12992 Multiparametric MRI targeted prostate biopsy: When omit systematic biopsy?
Pietro Pepe, Ludovica Pepe, Vincenzo Fiorentino, Mara Curduman, Filippo Fraggetta
13194 Effectiveness of cognitive fusion transrectal ultrasound prostate biopsy when compared with final prostatectomy histology
Ana Sofia Araújo, João Serra, Sara Anacleto, Ricardo Rodrigues, Catarina Tinoco, Andreia Cardoso, Mariana Capinha, Vera Marques, Paulo Mota
13257 Radical prostatectomy outcomes of prostate cancer cases: Insights from a leading surgeon's experience in Azerbaijan
Rashad Sholan
12829 Outcomes of transperineal reanastomosis as a salvage treatment for recurrent vesicourethral anastomosis stenosis after radical prostatectomy
Piotr Gwara, Łukasz Białek, Marta Rydzínska, Jakub Dobruch, Michał Skrzypczyk
12990 The learning cur ve for robotic-assisted pyeloplasty in urologists with no prior robotic experience using an ex-vivo model: A prospective, controlled study
12997 Role of inflammator y markers in predicting spontaneous passage of ureteral stones less than 10 mm
Ismaeel Aghaways, Rawa Bapir, Nabaz S Siwaily, Ahmed Mohammed Abdalqadir, Shakhawan Hamaamin Said, Ayman M Mustafa, Bryar Othman Muhammed, Hawbash M Rahim, Berun A Abdalla, Fahmi H Kakamad, Shvan H Mohammed
13295 Development and internal validation of El-Shazly-Buchholz’s nomogram to predict postoperative complications after PCNL: A multicenter study
Rawa Bapir, Kamran Bhatti, Mohamed El-Shazly, Juan Antonio Galan, Ahmed M Harraz, Sarwar Noori Mahmood, Renato N Pedro, Pablo Vargas, Athanasios Papatsoris, Alberto Trinchieri, Noor Buchholz
13158 Emergency treatment of obstructive pyelonephritis: A single center series
Bulent Kati, Eser Ordek, Omer Madsar, Eyyup Sabri Pelit
13163 Should patients with encrusted JJ stents involving the proximal/renal loop undergo primarily endoscopic combined intrarenal surger y?
Alexandra Rocha, Gonc ̧ alo Mendes, Sofia Mesquita, Mariana Madanelo, João Vital, Miguel Marques-Monteiro, Nuno Vinagre, Martinha Magalhães, Beatriz Oliveira, Guilherme Gonc ̧alves, Vítor Cavadas, Avelino Fraga
13156 Single site multi puncture supine (SMS) PCNL procedure in patient with complex renal stone: One incision, why should more?
Paksi Satyagraha, Reza Amorga, Taufiq Nur Budaya
12862 Analysis of the top-down HoLEP learning cur ve: A single-center experience of two clinical fellows
Karim Daher, Moustafa Fathy, Amr Hodhod, Parsa Nikoufar, Abdulrahman Alkandari, Loay Abbas, Ruba Abdul Hadi, Hazem Elmansy
12957 Altieri modified Nesbit corporoplasty for the treatment of penile cur vature: Comparison of local anesthesia vs loco-regional anesthesia on the clinical outcomes
Vincenzo Maria Altieri, Pietro Saldutto, Vittore Verratti, Roberto La Rocca, Ernesto Di Mauro, Giuseppe Celentano, Marco Capece, Vincenzo Morgera, Gianluigi Cacace, Walter Vena, Francesco Mastrangelo, Luigi Napolitano, Fabrizio Iacono
12894 Correlation between histopathology properties of dartos tissue and the severity of penile cur vature in hypospadias
Gede W K Duarsa, Pande M W Tirtayasa, Ni Wayan Winarti, Andy Michael, Komang H A Duarsa
12756 Evaluation of the effect of daily tadalafil 5 mg ver sus daily sildenafil 25 mg on neutrophil-lymphocyte and platelet-lymphocyte ratios in patients with erectile dysfunction: A comparative randomized controlled study
Abdel Rahman Bakry, Ali Mohamed Mahran, Hisham Diab Gaber, Mohamed Ismail Sedek, Sameh Fayek GamalEl Din, Ahmad Tarek Motawi, Mohamed Diab Mohamed, Ahmed Elshebany
EDITORIAL BOARD
EDITOR IN CHIEF
Alberto Trinchieri (Milan, Italy)
ASSOCIATE EDITORS
Emanuele Montanari, Department of Urology, IRCCS Foundation Ca’ Granda Ospedale Maggiore Policlinico, University of Milan, Italy – Gianpaolo Perletti, Department of Biotechnology and Life Sciences, Section of Medical and Surgical Sciences, University of Insubria, Varese, Italy; Department of Human Structure and Repair, Ghent University, Ghent, Belgium - Angelo Porreca, Robotic Urology and Mini Invasive Urologic Surgery Unit, Abano Terme Hospital, Abano Terme, Italy
EXECUTIVE EDITORIAL BOARD
Alessandro Antonelli, Department of Urology, Azienda Ospedaliera Universitaria Integrata (A O U I ), Verona, Italy - Antonio Celia, Department of Urology, San Bassiano Hospital, Bassano del Grappa, Italy - Luca Cindolo, Department of Urology, Villa Stuart Hospital, Rome, Italy - Andrea Minervini, Department of Urology, University of Florence, Unit of Oncologic Minimally-Invasive Urology and Andrology, Careggi Hospital, Florence, Italy - Bernardo Rocco, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy - Riccardo Schiavina, Department of Urology, University of Bologna, Bologna, Italy
ADVISORY EDITORIAL BOARD
Pier Francesco Bassi, Urology Unit, A Gemelli Hospital, Catholic University of Rome, Italy – Francesca Boccafoschi, Health Sciences Department, University of Piemonte Orientale in Novara, Italy – Alberto Bossi, Department of Radiotherapy, Gustave Roussy Institute, Villejuif, France –Tommaso Cai, S Chiara Hospital, Trento, Italy –Paolo Caione, Department of Nephrology-Urology, Bambino Gesù Pediatric Hospital, Rome, Italy – Luca Carmignani, Urology Unit, San Donato Hospital, Milan, Italy –Liang Cheng, Department of Urology, Indiana University School of Medicine, Indianapolis, IN; Department of Pathology and Laboratory Medicine, Indiana University School of Medicine, Indianapolis, IN – Giovanni Colpi, Retired Andrologist, Milan, Italy – Giovanni Corona, Department of Urology, University of Florence, Careggi Hospital, Florence, Italy – Antonella Giannantoni, Department of Surgical and Biomedical Sciences, University of Perugia, Italy – Paolo Gontero, Department of Surgical Sciences, Molinette Hospital, Turin, Italy – Steven Joniau, Organ Systems, Department of Development and Regeneration, KU Leuven, Belgium – Frank Keeley, Bristol Urological Institute, Southmead Hospital, Bristol UK – Laurence Klotz, Division of Urology, Department of Surgery, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, Ontario, Canada – Börje Ljungberg, Urology and Andrology Unit, Department of Surgical and Perioperative Sciences, Umeå University, Umeå, Sweden –Nicola Mondaini, Uro-Andrology Unit, Santa Maria Annunziata Hospital, Florence, Italy – Gordon Muir, Department of Urology, King's College Hospital, London, UK –Giovanni Muto, Urology Unit, Bio-Medical Campus University, Turin, Italy – Anup Patel, Department of Urology, St Mary's Hospital, Imperial Healthcare NHS Trust, London, UK – Glenn Preminger, Division of Urologic Surgery, Duke University Medical Center, Durham, NC, USA – David Ralph, St. Peter's Andrology Centre and Institute of Urology, London, UK – Allen Rodgers, Department of Chemistry, University of Cape Town, Cape Town, South Africa – Francisco Sampaio, Urogenital Research Unit, State University of Rio de Janeiro, Rio de Janeiro, RJ, Brazil – Kemal Sarica, Department of Urology, Kafkas University Medical School, Kars, Turkey – Luigi Schips, Department of Urology, San Pio da Pietrelcina Hospital, Vasto, Italy – Hartwig Schwaibold, Bristol Urological Institute, Southmead Hospital, Bristol, UK – Alchiede Simonato, Department of Urology, University of Verona, Azienda Ospedaliera Universitaria Integrata, Verona, Italy – Carlo Terrone, Department of Urology, IRCCS S Martino University Hospital, Genova, Italy – Anthony Timoney, Bristol Urological Institute, Southmead Hospital, Bristol, UK – Andrea Tubaro, Urology Unit, Sant’Andrea Hospital, “La Sapienza” University, Rome, Italy – Richard Zigeuner, Department of Urology, Medical University of Graz, Graz, Austria
BOARD OF REVIEWERS
Maida Bada, Department of Urology, S Pio da Pietrelcina Hospital, ASL 2 Abruzzo, Vasto, Italy - Lorenzo Bianchi, Department of Urology, University of Bologna, Bologna, Italy - Mariangela Cerruto, Department of Urology, Azienda Ospedaliera Universitaria Integrata (A O U I ), Verona, Italy - Francesco Chessa, Department of Urology, University of Bologna, Bologna, Italy - Daniele D’Agostino, Robotic Urology and Mini In-
vasive Urologic Surgery Unit, Abano Terme Hospital, Abano Terme, Italy - Fabrizio Di Maida, Department of Urology, University of Florence, Unit of Oncologic Minimally-Invasive Urology and Andrology, Careggi Hospital, Florence, Italy - Antonio Galfano, Urology Unit, Niguarda Hospital, Milan, Italy - Michele Marchioni, Department of Medical, Oral and Biotechnological Sciences, "G. d'Annunzio" University of Chieti, Laboratory of Biostatistics, Chieti, Italy - Andrea Mari, Department of Urology, University of Florence, Unit of Oncologic Minimally-Invasive Urology and Andrology, Careggi Hospital, Florence, Italy - Luigi Napolitano, Unit of Urology, Department of Neurosciences, Reproductive Sciences, and Odontostomatology University of Naples “Federico II”, Naples, Italy - Antonio Porcaro, Department of Urology, Azienda Ospedaliera Universitaria Integrata (A O U I ), Verona, Italy - Stefano Puliatti, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy - Daniele Romagnoli, Robotic Urology and Mini Invasive Urologic Surgery Unit, Abano Terme Hospital, Abano Terme, Italy - Chiara Sighinolf, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy - Tommaso Silvestri, Urology Clinic, Department of Medical, Surgical and Health Science, University of Trieste, Trieste, Italy - Petros Sountoulides, Aristotle University of Thessaloniki, Department of Urology, Thessaloniki, Greece - Alessandro Tafuri, Department of Urology, Vito Fazzi Hospital, Lecce, Italy
SIEUN EDITOR
Pasquale Martino, Department of Emergency and Organ Transplantation-Urology I, University Aldo Moro, Bari, Italy
SIEUN EDITORIAL BOARD
Emanuele Belgrano, Department of Urology, Trieste University Hospital, Trieste, ItalyFrancesco Micali, Department of Urology, Tor Vergata University Hospital, Rome, ItalyMassimo Porena, Urology Unit, Perugia Hospital, Perugia, Italy – Francesco Paolo Selvaggi, Department of Urology, University of Bari, Italy – Carlo Trombetta, Urology Clinic, Cattinara Hospital, Trieste, Italy – Giuseppe Vespasiani, Department of Urology, Tor Vergata University Hospital, Rome, Italy – Guido Virgili, Department of Urology, Tor Vergata University Hospital, Rome, Italy
UrOP EDITOR
Carmelo Boccafoschi, Department of Urology, Città di Alessandria Clinic, Alessandria, Italy
UrOP EDITORIAL BOARD
Renzo Colombo, Department of Urology, San Raffaele Hospital, Milan, Italy – Roberto Giulianelli, Department of Urology, New Villa Claudia, Rome, Italy – Massimo Lazzeri, Department of Urology, Humanitas Research Hospital, Rozzano (Milano), Italy – Angelo Porreca, Department of Urology, Polyclinic Abano Terme, Abano Terme (Padova), Italy –Marcello Scarcia, Department of Urology, "Francesco Miulli" Regional General Hospital, Acquaviva delle Fonti (Bari), Italy – Nazareno Suardi, Department of Urology, San Raffaele Turro, Milano, Italy
GUN EDITOR
Arrigo Francesco Giuseppe Cicero, Medical and Surgical Sciences Department, Sant’Orsola-Malpighi University Hospital, Bologna, Italy
GUN EDITORIAL BOARD
Gianmaria Busetto, Department of Urology, Sapienza University of Rome, Italy –Tommaso Cai, Department of Urology, Santa Chiara Regional Hospital, Trento, Italy –Elisabetta Costantini, Andrology and Urogynecological Clinic, Santa Maria Hospital of Terni, University of Perugia, Terni, Italy – Angelo Antonio Izzo, Department of Pharmacy, University of Naples, Italy – Vittorio Magri, ASST Nord Milano, Milano, Italy – Salvatore Micali, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy – Gianni Paulis, Andrology Center, Villa Benedetta Clinic, Rome, Italy – Francesco Saverio Robustelli della Cuna, University of Pavia, Italy – Giorgio Ivan Russo, Urology Department, University of Catania, Italy – Konstantinos Stamatiou, Urology Department, Tzaneio Hospital, Piraeus, Greece – Annabella Vitalone, Department of Physiology and Pharmacology, Sapienza University of Rome, Rome, Italy
Un'opera nuova e completa sul microbiota, il complesso consorzio di batteri che abita il nostro organismo e ne influenza lo status di salute omalattia. Centinaia di illustrazioni a colori, contenuti multimediali, aggiornati in progress continuo ed accessibili mediante QR code. Un Trattato imprescindibile per chi si occupa di salute interpretando i referti sul microbiota.
Costo di copertina €120,00, + spese di spedizione. Per informazioni ed eventuali ordini, scrivere a: info@edizioniscriptamanent.eu
ORIGINAL PAPERS
12951 Comparative study between intrathecal fentanyl and dorsal penile nerve block for controlling postoperative pain after inflatable penile prosthesis implantation
Adel Elatreisy, Yasser Ahmed, Ahmed Elgarhy, Mohamed Hindawy, Tamer Abouelgreed, Ismail Ahmed, Abdalla Abdalla, Hany Ramadan, Mohamed Aboelsuod, Khaled Shrief, Ayman Mohamed, Wael Ibrahim, Saeed Abdelhameed, Mohammad Alghamdi, Mohammed Alzahrani, Hamada Youssof
13119Pelvic floor contraction as an initial response to psycho-sensory sexual stimulation in men and a trigger for male sexual behaviour
Giuseppe La Pera, Sabrina Anticoli, Marilena Mangiardi, Stefano Livi
12427Reassessing cardiovascular risk stratification in men with erectile dysfunction
João Lorigo, Daniela M. Gomes, Ana R. Ramalho, Edgar T. Silva, Patrícia A. Mendes, Arnaldo Figueiredo
12891The effect of vitamin D in vitro supplementation on sperm deoxyribonucleic acid fragmentation
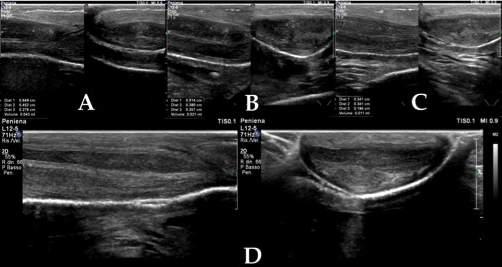
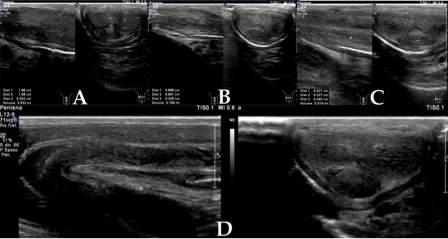
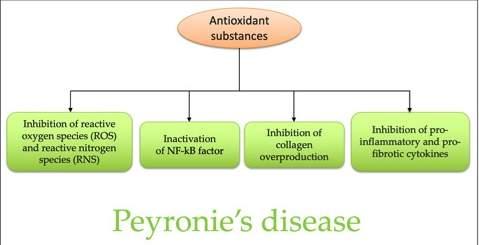
12956Healing of Peyronie's disease after multimodal antioxidant treatment. A case series
Gianni Paulis, Giovanni De Giorgio, Andrea Paulis
META-ANALYSIS
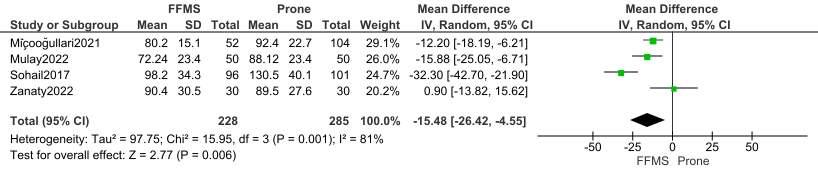
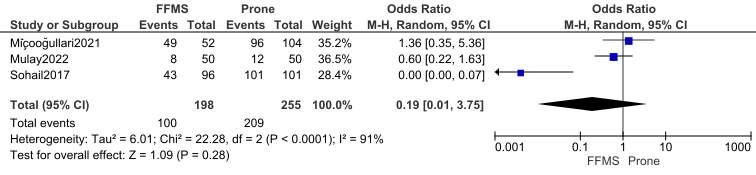
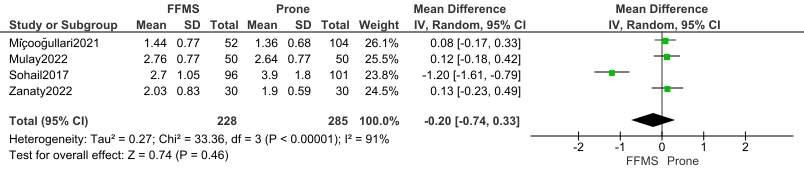
12944Barts flank-free modified supine position vs prone position in percutaneous nephrolithotomy: Systematic review and meta analysis
I Gede Yogi Prema Ananda, Kadek Budi Santosa, I Wayan Yudiana, Pande Made Wisnu Tirtayasa, Ida Bagus Putra Pramana, Nyoman Gede Prayudi, Gede Wirya Kusuma Duarsa
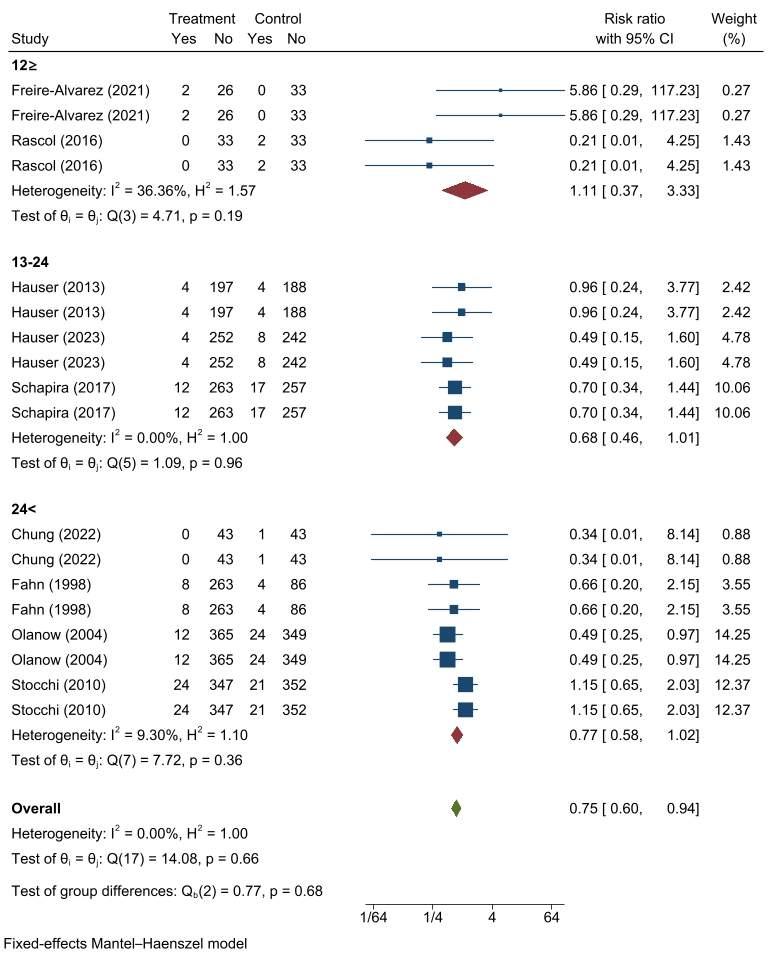
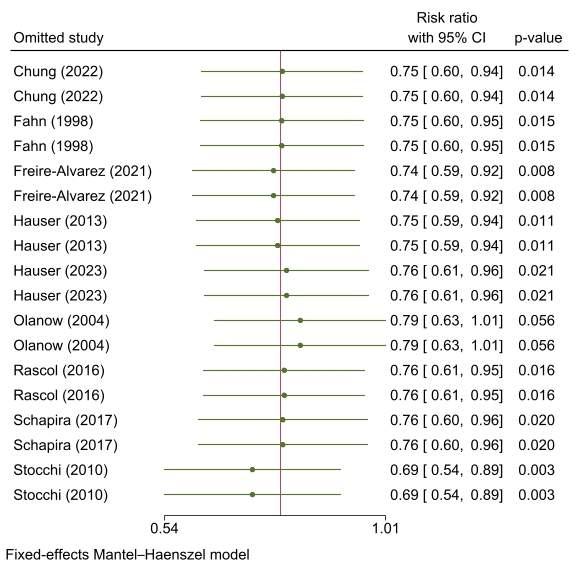
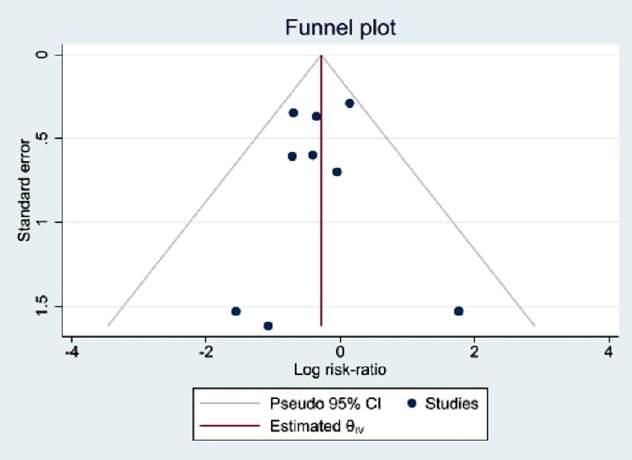
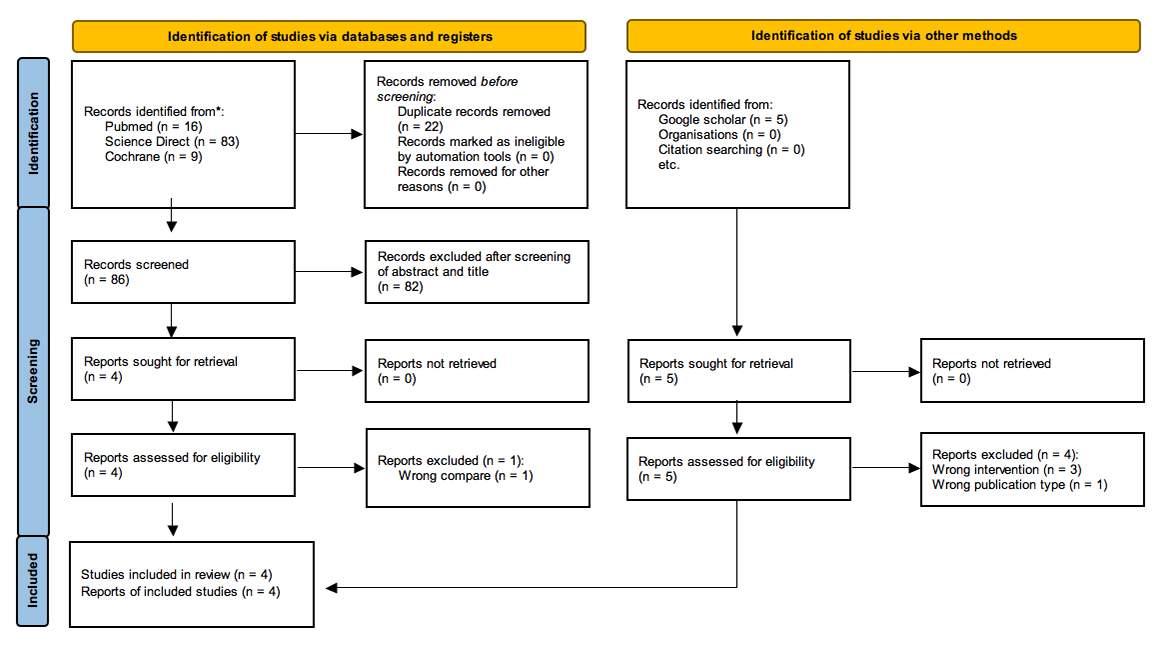
12833Effect of DOPA decarboxylase inhibitor supplements on the incidence of urinary tract infections in Parkinson’s disease patients: A systematic review and meta-analysis of randomized controlled trials
Ismaeel AlShoaibi, Basheer Abdo, Mohammed Abdullah, Khaled Alzanen, Mohammed Alhakamy, Mamoon Al-Namer, Abdulghani Al-Hagri, Morshed Salah, Afrah Salem, Mohammed Almogahed, Ibrahim Alnadhari, Faisal Ahmed
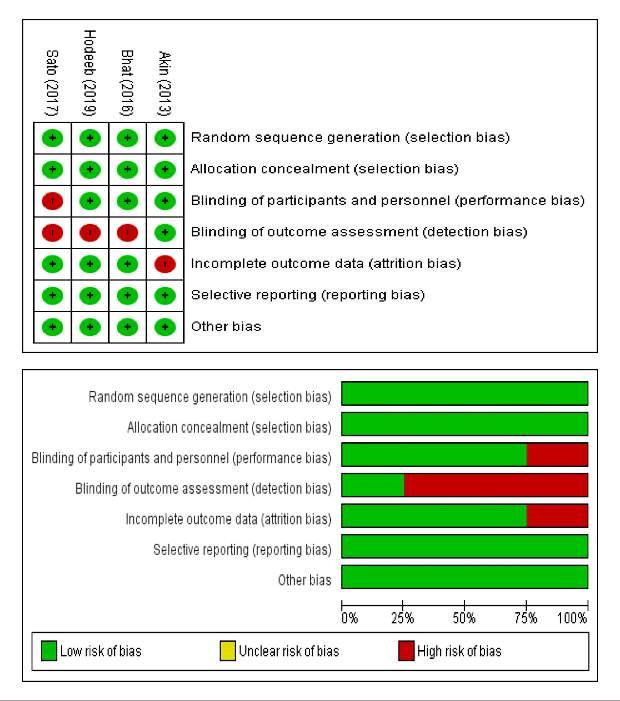
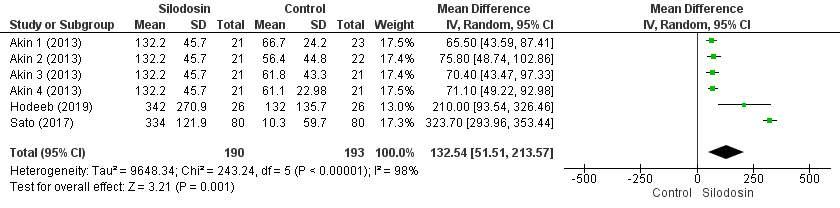
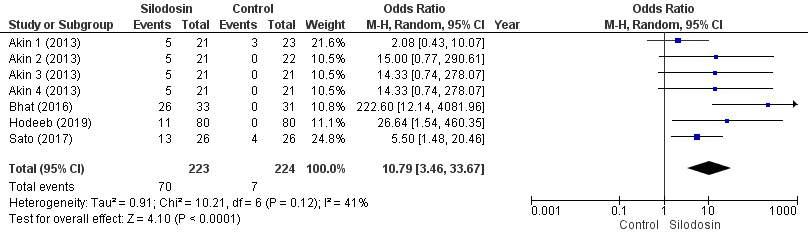
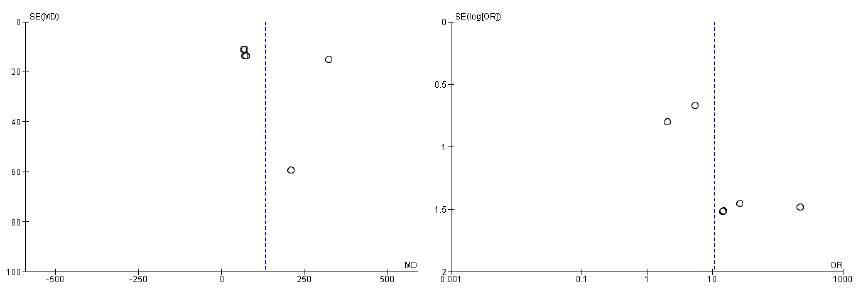
12984Promising selective alpha-1 blocker silodosin as a new therapeutic strategy for premature ejaculation and analysis of its drug adverse effect: A systematic review and meta-analysis of randomized controlled trials
Muhammad Ilham Fauzan, Besut Daryanto, Taufiq Nur Budaya, Moh. Anfasa Giffari Makkaraka, Muhammad Fakhri, Ilham Akbar Rahman
REVIEWS
13277Theobromine for treatment of uric acid stones and other diseases
Alberto Trinchieri
13098 Non-surgical management of BPH: An updated review of current literature and state of the art on natural compounds and medical therapy
Guglielmo Mantica, Francesca Ambrosini, Giovanni Drocchi, Zlata Zubko, Lorenzo Lo Monaco, Angelo Cafarelli, Alessandro Calarco, Renzo Colombo, Ottavio de Cobelli, Ferdinando De Marco, Giovanni Ferrari, Giuseppe Ludovico, Stefano Pecoraro, Domenico Tuzzolo, Carlo Terrone, Rosario Leonardi
LETTER
12975The psycho-sensory pelvic reflex: A new paradigm in the model of male sexual response
Giuseppe La Pera
Edizioni Scripta Manent s.n.c.
Via Melchiorre Gioia 41/A - 20124 Milano, Italy
Tel. +39 0270608060
e-mail: scriman@tin.it
web: www.edizioniscriptamanent.eu
Registrazione: Tribunale di Milano n. 289 del 21/05/2001
Direttore Responsabile: Pietro Cazzola
Direzione Marketing e PR: Donatella Tedeschi
Comunicazione e Media: Ruben Cazzola
Grafica e Impaginazione: Stefania Cacciaglia
Affari Legali: Avv. Loredana Talia (MI)
Ai sensi della legge 675/96 è possibile in qualsiasi momento opporsi all’invio della rivista comunicando per iscritto la propria decisione a: Edizioni Scripta Manent s.n.c. - Via Melchiorre Gioia, 41/A - 20124 Milano
The Publisher is not liable for the opinion expressed by the Authors of the articles and for images used by them.
GENERAL INFORMATION
AIMS AND SCOPE
“Archivio Italiano di Urologia e Andrologia” publishes papers dealing with the urological, nephrological and andrological sciences. Original articles on both clinical and research fields, reviews, editorials, case reports, abstracts from papers published elsewhere, book rewiews, congress proceedings can be published.
ORIGINAL PAPER
Multiparametric MRI targeted prostate biopsy: When omit systematic biopsy?
Pietro Pepe
1 ,
Ludovica Pepe
2 ,
Vincenzo Fiorentino
2 ,
Mara Curduman
3 , Filippo Fraggetta 4
1 Urology Unit, Cannizzaro Hospital, Catania, Italy;
2 Department of Human Pathology in Adult and Developmental Age “Gaetano Barresi”, University of Messina, Messina, Italy;
3 Pathology Unit, Cannizzaro Hospital, Catania, Italy;
4 Pathology Unit, ASP Catania, "Gravina" Hospital, Caltagirone, Italy
Summary
Introduction: To evaluate the detection rate for prostate cancer (PCa) performing multiparametric magnetic resonance imaging (mpMRI) fusion targeted biopsy (TPBx) combined only with ipsilateral systematic prostate biopsy (SPBx)
Materials and methods: From January 2023 to December 2023, 495 men with clinical suspicion of PCa underwent transperineal SPBx plus TPBx in the presence of PI-RADS score lesions ≥ 3.
Results: In 250/495 men (50 5%) a PCa was found, while 36/250 (14.4%) men had negative mpMRI. In comparison to TPBx, SPBx diagnosed a higher number of indolent PCa, 38 5 vs 5 8%, respectively; conversely, SPBx demonstrated a higher detection rate for clinically significant PCa (97 3 vs 85 4%) in the presence of ISUP Grade Group 2 (GG2). In details, rates were higher in the presence of GG2 (100 vs 76%), GG3 (85 7 vs 75 8%) and GG4 (100 vs 86 4%) tumors However, in GG5, both SPBx and TPBx diagnosed 100% of csPCa Furthermore, 89 4% of the cases showed csPCa on the negative mpMRI side
Conclusions: SPBx combined with TPBx maximized csPCa diagnosis; the use of reduced biopsy scheme limited to ipsilateral side of mpMRI lesion plus TPBx missed 11 6% csPCa Only in the presence of PI-RADS score 5 SPBx and TPBx diagnosed both 100% of csPCa
Submitted 30 August 2024; Accepted 16 September 2024
INTRODUCTION
Prostate cancer (PCa) is the most frequent tumor worldwide in the male population (1), with a high estimated risk of overdiagnosis and overtreatment for men enrolled in PSA screening In the last years, the use of multiparametric magnetic resonance imaging (mpMRI) combined with risk calculator including more clinical parameters allowed to improve the diagnosis of clinically significant PCa (csPCa) (2-7) In this respect, the diagnosis and treatment of PCa should be tailored for each patient to balance oncological and functional outcomes Although Active Surveillance (AS) protocols (8) have reduced overtreatment of low risk PCa and, in well informed patients, favorable intermediate risk (9, 10) PCa, the necessity of definitive treatment (radical prostatectomy or external radiotherapy) results to worse the quality of life Multiparametric MRI has improved the accuracy of sys-
tematic prostate biopsy in diagnosing csPCa and reducing unnecessary biopsies; the detection rate for csPCa is correlated with Prostate Imaging-Reporting and Data System (PI-RADS) score and in selected cases systematic biopsies could be omitted without harbor PCa diagnosis
In this study we have prospectively evaluated the detection rate for PCa performing only mpMRI/fusion targeted biopsy combined with ipsilateral systematic prostate biopsy
MATERIALS AND METHODS
From January 2023 to December 2023, we prospectively evaluated 495 men with clinical suspicion of PCa underwent transperineal systematic (SPBx: 20 cores in both prostatic lobes plus anterior zone) plus mpMRI/transrectal ultrasound (TRUS) fusion biopsy in the presence of PIRADS score lesions ≥ 3 (TPBx: 4 cores) (11, 12)
Clinical criteria for prostate biopsy were: PSA values > 4 ng/ml and/or suspicion digital rectal examination (DRE) or revaluation (scheduled biopsy) of men enrolled in AS protocol After institutional review board and ethical committee approval were granted, the informed consent was obtained from all individual participants included in the study Median PSA was 7 3 ng/ml (range: 3 8-152 ng/ml), digital rectal examination (DRE) was suspicion for PCa in 58/495 (11 7%) cases, 295 vs 200 underwent initial vs repeated biopsy, 48 men were enrolled in AS protocol for very low/low risk PCa (13) All the mpMRI index lesions characterized by a PI-RADS (version 2) ≥ 3 underwent targeted cores (TPBx: 4 cores); the procedure was performed transperineally using a tru-cut 18 gauge needle (Bard; Covington, GA, USA) under sedation and antibiotic prophylaxis The TPBx was done using an Hitachi 70 Arietta ecograph, Chiba, Japan) supplied by a bi-planar trans-rectal probe (14, 15)
The detection rate for PCa of SPBx in the controlateral “negative” mpMRI prostatic lobe of men has been evaluated; in detail, the opportunity to omit systematic biopsy in the hemigland without suspicion mpMRI lesions was evaluated
RESULTS
None had significant complications (Clavien-Dindo grade I) from prostate biopsy that needed hospital admission;
Table 1.
Biopsy findings in the 250 men with prostate cancer (PCa) submitted to systematic (SPBx) and targeted biopsy (TPBx).
1
5
2
2
46cases
GS: G eason score; PSA: Prostate specif c ant gen; GPC: greatest percentage of cancer; P -RADS: Prostate Imag ng-Reporting and Data System; GG: ISUP Grade Group; mpMRI: mult parametric magnet c resonance image
no patient had bilateral suspicious lesions at mpMRI In 250/495 (50 5%) men a PCa was diagnosed: 100 (40%) had an International Society of Urological Pathology (16) Grade Group 1 (ISUP GG1)/Gleason score 6, 50 (20%) a GG2/Gleason score 3+4, 28 (21 4%) a GG3/Gleason score 4+3, 26 (15 4%) a GG4/Gleason score 8 and 46 (18 4%) a GG5/Gleason score 9 36/250 (14 4%) men had negative mpMRI (PI-RADS score < 2): 38 9% (14 cases) were GG1, 33 3% (12 cases) GG2, 16 7% (6 cases) GG3, 11 1% (4 cases) GG4, and 0% GG5 SPBx in comparison with TPBx diagnosed a greater number of indolent PCa equal to 96/250 (38 5%) vs 14/250 (5 8%) men; on the contrary, SPBx showed an higher detection rate for csPCa (97 3 vs 85 4%) In details, rates were higher in the presence of GG2 (100 vs 76%), GG3 (85 7 vs 78 5%) and GG4 (100 vs 84 6%), whereas in GG5 SPBx vs TPBx diagnosed both 100% of csPCa (Table 1) SPBx in comparison with TPBx diagnosed 146/150 (97 3%) vs 128/150 (85 4%) csPCa, respectively
In total 16/150 (10 6%) men with csPCa had positive systematic cores located only in the ipsilateral side of suspicious mpMRI Out of them, 2/50 (4%) men with GG2 had PI-RADS 3; 10/28 (35 8%) with GG3 had PI-RADS score 3 (2 cases), 4 (6 cases) and 5 (2 cases), respectively; 2/26 (7 7%) and 2/46 (4 3%) with GG4 and GG5 had lesions PI-RADS score 4, respectively (Table 1)
P e r f o r m i n g o n l y T P B x w o u l d h a v e s p a re d 1 4 4 % (36/250) biopsies and adding systematic cores in the ipsilateral side of TPBx 11 6% csPCa located in the controlateral prostatic lobe with negative mpMRI would have missed
DISCUSSION
The use of mpMRI has increased the diagnosis of csPCa with a false negative rate equal to 15-20% of the cases; therefore, systematic biopsies, still today, should be combined with targeted cores to improve PCa diagnosis (17)
It remains unknown whether csPCa is missed due to the limited sensitivity of MRI, the suboptimal image fusion, the biopsy technique and strategy, expertise of the surgeon or a combination of these If the diagnosis of PCa is based on “MRI pathway” (18) the patients should be
advised of false negative rate for csPCa but, at the same time, the morbidity of the procedure could result less invasive because the lower number of needle cores
R e c e n t l y, a re d u c e d - c o re p ro s t a t e biopsy strategy confined to the ipsilateral emigland of suspicious mpMRI including “perilesional cores ” has been proposed to decrease the number of systematic cores, but, still today, the literature data are not in agreement and the detection rate for csPCa is correlated to different PI-RADS scores (19) Bourgeno et al (20) in 2 387 men submitted to different prostate biopsy schemes reported that the added value of contralateral systematic biopsy was negligible in terms of cancer detection (6 1% of the cases) and upgrading rates
Hegens et al (21) reported in 235 patients that TPBx plusperilesional biopsy approach detected 96 8% csPCa reducing the diagnosis of indolent PCa in 12 8% of the cases Deniffel et al (22) in 745 men submitted to mpMRI
TPBx plus systematic biopsy reported that standard cores could be avoided only in men with PI-RADS score 5 and/or previous negative biopsy, missing 1 vs 2% of csPCa and avoiding 27 vs 58% of systematic procedures On the other hand, Sawhney et al (23) reported in 490 men that about 20% of men with unilateral MRI lesions and csPCa on targeted biopsy were found to have controlateral csPCa on systematic biopsies Phelps et al. (24) in 212 men with mpMRI-visible intraprostatic lesions demonstrated that TPBx alone diagnosed 81 5% PCa, on the contrary 7 6% had controlateral involvement and 10 9% had bilateral PCa and concluded that TPBx combined with systematic biopsies maximizes csPCa diagnosis Hou et al (25) in 229 patients showed that the benefit of systematic biopsy added to TPBx was restricted to smaller PI-RADS score 3-4 resulting not useful for the diagnosis of csPCa in the presence of PI-RADS score lesions 5 and larger (> 1 cm) PI-RADS score 3-4 allowing to reduce systematic biopsies in 44 5% of the cases without compromising csPCa diagnosis The discordant data reported in literature are, probably, correlated with the clinical parameters (DRE, clinical stage, PSA values), PIRADS score values and number of needle cores performed by systematic prostate biopsy; in general, only in the presence of PI-RADS score 5 controlateral SPBx could be omitted Anyway, omitting controlateral SPBx a relevant number of csPCa could be definitively missed especially in men candidate to radiotherapy Recently, new prostate targeted strategies have been proposed; the use of transrectal microultrasound (26) and PSMA PET/CT (2730) demostrated good accuracy in diagnosing csPCa performing targeted biopsy when compared with mpMRI accuracy, but the results were obtained in men enrolled in clinical trials and/or in limited number of cases
In our series, among 250/495 (50 5%) PCa 150 (60%) where csPCa and 36 (14 4%) had negative mpMRI (PIRADS score ≤ 2) SPBx in comparison with TPBx diagnosed a greater number of indolent PCa (38 5 vs 5 8%);
P Pepe, L Pepe,
on the ther hand, SPBx showed an higher detection rate for csPCa (97 3 vs 85 4%)
In detail, only 16/150 (10 6%) men with csPCa had positive cores located only in the ipsilateral side of suspicious mpMRI: 2/50 (4%) men with GG2; 10/28 (35 8%) with GG3; 2/26 (7 7%) and 2/46 (4 3%) with GG4 and GG5, respectively Only men with PI-RADS score 5 had a detection rate for csPCa equal to 100% performing TPBx vs SPBx (Table 1) TPBx combined with ipsilateral SPBx alone would have missed 27 2% of PCa irrispective of PIRADS score and 11 6% were csPCa; in addition, quantitative histological findings useful for local staging of PCa and planification of definitive treatment (i e nerve sparing prostatectomy; intensity modulated radiotherapy) would have missed Finally, performing only TPBx would have spared 14 4% biopsies missing the presence of csPCa also in the negative mpMRI side in 89 4% of the cases
Regarding our results, some consideration should be done First, PCa diagnosis has been evaluated in biopsy finding and not in the entire prostate specimen; secondly, many patients had an indolent PCa because included in AS protocol and in these cases SPBx combined with TPBx is highly recommended Finally, a greater number of patients should be evaluated
CONCLUSIONS
SPBx combined with TPBx maximized csPCa diagnosis; the use of reduced biopsy scheme limited to TPBx plus ipsilateral systematic cores missed 11 6% of csPCa; only in the presence of PI-RADS score 5 SPBx and TPBx diagnosed all csPCa
REFERENCES
1 Bergengren O, Pekala KR, Matsoukas K, et al 2022 Update on Prostate Cancer Epidemiology and Risk Factors-A Systematic Review Eur Urol 2023; 84:191-206
2 Pepe P, Garufi A, Priolo GD, et al Is it Time to Perform Only Magnetic Resonance Imaging Targeted Cores? Our Experience with 1,032 Men Who Underwent Prostate Biopsy J Urol 2018; 200:774778
3 Roscigno M, Stabile A, Lughezzani G, et al The Use of Multiparametric Magnetic Resonance Imaging for Follow-up of Patients Included in Active Surveillance Protocol Can PSA Density Discriminate Patients at Different Risk of Reclassification? Clin Genitourin Cancer 2020; 18:e698-e704
4 Pepe P, D'Urso D, Garufi A, et al Multiparametric MRI Apparent Diffusion Coefficient (ADC) Accuracy in Diagnosing Clinically Significant Prostate Cancer In Vivo 2017; 31:415-418
5 Salemi M, Pettinato A, Fraggetta F, et al Expression of miR-132 and miR-212 in prostate cancer and metastatic lymph node: Case report and revision of the literature Arch Ital Urol Androl 2020; 92
6 Fiorentino V, Martini M, Dell'Aquila M, et al Histopathological Ratios to Predict Gleason Score Agreement between Biopsy and Radical Prostatectomy Diagnostics (Basel) 2020; 11:10
7 Pecci V, Troisi F, Aiello A, et al Targeting of H19/cell adhesion molecules circuitry by GSK-J4 epidrug inhibits metastatic progression in prostate cancer Cancer Cell Int 2024; 24:56
8 Pepe P, Cimino S, Garufi A, et al Confirmatory biopsy of men
under active surveillance: extended versus saturation versus multiparametric magnetic resonance imaging/transrectal ultrasound fusion prostate biopsy Scand J Urol 2017; 51:260-263
9 Russell JR, Siddiqui MM Active surveillance in favorable intermediate risk prostate cancer: outstanding questions and controversies Curr Opin Oncol 2022; 34:219-227
10 Pepe P, Pepe L, Pennisi M, Fraggetta F Oncological Outcomes in Men With Favorable Intermediate Risk Prostate Cancer Enrolled in Active Surveillance In Vivo 2024; 38:1300-1305
11 Pepe P, Pennisi M Morbidity following transperineal prostate biopsy: Our experience in 8 500 men Arch Ital Urol Androl 2022; 94:155-159
12 Pepe P, Candiano G, Pepe L, et al mpMRI PI-RADS score 3 lesions diagnosed by reference vs affiliated radiological centers: Our experience in 950 cases Arch Ital Urol Androl 2021; 93:139-142
13 Pepe P, Pepe L, Pennisi M, Fraggetta F Which Prostate Biopsy in Men Enrolled in Active Surveillance? Experience in 110 Men Submitted to Scheduled Three-Years Transperineal Saturation Biopsy Combined With Fusion Targeted Cores Clin Genitourin Cancer 2021; 19:305-308
14 Pepe P, Garufi A, Priolo G, Pennisi M Transperineal Versus Transrectal MRI/TRUS Fusion Targeted Biopsy: Detection Rate of Clinically Significant Prostate Cancer Clin Genitourin Cancer 2017; 15:e33-e36
15 Pepe P, Aragona F Prostate needle biopsy: 12 vs 18 cores -- is it necessary? Urol Int 2005; 74: 19-22
16 Offermann A, Hupe MC, Sailer V, et al The new ISUP 2014/ WHO 2016 prostate cancer grade group system: first résumé 5 years after introduction and systemic review of the literature World J Urol 2020; 38:657-662
17 Pepe P, Garufi A, Priolo G, Pennisi M Can MRI/TRUS fusion targeted biopsy replace saturation prostate biopsy in the re-evaluation of men in active surveillance? World J Urol 2016; 34:1249-1253, 2016
18 Chang SD, Ghai S, Kim CK, et al MRI Targeted Prostate Biopsy Te c h n i q u e s : A J R E x
Roentgenol 2021; 217:1263-1281
19 Yusim I, Mazor E, Frumkin E, et al Evaluation of the optimal strategy in men with a single unilateral suspicious lesion on MRI undergoing transperineal MRI/ultrasound fusion prostate biopsy Prostate 2023; 83:1255-1262
20 Bourgeno HA, Jabbour T, Baudewyns A, et al The Added Value of Side-specific Systematic Biopsy in Patients Diagnosed by Magnetic R
2024:S2588-9311(24)00031-2
21 Hagens MJ, Noordzij MA, Mazel JW, et al An Magnetic R e s o n a n c e I m a g i n g -
Approach for Prostate Cancer Diagnosis: "Less Is More" Eur Urol Open Sci 2022; 43:68-73
22 Deniffel D, Perlis N, Ghai S, et al Prostate biopsy in the era of MRItargeting: towards a judicious use of additional systematic biopsy Eur Radiol 2022; 32:7544-7554
23 Sawhney V, Huang R, Huang WC, et al Predictors of Contralateral Disease in Men with Unilateral Lesions on Multiparametric MRI Urology 2024:S0090-4295(24)00564-8
24 Phelps TE, Yilmaz EC, Harmon SA, et al Ipsilateral hemigland prostate biopsy may underestimate cancer burden in patients with u n i l a
48:1079-1089
25 Hou Y, Jiang KW, Zhang J, et al A clinical available decision support scheme for optimizing prostate biopsy based on mpMRI Prostate Cancer Prostatic Dis 2022; 25:727-734
26 Avolio PP, Lughezzani G, Anidjar M, et al The diagnostic accuracy of micro-ultrasound for prostate cancer diagnosis: a review World J Urol 2023; 41:3267-3276
27 Pepe P, Pepe L, Tamburo M, et al Targeted prostate biopsy: 68GaPSMA PET/CT vs mpMRI in the diagnosis of prostate cancer Arch Ital Urol Androl 2022; 94:274-277
28 Pepe P, Pennisi M Targeted Biopsy in Men High Risk for Prostate Cancer: 68Ga-PSMA PET/CT Versus mpMRI Clin Genitourin Cancer 2023; 21:639-642
29 Pepe P, Pepe L, Cosentino S, et al Detection Rate of 68Ga-PSMA PET/CT vs mpMRI Targeted Biopsy for Clinically Significant Prostate Cancer Anticancer Res 2022; 42:3011-3015
30 Pepe P, Roscigno M, Pepe L, et al Could 68Ga-PSMA PET/CT Evaluation Reduce the Number of Scheduled Prostate Biopsies in Men Enrolled in Active Surveillance Protocols? J Clin Med 2022; 11:3473
Correspondence
Pepe Pietro, MD (Corresponding Author) piepepe@hotmail com
Urology Unit, Cannizzaro Hospital, 95126 Catania, Italy
Ludovica Pepe, MD ludopepe97@gmail com
Vincenzo Fiorentino, MD vincenzo fiorentino@unime it
Department of Human Pathology in Adult and Developmental Age “Gaetano Barresi”, University of Messina, 98125 Messina, Italy
Mara Curduman, MD mara curduman@aoec it
Pathology Unit, Cannizzaro Hospital, 95126 Catania, Italy
Filippo Fraggetta, MD filippofra@hotmail com
Pathology Unit, ASP Catania, "Gravina" Hospital, 95041 Caltagirone, Italy
Conflict of interest: The authors declare no potential conflict of interest
P Pepe, L Pepe, V Fiorentino,
ORIGINAL PAPER
Effectiveness of cognitive fusion transrectal ultrasound prostate biopsy when compared with final prostatectomy histology
Ana Sofia Araújo 1 , João Serra 2 , Sara Anacleto 1 , Ricardo Rodrigues 1 , Catarina Tinoco 1 , Andreia Cardoso 1 , Mariana Capinha 1 , Vera Marques 1 , Paulo Mota 1, 2
1 Hospital de Braga, Dept of Urology, Braga, Portugal;
2 School of Medicine, University of Minho, Department of Urology, Braga, Portugal
Summary
Introduction and objectives: Prostate cancer (PCa) is the second most commonly diagnosed cancer in men Cognitive fusion transrectal ultrasound prostate biopsy is one of several modalities for diagnosing this disease However, no existing studies have shown the clear superiority of one image-guided technique over another. This investigation aimed to evaluate the efficacy of targeted biopsy through cognitive guidance, as well as to assess the accuracy of multiparametric magnetic resonance imaging (mpMRI) in the detection of PCa compared to the specimen obtained by radical prostatectomy (RP)
Materials and methods: We conducted a retrospective observational single-center study approved by the ethical committee, including men with prostate-specific antigen (PSA) levels between 2-10 mg/ml who underwent RP and cognitive fusion biopsy (CFB) between 2017 January and 2022 January
Results: A total of 639 patients were analyzed, 83 of whom met the inclusion criteria and were enrolled in this study The overall rate of PCa detection with CFB was 79 5% (median of specific PCa detection was 100%), and the rate of detecting clinically significant prostate cancer (csPCa) was 74 7% In addition, there was 42 2% agreement between the International Society of Urological Pathology (ISUP) score of the CFB and the RP specimen, which increased to 56 6% when the systematic biopsy was added. Regarding the accuracy of mpMRI, several parameters were evaluated with respect to RP sample histology. Of these, tumor location had a total match rate of 39.8% and a partial match rate of 55 4% Moreover, regarding extraprostatic extension (EPE), the present study found a significant association between the RP specimen and mpMRI (p = 0.002), with an agreement rate of 60% if it was present in the histology and 79 5% if it was not Additionally, larger prostates and tumors located in the transition zone were significantly associated with a lower CFB accuracy (p = 0 001 and p = 0.030, respectively). After adjusting for all variables evaluated, only prostate volume remains statistically significant (p = 0.029).
Conclusions: In this study, we conclude that mpMRI is highly accurate, allowing good characterization of suspicious tumors and reasonably guiding cognitive biopsy However, the use of both targeted biopsy through cognitive guidance and systematic biopsy increases the diagnostic accuracy for PCa Although there is no recommendation in the current literature for one guiding technique over another, we believe that cognitive-guid-
ed biopsy should only be reserved for centers with no access to ultrasound or magnetic resonance fusion software
Prostate cancer (PCa) is the second most common solid tumor in males worldwide and tends to be diagnosed mainly after 65 years of age (1) There is considerable variation between developed and developing countries regarding its incidence and mortality due to the hereditary component of the disease, the method of screening and diagnosis, and the involved environmental factors (2, 3) Approximately 95% of tumors are adenocarcinomas and tend to be located in the peripheral zone (PZ) of the prostate (4-6) PCa is diagnosed via direct sampling obtained by prostate biopsy, which can be performed transperineally or transrectally, both of which are comparable in terms of tolerability and the detection rate of clinically significant PCa (csPCa) (7) However, the first approach is preferred due to the lower risk of infection and associated rectal bleeding and the need for prophylactic antibiotic therapy (8-12) Other complications include urinary retention, haematuria, haematospermia, perineal pain, lower urinary tract symptoms, erectile dysfunction, and, very rarely, death (13)
The decision to perform a prostate biopsy is not only based on a particular prostate-specific antigen (PSA), but it is recommended to contextualize with PSA velocity and density, free/total PSA ratio, digital rectal examination (DRE), and with some patient risk factors such as age, ethnicity, family history, and associated comorbidities (14, 15)
The classical technique for obtaining a prostate sample is the standard ultrasound-guided double sextant prostate biopsy, where prostatic material (usually 12 samples) is randomly collected at predefined locations (10, 15-17)
The limitations associated with this technique include the high rate of clinically insignificant PCa (cisPCa) detection
A S Araújo, J Serra, S Anacleto, et al
and the failure to detect csPCa which leads to imprecision in stratifying this disease and may require a repeat of the procedure, delaying diagnosis and therapeutic decisionmaking (10, 12, 15, 16, 18)
Multiparametric magnetic resonance imaging (mpMRI) has shown superiority over individual MRI sequences, allowing the determination of a definitive correlation between the lesions identified by imaging and the tumor location in the specimens obtained from radical prostatectomy (RP) (10, 15, 19-21) mpMRI sequences include high-resolution T2-weighted imaging (T2W) to describe the anatomy of the prostate, typically combined with two functional MRI techniques, diffusion-weighted imaging (DWI) to display cell densities, and dynamic contrast-enhanced MRI (DCE-MRI), which can reveal the vascularization at the suspected location (7, 22, 23) The clinical indications for prostatic imaging include detection and localization of PCa, for guidance in mpMRI-guided biopsy (mpMRI-GB), local staging and stratification of the tumor, and assessment of PCa recurrence and local treatment (12, 14)
It has been demonstrated that the use of mpMRI before biopsy increases the detection of csPCa, and so the European Association of Urology (EAU) recommends performing mpMRI before biopsy for all eligible patients (8, 9, 15, 20, 24, 25)
The ability to detect and delineate lesions strongly suggestive of PCa on mpMR images has led to the development of new magnetic resonance imaging-guided biopsy (MRI-GB) techniques: cognitive fusion biopsy (CFB), biopsy performed during mpMRI imaging, and software fusion biopsy of the images previously obtained mpMRI with the images acquired during the ultrasound (7, 8, 15, 26) CFB consists of lesion identification and delineation on previously obtained mpMRI based on anatomical points that may exist near the lesion (7, 27)
Subsequently, through ultrasound, the operator can direct the biopsy needle to the suspected site, cognitively correlating the images obtained from mpMRI and ultrasound in real time (9, 28) This is an old, fast, simple, and accessible technique that does not require additional software to merge the mpMR images with those of the ultrasound (7, 10, 15, 28) The associated disadvantages are the limited accuracy of the biopsy in the absence of reference points, especially for smaller, anterior-located lesions (7, 9) CFB seems to be more useful for larger and more aggressive lesions, as well as diffuse abnormalities located in the PZ of the prostate (7, 9) The diagnostic accuracy of CFB depends on the visibility of the lesion on the ultrasound images, the position of the patient, and the location of the lesion on mpMRI because ultrasound and mpMRI do not employ the same exploration planes Furthermore, this technique depends on the operator and his experience in interpreting images and in transposing them to ultrasound (9, 10, 28)
Therefore, taking into account the associated advantages and disadvantages, the present study aims to evaluate the effectiveness of CFB in the detection of PCa in terms of accuracy and diagnosis of csPCa, as well as in comparison with the histological results obtained after RP; it also aims to evaluate the accuracy of mpMRI as well as the parameters that influence the probability of detecting PCa on mpMRI with respect to CFB histology
MATERIALS AND METHODS
The present study was approved by the Ethics Committee of Hospital de Braga (CEHB) (Appendix I) and the Department of Data Protection (Appendix II) The norms and recommendations of the Declaration of Helsinki, the Convention on Human Rights and Biomedicine, and the Guidelines on Good Clinical Practice were respected
We conducted a retrospective observational single-center study, including men who underwent RP and CFB between 2017 January and 2022 January In addition, the inclusion criteria for this study were: first biopsy, PSA levels between 2 and 10 ng/ml, and lesion categorization on mpMRI according to version 2 1 of the Prostate Imaging-Rating and Data System (PI-RADS) equal to or greater than 3 Patients who did not meet the inclusion criteria described above, as well as those whose outcome information was not fully available, were excluded
Data analysis was performed using IBM®SPSS® software, version 28 0 In the descriptive analyses, means (Ms) and standard deviations (SDs) are calculated for continuous variables with normal distributions, and medians (Mdns) with percentiles (P25-P75) are calculated otherwise The decision criteria were the skewness coefficient within the interval [-1; 1] and the analysis of the histogram
Categorical variables are described with numbers (n) and percentages (%) Ordinal variables are described as frequencies and percentages or as medians and percentiles, whichever was more intuitive for describing the variable
When comparing categorical variables, the chi-square test (𝝌2) was used in cases of compliance with Cochran's rules; otherwise, Fisher’s exact test was used
The standardized residuals, Ri = (O = observed frequency in the sample, E = expected frequency), were calculated in cases in which the association was statistically significant in tables with dimension (2 + n) X (2 + n), for n > 0 The residuals were said to be statistically significant when ri ≥ |1 96|, under the assumption of a normal distribution To assess the agreement of the evaluation methods, Cohen's kappa (κ) was calculated, in which 0 01 to 0 20 was considered minimal agreement, 0 21 to 0 40 fair agreement, 0 41 to 0 60 moderate agreement, 0 61 to 0 80 substantial agreement and 0 81 to 1 00 high agreement Logistic regression was used to evaluate the association of different variables with lower detection of PCa on CFB, first with univariate models and then with models adjusted to the variables with statistically significant results in the univariate analysis The odds ratio (OR) was calculated to assess the association between the variables Statistical significance was assessed using the 95% confidence interval (CI) for the OR and the associated p value Statistical significance was set at a p value < 0 05
Definitions
We defined as a csPCa when the International Society of Urological Pathology (ISUP) score was greater than or equal to 2 The presence of extraprostatic extension (EPE) was identified in the mpMRI report and in the pathological anatomy report of the specimens obtained by RP Regarding the characteristics of the lesions on mpMRI and in the histological analysis of the RP sample, 3 parameters were defined with regard to the location of the nodule
with the largest dimensions: zone (peripheral/transition/ both), laterality (right, left, both) and site (apex, middle, base, middle+base, middle+apex, base+apex, > 2 sites)
If the three location parameters agreed between mpMRI and the RP analysis, we consider a perfect match; if one of the three parameters was not in agreement, mpMRI was said to have no match A partial match was subdivided into false-positives (all those individuals whose tumor location in the mpMRI report was more extensive than that in the pathological anatomy report for the prostate specimen) and false-negatives (individuals whose imaging indicated a more restricted location than to the actual location of the tumor in the prostate)
RESULTS
Patient selection and sample characterization
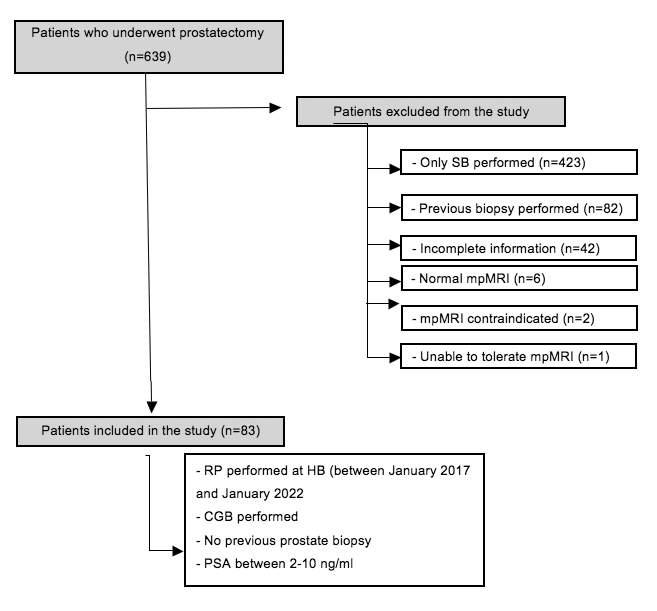
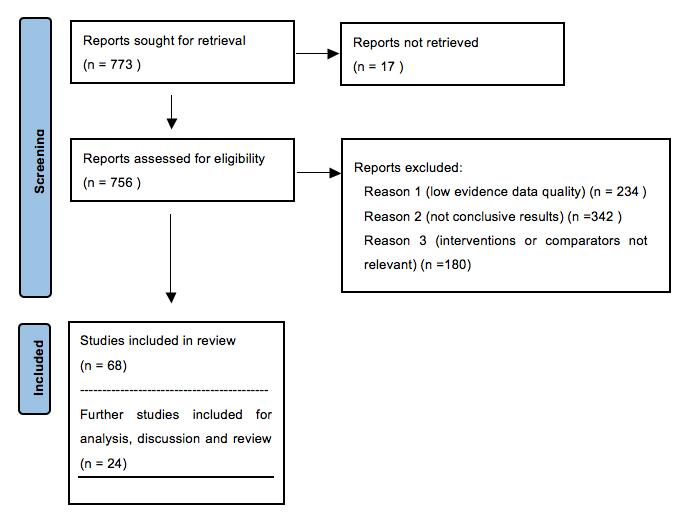
The patient selection process is described in the flowchart below (Figure 1)
Of the 639 patients initially analyzed, 83 with a mean age of 64 years were included, 34 of whom (41 0%) were suspected of PCa according to the DRE
The median total PSA was 6 62 ng/ml (P25-P75, 4 638 99), the median free/total PSA ratio was 13 00% (P25P75, 8 20%-19 00%) and the median PSA density was 0 15 ng/ml/cm3 (P25-P75, 0 10-0 21)
mpMRI analysis showed that most patients had only 1 suspicious nodule (n = 61, 73 5%), and the mean diameter of the largest identified lesion was 14 27 mm (SD = 4 60)
The median prostatic volume verified on mpMRI was
40 00 cm3 (P25-P75, 32 00-52 00), and the PI-RADS evaluation classified the largest nodule detected into three categories: 3 (n = 15, 18 1%), 4 (n = 36, 43 4%) and 5 (n = 32, 38 6%)
In most cases, two fragments (n = 58, 69 9%) were collected by CFB, with a range between 0 (n = 17, 20 5%) and 4 (n = 1, 1 2%) samples Most patients had two positive fragments (n = 36, 43 4%), and the median number of positive samples was 2 00 (P25-P75, 1 00-2 00)
Regarding SB, the most common number of fragments collected was 12 (n = 76, 91 6%) The tumor was detected in 0-2 (n = 15, 18 1%), 3-5 (n = 31, 37 3%), 6-7 (n = 19, 22 9%) and ≥ 8 samples (n = 18, 21 7%), with a median of 5 00 samples (P25-P75, 3 00-7 00)
On mpMRI, the nodules were mostly found in the PZ (n = 63, 75 9%), on the left (n = 37, 44 6%), and in the apical region (n = 23, 27 7%) In the RP sample, the tumor was detected more frequently in the PZ (n = 64, 77 1%), bilaterally (n = 45, 54 2%), and in more than 2 sites (n = 22, 26 5%)
The PCa ISUP score obtained for the samples collected from SB was distributed among categories 1 (n = 12, 14 5%) to 5 (n = 11, 13 3%), with most classified as category 4 (n = 17; 20 5%) The same results were observed for the tumors detected with CFB, with ISUP scores from 1 (n = 20, 24 1%) to 5 (n = 6, 7 2%), with category 4 being more frequent (n = 22, 26 5%) The overall ISUP scores were distributed among the same categories, from 1 (n = 15, 18 1%) to 5 (n = 13, 15 7%), where the highest frequency was observed for ISUP category 2 (n = 24, 28 9%)
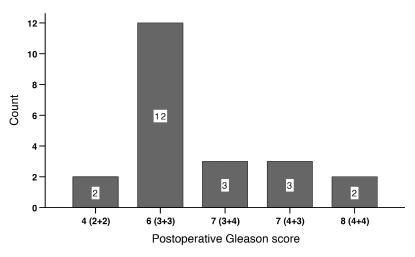
For the samples obtained from RP, the ISUP carcinoma scores ranged from 1 (n = 4, 4 8%) to 5 (n = 19, 22 9%), with most classified into category 2 (n = 29, 34 9%)
Regarding the presence of EPE, we found that 29 (34 9%) and 25 (30 1%) patients were positive on mpMRI and post-RP, respectively
Following SB, 16 individuals ( 1 9 3 % ) w e r e n e g a t i v e f o r tumor detection in the collected fragments, 12 (14 5%) were c l a s s i fi e d a s h a v i n g c i s P C a , and 55 individuals (66 3%) had csPCa
Figure 1.
Flowchart of the patient selection according to the inclusion and exclusion criteria for the study
A S Araújo, J Serra, S Anacleto, et al
Regarding the samples obtained by CFB, 20 (24 1%) and 62 men (74 7%) were said to have cisPCa and csPCa, respectively; only 1 patient (1 2%) had no diagnosis of PCa After removal of the prostate via RP, 4 men (4 8%) were diagnosed with cisPCa, and 79 individuals (95 2%) had csPCa (Table 1)
(obtained by the presence of ≥ 1 positive sample(s) in the total number of samples collected) was 79 5% The median of the specific rate of PCa detection, calculated by the formula (1 - ), was 100% (P25-P75, 50 0%-100 0%) For instance, if it was collected 3 fragments and all of them were positive [1 - ( 3 3 -3 )] = (1-0) = 1 or 100% Otherwise, if it was collected 3 fragments but none of them were positive [1 - ( 3 3 -0 )] = (1-1) = 0 or 0 0%
Association of PCa detection between CFB and SB
The association of cancer detection between CFB and SB showed moderate agreement (κ = 0 36), with statistical significance (p < 0 001), mainly for csPCa (80 6%) (Table 3) The standardized residues suggested that the number of samples considered to not have tumor tissue according to CFB and to have cisPCa according to SB was higher than expected (n = 1, 100%, Ri = 2 2%)
The proportion of cisPCa detected by both CFB and SB was 40 0%, with a positive residue of Ri = 3 0, suggesting a higher proportion than expected In contrast, the proportion of cisPCa from CFB classified as csPCa by SB (25 0%) was lower than expected (ri = -2 3) Although significant, 4 8% of csPCas detected with CFB were considered csPCa according to SB, which was lower than expected (ri = -2 0)
Comparison of the ISUP scores obtained with CFB and the Global ISUP score with the ISUP score obtained with RP histology
Table 4 compares the ISUP scores obtained for the samples collected with CFB with those described in the RP histology, using the formula (ISUP RP-ISUP CFB), with
Table 4.
Comparison of the ISUP scores obtained with CFB and the Global ISUP score with the ISUP score obtained with RP histology
total agreement observed for 35 (42 2%) The proportions of -/+1 and -/+2 errors were 45 7% (38 individuals) and 12% (10 individuals), respectively The same analysis was performed for the Global ISUP score, yielding a total agreement for 47 patients (56 6%), and proportions of -/+1, -/+2 and -/+3 errors of 30 1% (25 patients), 10 8% (9 patients) and 2 4% (2 patients), respectively
Rate of match considering mpMRI locations relative to RP histology
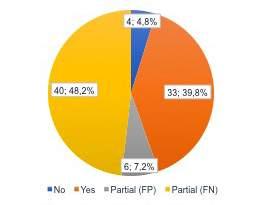
With respect to the RP samples, mpMRI had total match in tumor location in 33 patients (39 8%) Partial match was achieved for 46 patients (55 4%), 40 (48 2%) with false negatives and 6 (7 2%) with false positives No match at all was obtained for 4 patients (4 8%) (Figure 2)
Figure 2.
Rate of match considering mpMRI locations relative to RP histology
Table 3.
Association of PCa detection between CFB and SB.
csPCa0(0.0%)5(25.0%),Ri=-2.350(80.6%)
Association of laterality, tumor zone, site and EPE observed in RP histology with that observed on mpMRI
The laterality in the RP histology was statistically significantly associated with the laterality on mpMR (p < 001)
The agreement for right-, left-, and bilaterally located tumors was 73 7%, 94 7% and 28 9%,
Table 5
Association of laterality observed in RP histology with that observed on mpMRI.
RP histology laterality
Right Left
ZoneaccordingtompMRI
Both Fisher's Cohen's exact test κ
Right14(737%)0(00%)14(311%)p<0001035
Left1(53%)18(947%)18(400%)
Both4(211%)1(53%)13(289%)
Table 6.
Association of tumor zone in RP histology with that identified on mpMRI
The zone in which the tumor was found in RP histology was statistically significantly associated with that identified on mpMRI (p < 0 001) The agreement for the PZ, TZ, and both was 95 3%, 100% and 71 4%, respectively Cohen's κ was 0 84, indicating high agreement (Table 6)
Table 7 shows the associations of the RP histological site with that identified on mpMRI Statistically significant differences were found for apical (p = 0 026), middle (p < 0 001), and basal locations (p < 0 001) and > 2 sites (p < 0 001) Cohen's k showed the highest agreement for the basal location (κ = 0 80, high), with true negatives of 93 8% and true positives of 89 5% This was followed by agreement in middle locations (κ = 0 70, substantial), which had the highest proportion of true positives (89 7%), and in > 2 sites (κ = 0 43, fair), which had the highest proportion of true negatives (98 4%) Finally, apical sites had an agreement of 0 20, with 62 0% true negatives and 75 0% true positives
The association of EPE assessed by RP histology with that assessed on mpMRI was statistically significant (p = 0 002) (Table 8)
Regarding positive EPE as observed in RP histology, 60 0% of cases were also positive on mpMRI When EPE was not detected in the RP specimen, it was also not detected in 75 9% of the cases on imaging
The agreement between the two modalities was fair (κ = 0 34)
Table 9.
Association of different variables with lower detection of PCa on CFB, adjusted for covariates.
Table 7.
Association of tumor zone in RP histology with that identified on mpMRI
Apex RP histology Statistical test
ApexmpMRINoYes Χ2testCohen's κ
No44(620%)3(250%)p=0026020
Yes27(380%)9(750%)
Middle RP histology
MiddlempMRINoYes Χ2test
No45(83.3%)3(10.3%)p<0.0010.70
Yes9(167%)26(897%)
Base RP histology
BasempMRINoYes Χ2test
No60(938%)2(105%)p<0001080
Yes4(6.3%)17(89.5%)
> 2 sites RP histology
>2sitesmpMRINoYes Χ2test
No60(984%)14(636%)p<0001043
Yes1(16%)8(364%)
Table 8.
