12531 The impact of surgical technique on ver y ear ly functional outcomes after radical prostatectomy
Mladen Stankovic
12496 The association of anatomical renal mass complexity with surgical approach, Hb drop, and the rate of blood transfusion
Shakhawan Hama Amin Said, Lusan Abdulhameed Arkawazi Saiwan, Mzhda Sahib Jaafar, Nadhm Kanabi Majeed, Rawa Bapir, Ismaeel Aghaways, Abdullah A Qadir, Berun A Abdalla, Ayoob Asaad Mohammed Abid, Fahmi H Kakamad
12643 “Bottoms-up” minimally-invasive approach to inguinal lymph node dissection for penile cancer management. A single-center comparative study versus open approach and review
Vlad Horia Schitcu, Vlad Cristian Munteanu, Mihnea Bogdan Borz, Ion Cojocaru, Sergiu Vasile Labo, Andrei-Ionu ̦ t Ti ̦ se
12856 Programmed death-ligand expression and lymph node involvement in penile squamous cell carcinoma
12617 Efficacy of Flexible ureterorenoscopy in treating multiple renal stones: A cohor t study
Sarwar Noori Mahmood, Rawa Bapir, Khoshbin Faeq Mustafa, Ahmed Mohammed Abdalqadir, Shakhawan Hama Amin Said, Nali H Hama, Hiwa O Abdullah, Berun A Abdalla, Fahmi H Kakamad
12374 Adverse events related to laser fibers and laser machines during ureteroscopy and stone lithotripsy: Insights from an updated 10-year analysis of the US MAUDE database
Patrick Juliebø-Jones, Mathias Sørstrand Æsøy, Christian Beisland, Vincent De Coninck, Etienne Xavier Keller, Lazaros Tzelves, Peder Gjengstø, Christian Arvei Moen, Bhaskar K Somani, Øyvind Ulvik
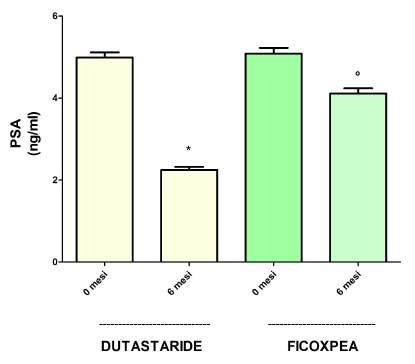
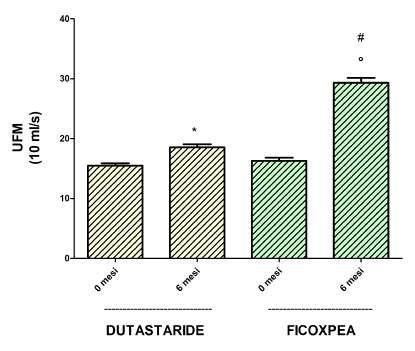
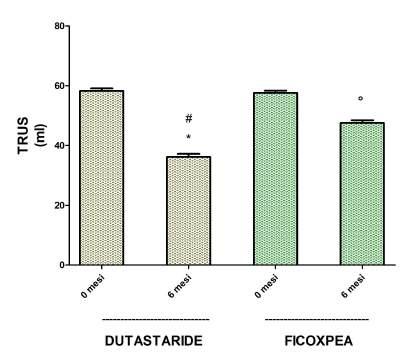
12869 Prospective obser vational study on the efficacy and tolerability of a complex of phytochemicals versus dutasteride in the treatment of Lower Urinar y Tract Symptomps (LUTS) due to Benign Prostatic Hyperplasia (BPH)
Giuseppe Saitta, Franco A Mantovani, Benedetto Calabrese, Camilla Aliboni, Giuseppe Di Paola, Attilio L Meazza, Mauro Seveso
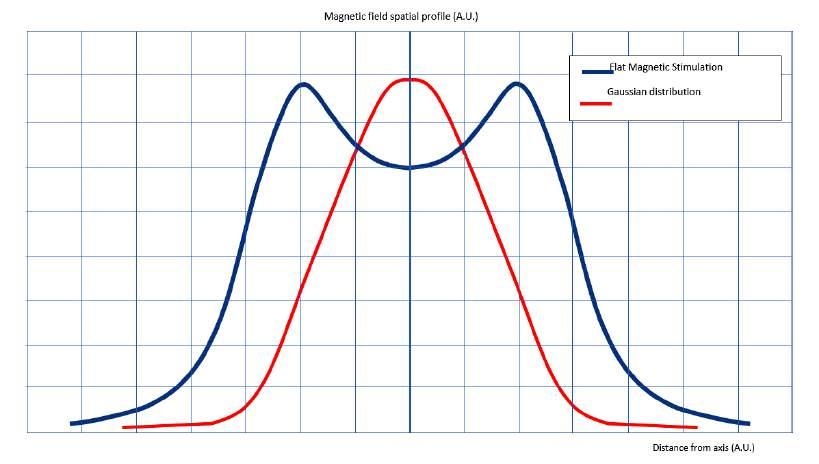
12623 Electromagnetic stimulation to reduce the hyper tonia of the pelvic floor muscles and improve chronic pelvic pain in women
Nicola Mondaini, Mauro Gacci, Tommaso Cai, Francesco Lotti, Vincenzo Li Marzi, Fabio Crocerossa, Francesco Cantiello, Sara Tanguenza, Alessandra Comito, Irene Fusco, Beatrice Marina Pennati, Rocco Damiano
12530 Utilizing ar tificial neural network system to predict the residual valve after endoscopic posterior urethral valve ablation
Mehdi Shirazi, Zahra Jahanabadi, Faisal Ahmed, Davood Goodarzi, Alimohammad Keshtvarz Hesam Abadi, Mohammad Reza Askarpour, Sania Shirazi
12661 Single-component ar tificial urinar y sphincter : Outcomes from one centre in Por tugal
João Aragão Vital, Miguel Marques Monteiro, Bernardo Lobão Teixeira, Gonc ̧ alo Grilo Mendes, Alexandra Rocha, Mariana Madanelo, Sofia Mesquita, Nuno Vinagre, Beatriz Oliveira, Martinha Magalhães, Ana Isabel Lopes, Carlos Ferreira, Paulo Príncipe, Avelino Fraga
12704 Functional outcome of the one-stage scrotal tunnel + ventral inver ted V incision + inver ted Y anastomosis technique to treat penile paraffinoma: A single center retrospective study
Muhammad Asykar Palinrungi, Syakri Syahrir, Syarif, Andhini L R Palinrungi, Muhammad Faruk
12899 Penoscrotal transposition: Long-ter m outcome in 29 patients
Dolev Perez, Stanislav Kocherov, Gaudat Jaber, Galiya Raisin, Boris Chertin
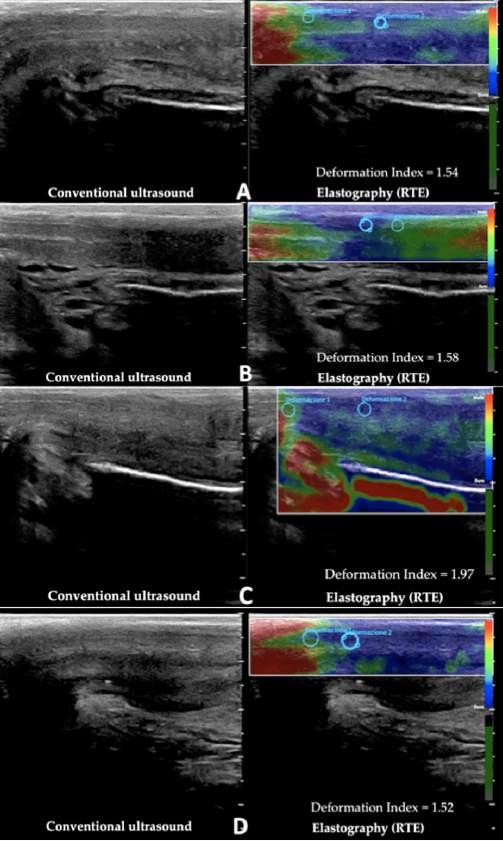
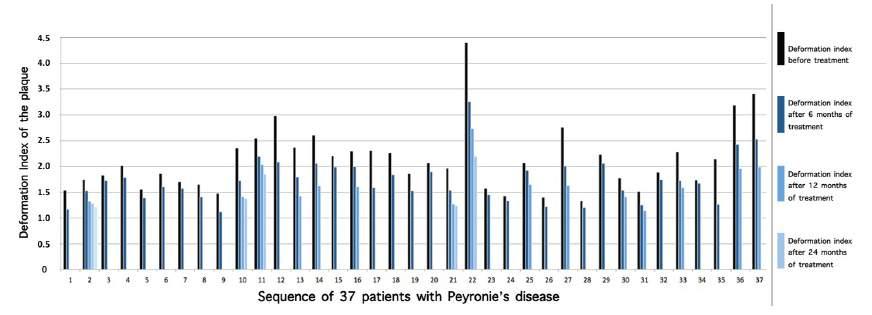
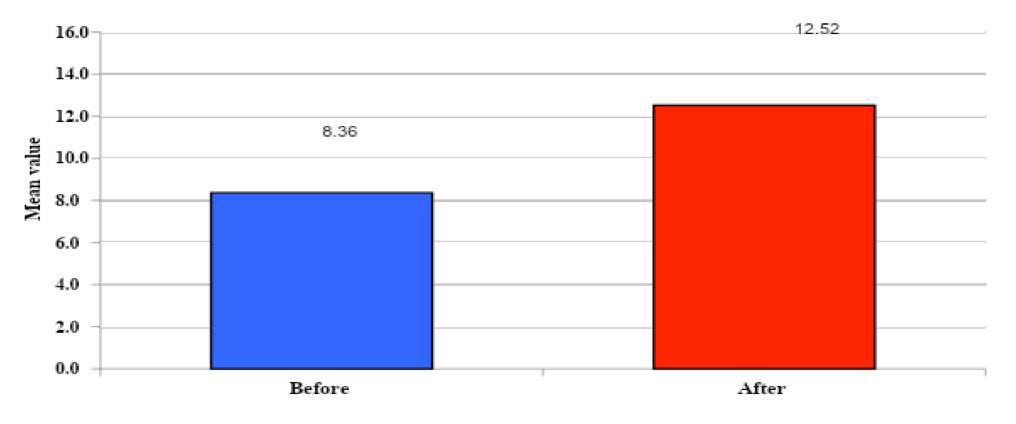
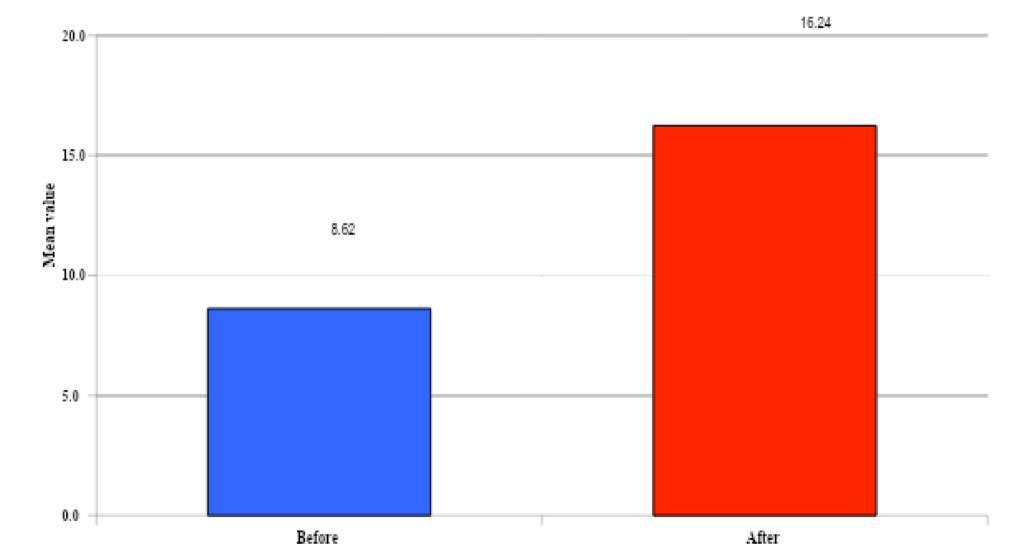
12690 Combining ultrasound and elastography for the detection of a non-palpable, non-sonographically visualized Peyronie's plaques. Our experience
Gianni Paulis, Giovanni De Giorgio, Andrea Paulis
12545 Can ser um 17-hydroxy progesterone predict an improvement in semen parameters following micro-varicocelectomy?: A prospective study
Mohamed Wael Ragab, Mohamed Abbas, Tarek Ramzy, Sameh Fayek GamalEl Din, Mohamed Yousry Elamir, Mohammad H Alkandari, Abdullah Salem Alshammari, Mohamed Ragab Shehata, Ashraf Zeidan
continued on page III
EDITORIAL BOARD
EDITOR IN CHIEF
Alberto Trinchieri (Milan, Italy)
ASSOCIATE EDITORS
Emanuele Montanari, Department of Urology, IRCCS Foundation Ca’ Granda Ospedale Maggiore Policlinico, University of Milan, Italy – Gianpaolo Perletti, Department of Biotechnology and Life Sciences, Section of Medical and Surgical Sciences, University of Insubria, Varese, Italy; Department of Human Structure and Repair, Ghent University, Ghent, Belgium - Angelo Porreca, Robotic Urology and Mini Invasive Urologic Surgery Unit, Abano Terme Hospital, Abano Terme, Italy
EXECUTIVE EDITORIAL BOARD
Alessandro Antonelli, Department of Urology, Azienda Ospedaliera Universitaria Integrata (A O U I ), Verona, Italy - Antonio Celia, Department of Urology, San Bassiano Hospital, Bassano del Grappa, Italy - Luca Cindolo, Department of Urology, Villa Stuart Hospital, Rome, Italy - Andrea Minervini, Department of Urology, University of Florence, Unit of Oncologic Minimally-Invasive Urology and Andrology, Careggi Hospital, Florence, Italy - Bernardo Rocco, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy - Riccardo Schiavina, Department of Urology, University of Bologna, Bologna, Italy
ADVISORY EDITORIAL BOARD
Pier Francesco Bassi, Urology Unit, A Gemelli Hospital, Catholic University of Rome, Italy – Francesca Boccafoschi, Health Sciences Department, University of Piemonte Orientale in Novara, Italy – Alberto Bossi, Department of Radiotherapy, Gustave Roussy Institute, Villejuif, France –Tommaso Cai, S Chiara Hospital, Trento, Italy –Paolo Caione, Department of Nephrology-Urology, Bambino Gesù Pediatric Hospital, Rome, Italy – Luca Carmignani, Urology Unit, San Donato Hospital, Milan, Italy –Liang Cheng, Department of Urology, Indiana University School of Medicine, Indianapolis, IN; Department of Pathology and Laboratory Medicine, Indiana University School of Medicine, Indianapolis, IN – Giovanni Colpi, Retired Andrologist, Milan, Italy – Giovanni Corona, Department of Urology, University of Florence, Careggi Hospital, Florence, Italy – Antonella Giannantoni, Department of Surgical and Biomedical Sciences, University of Perugia, Italy – Paolo Gontero, Department of Surgical Sciences, Molinette Hospital, Turin, Italy – Steven Joniau, Organ Systems, Department of Development and Regeneration, KU Leuven, Belgium – Frank Keeley, Bristol Urological Institute, Southmead Hospital, Bristol UK – Laurence Klotz, Division of Urology, Department of Surgery, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, Ontario, Canada – Börje Ljungberg, Urology and Andrology Unit, Department of Surgical and Perioperative Sciences, Umeå University, Umeå, Sweden –Nicola Mondaini, Uro-Andrology Unit, Santa Maria Annunziata Hospital, Florence, Italy – Gordon Muir, Department of Urology, King's College Hospital, London, UK –Giovanni Muto, Urology Unit, Bio-Medical Campus University, Turin, Italy – Anup Patel, Department of Urology, St Mary's Hospital, Imperial Healthcare NHS Trust, London, UK – Glenn Preminger, Division of Urologic Surgery, Duke University Medical Center, Durham, NC, USA – David Ralph, St. Peter's Andrology Centre and Institute of Urology, London, UK – Allen Rodgers, Department of Chemistry, University of Cape Town, Cape Town, South Africa – Francisco Sampaio, Urogenital Research Unit, State University of Rio de Janeiro, Rio de Janeiro, RJ, Brazil – Kemal Sarica, Department of Urology, Kafkas University Medical School, Kars, Turkey – Luigi Schips, Department of Urology, San Pio da Pietrelcina Hospital, Vasto, Italy – Hartwig Schwaibold, Bristol Urological Institute, Southmead Hospital, Bristol, UK – Alchiede Simonato, Department of Urology, University of Verona, Azienda Ospedaliera Universitaria Integrata, Verona, Italy – Carlo Terrone, Department of Urology, IRCCS S Martino University Hospital, Genova, Italy – Anthony Timoney, Bristol Urological Institute, Southmead Hospital, Bristol, UK – Andrea Tubaro, Urology Unit, Sant’Andrea Hospital, “La Sapienza” University, Rome, Italy – Richard Zigeuner, Department of Urology, Medical University of Graz, Graz, Austria
BOARD OF REVIEWERS
Maida Bada, Department of Urology, S Pio da Pietrelcina Hospital, ASL 2 Abruzzo, Vasto, Italy - Lorenzo Bianchi, Department of Urology, University of Bologna, Bologna, Italy - Mariangela Cerruto, Department of Urology, Azienda Ospedaliera Universitaria Integrata (A O U I ), Verona, Italy - Francesco Chessa, Department of Urology, University of Bologna, Bologna, Italy - Daniele D’Agostino, Robotic Urology and Mini In-
vasive Urologic Surgery Unit, Abano Terme Hospital, Abano Terme, Italy - Fabrizio Di Maida, Department of Urology, University of Florence, Unit of Oncologic Minimally-Invasive Urology and Andrology, Careggi Hospital, Florence, Italy - Antonio Galfano, Urology Unit, Niguarda Hospital, Milan, Italy - Michele Marchioni, Department of Medical, Oral and Biotechnological Sciences, "G. d'Annunzio" University of Chieti, Laboratory of Biostatistics, Chieti, Italy - Andrea Mari, Department of Urology, University of Florence, Unit of Oncologic Minimally-Invasive Urology and Andrology, Careggi Hospital, Florence, Italy - Luigi Napolitano, Unit of Urology, Department of Neurosciences, Reproductive Sciences, and Odontostomatology University of Naples “Federico II”, Naples, Italy - Antonio Porcaro, Department of Urology, Azienda Ospedaliera Universitaria Integrata (A O U I ), Verona, Italy - Stefano Puliatti, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy - Daniele Romagnoli, Robotic Urology and Mini Invasive Urologic Surgery Unit, Abano Terme Hospital, Abano Terme, Italy - Chiara Sighinolf, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy - Tommaso Silvestri, Urology Clinic, Department of Medical, Surgical and Health Science, University of Trieste, Trieste, Italy - Petros Sountoulides, Aristotle University of Thessaloniki, Department of Urology, Thessaloniki, Greece - Alessandro Tafuri, Department of Urology, Vito Fazzi Hospital, Lecce, Italy
SIEUN EDITOR
Pasquale Martino, Department of Emergency and Organ Transplantation-Urology I, University Aldo Moro, Bari, Italy
SIEUN EDITORIAL BOARD
Emanuele Belgrano, Department of Urology, Trieste University Hospital, Trieste, ItalyFrancesco Micali, Department of Urology, Tor Vergata University Hospital, Rome, ItalyMassimo Porena, Urology Unit, Perugia Hospital, Perugia, Italy – Francesco Paolo Selvaggi, Department of Urology, University of Bari, Italy – Carlo Trombetta, Urology Clinic, Cattinara Hospital, Trieste, Italy – Giuseppe Vespasiani, Department of Urology, Tor Vergata University Hospital, Rome, Italy – Guido Virgili, Department of Urology, Tor Vergata University Hospital, Rome, Italy
UrOP EDITOR
Carmelo Boccafoschi, Department of Urology, Città di Alessandria Clinic, Alessandria, Italy
UrOP EDITORIAL BOARD
Renzo Colombo, Department of Urology, San Raffaele Hospital, Milan, Italy – Roberto Giulianelli, Department of Urology, New Villa Claudia, Rome, Italy – Massimo Lazzeri, Department of Urology, Humanitas Research Hospital, Rozzano (Milano), Italy – Angelo Porreca, Department of Urology, Polyclinic Abano Terme, Abano Terme (Padova), Italy –Marcello Scarcia, Department of Urology, "Francesco Miulli" Regional General Hospital, Acquaviva delle Fonti (Bari), Italy – Nazareno Suardi, Department of Urology, San Raffaele Turro, Milano, Italy
GUN EDITOR
Arrigo Francesco Giuseppe Cicero, Medical and Surgical Sciences Department, Sant’Orsola-Malpighi University Hospital, Bologna, Italy
GUN EDITORIAL BOARD
Gianmaria Busetto, Department of Urology, Sapienza University of Rome, Italy –Tommaso Cai, Department of Urology, Santa Chiara Regional Hospital, Trento, Italy –Elisabetta Costantini, Andrology and Urogynecological Clinic, Santa Maria Hospital of Terni, University of Perugia, Terni, Italy – Angelo Antonio Izzo, Department of Pharmacy, University of Naples, Italy – Vittorio Magri, ASST Nord Milano, Milano, Italy – Salvatore Micali, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy – Gianni Paulis, Andrology Center, Villa Benedetta Clinic, Rome, Italy – Francesco Saverio Robustelli della Cuna, University of Pavia, Italy – Giorgio Ivan Russo, Urology Department, University of Catania, Italy – Konstantinos Stamatiou, Urology Department, Tzaneio Hospital, Piraeus, Greece – Annabella Vitalone, Department of Physiology and Pharmacology, Sapienza University of Rome, Rome, Italy
PARTNER CELEBRATING WITH US
Un'opera nuova e completa sul microbiota, il complesso consorzio di batteri che abita il nostro organismo e ne influenza lo status di salute omalattia. Centinaia di illustrazioni a colori, contenuti multimediali, aggiornati in progress continuo ed accessibili mediante QR code. Un Trattato imprescindibile per chi si occupa di salute interpretando i referti sul microbiota.
