the prostate that extended outside the gland
DISCUSSION
Multiparametric MRI has improved the cost-effectiveness of prostate biopsy by reducing the risk of overdiagnosis a n d n u m b e r o f u n n e c e s s a r y p ro c e d u re s ( 2 0 , 2 1 ) Although mpMRI is strongly recommended in men candidate to prostate biopsy or enrolled in active surveillance protocols (2, 22, 23), extended or SPBx should be always combined with mpMRI/TRUS fusion biopsy because the false negative rate of mpMRI (24) and the variable accuracy of mpMRI/TRUS fusion biopsy platforms (25) The correlation of the PI-RADS score to the diagnosis of aggressiveness cancer has been well established; Westphalen et al (7) and Otti et al. (8) showed in men with PI-RADS score 5 a detection rate for csPCa equal to 59 2 and 86%, respectively; we previously reported a detection rate of csPCa in the 86 7% of 105 men with PI-RADS score 5 who underwent repeated prostate biopsy (26) The systematic prostate biopsy detects only 3 4% of csPCa in case of negative MRI/TRUS targeted biopsy of PI-RAS score 5 lesions (27) Therefore, the presence of a negative histology of a PI-RADS score 5 lesion needs an accurate follow up to avoid the risk of missing a high grade csPCa; the use of PSA, PSAD, risk calculator, urinary genetic tests, and the repetition of mpMRI allow to reduce the risk of harboring a csPCa In this respect, a second opinion regarding initial mpMRI (28) and histology evaluation (29) should be performed to decrease the risk of false negative results Recently, PSMA-PET/CT has been proposed for the diagnosis of primary intraprostatic cancer (18, 19, 30, 31); the
P Pepe, L Pepe, M Pennisi
presence of focal uptake on PSMA-PET/CT (SUVmax) and the maximal dimensions of PET-avid lesions have been correlated with the presence of csPCa (32) Although there is a range of proposed cut-offs to detect csPCa from SUVmax (33-35), the concordance between preoperative PSMA PET/TC evaluation and definitive prostate specimen ranges from 81 2 (36) to 96% (37)
Many anatomic feature, benign conditions and technical pitfalls could mimic prostate cancer on mpMRI (38,39); the analysis of mpMRI parameters (DWI signal intensity and ADC values) combined with noninvasive test could help to separate benign lesions from csPCa (40-42)
Gottlieb et al (43) reported that men with previous specific granulomatous prostatitits the presence of a PI-RADS score ≤ 3 may not required prostate biopsy; in our experience, 16 men with initial PI-RADS score 5 and negative histology demonstrated six months later a PI-RADS score < 3 with normal clinical parameters (PSA, DRE, PSAD) (26) Recently, Wong et al (44) in 29 men with PIRADS score 4-5 and negative biopsy histology reported that a SUVmax > 20 was correlated with the presence of csPCa
In our series, 25/180 (13 9%) patients with PI-RADS score 5 had negative biopsy histology; six months from prostate biopsy the reduction of PSA and PSAD in 24/25 (96%) patients combined with the downgrading of PIRADS score from 5 to < 3 allowed to avoid a repeated prostate biopsy; at the same time, PSMA PET/CT evaluation showed SUVmax (median 7 5) values not suspicious for csPCa resulting in agreement with the mpMRI results
Only one man (4%) had an increased PSA value (31 ng/ml) with PI-RADS score 5, SUVmax of 32 and TPBx combined with systematic biopsy demonstrated the presence of a Gleason score 9/ISUP GG5 PCa
In definitive, the strict clinical follow up of men with negative histology of PI-RADS score 5 lesions reduce the risk of missing csPCa especially if PSMA PET/CT evaluation is in agreement with downgrading of mpMRI (PI-RADS score < 3)
Regarding our results some considerations should be done Firstly, the results were not evaluated on the entire prostate gland Secondly, we do not know if the presence of a mpMRI PIRADS score 3 (13 cases) was predictive of csPCa because a new biopsy was not performed Third, a greater number of patients should be evaluated Finally, a longer follow up is needed
CONCLUSIONS
A significant reduction of PSA and PSAD values combined with the downgrading of PI-RADS score to < 3 allow to avoid a repeated prostate biopsy in men with initial PIRADS 5 and negative biopsy; 68GaPSMA PET/CT evaluation, in our series, was in agreement with mpMRI results
REFERENCES
1 Lin Y, Yilmaz EC, Belue MJ, Turkbey B Prostate MRI and image Quality: It is time to take stock Eur J Radiol 2023; 161:110757
2 Pepe P, Garufi A, Priolo G, Pennisi M Can MRI/TRUS fusion targeted biopsy replace saturation prostate biopsy in the re-evaluation of men in active surveillance? World J Urol 2016; 34: 1249-1253
3 Rosenkrantz AB, Verma S, Choyke P, et al Prostate Magnetic Resonance Imaging and Magnetic Resonance Imaging Targeted Biopsy in Patients with a Prior Negative Biopsy: A Consensus Statement by AUA and SAR J Urol 2016; 196:1613-1618
4 Pepe P, Cimino S, Garufi A, et al Confirmatory biopsy of men under active surveillance: extended versus saturation versus multipar ametr ic mag ne ti c resonan ce im agi ng /transrectal u ltr asou nd fusion prostate biopsy Scand J Urol 2017; 51:260-263
5 Filson CP, Natarajan S, Margolis DJ, et al Prostate cancer detection with magnetic resonance-ultrasound fusion biopsy: The role of systematic and targeted biopsies Cancer 2016; 15:884-892
6 Pepe P, Garufi A, Priolo GD, et al Is it Time to Perform Only Magnetic Resonance Imaging Targeted Cores? Our Experience with 1,032 Men Who Underwent Prostate Biopsy J Urol 2018; 200:774778
7 Westphalen AC, Fazel F, Nguyen H, et al Detection of clinically significant prostate cancer with PIRADS v2 scores, PSA density, and ADC values in regions with and without mpMRI visible lesions Int Braz J Urol 2019; 45:713-723
8 Otti VC, Miller C, Powell RJ, et al The diagnostic accuracy of multiparametric magnetic resonance imaging before biopsy in the detection of prostate cancer BJU Int 2019; 123:82-90
9 Aragona F, Pepe P, Motta M, et al Incidence of prostate cancer in Sicily: results of a multicenter case-findings protocol Eur Urol 2005; 47:569-574
10 Fandella A, Scattoni V, Galosi A, et al Italian Prostate Biopsies Group: 2016 Updated Guidelines Insights Anticancer Res 2017; 37:413-424
11 Pepe P, Pennisi M Morbidity following transperineal prostate biopsy: Our experience in 8 500 men Arch Ital Urol Androl 2022; 94:155-159
12 Moore CM, Kasivisvanathan V, Eggener S, et al START Consortium Standards of reporting for MRI-targeted biopsy studies (START) of the prostate: recommendations from an International Working Group Eur Urol 2013; 64:544-552
13 Pepe P, Garufi A, Priolo G, Pennisi M Transperineal Versus Transrectal MRI/TRUS Fusion Targeted Biopsy: Detection Rate of Clinically Significant Prostate Cancer Clin Genitourin Cancer 2017; 15:e33-e36
14 Pepe P, Pennisi M, Fraggetta F How Many Cores Should be Obtained During Saturation Biopsy in the Era of Multiparametric Magnetic Resonance? Experience in 875 Patients Submitted to Repeat Prostate Biopsy Urology 2020; 137:133-137
15 Pepe P, Dibenedetto G, Pennisi M, et al Detection rate of anterior prostate cancer in 226 patients submitted to initial and repeat transperineal biopsy Urol Int 2014; 93:189-192
16 Epstein JI, Egevad L, Amin MB, et al Grading Committee The 2 0 1 4
(
) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System Am J Surg Pathol 2016; 40:244-52
17 Dindo D, Clavien PA Classification of surgical complications A new proposal with evaluation in a Cohort of 6336 patients and results of survey Ann Surg 2004; 2:205-213
18 Pepe P, Pennisi M Targeted Biopsy in Men High Risk for Prostate Cancer: 68Ga-PSMA PET/CT Versus mpMRI Clin Genitourin Cancer 2023; 21:639-642
19 Pepe P, Pepe L, Tamburo M, et al Targeted prostate biopsy:
68Ga-PSMA PET/CT vs mpMRI in the diagnosis of prostate cancer Arch Ital Urol Androl 2022; 94:274-277
20 Faria R, Soares MO, Spackman E, et al Optimising the Diagnosis of Prostate Cancer in the Era of Multiparametric Magnetic Resonance Imaging: A Cost-effectiveness Analysis Based on the Prostate MR Imaging Study (PROMIS) Eur Urol 2018; 73:23-30
21 Pepe P, Pepe G, Pepe L, et al Cost-effectiveness of Multiparametric MRI in 800 Men Submitted to Repeat Prostate Biopsy: Results of a Public Health Model Anticancer Res 2018; 38:2395-2398
22 Pepe P, Pepe L, Pennisi M, Fraggetta F Confirmatory transperineal saturation prostate biopsy combined with mpMRI decrease the reclassification rate in men enrolled in Active Surveillance: Our experience in 100 men submitted to eight-years scheduled biopsy Arch Ital Urol Androl 2022; 94:270-273
23 Kim H, Pak S, Park KJ, et al Utility of Multiparametric Magnetic Resonance Imaging With PI-RADS, Version 2, in Patients With Prostate Cancer Eligible for Active Surveillance: Which Radiologic Characteristics Can Predict Unfavorable Disease? Clin Genitourin Cancer 2020; 18:50-55
24 Cecchini S, Castellani D, Fabbietti P, et al Combination of Multiparametric Magnetic Resonance Imaging With Elastic-fusion Biopsy Has a High Sensitivity in Detecting Clinically Significant Prostate Cancer in Daily Practice Clin Genitourin Cancer 2020; 18:e501-e509
25 Westhoff N, Siegel FP, Hausmann D, et al Precision of MRI/ultrasound-fusion biopsy in prostate cancer diagnosis: an ex vivo comparison of alternative biopsy techniques on prostate phantoms World J Urol 2017; 35:1015-1022
26 Pepe P, Pennisi M Negative Biopsy Histology in Men With PIRADS Score 5 in Daily Clinical Practice: Incidence of Granulomatous Prostatitis Clin Genitourin Cancer 2020; 18:e684-e687
27 Arabi A, Deebajah M, Yaguchi G, et al Systematic Biopsy Does Not Contribute to Disease Upgrading in Patients Undergoing Targeted Biopsy for PI-RADS 5 Lesions Identified on Magnetic Resonance Imaging in the Course of Active Surveillance for Prostate Cancer Urology 2019; 134:168-172
28 Li JL, Phillips D, Towfighi S, et al Second-opinion reads in prostate MRI: added value of subspecialty interpretation and review at multidisciplinary rounds Abdom Radiol (NY) 2022; 47:827-837
29 Salvi M, Caputo A, Balmativola D, Scotto M Impact of Stain Normalization on Pathologist Assessment of Prostate Cancer: A Comparative Study Cancers (Basel) 2023; 15:1503
30 Pepe P, Pepe L, Tamburo M, et al 68Ga-PSMA PET/CT and Prostate Cancer Diagnosis: Which SUVmax Value? In Vivo 2023; 37:1318-1322
31 Pepe P, Fandella A, Barbera M, et al Advances in radiology and p a t h o l o g y o f p ro s t a t e c a n c e r : a
Pathologica 2024; 116:1-12
32 Pepe P, Pepe L, Cosentino S, et al Detection Rate of 68Ga-PSMA PET/CT vs mpMRI Targeted Biopsy for Clinically Significant Prostate Cancer Anticancer Res 2022; 42:3011-3015
33 Pepe P, Roscigno M, Pepe L, et al Could 68Ga-PSMA PET/CT Evaluation Reduce the Number of Scheduled Prostate Biopsies in Men Enrolled in Active Surveillance Protocols? J Clin Med 2022; 11:3473
34 Demirci E, Kabasakal L, Sahin OE, et al Can SUVmax values of Ga-68-PSMA PET/CT scan predict the clinically significant prostate cancer? Nucl Med Commun 2019; 40:86-91
35 Rüschoff JH, Ferraro DA, Muehlematter UJ, et al What's behind
68Ga-PSMA-11 uptake in primary prostate cancer PET? Investigation of histopathological parameters and immunohistochemical PSMA expression patterns Eur J Nucl Med Mol Imaging 2021; 48:4042-4053
36 Zhang LL, Li WC, Xu Z, et al 68Ga-PSMA PET/CT targeted biopsy for the diagnosis of clinically significant prostate cancer compared with transrectal ultrasound guided biopsy: a prospective randomized single-centre study Eur J Nucl Med Mol Imaging 2021; 48:483-492
37 Liu Y, Yu H, Liu J, et al A Pilot Study of 18F-DCFPyL PET/CT or PET/MRI and Ultrasound Fusion Targeted Prostate Biopsy for Intra-Prostatic PET-Positive Lesions Front Oncol 2021; 11:612157
38 Rais-Bahrami S, Nix JW, Turkbey B, et al Clinical and multiparametric MRI signatures of granulomatous prostatitis Abdom Radiol (NY) 2017; 42:1956-1962
39 Chatterjee A, Thomas S, Oto A Prostate MR: Pitfalls and benign lesions Abdom Radiol (NY) 2020; 45:2154-2164
40 Gordetsky JB, Ullman D, Schultz L, et al Histologic findings associated with false-positive multiparametric magnetic resonance imaging performed for prostate cancer detection Hum Pathol 2019; 83:159-165
41 Kawada H, Kanematsu M, Goshima S, et al Multiphase contrast-enhanced magnetic resonance imaging features of Bacillus Calmette-Guérin-induced granulomatous prostatitis in five patients Korean J Radiol 2015; 16:342-348
42 Pepe P, Pepe L, Curduman M, et al Ductal prostate cancer staging: Role of PSMA PET/CT Arch Ital Urol Androl 2024; 96:12132
43 Gottlieb J, Princenthal R, Cohen MI Multi-parametric MRI findings of granulomatous prostatitis developing after intravesical bacillus calmette-guérin therapy Abdom Radiol (NY) 2017; 42:1963-1967
44 Wong LM, Koschel S, Whish-Wilson T, et al Investigating PSMAPET/CT to resolve prostate MRI PIRADS4-5 and negative biopsy discordance World J Urol 2023; 463-469
Correspondence
Pietro Pepe, MD piepepe@hotmail com Ludovica Pepe, MD ludopepe97@gmail com Michele Pennisi, MD michepennisi2@virgilio it Urology Unit, Cannizzaro Hospital, via Messina 829, Catania, Italy
Conflict of interest: The authors declare no potential conflict of interest
P Pepe, L Pepe, M Pennisi
ORIGINAL PAPER
Does intravesical Bacillus Calmette-Guérin for bladder cancer protect from COVID-19?
Anastasia MacDonald 1 , Lexia Bao 2 , Vahid Mehrnoush 1 , Asmaa Ismail 1 , Livio Di Matteo 3 , Ahmed Zakaria 1 , Hazem Elmansy 1 , Peter Black 2 , Ahmed Kotb 1
1 Department of Urology, Northern Ontario School of Medicine University, Thunder Bay, ON, Canada;
2 Department of Urology, University of British Columbia, BC, Canada;
3 Department of Economics, Lakehead University, Thunder Bay, ON, Canada
Summary
Introduction: The study aimed to correlate the history of intravesical BCG as well as infantile BCG immunization with the incidence and severity of COVID-19 infection
Methods: Retrospective data collection of patients with high-risk non muscle invasive bladder cancer (NMIBC) from two Canadian centers Data collection included a history of BCG instillation, infantile immunization, and the development of COVID-19 infection Admission and/ or mortality because of COVID-19 was reported
Results: We could include data from 348 patients: including 188 and 160 patients from Ontario and British Columbia respectively COVID-19 affected 15% of these patients Intravesical BCG was used in 44% of these patients. Intravesical BCG and/or infantile BCG immunization did not correlate with the incidence of COVID-19 infection.
Conclusions: Previous intravesical BCG and/ or a history of infantile BCG vaccination were not more/ less frequent in patients who had COVID-19 infection
KEY WORDS: Bladder cancer; BCG; COVID-19
Submitted 4 March 2024; Accepted 28 March 2024
INTRODUCTION
The COVID-19 pandemic represented an unprecedented time in modern society, resulting in mortality and morbidity worldwide, as well as significant strain on healthcare resources and professionals Early in the pandemic, tremendous efforts were put forth to identify a vaccination against the etiologic agent in COVID-19 infection, SARSCoV-2 virus This infection is associated with deregulation of innate immune responses, ultimately resulting in systemic inflammation and mass virus replication (1) Trained immunity (TI) is a non-specific, protective inflammatory response generated from immunization against an unrelated pathogen (2) As such, TI was proposed as a mechanism to tackle infection and spread by creating an early immune response (1) Prior to the creation of COVID-19 specific immunizations, there was interest in the Bacillus CalmetteGuérin (BCG) vaccine for protection against COVID-19
The BCG immunization contains live-attenuated Mycobacterium bovis and is used to protect against tuberculosis in countries with high incidence (3) The BCG vaccine has reliably demonstrated TI, protecting against
numerous unrelated pathogens, including several respirator y infections such as influenza A and RSV (4) Interestingly, countries with higher rates of BCG immunization were observed to experience lower mortality rates from COVID-19 infections compared to countries with lower rates of immunization during the height of the pandemic (5) BCG therapy also represents an important role in the field of urology Intravesical BCG therapy is the goldstandard adjuvant therapy for non-muscle invasive bladder cancer (NMIBC) (6) Though its specific mechanism remains elusive, its therapeutic role in NMIBC has been attributed to local and systemic immune responses (7) Consequently, there was growing interest in a possible role for this therapy in protection against COVID-19 infection and symptom burden Some evidence has suggested NMIBC patients receiving intravesical BCG therapy had lower COVID-19 case-fatality rate than the overall population (8) Further research on the role of BCG immunization and intravesical therapy on COVID-19 infection has been limited As such, we sought to determine whether intravesical BCG and/or infantile BCG vaccination in patients with NMIBC affected the incidence of COVID-19 infection
METHODS
Retrospective data collection of patients with high-risk NMIBC diagnosed after January 1, 2015, from two Canadian centers Data collection included basic demographic (age/sex/race), clinical (smoking history/comorbidities/prior BCG vaccination or tuberculosis infection), pathologic (stage/grade of tumour), treatment (intravesical BCG/chemo) and outcome (recurrence/progression) variables Details on BCG including the number of instillations and duration of treatment were obtained
A simple survey was also sent to patients to record possible signs and symptoms of COVID-19, or a documented infection The severity of COVID-19 infection was measured by hospitalization, admission to ICU and death The survey was sent at the end of the pandemic
RESULTS
In this study, 348 patients who had been diagnosed with high-risk NMIBC were included All patients lived in Canada, however, 188 were from Ontario and 160 were
A MacDonald, L Bao, V Mehrnoush, A Ismail, et al
from British Columbia The mean age was 74 ± 10 Of the 348 participants, 44% (n = 152) had received intravesical BCG therapy History of BCG immunization could only be obtained from the Ontario cohort, with 60% (n = 113) being immunized It was observed that 24% (n = 45) of the Ontario cohort had received both intravesical BCG therapy and had a history of infantile BCG immunization Overall, 15% of participants were infected with COVID19 There was no significant difference in the incidence of COVID-19 infection between those with and without a history of infantile BCG immunization (p > 0 05) and between those who had and had not received intravesical BCG therapy (p > 0 05) Comparison of those with BCG immunization and/or BCG intravesical therapy and those with neither intervention did not identify a significant difference in COVID-19 (p > 0 05) Additionally, there was no significant difference in COVID-19 incidence between those with a combined history of intravesical BCG and BCG immunization with other participants (p > 0 05) Table 1 illustrates these findings The median number of BCG doses administered was the same in patients who had been infected with COVID-19 and those who had not (12 vs 12 doses; p > 0 05)
There was one incidence of mortality attributed to COVID-19 infection in a patient who did not receive intravesical BCG nor had infantile BCG Three cases required non-ICU hospital admission This included 2 patients who received both infantile and intravesical BCG and one patient who did not receive either The 3 cases recovered well
perhaps unsurprising as BCG therapy is administered locally to the bladder to prevent the recurrence of bladder cancer Studies have suggested the ability of intravesical BCG to confer TI against some respiratory infections, however, these have not been assessed in human studies9 While these installations are believed to generate both local and systemic inflammatory responses (5), the systemic response may not be strong or broad enough to directly prevent COVID-19 This may be supported by a study by Gallegos et al (2021), that identified a higher cumulative incidence of COVID-19 infection, but lower overall mortality in patients who completed intravesical BCG therapy for NMIBC compared to the general population These authors theorized that intravesical BCG immunization may confer protective benefits in terms of COVID-19 severity, rather than the development of infection (8)
Interestingly, Pichler et al (2023) assessed the ability of intravesical BCG to induce adaptive and innate immunity They found that repetitive BCG instillations were able to elicit an innate immune response and thus TI in a laboratory setting It was theorized that it would require a minimum of 6 weeks to elicit this response (10) In our study, those who developed COVID-19 infection and those who did not both received a median number of 12 doses of intravesical BCG, thus spanning a course longer than 6 weeks Despite this, there was no difference in the incidence of COVID-19 infection in those receiving BCG immunotherapy
Our data also demonstrated no correlation between BCG immunization and COVID-19 infection Given the many examples of TI protection from BCG immunization, there was strong speculation about its ability to protect against SARS-CoV-2 as well This was supported by the observation that countries with mandatory BCG immunization experienced a lower number of COVID-19 cases, in addition to reduced mortality (11) Despite this observation, the World Health Organization (WHO) declared that there was no evidence that the BCG vaccine can protect against COVID-19 (12) Before the development of COVID-19specific immunizations, several randomized control trials had been started to determine the efficacy of BCG immunization to protect against this infection (13)
DISCUSSION
Given the widespread implications of COVID-19 infection, significant efforts have been made to understand the relationships between this infection and well-established m e d i c a l p r a c t i c e s B C G i m m u n i z a t i o n h a s re l i a b l y demonstrated the ability to confer non-specific protection against various illnesses (4) The ability of intravesical BCG therapy to induce such protection remains unclear, although laboratory investigations have suggested intravesical BCG is capable of TI (9) High-risk NMIBC patients who had received intravesical BCG therapy represent a unique group of patients during the pandemic, as they had been treated with an agent hypothesized to confer protection against the SARS-CoV-2 virus
Our study did not identify a relationship between intravesical BCG administration and COVID-19 infection This is
There were several limitations to our study While intravesical BCG therapy was assessed at two centers, the history of immunization was only assessed at a single center and thus faced inevitable selection bias Further, our study did not account for the comorbidities of patients, w
COVID-19 infection In this study, we only assessed incidence of COVID-19 infection Future work may seek to categorize the severity and mortality of these patients
CONCLUSIONS
Overall, this study did not identify a relationship between the incidence of COVID-19 infection and a history of intravesical BCG therapy or BCG immunization in NMIBC patients The number of intravesical BCG doses received by those who were and were not infected did not vary Based on these results, it can be concluded that neither form of BCG therapy confers protection against this infection
Table 1
Correlation between BCG vaccination and the development of COVID-19 infection.
REFERENCES
1 Kaur G, Singh S, Nanda S, et al Fiction and Facts about BCG Imparting Trained Immunity against COVID-19 Vaccines 2022; 10:1006
2 Gong W, Aspatwar A, Wang S, et al COVID-19 pandemic: SARSCoV-2 specific vaccines and challenges, protection via BCG trained immunity, and clinical trials Expert Rev Vaccines 2021; 20:857-880
3 Okafor CN, Rewane A, Momodu II Bacillus Calmette Guerin 2023 Jul 3 In: StatPearls [Internet] Treasure Island (FL): StatPearls Publishing; 2024
4 Koneru G, Batiha GE, Algammal AM, et al BCG Vaccine-Induced Trained Immunity and COVID-19: Protective or Bystander? Infect Drug Resist 2021; 14:1169-1184
5 Miyasaka M Is BCG vaccination causally related to reduced COVID-19 mortality? EMBO Mol Med 2020; 12:e12661
6 Saginala K, Barsouk A, Aluru JS, et al Epidemiology of Bladder Cancer Med Sci (Basel) 2020; 8:15
7 Livak KJ, Schmittgen TD Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method Methods (San Diego, Calif ), 2001; 25:402-408
8 Gallegos H, Rojas PA, Sepúlveda F, et al Protective role of intravesical BCG in COVID-19 severity BMC Urology, 2021; 21:50
9 van Puffelen JH, Novakovic B, van Emst L, et al Intravesical BCG in patients with non-muscle invasive bladder cancer induces trained immunity and decreases respiratory infections J Immunother Cancer 2023; 11:e005518
10 Pichler R, Diem G, Hackl H, et al Intravesical BCG in bladder cancer induces innate immune responses against SARS-CoV-2 Front Immunol 2023; 14:1202157
11 Miller A, Reandelar MJ, Fasciglione K, et al (2020) Correlation between Universal BCG Vaccination Policy and Reduced Mortality for COVID-19 MedRxiv preprint doi: https://doi org/10 1101/ 2020 03 24 20042937
12 World Health Organization (2020) Bacille Calmette-Guérin ( B C G ) v a c c
nation-and-covid-19
13 Travassos TC, De Oliveira JMI, Selegatto IB, Reis LO COVID19 impact on bladder cancer-orientations for diagnosing, decision making, and treatment Am J Clin Exp Urol 2021; 9:132-139
Correspondence
Anastasia MacDonald anamacdonald@nosm ca
Vahid Mehrnoush vahidmehrnoush7@gmail com
Asmaa Ismail asmaaismail0782@gmail com
Ahmed Zakaria aszakaria81@yahoo com
Hazem Elmansy hazem mansy@rocketmail com
Ahmed Kotb; MD, PhD, FRCSC, FRCS Urol, FEBU Associate Professor drahmedfali@gmail com
Department of Urology, NOSM U, Thunder Bay, ON, Canada
Lexia Bao lexia bao@ubc ca
Peter Black peter black@ubc ca
Department of Urology, University of British Columbia, BC, Canada
Livio Di Matteo ldimatte@lakeheadu ca
Department of Economics, Lakehead University, Thunder Bay, ON, Canada
Conflict of interest: The authors declare no potential conflict of interest
Management of urinary stones: State of the art and future perspectives by Experts in Stone Disease
Athanasios Papatsoris 1, 25 , Alberto Budia Alba 2 , Juan Antonio Galán Llopis 3 , Murtadha Al Musafer 4 , Mohammed Alameedee 5 , Hammad Ather 6 , Juan Pablo Caballero-Romeu 7 , Antònia Costa-Bauzá 8 , Athanasios Dellis 9 , Mohamed El Howairis 10 , Giovanni Gambaro 11 , Bogdan Geavlete 12 , Adam Halinski 13 , Bernhard Hess 14 , Syed Jaffry 15 , Dirk Kok 16 , Hichem Kouicem 17 , Luis Llanes 18 , Juan M. Lopez Martinez 19 , Elenko Popov 20 , Allen Rodgers 21 , Federico Soria 22 , Kyriaki Stamatelou 23 , Alberto Trinchieri 24, 25 , Christian Tuerk 26
1 2nd Department of Urology, School of Medicine, Sismanoglio Hospital, National and Kapodistrian University of Athens, Athen;
2 Urology Department, La Fe University and Polytechnic Hospital, Valencia, Spain;
3 Department of Urology General University Hospital Dr Balmis, Alicante, Spain;
4 University of Basrah, Basrah, Iraq;
5 Diwaniya Teaching Hospital, Iraq;
6 Aga Khan University, Karachi, Pakistan;
7 Department of Urology, Miguel Hernández University, Alicante, Spain;
8 Laboratory of Renal Lithiasis Research, University Institute of Health Sciences Research (IUNICS-IdISBa), University of Illes Balears, Palma de Mallorca, Spain;
9 2nd Department of Surgery, Aretaieion Academic Hospital, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece;
10 Imperial college, London University, London, UK;
11 Division of Nephrology, Department of Medicine, University Hospital of Verona, Verona, Italy;
12 “Carol Davila” University of Medicine and Pharmacy & “Saint John" Emergency Clinical Hospital, Bucharest, Romania;
13 Private Medical Center “Klinika Wisniowa" Zielona Gora, Poland;
14 Internal Medicine & Nephrology, KidneyStoneCenter Zurich, Klinik Im Park, Zurich, Switzerland;
15 University Hospital Galway, Galway, Ireland;
16 Saelo Scientific Support, Oegstgeest, The Netherlands;
17 Private Clinic, Clinique Les Pins, Setif, Algeria;
18 Urology Department, University Hospital of Getafe, Getafe, Madrid, Spain;
19 Dept of Urology, University of Barcelona Clinic Hospital, Barcelona, Spain;
20 Department of Urology, UMHAT “Tzaritza Yoanna-ISUL", Medical University - Sofia, Sofia, Bulgaria;
21 University of Cape Town, Cape Town, South Africa;
22 Experimental Surgery Department, Ramón y Cajal University Hospital, Madrid, Spain;
23 MESOGEIOS Nephrology Center, Haidari Attica and NEPHROS EU Private Clinic, Athens, Greece;
24 School of Urology, University of Milan, Milan, Italy;
25 U-merge Scientific Office;
26 Urologic Department, Sisters of Charity Hospital and Urologic Praxis, Wien, Austria
Summary
Aim: To present state of the art on the management of urinary stones from a panel of globally recognized urolithiasis experts who met during the Experts in Stone Disease Congress in Valencia in January 2024 Options of treatment: The surgical treatment modalities of renal and ureteral stones are well defined by the guidelines of international societies, although for some index cases more alternative options are possible For 1 5 cm renal stones, both m-PCNL and RIRS have proven to be valid treatment alternatives with comparable stone-free rates The m-PCNL has proven to be more cost effective and requires a shorter operative time, while the RIRS has demonstrated lower morbidity in terms of blood loss and shorter recovery times SWL has proven to be less effective at least for lower calyceal stones but has the highest safety profile For a 6mm obstructing stone of the pelviureteric junction (PUJ) stone, SWL should be the first choice for a stone less than 1 cm, due to less invasiveness and lower risk of complications although it has a lower stone free-rate RIRS has advantages in certain conditions such as anticoagulant treatment, obesity, or body deformity.
Technical issues of the surgical procedures for stone removal: In patients receiving antithrombotic therapy, SWL, PCN and open surgery are at elevated risk of hemorrhage or perinephric hematoma URS, is associated with less morbidity in these cases An individualized combined evaluation of risks of bleeding and thromboembolism should determine the perioperative thromboprophylactic strategy Pre-interventional urine culture and antibiotic therapy are mandatory although UTI treatment is becoming more challenging due to increasing resistance to routinely applied antibiotics The use of an intrarenal urine culture and stone culture is recommended to adapt antibiotic therapy in case of postoperative infectious complications Measurements of temperature and pressure during RIRS are vital for ensuring patient safety and optimizing surgical outcomes although techniques of measurements and methods for data analysis are still to be refined. Ureteral stents were improved by the development of new biomaterials, new coatings, and new stent designs. Topics of current research are the development of drug eluting and bioresorbable stents.
Complications of endoscopic treatment: PCNL is considered the most invasive surgical option Fever and sepsis were observed in 11 and 0.5% and need for transfusion and embolization for bleeding in 7 and 0 4% Major complications, as colonic, splenic, liver, gall bladder and bowel injuries are quite rare but are associated with significant morbidity Ureteroscopy causes less complications, although some of them can be severe They depend on high pressure in the urinary tract (sepsis or renal bleeding) or application of excessive force to the urinary tract (ureteral avulsion or stricture)
Diagnostic work up: Genetic testing consents the diagnosis of monogenetic conditions causing stones It should be carried out in children and in selected adults In adults, monogenetic diseases can be diagnosed by systematic genetic testing in no more than 4%, when cystinuria, APRT deficiency, and xanthinuria are excluded. A reliable stone analysis by infrared spectroscopy or X-ray diffraction is mandatory and should be associated to examination of the stone under a stereomicroscope. The analysis of digital images of stones by deep convolutional neural networks in dry laboratory or during endoscopic examination could allow the classification of stones based on their color and texture. Scanning electron microscopy (SEM) in association with energy dispersive spectrometry (EDS) is another fundamental research tool for the study of kidney stones. The combination of metagenomic analysis using Next Generation Sequencing (NGS) techniques and the enhanced quantitative urine culture (EQUC) protocol can be used to evaluate the urobiome of renal stone formers. Twenty-four hour urine analysis has a place during patient evaluation together with repeated measurements of urinary pH with a digital pH meter. Urinary supersaturation is the most comprehensive physicochemical risk factor employed in urolithiasis research Urinary macromolecules can act as both promoters or inhibitors of stone formation depending on the chemical composition of urine in which they are operating At the moment, there are no clinical
INTRODUCTION
(Athanasios Papatsoris, Murtadha Al Musafer, Athanasios Dellis, Mohamed El Howairis)
Urolithiasis in the urinary tract is a worldwide prevalent disease, affected from several factors, especially diet- and climate-related, that shows increasing prevalence in all ages, races, and sexes They suggest a cause of significant morbidity despite scientific and technological advances As a result, the assessment of optimal diagnostic pathways and evidence-based management of urolithiasis and their incorporation into clinical practice is of utmost importance The purpose of this article is to accumulate up-to-date available knowledge and surgical tips and tricks from a panel of globally recognized urolithiasis experts who met during the Experts in Stone Disease Congress in Valencia in January 2024
This global multi-disciplinary approach in Urolithiasis was Noor Buchholz’s vision It is with regret to accept that Noor is no longer with us, and this article is a least farewell
Surgical stone management
The indications for the treatment of kidney and ureteral stones are well defined by
applications of macromolecules in stone management or prophylaxis. Patients should be evaluated for the association with systemic pathologies
Prophylaxis: Personalized medicine and public health interventions are complementary to prevent stone recurrence
Personalized medicine addresses a small part of stone patients with a high risk of recurrence and systemic complications requiring specific dietary and pharmacological treatment to prevent stone recurrence and complications of associated systemic diseases. The more numerous subjects who form one or a few stones during their entire lifespan should be treated by modifications of diet and lifestyle. Primary prevention by public health interventions is advisable to reduce prevalence of stones in the general population. Renal stone formers at "high-risk" for recurrence need early diagnosis to start specific treatment Stone analysis allows the identification of most “high-risk” patients forming non-calcium stones: infection stones (struvite), uric acid and urates, cystine and other rare stones (dihydroxyadenine, xanthine) Patients at “high-risk” forming calcium stones require a more difficult diagnosis by clinical and laboratory evaluation Particularly, patients with cystinuria and primary hyperoxaluria should be actively searched
Future research: Application of Artificial Intelligence are promising for automated identification of ureteral stones on CT imaging, prediction of stone composition and 24-hour urinary risk factors by demographics and clinical parameters, assessment of stone composition by evaluation of endoscopic images and prediction of outcomes of stone treatments The synergy between urologists, nephrologists, and scientists in basic kidney stone research will enhance the depth and breadth of investigations, leading to a more comprehensive understanding of kidney stone formation.
the main guidelines (Table 1), although some borderline cases remain amenable to different forms of treatment (13) These conditions may include kidney stones of 15 mm diameter and stones of 6 mm in the pyelo-ureteral joint Below are the potential benefits of each form of treatment
The 1.5 cm kidney stone
Mini-PCNL (Elenko Popov)
It is well established in international guidelines that most renal stones > 2 cm in diameter should be treated with percutaneous nephrolithotomy (PCNL) and those with a diameter < 1-2 cm with RIRS; however, mini-PCNL con-
Table 1.
Indications for treatment of 10-20 mm stones according to American and Europen associations guidelines
Stone Location Stone size EAU guidelines AUA guidelines
Upper/middle calyces/renal pelvis 10-20 PCNL/URS or SWL SWL or URS Lower pole 10-20 (favourable factors for SWL) SWL or URS/PCNL 10-20 (unfavourable factors for SWL) PCNL/URS as first line, SWL as second line
A Papatsoris, A Budia Alba, J A Galán Llopis, et al
stitutes a viable and effective minimally invasive treatment option for ever smaller stones, whereas the limits of RIRS are continuously pushed towards ever larger stones
In order to decrease the complications rate of PCNL, Jackman (1998) (4) developed the concept of minimallyi n v a s i v e p e r c u t a n e o u s n e p h r o l i t h o t o m y ( m i n i - p e r c ) , which is based on the assumption that the decrease of PCNL tract size (< 16 Fr) will lower the trauma on the renal parenchyma and hence the risk of bleeding
During the last decades, this tendency towards miniaturization (mini-PCNL, super-miniPCNL, ultra-mini PCNL and micro-PCNL) was steadily developed allowing for PCNL completion through a narrower and safer nephrostomy tract (5, 6)
A critical point for the success of this miniaturization was the introduction of medium and high-power lasers, which allows bigger stones to be treated with mini-PCNL
The ongoing experience with the mini-PCNL technique showed that mini-PCNL is not only a miniaturization but also a different method to remove the stones, as the stones come out of the calyceal system only by means of the irrigation flow without any further need of forceps or baskets (vacuum-cleaner effect or active aspiration sheath)
Standard PCNL still represents “the big gun ” to be used in cases of bulky nephrolithiasis being highly effective although with more significant complications (collateral damage) On the contrary miniaturized PCNL has the “the special forces” philosophy being small size, agile, flexible and with minimal surgical trauma A significant decrease of transfusion rate was observed with mPCNL
In the comparison with RIRS, new technological advancements favor the choice of mini-PCNL as new 7 5 F scopes, new bendable suction ureteral access sheaths (UASs), and new lasers with magnificent dusting abilities
Mini-PCNL is economically more feasible, without problems in cases of difficult retrograde access or need for prestenting; it requires fewer secondary procedures and guarantees much better flow that RIRS
RIRS (Bogdan Geavlete)
Starting from the last place in the list of therapeutic approaches for renal calculi smaller than 2 cm in 2010, retrograde intrarenal surgery (RIRS) can actually compete with all the other current stone treatment practices In 2023, the EAU Guidelines consecrated RIRS efficacy in treating stones up to 3 cm, depending on operator skills and frequently requiring staged procedures (2)
In comparison, despite the higher success rate in approaching lower pole calculi, mini-percutaneous nephrolithotomy (mini-PCNL) has been described as involving a higher rate of complications as well as a longer hospital stay (2)
The potential concern about the presence of residual fragments after the retrograde procedure proved to be clinically unjustified because more than four out of five cases of post-ureteroscopic renal stone fragments under 4 mm were found to either become stone-free due to spontaneous passage or retain asymptomatic stable-size fragments (7)
Aiming to reach an evidence-based comparison, a systematic review and meta-analysis including 18 eligible randomized-controlled clinical trials and involving over 1700 patients emphasized both mini-PCNL and RIRS as safe and effective alternatives in treating renal calculi of 1
to 3 cm It also acknowledged the mini-perc capacity to provide a higher stone-clearance rate with a shorter operation time On the other hand, the antegrade approach has been negatively characterized by significantly longer hospital stay, higher blood loss and transfusion rate, more severe complications, increased pain and higher hospital costs due to its invasive surgical profile (6)
Furthermore, a prospective cohort comparative study targeting precisely the current topic (average renal stone size of 15-16 mm) confirmed the few and not statistically significant differences between the two therapeutic alternatives Mini-PCNL was described as the more cost-effective option, with the drawback of substantially longer hospital stay, while comparable sone-free rates were obtained after a single session (93% versus 89%) (8) It has been consistently underlined that RIRS provides similar therapeutic efficacy in comparison to mini-perc, according to statistically similar stone-free rate, together with reduced perioperative morbidity (shown by the diminished blood loss as well as the shorter recovery time), and despite the longer operative time (9)
At last, but not least, RIRS seems to benefit from therapeutic superiority over extracorporeal shock-wave lithotripsy (ESWL), in light of the literature data supporting the significantly higher stone-free rate and lower re-treatment rate, without an increase in the incidence of complications (10)
Finally, the choice for any alternative minimally-invasive stone treatment should largely rely on some decisive factors, such as stone location, kidney anatomy, associated comorbidities and patient’s preference, as well as the urologist’s expertise and the available medical equipment Finally, it becomes increasingly clear that a patient-tailored therapeutic approach leads the way towards good clinical practice, while treatment algorithms and integrated management strategies are continuously evolving in the era of remarkable technological advances
SWL (Christian Tuerk)
The 15 mm kidney stones have an indication for interventional stone removal and according to the EAU guidelines, both SWL and endourological procedures are available as the first choice for this purpose In 2023, regularly updated systematic Cochrane reviews comparing SWL, ureteroscopy and percutaneous stone removal came to the conclusion that SWL may have lower three-month success rates but less complications compared to the alternatives (11) Another systematic review with network analysis, including 1674 patients, once more showed that SWL is the best option in terms of safety, although, at least for lower calyceal stones, the efficiency is worse (12) However, efficiency of SWL con be improved by proper patient selection and best practicing SWL-treatment Factors for prediction of SWL-success are skin to stone distance, Hounsfield units with stone heterogeneity, stone size/volume (13), anatomy of collecting system, etc In special situations SWL even could be the least burdensome way to treat depending on comorbidities, e g in patients with severe kyphoscoliosis including restrictive respiratory obstruction and anesthesia related difficulties (tracheal intubation) Best practicing SWL-treatment includes shock wave rate 1-1 5 Hz,
ramping of SW-intensity, correct coupling, careful monitoring of both, stone targeting and patients movements during SWL (US), proper analgesia (limits movements and respiratory excursions) (14) Besides proper patient selection and best clinical practice post-SWL measures can improve outcome, like medical expulsive therapy or diuresis-inversion-percussion (15)
Providing proper patient and stone selection and with best clinical SWL-practice the 1 5 cm kidney stone is definitely a case for SWL with low invasiveness and few complications
The 6 mm obstructing pelvi-ureteric junction (PUJ) stone
RIRS (Syed Jaffry)
Retrograde intrarenal surgery (RIRS) emerges as the optimal approach for managing a 6 mm Pelvi-ureteric Junction (PUJ) stone, despite the scarcity of data specific to this size This methodology's support comes from indirect evidence and a comprehensive evaluation of various critical factors influencing treatment decisions
Location plays a pivotal role in determining the approach for stone removal A stone positioned at the PUJ presents unique challenges due to its proximity to the kidney and the potential for causing significant obstruction RIRS, with its maneuverability and direct access capabilities, especially in cases with virgin ureters, either with or without the use of Ureteral access sheaths (UAS), offers a distinct advantage It enables effective push-back techniques and complete stone clearance, even in the face of PUJ obstruction or a tortuous alpha loop in the proximal ureter
The size of the stone, being 6 mm, resides in a grey zone where spontaneous passage is uncertain, thereby necessitating intervention RIRS, with its ability to address stones of this size with minimal complications and favorable outcomes, stands out as a particularly suitable option
Furthermore, the stone's composition, the presence and duration of obstruction, and whether the stone is impacted are all factors that RIRS can adeptly navigate RIRS also provides significant benefits in terms of patient safety and comfort It eliminates the need to stop anticoagulation therapy, which is crucial for patients at risk of thromboembolic events Additionally, for individuals with morbid obesity or body deformities, RIRS offers a safer alternative, reducing the risks associated with more invasive procedures
Moreover, in anatomically challenging conditions such as horseshoe kidneys, RIRS demonstrates superior adaptability and effectiveness While direct statistics for RIRS specifically targeting 6 mm PUJ stones are limited, the general success rate of RIRS for kidney stones supports the expectation of high stone free rates (SFRs) for such cases, adjusted for individual clinical scenarios Thus, RIRS stands as the preferred method for managing 6 mm PUJ stones, balancing efficacy, safety, and patient outcomes
Emergency SWL (eSWL) (Christian Tuerk)
In EAU-Guidelines shock wave lithotripsy is the first choice for interventional stone removal of up to 1 cm stones both, in the kidney pelvis and in ureter promising less invasiveness and complications but lower stone free rates (SFR) compared to endourological procedures To
address the current case of a 6 mm PUJ-stone the literature was examined with the question of the possible advantage of an early therapy
Back in 2014 Sarica et al showed in a retrospective case study that there is a highly significant relationship between ureteral wall thickness and the success rates of SWL (16)
The ureter wall thickness is a sign of impaction and depends on time A prospective randomized study comparing early (emergency) SWL with delayed treatment shows an impressive advantage of the eSWL over delayed SWL in both the SFR and the efficiency quotient after 1 day, 1 week, 1 month and 3 months (17) In 2023 a meta-analysis evaluating the efficacy of eSWL treating ureteral stones showed that SFR was statistically significant higher and faster in eSWL group with significant less auxiliary procedures (18) A matched-pair-analysis in 2021 from Switzerland compared immediate SWL vs delayed SWL after emergency stent insertion, including patient with PUJ-stones; e-SWL or stent respectively was performed within 48 hours after first presentation of patient; in this study once more SFR of 6-9 mm stones was significantly higher with lower reintervention rate compared to stent+delayed SWL (19)
In conclusion, the 6 mm obstructing PUJ-stone is definitely a case for emergency SWL showing low invasiveness, less complications and has much better results compared to delayed treatment, resulting in less loss of working days and being possible as an outdoor procedure depending on national health care
Technical issues of urinary stone management
Patients on anticoagulants (Hichem Kouicem)
In chronic anticoagulant users undergoing surgery, bleeding and thromboembolism are common and serious complications
There are two main classes of oral antithrombotic drugs: antiplatelet drugs (aspirin) and oral anticoagulants, including vitamin K antagonists (VKA) and direct-acting oral anticoagulants (DOAC) (Table 2)
The bleeding risk is associated with type of stone surgery and procedure as extracorporeal shock wave lithotripsy
Table 2.
Antithrombotic drugs
Anticoagulants agents V itamin K antagonists (VKA) Warfarin
Direct-acting oral anticoagulants (DOAC) Direct thrombin inhibitors Dabigatran Direct Xa inhibitors Apixiban Endoxaban Rivaroxaban
A Papatsoris, A Budia Alba, J A Galán Llopis, et al
(ESWL), percutaneous nephrolithotomy (PCNL), and open surgery
In case of low bleeding risk, the evidence suggests that VKA might not be stopped
Urgently needed surgery must take place under full antiplatelet therapy despite the increased bleeding risk
For high thrombotic risk, VKA must be stopped 5 days before surgery with bridging using full-dose of > lowm o l e c u l a r - w e i g h t h e p a r i n ( L M W H ) o r u n f r a c t i o n a t e d heparin (UFH) started 3 days before surgery LMWH or UFH will be stopped respectively one day and 4 to 6 hours before surgery VKA will be resumed 12 to 24 hours after the procedure For urologists, surgery performed on a patient under anticoagulant treatment led to manage the Risk-Risk Balance between bleeding and thromboembolism (20)
Antibiotic resistance (Adam Halinski)
UTIs are becoming increasingly difficult to treat owing to the rapid spread of drug resistance among Gram-negative organisms UTIs are at the forefront of the antibiotic resistance problem because 9% of all antibiotic prescriptions in the ambulatory setting in the USA are done for the treatment of UTI The problem is related to broadspectrum antibiotics that have been the drug of choice to treat both community- and hospital-associated UTIs
The increase of antibiotic resistance and appearance of multi-drug resistant (MDR) pathogens in the course of UTI is related to high rates of inadequate antibiotic empirical therapies prescribed without the antibiotic susceptibility testing and finally resulting in an ineffective UTI treatment
The risks of multi-drug resistant pathogens are: recurrent UTIs (21), hospitalization, age, genitourinary disturbances, prior use of antibiotics (22, 23), increased use of broadspectrum antibiotics leading to increased antimicrobial resistance and multi-resistance of bacteria (24)
Health care practitioners should be educated on the suitability of urine culture and should read the literature to compare it with local resistance rates Rapid molecular tests could shorten the waiting time for urine culture
Development of new antibiotics and probiotics can decrease the resistant rate On the other hand, antibioticsparing therapeutics including small-molecular inhibitors of bacterial adhesion, immunomodulatory therapy that alters the host response to infection and vaccinations against microbial targets could also be helpful
I n c o n c l u s i o n s , p r e - i n t e
e n t i o n a l u
n e c u l t u r e i s mandatory Antibiotic therapy is important in the UTI treatment but in recent years it is becoming more challenging due to increasing resistance to routinely applied antibiotics The use of an intrarenal urine culture and stone culture is recommended to adapt antibiotic therapy in case of postoperative infectious complications
Zero radiation ultrasound guided PCNL (Mohammed Alameedee)
PCNL is wide world used operation to remove renal stones , fluoroscopy is used as a guidance for PCNL, but it is limited by the risk of radiation, so ultrasound-guided PCNL is an option to replace fluoroscopic guidance avoiding the limitation of X-ray exposure It has multiple advantages with respect to fluoroscopic guidance as no
radiation, imaging of structures between skin and kidney to assess depth of the access needle and prevent organ injury , no need for contrast media (especially in case of failure of retrograde pyelogram due to difficult ureteric catheterization), safety in pediatric and pregnant patients, feasibility in supine position with no need for lithotomy position and ureter stent fixation, and cost-effectiveness
On the other hand, ultrasound guided PCNL is challenging to the surgeon because it needs good eye hand coordination with long training curve and because it can be difficult when perinephric fat make the identification of access needle tip difficult by ultrasound, especially in obese patients Hydro dissection can be used to overcome these difficulties by injection of normal saline through the access needle along the tract from skin to target calyx to dissect muscle layers and fatty tissue by saline which leads to easy identification of needle Optical hydro dissection allows easy identification of the access needle with concomitant continuous optical control by use of a 2 mm telescopic lens incorporated into an access needle associated with pressured saline infusion which dissect tissue layers along tract from skin to target calyx
Ultrasound-guided PCNL is an option to replace fluoroscopic guidance avoiding the limitation of X-ray exposure It has also multiple advantages as imaging of neighboring organs, no need for contrast media and ureteral catheterization safety in pediatric and pregnant patients and cost-effectiveness Optical hydrodissection by use of a 2 mm telescopic lens incorporated into an access needle allows easy identification of the needle with concomitant continuous optical control
Tubeless PCNL (Elenko Popov)
In the last decades, percutaneous nephrolithotomy (PCNL) experienced enormous technical advancements like miniaturization of the available armamentarium (2) To further decrease the invasiveness of this procedure, safety and efficacy of different exit strategies like the tubeless PCNL technique have been explored The presence of nephrostomy tube has several advantages potentially lowering complications rate as maintaining renal drainage, allowing for reintervention if needed; avoiding urine extravasation; and preventing continuous bleeding by compressing the dilatation tract Conversely, it also has significant drawbacks: prolonging hospitalization; increasing postoperative pain score and analgesic requirements; not being so suitable for ambulatory/day-case surgery
A significant problem in comparing use of nephrostomy after PCNL with tubeless PCNL in the literature is the standardization of nomenclature! Series can be different depending on type of PCNL (standard, mini, super-mini, micro, nano), characteristics of patients and stones, and types of nephrostomy (tube, small-bore tube, tubeless, not so tubeless, almost tubeless, totally tubeless) However, all meta-analyses comparing standard and tubeless PCNL reach similar conclusions (25-28): the key to effective outcome with tubeless PCNL is appropriate patient select, tubeless procedures are considered safe and effective in lowrisk patients, most of reported studies conclude that a tubeless procedure is associated with less patient discomfort and shorter hospital stay compared to the standard PCNL, the complication rate, including postoperative fever, haemat-
ocrit decrease, stone-free rate and urine extravasation usually did not differ between the different exit strategies
However, all of them report a risk of bias due to high heterogeneity of results
In conclusion, tubeless PCNL has several advantages and is relatively safe, but it may involve great risks if the patients are not carefully selected Therefore, the indications should be strictly controlled, and the technical requirements are relatively high The tubeless PCNL must also be implemented by experienced surgeons
Choice of Laser for Lithotripsy
(Elenko Popov)
The development of laser technologies is one of the main prerequisites in modern endourology Massive breakthroughs were achieved in the last years by second generation Holmium-YAG, Thullium fibre laser, pulsed Thulium laser (29-31)
The ideal laser for lithotripsy should be effective, safe, multitasking, fast, noiseless, ergonomic, and cost-effective
New Ho:YAG technologies as high power, high frequency and pulsed modulations have shown promising results for lithotripsy by reducing retropulsion with good ablation efficiency High peak power makes it particularly good for percutaneous nephrolithotomy High intrarenal temperatures and choice of correct setting are still concerning points Thulium fiber laser (TFL) has arrived to be one of the main players in flexible ureteroscopy Being highly efficient and quick, and by producing micro-dusting the laser is quickly heading to become a gold standard The new pulsed Thulium YAG is the newest laser
For now, only in-vitro studies show promising results with efficient lithotripsy As the peak power lies between Ho:YAG and TFL it may be able to adequately perform when needing high and low power lithotripsy
Pressure and temperature during RIRS (Syed Jaffry)
The review of temperature and pressure measurements during Retrograde intrarenal surgery (RIRS) highlights crucial insights and challenges inherent to the procedure These measurements are vital for ensuring patient safety and optimizing surgical outcomes, yet they present specific difficulties that demand a careful and informed approach
The challenges associated with accurately measuring and interpreting temperature and pressure levels during RIRS can significantly impact the procedure's efficacy and the patient's postoperative recovery Recognizing these challenges is the first step towards mitigating potential risks and enhancing the overall success of the surgery
To address these issues effectively, it is essential to focus on refining measurement techniques and developing novel methods for data analysis This includes improving the precision of intraoperative measurements and exploring advanced approaches for interpreting this data in realtime Moreover, establishing a clear correlation between these intraoperative metrics and long-term patient outcomes is crucial for validating the effectiveness of RIRS procedures
Collaboration between urologists, engineers, and data scientists is critical for advancing this field Together, they can work towards creating integrated systems that facilitate the seamless collection, analysis, and visualization of crucial surgical data Such systems would not only improve the
accuracy of temperature and pressure measurements but also enhance the decision-making process during RIRS
In the interim, adherence to current practices such as the use of Ureteral access sheaths (UAS) with or without suction devices, continuous fluid management monitoring, and the emphasis on surgeon skill development remain pivotal
These practices, alongside the optimal duration of surgery and a personalized approach to patient selection and procedure planning, are essential for maintaining the standard of care in RIRS Future research should thus prioritize these areas to ensure continued improvement in patient care and surgical outcomes in the realm of urology (32)
Urinary stent technology (Federico Soria)
The three pillars of stent improvement are the development of new biomaterials, new coatings, and new stent designs
Furthermore, the development of drug eluting stents is a topic on which many research groups are working
About the coatings, the aim is to prevent the formation of biofilm, which is associated with asymptomatic bacteriuria and urinary tract infection, as well as the encrustation of stents One fact researchers must be aware of is the severe antimicrobial resistance surveillance in Europe policy
The aim is to coat stents with substances that prevent the adhesion of bacteria and crystals on their surface To this end, different strategies have been developed, the most promising being the development of antimicrobial peptides with bactericidal capacity (33)
The great innovation in ureteral stents is mainly the development of research lines about drug-eluting stents The main idea in this topic is that the stents, in addition to improving urinary drainage and scaffolding, can perform other functions such as local drug delivery This could be in the near future with different applications There are experimental studies on drug-eluting stents releasing Rapamycin, Paclitaxel or Pirfenidone to inhibit relapse of ureteral strictures after endoureterotomy, in relation to inhibition of the mTOR pathway or reduction of TGF expression which inhibits collagen deposition (34, 35) In this regard, our research group developed a new coated mitomycin-eluting biodegradable ureteral stent for intracavitary instillation as an adjuvant therapy in upper urothelial carcinoma (36)
Thus, the development of drug-eluting stents is the near future, aiming to reduce the adverse effects of stents and to topical drug delivery to avoid systemic drug administration, thereby reducing complications
Bioresorbable stents (Federico Soria)
Unfortunately, the ideal ureteral stent has not yet been designed Nevertheless, several authors have outlined its characteristics very well, one of the features is related to ease of insertion and removal Obviously, the answer to easy removal is not having to remove them, which means that they would be biodegradable
The characteristics of an ideal biodegradable ureteral stent (BUS) should be: excellent biocompatibility; moderate mechanical properties; complete degradation without obstructive fragments; prevent migration; good flexibility for stent placement; radiopacity; visibility on ultrasound; controlled degradation rate; no mutagenic, antigenic, and carcinogenic activity; no degradation with toxic metabolites (37)
A Papatsoris, A Budia Alba, J A Galán Llopis, et al
About the current limitations to BUS development, there are some main points to improve
Degradation rate control: one of the most important factors in BUS development is the ability to control the degradation rate in order to develop a stent that will have the required duration
Biomechanical properties control: the balance between degradation and scaffold is very difficult to achieve
Fragmentation size control and non-obstructive fragments release: this is another essential requirement and has been the reason why the first BUS designs were not successful, as the degradation of the stents was often obstructive New designs, have managed to overcome this drawback thanks to the use of polymers and copolymers with different degradation rates
There are different research groups working on BUS Our research group has been developing a BUS for the last few years BraidStent is a braided stent made of synthetic polymers and copolymers that are degradable by hydrolysis This allows the suitable degradation rate, without obstructing fragments and the adjustment of degradation according to the needs of the individual patient (38, 39)
To summarize, it is certainly not a fiction Researchers have greatly improved BUSs and preclinical studies have already yielded very positive results In my opinion, the glass is half full and getting fuller
Complications of surgical stone treatment
Complications of PCNL (Hammad Ather)
Of the three minimally invasive surgical options (Shock wave lithotripsy/SWL, flexible ureteroscopy/fURS and percutaneous nephrolithotomy/PCNL), in the management of urolithiasis, PCNL is considered as the most invasive although it has high efficacy particularly for intermediate and large stones including staghorn calculi
In a review paper, Seitz et al (40) indicated that although no deviation from the normal postoperative course (Clavien 0) was observed in 76 7%, the rest had complications of various grades including death in 0 04% The two major most common complications include septic complications and bleeding Fever, and sepsis were observed in 11 and 0 5% respectively The bleeding related complications with need for transfusion and embolization were observed in 7 and 0 4% respectively Authors observed a wide variation in reporting of these complications in the absence of a specific tool for reporting procedure specific morbidity Clavien system is widely used to report urological complications, however, procedure specific scoring is more desirable In a paper published by de la Rosette et al (41) Authors observed that Clavien classification demonstrates high validity although inter-rater reliability is low for minor complications
Abdominal organ injury including colonic, splenic, liver, gall bladder and bowel injuries are fortunately quite rare but are associated with significant morbidity In a systematic review Ozturk et al (42) reported 51 colonic injuries out of 13000 patients undergoing both supine and prone PCNL All gall bladder injuries necessitated cholecystectomy, whereas liver injuries were mostly amenable to conservative treatment Laparotomy and diversion are rarely performed for colonic injuries, particularly in the absence
of signs of peritonitis Major bleeding complications are managed by embolization
In conclusion, PCNL related major complications are not frequent but significant Improvement in technique, equipment and better understanding have improved the outcome There is a downward trend in the incidence, but also most of the complications are managed conservatively
Management of PCNL complications (Alberto Budia Alba)
PCNL is a minimally invasive surgical technique, but it is not free of complications The reported complication rate is approximately 23 7% (40) Although the most frequent is fever (10 8%), serious complications can occur such as pleural lesions (1 5%), sepsis (0 5%), organ injury (0 4%) and even death (0 05%)
Perhaps, the best way to avoid them is to try to prevent t h e m
depending on the patient's position, adequate bridging treatment of anticoagulated or anti-aggregated patients, and preoperative cultures that allow the patient to arrive at surgery with sterile urine are effective measures to reduce the probability of complications
The complications of this technique are divided into intraoperative and postoperative Intraoperative complications can be prevented by accurate access through the calyceal papilla and performing delicate maneuvers in the dilation of the tract, which reduces intraoperative bleeding The use of a safety guide allows, in the event of failure to reach the urinary system, a new access using the safety guide without the need to re-puncture In case of perforation of the urinary tract during dilation, if the perforation is small, treatment can be completed, but if the leak is significant, it should be postponed after insertion of an urinary diversion The hydrothorax should be managed with pleural drainage; colon perforation, if it is intraperitoneal, requires surgical repair and, if it is extraperitoneal, it can be managed conservatively with urinary and retroperitoneal drainage
The most feared postoperative complication is urinary sepsis, more frequent in insulin-dependent patients, women and in case of large and infective lithiasis (43) An early identification and treatment is the key to a good therapeutic response
The second most serious postoperative complication is late hemorrhage, secondary to a pseusoaneurysm or arteriovenous fistula, which in most cases requires angioembolization
Therefore, although PCNL is a minimally invasive technique, it is not free of complications, some of them potentially serious, which should be identified early and treated properly
Complications of URS (Juan Pablo Caballero)
Ureteroscopy (URS) is a technique with a low frequency of severe complications (44, 45) But some complications can cause real nightmares We must emphasize the importance of complications generated by ureteral catheters Never place ureteral stents unnecessarily after ureteroscopy
We can identify URS-related complications until more than 6 months later Some of those that, due to their severity, we must avoid and know how to treat are those dependent on high pressure in the urinary tract, sepsis of
urinary origin, renal bleeding, and those secondary to applying excessive force to the urinary tract, as ureteral avulsion and ureteral stricture
Sepsis occurs more frequently in patients with a positive preoperative urine culture Therefore correct prophylaxis, or treatment, guided by the antibiogram and knowledge of local antibiotic resistances is mandatory Sepsis will occur more frequently if we exceed intrapelvic pressure levels greater than 30 mmHg
High pressure can also lead to bleeding from the renal parenchyma that will cause flank pain and a drop in hemoglobin levels Treatment will usually be by selective embolization of the renal parenchyma
One of the most devastating complications is ureteral avulsion, which can be proximal and/or distal (46, 47) Thinner or less compliant ureters are more sensitive to these complications, especially if we use larger caliber ureteroscopes
Urgent surgical repair by laparoscopy is essential
Ureteral stricture can occur up to 7 months after the intervention It requires a high degree of suspicion after ureteral injuries or impacted stones For its diagnosis we need imaging and functional tests, such as the isotopic renogram
ECIRS: indications and complications (Luis Llanes)
Endoscopic combined intrarenal surgery (ECIRS) combines retrograde and antegrade approaches using both flexible and rigid endoscopes for treating large or complex renal stones (48)
It was first described by Gaspar Ibarluzea in 2007 (49) and after, Cesare Scoffone created the acronym ECIRS (endoscopic combined intrarenal surgery) in 2008
The indications of ECIRS can be summarised in two (48):
1 To treat staghorn or complex kidney stones and limit the number of percutaneous accesses
2 To treat simultaneous multiple kidney and ureteral stones or an impacted pelvic stone
The modified supine position by Galdakao is the most extended patient position to do an ECIRS because two simultaneous surgeons are working and helping each other with total access to the urinary tract
Complications can potentially occur in the procedure: during access, procedure or exit process, and can be classified according to the modified Satava classification system (50):
• Grade 1: an error without consequences
• Grade 2a: an error was identified and corrected immediately with endoscopic surgery intraoperatively
• Grade 2b: a complication treated with endoscopic surgery in another operative session
• Grade 3: a complication that requires open or laparoscopic surgery
The postoperative complications of ECIRS, according to the Clavien-Dindo classification, are the same as in percutaneous nephrolithotomy (PCNL): haemorrhagic, infectious, obstructive, splanchnic injuries, infundibulum stenosis, surgical material retained and renocutaneous fistula Different metaanalyses and systematic reviews comparing ECIRS with PCNL for large and complex kidney stones show that overall complications, severe complications, postoperative fever, haemoglobin decrease, transfusion rate and Clavien Dindo complications are always in favour of ECIRS (51, 52)
Diagnostic work-up
Genetic testing (Giovanni Gambaro)
Genetic testing in nephrolithiasis patients consents the diagnosis of known genetic conditions causing stones and previously unknown gene causing renal stones
Many of the monogenetic diseases thus identified can develop CKD/end-stage renal disease and/or metabolic bone disease In this case, the genetic diagnosis has prognostic implications and is helpful for the prevention of nephropathy and osteopathy Few monogenic diseases identifiable with genetic testing also have specific therapies for personalized/precision therapy This is the case of primary hyperoxalurias, 1 25-(OH) D-24 hydroxylase deficiency- infantile hypercalcemia In the future, other therapies may be able to cure some other genetic defects causing nephrolithiasis Their identification is essential H
nephrolithiasis patients should undergo genetic testing
In studies in which genetic testing was systematically carried out to diagnose Mendelian diseases causing nephrolithiasis, the most frequent diagnosis was cystinuria
This is a diagnosis that can be made much more quickly and at much lower costs with the analysis of the morphology and composition of the stone, with the dosage of urinary cystine, with the observation of typical crystals in the urinary sediment, and finally, during a procedure of laser lithotripsy with the typical odor that emanates
Frequent genetic diagnoses can also be formulated based on specific easily determined laboratory test patterns (e g , distal renal tubular acidosis)
On the other hand, for the majority of monogenic diseases causing nephrolithiasis, there are no specific therapies
Another point to consider is that the prevalence of genetic nephrolithiasis in adult nephrolithiasis patients is lower than reported If cystinuria, APRT deficiency, and xanthinuria are excluded from the series in which genetic tests have been performed, a maximum of 4% of nephrolithiasis patients in tertiary reference centers are affected (53-55) If we move from the super-selected case series of tertiary reference centers to the general population of adult stone patients, less than 1% of them are carriers of genetic mutations other than cystinuria (56)
The success in identifying cases of genetic nephrolithiasis is the direct consequence of selecting cases with clinical characteristics that make one suspect its existence (Table 3) (57) It is in these adults that it is reasonable to per-
Table 3.
Warning elements on a possible genetic origin of nephrolithiasis
Early onset
Family cases
Consanguineous parents
Highly-active stone disease (bilateral, multiple stones, frequently recurrent)
Associated nephrocalcinosis
Renal hyperechogenicity
Tubular dysfunction and related manifestations (statural growth deficit, polyuria, bone disorders)
Particular stone composition and crystalluria (whewellite, cystine, dihydroxyadenine, xanthine)
A Papatsoris, A Budia Alba, J A Galán Llopis, et al
form genetic testing Since childhood age is one of the main elements for suspecting genetic stones, it is rational to carry out genetic tests in all children
Stone analysis (Alberto Trinchieri)
According to EAU guidelines (2), after stone passage a reliable stone analysis by infrared spectroscopy or X-ray diffraction is mandatory AUA guidelines (58) confirmed that, when a stone is available, a stone analysis should be obtained at least once A consensus conference (59) pointed out that infrared spectroscopy or X-ray diffraction to identify mineral types should be preceded by examination of the stone under a stereomicroscope to assess which part (or parts) of the stone should be taken for molecular analysis
Visual identification of stone morphology requires a skilled observer, therefore development of methods for evaluation of stone morphology are highly desirable
Examination of whole stones provides insight into how the stone has formed and grown, which is partly lost when examining a few fragments extracted from the urinary tract after lithotripsy
Unfortunately, in real-life some stone centers still perform the chemical examination of the stone and not all laboratories that perform the spectroscopic examination fulfill the quality requirements (60)
The analysis of digital images of stones by deep convolutional neural networks could allow the classification of stones based on their color and texture This technique can be used in the laboratory for the analysis of photographs of stones or fragments extracted from the urinary tract, but above all for the classification of stones during endoscopic examination in the operating room
Stone examination allows the diagnosis of rare stones such as cystine, dihydroxyadenine and xanthine stones; the diagnosis of stones with specific etiology such as uric acid, sodium or ammonium urate, struvite and brushite stones; the differentiation of subtypes of calcium stones (calcium oxalate monohydrate, calcium oxalate dihydrate and carbapatite); to provide information on the components of mixed stones
Stereoscopic microscopy (petroscopy) or the analysis of digital imaging allows the identification of subtypes of calcium oxalate or calcium phosphate stones with morphology associated with a specific etiology such as primary hyperoxaluria (COM 1c), enteric hyperoxaluria (COM 1e), renal tubular acidosis (Carbapatite type IV a2), struvite (type IV c) and brushite (type IV d) (61)
Endourological stone observation (Elenko Popov)
The analysis of the stone is a crucial step of the work up of renal stone forming patients as it provides relevant information on the pathogenic mechanisms of renal stone formation The analysis of the stone can be performed only after the spontaneous expulsion of the stone or its fragments or after its surgical removal Many efforts have been made to develop imaging modalities able to reliably diagnose in-vivo the physico-chemical composition of the stone before the procedure of stone removal
The increasing efficiency of lasers in “dusting” and “ popcorning” modes and the improved performance of endoscopic devices led to smaller stone fragments, which
reduce the accuracy of the stone analysis (microscopic morphology and infrared spectroscopy) by the lack of components representativeness considering that 48 6% of the stones have a mixed composition (62) Moreover, Keller et al (63) recently showed the impact of laserbased dusting on changes in stone composition with significant changes in the infrared spectra (particularly for weddellite, carbapatite, struvite, and brushite)
Consequently, examination by infrared spectroscopy of the stone powder by itself could not provide sufficient information of stone composition
This finding reinforces the need to observe the morphology of the stone before laser-induced destruction to preserve an etiological approach The examination should includ a visual observation of the stone surface first, before laser fragmentation, then visual observation of the section and the nucleus after laser stone section Endoscopic stone observation is feasible but necessitates significant experience, specific expertise, and training Even in in these optimal conditions the rate of concordance of endoscopic examination and microscopy is 80-90% for whewellite (Ia or Ib = 85%, Id = 92%, n = 12; Ie = 80%), 85% for weddellite (IIa or IIb = 85%), 91% for uric acid (IIIa or IIIb), 50% for carbapatite-struvite association (IVb), and 65% for brushite (IVd) (64)
The results of a multi-center expert setting (65), more resembling the real-world scenario, including 32 clinicians from 9 different countries, with significant expertise shows overall accuracy 39% (250 out of 640 predictions), with calcium oxalate dihydrate stones correctly detected in 69 8%, calcium oxalate monohydrate in 41 8%, uric acid in 33 3%, calcium oxalate/uric acid in 34 3%, cystine in 78 1% Precision rates for struvite (15 6%), calcium phosphate (0%) and mixed calcium oxalate/calcium phosphate (9 3%) were quite low
There is a significant tendency for improvement in endoscopic stone recognition in the future: advances in endoscope technology, such as Raman spectroscopy, polarization endoscopy and hyperspectral imaging; advances in digital technologies; potential implementation of artificial intelligence (AI) technologies for automated endoscopic stone recognition On the other hand, problems still need to be solved as bias in generating datasets, mathematical methods weaknesses, mixed stones, and significant difference between ex-vivo and in-vivo
In conclusion, the information that can currently be obtained from endoscopic observation of the stone is limited, as even expert surgeons may not be able to reliably predict the composition of the stone However, the imminent future technological innovations should allow an accurate prediction of the composition of the stone in its different components, thus adding information to that obtainable with the post-op analysis of the fragments after lithotripsy
For this reason, it should be emphasized the importance of an accurate description of the stone in the report of the endoscopic procedure that should be always accompanied with a photograph or video clip of the stone Urology residents should receive a specific training on the macroscopic aspect of urinary stones and should be encouraged in endoscopic recognition of the most frequent types of renal stones
Desktop scanning electron microscopy for urinary stones (A Costa-Bauzá)
Scanning electron microscopy (SEM) is a non-destructive technique that in the backscattered electron mode provides information about the three-dimensional structure of surface or sections of a kidney stone and a very clear characterization of crystals morphology
The methodology currently used for SEM consists of placing the stone on a sample holder, with no need to cover with gold After observation, the sample is in the same state as before SEM analysis Furthermore, SEM can be used with auxiliary techniques, especially X-ray scattering analysis energy dispersive spectrometry (EDS) This provides reliable data on the elemental composition of a specific point or a general area of a stone (66-68) A substance present in minute quantities, even at trace level, that is not detectable by IR spectroscopy can be identified Currently EDS can detect C, N and O, important elements for uric acid and ammonium urate identification
Thus, SEM-EDS can provide information about the:
- morphology of crystals in the stone allowing their unequivocal identification
- internal structure with location of crystalline phases and minor components
- identity of the initial area of calculus formation
- changes in the crystalline shape or composition
Currently, many renal calculi are fragmented prior to analysis, which implies a partial loss of information However, with stereoscopical microscopy, several representative fragments can be selected, and then use SEMEDS to provide additional information for determining stone etiology
Therefore, together with stereoscopical microscopy and IR spectroscopy, SEM-EDS is a fundamental tool for the study of kidney stones, and the information it provides has great clinical and practical importance SEM will be used more in the future due to the development of desktop models that are easy to use, more affordable, and provide results with the same quality as larger and more expensive models
Urinary and intestinal microbioma (Juan A Galán-Llopis)
Oxalobacter formigenes that has been largely studied in relation to its role in degrading oxalate and referred to as the main link between gut s microbiome and urinary stone disease However, not every species of Oxalobacter are related to stone disease and the latest studies suggest that the entire gut microbiome (GMB) seems to be involved in the pathophysiology of urolithiasis, and can have different roles supported by the presence of some short chain fatty acids, that will protect gut´s epithelium, also having an anti-inflammatory effect GMB dysbiosis exists in the kidney stone forming patients (more bacteroides, E Coli and shigella, less prevotella-9) and in order to restore this microbiome and prevent kidney stone formation, several measures including rational use of antibiotics, probiotic preparations and adjusted diet, and fecal microbial transplantation can be accomplished (69-72)
Urine is not sterile and some microorganisms, the urobiome, different in stone formers and healthy individuals, can be detected by the combination of metagenomic
analysis using Next generation sequencing (NGS) techniques (Amplicon, Shotgun) and the enhanced quantitative urine culture (EQUC) protocol (73) Differences between the stone and urine microbiota have been described, and that may indicate that certain bacteria contribute to urinary stone disease pathophysiology The microbiota of upper tract and bladder urine are similar, but there are differences between stone and urine microbiota, with a significant decrease of microbiota diversity in stone formers Urobiome can be regulated by pro and prebiotics, diet, and with immunomodulators Consensus will allow for proper future studies on urobiome research
Urinary pH (Juan A Galán-Llopis)
Urinary pH in humans shows a circadian rhythm and can be affected by different situations including diet, drugs, stress, gender, and genetic and metabolic diseases Apart from the balance between urinary stone promoters and inhibitors, both the time that the urine is within the urinary tract, and the urine pH are needed to form a stone A high urine pH (> 6 2), independent of diet, and hypocitraturia are the most important risk factors for calcium phosphate stones, especially in women (74) Fasting urine pH > 5 8 non-responding to acidification, associated to hypercalciuria, hypocitraturia, and the presence of apatite or brushite stones should direct suspicion to incomplete distal renal tubular acidosis (RTA) (75) Low urine pH (< 5 5), low urine volume and high uric acid (UA) osmolality will lead to UA stone formation (76) Cystine is highly soluble at urine pH higher than 7 5 The only stones that seem independent of urine pH are papillary calcium oxalate monohydrate (COM) and 2 8 dihydroxyadenine Urine pH should be properly measured with laboratory pH meters, preferably within two hours of collection and after 12 hours fasting, or else with a digital pH meter (Lit-Control) several times a day (fasting, and after meals) (77) A correct pH measurement will allow to treat and monitor the patient with prophylactic alkalizing drugs (potassium citrate, sodium bicarbonate) and/or preventing uric acid stone formation or increasing its dissolution with theobromine (78), and/or decreasing uric acid in urine with allopurinol/febuxostat Urine acidification can be achieved by using L-methionine and or ammonium chloride Phytate is the correct choice for kidney stones prevention whenever pH is neutral
24 Hour urine analysis (Dirk Kok)
Twenty-four hour urine analysis has a place during patient intake and during follow-up
Analysis of crystalluria can reveal the stone type which helps choosing preventive treatment and determining which urine parameters are relevant to monitor
For stones that are formed due to excessive crystal formation inside the nephron followed by plug formation (cystine, xanthine, uric acid, slightly soluble drugs, hyperoxaluria related calcium oxalate) the presence of the specific crystal type and the size of the crystals tell if the renal conditions in the patient are inducive of stone formation or not (79)
Treatment will be aimed at maintaining a low excretion rate for the stone components and at maintaining urine pH in a range where the solubility of the specific com-
A Papatsoris, A Budia Alba, J A Galán Llopis, et al
pound is high Urine analysis should comprise those factors
Most stones will consist of calcium oxalates and/ or calcium phosphates For these stones the relevant urine parameters are calcium, oxalate, phosphate, citrate, magnesium and pH These should be measured at patient intake, after stone removal and at the start of treatment
Treatment will consist of medication (e g alkali), drinking advice and lifestyle advice (80) Dietary advice includes avoidance of high oxalate content foods and balanced intake of protein (acid load) and fruit/vegetables (alkali load) (81) Urine pH and citrate content give information on the acid/base balance and the risk of forming calcium oxalate aggregates (82)
Finally, all stone formers will benefit from a drinking advice Monitoring urine volume always makes sense for all patients
Of course, the big catch in this is patient compliance (83) It is difficult to follow lifestyle advice especially when your problem of stone formation started decades earlier and everything at present appears to be normal (84) For this large group of patients, the most sensible manner of follow up will be to provide means for measuring urine volume (actual measurement of looking at the color) and measuring urine pH at home
Urinary Supersaturation Revisited:
A proposal for a simpler indicator of stone risk (Allen Rodgers) Despite shortcomings, urinary supersaturation (SS) is the most comprehensive of the numerous physicochemical risk factors employed in urolithiasis research (85) SS for calcium oxalate (CaOx) stones depends on the concentrations of free unbound calcium [Ca2+] and oxalate [Ox2-] species These species in turn depend on the speciation and pH of the urine solution itself As such, pH is correctly considered as an indirect measure of SS and a crucial indicator of stone risk Indeed, a commercially available meter for home use is available for measuring urinary pH in stone patients undergoing therapy (86) Urinary pH levels which should be targeted by the patients for reducing the risk of CaOx, calcium phosphate and uric acid crystallization are provided Given that lowering SS of CaOx is a strategic goal in the administration of therapeutic and prophylactic preparations, it is instructive to revisit the physicochemical aspects of this important urinary property and to recognize the aforementioned primary influencers of stone risk [Ca2+] and [Ox2-] Of these, the latter has been shown to be the limiting factor in CaOx crystal formation in urine (87) As such, stone formation is much more sensitive to changes in [Ox2-] than [Ca2+] Unfortunately, measurement of [Ox2-] cannot be routinely achieved Measurement of [Ca2+] is also difficult but easier It is proposed that the manufacturers of the pH-measuring device for home use consider incorporating a Ca-ion sensitive electrode into their current design to allow patients to monitor urinary pH and [Ca2+] simultaneously, notwithstanding that the factors are not independent
This will provide a double-check of risk leading to a more comprehensive assessment of treatment efficacy and risk of stone recurrence
Are there clinical applications of macromolecular stone promoters and inhibitors? (Allen Rodgers)
A major challenge for researchers investigating the possible role of urinary macromolecules (UMMs) as promoters or inhibitors of kidney stone formation is that many of these molecules play both roles depending on the chemical composition and properties of the urine in which they are operating (88, 89) Well known examples include Tamm-Horsfall protein which has been shown to promote and inhibit calcium oxalate (CaOx) aggregation depending on its degree of desialylation and osteopontin which in its phosphorylated form inhibits CaOx nucleation and aggregation (in different CaOx hydrates) but promotes aggregation in its phosphorylated -deficient form Besides acting on crystallization processes per se, urinary macromolecules also are able to influence crystalcell and crystal-crystal attachment processes, each one of which can modulate aspects of the stone formation process
Their activity depends on urine environment and the nature of crystal and cell surfaces Additionally, presence and absence of chemical, structural and conformational defects, increased or decreased expression, and the difficulty of finding consistent reproducible results from various experimental models exacerbate the challenge Given this myriad of factors which requires untangling and characterization, it seems unlikely that methods for controlling them by optimizing some and minimizing others is imminent At this stage, it is suggested that there are no realistic clinical applications of urinary macromolecules in stone management or prophylaxis
Nephrolithiasis as a systemic disorder (Bernhard Hess)
There is increasing evidence that many renal stone formers (SF) exhibit ‘non-urologic’ systemic metabolic abnormalities such as metabolic syndrome (MS), cardiovascular disease or bone disease A disease is defined as systemic if several organs/tissues or the whole body are affected (90) We analyzed additional anthropometric/metabolic data obtained from 531 non-selected consecutively referred renal stone formers, originally investigated for the prevalence of incomplete distal renal tubular acidosis (idRTA) (75)
Among them, 139 were primarily classified as having systemic disease: 8 cystine stone patients, 66 calcium stone formers with various secondary causes (bariatric surgery, primary hyperparathyroidism, inflammatory bowel disease, medullary sponge kidney, treatment with carboanhydrase inhibitors or HIV medication, glomerular disease) and 65 calcium stone formers with idRTA
The remaining 392 SF (320 idiopathic calcium, 63 uric acid, 9 infection SF) were screened for the following markers of systemic disease: 1) full MS or 2) traits thereof, 3) LDL-cholesterol > 3 0 mmol/l and 4) proteinuria > 150 mg/d as marker of cardiovascular risk, 5) very low urine volume < 1 2 L/d, likely due to reduced thirst sensitivity, and 6) low bone mass without idRTA
Only 3/63 (5%) of uric acid SF (UA-SF) were without any marker of systemic disease, compared with 39/320 (12%) of idiopathic calcium SF (ICSF), p < 0 0001
Among infection SF, only 1 out of 9 was without systemic markers
Table 4.
of systemic diseases in idiopathic calcium vs uric acid stone formers
A direct comparison of Idiopathic calcium vs uric acid stone formers is depicted in Table 4
Two or more systemic markers of systemic disease were more often present in UA-SF (49/63, 78%) than in ICSF (183/320, 57%), p < 0 0001 Overall, only 43 of 531 non-selected SF (8 1%) were without markers of systemic disease
The following conclusions can be drawn: 1) Nephrolithiasis should be considered a systemic disease, as 92% of SF exhibit markers of systemic disease 2) Recurrent CaSF and UA-SF should primarily be referred to internists or nephrologists for evaluation not only of urine chemistries, but systemic pathologies such as MS or traits thereof, elevated LDL-C, overt proteinuria, hyperparathyroidism, incomplete dRTA, bone disease, medullary sponge kidney, inflammatory bowel disease, bariatric surgery and lithogenic drugs
Screening of high-risk stone formers (Alberto Trinchieri)
Some renal stone formers are considered "high-risk" due to the high tendency to relapse with a consequent increased risk of obstructive episodes and surgeries which can cause a damage of renal function
In general, non-calcium stones have the greatest tendency to recur, although some subgroups of calcium stones also have high recurrence as calcium stones associated with
Table 5.