Association of EPE assessed by RP histology and that assessed on mpMRI
EPE RP histology
No Yes Χ2 test Cohen's κ EPEmpMRI
No44(759%)10(400%)p=0002034
Yes14(241%)15(600%)
Association of different variables with lower detection of PCa on CFB, adjusted for covariates
Table 9 shows the association of different variables with no detection of PCa on CFB, adjusted for covariates
In the univariate analysis, covariates referring to the presence of csPCa in the RP specimen (OR = 0 07 [95% CI = 0 07; 0 74], p = 0 027), a suspected tumor from DRE (OR
Dependent variable: No detection of PCa on CBF Unadjusted models (univariate) Ajusted model
= 0 14 [95% CI = 0 03; 0 67], p = 0 014) and PSA density (OR = 0 001 [95% CI = (0 00; 0 51)], p = 0 033) were significantly associated with detection of PCa on CFB A higher PI-RADS classification (OR = 0 46 [95% CI = 0 22; 098], p = 0 045) and tumor location in the PZ (OR = 0 25 [95% CI = (0 08-0 78)], p = 0 017) were also associated with detection of PCa on CFB
However, the volume of the prostate (OR = 1 06 [95% CI = 1 02; 1 09], p = 0 001) and nodule location in the TZ (OR = 3 96 [95% CI = 1 15; 13 66)], p = 0 030) were associated with no detection of PCa on CFB
When adjusting for all statistically significant variables from the univariate analysis, only prostate volume remained significant in the multivariate analysis (OR = 1 04 [95% CI = 1 01; 1 08)], p = 0 029); that is, for every 1 cm3 increase in the volume of the prostate, the odds of the CFB not hitting the mpMRI site increased by 4% The variable related to PSA density was not taken into account in the multivariate model, despite having a statistically significant result in the unadjusted model, as there was a loss of statistical power due to a wide confidence interval without statistical significance
DISCUSSION
The main objective of this study was to evaluate the effectiveness of CFB in the detection of PCa We observed an overall rate of PCa detection of 79 5%, consistent with previous investigations The median specific PCa detection rate in our investigation was 100%, i e , in 57 8% of the patients, all the biopsied samples were positive for the tumor A possible explanation for this high value may be the selection of patients with imaging results suggestive of PCa (PI-RADS ≥ 3) and elevated PSA values Dekalo et al showed that CFB had a PCa detection rate of 52% and 78% in individuals suspected only due to imaging and in men with changes in both analytical and mpMRI results, respectively (29) In the study published by Wang et al , there was a 67% detection rate of PCa through CFB (30)
A Portuguese study published in the Ata Urologica Portuguesa revealed an effectiveness of CFB of 73% in the detection of PCa (15) Recently, Kulis et al revealed a 52% success rate of CFB in patients with high PSA levels and persistent changes on imaging despite a previous negative SB (31)
Additionally, it was performed SB and CFB in the same patients which allow the association of these two routes of sample collection regarding the ability to identify prostatic lesions, and statistically significant differences were found with a moderate association between the two The two methods agreed in the detection of csPCa and cisPCa in 80 6% and 40 0% of cases, respectively
Based on the analysis of these data, CFB detected 62 cases (74 7%) of csPCa, while SB only detected 55 cases (66 3%) Nevertheless, we found that 9 and 3 patients classified as having no tumor and cisPCa, respectively, according to SB were identified as having csPCa with CFB, i e , approximately 19 3% of the patients with csPCa in our sample who underwent SB only would not have been correctly identified According to the available literature, the false-negative rate of SB is between 15 7-17%, especially for csPCa, corroborating the conclusions of several
studies that performing a prebiopsy mpMRI allows the detection of more cases of csPCa than with only SB (15, 18, 30-35) However, the 5 patients diagnosed with csPCa by SB but cisPCa according to CFB was greater than expected These results are in agreement with previous studies, where Kulis et al revealed that if only 5 patients (13 16%) had undergone CFB, the diagnosis would have failed; one of these patients had a Gleason scale score of 8 in the anatomopathological evaluation after RP (31) Thus, the data of the present study suggest that CFB could not detect all cases of csPCa, which is in agreement with previous studies; therefore, we do not advise completely replacing SB with CFB, but instead, they should be used in complementarity to reduce errors in the diagnosis of csPCa (10, 18, 30, 31, 35-38)
Based on the histology of the samples collected with CFB, the greatest Gleason score in the specimen was classified according to the ISUP score; a similar analysis was conducted for tumor tissue present in the prostate specimen collected by RP When comparing the differences between the ISUP values from RP and CFB for each patient, a total agreement of 42 2% (35 patients) was obtained Baco et al showed that the agreement in the Gleason score between SB and RP samples was 90% (20) This finding contrasts with the retrospective study by Diamand et al , which showed an agreement of 51 2%; however, the combination of SB and CFB increased the agreement with the final RP histology to 63 2% (39) This conclusion was observed in our study, showing that the combination of CFB and SB increased the agreement to 56 6%, a finding that is also corroborated by multicenter studies that confirmed the benefit of concomitant SB (39, 40)
Another objective of this study was to evaluate the accuracy of data provided from mpMRI in terms of tumor location with respect to the histology of the specimen obtained with RP A total match between the two was obtained in 39 8% (33 cases), a partial match was achieved in 55 4% (46 cases) and no match at all was found in 4 8% (4 cases) To date, no studies have been conducted comparing the 3 location parameters between mpMRI and RP specimens When analyzing each of the specific location parameters, we found high agreement with respect to laterality (73 7% on the right and 94 7% on the left) and zone (95 3% in the PZ and 100% in the TZ) With regard to site, Cohen's κ value showed a stronger agreement when the tumor was at the base (positive predictive value (PPV), 89 5%; negative predictive value (NPV), 93 8%), followed by the middle area (PPV 89 7%; NPV 83 3%) Therefore, there are high values in all parameters of the location; however, the total nonagreement can be explained because radiologists and pathologists do not use the same templates to correlate the locations, in addition to the fact that the in vivo and in vitro anatomical positions of the prostate also influence the interpretation of the affected site
Another way to assess the accuracy of mpMRI is through EPE, comparing it with that reported by the histology of the RP samples In the present study, agreements of 75 9% and 60% were obtained in detecting the absence and presence of EPE, respectively These data allow us to infer that in the present study, mpMRI had a specificity of 53% and a sensitivity of 18% In the study by Martins et al , a sensi-
A S Araújo, J Serra, S Anacleto, et al
tivity of 56% (CI, 39%-72%) and a specificity of 84% (CI, 75%-91%) were found Similar values were found in articles that evaluated the accuracy of mpMRI regarding EPE (41-44) Possible explanations for this wide variation in the accuracy of mpMRI in detecting mpMRI include the fact that there are several classification systems with different criteria for predicting the risk of EPE; however, in validation cohorts, none showed definitive superiority over others (12, 44), and therefore, different criteria can lead to different results Additionally, differences in the study design and in EPE prevalences among the populations, as well as differences in the experience of the radiologists and the center where the findings are interpreted, may influence the results (43)
We also intended to evaluate which factors (demographic, analytical, physical examination, mpMRI, and histological data of RP) were associated with a lower PCa detection on CFB
In the present study, age was not found to be a statistically significant predictor of PCa detection on CFB This can be explained by the findings of Bura et al , who showed that younger men exhibit lower signal intensity on T2W imaging, lower values on DWI, and diffuse enhancement on DCE-MRI, making the interpretation of PCa on mpMRI more difficult Although we are not aware of the existence of studies that associated DRE findings and the effectiveness of CFB, it is understood that there is a positive association between these two variables; therefore, when the DRE suggests a mass, CFB is more likely to hit the target tumor site
We also concluded that the PSA value did not affect the PCa detection of the CFB, a result that is corroborated by the study by Guang Xu (45) Possible explanations for this finding are due to the fact that larger prostates are also associated with a higher PSA level and as shown below, prostate volume is associated with a lower PCa detection on CFB However, PSA density was found to be a significant independent predictor of the correctness of CFB in the detection of PCa in the multivariate regression analysis, as Pang et al and Dekalo et al presented in their studies (10, 29)
Regarding factors related to mpMRI, in previous studies, it was demonstrated that for larger suspected nodules and higher values on the PI-RADS scale, the lesions were more frequently detected with CFB (10, 21, 36, 38, 45)
However, in our study, only higher values on the PIRADS scale were associated with higher PCa detection on CFB In addition, there was no preferential nodule location of the prostate with statistically significant in the univariate logistic regression model; however, it was demonstrated that malignant lesions in the anterior apical region of the prostate can be more frequently missed (46) With regard to prostate volume and the presence of cancer in the TZ, they were statistically significantly associated with less PCa detection on CFB These facts are corroborated by the current literature, since for larger prostates, there is greater difficulty in performing the biopsy (36) The association of TZ lesions with an inaccurate CFB may be due to the difficulty in distinguishing PCa from benign hyperplasia nodules (47) In contrast to TZ lesions, lesions located in the PZ were an independent predictor of PCa detection with CFB (36)
We also concluded that the existence of csPCa in the histology of RP samples was associated with a higher probability of correct PCa detection on CFB, which can be explained by the fact that higher Gleason scores are associated with greater tumor aggressiveness, allowing greater visibility on mpMRI (21, 47, 48) and, therefore, a higher probability of CFB PCa detection
This study demonstrated several limitations, including those related to its retrospective and nonrandomized nature, such as the potential bias in patient selection In addition, the small sample size could have implications r
Furthermore, factors associated with the performance of the biopsy, the lack of unified criteria in imaging and histology reports, and inconsistent experience by all professionals involved could have influenced these results
CONCLUSION
The present study concludes that mpMRI is highly accurate in characterizing the presence of suspicious nodules and reasonably in guiding cognitive biopsy However, the use of both targeted biopsy through cognitive guidance and systematic biopsy increases the diagnostic accuracy for PCa Although there is no recommendation in the current literature for one guiding technique over another, we believe that CFB should only be reserved for centers with no access to ultrasound or magnetic resonance fusion software Finally, more prospective, and randomized studies are needed to validate the results obtained
REFERENCES
1 Bray F, Ferlay J, Soerjomataram I, et al Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin 2018; 68:394-424
2 Rawla, P Epidemiology of Prostate Cancer World J Oncol 2019; 10:63-89
3 Haas G, Delongchamps N, Brawley O, et al The worldwide epidemiology of prostate cancer: perspectives from autopsy studies Can J Urol 2008; 15:3866-71
4 McNeal J, Redwine E, Freiha F, Stamey T Zonal distribution of prostatic adenocarcinoma Correlation with histologic pattern and direction of spread Am J Surg Pathol 1988; 12:897-906
5 Grignon J, Sakr W Zonal origin of prostatic adenocarcinoma: are there biologic differences between transition zone and peripheral zone adenocarcinomas of the prostate gland? J Cell Biochem Suppl 1994; 19:267-9
6 Mazhar D, Waxman J Prostate cancer Postgrad Med J 2002; 78:590-5
7 Puech P, Ouzzane A, Gaillard V, et al Multiparametric MRI-targeted TRUS prostate biopsies using visual registration Biomed Res Int 2014; 2014:819360
8 Immerzeel J, Israel B, Bomers J, et al Multiparametric Magnetic Resonance Imaging for the Detection of Clinically Significant Prostate Cancer: What Urologists Need to Know Part 4: Transperineal Magnetic Resonance-Ultrasound Fusion Guided Biopsy Using Local Anesthesia Eur Urol 2022; 81:110-117
9 Venderink W, Bomers J, Overduin C, et al Multiparametric Magnetic Resonance Imaging for the Detection of Clinically Significant
Prostate Cancer: What Urologists Need to Know Part 3: Targeted Biopsy Eur Urol 2020; 77:481-490
10 Pang C, Wang M, Hou H, et al Cognitive magnetic resonance imaging-ultrasound fusion transperineal targeted biopsy combined with randomized biopsy in detection of prostate cancer World J Clin Cases 2021; 9:11183-11192
11 Sugano D, Kaneko M, Yip W, et al Comparative Effectiveness of Techniques in Targeted Prostate Biopsy Cancers (Basel) 2021; 13:1449
12 EAU Guidelines Edn presented at the EAU Annual Congress Amsterdam 2022 ISBN 978-94-92671-16-5
13 Loeb S, Vellekoop A, Ahmed H, et al Systematic review of complications of prostate biopsy Eur Urol 2013; 64:876-92
14 Streicher J, Meyerson B, Karivedu V, Sidana A A review of optimal prostate biopsy: indications and techniques Ther Adv Urol 2019; 11:1756287219870074
15 Pina J, Dias J, Meirinha A, et al Biópsia prostática dirigida por fusão cognitiva após ressonância magnética multiparamétrica Comparação com a técnica habitual de biópsia aleatória Acta Urológica Portuguesa 2015; 32:101-107
16 Rodrigues S, Dores M, Metrogos V, et al Biópsia prostática orientada por fusão de imagem RMN-ETR: breve revisão a propósito de caso clínico Acta Urológica Portuguesa 2014; 31:88-91
17 Hsieh P, Chang T, Lin W, et al A comparative study of transperineal software-assisted magnetic resonance/ultrasound fusion biopsy and transrectal cognitive fusion biopsy of the prostate BMC Urol 2022; 22:72
18 Ahmed H, Bosaily A, Brown L, et al PROMIS study group Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confirmatory study Lancet 2017; 389:815-822
19 McHugh J, Saunders E, Dadaev T, et al Prostate cancer risk in men of differing genetic ancestry and approaches to disease screening and management in these groups Br J Cancer 2022; 126:1366-1373
20 Baco E, Ukimura O, Rud E, et al Magnetic resonance imagingtransectal ultrasound image-fusion biopsies accurately characterize the index tumor: correlation with step-sectioned radical prostatectomy specimens in 135 patients Eur Urol 2015; 67:787-94
21 Turkbey B, Mani H, Shah V, et al Multiparametric 3T prostate magnetic resonance imaging to detect cancer: histopathological correlation using prostatectomy specimens processed in customized magnetic resonance imaging based molds J Urol 2011; 186:1818-24
22 Israël B, Leest MV, Sedelaar M, et al Multiparametric Magnetic Resonance Imaging for the Detection of Clinically Significant Prostate Cancer: What Urologists Need to Know Part 2: Interpretation Eur Urol 2020; 77:469-480
23 Engels RRM, Israël B, Padhani AR, Barentsz JO Multiparametric Magnetic Resonance Imaging for the Detection of Clinically Significant Prostate Cancer: What Urologists Need to Know Part 1: Acquisition Eur Urol 2020; 77:457-468
24 Ploussard G, de la Taille A Prostate biopsies: let's move forward Eur Urol 2013; 64:893-4
25 Wegelin O, Exterkate L, van der Leest M, et al The FUTURE Trial: A Multicenter Randomised Controlled Trial on Target Biopsy Techniques Based on Magnetic Resonance Imaging in the Diagnosis of Prostate Cancer in Patients with Prior Negative Biopsies Eur Urol 2019; 75:582-590
26 Moore CM, Robertson NL, Arsanious N, et al Image-guided
prostate biopsy using magnetic resonance imaging-derived targets: a systematic review Eur Urol 2013; 63:125-40
27 Siddiqui MM, Rais-Bahrami S, Truong H, et al Magnetic reson a n c e i m a g i n g / u l t r a s o u n d - f u
prostate cancer versus systematic 12-core transrectal ultrasound biopsy Eur Urol 2013; 64:713-719
28 Bjurlin MA, Meng X, Le Nobin J, et al Optimization of prostate biopsy: the role of magnetic resonance imaging targeted biopsy in detection, localization and risk assessment J Urol 2014; 192:64858
29 Dekalo S, Matzkin H, Mabjeesh NJ High cancer detection rate using cognitive fusion - targeted transperineal prostate biopsies Int Braz J Urol 2017; 43:600-606
30 Wang L, Wang X, Zhao W, et al Surface-projection-based transperineal cognitive fusion targeted biopsy of the prostate: an original technique with a good cancer detection rate BMC Urology 2019; 19:107
31 Kuliš T, Zekulic T, Alduk AM, et al Targeted prostate biopsy using a cognitive fusion of multiparametric magnetic resonance imaging and transrectal ultrasound in patients with previously negative systematic biopsies and non-suspicious digital rectal exam Croat Med J 2020; 61:49-54
32 Yamada Y, Ukimura O, Kaneko M, et al Moving away from systematic biopsies: image-guided prostate biopsy (in-bore biopsy, cognitive fusion biopsy, MRUS fusion biopsy) -literature review World J Urol 2021; 39:677-686
33 Ryan J, Broe MP, Moran D, et al Prostate cancer detection with m a g n e t i c r e s o n a n c e i m a g i n g ( M R I ) / c o g n i t i v e f u s i o n b i o p s y : Comparing standard and targeted prostate biopsy with final prostatectomy histology Can Urol Assoc J 2021; 15:E483-e487
34 Watts KL, Frechette L, Muller B, et al Systematic review and meta-analysis comparing cognitive vs image-guided fusion prostate biopsy for the detection of prostate cancer Urologic Oncology: Seminars and Original Investigations 2020; 38:734 e19-734 e25
35 Lim LY, Tan GH, Zainuddin ZM, et al Prospective evaluation of using multiparametric magnetic resonance imaging in cognitive fusion prostate biopsy compared to the standard systematic 12-core biopsy in the detection of prostate cancer Urol Ann 2020; 12:276-282
36 Majchrzak N, Cieslinski P, Milecki T, et al Analysis of the usefulness of magnetic resonance imaging and clinical parameters in the detection of prostate cancer in the first systematic biopsy combined with targeted cognitive biopsy Cent European J Urol 2021; 74:321326
37 Oberlin DT, Casalino DD, Miller FH, et al Diagnostic Value of G u i d e d B i o p s i e s : F u s i o n a n d C
Resonance Imaging Versus Conventional Ultrasound Biopsy of the Prostate Urology 2016; 92:75-9
39 Diamand R, Oderda M, Al Hajj Obeid W, et al A multicentric study on accurate grading of prostate cancer with systematic and MRI/US fusion targeted biopsies: comparison with final histopathology after radical prostatectomy World J Urol 2019; 37:2109-2117
40 Ploussard G, Borgmann H, Briganti A, et al ; EAU-YAU Prostate Cancer Working Group Positive pre-biopsy MRI: are systematic biopsies still useful in addition to targeted biopsies? World J Urol 2019; 37:243-251
41 Martins M, Regusci S, Rohner S, et al The diagnostic accuracy of
A S Araújo, J Serra, S Anacleto, et al
multiparametric MRI for detection and localization of prostate cancer depends on the affected region BJUI Compass 2021; 2:178-187
42 de Rooij M, Hamoen EH, Witjes JA, et al Accuracy of Magnetic R e s o n
A Diagnostic Meta-analysis Eur Urol 2016; 70:233-45
43 Dinneen E, Allen C, Strange T, et al Negative mpMRI Rules Out Extra-Prostatic Extension in Prostate Cancer before Robot-Assisted Radical Prostatectomy Diagnostics (Basel) 2022; 12 1057
44 Park KJ, Kim MH, Kim JK Extraprostatic Tumor Extension: Comparison of Preoperative Multiparametric MRI Criteria and Histopathologic Correlation after Radical Prostatectomy Radiology 2020; 296:87-95
45 Xu G, Xiang L, Wu J, et al The accuracy of prostate lesion localization in cognitive fusion Clinical Hemorheology and Microcirculation 2020; 74:223-229
46 Rais-Bahrami S, Siddiqui MM, Turkbey B, et al Utility of multiparametric magnetic resonance imaging suspicion levels for detecting prostate cancer J Urol 2013; 190:1721-1727
47 Bratan F, Niaf E, Melodelima C, et al Influence of imaging and histological factors on prostate cancer detection and localisation on multiparametric MRI: a prospective study Eur Radiol 2013; 23:2019-29
48 Girouin N, Mège-Lechevallier F, Tonina Senes A, et al Prostate dynamic contrast-enhanced MRI with simple visual diagnostic criteria: is it reasonable? Eur Radiol 2007; 17:1498-509
Correspondence
Ana Sofia Araújo (Corresponding Author)
ana sofia araujo@hb min-saude pt
Sara Anacleto
sara anacleto@hb min-saude pt
Ricardo Rodrigues
ricardo matos rodrigues@hb min-saude pt
Catarina Tinoco
catarina sousa tinoco@hb min-saude pt
Andreia Cardoso
andreia filipa cardoso@hb min-saude pt
Mariana Capinha
mariana dias capinha@hb min-saude pt
Vera Marques
vera p marques@hb min-saude pt
Paulo Mota
paulo mota@hb min-saude pt
Hospital de Braga, Dept of Urology, Braga, Portugal
João Serra
serrajoao ricardo@gmail com
School of Medicine, University of Minho, Dept of Urology, Braga, Portugal
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Radical prostatectomy outcomes of prostate cancer cases: Insights from a leading surgeon's experience in Azerbaijan
Rashad Sholan
Scientific Research Center, State Security Service Military Hospital, Baku, Azerbaijan; Department of Kidney Diseases and Organ Transplantation, Republican Diagnostic Center, Baku, Azerbaijan
Summary
Objective: Prostate cancer is a significant health concern worldwide and ranks as the 4th most frequent cancer among men in Azerbaijan. While robot-assisted laparoscopic radical prostatectomy is the preferred surgical technique in many countries, open retropubic radical prostatectomy (ORP) remains the primary treatment option in Azerbaijan due to limited access to robotic surgical systems This study aims to analyze the outcomes of ORP in patients with local and locally advanced prostate cancer.
Methods: We retrospectively evaluated 95 men who underwent extraperitoneal retropubic ORP for prostate cancer at our center between May 2020 and December 2023 Comprehensive data on patient demographics, preoperative parameters, surgical details, and postoperative outcomes were collected Statistical analyses were conducted using IBM SPSS 27.0 software.
Results: The mean age of the patients was 65 9 years The median preoperative PSA level was 14 8 ng/mL, and lymph node enlargement was identified in 29 5% of patients A rectal injury occurred in one patient (1 1%) as the only intraoperative complication The mean intraoperative blood loss was 330 mL, and the median hospital stay was 6 days A positive surgical margin was observed in 38 9% of cases Diabetes mellitus and higher intraoperative blood loss were associated with prolonged hospital stays (≥ 7 days) Erectile dysfunction was reported in 52 6% of patients 6 months postoperatively, while urinary incontinence was observed in 2.2%.
Conclusions: ORP outcomes in Azerbaijan are comparable to those reported for laparoscopic and robot-assisted techniques in terms of perioperative and oncological results Despite the absence of advanced surgical technology, ORP remains an effective treatment option for prostate cancer when performed by experienced surgeons.
KEY WORDS: Prostate cancer; Open radical prostatectomy; Azerbaijan
Submitted 15 October 2024; Accepted 21 October 2024
INTRODUCTION
Prostate cancer is a major health concern for men worldwide, remaining one of the most prevalent malignancies affecting this population In Azerbaijan, prostate cancer has become increasingly common, ranking as the 4th most frequent cancer among men in 2022, with an incidence rate of 5 7% (1) Although prostate cancer treat-
ment has advanced over time, radical prostatectomy (RP) continues to be the standard surgical treatment for localized cases (2)
Over the past two decades, the surgical management of localized prostate cancer has undergone substantial changes Open radical prostatectomy (ORP) has been largely replaced by laparoscopic radical prostatectomy (LRP) and robot-assisted laparoscopic radical prostatectomy (RALP) in many parts of the world (3) RALP, in particular, has emerged as the leading surgical technique, accounting for over 61% of RP cases in some regions (4) Despite these technological advancements, ORP remains a crucial procedure in regions with limited access to robotic surgical systems, such as Azerbaijan, where RALP is not yet available The outcomes of ORP and minimally invasive techniques have been extensively studied Generally, RALP is associated with reduced blood loss and shorter hospital stays but incurs higher costs compared to ORP Both LRP and RALP have demonstrated favorable perioperative outcomes compared to ORP, with comparable long-term oncologic control (4) However, comprehensive studies examining ORP outcomes in the Azerbaijani population are lacking, and the effectiveness of this approach in early-stage prostate cancer within our region is not well documented In light of the absence of robot-assisted surgical methods in Azerbaijan and the scarcity of academic literature on prostatectomy outcomes for early-stage prostate cancer patients in this country, it is crucial to explore the experiences of surgeons proficient in the ORP technique This study aims to address this gap by providing insights from the perspective of an experienced surgeon on ORP outcomes in Azerbaijan We believe that sharing this experience will not only contribute valuable data to the limited academic literature on prostate cancer treatment in Azerbaijan but will also serve as a foundation for comparisons with international outcomes in prostate cancer surgery
METHODS
Study population and data collection
This study included men diagnosed with non-metastatic prostate cancer patients with T1-T3 tumors with or without lymph node involvement who underwent extraperi-
toneal retropubic ORP at our centers between May 2020 and December 2023 All procedures performed in the study involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments The study was approved by State Security Service Scientific Research Center Ethics Board (Decision no: ETEK: 24/03)
We collected comprehensive data on patients' baseline characteristics, including age, body mass index (BMI), comorbid diseases, smoking status, and family history of prostate cancer Preoperative parameters such as serum prostate-specific antigen (PSA) levels, prostate volume (measured via transrectal ultrasound or magnetic resonance imaging), imaging results, and needle biopsy findings were recorded
Surgical technique
All surgeries were performed using the open extraperitoneal retropubic approach, aiming to preserve urinary continence This technique was performed by an experienced surgeon following the standardized procedure described in the literature (5) After placing the patient in the supine position, a midline incision was made from the pubic symphysis to the umbilicus The extraperitoneal space was developed, and the prostate was carefully dissected, with an emphasis on preserving the neurovascular bundles whenever feasible, depending on the tumor's location and size Hemostasis was meticulously maintained throughout the procedure, and the dorsal vein complex was controlled using ligatures and sutures The bladder neck was dissected carefully to maintain its integrity, and the prostate was removed en bloc Bilateral pelvic lymph node dissection was performed in patients with a higher risk of lymph node involvement The urethrovesical anastomosis was completed using interrupted sutures A drain was placed in the pelvic cavity, and a urinary catheter was left in place for postoperative management
Intraoperative and postoperative data
During the surgery, data on the anesthesia method, duration of the operation, and estimated intraoperative blood loss were recorded Any intraoperative complications were documented Postoperative follow-up included monitoring for complications, such as bleeding, infection, or urinary leakage, as well as the duration of the hospital stay All prostatectomy specimens were examined by experienced pathologists, and pathological parameters such as Gleason score, surgical margin status, lymphovascular and/or perineural invasion, and lymph node involvement were assessed Serum PSA levels were measured at 3 months to evaluate early biochemical recurrence Erectile dysfunction (ED) was assessed six months postoperatively using an Azerbaijani translation of the third question from the International Index of Erectile Function, which inquired, “In the past 6 months, how often was your erection firm enough for penetration during sexual activity?” Erectile function was considered adequate if erections were sufficient for intercourse more than 50% of the time
Statistical analysis
Statistical analyses were performed using IBM SPSS 27 0 software Descriptive characteristics were presented as
frequency (%), mean ± SD, or median (range) Normal distribution of continuous variables was assessed using visual and analytical methods Chi-square or Fisher's exact test compared categorical groups Student t-test or Mann-Whitney U test compared independent continuous variables, while paired sample t-test or Wilcoxon test analyzed dependent variables A p-value < 0 05 was considered statistically significant
RESULTS
The mean age of the 95 patients included in the study was 65 9 ± 6 4 years (range: 52-83) The basic clinical characteristics of the patients are summarized in Table 1 The preoperative median PSA level was 14 8 ng/mL (range: 0 2-145), and the prostate volume was 55 mL (range: 28-
Table 1.
Baseline patient characteristics.
Characteristics
Total 95 patients *
Age(years)659±64
BMI(kg/m2)26.7±1.7
Comorbidities Diabetesmellitus34(358)
Coronaryarterydisease29(305)
Cholelithiasis7(74)
Artificialmitralvalve6(63)
Asthma5(53)
Renalstone4(4.2)
Heartfailure3(32)
COPD3(32)
Inguinalhernia3(32)
Others12(126)
Smoking37(389)
Familyhistoryofprostatecancer31(326)
* Findings are presented as n (%) or mean ± standard dev at on BM : Body mass ndex; COPD: Chronic obstruct ve pulmonary disease
Table 2.
Preoperative characteristics
Characteristics Total 95 patients *
PSA(ng/mL)148(02-145)
Prostatevolume(mL)55(28-110)
Lymphnodeenlargement28(295)
Needlebiopsyresults
ASAP22(232)
Adenocarcinoma73(768)
Gleasonscore
4(2+2)4(55)
5(2+3)2(27)
6(3+3)33(452)
7(3+4)4(55)
7(4+3)13(178)
8(4+4)16(21.9)
9(4+5)1(14)
Hemoglobinlevel(g/dL)14.6±1.6
* Findings are presented as n (%), mean ± standard dev ation or med an (min-max) ASAP: Atyp cal smal ac nar prol feration, PSA: Prostate-spec f c ant gen
110) Lymph node enlargement was detected on imaging in 28 patients (29 5%) Prostate needle biopsy identified atypical small acinar proliferation (ASAP) in 22 patients (23 2%) and prostate adenocarcinoma in 73 patients (76 8%) Among those with prostate adenocarcinoma, the Gleason score on preoperative biopsy was ≤ 6 in 53 4% of cases, 7 in 23 3%, and ≥ 8 in 23 3% (Table 2)
Intraoperative parameters and postoperative short-term surgical outcomes are presented in Table 3 One patient
Table 3.
Intraoperative parameters and postoperative surgical outcomes
Parameters Total 95 patients *
Anesthesiamethod
General87(916)
Epidural8(84)
Durationofsurgery(min)160(120-230)
Intraoperativebloodloss(mL)330(150-600)
Intraoperativecomplication1(1.1)**
ICUadmission1(11)**
Postoperativehemoglobinlevel(g/dL)131±09
Postoperativecomplication0(00)
Hospitalstay(days)6(5-14)
* F nd ngs are presented as n (%), mean ± standard dev at on or med an (min-max)
** A patient exper enced a rectal njury, wh ch was repaired ntraoperat ve y, and was subsequently monitored
n the ICU for one day
ICU: Intens ve care unit
Table 4.
Comparison of baseline and perioperative characteristics of patients with and without a hospital stay of ≥ 1 week Hospital stay * < 7 days (n = 49) ≥ 7 days (n = 46)
* Findings are presented as n (%), mean ± standard deviat on or median (m n-max)
BMI: Body mass index; COPD: Chronic obstructive pulmonary d sease
experienced a rectal injury, which was repaired intraoperatively; this patient was monitored in the ICU for one day No other postoperative complications or deaths occurred
Postoperative hemoglobin levels showed a significant decrease compared to preoperative levels (14 6 ± 1 6 g/dL vs 13 1 ± 0 9 g/dL; p < 0 001) The median hospital stay was 6 days (range: 5-14) A comparison between patients with a hospital stay of < 7 days (n = 49) and those with a stay of ≥ 7 days (n = 46) is shown in Table 4 Patients with a hospital stay of ≥ 7 days had a higher incidence of diabetes mellitus (47 8% vs 24 5%; p = 0 018) and greater median intraoperative blood loss (345 mL [range: 150600] vs 310 mL [range: 150-510]; p = 0 004)
In the postoperative pathological examination, a positive surgical margin was observed in 37 patients (38 9%), and the Gleason score was ≤ 6 in 27 4%, 7 in 55 8%, and ≥8 in 16 8% of cases For patients with a preoperative ASAP diagnosis (n = 22), the postoperative Gleason score was ≤6 in 63%, 7 in 27 3%, and ≥ 8 in 9 1% (Figure 1)
Regarding those with a preoperative Gleason score ≤ 6, 23 1% remained at ≤ 6 postoperatively; for patients with a preoperative Gleason score of 7, 64 7% retained a score of 7; and for those with a preoperative Gleason score of ≥ 8, 47 1% remained at ≥ 8 postoperatively (Figure 2)
Figure 1
Distribution of postoperative Gleason scores among patients initially diagnosed with atypical small acinar proliferation based on preoperative needle biopsy
Figure 2.
Comparison of preoperative and postoperative Gleason scores in patients diagnosed with prostate adenocarcinoma via preoperative needle biopsy
Lymph node metastasis was confirmed in 40 9% of patients with preoperative lymph node enlargement, compared to 6 6% of those without lymph node enlargement (p < 0 001) Detailed postoperative pathological outcomes
Table 5
Postoperative pathological outcomes
Parameters
Total 95 patients *
Surgicalmarginpositivity37(389)
Proximal10/37(270)
Distal12/37(324)
Both15/37(40.5)
Gleasonscore
4(2+2)2(2.1)
6(3+3)24(253)
7(3+4)30(316)
7(4+3)23(242)
8(4+4)7(74)
8(5+3)1(11)
9(4+5)7(74)
9(5+4)1(1.1)
Lymphovascularinvasion57(600)
Perineuralinvasion72(758)
Numberoflymphnodesremoved8(2-15)
Metastaticlymphnode15(158)
Numberofmetastaticlymphnodes(n=15)2(1-11)
* F nd ngs are presented as n (%) or median (min-max)
are provided in Table 5 The preoperative median PSA level of 14 8 ng/mL (range: 0 2-145) decreased to 0 0030 ng/mL (range: 0 0001-0 34) at the first postoperative month and remained stable at 0 0032 ng/mL (range: 0 0001-0 3) by the third postoperative month (Figure 3) While ED was present in 21 1% of patients before surgery, it was detected in 52 6% of patients 6 months after surgery Two (2 2%) patient developed urinary incontinence during postoperative follow-up
Figure 3.
Changes in prostate-specific antigen (PSA) levels measured preoperatively, as well as at the 1st and 3rd months postoperatively.
DISCUSSION
Our study provides a comprehensive analysis of the outcomes of ORP in men with local and locally advanced prostate cancer, offering valuable insights into the experi-
ences of a high-volume center in Azerbaijan While the adoption of LRP and RALP has grown rapidly worldwide, ORP continues to be a relevant surgical option, especially in settings where advanced technology is not available
Our study showed a median operative time of 160 minutes, comparable to the duration observed in LRP as reported by Çelen et al (6), where experience contributed to reduced operative times Our study had only one intraoperative complication (1 1%), which involved a rectal injury, consistent with the low complication rates reported in experienced centers performing ORP (7) Studies involving large ORP series have reported that mean intraoperative blood loss can range from 500 mL to over 2 liters (8) This variation is influenced by factors such as the surgical technique, whether nerve-sparing procedures are performed, the surgeon's level of experience, and the duration of the surgery (9) The intraoperative blood loss in our study was 330 mL, which was reported as 372 mL in a 2-year prospective LRP series by Leitao et al (10)
This suggests that while minimally invasive techniques offer some perioperative advantages, ORP remains a viable option, particularly when performed by an experienced surgeon The mean hospital stay for ORP in our cohort was comparable to that reported for minimally invasive techniques in other studies (10) Our analysis revealed that patients with diabetes mellitus and those with higher intraoperative blood loss experienced prolonged hospital stays Therefore, meticulous perioperative management is essential to minimize complications and optimize recovery following ORP
The positive surgical margin rate in our study was 38 9%, which is somewhat higher than the 23 7% reported by Çelen et al (6) for LRP but comparable to the rates reported in other ORP studies (3, 7) In comparing ORP outcomes with LRP and RALP, several studies have reported similar oncological results (11, 12) For instance, Ficarra et al (13) found no significant differences in positive surgical margin rates between ORP, LRP, and RALP, suggesting that all three techniques can provide effective cancer control when performed by experienced surgeons Furthermore, the positive surgical margin rates in our study were comparable to those reported for minimally invasive techniques (14)
This indicates that with adequate surgical expertise, ORP can achieve effective oncologic control, even in the absence of advanced technology
The median life expectancy after curative treatment for prostate cancer exceeds 10 years (15) As a result, it is vital to optimize long-term functional outcomes to enhance the postoperative quality of life for these men
The most frequent long-term complications following surgery are ED and urinary incontinence, both of which can significantly diminish patients' quality of life Pompe et al (16) found that the rate of functional erections significantly decreased after ORP While 78 4% of patients had functional erections at baseline, this dropped to 33 6% at 3 months post-surgery Gradual improvement was seen, reaching 44 7% at 12 months, 51 1% at 24 months, and 52 6% at 36 months While 78 9% of our patients described effective erection before the operation, this rate decreased to 47 4% 6 months after the operation Incontinence is often the most challenging and dis-
tressing complication associated with RP for both patients and clinicians Studies have reported postoperative continence rates ranging from 80% to 97% in contemporary surgical cases (7) In our series postoperative continence rate was 97 8%
When considering cost-effectiveness, ORP continues to have an advantage over RALP, particularly in lowresource settings Therefore, in countries like Azerbaijan, where robotic technology is not yet available, ORP remains an essential, effective, and cost-efficient option However, to ensure access to modern medical practices, companies offering robot-assisted surgical technologies s h o u l d a c t i v e l y c o l l a b o r a t e w i t h o u r c o u n t r y T h e expanding comprehensive health insurance system aims to enhance patient access to advanced treatments and improve overall health outcomes
A preoperative diagnosis of ASAP is known to be associated with varying rates of postoperative prostate cancer detection In one study, 42% of cases with a pathological diagnosis of ASAP were later confirmed to have prostate cancer (17) In another sudy, among 71 patients diagnosed with ASAP, 25 underwent pelvic bilateral lymphadenectomy and nerve-sparing RP immediately after the diagnosis (18) Remarkably, all 25 were confirmed to have adenocarcinoma in the final pathology, as verified by an independent review pathologist
In our cohort, 22 patients (23 2%) had preoperative needle biopsy results consistent with ASAP, with the diagnosis confirmed through repeat biopsies The decision to perform radical prostatectomy in these cases was driven by suspicious rectal exam findings and rising PSA levels
Radical surgery was undertaken after detailed discussions with patients about the potential benefits and risks Interestingly, all of these cases resulted in a postoperative diagnosis of prostate cancer In cases where ASAP is detected on biopsy, a comprehensive assessment that includes clinical, laboratory, and radiological findings is crucial Additionally, treatment decisions should take into account patient preferences, life expectancy, quality of life, and the psychological burden of the diagnosis
An important point to mention is that more than half of the patients in our cohort diagnosed with prostate cancer through preoperative biopsy had a Gleason score of 6 or lower However, due to the widespread negative perception of a cancer diagnosis in our society, active surveillance is not commonly accepted It also lacks sufficient support within the Ministry of Health's regulations This explains why RP was performed in these patients, despite their low Gleason scores Furthermore, the European Association of Urology (EAU) guidelines for active surveillance are somewhat limited due to the lack of data from prospective randomized controlled trials (19) When deciding between active surveillance and radical surgery, it's crucial to consider the patient's psychosocial status, anxiety levels, and societal views
CONCLUSIONS
In conclusion, our study provides valuable insights into the outcomes of ORP for prostate cancer in a setting without access to advanced laparoscopic or robotic techniques The findings underscore the importance of sur-
geon experience in achieving favorable outcomes and demonstrate that ORP remains a viable, effective, and potentially cost-efficient treatment option for prostate cancer
REFERENCES
1 Ferlay J, Ervik M, Lam F, et al (2024) Global Cancer Observatory: Cancer Today Lyon, France: International Agency for Research on Cancer Available from: https://gco iarc who int/today accessed [30 09 2024]
2 Costello AJ Considering the role of radical prostatectomy in 21st century prostate cancer care Nat Rev Urol 2020; 17:177-88
4 Healy KA, Gomella LG Retropubic, laparoscopic, or robotic radical prostatectomy: is there any real difference? Semin Oncol 2013; 40:286-96
5 Lepor H Radical retropubic prostatectomy Urol Clin North Am 2001; 28:509-19, viii
6 Çelen S, Özlülerden Y, Mete A, et al Laparoscopic radical prostatectomy: a single surgeon ’ s experience in 80 cases after 2 years of formal training African J Urol 2021; 27:57
7 Pereira R, Joshi A, Roberts M, et al Open retropubic radical prostatectomy Transl Androl Urol 2020; 9:3025-35
8 Yaxley JW, Coughlin GD, Chambers SK, et al Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: early outcomes from a randomised controlled phase 3 study Lancet 2016; 388:1057-66
9 Djavan B, Agalliu I, Laze J, et al Blood loss during radical prostatectomy: impact on clinical, oncological and functional outcomes and complication rates BJU Int 2012; 110:69-75
10 Leitão TP, Papatsoris AG, Mandron E Extraperitoneal laparoscopic radical prostatectomy: A prospective 2-year single-surgeon experience with 171 cases Arab J Urol 2012; 10:347-52
11 Lantz A, Bock D, Akre O, et al Functional and Oncological Outcomes After Open Versus Robot-assisted Laparoscopic Radical Prostatectomy for Localised Prostate Cancer: 8-Year Follow-up Eur Urol 2021; 80:650-60
12 Coughlin GD, Yaxley JW, Chambers SK, et al Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: 24-month outcomes from a randomised controlled study Lancet Oncol 2018; 19:1051-60
13 Ficarra V, Novara G, Fracalanza S, et al A prospective, nonrandomized trial comparing robot-assisted laparoscopic and retropubic radical prostatectomy in one European institution BJU Int 2009; 104:534-9
14 Ficarra V, Novara G, Artibani W, et al Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a systematic review and cumulative analysis of comparative studies Eur Urol 2009; 55:1037-63
15 Tward JD, Lee CM, Pappas LM, et al Survival of men with clini c a l l y l o c a l i z e d p r o s t a t e c a n c e r t r e a t e d w i t h p r o s t a t e c t o m y , brachytherapy, or no definitive treatment: impact of age at diagnosis Cancer 2006; 107:2392-400
16 Pompe RS, Tian Z, Preisser F, et al Short- and Long-term Functional Outcomes and Quality of Life after Radical Prostatectomy:
R Sholan
Patient-reported Outcomes from a Tertiary High-volume Center Eur Urol Focus 2017; 3:615-20
17 Mallén E, Gil P, Sancho C, et al Atypical small acinar proliferation: review of a series of 64 patients Scand J Urol Nephrol 2006; 40:272-5
18 Brausi M, Castagnetti G, Dotti A, et al Immediate radical prosta-
tectomy in patients with atypical small acinar proliferation Over treatment? J Urol 2004;172:906-8
19 Cornford P, van den Bergh RCN, Briers E, et al EAU-EANMESTRO-ESUR-ISUP-SIOG Guidelines on Prostate Cancer-2024
Update Part I: Screening, Diagnosis, and Local Treatment with Curative Intent Eur Urol 2024; 86:148-63
Correspondence
Rashad Sholan MD, PhD, DSci (Corresponding Author) sholanrashad@gmail com
Scientific Research Center, State Security Service Military Hospital, Baku, Azerbaijan AZ1000, Baku city, Badamdar, Mektebli street, 1
Conflict of interest: The authors declare no potential conflict of interest
Archivio Italiano di Urologia e Andrologia 2024; 96(4):13257
ORIGINAL PAPER
Outcomes of transperineal reanastomosis as a salvage treatment for recurrent vesicourethral anastomosis stenosis after radical prostatectomy
Piotr Gwara, Łukasz Białek, Marta Rydzi´nska, Jakub Dobruch, Michał Skrzypczyk
Department of Urology, Centre of Postgraduate Medical Education, Independent Public Hospital of Prof W Orlowski, Warsaw, Poland
Summary
Purpose: To evaluate transperineal reanastomosis (TRPA) combined with incontinence surgery as a complex treatment for recurring vesicourethral anastomosis stenosis (VUAS) after radical prostatectomy (RP).
Methods: Retrospective analysis of 8 patients who underwent TRPA for recurring VUAS. Detailed preoperative and follow up data were assessed
Results: Mean follow up lasted 47 months (range 17-77) with mean age being 63 4 years (range 61-70) All patients achieved patency and 87 5% (7/8) maintained it to the end of follow up However, four of them required additional procedures to retain patency Six underwent incontinence surgery – artificial urinary sphincter (AUS) implantation – after which one cuff erosion occurred In the end 62 5% (5/8) of patients achieved patent urethra and continence
Conclusions: TRPA combined with incontinence surgery is a reasonable treatment for patients with recurrent VUAS. Nonetheless, this is a set of difficult surgeries that may ultimately end in failure, i.e. the inability to restore urethral patency, urinary incontinence or urinary diversion, hence they should be performed by experienced surgeons.
Prostate cancer is the second most common cancer in men worldwide (1) With the rise of robot-assisted laparoscopic approach to radical prostatectomy (RP), the frequency of complications has been declining, one of them being vesicourethral anastomosis stenosis (VUAS) (2) Though rare, it is a serious condition of complicated nature Patients usually seek medical help upon having problems with micturition post-prostatectomy In more severe cases it may lead to acute urinary retention and require urgent care
Endoscopic procedures remain first line treatment that can be repeated if needed According to a recently published meta-analysis by Delchet et al their overall success rate is between 62 9% and 72 8% with a negative influence on the outcomes of previous radiotherapy (3) If the transurethral approach fails, the next line is open de novo reconstruction (reanastomosis) which can be performed via abdominal,
abdominoperineal or transperineal approach All VUAS treatment may aggravate existing urinary incontinence or cause one to occur de novo which patients should always be informed about before undergoing any VUAS-related surgery Following that, by consenting to the treatment of VUAS, the patient should be prepared for the necessity of further treatment for urinary incontinence
The aim of our study was to retrospectively evaluate the outcomes of transperineal reanastomosis (TPRA) as a salvage treatment option for a selected group of patients who still suffer from VUAS after either repeated, unsuccessful endoscopic procedures or the recurrence of VUAS after prior reanastomosis
METHODS
The study was designed as a retrospective case series study We searched our medical records database for patients who underwent TPRA between 2016 and 2022 Then, we collected the data regarding their medical history as well as cancer treatment history Follow up included evaluation of continence, sustenance of patency, and need for additional procedures All patients were treated with a transurethral procedure at least once prior to TRPA All patients had been informed and fully accepted the possibility of subsequent urinary incontinence after TRPA Patency was evaluated with retrograde urethrogram (RUG) and voiding cystourethrogram (VCUG) In case of any doubt, endoscopic evaluation of lower urinary tract was performed
Surgical technique
Patient is placed in a lithotomy position Through a median perineal incision the bulbous urethra is visualized Bulbocavernosus muscles are cut, and the bulb is mobilized both distally and proximally Both arteries of bulb of penis (if still existing) are cut and ligated The urethra is cut off at the distal end of stenosis - at the line between bulbous and membranous urethra, at the level of the diaphragm of pelvis A flexible cystoscope is inserted through the cystostomy into the bladder neck The scar tissue is incised under visual guidance of the cystoscope light All fibrous tissue is dissected, and the patency of the newly formed vesical orifice is tested with 30Fr bougie The scar tissue
P Gwara, Ł Białek, M Rydzinska, J Dobruch, M Skrzypczyk
around the bulbous urethra is dissected as well Eight Polysorb (5/0) sutures are placed on the bladder and the urethra, and the knots are tied tension-free After checking for leaks the 16Fr Foley transurethral catheter is placed Via a separate incision a Redon drain is installed with the end close to the anastomosis The wound is closed in three layers with absorbable, running 3/0 suture The skin is closed using absorbable, interrupted 3/0 sutures Finally, a 16Fr suprapubic catheter is placed (2, 4) After three to four weeks RUG and VCUG are performed and, if there is no leakage, both catheters are removed
RESULTS
Eight patients underwent TRPA between 02/2016 and 05/2022, all performed by the same surgeon (MS) Patients’ detailed overview is presented in Table (1) All patients received previous VUAS treatment with two havi n g u n d e r g o n e o p e n r e a n a s t o m o
approach All of them suffered from complete erectile dysfunction One patient underwent artificial urethral sphincter (AUS) placement before TRPA, which was complicated by cuff erosion and later AUS removal All patients presented with a patent anastomosis in RUG and VCUG post-TRPA All patients had a history of previous treatment with multiple transurethral procedures, including direct visual internal urethrotomy (DVIU), urethral dilatation, which were all failed The median stenosis length estimated in urethrography was 28 mm
Table (2) presents detailed overview of each patient’s treatment history and follow up All patients were incontinent after TPRA which was to be expected Half of them needed additional intervention due to stricture, after which all of them but one are stricture-free Out of seven patients with patent urethra six were willing to treat urinary incontinence and were treated with AUS implantation There was
Table 2.
Detailed patients’ treatment history and follow up.
one case of urethral erosion and required AUS removal He is scheduled for another AUS to be implanted The remaining 5 patients are socially continent One patient after
TUR: transurethra resection; UD: urethral d latation; TPRA: transperinea reanastomosis; DVIU: direct v s on nterna urethrotomy; TU : transurethral inc sion; TRAPA: transabdominoperineal reanastomos s; AUS: art f cial urinary sphincter; ACS: acute compartment syndrome; DVT: deep venous thrombos s; *Zephyr Surgica Implants, Geneva, Swittzerland; **Boston Sc ent fic, Malborough; Massachusetts, Un ted States of Amer ca
TRPA developed urethrocutaneous fistula which was later complicated by osteitis pubis Eventually he underwent urinary diversion with Bricker ileal conduit
DISCUSSION
VUAS is a complication of RP that is recently observed rarer After open RP its incidence has been reported to be between 2 6% (5) and 26% (6) but with the emergence of robot-assisted laparoscopic approach the incidence has declined to 0 2% (7)-1 6% (8) Britton et al (9) have found a positive correlation between VUAS frequency and adjuvant radiation, BMI, prostate volume, urine leak, blood transfusion and nonnerve-sparing technique They have also reported robot assistance and complete nerve sparing to be related to lower occurrence of stenosis (OR 0 39, p < 0 01 and OR 0 63, p < 0 01, respectively) A mean time of VUAS occurrence after RP is considered to be 3 4 months (9) Although rare, management of VUAS remains a significant surgical dilemma and substantially affect patients quality of life It also should be noted the treatment of VUAS affects continence in most patients, thus it is crucial to appropriately inform patients about possible consequences of treatment (10)
Endoscopic procedures remain a first line treatment for patients with non-obstructive VUAS It offers varied results with overall success rate between 13 and 73 (3, 11) Its low invasiveness and possible repeated nature are the reason for its wide acceptance by patients
Open reanastomosis remains a treatment option in the cases of recurrent stenosis after failed multiple endoscopic interventions Transperineal approach offers the best results with success rate of 93%, reaching 100% after a subsequent endoscopic procedure (12), compared to 60% (95% after subsequent endoscopic procedure) for abdominal (retropubic) approach (10) and 83% for abdominoperineal approach (13) While operating by retropubic access, one must manoeuvre in scar tissue after RP which hinders preparing the anastomosis Moreover, transperineal approach is much less invasive than retropubic approach or combined abdominoperineal approach
The concept of TRPA is similar to that of elaborate pelvic fracture urethral injury (PFUI) repair, involving complete mobilization of the bulbar urethra, crura separation, and in some cases inferior partial pubectomy for bladder neck access Nonetheless, Mundy and Andrich characterize TRPA as far more challenging than standard PFUI repair, necessitating a surgeon with substantial experience in complex PFUI procedures and the skill to employ various supplementary techniques when needed (4)
Unfortunately, mobilization of the urethra during the surgery usually leads to damaging the sphincter which typically leads to incontinence Thus, this access is commonly utilized in patients with preoperative urinary incontinence Favourably the incontinence can be treated afterwards with good effect with sling or AUS implantation (14) Ullate et al demonstrated that implanting the adjustable trans-obturator male system (ATOMS) in patients with urinary incontinence who were previously treated due to urethral stricture or bladder neck stenosis is not related with higher rate of complications such us surgical revision, device explantation or overactive bladder syndrome symptoms de novo
They observed, however, that 38% of the patients with treated stricture achieved continence (≤ 20 mL 24-h pad test) compared to 83% of those without Moreover, multivariate analysis revealed that previous stricture was one of the predictive factors of failure (15)
The AUS implantation may come with a range of complications However, with proper technique and surgical experience its risk can be significantly lowered Mechanical complications, regarding the device itself, occur at overall rate of 6 2% with the most susceptible part being cuff Among nonmechanical complications cuff erosion is the one requiring most consideration It is most frequent during first two years after AUS implantation with overall prevalence of 8 5% (16) The available literature data does not provide a clear answer to the question of optimal urethral management during AUS explantation, and the options include urinary diversion by transurethral and/or suprapubic catheterization, urethrorraphy, and in situ urethroplasty (17) There are conflicting data on the safety of AUS implantation in patients who have had transperineal surgery in the past It seems that previous unsuccessful sling procedure does not increase the risk of complications e g urethral injury or erosion (18, 19) On the other hand previous urethroplasty or AUS explantation due to erosion seems to negatively impact the risk of failure (20, 21) This could also be the reason for cuff erosion in the patient in our case series, who previously had three transperineal procedures
In our series 62 5% (5/8) of patients with refractory VUAS have fully achieved the goal of treatment - continence with patent urethra In addition, even a higher percentage of patients in our study declare satisfaction with the results of the treatment carried out This is in concordance with the study by Reiss et al (12), in which good results regarding quality of life after TRPA despite aggravation of incontinence in 60% of patients have been noted Extended follow-up also shows high success rate of TPRA and high percentage of AUS implantation (22) Nikolavsky et al (23) have reported a case series of 12 patients who underwent open reanastomosis with a patency rate of 93% (11/12) and continence in 72 7% (8/11) of the patients at the end of follow-up with a median time of 75 5 months Immediately after reconstruction only 33 3% (4/12) of patients were continent whereas 75% (6/8) were continent at the end of follow up, if incontinent patients had undergone incontinence treatment However, having used different approaches - abdominal, abdominoperineal and perineal, with only 25% (3/12) being perineal - their results are not easily compared to ours
There are also descriptions in the literature of case series in which buccal mucosa graft (BMG) was used in the treatment of VUAS Shahrour et al presented a series of 4 patients who underwent dorsal BMG urethroplasty for VUAS (24) Dolezel et al recently published descriptions of the treatment of VUAS via ventral BMG urethroplasty and endourethroplasty with BMG (25) These techniques are, however, reserved for the patients with non-obliterative strictures and the capability of its usage still needs confirmation
Limitations of this case series are its retrospective character as well as relatively small number of cases However, with VUAS being a rare condition, and compared to the available literature, such a small number is to be expected
CONCLUSIONS
TRPA is a valid treatment option for patients with obstructive, recurrent VUAS It offers satisfactory success rates and, at the same time, provides surgeons with optimal field visualisation and access unhindered by scar tissue However, achieving a patent urethra is only one step in VUAS treatment since reconstruction usually causes incontinence de novo or aggravates one existing prior With that in mind, patients should always be informed to expect two-step treatment - firstly open reconstruction and afterwards incontinence surgery (AUS or sling implantation, depending on patient’s preference and device availability) This way we limit patients’ dissatisfaction and improve their adherence What deserves to be emphasized, however, is that even for an experienced surgeon, this is a set of difficult surgeries that may ultimately end in failure, i e the inability to restore urethral patency, urinary incontinence or urinary diversion
REFERENCES
1 Bergengren O, Pekala KR, Matsoukas K, et al 2022 Update on Prostate Cancer Epidemiology and Risk Factors-A Systematic Review Eur Urol 2023; 84:191-206
2 R o s e n b a u m C M , F i s c h M , V e t t e r l e i n M W C o
p o r a r y Management of Vesico-Urethral Anastomotic Stenosis After Radical Prostatectomy Front Surg 2020; 7:587271
3 Delchet O, Nourredine M, González Serrano A, et al Post-prostatectomy anastomotic stenosis: systematic review and meta-analysis of endoscopic treatment BJU Int 2024; 133:237-45
4 Mundy AR, Andrich DE Posterior urethral complications of the treatment of prostate cancer BJU Int 2012; 110:304-25
5 Breyer BN, Davis CB, Cowan JE, et al Incidence of bladder neck contracture after robot-assisted laparoscopic and open radical prostatectomy BJU Int 2010; 106:1734-8
6 Hu JC, Gold KF, Pashos CL, et al Role of surgeon volume in radical prostatectomy outcomes J Clin Oncol Off J Am Soc Clin Oncol 2003; 21:401-5
7 Carlsson S, Nilsson AE, Schumacher MC, et al Surgery-related complications in 1253 robot-assisted and 485 open retropubic radical prostatectomies at the Karolinska University Hospital, Sweden Urology 2010; 75:1092-7
8 Parihar JS, Ha YS, Kim IY Bladder neck contracture-incidence and management following contemporary robot assisted radical prostatectomy technique Prostate Int 2014; 2:12-8
9 Britton CJ, Sharma V, Fadel AE, et al Vesicourethral Anastomotic Stenosis Following Radical Prostatectomy: Risk Factors, Natural History, and Treatment Outcomes J Urol 2023; 210:312-22
10 Pfalzgraf D, Beuke M, Isbarn H, et al Open retropubic reanastomosis for highly recurrent and complex bladder neck stenosis J Urol 2011; 186:1944-7
11 LaBossiere JR, Cheung D, Rourke K Endoscopic Treatment of Vesicourethral Stenosis after Radical Prostatectomy: Outcomes and Predictors of Success J Urol 2016; 195:1495-500
12 Reiss CP, Pfalzgraf D, Kluth LA, et al Transperineal reanastomosis for the treatment for highly recurrent anastomotic strictures as a last option before urinary diversion World J Urol 2014; 32:1185-90
13 Theodoros C, Katsifotis C, Stournaras P, et al Abdomino-perineal repair of recurrent and complex bladder neck-prostatic urethra contractures Eur Urol 2000; 38:734-740
14 Flynn BJ, Webster GD Evaluation and surgical management of intrinsic sphincter deficiency after radical prostatectomy Rev Urol 2004; 6:180-6
15 Ullate A, Arance I, Virseda-Chamorro M, et al ATOMS (Adjustable Trans-Obturator Male System) in Patients with PostP r o s t a t e c t o m y I n c o
Stricture or Bladder Neck Contracture J Clin Med 2022; 11:4882
16 Van der Aa F, Drake MJ, Kasyan GR, et al The artificial urinary sphincter after a quarter of a century: a critical systematic review of its use in male non-neurogenic incontinence Eur Urol 2013; 63:681-9
17 Białek Ł, Frankiewicz M, Adamowicz J, et al Urethral management after artificial urinary sphincter explantation due to cuff erosion Cent Eur J Urol 2023; 76:322-4
18 Lentz AC, Peterson AC, Webster GD Outcomes following artificial sphincter implantation after prior unsuccessful male sling J Urol 2012; 187:2149-53
19 Fisher MB, Aggarwal N, Vuruskan H, Singla AK Efficacy of artificial urinary sphincter implantation after failed bone-anchored male sling for postprostatectomy incontinence Urology 2007; 70:942-4
20 Lai HH, Boone TB Complex artificial urinary sphincter revision and reimplantation cases--how do they fare compared to virgin cases? J Urol 2012; 187:951-5
21 McGeady JB, McAninch JW, Truesdale MD, et al Artificial urinary sphincter placement in compromised urethras and survival: a comparison of virgin, radiated and reoperative cases J Urol 2014; 192:1756-61
22 Schuettfort VM, Dahlem R, Kluth L, et al Transperineal reanastomosis for treatment of highly recurrent anastomotic strictures after radical retropubic prostatectomy: extended follow-up World J Urol 2017; 35:1885-90
23 Nikolavsky D, Blakely SA, Hadley DA, et al Open reconstruction of recurrent vesicourethral anastomotic stricture after radical prostatectomy Int Urol Nephrol 2014; 46:2147-52
24 Shahrour W, Hodhod A, Kotb A, et al Dorsal Buccal Mucosal Graft Urethroplasty for Vesico-Urethral Anastomotic Stricture Postradical Prostatectomy Urology 2019; 130:210
25 Doležel J, Hrabec R, Uher M, et al Substitution Urethroplasty With Buccal Mucosal Graft in the Management of Stricture of Vesicourethral Anastomosis or Membranous Urethra: Single-institut i o n
Piotr Gwara, MD p gwara@wp pl Łukasz Białek, MD lukaszbtm@gmail com
Marta Rydzinska, MD martaaga drazkiewicz@gmail com
Jakub Dobruch, MD jdobruch@cmkp edu pl
Michał Skrzypczyk, MD, PhD (Corresponding Author) michalskrzypczyk@gmail com
Department of Urology, Centre of Postgraduate Medical Education, Independent Public Hospital of Prof W Orlowski, Czerniakowska Street 231, 00-416 Warsaw, Poland
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
The learning curve for robotic-assisted pyeloplasty in urologists with no prior robotic experience using an ex-vivo model: A prospective, controlled study
1 Department of Surgery, University of Bisha, Bisha, Saudi Arabia;
2 Department of Urology, University Hospital of Patras, Patras, Greece;
3 Medical University of Vienna, Vienna, Austria;
4 University Clinic of Urology Andrology, National University Hospital Center, Hubert Koutoukou MAGA of Cotonou, Benin
Summary
Introduction: Despite the increasing trend of utilizing robotic techniques in pyeloplasty, little is known about the learning curve for robot-assisted pyeloplasty (RAP) amongst urologists with no prior robotic experience Therefore, the present study aimed to evaluate the learning curve of residents in the last year or recently appointed urologists performing RAP using an ex-vivo model
Methods: A prospective ex-vivo model study was conducted including participants who were either residents in the last year or recently appointed urologists All participants had obtained the E-BLUS certification, or they were able to complete its 4 tasks successfully in a dry lab, without prior robotic experience Each participant performed four consecutive RAPs using the avatera system on an ex-vivo porcine model The primary endpoint of the present study was the change in the average time to complete the anastomosis from the first to the fourth attempt.
Results: Nine urologists and 8 residents were enrolled in this study. Each surgeon demonstrated a reduction in the time to complete anastomosis from the 1st to 4th attempt with an average of value of 4.41 ± 1.06 minutes (p = 0.003). The decrease in time was statistically significant in both urologists and residents subgroups (4.5 ± 1.41 minutes p = 0.049 and 4.33 ± 0 71 minutes p = 0 035 respectively)
Conclusions: The training on the ex-vivo model could lead, in only a few attempts, to a significant improvement in skills and in the required time of experienced-naïve surgeons to complete an RAP
KEY WORDS: Learning curve; Pyeloplasty; Robotic-assisted; Robotics; Avatera system
Submitted 30 August 2024; Accepted 6 September 2024
INTRODUCTION
The use of robotics in medical procedures has already been implemented in various medical specialties, including neuronavigation and stereotactic neurosurgery (1-3) In urology, applications of robotic systems have included laparoscopic camera control, percutaneous renal access, prostate biopsy, and transurethral resection of the prostate (4)
Laparoscopic pyeloplasty was initially proposed for the treatment of ureteropelvic junction (UPJ) obstruction, with a success rate of over 90% Besides, laparoscopic pyeloplasty is associated with reduced hospital stay and postoperative complications compared to the open approach (5)
However, intracorporeal suturing remains a technical challenge in the laparoscopic approach and may increase the operative time The tedious learning curve of laparoscopic pyeloplasty constitutes another limitation (6)
In this regard, robot-assisted pyeloplasty (RAP) has emerged as a feasible alternative to overcome the technical difficulties of conventional laparoscopic pyeloplasty (7) The RAP coveys all the advantages of conventional laparoscopic pyeloplasty while also decreasing the technical difficulties with intracorporeal suturing and shortening the operative time (8) It was reported that the high incidence of UPJ obstruction, which leads to a higher volume of cases, and the previous experience with laparoscopic surgery have improved the learning curve and outcomes of RAP (6)
The present study aimed to evaluate the learning curve of novice surgeons performing Robotic-assisted pyeloplasty using a recently introduced robotic system on an ex-vivo porcine model
PATIENTS AND METHODS
Study participants and robotic system
We conducted a prospective ex-vivo model study that enrolled residents in the last year or new urologists All participants were required to pass the European Training in Basic Laparoscopic Urological Skills (E-BLUS) training program or to achieve the goals in its four tasks in a similar dry lab We limited the participation in the present study to novice surgeons who did not have any prior experience with robotic surgery to perform four consecutive RAPs using the avatera system (avateramedical GmbH, Germany) The avatera system is a robotic system that is based on activated robotic force feedback The robotic cart is a four-arm component of the system that can be controlled by the surgeon and consists of three arms for controlling
the instruments (in a one-to-one master-slave fashion) and one arm to hold and control the endoscope The second component of the system is a separate control unit for the operating surgeon Because of this, it is easily adaptable to the majority of operating rooms It is equipped with a camera that has a resolution of full HD, while the single-use instruments are entirely articulated and can move in a range of 7 degrees of freedom Since the instruments are disposable, the possibility of crosscontamination is minimal, without the need for sterilization The special shape of the eyepiece, which leaves the surgeon's ear and mouth uncovered, is an additional advantage that has been developed This design makes it easier for the surgeon to communicate clearly with the operating team during surgical procedures (9)
Ethical standards
The study has been carried out in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments The experiments were carefully designed and preapproved by the Veterinary Administration of the Prefecture of Western Greece and conducted according to Directive 2010/63/EU (http:// eurlex europa eu/LexUriServ/LexUriServ do?uri= OJ:L:2010: 276:0033:0079:EN: PDF)
Animal model and experiment
The assessment of the learning curve was based on conducting four consecutive ex-vivo anastomoses on a porcine model, with strict compliance to relevant guidelines for the use of laboratory animals The porcine model consisted of the urinary bladder and both ureters, as described by Sanchez Hurtado et al (10) It was placed upside-down, while the bladder was considered as a dilated pelvis and the ureter as the proximal part of it (Figure 1) The normal ureterovesical junction (UVJ) was considered as a stenotic ureteropelvic junction (UPJ) The supply of porcine urinary bladders was performed by a slaughterhouse
A 4-hour theoretical educational training course was performed to all the participants by the avateramedical, presenting the use and care of the robotic system Afterward, each participant completed a 2-hour E-BLUS task-based training to familiarize themselves with the instruments and the function of the robotic system Three trocars were placed in an artificial insufflated abdominal model based on the set-up of the conventional robotic pyeloplasty, followed by the application of three robotic arms; one for
the endoscope, one for the Metzenbaum Scissors and the Needle Holder (the two instruments were exchanged during the procedure), and one for the Atraumatic Grasper (Figure 2) The three ports were used as none of the participants have previous experience with RAP
The ureter was resected horizontally in proximity to the renal hilum, followed by spatulation of its tip (Figure 3) The anastomosis was performed using a Vicryl 4-0 suture in a running way (Figure 4) Afterward, a 4F ureteral catheter was inserted from the distal part of the ureter, and indigo carmine (5 mL) was injected to ensure the patency and the water-tightness of the anastomosis The time between the first incision and the completion of the indigo carmine test was recorded as the time needed to complete the UP anastomosis The anastomosis leakage events were also recorded After the completion of the fourth attempt, the participants filled out a Likert-scaled Questionnaire
A Ayed, P Kallidonis, V Tatanis, et al
Figure 1. Ex- vivo pyeloplasty model set-up
Figure 2. Incision of the Ureteropelvic Junction
Figure 3. Spatulation of the ureter
Figure 4
Ureteropelvic anastomosis
Table 1. Postoperative evaluation questionnaire (1 being the lowest and 5 being the highest score)
Parameter Scores
Vision12345
Comfort12345
Confidence12345
evaluating the Vision, Comfort and Confidence to perform RAP after the training The overall questionnaire score ranged from 3-15 (1-5 points per question) (Table 1)
Statistical analysis
Data were analyzed using the Prism (GraphPad, Boston, USA) version 9 The time to complete the anastomosis
Figure 5.
and the reduction in time were described using mean, standard deviation (SD), median and range, while the percentage of change was calculated The overall questionnaire rating was described using mean, SD, median and range The trend of change in the time to complete the anastomosis was analyzed using paired t-test A twotailed p-value < 5% was considered statistically significant The learning curve factor (b factor) and the learning percentage (p percentage) is calculated based on the cumulative average model (Wright model) (11, 12)
RESULTS
The trend of change in time required to complete the pyeloplasty between the 1st and 4th attempts
Table 2
In total 9 urologists and 8 residents on the final year of residency were included into the study The urologists had a competency of basic laparoscopic operations (including laparoscopic varicocelectomy, laparoscopic hernia repair and laparoscopic nephrectomy), while the residents had a prior experience of participation in at least 20 laparoscopic operations (including radical nephrectomies, partial nephrectomies, radical prostatectomies and pyeloplasties)
The required time to complete the pyeloplasty in the 1st and 4th attempts (Paired t-test).
Each participant successfully completed the four attempts of RAP Each surgeon demonstrated a reduction in the time to complete anastomosis from the 1st to 4th attempts, as shown in Figure 5 There was a significant improvement, as demonstrated by the significant decrease in the average time to complete the anastomosis from 33 41 ± 3 8 minutes at the first attempt to 29 ± 4 2 minutes at the fourth attempt (p = 0 003) The mean reduction in the time to complete the pyeloplasty was 4 412 (4 96 to 3 87) minutes, with a percentage reduction of 13 5% (Table 2) Among the 1st attempt of all the participants, 4 events of anastomosis leakage occurred, while 2 events of anastomosis leakage were noticed among the 2nd attempts On the 3rd and 4th attempts, no anastomosis leakage was observed The mean overall score in the postoperative evaluation questionnaire was 11 94 ± 1 09 (median value: 12, range 10-14) In detail, the mean vision score, the mean comfort score and the mean confidence score were 4 41 ± 0 62, 4 18 ± 0 64 and 3 35 ± 0 49 respectively The b factor of the overall learning curve was -0 965 and the p learning percentage is 1 95
A stratification of the participants was performed into urologists and residents groups based on prior laparoscopic experience In both groups, the reduction in time was achieved at a statistically significant level In urologist groups, the 1st and 4th RAP was completed in a mean value of 32 89 ± 3 79 minutes and 28 56 ± 4 19 minutes respectively (p = 0 0351) The time to accomplish the anastomosis was diminished by a mean value of 13 44%, as it needed 4 33 ± 0 71 fewer minutes (Table 3) The mean overall score of the
Table 4.
The required time to complete the pyeloplasty in the 1st and 4th attempts in Residents Group (Paired t-test)
The b factor of the urologists subgroup’s learning curve was -2 90 In the residents group, the time needed to perform the 1st and 4th pyeloplasty was 34 ± 3 89 minutes and 29 5 ± 4 47 minutes respectively (p = 0 0497) The mean difference in time between the two attempts was 4 5 ± 1 41 minutes leading to a mean reduction ratio of 13 50% (Table 4)
The mean postoperative questionnaire score was 11 50 ± 0 93 (Vision 4 38 ± 0 52, Comfort 3 88 ± 0 64 and Confidence 3 25 ± 0 46) The b factor of the residents subgroup ’ s learning curve was -2 89
DISCUSSION
The results of the current study showed that the time of anastomosis reduced by 7 7% to 20 7%, with an average reduction of 13 5%, after four pyeloplasties A pilot study by Sung et al , compared robotic-assisted and laparoscopic pyeloplasty Based on the results, no significant difference in total surgical time (115 2 minutes for robotic and 94 5 minutes for laparoscopic, p = 0 2), anastomosis time (75 7 minutes for robotic and 64 3 minutes for laparoscopic, p = 0 3), and the number of suture bites per ureter (13 0 for robotic and 12 5 for traditional, p = 0 8) was noticed Five out of 6 robotic and 3 out of 4 laparoscopic pyeloplasties presented with immediate watertight anastomosis (13) Lorincz et al conducted a study to investigate the feasibility of robot-assisted minimally invasive pyeloplasty in piglets All seven piglets underwent the procedure without complications, and the results showed that robotic assistance enhanced surgical dexterity and precision The mean setup and anastomosis times were 19 minutes and 51 minutes, respectively The results demonstrated that robot-assisted pyeloplasty is a technically feasible procedure with acceptable morbidity in an animal model (14) Chammas Jr and his colleagues conducted a study to assess the learning curve for robotic pyeloplasty The study included in total 100 procedures performed on 127 patients and divided them into three groups (open pyeloplasty, laparoscopic pyeloplasty, and RAP) to analyze the learning curve The results showed a significant decrease in surgical time and hospital stay after 25 cases The median anastomosis time and operative time were decreased in the RAP as the number of procedures were increased, without significant difference (p > 0 05) (15) The reduction in anastomosis time in our study was observed earlier, indicating that using the avatera system could be associated with a shorter learning curve
The ex-vivo training model consisted of a porcine urinary bladder accompanied by both ureters This model was evaluated in details by Sanchez-Hurtado and his colleagues (10) The authors conducted the evaluation of face and content validity and enrolled 127 urologists who performed various Laparoscopic Ureteric Reconstructive Techniques
Afterward, the participants fulfilled a Likertscaled questionnaire The final rating range could be 1-10 points The mean rating was 9 19 ± 0 82, while the comments performed by the expert urologists who participated were positive In robotic pyeloplasty, the learning curve is particularly important as the procedure is technically demanding and requires a high level of dexterity and precision (16) The results of the study indicate that residents and new urologists can achieve a reduction in the time of anastomosis after four attempts at ex vivo robotic pyeloplasty using the avatera system The reduction in the time of anastomosis suggests that the participants were able to improve their proficiency in the performance of the procedure, resulting in a reduction in the overall time required to complete the anastomosis This improvement may be translated into ameliorated surgical outcomes, such as reduced complication rates and improved patient outcomes In contrast, in a retrospective study conducted by Sorensen et al , 33 children, who underwent RAP between 2006 and 2009, were compared to a matched group who underwent open pyeloplasty The results showed that the mean overall operative time was 90 minutes longer (38%) for the RAP arm After 15 to 20 robotic cases, the overall operative time was consistently within 1 SD of the average open pyeloplasty time with no significant difference in overall operative time The decrease in overall operative time was due to a decrease in anastomosis time rather than access time (17) The learning curve in robot-assisted laparoscopic pyeloplasty is influenced not only by individual surgical experience but also by the experience of the surgical team Sampinato et al. reported that junior surgeons were associated with a more rapid learning process with an earlier inflection point and comparable levels of expertise as senior surgeons after seven procedures (18) In our study, the progress of the less experienced residents’ group was greater than the urologists’ group More precisely, the mean decrease in time was 4 33 ± 0 71 minutes and 4 5 ± 1 41 minutes for the residents’ and urologists’ groups respectively
It is also worth noting that all participants in the study obtained the E-BLUS certification or could complete the four tasks in the dry lab, indicating that they had a basic level of proficiency in the use of laparoscopic surgery The certification and dry lab experience likely provided a foundation for the participants to build upon during the ex vivo pyeloplasty procedure, contributing to the observed reduction in the time of anastomosis Dothan et al reported that previous experience in open and laparoscopic pyeloplasty was associated with a shorter learning curve in the robotic approach (15)
We acknowledge the existence of some limitations in the present study The present study was based on ex-vivo models, which are limited in replicating the complexities of human anatomy, including blood flow, tissue response,
A Ayed, P Kallidonis, V Tatanis, et
and variability among patients As a result, the learning experience may not accurately reflect the challenges a surgeon would face during an actual procedure Besides, exvivo models do not allow for the possibility of encountering intraoperative complications, such as bleeding or unexpected anatomical variations This limits the urologist's ability to gain experience in managing these challenges in a real-life setting Lastly, in our study, all the participants had obtained or were capable to obtain the EBLUS certification Thus, the results of the ex-vivo study may not be generalizable to all urologists, as individual learning curves can vary based on prior experience, skill level, and other factors
CONCLUSIONS
In conclusion, our study demonstrates that ureteropelvic anastomosis was precisely, effectively, and comfortably performed using the robotic system Owing to its simplicity, residents and new urologists can improve their competency in the performance of robotic-assisted pyeloplasty using a porcine ex-vivo model
ACKNOWLEDGEMENT
The authors are thankful to the Deanship of Graduate Studies and Scientific Research at University of Bisha for supporting this work through the Fast-Track Research Support Program
REFERENCES
1 Mao JZ, Agyei JO, Khan A, et al Technologic Evolution of Navigation and Robotics in Spine Surgery: A Historical Perspective World Neurosurg 2021; 145:159-67
2 Stumpo V, Staartjes VE, Klukowska AM, et al Global adoption of r o b o t i c t e c h n o l o g y i n t o n e u r o s
Neurosurg Rev 2021; 44:2675-87
3 Qureshi YA, Mohammadi B Robotic oesophago-gastric cancer surgery Ann R Coll Surg Engl 2018; 100(6 sup):23-30
4 Thaly R, Shah K, Patel VR Applications of robots in urology J Robot Surg 2007; 1:3-17
5 Atalla MA, Dovey Z, Kavoussi LR Laparoscopic versus robotic pyeloplasty: man versus machine Expert Rev Med Devices 2010; 7:27-34
6 Morales-Lopez RA, Perez-Marchan M, Perez Brayfield M Current Concepts in Pediatric Robotic Assisted Pyeloplasty Frontiers in pediatrics 2019; 7:4
7 Kearns JT, Gundeti MS Pediatric robotic urologic surgery-2014 J Indian Assoc Pediatr Surg 2014; 19:123-8
8 Howe A, Kozel Z, Palmer L Robotic surgery in pediatric urology Asian J Urol 2017; 4:55-67
9 Liatsikos E, Tsaturyan A, Kyriazis I, et al Market potentials of robotic systems in medical science: analysis of the Avatera robotic system World J Urol 2022; 40:283-9
10 Sanchez Hurtado MA, Diaz-Guemes Martin-Portugues I, Correa Martin L, et al Development and assessment of an ex-vivo bench model aimed at laparoscopic ureteric reconstructive techniques J Pediatr Urol 2021; 17:753-5
11 Wright TP Factors Affecting the Cost of Airplanes Journal of the Aereonautical Science 1936; 3:122
12 Tilindis J, Kleiza V Learning curve parameter estimation beyond traditional statistic Applied Mathematical Modelling 2017; 45:768783
13 Sung GT, Gill IS, Hsu TH Robotic-assisted laparoscopic pyeloplasty: a pilot study Urology 1999; 53:1099-103
14 Lorincz A, Knight CG, Kant AJ, et al Totally minimally invasive robot-assisted unstented pyeloplasty using the Zeus Microwrist Surgical System: an animal study J Pediatr Surg 2005; 40:418-22
15 Dothan D, Raisin G, Jaber J, Kocherov S, Chertin B Learning curve of robotic-assisted laparoscopic pyeloplasty (RALP) in children: how to reach a level of excellence? J Robot Surg 2021; 15:93-7
16 Pakkasjärvi N, Krishnan N, Ripatti L, Anand S Learning Curves in Pediatric Robot-Assisted Pyeloplasty: A Systematic Review J Clin Med 2022; 11:6935
17 Sorensen MD, Delostrinos C, Johnson MH, et al Comparison of the learning curve and outcomes of robotic assisted pediatric pyeloplasty J Urol 2011; 185(6 Suppl):2517-22
18 Spampinato G, Binet A, Fourcade L, et al Comparison of the L
Between Senior and Junior Surgeons J Laparoendosc Adv Surg Tech A 2021; 31:478-483
Correspondence
Abdullah Ayed, MD (Corresponding Author) aayed@ub edu sa Department of Surgery, College of Medicine, University of Bisha, Bisha 61922, P O Box 551, Saudi Arabia
Panagiotis Kallidonis, MD Vasileios Tatanis, MD Angelis Peteinaris, MD Department of Urology, University Hospital of Patras, Patras, Greece
Evangelos Liatsikos, MD
Department of Anesthesiology and ICU, University Hospital of Patras, Patras, Greece
Medical University of Vienna, Vienna, Austria
Natchagande Gilles, MD
University Clinic of Urology Andrology, National University Hospital Center, Hubert Koutoukou MAGA of Cotonou, Benin
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Role of inflammatory markers in predicting spontaneous passage of ureteral stones less than 10 mm
Ismaeel Aghaways 1 , Rawa Bapir 2-4 , Nabaz S. Siwaily 2 , Ahmed Mohammed Abdalqadir 2 , Shakhawan Hamaamin Said 1 , Ayman M. Mustafa 3 , Bryar Othman Muhammed 5 , Hawbash M. Rahim 4, 6 , Berun A. Abdalla 3, 4 , Fahmi H. Kakamad 1, 3, 4 , Shvan H. Mohammed 4
1 College of Medicine, University of Sulaimani, Madam Mitterrand Street, Sulaimani, Kurdistan, Iraq;
2 Department of Urology, Sulaymaniyah Surgical Teaching Hospital, Sulaymaniyah, Iraq;
3 Smart Health Tower, Madam Mitterrand Street, Sulaimani, Kurdistan, Iraq;
6 Medical Laboratory Science Department, College of Health Sciences, University of Human Development, Sulaymaniyah, Kurdistan Region, Iraq;
Summary
Introduction: In ureterolithiasis, the prediction of spontaneous passage poses a challenge for urologists Moreover, there is controversy surrounding the preferred management approach, whether medical or surgical, as each approach has its disadvantages Procalcitonin and other inflammatory markers were studied for predicting stone passage spontaneously, but their significance remains controversial This study aims to assess the association between these markers, especially procalcitonin, and spontaneous ureteral stone passage
Materials and methods: In this multicenter prospective cohort study from March 2022 to October 2023, consecutive patients with a single unilateral distal ureteric stone less than 10 mm were enrolled Exclusion criteria were specified Patients underwent medical expulsive therapy (MET) and were monitored for stone passage The significance level was set at p < 0 05
Results: Out of 94 patients enrolled, 72.3% were male and 27 7% were female, with a mean age of 38 84± 10 41 years Stone sizes varied, with the most common range being 4 mm5 9 mm Participants were categorized based on spontaneous stone passage as spontaneous stone passage (SSP) and non-SSP. No significant differences were observed in most demographic and laboratory variables. However, serum procalcitonin and C-reactive protein showed significant differences between the SSP and non-SSP groups.
Conclusions: Although several inflammatory markers were studied to predict the spontaneous passage of the ureteral stone, the current study concluded that only elevated procalcitonin, C-reactive protein, and large stone diameter decrease the chance of spontaneous ureteral stone passage
KEY WORDS: Nephrolithiasis; Spontaneous stone passage; Inflammatory marker; Procalcitonin level; Renal stone surgery
Submitted 1 September 2024; Accepted 9 September 2024
INTRODUCTION
Nephrolithiasis is a common urinary tract disease, ranking third in terms of prevalence after urinary tract infection and benign prostate obstruction It affects around
5% to 10% of the population, leading many individuals to seek medical care for stone-related problems in emergency and general outpatient departments The lifetime possibility of experiencing urolithiasis is estimated to be around 13% for males and 7% for females
The incidence of urolithiasis is highest for males between the ages of 40 and 60, whereas for females, it peaks in the late 20s (1-3) A ureteric stone accounts for 20% of stones in the urinary tract, with 70% of these stones typically situated in the distal part of the ureter (3)
Major complaints such as urinary tract infection, vomiting, renal obstruction, nausea, hematuria (bloody urine), and abdominal or back pain in ureteral calculi can be noticed (4) A non-contrast computed tomography (NCCT) scan is the most preferred imaging technique for urolithiasis diagnosis in symptomatic patients The sensitivity and specificity of this diagnostic method were found to be approximately 100%, making it an extremely reliable diagnostic tool (4)
Regarding the management of stone passage, a considerable number of ureteral stones have the potential to pass on their own (5) Per the European Urological Association's and American Urological Association's recommendations, medical expulsive therapy (MET) is considered the primary treatment for ureteral stones measuring less than 10 mm (6) Not all patients taking MET can achieve spontaneous stone passage The key factors influencing predictability include the stone's size and its location As indicated by the American Urological Association, 68% of stones measuring less than 5 mm and 47% of stones exceeding 5 mm in size were noted to pass spontaneously (7) In cases where the stone cannot pass naturally, treatment alternatives such as extracorporeal shockwave lithotripsy (ESWL), ureteroscopy, and open surgery may be considered (4) Inflammatory markers are indicators of an inflammatory response in the human body The level of inflammation can be detected by various markers, such as serum procalcitonin, C-reactive protein (CRP), and others (8) Elevated levels of these markers are observed in various conditions, including COVID-19, cancer, and inflamma-
tory bowel disease (9) Newly conducted research has been released, demonstrating that biochemical indicators of inflammation can function as predictors for the spontaneous passage of stones (10) The relevance of inflammatory markers in the spontaneous passage of ureteral stones is a subject of debate among various studies (11) The current study aims to assess the association between serum procalcitonin, CRP, and other inflammatory markers with the possibility of passing stones spontaneously
MATERIALS AND METHODS
Study design and setting
This prospective observational cohort study was conducted from March 2022 to October 2023 Ethical approval was secured by the ethics committee with a degree No 5 3 a n d b o t h
obtained from each participant
Inclusion and exclusion criteria
The study focused on patients aged between 18 and 64 years, including both genders It only included patients diagnosed through a non-contrast-enhanced CT scan with single unilateral stones less than 10mm in size and located in the distal ureter below the lower border of the sacroiliac joint
Individuals with a single functioning kidney, more than 1 stone in the same ureter, bilateral ureteric and/or concurrent renal stones, severe hydronephrosis [defined as Grade 4 hydronephrosis based on the Onen classification systemwhich characterizes severe hydronephrosis as greater than 50% loss of renal parenchyma or a cyst-like kidney with no significant visible renal parenchyma (12)], impaired renal function, congenital or acquired anatomical anomaly of the urinary tract, pregnant patients, history of ureteral stenosis or reconstructive ureteral surgery, previous intervention for a stone or any other operation (within 2 months of inclusion in the study), or individuals who had ESWL and stent or nephrostomy insertion for a stone in the same ureter were not included
Furthermore, exclusion criteria were patients with diabetes, thyroid or hepatic disease, active malignancy, active inflammatory bowel disease, active infectious disease, immunological diseases, active chronic inflammatory disease, or patients who used antibiotic, steroid, NSAIDS, or immune suppressant medicines (within 2 weeks of inclusion in the study) or patients with documented infection clinically (fever > 38) or via investigations (positive urine culture) or patients who were also unable to comply with MET or had contraindications to MET therapy or side effects of the medications or patients who preferred immediate active treatment of stones, or who were lost follow-up during the study
Sample and data collection
Upon admission and throughout the acute phase, demographic information such as age, gender, body weight, and height were obtained from all patients This information was obtained as part of the initial assessment to characterize the study population Body mass index (BMI) was computed as the ratio of height in meter square to weight in
kilogram and expressed as kg/m2 A medical history and thorough physical examination were conducted on each participant to assess their overall health and identify any clinical signs As part of the initial assessment, inflammatory markers were measured, including complete blood count (white blood cells (WBCs), neutrophils (NCs), lymphocytes, neutrophil-to-lymphocyte ratio (NLR), platelet-tolymphocyte ratio (PLR), serum procalcitonin, C-reactive protein, and serum creatinine to evaluate disease severity All patients underwent NCCT scans of the kidney, ureter, and bladder Axial NCCT images with a slice thickness of 5 mm were obtained, utilizing specific imaging parameters such as a soft-tissue window with a width of 360, a pitch of 1 5, a tube voltage of 120 kV, and a tube current ranging from 70 to 90 mAs Radiological findings included a detailed analysis of stone characteristics, determining stone side (right versus left), site (proximal, mid, and distal), size (defined by the stone’s greatest diameter), and density measured in Hounsfield units In terms of hydronephrosis grading, the study utilized the Onen classification system This system categorized grades 0 and 1 as indicating no-to-mild hydronephrosis Conversely, grades 2, 3, and 4 were grouped to represent moderateto-severe hydronephrosis This classification allowed for a concise and clinically relevant assessment of the degree of hydronephrosis in the study population, providing a more detailed analysis of renal conditions and their implications (12) Concerning the anatomical position, the distal ureter was specified as the segment extending from the lower boundary of the sacroiliac joint to the bladder Stone size calculations were performed using both coronal and axial images obtained through cross-sectional imaging Finally, all the obtained data were recorded for further analysis
Follow-up
Patients without indications for interventional treatment underwent observation and MET, which involved a prescription of diclofenac sodium (75 mg/day) and tamsulosin (0 4 mg/day) for four weeks, along with a recommended daily fluid intake of 2-3 liters Those on MET attended weekly outpatient controls, excluding emergencies During these visits, patients were asked about the stone passage and any renal colic incidents For those unable to pass the stone, confirmation was sought through ultrasound/plain kidney-ureter-bladder at weeks one, two, and three, and at the fourth week using noncontrast abdominal CT Individuals failing to pass the stone were categorized as passage negative (NO SSP), while those successful were grouped as passage positive (SSP) Failure of passage was defined as the stone's presence on NCCT after four weeks or urgent intervention within the period due to stone-related complications, such as drainage, shockwave lithotripsy, or ureteroscopy (URS) Inflammatory markers were not reassessed during the follow-up period; instead, the follow-up focused on monitoring stone passage and patient progress
Statistical analysis
The acquired data were analyzed via Statistical Package for the Social Sciences software 25 0 Quantitative variables were analyzed by using an independent sample t-test and
I Aghaways, R Bapir, N S Siwaily, et al
chi-square; additionally, these data were presented in the form of means and standard deviations Qualitative data were presented as proportions and percentages In this study, a p-value of < 0 05 was considered significant
RESULTS
Demographic characteristics
Of the total patients enrolled in this study (n = 94), 68 (72 3%) were male and 26 (27 7%) were female They had a mean age of 38 84 ± 10 41 years (19-64 years), with the majority of the patients (33%) being between 29 and 38 years old The mean BMI of the participants was 26 3 ± 4 638, with the majority of participants falling within the normal range (18 5-24 9) Stone sizes were further classified into different classes; the most common stone size falls within the 4 mm-5 9 mm range, comprising the largest percentage of the sample (39 36%) Further characteristics of the enrolled participants are given in Table 1
Clinical characteristics and statistical analysis
The individuals enrolled in this study were divided into two main groups depending on whether they experienced spontaneous passage of stones or non-spontaneous passage of stones, with a mean age of 39 4 ± 10 8 and 37 78 ± 9 73, respectively The mean stone size ± SD in SSP was 5 41 ± 1 6, while the size of the stone in non-SSP was 6 37 ± 1 76
Inflammatory markers are regarded as predictive factors for the evaluation of spontaneous stone passage In this study, several demographics, laboratory, and radiological variables were analyzed to investigate their association with spontaneous stone passage No statistically significant differences among several variables between the NO SSP and SSP groups were found, including age, BMI, side (right or left) of the kidney stone, serum creatinine, PLR, white blood cells, granulocytes, and platelets
Regarding the association between inflammatory markers and the possibility of stone passage spontaneously, a high statistically significant difference in serum procalcitonin levels was found between the NO SSP and SSP groups (p < 0 001), with the mean of procalcitonin being higher (0 14 ± 0 089) among the NO SSP groups compared to the SSP group (0 05 ± 0 027) CRP, as another inflammatory marker, was found to have statistical significance between the NO SSP and SSP groups (p < 0 001), with the mean of CRP being lower among the SSP group (5 55 ± 5 06) compared to the NO SSP group (12 63 ± 11 03) Additionally, NLR and lymphocytes were found to have statistical significance difference between the NO SSP and SSP groups with a p-value of (0 032, and 0 032), respectively (Table 2)
Accordingly, the size of the stone also showed a statistically significant difference between the NO SSP and SSP groups (p-value =
0 009), with the mean stone size being higher among the NO SSP group (6 37 ± 1 76) compared to the SSP group (5 41 ± 1 6) Which indicated that larger stone sizes have less possibility of passing spontaneously Additionally, stone sizes were grouped into 2 major groups and analyzed
Table 1
Baseline characteristics
Table 2.
Analyzing demographic, laboratory, and radiological variables for predicting passage of stones spontaneously
Table 3. Association between procalcitonin level at admission and weeks of stone passage and Hydronephrosis grade
Parameters
Week10038±0016
Week20049±0022
Week30077±0013
Week40084±005
statistically to demonstrate their association with stone passage; a statistically significant difference was also found (p-value = 0 022) Hydronephrosis grade was determined for all the patients and further classified into mild and moderate to determine its association with the spontaneous passage of stones This variable was also found statistically significant (p-value = 0 018) Another factor that should be taken into account in this study is the significant difference in gender distribution between the NO SSP and SSP groups (p = 0 018) The SSP group had a higher percentage of males (77 8%) (Table 2)
Figure 1. Receiver operator curve analysis for Association between serum procalcitonin and stone passage.