Costo di copertina €120,00, + spese di spedizione. Per informazioni ed eventuali ordini, scrivere a: info@edizioniscriptamanent.eu
ORIGINAL PAPERS
12595 Effect of radiofrequency electromagnetic waves of mobile phone stations on male fer tility
Tarek Mohamed Gharib, Khaled Almekaty, Ashraf Mohamed Abdel Aal, Ibrahim Abdel-Al, Hazem Deif, Gamal M Hassan, Ahmed Haty, Ahmed Shafiea, Mohamed Elsayed Metwally, Elsayed Elawadey, Mohamed Abdelrahman Alhefnawy
12682 Vasectomy histolog y: Is it still useful?
Anthony Sim, Panagiotis Nikolinakos, Konstantinos Charitopoulos, Ivo Donkov, Samuel Bishara
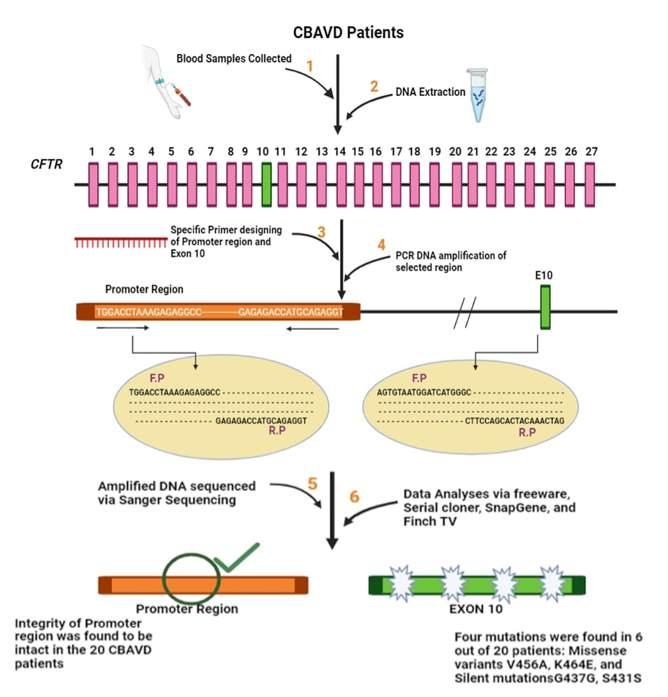
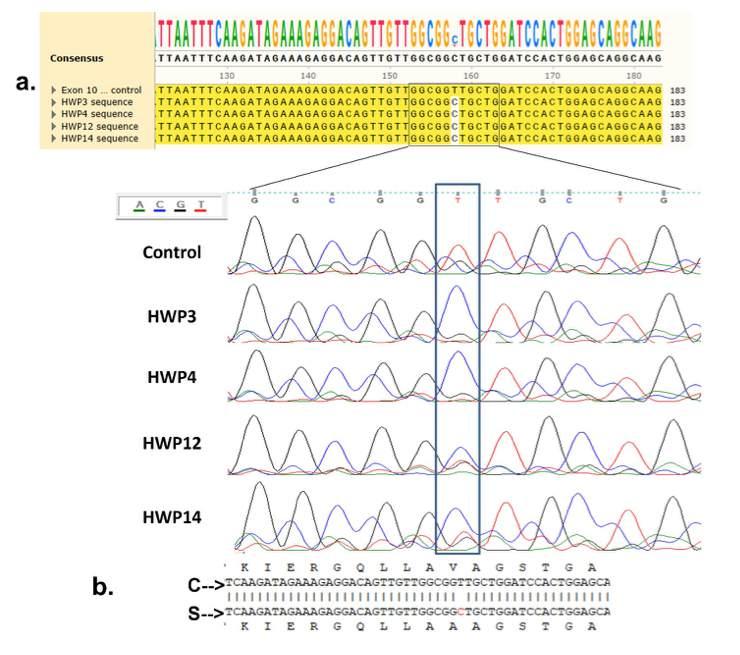
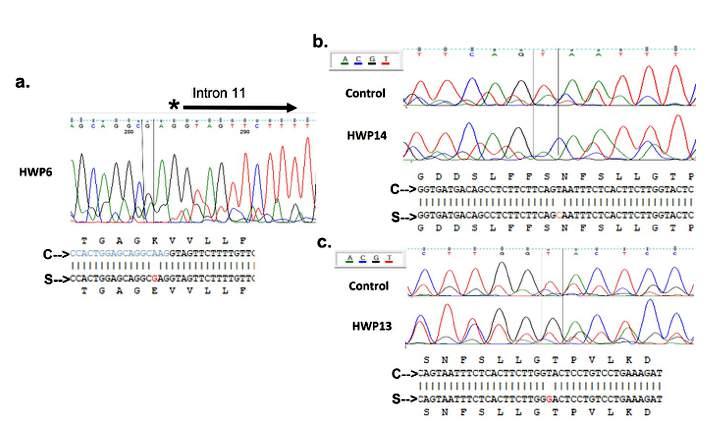
12464 CFTR Exon 10 deleterious mutations in patients with congenital bilateral absence of vas deferens in a cohor t of Pakistani patients
Khush Bakhat, Irsa Mateen, Hina Saif, Kanwal Anwar, Sadaf Sarfraz, Sheza Javaid, Khaleeq-ur-Rehman, Adnan Arshad, Muhammad Mustafa
12613 Kidney transplantation restores sex hor mone profile and improves sexual function in ESRD patients with erectile dysfunction
Hany M El Hennawy, Omar Safar, Abdullah S Al Faifi, Osama Shalkamy, Mahmoud Z El Madawie, Saad Thamer, Muath Almurayyi, Abdullah Mohammed Alqarni, Sami Saleh Amri, Ali Abdullah Hawan, Adel Elatreisy
12620 Sexual intercourse before embr yo transfer in assisted reproductive technolog y might enhance probability of pregnancy:
An obser vational study
Cennikon Pakpahan, Agustinus Agustinus, Ashon Sa’adi, Aucky Hinting, Lia Hinting, Christian Melka Parmanto, Andri Rezano
REVIEWS
12153 Surgical management of obstr ucting ureteral stones during pregnancy: A systematic review of different techniques
Catarina Laranjo-Tinoco, Maria João Oliveira, Ana Sofia Araújo, Andreia Cardoso, Carlos Oliveira, Paulo Mota, João Pimentel Torres
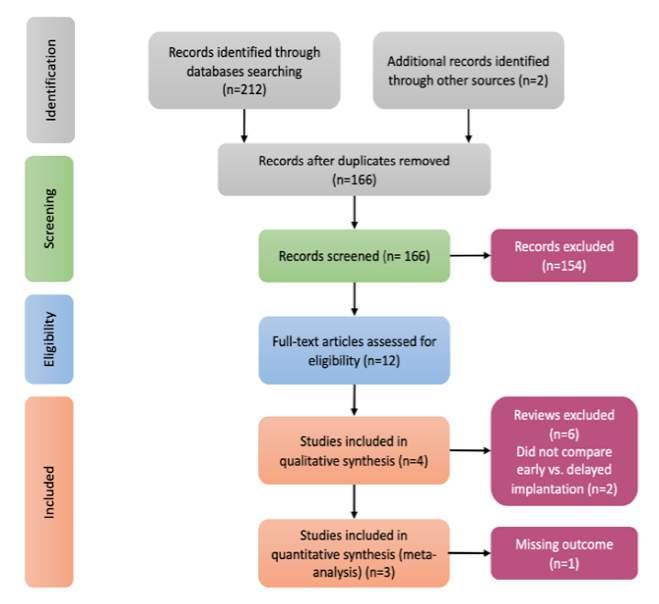
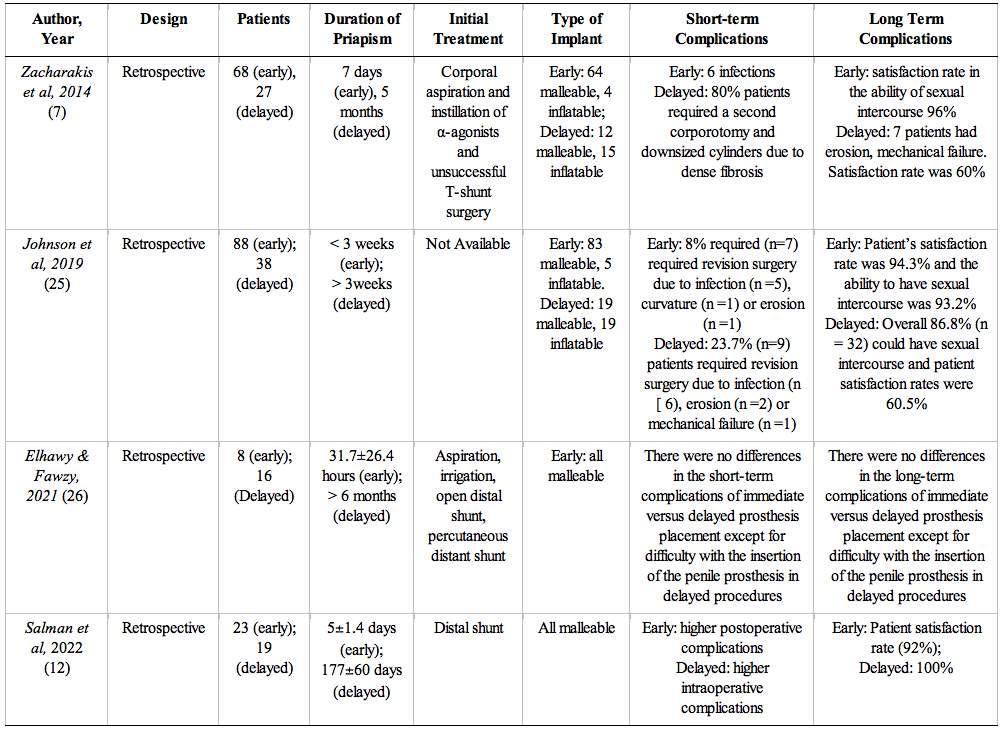
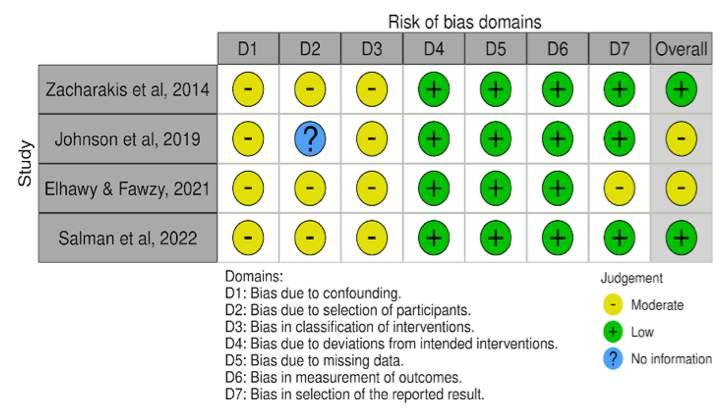
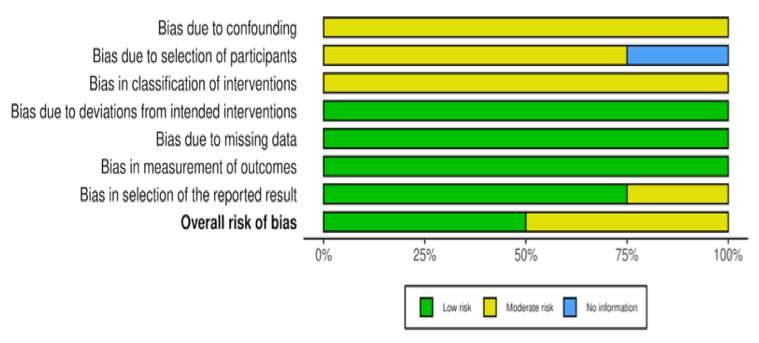
12576 A systematic review and meta-analysis of shor t- and long-ter m complications of ear ly versus delayed penile prosthesis implantation in patients with ischemic priapism
Agustin J Nanda De Niro, Gede Wirya Kusuma Duarsa, Marshal Harvy Wicaksono, Pande Made Wisnu Tirtayasa, Kadek Budi Santosa, I Wayan Yudiana, Nyoman Gede Prayudi
12687 The potential role of intracaver nosal injection of platelet-rich plasma for treating patients with mild to moderate erectile dysfunction: A GRADE-Assessed systematic review and meta-analysis of randomized controlled trials
Niwanda Yogiswara, Fikri Rizaldi, Mohammad Ayodhia Soebadi
12627 Redefining kidney transplantation procedure among adult Lupus nephritis: Expedient review approach and meta-analysis from the last couple of decades
Syah Mirsya Warli, Andi Raga Ginting, Naufal Nandita Firsty, Adrian Joshua Velaro, Stephani Clarissa Sembiring, Dewi Masyithah Darlan, Zaimah Zulkarnaini Tala
LETTERS
12784 Comment to “An unusual ‘linitis plastica’ like breast cancer bladder metastasis”
12837 How much does mitochondrial dysfunction affect male infer tility?
Ernesto Di Mauro, Gianluigi Cacace, Vincenzo Morgera, Roberto La Rocca, Luigi Napolitano, Pietro Saldutto, Vincenzo Maria Altieri
12936 Monkeypox: A new threat for healthcare and urolog y?
Rosario Leonardi, Angelo Cafarelli, Alessandro Calarco, Renzo Colombo, Ottavio de Cobelli, Ferdinando De Marco, Giovanni Ferrari, Giuseppe Ludovico, Stefano Pecoraro, Domenico Tuzzolo, Guglielmo Mantica on behalf of UrOP (Urologi Ospedalita Gestione Privata)
Edizioni Scripta Manent s.n.c.
Via Melchiorre Gioia 41/A - 20124 Milano, Italy
Tel +39 0270608060
e-mail: scriman@tin.it
web: www edizioniscriptamanent eu
Registrazione: Tribunale di Milano n 289 del 21/05/2001
Direttore Responsabile: Pietro Cazzola
Direzione Marketing e PR: Donatella Tedeschi
Comunicazione e Media: Ruben Cazzola
Grafica e Impaginazione: Stefania Cacciaglia
Affari Legali: Avv Loredana Talia (MI)
Ai sensi della legge 675/96 è possibile in qualsiasi momento opporsi all’invio della rivista comunicando per iscritto la propria decisione a: Edizioni Scripta Manent s n c - Via Melchiorre Gioia, 41/A - 20124 Milano
The Publisher is not liable for the opinion expressed by the Authors of the articles and for images used by them
GENERAL INFORMATION
AIMS AND SCOPE
“Archivio Italiano di Urologia e Andrologia” publishes papers dealing with the urological, nephrological and andrological sciences
Original articles on both clinical and research fields, reviews, editorials, case reports, abstracts from papers published elsewhere, book rewiews, congress proceedings can be published
ORIGINAL PAPER
The impact of surgical technique on very early functional outcomes after radical prostatectomy
Mladen Stankovic
Department of Urology, Salem Hospital, Academic Hospital, University of Heidelberg, Heidelberg, Germany
Summary
Introduction: To determine the very early functional as well as oncological outcomes after robot-assisted radical prostatectomy (RARP) and open radical prostatectomy (ORP) at a single institution
Methods: We identified patients who underwent RARP or ORP at our institution between August 2021 and July 2023 The main criterion for surgical technique selection was patient preference. Primary endpoints included anastomosis leakage rate, very early continence rate reported by standardized pad-test, and positive surgical margin rate Furthermore, we analyzed operation time, hospital stay, postoperative analgesia, and complication rates
Results: In this prospective study, we analyzed data from 222 radical prostatectomies (111 RARP and 111 ORP) There were no significant differences in preoperative age, prostate size, and risk stratification among the groups Patients who underwent RARP had lower anastomosis leakage rates (8.1% vs. 18.9%) and slightly lower early continence rates (76 6% vs 78 4%) when compared to patients who underwent ORP. Positive surgical margin rates were similar, and complication rates were also comparable. Operation time was similar for both techniques, but the hospital stay was significantly shorter in the RARP group (6.3 vs. 9.1 days, p = 0.03). The ORP group experienced significantly higher opioid administration postoperatively (p < 0 001)
Conclusions: From a functional and oncological point of view, both techniques are safe and provide excellent outcomes when performed by experienced surgeons Nevertheless, patients are likely to benefit from a shortened hospital stay and reduced postoperative pain after RARP
Prostate cancer is a major health concern and represents the second most commonly diagnosed cancer in men, with an estimated 1 4 million new cases worldwide in 2020; incidence is mainly dependent on age (1) The main goal of radical prostatectomy by any approach is the eradication of cancer while, whenever possible, preserving pelvic organ function (2) The initial transperineal open technique was described more than 100 years ago (3), but it was not until the '80s with the retropubic
approach, which allowed for nerve-sparing, that the procedure gained popularity (4) The retropubic open approach was considered the gold standard for more than two decades, until about 25 years ago when the first laparoscopic radical prostatectomy was performed (5) Further innovations were to follow, and soon after, in 2002, the first reports of robot-assisted procedures started to emerge (6) Since then, the surgical management of prostate cancer has changed drastically Nevertheless, the uptake of robotic systems varies even today from country to country and mostly depends on cost, insurance coverage, and government healthcare approval (7) Still, the market share of RARP is extremely high, with up to 85% in the USA and more than 92% in England (8), which does not leave much room for ORP Considering the immense expansion of robotics in urology, justified questions emerged: should this open surgical technique be performed at all in the robotics era? While RARP is generally accepted to have a shorter hospital stay, there is conflicting evidence regarding functional outcomes and no reliable data on oncological outcomes (9) when the two techniques are compared The main goal of this prospective study was to assess the safety, functional outcomes, and oncological outcomes after ORP and RARP performed by two experienced surgeons at one institution
METHODS
We prospectively analyzed the records of patients who u n d e r w e n t r a d i c a l p ro s t a t e c t
between August 2021 and July 2023
The ethics committee of the State Medical Chamber of Baden-Württemberg approved the project (F-2023-120)
The data were obtained from the patient data management software (CGM Clinical®), in which all relevant data such as preoperative staging, external imaging findings, therapy-relevant parameters, and complication rates are prospectively updated The main criterion for surgical technique selection was patient preference Patients were informed about the available surgical options for their condition during their preoperative consultations with their respective referring urologists During these consultations, patients were provided with comprehensive information about each surgical approach, including its benefits, risks, and potential outcomes Patients were
encouraged to express their preferences based on their individual medical history, personal preferences, and understanding of the procedures We obtained data from 263 patients but excluded 41 to standardize surgical variables, resulting in a final cohort of 222 patients treated by two highly experienced surgeons, each having performed over 2000 procedures in representive technique During ORP, the retropubic access was used, the endopelvic fascia was incised, and the prostate dissected in ascending order The vesicourethral anastomosis was performed using six independent single sutures During RARP, the transperitoneal approach was used, the endopelvic fascia was also incised, but the prostate was dissected in descending order The vesicourethral anastomosis was performed using one running suture with two needles S
approach The catheter was removed directly after the cystography was performed (day 5-6 after RARP and day 7-8 after ORP) given no urinary leakage was evident In case of leakage, the catheter remained for another 1-2 days, depending on the leakage severity Upon catheter removal, patients had one day for pelvic floor muscle exercises, explained and taught by a physical therapist The very early continence was then documented using a standardized pad test This test measures the amount of involuntary urine loss while performing predefined physical activities with a full bladder within 1h The urine pad was weighed before and after the test Full continence was defined as urine loss of 0-10g and one urine pad per day Mild urinary incontinence grade I and grade II were defined as urine loss of 10-25 g and 25-50 g, respectively Urine loss of > 50 g represented severe incontinence
The pathologist graded the tumors according to the Gleason system (10), analyzing the entire prostate including every tumor focus The complication rates were documented using the Clavien-Dindo classification (11) The statistics were performed using SPSS Software v23 The significance level was set at 0 05
RESULTS
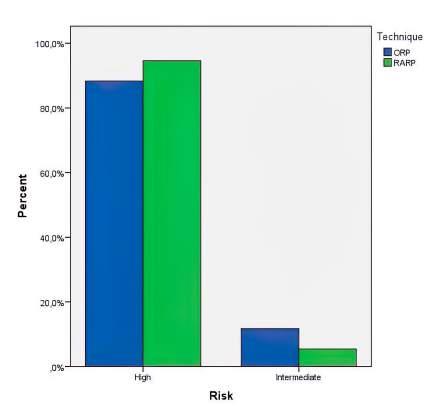
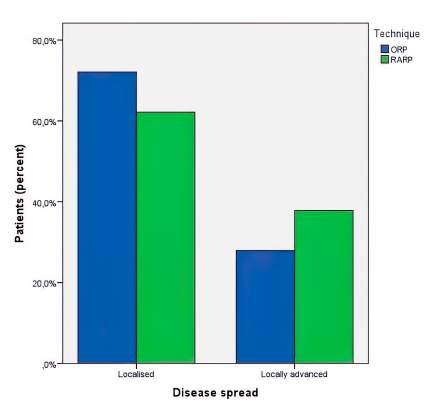
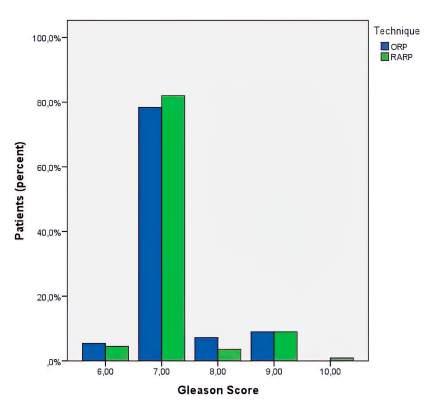
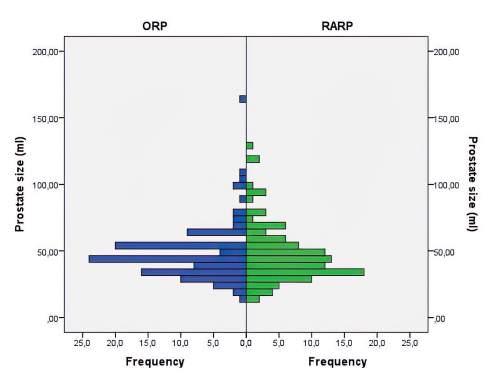
Between August 2021 and July 2023, 222 men with histologically proven prostate cancer underwent radical prostatectomy, of whom 111 underwent ORP and 111 underwent RARP The main patient characteristics are listed in Table 1 There were no significant differences in preoperative age, PSA, and IPSS between the RARP and ORP groups Based on D’Amico's (12) risk classification of prostate cancer, 13 patients (11 7%) had intermediaterisk and 98 patients (88 3%) had high-risk cancer in the ORP group, as represented in Figure 1 In the RARP group, 6 patients (5 4%) and 105 patients (94 6%) had intermediate- and high-risk cancer, respectively Figures 2 and 3 show the disease spread and Gleason score among the groups Most of the patients had a preoperative prostate volume of ≤ 70 ml on the transrectal ultrasound (RARP 84 6% vs ORP 86 1%) as shown in Figure 4 Nerve sparing was able to be performed on 37 8% of patients in the RARP group and on 39 6% of patients in the ORP group Pelvic lymph node dissection (PLND) was performed on all patients The duration of
Table 1.
Patient characteristics
M Stankovic
Figure 1. D’Amico Risk stratification.
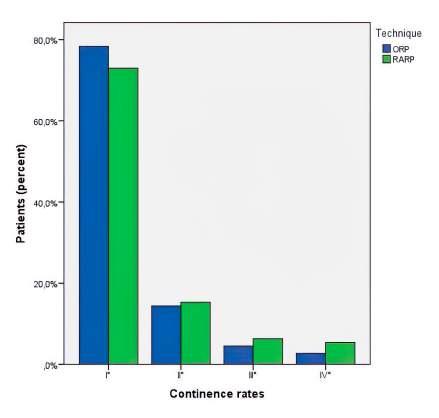
the procedure was similar among the groups, as were the positive surgical margin rates (13 6% RARP vs 15 3% ORP) Patients who underwent RARP had lower anastomosis leakage rates (8 1% vs 18 9%) and slightly lower early full continence rates (76 6% vs 78 4%) when compared to patients who underwent ORP, though the differences were not significant (Figure 5) Nevertheless, the hospital stay was significantly shorter in the RARP group (6 3 vs 9 2 days, p = 0 03) and the ORP group experienced significantly higher opioid administration rates postoperatively (1 vs 81 patients, p < 0 001) Finally, the complication rates were assessed and the vast majority of
patients in both groups (93 7% for RARP and 91% for ORP) did not experience any deviation from the normal postoperative course
DISCUSSION
Despite the paucity of data on anastomosis leakage rates following radical prostatectomy due to many institutions no longer performing contrast cystography, our department remains one of the few that continues this practice Additionally, we have consistently employed a standardized pad test for the past two decades This allows us to confidently present our radiologically obtained leakage
Figure 2. Diasease spread
Figure 4. Distribution of prostate size among groups
Figure 3. Distribution of Gleason Score among groups
Figure 5. Early continence rates based on standardized Pad-Test
results as a reliable measure Contrary to a prominent meta-analysis suggesting superior early functional outcomes for RARP compared to ORP (13), our research did not corroborate this We discovered no significant discrepancies regarding the early continence rate between the two procedures Continence is typically evaluated 12 months post-surgery, with average late continence rates generally being around 80% (14, 15) However, our findings demonstrate exceptionally high early continence rates upon catheter removal of 76 6% for RARP and 78 4% for ORP (16) Furthermore, our severe early incontinence rates barely reached 6% for both techniques, markedly lower than the average 15% cited in existing literature (17, 18) Mirroring another meta-analysis (19), our study detected no significant divergence in positive surgical margin rates between the two techniques Notably, surgical margin status is a crucial prognostic indicator for biochemical recurrence (20), and positive surgical margin rates can fluctuate considerably, from 7% to 44%, depending on the surgeon's experience (2123) Regardless of factors such as patient and tumour characteristics and the size of lymph node packets removed, which influence the number of lymph nodes reported in histology (24, 25), our study found an insignificant difference in the number of lymph nodes removed per procedure (median 15 4 vs 16 1; ORP vs RARP) All patients underwent the same tissue processing and blocking procedures in the same laboratory The disparity in preoperative prostate size, which can act as a predictive factor for functional outcomes, was not a concern as the majority of patients exhibited a preoperative prostate volume of ≤ 70 ml on transrectal ultrasound (RARP 84 6% vs ORP 86 1%) Additionally, both procedures consumed similar operative time
Hospital stay was significantly shorter after RARP and O R P g ro u p e x p e r i e n c e d s i g n i f i c a n
h i g h e r o p i o i d administration rates postoperatively, Our data showed that patients undergoing RARP had a significantly shorter hospital stay and fewer postoperative opioid requirements than the ORP group, proving the benefit of minimally invasive surgical approach, as already in literature reported (26) Nonetheless, the vast majority of patients in both groups did not experience any deviation from the normal postoperative course
We acknowledge that our study has its limitations Single centre study with just two surgeons evaluated and lack of randomisation being some of them, so that the results might not generalise to other settings Lack of intraoperative blood loss data and missing potency data being the other limitations It should be mentioned that no patient required an intraoperative blood transfusion in either group However, despite these limitations, our study has its strengths We were able to prospectively analyse two almost identical patient groups who underwent two different surgical techniques Furthermore, in addition to minimising variability by having standardised procedures, we were also able to have somewhat of a surgeon heterogenity by having one expert in the respective surgical approach, performing all the procedures As some authors have already stated, the patients should be ancouraged to choose an experianced surgen rather that a specific surgical approach (27)
Our study can be interpreted as a small contribution to a never ending-debate
CONCLUSIONS
The two techniques yield very similar early functional and oncological outcomes when performed by very experienced surgeons ORP will probably continue to be performed in institutions with financial limitations and limited access to robotics Nevertheless, patients are likely to benefit from a shortened hospital stay and reduced postoperative pain after RARP
REFERENCES
1 Culp MB, Soerjomataram I, Efstathiou JA, et al Recent Global Patterns in Prostate Cancer Incidence and Mortality Rates Eur Urol 2020; 77:38-52
2 Adolfsson J Watchful waiting and active surveillance: the current position BJU Int 2008; 102:10-14
3 Hatzinger M, Hubmann R, Moll F, Sohn M Die Geschichte der Prostatektomie - Von den Anfängen bis DaVinci (The history of prostate cancer from the beginning to DaVinci) Aktuelle Urol 2012; 43:228-230
4 Walsh PC, Donker PJ Impotence following radical prostatectomy: insight into etiology and prevention J Urol 1982; 128:492-497
6 B i n d e r J , J o n e s J , B e n t a s W, e t a l R o b o t
Laparoskopie in der Urologie Radikale Prostatektomie und rekonstruktive retroperitoneale Eingriffe (Robot-assisted laparoscopy in urology Radical prostatectomy and reconstructive retroperitoneal interventions) Urologe A 2002; 41:144-149
7 Chandrasekar T, Tilki D Robotic-assisted vs open radical prostatectomy: an update to the never-ending debate Transl Androl Urol 2018; 7(Suppl 1):S120-S123
8 Luciani LG, Mattevi D, Cai T, Malossini G Robotics in Urology: No More Shadows? Uro 2021; 1: 254-265
9 Novara G, Ficarra V, Rosen RC, et al Systematic review and meta-analysis of perioperative outcomes and complications after robot-assisted radical prostatectomy Eur Urol 2012; 62:431-52
10 Gleason DF, Mellinger GT Prediction of prognosis for prostatic adenocarcinoma by combined histological grading and clinical staging J Urol 1974; 111:58-64
11 Dindo D, Demartines N, Clavien PA Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey Ann Surg 2004; 240:205-213
12 D'Amico AV, Whittington R, Malkowicz SB, et al Pretreatment nomogram for prostate-specific antigen recurrence after radical prostatectomy or external-beam radiation therapy for clinically localized prostate cancer J Clin Oncol 1999; 17:168-172
13 Ficarra V, Novara G, Rosen RC, et al Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy Eur Urol 2012; 62: 405-17
14 Haglind E, Carlsson S, Stranne J, et al Urinary Incontinence and Erectile Dysfunction After Robotic Versus Open Radical Prostatectomy:
A Prospective, Controlled, Nonrandomised Trial Eur Urol 2015; 68:216-225
15 Gresty H, Walters U, Rashid T Post-prostatectomy incontinence: multimodal modern-day management Br J Community Nurs 2019; 24:154-159
16 Theissen L, Preisser F, Wenzel M, et al Very Early Continence After Radical Prostatectomy and Its Influencing Factors Front Surg 2019; 6:60
17 Hoeh B, Preisser F, Wenzel M, et al Correlation of Urine Loss after Catheter Removal and Early Continence in Men Undergoing Radical Prostatectomy Curr Oncol 2021; 28:4738-4747
18 Heidenreich A, Fossati N, Pfister D, et al Cytoreductive Radical Prostatectomy in Men with Prostate Cancer and Skeletal Metastases Eur Urol Oncol 2018; 1:46-53
19 Novara G, Ficarra V, Mocellin S, et al Systematic review and meta-analysis of studies reporting oncologic outcome after robotassisted radical prostatectomy Eur Urol 2012; 62: 382-404
21 Yossepowitch O, Briganti A, Eastham JA, et al Positive surgical margins after radical prostatectomy: a systematic review and contemporary update Eur Urol 2014; 65: 303-13
22 Eastham JA, Kattan MW, Riedel E, et al Variations among individual surgeons in the rate of positive surgical margins in radical prostatectomy specimens J Urol 2003; 170: 2292-95
23 Suardi N, DellOglio P, Gallina A, et al Evaluation of positive surgical margins in patients undergoing robot-assisted and open radical prostatectomy according to preoperative risk groups Urol Oncol 2016; 34: 57
24 Liss MA, Palazzi K, Stroup SP, Jabaji R, et al Outcomes and complications of pelvic lymph node dissection during robotic-assisted radical prostatectomy World J Urol 2013; 31: 481-88
Conflict of interest: The authors declare no potential conflict of interest
26 Gandaglia G, Sammon JD, Chang SL, et al Comparative effectiveness of robot-assisted and open radical prostatectomy in the postdissemination era J Clin Oncol 2014; 32: 1419-26
27 Yaxley JW, Coughlin GD, Chambers SK, et al Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: early outcomes from a randomised controlled phase 3 study Lancet 2016; 388:1057-1066
ORIGINAL PAPER
The association of anatomical renal mass complexity with surgical approach, Hb drop, and the rate of blood transfusion
Shakhawan Hama Amin Said 1 , Lusan Abdulhameed Arkawazi Saiwan 1 , Mzhda Sahib Jaafar 1 , Nadhm Kanabi Majeed 1 , Rawa Bapir 2, 3, 4 , Ismaeel Aghaways 1 , Abdullah A. Qadir 1, 2 , Berun A. Abdalla 2, 4 , Ayoob Asaad Mohammed Abid 1 , Fahmi H. Kakamad 1, 2, 4
1 College of Medicine, University of Sulaimani, Sulaymaniyah, Kurdistan, Iraq;
2 Smart Health Tower, Madam Mitterrand Street, Sulaymaniyah, Kurdistan, Iraq;
3 Department of Urology, Sulaymaniyah Teaching Hospital, Sulaymaniyah, Kurdistan, Iraq;
Introduction: The third most prevalent malignant neoplasm involving the urinary tract is renal cell carcinoma (RCC), encompassing nearly 3 5% of the entire cancers afflicting the body. The aim of this research was to explore how the R E N A L nephrometry score relates to the decisions made regarding surgery in individuals with localized RCC Methods: This prospective study, assessed patients with localized parenchymal renal masses (stages I and II) tentatively diagnosed as RCC. Utilizing preoperative multiphasic renal CT scans and MRI, the R E N A L score categorized masses for nephrometry values Inclusion criteria involved collecting patient data, and data collection utilizing a structured format focusing on the nephrometry grading system.