Panel of candidate genes related to nephrolithiasis.
Calcium metabolism
Hypercalciurias and Renal Tubular Acidosis
some genetic diseases (hereditary hypercalciurias, hereditary distal tubular acidosis, primary hyperoxaluria) or acquired diseases (primary hyperparathyroidism, sarcoidosis, distal tubular acidosis secondary to autoimmune diseases, immobilization syndrome and other bone diseases, therapy with carbonic anhydrase inhibitors, enteric hyperoxalurias associated with ileal resection, chronic inflammatory bowel disease and some types of bariatric surgery)
High-risk renal stone formers need early diagnosis to start specific treatments Stone analysis allows the identification of most non-calcium stones: infection stones (struvite), uric acid and urates, cystine and other rare stones (dihydroxyadenine, xanthine)
Most forms of calcium stones secondary to specific acquired diseases can be diagnosed by a thorough history associated with biochemical tests for the evaluation of calcium phosphate metabolism and measurement of fasting urinary pH
Some forms of stones are secondary to monogenic hereditary defects which can be diagnosed by searching for mutations in a large panel of candidate genes (91) (Table 5)
The study of this panel of genes (or similar panels) allowed the diagnosis of a monogenic hereditary defect in 16 8-30% of pediatric series with nephrolithiasis In a large pediatric series with a very low average age of 2 5 years, a monogenic defect was demonstrated in 39% (92) Conversely, in adult populations the rate of monogenic hereditary defects does not exceed 7%, including genetic defects associated with cystinuria which are relatively frequent (92) On the other hand, the cost of these investigations still represents a limiting factor in their routine use, although there has been a significant decline in costs with next-generation sequencing (NGS) approaches
For this reason, it has been suggested that intensive research into genetic etiology should be reserved for children who form kidney stones before 5 years of age, especially if coexisting nephrocalcinosis and/or consanguinity are present For children > 5 years and adults, the genetic study must be preceded by a careful assessment of the phenotype to select cases in which a genetic defect is suspected (93)
Orher candidates genes for association with nephrolithiasis AMMECR1, AP2S1, CLDN10, GDNF, GNA11, OXGR1, SLC13A5, SLC26A6, SLC26A7, SLC7A13, TRPV5, TRPV6
The study of the phenotype is of particular importance for the diagnosis of cystinuria and primary hyperoxaluria Early diagnosis of cystinuria is mandatory due to the relative frequency of the disease (1/7000 newborns) and of cystine stones (approximately 6-8% in pediatric series, 1% in adults) Cystinuria is caused by mutations of SLC3A1 and SLC7A9 genes encoding for the two subunits of the transporter of cysteine, ornithine, lysine and arginine in the proximal tubule which cause elevated urinary excretion of cystine The phenotype of these patients is potentially easy to identify through stone analysis, the use of a colorimetric test in urine (which is limited by the toxicity of one of the reagents), the demonstration of typical crystalluria and ion chromatography (for diagnostic confirmation) However, in real life the diagnosis of cystinuria is still delayed compared to the first
A Papatsoris, A Budia Alba, J A Galán Llopis, et al
Markers
episode of stones and the percentage of patients with renal failure is high despite the availability of effective pharmacological treatments (94) Greater organization and attention from clinicians should therefore be required for the diagnosis of this disease, especially when the onset occurs after the age of 16 An interesting option could be postnatal screening which seems to be justified by the prevalence of the disease and the availability of effective therapy Post-natal diagnosis has been tested in some communities in Spain where the disease has been diagnosed in 1/4129 newborns (95) and cystine stones were observed in 10 5% of cases after a 17 years follow up (96)
Colon hyperechogenicity at prenatal ultrasound examination has been reported in some patients who presented with cystinuria and could be used to select newborns to screen for the genetic defect (97)
Primary hyperoxaluria is the result of 3 rare genetic defects of hepatic oxalate metabolism which cause an exaggerated excretion of oxalate in the urine An effective therapy for the treatment of primary hyperoxaluria type I (lumasiran) has recently been introduced (98)
The phenotype is not always easily identifiable as it is associated with the formation of calcium oxalate monohydrate stones with the same chemical composition as idiopathic calcium oxalate stones
Diagnosis is easier in cases with early and severe presentation with nephrocalcinosis, renal failure and manifestations of systemic oxalosis In cases with onset in adulthood and without nephrocalcinosis the diagnosis is often delayed after 5 years from initial presentation and at end stage renal disease (in 30-60% of cases) (99)
The recognition of the phenotype is usually based on the measurement of 24-hour oxaluria which is not always easily accessible and can be cumbersome for pre-analytical reasons of sample collection and preservation
These problems could be overcome with the development and diffusion of rapid qualitative diagnostic tests for the recognition of oxaluria which have already been described in numerous reports (100)
A l t e r n a t i v e l y , t h e g r e a t e r d i f f u s i o n o f s t e r e o s c o p i c microscopy for the analysis of stones, in addition to infrared spectroscopy or X-ray diffractometry, could help to recognize the pathognomonic morphology of calcium oxalate monohydrate stones of patients with primary hyperoxaluria which present different color and structure with respect to idiopathic COM stones (101)
Prevention strategies
Personalized medicine (Giovanni Gambaro)
Personalized or precision medicine is not only aimed at specific molecular targets of that specific patient We have e x a m p l e s o f s u c h m e d i c i n e i n t h e t r e a t m e n t o f nephrolithiasis This is the case of Thiopronine for cystinuria, of Rifampin in Infantile Hypercalcemia CYP24A1 gene mutation, and finally of Lumasiran and Nedosiran in primary Hyperoxalurias However, the meaning of precision or personalized medicine is much broader These terms mean a prevention and treatment approach considering individual genetic variations and environmental and lifestyle conditions It is a concept that those involved in the prevention of nephrolithiasis know well The EAU
guidelines have well interpreted the concept of personalized medicine when they state that the individual risk of recurrence and systemic complications of stones must be assessed globally because this is imperative for pharmacological treatment (14)
No antithesis exists between personalized medicine and public health interventions to prevent stones The first addresses a small part of stone patients with a high risk of recurrence and systemic complications, which must be identified among the more numerous subjects who form one or a few stones during their entire lifespan Just to give an example (please consider that the following percentages are approximate and for illustrative purposes only), let's assume that the prevalence of nephrolithiasis in the general population is 10%; only 10% of these could be genuinely recurrent stone patients Among these, only 10% might have secondary forms Well, personalized treatment should only be reserved for these last two categories of subjects
The AUA and EAU guidelines suggest a selective approach to pharmacological prevention and recommend conducting a metabolic study on the 24-hour urine of stone patients (14, 59) Unfortunately, although this is only part of the overall risk assessment of a stone patient, the metabolic study is often ignored in clinical practice (102, 103) However, there is an antithesis between personalized medicine and an empirical approach to preventing nephrolithiasis The empiric approach (104), including lifestyle, nutritional, and pharmacological measures administered to stone patients, is based solely on stone composition with minimal or no metabolic urinary investigations This exposes the renal stone patients to a risk of under-diagnosis and under-treatment, i e , missing the chance to properly diagnose and treat that minority of those with nephrolithiasis who could benefit from specific and/or ancillary treatments (e g , parathyroidectomy or treatments for slowing the progression of chronic kidney disease), the inherited and secondary forms Furthermore, other problems with such an approach are unwanted adverse events and un-loyalty of patients (105)
In a nephrolithiasis patient, a complete diagnostic workup should be carried out with the aim of:
• Identification of secondary forms of nephrolithiasis
• Diagnosis of idiopathic calcium nephrolithiasis
• Risk assessment of chronic kidney disease and metabolic bone disease
• Identification of patients who need to be treated to prevent stones and systemic complications (6) At the end of the work-up, only a minority of patients will need a personalized treatment
The risk of considering nephrolithiasis only as a problem of public health policies is that this is interpreted as a renunciation of the commitment to identify the few patients who, on the contrary, require personalized therapies
Public Health Policy (Alberto Trinchieri)
In the last three decades, the prevalence of kidney stones has increased worldwide Higher prevalence rates are observed in developed countries although increase of prevalence rates are also expected in developed countries (106) The increase in the prevalence of kidney stones is linked to the greater impact of environmental risk factors
(diet, lifestyle, climate), while the impact of genetic factors remains unchanged In particular, the role of climate factors is increasing because of global warming and urbanization which exaggerates the effect of increasing global surface temperatures (urban heat islands) (107, 108) The increase in the prevalence of kidney stones is associated with the change in the clinical presentation of the disease and in the spectrum of stone composition due to the increased impact of environmental factors compared to genetic factors The comparison of case series studied in the same country in different periods of time demonstrates that the average age of patients with urinary stones has increased over the last 30 years from the 5th to the 6th decade (109) The spectrum of stone composition also changed during this period The frequency of infection stones (struvite) has decreased in most geographical areas thanks to the improvement of social and health conditions
Furthermore, a trend towards a reduction in calcium phosphate stones in favor of an increase in the frequency of calcium oxalate was observed In the context of calcium oxalate stones, an increase in the frequency of calcium oxalate monohydrate stones and a reduction in calcium oxalate dihydrate stones was also observed In some southern areas of Western countries (Texas, Southern Europe) an increase in the frequency of uric acid-containing stones has been observed, while this trend has not been observed in more northern geographical areas The frequency of uric acid-containing stones tends to be positively correlated with the increase in environmental temperature
Furthermore, the prevalence of hypercalciuria, the urinary saturation values with respect to calcium oxalate, calcium phosphate and uric acid have progressively reduced over time Finally, the average interval between the first episode of stone disease and subsequent episodes of recurrent stone disease tends to lengthen (110, 111)
The “ new ” presentation of urinary stone disease is characterized by higher renal stone prevalence, higher age at stone onset, longer interval between stone episodes, more frequent calcium oxalate monohydrate and/or uric acid stones, less frequent hypercalciuria, and lower urinary saturation
At present, renal stone prevalence is higher but most renal stone formers present a mild to moderate disease with late onset of stone formation This trend is mostly related to a change of environmental risk factors for atone formation
This trend cannot be countered only by increasing the provision (and costs) of curative services
On the contrary, measures of primary prevention are h i g h l y n e e d e d ( g e n e r a l p r a c t i t i o n e r s , m e d i a , s o c i a l media) In fact, patients who form the first stone at middle-age or after need a simplified screening including clinical history, stone analysis, measure of calcium/phosphate metabolism, urinary pH, and urine culture They usually only require general measures such as high fluid intake, diet and alkalinization
Furthermore, lifestyle adaptation to climate change is also requested at institutional level (landscape, urban and building strategies to augment adaptive capacity to hot weather) and at individual level
Personalized medicine or public health policy? (Dirk Kok)
The answer to this question depends on the process by
which the stone was formed: fixed or free particle mechanism (112)
Both require supersaturation of the surrounding fluid, being urine inside the nephron, urine in the urinary tract or interstitial fluid
Personalized medicine can prevent stones that start inside the nephron or in the urinary tract
An example is infection stones that are formed from high concentrations of calcium, magnesium, phosphate and ammonium and a high pH Effective prevention requires removal of all stone fragments (resident bacteria), supplying the correct antibiotics and drugs that reduces urine pH and urease activity You need to be aware that a negative urine culture does not exclude the presence of urease producing bacteria, because they may reside inside crystal material or urothelial cells (113)
Similarly, we also know how to prevent stones that start by crystallization in the nephron because of high blood values plus local nephron conditions For instance, drugs of which supersaturation increases at high pH may form crystals in the loop of Henle This can be detected by looking for drug crystals in the urine (114, 115) When the numbers of crystals formed become too high, aggregates may block the duct of Bellini and start stone formation For such drugs it should be remembered that there exists a window of plasma levels with a lower limit determined by the desired effectivity and a higher limit determined by the crystallization risk It might be wise to monitor crystalluria for any new drug in order to detect future risks of stone formation Cystine, xanthine and uric acid stones are other stone types that start from high plasma values and abnormal urine conditions Limitation of the excretion of metabolites in combination with steering urine pH in the appropriate direction plus, if possible, adding compounds that bind the stone forming material will prevent new stone formation and examining crystalluria has a good monitoring function
For some of stones made of calcium oxalate and phosphate salts where high plasma values are involved (genetic hyperoxaluria, hyperparathyroidism, extreme intake of oxalate or oxalate precursors) the same principles as described above can be maintained
On the contrary, the problem lies with the calcium stones that are related to lifestyle and may start with renal plaques
The whole process can take up to decades (116) Here prevention involves long term adaptation of the stone former to a lifestyle that poses less of a stone forming risk This is a very difficult task that requires a combination of personal attention by the doctor and public health or commercial initiatives that aim to direct people towards a healthier lifestyle (117-119) Someone who is forming the first stone can only be helped by the latter two
Future research
Artificial Intelligence (AI) -
A window to the future (Alberto Trinchieri)
Artificial intelligence is a branch of computer science that develops systems capable of performing tasks that would require human intelligence such as learning, reasoning, problem solving, perception and understanding language
Artificial intelligence is expressed through various tech-
A Papatsoris, A Budia Alba, J A Galán Llopis, et al
nologies such as machine learning, expert systems, natural language processing, computer vision and robotics
In particular, machine learning consists of the development of algorithms to make predictions or decisions based on patterns identified in the analyzed data without explicit programming A subset of machine learning is deep learning through algorithms organized in complex layered neural networks that are exercised by analyzing unstructured or unlabeled data
Artificial intelligence is used in medicine with various applications for the purpose of collecting medical history through voice or text analysis to create real-time transcriptions of the conversation between physician and patient, detection of clinical signs, automated image analysis, classification, and categorization of pathological, radiological, and endoscopic images
The applications of artificial intelligence in the management of the renal stone patients have several purposes: automated identification of ureteral stones on CT imaging, prediction of stone composition by clinical parameters, prediction of 24-hour urinary risk factors by demographics and clinical parameters, and assessment of stone composition by evaluation of images (photographs, endoscopic videos) (120)
The analysis of digital photographs or endoscopic intraoperative views by deep convolutional neural networks (CNNs) can allow the identification and classification of kidney stones
A recent meta-analysis has shown that in the last 5 years the predictive positive value has increased for different types of stones from 50-75% to 96-99% (121)
An application for smartphones equipped with a miniaturized microscope was also developed which demonstrated an accuracy of 88% (122)
Artificial intelligence techniques have also been used for the prediction of postprocedural outcomes such as the prediction of spontaneous passage of ureteral stones, the stone-free status after SWL, the lower pole stone clearance after SWL, the stone growth after SWL, the prediction of success after PCNL
In conclusion, the extensive application of artificial intelligence in Urology will revolutionize the decision-making process Efficiency, accuracy and precision will be enhanced with decreased workload for clinicians
Synergy between urologists, nephrologists and scientists in basic stone research (Kyriaki Stamatelou)
Urology is currently the dominant specialty involved in the management of kidney stones Depending on the particular setting of care and the individual referral practices, the role of Nephrologists in urolithiasis is usually limited Nephrologists are generally involved in the medical management of kidney stones only when repeated recurrences or a noticeable kidney injury or kidney failure occur In recent years collaboration between Basic Research scientists and urologists and nephrologists happens in very few places in the world, mainly kidney stone clinics, academic research centers and centres of excellence for urolithiasis (123-125)
Yet, it is apparent that basic scientists, including biochemists, geneticists, and physiologists, can contribute to our understanding of the fundamental mechanisms of
kidney stone formation uncovering molecular pathways, genetic factors, and physiological processes that are involved in stone development but remain incomprehensible
Synergy between clinical practitioners and basic scientists can extend to translational research, where findings from basic science are translated into clinical applications and help develop targeted therapies and preventive strategies based on the latest scientific insights Synergy in clinical trials is also essential for evaluating new surgical techniques, medical treatments, or preventive strategies
Synergy can also include the formation of Interdisciplinary Teams that would address all aspects of disease management including acute stone events, recurrences, co-morbidities, preventive measures and patient education
An excellent example of contemporary meaningful synergy is the development of a revolutionary drug for the treatment of Primary Hyperoxaluria Type 1 The application of a biotechnology breakthrough, small RNA interference molecules for silencing a gene coding a protein, that stops the production of oxalate and alleviates the symptoms of the catastrophic disease
In conclusion, the synergy between urologists, nephrologists, and scientists in basic kidney stone research enhances the depth and breadth of investigations, leading to a more comprehensive understanding of kidney stone formation, risk factors, and treatment options This collaboration is essential for developing effective strategies to prevent kidney stones and improve the overall care of affected individuals
CONCLUSIONS
(Athanasios Papatsoris)
Urolithiasis is a multifactorial disease, increasing in prevalence worldwide At the same time, minimally invasive treatment techniques are under constant evolution, changing the landscape of optimal management The present article aimed in covering all aspects in diagnosis and management of urolithiasis, using high-quality, evidence-based material, in order to help urologists tailoring the stone disease management Given the continuous improvement in all aspects of endourology, future studies are needed to provide urologists with updated material in treatment incorporating individual patient preferences along with surgical expertise
ACKNOWLEDGMENTS
This work was born from the great organizational skills and scientific vision of Noor Buchholz, who, despite being seriously ill, wanted to organize yet another edition of the Experts in Stone Disease meeting until the end The first edition of ESD was held in Dubai in 2012 It was f o l l o w e d b y n u m e r o u s o t h e r editions in Cape Town, Dubai, Shanghai, Athens and finally in Valencia Noor was unable to be present in Valencia but his spirit hovered among the participants
of the event who remembered him several times The program was inspired by his scientific philosophy in particular the collaboration between urologists, nephrologists and scientists in basic stone research and the creation of relationships between experts from both, developed as well as developing countries Noor died on 13 February 2024 two weeks after his last successful meeting We also thank Vicky Nickolopoulou who helped to superbly organize all the editions of ESD and we thank Devicare SL for its unconditioned support to the organization of the ESD Congress in Valencia
REFERENCES
1 Assimos D, Krambeck A, Miller NL, et al Surgical management of stones: American Urological Association/Endourological Society Guideline, part II J Urol 2016; 196:1161
2 Skolarikos A, Jung H, Neisius A, et al EAU Guidelines 2023 on Urolithiasis Edn presented at the EAU Annual Congress Milan 2023 ISBN 978-94-92671-19-6 EAU Guidelines Office, Arnhem, The Netherlands http://uroweb org/guidelines/compilations-of-all-guidelines/
3 Akram M, Jahrreiss V, Skolarikos A, et al Urological Guidelines for Kidney Stones: Overview and Comprehensive Update J Clin Med 2024; 13:1114
4 Jackman SV, Docimo SG, Cadeddu JA, et al The “mini-perc” technique: a less invasive alternative to percutaneous nephrolithotomy World J Urol 1998; 16:371-374
5 Lahme S Miniaturisation of PCNL Urolithiasis 2017; 46:99-106
6 Liu Y, Zhang H, Wen Z, et al Efficacy and safety of minimally invasive percutaneous nephrolithotomy versus retrograde intrarenal surgery in the treatment of upper urinary tract stones (> 1 cm): a systematic review and meta-analysis of 18 randomized controlled trials BMC Urol 2023; 23:171
7 Rebuck DA, Macejko A, Bhalani V, et al The natural history of renal stone fragments following ureteroscopy Urology 2011; 77:564-8
8 Mahmood SN, Ahmed CJ, Tawfeeq H, et al Evaluation of mini-PCNL and RIRS for renal stones 1-2 cm in an economically challenged setting: A prospective cohort study Ann Med Surg (Lond) 2022; 81:104235
9 Jiao B, Lai S, Xu X, et al The efficacy of flexible ureteroscopy lithotripsy and miniaturized percutaneous nephrolithotomy for the treatment of renal and proximal ureteral calculi of ≤ 2 cm: A retrospective study Medicine (Baltimore) 2019; 98:e14535
10 Zheng C, Yang H, Luo J, et al Extracorporeal shock wave lithotripsy versus retrograde intrarenal surgery for treatment for renal stones 1-2 cm: a meta-analysis Urolithiasis 2015; 43:549-56
11 Setthawong V, Srisubat A, Potisat S, et al Extracorporeal shock wave lithotripsy (ESWL) versus percutaneous nephrolithotomy (PCNL) or retrograde intrarenal surgery (RIRS) for kidney stones Cochrane Database Syst Rev 2023; 8:CD007044
12 Hou J, Xu F, Du H, et al Efficacy and safety of the surgical treatments for lower calyceal stones: a systematic review and network metaanalysis Int J Surg 2023; 109:383-8
13 Güler Y Non-contrast computed tomography-based factors in predicting ESWL success: A systematic review and meta-analysis Progr Urol 2023; 33:27-47
14 Geraghty RM, Davis NF, Tzelves L, et al Best practice in interventional management of urolithiasis: an update from the European Association of Urology Guidelines Panel for Urolithiasis 2022 Eur Urol Focus 2023; 9:199-208
15 Peng L, Wen J, Zhong W, Zeng G Is physical therapy effective following extracorporeal shockwave lithotripsy and retrograde intrarenal surgery: a meta-analysis and systematic review BMC Urology 2020; 20:1-11
16 Sarica K, Kafkasli A, Yazici Ö, et al Ureteral wall thickness at the impacted ureteral stone site: a critical predictor for success rates after SWL Urolithiasis 2015; 43:83-8
17 Bucci S, Umari P, Rizzo M, et al Emergency extracorporeal shockwave lithotripsy (eSWL) as opposed to delayed SWL (dSWL) for the treatment of acute renal colic due to obstructive ureteral stone: a prospective randomized trial Minerva Urol Nefrol 2018; 70:526-33
18 Peng C-X, Lou Y-K, Xu L, et al Efficacy of emergency extracorporeal shock wave lithotripsy in the treatment of ureteral stones: a metaanalysis BMC Urology 2023; 23:56
19 Cornelius J, Zumbühl D, Afferi L, et al Immediate shockwave lithotripsy vs delayed shockwave lithotripsy after urgent ureteral stenting in patients with ureteral or pyeloureteral urolithiasis: a matched-pair analysis J Endourol 2021; 35:721-7
20 Bourdoumis A, Stasinou T, Kachrilas S, et al Thromboprophylaxis and bleeding diathesis in minimally invasive stone surgery Nat Rev Urol 2014; 11:51-8
21 Walker E, Lyman A, Gupta K, et al Clinical management of an increasing threat: outpatient urinary tract infections due to multidrugresistant pathogens Clin Infect Dis 2016; 63:960-965
22 Tenney J, Hudson N, Alnifaidy H, et al Risk factors for aquiring multidrug-resistant organisms in urinary tract infections: A systematic literature review Saudi Pharm J 2018; 26:678-684
23 Wagenlehner FM, Vahlensieck W, Bauer HW, et al Prevention of recurrent urinary tract infections Minerva Urol Nefrol 2013; 65:9-20
24 Cek M, Tandogdu Z, Wagenlehner F, et al Healthcare-associated urinary tract infections in hospitalized urological patients - a global perspective: results from the GPIU studies 2003-2010 World J Urol 2014; 32:1587-1594
25 Gauhar V, Traxer O, García Rojo E, et al Complications and outcomes of tubeless versus nephrostomy tube in percutaneous nephrolithotomy: a systematic review and meta-analysis of randomized clinical trials Urolithiasis 2022; 50:511-522
26 Chen ZJ, Yan YJ, Zhou JJ Comparison of tubeless percutaneous nephrolithotomy and standard percutaneous nephrolithotomy for kidney stones: A meta-analysis of randomized trials Asian J Surg 2020; 43:6068
27 Li Q, Gao L, Li J, et al Total tubeless versus standard percutaneous nephrolithotomy: a meta-analysis Minim Invasive Ther Allied Technol 2019; 29:61-69
28 Xun Y, Wang Q, Hu H, et al Tubeless versus standard percutaneous nephrolithotomy: an update meta-analysis BMC Urol 2017; 17:102
29 Kim HJ, Ghani KR Which Is the Best Laser for Lithotripsy? Holmium Laser Eur Urol Open Sci 2022; 44:27-29
30 Emiliani E, Kanashiro A, Angerri O Lasers for stone lithotripsy: advantages/disadvantages of each laser source Curr Opin Urol 2023; 33:302-307
31 Ortner G, Somani BK, Güven S, et al Experts' recommendations in laser use for the treatment of urolithiasis: a comprehensive guide by the European Section of Uro-Technology (ESUT) and Training-Research in Urological Surgery and Technology (T R U S T )-Group World J Urol 2024; 42:33
32 Panthier F, Pauchard F, Traxer O Retrograde intra renal surgery and safety: pressure and temperature A systematic review Curr Opin Urol 2023; 33:308-317
A Papatsoris, A Budia Alba, J A Galán Llopis, et al
33 Yao Q, Zhang J, Pan G, Chen B Mussel-Inspired Clickable Antibacterial Peptide Coating on Ureteral Stents for Encrustation Prevention ACS Appl Mater Interfaces 2022; 14:36473-36486
34 Ho DR, Su SH, Chang PJ, et al Biodegradable Stent with mTOR Inhibitor-Eluting Reduces Progression of Ureteral Stricture Int J Mol Sci 2021; 22:5664
35 Hu J, Wang Z, Hu H, et al In vitro and in vivo assessment of a bilayered degradable rapamycin-eluting stent for ureteral stricture caused by holmium: YAG laser lithotripsy Acta Biomater 2023; 172:321-329
36 Soria F, Delacruz JE, Aznar-Cervantes SD, et al Animal model assessment of a new design for a coated mitomycin-eluting biodegradable ureteral stent for intracavitary instillation as an adjuvant therapy in upper urothelial carcinoma Minerva Urol Nephrol 2023; 75:194-202
37 Soria F, de la Cruz JE, Budia A, et al Experimental Assessment of New Generation of Ureteral Stents: Biodegradable and Antireflux Properties J Endourol 2020; 34:359-365
38 de la Cruz JE, Soto M, Martínez-Plá L, et al Biodegradable ureteral stents: in vitro assessment of the degradation rates of braided synthetic polymers and copolymers Am J Clin Exp Urol 2022; 10:1-12
39 Soria F, de La Cruz JE, Budia A, et al Iatrogenic Ureteral Injury Treatment with Biodegradable Antireflux Heparin-Coated Ureteral StentAnimal Model Comparative Study J Endourol 2021; 35:1244-1249
40 Seitz C, Desai M, Häcker A, et al Incidence, prevention, and management of complications following percutaneous nephrolitholapaxy Eur Urol 2012; 61:146-58
41 de la Rosette JJ, Opondo D, Daels FP, et al CROES PCNL Study Group Categorisation of complications and validation of the Clavien score for percutaneous nephrolithotomy Eur Urol 2012; 62:246-55
42 Öztürk H Gastrointestinal system complications in percutaneous nephrolithotomy: a systematic review J Endourol 2014; 28:1256-67
43 Lorenzo-Soriano L, Ordaz-Jurado DG, Pérez Ardavín J, et al Predictive factors of infectious complications in the postoperative of percutaneous nephrolithotomy Actas Urol Esp 2019; 43:131-136
44 Perez Castro E, Osther PJ, Jinga V, et al CROES Ureteroscopy Global Study Group Differences in ureteroscopic stone treatment and outcomes for distal, mid-, proximal, or multiple ureteral locations: the Clinical Research Office of the Endourological Society ureteroscopy global study Eur Urol 2014; 66:102-9
45 Ma YC, Jian ZY, Yuan C, et al Risk Factors of Infectious Complications after Ureteroscopy: A Systematic Review and MetaAnalysis Based on Adjusted Effect Estimate Surg Infect (Larchmt) 2020; 21:811-822
46 Gaizauskas A, Markevicius M, Gaizauskas S, Zelvys A Possible complications of ureteroscopy in modern endourological era: two-point or "scabbard" avulsion Case Rep Urol 2014; 2014:308093
47 Taie K, Jasemi M, Khazaeli D, Fatholahi A Prevalence and management of complications of ureteroscopy: a seven-year experience with introduction of a new maneuver to prevent ureteral avulsion Urol J 2012; 9:356-60
48 Estrade V, Meria P, Almeras C; Lithiasis Committee of the French Association of Urology (CLAFU) 2022 Recommendations of the AFU Lithiasis Committee: Combined approach for the management of kidney and ureteral stones (Endoscopic Combined IntraRenal Surgery, ECIRS) Prog Urol 2023; 33:871-874
49 Ibarluzea G, Scoffone CM, Cracco CM, et al Supine Valdivia and modified lithotomy position for simultaneous anterograde and retrograde endourological access BJU Int 2007; 100:233-236
50 Oguz U, Resorlu B, Ozyuvali E, et al Categorizing intraoperative complications of retrograde intrarenal surgery Urol Int 2014; 92:164168
51 Liu YH, Jhou HJ, Chou MH, et al Endoscopic Combined Intrarenal Surgery Versus Percutaneous Nephrolithotomy for Complex Renal Stones: A Systematic Review and Meta-Analysis J Pers Med 2022; 12:532
52 Widyokirono DR, Kloping YP, Hidayatullah F, et al Endoscopic Combined Intrarenal Surgery vs Percutaneous Nephrolithotomy for Large and Complex Renal Stone: A Systematic Review and MetaAnalysis J Endourol 2022; 36:865-876
53 Halbritter J, et al Fourteen monogenic genes account for 15% of nephrolithiasis/nephrocalcinosis J Am Soc Nephrol 2015; 26:543-551
54 Braun DA, et al Prevalence of Monogenic Causes in Pediatric Patients with Nephrolithiasis or Nephrocalcinosis Clin J Am Soc Nephrol 2016; 11:664-72
55 Daga A, et al Whole exome sequencing frequently detects a monogenic cause in early onset nephrolithiasis and nephrocalcinosis Kidney Int 2018; 93:204-213
56 Santoro G, et al Association analysis of 10 candidate genes causing Mendelian calcium nephrolithiasis in the INCIPE study: a South European general population cohort Clin Kidney J 2023; 16:521-527
57 Ferraro PM, et al When to suspect a genetic disorder in a patient with renal stones, and why Nephrol Dial Transplant 2013; 28:811-820
58 Pearle MS, Goldfarb DS, Assimos DG, et al American Urological Assocation Medical management of kidney stones: AUA guideline J Urol 2014; 192:316-24
59 Williams JC Jr, Gambaro G, Rodgers A, et al Urine and stone analysis for the investigation of the renal stone former: a consensus conference Urolithiasis 2021; 49:1-16
60 Siener R, Buchholz N, Daudon M, et al EAU Section of Urolithiasis (EULIS) Quality Assessment of Urinary Stone Analysis: Results of a Multicenter Study of Laboratories in Europe PLoS One 2016; 11:e0156606
61 Cloutier J, Villa L, Traxer O, Daudon M Kidney stone analysis: "Give me your stone, I will tell you who you are!" World J Urol 2015; 33:157-69
62 Estrade V, De Senneville BD, Meria P, et al Toward improved endoscopic examination of urinary stones: A concordance study between endoscopic digital pictures vs microscopy BJU Int 2020
63 Keller EX, De Coninck V, Doizi S, et al Thulium fiber laser: ready to dust all urinary stone composition types? World J Urol 2020; 38:188394
64 Almeras C, Pradere B, Estrade V Meria P On behalf of the Lithiasis Committee of the French Urological Association Endoscopic Papillary Abnormalities and Stone Recognition (EPSR) during Flexible Ureteroscopy: A Comprehensive Review J Clin Med 2021; 10:2888
65 Sampogna G, Basic D, Geavlete P, et al En representación del grupo SEGUR Endoscopic identification of urinary stone composition: A study of South Eastern Group for Urolithiasis Research (SEGUR 2) Actas Urol Esp (Engl Ed) 2021; 45:154-159
66 Costa-Bauzá A, Grases F, Julià F The power of desktop scanning electron microscopy with elemental analysis for analyzing urinary stones Urolithiasis 2023; 51:50
67 Racek M, Racek J, Hupáková I Scanning electron microscopy in analysis of urinary stones Scand J Clin Lab Invest 2019; 79:208-217
68 Bazin D, Bouderlique E, Daudon M, et al Scanning electron microscopy-a powerful imaging technique for the clinician C R Chimie 2022; 25:37-60
69 Ticinesi A, Nouvenne A, Meschi T Gut microbiome and kidney stone disease: not just an Oxalobacter story Kidney Int 2019; 96:25-27
70 Lee JA, Stern JM Understanding the Link Between Gut Microbiome and Urinary Stone Disease Curr Urol Rep 2019; 20:19
71 Kachroo N, Lange D, Penniston KL, et al Standardization of microbiome studies for urolithiasis: an international consensus agreement Nat Rev Urol 2021; 18:303-311
72 Yuan T, Xia Y, Li B, et al Gut microbiota in patients with kidney stones: a systematic review and meta-analysis BMC Microbiol 2023; 23:143
73 Wolfe AJ, Toh E, Shibata N, et al Evidence of uncultivated bacteria in the adult female bladder J Clin Microbiol 2012; 50:1376-83
74 Adomako EA, Li X, Sakhaee K, et al Urine pH and Citrate as Predictors of Calcium Phosphate Stone Formation Kidney360 2023; 4:1123-1129
75 Sromicki J, Kacl G, Föhl M, Hess B Prospective long-term evaluation of incomplete distal renal tubular acidosis in idiopathic calcium nephrolithiasis diagnosed by low-dose NH4CL loading - gender prevalences and impact of alkali treatment J Nephrol 2022; 35:1619-1626
76 Wiederkehr MR, Moe OW Uric Acid Nephrolithiasis: A Systemic Metabolic Disorder Clin Rev Bone Miner Metab 2011; 9:207-217
77 Grases F, Costa-Bauzá A, Gomila I, et al Urinary pH and renal lithiasis Urol Res 2012; 40:41-6
78 Julià F, Costa-Bauza A, Berga F, Grases F Effect of theobromine on dissolution of uric acid kidney stones World J Urol 2022; 40:2105-2111
79 Daudon M, Frochot V "Crystalluria" Clinical Chemistry and Laboratory Medicine (CCLM)[Internet] 2015; 53: s1479-s1487
80 Siener R Nutrition and Kidney Stone Disease Nutrients 2021; 13:1917
81 Kok DJ Metaphylaxis, diet and lifestyle in stone disease Arab J Urol 2012; 10:240-9
82 Kok DJ, Papapoulos SE, Bijvoet OLM Excessive crystal agglomeration with low citrate excretion in recurrent stone formers Lancet 1986; i:1056-1058
83 Kok DJ The preventive treatment of recurrent stone-formation: how can we improve compliance in the treatment of patients with recurrent stone disease? Urolithiasis 2016; 44:83-90
84 Kok DJ, Boellaard W, Ridwan Y, Levchenko VA Timelines of the “free-particle” and “fixed particle” models of stone-formation: theoretical and experimental investigations Urolithiasis 2017; 45:33-41
85 Laube N, Kleinen L Risk indices In Rao PN, Preminger GM, Kavanagh JP (eds ), Urinary Tract Stone Disease, Springer-Verlag, London 2011; pp 355-368
86 Galan J New medical device to monitor the urine pH of stone former patients 14th Meeting of the International Urolithiasis Society in conjunction with the 5th Experts in Stone Disease Conference , June 10-11, Athens, Greece 2022
87 Robertson WG, Peacock M The cause of idiopathic calcium stone disease: hypercalciuria or hyperoxaluria? Nephron 1980; 26:105-10
88 Rimer JD, Kolbach-Mandel AM, Ward MD, Wesson JA The role of macromolecules in the formation of kidney stones Urolithiasis 2017; 45:57-74
89 Negri AL, Spivacow FR Kidney stone matrix proteins: Role in stone formation World Journal of Nephrology 2023; 12:21
91 Schönauer R, Scherer L, Nemitz-Kliemchen M, et al Systematic assessment of monogenic etiology in adult-onset kidney stone formers undergoing urological intervention-evidence for genetic pretest probability Am J Med Genet C Semin Med Genet 2022; 190:279-288
92 Liu Y, Ge Y, Zhan R, et al Identification of mutations in 15 nephrolithiasis-related genes leading to a molecular diagnosis in 85 Chinese pediatric patients Pediatr Nephrol 2023; 38:3645-3661
93 Langman CB A rational approach to the use of sophisticated genetic analyses of pediatric stone disease Kidney Int 2018; 93:15-18
94 Prot-Bertoye C, Lebbah S, Daudon M, et al French Cystinuria Group CKD and Its Risk Factors among Patients with Cystinuria Clin J Am Soc Nephrol 2015; 10:842-51
95 Sánchez Pintos P, Cocho de Juan JÁ, et al Evaluación y perspectiva de 20 años de cribado neonatal en Galicia Resultados del programa [Evaluation and perspective of 20 years of neonatal screening in Galicia Program results ] Rev Esp Salud Publica 2020; 94:e202012161
96 Piñero-Fernández JA, Vicente-Calderón C, Lorente-Sánchez MJ, et al Phenotypic characterization of a pediatric cohort with cystinuria and usefulness of newborn screening Pediatr Nephrol 2023; 38:1513-1521
97 Fuchs F, Rodriguez A, Mousty E, et al Postnatal outcome of children with antenatal colonic hyperechogenicity Prenat Diagn 2024; 44:28-34
98 Dejban P, Lieske JC New therapeutics for primary hyperoxaluria type 1 Curr Opin Nephrol Hypertens 2022; 31:344-350
99 van Woerden CS, Groothoff JW, Wanders RJ, et al Primary hyperoxaluria type 1 in The Netherlands: prevalence and outcome Nephrol Dial Transplant 2003; 18:273-9
100 Chen P, Cen L, Wang Y, et al Rapid binary visual detection of oxalate in urine samples of urolithiasis patients via competitive recognition and distance reading test strips J Mater Chem B 2023; 11:25302537
101 Daudon M, Estepa L, Lacour B, Jungers P Unusual morphology of calcium oxalate calculi in primary hyperoxaluria J Nephrol 1998; 11(Suppl 1):51-5
102 Ganesan C, et al Prevalence of twenty-four hour urine testing in Veterans with urinary stone disease PLoS One 2019; 14:e0220768
103 Ferraro PM, et al Practice patterns of kidney stone management across European and non European centers: an in-depth investigation from the European Renal Stone Network (ERSN) J Nephrol 2021; 34:1337-1346
109 Trinchieri A, Maletta A, Simonelli G, et al Time changes in the spectrum of urinary stone composition: a role for climate variations? BMC Nephrol 2020; 21:535
110 Rendina D, De Filippo G, De Pascale F, et al The changing profile of patients with calcium nephrolithiasis and the ascendancy of overweight and obesity: a comparison of two patient series observed 25 years apart Nephrol Dial Transplant 2013; 28(Suppl 4):iv146-51
111 Nouvenne A, Ticinesi A, Allegri F, et al Twenty-five years of idiopathic calcium nephrolithiasis: has anything changed? Clin Chem Lab Med 2014; 52:337-44
112 Kok DJ, Khan SR Calcium oxalate Nephrolithiasis, a free or fixed particle disease Kidney International 1994; 46:847-854
113 Mathoera RB, Kok DJ, Verduin K, Nijman RJM Pathological and therapeutical significance of cellular invasion by Proteus Mirabilis in an
A Papatsoris, A Budia Alba, J A Galán Llopis, et al
enterocystoplasty infection stone model Infect Immun 2002; 70:70227032
114 Salahuddin S, Hsu YS, Buchholz NP, et al Is Indinavir crystalluria an indicator for indinavir stone formation? AIDS 2001; 15:1079-1080
115 Dieleman JP, Salahuddin S, Hsu YS, et al Indinavir crystallisation under loop of Henle conditions: experimental evidence J Acq Immun Def Synd 2001; 28:9-13
116 Kok DJ, Boellaard W, Ridwan Y, Levchenko VA Timelines of the “free-particle” and “fixed particle” models of stone-formation: theoretical and experimental investigations Urolithiasis 2017; 45:33-41
117 Kok DJ The preventive treatment of recurrent stone-formation: how can we improve compliance in the treatment of patients with recurrent stone disease? Urolithiasis 2016; 44:83-90
118 Kok DJ Metaphylaxis, diet and lifestyle in stone disease Arab J Urol 2012; 10:240-9
119 Kok DJ The preventive treatment of recurrent stone-formation: how can we improve compliance in the treatment of patients with recurrent stone disease? Urolithiasis 2016; 44:83-90
Correspondence
Athanasios Papatsoris, MD, MSc, MSc, PhD, FEBU, FESagpapatsoris@yahoo gr
2nd Department of Urology, School of Medicine, Sismanoglio Hospital, National and Kapodistrian University of Athens, Athens; U-merge Scientific Office
Alberto Budía Alba, MD - alberto budia@hotmail com Head of Urology Department, La Fe University and Polytechnic Hospital Associate Professor of Valencia University, Valencia, Spain
Juan Antonio Galán-Llopis, MD, PhD - jagalanllopis@gmail com Department of Urology, General University Hospital Dr Balmis, ISABIAL, Alicante, Spain
Murtadha Almusafer, MD, FICMS, FACS - murtadha majeed@uobasrah edu iq Professor of Urology, University of Basrah, Basrah, Iraq
Mohammed Alameedee, MD - mohammedalameedee@yahoo com Consultant urologist, Diwaniya Teaching Hospital, Iraq
Hammad Ather, MBBS, FCPS (Urol), FRCS (Glas ), FEBUhammadather@gmail com
Akberali Hashwani & Family Endowed Professor of Urology Aga Khan University, Karachi, Pakistan
Juan Pablo Caballero-Romeu, MD - drjpcaballero@gmail com Alicante Institute for Health and Biomedical Research (ISABIAL); Department of Urology, Miguel Hernández University, Alicante, Spain
Antònia Costa-Bauzá - antonia costa@uib es Laboratory of Renal Lithiasis Research, University Institute of Health Sciences Research (IUNICS-IdISBa), University of Illes Balears, Palma de Mallorca, Spain
Athanasios E Dellis, MD, PhD, FEBU - aedellis@gmail com Professor in Urology, 2nd Department of Surgery, Aretaieion Academic Hospital, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece
Mohamed El Howairis, MD, MBBS, FRCSed, MSc, DIc, Honorary Professor of Urology - londonclinic1@gmail com
Imperial college, London University, London, UK
Giovanni Gambaro, MD, PhD, FERAgiovanni gambaro@univr it; giovanni gambaro@hotmail it
Div of Nephrology, Dept of Medicine, University Hospital of Verona, Verona, Italy
Geavalete Bogdan Geavlete, MD, PhD - bogdan geavlete@yahoo com Professor of Urology, “Carol Davila” University of Medicine and Pharmacy Medical Director, "Saint John" Emergency Clinical Hospital 13 Vitan Barzesti Street, District 4, 042122 Bucharest, Romania
Conflict of interest: The authors declare no potential conflict of interest
120 Hameed BMZ, Shah M, Naik N, et al The Ascent of Artificial Intelligence in Endourology: a Systematic Review Over the Last 2 Decades Curr Urol Rep 2021; 22:53
121 El Beze J, Mazeaud C, Daul C, et al Evaluation and understanding of automated urinary stone recognition methods BJU Int 2022; 130:786-798
122 Onal EG, Tekgul H Assessing kidney stone composition using smartphone microscopy and deep neural networks BJUI Compass 2022; 3:310-315
123 Rodgers A, Trinchieri A Fifty years of basic and clinical renal stone research: have we achieved major breakthroughs? A debate Curr Opin Nephrol Hypertens 2023; 32:177-182
124 Jungers P, Joly D, Blanchard A, et al Lithiases rénales héréditaires monogéniques : récents acquis diagnostiques et thérapeutiques [Inherited monogenic kidney stone diseases: recent diagnostic and therapeutic advances] Nephrol Ther 2008; 4:231-55
125 Tiselius HG, Daudon M, Thomas K, Seitz C Metabolic Work-up of Patients with Urolithiasis: Indications and Diagnostic Algorithm Eur Urol Focus 2017; 3:62-71
Adam Halinski, MD - adamhalinski@gmail com
Private Medical Center "Klinika Wisniowa" Zielona Gora, Poland
Bernhard Hess, MD - bernhard hess@hirslanden ch
Internal Medicine & Nephrology, KidneyStoneCenter Zurich, Klinik Im Park, Zurich, Switzerland
Saelo scientific support, Oegstgeest, The Netherlands
Hichem Kouicem, MD - hkouicem uro@yahoo fr
Physician Urologist Surgeon, Private clinic, Clinique Les Pins, Setif, Algeria
Luis Llanes, MD, Associate Professor of Urologyluis llanes@yahoo es; luis llanes@salud madrid org
Francisco de Vitoria University (Madrid)
Head of Urology Department, University Hospital of Getafe Carretera Toledo km 12 500, 28905 Getafe Madrid, Spain
Juan M Lopez Martinez, MD - urodrlopez@gmail com
Dept of Urology, University of Barcelona Clinic Hospital, Barcelona, Spain
Elenko Popov, MD, Ph D , FEBU, Assoc Prof - shennyp@yahoo com
Department of Urology, UMHAT "Tzaritza Yoanna- ISUL", Medical University, Sofia, Sofia, Bulgaria
Allen Rodgers, MSc, PhD - allen rodgers@uct ac za
Emeritus Professor and Senior Research Scholar, University of Cape Town, South Africa
Federico Soria, MD PhD - fsoria research@gmail com
Head of Experimental Surgery Department, Profesor Investigador, Universidad de Alcalá
Ramón y Cajal University Hospital, IRYCIS Madrid, Spain
Kyriaki Stamatelou, MD, Nephrologist MBAkstamatelou@mesogeios gr, dr stamatelou@gmail com
Scientific Director MESOGEIOS Nephrology Center, Haidari Attica and NEPHROS EU Private Clinic
104 Vasilissis Sofias Avenue, 11527 Athens Greece
Alberto Trinchieri, MD - alberto trinchieri@gmail com
School of Urology, University of Milan, Milan, Italy; U-merge Scientific Office
Christian Türk, MD - office@tuerk at Urologic department, Sisters of Charity Hospital, 1060 Vienna, Austria and Urologic Praxis, 1030 Vienna, Urologische Praxis, Ziehrerplatz 7/7, A-1030 Wien, Austria
ORIGINAL PAPER
Factors associated to hemoglobin decrease after percutaneous nephrolithotomy: A retrospective study
Syarif 1 , Abdul Azis 1 , Saidah Rahmat A 2 , Ahmad Taufik Fadillah Zainal 3 , Ade Nusraya 3
1 Division of Urology, Department of Surgery, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia;
2 Faculty of Medicine, Muhammadiyah Malang University, Malang, Indonesia;
3 Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
Summary
Objective: This study aims to determine the preoperative and perioperative risk parameters associated with a decrease in hemoglobin (Hb) in patients undergoing percutaneous nephrolithotomy (PCNL)
Methods: We collected prospective data of consecutive patients who underwent PCNL from January 2018 to December 2022
The median decrease in post-operative hemoglobin levels compared to pre-operative was found to be 1 5 g/dl This value was the cut-off value that divided the sample into two groups. Group 1 has a decrease in Hb levels that is higher or equal to the cutoff, group 2 has a decrease in Hb levels that is lower than the cut-off All preoperative, stone characteristics and perioperative factors were recorded.
Results: A total of 273 patients were included in the study, 141 in Group 1 and 132 in Group 2. The mean age of Group 1 was significantly higher (55 48 ± 8 73 vs 45 9 ± 10 75 years, p < 0 05) The mean bleeding of Group 1 was significantly higher (285 85 ± 113 68 vs 135 ± 77 54 ml, p < 0 05) There was a significant difference in mean operation time between groups (86 35 ± 32 05 vs 64 89 ± 27 83 min, p < 0 05)
Multivariate analysis showed that the variables age, comorbid diabetes mellitus, intraoperative bleeding amount, and operation time had a significant relationship with Hb reduction in patients undergoing PCNL (p < 0 05)
Conclusions: Older age, comorbid diabetes mellitus, large amounts of intraoperative bleeding, and longer operating time are factors associated with PCNL-related postoperative hemoglobin decrease.
Submitted 13 February 2024; Accepted 24 February 2024
INTRODUCTION
Percutaneous nephrolithotomy (PCNL) is an effective, safe, and minimally invasive treatment method with low rate of renal and ureteral calculi complications (1, 2) Indications for PCNL were determined as the presence of larger than 2 cm stones in the upper urinary tract or stones larger than 1 5 cm in the renal lower pole resistant to extracorporeal shock wave lithotripsy (3) High success rates that exceed 90% have been reported with percutaneous nephrolithotomy However, despite the high success rate, several complications still often occur due to PCNL procedures (4)
Complications from PCNL can arise due to various factors Stone characteristics are among the factors contributing to complications In fact, size, location, and complexity of the kidney stones can increase the risk of complications during PCNL Larger stones may require more extensive procedures, increasing the chances of complications Other risk factors are related to patient characteristics, such as obesity, older age, or pre-existing medical conditions like diabetes or hypertension, that can increase the risk of complications during PCNL (5, 6) Bleeding is still one of the most common and significant morbidities, with reports showing an average hemoglobin drop ranging from 2 1 to 3 3 g/dL (7-12)
Bleeding complications are one of the potential risks associated with PCNL Sources of bleeding during PCNL can be multifactorial including injury to the renal vessels during the procedure, bleeding at the puncture site, trauma to surrounding tissue when crushing and removing kidney stones It is important to identify the factors associated to intraoperative bleeding and massive post-operative hemoglobin reduction so that transfusion therapy can be prepared if necessary (5, 6, 13)
In this study, we aim to determine the factors associated with PCNL-related hemoglobin decrease
MATERIALS AND METHODS
This research is a retrospective analytical observational study of patients undergoing PCNL at Siloam Hospital Makassar, South Sulawesi, Indonesia This study used secondary electronic medical records on patients who underwent PCNL from January 2018 to December 2022
The inclusion criteria in this study were being patients aged 23-78 years who underwent unilateral PCNL and had complete medical record data, while the exclusion criteria were being patients with complete staghorn stones, chronic kidney disease, anatomical or functional abnormalities of the urinary tract system, receiving a transfusion before or during the surgical procedure, being on anti-coagulant therapy, being submitted another surgical procedure or to bilateral PCNL surgery in the same session All patients who met the exclusion criteria were removed from the research sample
All PCNL procedures in this study sample were performed using a 24 F Amplatz sheath for renal calculi; surgery was
performed in complete supine position under subarachnoid spinal block; the tract was dilatated using serial metallic dilatators and stone fragmentation was done by Lithoclast® Master (EMS, Nyon, Switzerland); residual fragments were cleared using a flexible nephroscope; experience of surgeons was more than five year At the end of the procedure, a 18 Fr Foley urethral catheter with the balloon inflated was placed Operative time was considered from the beginning of the cystoscopy for ureteral catheter insertion to the end of the placement of nephrostomy catheter
A non-contrast Computerized tomography (CT scan) and routine serum exams were performed during the first postoperative day in all cases The success rate was defined as the absence of residual symptomatic fragments > 4 mm in the CT of the first postoperative day
Characteristic data collected included age, gender, body mass index (BMI) (normal value: 18 5-25 0), stone characteristics (stone side and location, degree of hydronephrosis, stone burden, and stone complexity using Guy's Stone Score (GSS) based on preoperative CT scan analysis)
Intraoperative factors include operative time and amount of bleeding The amount of bleeding was calculated by the anesthesiologist team from the initial flank incision to access the kidney to the closure of the incision site with sutures or adhesive strips The amount was calculated by the total blood volume collected in the suction canister (taking into account the fluid used for irrigation) and the estimated bleeding from the gauze/sponge used during the operation
Comorbidities including hypertension and diabetes mellitus were also registered
Hemoglobin (Hb) levels (normal value: male 13-17 g/dl; female 12-16 g/dl) of all patients were tested 3-5 days before the surgery After PCNL is carried out, hemoglobin measurement was carried out again 2 hours after surgery The decrease in hemoglobin levels was assessed by the difference between hemoglobin before and after surgery The median reduction of hemoglobin level was 1 5 g/dl; this value was accepted as the cut-off value Patients were divided into two groups based on the threshold value Patients with reductions in hemoglobin levels by more than 1 5 g/dl were assigned to Group 1, and patients with reductions by less than the cut-off value were assigned to Group 2
Statistics
Variables with categorical data are reported as frequencies and percentages Meanwhile, continuous data variables are reported in the form of mean and standard deviation The data normality test was carried out using the Kolmogorov-Smirnov test The chi-square test was performed to assess the association of categorical variables Alternatively, Fisher's exact test was used if chi-square requirements were not met To test comparisons of numerical data, an independent t test was carried out for normally distributed data and the Mann-Whiteney test for non-normally distributed data The Pearson correlation test was carried out if the data were normally distributed, while the Spearman correla-
tion test was carried out if the data were not normally distributed
Ethical approval
This research has received ethical approval from the Health Research Ethics Committee Siloam Hospital, Makassar (No 068/KE-RS/SHMK/IX/2023)
RESULTS
A total of 368 electronic medical records were collected, 95 of which met one of the exclusion criteria, leaving 273 samples who met the criteria and were included in this study Of the 273 samples, 141 samples were in group 1 and 132 samples were in group 2 The average decrease in post-operative Hb in the total study sample was 1 5 g/dl The average age in the total study sample was 50 85 years The majority of patients were males (74 4%) A total of 37 4% of patients had comorbid hypertension and 9 2% diabetes mellitus The average body mass index (BMI) was 26 45 kg/m2 The average total bleeding during surgery was 212 ml and the average operative time was 75 97 minutes Data characteristics of this research sample are available in Table 1 Several variables were found to have a significant relationship with post-operative Hb reduction, namely age, comorbid diabetes mellitus, comorbid hypertension, intraoperative amount of bleeding and operation time The mean age of Group 1 was significantly higher than in Group 2 (55 48 ± 8 73 vs 45 9 ± 10 75 years, p < 0 001) Mean bleeding amount in Group 1 was significantly higher than Group 2 (285 85 ± 113 68 vs 135 ± 77 54 ml, p < 0 001) There was a significant difference also in mean operation time between groups (Group 1 86 35 ± 32 05 vs Group 2 64 89 ± 27 83 minutes, p < 0 001) The characteristics of stones and their distribution are presented in Table 2 Most stones were found in the right urinary tract (56%) and the majority of patients were accompanied by moderate hydronephrosis (41 4%) Stone location was most commonly reported at the lower pole (42 9%) In most patients, stone burden was around 30-50 mm2 (58 2%) Stone complexity was most commonly reported as grade 2 (51 6%) Bivariate analysis showed that of all stone characteristics, only stone burden was reported
Table 1.
Clinical characteristics of patients and distribution according to decreases of Hb.
Syarif, A Azis, S Rahmat A , et al
Table 2
Stone characteristics and distribution according to decreases of Hb
to have a significant relationship with post-operative Hb reduction, because patients with a higher stone burden tended to have a greater decrease in Hb (p < 0 05)
The results of multivariate analysis showed that the variables age, comorbid DM, bleeding amount, and operation
Table 3
Multivariate analysis of factors associated with hemoglobin decrease
HT 1 454 0 706 - 2 994 0 309
DM 3 574 1
CI: Confidence Interval;
Table 4
Diabetes mell tus; HT: Hypertens on
Correlation analysis between factors associated with hemoglobin decrease. Variable
time significantly influenced the reduction in post-operative Hb (p < 0 05) (Table 3) Next, a correlation test was carried out to assess the strength and direction of the correlation between Hb decrease and age, intraoperative bleeding amount and operation time The results showed that age had a weak positive correlation with decrease in Hb (R: 0 337, p < 0 001), intraoperative bleeding amount had a strong positive correlation with decrease in Hb (R: 0 669, p < 0 001), and operation time had a moderate positive correlation with decrease in Hb (R: 0 432, p< 0 001) (Table 4) These results show that older age, greater amount of bleeding, and longer operation time are associated with a higher decrease in post-operative Hb levels
DISCUSSION
D
nephrolithotomy (PCNL), bleeding complic
decreased hemoglobin levels Factors associated with bleeding consist of age, diabetes mellitus, operation time and intraoperative bleeding amount (14)
A study by Taylot et al found that patients with diabetes mellitus had a higher risk of bleeding complications during PCNL due to impaired platelet function and altered coagulation factors (15) The significant association between diabetes mellitus and increased blood loss during PCNL leads to a greater decrease in hemoglobin level Furthermore, diabetes mellitus affects the entire vascular system, causing microangiopathies and an increased tendency for bleeding In univariate analyses in their study, Tefekli et al found that diabetes mellitus and hypertension correlated with decreased hemoglobin levels (14, 16) The multivariate regression analysis revealed that diabetes mellitus is an independent risk factor for bleeding Our study also found diabetes mellitus as a significant risk factor in multivariate regression analysis Significant correlations were found between advanced age and increased risk of bleeding complications and subsequent hemoglobin decrease in PCNL procedures (14) Reduced ability to recover after injury and changes in cardiovascular system may be possible mechanisms for increased bleeding (17) Therefore, age has to be considered an high-risk factor for decreasing hemoglobin after PCNL
+ Pearson correlations; R: Correlat on coefficient
There are several studies indicating that stone burden is another risk factor for decreasing hemoglobin after PCNL In their study, Kukreja et al demonstrated that a larger stone burden was associated with an increased risk of bleeding complications during PCNL, resulting in a greater decrease in hemoglobin levels Syahputra et al , suggested that the size of the kidney stone positively correlated with the amount of blood loss during PCNL (18, 19) However, in our study, multivariate regression showed no significant correlation between stone burden and decrease of hemoglobin A study by Wilson et al found that longer operation
times were associated with a higher risk of bleeding complications during PCNL, leading to a more significant decrease in hemoglobin levels Chen et al reported a positive correlation between operation duration and blood loss during PCNL (20, 21) and Lee et al demonstrated a significant correlation between the amount of blood loss during PCNL and the decrease in hemoglobin levels postoperatively Kumar et al also reported that higher blood loss during PCNL was associated with a greater decrease in hemoglobin levels (22, 23)
The analysis of the selected studies revealed several significant findings Firstly, advanced age was consistently associated with an increased risk of bleeding complications and subsequent hemoglobin decrease in PCNL procedures Secondly, patients with a history of hypertension demonstrated a higher incidence of bleeding and greater hemoglobin decrease than normotensive individuals Furthermore, diabetes mellitus was found to be an independent risk factor for bleeding complications Stone size, operative duration, and blood loss significantly influenced bleeding in PCNL procedures
The present research has several advantages, including a fairly large sample size and an analysis which was carried out comprehensively and sequentially However, apart from that, this study also has limitations, including using secondary data from medical records and considering PCNL carried out by different surgeons with different experience so that this could be a confounding factor in this study
CONCLUSIONS
This comprehensive study highlights the importance of considering various factors associated with bleeding complications and hemoglobin reduction in PCNL procedures Older age, comorbid diabetes mellitus, more perioperative bleeding, and long operative time are significantly associated with decreasing Hb post-PCNL surgery These findings emphasize the need for careful patient selection, careful surgical technique, and appropriate precautions to minimize bleeding complications in PCNL procedures
REFERENCES
1 Yu J, Park HK, Kwon HJ, et al Risk factors for acute kidney injury after percutaneous nephrolithotomy: Implications of intraoperative hypotension Medicine (Baltimore) 2018; 97:e11580
2 Batagello CA, Vicentini FC, Monga M, et al Tranexamic acid in patients with complex stones undergoing percutaneous nephrolithotomy: a randomised, double-blinded, placebo-controlled trial BJU Int 2022; 129:35-47
3 de la Rosette JJMCH, Opondo D, Daels FPJ, et al Categorisation of complications and validation of the Clavien score for percutaneous nephrolithotomy Eur Urol 2012; 62:246-55
4 Sharma A, Parab S, Goyal G, et al Comparison of single-step renal dilatation and serial renal dilatation in percutaneous nephrolithotomy: A retrospective case-control study Urol Ann 2021; 13:374-7
5 Türk C, Petrík A, Sarica K, et al EAU Guidelines on Interventional Treatment for Urolithiasis Eur Urol 2016; 69:475-82
6 Skolarikos A, Gross AJ, Krebs A, et al Outcomes of Flexible Ureterorenoscopy for Solitary Renal Stones in the CROES URS Global Study J Urol 2015; 194:137-43
7 Alken P, Hutschenreiter G, Günther R Percutaneous kidney stone removal Eur Urol 1982; 8:304-11
8 Segura JW, Patterson DE, LeRoy AJ, et al Percutaneous removal of kidney stones: review of 1,000 cases J Urol 1985; 134:1077-81
9 Tiselius HG, Ackermann D, Alken P, et al Guidelines on urolithiasis Eur Urol 2001; 40:362-71
10 Matlaga BR, Kim SC, Lingeman JE Improving outcomes of percutaneous nephrolithotomy: Access EAU Update Series 2005; 3:37-43
11 Davidoff R, Bellman GC Influence of technique of percutaneous tract creation on incidence of renal hemorrhage J Urol 1997; 157:1229-31
12 Michel MS, Trojan L, Rassweiler JJ Complications in percutaneous nephrolithotomy Eur Urol 2007; 51:899-906
13 Stoller ML, Wolf JS, St Lezin MA Estimated blood loss and transfusion rates associated with percutaneous nephrolithotomy J Urol 1994; 152:1977-81
14 Eksi M, Ozlu DN, Kargi T, et al Pre-Operative Parameters
Nephrolithotomy Sisli Etfal Hastan Tip Bul 2022; 56:70-6
15 Taylor E, Miller J, Chi T, Stoller ML Complications associated with percutaneous nephrolithotomy Transl Androl Urol 2012; 1:223-8
16 Tefekli A, Ali Karadag M, Tepeler K, et al Classification of percutaneous nephrolithotomy complications using the modified clavien grading system: looking for a standard Eur Urol 2008; 53:184-90
17 Du N, Ma JQ, Luo JJ, et al The Efficacy and Safety of Transcatheter Arterial Embolization to Treat Renal Hemorrhage after Percutaneous Nephrolithotomy Biomed Res Int 2019; 2019:6265183
18 Kukreja R, Desai M, Patel S, et al Factors affecting blood loss during percutaneous nephrolithotomy: prospective study J Endourol 2004; 18:715-22
19 Syahputra FA, Birowo P, Rasyid N, et al Blood loss predictive factors and transfusion practice during percutaneous nephrolithotomy of kidney stones: a prospective study F1000Res 2016; 5:1550
20 Wilson R, et al Predictors of blood loss during percutaneous nephrolithotomy Journal of Endourology 2015; 29:402-6
21 Chen Q, et al Risk factors for bleeding during percutaneous nephrolithotomy: A retrospective study J Endourol 2017; 31:581-6
22 Lee C, et al Predictors of postoperative hemoglobin decrease and blood transfusion in percutaneous nephrolithotomy World J Urol 2018; 36:263-9
23 Kumar A, et al Predictors of blood transfusion in percutaneous nephrolithotomy: A prospective study J Urol 124:153-9
Correspondence
Syarif, MD
syarifbakri@hotmail com Division of Urology, Department of Surgery, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
Perintis Kemerdekaan St KM 10, Tamalanrea, Makassar, Indonesia
(Postal Code: 90245)
Abdul Azis, MD
Saidah Rahmat A , MD
Faculty of Medicine, Muhammadiyah Malang University, Malang, Indonesia
Ahmad Taufik Fadillah Zainal, MD
Ade Nusraya, MD
Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
Conflict of interest: The authors declare no potential conflict of interest
Syarif, A Azis, S Rahmat A , et al
ORIGINAL PAPER
Comparison of two percutaneous nephrolithotomy methods for the treatment of pediatric kidney stones: Mini-percutaneous nephrolithotomy and standard percutaneous nephrolithotomy
Kadir Karkin 1 , Mubariz Aydamirov 2 , Bug ˘ ra Aksay 1 , Eyüp Kaplan 3 , Güçlü Gürlen 1 , Adem Altunkol 1 , Ferhat Ortaog ˘ lu 1 , Ömer Faruk Akgün 1 , Ediz Vurus ¸ kan 1 , Zafer Gökhan Gürbüz 1
1 Health Sciences University, Adana City Training and Research Hospital Urology Clinic, Adana, Turkey; ² Bas ¸ kent University, Alanya Application and Research Center, Alanya, Turkey; ³ Abdulkadir Yüksel State Hospital Urology Clinic, Gaziantep, Turkey
Summary
Objective: In this study, the aim was to compare the results of mini and standard percutaneous nephrolithotomy (PCNL) for the treatment of pediatric kidney stones.
Materials and Methods: Data for 128 patients < 18 years of age who underwent mini and standard PCNL due to pediatric kidney stones were retrospectively examined Patients were divided into two groups: mini-PCNL (16-20 Fr) and standard PCNL (26 Fr) Surgery time, number of punctures to the pelvicalyceal system, hospital stay, postoperative hemoglobin drop, complications and stone-free status (SFR) were compared between the groups Additional surgical intervention (double-J stent, ureterorenoscopy, secondary PCNL) performed after the surgery was recorded The absence of residual stones or < 3 mm residual stones on kidney, ureter and bladder radiography (KUB) and ultrasonography (USG) performed in the third postoperative month were accepted as success criteria.
Results: There were 32 (43 8%) patients in the mini-PCNL group and 41 (56.2%) patients in the standard PCNL group. The mean age was 9 3 ± 4 1 years in the mini-PCNL group and 10.1 ± 5.4 years in the standard PCNL group. Mean stone size in the mini-PCNL group was 2 1 ± 1 2; while for standard PCNL it was 2.3 ± 1.4. The mean surgery time was statistically significantly higher in the mini-PCNL group (p = 0 005) There was no difference between the groups in terms of intraoperative double J stent use, postoperative complications and SFR A double J stent was inserted in two patients in the mini-PCNL group and in one patient in the standard PCNL group due to urine leakage from the nephrostomy tract in the postoperative period. Although the postoperative hemoglobin drop was found to be significantly higher in standard PCNL (p = 0.001), hematuria and blood transfusion rates were low in both groups Mean hospital stay was shorter in the mini-PCNL group compared to standard PCNL (3 6 ± 1 2 days vs 2 5 ± 1 1; p = 0 018)
Conclusions: Although mini-PCNL has longer surgery time compared to standard PCNL, it should be preferred for the treatment of pediatric kidney stones due to advantages such as similar success and complication rates to standard PCNL, short hospital stay and less postoperative hemoglobin drop
KEY WORDS: Mini percutaneous nephrolithotomy; Standard percutaneous nephrolithotomy; Pediatric Kidney Stones
Submitted 8 February 2024; Accepted 17 February 2024
INTRODUCTION
Although kidney stones are less common in children compared to adults, their recurrence rate is higher (1,2) Therefore, in this age group, complete removal of stones with a less traumatic method is important for future kidney health In the past, pediatric kidney stones were treated with open surgery However, today, extracorporeal shock wave lithotripsy (SWL) treatment is widely used for most pediatric kidney stones (3) The main disadvantages of the SWL method are that it is performed under general anesthesia and requires a high number of sessions (4) Percutaneous nephrolithotomy (PCNL) is a frequently used treatment method, especially for the treatment of large and complex stones (3) EAU guidelines recommend PCNL as the first treatment option for pediatric kidney stones larger than 2 cm and stones larger than 1 cm in the lower calyx However, the possibility of bleeding requiring transfusion increases as the sheath diameter, number of punctures, and surgery time increase in PCNL (5, 6) This is why mini-PCNL has become popular today With the mini-PCNL method, it is expected that there will be less renal parenchymal damage and fewer complications since the working channel is smaller Because pediatric kidneys are small and mobile, have thin parenchyma, and the pelvicalyceal area has small volume, the large instruments used in standard PCNL can be traumatic (7)
Therefore, the importance of mini-PCNL increases for these patients Our study aimed to compare the results of mini and standard PCNL, along with their morbidity and success rates, for pediatric kidney stones
MATERIALS AND METHODS
The data for 128 patients < 18 years of age who underwent PCNL for pediatric kidney stones between June 2013 and December 2022 were retrospectively examined Patients who had previously undergone PCNL, had chronic kidney disease, were operated for ureteral stones in the same session, had skeletal anomalies, and with missing postoperative follow-up data were excluded from the study Patients were divided into two groups: mini-PCNL
(16-20 Fr) and standard PCNL (26 Fr) Preoperatively, urinalysis, urine culture, complete blood count, kidney and liver function tests, coagulation tests, urinary ultrasonography (USG), kidney, ureter and bladder radiography (KUB) and non-contrast whole abdominal computed tomography (NCCT) were performed on all patients Those with active urinary tract infection were treated with appropriate antibiotics, and those with no growth in the control urine culture were taken for surgery Stone size was defined as the maximum diameter of the stone In the presence of multiple stones, the sum of the longest diameter of each stone was accepted as the stone size
In both groups, the surgeries were performed in prone position under general anesthesia and with antibiotic (cephalosporin) prophylaxis Previously, a 4-6 Fr ureteral catheter was inserted in patients in the lithotomy position Diluted opaque material was administered through the ureteral catheter to visualize the collecting system
Then, after determining the appropriate calyx under fluoroscopy, entry was made with a two-piece needle with an 18-gauge trocar tip (Cook Urological, Bloomington, IN, USA) When necessary, additional entries were made before dilation began A 0 035 inch hydrophilic nitinol (Terumo, Tokyo, Japan) guide wire was sent through the needle to the collector system In the mini-PCNL group, 16-20 Fr dilatation was performed over the guide wire with the help of Amplatz dilators and a sheath was placed The kidney was entered with a 15 Fr rigid nephroscope (Olympus), and a pneumatic lithotripter was used when necessary, along with a holmium laser, to break up the stones The broken stone pieces were removed by washing, using forceps and a basket Patients in the standard PCNL group underwent 26 Fr dilation and surgeries were performed with a 24 Fr nephroscope
A pneumatic lithotripter was used to break up the stones At the end of the procedures, the presence of residual stones was checked with fluoroscopy If no residual stone could be seen during both fluoroscopy and endoscopic examination, the operation was considered completed Double-J stents were emplaced antegradely in those who were thought to have infection stones, with injuries in the renal pelvis, and stenosis in the ureteropelvic junction At the end of the procedure, a 12-14 Fr Foley catheter was inserted as a nephrostomy tube On the first postoperative day, all patients underwent KUB and their urethral catheters were removed; the nephrostomy tube was removed on the first or second day Patients who had no fever, hematuria, or discharge from the nephrostomy tract during follow-up were discharged Surgery time, number of punctures to the pelvicalyceal system, hospital stay, postoperative hemoglobin drop, complications and stone-free status (SFR) were compared between the groups In both groups, the duration of surgery was defined as the time from the first puncture of the pelvicalyceal system until the placement of the nephrostomy catheter The first follow-up after discharge was performed two weeks later (those with a DJ stent had their stents removed) The success criteria were defined as no additional postoperative surgical intervention (double-J stent, ureterorenoscopy, secondary PCNL), no residual stones or < 3 mm stones at KUB and USGs performed 3 months later
S t at ist ic al an alysis
Data were analyzed using SPSS The chi-square test was used to compare proportions Fisher's exact test was used when the expected number of > 20% of cells in the table fell below five Student t test was used to compare the means of two groups A P value of 0 05 was considered statistically significant Univariate analyses were performed to detect a significant relationship between each of the dependent and independent variables A 95% confidence interval was also calculated
RESULTS
A total of 73 pediatric patients were included in the study
There were 32 (43 8%) patients in the mini-PCNL group and 41 (56 2%) patients in the standard PCNL group
The mean age was 9 3 ± 4 1 years in the mini-PCNL group and 10 1 ± 5 4 years in the standard PCNL group
Mean stone size for mini-PCNL was 2 1 ± 1 2; for standard PCNL it was 2 3 ± 1 4 There were no differences between the groups in terms of demographic, clinical and radiological stone characteristics of the patients (Table 1)
The mean surgery time was statistically significantly higher in the mini-PCNL group (p = 0 005) There was no difference between the groups in terms of intraoperative double J stent use, postoperative complications and SFR
The overall SFR was 81 2% in mini-PCNL and 85 4% in standard PCNL Complications were generally managed with medical treatment A double J stent was placed in two patients in the mini-PCNL group and in one patient in the standard PCNL group due to urine leakage from the nephrostomy tract in the postoperative period
Although puncture rates were slightly higher in the miniPCNL group, this was not statistically significant (p = 0 076) Although postoperative hemoglobin drop was found to be significantly higher in standard PCNL (p = 0 001), hematuria and blood transfusion rates were low in both groups Blood transfusion was performed in one patient in the mini-PCNL group and in two patients in the standard PCNL group The mean hospital stay was
Table 1.