Table 4.
Receiver operating characteristic (ROC) for the association between procalcitonin and stone passage
Parameters Area 95% confidence Cut off P-value under cur ve inter val value
Regarding the association between procalcitonin level at a d m i s s i o n w i t h t h e w e
d hydronephrosis grade, it was found that procalcitonin levels vary significantly across different weeks of stone passage (p < 0 001) Procalcitonin levels were lowest at Week 0 (0 021 ± 0 002) and increased progressively in subsequent weeks: Week 1 (0 038 ± 0 016), Week 2 (0 049 ± 0 022), Week 3 (0 077 ± 0 013), and Week 4 (0 084 ± 0 059) However, no significant difference in procalcitonin levels between different hydronephrosis grades was found (p = 0 093) (Table 3)
Receiver operating characteristic (ROC) for the association between procalcitonin and stone passage showed an area of 0 925 (%95 C I 0 866-0 984) with a cut-off value of 0 076, a sensitivity of 82%, a specificity of 88%, and a p-value < 0 001 (Figure 1) (Table 4)
DISCUSSION
Nephrolithiasis is a commonly occurring urinary tract condition, which is the third most prevalent disease after infections in the urinary tract and benign obstruction in the prostate (1) Various therapeutic approaches and treatment methods exist for the management of stones in the ureter, depending on factors such as the size of the stone, location, composition, and clinical aspects (11) These treatment options range from conservative treatment or non-surgical treatment (with analgesics with or without MET to assist spontaneous stone passage) to invasive treatments such as ESWL and ureteroscopy (URS-L) (flexible or semi-rigid) (6, 13, 14) Medical treatment is considered cost-effective, alleviating the need for surgical procedures and leading to minimal complications Potential disadvantages of MET may include recurring colic and urinary tract infections (11) Conversely, invasive procedures lead to a safer and more efficient stone removal rate, with a higher cost compared to medical treatment Furthermore, potential complications in the urinary system, such as the formation of hematomas, urinary infections, and urinary extravasation, should be taken into account as adverse effects of this treatment approach (15)
The success of ESWL and URS-L treatments depends on the stone's location and size, with reported success rates ranging from 68% to 90% for ESWL and 80% to 97% for URS-L (6) Likewise, delaying surgical intervention until medical therapy fails can be stressful for the patient and increase treatment costs compared to the immediate surgical removal of a stone (11) These controversies about c h o o s i n g t h e m a n a g e m e n t m e t h o d h a v e l e d m a n y researchers to study inflammatory markers These markers can help clinicians decide on the most effective treatment method for patients
Medical expulsive therapy (MET) involves the administration of medications to facilitate the expulsion of ureteric stones Various drugs, including alpha-blockers, calcium c h a n n e l s b l o c k e r s , c o r t i c o s t e r o i d s , a n d p h o s p h o d iesterase-5 inhibitors, have undergone thorough examination Recent guidelines recommend alpha-blockers as an effective standalone therapy for the medical removal of stones in the ureter On the other hand, there isn't enough evidence to consider other drugs mentioned as
I Aghaways, R Bapir, N S Siwaily, et al
standalone therapies (14) According to the recent guidelines from the European Association of Urology (EAU), for distal ureteric stones larger than 5 mm, alpha-blockers are recommended as MET (15, 16) Most studies in the literature assess MET outcomes over a four-week duration, and there is no data available to support other time intervals currently In the present study, patients were given diclofenac sodium (75 mg/day,) as an analgesic to reduce pain and tamsulosin (0 4 mg/day) for four weeks, along with a daily fluid intake of 2-3 liters
The possibility of passing ureteral stones naturally is highly influenced by two crucial factors, its size and location The relationship between stone size and spontaneous stone passage (SSP) is inversely proportional Stones measuring less than 5 mm have a 75% chance of passing naturally, with the possibility of passage decreasing as the size increases For ureteral stones between 5 and 10 mm, the chance of spontaneous passage ranges from 25 to 46% Additionally, it has been reported that for stones less than 4mm, there is a 95% possibility of spontaneous passage within 40 days (1, 11, 17) The European Association of Urology and American Urological Association (EAU/AUA) panel examined spontaneous passage rates through a recent meta-analysis, revealing rates of 68% for stones smaller than 5 mm and 48% for stones ranging from 5 to 10 mm (18) One study by Demehri et al classified patients into 3 groups based on stone sizes, groups were less than or equal to 5 mm, between 5 and 10 mm, and greater than 10 mm A spontaneous passage rate of 92% for stones less than 5 mm and 9 1% for stones larger than 10 mm was observed (19) The current study revealed an overall SSP rate of 67%; additionally, the mean size of the stone was 5 41 ± 1 6 among SSP groups and 6 37 ± 1 76 among NO SSP groups, with a p-value of 0 009, which indicates a statistically significant difference between the two groups in terms of stone size Likewise, patients in this study were classified into two groups based on stone size, and statistical analysis showed a pvalue of 0 022 with the highest rate of SSP (73 77%) for stones less than 6mm
Several studies have consistently demonstrated that demographic characteristics do not exert a significant influence on the probability of ureteral stones passage spontaneously A study conducted by Mohammad et al involving 73 patients with distal ureteric stones sized 4-8 mm revealed no significant difference in age, BMI, or gender between the SSP and non-SSP groups statistically (3) In another study, which was conducted on 54 patients with single ureteral stones, no significant difference was found in demographic characteristics between the SSP and NO SSP groups (1) However, according to a study conducted by Puntub et al , which included 139 patients with ureteral stones < 10 mm, demographic characteristics such as age and gender showed statistically significant differences between the SSP and NO SSP groups The study found that individuals with SSP had a mean age of 44 53 years, while those with NO SSP had an average age of 52 62 years The study also observed that males had a better chance of SSP than females The statistical analysis showed a significant relationship between age, gender and stone passage with a p-value of 0 003 and 0 031, respectively (4) In the present study, considering various
demographic characteristics, only gender exhibited a statistically significant difference between the SSP and nonSSP groups The incidence of SSP was significantly higher among males (77 8%) compared to females (22 2%), and this was found to be statistically significant with a pvalue of 0 018
Regarding the side of the stone, in one study by Jain et al conducted on 185 patients with stones in the ureter, the side of the stone showed no significant difference among the SSP and NO SPP groups (20) In another study in which 156 patients enrolled, the side of the stone showed no statistically significant difference among the SSP and NO SSP groups with a p-value of 0 1 (7) In this study, statistical analysis showed no significant difference in the spontaneous passage of ureteral stones between left- and right-sided stones with a p-value of 0 717
Regarding the association between inflammatory markers and ureteral stone passage, several inflammatory markers have been studied In a study involving 156 patients conducted by Sfoungaristos et al , elevated levels of WBCs and NC during the acute phase of renal colic were linked to an elevated possibility of ureteral stones passing spontaneously (7) Likewise, in another study by Özcan et al , which was conducted on 251 renal colic patients, statistical analysis showed a significant difference in WBCs and neutrophils among groups that pass their stones spontaneously and those that do not pass their stones, with the level being higher among NO SSP groups compared to SSP groups (21) In another study, which was performed on 192 patients, WBCs and NCs were decreased among SSP groups compared to NO SSP groups, with a p-value of 0 0005 for both markers (14) Additionally, in a study by Park et al , in which a total of 182 patients were enrolled, it was reported that an elevated level of NC percentage leads to a spontaneous decrease in the rate of ureteral stone passage (22) A possible causation for this finding is that ureteral stone presence leads to swelling of the ureteral mucosa, ultimately resulting in obstruction These interactions may contribute to increased inflammatory reactions and an elevated percentage of neutrophils and white blood cells (4)
The neutrophil-to-lymphocyte ratio (NLR) and platelet-tolymphocyte ratio (PLR) are other markers that can be used as predictors of ureteral stone passage Different studies suggested that elevated NLR and PLR are associated with a decreased possibility of spontaneous ureteral stone passage Statistical analysis showed that there is an inverse relationship between NLR and PLR levels and the spontaneous passage of ureteral stones, as indicated by a p-value of less than 0 005 in various studies (5, 8, 11, 23)
However, in contrast to the above-mentioned studies, according to a study by Ahmed et al , which was performed on 163 patients for spontaneous passage prediction of stones less than 10 mm, it was reported that serum WBCs did not show a significant difference between SSP and non-SSP groups (12) Likewise, in a retrospective study performed on 279 patients, it was found that inflammatory markers, particularly WBCs, NC, and NLR, do not serve as meaningful parameters for passage prediction of ureteral stones as they did not show any difference between both groups significantly (24) Additionally, in a prospective study that was performed
to find the relationship between stone passage and inflammatory markers, in which 139 patients were enrolled, it was concluded that both WBCs and NCs did not play a role in predicting the passage of stones spontaneously, with a p-value of 0 97 and 0 58, respectively (4) The current study findings are in contrast with these studies We observed elevated NLR and decreased lymphocyte count among patients who pass their stones spontaneously (SSP), with mean values of 3 75 ± 2 37 and 2 61 ± 1 20, respectively, compared to NO SSP groups with mean values of 2 74 ± 1 61 and 4 17 ± 5 38, respectively The statistical analysis of both variables showed a pvalue of 0 032 Additionally, the current study findings did not show any statistically significant differences in WBCs, PLR, NCs, and platelets among the SSP and NO SSP groups
Another inflammatory parameter that serves as a meaningful parameter for predicting ureteral stone passage is CRP, which is primarily produced by the liver in response to tissue damage and serves as a sensitive indicator of inflammation (25) Previous studies have established associations between CRP and various inflammatory conditions, including diabetic nephropathy (26), subacute thyroiditis (27), and hepatitis (28) In numerous studies, the serum CRP level appeared as a significant predictor for the spontaneous passage of ureteral stones These studies consistently observed a significant elevation in serum CRP levels among patients who did not experience spontaneous ureteral stone passage (2-4, 20-22) One potential explanation of the mentioned results could be that the rise in these levels reflects the extent of inflammation induced in the ureteral mucosa as a stone passes through This is supported by the observation that the interaction between the mucosa of the ureter and the stone leads to inflammation at the site where the stone is located (29)
However, in contrast to these findings, a study conducted by Hassan et al , in which 195 patients were enrolled, reported that the spontaneous passage rate of ureteral stones among individuals with high CRP levels was higher, with a statistically significant p-value of less than 0 05 (30) The current study reported that CRP is a strong inflammatory marker to predict spontaneous passage of ureteral stones, with the level being elevated among those who did not pass their stones spontaneously (12 63 ± 11 03), compared to SSP groups (5 55 ± 5 06) with a p-value of < 0 001
Apart from stone size, location, WBC indices, and CRP, to our knowledge, there are limited studies in genuine literature that examine the effects of procalcitonin on stone passage (31) Procalcitonin is a peptide composed of 116 amino acids, possessing a molecular weight of approximately 13 kilodaltons Ghillani et al initially characterized this hormone in 1989 as a precursor to calcitonin, a thyroid gland-produced hormone consisting of 32 amino acids (32) The normal range for procalcitonin in the general population is recognized as being below 0 05 ng/mL During systemic infections, it may elevate to levels of 2 ng/mL, and in cases of sepsis, it can reach levels higher than 10 ng/mL (33) Likewise, procalcitonin has been identified as useful in establishing a relationship between infections in the urinary tract and obstructed ureteral
stones According to Papa Giannopoulos et al , they found that procalcitonin levels exceeding 100 pg/ml (0 1 ng/ml) were observed in 18% of patients treated with medical expulsive therapy (MET), 45% of those had undergone procedures such as ureteroscopy with laser lithotripsy (URSL) or the placement of a ureteral stent (34) In a study conducted by Cilesiz et al to examine the role of procalcitonin in predicting the possibility of spontaneous passage of ureteral stones, in which 54 patients were enrolled, it was reported that the procalcitonin levels were significantly elevated in groups that did not experience spontaneous stone passage (0 207 ± 0 145 ng/ml) compared to those with successful spontaneous stone passage (0 133 ± 0 028 ng/ml) with a p-value of < 0 001 (1) In the current study, in which 94 patients were involved, it was found that procalcitonin levels were significantly higher among groups failing to pass their stones spontaneously (0 14 ± 0 089) compared to those who passed their stones spontaneously (0 05 ± 0 027), with a p-value of < 0 001 In this study, the determined cutoff value for procalcitonin in predicting stone passage was established at 0 076 ng/ml with an AUC of 0 925, a sensitivity of 82%, and a specificity of 88% (95% CI 0 8660 984) The possible explanation for elevated procalcitonin among NO SSP groups is linked to an excess of mucosal inflammation This excess mucosal inflammation might have increased the possibility of stone impaction in the future, making their passage more challenging (1) In this study, the association between procalcitonin levels and weeks of passage among SSP groups was examined at the time Patients were classified based on weeks of stone passage into five groups Statistical analysis showed that procalcitonin levels vary significantly across different weeks of stone passage (p < 0 001) Procalcitonin levels are lowest at Week 0 (0 021 ± 0 002) and increase progressively in subsequent weeks: Week 1 (0 038 ± 0 016), Week 2 (0 049 ± 0 022), Week 3 (0 077 ± 0 013), and Week 4 (0 084 ± 0 059)
The association between stone passage and hydronephrosis grade is a subject of controversy, yet individuals with no or mild hydronephrosis were more likely to pass their s t o n e s s p o n t a n e o u s l y t h a n t h o s e w i t h m o d e r a t e hydronephrosis, according to a study conducted on 163 patients (13) In contrast, in a study by Jendeberg et al , which was performed on 392 patients retrospectively, it was reported that stones inducing moderate to significant hydronephrosis exhibited a greater likelihood of spontaneous passage compared to stones causing either no hydronephrosis or only mild hydronephrosis, with a pvalue of 0 002 (35) In the present study, hydronephrosis grade was significantly different among SSP and NO SSP groups Statistical analysis showed an increased chance of SSP when dealing with mild hydronephrosis (80 3%) compared to moderate hydronephrosis (19 7%), with a p-value of 0 018
A notable limitation of this study is that we did not assess the time length from the onset of symptoms to the first admission Consequently, we did not analyze how this time interval might relate to inflammatory markers Future research should consider evaluating this aspect to provide further insights into the progression of inflammation and its impact on inflammatory indexes
I Aghaways, R Bapir, N S Siwaily, et al
Role of inflammatory markers in predicting spontaneous passage of ureteral stones less than 10 mm
CONCLUSIONS
The findings suggest that elevated levels of procalcitonin may be a contributing factor in complicating the stone's passage and lengthening the duration of the stone passage Likewise, elevated CRP and larger stones were found to decrease the chance of SSP The validity and confirmation of the current findings require further studies
REFERENCES
1 Çilesiz NC, Arslan B, Balcı MB, et al The role of procalcitonin and other markers of inflammation in predicting spontaneous passage of ureteral stones Journal of Academic Research in Medicine 2021; 11:179-18
2 Hada A, Yadav SS, Tomar V, et al Assessment of factors affecting the spontaneous passage of lower ureteric calculus on the basis of lower ureteric calculus diameter, density, and plasma C-reactive protein level Urol Ann 2018; 10:302
3 Mohammad EJ, Abbas KM, Hassan AF, Abdulrazaq AA Serum creactive protein as a predictive factor for spontaneous stone passage in patients with 4 to 8 mm distal ureteral stones International Surgery Journal 2018; 5:1195-200
4 Puntub A, Lerdpraiwan W Relationship between the spontaneous passage rates of ureteral stones less than 10 mm and serum C-reactive protein levels, white blood cell counts and neutrophil percentages Insight Urology 2018; 39:42-9
5 Abou Heidar N, Labban M, Bustros G, Nasr R Inflammatory serum markers predicting spontaneous ureteral stone passage Clin Exp Nephrol 2020; 24:277-83
6 Türk C, Petrík A, Sarica K, et al EAU guidelines on diagnosis and conservative management of urolithiasis Eur Urol 2016; 69:468-74
7 Sfoungaristos S, Kavouras A, Katafigiotis I, Perimenis P Role of white blood cell and neutrophil counts in predicting spontaneous stone passage in patients with renal colic BJU Int 2012; 110:E33945
8 Aldaqadossi HA Stone expulsion rate of small distal ureteric calculi could be predicted with plasma C-reactive protein Urolithiasis 2013; 41:235-9
9 Abdullah HO, Braim SA, Rasool MA, et al Role of Inflammatory Markers in Severity, ICU Admission, and Mortality in COVID-19: A Systematic Review and Meta-analysis of 79,934 Patients Barw Med J 2024; 2:65-83
10 Kim BH the authors reply: relationship between spontaneous passage rates of ureteral stones less than 8 mm and serum C-reactive protein levels and neutrophil percentages Korean J Urol 2013; 54:889-90
11 Aghaways I, Ibrahim R, Bapir R, et al The role of inflammatory serum markers and ureteral wall thickness on spontaneous passage of ureteral stone < 10 mm: A prospective cohort study Ann Med Surg 2022; 80:104198
12 Kim SY, Kim MJ, Yoon CS, et al Comparison of the reliability of two hydronephrosis grading systems: the Society for Foetal Urology grading system vs the Onen grading system Clin Radiol 2013; 68:e484-90
13 Ahmed AF, Gabr AH, Emara AA, et al Factors predicting the spontaneous passage of a ureteric calculus of 10 mm Arab J Urol 2015; 13:84-90
14 Ramasamy V, Aarthy P, Sharma V, Thakur AP Role of inflammatory markers and their trends in predicting the outcome of med-
ical expulsive therapy for distal ureteric calculus Urol Ann 2022; 14:8
15 Bultitude M, Smith D, Thomas K Contemporary management of stone disease: the new EAU urolithiasis guidelines for 2015 Eur Urol 2016; 69:483-4
16 Türk C, Knoll T, Seitz C, et al European Association of Urology Medical expulsive therapy for ureterolithiasis: the EAU recommendations in 2016 Eur Urol 2017; 71:504-7
17 Skolarikos A, Laguna MP, Alivizatos GE, et al The role for active monitoring in urinary stones: a systematic review J Endourol 2010; 24:923-30
18 Preminger GM, Tiselius HG, Assimos DG, et al Guideline for the management of ureteral calculi J Urol 2007; 178:2418-34
19 Demehri S, Steigner ML, Sodickson AD, et al CT-based determination of maximum ureteral stone area: a predictor of spontaneous passage AJR Am J Roentgenol 2012; 198(3):603-8
20 Jain A, Sreenivasan SK, Manikandan R, et al Association of spontaneous expulsion with C-reactive protein and other clinicod e m o g r a p h i c f a c
Urolithiasis 2020; 48:117-22
21 Özcan C, Aydogdu O, Senocak C, et al Predictive factors for spontaneous stone passage and the potential role of serum C-reactive protein in patients with 4 to 10 mm distal ureteral stones: a prospective clinical study J Urol 2015; 194:1009-13
22 Park CH, Ha JY, Park CH, et al Relationship between spontaneous passage rates of ureteral stones less than 8 mm and serum Creactive protein levels and neutrophil percentages Korean J Urol 2013; 54:615-8
23 Lee KS, Ha JS, Koo KC Significance of neutrophil-to-lymphocyte ratio as a novel indicator of spontaneous ureter stone passage Yonsei Med J 2017; 58:988-993
24 Senel C, Aykanat IC, Asfuroglu A, et al What is the role of inflammatory markers in predicting spontaneous ureteral stone passage? Aktuelle Urologie 2022; 53:448-53
25 Wang L, Li Y, Wang C, et al C-Reactive protein, infection, and outcome after acute ischemic stroke: a registry and systematic review Curr Neurovasc Res 2019; 16:405-15
26 Bilgin S, Kurtkulagi O, Tel BM, et al Does C-reactive protein to serum Albumin Ratio correlate with diabetic nephropathy in patients with Type 2 diabetes mellitus? The CARE TIME study Prim Care Diabetes 2021; 15:1071-4
27 Baruah MP, Bhattacharya B, Baruah UM C-Reactive protein level can be a better indicator than erythrocyte sedimentation rate in assessing the severity of inflammation and guiding glucocorticoid therapy in subacute thyroiditis Indian J Endocrinol Metab 2022; 26:328
28 Demirkol ME, Aktas G, Bilgin S, et al C-reactive protein to lymphocyte count ratio is a promising novel marker in hepatitis C infection: the clear hep-c study Rev Assoc Med Bras (1992) 2022; 68:838-841
29 Nuss GR, Rackley JD, Assimos DG Adjunctive therapy to promote stone passage Rev Urol 2005; 7:67
30 Hassan M, Hayat S, Shahzad M Frequency of spontaneous expulsion of lower ureteric stones in patients with raised C-protein KJMS 2019; 12:469
31 Abdullah HO, Abdalla BA, Kakamad FH, et al Predatory Publishing Lists: A Review on the Ongoing Battle Against Fraudulent Actions Barw Med J 2024; 2:26-30
32 Ghillani PP, Motté P, Troalen F, et al Identification and measurement of calcitonin precursors in serum of patients with malignant diseases Cancer Res 1989; 49:6845-51
33 Claeys R, Vinken S, Spapen H, et al Plasma procalcitonin and C-reactive protein in acute septic shock: clinical and biological correlates InAdvances in Critical Care Testing: The 2002 IFCC-Roche Diagnostics Award 2004, Springer Berlin Heidelberg, pp 17-31
34 Papagiannopoulos D, Whelan P, Ahmad W, et al Procalcitonin is a strong predictor of urine culture results in patients with obstructing ureteral stones: a prospective, pilot study Urol Ann 2016; 8:277-80
35 Jendeberg J, Geijer H, Alshamari M, et al Size matters: The width and location of a ureteral stone accurately predict the chance of spontaneous passage Eur Radiol 2017; 27:4775-85
Correspondence
Ismaeel Aghaways ismaeelagha@hotmail com
Shakhawan Hamaamin Said shakhwan said@gmail com
College of Medicine, University of Sulaimani, Madam Mitterrand Street, Sulaimani, Kurdistan, Iraq
Rawa Bapir
Dr rawa@yahoo com
Nabaz S Siwaily nabaz@gmail com
Ahmed Mohammed Abdalqadir ahmed abdalqadir@gmail com
Department of Urology, Sulaymaniyah Surgical Teaching Hospital, Sulaymaniyah, Iraq
Ayman M Mustafa aymanmajid75@gmail com
Berun A Abdalla berun anwer95@gmail com
Smart Health Tower, Madam Mitterrand Street, Sulaimani, Kurdistan, Iraq
Bryar Othman Muhammed muhammed ali@gmail com
Smart Health Tower/Raparin, Madam Mitterrand Street, Sulaimani, Kurdistan, Iraq
Fahmi Hussein Kakamad (Corresponding Author) fahmi hussein@univsul edu iq
Doctor City, Building 11, Apartment 50, Sulaimani, Kurdistan, Iraq
Conflict of interest: The authors declare no potential conflict of interest
I Aghaways, R Bapir, N S Siwaily, et al
ORIGINAL PAPER
Development and internal validation of El-Shazly-Buchholz’s nomogram to predict postoperative complications after PCNL: A multicenter study
Rawa Bapir 1, 2 , Kamran Bhatti 3 , Mohamed El-Shazly 4 , Juan Antonio Galan 5 , Ahmed M Harraz 6, 7 , Sarwar Noori Mahmood 8 , Renato N Pedro 9 , Pablo Vargas 10 , Athanasios Papatsoris 11, 12 , Alberto Trinchieri 12 , Noor Buchholz 12
1 Department of Urology, Sulaymaniyah Surgical Teaching Hospital, Sulaymaniyah, Iraq;
2 Smart Health Tower, Madam Mitterrand Street, Sulaymaniyah, Iraq;
3 HMC Medical Corporation, Al Khor, Qatar;
4 Menoufia University, Shebin Elkom 32714, Egypt;
5 Department of Urology, Dr Balmis General University Hospital, Alicante Institute for Health and Biomedical Research (ISABIAL), Alicante, Spain;
6 Mansoura University Urology and Nephrology Center, Mansoura, Egypt;
7 Farwaniya Hospital and Sabah Al Ahmad Urology Center, Kuwait City, Kuwait;
8 Department of Surgery, College of Medicine, University of Sulaymaniyah, Sulaymaniyah, Iraq;
9 Division of Urology, Faculdade de Medicina São Leopoldo Mandic de Campinas, Sao Paulo, Brazil;
10 Marina Baixa Hospital La Vila Joiosa Alicante Spain;
11 2nd Department of Urology, School of Medicine, Sismanoglio Hospital, National and Kapodistrian University of Athens;
12 U-merge Scientific Office
Summary
Introduction: A model to predict the risk of surgical complications following percutaneous nephrolithotomy (PCNL) could be a useful tool to guide clinical decision-making The aim of this study was to develop a simple and widely applicable stratification tool to be used for patient counseling, surgical planning, evaluation of outcomes, and academic reporting.
Methods: Data of patients who underwent PCNL were retrieved from the database of the collaborating centers including demographics of patients, characteristics of their stones and urinary tracts, and perioperative data The primary outcome was the development of postoperative complications Data were randomly split into a training dataset (85%) and a validation dataset (15%). A univariate and multivariate logistic regression analysis of the training dataset was performed to identify independent predictors of postoperative complications Model variables were used to construct a nomogram that was internally validated on the testing dataset by measuring calibration, discrimination, and plotting the decision curve
Results: Six hundred thirty one patients (245 Males) with a median (IQR) age of 49 (37-56) years were included. Post-operative complications occurred in 147 (23.3%) patients. Significant predictors of complications included preoperative urine culture (p < 0 001), largest stone diameter (p = 0 02), and intraoperative blood loss (p = 0 002) A nomogram was developed from the predictors and applied to the validation dataset showing an area under the curve (95%CI) of 66 4% (52 2;80 6)
Conclusions: This new scoring system emphasized patient characteristics and operative details rather than stone characters to predict the morbidity of PCNL Furthermore, it should facilitate risk adjustment, enabling physicians to better define the nephrolithiasis disease continuum and identify patients who should be referred to tertiary care centers
KEY WORDS: Percutaneous nephrolithotomy; Complications; Urine culture; Stone diameter; Intraoperative blood loss
Submitted 24 October 2024; Accepted 28 October 2024
INTRODUCTION
Percutaneous nephrolithotomy (PCNL) is the gold standard procedure to treat relatively large renal stones (> 2 cm) with a high success rate but still with significant morbidity despite technical advances There is no consensus on an ideal predictive model of morbidity outcomes following PCNL Available predictive tools aim at assessing the kidney stone complexity to predict the stone-free rate They include the Guy’s Stone Score, the CROES nomogram, S T O N E nephrolithometry, Seoul National University Renal Stone Complexity (S-ReSC) score, and the Simple Stone Score (SSS) (1-5) In our opinion, the risk of surgical complications is an important variable that should guide clinical decision-making In comparative studies, none of the available scoring systems was fully satisfactory in predicting surgical complications (6) Considering the deficient literature in assessing post-PCNL morbidity, this study was conducted to develop a widely applicable, simple disease stratification tool that will greatly improve patient counseling, surgical planning, evaluation of outcomes, and academic reporting
METHODS
Patient data
A total of 631 patients who underwent PCNL at the collaborating centers were retrospectively analyzed The pro-
R Bapir, K Bhatti, M El-Shazly, et al
cedures used in this study adhere to the tenets of the Declaration of Helsinki (as revised in 2013) Approval was obtained from the Research Ethics Committees of Medical Research Center HMC (MRC-01-20-385) Because of its retrospective nature, the consent was waived from the participants All the information collected during the research project remained confidential to the extent required and provided by law Patient data were anonymized, coded, and kept by the principal investigator
The preoperative clinical data included age, gender, body mass index (BMI), recurrent stone status, previous renal surgery in the ipsilateral kidney, associated comorbidities, the American Society of Anesthesia (ASA) score, preoperative urine culture, and diagnostic imaging (modality) Stone characteristics were the stone diameter, burden, density (Hounsfield Unit), and the number of involved calyces
Intraoperative documented data included PCNL position, operative time, number of tracts, size of the tract, intraoperative blood loss (Hb loss > 2 gr/dl), pus on the puncture, residual fragments size and number, exit strategy, combination with retrograde intrarenal surgery (RIRS), and the caseload of surgeon per year Postoperatively, collected data were fever, urine culture, sepsis, bleeding, postoperative transfusion, length of hospital stay, and stone-free status/residual fragments
Study outcome
The primary outcome was the development of postoperative complications by Clavien-Dindo system (7) A secondary outcome was the development of postoperative infectious complications
Statistical analysis
The data were randomly split into a training dataset (85%) and a validation dataset (15%) In the training dataset, a univariate and multivariate logistic regression analysis was performed to identify independent predictors of the occurrence of any postoperative complication
Statistical significance was determined using the Chisquare or Fischer's exact tests for categorical variables whenever appropriate Mann-Whitney U or Student ttests were used for non-parametric and parametric variables, respectively Model variables were used to construct a nomogram The nomogram was internally validated by measuring calibration, discrimination, and plotting the decision curve A calibration plot was generated to identify how much predicted nomogram probabilities match the actual post-operative complications values The discrimination was evaluated by calculating the area under the curve (desired when more than 50%) Decision curve analysis reveals the net benefit of using the model to detect postoperative complications
The decision curve compares the ability of the nomogram to distinguish the occurrence or absence of complications according to a range of threshold probabilities If the decision curve shows a higher net benefit, it is clinically beneficial
Statistical analysis was performed using R programming language version 4 1 2 with p-value less than 0 05 was considered statistically significant
RESULTS
Patients’ demographics
A total of 631 patients with a median (IQR) age of 49 (37:56) years were included Female patients constituted 38 83% while obese patients (> 30 BMI) accounted for 43 26% Four institutions contributed to the current study [J: 100 (15 85%), M: 99 (15 69%), R: 332 (52 61%), and U: 100 (15 85%) patients]
Postoperative complications occurred in 147 (23 3%) patients After random splitting, there was no significant difference between both groups The difference between both groups is shown in Table 1
Table 1.
Comparison between training and validating datasets for patients who underwent percutaneous nephrolithotomy in 4 institutions. Parameter Train Validate p-value
BMI: Body mass index; ASA: Amer can soc ety of anesthesiology; LSD: Largest stone diameter; HU: Hounsfield units; OR: Operat on; LOS: Length of stay
* Mode of drainage after the procedures
Predictors of complications in the training dataset
Significant variables include preoperative urine culture [positive: 24 (5 78%) versus 22 (18 18%), p < 0 001], median (IQR) largest stone diameter [30 (20:40) versus 35 (22:48), p = 0 02], intraoperative blood loss [24 (5 78%) versus 18 (14 88%), p = 0 002] Data are displayed in Table 2 On multivariate logistic regression analysis, independent predictors were intra-operative blood loss [odds ratio (OR) and 95% confidence interval (CI): 2 5 (1 2:4 9), p = 0 007], preoperative urine culture [OR (95%CI): 3 2 (1 6:6), p < 0 001] (Table 3)
Nomogram development and validation
A nomogram was developed from the predictors and is displayed in Figure 1 The nomogram is applied to the validation dataset The area under the curve (95%CI) was 66 4 (52 2; 80 6) Regarding calibration, the nomogram's predicted probabilities slightly overestimated the post-opera-
Figure 1. Nomogram for the evaluation of the risk of complications after PCNL.
Table 2.
Univariate and logistic regression analysis for predictors of post-PCNL complications
B: Regression coefficient; OR: Odds rat o; CI: Confidence interval
tive complications' actual occurrence The Calibration plot is displayed in Figure 2A The decision curve shows a higher net benefit of the model in a wide range of thresholds (25%-75%) Therefore, the model is performing better in this range of thresholds than if treatment of complications is considered in all patients or in none of the patients Results are displayed in Figure 2B
Calibration plot (A) and Range of Threshold
DISCUSSION
Literature exhibits multiple stone scoring systems for evaluating outcomes of percutaneous nephrolithotomy including the Guy’s stone score, the Clinical Research Office of the Endourological Society (CROES) nomogram, the S T O N E score, and the S-ReSC score (1-5) The pivotal variables in all the scoring systems are stone location, stone number, and the presence of staghorn calculi
The Guy’s stone score stratifies patients into four grades, where grade I indicates a solitary stone with simple anatomy (mid-lower pole or renal pelvis), grade II a solitary stone in the upper pole or multiple stones with simple anatomy or a solitary stone with abnormal anatomy, grade III multiple stones with abnormal anatomy or stones in a calyceal diverticulum or partial staghorn stone, and grade IV staghorn stone or any stone in a patient with spina bifida or spinal injury The S T O N E score classifies patients into low-, moderate-, and highrisk groups according to stone size (S), tract length (T), obstruction (O), number of involved calyces (N), and essence (E) (composition or stone density) The CROES nomogram grades risk across a continuous scale considering the stone burden, location, number, and surgical volume The S-ReSC scoring system subdivides the pelvicaliceal system in nine locations and the score is the cumulative sum of the locations involved by the stone
Several studies evaluated the efficacy of these stone-scoring systems in predicting the stone-free status and the incidence of complications after percutaneous nephrolithotomy A systematic review (6) of ten studies (8-17) with metanalysis compared the efficacy of the stone scoring systems in predicting stone-free rate after PCNL most of them confirming their equal predictive efficacy of the stone-free rate
Stone free status was negatively related to Guy’s (WMD = -0 64, p < 0 0001) and S T O N E score (WMD = -1 23, p < 0 0001) and positively to the score of CROES nomogram (WMD = 29 48, p = 0 003) No significant difference between the three stone scoring nomogram was
found at comparison of area under curves (AUC) of predicting stone free rate
A secondary outcome of the systematic review of Jiang et al (6) was the comparison of the efficacy of the stone score systems in predicting complications after PCNL Tailly et al (16) and Sfoungaristos et al (15) did not find correlation between stone scores and complication rates Similarly, Noureldin et al (14) and Kocaaslan et al (12) observed no significant correlation of Guy score and S T O N E score with complications after PCNL Only Bozkurt et al (8) observed a correlation of Guy’s score and the CROES nomogram with complication rates after PCNL In addition, Choi et al (10) compared the predictability of the outcomes of tubeless PCNL using the Guy score, CROES nomogram, and S T O N E score showing that only the Guy score was able to predict the complication rate after PCNL The metanalysis showed that only the Guy’s score was able to predict complications after PCNL (WMD =0 29, 95% CI: -0 57 to -0 02, p = 0 03)
A systematic review (18) specifically focused on the correlation between stone scoring systems and postoperative complications after PCNL in adult patients adding six studies (19-24) to the 5 studies (9, 10, 13, 16, 17) previously considered by the systematic review of Jiang et al (6) A significant correlation with complications was obtained with Guy’s stone score in 6 out 9 studies, with S T O N E nephrolithometry score in 4 out 11 studies, with CROES score in 3 out 9 studies and with S-ReSC score in one of two studies, respectively Other studies (16, 19-21) showed no correlation between nomograms and post-surgical complications graded using the Clavien-Dindo (CD) classification system modified for PCNL (8)
Biswas et al (22) found significative correlations between GSS, S T O N E nephrolithometry score, and CROES score with post-operative complications including EBL Labadie et al (13) reported no significant correlation at logistic regression analysis of GSS, S T O N E nephrolithometry score and CROES score with most post-operative complications, although GSS and S T O N E nephrolithometry were cor-
R Bapir, K Bhatti, M El-Shazly,
Figure 2
Development and internal validation of El-Shazly-Buchholz’s nomogram to predict postoperative complications after PCNL
related with EBL Choi et al (9) found a correlation between GSS and post-operative complications, while S T O N E nephrolithometry score and CROES score were not correlated Similar results were obtained by the same authors in a cohort of tubeless PCNL (10) Al Adl et al (23) evaluated the correlation between all four nomograms and complications observing a modest correlation of S T O N E nephrolithometry score, GSS, S-ReSC score, and CROES score with complications according to CD, although only GSS, S-ReSC score and CROES score correlated with EBL Khan et al (24) reported significant correlation between both S T O N E nephrolithometry score and GSS with overall complication rates at multivariate analysis Overall results demonstrated that stone morphology, as accurately described by the stone scoring systems, seemed to be not sufficient by itself to accurately predict the risk of complications after PCNL
Our nomogram adds to a measure of stone size, as stone diameter, other two easily obtained measures as positivity of preoperative urine culture and intraoperative blood loss Preoperative urine culture is mandatory before PCNL although it was well demonstrated that a negative midstream urine culture cannot exclude the presence of infection in the stone or the urinary tract upstream of the stone (25)
A systematic review of 19 studies demonstrated that positivity of stone culture was associated with higher odds of developing a Systemic Inflammatory Response Syndrome (SIRS) after PCNL in comparison with preoperative midstream urine culture (PMUC), although the odds of developing sepsis were not significantly different between positivity of stone culture or PMUC (26)
In another study, high procalcitonin (PCT) values, IL-6 (> 264 pg/ml), SIRS score (> 2 5), National Early Warning Score (NEWS) (> 2 5), quick Sequential Organ Failure Assessment (qSOFA) (> 0 50) and surgical time were independent risk factors for septic shock (27) Finally, at multivariate analysis, renal pelvic pressure ≥ 30 mmHg during PCNL procedure was included among the more relevant risk factors for urosepsis together with operative time, bladder urine culture and hydronephrosis (28)
Intraoperative blood loss is a parameter that can be only obtained at the end of the procedure therefore it cannot be used in the choice and the planning of the treatment although it can be useful to identify those patients that are at higher risk of complications requiring a strict followup for prevention and early treatment of complication
The strength of this study is the homogeneity of the series that was analyzed, which comes from only 4 centres that contributed at least 100 cases each The number of cases studied is relatively high although for the prediction of less frequent and more serious complications it could be even too small Furthermore, the retrospective design constitutes another limitation
Finally, for the prediction of infectious complications, some microbiological parameters were not available (culture of the pelvic urine and of the stone) as well as some laboratory tests (C-reactive protein, procalcitonin) and symptomatic scores predictive of the systemic inflammatory response or sepsis For these reasons, the efficacy of the nomogram will have to be confirmed by prospective studies of larger series
CONCLUSIONS
This new scoring system (the El-Shazly-Buchholz’s nomogram) emphasized on patient characteristics and operative details rather than stone features as in previous scores It should allow reliable and accurate comparisons of treatment efficacy and quality of surgical care by predicting the morbidity of PCNL Furthermore, it should facilitate risk adjustment, enabling physicians to better define the nephrolithiasis disease continuum and identify patients who should be referred to tertiary care centers
ACKNOWLEDGMENTS
This study was designed by Noor Buchholz who organized its initial phase and contributed an important surgical case series After he passed away on February 13, 2024, his collaborators and friends wanted to complete his work so that the memory of his enthusiastic activity in the study and treatment of kidney stones is maintained over time
REFERENCES
1 Thomas K, Smith NC, Hegarty N, Glass JM The Guy's stone score grading the complexity of percutaneous nephrolithotomy procedures Urology 2011; 78:277-81
2 Okhunov Z, Friedlander JI, George AK, et al S T O N E nephrolithometry: novel surgical classification system for kidney calculi Urology 2013; 81:1154-9
3 Smith A, Averch TD, Shahrour K, et al A nephrolithometric nomogram to predict treatment success of percutaneous nephrolithotomy J Urol 2013; 190:149-56
4 Jeong CW, Jung JW, Cha WH, et al Seoul National University renal stone complexity score for predicting stone-free rate after percutaneous nephrolithotomy PLoS One 2013; 8:e65888
5 Harraz AM, El-Nahas AR, Nabeeh MA, et al Development and validation of a simple stone score to estimate the probability of residual stones prior to percutaneous nephrolithotomy Minerva Urol Nephrol 2021; 73:525-531
6 Jiang K, Sun F, Zhu J, et al Evaluation of three stone-scoring systems for predicting SFR and complications after percutaneous nephrolithotomy: a systematic review and meta-analysis BMC Urol 2019; 19:57
7 de la Rosette JJ, Opondo D, Daels FP, et al Categorisation of complications and validation of the Clavien score for percutaneous nephrolithotomy Eur Urol 2012; 62:246-55
8 Bozkurt IH, Aydogdu O, Yonguc T, et al Comparison of guy and c l i n
y Nephrolithometry Scoring Systems for predicting stone-free status and complication rates after percutaneous Nephrolithotomy: a single centerstudy with 437 cases J Endourol 2015; 29:1006-10
9 Choi SW, BaeWJ, Ha US, et al Prognostic impact of stone-scoring systems after percutaneous Nephrolithotomy for staghorn calculi: a single Center's experience over 10 years J Endourol 2016; 30:97581
10 Choi SW, Bae WJ, Ha US, et al Prediction of stone-free status and complication rates after tubeless percutaneous nephrolithotomy: a comparative and retrospective study using three stone-scoring systems and preoperative parameters World J Urol 2017; 35:449-457
11 Jaipuria J, Suryavanshi M, Sen TK Comparative testing of reliability and audit utility of ordinal objective calculus complexity
scores Can we make an informed choice yet? BJU Int 2016; 118:958-68
12 Kocaaslan R, Tepeler A, Buldu I, et al Do the urolithiasis scoring systemspredict the success of percutaneous nephrolithotomy in cases with anatomical abnormalities? Urolithiasis 2016; 45:305-10
13 Labadie K, Okhunov Z, Akhavein A, et al Evaluation and comparison of urolithiasis scoring systems used in percutaneous kidney stone surgery J Urol 2015; 193:154-9
14 Noureldin YA, Elkoushy MA, Andonian S Which is better? Guy's versus S T O N E nephrolithometry scoring systems in predicting stone-free status postpercutaneous nephrolithotomy World J Urol 2015; 33:1821-5
15 Sfoungaristos S, Gofrit ON, Pode D, et al Percutaneous nephrolithotomy for staghorn stones: which nomogram can better predict postoperative outcomes? World J Urol 2016; 34:1163-8
16 Tailly TO, Okhunov Z, Nadeau BR, et al Multicenter external validation and comparison of stone scoring Systems in Predicting Outcomes after Percutaneous Nephrolithotomy J Endourol 2016; 30:594-601
17 Yarimoglu S, Polat S, Bozkurt IH, et al Comparison of S T O N E and CROES nephrolithometry scoring systems for predicting stone-free status and complication rates after percutaneous nephrolithotomy: a single center study with 262 cases Urolithiasis 2017; 45:489-494
18 Mazzon G, Choong S, Celia A Stone-scoring systems for predicting complications in percutaneous nephrolithotomy: A systematic review of the literature Asian J Urol 2023; 10:226-238
19 Ozgor F, Yanaral F, Savun M, et al Comparison of STONE, CROES and Guy’s nephrolithometry scoring systems for predicting s t o n e - f r e e s t a t u s a n d c o m p l i c a t i
nephrolithotomy in obese patients Urolithiasis 2018; 46:471-7
20 Farhan M, Nazim SM, Salam B, Ather MH Prospective evaluation of outcome of percutaneous nephrolithotomy using the ‘STONE’ nephrolithometry score: a single-centre experience Arab J Urol 2015; 13:264-9
21 Yarimoglu S, Bozkurt IH, Aydogdu O, et al External validation and comparisons of the scoring systems for predicting percutaneous nephrolithotomy outcomes: a single center experience with 506 cases J Laparoendosc Adv Surg Tech 2017; 27:1284-9
22 Biswas K, Gupta SK, Tak GR, et al Comparison of STONE score, Guy’s stone score and Clinical Research Office of the Endourological Society (CROES) score as predictive tools for percutaneous nephrolithotomy outcome: a prospective study BJU Int 2020; 126:494-501
23 Al Adl AM, Mohey A, Abdel Aal A, et al Percutaneous nephrolithotomy outcomes based on S T O N E , GUY, CROES, and S-ReSC scoring systems: the first prospective study J Endourol 2020; 34:1223e8
24 Khan N, Nazim SM, Farhan M, et al Validation of S T O N E nephrolithometry and Guy’s stone score for predicting surgical outcome after percutaneous nephrolithotomy Urol Ann 2020; 12:324e30
25 Mariappan P, Smith G, Bariol SV, et al Stone and pelvic urine culture and sensitivity are better than bladder urine as predictors of urosepsis following percutaneous nephrolithotomy: a prospective clinical study J Urol 2005; 173:1610-4
26 Li Y, Xie L, Liu C Prediction of systemic inflammatory response syndrome and urosepsis after percutaneous nephrolithotomy by urine culture, stone culture, and renal pelvis urine culture: Systematic review and meta-analysis Heliyon 2024; 10:e33155
27 Yuxin Liu Y, Sun Q, Long H, et al The value of IL-6, PCT, qSOFA, NEWS, and SIRS to predict septic shock after Percutaneous nephrolithotomy BMC Urology 2024; 24:116
28 Haoxiang Xu H, Wang K, Cao Z, et al Nomogram including renal pelvic pressure to predict the occurrence of urosepsis following percutaneous nephrolithotomy: a dual center retrospective study of 1,448 patients Transl Androl Urol 2024; 13:667-678
Correspondence
Rawa Bapir, MD dr rawa@yahoo com
Department of Urology, Sulaymaniyah Surgical Teaching Hospital, Sulaymaniyah, Iraq
Smart Health Tower, Madam Mitterrand Street, Sulaymaniyah, Iraq
Kamran Bhatti, MD, MS, FACS kamibhatti92@gmail com
HMC Medical Corporation, Al Khor, Qatar
Assistant Professor of Urology, Qatar University, Qatar Specialist Urology, HMC Medical Corporation, Al Khor, Qatar
Mohamed El-Shazly, MD mshazly2001@yahoo com
Assistant Professor of Urology, Menoufia University, Shebin Elkom 32714, Egypt
Juan Antonio Galan, MD jagalanllopis@gmail com
Department of Urology, Dr Balmis General University Hospital, Alicante Institute for Health and Biomedical Research (ISABIAL), Alicante, Spain
Ahmed M Harraz, MD, MS, FRCS, EBU ahmed harraz@hotmail com
Professor, Urology and Nephrology Center, Mansoura University, Mansoura, Egypt
Consultant, Farwaniya Hospital and Sabah Al Ahmad Urology Center, Kuwait City, Kuwait
Sarwar Noori Mahmood, MD sarwarchalabi@yahoo com
Department of Surgery, College of Medicine, University of Sulaymaniyah, Sulaymaniyah, Iraq
Renato N Pedro, MD rnpedro@gmail com Division of Urology, Faculdade de Medicina São Leopoldo Mandic de Campinas, Sao Paulo, Brazil
Pablo Vargas, MD pavaran5@gmail com
Marina Baixa Hospital, La Vila Joiosa, Alicante, Spain
Athanasios Papatsoris, MD agpapatsoris@yahoo gr
2nd Department of Urology, School of Medicine, Sismanoglio Hospital, National and Kapodistrian University of Athens, U-merge Scientific Office
Alberto Trinchieri, MD
alberto trinchieri@gmail com
Noor Buchholz, MD U-merge, Scientific Office
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Emergency treatment of obstructive pyelonephritis: A single center series
Bulent Kati 1 , Eser Ordek 2 , Omer Madsar 1 , Eyyup Sabri Pelit 1
1 Harran University, Faculty of Medicine, Urology Department, Sanliurfa, Turkey;
2 Mustafa Kemal University, Faculty of Medicine, Urology Department, Hatay, Turkey
Summary
Objective: This study aims to compare two different drainage methods, percutaneous nephrostomy (PCN) and retrograde ureteral double-J (DJ) stent insertion, in patients with obstructive pyelonephritis (OP)
Methods: The study included 77 patients who presented to the emergency department due to stones Type of decompression treatment (PCN or DJ stent), fever, white blood cell count (WBC), C-reactive protein (CRP) levels, urine culture, blood culture, presence of additional diseases, and antibiotic treatment were evaluated for these patients Emergency decompressive treatment was not randomly assigned. The clinician chose the appropriate treatment method based on the patient’s condition after obtaining an informed consent. Patients under the age of 18 were categorized into three subgroups: infants, children under 10 years, and adolescents.
Results: Of the 77 patients, 31 were in the DJ stent group and 46 were in the PCN group Patients in the PCN group exhibited significantly higher fever levels before the procedure (37 6 ± 1 0°C) Additionally, the positivity rate of urine and blood cultures was higher in the PCN group The average time to stone treatment after infection and medical treatment, as well as fever control, was shorter in the PCN group (9 ± 2 3 days)
Empiric treatment with Ceftriaxone (1 g IV) was confirmed by sensitivity results of urine or blood culture in 45% of cases None of the patients developed advanced urosepsis after the procedure, but the resolution of infection parameters was faster in the PCN group (7 ± 3 3 days)
Conclusions: Both PCN and DJ stent insertion are effective and safe methods for managing obstructive pyelonephritis It was observed that the PCN method under local anesthesia was useful in quickly controlling fever and allowing early surgical treatment. Finally, third-generation cephalosporin antibiotics are beneficial for empiric initial treatment
KEY WORDS: Kidney stone; Obstruction; Pyelonephritis; DJ stent; Percutaneous nephrostomy
Submitted 26 September 2024; Accepted 10 October 2024
INTRODUCTION
Pyelonephritis is termed as obstructive pyelonephritis (OP) when it is associated with urinary tract obstruction The primary cause of OP is typically an urinary stone that obstruct the urinary system Acute OP due to urolithiasis represents a medical-surgical emergency and often leads
to critical complications (1) The mortality rate among patients with sepsis secondary to acute complex OP is reported to be approximately 2% (2) Emergency decompression of the renal collecting system is required for two types of patients with obstructive urolithiasis: those with advanced urinary tract infection and those who develop renal failure The main methods for treating them are double-J (DJ) ureteral stent or percutaneous nephrostomy (PCN) tube insertion (3) The superiority between these two methods in resolving the problem remains controversial Factors such as the suitability or ease of the method, clinical resources, experience, evolving complications, and their severity are still uncertain and debatable (4) While it is generally accepted that the stone should not be treated at the same time of decompression of the urinary system, there is no consensus on whether stone surgery should be performed after decompression (5) To address this gap in the literature and determine the feasibility of the chosen method, it is crucial to consider the risks of complications, the recovery process, the occurrence of urosepsis, the appropriate timing of stone treatment, and the modality of antibiotic management
MATERIALS AND METHODS
P at ien t selec t io n
This retrospective study included patients with obstructive pyelonephritis (OP) secondary to urolithiasis who underwent PCN or retrograde ureteral DJ stent insertion between January 2020 and January 2022 The study utilized hospital archive records and was approved by the University Local Ethics Committee The study protocol was reviewed and approved by the Institutional Review Board of our University College of Medicine (approval number: 58119) Informed consent was obtained by all subjects when they were enrolled
A total of 77 patients were included, encompassing individuals of more than 6 months of age with complete hospital records Pregnant women were excluded from this study None of the patients had undergone treatment of obstructive stones before medical intervention Patients were categorized into two groups based on the drainage method Upon presentation to the emergency room or urology outpatient clinic, patients with stones were evalu-
ated for fever, white blood cell count (WBC), C-reactive protein (CRP) levels, urine culture, blood culture, presence of additional diseases, and antibiotic treatment (Table 1)
Complications, treatment duration, and post-treatment stone surgery timing were recorded for patients undergoing DJ stent or PCN insertion, and the suitability and success rates of the methods were compared
S u r g ic al t ec h n iq u e f o r DJ st en t in ser t io n
Patients received comprehensive information regarding the interventional procedure and provided informed consent by signing a consent form Prior to the procedure, all patients received 1 g of ceftriaxone intravenously as antibiotic prophylaxis Under sterile conditions and either local or spinal anesthesia, a 17 Fr cystoscope was inserted into the bladder through the urethral orifice Subsequently, a 4 7 Fr, 26 cm DJ stent was inserted using a guide wire for adult patients, while the size of the DJ stent for patients under 12 years of age was adjusted accordingly Fluoroscopy was utilized to verify the accurate positioning of the DJ stent
S u r g ic al t ec h n iq u e f o r p er c u t an eo u s n ep h r o st o m y
After obtaining patient information and consent, the renal system was visualized using ultrasonography under local anesthesia Following identification of a suitable calix, access to the system was achieved using a Chiba needle The system was visualized under fluoroscopy with the administration of contrast agent A suitable guidewire was passed through the skin, and dilatation was performed to facilitate the insertion of a 16 Fr nephrostomy tube (8-10 Fr for children) into the kidney
S t at ist ic al m et h o d s
Mean, standard deviation, median, minimum, maximum, frequency, and ratio values were used in the descriptive statistics of the data The distribution of variables was measured using the Kolmogorov-Smirnov test
Independent sample t-tests and Mann-Whitney U-tests were used in the analysis of quantitative independent data The chi-square test was used in the analysis of qualitative independent data, and the Fischer test was used when the chi-square test conditions were not met The SPSS 27 0 program was used in the analysis
RESULTS
The characteristics of patients who received decompression treatment by the two methods are summarized in Table 1 and Table 2, which also include data on the time interval to stone treatment after infection, and on the time for infection parameters to subside
Patients under the age of 18 were categorized into three subgroups: infants, children under 10 years, and adolescents We treated 12 pediatric patients under the age of 18 divided into three groups: infants (0-2 years), children under 10 years (3-9 years), and adolescents (10-18 years) The majority of the pediatric patients were adolescents, who showed a clinical presentation similar to adult cases Specifically, 1 patient was an infant (8 3%), two patients were children under 10 years (16 7%), and nine patients were adolescents (75%)
We analyzed the antibiotic sensitivity profiles of the pathogens isolated from both urine and blood cultures The most commonly isolated pathogen was Escherichia coli, which exhibited high sensitivity to beta-lactam antibiotics, particularly ceftriaxone, with a sensitivity rate of 85% This aligns with our empirical use of ceftriaxone as first-line therapy in obstructive pyelonephritis cases Other pathogens such as Klebsiella pneumoniae and Pseudomonas aeruginosa showed variable sensitivity, w i t h K l e b s i e l l a d e m o n s t r a t i n g 7 0 % s e
o Ertapenem and Pseudomonas showing significant resistance to many common antibiotics but retaining sensitivity to Ceftazidime and Piperacillin-tazobactam Candida species, detected in a subset of patients, responded well to Fluconazole This data underscores the importance of culture-based antimicrobial stewardship in the management of obstructive pyelonephritis, ensuring that empirical treatment is adjusted based on pathogen sensitivity profiles to improve outcomes and reduce resistance development
Table 1.
General characteristics of patients who underwent PCN and DJ stent (n:77).
Fever360-393379374±10
Pulse680-1220920940±129
WBC40-410110131±69
CRP00-42067103±102
Urinecu
lebsiella397
Psodomonas265%
Enterobacter132%
Enterokok132%
Bloodculture(-)68883% (+)9117%
Candida7778%
EColi111.1%
Klebsiella1111%
Comorbidity(-)34442%
(+)43558%
AppliedantibioticsCeftriazone36468%
Ertapenem23299%
Cephaxon339%
Amikacin226%
Cilapem226%
Fluconazole226%
Vancomicin+Imipenem226%
Gentamicin113%
Ceftazidime113%
Meropenem113%
Meropenem+Tazocin113%
Cilanem113%
Imipenem113%
Ceftriazone+Metronidazole113%
B Kati, E Ordek, O Madsar, E Sabri Pelit
Percutaneous nephrostomy Dj Stent P Mean ± ss/n-% Median Mean ± ss/n-% Median
Age336±252290373±2303300518t
GenderFemale2043.5%1548.4%0.67X2
Male26565%16516%
Fever376±10380371±103700048m
Pulse975±130955887±1108800006m
WBC141±81120116±431100352m
CRP115±10510084±95500190m
Urineculture(-)25543%21677%0240X2
(+)21457%10323%
EColi14667%5500%
Candida3143%2200%
Klebsiella295%1100%
Psodomonas148%1100%
Enterobacter000%1100%
Enterokok14.8%00.0%
Bloodculture(-)39848%29935%0240X2 (+)7152%265%
Candida5714%21000%
EColi1143%000%
Klebsiella1143%000%
Comorbidity(-)21457%13419%0747X2
(+)25543%18581%
Timetostonetreatmentandfevercontrol(day)9±2311±25 0 047 m
Statistical comparison of the information of patients who underwent PCN and DJ stent
Table 3. Comparative analysis of urine culture or blood culture results and antibiotic treatments administered between groups accordingly Percutaneous nephrostomy Dj Stent P
CRP11.5±10.510.00.0-42.01.9-19.58.4±9.
Urineculture(-)25543%21677%0240X2
(+)21457%10323%
EColi14667%5500%
Candida3143%2200%
Klebsiella295%1100%
Psodomonas148%1100%
Enterobacter000%1100%
Enterokok148%000%
Bloodculture(-)39848%29935%0240X2
(+)7152%265%
Candida5714%21000%
EColi1143%000%
Klebsiella1143%000%
Comorbidity(-)21457%13419%0747X2
(+)25543%18581%
AppliedantibioticsCeftriazon1737.0%1961.3%
Ertapenem1532.6%825.8%
Cephaxon36.5%00.0%
Amikacin243%000%
Cilapem243%000%
Fluconazole243%000% Vancomicin+Imipenem243%000%
Gentamicin000%132%
Ceftazidime000%132%
Meropenem122%000%
Meropenem+Tazocin122%000%
Cilanem000%132% Imipenem122%000%
Ceftriazon+Metronidazole000%132%
DISCUSSION
It has been determined that both methods are successful and safe in treating obstructive pyelonephritis before treatment directed to removal of the stone
Upper urinary tract (UUT) stones commonly lead to pain and drug-resistant pain pyelonephritis, potentially resulting in kidney unit loss and life-threatening situations in case of severe infections (6)
The European Association of Urology (EAU) guidelines for lithiasis suggest to delay definitive stone treatment after the resolution of infection or sepsis (7) In our clinical practice, stone treatment was not performed in association with decompression therapy
PCN was initially described by the urologist Dr Willard Goodwin in 1955 as a minimally invasive, X-ray-guided procedure, either temporary or permanent, offering an alternative to traditional surgery for patients with hydronephrosis (8) Since then, there has been an increase in the use of fluoroscopy and ultrasonography in PCN among urologists and interventional radiologists A survey study involving urologists and radiologists assessing pelvic system decompression concluded that preferences for PCN or DJ stent placement are generally based on personalized treatment according to the degree of hydronephrosis in the obstruction (9) In our study, the PCN procedure was commonly performed by interventional radiologists (87% of cases)
However, in determining the treatment approach, aside from the degree of hydronephrosis, we aimed to a comprhensive evaluation focusing on the identification of the patient's clinical factors and to subsequent administration of antibiotic treatment until primary stone therapy
Retrograde DJ stent placement offers the advantage of being a feasible option, which is preferred in routine practice by urologists Compared to PCN, DJ stent placement is considered more cosmetically favorable for patients However, many patients undergoing DJ stent placement experience lower urinary tract symptoms (LUTS), including post-operative pain, polyuria, and dysuria Consequently, because of the resulting reduction in quality of life, some patients may not prefer this procedure (10) According to the European Guideline, it is recommended that upon the patient's initial presentation, a urinary culture analysis is promptly conducted, with a subsequent reanalysis of the urinary culture following urological intervention Following this general principle, in our study, we conducted two separate urine culture analyses before and after drainage treatment Our results indicated that 40% of these cultures were positive, with culture positivity detected in 21 patients with nephrostomy and 10 patients with DJ stent placement In the study conducted by Anıl H et al , a culture positivity rate of 66 7% was observed, and the most frequently isolated pathogen in urinary tract infections was Escherichia coli (11) Similarly, in our study, Escherichia coli was the most frequently observed organism at 24 6% Additionally, Pseudomonas aeruginosa and Klebsiella pneumoniae were among the other common pathogens, while Candida infection, which is also described in the literature, was also frequently observed (12, 13)
The relatively low rate of positive urine cultures (40 3%) and blood cultures (11 7%) in our study can be attributed to several factors First, obstructive pyelonephritis often
triggers an inflammatory response, which may not always lead to detectable bacteriuria or bacteremia by the time cultures are taken This can happen due to the intermittent shedding of bacteria into the urine or bloodstream, resulting in negative culture results despite the presence of infection Additionally, many patients might have received empirical antibiotic treatment prior to hospital admission or sample collection, which could suppress bacterial growth and lead to false-negative cultures Furthermore, the obstruction itself may limit the dispersion of bacteria into the bloodstream or urinary tract, reducing the likelihood of positive cultures Moreover, variations in the timing and quality of sample collection can also play a role In some cases, cultures may have been taken after the initiation of antibiotic therapy or during phases of fluctuating bacteremia, reducing culture sensitivity It is also possible that some cases involved non-bacterial causes of infection, such as fungal infections, which were detected in a subset of patients These factors, along with the complex nature of obstructive urolithiasis and pyelonephritis, likely contributed to the relatively low culture positivity rates observed in our study
Patients were administered broad-spectrum antibiotic treatment in accordance with European guidelines before the culture results are available (14)
In our clinical practice, the obstructive pyelonephritis patients which apply to the emergency room or outpatient clinic, are immediately started with the broad-spectrum antibiotic Ceftriaxone (1 g IV) However, following the results of the urinary culture antibiogram, the appropriate treatment is then prescribed from the infectious diseases department The most common treatments were Ceftriaxone and Ertapenem In a study conducted by Subramanian et al , antibiotic sensitivity was evaluated after initial empirical treatment in patients with urosepsis, and it was concluded that 41 of 63 patients (65%) were sensitive to beta-lactam antibiotics according to urine culture (13) We have observed that sensitivity to intial empirical broad spectrum Ceftriaxone treatment has been confirmed in 46 75% of cases, so we administered this treatment regimen in our clinic
Urinary Candida species are a common clinical finding, especially among hospitalized patients In fact, some reports indicate that 90% of Candida urinary tract infection (UTI) cases occur in hospitalized patients with a urinary catheter (15) According to urine and blood culture results, we observed Candida positivity in 12 patients (38 7%) Half of these patients had diabetes (DM) and 8 patients were either hospitalized or had a urinary catheter installed Only 2 patients were recommended fluconazole treatment as antifungal therapy by the infectious diseases department after confirmation by new urine or blood culture tests In addition, recommendations were made for regulating blood sugar level and changing the catheter There are some limitations in our study The small number of patients may be related to the fact that the study coincided with the Covid-19 pandemic period Moreover, patients may be also treated in other centers so limiting our access to accurate information In addition, the results of urine and blood cultures may be affected by regional and geographical factors Therefore, it is important to highlight that the spectrum of pathogens and sen-
B Kati, E Ordek, O Madsar, E Sabri Pelit
sitivity to antibiotic that we have observed are specific for patients from our region
CONCLUSIONS
PCN and DJ stent techniques show comparable effectiveness in the treatment of cases of sepsis resulting from obstructive uropathy Although the PCN technique is more invasive, it helps to quickly obtain an urine sample from the upper urinary tract in order to diagnose the causative microorganism, facilitating the rapid and accurate implementation of treatment protocols Empiric antibiotic therapy with ceftriaxone shows sensitivity to pathogens in almost half of patients Finally, PCN can accelerate timing of stone treatment and be used as a guide for subsequent surgeries
REFERENCES
1 Abi Tayeh G, Safa A, Sarkis J, et al Determinants of pyelonephritis onset in patients with obstructive urolithiasis Urologia 2022; 89:100-103
2 Ryan J, O'Neill E, McLornan L Urosepsis and the urologist! Curr Urol 2021; 15:39-44
3 Türk C, Knoll T, Seitz C, et al European Association of Urology M e d i c a l E x p u l s i v e T h e r a p y f o r U re t e ro l i t h i a s i s : T h e E A U Recommendations in 2016 Eur Urol 2017; 71:504-507
4 Pearle MS, Pierce HL, Miller GL, et al Optimal method of urgent decompression of the collecting system for obstruction and infection due to ureteral calculi J Urol 1998; 160:1260-4
5 Itami Y, Miyake M, Owari T, et al Optimal timing of ureteroscopic lithotripsy after the initial drainage treatment and risk factors for postoperative febrile urinary tract infection in patients with obstructive pyelonephritis: a retrospective study BMC Urol 2021; 21:10
6 Pandey S, Sharma D, Sankhwar S, et al Are there any predictive risk factors for failure of ureteric stent in patients with obstructive urolithiasis with sepsis? Investig Clin Urol 2018; 59:371-375
7 Türk C, Petrík A, Sarica K, et al EAU Guidelines on Diagnosis and Conservative Management of Urolithiasis Eur Urol 2016; 69:468-74
8 Preminger GM, Tiselius HG, Assimos DG, et al EAU/AUA Nephrolithiasis Guideline Panel 2007 guideline for the management of ureteral calculi J Urol 2007; 178:2418-34
9 Pietropaolo A, Seoane LM, Abadia AA, et al Emergency upper urinary tract decompression: double-J stent or nephrostomy? A European YAU/ESUT/EULIS/BSIR survey among urologists and radiologists World J Urol 2022; 40:1629-1636
10 Joshi HB, Stainthorpe A, MacDonagh RP, et al Indwelling ureteral stents: evaluation of symptoms, quality of life and utility J Urol 2003; 169:1065-9
11 Anıl H, Sener NC, Karamık K, et al Comparison of Percutaneous Nephrostomy and Ureteral DJ Stent in Patients with Obstructive Pyelonephritis: A Retrospective Cohort Study J Invest Surg 2022; 35:1445-1450
12 Bonkat G, Cai T, Veeratterapillay R, et al Management of Urosepsis in 2018 Eur Urol Focus 2019; 5:5-9
13 Subramanian A, Bhat S, Mookkappan S, et al Empiric antibiotic and in-vitro susceptibility of urosepsis pathogens: do they match? The outcome of a study from south India J Infect Dev Ctries 2021; 15:1346-1350
14 Bonkat G, Pickard R, Bartoletti R, et al "EAU guidelines on urological infections " EAU Guidelines Office, 2018, Arnhem, the Netherlands
15 Fisher JF, Kavanagh K, Sobel JD, et al Candida urinary tract infection: pathogenesis Clin Infect Dis 2011; 52(Suppl 6):S437-51
Correspondence
Bulent Kati Associate Prof M D FEBU (Corresponding Author) bulentkati@harran edu tr Omer Madsar omermadsar46@gmail com
Eyyup Sabri Pelit dreyyupsabri@hotmail com
Harran University, Faculty of Medicine, Urology Department, 63440 Sanliurfa, Turkey
Eser Ordek dr eseser@hotmail com
Mustafa Kemal University, Faculty of Medicine, 31100 Urology Department, Hatay, Turkey
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Should patients with encrusted JJ stents involving the proximal/renal loop undergo primarily endoscopic combined intrarenal surgery?
Alexandra Rocha, Gonçalo Mendes, Sofia Mesquita, Mariana Madanelo, João Vital, Miguel Marques-Monteiro, Nuno Vinagre, Martinha Magalhães, Beatriz Oliveira, Guilherme Gonçalves, Vítor Cavadas, Avelino Fraga
Urology Department, Centro Hospitalar e Universitário de Santo António, Unidade Local de Saúde de Santo António, Porto, Portugal
Summary
Background: Ureteral stents are one of the most used devices in Urology, allowing drainage of the upper urinary system, and can be used either in elective or emergency procedures However, as a foreign body inside the urinary system, they are subject to encrustation. Encrustation is one of the burdens seen with double-J stents and, to date, there is no consensus about its best management. This study aims to prove that Endoscopic Combined Intra-Renal Surgery (ECIRS) is the best choice when there’s an encrusted proximal loop of a ureteral stent
Methods: The authors conducted a retrospective cohort study of patients with an encrusted proximal loop of the ureteral stent who underwent surgery at a single center, comparing ECIRS with other procedures
Results: Between July 2011 and June of 2024, 33 patients (18 females and 15 males) were submitted to surgery The median indwelling time of the stent was 11 (8-19) months and a stentfree rate of 100% was achieved. The authors demonstrated a significant stone-free rate of 61 1% following ECIRS compared to merely 20% with other procedures (p = 0.023). Notably, while the complication rate was low across all procedures, the ECIRS group exhibited fewer complications (5.6%) than those undergoing alternate techniques (13 3%), though this difference was not statistically significant (p = 0.439).
Conclusions: Our study advocates for ECIRS as the preferred initial treatment for encrusted proximal ureteral stents, as it facilitates superior stone clearance, minimizes complications, and maintains comparable operative efficiency. This research contributes valuable insights into the management of challenging cases involving encrusted ureteral stents, calling for future studies to further validate these findings
KEY WORDS: Encrusted stent; Lithiasis; Endoscopic combined intra-renal surgery
Submitted 26 September 2024; Accepted 27 September 2024
INTRODUCTION
Ureteral stents are one of the most used devices in Urology They allow the drainage of the upper urinary system and are a powerful tool to use either in elective or emergency procedures However, as a foreign body inside the urinary system, they are subject to encrustation Encrustation is one of the burdens seen with double-J
stents (1) An encrusted stent is defined as one that cannot be removed simply by cystoscopy due to calcification or stone formation around the stent (1, 2) Several risk factors have been described, namely indwelling time and bacterial colonization, as well as patient specific factors and the physical characteristics of the stent (3) El-Faqih et al proved that the incidence of stent encrustation increases with indwelling time, reporting 9 2% of stents removed before 6 weeks were encrusted compared to 47 5% removed between 6 to 12 weeks (4)
Nowadays there is no consensus around the best management of this type of complication Its approach depends on the severity and location of the encrustation Some classification for the encrusted stents (ESs) had been published in the last years, namely the KUB score and the forgotten, encrusted and calcified (FECal) grading system The first one, KUB system is based on the degree of encrustation of the stent in the kidney, ureter and bladder, grading it from 1 to 5, and it’s supposed to identify those that will be surgically challenging to remove (5) The later, is based on the stone size, location and degree of stent encrustation, and graded from 1 to 5, proposing also a treatment algorithm (2, 6) In 2021, Manzo et al proposed a novel system, the V-GUES, which aims to propose a visual classification for ESs that help to guide the choice of the appropriate treatment This system is based on visual interpretation of CT scans and divides it into 4 categories: group A includes distal calcification, sparing the ureteral and proximal portions of the stent; group B includes calcification of the distal and ureteral portions of the stent, sparing the proximal loop; group C includes proximal calcification, with or without calcification of the distal portion, but sparing the ureteral portion of the stent; and finally group D includes calcification of the proximal and ureteral portions of the stent, with or without calcification of the distal portion The authors advocate that their classification system is associated with the number of procedures required for a patient to be stent-free, stone-free rate and complications They suggested that this classification will allow urologist to choose the most reliable intervention (1)
Based on the aforementioned studies, the authors intended to prove that the Endoscopic Combined Intra-Renal Surgery (ECIRS) is the best choice when there’s an encrusted proximal loop of a ureteral stent
MATERIALS AND METHODS
We conducted a retrospective cohort study of all patients who were found to have an encrusted JJ stent and underwent surgical procedures for its removal in our center between July 2011 and June of 2024 (54 patients) From this group of patients, the ones with proximal loop encrustation were selected, based on preoperative CT scans and the V-GUES classification The patients selected belonged to the C and D groups from this classification All patients without a preoperative CT scan were excluded
All clinical and surgical data were collected from patients' files, focusing on age, sex, height and weight and renal function (serum creatinine levels) We also gathered information about the procedure during which the stent was initially placed, the time of diagnosis of the encrustation and the duration of the catheterization We registered the type and number of procedures needed to achieve a stone free status, that was defined as the absence of any fragments in the postoperative imaging studies, and a stent-free status
All patients underwent surgery in our hospital, by a single surgeon Treatment decisions were based on the surgeon ’ s preference The surgeries performed were semirigid ureteroscopy (srURS), flexible ureteroscopy (fURS), percutaneous nephrolithotomy (PCNL) and endoscopic combined intrarenal surgery (ECIRS) All patients with positive cultures were treated with antibiotics before the surgery, and all were given perioperative antibiotic prophylaxis Other data collected included the postoperative complications, including the first 30 days, and classified according to the Clavien-Dindo classification
Data was collected in a SPSS file We conducted descriptive statistics for all the variables, presenting their means or median according to the presence (or not) of a normal distribution The categorical and nominal variables are p re s e n t e d i n f re q u e n c y t a b l e s To c o m p a re m e a n s between variables we used a t-sample test The correlation between variables was ascertained using Pearson correlation and logistic regression was made to obtain odds ratio of the variables, were applicable Differences were considered statistically significant if p < 0 05
The study was made in were in accordance with the Helsinki Declaration
RESULTS
Between July 2011 and June of 2024, 33 patients with an encrusted proximal/kidney loop of a ureteral stent were submitted to surgery in our centre There were 18 females and 15 males, with a mean age of 53 9 (± 19 0) years The mean height and weight were 1 62 (± 0 1) m and 74 1 (± 19 4) kg, respectively The mean BMI was 27 8 (± 6 0) In 11 cases the encrusted JJ stent was on the left and in 20 cases on the right; we had 2 cases of encrusted stents in a renal transplant The preoperative serum creatinine levels were 1 1 (± 0 6) mg/dl and the postoperative was 1 1 (± 0 4) mg/dl We found no statistically significant difference in the creatinine levels pre- and post-operatively (p = 0 961)
Preoperative urine cultures were also taken, with a positive result in 10 cases and negative in 9 In 12 cases the lab was not able to isolate the bacteria probably due to contamination of the sample In the other 2 cases the pre-
Table 1
Results of urine cultures
Urine culture Frequency (%)
Ecoli6(607%)
Pmirabilis3(30%)
Calbicans1(10%)
Table 2.
Frequency table of the surgeries performed.
Surger y Frequency (%)
Co
PCNL8(242%)
Flexibleureteroscopy6(182%)
Semirigidureteroscopy1(3%)
operative urine culture was not available The isolated strain was Escherichia coli in 6 patients, followed by Proteus mirabilis in 3 cases, and 1 case of Candida albicans These results can be consulted on Table 1
The median indwelling time of the stent was 11 (8-19) months, varying between 5 and 71 months We found no correlation between indwelling time and the occurrence of complications (p = 0 830) or the stone-free rate (p = 0 423)
Regarding surgical approach, the most performed surgery was endoscopic combined intrarenal surgery in 18 cases of 35 (54 5%), as can be seen on table 2 In 8 patients (24 2%) the surgery chosen was PCNL, 6 patients (18 2%) underwent fURS and 1 patient (3%) underwent srURS
The mean time of procedure was 121 1 (± 44 3) min When comparing ECIRS with other procedures, the authors found a mean time for combined surgery of 123 6 (± 50 9) min and a mean time a 118 1 (± 36 5) min for other surgeries
There was no statically significant difference between the groups (p = 0 727) We also found no difference between the procedure time and the occurrence of complications (p = 0 523) and the stone-free rate (p = 0 487)
In all the cases (100%) the encrusted stent was removed in the first procedure
Regarding the stone-free state, 14 patients (42 4%) were stone free after the first procedure, with 19 (57 6%) patients not achieving this state Comparing the ECIRS procedure with the other surgeries performed, a stone-free rate of 61 1% was achieved with the ECIRS procedure, while other procedures resulted in a 20% stone-free rate
Comparing these rates, we found a correlation between the choice of ECIRS and the stone-free rate (p = 0 023, OR 6 3, 95% CI:1 3-30 5) This data can be seen on Table 3
Table 3.
Comparing ECIRS with other procedures regarding stent-free, stone-free and complication rate
Combined procedure Other procedures P
A Rocha, G Mendes, Sofia Mesquita, et L
Table 4
Description of complications
The median hospital stay was 3 (2-3) days Overall, there were 3 cases (9 1%) of postoperative complications in the first 30 days Two cases of fever with urinary tract infection (UTI) and 1 case of urinary leakage Regarding the Clavien-Dindo classification, all fall into the II classification Comparing ECIRS with other procedures, we found a complication rate of 5 6% with ECIRS and a 13 8% rate with other procedures; we found no statistically significant correlation between these variables (p = 0 439) The complications and its frequencies can be seen on table 4 Regarding the necessity of a second procedure, 2 patients needed other surgery - 1 patient a fURS (first procedure was a mini-PCNL), 1 mini-PCNL (first procedure was fURS) No complication was reported on these cases
DISCUSSION
Encrusted ureteral stents are a complex problem to manage and it may be difficult and risky to treat it (7, 8)
Classification systems appear to facilitate the approach of this type of patients According to Juliebø-Jones et al. (7), it is recommended to use one of the classification systems available In this study, the authors chose to use the VGUES classification system as it appears as the most reliable and useful The KUB system is based on X-ray images alone, which may render some limitations The FECal system, despite its more broaden classification, it is only based on 9 patients (1, 2) The classification was used to select patients to enter the study, and only the ones categorized as C or D were selected - which means with the presence of encrusted proximal loop of the stent was the selection criteria
Some authors already proposed that the location of the e n c r u s t a t i o n w i l l d e t e r m i n e t h e s u rg i c a l m o d a l i t y required for the management of the ureteral stent, and the authors from V-GUES already suggest that combined surgery was associated with best stone-free and stent-free rate (1, 2) The main objective of this study is to propose ECIRS, with combined percutaneous surgery and retrograde endoscopic surgery, as the best first approach to managed encrusted proximal loops of ureteral stents
This study harbours some limitations inherent to its retrospective design and relatively small patient cohort
However, due to the nature of this type of cases and its relative scarcity, the authors believe that a prospective study is not feasible The cases were all performed by the same surgeon, with plenty of experience in lithiasis surgery, which could help to explain the good results
The data collected gathered information from patients with an encrusted proximal/kidney loop of a ureteral stent that were submitted to surgery in our centre for a
period of roughly 13 years The sample obtained was 33 patients, with 18 women and 15 men Given the scarcity of reports on these subject, and its relative infrequent occurrence, this number are in line with other single center reports
The median indwelling time of the stent was 11 (8-19) months It is known that the prolonged indwelling time of stents increases the prevalence and severity of all complications (8) However, we could not find a correlation between the occurrence of complications or stonefree rate and the indwelling time of the ureteral stent We hypothesize that this could be explained by the low level of complications present in the sample
The mean time of procedure for ECIRS was 123 6 (± 50 9) min, that was not statistically significantly different from the mean time of the other procedures (p = 0 727) This shows that, even when comparing operative time, the use of a more complex surgery, like the combined approach, does not imply longer operative times, advocating for its use
There was a 100% rate of stent-free patients after the first procedure, independently of the procedure used This excellent stent-free rate can be explained by the relative short number of cases and the experience of the surgeon
When focusing on the stone-free state, 42 4% of the patients achieved this state after the first procedure
When comparing the two groups, we found a higher stone-free rate when using ECIRS comparing to other procedures (61 1% vs 20%, respectively) In this case, we found a positive correlation between the use of ECIRS and the stone-free status, with a OR of 6 3 (p = 0 023, 95% CI:1 3-30 5) This shows that ECIRS is a more effective procedure comparing to the other procedures, in cases of encrusted stent, namely with proximal loop encrustation Some authors already proposed that PCNL should be used in encrusted proximal loops stent Pais et al. state that only 8% of the stents could be removed by PCNL alone, suggesting that additional procedures may be needed (9) Our results show that in proximal loops, ECIRS should be preferred as first-line as it is the most successful surgery
When looking at the complications rate, the group had a very low complication rate and only with Clavien-Dindo II Once again, this could probably be explained by the experience of the surgeon and the limited number of cases analysed Despite not being statistically significant, the complication rate was lower when using the combined approach, supporting its primary use
There was need for a second procedure in 2 patients All the patients needed at least one procedure with a percutaneous access and others with retrograde endoscopic surgery This is also in favour with the proposed theory (all needed combined surgery), even if it was in two separate procedures This supports the theory of using combined approach as the first choice in this type of patients
In the remaining patients, the residual stone burden was very little and didn’t need other procedure
Weeding et al reported that patient with proximal encrusted stents required more procedures to remove the stent and the stone burden (10) Our study group reports that
Rocha,
the used of combined surgery approach can improve outcomes and reduce the number of surgeries needed to treat this type of patients
CONCLUSIONS
Encrusted ureteral stents poses a significant challenge for urologist There is a lack of standardized treatment in this area The authors propose combined surgery as the first choice for the treatment of encrusted proximal loops of ureteral stents, as it is associated with better stone-free rate and fewer complications, while not increasing operative time
REFERENCES
1 Manzo BO, Alarcon P, Lozada E, et al A Novel Visual Grading for U re t e r a l E n c r u s t e d S t
C
Endourologic Treatment J Endourol 2021; 35:1314-9
2 Acosta-Miranda AM, Milner J, Turk TMT The FECal Double-J: A Simplified Approach in the Management of Encrusted and Retained Ureteral Stents J Endourol 2009; 23:409-15
3 Tomer N, Garden E, Small A, Palese M Ureteral Stent Encr ustation: Epidemiology, Pathophysiology, Management and Current Technology J Urol 2021; 205:68-77
4 El-Faqih SR, Shamsuddin AB, Chakrabarti A, et al Polyurethane Internal Ureteral Stents in Treatment of Stone Patients: Morbidity Related to Indwelling Times J Urol 1991; 146:1487-91
5 Arenas JL, Shen JK, Keheila M, et al Kidney, Ureter, and Bladder (KUB): A Novel Grading System for Encrusted Ureteral Stents Urology 2016; 97:51-5
6 Guner E, Gokhan Seker K Comparison of Two Different Scoring Systems in Encrusted Ureteral Stent Management: A Single-Center Experience Urol J 2020; 17:248-251
7 Juliebø-Jones P, Pietropaolo A, Sørstrand Æsøy M, et al Endourological management of encrusted ureteral stents: An up-todate guide and treatment algorithm on behalf of the European Association of Urology Young Academic Urology Urolithiasis Group Cent European J Urol 2021; 74:571-8
8 Adanur S, Ozkaya F Challenges in Treatment and Diagnosis of forgotten/encrusted double-J Ureteral stents: the Largest single-center Experience Ren Fail 2016; 38:920-6
9 Pais VM, Chew B, Shaw O, et al Percutaneous Nephrolithotomy for Removal of Encrusted Ureteral Stents: A Multicenter Study J Endourol 2014; 28:1188-91
10 Weedin JW, Coburn M, Link RE The Impact of Proximal Stone Burden on the Management of Encrusted and Retained Ureteral Stents J Urol 2011; 185:542-7
Correspondence
Maria Alexandra Ferreira Rocha (Corresponding Author) marialexandrarocha@gmail com
Gonçalo Mendes goncalo grilomendes@gmail com
Sofia Mesquita sofiaoplmesquita@gmail com
Mariana Madanelo marianacmadanelo@gmail com
João Vital joaopvital@gmail com
Miguel Marques-Monteiro mmonteiro iam@gmail com
Nuno Vinagre nunomrvinagre@gmail com
Martinha Magalhães martinha a magalhaes@gmail com
Beatriz Oliveira
ana bia 5@hotmail com
Guilherme Gonçalves guilha gon@gmail com
Vitor Cavadas vcavadas@gmail com
Avelino Fraga avfraga@gmail com
Urology Department, Centro Hospitalar e Universitário de Santo António, Unidade Local de Saúde de Santo António, Porto, Portugal
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Single
site multi puncture supine (SMS) PCNL procedure in patient with complex renal stone: One incision, why should more?