Results: The study included 64 patients aged (Mean ± SD) 49 78 ± 12 35 yrs Undergoing renal mass surgery, there were 17 (26 5%) low, 28 (43 8%) moderate and 19 (29 7%) high-complexity lesions. All patients with a low Nephrometry score (n = 17) underwent partial nephrectomy, and all cases with a high score (n = 19) underwent radical nephrectomy For those with a moderate Nephrometry score (n = 28), 13 (46 4%) underwent partial nephrectomy, while the remaining 15 (53.6%) cases underwent radical nephrectomy. Morbidity was low, and no mortality occurred at 180 days Patients who had lesions fully above or below polar lines were less likely to need blood transfusions A trend towards higher Fuhrman grades in patients receiving transfusions suggests a potential link between tumor aggressiveness and bleeding risk
Conclusions: Our findings provide insight on the utilization of the R E N A L nephrometry score in forecasting perioperative, post-surgical, and oncological results. Such data might help optimize surgical methods and pre-operative patient counseling
KEY WORDS: R E N A L nephrometry score; Renal mass complexity; Surgical approach; Hemoglobin drop; Blood transfusion prediction
Submitted 24 March 2024; Accepted 6 April 2024
INTRODUCTION
The third most prevalent malignant neoplasm involving the urinary tract is renal cell carcinoma (RCC), encompassing nearly 3 5% of the entire cancers afflicting the body (1)
As a result of the extensive utilization of the more available and higher precision imaging techniques, the prevalence of renal cell carcinoma is on the rise, particularly notable in tumors ranging between 2 to 4 cm (2, 3) The RCC’s biology is intricate, and although nearly 33% of all kidney masses first present signs of systemic disease, yet a significant number of localized renal masses show a tendency to progress slowly (4) Surgical management is still the primary treatment option Due to the ongoing evolution of imaging technologies, particularly the enhancements seen in ultrasonography, there has been a discernible augmentation in the identification of RCCs at an early stage (5) There are numerous therapeutic options for kidney tumors, including excision via partial nephrectomy (PN) or radical nephrectomy (RN), ablative procedures, or active observation (6) The determination of surgical approaches is substantially impacted by factors such as the volume and precise anatomical location of the neoplasm Further considerations shaping the chosen surgical approach and intervention include the skillset and experience of the surgeon, the capabilities of the operating facility, and established procedural norms within the medical practice (7) Increasing evidence implies a link connecting the pathological and anatomical characteristics of the renal tumors (8-10), however objective measurements of renal mass anatomy have only recently been described (7, 11-13) In recent times, there has been a discernible demand for precise anatomical characterization of renal masses, prompting the emergence of new scoring systems tailored to offer objective guidance in surgical decision-making processes Two predominant systems have garnered widespread attention: the RENAL nephrometry score (RNS) which was established by Kutikov and Uzzo (2009) and objectively quantifies relevant kidney tumor anatomy characteristics using a scoring system; the Preoperative Aspects and Dimensions Used for Anatomical Classification (P A D U A ) approach which was proposed by Ficarra et al (2009) and closely resembles the RENAL score, offering an alternative anatomical assessment (7, 14, 15) Scoring algorithms have been created and verified to appropriately evaluate the likelihood of postsurgical adverse events and to reflect the
complexity of renal tumors (16) The aim of this research was to explore how the R E N A L nephrometry score relates to the decisions made regarding surgery in individuals with localized RCC
METHODS
Study design
This prospective study design was approved by the Institutional Research Ethics Committee, and all patients were granted informed consent Preoperative multiphasic renal CT scans with intravenous contrast injection were performed on all patients, with magnetic resonance imaging (MRI) serving as additional imaging R E N A L score was used to assess the kidney tumor Masses with nephrometry values of 4 to 6 were categorized as to be mildly complicated for resection, those with scores ranging from 7 to 9 were classed as moderate complexity, and those with scores between 10 to 12 were labeled high complexity
The nephrometry score of a kidney tumor might vary from 4a (1+1+1+a+1) to 12ph (3+3+3+ph+3) [1] In this investigation, the R E N A L score was utilized to evaluate patients with renal tumors managed at our hospital with radical nephrectomy or partial nephrectomy, conducted through both open and laparoscopic approaches
Inclusion and exclusion criteria
Data for inclusion criteria regarding clinical features, histopathological specimens, and cross-sectional images, as well as surgical and postsurgical outcomes, were gathered from the medical database
Sample size & sampling procedures
This study was done prospectively on 64 patients who had localized parenchymal renal mass (stages I and II) that was tentatively diagnosed as RCC and were planned for surgery
Data collection procedures
A structured data abstraction format with items targeting the nephrometry grading system was applied The R E N A L score was established in 2009 (7) and is based on the five most repeatable aspects of a solid renal mass's anatomy: (R)adius (the largest diameter of the tumor in centimeters) to which points were assigned as 1 (≤ 4 cm), 2 (> 4 but < 7 cm), and 3 (≥ 7 cm); (E)xophytic/endophytic properties (points were designated as 1 in cases where 50% or more of the tumor exhibited exophytic growth, 2 when less than 50% of the tumor demonstrated exophytic characteristics, and 3 in instances where the tumor displayed entirely endophytic characteristics); (N) component (nearness) of the tumor to the collecting system or sinus and for which points were assigned as 1 (≥ 7 mm), 2 (> 4 but < 7 mm), and 3 (invading, touching, or within 4 mm); (A) indicates the anterior or posterior location of the tumor which was designated as a non-numerical suffix that describes the location of the tumor with respect to the kidney midline plane as assessed on axial images (the tumor is designated with the suffix “ x ” when it cannot be specified as either anterior or posterior; (L) designates the location of tumor in relation to polar lines Standardized points (1-3
points per descriptor) were given to each parameter, excluding the anterior or posterior component An additional suffix “h” is used to highlight a hilar tumor
The literature review was done by carefully selecting papers from reputable journals and omitting those from predatory sources based on predetermined criteria of Kscien’s list (17)
RESULTS
In this study, a total of 64 patients were included, encompassing 28 males and 36 females The patients had the surgery through an open approach except for five (7 8%)
Table 1.
Presents clinical characteristics of the 64 patients enrolled in this study
Variables
(43 8%)
(56 2%) Tumors
(43.8%)
(56 2%)
medical history
(59 4%)
(25%)
(6.3%)
(9 4%)
BMI < 18 5 0 (0%)
5-24 9
(31 3%) 25-29 9
Blood transfusion
of management
(46 9%)
(21 9%)
(25%)
(75%)
(53 1%)
(46 9%) Presentation on symptomatic
(64 1%)
(35 9%)
Symptom of presentation
Asymptomatic
(60 9%) Right loin pain
ASA 1
(12 5%) Left loin pain
(15 6%)
Anemia 2 (3 1%) Hematuria 5 (7 8%)
(45 3%)
(39 1%)
(14 1%)
1 (1 6%)
(78 1%)
(21 9%)
Nephrometry score
(26 5%)
(43 8%)
(29 7%)
S Hama Amin Said, L Abdulhameed Arkawazi Saiwan, M Sahib Jaafar
Table 2.
Surgical approach stratified by nephromtery score and relationships between Hb-drop and postoperative creatinine change with Nephrometery score Variables
patients who had laparoscopic surgery Among them 30 (46 9%) patients underwent partial nephrectomy, while 34 patients (53 1%) underwent radical nephrectomy
Among these patients, 41 (64 1%) had an incidental finding of a renal tumor, while 23 (35 9%) presented with symptoms Of these, 28 (43 8%) had a right-sided renal tumor, while 36 (56 2%) had a left-sided renal tumor
Most of our patients were diagnosed with clear-cell RCC on final histopathology (n = 60) The remaining cases consisted of multilocular cystic RCC (n = 1), renal oncocytoma (n = 2), and renal angiomyolipoma (n = 1) Sixteen patients (25%) received perioperative blood transfusions, while 48 (75%) did not (Table 1) The general 180-day morbidity in the current investigation was low, including pleural injury (n = 3), urinary leakage (n = 1), and patients requiring postoperative blood transfusion (n = 6) The mortality rate was zero after 180 days of follow-up
There were 17 (26 5%) low, 28 (43 8%) moderate and 19 (29 7%) high-complexity lesions (Table 1) All patients with a low Nephrometry score (n = 17) underwent partial nephrectomy, and all cases with a high score (n = 19) underwent radical nephrectomy For those with a moderate Nephrometry score (n = 28), 13 (46 4%) underwent partial nephrectomy, while the remaining 15 (53 6%) cases underwent radical nephrectomy (Table 2) Additionally, Table 2
Table 3.
Anatomical characteristics of dimension nephrometry scores.
provides post-operative follow-up data, examining the connections between Hbdrop and postoperative creatinine change with different nephrometry scores The Nephrometry scores were categorized as low, moderate, and high, and the data are reported as mean ± SD For the variable "Hb drop" , the following values were observed: for low Nephrometry score: 1 02 ± 0 65, for moderate Nephrometry score 1 50 ± 0 83; for high Nephrometry score 1 53 ± 0 78 (with a p-value of 0 093)
For the variable “postoperative creatinine change" , the data aer as follows: for low Nephrometry Score 0 14 ± 0 19; for moderate Nephrometry score 0 12 ± 0 20; for high Nephrometry score 0 08 ± 0 21 (with a p-value of 0 705 ) (Table 2)
The anatomical location data based on the nephrometry score reveals important details about the renal masses under study The mean maximum dimension and standard deviation (SD) was measured at 1 96 ± 0 73 The nature of the masses is described in terms of endophytic and exophytic characteristics, with 37 5% of the masses being predominantly exophytic, 48 5% showing a 50% exophytic nature, and 14 1% being primarily endophytic (Table 3) Regarding their location, 31 3% of the masses are prioritized anteriorly [designated as 'Priority (a)'], while the same percentage is located posteriorly ['Priority (p)'] An additional 37 4% of the masses are categorized as 'Uncertain (x) ' The proximity of the masses to the renal hilum is also noted, with 12 5% located at or above 7 units away, 15 6% situated between 4 and 7 units, and the majority, 71 9%, being located within 4 units of the hilum (Table 3)
Polar relationships further characterized the masses, with 53 1% positioned exclusively under or upwards of the polar lines Another 20 3% of the masses crossed the polar line, while the remaining 26 6% were distributed such that 50% of the mass either crosses the polar line, extends across the axial renal midline, or is fully situated amidst the polar lines These factors collectively provide insights into the lesion's size, endophytic or exophytic nature, its specific location, proximity to the hilum, and its relationship to the polar lines This data distribution is detailed in Table 3
A comparative analysis was conducted between patients who received blood transfusions and those who did not The mean maximum diameter for patients receiving blood transfusions was 2 25 ± 0 77, while those who did not receive transfusions had a mean diameter of 1 87 ± 0 70 (p = 0 077) Patients with tumors ≥ 50% exophytic nature received transfusion in 4/24, those with < 50% exophytic nature tumors received in 7/32, and patients with endophytic tumors on 5/9 (p = 0 065) Patients with tumors in anterior location had transfusion in 5/20, patients with tumors in posterior location in 5/20 and patients with tumors in unknown location in 6/24 (p =1 00) In regards to the nearness with hilum, patients with a distance ≥ 7 units received blood in 1/8, and those with distances > 4 but < 7 units in 1/10, and for distances ≤ 4 units, 14/46 received blood (p = 0 274) In regard to polar relation, the
Table 4
Comparison
(p) 5 (25) 15 (75)
Table 5.
Surgical approach of renal cell carcinoma
Table 6
Relationship between Nephrometry score and Hb drop with blood transfusion and Relationship of blood transfusion with Fuhrman grade
analysis showed that 5/34 of the cases with mass entirely above or below the polar lines received a blood transfusion, whereas transfusion were received in 3/13 of those with lesions that crossed polar lines (p = 0 042) The results from this comparative evaluation are summarized (Table 4)
The number of patients by type of management, radical or partial, revealed that the type of surgery was based on the anatomical scores (Table 5)
nephrometry scores and hemoglobin decline in the context of blood transfusion The transfusion rate was correlated with Nephrometry score (Table 6) Patients with low, moderate, and high nephrometry scores had transfusions in 2/15, 6/28, and 8/19, respectively (p = 0 093 Additionally, mean ± SD values for Hb drop for those who received a blood transfusion or not are presented in (Table 6) Furthermore, Table 6 delved into the investigation of the relationship between blood transfusion and Fuhrman grade, with information presented as counts and percentages (N%)
For patients who did not receive blood, Fuhrman Grade 1 accounted for 60 9% (28 cases), Fuhrman Grade 2 for 37% (17 cases), and Fuhrman Grade 3 for 2 1% (1 case) Patients who received blood were 5/33 in Fuhrman grade 1 group, 11/28 in Fuhrman grade 2 group and 0/1 in Fuhrman grade 3 group (p = 0 094) These findings are comprehensively presented in (Table 6), contributing to the insight into the interplay between nephrometry scores, hemoglobin decline, and Fuhrman grade in the studied cohort
DISCUSSION
The third most prevalent malignant neoplasm involving the urinary tract is RCC, encompassing nearly 3 5% of the entire cancers afflicting the body (1) An approximate 54 390 new diagnoses and 13 010 mortalities in 2008 were attribu t e d t o R C C ( 1 8 ) M o s t d i a g n o s e s nowadays are unintentional In the past, symptoms such as weight loss, hematuria, or a palpable flank bulge would indicate the condition The reason for this change is because more cross-sectional diagnostic imaging is being used As a result, at least 48-66% of RCC diagnoses have been established based on asymptomatic, incidental renal masses
S Hama Amin Said, L Abdulhameed Arkawazi Saiwan, M Sahib Jaafar
(19) Both the incidence of RCC and the rate of RCC therapies have risen consistently over the last three decades with lower-stage migration (20) The treatment of localized RCC is a therapeutic challenge due to the diversity of tumor appearances and unique patient circumstances
Surgical management, such as PN and RN, is the main treatment option for localized RCC A number of factors, including the size, location, and intricacy of the tumor, influence the decision to perform a particular surgery (21) The R E N A L nephrometry score employs imaging-derived characteristics of kidney tumors to measure t u m o r c o m p l e x i t y o b j e c t i v e l y , f a c i l i t a t i n g d e c i s i o n s regarding the selected technique and strategy
Postoperative results in individuals receiving open or minimally invasive PN have been correlated with the R E N A L score The current study underscores the effectiveness of the R E N A L nephrometry score in forecasting surgical complexity and postsurgical morbidity
The results of this investigation correspond with past studies that have highlighted the connection between surgical technique selection and tumor architecture One standardized and objective tool for preoperative decisionmaking is the R E N A L-NS It gives urologists a useful tool for determining the optimal surgical approach and evaluating the complexity of renal masses These findings provide credence to the hypothesis that anatomicallybased tailored renal mass surgery might lead to improved clinical outcomes (22) According to this study, anatomic tumor features like size and location have a profound effect on preoperative outcomes and the prognosis that follows surgery According to our findings, renal masses' preoperative radiographic and anatomic characteristics can predict the mass's pathologic characteristics The R E N A L Nephrometry score, as the primary rating algorithm established to gauge renal tumor architecture concerning surgical resectability, was utilized in this study
Excision is the usual course of treatment for individuals with a solid renal tumor Active observation, operative excision, and thermal ablative procedures are all effective therapeutic options for suitably chosen individuals with a c l i n i c a l s t a g e T 1 k i d n e y t u m o r , a s n e w A m e r i c a n
Urological Association guidelines have shown (23)
R E N A L nephrometry scores range through 4 to 12 points Lesions that have a collective score of 4, 5, or 6 on nephrometry are classified as low complexity Meanwhile tumors with cumulative points of 7 to 9 points are considered intermediate complexity, and masses scored between 10 to 12 are classified as high complexity lesions A suffix of a or p, and x adds a descriptive component to the system, signifying the anterior or posterior location of the mass, whereas a h is used for hilar tumors (7) Of the 68 patients in the current study, 34 (53 1%) underwent RN and 30 (46 9%) underwent PN based on their nephrometry scores: 17 (26 5%) were low complexity, followed by 28 (43 8%) intermediate complexity and 19 (29 7%) high complexity
Haidar et al found a relationship connecting R E N A L score and surgical technique choice PN was done in 75 6% of cases with low score, 54 6% of instances with moderate level (p = 0 004), and only 11 7% of those with high score (p < 0 001) (24) In our study, 46 9% of 68 patients underwent partial nephrectomy, with 56 6%
having a low score and 43 3% having a moderate score
The remaining patients underwent radical nephrectomy, with 44 1% and 55 8% having intermediate and high scores, respectively
To define the anatomical aspects of a kidney mass, another approach called Preoperative Aspects and Dimensions Used for an Anatomical (PADUA) was established With the exception of defining the sinus lines and assessing the physical connection between the tumor and the renal sinus, or urine collecting system, this system is comparable to the nephrometry score The C-Index Method was finally presented to ascertain the centrality of a tumor
The distance separating the mass and the kidney centers must be calculated using a sophisticated geometric approach utilizing cross-sectional imaging (25, 26)
Whenever medically feasible, most globally recognized standards recommend doing a partial nephrectomy for T1a tumors Approaches to solid renal tumor care include deciding whether to remove the entire kidney or only the tumor with a clean surgical margin, as well as whether to use an open or laparoscopic surgical technique It was demonstrated that tumor volume increases the likelihood of malignant vs benign pathology, high-grade versus lowgrade illness, and clear cell versus papillary histology (27) In our study, all patients with a low Nephrometry score got partial nephrectomy, while all patients with a high score had radical nephrectomy Those with a moderate score (46 4%) got partial nephrectomy, while the rest (53 6%) had radical nephrectomy
One of the most difficult components of RCC therapy is preventing perioperative problems while maintaining patient safety (28) The study identified just a few cases of pleural injury, urinary incontinence, and the need for postoperative blood transfusions The lack of mortality throughout the 180-day follow-up period is reassuring, showing that anatomically complex surgical decisions do not threaten patient safety
In terms of perioperative blood transfusions, the study revealed that a quarter of the patients needed them, although the rest did not This study stresses the need of accurately calculating perioperative blood loss, which can affect surgical technique and postoperative therapy In challenging cases, efforts to decrease blood loss and the need for transfusions, such as precision surgical techniques and advanced hemostatic therapies, should be considered Haider et al. revealed that individuals with an elevated R E N A L score experienced more adverse perioperative results in comparison to those with a lower score Subjects with a high R E N A L score (19 4% vs 6 3%, p = 0 018) were three folds more likely to get blood transfusions than those with a low score (24) Out of the 68 patients in the current study, 16 had blood transfusions, the majority, 8 (50%) had high scores, followed by 6 (37 5%) with moderate scores and 2 (12 5%) with low scores
There is ongoing debate regarding the ability of the R E N A L nephrometry scoring technique to reliably forecast malignancy and high histopathological grades in small kidney tumors Osawa et al found that despite the fact that R E N A L nephrometry scores were effective in distinguishing the benign and malignant kidney masses, as well as low- and high-grade kidney tumors, histopatho-
logical examination yielded superior performance in this regard (29) Further investigations have demonstrated a profound relationship between the R E N A L score and both tumor grade (p < 0 0001) and histology (p < 0 0001) This suggests that as tumor volume rises, there is a higher probability of malignancy, particularly highgrade and clear-cell tumors, upon histological examination (30) The consequence of RCC tumor complexity on oncologic results remains to be definitively made This current research revealed that the R E N A L score played a predictive role in key oncologic outcomes For instance, individuals exhibiting lower R E N A L scores demonstrated markedly higher survival rates in contrast to those presenting higher nephrometry scores Similarly, tumors with elevated R E N A L scores showed more likelihood of experiencing recurrence and progression
CONCLUSIONS
The R E N A L nephrometry scoring system offers a versatile, advantageous, and replicable tool for quantifying the key aspects of renal anatomy The cumulative nephrometry score was shown to be linked with operative decision-making Specifically, the anatomical characteristics of a kidney tumor foretell the utilization of different surgical approaches
REFERENCES
1 Shaaban MS, Abou Youssif TM, Mostafa A, et al Role of RENAL nephrometry scoring system in planning surgical intervention in patients with localized renal masses Egy J Radiol Nucl Med 2015; 46:1175-81
2 Chow WH, Devesa SS, Warren JL, Fraumeni Jr JF Rising incidence of renal cell cancer in the United States JAMA 1999; 281:1628-31
3 Hollingsworth JM, Miller DC, Daignault S, Hollenbeck BK Rising Incidence of Small Renal Masses: A Need to Reassess Treatment Effect J Natl Cancer Inst 2006; 98:1331-4
4 Yousif A, Mohsin SA malignant renal tumors in Iraq (clinical & epidemiological study) Univ Thi-Qar J Med 2011; 5:117-26
5 Van Poppel H, Da Pozzo L, Albrecht W, et al A Prospective, Randomised EORTC Intergroup Phase 3 Study Comparing the Oncologic Outcome of Elective Nephron-Sparing Surgery and Radical Nephrectomy for Low-Stage Renal Cell Carcinoma Eur Urol 2011; 59:543-52
6 Kunkle DA, Egleston BL, Uzzo RG Excise, Ablate or Observe: The Small Renal Mass Dilemma A Meta-Analysis and Review J Urol 2008; 179:1227-34
7 Kutikov A, Uzzo RG The RENAL nephrometry score: a comprehensive standardized system for quantitating renal tumor size, location and depth The Journal of urology 2009; 182:844-53
8 Weizer AZ, Gilbert SM, Roberts WW, et al Tailoring technique of laparoscopic partial nephrectomy to tumor characteristics J Urol 2008; 180:1273-8
9 Schachter LR, Bach AM, Snyder ME, et al The impact of tumour location on the histological subtype of renal cortical tumours BJU int 2006; 98:63-6
10 Venkatesh R, Weld K, Ames CD, et al Laparoscopic partial
nephrectomy for renal masses: effect of tumor location Urol 2006; 67:1169-74
11 Ficarra V, Novara G, Secco S, et al Preoperative aspects and dimensions used for an anatomical (PADUA) classification of renal tumours in patients who are candidates for nephron-sparing surgery Eur Urol 2009; 56:786-93
12 Simmons MN, Ching CB, Samplaski MK, et al Kidney tumor location measurement using the C index method J Urol 2010; 183:1708-13
13 Ficarra V, Novara G, Secco S, et al Preoperative aspects and dimensions used for an anatomical (PADUA) classification of renal tumours in patients who are candidates for nephron-sparing surgery
Eur Urol 2009; 56:786-93
14 Hsieh PF, Chang CH, Yang CR, et al C index is associated with both short-term and long-term renal functional outcome after partial nephrectomy Urol Sci 2013; 24:46-50
15 Simmons MN, Ching CB, Samplaski MK, et al Kidney tumor location measurement using the C index method J Urol 2010; 183:1708-13
16 Jemal A, Siegel R, Ward E, et al Cancer statistics, 2008 CA J Clin 2008; 58:71-96
17 Muhialdeen AS, Ahmed JO, Baba HO, et al Kscien’s List; A New Strategy to Discourage Predatory Journals and Publishers (Second Version) BMJ 2023; 1:24-26
18 Parsons JK, Schoenberg MS, Carter HB Incidental renal tumors: casting doubt on the efficacy of early intervention Urol 2001; 57:1013-5
19 Hollenbeck BK, Taub DA, Miller DC, et al National utilization trends of partial nephrectomy for renal cell carcinoma: a case of underutilization? Urol 2006; 67:254-9
20 Chen DY, Uzzo RG Optimal management of localized renal cell carcinoma: surgery, ablation, or active surveillance J Natl Compr Canc Netw 2009; 7:635-43
21 Simhan J, Smaldone MC, Tsai KJ, et al Objective measures of renal mass anatomic complexity predict rates of major complications following partial nephrectomy Eur Urol 2011; 60:724-30
22 Novick AC Guideline for Management of the Clinical Stage1 Renal Mass AUA Educ Res 2009, Linthicum, USA 2009
23 Kutikov A, Uzzo RG The RENAL nephrometry score: a comprehensive standardized system for quantitating renal tumor size, location and depth J Urol 2009; 182:844-53
24 Abou Heidar N, Hakam N, El-Asmar JM, et al The RENAL score ’ s relevance in determining perioperative and oncological outcomes: a Middle-Eastern tertiary care center experience Arab J Urol 2022; 20:115-20
25 Canter D, Kutikov A, Manley B, et al Utility of the RENAL nephrometry scoring system in objectifying treatment decision-making of the enhancing renal mass Urol 2011; 78:1089-94
26 Sciorio C, Prontera PP, Scuzzarella S, et al Predictors of surgical outcomes of retroperitoneal laparoscopic partial nephrectomy Arch Ital Urol Androl 2020; 92
27 Bamias A, Escudier B, Sternberg CN, et al Current clinical practice guidelines for the treatment of renal cell carcinoma: a systematic review and critical evaluation Oncol 2017; 22:667-79
28 Krabbe LM, Bagrodia A, Margulis V, Wood CG Surgical management of renal cell carcinoma Semin Intervent Radiol 2014; Vol 31, No 01, pp 027-032 Thieme Medical Publishers
S Hama Amin Said, L Abdulhameed Arkawazi Saiwan, M Sahib Jaafar
29 Osawa T, Hafez KS, Miller DC, et al Comparison of percutaneous renal mass biopsy and RENAL nephrometry score nomograms for determining benign vs malignant disease and low-risk vs high-risk renal tumors Urol 2016; 96:87-92
30 Kutikov A, Smaldone MC, Egleston BL, et al Anatomic features of enhancing renal masses predict malignant and high-grade pathology: a preoperative nomogram using the RENAL Nephrometry score Eur Urol 2011; 60:241-8
Correspondence
Shakhawan Hama Amin Said
Lusan Abdulhameed Arkawazi Saiwan
Mzhda Sahib Jaafar
Nadhm Kanabi Majeed
Ismaeel Aghaways
Abdullah A Qadir
Ayoob Asaad Mohammed Abid College of Medicine, University of Sulaimani, Sulaymaniyah, Kurdistan, Iraq
Rawa Bapir
Berun A Abdalla berun anwer95@gmail com
Smart Health Tower, Madam Mitterrand Street, Sulaymaniyah, Kurdistan, Iraq
Fahmi H Kakamad (Corresponding Author) fahmi hussein@univsul edu iq
Doctors City, Building 11, Apartment 50, Sulaimani, Iraq
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
“Bottoms-up” minimally-invasive approach to inguinal lymph node dissection for penile cancer management. A single-center comparative study versus open approach and review
Vlad Horia Schit ̦cu, Vlad Cristian Munteanu, Mihnea Bogdan Borz, Ion Cojocaru, Sergiu Vasile Labo, Andrei-Ionut ̦ Tis ̦ e
Department of Urology, Institute of Oncology “Prof Dr Ion Chiricuta”, Romania
Summary
Purpose: Open inguinal lymph node dissection (OILND) plays a crucial role in penile cancer management, but in order to improve patient outcomes, minimally-invasive (MILND) approaches were developed. Our “bottoms-up” MILND is a novel endoscopic technique, changing the way the sequence of dissection is performed. This study aims to compare our approach to the current standard of OILND in terms of oncologic and perioperative outcomes.