Comparison of patients' demographic, clinical and radiological parameters
Variables Mini PCNL (n = 32) Standard PCNL (n = 41) p
shorter in the mini-PCNL group compared to standard PCNL (3 6 ± 1 2 days vs. 2 5 ± 1 1; p = 0 018) (Table 2)
DISCUSSION
In this study, it was planned to compare the results of standard and mini-PCNL for pediatric kidney stones Although the surgery time was longer in mini-PCNL, the hospital stay and average postoperative hemoglobin drop were less SFR and complication rates were similar between the groups The prevalence of pediatric kidney stones with high recurrence rates is increasing day by day (8) PCNL is a standard treatment method in this age group, especially for the treatment of large kidney stones Mini-PCNL is the most popular technique in recent times With this technique, the aim is to cause less damage to the kidney parenchyma, reduce complications, and achieve high SFR by using small-diameter sheaths (9-11) In many studies, the SFR in standard PCNL is 50-98% (5, 10-14) In miniPCNL, this rate was reported to be 80-85% (5, 8, 14) In similar literature studies comparing mini and standard PCNL in the pediatric population, there was no significant difference between the two techniques in terms of SFR (1517) If we look at the SFR in our study, it was similar to the literature with rates of 81 2% in the mini-PCNL group and 85 4% in the standard PCNL group Many studies showed that the operation time in miniPCNL is longer than standard PCNL (13, 18, 19) In our study, the operation time was longer in the mini-PCNL group We think that surgery times are prolonged in miniPCNL due to reasons such as the slow flow of irrigation fluid due to the use of small-diameter instruments, the
limited visual field due to the use of miniaturized endoscopic devices, and the preference for stones to be broken into smaller pieces for removal or grinding, instead of active stone crushing One of the complicated situations in studies comparing both standards in the literature is the length of hospital stay Although some studies showed that the postoperative hospital stay is similar for both methods (13, 18-20), some reported that the length of stay is shorter for mini-PCNL (15) In our study, the length of stay after mini-PCNL was found to be significantly shorter We think that the smaller size of the nephrostomy tract and the resulting reduction in postoperative pain and bleeding result in a shorter hospital stay After PCNL surgery, patients may experience complications such as fever, urinar y tract infection and bleeding Complication rates in the literature vary between 15-25% (21-26) Although some studies say that complication rates are similar (19, 20), there are also studies showing that intraoperative bleeding, postoperative hemoglobin drop and blood transfusion rates are significantly higher in standard PCNL (13, 18) In our study, although the number of punctures seemed to be slightly higher with mini-PCNL, the postoperative hemoglobin drop was found to be significantly higher with standard PCNL However, there was no statistically significant difference between the groups in terms of general postoperative complications Our study has some limitations Firstly, our study was a retrospective study and the number of patients was small Secondly, no subgroup analysis was performed according to stone complexity Thirdly, due to the small number of patients, analysis was not made according to age groups Additionally, computed tomography could not be used in follow-up imaging to avoid further radiation exposure
CONCLUSIONS
Although mini-PCNL has a longer surgery time compared to standard PCNL, it has similar success and complication rates In addition, it is a safe and effective method that should be preferred for the treatment of pediatric kidney stone patients due to important advantages such as short hospital stay and less postoperative hemoglobin drop
REFERENCES
1 Smaldone MC, Docimo SG, Ost MC Contemporary surgical management of pediatric urolithiasis Urol Clin North Am 2010; 37:253-67
2 Veeratterapillay R, Shaw MB, Williams R, et al Safety and efficacy of percutaneous nephrolithotomy for the treatment of paediatric urolithiasis Ann R Coll Surg Engl 2012; 94:588-92
3 Tekgül S, Stein R, Bogaert G, et al European Association of Urology and European Society for Paediatric Urology Guidelines on Paediatric Urinary Stone Disease Eur Urol Focus 2022; 8:833-39
4 Zeren S, Satar N, Bayazit Y, et al Percutaneous nephrolithotomy in the management of pediatric renal calculi J Endourol 2002; 16:75-8
5 Guven S, Istanbulluoglu O, Gul U, et al Successful percutaneous nephrolithotomy in children: multicenter study on current status of its use, efficacy and complications using Clavien classification J Urol 2011; 185:1419-24
6 Onal B, Dogan HS, Satar N, et al Factors affecting complication
rates of percutaneous nephrolithotomy in children: results of a multiinstitutional retrospective analysis by the Turkish pediatric urology society J Urol 2014; 191:777-82
7 Kapoor R, Solanki F, Singhania P, et al Safety and efficacy of percutaneous nephrolithotomy in the pediatric population J Endourol 2008; 22:637-40
8 Hesse A, Brändle E, Wilbert D, et al Study on the prevalence and incidence of urolithiasis in Germany comparing the years 1979 vs 2000 Eur Urol 2003; 44:709-13
9 Samad L, Aquil S, Zaidi Z Paediatric percutaneous nephrolithotomy: setting new frontiers BJU Int 2006; 97:359-63
10 Jackman SV, Hedican SP, Peters CA, et al Percutaneous nephrolithotomy in infants and preschool age children: experience with a new technique Urology 1998; 52:697-701
11 Dogan B, Atmaca AF, Canda AE, et al Efficiency of percutaneous nephrolithotomy in pediatric patients using adult-type instruments Urol Res 2012; 40:259-62
12 Salah MA, Tóth C, Khan AM, et al Percutaneous nephrolithotomy in children: experience with 138 cases in a developing country World J Urol 2004; 22:277-80
13 Unsal A, Resorlu B, Kara C, et al Safety and efficacy of percutaneous nephrolithotomy in infants, preschool age, and older children with different sizes of instruments Urology 2010; 76:247-52
14 Goyal NK, Goel A, Sankhwar SN, et al A critical appraisal of complications of percutaneous nephrolithotomy in paediatric patients using adult instruments BJU Int 2014; 113:801-10
15 Mahmood SN, Aziz BO, Tawfeeq HM, et al Mini- versus standard percutaneous nephrolithotomy for treatment of pediatric renal stones: is smaller enough? J Pediatr Urol 2019; 15:664 e1-664 e6
16 Mahajan AD, Mahajan SA Comparison of Mini-Percutaneous Nephrolithotomy by Standard and Miniperc Instruments in Pediatric Population: A Single-Center Experience J Pediatr Urol 2021; 26:37479
Correspondence
Kadir Karkin, MD, FEBU (Corresponding Author) kadir karkin@msn com Department of Urology, Health Sciences University, Adana City Training and Research Hospital, Adana, Türkiye
Mubariz Aydamirov, MD aydemirov 89@mail ru Bas ¸ kent University, Alanya Application and Research Center, Alanya, Türkiye
Bug ra Aksay, MD bgraksay@gmail com
Güçlü Gürlen, MD guclugurlen@hotmail com
Adem Altunkol, MD ademaltunkol@hotmail com
Ferhat Ortoglu, MD ferhatort@hotmail com
Ömer Faruk Akgün, MD dromerfarukakgun@gmail com
Ediz Vurus¸ kan, MD evuruskan@hotmail com
Zafer Gökhan Gürbüz, MD zafergokhangurbuz@yahoo com
Eyüp Kaplan, MD dreyup001@hotmail com
Abdulkadir Yüksel State Hospital Urology Clinic, Gaziantep, Türkiye
Conflict of interest: The authors declare no potential conflict of interest
17 Kumar N, Yadav P, Kaushik VN, et al Mini-versus standard percutaneous nephrolithotomy in pediatric population: A randomized controlled trial J Pediatr Urol 2023; 19:688-95
18 Bilen CY, Koçak B, Kitirci G, et al Percutaneous nephrolithotomy in children: lessons learned in 5 years at a single institution J Urol 2007; 177:1867-71
19 Celik H, Camtosun A, Dede O, et al Comparison of the results of pediatric percutaneous nephrolithotomy with different sized instruments Urolithiasis 2017; 45:203-208
20 Altintas R, Oguz F, Tasdemir C, et al The importance of instrument type in paediatric percutaneous nephrolithotomy Urolithiasis 2014; 42:149-153
21 Ozden E, Mercimek MN, Yakupoglu YK, et al Modified Clavien classification in percutaneous nephrolithotomy: assessment of complications in children J Urol 2011; 185:264-68
22 Zeng G, Zhao Z, Zhao Z, et al Percutaneous nephrolithotomy in infants: evaluation of a single-center experience Urology 2012; 80:408-11
23 Resorlu B, Unsal A, Tepeler A, et al Comparison of retrograde intrarenal surgery and mini-percutaneous nephrolithotomy in children with moderate-size kidney stones: results of multi-institutional analysis Urology 2012; 80:519-23
24 Yan X, Al-Hayek S, Gan W, et al Minimally invasive percutaneous nephrolithotomy in preschool age children with kidney calculi (including stones induced by melamine-contaminated milk powder) Pediatr Surg Int 2012; 28:1021-24
25 Izol V, Satar N, Bayazit Y, et al Which factors affect the success of pediatric PCNL? Single center experience over 20 years Arch Ital Urol Androl 2020; 18:345-49
26 Eslahi A, Ahmed F, Hosseini MM, et al Minimal invasive percutaneous nephrolithotomy (Mini-PCNL) in children: Ultrasound versus fluoroscopic guidance Arch Ital Urol Androl 2021; 28:173-77
K Karkin, M Aydamirov, B Aksay, et al
ORIGINAL PAPER
Dynamic
renal scans as a modality for follow-up of flexible ureteroscopy
Murad Asali 1, 2 , Osman Hallak 1
1 Urology Department, Barzilai Medical Center, Ben Gurion University of the Negev, Beer Sheva, Israel;
2 Assuta Medical Center, Ramat Hyal, Ben Gurion University of the Negev, Beer Sheva, Israel
Summary
Objective: To determine whether dynamic renal scans – DTPA or MAG3 – routinely performed after flexible ureteroscopies (f-URS) could detect the development of an obstruction and thus promote prompt early intervention for kidney preservation
Patients and methods: In this retrospective study, with all the data recorded prospectively between April 2010 and October 2023, 250 renal units in 242 patients with upper urinary tract stones (UUTS) who underwent ureterorenoscopy by one surgeon in the same medical center were evaluated Stone-free rate (SFR) was defined as no residual fragments at all using an intraoperative “triple test” The following characteristics were examined: gender, BMI, age, Hounsfield unit, stone diameter, laterality, renal/ureteral stones, stone-free rate, and auxiliary procedures per renal unit. The Clavien-Dindo classification was used to report complications Renal units with residual stones were scheduled for a 2nd f-URS. Post- flexible ureteroscopy ureteral obstruction and renal function were detected using renal scan DTPA or MAG-3. The primary outcome was renal/ ureteral obstruction.
Results: The mean patient age was 53 years The mean stone size was 12.3 mm. Stones in renal pelvis, upper, middle and lower calyces were treated in 9 2% (23), 27 6% (69), and 30 8% (77) of cases, respectively; 44% (110) ureteral stones were also treated. The single- and second-session SFRs were 94 8% and 99 7%, respectively. A third auxiliary procedure was needed in one renal unit (0 4%) The mean number of procedures per renal unit was 1.06 (264/250). Ureteral double-J stents were inserted in 53.6% (134) of the cases In 37 (14 8%) cases, a stent was placed before surgery. Post-operative complications were minor, with readmission and pain control needed in only two patients (0 8%) No avulsion or perforation of the ureters was observed. In six patients with t1/2 between 10-20 minutes, a second renal scan revealed spontaneous improvement and no obstruction in five patients One patient with large stones and a history of prior ureteroscopy developed a ureteral stricture (0 4%) and needed treatment with laser endoureterotomy
Conclusions: Post-flexible ureteroscopy obstruction due to ureteral stricture is very rare A routine renal scan post-operatively may be used in potentially high-risk patients
Submitted 17 February 2024; Accepted 31 March 2024
INTRODUCTION
As known, nephrolithiasis is a common disease in Asia with a rate of 1%-5% (1) With the development of small
flexible ureteroscopes and the improvement of laser lithotripsy, flexible ureteroscopy has become the standard of care for treating urolithiasis less than 2 cm (2, 3) In the early 1970s, Takagi et al (4) and Takayasu et al (5) first reported the clinical application of a fiberoptic pyeloureteroscope With technological advancements in endourology, including new lasers, and advanced flexible ureteroscopes, the treatment indications for retrograde intrarenal surgery (RIRS) have expanded to include not only large stones but also upper urinary tract urothelial carcinoma, ureteral stricture, and a diagnostic tool for hematuria
In 1991, Grasso et al presented an advanced flexible ureteroscope with a 7 5-Fr tip and an up 120º/down 170º deflection system In 1998, they published a clinical study of 492 patients treated with a flexible ureteroscope with a larger 3 6-Fr working channel (7) Later, in 2001, a f-URS with a two-way deflection system (270º/270º) and stronger durability was introduced to the market, improving access to the pelvicalyceal system (8) Surgeons must consider the risk of various complications due to ureteroscopy including thermal injury, ureteral injury caused by the ureteral access sheath, and strictures (6)
Ureteral stricture is a late complication that may cause severe damage to a patient’s health The incidence rate of postoperative ureteral stricture varies from 0 23 to 2 97% (9-13) Subsequent treatment of the stricture should be tailored according to the stricture length and severity of hydronephrosis Strictures longer than 1 cm with severe hydronephrosis should be treated with reconstructive surgery and not by endourological interventions (6, 14)
This study presents the results of diagnosis of possible complications associated with f-URS for treating upper urinary tract stones (UUTS) in particular renal/ ureteral obstruction, using dynamic renal scans using either diethylenetriaminepentaacetic acid (DTPA) or mercapto acetyl tri glycine (MAG-3), in order to answer the question if there is a need of routine renal scan after f-URS
DTPA = diethylenetriaminepentaacetic acid
MAG3 = mercapto acetyl tri glycine
PATIENTS AND METHODS
One surgeon performed ureterorenoscopy on 917 renal units in patients with UUTS in the same medical center between April 2010 and October 2022
A 7 5 Fr flexible ureteroscope was utilized with Holmium: YAG (yttrium aluminum garnet) laser for lithotripsy in all
patients The laser fibers used were 200 µ, 230 µ, and 272 µ, with an energy of 0 3-1 joule and a frequency of 8-80 Hz The calculi fragments were taken out with a basket
The ureteral access sheath (UAS) was always placed below the ureteral stone and moved up to the middle or proximal ureter for renal stone treatment
A total of 267 patients who underwent a post-operative dynamic renal scan using either DTPA or MAG3 were included in the study
Out of them, 13 needed a second session, one needed a third session
The patients were included in the study after meeting our inclusion criteria, as follows:
1 Upper urinary tract stones
2 Use of the same 7 5Fr flexible ureteroscope (flexible uretero-renoscope Flex- X2s [Karl Storz & Co KG, Tuttlingen, Germany])
3 Use of a Holmium: YAG laser with consistent energy, frequency, and fibers ( 200 µ, 230 µ, and 272 µ) usage
4 Use of Sphinx JR 30-watt [LISA Laser Products GmbH, Germany], Mega Plus 15 Watt [Richard Wolf GmbH, Knittlingen, Germay], or Luminis 120-watt [Luminis, Yokneam, Israel] laser generator
5 Use of a UAS (Flexor ureteral access sheath 12/14F, 28, 35, 45 cm; FUS- Cook Medical, Bloomington, IN, USA)
6 All data recorded
7 Adults aged 18 years and older
8 A dynamic renal scan, either DTPA or MAG3 was done postoperatively
The exclusion criteria were as follows:
1 Using other flexible ureteroscopes
2 Missed data
4 No other access sheath type use
5 Using a rigid ureteroscope
6 Single kidney
At the end of the operation, a triple test was done for all calyces, using 1) a plain abdominal radiograph of the kidneys, ureters, and bladder, 2) using the scope and the Carm while injecting contrast intraoperatively as a retrograde pyelography and 3) screening every calyx using the endoscope and following the anatomy on the C-arm screen as described in Asali et al article (15)
In all the patients, the following characteristics were evaluated: gender, BMI, age, stone radiopacity (Hounsfield unit), stone diameter, stone laterality (Table 1), stone location (renal/ureteral), stone-free rate (Table 2), auxiliary procedures per renal unit (Table 3), double-J stent insertion, and perioperative complications (Table 4) Stone-free status was defined as complete stone removal
This study was retrospective, and all the data (demographics data, stone characteristics, operative and postoperative data) were recorded prospectively
Postoperative follow-up was scheduled one month later with a dynamic renal scan DTPA/ MAG3, urine culture, and renal function The results were divided into obstructed (t1/2 more than 20 minutes), equivocal (t1/2 10-20 minutes), and non-obstructed (t1/2 less than 10 minutes)
The primary endpoint was a renal/ureteric obstruction demonstrated by a renal scan with a t1/2 of more than 20 minutes
Patients with residual stones were scheduled for a 2nd f-URS/RIRS (retrograde intrarenal surgery), and patients with obstruction were scheduled for re-intervention
The Clavien-Dindo classification was used to report complications (16)
All procedures performed in this study were performed after receiving informed consent from all the patients
RESULTS
The mean patient age was 53 years The mean maximum stone diameter was 12 3 mm (Table 1) Stones were in the renal pelvis, upper, middle, and lower calyces stones in 9 2% (23), 27 6% (69), and 30 8% (77) of cases, respectively (Table 2); 44% (110) were ureteral stones
The mean stone diameter of stones of the renal pelvis, upper and middle calyces, lower pole, upper ureter, middle ureter, and lower ureter was 11 3 mm, 8 2 mm, 7 9 mm, 8 8 mm, 7 8 mm, and 8 2 mm, respectively The characteristics of renal and ureteral stone are shown in Table 2
The single- and second-session SFRs were 94 8% and 99 7%, respectively A third auxiliary procedure was needed in one renal unit (0 4%) (Table 3)
Table 1.
Patient demographic and stone characteristics
Table 2. Renal and ureteral stone location and diameter
Table 3.
M Asali, O Hallak
Table 4 Complications
Intramuscu ar; IV Intravenous
The mean number of procedures per renal unit was 1 06 (264/250)
Ureteral double-J stents were inserted in 53 6% (134) of the cases In 37 (14 8%) cases, a stent was placed before the surgery
Post-operative complications were minor, with readmission for pain control needed in only two patients (0 8%) while two patients (0 8%) had intermittent haematuria secondary to the stent No avulsion or perforation of the ureters was observed (Table 4) Grade I complications according to Clavien-Dindo classification were observed in nine cases (3 6%) (9/250) No grades II, IV, or V were observed
The mean hospital stay was one day
At postoperative renal scan 244 renal units demonstrated t1/2 less than 10 minutes and six patients a t1/2 between 10-20 minutes; a second renal scan revealed improvement and no obstruction in five patients One patient developed ureteral stricture (0 4%) and needed treatment with laser endoureterotomy (Table 4)
DISCUSSION
Advances in flexible ureteroscope designs, accessory instrumentations, and new laser generators have allowed endoscopic treatment for more challenging cases Using the UAS makes it easier to enter and exit the ureter, renal pelvis, and calyces during the operation and even more when handling large stones
RIRS is a safe and valuable modality of treatment for renal stones It is a well-established procedure under constant evolution with advances in technique and technology It has gained worldwide popularity due to its minimal invasiveness and satisfactory outcomes (17) Flexible URS has become the standard of care for treating urolithiasis less than 2 cm (2, 3) There is no doubt that f-URS surgery has become very common in the treatment of UUTS even though the SFR is higher after percutaneous nephrolithotomy (PCNL) Furthermore, f-URS is also an option for renal stones larger than 2 5 cm with low morbidity (18)
Despite this, ureteral strictures are still observed after fURS as a result of injury from impacted stones, ureteral perforations, or unclear intraoperative vision (19, 20) Darwish et al concluded that post-URS ureteral stricture incidence is low and that impacted stones are the most common cause of URS complications and stricture formation (21) Traxer et al reported a higher risk of severe ureteral injury secondary to UAS use (22) However, Özsoy et al 's experimental animal model demonstrated that after two weeks, only minimal inflammatory changes were evident in the ureter suggesting negligible long-term impacts secondary to UAS use (23) According to Manger et al , ureteral strictures typically appear during the first four weeks of follow-up postoperatively (24) Renal loss can result from ureteral strictures, therefore, we need to be aware of this risk throughout our postoperative followup Even if our standard approach involves the use of UAS and small-diameter flexible ureteroscopes, our concern is how to diagnose an obstruction secondary to strictures as early and as feasibly as possible
In this study, a dynamic renal scan was routinely performed post-operatively
Early diagnosis and treatment of ureteral stricture is the cornerstone of its management So, could routine postoperative imaging help in the early diagnosis of ureteral stricture and prevent renal loss? Patients with high-risk indicators for the development of stenosis, such as impacted stones, should undergo postoperative imaging, according to May et al (25) Jung et al compared two groups of patients who underwent mini-PCNL or RIRS and were monitored by 99mTc-DTPA preoperatively and postoperatively No differences in renal function between the groups were noticed (26) Piao et al reported their results using 99mTc-DTPA to check the relative renal function after minimal invasive renal surgery, although their purpose was not to diagnose ureteral stricture (27) In this study, a UAS was standardly used, and a routine scan was done postoperatively; 244 renal units demonstrated no obstruction, while in six patients t1/2 was between 1020 minutes In these patients, a second renal scan was done, and improvement was achieved However, one symptomatic patient underwent a retrograde pyelography (1/250) which diagnosed a ureteric stricture and was subsequently treated endoscopically with laser endoureterotomy and placement of a temporary stent
We showed that renal or ureteral obstruction post-f-URS is very rare (2 4% of the renal units), when renal retention was suggested by a dynamic renal scan with t1/2 between 10-20 minutes, but only one out of six patients needing treatment
The advantages of our study include: outcomes may be more easily compared because all surgeries were carried out by the same surgeon using the same equipment, personnel, ureteroscope, holmium laser energy and UAS from the same company The disadvantages include: its retrospective design, absence of a control group, and the untested duration of the surgery, which may be a risk factor for stricture formation
To our knowledge, there are no studies that investigated the use of a routine dynamic renal scan post-f-URS to diagnose ureteral strictures and suggest an early evaluation and treatment
We showed that f-URS was successful in 94 8% (237/250) of cases in the first session, and cumulative SFR in a twostage procedure was 99 7% (249/250) A third auxiliary procedure was done successfully in one patient In this study, favourable results were achieved, even if it included 30 8% (77/250) of lower pole stones The mean number of procedures per renal unit was 1 06 According to the Clavien-Dindo classification, no major complications were observed
CONCLUSIONS
O b s t r u c t i o n d u e t o u re t e r a l s t r i c t u re p o s t - f l e x i b l e ureteroscopy is very rare, a dynamic renal scan post-operatively may be used in high-risk patients
REFERENCES
1 Sorokin I, Mamoulakis C, Miyazawa K, et al Epidemiology of stone disease across the world World J Urol 2017; 35:1301-1320
2 de la Rosette J, Denstedt J, Geavlete P, et al CROES URS Study Group The clinical research office of the endourological society ureteroscopy global study: indications, complications, and outcomes in 11,885 patients J Endourol 2014; 28:131-9
3 Kılıç Ö, Akand M, Van Cleynenbreugel B Retrograde intrarenal surgery for renal stones - Part 2 Turk J Urol 2017; 43: 52-260
4 Takagi T, Go T, Takayasu H, Aso Y Fiberoptic pyeloureteroscope Surgery 1971; 70:661-3
5 Takayasu H, Aso Y, Takagi T, Go T Clinical application of fiberoptic pyeloureteroscope Urol Int 1971; 26:97-104
6 Xiong M, Zhu X, Chen D, et al Post ureteroscopic stone surgery ureteral strictures management: a retrospective study Int Urol Nephrol 2020; 52:841-849
7 Grasso M, Bagley D Small diameter, actively deflectable, flexible ureteropyeloscopy J Urol 1998; 160:1648-53
8 Ankem MK, Lowry PS, Slovick RW, et al Clinical utility of dual active deflection flexible ureteroscope during upper tract ureteropyeloscopy Urology 2004; 64:430-4
9 Mario S, Watterson JD, Wollin TA, et al Holmium:YAG laser lithotripsy for upper urinary tract calculi in 598 patients J Urol 2002; 167:31-34
10 Weizer AZ, Auge BK, Silverstein AD, et al Routine postoperative imaging is important after ureteroscopic stone manipulation J Urol 2002; 168:46-50
11 Elashry OM, Elgamasy AK, Sabaa MA, et al Ureteroscopic management of lower ureteric calculi: a 15-year single-centre experience BJU Int 2010; 102:1010-1017
12 El-Abd AS, Suliman MG, Farha MOA, et al The development of ureteric strictures after ureteroscopic treatment for ureteric calculi: a long-ter m study at two academic centres Arab J Urol 2014; 12:168-172
13 Li L, Pan Y, Weng Z,, et al A Prospective randomized trial comparing pneumatic lithotripsy and holmium laser for management of middle and distal ureteral calculi J Endourol 2015; 29:883-7
14 DiMarco DS, LeRoy AJ, Thieling S, et al Long-term results of treatment for ureteroenteric strictures Urology 2001; 58:909-13
15 Asali M Sheathed flexible retrograde intrarenal surgery without safety guide wire for upper urinary tract stones Arch Ital Urol Androl 2022; 94:186-189
16 Dindo D, Demartines N, Clavien PA Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey Ann Surg 2004; 240:205-13
17 Sanguedolce F, Bozzini G, Chew B, et al The Evolving Role of Retrograde Intrarenal Surgery in the Treatment of Urolithiasis Eur Urol Focus 2017; 3:46-55
18 Breda A, Angerri O Retrograde intrarenal surgery for kidney stones larger than 2 5 cm Curr Opin Urol 2014; 24:179-83
19 Roberts WW, Cadeddu JA, Micali S, et al Ureteral stricture formation after removal of impacted calculi J Urol 1998; 159:723-6
20 Brito AH, Mitre AI, Srougi M Ureteroscopic pneumatic lithotripsy of impacted ureteral calculi Int Braz J Urol 2006; 32:295-9
21 Darwish AE, Gadelmoula MM, Abdelkawi IF, et al Ureteral stricture after ureteroscopy for stones: A prospective study for the incidence and risk factors Urol Ann 2019; 11:276-281
22 Traxer O, Thomas A Prospective evaluation and classification of ureteral wall injuries resulting from insertion of a ureteral access sheath during retrograde intrarenal surgery J Urol 2013; 189:5804
23 Özsoy M, Kyriazis I, Vrettos T, et al Histological changes caused by the prolonged placement of ureteral access sheaths: an experimental study in porcine model Urolithiasis 2018; 46:397-404
24 Manger JP, Mendoza PJ, Babayan RK, Wang DS Use of renal ultrasound to detect hydronephrosis after ureteroscopy J Endourol 2009; 23:1399-402
25 May PC, Hsi RS, Tran H, et al The morbidity of ureteral strictures in patients with prior ureteroscopic stone surgery: multi-institutional outcomes J Endourol 2018; 32:309-314
26 Jung JH, Yoo S, Park J, et al Postoperative renal functional changes assessed by 99mTc-DTPA scintigraphy and predictive factors after miniaturized percutaneous nephrolithotomy and retrograde intrarenal surgery: An observational 1-year follow-up study Investig Clin Urol 2020; 61:59-66
27 Piao S, Park J, Son H, et al Evaluation of renal function in patients with a main renal stone larger than 1 cm and perioperative renal functional change in minimally invasive renal stone surgery: a prospective, observational study World J Urol 2016; 34:725-32
Correspondence
Murad Asali, MD (Corresponding Author) dr muradasali@gmail com Department of Urology, Barzilai Medical Center, Ben Gurion University of the Negev, Beer Sheva, Sokolov 26/99, 8430905
Osman Hallak, MD
Urology Department, Barzilai Medical Center, Ben Gurion University of the Negev, Beer Sheva, Israel
Conflict of interest: The authors declare no potential conflict of interest
M Asali, O Hallak
ORIGINAL PAPER
Exploring the potential of combined B-mode features and color Doppler
ultrasound in the diagnosis of ureteric stone as an alternative to ionizing radiation exposure by computed tomography
Ahmed M Abdel Gawad 1 , Bahaa-Eldin A Moustafa 2 , Tamer A Abouelgreed 3 , Esam A Elnady 1 , Saed Khater 1 , Mohamed Rehan 1 , Mohamed F Elebiary 3 , Basem A Fathy 3 , Ahmed Shaalan 4 , Nasser Ramadan 5 , Mohamed Hindawy 3 , Salma F Abdelkader 6
1 Department of Urology, Faculty of Medicine, Al-Azhar University, Damietta, Egypt;
2 Department of Radiology, Faculty of Medicine, Al-Azhar University, Damietta, Egypt;
3 Department of Urology, Faculty of Medicine, Al-Azhar University, Cairo, Egypt;
4 Department of Radiology, Faculty of Medicine, Al-Azhar University, Cairo, Egypt;
5 Department of Urology, NMC Royal hospital, Sharjah, UAE;
6 Department of Radiology, Faculty of Medicine, Ain shams University, Cairo, Egypt
Summary
Objective: To assess the diagnostic efficacy of integrating B-mode and color Doppler capabilities of ultrasound (US) to establish a robust standalone diagnostic tool for the diagnosis of ureteric stones as an alternative to non-contrast-enhanced computed tomography (NCCT)
Methods: A total of 140 consecutive patients diagnosed with ureteric stones using NCCT were enrolled On the same day, US in both B-mode and Color Doppler was performed by an experienced radiologist who was blinded to the NCCT scan results The diagnostic rate of US for stone detection was recorded. Additionally, baseline patient and stone characteristics were analyzed for their association with the accuracy of stone detection using US
Results: US exhibited a high sensitivity of 91.43%, detecting 128 out of 140 stone foci Notably, ureteric stones in the proximal and uretero-vesical junction (UVJ) segments were readily identifiable compared to those in the pelvic region (p = 0 0003)
Additionally, hydronephrosis enhanced the US's ability to detect stones (p < 0 0001) Conversely, abdominal gases and obesity adversely affected US capabilities (p < 0 0001 and p = 0 009, respectively) Stone side, size, and density showed no statistically significant impact (p > 0 05)
Conclusions: US with its color Doppler capabilities could serve as a reliable and safe alternative imaging modality in the diagnostic work up of patients with ureterolithiasis Factors including stone location, Hydronephrosis, weight and abdominal gases significantly influenced its accuracy.
Urolithiasis is a common health issue, with prevalence rates varying worldwide, ranging from 1% to 20% (1, 2) Patients with ureteral stones typically present repeatedly to the emergency room (ER) with acute abdominal pain, necessitating prompt evaluation Non-contrast-enhanced computed
tomography (NCCT) is the standard for diagnosing urinary stones However, utilizing NCCT for all patients may pose challenges since it has the inherent property of releasing ionizing radiation even with the usage of low-dose CT protocols with possible undesirable effects on the human body This directed research efforts towards the utilization of other safe diagnostic tools, such as ultrasonography (US) (1-3) US is now established as the primary diagnostic imaging modality in patients with ureteric colic It is safe (no radiation risk), reproducible, inexpensive, and widely available It can identify urinary stones, upper urinary tract (UUT) dilatation, as well as other causes of acute abdomen like ovarian problems and appendicitis (4) However, Bmode US is deemed lesser than CT in diagnosing ureteral stones US has a sensitivity of 45% and a specificity of 94%, compared to 93 1% and 96 6% for low-dose CT (1, 5) Changes in gain and depth, along with other modes such as angling, S (stone-specific) mode, and color Doppler capabilities like twinkling artifact (TA), are key variables enhancing US accuracy for stone detection (6, 7) In this study, we aimed to assess the diagnostic efficacy of integrating B-mode and color Doppler capabilities of US to establish a robust standalone diagnostic tool for the diagnosis of ureteric stones as an alternative to NCCT
PATIENTS AND METHODS
This is an interventional prospective study carried out between March 2022 and June 2023, including 140 consecutive patients diagnosed with ureteric stones by NCCT We excluded pregnant women, patient with sonographically detected issues responsible of the pain other than ureteric calculi like appendicitis, oophoritis, ovarian cyst and diverticulitis, and patients with double-J ureteric stents
Procedures
All studied patients initially underwent systematic examination by NCCT then US in B-mode and color Doppler
A M Abdel Gawad, B -E A Moustafa, T A Abouelgreed, et al
The examination occurred at Al-Azhar University Hospital, New Damietta
NCCT technique
CT imaging was performed using Toshiba aquilion 160 slices scanner, Japan, 2015 Patients were examined with full urinary bladder in supine position The coverage area extended from the upper pole of both kidneys to the base of the urinary bladder Tube potential of 100-120 kVp and automatic tube current modulation with mA range of 80500 was frequently used; however, the scan acquisition protocols were tailored to the patient body weight and CT scanner technology Axial sections of 5mm thickness were taken, complimented with 3 mm coronal/sagittal reformatted images Stone size was estimated by measuring largest dimension Measurements were made on the soft tissue window (window width - 400 HU and window level - 30 HU)
US (B-mode & color Doppler) technique
US imaging was performed using a real-time US machine
Figure 1
(Accuvix XG, Samsung Medison co , Korea 2018) which was equipped with an abdominal curved probe (C2-8 convex probe 2-8 MHz) and linear probe (11L-D High Frequency 2D Probe 4-10 MHz) Patients were examined with full urinary bladder After applying US gel on the abdomen, US imaging series were acquired aiming to scan the urinary tract as well as other abdominopelvic organs that may be responsible for the complaint The size and echogenicity of the renal parenchyma (normal, increased, or decreased) and the presence of any detectable parenchymal calcifications or abnormality were noted Starting with the identification of fluid-filled (an-echoic) calyces and renal pelvis, we went ahead to the ureter tracking it in its anatomical site which is also a fluid-filled tubular structure with absent flow signal in color mapping study The degree of dilatation of the pelvicalyceal system was graded (mild, moderate, and severe), and the ureters were visualized for dilatation The gases in the intestine that handicapped the visualization of the ureter were fought by gentle pressure by the probe as well as making the patient lie on the contralateral side Identification of calculi in the ureter was by
US images from a 45-year-old female patient with Distal Ureteric Stone (A) B-mode US scan of the right kidney in the longitudinal plane showing moderately dilated Pelvi-Caliceal System (PCS) (B) B-mode US scan of the urinary bladder and distal ureter (which is an-echoic tubular structure) in the longitudinal oblique plane, showing an echogenic stone with posterior acoustic shadowing inside the distal ureter. (C) Color Doppler scan on the previous plane exhibiting absent flow signal in the tubular structure (ensuring being ureter) & TA caused by the distal ureteric stone (D) Dual (B & Color) modes of the same plane
Figure 2.
US images from a 38-year-old male patient with Mid-Ureteric Stones. (A) B-mode US scan of the right kidney in the longitudinal plane showing mild HUN (B) B-mode US scan on the mid-ureter (which is an-echoic tubular structure) in the longitudinal oblique plane showing two hyperechoic stones with posterior acoustic shadowing inside it (Blue Arrows).
(C) Color Doppler scan on the previous plane exhibiting absent flow signal in the tubular structure (ensuring being ureter), TA of the two stones & blood flow color signals in iliac vessels (Yellow Arrow)
detection of abnormal objects with increased echoes on grayscale US that casts posterior acoustic shadowing Color Doppler US came after to detect TA presence utilizing a red-blue color map (Figures 1, 2)
Outcome measures
Data about patients’ age, sex, BMI and stone characteristics (side, size, location, density and hydroureteronephrosis) were collected In addition, the diagnostic rate of US (B-mode in combination with color Doppler) for stone detection was recorded
Sample size and statistical analyses
An online statistical calculator “https://statulator com/ SampleSize/ss1P html” was used to estimate the sample size considering the following factors: assuming that 10% of the subjects in the population suffer from urolithiasis (1, 2), 5% absolute precision, and 95% confidence
Allowing for a 10% dropout rate, a total sample size of 139 patients was estimated Data were tabulated and analyzed using the SPSS package 25 (IBM Corp, Armonk, NY, USA) Univariate analyses of continuous and categorical variables were done using the independent sample t-test and chi-square test, respectively The sensitivity of US (Bmode in combination with color Doppler) for stone
detection was calculated with 95% CI (confidence interval), with statistical significance considered at p < 0 05 Informed consent was obtained from all participants in the study, and the protocol for this research project was a p
This study included 140 consecutive patients diagnosed with ureteric stones using NCCT The patients' age ranged from 14 years to 77 years with a mean of 41 years The pre-procedural patients’ demographics (age, sex and BMI) and stone characteristics (side, size, location, density and hydroureteronephrosis) are detailed in Table 1 When B-mode and color Doppler US were employed, the US demonstrated a high sensitivity of 91 43% (95% CI: 85 51% to 95 49%), detecting 128 out of 140 stone foci, which indicates its effectiveness in accurately identifying true positive cases For further analysis, we assessed all factors potentially influencing US accuracy for stone detection, including baseline patients' and stone characteristics (Table 2) Interestingly, stone-related variables (side, size, and density) showed no statistically significant impact (p > 0 05) Conversely, patient-related variables
A M Abdel Gawad, B -E A Moustafa, T A Abouelgreed, et al
statistically significant association Ureteral stones in the proximal and uretero-vesical junction (UVJ) segments were readily identifiable compared to those in the pelvic region ( p = 0 0 0 0 3 ) A d d i t i o n a l l y , t h e p r e s e n c e o f H U N enhanced the US's ability to detect stones (p < 0 0001) Conversely, the presence of gases in the abdomen and obesity negatively impacted on US capabilities (p < 0 0001 and p = 0 009, respectively)
DISCUSSION
(27 14)
(55 72) Mod (Gr 2)
Sever (Gr 3) 7 (5)
Stone Size, mean ± SD (range), mm 8 5 ± 1 19 (3 74-21 2)
Stone Density, mean ± SD (range), HU 693 17 ± 590 35 (110-1440)
Location, n (%)
Lumber 42 (30)
Pelvic 81 (57 86)
17 (12
Uretero-Ves ca Junction
Table 2
Categorical variables tested against US accuracy for stone detection.
Junct on
(BMI and gaseous abdomen), stone location, and the degree of hydroureteronephrosis (HUN) demonstrated a
It is now a common practice to conduct imaging studies in all patients with suspected renal colic admitted to the emergency room This trend may stem from concerns about overlooking potentially life-threatening conditions that resemble renal colic, such as a ruptured aortic aneurysm, ovarian torsion, or appendicitis Additionally, there is a necessity for imaging confirmation to determine the underlying cause of symptoms before considering discharge (8, 9) NCCT is the official method for diagnosing urinary stones due to its benefits, being unaffected by intestinal gas and posing excellent accuracy in detecting ureteral stones However, concerns about the over-utilization of CT are growing because of increasing health care costs and, more importantly, exposure to ionizing radiation A study published in the Journal of the American Medical Association estimated that 1 in 1400 people over the age of 60 who receive NCCT may develop cancer or leukemia (10) It is noteworthy that radiation exposure has cumulative effects, raising the risk of future cancers This cumulative impact builds up over time Consequently, young individuals and pregnant women should minimize exposure to radiation whenever possible (11) Currently, there is a growing emphasis on radiation protection when imaging patients with suspected renal colic This focus has extended beyond the radiological community (12, 13) and emergency physicians (14, 15) to include urologists In the 2023 guidelines on urolithiasis of the European Association of Urology, it is stated that US should be the primary diagnostic imaging tool in patients with renal colic, and NCCT should be reserved for cases where the diagnosis is doubtful (1) US is a safe, cost-effective, non-invasive, and readily available technique for assessing patients with renal colic Importantly, prioritizing US usage can prevent radiation exposure in approximately 70% of cases and possesses the ability to identify alternative diagnoses mimicking renal colic (9, 16)
Nevertheless, its application remains a subject of debate as it effectively detects dilatation of the excretory system even in inexperienced hands (14) However, challenges arise in directly visualizing stones, particularly in the pelvic ureters, making it operator-dependent for stone detection and relying on “indirect findings” for diagnosis
Additionally, the absence of these “indirect findings” does not rule out ureteral stones (17) The performance of US studies by radiologists and modifications in gain and depth settings, along with the utilization of various modes such as angling, S (stone-specific) mode, and color Doppler features like TA, have been reported to enhance the precision of US for stone detection (6-8 & 18-20) The color Doppler TA manifests as a rapidly alternating signal in color Doppler imaging, resembling turbulent flow It is
often observed when scanning a stationary object with an irregular surface, such as urinary stones, which reflects the Doppler signal In Doppler imaging, this phenomenon presents as a jumbled pattern The spectral analysis of twinkling may reveal aliasing (7) It is very useful to confirm findings of grey-scale, especially in doubtful cases due to the small size of the stone or when its location is in difficult-to-visualize ureteral portions However, careful interpretation is essential since the jumbled pattern of twinkling may mimic turbulent flow, which could be confusing and may lead to errors in diagnosis Additionally, the presence of aliasing in the twinkling spectrum could further complicate the interpretation, potentially making it challenging to distinguish between true flow abnormalities and artifacts Therefore, it should be interpreted along with other clinical information and imaging modalities to ensure an accurate diagnosis (17) Several studies have highlighted the usefulness of US compared to NCCT in the initial diagnosis and management of renal colic patients, without a notable increase in complications, serious adverse events, return emergency department visits, or hospitalizations (18-20) In our study, the sensitivity of US for detection of ureteric stones was about 91 43%, detecting 128 out of 140 stone foci (95% CI: 85 51% to 95 49%) which is in accordance with previous reports (21-23) The role of patient’s and stone-related variables in the US detection of ureteric stones has been extensively evaluated in previous reports Factors such as the presence of HUN, vascular calcifications and other artifacts that may also be mistaken for stones, experience and knowledge of the urinary tract anatomy and the presence of bowel gas, which may obscure the ureteral calculi, as well as stone size, location, and density, can affect the detection of ureteric stones For instance, Ahmed et al reported an overall sensitivity of US of 75 4% The detection rate of mid and distal ureteral stone was lower than that at proximal locations, and the detection rate increased with stone size and the degree of HUN Conversely, US is of limited value, particularly when used by an inexperienced radiologist, and in the case of smaller stone size, increased weight, and low grade of HUN (22) Another study by Sen et al reported a sensitivity of US of 86 8 %, with better success noted in proximal ureteral stones (95 6 %) (21) Goertz and Lotterman also found that the increasing degree of HUN was associated with an increased likelihood of diagnosing ureteric stones using US (24) In a more recent report on the diagnostic value of US in ureteric stones ≤ 10 mm by Krakhotkin et al , while the US demonstrated a sensitivity rate exceeding 90% for stones ≥ 5 mm located in the proximal and distal ends of the ureter, its accuracy was notably restricted, not exceeding 53%, for stones sizing 1-3 mm and those situated in the middle ureter possibly due to bowel interposition (25) Our results closely align with previous reports, indicating that the stone location and increasing degree of HUN were associated with increasing detection rate of ureteric stone in US (p = 0 0003 and < 0 0001, respectively) On the other hand, the presence of bowel gases negatively impacted US capabilities (p < 0 0001) Of note all US assessments in our study were conducted solely by an experienced radiologist Regarding the impact of BMI on the sensitivity of US and color Doppler capabilities, some
studies have reported that higher BMI values decrease the sensitivity of both modalities (22, 26, 27), consistent with our findings (p = 0 009) However, others have not found any correlation (18, 21, 28), possibly due to the small number of patients with BMI > 30 kg/m² As for the role of stone size, it was evaluated in several studies Winkel et al (16) and Mitterberger et al (19) found no correlation However, Sen et al (21), Ahmed et al (22), Krakhotkin et al (25), and Sorensen et al (29) reported that as the stone size increased, the sensitivity of US also increased In our study, the ureteral stone side, size, and density exhibited no statistically significant impact (p > 0 05)
Limitations
Our study possesses certain limitations Firstly, color Doppler US relies heavily on the examiner's skill; specific training of healthcare professionals may be required to develop sufficient skills and be aware of its strengths and limitations Also, our study was single-blinded; future double-blinded research investigations may shed more light on the preference of US over NCCT Furthermore, future studies examining US outcomes in relation to different operators rather than a single expert, as well as investigating the role of stone composition and surface roughness are warranted
CONCLUSIONS
US with its color Doppler capabilities could serve as a promising and safe alternative imaging modality in the diagnostic work up of patients with ureterolithiasis However, factors such as stone location, HUN, weight, and the presence of abdominal gases, along with the examiner’s competence significantly influence its accuracy
REFERENCES
1 A Skolarikos, H Jung, A Neisius, et al (2023) EAU Guidelines on Urolithiasis - Limited Update March 2023 European Association of Urology, Arnhem, the Netherlands ISBN 978-94-92671-19-6 Retrieved from https://uroweb org/guidelines/urolithiasis/
2 Sorokin I, Mamoulakis C, Miyazawa K, et al Epidemiology of stone disease across the world World J Urol 2017; 35:1301-1320
3 Zou B, Zhou Y, He Z, et al A critical appraisal of urolithiasis clinical practice guidelines using the AGREE II instrument Transl Androl Urol 2023; 12:977-988
4 Wang M, Ma Q, Chen Y, et al Value of the color Doppler imaging mode in improving physicians' diagnostic performance in patients with mid-ureteric stones larger than 5 mm: a retrospective study Urolithiasis 2021; 49:463-469
5 Xiang H, Chan M, Brown V, et al Systematic review and metaanalysis of the diagnostic accuracy of low-dose computed tomography of the kidneys, ureters and bladder for urolithiasis J Med Imaging Radiat Oncol 2017; 61:582-590
6 Dunmire B, Lee FC, Hsi RS, et al Tools to improve the accuracy of kidney stone sizing with ultrasound J Endourol 2015; 29:1471452
7 Sternberg KM, Eisner B, Larson T, et al Ultrasonography Significantly Overestimates Stone Size When Compared to Low-dose, Non-contrast Computed Tomography Urology 2016; 95:67-71
8 May PC, Haider Y, Dunmire B, et al Stone-Mode Ultrasound for Determining Renal Stone Size J Endourol 2016; 30:958-62
9 Moore CL, Carpenter CR, Heilbrun ML, et al Imaging in Suspected Renal Colic: Systematic Review of the Literature and Multispecialty Consensus J Urol 2019; 202:475-483
10 Rehab Abdel Rahman El Bakry Prospective comparative study between un-enhanced multi-detectors computed tomography and ultrasonography in evaluation of acute renal colic, Alexandria Journal of Medicine 2017; 53:367-371
11 Schmid E, Leeson K, Xu KT, et al CT imaging history for patients presenting to the ED with renal colic--evidence from a multi-hospital database BMC Emerg Med 2019; 19:24
12 Moore CL, Scoutt L Sonography first for acute flank pain? J Ultrasound Med 2012; 31:1703-11
13 Patatas K, Panditaratne N, Wah TM, et al Emergency department imaging protocol for suspected acute renal colic: re-evaluating our service Br J Radiol 2012; 85:1118-22
14 Dalziel PJ, Noble VE Bedside ultrasound and the assessment of renal colic: a review Emerg Med J 2013; 30:3-8
15 Smith-Bindman R, Aubin C, Bailitz J, et al Ultrasonography versus computed tomography for suspected nephrolithiasis N Engl J Med 2014; 371:1100-10
16 van Randen A, Laméris W, van Es HW, et al OPTIMA Study Group A comparison of the accuracy of ultrasound and computed tomography in common diagnoses causing acute abdominal pain Eur Radiol 2011; 21:1535-1545
17 Nicolau C, Claudon M, Derchi LE, et al Imaging patients with renal colic-consider ultrasound first Insights Imaging 2015; 6:441447
18 Winkel RR, Kalhauge A, Fredfeldt KE The usefulness of ultrasound colour-Doppler twinkling artefact for detecting urolithiasis compared with low dose nonenhanced computerized tomography Ultrasound Med Biol 2012; 38:1180-1187
19 Mitterberger M, Aigner F, Pallwein L, et al Sonographic detection of renal and ureteral stones Value of the twinkling sign Int Braz J Urol 2009; 35:532-539
20 Ripollés T, Martínez-Pérez MJ, Vizuete J, et al Sonographic diagnosis of symptomatic ureteral calculi: usefulness of the twinkling artifact Abdom Imaging 2013; 38:863-869
21 Sen V, Imamoglu C, Kucukturkmen I, et al Can Doppler ultrasonography twinkling artifact be used as an alternative imaging modality to non-contrast-enhanced computed tomography in patients with ureteral stones? A prospective clinical study Urolithiasis 2017; 45:215-219
22 Ahmed F, Askarpour MR, Eslahi A, et al The role of ultrasonography in detecting urinary tract calculi compared to CT scan Res Rep Urol 2018; 10:199-203
23 Patlas M, Farkas A, Fisher D, et al Ultrasound vs CT for the detection of ureteric stones in patients with renal colic Br J Radiol 2001; 74:901-4
24 Goertz JK, Lotterman S Can the degree of hydronephrosis on ultrasound predict kidney stone size? Am J Emerg Med 2010; 28:813-6
25 Krakhotkin DV, Chernylovskyi VA, Sarica K, et al Diagnostic value ultrasound signs of stones less than or equal to 10 mm and clinico-radiological variants of ureteric colic Asian J Urol 2023; 10:3949
26 Asbeutah AM, Bakir YY, Swamy N, et al Subject body mass index affects Doppler waveform in celiac artery by duplex ultrasound Open Cardiovasc Med J 2013; 7:40-45
27 Pichler R, Skradski V, Aigner F, et al In young adults with a low body mass index ultrasonography is sufficient as a diagnostic tool for ureteric stones BJU Int 2012; 109:770-774
28 Kielar AZ, Shabana W, Vakili M, Rubin J Prospective evaluation of Doppler sonography to detect the twinkling artifact versus unenhanced computed tomography for identifying urinary tract calculi J Ultrasound Med 2012; 31:1619-1625
29 Sorensen MD, Harper JD, Hsi RS, et al B-mode ultrasound versus color Doppler twinkling artifact in detecting kidney stones J Endourol 2013; 27:149-153
Correspondence
Ahmed M Abdel Gawad (Corresponding Author) ahgawad84@gmail com
Esam A Elnady esammohsen@gmail com
Saed Khater dr saedkhater@gmail com
Mohamed Rehan mrehan4040@gmail com
Department of Urology, Faculty of Medicine, Al-Azhar University, Damietta, Egypt
Bahaa-Eldin A Moustafa dr bhaa@gmail com
Department of Radiology, Faculty of Medicine, Al-Azhar University, Damietta, Egypt
Tamer A Abouelgreed dr tamer ali@yahoo com
Mohamed F Elebiary dr elebiary@yahoo com
Basem A Fathy basemhara@Gmail com
Mohamed Hindawy hindawy78@gmail com
Department of Urology, Faculty of Medicine, Al-Azhar University, Cairo, Egypt
Ahmed Shaalan dr ahmedshallan@yahoo com
Department of Radiology, Faculty of Medicine, Al-Azhar University, Cairo, Egypt
Nasser Ramadan nasseruro99@gmail com
Department of Urology, NMC Royal Hospital, Sharjah, UAE
Salma F Abdelkader salmafathy4@gmail com
Department of Radiology, Faculty of Medicine, Ain Shams University, Cairo, Egypt
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Role of urine glycosaminoglycan levels in the diagnosis and follow-up in men with lower urinary tract symptoms
Hasan Riza Aydin 1 , Cagri Akin Sekerci 2 , Huseyin Kocakgol 3 , Banu Isbilen Basok 4 , Fevzi Bedir 3 , Ahmet Ozgur Guctas 5 , Firat Akdeniz 6 , Hamit Zafer Aksoy 1 , Mehmet Akif Ramazanoglu 7 , Yiloren Tanidir 2
1 Department of Urology, Trabzon Faculty of Medicine, University of Health Sciences, Trabzon, Turkey;
2 Department of Urology, School of Medicine, Marmara University, Istanbul, Turkey;
3 Department of Urology, Erzurum Training and Research Hospital, Erzurum, Turkey;
4 Department of Biochemistry, Tepecik Training and Research Hospital, University of Health Sciences, Izmir, Turkey;
5 Department of Urology, Marmara Pendik Training and Research Hospital, Istanbul, Turkey;
6 Medical Park Hospital, Trabzon Turkey;
7 Department of Urology, Trabzon Kanuni Training and Research Hospital, Trabzon, Turkey
Summary
Objective: The aim of this study was to investigate whether urinary glycosaminoglycans (GAG) levels reflect clinical status in men with lower urinary tract symptoms and if they could be used as a marker in management of overactive bladder (OAB).
Methods: A total of 34 patients were recruited who were admitted with LUTS and diagnosed as having clinically bladder outlet obstruction (BOO) due to prostate enlargement These newly diagnosed, never treated patients underwent routine investigation, consisting of history, physical examination, PSA, ultrasound, uroflowmetry, assessment of symptoms scored by both International Prostate Symptom Score (IPSS) and MarmaraOveractive Bladder Questionnaire (M-OBQ). The patients were divided into two groups as those with an initial M-OBQ score < 12 (group 1) and ≥ 13 (group 2). Alfa blocker was initiated in eligible patients Further evaluations included prostate volume measurement, pre- and post-treatment urinary GAG levels, IPSS and M-QAOB values and maximum urine flow rate (Qmax)
Results: Before treatment, urinary GAG level was 21 5 mg/gCr (6 1-45 5) in Group 1, and 23 35 mg/gCr (15 6-32 6) in Group 2 (p =0 845) After the treatment, the GAG level in Group 1 and Group 2 were found to be 19 8 mg/gCr (7 4-70 5) and 18 (7 641 7), respectively (p = 0 511) No difference in GAG levels was found in subgroup analysis for patients with or without OAB
Conclusions: In recent years, there have been many studies investigating the relationship between LUTS and urinary markers However, in our prospective study, no relationship was found between pre- and post- treatment urinary GAG levels in patients with LUTS with or without OAB
Submitted 2 February 2024; Accepted 18 February 2024
INTRODUCTION
Lower urinary tract symptoms (LUTS) are one of the most common conditions in the urology clinic, affecting at least one in four men after 40 years of age (1) Bladder dysfunction (detrusor overactivity or underactivity) and blad-
der outlet obstruction (BOO) are two main pathologies involved in the etiology of LUTS (2) LUTS is often associated with BOO caused by prostate enlargement in men Moderate and severe LUTS are reported as 26% in men aged 40-49, while this rate doubles in the group aged 70 and older (3) The International Prostate Symptom Score (IPSS) from 8 to 19 indicates moderate LUTS (4), while a m a x i m u m f l o w ( Q max) o f l e s s t h a n 1 5 m l / s e c i n uroflowmetry has 82% sensitivity for BOO (5) According to European Association Urology (EAU) Guidelines (6), alpha blockers are recommended as the first-line medical treatment in patients clinically diagnosed with BOO (7) In recent years, many studies have been published on the relationship of urinary biomarkers with LUTS Nerve growth factor and brain derived neurotrophic factor, which are among most studied markers, have been shown to be closely associated with neurogenic or nonneurogenic detrusor overactivity and significant improvements were observed after treatment (8-11) The relationship between urinary glycosaminoglycan (GAG) and overactive bladder (OAB) has been demonstrated and it has been reported that the values have decreased after treatment (12) Men with prostate enlargement (PE) and LUTS often have symptoms of overactive bladder However, to our knowledge, there is no previous study in the literature examining the utility of urinary GAG levels in this patient group The aim of this study was to investigate the relationship between urinary GAG levels and patients with LUTS
MATERIALS AND METHODS
Patients who were seen in the outpatient clinic due to LUTS and diagnosed as clinically BOO due to PE were included in the study Ethical approval was obtained from the local ethics committee (2018/53) The study was designed prospectively and submitted to ClinicalTrials gov (Identifier: NCT03955484) Before starting an alphablocker medication, patients were enrolled to the study All patients were evaluated under the guidance of EAU guide-
lines (6) Patients received routine investigation, consisting of medical history taking, physical examination including digital rectal examination, prostate-specific antigen (PSA), urinalysis and urine culture, ultrasound imaging, and uroflowmetric study, measurement of post void residual urine (PVR) assessment of symptoms scored by both International Prostate Symptom Score (IPSS) and MarmaraOveractive Bladder Questionnaire (M-OABQ) (13)
Male patients who applied to the urology outpatient clinic with LUTS, and had an IPSS of 8 and above, and a prostate volume greater than 40 ml and a maximum flow of less than 15 ml/sec, were diagnosed with clinically BOO due to prostate enlargement Of these patients, those who did not receive any medical and/or surgical treatment for LUTS were found to be eligible for the study
Patients with a history of medical and/or surgical treatment for LUTS, or with a diagnosis of urethral stenosis, prostate cancer, neurologic diseases, spinal cord trauma or an absolute indication for surgical treatment at first admission (macroscopic hematuria, bladder stones, urinar y retention, upper urinar y tract dilatation) were excluded from the study Also, patients who required prostate biopsy according to rectal examination and PSA were not included the study In the initial evaluation, those who were not suitable for alpha-blocker treatment and needed urodynamic examination were excluded from the study Apart from the study group, 10 healthy adult males were selected as the controls for the assessment of baseline urinary GAG levels
The study group were divided into two subgroups, according to M-OABQ score before the alpha-blocker medication: a score of 12 and less (group 1) and a score of 13 and higher (group 2) The M-OABQ is a tool to assess OAB symptoms M-OAB questionnaire consists of eight questions and it has the highest sensitivity (97%) and specificity (94%) for the diagnosis of OAB when a cut off value of 12 5 for the total score is used (13) After one month of alpha blocker treatment, all patients underwent re-evaluated with uroflowmetry, PVR, IPSS, M-OABQ Pre- and post-treatment urinary GAG values, prostate volumes, IPSS and MOABQ values and Qmax were compared
B io c h em ic al an alysis
Midstream mor ning urine samples were collected into sterile urine collection tubes and each urine sample was centrifuged at 5000 g for 10 minutes, the super natant was aliquoted in 1 5-mL microcentrifuge tubes and stored at -800C until further analysis
Total GAG levels in supernatants were determined using the Blyscan Sulfated Glycosaminoglycan assay (Blyscan Assay, Biocolor Ltd , Northern Ireland, UK) according to the manufacturer’s instructions (14) The Blyscan Assay as a direct colorimetric method quantifying urinar y glycosaminoglycan excretion exploits the specific binding of 1,9-dimethylmethylene blue that provides a specific label for the sulfated polysaccharide component of proteoglycans or the protein-free sulfated glycosaminoglycan chains (15) The detection limit of assay was 2 5 µg/mL Urinary creatinine (Cr) concentration was determined on each sample using the kinetic Jaffe method in the AU5800 clinical chemistry system (Beckman Coulter Inc ,
CA, USA) The urinary concentrations of GAG were normalized to the concentration of urinary Cr and results were expressed as, milligram per gram of Cr
S t at ist ic al an alysis
Data were analyzed using the IBM Statistical Package for the Social Sciences version 22 (IBM SPSS Statistics for Windows, Chicago, IL, USA) The normality of the distribution of the variables was evaluated using the ShapiroWilk test As the distribution of continuous variables did not show a normal distribution, continuous data were p
Comparison of independent and dependent groups were done with Mann-Whitney U test and Wilcoxon Signed Ranks Test, respectively The p value < 0 05 was accepted as statistically significant
RESULTS
Thirty-four patients with a median age of 59 5 (42-74) years were included in the study There were 22 patients in group 1 and 12 patients in group 2 The median age of the control group was 44 5 (44-52) years The median age of group 1 was 60 (48-72) years, and of group 2 was 58 (54-74) (p = 0 845) Pre-treatment normalized urinary GAG level was found to be 20 8 (6 1-45 5) mg/gCr in study group and 17 8 (11 5-22 26) mg/gCr in control group (p = 0 183) The normalized urinary GAG level of the study group after the treatment was found to be 19 7 (7 53-70 5) mg/gCr and did not show a statistical difference compared to the pre-treatment level (p = 0 530) Initial normalized urinary GAG value of group 1 and 2 were as 21 5 (6 1-45 5) mg/gCr and 23 35 (15 6-32 6) mg/gCr, respectively (p = 0 845) (Table 1) Both IPSS and M-OBQ score were found to be higher in group 2 compared to group 1 (p = 0 009, p < 0001, respectively) (Table 1) Baseline prostate volume (ml), PSA (mg/dl), PVR (ml), Qmax (ml/sec) were found to be similar in both groups (p = 0 136, p = 0 383, p = 0 276, p = 0 790, respectively) (Table 1)
Table 1.
Comparison of age, prostate volume, symptom scores, PVR, Qmax and urinary GAG values between the two groups before medical treatment
PSA: Prostate Specific Antigen; IPSS: Internat ona Prostate Symptom Score; QL: Qua ity of L fe; M-OABQ: Marmara-Overactive B adder Questionnaire; PVR: Post Void Residua Urine Vo ume; Qmax: Max mum Urine F ow Rate; GAG: G ycosam noglycan
H Riza Aydin, C Akin Sekerci, H Kocakgol, et al
Table 2.
Comparison of symptom scores, PVR, Qmax and urinary GAG values between the two groups after medical treatment
Post-treatment Group 1 (n: 22) Group 2 (n: 12) p value
IPSS: Internat onal Prostate Symptom Score; QL: Qual ty of Life; M-OABQ: Marmara-Overact ve Bladder Quest onnaire; PVR: Post Vo d Residual Ur ne Volume; Qmax: Maximum Ur ne Flow Rate; GAG: Glycosaminog ycan
After the alpha-blocker treatment, the normalized urinary GAG levels in group 1 and 2 was found to be statistically similar as 19 8 (7 4-70 5) mg/gCr and 18 (7 6-41 7) mg/gCr, respectively (p = 0 511) (Table 2) Interestingly, only M-OBQ score was still found to be higher in group 2 compared to group 1 (p < 0 0001), but IPSS, PVR and Qmax were found to be statistically similar (p=0 204, p= 0 309, p = 0 245, respectively) (Table 2)
DISCUSSION
Recently, several urinary biomarkers have been frequently studied in the assessment of LUTS In general, urinary biomarker levels are frequently studied in various disease as they can be measured both noninvasively and easily GAGs, a polysaccharide molecule produced in every cell in the human body, exist in two main structures as sulfated and non-sulfated (16, 17) Non-sulfated GAG contains hyaluronic acid, while sulfated GAGs include chondroitin sulfate, dermatan sulfate, keratan sulfate, heparan sulfate, and heparin GAGs are in the structure of the basal lamina of the urethra, and damage to the GAG layer can affect the basal functions of the urothelium (17, 18) This process may result in the bladder surface being exposed to microcrystals, proteins, calcium, toxic metabolic products, and carcinogens of the urine (19) Thus, GAGs have been studied in overactive bladder (OAB) and found to have an association with OAB (12)
Intriguingly, urinary GAG levels are affected differently in patients with LUTS symptoms In a study conducted with 45 patients with OAB, urinary GAG levels were found to be higher in the patients with OAB compared to the healthy subjects One month of solifenacin treatment did help to decrease GAG levels but no significant difference was found between responders and non-responders (12)
Yet, in another study involving 25 patients with LUTS (mean age 65 75 years) and urodynamically proven detrusor overactivity, urinary GAG values were shown to be low compared to the healthy control group (20) In interpreting this finding, the authors speculated that high-amplitude and prolonged overactive detrusor contractions may be associated with the ischemic process in the bladder epithelium, which in turn could reduce urinary GAG excretion
The relationship between interstitial cystitis (IC), another
pathology, and urinary GAG level has also been studied Like in OAB, levels of urinary GAG were differently reported Lokeshwar et al reported urinary GAG levels to be higher in patients with IC compared to healthy controls and even higher in patients with severe IC symptoms compared to those with mild symptoms (21) Controversially, Lucon et al reported urinary GAG levels to be low in patients with IC compared to patients with stress urinary incontinence However, these authors also evaluated GAG in tissue samples and could not show a decrease in the GAG content of the urothelium in any groups (22) Nocturnal enuresis appears to be another pathology associated with changes of urinary GAG values Researchers have shown that urinary GAG excretion is increased in children with nocturnal enuresis compared to healthy children (23, 24) Urinary GAG has also been reported to be associated with other urological pathologies such as renal cell carcinoma, acute renal failure, and bladder cancer, apart from lower urinary tract pathologies
In the current study, no significant difference was found between urinary GAG values in BOO patients with and without OAB symptoms Most significant limitation of our prospective study is the small sample size; it could be responsible for the failure to show statistical difference in various situations Another limitation is the lack of urodynamics to diagnose detrusor over activity and BOO Additionally, the control group was younger and was not formally assessed as the study group with medical history taking, physical examination including digital rectal examination, PSA, ultrasound imaging, and uroflowmetric study, measurement of PVR and assessment of symptoms by IPSS and M-OABQ
CONCLUSIONS
No potential role of measurement of urinary GAG was found in the evaluation of patients with LUTS in this study We consider that this result may have been affected by the small number of the sample of patients and should be confirmed by studies with a higher number of subjects
REFERENCES
1 Robertson C, Link CL, Onel E, et al The impact of lower urinary tract symptoms and comorbidities on quality of life: the BACH and UREPIK studies BJU Int 2007; 99:347-54
2 Chapple CR, Wein AJ, Abrams P, et al Lower urinary tract symptoms revisited: a broader clinical perspective Eur Urol 2008; 54:563-9
3 Speakman M, Kirby R, Doyle S, Ioannou C Burden of male lower urinary tract symptoms (LUTS) suggestive of benign prostatic hyperplasia (BPH) - focus on the UK BJU Int 2015; 115:508-19
4 Barry MJ, Fowler FJ, Jr , O'Leary MP, et al The American Urological Association symptom index for benign prostatic hyperplasia The Measurement Committee of the American Urological Association J Urol 1992; 148:1549-57
5 Reynard JM, Yang Q, Donovan JL, et al The ICS-'BPH' Study: uroflowmetry, lower urinary tract symptoms and bladder outlet obstruction Br J Urol 1998; 82:619-23
6 Cornu JN, Gacci M, Hashim H, et al Eau Guidelines on Non-
Neurogenic Male Lower Urinary Tract Symptoms (LUTS), incl Benign Prostatic Obstruction (BPO) EAU Guidelines Edn presented at the EAU Annual Congress Milan March 2023, EAU Guidelines Office, Arnhem, the Netherlands
7 Gravas S, Cornu J, Gacci M, et al Management of non-neurogenic male lower urinary tract symptoms (LUTS), incl benign prostatic obstr uction (BPO) 2019 https://uroweb org/guidelines/management-of-non-neurogenic-male-luts
8 Suh YS, Ko KJ, Kim TH, et al Urinary Nerve Growth Factor as a Potential Biomarker of Treatment Outcomes in Overactive Bladder Patients Int Neurourol J 2017; 21:270-81
9 Cekerci Ç A, Isbilen B, Isman F, et al Urinary NGF, TGF-b1, TIMP-2 and bladder wall thickness predict neurourological findings in children with myelodysplasia J Urol 2014; 191:199-205
10 Wang LW, Han XM, Chen CH, et al Urinary brain-derived neurotrophic factor: a potential biomarker for objective diagnosis of overactive bladder Int Urol Nephrol 2014; 46:341-7
11 Sekerci CA, Tanidir Y, Toprak T, et al Value of Urinary BrainDerived Neurotrophic Factor Levels on the Assessment of Botulinum Toxin Type A Treatment for Neurogenic Detrusor Overactivity in Children with Myelodysplasia J Urol 2019; 201:174-80
12 Alkis O, Zumrutbas AE, Toktas C, et al The use of biomarkers in the diagnosis and treatment of overactive bladder: Can we predict the patients who will be resistant to treatment? Neurourol Urodyn 2017; 36:390-3
13 Mesane MAA, Formunun S Constitution and validation of a new s y m p t o m a s s e s s m e n t t o o l f
r : M
a r a Overactive Bladder Questionnaire (M-OBQ) Journal of Urological Surgery 2014; 1:24-7
14 Mashima R, Sakai E, Tanaka M, et al The levels of urinary glycosaminoglycans of patients with attenuated and severe type of mucopolysaccharidosis II determined by liquid chromatography-tandem mass spectrometry Mol Genet Metab Rep 2016; 7:87-91
15 Whitley CB, Ridnour MD, Draper KA, et al Diagnostic test for mucopolysaccharidosis I Direct method for quantifying excessive urinary glycosaminoglycan excretion Clin Chem 1989; 35:374-9
16 Gandhi NS, Mancera RL The structure of glycosaminoglycans and their interactions with proteins Chem Biol Drug Des 2008; 72:455-82
17 Ustundag Y, Huysal K, Guzelsoy M, et al Urine and serum glycosaminoglycan levels in the diagnosis of urological diseases and conditions: A narrative review of the literature Urologia 2021; 88:103-9
18 Costantini E, Lazzeri M, Porena M GAGs and GAGs diseases: when pathophysiology supports the clinic Urologia 2013; 80:173-8
19 Nickel JC, Emerson L, Cornish J The bladder mucus (glycosaminoglycan) layer in interstitial cystitis J Urol 1993; 149:716-8
20 Siracusano S, Cucchi A, Ciciliato S, et al Urinary levels of glycosaminoglycans in patients with idiopathic detrusor overactivity Int Urogynecol J Pelvic Floor Dysfunct 2009; 20:1477-80
21 Lokeshwar VB, Selzer MG, Cerwinka WH, et al Urinary uronate and sulfated glycosaminoglycan levels: markers for interstitial cystitis severity J Urol 2005; 174:344-9
22 Lucon M, Martins JR, Leite KR, et al Evaluation of the metabolism of glycosaminoglycans in patients with interstitial cystis Int Braz J Urol 2014; 40:72-9
23 Ferrara P, Rigante D, Lambert-Gardini S, et al Urinary excretion of glycosaminoglycans in patients with isolated nocturnal enuresis or combined with diurnal incontinence BJU Int 2000; 86:824-5
24 Budak YU, Huysal K, Guray A Urinary glycosaminoglycan excretion in patients with primary nocturnal enuresis Ital J Pediatr 2010; 36:13
Correspondence
Hasan Riza Aydin, MD (Corresponding Author) hrizaaydin@gmail com
Hamit Zafer Aksoy, MD
hamitzaferaksoy@hotmail com
Department of Urology, Trabzon Faculty of Medicine, University of Health Sciences, Trabzon, Turkey
Cagri Akin Sekerci, MD cagri sekerci@hotmail com
Yiloren Tanidir yiloren@yahoo com
Department of Urology, School of Medicine, Marmara University, Istanbul, Turkey
Huseyin Kocakgol, MD hsynkocakgl@gmail com
Fevzi Bedir, MD fevzibedir84@gmail com
Department of Urology, Erzurum Training and Research Hospital, Erzurum, Turkey
Banu Isbilen Basok, MD drisbilen@yahoo com
Department of Biochemistry, Tepecik Training and Research Hospital, University of Health Sciences, Izmir, Turkey
Ahmet Ozgur Guctas, MD aoguctas@gmail com
Department of Urology, Marmara Pendik Training and Research Hospital, Istanbul, Turkey
Firat Akdeniz, MD dr frt5535@gmail com
Medical Park Hospital, Trabzon Turkey
Mehmet Akif Ramazanoglu, MD maramazanoglu@hotmail com
Department of Urology, Trabzon Kanuni Training and Research Hospital, Trabzon, Turkey
Conflict of interest: The authors declare no potential conflict of interest
H Riza Aydin, C Akin Sekerci, H Kocakgol, et al
ORIGINAL PAPER
Efficacy of
Palmitoylethanolamide, Epilobium
and Calendula suppositories for the treatment of patients with chronic prostatitis/chronic pelvic pain syndrome type III
Giuseppe Morgia 1 , Arturo Lo Giudice 1 , Maurizio Carrino 2 , Salvatore Voce 3 , Andrea Cocci 4 , Giulio Reale 3 , Andrea Minervini 4 , Sebastiano Cimino 5 , Giorgio Ivan Russo 5 , Francesca Zingone 1
1 Unit of Urology, Mediterranean Oncological Institute (IOM), University of Catania, Italy;
2 Unit of Urology, Cardarelli Hospital, Naples, Italy;
3 Unit of Urology, Ravenna Hospital, Italy;
4 Department of Urology, University of Florence, Italy;
5 Department of Urology, University of Catania, Italy
Summary
Objective: The management of chronic prostatitis/chronic pelvic pain syndrome type III (CP/CPPS) has been always considered complex due to several biopsychological factors underlying the disease In this clinical study, we aimed to evaluate the efficacy of the treatment with Palmitoylethanolamide, Epilobium and Calendula extract in patients with CP/CPPS III
Materials and methods: From June 2023 to July 2023, we enrolled 45 consecutive patients affected by CP/CPPS type III in three different institution We included patients aged between 18 and 75 years with symptoms of pelvic pain for 3 months or more before the study, a total National Institutes of Health Chronic Prostatitis Symptom Index (NIH-CPSI) score ≥ 12 point and diagnosed with NIH category III, according to 4-glass test Meares-Stamey test. Patients were then allocated to receive rectal suppositories of PEA, Epilobium and Calendula, 1 suppository/die for 1 month. All patients have been tested with standard urinalysis in order to assess urinary leukocytes (U-WBC)
The primary endpoint of the study was the reduction of NIHCPSI The secondary outcomes were the change of peak flow, post-void residual (PVR), IIEF-5, VAS score, PSA and decrease of U-WBC
Results: A total of 45 patients concluded the study protocol. At baseline, the median age of all the patients included in the cohort was 49 years, the median PSA was 2.81 ng/ml, the median NIH-CPSI was 18 55, the median IIEF-5 was 18 27, the median U-WBC was 485 3/mmc, the median VAS score was 6 49, the median PVR was 26 5 ml and the median peak flow was 16 3 ml/s After 1 month of therapy we observed a statistically significant improvement of NIH-CPSI, U-WBC, PSA, IIEF-5, peak flow, PVR and VAS
Conclusions: In this observational study, we showed the clinical efficacy of the treatment with PEA, Epilobium and Calendula, 1 suppository/die for 1 month, in patients with CP/CPPS III
The benefits of this treatment could be related to the reduction of inflammatory cells in the urine that could imply a reduction of inflammatory cytokines These results should be confirmed in further studies with greater sample size.
Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) stands as one of the prevalent conditions affecting men, often related with benign prostatic hyperplasia (BPH), posing significant financial burdens on healthcare systems (1-4) Despite its prevalence and the progress in treatment of BPH (5), the understanding of CP/CPSS underlying mechanisms remains incomplete due to diverse risk factors and associated conditions Psychological factors and various triggers, such as infection or inflammation, can exacerbate CP/CPPS mechanisms, ultimately impacting patients' quality of life (QoL) and psychological wellbeing (6) Consequently, treatment approaches vary and may not consistently yield clinical efficacy, as shown by the variability in reported treatment effects across case series and controlled trials, often influenced by placebo effects or publication biases (7) Among the spectrum of therapies, some new treatments emerged in last years, such low-intensity shockwave therapy and acupuncture (8, 9) although there is not enough strong evidence to adopt these therapies in clinical practice The core of treatment of CP/CPSS is still phytotherapy, or herbal medicine, particularly in alleviating pain and enhancing QoL, alongside mild anti-inflammatory effects Additionally, rectal therapies involving corticosteroids have shown promise in CP/CPPS patients, with beclomethasone di-propionate suppositories demonstrating a favorable safety profile and efficacy in ameliorating storage symptoms and clinical findings associated with lower urinary tract inflammation (10) In a previous study we demonstrated the efficacy of Curcumina and Calendula suppositories for the treatment of patients with chronic prostatitis/chronic pelvic pain syndrome type III (11) However, there is a growing body of evidence regarding the therapeutic benefits of Palmitoylethanolamide and Epilobium on BPH and CP/CPSS, due their anti-inflammatory effect and inhibition on NF-KB (12, 13) Based on these premises, the aim of this study is investigating the efficacy of Palmitoylethanolamide, Epilobium, Curcumina and Calendula suppositories for the treatment of patients with chronic prostatitis/chronic pelvic pain syndrome type III
MATERIALS AND METHODS
From June 2023 to July 2023, we enrolled 45 consecutive patients affected by CP/CPPS III in three different institutions Inclusion criteria were age between 18 and 75 years old, symptoms of pelvic pain for 3 months or more before the study according to European Association of Urology (EAU) guidelines, a negative 4-glass test Meares-Stamey test and a total National Institutes of Health Chronic Prostatitis Symptom Index (NIH-CPSI) score ≥ 12 point Patients diagnosed with NIH category IIIA and IIIB using the PPMT (pre- and post-massage test) have been enrolled Category IIIA refers to the presence of white blood cells (WBC) after a prostate massage urine specimen (VB3) (WBC in VB3 > 10/hps) Category IIIB refers to patients with pelvic pain with no evidence of inflammation on VB3 Exclusion criteria were urinary tract infection, urethritis, sexually transmitted disease (STD), treatment with phytotherapeutic agents, alpha-blockers or antibiotics, urogenital cancer At baseline subjects underwent uroflowmetry to evaluate the peak flow and the post void residual (PVR), they filled out the International Index of Erectile Function questionnaire (IIEF-5), the NIH-CPSI and the visual analogue score (VAS) PSA test and urinary white blood cells count (U-WBC) have also been performed All subjects gave written informed consent before entering the study, which was conducted in accordance with the Declaration of Helsinki Patients underwent treatment consisting of rectal suppositories of PEA, Epilobium and Calendula (Riflog CM), 1 suppository/die for 1 month
Statistical analysis
The primary endpoint of the study was the reduction of NIH-CPSI The secondary outcomes were the change of U-WBC, peak flow, IIEF-5 and VAS The Student T-Test was used for comparisons in the distribution of nonnormal variables between baseline and follow-up A twosided p-value < 0 05 was considered statistically significant in all the tests used Statistical analyses were performed using STATA®16 software (StataCorp LLC, US)
RESULTS
We enrolled 45 patients in study, at baseline, average age was 48 75 (S D 13 44; IQR 29-68), average NIH-CPSI score was 18 55 (S D 3 71; IQR 12-24), average IIEF5 score was 18 27 (S D 5 18; IQR 11-25), average peak flow was 16 3 ml/s (S D 7 78; IQR 8 6-31), average PVR was 26 5 ml (S D 29 5; IQR 0-70), average VAS score was 6 49 (S D 1 55; IQR 4-8), average U-WBC was 485 3/mmc (S D 407 98; IQR 0-1153), average PSA was 2 81 ng/ml (S D 1 76; IQR 0 57-5 4) After 1 month of follow-up, average NIH-CPSI score reduced to 9 36 (S D 4 63; IQR 2-15), average IIEF5 score augmented to 19 53 (S D 5 46; IQR 11-25), average VAS score reduced to 2 84 (S D 1 75; IQR 0-5) and average PSA reduced to 1 74 ng/ml (S D 1 26; IQR 0 4-3 8) (Figure 1)
Furthermore, at follow-up average peak flow augmented to17 63 ml/s (S D 7 63; IQR 9 4-32), average PVR reduced to 19 48 ml ( S D 26 83; IQR 0-50), average UWBC reduced to 306 85/mmc (S D 359 65; IQR 0-837) (Figure 2) All the changes were statistically significant
since the mean difference in NIH-CPSI score was -9 2 (95%CI -7 57; -10 82, p < 0 05); the mean difference in IIEF5 score was 1 27 (95%CI 0 67; 1 85, p < 0 05); the mean difference in VAS score was -3 65 (95%CI -4 23; -3 07, p < 0 05); the mean difference in peak flow was 1 34 (95%CI 0 52; 2 15, p < 0 05); the mean difference in PVR was -7 05 (95%CI -9 92; -4 17, p < 0 05); the mean difference in U-WBC score was -178 45 (95%CI -225 39; -131 52, p < 0 05); the mean difference in PSA score was -1 06 (95%CI -1 40; -0 72, p < 0 05)
Figure 1.
NIH-CPSI score, IIEF-5 score, VAS score and PSA at baseline and follow-up
Figure 2.
Peak flow, post-void residual and U-WBC at baseline and follow-up
G Morgia, A Lo Giudice, M Carrino, et al
DISCUSSION
CP/CPPS stands as one of the most common ailments affecting males under the age of 50 It is distinguished by a diverse range of risk factors and subsequent clinical presentations Various treatments, such as alpha-blockers, antibiotics, anti-inflammatory drugs, and other agents like finasteride, phytotherapy, and gabapentinoids, are regularly employed Nonetheless, the effectiveness of these treatments remains contentious due in part to the limited size and statistical power of many clinical trials assessing their efficacy (14)
In this study, we demonstrated that the utilization of rectal suppositories containing of PEA, Epilobium and Calendula (Riflog CM) proved to be clinically effective in alleviating pain, improving voiding symptoms, and enhancing urinary flow after one month of treatment; on the other hand, we demonstrated the reduction of UWBC and PSA values, as an effect of reducing inflammation The underlying rationale behind such therapy likely stems from its anti-inflammatory properties, which could exert multiple beneficial effects
The extract from Calendula officinalis flowers demonstrated significant anti-inflammatory properties In a chronic inflammation model using formalin, administration of Calendula extract at doses of 250 and 500 mg/kg body weight resulted in inhibitions of 32 9% and 62 3%, respectively, compared to control groups Additionally, Calendula extract significantly suppressed TNF-alpha p r o d u c t i o n b y m a c r o p h a g e c u l t u r e s t r e a t e d w i t h lipopolysaccharide (LPS) Furthermore, the extract significantly inhibited the elevated levels of pro-inflammatory cytokines IL-1beta, IL-6, TNF-alpha, and IFN-gamma, as well as the acute phase protein C-reactive protein (CRP) induced by LPS injection in mice Treatment with the extract also led to inhibition of LPS-induced cyclooxygenase-2 (Cox-2) levels in mice spleens (15)
The analgesic effects of PEA are exerted through various pathways PEA directly targets PPARα and GPR55 receptors and indirectly influences CB1, CB2, and TRPV1 receptors It suppresses inflammation by hindering MC activation, downregulating mediators like NGF, COX-2, TNF-α, and iNOS, and inhibiting microglia and astrocyte activation In chronic inflammatory conditions, this enables PEA to maintain peripheral nerve structure, decrease endoneural edema, and mitigate macrophage infiltration
Currently, PEA has a recognized role as an analgesic in various clinical conditions, such as headache and menstrual pain (16)
Epilobium has a recognized role in BPH treatment due to his anti-inflammatory effects inhibiting COX and NF-kB (12, 17) Some bias of our study are that it is not a randomized trial, the small sample size and the lack of comparison with placebo, however our previous randomized trial has demonstrated the superiority of phytotherapy versus placebo in similar setting; some strengths are the investigations of new compounds for CP/CPPS treatment, the “real life” design and the consideration of objective indicators of urinary inflammation such as UWBC
In conclusion we demonstrated the efficacy of rectal suppositories with PEA, Epilobium and Calendula (Riflog CM)
for the treatment of CP/CPPS, in terms of pain and urinary symptoms; these results should be confirmed in further studies with, perhaps, greater sample size and randomized placebo-controlled trial design
REFERENCES
1 Russo GI, Cimino S, Fragalà E, et al Relationship between nonalcoholic fatty liver disease and benign prostatic hyperplasia/lower urinary tract symptoms: new insights from an Italian cross-sectional study World J Urol 2015; 33:743-51
2 Morgia G, Mucciardi G, Galì A, et al Treatment of chronic prostatitis/chronic pelvic pain syndrome category IIIA with Serenoa repens plus selenium and lycopene (Profluss) versus S repens alone: an Italian randomized multicenter-controlled study Urol Int 2010; 84:400-6
3 Morgia G, Cimino S, Favilla V, et al Effects of Serenoa Repens, Selenium and Lycopene (Profluss®) on chronic inflammation associated with Benign Prostatic Hyperplasia: results of “FLOG” (Flogosis and Profluss in Prostatic and Genital Disease), a multicentre Italian study International Braz J Urol 2013; 39:214-21
4 Rees J, Abrahams M, Doble A, Cooper A Diagnosis and treatment of chronic bacterial prostatitis and chronic prostatitis/chronic pelvic pain syndrome: a consensus guideline BJU Int 2015; 116:509-25
5 Cocci A, Bocchino AC, Cito G, et al Role of Rezum in the treatment of benign prostate hyperplasia: A review of the literature Turk J Urol 2021; 47:452-460
6 Vanella L, Russo GI, Cimino S, et al Correlation Between Lipid Profile and Heme Oxygenase System in Patients With Benign Prostatic Hyperplasia Urology 2014; 83:1444 e7-1444 e13
7 Morozov A, Bazarkin A, Babaevskaya D, et al A systematic review and meta-analysis of placebo effect in clinical trials on chronic prostatitis/chronic pelvic pain syndrome Prostate 2022; 82:63356
8 Mykoniatis I, Pyrgidis N, Sokolakis I, et al Low-intensity shockwave therapy for the management of chronic prostatitis/chronic pelvic pain syndrome: a systematic review and meta-analysis BJU Int 2021; 128:144-52
9 Pan J, Jin S, Xie Q, et al Acupuncture for Chronic Prostatitis or Chronic Pelvic Pain Syndrome: An Updated Systematic Review and Meta-Analysis Pain Res Manag 2023; 2023:1-13
10 Bozzini G, Provenzano M, Buffi N, et al An observational study of the use of beclomethasone dipropionate suppositories in the treatment of lower urinary tract inflammation in men BMC Urol 2016; 16:25
11 Morgia G, Russo GI, Urzì D, et al A phase II, randomized, single-blinded, placebo-controlled clinical trial on the efficacy of Curcumina and Calendula suppositories for the treatment of patients with chronic prostatitis/chronic pelvic pain syndrome type III Arch Ital Urol Androl 2017; 89:110
12 Cicero AFG, Allkanjari O, Busetto GM, et al Nutraceutical treatment and prevention of benign prostatic hyperplasia and prostate cancer Arch Ital Urol Androl 2019; 91:139
13 Deng L, Zong W, Tao X, et al Evaluation of the therapeutic effect against benign prostatic hyperplasia and the active constituents from Epilobium angustifolium L J Ethnopharmacol 2019; 232:1-10
14 Magistro G, Wagenlehner FME, Grabe M, et al Contemporary
15 Preethi KC, Kuttan G, Kuttan R Anti-inflammatory activity of flower extract of Calendula officinalis Linn and its possible mechanism of action Indian J Exp Biol 2009; 47:113-20
Correspondence
Giuseppe Morgia, MD (Corresponding Author) giuseppe morgia@unict it
Arturo Lo Giudice, MD arturologiudice@gmail com Francesca Zingone, MD francesca zingone@grupposamed com
University of Catania, Mediterranean Oncological Institute (IOM) Unit of Urology, Catania (Italy)
Maurizio Carrino, MD maurizio carrino@aocardarelli it Cardarelli Hospital, Unit of Urology, Naples (Italy)
Salvatore Voce, MD salvatore voce@auslromagna it Giulio Reale, MD dottorgreale@gmail com Ravenna Hospital, Unit of Urology, Ravenna (Italy)
Andrea Cocci, MD cocci andrea@gmail com
Andrea Minervini, MD andrea minervini@unifi it
University of Florence Department of Urology, Florence (Italy)
Sebastiano Cimino, MD ciminonello@hotmail com
Giorgio Ivan Russo, MD giorgioivan1987@gmail com
University of Catania, Department of Urology, Catania (Italy)
Conflict of interest: The authors declare no potential conflict of interest
16 Clayton P, Hill M, Bogoda N, et al Palmitoylethanolamide: A Natural Compound for Health Management Int J Mol Sci 2021; 22:5305
17 Deng L, Zong W, Tao X, et al Evaluation of the therapeutic effect against benign prostatic hyperplasia and the active constituents from Epilobium angustifolium L J Ethnopharmacol 2019; 232:1-10
G Morgia, A Lo Giudice, M Carrino, et
ORIGINAL PAPER
Reliability and validity analysis of Turkish version of the Symptoms of Lower Urinary Tract Dysfunction Research Network Symptom Index-10 questionnaire
Serkan Akan 1 , Hasan Huseyin Tavukcu 2 , Meftun Culpan 3 , David Cella 4
1 Department of Urology, University of Health Sciences, Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey;
2 Department of Urology, Medipol University Camlica Hospital, Istanbul, Turkey;
3 Department of Urology, Faculty of Medicine, Istanbul Medeniyet University, Istanbul, Turkey;
4 Department of Medical Social Sciences, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, USA
Summary
Introduction: To evaluate the validity and reliability of the Turkish version of the Symptoms of Lower Urinary Tract Dysfunction Research Network Symptom Index-10 (LURN SI-10)
Materials and methods: In this, single-centre study, patients between 18 and 65 years old, who were suffering from lower urinary tract symptoms (LUTS) without any known urinary tract disease and on no medication, were enrolled The control group consisted of participants, who were admitted to our clinic suffering from any complaint except LUTS and met all of the other inclusion and exclusion criteria Participants’ demographics such as age, sex, and level of education were recorded.
The Turkish version of the LURN SI-10, International Prostate Symptom Score (IPSS) and Overactive Bladder Questionnaire (OAB-V8) were administered to all participants Construct validity was evaluated by confirmatory factor analysis and concurrent validity was evaluated with correlations to similar measures. Internal consistency (Cronbach's alpha) was used to establish the scale's internal consistency reliability
Results: A total of 164 participants were included in the final analysis Of those, 57% were male The individuals were identified as being in the “patient group” (n = 86) and a “control group” (n = 78) The mean age was 48 24 ± 14 30 years
The median total LURN SI-10 scores of patient group and control group were 12 0 (9-18 25) and 4 0 (2 75-6), respectively
The LURN SI-10 questionnaire showed a high correlation with the IPSS and the OAB-V8 questionnaires (r: 0 761; p: 0 001; r: 0 737; p: 0 001, respectively) in concurrent validity analysis Cronbach’s alpha coefficient of the LURN SI-10 was 0 850
Conclusions: This promising measurement tool can be used to evaluate LUTS in Turkish women and men Further studies should be conducted to assess the clinical usefulness of this questionnaire
Submitted 22 February 2024; Accepted 28 March 2024
INTRODUCTION
Lower urinary tract symptoms (LUTS), which include storage, voiding, and post-micturition symptoms, are related with lower urinary tract dysfunction Above 40 years of
age, LUTS are common in both females and males with similar incidences Rates of storage, voiding, and postmicturition symptoms in females and males are 51 3% vs 59 2%, 25 7% vs 19 5%, and 16 9% vs 14 2%, respectively (1)
These patients admit to clinic suffering from usually more than one symptom Therefore, symptom scores obtained from questionnaires are often used for evaluation of these patients (2)
The International Prostate Symptom Score (IPSS) has been a well-known and frequently used symptom index for many years Despite its prevalent utilization, there are some drawbacks of the IPSS It was devised for males and does not interrogate symptoms such as incontinence and post-void dribbling On the other hand, Overactive Bladder Questionnaire V8 (OAB-V8), which is also commonly used, inquiries about frequency, urgency, urge or stress incontinence, and nocturia It was conceived for both males and females, but it covers predominantly storage symptoms and does not question voiding difficulty
As a result, a questionnaire which evaluates both males and females and involves all the important lower urinary tract symptoms will be of benefit for clinicians
“ C
Symptoms (CASUS)” questionnaire, which consists of 93 questions covering a wider spectrum of symptoms when compared with other questionnaires, was developed to enhance phenotypical analyses of the patients with LUTS by The Lower Urinary Tract Dysfunction Research Network (LURN) (3) Based upon CASUS, which is impractical in clinical use because of its length, Cella and colleagues devised and reported first the LURN symptom index of 29 items (LURN SI-29) and thereafter LURN symptom index of 10 items (LURN SI-10) by abridging the former (4)
In these studies, it is stated that a shorter and successful measure (LURN SI-10) in correlation with the clinical presentation is obtained, which is also more comprehensive than present LUTS questionnaires and applicable to both males and females (5)
In this study, we aimed to investigate the validity and reliability of the LURN SI-10 questionnaire, which was translated into Turkish before, in patients with LUTS
MATERIALS AND METHODS
We obtained a written approval of the developers of the LURN SI-10 index for validating it in Turkish language The local ethics committee endorsed the study with decision number 2022/70 in accordance with the Helsinki Declaration A written informed consent was signed by all individuals
Patient population
We planned to enrol a minimum of 70 patients, who admit to our clinic suffering from LUTS, and a minimum of 70 participants for control group between September 2022 and October 2023 prospectively Our inclusion criteria were: [1] admission to our clinic with clinically significant LUTS, [2] age between 18 and 65 years, [3] answering all the questions in each questionnaire, [4] signing the written informed consent Our exclusion criteria were: [1] using medications such as alpha blockers, antimuscarinic agents, beta-mimetics, pain killers or drugs potentially impairing lower urinary tract functions, [2] a history of overactive bladder, bladder cancer, chronic pelvic pain syndrome, chronic prostatitis, prostate cancer, and a neurological disorder potentially causing lower urinary tract dysfunction, [3] presence of temporary or permanent urethral or ureteral catheter, [4] presence of a debilitative disorder, [5] being unable to communicate
The control group consisted of participants, who admitted to our clinic suffering from any complaint expect LUTS and met all the other inclusion and exclusion criteria
Tools for data collection
Demographic data of the participants such as age, sex, education level were collected All individuals took The Turkish version of the LURN SI-10 and validated Turkish versions of the IPSS and OAB-V8 questionnaires (6, 7) They were requested to complete the questionnaires on their own without professional aid at first application
LURN SI-10
The LURN SI-10, first published in 2020, was conceived as a self-reported outcome questionnaire for clinical use with patients to assess LUTS 2020 (5) It includes 10 questions about frequency, nocturia, urgency, incontinence, bladder pain, voiding, and post-micturition symptoms as well as an additional question measuring dissatisfaction with LUTS Each question scores between zero and four according to frequency of the symptom (Nineth and tenth questions between zero and three) The total score is calculated as “the total score of ten questions x 10/number of the questions answered” (maximum score 38) Last question about dissatisfaction with LUTS is about quality of life and does not affect the total score
IPSS
The IPSS consists of eight questions and is usually used for screening, diagnosing and treatment planning of benign prostate obstruction (BPO) Seven questions investigate incomplete emptying of the bladder, frequency, intermittency, urgency, weak stream, straining, and nocturia The eighth question is about overall quality of life
A score between zero and seven means mild, between eight and 19 means moderate, and between 20 and 35
means severe symptoms Although IPSS is generally used in males with the diagnosis of BPO, it is not specific for males or prostate diseases (8)
OAB-V8
The Overactive Bladder Questionnaire (OAB-Q) was developed in 2002 by Coyne and colleagues as a questionnaire for OAB symptoms and quality of life (9) It can be used in patients with a provisional diagnosis of both wet and dry OAB The OAB-V8 consists of the first eight questions of the OAB-q and is recommended as a screening and awareness test for OAB (10) A score between zero and seven indicates mild symptoms and eight and 40 indicates severe symptoms Tarcan and colleagues validated OAB-V8 in Turkish language in 2012 (11)
Linguistic validation
We obtained a written approval of the developers of the LURN SI-10 index for validating it in Turkish language
The Turkish LURN SI-10 questionnaire, which was not validated in Turkish language but developed based upon Turkish LURN SI-29 questionnaire (12), which was validated in Turkish and published in 2021, was sent to the corresponding author by developers of LURN SI-10 and used in this study
Statistical analysis
For statistical analyses, IBM SPSS Statistics 22 and AMOS 22 computer programs were used Normally distribution of the data was controlled by Kolmogorov-Smirnov test Findings were represented with descriptive statistical methods (minimum, maximum, mean, standard deviation, median, frequency) In comparison of quantitative data, normally distributed groups were compared by using Student t test and non-normally distributed groups w e
Qualitative data were compared by using Chi-square test
Exploratory factor analysis (EFA) was performed to test the construct validity of the LURN SI-10 Kaiser-Meyer-Olkin (KMO) test was used to assess the sufficiency of the sample for the factor analysis Bartlett test demonstrated the correlation among variables For evaluating the construct validity, c o n fi r m a
(CFA) test was applied Model fit was tested by using the χ2 goodness of fit test (χ2, χ2/degree of freedom [df]), the goodness of fit index (GFI), root mean square error of approximation (RMSEA), the comparative fit index (CFI), and the nonnormed fit index (NNFI) Cronbach’s alpha coefficient was calculated for reliability of the scale Association between non-normally distributed parameters was controlled by using Spearman’s rho correlation test Partial correlation analysis was performed for evaluating the correlation between scores after adjustment for age A p value less than 0 05 was considered statistically significant
RESULTS
Due to incomplete questionnaires, nine participants were excluded A total of 164 individuals between the age of 18 and 65 years were enrolled in the study Of those, 71 (43 3%) were female, 93 (56 7%) were male, 86 were in
S Akan, H Huseyin Tavukcu, M Culpan, D Cella
the patient group, and 78 were in the control group The ratio of the females in the patient group was significantly higher than that in the control group (55 8% vs 29 5%, p < 0 05) The mean age of all participants was 48 24 ± 14 30 years In the patient and control groups, the mean ages were 50 95 ± 11 79 and 45 24 ± 16 20 years, respec-
Table 1.
Comparison of total scores of the LURN SI-10, IPSS, and OAB-V8 between groups
1 Student t test; 2 Ki-kare test; 3 Mann Wh tney U test; * p < 0 05
Table 2
Correlation of the LURN SI-10 with the IPSS and OAB-V8
Total Patient Control
IPSS r 0 761 0 628 0 472 p 0 001* 0 001* 0 001*
OAB-V8 r 0.737 0.597 0.490 p 0 001* 0 001* 0 001*
Spearman’s corre ation; *p < 0 05
Figure 1
Total scores of the LURN SI-10, IPSS and OAB-V8 in groups
tively The mean age of the patient group was higher than that of the control group significantly (p < 0 05)
The median total LURN SI-10 scores were 12 0 (9-18 25) vs 4 0 (2 75-6) in patient group and control group, respectively (p < 0 001) The median total IPSS scores were 14 0 (9-21 25) vs 4 5 (2-7) in patient group and control group, respectively (p < 0 001) The median total OAB-V8 scores were 20 5 (12-28) vs 7 0 (4 75-9 25) in patient group and control group, respectively (p < 0 001) Table 1 and Figure 1 demonstrate the LURN SI10, IPSS and OAB-V8 scores and scale graphs of the groups, respectively
The validity of the scale
Exploratory factor analysis (EFA) was performed to test the construct validity of the scale Principal component analysis and varimax rotation were used in the factor analysis
Associations of LURN SI-10 total score with IPSS and OAB-V8 were assessed for concurrent validity The LURN SI-10 total score demonstrated a high correlation with those of IPSS and OAB-V8 (r = 0 761, p < 0 001 and r = 0 737, p < 0 001, respectively) Figure 2 shows the correlations of LURN SI-10 with IPSS and OAB-V8
When all individuals were assessed, a high, positive, and statistically significant correlation between both LURN SI-10 vs IPSS (0 76) and LURN SI-10 vs OAB-V8 (0 73) were observed (p < 0 001) The correlation analyses in patient and control groups are shown in Table 2
In addition, the correlations of the LURN SI-10 total score with the IPSS and the OAB-V8 were investigated in male and female participants separately In all females, a high, positive, and statistically significant correlation between
Figure 2.
Correlation of the LURN SI-10 with the IPSS and OAB-V8
both LURN SI-10 vs IPSS (0 75) and LURN SI-10 vs OABV8 (0 79) were observed (p < 0 001) Besides, a high, positive, and statistically significant correlation was found between the LURN SI-10 total score and both IPSS and OAB-VS in the female patient group (p < 0 001) In the female control group, a high, positive, and statistically significant correlation was found between LURN SI-10 total score and OAB-V8 (p < 0 001) In all males, a high, positive, and statistically significant correlation was found between the LURN SI-10 total score and both IPSS and OAB-V8 (78% and 67%, respectively) (p < 0 001) Besides, a high, positive, and statistically significant correlation was found between the LURN SI-10 total score and both IPSS and OAB-VS in the male patient group (p < 0 001) In the male control group, a high, positive, and statistically significant correlation was found between LURN SI-10 total score and IPSS (p < 0 001) In the male control group, a low, positive, and statistically significant correlation was found between the LURN SI-10 total score and OAB-V8 (p = 0 031) (Table 3)
The reliability of the scale
Cronbach’s coefficient of the LURN SI-10 for the internal consistency of the scale was 0 850 Descriptive data and Cronbach’s coefficients of the LURN SI-10, IPSS and OAB-V8 questionnaires are shown in Table 4
DISCUSSION
In this study, the validity and reliability assessment of the LURN SI-10 questionnaire in Turkish was performed to make it applicable in patients with LUTS According to results of our study, version of the LURN SI-10 demonstrated good internal consistency reliability and concurrent validity, consistent with the results of the original study conducted by LURN group (5) We hope that our study will contribute to standard reporting of symptoms in Turkish-speaking patients and lead to improved evaluation of male and female patients with LUTS
Table 3.
The correlations of LURN-10 with IPSS and OAB-VS in females and males
SI‐10
Male patients with LUTS usually admit to clinic suffering from differing types of involuntary loss of urine, which are not adequately caught by the IPSS (13) Thus, by using the IPSS solely, these symptoms, which substantially impair the quality of life, could be overlooked and the patient could miss the appropriate counselling opportunity On the other hand, OAB-V8 is an excellent questionnaire for evaluating various types of involuntary loss of urine but cannot assess voiding symptoms if used solely When compared with other questionnaires, LURN SI10, which was validated in Turkish, has several advantages First, it can be applied to both male and female patients with LUTS successfully In addition, LURN SI-10 completely interrogates incontinence and post-void dribbling/pain, which are not included in the IPSS, and LUTS such as voiding difficulty, which are not included in the OAB-V8 It can prevent waste of time and effort, for both clinicians and patients, to be able to interrogate all LUTS by application of this questionnaire of only 10 questions without using other scales In this study, regarding criterion-related validity was assessed with associations of LURN SI-10 with IPSS and OAB-V8 It was found that LURN SI-10 was highly correlated with IPSS and OAB-V8 questionnaires (r = 761 and r = 737, respectively)
In our results, Cronbach’s alpha internal consistency coefficients of the LURN SI-10, IPSS and OAB-V8 were consistently high (0 850, 0 847, and 0 921, respectively) However, in the control group, internal consistency coefficients were notably lower (0 529, 0 616, and 0 613, respectively) These tools clearly perform better as single total scores in clinical samples, an important consideration when planning future studies
Spearman s correlation; *p < 0 05
Table 4.
Descriptive statistics and Cronbach’s alpha coefficients of the LURN SI-10, IPSS and OAB-V8.
To the best of our knowledge, this is the first study that assesses the validity and reliability of the LURN SI-10 in a non-English language Recently, the validity of the LURN SI-10 has been tested by comparing with the IPSS and its significant correlation has been reported (14) However, that study included only male patients with LUTS In our study, comparisons with the control group were made for both male and female patients and a significant correlation was demonstrated A statistically significant, positive correlation was found between the LURN SI-10 and the IPSS in both groups (p: 0 001)
In 2021, the LURN SI-29 was translated into Turkish and its validation was completed by comparing with the IPSS and Urogenital Distress Inventory (UDI-
S Akan, H Huseyin Tavukcu, M Culpan, D Cella
6) (12) However, it was developed for use in clinical studies and outcomes research Conversely, the LURN SI10 was designed as a concise (single-page) form for simple administration in clinical practice To the best of our knowledge, there is no study investigating the correlation between the LURN SI-10 and OAB-V8 in English literature In this study, we opted for the OAB-V8, which covers rather storage symptoms, because it was validated in Turkish language in 2012 and has been used for more than ten years in our country A statistically significant, positive correlation was found between the LURN SI-10 and the OAB-V8 in both patient and control groups (p: 0 001)
There are some limitations of this study We designed the study as a quality improvement initiative to compare the IPSS and OAB-V8 with the LURN SI-10 and for that reason main clinical data such as comorbidities, race/ethnicity, and body mass index are not included in the present analyses Moreover, we were not able to attain the age and sex similarity between the patient and control group since this was a pilot study Further prospective studies, evaluating test-retest reliability, the effects of comorbidities, and any changes in answers in LURN SI-10 questionnaire after medical treatment are needed
CONCLUSIONS
In this study, the validity and reliability of the LURN SI10 questionnaire in Turkish language and its use in patients with LUTS were assessed This promising measurement tool is concise and simple, with initial evidence for reliability and validity in clinical samples and can be used to evaluate LUTS in Turkish women and men Further studies should be conducted to assess the clinical usefulness of this questionnaire
REFERENCES
1 Irwin DE, Milsom I, Hunskaar S, et al Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study Eur Urol 2006; 50:1306
2 Selekman RE, Harris CR, Filippou P, et al Validation of a Visual Prostate Symptom Score in Men With Lower Urinary Tract Symptoms in a Health Safety Net Hospital Urology 2015; 86:354-8
3 Yang CC, Weinfurt KP, Merion RM, et al Symptoms of Lower Urinary Tract Dysfunction Research Network J Urol 2016; 196:146-152
4 Cella D, Smith AR, Griffith JW, et al A new outcome measure for LUTS: Symptoms of Lower Urinary Tract Dysfunction Research N e t w o r k S y m p t o m I n d e x - 2 9 ( L U R N S I - 2 9 ) q u e s t i o n n a i r e Neurourol Urodyn 2019; 38:1751-1759
5 Cella D, Smith AR, Griffith JW, et al LURN Study Group A New Brief Clinical Assessment of Lower Urinary Tract Symptoms for Women and Men: LURN SI-10 J Urol 2020; 203:164-170
6 Bozlu M, Doruk E, Akbay E, et al Effect of administration mode (patient vs physician) and patient's educational level on the Turkish version of the International Prostate Symptom Score Int J Urol 2002; 9:417-421
7 Tarcan T, Mangır N, Özgür MO, et al Constitution and Validation
of a New Symptom Assessment Tool for Overactive Bladder: Marmara Overactive Bladder Questionnaire (M-OBQ) Journal of Urological Surgery 2014; 1:24-27
8 Okamura K, Nojiri Y, Osuga Y, Tange C Psychometric analysis of international prostate symptom score for female lower urinary tract symptoms Urology 2009; 73:1199-202
9 Coyne K, Revicki D, Hunt T, et al Psychometric validation of an overactive bladder symptom and health-related quality of life questionnaire: the OAB-q Qual Life Res 2002; 11:563
10 Coyne KS, Zyczynski T, Margolis MK, et al Validation of an overactive bladder awareness tool for use in primary care settings Adv Ther 2005; 22:381-94
11 Tarcan T, Mangır N, Özgür MÖ, Akbal C OAB-V8 As¸ırı Aktif Mesane Sorgulama Formu Validasyon Çalısması Üroloji Bülteni 2012; 21:113-116
12 Culpan M, Acar HC, Cella D, et al Turkish validation and reliability of the symptoms of Lower Urinary Tract Dysfunction Research Network Symptom Index-29 (LURN SI-29) questionnaire in patients with lower urinary tract symptoms Neurourol Urodyn 2021; 40:2034-2040
13 Helfand BT, Smith AR, Lai HH, et al Prevalence and characteristics of urinary incontinence in a treatment seeking male prospective cohort: results from the LURN study J Urol 2018; 200:397-404
14 Glaser AP, Kristof TW, Judge C, et al The 10-item LURN Symptom Index (LURN SI-10) Detects Additional Symptoms and Shows Convergent Validity With the IPSS in Men Presenting With Lower Urinary Tract Symptoms Urology 2023; 171:184-189
Correspondence
Serkan Akan, MD, Associate Professor (Corresponding Author) drserkanakan@hotmail com
Department of Urology, University of Health Sciences, Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey
Hasan Huseyin Tavukcu, MD, Associate Professor hhtavukcu@yahoo com
Department of Urology, Medipol University Camlica Hospital, Istanbul, Turkey
Meftun Culpan, MD, Associate Professor mculpan@gmail com
Department of Urology, Faculty of Medicine, Istanbul Medeniyet University, Istanbul, Turkey
David Cella, PhD, Professor d-cella@northwestern edu
Department of Medical Social Sciences, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, USA
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Differences in bladder neck angles between female patients with overactive bladders and healthy peers
Mehmet Yoldas, Mehmet Zeynel Keskin
1
Tepecik Training and Research Hospital Urology Clinic, Izmir, Turkey
Summary
Aim: The aim of this study was to compare the differences between angles of bladder neck in girls with overactive bladder and those in healthy ones using transabdominal ultrasonography
Materials and Methods: This study consists of 28 girls complicated with overactive bladder (Group I) and 40 healthy girls (Group II) The anteroposterior vesical wall angle (APVA), urethroposterior vesical wall angle (UPVA), urethroanterior vesical wall angle (UAVA), thickness of bladder mucosa, distance of urethral orifices, and distance between ureter and urethra orifice were measured in supine position using transabdominal ultrasonography. The results were compared between the two groups
Results: UAVA in Group I was higher than Group II (135.2 ± 12 2 mm vs 117 4 ± 14 0 mm; p = 0 009) UPVA was smaller in Group I than Group II (114.6 ± 19.5 mm vs. 135.3 ± 16.5 mm; p = 0 014) The distance between the ureteral orifices was 31 8 ± 8.5 mm in Group I and 17.0 ± 4.1 mm in Group II (p < 0 001) There was no statistically significant difference between groups in terms of APVA, bladder mucosa thickness, and distance between ureter and urethra orifice (p > 0 05)
Conclusion: Bladder neck dynamics may play an important role in overactive bladder pathophysiology due to differences in UPVA, UAV, and location of ureteral orifices in this patient population
Submitted 18 January 2024; Accepted 15 February 2024
INTRODUCTION
Overactive bladder (OAB) is a dysmotility disorder characterized by various symptoms, including a sudden urge to urinate, urinary incontinence, and frequent urinary tract infections It is associated with the overstimulation of the detrusor muscle during the bladder's filling phase In some cases, individuals, especially women, may contract pelvic floor muscles voluntarily by squatting and applying pressure to the urethra with their heels to prevent urinary incontinence (1) While factors such as age, chronic neurological diseases, diabetes, and spinal injuries can contribute to OAB in adults, the etiology of this disorder in women is not fully understood Diagnosing OAB in women involves a comprehensive approach, including lower urinary tract ultrasonography (US), urodynamic examination, and a detailed patient history (2)
Transabdominal ultrasound (US) as a preferred non-invasive radiological imaging method for evaluating the urinary system Transabdominal ultrasound (US) as a preferred non-invasive radiological imaging method for evaluating the urinary system Limitations of transabdominal US in providing detailed information about bladder dynamics are acknowledged, especially concerning the morphology of bladder neck, which can vary based on factors such as body position and urine volume Recent studies on ultrasonographic examination of bladder neck dynamics in women highlight the importance of understanding these dynamics (3, 4) The specific aspects evaluated in these studies, such as mucosal thickness, morphology of trigonum and bladder floor, and anteroposterior angle of the bladder wall, demonstrate the complexity of assessing bladder function (3-6) This suggests a focus on understanding how the bladder neck behaves in patients with OAB compared to those without this condition
METHODS
Before study initiation, approval was obtained from the ethics committee of T e p e c i k E d u c a t i o n a n d R e s e a r c h Hospital (Approval number: 2023/08-31), and consent forms from the patients who agreed to participate in the study were obtained The study was conducted in accordance with the principles of the Declaration of Helsinki Patients with kidney disease, stone disease, a history of urinary system interventions, active urinary tract infections, a history of multiple drug use, and anomalies detected in urinary system by ultrasound were excluded from the study
This prospective study was conducted between October 2023 and December 2023 Among the patients who visited our clinic due to urinary symptoms between the mentioned dates, 29 female patients diagnosed with Overactive Bladder (OAB) were planned to be included in the study group (Group I) Additionally, 30 female patients who did not exhibit urinary symptoms were planned to be included in the control group (Group II)
Ultrasonographic examination
The patients were assessed in the supine position, as it provides the most stable bladder conditions during the examination Following a period for allowing patients to
achieve bladder fullness, the examination was conducted by scanning the suprapubic abdominal wall in both sagittal and transverse planes Initially, the three-dimensional measurement of urine in the bladder was performed, followed by the calculation of bladder volume
Firstly, we assessed bladder volume, bladder wall thickness, the presence of trabeculation, and any additional pathology Subsequently, we examined the localization of both kidneys, their contours, and the structure of the pelvicalyceal system Following that, we measured kidney sizes and parenchymal thicknesses The mucosal thickness of the bladder wall was measured within a distance of up to 2 cm from the bladder neck, while the distance between the bladder smooth muscle layer and the mucosal surface was measured to include the mucosal-submucosal low-echo area The diameters of both ureteral orifices were then measured at the axial plane Additionally, we determined whether the ureteral orifices opened to the bladder in the normal position
The bladder neck was easily visualized as a 'V' depression in the sagittal plane, and the urethrovesical junction was identified A line parallel to the urethra was drawn throughout the urethra from the level of the urethrovesic a l j u n c t i o n T h e a n t e r o p o s t e r i o r v
(APVA), urethroposterior vesical wall angle (UPVA), and urethroanterior vesical wall angle (UAVA) were measured
The APVA of the bladder neck was calculated by measuring the angle between the anterior wall (anterior base plate) and the posterior wall in the sagittal plane The
UPVA between the urethra and the posterior vesical wall and the UAVA between the urethra and anterior wall were then measured Subsequently, the distance between the ureteral orifices and between the ureteral and uret h r a l o r i fi c e s w a s m e a s u r e d o n t h e a x i a l p l a n e
Measurement is shown in Figure 1
Statistical analysis
All data were analyzed using PASW version 18 0 (SPSS Inc , Chicago, IL, USA) Descriptive data were expressed as mean ± SD Differences between the two groups were assessed using the Mann-Whitney U test for categorized variables and Student’s t-test for continuous variables A p-value of < 0 05 was considered statistically significant
RESULTS
The age range of the patients was 25 to 49 years, with no difference in age and weight observed between the two groups (Table 1) UAVA was higher in Group I than in Group II (138 4° ± 11 2° vs 115 2° ± 13 4°, respectively; p = 0 008), whereas UPVA was lower in Group I than in Group II (118 1° ± 18 5° vs 138 2° ± 17 7°, respectively; p = 0 012) The mean distance between the ureteral orifices was 41 7 ± 7 5 mm in Group I and 25 0 ± 3 2 mm in Group II (p = 0 000) No significant difference in the results of other measurements for the lower urinary system was observed between the two groups (p > 0 05; Table 1)
Figure 1. Measurement of anteroposterior vesical wall angle (APVA), urethroposterior vesical wall angle (UPVA), and urethroanterior vesical wall angle (UAVA)
M Yoldas, M Zeynel Keskin
Table 1.
Comparison of demographic and study results between both groups Parameter
Data were expressed n
DISCUSSION
The current study revealed that patients with Overactive B l a d d e r ( O A B ) e x h i b i t e d d e c r e a s e d U P V A v a l u e s , increased UAVA values, and an increased distance between orifices A prior study, albeit with a limited number of adult patients, identified bladder neck changes associated with post-hormonal alterations in bladder neck fibroblast activity (5)
Considering that our participants were female patients in the hormonally active period, we support the validity of this hypothesis for the OAB patient group in our study
We propose that the variances in UPVA and UAVA of the bladder neck among OAB patients may be linked to changes in the bladder wall attributed to excessive detrusor activity Sugaya et al , who determined Anteroposterior Vesical Wall Angle (APVA) values in healthy individuals aged 0-29 years (6), found that children under 10 years old had lower APVA values Those over 10 years old, however, exhibited values similar to adults that were associated with hormonal changes However, at present, no study has comprehensively investigated bladder neck angles during adulthood
Lower urinary tract disorders are prevalent in childhood, with anatomical issues, neurological impairments, and behavioral disorders in toilet training identified as etiological factors (7) Additionally, Goessaert et al. demonstrated that children experiencing daytime urinary incontinence had a twofold increased risk of sudden feelings of urination and urinary incontinence in adulthood Furthermore, Song et al (8) found that individuals with complaints of constipation and urinary incontinence in adulthood had similar issues during childhood These studies suggest a potential pathological link between childhood and adult disorders If symptoms persist from childhood to adulthood, as suggested by the aforementioned studies, it becomes crucial to understand the pathophysiology of the disease during childhood and implement appropriate treatment, prioritizing the lifelong well-being of the patient
The strength of our study lies in being the first to explore bladder neck angles in women, confirming that women diagnosed with OAB exhibit alterations in bladder neck angles However, a notable limitation of the current study
is the relatively small number of cases and our exclusive focus on women
CONCLUSIONS
Despite the link between OAB in childhood and similar urinary symptoms in adulthood, the pathophysiology of this relationship has not been fully elucidated We posit that a more detailed investigation of the bladder neck and its dynamics could yield significant insights not only for the diagnosis and treatment of the disorder during childhood but also for addressing similar symptoms in adulthood Our findings, indicating changes in bladder neck angles among women diagnosed with OAB, suggest a potential role of these changes in the pathophysiology of OAB in girls Additionally, the measurement of bladder neck angles could serve as a diagnostic tool for OAB Therefore, further large-scale studies are needed to uncover different approaches for the treatment of this disease
REFERENCES
1 Drake MJ Fundamentals of terminology in lower urinary tract function Neurourol Urodyn 2018; 37:13-19
2 Chen LC, Kuo HC Pathophysiology of refractory overactive bladder Lower urinary tract symptoms 2019; 11:177-181
3 Sugaya K, Nishijima S, Oda M, et al Transabdominal vesical sonography of urethral syndrome and stress incontinence Int J Urol; 2003: 10:36-42
4 Tafuro L, Montaldo P, Iervolino LR, et al Ultrasonographic bladder measurements can replace urodynamic study for the diagnosis of nonmonosymptomatic nocturnal enuresis BJU Int 2010; 105:108-111
5 Lo TS, Ng KL, Hsieh WC, et al Ultrasonography and clinical outcomes following anti-incontinence procedures (Solyx™ tape): a 3year post-operative review Int Urogynecol J 2022; 33:2749-2759
6 Sugaya K, Nishijima S, Oda M, et al Ultrasonographic changes of the female bladder neck during development Int J Urol 2002; 9:668671
7 Fotter R, Riccabona M Functional disorders of the lower urinary tract in children Radiologe 2005; 45:1085-1091
8 Goessaert AS, Schoenaers B, Opdenakker O, et al Long-term followup of children with nocturnal enuresis: increased frequency of nocturia in adulthood J Urol 2014; 191:1866-1870
9 Song QX, Wang L, Cheng X, et al The clinical features and predictive factors of nocturnal enuresis in adult men BJU Int 2020; 126:472-480
Correspondence
Mehmet Yoldas, MD (Corresponding Author) yoldas 2297@hotmail com
Mehmet Zeynel Keskin, MD zeynel akd@hotmail com
Republic of Turkey Ministry of Health Izmir Provincial Health Directorate Izmir University of Health Sciences Tepecik Training and Research Hospital Urology Clinic, Izmir, Turkey; Yenis ehir, Gaziler Cd No:468, 35020 Konak/Izmir
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
The use of urodynamic to assess the mechanism of incontinence in patients with Yang-Monti based catheterizable cutaneous stomas
M. Abdelwadood 1 , Eman H. Ibrahim 2, 3 , Tamer A. Abouelgreed 4 , Yasser M. Haggag 5 , Mohamed M. Yassin 1 , Mohamed A. Elhelaly 4 , El-Sayed I. El-Agamy 4 , Basem Fathi 4 , Salma F. Abdelkader 6 , Sameh S. Ali 7 , Naglaa M Aboelsoud 8 , Nasser Ramadan 9 , Mohamed Sobhy 10 , Tarek Gharib 11
1 Department of Urology, Faculty of Medicine, Ain Shams University, Cairo, Egypt;
2 Department of Biomedical Sciences, College of Medicine, Gulf Medical University, Ajman, UAE;
3 Department of Pathology Faculty of Medicine, Al-Azhar University, Cairo, Egypt;
4 Department of Urology, Faculty of Medicine, Al-Azhar University, Cairo, Egypt;
5 Department of Urology, Faculty of Medicine, Al-Azhar University, Asyut, Egypt;
6 Department of Radiology, Faculty of Medicine, Ain Shams University, Cairo, Egypt;
7 Department of Radiology, Sheikh Khalifa General Hospital, UAQ, UAE;
8 Department of Radiology, Faculty of Medicine, Al-Azhar University, Cairo, Egypt;
9 Department of Urology, NMC Royal Hospital, Sharjah, UAE;
10 Department of Surgery, Faculty of Medicine, Gulf medical University, Ajman, UAE;
11 Department of Urology, Faculty of Medicine, Benha University, Benha, Egypt
Summary and peristaltic contraction of the conduit has no effect on continence mechanism
Objective: To analyze the static and dynamic urodynamic parameters of reservoirs and continent conduits in continent cutaneous urinary diversion with catheterizable stoma.
Materials and methods: 76 patients had augmented ileocystoplasty or continent urinary diversion with catheterizable urinary stoma based on Mitrofanoff principle and Yang-Monti procedure using subserous tunnel as continence mechanism. They were followed up for at least 6 months post-operatively for continence through stoma and divided into two groups (continents vs non-continent) according to stomal continence Both groups had urodynamic assessment performed via the stoma to assess reservoir capacity, pressure and contractions, efferent limb functional length, reservoir overactivity, static and dynamic maximal closure pressures and leak point pressure
Results: Continence rate was 87% Continent group included 66 patients and incontinent group included 10 patients In both groups at rest, the reservoir pressure after filling did not exceed 25 cm H2O During peristaltic contraction, the pressure did not exceed 30 cm H2O and the duct remained continent After Valsalva maneuver, the reservoir pressure increased up to 34 (+ 7 4) cm H2O and leakage occur in 10 patients (13%)
Reservoir (wall) overactivity was recorded in 54 patients, with insignificant rise in intraluminal pressure during the contractions. In both groups, the efferent tract closing pressure was always higher than the reservoir pressure The mean of maximal closing pressure at Valsalva was 82.5 (+ 4.18) cm H2O in the continent group and 61 66 (+ 8 16) cm H2O in the incontinent group. The mean functional length of the conduit was 4.95 + 1 62 in the continent group and 2 80 + 1 50 cm in the incontinent group.
Conclusions: Urodynamic evaluation of continent catheterizable cutaneous stoma after Yang-Monti procedure has a practical significance Functional length of the conduit seems to be the most influential factor for continence reflecting static & dynamic maximal closure pressure Higher conduit closing pressure is associated with better continence. Contractions of the pouch
Continent cutaneous diversion has proven to be an effective way of urinary diversion Yang-Monti ileovesicostomy technique uses ileal segment as a conduit instead of appendix as originally described in Mitrofanoff principle if appendix is not accessible Urodynamic is a clinical test or a series of clinical tests used to describe the current function or dysfunction of the lower urinary tract In theory and in practice, the clinician utilizes the results of urodynamic testing to direct therapy whether surgical, medical, or behavioral alone or in combination Current methods include water filled urodynamic, ambulatory urodynamic, and video urodynamic Regardless of the method, urodynamic examines the functional anatomy of the bladder or urethra or both and their response to filling, storing, and voiding (1) Urodynamic testing is an important tool in urology providing objective descriptions concerning the patient’s incontinence and voiding dysfunction (2) Therefore, the objectives of this study was to analyze the static and dynamic urodynamic parameters of the reservoir and conduit affecting continence after continent cutaneous urinary diversion with catheterizable stoma using Yang-Monti technique
MATERIALS AND METHODS
Between June 2018 and May 2023, 76 patients who had continent urinary diversion and catheterizable urinary stoma based on Mitrofanoff principle and Yang-Monti tech-
M Abdelwadood, Eman H Ibrahim, Tamer A Abouelgreed, et al
nique in the institution of the Authors were included in this study and prospectively studied and followed up post-operatively for continence through the stoma for a minimum of 6 months The mean age of the patients at time of surgery was 19 years (5-59 years); 51 patients were males and 25 patients were females The indications for continent diversion were (neurogenic bladder in 59 patients, bladder cancer in 13 patients, and congenital anomalies in 4 patients) Sixty-one cases had augmented ileocystoplasty with a patch of detubularised ileum and 15 cases had their native bladder replaced by intestinal reservoir An ileal segment with average length of 45 cm was detubularised and used as a reconfigured spherical reservoir for the ileovesicostomy procedure Surgery for bladder neck closure was performed in 37 patients of the augmented group The patients were divided into two groups according to stomal continence Both groups had ascending pouchography and urodynamic study assessment performed via the stoma to assess reservoir capacity, pressure and contractions, efferent limb functional length, overactivity, static and dynamic maximal closure pressures and leak point pressure The assessment was performed 15 days after the withdrawal of anticholinergic drugs and treatment of urinary tract infection The patients who presented with reflux are excluded State of continence was documented at 6 months and every 3 months later till end of the study Mean follow up period was 30 6 months (ranging from 9 to 48 months)
Urodynamic study was performed using a trans-stomal 6 French dual catheter and a 14 French rectal balloon catheter for pouchometry and pressure profilometry of the efferent tract The rate of filling used was 50 ml/minute and the capacity measured at sense of discomfort or notice of leakage The withdrawal of sensors was done with an electric arm at a speed of 2 ml/min The static profile maximum closure pressure of the efferent limb was obtained by subtracting the baseline (empty) reservoir pressure from the maximum inner pressure of the efferent limb The catheter was again passed into the reservoir and the side hole of the catheter was manually positioned at the point of the static profile maximal closure pressure of the conduit The pouch was filled and the response of the conduit pressure to a reservoir contraction and/or abdominal strain (cough or Crede) was recorded The presence of involuntary reservoir contractions or conduit leak was noted Abrupt increase in conduit pressure without simultaneous changes in reservoir or abdominal pressure was considered evidence of peristaltic activity of the conduit The dynamic profile maximal reservoir pressure was recorded, and dynamic profile maximal closure pressure of the efferent limb was derived by subtracting the greatest filling phase conduit pressure from simultaneous reservoir pressure Leak point pressure, compliance and reservoir capacity were evaluated The functional length of the efferent limb was defined as the continuous length of the efferent limb in which the pressure was higher than the reservoir pressure
Protocols and written informed consent for all participants were approved by the Research Ethics Committee of Thumbay University Hospital (affiliated with Gulf Medical University, REC #: 52/2018)
S t at ist ic al m et h o d s
Demographic data, reservoir capacity, functional length, closure pressures were reported using mean + standard deviation (SD) Differences in means were assessed by Student t test for significance Correlation among the continuous variables was analyzed using Pearson correlation coefficient Dichotomous variables as continence status, contractions, functional length greater than 2 0 cm versus less were analyzed using Chi-square test
RESULTS
Continence rate was 87% Continent group included 66 patients and incontinent group included 10 patients
No major surgical complications or mortality observed in the study Stomal complications were observed in 4 patients in form of stomal stenosis in 2 patients and difficult catheterization in further 2 patients Surgical revision was performed for 7 patients; in the 4 cases with stomal complications other than incontinence and in 3 cases with incontinence that were treated with injection of bulking agents with 2 successes and 1 failure after submucosal injection of bulking agent The rest of the incontinent group were managed by frequent catheterization
All procedures performed in this study complied with institutional and/or national research council ethical standards as well as the 1964 Declaration of Helsinki and its subsequent amendments or similar ethical standards
The capacity of the reservoir was 496 8 (+180 27) ml (range 100-900) It was smaller in the incontinent group without a statistically significant difference In both groups, the reservoir pressure at rest after filling did not exceed 25 CmH2O; the mean value was 20 72+6 05 cmH2O with no significant difference between continent and incontinent groups (Table 1) Peristaltic contractions of the reservoir were noted in 6 cases During contractions, the pressure did not exceed 30 CmH2O and the duct remained continent After Valsalva maneuver, the reservoir pressure increased up to 41 4 CmH2O without significant difference between continence groups (Table 1) and leakage occur in 10 patients All patients had positive static and dynamic maximal conduit closure pressures In every case the dynamic was greater than the static pressure reflecting a positive conduit to reservoir pressure gradient as the reservoir was filled to its capacity The mean static and dynamic maximal closure pressures of the incontinent group were lower compared to those of the continent patients but the differences were not statistically significant (Table 1) In both groups, the efferent tract closing pressure was always higher than the reservoir pressure The mean efferent closing pressure at Valsalva was 82 5 (+ 4 18) CmH2O in the continent group and 61 66 (+ 8 16) CmH2O in the incontinent group which demonstrated a highly significant difference (Table 1) Overactivity was recorded in 54 patients, with insignificant rise in intraluminal pressure during the contractions (Table 2) The mean functional profile length of the conduit was 4 6 + 1 77 cm (ranging from 1 7 cm to 7 5 cm) and was correlated positively to continence status (Table 3) The mean functional length of the continent and incontinent groups were 4 95 (+1 62) cm and 2 80 (+1 50) cm respectively with a highly significant difference (Table 1) All the
Table 1
Urodynamic data of the continent group in comparison to incontinent group.
In our study, one patient was managed by surgical elongation of the tunnel and become completely dry on five hours interval between catheterization
DISCUSSION
Mitrofanoff principle was described to achieve continent urinary diversion through an appendiceal stoma in cases of compromised vesico-urethral function with inaccessible urethra (3) An alternative approach (Yang-Monti technique) using an opened ileal segment closed transversely was described later when the appendix could not be used o r p
Table 2.
Intraluminal
patients with conduit functional profile length of 2 cm or less were incontinent Further analysis of patients with functional length lower than 2 cm revealed a lower static profile maximal closure pressure compared to those with a functional profile length of greater than 2 cm Also, functional length was positively correlated to dynamic closure pressure (Table 4) Conduit peristalsis was observed in 29 patients However, there was no statistically significant difference between incidence of conduit peristalsis in continent (23 patients/66) and incontinent (6 patients/10), by the measurement of functional profile length, static or dynamic maximal closure pressure (Table 5)
Table 3.
Correlation between functional length and continence status.
Significance (2-tailed)
* Correlation is significant at the 0 05 leve
Table 4.
Correlations between functional length and maximal closure pressure
Table 5.
Conduit peristaltic contraction in relation to urodynamic data
(MACE) (4) The Monti ileovesicostomy has become an integral component of lower urinary tract reconstruction and more recently laparoscopic and robotically assisted techniques have been described also (5, 6)
In the present study, the continence rate was 87%, that is lower than those achieved by studies which used appendicovesicostomy with continence rates ranging from 91 to 96% (7-9) Other studies on Monti technique suggested continence rates comparable to appendicovesicostomy (10) This result may be attributed to the high conduit intraluminal pressure achieved by appendiceal stoma (11) or inadequate surgical technique as inadequate flap valve mechanism, internal fistula or inadequate reservoir (12) The reservoir capacity was adequate in most cases with a mean cystometric capacity at 6 months of 496 ml due to detubularisation Smaller reservoir capacity was observed in incontinent group but without statistical significance, although seven patients of the incontinent group showed a capacity of 250-300 ml These patients had to catheterize their pouch every two hours to avoid urine leak and during nighttime, an indwelling catheter had to be placed to avoid sleep interruption The incontinence in the other three patients with adequate capacity can be explained by insufficient tunnel length, inadequate fixation of efferent channel to rectus sheath or angulation One patient was managed by surgical elongation of the tunnel becoming completely dry at five hours interval between catheterizations Two cases were managed by submucosal injection of bulking agent which achieved temporary continence only for 2 months and required subsequent revision of the conduit to regain continence These results support poor results observed in literature for bulking agent injection in ileal stomal incontinence (13, 14) Stomal complications in this study were minimal (5 2%) in comparison to results of appendicovesicostomy observed in literature (15) and better than reports of other studies that suggested same rate of stomal complications for Monti technique compared to appendicovesicostomy (11 to 19%) (10) The urodynamic study at rest showed low reservoir pressure due to detubularisation which delays and reduces the amplitude of the pressure rise caused by partial contractions and consequently accommodates higher volumes and prevents leakage Detrusor overactivity was detected in many patients but did not cause a significant rise in the reservoir pressure or associated leakage The conduit pressure was an important factor contributing in efficacy of continent catheterizable stomas, being the higher the conduit pressure, the more the continence mechanism The mean static and dynamic closure pressure of the conduit were lower in
M Abdelwadood, Eman H Ibrahim, Tamer A Abouelgreed, et al
incontinent cases but the difference was not statistically significant These results are similar to the results achieved by other studies (11, 16) The efferent tract closing pressure (with full reservoir) in our study was 75 CmH2O This result is similar to the result obtained by appendicovesicostomy However, most long-term studies supported durable results of appendicovesicostomy (11) where this is still to be proven for ileovesicostomy by future long term studies The mean functional length was 4 6 cm and it showed a highly significant difference between continent and incontinent group Although static and dynamic closure pressures were not significantly different between continent and incontinent groups, there was a significant correlation between functional length and the maximum closure pressure Thus, the cause of incontinence can be attributed to length of the conduit more than reservoir capacity Strong peristaltic contractions of the conduits were demonstrated in some individuals but the overall effect of these pressure waves did not correlated with clinical continence or with any other urodynamic factor
CONCLUSIONS
Urodynamic evaluation of continent catheterizable cutaneous stoma after Yang-Monti procedure has a practical significance Functional length of the conduit seems to be the most influential factor for continence reflecting static and dynamic maximal closure pressure Higher conduit closing pressure is associated with better continence Contractions of the pouch and peristaltic contraction of the conduit has no effect on continence mechanism
ACKNOWLEDGMENTS
Thanks to Prof Dr Hossam Hamdy, President of Gulf Medical University for his suggestion
REFERENCES
1 Abouelgreed T, Saleh D, Abdelaal M, et al Urodynamic changes following laparoscopic versus vaginal hysterectomy Arch Ital Urol Androl 2022; 94:315-318
2 Kupec T, Pecks U, Gräf CM, et al Size Does Not Make the Difference: 3D/4D Transperineal Sonographic Measurements of the Female Urethra in the Assessment of Urinary Incontinence Subtypes Biomed Res Int 2016; 2016:1810352
3 Ramanan V, Kapoor R, Srinadh ES, et al Mitrofanoff principle for continent urinary diversion Urol Int 1997; 58:108-112
4 Monti PR, de Carvalho JR Transverse tubulization of intestinal s
Mitrofanoff procedure Prog Urol 2001; 11:382-384
5 Thakre AA, Yeung CK, Peters C Robot-assisted Mitrofanoff and Malone antegrade continence enema reconstruction using divided appendix J Endourol 2008; 22:2393-2396
7 Elshal AM, Abol-Enein H, Sarhan O, et al Catheterizable serous lined urinary outlet in children and adolescents: a choice when other treatments fail J Urol 2011; 185:1083-1087
8 Mhiri MN, Bahloul A, Chabchoub K Mitrofanoff appendicovesicostomy in children: indication and results Prog Urol 2007; 17:245-249
9 Surer I, Ferrer FA, Baker LA, Gearhart JP Continent urinary diversion and the exstrophy-epispadias complex J Urol 2003; 169:11021105
10 Clark T, Pope JC 4th, Adams mC, et al Factors that influence outcomes of the Mitrofanoff and Malone antegrade continence enema reconstructive procedures in children J Urol 2002; 168:1537-1540
11 Chabchoub K, Ketata H, Fakhfakh H, et al Continent urinary diversion (Mitrofanoff principle) Physical mechanisms and urodynamic explanation of continence Prog Urol 2008; 18:120-124
12 Cain MP, Andrew MD, Anthany JG, et al Updated experience with the Monti catheterizable channel Pediatric Urology 2008; 72:782-785
13 Gowda BO, Agrawal V, Harrison SC The continent catheterizable abdominal conduit in adult urological practice BJU Int; 2008; 102:1688-1692
14 Welk BK, Afshar K, Rapoport D, MacNeily AE Complications of the catheterizable channel following continent urinary diversion: Their nature and timing J Urol 2008; 180:1856-1860
15 Van der AF, Joniau S, De Baets K, De Ridder D Continent catheterizable vesicostomy in an adult population: success at high costs Neurourol Urodyn 2009; 28:487-4891
16 Watson HS, Bauer SB, Peters CA, et al Comparative urodynamics of appendiceal and ureteral Mitrofanoff conduits in children J Urol 1995; 154:878-882
Correspondence
Eman H Ibrahim, MD (Corresponding Author)
dr eman@gmu ac ae
Department of Biomedical Sciences, College of Medicine, Gulf Medical University, Ajman, UAE & Department of Pathology, Faculty of Medicine, Al-Azhar University, Cairo, Egypt
M Abdelwadood, MD - wadoodaref@gmail com
Mohamed M Yassin, MD - yassinmmm@med asu edu eg
Department of Urology, Faculty of Medicine, Ain Shams University, Cairo, Egypt
Tamer A Abouelgreed, MD - dr tamer ali@yahoo com
Mohamed A Elhelaly, MD - elhelalymohammed@yahoo com
El-Sayed I El-Agamy, MD - abuamr1978@yahoo com
Basem Fathi, MD - basemhara@Gmail com
Department of Urology, Faculty of Medicine, Al-Azhar University, Cairo, Egypt
Yasser M Haggag, MD - uro doc@yahoo com
Department of Urology, Faculty of Medicine, Al-Azhar University, Asyut, Egypt
Salma F Abdelkader, MD - salmafathy4@gmail com
Department of Radiology, Faculty of Medicine Ain Shams University, Cairo, Egypt
Sameh S Ali, MD - drsamehsaied@yahoo com
Department of Radiology, Sheikh Khalifa General Hospital, UAQ, UAE
Naglaa M Aboelsoud, MD - nglaa mahmoud@gmail com
Department of Radiology, Faculty of Medicine, Al-Azhar University, Cairo, Egypt
Nasser Ramadan, MD - nasseruro99@gmail com
Department of Urology, NMC Royal Hospital, Sharjah, UAE
Mohamed Sobhy, MD - mss54482000@yahoo com
Department of Surgery, Faculty of Medicine, Gulf Medical University, Ajman, UAE
Tarek Gharib, MD - tarekgh78@yahoo com
Department of Urology, Faculty of Medicine, Benha University, Benha, Egypt
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Robotic-assisted laparoscopic pyeloplasty for the treatment of ureteropelvic junction obstruction –
How should success be determined?
Marie Lien 1 , Mathias Sørstrand Æsøy 1, 2 , Karin Hjelle 1, 2 , Bjarte Almås 2 , Patrick Juliebø-Jones 1, 2 , Øyvind Ulvik 1, 2
1 Department of Clinical Medicine (K1), University of Bergen, Bergen, Norway;
2 Helse Bergen HF, Department of Urology, Haukeland University Hospital, Bergen, Norway
Summary
Background: Ureteropelvic junction obstruction (UPJO) is characterised by stenosis of the ureteral lumen at the level of the renal pelvis and proximal ureter. At Haukeland University Hospital, robotic-assisted laparoscopic pyeloplasty (RLP) for UPJO has been performed since 2014. The aim of this study was to evaluate the results of the treatment and consider what determines treatment success
Materials and methods: Retrospective review was performed of consecutive patients undergoing RLP between 2014-2022
Outcomes of interest included symptom relief, complication rates and renographic findings at follow-up Treatment success was defined in terms of symptom improvement and/or improvement as well as relief of obstruction on renography
Results: In total, 95 RLPs were performed in 54 women and 41 men, with a mean age of 40 years (IQR: 21-58) Flank pain was the most frequent presenting complaint (n = 81, 85%) followed by infection (n = 33, 35%) More than one indication for surgery was present in 1/3 of the patients Urodynamic relevant obstruction on renography was found in 62 patients (65%) preoperatively Mean operative time was 123 minutes (range 60-270)
Two patients experienced minor intraoperative complications
At three months follow-up, 91% of patients had symptom relief, and no obstruction on renography was recorded in 64% There was no significant association between improvement in symptoms and renography findings at follow-up, p = 1.
Conclusions: RLP can deliver a high success rate in terms of symptom relief and few complications. There was no association between renography findings and symptom relief at follow-up Success after surgery should be determined by symptom relief rather than renography findings
Submitted 26 February 2024; Accepted 28 March 2024
INTRODUCTION
Ureteropelvic junction obstruction (UPJO) is a condition where the flow of urine from the renal pelvis to the ureter is impaired at the anatomical transition between the renal pelvis and proximal ureter (1) While most cases are congenital, other possible causes include kidney stone dis-
ease, urothelial neoplasms and as a result of inflammatory processes Postoperative scarring and ischemia can also serve as precipitants Congenital aetiologies encompass a range of possible causes, including physiological defects such as aperistaltic segments and anatomical factors such as the presence of crossing vessels (2) Moreover, UPJO is considered the most common congenital abnormality of the ureter (2) This particular impairment can lead to the development of hydronephrosis as well as a progressive deterioration in renal function (3) From a clinical perspective, the most common presenting complaint is intermittent abdominal or flank pain, which is often associated with an excess intake of fluid This may also be accompanied by nausea and vomiting (2) The diagnosis can be subsequently confirmed through imaging modalities such as ultrasound and computed tomography (CT) urography (4) Additionally, isotopic renography is commonly used for diagnostic purposes, although consensus regarding the exact criteria for defining obstruction is lacking (5) Symptomatic obstruction of the ureteropelvic junction should be treated surgically (6)
Indications for surgery include the presence of symptoms associated with the obstruction, a progressive impairment of renal function or infection in the upper urinary Historically, the preferred surgical procedure has been dismembered pyeloplasty when intervention is warranted (2) Initially, open surgery was the sole option; however, advancements in surgical technology over recent decades have allowed for minimally invasive approaches, such as laparoscopic and robotic pyeloplasty, to now standard as the reference interventions (7)
Currently, robotic assisted laparoscopic pyeloplasty (RLP) is reported to yield success rates exceeding 90% (8-11) The robotic-assisted approach for pyeloplasty is further associated with short hospital stay and low complication rates (12) Consensus is also lacking regarding how treatment success should be defined
At our institution, the Da Vinci Robotic system (Intuitive Surgical, Sunnyvale, CA, USA) is currently utilized in the surgical management of UPJO In the present study, we aimed to evaluate the outcomes associated with RLP since beginning with this approach In addition, we wanted to explore the relationship between the result of the follow
M Lien, M Sørstrand Æsøy, K Hjelle, et al
up isotopic renography in comparison to symptom improvement in order to better understand how treatment success should be defined
MATERIALS AND METHODS
Study population and setting
Since 2014, RLP has been the standard treatment for UPJO at Haukeland University Hospital, a regional centre in Western Norway Retrospective review of the electroni c m e d i c a l r e c
patients undergoing RLP between 2014 and 2022
Outcomes of interest included symptom relief, complication rates and renographic findings at three months follow-up Patient demographics and preoperative characteristics are shown in Table 1 The American Society of A n e s t h e s i o l o g i s t (ASA) score was used assessing the patient’s general condition
Indications for surgery included flank pain, infection, and impaired renal function These indications did not change over the study period An evaluation of the symptom burden was made by each urologist in consultation with the patient
During the preoperative work up, all patients underwent imaging with ultrasonography and cross-sectional imaging such as CT A preoperative nuclear scan (MAG3 diuretic renogram) was performed in order to determine split- and total renal function, as well as to assess the degree of obstruction Urodynamic relevant obstruction was defined as no emptying of the renal pelvis within 15 minutes after intravenous administration of diuretics
Physiological obstruction was determined by delayed emptying of the renal pelvis within 15 minutes after diuretic administration Serum creatinine and eGFR were measured both preoperatively and at follow-up
Surgical procedure
The Da Vinci Robotic Surgical System was used to perform an Anderson-Hynes dismembered pyeloplasty with resection of excess renal pelvis and re-anastomosis to the ureter A postoperative JJ-stent was routinely placed before completing the anastomosis and remained in place for four weeks before removal in the outpatient clinic An abdominal drain at the conclusion of the surgery was placed at the surgeon s discretion in the early procedures Postoperative complications were assessed using the Clavien-Dindo grading system (13)
All patients were scheduled for follow-up at least three months postoperatively The follow-up included repeat isotopic renography as well as consultation with a urologist Further follow-up was repeated whenever deemed necessary by the surgeon, respectively 12 months postoperatively
Treatment success
Treatment success was determined based on the following criteria:
1 Patient-reported improvement: Surgical success was categorised if patients reported a clinically significant improvement in their symptoms or complete symptom relief at the three-month follow-up assessment
2 Radiological assessment: Radiological success was categorised as the absence of urodynamic relevant obstruction on isotopic renography conducted at least three months postoperatively
Statistics
Independent samples t-tests were performed to compare continuous variables, such as renal split function and cre-
Associations between categorical variables, i e , symptom relief and findings at isotopic renography at follow-up, were assessed using exact chi-squared tests or Fischer s exact tests IBM SPSS Statistics 28 (IBM, Armonk, NY) was used for statistical analysis The p-value was considered significant when < 0 05
Ethics and approvals
In accordance with institutional and Norwegian regulations, the study was registered as a clinical audit (eProtocol, project ID 3470) and as such, was exempted from further ethical approval
Table 1.
Preoperative characteristics.
in kg, mean (range, IQR)
Creatinine in mmol/L, mean (IQR)
(32-160, 62-87)
(39-135, 64-90)
– flowchart.
RESULTS
Between April 2014 and December 2022, 95 RLP procedures were performed by five urologists In total, 54 (57%) women and 41 (43%) men with a mean age of 40 years (IQR: 21-58) underwent surgery Preoperative characteristics are provided in Table 1
Flank pain was the most frequent cause of surgery (81 cases, 85%) followed by infection (33 cases, 35%) and impaired renal function (19 cases, 20%) In 32 patients (34%), more than one indication for surgery was present
An isotopic renography prior to surgery was performed in 93 patients (98%), and urodynamic relevant obstruction was found in 62 (67%) In the remaining 31 (33%), renography was inconclusive or revealed physiological obstruction only (Figure 1) There was no statistically significant association between flank pain and urodynamic relevant obstruction on preoperative isotopic renography, p = 0 35 Anderson-Hynes pyeloplasty with re-anastomosis between the ureter and the renal pelvis was performed in all patients, except for one patient who underwent adhesioloysis around the ureteropelvic junction only Antegrade JJstent was placed in all but two patients In one of these cases, placement of the stent was unsuccessful, and a nephrostomy tube was inserted In the other case, insertion of a JJ-stent was deemed unnecessary as no new anastomosis was made An abdominal drain was placed at the end of the surgery in the first 11 patients undergoing RLP when the robotic approach was first started In these cases, the drain was removed on the first postoperative day For the latter 84 patients, no abdominal drain was placed Details regarding the surgical procedures are listed in Table 2 Intraoperative complications occurred in two patients
(2%), both involved minor bleeding from either a tear in the renal parenchyma or the renal pelvis The surgical procedures were successfully completed in both patients Four patients (4%) developed post operative infection
Table 2 The surgical procedure
Figure 1. Renography findings
Lien,
Table 3.