Paksi Satyagraha, Reza Amorga, Taufiq Nur Budaya
Urology Department, Faculty of Medicine, Universitas Brawijaya, Saiful Anwar General Hospital, Malang, Indonesia
Summary
Introduction: Since percutaneous nephrolithotomy (PCNL) was introduced in 1976, it has been the standard procedure for large renal stones
Over time, the PCNL technique changed and developed into various techniques We introduce single site multipuncture supine (SMS) PCNL to give cosmetic advantage due to less tissue injury in complex renal stone This study aimed to determine the outcome SMS PCNL procedure in patients with complex renal stones diseases
Materials and methods: This study was a retrospective study including all patients with kidney stones who had undergone SMS PCNL at the Urology Department of Saiful Anwar General Hospital from March 2019 until December 2022 All SMS PCNL procedures were performed by a single operator. The patients were divided into three groups that included that were treated with 2, 3, and 4 punctures. The data were collected using SPSS ver 25
Result: Ninety-three patients were included in this study. The characteristics of the patient such as gender, age, BMI were not significantly different among the groups. The outcome of SMS PCNL procedure showed low complication rate during operation in 2-,3-,and 4-puncture groups (3.2%, 7.4%, 0%, respectively). The Stone Free Rate (SFR) showed no significant difference between the 3 groups (p = 0.496). The SFR was 85.7% in 2-puncture, 77 8% in 3-puncture, 66 7% in 4-puncture group
The AUC of Guy’s Stone Score with cut off value was 3.5 (AUC = 0 549, p-value = 0 541, CI 95%)
Conclusions: Single Site Multi Puncture PCNL is safe and efficient approach to complex renal stones Single Site Multipunctures Supine PCNL is comparable with other techniques of PCNL and gives minimal tissue injury that would benefit for cosmetic
KEY WORDS: Multipunctures; Outcome; PCNL; Renal stone
Submitted 26 September 2024; Accepted 28 September 2024
INTRODUCTION
In urologic practice, renal stone disease is challenging because of its enormous stone burden and recurrence
The goal of renal stone management is a minimally invasive, effective, and with minor complication surgery (1) Since Fernstrom described percutaneous nephrolithotomy (PCNL) in 1976, it has been the standard procedure for large renal stones, usually more than 2 cm Patients with
complex multiple renal stones face various problems during PCNL, including a higher occurrence of residual calculus and the need for multiple tracts Compared to procedures using single tracts, multiple percutaneous tracts have a higher risk of bleeding and complication rates (2, 3) Over time, the PCNL technique changed, moving from multisite multi puncture, single-site single puncture to single-site multi puncture
In 2011, M Lezrek reported renal displacement procedure to make superior calyx easily reached (4) As the years go, in 2018, Single Site Multi puncture supine (SMS) PCNL modified the renal displacement technique by Lezrek using a 18G needle to reach superior calyx easily to performed access the lower, middle, and upper renal pole to treat staghorn and multiple renal stones through a single skin incision giving cosmetic advantage due to less tissue injury (Figure 1) This study aimed to determine the outcomes SMS procedure in patients with complex renal stones
METHODS
Study population
The design of this study is a cohort retrospective study Data on patient demography, surgical technique, and outcome of operation was acquired through medical records All cases were sampled to acquire the number of patients required The inclusion criteria for this study was being a patient who underwent SMS PCNL from March 2019 to December 2022 Patients with anatomical abnormalities were excluded from the study The patients were divided into 3 groups: 2 punctures, 3 punctures, and 4 punctures Data on gender, age, body mass index (BMI), comorbidity, and stone size were collected preoperatively Evaluation of outcome after procedure was done two weeks after the procedure with kidney-ureter-bladder (KUB) X-ray Guy’s Stone System (GSS) score was obtained on the base of NCCT images GSS used was as follows (5): Grade I: A solitary stone in the mid/lower pole with simple anatomy or a solitary stone in the pelvis with simple anatomy; Grade II: A solitary stone in the upper pole with simple anatomy or multiple stones in a patient with simple anatomy or any solitary stone in a patient with abnormal anatomy; Grade III: Multiple stones in a patient with
Figure 1.
A Post operative scar with one incision
B Post operative scar with two incision
abnormal anatomy or stones in a calyceal diverticulum or partial staghorn calculus; Grade IV: Staghorn calculus or any stone in patient with spina bifida or spinal injury
Any complication during the operation or untoward event was noted using the Clavien-Dindo classification (6) The outcome of SMS PCNL was determined by the stone free rate, operative time, delta hemoglobin, delta creatinine, and hospital stay Data were collected and analyzed statistically using the SPSS Software ver 25 Quantitative data were expressed as mean ± standard deviation (SD) and median Qualitative data were expressed as frequency and percentage Gender, comorbidity and Guy’s Stone System were analyzed with chi square BMI, stone size, delta hemoglobin, delta creatinine, operative time and hospital stay were analyzed with Kruskall Wallis and Dunn This study was approved by the H e a l t h R e s e a r c h E t h i c s Commission of Saiful Anwar General Hospital
Surgical technique
The PCNL procedures were performed under general or epidural anesthesia We used the Barts' Flank-Free' modified supine position A relatively horizontal tract allows low intrarenal pressures and easy washout of fragments
An 18-gauge needle was used to perform the percutaneous puncture under C-Arm-guidance and fluoroscopy after retrograde pyelography (RPG) from ureteral catheter; then a guidewire with a J-Tip super stiff rigid shaft was inserted Under continuous fluoroscopic observation, the needle's proximal end was steadily moved in the cephalic direction (Figure 2)
Figure 3
The first needle's body is progressively bent and secured to the drape The superior calyx is punctured at the point where the first needle enters
As a result of the Lezrek maneuver, the kidney was moved caudally At the same time, a forceps twists the needle's body and secures it to the drape (Figure 3)
The calyx of the upper pole is punctured, and a tract was made (Figure 4) Furthermore, the natural axis of the kidney was slightly inverted, with the lower pole tilted medially and the upper pole oriented laterally The upper calyxes were redirected downward and closer to the cutaneous entry as a result Therefore, the targeted calyx was shown more clearly The next punctures that needed to reach the stone are entered through the same incision as the first puncture and dilation is conducted using Alken dilator until 30 Fr and Amplatz 30 Fr was inserted, followed by the insertion of standard size 26 Fr nephroscope or even 12 Fr nephroscope (mini PCNL)
Lithotripsy with following fragments’ evacuation was done The operations were completed with the insertion of a 20-Fr nephrostomy tube or 12 Fr naso-gastric tube into the tract This technique which describes multipunctures PCNL was done through a single skin incision (7) KUB was performed to evaluate the residual stone Stone more than 5 mm were defined as residual stone (8)
Figure 2.
A guidewire was inserted through a middle calyx puncture to protect the urothelium from the needle distal end during needle bending
Figure 4. The kidney is several millimeters lower after caudal renal displacement, and the upper pole calyx is available
RESULTS
Of 98 patients with renal stones who had undergone SMS PCNL, 93 patients were included in this study Five
Table 1 Patient characteristic
Asthma116%
DiabetesMellitus9143%274%13333%
Hypertension463%
Obesity463%137%
StoneSize,cm,mean±SD309±136405±133516±1250001
Guy’sScoringSystem(GSS)0893
GradeI000000
GradeII22349%1037%1333%
GradeIII32508%12445%1333%
GradeIV914.3%518.5%133.3%
anatomical abnormality (n = 5) The patients were divided into three groups based on the number of punctures done during PCNL operation: 63 patients with 2 punctures, 27 patients with 3 punctures, 3 patients with 4 punctures Comparison of the patient’s age at the time of surgery between the groups showed a value of 0 491 (p > 0 05), which mean no significant difference In this study, the number of male patients (55 6%, 70 4%, 66 7% respectively) was more than females in all the 3 groups (44 4%, 29 6%, 33 3% respectively) Both body mass index (BMI) and gender showed no significant difference between 2-, 3-, and 4- puncture groups (p 0 410, p 0 800, respectively) In our study, the comparison of the presence of comorbidities showed 0 874 (p < 0 05), indicating that there was no significant difference Mean stone size was larger in 4 puncture group (5 16 cm) than 2 and 3 puncture group (3 09 cm, 4 05 cm, respectively) The comparison of stone complexity (Guy’s scoring system) showed that there was a not significant difference between the 3 groups (p = 0 893) (Table 1)
We analyze the outcome between 2-puncture, 3-punc-
ture, and 4-puncture groups There was no significant difference in the complications between the three groups (p = 0 618) In the 2- and 3-puncture groups there were 2 patient in each group (3 2%, 7 4%, respectively) who had complications; differently from the 4-puncture group where there was no complication Three patients (one patient who underwent 2-puncture procedure and 2 patients who underwent 3-puncture procedure) needed blood transfusion (Clavien grade II) because hemoglobin dropped more than 2 mg/dL in the first 24 h post-operatively One patient in the 2-puncture group developed septic condition (Clavien Grade IVb) Stone-free status was achieved in 85 7%, 77 8%, 66 7% of patients in 2-, 3-, and 4-puncture group, respectively (Table 2)
There was a significant difference (p = 0 000) in operation time between 3 groups Two-puncture group has less operative time (55 min) than the 3- and 4-puncture groups (76 and 86, respectively) Hospital stay of patients has a significant difference (p = 0 000), whereas fourpuncture group had a longer median hospital stay (4 days) than 2-puncture and 3-puncture groups (2 and 3 days, respectively) There was no significant difference
Complication:0618
Table 2. The outcome between 2 punctures, 3 punctures, and 4 punctures of the SMS procedure The number of puncture of SMS 234P Freq % Freq % Freq %
The comparison of operative time, hospital stay, delta hemoglobin, and creatinine between 2, 3, and 4 punctures of the SMS procedure
Table 4.
The outcome between 2 punctures, 3 punctures, and 4 punctures of the SMS procedure
in ∆Hb (p = 0 165), ∆creatinine (p = 0 418) between 2-, 3-, and 4- puncture groups (Table 3) Comparison of stone free and complication rates based on stone complexity grade (Guy’s stone scoring system) are shown in Table 4
Guy’s scoring system (GSS) was a valuable tool to predict the stone free rate and complication associated with SMS PCNL
In this study, area under curve (AUC) of GSS with a cut off value of 3 5 was 0 549 (p-value = 0 541, CI 95%)
The ROC analysis revealed that GSS predicted complica-
tion with a level of prediction accuracy of 79 57% and predicted the stone free with a prediction accuracy of 68 82% (Figure 5)
DISCUSSION
PCNL is considered the first-line management for renal stones larger than 2 cm and also for complex renal stone
Percutaneous renal surgery has seen a rise in success rates and a decrease in complications because to advancements in endourologic equipment and lithotripsy devices
Patients with complex multiple renal calculi are a special challenge for PCNL because they more likely have residual stone
Multiple access approach (puncture or tracts) is still controversial
Multiple punctures are necessary to prevent second-look procedure (RIRS or ESWL) although they are frequently linked to an increased risk of bleeding (3) Successful puncture is always the first step in a safe and efficient PCNL, especially for complex renal stones In our study, there was no sig-
Figure 5. Analysis receiver operating characteristic curve for Guy’s stone score for prediction of stone free and complications of percutaneous nephrolithotomy.
nificant difference of complication rate among the 3 groups (p = 0 618)
Similarly to previous studies, multi-tract when compared with single tract PCNL, showed no significant difference in term of complication (2)
In this study 1 patient in the 2-puncture group (1 6%) and 2 patients (7 4%) in the 3-puncture group required blood transfusion showing a low rate in comparison with the rate reported by Hegarty and Desai, who observed a transfusion rate of 12 4% (9)
Bleeding is the most reported major complication of PCNL In present study, we compared the ∆hemoglobin between the 3 groups There was no significant difference between the 3 groups Akman et al reported that the number of accesses is one of the two predictive indicators for total blood loss and request of transfusion
Furthermore, multiple accesses increased transfusion requirements 4 46 times compared with single tract approaches The mean decrease of Hb was 1 67 g/dL in the single tract group and 2 25 g/dL in the multiple tract group (10) In the present study, mean ∆Hb in 3-puncture group (1 17 g/dL) was slightly higher than the mean ∆Hb in 2- and 4-puncture group (0 94 g/dL, 1 07 g/dL, respectively) and showed to be not different with differences of hemoglobin reported in other studies
There was an improvement in serum creatinine levels in the 3 groups This result is similar to a previous study, which showed a significant improvement 2 weeks after the procedure of serum creatinine level with respect to preoperative values (11) This could be explained by the obstructive nature of stones in our study, despite prior reports showing there was a significant rise in serum creatinine in cases of multiple puncture PCNL for patients who are known cases of renal insufficiency
Various factors including larger stones, complex stones, and multiple accesses require longer operative times, which usually result in enhanced complication rates, such as bleeding In present study, there was a significant difference of the operative time between the 3 groups (p = 0 000) Four-puncture group had longer operative time (86 min) than 2-puncture group (55 min) and 3-puncture group (76 min) The operative times in 4-puncture was longer because the stones are more complex and larger Previous studies established a cut off point of operative time of 58 minutes for necessitating blood transfusion For operative time more than 58 minutes, blood transfusion requirement increased 2 81 times (10)
Differently by the present study, Jiao et al reported no significant different operative time between single access and multi access PCNL (MD = -42 78 min, 95% CI (0-85 49 to -0 07), p = 0 05) (12)
Multiple punctures may be associated with an increased risk of bleeding This can also affect the length of inpatient stay In the present study, there was a significant difference (p = 0 000) of hospital stay between the 3 groups (2 2 days, 2 96 days, 3 67 days, respectively) Differently from the present study, Jiao et al showed that single access and multi access group were similar (MD = -0 59, 95% CI (-3 59 to 2 41), p = 0 70) (12)
Labadie et al in their retrospective study showed the low GSS score to be significantly associated with stone free rate (p = 0 002) and the AUC was 0 634 (95% CI 0 566-
0 702) (13) In another retrospective study it was found that the AUC of GSS was 0 739 (95%CI, 0 665-0 813) and it was demonstrated that GSS has a good predictive rate for stone free rate (14) Differently, in our study, GSS showed a cut off value of 3 5 with AUC of 0 549 (p-value = 0 541, 95%CI) that was not enough strong to predict stone free status and complications, because there were some confounding factor such as presence of comorbidity that can affect outcome of multiple punctures
We encountered several limitations in our study, including lack of stone composition, short follow-up, and small population samples especially in 4-puncture group Further, large scale multicenter prospective studies and reduction of confounding factors can help in predicting stone free and complication rates
CONCLUSIONS
Single Site Multi Puncture PCNL is an approach to larger and complex renal stone This method is safe and efficient
This technique is comparable with others technique of PCNL and creates less tissue injury that would benefit cosmetic result
REFERENCES
1 Shalaby MM, Abdala MA, Aboul-Ella HA, et al Single Puncture Percutaneus Nephrolithomy for Management of Complex Renal Stones BMC Res Notes 2009; 2:62
2 Liang T, Zhao C, Wu G, et al Multi tract Percutaneus Nephrolithotomy Combined with EMS Lithotripsy for Bilateral Complex Renal Stones: Our Experience BMC Urology 2017; 17:1-5
3 Verma A, Tomar V, Yadav S Complex Multiple Renal Calculi: Stone Distribution, Pelvicalyceal Anatomy and Site of Puncture as Predictor of PCNL Outcome Springerplus 2016; 5:1356
4 Lezrek M, Bazine K, Ammani A, et al Needle Renal Displacement Techinque for the Percutaneus Approach to the Superior Calix J Endourol 2011; 25:1723-1726
5 Thomas K, Smith NC, Hegarty N, Glass JM The Guy’s stone score- Grading the complexity of percutaneous nephrolithotomy procedures Urology 2011; 78:277-81
6 Clavien PA, Barkun J, de Oliveira ML, et al The Clavien-Dindo classification of surgical complications: five-year experience Ann Surg 2009; 250:187-196
7 Ilham M Paksi S, Andri K A Novel Technique Single Site Multipunctures Supine PCNL: Case Series Report Jurnal Urologi Indonesia 2024; 31:55-60
8 Ermis O, Bhaskar S, Thomas R, et al Definition, treatment and outcome of residual fragments in staghorn stones Asian J Urol 2020; 7:116-21
9 Hegarty NJ, Desai MM Percutaneus Nephrolithotomy Requiring Multiple Tracts: Comparison of Morbiditiy with Single Tract Procedures J Endourol 2006; 20:753-60
10 Akman T, Binbay M, Sari E, et al Factor Affecting Bleeding During Percutaneus Nephrolithotomy: Single Surgeon Experience J Endourol 2011; 25:327-333
11 Elawady H, Mostafa DE, Mahmoud MA, et al Is multiple tracts percutaneous nephrolithotomy (PCNL) safe modality in management
of complex renal stones? A prospective study: Single center experience African J Urol 2018; 24:308-314
12 Jiao B, Ding Z, Luo Z, et al Single- versus Multiple-tract percutaneous nephrolithotomy in the surgical management of staghorn stones or complex caliceal calculi: A systematic review and metaanalysis Biomed Res Int 2020; 2020:8817070
13 Labadie K, Okhunov Z, Akhavein A, et al Evaluation and Comparison of Urolithiasis Scoring Systems Used in Percutaneous Kidney Stone Surgery J Urol 2015; 193:154-159
14 Kumar U, Tomar V, Yadav SS, et al STONE score versus Guy's Stone Score - prospective comparative evaluation for success rate and complications in percutaneous nephrolithotomy Urol Ann 2018; 10:76-81
Correspondence
Paksi Satyagraha (Corresponding Author) uropas fk@ub ac id
Taufiq Nur Budaya taufiq uro fk@ub ac id
Reza Amorga amorga reza@gmail com
Urology Department, Saiful Anwar General Hospital Malang, Jalan Jaksa Agung Suprapto 2, Klojen, Malang, East Java 65112, Indonesia
Conflict of interest: The authors declare no potential conflict of interest
Archivio Italiano di Urologia e Andrologia 2024; 96(4):13156
P Satyagraha, R Amorga, T Nur Budaya
ORIGINAL PAPER
Analysis of the top-down HoLEP learning curve: A single-center experience of two clinical fellows
Karim Daher 1 , Moustafa Fathy 1, 2 , Amr Hodhod 3 , Parsa Nikoufar 1 , Abdulrahman Alkandari 1 , Loay Abbas 1, 4 , Ruba Abdul Hadi 1 , Hazem Elmansy 1
1 Urology Department, Thunder Bay Regional Health Sciences Centre, Northern Ontario School of Medicine, Thunder Bay, Ontario, Canada;
3 Urology Department, King Abdulaziz Medical City, National Guard Hospitals Affairs, Riyadh, Saudi Arabia;
4 Urology Department, Theodor Bilharz Research Institute, Giza, Egypt
Summary
Introduction: Holmium laser enucleation of the prostate (HoLEP) is known to have a steep learning curve The top-down technique was introduced to lessen the number of procedures required to master HoLEP. We aimed to present the experiences of two successive clinical fellows with the top-down HoLEP learning curve and compare their performance with the supervisor
Methods: We conducted a prospective study of 40 patients who underwent top-down HoLEP performed by two successive fellows at our institution from September 2020 to November 2022
Before data collection, each learner observed three top-down HoLEP procedures and assisted with seven additional cases before independently performing top-down HoLEP under supervision We collected data from each fellow’s first 20 consecutive top-down HoLEP procedures The learners’ cases were grouped according to chronological order (Cases 1-10 and 11-20)
The primary outcome was defined as the number of cases before the fellow could independently complete all steps of top-down HoLEP without any major intraoperative complications.
The secondary outcomes included the intraoperative and postoperative outcomes of both groups The fellows’ 40 cumulative cases were then compared against retrospective data from 148 procedures conducted by their supervisor
Results: There were no significant differences in patient demographics for both clinical fellows Each learner performed the first 20 cases independently without needing the supervisor to intervene. No major intraoperative complications were recorded, and there were no statistically significant differences in intraoperative and postoperative outcomes between fellows’ cases
There was a statistically significant difference between the fellows and their supervisor in terms of operative efficiency and enucleation efficiency (p < 0 001) We did not find a significant difference between the fellows and the supervisor regarding intraoperative complications, major postoperative complications, or postoperative subjective and objective parameters
Conclusions: Top-down HoLEP shows promising and reproducible results in shortening HoLEP’s learning curve Larger comparative and multi-institutional studies are warranted
Holmium laser enucleation of the prostate (HoLEP) is a sizeindependent gold-standard surgical treatment for benign prostatic hyperplasia (BPH) (1, 2) It offers comparable outcomes to open prostatectomy (OP) and transurethral resection of the prostate (TURP), with shorter hospital stays and lower morbidity rates (3, 4) Improvements in longterm outcomes post-HoLEP are durable, with minimal late complications and low reoperation rates (5) Various barriers hinder HoLEP's widespread adoption, as mastering it requires proficiency in endoscopic techniques and presents significant challenges (6-9)
HoLEP's learning curve typically involves 25-50 procedures (10) However, a well-structured mentorship program may reduce the number of cases, allowing for faster proficiency (6, 10) Several studies attempted to determine the threshold of procedures defining the learning phase, considering factors like surgical duration, enucleation efficiency, energy expenditure, prostate-specific antigen (PSA) level reduction, and complication rates (9, 11, 12)
Efforts to address traditional HoLEP's steep learning curve include modifications to simplify the procedure and reduce operative time (13-17) York et al introduced the top-down technique in 2017 Advantages of topdown HoLEP include minimizing the risk of overstretching the sphincter during distal mucosal flap cutting and eliminating the encircling technique (18) Our study aims to enhance understanding of HoLEP's learning trajectory by comparing two successive fellows and their supervisor performing top-down HoLEP We endeavor to provide insights to shape training protocols and advance HoLEP's adoption in urological practice
MATERIALS AND METHODS
Following ethics board approval, we conducted a prospective study of 40 patients who underwent top-down HoLEP performed by two successive clinical fellows at our institution from September 2020 to November 2022
The study also included retrospective data from 148 cases performed by a HoLEP expert (H E ) from October 2017 to September 2020 prior to establishing a clinical fellowship program
Before data collection, each fellow observed three topdown HoLEP cases and assisted with seven (totaling 10 cases) Once the supervisor determined the learner attained a reasonable level of confidence in technical aspects, a prospective study was initiated After 10 procedures, the supervisor ceased actively participating in surgery but remained present to observe and assist if needed
Our study involved the initial 20 consecutive procedures by 2 successive fellows (20 cases/fellow) Fellow 1 operated from September 2020 to June 2021, while Fellow 2 completed procedures from February to November 2022
Participants were divided into Group 1 (patients 1-10) and Group 2 (patients 11-20) We also compared the fellows' 40 cases to their supervisor's 148 cases
The primary outcome was the number of cases needed for the fellow to independently complete all top-down HoLEP steps without major intraoperative complications
Intraoperative safety measures included capsular perforation, bleeding requiring transfusion, and bladder injury during morcellation
Secondary outcomes encompassed intraoperative parameters such as operative efficiency, enucleation efficiency, morcellation time, resected weight, and postoperative results Operative efficiency, defined as the rate of prostate tissue removal during the entire HoLEP procedure (including both enucleation and morcellation phases), was calculated by dividing the total weight of enucleated tissue (grams) by the total operative time (minutes), and expressed as grams per minute (g/min) Similarly, enucleation efficiency measured the rate of tissue removal during the enucleation phase alone, excluding morcellation time
This was calculated by dividing the weight of enucleated tissue (grams) by the enucleation time (minutes), also expressed as grams per minute (g/min)
We utilized a 100-W holmium:YAG laser (VersaPulse PowerSuite™, Lumenis, Yokneam, Israel) Both techniques employed a 550-μm laser fiber and a 28-F continuous flow resectoscope (Karl Storz SE & Co KG, Tuttlingen, Germany) Enucleated tissue was morcellated with a Karl Storz® DrillCut™ morcellator Primary laser settings for enucleation were 2 J and 40 Hz and 2 J and 20 Hz for hemostasis
Study population
The inclusion criteria comprised males aged > 50 years with medically refractory LUTS due to BPH, International Prostate Symptom Score (IPSS) ≥ 15, Quality of Life (QoL) score ≥ 3, and maximum flow rate (Qmax) < 15 mL/sec
Patients were excluded if they had previous surgical BPH treatment, a history of prostate cancer, urethral stenosis, or neurogenic bladder, the inability to withhold anticoagulant or antiplatelet medication, and an active urinary tract infection (UTI)
The preoperative evaluation encompassed patient demographics, a physical examination, and a detailed medical history, including anticoagulant or antiplatelet use, history of urinary retention, and prior prostate procedures
Symptom assessment included IPSS and QoL questionnaires All patients received PSA testing, uroflowmetry, a post-void residual (PVR) bladder scan, and transrectal ultrasound (TRUS) for prostate volume estimation
Patients were advised that if medically feasible, they should
temporarily withold their anticoagulant and antiplatelet medications before surgery for 3 days and 7 days, respectively Intraoperative parameters, postoperative outcomes, and readmission data were recorded Data on surgical parameters such as enucleation time, morcellation time, operative and enucleation efficiencies, resected weight, intraoperative complications, and the need for blood transfusion were collected Early postoperative complications with emergency room (ER) visits and a failed trial of void (TOV) were also recorded
Surgical technique
All HoLEP procedures were performed using the topdown technique as previously described (19) Briefly, the distinction between the traditional and top-down HoLEP techniques lies in the direction and approach of enucleation In both traditional and top-down HoLEP, a single incision is made at the 6 o ’clock position of the bladder neck for a bilobar prostate configuration With a trilobar configuration, the bladder neck incision is made at either 5 or 7 o ’clock to establish the capsular plane The lateral lobes are then enucleated using a two-lobe approach, where one lateral lobe is followed by the combined enucleation of the other lateral lobe and the median lobe In traditional HoLEP, dissection follows a bottom-up approach For the top-down technique, the anterior commissure mucosa is then incised using 2 J/20 Hz, starting from the bladder neck at 12 o ’clock The incision is deepened to separate the area between the right and left adenoma until the surgical capsule is reached Once the plane between the adenoma and the surgical capsule is established, a top-down lateral lobe dissection is performed and extended anteroposteriorly towards the apical adenoma at 6 o ’clock The enucleated tissue is then morcellated using a Karl Storz DrillCut™ (Germany) morcellator
Postoperative care
A 3-way catheter (22 F, with 75 mL of sterile water in the balloon) was inserted postoperatively for all patients They were kept on continuous bladder irrigation (CBI) with an overnight admission, followed by a trial of void (TOV) within 24 hours
Follow-up
Patients were followed up at 1, 3, and 6 months, and PSA testing was performed at 3 months Postoperative complications included persistent hematuria, clot retention, urethral strictures, and bladder neck contraction Stress urinary incontinence (SUI) was assessed by a history of involuntary urine leakage during coughing or sneezing and the use of pads to prevent wetting Additionally, SUI was evaluated by directing the patient to cough with a full bladder and observing urine passage
Statistical analyses
Data collection and statistical analysis were performed using the Statistical Package for the Social Sciences (SPSS® IBM®) version 26 Categorical variables were reported as numbers and percentages and analyzed using the Chi-squared test, while continuous data were presented as medians and ranges and evaluated using the Mann-Whitney U test A pvalue of < 0 05 was considered statistically significant
K Daher, M Fathy, A Hodhod, et al
Table 1A
Comparison of patient demographics, perioperative and early postoperative outcomes between the fellows’ 20 cases
RESULTS
No significant differences in demographics and preoperative data were observed between the early and later cases for both fellows Similarly, when comparing the 20 cases of Fellow 1 and Fellow 2, no differences were observed in patient demographics, perioperative, or early postoperative outcomes (Table 1A)
Operative and postoperative outcomes
Operative efficiency, enucleation time, and enucleation efficiency were not significantly different between the initial and subsequent 10 cases for both fellows Fellow 1's median enucleation efficiency was 0 94 g/min for initial cases and 1 12 g/min for subsequent cases (p = 0 739) The second fellow's median enucleation efficiency was 1 11 g/min for the first 10 cases and 0 85 g/min for subsequent procedures (p = 0 436) When comparing the two fellows, there were no significant differences in operative efficiency, enucleation time, or enucleation efficiency Fellow 1's median enucleation efficiency was 1 02 g/min, compared to Fellow 2's median of 1 07 g/min (p = 0 947)
LUTS: Lower urinary tract symptoms; ASA: American Society of Anesthes o ogists; TRUS: Transrectal u trasound; IPSS: Internationa Prostate Symptom Score; QoL: qual ty of ife; Qmax: Maximum urinary flow rate; PVR: Post-vo d res dual urine test; TOV: Tria of void; PSA: Prostate-specif c ant gen
No intraoperative complications or need for blood transfusion were recorded in either group Successful first TOV, as well as readmission and retreatment rates, were similar across both fellows' cases None of the patients in either group experienced Clavien II-V complications However, one participant from each fellow's cohort had a failed TOV (Clavien I), both of whom passed their TOV within one week Five incidents of prolonged or severe hematuria requiring ER visits were recorded (2 for Fellow 1 and 3 for Fellow 2), all of which were managed conservatively with Foley catheter reinsertion and CBI (Clavien I); three patients were readmitted None of the patients experienced any cardiovascular events or UTIs
No significant differences in prostate weight or PSA reduction percentages were observed between both learners (Table 1A) Additionally, postoperative outcomes at 1, 3, and 6 months showed no significant differences between the two fellows SUI rates were low and comparable across all groups (Table 1B) Tables 1A and 1B demonstrate that both learners had comparable perioperative and postoperative outcomes for all 20 procedures, with no statistically significant differences
Comparison with supervisor's performance
Table 2 compares clinical outcomes between cases managed by the fellows and their supervisor Regarding operative efficiency, the supervisor demonstrated a median of
Table 1B
Comparison of postoperative outcomes between the fellows’ 20 cases at 1, 3 and 6 months
Parameters Fellow 1 Fellow 2 P 20 Cases 20 Cases
1 month postoperative
IPSSmedian(range)85(1-24)8(2-18)0988
QoLmedian(range)25(0-6)2(0-5)0696
Qmax mL/smedian(range)23(11-50)17(6-40)031
PVRmLmedian(range)44(0-390)47(0-160)0897
SUIn(%)3(15)3(15)05
3 months postoperative
IPSSmedian(range)75(0-24)55(1-23)0347
QoLmedian(range)25(0-5)1(0-5)0081
Qmax mL/smedian(range)20(11-34)21(13-45)072
PVRmLmedian(range)40(0-130)63(0-150)0281
SUIn(%)1(5)2(10)05
6 months postoperative
IPSSmedian(range)6(2-16)5(1-10)0126
QoLmedian(range)2(0-4)1(0-3)0111
Qmax mL/smedian(range)20(8-39)22(15-41)0532
PVRmLmedian(range)49(0-130)24(0-110)0.48
SUIn(%)00-
IPSS: Internat onal Prostate Symptom Score; QoL: qual ty of ife; Qmax: Maximum urinary flow rate; PVR: Post-void res dua ur ne test; TOV: Tria of void; SUI: Stress urinary incontinence
LUTS: Lower urinary tract symptoms; ASA: Amer can Society of Anesthesiolog sts; TRUS: Transrecta ultrasound; IPSS: International Prostate Symptom Score; QoL: quality of l fe; Qmax: Max mum ur nary flow rate; PVR: Post-void residua ur ne test; TOV: Trial of void; PSA: Prostate-specific antigen; SUI: Stress ur nary ncont nence
1 41 g/min, exceeding the fellows' 0 83 g/min, p < 0 001
Figure 1 illustrates the differences in enucleation efficiency between the two fellows and their supervisor
Two patients in the supervisor's cohort experienced intraoperative superficial bladder mucosal injury during morcellation
Table 2
Comparison of patient demographics, perioperative and postoperative outcomes between the fellows’ and supervisor’s cases
Postoperative outcomes, including successful first TOV, did not show statistical significance Clavien I complications were lower in the supervisor's cohort (9 5%) compared to the learners' group (17 5%), p = 0 001 Conversely, two cases of prolonged or severe hematuria were recorded in the supervisor's group, with one occurring after the patient resumed antiplatelet therapy and was managed conservatively In the first postoperative month, SUI occurred in 15% of the fellows' cases, significantly higher than the 6 1% observed in the supervisor's group, p = 0 030 At three months follow-up, SUI was present in 7 5% of the fellows' cases compared to 2 7% in the supervisor's cases One patient (0 7%) from the supervisor's cohort had SUI at 6 months postoperative, while no cases of SUI were reported in the fellows' group
DISCUSSION
Although the term “learning curve ” lacks a standardized definition, it's often described as the number of cases required to accomplish procedures efficiently, with acceptable complication rates and fair health outcomes (20)
Our study sought to assess whether the topdown technique could decrease HoLEP's learning curve by comparing the performance and outcomes of two fellows with their experienced supervisor To our knowledge, this is the first comparative study assessing procedural efficacy, safety profiles, and learning curves of top-down HoLEP in a supervised training environment
Both fellows had prior experience with TURP Each learner observed 3 cases while receiving practical instructions The fellows progressively assisted and performed parts of surgery under supervision (7 cases/fellow), leading to eventual independent performance This teaching approach is comparable to El-Hakim and Elhilali (21), where a urology resident observed 10 HoLEP procedures performed by an experienced supervisor Afterwards, the resident operated on 27 patients, divided into two groups (15 and 12 participants), with minimal to moderate mentor intervention The greater number of observed cases reported by El-Hakim and Elhilali (21) compared to our study (10 vs 3, respectively) underscores the "easierto-grasp" characteristic of the top-down technique over traditional HoLEP Similar to our study, the performance and outcomes of both initial and subsequent cases exhib-
Comparison of median enucleation efficiency between the fellows and their supervisor.
ited no significant differences, indicating consistency and rapid mastery of the procedural skill set
Conversely, Seki et al suggested that HoLEP could be learned without a qualified instructor, but achieving competence typically required > 50 cases of operational experience (22) The higher number of cases to achieve competency compared to our study confirms that the topdown approach, combined with structured training, may ease and shorten the HoLEP learning curve for novices
Despite training at different intervals, the fellows exhibited no significant differences in cumulative case experiences, affirming the efficacy and consistency of our teaching approach Kim et al demonstrated the reproducibility of conventional HoLEP by assessing the procedure at two hospitals on different continents (23)
Prostate volume is considered pivotal in the early learning phase Shah and colleagues reported that operators achieved proficiency in HoLEP after a mean of 20 cases, but only for small prostates (8) Further learning was required to advance from small to intermediate glands and larger prostates
This observation was supported by a larger retrospective study involving 1,113 patients and 39 surgeons (24), which also corroborated the findings of Moody et al (25)
The latter study suggested completing at least 30 procedures on smaller glands (< 50 g) before attempting to enucleate larger adenomas with standard HoLEP The mean prostate volume of patients operated on by both fellows in our study exceeded 90 cc, surpassing the average volumes reported in various publications assessing the HoLEP learning curve for inexperienced surgeons or trainees From our observations, attempting to enucleate glands < 50 g would be challenging and not advisable for novice HoLEP learners
Our findings indicate no significant differences in operative efficiency, enucleation time, or enucleation efficiency between both fellows’ initial and subsequent cases These findings contrast with Seki et al.'s data, which demonstrated a significant increase in enucleation efficiency with growing experience when comparing initial to last standard HoLEP cases (22) They reported that the average tissue enucleation efficiency significantly increased from 0 29 g/min to 0 75 g/min between the initial and final 10 cases, respectively
Moreover, Placer et al. studied 125 patients and found that enucleation efficiency increased with the number of procedures, eventually reaching a plateau (9) These results indicate potential differences in operative efficiency improvement patterns between conventional and top-down HoLEP with increasing experience, suggesting that standard HoLEP may show more improvement with additional cases Consistent performance across early and later cases in our study extends to postoperative outcomes Our results align with those of Seki et al , who found no change in postoperative parameters (22)
Comparative analysis of performance with supervisor
Comparative analysis of both fellows to their supervisor when performing the top-down technique revealed valuable insights, particularly concerning surgical efficiency and postoperative outcomes Regarding enucleation efficiency, an objective parameter for gauging operative learning, the fellows had a median of 1 06 g/min, lower than their supervisor's median of 1 6 g/min These findings emphasize the importance of progressive experience for enhancing operative efficiency in HoLEP, regardless of the technique utilized Despite using a similar approach to condensing the learning process into a short, supervised
FIgure 1.
period, El-Hakim and Elhilali found that resident-performed cases yielded outcomes comparable to those of an experienced urologist, possibly due to increased supervisor intervention in the initial cases of their study (21)
Although we noted differences in operative performance, early postoperative outcomes such as successful TOV were similar between the learners and their supervisor Similarly, no significant differences were observed in postoperative parameters, including IPSS, QoL, Qmax, and PVR These findings align with data from Shah et al (8) and Shigemura and colleagues (24), which showed no change or improvement in these parameters with increasing surgical experience
In the initial 4 weeks post-HoLEP, transient SUI can significantly bother patients Predictors of transient SUI following HoLEP are multifaceted and can be associated with either the patient or the procedure, as reported by several studies (12, 13, 26-29)
One purported benefit of top-down HoLEP is reducing sphincter overstretching by cutting the mucosal flap attached to it, potentially reducing transient SUI
However, our recent randomized controlled trial comparing top-down and traditional HoLEP demonstrated that at 3 months postoperative, two patients (4 1%) in the conventional and one (2 2%) in the top-down HoLEP group experienced SUI without significant difference (30)
In our analysis, SUI rates one month postoperatively were higher in the fellows' cumulative cases (15%) compared to the supervisor's (6 1%), p = 0 030 However, no differences were observed at the three-month follow-up
The high SUI rate initially among the fellows' group may be attributed to challenges of the early learning curve, as noted by Placer et al (9) However, these early findings may not fully demonstrate the impact of experience on incontinence rates, as transient SUI is typical in the early postoperative phase The comparable SUI rates at 3 months indicate that with 20 cases, the fellows attained an early proficiency level, yielding low SUI rates similar to experienced surgeons
Numerous studies have demonstrated that achieving low SUI rates requires an initial experience of 20 cases Shigemura et al (24) reported that surgeons' experience beyond 20 procedures significantly reduced SUI at three months Elshal et al 's prospective study also noted a significant decrease in SUI rates after 20 procedures (12)
Limitations
We acknowledge certain limitations of our research; it is a single-center study with a small sample size, which may restrict the generalizability of our findings Additionally, the study involved retrospective data for the supervisor, which may introduce bias and confounding variables However, it involved prospective data collection for both fellows Larger prospective studies are needed to effectively validate findings and compare traditional versus top-down HoLEP techniques
CONCLUSIONS
Our findings suggest that implementing the top-down HoLEP technique in a supervised educational program ensures safety and comparable outcomes to experienced
supervisors, regardless of trainees' familiarity with conventional HoLEP This approach accelerates learning and demonstrates potential in urological training Further research is needed to validate its efficacy and safety across diverse clinical settings
ACKNOWLEDGMENT
We would like to thank Dr Walid Shahrour and Dr Husain Alaradi for their valuable advice
REFERENCES
1 Elzayat EA, Habib EI, Elhilali MM Holmium laser enucleation of the prostate: a size-independent new "gold standard" Urology 2005; 66(5 Suppl):108-13
2 van Rij S, Gilling PJ In 2013, holmium laser enucleation of the prostate (HoLEP) may be the new 'gold standard' Curr Urol Rep 2012; 13:427-32
3 Yin L, Teng J, Huang CJ, et al Holmium laser enucleation of the prostate versus transurethral resection of the prostate: a systematic review and meta-analysis of randomized controlled trials J Endourol 2013; 27:604-11
4 Naspro R, Suardi N, Salonia A, et al Holmium laser enucleation of the prostate versus open prostatectomy for prostates >70 g: 24month follow-up Eur Urol 2006; 50:563-8
5 Ibrahim A, Alharbi M, Elhilali MM, et al 18 Years of Holmium Laser Enucleation of the Prostate: A Single Center Experience J Urol 2019; 202:795-800
6 Robert G, Cornu JN, Fourmarier M, et al Multicentre prospective evaluation of the learning curve of holmium laser enucleation of the prostate (HoLEP) BJU Int 2016; 117:495-9
7 Brunckhorst O, Ahmed K, Nehikhare O, et al Evaluation of the Learning Curve for Holmium Laser Enucleation of the Prostate Using Multiple Outcome Measures Urology 2015; 86:824-9
8 Shah HN, Mahajan AP, Sodha HS, et al Prospective evaluation of the learning curve for holmium laser enucleation of the prostate J Urol 2007; 177:1468-74
9 Placer J, Gelabert-Mas A, Vallmanya F, et al Holmium laser enucleation of prostate: outcome and complications of self-taught learning curve Urology 2009; 73:1042-8
10 Kampantais S, Dimopoulos P, Tasleem A, et al Assessing the learning curve of holmium laser enucleation of prostate (HoLEP): A systematic review Urology 2018; 120:9-22
11 Kim KH, Kim KT, Oh JK, et al Enucleated weight/enucleation time, is it appropriate for estimating enucleation skills for holmium laser enucleation of the prostate? A consideration of energy consumption World J Mens Health 2018; 36:79
12 Elshal AM, Nabeeh H, Eldemerdash Y, et al Prospective assessment of learning curve of holmium laser enucleation of the prostate for treatment of benign prostatic hyperplasia using a multidimensional approach J Urol 2017; 197:1099-107
13 Endo F, Shiga Y, Minagawa S, et al Anteroposterior dissection HoLEP: a modification to prevent transient stress urinary incontinence Urology 2010; 76:1451-1455
14 Minagawa S, Okada S, Sakamoto H, et al En-bloc technique with anteroposterior dissection holmium laser enucleation of the prostate allows a short operative time and acceptable outcomes Urology 2015; 86:628-633
K Daher, M Fathy, A Hodhod, et al
15 Gong YG, He DL, Wang MZ, et al Holmium laser enucleation of the prostate: a modified enucleation technique and initial results J Urol 2012; 187:1336-1340
16 Rivera ME, Lingeman JE, Krambeck AE Holmium laser enucleation of the prostate J Endourol 2018; 32(Suppl 1):S7-9
17 Press B, Ghiraldi E, Kim DD, et al "En-Bloc" enucleation with early apical release compared to standard holmium laser enucleation of the prostate: A retrospective pilot study during the initial learning curve of a single surgeon Urology 2022; 165:275-9
18 York NE, Dauw CA, Borofsky MS, et al V5-08 “TopDown” holmium laser enucleation of the prostate (Holep) technique J Urol 2017; 197:e601
19 Hodhod A, Oquendo F, Tablowski T, et al 'Top-Down' holmium laser enucleation of the prostate Report of initial cases performed by a single surgeon Arab J Urol 2020; 19:130-6
20 Herrell SD, Smith JA, Jr Robotic-assisted laparoscopic prostatectomy: what is the learning curve? Urology 2005; 66(5 Suppl):105-7
21 El-Hakim A, Elhilali MM Holmium laser enucleation of the prostate can be taught: the first learning experience BJU Int 2002; 90:863-9
22 Seki N, Mochida O, Kinukawa N, et al Holmium laser enucleation for prostatic adenoma: analysis of learning curve over the course of 70 consecutive cases J Urol 2003; 170:1847-50
23 Kim SC, Matlaga BR, Kuo RL, et al Holmium laser enucleation
of the prostate: a comparison of efficiency measures at two institutions J Endourol 2005; 19:555-8
24 Shigemura K, Yamamichi F, Kitagawa K, et al Does surgeon experience affect operative time, adverse events and continence outcomes in holmium laser enucleation of the prostate? A Review of More Than 1,000 Cases J Urol 2017; 198:663-70
25 Moody JA, Lingeman JE Holmium laser enucleation for prostate adenoma greater than 100 gm : comparison to open prostatectomy J Urol 2001; 165:459-62
26 Tunc L, Yalcin S, Kaya E, et al The "Omega Sign": a novel HoLEP technique that improves continence outcomes after enucleation World J Urol 2021; 39:135-41
27 Lerner LB, Tyson MD, Mendoza PJ Stress incontinence during the learning curve of holmium laser enucleation of the prostate J Endourol 2010; 24:1655-8
28 Cornwell LB, Smith GE, Paonessa JE Predictors of Postoperative Urinary Incontinence After Holmium Laser Enucleation of the Prostate: 12 Months Follow-Up Urology 2019; 124:213-7
29 Elmansy HM, Kotb A, Elhilali MM Is there a way to predict stress urinary incontinence after holmium laser enucleation of the prostate? J Urol 2011; 186:1977-81
30 Elmansy H, Abbas L, Fathy M, et al Top-down holmium laser enucleation of the prostate (HoLEP) versus traditional HoLEP for the treatment of benign prostatic hyperplasia (BPH): 1-year outcomes of a randomized controlled trial Prostate Cancer Prostatic Dis 2024; 27:462-8
Correspondence
Karim Daher
Karim daher01@lau edu
Moustafa Fathy moustafa mf9@gmail com
Parsa Nikoufar
parsa nikoofar@gmail com
Abdulrahman Alkandari dr aaa 186@gmail com
Loay Abbas loay46@gmail com
Ruba Abdul Hadi ruba ahadi@gmail com
Urology Department, Thunder Bay Regional Health Sciences Centre, Northern Ontario School of Medicine, Thunder Bay, Ontario, Canada
Amr Hodhod amrwuk@yahoo co uk
Urology Department, King Abdulaziz Medical City, National Guard Hospitals Affairs, Riyadh, Saudi Arabia
Hazem Elmansy, MD, MSc, FRCSC (Corresponding Author) hazem mansy@rocketmail com
Associate Professor & Program Director of the Minimally Invasive Urologic Surgery Fellowship Program, Thunder Bay Regional Health Sciences Centre, Northern Ontario School of Medicine, Thunder Bay, Ontario, Canada
146 Court Street South, Thunder Bay, ON, P7B 2X6
Conflict of interest: H Elmansy is an Investigator for Urotronic Inc (Laborie) and Zenflow Inc He previously received honoraria and a research grant from Boston Scientific
The other co-authors do not have a conflict of interest to disclose
ORIGINAL PAPER
Altieri modified Nesbit corporoplasty for the treatment of
penile curvature: Comparison of local anesthesia vs loco-regional anesthesia on the clinical outcomes
Vincenzo Maria Altieri 1, 2 , Pietro Saldutto 2 , Vittore Verratti 3 , Roberto La Rocca 4 , Ernesto Di Mauro 4 , Giuseppe Celentano 4 , Marco Capece 4 , Vincenzo Morgera 4 , Gianluigi Cacace 4 , Walter Vena 2 , Francesco Mastrangelo 4 , Luigi Napolitano4, Fabrizio Iacono 1
1 Department of Medicine and Health Sciences "V Tiberio", University of Molise, Campobasso, Italy;
2 Department of Urology, Humanitas Gavazzeni, Bergamo, Italy;
3 Department of Psychological, Health and Territorial Sciences, University "G D'Annunzio" Chieti-Pescara, Chieti, Italy;
4 Unit of Urology, Department of Neurosciences, Reproductive Sciences, and Odontostomatology University of Naples “Federico II”, Naples, Italy
Summary
Objective: To compare the safety profile and clinical outcomes of Altieri-modified Nesbit corporoplasty using two different anesthesia methods including spinal anesthesia and local anesthesia
Materials and methods: A total of 40 patients with congenital penile curvature (CPC) and Peyronie’s disease (PD) underwent Altieri-modified Nesbit corporoplasty. Group 1 (n = 20) received spinal anesthesia, and Group 2 (n = 20) received local anesthesia. The patients were categorized into age groups (< 30 years, 31-45 years, 46-60 years, and 61-75 years) for analysis
Clinical outcomes, post-operative complications, hospital stay, pain levels, and other parameters were assessed
Results: The results showed that 2 patients (10%) reported postoperative complications, including headache, arterial hypotension, and penile foreskin necrosis from the spinal anesthesia group Whereas, in the local anesthesia group, 1 patient (5%) reported scar phimosis. Further, post-operative pain was predominantly very mild, with 16 patients (80%) in the spinal anesthesia group and 14 patients (70%) in the local anesthesia group experiencing minimal discomfort Age did not significantly impact hospital stay, post-operative intestinal disorders, constipation, lower urinary tract symptoms, voiding burning, or dysuria
Conclusions: Spinal anesthesia may lead to more post-operative complications and longer hospital stays compared to local anesthesia Age does not significantly affect most clinical outcomes but can influence post-operative pain in patients receiving local anesthesia.
Congenital penile curvature (CPC) is a rare condition with an incidence of less than 1% (1) Peyronie’s disease (PD) is a fibrotic disorder of the tunica albuginea of the penis characterized by the presence of fibrotic plaques often leading to penile deformity, with or without concomitant
pain Men with PD are most commonly present in their sixth decade of life, with a mean age of 52-57 years old (2-5) PD impacts sexual function and is also associated with psychosocial distress in patients and their partners Once thought to be rare, PD now has a reported prevalence of up to 20 3% in adult men (6) whose conservative treatment is usually successful during the active phase (7) Treatment of PD utilizes both medical and surgical approaches and includes a diverse group of systemic and locally administered drugs Approaches to PD have included observation, small molecule and biologic drugs a d m i n i s t e r e d o r a l l y , t o p i c a l l y , a n d i n t r a l e s i o n a l l y , mechanical therapies, and surgery Counseling and observation alone may be appropriate for patients with minimal curvature that does not impede sexual intercourse and with no erectile dysfunction (ED) (8); other patients will elect to proceed with treatment If the curve in the penis continues during the stable phase and plaques are completely stabilized, surgery is generally the best treatment, mainly if there are problems with having sexual intercourse (9) Orally treatments with vitamin E, potassium para-aminobenzoate and tamoxifen have been used in the initial phase with low success rates (10) Penile shortening procedures are used when the curvature is less severe and include the Nesbit wedge resection and the plication techniques performed on the convex unaffected side of the penis Penile lengthening procedures are performed on the concave side of the penis and require the use of a graft (11-14) Altieri modified Nesbit corporoplasty avoids intraoperative use of tourniquet without risk of bleeding, to reduce penile ischemic anatomical and functional damages such as long-term erectile dysfunction (15)
Surgical procedures can be performed under local block anesthesia, general, or regional anesthesia
The choice of anesthetic technique has a major impact on how the patient responds during the postoperative period Local anesthesia is cheaper, avoids the hazards of general or spinal anesthesia, and may be the only option in patients in whom general/spinal anesthesia is deemed too
r i s k y R e g i o n a l a n e s t h e s i a h a s b e e n i n c r e a s i n g l y employed in the outpatient setting, given its unique characteristics of selectivity and efficacy in the control of acute postoperative pain Outpatient regional anesthesia economic externalities have been investigated by some studies, which have associated its systematic adoption with a decrease in anesthesia-controlled operating room time and thus in the operating room fixed costs, potentially translating into a significant increase in patient turnover and ultimately hospital revenues (16, 17) However, some patients may not get complete pain relief from local block anesthesia Spinal anesthesia has been shown to decrease postoperative pain after inguinal herniorrhaphy when compared with general anesthesia; local anesthesia has been shown to reduce hospital time, lower the cost of treatment, and has no or fewer side effects compared with spinal and general anesthesia (19, 20) Little information is available on the use of local anesthesia and loco-regional anesthesia on the clinical outcomes of Peyronie’s disease and congenital penile curvature Therefore, present study, was to compare the safety profile and the outcomes of spinal and local anesthesia for surgical treatment of Peyronie’s disease and congenital penile curvature
METHODS
Study design
The present study compared the clinical outcomes of two groups of patients undergoing Altieri-modified Nesbit corporoplasty for the treatment of penile curvature using local vs loco-regional anesthesia Group 1 consists of 20 patients with an age ranging from 17 to 71 years who underwent surgery under spinal anesthesia between January 2010 and March 2019 While Group 2 consists of 20 patients with an age range from 18 to 68 years who underwent surgery under local anesthesia between January 2010 and March 2019 The comparison of patients’ clinical outcomes was also studied based on different age groups (< 30 years, 3145 years, 46-60 years, 61-75 years) and with respect to local vs loco-regional anesthesia All patients underwent surgery using the same adapted Nesbit method and had a year-long following evaluation A short-term post-operative assessment was performed every week to look for any early complications until the incision had fully healed
Inclusion and exclusion criteria
In this research, patients with Peyronie's disease and congenital penile curvature were included Patients who didn't improve after taking their medications were treated with prosthesis insertion and were left out of the research Another criteria for exclusion was the existence of complex penile curvatures (PC) in patients, which required elongation operations involving plaque incision and bovine pericardial grafting to fill the albugineal defect Additionally, patients with follow-ups of less than 12 months were excluded from the study
Ethical approval
The "G D'Annunzio" University of Chieti and Pescara (01/26-01-2017) and the Ethics Committee for Biomedical Research of the districts of Chieti and Pescara authorized the
research, which was carried out in line with the Declaration of Helsinki (revised in 2013) All patients provided documented, fully informed consent
Clinical outcomes
Following a year of monitoring, a thorough physical examination was conducted among both the treatment groups, including assessments of the degree of full straightness, remaining curvature (> 15°), penile shortening, and a visible suture knot Additionally, patient happiness, erectile performance as measured by the IIEF-5, and penile Doppler ultrasonography were also assessed
We used five questions to gauge patient happiness, asking respondents to indicate their degree of satisfaction on a scale from "very dissatisfied" to "very satisfied"(21) Clinical outcome was evaluated by the change in ED and penile vibratory stimulation (PVS) along with the severity at the baseline and the end of the study The comparison of clinical outcomes among local vs loco-regional anesthesia groups was done through post-operative complications, along with hospital stay, post-operative pain, constipation, intestinal disorders, bladder catheterization, lower urinary tract symptoms, voiding burning and dysuria
Statistical analysis
The clinical outcomes for both groups were analyzed considering p ≤ 0 05 as statistical significance and analyzing the results with the SPSS software (Version 25 0, SPSS Inc , Chicago, IL, USA)
RESULTS
The evaluation of patients undergoing Altieri-modified Nesbit corporoplasty for the treatment of penile curvature in spinal anesthesia and local anesthesia groups showed that 2 patients who were given spinal anesthesia and 4 patients who were given local anesthesia were in a group with less than 30 years of age Three patients for each type of anesthesia were found in the age group of 31-45 years In the age group 46-60 years, six and seven patients were given spinal and local anesthesia respectively In the age group 61-75 years, nine and six patients were given spinal and local anesthesia respectively Data are presented in Figure 1
Age distribution of patients with penile curvature in spinal anesthesia and local anesthesia groups,
V M Altieri, P Saldutto, V Verratti, et al
Figure 1.
Figure 2.
The satisfaction rate of patients with penile curvature in spinal anesthesia and local anesthesia groups
*Satisfaction was self-assessed by patients using a 5-point rating scale, with a score of 1 indicating very dissatisfied and 5 indicating very satisfied
Two of the patients in the spinal anesthesia group reported post-operative complications, one had headache and arterial hypotension while the second had penile foreskin necrosis Only one patient in the local anesthesia group reported scar phimosis as post-operative complication
The results showed only one patient from each group was somewhat dissatisfied with the procedure, while 2 from the spinal anesthesia group and 5 from the local anesthesia group were neither satisfied nor dissatisfied On the other hand, 17 from the spinal anesthesia group and 14 from the local anesthesia group were somewhat satisfied with the procedure as presented in the Figure 2 However, Pearson chi-square showed a non-significant difference (p = 0 455) among the treatment groups
The results also showed that one patient from the local anaesthesia group and two patients from spinal anaesthesia group showed noticeable and distracting pain, while, 2 from the spinal anesthesia group and 5 from the local anesthesia group showed minor pain On the other hand, 16 from the spinal anesthesia group and 14 from the local anesthesia group were having very mild pai as presented in Figure 3 However, Pearson chi-square showed a nonsignificant difference (p = 0 416) among the treatment groups
Other clinical outcomes were not significantly different between spinal and local anesthesia groups, including penile shortening, post-operative intestinal disorders, post-
Figure 3
Post-operative pain among patients with penile curvature in spinal anesthesia and local anesthesia groups.
operative constipation, post-operative lower urinary tract symptoms, voiding burning, and dysuria Hospital stay and post-operative bladder catheterization showed significant differences between spinal anesthesia and local anesthesia groups as shown in Table 1 There was a non-significant difference (p = 0 964) in penile shortening when spinal and local anesthesia groups were compared There was no shortening in 35% and 30% of the patients given local anesthesia and spinal anesthesia, respectively Only 5% of the patients from each group showed 0 5 cm shortening in penile length In the spinal anesthesia group, 30%, 20%, and 15% of patients showed penile shortening of 1 0, 1 5, and 2 0 cm, respectively Similarly, 20%, 25%, and 15% of patients in the local anesthesia group showed penile shortening of 1 0, 1 5, and 2 0 cm, respectively (Table 1) There was a significant difference (p = 0 000) in length of hospital stay when comparing spinal and local anesthesia groups, as 100% of the patients had to stay in the hospital after the procedure in the spinal anesthesia group while none after the procedure in local anesthesia group (Table 1)
The chi-square test showed non-significant difference (p = 0 147) in post-operative intestinal disorders and post-operative constipation when comparing patients in spinal and local anesthesia groups Only 10% of the patients who showed post-operative intestinal disorders and post-operative constipation were given spinal anes-
Table 1.
Clinical outcomes among patients with congenital penile curvature in spinal anesthesia and local anesthesia groups
Penileshortening(cm)0964
006(30%)7(35%)
051(5%)1(5%)
106(30%)4(20%)
154(20%)5(25%)
203(15%)3(15%)
HospitalStay0000
Yes20(100%)0(0%)
No0(0%)20(100%)
Post-operativeintestinaldisorders0147
Yes2(10%)0(0%)
No18(90%)20(100%)
Post-operativeconstipation0147
Yes2(10%)0(0%)
No18(90%)20(100%)
Post-operativebladdercatheterization0000
Yes20(100%)0(0%) No0(0%)20(100%)
Post-operativelowerurinarytractsymptoms0147
Yes2(10%)0(0%) No18(90%)20(100%)
Voidingburning0311
Yes1(5%)0(0%)
No19(95%)20(100%)
Dysuria0311
Yes1(5%)0(0%)
No19(95%)20(100%)
** Pearson Ch -Square
thesia while none of the patients showed any intestinal disorder from local anesthesia group (Table 1)
There was a significant difference (p = 0 000) in postoperative bladder catheterization rate when comparing spinal and local anesthesia groups, as 100% of the patients had post-operative bladder catheterization in the spinal anesthesia group while none of the patients had it in local anesthesia group (Table 1)
The results showed non-significant difference (p = 0 147) in post-operative lower urinary tract symptoms when comparing patients in spinal and local anesthesia groups Only 10% of the patients in the spinal anesthesia group showed post-operative lower urinary tract symptoms while none of the patients showed post-operative lower urinary tract symptoms in the local anesthesia group (Table 1)
The results showed also non-significant difference (p = 0 311) in burning at voiding and dysuria when comparing patients in spinal and local anesthesia groups Only 5% of the patients in the spinal anesthesia group showed burning at voiding and dysuria while none of the patients showed such symptoms in the local anesthesia group (Table 1)
The age group comparison of the length of hospital stay showed that among patients of spinal anaesthesia group having age less than 30 only two had to stay in hospital while in age group 31-45 years, three patients had a hospital stay In group 46-60 years, six patients have hospital stay while, in group 61-75 years, nine patients have a hospital stay On the other hand, none of the patients from local anaesthesia group stay in the hospital There was a non-significant difference (p = 0 719) among age groups for hospital stay as shown in Table 2
In the age group less than 30 years given spinal anaesthesia, only 2 patients had very mild post-operative pain, whereas, in group 31-45 years, three patients had very mild pain Similarly, in age group 46-60 years, four patients had very mild pain, one had minor, and one had noticeable and distracting pain In group 61-75 years, seven patients had very mild pain, one had minor pain, and one had noticeable and distracting pain There was non-significant (p = 0 925) difference among the age groups On the other hand, among age group less than 30 years given local anaesthesia, four patients had very mild pain and in age group 31-45 years, three patients had minor pain In age group 46-60 years, six patients had very mild pain and one had minor pain In age group 61-
Table 2.
Pearson Chi-Square test for the relation of age groups with anaesthesia types and hospital stay
Anesthesia
S
31-45years03
46-60years06 61-75years09
Localanesthesia<30years40
31-45years30
46-60years70
61-75years60
Table 3.
Pearson Chi-Square test for the relation of age groups with anaesthesia types and post-operative pain
Anesthesia type Age group Post-operative pain Pearson Very mild Minor Noticeable Chi-Square and distracting
Spinalanesthesia<30years2000.925
31-45years300
46-60years411
61-75years711
Localanesthesia<30years4000037
31-45years030
46-60years610
61-75years411
75 years, four patients had very mild pain, one patient had minor pain and one had noticeable and distracting pain There was a significant difference (p = 0 037) among age groups given local anaesthesia for post-operative pain (Table 3)
The results of age group comparison for the post-operative intestinal disorder in patients given spinal anaesthesia showed that there were only two patients in age group 61-75 years had post-operative intestinal disorder None of the patients in other age groups have such disorder On the other hand, there was no patients having post-operative intestinal disorder in local anaesthesia group The Pearson chi-square test showed a non-significant (p = 0 438) difference for post-operative intestinal disorder by type of anaesthesia and age (Table 4)
Table 4.
Pearson Chi-Square test for the relation of age groups with anesthesia types and post-operative intestinal disorder
Anesthesia type Age group Post-operative intestinal disorder Pearson No Yes Chi-Square
Spinalanesthesia<30years20
31-45years30
46-60years60
61-75years72
Localanesthesia<30years40
31-45years30
46-60years70
61-75years60
The results of age group comparison for the post-operative constipation in patients given spinal anaesthesia showed that there were only two patients in age group 61-75 years who were having post-operative constipation however, none of the patients in other age group have such disorder On the other hand, there was no patients having post-operative constipation in local anaesthesia group The Pearson Chi-Square test showed a non-significant (p = 0 438) difference among anaesthesia, age groups and post-operative intestinal disorder (Table 5)
The results of age group comparison for post-operative bladder catheterization rate in patients given spinal anaesthesia showed that 2, 3, 6 and 9 patients in age groups < 30 years, 31-45 years, 46-60 years and 61-75
V M Altieri, P Saldutto, V Verratti, et al
Table 5.
Pearson Chi-Square test for the relation of age groups with anesthesia types and post-operative constipation
Anesthesia type Age group Post-operative constipation Pearson No Yes Chi-Square
Spinalanesthesia<30years200438
31-45years30
46-60years60
61-75years72
Localanesthesia<30years40
31-45years30
46-60years70
61-75years60
years respectively, had post-operative bladder catheterization None of the patients in the local anaesthesia group have post-operative bladder catheterization There was non-significant (p = 0 719) difference for post-operative bladder catheterization by type of anaesthesia and age (Table 6)
The results of age group comparison for the post-operative lower urinary tract symptoms in patients given spinal anaesthesia showed that there was only one patient in age group 31-45 years and one patient in age group 46-60 years showing post-operative lower urinary tract symptoms None of the patients in the local anaesthesia group have post-operative lower urinary tract symptoms There was non-significant (p = 0 343) difference for lower urinary tract symptoms by type of anaesthesia and age (Table 7)
Table 6.
Pearson Chi-Square test for the relation of age groups with anaesthesia types and post-operative bladder catheterization
Anesthesia type Age group Post-operative bladder catheterization Pearson No Yes Chi-Square
Spinalanesthesia<30years020719
31-45years03
46-60years06
61-75years09
Localanesthesia<30years40
31-45years30
46-60years70
61-75years60
Table 7
Pearson Chi-Square test for the relation of age groups with anesthesia types and post-operative lower urinary tract symptoms
Anesthesia type Age group Post-operative lower urinary Pearson tract symptoms Chi-Square No Yes
Spinalanesthesia<30years200.343
31-45years21
46-60years51
61-75years90
Localanesthesia<30years40
31-45years30
46-60years70
61-75years60
Table 8
Pearson Chi-Square test for the relation of age groups with anaesthesia types and voiding burning
Anesthesia type Age group Voiding burning Pearson No Yes Chi-Square
Spinalanesthesia<30years200438
31-45years30
46-60years51
61-75years90
Localanesthesia<30years40
31-45years30
46-60years70
61-75years60
Table 9.
Pearson Chi-Square test for the relation of age groups with anesthesia types and dysuria
Anesthesia type Age group Dysuria Pearson No Yes Chi-Square
Spinalanesthesia<30years200113
31-45years21
46-60years60
61-75years90
Localanesthesia<30years40
31-45years30
46-60years70
61-75years60
The results of age group comparison for burning at voiding in patients given spinal anaesthesia showed that there was only one patient in age group 46-60 years who showed symptoms of burning None of the patients in the local anaesthesia group had burning at voiding There was non-significant (p = 0 438) difference of burning at voiding by type of anaesthesia and age (Table 8)
The results of age group comparison for the dysuria in patients given spinal anaesthesia showed that there was only one patient in age group 31-45 years who showed symptoms of dysuria None of the patients in the local anaesthesia group had dysuria There was non-significant (p = 0 113) difference for dysuria by type of anaesthesia and age (Table 9)
DISCUSSION
Altieri modified Nesbit corporoplasty for the treatment of penile curvature utilizes surgical approaches in patients with CPC or PD that are naïve to treatment or have previously used locally or systemic and drugs
The choice of anesthetic technique to perform Altieri modified Nesbit corporoplasty has a major impact on how the patient responds during the postoperative period (22) In the present study, we compared the safety profile and the outcomes of local anesthesia vs loco-regional anesthesia for surgical treatment of penile curvature The distribution of patients by age groups in the present study showed that most of the patients were in the elderly age group (61-75 years) which might be due to the reason that elderly population is at a high risk of diseases (23)
V M Altieri, P Saldutto, V Verratti, et al
Additionally, our results also showed that more patients showed only mild pain in the spinal anesthesia group compared to the local anesthesia group which should be due to the section in the ligaments, fascia, or bone with localized bleeding (24) In the present study, the comparison of spinal and local anesthesia in the context of post-operative outcomes reveals that local anesthesia appears to be associated with a shorter hospital stay, potentially making it a more favorable choice for this particular procedure There was a non-significant difference in penile shortening when it was compared in spinal and local anesthesia groups These findings are consistent with the study conducted by Ana et al who reported that surgical treatment of penile curvature under local anesthesia improves the cost-effectiveness ratio with the same quality of care, degree of satisfaction and postoperative functional results, maintaining a similar rate of intra/posto p e r a
showed that 10% of patients in the spinal anesthesia group showed post-operative intestinal disorders and post-operative constipation compared to the local anesthesia group which might be due to the shorter time needed to return of bowel function (26) These results are in-line with the previous studies reporting post-operative constipation (27-28) Our results also showed a significant difference in post-operative bladder catheterization time when comparing spinal and local anesthesia groups as 100% of the patients had post-operative bladder catheterization in the spinal anesthesia group while none of the patients had post-operative bladder catheterization in local anesthesia group Need of post-operative bladder catheterization after spinal anesthesia was due to the urinary retention (29) In the present study, due to the urinary retention, patients who had spinal anesthesia also showed signs of post-operative lower urinary tract symptoms These findings are consistent with the previously reported studies (30, 31) Similarly, patients after surgery conducted by using spinal anesthesia also showed signs of voiding burning and dysuria It has been reported that spinal anesthesia commonly leads to urinary retention because the patient is unable to feel the bladder sensation and to initiate voiding after the surgery Bladder and sphincter muscles are unable to respond for voiding reflex (32, 33)
Altieri-modified Nesbit corporoplasty and minimally invasive techniques can offer effective solutions for penile curvature with high patient satisfaction rates and minimal complications (34) However, it has to be considered the specific patient population, the severity of the curvature, and the desired outcomes when choosing the most appropriate surgical technique and anesthesia type The choice of anesthesia, whether spinal or local, should also consider the potential post-operative complications and the patient's overall health status Further, the results of present study also showed that most patients in age group 61-75 years who were given spinal anaesthesia had hospital stay due to the deep sedation during spinal anaesthesia in older age group (35, 36) Furthermore, noticeable and distracting post-operative pain was observed among higher age group patients who were given spinal anesthesia that might be due to numbness, and motor weakness among older patients (37) Similarly, age group
comparison for the post-operative intestinal disorders showed more intestinal disorders among 61-75 years age group patients who were given spinal anaesthesia which could be due to increased colonic transit time among older patients (38) Our results also showed that patients in age group 61-75 years had post-operative constipation with spinal anaesthesia These findings are consistent with previously reported studies (39)
Our findings showed that post-operative lower urinary tract symptoms were observed in patients with age groups 31-45 years and 46-60 years given spinal anaesthesia Symptoms of voiding burning were observed in patients with age group 46-60 years wereas dysuria was observed in patients with age group 31-45 years These findings are comparable to the previously reported studies (41, 42)
In conclusion, the choice of anesthesia technique for surgical treatment of penile curvature, particularly utilizing the Altieri modified Nesbit corporoplasty method, plays a pivotal role in determining postoperative outcomes Our findings also support the preference for local anesthesia in terms of shorter hospital stays and less post-operative complications Particularly, spinal anesthesia was associated with a higher risk of post-operative complications such as urinary retention and constipation In summary, the choice of anesthesia method should be a well-considered decision that considers the individual patient's characteristics, the surgical technique to be employed, and the potential implications for postoperative outcomes, making it essential for healthcare professionals to make informed choices in the best interest of their patients Moreover, long-term follow-up studies are required for making informed decisions about the choice of anesthesia Future research should focus on collecting patientreported outcomes to assess quality of life, psychological well-being, and sexual function after surgery Additionally, as surgical techniques and technology advance, the potential for minimally invasive procedures and innovations in anesthesia protocols may provide safer and more efficient options for patients Collaboration through multi-center studies and international comparisons will help identify best practices and regional variations, ultimately leading to more personalized, effective, and globally accessible care for individuals seeking treatment for penile curvature
CONCLUSIONS
This study comparing Altieri-modified Nesbit corporoplasty outcomes with spinal anesthesia and local anesthesia for congenital penile curvature and Peyronie's disease with spinal anesthesia and local anesthesia confirms the effectiveness of the surgical procedure and demonstrates that both approaches yield high patient satisfaction and minimal post-operative pain However, spinal anesthesia was associated with a slightly higher rate of post-operative complications and significantly longer hospital stays compared to local anesthesia Importantly, age did not significantly influence most clinical outcomes, except for post-operative pain, where older patients in the local anesthesia group reported slightly more discomfort These findings provide valuable insights for clinicians,
aiding in the selection of anesthesia methods to optimize patient outcomes and enhance their overall surgical experience
REFERENCES
1 Montag S, Palmer LS Abnormalities of penile curvature: chordee and penile torsion ScientificWorldJournal 2011; 11:1470-8
2 El-Sakka AI Prevalence of Peyronie's disease among patients with erectile dysfunction Eur Urol 2006; 49:564-9
3 Spirito L, Manfredi C, La Rocca R, et al Daily low-dose tadalafil may reduce the penile curvature progression rate in patients with acute Peyronie's disease: a retrospective comparative analysis Int J Impot Res 2024; 36:129-134
4 Spirito L, Manfredi C, La Rocca R, et al Long-term outcomes of extracorporeal shock wave therapy for acute Peyronie's disease: a 10-year retrospective analysis Int J Impot Res 2024; 36:135-139
5 Kadioglu A, Sanli O, Akman T, et al Factors affecting the degree of penile deformity in Peyronie disease: an analysis of 1001 patients J Androl 2011; 32:502-8
6 Nehra A, Alterowitz R, Culkin DJ, et al ; American Urological Association Education and Research, Inc , Peyronie's Disease: AUA Guideline J Urol 2015; 194:745-53
7 Brimley SC, Yafi FA, Greenberg J, et al Review of Management Options for Active-Phase Peyronie's Disease Sex Med Rev 2019; 7:329-337
8 Carson CC, Levine LA Outcomes of surgical treatment of Peyronie's disease BJU Int 2014; 113:704-13
9 Egydio PH, Sansalone S Peyronie's reconstruction for maximum length and girth gain: geometrical principles Adv Urol 2008; 2008:205739
1 0 C h u n g E , R a l p h D , K a g i o g l u A , e t a l E v i d e n c e - B a s e d Management Guidelines on Peyronie's Disease J Sex Med 2016; 13:905-23
11 Hatzimouratidis K, Eardley I, Giuliano F, et al European Association of Urology EAU guidelines on penile curvature Eur Urol 2012; 62:543-52
12 Langston JP, Carson CC 3rd Peyronie disease: plication or grafting Urol Clin North Am 2011; 38:207-16
13 Nesbit RM Congenital curvature of the phallus: report of three cases with description of corrective operation J Urol 1965; 93:230-2
14 Sasso F, Vittori M, D'Addessi A, Bassi PF Penile curvature: an update for management from 20 years experience in a high volume centre Urologia 2016; 83:130-138
15 Altieri VM, Greco F, Lisanti RC, et al Clinical and penile Doppler outcomes using a modified, tourniquet free, Nesbit plication for severe Peyronie's disease Transl Androl Urol 2021; 10:28572870
1 6 R o c c o G N o n - i n t u b a t e d u n i p o r t a l l u n g s u r g e r y † E u r J Cardiothorac Surg 2016; 49(Suppl 1):i3-5
17 Furák J, Szabó Z, Horváth T, et al Non-intubated, uniportal, video assisted thoracic surgery [VATS] lobectomy, as a new procedure in our department Magy Seb 2017; 70:113-117
18 Callesen T, Bech K, Kehlet H One-thousand consecutive inguinal hernia repairs under unmonitored local anesthesia Anesth Analg 2001; 93:1373-6
19 Kehlet H, Aasvang E Groin hernia repair: anesthesia World J Surg 2005; 29:1058-61
20 Sungurtekin H, Sungurtekin U, Erdem E Local anesthesia and midazolam versus spinal anesthesia in ambulatory pilonidal surgery J Clin Anesth 2003; 15:201-5
21 Likert R A technique for the measurement of attitudes Archives of Psychology, 1932: 22: 140-55
22 Sidhom K, Chung D, Patel P Case series - Tolerability of penile fracture repair under conscious sedation Can Urol Assoc J 2023; 17:E218-E220
23 Cuvillon P, Lefrant JY, Gricourt Y Considerations for the Use of Local Anesthesia in the Frail Elderly: Current Perspectives Local Reg Anesth 2022; 15:71-75
24 Benzon HT, Asher YG, Hartrick CT Back Pain and Neuraxial Anesthesia Anesth Analg 2016; 122:2047-58
25 Ana MM, Carlos FP, Teresa MSM, et al Corporoplasty under local anesthesia: Cost-effective improvement of the surgical treatment of Peyronie's disease Rev Int Androl 2022; 20:231-236
26 Stevens RA, Mikat-Stevens M, Flanigan R, et al Does the choice of anesthetic technique affect the recovery of bowel function after radical prostatectomy? Urology 1998; 52:213-8
27 Celik S, Atar NY, Ozturk N, et al Constipation Risk in Patients Undergoing Abdominal Surgery Iran Red Crescent Med J 2015; 17:e23632
28 Stienen MN, Smoll NR, Hildebrandt G, et al Constipation after thoraco-lumbar fusion surgery Clin Neurol Neurosurg 2014; 126:137-42
29 Kreutziger J, Frankenberger B, Luger TJ, et al Urinary retention after spinal anaesthesia with hyperbaric prilocaine 2% in an ambulatory setting Br J Anaesth 2010; 104:582-6
30 Haleem S, Ozair A, Singh A, et al Postoperative urinary retention: A controlled trial of fixed-dose spinal anesthesia using bupivacaine versus ropivacaine J Anaesthesiol Clin Pharmacol 2020; 36:94-99
31 Yilmaz G, Akca A, Kıyak H, et al Spinal Anesthesia Is Associated With Postoperative Urinary Retention In Women Undergoing Urogynecologic Surgery Eastern Journal of Medicine 2020; 25:293298
32 Mahan KT, Wang J Spinal morphine anesthesia and urinary retention J Am Podiatr Med Assoc 1993; 83:607-14
33 Wang LL, Kang M, Duan LX, et al Effect of single spinal anesthesia with two doses ropivacaine on urinary retention after hemorrhoidectomy in male patients Front Surg 2023; 9:1077575
34 Rossi A, Alei G, Viscuso P, et al An original mininvasive corporoplasty technique for penile curvature without circumcision Arch Ital Urol Androl 2022; 94:334-338
35 Sieber FE, Zakriya KJ, Gottschalk A, et al Sedation depth during spinal anesthesia and the development of postoperative delirium in elderly patients undergoing hip fracture repair Mayo Clin Proc 2010; 85:18-26
36 Neuman MD, Feng R, Carson JL, et al ; REGAIN Investigators Spinal Anesthesia or General Anesthesia for Hip Surgery in Older Adults N Engl J Med 2021; 385:2025-2035
37 Bafna U, Rajarajeshwaran K, Khandelwal M, Verma AP A comparison of effect of preemptive use of oral gabapentin and pregabalin for acute post-operative pain after surgery under spinal anesthesia J Anaesthesiol Clin Pharmacol 2014; 30:373-7
38 Tu C-P, Tsai C-H, Tsai C-C, et al Postoperative Ileus in the Elderly International Journal of Gerontology 2014; 8:1-5
39 Lang-Illievich K, Bornemann-Cimenti H Opioid-induced constipation: a narrative review of therapeutic options in clinical management Korean J Pain 2019; 32:69-78
40 Yılmaz E, Arı M Impact of Pre-Operative Anxiety on PostOperative Constipation Turk J Colorectal Dis 2016; 26:39-46
41 Basques BA, Bohl DD, Golinvaux NS, et al General versus spinal anaesthesia for patients aged 70 years and older with a fracture of the hip Bone Joint J 2015; 97-B:689-95
42 Hernandez NS, Wang AY, Kanter M, et al Assessing the impact of spinal versus general anesthesia on postoperative urinary retention in elective spinal surgery patients Clin Neurol Neurosurg 2022; 222:107454
Correspondence
Vincenzo Maria Altieri, MD vincenzomaria altieri@gmail com
Fabrizio Iacono, MD info@fabrizioiacono it
Department of Medicine and Health Sciences "V Tiberio", University of Molise, 86100 Campobasso, Italy
Pietro Saldutto, MD pietro saldutto@gavazzeni it
Walter Vena, MD walter vena@gavazzeni it
Department of Urology, Humanitas Gavazzeni, 24125 Bergamo, Italy
Vittore Verratti
vittore verratti@unich it
Department of Psychological, Health and Territorial Sciences, University "G d'Annunzio" Chieti-Pescara, 66100 Chieti, Italy
Roberto La Rocca, MD robertolarocca87@gmail com
Giuseppe Celentano, MD dr giuseppecelentano@gmail com
Marco Capece, MD drmarcocapece@gmail com
Ernesto Di Mauro, MD
ernesto dimauro@unina it
Vincenzo Morgera, MD vincemorgera87@gmail com
Gianluigi Cacace, MD cacace gianlu@gmail com
Francesco Mastrangelo, MD fmastrangelo91@gmail com
Unit of Urology, Department of Neurosciences, Reproductive Sciences, and Odontostomatology University of Naples “Federico II”, Naples, Italy
Luigi Napolitano, MD (Corresponding Author) dr luiginapolitano@gmail com
Unit of Urology, Department of Neurosciences, Reproductive Sciences, and Odontostomatology University of Naples “Federico II”
Via Sergio Pansini 5, 80131 Naples, Italy
Conflict of interest: The authors declare no potential conflict of interest
V M Altieri, P Saldutto, V Verratti,
ORIGINAL PAPER
Correlation between histopathology properties of dartos tissue and the severity of penile curvature in hypospadias
Gede W K Duarsa 1 , Pande M W Tirtayasa 2 , Ni Wayan Winarti 3 , Andy Michael 4 , Komang H A Duarsa 5
1 Department of Urology, Faculty of Medicine Universitas Udayana/Prof dr I G N G Ngoerah General Hospital, Denpasar, Indonesia;
2 Department of Urology, Faculty of Medicine Universitas Udayana/Universitas Udayana Teaching Hospital, Denpasar, Indonesia;
3 Department of Pathology Anatomy, Faculty of Medicine Universitas Udayana/Prof dr I G N G Ngoerah General Hospital, Denpasar, Indonesia;
4 Department of Surgery, Faculty of Medicine Universitas Udayana/Prof dr I G N G Ngoerah General Hospital, Denpasar, Indonesia;
5 Medical Doctor Study Program, Faculty of Medicine Universitas Udayana, Denpasar, Indonesia
Summary
Purpose: Hypospadias, one of the congenital anomalies commonly associated with some degrees of ventral penile curvature that may arise from malformation of dartos fascia, the chordee. Our study aims to determine the correlation between the histopathology properties of dartos fascia and the severity of ventral penile curvature in hypospadias
Materials and methods: One hundred hypospadias patients with various degrees of ventral penile curvature were included in this cross-sectional analytical study from 2020 to 2022 During hypospadias repair, ventral dartos fascia was excised and analyzed for the degree of collagen thickness and the severity of the fibrotic condition
Results: Out of 100 patients, the mean age was 6 58 + 4 28 years, who were classified as mild to moderate (66%) and severe (34%) ventral curvature cases The analyses showed significant differences in the severity of fibrotic condition and collagen thickness of dartos fascia to the severity of penile ventral curvature with p-values of 0.002 and 0.017, respectively. Conclusions: The difference in histopathology properties of dartos fascia may affect the severity of penile curvature in hypospadias patients
Hypospadias is a congenital anomaly found in children characterized by an abnormal location of urethral opening on the ventral side of the penis The incidence of hypospadias varies around the world, with a prevalence of about 1 case in every 250 male newborn babies This malformation is caused by abnormal development of the ventral side of the penis, hence an abnormal proximal position of the urethral opening (1)
The abnormality has been classified into several categories Based on the position of the urethral opening, hypospadias can be differentiated into proximal and distal types Ventral curvature, the chordee, is another asso-
ciated condition found in hypospadias, mostly the proximal type, which is the proximal part of urethral folds that were fused incompletely and left an opening in the ventral penis in males (2, 3) Chordee may arise from the inadequacy or disorder of the dartos fascia, on the ventral side of the penis The severity of the chordee may be associated with the degree of dartos fascia abnormality (4) In hypospadias patients, the composition of the extracellular matrix (ECM) was varied and different compared to the non-hypospadias patients, in which the main components are collagens, elastic fibers, and proteoglycans/glycosaminoglycans (GAGs) These composition changes might contribute to the thickening and stiffness of the tissue A previous study reported that the dartos fascia in hypospadias had thicker collagen fibers than a normal penis (5) To the best of our knowledge, there is no study reporting if there is any correlation between the degree of collagen thickness and the severity of the fibrotic condition of dartos fascia to the severity of ventral curvature Therefore, this study aimed to compare the degree of collagen thickness and the severity of the fibrotic condition to the severity of ventral curvature in hypospadias
MATERIALS AND METHODS
A cross-sectional analytical study was performed on 100 hypospadias patients with various degrees of chordee who underwent urethroplasty between 2020 and 2022 Patients were differentiated into two groups based on the severity of penile curvature degree, namely mild to moderate (< 60 degrees) and severe (> 60 degrees) The penile curvature degree was measured, twice at least, using a goniometer intraoperatively before performing urethroplasty and a single surgeon (GWKD) performed urethroplasty for this study Excision of ventral dartos fascia, including tunica albuginea, which manifests as chordee, was performed during surgery with a U-shape incision, which was a wide excision of urethra of about 8 mm in length, which started at 2 mm from proximal tip of urethral meatus to 2 mm from distal urethral meatus These tissues were sent to the pathology laboratory to assess the fibrotic and collagen density conditions Patients who underwent re-urethro-
plasty due to a failed previous operation were excluded
The study has been approved by the research ethics committee of the Faculty of Medicine, Universitas Udayana, Prof I G N G Ngoerah General Hospital, Denpasar with No 2773/UN14 2 2VII 14/ LT/2022, and written informed consent has been acquired from the parents
The staining and evaluation of dartos specimens were conducted by a single pathologist (NWW) without prior information regarding the clinical condition of patients The Masson’s trichrome (MST) and hematoxylin and eosin (H&E) staining were performed to assess the collagen fibers thickness and the severity of the fibrosis, respectively The images were then enlarged 200 times and five random points were marked to evaluate the specimen thoroughly Regarding the t h i c k n e s s o f c o l l a g e n , p a t i e n t s w e re divided into two groups: thin to moderate and thick
Figure 1.