Materials and methods: In our database, from 2016 to 2023, 12 patients underwent OILND and 16 had a “bottoms-up” MILND, which is performed with a three port configuration, starting the dissection under the fascia lata, dissecting the femoral vessels in the most distal part of the femoral fossa, followed by dissection of the proximal and superficial lymph nodes at the top of the femoral triangle
Results: For MILND, median operation time per groin was shorter (58 vs 64 minutes, p = 0 34), patients presented shorter hospital stays (10 vs 18 days, p = 0.32) and fewer days with drains (14 vs 24 days, p = 0 01) Median lymph node yield per groin was higher for MILND (10 vs 9 nodes, p = 0.7), but OILND had a higher median of positive lymph nodes (4 vs 3 nodes, p = 0 63) MILND patients experienced a lower incidence of major complications (33% vs 58%, p = 0 007) Conclusions: We have proved that our technique of MILND is not inferior to the current standard and we believe that it can further improve patient outcomes with a safer, simplified and easily reproducible approach
KEY WORDS: Penile cancer; Inguinal lymphadenectomy; Minimally invasive; Video endoscopic
Submitted 6 May 2024; Accepted 6 June 2024
INTRODUCTION
Penile cancer is a rare disease with an annual incidence below 1 case per 100 000 men, representing less than 1% of malignancies in men (1) Following the routes of anatomical drainage, regional lymphatic metastases first occur at level of the superficial and deep inguinal lymph nodes, usually in medial-superior zone, followed by the pelvic lymph nodes (2, 3) While inguinal spread can be either unilateral or bilateral and crossover to the contralat-
eral groin is possible, distant lymphatic spread above the pelvic lymph nodes to the retroperitoneal nodes is classified as metastatic disease (4) Conversely, metastatic spread from the inguinal lymph nodes to the contralateral pelvic nodes was not reported, nor crossover from the pelvic nodes to the opposite side of the pelvis (5) Inguinal lymph node dissection (ILND) is indicated for proper cancer staging and has a curative role when the cancer is limited to the penis and regional nodes The EAU guidelines endorse performing open ILND for clinically node positive patients or after nodal metastasis is confirmed after image-guided biopsy For cN0 disease with high metastatic risk, surgical staging is recommended, preferably by dynamic sentinel node biopsy rather than ILND (4) Unfortunately, recovery after ILND is hindered by postoperative complications occurring in up to 77% of cases, including: wound infections, skin or flap necrosis, seroma, lymphoedema, lymphocele, etc (6) In order to overcome the morbidity of the open ILND, in 2002, Ian M Thompson developed a minimally invasive endoscopic subcutaneous approach for ILND and the first endoscopic subcutaneous modified ILND was performed in 2003 (7)
The endoscopic approach was further developed with the incorporation of 3D and robotic-assisted systems Compared to open ILND, minimally-invasive inguinal lymph node dissection (MILND) improves the lymph-node yield, facilitates a shorter hospital stay with fewer skin complications, lymphoedema and other major complications (8)
The most widespread technique utilized for MILND (7) involves two stages of dissection, first above the fascia lata for the superficial nodes and the second under the fascia lata for the deep inguinal lymph nodes around the femoral vessels We believe that the MILND procedure can be simplified by first approaching the deep and distal part of the femoral triangle, following the femoral vascular bundle and its branches cranially and superficially for a complete inguinal lymphadenectomy
The purpose of our study is to assess the results of the ILND procedures performed in our centre, both by open and minimally invasive approach, to determine whether our novel technique of MILND is non-inferior to the current standard of treatment, the OILND
MATERIALS AND METHODS
We retrospectively reviewed our database of patients who underwent ILND in our center, starting from 2016 to 2023 All patients included in our study were diagnosed with penile cancer with indication for ILND based on the guidelines at that time (cN1/cN2 disease or cN0 with highrisk primary tumor for which dynamic sentinel node biopsy was not available) Patients with bulky or ulcerated inguinal lymph nodes were excluded from the study
During the analyzed period, all ILND procedures were performed by a single surgeon (V S ), who operated initially only by open approach and then switched to performing only the minimally invasive approach whenever indicated
In case metastatic spreading to the pelvic lymph nodes was suspected on pre-operative imaging (computer tomography or positron emission tomography scan), laparoscopic extended pelvic lymph node dissection was performed in the same session
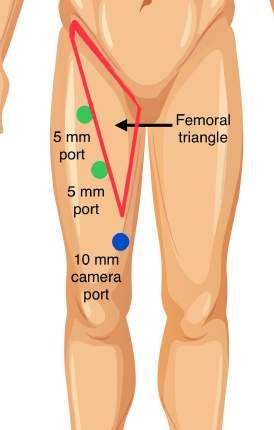
For the minimally invasive approach, the patient was placed in dorsal decubitus position with the upper limbs alongside the body, and the lower limbs in a “frog-legged” position (Figure 1) A three-port configuration was implemented with one 10 mm port for the camera, and two 5 mm ports for the instruments The optical port is placed first at 2 cm caudally from the apex of Scarpa’s triangle using an open technique and the other two 5 mm ports are placed on the lateral border of the triangle (Figure 2) In order to ensure a wide space for work and a safe introduction of the working trocars, the subcutaneous space is further developed with the Gaur balloon
Dissection was carried out with a bipolar clamp and 5 mm polymer clips that were used to secure lymph vessels
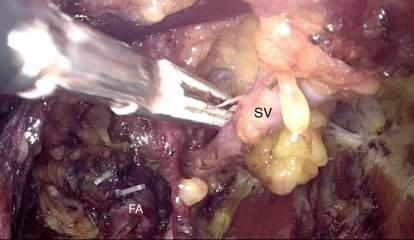
The deep lymph nodes around the femoral neurovascular bundle were first dissected (Figure 3), starting at the apex of the femoral triangle, thus ensuring vascular control from the start of the procedure Following the femoral vessels cranially, the deep lymph node dissection is completed, including the excision of the Cloquet node The sapheno-femoral junction is isolated and, by following the saphenous vein, the superficial lymph nodes are dissected up to the inguinal ligament Thus, the ILND is performed starting from the “bottom” , at the deepest and most caudal region of the femoral triangle, and finishing “ up ” at the level of the inguinal ligament
Open inguinal lymph node dissection (OILND) was carried out classically, with an incision below and parallel to the inguinal ligament For both approaches, saphenous vein sparing was performed whenever possible in order to improve post-operative recovery (Figure 4) Negative pressure wound drainages were installed at the end of the surgery and were replaced with passive drains after 3 days After draining less than 30 mL in 24 hours, passive tubes were removed
Figure 3
Minimally invasive lymph node dissection proximal to the femoral vessels FA: femoral artery; FV: femoral vein; ILN: inguinal lymph nodes
V Horia Schitcu, V Cristian Munteanu, M Bogdan Borz, et al
Figure 1. Patient positioning and port placement
Figure 2. Port placement relative to the femoral triangle.
Statistical analysis was performed using the SPSS software package Descriptive analysis was carried out using frequencies, means, medians, interquartile ranges and standard deviations For group comparisons of continuous variables, Student’s t-test or the Mann-Whitney U test was performed depending on the results of the KolmogorovSmirnov test The chi-squared test was used to examine categorical variables
Ethical approval
This retrospective study was conducted using anonymized data retrieved the Institute of Oncology “Prof Dr Ion Chiricut ̦ a” patient registry Ethical approval for this study was obtained from the institute’s Ethics Committee, with waiver of informed consent granted due to the retrospective nature of the study and the use of de-identified data in accordance with local regulations and institutional guidelines
RESULTS
Our database of ILND is comprised of 28 cases of patients diagnosed with penile cancer requiring inguinal lymph node staging From 2016 to 2023, 12 patients underwent OILND and 16 had a “bottoms-up” MILND
In total, OILND and MILND were performed on 24 and 32 groins, respectively
The median age of the patients included in our study was 63 years (range 59-66) For the OILND group, the median age was 61 years (range 54-67) and for the MILND 63 years (range 57-66), with no statistically significant difference (p = 0 69) All cases were diagnosed with penile squamous cell carcinoma and the MILND and OILND groups were comparable in pathological T stage (p = 0 52) Saphenous vein preservation was attempted whenever feasible and was achieved for 12 groins (50%) in the OILND group and 18 (56 25%) in the MILND group, with no significant difference (p = 0 3) Median operation time for one groin was 58 minutes (IQR 48-68 minutes) in the MILND group, shorter that 64 minutes (IQR 55-73 minutes) for OILND, but statistically insignificant (p = 0 34) Patients who underwent MILND had a shorter median hospital stay (10 vs 18 days, p = 0 32) and a significantly shorter median
number of days until drainage tubes were removed (14 vs 24 days, p = 0 01)
Median lymph node yield per groin was slightly higher in the MILND group (10 vs 9 nodes, p = 0 7), but OILND yielded a marginally higher median of positive lymph nodes per groin (4 vs 3 nodes, p = 0 63) for each groin
Regarding the pathology result, there were no significant differences between pN staging regardless of surgical approach (p = 0 55)
Patients treated with MILND experienced a significantly lower incidence of major complications ranked ClavienDindo > II (31 25% vs 58 3%, p < 0 007) The complications encountered in the OILND group were three cases of lymphocele that required percutaneous drainage, one case of wound infection and three cases of wound dehiscence
In the MILND group, one patient experienced delayed wound healing due to wound dehiscence and three other cases required percutaneous drainage for lymphocele
If saphenous vein preservation was accomplished, the median time duration until drainage tubes were removed was significantly shorter compared to cases where saphenous vein sparing was not possible (13 vs 23 days, p = 0 03) and the median duration of hospital stay was reduced (11 5 vs 18 days, p = 0 06), although insignificantly
The Table 1 summarizes patient demographics, tumor characteristics, operative parameters, initial patient outcomes and pathological data
DISCUSSION
ILND represents a critical aspect of cancer treatment and staging for patients with penile cancer Despite its importance in oncological care, ILND is considered a highly morbid procedure A systematic review and meta-analysis (9)
Table 1.
Patient demographics, tumor characteristics, operative parameters, initial patient outcomes and pathological data
Saphenous vein preservation, no of groins (%) 10 (41 6%) 15 (46 8%)
V Horia Schitcu, V Cristian Munteanu, M Bogdan Borz, et al
found that perioperative adverse events were common in patients undergoing ILND, with high BMI, comorbidities, and diabetes identified as independent predictors for complications
Historically, OILND has been the standard of care However, due to potential complications and morbidity associated with OILND, there has been growing interest in minimally invasive techniques, such as video-endoscopic or robot-assisted ILND These techniques are suggested to achieve comparable oncologic outcomes to OILND, with lower rates of complications (8, 10)
We present our approach for MILND which is different from the already established MILND technique described in the literature, demonstrating unique advantages The initial space developed under the fascia lata with the Gaur balloon provides adequate space for safe port placement and tissue manipulation, reducing the need for other aid ports and instruments By approaching first the apex of the inguinal triangle, early vascular control of the femoral bundle is achieved, thus reducing the hemorrhagic risk of this procedure Continuing the dissection proximally, around the femoral artery, the femoral vein and the saphenofemoral junction can then be easily and safely isolated, facilitating the preservation of the saphenous vein Conversely, the invasion of the saphenous vein is easily identified before commencing its dissection, thus making the decision to preserve or to sacrifice quick and early during the procedure
In our high-volume center, we compared the early results following the adoption of our technique of MILND with the outcomes of the well-established OILND Our study included 28 patients with penile cancer requiring ILND, with 12 patients undergoing OILND and 16 MILND The results showed no significant differences between the two groups in age, pathological T stage, saphenous vein preservation rate and median operation time However, patients who underwent minimally invasive procedures had shorter hospital stays and required fewer days with drains in place The minimally invasive group also had a slightly higher median lymph node yield per groin, though the open group had a marginally higher median number of positive lymph nodes per groin No significant differences were observed in pN staging between the two surgical approaches However, patients in the minimally invasive group experienced a significantly lower incidence of major complications (Clavien-Dindo > II) In addition, successful saphenous vein sparing reduced the duration of hospital stay and decreased the period for wound drainage significantly
Previous systematic reviews and meta-analyses have reported better perioperative outcomes and comparable shortterm oncological outcomes for minimally invasive techniques A 2019 systematic review and meta-analysis (10) compared video endoscopic ILND (VE-ILND) and OILND in the management of penile cancer The results indicated that the VE-ILND group had less intraoperative blood loss, shorter hospital stay, shorter drainage time, reduced wound infection rate, reduced skin necrosis rate, and lower lymphedema rate compared to the OILND group However, the number of dissected lymph nodes was slightly higher in the OILND group Lymphocele rate and recurrence rate were found to be similar between the two groups
A 2022 systematic review and meta-analysis (8) compared robot-assisted video endoscopic ILND (RAVEIL/VEIL) with OILND in penile carcinoma management RAVEIL and VEIL techniques increased the operative time (MD = 15 28) but reduced hospital stay (MD = -1 06), and decreased the duration of drainage (MD = -2 82) It also demonstrated lower rates of wound infection (OR = 0 15), skin necrosis (OR = 0 12), lymphedema (OR = 0 41), and major complications (OR = 0 11) compared to OILND Recurrence rates and number of deaths were comparable, but RAVEIL/VEIL had a slightly larger lymph-node yield (MD = 0 44) RAVEIL/VEIL demonstrated fewer complications and better lymph-node yield, with comparable oncological outcomes to OILND
Thyavihally et al (11) compared video endoscopic inguinal lymphadenectomy (VEIL) and open ILND (O-ILND) in terms of perioperative and survival outcomes Results from 79 patients showed wound complications were higher in OILND (65 6%) than VEIL (27 7%) (p = 0 001) Median overall survival was 80 months for O-ILND and 88 months for VEIL (p = 0 840), with five-year survival rates of 65% and 66 8% (p = 0 636) and disease-specific survival rates of 76 6% and 73 9% (p = 0 96), respectively
A 2023 systematic review assessed the clinical effectiveness of treatment options available for the management of inguinal and pelvic lymphadenopathy in men with penile cancer and reinforced the idea that early ILND improves survival in nodal disease in penile cancer and, furthermore, MILND may offer comparable survival outcomes to open ILND with lower wound-related morbidity (12)
As observed, minimally invasive surgery provides an economic benefit in reducing costs of hospitalization and an earlier return to activity, when compared with open surgery (13) It is very probable that this is as also the case for MILND, but we also believe that our method of VEIL can provide further financial advantage when compared to the associated costs of RAVEIL Although additional studies would be needed to demonstrate this hypothesis, a lower financial-impact procedure that is simplified and with reproducible favorable outcomes would serve as additional reasons for adoption, especially in developing countries
Following the latest recommendations by the EAU-ASCO guidelines, for cN0 disease that requires inguinal lymph node staging, dynamic sentinel node biopsy (DSNB) is preferred in order to avoid unnecessary formal ILND and its associated morbidity (4) An updated systematic review and meta-analysis by Zou et al (14) assessed the accuracy of radiocolloid-based DSNB in penile cancer with clinically negative groin (cN0) disease and found a pooled sensitivity of 88% and a negative predictive value of 99%
Factors such as preoperative ultrasonic scan (USS), fine-needle aspiration cytology (FNAC), surgical exploration of the wound for suspicious lymph nodes, immunohistochemistry and extensive experience were associated with improved DSNB sensitivity
A 2022 systematic review, Fallara et al (15) assessed the diagnostic accuracy of DSNB and ILND in detecting lymph node metastasis in penile cancer patients with cN0 disease
It found that DSNB had a pooled weighted sensitivity of 0 87, but for detecting further positive lymph nodes at ILND, DSNB had a pooled weighted sensitivity of 0 50
The study concluded that a positive DSNB is poorly able to
“Bottoms-up” minimally-invasive approach to inguinal lymph node dissection for penile cancer management
discriminate which patients will have further metastatic involvement at the completion of ILND, suggesting that better patient stratification could help avoid unnecessary overtreatment and postoperative comorbidities For this, Kumar et al demonstrated that outcomes can be further improved with additional inguinal ultrasound, fine needle aspiration and cross-sectional imaging to select patients for either INLD or DSNB, leading into a DSNB procedure with a sensitivity of 100% at a mean follow-up of 5 years (16) Our study demonstrates that our novel technique for MILND provides benefits such as shorter hospital stay and reduced complications compared to the well-established open approach The findings align with those of previous systematic reviews and meta-analyses, which have also reported better perioperative outcomes and comparable short-term oncological outcomes for minimally invasive techniques However, our study has several limitations The sample size is relatively small and the data is provided from a single center with a single surgeon, which may hinder the extrapolation of the results Additionally, our study focused on early post-operative results and did not assess long-term oncological outcomes Future research should involve larger, multicenter studies with more diverse patient populations and longer follow-up periods to better understand the safety, efficacy, and long-term outcomes of minimally invasive approaches for ILND
CONCLUSIONS
Our study compared our novel 'bottoms-up' minimally invasive inguinal lymph node dissection in penile cancer management with the current standard of treatment, the open approach Our approach is less invasive, resulting in a shorter operating time (58 vs 64 mins, IQR 55-73 minutes vs 48-68 minutes), shorter hospital stays (10 vs 18 days, IQR 7-17 days vs 8-20 days), fewer days with drains (14 vs 24 days, IQR 8-20 vs 19-30 days), and fewer major complications (33% vs 58%) We retrieved more lymph nodes (10 vs 9) but had similar cancer-related outcomes This suggests our approach is non-inferior to the standard of treatment, but safer and simpler for patients and surgeons alike
REFERENCES
1 Montes Cardona CE, García-Perdomo HA Incidence of penile cancer worldwide: systematic review and meta-analysis Revista Panamericana de Salud Pública 2017; 1-10
2 Leijte JAP, Kirrander P, Antonini N, et al Recurrence patterns of squamous cell carcinoma of the penis: recommendations for followup based on a two-centre analysis of 700 patients Eur Urol 2008; 54:161-8
3 Alnajjar HM, Lam W, Bolgeri M, et al Treatment of Carcinoma In Situ of the Glans Penis with Topical Chemotherapy Agents European Urology 2012; 62:923-8
4 Brouwer OR, et al EAU-ASCO Penile Cancer Guidelines Edn presented at the EAU Annual Congress Milan 2023 Arnhem, The Netherlands: EAU Guidelines Office; 2023
5 Smith JA, Howards SS, Preminger GM, Dmochowski RR Hinman"s Atlas of Urologic Surgery Revised Reprint Elsevier Health Sciences; 2019
6 Stuiver MM, Djajadiningrat RS, Graafland NM, et al Early
Wound Complications After Inguinal Lymphadenectomy in Penile Cancer: A Historical Cohort Study and Risk-factor Analysis Eur Urol 2013; 64:486-92
7 Sotelo R, Sánchez-Salas R, Carmona O, et al Endoscopic Lymphadenectomy for Penile Carcinoma J Endourol 2007; 2:364-7
8 Patel KN, Salunke A, Bakshi G, et al Robotic-Assisted VideoE
Endoscopic Inguinal Lymphadenectomy (VEIL) versus Open Inguinal L y m p h - N o d e D i s s e c t i
Comparison of perioperative outcomes, complications and oncological outcomes A systematic review and meta-analysis Urol Oncol 2022; 40:112 e11-112 e22
9 Cacciamani GE, Medina LG, Sayegh AS, et al Complications and Adverse Events in Lymphadenectomy of the Inguinal Area (CALI) project, the International Consensus Panel on Complications in Urology (ICPCU), and the Intraoperative Complications assessment and reporting with Universal Standards (ICARUS) Global Surgical Collaboration Assessment and Reporting of Perioperative Adverse Events and Complications in Patients Undergoing Inguinal Lymphadenectomy for Melanoma, Vulvar Cancer, and Penile Cancer: A Systematic Review and Meta-analysis World J Surg 2023; 47:962-974
10 Hu J, Li H, Cui Y, et al Comparison of clinical feasibility and oncological outcomes between video endoscopic and open inguinal lymphadenectomy for penile cancer: a systematic review and metaanalysis World J Urol 2020; 38:1301-1311
11 Thyavihally YB, Dev P, Waigankar SS, et al Comparative study of perioperative and survival outcomes after video endoscopic inguinal lymphadenectomy (VEIL) and open inguinal lymph node dissection (O-ILND) in the management of inguinal lymph nodes in carcinoma of the penis J Robotic Surg 2021; 15:695-703
12 Sachdeva A, McGuinness L, Zapala Ł, et al Node-positive Penile Cancer: A Systematic Review Eur Urol 2024; 85:257-273
13 Ho C, Tsakonas E, Tran K, et al Robot-Assisted Surgery Compared with Open Surgery and Laparoscopic Surgery: Clinical Effectiveness and Economic Analyses Internet) Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2011 Sep (CADTH Technology Report, No 137 ) 5, Economic Analysis Available from: https://www ncbi nlm nih gov/books/NBK168933/
14 Zou ZJ, Liu ZH, Tang LY, et al Radiocolloid-based dynamic sentinel lymph node biopsy in penile cancer with clinically negative inguinal lymph node: an updated systematic review and meta-analysis Int Urol Nephrol 2016; 48:1951-1962
15 Fallara G, Pozzi E, Onur Cakir O, et al EAU-YAU Penile and Testis Cancer Working Group Diagnostic Accuracy of Dynamic Sentinel Lymph Node Biopsy for Penile Cancer: A Systematic Review and Meta-analysis Eur Urol Focus 2023; 9:500-512
16 Kumar V, Kumar PR, Juette A, et al Improved outcome in penile cancer with radiologically enhanced stratification protocol for lymph node staging procedures: a study in 316 inguinal basins with a mean follow-up of 5 years BMC Urol 2023; 23:137
Correspondence
Vlad Horia Schit ̦cu, MD - schitcu@yahoo com
Vlad Cristian Munteanu, MD - vladcristian munteanu@gmail com
Mihnea Bogdan Borz, MD - borz m bogdan@gmail com
Ion Cojocaru, MD - cojocaruion90@yahoo com
Sergiu Vasile Labo, MD - atolica@gmail com
Andrei-Ionut ̦ Tis ̦e, MD (Corresponding Author) andreitisemd@gmail com
Department of Urology, Institute of Oncology “Prof Dr Ion Chiricuta”, Romania - Str Republicii 34-36, Cluj-Napoca 400015, Romania
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Programmed death-ligand expression and lymph node involvement in penile squamous cell carcinoma
1 Portuguese Institute of Oncology in Lisbon, Urology, Lisbon, Portugal
2 Portuguese Institute of Oncology in Lisbon, Pathology, Lisbon, Portugal
Summary
Purpose: Our objective was to investigate the association between programmed death-ligand (PD-L1) immunoexpression measured as a combined positive score and clinical outcomes in penile SqCC.