Postoperative complications occurring within 3 months after surgery
during the hospital stay and one patient (1%) experienced postoperative pain before discharge beyond that expected All the postoperative complications were categorised as Clavien-Dindo grade 1 or 2 Median post operative hospital stay was two days (IQR: 1-2)
Follow-up after three months with an isotope renography was registered in 88 cases (94%), and no obstruction was found in 56 cases (64%) In the remaining 32 patients (36%), 22 (25%) still had signs of urodynamic relevant obstruction and an additional 10 (11%) had inconclusive tests (Figure 1)
The renal split function did not change from the preoperative (right 51 1%/left 48 9%) to the three months follow up renography (right 51 1%/left 48 9%), p = 1 No difference was observed regarding serum-creatinine when preoperative blood analysis (85 mmol/L) was compared to blood test at follow-up (84 mmol/L), p = 0 5 The same result was found comparing GFR before and after surgery (82 mL/min and 83 mL/min, respectively), p = 0 7
In total, 91% of all patients experienced complete resolution of their symptoms (n = 45) or reported overall symptom improvement (n = 33) Of note, 30 out of 32 patients with inconclusive renography findings or persistent urodynamic relevant obstruction after three months, nevertheless reported symptom free status (n = 14) or experienced overall improvement in their symptom burden (n = 16) There was no significant association between symptom improvement or becoming symptom free after surgery and the finding of no obstruction on follow-up isotopic renography, p = 1 Table 3 summarises postoperative complications occurring within the first three months after surgery
A total of 54 patients (57%) underwent 12 months follow up including additional isotopic renography (Figure 1) No obstruction was registered in 46 patients (85%), and inconclusive findings in two patients (4%) Urodynamic obstruction was registered in six patients (11%) In three of these, signs of obstruction had appeared since the previous follow-up Despite the renographic finding, all three experienced symptom resolution
In 12 patients (71%) with urodynamic obstruction or inconclusive finding at three months follow-up, no obstruction was registered at the 12-month renography Furthermore, 93 % of the patients experienced complete symptom resolution or reported an overall improvement
in their symptoms at 12 months follow up Patients with persistent obstruction after 12 months were planned for further follow-up with renography and endoscopic assessment whenever indicated No patients needed repyeloplasty
DISCUSSION
In this study, we have examined the outcomes of RLP conducted at our institution over a period of nearly 8 years Flank pain was the most frequent indication for surgery However, more than one indication for surgery was identified in one third of the patients AndersonHynes dismembered pyeloplasty was performed in all but one patient In total, 91% of the patients reported resolution of their pain at follow-up Two patients had minor intraoperative bleeding, which ultimately had no impact on completing the surgery In addition, four patients experienced a post operative urinary infection and received antibiotic therapy Our results align with previous research, which supports RLP as a safe procedure with a high success rate in terms of symptom relief and the complication burden (8, 9, 14, 15)
At three months follow-up, no obstruction on isotopic renography was found in 64% of the patients In the r e m a i n i n g 3 6 % , e v i d
obstruction was either still present, or the test was inconclusive Our radiological success rate is lower compared to other reports in the literature, which is likely attributable in part to variations in the definitions employed for renographic success (8, 15, 16) While we determined radiological success as the absence of urodynamic significant obstruction on renography three months after surgery, defined as no emptying of the renal pelvis within 15 minutes after intravenous administration of diuretics, Etafy et al defined radiological success as a half-time (t½) isotope excretion of less than 10 minutes on diuretic renogram performed five to six weeks postoperatively (14) In that study, 82 5% of the patients were considered to be successfully treated based on the diuretic renogram (14) Wood et al reported a success rate of 97 6% from a radiological perspective, with improvement or the arrest of deteriorating drainage, as the given criteria for success but with no further details (8) The lack of a common definition for treatment success after pyeloplasty thus makes it difficult to compare results across different studies
In the present study, while flank pain was preoperatively reported in 81 cases, preoperative isotopic renography indicated urodynamic relevant obstruction in 62 cases only Surprisingly, no statistically significant association between the presence of preoperative flank pain and detection of urodynamic relevant obstruction was found, p = 0 35 This might be explained by the strict definition for obstruction at renography used at our institution
On the other hand, patients may experience intermittent flank pain due to UPJO that may not be recognized as relevant obstruction in time periods with no symptoms
This may also explain why 30 of the 32 patients in our study displaying persistent urodynamic relevant obstruction or inconclusive findings at follow-up isotopic renography, reported symptom improvement or complete resolution
M
M Sørstrand Æsøy, K Hjelle, et al
Robotic-assisted
Furthermore, although the obstruction is relieved by the surgery, persistent hydronephrosis due to a flaccid renal pelvis may cause delayed emptying and thereby mimic obstruction
Although no association between obstruction on renography and symptom relief was found, renal split function before and after surgery may add information to the result of the surgery In the present study, renal split function was unchanged between preoperative and follow-up tests, indicating that the surgery did not deteriorate the function of the affected kidney Other author groups have also reported on the diagnostic value of split renal function when determining success after pyeloplasty (5, 15)
The difficulty in defining obstruction at renography, and the finding of no association between symptoms and renographic obstruction in the present study, have led us to question the clinical role of isotopic renography in UPJO besides determining renal split function
Previous studies have shown that RLP is associated with a markedly reduced postoperative hospital stay when compared to conventional laparoscopic pyeloplasty This highlights the efficiency and potential benefits of adopting a robotic approach in the setting of urological procedures (17, 18) Our median inpatient stay was 2 days (IQR: 1-2), which is similar to findings from other studies (8, 14, 16, 19-21)
The present study has several limitations The retrospective design may have impeded complete data collection for all patients A few patients were lost to follow-up as they were referred from external centres and underwent follow up at their local hospital Despite this, complete follow-up data was available for 94% of the patients, which is a strength of the study The sample size is relatively small, but the vast majority of published series originate from nations with much larger populations
The majority of patients (91%) reported either improvement or complete resolution of their symptoms at three months follow-up However, no validated tool for subjective pain assessment was employed in this study The assessment of preoperative symptoms and postoperative symptom relief was therefore based solely on patients individual accounts to the urologist and the documentation accordingly This lack of standardisation is a clear limitation of the study but does reflect real world practice While a lack of a standardised definition for urodynamic relevant obstruction on isotopic renography in the literature presents a further challenge when conducting research in this particular area, a definition was applied in this study that was implemented at our institution prior to the study start date and has remain unchanged over the whole period
CONCLUSIONS
RLP can be performed with high success rates in terms of symptom relief and the morbidity profile Of particular relevance to clinical practice is that this study highlights the disparity between renographic findings and symptom improvement Of note, an absence of correlation between preoperative pain and isotopic renography findings was found, and there was no discernible link between renography results and symptom relief at follow-up Therefore,
we argue that defining treatment success should place a greater emphasis on symptom improvement rather than only relying on renography findings
REFERENCES
1 Al-Salem AH Pelviureteric Junction Obstruction Atlas of Pediatric Surgery: Principles and Treatment Cham: Springer International Publishing; 2020; p 819-27
2 Wein A KL, et al Campbell-Walsh Urology 10th edition Elsevier Saunders 2012; p 1122-47
3 Koff SA MK Anomalies of the kidney In: Gillenwater JY, Grayhack JT, Howards SS, editors Adult and Pediatric Urology Philadelphia, Unites States: Lippincott Williams & Wilkins 2001; p 2129
4 Hemal AM, M, editor Robotics in Genitourinary Surgery: Springer 2011
5 Piepsz A The predictive value of the renogram Eur J Nucl Med Mol Imaging 2009; 36:1661-4
6 Tanagho EM, JW Smith’s General Urology 17 ed: McGraw-Hill Medical; 17th edition 2007; p 768
7 Shah KK, Louie M, Thaly RK, Patel VR Robot assisted laparoscopic pyeloplasty: a review of the current status Int J Med Robot 2007; 3:35-40
8 Wood TC, Raison N, El-Hage O, et al Robot-assisted laparoscopic pyeloplasty: a single-centre experience Surg Endosc 2018; 32:4590-6
9 Zhang P, Shi T, Fam X, et al Robotic-assisted laparoscopic pyeloplasty as management for recurrent ureteropelvic junction obstruction: a comparison study with primary pyeloplasty Transl Androl Urol 2020; 9:1278-85
10 Gupta NP, Nayyar R, Hemal AK, et al Outcome analysis of robotic pyeloplasty: a large single-centre experience BJU Int 2010; 105:980-3
11 Bird VG, Leveillee RJ, Eldefrawy A, et al Comparison of robotassisted versus conventional laparoscopic transperitoneal pyeloplasty for patients with ureteropelvic junction obstruction: a single-center study Urology 2011; 77:730-4
1 2 C a i P Y , L e e R S U
/ Hydronephrosis Urol Clin North Am 2023; 50:361-9
13 Dindo D, Demartines N, Clavien PA Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey Ann Surg 2004; 240:205-13
14 Etafy M, Pick D, Said S, et al Robotic pyeloplasty: the University of California-Irvine experience J Urol 2011; 185:2196-200
15 Schwentner C, Pelzer A, Neururer R, et al Robotic AndersonHynes pyeloplasty: 5-year experience of one centre BJU Int 2007; 100:880-5
16 Thom MR, Haseebuddin M, Roytman TM, et al Robot-assisted pyeloplasty: outcomes for primary and secondary repairs, a single institution experience Int Braz J Urol 2012; 38:77-83
17 Braga LH, Pace K, DeMaria J, Lorenzo AJ Systematic review and meta-analysis of robotic-assisted versus conventional laparoscopic pyeloplasty for patients with ureteropelvic junction obstruction: effect on operative time, length of hospital stay, postoperative complications, and success rate Eur Urol 2009; 56:848-57
18 Carmona O, Dotan ZA, Haifler M, et al Laparoscopic Versus
Lien, M Sørstrand Æsøy, K Hjelle, et al
Robot-Assisted Pyeloplasty in Adults-A Single-Center Experience J Pers Med 2022; 12
19 Patel V Robotic-assisted laparoscopic dismembered pyeloplasty
Urology 2005; 66:45-9
20 Mufarrij PW, Woods M, Shah OD, Palese MA, Berger AD,
Thomas R, et al Robotic dismembered pyeloplasty: a 6-year, multiinstitutional experience J Urol 2008; 180:1391-6
21 Sivaraman A, Leveillee RJ, Patel MB, et al Robot-assisted laparoscopic dismembered pyeloplasty for ureteropelvic junction obstruction: a multi-institutional experience Urology 2012; 79:351-5
Correspondence
Marie Lien, medical student makrlien@gmail com
Department of Clinical Medicine (K1), Faculty of Medicine, University of Bergen - Postboks 7804, 5020 Bergen, Norway
Mathias Sørstrand Æsøy, MD mathias asoy@gmail com
Karin Hjelle, MD PhD Assoc Professor
karin margrethe hjelle@helse-bergen no
Bjarte Almås, MD PhD bjarte almaas@helse-bergen no
Patrick Juliebø-Jones, MD PhD jonesurology@gmail com
Øyvind Ulvik, MD PhD Assoc Professor (Corresponding Author) doc ulvik@online no
Helse Bergen HF, Department of Urology, Haukeland University Hospital Postboks 1400, 5021 Bergen, Norway
Conflict of interest: The authors declare no potential conflict of interest
Archivio Italiano di Urologia e Andrologia 2024; 96(2):12431
M
ORIGINAL PAPER
Pediatric renal transplantation: A single center experience
Shakhawan Hama Amin Said 1 , Saiwan Hayas Agha 1 , Goran Fryad Abdulla 1 , Mzhda Sahib Jaafar 1 , Rawa Bapir 2-4 , Nali H Hama 1, 2 , Ismaeel Aghaways 1 , Aso Omer Rashid 1 , Berun A Abdalla 2, 4 , Fahmi H Kakamad 1, 2, 4
1 College of Medicine, University of Sulaimani, Sulaymaniyah, Kurdistan, Iraq;
2 Smart Health Tower, Madam Mitterrand Street, Sulaymaniyah, Kurdistan, Iraq;
3 Department of Urology, Sulaymaniyah Teaching Hospital, Sulaymaniyah, Kurdistan, Iraq;
Introduction: The rising prevalence of global end-stage renal disease (ESRD) is a significant health concern, especially among children. Although renal replacement therapy is available, children with ESRD are at an increased risk of mortality. Kidney transplantation is the preferred modality of treatment and surpasses renal replacement therapy in terms of survival. However, pediatric renal transplantation could prove difficult due to factors like smaller recipients and donor-recipient mismatches leading to higher complications
Materials and methods: A retrospective single-group case series study was conducted on children with ESRD who were planned to undergo kidney transplantation from living donors between 2015 and 2021 The data was collected from two centers in the city of Sulaymaniyah
Results: The study comprised a predominantly male patient population, with a total of 39 individuals (n = 39) and 13 female patients. The donors were mostly males between 25-40 years old The majority of participants were 15-18 years old In majority of the patients Thymoglobulin was the immunosuppressive agent used in induction The most common etiology for renal failure was reflux nephropathy and artery anastomosis was performed to the external iliac artery in the majority of patients. Only 9 patients had complications following the transplantation and 3 patients had an episode of acute rejection
Conclusions: Renal transplantation is the preferred treatment of renal failure in pediatric patients in the city of Sulaymaniyah The most common etiology for pediatric renal failure was reflux nephropathy which was different from the findings of North American Pediatric Renal Trials and Collaborative Studies.
Submitted 15 February 2024; Accepted 22 February 2024
INTRODUCTION
The global incidence of end-stage renal disease (ESRD) is currently escalating and posing a significant health concern worldwide Chronic kidney disease (CKD) is a condition characterized by irreversible injury to the kidneys that can advance to ESRD, the final stage of renal deterioration ESRD is a devastating disorder associated with high mortality rates and cardiovascular complications
The disease in children is more complex than in adults, leading to specific challenges such as poor growth, cognitive problems, bladder dysfunction, and special dietary needs, which profoundly impact their quality of life (1, 2) Despite the availability of renal replacement therapy (RRT), children with severe renal failure face a significantly increased risk of mortality, approximately 30 times h i g h
Furthermore, children with hemodialysis experience low self-esteem, loss of identity, compromised body integrity, diminished control, and reduced independence (2) Kidney transplantation (KTx) remains the preferred treatment for both adults and children with ESRD It offers
enhanced quality of life compared to RRT However, despite KTx being a well-established procedure for adults, it is relatively rare in children (3) Even though there have been significant improvements in graft and patient outcomes, KTx remains a challenging procedure for pediatric patients This is primarily due to factors like smaller recipients, congenital anomalies, and donorrecipient mismatches that lead to an increased risk of postoperative complications (3) It has also been reported that long-term graft survival rates in the pediatric population have not shown significant improvement, primarily due to factors like infections, episodes of acute rejection, and suboptimal adherence to medication regimens (4) The existing literature on pediatric KTx predominantly focuses on long-term outcomes for grafts and patients However, there is a scarcity of data regarding the impact of pre-transplantation factors, donor-recipient mismatching, and the occurrence and consequences of surgical complications (3, 5)
The present study is a case series aimed to show the experience of the city of Sulaymaniyah regarding pediatric renal transplantation
METHODS
Study design
A retrospective single-group case series study was conducted on children with ESRD who were planned to undergo KTx from living donors between 2015 and
2021 The consent for participation and publication of data was obtained from the parents of patients Ethical approval of the study was provided by the ethical committee of the University of Sulaimani
Inclusion criteria
All children younger than 18 years who underwent renal transplantations from living donors due to ESRD
Exclusion criteria
Renal transplant cases older than 18 years old
Data collection
The data was collected from two centers, Shar Hospital and Faruk Medical City, by reviewing the medical records of patients or filling out a specific questionnaire form by patients or their families The extracted variables were patient demographics, etiology of renal failure, history of dialysis before transplantation, donor characteristics, the surgical technique of renal transplantation including the type of vascular and ureteric reconstruction, ischemia time, patient and graft survival, acute rejection episodes, reasons for graft failure, and cause of death Doppler ultrasound of the graft had been performed within 24 hours of transplantation Graft function had been monitored daily using plasma creatinine levels The applied i m m u n o s u p p r e s s i o n p r o t o c o l (
d maintenance therapy) had been documented Operative and postoperative adverse events had been graded using the Modified Clavien Dindo Scale of Complication Severity (6) Graft failure was defined as the failure of a renal transplant with a return to dialysis or the performance of a second preemptive transplant Acute rejection episode was defined as a rise in serum creatinine of at least 30% from baseline levels, accompanied by clinical symptoms and signs (fever, oliguria), and pathologic proof with a renal biopsy
Data analysis
Data entry and coding were done using Microsoft Excel (Version 2010) Data analysis was performed using Statistical Package for the Social Sciences (SPSS) Version 24 Standard descriptive statistics, including percentages and mean ± standard deviation, were performed to analyze the data
RESULTS
Our patients were grouped into 3 age categories Only 9 (17 3%) of them were younger than 10 years old while the majority 31 patients 59 6% were between 15-18 years old The remaining 12 (23 1%) patients were between 11-14 years old Thirty-nine patients were male and constituted 75% of our data while the remaining 25% (13 patients) were females The mean Body Mass Index (BMI) of our patients was 21 3 ± 1 69 The immunosuppressive pharmacologic agents used for induction were Thymoglobulin (used in 88 5% of our patients) and Basiliximab (used in only 6 patients) Only two patients had a history of previous transplantation and the other 50 patients were having their first attempt at renal transplantation
The majority of the donors were 25-40 years old and a minority of 5 donors were older than 40 years old The majority (42, 80 8%) of the donors were male and the rest were female Only 8 of the donors were related to the patients and the other 44 donors were non-related
The most common etiology for renal failure was reflux nephropathy which accounted for 21 2% of the patients
This was followed by Focal Segmental Glomerulosclerosis which accounted for 17 3% of the patients Forty-six patients had a single graft artery which accounted for 88 5% of the cases The rest of the patients had double artery grafts
Artery anastomosis was performed to the external iliac artery in the majority of the patients, accounting for 63 5% of them, and in the remaining patients it was anastomosed to the common iliac artery Thirty-eight patients had the venous anastomosis done with the external iliac vein and in only 2 patients the anastomosis was performed with the Inferior Vena Cava (IVC)
Post-operative evaluation of our patients showed only 9 patients had complications following the transplantation and 3 patients had an episode of acute rejection Table 1 shows the recipient characteristics, etiologies of renal failure, surgical techniques and post-operative data
Table 1.
Recipient and Donor characteristics, etiology of renal failure, surgical technique
S Hama Amin Said, S Hayas Agha, G Fryad Abdulla, et al
(1 9)
(17 3)
(9 6)
(88 5)
(63 5)
(36 5)
(73 1)
(9 6)
(3 8)
8)
9)
9)
DISCUSSION
Renal transplantation is the preferred modality for the treatment of ESRD If possible, pre-emptive renal transplantation, which is transplantation before the need for dialysis, shows better results than early renal transplantation
The analysis of our pediatric renal transplant patient data reveals a predominant demographic within the age bracket of 15-18 years, comprising 59 6% of the data Subsequently, the following demographic consists of patients aged between 11-14 years, representing 23 1% of the total, while those under 10 years old account for 17 3% This distribution of age segments aligns with the conclusions drawn from a study conducted by Chacko and colleagues Their findings similarly underscore a prevalence of older pediatric recipients in renal transplantation, with a mean age of 15 years Consequently, it suggests a propensity for renal transplantation among older children and adolescents (7)
In terms of gender distribution, our data showed that 75% of the patients (n = 39) were male while only 25% were female (n = 13) In accordance with the data recorded in the North American Pediatric Renal Trials and Collaborative Studies (NAPRTCS) registry, it has been observed that there exists an inverse correlation between the age group of patients and the male-to-female ratio
Specifically, as the age group of patients advances, the ratio of male to female patients tends to decrease During infancy, the male patients made up 70% of the NAPRTCS data At ≥ 18-year-old, this ratio decreases to 54 3% for males and 45 7% for female (8) Chacko et al also found a disparity in male to female ratio in pediatric renal transplantation, where 65% of the patients in their study were male and only 35% were female (7) This was in contrast to a study by Barlas et al , in which a gender disparity was not as obvious and only 51 2% of their data were male (9) Also, in a paper by Kavas and colleagues, out of 37 patients, 20 of them were male and 17 were female (10) In a study conducted by Hogan and colleagues that investigated gender disparities in access to pre-emptive pediatric renal transplantation in Europe, revealed a significant gender disparity, indicating that girls were 23% less likely to undergo a pre-emptive renal transplant when compared to boys This outcome underscores the existence of genderrelated discrepancies in the accessibility of pre-emptive renal transplantation within the pediatric population in Europe, warranting further exploration into the factors contributing to this observed disparity (11)
The most common cause of renal failure in our patients was reflux nephropathy which accounted for 21 2% of the patients While the second most common cause was Focal Segmental Glomerulosclerosis (FSGS) which accounted for 17 3% of the patients In accordance with the NAPRTCS registry, it is noteworthy to underscore that renal dysplasia in infants emerges as the predominant etiology of renal failure within the pediatric age group However, as age advances, the probability of renal dysplasia serving as the primary causative factor for renal failure diminishes Notably, upon reaching the age of 18 years and beyond, focal segmental glomerulosclerosis (FSGS) emerges as the predominant cause of renal failure Subsequently, obstructive uropathy ranks second in prevalence, while renal dysplasia occupies the third position in the hierarchy of causative factors for renal failure (8)
Our findings were in contrast to a paper by Kavaz et al. where the most common cause of ESRD was juvenile nephronophthisis (N = 11 out of 37 patients) Reflux nephropathy was found to be the cause of renal failure in only 2 patients and Focal segmental glomerulosclerosis was determined to the cause in 4 patients (10)
In the study conducted by Barlas and colleagues, it was identified that vesicoureteral reflux and primary glomerular disease were the predominant etiologies leading to ESRD (9) The similarity in our findings prompts questions regarding whether the high prevalence of reflux nephropathy and primary glomerular disease as primary causes of ESRD is attributable to a smaller sample size within our centers, or if it is a consequence of the geographic proximity of the two centers, where both are located in neighboring countries
While most of our patients had no complication post-operatively, the most common complication in our data proved to be urinary tract infection which accounted for 9 6% (n = 5) of our complications The most common complications in a study by Beetz et al were vascular complications for which 34 (15 4%) patients needed surgical revision of their transplantations Also, urinary tract infections accounted for 6 3% of their overall complications (3) Hemorrhage
accounted for 3 8% of our complications This goes in line with the complications of a study done by Irtan et al , where only 2 out of 202 patients had hemorrhage (12) The difference among these numbers could be explained by the difference in sample size, where Beetz et al had a larger sample size of 221 patients and Irtan et al had a sample size of 202 patients (3, 12)
The main limitation of our study was a lack of a comparison group, hence correlating the preoperative variables to graft survival could not be done appropriately and establishing causations was not possible The sample size was small and cannot be generalized for the whole population Also, the retrospective nature of the study is another limitation
CONCLUSIONS
Renal transplantation is the preferred treatment of renal failure in pediatric patients in the city of Sulaymaniyah
The most common etiology for pediatric renal failure was reflux nephropathy which was different from the findings of NAPRTCS
REFERENCES
1 Ghelichi-Ghojogh M, Mohammadizadeh F, Jafari F, et al The global survival rate of graft and patient in kidney transplantation of children: a systematic review and meta-analysis BMC Pediatr 2022; 22:503
2 Agerskov H, Thiesson HC, Pedersen BD Everyday life experiences in families with a child with kidney disease J Ren Care 2019; 45:205-211
3 Beetz O, Weigle CA, Nogly R, et al Surgical complications in pedi-
Correspondence
Shakhawan Said, MD
shakhwan said@gmail com
Saiwan Agha, MD
saiwan agha@gmail com
Goran Abdullah, MD
goran abdullah@gmail com
Mzhda Jafaar, MD
mzhda jafaar@gmail com
Nali Hama, MD
nali hama12@gmail com
Ismaeel Aghaways, MD ismaeelagha@hotmail com
Aso Rashid, MD
aso rashid@univsul edu iq
Fahmi Kakamad, MD (Corresponding Author)
fahmi hussein@univsul edu iq
College of Medicine, University of Sulaimani, Sulaymaniyah, Kurdistan, Iraq
Doctors City, Building 11, Apartment 50, Sulaimani, 46001 Iraq
Rawa Bapir, MD
dr rawa@yahoo com
Berun Abdalla, MD
berun anwer95@gmail com
Smart Health Tower, Madam Mitterrand Street, Sulaymaniyah, Kurdistan, Iraq
Conflict of interest: The authors declare no potential conflict of interest
atric kidney transplantation-Incidence, risk factors, and effects on graft survival: A retrospective single-center study Pediatr Transplant 2021; 25:e13871
4 Naderi G, Latif A, Karimi S, et al The Long-term Outcome of Pediatric Kidney Transplantation in Iran: Results of a 25-year Single-Center Cohort Study Int J Organ Transplant Med 2017; 8:85-96
5 Loes Oomen, Huib de Jong, Antonia HM Bouts, et al A pre-transplantation risk assessment tool for graft survival in Dutch pediatric kidney recipients Clin Kidney J 2023; 16:1122-1131
6 Clavien PA, Barkun J, De Oliveira ML, et al The Clavien-Dindo classification of surgical complications: five-year experience Ann Surg 2009; 250:187-96
7 Chacko B, Rajamanickam T, Neelakantan N, et al Pediatric renal transplantation--a single center experience of 15 yr from India Pediatr Transplant 2007; 11:844-9
8 Chua A, Cramer C, Moudgil A, et al NAPRTCS investigators Kidney transplant practice patterns and outcome benchmarks over 30 years: The 2018 report of the NAPRTCS Pediatr Transplant 2019; 23:e13597
9 Barlas IS, Demir M, AKIN EB A single-center nine-year experience in pediatric kidney transplantation Cumhuriyet Medical Journal 2020; 42:126-35
10 Hogan J, Couchoud C, Bonthuis M, et al ESPN/ERA-EDTA Registry Gender Disparities in Access to Pediatric Renal Transplantation in Europe: Data From the ESPN/ERA-EDTA Registry Am J Transplant 2016; 16:2097-105
11 Kavaz A, Özçakar ZB, Bulum B, et al Pediatric renal transplantation: a single center experience Transplant Proc 2008; 40:1095-8
12 Irtan S, Maisin A, Baudouin V, et al Renal transplantation in children: critical analysis of age related surgical complications Pediatr Transplant 2010; 14:512-9
S Hama Amin Said, S Hayas Agha, G Fryad Abdulla, et al
ORIGINAL PAPER
Evaluating prognostic indicators for in-Hospital mortality in Fournier's gangrene: A 7-year study in a tertiary Hospital
Soetojo Wirjopranoto 1, 2* , Mohammad Reza Affandi 1* , Faisal Yusuf Ashari 3, 4 , Yufi Aulia Azmi 2, 5 , Kevin Muliawan Soetanto 6
1 Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia;
2 Department of Urology, Faculty of Medicine, Universitas Airlangga- Dr Soetomo General Academic Hospital, Surabaya, Indonesia;
3 Department of Biomedical Sciences, Faculty of Medicine Universitas Airlangga, Surabaya, Indonesia;
4 Faculty of Biology, Medicine and Health, University of Manchester, Manchester, United Kingdom;
5 Department of Health Sciences, University of Groningen, University Medical Center Groningen, Groningen, Netherlands;
6 Department of Immunology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
* These authors equally contributed as first co-authors
Summary
Background: Fournier's Gangrene Scoring Index (FGSI), Simplified FGSI (SFGSI), Uludag FGSI (UFGSI), Laboratory Risk Indicator for Necrotizing (LRINEC), Neutrophil-Lymphocyte ratio (NLR), and Platelet-lymphocyte ratio (PLR) have been devised to assess the risk of mortality in Fournier's Gangrene (FG) patients. However, the effectiveness of these indicators in predicting mortality at the time of admission remains uncertain The aim of this study is to assess the prognostic efficacy of FG’s various indicators on in-hospital mortality
Methods: This study analyzed 123 patients from Dr Soetomo General Hospital’s emergency department in Indonesia from 2014 to 2020 Data included demographics, wound cultures, and parameters like FGSI, UFGSI, SFGSI, NLR, PLR, and LRINEC
In-hospital mortality status was also recorded The data was subjected to comparative, sensitivity, specificity and regression analyses.
Results: In our study of 123 patients, the median age was 52, with a mortality rate of 17.9%. The majority of patients were male (91 1%) and the most common location was scrotal (54.5%). Non-survivors had a shorter median stay (6.5 days) compared to survivors (14 days) Diabetes was the most prevalent comorbidity (61.8%). The highest sensitivity and specificity were found in FGSI and UFGSI indicators Multivariate logistic regression identified LoS and FGSI as independent predictors of mortality
Conclusions: FGSI and UFGSI, upon admission, demonstrated the highest sensitivity and specificity, with hospital stay duration and FGSI as key mortality determinants.
KEY WORDS: Fournier's gangrene; Indicator; Neutrophil/lymphocyte ratio (NLR); Platelet to lymphocit ratio
Submitted 14 January 2024; Accepted 19 February 2024
INTRODUCTION
Despite significant strides in technological advancement, Fournier’s Gangrene (FG) continues to pose a formidable challenge with mortality rates oscillating between 5% and 65% (1) An array of prognostic indicators, encompassing F o u r n i e r ’ s G a n g r e n e S e v e r i t y I n d e x ( F G S I ) , U l u d a g Fournier’s Gangrene Severity Index (UFGSI), Simplified
Fournier’s Gangrene Severity Index (SFGSI), Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC), Neutrophil-tolymphocyte Ratio (NLR), and Platelet-to-lymphocyte Ratio (PLR), have been formulated to estimate the mortality risk in FG patients (2-6) These predictive instruments are invaluable for healthcare professionals, especially urologists and surgeons, as they enable the initiation of more aggressive interventions at an early stage Some of these indicators, engineered for ease of use and practicality, rely solely on laboratory data (SFGSI, LRINEC, NLR, and PLR), while others are more sophisticated, amalgamating both laboratory and clinical data (FGSI and UFGSI) In the quest for an indicator that harmonizes precision and simplicity, a comparative evaluation of these indicators is indispensable However, the sensitivity and specificity of these scoring systems remain undetermined This study seeks to assess the efficacy of FGSI, UFGSI, SFGSI, LRINEC, NLR, and PLR at the point of admission in forecasting mortality outcomes in FG patients
MATERIALS AND METHODS
A retrospective cross-sectional study from January 2014 to December 2020 was conducted following approval from the Hospital Review Board (No 0528/LOE/301 4 2/VII/ 2021) The study included all patients with FG admitted to Dr Soetomo Hospital Patient data was retrieved from the hospital's electronic medical records system All participants provided written informed consent for the use of their clinical information for research purposes The study included patients diagnosed with FG by a urologist, excluding those with incomplete data
Scoring was done at admission, reflecting the emergency assessment when the patient arrived at the hospital If a patient had test results from another healthcare institution, these tests were repeated
The data examined included demographics (age, sex, etiology, comorbidities, and wound culture results) and parameters (FGSI, UFGSI, SFGSI, LRINEC, PLR, and NLR) Participants were segregated into two categories: those who survived and those who did not A comparative analysis was conducted between these groups con-
S Wirjopranoto, M Reza Affandi, F Yusuf Ashari, Y Aulia Azmi, K Muliawan Soetanto
cerning demographic information and scoring The FGSI, UFGSI, SFGSI, LRINEC, NLR, and PLR were calculated using various parameters (5, 7, 8)
Statistical analysis
Group comparisons were performed using chi-square and Mann Whitney U test as approp r i a t e T h e a r e a u n d e r t h e receiver operating characteristic (ROC) curve was used to assess sensitivity and specificity, and the Youden index was used to determine the optimal cutoff v a l u e M u l t i v a r i a b l e l o g i s t i c regression models were cons t r u c t e d u s i n g t h e s t e p w i s e backward LR method A significance level of p < 0 05 was considered statistically significant Data analyses were perf o r m e d u s i n g I B M S P S S
Statistics for Windows version 24 0 (IBM Corp , Armonk, NY, USA)
RESULTS
The ROC curve for FGSI, SFGSI, NLR, PLR, and LRINEC
Throughout the period under investigation, spanning from January 2014 to December 2020, the emergency department received a total of 135 patients with FG However, the analysis only incorporated 123 patients (Figure 1) The patients had a median age of 52 (44-61), and the mortality rate was recorded at 17 9% The study population was predominantly male (91 1%), and the most common location was scrotal (54 5%) Non-survivors had a shorter median duration of stay compared to survivors, with lengths of 6 5 (3-14) days and 14 (7-21) days, respectively (Table 1) Diabetes was identified as the most prevalent comorbidity, present in 61 8% of patients
1. Algorithm for the Inclusion and exclusion of patients.
Table 1
Prognostic correlation with
Length of
The microorganisms most frequently encountered in our study population were Pseudomonas spp , Klebsiella pneumonia, E coli, and Acinetobacter spp (Table 2)
As illustrated in Figure 2, the ROC analysis unveiled cutoff values (sensitivity, specificity) for FGSI, SFGSI, UFGSI, NLR, PLR, and LRINEC predicting mortality as follows: 9 (100%, 83 2%), 2 5 (50%, 74 3%), 10 5 (100%, 83 2%), 7 5 (95 5%, 47 5%), 264 69 (68 2%, 57 4%), and 3 5 (50%, 56 4%), respectively To identify independent predictors of mortality, a multivariate logistic regression analy-
Evaluation of the predictive capacity of FGSI, SFGSI, UFGSI, NLR, PLR, and LRINEC through univariate analysis. Variable Total Sur vivor Non-sur vivor p value
Outcomes of the multivariate logistic regression analysis.
DISCUSSION
During the study interval, it was observed that the majority of patients were male, with the scrotum being the most frequent site of origin The length of hospital stay, prevalence of diabetes, and incidence of Pseudomonas spp were also noteworthy among patients An analysis of sensitivity, specificity, and independent risk factors for mortality revealed that both FGSI and UFGSI demonstrated the highest sensitivity and specificity Furthermore, the length of hospital stay and FGSI were identified as independent prognostic value Despite significant advancements, the mortality associated with FG remains alarmingly high (9-11) Our study, conducted at a tertiary hospital in Indonesia's secondlargest city, yielded a mortality rate of 17 9%, which could be attributed to the availability of advanced medical facilities and expertise Notably, the demographics between groups were comparable, with the exception of LoS, which was significantly lower among non-survivors
In this study, we investigated established indicators employed at admission to predict FG mortality, including FGSI, SFGSI, NLR, PLR, and LRINEC FGSI, recognized as the earliest and most frequently utilized indicator, is designed to assess the likelihood of mortality in FG patients (12) Our findings indicated that individuals who did not survive exhibited elevated FGSI values compared to those who did The optimal cut-off for FGSI, along with its sensitivity and specificity, was identified as 9, 100%, and 83 2%, respectively These results outperformed those of previous studies, which reported sensitivity range of 69% to 100% and specificity range of 57% to 97% (4, 7, 13) The established cut-off of 9 at admission aligns with the accepted threshold for mortality prediction Therefore, FGSI with this recognized cut-off can be effectively utilized for early assessment and aggressive intervention
sis was conducted, including variables that were significantly associated with mortality in the univariate analysis (p < 0 05) (Table 3) Among these variables, only length of stay (LoS) and FGSI remained significant predictors of mortality in the multivariate analysis (Table 4)
An analysis of the SFGSI, a simplified version of the FGSI that utilizes only three variables, revealed no differences between groups The optimal cut-off, sensitivity, and specificity for SFGSI were determined to be 2 5, 50%, and 74 3%, respectively The cut-off was similar to the consensus, which considered values above 2 as indicating a high risk of mortality (4) However, the reliability of SFGSI on admission to predict mortality in FG patients could not be confirmed
The UFGSI, a version of FGSI that includes age and disease extent, was studied UFGSI values were found to be
Supplementary Table 1. Measured parameters and cut-off score of each scoring system from the literature
FGSI: Fournier’s Gangrene Sever ty Index; UFGSI: Uludag Fournier’s Gangrene Sever ty Index; SFGSI: Simpl f ed Fournier’s Gangrene Sever ty Index; NLR: Neutrophi -to-lymphocyte Ratio (NLR); PLR: Platelet-to-lymphocyte Ratio (PLR); LRINEC: Laboratory Risk Ind cator for Necrot zing Fasci t s
S Wirjopranoto, M Reza Affandi, F Yusuf Ashari, Y Aulia Azmi, K Muliawan Soetanto
higher in non-survivors The optimal cut-off, sensitivity, and specificity for UFGSI were identified as 10 5, 100%, and 83 2%, respectively These values were similar to those of the FGSI While previous research suggested that UFGSI performs better than FGSI, the difference in our findings could be due to the lack of pelvic and beyond involvement in our study population (3)
NLR and PLR have been used as mortality predictors in FG patients in previous studies (5, 6, 14) High NLR and PLR have been linked with mortality predictors in FG patients (5, 14) One study found NLR and PLR to be better than FGSI (14), while another found NLR to be better than PLR (6) However, our study showed significantly higher NLR levels in non-survivors compared to survivors Despite this, neither NLR nor PLR predicted inhospital mortality in our study NLR and PLR are known markers of inflammation and infection (15) The divergence in results suggests that NLR and PLR may be influenced by the disease phase, whether acute or chronic, a distinction challenging to ascertain in a tertiary hospital setting primarily consisting of referred patients (16)
The LRINEC score, which overlaps with FGSI in some variables, is a laboratory-centric indicator employed to evaluate mortality in patients suffering from FG While certain studies have identified a significant correlation between elevated LRINEC scores and mortality (5, 17), our research did not discern a notable difference between survivors and non-survivors, nor could it prognosticate in-hospital mortality for FG These findings may be profoundly influenced by the specific laboratory equipment utilized and the disease’s stage at the time of examination Given the inconsistent results obtained using laboratorybased indicators like SFGSI, LRINEC, NLR, and PLR, employing a scoring system (FGSI and UFGSI) at the time of admission could potentially provide a more accurate prediction of mortality for FG patients
Despite its strengths, this study has certain limitations First, it utilized a retrospective design, which restricted to influence the laboratory blood draws Second, the study analysed data from a single tertiary referral center, potentially leading to a sample population skewed towards more severe cases Thirdly, each patient may have been in a distinct disease stage upon admission, given our hospital's tertiary status and frequent intake of referred patients Lastly, despite the confirmation of all FG cases through a thorough review of medical and surgical records, some positive cases might have been missed due to the absence of comprehensive retrospective records Future prospective studies involving multiple centers are imperative to identify the most sensitive parameters for predicting patient mortality
CONCLUSIONS
In this study, it was observed that FGSI and UFGSI showed the highest sensitivity and specificity among the current indicators upon admission The duration of hospital stay and FGSI were recognized as independent determinants of mortality These indicators could potentially offer a more accurate prediction of mortality However, it is essential to exercise caution when interpreting laboratory-only indicators in a tertiary hospital
setting due to possible biases arising from disease stage To validate these results, a multicenter prospective study is recommended This would aid in verifying the reliability and applicability of these indicators across various settings and patient demographics
ACKNOWLEDGMENTS
All Medical Recors Staff’s of Soetomo General Academic Hospital and Faculty of Medicine, Universitas Airlangga
REFERENCES
1 Sorensen MD, Krieger, JN, Rivara FP, et al Fournier's Gangrene: Management and Mortality Predictors in a Population Based Study J Urol 2009; 182:2742-2747
2 Laor E, Palmer LS, Tolia BM, et al Outcome Prediction in Patients with Fournier's Gangrene J Urol 1995; 89-92
3 Yilmazlar T, Ozturk E, Ozguc H, et al Fournier's gangrene: an analysis of 80 patients and a novel scoring system Tech Coloproctol 2010; 14:217-223
4 Lin TY, Ou CH, Tzai TS, et al Validation and simplification of Fournier's gangrene severity index Int J Urol 2014; 21:696-701
5 Bozkurt O, Sen V, Demir O, Esen A Evaluation of the utility of different scoring systems (FGSI, LRINEC and NLR) in the management of Fournier’s gangrene Int Urol and Neph 2015; 47:243-248
6 Wirjopranoto S Comparison between neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as predictors of mortality on Fournier's gangrene cases Indian J Urol 2023; 39:121-125
7 Ureyen O, Acar A, Gokcelli U, et al Usefulness of FGSI and UFGSI scoring systems for predicting mortality in patients with Fournier's gangrene: A multicenter study Ulus Travma Acil Cerrahi Derg 2017; 23:389-394
8 Tutino R, Colli F, Rizzo G, et al Which Role for Hyperbaric Oxygen Therapy in the Treatment of Fournier's Gangrene? A Retrospective Study Front Surg 2022; 9:850378
9 Rieger C, Huber M, Kastner L, et al Center-based First-line Therapy Is a Significant Predictor for Mortality of Fournier Gangrene JU Open Plus 2023; 1
10 Bermani BF, Rizaliyana S, Handriani I Predisposition Factors Analysis for Fournier’s Gangrene Defects Closure Complication J Rekon Est 2021; 5:13
11 Radcliffe RS, Khan MA Mortality associated with Fournier's gangrene remains unchanged over 25 years BJU Int 2020; 125:610616
12 Laor E, Palmer LS, Tolia BM, et al Outcome Prediction in Patients with Fournier's Gangrene J Urol 1995; 154:89-92
13 Noegroho BS, Siregar S, Mustafa A, Rivaldi MA Validation of FGSI Scores in Predicting Fournier Gangrene in Tertiary Hospital Res Rep Urol 2021; 13:341-346
14 Yim SU, Kim SW, Ahn JH et al Neutrophil to Lymphocyte and Platelet to Lymphocyte Ratios Are More Effective than the Fournier's Gangrene Severity Index for Predicting Poor Prognosis in Fournier's Gangrene Surg Infect 2016; 17:217-223
15 Kosidlo JW, Wolszczak-Biedrzycka B, Matowicka-Karna J, et al Clinical Significance and Diagnostic Utility of NLR, LMR, PLR and SII in the Course of COVID-19: A Literature Review J Inflamm Res 2023; 16:539-562
16 Kose N, Yildirim T, Akin F, et al Can NLR, PLR and LMR be used as prognostic indicators in patients with pulmonary embolism? Author's reply on commentary Bosn J Basic Med Sci 2021; 21:502
17 Kincius M, Telksnys T, Trumbeckas D, et al Evaluation of LRINEC Scale Feasibility for Predicting Outcomes of Fournier Gangrene Surg Infect 2016; 17:448-453
Correspondence
Prof Soetojo Wirjopranoto, MD (Corresponding Author) stjowirjopranoto@gmail com
Department of Urology, Faculty of Medicine, Universitas AirlanggaDr Soetomo General Academic Hospital, Surabaya, Indonesia
Mohammad Reza Affandi, MD rezaaffandi@outlook com
Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia
Faisal Yusuf Ashari, MD faisal ashari@postgrad manchester ac uk
Department of Biomedical Sciences, Faculty of Medicine Universitas Airlangga, Surabaya, Indonesia
Jl Mayjen Prof Dr Moestopo No 6-8, Surabaya, East Java, Indonesia, 60286 Faculty of Biology, Medicine and Health, University of Manchester, Manchester, UK
Yufi Aulia Azmi, MD
yufiazmi@gmail com; y aulia azmi@umcg nl
Department of Urology, Faculty of Medicine, Universitas AirlanggaDr Soetomo General Academic Hospital, Surabaya, Indonesia
Department of Health Sciences, University of Groningen, University Medical Center Groningen, Groningen, Netherlands
Kevin Muliawan Soetanto, MD kmskevinmuliawan@gmail com
Department of Immunology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Effects of antisperm antibodies post vasectomy reversal on pregnancy rates
Tamer A. Abouelgreed 1 , Mohamed A. Amer 2 , Hassan Mamdouh 2 , Ahmed F. El-Sherbiny 3 , Hany Aboelwafa 2 , Omar A. Omar 2 , Mohammed Abdelshakour 2 , Mohammad Elesawy 2 , Mohamed Sonbol 2 , Ahmed N. Maawad 2 , Elsayed M. Zayed 2 , Mostafa T. Eldestawy 2
1 Department of Urology, Al-Azhar University, Cairo, Egypt & Gulf medical university, Ajman, UAE;
2 Department of Dermatology & Andrology, Al-Azhar University, Cairo, Egypt;
3 Department of Andrology, International Islamic Center for Population Studies and Research, Al-Azhar University, Cairo, Egypt
Summary
Objective: To investigate the correlation between antisperm antibodies (ASAs), pregnancy rates, and the method of conception following vasectomy reversal. This is particularly relevant as patients undergoing vasectomy reversal often express concerns about the potential inhibitory effects of ASAs on achieving pregnancy. Additionally, the American Urological Association guidelines for vasectomy emphasize the need for further research to address this question
Patient and Methods: We conducted a retrospective analysis involving chart reviews and phone interviews with individuals who underwent vasectomy reversal at our institution between May 2015 and April 2023 Patients who underwent vasectomy reversal for reasons other than fertility, as well as those lacking postoperative semen analysis with ASA data, were excluded We classified patients based on low (below 50%) or high (50% or above) ASA levels determined by their initial postoperative semen analysis The primary outcome measured was the pregnancy rate, including details on the method of conception
Results: A total of 145 patients were subjected to chart review The median age at the time of surgery was 43 years, with a median obstruction interval of 7 7 years The median age of their partners was 29 years The majority (80%) of patients underwent bilateral vasovasostomy Among them, 60 patients (41.4%) exhibited low (< 50%) ASA levels, while 85 (58.6%) had high (≥ 50%) ASA levels Follow-up phone interviews were completed by 48 patients. Among them, the 19 men with low ASA levels, 13 (68 4%) achieved pregnancy, with 6 (31 6%) experiencing spontaneous conception. For the 29 men with high ASA levels, 21 (72 4%) achieved pregnancy, including 11 (38%) through spontaneous conception. The p-value from Fisher’s exact test was 0 2
Conclusions: Our findings suggest that ASA levels do not show a significant association with either the pregnancy rate or the method of conception following vasectomy reversal.
Submitted 31 January 2024; Accepted 15 February 2024
INTRODUCTION
Vasectomy is conducted around 500,000 times annually in the United States, being a secure and efficient method of permanent male contraception (1) About 6% of men
opting for vasectomy subsequently expresses a desire for additional pregnancies (2) For these individuals, there are four choices for expanding their families: vasectomy reversal, sperm extraction with in-vitro fertilization (IVF), donor sperm insemination, and adoption Various factors, including parental age, female factor infertility, desired number of children, and cost, play a role in decidi n g b e t w e e
patients annually choose vasectomy reversal (3) Among those considering vasectomy reversal, a key question is the impact of seminal antisperm antibody (ASA) levels on postoperative pregnancy rates Seminal ASAs in the general infertility population can cause immunologic infertili t y b y
However, it remains unclear if seminal ASAs also result in infertility after vasectomy reversal (4, 5) Despite the presumed high seminal ASA levels in individuals who have undergone vasectomy reversal, the pregnancy rates are substantial, with about 73% achieving pregnancy (6) Given these considerations, the clinical significance of seminal ASA levels after vasectomy reversal warrants further investigation (7, 8) Previous research on this topic, conducted in the 1980s, predates advancements in microscopic vasectomy reversal techniques and relies on outdated testing methods for seminal ASA levels (9) The 2015 American Urologic Association (AUA) vasectomy guidelines highlight the need for additional research on the impact of antisperm antibodies and their influence on fertility rates after vasectomy reversal (10, 11) Our laboratory routinely conducts IgG ASA testing on all semen samples with progressive motile sperm concentrations of ≥ 2M/ml, including post-vasectomy reversal samples This presents a unique opportunity for us to assess the relationship between seminal ASA levels following vasectomy reversal and pregnancy rates, as well as the methods of conception Through retrospective chart reviews and phone interviews of patients who underwent vasectomy reversal at our institution, we aim to explore the potential association between seminal ASA levels and pregnancy rates, methods of conception, and semen analysis parameters Our hypothesis was that seminal ASA levels were not correlated with pregnancy rates or methods of conception after vasectomy reversal
PATIENT AND METHODS
In this study, we enrolled consecutive patients who underwent vasectomy reversal at our institution between May 2012 and April 2020, under the care of two surgeons Patients undergoing vasectomy reversal for pain or those lacking postoperative semen analysis with ASA were excluded from the study All procedures performed in this study complied with institutional and/or national research council ethical standards as well as the 1964 Declaration of Helsinki and its subsequent amendments or similar ethical standards Protocols and written informed consent for all participants were approved by the Research Ethics Committee of Thumbay University Hospital (affiliated to Gulf Medical University, REC #: 21/2015)
Data collection
To gather comprehensive data, we conducted a chart review encompassing patient and partner demographics (such as age, number of prior pregnancies, and obstruction interval at the time of vasectomy reversal), details about the surgical technique, intraoperative vasal fluid quality, postoperative complications, and parameters from follow-up semen analyses Chart review and phone interviews were the primary methods employed Patients meeting the inclusion criteria were invited to participate in a phone interview, and notifications were sent via SMS to alert them about an expected call from the study team The study team made up to three attempts to contact each patient for the phone interview During the interview, a standardized script was utilized, addressing inquiries about pregnancies post-vasectomy reversal and the methods of conception
ASA testing and semen analysis
Standard semen analysis, including volume, concentration, motility, total motile sperm count, and strict morphology, was performed on all samples using World Health Organization (WHO) reference techniques and appropriate ranges based on the year of the semen analysis Additionally, IgG Sperm MAR ASA testing was routinely conducted on all semen samples with progressive motile sperm concentrations of ≥ 2M/ml, a technique first described in 1992 (12) Our laboratory, in accordance with WHO 5th edition reference range for ASA levels, performed IgG ASA testing on semen samples with a 50% cut-off to categorize low (below 50%) and high (≥ 50%) ASA levels Furthermore, we evaluated seminal ASA levels as a continuous variable to explore if an alternative cut-off could more accurately predict pregnancy rates
Outcomes
Our primary objectives cantered on assessing the pregnancy rate and the method of conception, including details such as intercourse, intrauterine insemination (IUI), IVF, and other methods like donor insemination, as reported by the patients during the phone interviews Secondary outcomes focused on the semen analysis parameters obtained from the initial postoperative semen analysis
Statistical analyses
Statistical analyses were conducted using descriptive statistics to evaluate demographic and clinical characteristics of
patients meeting inclusion criteria, comparing those who completed phone interviews to the overall cohort The Wilcoxon signed-rank test was employed to assess differences in semen analysis parameters between individuals with low and high seminal ASA levels To analyse pregnancy rates and methods of conception among men with different seminal ASA levels, Fisher's exact test was utilized Considering the potential confounding effect of the time interval since vasectomy on pregnancy outcomes, the relationship between seminal ASA levels and obstructive interval was evaluated using the Wilcoxon signed-rank test Additionally, a logistic model was employed to explore whether an alternative seminal ASA level cut-off, apart from the conventional 50%, could provide better predictive value for pregnancy rates Sensitivity analyses were incorporated to address two decisions made in our primary analyses Firstly, we conducted a sensitivity analysis to determine the impact of using continuous seminal ASA levels instead of dichotomized low and high levels Secondly, to assess the influence of using the last postoperative semen analysis (rather than the first) on our findings, we reanalysed the primary outcomes using the last postoperative semen analysis for patients with multiple postoperative analyses All statistical analyses were carried out using SAS version 9 4 (SAS Institute Inc ), and a p-value below 0 05 was considered statistically significant
cloudy/opaque/opalescent/milky n (%) 80 (55 2%) 24 (50%)
thick/yellow/toothpaste/creamy/pasty n (%) 20 (13 8%) 9 (18 75%) scant/paucity n (%) 9 (6 2%) 2 (4 2%)
Missing n (%) 14 (9 6%) 5 (10 45%)
Motility
Motile n (%) 30 (21%) 15 (31 2%) Nonmotile n (%) 35 (24%) 15 (31 2%) Missing n (%) 80 (55%) 18 (37 6%)
Postoperative complications None n (%) 137 (94.4%) 44(91.6%)
Follow up semen analysis parameters
of follow up SAs
3 d n (%) 22 (15%) 6 (12 5%)
First semen analysis (SA) values Time to first SA (weeks)
(IQR) 11 (8 1-20) 10 (8-19) Concentration (M/ml)
(IQR) 33 (13-70) 32 (10-69) Total motility (%)
Total motile sperm count (M/ejaculate) Median (IQR) 27 (9-64) 21 (7- 57) Normal morphology (%) Median (IQR) 7 (4-9) 8 (6-11)
Antisperm antibody (%) Median (IQR) 48 (13-88) 46 (11- 87)
< 50% n (%) 60 (42%) 20(41 66%)
≥ 50% n (%) 84 (58%) 28 (59 34%)
RESULTS
After applying the specified inclusion and exclusion criteria, we identified a cohort comprising 145 patients who underwent vasectomy reversal at our institution between May 2012 and April 2020 The median age at the time of surgery for this cohort was 43 years, with a median obstruction interval of 7 7 years The median age of their partners was 29 years Among the 145 patients, 116 (80 %) underwent bilateral vasovasostomy, 24 (16 6%) underwent a combination of vasovasostom y a n d v a s o e p i d i d y m o s t o m y , 3 ( 2 % ) underwent unilateral vasovasostomy, and 2 (1 4%) underwent bilateral vasoepididymostomy (Table 1) Forty eight (33%) participated in a phone interview The demographic and clinical characteristics, including obstruction interval, vasectomy reversal technique, intraoperative vasal fluid quality, and postoperative complications, w e r e c o m p a r a b l e b e t w e e n t h e o v e r a l l cohort of 145 patients and the subgroup of 48 patients who completed the phone interview Of the 145 patients, 60 had low seminal ASA levels (< 50%), while 85 had high seminal ASA (≥ 50%) levels There were no statistically significant differences in obstruction interval, vasectomy reversal technique, or semen analysis parameters
(e g , concentration, total motility, total motile sperm count, strict morphology) between the low and high seminal ASA groups (Table 2) Of the 48 patients who completed the phone interview, 19 (39 6%) had low seminal ASA levels, and 29 (60 4%) had high seminal ASA levels (Table 3) The median time from vasectomy reversal to the date of completing the phone interview was 8 2 years for the low seminal ASA group and 7 9 years for the high seminal ASA group Among the men with low seminal ASA levels, 13 (68 4%) achieved a pregnancy, with 9 (47 3%) having spontaneous pregnancies and 4 (21 1%) using IVF Among the men with high seminal ASA levels, 22 (75 8%) achieved a pregnancy, with 12 (41 4%) having spontaneous pregnancies, 3 (10 4%) using intrauterine insemination (IUI), and 7 (24%) using IVF The Fisher’s exact test p-value for differences in pregnancy rates and methods of conception was 0 2 No statistically significant relationship was found between obstruction interval and pregnancy rates (Wilcoxon test p-value = 0 5) (Table 3) To assess whether a different seminal ASA level cut-off could better predict pregnancy rates, we employed a logistic model to examine the relationship between seminal ASA levels as a continuous variable and pregnancy rates The analysis revealed no association between seminal ASA levels and pregnancy rates, with a p-value of 0 98 In sensitivity analyses, our findings remained consistent when using continuous seminal ASA levels instead of dichotomized levels (Wilcoxon p-value 0 97) Among the 79 patients with multiple postoperative semen analyses, 17 (22%) experienced changes in their seminal ASA categories across analyses Specifically, 9 (53%) patients shifted from the low to the high seminal ASA group, 7 (41%) shifted from the high to the low seminal ASA group, and 1 (6%) changed across groups in both directions
Furthermore, our results were unchanged when using seminal ASA levels from the last postoperative semen analyses instead of those from the first postoperative semen analysis (Signed rank test, p-value = 0 5)
Table 2.
Vasectomy reversal technique, obstruction interval, and follow up semen analysis parameters for studied patients
Technique of vasectomy reversal
Follow up semen analysis parameters
Number of follow up SAs
Table 3.
Pregnancy rates and methods of conception for studied patients, based on the first postoperative semen analysis
DISCUSSION
We have three main findings Firstly, there is no association between seminal ASA levels after vasectomy reversal and pregnancy rates or methods of conception Secondly, men with low and high seminal ASA levels showed no differences in postoperative semen analysis parameters Thirdly, we were unable to identify a specific cut-off level for postoperative seminal ASA levels that strongly correlates with pregnancy rates Overall, these findings indicate that seminal ASA levels are not linked to pregnancy rates, the method of conception, or semen analysis parameters following vasectomy reversal These insights can enhance the counselling of patients before and after undergoing vasectomy reversal
Our discovery that seminal ASA levels after vasectomy reversal are not associated with pregnancy rates or methods of conception contrasts with earlier studies from the 1980s (10, 13) In particular, Thomas et al (13) found no association between serum or seminal ASA titres and pregnancy rates in 35 men who underwent vasectomy reversal at a single centre with at least 1 year of follow-up Parslow et al (10) in their evaluation of 130 men at two canters, observed that higher preoperative serum ASA titres were linked to lower pregnancy rates, while postoperative seminal ASA titres were not associated with pregnancy rates after at least 1 year of follow-up Belker et al., cited by Nam et al. (14), in their prospective study of patients who had undergone vasovasostomy, found that 66% of those who achieved pregnancy had no measurable serum ASA levels, while 71% of those unable to achieve pregnancy had measurable serum ASA levels
These studies suggested that patients with serum ASA levels exceeding 2 million per millilitre might require IVF to achieve pregnancy, irrespective of seminal ASA levels Our study had longer follow-up than studies previously mentioned and used the modern day IgG SpermMAR technique to measure seminal ASAs, as recommended by the WHO laboratory manual (12) Despite these earlier findings, our study highlights that seminal ASA levels foll o
decreased pregnancy rates This information can offer reassurance to patients seeking to have children after a vasectomy For healthcare providers, our results can serve a
patients before and after vasectomy reversal Furthermore, we observed no significant differences in postoperative semen analysis parameters between men with low and high ASA levels The impact of seminal ASA on semen analysis parameters in the g
h a s shown mixed findings Some studies have r e p o
seminal ASA levels and increased sperm agglutination, (15, 16) decreased sperm concentration, (17, 18) and reduced sperm motility (4, 16-18) However, the influence of seminal ASA levels on semen analysis parameters within the vasectomy reversal patient population has not been thoroughly evaluated In our study, there was no statistically significant distinction in semen analysis parameters, including concentration, total motility, total motile sperm count, and strict morphology, between men with low and high seminal ASA levels, using either the first or the last postoperative semen analysis These findings underscore the necessity of establishing specific semen analysis reference values for vasectomy reversal patients, enabling more accurate counselling of postoperative patients on their likelihood of spontaneous conception (19) Finally, we were unable to identify a specific cut-off level for postoperative seminal ASA levels strongly associated with pregnancy rates The 2010 WHO laboratory manual recommended ASA testing as a routine component of semen analyses with a 50% cut-off to categorize low and high ASA levels However, limited evidence supports this 50% cut-off, and the 2010 WHO laboratory manual acknowledges it as a "consensus" threshold value The 2021 WHO laboratory manual discussed the limited evidence behind ASA reference values and cautioned against over interpreting ASA values as causative of subfertility Despite efforts using a logistic model to find a more effective seminal ASA cut-off for predicting pregnancy rates after vasectomy reversal, we were unable to identify a cutoff that reliably predicted a couple's likelihood of achieving pregnancy (20) Our study comes with several limitations Firstly, the data were retrospectively obtained from a single institution, potentially limiting the generalizability of our observations to other settings Nevertheless, our study presents a contemporary analysis compared to earlier studies from the 1980s, featuring a longer follow-up and the use of modern, WHO-recommended laboratory techniques for measuring ASA levels Secondly, approximately one-third of the included patients participated in a phone interview, introducing the potential for selection bias However, the demographic and clinical characteristics of the interviewed men were similar to those of the overall cohort Thirdly, postoperative semen analyses were conducted at varying time points after surgery, with some patients undergoing multiple analyses We chose to utilize the first postoperative semen analysis to categorize patients as having low or high seminal ASA levels Although 22% of the cohort exhibited movement across seminal ASA groups over time, our sensitivity analysis
using the last postoperative semen analysis did not alter our findings Fourthly, since our laboratory routinely performs ASA testing on semen samples with progressive motile sperm concentrations of ≥ 2 million per millilitre, there may be a selection bias as patients with severe oligoasthenospermia were excluded from our analysis
However, we identified 17 samples with sperm concentrations < 2 million per millilitre and available seminal ASA levels, as ASA testing on semen samples was conducted at the laboratory's discretion for all samples
Additionally, men with progressive motile sperm concentrations < 2 million per millilitre are likely to require IVF to achieve pregnancy, irrespective of seminal ASA levels Notwithstanding these limitations, our study holds significant implications for both patients and healthcare providers For individuals seeking to conceive after a vasectomy, our findings provide assurance that high seminal ASA levels after vasectomy reversal are not linked to decreased pregnancy rates
CONCLUSIONS
Postoperative seminal ASA levels are not associated with pregnancy rates, methods of conception, or semen analysis parameters after vasectomy reversal surgeries Accordingly we highly recommend pre- and post-operative patient counselling in the context of vasectomy reversal
ACKNOWLEDGMENTS
We would like to thank prof Dr Hossam Hamdy (the Chancellor of Gulf Medical University) for his valuable support
REFERENCES
1 Ostrowski KA, Holt SK, Haynes B, et al Evaluation of Vasectomy Trends in the United States Urology 2018; 118:76-79
2 Sandlow JI, Nagler HM Preface Urol Clin North Am 2009; 36:xiii-xiv
3 Dubin JM, White J, Ory J, et al Vasectomy reversal vs sperm retrieval with in vitro fertilization: a contemporary, comparative analysis Fertil Steril 2021; 115:1377-1383
4 Silva AF, Ramalho-Santos J, Amaral S The impact of antisperm antibodies on human male reproductive function: an update Reproduction 2021; 162:R55-R71
5 El-Sherbiny AF, Ali TA, Hassan EA, et al The prognostic value of seminal anti-sperm antibodies screening in men prepared for ICSI: a call to change the current antibody-directed viewpoint of sperm autoimmunity testing Ther Adv Urol 2021; 13:1756287220981488
6 Royle MG, Parslow JM, Kingscott MM, et al Reversal of vasectomy: the effects of sperm antibodies on subsequent fertility Br J Urol 1981; 53:654-9
7 Herrel LA, Goodman M, Goldstein M, et al Outcomes of Microsurgical Vasovasostomy for Vasectomy Reversal: A Metaanalysis and Systematic Review Urology 2015; 85:819-825
8 Hellema HW, Samuel T, Rumke P Sperm autoantibodies as a consequence of vasectomy II Long-term follow-up studies Clin Exp Immunol 1979; 38:31-36
9 Tung KS Human sperm antigens and antisperm antibodies I Studies on vasectomy patients Clin Exp Immunol 1975; 20:93-104
10 Parslow JM, Royle MG, Kingscott MM, et al The effects of sperm antibodies on fertility after vasectomy reversal Am J Reprod Immunol (1980) 1983; 3:28-31
11 Silber SJ, Grotjan HE Microscopic vasectomy reversal 30 years later: A summary of 4010 cases by the same surgeon J Androl 2004; 25:845-859
12 Cooper TG, Aitken J, Auger J, et al WHO ASA World Health Organization Published online 2010
13 Thomas AJ Jr, Pontes JE, Rose NR, et al Microsurgical vasovasostomy: immunologic consequences and subsequent fertility Fertil Steril 1981; 35:447-50
14 Nam CS, Tooke BP, Strasser O, et al Antisperm Antibody Levels After Vasectomy Reversal Are Not Associated With Pregnancy Rates o r M e t h o d o f C o n c e p
4295(24)00124-9
15 Barbonetti A, Castellini C, D’Andrea S, et al Prevalence of antisperm antibodies and relationship of degree of sperm auto-immunization to semen parameters and post-coital test outcome: a retrospective analysis of over 10 000 men Human Reproduction 2019; 34:834-841
16 Tomlinson M, Lewis S, Morroll D Sperm quality and its relationship to natural and assisted conception: British Fertility Society Guidelines for practice Hum Fertil 2013; 16:175-193
17 Verón GL, Molina RI, Tissera AD, et al Incidence of Sperm S
Parameters and Sperm Kinematics Am J Reprod Immunol 2016; 76:59-69
18 Cui D, Han G, Shang Y, et al Antisperm antibodies in infertile men and their effect on semen parameters: A systematic review and meta-analysis Clin Chim Acta 2015; 444:29-36
19 Majzoub A, Tadros NN, Polackwich AS, et al Vasectomy reversal semen analysis: new reference ranges predict pregnancy Fertil Steril 2017; 107:911-915
20 Bjorndahl L, Apolikhin O, Baldi E, et al WHO Laboratory Manual for the Examination and Processing of Human Semen Sixth Edition
Correspondence
Tamer A Abouelgreed, MD (Corresponding Author) dr tamer ali@yahoo com; tamerali 8@azhar edu eg Department of Urology, Al-Azhar University, Cairo, Egypt & Gulf medical university, Ajman, UAE
Mohamed A Amer, MD - amerrom@yahoo com
Hassan Mamdouh, MD - hsdermaclinic@yahoo com
Hany Aboelwafa, MD - dr hanyos138@yahoo com
Omar A Omar, MD - omarabdelhady 236@azhar edu eg
M Abdelshakour, MD - Dr mohammed 121@yahoo com
Mohammad Elesawy, MD - elesawy288@gmail com
Mohamed Sonbol, MD - bosombol1185@gmail com
Ahmed N Maawad, MD - ah nabil70@gmail com
Elsayed M Zayed, MD - sayedmzayed@gmail com
Mostafa T Eldestawy, MD - mostafa eldestawy@azhar edu eg
Department of Dermatology & Andrology Al-Azhar University, Cairo, Egypt
Ahmed F El-Sherbiny, MD - Ahmed derma@yahoo com
Department of Andrology, International Islamic Center for Population Studies and Research, Al-Azhar University, Cairo, Egypt
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Pentoxifylline
treatment as a safe method
for selecting viable testicular spermatozoa before cryopreservation of a small numbers of spermatozoa in azoospermia individuals
1 International Campus, Shahid Sadoughi University of Medical Science, Yazd, Iran;
2 Research and Clinical Center for Infertility, Yazd Reproductive Sciences Institute, Shahid Sadoughi University of Medical Sciences, Yazd, Iran;
3 Andrology Research center, Yazd Reproductive Sciences Institute, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
Summary
Background: Single sperm cryopreservation (SSC) is a specific technique especially used in individuals with small numbers of sperm who suffered from non-obstructive azoospermia (NOA) Testicular specimens possess poor motility and low population of viable spermatozoa Therefore, sperm selection methods such as applying pentoxifylline (PTX) may improve motility in these cases The main aim of this study was to evaluate the protective effects of PTX on testicular spermatozoa before and after performing SSC. Methods: Thirty testicular samples were obtained from men with azoospermia. This study was conducted in two phases. Phase 1 evaluated the effect of PTX for sperm selection before SSC. Twenty testicular samples were divided to two experimental groups: SSC without (I) and with PTX treatment (II) For PTX treatment spermatozoa were incubated with PTX at 37°C for 30 min and only motile spermatozoa were selected for SSC In phase 2, ten testicular samples were cryopreserved with SSC and warming procedure was carried out in droplet with and without PTX. Motility and viability rates, morphology by motile sperm organelle morphology examination (MSOME), DNA fragmentation by sperm chromatin dispersion test (SCD) and mitochondrial membrane potential (MMP) were evaluated
Results: In phase 1, post warm motility rate was higher in PTX exposed group compared to the unexposed group (25 6 ± 8 13 vs. 0.85 ± 2.1) (p > 0.00). Recovery rate, viability and morphology were not significantly different between groups DNA integrity and MMP were also similar between both groups In phase 2 although motility increased in PTX group compared to without PTX group (29 30 ± 12 73 vs 1 90 ± 2 64) (p > 0 00), the viability rate was not different (70 40 ± 12 12 vs 65 30 ± 11 87) All above mentioned parameters were similar between the two SSC groups
Conclusions: Supplementation of testicular spermatozoa with PTX before cryopreservation increases motility and did not have adverse effects on viability, morphology, DNA integrity and MMP. PTX could be used as sperm selection method before single sperm cryopreservation, but PTX could not maintain motile the most of viable testicular sperms.
KEY WORDS: Non-obstructive azoospermia; Pentoxifylline; Testicular sperm; Single sperm cryopreservation
Submitted 29 March 2024; Accepted 6 April 2024
INTRODUCTION
Azoospermia, defined as lack of spermatozoa in ejaculate samples, affects 1% of all men and 10-15% of individuals with infertility (1, 2) Moreover, about 60% of men with azoospermia have non-obstructive azoospermia (NOA) that occurs by severe defects during spermatogenesis procedure (3) Cryopreservation of spermatozoa after biopsy of testicular tissue prevent from repetitions of biopsy in azoospermic cases (4) Conventional cryopreservation methods are not appropriate in these cases owing to limited numbers of spermatozoa which are lost during freezing and thawing techniques (5) Therefore, the concept of single spermatozoa cryopreservation (SSC) was proposed in 1997 by Cohen et al (6) who used empty zona pellucida for freezing After that, various cr yo-devices and methods were designed to increase fertilization chance in cases with limited number of sperm (7) In this regard, some details of this technique, such as selecting proper spermatozoa before freezing, requir much more attention In these cases, sperm specimen obtained from testicular tissue usually poses little or no motility Using spermatozoa with no motility in ICSI procedure negatively affects clinical outcomes (8) Therefore, it is noteworthy to find a method for selecting viable spermatozoa before freezing in order to optimize thawing outcomes (especially sperm motility) with less possible adverse effects on sperm biological characteristics
In case of absent or poor movement of testicular sperm specimen, different methods including hypo- osmotic swelling test (HOS), sperm tail flexibility test and in-vitro culturing are available to enhance motility of testicular sperm (9, 10) The mentioned methods might adversely affect sperm functions and biological characteristics For instance, HOS test causes water entrance to spermatozoa resulting in membrane expansion which finally leads to cell membrane lysis and death (11) Pentoxifylline (PTX), sperm activation chemical agent, is a phosphodiesterase (PDE) inhibitor that is able to improve sperm motility by increasing cyclic adenosine monophosphate (c-AMP) levels and protein kinase A (PKA) activity PTX is a user-friendly and easy method to identify viable spermatozoa from immotile spermatozoa (12)
K Lorian, S Vahidi, F Dehghanpour, F Anbari, A Agha-Rahimi
To our knowledge, PTX as sperm selection method has not been used in SSC technique The main aim of this study is to investigate the effect of PTX on sperm motility, morphology, viability, DNA fragmentation and mitochondrial membrane potential by incubation of NOA testicular samples in PTX (as sperm selection method) before and after applying SSC technique using Cryo-vial device
METHODS AND MATERIALS
S t u d y d esig n
This study was performed from 22 June 2023 to 28 September 2023 at Yazd Reproductive Sciences Institute It was was approved by ethics committee of Shahid Sadoughi University of Medical Sciences (IR SSU MEDICINE REC 1401 016) Written informed consents were obtained from the men who referred to Yazd infertility center for treatment before collection of samples The study was conducted in two phases
Phase 1:
1 Testicular sperm specimens were collected surgically by TESE and micro-TESE from 20 azoospermic men 2 Selected spermatozoa were randomly divided into two experimental groups: (I): SSC without PTX treatment (control) and (II): SSC with PTX treatment 3 Testicular spermatozoa were prepared, and the suspension was divided and poured in two culture dishes (one for control group and the other one for PTX group 4 In both groups the spermatozoa were selected first based on tail movement and then by tail flexibility gently by a ICSI injection micropipette (Nikon, Japan) equipped with a micromanipulator 5 In control group, twenty spermatozoa were randomly selected and placed in HOS medium and the percentage of viable spermatozoa was determined 6 The viability and motility of fresh testicular samples were also reported 7 The remaining spermatozoa were cryopreserved 8 In PTX group, the selected spermatozoa transferred to the PTX droplets and after that, only motile spermatozoa were selected for SSC
Phase 2:
1 In this phase, spermatozoa were selected from TESE and micro-TESE samples from 10 azoospermic men 2
About one-hundred testicular spermatozoa or more were selected as previous described and cryopreserved by SSC technique on several cryotops 3 For warming, Cryotops were randomly divided to be warmed in (I): sperm washing medium without PTX (control) or (II) in sperm washing medium with PTX in the same concentration as phase 1 (Figure 1)
Testicular sperm preparation and processing
Seminiferous tubules fragments were poured in large culture dishes consisting of sperm washing medium (Bio chrome, Berlin, Germany) supplemented with 5 mg/mL Human serum albumin (HSA, Vitrolife, Englewood, CO) Seminiferous tubules were recognized by applying a stereomicroscope and the stainless blades were used to remove blood clots After that, extruded testicular tissue
was washed in sperm washing medium supplemented with 5 mg/mL HSA to remove the blood and then placed to the central-well dish (Falcon, USA) consisting of fresh sperm medium Tubules mechanical dispersion was performed by mincing repeatedly using stainless blades The media containing spermatozoa was centrifuged at 300g for 10 min After removing the supernatant, the collected pellet was resuspended in 1 mL of sperm washing medium supplemented with 5 mg/mL HSA and used for single sperm cryopreservation (13)
Single sperm cryopreservation and warming procedure
Testicular samples (1-3 μL droplet) were added to 5 μL droplet of sperm washing medium supplemented with 5 mg/ mL HSA on ICSI dish (Falcon, 1006 dish) (Figure 1B) Sperm cells were collected using ICSI injection micropipette (Nikon, Japan) equipped with a micromanipulator (Figure 1C) For single sperm cryopreservation Cryotop Vial Device (CVD) was used In previous study, we designed a new carrier which contains cryotop (Kitazato, Japan) and cryovial (Nest, China) (14) (Figure 1A) Selected spermatozoa were placed on 0 5 M sucrose (Sigma-Aldrich) diluted 1:1 with sperm washing medium (final concentration 0 25 m sucrose) droplet on the Cryotop strip by using the ICSI pipette (Figure 1D, E) Then, the polypropylene strip was placed into the cryovial and closed carefully (Figure 1F) Cryovial directly plunged into liquid nitrogen (Figure 1G) The samples were maintained in liquid nitrogen at least 72 h pre warming (15) For warming procedure, Cryotops were removed from cryovials and Cryotop strip was placed directly in a pre-warmed 5 μL droplet of sperm washing medium supplemented with 5 mg/ mL HSA on ICSI dish at 37°C Cryotop was washed with 10 μL droplets to remove all spermatozoa remain on Cryotop strip (Figure 1I) Pre-warmed oil (Ovoil; vitrolife, Sweden) was poured on droplet with spermatozoa After 30 min incubation at 37°C, to aspirate sperm cells a micropipette equipped with micromanipulator on an inverted microscope was used Finally, retrieved spermatozoa were transferred to a new droplet of sperm washing medium supplemented with 5 mg/mL HSA (15) In phase 2, in addition to warming in sperm washing medium, warming was also performed in PTX droplet (Figure 1J)
Treatment of testicular spermatozoa with PTX
For PTX preparation, 3 6 mM stock solution of PTX (Sigma, St Louis, MO, USA) was provided by adding 1 mg PTX powder to 1 mL sperm washing medium supplemented with 5 mg/ml HAS This solution can be stored at 4°C for up to 7 days
To prepare working solution, the stock solution was diluted 1:1 with sperm washing medium The final concentration of PTX in the specimen was 1 76 mM Selected spermatozoa by ICSI injection micropipette (Nikon, Japan) equipped with a micromanipulator were added to the PTX droplet, which was overlaid with pre-warmed oil (Ovoil; vitrolife, Sweden) Testicular sperm samples were incubated in PTX droplets at 37°C for 30 min The droplet was investigated for viable and motile spermatozoa and then, selected by ICSI injection micropipette and transferred to the new droplet for freezing (16) In phase 2, if spermatozoa were not motile, the viability was checked with HOS test
Figure 1.
Steps of study design CVD: Cryotop vial device, PVP: Polyvinylpyrrolidone, ICSI: intracytoplasmic sperm injection, LN: liquid nitrogen, HSA: human serum albumin (Figure is original and never used before)
A
Cryotop vial device (CVD) was used for single sperm cryopreservation
This device consists of vial, a screw cap, Cryotop, soft foam and a fine polypropylene strip
C
B. Droplets of testicular spermatozoa and PVP droplet for needle stabilization
F.
Spermatozoa incubated with and without PTX were placed into the sucrose droplet on the tip of the Cryotop and then, the Cryotops were inserted into cryovial and closed with screw cap tightly
G. Cryovials were transferred to the LN tank
Sperm cells were collected using a ICSI injection micropipette equipped with a micromanipulator
D.
Sperm cells were placed into the PTX droplet and in the droplets without PTX.
E. Both culture dishes were transferred to the incubator
H For warming cryovials were removed from LN tank and placed into the LN foam box.
I.
Cryotops were removed from cryovials and Cryotop strip was placed directly in a pre-warmed 5 μL droplet of sperm washing medium supplemented with 5 mg/mL HSA on ICSI dish at 37◦C
K Lorian, S Vahidi, F Dehghanpour, F Anbari, A Agha-Rahimi
Sperm parameters evaluation
To assess sperm recovery, motility and viability an inverted microscope system was used Sperm recovery rate was recorded by below formula: number of post-warm sperm /number of cryopreserved sperm × 100 Sperm motility and viability were determined by post-thaw motility and viability, respectively (15) For viability assessment after thawing, motile spermatozoa were considered viable, while for immotile spermatozoa hypo-osmotic swelling test (HOS) was performed The sum of motile and nonmotile sperms in the medium was calculated
Hypo-osmotic swelling test (HOS)
The spermatozoa were selected by using a ICSI injection micropipette (Nikon, Japan) equipped with a micromanipulator and then the tail of spermatozoa was placed in 5µl of hypo-osmotic droplet Coiled tail patterns Viable spermatozoa indicated For preparing HOS medium, the sperm washing medium was diluted 1:1 with distilled water (17)
Fine sperm morphology evaluation
The morphology of spermatozoa was evaluated applying an inverted microscope at high magnification using motile sperm organelle morphology examination (MSOME) technique (Nikon ECLIPSE TE300) Medium droplets were placed into the glass-bottom dish (GWSt 1000; Will Co ) and sperm cells were transferred to it by using a ICSI pipette equipped with a micromanipulator Sperm cells were then assessed under high magnification (6600 ×) using an inverted microscope with high-power differential interference contrast optics Morphological assessment was carried out on monitor and spermatozoa were categorized in to three groups (high, medium and lowquality) according to the shape of the spermatozoa (sperm head, vacuoles, and base) (18)
DNA fragmentation evaluation
The SDFA kit (Tehran, Iran) was used to assess sperm DNA fragmentation by Sperm Chromatin Dispersion (SCD) test Briefly, low-melting-point agarose gel droplet (5 μl)
Figure 2.
was placed onto the pre-coated slide Selected spermatoz o a b y I C S I i n j e c t i o n m i c ro p i p e t t e ( N i k o n , J a p a n ) equipped with a micromanipulator were gently added to the agarose gel droplet and small coverslips were placed on the slide After that, the staining procedure was done according to the kit instructions Then, slides were assessed by a bright field microscope according to the halo size Spermatozoa with no or small halos showed DNA fragmentation while, spermatozoa with medium or large halos considered as intact DNA Percentage of spermatozoa with DNA fragmentation was recorded (16)
Sperm mitochondrial membrane potential (MMP) was assessed by tetraethylbenzimidazolylcarbocyanine iodide (JC-1) mitochondrial membrane potential assay kit (Cayman Chemical Co, Ann Arbor, MI, USA; cat #10009172) The sperm cells were placed in JC-1 working solution droplets by the ICSI pipette equipped with micromanipulator After that, samples were incubated at 37°C for 30 min in dark environment Then, the cells were examined by fluorescence microscope (Olympus BX51, Japan) according to manufacturer’s instructions Spermatozoa with an orange fluorescence dye were considered as having high mitochondrial membrane potential (active mitochondria, JC1+) The percentage of cells with a high mitochondrial membrane potential were recorded (15)
Statistical analysis
Data were analyzed by the Statistical Package for the Social Sciences (SPSS) version 20 (IBM, California, United States) Data were expressed as mean ± SD Kolmogorov-Smirnov test was used to test the normality of data Independent sample T test and Mann-Whitney Test were used for comparing the data with normal and abnormal distribution, respectively between two cryo-groups groups Paired sample T test was used for comparing the fresh group with cryo-groups Plotted graphs were carried out with GraphPad Prism 8 4 2 (GraphPad Software, Inc., San Diego, CA, USA) P < 0 05 was considered significant
Sperm parameters Recovery (A), viability (B) and motility (C) of testicular spermatozoa incubated with PTX before single sperm cryopreservation (Phase 1). Data are presented as mean ± SD. ***P<0.001 (analysis by Mann-Whitney Test). A and B analysis by Independent Samples T Test
RESULTS
Phase 1 (PTX treatment before cryopreservation)
Post-warmed spermatozoa parameters
In phase 1 results of sperm parameters showed that recovery rate after SCC was similar between PTX and control groups (87 00 ± 7 07 vs 87 70 ± 6 74) (Figure 2A) The viability of fresh testicular samples, which was at first selected by tail flexibility and twitching movement and then confirmed by HOS test, was about 98% The percentage of viable spermatozoa decreased in PTX and control groups compared to the fresh group (71 55 ± 11 36 vs 66 80 ± 11 09 and vs 98 8 ± 3 15, p > 0 001)
No remarkable changes were observed in viability rates between the two SSC groups (Figure 2B) The percentage of fresh motile testicular spermatozoa was about 11 75%
After incubation with PTX, only the motile spermatozoa (approximately, 100% motile spermatozoa) were selected for SSC in the PTX group Exposure of testicular samples with PTX before freezing significantly increased the
motility rate of post-thawed spermatozoa compared to the unexposed group (25 65 ± 8 13 vs 0 85 ± 2 10) (Figure 2C p > 0 001)
Post-warmed sperm DNA fragmentation and mitochondrial membrane potential
In phase 1, comparison of DNA fragmentation results between cryopreservation groups showed that PTX did not significantly alter DNA fragmentation percentage (32 6 ± 4 18 vs 31 10 ± 4 15) (Figure 3A)
The percentage of spermatozoa with active mitochondrial membrane potential in phase 1 was not different between two cryopreservation groups (50 20 ± 9 15 vs 49 25 ± 9 12) (Figure 3B)
Post-warmed fine sperm morphology
The percentages of high (10 40 ± 6 85 vs 9 30 ± 6 30), medium (53 30 ± 15 71 vs 51 30 ± 15 52) and low (33 90 ± 14 48 vs 38 00 ± 13 91) quality spermatozoa in phase 1 were not different between PTX and control groups (Figure 4A-C)
Figure 3. DNA fragmentation index (DFI) (A) and mitochondrial membrane potential (MMP) (B) after incubation with PTX before single sperm cryopreservation (Phase 1)
Data are presented as mean ± SD and analysis by Independent Samples T Test
4. Fine sperm morphology Morphology of sperm classified in three groups high (A), medium (B) and low (C) quality after incubation in PTX before single sperm cryopreservation (phase 1) Data are presented as mean ± SD and analysis by Independent Samples T Test
Archivio
Figure
K Lorian, S Vahidi, F Dehghanpour, F Anbari, A Agha-Rahimi
Figure 5.