The MST staining of collagen fibers (200x), the green arrow points to the thin to moderate collagen fibers in Figure (A) and thick collagen fibers in Figure (B) The H&E staining of fibrotic changes (200x), the green arrow points to the mild to moderate fibrosis in Figure (C) and severe fibrosis in Figure (D)
Moreover, patients were also assigned into two groups in terms of the severity of fibrotic conditions, namely mild to moderate and severe The cut-off points of thin to moderate and thick/severe are below or above 60% per high power field (HPF) for both variables These percentages were obtained by dividing the area occupied by collagen by the area of the entire high power field
The Chi-square and the alternative Fisher’s exact tests were used to analyze the relationship between the severity of chordee and collagen thickness and fibrotic severity on dartos tissue P-value < 0 05 was considered statistically significant
RESULTS
The characteristics of all patients in our institution are shown in Table 1 The mean age of 100 patients was 6 58 + 4 28 years and they were classified into mild to moderate (66%) and severe (34%) ventral curvature cases Moreover, in terms of collagen thickness of dartos fascia, there were 76% and 24% cases with thin to moderate and
Table 1. Characteristics of all patients
Variable
Hypospadiaspatients(n=100)
Meanage(year+SD)658+428
Ventralcurvature,n(%)
Mild-moderate66(66)
Severe34(34)
Fibroticseverityofdartosfascia,n(%)
Mild-moderate87(87)
Severe13(13)
Collagenthicknessofdartosfascia,n(%)
Thin-moderate76(76)
Thick24(24)
thick collagen density, respectively In addition, 87% and 13% of patients suffered from mild to moderate and severe fibrotic conditions of their dartos fascia, respectively Representation of thin to moderate and thick collagen density as well as mild to moderate and severe fibrosis, shown in Figure 1
The analyses showed significant differences in the severity of fibrotic and collagen thickness of dartos fascia to the severity of ventral curvature with p-values of 0 002 and 0 017 respectively, shown in Table 2
Table 2. Analysis of collagen thickness and fibrotic severity on ventral curvature
a
Thin-moderate55210017** Thick1113
* : signif cant resu t (F sher’s exact test); ** : s gnificant resu t (Chi-square test)
DISCUSSION
A previous study revealed that the number collagen fibers of dartos fascia was significantly lower but the fibers were thicker in hypospadias compared to normal penis Moreover, the reticulin to total collagen ratio was higher in hypospadias compared to normal penis Reticulin, a type III collagen fibers, was found to increase during early stage of life and early healing condition (6) At the molecular level, Yuri et al showed the downregulation of several types of collagen gene expressions compared to normal patients COL1A1 and COL6A1 were also significantly downregulated in the moderate and severe chordee
G W K Duarsa, P M W Tirtayasa, N Wayan Winarti, et al
groups compared to the mild chordee groups, with p-values of 0 003 and 0 037, respectively (7, 8) Therefore, we assessed the thickness of collagen fibers in hypospadias in several degrees of ventral curvature Our study reported that collagen fibers of dartos fascia in hypospadias were significantly thicker in severe compared to mild to moderate ventral curvature As far as we know, this is the first study comparing the histopathology aspect of dartos fascia in various degrees of ventral curvature of hypospadias
Fibrotic tissue leads to thickening and scarring of the tissue it affects (9, 10) Fibrotic tissue is a collection of extracellular matrix (ECM) and it may appear in various degree of elasticity and thickness that depends on its properties of collagen and elastin (11) Fibrosis is known as a disproportionate development of connective tissue that disrupts the structure and function of any tissue (12) Chordee exists due to the fibrosis of dartos fascia that results in elasticity disruption and leads to penile bending (13) Moreover, we reported the distinction of dartos fascia properties in various degrees of ventral curvature of hypospadias patients, especially in collagen thickness and fibrosis severity The more severe ventral curvature degree patients suffered, the more severe and thicker the fibrotic condition and collagen thickness they would have
Hypospadias patients with severe ventral curvature had more abnormal and inelastic dartos fascia tissue that led to more severe ventral bending of the penile
Histopathology study on the hypospadias urethral plate revealed the characteristic of well-built connective tissue with adequate vascularization and no signs of fibrosis on the urethral plate (14) Moreover, there was no difference in collagen density in patients with hypospadias compared to the normal patient (15) However, the readouts of our study are different from those of previous studies
Previous studies evaluated the histopathology of the urethral plate, on the other hand, our study assessed the histopathology of the dartos fascia especially taken from the ventral side of the penile
In the current literature, there are no guidelines about the definition of collagen fiber thickness and fibrotic changes in micrometers, which might be a potential bias due to tissue sampling and handling for microscope analysis differences in size
Several pieces of literature have reported the abnormality of dartos fascia in hypospadias, buried penis and also in epispadias cases (3, 16) Atmoko et al. showed a reduction of total collagen to elastin and also an increased ratio of reticulin fibers in dartos fascia of hypospadias and buried penis (3) Moreover, there were thicker collagen and abnormal smooth muscle action distribution in hypospadias and buried penis compared to normal penile (3, 16)
To the best of our knowledge, this is the first study to compare the histopathology of dartos fascia based on the severity of ventral curvature in hypospadias patients This study showed that severe ventral curvature is correlated with thicker collagen fibers and more severe fibrosis condition of dartos fascia compared with mild to moderate ventral curvature in hypospadias patients A more progressive excision of the chordee is warranted in severe ventral curvature penile during hypospadias repair In fact, total excision of the chordee is mandatory during urethroplasty regardless of the degree of penile curvature
as this is an abnormal tissue Leaving even a small remnant of chordee during reconstructive surger y may increase the risk of complications following surgery (17) We realized that there was a more objective measurement of fibrosis based upon immunohistochemical staining and/or quantification of relative protein expression such as collagen types and elastin Therefore, we recommended that further study is needed to evaluate the composition of collagen in dartos fascia based on the severity of chordee using an electron microscope with specific immunohistochemical staining Since we did not focus on and discuss the surgical outcomes in our study, we also recommended further study to assess the complication post-surgical to evaluate the outcome, which is not only studies at the protein level and molecular studies
CONCLUSIONS
There is a difference in the properties of dartos fascia in severe ventral curvature compared with mild to moderate ventral curvature of hypospadias patients, especially in the thickness of collagen fibers and severity of the fibrotic condition The difference in histopathology properties of dartos fascia may affect the severity of penile curvature in hypospadias patients
REFERENCES
1 Waterloos M, Hoebeke P, Spinoit AF Hypospadias variants In: Congenital anomalies of the penis Berlin: Springer; 2017
2 Palmer LS, Palmer JS Management of abnormalities of external genitalia in boys In: Wein AJ, Kavoussi LR, Partin AW, Peters CA (Eds ) Campbell-Walsh urology 11th ed Philadelphia: Elsevier Ltd; 2016, pp 3374-6
3 Abbas M, Liard A, Elbaz F, Bachy B Outcome of surgical management of concealed penis J Pediatr Urol 2007; 3:490-4
4 Van Der Putte SCJ Hypospadias and associated penile anomalies: a histopathological study and a reconstruction of the pathogenesis J Plast Reconstr Aesthet Surg 2007; 60:48-60
5 Atmoko W, Shalmont G, Situmorang GR, et al Abnormal dartos fascia in buried penis and hypospadias: evidence from histopathology J Pediatr Urol 2018; 14:536 e1-536 e7
6 Cheng W, Yan-hua R, Fang-gang N, Guo-an Z The content and ratio of type I and III collagen in skin differ with age and injury African J Biotechnol 2011; 10:2524-9
7 Yuri P, Gunadi G, Lestari RP, et al The impact of COL1A1 and COL6A1 expression on hypospadias and penile curvature severity BMC Urol 2020; 20:189
9 Almine JF, Bax DV, Mithieux SM, et al Elastin based materials Chem Soc Rev 2010; 39:3371-9
10 Daamen WF, Veerkamp JH, Van Hest JCM, Van Kuppevelt TH Elastin as a biomaterial for tissue engineering Biomaterials 2007; 28:4378-98
11 Neary R, Watson CJ, Baugh JA Epigenetics and the overhealing wound: the role of DNA methylation in fibrosis Fibrogenesis Tissue Repair 2015; 8:1-13
12 Karsdal MA Biochemistry of collagens, laminins and elastin structure, function and biomarkers Berlin: Springer; 2016
13 Montag S, Palmer LS Abnormalities of penile curvature: chordee and penile torsion Sci World J 2011; 11:1470-8
14 Snodgrass W, Patterson K, Plaire JC, et al Histology of the urethral plate: implications for hypospadias repair J Urol 2000; 164:988-90
15 Erol A, Baskin LS, Li YW, Liu WH Anatomical studies of the ure-
thral plate: why preservation of the urethral plate is important in hypospadias repair BJU Int 2000; 85:728-34
16 Spinoit AF, Van Praet C, Groen LA, et al Congenital penile pathology is associated with abnormal development of the dartos muscle: a prospective study of primary penile surgery at a tertiary referral center J Urol 2015; 193:1620-4
17 Halaseh SA, Halaseh S, Ashour M Hypospadias: A Comprehensive Review Including Its Embryology, Etiology and Surgical Techniques Cureus 2022; 14:e27544
Correspondence
Gede Wirya Kusuma Duarsa (Corresponding Author) gwkurology@gmail com
Department of Urology, Faculty of Medicine, Universitas Udayana, Prof Dr I G N G Ngoerah General Hospital, Denpasar, Bali, Indonesia
Pande Made Wisnu Tirtayasa wisnu tirtayasa@unud ac id
Department of Urology, Faculty of Medicine Universitas Udayana/ Universitas Udayana Teaching Hospital, Denpasar, Indonesia
Ni Wayan Winarti nw winarti@unud ac id
Department of Pathology Anatomy, Faculty of Medicine Universitas Udayana/Prof dr I G N G Ngoerah General Hospital, Denpasar, Indonesia
Andy Michael
andymichael91 am@gmail com
Department of Surgery, Faculty of Medicine Universitas Udayana/ Prof dr I G N G Ngoerah General Hospital, Denpasar, Indonesia
Komang Harsa Abhinaya Duarsa abhinaya duarsa@gmail com
Medical Doctor Study Program, Faculty of Medicine Universitas Udayana, Denpasar, Indonesia
Conflict of interest: This study was supported by the PNBP Universitas Udayana funding grant 2022 No B/78 174/UN14 4/PT/01/03/2022
G W K Duarsa, P M W Tirtayasa, N Wayan Winarti, et al
ORIGINAL PAPER
Evaluation of the effect of daily tadalafil 5 mg versus
daily sildenafil
25 mg on neutrophil-lymphocyte and platelet-lymphocyte ratios in patients with erectile dysfunction: A comparative randomized controlled study
Abdel Rahman Bakry 1 , Ali Mohamed Mahran 1 , Hisham Diab Gaber 1 , Mohamed Ismail Sedek 2 , Sameh Fayek GamalEl Din 3 , Ahmad Tarek Motawi 3 , Mohamed Diab Mohamed 1 , Ahmed Elshebany 1
1 Department of Andrology & STDs, Faculty of Medicine, Assiut University, Assiut, Egypt;
2 Department of Clinical Pathology, Faculty of Medicine, Assiut University, Assiut, Egypt;
3 Department of Andrology & STDs Kasr Alainy Faculty of Medicine, Cairo University, Giza, Egypt
Summary
Background: Previous studies had shown that the neutrophils/lymphocytes (NLR) and platelets/lymphocytes (PLR) ratios could be used as markers of inflammatory load as well as prognostic factors in several medical conditions The current study aimed to compare between the effect of using daily tadalafil 5 mg/day versus daily sildenafil 25 mg/day in improving erectile function as well as their ability to reduce NLR and PLR
Methods: One hundred and four participants were recruited. Seventy-four randomized patients with erectile dysfunction were equally divided into 2 groups. Patients in group A used daily tadalafil 5 mg for 2 months while patients in group B used daily sildenafil 25 mg for 2 months. Patients were collected from June 2022 to June 2023 Thirty healthy individuals served as controls. All patients and controls were evaluated using the validated Arabic version of the international index of erectile function (ArIIEF-5) at baseline and after 2 months of medical treatment. Five cc of venous blood sample was obtained before and after 2 months of medical treatment to compare the effect of phosphodiestrase type 5 inhibitors (PDE-5Is) intake for erectile dysfunction on PLR and NLR before and after treatment.
Results: The current study showed that there were no statistically significant differences between the cases and the controls apart from the ArIIEF-5 scores Moreover, there was no significant difference between patients in group A and those in group B regarding PLR and NLR post administration of PDE-5Is
Interestingly, patients in group A demonstrated a highly significant difference between the ArIIEF-5 scores as well as the PLR and the NLR before and 2 months after administration of daily tadalafil 5 mg On the other hand, patients in group B who were administrated daily sildenafil 25 mg for 2 months demonstrated only a highly significant difference between the ArIIEF-5 scores before and after administration Meanwhile, patients in group B did not reveal any statistically significant difference in the PLR and the NLR before and 2 months after administration of sildenafil 25 mg. Further regression analysis after adjustment of different variables of the study showed a significant correlation between ArIIEF-5 and PLR in patients who received daily tadalafil 5 mg (r = 0 430, p = 0 004)
Conclusions: Tadalafil and sildenafil have similar clinical efficacy in treating erectile dysfunction However, tadalafil is more effective in lowering PLR and NLR compared to sildenafil.
Erectile dysfunction (ED) is an inability to provide adequate erection to initiate or maintain any sexual activity (1) ED prevalence in adult males is approximately 20% (2) Previous studies had shown that the neutrophils/lymphocytes (NLR) and platelets/lymphocytes (PLR) ratios could be used as markers of inflammatory load as well as prognostic factors in several medical conditions (3-4) The common pathophysiological conditions underlying ED, CVD and other vascular diseases included inflammation, atherosclerosis and endothelial dysfunction (5) The NLR and PLR were known to be potential markers of inflammation in vascular diseases and inflammation play a critical role in the initiation and development of vascular endothelial dysfunction and atherosclerosis (6) Neutrophils produce and secrete several inflammatory mediators including myeloperoxidase (MPO) and reactive oxygen species (ROS) which can be responsible of myocardial and non-myocardial tissue damages (7) Additionally, platelets release numerous inflammatory mediators that modify leukocyte and endothelial responses via different inflammatory stimuli (8)
A modern study had revealed that NLR and PLR had been proposed as biomarkers of subclinical inflammation and many studies had investigated these ratios (9) A previous study had demonstrated that onset and severity of ED had been attributed to increased levels of inflammatory biomarkers (10) In the same context, NLR and PLR were used as signs of inflammation together with a significant relationship between development of ED and these inflammatory markers (11) Previous studies reported a chronic effect of sildenafil and tadalafil on endothelial function and pro-inflammatory markers (12) Das (2007) stated that different cohorts of ED patients were associat-
ed with increased levels of inflammatory markers as well as the significant ability of oral phosphodiesterase-5 inhibitors (PDE-5Is) to decrease these markers (13) The current study aimed to compare between the effect of using daily tadalafil 5 mg/day versus daily sildenafil 25 mg/day in improving erectile function as well as their ability to reduce NLR and PLR
PATIENTS AND METHODS
One hundred and four participants with erectile dysfunct i o n ( E D ) w e r e r e c r u i t e d S e v e n t y - f o u r r a n d o m i z e d patients were equally divided into 2 groups Thirty healthy individuals served as controls Patients in group
A used daily tadalafil 5 mg for 2 months while patients in group B used daily sildenafil 25 mg for 2 months Patients were collected from the andrology outpatient clinic, Assiut University Hospital from June 2022 to June 2023
The institutional review board approved the study (17101846) that conforms to Helsiniki declaration 2013 (14) All Patients signed a written informed consent after explaining the steps and the aim of the study They were randomized by simple numbering method
Inclusion criteria of the patients
Any male patient aged 25 to 60 years in a stable relationship and suffering from ED was included
Exclusion criteria of the patients
Patients who suffered from severe uncontrolled medical conditions, patients under treatment with sublingual nitrate, patients with blood diseases that affect sexual function and patients using cytotoxic drugs or immunosuppressive drugs were excluded Also, patients without partners were excluded
Inclusion criteria of the controls
They were age matched potent controls who attended the outpatient clinic for fertility checkup
All participants were subjected to the following steps Medical as well as sexual and surgical histories were obtained General and local examinations were done All patients and controls were evaluated using the validated Arabic version of the international index of erectile function (ArIIEF-5) at baseline and after 2 months of medical treatment (15) Five cc of venous blood sample was obtained before and after 2 months of medical treatment by using sterile 5 ml syringe then the sample poured into EDTA vacuum tube Then gentle mixing was performed to obtain complete blood count using CELL-DYN haematology analyzer device to compare the effect of PDE-5Is intake for ED on PLR and NLR before and after treatment Patients in group A received daily tadalafil 5 mg while patients in group B received daily sildenafil 25 mg for 2 months
Statistical analysis
Data were fed to the computer and analyzed using IBM SPSS software package version 20 0 (Armonk, NY: IBM Corp) Qualitative data were described using number and percent The Kolmogorov-Smirnov test was used to verify the normality of distribution Quantitative data were described using range (minimum and maximum), mean,
standard deviation, median and inter-quartile range (IQR) Chi-square test was used for categorical variables, to compare between different groups Student t-test was used for normally distributed quantitative variables and to compare between two studied groups Paired t-test was used for normally distributed quantitative variables and to compare between two repeated measures Mann-Whitney test was used for nonparametric quantitative variables and to compare between two studied groups Wilcoxon test was used for nonparametric quantitative variables and to compare between two repeated measures Significance of the obtained results was judged at the 5% level
RESULTS
Table 1 showed that there were no statistically significant differences between the cases and the controls apart from the ArIIEF-5 scores Furthermore, the current study revealed that there was no statistically significant difference between patients in group A and those in group B regarding the ArIIEF-5 prior to administration of PDE5Is (Table 2) Also, the current study demonstrated that there were no statistically significant differences between patients in group A and those in group B regarding PLR and NLR prior to administration of PDE5-Is (Table 2) Conversely, there was no statistically significant difference between patients in group A and those in group B regarding the ArIIEF-5 after intake of PDE5-Is (Table 3)
Table 1.
Socio-demographic data of the participants Tadalafil Sildenafil Controls P-value Mean SD Mean SD Mean SD Age442±69457±61451650602
ArIIEF5before108±47102±48239±090000
PLRbefore1263±361173±369110±4690206
NLRbefore22±1172±11919±140686
ArIIEF5 = the val dated Arabic version of the nternationa ndex of erectile function; PLR = p ate ets/ ymphocyte rat o; NLR = neutroph ls/lymphocyte ratio
Table 2.
ArIIEF-5 and NLR and PLR among studied cases before intervention.
Group A - Tadalafil Group B - Sildenafil P (n = 37) (n = 37)
ian(IQR)9(7-15)8(6-15)
rectiledysfunctionN%N% No00000741
Mild71897189
Moderate1745914378
Severe1335116432
PLRRange456-18560-1940296
Mean±SD12625±360411733±3691
NLRRange048-39056-430384
Median(IQR)21(1-32)18(08-31)
ArIIEF5 = the va idated Arabic version of the international index of erect le function; PLR = platelets/lymphocyte ratio; NLR = neutrophi s/ ymphocyte ratio
A Rahman Bakry, A Mohamed Mahran, H Diab Gaber, et al
Table 3.
ArIIEF-5 and NLR and PLR among studied cases post intervention
Group A - Tadalafil Group B - Sildenafil P (n = 37) (n = 37)
ArIIEF5 the va idated Arab c version of the international ndex of erect le funct on; PLR platelets/lymphocyte ratio; NLR neutrophi s/ ymphocyte rat o; IQR: Interquarti e range
Table 4.
ArIIEF-5 and NLR and PLR pre and post-intervention in group A
Group A who received Pre-inter vention Post-inter vention P tadalafil 5 mg (n = 37) (n = 37)
ArI EF5 the val dated Arabic vers on of the nternat ona index of erecti e function; PLR p ate ets/ ymphocyte rat o; NLR neutroph ls/lymphocyte ratio; IQR: Interquart le range
Moreover, there was no significant difference between patients in group A and those in group B regarding PLR and NLR post administration of PDE5-Is (Table 3)
Interestingly, patients in group A demonstrated a highly significant difference between the ArIIEF-5 scores as well as the PLR and the NLR before and 2 months after administration of daily tadalafil 5 mg (Table 4)
On the other hand, patients in group B who were administrated daily sildenafil 25 mg for 2 months demonstrated only a highly significant difference between the ArIIEF-5 scores before and after administration (Table 5)
Meanwhile, patients in group B did not reveal any statistically significant difference in the PLR and the NLR before and 2 months after administration of sildenafil 25 mg (Table 5)
Further regression analysis after adjustment of different variables of the study showed a significant correlation between ArIIEF-5 and PLR in patients in group A who received daily tadalafil 5 mg (r = 0 430, p = 0 004) (Table 6) It should be mentioned that no other correlation was observed (Table 6)
Table 5.
ArIIEF-5 and PLR and NLR pre and post-intervention in group B
Group B who received Pre-inter vention Post-inter vention P tadalafil 25 mg (n = 37) (n = 37)
ArIIEF5 the validated Arab c version of the internationa ndex of erect le funct on; PLR platelets/lymphocyte ratio; NLR = neutrophi s/ ymphocyte rat o; IQR: Interquarti e range
Table 6
PLR and NLR and smoking in both groups and tadalafil and sildenafil post intervention.
ArIIEF5 = the val dated Arabic vers on of the nternationa index of erectile function; PLR = p ate ets/ ymphocyte rat o
DISCUSSION
The current study demonstrated that baseline PLR and NLR were higher in the patients compared to the controls However, they did not show any significant difference Consistently, Demirci and Ozgur (2019) found that the median NLR level and PLR level were higher when compared to controls in mild-moderate ED and severe ED groups (16) Similarly, Aslan et al (2019) found that NLR was higher in the patients compared to the controls (17) and that it also predicted ED and it might be helpful in diagnosing ED (17) Zhang et al (2022) reported that NLR and PLR were significantly higher in ED patients compared with healthy controls (18) and Ventimiglia et al. (2018) determined that NLR was 3 times higher in severe ED patients and that they were independent predictors (19) A modern retrospective study conducted by Akbas¸ et al (2016) showed that the PLR value increased proportionately with the severity of ED (20)
Our study did not show any statistically significant difference between the studied groups regarding PLR and NLR post-intervention Kilic et al (2023) reported that there was no significant difference in NLR or PLR between ED patients who did not respond to PDE5I treatment and controls who responded to treatment (21) and that there was a highly significant difference between ArIIEF-5 scores before and after intervention in the studied groups who received daily tadalafil 5 mg and daily sildenafil 25 mg Similarly, Gong et al (2017) revealed that sildenafil and tadalafil had equivalent abilities to improve IIEF
scores (22) However, Rubio-Aurioles et al (2012) revealed that the time concerns domain score of the Psychological and Interpersonal Relationship Scales (PAIRS) was significantly lower for daily tadalafil 5 mg compared with sildenafil on demand treatment (23) showing that tadalafil improves sexual confidence more efficiently than sildenafil (23)
Interestingly, our patients in group A who received daily tadalafil 5 mg for 2 months showed a high statistically significant difference between pre and post-intervention PLR and NLR Meanwhile, patients in group B who received daily sildenafil 25 mg for 2 months did not show any statistically significant difference between pre and post-intervention PLR and NLR Consistently, La Vignera et al (2014) showed that tadalafil has a preventive effect on both endothelial apoptosis and excessive platelet adhesion in ED patients (24) Furthermore, a recent Egyptian study demonstrated that daily tadalafil 5 mg supplementation lowers these markers with significant improvement in the erectile function (25) The superiority of tadalafil versus sildenafil in lowering PLR and NLR in the current study might be explained by the shorter half-life of sildenafil but no available data support this hypothesis that needs further investigations
Although tadalafil and sildenafil showed significant improvement in improving the ArIIEF-5 scores, yet, tadalafil was superior to sildenafil in lowering the studied inflammatory markers A previous systematic review conducted by Mirone et al (2008) stated that tadalafil was preferred by the patients compared to sildenafil for several reasons (26) Firstly, patients preferred tadalafil owing to its flexibility (27) Secondly, tadalafil was also preferred owing to its better tolerance (28) Finally, tadalafil was preferred by the patients for its higher efficacy (28-29) To the best of our knowledge, the current study is one of the first to demonstrate higher efficacy of tadalafil compared to sildenafil in lowering NLR and PLR However, there were several limitations of the current study that should be acknowledged The sample size was relatively small and the patients were followed up for short duration
CONCLUSIONS
Tadalafil and sildenafil have similar clinical efficacy in treating ED However, tadalafil is more effective in lowering PLR and NLR compared to sildenafil Future studies are required to replicate this finding as it may add superiority to tadalafil compared to sildenafil
REFERENCES
1 Impotence NIH Consensus Development Panel on Impotence JAMA1993; 270:83-90
2 Burnett AL Evaluation and management of erectile dysfunction
In Kavoussi LR, Novick AC, Partin AW, & Peters Içinde CA (Eds ), Campell-Walsh Urology Philadelphia, PA: Elsevier 2012; pp 721748
3 Bhat T, Teli S, Rijal J, et al Neutrophil to lymphocyte ratio and cardiovascular diseases: a review Expert Rev Cardiovasc Ther 2013; 11:55-9
4 Feng JR, Qiu X, Wang F, et al Diagnostic Value of Neutrophil-to-
Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio in Crohn's Disease Gastroenterol Res Pract 2017; 2017:3526460
5 Zhang Y, Feng X, Wu X, et al A systematic review and metaanalysis of the relationship between erectile dysfunction and the neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios Andrologia 2022; 54:e14337
6 Liao Z, Tang Y, Li X, Li D The relationship between hematologic parameters and erectile dysfunction Sex Med 2021; 9:100401
7 Winterbourn CC, Kettle AJ, Hampton MB Reactive Oxygen Species and Neutrophil Function Annu Rev Biochem 2016; 85:765-92
8 Thomas MR, Storey RF The role of platelets in inflammation Thromb Haemost 2015; 114:449-58
9 K a r a b a k a n M , B o z k u r
Dysfunction, the Neutrophil-to-Lymphocyte Ratio, and the Plateletto-Lymphocyte Ratio J Acad Res Med 2019; 9:27-31
10 Furuncuoglu Y, Tulgar S, Dogan AN, et al How obesity affects the neutrophil/lymphocyte and platelet/lymphocyte ratio, systemic immune-inflammatory index and platelet indices: a retrospective study Eur Rev Med Pharmacol Sci 2016; 20:1300-6
11 Diniz LR, de Lima SG, de Amorim Garcia JM and de Oliveira Diniz KL Neutrophil to Lymphocyte Ratio as a Prognostic Predictor in Older People With Acute Coronary Syndrome Angiology 2019; 70:264-71
12 Santi D, Giannetta E, Isidori AM, et al Therapy of endocrine disease: effects of chronic use of phosphodiesterase inhibitors on endothelial markers in type 2 diabetes mellitus: a meta-analysis Eur J Endocrinol 2015; 172:R103-14
13 Das UN Is erectile dysfunction a low-grade systemic inflammatory condition? Eur Heart J 2007; 28:642-3
1 4 W o r l d M e d i c a l A s s o c
Declaration of Helsinki: Ethical principles for medical research involving human subjects JAMA 2013; 310: 2191-2194
15 Shamloul R, Ghanem H, Abou-Zeid A Validity of the Arabic version of the sexual health inventory for men among Egyptians Int J Impot Res 2004; 16:452-5
16 Demirci A, Ozgur BC The effect of using tadalafil 5 mg/day on neutrophil-lymphocyte and platelet-lymphocyte ratios in mild-medium and severe erectile dysfunction patients; and comparison of clinical response Andrologia 2019; 51:e13347
17 Aslan A, Kaya Y, Cirakoglu A, et al Neutrophil-Lymphocyte Ratio Could Be a Marker for Erectile Dysfunction Urol J 2019; 16:216-20
18 Zhang Y, Feng X, Wu X, et al A systematic review and metaanalysis of the relationship between erectile dysfunction and the neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios Andrologia 2022; 54:e14337
19 Ventimiglia E, Cazzaniga W, Pederzoli F, et al The role of neutrophil-to-lymphocyte ratio in men with erectile dysfunction preliminary findings of a real-life cross-sectional study Andrology 2018; 6:559-63
20 Akbas A, Gulpınar MT, Sancak EB, et al The relationship between platelet-lymphocyte ratio and severity of erectile dysfunction Kaohsiung J Med Sci 2016; 32:91-5
21 Kilic M, Erkan A, Zengin S, et al Inflammatory biomarkers may predict response to phosphodiesterase type 5 inhibitor treatment in patients with erectile dysfunction Investig Clin Urol 2023; 64:404-411
22 Gong B, Ma M, Xie W, et al Direct comparison of tadalafil with
A Rahman Bakry, A Mohamed Mahran, H Diab Gaber, et al
Evaluation of the effect of daily tadalafil 5 mg versus daily sildenafil 25 mg on neutrophil-lymphocyte and platelet-lymphocyte ratios
sildenafil for the treatment of erectile dysfunction: a systematic review and meta-analysis Int Urol Nephrol 2017; 49:1731-40
23 Rubio-Aurioles E, Porst H, Kim ED, et al A randomized openlabel trial with a crossover comparison of sexual self-confidence and other treatment outcomes following tadalafil once a day vs tadalafil or sildenafil on-demand in men with erectile dysfunction J Sex Med 2012; 9:1418-29
24 La Vignera S, Condorelli RA, Burgio G, et al Functional characterization of platelets in patients with arterial erectile dysfunction Andrology 2014; 2:709-15
25 GamalEl Din SF, Nabil Ismail N, Moawad HH, et al Evaluation of tadalafil supplementation on the neutrophil/lymphocyte and the platelet/lymphocyte ratios in patients with erectile dysfunction: A prospective study Urologia 2024; 91:598-603
26 Mirone V, Fusco F, Rossi A, et al Tadalafil and vardenafil vs sildenafil: a review of patient-preference studies BJU Int 2009; 103:1212-7
27 Von Keitz A, Rajfer J, Segal S, et al A multicenter, randomized, double-blind, crossover study to evaluate patient preference between tadalafil and sildenafil Eur Urol 2004; 45:499-509
28 Eardley I, Montorsi F, Jackson G, et al Factors associated with preference for sildenafil citrate and tadalafil for treating erectile dysfunction in men naive to phosphodiesterase 5 inhibitor therapy: post hoc analysis of data from a multicentre, randomized, open-label, crossover study BJU Int 2007; 100:122-9
29 Eardley I, Mirone V, Montorsi F, et al An open-label, multicentre, randomized, crossover study comparing sildenafil citrate and tadalafil for treating erectile dysfunction in men naïve to phosphodiesterase 5 inhibitor therapy Sex Med 2005; 96:1323-32
30 Rodriguez Tolra JR, Cuadrado Campaña JM, Fumadó Ciutat L, Franco Miranda E Prospective, randomized, open-label, fixed dose, crossover study to establish preference of patients with erectile dysfunction after taking the three PDE-5 inhibitors J Sex Med 2006; 3:901-9
Correspondence
Abdel Rahman Bakry, MD
Ali Mohamed Mahran, MD
Hisham Diab Gaber, MD
Mohamed Diab Mohamed, MSc
Ahmed Elshebany, MD
Department of Andrology & STDs, Faculty of Medicine, Assiut University, Assiut, Egypt
Mohamed Ismail Sedek, MD
Department of Clinical Pathology, Faculty of Medicine, Assiut University, Assiut, Egypt
Ahmad Tarek Motawi, MD
Sameh Fayek GamalEl Din, MD (Corresponding Author) samehfayek@kasralainy edu eg
Department of Andrology & STDs Kasr Al-Ainy, Faculty of Medicine Cairo University, Al-Saray Street, El Manial, Cairo, 11956, Egypt
Conflict of interest: The authors declare no potential conflict of interest
Comparative study between intrathecal fentanyl and dorsal penile nerve block for controlling postoperative pain after inflatable penile prosthesis implantation
Adel Elatreisy 1, 2, Yasser Ahmed 1, Ahmed Elgarhy 3, Mohamed Hindawy 1, Tamer Abouelgreed 1 , Ismail Ahmed 3, Abdalla Abdalla 3, Hany Ramadan 3, Mohamed Aboelsuod 3, Khaled Shrief 3 , Ayman Mohamed 3, Wael Ibrahim 3, Saeed Abdelhameed 3, Mohammad Alghamdi 2 , Mohammed Alzahrani 2, Hamada Youssof 4
1 Urology Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt;
2 Urology Department, King Fahd Armed Forces Hospital, Jeddah, Saudi Arabia;
3 Anesthesia Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt;
4 Urology Department, Faculty of Medicine, Fayoum University, Fayoum, Egypt.
Summary
Objectives: To compare the efficacy of intrathecal fentanyl and dorsal penile nerve block for postoperative pain management in patients undergoing inflatable penile prosthesis (IPP).
Patients and methods: A prospective single-center study included 80 patients amenable to IPP. Patients were divided equally into two groups. Group I included 40 patients who were managed with spinal anesthesia with intrathecal fentanyl before undergoing IPP. Group II comprised 40 patients who received spinal anesthesia with dorsal penile block before IPP. Study groups were compared regarding postoperative VAS (Visual Analog Scale) scores, total narcotics consumption, patient satisfaction levels, and perioperative complications.
Results: The study groups were comparable regarding baseline patients’ criteria. The operative time was comparable between the study groups, with group I and group II having respective median times of 64 minutes (interquartile range: 55-78) and 67 minutes (interquartile range: 56-81) (p = 0.65). Additionally, both groups demonstrated similar distributions in IPP implant cylinder and reservoir size (p = 0.9). Postoperative pain was higher in group I, with a statistically significant difference (p<0.001). Eight patients in group I (20%) called the physician’s office asking for pain medication, compared to two patients in group II (5%) (p = 0.04). 85% of patients in group II were highly satisfied compared to 50 % in group I (p = 0.003).
We reported a 5% complication rate in group I compared to 2.5% in group II (p = 0.6).
Conclusions: The present study found that the dorsal penile nerve block offers superior postoperative pain control and patient satisfaction compared to intrathecal fentanyl for patients undergoing inflatable penile prosthesis insertion.
Inflatable penile prosthesis (IPP) represents a gold-standard surgical treatment for medically refractory erectile dysfunc-
tion (1). Postoperative pain control after IPP surgery can be enhanced by targeting nerve endings and receptors in penile tissues. The dorsal penile nerve, formed by converging nerve fibers, carries signals through the pudendal nerve to the spinal cord (S2-S4), then to the thalamus and sensory cortex. Anesthesia can be applied at various points along this pathway, including the dorsal nerve, perineal nerve, pudendal nerve, and S2-S4 nerve roots (2). Several studies explored intraoperative analgesia for postoperative pain control. Raynor et al., for instance, found that the dorsal penile nerve block (DPNB) reduced early postoperative pain but did not impact postoperative narcotic use (3). Additionally, Xie et al. studied the effectiveness of a combination of penile dorsal nerve and ring blocks, while Hsu et al. investigated the efficacy of a crural block. Both studies noted a decrease in early postoperative pain, although rates of postoperative narcotic use were not reported (4, 5). The opioid fentanyl, possessing lipophilic properties, exhibits rapid onset and demonstrates up to 20 times greater potency when administered via the intrathecal route in comparison to the intravenous route (6). However, the use of intrathecal fentanyl has been linked to an increase in intravenous opioid requirement during the postoperative period, potentially attributable to subtle opioid tolerance or opioid-induced hyperalgesia (7). Additionally, it has been noted that intrathecal fentanyl doses exceeding 0.25 µg/kg may reach a "ceiling effect," indicating that higher doses do not enhance intraoperative analgesia and may amplify adverse effects (8). Our study compares intrathecal fentanyl and dorsal penile nerve block for controlling postoperative pain in patients undergoing insertion of an inflatable penile prosthesis.
PATIENTSANDMETHODS
A concurrent cohort study was conducted at the Urology and anesthesia Departments, Faculty of Medicine, Al-Azhar University, Cairo, Egypt. The study spanned from February 2022 to February 2024 and included 80 eligible patients
for elective inflatable penile prosthesis implantation with ASA I, II, and III at the facility The study protocol received approval from the institutional review board Informed written consent was obtained from all participants in compliance with ethical guidelines and regulations to ensure patient safety and confidentiality
Inclusion criteria
IPP was considered for patients with ED after the failure of conservative therapy, including phosphodiesterase inhibitors, alprostadil urethral suppositories, vacuum erection devices, and intracavernosal injections
Exclusion criteria
Patients with ASA IV and coagulopathy were excluded from the study
The study cohort was divided into two equally sized groups The patients were prospectively allocated to treatment groups without randomization The choice between intrathecal fentanyl or DPNB was made through mutual agreement by the patients and physicians Group I consisted of 40 patients who underwent spinal anesthesia with intrathecal fentanyl before undergoing IPP In comparison, Group II comprised 40 patients who received spinal anesthesia with DPNB before IPP
Anesthesia technique
Upon establishing an Intravenous (IV) line, a pre-load of normal saline was administered before the initiation of spinal anesthesia Cardiorespiratory monitoring, including heart rate (HR), peripheral oxygen saturation (SPO2), and blood pressure (BP), was commenced for all patients In the case of group, I, spinal anesthesia was induced using a 25-gauge BD Quinck spinal needle following the sterilization of the back and identification of the anatomical landmark The needle was then inserted using a paramedian approach at the L3-4 intervertebral lumbar space level Upon successful confirmation of cerebrospinal fluid (CSF) flow, a combination of 15 mg (3 ml) of heavy bupivacaine and 0 25 mcg/kg (0 5 ml) of Fentanyl was intrathecally injected
For group II, spinal anesthesia induction involved the use of 3 5 ml (3 ml heavy bupivacaine plus 0 5 ml water for injection), followed by a dorsal penile nerve block performed by inserting an 18-gauge needle connected to a 20 CC syringe between the suspensory ligament and the base of the penis A total volume of 20 bupivacaine was injected at the 2- and 10-o'clock positions (10 ml for each side) for the right and left dorsal penile nerves All penile implant procedures were conducted by a single surgeon using a penoscrotal approach, employing Coloplast titan and Rigicon prostheses
Postoperative pain assessment was conducted using a visual analog scale (VAS) after the IPP surgeries at 2, 4, 8, 12, 16, 20, 24 and 36 hours Patient satisfaction was evaluated using the 5-point Likert scale, ranging from dissatisfied (1) to completely satisfied (5)
Outcome
In the comparative analysis of the study groups, the parameters considered encompassed patients' demographics, postoperative Visual Analog Scale (VAS) scores, total nar-
cotics consumption, patient satisfaction levels regarding postoperative pain management, and perioperative complications according to Modified Clavien Classification System (MCCS) (9)
Statistical analysis
We analyzed the data using the Statistical Package for Social Science (SPSS) software, version 29 (SPSS Inc , Chicago data The descriptive statistics included percentages, frequencies, means, and medians We compared categorical variables between the two groups using the Fisher exact test Additionally, for normally and abnormally distributed continuous variables, we used the Student’s t-test or the Mann-Whitney U test, respectively Statistical significance was defined as a two-tailed p-value of less than 0 05
RESULTS
Group I included 40 patients who underwent spinal anesthesia with intrathecal fentanyl before undergoing IPP, while Group II included 40 patients who received spinal anesthesia with dorsal penile block before IPP The s t u d y g r
s e l i n e patients’ criteria, as depicted in Table 1 The smoking status and prevalence of prior prostatectomy, pelvic radiation therapy, Peyronie’s disease, diabetes, and hypertension were similar across the study groups (p = 0 87) The o p e r a t i v e t i m e w a s c o m p a r a b l e b e t w e e n t h e s t u d y groups, with group I and group II having respective median times of 64 minutes (interquartile range: 55-78)
a n d 6 7 m i n u t e s ( i n t e r q u a r t i l e r a n g e : 5 6 - 8 1 ) ; t h e between-group difference was not statistically significant (p = 0 65) Additionally, both groups demonstrated similar distributions in implant cylinder size and reservoir size (p = 0 9), as shown in Table 1
As measured with the VAS score, post-operative pain was higher in group I, with a statistically significant difference
Table 1
Comparison between the study groups regarding baseline patients’ criteria.
Parameter Group I Group II P-value (n = 40) (n = 40)
(p < 0.001), as shown in Table 2. Eight patients in group I (20%) called the physician’s office asking for pain medication, compared to two patients in group II (5%) with a statistically significant difference (p = 0.04).
Regarding patients’ satisfaction with post-surgery pain control, 85% of patients in group II were highly satisfied compared to 50 % in group I. On the other hand, 25% of group I reported low satisfaction on the 5-point Likert scale compared to 5% in group II, with a significant p-value (p = 0.003) (Table 2).
The 90-day perioperative complication rates were comparable between the study groups, as shown in Table 2. We reported a 5% complication rate in group I compared to 2.5% in group II (p = 0.6).
DISCUSSION
Pain control after IPP surgery has been well studied and includes a multimodal analgesic approach that utilizes combinations of different non-opioid analgesics (10).
Given the significant impact of the opioid epidemic, there is a growing emphasis on reducing narcotic use in postoperative care. Consequently, nerve blocks are increasingly employed in urological procedures as an essential strategy for achieving this goal (11).
There are multiple studies about the intra-operative use of local anesthesia to improve pain control during penile prosthesis surgery. Nagao and colleagues studied the utilization of dorsal penile nerve block with 10 mL of bupivacaine as a single pain control approach during noninflatable prosthesis insertion in 20 patients at a mean follow-up of 3.4 years; they did not report any patient with chronic penile pain (12).
Ghanem and Fouad reported a series of 159 patients who received a dorsal penile nerve block for anesthesia during
implantation of a penile prosthesis; additional general anesthesia was reported in 1.8%, and 5% of their cohort required additional local anesthesia (13). However, they did not report postoperative pain control.
Raynor and colleagues investigated the efficacy of dorsal penile block in pain control compared to placebo after 30 penile prosthesis implants; they found that VAS scores were significantly lower in patients with penile block (14).
In their study, Gürkan and colleagues compared an ultrasound-guided penile nerve block administered to patients undergoing implantation under spinal anesthesia and a control group who did not receive local anesthesia. The results indicated that patients who received the penile nerve block exhibited lower VAS scores and reduced opioid consumption during all observed time intervals up to 24 hours (15).
Numerous studies have indicated that the use of intrathecal fentanyl in combination with bupivacaine results in reduced requirements for intraoperative supplemental analgesia, a decreased incidence of intraoperative nausea/vomiting, and an extended duration until the first analgesic request (30).
The aggregated data from 14 studies revealed an 8% incidence of pruritus in patients administered intrathecal fentanyl, in contrast to 0.6% in the placebo cohort (30).
In the present study, we conducted a comparative analysis of the effectiveness of dorsal penile block and intrathecal fentanyl in managing postoperative pain among patients undergoing inflatable penile prosthesis insertion. Our findings indicate that DPNB demonstrated superior efficacy in pain reduction, accompanied by a significant decrease in postoperative narcotic usage and greater overall patient satisfaction. There were no adverse events with intrathecal fentanyl, and the incidence of perioperative morbidities was comparable to DPNB.
Limitations of the study
The current study introduces a novel prospective comparison between dorsal penile block and intrathecal fentanyl. However, it is essential to note that the study has certain limitations, such as the absence of randomization and a relatively small sample size.
CONCLUSIONS
Our research illustrates that the dorsal penile block offers superior postoperative pain management and patient satisfaction compared to intrathecal fentanyl for patients undergoing inflatable penile prosthesis insertion.
Ethical approval
All procedures conducted in this study complied with the Institution and National Research Committee's ethical standards, the 1964 Declaration of Helsinki, and its subsequent amendments or equivalent ethical standards. The institutional review board approved the protocol for the current study of the Anesthesia Department at the Faculty of Medicine, Al-Azhar University Hospital Informed written consent was obtained from all participating patients.
REFERENCES
1 Burnett AL, Nehra A, Breau RH, et al Erectile dysfunction: AUA guideline J Urol 2018; 200:633-41
2 Zhu M, Labagnara K, Loloi J, et al Pudendal nerve block decreases narcotic requirements and time spent in post-anesthesia care units in patients undergoing primary inflatable penile prosthesis implantation Int J Impot Res 2024; 1-6
3 Raynor MC, Smith A, Vyas SN, et al Dorsal penile nerve block prior to inflatable penile prosthesis placement: a randomized, placebo-controlled trial J Sex Med 2012; 9:2975-9
4 Xie D, Nicholson M, Azaiza M, et al Effect of operative local anesthesia on postoperative pain outcomes of inflatable penile prosthesis: prospective comparison of two medications Int J Impot Res 2018; 30:93-96
5 Hsu GL, Hsieh CH, Wen HS, et al Outpatient penile implantation with the patient under a novel method of crural block Int J Androl 2004; 27:147-51
6 Uppal, Vishal FRCA, Retter, Susanne MD, Casey, Margaret MD, et al Efficacy of Intrathecal Fentanyl for Cesarean Delivery: A Systematic Review and Meta-analysis of Randomized Controlled Trials with Trial Sequential Analysis Anesthesia & Analgesia 2020; 130:111-125
7 Carvalho B, Drover DR, Ginosar Y, et al Intrathecal fentanyl added to bupivacaine and morphine for cesarean delivery may induce a subtle acute opioid tolerance Int J Obstet Anesth 2012; 21:29-34
8 Belzarena SD Clinical effects of intrathecally administered fentanyl in patients undergoing cesarean section Anesth Analg 1992; 74:653-657
9 Dindo D, Demartines N, Clavien PA Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey Ann Surg 2004; 240:205-213
10 Lucas J, Gross M, Yafi F, et al A Multiinstitutional Assessment of Multimodal Analgesia in Penile Implant Recipients Demonstrates Dramatic Reduction in Pain Scores and Narcotic Usage J Sex Med 2020; 17:518-25
11 García Rojo E, Garcíia Gómez B, Manfredi C, al Efficacy and safety of dorsal penile nerve block before collagenase of clostridium histolyticum injections in peyronie’s disease patients: Results from a prospective pilot study Andrologia 2020; 52:e13740
12 Nagao K, Ishii N, Miura K, et al One-day penile prosthesis surgery by penile block Int J Urol 2000; 7:S56-60
13 Ghanem H, Fouad G Penile prosthesis surgery under local penile block anaesthesia via the infrapubic s space Int Androl 2000; 23:357-9
14 Raynor MC, Smith A, Vyas SN, et al Dorsal Penile Nerve Block Prior to Inflatable Penile Prosthesis Placement: A Randomized, Placebo-Controlled Trial J Sex Med 2012; 9:2975-9
15 Gürkan Y, Kus ¸ A, Aksu C, et al Ultrasonography- guided penile block for adult penile surgery Can J Anesth 2016; 63:780-81
16 Uppal, Vishal, Retter, Susanne, Casey Margaret, et al Efficacy of Intrathecal Fentanyl for Cesarean Delivery: A Systematic Review and Meta-analysis of Randomized Controlled Trials with Trial Sequential Analysis Anesthesia & Analgesia 2020; 130:111-125
Correspondence
Adel Elatreisy, MD, MSc, PhD (Urol), FRCS (Urol) (Corresponding Author) dr adelelatreisy@yahoo com
Adel elatreisy@azhar edu eg
Urology Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt Urology Department, King Fahd Armed Forces Hospital, Jeddah, Saudi Arabia
Flat 1, 3245 Manazil Aleuzama’ Street, Ar Ruwais Dist, Jeddah, Saudi Arabia
Postal code: 23211
Yasser Ahmed dryasserbadran@gmail com
Mohamed Hindawy hindawy78@gmail com
Tamer Abouelgreed dr tamer ali@yahoo com Urology Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt
Ahmed Elgarhy elgarhy 79@yahoo com
Ismail Ahmed ismailabdelgawad 623@azhar edu eg Abdalla Abdalla abdalla201@yahoo com
Hany Ramadan hanysaid icu@gmail com
Mohamed Aboelsuod abosoad mohamed2017@gmail com
Khaled Shrief khaledshrief2@gmail com
Ayman Mohamed ayman icu@yahoo com
Wael Ibrahim waelelmahdy@gmail com
Saeed Abdelhameed dr said mostafaa@yahoo com dr said mostafaa@yahoo com
Anesthesia Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt
Mohammad Alghamdi mmss 19903@hotmail com
Mohammed Alzahrani mohdsaleh9@hotmail com
Urology Department, King Fahd Armed Forces Hospital, Jeddah, Saudi Arabia
Hamada Youssof hay02@fayoum edu eg
Urology Department, Faculty of Medicine, Fayoum University, Fayoum, Egypt
Conflict of interest: The authors declare no potential conflict of interest
A Elatreisy, Y Ahmed, A Elgarhy, et
ORIGINALPAPER
Pelvic floor contraction as an initial response to psycho-sensory sexual stimulation in men and a trigger for male sexual behaviour
Giuseppe La Pera 1, Sabrina Anticoli 2, Marilena Mangiardi 2, Stefano Livi 3
1 Consultant Urologist, Rome, Italy;
2 Stroke Unit - Head Neck and Neuroscience Department, San Camillo Hospital, Rome, Italy;
3 Social and Developmental Psychology, University of Rome "La Sapienza", Rome, Italy.
Summary
Introduction: This study is based on the hypothesis that, in men, the initial sexual response to erotic stimuli is triggered by a psycho-sensory pelvic reflex, mediated by the contraction of the pelvic floor muscles (PFM), rather than by an erection.
Objective: The objective is to determine, using a questionnaire that evokes an erotic image, whether there is a correlation between an erotic psycho-sensory stimulus and PFM contraction in men and females and whether this contraction encourages the subject to seek sexual activity.
Materials and methods: An online questionnaire was administered to 270 respondents (134 males, 136 females; mean age = 36.53, SD = 10.7; range 19-63). The questionnaire assessed the relationship between the perception of anterior PFM contraction and an evocative erotic image.
Results: The results show that following an evoked erotic stimulus, there is a significantly higher prevalence of perceived genital sexual responses in males compared to females through PFM contraction. A statistically significant difference was also observed in the desire to engage in sexual activity when perceiving PFM contraction (mean: Males 2.04 ± 0.95 vs. Females 1.02 ± 0.88; p < 0.001).
Conclusions: In this sample, an evocative erotic image triggers the perception of the genital sexual response via PFM contraction in more males than females. Additionally, PFM contraction, when perceived, prompts more males to seek sexual activity. These findings support the hypothesis that Pelvic Floor Muscles contraction is the initial response to psycho-sensory stimulation in men and a trigger for male sexual behaviour.
KEYWORDS: Psycho-sensory sexual pelvic reflex; Male sexual response; Male genital response; Pelvic floor; Neurological reflex; Male sexual behaviour; Genital perception; Ejaculatory urgency.
Submitted 19 September 2024; Accepted 10 October 2024
INTRODUCTION
The genital sexual response to erotic stimuli refers to the physiological and psychological changes in the genital organs that occur in response to sexual stimuli. It depends on multiple psychological, emotional, and physiological factors. Each of these factors can trigger a genital sexual response, which is considered an indicator of male arousal (1) and a motivational mechanism in the pursuit of sex-
ual activity (2). The psychophysiological model introduced by Masters and Johnson in the 1960s (3), which correlates simultaneous genital sexual response with the subjective perception of arousal, often shows great variability, despite frequent correlations. This finding has sparked debate among researchers, particularly regarding the explanation of the motivational mechanisms that drive individuals to seek sex. In fact, the subjective perception of genital arousal does not always align with the actual genital sexual response in male, such as increased volume and penile rigidity (4). As reported by Rieger and colleagues (4), in some situations, certain men, while feeling aroused, do not exhibit a simultaneous genital sexual response; in other words, the penis does not reflect an arousal state corresponding to the perceived sensation of excitement. In this experiment, some subjects without erectile dysfunction were asked to perform mathematical calculations during visual erotic stimulation, leading to a reduction in erection but not in the state of arousal (4, 5). In other cases, the opposite was observed: a genital sexual response occurred without an actual arousal state, as happens during nocturnal erections in the REM phase of sleep, which are not always associated with erotic dreams or arousal states (1, 6). This also occurs in patients with priapism, where an erection is present by definition, but without sexual arousal (7). The same phenomenon can be observed during cavernous pharmacological infusion with papaverine, as occurred during Virag's experiment, in which an erection was obtained under general anesthesia without the subject being aroused or aware of it (8). There are numerous explanations in the literature for this lack of simultaneous correspondence between selfreported arousal perception following visual stimulation and the genital arousal response. Among the various causes that could explain this discrepancy between perceived arousal and the objective genital arousal response, several hypotheses have been considered, including, but not limited to, methodological errors in the quality and duration of the erotic stimulus, the method of measuring self-reported arousal, and the objective measurement of the genital arousal response (9).
The lack of this simultaneous correlation, at least in men, could be due to the possibility that a pelvic reflex is elicited by psycho-sensory sexual stimulation (10). The direct
consequence of the presence of this psycho-sensory pelvic reflex implies that the perception of the genital response after visual erotic stimulation may not simply be the perception of an erection, as hypothesized in the excitement phase described by Masters and Johnson, but rather the perception of the involvement of another structure, which, according to this hypothesis, is constituted by the pelvic floor This contraction would cause an increase in pressure within the corpus cavernous and the corpus spongiosum of the urethra, which is then transmitted to the receptors in the glans This increase in pressure in these structures may lead to a conscious perception of the genital response, which is interpreted as the occurrence of a sexual response of the genitals In other words, the perception of the pelvic floor contraction, particularly of the ischiocavernosus, bulbourethral, and bulbocavernosus muscles, might serve as one of the indicators of sexual response to visual or imagined stimuli
This could explain why changes in penile volume, blood flow, or rigidity the primary indicators of genital arousal response in men may not be and may lay the foundation for a revised psychophysiological model that incorporates this new parameter: pelvic floor muscle contraction as initial response to psycho-sensory sexual stimulation
The aim of this study is to evaluate, through a questionnaire that evokes an erotic image: whether there is a correlation in men and females between an evoked erotic image and pelvic floor contraction, and whether this contraction prompts the individual perceiving this sensation to seek sexual activity
MATERIALS AND METHODS
Procedure and sample
We administered a questionnaire via the Prolific platform (www prolific com) Prolific is an online platform that connects researchers with high-quality participants for academic studies, offering a diverse and reliable pool It ensures ethical standards by providing fair compensation and robust data quality, making it a preferred tool for behavioral and social sciences research (11, 12) All respondents provided informed consent beforehand, in which the anonymity of responses was guaranteed, following the guidelines of the Helsinki Declaration of 2013 (Ethical Principles for Medical Research Involving Human Subjects)
Four-hundred subjects answered the survey All respondents were asked about their sexual preferences, specifically whether they identified as heterosexual, homosexual, bisexual, or other (pansexual or undeclared) Sixtythree respondents, who identified as homosexual, bisexual, or other were excluded Only those who answered all the presented questions were retained, in order to maintain comparability of responses The final sample consisted of 270 respondents with an average age of 36 53 years (SD = 10 7; range 19-63), comprising 134 males (49 6%; average age 35 93, SD 10 12; range 1963) and 136 females (50 4%; average age 37 13, SD 11 22; range 21-63)
All respondents read a description of the pelvic floor muscles, their function, and typical use during urination Subsequently, they were asked if they understood what
the pelvic floor and pelvic floor contraction were, and all responded affirmatively
Measures
Male respondents were administered the following five questions: “Do you feel you have experienced increased tension in the penis and glans (or increased tension in the clitoris in the female version) due to pelvic floor contraction when: “with a 5-point response scale: Never (0), Rarely (1), Sometimes (2), Often (3), Always (4), and “I have not been in this situation” (the latter treated as a missing value)
The items considered in the five questions were:
ITEM 1 W h e n y o u r p a r t n e r d r
provocative manner;
ITEM 2 When you encounter a particularly attractive woman;
ITEM 3 When you see an erotic scene (e g , a film);
ITEM 4 When your partner sends you sexually provocative photos;
ITEM 5 When you see a particularly attractive woman, do you immediately feel the desire to have sexual intercourse
Subsequently, in order to determine the presence or absence of sexual disorders, male respondents were asked to respond to the following questionnaires: 1) The International Index of Erectile Function (IIEF5) (13) as well as questions related to sexual desire extracted from the IEEF15 (14), specifically q11 “How often have you felt sexual desire in the past four weeks?” and q12 “How would you rate your level of sexual desire?” Additionally, they were asked to complete the Premature Ejaculation Diagnostic Tool (PEDT) (15)
Female respondents were asked to respond to two questionnaires: the Female Sexual Dysfunction (FSD) (16) and the Female Sexual Distress Scale for the study of psychological distress (FSDS) (17)
Statistical methods
The responses to the questionnaire from males and females were subjected to the A n a l y s i s o f V a r i a n c e (ANOVA) All analyses were conducted using IBM SPSS Statistics for Windows, Version 25 0 with a two-level factor (male/female) for each of the five questions
RESULTS
Data analysis
Regarding the IIEF 5 questionnaire, we considered subjects with a total score of 21 or higher on the five questions to be normal (14)
Their distribution was as follows: Normal (14) ≥ 21: n 95 subjects, accounting for 70 9%; Pathological (14) < 21: n 39 subjects, accounting for 29 1%
Regarding the PEDT questionnaire, we considered subjects without premature ejaculation to be those who scored 9 or less on the five questions
Subjects with a score of 10 or higher (16) were considered likely to have premature ejaculation, and those with a score above 11 were considered to have premature ejaculation
In our sample, the distribution was as follows: Normal ≤ 9: n 105 subjects, accounting for 78 4%; Pathological or likely pathological > 9: n 29 subjects, accounting for 21 6%
G La Pera, S Anticoli, M Mangiardi, S Livi
Table 1a
Means and frequencies related to the degree of arousal (percentages in parentheses)
Differences in means between males and females in the degree of arousal (standard deviation in parentheses)
Do you fee you have exper enced increased tension in the pen s and g ans (or increased tension in the c itoris in the fema e version) due to pe vic f oor contract on The d fference between male and female responses has been statistical y sign ficant n al Items
Regarding the questions related to male sexual desire, we extracted from the IIEF15 questionnaire (15), when the response to one or both of these questions was less than 3, we considered the subject to have low sexual desire
The distribution of subjects was as follows: Normal ≥ 3: n 127, accounting for 94 8%; Pathological < 3: n 7, accounting for 5 2%
In order to identify dysfunctions in the female sample, we used the 6-item FDS questionnaire (17) instead of the tra-
ditional 19-item FDS questionnaire, which has c o m p a r a b l e p s y c h o m e t r i c p r o p e r t i e s b u t i s quicker to use, making the survey easier
The distribution between normal and pathological in our sample was as follows: Normal ≥ 19: n 98, accounting for 72 1%; Pathological < 19: n 38, accounting for 27 9%
We also used the FSDS-R questionnaire (18) to measure female sexual distress, with a cut-off value of less than 11 to distinguish normal from pathological
In our sample, the distribution was as follows: Normal < 11: n 73, accounting for 53 74%; Pathological ≥ 11: n 63, accounting for 46 3%
Means and frequencies related to the degree of arousal were calculated for the responses to each item (see Tables Ia, Ib) The results were statistically different between men and women, indicating that an evoked erotic stimuli in men was more frequently accompanied by pelvic floor muscle contraction compared to women (see Figure 1 and Table 1b)
Figure 1. Differences between males and females in the degree of perceived arousal
Do you feel you have experienced increased tension in the penis and glans (or increased tension in the clitoris in the female version) due to pelvic floor contraction
The difference between male and female responses has been statistically significant in all Items
Table 2
Differences in means between male participants with and without erectile dysfunction (IEEF5) (standard deviation in parentheses).
P=095P=707P=6
Do you fee you have exper enced increased tension in the pen s and g ans (or increased tension in the c itoris in the fema e version) due to pelvic f oor contract on There are no stat stica ly s gnificant d fferences in any tem between males w th and w thout ED
Table 3.
Differences in means between male participants with and without premature ejaculation (PE) (standard deviation in parentheses)
Do you feel you have experienced increased tens on n the penis and glans (or ncreased tension n the cl tor s n the female vers on) due to pelv c floor contraction There are no statistically sign f cant differences n any item between males with and without PE
The differences in mean arousal were significant for all the questions asked: males expressed more frequent contraction in Item 1 (“When your partner dresses in a sexually provocative manner”) (M = 2 06 vs 1 46 (F(1 268) = 91 90, p < 001); Item 2 (“When you encounter a particularly attractive woman/man”) (M = 1 77 vs 1 28 (F(1 268) = 15 73, p < 001); Item 3 (“When you see an erotic scene (e.g.,
a film)”) (M = 2 54 vs 2 28 (F(1 268) = 4 92, p = 027); Item 4 (“When your partner sends you sexually provocative photos") (M = 3 05 vs 1 81 (F(1 268) = 72 25, p < 001); Item 5 ("When you see a particularly attractive woman/man, do you immediately feel the desire to have sexual intercourse ”) (M = 2 04 vs 1 12 (F(1 268) = 69 46, p < 001)
The Analysis of Variance was then applied to compare healthy subjects with those having sexual disorders as defined by the test For both erectile dysfunction (ED) and premature ejaculation (PE) (see Tables and Figures 2, 3) the comparison between normal male subjects and those with one or more pathological test results concerning the responses to the five questions did not show statistically significant differences Regarding desire disorder, statistically significant differences were found in arousal in the questions related to “When your partner dresses in a sexually provocative manner” and “When my partner sends me sexually provocative photos” , that is, in questions related to one's partner In both cases, those without a desire disorder reported a higher degree of arousal compared to those with a desire disorder (see Table and Figure 4) For Item 1 (“When your partner dresses in a sexually provocative manner”) (M = 2 70 vs 1 86 (F(1 132) = 5 05, p = 026) and for Item 4 (“When your partner sends you sexually provocative photos”) (M = 3 09 vs 2 29 (F(1 132) = 4 40, p = 038) This section is limited to men who answered questions q11 and q 12 of the IIEF-15 questionnaire
Figure 2.
Differences in means between male participants with and without erectile dysfunction (IEEF-5)
Do you feel you have experienced increased tension in the penis and glans (or increased tension in the clitoris in the female version) due to pelvic floor contraction
There are no statistically significant differences in any item between males with and without ED
Figure 3
Differences in means between male participants with and without premature ejaculation (PE) (standard deviation in parentheses)
Do you feel you have experienced increased tension in the penis and glans (or increased tension in the clitoris in the female version) due to pelvic floor contraction
In all Items there is no statistical difference between respondents with PE and non-PE
G La Pera, S Anticoli, M Mangiardi, S Livi
4.
Do you fee you have exper enced ncreased tension in the pen s and g ans (or increased tension in the cl toris in the fema e version) due to pe vic f oor contractio In this sect on im ted to men who answered to quest on q11 and q 12 of the IIEF-15 questionnaire there s statist cal different sign ficant n Item 1 and Item 4 between men w th an without des re disorders
Table 5
Differences in means between female participants regarding female sexual dysfunctions (FSD) (standard deviation in parentheses).
NoFSD(n=98)166(103)130(101)243(093)203(
FSD(n=38)092(100)124(110)189(111)124(112)089(
Do you fee you have exper enced ncreased tension in the pen s and g ans (or increased tension in the cl toris in the fema e version) due to pe vic f oor contraction The d fference between female with and with FSD has been statistical y sign f cant n Items 1, 3 and 4
Regarding the comparison of normal female subjects with those having FSDI-6 (female sexual dysfunction) or FDSS-R (distress) pathological, the results indicated some statistically significant differences (see Tables and Figures 5, 6) In particular, females without disorders exhibited
higher arousal, except for item 2 (“When you encounter a particularly attractive woman/man”) For these items, women without sexual disorders showed a higher degree of arousal: in this case, females expressed more arousal in Item 1 (“When your partner dresses in a sexually provocative manner ”) (M = 1 66 vs 0 92 (F(1 134) = 14 37, p < 001); Item 3 (“When you see an erotic scene (e g , a film)”) (M = 2 43 vs 1 89 (F(1 134) = 8 07, p = 005); Item 4 (“When your partner sends you sexually provocative photos”) (M = 2 03 vs 1 24 (F(1 134) = 3 46, p < 001)
Regarding female sexual distress (see Table and Figure 5), no statistically significant differences were recorded except for Item 3 (“When you see an erotic scene (e g , a film)”) In this case, women with a sexual disorder showed a greater pelvic floor contraction associated with viewing these erotic scenes (M = 2 51 vs 2 08 (F(1 134) = 6 26, p = 01)
The results indicate that there are no differences among men between those without sexual disorders and those with ED or PE However, some statistically significant differences emerge in the greater arousal of those without desire disorders related to pelvic floor contraction during visual erotic stimuli experienced with their partner
Regarding the female sample, respondents with sexual dysfunction showed a greater contraction in normal subjects compared to those with sexual disorders (similar to what was observed in the male sample) However, female respondents with sexual distress exhibited higher con-
Figure 4.
Differences in means between male participants with and without desire disorder
Do you feel you have experienced increased tension in the penis and glans (or increased tension in the clitoris in the female version) due to pelvic floor contraction
In this section limited to men who answered to question q11 and q12 of the IIEF-15 questionnaire there is statistical different significant in Item 1 and Item 4 between men with and without desire disorders
Figure 5.
Differences in means between female participants regarding Female Sexual dysfunctions (FSD)
Do you feel you have experienced increased tension in the penis and glans (or increased tension in the clitoris in the female version) due to pelvic floor contraction
The difference between female with and with FSD has been statistically significant in Items 1, 3 and 4
Table 6.
Differences in means between female participants regarding female sexual distress (FSDS)
Do you fee you have exper enced increased tension in the pen s and g ans (or increased tension in the c itoris in the fema e version) due to pe vic f oor contract on The d fference between females with and with FSDS has been stat st cally signif cant only n Items 1
traction values compared to those without sexual distress
Overall, there is a tendency in both male and female samples to show greater tension in the penis or clitoris due to pelvic floor contraction in normal subjects compared to pathological ones, except in the case of female sexual distress, where the trend is reversed
DISCUSSION
A first consideration arising from these data is inspired by numerous studies that have highlighted that, in the psychophysiological response to erotic stimuli, there is a correlation between genital arousal and its simultaneous conscious perception (7) This agreement between genital sexual response and its perception is much more frequent in men than in women (7), and there is a difference between women with sexual dysfunction and those without (18)
These studies have never clarified the potential anatomical structure that enables this agreement in the perception of arousal in men According to our study, what facilitates the perception of arousal is the contraction of the pelvic floor, which in turn triggers the sexual response, generating a need for sexual activity The initial hypothesis is based on the idea that, following visual or psychosensory sexual stimulation, the psychophysiological response initiates, like a neurophysiological reflex, the contraction of the pelvic floor, specifically the bulbourethral, bulbocavernosus, and ischiocavernosus muscles The reflex contraction of these muscles would cause a "squeezing" of the corpus spongiosum of the urethra and the corpus cavernosum, leading to the perception of arousal
Consequently, the individual might seek a solution for this arousal, experiencing an urgent desire for sexual
Figure 6.
Differences in means between female participants regarding Female Sexual Distress (FSDS)
Do you feel you have experienced increased tension in the penis and glans (or increased tension in the clitoris in the female version) due to pelvic floor contraction
The difference between females with and with FSDS has been statistically significant only in Items 1
activity, similar to the need to urinate or defecate when the bladder or rectum is full
These findings could explain the difference in sexual response behaviors between men and women, as demonstrated in anatomical studies of the anterior pelvic floor The male pelvic floor muscles are significantly stronger and more effective in contracting the corpus spongiosum of the urethra and the corpus cavernosum than the thin muscle fibers of the female pelvic floor, which reach only a small portion of the clitoral cavernous bodies (19)
Furthermore, continuing with the analysis suggested by these data, it is useful to consider the epidemiological data on pelvic floor disorders, which reinforce our observations It is well-documented in medical literature that pelvic floor disorders are more common among women (20) and are associated with female sexual dysfunction (21)
Finally, when analyzing these data, it is important to remember that there are variables not considered in our study that could negatively influence the observed results, such as the cultural differences that lead women to express their sexual preferences and arousal less frequently in public (self-censorship, social modesty) Although this could represent a source of bias, the guarantee of anonymity provided by an online questionnaire may have mitigated this issue (22, 23)
CONCLUSIONS
The data presented here highlight a statistically significant difference between heterosexual males and females in the perception of visual arousal and, among females, a statistically significant difference between those with sexual disorders and those without via the pelvic floor muscle contraction Additionally, there is a difference between males and females in the perception of the urgent need to have sex following visual arousal and pelvic floor contraction
This study aligns and support the hypothesis that the initial response of the male sexual reaction to visual erotic stimuli is mediated by a reflex contraction of the anterior pelvic floor muscles Furthermore, these data support the hypothesis that there is a difference in visual arousal between males and females, which triggers the so-called "desire" for sex, similar to the perception of an urgent need to urinate or defecate when the bladder or rectum is full
G La Pera, S Anticoli, M Mangiardi, S Livi
Further studies, including neurophysiological tests and additional data, are necessary to confirm the hypothesis of the psycho-sensory pelvic reflex in response to erotic stimuli and the new paradigm of human sexual response
ACKNOWLEDGMENTS
I thank Martha B Scherr for her help in translating the text into English
REFERENCES
1 Janssen E, Everaerd W Determinants of male sexual arousal Annual Review of Sex Research 1993; 4:211-246
2 Bailey JM What is sexual orientation and do women have one? Nebr Symp Motiv 2009; 54:43-63
3 Masters WH, Johnson VE Human Sexual Response Little, Brown and Company, New York 1966
4 Rieger G, Chivers ML, Bailey JM Sexual arousal patterns of bisexual men Psychol Sci 2005; 16:579-84
5 van Lankveld JJ, van den Hout MA Increasing neutral distraction inhibits genital but not subjective sexual arousal of sexually functional and dysfunctional men Arch Sex Behav 2004; 33:549-58
6 Bach AK, Brown TA, Barlow DH The effects of false negative feedback on efficacy expectancies and sexual arousal in sexually functional males Behavior Therapy 1999; 30:79-95
7 Chivers ML, Seto MC, Lalumière ML, et al Agreement of selfreported and genital measures of sexual arousal in men and women: A meta-analysis Arch Sex Behav 2010; 39:5-56
8 Silberman M, Stormont G, Leslie SW, Hu EW Priapism StatPearls [Internet] Treasure Island (FL): StatPearls Publishing 2023; 30:1-11
9 Porst H, Lewis R, Virag R, Goldstein I A comprehensive history of injection therapy for erectile dysfunction, 1982-2023 Sex Med Rev 2024; 12:419-433
10 La Pera G The Psycho-Sensory Pelvic Reflex: A New Paradigm in the Model of Male sexual response Arch Ital Urol Androl 2024; 96:12975
11 Palan S, Schitter C Prolific ac–A subject pool for online experiments J Behav Exp Financ 2018; 17:22-27
12 Peer E, Brandimarte L, Samat S, Acquisti A Beyond the Turk: Alternative platforms for crowdsourcing behavioral research J Exp Soc Psychol 2017; 70:153-163
13 Rosen RC, Cappelleri JC, Smith MD, et al Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction Int J Impot Res 1999; 11:319-26
14 Rosen RC, Riley A, Wagner G, et al The International Index of Erectile Function (IIEF): a multidimensional scale for assessment of erectile dysfunction Urology 1997; 49:822-830
15 Symonds T, Perelman MA, Althof S, et al Development and validation of a premature ejaculation diagnostic tool Eur Urol 2007; 52:565-73
16 Isidori AM, Pozza C, Esposito K, et al Development and validation of a 6-item version of the female sexual function index (FSFI) as a diagnostic tool for female sexual dysfunction J Sex Med 2010; 11:39-46
17 DeRogatis L, Clayton A, Lewis-D’Agostino D, et al Validation of
the female sexual distress scale revised for assessing distress in women with hypoactive sexual desire disorder J Sex Med 2008; 5:357-364
18 Handy AB, Stanton AM, Pulverman CS, Meston CM Differences in Perceived and Physiologic Genital Arousal Between Women with and without Sexual Dysfunction J Sex Med 2018; 15:52-63
19 Rocca Rossetti S , Functional anatomy of pelvic floor Arch Ital Urol Androl 2016; 88:28-37
20 Lakhoo J, Hhatri G, Chernyak V et al MRI of the Male Pelvic Floor Radiographics 2019; 39:2003-2022
21 Handa VL, Cundiff G, Chang HH et al Female sexual function and pelvic floor disorders Obstet Gynecol 2008; 111:1045-1052
22 Fortenberry JD, Hensel DJ Sexual modesty in sexual expression and experience: A scoping review, 2000-2021 J Sex Res 2022; 59:1000-1014
23 Morokoff PJ Effects of sex guilt, repression, sexual ‘‘arousability’’ and sexual experience on female sexual arousal during erotica and fantasy J Pers Soc Psychol 1985; 49:177-187
Correspondence
Giuseppe La Pera, MD (Corresponding Author) dr giuseppelapera@gmail com
Via delle Mura Gianicolensi 67 c/o UPMC Salvator Mundi International Hospital, Rome, Italy
Sabrina Anticoli
Marilena Mangiardi
Stroke Unit - Head Neck and Neuroscience Department San Camillo Hospital, Rome, Italy
Stefano Livi
Social and Developmental Psychology, University of Rome "La Sapienza", Rome, Italy
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Reassessing cardiovascular risk stratification in men with erectile dysfunction
João Lorigo 1 , Daniela M. Gomes 2, 3 , Ana R. Ramalho 1, 3 , Edgar T. Silva 1, 3 , Patrícia A. Mendes 1, 3 , Arnaldo Figueiredo 1, 3
1 Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal;
2 Unidade de Saúde Familiar Serra da Lousã, Vilarinho, Portugal;
3 Faculdade de Medicina da Universidade de Coimbra, Coimbra, Portugal
Summary
Background and objectives: Erectile dysfunction (ED) is an independent and strong marker of cardiovascular disease (CVD) risk The Princeton Consensus aimed to evaluate and manage cardiovascular risk in men with ED and no known cardiovascular disease, focusing on identifying those requiring additional cardiologic work-up. It has recently been updated to the American population demographics, but European recommendations are needed.
Methods: It was developed a cross-sectional investigation including erectile dysfunction patients. Data were collected from hospital registries Two risk stratification models were employed and compared: Princeton Consensus Criteria (PC) and European Society of Cardiology (ESC) CVD Risk Criteria
The objective was to stress the importance of the changes in IV Princeton Consensus recommendations in stratifying CVD risk in men with erectile dysfunction using a model validated in European men
Results: A total of 137 patients with ED, with a mean age of 57 1 years old, were included According to the PC criteria, 39.7% of the patients were “Low Risk”. When using ESC criteria, the proportion of “Low Risk” patients were significantly lower (12%, p < 0 05) Among “Low Risk” patients according to the PC, 52 5% and 20% were classified as High and Very high risk according to ESC criteria, respectively One myocardial infarction was reported The patient was classified as “Low Risk” according to the PC, but the ESC criteria categorized him as “high risk”
Conclusions: PC is less sensitive than ESC recommendations detecting CVD It raises concerns that Urologists could be overlooking patients with undiagnosed CVD, consequently missing out on opportunities for prevention of major cardiovascular events (MACEs) and premature deaths
KEY WORDS: Erectile dysfunction; Cardiovascular disease; IV Princeton consensus
Submitted 25 February 2024; Accepted 1 June 2024
INTRODUCTION
Erectile dysfunction (ED), defined as a man ’ s consistent or recurrent inability to attain and/or maintain penile erection enough for successful vaginal intercourse (1), is a common problem in men as they age Epidemiological data shows a high prevalence and incidence of ED world-
wide (2) It is estimated by the year 2025, 322 million men will suffer from ED (3) In a European study of men aged 30-80 years, the prevalence of ED was 19 2%, with a steep age-related increase from 2 3% to 53 4% (4)
Cardiovascular disease (CVD) is a leading cause of death and disability in men (5) In Europe, deaths from CVD in those aged < 70 years old are a particular concern, with > 60 million potential years of life lost to CVD annually (6)
The link between ED and CVD has been previously characterized primarily by shared risk factors (7-9) However, an emerging set of data indicates that ED is in fact an independent and strong marker of CVD risk (10-22) As we know, both diseases are consequences of systemic vascular disease and shared common risk factors
Furthermore, they share the same pathological process: endothelial dysfunction (18) Knowledge of this association justified the introduction in 2021 in the European Society of Cardiology (ESC) guidelines on cardiovascular disease prevention in clinical practice of the recommendation to assess cardiovascular risk in men with evidence of erectile dysfunction, with recommendation level IIa and evidence C (23) Because of the quality of life (QoL) burden it carries, ED may drive men to seek medical attention in the absence of other cardiovascular symptoms Thus, the presence of ED may provide the opportunity for CVD assessment and mitigation of its risks The importance of evaluating cardiovascular risk in men with ED is now a critical factor for overall early stage management of CVD, especially in younger men (7, 9)
In accordance with the European Association of Urology (EAU) guidelines, sexual rehabilitation should only commence after a meticulous evaluation of the cardiovascular risk, alongside with an assessment of the individual's capabilities to engage in physical activity (7) Despite these recommendations, recent research highlighted a deficiency in the evaluation of CVDs in patients with ED by urologists: alarmingly, fewer than half of these clinicians undertook a combined assessment encompassing both CVD and ED (24)
The Princeton consensus (Expert Panel) Conference, is a multispecialty collaborative tradition dedicated to optimizing sexual function and preserving cardiovascular health (9) The III Princeton consensus (Princeton 3) were published over a decade ago (9), and since then, several
Lorigo, D M Gomes, A R Ramalho, et al
alternative risk models have been revised and validated for the prediction of cardiovascular risk in individual patients, according to their demographic background The IV Princeton consensus (Princeton 4) were recently updated, addressing this disparity (25) The Princeton 4 recommends the use of Atherosclerotic Cardiovascular Disease (ASCVD) model introduced by the American College of Cardiology/American Heart Association (AHA/ACC) in 2013 (26) to estimate the CVD risk in all patients with organic vasculogenic ED However, the ASCVD score is not validated to the European population Of particular interest is the SCORE2/SCORE2-OP developed by the ESC, that was last updated in 2021 and is distinct for being the developed and validated for the European population (27)
The present study aimed to stress the importance of the changes in Princeton 4 recommendations in stratifying CVD risk in men with erectile dysfunction using a model validated in European men
METHODS
This study was designed as a cross-sectional study to evaluate the adequacy of the Princeton consensus (PC) for strat-
ifying men with ED based on their CVD risk The study drew upon a clinical series of patients with ED to conduct a comprehensive review The study included all patients referred to the andrology department at a Central Hospital in Portugal for the assessment and treatment of erectile dysfunction within the designated study timeframe (three-year period, from December 2019 to December 2022) All patients included in the analysis were diagnosed with organic ED according to the clinical data and all of them were interviewed by the same expert in andrological care to ensure consistency in data collection and evaluation
We collected demographic data, medical history, and CVD risk factors recorded in the hospital registries during a minimum follow-up period of 12 months The proportion of positive stress test results and subsequent invasive cardiac procedures was documented The occurrence of major adverse cardiovascular events (MACEs) was monitored during the study period
Two risk stratification models were employed: Classic Princeton criteria (PC) and ESC CVD Risk Criteria To facilitate meaningful comparisons and clinical applicability, patients were subsequently categorized into "low risk" and "Non-low risk" groups for all risk assessments Specifically, PC and ESC Lowest risk categories, PC low risk and ESC Low to Moderate risk patients, respectively, were placed in the "low risk" category, whereas the leftovers were grouped under "non-low risk" For a visual representation of the risk groups recommended by the ESC CVD Risk Stratification Criteria, please refer to Figure 1 (23)
The ESC guidelines (23) served as the basis for patient stratification in this study Following the ESC panel's recommendations, individuals with a history of CVD were automatically categorized as not being at low risk for future MACEs, as depicted in Figure 1 Consequently, all patients with documented CVD were classified as "nonlow risk" for the analysis Those witho u t p re v i o u s C V D w e re s t r a t i f i e d based on the SCORE2/SCORE2-OP system We utilized the HeartScore calculator available on the ESC online platform (https://www heartscore org/), which necessitates input regarding patients' age, sex, blood pressure, total HDL and LDL cholesterol levels, and smoking status All relevant data were extracted from hospital registries
Figure 1
Patients’ categories and associated CVD risk according to ESC guidelines
J
The data were managed on and analysed using SPSS for Windows All values were expressed as mean (± standard deviation) or as percentages Standard descriptive analysis was performed to analyse the baseline characteristics of the study population The categorized risk estimates derived from the different risk scores were compared using McNemar test (as the risk scores were dichotomized as “low risk” or “high risk”) A p value < 0 05 was considered statistically significant The study was conducted following the principles outlined in the Declaration of Helsinki Approval from the Institutional review board were obtained
RESULTS
Our study included 137 patients with ED with a mean age of 57 1 ± 10 5 years old The average Body mass index (BMI) was 27 7 ± 4 1 kg/m2, and each patient had a median of 3 CVD risk factors Of the total population, 28 5% had diabetes mellitus (DM), 12 4% had chronic kidney dis-
ease (CKD), 6 6% had a previous stroke and 4 4% had a myocardial infarction (MI) Baseline characteristic of the population are summarized in Table 1 Table 2 presents the categorization of patients based on various risk models, and Table 3 provides a comparison between these models Figure 2 gives a visual representation of the distribution according to the model applied According to the PC, approximately 39 7% of patients were classified as "low risk" However, when using alternative risk scores (ESC criteria), the percentage of patients classified as being at the lowest risk group was significantly lower (12%, p < 0 05) Within the "low risk" group according to the PC, 52 5% and 20% were classified as high and very high risk according to the ESC criteria, respectively
Patients without previously known CVD showed a mean 10-year risk of CVD events of 6 5% ± 3 5% according to the SCORE2/SCORE2-OP Moreover, Low, Intermediate and high-risk patients according to PC showed a 10-year risk calculated with the SCORE2/SCORE2-OP formula of 5 4% ± 3 2%, 7 6% ± 3 6% and 8 5% (n = 1), respectively
To address arbitrary cutoff values used for categorization in the SCORE2/SCORE2-OP model, we utilized a ROC curve (Figure 3) Our analysis pinpointed a 5% 10-year CVD risk threshold from the SCORE2/SCORE2-OP model, offering
2.