Materials and methods: We retrospectively reviewed all penile SqCC cases diagnosed in our institution between 2018 and 2023 PD-L1 immunohistochemistry was performed as a qualitative assay Immunoexpression in both tumor and immune cells equal or superior to 1 was considered positive
Results: A total of 34 patients with conventional penile SqCC were included Eleven cases were HPV-associated (32 4%)
Twelve cases were PD-L1 CPS < 1 and twenty-two were PD-L1 CPS ≥ 1 Nine cases (32 4%) were PD-L1 CPS ≥ 1 and p16 positive, but this did not translate in worse clinicopathological features. Larger tumors (3.0 cm in PD-L1 CPS ≥ 1 vs 2.5 cm in PD-L1 CPS < 1; p = 0 662), vascular invasion (36 4% in PD-L1 CPS ≥ 1 vs. 25.0% in PD-L1 CPS < 1; p = 0.705) and perineural invasion (40 9% in PD-L1 CPS≥1 vs 16 7% in PD-L1 CPS < 1; p = 0.252) were associated with PD-L1 expression. Among the high-risk features, only lymph node involvement had statistical significance, with 14 out of 22 PD-L1 CPS ≥ 1 patients (63.6%) having lymph node metastases when lymphadenectomy was performed (p = 0.031). With a median follow-up of 16 months (IQR 27 5), PD-L1 CPS ≥ 1 patients had worse overall survival (53 4 months vs 75.9 months), but no statistical significance could be inferred (p = 0 188)
Conclusions: It is noteworthy the clinical significance of lymph node involvement in PD-L1 CPS ≥ 1 cases and a trend towards worse overall survival in this group of patients.
Penile cancer (PC) is a rare form of cancer in Western nations, with squamous cell carcinoma (SqCC) being the most common type, accounting for around 95% of cases (1) The global incidence of PC varies due to differences in socioeconomic and religious factors, representing less than 1% of all malignancies in Western Europe (2) Regions with high rates of human papillomavirus (HPV) infection are most affected by penile cancer, with approximately one third to half of cases attributed to HPV-related causes (3) The management of penile cancer presents a significant challenge for clinicians This malignancy is highly aggres-
sive, and there is a lack of well-defined strategies for patients whose metastatic penile carcinoma progresses or recurs after front-line cisplatin-based chemotherapy (4)
The ability of tumor cells to evade the immune system is one of the many characteristics of tumor cells recognized as a hallmark of cancer (5) The programmed cell death 1 and its ligand (PD-1/PD-L1) pathway is one of the primary immune checkpoint targets that has been extensively studied in clinical research in recent years (6)
PD-L1 acts as a co-stimulatory ligand, which, upon binding with its receptor PD-1, functions as a negative regulator of T-cell-mediated antitumor immunity (7) Although PD-L1 expression is typically induced in cells of the macrophage lineage and T cells, abnormal PD-L1 expression has been detected in various types of cancer This has led to the hypothesis that PD-L1 expression in either tumor cells or tumor-infiltrating immune cells (TIICs) might facilitate tumor progression by inhibiting the antitumor immune response (7)
Currently, several clinical studies evaluating PD-1/PD-L1 inhibitors have been conducted in several different tumor types including melanoma, breast cancer, non-small-cell lung cancer, and head and neck cancer PD-L1 expression has also been extensively studied in a number of urological malignancies such as bladder, kidney, and prostate cancer However, there have been relatively few studies on PD-L1 expression in penile squamous cell carcinoma (8-10) Given the aforementioned difficulty in treating recurrent and/or metastatic penile SQCC, the targeting of PD-L1 may offer a novel therapeutic avenue for those patients who exhibit PD-L1 expression upon recurrence or progression after first-line chemotherapy
The aim of our study is to investigate the association between PD-L1 immunoexpression as a combined positive score and clinical outcomes in penile squamous cell carcinoma
METHODS
Patients and samples
We retrospectively reviewed all penile SqCC cases treated in our institution between 2018 and 2023 Tumors were classified according to the 5th edition of the World Health Organization Urinary and Male genital tumors 2004 TNM classification Exclusion factors included a non-squamous cell carcinoma diagnosis and cases without available
material for additional immunohistochemistry studies and without clinical follow-up Baseline patient and dise a s e c h a r a c t e r i s t i c s w e r e a s s e s s e d f o r t h e s e l e c t e d patients All penile specimens were reviewed by a pathologist specialized in genitourinary pathology
All research was performed in accordance with relevant national and international regulations and informed consent to use the pathology material was obtained from all participants The research was performed in accordance with the Declaration of Helsinki
Immunohistochemistry
PD-L1 expression was assessed by immunohistochemistry (IHC) in formalin-fixed, paraffin-embedded (FFPE) tumor samples at our institution PD-L1 IHC 22C3 pharmDx assay was performed using a monoclonal mouse anti-PDL1 clone 22C3 and a validated protocol for Ventana BenchMark Ultra platform PD-L1 protein expression was determined by using a Combined Positive Score (CPS), counting the number of PD-L1 staining cells (tumor cells, lymphocytes, macrophages) divided by the total number of viable tumor cells, multiplied by 100 (e g if 1 staining cell was found out of 100 viable cells the score was 1/100 x 100 = 1) A minimum of 100 viable tumor cells was present in each stained slide for adequate PD-L1 evaluation PD-L1 staining was evaluated as membranous tumor cell staining and membranous/cytoplasmic staining of mononuclear inflammatory cells (MICs) within tumor nests and adjacent supporting stroma PD-L1 CPS ≥ 1 cases were considered when CPS ≥ 1 Also, in all cases before 2021 IHC for P16 was performed on Ventana® Benchmark ULTRA equipment with the Ventana® optview DAB IHC detection kit (ref 760-700) CC1 was used for antigen retrieval (AR) and anti-P16 (Roche Ventana® - clone E6H4) was used Positive cases were considered if a strong block positivity for p16 was observed
Statistical analysis
C o n t i n u o u s d a t a w e r e d e s c r i b e d b y m e d i a n a n d interquartile range (IQR) Categorical data were presented by counts and percentages Comparisons between continuous data were performed by the Mann-Whitney U test and categorical data by Pearson's chi-squared or Fisher's exact test, accordingly Kaplan-Meier curves were obtained to estimate the survival rates with statistical significance evaluated by the log-rank test A p < 0 05 was defined as statistically significant Data was processed and analysed with IBM-SPSS software version 22 0
RESULTS
Patient characteristics
A total of 34 patients were eligible for analysis in this study The median age at diagnosis was 67 years (IQR 20) The median size of the tumor was 3 0 cm (IQR 3 3)
Among the patients, 11 were classified as HPV-associated (p16 positive) Twenty-two cases were considered to be PD-L1 CPS ≥ 1
The study uniformly recorded cases across all grades Regarding pathological stages, no pT1b tumors were
observed, but all other stages were represented A partial penectomy was performed in the majority of the cases (70 6%) and none of the patients had adjuvant treatments
Clinicopathological and demographic characteristics of the cohort are presented in Table 1
Association of PD-L1 expression with clinicopathological features
Larger tumors (3 0 cm in PD-L1 CPS ≥ 1 vs 2 5 cm in PDL1 CPS < 1; p = 0 662), vascular invasion (36,4% in PDL1 CPS ≥ 1 vs 25,0% in PD-L1 CPS < 1; p = 0 705) and perineural invasion (40 9% in PD-L1 CPS ≥ 1 vs 16,7% in PD-L1 CPS < 1; p = 0 252) were associated with PDL1 expression, but with no statistical significance
Twenty-three patients underwent lymphadenectomy, with lymph node involvement detected in 17 of them
Among those with lymph node involvement, 16 patients were found to be PD-L1 CPS ≥ 1
Among the high-risk features, only lymph node involvement had statistical significance, with 14 out of 22 PD-L1 CPS ≥ 1 patients (63 6%) having lymph node metastases when lymphadenectomy was performed (p = 0 031)
These associations are presented in Table 2
Association of PD-L1 expression with survival outcomes: With a median follow-up of 16 months (IQR 27 5), PDL1 CPS ≥ 1 patients had worse overall survival (53 4
Table 1.
Clinical and pathological characteristics.
Characteristic
Median age at surgery, yr
High-risk HPV status, n (%) Negative
sample (n = 34)
(IQR 20)
(67 6%) Positive 11 (32 4%)
PD-L1 status, n (%)
CPS < 1
(35 3%)
CPS ≥ 1 22 (64 7%)
Median tumor size, cm 3 (IQR 3 3)
Tumor grade, n (%)
11 (32 4%) 2 14 (41 2%) 3 8 (23 5%) 4 1 (2 9%)
Vascular invasion, n (%)
Perineural invasion, n (%)
pT stage, n (%)
(67 6%)
(32 4%)
(67 6%)
(32 4%)
(26 5%)
(32 4%) 3
Lymph node involvement, n (%)
(41 2%)
17 (50 0%) Yes 17 (50 0%)
Treatment, n (%)
Glansectomy 6 (17.6%)
Partial penectomy 24 (70 6%)
Total penectomy 4 (11 8%)
I Peyroteo, F Santos, C Marialva, R Ramos
Table 2.
Association of PD-L1 expression with clinicopathological features
acteristics of penile SqCC, as well as associated prognostic implications In fact, our results showed a trend towards worse clinical features and worse survival in PDL1 CPS ≥ 1 patients, as well as a significant association between PD-L1 status and lymph node involvement
The association between PD-L1 expression and clinicopathological features observed in our study is consistent with previous research in various cancer types, including studies conducted in penile cancer (9, 10)
We found a trend towards larger tumor size, vascular invasion, and perineural invasion in patients with PD-L1 CPS ≥ 1 tumors, although statistical significance was not achieved, probably due to the low number of patients in our cohort These findings are consistent with the largest c
p = 0 705
p = 0 252
pT stage, n (%) p 0 989
pT1a 3 (25 0%) 6 (27 3%)
pT2 4 (33 3%) 7 (31 8%)
pT3 5 (41 7%) 9 (40 9%)
Lymph node involvement, n (%)
No 9 (75 0%) 8 (50 0%)
Yes 3 (25 0%) 14 (63 6%)
p = 0 031
months vs 75 9 months), but statistical significance could not be inferred (p = 0 188) The survival curves are presented in Figure 1
DISCUSSION
The rarity of penile cancer in Western countries poses challenges in understanding its biology and optimal management strategies Our study aimed to find an association between PD-L1 status and clinicopathological char-
Davidsson and colleagues, who analysed 222 cases of penile squamous cell carcinoma (SqCC) (8) This suggests a potential link between PD-L1 expression and aggressive tumor behaviour, which poses the question regarding the need for a different treatment pathway in these patients
A novel observation in our study is the significant associa
involvement We found that a higher proportion of patients with PD-L1 CPS ≥ 1 tumors had lymph node metastases upon lymphadenectomy compared to those with PD-L1 CPS < 1 tumors, with 14 out of 22 PD-L1 CPS ≥ 1 patients (63 6%) having lymph node metastases when lymphadenectomy was performed (p = 0 031) and only 3 out of 12 PD-L1 CPS < 1 patients having lymph node involvement
These findings are in line with those from Udager and colleagues that were among the first to investigate PD-L1 expression in a cohort of 37 patients with penile SqCC They discovered that PD-L1 expression was detected in 62 2% of penile SqCC Despite the limited sample size, they noted a trend towards worse clinical clinicopathological features and worse overall survival but, at least to our knowledge, no statistically significant association has been established yet (9) This finding suggests a potential
1. Overall survival stratified by PD-L1 status.
Figure
role for PD-L1 expression in promoting tumor metastasis and aggressiveness However, the underlying mechanisms driving this association remain unclear and warrant further investigation through mechanistic studies
The lack of a standard second-line treatment for patients with metastatic penile SCC underscores the urgent need f o r n o v e l t h e r a p e u t i c s t r a t e g i e s T h e e m e r g e n c e o f immune checkpoint inhibitors targeting the PD-1/PD-L1 pathway has revolutionized cancer treatment across various tumor types Our study adds to the growing body of evidence supporting the clinical relevance of PD-L1 expression as a potential biomarker for immunotherapy response in penile SqCC
In our study, we observed a high proportion of patients with PD-L1 CPS ≥ 1 (64,7%), which is in line with the current literature (8, 9) Until now, the main focus has been on HPV related penile carcinoma that in our sample was only 32,4%, which is also in line with the current evidence (3) Given the much higher prevalence of PD-L1 expression there is potential for identifying a novel therapeutic target since the literature indicates that tumors expressing high levels of PD-L1 are more likely to respond to immunotherapy
Additionally, In the future, it will be of interest to observe the potential impact of male HPV vaccination on the incidence and oncological outcomes of penile cancer HPVrelated penile cancers are believed to have better outcomes (3) If the incidence of HPV-related cancers decreases as a result of vaccination efforts, we may encounter a higher proportion of aggressive cases Therefore, the importance of novel strategies will become even more significant
F u r t h
chemotherapy over time, yet they may still be suitable candidates for immunotherapy Offering such patients an alternative treatment could prevent disease progression If clinical benefits are demonstrated in this advanced setting, there is potential to pursue approval for this therapy in earlier stages as an adjuvant treatment for tumors with high-risk features, similar to current discussions regarding kidney cancer treatment protocols
Despite the promising role of PD-L1 expression as a prognostic biomarker, our study did not find a statistically significant association between PD-L1 expression and overall survival This may be attributed to the relatively small sample size and short follow-up duration The survival curves show a trend towards separation, suggesting that with a larger sample size, the survival outcomes would likely achieve statistical significance Larger studies with longer follow-up periods are warranted to validate our findings and assess the impact of PD-L1 expression on survival outcomes in penile SqCC
Several limitations should be considered when interpreting our results First, our study was retrospective and conducted at a single institution, which may introduce selection bias and limit generalizability Second, the assessment of PD-L1 expression was based on immunohistochemistry, which has inherent variability and subjectivity Future studies incorporating more robust techniques, such as RNA sequencing or multiplex immunofluorescence, could provide deeper insights into the tumor microenvironment and immune landscape in penile SqCC
Despite de low number of cases, reflecting the rarity of this tumor, our data comes from a tertiary cancer center in Portugal, where all decisions are based on multidisciplinary tumor boards Besides this, we exclusively analysed conventional squamous cell carcinoma and omitted other histologies to avoid confounding the results with histologies known to have a different prognosis
CONCLUSIONS
Our study highlights the association between PD-L1 expression and worse clinical outcomes in penile SqCC It is noteworthy the clinical significance of lymph node involvement in PD-L1 CPS ≥ 1 cases, suggesting a potential role of PDL1 as a predictive biomarker for metastatic disease
REFERENCES
1 EAU Guidelines (2024) Edn presented at the EAU Annual Congress Paris 2024
2 Bleeker MCG, Heideman DAM, Snijders PJF, et al Penile cancer: epidemiology, pathogenesis and prevention World J Urol 2009; 27:141-150
3 Backes DM, Kurman RJ, Pimenta JM, Smith JS Systematic review of human papillomavirus prevalence in invasive penile cancer Cancer Causes Control 2009; 20:449-457
4 Brouwer OR, Rumble RB, Ayres B, et al Penile Cancer: EAUASCO Collaborative Guidelines Update Q and A JCO Oncol Pract 2024; 20:33-37 h
5 Topalian SL, Hodi FS, Brahmer JR, et al Safety, Activity, and Immune Correlates of Anti-PD-1 Antibody in Cancer N Engl J Med 2012; 366:2443-2454
6 Brahmer JR, Tykodi SS, Chow LQM, et al Safety and Activity of Anti-PD-L1 Antibody in Patients with Advanced Cancer N Engl J Med 2012; 366:2455-2465
7 El-Mouallem N, Paul AK Immune Checkpoint Inhibitors for Urothelial Cancer: An Update on New Therapies Fed Pract 2018; 35:S62
8 Davidsson S, Carlsson J, Giunchi F, et al PD-L1 Expression in Men with Penile Cancer and its Association with Clinical Outcomes Eur Urol Oncol 2119; 2:214-221
9 U Udager AM, Liu TY, Skala SL, et al Frequent PD-L1 expression in primary and metastatic penile squamous cell carcinoma: potential opportunities for immunotherapeutic approaches Ann Oncol 2016; 27:1706-12
10 Bacco MW De, Carvalhal GF, MacGregor B, et al PD-L1 and p16 Expression in Penile Squamous Cell Carcinoma From an Endemic Region Clin Genitourin Cancer 2020; 18:e254-e259
Correspondence
Inês Peyroteo (Corresponding Author) ipeyroteo@gmail com
Celso Marialva
Rodrigo Ramos
Portuguese Institute of Oncology in Lisbon, Urology, Lisbon, Portugal
Filipa Santos
Portuguese Institute of Oncology in Lisbon, Pathology, Lisbon, Portugal
Conflict of interest: The authors declare no potential conflict of interest This work was presented at American Association of Urology Congress in 2024
I Peyroteo, F Santos, C Marialva, R Ramos
ORIGINAL PAPER
Efficacy of Flexible ureterorenoscopy in treating multiple renal stones: A cohort study
Sarwar Noori Mahmood 1, 2 , Rawa Bapir 3, 4, 5 , Khoshbin Faeq Mustafa 4 , Ahmed Mohammed Abdalqadir 4 , Shakhawan Hama Amin Said 1 , Nali H Hama 1, 3 , Hiwa O Abdullah 3, 5 , Berun A Abdalla 3, 5 , Fahmi H Kakamad 1, 3, 5
1 College of Medicine, University of Sulaimani, Sulaymaniyah, Kurdistan, Iraq;
2 Mercy Medical City, Malik Mahmood Street, Sulaymaniyah, Kurdistan, Iraq;
3 Smart Health Tower, Madam Mitterrand Street, Sulaymaniyah, Kurdistan, Iraq;
4 Department of Urology, Sulaymaniyah Teaching Hospital, Sulaymaniyah, Kurdistan, Iraq;
Introduction: While the efficacy of flexible ureterorenoscopy (URS) in managing solitary kidney stones (KSs) is widely acknowledged, its effectiveness in treating multiple stones has scarcely been investigated This study aims to assess the effectiveness and safety of retrograde intrarenal surgery (RIRS) utilizing flexible URS and laser lithotripsy in the management of multiple KSs.
Methods: This study was a single-group cohort study conducted on patients with multiple KSs who underwent treatment with RIRS using flexible URS and laser lithotripsy Stone-free status was considered as the lack of residual stone fragments or any residual stone of any size The first follow-up appointment was arranged 3-4 weeks following the procedure If significant residual stones were present, patients underwent reintervention within 2-4 weeks
Results: A total of 110 patients with multiple KSs were included The mean stone burden was 27 5 ± 7 9 mm, and the mean duration of the operation was 54.9 ± 19.7 minutes. Seven cases (6 3%) experienced intraoperative complications, while postoperative complications were found in eight cases (7.3%). After four weeks, a stone-free rate (SFR) was documented in 80 9% of the cases, and this rate increased to 93.6% after three months. The SFR after three months was significant with Guy’s stone score (p < 0.001); however, it did not reach a significant level with any other parameters
Conclusions: The RIRS with flexible URS may be an effective and potentially safe procedure for treating multiple KSs It may yield a favorable SFR with an acceptable complication rate.