Sperm parameters Recovery (A), viability (B) and motility (C) of testicular spermatozoa incubated with PTX after single sperm cryopreservation (phase 2) Data are presented as mean ± SD and analysis by Independent Samples T Test ***P < 0 001 versus control and PTX groups
Phase 2 (PTX treatment after cryopreservation)
Post-warmed spermatozoa parameters
In phase 2, recovery rate was similar between PTX and control groups (84 70 ± 11 26 vs 85 80 ± 9 15) (Figure 5A) The percentage of fresh viable testicular spermatozoa, which were selected as in phase 1, was about 98 5% and decreased in both SSC groups compared to the fresh group (70 40 ± 12 12 vs 65 30 ± 11 87 and vs 98 5 ±
This result showed that after PTX not all viable spermatozoa could be motile
Post-warmed sperm DNA fragmentation and mitochondrial membrane potential
In phase 2, DNA fragmentation was similar between the two SSC groups (28 70 ± 4 64 vs 29 50 ± 3 97) (Figure 6A)
2 10, p > 0 001) Moreover, there were no significant changes between the two SSC groups in viability rate (Figure 5B) the percentage of fresh motile testicular spermatozoa was about 10% After warming, the percentage of motile spermatozoa which were incubated with PTX was significantly increased compared to the spermatozoa without PTX incubation (29 30 ± 12 73 vs 1 90 ± 2 64) (Figure 5C p > 0 001) Comparison of motility (29 30 ± 12 73) and viability (70 40 ± 12 12) in PTX group in phase 2 were significantly different (p > 0 001)
Figure 6.
DNA fragmentation index (DFI) (A) and mitochondrial membrane potential (MMP) (B) after incubation with PTX before single sperm cryopreservation (Phase 1)
Data are presented as mean ± SD and analysis by Independent Samples T Test.
In phase 2, spermatozoa with active mitochondrial membrane potential were similar in the two cryopreservation groups (55 30 ± 6 73 vs 55 40 ± 5 81) (Figure 6B)
Post-warmed fine sperm morphology
In phase 2, high (17 50 ± 11 50 vs 16 10 ± 11 68), medium (51 60 ± 12 86 vs 52 70 ± 15 16) and low (30 90 ± 11 51 vs 31 20 ± 17 47) quality testicular spermatozoa rates were similar between PTX and control groups (Figure 7A-C)
Figure 7
Fine sperm morphology Morphology of sperm classified in three groups high (A), medium (B) and low (C) quality incubated in PTX after single sperm cryopreservation (phase 2).
Data are presented as mean ± SD and analysis by Independent Samples T Test
DISCUSSION
The cryopreservation of sperm with SSC technique is beneficial to reduce the times of sperm retrieval techniques by freezing spermatozoa (without testicular tissues, debris and round cells) on a significant number of Cryotop Therefore, using this method increased the oocyte retrieval times in these groups of patients We previously reported that SSC using CVD (14) and sucrose medium (15) was a suitable strategy for cryopreservation of testicular sperm TESE or micro-TESE samples may have 10 or more than 100 spermatozoa, which it is not practical to place all together on a Cryotop In this regard, viable spermatozoa with good morphology should be selected Selecting v i a b l e s p e r m a t o z o a b a s e d o n s p e r m t a i l f l e x i b i l i t y depends on skill and experience of the embryologist Using safe chemical substance like PTX could resolve the weakness of sperm tail flexibility method (19) Although some studies evaluated the safety of PTX on cryopreserved testicular sperms after thawing in conventional freezing method, it is not clear whether testicular sperm exposure to PTX before cryopreservation make it more vulnerable to cryo-damage Mahaldashtian et al concluded that PTX exerts beneficial effects on post-thawed sperm motility and increased 2PN and embryo formation without detrimental impacts on sperm DNA integrity (16) Xian et al supplemented the sperm freezing media with PTX for assessing testicular sperm motility during cryopreservation and warming procedures and reported that PTX enhances testicular sperm motility (20) The recovery rate, number of spermatozoa that were retrieved after freezing, is an essential factor that can show the efficacy of cryo-devices Our recovery rate was about 87% which is in accordance with other researches that applied similar cryo-devices (21, 22) Also, the viability rate after SSC in both phases was about 60% in agreement with our previous report (15) In both phases of this study, at first, tail movement and flexibility method was applied to select viable spermatozoa The HOS test showed that about 98% of these spermatozoa were viable This indicat-
ed that, if these methods are used properly, a significant number of viable spermatozoa could be selected Moreover, we showed that the incubation of testicular sperm, before and after SSC, with PTX enhances sperm motility, although no significant difference was observed between groups in sperm viability The similarity of post-warming viability between groups showed that PTX does not exert detrimental effects on sperm in cryo-warmed process In phase two, 26% of spermatozoa were motile after warming in PTX, while the viability rate was more than 60% Probably the cryo-damage to spermatozoa caused that most of viable sperm cannot be motile after PTX exposure Therefore, using PTX after SSC when the numbers of spermatozoa are limited is not practical for selecting viable spermatozoa Exposure of testicular spermatozoa to PTX before and after SSC did not show adverse effect on fine morphology Nabi et al incubated ejaculated spermatozoa samples with 3 6 mmol/L PTX for 30 min at 37ºC after vitrification warming and showed that PTX did not alter ultrastructural aspects of spermatozoa (23) In another study, Mahaldashtian et al reported that treatment of oligoasthenoteratozoospermic samples with PTX did not change the vacuole status of sperm head (24)
Sperm chromatin integrity and structure are a determining factor in fertility potential It is vital to inseminate the oocytes with spermatozoa that have intact DNA Our results showed that PTX did not alter DNA integrity of testicular samples when applied before and after freezing between groups This finding is in agreement with other studies that showed PTX does not have harmful impacts on DNA/chromatin status in TESE (16) and asthenozoospermic cases (25, 26)
MMP is related to normal sperm parameters including motility and viability Mitochondria are the main source of adenosine triphosphate generation that is vital for sperm motility and cellular phenomena including capacitation, hyper activation and acrosome reaction (27) According to our results, MMP was similar between PTX exposed and non-exposed group before and after SSC Previously it was
K Lorian, S Vahidi, F Dehghanpour, F Anbari, A Agha-Rahimi
reported that PTX did not exert any detrimental effect on sperm MMP (24)
CONCLUSIONS
Adding PTX at safe concentration as sperm selection method before SSC of testicular samples, could select the viable sperm without intensifying the adverse effects of cryo-damage However, it seems that using PTX after warming, when numbers of spermatozoa are limited, is not practical for selecting viable spermatozoa, because the most of viable sperm cannot be motile after PTX exposure during warming procedure
REFERENCES
1 Cetinkaya M, Onem K, Zorba OU, et al Evaluation of microdissection testicular sperm extraction results in patients with nonobstructive azoospermia: independent predictive factors and best cutoff values for sperm retrieval Urology Journal 2015; 12:2436-43
2 Cocuzza M, Alvarenga C, Pagani R The epidemiology and etiology of azoospermia Clinics 2013; 68:15-26
3 Modarresi T, Hosseinifar H, Hampa AD, et al Predictive factors of successful microdissection testicular sperm extraction in patients with presumed sertoli cell-only syndrome Int J Fertil Steril 2015; 9:107-12
4 AbdelHafez F, Bedaiwy M, El-Nashar SA, et al Techniques for cryopreservation of individual or small numbers of human spermatozoa: a systematic review Hum Reprod Update 2009; 15:153-64
5 Liu S, Li F Cryopreservation of single-sperm: where are we today? Reprod Biol Endocrinol 2020; 18:41
6 Cohen J, Garrisi GJ, Congedo-Ferrara TA, et al Cryopreservation of single human spermatozoa Hum Reprod 1997; 12:994-1001
7 Endo Y, Fujii Y, Motoyama H Clinical and neonatal outcomes of individually vitrified human sperm with Cryotop and Cell Sleeper Cryobiology 2022; 108:78-81
8 Karacan M, Alwaeely F, Erkan S, et al Outcome of intracytoplasmic sperm injection cycles with fresh testicular spermatozoa obtained on the day of or the day before oocyte collection and with cryopreserved testicular sperm in patients with azoospermia Fertil Steril 2013; 100:975-80
9 Verheyen G, Joris H, Crits K, et al Comparison of different hypoosmotic swelling solutions to select viable immotile spermatozoa for potential use in intracytoplasmic sperm injection Hum Reprod Update 1997; 3:195-203
10 Gholizadeh L, Khalili MA, Maleki B, et al Quality of testicular spermatozoa improves with changes in composition of culture medium Basic Clin Androl 2023; 33:22
11 Luo Y, Peng F, Li L, et al Sperm Activation with Pentoxifylline Is B e n e f i c i a l F o r N o n - O b s t r u c t i v e A z
Testicular Sperm before Intracytoplasmic Sperm Injection Int J Women’s Health Care 2022; 7:73
12 Mahaldashtian M, Khalili MA, Nottola SA, et al Does in vitro application of pentoxifylline have beneficial effects in assisted male reproduction? Andrologia 2021; 53:e13722
13 Esteves SC, Varghese AC Laboratory handling of epididymal and testicular spermatozoa: what can be done to improve sperm injections outcome J Hum Reprod Sci 2012; 5:233
14 Bagheripour N, Khalili MA, Nabi A, et al A new cryotop vial device system provides an aseptic cryoprotectant-free and centrifugefree cryopreservation of human spermatozoa (a closed system) Cryobiology 2023; 111:70-75
15 Maleki B, Khalili MA, Gholizadeh L, et al Single sperm vitrification with permeable cryoprotectant-free medium is more effective i
Cryobiology 2022; 104:15-22
16 Mahaldashtian M, Khalili MA, Mangoli E, et al Pentoxifylline treatment had no detrimental effect on sperm DNA integrity and clinical characteristics in cases with non-obstructive azoospermia Zygote 2023; 31:8-13
17 Sallam HN, Farrag A, Agameya A-F, et al The use of the modified hypo-osmotic swelling test for the selection of immotile testicular spermatozoa in patients treated with ICSI: a randomized controlled study Hum Reprod 2005; 20:3435-40
18 Cassuto NG, Bouret D, Plouchart JM, et al A new real-time morphology classification for human spermatozoa: a link for fertilization and improved embryo quality Fertil Steril 2009; 92:1616-25
19 Nordhoff V How to select immotile but viable spermatozoa on the day of intracytoplasmic sperm injection? An embryologist's view Andrology 2015; 3:156-62
20 Xian Y, Jiang M, Liu B, et al A cryoprotectant supplemented with pentoxifylline can improve the effect of freezing on the motility of human testicular sperm Zygote 2022; 30:92-7
21 Endo Y, Fujii Y, Shintani K, et al Single spermatozoon freezing using Cryotop Journal of Mammalian Ova Research 2011; 28:47-52
22 Sun J, Chen W, Zhou L, et al Successful delivery derived from cryopreserved rare human sper matozoa with novel cryopiece Andrology 2017; 5:832-7
23 Nabi A, Khalili MA, Talebi AR, et al In-vitro application of pentoxifylline preserved ultrastructure of spermatozoa after vitrification in asthenozoospermic patients Urology Journal 2017; 14:4038-43
24 Mahaldashtian M, Khalili MA, Vatanparast M, et al The effect of pentoxifylline and calcium ionophore treatment on sperm cell biology in oligoasthenoteratozoospermia samples Zygote 2023; 31:85-90
25 Asokan Y, Honguntikar SD, Uppangala S, et al In situ viability detection assays induce heat-shock protein 70 expression in spermatozoa without affecting the chromatin integrity Andrologia 2015; 47:958-65
26 Nabi A, Khalili MA, Fesahat F, et al Pentoxifylline increase sperm motility in devitrified spermatozoa from asthenozoospermic patient without damage chromatin and DNA integrity Cryobiology 2017; 76:59-64
27 Boguenet M, Bouet P-E, Spiers A, et al Mitochondria: their role in spermatozoa and in male infertility Hum Reprod Update 2021; 27:697-719
Correspondence
Keivan Lorian, PhD
International Campus, Shahid Sadoughi University of Medical Science, Yazd, Iran
Serajoddin Vahidi, MD
Andrology Research center, Yazd Reproductive Sciences Institute, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
Fatemeh Dehghanpour, PhD
Fatemeh Anbari, PhD
Azam Agha-Rahimi, PhD (Corresponding Author)
63rahimi@gmail com
Research and Clinical Center for Infertility, Yazd Reproductive Sciences Institute, Shahid Sadoughi University of Medical Sciences, Bouali Avenue, Safayieh, Yazd, Iran
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Efficacy and safety of malleable penile prosthesis compared to inflatable penile
1 Department of Urology, Faculty of Medicine, Universitas Airlangga, Indonesia;
2 Dr Soetomo General-Academic Hospital, Surabaya, East Java, Indonesia;
3 Universitas Airlangga Teaching Hospital, Surabaya, East Java, Indonesia
Summary
Introduction: Erectile dysfunction can cause self-withdrawal and decreased quality of life Patients who do not respond to pharmacological therapy and other conservative treatments are urged to undergo penile prosthesis implantation Malleable penile prosthesis was the first prosthesis developed, but then inflatable penile prosthesis was developed to give a more natural erection There is no metaanalysis comparing inflatable and malleable penile prostheses in terms of safety and efficacy This study is conducted to evaluate patient and partner satisfaction, ease of use, mechanical failure, and infection rate in patients who underwent penile prosthesis implantation.
Method: This meta-analysis followed Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) protocols. Five eligible studies were included from Pubmed, Scopus, ScienceDirect, and SemanticScholar databases.
Result: In this study, patient and partner satisfaction are significantly better (OR 3.39, 95% CI 1.66-6.93, p = 0.0008)
(OR 2 32, 95% CI 1 75-3 08, p < 0 00001) Mechanical failure is also significantly higher in inflatable penile prostheses (OR 5 60, 95% CI 2 02-15 53, p = 0 0009) There is no significant difference in terms of ease of use and infection rate in inflatable or malleable penile prostheses
Conclusions: This study concluded that inflatable penile prosthesis is better in terms of patient and partner satisfaction, but mechanical failures occur more frequently in this type of prosthesis
Submitted 5 February 2024; Accepted 10 February 2024
INTRODUCTION
Inadequate penile erection, otherwise known as erectile dysfunction (ED), is defined as the inability to achieve or maintain sufficient penile erection for vaginal penetration until orgasm (1) The prevalence of ED in men aged 20 to 80 years in Jakarta reached 35 6% (2) Erectile dysfunction is not a life-threatening condition, but it can result in withdrawal from sexual intimacy, decreased quality of life, and decreased work productivity (3) Erectile dysfunction causes many negative effects Thus, proper han-
dling and management are needed to improve the state and quality of life of the patients
ED management includes control of risk factors (tobacco consumption, obesity, sedentary lifestyle, chronic alcohol consumption, comorbidities, and depression) and appropriate pharmacological therapy The first-line treatment for ED is oral therapy with Cyclic Guanosine Monophosphate (cGMP) inhibitors and Phosphodiesterase 5 inhibitors (PDE5 inhibitors) (4) Prior to the development of PDE5 inhibitors, intracavernosal injection was the first-line treatment for patients with ED However, at present, intracavernosal injection can be used as an important second-line treatment option and as the core of the DE diagnostic examination (5) Intraurethral Prostaglandin E1 (PGE1) [alprostadil, Medicated Urethral System for Erection (MUSE); Vivus, Menlo Park, Calif] was introduced in 1997 MUSE, uses PGE1 which directly affects the trabecular smooth muscle binding to specific receptors and thereby increasing the synthesis of cyclic Adenosine Monophosphate (cAMP) (6) Vacuum Erectile Device (VED), a means of therapy for ED patients, uses negative pressure to dilate the sinusoids of corpora cavernosa and increase blood flow to penile VED can be used together with an external constriction ring placed at the bulb of the penile to prevent outward blood flow in order to maintain erection for sexual intercourse (7)
The implantation of penile prostheses remains a relevant therapeutic option and is in demand, especially among uncured ED patients who have undergone conservative treatments A study suggested that penile prosthesis implantation may be considered in ED patients who do not exhibit positive respond to pharmacotherapy or who wish for a permanent solution to their problem (8, 9)
The first penile prosthesis implantation surgery was performed by a Russian surgeon named Nikolaj A Bogaraz in 1936 Currently, penile prostheses become the gold standard in patients experiencing recurrent ED after being given medicamentosa therapy and in patients with penile trauma (10)
There are three types of penile prostheses available: semirigid or malleable, two-piece inflatable, and threepiece inflatable penile prosthesis (IPP) At present, the inflatable three-piece penile prosthesis is the most widely used and recommended due to high patient and part-
ner satisfaction, natural cosmetic appearance, and its ability to enable patients to get or lose an erection at will
The implantation of an IPP has several side effects, namely perforation of corpus cavernosum, urethral damage, mechanical failure, infection, as well as bladder, intestinal, and vascular trauma (11)
The implantation of a malleable penile prosthesis (MPP) is easier to do In addition, MPP rarely experiences mechanical failures and is affordable Complications may occur during or after surgery The most common complications during surgery are urethral and corpus cavernosum trauma, while those occurring post-surgery are hematoma, infection, penile deformity, pain, and penile erosion (8)
Despite their advantages, inflatable penile prostheses have some limitations, such as expensive price, being hard to use, difficult implantation techniques, and high risk of infection Inflatable penile prostheses have a risk of being damaged after being used for more than 10 years and require replacement
Malleable penile prostheses are cheaper and easier to use even though they do not provide cosmetic and erection naturalness as well as inflatable penile prostheses
Malleable prostheses are less prone to damage and infection compared to inflatable penile prostheses
There is a systematic review by Karl H Pang in 2021 concerning complications and satisfaction after penile prosthesis implantation in patients with spinal cord injury
Several weaknesses are present in this study, as it only includes old studies written in English Furthermore, quantitative analysis cannot be conducted in this study due to the heterogeneous nature of the output and lack of control population (12)
There is currently no meta-analysis study comparing the efficacy and safety of the use of inflatable and m a l l e a b l e p e n i l e p r o s t h e s e s i n patients with ED Therefore, the a u t h o r s c a r r y o u t a s y s t e m a t i c review and meta-analysis study to compare the efficacy and safety of the use of inflatable penile prostheses compared to malleable prostheses in patients with ED
Table 1.
MATERIALS AND METHODS
Search strategy and study selection
The study used the quantitative method according to the Preferred Reporting Items for Systematic reviews and Metaanalysis (PRISMA) protocol The search process was carried out to ensure that the meta-analysis was in line with the topic or PICO (participant, intervention, comparison, outcome) The inclusion criteria of this study were observational design studies (cohort, case control, and cross sectional), studies that compared malleable and inflatable penile prostheses in patients with ED caused by diabetes mellitus, vascular disease, history of radical prostatectomy surgery, history of surgery in the pelvic area, as well as Peyronie’s, neurogenic, and priapism diseases The exclusion criteria of this study were duplicate articles, articles not written in English, articles that were not available in fulltext, patients with ED caused by other than diabetes mellitus, vascular disease, history of radical prostatectomy sur-
Results of article search using several international databases
Database Keywords n PubMed/MEDLINE ("erectile dysfunction" OR "sexual dysfunction" OR "impotence" OR "impotency") AND ("inflatable") 49 AND ("malleable" OR "Malleable" OR "semi-rigid" OR "semi rigid" OR "non-inflatable" OR "non inflatable") AND ("penile prosthesis" OR "penile-prosthesis" OR "penile prosthesis") AND [("satisfaction") OR ("complication”)]
Scopus [TITLE-ABS-KEY (erectile AND dysfunction) AND TITLE-ABS-KEY (inflatable AND penile AND prosthesis) 113 AND TITLE-ABS-KEY (malleable AND penile AND prosthesis)]
ScienceDirect ("inflatable penile prosthesis") AND ("malleable penile prosthesis") AND ("erectile dysfunction" OR "ED") 82 AND ("satisfaction" OR "complication”)
Semantic Scholar ED erectile dysfunction penile prosthesis
H Satwikananda, T Bagus Laksita, W Djatisoesanto, D Moesbadianto Soebadi
Figure 1.
PRISMA diagram of the study search and selection process
and safety of malleable penile prosthesis compared to inflatable penile prosthesis
gery, history of surgery in the pelvic area, as well as Peyronie’s, neurogenic, and priapism diseases The study selection was carried out by conducting eligible study search on PubMed, Scopus, ScienceDirect, and Semantic Scholar databases The search was carried out up to February 2023
The keywords we used include “erectile dysfunction” , “penile prostheses” , “malleable” , “inflatable” , “efficacy” , “satisfaction” , and “compliance” The keywords used in the study search are displayed in Table 1 Study search and selection were conducted based on PRISMA guidelines (Figure 1)
Quality assessment and data extraction
Data extraction was carried out by two authors independently in accordance with the specified examples In case of differences in data extraction results, they were discussed and settled by a third author The data extracted comprised the characteristics and methodologies of the study, namely the name of the first author, year of publication, number of patients, age of patients, and design of the study In addition, there were research interventions that were divided into the types of intervention given, namely the implantation of inflatable penile prostheses and malleable penile prostheses The outcome extracted were patient satisfaction, partner satisfaction, ease of use, mechanical failure rates, and infection rates The risk of bias of the study was assessed using the Newcastle Ottawa Scale
Statistical analysis
The data obtained was then inputted and analyzed using
Table 2.
Basic characteristics of the included studies
Author's
Natali, 2008 (26)
Berto, 2014 (28) Spain
the Review Manager 5 4 software The outcome evaluated in this study comprised postoperative complications consisting of mechanical failure and penile prosthesis infection Chi-square and I2 tests were used to evaluate the heterogeneity between studies If the result of the heterogeneity test was high (I2 test > 50% and chi-square p < 0 05), then the random-effects model was used On the other hand, if the result of the heterogeneity test was low (I2 < 50%, chi-square p > 0 05), the fixed-effect model was instead used The results comprised dichotomous data Thus, analysis using pooled odds ratio (OR) with 95% confidence interval (CI) is used in the presentation of the data The results of the analysis is presented in the form of Forest plots and explained in the form of a narrative review The publication bias was assessed using a funnel plot
RESULTS
Based on initial search results through PubMed, Scopus, ScienceDirect, and Semantic Scholar databases, the authors identified 708 articles The authors screened 598 titles and abstracts after carrying out the process of removing duplicate articles and automation Based on predetermined eligibility criteria, the authors excluded 590 articles by reading their titles and abstracts Based on further review conducted by reading the full texts, the authors included 5 studies that met the eligibility criteria The characteristics of the 5 included studies are described in Table 2
This review includes studies evaluating comparison of the use of IPP and MPP, covering a total of 1 234 adult patients, published between 2008 and 2019 All of the studies included are retrospective cohort studies conducted in Germany, Italy, Spain, and Turkey The average age of patients who were subjects in these 5 studies was between 52 6 and 58 9 years
The data extracted from the five studies included names of the researchers and years of the publication of the studies, designs of the studies, number of samples, types and brands of penile prostheses, duration of follow-up, etiology of ED, average age of samples, patient satisfaction, partner satisfaction, ease of use, mechanical failures, and number of infections
The quality assessment of the study was conducted using the Newcastle-Ottawa Scale (NOS) parameter as all the studies included use an observational study design In the selection aspect, all the studies that are included employ a good selection process as the participants involved were quite representative of cases in the adult population and most of the data was acquired using medical records and validated questionnaires In addition, the studies included also possess good comparative and exposure aspects as they had adequate follow-up duration and low dropout numbers Based on the final assessment, all the studies included have NOS scores between 7 and 8, signifying that they are of good quality The quality assessment are presented in Table 3
Comparison of IPP and MPP with regard to patient satisfaction
In this analysis, four articles involving a total of 1 484 patients who underwent penile prosthesis implantation procedure were included to assess and compare patient satisfaction with regard to the use of IPP and MPP For statistical analysis, fixed-effect models were used as the degree of
heterogeneity between studies in this analysis is low In subgroup 1, the authors compared the satisfaction of patients who used Two-piece IPP with those who used MPP The analysis results show an OR of 2 40 [95% CI 1 31, 4 40] There is a moderate degree of heterogeneity with a chisquare of 4 84, degrees of freedom (df) of 3 (p = 0 18), and I2 value of 38% The test for overall effect demonstrates statistically significant results with p = 0 005 This suggests a more favorable outcome for the Two-piece IPP Subgroup 2 compares the Three-piece IPP with MPP, resulting in an OR of 4 16 [95% CI 2 85, 6 06] There is a very low degree of heterogeneity with a chi-square of 0 01, df of 1 (p = 0 94), and I2 value of 0% The test for overall effect demonstrates statistically very significant results with p < 0 00001, indicating the advantage of the use of Three-piece IPP
By combining these two subgroups, a total OR of 3 55 [95% CI 2 58, 4 89] was obtained, demonstrating the superiority of IPP over the MPP The degree of heterogeneity remains relatively low, with a chi-square of 6 61, df of 5 (p = 0 25), and I2 value of 24% The test for overall effect demonstrates statistically significant results with p = 0 00001 The subgroup difference test was carried out to assess whether there were significant differences between the two subgroups The test results showed that there were no significant differences between the two subgroups, with chi-square of 2 28, df of 1 (p = 0 13), and I2 of 56 2%
These findings suggest that overall, patients tend to be more satisfied with the use of IPP compared to MPP, with statistically significant results The heterogeneity between studies we included in this analysis is relatively low, which adds confidence to the results of this study (Figure 2)
Comparison of IPP and MPP with regard to partner satisfaction
In this analysis, four articles involving a total of 1 517 patients who underwent a penile prosthesis implantation
H Satwikananda, T Bagus Laksita, W Djatisoesanto, D Moesbadianto Soebadi
procedure are included This study aims to evaluate and compare partner satisfaction with regard to the use of Two-piece IPP and MPP Fixed-effect models were used in statistical analysis as the degree of heterogeneity between studies in this analysis is low
In subgroup 1, the authors compared the partner satisfaction between the Two-piece IPP and MPP The analysis results show an OR of 1 26 [95% CI 0 73, 2 18] There is a low degree of heterogeneity with a chi-square of 3 00, df of 3 (p = 0 39), and I2 value of 0% The test for overall
effect demonstrates statistically insignificant results (p < 0 41), showing the advantage of the use of Two-piece IPP Subgroup 2 is focused on the comparison between Threepiece IPP and MPP, where an OR of 2 42 [95% CI 1 79, 3 26] is obtained In this subgroup, there is a very low degree of heterogeneity with a chi-square of 0 15, df of 1 (p = 0 70), and I2 value of 0% The test for overall effect demonstrates statistically very significant results (p < 0 00001), indicating the advantage of the use of Threepiece IPP (Figure 3)
Figure 2. Forest plot of patient satisfaction.
Figure 3 Forest plot of partner satisfaction
H Satwikananda, T Bagus Laksita, W Djatisoesanto, D Moesbadianto Soebadi
Comparison of IPP and MPP with regard to ease of use
The authors assessed the comparison between the ease of use of IPP and MPP prostheses in four studies involving a total of 1,484 patients
The results of the analysis also demonstrate that the studies included have a high degree of heterogeneity (I2 = 86%, p < 0 0001) Thus, the analysis method used was the random-effects model
In subgroup 1, the authors compared the ease of use of Two-piece IPP and MPP The analysis results show an OR of 0 59 [95% CI 0 13, 2 82] There is a high degree of heterogeneity with a chi-square of 19 18, df of 3 (p = 0 0003), and I2 value of 84% The test for overall effect demonstrates statistically insignificant results (p < 0 51), showing the advantage of the use of Two-piece IPP
Subgroup 2 compares the ease of use of three-piece IPP and MPP An OR of 0 24 [95% CI 0 16, 0 35] was obtained There is a high degree of heterogeneity in this subgroup with a chi-square of 0 04, df of 1 (p = 0 84), and I2 value of 0%
A s t a t i s t i c a l l y s i g n i fi c a n t r e s u l t ( p = 0 0 0 0 1 ) w a s obtained, indicating the superiority of MPP (Figure 4)
Comparison of IPP and MPP with regard to mechanical railure
The comparison of mechanical failures is analyzed by including two studies involving a total of 1 081 patients Heterogeneity analysis using I2 indicates that the degree of heterogeneity between studies is low (I2 = 55%, p = 0 14)
As such, the fixed-effects model analysis method used was used Based on the results of the analysis on 1,081 patients who underwent penile prostheses implantation, the rate of mechanical failure of IPP and MPP differs significantly (OR 5 60 95% CI 2 02-15 53, p = 0 0009) (Figure 5)
Comparison of IPP and MPP with regard to infection rate
The infection rate is analyzed by including three studies involving a total of 449 patients Heterogeneity analysis using I2 demonstrates that the degree of heterogeneity between studies is low (I2 = 0%, p = 0 87) Therefore, the fixed-effects model analysis method was used Based on the results of the analysis on 449 patients who underwent penile prostheses implantation, there is no significant difference in the rate of infection between IPP and MPP (OR 1 26 95% CI 0 56-2 86, p = 0 58) (Figure 6)
Figure 4 Forest plot of ease of use
Figure 5. Forest plot of mechanical failure
DISCUSSION
Erectile dysfunction has been linked to loss of work productivity and poor quality of life in men associated with mental and psychological health cndition, especially compared to men who do not suffer from ED Partners of patients with ED often complain of having problems in relationships, decreased sexual activity, and decreased sexual satisfaction The burden associated with ED can negatively affect men and their partners (13)
Currently, according to the American Urology Association (AUA) (2018), therapies commonly used for patients with ED include oral PDE5i, VED, intraurethral Alprostadil, intracavernosal injection, and penile prosthesis (14) Guidelines from the European Association of Urology (EAU) from 2016 to 2023 state that penile prosthesis implantation is one of the best options in terms of satisfaction levels (92-100% in patients and 91-95% in their partners) regardless of the indication when compared to other therapeutic options (8) The EAU guidelines also state that penile prosthesis implantation is a valid third-line therapeutic option for the treatment of ED when drugs and VED are shown to be ineffective, unsatisfactory, or contraindicated due to comorbidities of the patients (15)
In literature, penile prostheses have been reported as the most successful surgical treatment with the highest satisfaction level among therapeutic options for ED Each type of penile prosthesis has different advantages and disadvantages that can affect patient satisfaction Malleable penile prostheses have a structure that can be bent while wearing clothes and urinating as well as can be erected prior to having sexual intercourse Advantages of malleable penile prostheses include low rate of mechanical failures, easier surgical procedures, shorter operating times, and relatively cheaper prices On the other hand, patients using malleable prostheses will face difficulty if they need to undergo endourological treatment Inflatable penile prostheses have an upper edge in terms of cosmetic appearance Its method of increasing penile length and thickness is also close to natural erections The most critical disadvantage to this type of prosthesis is its possibility to suffer mechanical damage (16)
This meta-analysis involved a total of 1,234 adult patients from studies comparing IPP and MPP All of the studies included are retrospective cohort studies conducted in Germany, Italy, Spain, and Turkey The average age of patients who were included in these 5 studies was between 52 6 and 58 9 years
Patient satisfaction rate for inflatable penile prosthesis is higher than that of malleable penile prosthesis Patient satisfaction can be affected by several factors, such as expectations about penile prostheses before implantation, incidence of post-operative pain and edema, adverse effects, usefulness of penile prostheses, ease of use, and acceptance by partners (17) A study conducted by Jorissen et al in 2019 states that three-piece inflatable penile prostheses have the highest satisfaction rate In the study, the patient satisfaction rate was 80 4% for AMSLGX and 91 1% for Coloplast Titan The study also suggests that patient sexual satisfaction is strongly influenced by partner satisfaction (18)
In our study, higher partner satisfaction rates for inflatable penile prostheses are obtained The results of this metaanalysis correlate with a study conducted by Vakalopoulos et al., which discovered high average EDITS scores in terms of partner satisfaction and underlined a high level of satisfaction in the management of their male partners Regression analysis in the study shows a direct linear correlation of the satisfaction levels of male patients with female partners (19) Even though patients who underwent malleable penile prosthesis implantation feel dissatisfied with the constant stiffness in the first few days after the implantation, they will accept such condition state over time (16) A study carried out by Akin-Olugbade et al discovers that patients with Peyronie’s, post-radical prostatectomy, and BMI > 30 kg/m2 demonstrate lower levels of satisfaction compared to other patients who underwent penile prosthesis implantation Decreased satisfaction levels in patients with Peyronie’s disease and post-radical prostatectomy are caused by decreased penile length Meanwhile, in patients with BMI > 30 kg/m2, dissatisfaction with penile prostheses is not very apparent However, mechanical problems related to the size of prepubic fat have been observed in this patient group Dissatisfaction with penile prostheses in patients over 70 years of age can be attributed to proficiency in using penile prostheses (20)
Some of the negative aspects of dissatisfaction with penile prostheses are caused by unrealistic expectations about penile prostheses, reduced penile size, and unnatural erections Carvalheira (2015) states that unrealistic expectations about penile prostheses were reported in 11 cases and related to the wishful thinking that penile prostheses implantation could solve the patient’s problems and that the prosthesis implantation could reinvigorate the desired sexual relationship Such expectations are also present in
Figure 6
Forest plot of infection comparison
men who desire unprecedented sexual intercourse experience Another study also suggests that low expectations about penile prostheses could lead to higher patient satisfaction (21)
Our meta-analysis also assesses the ease of using penile prostheses experienced by patients Subgroup analysis comparing three-piece IPP and MPP discovered statistically significant results about the superiority of MPP in terms of ease of use Inflatable penile prosthesis requires dexterity while using it, and one of the advantages of MPP over IPP is its ease of use (22, 23)
In other studies, it is found that at the beginning of MPP implantation, many patients felt dissatisfied due to persistent stiffness in the first few days However, over time, MPP users exhibit high levels of satisfaction and ease because they are able to ensure fast and maximum hardness compared to IPP This difference is based on pain and discomfort due to the presence of IPP pump in the scrotum, causing patients to become fearful and requiring them to learn more at clinics to use IPP optimally (16, 24)
The design of penile prostheses has evolved from semirigid and malleable to two-piece shafts and then evolved again into three-piece inflatable penile prostheses The ideal penile prosthesis is one that can provide the most natural flaccid and erect state Three-piece penile prosthesis can meet such criteria, but with the added mechanical components compared to the malleable prosthesis, it bore an increased risk of mechanical failures (25)
According to the meta-analysis conducted by the authors, inflatable penile prostheses are more prone to mechanical failures More mechanical failures were observed in threepiece inflatable penile prostheses, which occurred in 38 patients In their study, Natali et al state that the average incidence of prosthesis leakage occurs 25 2 months after implantation Of the 10 cases of mechanical failure in this study, the most frequent causes of mechanical failure were leaks in the prosthesis tube (40%), leaks in the saline reservoir (40%), and leaks from the connecting tube (20%) In general, there are fewer mechanical failures in malleable prostheses as their mechanical structure is simpler (26)
A study conducted by Ashton M Smelser et al found that 56% of cases where revision was performed on patients with penile prostheses were caused by mechanical failure
The damaged parts of the penile prostheses vary, while all components are at risk of being damaged including the pump, connecting hose, reservoir, and prosthesis cylinder Leaks in the connecting tube and cylinder are the most frequent cause of damage to inflatable penile prostheses (27)
Leaks in the connecting tube usually occur on the bendproof outer part of the hose connection Ashton et al assume that damage to the connecting tube is caused by the pump mechanism and ease of use for the patients
One type of inflatable penile prosthesis has a pump design that makes it more difficult to deflate the penile prosthesis Thus, the connecting tube tends to bend more frequently, resulting in leaks (27)
Infection is one of the complications that need to be assessed from the results of surgery We conducted a metaanalysis of two studies to obtain output regarding infection rates In the meta-analysis results, there was no significant difference in the infection rates after prosthesis implanta-
tion surgery in the inflatable and malleable penile prosthesis groups This is also in line with a study conducted by Berto et al , indicating that there is no significant difference in the incidence of postoperative infection In general, infection in prosthesis implantation presents at a rate of 1012% In the study, it was also stated that all patients who experience infection in prostheses have comorbidities in the form of diabetes mellitus with metabolic disorders and increased glycosylated hemoglobin levels (28) Another study carried out by Jorissen et al suggests that although rare, infection generally does not occur immediately after penile prosthesis implantation but can become very severe This is influenced by the patients’ comorbidities such as diabetes mellitus or others (18)
The infection rate in penile prostheses has decreased over time Around 1980s and 1990s, the infection rate in penile prostheses ranged from 8% to 11% Meanwhile, in early 2000, it ranged from 3% to 5% The introduction of penile prostheses with antibiotics coating and the development of surgical techniques have decreased infection rates by about 0 3% to 2 7% (28)
In 2000, American Medical Systems (AMS) introduced a penile prosthesis with an Inhibizone™ coating, containing the antibiotics Minocycline and Rifampin that coats the surface of the prosthesis and inhibits bacterial growth In 2004, a study by Carson explained that in the 60 days a
Inhibizone™-coated penile prostheses was 0 28% compared to 1 59% in patients with non-coated penile prostheses; six months after surgery, the penile prosthesis infection rate was 0 68% in the coated penile prosthesis group compared to 1 61% in the control group (29)
In 2002, Mentor (now Coloplast) introduced Titan, which had a hydrophilic coating that can reduce bacterial attachment and apply antibiotics to the entire surface of the prosthesis when dipped into an antibiotic solution during surgery In 2004, Wolter and Hellstrom published data on infections from Mentor’s database and the FDA’s report on penile prostheses removal One year after implantation, the infection rate on Titan prosthesis implants was 1 06% (25/2357), while that of non-coated prostheses was 2 07% (10/482) (p 0 033) (29)
The three parameters analyzed in the study (patient satisfaction, partner satisfaction, and ease of use) were analyzed using the EDITS questionnaire (30) The questionnaire was first validated in 1999 as an instrument that can be used to assess the satisfaction of patients who underwent ED therapy and their partners EDITS questionnaire can assess subjective acknowledgment of patient satisfaction and it includes more than the efficacy of patient management (30) EDITS are validated questionnaires developed by Althof et al to assess satisfaction after receiving medicamentosa management (31) This questionnaire was later modified by Levine to assess satisfaction after penile prosthesis implantation The questions listed in this questionnaire assess overall patient satisfaction, the extent to which the penile prosthesis met the patients’ expectations, the possibility of continued use, ease of use of the device, confidence in the ability to engage in sexual activity, patient assessment of partner satisfaction, patient assessment of their partners’ feelings about continued use of the prosthesis, stiffness, and appearance (32)
H Satwikananda, T Bagus Laksita, W Djatisoesanto, D Moesbadianto Soebadi
This study has several limitations, among which is the fact that the studies included herein are observational studies The reason being, to date, there is no Randomized Control Trial (RCT) study that examines penile prostheses This study also does not have many reference articles The output of this study is a general comparison of inflatable penile prostheses and malleable prostheses This study does not specifically compare each type of inflatable penile prosthesis, be it two-piece or three-piece Therefore, more reference articles, large-scale multicenter observational studies, and RCT research are needed to improve this study
CONCLUSIONS
This study concludes that inflatable penile prostheses are better in terms of patient and partner satisfaction Even though mechanical failure is more common in inflatable penile prostheses than malleable penile prostheses, there is no significant difference in the incidence of infection
This study will make a major contribution as one of the basic considerations to produce recommendations for surgeons and urologists in considering appropriate prostheses Further studies can make a more specific comparison of the types and success rate of pregnancy between prostheses
REFERENCES
1 Shamloul R, Ghanem H Erectile dysfunction Lancet 2013; 381:153-165
2 Birowo P, Deswanto IA, Rasyid N Epidemiology of erectile dysfunction: A cross-sectional web-based survey conducted in an Indonesian national referral hospital, F1000Research 2019; 8:817
3 Elterman DS, Bhattacharyya SK, Mafilios M, et al The Quality of Life and Economic Burden of Erectile Dysfunction Res Rep Urol 2021; 13:79-86
4 Droupy S, Colson MH Assessment of a New Formulation of Sildenafil on Common Practice: An Observational Study Int J Reprod Med 2022; 2022:9122099
5 Belew D, Klaassen Z, Lewis RW Intracavernosal Injection for the Diagnosis, Evaluation, and Treatment of Erectile Dysfunction: A Review Sex Med Rev 2015; 3:11-23
6 Raina R, Nandipati KC, Agarwal A, et al Combination therapy: medicated urethral system for erection enhances sexual satisfaction in sildenafil citrate failure following nerve-sparing radical prostatectomy J Androl 2005; 26:757-760
7 Lin H, Wang R The science of vacuum erectile device in penile rehabilitation after radical prostatectomy Transl Androl Urol 2013; 2:61-66
8 Vendeira P Penile prosthesis surgery: Indications and penoscrotal approach Implante de prótesis peneana: indicaciones y abordaje penoescrotal Actas Urol Esp (Engl Ed) 2020; 44:377-381
10 Polchert M, Dick B, Raheem O Narrative review of penile prosthetic implant technology and surgical results, including transgender patients Transl Androl Urol 2021; 10:2629-2647
11 Wang VM, Levine LA Safety and Efficacy of Inflatable Penile
Prostheses for the Treatment of Erectile Dysfunction: Evidence to Date Med Devices (Auckl) 2022; 15:27-36
12 Pang KH, Muneer A, Alnajjar HM A systematic review of penile prosthesis insertion in patients with spinal cord injury Sex Med Rev 2022; 10:468-477
13 Li JZ, Maguire TA, Zou KH, et al Prevalence, Comorbidities, and Risk Factors of Erectile Dysfunction: Results from a Prospective Real-World Study in the United Kingdom Int J Clin Pract 2022; 2022:5229702
14 Muncey W, Sellke N, Kim T, et al Alternative Treatment for Erectile Dysfunction: a Growing Arsenal in Men's Health Curr Urol Rep 2021; 22:11
15 Hatzichristou D, Kirana PS, Banner L, et al Diagnosing Sexual Dysfunction in Men and Women: Sexual History Taking and the Role of Symptom Scales and Questionnaires J Sex Med 2016; 13:11661182
16 Bayrak O, Erturhan S, Seckiner I, et al Comparison of the patient's satisfaction underwent penile prosthesis; Malleable versus Ambicor: Single center experience Arch Ital Urol Androl 2020; 92:25-29
17 Kılıçarslan H, Kaynak Y, Gökcen K, et al Comparison of patient satisfaction rates for the malleable and two piece-inflatable penile prostheses Turk J Urol 2014; 40:207-210
18 Jorissen C, De Bruyna H, Baten E, Van Renterghem K Clinical Outcome: Patient and Partner Satisfaction after Penile Implant Surgery Curr Urol 2019; 13:94-100
19 Vakalopoulos I, Kampantais S, Ioannidis S, et al High patient satisfaction after inflatable penile prostheses implantation correlates with female partner satisfaction J Sex Med 2013; 10:2774-2781
2 0 A k i n - O l u g b a d e O , P a r k e r M , G u h r i n g P , M u l h a l l J
Determinants of patient satisfaction following penile prosthesis surgery J Sex Med 2006; 3:743-748
21 Carvalheira A, Santana R, Pereira NM Why Are Men Satisfied or Dissatisfied with Penile Implants? A Mixed Method Study on Satisfaction with Penile Prosthesis Implantation J Sex Med 2015; 12:2474-2480
22 Habous M Malleable (Semi-Rigid) Penile Prosthesis (MPP) J Sex Med 2015; 12:1984-1988
23 Bettocchi C, Palumbo F, Spilotros M, et al Patient and partner satisfaction after AMS inflatable penile prosthesis implant J Sex Med 2010; 7:304-9
24 Braun AE, Swerdloff D, Sudhakar A, et al Defining the incidence and management of postoperative scrotal hematoma after primary and complex three-piece inflatable penile prosthesis surgery Int J Impot Res 2023:1-5
25 Bartley J, Zimmerman WB, Dhabuwala CB Inflatable penile prosthesis and salvage protocol for mechanical failure: is it really necessary? J Sex Med 2012; 9:2175-2181
26 Natali A, Olianas R, Fisch M Penile implantation in Europe: s u c c e s s e s a n d c o m p l i c a t i o n s w i t h 2 5 3 i m p l a n t s i n I t a l y a n d Germany J Sex Med 2008; 5:1503-1512
27 Smelser AM, VanDyke ME, Nealon SW, et al Mechanical indications for inflatable penile prosthesis revision: analysis and implications for revision surgery J Sex Med 2023; 20:1044-1051
28 Bertó RR, López-Acón JD, Marco SL, et al Penile prosthesis: Patient satisfaction, use and preference for malleable vs inflatable World J Clin Urol 2014; 3:134-138
29 Gon LM, de Campos CCC, Voris BRI, et al A systematic review
H Satwikananda, T Bagus Laksita, W Djatisoesanto, D Moesbadianto Soebadi
of penile prosthesis infection and meta-analysis of diabetes mellitus role BMC Urol 2021; 21:35
30 Bernal RM, Henry GD Contemporary patient satisfaction rates for three-piece inflatable penile prostheses Adv Urol 2012; 2012:707321
31 Althof SE, Corty EW, Levine SB, et al EDITS: development of questionnaires for evaluating satisfaction with treatments for erectile dysfunction Urology 1999; 53:793-799
32 Levine LA Diagnosis and treatment of erectile dysfunction Am J Med 2000; 109 Suppl 9A:3S-30S
33 Çayan S, Ascı R, Efesoy O, et al Comparison of Long-Term Results and Couples' Satisfaction with Penile Implant Types and Brands: Lessons Learned From 883 Patients With Erectile Dysfunction Who Underwent Penile Prosthesis Implantation J Sex Med 2019; 16:10921099
Correspondence
Handaru Satwikananda handaru satwikananda@gmail com
Department of Urology, Faculty of Medicine, Universitas Airlangga Dr Soetomo General-Academic Hospital, Surabaya, East Java, Indonesia
Tetuka Bagus Laksita dr tetuka@gmail com
Doddy Moesbadianto Soebadi dmsoebadi@gmail com
Wahjoe Djatisoesanto (Corresponding Author) wahjoe djatisoesanto@fk unair ac id
Department of Urology, Faculty of Medicine, Universitas Airlangga Universitas Airlangga Teaching Hospital, Surabaya, East Java, Indonesia
Jl Mayjen Prof Dr Moestopo No 6-8, Surabaya, East Java, Indonesia, 60286
Conflict of interest: The authors declare no potential conflict of interest
Archivio Italiano di Urologia e Andrologia 2024; 96(2):12353
ORIGINAL PAPER
Novel emerging therapy for erectile dysfunction: Efficacy and safety of flat magnetic stimulation
Daniel Galimberti 1 , Agustina Vila Echague 2 , Ery A Ko 3 , Laura Pieri 4 , Alessandra Comito 4 , Irene Fusco 4 , Tiziano Zingoni 4
1 Coordinador de Láser de Derma Internacional Centre, Buenos Aires, Argentina;
2 Médica Dermatologa, Directora de Grupo de Láser SAD (Sociedad Argentina de Dermatología), Buenos Aires, Argentina;
3 Dermatóloga, Fellow de Láser y Estética Derma Internacional, Buenos Aires, Argentina;
4 El En Group, Calenzano, Italy
Summary
Background: The erectile dysfunction (ED), which is the inability to achieve and/or sustain a penile erection sufficient to result in a satisfying sexual performance, represents a very common complaint for men over forty years old. The aim of the study was to evaluate if Flat Magnetic Stimulation (FMS) technology could help individuals with symptomatic erectile dysfunction.
Methods: Twenty patients with erectile dysfunction, underwent eight sessions of about 30 minutes each in a twice a week frequency with the study device During treatments, every potential side effect was assessed The International Index of Erectile Function (IIEF) was compiled by all patients at the beginning, after the eighth treatment and at 1 month from the end of the last treatment The questionnaire scores were presented as median values along with the interquartile range (IQR) and we set the significance threshold at 0 01
Results: After the treatment and at 1-month follow-up, the increase in questionnaire scores was statistically significant compared to the baseline, thus supporting the clinical usefulness of this treatment. In particular, the result of the study indicates a statistically significant difference between IIEF score before treatment (Median = 34) and IIEF score after the end of treatment (Median = 45) and between IIEF score before treatment and IIEF score at 1-month follow-up (Median = 54).
Conclusions: The study findings showed that FMS represents a promising treatment option to individuals affected by symptomatic erectile dysfunction
KEY WORDS: Symptomatic erectile dysfunction; Flat magnetic stimulation; Emerging therapy
Submitted 26 March 2024; Accepted 18 April 2024
INTRODUCTION
The inability to achieve and/or sustain a penile erection sufficient to result in a satisfying sexual performance is known as erectile dysfunction (ED) (1) ED can have a substantial negative effect on physical and mental health of patients as well as the quality of life for their partners (2) Men who have ED are frequently feeling guilty about their condition and avoid seeking professional help (3) ED can be effectively treated with available therapies However, it cannot be cured, except for psychogenic ED, post-traumatic arteriogenic ED in younger patients, and hormonal causes (1)
While oral Phosphodiesterase type 5 inhibitors (PDE5Is) have long been recommended as the initial treatment option, some patients did not respond well to this therapy As a result, non-surgical treatment alternatives like vasodilating agents, intraurethral alprostadil, vacuum erection devices (VEDs) and intracavernosal injections (ICIs) are available (4) Nevertheless, those therapeutic approaches are not able to change the underlying pathophysiology of the erectile mechanism and have several serious drawbacks (5) Nowadays, it is established that specific pelvic floor muscles play a part in the ejaculatory and erectile mechanisms (6) As previously shown in the literature, pelvic floor electromagnetic/magnetic therapy can be a non-invasive option for men with the syndrome of chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) (7) Relevant advances in magnetic stimulation technology have been made recently, including Flat Magnetic Stimulation (FMS) (8)
Even before FMS, the goal of pelvic floor muscle training (PFMT) was to restore the pelvic floor muscles by enhancing proprioception, relaxation, and muscle tone Exercises targeting the pelvic floor muscles have been shown to enhance erection, particularly in post-prostatectomy ED patients (9) Mondaini et al have recently demonstrated that FMS improved CP/CPPS symptoms (pelvic/genital pain, ejaculatory pain, and urinary symptoms) (10) In light of these evidence, our goal was to investigate if FMS could help individuals with symptomatic erectile dysfunction
MATERIALS AND METHODS
A prospective single-group study was carried out from February to November 2023, in a private medical centre, in Argentina, using Dr Arnold (DEKA M E L A , Calenzano, Italy) device that includes a chair applicator and a main unit An electromagnetic field with a homogenous profile produces the stimulation Greater muscle fibre recruitment is made possible by the uniformity of the magnetic field distribution, which prevents any region of unequal stimulation intensity
Twenty patients with erectile dysfunction in total, were enrolled in this study Their mean (± SD) age was 56 89 (± 6 63) years, ranging from 46 to 66 years Patients with severe neurological diseases, malignant tumours, obesity, pacemakers, or metal implants were included among the
Galimberti, A Vila Echague, E A Ko, et al
exclusion criteria Before beginning the treatment, PDE5I users had to endure a three-week wash-out period For the duration of the treatment session, all patients agreed to abstain from using PDE5I or any other ED therapies Patients underwent eight sessions of about 30 minutes each in a twice a week frequency The following FMS schedule was used: sessions 1 to 4 followed the Hypotonus/ Weakness 1 protocol whereas sessions 5 to 8 followed the Hypotonus/Weakness 2 protocol The Hypotonus/ Weakness 1 protocol consists of about 30 minutes warm-up and muscle activation phase, followed by a muscle work phase focused on restoring tropism and muscle tone (2030Hz) in a trapezoidal shape For a total of about 30 minutes, the Hypotonus/Weakness 2 protocol consists of a warm-up and muscle activation phase, a muscle work phase targeted at increasing tropism (volume), and a muscle strength phase (40-50Hz) in a trapezoidal shape
D u r i n g t re a t m e n t s , e v e r y p o t e n t i a l s i d e e ff e c t w a s assessed, including skin redness, local erythema, tendon pain, muscle pain, and transient muscle spasms
The Inter national Index of Erectile Function (IIEF) is a psychometrically and cross-culturally valid tool to identify treatment-related alterations in erectile dysfunction patients which showed high sensitivity and specificity It comprises 15 items and 5 domains and is an accurate and valid psychometric tool for assessing efficacy of ED treatment The IIEF has a possible score range from 5 to 25, and ED is classified into five categories based on the scores: severe (57), moderate (8-11), mild to moderate (12-16), mild (17-21), and no ED
Table 1.
(22-25) In the IIEF there are six items in the erectile function domain (EF-score), two items in the orgasmic function domain (OF-score), two items in the sexual desire domain (SD-score), three items in the intercourse satisfaction domain (IS-score), and two items in the overall sexual satisfaction domain (OS-score) (11)
An higher post-test IIEF score compared with the pre-test score was considered an improvement in ED
The IIEF was compiled by all patients at the beginning, after the eighth treatment and at 1 month from the end of the last treatment (1MFU)
The questionnaire scores were presented as median values along with the interquartile range (IQR) Significance threshold was set at 0 01 Student’s t-test, SPSS (IBM Corp , New York, NY, USA) and R 4 1 (the R Core Team, Vienna, Austria, 2021) were used to perform statistical analysis
The article is in accordance with the Declaration of Helsinki on Ethical Principles for Medical Research involv-
Median values and interquartile range at baseline, at the end of the treatment sessions (after the eighth treatment), and at 1-month follow-up, related to international index of erectile function (IIEF), erectile function (EF) score, orgasmic function (OF) score, sexual desire (SD) score, intercourse satisfaction (IS) score and overall satisfaction (OS) score.
Figure 1.
Box plot for score at baseline, at the end of the treatment sessions (after the eighth treatment, and 1-month follow-up for international index of erectile function (IIEF).
D
Figure 2.
Box plots at baseline, at the end of the treatment sessions (after the eighth treatment), and 1-month follow-up related to erectile function (EF) score, orgasmic function (OF) score, sexual desire (SD) score, and intercourse satisfaction (IS) score
ing human subjects Ethical approval is not necessary as the study device is already CE marked since 2020 Written informed consent has been obtained from the patients to publish this paper
RESULTS
Outcome measures of questionnaire score at the baseline, end of treatment, and 1-month follow-up are summarized in Table 1, Figure 1 and Figure 2 After the treatment and at 1-month follow-up, the increase in scores was statistically significant compared to the baseline, thus supporting the clinical usefulness of this treatment In particular, the test result indicates a statistically significant difference between IIEF score before treatment (Median = 34) and IIEF score after the end of treatment (Median = 45) and between IIEF score before treatment and IIEF score at 1-month follow-up (Median = 54)
The improvement was confirmed in all IIEF domains (see Table 1) Although the erectile function domain showed the largest change, significant modifications were noted in all the domains in the patients after treatment
The ED severity is shown in Figure 3 and Table 2 Among the 20 participants of this study during the pre-test, we found that 20% of patients had severe ED (score range 6-
10), 70% moderate ED (score range 11-16), 5% mildmoderate ED (score range 17-21), and 5% mild ED (score range 22-25) None of them was found without dysfunction (score range 26-30)
After the treatment, 5% of participants were found to have severe ED, 20% had moderate ED, 65% had mild-moderate ED, 5% mild ED (score range 22-25), and lastly, 5% were found without dysfunction (score range 26-30)
During the post-test (after one month of the last treatment session), no participant was found to have severe ED Few (10%) had moderate ED, the majority (45% and 40%) had mild-moderate ED and mild ED respectively, while 5% were found without dysfunction (see Table 2)
Table 2.
% of patients divided into 5 categories of ED classification
ED classification Before End of treatment 1MFU
Severe (range score: 6-10) 4/20 (20%) 1/20 (5%) 0/20 (0%)
No ED (range score: 26-30) 0/20 (0%) 1/20 (5%) 1/20 (5%)
DISCUSSION
The current pharmacological treatment of ED and nonsurgical treatment alter natives (such as vasodilating agents, intraurethral alprostadil, vacuum erection devices and intracavernosal injections) do not appear to improve endothelial dysfunction, restoring physiological erectile function, or significantly changing the underlying pathophysiology of the erectile function (EF) (12) These therapeutic approaches have a lot of drawbacks (side effects, low response rates) and a steady discontinuation rate of them was displayed (13) On the other hand, a penile prosthesis implant is an irreversible form of treatment and, even after the implantation, a man will never again be able to achieve a spontaneous erection
The low-intensity extracorporeal shock wave therapy (LiESWT) has been proposed as a promising treatment for vasculogenic ED in recent years
Since Vardi et al (14) initially reported the use of LiESWT in the treatment of ED in 2010, several studies have assessed the effectiveness of Li-ESWT in various form of ED, whether they are organic (vasculogenic or neurogenic) or mixed (15) The patients included in the studies exhibit significant differences regarding cardiovascular risk factors, response to PDE5I, duration, and severity of ED Additionally, there is a great deal of variation in the shockwave generators, the kind of shockwaves released, the parameters set, and the treatment plans employed (1) It is challenging to determine whether LiESWT is a practical option for the management of ED overall given the heterogeneous data Several sexual medicine societies have cautiously accepted Li-ESWT as a treatment for men with ED in the past year It is safe and
Figure 3
The percentage of patients is divided into 5 categories of ED classification No ED (EF score 26-30), mild (EF score 22-25), mild to moderate (EF score 17-21), moderate (EF score 11-16) at baseline, at the end of the treatments and 1 month after the last session
reasonably effective, but it should only be used in the context of clinical research (12, 16)
Overall, there was an improvement in the IIEF-EF score according to the pooled data from meta-analyses, but the estimates are low (ranging from roughly 2-4 IIEF-EF points) and the heterogeneity is high (16) Most of the research that has been published only included follow-up data for two years (12) and this raises the question of whether the early improvements in EF can be maintained over the long run The results of the long-term study by Chung and Cartmill, indicate that, 48-60 months after the end of Li-ESWT, the clinical improvement in EF that was previously seen is still declining and appears to plateau at 40% clinical efficacy (17)
The idea of "regenerative" therapies for the treatment of ED has drawn a lot of attention in recent years This concept makes sense because ED causes the erectile tissue to undergo anatomical and functional changes that are typified by progressive cavernosal fibrosis (18) Stem cell injections, platelet-rich plasma, and low-intensity shockwave therapy (Li-SWT) are examples of regenerative treatments Angiogenesis and neurogenesis may be induced by these methods, "restoring" malfunctioning erectile tissue, according to accumulating animal data (19)
Regenerative therapies are a viable treatment option for erectile dysfunction, but there is currently little human data to support this claim (20)
We can also include magnetic stimulation in the list of regenerative therapies In patients with urinary incontinence and pelvic floor disorders, magnetic stimulation has already been used to treat the human pelvic floor with great success There have been no negative side effects or dis-
D Galimberti, A Vila Echague, E A Ko, et al
comfort and the pelvic floor muscle (PFM) tone and strength have significantly improved The demonstration was conducted both quantitatively, using ultrasound exams, and qualitatively, using validated questionnaires (21)
Magnetic stimulation is a type of passive rehabilitation where there is no need for the patient to get undressed during treatment Patients sit in an ergonomic chair that has a height-adjustable backrest, allowing them to experience total comfort and relaxation at every session This innovative device targets neuromuscular tissue by creating an electric current that causes PFM to contract passively and strongly
Electric currents associated with magnetic stimulation led to neuron depolarization, which triggers concentric contractions and lifts all PFMs This results in profound stimulation and the regeneration of neuromuscular control
Indeed, the entire procedure causes the muscle structure to change because the fibres tend to become hypertrophic and hyperplasic (8, 22) In addition to having a specific protocol for muscle hypertonicity, the device used in our study was appropriate for treating pelvic floor muscle dysfunction and ED Indeed, by using lower frequencies (about 10 Hz) in the overtone protocol for hypertonic management, the electromagnetic field is distributed uniformly and does not produce areas of varying stimulation intensity
Frigerio and colleagues showed that FMS significantly increased the size of the urethral rhabdosphincter, leading to a 15 4% increase in muscle volume, increasing the quality of life scores related to urination (8) It has also been demonstrated that strengthening the pelvic floor muscles greatly enhances post-prostatectomy urine continence, post-micturition dribble and erectile function (22)
FMS technology has also a comparable impact on different skeletal muscles In a study by Leone et al , the effectiveness of similar device, which uses FMS technology, was assessed on the abdomens of 15 patients (23) This study showed that one month following the last treatment, all treated areas had experienced hypertrophy in terms of the thickness of abdominal muscle tissue
Smooth muscle tissue makes up about 45% of the cavernous volume, with collagen making up most of the non-muscle component The most crucial component of the hemodynamic processes that underlie an erection is the smooth muscle of the penis, consequently, magnetic stimulation, may be crucial in the treatment of ED, restoring fibromuscular pathological changes within the corpus cavernosum
In 2003, Van Kampen et al carried out a literature review whose results suggested that perineal rehabilitation could be an effective treatment for erectile dysfunction (24)
In human studies, Karacan et al have shown that peaks in blood flow recordings coincided with bursts in the perineal muscles' EMG activity during nocturnal penile tumescence (25)
Our findings support the notion that pelvic floor rehabilitation plays a part in erectile dysfunction and are consistent with those of Rival and Clapeau (6) Indeed the improvement in IIEF-scores after the treatment and at the one-month follow-up was statistically significant when compared to the baseline, indicating the treatment's clin-
ical utility The mechanisms supporting the potential role of strengthening the pelvic floor in erection would be an increase in endocavernous pressure and the limitation of venous return from the penis Awareness of the region would also allow the patient to regain control of this part of their body
Some authors have proposed including perineal rehabilitation as a first-line treatment for erectile dysfunction (26) This approach has no side effects, is cost-controlled and it can be combined with recommended approaches in the management of erectile dysfunction
However, we do agree that more investigation is needed to look at different pathophysiological changes associated with FMS on penile tissue, including long-term histological changes
In addition to muscular involvement, many studies have indicated that endothelial dysfunction or vascular damage is a key mechanism of ED (27)
In animal models, it has been shown that by shifting astrocytic phenotypes (A1-A2), magnetic stimulation can reduce the production of the pro-inflammatory cytokine TNF-alpha and promote the production of the anti-inflammatory cytokine IL-10 In A2 astrocytes, magnetic stimulation also promoted the release of angiogenesis-related factors TGFb and VEGF, which can support angiogenesis
In a prior study, angiogenesis-related genes (VEGFA and BAI1) were found to be upregulated in rats following magnetic stimulation (28) Lee and colleagues, following a stroke in an animal model, argued that magnetic stimulation, on the affected hemisphere, caused modifications in the angiogenic pathways; indeed, magnetic stimulation significantly raised endothelial nitric oxide synthase (eNOS) phosphorylation, which enhances angiogenesis (29) Since nitric oxide (NO) is essential for a physiological penile erection (as well as the mechanism through which PDE5Is act), we could speculate that FMS, besides the positive muscular effects, might have some NO-dependent benefits in angiogenesis, making it advantageous for patients with vasculogenic ED and low PDE5I response
Furthermore, sperm motility is increased when human spermatozoa are exposed to a very low-frequency electromagnetic field (30)
While it's true that a person with erectile dysfunction might not have any difficulties to procreating, there are general characteristics and shared risk factors that lead to the development of infertility and erection dysfunction, so we can also conjecture about the potential positive impact of FMS on spermatozoa motility
Filippini's study [which showed a significant improvement in PFM tone and strength in patients with urinary incontinence and pelvic floor disorders, both qualitatively and quantitatively with ultrasound exams (21)] and Mondaini's study [which showed improved erectile functioning, with the total mean IIEF-5 score significantly increasing from 21 3 ± 2 7 at baseline to 24 3 ± 0 5 at 1 moth follow up after the last treatment session, p < 0 001 (10)] contributed to the concept of using FMS for ED treatment
Our preliminary clinical findings were validated using prospectively questionnaires and, the outcome measures were the significant improvement of IIEF, without any significant adverse events
Galimberti, A Vila Echague, E A Ko, et al
Our device offers a number of significant benefits, including the ability to stimulate muscles without the need for a probe and the ability for patients to remain fully clothed while seated in an ergonomic and comfortable position due to the gradually correct emission of supplied energy
Finally, Dr Arnold can be defined as an "educator" system because it helps the patient perceive the muscles involved in the treatment; additionally, other pharmaceutical or physical techniques can be used in conjunction with this new technology
We recognized that our study had several limitations, including a small sample size, the absence of a sham treatment arm, and the lack of objective measurements of penile hemodynamics like penile colour duplex ultrasonography
However, prior research (12) has shown a strong correlation between the subjective report of EF recovery and objective penile hemodynamic improvements
In conclusion, perineal physiotherapy seems to have its place in the management of erectile dysfunction
Furthermore, magnetic stimulation of the muscle within the corpus cavernosum certainly induces muscle hypertrophy and the physiology of erection underlies the need for effective contraction of the ischiocavernosus; the treatments turned out with no side effects and with a high degree of patient acceptance
Undoubtedly, our experience has shown that FMS is a safe and effective option for improving ED with certainly muscular effects and with a potential interference in angiogenesis and spermatozoa motility
For most men with ED, the ideal result is a lasting solution, which is something that FMS can potentially accomplish
The long-term safety and efficacy of this therapy, which is still in the experimental stage, require further research in this area Therefore, from a theoretical standpoint, this method can restore erectile function when compared to other previously used treatment methods
CONCLUSIONS
The study findings showed that FMS represents a successful treatment option to individuals affected by symptomatic erectile dysfunction
REFERENCES
1 European Association of Urology EAU Guidelines Edn Presented at the EAU Annual Congress Amsterdam Arnhem: EAU Guidelines Office; 2022; 46-71
2 Hatzimouratidis K, Amar E, Eardley I, et al European Association of Urology Guidelines on male sexual dysfunction: erectile dysfunction and premature ejaculation Eur Urol 2010; 57:804-14
3 Ariba AJ, Oladapo OT, Iyaniwura CA, Dada OA Management of erectile dysfunction: perceptions and practices of Nigerian primary care clinicians South African Family Practice 2014; 49:16-16d
4 Burnett AL, Nehra A, Breau RH, et al Erectile dysfunction: AUA guideline J Urol 2018; 200:633-41
5 Yee CH, Chan ES, Hou SS, Ng CF Extracorporeal shockwave therapy in the treatment of erectile dysfunction: a prospective, randomized, double-blinded, placebo controlled study Int J Urol 2014; 21:1041-5
6 Rival T, Clapeau L Efficacité de la rééducation du plancher pelvien dans la dysfonction érectile: revue de la littérature Prog Urol 2017; 27:1069-1075
7 Rowe E, Smith C, Laverick L, et al A prospective, randomized, placebo controlled, double-blind study of pelvic electromagnetic therapy for the treatment of chronic pelvic pain syndrome with 1 year of followup Clin Trial J Urol 2005; 173:2044-7
8 Frigerio M, Barba M, Cola A, et al Flat Magnetic Stimulation for Stress Urinary Incontinence: A Prospective Comparison Study Bioengineering (Basel) 2023; 10:295
9 Wong C, Louie DR, Beach C A systematic review of pelvic floor muscle training for erectile dysfunction after prostatectomy and recommendations to guide further research J Sex Med 2020; 17:737748
10 Mondaini N, Gacci M, Cai T, et al Efficacy of top flat magnetic stimulation for chronic pelvic pain in men: preliminary results Int J Impot Res 2024
11 Rosen RC, Cappelleri JC, Smith MD, et al Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction Int J Impot Res 1999; 11:319-26
12 Chung E, Lee J, Liu CC, et al Clinical Practice Guideline Recommendation on the Use of Low Intensity Extracorporeal Shock Wave Therapy and Low Intensity Pulsed Ultrasound Shock Wave Therapy to Treat Erectile Dysfunction: The Asia-Pacific Society for Sexual Medicine Position Statement World J Mens Health 2021; 39:1-8
13 Yee CH, Chan ES, Hou SS, Ng CF Extracorporeal shockwave therapy in the treatment of erectile dysfunction: a prospective, randomized, double-blinded, placebo controlled study Int J Urol 2014; 21:1041-5
14 Vardi Y, Appel B, Jacob G, et al Can low intensity extracorporeal shockwave therapy improve erectile function? A 6-month follow-up pilot study in patients with organic erectile dysfunction Eur Urol 2010; 58:243-8
15 Ergün M, Akyüz O Is Li-ESWT effective in diabetic patients with severe erectile dysfunction? Asian J Androl 2022; 24:521-4
16 Capogrosso P, Frey A, Jensen CFS, et al Low-intensity shock wave therapy in sexual medicine Clinical recommendations from the European Society of Sexual Medicine (ESSM) J Sex Med 2019; 16:1490-1505
17 Chung E, Cartmill R Evaluation of Long-Term Clinical Outcomes and Patient Satisfaction Rate Following Low IntensityShock Wave Therapy in Men With Erectile Dysfunction: A Minimum 5-Year Follow-Up on a Prospective Open-Label Single-Arm Clinical Study Sex Med 2021; 9:100384
18 Iacono F, Giannella R, Somma P, et al Histological alterations in caver nous tissue after radical prostatectomy J Urol 2005; 173:1673-6
19 Liu MC, Chang ML, Wang YC, et al Revisiting the Regenerative Therapeutic Advances Towards Erectile Dysfunction Cells 2020; 9:1250
20 Alhefnawy MA, Salah E, Bakry S, et al Autologous mesenchymal stem cell therapy for diabetic men with erectile dysfunction Is it promising? A pilot study Arch Ital Urol Androl 2023; 95:11669
21 Filippini M, Biordi N, Curcio A, et al A Qualitative and Quantitative Study to Evaluate the Effectiveness and Safety of Magnetic Stimulation in Women with Urinary Incontinence Symptoms and Pelvic Floor Disorders Medicina (Kaunas) 2023; 59:879
D
22 Dorey G Restoring pelvic floor function in men: review of RCTs Br J Nurs 2005; 14:1014-8, 1020-1
23 Leone A, Piccolo D, Conforti C, et al Evaluation of safety and efficacy of a new device for muscle toning and body shaping J Cosmet Dermatol 2021; 20:3863-3870
24 Van Kampen M, De Weerdt W, Claes H, Feys H Treatment of erectile dysfunction by perineal exercise, electromyo-graphic biofeedback and electrical stimulation Phys Ther 2003; 83:536
25 Karacan I, Aslan C, Hirshkowitz M Erectile mechanisms in man Science, 1983; 220:1080-2
26 Silva AB, Sousa N, Azevedo LF, Martins C Physical activity andexercise for erectile dysfunction: systematic review and metaanalysis Br J Sports Med 2017; 51:1419-1424
27 Gandaglia G, Briganti A, Jackson G, et al A systematic review of the association between erectile dysfunction and cardiovascular disease Eur Urol 2014; 65:968-978
28 Ljubisavljevic MR, Javid A, Oommen J, et al The effects of different repetitive transcranial magnetic stimulation (rTMS) protocols on cortical gene expression in a rat model of cerebral ischemic-reperfusion injury PLoS One 2015; 10:e0139892
29 Lee Y, Oh BM, Park SH, Han TR Low-Frequency Repetitive Transcranial Magnetic Stimulation in the Early Subacute Phase of Stroke Enhances Angiogenic Mechanisms in Rats Ann Rehabil Med 2022; 46:228-236
30 Iorio R, Delle Monache S, Bennato F, et al Involvement of mitochondrial activity in mediating ELF-EMF stimulatory effect on human sperm motility Bioelectromagnetics 2011; 32:15-27
Correspondence
Daniel Galimberti daniel galimberti@gmail com Coordinador de Láser de Derma Internacional Centre, Buenos Aires, Argentina
Agustina Vila Echague agus1511@yahoo com
Médica dermatóloga, Directora de Grupo de Láser SAD (Sociedad Argentina de Dermatología)
Ery A Ko erykohiba@gmail com
Dermatóloga, Fellow de Láser y Estética Derma Internacional, Buenos Aires, Argentina
Laura Pieri l pieri@deka it
Alessandra Comito a comito@elen it
Irene Fusco (Corresponding Author) i fusco@deka it
Tiziano Zingoni t zingoni@elen it
El En Group, 50041 Calenzano, Italy
Conflict of interest: Authors TZ, AC, LP and IF were employed by El En Group The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest
ORIGINAL PAPER
Surgeon’s point of view in vesico-vaginal fistula management
1 Department of Urology, Faculty of Medicine, Universitas Udayana, Indonesia;
2 Prof Dr I G N G Ngoerah General Hospital, Denpasar, Indonesia;
3 Department of Surgery, Faculty of Medicine, Universitas Udayana, Indonesia;
4 Department of Urology, Faculty of Medicine, Universitas Airlangga, Indonesia;
5 Department of Urology, Faculty of Medicine, Universitas Indonesia, Cipto Mangunkusumo General Hospital, Jakarta, Indonesia;
6 Department of Urology, Bhayangkara Anton Soedjarwo Hospital, Pontianak, Indonesia
Summary
Objectives: Vesicovaginal fistulas (VVF) are the most commonly acquired fistulas of the urinary tract The management of VVF is mainly based on expert opinion and surgeon experience. This study aims to provide the practice patterns and outcomes of vesicovaginal fistula (VVF) management in Indonesia.
Methods: This study utilizes the results of a survey among the surgeons who performs VVF repair in referral hospitals throughout Indonesia between June and July of 2021 Data analysis was carried out with SPSS descriptively by displaying the relative frequency of the answers to each question of the questionnaire form
Results: We collected responses from 93 respondents consisting of 68 urologists and 25 gynecologists The most commonly reported cause of VVF was obstetric (50 5%) Most respondents confirmed the diagnosis of VVF by cystoscopy (81 7%) Waiting time to repair VVF was generally 12 weeks (79.6%), while the transvaginal approach repair was more often performed (77.4%). An additional procedure, such as tissue interposition was performed in 50 5% of cases Tissue interposition was mostly indicated in recurrent VVF (81%), with omentum being the most selected tissue interposition (71%) When indicated, the most selected method of transabdominal approach was open transvesical (54,84%) A laparoscopic approach was performed only in 7.5% of cases. Overall, the success rate for VVF repair in Indonesia was 70-100% at first attempt
Conclusions: The transvaginal approach is preferred, either with or without an interposition tissue flap The success rate at the first attempt is satisfactory.
Vesicovaginal fistulas (VVF) are the most commonly acquired fistulas of the urinary tract (1) Although rarely fatal, VVF causes great concern because of its disturbance to a patient’s quality of life, encompassing physical, emotional, psychological, and economic aspects To date, there has never been a comprehensive worldwide survey designed to precisely determine the information on vesi-
covaginal fistula The incidence is pinpointed because of underdiagnosis and lack of awareness of this condition
Previous research has found that VVF incidence is higher in low-and middle-income countries, although there is also a relatively high incidence in high-income countries (1-3) At least 3 million women in third-world countries are affected by this condition (4) In African countries alone, up to 130 000 new cases are found each year (5) Indonesia, a developing country, also suffers greatly from the high prevalence of VVF (6) Therefore, many women with VVF are undiagnosed and untreated, leaving quite a complex healthcare problem (5, 6)
Despite its significant impact, there has yet to be a consensus on the optimal approach to treat VVF The choice of therapy is mainly based on expert opinion and surgeon experience Currently, the European Association of Urology guidelines have no specific algorithm for VVF repair (7) Furthermore, it is lacking a surgical treatment algorithm based on the characteristics of the fistula The purpose of this study was to review practice patterns and outcomes of VVF treatment in Indonesia to aid practitioners in selecting appropriate management for their patients
METHODS
This research is an observational study with a cross-sectional design The sample selection was carried out by voluntary reply to a survey link which was sent to surgeons who performs VVF repair in referral hospitals throughout Indonesia The invited surgeons were urogynecologists, female urologists, and general urologists who had a course of VVF repair The Indonesian Urology
A s s o c i a t i o n a n d I n d o n e s i a n O b s t e t r i c s a n
Association facilitated the research by listing the surgeon performing VVF repair This study was conducted between June and July 2021 Data collection was limited to one year prior to survey completion We tried to increase the sample after the end of the pandemic era, but the additional data did not meet the inclusion criteria The assessment of all variables was carried out using a structured questionnaire in electronic form Data collected in the survey period were downloaded from the serv-
er in the format of Excel data Data analysis was carried out with SPSS descriptively by displaying the relative frequency of the answers to each question of the questionnaire form
RESULTS
VVF in Referral Hospitals in Indonesia
Ninety-three respondents were surgeons who performed VVF repair in various referral hospitals in Indonesia Most of the surgeons were urologists (51 6%) The number of VVF cases managed by each practitioner was generally less than 10 cases in 1 year (91 4%), with the most common etiologies being obstetric etiology, which consist of vaginal delivery, caesarean section procedure, and caesarean hysterectomy (50 5%) and iatrogenic etiology, which is related to urinary tract injuries during abdominal surgery (Table 1)
The choice of modalities used for diagnosing VVF varied, with cystoscopy being the most common examination used by 81 7% of surgeons (Figure 1) It was followed by t h e d y e / m e t h y l e n e b l u e t e s t ( 6 4 5 % ) , c y s t o g r a p h y (60 2%), pelvic examination (53 8%), and intravenous
The Characteristics of VVF Cases at the Referral Hospitals in Indonesia
K Budi Santosa, S Novia Marta, Ronald Sugianto, et al
Table 1.