Patient distribution according to the models applied
s
)9
lcholesterol(mg/dL)1758±395
HDLcholesterol(mg/dL)512±185
LDLcholesterol(mg/dL)1037±464
Cardiovascularriskfactors(%) ≤ 2419% ≥ 3581%
Table 2.
Patients’ distribution according to the risk models applied
Characteristics of patients who underwent a cardiac procedure or a major adverse cardiovascular event (MACE).
Patients MACE Cardiac III Princeton ESC inter vention consensus guidelines
1N
to
2O
3O
4N
5N
the optimal balance of sensitivity and specificity when compared to the PC Of the men without CVD, 40 7% showed a 10-year risk below 5%, aligning with the proportion classified as “low risk” by the PC (39 7%) Notably, within the PC "low risk" group, 40 7% still exhibited a 10year MACE risk surpassing this threshold Among men who underwent stress testing, 10 patients (21 7%) tested positive for ischemia and were referred to the Cardiology department During follow-up, two MACEs were reported: 1 myocardial infarction (MI) and 1 ventricular tachycardia (VT) Out of the 137 included patients, five underwent cardiac interventions (1 angioplasty, 1 bypass, 1 implantable cardioverter defibrillator (ICD), 1 MitraClip and 1 valvuloplasty) The sole MI reported occurred in a patient classified as "low risk" according to the PC However, the 47-year-old male with DM, according to the ESC guidelines, was categorized as "high risk" Nevertheless, there was no significant difference in the MI rate between the two models (p < 0 05) Further information on these patients can be seen in Table 4
DISCUSSION
The association between ED and undiagnosed CVD has been extensively investigated since its initial recognition as an independent risk factor A meta-analysis encompassing 12 prospective cohort studies identified ED as a predictive indicator for various cardiovascular outcomes: cardiovascular events (HR 1 44, 95% CI 1 27-1 63), cardiovascular mortality (HR 1 19, 95% CI 0 97-1 46), myocardial infarction (HR 1 62, 95% CI 1 34-1 96), cerebrovascular events (HR 1 39, 95% CI 1 23-1 57), and allcause mortality (HR 1 25, 95% CI 1 12-1 39) (28)
Another comprehensive literature review highlighted that ED precedes cardiac events by a period of 3 to 5 years, which responds to an important window of opportunity in the prevention of cardiovascular events (21) An umbrella review of systematic reviews and meta-analyses underscored the consistent finding that ED frequently precedes symptomatic CVD This recognition equips healthcare practitioners with the opportunity to screen and identify high-risk patients at an early stage, ultimately contributing to prevent morbidity and mortality (27) Similarly, Gandaglia et al found that ED patients with cardiovascular risk factors should be considered high risk, warranting comprehensive cardiovascular evaluations due to potential silent coronary artery disease (30) Raheem et al emphasized the responsibility of urologists, general practitioners, and primary care physicians to
identify high-risk patients and refer them to cardiologists for assessment (31)
Due to the robust association between ED and CVD, major urological associations such as EAU, AUA and, more recently, ESC advocate for systematic assessment of ED patients regarding their CVD risk (7, 23, 32) This approach recommends sexual rehabilitation exclusively for patients categorized as low risk, while those at higher risk require further cardiologic evaluation This evaluation does not primarily focus on the patient's ability to tolerate pro-erectile medication, given the generally safe nature of these therapies (33) Instead, it aims to determine the patient's physical capability to sustain the exercise intensity demanded by sexual activity Sexual activity between couples in a longstanding relationship equates to approximately 3 Mets (metabolic equivalent of task), therefore completing 4 minutes of the standard Bruce t
arrhythmias, or a fall in systolic blood pressure (BP) confirms the safety of sexual activity (7, 9)
The Princeton 3 underscored that intermediate risk patients should undergo stress test to gauge exercise capacity prior to initiating proerectile therapy High-risk patients are advised to undergo a thorough cardiologist assessment and optimization before embarking on rehabilitation (7, 32) A limitation of the Princeton 3 was its insufficient consideration of varying degrees of severity associated with specific risk factors, such as age, DM, and lipid profile While uncontrolled hypertension designates individuals as high risk, the Consensus overlooked the progressive impact of aging, current lipid profile and glycaemic status, regarding them to mere contributors within the cumulative risk factor count In contrast, the ESC criteria (as shown in this study) and the ASCVD score (as proposed in the Princeton 4) demonstrates a more comprehensive, personalized and sensitive approach
As recently published (25), the Princeton 4 suggests assessing all vasculogenic ED patients based on their 10year risk of CVD using the ASCVD score If the 10-year risk is 5-20%, coronary artery calcium (CAC) testing is reco m m e n d e
Patients with an abnormal CAC test or an initial risk over 20% should be referred to preventive cardiology for rigorous risk factor control Our study supports and reinforces this new recommendation
The ESC criteria encompass the exact age, blood pressure, lipid profile in risk evaluation, CKD stage and current glycaemic control For instance, under the PC, a 40year-old smoker with hypertension and dyslipidaemia is classified as intermediate risk (owing to the presence of three risk factors, excluding sex) Conversely, a 75-yearold smoker without comorbidities is labelled low risk
However, considering both individuals show normal lipid profile and blood pressure, the SCORE2/SCORE2-OP model presents divergent outcomes The first patient is designated low risk with a 2% 10-year cardiovascular event risk, while the second patient faces a substantially higher risk of 18% over the same period However, the clinical significance of these disparities remains uncertain While it is accepted that patients classified as Intermediate Risk by the PC should undergo a physical capacity assessment, there hasn't been a direct compari-
son with other risk models, nor has a definitive threshold for the 10-year CVD event risk, needing stress testing, been explored Yet, this approach appears the most patient-focused method for evaluating these patients
Notably, there was only one reported case of myocardial infarction, and it occurred in a patient classified as "low risk" according to the PC criteria In contrast, the ESC criteria categorized that patient as "high risk" However, despite the different risk stratifications, the study did not find significant differences in the risk of MACEs between the "low risk" and "non-low risk" groups This can be attributed to the infrequency of these events during the relatively brief study period, or, to a lesser extent, to a well-timed preventive intervention
Using ROC curves helped us pinpoint a 5% 10-year CVD risk threshold from the SCORE2/SCORE2-OP model, which struck a balance between sensitivity and specificity when compared to the PC However, we observed that for "low risk" patients defined by the PC, 40 7% of patients still exhibited a 10-year MACE risk surpassing 5% This finding underscore, again, the significant differences between these two models and the importance of selecting the appropriate model and cutoff values when assessing cardiovascular risk
This study possesses some limitations Firstly, its retrospective design renders it susceptible to potential biases in data collection Nonetheless, it's important to note that all patients underwent interviews conducted by the same Urologist, and the quality of registries was classified as highly reliable Secondly, while the collected risk factors were considered dependable, the reference to the presence of family history of premature coronary artery disease were inconsistent and was consequently excluded from the analysis as a potential risk factor Finally, the limitations stemming from the sample size, potential data loss during follow-up, and its duration proved inadequate for comprehensively assessing the clinical implications regarding the incidence of MACEs between the models Ultimately, alternative risk models like the ESC recommendations may enhance the assessment of patients with CVD This stresses the pertinence of the updates in Princeton 4, from the previous Princeton 3
CONCLUSIONS
The study underscores that the PC exhibits lower sensitivity compared to the ESC recommendations to stratify the CVD risk of European men This disparity raises concern that Urologists could be overlooking patients with undiagnosed cardiovascular disease, thereby missing critical opportunities for timely prevention of MACEs and premature deaths This underscores the relevance of the u p d a t e s i n P r i n c e t o n 4 c o m p a re d t o t h e p re v i o u s Princeton 3 The EAU guidelines should be revised accordingly, taking into account the optimal risk model for the European patient population
REFERENCES
1 Partin AW, Peters CA, Kavoussi LR, et al Campbell Walsh Wein Urology: 3-Volume Set Elsevier; 2020
2 Selvin E, Burnett AL, Platz EA Prevalence and risk factors for erectile dysfunction in the US Am J Med 2007; 120:151-157
3 Ayta IA, McKinlay JB, Krane RJ The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences BJU Int 1999; 84:50-56
4 Braun M, Wassmer G, Klotz T, et al Epidemiology of erectile dysfunction: results of the “Cologne Male Survey ” Int J Impot Res 2000; 12:305-311
5 Loscalzo J, Fauci AS, Kasper DL, et al Harrison’s Principles of Internal Medicine, Twenty-First Edition (Vol 1 & Vol 2) McGraw Hill Professional; 2022
6 Townsend N, Kazakiewicz D, Lucy Wright F Epidemiology of cardiovascular disease in Europe Nat Rev Cardiol Published online 2022 doi:10 1038/s41569-021-00607-3
7 Sexual and Reproductive Health Uroweb - European Association of Urology Accessed August 23, 2023 https://uroweb org/guidelines/sexual-and-reproductive-health
8 How To Evaluate Cardiovascular Risk in a Patient With Erectile Dysfunction American College of Cardiology Accessed August 23, 2023 https://www acc org/latest-in-cardiology/articles/2014/07/18/ 16/01/how-to-evaluate-cardiovascular-risk-in-a-patient-with-erectile-dysfunction
9 Nehra A, Jackson G, Miner M, et al The Princeton III Consensus recommendations for the management of erectile dysfunction and cardiovascular disease Mayo Clin Proc 2012; 87:766-778
10 Thompson IM, Tangen CM, Goodman PJ, et al Erectile dysfunction and subsequent cardiovascular disease JAMA 2005; 294:29963002
11 Schouten BW, Bohnen AM, Bosch JL, et al Erectile dysfunction prospectively associated with cardiovascular disease in the Dutch general population: results from the Krimpen Study Int J Impot Res 2008; 20:92-9
12 Gazzaruso C, Solerte SB, Pujia A, et al Erectile dysfunction as a predictor of cardiovascular events and death in diabetic patients with angiographically proven asymptomatic coronary artery disease: a p o t e n t i a l p ro t e c t i v e ro l e f o r s t a t i n s a n d 5 - p h o s p h o d i e s t
inhibitors J Am Coll Cardiol 2008; 51:2040-4
13 Araujo AB, Hall SA, Ganz P, et al Does Erectile Dysfunction Contribute to Cardiovascular Disease Risk Prediction beyond the Framingham Risk Score? J Am Coll Cardiol 2010; 55:350-6
14 Böhm M, Baumhäkel M, Teo K, et al Erectile dysfunction predicts cardiovascular events in high-risk patients receiving telmisartan, ramipril, or both: The ONgoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial/Telmisartan Randomized AssessmeNt Study in ACE iNtolerant subjects with cardiovascular Disease (ONTARGET/TRANSCEND) Trials Circulation 2010; 121:1439-46
15 Jackson G, Boon N, Eardley I, et al Erectile dysfunction and coronary artery disease prediction: evidence-based guidance and consensus Int J Clin Pract 2010; 64:848-57
16 David Batty G, Li Q, Czernichow S, et al Erectile dysfunction and later cardiovascular disease in men with type 2 diabetes: prospective cohort study based on the ADVANCE trial J Am Coll Cardiol 2010; 56:1908-13
17 Dong JY, Zhang YH, Qin LQ Erectile dysfunction and risk of cardiovascular disease: meta-analysis of prospective cohort studies J Am Coll Cardiol 2011; 58:1378-85
18 Diaconu CC, Manea M, Marcu DR, et al The erectile dysfunction as a marker of cardiovascular disease: a review Acta Cardiol 2020; 75:286-292
19 Corona G, Rastrelli G, Isidori AM, et al Erectile dysfunction and cardiovascular risk: a review of current findings Expert Rev Cardiovasc Ther 2020; 18:155-164
20 Yannas D, Frizza F, Vignozzi L, et al Erectile Dysfunction Is a Hallmark of Cardiovascular Disease: Unavoidable Matter of Fact or Opportunity to Improve Men’s Health? J Clin Med Res 2021; 10:2221
21 Imprialos K, Koutsampasopoulos K, Manolis A, Doumas M Erectile Dysfunction as a Cardiovascular Risk Factor: Time to Step Up? Curr Vasc Pharmacol 2021; 19:301-312
22 Seidu S, Cebrián A, Kunutsor SK, Khunti K Erectile dysfunction, phosphodiesterase-5 inhibitor use and risk of cardiovascular disease and mortality in people with diabetes: A systematic review and metaanalysis Prim Care Diabetes 2022; 16:601-613
23 Visseren FLJ, Mach F, Smulders YM, et al 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice Eur Heart J 2021; 42:3227-3337
24 Kloner RA, Burnett AL, Miner M, et al Princeton IV consensus guidelines: PDE5 inhibitors and cardiac health J Sex Med 2024; 21:90-11
25 Goff DC Jr, Lloyd-Jones DM, Bennett G, et al 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines Circulation 2014; 129(25 Suppl 2):S49-S73
26 Li D, Li X, Peng E, et al Do Urologists Really Recognize the
Disease? Sex Med Today 2020; 8:195-204
27 SCORE2 working group and ESC Cardiovascular risk collaboration SCORE2 risk prediction algorithms: new models to estimate 10year risk of cardiovascular disease in Europe Eur Heart J 2021; 42:2439-2454
28 Vlachopoulos CV, Terentes-Printzios DG, Ioakeimidis NK, et al Prediction of cardiovascular events and all-cause mortality with erectile dysfunction: a systematic review and meta-analysis of cohort studies Circ Cardiovasc Qual Outcomes 2013; 6:99-109
29 Mostafaei H, Mori K, Hajebrahimi S, et al Association of erectile dysfunction and cardiovascular disease: an umbrella review of systematic reviews and meta-analyses BJU Int 2021; 128:3-11
30 Gandaglia G, Briganti A, Jackson G, et al A systematic review of the association between erectile dysfunction and cardiovascular disease Eur Urol 2014; 65:968-978
31 Raheem OA, Su JJ, Wilson JR, Hsieh TC The Association of Erectile Dysfunction and Cardiovascular Disease: A Systematic Critical Review Am J Mens Health 2017; 11:552-563
32 Erectile Dysfunction (ED) Guideline - American Urological Association Accessed August 28, 2023 https://www auanet org/ guidelines-and-quality/guidelines/erectile-dysfunction-(ed)-guideline
33 Kostis JB, Jackson G, Rosen R, et al Sexual Dysfunction and Cardiac Risk (the Second Princeton Consensus Conference) Am J Cardiol 2005; 96:313-321
Correspondence
João Diogo Abreu Lorigo (Corresponding Author) joaolorigo@gmail com
Centro Hospitalar e Universitário de Coimbra
Rua Vale Rosal, Lote 18, 1D, 3040-321, Coimbra, Portugal
Daniela Gomes
Unidade de Saúde Familiar Serra da Lousã, Vilarinho, Portugal danielasmgomes20@gmail com
Ana Rita Ramalho arita gcr@gmail com
Edgar Silva edsilva elv@gmail com
Patrícia Mendes
patricia a mendes@chuc min-saude pt
Arnaldo Figueiredo
ajcfigueiredo@gmail com
Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
The effect of vitamin D in vitro supplementation on sperm deoxyribonucleic acid fragmentation
Andri Rezano 1, 2 , Ditto Rezkiawan 2 , Vellyana Lie 2 , Arya Srisadono 2 , Rafly Mochamad Rivaldo 3 , Amelia Reta Purba 3 , Melia Juwita Adha 4 , Tjahjo Djojo Tanojo 2, 5 , Maria P B D Pramesti 2, 6
1 Department of Biomedical Sciences, Faculty of Medicine, Universitas Padjadjaran, Sumedang, West Java, Indonesia;
2 Andrology Study Program, Faculty of Medicine, Universitas Airlangga, Surabaya, East Java, Indonesia;
3 Medical Study Program, Faculty of Medicine, Universitas Padjadjaran, Sumedang, West Java, Indonesia;
4 Holistic General Hospital, Purwakarta, West Java, Indonesia;
5 Andrology Clinic, Dr Soetomo Academic Hospital, Surabaya, East Java, Indonesia;
6 Department of Biomedical Sciences, Faculty of Medicine, Universitas Airlangga, Surabaya, East Java, Indonesia
Summary
Objective: This study aimed to identify the direct effect of vitamin D on sperm DNA integrity after swim-up preparation
Materials and methods: Normozoospermia samples were gathered from 12 men and assessed for their baseline characteristics, including DNA Fragmentation Index (DFI). Each sample was then prepared using the swim-up method Half of the samples were incubated with vitamin D, while the other half were incubated with a standard sperm-washing medium
Results: Vitamin D significantly reduced the DFI compared to the baseline (5 5 ± 3 4% versus 17 6 ± 4 2%; p < 0 001) and the swim-up-only group (5 5 ± 3 4% versus 12 0 ± 4 2%; p < 0 001)
Microscopic examination reflected these results, showing a reduction in the number of small halos and no halos with an increased appearance of large to medium-sized halos
Conclusions: These results suggest that vitamin D incubation is valuable in protecting sperm from DNA damage that develops during sperm preparation However, additional investigation is warranted to explore other preparation methods and to elucidate the underlying mechanisms
KEY WORDS: Assisted reproductive technology; DNA damage; Male infertility; Swim up
Submitted 2 August 2024; Accepted 26 August 2024
INTRODUCTION
Infertility is a significant global health issue, affecting approximately 1 in 7 couples, with contributions from both male and female factors equally distributed (1-3)
Among the various factors contributing to male infertility, damage to sperm DNA is a critical concern, impacting 20-40% of subfertile men This DNA damage can arise from several sources, including imperfections in the apoptosis process during spermatogenesis (4), protamination during spermiogenesis (5), and oxidative stress from various endogenous and exogenous factors (6)
Excessive production of reactive oxygen species (ROS) beyond the body’s antioxidant capacity can lead to significant damage to sperm function, causing lipid peroxidation, protein oxidation, mitochondrial dysfunction, and DNA damage (7, 8)
In the context of assisted reproductive technology (ART), sperm preparation aims to isolate spermatozoa with optimal morphology and motility for successful fertilization (9) However, the cellular structure and function of spermatozoa can be compromised during sperm preparation due to repeated centrifugation cycles, which induce ROS formation and result in the loss of seminal plasma antioxidants (10) Studies have shown that ROS production in normal spermatozoa can increase 2-5 times after indirect swim-up preparation, with exposure to ROS from 1-2 hours leading to a 2-4-fold increase in DNA damage (11)
To mitigate these effects, sperm selection methods such as the swim-up technique are employed to reduce the main sources of intracellular ROS, namely leukocytes and immature sperm (12) According to the WHO laboratory manual, the swim-up method is a simple method that allows motile sperm to swim into an overlaid medium, separating them from non-motile spermatozoa This method enhances sperm motility, average velocity, normal morphology and fertilization rates in vitro in mammals in compared to a lower fraction (13) However, simple washing or swim-ups from the pellet have been associated with a sudden burst of ROS production, reduced motility, and impaired sperm-oocyte fusion in the zonafree hamster oocyte penetration test (14)
Despite these challenges, the swim-up method has been shown to maintain better sperm DNA integrity compared to other procedures, such as density gradient centrifugation, demonstrating reduced DNA fragmentation and vacuolization (15, 16)
Antioxidant administration, including vitamins C, E, catalase and glutathione, has been suggested to protect sperm DNA integrity during preparation (17)
Specifically, serum vitamin D levels have been correlated with improvements in sperm number, motility, morphology, and DNA fragmentation (18) Vitamin D plays a crucial role in calcium regulation within the male reproductive system, and its activation in semen has been shown to enhance intracellular calcium levels, motility and acrosome reaction in spermatozoa (19) Additionally, vitamin D functions as a membrane antioxidant (20) and influences gene expression related to cell proliferation, differ-
entiation, apoptosis and oxidative stress through its receptors in the nucleus and post-acrosome of spermatozoa (21-23)
Although numerous studies have explored the role of vitamin D in the reproductive system, research specifically examining its impact on reducing the DNA fragmentation index (DFI) of human spermatozoa remains limited The DFI is a crucial indicator of semen quality, reflecting the integrity and damage to sperm DNA, thereby detecting potential sperm damage (24) Blaseg et al (2022) found no association between circulating vitamin D levels and human DFI However, though the study was limited by using circulating vitamin D as a proxy for intratesticular levels (25) Additionally, many studies have not considered ART factors in their analyses (26, 27)
Therefore, this study aims to investigate the effect of vitamin D in vitro administration on sperm DFI in normozoospermic samples following sperm preparation using the swim-up method, addressing a critical gap in current reproductive research
MATERIALS AND METHODS
A total of 12 semen samples (n = 12) were included in this study, each with a volume of 3 mL The inclusion criteria for selecting samples were men aged 26-35 years who agreed to participate and signed the informed consent, had abstained from ejaculation for 2-7 days, and were diagnosed with normozoospermia, characterized by a semen volume greater than 2 ml Baseline (BL) characteristics assessed for each sample included patient age, body mass index, semen volume, sperm concentration, progressive motility, non-progressive motility, and DFI
Samples were collected using sterile, clean instruments maintained at the same temperature as the spermatozoa to prevent bacterial contamination, which can reduce sperm quality All tools were sterilized, disinfected, wrapped in aluminium foil, and stored at 37°C until use Following the WHO protocols (2021) Samples were collected via masturbation onto a sterile glass container and allowed to liquefy for 20-30 minutes Semen volume, motility, and total sperm count were measured to ensure normal values before inclusion in the study After the initial assessment, sperm samples were prepared using the swim-up method The prepared samples were
then divided into two groups: one undergoing swim-up preparation with vitamin D incubation (SD) and the other undergoing swim-up preparation only (SU) Unprepared samples (BL) were also included in the evaluation Spermatozoa from all groups (BL, SD, and SU) were evaluated for DNA fragmentation index
Sperm preparation
Sperm preparation using the swim-up method was performed by mixing semen and Sperm Rinse™ medium (Vitrolife, USA) in a 1:1 ratio in a 5 ml tube The mixture was then centrifuged at a speed of 400 G for 10 minutes After centrifugation, the supernatant was discarded, and the pellet was resuspended with 2 ml of Sperm Rinse™ medium The resuspended pellet was centrifuged again at a speed of 400 G for 5 minutes The supernatant was discarded, and 2 ml of SpermRinse™ medium was gently added to the pellet along the tube wall The tube was then placed at 45° angle and incubated at 37°C for 45 minutes Finally, 1 ml of the upper medium fraction was carefully transferred to two new tubes, with 500 µl in each tube, for further analysis (13)
Vitamin D incubation
A solution of active vitamin D, 1 25(OH)2D3 (Calcitriol, molecular weight 416 64), was prepared in 100% ethanol with a stock concentration of 10 μg/ml (24 μM) and stored in a -20°C To analyse the effect of in vitro vitamin D administration on DNA fragmentation, 500 uL postpreparation spermatozoa were incubated with 1 nM 1 25(OH)2D3 at 37°C, for 45 minutes (19) The working solution concentration was prepared in stages starting from 1 mM, 10 μM, 10 nM, and finally 1 nM The control group without vitamin D was incubated with SpermRinse™ medium under the same conditions
DNA fragmentation index
D N A
FIgure 1.
Determination of DNA fragmentation based on halo size (28).
1) The diameter of the core as the determinant of DNA fragmentation
2) Large halo and 3) medium halo show spermatozoa without DNA fragmentation.
4) Small halo and 5) no halo indicating spermatozoa DNA fragmentation.
D N A
Fragmentation Kit (SpermFunc®, BRED-002, BRED Life Science Technology Inc ), following the manufacturer’s protocol Observations were made using a light microscope at 400X magnification to distinguish between unfragmented DNA (big and medium halos) and fragmented DNA (small halos, no halos, and damaged spermatozoa) in 500 spermatozoa cells Normal sperm DNA presented
A Rezano, D Rezkiawan, V Lie, et al
as medium (halo thickness smaller than the length but greater than one-third of the core minor diameter) to big halos (halo thickness equal to or greater than the length of the core minor diameter) In contrast, damaged/fragmented sperm DNA presented as no halos or small halos (halo thickness equal to or less than one-third of the core minor diameter) (Figure 1) The percentage of spermatozoa with DNA fragmentation was calculated as the DNA Fragmentation Index (DFI)
Statistics
Data were recorded and analysed to compare the effect of vitamin D incubation on sperm DNA integrity between the vitamin D-treated group (SD), the control group (SU), and the unprepared samples (BL) This comparison aimed to determine whether vitamin D supplementation during sperm preparation could enhance DNA integrity in spermatozoa, thus potentially improving outcomes in ART Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 26 0 for Windows The Shapiro-Wilk test was used to determine whether the data were normally distributed (p > 0 05) or not normally distributed (p < 0 05) Differences in DFI values between groups were tested using paired t-test, and results were expressed as mean ± standard deviation A pvalue of less than 0 05 was considered statistically significant
Ethical approval
The study was approved by the Health and Humanities Research Ethics Committee, Faculty of Medicine, Universitas Airlangga (Code: 242/EC/KEPK/FKUA/2023) Samples were collected between August-October 2023
RESULTS
Patient characteristics
A total of 12 volunteers participated during the study period All DFI data between groups were found to be normally distributed (p > 0 05) The mean age of volunteers was 30 9 years (30 9 ± 2 6), reflecting the reproductive age of men The body mass index (BMI) was 27 4 kg/m2 (27 4 ± 4 1), classified as level 1 obesity; the mean baseline DFI value was 17 6 ± 4 2%, which falls within the normal range Baseline characteristics are summarized in Table 1
2.
Table 1.
Age and semen profile of the study subjects.
Subject characteristics Mean ± SEM (n = 12)
Patientage(inyears)309±26
BodyMassIndex(kg/m2)274±41
Semenvolume(ml)3.4±1.0
Spermconcentration(million/ml)487±251
Progressivemotility(%)524±134
Non-progressivemotility(%)68±37
DNAfragmentationindex(%)176±42
Table 2.
Paired t-test results from each treatment group on DFI.
Variable Group 1 Group 2 P-value (Mean ± SD) (Mean ± SD)
DFIBL(176±42)SU(120±42)<0001
SU(120±42)SD(55±34)<0001
BL(176±42)SD(55±34)<0001
DFI between groups
A paired t-test was conducted to compare the DFI within each sample group (Table 2) The SU group exhibited a significantly reduced DFI (12 0 ± 4 2%) compared to the BL characteristics (17 6 ± 4 2%) Furthermore, the DFI was significantly decreased in the SD group (5 5 ± 3 4%) compared to both the SU group (12 0 ± 4 2%) and the initial BL (17 6 ± 4 2%), with mean reductions of 6 5% and 12 1% respectively These findings suggest that vitamin D incubation during sperm preparation resulted in a significant improvement in sperm DNA integrity compared to the control groups
Evaluation of spermatozoa DNA fragmentation examination
In each group, variations in the appearance of a large halos, medium halos, small halos and no halos were observed in semen samples before and after preparation Specifically, the presence of small halos and no halos was noticeably reduced in the post-preparation samples of the SD group (Figure 2)
Evaluation of spermatozoa’s DNA fragmentation in the BL, SU and SD groups.
FIgure
Image caption: a Large halos; b Medium halos; c Small halos; d No halos
DISCUSSION
The decline in sperm quality and function due to increasing reproductive disorders globally is a significant concern in reproductive health A recent study highlighting the impact of vitamin D deficiency on mouse fertility and subsequent improvements in semen parameters has shed new light on the role of vitamin D in male reproductive function (29) Numerous studies have emphasized the role of vitamin D in male reproductive health, particularly in enhancing sperm quality and motility (30)
Infertility affects approximately 15-20% of couples of reproductive age, with male factors contributing to around 50% of cases (31, 32) In our study, the average age of the sample population was 30 9 ± 2 6 years, consistent with previous research (33) Additionally, the average BMI of the participants fell within the category of level 1 obesity Obesity is known to increase the risk of sperm DNA damage in infertile men due to its association with increased oxidative stress (34, 35)
Sperm DNA integrity is critical to successful fertilization and embryogenesis (36) However, previous studies have been limited in evaluating the functional status of spermatozoa (37), indicating the need for further research In our study, despite having normal semen parameters, semen samples exhibited a DFI of 17 6 ± 4 2% This finding aligns with previous research conducted by Halim et al , where the DFI before semen processing was 16 12% (13 4819 04) (38) Oxidative stress levels that are insufficient to induce cell death can still disrupt sperm function, highlighting the importance of addressing DNA fragmentation in infertility (39) The extent of DNA fragmentation’s impact on fertilization depends on both the level of DNA damage and the DNA repair capacity of the oocyte (40)
Our study revealed that supplementation of vitamin D, calcitriol [1 25(OH)2D3] at a concentration of 1 nM after sperm preparation, led to a significant reduction in sperm DNA fragmentation by 6 5% Notably, there was a synergistic effect between sperm preparation and vitamin D administration in decreasing DNA fragmentation compared to baseline levels These findings differ from a study by Moghadam et al (2019), which reported no repair of DNA damage with vitamin D administration after swim-up (41) This discrepancy may be attributed to differences in the DNA damage examination methods used, with the sperm chromatin dispersion method proving more effective than the TUNEL method in diagnosing sperm DNA damage in unexplained infertility (40) The protective mechanism of vitamin D on sperm DNA integrity can be explained in several ways Firstly, the hydrophobic part of vitamin D binds to fatty acid residues on the spermatozoa membrane, thereby protecting membrane integrity (20) Additionally, vitamin D has been shown to enhance the integrity of spermatozoa membranes during cryopreservation by reducing intracellular ROS levels (41) VDR expression in testes and spermatozoa, along with cellular uptake of circulating vitamin D, play crucial roles in regulating spermatozoa motility and acrosome function (19) Moreover, administration of 20,000 nM of vitamin D has been associated with increased expression of heat shock protein 70 (HSP70), a marker of oxidative stress and lipid peroxidation, indicating a dose-response relationship of vitamin D as an antioxidant (42)
While our study supports the role of antioxidants in maintaining sperm chromatin integrity during sperm preparation, definitive conclusions cannot be drawn due to certain limitations This study did not directly examine intraspermatozoal ROS levels and endogenous antioxidants Future research should address these factors and analyse abnormal semen samples to further elucidate the role of vitamin D in infertility Additionally, investigations into other variables, such as ROS levels, antioxidants, lipid peroxidation, and acrosome reactions, as well as their impacts on fertilization outcomes, pregnancy, and embryo development, are warranted Comparative studies between swim-up and other sperm selection procedures, such as density gradient centrifugation, are also needed to evaluate their efficacy and drawbacks in reducing DNA damage with vitamin D administration
CONCLUSIONS
This study demonstrated that DFI significantly decreased following sperm preparation using the swim-up method Additionally, the DFI further decreased significantly in the group treated with vitamin D compared to both the pre-preparation and post-preparation without vitamin D administration groups
These findings highlight the protective role of vitamin D against DNA damage incurred during sperm preparation However, further studies are necessary to elucidate the underlying mechanism of this protective effect and to compare the efficacy of vitamin D supplementation with o t h e r s p e r m p r e p a r a t i o n m e t h o d s F u t u r e r e s e a r c h should also consider examining different variables such as ROS levels, antioxidants, lipid peroxidation, acrosome reactions, and their impacts on fertilization outcomes, pregnancy, and embryo development
ACKNOWLEDGMENTS
The authors express sincere gratitude to the staff at the Department of Biomedical Sciences Faculty of Medicine Universitas Airlangga and Andrology Clinic, Dr Soetomo Academic Hospital, for their invaluable assistance and support throughout this study
REFERENCES
1 Agarwal A, Baskaran S, Parekh N, et al Male infertility Lancet 2021; 397:319-33
2 Turner KA, Rambhatla A, Schon S, et al Male Infertility is a Women’s Health Issue-Research and Clinical Evaluation of Male Infertility Is Needed Cells 2020; 9:990
3 World Health Organization 2020 Infertility Available at: h t t p s : / / w w w w h o i n
accessed May 2024
4 Asadi A, Ghahremani R, Abdolmaleki A, Rajaei F Role of sperm apoptosis and oxidative stress in male infertility: A narrative review Int J Reprod Biomed 2021; 19:493-504
5 Agarwal A, Selvam MK, Baskaran S, Cho CL Sperm DNA damage and its impact on male reproductive health: a critical review for clinicians, reproductive professionals and researchers Expert Rev Mol Diagn 2019; 19:443-57
A Rezano, D Rezkiawan, V Lie, et al
6 Ribas-Maynou J, Yeste M Oxidative Stress in Male Infertility: Causes, Effects in Assisted Reproductive Techniques, and Protective Support of Antioxidants Biology (Basel) 2020; 9:77
7 Gualtieri R, Kalthur G, Barbato V, et al Sperm Oxidative Stress during In Vitro Manipulation and Its Effects on Sperm Function and Embryo Development Antioxidants (Basel) 2021; 10 1025
8 Dutta S, Majzoub A, Agarwal A Oxidative stress and sperm function: A systematic review on evaluation and management Arab J Urol 2019; 17:87-97
9 Marzano G, Chiriacò MS, Primiceri E, et al Sperm selection in assisted reproduction: A review of established methods and cuttingedge possibilities Biotechnol Adv 2020; 40:107498
10 Aitken RJ, Drevet JR The Importance of Oxidative Stress in Determining the Functionality of Mammalian Spermatozoa: A TwoEdged Sword Antioxidants 2020; 9:111
11 Natali, I Sperm Preparation Techniques for Artificial Insemination - Comparison of Sperm Washing, Swim Up, and Density Gradient Centrifugation Methods In: Manafi, M, eds Artificial Insemination in Farm Animals IntechOpen; 2011; Available from: https://www intechopen com/chapters/16102
12 Wildy ML, Boyd L, Fourie J, et al The Development of a Simplified Swim-up Method for Sperm Processing Journal of Infertility and Reproductive Biology 2021; 9:160-7
13 World Health Organization WHO laboratory manual for the examination and processing of human semen Geneva: World Health Organization 2021; 6:1-276
15 Xue X, Wang WS, Shi JZ, et al Efficacy of swim-up versus density gradient centrifugation in improving sperm deformity rate and DNA fragmentation index in semen samples from teratozoospermic patients J Assist Reprod Genet 2014; 31:1161-6
16 Raad G, Bakos HW, Bazzi M, et al Differential impact of four sperm preparation techniques on sperm motility, morphology, DNA fragmentation, acrosome status, oxidative stress, and mitochondrial activity: A prospective study Andrology 2021; 9:1549-59
17 Beygi Z, Forouhari S, Mahmoudi E, et al Role of Oxidative Stress and Antioxidant Supplementation in Male Fertility Curr Mol Med 2021; 21:265-82
18 Güngör K, Güngör ND, Ba ar MM, et al Relationship between serum vitamin D levels semen parameters and sperm DNA damage in men with unexplained infertility Eur Rev Med Pharmacol Sci 2022; 26:499-505
19 Jensen MB, Bjerrum PJ, Jessen TE, et al Vitamin D is positively associated with sperm motility and increases intracellular calcium in human spermatozoa Hum Reprod 2011; 26:1307-17
20 Wiseman H Vitamin D is a membrane antioxidant Ability to inhibit iron-dependent lipid peroxidation in liposomes compared to cholesterol, ergosterol and tamoxifen and relevance to anticancer action FEBS Lett 1993; 326:285-8
21 Zmijewski MA Nongenomic Activities of Vitamin D Nutrients 2022; 14:5104
22 Hanel A, Carlberg C Vitamin D and evolution: Pharmacologic implications Biochem Pharmacol 2020; 173:113595
23 Gasperini B, Falvino A, Piccirilli E, et al Methylation of the
Vitamin D Receptor Gene in Human Disorders Int J Mol Sci 2024; 25:107
24 Yang H, Li G, Jin H, et al The effect of sperm DNA fragmentation index on assisted reproductive technology outcomes and its relationship with semen parameters and lifestyle Transl Androl Urol 2019; 8:356
25 Blaseg E, Wald TV, Hansen KA Vitamin D levels and human sperm DNA fragmentation: a prospective, cohort study Basic Clin Androl 2022; 32:14
26 Banks N, Sun F, Krawetz SA, et al Male vitamin D status and male factor infertility Fertil Steril 2021; 116:973-9
27 Maghsoumi-Norouzabad L, Zare Javid A, Mansoori A, et al Evaluation of the effect of vitamin D supplementation on spermatogram, seminal and serum levels of oxidative stress indices in asthenospermia infertile men: a study protocol for a triple-blind, randomized controlled trial Nutrition Journal 2021; 20:1-11
2 8 Z e q i r a j A , B e a d i n i S , B e a d i n i N , e t a l S p e r m D N A Fragmentation, Determined Using the Sperm Chromatin Dispersion (SCD) Test, A Study in Republic of Kosovo Population Int J Biol 2018; 10:14-8
29 Cito G, Cocci A, Micelli E, et al Vitamin D and Male Fertility: An Updated Review World J Mens Health 2020; 38:164-77
30 Adamczewska D, Słowikowska-Hilczer J, Walczak-Jedrzejowska R The Association between Vitamin D and the Components of Male Fertility: A Systematic Review Biomedicines 2022; 11:90
31 Amorini AM, Listorti I, Bilotta G, et al Antioxidant-Based Therapies in Male Infertility: Do We Have Sufficient Evidence Supporting Their Effectiveness? Antioxidants 2021; 10:220
32 Babakhanzadeh E, Nazari M, Ghasemifar S, Khodadadian A Some of the Factors Involved in Male Infertility: A Prospective Review Int J Gen Med 2020; 13:29-41
33 Halim B, Girsang E, Nasution SLR, Manalu P Hambatan Akses Pelayanan Infertilitas pada Pasien dari Kawasan Urban dan Rural yang Berobat di Klinik Bayi Tabung Halim Fertility Center RSIA Stella Maris Media Kesehatan Masyarakat Indonesia 2020; 19:272-8
34 Pakpahan C, Rezano A, Margiana R, et al The Association Between Lipid Serum and Semen Parameters: a Systematic Review Reprod Sci 2023; 30:761-71
35 Karimi E, Heshmati J, Shirzad N, et al The effect of synbiotics supplementation on anthropometric indicators and lipid profiles in women with polycystic ovary syndrome: a randomized controlled trial Lipids Health Dis 2020; 19:60
36 Barbarosie C, Agarwal A, Henkel R Diagnostic value of advanced semen analysis in evaluation of male infertility Andrologia 2021; 53:e13625
37 Ayad BM, Oyeyipo IP, Van der Horst G, Du Plessis SS Cementing the relationship between conventional and advanced semen parameters Middle East Fertil Soc J 2021; 26:1-10
38 Aitken RJ Impact of oxidative stress on male and female germ cells: implications for fertility Reproduction 2020; 159:R189-201
39 Halim B, Angellee J, Lubis HP, Bachsinar B Sperm Quality and D e o x y
Centrifugation with Swim-Up Processing Technique: A Prospective Cohort Study Open Access Maced J Med Sci 2021; 9:626-30
40 Agarwal A, Farkouh A, Saleh R, et al Technical Aspects and Clinical Limitations of Sperm DNA Fragmentation Testing in Male Infertility: A Global Survey, Current Guidelines, and Expert Recommendations World J Mens Health 2024; 42:202-15
41 Moghadam MT, Fard YA, Saki G, Nikbakht R Effect of vitamin D on apoptotic marker, reactive oxygen species and human sperm parameters during the process of cryopreservation Iran J Basic Med Sci 2019; 22:1036
42 Moghadam MT, Hamidian O, Mansouri E, Nikbakht R Effects of vitamin D3 on the level of heat shock protein 70 and oxidative stress in human sperm: a pilot study Middle East Fertil Soc J 2020; 25:1-8
Correspondence
Andri Rezano, MD-Andrologist, PhD, Associate Professor andri rezano@unpad ac id
Department of Biomedical Sciences, Faculty of Medicine Universitas Padjadjaran Jl Ir Soekarno KM 21 Jatinangor, Sumedang 45363, West Java, Indonesia
Ditto Rezkiawan
ditto rezkiawan-2021@fk unair ac id Vellyana Lie vellyana lie-2022@fk unair ac id
Arya Srisadono
arya srisadono-2022@fk unair ac id Tjahjo Djojo Tanojo tjahjodjojo@gmail com
Maria PBD Pramesti pramestidyan@gmail com Andrology Study Program, Faculty of Medicine, Universitas Airlangga, Surabaya 60132, East Java, Indonesia
Mochamad Rivaldo rafly22001@mail unpad ac id Medical Study Program, Faculty of Medicine, Universitas Padjadjaran, Sumedang, 45363, West Java, Indonesia
Amelia Reta Purba amelia23007@mail unpad ac id Medical Study Program, Faculty of Medicine, Universitas Padjadjaran, Sumedang 45363, West Java, Indonesia
Melia Juwita Adha meliarezano@gmail com
Holistic General Hospital, Purwakarta 41115, West Java, Indonesia
Conflict of interest: The authors declare no potential conflict of interest
A Rezano, D Rezkiawan, V Lie, et al
CASE SERIES
Healing of Peyronie's disease after multimodal antioxidant treatment. A case series
Gianni Paulis 1 , Giovanni De Giorgio 2 , Andrea Paulis 3
1 Department of Urology and Andrology, Peyronie’s Care Center, Castelfidardo Clinical Analysis Center, Rome, Italy;
2 Department of Urology and Andrology, Section of Ultrasound Diagnostics, Castelfidardo Clinical Analysis Center, Rome, Italy;
3 Bambino Gesù Children’s Hospital, IRCCS (Istituti di Ricovero e Cura a Carattere Scientifico), Rome, Italy
Summary
Introduction: Peyronie’s disease (PD) is characterized by fibrosis of the penile tunica albuginea. Conservative treatment options may involve oral and/or injectable medications
Materials and methods: This case series includes four patients with PD in the first phase The diagnosis of PD included a medical history; penile palpation; a physical examination of the penis, documenting penile deformity (Kelâmi method); penile dynamic Doppler ultrasound (PDDU) + elastography, measuring the plaque and calculating its volume (cm3), and the deformation index (strain ratio); and the completion of the following questionnaires: IIEF to assess erectile function, VAS to assess pain, and Peyronie's Disease Questionnaire (PDQ) symptom bother to evaluate the psychosexual impact of the disease
Diagnostic follow-up evaluations were conducted before and every 6-12 months throughout the conservative treatment
The four patients were treated at our andrology clinic between January 2019 and November 2023 Our treatment included the following: bilberry, propolis, ginkgo biloba, silymarin, L-carnitine, coenzime Q-10, Boswellia, superoxide dismutase, vitamin E, vitamin C, topical diclofenac gel, propolis cream, and perilesional penile injections with pentoxifylline for cases involving penile plaques with volumes of > 0 100 cm3
Results: Complete resorption of the PD plaque after treatment occurred in all cases The disappearance of Peyronie's plaque occurred over a period ranging from 18 to 36 months, in relation to the volume of the plaque
Conclusions: Despite the limited sample size in our study, these patients verifiably achieved the complete resorption of the affected disease area. Our results will provide useful insights for uroandrological clinical practice Nevertheless, randomized controlled trials with a larger number of PD patients are needed to demonstrate the effectiveness of multimodal antioxidant treatment.
Submitted 26 August 2024; Accepted 2 September 2024
INTRODUCTION
PD is a genetically based chronic inflammatory condition that affects the tunica albuginea of the penile corpora cavernosa in genetically predisposed males, leading to the formation of an inelastic and fibrous penile plaque that
inevitably causes various types of penile deformation Its prevalence ranges from 3 2% to 13 1% and is less common in Asian countries (0 6-5 0%) and among populations of black African descent (0 1-3 5%) (1-8) PD typically affects middle-aged men, but cases have increased among younger patients in recent years In 2001, two authors reported the prevalence of PD in young people under the age of 40 as 1 5% and 4 8% (2, 9) Some authors have noted an increase in the incidence of PD in younger patients, with their study showing an 18 6% incidence in individuals under 40 compared with the 24 2% incidence found in our most recent study (10, 11) PD symptoms include penile deformity (in more than 90% of cases), penile pain (in between 20% and 70% of cases), erectile dysfunction (in over 30% of cases), and psychological distress, such as anxiety and depression (in approximately 48% of cases) (12, 13) Penile deformities can manifest as curvature, shortening, twisting, indentations, hourglass deformities, and in more severe cases, "flail penis"
Traumatic theory appears to be the most widely accepted of the several etiopathogenetic hypotheses According to this theory, the local accumulation of fibrin resulting from trauma (whether micro- or macro-trauma) is believed to initiate the disease process by triggering the production of free radicals (oxidative stress) and fibrogenic cytokines, leading to excessive collagen production and deposition (plaque) (14-22) The disease progresses in two phases: The inflammatory ("active") phase comes first, lasting for approximately 12-18 months, during which plaque formation and remodeling occur (23-30) Conservative medical therapy is recommended during this first phase The second phase is the "stabilization" stage, wherein the disease stops progressing, the plaque stops growing, and any pain usually subsides Surgical treatment is recommended during this second phase if there is a severe penile deformity that hinders sexual intercourse or if severe erectile dysfunction is present (23, 24, 26, 27,30-34)
The conservative medical treatment in the first phase of PD includes oral therapies, penile infiltrations, including vitamin E, colchicine, potaba, tamoxifen, pentoxifylline (PTX), bioactive food extracts with an antioxidant action (L-arginine, carnitine, propolis, bilberry, coenzyme Q10, etc ), non-steroidal anti-inflammatory drugs (NSAIDs), phosphodiesterase 5 (PDE-5) inhibitors, penile infiltrations (verapamil, corticosteroids, interferon-α2b (IFNa2b), pentoxi-
The physical treatment in the first phase of PD includes extracorporeal shock wave therapy (ESWT), iontophoresis, and penile traction and vacuum devices (26, 33, 59, 60)
Surgical treatments for PD are targeted to each patient's specific needs and may include corporoplasty, with or without grafts, and the possible insertion of a penile prosthesis (28, 31, 32, 34, 36, 41)
PD diagnostics involves penile palpations, photographic documentation of the deformation (according to the Kelâmi guidelines), penile dynamic Doppler ultrasound (PDDU), and the completion of questionnaires for pain (VAS), erectile function (IIEF), and psychometric evaluations like the Peyronie's Disease Questionnaire (PDQ) (10, 42-47)
The scientific literature reports eleven human patients with PD who have recovered following medical treatment with antioxidants (48-51) Cases of PD resolution have been published before, but only in experimental studies in rats (52-54) The scientific literature has always reported the possibility of the spontaneous resolution of PD (31, 55-57) However, some studies do not agree with this possibility (58-59) We believe that treating oxidative stress (a key mechanism of inflammation) with antioxidants is the best therapeutic approach to treat PD (35, 60-62)
Multimodal treatment aims to achieve superior outcomes compared with using a single substance or therapy alone
All the antioxidants we use have anti-inflammatory and antifibrotic properties by blocking the activity of the NF-kB factor In our multimodal treatment, we have also used NSAID (diclofenac), although administered locally to avoid possible long-term toxic effects due to oral administration (63, 64)
This case report aimed to present four cases of patients with PD who experienced plaque regression following “multimodal” antioxidant therapy (with oral antioxidants, topical diclofenac gel, and penile perilesional injections with 60 mg of pentoxifylline)
Our recent four articles have shown that the duration of m u l t i m o d a l t re a t m e n t n e e d e d t o re g re s s P e y ro n i e ' s plaque directly depends on the plaque's size (48-51) Therefore, larger plaques require a relatively longer time to completely regress In our recent case report, a patient with PD achieved complete plaque regression in just four months of combined antioxidant therapy, as his plaque was small (51)
METHODS
This case series includes four cases of patients with PD in the first phase who experienced the plaque's disappearance following "multimodal" antioxidant therapy including various oral antioxidants, topical diclofenac gel and propolis cream, and penile perilesional injections with a potent antioxidant and antifibrotic substance, pentoxifylline, specifically for cases involving penile plaques with volumes of > 0 100 cm3
The complete list of antioxidant substances used is shown in the following tables 1, 2, 3, and 4 The diagnosis of PD included a detailed medical history; penile palpation; a physical examination of the penis, documenting penile deformity using the Kelâmi method and measuring the
angulation; penile dynamic Doppler ultrasound (PDDU) + elastography, measuring the plaque in three dimensions and calculating its volume (cm3) using the ellipsoid formula (volume = 0 524 × length × width × thickness) and the deformation index (strain ratio); and the completion of the following questionnaires: IIEF to assess erectile function, VAS to assess pain, and the Questionnaire (PDQ symptom bother) to evaluate the psychosexual impact of the disease (10, 42-47, 65, 66)
The strain ratio (or deformation index), indicating the plaque's stiffness was detected via echo-elastography The strain ratio, expressed as a number, represents the ratio between the stiffness of the pathological tissue (plaque) and that of the adjacent normal tissue The four patients were treated at our andrology clinic between January 2019 and November 2023 All patients signed an informed consent form for the multimodal treatment During the consent process, patients were informed that the treatment for PD would be lengthy due to the chronic nature of the disease
The patients also agreed to the publication of their clinical data, provided that they be published anonymously All these patients did not consent to the publication of photos of their penises, even though they would have been published anonymously
A single andrologist operator performed and assessed PDDU with elastography on all patients in a single session
We used the Philips HD 15 machine (Washington, United States) that was later upgraded to a Philips Affinity 70 G (Washington, United States) In each of the 4 cases described, we reported the type of ultrasound machine used Diagnostic follow-up evaluations were conducted before and approximately every 6-12 months throughout the conservative treatment
RESULTS
C ase ser ies p r esen t at io n
In each case presented, several treatment cycles combined with antioxidants were necessary before reaching complete plaque reabsorption We describe the four individual cases in detail, with their personal clinical characteristics present before and at the end of treatment when the therapeutic goal was achieved A table listing the individual variations obtained after each treatment cycle is included for each clinical case presentation
Case 1
Case 1 was a 57-year-old Caucasian man, a non-smoker, suffering from chronic prostatitis, with the presence at the origin of a congenital penile curvature (dorsal of 25 degrees, left lateral of 5 degrees, and right lateral of 5 degrees), before the appearance of PD The patient did not report any traumatic events involving his penis in the previous 6-12 months He reported that he had started to notice a penile curvature, different from usual, approximately 6-8 months earlier At the time of our visit, the patient did not report any penile pain (VAS score = 0) nor complained of erectile dysfunction The IIEF score was 26 The PDQ symptom bother score was 11 In our observations, the penile deformation presented as a multiplanar curve, with a significantly reduced penile diameter in its distal third The goniometric
G Paulis, G De Giorgio, A Paulis
Table 1
Case 1: clinical data collected before, during, and after antioxidant treatment
UltrasoundmeasurementsPlaquestrainrati
Basalplaque:Basalplaque1802611
121 × 104 × 423mm(volume=0279cm3
Distalplaque:Distalplaque=253
240 × 293 × 435mmwithtwointernal
calcificationsmeasuring52 × 93mm
and50 × 80mm(volume=160cm3)
Totalvolumeofthetwoplaques1879cm3
F irst cycle Orally:L-carnitine1000mg+Propolis700mg+Ginkgobiloba240mg of multimodal treatment with antioxidants +Bilberry180mg+CoenzymeQ-10100mg+Silymarin400mg (6 months)
+Superoxidedismutase11000IU/g10mg/daily/for6months; +Topically:Propoliscream/2xdaily+Diclofenacgel4%/daily/for18months; +Peri-lesionalpenileinjections:Pentoxifylline60mg(with30Gneedle), 1penileinjectionevery2monthsfor12months PenileplaqueswerenolongerdetectableAbsenceofnon-elasticAftertheregressionTotaltherapydurationuntilplaque’sdisappearance30months pe
VAS = visua ana og scale, a pain measurement questionna re (score range: 0-10) (45); IIEF = Internat onal Index of Erect le Funct on, a quest onnaire for assessing erectile funct on with a score range of 0-30, indicating d fferent ED severity evels (no ED, score range: 26-30) (46); PDQ symptom bother PD Questionna re symptom bother for eva uating the psychosexua mpact, with a score range of 0-30 (10, 47, 66) The stra n rat o (deformat on ndex), detected via echo-elastography, indicates the plaque's st ffness (65) It s expressed as a number, representing the rat o between the st ffness of the patholog cal t ssue (plaque) and that of the ad acent normal tissue When e astography does not detect any anelastic area (p aque), the strain ratio index corresponds to 1 In th s case, the mage d splayed on the ultrasound machine screen does not show any index
measurements showed a dorsal curve of 41 degrees, a right lateral curve of 17 degrees, and a left lateral curve of 17 degrees Upon palpation, two basal and distal penile plaques of approximately 10 mm and 20 mm in length were detected, respectively, both with a fibrous consistency Two plaques were present in the penile eco-elastography examination The first penile plaque was located in the basal third and measured 12 1 × 10 4 × 4 23 mm (volume = 0 279 cm3), while the second plaque was located in the distal third and measured 24 0 × 29 3 × 4 35 mm (volume = 1 60 cm3)
Two calcifications in the second plaque measured 5 2 × 9 3 mm and 5 0 × 8 0 mm The total volume of the two plaques was 1 879 cm3 The ultrasound appearance of the basal
plaque was iso-hyperechoic, and that of the distal plaque was iso-hyperechoic-calcific
The strain ratios of the two basal and distal penile plaques were 1 8 and 2 53, respectively The cavernous arteries showed a normal arterial flow and end-diastolic velocity in the PDDU examination (with a penile injection of 10 mcg of alprostadil) The patient then underwent multimodal therapy with antioxidants The complete list of antioxidant substances in the multimodal treatment administered to the patient, alongside the pre-treatment clinical data and those related to each subsequent follow-up after the three treatment cycles, is shown in Table 1
After completing the third cycle of six perilesional penile injections with 60 mg of pentoxifylline (every 2 months), the patient delayed the scheduled follow-up after 12 months and continued oral and local home therapy for an additional 6 months The follow-up was then performed 18 months after the last check-up I
before, during, and after treatment are presented in Figure 1
After three treatment cycles, totaling 36 months of multimodal antioxidant therapy, the patient underwent a complete follow-up, and no penile nodules were palpable No plaque was detected in the ultrasound examination
The patient did not report any penile pain (VAS score = 0) nor complained of erectile dysfunction The IIEF score was 27 The PDQ symptom bother score was four
The patient had an excellent psychological state, and the penis's appearance was comparable to the condition before PD (congenital curvature of the penis), The patient expressed satisfaction with the excellent results achieved at the end of our treatment
Case 2
A 48-year-old Caucasian man, a non-smoker, reported that he had suffered from prostatitis in the past but had no related symptoms at the time of the visit The patient reported that he already had a congenital penile curvature before the onset of PD The congenital penile deformity consisted of a mild dorsal curvature of 10 degrees
The patient did not report any traumatic events involving his penis in the previous 612 months He reported that he had started to notice a penile curvature, different from usual, approximately 9 months earlier The patient did not report any penile pain (VAS score = 0) nor complained of erectile dysfunction at the time of our visit The IIEF score was 27 The PDQ symptom bother score was 10 In our observation, the penile deformation presented with a dorsal curve of 45 degrees Upon palpation, two plaques were detected at the basal third level and the distal level of the penis, approximately 10
G Paulis, G De Giorgio, A Paulis
Figure 1. Images of the ultrasound exam (longitudinal and transverse scan) are shown before (A), during (B) and (C), and after multimodal treatment (D)
mm and 15 mm in length, respectively Both plaques had a fibrous consistency Two plaques were present in the penile eco-elastography examination The first penile plaque was located at the basal third and measured 9 28 × 10 9 × 3 99 mm (volume = 0 212 cm3), while the second plaque was located in the distal third and measured 14 3 × 11 7 × 2 86 mm (volume = 0 252 cm3) The total volume of the two plaques was 0 464 cm3 The ultrasound appearance of the two plaques was iso-hyperechoic The strain ratios of the
two basal and distal penile plaques were 2 1 and 1 89, respectively The cavernous arteries exhibited a normal arterial flow and end-diastolic velocity in the PDDU examination (a penile injection of 10 mcg of alprostadil) The patient then underwent multimodal therapy with antioxidants However, the patient did not consent to the publication of photos of his penis, even if published anonymously
Table 2 displays the full list of antioxidant substances
Table 2. Case 2: clinical data collected before, during, and after antioxidant treatment.
Basalplaque:B
928 × 109 × 399mm(volume=0212cm3)
Distalplaque:Distalplaque=189
143 × 117 × 286mm(volume=0252cm3)
Totalvolumeofthetwoplaques0464cm3 F irst cycle Orally:L-carnitine1000mg+Propolis700mg+Ginkgobiloba240mg of multimodal treatment with antioxidants +Bilberry180mg+CoenzymeQ-10100mg+Silymarin400mg (6 months) +Boswellia200mg+VitaminC50mg+VitaminE48mg +Superoxidedismutase11000IU/g10mg/daily/for6months; +Topically:Propoliscream/2xdaily+Diclofenacgel4%/daily/for6months;
VAS = visual ana og scale, a pain measurement questionna re (score range: 0-10) (45); IIEF = International Index of Erectile Funct on, a questionna re for assessing erectile function with a score range of 0-30, nd cat ng d fferent ED severity levels (no ED, score range: 26-30) (46); PDQ symptom bother = PD Questionna re symptom bother for evaluating the psychosexual impact, with a score range of 0-30 (10, 47, 66) The stra n rat o (deformat on ndex), detected v a echo-elastography, indicates the p aque's stiffness (65) It is expressed as a number, represent ng the ratio between the stiffness of the pathologica tissue (p aque) and that of the adjacent norma t ssue When elastography does not detect any ane ast c area (plaque), the stra n rat o index corresponds to 1 In this case, the image disp ayed on the u trasound machine screen does not show any ndex
included in the multimodal treatment given to the patient, alongside the clinical data before treatment and at each follow-up after the treatment cycles
The images from the ultrasound examination before, during, and after treatment are presented in Figure 2
After undergoing three cycles of treatment, which lasted a total of 30 months, the patient had a comprehensive follow-up assessment that revealed no palpable penile nodules The ultrasound examination did not detect any plaque The patient did not report any penile pain (VAS score = 0) nor complained of erectile dysfunction, the IIEF
score was 27 The PDQ symptom bother score was four The patient's psychological well-being was excellent, and the penis's appearance was similar to its pre-PD state (a congenital dorsal curvature of the penis of 10 degrees) The patient expressed satisfaction with the outstanding results obtained after completing our antioxidant treatment
Case 3
The images from the ultrasound examination (longitudinal and transverse scans) are shown in sequence: before (A), during (B) and (C), and after (D) the multimodal treatment.
A 42-year-old Caucasian man, a non-smoker, reported having fibromyalgia The patient mentioned experiencing a traumatic event to his penis during sexual intercourse approximately 4 months before He noticed a slight dorsal curvature of the penis under the glans, at the distal third of the penis, approximately 2 months ago He also reported feeling pain in the penis during erection and sometimes at rest for the past 2 months
During the visit, the patient reported penile pain during erection (VAS score = 5) but did not mention erectile dysfunction His IIEF score was 26, and the PDQ symptom bother score was 14 The penile deformity observed was a 20-degree sub-glandular dorsal curve No penile plaque was detected upon palpation
A plaque was detected in the penile echoelastography examination The plaque was located in the distal third of the penis and measured 6 49 × 4 52 × 2 79 mm (volume = 0 043 cm3) The ultrasound appearance of the plaque was isoechoic with mild hyperechogenicity in its distal portion The plaque strain ratio was 1 8 The cavernous arteries showed normal arterial flows and end-diastolic velocities during the PDDU examinat i o n (
alprostadil) The patient underwent multimodal therapy with antioxidants but without penile injections of pentoxifylline due to the plaque's small size Table 3 shows the
administered to the patient, alongside the clinical data before treatment and at each follow-up after the treatment cycles
The images from the ultrasound examination before, during, and after treatment are presented in Figure 3
After undergoing three cycles of treatment, which lasted a total of 18 months, the p
assessment that revealed no palpable penile nodules The ultrasound examination did not detect any plaque, the patient did not complain of penile pain (VAS score = 0), and the IIEF score was 27 The PDQ symptom bother score was four The patient's psychological state was excellent, and no curvature of the penis was noticeable during the erectile phase The patient expressed satisfaction with the outstanding results obtained after completing the antioxidant treatment
G Paulis, G De Giorgio, A Paulis
Figure 2.
Table 3
Case 3: clinical data collected before, during, and after antioxidant treatment
withtheinitialsituation Third cycle orally:L-Carnitine1000mg+Propolis700mg+Ginkgobiloba240mg of multimodal treatment with antioxidants +Bilberry180mg+C
VAS visua analog scale, a pa n measurement quest onnaire (score range: 0-10) (45); IEF Internat onal Index of Erect le Function, a quest onnaire for assessing erect le funct on with a score range of 0-30, indicating different ED sever ty evels (no ED, score range: 26-30) (46); PDQ symptom bother PD Quest onnaire symptom bother for evaluat ng the psychosexual impact, w th a score range of 0-30 (10, 47, 66) The strain ratio (deformation index), detected v a echo-elastography, indicates the plaque's stiffness (65) It is expressed as a number, representing the rat o between the stiffness of the patho ogical tissue (plaque) and that of the adjacent normal tissue When elastography does not detect any anelastic area (plaque), the strain ratio ndex corresponds to 1 In this case, the image d splayed on the ultrasound mach ne screen does not show any index
Figure 3
The images from the ultrasound examination (longitudinal and transverse scans) are shown in sequence: before (A), during (B) and (C), and after (D) the multimodal treatment.
Case 4
A 47-year-old Caucasian man, a non-smoker, reported having irritable bowel syndrome He reported that he had been suffering from erectile dysfunction for approximately 10 years The patient had been taking a 10 mg tadalafil tablet before sexual intercourse for this disorder for several years
The patient did not remember any traumatic event involving his penis He reported noticing the appearance of penile deformity and penile pain during erection for approximately 9 months Upon penile examination, a 15 mm long nodule with a fibrous consistency was palpable
The VAS score was three The patient’s IIEF score was 20, and the PDQ symptom bother score was 15 The penile deformity observed consisted of a 30-degree dorsal curvature of the penis associated with another curvature to the left of the same degree The middle third level of the penile shaft had an “hourglass” appearance A plaque was detected in the penile echo-elastography examination in the middle third of the penis and measured 18 8 × 15 8 × 3 42 mm (volume = 0 532 cm3) The ultrasound appearance of the plaque was iso-hyperechoic The plaque strain ratio
was 2 3 In the PDDU examination (a penile injection of 10 mcg of alprostadil), the cavernous arteries showed normal arterial flows, while the end-diastolic speeds were high (12 2 cm/s on the right; 10 6 cm/s on the left), indicating veno-occlusive insufficiency The patient underwent multimodal therapy with antioxidants, including periodic perilesional penile injections with 60 mg of pentoxifylline
However, we allowed the patient to continue taking one 10 mg tadalafil tablet before sexual intercourse
Table 4 shows the complete list of antioxidant substances included in the multimodal treatment administered to the patient, alongside the clinical data before treatment and at each follow-up after the treatment cycles
The images from the ultrasound examination before, during, and after treatment are presented in Figure 4
After completing three treatment cycles over 30 months, the patient underwent a thorough follow-up evaluation that showed no palpable penile nodules An ultrasound examination also did not find any plaque During the PDDU examination (a penile injection of 10 mcg of alprostadil), the cavernous arteries showed normal arterial flows, while the end-diastolic velocities remained elevated
Case 4: clinical data collected before, during, and after antioxidant treatment
188 × 158 × 342mm(volume0532cm3)23of30degrees32015 F irst cycle Orally:L-carnitine1000mg+Propolis700mg+Ginkgobiloba240mg of multimodal treatment with antioxidants +Bilberry180mg+CoenzymeQ-10100mg+Silymarin400mg
VAS visua ana og scale, a pain measurement questionna re (score range: 0-10) (45)); IIEF Internationa Index of Erecti e Function, a questionnaire for assess ng erecti e function w th a score range of 0-30, ndicat ng
leve s (no ED, score range: 26-30) (46); PDQ symptom bother = PD Quest onnaire symptom bother for evaluating the psychosexual impact, with a score range of 0-30 (10, 47, 66) The stra n ratio (deformat on index), detected v a echo-elastography, indicates the p aque's stiffness (65) It is expressed as a number, representing the ratio between the stiffness of the patho ogical tissue (plaque) and that of the adjacent norma tissue When elastography does not detect any ane ast c area (plaque), the strain ratio index corresponds to 1 In this case, the image disp ayed on the u trasound machine screen does not show any ndex
G Paulis, G De Giorgio, A Paulis
Table 4
(8 8 cm/s on the right; 8 6 cm/s on the left), indicating persistent occlusive insufficiency, albeit modestly improved after our treatments The IIEF score was 22, while it was 20 before our treatment Erectile dysfunction was moderately improved because, initially, the plaque likely deprived the penis of a portion of functioning erectile tissue The patient did not report any penile pain (VAS score = 0) After the plaque completely regressed, we observed a residual penile deformity characterized by a dorsal curve of 10 degrees and a left lateral curve of 5 degrees Before our treatment, the initial penile deformity consisted of a dorsal curve of 30 degrees and a left lateral curve of 30 degrees The PDQ symptom bother score was four The patient's psychological state had certainly improved compared with pre-treatment; however, the erectile dysfunction still caused some concern for the patient The patient reported that the slight residual penile deformation no longer worried him The patient was pleased with the good results achieved after finishing the antioxidant treatment
Complete resorption of the PD plaque after treatment occurred in all cases The disappearance of Peyronie's plaque occurred over a period ranging from 18 to 36 months, in relation to the volume of the plaque
DISCUSSION
The scientific literature has documented eleven PD human patients who have recovered following medical treatment with bioactive food extracts with antioxidant properties (48-51) All 11 cases already published that had achieved complete plaque reabsorption after antioxidant treatment involved men in the first phase of PD
Before these experiences, cases of PD healing had been published, but these were experimental studies on rats in which PD-like plaques were induced with solutions of human fibrin and thrombin or with transforming growth factor-b1 (52-54)
Before these healing experiences, the scientific literature had always reported the possible spontaneous resolution of the disease in 3 2-13% of cases, as expression of the natural history of PD (31, 55-57) However, some of these studies were not based on instrumental exams but on patient self-reports via questionnaires Like other authors with extensive experience in this disease, we believe PD cannot resolve spontaneously (58, 59) In a study published in 2013, we demonstrated that penile curvature can improve without the disease regressing Without treatment, Peyronie's plaque in its progression can extend to the contralateral side of the curve and cause a reduction in the elasticity of the cavernous tissue, resulting in a paradoxical improvement of the penile curvature (29)
Numerous articles in the scientific literature on PD consider surgical treatment the "gold standard" and the ideal and definitive therapeutic option Unfortunately, these considerations have led most uroandrologists to believe that PD is an incurable disease, resulting in a widespread pessimistic attitude and resistance to medical therapy for PD On the contrary, we have always believed that since PD is related to chronic inflammation, the best treatment would be to treat this disease like any other chronic inflammatory disease
Long-term treatment of PD patients with NSAIDs, corticosteroids, or other drugs can lead to chronic damage or toxicity in organs such as the liver, kidneys, immune system, and gastrointestinal system Therefore, we have
Figure 4
The images of the ultrasound examination (longitudinal and transverse scans) are shown in sequence: before (A), during (B) and (C), and after (D) the multimodal treatment.