Nephrolithiasis, also known as kidney stone (KS), is a common condition with a global concern (1) Following urinary tract infections and prostate diseases, KS is the most presented urinary tract disease Regarding epidemiology, KSs affect about 5% of females and 12% of males over their lifetimes (2, 3) Variations in risk factors for KSs can be observed among different population groups (4) The inci-
dence of KSs is influenced by multiple factors, including environmental factors, gender, race, geographical location, occupation, exposure to hot climates, family history, unhealthy diet, obesity, smoking, alcohol consumption, and low fluid intake (5) Additionally, comorbid metabolic disorders, such as hypertension, diabetes mellitus, cardiovascular disease, and chronic kidney disease can be associated with an elevated risk (3, 4, 6, 7) The symptoms of KSs exhibit variability based on their location whether within the kidney, ureter, or urinary bladder (8) Common sites for stone dislodgement include the vesicoureteric junction, mid-ureter, and pelvoureteric junction (9) Clinical presentations encompass renal colic and flank pain, often accompanied by gross hematuria, a burning sensation during urination, nausea, vomiting, and fever (9-11) Over the last three decades, there have been notable advancements in KS treatment Currently, treatment options include minimally invasive methods such as extracorporeal shock wave lithotripsy (ESWL), percutaneous nephrolithotomy (PCNL), and retrograde intrarenal surgery (RIRS), as opposed to conventional open surgery (12) The applications of RIRS in treating KSs have expanded significantly due to recent advances in endoscopic technology (13) Although the efficacy of flexible ureterorenoscopy (URS) in managing solitary KS is widely acknowledged in the literature, its effectiveness in treating multiple stones has scarcely been investigated (14) The present study aims to assess the effectiveness and safety of RIRS utilizing flexible URS and laser lithotripsy in the management of multiple KSs
METHODS
Setting and design
This single-group cohort study was carried out on patients with multiple KSs who underwent treatment with RIRS with flexible URS and laser lithotripsy at a single center between September 2020 and July 2023 The Iraqi Council for Medical Specializations granted ethical approval for the study Patients underwent comprehensive counseling concerning various treatment approaches, the risk of complications, and the potential necessity for
a staged or auxiliary procedure to ensure an optimal stone-free rate
Eligibility criteria
The inclusion criteria comprised the following: 1) Patients aged ≥ 18, presenting with multiple KSs sized between 11 and 30 mm 2) Stones distributed anywhere within the pelvicalyceal system 3) Conducting RIRS was based on patient preference and several characteristics, such as morbid obesity, congenital renal anomalies, coagulopathy, and treatment failure with PCNL or ESWL Patients with calyceal diverticular stones, ipsilateral ureteric stones or strictures, staghorn stones, pelvic-ureteric junction obstruction, or a medullary sponge kidney were excluded
Patient examination and data collection
Patients underwent preoperative assessment through noncontrast computed tomography (CT) Stone sizes were determined by calculating the sum of the greatest dimensions of each stone observed on non-contrast CT scans The collected data encompassed patients’ demography, family history for KS, history of KS intervention, comorbidities, renal ultrasonography (U/S), non-contrast CT Kidney-UreterBladder (KUB), the indication of RIRS, stone parameters (laterality, number, size), operation time, complications, and stone-free status Complications were classified based on the Modified Clavien Classification System (MCCS) (15)
Stone-free status was considered as the lack of residual stone fragments or any residual stone of any size, as determined by U/S and KUB imaging The outcomes of interest encompassed stone-free rate (SFR) and complication rates
Stones exceeding the 400-600 HU threshold were more likely classified as radiopaque, whereas those falling below were considered radiolucent, although assessment based solely on HU values may have limitations and clinical correlation with additional imaging modalities or stone analysis was often necessary for accurate characterization
Intervention
Under either general or spinal anesthesia and with patients positioned in lithotomy, a semi-rigid ureteroscope (8-9 5F, Karl Storz Endoscopy, Tuttlingen, Germany) was utilized for all procedures This facilitated the passive dilation of the ureter, enabling the evaluation of the presence of concurrent ureteral stones or strictures A Zebra nitinol guidewire (0 032/0 035 inches) (Boston Scientific, USA) was threaded into the pelvicalyceal system through the ureteroscope Following this, a 7 5 Fr flexible URS (Storz Flex-X2S, Tuttlingen, Germany), or a digital singleuse ureteroscope (HU32, Shenzhen Huge Med Medical Technical Development, China), was advanced along the guidewire in a monorail manner In patients pre-stented, a ureteral access sheath (UAS) was placed over the guidewire, followed by the advancement of the flexible URS through the UAS Stone fragmentation was achieved using either the Holmium: YAG laser (Cyber-Ho 60 Holmium laser system, Quanta System, Milan, Italy) or the Calculase III (Storz, Tuttlingen, Germany) This involved applying 0 5-0 8 J power at a frequency of 15-30 Hz through a 200 μm fiber To obviate the necessity for stone retrieval, a stone dusting technique was utilized, frag-
menting the stones into minuscule pieces or fine powder Following the completion of lithotripsy, a visual assessment of the pelvicalyceal system was conducted to detect any residual stone fragments To prevent overlooking substantial pieces or fragments, fluoroscopy was utilized Under direct endoscopic vision, the guidewire was carefully inserted into the renal pelvis or collecting system Following this, the flexible ureteroscope was gradually retracted, allowing for a thorough examination of the entire ureter to identify larger calculi, fragments, and any instances of significant ureteral damage Subsequent to the procedure, a double-J (DJ) stent with dimensions 5-6 F and a length of 26 cm was inserted in all cases Additionally, an indwelling Foley catheter was left in place for approximately 6-12 hours If the postoperative course was uncomplicated, patients were discharged on the postoperative day with prescribed oral antibiotics
Follow-up
The first follow-up appointment was arranged 3-4 weeks after the procedure The KUB examination was conducted, and the DJ stent was removed in the absence of any complications In the presence of significant residual stones and substantial complications, patients underwent reintervention within 2-4 weeks Conversely, patients without complications but with residual stones remained under observation for three months Subsequent evaluations, utilizing renal U/S and KUB X-ray, took place three months after the intervention CT scans were excluded from the diagnostic protocol to minimize expenses and reduce radiation exposure At the three-month mark following the intervention, the SFR was determined This categorization included either complete stone-free status, indicating the lack of residual stone fragments, or the presence of residual stones, identified through U/S and KUB X-rays
Statistical analysis
The data were organized in Microsoft Excel (2019) Subsequently, they were analyzed using the Statistical Package for the Social Sciences (SPSS) (Version 22, IBM SPSS Statistics Inc , USA) The data are presented as frequency, percentage, range, mean, and standard deviation The chi-square test and independent samples T-test were employed to identify significant relationships between the SFR and other variables Statistical significance was defined as p-values less than 0 05
RESULTS
A total of 110 patients with multiple KSs were included, with a mean age of 45 ± 13 82 years and a mean BMI of 25 ± 3 39 kg/m2 The majority of the cases (66 4%) were male A positive history of KS intervention was found in 26 4% of cases Hypertension was the most common comorbidity (74 5%) Ten patients (9 1%) had a history of ischemic heart disease, and nine of them were receiving anticoagulant medications The degree of hydronephrosis was commonly distributed between mild (39 1%) and moderate (31 8%) Renal malformation was present in 18 2% of the patients, while renal malfunction was observed in 20% The indication for RIRS was predomi-
S, Noori Mahmood, R, Bapir, K, Faeq Mustafa, et al
nantly primary (80 9%) Half of the cases (50%) presented with two stones, 38 (34 5%) with three stones, and 17 cases (15 5%) had more than three stones The mean stone burden was 27 5 ± 7 9 mm and the majority of them were unilateral (91 8%) Radiopaque was the prevalent radiologic characteristic of the stones (74 5%) According to Guy’s stone score (GSS), the majority of the stones were categorized as grade 2 (87 3%) Intraoperative fluoroscopy was utilized in 52 (47 3%) patients The mean duration of the operation and laser operating time were 54 9 ± 19 7 minutes and 31 8 ± 15 8 minutes, respectively Seven cases (6 3%) experienced intraoperative complications, including bleeding in four cases (3 6%) and ureteral injury in three cases (2 7%) Postoperative complications were urinary tract infection (5 5%) and hematuria (1 8%), of which seven cases (6 4%) were re-admitted to the hospital and managed conservatively Five cases (4 5%) needed the second stage of RIRS due to residual stones After four weeks, stone free status was achieved in 80 9% of the cases, and this increased to 93 6% after three months (Table 1) The SFR after three months was significant with GSS; however, it did not reach a significant level with any other parameters (Tables 2 and 3)
DISCUSSION
Renal stones have several treatment options, each with its advantages and drawbacks PCNL is a method known for effectively treating large KSs (16) However, it involves accessing the kidney through the renal parenchyma Furthermore, the widely used prone position during the procedure may increase the risks associated with anesthesia and result in a decline in oxygen saturation levels, especially in patients who are obese or elderly and already have respiratory disorders (17) Complications, including hemorrhage, hydrothorax, septicemia, bowel and major vessel injuries, and renal collecting system perforation, pose significant risks during and after this procedure This has driven heightened interest in alternative treatment modalities (18, 19) Recently, there has been a growing discussion about using RIRS for multiple KSs Several studies have investigated the feasibility and effectiveness of RIRS in treating the issue (20, 21) Çakıcı et al compared the efficacy of RIRS and PCNL in treating multicalyceal stones PCNL was the preferred treatment modality unless patients had comorbidities such as anesthesia risk, bleeding diathesis, or anatomical issues where PCNL was unsuitable (20) Alazaby et al assessed RIRS for the treatment of multiple KSs and reached a positive conclusion regarding its efficacy They recommended the utilization of RIRS for patients with multiple KSs, especially in cases where prior treatments such as ESWL and PCNL have been unsuccessful (21) In the present study, the results indicated a favorable outcome, with the SFR reaching 93 6% at 3 months postoperatively The mean operation time was 54 9 ± 19 7 minutes No significant correlations were identified between the mean operation time and the SFR at both 4 weeks and 3 months postoperatively Ozgor et al reported a mean operation time of 47 8 ± 22 2 minutes Also, they reported no significant
c o r r e l a t i o n b e t w e e n i t a n d S F R ( 2 2 ) I n c o n t r a s t , Demirbas et al reported a mean operative time of 62 8 ±
SD: Standard deviation; KS: Kidney stone; Min: m nute * A primary indication means that the patient underwent RIRS for the f rst t me, whi e a secondary ind cation means the patient had a positive history of RIRS # Grade II accord ng to Mod fied C avien Classification System
17 57 minutes and identified a highly significant correlation between the procedure time and SFR (23) A mean operation time of 51 97 ± 20 18 minutes has also been reported (24) Variations in the duration of procedures among different studies may reflect the overall proficiency and the inherent complexities of the surgical tasks It is crucial to recognize that these differences may also arise from varying methodologies used to estimate operative time Notably, some practitioners begin their time assessment with the initiation of cystoscopy, while others commence the measurement at the start of URS
The SFR in the current study was similar to that Alazaby et al reported (92 8%) (21) The similarity may be attributed to the close resemblance in mean stone burden Our reported stone burden was 27 5 mm, and Alazaby et al reported a mean stone burden of 25 7 mm (21) In the present study, although SFR was higher with fewer stones per renal unit, the difference was not statistically significant when comparing two stones with three or more at three months post-procedure This contrasts with Alazaby et al , who reported significant differences: 100% SFR for two stones, 77 7% for three, and 50% for four stones In our cohort, SFR was 98 2% for two stones, 86 8% for three stones, and 94 1% for more than three stones This discrepancy may be attributed to the larger sample size in this study and differences in the definition of SFR The current study considered patients as stone-free when no stone fragments were detected by US and KUB, while Alazaby et al considered SFR when fragments of 3 mm or less detected in CT-KUB (21)
The current study unveiled a significant correlation between the SFR observed three months post-operation and the GSS This may suggest that as the complexity of stones increases, the probability of achieving stone-free status diminishes within the three months following the operation This aligns with the conclusions drawn by
Table 2.
Correlation of SFR with RIRS indication, stone characteristics, stent placement, and ureteric access sheath
Table 3.
Correlation of stone burden and operation time with SFR.
Karsiyakali et al , who also found a significant correlation between SFR and GSS grade 3 (25) Notably, their study questioned the GSS scoring system's effectiveness in predicting SFR after RIRS This is due to the reduced utility for GSS grade 1 and grade 4 stones, making the system less effective across the entire stone complexity spectrum As a result, their findings highlight the necessity for a nuanced approach to predict SFR post-RIRS (25) In this study, the assessment of radiopacity in stones showed no significant correlation with SFR at four weeks and three months postoperation This aligns with Lim et al 's findings on the relationship between stone radiopacity and SFR after RIRS procedures (26) Ozgor et al. similarly concluded that there was no significant correlation between these parameters (22) These outcomes emphasize the need for a nuanced consideration of factors influencing SFR beyond focusing solely on stone radiopacity in the postoperative context With decreased instrument size, potential complications like ureteral avulsion are now extremely rare Our study found no major complications, but 15 patients (13 6%) experienced manageable minor complications seven intraoperative and eight postoperative This aligns with Alazaby et al , reporting 16 6% minor complications (21) In contrast, Atis et al documented 3 4% minor complications in their RIRS group; this variance may be due to varying sample sizes, and notably, our cohort included intraoperative complications (27) This research is subject to several limitations, including the study's small sample size, which limits its generalizability The definition of stone burden varies, introducing potential inconsistencies Additionally, the absence of a comparison with alternative stone treatment methods hinders a comprehensive assessment The study's short follow-up duration restricts the evaluation of long-term outcomes To avoid citing nonpeer-reviewed data, the authors ensured the credibility of the referenced studies (28)
S, Noori Mahmood, R, Bapir, K, Faeq Mustafa, et al
In conclusion, RIRS with flexible URS may be an effective and potentially safe procedure for treating multiple KSs It may yield an excellent SFR with an acceptable complication rate
REFERENCES
1 Said SH, Al Kadum Hassan MA, Ali RH, et al Percutaneous nephrolithotomy; alarming variables for postoperative bleeding Arab J Urol 2017; 15:24-29
2 Bhatti KH, Bapir R, Bhatti WS, et al Efficacy of sexual intercosurse in the spontaneous passage of distal or intramural ureteral stones: a randomsized controlled trial Ann Med Surg (Lond) 2023; 85:5972-5976
3 Guan F, Han W, Ni T, et al Genetic polymorphisms of RGS14 and renal stone disease Arch Med Res 2021; 52:332-8
4 Safarinejad MR Adult urolithiasis in a population-based study in Iran: prevalence, incidence, and associated risk factors Urol Res 2007; 35:73-82
5 Bhatti KH, Rawa Bapir, Nadeem Sohail, et al Occupational hazard in urolithiasis patients in Qatar:A single-center cross-sectional study Arch Ital Urol Androl 2024; 96:12022
6 Ferraro PM, Taylor EN, Gambaro G, Curhan GC Vitamin D intake and the risk of incident kidney stones J Urol 2017; 197:405-10
7 Romero V, Akpinar H, Assimos DG Kidney stones: a global picture of prevalence, incidence, and associated risk factors Rev Urol 2010; 12:e86
8 Kumar A, Kumar N, Vasudeva P, et al A prospective, randomized comparison of shock wave lithotripsy, retrograde intrarenal surgery and miniperc for treatment of 1 to 2 cm radiolucent lower calyceal renal calculi: a single center experience J Urol 2015; 193:160-4
9 Aggarwal R, Srivastava A, Jain SK, et al Renal stones: a clinical review EMJ Urol 2017; 5(1):98-103
10 Khan SR, Pearle MS, Robertson WG, et al Kidney stones (Primer) Nat Rev Dis Primers 2016; 2:1
11 Teichman JM Acute renal colic from ureteral calculus N Engl J Med 2004; 350:684-93
12 Chung DY, Kang DH, Cho KS, et al Comparison of stone-free rates following shock wave lithotripsy, percutaneous nephrolithotomy, and retrograde intrarenal surgery for treatment of renal stones: A systematic review and network meta-analysis PloS one 2019; 14: e0211316
13 Ucer O, Erbatu O, Albaz AC, et al Comparison stone-free rate and effects on quality of life of percutaneous nephrolithotomy and retrograde intrarenal surgery for treatment of renal pelvis stone (24 cm): A prospective controlled study Curr Urol 2022; 16:5-8
14 Yanaral F, Ozgor F, Kucuktopcu O, et al Comparison of flexible ureterorenoscopy and mini percutaneous nephrolithotomy in the management of multiple renal calculi in 10-30 mm size Urol J 2019; 16:326
15 Tevis SE, Kennedy GD Postoperative complications and implications on patient-centered outcomes J Surg Res 2013; 181:106-13
16 Kasap Y, Senel S, Uzun E, et al Does surgical position affect infective complications in percutaneous nephrolithotomy? Urolithiasis 2022; 50:765-71
17 Saltirov I, Petkova K Complications Related with PCNL and Their Management In: Zeng G, Sarica K (eds) Percutaneous Nephrolithotomy Springer, Singapore 2020
18 Chandrasekera S Percutaneous Nephrolithotomy: Management of Complications In: Ng ACF, Wong MY, Isotani S (eds) Practical Management of Urinary Stone Springer, Singapore 2021
19 Breda A, Ogunyemi O, Leppert JT, et al Flexible ureteroscopy and laser lithotripsy for single intrarenal stones 2 cm or greater is this the new frontier? J Urol 2008; 179:981-4
20 Cakici M, Sari S, Ozok H, et al Comparison of Retrograde Intrarenal Surgery and Percutaneous Nephrolithotomy in the Treatment of 2-3 cm Multicalyceal Kidney Stones J Urol Surg 2018; 5: 143-48
21 Alazaby H, Khalil M, Omar R, et al Outcome of retrograde flexible ureterorenoscopy and laser lithotripsy for treatment of multiple renal stones Afr J Urol 2018; 24:146-51
22 Ozgor F, Kucuktopcu O, Ucpinar B, et al Is there a difference between presence of single stone and multiple stones in flexible ureterorenoscopy and laser lithotripsy for renal stone burden< 300mm 2? Int Braz J Urol 2016; 42:1168-77
23 Demirbas A, Yazar VM, Ersoy E, et al Comparision of percutaneous nephrolithotomy and retrograde intrarenal surgery for the treatment of multicalyceal and multiple renal stones Urol J 2018; 15:318-22
24 Sercan SA, Selmi V, Caniklioglu M, et al Our retrograde intrarenal surgery experience in the treatment of multi-caliceal and multiple kidney stones Kırıkkale Üniversitesi Tıp Fakültesi Dergisi 2020; 22:406-10
25 Karsiyakali N, Karabay E, Erkan E, Kadihasanoglu M Evaluation of nephrolithometric scoring systems to predict outcomes of retrograde intrarenal surgery Urol J 2020; 17:352-7
26 Lim SH, Jeong BC, Seo SI, et al Treatment outcomes of retrograde intrarenal surgery for renal stones and predictive factors of stone-free Korean J Urol 2010; 51:777
27 Atis G, Culpan M, Pelit ES, et al Comparison of percutaneous nephrolithotomy and retrograde intrarenal surgery in treating 20-40 mm renal stones Urol J 2017; 14:2995-9
28 Muhialdeen AS, Ahmed JO, Baba HO, et al Kscien’s List; A New Strategy to Discourage Predatory Journals and Publishers (Second Version) Barw Med J 2023; 1:24-26
Correspondence
Sarwar Noori Mahmood, MD
Shakhawan Hama Amin Said, MD
Nali H Hama, MD
College of Medicine, University of Sulaimani, Sulaymaniyah, Kurdistan, Iraq
Rawa Bapir, MD
Hiwa O Abdullah, MD
Berun Abdalla, MD
berun anwer95@gmail com
Smart Health Tower, Madam Mitterrand Street, Sulaymaniyah, Kurdistan, Iraq
Khoshbin Faeq Mustafa, MD
Ahmed Mohammed Abdalqadir, MD
Department of Urology, Sulaymaniyah Teaching Hospital, Sulaymaniyah, Kurdistan, Iraq
Fahmi Hussein Kakamad, MD (Corresponding Author) fahmi hussein@univsul edu iq
Doctors City, Building 11, Apartment 50, Sulaimani, Iraq
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Adverse events related to laser fibers and laser machines during ureteroscopy and stone lithotripsy: Insights from an updated 10-year analysis of the US MAUDE database
Patrick Juliebø-Jones 1, 2, 7 , Mathias Sørstrand Æsøy 1 , Christian Beisland 1, 2 , Vincent De Coninck 3, 7 , Etienne Xavier Keller 4, 7 , Lazaros Tzelves 5, 7 , Peder Gjengstø 1 , Christian Arvei Moen 1 , Bhaskar K Somani 6 , Øyvind Ulvik 1, 2
1 Department of Urology, Haukeland University Hospital, Bergen, Norway;
2 Department of Clinical Medicine, University of Bergen, Bergen, Norway;
3 Department of Urology, AZ Klina, Brasschaat, Belgium;
4 Department of Urology, University Hospital Zurich, University of Zurich, Zurich, Switzerland;
5 Second Department of Urology, National and Kapodistrian University of Athens, Sismanogleio General Hospital, Athens, Greece;
6 Department of Urology, University Hospital Southampton, UK;
7 EAU YAU Urolithiasis group
Summary
Introduction: Ureteroscopy has become increasingly chosen as a treatment of choice for patients with kidney stone disease and laser as the energy source for stone lithotripsy is a key part of this. Our aim was to analyse a national database to evaluate the burden of adverse events related to laser fibers and laser machines
Methods: Search was performed of the Manufacturer User and Facility Device Experience (MAUDE) database in the United States for all events related to holmium laser fibers and holmium laser machines during ureteroscopy between 2012-2021. Information collected included the following: problem, timing, prolonged anaesthesia, early termination of procedure, injury and retained parts
Results: 699 holmium laser fiber events were reported and these had been manufactured by 13 different companies The commonest problems were breakage outside the patient while in use (26.3%) and breakage of the laser fiber tip (21.2%).
Manufacturers concluded root cause to be device failure in 8.9%. 29% of issues occurred before the laser had been activated 5 2% of cases had to be cancelled as a result of an event Significantly more injuries were sustained intra-operatively by operating staff compared to patients (6% vs 0 2%, p < 0 001) All these injuries were superficial burns to the skin with the hand being the most affected body part (88.1%). Zero ocular injuries were reported. Only eight events were related to laser machines and all involved sudden hardware failure but no patient injury
Conclusions: Laser fibers are fragile Most adverse events are due to operator error Direct patient injury from laser fiber is scarce but operating staff should be aware of the risk of sustaining minor burns Laser machines rarely incur problems and, in this study, did not result in any safety issues beyond need to abort the procedure due to lack of spare equipment.
Submitted 9 February 2024; Accepted 15 February 2024
INTRODUCTION
Ureteroscopy is increasingly chosen as a treatment of choice for patients with kidney stone disease (KSD) (1) Multiple national registries have recorded that it is the surgical intervention for KSD, which has seen the greatest uptake in recent years (2, 3) A key reason for this shift in practice pattern has been the advancements related to the energy source employed for intracorporal endoscopic stone lithotripsy and more specifically, the advent of laser (Light Amplification by Stimulated Emission of Radiation) to urological practice (4-6) The Manufacturer User and Facility Device Experience (MAUDE) database is a registry in the United States that catalogues failures including damages related to surgical devices (7) This database, which is essentially a library of adverse events can therefore be examined to gain understanding in surgical fields (8) To date, and in contrast to other areas of urology, little has been explored in the area of lasers used in URS and stone lithotripsy (9) Our aim was to analyse this database and evaluate the events recorded with the principal purpose of evaluating its safety, insights and lessons learned from it relevant to laser machines and fibers
MATERIALS AND METHODS
Search was performed of the MAUDE database for all events related to holmium laser fibers and laser machines between January 1st 2012 to December 31st 2021 (10) Search terms used were “laser” , “laser fiber” , “holmium laser” , “ureteroscopy” and “laser machine” This yielded 5450 events Event reports combine the information given by health professional as well as a manufacturer summary and verdict on root cause Each report was individually reviewed, and the following information was collected: problem related to the event, timing, prolonged anaesthesia, early termination of procedure, patient injury, surgeon
P Juliebø-Jones, M Sørstrand Æsøy, C Beisland, et al
injury, retained parts and manufacturers´ final verdict on root cause Reports were excluded if there was insufficient information (n = 37) and/or where the wording lacked clarity (n = 9) This also applied to any duplicates (n = 59) All information in this particular database is unrestricted and freely available to the public worldwide and completely anonymised As such, ethical approval was not deemed necessary Data was collected and analysed using SPSS Statistics v 26 (IBM, Armonk, NY) Where deemed appropriate, categorical variables were compared using Chi-square test with p-values < 0 05 considered to be statistically significant
RESULTS
Laser fibers
Over the study period, 699 were events reported related to laser fibers manufactured by 13 different companies (Table 1)
The commonest problems were inadvertent breakage outside the patient while in use (26 3%), breakage of the laser fiber tip inside the patient´s body (21 2%) and laser fiber that suddenly stopped working (16 7%) When laser fibers were reported to suddenly stop working, the cause was found to be micro cracks If overheating of the laser fiber was reported (3 9%), the underlying cause was also found to be micro cracks Manufacturers reported the laser fiber problem to have been caused by manufacturing fault, in 8 9% of the events In that latter group, two skin burns to staff were recorded but no patient injuries None of the procedures had been terminated but two had incurred prolonged anaesthesia While most issues arose while the laser had been activated and in use, 29% occurred before this happened The most frequently reported reasons for the latter were either the laser being broken in the packaging (16 6%) or inadvertently broken by the assistant during preparation or assembly While more than 9 in 10 of these events did not affect the procedure being successfully completed, it remained the case that 5 2% had to be cancelled and 14 7% required prolonged anaesthesia The latter was typically due to the additional time required for basket retrieval of the detached laser fiber tip, which is not always straightforward Overall, 5% of patients had a fiber fragment retained in the urinary system at the end of the case Onward treatment plan for this issue appeared to come down to surgeon preference While 60% of these retained fragments led to the patients being re-listed for elective URS and active retrieval, the remainder were left to pass spontaneously In 10% of the latter group, a supplementary report had been filed to provide an update that the patient had been re-admitted with pain and required emergency URS and retrieval of the residual fragment Details were not available to provide a further update on whether surgery to remove residual fragments was successful
In 4 7% of the events, the ureteroscope was damaged Cases were terminated early to insufficient spare equipment being readily available at the time of surgery rather than safety concerns except for one case That particular event involved the surgical drapes catching fire while the
Table 1
Summary of events
Characteristic
Problem
Broken outside patient while in use
Broken in packaging
Broken in preparation or assembly
Overheating
Broken on entry to scope
Broken within body of scope
Not registering
(3 9%)
(3%)
(2 3%)
(0 4%)
Broken after reported stuck in machine 3 (0 4%)
Misfiring 1 (0.1%)
Visible location of laser fiber breakage while in use
Distal section
Middle section (i e , within scope)
Proximal section (i e , outside patient)
Damage to ureteroscope
Timing of problem
(45.4%)
(4 3%)
(50 3%)
(4 7%)
Before laser used 203 (29%)
During laser use 488 (69 8%)
After completion laser usage 8 (1 2%)
Successful completion of procedure Yes 662 (94 8%)
Prolonged anaesthesia Yes 103 (14 7%)
Lost laser fiber tip left in patient at end of the case Yes 35 (5%)
Management: Conservative
(40%) Re-listed for planned URS and removal
(60%)
laser fiber was resting against them while in use and was found to be broken Limited details beyond this were available but it was confirmed that it was successfully extinguished, and no injury was sustained to the patient or staff Significantly more injuries were sustained intra-operatively by operating staff compared to patients (6% vs 0 2%, p < 0 001) (Table 2)
The distribution of injuries to surgeon and assistant/nurse was 45 2% and 54 8%, respectively All these injuries were superficial burns to the skin with the hand being the most affected body part (88 1%) No ocular injuries were reported Only two intra-operative injuries were recorded in patients These consisted of a superficial skin burn to their leg and a case of thermal injury to the ureteric mucosa resulting in stenting
Laser machines
There were few events related specifically to the holmium laser machine itself In total, there were eight reported, and all involved a sudden shut down of the machine These occurred after laser activation had been commenced These all related in prolonged anaesthesia While no patient or operating staff injuries were record-
Table 2.