Figure 1. Diagnostic modalities of VVF
Figure 2. The abdominal approach in VVF repair
Indication for the use of interposition tissue
pyelography (IVP) (2 2%) In the case of iatrogenic VVF, the majority of surgeons (65 6%) did not routinely perform an IVP as the first examination
Most of the surgeons (79 6%) choose 12 weeks to perform VVF repair The transvaginal approach for VVF repair was carried out by 77 4% of respondents When indicated the most selected method of transabdominal approach was open transvesical (54 84%), as shown in Figure 2
As many as 50 5% of surgeons did not use tissue interposition for VVF repair Tissue interposition was indicated for recurrent VVF (81%), complex VVF (64 3%), in all cases (35 7%), and radiation cases (35 7%) (Figure 3)
The most widely used interposition was the omentum (71%) (Figure 4), followed by labial fat-fibrose tissue (55%), and peritoneum (17%)
Most surgeons did not routinely give antimuscarinic to the patient after VVF repair (72%)
In comparison, respondents' opinion was quite divided on the use of ureteral protection during VVF repair: 50 5% did not do it routinely, while 46 2% did it routinely Overall, the first attempt at VVF repair was quite successful, with only 16 1% of respondents having < 70% success (Table 2)
Figure 3
Figure 4. Tissue interposition for VVF repair.
Table 2
Overview of the Management of VVF at the Referral Hospital in Indonesia
>
DISCUSSION
Vesico vaginal fistula is the most common fistula found in the daily clinical setting (> 72%), occurring mainly from obstetrical complications (80%) (5, 6, 8) This research confirms this finding with obstetrical complication being the most common cause for VVF (50 5%), followed with iatrogenic (48 1%) In this survey, cystoscopy was the most frequent diagnostic modality used by respondents to diagnose VVF (81 7%), followed by dye/methylene blue (64 5%) and cystography (60 2%) Patients with vesicovaginal fistula usually present with symptoms of continuous urinary leakage The severity of the clinical manifestation depends on the size of the fistula In the examination, the surgeons must evaluate the fistula's size, number, and site to plan treatment (3) Through previous clinical experience, it was found that diagnostic modalities differ in each management area, and urologists tend to confirm VVF by performing cystoscopy Meanwhile, intravenous pyelography is another modality used to diagnose a concurrent ureteral injury However, only 34 4% of surgeons apply this modality Evaluation of the upper urinary tract might be essential because up to 12% of postsurgical VVFs have an associated ureter injury (9) The choice of the diagnostic modality highly depends on resource availability and operator judgment
The timing of VVF repair is of utmost importance because the first attempt of treatment is correlated with the best possible outcome (3, 10) Timing of repair is subject to numerous factors, such as current illness, other comorbidities, nutritional status, and immunity of the patient This research also observes that the common waiting time from VVF diagnosis to repair was 12 weeks (79 6%) This finding is in agreement with the literature, reporting an expected waiting time of 12 weeks (3) Other waiting timing options reported were 2, 4, and 8 weeks with an equal response rate of 5% (3) The only exception to this timing is VVF caused by radiation, which usually needs about six months to 1 year of waiting time from diagnosis to repair (3, 4) This timing also considers tissue necrosis and subsi-
dence of inflammation after childbirth and postsurgical VVF (3) Other things that need to be considered are hemostasis and adequate vascular supply, sufficient exposure and tissue mobilization, and also tensionless suture (3) The transvaginal approach is also more favored in the repair of VVF, as also observed in previous studies (3, 4, 11, 12) In this research, 77 4% of surgeons choose transvaginal approach in VVF repair Furthermore, 30 7% of surgeons use a transvaginal approach in 100%, whereas 28% of surgeons use it in 75-100% of cases We found that all participants who did not perform the transvaginal approach were urologists, who usually preferred for the transabdominal approach based on familiarity and preferences acquired during residency This difference is becoming increasingly blurred as urologists gain more experience and comfort in transvaginal surgery for various d i s
favored because it significantly reduces the risk of hemorrhage, offers numerous interposition flaps options, implies a shorter surgery time and rapid recovery (3) However, abdominal approach should be considered if there are contraindications for transvaginal approach It should be also considered in presence of associated bladder stones or in the case of high-position fistula with an anatomically narrow vagina The most recommended transabdominal approach, which once was the gold standard for VVF repair, is the O’Connor procedure which includes an intraperitoneal approach The most used transabdominal method for VVF repair in the present study was the open t r a n s v e s i c a l a p p r o a c h ( 5 4 8 4 % ) f o l l o w e d b y o p e n transperitoneal transvesical (21 5%) and open transperitoneal extravesical approach (21 5%) In 7 5% of all cases, a laparoscopic approach was chosen The laparoscopic approach is relatively more efficient and less invasive, with less downtime and complications (14) There are still debates about the best transabdominal method, although it can be concluded that the most recommended procedure is most probably the procedure in which the operator feels most confident and trained (3, 4, 10)
Application of tissue transposition is made by only 45 2% of surgeons participating in the survey, whereas 50 5% surgeons do not There are differences in the type of tissue interposition between urologists and gynecologists, where 53 6% of urologists prefer to use omentum (65%) and labia fat fibrous tissue (46%) In comparison, only 20% of urogynecologists perform transposition flaps and prefer to use omentum and labial fat for tissue transposition equally Evans et al (12), found that a 100% success rate was observed in applying tissue transposition in repair, whereas a 63% success rate was observed in repair without tissue transposition However, a study by Pshak et al (15) found that the cure rate without tissue transposition application is 100% In our survey, surgeons mainly apply tissue transposition in the cases of recurrent VVF (81%), complex VVF (64 3%), and VVF due to radiation (35 7%)
The anatomical organ mostly used for tissue transposition is the omentum (71%), followed by labial fat-fibrous tissue and peritoneum Other tissue transposition flaps that can be used are gracilis muscle, and urinary bladder mucosa advancement flaps (10) As an alternative Floseal hemostatic matrix can be used Previous studies have stated that no technique is superior than another, and tissue
K Budi Santosa, S Novia Marta, Ronald Sugianto, et al
used for transposition depends on technical approach, surgeon ’ s clinical experience, and preference (4)
In our survey, only 46 2% surgeons routinely insert a ureteral catheter for ureter protection, whereas 50 5% do not This choice depends on considering the risk of ureteral injury during the dissection and suturing of the fistula Antimuscarinic medication benefits the patient by alleviating discomfort postoperatively and reducing bladder spasms (6, 16) Still, some surgeons choose to give antimuscarinics only if there is a complaint of urgency or discomfort during the use of the catheter instead of giving it routinely as seen in the results of our survey, where only 23 7% of surgeons administer antimuscarinic medication for patients during the use of the catheter
The overall success rate is defined as the overall percentage of all patients recovering completely, as clinically demonstrated by termination of constant leaking of urine after removal of the postoperative catheter (4) In this research, most surgeons report a 70-100% success rate at first attempt, regardless of the repair technique A similar success rate in the first attempt repair (70-100%), was found throughout the literature for both vaginal and abdominal approaches (17) One of the latest studies by Warner et al found a success rate at first attempt repair of 91% (vaginal) and 86% (abdominal) (18) However, success rates can be as low as 42% in other studies, which are negatively affected by the difficulty of repair (19)
Factors of repair failure are vaginal delivery and partial or total damage of the urethra, and also malignant etiology of the fistula and its further management by chemotherapy and radiotherapy that could delay the healing phase of the fistula repair (20) There are several nonrandomized cohort studies reporting results from both abdominal and vaginal procedures with overall closure rates at the first operation of 89% and 87%, respectively (21, 22) The authors considered a limitation of this study the fact that being the most preferred technique did not guarantee its superiority However, this is the first study that assesses the VVF treatment from the surgeon ’ s point of view, which might help and guide the VVF treatment based on Indonesian experiences The location of the hospital and the resources of the hospital may affect a differing clinical judgment in each case We recommended further research on VVF repair with population-based research and global surveys of fistula patient management in each hospital
CONCLUSIONS
Management of VVF in Indonesia was initiated with cystoscopy Most operators choose to repair VVF after 12 weeks, with the transvaginal technique being the most common approach The use of tissue interposition is usually done in a complex VVF Overall, the success rate for VVF repair in Indonesia is 70-100% at first attempt
ETHICAL APPROVAL
Ethical approval has been acquired in this study by Health Research Ethics Committee of Prof I G N G Ngoerah General Hospital, Denpasar, Indonesia with no 2267/ UN14 2 2 VII 14/LT/2023
REFERENCES
1 El-Azab AS, Abolella HA, Farouk M Update on vesicovaginal fistula: a systematic review Arab J Urol 2019; 17:61-8
2 Haroun A, Ali Mahamat M, Abdel Salam S, Cherif H, Jalloh M, Niang L, et al The epidemiological, clinical and therapeutical aspects of the vesico-vaginal fistula at the national fistula treatment center in N'apos Djamena Int J Clin Urol 2020; 4:34
3 Rajaian S, Pragatheeswarane M, Panda A Vesicovaginal fistula: review and recent trends Indian J Urol 2019; 35:250
4 Abrams P, de Ridder D, deVries C, Elneil S, Esegbona G, Mourad S, et al Obstetric fistula in the developing word ICUD-SIU International consultation, Marrakech, Morocco, October 13-16, 2010
5 Lo TS, Chua S, Wijaya T, Kao CC, Uy-Patrimonio MC Clinical relevance and treatment outcomes of vesicovaginal fistula (VVF) after obstetric and gynecologic surgery Taiwan J Obstet Gynecol 2019; 58:111-6
6 Mukti NA, Mochtar AA, Wiyati PS Kejadian fistula urogenital pada perempuan di RSUP Dr Kariadi Semarang 2018; 7:16
7 Harding CK, Lapitan MC, Arlandis S, Bo K, Cobussen-Boekhorst H, Costantini E, et al EAU Guidelines on Management of NonN e u r o g
Guidelines 2023 2023:91-95
8 Adibarata MA, Aditya R, Gumilar KE, Pascawardhana M, Wicaksono B, Ernawati, et al Bacterial vaginosis in gynecologic outpatient clinic Dr Soetomo Hospital January - June 2017: A Cross Sectional Study In Proceedings of the 23rd Regional Conference of Dermatology (RCD 2018), Scitepress 2021, pp 307-311
9 Goodwin WE, Scardino PT Vesicovaginal and ureterovaginal fistula: a summary of 25 years of experience J Urol 1980; 123: 370-4
10 Shrestha DB, Budhathoki P, Karki P, Jha P, Mainali G, Dangal G, et al Vesico-vaginal fistula in females in 2010-2020: a systemic review and meta-analysis Reprod Sci 2022; 29:3346-3364
11 Margules AC, Rovner ES The use of tissue flaps in the management of urinary tract fistulas Curr Urol Rep 2019; 20:32
12 Singh V, Mehrotra S, Bansal A, Akhtar A, Sinha RJ Prospective randomized comparison of repairing vesicovaginal fistula with or without the interposition flap: result from a tertiary care institute in Northern India Turk J Urol 2019; 45:377-83
13 Warner R, Beardmore-Gray A, Pakzad M, Hamid R, Ockrim J, Greenwell T The cost effectiveness of vaginal versus abdominal repair of vesicovaginal fistula Int Urogynecology J 2020; 31:1363-9
14 Giannakopoulos S, Arif H, Nastos Z, Liapis A, Kalaitzis C, Touloupidis S Laparoscopic transvesical vesicovaginal fistula repair with the least invasive way: only three trocars and a limited posterior cystotomy Asian J Urol 2020; 7:351-6
15 Pshak T, Nikolavsky D, Terlecki R, Flynn BJ Is tissue interposition always necessary in transvaginal repair of benign, recurrent vesicovaginal fistula? Urology 2013; 82:707-12
16 Breen M, Ingber M Controversies in the management of vesicovaginal fistula Best Pract Res Clin Obstet Gynaecol 2019; 54:61-72
1 7 S t a m a t a k o s M , S a r g e d i C , S t a s i n o u T , K o n t z o g l o u K Vesicovaginal Fistula: diagnosis and management Indian J Surg 2014; 76:131-6
18 Warner R, Beardmore-Gray A, Pakzad M, Hamid R, Ockrim J, Greenwell T The cost effectiveness of vaginal versus abdominal repair of vesicovaginal fistula Int Urogynecology J 2020; 31:1363-9
19 Bernard L, Giles A, Fabiano S, Giles S, Hudgins S, Olson A, et al
Predictors of obstetric fistula repair outcomes in Lubango, Angola J Obstet Gynaecol Can 2019; 41:1726-33
20 Delamou A, Delvaux T, Beavogui AH, Toure A, Kolié D, Sidibé S, et al Factors associated with the failure of obstetric fistula repair in Guinea: implications for practice Reprod Health 2016; 13:135
Correspondence
Kadek Budi Santosa (Corresponding Author) busanbsa@gmail com
Department of Urology, Faculty of Medicine, Universitas Udayana
Prof Dr I G N G Ngoerah General Hospital, Denpasar Jl PB Sudirman, Denpasar 80232, Bali, Indonesia
Stacia Novia Marta stacianoviamarta@gmail com
Prof Dr I G N G Ngoerah General Hospital, Denpasr Department of Surgery, Faculty of Medicine, Universitas Udayana
Ronald Sugianto ronald sugianto-2023@fk unair ac id
Prof Dr I G N G Ngoerah General Hospital, Denpasar Department of Urology, Faculty of Medicine, Universitas Airlangga
Fina Widia finawidia@yahoo com
Department of Urology, Faculty of Medicine, Universitas Indonesia, Cipto Mangunkusumo General Hospital, Jakarta
Parsaoran Nababan saornbbn@gmail com
Department of Urology, Bhayangkara Anton Soedjarwo Hospital, Pontianak
Harrina Erlianti Rahardjo harrinaerlianti@gmail com
Department of Urology, Faculty of Medicine, Universitas Indonesia, Cipto Mangunkusumo General Hospital, Jakarta
Conflict of interest: The authors declare no potential conflict of interest
21 Hilton P Urogenital fistula in the UK: a personal case series managed over 25 years BJU Int 2011; 110:102-10
22 Ockrim JL, Greenwell TJ, Foley CL, Wood DN, Shah PJR A tertiary experience of vesico-vaginal and urethro-vaginal fistula repair: factors predicting success BJU Int 2009; 103:1122-6
K Budi Santosa, S Novia Marta, Ronald Sugianto, et al
CASE SERIES
Prostatic artery embolization for intractable hematuria in patients with unregulated coagulation parameters: Three case reports
1 Department of Surgery, Division of Urology, McGill University Health Center, Montreal, Canada;
2 Department of Surgery, Faculty of Medicine, Rabigh, King Abdulaziz University, Jeddah, Saudi Arabia;
3 Department of Urological Sciences, University of British Columbia, Vancouver, Canada;
4 Department of Radiology, McGill University, Montreal, Canada
* Co-First Author
Summary
Introduction: Benign prostatic hyperplasia is a prevalent disease that could be responsible of severe intractable hematuria requiring invasive surgical management.
Case presentation: We report three high-risk cases presented with intractable hematuria of prostatic origin with high medical co-morbidities treated safely and effectively by prostatic artery embolization with favorable outcomes
Conclusions: In non-surgical, anticoagulated patients, prostatic artery embolization represents a safe and effective intervention for the treatment of intractable hematuria related to benign prostatic hyperplasia
Submitted 24 February 2024; Accepted 9 February 2024
INTRODUCTION
Benign prostatic hyperplasia (BPH) is a prevalent disease, affecting up to 50% of men over the age of 50, usually associated with lower urinary tract symptoms (LUTS) (1) Intractable hematuria represents a severe complication of BPH, which often requires invasive management (2) W h i l e t r a n s
( T U R P ) remains the mainstay therapy for BPH, laser enucleation techniques represent the standard of care for the surgical treatment of larger prostates or in anticoagulated patients (3, 4) However, elderly or co-morbid patients may be at high medical risk for the prolonged anesthesia-time associated with laser TURP In these cases, non-surgical treatment for BPH, such as prostatic artery embolization (PAE), may be considered PAE consists of embolization of selected prostatic arteries to produce ischemic necrosis and shrinkage of the prostate gland (5, 6) Arterial embolization has previously been described for treatment of intractable hematuria due to prostate and bladder pathologies (7, 8) However, to the best of our knowledge, PAE for the treatment of intractable hematuria in co-morbid BPH patients with unregulated coagulation
parameters has yet to be described This case series presents three patients of high medical risk with intractable hematuria of prostatic origin, where PAE was performed and resulted in the resolution of prostatic hemorrhage
CASE PRESENTATION
Case 1
A 91-year-old man presented with a 48-hour history of p a i n l e s s g r o s s h
included BPH with voiding LUTS, atrial fibrillation on Edoxaban, left cortical stroke, dyslipidemia, hypertension and right-sided heart failure with ascites Hemoglobin was 111 g/L at arrival, while pre-procedure hemoglobin was 89 g/L (baseline 120 g/L) Anticoagulation was held at arrival and daily subcutaneous thromboprophylaxis was prescribed The prostate gland volume was 200cc on computed tomography (CT) (Figure 1) Cystoscopy confirmed the prostate gland was the origin of the hematuria Continuous bladder irrigation (CBI) was performed for 10 days, with no resolution of symptoms Given the multiple medical comorbidities, this patient was not a candidate for surgery and was offered PAE, which he accepted The patient was on CBI for 5 days post-PAE before the resolution of the gross hematuria and passed the trial of void on day 6 Anticoagulation therapy was resumed on day 7 post-PAE At 6-month follow-up, the patient was voiding well and had no recurrence of hematuria
Case 2
An 85-year-old man presented with recurrent gross hematuria for one month with clots, complicated by urinary retention and infection Previous medical history included BPH, atrial flutter on Apixaban, sick sinus syndrome with pacemaker, coronary artery bypass surgery, type 2 diabetes mellitus and hypertension At presentation, hemoglobin was 84 g/L (baseline 115 g/L) and required transfusion of 2 units of packed red blood cells (PRBC) The prostate gland volume was 120cc on CT
scan Cystoscopy confirmed the prostate as the source of the bleeding Symptoms did not resolve after 7 days of CBI Given the multiple cardiac comorbidities and minimal LUTS prior to presentation, PAE was preferred by the patient The anticoagulation was held 24 hours prior to the intervention The patient had no reoccurrence of hematuria and passed trial of void at day 1 post PAE intervention; anticoagulation therapy was resumed then, and he was discharged from hospital on post-intervention day 2 At 1-month follow-up, he reported an improvement in LUTS and no recurrence of hematuria; he was subsequently lost to follow-up
Case 3
A 78-year-old man was transferred to our center in the context of an intractable prostatic hemorrhage nonresolving after 30 days of CBI Patient was previously known for atrial fibrillation on Warfarin, hypertension, type 2 diabetes mellitus, morbid obesity, and chronic urinary retention secondary to BPH The prostate volume was 150cc measured on CT On arrival, hemoglobin level was 78 g/L (baselines 121 g/L) and raised to 96 g/L after receiving 2 units of PRBC transfusion The cystoscopy confirmed the bleeding originated from the prostate Surgery did not represent a safe treatment option for this patient given the significant medical comorbidities and associated anesthetic risk As such, PAE was offered and
Figure 1.
Prostate gland measurements pre-angioembolization for patient described in Case 1 (axial and sagittal views)
accepted by the patient Anticoagulation therapy was held 24 hours prior to the intervention The patient had resolution of gross hematuria on post-procedure day 1 He resumed anticoagulation therapy day 1 post-intervention At 6-month follow-up, he had no reoccurrence of gross hematuria and LUTS had also improved
Prostatic artery embolization technique description Technically, PAE was achieved under local anesthetic ( X y l
Ultrasound was performed prior to the puncture to assess f o r t h
Subsequently, the right common femoral artery was punctured, permitting the insertion of a 5-French regular vascular sheath A 5-French Cobra (Cook, Bloomington, IN, USA) catheter was used for the internal iliac artery catheterizations and a 2-French ProGreat microcatheter (Terumo, Somerset, NJ, USA) and Fathom™ 0 016 inch wire (Boston Scientific, Marlborough, MA, USA) were used for the catheterization of the prostatic arteries The microcatheter was advanced in the prostatic arteries beyond any significant side branches supplying the bladder, rectum or penis and its placement was confirmed using cone-beam CT The PErFecTED technique (Proximal Embolization First, Then Embolize Distal) was performed This technique, when possible, has been associated with greater degree of prostatic ischemia and infarc-
Figure 2a.
Angiogram of prostatic arteries right lobe of the prostate pre and post angioembolization, respectively (patient in case 1). Note the absence of the prostatic parenchymal blush (arrow) post embolization.
M Belmonte, A Khogeer, G Moussaoui, et al
3
Figure 2b. Angiogram of the left lobe of the prostate pre and post angioembolization, respectively (patient in case 1)
Visualization of the penile arteries (arrows) prior to angioembolization of the left prostatic artery (block arrow)
tion, thus leading to better clinical outcomes (13) Embolization was performed using Embospheres 300500 um (Merit Medical, South Jordan, UT, USA) diluted in 20 mL 1:1 ratio of contrast to saline injected in 1 ml aliquots followed by 3 ml normal saline flush between aliquots until complete stasis was obtained (Figure 2a) A similar technique was performed on both sides, always making sure to avoid non-targeted embolization via collaterals to other critical arterial structures such as the penile arteries (Figures 2b, 3)
DISCUSSION
Prostate hemorrhage represents a severe complication of BPH, and rapid control of the bleeding is necessary to avoid morbidity associated with intractable gross hematuria Medical therapies, such as 5-alpha reductase inhibitors, have previously been proposed as treatment avenues in BPH-related gross hematuria (9) However, time to response, particularly in patients with larger prostates, has been reported to be on average 10 days or longer (9) When conservative management fails, surgical procedures such as TURP or Holmium laser enucleation of the prostate often represent the best treatment option for patients While regional anesthesia is preferred for these interventions, it may be contraindicated due to patients’ anticoagulation status Consequently, prolonged general anesthesia is used, which increases the risk for
perioperative complications in anticoagulated patients with cardiac or metabolic comorbidities (10) PAE represents a minimally invasive procedure performed under local anesthesia Embolization of the prostatic arteries was previously shown to improve LUTS and preserve sexual function scores in patients with BPH (11) A previous study, where patients with unregulated coagulation parameters were excluded, has reported on the use of PAE for the treatment of BPH related gross hematuria and found the intervention to be safe for non-surgical candidates (7) In this case series, we presented three non-surgical candidates on anticoagulation therapy who successfully underwent PAE In all 3 cases, no immediate complications occurred None of the patients developed infection, and groin pain was not a complaint our participants reported
Complete resolution of the intractable hematuria was seen in all cases, with no reoccurrence at a minimum of 6-months’ follow-up While PAE represents a non-inferior alternative to TURP, it is not void of limitations (12)
The access to this procedure in the community is limited and anatomical variants or severe atherosclerotic disease render the procedure difficult and sometimes impossible
The follow-up times for the patients in our series is short, limiting the assessment of the durability of the hemostatic effect of PAE
CONCLUSIONS
PAE represents a safe and effective intervention for the treatment of BPH-related intractable hematuria in nonsurgical and anticoagulated patients Our experience with PAE in high-risk patients has been favourable and warrants further investigation with a larger cohort and longer follow-up
REFERENCES
1 Berry SJ, Coffey DS, Walsh PC, Ewing LL The development of human benign prostatic hyperplasia with age J Urol 1984; 132:474-9
Figure
2 Ramyil VM, Dakum NK, Liman HU, Udeh EI The management of prostatic haematuria Niger J Med 2008; 17:439-42
3 Elzayat EA, Elhilali MM Holmium laser enucleation of the prostate (HoLEP): the endourologic alternative to open prostatectomy Eur Urol 2006; 49:87-91
4 Elzayat E, Habib E, Elhilali M Holmium laser enucleation of the prostate in patients on anticoagulant therapy or with bleeding disorders J Urol 2006; 175:1428-32
6 Kuang M, Vu A, Athreya S A Systematic Review of Prostatic Artery Embolization in the Treatment of Symptomatic Benign Prostatic Hyperplasia Cardiovasc Intervent Radiol 2017; 40:655663
7 Tian W, Zhou C, Leng B, et al Prostatic Artery Embolization for Control of Gross Hematuria in Patients with Benign Prostatic Hyperplasia: A Single-Center Retrospective Study in 20 Patients J Vasc Interv Radiol 2019; 30:661-667
8 Mohan S, Kumar S, Dubey D, et al Superselective vesical artery embolization in the management of intractable hematuria secondary to hemorrhagic cystitis World J Urol 2019; 37:2175-2182
9 Kearney MC, Bingham J, Bergland R, et al Clinical predictors in the use of finasteride for control of gross hematuria due to benign prostatic hyperplasia J Urol 2002; 167:2489-2491
10 Hanson RA, Zornow MH, Conlin MJ, Brambrink AM Laser resection of the prostate: implications for anesthesia Anesth Analg 2007; 105:475-9
11 Feng S, Tian Y, Liu W, et al Prostatic Arterial Embolization
Cardiovasc Intervent Radiol 2017; 40:22-32
12 Abt D, Hechelhammer L, Müllhaupt G, et al Comparison of prostatic artery embolisation (PAE) versus transurethral resection of the prostate (TURP) for benign prostatic hyperplasia: randomised, open label, non-inferiority trial BMJ 2018; 361:k2338
13 Carnevale FC, Moreira AM, Antunes AA The "PErFecTED technique": proximal embolization first, then embolize distal for benign prostatic hyperplasia Cardiovasc Intervent Radiol 2014; 37:1602-5
Correspondence
Manuel Belmonte, MD manuel belmontecg@gmail com
Mélanie Aubé-Peterkin, MD, FRCSC (Corresponding Author) melanie aube-peterkin@muhc mcgill ca Carrier Serge, MD serge carrier@mcgill ca McGill University Health Centre 1001 Décarie Blvd, Montreal, Quebec H4A 3J1, Canada
Abdulghani Khogeer, MD dr-abdulghani@hotmail com
Department of Surgery, Faculty of Medicine, Rabigh, King Abdulaziz University, Jeddah, Saudi Arabia
Ghizlane Moussaoui, MD ghizlane moussaoui@mail mcgill ca
Department of Urological Sciences, University of British Columbia, Vancouver, Canada
Rafael Melo, MD rcardosodemelo@gmail com
Louis-Martin Boucher, MD lmboucher@yahoo com
Tatiana Villalpando-Cabrera, MD tacaal@hotmail com
Department of Radiology, McGill University, Montreal, Canada
Conflict of interest: The authors declare no potential conflict of interest
M Belmonte, A Khogeer, G Moussaoui, et al
CASE REPORT
An unusual “linitis plastica” like breast cancer bladder metastasis
1 Department of Surgery, Unit of Urology, ARES Sardegna, ASL Sulcis, Sirai Hospital, Carbonia, Italy; 2 Pathology Department, ARES Sardegna - ASL Cagliari, SS Trinità Hospital, Cagliari, Italy
Summary
Breast cancer (BrC) is the most frequently diagnosed malignancy in woman and most BrC related deaths are due to metastasis. BrC frequently metastasizes to the lymph nodes, liver, lung, bone and brain while the urinary bladder is considered as an unusual site for breast metastasis We report a case of bladder metastasis identified in a patient with past BrC history, presenting with hematuria, low urinary tract symptoms, and hydronephrosis
KEY WORDS: Bladder metastasis; Breast cancer; Breast cancer metastasis
Submitted 16 March 2024; Accepted 28 March 2024
INTRODUCTION
BrC is the most frequently diagnosed malignancy in women with an estimated 1 6 million new cancer cases diagnosed worldwide (1) Incidence of BrC show variability across different countries It is highest in Australia, Europe and North America, reflecting discrepancies in early diagnosis and in the entity of risk factors Although we actually have effective screening programs and therapies, it remains the leading cause of death because of metastatic disease BrC in fact usually metastasizes to lymph nodes, bone, lung and liver, while bladder metastasis is very uncommon, accounting for about 2 4% of all bladder metastasis (2) We present the case of 75-year-old woman with severe hematuria and a history of breast cancer
CASE REPORT
In January 2023 we hospitalized a 75-year-old woman suffering from dementia from the Emergency Department due to the appearance of severe hematuria and dysuria Her past medical history showed hypothyroidism, hypercholesterolemia, bilateral hearing loss In 2018 she underwent a left nipple sparing mastectomy and contextual axillary lymphadenectomy Histopathological examination showed an infiltrating lobular carcinoma pT2G2N2 (6/15 positive lymph nodes, RE=90% RPg=34% Ki67=18% Her2: +--)
The patient at the time was not eligible for adjuvant chemotherapy due to the time since diagnosis, so she received letrozole and locoregional radiotherapy from 03/27/2019 to 05/03/2019 The patient then adequately adhered to the follow-up protocol At the emergency-
urgency department she underwent an abdominal ultrasound which showed a markedly thickened urinary bladder (max 10 4 mm), with finely corpuscular contents as of blood nature and bilateral hydronephrosis (Figure 1)
Blood tests demonstrated a slight increase in serum creatinine (1 42 mg/dL) and mild anemia (HBG 11 3 g/dL)
Contrast- enhanced CT scan showed diffuse and marked thickening of the entire urinary bladder (10 4 mm max) with contextual inhomogeneity of the perivesical fat, particularly affecting the Retzius space, bilateral hydronephrosis and numerous osteolytic skeletal lesions affecting the vertebral metameres from D10 to L2, proximal diaphysis of the left femur and left iliac wing (Figure 2) We decided to proceed with a transurethral resection of the bladder Cystoscopy showed a bladder with little distensibility and erythematous mucosa, in the absence of clear vegetating neoplasms The ureteral meatuses could not be recognized We then proceeded to perform a TURB for hemostatic and biopsy purposes TURB specimen showed proliferation of cells CK19+, CK34BE12+, PgR+, ER- (Figure 3) compatible with poorly differentiated epithelial neoplasia and suspected of breast cancer primitiveness The poor performance status made the patient ineligible for any oncological therapy
DISCUSSION
BrC is the most frequent cancer in women worldwide The most common sites of metastasis are bone, lung, liver and brain The urinary bladder is rarely involved, being only about 4 5% of all bladder metastases derived from solid tumors (2) and typically the majority of cases are secondary to direct invasion by pelvic neoplasms (3) Bladder metastases deriving from BrC accounts for about 2 4% of all bladder metastases (2), they usually are expression of systemic disease (9) and rarely occur as solitary metastases (4) A review of the literature showed about 65 cases of BrC bladder cancer metastases published (5) The majority of BrC bladder metastases derives from an invasive lobular carcinoma (ILC) rather than an invasive ductal carcinoma (IDC): ILC has in fact a particular tropism for serosal surfaces such as gastrointestinal and gynecological tracts, and from these two last sites metastases can then spread to the bladder (6) They can present as exophytic mass, thickening of the bladder wall or nonspecific mucosal phlogistic areas
1. Ultrasound of the bladder showing diffuse bladder wall thickening
2 CT scan demonstrating thickening of urinary wall.
The most common clinical presentation is characterized by asymptomatic gross hematuria, lower urinary tract symptoms in case of detrusor involvement, flank pain because of hydronephrosis with renal failure and sepsis, but early stages can be asymptomatic (7)
The diagnostic workshop of the patient must include ultrasounds, CT scans and cystoscopy Endoscopy can be used to stop hematuria by transurethral resection of bladder (TURB) (7), possibly to visualize ureteral meatus in case of need for ureteral stent placement, but most of all to obtain biopsy samples Despite of all, the past clinical history of the patient remains fundamental in formulating the suspicion of bladder metastases
Prognosis is similar to that of any metastatic BrC, with an average survival of 18-30 months (8), while the gold standard treatment is a combination of endocrine therapy and chemotherapy Radiotherapy also can have a role in controlling hematuria
R Farci, S Tolu, M Trombetta, et al
Figure
Figure
Figure 3. Histopathology image of specimen: demonstration of PR positive BrC cells
CONCLUSIONS
BrC urinary bladder metastases are a rare disease and the differential diagnosis compared to other pathologies with similar symptoms can be complex, and the Physician need to take into consideration this possibility in all women with past history of BrC presenting with urinary symptoms (9)
REFERENCES
1 Torre LA, Bray F, Siegel RL, et al Global Cancer Statistics, 2012 CCA Cancer J Clin 2015; 65:87-108
2 Bates AW, Baithun SL The significance of secondary neoplasms of the urinary and male genital tract Virchows Arch 2002; 440:640-647
3 Cormio L, Sanguedolce F, Di Fino G, et al Asymptomatic bladder metastasis from breast cancer Case Rep Urol 2014; 2014:672591
4 Zagha RM, Hamawy KJ Solitary breast cancer metastasis to the bladder: an unusual occurrence Urol Oncol 2007; 25:236-239
5 Karjol U, Jonnada P, Cherukuru S, et al Bladder metastasis from breast cancer: a systematic review Cureus 2020; 12:e7408
6 Ferlicot S, Vincent-Salomon A, Médioni J, et al Wide metastatic spreading in infiltrating lobular carcinoma of the breast Eur J Cancer 2004; 40:336-341
7 Ramsey J, Beckman EN, Winters JC Breast cancer metastatic to the urinary bladder Ochsner Journal information 2008; 8:208-212
8 Gennari A, Conte P, Rosso R, et al Survival of metastatic breast carcinoma patients over a 20-year period: a retrospective analysis based on individual patient data from six consecutive studies Cancer 2005; 104:1742-1750
9 De Rose AF, Balzarini F, Mantica G, et al Late urinary bladder metastasis from breast cancer Arch Ital Urol Androl 2019; 91:60-62
Correspondence
Riccardo Farci, MD (Corresponding Author) riccardo farci@aslsulcis it - Urology Department Andrea Solinas, MD - Urology Department andreasolinas@aslsulcis it Simona Tolu, MD
simona tolu@aslsulcis it - Oncology Department Alessandro Murgia, MD alessandro murgia@aslsulcis it - Radiology Department ARES Sardegna - ASL Sulcis, Sirai Hospital Via Ospedale, 09013 Carbonia, Italy
Matilde Trombetta, MD matilde trombetta@aslcagliari it
Pathology Department, ARES Sardegna - ASL Cagliari, SS Trinità Hospital Via Is Mirrionis 92, 09121 Cagliari, Italy
Conflict of interest: The authors declare no potential conflict of interest
CASE REPORT
Management of an elderly patient with retention of a steel nail in the scrotum: A case report
Background: The retention of foreign bodies inside the body during ludic/sexual procedures or for traumatism represents one of the causes of visits to accident and emergency departments that often requires surgical removal of the foreign body. However, there are cases where the discovery of such foreign bodies takes place after many years, as in patients that are slightly compromised from a neuro-sociological point of view
Case presentation: A 76-year-old male presented to an outpatient urological examination due to an increase in scrotal volume. At the ultrasound check, an acoustic interference from a solid object was detected, for which computed tomography was requested. The computed tomography scan revealed the presence of an elongated metal body in the perineum
The removal of the foreign body in the operating theatre was then scheduled A 10 cm long stainless-steel nail located within an abscessed foreign body granuloma was identified and removed via a scrotal access
Four days later, a new surgical toilet was performed due to minimal necrosis of the skin flaps The patient then performed three more dressings in the operating theatre during the following week Healing took place by secondary intention until a perfect healing of the surgical wound was obtained
Conclusions: Removal of foreign bodies from the perineum in case of infection can be challenging Careful attention and postoperative dressings are crucial for the success of the case.
Submitted 6 February 2024; Accepted 10 February 2024
INTRODUCTION
The choice of access, strategy, and timing for the removal of foreign bodies is determined by their shape, size, location, and potential mobility They often require careful and sometimes multidisciplinary planning for strategy optimization Although it remains uncommon in everyday practice, a rapid surgical exploration of penetrating scrotal injury is nevertheless required to accurately evaluate the involvement of genitourinary and reproductive organs (1)
In this paper, we describe the sensitive management of a patient with a rare finding of a nail of about 12 cm lodged in the scrotum and enclosed within an abscess
CASE REPORT
A 76-year-old man presented as an outpatient at Apuane Hospital (Massa, Italy) in January 2022, having noticed a volumetric increase in the scrotum for some years (Figure 1)
His past medical history was significant only for a remote history of childhood exanthematous diseases and a picture of initial decline in cognitive function The patient did not report recent trauma or episodes of scrotum-perineal pain
On physical examination, an enlarged scrotum with a firm mass that was not tender to palpation was noted An in-office ultrasound identified uneven tissue and the presence of a reflective foreign body An abdominal-pelvic CT scan confirmed the presence of a radio-opaque, ‘beaded’ foreign body in the scrotum (Figure 2) with testicles in place and uninjured
One week later, he was admitted to the hospital Under assisted spinal anesthesia in the lithotomy position, a scrotoperineal access was performed using a cruciate ‘Mercedes-like’ incision
The median incision of the cross allowed the opening of the scrotal bags and the vaginal tunics, with isolation of the right and left spermatic cords, and of the testicles, bilaterally The spermatic cords were isolated and the testicles secured and lateralized with a wider exposure of the operative field
Surgical exploration revealed the presence of an abscess with a capsule adherent to the surrounding tissues that was clearly identifiable The capsule was gently detached from the surrounding planes where it had created strong adhesions The detachment was guided by the finger with tactile perception of the foreign body retained inside the abscess During the procedure, the abscess capsule burst open, causing brown pus to ooze out; liquid cultures were sent The foreign body was kept in place until complete excision of the sheath to create a guide for the direction of the abscess capsule in order to completely excise it
The foreign body was found to be a 10-cm stainless steel nail (Figure 3)
Once the abscess and the foreign body were removed, a surgical toilet was performed, including multiple washings of the field with povidone iodine and hydrogen peroxide The final washing was carried out with abundant saline solution A povidone iodine gauze and two suction
Iacopo Meneghetti 1 , Novella Cesta 2 , Luca Mosillo 1 , Simone Belli 1 , Daniele Bianchi 1 , Maurizio De Maria 1
Figure 1.
Aspect of the preoperative clinical picture of the case
Note the increase in scrotal volume due to the retention of the foreign body.
2.
Figure 3
Extracted stainless steel nail and capsules of the abscess surrounding the foreign body
CT scan evidenced the presence of an abundant, apparently biloculated effusion in the scrotal area which cranially reached the left gluteal region In the scrotal area, the presence of a linear metallic image was also noted
drains (airtight) were left in place with partial closure of the superficial planes A second look was scheduled on the fourth postoperative day During the second look, the tips of the skin flaps appeared blackish as a sign of ischemic suffering for a few millimeters from the free edge, so they were trimmed with a cold knife until bleeding vital tissue was reached The wound was again cleaned with povidone iodine, and one suction drain was again applied Two days later, a third look found vital tissues, so deep-tissue debridement of the wound was performed At fourth and fifth look in the operating theatre on the eighth and tenth days, respectively, a deep disinfection of the field was performed and the skin flaps were brought together so that there was no tension, leaving a very small space in the center of the star with the aim of healing by secondary intention
During the remaining hospitalization, the patient was treated daily with povidone iodine disinfection He was discharged on the 16th postoperative day with a bladder catheter
A n t i b i o t i c t h e r a p y w i t h i
avenous ceftriaxone 2gr q24h was empirically started A blood culture was negative for bacteria, and no microbiological growth was detected in the samples collected during surgery
Because of the persistence of elevated serum C-reactive protein (17 ng/ml), on the third postoperative day, the therapy was modif i e d
4 5 gr q8h by the infectious diseases consultant and continued for three weeks
The patient removed the bladder catheter on the 30th day as an outpatient, with clear urine output and no postvoiding residue Dressings were applied at home by the patient daily and every week in the clinic for six weeks At the final check-up at two months, the wound was completely healed and the patient was fine
DISCUSSION
An operation to remove a foreign body must always be planned in detail A CT is essential to evaluate the location of the foreign body and associated abscess structures and the organs involved The surgeon also needs a CT to be able to choose the best access to ensure adequate exposure of the fields, as not completely cleaning of an infected area is the first step for the therapeutic failure
I Meneghetti, N Cesta, L Mosillo, et al
Figure
The ‘Mercedes-like’ scrotal incision was a winning choice, as it allowed a wide exposure of the field on the perineal plane with the incision on the scrotal raphe, along with bilateral exposure of the testicles with a single median cut Each arm of the cross measured approximately 5 cm, with vertical midline incision on the scrotal raphe to the base of the scrotum, the point at which the center of the cross was therefore located The other two arms were directed laterally, thus distancing themselves from the anus In our opinion, a strong point of the procedure was the complete removal of the surrounding abscess capsule, thanks to the use of the tactile sensation, which, in following the nail, allowed a delicate and relatively safe excision Unfortunately, with the opening of the abscess cavity, the surrounding tissues became contaminated These were promptly washed thoroughly in order to reduce the risk of spreading the infection to the surrounding field
A key concept for the healing all wounds, with particular attention to dirty areas such as the perineal region, is keeping them clean and uncontaminated (2)
Also, Hartz et al reported that in their experience of 100 patients with perineal wounds, those who received primary closure with immediate suction drainage had the best outcomes compared to those left open with simple p a c k i n g a n d t h o s e w h o h a d n o n - s u c t i o n p
n e a l drainage (3) We used hydrogen peroxide in the first procedure and the two following daily dressings in the ward due to its action on anaerobic bacteria However, its aggressive action on the tissues prompted us to limit its use in subsequent dressings for fear of injuring the tissues and delaying their healing In fact, uncontrolled hydrogen peroxide generation in tissues can result in chronic inflammation, which could contribute to delayed healing of the wound (4)
In our centre, we tend to use and prefer the use of povidone iodine both for the dressing of infected wounds and for the dressing of ordinary surgical wounds, due to its broad antimicrobial spectrum, lack of resistance, efficacy against biofilms, good tolerability, and effect on excessive inflammation (5)
The prompt identification and cleaning of the ischemic flaps were crucial for a speedy recovery and improved survival During the first three postoperative days, there were no signs of local or systemic worsening of the picture, and for this reason, we waited until the fourth postoperative day when the ischemic flaps were promptly identified An earlier debridement, in our opinion, would not have allowed us to identify the affected areas where curettage should be carried out Kline et al suggested a low threshold for returning to the operating room for examination under anesthesia and additional surgical debridement within 24 to 48 hours, especially in patients with extensive initial debridement (6)
We extended the antibiotic therapy from the time of the procedure until discharge on day 21
In principle, it is recommended that antibiotic therapy be interrupted when operative procedures other than a dressing are no longer indicated and control of the infectious source has been achieved Lauerman et al , evaluating antibiotic duration and outcomes in Fournier’s gangrene, showed no difference in outcomes in patients receiving
fewer than seven days of therapy compared with longer durations (7)
CONCLUSIONS
The management of patients with foreign bodies inserted into the perineum must be guided by common sense and cardinal principles, as each case is a story unto itself When the case is complicated by an infection, great attention and care must be taken to prevent it from evolving into a situation of extensive or systemic infection that is much more complex to manage
REFERENCES
1 Morey AF, Metro MJ, Carney KJ, et al Consensus on genitourinary trauma: external genitalia BJU Int 2004; 94:507-15
2 Del Pino A, Abcarian H The difficult perineal wound Surg Clin North Am 1997; 77:155-74
3 Hartz RS, Poticha SM, Shields TW Healing of the perineal wound Arch Surg 1980; 115:471-4
4 Zhu G, Wang Q, Lu S, et al Hydrogen Peroxide: A Potential Wound Therapeutic Target? Med Princ Pract 2017; 26:301-308
5 Bigliardi PL, Alsagoff SAL, El-Kafrawi HY, et al Povidone iodine in wound healing: A review of current concepts and practices Int J Surg 2017; 44:260-268
6 Kline BP, Jeganathan NA Necrotizing Soft Tissue Infections of the Perineum Clin Colon Rectal Surg 2022; 35:237-243
7 Lauerman MH, Kolesnik O, Sethuraman K, et al Less is more? Antibiotic duration and outcomes in Fournier’s gangrene J Trauma Acute Care Surg 2017; 83:443-448
Correspondence
Iacopo Meneghetti, MD, FEBU (Corresponding Author) iacopo meneghetti@tiscali it
Conflict of interest: The authors declare no potential conflict of interest
REVIEW
The role of immunotherapy in urological cancers
Efe Bosnali 1 , Enes Malik Akdas 2 , Engin Telli 2 , Kerem Teke 2 , Onder Kara 2
1 Department of Urology, University of Health Sciences, Derince Training and Research Hospital, Kocaeli, Turkey;
2 Department of Urology, School of Medicine, Kocaeli University, Turkey
Summary
Immunotherapy is defined as a therapeutic approach that targets or manipulates the immune system A deeper understanding of the cellular and molecular composition of the tumour environment, as well as the mechanisms controlling the immune system, has made possible the development and clinical investigation of many innovative cancer therapies Historically, immunotherapy has played an essential role in treating urologic malignancies, while in the modern era, the development of immune checkpoint inhibitors (ICIs) has been critical to urology
Urothelial carcinoma is a common type of cancer in the genitourinary system, and treatment strategies in this area are constantly evolving. Intravesical and systemic immunotherapeutic agents have begun to be used increasingly frequently in treating urothelial carcinoma. These agents increase the anti-tumour response by affecting the body's defence mechanisms
Immunotherapeutic agents used in urothelial carcinoma include various options such as BCG, interferon, anti-PD-1 (pembrolizumab, nivolumab) and anti-PD-L1 (atezolizumab, avelumab, durvalumab)
Renal cell carcinoma (RCC) has been known for many years as a tumour with unique sensitivity to immunotherapies The recent emergence of ICIs that block PD-1/PD-L1 (pembrolizumab, nivolumab, atezolizumab) or CTLA4 (ipilimumab) signalling pathways has reestablished systemic immunotherapy as central to the treatment of advanced RCC In light of randomized clinical trials conducted with increasing interest in the application of immunotherapies in the adjuvant setting, combination therapies (nivolumab/ipilimumab, nivolumab/cabozantinib, pembrolizumab/axitinib, pembrolizumab/lenvantinib) have become the standard first-line treatment of metastatic RCC
Prostate cancer is in the immunologically "cold" tumour category; on the contrary, in recent years, immunotherapeutic agents have come to the fore as an essential area in the treatment of this disease Especially in the treatment of castration-resistant prostate cancer, immunotherapeutic agents constitute an alternative treatment method besides androgen deprivation therapy and chemotherapy. Ipilimumab, nivolumab, pembrolizumab, atezolizumab, and Sipuleucel T (Vaccine-based) are promising alternative treatment options.
Considering ongoing randomized clinical trials, immunotherapeutic agents promise to transform the uro-oncology field significantly In this review, we aimed to summarize the role of immunotherapy in urothelial, renal and prostate cancer in the light of randomized clinical trials
Submitted 24 January 2024; Accepted 10 February 2024
INTRODUCTION
The immune system plays a vital role in preventing and defending against cancer In recent years, significant advances have been made in understanding the immune system and its role in cancer
Immunotherapy is the golden child of medical oncology and a new approach to cancer treatment (1) The origin of immunotherapy in urological cancers was found in 1976 by Morales et al It started with the introduction of Bacillus Calmette-Gueren (BCG) treatment for superficial bladder cancer (BC) (2) This development was followed by the introduction of cytokines such as interferon and interleukin-2 (IL-2) in the treatment of metastatic renal cell carcinoma (mRCC) One of the first reports demonstrating the potential application of immune modulation in cancer treatment was in 1984, when the administration of IL-2 in a patient diagnosed with melanoma reduced the tumour burden This report has since led to significant interest in the field of immunology and its role in managing various malignancies (3) In 2010, it joined the field of prostate cancer immunotherapy with the approval of the autologous cancer vaccine Sipuleucel-T More recently, immune checkpoint inhibitors (ICIs) have been introduced with striking results for urology-specific malignancies
The introduction of ICIs over the past decade has led to significant advances in cancer treatment Recent advances in immunotherapy treatment promise to significantly transform the field of uro-oncology In this review, we aimed to summarize the use of immunotherapeutic agents in treating urothelial, renal and prostate cancer in the light of clinical studies
Urothelial carcinoma
Urothelial carcinoma can occur along the entire urothelium, which anatomically extends from the kidney to the urethra Urothelial carcinomas can generally be examined under two main headings: upper urinary tract urothelial carcinomas (UTUC) and lower urinary tract urothelial carcinomas It is often not possible to evaluate these two main topics independently
BC accounts for 90-95% of urothelial carcinomas, UTUC accounts for 5-10%, and urethral cancer accounts for 1% (4) Today, in most studies on the role of immunotherapy in urothelial carcinoma, BC and UTUC have been evaluated together BC is the 10th most common cancer in the entire population and the 7th most common cancer in men
BC is responsible for 2 1% of cancer-related deaths and is the 13th deadliest cancer (5) At the time of initial diagno-
sis, 75% of the patients are diagnosed with non-muscleinvasive bladder cancer (NMIBC) (Ta, T1, CIS) and 25% with muscle-invasive bladder cancer (MIBC) (T2-T4) (6)
UTUC is a malignant change in urothelial cells extending from the renal pelvis and calyces to the ureteral orifice
The exact incidence of UTUC is challenging to determine because it is often associated with renal pelvis and ureteral malignancies; they are reported in a single category as renal tumours (7) The estimated incidence of UTUC in Western countries is 2/100,000 cases per year, and its incidence is highest between the ages of 70 and 90 (8)
Immunotherapeutic Agents Used in Urothelial Carcinoma (Intravesical and Systemic)
The main goal of immunotherapeutic agents is to increase the anti-tumour response by acting on the body's defence cells The main immunotherapeutic agents used in urothelial carcinoma are;
• Interferon
• BCG } BC (Intravesical Therapy)
• Anti-PD-1 (pembrolizumab, nivolumab)}BC and UTUC
immunotherapy in urothelial carcinoma is intravesical BCG treatment in BC BCG stimulates the immune system in two separate ways First, it enhances the anti-tumour response via Toll-like receptors, inflammatory cytokines, and tumour necrosis factors Secondly, it increases the immune response against the tumour by stimulating CD4+ T Helper cells
In addition to these mechanisms, BCG is cytotoxic against tumour cells (9) Interferon is an immunotherapeutic agent that can be used alone or in combination with BCG Its mechanism of action is lymphocyte activation and strengthening of the T-helper type I immune response (10)
Nowadays, systemic immunotherapeutic agents are increasingly used to treat urothelial carcinoma This group of drugs acts through PD-1 and PD-L1 receptors The interaction between PD-1 and PD-L1 triggers immune suppressive mechanisms when T cells encounter tumour cells In this way, PD-L1 checkpoint blockade may interfere with tumour/immune cell interactions for some tumours and thus improve anti-tumour immune responses There are four immunotherapeutic agents approved by the Food and Drug Administration (FDA) for use in patients diagnosed with metastatic urothelial carcinoma (mUC) and progressing following platinum-based chemotherapy (CT) (pembrolizumab, nivolumab, atezolizumab, avelumab)
Pembrolizumab
In light of the data obtained from the Keynote-057 trial in phase II, The FDA approved the use of pembrolizumab in 2020 for the treatment of BCG-refractory high-risk, NMIBC-diagnosed patients who are not suitable for radical cystectomy or who refuse radical cystectomy (11) This study showed that pembrolizumab treatment has acceptable response rates in first-line treatment in patients with locally advanced or metastatic urothelial cancer with high comorbidity rates who cannot receive platinumbased CT Use with this indication was approved by the FDA in 2017 (12)
In a phase II trial (PURE-01) conducted on patients diagnosed with MIBC, regardless of their suitability for platinum-based CT, pembrolizumab neoadjuvant therapy alone has been shown to reduce tumour downstaging at radical cystectomy pathology (13) Another study showed that adding pembrolizumab to platinum-based CT in neoadjuvant treatment improved pathological response rates (14) In another study, the effectiveness of maintenance treatment with pembrolizumab was evaluated in patients who were given platinum-based CT in first-line treatment and stable disease was achieved There was a benefit in progression-free survival (PFS) (5 4 vs 3 mo , p = 0 04) (15) In another phase III randomized controlled trial (RCT), pembrolizumab monotherapy in second-line treatment showed improvement in overall survival (OS) compared to CT (10 3 vs 7 4 mo , p = 0 002) (16) However, there are also studies reporting that adding pembrolizumab to standard adjuvant CT in patients with advanced urothelial carcinoma does not increase treatment effectiveness (12)
Nivolumab
According to a phase II single-arm trial results in 270 patients diagnosed with surgically unresectable locally advanced or mUC, an objective response rate (ORR) of 19 6% was achieved in patients receiving nivolumab monotherapy It was shown to provide clinical benefit regardless of PD-L1 expression Based on the results of this study, the PD-1 inhibitor nivolumab has been approved for second-line treatment in patients diagnosed with mUC who have not received an adequate response to platinum-based CT (17) According to the phase I-II trial results conducted in patients with mUC who did not respond adequately to platinum-based CT, nivolumab/ipilimumab combination therapy had an ORR of up to 38% (18) According to EAU guidelines, adjuvant nivolumab treatment is recommended for patients with pT3, pT4, and pN+ UTUC who cannot receive adjuvant platinum-based CT (19) In the CheckMate-274 trial, 709 patients with a high risk of recurrence and diagnosed with locally advanced urothelial cancer were randomized In this study, adjuvant nivolumab was given to one group and placebo to the other group, and a statistically significant improvement in disease-free survival (DFS) was detected in the treatment arm (10 8 vs 20 8 mo p < 0 001) (20) Based on data from the study, nivolumab was approved by the FDA for the adjuvant treatment of urothelial carcinoma
Atezolizumab
Atezolizumab is a monoclonal antibody that inhibits antiPD-L1 In light of the data from RCTs, the use of atezolizumab in the first-line treatment of patients diagnosed with locally advanced or mUC who are not suitable for platinum-based CT and in the second-line treatment of patients whose disease progresses despite platinum-based CT and who cannot undergo surgical resection has been approved by the FDA and European Medicines Agency (EMA) (21, 22)
The recently published ABACUS study evaluated the effectiveness of neoadjuvant atezolizumab treatment in patients unsuitable for cisplatin treatment According to the results of this study, 2-year DFS and OS were reported as 68% and 77%, respectively In another single-arm phase II clinical study, in the neoadjuvant treatment of patients with cT2-
E Bosnali, E Malik Akdas, E Telli, K Teke, O Kara
T4aN0M0 stage tumours, the addition of atezolizumab to gemcitabine-cisplatin combination has been shown to provide a relapse-free survival advantage (23)
In the multicenter randomized controlled phase III study (IMvigor 130), 1213 patients with locally advanced or mUC were divided into three groups Survival analyses were compared by giving platinum-based CT/atezolizumab to group A, atezolizumab to group B, and platinumbased CT/placebo to group C The median OS times of patients in groups A and C were reported as 16 mo and 13 4 mo , respectively, and there was a statistically significant difference between both groups (0 83, 95% CI 0 69-1, p = 0 027) The median OS times of patients in groups B and C were 15 7 mo , and 13 1 mo , respectively, and it was reported that there was no statistically significant difference between the two groups As a result, it has been reported that adding atezolizumab to platinumbased CT in first-line treatment provides a survival advantage in patients diagnosed with mUC (24)
Avelumab
Avelumab is a humanized monoclonal antibody that acts by binding to PD-L1, similar to atezolizumab and durvalumab In the JAVELIN Bladder 100 trial, patients with locally advanced/mUC whose disease was stable or had clinical improvement after 4-6 courses of platinum-based CT were divided into two groups One group was given supportive treatment, and the other group was given avelumab treatment In the avelumab arm, a statistically significant improvement in OS was detected (14 3 vs 21 4 mo ) (25) Based on the data of this study, the use of avelumab in maintenance therapy in patients with locally advanced or mUC has been approved by the FDA (26) In the EAU 2023 guideline, maintenance avelumab treatment is strongly recommended in patients diagnosed with mUC whose disease is stable after first-line platinum-based CT (19)
Durvalumab
Durvalumab is a humanized monoclonal antibody that
acts by binding to PD-L1 and blocking the PD-1-CD80 interaction It received accelerated approval from the FDA in 2017 for patients with urothelial carcinoma who did not respond adequately to neoadjuvant or adjuvant treatment (26)
The DANUBE phase III clinical study compared durvalumab monotherapy with durvalumab/tremelimumab and platinum-based CT The superiority of the tried treatments over CT has not been determined (27) After the report of the DANUBE study was published, the indication of durvalumab in BC was withdrawn (28) Clinical trials of various urothelial cancer immune therapies were summarized in Table 1 (29)
Role of immunotherapy in urothelial carcinoma
Urothelial carcinoma is a common type of cancer in the genitourinary system, and treatment strategies in this area are constantly evolving Agents used in immunotherapy in urothelial carcinoma include various options such as BCG, interferon, anti-PD-1 (nivolumab, pembrolizumab), anti-PD-L1 (atezolizumab, durvalumab, avelumab) These agents increase the anti-tumour response by affecting the body's defence mechanisms They show effectiveness at different treatment stages in BC and UTUC
Cisplatin-based CT has been used as standard therapy in the treatment of urothelial carcinoma for many years The results of clinical studies with systemic immunotherapeutic agents show that the use of immunotherapeutic agents in treating urothelial carcinoma is becoming increasingly widespread and is considered an effective alternative in patients who are resistant or unsuitable for platinumbased CT Comparisons between these agents should consider clinical outcomes such as ORR, OS, and DFS When determining the areas of use and advantages of each agent, the characteristics of the patients and their pre-treatment conditions should be considered The usage recommendations regarding immunotherapeutic agents employed in urothelial carcinoma in the EAU guidelines are presented in Table 2 (19) Immunotherapy has become an increasingly important
Atezolizumab IMvigor210 Second-line mUC, after platinum CT May 2016
Atezolizumab IMvigor210 First-line mUC, platinum-ineligible April 2017
Pembrolizumab Keynote-052 First-line mUC, platinum-ineligible May 2017 ORR 24% Balar 2017 and Vuky 2020
Pembrolizumab Keynote-057 Recurrent NMIBC January 2020 CRR 41% Balar 2021
Avelumab JAVELIN Bladder 100 Maintenance, mUC June 2020
Nivolumab Checkmate-274 Adjuvant, MIBC August 2021
Median OS Powles 2020 21 vs 14 mo of the control
Median DFS Ba orin 2021 20 8 vs 10 8 mo of the control
The PD-L1 inhibitors atezolizumab and nivolumab and the PD-1 inhibitor pembrolizumab have been approved for patients whose disease has progressed despite platinum-based CT and who have not received prior immunotherapy
The PD-L1 inhibitor atezolizumab and the PD-1 inhibitor pembrolizumab are approved for patients with advanced or mUC unsuitable for first-line platinum-based CT
Offer patients with PD-L1-positive tumours the checkpoint inhibitors pembrolizumab or atezolizumab
Offer adjuvant nivolumab to selected patients with pT3/4 and/or pN+ disease who are ineligible for or refuse adjuvant cisplatin-based CT
For patients who achieve stable disease after first-line platinum-based CT, use maintenance treatment with the PD-L1 inhibitor avelumab
Table 1. Clinical trials of varying treatment plans for urothelial carcinoma (29)
Table 2.
Summary of the use of immunotherapeutic agents in the treatment of urothelial carcinoma according to EAU guidelines (19)
treatment modality in urothelial carcinoma However, further RCTs and long-term follow-up periods will strengthen our knowledge of the effectiveness and safety of these agents In the future, the role of immunotherapy will be better understood by focusing on more specific treatment strategies and personalized treatments for disease subtypes
Renal cell carcinoma
Renal cell carcinoma (RCC) accounts for 2-3% of adult cancers, although its incidence is increasing in Western countries (30) According to the American Cancer Society data for 2023, it is predicted that approximately 81 800 new cases will be diagnosed in the United States, and 14 890 of the patients will die from kidney cancer (31)
Approximately 70% of kidney cancer cases are diagnosed at a localized or locally advanced stage, and the standard of care for these patients is radical or partial nephrectomy (32) Despite this, approximately 35% of patients initially present with advanced or metastatic RCC (mRCC), and 30% of patients presenting with localized disease experience recurrence (33)
RCC has been known for many years as a tumour with unique sensitivity to immunotherapies (34) Systemic first-line treatment for mRCC is rapidly evolving, with multiple approved strategies and new clinical trials ongoing The introduction of mainly new ICIs has led to a paradigm shift in the treatment of this disease (35) RCC immunotherapy agents inhibit receptor-ligand pairs that modulate the congenital or acquired immune system These molecular pairs, known as immune checkpoints, include PD-1 and PD-L1 and CTLA4 multiple ligands, i n c l u d i n g c y t o t o x
4 (CTLA4), CD80, and CD86 (36) The recent emergence of ICIs that block the PD-1/PD-L1 or CTLA4 signalling pathways has re-established systemic immunotherapy as central to the medical treatment of advanced RCC, resulting in increasing interest in the application of immunotherapies in the adjuvant setting Many RCTs are being conducted (34)
Treatment of locally advanced RCC (Neoadjuvant/adjuvant therapy)
Given the recent success of ICIs in mRCC, these therapies are now being studied in the (neo)adjuvant setting to treat localized RCC The rationale for using neoadjuvant ICIs stems from the hypothesis that intact kidney tissue may provide a source of antigen for the persistent cancerspecific immune response (37) The advantage of adjuvant immunotherapy is that it can maintain efficacy and eliminate micrometastases even after treatment discontinuation (38) This section aims to provide an overview of completed or ongoing clinical trials on adjuvant treatment of RCC, accompanied by the 2023 EAU guideline and current reviews
Keynote-564 Trial (Pembrolizumab)
Pembrolizumab is a humanized monoclonal IgG4 antibody and is also a PD-1 inhibitor Keynote-564 study included intermediate-high risk (pT2, grade 4 or sarcomatoid, N0, M0 or pT3, any grade, N0, M0) or high risk of recurrence (pT4, any grade, N0, M0 or any pT, any
grade, pN+, M0, or no evidence of disease after resection of oligometastatic sites < 1 year after nephrectomy or NED) It was a phase III clinical trial in which pembrolizumab (17 cycles of 3 weeks of treatment) was randomized vs placebo as adjuvant therapy in 994 patients (39) In this study, M1 NED was defined as complete resection of oligometastasis simultaneously or within one year after nephrectomy At a median follow-up of 24 mo , DFS was 77 1% vs 68 1% (HR 0 68, 95% CI: 0 53-0 87; p = 0 0010), and this rate was maintained at 30 mo follow-up In subgroup analyses of the study, patients with M0 tumours (HR 0 74, 95% CI: 0 57-0 96) and patients with M1 tumours with NED (HR 0 29, 95% CI: 0 120 69) DFS benefit was observed and the DFS benefit of pembrolizumab was observed in patients with PD-L1 combined positive score (CPS) ≥ 1 (HR 0 67, 95% CI 0 510 88) compared to patients with PD-L1 CPS < 1 (HR 0 83, 95% CI 0 45-1 51) In this context, Keynote-564 is the first study of adjuvant ICI to report a positive primary endpoint of DFS Median OS was not reached in both groups The most common adverse effects (AEs) in the pembrolizumab group were fatigue (1%), diarrhoea (1 6%) and skin rash (0 8%), and grade 4-5 AEs were not observed in both study arms (40)
The study's results led to FDA approval of single-agent pembrolizumab for the adjuvant treatment of patients with resected ccRCC, intermediate-high risk, or high risk of recurrence In 2021, the EAU RCC guideline issued a weak recommendation for pembrolizumab as adjuvant therapy for ccRCC with intermediate to high risk of recurrence, as defined by the study, until final OS data and results from other studies are available Keynote-564 data should also be interpreted in the context of several significant randomized phase III clinical trials investigating RCC treatment with immunotherapy in the adjuvant setting, pending or ongoing for data to be published These include clinical studies IMmotion010 (NCT03024996), CheckMate 914 (NCT03138512), and PROSPER (NCT03055013) (Table 3) (41) Not all data published in peer-reviewed journals are available for these clinical studies, but limited data were presented for IMmotion010, CheckMate 914, and PROSPER at the European Society of Medical Oncology (ESMO) Congress in September 2022
IMmotion010 Trial (Atezolizumab)
IMmotion010 is a randomized placebo-controlled phase III trial evaluating the PD-L1 inhibitor atezolizumab as an adjuvant treatment option in 778 RCC patients with a clear cell or sarcomatoid component and a high risk of recurrence
IMmotion010 is the first adjuvant ICI study to investigate the efficacy of a PD-L1 inhibitor in terms of DFS and OS in RCC However, the study did not reach its primary endpoint, with a mean DFS of 57 2 mo in the atezolizumab arm vs 49 5 mo in the placebo arm [HR 0 93 95% CI 0 751 15; p = 0 495] (42) No DFS improvement was detected with atezolizumab in any investigational subgroups Grade ≥ 3 AEs were reported in 27% and 21% of patients in the atezolizumab and placebo groups, respectively The most common grade 3-4 AEs were hypertension, hyperglycemia (3% vs 2%), and diarrhoea (1% vs 2%), observed in 2% vs
E Bosnali, E Malik Akdas, E Telli, K Teke, O Kara
Table 3.
Clinical trials investigating immunotherapy in the adjuvant setting in RCC (41).
Trial identifier Therapeutic agent
Keynote-564 NCT03142334
IMmotion010 NCT03024996
CheckMate 914 NCT03138512
PROSPER NCT03055013
RAMPART NCT03288532
Pembrolizumab 200 mg IV every 3 weeks for up to 17 cycles
Atezolizumab 1 200 mg every 21 days for 1 year
Part A: Nivolumab 240 mg IV every 2 weeks, up to 12 doses, ipilimumab 1 mg/kg IV, up to four doses given in cycles 1, 4, 7 and 10
Part B: Nivolumab 240 mg intravenously every 2 weeks, up to 12 doses
Nivolumab 480 mg IV, one dose given before surgery, up to nine doses given every 28 days following surgery
Part A: Durvalumab 1 500 mg every 28 days for 1 year
Part B: Durvalumab 1.500 mg every 28 days for 1 year + tremelimumab 75 mg on weeks 1 and 4
Inclusion criteria Histolog y The primar y endpoint(s) Estimated primar y (tumour stage and grade) and results completion date
ccRCC might include sarcomatoid features All histological subtypes included
DFS for treatment vs placebo: (HR 0 68, 95% CI 0 53–0 87; P 0 0010)
DFS (assessed through IRF) for atezolizumab vs surgery alone: (HR 0 97, 95% CI 0 74–1 28; P= 0 43)
DFS (assessed through BICR) for nivolumab or ipilimumab vs placebo
Part A: (HR 0 92, 95% CI 0 71–1 19; P = 0 5347)
Part B: results pending EFS for nivolumab (HR 0 97, 95% CI 0 74–1 28; P = 0 43)
DFS, OS (results pending)
Dec 2020
May 2022
Ju y 2024
Nov 2023
Ju y 2024
BICR: Bl nded independent central rev ew; ccRCC: C ear cell renal cel carc noma; DFS: Disease-free survival; EFS: Event-free survival; G: Tumour grade; IRF: Independent review fac l ty; IV: Intravenously; N: Noda stage; NED: No evidence of disease; OS: Overal surviva ; p: Patholog cal; T: Tumour stage
15% of patients in the atezolizumab vs the placebo group, respectively (43)
CheckMate 914 Trial (Nivolumab/Ipilimumab)
CheckMate 914 is a phase III randomized placebo-controlled two-part study examining the effectiveness of a d j u v a n t n i v o l u m a b a n d n i v o l u m a b / i p i l i m u m a b i n patients with clear cell RCC at high risk of recurrence after nephrectomy (44) Results of the part A study were reported at ESMO Congress 2022; 816 patients were randomized to nivolumab/ipilimumab or placebo
The study evaluated 12 cycles of nivolumab at 240 mg every two weeks for six mo plus ipilimumab at 1 mg/kg every six weeks for four cycles vs placebo as adjuvant therapy for 816 patients At a median follow-up of 37 mo , DFS was similar between patients in both arms, and the study did not meet its primary endpoint (HR 0 92, 95% CI 0 71-1 91; p = 0 5347) OS analysis could not be performed due to a hierarchical study design The incidence of treatment-related grade 3 AEs was 29% in the nivolumab/ipilimumab group and 2% in the placebo group, with 4 (1%) deaths considered to be related to combination therapy The high discontinuation rate of 33% in CheckMate 914 is concerning and may negatively impact the study's effectiveness (45, 46) Based on these data, ICI/ICI combination therapy appears to increase risk rather than benefit and is unlikely to be introduced into clinical practice
PROSPER Trial (Peroperative Nivolumab)
PROSPER is a perioperative phase III randomized study comparing neoadjuvant nivolumab (1 cycle) followed by radical/partial nephrectomy and postsurgical follow-up with the group receiving nine doses of adjuvant nivolumab (480 mg IV every four weeks)
The study included 819 high-risk patients, defined as ≥T2 or T any pN+ RCC of any histology, for whom radical/partial nephrectomy was planned Most patients had clear cell histology (78%), 8% had papillary, and 7% had
chromophobe histology The primary endpoint of the study was relapse-free survival An interim analysis at 16 mo of follow-up showed that the addition of perioperative nivolumab did not improve relapse-free survival compared with standard of care surgery, and the study was stopped early due to lack of efficacy (HR 0 97 [95% CI: 0 74-1 28], p = 0 43) (37) As a result, single-agent neoadjuvant immunotherapy does not currently have any role in the treatment of ccRCC
Treatment of mRCC
(ICI Monotherapy/Combination Therapy)
Several positive phase III trials of ICI/ICI or ICI/tyrosine kinase inhibitor (TKI) dual combinations have established the current treatment paradigm for mRCC, all demonstrating superior clinical benefits, including OS, compared to sunitinib monotherapy (47) ICI combination therapies have become the standard fi r s t - l i n e t r e a t m e n t o f m R C C T h e s e c o m b i n a t i o n s include a dual ICI blockade or a single ICI combined with a TKI (48) A direct comparison between combination regimes is not currently available; therefore, the choice of first-line treatment for each patient is based on numerous individualized variables, including comorbidities, disease location and burden, and psychosocial and economic factors (49) In recent years, advances have been seen in the diagnosis, management, and treatment of the ccRCC subtype resulting from various randomized and prospective phase III clinical studies, including combined therapy effective on immune checkpoints such as PD-1, CTLA-4, and PDL-1 (CheckMate-9ER, Keynote-426, CLEAR and CheckMate-214)
ICI monotherapy in the treatment of mRCC
Nivolumab is a humanized monoclonal PD-1 antibody approved for various metastatic tumours The use of the d r u g i n t r e a t i n g m R C C w a s b a s e d o n d a t a f r o m CheckMate-025 (NCT01668784) In this phase III clinical trial comparing nivolumab with everolimus in the
treatment of mRCC with clear cell subtype refractory to vascular endothelial growth factor (VEGFR)-targeted therapy, nivolumab had longer OS, better quality of life and lesser grade 3-4 AEs than everolimus Despite the OS advantage of nivolumab, no PFS advantage was detected in this study (50) PFS does not appear to be a reliable outcome indicator for PD-1 therapy in RCC No RCTs supporting single-agent ICIs in treatment-naïve patients have been reported
Keynote-427 (NCT02853344), published in 2021, is a prospective phase II single-arm clinical study using pembrolizumab in mRCC patients consisting of two cohorts (ccRCC and nccRCC) (51) The nivolumab study included patients who had received prior treatment, while the pembrolizumab study included patients who had not received prior treatment Moreover, the subtypes included in these clinical studies and their representation percentages differed Therefore, each study's subtype that responds better to immunotherapy differs because the populations studied are heterogeneous (52) Given these results and without randomized phase III data, singleagent ICI therapy is not recommended as an alternative in the first-line treatment setting (48)
Combination therapy in the treatment of mRCC (ICI/ICI-ICI/TKI)
The beneficial results obtained in clinical trials with immunotherapy treatment have allowed combining such treatments with others using different mechanisms to enhance immunomodulatory effects (53) The contemporary standard of care for metastatic clear cell RCC (ccmRCC) is the use of TKIs dually (ICI/ICI) or in combination with ICI (54) In the first-line treatment of cc-mRCC, ICI and VEGFR-targeted TKIs have been shown to improve OS compared to TKI monotherapy in randomized studies However, each combination regimen is thought to be highly effective, with ORR ranging from 42% to 71% (55-58)
Several studies have evaluated combination therapies in cc-mRCC and demonstrated improvement in overall response rate, PFS, and OS compared to standard treatment (sunitinib) These studies were Checkmate-9ER (58) (nivolumab/cabozantinib), Keynote426 (57) (pembrolizumab/axitinib), and CLEAR (55) (pembrolizumab/lenvatinib), all of which focused on ccRCC and did not include less common subtypes of kidney cancer In recent years, new prospective trials have been conducted to evaluate the effectiveness of ICI/TKI combinations in less common subtypes (Table 4) (59)
CheckMate-9ER Trial (Nivolumab/Cabozantinib)
CheckMate-9ER is a phase III RCT comparing nivolumab/cabozantinib (n = 323) combination therapy with sunitinib (n = 328) in 651 treatment-naive patients diagnosed with cc-mRCC During a mean follow-up period of 32 9 mo , the median OS was 37 7 mo in the group treated with nivolumab/cabozantinib and 34 3 mo in the patients treated with sunitinib, and as a result, no statistically significant difference was observed While the median PFS was 16 6 mo in the group receiving nivolumab/cabozantinib treatment, PFS was 8 3 mo in sunitinib treatment alone As a result, a statistically sig-
nificant survival increase in PFS was observed in favour of combination treatment
Treatment-related AEs (> grade 3) occurred in 61% of patients receiving nivolumab/cabozantinib and 51% receiving sunitinib alone Treatment-related death was reported in one patient in the nivolumab/cabozantinib arm and two patients in the sunitinib arm (58)
Keynote-426 Trial (Pembrolizumab/Axitinib)
The Keynote-426 trial compared the outcomes of pembrolizumab/axitinib combination therapy with sunitinib monotherapy in 861 treatment-naïve cc-mRCC patients During a median follow-up of 42 8 mo , pembrolizumab/axitinib combination therapy showed an OS advantage for the intention to treat group (HR: 0 73, 95% CI: 0 600 88, p < 0 001)
Median OS was 45 7 months in the pembrolizumab/axitinib arm and 40 1 months in the sunitinib arm, and a PFS advantage was also demonstrated in the combination arm in IMDC subgroups Treatment-related AEs (> grade 3) occurred in 63% of patients receiving combination t h e
Treatment-related deaths were reported at a rate of approximately 1% in both arms (57)
The CLEAR randomized phase III clinical trial compared everolimus/lenvantinib or pembrolizumab/lenvantinib combination therapy with sunitinib alone in treating advanced RCC CLEAR randomized a total of 1,069 patients (in a 1:1:1 ratio) to pembrolizumab/lenvatinib (n = 355), everolimus/lenvatinib (n = 357), and sunitinib (n = 357) In the study, the pembrolizumab/lenvatinib arm reached its primary endpoint compared to sunitinib, with a median PFS of 9 2 mo vs 23 9 mo (HR: 0 39, 95% CI: 0 32-0 49, p < 0 001) Compared to sunitinib, OS was significantly improved with pembrolizumab/lenvatinib (HR: 0 66, 95% CI: 0 49-0 88, p = 0 005) Efficacy was observed in all IMDC risk groups, regardless of PD-L1 status Grade 3 or higher AEs associated with treatment with pembrolizumab/lenvatinib were 72% Treatmentrelated deaths occurred in four patients in the pembrolizumab/lenvatinib arm and one patient in the sunitinib arm (55)
CheckMate-214 Trial (Ipilimumab/Nivolumab)
The combination of ipilimumab/nivolumab, targeting anti-CTLA4 and anti-PD-1, showed improvements in PFS and OS compared to sunitinib based on data from the phase III CheckMate-214 trial, which led to its approval by the International Metastatic RCC Database Consortium (IMDC) for the treatment of low and intermediate risk ccmRCC At 60 mo of follow-up in the CheckMate-214 trial, OS rates were 43% in the ipilimumab/nivolumab arm and 31% in the sunitinib arm, respectively Grade 34 toxicity was reported in 46% and treatment-secondary death in 1 5% in the ipilimumab/nivolumab arm (56) Therefore, immune combination therapy should be applied within the scope of a multidisciplinary team in centres with appropriate supportive care experience (Table 5) (48)
E Bosnali, E Malik Akdas, E Telli, K Teke, O Kara
Table 4
First-line immune checkpoint inhibitor combination trials for clear-cell RCC (59)
Study N Experimental ar m Primar y endpoint Risk groups PFS (mo)
CheckMate 9ER NCT03141177
Median follow-up of 23 5 mo
Keynote-426 NCT02853331
Median follow-up of 42.8 mo.
CLEAR NCT02811861
Median follow-up of 33 4 mo
Checkmate 214 NCT02231749
Median follow-up of 60 mo.