always believed that targeting oxidative stress, a key mechanism in inflammation, with antioxidants is the best therapeutic approach for interrupting the inflammatory process of this disease (35, 60-62) Although antioxidants are not included in the current EAU European Association of Urology (EAU) and American Urological Association (AUA) guidelines for treating PD, three randomized studies in the literature have discussed the use of antioxidant substances in PD patients (31, 32, 68-70) Additionally, several controlled studies have shown positive outcomes when antioxidants have been used in combination (61, 62, 67) The EAU and AUA guidelines strongly recommend infiltrative therapy with collagenase clostridium histolyticum (CCH) or interferon alpha-2b (31, 32, 39) However, we did not employ CCH in treatment as it is indicated for PD in the "stabilization phase" On the contrary, our PD patients were all in the active phase of the disease Furthermore, in Italy, the drug Xiapex (CCH) has been withdrawn from the market by the Italian Medicines Agency (AIFA) as of January 1, 2020 Additionally, we did not utilize interferon alpha-2b due to its high cost and potential side effects, including fever and flu-like symptoms, fatigue, nausea, diarrhea, vomiting, and dizziness
The positive response to our treatments is attributed to the antioxidant properties of the substances used, which can interrupt inflammation and negatively interfere with oxidative stress, a key factor in fibrogenesis (19, 20)
Figure 5 shows the interfering activities of antioxidants on the various pathogenetic mechanisms involved in PD
Propolis, bilberry, silymarin, boswellia, coenzyme Q-10, carnitine, and Ginkgo biloba exhibit antioxidant and antifibrotic activity, inhibit pro-inflammatory cytokines, metalloproteins with anti-elastic properties, the COX-2 enzyme, and NF-kappa-B factor (22) Coenzyme Q-10
also protects cellular membranes from lipid peroxidation caused by reactive species, and regenerates vitamin E to its natural and non-oxidized state after it has oxidized from exerting its antioxidant action (22) Carnitine also reduces the production of inducible nitric oxide synthase (iNOS), inhibits fibroblast proliferation and their differentiation into osteoblasts, and induces vasodilation through an endothelial mechanism that utilizes the nitric oxide pathway (22)
Superoxide dismutase (SOD) protects the human body from tissue damage caused by ROS by removing superoxide anion SOD has anti-inflammatory action and inhibits fibroblast proliferation (22, 71) Vitamin C acts as a scavenger against reactive species and inhibits pro-inflammatory cytokines, and fibroblast proliferation (22) Vitamin E is a ROS scavenger and inhibits NF-kB factor, COX-2, proinflammatory cytokines, PDGF, and fibroblast proliferation (22, 35) Pentoxifylline (PTX) inhibits ROS, myofibroblastic differentiation, collagen deposition, NF-kB factor, proinflammatory cytokines, TGF-beta-1, COX-2, iNOS protein expression, and PAI-1 and stimulates fibroblast apoptosis In our multimodal treatment, we also used diclofenac (an NSAID) administered locally to avoid potential organ damage associated with long-term oral therapy (29, 30) Diclofenac also has antioxidant properties and has been demonstrated to penetrate tissues deeply (63, 64)
The multimodal antioxidant treatment for PD described in this article is the same as described in our recent articles and differs only in the dose of PTX used for penile injections, which is 60 mg instead of 100 mg We noticed that by reducing the dose of PTX, we achieved the same results as in the past with higher doses of PTX
The treatment lasted for an extended period in three of the four cases described here (30-36 months) A pro-
G Paulis, G De Giorgio, A Paulis
Figure 5
Inhibitory action of antioxidant agents on the main pathogenetic mechanisms of Peyronie's disease
longed treatment duration is essential due to the chronic inflammatory nature of PD, which requires time for complete plaque resorption The treatment duration may also be affected by the size of the PD plaque The excellent result obtained in the third case, with a shorter treatment time (a year and six months) compared with the other three cases, is likely because of the early diagnosis (four months after the penile trauma) In this case, we were able to provide the patient with a shorter course of treatment without periodic penile injections, as the plaque was small (0 043 cm3) because the PD was in an early stage In our treatment plan involving penile injections, we progressively extended the time between each pentoxifylline injection throughout the treatment process This approach was based on the understanding that even minor peri-lesional injections can cause trauma, which is a known trigger for developing PD We preferred increasing the intervals between injections (every 2 weeks > every month > every 2 months) whenever regression of the disease was observed during scheduled follow-ups to minimize the risk of new traumas
It has been reported in the literature that ultrasound evaluation of the penis in PD cannot provide adequate plaque measurements We believe, however, that an accurate plaque size can be obtained if a highly sensitive and upto-date ultrasound machine with an elastographic module is used and, above all, if an expert clinician with great experience in this disease performs the evaluation (31, 65, 72, 73)
Therefore, we believe that our findings resulted from both the treatment substances and the specific ultrasound evaluation method we employed This method enabled us to accurately diagnose the affected area (plaque) and closely monitor its progression during scheduled follow-ups
CONCLUSIONS
Despite the small sample size in this case report, our multimodal antioxidant treatment yielded highly satisfactory outcomes, allowing for the complete disappearance of the penile plaques in the disease area We believe that the excellent responses to our therapy were due to the appropriate use of antioxidant substances, as well as the use of a very sensitive and up-to-date ultrasound machine capable of recognizing the plaques and providing their locations and precise dimensions Additionally, having a clinician with great experience in PD conduct the echoelastography examinations contributed to the positive outcomes Specialists may find this case series of great interest for uroandrological practice, despite the limited number of cases presented However, randomized controlled trials with a larger number of PD patients are needed to demonstrate the efficacy of the multimodal antioxidant treatment
REFERENCES
1 Bias WB, Nyberg LM Jr, Hochberg MC, et al Peyronie’s disease: A newly recognized autosomal-dominant trait Am J Med Genet 1982; 12:227-235
2 Schwarzer U, Sommer F, Klotz T, et al The prevalence of Peyronie’s disease: Results of a large survey BJU Int 2001; 88:727-730
3 Rhoden EL, Teloken C, Ting HY, et al Prevalence of Peyronie’s disease in men over 50-y-old from Southern Brazil Int J Impot Res 2001; 13:291-293
4 La Pera G, Pescatori ES, Calabrese M, et al Peyronie’s disease: Prevalence and association with cigarette smoking A multicenter population- based study in men aged 50-69 years Eur Urol 2001; 40:525-530
5 DiBenedetti DB, Nguyen D, Zografos L, et al A Population-Based Study of Peyronie’s Disease: Prevalence and Treatment Patterns in the United States Adv Urol 2011; 2011:282503
6 Shiraishi K, Shimabukuro T, Matsuyama H The prevalence of Peyronie’s disease in Japan: A study in men undergoing maintenance hemodialysis and routine health checks J Sex Med 2012; 9:27162723
7 Stuntz M, Perlaky A, des Vignes F, et al The Prevalence of Peyronie’s Disease in the United States: A Population-Based Study PLoS ONE 2016; 11:e0150157
8 Kyei MY, Mensah JE, Asante E, et al Peyronie’s Disease in People of African Origin: A Mini Review J Ger Ag Res 2017, 1, 104 Av
gin A Mini Review (accessed on 21 August 2024)
9 Levine LA, Estrada CR, Storm DW, et al Peyronie disease in younger men: characteristics and treatment results J Androl 2003; 24:27-32
10 Cilio S, Fallara G, Capogrosso P, et al The symptomatic burden of Peyronie's disease at presentation according to patient age: A critical analysis of the Peyronie's disease questionnaire (PDQ) domains Andrology 2023; 11:501-507
11 Paulis G, De Giorgio G, Paulis A Clinical Presentation of Peyronie's Disease: A Retrospective Study of 564 Cases Diagnostics (Basel) 2024; 14:1125
12 Weidner W, Schroeder-Printzen I, Weiske WH, et al Sexual dysfunction in Peyronie’s disease: An analysis of 222 patients without previous local plaque therapy J Urol 1997; 157:325-328
13 Nelson CJ, Diblasio C, Kendirci M, et al The chronology of depression and distress in men with Peyronie’s disease J Sex Med 2008; 5:1985-1990
14 Devine CJ Jr, Somers KD, Ladaga LE Peyronie’s disease: Pathophysiology Prog Clin Biol Res 1991; 370:355-358
15 Devine CJJ, Somers KD, Jordan GH, et al Proposal: Trauma as a cause of Peyronie’s lesion J Urol 1997; 157:285-290
16 Jarow JP, Lowe FC Penile trauma: An etiologic factor in Peyronie’s disease and erectile dysfunction J Urol 1997; 158:13881390
18 Moreland RB, Nehra A Pathophysiology of Peyronie's disease Int J Impot Res 2002; 14:406-410
19 Sikka SC, Hellstrom WJ Role of oxidative stress and antioxidants in Peyronie’s disease Int J Impot Res 2002; 14:353-360
20 Bivalacqua TJ, Champion HC, Hellstrom WJ Implications of nitric oxide synthase isoforms in the pathophysiology of Peyronie’s disease Int J Impot Res 2002; 14:345-352
21 El-Sakka AI, Salabas E, Dinc ̧ er M, et al The pathophysiology of Peyronie’s disease Arab J Urol 2013; 11:272-277
22 Paulis G, De Giorgio G, Paulis L Role of Oxidative Stress in
P e y ro n i e ’ s D i s e a s e : B i o c h e m i c a l E v i d e n c e a n d E x p e r i e n c e s o f
Treatment with Antioxidants Int J Mol Sci 2022, 23, 15969 https://doi org/10 3390/ijms232415969
23 Jalkut, M, Gonzalez-Cadavid, N, Rajfer, J Peyronie's Disease: A Review Rev Urol 2003; 5:142-148
24 Kadioglu A, Akman T, Sanli O, et al Surgical Treatment of Peyronie’s Disease: A Critical Analysis Eur Urol 2006; 50:235-248
25 Mulhall JP, Schiff J, Guhring P An analysis of the natural history of Peyronie's disease J Urol 2006; 175:2115-2118
26 Ralph D, Gonzalez-Cadavid N, Mirone V, et al The management of Peyronie's disease: evidence-based 2010 guidelines J Sex Med 2010; 7:2359-2374
27 Levine LA, Burnett AL Standard operating procedures for Peyronie’s disease J Sex Med 2013, 10, 230-244
28 Garaffa G, Trost LW, Serefoglu EC, et al Understanding the course of Peyronie's disease Int J Clin Pract 2013; 67:781-788
29 Paulis G, Cavallini G Clinical evaluation of natural history of Peyronie's disease: our experience, old myths and new certainties Inflamm Allergy Drug Targets 2013; 12:341-348
30 Bella AJ, Lee JC, Grober ED, et al 2018 Canadian Urological Association guideline for Peyronie's disease and congenital penile curvature Can Urol Assoc J 2018, 12(5), E197-E209
31 Hatzimouratidis K, Eardley I, Giuliano F, et al EAU guidelines on penile curvature Eur Urol 2012; 62:543-552
32 Nehra A, Alterowitz R, Culkin DJ, et al Peyronie's Disease: AUA Guideline J Urol 2015; 194:745-753
33 Levine LA, Larsen S Diagnosis and Management of Peyronie Disease In: Campbell-Walsh Urology 11th Ed , Wein AJ, Kavoussi LR, Partin AW, Peters CA, Eds,; Elsevier Saunders: Philadelphia (PA), 2015 Volume 1 (Chapter 31); 722-748
34 Kendirci M, Hellstrom WJ Critical analysis of surgery for Peyronie's disease Curr Opin Urol 2004; 14:381-388
35 Paulis G, Brancato T, D'Ascenzo R, et al Efficacy of vitamin E in the conservative treatment of Peyronie's disease: legend or reality? A controlled study of 70 cases Andrology 2013; 1:120-128
36 Chung E, Ralph D, Kagioglu A, et al Evidence-based management guidelines on Peyronie’s disease J Sex Med 2016; 13:905-923
37 Gennaro R, Barletta D, Paulis G Intralesional hyaluronic acid: an innovative treatment for Peyronie's disease Int Urol Nephrol 2015; 47:1595-1602
38 Zucchi A, Costantini E, Cai T, et al Intralesional Injection of Hyaluronic Acid in Patients Affected With Peyronie's Disease: Preliminary Results From a Prospective, Multicenter, Pilot Study Sex Med 2016; 4: e83-e88
39 Nguyen HNT, Anaissie J, DeLay KJ, et al Safety and efficacy of collagenase Clostridium histolyticum in the treatment of acute-phase Peyronie’s disease J Sex Med 2017; 14:1220-1225
40 Cilio S, Rocca R, Celentano G, et al Intraplaque injections of hyaluronic acid for the treatment of stable-phase Peyronie's disease: a retrospective single-center experience Asian J Androl 2024; 26:268-271
41 Osmonov D, Ragheb A, Ward S, et al ESSM Position Statement on Surgical Treatment of Peyronie's Disease Sex Med 2022; 10:100459
42 Kelâmi A Autophotography in evaluation of functional penile disorders Urology 1983; 21:628-629
43 Eri LM, Thomassen H, Brennhovd B, et al Accuracy and repeatability of prostate volume measurements by transrectal ultrasound Prostate Cancer Prostatic Dis 2002; 5:273-278
44 Lee JS, Chung BH Transrectal ultrasound versus magnetic resonance imaging in the estimation of prostate volume as compared with radical prostatectomy specimens Urol Int 2007; 78:323-327
45 Kahl C, Cleland JA Visual analogue scale, numeric pain rating scale and the McGill pain Questionnaire: An overview of psychometric properties Phys Ther Rev 2005; 10:123-128
46 Rosen RC, Riley A, Wagner G, et al The international index of erectile function (IIEF): A multidimensional scale for assessment of erectile dysfunction Urology 1997; 49:822-830
47 Hellstrom WJ, Feldman R, Rosen RC, et al Bother and distress associated with Peyronie's disease: validation of the Peyronie's disease questionnaire J Urol 2013, 190, 627-634
48 Paulis G, De Giorgio G Complete Plaque Regression in Patients w
23:e936146
49 Paulis G, De Giorgio G Full Regression of Peyronie’s Disease Plaque Following Combined Antioxidant Treatment: A Three-Case Report Antioxidants 2022; 11:1661
50 Paulis G, De Giorgio G Patients with Peyronie’s disease achieve complete plaque regression after multimodal treatment with antioxidants: A case series J Med Case Rep 2022; 16:359
51 Paulis G, De Giorgio G Disappearance of Plaque Following Treatment with Antioxidants in Peyronie's Disease Patients-A Report of 3 Cases Clin Pract 2022; 12:1020-1033
52 Kwon KD, Choi MJ, Park, JM, et al Silencing histone deacetylase 2 using small hairpin RNA induces regression of fibrotic plaque in a rat model of Peyronie’s disease BJU Int 2014; 114:926-936
53 Song KM, Chung DY, Choi MJ, et al Vactosertib, a Novel, Orally Bioavailable Activin Receptor-Like Kinase 5 Inhibitor, Promotes Regression of Fibrotic Plaques in a Rat Model of Peyronie's Disease World J Mens Health 2020; 38:552-563
54 Ryu JK, Piao S, Shin HY, et al IN-1130, a novel transforming growth factor-beta type I receptor kinase (activin receptor-like kinase 5) inhibitor, promotes regression of fibrotic plaque and corrects penile curvature in a rat model of Peyronie's disease J Sex Med 2009; 6:1284-1296
55 Gelbard MK, Dorey F, James K The natural history of Peyronie's disease J Urol 1990; 144:1376-1379
56 Kadioglu A, Tefekli A, Erol B, et al A retrospective review of 307 men with Peyronie's disease J Urol 2002; 168:1075-1079
57 Weidner W, Hauck EW, Schnitker J, Peyronie's Disease Study Group Potassium paraaminobenzoate (POTABA™) in the treatment of Peyronie's disease: a prospective, placebo-controlled, randomized study Eur Urol 2005; 47:530-536
58 Bekos A, Arvaniti M, Hatzimouratidis K, et al The natural history of Peyronie's disease: an ultrasonography-based study Eur Urol 2008; 53:644-650
59 Levine LA Peyronie's disease: contemporary review of non-surgical treatment Transl Androl Urol 2013; 2:39-44
60 Paulis G, D'Ascenzo R, Nupieri P, et al Effectiveness of antioxidants (propolis, blueberry, vitamin E) associated with verapamil in the medical management of Peyronie's disease: a study of 151 cases Int J Androl 2012; 35:521-527
61 Paulis G, Cavallini G, De Giorgio G, et al Long-term multimodal therapy (verapamil associated with propolis, blueberry, vitamin E and local diclofenac) on patients with Peyronie’s disease (chronic inflammation of the tunica albuginea) Results of a controlled study Inflamm Allergy Drug Targets 2013; 12:403-409
62 Paulis G, Barletta D, Turchi P, et al Efficacy and safety evaluation of pentoxifylline associated with other antioxidants in medical treatment of Peyronie’s disease: A case-control study Res Rep Urol 2016; 8:1-10
63 Tang YZ, Liu ZQ Evaluation of the free-radical-scavenging activity of diclofenac acid on the free-radical-induced haemolysis of human erythrocytes J Pharm Pharmacol 2006; 58:625-631
64 Radermacher J, Jentsch D, Scholl MA, et al Diclofenac concentrations in synovial fluid and plasma after cutaneous application in inflammatory and degenerative joint disease Br J Clin Pharmacol 1991; 31:537-541
65 Paulis G, De Giorgio G, Paulis A Ultrasound Elastography as a Diagnostic Tool for Peyronie's Disease: A State-of-the-Art Review Diagnostics (Basel) 2024; 14:665
66 Cocci A, Verze P, Zucchi A, et al Validation of the Italian version of the Peyronie's Disease Questionnaire (PDQ) Int J Impot Res 2023, 10 1038/s41443-023-00792-4 Available online: https://doi org/10 1038/s41443-023-00792-4 (accessed on 21August 2024)
67 Gallo L, Sarnacchiaro P Ten-year experience with multimodal treatment for acute phase Peyronie’s disease: A real life clinical report Actas Urol Esp (Engl Ed) 2019; 43:182-189
68 Favilla V, Russo GI, Privitera S, et al Combination of intralesional verapamil and oral antioxidants for Peyronie’s disease: A prospective, randomised controlled study Andrologia 2014; 46:936-942
69 Riedl CR, Sternig P, Gallé G, et al Liposomal recombinant human superoxide dismutase for the treatment of Peyronie’s disease: A randomized placebo-controlled double-blind prospective clinical study Eur Urol 2005; 48:656-661
70 Alizadeh M, Karimi F, Fallah, MR Evaluation of verapamil efficacy in Peyronie’s disease comparing with pentoxifylline Glob J Health Sci 2014; 6:23-30
71 Carillon J, Rouanet JM, Cristol JP, Brion, R Superoxide dismutase administration, a potential therapy against oxidative stress related diseases: several routes of supplementation and proposal of an original mechanism of action Pharm Res 2013; 30:2718-2728
72 McCauley JF, Dean RC Diagnostic utility of penile ultrasound in Peyronie’s disease World J Urol 2020; 38:263-268
73 Parmar M, Masterson JM, Masterson, TA, 3rd The role of imaging in the diagnosis and management of Peyronie’s disease Curr Opin Urol 2020; 30:283-289
Correspondence
Gianni Paulis, MD paulisg@libero it
Department of Urology and Andrology, Peyronie’s Care Center, Castelfidardo Clinical Analysis Center, 00185 Rome, Italy
Giovanni De Giorgio, MD
Department of Urology and Andrology, Section of Ultrasound Diagnostics, Castelfidardo Clinical Analysis Center, 00185 Rome, Italy
Andrea Paulis
andrea fx 94@gmail com
Bambino Gesù Children’s Hospital, IRCCS (Istituti di Ricovero e Cura a Carattere Scientifico), Rome, Italy
Conflict of interest: The authors declare no potential conflict of interest
META-ANALYSIS
Barts flank-free modified supine position vs prone position in percutaneous nephrolithotomy: Systematic review
and meta analysis
I Gede Yogi Prema Ananda 1 , Kadek Budi Santosa 1, 2 , I Wayan Yudiana 1, 2 , Pande Made Wisnu Tirtayasa 1, 3 , Ida Bagus Putra Pramana 1, 3 , Nyoman Gede Prayudi 1, 2 , Gede Wirya Kusuma Duarsa 1, 2
1 Department of Urology, Faculty of Medicine, Universitas Udayana, Denpasar, Bali, Indonesia;
2 Prof Dr I G N G Ngoerah Hospital, Denpasar, Bali, Indonesia;
3 Universitas Udayana Teaching Hospital, Badung, Bali, Indonesia
Summary
Introduction: Percutaneous Nephrolithotomy (PCNL) has been performed in various positions, including prone position and several modifications of supine position. The Barts flank-free modified supine (FFMS) position is a newly enhanced version of the supine positions
This study aims to compare the outcomes of Barts FFMS and prone position in PCNL
Methods: This study followed PRISMA 2020 guideline and was registered to PROSPERO CRD42024530426 Comprehensive search in PubMed, Sciencedirect, and Scopus was conducted until May 2024 Stone-free rates, complications, surgery duration, fluoroscopy duration, use of nephrostomy, and length of stay were collected Data were analyzed using RevMan 5 4
Results: A total of 4 studies were included in this review. There was no significant difference in stone-free rates between Barts FFMS and prone positions (OR = 1.12, 95% CI 0.64-1.95, p = 0 70) There were no significant difference in incidence of fever (OR = 0.91, 95% CI 0.38-2.18, p = 0.84), need for blood transfusion (OR = 0 46, 95% CI 0 11-1 88, p = 0 28), and urine leakage (OR = 0.41, 95% CI 0.16-1.05, p = 0.06). The surgery duration was significantly shorter in Barts FFMS position than in prone position (MD = -15 48, 95% CI [(-26 42)-(-4 55)], p = 0 006) There was no significant difference in patients requiring nephrostomy (OR = 0 19, 95% CI 0 01-3 75, p = 0 28) There were no significant difference in fluoroscopy duration (MD = 0 27, 95% CI [(-6 85)-7 40], p = 0 94) and the length of hospital stay (MD = -0 20, 95% CI [(-0 74)-0 33], p = 0 46)
Conclusions: The surgery duration was significantly shorter in Barts FFMS position than in prone position There were no significant differences regarding stone-free rates, complications, fluoroscopy duration, use of nephrostomy, and length of hospital stay This indicates that neither Barts FFMS nor prone position is superior, and the choice should be based on the surgeon's preference and the patient's clinical status
KEY WORDS: Barts; Flank-free; Supine; Prone; PCNL
Submitted 19 August 2024; Accepted 31 August 2024
INTRODUCTION
Nephrolithiasis is among the most prevalent urological conditions, impacting around 12% of the global popula-
tion (1) Its prevalence varies worldwide, starting from 15% in Asia, 5-9% in Europe, and 7-13% in North America (2) The global morbidity and disability-adjusted life years (DALYs) of nephrolithiasis increased substantially between 1990 and 2019 (3) The majority of kidney stones are composed of calcium, primarily in the form of c a l c i u m o x a l a t e o r c a l c i u m p h o s p h a t e s t o n e s ( 2 ) Nephrolithiasis is often symptomatic (4)
Percutaneous nephrolithotomy (PCNL) is the primary treatment in patients with symptomatic nephrolithiasis larger than 2 cm (5) Over time, PCNL has been through many alterations in patient positioning The first ever PCNL was done by Fernström et al in prone position, back in 1976 The prone position was believed to be safely avoiding vital organs, such as the colon (6) Later, the first report of supine PCNL was introduced by Valdivia et al in 1990 (7) and further elaborated in 1998 (8) Since then, the supine position has undergone variable modifications This includes the flank roll position, Galdakaomodified Valdivia position, crossed-leg supine position, complete supine position, and the most recent Barts FFMS position (9) All of them have been reported to decrease the duration of PCNL procedures by eliminating the need for patient repositioning and allowing quick airway access (10)
Barts flank-free modified supine (FFMS) position is a newly enhanced version of the traditional supine position, with better access to the kidney (10) It offers several advantages compared to the prone position, including easier fluoroscopy access, more comfortable patient positioning, simpler tract dilation, reduced kidney pressure, improved fragment clearance, and easier transition to RIRS (11) Given these potential benefits, it is crucial to determine whether Barts FFMS is superior to the prone position in terms of clinical outcomes
This study aims to compare the Barts FFMS and prone positions in PCNL, focusing on key clinical outcomes such as stone-free rates, complications, and surgery duration By identifying the optimal patient positioning for PCNL, this study seeks to contribute to the improvement of patient care and surgical efficiency in the treatment of nephrolithiasis
METHODS
Study design
This systematic review and meta-analysis followed PRISMA 2020 guidelines and was registered to PROSPERO CRD42024530426
Search strategy
Comprehensive search by the authors in scientific databases such as PubMed, Sciencedirect, and Scopus was conducted until May 2024 The keywords used were "PCNL" AND ("flank-free" OR "Barts") The authors engaged in discussions to settle any disagreements
Eligibility criteria
Inclusion criteria cover studies in English, RCT or cohort studies, and adult patients who had undergone standard PCNL in Barts FFMS compared to prone position The definition of Barts FFMS position included in this study is a supine position with a 15° tilt of the ipsilateral flank, achieved by placing a 3-liter saline bag under the rib cage and a gel pad under the pelvis, thus creating the 'flankfree' position (8)
Stone-free rates, postoperative complications, and duration of surgery were the expected prim a r y o u t c o m e s , w h i l e fl u o r o s c o p y duration, need for nephrostomy, and length of stay were chosen as secondary outcomes Exclusion criteria cover non-English articles, study designs other than RCTs or prospective studies, non-standard PCNL procedures, and PCNL positions other than Barts FFMS and prone position
Data extraction
Information was systematically collected using a structured format as first author, publication year, study design, sample size, age, body mass index (BMI), stone size, stone-free rates, complications, duration of surgery, duration of fluoroscopy, number of patients needing nephrostomy, and length of hospital stay
Data analysis
The analysis for this study was conducted using Review Manager version 5 4 (The Cochrane Collaboration, The Nordic Cochrane Centre, Copenhagen, Denmark) For continuous data, the Mean Difference (MD) was utilized, while dichotomous data were analyzed using the Odds Ratio (OR) Meta-analysis was performed when two or more studies provided the same type of data
To assess the heterogeneity among the included studies, Cochran’s Q and I² s t a t i s t i c s w e r e e m p l o y e d A fi x e deffects model was used when there was statistical homogeneity (defined as p-
value > 0 1 and I² < 50%) In cases where heterogeneity was present (p-value ≤ 0 1 or I² ≥ 50%), a random-effects model was applied Statistical significance was determined with a threshold of p < 0 05
Quality appraisal
To assess the selected studies, we utilized two different tools We utilized two different tools: the Jadad score for randomized controlled trials (RCTs) and the NewcastleOttawa Scale (NOS) for cohort studies If any discrepancies arose in bias assessments or justifications, they will be resolved through discussions among the authors until a consensus was reached
RESULTS
Study selection
T h e s e a r c h y i e l d e d 2 6 3 r e s u l t s , w i t h 2 3 1 r e c o r d s removed due to duplicates and irrelevance After this removal, 32 potentially relevant articles remained A thorough examination of the full texts resulted in 4 studies meeting the inclusion criteria for this review The process is illustrated in the PRISMA flow chart (Figure 1)
I Gede Yogi Prema Ananda, K Budi Santosa, I W Yudiana, et al
Figure 1. PRISMA flowchart
Table 1
Assessment of the studies included
Author
Mulay et al , 2022 (12)RCT1-
Míçoog ul ar et a , 2021 (13)Cohort-7
Sohail et al., 2017 (14)Cohort-7
Zanaty et al , 2022 (15)RCT2-
Table 2. Baseline characteristics of the studies included.
Study
Stone-free rates
Based on the forest plot presented in Figure 2, which included all 4 studies, there was no significant difference in the stone-free rate between Barts FFMS and the prone position (OR = 1 12, 95% CI 0 64-1 95, p = 0 70)
Soha l et a (2017) BartsFFMS96389±101279±72299±12685-
Prone101452±95287±65297±15179o
Míçoogullari et al (2021) BartsFFMS52439±162244±29321±07392Residua
Figure 2. Stone-free rates.
n
s<3mm1month Prone104408±146248±29327±08294
Study assessment
Two RCTs were included, assessed using the Jadad score and classified as poor quality Two cohort studies were assessed using the Newcastle-Ottawa Scale, all rated as good quality The assessment details are presented in Table 1
Study characteristics
There were 4 studies with a total of 228 PCNL patients operated in the Barts FFMS position and 285 patients in the prone position
The data in Table 2 provides a summary of the subject's baseline characteristics
From the 4 studies, only 3 of them showed proper data to account for the mean age of the patients One study by Zanaty et al lacked the standard deviation (SD) in mean age data The baseline characteristics such as the sample size, mean age, BMI, stone size, stone-free rate, the definition of stone-free status, and follow up time were available in Table 2
fer significantly between Barts FFMS and the prone position (OR = 0 91, 95% CI 0 38-2 18, p = 0 84)
Blood loss requiring transfusion (Clavien-Dindo Grade 2)
Only 3 studies reported blood transfusion
Forest plot in Figure 4 demonstrates that there was no significant difference in the incidence of blood loss requiring transfusion between patients in the Barts FFMS and prone positions (OR = 0 46, 95% CI 0 11-1 88, p = 0 28)
Urine leakage (Clavien-Dindo Grade 3)
Figure 5 illustrates that the incidence of urine leakage was not significantly different between the Barts FFMS and prone position groups, as shown in the Forest plot of 3 studies (OR = 0 41, 95% CI 0 16-1 05, p = 0 06)
Surgery duration
The duration of surgery was significantly shorter in Barts
FFMS position than in prone position, as indicated in Figure 6 (MD = -15 48, 95% CI [(-26 42)-(-4 55)], p = 0 006) It also showed the studies were heterogeneous
Use of nephrostomy
In Figure 7, the forest plot of 3 studies displayed that the use of nephrostomy after PCNL did not differ significant-
Archivio Italiano di Urologia e Andrologia 2024; 96(4):12944
I Gede Yogi Prema Ananda, K Budi Santosa, I W Yudiana, et al
Figure 4. Blood loss requiring transfusion.
Figure 5 Urine leakage
Figure 6. Duration of surgery
Figure 3 Fever
ly in Barts FFMS and prone position (OR = 0 19, 95% CI 0 01-3 75, p = 0 28)
The studies were heterogeneous
Fluoroscopy duration
Only 2 studies reported the duration of fluoroscopy used in PCNL, and they were heterogeneous As shown in Figure 8, the duration of fluoroscopy did not significantly differ between the Barts FFMS and prone position groups (MD = 0 27, 95% CI [(-6 85)-7 40], p = 0 94)
Length of hospital stay
The included studies in this outcome were heterogeneous There was no significant difference between patients in the Barts FFMS and prone positions, as shown in Figure 9 (MD = -0 20, 95% CI [(-0 74)-0 33], p = 0 46)
DISCUSSION
When choosing between the Barts FFMS and prone positions, it is important to note that all supine positions,
regardless of the modification, offer several advantages over the prone position These include easier positioning for anesthesia, reduced risk of nervous system injury, and suitability for patients with comorbidities such as cardiovascular disease, risk of infection, and obesity (16) Additionally, the total cost of supine PCNL is lower than that of prone PCNL, due to savings on surgical equipment and anesthesia expenses (17)
To determine whether the Barts FFMS or prone position is superior, this review focused on stone-free rates, complications, and surgery duration as primary outcomes
The stone-free rates were not significantly different between the Barts FFMS and prone positions While a meta-analysis by Birowo et al (18) found higher stonefree rates for supine positions in general, Li et al (19) reported no significant difference between supine and prone positions
Complications were classified using the Clavien-Dindo system: fever as grade 1, blood loss requiring transfusion as grade 2, and urine leakage as grade 3 The incidences of fever, transfusion due to blood loss, and urine leakage
Figure 8
Duration of fluoroscopy
Figure 9
Length of hospital stay
Figure 7. Nephrostomy
were not significantly different between the Barts FFMS and prone positions However, Li et al (19) found no significant difference in complication rates between supine and prone positions, while Birowo et al (18) reported significantly lower major complications in supine positions
These discrepancies may be due to inconsistencies in outcome reporting, as not all studies used the Clavien-Dindo classification
In this review, the duration of PCNL was significantly shorter in the Barts FFMS position compared to the prone position This aligns with Li et al (19), who also found shorter durations in supine positions, but contrasts with Birowo et al (18) who reported no significant difference
Literature suggests that supine positions should reduce operation time by eliminating the need for patient repositioning and allowing quick airway access (10)
Additionally, supine positions facilitate easier anesthesia, further shortening the duration of surgery (16)
The insertion of a nephrostomy tube after PCNL remains as a standard procedure It served as drainage, a means to tamponade bleeding after surgery, and an access for a second exploration if necessary (20)
In this review, the use of nephrostomy was reported in three articles and showed no significant difference between the Barts FFMS and prone positions
The use of fluoroscopy is a crucial step in PCNL, allowing urologists to guide the needle to a safe location The imaging helps them to navigate into Brodel’s line of bloodless incision, minimizing the probability of bleeding (21) Fluoroscopy duration was reported in only two studies in this review, showing no significant difference between Barts FFMS and prone patients
In this study, the length of hospital stay did not significantly differ between the Barts FFMS and prone positions This is consistent with meta-analyses by Birowo et al (18) and Li et al (19)
This review article provides valuable information to assist surgeons in choosing between the two positions However, this study has limitations, including a small number of included studies, inconsistencies in outcome reporting, and high heterogeneity in some outcomes Future research should explore the cost-benefit analysis and potential advantages of the Barts FFMS position to optimize PCNL procedures
CONCLUSIONS
The surgery duration was significantly shorter in Barts FFMS position than in prone position There were no significant differences regarding stone-free rates, complications, fluoroscopy duration, use of nephrostomy, and length of hospital stay
Overall, the Barts FFMS position was not superior to the prone position It offers a viable alternative to the prone position in PCNL, with no significant differences in clinical outcomes Therefore, the choice of patient position should be based on the surgeon's preference and the patient's clinical condition
Surgery, Urology Division, Prof Dr I G N G Ngoerah General Hospital for their support
REFERENCES
1 Alelign T, Petros B Kidney Stone Disease: An Update on Current Concepts Adv Urol 2018; 2018:3068365
2 Sorokin I, Mamoulakis C, Miyazawa K, et al Epidemiology of stone disease across the world World J Urol 2017 Sep; 35(9):1301-1320
3 Zhang L, Zhang X, Pu Y, et al Global, Regional, and National Burden of Urolithiasis from 1990 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019 Clin Epidemiol 2022; 14:971-983
4 Edvardsson VO, Indridason OS, Haraldsson G, et al Temporal trends in the incidence of kidney stone disease Kidney Int 2013; 83:146-52
5 Assimos D, Krambeck A, Miller N Surgical Management of Stones: AUA/Endourology Society Guideline (2016), part II Journal of Urology 2016; 196: 1-50
6 Fernström I, Johansson B Percutaneous pyelolithotomy Scand J Urol Nephrol 1976; 10:257-9
7 Valdivia JG, Valer J, Villarroya S, et al Why is Percutaneous Nephroscopy Still Performed with the Patient Prone? Journal of Endourology 1990; 4: 269-277
8 Valdivia Uría J G, Valle Gerhold J, López López JA, et al Technique and complications of percutaneous nephroscopy: experience with 557 patients in the supine position J Urol 1998; 160:1975-1978
9 Karaolides T, Moraitis K, Bach C, et al Positions for percutaneous nephrolithotomy: Thirty-five years of evolution Arab Journal of Urology 2012; 10: 307-316
10 Kumar P, Bach C, Kachrilas S, et al Supine percutaneous nephrolithotomy (PCNL): ’In vogue ’ but in which position? BJU International 2012; 110: 1-4
11 Bach C, Goyal A, Kumar P, et al The Barts 'flank-free' modified supine position for percutaneous nephrolithotomy Urol Int 2012; 89:365-8
12 Mulay A, Mane D, Mhaske S, et al Supine versus prone percutaneous nephrolithotomy for renal calculi: Our experience Curr Urol 2022; 16:25-29
13 Miçoogulları U, Kamacı D, Yıldızhan M, et al Prone versus Barts “flank-free” modified supine percutaneous nephrolithotomy: a match-pair analysis Turk J Med Sci 2021; 51:1373-1379
1 4 S o h a i l N , A l b o d o u r A , A b d e l r a h m a n K M P e r c u t a n e o u s nephrolithotomy in complete supine flank-free position in comparison to prone position: A single-centre experience Arab J Urol 2016; 15:42-47
15 Zanaty F, Mousa A, Elgharabawy M, et al A prospective, randomized comparison of standard prone position versus flank-free modified supine position in percutaneous nephrolithotomy: A singlecenter initial experience Urol Ann 2022; 14:172-176
16 Proietti S, Rodríguez-Socarrás ME, Eisner B, et al Supine percutaneous nephrolithotomy: tips and tricks Transl Androl Urol 2019; 8(Suppl 4):S381-S388
17 Satyagraha P, Alluza HHD, Daryanto B, Nurhadi P Prone vs Supine PCNL: What about the Cost? J Med - Clin Res & Rev 2018; 2: 1-6 https://doi org/10 33425/2639-944X 1067
ACKNOWLEDGMENTS
We would like to thank all the staff at the Department of
18 Birowo P, Tendi W, Widyahening IS, et al Supine versus prone
I Gede Yogi Prema Ananda, K Budi Santosa, I W Yudiana, et al
position in percutaneous nephrolithotomy: a systematic review and meta-analysis F1000Res 2020; 9:231
19 Li J, Gao L, Li Q, et al Supine versus prone position for percutaneous nephrolithotripsy: A meta-analysis of randomized controlled trials Int J Surg 2019; 66:62-71
Correspondence
I Gede Yogi Prema Ananda (Corresponding Author) yogiprema16@gmail com
Department of Urology, Faculty of Medicine, Universitas Udayana, Denpasar, Bali, Indonesia
Kadek Budi Santosa busanbsa@gmail com
I Wayan Yudiana yanyud@yahoo com
Nyoman Gede Prayudi prayudi blonx@yahoo com
Gede Wirya Kusuma Duarsa gwkduarsa@yahoo com
Prof Dr I G N G Ngoerah Hospital, Denpasar, Bali, Indonesia
Pande Made Wisnu Tirtayasa wisnu tirtayasa@gmail com
Ida Bagus Putra Pramana bagusputra@unud ac id
Universitas Udayana Teaching Hospital, Badung, Bali, Indonesia
Conflict of interest: The authors declare no potential conflict of interest
20 Türk C, Petrík A, Sarica K, et al EAU Guidelines on Interventional Treatment for Urolithiasis Eur Urol 2016; 69:475-82
21 Sharma GR, Maheshwari PN, Sharma AG, et al Fluoroscopy guided percutaneous renal access in prone position World journal of clinical cases 2015; 3: 245-264
META-ANALYSIS
Effect of DOPA decarboxylase inhibitor supplements on the incidence of urinary tract infections in Parkinson’s disease patients: A
systematic review and meta-analysis of randomized controlled trials
Ismaeel AlShoaibi 1 , Basheer Abdo 1 , Mohammed Abdullah 1 , Khaled Alzanen 1 , Mohammed Alhakamy 1 , Mamoon Al-Namer 1 , Abdulghani Al-Hagri 2 , Morshed Salah 3 , Afrah Salem 1 , Mohammed Almogahed 1 , Ibrahim Alnadhari 4 , Faisal Ahmed 5
1 Department of Internal Medicine, School of Medicine, Ibb University, Ibb, Yemen;
2 Student Research Committee, Faculty of Medicine and Health Sciences, Sana'a University, Sana'a, Yemen;
3 Urology Section, Surgery Department, Hazm Mebaireek General Hospital, Hamad Medical Corporation, Doha, Qatar
4 Department of Surgery, School of Medicine, Qatar University, Doha, Qatar;
5 Department of Urology, School of Medicine, Ibb University, Ibb, Yemen
Summary
Objectives: Parkinson’s disease is the most common neurodegenerative disease
Combining levodopa with other drugs, including decarboxylase inhibitors (DCI) is its most effective treatment Urinary tract infection (UTI) is the most common cause of hospitalization in Parkinson’s patients, making it crucial to find an appropriate treatment to reduce the incidence of this complication. This study aimed to investigate UTIs in Parkinson’s patients using levodopa with DCI supplements.
Methods: In this systematic review and meta-analysis, databases such as PubMed, Scopus, Embase, Cochrane, and Web of Science were searched up to March 2024 Only randomized controlled trials involving Parkinson’s patients were included in the present study Parkinson’s patients who used levodopa along with carbidopa or benserazide were considered the intervention group, while those who used levodopa with another drug were considered the control group.
Results: Nine interventional studies were ultimately analyzed The relative risk (RR) of UTI in patients taking DCI was 26% lower than those who did not (RR Treatment/Control = 0 74, 95% CI: 0.58-0.95, p = 0.019). Furthermore, observations at different times of follow-up showed that at 13-24 weeks and at > 24 weeks of treatment with DCI, there was a reduction in the incidence of UTI (RR = 0 68, 95% CI: 0 46-1 01 and RR = 0 77, 95% CI: 0.58-1.0, respectively). On the contrary, there was an increase of the risk of UTI in the first 12 weeks of treatment with DCI (RR = 1.11, 95% CI: 0.37-3.33).
Conclusions: The results of this study indicated that using DCI drugs is associated with a reduced relative risk of developing UTIs The beneficial effect of the drug showed after 12 weeks of treatment after an initial negative effect on the risk of UTI
Parkinson's disease (PD) is one of the most common neurodegenerative diseases, primarily caused by the degeneration of dopamine-producing neurons and α-synuclein accumulation in the substantia nigra and the formation of Lewy bodies However, various mechanisms and pathway dysfunctions contribute to Parkinson's disease pathogenesis, including oxidative stress, malfunctioning mitochondria, cellular calcium imbalance, neuroinflammation, and other neurotransmitter system abnormalities (1, 2) The main symptoms of this disease include bradykinesia, rigidity, tremors, and postural instability (3) The risk of PD increases almost exponentially with age, with most patients being over 65 years old Globally, the incidence and prevalence of this disease from 1990 to 2019 have been reported to be 13 43 and 106 28 per 100 000 population, respectively, with a rising global trend in the burden of PD (4) Since there is currently no definitive cure for PD, symptom control – primarily through dopamine agonists and dopamine replacement therapy – remains the only treatment approach (5) Levodopa is one of the most effective drugs, having been used in PD treatment for over five decades (6) The metabolism of this drug occurs through four pathways: decarboxylation, O-methylation, transamination, and oxidation (7) Seventy percent of oral levodopa is metabolized by the enzyme AAAD (aromatic amino-acid decarboxylase) in the gut and liver (8) To increase the drug's half-life and concentration levels, DOPA decarboxylase inhibitors (DCI) such as carbidopa and benserazide are prescribed alongside levodopa (9) The main side effects of PD medications include gastrointestinal issues like nausea and psychiatric disorders such as psychosis and dyskinesia (10) A recent retrospective study by Gremke et al indicated that the incidence of urinary tract infection (UTI) during one year of treatment with DCI drugs exceeds ten percent (11) Urinary tract infection (UTI) is a common factor in worsening the neurological status of patients with PD UTI can be one of the leading causes of delirium, decreased functional-
ity, falls, and hospitalizations in these patients (12) Various clinical features of PD, including autonomic dysfunction, urodynamic changes, weakness, cognitive impairment, and the need for bladder catheterization, contribute to the increased risk of UTI (13) Moreover, untreated UTI can lead to urosepsis, a major complication in PD The use of clean methods for catheterization when requested, antibiotics, and supplements are among the preventive strategies for UTI in PD patients (13) Various studies have reported UTI as a side effect of DCI drugs in Parkinson's patients (1416) However, given that this significant complication has not been addressed explicitly in different studies, we aimed to conduct a systematic review and meta-analysis to investigate and compare the incidence of UTI due to DCI drugs with other Parkinson's medications
MATERIALS AND METHODS
Research design
This systematic review and meta-analysis were registered with PROSPERO (registration number: CRD42024560930) and were done according the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (17) Additionally, this study was reported in compliance with the AMSTAR (A Measurement Tool to Assess Systematic Reviews) methodological quality guidelines
Research question
Does the incidence of UTI in patients treatment with DCI drugs differ compared to patients on other Parkinson's medications?
Research criteria and study selection
Two researchers independently imported the search results from each database into EndNote software Using EndNote, duplicates were identified and removed Subsequently, two researchers screened all remaining articles to identify eligible studies A third researcher reviewed and resolved any controversies between the two researchers
This study's inclusion criteria were randomized clinical trials (RCTs) published as full articles Exclusion criteria included reviews, book chapters, conference abstracts, in vivo and in vitro studies, cross-sectional, case-control, and cohort studies Additionally, studies with a lack of full text and unclear data, including patients with prostate carcinoma or uncontrolled diabetes, patients with other urinary problems, or studies with small sample size (n < 20), were excluded The relative risk (RR) was calculated as the effect size based on the reported incidence of UTI in the intervention and control groups
The intervention group comprised PD patients who received DCI drugs (carbidopa or benserazide) alongside levodopa The control group included PD patients who took levodopa with other medications (e g , Rotigotine, Safinamide, or Entacapone) We labeled them as "Other" to indicate the use of drugs other than the intervention drugs
Search strategy - Data sources
We researched the PubMed/Medline, Scopus, Embase, Cochrane Library, and Web of Science databases up to March 2024 Gray literature was also reviewed to identify
additional relevant studies The search was performed without any time or language restrictions The MeSH (Medical Subject Heading) and non-MeSH keywords used included: “Parkinson's Disease, Parkinson, Parkinsonism, Carbidopa, Benserazide, Aromatic Amino Acid Decarboxylase Inhibitors, DOPA decarboxylase inhibitor, DCI, Urinary Tract Infections, Cystitis, Pyelonephritis, lower urinary tract symptoms, urinary, and urosepsis” A multi-stage process was employed to determine the search keywords and design the search syntax, utilizing common free-text keywords and MeSH terms
Data extraction
The outcome was the incidence of UTI complications in the intervention and control groups Data extracted from each study included the first author's name, publication date, start date of data collection, intervention or control designation, form of drug administration, collaborating countries in data collection, sample size, and incidence of UTI in both groups
Quality Assessment (Risk of Bias assessment)
A systematic assessment of bias in the included RCTs was conducted using the Cochrane RoB 2 0 tool (introduced in 2016 and last revised on August 22, 2019) to assess the risk of bias in randomized trials (18) The following domains were used to evaluate each study: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result Studies were categorized as low risk of bias, high risk of bias, or with some concerns Two researchers independently performed screening, study selection, validation, data extraction, and methodological quality assessment, with any disagreements resolved by a third reviewer
Publication Bias
Publication bias was assessed using funnel plots and Eggar's weighted regression (19) A p-value greater than 0 05 indicated no publication bias
Subgroup and sensitivity analysis
Sensitivity analysis was conducted using a leave-one-out approach to assess the impact of individual studies on the overall effect size Subgroup analysis was performed based on variables such as follow-up duration and type of treatment
Statistical analyses
Data were entered into a statistical program and analyzed using STATA 17 0 (Stata Corporation, College Station, TX) A random effects model was used to account for heterogeneity between studies Heterogeneity was assessed using Cochran’s test and the Higgins I2 test, and the differences between studies by the researchers were evaluated using qualitative evaluation Forest plots were used to display the effect size of each study and pooled estimates A p-value of less than 0 05 was considered statistically significant
RESULTS
Study selection and characteristics
After searching all international databases, 1407 articles
I AlShoaibi, B Abdo, M Abdullah, et al
were found After removing duplicate articles, 1328 were screened for title and abstract review Following the screening phase, 150 articles were selected for the next phase, where full-text articles were assessed, and nine articles were included in the final analysis (20-28)
Additionally, the references of the included articles were examined to identify and include related studies The study selection process is illustrated in Figure 1
The included studies were up to March 2024 Nine studies comprising 18 records within the time frame were eligible, and they specifically addressed UTI as a side effect of DCI use in Parkinson's disease patients Descriptive data of these studies are presented in Table 1 (20-28)
Risk of Bias Assessment
Figure 2 shows the quality assessment results Based on the quality evaluation checklist used, 7 articles were of good quality (low risk), 2 articles had some concerns, and none were of poor quality (high risk) It is noteworthy that all the reviewed studies were randomized trials In 7 studies, blindness was double-masked, and five studies were phase 3 trials
Heterogeneity
The results of the Chi-squared test and the I2 index indicated no heterogeneity regarding side effects among the studies (I2 = 7 52%, Q-value = 14 07, p = 0 661) However, due to the inherent qualitative differences between the studies, a random effects model was used for the analyses
The results of the fixed effects model were also reported
The relative risk of UTI side effects
Based on the random effects model, the relative risk (RR) of UTI in patients taking DCI (carbidopa) was 26% lower than in patients not taking it, and this reduction was statistically significant (RR Treatment/Control = 0 74, 95% CI: 0 58-0 95, p = 0 019) (Figure 3) Similarly, based on the fixed effects model, the results were consistent, showing a 25% lower relative risk of UTI in patients taking DCI (carbidopa) compared to those not taking it (RR Treatment/Control = 0 75, 95% CI: 0 60-0 94, p = 0 012) (Appendix 1)
Subgroup analysis
The subgroup analysis results based on the type of intervention (DCI group vs Other groups) were consistent In the DCI group, the relative risk of UTI was 26% lower (RR = 0 74, 95% CI: 0 54-1 03), and in the other group, it was 24% lower (RR = 0 76, 95% CI: 0 56-1 03) (Appendix 2) However, the results varied based on the follow-up duration For follow-ups from 13 to 24 weeks and over 24 weeks, the relative risk was 32% lower (RR = 0 68, 95% CI: 0 46-1 01) and 23% lower (RR = 0 77, 95% CI: 0 58-1 02), respectively For follow-ups up to 12 weeks, the relative risk was 11% higher (RR = 1 11, 95% CI: 0 37-3 33) (Appendix 3)
Sensitivity analysis
The sensitivity analysis showed that the effect size did not change significantly after excluding any individual study, and the results remained statistically significant (Appendix 4)
Preferred Reporting Items for a Systematic Review and Meta-Analysis (PRISMA) 2020 flow diagram for new systematic reviews, including database, registers, and other source searches
FIgure 1.
I AlShoaibi, B Abdo, M Abdullah, et al
Table 1.
Demographic characteristics of the included studies in the systematic review.
D Author Year of Year of starting Inter vention Consumption Countr y Sample Follow-up publication data collection or control form size time
(A) Risk of bias summary of all included randomized clinical trials (RCTs); (B) Detailed risk of bias
FIgure 3. Meta-analysis of the relative risk of urinary tract infection complications in Parkinson's disease patients; CI: Confidence interval
APPENDIX
Archivio Italiano di Urologia e Andrologia 2024; 96(4):12833
Appendix 1
Meta-analysis of the relative risk of urinary tract infection in Parkinson’s disease patients using decarboxylase inhibitors (Carbidopa); CI: Confidence interval
Appendix 2.
Subgroup meta-analysis of the relative risk of urinary tract infection in Parkinson’s disease patients using decarboxylase inhibitors (Carbidopa) based on type of intervention; CI: Confidence interval
I AlShoaibi, B Abdo, M Abdullah, et al
Appendix 3.
Subgroup meta-analysis of the relative risk of urinary tract infection in Parkinson’s disease patients using decarboxylase inhibitors (Carbidopa) based on treatment duration; CI: Confidence interval
Appendix 4.
Sensitivity analysis results of the studies included in the meta-analysis with the exclusion of one study; CI: Confidence interval
Publication bias
Finally, a funnel plot was created to assess publication bias for the UTI complication of DCI Egger's test results did not confirm the presence of publication bias for UTI complications (bias: -0 19, SE = 0 48, p = 0 693) (Figure 4)
DISCUSSION
Our study results indicated that the use of DCI drugs in P D p a t i e n t s i s a p r o t e c t i v e f a c t o r a g a i n s t U T I
Furthermore, the duration of treatment is significantly essential, because DCI use for less than 12 weeks is associated with an increased relative risk of developing UTI in PD patients whereas long-term use has shown a protective effect against UTI
Findings from a prospective cross-sectional study by Chaudhuri et al indicated that the occurrence of UTI in PD patients using carbidopa gel is 3% (20) Additionally, a cross-sectional survey by Fernandez et al reported a UTI i n c i d e n c e o f 1 1 4 % d u e t o L e v o d o p a - C a r b i d o p a
Intestinal Gel use in PD patients (21) Another study by Fernandez et al reported that the occurrence of UTI in carbidopa users was 7 8% (29) Different results regarding UTI incidence have been obtained in randomized and controlled studies A 134-week prospective double-blind trial by Stocchi et al (28) reported that UTI occurrence in patients using levodopa and carbidopa was 1% higher than in the control group Conversely, in a prospective, double-anonymized, placebo-controlled trial, Olanow et al (25) reported that UTI occurrence was half as frequent in the levodopa and carbidopa group compared to the control group Both studies compared entacapone in PD patients using levodopa and carbidopa, but differences in sample size, length of follow-up, and the duration of Parkinson's disease may explain the divergent results
Our study demonstrated that although levodopa with DCI was associated with a reduced incidence of UTI, it did not
FIgure 4.
Funnel plot for the studies assessing urinary tract infection complication of carbidopa; CI: Confidence interval
significantly differ from other drugs used with levodopa in reducing UTI occurrence Mechanistically, carbidopa increases the conversion of levodopa to dopamine in the central nervous system (CNS), reducing peripheral side effects during PD treatment (30) Although the effects of levodopa on urinary infections are not well-defined, some previous animal and human studies have shown that acute activation of D2 receptors worsens bladder function (31, 32) Conversely, a survey of Parkinsonian monkeys demonstrated that tonic activation of D1 receptors prevents bladder voiding (33) Residual urine can be associated with urinary infections (34, 35) Therefore, by preventing the peripheral conversion of levodopa, carbidopa causes a greater amount of levodopa to reach the brain, and as a result, the dose of levodopa consumed is reduced and its side effects are avoided (36)
Another mechanism suggests that inflammatory genes are expressed in PD, leading to immune cell infiltration into the brain and increased activated/memory T cells (37) In a laboratory study by Zhu et al (30), carbidopa was shown to inhibit T cell responses and autoimmunity in two animal models of Parkinson's, potentially increasing infection risk They concluded that this indicates the immunosuppressive activity of this DCI Further studies are needed to better understand the relationship between carbidopa and urinary tract infection
A cross-sectional study by Gremke et al (11) used another DCI, benserazide, instead of carbidopa The study (11) did not show a significant relationship between the two DCI drugs, but benserazide had better protective effects compared to carbidopa Due to a lack of studies for comparison, we did not focus on benserazide, and most of our results pertain to carbidopa Nonetheless, we recommend future studies to investigate urinary complications, particularly UTI, in PD patients using benserazide
A phase 3 interventional study by Freire-Alvarez et al (22) reported that UTI occurrence in PD patients was 7%
higher in the group treated with carbidopa-levodopa for 12 weeks compared to the control group Fernandez et al also noted an increasing trend in UTI occurrence up to week 13, followed by a decreasing trend until week 54 (29) Our study also found that treatment with levodopa and DCI (carbidopa) increased the risk of UTI within 12 weeks, while the risk decreased in the 13-24 week and ¬> 24-week periods An open-label phase 3b study by Standaert et al , examining non-motor symptoms in PD patients using carbidopa gel over 60 weeks, reported a significant reduction in urinary symptoms up to week 12, but this reduction was not sustained They used the NonMotor Symptoms Scale (NMSS) scoring system, which only assesses urgency, frequency, and nocturia, whereas our study focused solely on UTI occurrence UTI is a significant cause of hospitalization and mortality in PD patients Management strategies for UTI in PD patients mainly involve preventive measures, including vitamin supplements, estrogen supplements, prophylactic antibiotics, and hygiene practices in catheterization cases (38) Given our study's finding of a 32% relative risk reduction in UTI occurrence in PD patients using DCI (carbidopa) during weeks 13-24, we recommend future studies focus on DCI drugs in patients with Parkinson's disease who suffer from urinary symptoms, especially UTI, in this treatment period so that they can benefit from the maximum protective effects of DCI drugs, especially carbidopa Further research is necessary to optimize PD treatment, considering the associated urological complications and infections
Limitations and Strengths: This study is the first systematic review and meta-analysis examining UTI occurrence in PD patients using DCI drugs However, it has some limitations Firstly, many studies were excluded due to the need of randomization and control groups Secondly, control groups in the studies were highly heterogeneous, potentially affecting the comparison of DCI drug effects Thirdly, not all studies provided detailed information on specific variables, so the intended outcome in this study was not reported in terms of the dosage of the drugs used, and it was impossible to estimate the relative risk based on the dosage
CONCLUSIONS
Our study showed that DCI use, along with levodopa in PD patients, is associated with a reduced relative risk of UTI occurrence However, this reduction was not specific to DCI drugs, as other medications used with levodopa also reduced UTI occurrence Subgroup analysis indicated that the relative risk of UTI significantly decreased starting from the 13 to 24-week treatment period with DCI These findings can help researchers better manage the primary cause of hospitalization and mortality in PD patients that is UTI Additionally, researchers can use these findings to design future studies more effectively, focusing on the type of drug and treatment duration with DCI drugs, especially carbidopa
ACKNOWLEDGMENTS
The authors would like to thank the General Manager of
Althora General Hospital, Ibb, Yemen, Dr Abdulghani Ghabisha, for editorial assistance
REFERENCES
1 DeMaagd G, Philip A Parkinson's Disease and Its Management: Part 1: Disease Entity, Risk Factors, Pathophysiology, Clinical Presentation, and Diagnosis P T 2015; 40:504-32
2 Aarsland D, Batzu L, Halliday GM, et al Parkinson disease-associated cognitive impairment Nat Rev Dis Primers 2021; 7:47
3 Bloem BR, Okun MS, Klein C Parkinson's disease Lancet 2021; 397:2284-303
4 Ou Z, Pan J, Tang S, et al Global Trends in the Incidence, Prevalence, and Years Lived With Disability of Parkinson's Disease in 204 Countries/Territories From 1990 to 2019 Front Public Health 2021; 9:776847
6 Supriya P, Rajaram S Literature Review on History and Pharmacotherapy of Parkinsons Disease J Pharm Res Int 2021; 33:839-49
7 Beckers M, Bloem BR, Verbeek MM Mechanisms of peripheral levodopa resistance in Parkinson's disease NPJ Parkinsons Dis 2022; 8:56
8 Amjad F, Bhatti D, Davis TL, et al Current Practices for Outpatient Initiation of Levodopa-Carbidopa Intestinal Gel for Management of Advanced Parkinson's Disease in the United States Adv Ther 2019; 36:2233-46
9 Montioli R, Voltattorni CB, Bertoldi M Parkinson's Disease: Recent Updates in the Identification of Human Dopa Decarboxylase Inhibitors Curr Drug Metab 2016; 17:513-8
10 Chou KL Adverse events from the treatment of Parkinson's disease Neurol Clin 2008; 26(3 Suppl):S65-83
11 Gremke N, Griewing S, Printz M, et al Association between Parkinson's Disease Medication and the Risk of Lower Urinary Tract Infection (LUTI): A Retrospective Cohort Study J Clin Med 2022; 11:7077
12 Okunoye O, Kojima G, Marston L, et al Factors associated with hospitalisation among people with Parkinson's disease - A systematic review and meta-analysis Parkinsonism Relat Disord 2020; 71:66-72
13 Hogg E, Frank S, Oft J, et al Urinary Tract Infection in Parkinson's Disease J Parkinsons Dis 2022; 12:743-57
14 Fernandez HH, Boyd JT, Fung VSC, et al Long-term safety and efficacy of levodopa-carbidopa intestinal gel in advanced Parkinson's disease Mov Disord 2018; 33:928-36
15 Espay A, Hauser R, Dhall R, et al Long-term Safety and Efficacy of IPX203 in Parkinson’s Disease Patients with Motor Fluctuations: A 9-Month Open-label Extension Trial (S32 006) Neurology 2023; 100(17 suppl 2):2472
16 Boyd JT, Zadikoff C, Benesh JA, et al A post hoc comparison of levodopa-carbidopa intestinal gel daytime monotherapy vs polytherapy safety and efficacy in patients with advanced Parkinson's disease: Results from 6 phase 3/3b open-label studies Clin Park Relat Disord 2020; 2:25-34
17 Page MJ, McKenzie JE, Bossuyt PM, et al Updating guidance for reporting systematic reviews: development of the PRISMA 2020 statement J Clin Epidemiol 2021; 134:103-12
18 Sterne JAC, Savovic J, Page MJ, et al RoB 2: a revised tool for assessing risk of bias in randomised trials BMJ 2019; 366:l4898
19 Begg CB, Berlin JA Publication bias and dissemination of clinical research J Natl Cancer Inst 1989; 81:107-15
20 Chung SJ, Calopa M, Ceravolo MG, et al Effects of Levodopa-
Disease: INSIGHTS Study Parkinsons Dis 2022; 2022:1216975
21 Fahn S, Oakes D, Shoulson I, et al Levodopa and the progression of Parkinson's disease N Engl J Med 2004; 351:2498-508
22 Freire-Alvarez E, Kurca E, Lopez Manzanares L, et al LevodopaCarbidopa Intestinal Gel Reduces Dyskinesia in Parkinson's Disease in a Randomized Trial Mov Disord 2021; 36:2615-23
23 Hauser RA, Hsu A, Kell S, et al Extended-release carbidopa-levodopa (IPX066) compared with immediate-release carbidopa-levodopa in patients with Parkinson's disease and motor fluctuations: a phase 3 randomised, double-blind trial Lancet Neurol 2013; 12:346-56
24 Hauser RA, Espay AJ, Ellenbogen AL, et al IPX203 vs Immediate-Release Carbidopa-Levodopa for the Treatment of Motor Fluctuations in Parkinson Disease: The RISE-PD Randomized Clinical Trial JAMA Neurol 2023; 80:1062-9
25 Olanow CW, Kieburtz K, Stern M, et al Double-blind, placebocontrolled study of entacapone in levodopa-treated patients with stable Parkinson disease Arch Neurol 2004; 61:1563-8
26 Rascol O, Zesiewicz T, Chaudhuri KR, et al A Randomized Controlled Exploratory Pilot Study to Evaluate the Effect of Rotigotine Transdermal Patch on Parkinson's Disease-Associated Chronic Pain J Clin Pharmacol 2016; 56:852-61
27 Schapira AH, Fox SH, Hauser RA, et al Assessment of safety and efficacy of safinamide as a levodopa adjunct in patients with Parkinson disease and motor fluctuations: a randomized clinical trial JAMA neurology 2017; 74:216-24
28 Stocchi F, Rascol O, Kieburtz K, et al Initiating levodopa/carbidopa therapy with and without entacapone in early Parkinson disease: the STRIDE-PD study Ann Neurol 2010; 68:18-27
29 Fernandez HH, Vanagunas A, Odin P, et al Levodopa-carbidopa intestinal gel in advanced Parkinson's disease open-label study: interim results Parkinsonism Relat Disord 2013; 19:339-45
30 Zhu H, Lemos H, Bhatt B, et al Carbidopa, a drug in use for management of Parkinson disease inhibits T cell activation and autoimmunity PLoS One 2017; 12:e0183484
31 Uchiyama T, Sakakibara R, Hattori T, Yamanishi T Short-term effect of a single levodopa dose on micturition disturbance in Parkinson's disease patients with the wearing-off phenomenon Mov Disord 2003; 18:573-8
32 Brusa L, Petta F, Pisani A, et al Central acute D2 stimulation worsens bladder function in patients with mild Parkinson's disease J Urol 2006; 175:202-6
33 Yoshimura N, Mizuta E, Yoshida O, Kuno S Therapeutic effects of dopamine D1/D2 receptor agonists on detrusor hyperreflexia in 1methyl-4-phenyl-1,2,3,6-tetrahydropyridine-lesioned parkinsonian cynomolgus monkeys J Pharmacol Exp Ther 1998; 286:228-33
34 Byron JK Urinary Tract Infection Vet Clin North Am Small Anim Pract 2019; 49:211-21
35 Storme O, Tiran Saucedo J, Garcia-Mora A, et al Risk factors and predisposing conditions for urinary tract infection Ther Adv Urol 2019; 11:1756287218814382
36 Gilbert JA, Frederick LM, Ames MM The aromatic-L-amino
acid decarboxylase inhibitor carbidopa is selectively cytotoxic to human pulmonary carcinoid and small cell lung carcinoma cells Clin Cancer Res 2000; 6:4365-72
37 Tan EK, Chao YX, West A, et al Parkinson disease and the immune system - associations, mechanisms and therapeutics Nat Rev Neurol 2020; 16:303-18
38 Aslam S, Albo M, Brubaker L Recurrent Urinary Tract Infections in Adult Women JAMA 2020; 323:658-9
Correspondence
Ismaeel AlShoaibi, MD drismsho@gmail com
Basheer Abdo Abdobasheer500@gmail com
Mohammed Abdullah, MD Dr moh moqbel@gmail com
Khaled Alzanen, MD Khaledhamoud409@gmail com
Mohammed Alhakamy, MD wwkkh2018@gmail com
Mamoon Al-Namer, MD m namer@yaho com
Afrah Salem, MD salemafrah111@gmail com
Mohammed Almogahed, MD mugahedmoham123@gmail com
Department of Internal Medicine, School of Medicine, Ibb University, Ibb, Yemen
Abdulghani Al-Hagri, MD alhagriabdulghani@gmail com
Student Research Committee, Faculty of Medicine and Health Sciences, Sana'a University, Sana'a, Yemen
Urology Office, Althora General Hospital, Alodine Street, Ibb (Yemen)
Morshed Salah, MD morshed salah@gmail com
Urology Section, Surgery Department, Hazm Mebaireek General Hospital, Hamad Medical Corporation, Doha, Qatar
Ibrahim Alnadhari, MD ibrahimah1978@yahoo com
Department of Surgery, School of Medicine, Qatar University, Doha, Qatar
Al Wakra Hospital, Hamad Medical Corporation, Al Wakra, (Qatar)
Faisal Ahmed, MD (Corresponding Author) fmaaa2006@yahoo com
Department of Urology, School of Medicine, Ibb University, Ibb, Yemen
Conflict of interest: The authors declare no potential conflict of interest
META-ANALYSIS
Promising selective alpha-1 blocker silodosin as a new therapeutic strategy for premature ejaculation and analysis of its drug adverse effect: A systematic review and meta-analysis of randomized controlled trials
Muhammad Ilham Fauzan 1 , Besut Daryanto 1 , Taufiq Nur Budaya 1 , Moh Anfasa Giffari Makkaraka 2 , Muhammad Fakhri 3 , Ilham Akbar Rahman 4
1 Department of Urology, Faculty of Medicine, Universitas Brawijaya, Dr Saiful Anwar General Hospital, Malang, Indonesia;
2 Andi Djemma Masamba Hospital, South Sulawesi, Indonesia;
3 Aceh Singkil Hospital, Aceh, Indonesia;
4 Department of Urology, Faculty of Medicine, Airlangga University, Surabaya, Indonesia
Summary
Introduction and objectives: Premature Ejaculation (PE) occurs in 31% of men aged 18-59 years, leading to disappointment and avoidance of sexual relations The current guideline of treatment for PE is Dapoxetine, which possesses several adverse effects causing the limitation of its long-term use Silodosin, an alpha-1 blocker, has been proposed as a new option for treating PE due to its minimal side effects Therefore, our study aims to assess the efficacy of silodosin in treating PE.
Materials and methods: This systematic review and meta-analysis was in accordance with Cochrane Handbook guidelines. Comprehensive literature search was conducted in several databases including PubMed, ScienceDirect, and Cochrane Central Register of Controlled Trials The studies were included if they met the following criteria: (1) Involving premature ejaculation patients; (2) Intervention using silodosin; (3) Comparing placebo or other therapies for PE (4) Outcome includes the Intravaginal Ejaculation Latency Time (IELT) and reported adverse events related to the therapy Study quality was assessed using Cochrane risk-of-bias criteria Statistical analysis in this study was performed using Review Manager 5 4
Results: A total of four studies were included in this meta-analysis Our study showed that patients who received silodosin had a significantly longer IELT compared to control (MD: 132 54, 95% CI 51 51-213 57, p < 0 001) However, patient treated with silodosin also possessed significantly higher risk of adverse event for developing reduced semen ejaculation (OR 10 79, 95% CI 3.46-33.67, p < 0.0001).
Conclusions: Silodosin significantly increased IELT However, it also reduced semen ejaculation as its drug adverse effect. This result supports the clinical use of silodosin as an alternative treatment for premature ejaculation.
Ejaculation involves complex physiological processes Premature ejaculation (PE) is defined as inability to delay
ejaculation upon vaginal penetration and classified into lifelong and acquired PE (1, 2) PE affects about 31% of men aged 18-59, causing psychological effects such as disappointment, hopelessness, and avoidance of sexual relations (3)
, including behavioral, psychological, and pharmacological approaches SSRIs including dapoxetine and paroxetine are the gold standard, but their long-term use is limited due to several adverse effects, including psychiatric and neurological complications (4, 5) Silodosin, an alpha-1 blocker, offers a new option for treating PE with minimal side effects (6) Alpha-1 blockers, as primary treatment for benign prostatic hyperplasia, are also linked to PE treatment Recent studies show they suppress seminal emission by inhibiting smooth muscle contraction, potentially delaying ejaculation (7) Limited research exists on silodosin's effectiveness in treating PE Investigating silodosin as an alternative treatment for PE is crucial Hence, we aim to assess its efficacy in treating PE
METHODS
Literature search
On December 23, 2023, four reviewers (M A , M F , I F , I A ) c o n d u c t e d a l i t e r a t u r e s t u d y u s i n
P
M e d , ScienceDirect, and Cochrane Library, including additional valid studies and screening reference lists for relevant research outside of the databases if they met the criteria
Eligibility criteria
The search was performed using keywords ‘(Silodosin) AND (Premature Ejaculation)’ Followed the PICO criteria: (1) populations with premature ejaculation; (2) silodosin therapy; (3) comparison with placebo or other therapies; (4) outcomes including Intravaginal Ejaculation Latency Time (IELT) and therapy-related adverse events; (5) randomized controlled studies; (6) published in English
Selection process
Duplicate studies were excluded after the initial search
Four independent reviewers screened titles and abstracts for eligibility, including studies that met criteria and excluding those that didn't
Conflicts were resolved through discussion The screening results follow Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines
Data collection
Each author independently extracted data, which was then cross-examined by others Discrepancies were resolved through discussion Authors were contacted for unclear information; non-responsive studies were withdrawn with reviewer consent Collected data include author, year, location, design, population, sample size, mean age, intervention, control, outcomes, and adverse events
Quality assessment
Study quality was assessed using the Cochrane risk-ofbias tool with Review Manager 5 4, classifying each point as low, high, or unclear risk
Statistical analysis
Data were processed using Review Manager 5 4 Two meta-analyses assessed the effect and odds of silodosin versus placebo or other therapies The first analysed mean differences in IELT scores, and the second analysed adverse event odds ratios, both with 95% CIs Heterogeneity was assessed by I2 value; a fixed-effects model was used if I2 < 50%, and a random-effects model if I2 ≥50% Results are shown in a Forest plot, with sig-
Figure 1
nificance at p < 0 05 A funnel plot was used to evaluate publication bias Asymmetrical distribution indicates high bias, while symmetrical distribution indicates low bias
RESULTS
Literature search and screening results
Using keywords, 108 studies were identified from databases, plus 5 studies outside the databases, totaling 113 After removing 22 duplicates, two reviewers screened 91 titles and abstracts, excluding 86 that didn't meet criteria Four studies met the criteria for analysis Full search and filter details are in Figure 1
Characteristics of eligible studies
The four included RCTs were conducted in three countries, with a total of 358 PE patients Most studies diagnosed PE using DSM-IV-TR and ISSM criteria All studies administered 4 mg of silodosin 1-3 hours before intercourse Controls included placebo (Hodeeb et al , Bhat et al ), Naftopidil 25 mg (Sato et al ), and other alpha blockers (Akin et al ) Outcomes measured included IELT in all studies, CGIC in three (Sato, Bhat, Akin et al ), PE Profile in two (Sato, Bhat et al ), and QOL index in one (Akin et al ) The most common side effect was reduced semen ejaculation Full study characteristics are in Table 1
Quality assessment result
The risk of bias assessment using Review Manager 5 4 showed that all studies generally had a low risk of bias (Figure 2) However, blinding bias was high in some studies due to the lack of double-blind procedures
Flow diagram of literature search and selection based on Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA).
3 Bhat et al (2016)ChinaRCTDiagnosedPE326±353287±31464Silodosin4mgPlacebo1IELT1Reduced patientreported(31 vs 33)(3hoursbefore(3hoursbefore2CGICsemenvolume unsatisfiedwithintercourse)intercourse)3PEProfile2Uncomfortably ‘ondemand’delayedejaculation dapoxetine3Dizziness
4 Akin et al (2013)USARCTPEpatient494±1181433±89108Silodosin4mg1Tamsulosin04mg1IELTReduced diagnosedwith2.46±8.6(21
db-RCT: Doub e B ind-Randomized Controlled Study; PE: Premature E aculat on; DSM IV-TR: D agnostic and Stat st cal Manual of Menta Disorders IV-Text Revision; ISSM: Internat onal Society of Sexual Med c ne; IELT: ntravaginal E aculation Latency T me; CGIC: Cl n ca Globa Impression of Change; QoL: Qual ty of Life
Statistical analysis (Meta-Analysis)
Efficacy of Silodosin on IELT scores
Meta-analysis of four RCTs found that silodosin recipients had significantly longer IELT than controls (MD: 132 54, 95% CI 51 51-213 57, p < 0 001) Heterogeneity exceeded 50% (p < 0 00001, I2 = 98%), so the random-effects model was applied (Figure 3)
Silodosin reported adverse event analysis
All studies reported reduced semen ejaculation as an adverse event postsilodosin Figure 4 displays the pooled effect size
The Forest plot indicated heterogeneity below 50% (p = 0 12, I2 = 4 1 % ) , f a v o r
t s model Silodosin treatment significantly increased the risk of reduced semen ejaculation (OR 10 79, 95% CI 3 46-33 67, p < 0 0001)
Funnel Plot analysis
The funnel plot in Figures 5A and 5B shows the symmetrical shape of the study distribution, indicating a low risk of publication bias in this metaanalysis
Figure 2.
Risk of bias assessment using the Cochrane risk-of-bias tool for randomized trials.
Table 1
M Ilham Fauzan, B Daryanto, T Nur Budaya, et al
Figure 3.
Forest plot analysis of the silodosin effect in Intravaginal Ejaculation Latency Time (IELT).
M-H: Mantel–Haenszel, CI: Confidence interval
Figure 4.
Forest plot analysis of reduced semen ejaculation as a silodosin adverse event
M-H: Mantel–Haenszel, CI: Confidence interval
Figure 5
Funnel plot analysis: A) Effect of silodosin on IELTs B) Reduced semen ejaculation as silodosin adverse event
SE: Standard Error; MD: Mean Difference; OR: Odds Ratio
DISCUSSION
PE is the most prevalent male sexual disorder, affecting 30% to 50% of men globally (8) PE is a common male sexual disorder, leads to negative effects including avoidance of sexual intimacy, frustration, reduced confidence with partners, and decreased quality of life (2, 3) PE treatments include oral medications like SSRIs and alpha blockers, as well as topical and behavioral therapies (9) Dapoxetine, an SSRI, treats PE by inhibiting the ejaculatory reflex However, its significant adverse effects, like nausea, dizzi-
ness, and loss of libido, negatively impact patients' QOL (3-5) Silodosin, an alpha blocker for BPH, is highly selective for α1a adrenergic receptors and effective in treating PE (10)
In this meta-analysis, patients receiving silodosin before intercourse showed improved IELT compared to controls or those on placebo (MD: 132 54, p < 0 001) Alpha blockers, including silodosin, are gaining attention as alternative treatments for their ability to inhibit contractions of seminal vesicles, vas deferens, prostate, and asso-
c i a t e d m u s c l e s , p e r i p h e r a l e f f e c t o r s i n e j a c u l a t i o n
Silodosin's strong suppressive action on seminal emission, via its high α1A selectivity, may prolong IELT and improve ejaculatory control (11-13) While effective for PE, Silodosin may cause mild anejaculation discomfort and reduced semen ejaculation α1Aadrenoreceptor antagonists, including Silodosin, suppress seminal emission, possibly reducing semen production and prolonging ejaculation (12) Roehrborn et al discovered that 28 1% of those experiencing retrograde ejaculation during silodosin treatment showed significant symptom improvement and enhanced peak flow rate compared to those without this side effect This suggests silodosin effectively relaxes smooth muscles in the lower urinary and genital tracts, leading to retrograde ejaculation (14) Silodosin has fewer systemic adverse events and is more effective in treating PE than other alpha blockers (9) Akin et al compared PE patients given 4 mg silodosin 2-3 hours before intercourse with those on other alpha blockers: tamsulosin hydrochloride 0 4 mg, alfuzosin 10 mg, terazosin 5 mg, and doxazosin mesylate 4 mg Silodosin significantly improved QoL, increased IELT, and decreased PEP (9) Silodosin's selectivity for alpha 1 receptors in the prostate makes it more effective in treating PE Studies by Sato Y et al and Hodeeb et al support silodosin's greater improvement in PE patients, offering a promising, effective, affordable, and safe treatment avenue (11, 15) This study has several limitations Firstly, due to silodosin's novelty, relevant literature sources were still scarce Secondly, the literatures that existed did not yet compare silodosin to dapoxetine, the main therapy for premature ejaculation therefore comparison of head-tohead was not available in this study Thirdly, sample sizes varied, causing significantly high heterogeneity
CONCLUSIONS
Silodosin significantly increased IELT However, it causes reduced semen ejaculation as its drug adverse effect This result supports the clinical use of silodosin as an alternative treatment for premature ejaculation Further clinical studies evaluate the comparison of silodosin and SSRI are warranted
REFERENCES
1 Parnham A, Serefoglu EC Classification and definition of premature ejaculation Transl Androl Urol 2016; 5:416-23
2 Crowdis M, Leslie SW, Nazir S Premature Ejaculation 2023 May 30 In: StatPearls (Internet) Treasure Island (FL): StatPearls Publishing; 2024
3 Hatzimouratidis, K Giuliano, F Moncada, et al EAU Guidelines on Erectile Dysfunction, Premature Ejaculation, Penile Curvature and Priapism In: European Association of Urology Guidelines, EAU Guidelines Office, Arnhem, the Netherlands, Published online 2019:1-28
4 Hisasue S The drug treatment of premature ejaculation Transl Urol Androl 2016; 5:482-486
5 McMahon CG Dapoxetine: a new option in the medical management of premature ejaculation Ther Adv Urol 2012; 4:233-51
6 Bhat GS, Shastry A Effectiveness of 'on demand' silodosin in the treatment of premature ejaculation in patients dissatisfied with dapoxetine: a randomized control study Cent European J Urol 2016; 69:280-284
7 Martin C, Nolen H, Podolnick J, Wang R Current and emerging therapies in premature ejaculation: Where we are coming from, where we are going Int J Urol 2017; 24:40-50
8 Gao J, Zhang X, Su P, et al Prevalence and impact of premature ejaculation in outpatients complaining of ejaculating prematurely: Using the instruments of intravaginal ejaculatory latency time and patient-reported outcome measures Int J Impot Res 2014; 26:94-99
9 Akin Y, Gulmez H, Ates M, et al Comparison of alpha blockers in treatment of premature ejaculation: a pilot clinical trial Iran Red Crescent Med J 2013; 15:e13805
10 Maladkar M, Awate S, Bramhe P Exploring Alpha-Blockers as an Effective Intervention for Premature Ejaculation The Indian practitioner 2024; 77:31-36
11 Sato Y, Otani T, Amano T, et al Silodosin versus naftopidil in the treatment of premature ejaculation: A prospective multicenter trial Int J Urol 2017; 24:626-631
12 Sato Y, Tanda H, Nakajima H, et al Silodosin and its potential for treating premature ejaculation: a preliminary report Int J Urol 2012; 19:268-72
13 Kobayashi K, Masumori N, Hisasue SI, et al Inhibition of seminal emission Is the main cause of anejaculation induced by a new highly selective α1A-Blocker in normal volunteers J Sex Med 2008; 5:2185-2190
14 Roehrborn CG, Lepor H, Kaplan SA Retrograde Ejaculation Induced By Silodosin Is the Result of Relaxation of Smooth Musculature in the Male Uro-Genital Tracts and Is Associated With Greater Urodynamic and Symptomatic Improvements in Men LUTS Secondary to BPH J Urol 2009; 181:694-695
15 Mohamed Y, Hodeeb I, Saeed M, Hasan M Effectiveness and Safety of Silodosin in Treatment of Premature Ejaculation : Placebo Double Blind Control Study The Egyptian Journal of Hospital Medicine 77:5482-5487
Correspondence
Muhammad Ilham Fauzan ilhmfauzn18@gmail com
Taufiq Nur Budaya taufiq uro fk@ub ac id
Department of Urology, Faculty of Medicine, Universitas Brawijaya, Dr Saiful Anwar General Hospital, Malang, Indonesia
Besut Daryanto (Corresponding Author) urobes fk@ub ac id
Department of Urology, Dr Saiful Anwar General Hospital Malang Jalan Jaksa Agung Suprapto 2, Klojen, Malang, East Java 65112, Indonesia
Moh Anfasa Giffari Makkaraka fasagifari@gmail com
Andi Djemma Masamba Hospital, South Sulawesi, Indonesia
Muhammad Fakhri muhammadfakhri md@gmail com
Aceh Singkil Hospital, Aceh, Indonesia
Ilham Akbar Rahman ilhamakbaarr@gmail com
Department of Urology, Faculty of Medicine, Airlangga University, Surabaya, Indonesia
Conflict of interest: The authors declare no potential conflict of interest
REVIEW
Theobromine for treatment of uric acid stones and other diseases
Alberto Trinchieri
C d C Ambrosiana, Cesano Boscone, Milan, Italy
Summary
Theobromine (or 3,7-dimethylxanthine) is a natural alkaloid present in cocoa plant and its derivatives, such as chocolate. About 20% of ingested theobromine is excreted unchanged in the urine Theobromine also derived from caffeine that is metabolized into theobromine by 12% The primary metabolites of theobromine are 3-methylxantine, 7-methylxantine, 7-methyluric acid and 3,7-dimethyluric acid Theobromine has an inhibitory activity of uric acid crystallization, because it has a structural pattern very similar to uric acid and can substitute uric acid molecules in the corresponding uric acid crystals, making them longer and thinner and decreasing their growth rate Theobromine also favors the dissolution of crystals by decreasing supersaturation of uric acid by forming aggregates with uric acid through hydrogen bonds and aromatic stacking interactions (-stacking bonds) increasing urinary solubility of uric acid Theobromine can be used for uric acid stone dissolution in combination with alkalinization to reduce the dose of citrate, thus preventing excessive alkalinization and the risk of formation of sodium urate crystals Theobromine could also be used to treat patient with xanthine stones that cannot be dissolved by alkalinization because the solubility of xanthine is relatively independent of urinary pH A metabolite of theobromine, 7-methylxanthine, has the potential to be used for the prevention of the formation of sodium urate crystals in the synovial fluid of gouty patients
Submitted 21 October 2024; Accepted 24 October 2024
INTRODUCTION
Theobromine (or 3,7-dimethylxanthine) is a natural alkaloid present in Theobroma cacao (cocoa plant) and its derivatives It is found in chocolate, and it is also present in small quantities in tea leaves (1, 2)
Chemically it is a xanthine, a derivative of purine, whose related compounds include theophylline, caffeine, paraxanthine, and 7-methylxanthine, each of which differ in the number or placement of the methyl groups Theobromine is derived from the nucleoside xanthosine by cleavage of the ribose and N-methylation to 7-methylxanthosine
Theobromine is slightly water-soluble but more fat-soluble, therefore requires 2-3 hours to peak, while caffein is highly water-soluble and peaks after only 30 minutes In the liver, it is metabolized into xanthine and subsequently into methyluric acid
The elimination half-life of theobromine is between 6 and 8 hours The primary metabolites of theobromine are 3-methylxantine, 7-methylxantine, 7-methyluric acid and 3,7-dimethyluric acid, with 18-21% of theobromine excreted unchanged in the urine (3-5)
Theobromine also derives from caffeine that is metabolized in the liver into paraxanthine (84%), theobromine (12%), and theophylline (4%) For this reason, individuals that non ingest theobromine (or chocolate) could have low, though detectable, urinary levels of theobromine (6, 7)
Theobromine has stimulating action on the central nervous system by intervening on the synapses, but this effect is weaker than caffeine (8)
It has negligible toxicity in humans, because it is metabolized very quickly In other mammals, such as dogs and cats, it becomes toxic because they metabolize theobromine very slowly The symptoms of intoxication are excitation, lowered heart rate, convulsions and in the most serious cases death (9)
Theobromine has several various pharmacological applications including cough suppression, increase of plasma HDL cholesterol and decrease of plasma LDL cholesterol, protection of enamel surface (10-13) A derivative of theobromine, 7-methylxanthine, has been used for the treatment of myopia (14)
Theobromine should be administered as extract of cocoa beans rather than chocolate that contains large amounts of sugar and oxalate, that should be avoided in subjects with diabetes type 2 or metabolic syndrome and calcium oxalate renal stone formers
TREATMENT AND PREVENTION OF URIC ACID STONES
Uric acid urinary stones account for about 10% of all the urinary stones although it is predictable an increase of their prevalence because of demographic and climate changes (15, 16)
Uric acid stones form by crystallization of urinary uric acid when its concentration is above the threshold of solubility which depends on pH It ranges from 110 mg/L for urinary pH below 5 0 to 250 mg/L for pH 5 5 and up to 600 mg for a pH over 6 0
Urinary saturation for uric acid depends on urinary pH and urinary uric acid concentration (17-19) When urine is supersaturated with respect to uric acid, crystal formation is possible, although above this threshold there is an interval of saturation values at which the solution is
A Trinchieri
metastable that means that preformed crystals can grow but there is no formation of new crystals Above the upper limit of the metastable zone of saturation crystals form spontaneously Other factors can interfere with uric acid crystallization in the urine as the presence of heterogeneous nuclei that can facilitate crystal formation or inhibitors of crystallization Uric acid stones can be dissolved when urinary saturation is under the threshold of supersaturation
Alkalinization
Alkalinization by high doses of citrate and bicarbonate is commonly used for uric acid dissolution (20) Urinary pH should be raised over 6, although higher values are not recommended because a urinary pH above 6 2 can cause the formation of an outer shell of insoluble calcium phosphate salts that are less soluble for higher pH values Furthermore, in the presence of hyperuricosuria, deposits of sodium and/or potassium urate can form, because of reduced solubility of such urate salts at higher pH values (contrary to what happens for uric acid) Finally, long-term treatment with citrate can cause gastrointestinal disturbances
Other substances
N-acetylcysteine (NAC) has been proposed for its alkalinizing and mucolytic effect due to the cleavage of disulfide bridges of mucoproteins contained in the deposits of organic matter covering stone crystals (21, 22)
In vitro studies suggested the use of some glycosaminoglycans, glycoproteins and saponins (such as ginseng extract) to interfere with crystallization of uric acid (23) However, these substances are not properly inhibitors because they act by modifying the surface tension of water and do not show dose-response relationships
THEOBROMINE
More recently, in vitro studies showed that theobromine is a very effective inhibitor of uric acid crystallization (24, 25) This effect is clinically significant for urinary concentration over 15 mg/L or higher, although higher concentrations (80 mg/L) provided no additional benefit Urinary concentrations in the therapeutical range are obtained after oral administration of 300 mg of theobromine with approximately 60 mg excreted unchanged in the urine Caffeine, theophylline and paraxanthine showed no similar effects In fact, they had a structure very similar to theobromine, but minimal modification of their chemical structure makes them ineffective as inhibitors Theobromine inhibits nucleation of uric acid crystals being absorbed onto the faces of the crystals and modifying their morphology making them longer and thinner In particular, theobromine may inhibit growth at only one of the faces of the crystal (210), but not at the others (001 and 201) Because uric acid and theobromine molecules have very similar structural patterns, theobromine can substitute uric acid molecules in the corresponding uric acid crystals The incorporation of this molecule to the uric acid crystal lattice modifies the structure of some layers so increasing their energy and decreasing their growth rate In the presence of theobromine crystals formed on the surface of the uric acid
were smaller Thus, theobromine may be clinically useful in preventing the regrowth of uric acid calculi fragments
Theobromine also favors the dissolution of crystals by decreasing supersaturation of uric acid (26)
The velocity of stone dissolution depends on the size and location of the stone and on flow of irrigation
Furthermore, the microstructure of the stone, as observed at scanning electronic microscopy can influence the process of dissolution In fact, stones that appeared macroscopically similar, may have major differences in microstructure by the presence of porosities, the distribution of organic matter and the size of crystals The dissolution can be made difficult by the presence of shells of sodium/potassium urate or apatite as consequence of very high pH (above 7) and high uric acid concentration (27)
Combined treatment
The combination of alkalization with citrate and theobromine patented and commercialized by the company Devicare in its Lit-Control pH Up treatment (28, 29), allows to use lower doses of citrate, thus preventing excessive alkalinization to avoid formation of sodium urate crystals (30)
Furthermore, the reduced dose of potassium citrate administration decreases the risk of hyperkaliemia in patients with kidney failure or heart disease
THEOBROMINE AND XANTHINURIA
Xanthinuria is a rare hereditary disorder related to a deficiency of xanthine dehydrogenase/oxidase (XDH/OX) causing an accumulation of hypoxanthine and xanthine due to a reduced degradation of these two precursors to uric acid This results in hypouricemia, hypouricosuria, xanthinuria and formation of xanthine urinary stones (31, 32) There are different types of xanthinuria due to mutations of different genes (33-35) The classical type I is caused by a mutation in XDH/XO gene mapped to chromosome 2p23 1 Type II depends on mutations in molybdenum cofactor sulfurase gene (MOCOS) localized on chromosome 18q12 2 that cause a defect of XDH/OX and aldehyde oxidase (AO) Triple deficiency of XDH, AOX and sulfite oxidase is caused by molybdenum cofactor deficiency type A (OMIM 252150) due to mutations in MOCS1 gene (6p21 1)
The classical presentation occurs at any age with renal colic, hematuria and urinary tract infection associated to xanthine stones Less frequently the presentation is more severe with renal failure, muscle-skeletal and gastrointestinal symptoms Traditional diagnosis with allopurinol loading test or liver biopsy has been replaced by genetic testing in stone patients with extremely low serum and low urinary uric acid replaced by xanthine
The treatment for patients with xanthinuria is a low purine diet and high intake of fluids In contrast to patients with uric acid stones, urine alkalinization is not effective because the solubility of xanthine is relatively independent of urinary pH
A recent study showed that 1-methylxanthine (1-MX), 7-methylxanthine (7-MX), and 3-methylxanthine (3-MX) significantly inhibited xanthine crystallization in vitro in a concentration dependent manner (36)
Two of these molecules are major metabolites of theobromine whereas the third is a metabolite of caffeine In fact, after theobromine ingestion, 20% is excreted as theobromine, 21 5% as 3-MX, and 36% as 7-MX and after consumption of caffeine, 19% of it is excreted as 1-MX
Hypoxanthine (HX), theophylline (TP), paraxanthine (PX), theobromine (TB), caffeine (CF), 1-methyluric acid (1-MU), and 1,3-dimethyluric acid (1,3-DMUA) showed no significant inhibitory effect on xanthine crystallization because only methyl derivatives of xanthine can be incorporated into the xanthine crystal lattice modifying its structure and slowing crystal growth (by increasing Gibbs free energy) However, even if theobromine did not inhibit xanthine crystallization by itself, it could be used for prevention of xanthine stones by the effects of its metabolites
THEOBROMINE AND GOUT
Gout is a rheumatic disease presenting with pain, swelling, and redness in the peripheral joints, especially in the metatarsophalangeal joint in the big toe and other joints in the feet and hands (37)
The disease is due to accumulation of monosodium urate (NaU) needle-shaped crystals in the affected joints
Synovial fluid is an ultrafiltrate from plasma with a pH of 7 4 and a sodium level of about 150 mmol/L At a pH of 7 4 most uric acid is present as univalent anionic urate, whereas at serum urate level below 6 mg/dl sodium urate crystals do not form because sodium urate solubility threshold is 6 6 mg/dl When urate levels are over the solubility limit of 6 6 mg/dl sodium urate crystals start to form Furthermore, solubility of sodium urate is related to temperature and tends to decrease at temperature lower than 37°C, being only 3 7 mg/dl at 26°C This explains why crystal formation is more common in the joints of the hands and feet where temperature tends to be lower (38)
The pathophysiology of crystal formation in synovial fluids is peculiar because the circulation of fluids in the cavities of synovial joints is quite limited with a much slower renewal of fluids compared to urinary tract where the flow of urine is continuous and relatively fast
Consequently, inhibitors that can prevent crystal formation for a period up to 30-40 minutes can be useful in continuous flow of urine, but they are ineffective in absence of renewal of fluid as in the joint cavities
Treatment of gout is based on anti-inflammatory drugs and the reduction of serum urate levels by a low purine diet, or drugs decreasing the production of uric acid, as allopurinol and febuxostat or drugs increasing the urinary excretion of uric acid, such as probenecid
An alternative approach could be increasing urate solubility or inhibit sodium urate crystallization
Some in vitro studies demonstrated that the combination of arginine-rich peptide and copper ions was able to delay the crystallization of sodium urate (39, 40) Similarly, the addition of trimethoprim to urate solutions delayed sodium urate crystallization because trimethoprim acted as competing binding agent forming a more soluble co-crystal with sodium urate (41)
Theobromine can form aggregates with uric acid through hydrogen bonds and aromatic stacking interactions (-stacking bonds) increasing urinary solubility of uric
acid (42) Similarly, the solubility of uric acid increased in the presence of vitamin C (43) Furthermore, theobromine is also able to interact with uric acid crystals changing their morphology
Epidemiological studies demonstrated that coffee and chocolate consumption decreased the risk of gout (44, 45)
An in vitro study suggested that 7-methylxanthine, a metabolite of theobromine, has the potential to be used for the prevention of gout (46) The same study found that 3-methylxanthine also prevented crystallization, although this happens at a four-fold-greater concentration than with 7-methylxanthine; 7-methyluric acid has a slightly stronger effect than 3-methylxanthine, but its plasma levels are negligible
For this reason, consumption of 7-methylxanthine (or theobromine) has the potential for preventing the crystallization of sodium urate and the development of gout
Regarding the safety of the treatment of 7-methylxanthine, studies documented that it has no toxic effects up to an oral dose of 1000 mg/kg of weight indicating that the consumption of 400 mg three times per day that should be requested to prevent gout seems to be safe
CONCLUSIONS
Theobromine is a natural product that has several potential therapeutic applications The use for the treatment of uric stones is the most promising because it allows the dissolution of uric acid stones faster with the use of lower doses of alkalizers However, clinical efficacy must be confirmed by randomized clinical trials Treatment with theobromine or its derivatives could be used in the treatment of xanthinuria or gout
REFERENCES
1 Craig WJ, Nguyen TT Caffeine and theobromine levels in cocoa and carob products J Food Sci 1984; 49:302-303
2 M a r t í n e z - L ó p e z S , S a r r i á B , G ó m e z - J u a r i s t i M , e t a l Theobromine, caffeine, and theophylline metabolites in human plasma and urine after consumption of soluble cocoa products with different methylxanthine contents Food Res Int 2014; 63:446-455
3 Gates S, Miners JO Cytochrome P450 isoform selectivity in human hepatic theobromine metabolism Br J Clin Pharmacol 1999; 47:299-305
4 Tarka SM, Arnaud MJ, Dvorchik BH, Vesell ES Theobromine kinetics and metabolic disposition Clin Pharmacol Ther 1983; 34:546-555
5 Rodopoulos N, Höjvall L, Norman A Elimination of theobromine metabolites in healthy adults Scand J Clin Lab Invest 1996; 56:373383
6 Lelo A, Birkett DJ, Robson RA, Miners JO Comparative pharmacokinetics of caffeine and its primary demethylated metabolites paraxanthine, theobromine and theophylline in man Br J Clin Pharmacol 1986; 22:177-182
7 Tang-Liu DS, Williams RL, Riegelman S Disposition of caffeine and its metabolites in man J Pharm Exp Ther 1983; 224:180-185
8 Mitchell ES, Slettenaar M, vd Meer N, et al Differential contributions of theobromine and caffeine on mood, psychomotor performance and blood pressure Physiol Behav 2011; 104:816-822
9 Finlay F, Guiton S Chocolate poisoning BMJ 2005; 331:633
Theobromine
10 Halfdanarson TR, Jatoi A Chocolate as a cough suppressant: rationale and justification for an upcoming clinical trial Support Cancer Ther 2007; 4:119-122
11 Khan N, Monagas M, Andres-Lacueva C, et al Regular consumption of cocoa powder with milk increases HDL cholesterol and reduces oxidized LDL levels in subjects at high-risk of cardiovascular disease Nutr Metab Cardiovasc Dis 2012; 22:1046-1053
12 Neufingerl N, Zebregs YE, Schuring EA, Trautwein EA Effect of cocoa and theobromine consumption on serum HDL-cholesterol concentrations: a randomized controlled trial Am J Clin Nutr 2013; 97:1201-1209
13 Kargul B, Ozcan M, Peker S, et al Evaluation of human enamel surfaces treated with theobromine: a pilot study Oral Health Prev Dent 2012; 10:275-282
14 Lai L, Trier K, Cui DM Role of 7-methylxanthine in myopia prevention and control: A mini-review Int J Ophthalmol 2023; 16:969976
15 Trinchieri A, Montanari E Prevalence of renal uric acid stones in the adult Urolithiasis 2017; 45:553-562
16 Brikowski TH, Lotan Y, Pearle MS Climate-related increase in the prevalence of urolithiasis in the United States Proc Natl Acad Sci U S A 2008; 105:9841-9846
17 Trinchieri A, Montanari E Biochemical and dietary factors of uric acid stone formation Urolithiasis 2018; 46:167-172
18 Wagner CA, Mohebbi N Urinary pH and stone formation J Nephrol 2010; 23(Suppl 16):S165-169
19 Grases F, Costa-Bauza A, Gomila I, et al Urinary pH and renal lithiasis Urol Res 2012; 40:41-46
20 Trinchieri A, Esposito N, Castelnuovo C Dissolution of radiolucent renal stones by oral alkalinization with potassium citrate/potassium bicarbonate Arch Ital Urol Androl 2009; 81:188-91
21 Burns JR, Gauthier JF, Finlayson B Dissolution kinetics of uric acid calculi J Urol 1984; 131:708-711
22 Sadowska AM N-acetylcysteine mucolysis in the management of chronic obstructive pulmonary disease Ther Adv Respir Dis 2012; 6:127-135
23 Grases F, Ramis M, Villacampa AI, Costa-Bauzá A Uric acid urolithiasis and crystallization inhibitors Urol Int 1999; 62:201204
24 Grases F, Rodriguez A, Costa-Bauza A Theobromine inhibits uric acid crystallization A potential application in the treatment of uric acid nephrolithiasis PLoS ONE 2014; 9:e111184
25 Costa-Bauza A, Grases F, Calvó P, et al Effect of Consumption of Cocoa-Derived Products on Uric Acid Crystallization in Urine of Healthy Volunteers Nutrients 2018; 10:1516
26 Chattaraj KG, Paul S Inclusion of theobromine modifies uric acid aggregation with possible changes in melamine-uric acid clusters responsible for kidney stones J Phys Chem B 2019; 123:10483-10504
27 Sadi MV, Saltzman N, Feria G, Gittes RF Experimental observations on dissolution of uric acid calculi J Urol 1985; 134:575-579
28 Grases F, et al Combination of a urinary basifying agent and an uric acid crystallisation inhibitor for the treatment and prevention of renal lithiasis EP3130337B1, 2019
29 Grases F, et al Theobromine or its derivatives for the treatment or prevention of uric acid renal lithiasis EP3150208B1, 2023
30 Hernandez Y, Costa-Bauza A, Calvó P, et al Comparison of two
dietary supplements for treatment of uric acid renal lithiasis: citrate vs citrate + theobromine Nutr 2020; 12:2012
31 Carpenter TO, Lebowitz RL, Nelson D, Bauer S Hereditary xanthinuria presenting in infancy nephrolithiasis J Pediatr 1986; 109:307-309
32 Mateos FA, Puig JG, Jimenez ML, Fox IH Hereditary xanthinuria: Evidence for enhanced hypoxanthine salvage J Clin Invest 1987; 79:847-852
33 Ichida K, Amaya Y, Okamoto K, Nishino T Mutations associated with functional disorder of xanthine oxidoreductase and hereditary xanthinuria in humans Int J Mol Sci 2012; 13:15475-15495
34 Ichida K, Matsumura T, Sakuma R, et al Mutation of human molybdenum cofactor sulfurase gene is responsible for classical xanthinuria type II Biochem Biophys Res Commun 2001; 282:1194-1200
35 Mraz M, Hurba O, Bartl J, et al Modern diagnostic approach to hereditary xanthinuria Urolithiasis 2015; 43:61-67
36 Grases F, Costa-Bauza A, Roig J, Rodriguez A Xanthine urolithiasis: Inhibitors of xanthine crystallization PLoS ONE 2018; 13:e0198881
37 Archer HE, Rhoden E Uric-acid levels in blood and plasma Br Med J 1951; 2:947
38 Kippen I, Klinenberg JR, Weinberger A, Wilcox WR Factors affecting urate solubility in vitro Ann Rheum Dis 1974; 33:313-317
39 Liu Y, Zhang Q, Du J, Guo R Arginine-rich peptides as crystallization inhibitors for sodium urate J Mater Chem B 2023; 11:73897400
40 Liu Y, Zhang Q, Li N, et al Efficient synergistic cooperation of an arginine-rich peptide and copper ions in sodium urate crystallization inhibition Langmuir 2023; 39:9942-9951
41 Hall VM, Thornton A, Miehls EK, et al Uric acid crystallization interrupted with competing binding agents Cryst Growth Des 2019; 19:7363-7371
42 Chattaraj KG, Paul S Appraising the potency of small molecule inhibitors and their graphene sur face-mediated organizational attributes on uric acid-melamine clusters Phys Chem Phys 2022; 24:1029-104
43 Chattaraj KG, Paul S The miscibility and solubility of uric acid and vitamin C in the solution phase and their structural alignment in the solid-liquid interface Phys Chem Chem Phys 2021; 23:1516915182
44 Choi HK, Curhan G Coffee consumption and risk of incident gout in women: The Nurses’ Health Study Am J Clin Nutr 2010; 92:922-927
45 Dillinger TL, Barriga P, Escárcega S, et al Food of the gods: Cure for humanity? A cultural history of the medicinal and ritual use of chocolate J Nutr 2000; 130(Suppl S8):2057S-2072S
46 Costa-Bauza A, Grases F 7-methylxanthine inhibits the formation of monosodium urate crystals by increasing its solubility Biomolecules 2023; 13:1769
Correspondence
Alberto Trinchieri, MD (Corresponding Author) alberto trinchieri@gmail com C d C Ambrosiana, Cesano Boscone, Milan, Italy
Conflict of interest: The authors declare no potential conflict of interest
Non-surgical management of BPH: An updated review of current literature and state of the art on natural compounds and
medical therapy
Guglielmo Mantica 1, 2 , Francesca Ambrosini 2 , Giovanni Drocchi 1 , Zlata Zubko 1 , Lorenzo Lo Monaco 1 , Angelo Cafarelli 3 , Alessandro Calarco 4 , Renzo Colombo 5 , Ottavio de Cobelli 6 , Ferdinando De Marco 7 , Giovanni Ferrari 8 , Giuseppe Ludovico 9 , Stefano Pecoraro 10 , Domenico Tuzzolo 11 , Carlo Terrone 1, 2 , Rosario Leonardi 12
1 Department of Surgical and Diagnostic Integrated Sciences (DISC), University of Genova, Genova, Italy;
2 IRCCS Ospedale Policlinico San Martino, Genova, Italy;
3 Urology Unit, Villa Igea, Ancona, Italy;
4 Department of Urology, San Carlo di Nancy Hospital, Rome, Italy;
5 Department of Urology, Vita e Salute San Raffaele University, Milan, Italy;
6 Department of Urology, IEO European Institute of Oncology, IRCCS, Milan, Italy;
7 I N I Grottaferrata, Rome, Italy;
8 Hesperia Hospital, Modena, Italy;
9 Ospedale Miulli, Acquaviva delle Fonti, Bari, Italy;
12 Casa di Cura Musumeci-Gecas, Gravina di Catania, Italy
Summary
Introduction: Benign prostatic hyperplasia (BPH) is a common urological disease that is strongly associated with the aging process and can lead to lower urinary tract symptoms (LUTS). LUTS due to BPH can significantly affect the quality of life of many patients Among the treatments available for BPH to improve symptoms and functional outcomes, drug therapy and surgical therapy are the options of choice. However, for most patients with symptomatic BPH, medical management remains the cornerstone of treatment. Pharmacologic interventions are often preferred as a first approach, being less invasive compared to surgery Although the medical treatment of BPH is currently defined by the algorithms of international guidelines, the need for a more personalized approach is increasingly recognized given the wide and heterogeneous range of therapeutic options available
Materials and methods: A review of medical therapy for BPH was conducted using relevant articles in PubMed, Scopus, and the Cochrane Central Register of Controlled Trials In this review, all drug treatments currently available on the international market whose efficacy is scientifically proven are reviewed and described (phytotherapy, alpha-blockers, muscarinic receptor antagonists, 5-alpha-reductase inhibitors, combination therapies, etc )
Results: A total of 17 randomized clinical trials were selected for review. Further 75 studies were included for analysis and discussion
Conclusions: As the treatment landscape continues to evolve, tailoring therapy to individual patient needs and preferences is likely to become increasingly important to ensure that treatment strategies are both effective and meet patient expectations
KEY WORDS: Benign prostatic hyperplasia; Medical therapy; Alpha-blockers; Antimuscarinics; Phytotherapy
Submitted 13 September 2024; Accepted 23 November 2024
INTRODUCTION
Benign prostatic hyperplasia (BPH) is a common urological disease that is strongly associated with the aging process (1) Prostate growth is influenced by a combination of intrinsic and extrinsic factors that interact in a complex manner The pathophysiological pathway includes hormone and androgen exposure as well as growth factors, chronic inflammation and genetics (2) Lower urinary tract symptoms (LUTS) due to BPH can have a significant impact on patients’ quality of life (3) For most patients with symptomatic benign prostatic hyperplasia, medical m
Pharmacologic measures are often preferred as a first approach as they can relieve symptoms and improve the patient’s well-being (4) The landscape of medical treatment for BPH is constantly evolving The efficacy of overthe-counter medications, plant extracts and natural supplements has not yet been adequately researched and their benefits are still unclear At the same time, ongoing studies of new pharmacologic agents, such as beta-3 agonists, have the potential to expand the available therapeutic options, providing hope for more targeted and effective strategies in the future With this review, we aimed to provide an up-to-date overview of the most common medical treatments for LUTS including phytotherapy in the context of BPH
MATERIALS AND METHODS
In July 2024, a systematic review of medical therapy for BPH was conducted using relevant articles in PubMed, Scopus, and the Cochrane Central Register of Controlled Trials The review focused on phytotherapy and medical
treatment of BPH Three authors (GM, FA, GD) independently screened the titles and abstracts of the datasets for eligibility Reviews, original articles, and case reports were included, while other types of articles were excluded Evidence was limited to human data and experimental animal studies Only publications in English were considered In addition, manuscripts that were not focused on the purpose of the review were not included The original list of selected articles was supplemented by individual suggestions from the co-authors of the present review Similarly, articles published before 1990 but considered interesting for the purpose of the review were suggested by the authors and assessed by the screening team
The reference lists of the selected articles/systematic reviews/meta-analyses were also screened to identify further potentially relevant studies, using the same criteria as for the initial search
RESULTS
The search strategy has been highlighted using the PRISMA flowchart (5) (Figure 1) and PICO model (6) (Supplementary matherial) to summarize the results The risk of bias of the 17 randomized controlled trials included has been evaluated using the ROB 2 – revised tool (7) (Figure 2)
Figure 1
PRISMA flowchart
Source: Page MJ, et al. BMJ 2021; 372: n71
Figure 2.