Operating staff injury Yes
(6%)
(45 2%) Nurse/assistant
(54 8%) Injury
(100%)
(88 1%)
2 (4 8%)
(4 8%)
(2 4%)
(0 2%)
ed as a result, six out of eight of these cases had to be cancelled as no spare laser machine was available
Manufacturer claimed responsibility for this issue in only two cases Reasons given by the manufacturer as to why responsibility could not be accepted in the other cases included previous repair having been performed by an external company and failure to service the machine in a timely manner
DISCUSSION
This study has found that the safety profile related to use of laser fibers is favourable Risk of intra-operative injury to a patient related to a laser fiber problem seems to be a rare event The risk for injury to operating staff is higher in comparison, but still relatively low Likelihood of manufacturing failure is low, and most problems are the result of user error including mishandling of the fiber While more than one in ten cases incurred prolonged anaesthesia, over 90% of cases were completed successfully despite the event Lack of spare equipment being readily available leads to cancellation of cases mid procedure
Our study revealed limited results for laser machines, which would suggest that in comparison, that such hardware problems are rare and while they do not result in patient injury, having spare laser unit would prevent aborting the operation
These findings from the MAUDE database confirm the fragility of laser fibers Surgeons and operating staff alike should invest time in learning how to use and handle them safely and appropriately (11) Key points include being gentle when feeding the fiber into the scope as well as securing the fiber with a damp swab rather than with a glove or instrument (Table 3) (12)
Awareness of risk factors for fiber fracture can help minimise the risk of occurrence These include increased angle of deflection, shorter pulse duration, higher core diameter and higher pulse energy (11) The soft, polyte-
trafluoroethylene lining of the flexible ureteroscope is extremely sensitive to damage such as by uncontrolled energy loss occurring during fiber fracture or the silicate tip itself Relevant to this, is observing the safety distance concept of the laser tip in relation to the ureteroscope tip to prevent iatrogenic damage from the laser´s cavitation bubble or direct laser energy impact It is worth noting a relatively low rate of damages to the ureteroscope in our analysis (4 7%), compared to a fourfold higher rate of breakage of the laser fiber tip (21 2%)
This observation suggests that the laser fiber tip may have broken relatively far away from the instrument in most cases, an event known to happen when working with a transparent fiber tip Interestingly, a theme from the reports of the MAUDE database was that if the glass tip had not been clipped beforehand, identification and retrieval was more difficult This is precisely the reason why some authors have suggested to cut the fiber tip though the coloured plastic jacket, discarding the transparent fiber tip and its risk of breakage and retainment (11) Note the laser pilot beam can be activated prior to use to help identify coating damage Management of broken laser fiber tip appears to vary and indeed there is no precedent in terms of evidence to really guide how this should be While this study has not compared single use and re-usable fibers, when using the latter, these should be carefully inspected and checked for cracks or damages, which can cause subsequent energy leakage (13) In this regard, single-use fibers may lower the risk of unintended laser energy leakages compared to re-usable fibers and would be readily available in case of fiber failure
Our findings serve as a reminder that damage can occur outside the operating theatre such as during packaging and sterilisation process While this remains an area where there is limited research to guide clinical practice, the authors recommend implementation of safety training courses locally for dedicated personnel training as well as hospital protocols for safe use of laser A previous survey of endourologists revealed that institutional laser safety training was only present among 63% of the respondents hospitals and likewise, a formal committee was only found in 34% (14)
The potential for ocular injuries attracts a lot of attention and had led to continued debate regarding the absolute
Table 3.
Summary of prevention strategies for laser machine and fiber failure
Problem Prevention
Machine failure
Laser fiber failure
Laser machine testing prior to procedure
Spare machine (if available)
Regular servicing and testing of machine
Careful removal from packagiung to acoid breakage
Careful insertion of fiber into the scope
Secure fiber on outside with wet swab
Cutting the distal tip of the fiber after use (for resuable fiber)
Laser fibers should not be wrapped too tight If a lesion is detected, cut the fiber proximal to this lesion
Activate laser pilot beam prior to use to help identify coating damage
Intra-operative injuries
P Juliebø-Jones, M Sørstrand Æsøy, C Beisland, et al
need for protective eyewear (14) Operating staff injuries were mostly limited to skin burns, with no eye injury at all This data adds to the evidence supporting the possibility of omitting wearing protective glasses for laser interventions in urology, except for Greenlight laser where the risk of injury to the retina remains a safety hazard Similarly, a previous review has found that no injuries of this kind related to Ho:YAG have ever been reported in the literature over the past 20 years (15) Villa et al found the critical laser fiber tip to eye distance for injury to be 5 cm when using Ho:YAG (16)
Limitations
There are drawbacks to acknowledge in this study Firstly, the total number of cases performed over this study period is not known and therefore the incidence of these events cannot be calculated Given manufacturers were providing evaluations on their own equipment, inherent bias can be present There was only one case of thermal injury to the ureter reported, which is acknowledged to not be representative of its true burden Similarly, late complications such as ureteral stricture, which can occur because of thermal injury have not been captured in this data set and this is also a limitation
The data in MAUDE is added prospectively, however, the intention for its use is not primarily for academic research purposes Research groups wishing to study this data are reliant on trusting the quality of information provided In this regard, we were strict to exclude events where information was limited or deemed of insufficient quality The database also does not register certain parameters such as hospital setting (e g , community versus academic), surgeon experience nor any information regarding patient characteristics such as comorbidities, stone burden or anticoagulation status (17) Also, specific details on prolonged anaesthesia such as precise timings were not available However, there are valuable insights that arise from reviewing this database, which is relatively unique in nature and the largest of its kind globally Our study sheds light on events that while they may have been heard of or reported in individual case reports, such data lies outside the standard parameters that are recorded in clinical studies Moreover, nearly all studies that evaluate the intricacies of laser properties are exclusively performed in the pre-clinical setting
A strength of databases such as MAUDE is that they are well suited for reporting events that are often related to user error as the information can be shared anonymously It is such that authors rarely strive to publish results, which could potentially place their own reputation and their hospital´s in an unfavourable light, which may in turn lead to underreporting go these events
CONCLUSIONS
Laser fibers are fragile, and the vast majority of adverse events related to them are not caused by a manufacturing fault, but rather operator and handling errors Damage to a patient specifically from the physical laser fiber is very seldom but operating staff should be aware of the risk of sustaining minor burns when handling the laser fiber while in use Laser machines rarely incur problems intra-
operatively and in this study did not result in any safety issues beyond the need to abort the procedure due to lack of spare equipment
REFERENCES
1 Herout R, Baunacke M, Groeben C, et al Contemporary treatment trends for upper urinary tract stones in a total population analysis in Germany from 2006 to 2019: will shock wave lithotripsy become extinct? World J Urol 2022; 40:185-91
2 Jour I, Lam A, Turney B Urological stone disease: a 5-year update of stone management using Hospital Episode Statistics BJU Int 2022; 130:364-9
3 Geraghty RM, Jones P, Somani BK Worldwide Trends of Urinary Stone Disease Treatment Over the Last Two Decades: A Systematic Review J Endourol 2017; 31:547-56
4 Staehler G, Hofstetter A, Gorisch W, et al Endoscopy in experimental urology using an argon-laser beam Endoscopy 1976; 8:1-4
5 Kronenberg P, Cerrato C, Juliebo-Jones P, et al Advances in lasers for the minimally invasive treatment of upper and lower urinary tract conditions: a systematic review World J Urol 2023; 41:381727
6 Juliebø-Jones P, Keller EX, Haugland JN, et al Advances in Ureteroscopy: New technologies and current innovations in the era of Tailored Endourological Stone Treatment (TEST) Journal of Clinical Urology 0(0):20514158221115986
7 Gurtcheff SE Introduction to the MAUDE database Clin Obstet Gynecol 2008; 51:120-3
8 Lee J, Kaplan-Marans E, Jivanji D, et al Post-cystoscopy infections and device malfunctions in reprocessed flexible cystoscopes in a national database Can J Urol 2022; 29:11361-5
9 Althunayan AM, Elkoushy MA, Elhilali MM, Andonian S Adverse events resulting from lasers used in urology J Endourol 2014; 28:256-60
10 Administration UFaD MAUDE - Manufacturer and User F a c i l i t y D e v i c e E x p e r i e n c e 2 0 2 3 [ A v a i l a b l e f r o m : h t t p s : / / www accessdata fda gov/scripts/cdrh/cfdocs/cfmaude/textsearch cfm
11 Keller EX, Kronenberg P, Tailly T, et al Laser accessories: surgical fibers, strippers, cleavers, and protective glasses Curr Opin Urol 2022; 32:330-338
12 Talso M, Emiliani E, Haddad M, et al Laser Fiber and Flexible Ureterorenoscopy: The Safety Distance Concept J Endourol 2016; 30:1269-74
13 Juliebo-Jones P, Somani BK, Gjengsto P, et al Holmium and Thulium Fiber Laser Safety in Endourological Practice: What Does the Clinician Need to Know? Curr Urol Rep 2023; 24:409-15
14 Paterson NR, Fitzpatrick R, Blew B, et al Perceptions and Practice Patterns of Holmium Laser Goggles in Endourological Procedures: An Unnecessary Evil? J Endourol 2019; 33:146-50
15 Bhojani N, Andonian S, Watterson JD, et al Canadian Urological Association best practice report: Holmium:YAG laser eye safety Can Urol Assoc J 2020; 14:380-2
16 Villa L, Cloutier J, Comperat E, et al Do We Really Need to Wear Proper Eye Protection When Using Holmium:YAG Laser During Endourologic Procedures? Results from an Ex Vivo Animal Model on Pig Eyes J Endourol 2016; 30:332-7
17 Gopal N, Long B, Phillips J, Eshghi M Endovascular Stapler
Complications During Minimally Invasive Nephrectomy: An Updated
Correspondence
Patrick Juliebø-Jones, MD (Corresponding Author) jonesurology@gmail com
Resident Department of Urology, Haukeland University Hospital, Bergen, Norway
Mathias Sørstrand Æsøy, MD
mathias asoy@gmail com
Peder Gjengstø, MD peder gjengsto@helse-bergen no
Christian Arvei Moen, MD
christian arvei moen@gmail com
Consultant urological surgeon Department of Urology, Haukeland University Hospital, Bergen, Norway
Christian Beisland, MD
christian beisland@helse-bergen no
Consultant urological surgeon, Professor of Urology Department of Urology, Haukeland University Hospital, Bergen, Norway
Vincent De Coninck, MD vdconinck@gmail com
Consultant Urologist
Department of Urology, AZ Klina, Brasschaat, Belgium
Etienne Xavier Keller, MD etienne xavier keller@gmail com
Consultant urological surgeon
Department of Urology, University Hospital Zurich, University of Zurich, Zurich, Switzerland
Lazaros Tzelves, MD lazarostzelves@gmail com
Consultant Urologist
Second Department of Urology, National and Kapodistrian University of Athens, Sismanogleio General Hospital, Athens, Greece
Bhaskar K Somani, MD bhaskarsomani@yahoo com
Consultant urological surgeon, Professor of Urology Dept of Urology, University Hospital Southampton, UK
Øyvind Ulvik, MD doc ulvik@online no
Consultant urological surgeon, Associate Professor of Urology Department of Urology, Haukeland University Hospital, Bergen, Norway
Conflict of interest: Øyvind Ulvik has acted as a consultant for Olympus
The other authors have nil to declare
Review of the FDA MAUDE Database From 2009-2019 Urology 2021; 153:181-4
ORIGINAL PAPER
Prospective observational study on the efficacy and tolerability of a complex of phytochemicals versus dutasteride in the treatment of Lower Urinary Tract Symptomps due to Benign Prostatic Hyperplasia
Giuseppe Saitta 1 , Franco A Mantovani 1 , Benedetto Calabrese 1, 2 , Camilla Aliboni 1, 2 , Giuseppe Di Paola 1 , Attilio L Meazza 1 , Mauro Seveso 1
Introduction: The aim of our study was to treat 2 similar groups of patients suffering from benign prostatic hyperplasia (BPH): one group with a complex of phytochemicals based on phycocyanin, Palmitoylethanolamide (PEA) and selenium; the other group with dutasteride. The effectiveness of these treatments was checked, especially regarding the improvement of lower urinary tract symptoms (LUTS) and the reduction of prostatic specific antigen (PSA) and prostate volume
Materials and methods: We included 104 patients in the study
All patients were aged between 50 and 70 years, with PSA values between 4 and 10 ng/ml, prostate volume, as calculated by transrectal ultrasound between 50 and 70 cc, maximum flow value greater than or equal to 10 ml/s at flowmetry, no suspicious nodules on difital rectal examination (DRE), no suspicious lesions on magnetic resonance imaging MRI (PI-RADS 1-2), negative previous prostatic biopsies or never biopsied, moreover absence of diabetes mellitus or chronic renal failure (blood creatinine > 2 mg/dl). We considered: Group A of 54 men who used the complex of phytochemicals; Group B of 50 patients treated with dutasteride. We followed all the patients for 6 months after starting therapy, considering the following parameters: PSA, prostate volume, and flowmetry.
Results: Our results showed that both dutasteride and the phytochemicals complex decreased PSA levels (p < 0.0001 for both), with a more significant effect of dutasteride (mean decrease of -2.743 ng/ml vs -0.971 ng/ml). Uroflowmetry also improved in both groups ( p < 0 0001) with a mean increase in maximum flow of urine of + 3.03 ml/min for the dutasteride group and + 13 02 ml/min for phytochemicals complex group Lastly, dutasteride proved to be highly effective on reducing the prostate volume on transrectal ultrasound (TRUS) (-22 14 ml, p < 0.0001) compared to the complex of phytochemicals, which showed a mean decrease of -10 04 ml (p < 0 0001) Moreover, the reduction in prostate volume obtained through the use of dutasteride proved to be more consistent than the one obtained by using the complex of phytochemicals even at statistical analysis (p < 0 0001)
Conclusions: Both the complex of phytochemicals and dutasteride showed reduction of PSA values after 6 months of treatment The complex based on phycocyanin, PEA and selenium showed a statistically significant improvement in urinary flow, while dutasteride acted more on the volume of the prostate
However, the natural complex is a product with good efficacy on the phlogistic component and does not have the side effects of dutasteride (eg gynecomastia, reduced libido). Therefore, we believe it can be used by a large part of the population with BPH, in order to reduce LUTS and PSA and improve urinary flow, without side effects
Submitted 5 August 2024; Accepted 12 September 2024
INTRODUCTION
Benign Prostatic Hyperplasia (BPH) is a common urological disease among older men It consists of a progressive enlargement of the prostatic tissue, especially its central portion The resulting bladder outlet obstruction, coupled with increased muscle tone of the bladder and secondary dysfunction of the detrusor, produce lower urinary tract symptoms (1) Medical treatment is the first-line therapeutical option for this condition Commonly administered drugs are alphablockers, 5-Alpha Reductase Inhibitors (5-ARIs) and phosphodiesterase 5-Inhibitors (PDE5-I) If men have persistent irritative storage symptoms after first line BPH therapy then OverActive Bladder (OAB) medications can be added or used as a replacement
Combination therapies usually allow to increase the efficacy of medical treatments and delay the need for corrective surgery (2, 3) Most said drugs, however, show a consistent rate of side effects in those who use them This is why there is a massive increase of interest for herbal and nutraceutical treatments Serenoa Repens, for instance, is one of the oldest and most effective nutraceutical drugs used to treat BPH-related symptoms In vitro, Serenoa repens extract (320 mg once a day) has demonstrated anti-inflammatory, antiandrogenic, and estrogenic effects along with a decrease in sexual hormone-binding globulin; inhibition of 5α-reductase, muscarinic cholinoreceptors, dihydropyridine receptors, and vanilloid receptors; neutralization of free radicals As of today, Serenoa Repens is considered
equally effective compared to the alpha- blocker tamsulosin for what concerns the improvements on International Prostate Symptom Score (IPSS), Quality of Life (QoL), maximum urinary flow rate, postvoid residual volume and Prostate Specific Antigen (PSA) levels (4, 5)
Combination therapy of alpha-blockers and Serenoa Repens, furthermore, proved even more effective than monotherapy (6)
Palmitoylethanolamide (PEA) is an endogenous fatty acid amide-signaling molecule with anti-inflammatory and neuroprotective effects that has an interesting role in the management of chronic pelvic pain syndrome and chronic urological pain (7) PEA exerts its clinical effects through different mechanisms: the down-regulation of mast cell activation; the direct activation at least two different receptors: the peroxisome proliferator-activated receptors-alfa (PPAR-α) and the orphan G-protein coupled receptors 55 (GPCR 55): GPR55; more recently, it has also been demonstrated that PEA can activate transient receptor potential vanilloid 1 (TRPV1) channels or increase the expression of cannabinoid receptor 2 (CB2) receptors, of which PEA has been demonstrated to be a weak agonist, via PPAR-α receptors This results in a neuroprotective and anti-nociceptive effect of PEA, decreasing hyperalgesic responses in the chronic constriction injury (CCI) model of neuropathic pain (8, 9) In a female rat model of cyclophosphamideinduced cystitis, it has been reported that pain behavior, bladder inflammation and voiding dysfunction were associated with increased bladder levels of PEA, up-regulation of cannabinoid receptor 1 (CB1) receptor expression and down-regulation of PPAR-α expression Oral administration of ultra micronized PEA produced both anti-inflammatory and analgesic effects (10) Such results suggest that PEA could also be used in BPH-related voiding dysfunctions and irritative lower urinary tract symptoms (LUTS) In fact, D’Amico et al demonstrated that daily administration of PEA in BPH-affected rats considerably reduced the levels of testosterone and dihydroetestosterone (DHT), main characters of BPH Also, it substantially reduced 5α-reductase-2 expression and obtained a significant decrease in tumor growth factor-beta (TGF-b) expression, leading to a better cellular growth/apoptosis ratio (11)
Phycocyanin (PC) is a protein that derives from spirulina It has been widely demonstrated that PC exerts its antiinflammatory and antioxidant activity through the inhibition of cyclooxygenase-2 (COX-2) enzymatic activity The same inhibitory effect of COX-2 was observed in the model of human prostate epithelial cells, in which PC also showed a synergic effect with PEA by abating the synthesis of prostaglandin E2 (PGE2) (12, 13)
Selenium (Se) and Tomato Extracts (TE) are important trace elements in health, and their role has been widely evaluated even for BPH and prostate cancer Se may be able to prevent, inhibit or reverse the transition of the epithelial cells to the mesenchymal phenotype Both Se and TE proved to modify anatomopathological results when comparing a hyperplastic hypertrophic prostate treated with both elements and a healthy one In particular, mild hyperplasia with predominance of no presence of glandular hyperplasia and stromal restructuring and decrease in the thickness of the epithelium was observed Furthermore, the combination
on Se and TE proved to be synergic In the oxidative stress markers of the BPH group, there was a significant increase in malondialdehyde (MDA) and nitrites (NO2) with respect to the control group Oral administration of Se and TE, especially when combined, proved to significantly decrease the levels of those markers, thus showing an antioxidant effect (14, 15)
The aim of our study was to compare two groups of patients affected by BPH: the first was treated with the 5ARI Dutasteride, the second, instead, with a combination of nutraceuticals: Palmitoylethanolamide (200 mg), Phycocianin (250 mg) and Selenium (55 mcg)
Although synergic effects between such elements have been hypothesized and, to some extent, demonstrated, our aim is to contribute to the present literature by describing the results in this cohort of patients
MATERIAL AND METHODS
We included in the study 104 patients who presented to the Istituto Clinico Città Studi (ICCS) in Milan, Italy, complaining of symptoms related to BPH
All patients were aged between 50 and 70 years, with Prostate Specific Antigen (PSA) values between 4 and 10 ng/mL, prostate volume, calculated through transrectal ultrasound (TRUS), between 50 and 70 ml, a maximum flow of urine value greater than or equal (4) to 10 ml/s at uroflowmetry, no suspicious nodules on digital rectal examination (DRE), no suspicious lesions on MRI (Prostate Imaging - Reporting and Data System score: 1-2), negative previous prostatic biopsies or never biopsied Patients with diabetes mellitus or chronic renal failure were excluded
We divided our patients into two groups: group A including 54 men who were treated using a complex containing phycocyanin, palmitoylethanolamide and selenium [Ficoxpea (F), by KURA®], and group B including 50 men who were treated using Dutasteride alone (D) We re-evaluated all patients after 6 months of therapy, considering the following parameters: PSA levels, uroflowmetry (UFM), prostate volume
Statistical analysis
Data were collected using Microsoft Excel (v 12 2 4) and analyzed using the SPSS Statistics v 29 software (IBM Corporation New York, USA) Statistical analysis of data was performed using ANOVA test with Tukey’s post-hoc correction P values < 0 05 were considered significant All data are expressed as mean ± Structural Equation Models (SEM)
RESULTS
Our results showed a significant decrease in PSA value both for the dutasteride (-2 743 ng/mL after 6 months of treatment) and phytochemicals complex (-0 9712 ng/mL after 6 months of treatment) groups (Figure 1) There was a significant difference among the PSA values between the two groups after 6 months of treatment (+1 865 ng/mL higher for the phytochemicals complex group) (Figure 1) Regarding UFM, there was a slight but significant increase in the flow of urine (ml/s) for the dutasteride group (mean increase of +3 029 ml/s after 6 months of treat-
G Saitta, F A Mantovani, B Calabrese, et al
Figure 1.
Difference of basal and 6-month follow up PSA values in dutasteride and phytochemical complex groups: significant decrease in both groups * . Lower mean PSA in dutasteride group at 6 month follow up
ment) The phytochemicals complex group, on the other hand, showed a greater improvement after the administration of the complex with a mean increase of +13 03 ml/s (p < 0 001) after 6 months of treatment (Figure 2) The improvement in the flow of urine was statistically higher than that of the dutasteride group (+13 03 ml/s vs +3 029 ml/s, p < 0 001) (Figure 2)
The mean voided volume (VV) was greater than 150 ml (154-347 ml) at the first observation and also after the medical therapy (157-418 ml) The post void residual
Figure 2.
Difference of basal and 6-month follow up uroflowmetry values in dutasteride and phytochemical complex groups: significant improvement in both groups * . Higher mean Qmax values in the phytochemical complex group at 6-month follow up #
Figure 3.