JAVELIN 101 NCT02684006
Median follow-up 19 mo
IMmotion151 NCT02420821
Median follow-up 24 mo
1096 886 915
NIVO 240 mg fixed dose IV every 2 wk plus CABO 40 mg PO daily vs SUN 50 mg PO QD 4/2 wk
PFS in the ITT by BICR
IMDC
FAV 22%
IMD 58%
POOR 20%
MSKCC
Not determined
PEMBRO 200 mg IV Q3W plus AXI 5 mg PO BID vs SUN 50 mg PO QD 4/2 wk
PEMBRO 200 mg IV Q3W plus LEN 20 mg PO QD vs SUN 50 mg PO QD 4/2 wk NIVO 3 mg/kg plus IPI 1 mg/kg IV Q3W for 4 doses then NIVO 3 mg/kg IV Q2W vs SUN 50 mg PO QD 4/2 wk
AVE 10 mg/kg IV Q2W plus AXI, 5 mg PO BID vs SUN 50 mg PO QD 4/2 wk
PFS and OS in the ITT by BICR
IMDC
FAV 31%
IMD 56%
POOR 13%
MSKCC
Not determined
PFS in the ITT by BIRC
IMDC
FAV 31% IMD 59% POOR 9% NE 1%
MSKCC
PFS and OS in the IMDC intermediate and poor risk population by BICR
PFS in the PD-L1+ population and OS in the ITT by BICR
BATEZO = atezol zumab; AVE = avelumab; AXI = axitinib; BEV = bevacizumab; BICR = b inded ndependent centra rev ew; BID = twice a day; CABO = cabozantinib; CI = confidence interval; FAV = favourable; HR = hazard rat o; IPI = pi imumab; IMD = intermed ate; IMDC = Metastatic Rena Cancer Database Consort um; IR = nvestigator review; TT = intention-to-treat; IV = intravenous; LEN = lenvatin b; mo = months; MSKCC = Memoria S oan Ketter ng Cancer Center; NE = non-estimable; NR not reached; NIVO n vo umab; OS overall surviva ; PEMBRO pembrolizumab; PFS profession-free surv val; PITT PFS intention-to-treat; PO by mouth; Pts pat ents; QD once a day; Q2W every 2 weeks; Q3W every 3 weeks; SUN sun t nib; wk weeks
Table 5.
Updated EAU Guidelines recommendations for the first-line treatment of cc-mRCC (48)
Standard of Care Alter native in patients who can not receive or tolerate immune checkpoint inhibitors
IMDC The International Metastat c Renal Ce l Carcinoma Database Consortium *pazopanib for intermediate-risk disease on y [1b] = based on one randomised control ed phase III tr al [2a] = based on a we l-des gned study w thout random sat on or subgroup analys s of a random sed contro led tria
Immunotherapy in Metastatic Non-clear cell RCC
Among diagnosed renal tumours, clear cell RCC is the most common type (80%); the remaining 20% is nonclear cell renal cell carcinoma (nccRCC), a rare and histopathologically heterogeneous group of tumours (31) In most kidney cancer trials, nccRCC tumours are not included or only marginally represented Therefore, little is known about the best management of nccRCC types Treatment options for nccRCC are limited as few specific studies are available Although nccRCC subtypes have not been included in pivotal ccRCC clinical trials, their treatments are based on data from ccRCC clinical trials No phase III clinical trials have been reported for patients diagnosed with metastatic nccRCC (60) The EAU 2023 guideline made a weak recommendation for pembrolizumab alone or pembrolizumab/lenvantinib or nivolumab/cabozantinib treatment for papillary RCC patients based on small single-arm studies
Conducting clinical trials on more patients with different histologies and investigating new biomarkers that will help predict response to treatment remain questions that researchers need to answer in the treatment of nccRCC
Undoubtedly, future clinical trials will play a key role in treating these patients (61)
Role of Immunotherapy in RCC
Immunotherapy is the cornerstone of mRCC treatment
These agents are currently used in clinical trials in the (neo)adjuvant setting for high-risk localized RCC to achieve primary tumour response, reduce the risk of recurrence, and improve long-term oncological outcomes
In addition to shrinking the primary tumour and enabling nephron-sparing surgeries, neoadjuvant ICIs could theoretically generate a durable immune response given the presence of antigens in intact kidney tissue (32) However, whether neoadjuvant ICI/TKI use is associated with longterm DFS or OS benefit is not yet known
Immunotherapy treatment in the adjuvant setting is promising, but the risk of disease recurrence remains high In the Keynote-564 (39) trial, relapse was observed in 22 7% of patients in the pembrolizumab group The heterogeneity observed between adjuvant ICI studies may include differences in study groups (e g , the inclusion of M1 NED in Keynote-564 and IMmotion010 and no inclusion in CheckMate 914), drug tolerability, and factors that may affect adequate drug distribution (e g , Checkmate 914) (43% medication discontinuation rate)
m
including T2a/grade 3 patients in the CheckMate 914 study, who were assumed to have lower malignancy than the other two, may have significantly affected the study results These differences in inclusion criteria between ongoing clinical trials may affect the risk of disease recurrence and, ultimately, negatively contribute to disease progression Additionally, differences in treatment-limiting toxicity rates across studies may alter the treatment received and impact DFS results One of the reasons why the IMmotion010 (43) trial failed to meet the primary endpoint compared to the Keynote-564 study may be that the anti-PD-1 and PD-L1 antibodies used in the studies showed a difference in efficacy Liu et al discuss the incidence of renal adverse events (rAEs) for ICI-based reg-
imens vs targeted or chemotherapies, including 95 RCTs totalling more than 40,000 patients (62) Grade 3 or higher rAEs incidence was 4 3% Among ICI monotherapies, anti-CTLA4 was found to have a higher risk of ≥ grade 3 rAEs compared to anti-PD-1/PD-L1 Diagnostic and management challenges for ICI-associated toxicities highlight the value of a multidisciplinary approach to the management of high-grade rAEs
Currently, there are no standard or validated biomarkers to help treat RCC Discovering one or more of these biomarkers is probably at the top of every researcher's wish list If biomarkers can be identified in patients who have not received CT or at an earlier time when cancer is diagnosed, opportunities for the use of neoadjuvant or early adjuvant immunotherapy will increase
Although DFS benefit in the adjuvant setting is a meaningful primary endpoint supported by the FDA and the European Medical Association, treatment-related toxicities should not be ignored by patients and clinicians While the DFS benefit of pembrolizumab was maintained in long-term follow-up, against the background of many negative adjuvant clinical trials, clinicians await the study's long-term OS data before recommending adjuvant pembrolizumab to patients In the meantime, adjuvant pembrolizumab remains a reasonable option for patients with high-risk RCC in light of the EAU 2023 guideline When discussing adjuvant treatment options with a patient with high-risk RCC, clinicians should discuss available data supporting the use of adjuvant ICIs and outline questions that will be answered over time Until we get answers to these crucial questions, adjuvant immunotherapy application appears to be a personalized decision
Prostate cancer
Prostate cancer is the 2nd most common type of cancer in men and ranks 5th among cancer-related deaths Prostate cancer is the most frequently diagnosed cancer in 112 countries in the world, followed by lung cancer in 36 countries and colorectal cancer in 11 countries (63) The widespread use of prostate-specific antigen (PSA) has led to a significant increase in the incidence of prostate cancer This has resulted in increased detection of indolent disease and decreased detection of metastatic prostate cancer (64) The most important risk factors in the aetiology of prostate cancer are, as many studies have shown, advanced age, geography, ethnicity, family history and genetic predisposition (65-67)
In recent years, immunotherapy has emerged as an essential field in the treatment of prostate cancer Prostate cancer is an immunological tumour to a lesser extent compared to other types of urological cancer The reasons for this are that prostate cancer has a low rate of tumour mutation, PDL1 expression and T-cell infiltration (68) Therefore, although immunotherapy has a limited place in prostate cancer, some immunotherapeutic agents have become part of standard treatment in the past few years It provides an alternative treatment method, especially for castrationresistant prostate cancer (CRPC), in addition to standard methods such as androgen deprivation therapy and CT (69, 70) A particular subgroup of patients, including mismatch repair (dMMR) deficient, CDK12-mutated tumours in addition to high PD-L1 tumour expression, tumour muta-
E Bosnali, E Malik Akdas, E Telli, K Teke, O Kara
tional burden, and microsatellite instability (MSI), have recently shown good responses to ICI therapy (68, 71)
The main immunotherapeutic agents used in prostate cancer are:
• Ipilimumab
• Nivolumab
• Pembrolizumab
• Atezolizumab
• Sipuleucel-T (Vaccine based)
Ipilimumab
Ipilimumab is a monoclonal antibody that increases the immune system's response to tumour cells by targeting the CTLA-4 receptor It is the first FDA-approved ICI for prostate cancer When administered as monotherapy, ipilimumab has been shown to significantly increase the proportion of regulatory effector T lymphocytes present in the tumour microenvironment (TME) (72)
In the literature, phase I trials have shown that ipilimumab and its combinations provide PSA reduction in patients and prolong the PSA doubling time (73-76)
Slovin et al shared the results of 50 patients diagnosed with metastatic CRPC (mCRPC) who received ipilimumab alone or ipilimumab/radiotherapy (RT) combination therapy A more than 50% decrease in PSA was observed in eight patients, a complete response was achieved in 1 patient, and no progression was observed in 6 patients (77) Kwon et al , in a randomized controlled phase III study, 799 mCRPC patients received palliative RT therapy Then, the patients were divided into two groups, one receiving ipilimumab and the other receiving placebo
Although a significant improvement in PFS was detected in the ipilimumab arm between the two groups, no significant difference was detected in OS data (70) After three years, an approximately two- to three-fold higher OS benefit was detected in the ipilimumab arm (78) Beer et al reported increased PFS and a higher PSA response rate (23% vs 8%) in the ipilimumab arm (5 6 mo ) compared to the placebo arm (3 8 mo ) in mCRPC (79)
Nivolumab
The interaction of PD-1 with its ligand prevents the activation of T cells, and, as a result, the destruction of can-
Table 6.
Clinical trials of varying treatment plans for mCRPC (91)
Pembrolizumab
Pembrolizumab
Pembrolizumab plus Docetaxel and Prednisone
Pembrolizumab plus Enzalutamide
Atezolizumab
Atezolizumab with Sipuleucel-T
Avelumab
Nivolumab plus Ipilimumab mCRPC mCRPC Advanced prostate adenocarcinoma
cer cells by the immune system is prevented Nivolumab is an IgG4 monoclonal antibody that demonstrates antitumor response by blocking PD-1 (80, 81)
In the CheckMate 650 phase II clinical trial investigating the combined effects of ipilimumab and nivolumab in patients with mCRPC, combination therapy demonstrated an ORR of 25% (81)
Shenderov et al , in patients with AR-V7 positive mCRPC, which is associated with poor prognosis, investigated the effectiveness of nivolumab/ipilimumab combination therapy Although this study showed that combination therapy may benefit AR-V7 positive PCa patients, sufficient evidence was not obtained for routine use (82)
Pembrolizumab
Pembrolizumab is an anti-PD-1 antibody that acts similarly to nivolumab In the Keynote-365 study, CT-refractory mCRPC patients receiving abiraterone or enzalutamide were given pembrolizumab/docetaxel and prednisone combination therapy The PSA response rate was 34%, the radiological mean PFS was 8 5 mo , and the OS was 20 2 mo (83)
In a phase II clinical study (Keynote-199) involving multiple cohorts, pembrolizumab monotherapy was administered to 258 patients diagnosed with mCRPC who had bone-predominant metastases measurable by Response Evaluation Criteria In Solid Tumors (RECIST) and received docetaxel and targeted endocrine therapy Patients with positive PD-L1 expression showed an ORR of 5%, and patients with negative expression showed an ORR of 3% Median OS was reported as 9 5 mo in PD-L1 expressionpositive patients and 7 9 mo in negative patients (84) With these results, it is thought that pembrolizumab treatment may be more effective in tumours with high PD-L1 expression
Atezolizumab
Atezolizumab, avelumab and durvalumab, which target PD-L1, work by blocking the interaction of PD-L1 with PD-1 These agents have been investigated as an option in the treatment of advanced prostate cancer (85-89) In IMbassador 250 study, 759 patients with mCRPC or locally advanced CRPC refractory to abiraterone and doxetaxel were treated with the combination of atezolizumab
One dose of RT followed by 10 mg/kg ipilimumab every 3 weeks
200 mg every 3 weeks
10 mg/kg every 2 weeks
200 mg pembrolizumab and 75 mg/m2 docetaxel every 3 weeks, 5 mg prednisone BID
200 mg pembrolizumab every 3 weeks with 4 doses of enzalutamide Every 3 weeks
1200 mg azetolizumab every 3 weeks, sipuleucel-T every 2 weeks
10 mg/kg every 2 weeks
1 mg/kg nivolumab and 3 mg/kg ipilimumab IV followed by 480 mg nivolumab every 4 weeks
Overall increased survival rates for patients given ipilimumab
OS of 14.1 mo. with acceptable safety
OS of 7 9 mo
OS of 29 2 mo with acceptable safety
OS of 41.7 mo.
OS of 14 7 mo with acceptable safety
OS of 23 6 mo
OS of 7.4 mo.
OS of 19 0 mo
et al
Antonarakis et al
Hansen et al
Yu et al
Graff et al
Petrylak et al
Dorff et al
Brown et al
Sharma et a
Fizazi
and enzalutamide or enzalutamide alone Similar OS rates were detected in both treatment arms Subgroup analyses reported that combination therapy may benefit patients with high PD-L1 expression (86)
Sipuleucel-T
There are also immunotherapeutic vaccines used in the treatment of prostate cancer However, many of these vaccines are still in the experimental stage FDA approval of Sipuleucel-T is considered the first a p p l i c a t i o n o f i m m u n o t h e r a p y i n p r o s t a t e c a n c e r
Sipuleucel-T is the only FDA-approved vaccine approved for use against prostate cancer It has been shown in the literature that Sipuleucel-T is effective in mCRPC (69, 90) According to a study conducted by Kantoff et al in mCRPC patients, sipuleucel-T treatment prolonged OS by an average of 4 1 mo and resulted in a 22% reduction in the risk of death (69) These results may guide new immunotherapeutic vaccine trials Clinical trials of various prostate cancer immune therapies were summarized in Table 6 (91)
Role of Immunotherapy in Prostate Cancer
As it is known, prostate cancer is in the category of immunologically "cold" tumours, so patients must be evaluated according to their individual immunogenicity status in order to receive effective immunotherapy treatment (91)
More successful treatment results can be achieved in larger patient populations with combination treatments with different agents Another critical issue is that immunological interventions are generally applied only to those with advanced disease, although, as the disease progresses, the n u m b e r o f T c e l l s d e c r e a s e s T h e r e f o r e , a p p l y i n g immunotherapy at the early stage of the disease may provide a more effective response to treatment
Immunotherapy is a promising alternative treatment option, especially in some CRPC patients ICI treatment success is higher in prostate cancer patients with high MSI/dMMR or CDK12 mutations A better understanding of TME and ICI mechanisms through high-volume prospective RCTs may pave the way for new immunotherapeutic approaches in advanced prostate cancer
CONCLUSIONS
Given the limited research experience to date, it remains unclear whether the persistence of the primary tumour will impact attempts to modulate the metastatic cascade or whether different immunotherapy agents have different degrees of efficacy in adjuvant or neoadjuvant settings
Cisplatin-based CT has long been used as standard therapy in the treatment of urothelial carcinoma With the promising results obtained in locally advanced and mUC, systemic immunotherapeutic agents have begun to take their place in the standard treatment of the disease
However, more RCT evidence and extended follow-up periods are needed
Data from large clinical trials to evaluate immunotherapy and TKIs for treating RCC in the adjuvant setting remain largely conflicting regarding the DFS benefit of either
treatment modality However, a comprehensive biological rationale exists for administering TKIs and immunotherapy agents in the adjuvant setting However, questions regarding the optimal adjuvant treatment regimen and appropriate method in RCC still remain to be answered
Prostate cancer, which is considered an immunological "cold" tumour, is not as sensitive to immunotherapy as o t h e r u r o
g results have been obtained in some identified prostate cancer patients In the light of new prospective RCTs, treatment procedures that reach sufficient evidence levels do not seem far away
To make an informed decision about the individualized use of adjuvant immunotherapy, clinicians should discuss the available data with patients and actively make the decision Further research and development of biomarkers are needed to answer these questions and improve outcomes for uro-oncology Although it is challenging to stay up to date on innovations in immunotherapy, given the ongoing RCTs, there is no doubt that we will have more options available to our patients who need this treatment in the next decade
REFERENCES
1 Elena Dreyzin AK Kidney Cancer and Its Treatment In: Edouard J Trabulsi CDL, Anne E Lizardi-Calvaresi, editor Chemotherapy and Immunotherapy in Urologic Oncology Switzerland: Springer Nature; 2021 p 231-7
2 Morales A, Eidinger D, Bruce AW Intracavitary Bacillus Calmette-Guerin in the treatment of superficial bladder tumors J Urol 1976; 116:180-3
3 Rosenberg SA, Lotze MT, Muul LM, et al Observations on the systemic administration of autologous lymphokine-activated killer cells and recombinant interleukin-2 to patients with metastatic cancer New Engl J Med 1985; 313:1485-92
4 Cassell A, 3rd, Manobah B, Willie S Diagnostic and Therapeutic Challenges of Rare Urogenital Cancers: Urothelial Carcinoma of the Renal Pelvis, Ureters and Urethra World journal of oncology 2021; 12:20-7
5 Bray F, Ferlay J, Soerjomataram I, et al Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin 2018; 68:394424
6 Babjuk M, Burger M, Comperat EM, et al European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ) - 2019 Update Eur Urol 2019; 76:639-57
7 Siegel RL, Miller KD, Jemal A Cancer statistics, 2019 CA Cancer J Clin 2019; 69:7-34
8 Petros FG Epidemiology, clinical presentation, and evaluation of u p p e r - t r a c t
; 9:1794-8
9 W a r d G r a d o s D F , A h m a d i H , G r i f fi t h T S , W a r l i c k C A Immunotherapy for Bladder Cancer: Latest Advances and Ongoing Clinical Trials Immunol Invest 2022; 51:2226-51
10 Naitoh J, Franklin J, O'Donnell MA, Belldegrun AS Interferon alpha for the treatment of superficial bladder cancer Adv Exp Med Biol 1999; 462:371-86
11 Balar AV, Kamat AM, Kulkarni GS, et al Pembrolizumab
E Bosnali, E Malik Akdas, E Telli, K Teke, O Kara
monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): an openlabel, single-arm, multicentre, phase 2 study Lancet Oncol 2021; 22:919-30
12 Balar AV, Castellano D, O'Donnell PH, et al First-line pembrolizumab in cisplatin-ineligible patients with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052): a multicentre, single-arm, phase 2 study Lancet Oncol 2017; 18:1483-92
13 Necchi A, Anichini A, Raggi D, et al Pembrolizumab as Neoadjuvant Therapy Before Radical Cystectomy in Patients With Muscle-Invasive Urothelial Bladder Carcinoma (PURE-01): An Open-Label, Single-Arm, Phase II Study J Clin Oncol 2018; 36:3353-60
14 Rose TL, Harrison MR, Deal AM, et al Phase II Study of Gemcitabine and Split-Dose Cisplatin Plus Pembrolizumab as Neoadjuvant Therapy Before Radical Cystectomy in Patients With Muscle-Invasive Bladder Cancer J Clin Oncol 2021; 39:3140-8
15 Galsky MD, Mortazavi A, Milowsky MI, et al Randomized Double-Blind Phase II Study of Maintenance Pembrolizumab Versus Placebo After First-Line Chemotherapy in Patients With Metastatic Urothelial Cancer J Clin Oncol 2020; 38:1797-806
16 Bellmunt J, de Wit R, Vaughn DJ, et al Pembrolizumab as Second-Line Therapy for Advanced Urothelial Carcinoma New Engl J Med 2017; 376:1015-26
17 Sharma P, Retz M, Siefker-Radtke A, et al Nivolumab in metastatic urothelial carcinoma after platinum therapy (CheckMate 275): a multicentre, single-arm, phase 2 trial Lancet Oncol 2017; 18:312-22
18 Sharma P, Siefker-Radtke A, de Braud F, et al Nivolumab Alone and With Ipilimumab in Previously Treated Metastatic Urothelial Carcinoma: CheckMate 032 Nivolumab 1 mg/kg Plus Ipilimumab 3 mg/kg Expansion Cohort Results J Clin Oncol 2019; 37:1608-16
19 Rouprêt M, Seisen T, Birtle AJ, et al European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2023 Update Eur Urol 2023; 84:49-64
20 Bajorin DF, Witjes JA, Gschwend JE, et al Adjuvant Nivolumab versus Placebo in Muscle-Invasive Urothelial Carcinoma New Engl J Med 2021; 384:2102-14
21 Rosenberg JE, Hoffman-Censits J, Powles T, et al Atezolizumab in patients with locally advanced and metastatic urothelial carcinoma who have progressed following treatment with platinum-based chemotherapy: a single-arm, multicentre, phase 2 trial Lancet 2016; 387:1909-20
22 Balar AV, Galsky MD, Rosenberg JE, et al Atezolizumab as firstline treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: a single-arm, multicentre, phase 2 trial Lancet 2017; 389:67-76
2 3 F u n t S A , L a t t a n z i M , W h i t i n g K , e t a l N e o a d j u v a n t
Atezolizumab With Gemcitabine and Cisplatin in Patients With Muscle-Invasive Bladder Cancer: A Multicenter, Single-Arm, Phase II Trial J Clin Oncol 2022; 40:1312-22
24 Galsky MD, Arija JAA, Bamias A, et al Atezolizumab with or without chemotherapy in metastatic urothelial cancer (IMvigor130): a multicentre, randomised, placebo-controlled phase 3 trial Lancet 2020; 395:1547-57
25 Powles T, Park SH, Voog E, et al Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma New Engl J Med 2020; 383:1218-30
26 Erck A, Aragon-Ching JB Maintenance avelumab for metastatic
urothelial cancer: a new standard of care Cancer Biol Ther 2020; 21:1095-6
27 Powles T, van der Heijden MS, Castellano D, et al Durvalumab alone and durvalumab plus tremelimumab versus chemotherapy in previously untreated patients with unresectable, locally advanced or metastatic urothelial carcinoma (DANUBE): a randomised, openlabel, multicentre, phase 3 trial Lancet Oncol 2020; 21:1574-88
28 Rhea LP, Aragon-Ching JB Advances and Controversies With Checkpoint Inhibitors in Bladder Cancer Clin Med Insights Oncol 2021; 15:11795549211044963
29 Abd El-Salam MA, Smith CEP, Pan CX Insights on recent innovations in bladder cancer immunotherapy Cancer Cytopathol 2022; 130:667-83
30 Ferlay J, Colombet M, Soerjomataram I, et al Cancer incidence and mortality patterns in Europe: Estimates for 40 countries and 25 major cancers in 2018 Eur J Cancer 2018; 103:356-87
31 Siegel RL, Miller KD, Wagle NS, Jemal A Cancer statistics, 2023 CA Cancer J Clin 2023; 73:17-48
32 Kaur J, Patil G, Geynisman DM, Ghatalia P Role of perioperative immunotherapy in localized renal cell carcinoma Ther Adv Med Oncol 2023; 15:17588359231181497
33 Gill DM, Hahn AW, Hale P, Maughan BL Overview of Current and Future First-Line Systemic Therapy for Metastatic Clear Cell Renal Cell Carcinoma Curr Treat Options Oncol 2018; 19:6
34 Tykodi SS, Pichler R Editorial: Immune checkpoint inhibitors in renal cell carcinoma Front Oncol 2023; 13:1203463
3 5 Q u h a l F , M o r i K , B r u c h b a c h e r A , e t a l F i r s t - l i n e Immunotherapy-based Combinations for Metastatic Renal Cell Carcinoma: A Systematic Review and Network Meta-analysis Eur Urol Oncol 2021; 4:755-65
36 Sharma P, Allison JP Immune checkpoint targeting in cancer therapy: toward combination strategies with curative potential Cell 2015; 161:205-14
37 Allaf M, Kim S, Harshman L, et al Phase III RandOmized Study Comparing PErioperative Nivolumab (Nivo) versus Observation in Patients with Renal Cell Carcinoma Undergoing Nephrectomy (PROSPER, ECOG-ACRIN EA8143), a National Clinical Trials Network trial Annal Oncol 2022; 23:S1432-33
38 Tacconi EMC, Tuthill M, Protheroe A Review of Adjuvant Therapies in Renal Cell Carcinoma: Evidence to Date Onco Targets Ther 2020; 13:12301-16
39 Powles T, Tomczak P, Park SH, et al Pembrolizumab versus placebo as post-nephrectomy adjuvant therapy for clear cell renal cell carcinoma (KEYNOTE-564): 30-month follow-up analysis of a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial Lancet Oncol 2022; 23:1133-44
40 Choueiri TK, Tomczak P, Park SH, et al Adjuvant pembrolizumab after nephrectomy in renal-cell carcinoma New Engl J Med 2021; 385:683-94
41 Fitzgerald KN, Motzer RJ, Lee C-H Adjuvant therapy options in renal cell carcinoma targeting the metastatic cascade Nat Rev Urol 2023; 20:179-93
42 Bex A, Uzzo R, Karam J, et al LBA66 IMmotion010: Efficacy and safety from the phase III study of atezolizumab (atezo) vs placebo (pbo) as adjuvant therapy in patients with renal cell carcinoma (RCC) at increased risk of recurrence after resection Ann Oncol 2022; 33:S1431-S2
43 Pal SK, Uzzo R, Karam JA, et al Adjuvant atezolizumab versus
placebo for patients with renal cell carcinoma at increased risk of recurrence following resection (IMmotion010): a multicentre, randomised, double-blind, phase 3 trial Lancet 2022; 400:1103-16
44 Bex A, Russo P, Tomita Y, et al A phase III, randomized, placebo-controlled trial of nivolumab or nivolumab plus ipilimumab in patients with localized renal cell carcinoma at high-risk of relapse after radical or partial nephrectomy (CheckMate 914) J Clin Oncol 2018; 29 (Suppl 8):VIII330
45 Motzer RJ, Russo P, Grunwald V, et al Adjuvant nivolumab plus ipilimumab versus placebo for localised renal cell carcinoma after nephrectomy (CheckMate 914): a double-blind, randomised, phase 3 trial Lancet 2023; 401:821-32
46 Motzer R, Russo P, Gruenwald V, et al LBA4 Adjuvant nivolumab plus ipilimumab (NIVO+ IPI) vs placebo (PBO) for localized renal cell carcinoma (RCC) at high risk of relapse after nephrectomy: Results from the randomized, phase III CheckMate 914 trial Ann Oncol 2022; 33:S1430
47 Motzer RJ, Jonasch E, Agarwal N, et al Kidney Cancer, Version 3 2022, NCCN Clinical Practice Guidelines in Oncology J Natl Compr Canc Netw 2022; 20:71-90
48 Ljungberg B, Albiges L, Abu-Ghanem Y, et al European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update Eur Urol 2022; 82:399-410
49 Fitzgerald KN, Lee CH Personalizing First-Line Management of Metastatic Renal Cell Carcinoma: Leveraging Current and Novel Therapeutic Options J Natl Compr Canc Netw 2022; 20(13)
50 Motzer RJ, Escudier B, McDermott DF, et al Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma New Engl J Med 2015; 373:1803-13
51 McDermott DF, Lee J-L, Bjarnason GA, et al Open-label, singlearm phase II study of pembrolizumab monotherapy as first-line therapy in patients with advanced clear cell renal cell carcinoma J Clin Oncol 2021; 39:1020
52 Vogelzang NJ, Olsen MR, McFarlane JJ, et al Safety and efficacy of nivolumab in patients with advanced non–clear cell renal cell carcinoma: results from the phase IIIb/IV CheckMate 374 study Clin Genitourin Cancer 2020; 18:461-8 e3
5 3 K a d o w a k i N [ C o m b i n a t i o n o f T a r g e t e d T h e r a p y a n d I m m u n o t h e r a p y f o r C a n c
42:1046-9
5 4 R a t h m e l l W K , R u m b l e R B , V a n V e l d h u i z e n P J , e t a l Management of Metastatic Clear Cell Renal Cell Carcinoma: ASCO Guideline J Clin Oncol 2022; 40:2957-95
5 5 M o t z e r R , A l e k s e e v B , R h a S Y , e t a l L e n v a t i n i b p l u s Pembrolizumab or Everolimus for Advanced Renal Cell Carcinoma
New Engl J Med 2021; 384:1289-300
56 Motzer RJ, Tannir NM, McDermott DF, et al Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma
New Engl J Med 2018; 378:1277-90
57 Rini BI, Plimack ER, Stus V, et al Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma New Engl J Med 2019; 380:1116-27
58 Choueiri TK, Powles T, Burotto M, et al Nivolumab plus C a b o z a n t i n i b v e r s u s S u n i t i n i b f o r A d v a n c e d R e n a l - C e l l Carcinoma New Engl J Med 2021; 384:829-41
59 Ljungberg B, Albiges L, Bedke J, et al EAU Guidelines on Renal Cell Carcinoma Limited March 2023 ed Arnhem, The Netherlands : EAU Guidelines Office; 2023; p 29-62
60 Climent C, Soriano S, Bonfill T, et al The role of immunotherapy in non-clear cell renal cell carcinoma Front Oncol 2023; 13:941835
61 Bergmann L, Weber S, Hartmann A, Ahrens M Pathology and systemic therapy of non-clear cell renal cell carcinoma: an overview Expert Rev Anticancer Ther 2021; 21:1273-86
62 Liu K, Qin Z, Xu X, et al Comparative Risk of Renal Adverse Events in Patients Receiving Immune Checkpoint Inhibitors: A Bayesian Network Meta-Analysis Front Oncol 2021; 11:662731
63 Sung H, Ferlay J, Siegel RL, et al Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries CA Cancer J Clin 2021; 71:209-49
64 Welch HG, Albertsen PC Prostate cancer diagnosis and treatment after the introduction of prostate-specific antigen screening: 1986-2005 J Natl Cancer Inst 2009; 101:1325-9
65 Bratt O, Drevin L, Akre O, et al Family History and Probability of Prostate Cancer, Differentiated by Risk Category: A Nationwide Population-Based Study J Natl Cancer Inst 2016; 108:djw110
66 Krstev S, Knutsson A Occupational Risk Factors for Prostate Cancer: A Meta-analysis J Cancer Prev 2019; 24:91-111
67 Campi R, Brookman-May SD, Subiela Henriquez JD, et al Impact of Metabolic Diseases, Drugs, and Dietary Factors on Prostate Cancer Risk, Recurrence, and Survival: A Systematic R
68 Bilusic M, Madan RA, Gulley JL Immunotherapy of Prostate Cancer: Facts and Hopes Clin Cancer Res 2017; 23:6764-70
69 Kantoff PW, Higano CS, Shore ND, et al Sipuleucel-T immunotherapy for castration-resistant prostate cancer New Engl J Med 2010; 363:411-22
70 Kwon ED, Drake CG, Scher HI, et al Ipilimumab versus placebo after radiotherapy in patients with metastatic castration-resistant prostate cancer that had progressed after docetaxel chemotherapy (CA184-043): a multicentre, randomised, double-blind, phase 3 trial Lancet Oncol 2014; 15:700-12
71 Markowski MC, Shenderov E, Eisenberger MA, et al Extreme responses to immune checkpoint blockade following bipolar androgen therapy and enzalutamide in patients with metastatic castration resistant prostate cancer Prostate 2020; 80:407-11
72 Fellner C Ipilimumab (yervoy) prolongs survival in advanced melanoma: serious side effects and a hefty price tag may limit its use P T 2012; 37:503-30
73 Small EJ, Tchekmedyian NS, Rini BI, et al A pilot trial of CTLA4 blockade with human anti-CTLA-4 in patients with hormonerefractory prostate cancer Clin Cancer Res 2007; 13:1810-5
74 McNeel DG, Smith HA, Eickhoff JC, et al Phase I trial of tremelimumab in combination with short-term androgen deprivation in patients with PSA-recurrent prostate cancer Cancer Immunol Immunother 2012; 61:1137-47
75 Jochems C, Tucker JA, Tsang KY, et al A combination trial of vaccine plus ipilimumab in metastatic castration-resistant prostate cancer patients: immune correlates Cancer Immunol Immunother 2014; 63:407-18
76 Hegde A, Jayaprakash P, Couillault CA, et al A Phase I DoseE
Evofosfamide in Combination with Ipilimumab in Advanced Solid Malignancies Clin Cancer Res 2021; 27:3050-60
77 Slovin SF, Higano CS, Hamid O, et al Ipilimumab alone or in
E Bosnali, E Malik Akdas, E Telli, K Teke, O Kara
combination with radiotherapy in metastatic castration-resistant prostate cancer: results from an open-label, multicenter phase I/II study Ann Oncol 2013; 24:1813-21
78 Fizazi K, Drake CG, Beer TM, et al Final Analysis of the Ipilimumab Versus Placebo Following Radiotherapy Phase III Trial in Postdocetaxel Metastatic Castration-resistant Prostate Cancer Identifies an Excess of Long-term Survivors Eur Urol 2020; 78:822-30
79 Beer TM, Kwon ED, Drake CG, et al Randomized, DoubleBlind, Phase III Trial of Ipilimumab Versus Placebo in Asymptomatic or Minimally Symptomatic Patients With Metastatic ChemotherapyNaive Castration-Resistant Prostate Cancer J Clin Oncol 2017; 35:40-7
80 Sharma P, Pachynski RK, Narayan V, et al Initial results from a phase II study of nivolumab (NIVO) plus ipilimumab (IPI) for the
81 Caruso C Anti–PD-1–CTLA4 Combo Hits Prostate Cancer Cancer Discov 2019; 9:569-70
82 Shenderov E, Boudadi K, Fu W, et al Nivolumab plus ipilimumab, with or without enzalutamide, in AR-V7-expressing metastatic castration-resistant prostate cancer: A phase-2 nonrandomized clinical trial Prostate 2021; 81:326-38
83 Evan YY, Kolinsky MP, Berry WR, et al Pembrolizumab plus docetaxel and prednisone in patients with metastatic castrationresistant prostate cancer: long-term results from the phase 1b/2 KEYNOTE-365 cohort B study Eur Urol 2022; 82:22-30
84 Antonarakis ES, Piulats JM, Gross-Goupil M, et al Pembrolizumab for Treatment-Refractory Metastatic Castration-Resistant Prostate
Cancer: Multicohort, Open-Label Phase II KEYNOTE-199 Study J Clin Oncol 2020; 38:395-405
85 Petrylak DP, Loriot Y, Shaffer DR, et al Safety and Clinical Activity of Atezolizumab in Patients with Metastatic CastrationResistant Prostate Cancer: A Phase I Study Clin Cancer Res 2021; 27:3360-9
86 Powles T, Yuen KC, Gillessen S,, et al Atezolizumab with enzalutamide versus enzalutamide alone in metastatic castration-resistant prostate cancer: a randomized phase 3 trial Nat Med 2022; 28:144-53
87 Fong L, Morris MJ, Sartor O, et al A Phase Ib Study of Atezolizumab with Radium-223 Dichloride in Men with Metastatic Castration-Resistant Prostate Cancer Clin Cancer Res 2021; 27:4746-56
88 Kwan EM, Spain L, Anton A, et al Avelumab Combined with Stereotactic Ablative Body Radiotherapy in Metastatic Castrationresistant Prostate Cancer: The Phase 2 ICE-PAC Clinical Trial Eur Urol 2022; 81:253-62
89 Karzai F, VanderWeele D, Madan RA, et al Activity of durvalumab plus olaparib in metastatic castration-resistant prostate cancer in men with and without DNA damage repair mutations J Immunother Cancer 2018; 6:1-12
90 Cheever MA, Higano CS PROVENGE (Sipuleucel-T) in prostate cancer: the first FDA-approved therapeutic cancer vaccine Clin Cancer Res 2011; 17:3520-6
91 Wang I, Song L, Wang BY, et al Prostate cancer immunotherapy: a review of recent advancements with novel treatment methods and efficacy Am J Clin Exp Urol 2022; 10:210-33
Correspondence
Efe Bosnalı, MD (Corresponding Author) efebosnali415@gmail com
Department of Urology, University of Health Sciences, Derince Training and Research Hospital, Turkey, 41380
Enes Malik Akdas, MD
Turkey enesmalikakdas@gmail com
Engin Telli, MD
Turkey engintelli@gmail com
Kerem Teke, MD
Turkey drtekekerem@gmail com
Onder Kara, MD
Turkey onerkara@yahoo com
Kocaeli University, School of Medicine, Department of Urology, Kocaeli, Turkey
Conflict of interest: The authors declare no potential conflict of interest
REVIEW
The influence of oral antioxidants on men with infertility: A systemic review
Tamer A. Abouelgreed 1 , Mohamed A. Amer 2 , Hassan Mamdouh 2 , Ahmed F. El-Sherbiny 3 , Hany Aboelwafa 2 , Sameh F. Fahmy 2 , Omar A. Omar 2 , Mohammed Abdelshakour 2 , Mohammad Elesawy 2 , Mohamed Sonbol 2 , Ahmed N. Maawad 2 , Osama K. Elsayed 2
1 Department of Urology, Al-Azhar University, Cairo, Egypt;
2 Department of Dermatology & Andrology, Al-Azhar University, Cairo, Egypt;
3 Department of Andrology, International Islamic Center for Population Studies and Research, Al-Azhar University, Cairo, Egypt
Summary
Objective: This study aims to investigate the current evidence regarding the impact of oral antioxidant supplementation on semen parameters of infertile men.
Materials and methods: We conducted a systematic search of PubMed, and Cochrane electronic databases, adhering to modified Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The focus was on studies exploring the effects of antioxidant therapy on infertile men, with an examination of antioxidants in terms of types, doses, rationale for use, and their impact on semen parameters measures.
Results: A total of 18 studies that met the inclusion criteria were included in this study. Out of these, 14 studies reported a significantly positive influence of antioxidant therapy on basic semen parameters and advanced sperm function These comprised 11 randomized clinical trials and 7 prospective studies Commonly utilized antioxidants included Vitamin E, Vitamin C, carnitines, co-enzyme Q10, N-acetyl cysteine, zinc, selenium, folic acid, and lycopene
Conclusions: Overall, antioxidants generally demonstrate a favorable effect on semen parameters of infertile men However, further research is necessary to pinpoint the optimal antioxidant regimen that can be applied safely and effectively in clinical practice.
Submitted 30 January 2024; Accepted 18 February 2024
INTRODUCTION
Infertility is defined as the inability to conceive after at least 12 months of regular, unprotected intercourse, a f f e c t i n g a p p r o x i m a t e l y 1 5 % o f c o u p l e
l y Notably, male factors contribute to nearly half of the reported cases, often linked to disturbances in testicular function or blockage of reproductive passages (1, 2) Consequently to the efforts to unravel the molecular-level of idiopathic male infertility, the substantial role played by oxidative stress (OS) has been underscored OS refers to the imbalance in the body's redox state, arising from either excessive oxidants or insufficient antioxidants
Reactive oxygen species (ROS), commonly known as 'free
radicals,' are highly reactive oxygen-derived molecules characterized by unpaired electrons in their outer valence orbital These include oxygen-centered radicals (hydroxyl radical, nitric oxide radical, and superoxide anion radical) and non-radical derivatives (hydrogen peroxide, peroxynitrite anion, and hypochlorous acid) (3, 4) Various endogenous (e g , immature spermatozoa, leukocytes, varicocele) and exogenous (e g , testicular hyperthermia, environmental and habitual exposures) factors have been identified as potential causes of increased ROS production To counterbalance ROS, antioxidants play a crucial role in maintaining the desired redox equilibrium for optimal sperm function (5) Seminal fluid is rich in antioxidants that nourish and protect sperm, existing in two forms: enzymatic and non-enzymatic antioxidant systems (6) The enzymatic system comprises naturally occurring antioxidants, including glutathione peroxidase, superoxide dismutase, and catalase, believed to originate from the prostate and found in sperm cells or seminal plasma In contrast, the non-enzymatic system consists of various compounds obtained through diet or supplements When an excess of ROS is produced or antioxidant activity is insufficient, OS occurs, disrupting the e q u i l i b r i u m
n Spermatozoa are particularly susceptible to OS due to their low levels of enzymatic antioxidants, originating from the prostate Additionally, the high concentration of polyunsaturated fatty acids, notably docosahexaenoic acid, in the sperm cell's plasma membrane makes them attractive targets for ROS-induced oxidation reactions Recent decades have witnessed significant progress in understanding male infertility, incorporating tests like sperm DNA fragmentation (SDF) and measures of OS to enhance clinicians' insights into male fertility potential (7,8) Advances in assisted reproductive therapy (ART) have allowed previously infertile men to father biological children However, OS remains a critical factor influencing reproductive outcomes, both in natural conception and with ART Approximately 25% of infertile men exhibit significant levels of ROS in their semen compared to fertile counterparts (9) OS negatively impacts semen parameters, fertilization rates, embryonic development, and pregnancy rates (10, 11)
The impact of antioxidants on fertility depends by substantial variations in antioxidant forms, dosages, combinations, and outcome measures across studies This literature review aims to explore the most commonly used antioxidants in treating male infertility and investigate the effect of their doses that may confer benefits on basic semen parameters, advanced sperm function tests, outcomes of ART, and live-birth rates
MATERIALS AND METHODS
Research strategy
The research strategy adhered to modified Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (12) A literature search was conducted on PubMed, and Cochrane electronic databases to identify studies exploring the effectiveness of antioxidants in treating male infertility Keywords and Medical Subject Heading (MeSH) phrases included 'antioxidants,' 'male infertility,' semen parameters'
Study selection
Screening of articles was performed based on title and abstract by all authors followed by examination of relevant full papers Additionally, review articles were scrutinized for potential inclusion (male patients, human studies) Exclusion criteria were based on study methods (retrospective, case report, editorial, or commentary) Data extraction was cross-checked and verified
Outcome measures
The outcomes of interest included the type and dosage of antioxidants, their mechanism of action, impact on basic semen parameters and advanced sperm function tests
RESULTS
The search strategy identified 380 articles, with 315 excluded based on title and/or abstract The remaining 65 articles underwent screening, leading to the identification of 18 studies that met the inclusion and exclusion criteria These comprised 11 randomized clinical trials (1323) and 7 prospective studies (24-30) Out of these, 14
Table 1.
The mode of action of commonly used antioxidants
Antioxidant compound
Mechanism of action
Ascorbic acid (vitamin C) Neutralises free radicals
studies (13-19, 24-30) reported a significant positive effect of antioxidant therapy on various parameters such as basic semen parameters, advanced sperm function tests Commonly investigated antioxidants included vitamin E, vitamin C, carnitines, N-acetyl cysteine (NAC), coenzyme Q10 (CoQ10), zinc, selenium, folic acid, and lycopene The doses and mechanisms of action for each antioxidant are presented in Table 1 Additionally, Table 2 outlines the outcomes of antioxidant treatment that were assessed across studies (13-30)
DISCUSSION
A n t i o x i d a n t s , w h e t h e r b i o l o g i c a l o r c h e m i c a l c o mpounds, act scavenging free radicals, neutralizing their
T A Abouelgreed, M A Amer, H Mamdouh, et al
effects, and disrupting the chain reaction leading to OS in body tissues In the context of male fertility, antioxidants are commonly prescribed for their accessibility and relatively low cost However, conflicting results have been observed in studies assessing the impact of antioxidant therapy on male fertility While some studies reported positive effects on semen parameters, sperm function, and pregnancy rates, others failed to confirm such benefits or even indicated a negative influence on male fertility The heterogeneity across studies and the unknown optimal balance of the redox system for sperm function contribute to these discrepancies Overconsumption of antioxidants may lead to reductive stress with potential detrimental effects on human health, including impairment of mitochondrial activity (31-33)
Antioxidants: Mechanism of action and rationale for use
Numerous compounds with antioxidant properties have been explored for treating male infertility (Table 1)
Understanding the mechanisms of action of commonly used compounds is crucial before delving into the associated evidence in clinical practice
Vitamin E (a-tocopherol): This potent chain-breaking antioxidant is a fat-soluble compound predominantly located in cell membranes It quenches free hydroxyl radicals and superoxide anions, reducing lipid peroxidation initiated by ROS at the plasma membrane level Vitamin E levels found to be correlated to the percentage of motile spermatozoa in semen Lower vitamin E levels were observed in the semen of infertile men (34)
Vitamin C (ascorbic acid): A water-soluble compound that is found in high concentrations in seminal plasma more than in blood serum It neutralizes hydroxyl, superoxide, and hydrogen peroxide radicals, offering protection against endogenous oxidative damage Seminal fluid analyses from infertile men with asthenozoospermia revealed lower vitamin C levels and higher ROS levels compared to fertile controls (35)
Carnitines (L-carnitine and L-acetyl carnitine): These watersoluble antioxidants are involved in sperm metabolism, fueling essential activities like sperm motility Carnitines exhibit antioxidant activities by scavenging superoxide anions and hydrogen peroxide radicals, inhibiting lipid peroxidation Semen samples from infertile men with oligoasthenoteratozoospermia showed significantly lower carnitine levels (36)
CoQ10: This vital antioxidant is present in almost all body tissues, particularly in sperm mitochondria involved in cellular respiration and energy production CoQ10's role in promoting motility and acting as an antioxidant is rationalized by its inhibitory effect on superoxide formation (37)
NAC (N-acetyl cysteine): This amino acid, converted to cysteine in body tissues, acts as a precursor of glutathione, a crucial naturally occurring antioxidant that neutralizes various ROS NAC directly reduces OS by scavenging hypochlorous acid and hydroxyl radicals Studies have documented its positive influence on germ cell survival, showcasing reductions in ROS levels and improvements in sperm motility after incubation with NAC (38)
Selenium: An essential trace element, selenium's role in spermatogenesis is linked to its ability to protect sperm
DNA against OS damage Selenium's antioxidant properties are associated with its augmentation of glutathione function Selenoenzymes, including phospholipid hydroperoxide glutathione peroxidase (PHGPX) and sperm capsular selenoprotein glutathione peroxidase, contribute to maintaining sperm structural integrity Selenium deficiency is often correlated with morphological sperm abnormalities and impaired motility (39)
Zinc: Another essential trace element, zinc, plays vital roles in RNA and DNA metabolism, signal transduction, gene expression, and apoptosis regulation Its antioxidant properties stem from its ability to decrease the production of hydrogen peroxide and hydroxyl radicals by antagonizing redox-active transition metals like iron and copper Higher zinc concentrations in seminal plasma are observed in fertile men compared to subfertile men, and zinc deficiency is associated with various sperm structural abnormalities (40)
Folic Acid (Vitamin B9): Involved in nucleic acid synthesis and amino acid metabolism, folic acid is used in male infertility treatment for its free radical scavenging abilities Folic acid intake is linked to an increased reducedto-oxidized glutathione ratio (41)
Lycopene: A naturally synthesized carotenoid found in fruits and vegetables, lycopene contributes significantly to the human redox defense system due to its potent ROS quenching abilities (42)
Antioxidant effect on basic semen parameters
Semen analysis remains a fundamental test for assessing male fertility due to its simplicity and wide availability However, continuous updates in reference values pose challenges in interpreting the evidence surrounding the potential impact of antioxidants, as changes in criteria may label patients differently Despite these challenges, studies have reported improvements in basic semen parameters following oral antioxidant intake, either alone or in combination
Vitamin E: Used in combination with other vitamins and minerals, vitamin E alone (300 mg daily) showed a significant improvement in sperm motility in infertile men (23) A study comparing vitamin E, clomiphene citrate, and a combination of both treatments in patients with idiopathic oligoasthenozoospermia reported a significant improvement in sperm concentration and motility with the combined regimen (13) Another study using vitamin E (400 mg) + selenium (200 µg) for 100 days showed a significant improvement in sperm motility, morphology, or both in infertile men (34) However, some studies failed to reproduce significant effects on semen parameters using vitamin E alone or in combination with other antioxidants (28, 30)
Vitamin C: Studies demonstrated the positive effects of vitamin C, particularly in heavy smokers, showing dosedependent improvements in sperm quality (43) Vitamin C as an adjunct therapy post-varicocelectomy resulted in a statistically significant improvement in sperm motility and morphology compared to a placebo group (44) Several antioxidant supplements containing vitamin C have been investigated, showing significant improvement in sperm motility with combinations including zinc and vitamin E (19)
Carnitines: Studies confirmed the significant influence of carnitines, especially on sperm motility (45) A placebocontrolled trial demonstrated significant improvement in all semen parameters, with the most significant increase in sperm motility, using a combined treatment of L-carnitine (2 g) and L-acetyl carnitine (1 g) (20) LC and LAC treatment showed significant improvement in semen parameters, particularly in patients with lower baseline values of motility (46)
CoQ10: CoQ10 significantly improved sperm concentration and motility compared to placebo in men with idiopathic oligoasthenozoospermia (16) A clinical trial demonstrated improvements in sperm morphology, catalase, and superoxide dismutase with CoQ10 treatment (47) These findings highlight the potential benefits of antioxidant supplementation in improving sperm parameters, but variations in study outcomes emphasize the need for further research and standardization A systematic review of three randomized controlled clinical trials involving 332 infertile men indicated that CoQ10 treatment (200-300 mg daily) led to a significant increase in sperm concentration (MD 5 33 x 10^6 sperm/mL, p < 0 001) and motility (MD 4 5%, p < 0 001) (48)
NAC (N-acetyl cysteine): In a randomized placebo-controlled study of 120 patients with idiopathic infertility, daily treatment with 600 mg NAC for 3 months resulted in a significant improvement in volume, motility, and viscosity of semen compared to placebo (21) Combining 600 mg NAC with 200 mg selenium showed a significant improvement in all semen parameters, with a dosedependent positive correlation between the sum of selenium and NAC concentrations and mean sperm concentration, motility, and normal morphology (17)
Folic Acid: In a double-blind, placebo-controlled interventional study, subfertile men receiving combined therapy of folic acid and zinc showed a statistically significant 74% increase in total normal sperm concentration after 26 weeks of treatment (18)
Selenium: A randomized placebo-controlled clinical trial involving 468 infertile men with idiopathic oligoasthenozoospermia demonstrated significant improvements in all semen parameters with selenium (200 mg) alone, NAC (600 mg) alone, or a combination of both supplements compared to placebo (17) The combination of selenium with vitamin E resulted in increased sperm motility (24) However, a study with normozoospermic men using selenium (300 mg) daily for 48 weeks did not show a significant influence on semen parameters (29)
Zinc: In a prospective trial with asthenozoospermic men, zinc supplementation for 3 months led to a significant improvement in sperm concentration, progressive motility, fertilizing capacity, and a reduction in the incidence of anti-sperm antibodies (19) Oral zinc supplementation restored seminal catalase-like activity and improved sperm concentration and progressive motility in asthenozoospermic men (49)
Lycopene: In a study involving 30 men with idiopathic oligoasthenozoospermia, treatment with 2 mg lycopene twice daily for 3 months resulted in statistically significant improvements in sperm concentration and motility in 66% and 53% of patients, respectively (33) A similar dose of lycopene was used in the treatment of 50 patients
with idiopathic oligoasthenozoospermia, and after a 1year follow-up, sperm concentration, motility, and morphology improved in 70%, 54%, and 38% of patients, respectively (35)
Antioxidant influence on advanced sperm function tests
The conventional semen analysis has faced criticism for its limited ability to predict fertility accurately While it offers valuable information on sperm production, accessory organ secretions, ejaculation, and emission, it falls short in predicting fertility (50) It does not provide insights into the functional potential of sperm to successfully fertilize an ovum or undergo the necessary maturation processes for fertilization To address this limitation, advanced tests of sperm function were developed to enhance the predictive power of semen studies Among these advanced tests, SDF and OS measures have been the most widely studied Recent research has expanded our understanding of the implications of SDF on male fertility (8) Human sperm DNA, mostly bound to protamine, forms a condensed chromatin that is easily transportable through the sperm head and more resistant to damage during transit through the reproductive tracts (51) However, SDF can occur due to errors in chromatin packaging during spermatogenesis or exposure to seminal OS during epididymal transit (52) Both in vitro and in vivo studies confirm that elevated SDF can negatively impact fertility at various stages, including fertilization, early embryo development, implantation, and pregnancy (53,54) Therefore, addressing OS appears to be a justifiable approach to minimize SDF incidence in semen samples Several studies have investigated the impact of dietary antioxidant supplementation on sperm DNA integrity (22, 25, 36, 55) While these studies generally assessed small-sized samples and had short treatment durations, they consistently reported a positive effect on SDF measures For instance, Greco et al (20) found a significant reduction in SDF percentage (p < 0 001) in patients with unexplained infertility and elevated SDF levels treated with vitamin C and vitamin E Another study reported a 19% decrease in SDF (p < 0 001) with a combination of antioxidants containing zinc and selenium (36) Abad et al (29) examined the effects of oral antioxidant therapy on SDF dynamics, revealing significant reductions at each experimental time-point (p < 0 05) Studies also explored antioxidant therapy in patients with high SDF due to varicocele In one study, a c
decrease in SDF levels (22 1%, p = 0 02) and an increase in sperm concentration (p = 0 04) (38) Assessing seminal OS levels has become integral in evaluating infertile men, considering its utility in various clinical scenarios (56) However, routine clinical use is hindered by factors such as test availability, complexity, cost-effectiveness, and a lack of universally accepted analysis methods Various assays, classified as direct (e g , chemiluminescence and flow cytometry assays) and indirect (e g , myeloperoxidase test, lipid peroxidation levels), are available to measure OS Each type has its advantages and disadvantages, with direct assays providing accurate measures but being expensive and requiring expertise, while indirect assays are simpler and more cost-effective but
T A Abouelgreed, M A Amer, H Mamdouh, et al
assess an end state influenced by various unknown pathological processes (57-59) Numerous studies investigating the impact of antioxidant therapy on male fertility have evaluated its effects on OS as a key outcome measure For instance, a 6-month regimen of vitamin E (300 mg daily) significantly reduced lipid peroxidation in semen samples from 110 asthenozoospermic men (23) Similarly, Comhaire et al (24) reported a significant decrease in seminal ROS levels with a combination of 180 mg vitamin E and 30 mg β-carotene in 27 infertile men Omu et al (17) examined the effectiveness of daily supplementation with vitamin E (20 mg), vitamin C (10 mg), and zinc (400 mg) over 3 months in 45 asthenozoospermic men, observing a twofold reduction in malondialdehyde (an indicator of lipid peroxidation) (p < 0 01), a significant decrease in pro-apoptosis markers (p < 0 05), and a substantial increase in total antioxidant capacity (P < 0 01) Another study revealed that vitamin E (400 mg) and selenium (225 mg) intake for 3 months led to significant reductions in malondialdehyde levels, coupled with improvements in sperm motility and viability (24) Furthermore, Oeda et al (60) observed a direct dose- and time-dependent reduction in seminal ROS when semen samples were incubated with N-acetylcysteine (NAC), suggesting the potential usefulness of NAC in reducing OS In a randomized placebo-controlled study involving 120 patients with idiopathic infertility, those receiving 600 mg of NAC daily showed significant improvements in sperm motility compared to the placebo group (61) Additionally, Gharagozloo and Aitken (62) conducted a systematic review of 20 trials, indicating a significant reduction in OS or sperm DNA damage after antioxidant treatment in 19 of them
CONCLUSIONS
Numerous research has investigated the impact of antioxidant therapy on male fertility, demonstrating its potent i a l i n r e v e r s i n g O S - i n d u c e d s p e r m d y s f u n c t i o n Commonly used compounds include vitamin E, vitamin C, carnitines, zinc, selenium, NAC, CoQ10, folic acid, and lycopene However, the identification of an ideal antioxidant treatment method is hindered by study design heterogeneity and the unknown normal physiological level of the fine redox balance Further studies are necessary to determine the optimal and safe antioxidant preparation for managing male infertility
REFERENCES
1 Ahmad Majzoub and Ashok Agarwal Systematic review of antioxidant types and doses in male infertility: Benefits on semen parameters, advanced sperm function, assisted reproduction and live-birth rate Arab J Urol 2018; 16:113-124
2 Agarwal A, Mulgund A, Hamada A, Chyatte MR A unique view on male infertility around the globe Reprod Biol Endocrinol 2015; 13:37
3 Halliwell B Free radicals and vascular disease: how much do we know? BMJ 1993; 307:885-886
4 Brooker RJ Genetics: analysis and principles 4th ed Ohio, USA: McGraw-Hill Higher Education; 2011
5 Aitken RJ, Clarkson JS, Fishel S Generation of reactive oxygen species, lipid peroxidation, and human sperm function Biol Reprod 1989; 41:183-197
6 Sies H Strategies of antioxidant defence Eur J Biochem 1993; 215:213-219
7 Agarwal A, Majzoub A, Esteves SC, et al Clinical utility of sperm DNA fragmentation testing: practice recommendations based on clinical scenarios Transl Androl Urol 2016; 5:935-950
8 Agarwal A, Sharma RK, Nallella KP, et al Reactive oxygen species as an independent marker of male factor infertility Fertil Steril 2006; 86:878-885
9 Agarwal A, Saleh RA, Bedaiwy MA Role of reactive oxygen species in the pathophysiology of human reproduction Fertil Steril 2003; 79:829-843
10 Gharagozloo P, Gutierrez-Adan A, Champroux A, et al A novel antioxidant formulation designed to treat male infertility associated with oxidative stress: promising preclinical evidence from animal models Hum Reprod 2016; 31:252-256
11 ElSheikh MG, Hosny MB, Elshenoufy A, et al Combination of vitamin E and clomiphene citrate in treating patients with idiopathic oligoasthenozoospermia: a prospective, randomized trial Andrology 2015; 3:864-867
12 Paradiso Galatioto G, Gravina GL, Angelozzi G, et al May antioxidant therapy improve sperm parameters of men with persistent oligospermia after retrograde embolization for varicocele? World J Urol 2008; 26:97-102
13 Peivandi S, Karimpour A, Moslemizadeh N Effects of L-carnitine on infertile men ’ s spermogram; a randomized clinical trial J Reprod Infertil 2010; 10:245-251
14 Safarinejad MR Efficacy of coenzyme Q10 on semen parameters, sperm function and reproductive hormones in infertile men J Urol 2009; 182:237-248
15 Safarinejad MR, Safarinejad S Efficacy of selenium and/or Nacetyl-cysteine for improving semen parameters in infertile men: a double-blind, placebo controlled, randomized study J Urol 2009; 181:741-751
16 Wong WY, Merkus HM, Thomas CM, et al Effects of folic acid and zinc sulfate on male factor subfertility: a double-blind, randomized, placebo-controlled trial Fertil Steril 2002; 77:491-498
17 Omu AE, Al-Azemi MK, Kehinde EO, et al Indications of the mechanisms involved in improved sperm parameters by zinc therapy Med Princ Pract 2008; 17:108-116
18 Lenzi A, Sgrò P, Salacone P, et al A placebo-controlled doubleblind randomized trial of the use of combined l-carnitine and lacetyl-carnitine treatment in men with asthenozoospermia Fertil Steril 2004; 81:1578-1584
19 Ciftci H, Verit A, Savas M, et al Effects of Nacetylcysteine on semen parameters and oxidative/antioxidant status Urology 2009; 74:73-76
20 Greco E, Iacobelli M, Rienzi L, et al Reduction of the incidence of sperm DNA fragmentation by oral antioxidant treatment J Androl 2005; 26:349-353
21 Suleiman SA, Ali ME, Zaki ZM, et al Lipid peroxidation and human sperm motility: protective role of vitamin E J Androl 1996; 17:530-537
22 Keskes-Ammar L, Feki-Chakroun N, Rebai T, et al Sperm oxidative stress and the effect of an oral vitamin E and selenium supplement on semen quality in infertile men Arch Androl 2003; 49:83-94
23 Tremellen K, Miari G, Froiland D, Thompson J A randomised control trial examining the effect of an antioxidant (Menevit) on pregnancy outcome during IVF-ICSI treatment Aust N Z J Obstet Gynaecol 2007; 47:216-221
24 Comhaire FH, Christophe AB, Zalata AA, et al The effects of combined conventional treatment, oral antioxidants and essential fatty acids on sperm biology in subfertile men Prostaglandins Leukot Essent Fatty Acids 2000; 63:159-165
25 Gupta NP, Kumar R Lycopene therapy in idiopathic male infertility - a preliminary report Int Urol Nephrol 2002; 34:369-372
26 Moslemi MK, Tavanbakhsh S Selenium-vitamin E supplementation in infertile men: effects on semen parameters and pregnancy rate Int J Gen Med 2011; 4:99-104
27 Mohanty NK, Kumar S, Jha AK, Arora RP Management of idiopathic oligoasthenospermia with lycopene Indian J Urol 2001; 18:57-61
28 Ménézo YJ, Hazout A, Panteix G, et al Antioxidants to reduce sperm DNA fragmentation: an unexpected adverse effect Reprod Biomed Online 2007; 14:418-421
29 Abad C, Amengual MJ, Gosálvez J, et al Effects of oral antioxidant treatment upon the dynamics of human sperm DNA fragmentation and subpopulations of sperm with highly degraded DNA Andrologia 2013; 45:211-216
30 Gual-Frau J, Abad C, Amengual MJ, et al Oral antioxidant treatment partly improves integrity of human sperm DNA in infertile grade I varicocele patients Hum Fertil (Camb) 2015; 18:225229
31 Singh F, Charles AL, Schlagowski AI, et al Reductive stress impairs myoblasts mitochondrial function and triggers mitochondrial hormesis BBA 2015; 1853:1574-1585
32 Mentor S, Fisher D Aggressive antioxidant reductive stress impairs brain endothelial cell angiogenesis and blood brain barrier function Curr Neurovasc Res 2017; 14:71-81
33 Lamosova D, Jurani M, Greksak M, et al Effect of Rooibos tea (Aspalathus linearis) on chick skeletal muscle cell growth in culture Comp Biochem Physiol C: Pharmacol Toxicol Endocrinol 1997; 116:39-45
34 Omu AE, Fatinikun T, Mannazhath N, Abraham S Significance of simultaneous determination of serum and seminal plasma alphatocopherol and retinol in infertile men by high-performance liquid chromatography Andrologia 1999; 31:347-354
35 Jacob RA, Pianalto FS, Agee RE Cellular ascorbate depletion in healthy men J Nutr 1992; 122:1111-1118
36 Banihani S, Agarwal A, Sharma R, Bayachou M Cryoprotective effect of L-carnitine on motility, vitality and DNA oxidation of human spermatozoa Andrologia 2014; 46:637-641
37 Lewin A, Lavon H The effect of coenzyme Q10 on sperm motility and function Mol Aspects Med 1997; 18(Suppl ):S213-219
38 Erkkila K, Hirvonen V, Wuokko E, et al N-acetyl-L-cysteine inhibits apoptosis in human male germ cells in vitro J Clin Endocrinol Metab 1998; 83:2523-2531
39 Ursini F, Heim S, Kiess M, et al Dual function of the selenoprotein PHGPx during sperm maturation Science 1999; 285:13931396
40 Hambidge KM, Krebs NF Zinc deficiency: a special challenge J Nutr 2007; 137:1101-1105
41 Joshi R, Adhikari S, Patro BS, et al Free radical scavenging
behavior of folic acid: evidence for possible antioxidant activity Free Radic Biol Med 2001; 30:1390-399
42 Agarwal A, Sekhon LH Oxidative stress and antioxidants for idiopathic oligoasthenoteratospermia: Is it justified? Indian J Urol 2011; 27:74-85
43 Cooper TG, Noonan E, von Eckardstein S, et al World Health Organization reference values for human semen characteristics Hum Reprod Update 2010; 16:231-245
44 Dawson EB, Harris WA, Teter MC, Powell LC Effect of ascorbic acid supplementation on the sperm quality of smokers Fertil Steril 1992; 58:1034-1039
45 Cyrus A, Kabir A, Goodarzi D, Moghimi M The effect of adjuvant vitamin C after varicocele surgery on sperm quality and quantity in infertile men: a double blind placebo controlled clinical trial Int Braz J Urol 2015; 41:230-238
46 Balercia G, Regoli F, Armeni T, et al Placebo-controlled doubleblind randomized trial on the use of L-carnitine, L-acetylcarnitine, or combined L-carnitine and L-acetylcarnitine in men with idiopathic asthenozoospermia Fertil Steril 2005; 84:662-671
47 Nadjarzadeh A, Shidfar F, Amirjannati N, et al Effect of Coenzyme Q10 supplementation on antioxidant enzymes activity and oxidative stress of seminal plasma: a double-blind randomised clinical trial Andrologia 2014; 46:177-183
48 Lafuente R, González-Comadrán M, Solà I, et al Coenzyme Q10 and male infertility: a meta-analysis J Assist Reprod Genet 2013; 30:1147-1156
49 Hadwa MH, Almashhedy LA, Alsalman AR Oral zinc supplementation restores superoxide radical scavengers to normal levels in spermatozoa of Iraqi asthenospermic patients Int J Vitam Nutr Res 2015; 85:165-173
50 Esteves SC Clinical relevance of routine semen analysis and controversies surrounding the 2010 World Health Organization criteria for semen examination Int Braz J Urol 2014; 40:443-453
51 Erenpreiss J, Spano M, Erenpreisa J, et al Sperm chromatin structure and male fertility: biological and clinical aspects Asian J Androl 2006; 8:11-29
52 Shamsi MB, Kumar R, Dada R Evaluation of nuclear DNA damage in human spermatozoa in men opting for assisted reproduction Indian J Med Res 2008; 127:115-123
53 Sharma RK, Said T, Agarwal A Sperm DNA damage and its clinical relevance in assessing reproductive outcome Asian J Androl 2004; 6:139-148
54 Saleh RA, Agarwal A, Sharma RK, et al Evaluation of nuclear DNA damage in spermatozoa from infertile men with varicocele Fertil Steril 2003; 80:1431-1436
55 Saleh RA, Agarwal A, Nada EA, et al Negative effects of increased sperm DNA damage in relation to seminal oxidative stress in men with idiopathic and male factor infertility Fertil Steril 2003; 79(Suppl 3):1597-1605
56 Agarwal A, Cho CL, Esteves SC Should we evaluate and treat sperm DNA fragmentation? Curr Opin Obstet Gynecol 2016; 28:164-171
57 Gil-Villa AM, Cardona-Maya W, Agarwal A, et al Role of male factor in early recurrent embryo loss: do antioxidants have any effect? Fertil Steril 2009; 92:565-571
58 Agarwal A, Makker K, Sharma R Clinical relevance of oxidative stress in male factor infertility: an update Am J Reprod Immunol 2008; 59:2-11
59 Agarwal A, Tvrda E, Sharma R Relationship amongst terato-
zoospermia, seminal oxidative stress and male infertility Reprod Biol Endocrinol 2014; 12:45
60 Oeda T, Henkel R, Ohmori H, Schill WB Scavenging effect of Nacetyl-L-cysteine against reactive oxygen species in human semen: a possible therapeutic modality for male factor infertility? Andrologia 1997; 29:125-131
Correspondence
Tamer A Abouelgreed, MD (Corresponding Author) dr tamer ali@yahoo com; tamerali 8@azhar edu eg Department of Urology, Al-Azhar University, Cairo, Egypt & Gulf medical university, Ajman, UAE
Mohamed A Amer, MD amerrom@yahoo com
Hassan Mamdouh, MD hsdermaclinic@yahoo com
Hany Aboelwafa, MD dr hanyos138@yahoo com
Sameh F Fahmy samehmohamed74@azhar edu eg
Omar A Omar, MD omarabdelhady 236@azhar edu eg Mohammed Abdelshakour, MD Dr mohammed 121@yahoo com
Mohammad Elesawy, MD elesawy288@gmail com
Mohamed Sonbol, MD bosombol1185@gmail com
Ahmed N Maawad, MD ah nabil70@gmail com
Osama K Elsayed Osamaandroderma@gmail com
Department of Dermatology & Andrology Al-Azhar University, Cairo, Egypt
Ahmed F El-Sherbiny, MD - Ahmed derma@yahoo com
Department of Andrology, International Islamic Center for Population Studies and Research, Al-Azhar University, Cairo, Egypt
Conflict of interest: The authors declare no potential conflict of interest
61 Benatta M, Kettache R, Buchholz N, Trinchieri A The impact of nutrition and lifestyle on male fertility Arch Ital Urol Androl 2020; 92 121-131
62 Gharagozloo P, Aitken RJ The role of sperm oxidative stress in male infertility and the significance of oral antioxidant therapy Hum Reprod 2011; 26:1628-1640
INSTRUCTIONS TO AUTHORS – ARCHIVIO ITALIANO
OPEN ACCESS
Open access publishing does have its costs. Information regarding authors’ payment are not made available to editors and reviewers ensuring that they cannot be influenced in their selection of papers for publication by payment conditions or limitations. The Article Processing Charge for publication in this journal is EUR 300,00 (plus VAT, if applicable).
Our fees cover the costs of peer review, copyediting, publication, different format of publication (HTML, PDF), inclusion in many Open Access databases.
All bank charges shall be borne by the payer. Please note that our fees do not include taxes (VAT):
- Private or public ITALIAN customers (individuals, universities, hospitals, other organizations) must ALWAYS add VAT (IVA) at standard rate (4%);
- European Union PRIVATE customers must add the standard rate of their own country VAT tax;
- European Union private/public ORGANIZATIONS (universities, hospitals, others with regular VAT number) should not add any taxes at standard rate, provided that they indicate their VAT number;
- Outside the European Union, individuals and organizations should not add any taxes at standard rate.
Important: Authors are NOT required to pay at the moment of submission. If the paper is accepted, the Managing Editor of Open Access Edition will guide the Authors through the payment procedure. No article will be published before waiver or payment.
According to the United Nations list of Least Developed Countries (LCDs) available from: http://www.un.org/en/development/desa/policy/cdp/ldc2/ldc_countries.shtml Authors coming from those countries are entitled to ask for a discount.
A “Formal Request for discount” has to be forwarded to the Managing Editor of Open Access Edition, after receiving the acceptance letter. The Editorial Committee will then evaluate the merits of each individual case.
Any other informal request (such as comments at the moment of submission, or made in the covering letter of the revised version) will not be taken into consideration.
FAST-TRACK PEER REVIEW
All papers published in Archivio Italiano di Urologia e Andrologia (AIUA) are peer reviewed. Fast-track peer review (4 weeks) can be obtained by supplementary fee of € 488 (VAT included).
METHODS OF PAYMENT Authors can pay their fees by: PayPal is the most recommended and secure payment system. It enables you to pay getting your payment receipt immediately and without sharing your financial information. Other methods of payment are:
Bank transfer
BANK NAME: Banca Popolare di Sondrio, Branch #1, Strada Nuova 75, I-27100 Pavia, Italy
ACCOUNT HOLDER: PAGEPress Srl
BIC/SWIFT: POSOIT22
IBAN: IT85Y0569611301000005086X83
Credit Card The credit card form to be filled and returned either via e-mail or via fax is available for download here.
Check sent by surface mail Checks must be made payable to PAGEPress Srl and must be sent to our full postal address: PAGEPress Publications, via A. Cavagna Sangiuliani 5, 27100 Pavia, Italy.
Note: In any method of payment you choose, kindly specify: 1. journal name; 2. paper ID number; 3. first author.
IMPORTANT TO KNOW
REGISTERED DRUGS, DIET SUPPLEMENTS, NUTRACEUTICALS, MEDICAL DEVICES
Authors of papers that contain references to registered drugs, diet supplements, nutraceuticals and medical devices are requested to buy a minimum amount of 100 reprints at a cost of € 1.500 (1 to 4 pages) or € 2.000 (5 to 8 pages). Prices for the purchase of number of reprints greater than 100 can be negotiated with Edizioni Scripta Manent At present, Edizioni Scripta Manent let everyone to read, print and download papers from website, but retains copyright for republishing and distribution rights for commercial purpose.
TRANSLATION
Translation of manuscripts in Italian language is offered on payment.
Translation and reprints can be requested to Edizioni Scripta Manent by e-mail to info@edizioniscriptamanent.eu
AUTHORS’ RESPONSIBILITIES
Manuscripts are accepted with the understanding that they have not been published or submitted for publication in any other journal.
Authors must submit the results of clinical and experimental studies conducted according to the Helsinki Declaration on clinical research and to the Ethical Code on animal research set forth by WHO (WHO Chronicle 1985; 39:51). The Authors must obtain permission to reproduce figures, tables and text from previously published material. Written permission must be obtained from the original copyright holder (generally the Publisher).
MANUSCRIPT PRESENTATION
Authors must submit their manuscripts (MAC and WINDOWS Microsoft Word are accepted) after registration and login to the link: http://www.aiua.it. Surface or e-mail submission are not accepted.
Manuscripts must be written in English language in accordance with the “Uniform Requirements for Manuscripts submitted to biomedical journals” defined by The International Committee of Medical Journal Editors (http://www.ICMJE.org). Manuscripts
in Italian language can be published after translation (expenses will be charged to the Authors). Manuscripts should be typed double spaced with wide margins. They must be subdivided into the following sections:
TITLE PAGE
It must contain: a) title; b) a short (no more than 40 characters) running head title; c) first, middle and last name of each Author without abbreviations; d) University or Hospital, and Department of each Author; e) last name, address and e-mail of all the Authors; f) corresponding Author; g) acknowledgement of conflict of interest and financial support.
SUMMARY
Authors must submit a summary (300 words, 2000 characters) divided by subheadings as follows: Objective(s), Material and method(s), Result(s), Conclusion(s). After the summary, three to ten key words must appear, taken from the standard Index Medicus terminology.
TEXT
For original articles concerning experimental or clinical studies, the following standard scheme must be followed: Summary - Key Words - Introduction - Material and Methods - Results - Discussion - Conclusions - References - Tables - Legends - Figures.
Case Report should be divided into: Summary - Introduction (optional) - Case report(s) - Conclusions - References
Supplementary Materials can be added for online publication.
SIZE OF MANUSCRIPTS
Literature reviews, Editorials and Original articles should not exceed 3500 words with 3-5 figures or tables, and no more than 30 references.
Case reports, Notes on surgical technique, and Letters to the editors should not exceed 1000 words (summary included) with only one table or figure, and no more than three references. No more than five authors are permitted.
REFERENCES
References must be sorted in order of quotation and numbered with arabic digits between parentheses. Only the references quoted in the text can be listed. Unpublished studies cannot be quoted, however articles “in press” can be listed with the proper indication of the journal title, year and possibly volume. References must be listed as follows.
JOURNAL ARTICLES
All Authors if there are six or fewer, otherwise the first three, followed by “et al.”. Complete names for Work Groups or Committees. Complete title in the original language. Title of the journal following Index Medicus rules. Year of publication; Volume number: First page. Example: Starzl T, Iwatsuki S, Shaw BW, et al. Left hepatic trisegmentectomy Surg Gynecol Obstet. 1982; 155:21.
BOOKS
Authors - Complete title in the original language. Edition number (if later than the first). City of publication: Publisher, Year of publication. Example: Bergel DIA. Cardiovascular dynamics. 2nd ed. London: Aca de mic Press Inc., 1974.
BOOK CHAPTERS
Authors of the chapters - Complete chapter title. In: Book Editor, complete Book Title, Edition number. City of publication: Publisher, Publication year: first page of chapter in the book. Example: Sagawa K. The use of central theory and system analysis. In: Bergel DH (Ed), Cardiovascular dynamics. 2nd ed. London: Aca demic Press Inc., 1964; 115.
TABLES
Tables must be numbered in Arabic digits and referred to in the text by progressive numbers. Every table must be accompanied by a brief title. The meaning of any abbreviations must be explained at the bottom of the table itself.
FIGURES
(Graphics, algorithms, photographs, drawings). Figures must be numbered and quoted in the text by number. The meaning of symbols or abbreviations must be indicated. Histology photograph legends must include the enlargement ratio and the staining method. Legends must be collected in one or more separate pages.
• Do not include any illustrations as part of your text file. • Do not prepare any figures in Word as they are not workable. • Line illustrations must be submitted at 600 DPI.
• Halftones and color photos should be submitted at a minimum of 300 DPI. • Power Point files cannot be uploaded. • If possible please avoid transmitting electronic files in JPEG format or save the JPEG at the highest quality available • PDF files may be uploaded.
MANUSCRIPT REVIEW
Manuscripts are evaluated by the Editorial Board and/or by two referees designated by the Editors. The Authors are informed in a time as short as possible on whether the paper has been accepted, rejected or if a revision is deemed necessary. The Editors reserve the right to make editorial and literary corrections with the goal of making the article clearer or more concise, without altering its contents. Submission of a manuscript implies acceptation of all above rules.
PROOFS
Authors are responsible for ensuring that all manuscripts are accurately typed before final submission. Galley proofs will be sent to the first Author. Proofs should be returned within seven days from receipt.
Salutepertutti.it è un progetto indipendente. Abbonati per i tuoi pazienti in sala d’aspetto.