Risk of bias of the 17 randomized controlled trials evaluated using the ROB 2 –revised tool
Archivio Italiano di Urologia e Andrologia 2024; 96(4):13098
G Mantica, F Ambrosini, G Drocchi, et al
Watchful waiting and dietary lifestyle
Many men with mild LUTS do not find their symptoms bothersome enough to warrant medical treatment or surgery In addition, many patients are concerned about the potential complications associated with taking medication In selected cases without clinical complications (renal insufficiency, hematuria, hydronephrosis, urinary tract infections, acute urinary retention ), Watchful Waiting (WW) might therefore be an even more attractive choice In patients with mild LUTS (International Prostate Symptom Score - IPSS), the condition can remain stable many times without complications such as acute urinary retention (8) The key issues in the treatment of BPH with WW are the establishment of patient selection criteria and the assessment of risk factors for disease progression Longitudinal studies such as the Baltimore Longitudinal Study of Aging (9) and the Olmstead County Study (10) have shown that advanced age, a larger prostate, and decreased urinary flow can predict the need for treatment The Veterans Administration Cooperative Study has shown that in properly selected patients, especially those with low baseline values, watchful waiting can be a viable and safe strategy (11) Before or alongside treatment, lifestyle counseling and self-care information can positively impact men with LUTS due to BPH (12) Key components of this strategy include patient education, reassurance and regular monitoring, combined with specific lifestyle advice aimed at reducing urinary symptoms (12) It is often recommended to reduce fluid intake at times that minimize discomfort, such as before bedtime, and to limit the consumption of caffeine and alcohol, which can exacerbate symptoms such as frequency, urinary urgency and nocturia due to their diuretic effects (13) Techniques such as double voiding, urethral milking and bladder training are also recommended to improve bladder control and reduce dribbling (14) Another important measure is to avoid constipation and situations in which a person has to hold urine Systematic reviews and meta-analyzes have found that self-management measures that include these lifestyle changes can significantly reduce the severity of symptoms and slow the progression of the disease, thus providing relief (14) This holistic approach not only improves quality of life, but also empowers patients to actively manage their disease
Phytotherapy
Phytotherapy is a science that uses plant extracts, from leaves to roots to seeds, to achieve benefits in the treatment of diseases (15-17) There are numerous in vitro studies in the literature on the potential benefits of phytotherapy in the treatment of BPH, but little is known about the actual in vivo effects
Serenoa repens
Serenoa Repens, also known as saw palmetto, is probably the best-known plant available for the treatment of BPH (18) The dried, ripe berry is used for the extraction Serenoa repens has anti-androgenic activity with inhibition of 5α-reductase and therefore reduces prostate volume; its activity is associated with the action of free fatty acids such as lauric and palmitic acid, which are also responsible for reducing inflammation For these reasons,
saw palmetto can slow down the development of BPH and improve patients' quality of life (QoL), IPSS and symptoms (19) There are many different types of extraction from the plant Hexane extraction has proven to be the most reliable and provides the best results Currently, Serenoa repens is the only phytotherapy recommended in most of the major international guidelines for the treatment of BPH and its symptoms (20, 21) Most tablets available on the market are 320 mg and are taken once daily Nevertheless, the dose and efficacy also depend on the extraction method itself
Cucurbita
The seeds of Cucurbita pepo L appear to have the property of inhibiting 5α-reductase and testosterone-induced hypertrophy by lowering dihydrotestosterone (DHT) levels Some clinical studies showed an improvement in quality of life and IPSS without altering patients’ sexual function during treatment (22, 23)
Urtica
Urtica dioica, the active ingredient of which is the dried root, is frequently used in traditional European medicine for the treatment of BPH Urtica can reduce the conversion of testosterone into DHT Several studies have shown a proliferation-inhibiting effect by binding to the membrane receptors of the prostate, thereby inhibiting its proliferative activity in prostate tissue In vivo studies in rats showed a possible inhibition of 5α-reductase However, more extensive studies in humans are needed to confirm its benefits (24-26)
Curcuma
Curcuma longa Linn is often used to treat urinary tract diseases due to its antioxidant and anti-inflammatory properties In a recent study (27), this plant was able to improve LUTS symptoms, IPSS and Qmax score An improvement was observed both in untreated patients and in patients already treated with alpha-blockers and/or 5α-reductase inhibitors (5-ARI)
Pygeum africanum
Pygeum africanum (Prunus) is known among the indigenous population of Africa for its antiproliferative and antiinflammatory properties It appears to be able to inhibit prostate growth factors and reduce the production of prostaglandins in the prostate (28) This leads to a reduction in chronic prostatitis and the inflammatory symptoms of BPH The evidence in the literature regarding the mechanism of actions and the clinical effect is weak
Pollens
Cernitin, the best-known pollen, is an extract of Secale cereale that has an interesting effect on BPH and can improve both irritative and obstructive symptoms (29) Its effect is achieved by relaxing the smooth muscles of the urethra and apoptosis of the cells of the prostatic transition zone Some studies based on small samples showed an improvement in IPSS and a decrease in prostate volume after long-term treatment with pollen (30, 31) Peony pollen, the pollen of Paeonia suffruticosa, also appears to be able to attenuate oxidative stress and
inflammation They could be directly involved in the regulation of the gut microbiota In addition, some pollen in combination with vitamins (Deprox 500®) showed an improvement in the IPSS and the NIH Chronic Prostatitis Symptom Index (NIHCPSI), alone or in combination with Serenoa repens (32-35) The literature lacks strong evidence on this drug
Epilobium
Epilobium species are perennial plants whose flowers and leaves are used for the presence of some substances such as phenolic acids, flavonoids, and tannins The therapeutic effect of Epilobium has been demonstrated in vitro, with a reduction in PSA levels and a reduction in the inflammatory response and oxidative stress of prostate cells In a randomized, placebo-controlled trial, epilobium was shown to improve post-void residual (PVR), increase IPSS, and reduce nocturia (36) Other studies have investigated the efficacy of epilobium and showed similar results (37)
Palmitoylethanolamide (PEA)
PEA is an endocannabinoid-like bioactive lipid mediator that belongs to the N-acylethanolamine family The properties of PEA include a known anti-inflammatory effect and the reduction of testosterone and DHT levels in both the prostate and serum In addition, PEA can reduce the upregulation of 5α-reductase 2 and androgen receptor induced by BPH (38-40) Most of the available studies were conducted in vitro, while the literature contains only a few in vivo studies
Other plants
Other plant extracts are used in traditional medicine to treat BPH and its symptoms Some of these plants are: Hypoxis hemerocallidea, Pinus pinaster, Roystonea regia, Solanum lycopersicum The substances extracted from these plants appear to have a positive effect on BPH thanks to their antioxidant, anti-inflammatory and anticarcinogenic properties However, the current literature is minimal and of limited significance (41-43)
Conventional therapies
Alpha blockers
Among the drugs available for the treatment of LUTS and bladder outlet obstruction (BOO) due to BPH, alpha-blockers are the most frequently used The literature is full of data evaluating the therapeutic benefits of these drugs, which are also recommended in the most widely followed guidelines (12, 44-45) Their mechanism of action is closely related to the presence of many smooth muscle cells in the prostate that are amenable to alpha-adrenergic stimulation (46) This stimulation leads to relaxation of the prostate and bladder neck The bladder and prostate contain predominantly alpha-1 receptors, which enables the use of selective blockers The most commonly sold alpha-blockers today are tamsulosin, alfuzosin, doxazosin, silodosin, naftodipil and terazosin (47) The data available in the literature show that alpha-blockers can reduce the IPSS score by 30-40% and improve Qmax by 20-25% One of their most important effects is to reduce the risk of
acute urinary retention (48) Unfortunately, these drugs are not free of side effects, such as hypotension and retrograde ejaculation, which are often significant for some patients
Alpha reductase inhibitors
Another important drug for the treatment of BPH are 5alpha-reductase inhibitors (5-ARI) There are two types of 5α-reductase enzymes, but type 2 is most common in the prostate This enzyme converts a portion of testosterone into dihydrotestosterone (DHT), which plays a role in prostate growth (49) The 5-ARIs act by suppressing the enzyme 5α-reductase Dutasteride and finasteride are the most commonly used 5-ARIs and are equivalent in terms of results and effect The PLESS study has shown that finasteride reduces the relative long-term risk of acute urinary retention and the need for surgery compared to placebo 5-ARIs are able to improve LUTS and Qmax (5052) and their effect may also be important before surgery by reducing prostate bleeding during TURP (53, 54) 5ARIs are not free from potential side effects such as d e
depression and anxiety One of the properties of 5-ARIs is the lowering of PSA levels This effect, which has already been observed with other drugs (55) with a different mechanism, is much more pronounced with 5ARIs Therefore, the use of 5-ARIs must always be considered in the diagnosis of prostatic neoplasia in order to best select patients with a clinically significant risk of prostatic neoplasia who are candidates for prostate biopsy (56-58)
Muscarinic receptor antagonists
Normal physiological bladder emptying depends on the activation of the contractile muscarinic receptors on the smooth muscle of the bladder tricuspid This activation is triggered by the neurotransmitter acetylcholine Five subtypes of G-protein-coupled muscarinic receptors (M1; M2; M3; M4; M5) have been characterized pharmacologically Most muscarinic receptors in the detrusor muscle are M2 (70%) and M3 (30%) (59) Currently, the most commonly used antimuscarinic drugs are oxybutynin, propiverine, tolterodine and solifenacin (60, 61)
The current EAU guidelines recommend the use of muscarinic receptors in men with moderate to severe LUTS who have mainly bladder storage symptoms (12) A considerable number of muscarinic receptors are located in different parts of the body (salivary glands, gastrointestinal tract and central nervous system) Therefore, the side effects of antimuscarinics may affect these areas (62) The most frequently reported adverse effects include blurred vision, constipation and dry mouth (61) Their main effect is to reduce the urge to urinate and the frequency of urination
In addition, they are able to increase bladder capacity, allowing patients to hold urine for longer periods of time without discomfort This improvement can significantly increase the quality of life of BPH patients as they need to urinate less frequently Usually, these drugs are used in combination with alpha-blockers This combination can be particularly effective in treating both the obstructive and irritative symptoms of BPH
G Mantica, F Ambrosini, G Drocchi, et al
Beta 3 agonists
Humans have three different subtypes of β-adrenoceptors (β1, β2 and β3) In human bladder tissue, β3-adrenoceptors are predominantly expressed (63) Activation of this receptor is associated with detrusor smooth muscle relaxation during the storage phase of micturition and therefore improves bladder compliance and capacity Mirabegron is the first β3-adrenoceptor agonist approved in clinical practice and may be an alter native treatment option to antimuscarinics for patients with overactive bladder symptoms (64-66) The efficacy and safety of mirabegron 50 mg compared to placebo and antimuscarinics was evaluated in male patients with overactive bladder in five phase III studies Mirabegron showed significant improvements in the reduction of micturition frequency compared to placebo Mirabegron 50 mg has been shown to be relatively safe Gastrointestinal symptoms and dry mouth are the most commonly reported adverse effects Mirabegron 100 mg, on the other hand, showed a slightly increased risk of high blood pressure and cardiac arrhythmia (68)
Phosphodiesterase 5 inhibitors
Phosphodiesterase type 5 (PDE5) inhibitors (sildenafil, tadalafil, vardenafil and avanafil) are the gold standard in the treatment of patients with erectile dysfunction (ED) These drugs block the enzyme PDE5 and thus regulate the level of cyclic guanosine monophosphate (cGMP) by breaking it down to inactive 5′-guanosine monophosphate (5′-GMP) This process leads to smooth muscle relaxation in the corpus cavernosum of the penis (69, 70) This relaxation increases the arterial inflow into the penis, which is necessary to achieve and maintain an erection In addition, tadalafil relaxes the smooth muscles of the bladder and prostate and can thus improve LUTS (71) Therefore, the daily intake of 5 mg tadalafil has been approved for the treatment of BPH Compared to a placebo, 5 mg tadalafil once daily as monotherapy or in combination with alpha-blockers can significantly improve quality of life and IPSS (72, 73) Phosphodiesterase type 5 inhibitors are generally well tolerated, especially at low doses The most common side effects are headache, redness of the skin, and nasal congestion (69, 70)
Combination therapy
Although alpha blockers are the treatment of choice in most cases, in many cases their effect alone is not sufficient to relieve the symptoms of BPH It is therefore poss i b l e t o c o m b i n e t h i s t h e r a p y w i t h 5 - A R I s , P D E 5 inhibitors, Mirabegon, antimuscarinics and, of course, phytotherapy, which generally leads to good results Studies such as COMBAT and CONDUCT have shown that dutasteride plus tamsulosin can improve Qmax and IPSS and reduce the risk of acute urinary retention (74, 75) Therefore, combination therapy with 5-ARI and alpha-blockers could be an option for patients with large prostate volume and severe LUTS Similar studies looking at the combination of alpha-blockers and PDE5 inhibitors (tadalafil), alpha-blockers and mirabegone or alphablockers and antimuscarinics have shown that combination therapy is able to reduce LUTS without a significant increase in side effects (76, 77)
DISCUSSION
Medical treatment for BPH has evolved significantly over the years, offering a variety of treatment options aimed at alleviating symptoms and improving overall patient outcomes (78-80) In selected uncomplicated cases, WW and lifestyle changes can play a positive role in the management of BPH symptoms (14) Systematic reviews and meta-analyzes have shown that such self-management measures can significantly alleviate symptoms and control the progression of the disease (14) Nevertheless, the elements of self-care management have not been assessed individually and the lifestyle advice is derived from a formal consensus method, so further research is needed in this area (12) Among the approved drugs for the medical management of BPH, alpha-blockers have been considered a cornerstone of BPH treatment for many years They provide rapid relief of symptoms, often within a few weeks, and are generally well tolerated (81) However, some patients may experience side effects such as dizziness, orthostatic hypotension, and ejaculatory dysfunction (82) Despite these potential problems, alpha-blockers remain a widely used drug due to their efficacy and rapid onset of action (12) 5-ARI, by lowering dihydrotestosterone levels, can shrink the prostate and improve LUTS over time (12) However, relief may be slower to come compared to alpha-blockers, and potent i
) Moreover, their impact on PSA needs to be considered in relation to prostate cancer screening (12) Despite these concerns, they are a valuable option for the treatment of BPH, especially in patients with prostate enlargement > 40 mL Treatments with phosphodiesterase-5 inhibitors such as tadalafil, have also shown promise in the management of BPH These drugs can provide additional relief from symptoms such as urinary urgency and frequency, improve erectile function and help to maintain ejaculatory function (84) They offer a different mechanism of action to conventional BPH therapies and can be particularly useful for patients suffering from both BPH and erectile dysfunction However, they can cause side effects such as headaches and gastrointestinal discomfort, and interactions with other medications must be carefully monitored Research on newer agents such as beta-3 agonists, such as mirabegron, is ongoing These medications target bladder function rather than prostate size and may help relieve storage symptoms such as urinary urgency and frequency Although the long-term efficacy and safety of these drugs are still under investigation, the available literature suggests that beta-3 agonists may be an effective addition to the BPH treatment options (12) A further possibility that has emerged in recent years is that of suspension therapy for fragile patients or for patients with a combination of different therapies in order to reduce the risk of side effects However, still few studies are currently available on the topic (85, 86)
One of the most evolving and extensive fields related to the medical treatment of BPH is phytotherapy Several plantderived substances are commercially available, including both herbal medicines and dietary supplements (87) Phytotherapy has undeniable advantages, including high tolerability and low side effects (16) They are also easily available online or over the counter Sometimes patients
find it difficult to adhere to the treatments because the side effects, including retrograde ejaculation, can significantly affect the patient’s psychological well-being, leading them to prefer phytotherapy On the other hand, the evidence on phytotherapy is not conclusive, the mechanism of action is not always fully understood and many of these substances have not undergone the rigorous testing that drugs normally receive Considering their mostly moderate efficacy, which is inferior to that of approved drugs, there is a lack of strong recommendations in European (EAU) or American Urological Association (AUA) guidelines (12) However, in a historical period in which there is the threat of further pandemics (88) which can cause an increase in the waiting list of patients suffering from BPH, a correct knowledge of the medical therapy of BPH is of fundamental importance, allowing to manage the patient also through telemedicine and while waiting for surgery (89-91)
CONCLUSIONS
In conclusion, the medical management of BPH is currently defined by the algorithms of the EAU and AUA guidelines (12, 92) However, given the broad and heterogeneous range of therapeutic options available, the need for a more personalized approach is increasingly recognized As the treatment landscape continues to evolve, tailoring therapy to individual patient needs and preferences is likely to become increasingly important to ensure that treatment strategies are both effective and meet patient expectations
REFERENCES
1 GBD 2019 Benign Prostatic Hyperplasia Collaborators The global, regional, and national burden of benign prostatic hyperplasia in 204 countries and territories from 2000 to 2019: a systematic analysis for the Global Burden of Disease Study 2019 Lancet Healthy Longev 2022; 3:e754-e776
2 Devlin CM, Simms MS, Maitland NJ Benign prostatic hyperplasia - what do we know? BJU Int 2021; 127:389-399
3 Montiel-Jarquín ÁJ, Gutiérrez-Quiroz CT, Pérez-Vázquez AL, et al Quality of life and erectile dysfunction in patients with benign prostatic hyperplasia Cir Cir 2021; 89:218-222
4 Haile ES, Sotimehin AE, Gill BC Medical management of benign prostatic hyperplasia Cleve Clin J Med 2024; 91:163-170
5 Page MJ, McKenzie JE, Bossuyt PM, et al The PRISMA 2020 statement: an updated guideline for reporting systematic reviews BMJ 2021; 372:n71
6 Frandsen TF, Bruun Nielsen MF, Lindhardt CL, Eriksen MB Using the full PICO model as a search tool for systematic reviews resulted in lower recall for some PICO elements J Clin Epidemiol 2020; 127:69-75
7 Sterne JAC, Savovic J, Page MJ, et al RoB 2: a revised tool for assessing risk of bias in randomised trials BMJ 2019; 366:l4898
8 Djavan B, Fong YK, Harik M, et al Longitudinal study of men with mild symptoms of bladder outlet obstruction treated with watchful waiting for four years Urology 2004; 64:1144-8
9 Arrighi HM, Metter EJ, Guess HA, Fozzard JL Natural history of
benign prostatic hyperplasia and risk of prostatectomy The Baltimore Longitudinal Study of Aging Urology 1991; 38(Suppl 1):4-8
10 Jacobsen SJ, Jacobson DJ, Girman CJ, et al Treatment for benign prostatic hyperplasia among community dwelling men: the Olmsted County study of urinary symptoms and health status J Urol 1999; 162:1301-6
11 Wasson JH, Reda DJ, Bruskewitz RC, et al A comparison of transurethral surgery with watchful waiting for moderate symptoms of benign prostatic hyperplasia The Veterans Affairs Cooperative Study Group on Transurethral Resection of the Prostate N Engl J Med 1995; 332:75-9
12 EAU Guidelines Edn presented at the EAU Annual Congress Paris April 2024 ISBN 978-94-92671-23-3
13 Brown CT, Yap T, Cromwell DA, et al Self management for men with lower urinary tract symptoms: randomised controlled trial BMJ 2007; 334:25
14 Albarqouni L, Sanders S, Clark J, et al Self-Management for Men With Lower Urinary Tract Symptoms: A Systematic Review and Meta-Analysis Ann Fam Med 2021; 19:157-167
16 Kim SW Phytotherapy: emerging therapeutic option in urologic disease Transl Androl Urol 2012; 1:181-91
17 Antoniou V, Gauhar V, Modi S, Somani BK Role of Phytotherapy in the Management of BPH: A Summary of the Literature J Clin Med 2023; 12:1899
18 Nickel JC, Chughtai B, De Nunzio C, et al Rethinking the Role of Saw Palmetto Extract for Men with Lower Urinary Tract Symptoms in North America Uro 2022; 2:137-150
19 Tacklind J, Macdonald R, Rutks I, et al Serenoa repens for benign prostatic hyperplasia Cochrane Database Syst Rev 2012; 12:CD001423 Update in: Cochrane Database Syst Rev 2023; 6:CD001423
20 Barry MJ, Meleth S, Lee JY, et al Effect of Increasing Doses of Saw Palmetto Extract on Lower Urinary Tract Symptoms: A Randomized Trial JAMA 2011; 306:1344-1351
21 Giulianelli R, Pecoraro S, Sepe G, et al Multicentre study on the efficacy and tolerability of an extract of Serenoa repens in patients with chronic benign prostate conditions associated with inflammation Arch Ital Urol Androl 2012; 84:94-8
22 Theil G, Richter M, Schulze M, et al Extract from Cucurbita pepo improves BPH symptoms without affecting sexual function: a 24-month noninterventional study World J Urol 2022; 40:17691775 Erratum in: World J Urol 2022; 40:2589-2590
23 Damiano R, Cai T, Fornara P, et al The role of Cucurbita pepo in the management of patients affected by lower urinary tract symptoms due to benign prostatic hyperplasia: A narrative review Arch Ital Urol Androl 2016; 88:136-43
24 Moradi HR, Erfani Majd N, Esmaeilzadeh S, Fatemi Tabatabaei SR The histological and histometrical effects of Urtica dioica extract on rat's prostate hyperplasia Vet Res Forum 2015; 6:23-9
25 Bougueroua K, Boufadi MY, Latreche B, et al Effects of algerian nettle (Urtica dioica L ) on benign prostatic hyperplasia and their mechanism of action elucidation: in vivo and in silico approaches Nat Prod Res 2024; 38:4017-4027
26 Sens-Albert C, Weisenburger S, König BC, et al Effects of a pro-
G Mantica, F Ambrosini, G Drocchi, et al
prietary mixture of extracts from Sabal serrulata fruits and Urtica dioica roots (WS® 1541) on prostate hyperplasia and inflammation in rats and human cells Front Pharmacol 2024; 15:1379456
27 Crocerossa F, Cantiello F, Bagalá L, et al Clinical Effects of Oral Supplementation of Gamma-Cyclodextrin Curcumin Complex in M a l e P a t i e n t
Hyperplasia-Related Lower Urinary Tract Symptoms Urol Int 2023; 107:924-934
28 Rubegeta E, Makolo F, Kamatou G, et al The African cherry: A review of the botany, traditional uses, phytochemistry, and biological activities of Prunus africana (Hook f ) Kalkman J Ethnopharmacol 2023; 305:116004
29 Antonelli M, Donelli D, Firenzuoli F Therapeutic efficacy of orally administered pollen for nonallergic diseases: An umbrella review Phytother Res 2019; 33:2938-2947
30 Yasumoto R, Kawanishi H, Tsujino T, et al Clinical evaluation of long-term treatment using cernitin pollen extract in patients with benign prostatic hyperplasia Clin Ther 1995; 17:82-7
31 F Chen, X Zhang, J Bai, et al Anti-proliferative effect and mechanisms of Peony pollen on BPH via inhibition of inflammatory factors, oxidative damage and modulation of gut microbiota and SCFAs metabolism, Pharmacological Research - Modern Chinese Medicine, 2024; 12:100472
32 Macchione N, Bernardini P, Piacentini I, et al Flower Pollen Extract in Association with Vitamins (Deprox 500®) Versus Serenoa repens in Chronic Prostatitis/Chronic Pelvic Pain Syndrome: A Comparative Analysis of Two Different Treatments Antiinflamm Antiallergy Agents Med Chem 2019; 18:151-161
33 Cai T, Luciani LG, Caola I, et al Effects of pollen extract in association with vitamins (DEPROX 500®) for pain relief in patients affected by chronic prostatitis/chronic pelvic pain syndrome: results from a pilot study Urologia 2013; 80(Suppl 22):5-10
34 Cai T, Wagenlehner FM, Luciani LG, et al Pollen extract in association with vitamins provides early pain relief in patients affected by chronic prostatitis/chronic pelvic pain syndrome Exp Ther Med 2014; 8:1032-1038
35 Maurizi A, De Luca F, Zanghi A, et al The role of nutraceutical medications in men with non bacterial chronic prostatitis and chronic pelvic pain syndrome: A prospective non blinded study utilizing flower pollen extracts versus bioflavonoids Arch Ital Urol Androl 2019; 90:260-264
36 Esposito C, Santarcangelo C, Masselli R, et al Epilobium angustifolium L extract with high content in oenothein B on benign prostatic hyperplasia: A monocentric, randomized, double-blind, placebo-controlled clinical trial Biomed Pharmacother 2021; 138:111414
37 Deng L, Zong W, Tao X, et al Evaluation of the therapeutic effect against benign prostatic hyperplasia and the active constituents from Epilobium angustifolium L J Ethnopharmacol 2019; 232:1-10
38 Cicero AFG, Allkanjari O, Busetto GM, et al Nutraceutical treatment and prevention of benign prostatic hyperplasia and prostate cancer Arch Ital Urol Androl 2019; 91:139
39 D'Amico R, Genovese T, Cordaro M, et al Palmitoylethanolamide/ Baicalein Regulates the Androgen Receptor Signaling and NF-κB/Nrf2 Pathways in Benign Prostatic Hyperplasia Antioxidants (Basel) 2021; 10:1014
40 Cordaro M, Impellizzeri D, Siracusa R, et al Effects of a comicronized composite containing palmitoylethanolamide and polydatin in an experimental model of benign prostatic hyperplasia Toxicol Appl Pharmacol 2017; 329:231-240
41 Drewes SE, Elliot E, Khan F, et al Hypoxis hemerocallidea--not merely a cure for benign prostate hyperplasia J Ethnopharmacol 2008; 119:593-8
42 Carbajal D, Molina V, Mas R, Arruzazabala ML Therapeutic effect of D-004, a lipid extract from Roystonea regia fruits, on prostate hyperplasia induced in rats Drugs Exp Clin Res 2005; 31:193-7
43 Lambertini L, Di Maida F, Tellini R, et al Impact of the Treatment of Serenoa repens, Solanum lycopersicum, Lycopene and Bromelain in Combination with Alfuzosin for Benign Prostatic Hyperplasia Results from a Match-Paired Comparison Analysis Uro 2021; 1:228-237
44 Michel MC, Vrydag W Alpha1-, alpha2- and beta-adrenoceptors in the urinary bladder, urethra and prostate Br J Pharmacol 2006; 147(Suppl 2):S88-119
45 Kortmann BB, Floratos DL, Kiemeney LA, et al Urodynamic effects of alpha-adrenoceptor blockers: a review of clinical trials Urology 2003; 62:1-9
46 Michel MC, Mehlburger L, Bressel HU, Goepel M Comparison of tamsulosin efficacy in subgroups of patients with lower urinary tract symptoms Prostate Cancer Prostatic Dis 1998; 1:332-335
47 Karavitakis M, Kyriazis I, Omar MI, et al Management of Urinary Retention in Patients with Benign Prostatic Obstruction: A Systematic Review and Meta-analysis Eur Urol 2019; 75:788-798
48 Gwon YN, Park JJ, Yang WJ, et al Comparing effects of alphablocker management on acute urinary retention secondary to benign prostatic hyperplasia: A systematic review and network meta-analysis Prostate Int 2023; 11:91-99
49 Andriole G, Bruchovsky N, Chung LW, et al Dihydrotestosterone and the prostate: the scientific rationale for 5alpha-reductase inhibitors in the treatment of benign prostatic hyperplasia J Urol 2004; 172:1399-403
50 Nickel JC, Fradet Y, Boake RC, et al Efficacy and safety of finasteride therapy for benign prostatic hyperplasia: results of a 2-year randomized controlled trial (the PROSPECT study) PROscar Safety Plus Efficacy Canadian Two year Study CMAJ 1996; 155:1251-9
51 Naslund MJ, Miner M A review of the clinical efficacy and safety of 5alpha-reductase inhibitors for the enlarged prostate Clin Ther 2007; 29:17-25
452 Roehrborn CG, Siami P, Barkin J, et al The effects of dutasteride, tamsulosin and combination therapy on lower urinary tract symptoms in men with benign prostatic hyperplasia and prostatic enlargement: 2-year results from the CombAT study J Urol 2008; 179:616-21 Erratum in: J Urol 2008; 180:1191
53 Khwaja MA, Nawaz G, Muhammad S, et al The Effect of Two Weeks Preoperative Finasteride Therapy in Reducing Prostate Vascularity J Coll Physicians Surg Pak 2016; 26:213-5
54 Hirshburg JM, Kelsey PA, Therrien CA, et al Adverse Effects and Safety of 5-alpha Reductase Inhibitors (Finasteride, Dutasteride): A Systematic Review J Clin Aesthet Dermatol 2016; 9:56-62
55 Mantica G, Chierigo F, Cassim F, et al Correlation Between Long-Term Acetylsalicylic Acid Use and Prostate Cancer Screening with PSA Should We Reduce the PSA Cut-off for Patients in Chronic Therapy? A Multicenter Study Res Rep Urol 2022; 14:369-377
56 De Nunzio C, Lombardo R, Baldassarri, et al Rotterdam mobile phone app including MRI data for the prediction of prostate cancer: A multicenter external validation Eur J Surg Oncol 2021; 47:26402645
57 Cindolo L, Bertolo R, Minervini A, et al External validation of
Cormio nomogram for predicting all prostate cancers and clinically significant prostate cancers World J Urol 2020; 38:2555-2561
58 Mantica G, Pacchetti A, Aimar R, et al Developing a five-step training model for transperineal prostate biopsies in a naïve residents' group: a prospective observational randomised study of two different techniques World J Urol 2019; 37:1845-1850
59 Hegde SS, Eglen RM Muscarinic receptor subtypes modulating smooth muscle contractility in the urinary bladder Life Sci 1999; 64:419-28
60 Mansfield KJ, Liu L, Mitchelson FJ, et al Muscarinic receptor subtypes in human bladder detrusor and mucosa, studied by radioligand binding and quantitative competitive RT-PCR: changes in ageing Br J Pharmacol 2005; 144:1089-99
61 Abrams P, Andersson KE Muscarinic receptor antagonists for overactive bladder BJU Int 2007; 100:987-1006
62 Abrams P, Andersson KE, Buccafusco, et al Muscarinic receptors: their distribution and function in body systems, and the implications for treating overactive bladder Br J Pharmacol 2006; 148:565-78
63 Andersson KE, Wein AJ Pharmacology of the lower urinary tract: basis for current and future treatments of urinary incontinence Pharmacol Rev 2004; 56:581-631
64 Andersson KE, Martin N, Nitti V Selective β₃- adrenoceptor agonists for the treatment of overactive bladder J Urol 2013; 190:1173-80
65 Chapple CR, Cardozo L, Nitti VW, et al Mirabegron in overactive bladder: a review of efficacy, safety, and tolerability Neurourol Urodyn 2014; 33:17-30
66 Chapple CR, Siddiqui E Mirabegron for the treatment of overactive bladder: a review of efficacy, safety and tolerability with a focus on male, elderly and antimuscarinic poor-responder populations, and patients with OAB in Asia Expert Rev Clin Pharmacol 2017; 10:131-151
67 Tubaro A, Batista JE, Nitti VW, et al Efficacy and safety of daily mirabegron 50 mg in male patients with overactive bladder: a critical analysis of five phase III studies Ther Adv Urol 2017; 9:137-154
68 Sebastianelli A, Russo GI, Kaplan SA, et al Systematic review and meta-analysis on the efficacy and tolerability of mirabegron for the treatment of storage lower urinary tract symptoms/overactive bladder: Comparison with placebo and tolterodine Int J Urol 2018; 25:196-205
69 Huang SA, Lie JD Phosphodiesterase-5 (PDE5) Inhibitors In the Management of Erectile Dysfunction P T 2013; 38:407-19
7 0 E l H a d y A K , E l - G a m i l D S , A b d e l - H a l i m M , A b a d i A H Advancements in Phosphodiesterase 5 Inhibitors: Unveiling Present and Future Perspectives Pharmaceuticals (Basel) 2023; 16:1266
71 Yokoyama O, Igawa Y, Takeda M, et al Tadalafil for lower urinary tract symptoms secondary to benign prostatic hyperplasia: a review of clinical data in Asian men and an update on the mechanism of action Ther Adv Urol 2015; 7:249-64
72 Cui J, Cao D, Bai Y, et al Efficacy and Safety of 12- week Monotherapy With Once Daily 5 mg Tadalafil for Lower Urinary Tract Symptoms of Benign Prostatic Hyperplasia: Evidence-based Analysis Front Med (Lausanne) 2021; 8:744012
73 Brock G, Broderick G, Roehrborn CG, et al Tadalafil once daily in the treatment of lower urinary tract symptoms (LUTS) suggestive of benign prostatic hyperplasia (BPH) in men without erectile dysfunction BJU Int 2013; 112:990-7
74 Siami P, Roehrborn CG, Barkin J, et al Combination therapy with dutasteride and tamsulosin in men with moderate-to-severe benign prostatic hyperplasia and prostate enlargement: the CombAT (Combination of Avodart and Tamsulosin) trial rationale and study design Contemp Clin Trials 2007; 28:770-9
75 Roehrborn CG, Oyarzabal Perez I, Roos EP, et al Efficacy and safety of a fixed-dose combination of dutasteride and tamsulosin treatment (Duodart®) compared with watchful waiting with initiation of tamsulosin therapy if symptoms do not improve, both provided with lifestyle advice, in the management of treatment-naïve men with moderately symptomatic benign prostatic hyperplasia: 2-year CONDUCT study results BJU Int 2015; 116:450-9
76 Brasure M, MacDonald R, Dahm P, et al Newer Medications for Lower Urinary Tract Symptoms Attributed to Benign Prostaic Hyperplasia: A Review [Internet] Rockville (MD): Agency for Healthcare Research and Quality (US); 2016 May Report No : 16EHC024-EF
77 Kakizaki H, Lee KS, Yamamoto O, et al Mirabegron Add-on Therapy to Tamsulosin for the Treatment of Overactive Bladder in Men with Lower Urinary Tract Symptoms: A Randomized, Placebocontrolled Study (MATCH) Eur Urol Focus 2020; 6:729-737
78 Stewart KL; Lephart ED Overview of BPH: Symptom Relief with Dietary Polyphenols, Vitamins and Phytochemicals by Nutraceutical Supplements with Implications to the Prostate Microbiome Int J Mol Sci 2023; 24:5486
79 Kaltsas A, Kratiras Z, Zachariou A, et al Evaluating the Impact of Benign Prostatic Hyperplasia Surgical Treatments on Sexual Health Biomedicines 2024; 12:110
80 Hughes T, Harper P, Somani BK Treatment Algorithm for Management of Benign Prostatic Obstruction: An Overview of Current Techniques Life 2023; 13:2077
81 Barendrecht MM, Abrams P, Schumacher H, et al Do alpha1adrenoceptor antagonists improve lower urinary tract symptoms by reducing bladder outlet resistance? Neurourol Urodyn 2008; 27:226-230
82 Nickel JC, Sander S, Moon TD A meta-analysis of the vascularrelated safety profile and efficacy of alpha-adrenergic blockers for symptoms related to benign prostatic hyperplasia Int J Clin Pract 2008; 62:1547-1559
83 Corona G, Tirabassi G, Santi D, et al Sexual dysfunction in subjects treated with inhibitors of 5α-reductase for benign prostatic hyperplasia: a comprehensive review and meta-analysis Andrology 2017; 5:671-678
84 Gacci M, Corona G, Salvi M, et al A systematic review and meta-analysis on the use of phosphodiesterase 5 inhibitors alone or in combination with α-blockers for lower urinary tract symptoms due to benign prostatic hyperplasia Eur Urol 2012; 61:994-1003
85 van der Worp H, Jellema P, Hordijk I, et al Discontinuation of alpha-blocker therapy in men with lower urinary tract symptoms: a systematic review and meta-analysis BMJ Open 2019; 9:e030405
86 Sebastianelli A, Spatafora P, Frizzi J, et al Which Drug to Discontinue 3 Months After Combination Therapy of Tadalafil plus Tamsulosin for Men with Lower Urinary Tract Symptom and Erectile Dysfunction? Results of a Prospective Observational Trial Eur Urol Focus 2021; 7:432-439
87 Morgia G, Lo Giudice A, Carrino M, et al Efficacy of Palmitoylethanolamide, Epilobium and Calendula suppositories for the treatment of patients with chronic prostatitis/chronic pelvic pain syndrome type III Arch Ital Urol Androl 2024; 96:12582
G Mantica, F Ambrosini, G Drocchi, et al
88 Leonardi R, Bellinzoni P, Broglia L, et al Hospital care in Departments defined as COVID-free: A proposal for a safe hospitalization protecting healthcare professionals and patients not affected by COVID-19 Arch Ital Urol Androl 2020; 92:67
89 Ambrosini F, Di Stasio A, Mantica G, et al COVID-19 pandemic and uro-oncology follow-up: A "virtual" multidisciplinary team strategy and patients' satisfaction assessment Arch Ital Urol Androl 2020; 92:78
90 Mirone V, Di Bello F, Morra S, et al Telemedicine and social
media: A contemporary analysis of the most shared content by internet users Arch Ital Urol Androl 2024; 96:11206
91 Carrión DM, Gómez Rivas J, Rodríguez-Socarrás ME, et al Implementación de la teleconsulta en la práctica urológica durante la era Covid-19: ¿qué hemos aprendido? [Implementation of Remote Clinics in urology practice during the COVID-19 era: What have we learned?] Arch Esp Urol 2020; 73:345-352
92 Sandhu JS, Bixler BR, Dahm P, et al Management of Lower Urinary Tract Symptoms Attributed to Benign Prostatic Hyperplasia (BPH): AUA Guideline Amendment 2023 J Urol 2024; 211:11-19
Correspondence
Guglielmo Mantica (Corresponding Author) guglielmo mantica@gmail com Giovanni Drocchi g drocchi@hotmail it
Zlata Zubko zlata@zubko it
Lorenzo Lo Monaco lomonaco lorenzo@libero it
Carlo Carlo Terrone carlo terrone@med uniupo it
Department of Surgical and Diagnostic Integrated Sciences (DISC), University of Genova, Genova, Italy
Francesca Ambrosini IRCCS Ospedale Policlinico San Martino, Genova, Italy f ambrosini1@gmail com
Angelo Cafarelli info@angelocafarelli it Urology Unit, Villa Igea, Ancona, Italy
Alessandro Calarco segreteria@alessandrocalarco com Department of Urology, San Carlo di Nancy Hospital, Rome, Italy
Renzo Colombo colombo renzo@hsr it Department of Urology, Vita e Salute San Raffaele University, Milan, Italy
Ottavio de Cobelli ottavio de-cobelli@ieo it Department of Urology, IEO European Institute of Oncology, IRCCS, Milan, Italy
Ferdinando De Marco info@clinicavillamargherita it I N I Grottaferrata, Rome, Italy
Giovanni Ferrari visite@giovanniferrariurologo it Hesperia Hospital, Modena, Italy
Giuseppe Ludovico g ludovico@miulli it Ospedale Miulli, Acquaviva delle Fonti, Bari, Italy
12 Casa di Cura Musumeci-Gecas, Gravina di Catania, Italy
Resection of the Prostate. N Engl J Med.
Brown CT, Yap T, Cromwell DA, et al. Self management for men with lower urinary tract symptoms: randomised controlled trial. BMJ. 2007 Jan
20 Barry M.J., Meleth S., Lee J.Y., et al. Effect of Increasing Doses of Saw Palmetto Extract on Lower Urinary Tract Symptoms: A Randomized Trial. JAMA. 2011
27 Crocerossa F, Cantiello F, Bagalá L, et al. Clinical Effects of Oral Supplementation of Gamma-Cyclodextrin Curcumin Complex in Male Patients with Moderate-To-Severe Benign Prostatic Hyperplasia-Related Lower Urinary Tract Symptoms. Urol Int. 2023
30 Yasumoto R, Kawanishi H, Tsujino T, et al. Clinical evaluation of long-term treatment using cernitin pollen extract in patients with benign prostatic hyperplasia. Clin Ther. 1995 Jan-Feb
10 Jacobsen SJ, Jacobson DJ, Girman CJ, et al. Treatment for benign prostatic hyperplasia among community dwelling men: the Olmsted County study of urinary symptoms and health status
2115 men Instrumental follow up No instreumental follow up Urological measurements may have influenced treatment
Wasson JH, Reda DJ, Bruskewitz RC, Elinson J, Keller AM, Henderson WG. A comparison of transurethral surgery with watchful waiting for moderate symptoms of benign prostatic hyperplasia. The Veterans Affairs Cooperative Study Group on Transurethral
33 Cai T, Luciani LG, Caola I, et al. Effects of pollen extract in association with vitamins (DEPROX 500®) for pain relief in patients affected by chronic prostatitis/chronic pelvic pain syndrome: results from a pilot study. Urologia. 2013 Apr 24
35 Maurizi A, De Luca F, Zanghi A, et al. The role of nutraceutical medications in men with non bacterial chronic prostatitis and chronic pelvic pain syndrome: A prospective non blinded study utilizing flower pollen extracts versus bioflavonoids. Arch Ital Urol Androl. 2019 Jan
36 Maurizi A, De Luca F, Zanghi A, et al. The role of nutraceutical medications in men with non bacterial chronic prostatitis and chronic pelvic pain syndrome: A prospective non blinded study utilizing flower pollen extracts versus bioflavonoids. Arch Ital Urol Androl. 2019 Jan
50 Nickel JC, Fradet Y, Boake RC, et al. Efficacy and safety of finasteride therapy for benign prostatic hyperplasia: results of a 2-year randomized controlled trial (the PROSPECT study). PROscar Safety Plus Efficacy Canadian Two year Study. CMAJ. 1996 Nov 1;155(9):1251-9. PMID: 8911291; PMCID: PMC1335066.
613 patients patients were given finasteride (5 mg/d) for 2 yers
53 Khwaja MA, Nawaz G, Muhammad S, Jamil MI, Faisal M, Akhter S. The Effect of Two Weeks Preoperative Finasteride Therapy in Reducing Prostate Vascularity. J Coll Physicians Surg Pak. 2016 Mar;26(3):213-5. PMID: 26975954.
67 Tubaro A, Batista JE, Nitti VW, et al. Efficacy and safety of daily mirabegron 50 mg in male patients with overactive bladder: a critical analysis of five phase III studies. Ther Adv Urol. 2017 May 10;9(6):137-154. doi: 10.1177/1756287217702797. PMID: 28588652; PMCID: PMC5444577.
73 Brock G, Broderick G, Roehrborn CG, Xu L, Wong D, Viktrup L. Tadalafil once daily in the treatment of lower urinary tract symptoms (LUTS) suggestive of benign prostatic hyperplasia (BPH) in men without erectile dysfunction. BJU Int. 2013 Nov;112(7):990-7. doi: 10.1111/bju.12251. Epub 2013 Aug 13. PMID: 23937669.
74 Siami P, Roehrborn CG, Barkin J, et al. Combination therapy with dutasteride and tamsulosin in men with moderate-to-severe benign prostatic hyperplasia and prostate enlargement: the CombAT (Combination of Avodart and Tamsulosin) trial rationale and study design. Contemp Clin Trials. 2007 Nov;28(6):770-9. doi: 10.1016/j.cct.2007.07.008. Epub 2007 Aug 2. PMID: 17761460.
80 patients The finasteride group (Group A) was prescribed oral 5 mg of finasteride daily for 2 weeks before surgery.
The control group (Group B) did not receive any agent Finasteride reduces microvessel density and hence prostate vascularity with only 2-week therapy and the mean MVD is clearly correlated with size of prostate.
771 patients Mirabegron 50 mg (393 patients) versus placebo (378 patients) Mirabegron 50 mg demonstrated superiority versus placebo (treatment difference: 0.37 [95% confidence interval (CI): 0.74, 0.01]) for reducing micturition frequency; improvements in urgency and incontinence were not significantly different between mirabegron 50 mg and placebo.
1089 men without ED (n = 338) and with ED (n = 751)
Tadalafil once daily in men withoutor with erectile dysfunction (ED)
versus placebo
Tadalafil 5 mg once daily improved BPH-LUTS in men without ED by a magnitude similar to that observed in men with ED. The adverse event profile in men without ED was consistent with that observed in men with ED.
4838 patients Combination therapy with dutasteride and tamsulosin versus the monotherapies Combination therapy was significantly superior to tamsulosin monotherapy but not dutasteride monotherapy at reducing the relative risk of AUR or BPH-related surgery. Combination therapy was also significantly superior to both monotherapies at reducing the relative risk of BPH clinical progression. Combination therapy provided significantly greater symptom benefit than either monotherapy at 4 yr.
Study
75 Roehrborn CG, Oyarzabal Perez I, Roos EP, et al. Efficacy and safety of a fixed-dose combination of dutasteride and tamsulosin treatment (Duodart(®) ) compared with watchful waiting with initiation of tamsulosin therapy if symptoms do not improve, both provided with lifestyle advice, in the management of treatment-naïve men with moderately symptomatic benign prostatic hyperplasia: 2year CONDUCT study results. BJU Int. 2015 Sep;116(3):450-9. doi: 10.1111/bju.13033. Epub 2015 Jan 29. PMID: 25565364.
77 Kakizaki H, Lee KS, Yamamoto O, et al. Mirabegron Add-on Therapy to Tamsulosin for the Treatment of Overactive Bladder in Men with Lower Urinary Tract Symptoms: A Randomized, Placebo-controlled Study (MATCH). Eur Urol Focus. 2020 Jul 15;6(4):729-737. doi: 10.1016/ j.euf.2019.10.019. Epub 2019 Nov 11. PMID: 31718957
86 Sebastianelli A, Spatafora P, Frizzi J, et al. Which Drug to Discontinue 3 Months After Combination Therapy of Tadalafil plus Tamsulosin for Men with Lower Urinary Tract Symptom and Erectile Dysfunction? Results of a Prospective Observational Trial. Eur Urol Focus. 2021 Mar;7(2):432-439. doi: 10.1016/j.euf. 2019.09.015. Epub 2019 Oct 10. PMID: 31606473.
Population Intervention Comparision Stated outcome/findings
742 patients FDC (369 patients) followed for 24 months. versus WW-All (373) followed for 24 months.
568 patients The mirabegron add-on therapy to tamsulosin versus placebo, as add-on to tamsulosin.
FDC therapy with dutasteride and tamsulosin, plus lifestyle advice, resulted in rapid and sustained improvements with significantly greater symptom and QoL improvements and a significantly reduced risk of BPH progression compared with WW plus initiation of tamsulosin as per protocol.
The mirabegron add-on therapy to tamsulosin for 12 wk in men with LUTS and OAB symptoms demonstrated superior efficacy to placebo and was well tolerated.
versus 25 patients discontinued tadalafil (Group TAM).
After 12 wk of combination therapy, monotherapy with tadalafil for further 12 wk allows to preserve the improvement of storage IPSS and IIEF-5, in addition to total IPSS.
The psycho-sensory pelvic reflex: A new paradigm in the model of male sexual response
Giuseppe La Pera
Consultant Urologist, Rome, Italy
KEY WORDS: Pelvic reflex; Male sexual response; Male genital response; Pelvic floor; Neurological reflex; Genital excitatory response; Genital perception; Ejaculatory urgency
Submitted 26 August 2024; Accepted 31 August 2024
To the Editor,
What are the male anatomical structures that trigger the so-called "desire" to have sex? What are the male anatomical structures that determine the perception of arousal in men?
The most prevalent models of male sexuality to date, those of Masters W, Johnson VE (1) and Kaplan HS (2), while revolutionary for their time and introducing important physiological concepts, begin the entire process with erection and its perception as the first anatomical sign of male arousal and desire However, erection as the first response of male reactivity does not always coincide with arousal, understood as the psychological and physiological arousal that a male experiences in response to sexual stimuli It also does not always coincide with the perception of arousal, meaning the perception of occurrence of an erection, or more accurately, the excitatory response of the genitals
In fact, the subjective perception of the excitatory response of the genitals does not always correspond simultaneously with the actual genital response, such as an increase in penile volume and rigidity (3, 4) For instance, a study by Rieger (5) reported that some men without erectile dysfunction, when asked to perform mathematical calculations during visual erotic stimulation, experienced a reduction in erection but not in self-reported arousal In other situations, the opposite was found: a genital excitatory response, such as an erection, occurred without a subjective state of arousal This is what happens during nocturnal erections in the REM phase of sleep, which are not always associated with erotic dreams or arousal states (6, 7)
Another example where erection does not lead to subjective arousal and its perception is the phenomenon of priapism, which is characterized by an erection without arousal (8) The same phenomenon can be observed during cavernous pharmacological infusion with papaverine, as occurred during Virag's experiment, in which an erection was obtained under general anesthesia without the subject being aroused or aware of it (9)
This lack of simultaneous correspondence, at least in men, may be due to the fact that the perception of the genital response after visual or psycho-sensory stimulation may not be a simple perception of erection, but rather a consequence of the involvement of another structure, which, according to my hypothesis, is the pelvic floor
There are three clues that have led me to hypothesize that the first response to psycho-sensory stimulation, understood as all visual or mental erotic stimuli, could involve an initial response mediated through pelvic floor contraction, making the male subject aware of the genital excitatory response
The first clue arises from the negative consequences on sexuality following radical prostatectomy for cancer This “ experimental model” , which I place in quotation marks out of respect for the patients who have undergone cancer surgery, highlights two phenomena that have so far only been described as contemporaneous but not yet proven to be in a cause-andeffect relationship: damage to the pelvic floor (10) with static alterations due to vesicourethral anastomosis (11) and a decrease in libido by 50% (12), even when erection is restored postoperatively (13)
The second clue that supports my hypothesis is based on studies by Shafik published in 2001 (14), in which the author demonstrated that both the bladder and rectum exhibit an excitatory reflex involving the levator ani muscle and an inhibitory reflex involving the pubo-rectalis muscle, which regulates the perception of urgency and the mechanism of evacuation and urination This study raises the question: if the bladder, rectum, and penis share common nerve bundles and blood vessels, and if these structures are all traversed by the pelvic floor muscles, why should these same muscles not play a similar role in male arousal, not just in erection and ejaculation, as has been demonstrated so far? (15-17)
The third piece of evidence for this new theory on male sexual response is based on research conducted by La Pera (18) and colleagues, in which 270 subjects, responding to a questionnaire that evoked an erotic image, highlighted a correlation between initial arousal and pelvic floor contraction
The purpose of this work is to propose a new pathophysiology of the male sexual response, integrating the model of Masters
and Johnson, which includes excitement, plateau, orgasm, and resolution In this new hypothesis, their model is complemented by a fifth step represented by the psycho-sensory pelvic reflex, mediated by the contraction of the pelvic floor
Pathophysiology of the male sexual response
To illustrate the proposal of this new model, which integrates the pioneering work of Masters and Johnson, we analyze two aspects that have not been considered until now and which, in our opinion, although not yet demonstrated, could be fundamental to the first male sexual response: the psycho-sensory sexual reflex and the perception of the male genital response
The psycho-sensory sexual pelvic reflex
The hypothesis proposed here is based on the reflexive involvement of the pelvic floor in response to psycho-sensory erotic stimulation This reflex response, in my view, consists in the contraction of the pelvic floor, which makes the subject aware of the excitatory response According to this new model, when a man receives visual or imagined erotic stimulation, a reflexive contraction of the pelvic floor occurs This reflex not only causes the contraction of the levator ani muscle, but also triggers the contraction of the bulbourethral, bulbocavernosus, and ischiocavernosus muscles
In this proposal, following psycho-sensory stimulation, the contraction of these muscles results in the compression of the intra-abdominal part of the penis, increasing the pressure within the corpus spongiosum and corpus cavernosum
Furthermore, this increase in pressure within the corpus spongiosum of the urethra is transmitted to the glans and its receptors, resulting in the perception of the genital response According to this hypothesis, the psychophysiological reflex is the missing link – the mechanism – in the sequence of events that leads from visual or imagined erotic stimulation to a genital response and its perception
The perception of the male genital response
If the sequence of events is as described above, we should ask ourselves how the perception of the sensation of the first genital excitatory response occurs and how we should define this initial genital excitatory response
Continuing with this hypothesis, the perception of this genital excitatory response – the process through which we interpret, organize, and give meaning to the sensations originating from the genitals – occurs because the pelvic floor muscles, including the bulbourethral, bulbocavernosus, and ischiocavernosus muscles, reflexively contract in response to a psycho sensorial stimulus, causing a “compression” of the internal part of the penis, consisting of the corpus cavernosum and the corpus spongiosum of the urethra The contraction of these muscles increases pressure within the penis, corpus cavernosum and corpus spongiosum of the urethra, and is transmitted to the receptors of the glans This contraction and increase in pressure inside the penis determine the perception of the genital response
From this psycho-physiological mechanism, we can deduce how to define the first genital excitatory response, which should therefore be defined as the contraction of the pelvic floor muscles and increase in pressure within the corpus cavernosum and corpus spongiosum of the urethra in response to psycho-sensory erotic stimulation
DISCUSSION
Once the perception of the contraction of the pelvic floor and increase in pressure within the corpus cavernosum and corpus spongiosum of the urethra becomes conscious, there is a need to engage in sex and seek mechanical genital stimulation that leads to orgasm
This need constitutes an “Ejaculatory urgency ” , similar to the sensation experienced when the bladder is full and there is an urgency to find an appropriate place to void the bladder and relieve the sensation of urgency The antagonist of this psycho-sensory sexual pelvic reflex could be the pubo-rectalis muscle, which, similar to how it inhibits contraction for urination and defecation, inhibits the sensation of urgency to evacuate (14)
When such a “need” becomes conscious through this sensation, the brain decides case-by-case how to proceed to find a solution to satisfy this need, using the tools at its disposal
The contraction of the pelvic floor, generating the sensation of genital response, would signal the need to "take action" and engage in behaviors that enable mechanical stimulation of the genitals – in other words, to have sex The perception of the contraction of the pelvic floor and the increase in pressure within the corpus cavernosum and corpus spongiosum initiates a series of behaviors aimed at achieving mechanical stimulation of the genitals that lead to ejaculation
This is a “cascade” of events that begins with the psycho-sensory pelvic reflex and ends with ejaculation The perception of this contraction, due to the psycho-sensory pelvic reflex, as reconstructed here, could be one of the triggers or one of the possible motivations that initiates the search for sexual activity
The new
five-phase
model of male sexual response
The sequence of events describing the new model of the male sexual response consists of five phases At present, it is not known how much each of these phases may overlap with the previous one and continue subsequently after the end of its action According to this proposal, the classic Masters and Johnson model is supplemented by a preliminary phase called the phase of reflex and perception
Phase of the psycho-sensory sexual pelvic reflex and its perception
The phase of reflex and perception that precedes the four stages of the male sexual response described by Masters and Johnson consists of the following six moments:
Giuseppe La Pera
1 Trigger phase: The subject has a thought or sees an erotic image capable of eliciting a genital excitatory response
2 Phase of the psycho-sensory pelvic reflex: In this phase, the erotic stimulus triggers a neurological reflex that leads to an involuntary contraction of the pelvic floor, particularly the levator ani, bulbourethral, bulbocavernosus, and ischiocavernosus muscles
3 Compression phase: The intra-abdominal part of the penis and urethra, where the bulbourethral, bulbocavernosus, and ischiocavernosus muscles insert, are compressed by the contraction of these muscles
4 Pressure increase phase: Following the compression in the previous phase, an increase in pressure occurs within the corpus cavernosum and corpus spongiosum
5 Perception phase: The increase in pressure in the corpus cavernosum and corpus spongiosum of the urethra, the stimulation of the receptors of the glans, and the contraction of the pelvic floor are consciously perceived
6 Trigger phase: Once it is perceived that a genital response has occurred, the subject begins to feel the need to have sex and engages in behaviors aimed at achieving the mechanical stimulation necessary for a full erection, to then progress to the plateau phase, and subsequently to orgasm with ejaculation
CONCLUSIONS
In this article, a new paradigm for the male sexual response is proposed and hypothesized, integrating a fifth step into the Masters and Johnson model This new model consists of the psycho-sensory sexual pelvic reflex and perception of pelvic floor contraction, which triggers the “cascade” of the subsequent four phases of the male sexual response: excitement, plateau, orgasm, and resolution In this model, the subjective perception of pelvic floor contraction could be the trigger that initiates the motivation to seek mechanical genital stimulation to achieve ejaculation
ACKNOWLEDGMENTS
I thank Martha B Scherr for her help in translating the text into English
REFERENCES
1 Masters WH, Johnson VE Human Sexual Response Little, Brown and Company, New York, 1966
2 Kaplan HS The New Sex Therapy Brunner/Mazel, 1974
3 Janssen E Sexual arousal in men: A review and conceptual analysis Hormones and Behavior 2011; 59:708-716
4 Van Lankveld J, van den Hout MA Increasing neutral distraction inhibits genital but not subjective sexual arousal of sexually functional and dysfunctional men Archives of Sexual Behavior 2004; 33:549-558
5 Rieger G, Chivers ML, Bailey JM Sexual arousal patterns of bisexual men Psychological Science 2005; 16:579-584
6 Bach AK, Brown TA, Barlow DH The effects of false negative feedback on efficacy expectancies and sexual arousal in sexually functional males Behavior Therapy 1999; 30:79-95
7 Janssen E, Everaerd W Determinants of male sexual arousal Annual Review of Sex Research 1993; 4:211-246
8 Silberman M, Stormont G, Leslie SW, Hu EW Priapism StatPearls [Internet] Treasure Island (FL): StatPearls Publishing 2023; 30:1-11
9 Porst H, Lewis R, Virag R, Goldstein I A comprehensive history of injection therapy for erectile dysfunction, 1982-2023 Sexual Medicine Reviews 2024; 12:419-433
10 Cui J, Guo H, Li Y, Chen S, et al Pelvic floor reconstruction after radical prostatectomy: A systematic review and meta-analysis of different surgical techniques Scientific Reports 2107; 7:2737
11 Kadono Y, Nohara T, Kawaguchi S, et al Impact of pelvic anatomical changes caused by radical prostatectomy Cancers (Basel) 2022;14:3050
12 Messaoudi R, Menard J, Parquet H, et al Modification of sexual desire and orgasm after radical prostatectomy for prostate cancer Progrès en Urologie 2011; 21:48-52
13 Dalkin BL, Christopher BA Potent men undergoing radical prostatectomy: A prospective study measuring sexual health outcomes and the impact of erectile dysfunction treatments Urologic Oncology 2008; 26:281-285
14 Shafik A Effect of pelvic floor muscles contraction on vesical and rectal function with identification of puborectalis-rectovesical inhibitory reflex and levator rectovesical excitatory reflex World Journal of Urology 2001;19:278-284
15 Shafik A Response of the urethral and intracorporeal pressures to cavernosus muscle stimulation: role of the muscles in erection and ejaculation Urology 1995; 46:85-88
16 Gerstenberg TC, Levin RJ, Wagner G Erection and ejaculation in man: Assessment of the electromyographic activity of the bulbocavernosus and ischiocavernosus muscles British Journal of Urology 1990; 65:395-402
17 de Groat WC, Booth AM Physiology of male sexual function Annals of Internal Medicine 1980; 92:329-331
18 La Pera G, Anticoli S, Mangiardi M, Livi S Pelvic floor contraction as an initial response to psycho-sensory sexual stimulation in men and a trigger for male sexual behaviour Arch Ital Urol Androl 2024; 96:13119
Correspondence
Giuseppe La Pera MD (Corrisponding Author) – dr giuseppelapera@gmail com
Via delle Mura Gianicolensi 67 c/o UPMC Salvator Mundi International Hospital, Rome, Italy
Conflict of interest: The authors declare no potential conflict of interest
INSTRUCTIONS TO AUTHORS – ARCHIVIO ITALIANO
OPEN ACCESS
Open access publishing does have its costs. Information regarding authors’ payment are not made available to editors and reviewers ensuring that they cannot be influenced in their selection of papers for publication by payment conditions or limitations. The Article Processing Charge for publication in this journal is EUR 300,00 (plus VAT, if applicable).
Our fees cover the costs of peer review, copyediting, publication, different format of publication (HTML, PDF), inclusion in many Open Access databases.
All bank charges shall be borne by the payer. Please note that our fees do not include taxes (VAT):
- Private or public ITALIAN customers (individuals, universities, hospitals, other organizations) must ALWAYS add VAT (IVA) at standard rate (4%);
- European Union PRIVATE customers must add the standard rate of their own country VAT tax;
- European Union private/public ORGANIZATIONS (universities, hospitals, others with regular VAT number) should not add any taxes at standard rate, provided that they indicate their VAT number;
- Outside the European Union, individuals and organizations should not add any taxes at standard rate.
Important: Authors are NOT required to pay at the moment of submission. If the paper is accepted, the Managing Editor of Open Access Edition will guide the Authors through the payment procedure. No article will be published before waiver or payment.
According to the United Nations list of Least Developed Countries (LCDs) available from: http://www.un.org/en/development/desa/policy/cdp/ldc2/ldc_countries.shtml Authors coming from those countries are entitled to ask for a discount.
A “Formal Request for discount” has to be forwarded to the Managing Editor of Open Access Edition, after receiving the acceptance letter. The Editorial Committee will then evaluate the merits of each individual case.
Any other informal request (such as comments at the moment of submission, or made in the covering letter of the revised version) will not be taken into consideration.
FAST-TRACK PEER REVIEW
All papers published in Archivio Italiano di Urologia e Andrologia (AIUA) are peer reviewed. Fast-track peer review (4 weeks) can be obtained by supplementary fee of € 488 (VAT included).
METHODS OF PAYMENT Authors can pay their fees by: PayPal is the most recommended and secure payment system. It enables you to pay getting your payment receipt immediately and without sharing your financial information. Other methods of payment are:
Bank transfer
BANK NAME: Banca Popolare di Sondrio, Branch #1, Strada Nuova 75, I-27100 Pavia, Italy
ACCOUNT HOLDER: PAGEPress Srl
BIC/SWIFT: POSOIT22
IBAN: IT85Y0569611301000005086X83
Credit Card The credit card form to be filled and returned either via e-mail or via fax is available for download here.
Check sent by surface mail Checks must be made payable to PAGEPress Srl and must be sent to our full postal address: PAGEPress Publications, via A. Cavagna Sangiuliani 5, 27100 Pavia, Italy.
Note: In any method of payment you choose, kindly specify: 1. journal name; 2. paper ID number; 3. first author.
IMPORTANT TO KNOW
REGISTERED DRUGS, DIET SUPPLEMENTS, NUTRACEUTICALS, MEDICAL DEVICES
Authors of papers that contain references to registered drugs, diet supplements, nutraceuticals and medical devices are requested to buy a minimum amount of 100 reprints at a cost of € 1.500 (1 to 4 pages) or € 2.000 (5 to 8 pages). Prices for the purchase of number of reprints greater than 100 can be negotiated with Edizioni Scripta Manent At present, Edizioni Scripta Manent let everyone to read, print and download papers from website, but retains copyright for republishing and distribution rights for commercial purpose.
TRANSLATION
Translation of manuscripts in Italian language is offered on payment.
Translation and reprints can be requested to Edizioni Scripta Manent by e-mail to info@edizioniscriptamanent.eu
AUTHORS’ RESPONSIBILITIES
Manuscripts are accepted with the understanding that they have not been published or submitted for publication in any other journal.
Authors must submit the results of clinical and experimental studies conducted according to the Helsinki Declaration on clinical research and to the Ethical Code on animal research set forth by WHO (WHO Chronicle 1985; 39:51). The Authors must obtain permission to reproduce figures, tables and text from previously published material. Written permission must be obtained from the original copyright holder (generally the Publisher).
MANUSCRIPT PRESENTATION
Authors must submit their manuscripts (MAC and WINDOWS Microsoft Word are accepted) after registration and login to the link: http://www.aiua.it. Surface or e-mail submission are not accepted.
Manuscripts must be written in English language in accordance with the “Uniform Requirements for Manuscripts submitted to biomedical journals” defined by The International Committee of Medical Journal Editors (http://www.ICMJE.org). Manuscripts
in Italian language can be published after translation (expenses will be charged to the Authors). Manuscripts should be typed double spaced with wide margins. They must be subdivided into the following sections:
TITLE PAGE
It must contain: a) title; b) a short (no more than 40 characters) running head title; c) first, middle and last name of each Author without abbreviations; d) University or Hospital, and Department of each Author; e) last name, address and e-mail of all the Authors; f) corresponding Author; g) acknowledgement of conflict of interest and financial support.
SUMMARY
Authors must submit a summary (300 words, 2000 characters) divided by subheadings as follows: Objective(s), Material and method(s), Result(s), Conclusion(s). After the summary, three to ten key words must appear, taken from the standard Index Medicus terminology.
TEXT
For original articles concerning experimental or clinical studies, the following standard scheme must be followed: Summary - Key Words - Introduction - Material and Methods - Results - Discussion - Conclusions - References - Tables - Legends - Figures.
Case Report should be divided into: Summary - Introduction (optional) - Case report(s) - Conclusions - References
Supplementary Materials can be added for online publication.
SIZE OF MANUSCRIPTS
Literature reviews, Editorials and Original articles should not exceed 3500 words with 3-5 figures or tables, and no more than 30 references.
Case reports, Notes on surgical technique, and Letters to the editors should not exceed 1000 words (summary included) with only one table or figure, and no more than three references. No more than five authors are permitted.
REFERENCES
References must be sorted in order of quotation and numbered with arabic digits between parentheses. Only the references quoted in the text can be listed. Unpublished studies cannot be quoted, however articles “in press” can be listed with the proper indication of the journal title, year and possibly volume. References must be listed as follows.
JOURNAL ARTICLES
All Authors if there are six or fewer, otherwise the first three, followed by “et al.”. Complete names for Work Groups or Committees. Complete title in the original language. Title of the journal following Index Medicus rules. Year of publication; Volume number: First page. Example: Starzl T, Iwatsuki S, Shaw BW, et al. Left hepatic trisegmentectomy Surg Gynecol Obstet. 1982; 155:21.
BOOKS
Authors - Complete title in the original language. Edition number (if later than the first). City of publication: Publisher, Year of publication. Example: Bergel DIA. Cardiovascular dynamics. 2nd ed. London: Aca de mic Press Inc., 1974.
BOOK CHAPTERS
Authors of the chapters - Complete chapter title. In: Book Editor, complete Book Title, Edition number. City of publication: Publisher, Publication year: first page of chapter in the book. Example: Sagawa K. The use of central theory and system analysis. In: Bergel DH (Ed), Cardiovascular dynamics. 2nd ed. London: Aca demic Press Inc., 1964; 115.
TABLES
Tables must be numbered in Arabic digits and referred to in the text by progressive numbers. Every table must be accompanied by a brief title. The meaning of any abbreviations must be explained at the bottom of the table itself.
FIGURES
(Graphics, algorithms, photographs, drawings). Figures must be numbered and quoted in the text by number. The meaning of symbols or abbreviations must be indicated. Histology photograph legends must include the enlargement ratio and the staining method. Legends must be collected in one or more separate pages.
• Do not include any illustrations as part of your text file. • Do not prepare any figures in Word as they are not workable. • Line illustrations must be submitted at 600 DPI.
• Halftones and color photos should be submitted at a minimum of 300 DPI. • Power Point files cannot be uploaded. • If possible please avoid transmitting electronic files in JPEG format or save the JPEG at the highest quality available • PDF files may be uploaded.
MANUSCRIPT REVIEW
Manuscripts are evaluated by the Editorial Board and/or by two referees designated by the Editors. The Authors are informed in a time as short as possible on whether the paper has been accepted, rejected or if a revision is deemed necessary. The Editors reserve the right to make editorial and literary corrections with the goal of making the article clearer or more concise, without altering its contents. Submission of a manuscript implies acceptation of all above rules.
PROOFS
Authors are responsible for ensuring that all manuscripts are accurately typed before final submission. Galley proofs will be sent to the first Author. Proofs should be returned within seven days from receipt.
Salutepertutti.it è un progetto indipendente. Abbonati per i tuoi pazienti in sala d’aspetto.