Difference of basal and 6-month follow up prostate volume values in dutasteride and phytochemical complex groups: significant decrease in both groups * Lower mean volume in dutasteride group at 6-month follow up #
(PVR) volume was greater than 50 ml (55-165 ml) before treatment and slightly decreased in both groups after 6 months (45-150 ml) No particular differences were found between the 2 groups regarding these parameters Lastly, prostate volume evaluated through TRUS showed significant improvements in both groups For the dutasteride group, a mean volume decrease of -22 14 ml (p < 0 001) after 6 months of treatment was found; for the phytochemicals complex group, despite being still significant from a statistical point of view, the mean decrease was much lower: -10 04 ml (p < 0 001) after 6 months of treatment (Figure 3) The difference in mean volume decrease was much higher in the dutasteride group, when compared to the phytochemicals complex group (-22 14 ml vs -10 04 ml, p < 0 001) (Figure 3)
DISCUSSION
The efficacy of nutraceuticals for the treatment of BPHrelated urinary symptoms is a wide field of interest in urology Our study aims to enriching the present literature for what concerns the comparison between commonly used drugs, like 5-ARI Dutasteride, and a combin a t i o n o
, Selenium and Phycocianin
Our results show that both the alternatives are valid for the treatment of such symptoms and suggest that treating BPH does not necessarily require the administration of drugs, such as 5-ARIs, that usually heavily impact the QoL because of their side effects
5-ARI Dutasteride is well-known for its capability in reducing PSA values, the prostate volume and improving U F M p a r a m e t
However, 5α-reductases (5α-Rs), a family of several isozymes whose activity is inhibited by the administration of 5-ARIs, play an important role in human physiology by
regulating cellular metabolism of androgens, glucocorticoids and other steroids Along with hypoactive sexual desire, erectile dysfunction, gynecomastia and psychiatric side effects such as a higher risk of major depression, some studies suggest that such treatments may result in development of non-alcoholic fatty liver diseases (NAFLD), insulin resistance (IR), type 2 diabetes (T2DM), dry eye disease, potential kidney dysfunction, among other metabolic dysfunctions (16, 17)
Not many studies in literature have evaluated the role of less known nutraceuticals in the treatment of BPH (PEA, Selenium, Phycocyanin, etc ) However, based on the biochemical activities of such molecules, it is reasonable to suppose that their main action is towards inflammation and its pathways Today, it is only possible to estimate the effects of such chemicals on the prostate function
For instance, PEA has been demonstrated to play a significant neuroprotective effect on chronic pelvic pain, but it may also play an important role in reducing inflammation by interfering with the androgenic pathways As previously said, daily administration of PEA is capable of reducing the levels of testosterone, DHT and decreasing the expression of markers like PSA and 5αreductases in the prostate tissue (11) This mechanism may lead to the reduction in prostate weight and inflammation markers that eventually is responsible for the i m p ro v e m e n t o f B P H - r e l a t e d L U T S t h a t w e h a v e observed in our results
According to our data, even if analysis is biased by the low number of patients taken into consideration, our results show that the complex was able to improve the maximum flow of urine by +13 03 ml/s after 6 months of treatment without dramatically reducing the prostate volume in the meantime Not only is this evidence significant, but it is also very puzzling when compared to the +3 029 ml/s increase in patients treated with dutasteride
Even though this result may be paradoxical to some extent, it is possible to deduce that this combination of nutraceuticals may have a stronger impact on UFM parameters than on prostate weight or PSA serum levels, where dutasteride seemed to perform better, because of their effect on inflammation
This result supposedly highlights the importance of inflammation pathways in determining urinary symptoms and the fact that such combination of nutraceuticals may have an equal or even slightly stronger anti-inflammatory effect compared to that of 5-ARI Dutasteride in BPH, thus undermining the importance of the absolute value of the prostate volume, main target of 5-ARIs, in causing BPH-related LUTS
However, it is important to acknowledge the intrinsic limits of this study The limited number of patients, and the fact that most of them had seen a urologist prior to the inclusion in the study, hence probably being exposed to Serenoa Repens and/or modifications of their lifestyle, could have affected the astonishing result that we have obtained regarding the UFM parameters
The role of prostate inflammation in determining BPHrelated LUTS is controversial and many studies are being conducted as to explain its exact role in the pathophysiology of BPH It is well known that prostate tissue affected by BPH carries a particular kind of inflammatory infil-
trate (CD3+ T lymphocytes, CD19 or CD20 B lymphocytes, and macrophages) Most T cells in the inflammatory areas are CD4+ that are not present in normal prostate tissue (scattered stromal and intraepithelial T, 70% of which are CD8+, and B lymphocytes, macrophages, and mast cells) However, the stimulus for an inflammatory response in the prostates of older males is not fully understood and it is likely to be multifactorial (18) In an interesting clinical study, Kwon et al observed that in patients with high-grade prostatic inflammation, the use of ablockers with 5-ARIs can be insufficient to reduce symptom severity Patients with high- grade chronic inflammation reported significantly lower changes in IPSS and storage symptom scores compared to patients with lowgrade inflammation (19) A meta-analysis of three randomized controlled trials showed that non-steroidal antiinflammatory drugs (NSAIDs), when given over periods of 4-24 weeks, improved symptoms by 2 9 IPSS points and flow by 0 89 ml/second (20)
These studies suggest the need to treat inflammation accordingly, a field in which nutraceuticals seem to have convincing possibilities
CONCLUSIONS
Both nutraceutical complex and dutasteride showed reduction of PSA values after 6 months of treatment The complex based on phycocyanin, PEA and selenium showed a statistically significant improvement in urinary flow, while dutasteride acted more on the volume of the prostate
However, the natural complex is a product with good efficiency on the phlogistic component and does not have the side effects reported for dutasteride (such as gynecomastia, reduced libido) Therefore, we believe it can be used by a large part of the BPH population, in order to reduce LUTS and PSA and improve urinary flow, without side effects
ACKNOWLEDGEMENTS
First of all, we thank the patients who participated giving us the possibility to observe and analyze the effects of the therapies We are grateful to all the staff of our Institute for the support in the successful completion of this study
Of course we appreciate who provide financial support to publish this manuscript
DECLARATION
The introduction of Ficoxpea® in the commerce was ethically approved and officially notified at the Italian Ministry of Health on 16th October 2020
All patients followed by us accepted anonymous data collection and agreed on its possible use for scientific purposes
REFERENCES
1 GBD 2019 Benign Prostatic Hyperplasia Collaborators The global, regional, and national burden of benign prostatic hyperplasia in 204 countries and territories from 2000 to 2019: a systematic analysis for the Global Burden of Disease Study 2019 Lancet Healthy Longev 2022; 3:e754-e776
G Saitta, F A Mantovani, B Calabrese, et al
2 Blankstein U, Van Asseldonk B, Elterman DS BPH update: medical versus interventional management Can J Urol 2016; 23(Suppl 1):10-5
3 Van Asseldonk B, Barkin J, Elterman DS Medical therapy for benign prostatic hyperplasia: a review Can J Urol 2015; 22 Suppl 1:7-17
4 Alcaraz A, Rodríguez-Antolín A, Carballido-Rodríguez J, et al Efficacy and tolerability of the hexanic extract of Serenoa repens compared to tamsulosin in moderate-severe LUTS-BPH patients Sci Rep 2021; 11:19401
5 Cai T, Cui Y, Yu S, et al Comparison of Serenoa repens With Tamsulosin in the Treatment of Benign Prostatic Hyperplasia: A Systematic Review and Meta-Analysis Am J Mens Health 2020; 14:1557988320905407
6 Alcaraz A, Rodríguez-Antolín A, Carballido-Rodríguez J, et al The Qualiprost Study Group OBO Clinical Benefit of Tamsulosin and the Hexanic Extract of Serenoa Repens, in Combination or as Monotherapy, in Patients with Moderate/Severe LUTS-BPH: A Subset Analysis of the QUALIPROST Study J Clin Med 2020; 9:2909
7 Cicero AFG, Allkanjari O, Busetto GM, et al Nutraceutical treatment and prevention of benign prostatic hyperplasia and prostate cancer Arch Ital Urol Androl 2019; 91:139
8 P e t r o s i n o S , D i M a r z o V T h e p h a r m a c o l o g y o f p a l m itoylethanolamide and first data on the therapeutic efficacy of some of its new formulations Br J Pharmacol 2017; 174:1349-1365
9 LoVerme J, Russo R, La Rana G, et al Rapid broad-spectrum analgesia through activation of peroxisome proliferator-activated receptor-alpha J Pharmacol Exp Ther 2006; 319:1051-61
10 Pessina F, Capasso R, Borrelli F, et al Protective effect of palmitoylethanolamide in a rat model of cystitis J Urol 2015; 193:1401-8
11 D'Amico R, Genovese T, Cordaro M, et al Palmitoylethanolamide/ Baicalein Regulates the Androgen Receptor Signaling and NF-κB/Nrf2 Pathways in Benign Prostatic Hyperplasia Antioxidants 2021; 10:1014
12 Bergandi L, Apprato G, Silvagno F Antioxidant and AntiI n fl a m m a t o r y A c t i v i t y o f C o m b i n e d P h y c o c y a
Palmitoylethanolamide in Human Lung and Prostate Epithelial Cells
Antioxidants 2022; 11:201
13 Cordaro M, Impellizzeri D, Siracusa R, et al Effects of a comicronized composite containing palmitoylethanolamide and polydatin in an experimental model of benign prostatic hyperplasia
Toxicol Appl Pharmacol 2017; 329:231-240
14 Arias-Chávez DJ, Mailloux-Salinas P, Ledesma Aparicio J, et al Selenium in combination with a tomato lipid extract as a therapy for benign prostatic hyperplasia and its alterations in rats with induced BPH J Cell Mol Med 2023; 27:3147-3156
15 Kok DE, Kiemeney LA, Verhaegh GW, et al A short-term intervention with selenium affects expression of genes implicated in the epithelial-to-mesenchymal transition in the prostate Oncotarget 2017; 8:10565-10579
16 Traish AM Health Risks Associated with Long-Term Finasteride and Dutasteride Use: It's Time to Sound the Alarm World J Mens Health 2020; 38:323-337
1 7 G a r c i a - A r g i b a y M , H i y o s h i A , F a l l K , M o n t g o m e r y S Association of 5α-Reductase Inhibitors With Dementia, Depression, and Suicide JAMA Netw Open 2022; 5:e2248135
18 Ficarra V, Rossanese M, Zazzara M, et al The role of inflammation in lower urinary tract symptoms (LUTS) due to benign prostatic hyperplasia (BPH) and its potential impact on medical therapy Curr Urol Rep 2014; 15:463
19 Kwon YK, Choe MS, Seo KW, et al The effect of intraprostatic chronic inflammation on benign prostatic hyperplasia treatment Korean J Urol 2010; 51:266-70
20 Kahokehr A, Vather R, Nixon A, Hill AG Non-steroidal antiinflammatory drugs for lower urinary tract symptoms in benign prostatic hyperplasia: systematic review and meta-analysis of randomized controlled trials BJU Int 2013; 111:304-11
Correspondence
Giuseppe Saitta, MD (Corresponding Author) gsaitta@hotmail it
ICCS Istituto Clinico Città Studi, Milan (Italy)
Viale Sabotino 19, 20135, Milan (Italy)
Franco A Mantovani, MD mantovanifranco@yahoo it
Benedetto Calabrese, MD calabrese benedetto98@gmail com
Camilla Aliboni, MD
camilla aliboni@gmail com
Giuseppe Di Paola, MD giuseppe dipaola@ic-cittastudi it
Attilio L Meazza, MD
attilio meazza@ic-cittastudi it
Mauro Seveso, MD
mauro seveso@ic-cittastudi it
ICCS Istituto Clinico Città Studi, Milan (Italy)
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Electromagnetic stimulation to
reduce the hypertonia of the pelvic floor muscles and improve chronic pelvic pain in women
Nicola Mondaini 1 , Mauro Gacci 2 , Tommaso Cai 3 , Francesco Lotti 4 , Vincenzo Li Marzi 2 , Fabio Crocerossa 1 , Francesco Cantiello 1 , Sara Tanguenza 5 , Alessandra Comito 6 , Irene Fusco 6 , Beatrice Marina Pennati 6 , Rocco Damiano 1
1 Department of Urology, Magna Graecia University of Catanzaro, Catanzaro, Italy;
2 Department of Minimally Invasive and Robotic Urologic Surgery and Kidney Transplantation, University of Florence, Florence, Italy;
3 Department of Urology, Santa Chiara Regional Hospital, Trento, Italy;
4 Sexual Medicine and Andrology Unit, Department of Experimental and Clinical Biomedical Sciences, University of Florence, Florence, Italy;
5 Pelvic Pain Centre, Florence, Italy;
6 El En Group, 50041 Calenzano, Italy
Summary
Background: The increased hypertonicity or activity of pelvic floor muscles can lead to chronic pelvic pain (CPP). It represents an aspecific and persistent pain with no apparent clinical reason, affecting an estimated 6% to 16% of women worldwide. This study aimed to evaluate with validated questionnaires the efficacy and the safeness of a new device that uses Top flat Magnetic Stimulation for the management of muscular hypertonia in women with CCP
Methods: All patients underwent 8 sessions of treatment with a non-invasive electromagnetic therapeutic device The device produces a TOP Flat Magnetic Stimulation with a uniform profile so, the muscle work aims to reduce pain while also inhibiting muscle activity. The PISQ-12 questionnaire was used for the evaluation of improvements Side effects were monitored
Results: The PISQ-12 total mean score decreases from 29.2 (± 3 3) to 17 (± 2) Regarding the behavioural-emotive items (1-4), a decrease from 12 (± 2) to 7 (± 0 9) was observed Physical items (5-9) decrease from 10 6 (± 1 8) to 6 (± 1 4) and the Partner Related items (10-12) from 6 6 (± 1 6) to 3 9 (± 0 4)
Conclusions: The device we used in this research demonstrated to be a valid tool for the treatment of chronic pelvic pain in female patients
The increased hypertonicity or activity of pelvic floor muscles can lead to chronic pelvic pain (CPP) or myofascial syndrome when the type of pelvic floor dysfunction called Pelvic floor tension myalgia (PFTM) occurs (1) CPP management is a tremendous concern for healthcare professionals and a significant financial burden for healthcare systems because it represents an aspecific and persistent pain with no apparent clinical reason The World Health Organisation (WHO) has lately recognised chronic pain as
a separate condition, defining chronic primary pain as any pain without a clear cause (2) An estimated 4% to 16% of women worldwide (3, 4) are thought to experience chronic pelvic pain in their lives, which is also known as persistent noncancer pelvic discomfort This condition frequently results in discomfort during sex (dyspareunia), orgasmic dysfunction, and decreased desire, arousal, and lubrication in addition to producing pain in or perceived to be in the pelvic tissues (5) Pelvic discomfort and symptoms of the lower urinary tract are the two main clinical hallmarks of chronic pelvic pain syndrome (CPPS) Different aspects of the CPP have been investigated through the years According to scientific research in the literature, compared to women without chronic pelvic pain, women with chronic pelvic pain exhibited increased pelvic floor muscular tone, stronger resistance to pressure application, and slower stretching of the pelvic floor muscles by the index finger (6, 7) Additionally, they demonstrated lower pelvic floor muscular flexibility and increased pelvic floor muscle stiffness Finally, electromyography (EMG) analysis revealed that the women with persistent pelvic discomfort had increased myoelectrical activity in both the superficial and deep pelvic floor muscles (6, 8) Although there are many theories on the aetiology of myofascial pain, none of them have been proven in the literature According to one idea, metabolic alterations at the level of the motor endplate that result in muscular hyperactivity or microscopic muscle injury are the source of myofascial pain (9, 10) Additionally, it has been postulated that myofascial pain involves alterations in the central nervous system, such as glial cell proliferation and neuronal cell death, which could account for the referred pain patterns observed in myofascial pain pathologies (9, 11) Finally, it has been proposed that the persistent muscle spasm and contraction associated with myofascial pain represents a compensating strategy for pelvic floor dysfunction or defects in the design of the levator ani muscle (9, 10)
Table 1.
1
2
3
4
5
Myofascial pain is the most common symptom in patients with CPP and it can be the primary source of pain, unrelated to organ disease, or it can be a secondary source of pain elicited by a reflex response (visceral-muscle reflex) (3) Trigger points often develop in the affected muscles Trigger points are specific areas of tenderness that develop in the muscle wall and can begin as just a symptom of pelvic pain, or they can be the main source of the pain For this reason, treating trigger points can significantly reduce pain
In addition, it has been noted that it is a very common finding that the origin of the pain area was previously affected by gynaecological (ovarian cysts, endometriosis, dyspareunia, vulvodynia, recurrent candidiasis), or urological (interstitial cystitis/painful bladder syndrome, urgency/frequency, urge incontinence), or colorectal (constipation, proctalgia fugax, irritable bowel syndrome), or tissue adherence (scarring following surgery) disorders, or other musculoskeletal or neural (pudendal neuralgia, coccygodynia, post-surgical or postnatal pelvic pain) conditions (12)
However, there is currently no standardized and reliable technique for evaluating myofascial pain An evidencebased physical examination for myofascial pain is required considering the mounting evidence linking myofascial pain to chronic pelvic pain syndromes and new information pointing to a connection between subclinical myofascial pain and lower urinary tract symptoms (LUTS) In addition, although some aspects of the pelvic floor myofascial evaluation may be the same in men and women, the method used to access these muscles differs, hence for the purposes of this research study, we chose to concentrate on examination techniques in women (13, 14)
There are numerous treatment methods for managing PFTM and CPP, including pharmaceutical (analgesics and muscle relaxants) and non-pharmacological therapies Between these, there are high-voltage electro-galvanic stimulation (HVGS), transcutaneous electrical nerve stimulation (TENS) devices, ultrasound, short wave diathermy, massages, posture training and strengthening exercises, biofeedback, botulin toxin injections, hydrotherapy, and sitz baths seem to be the most effective treatments Nevertheless, some women do not react to conventional
treatments such as medical/pharmacological management, physical therapy methods or surgery (15, 16)
It is important to remember that all these levels of pain should be treated together with a multidisciplinary therapy approach to be effective The treatment can therefore include, in addition to the rehabilitation treatment with a midwife, also a psychological, and medical consultation and/or the use of supplements or drugs It may happen that it is not possible to completely solve the pain An effective treatment means that the pain has decreased to a level where you can once again enjoy your life and the activities you did before the pain began (17, 18)
In this study, we explored the effectiveness of extracorporeal Top flat Magnetic Stimulation (FMS) for improving chronic pelvic pain conditions After its approval by the FDA in 1998, FMS is now mostly used for the treatment of Urge Urinary Incontinence (UUI) It is a viable option with the significant advantage of letting patients remain comfortable in their clothes throughout a procedure
Depending on the protocol, the FMS technology allows the improvement of muscle mass by neuromuscular stimulation since it depolarizes motor neurons, inducing large and deep muscle contractions On the other hand, it can help in the treatment of muscular hypertonia inducing fibres relaxation while maintaining a uniform profile and preventing any areas of irregular stimulation intensity (19) Moreover, because magnetic stimulation has no impact on cutaneous receptors, the discomfort associated with electrostimulation is also avoided
This study aimed to evaluate with validated questionnaires the efficacy and the safeness of a new device that uses Top flat Magnetic Stimulation for the management of muscular hypertonia in women with CCP
MATERIALS AND METHODS
A retrospective evaluation study was conducted at the Pelvic Pain Centre, Florence, Italy between January, and September 2023
S t u d y p o p u lat io n
Patients presenting secondary chronic pelvic pain due to cystitis, endometriosis or vulvodynia, and non-responders to the current available pharmacological or physical solutions, were considered in this study To make a precise diagnosis of chronic pelvic pain, we have ruled out all other pathologies that might be causing the same kind of excruciating symptoms These conditions included menopause, pelvic organ prolapses, genital infections, menstruation, malignant tumours, severe neurological diseases, pregnancy, obesity, and those who had metal implants or pacemakers Patients with hypertonicity of the pelvic floor and persistent pelvic discomfort met the inclusion criteria An experienced gynaecologist manually evaluated the pelvic floor muscles in all patients to diagnose hypertonic pelvic floor (19) Also, any previous gynaecological surgery was considered as an exclusion criterion for enrolment in the investigation Lastly, patients were asked to avoid any other pharmacological (also painkillers) and non-pharmacological medications from 15 days before the study began and for the whole duration of the study Other contraindications include the presence of cardiac pacemakers, implanted defibrillators/
N Mondaini, M Gacci, T Cai, et al
neurostimulators, electronic or metal implants, bleeding conditions, cardiac diseases, pulmonary deficiency, malignant cancerous lesions, pregnancy, severe inflammatory conditions, fever and weight over 160 kilograms
S t u d y d ev ic e
For this study, was used a non-invasive electromagnetic t h e r a p e u t i c d e v i c e ( D R A R N O L D , D E K A M E L A Calenzano, Italy) with a chair applicator and a main unit
The chair has a coil in the centre of the seat to target the deep pelvic floor area Before each session, a gynaecologist set the patient's position to guarantee the best result
The patient's legs are set up perpendicularly so that the thighs are parallel to the floor and the feet are flat
Patients should bend their knees to a 90-degree angle or slightly higher This way, the perineum of the patient is perfectly aligned with the centre of the seat, and the local stimulation of the sphincter muscles and pelvic floor is at maximum The device produces a TOP Flat Magnetic Stimulation electromagnetic field with a uniform profile
The magnetic fields transmit current directly to the muscle tissue in-, contracting or relaxing it The electromagnetic stimulation's spatial profile (Figure 1) distinguishes DR ARNOLD from other devices It covers a larger area, is uniformly dispersed Because of this configuration, electromagnetic radiation can be distributed deeply, symmetrically, and uniformly, reaching deep neural areas inside the pelvis without dispersing superficially
S t u d y p r o t o c o ls
Procedure protocols for reducing hypertonicity with lowfrequency stimulations (around 10 Hz), were used A total of 8 treatment sessions for every patient were performed Sessions were held twice weekly for 4 weeks in a row, lasting ca 30 minutes depending on the patient's
muscle condition After the first two minutes of warm-up for all patients, the Overtone/Pain protocol was chosen (19) The warm-up phase is a gentle muscle activation; it is a preparation step in which blood circulation is increased with low frequencies (about 5 Hz) Using frequencies of about 10 Hz, the overtone/pain protocol produces low-level electric currents on neuromuscular tissue, which depolarizes neurons and causes decontraction of the pelvic floor muscles So, the muscle work aims to reduce pain (hyperactivity and hypertonia) while also inhibiting muscle activity Data were gathered at the beginning of the study, at the end of each treatment session, and three months later
Potential side effects and adverse events such as muscle soreness, momentary muscle spasms, joint/tendon pain, or local erythema/skin redness were monitored throughout the treatment period
Valid at ed q u est io n n air es
CPP was assessed using the Pelvic Organ Prolapse/Urinary Incontinence Sexual Function Questionnaire (PISQ-12) (20)
It is a test of sexual function and a condensed version of the PISQ-31 (21) The PISQ-12 has three domains: partnerrelated (items 10-12), physical (items 5-9), and behavioural-emotive (items 1-4) Lower scores imply enhanced sexual function Scores are calculated by totalling the scores for each question, going from 0-never to 4-always Reverse scoring is used for items 1, 2, 3 and 4 (20) It was administered before the first treatment and right after the last session
Moreover, a Visual Analogue Scale (VAS) was used to collect information from every patient about the pain intensity perceived before and after the last treatment The scores ranged from 0 (No Pain) to 10 (Very Painful, not bearable)
Figure 1
Spatial profile of the uniform distribution of Flat Magnetic stimulation Courtesy of DEKA M E L A company
Table 2.
PISQ-12 questionnaire mean results divided by different items (behavioural-emotive (items 1-4), physical (items 5-9), and partner-related (items 10-12) pre- and post-treatments.
PISQ-12 Questionnaire
VAS Questionnaire
Figure 2.
Moreover, most of them have had surgical events in the past Generally, no side effects were observed during the study When the results of the questionnaires are considered, the PISQ-12 total mean score proved to be statistically significant different (p < 0 05) and decreases from 29 2 (± 3 3) to 17 (± 2) at the end of the study The same statistical significance is found when analysing the single items Regarding the behavioural-emotive items (1-4), a decrease from 12 (± 2) to 7 (± 0 9) was observed Physical items (5-9) decrease from 10 6 (± 1 8) to 6 (± 1 4) and the Partner Related items (10-12) from 6,6 (± 1 6) to 3 9 (± 0 4) (see Table 2 and Figure 2)
The VAS questionnaire scores were collected by every patient at baseline (before the first treatment) and right after the last treatment The mean score decreased from 8
Graphical representation of the PISQ-12 questionnaire: mean results divided by different items (behavioural–emotive (items 1-4), physical (items 5-9), and partner-related (items 10-12) at baseline (pre-first treatment) and after the last treatment
S t at ist ic al an alysis
The statistical analysis was performed with SPSS (IBM Corp , New York, USA) Specifically, the Student t-test (p < 0 05 for significance) was conducted (means and ± SDs)
RESULTS
In total, 40 women presenting secondary chronic pelvic pain were considered Some general demographic information is reported in Table 1 The population median age was 34 7± 8 1 year (from the youngest, 19 years old, to the eldest, 45 years old) The great majority of the subjects were married (82 5%) and with a higher education (77 5%)
Table 3.
VAS questionnaire mean results at baseline (before the first treatment) and after the last treatment are reported
VAS Questionnaire
Significance
(± 1 3) to 3 (± 0 6) with statistical significance (p < 0 05) (see Table 3 and Figure 3)
Figure 3.
Graphical representation of the VAS questionnaire for the pain intensity evaluation. The mean results pre- and post-treatment are shown
Figure 4.
Graphical representation of the correlation between the patient’s age and different PISQ-12 item score results.
No correlation between the patient’s age and different PISQ12 item score results was remarkable (see Figure 4) Magnetic stimulation appears to be effective in the observed improvement of sexual function and health regardless of patient age as shown by the consistent reduction of the PISQ-12 questionnaire scores
DISCUSSION
In women, when the pelvic floor muscles show an increased hypertonicity or activity, it can lead to CPP The magnetic stimulation technique deeply interests the muscles of the pelvic floor, restoring neuromuscular control (22) The interaction with the tissue can result in muscle contraction or relaxation, depolarization of neuronal cells, and changes to the blood circulation system According to the scientific literature (23-27), this technology may have an impact on the sexuality and health of a large patient population Based on the subjective assessment, patients also reported additional therapeutic advantages, such as improved urine control (28-30) and higher sexual satisfaction (31) In fact, the overtone/pain protocol for hypertonic management may use lower frequencies (around 10 Hz) to produce an electromagnetic field distribution that is homogeneous and does not produce regions of different stimulation intensity, preventing overstimulation of the already hypersensitive receptors and sensory nerves typical of chronic pelvic pain Because no probe is placed into the vaginal channel during muscle stimulation, the device we employed is considered non-invasive Thanks to the steady emission of energy that is progressively given, patients can continue to be fully clothed in a comfortable and supportive chair and resume their daily activities straight immediately following sessions
The DR ARNOLD system can also be seen as an "educator" system because it enables the patient to sense the relaxation of the treated muscles, allowing them more autonomy and awareness to choose when to repeat the next treatment session Furthermore, the use of this novel technology can be combined with existing pharmacological or physical methods (32) The etiopathology of CPP is not fully understood Indeed, genito-pelvic pain/penetration disorders, vulvodynia, interstitial cystitis/bladder pain syndrome and endometriosis, are just a few of the illnesses that can produce CPP However, it's possible that women with any of these diseases have identical pelvic floor muscle tone and functionality Studying the correlation between personal and social characteristics such as the marital status or the education level and the presence of CPP, was not matter of this research study But, according to other investigation in literature, pelvic floor muscle strength (PFMS) declines with age and ageing increases the likelihood of incontinence and genital organ prolapses and also CPP development (33, 34)
Furthermore, a number of studies have demonstrated a strong correlation between pelvic floor diseases and educational attainment [34-36) Similar findings were made by Gümüssoy et al (2021) [37), where it was discovered that as women's educational levels rose, so did their PFMS values This finding implies that women's awareness of PFMS is raised by education According to the results of this study, women with lower income levels or without employment had lower PFMS values
Overholt et al (2019) (38) described a clinical case providing support to evaluate the efficacy of pulsed electromagnetic field therapy for the management of chronic pelvic pain in interstitial cystitis/bladder pain syndrome Indeed, for urinary incontinence higher frequencies (fre-
N Mondaini, M Gacci, T Cai, et al
quencies ≥ 20 Hz) are needed to target the muscles and improve muscular tone In this study, device protocols with a low-frequency (10Hz) emission were used By using the Top FMS technology, the distribution of the magnetic vibrations is homogeneous in the treated area Indeed, these low frequencies are able to create a homogeneous distribution of the electromagnetic field that does not create regions of different stimulation intensity avoiding an overstimulation/overactivation of the pelvic floor muscles In this way, no energy-peak can be produced This is important because, in patients presenting CCP, these energy-peaks can cause opposite outcomes, resulting in the worsening of the pain feeling due to an overactivation of the pelvic floor muscles
With this study we wanted to evaluate with validated questionnaires the efficacy and the safeness of a new device that uses Top flat Magnetic Stimulation for the management of muscular hypertonia in women with CCP Our results indicated that the patient's symptoms of muscular hypertonia and chronic pelvic pain were improved As support, the PISQ-12 questionnaire was used because of its internal consistency, test-retest reliability, and validity After the final therapy, we have seen a considerable decrease in the PISQ12 mean score When the single items are considered, the trend is comparable Also, results from the VAS questionnaires revealed a statistically significant reduction of the patient pain perception after the conclusion of the treatment cycle No correlation between the patient’s age and different PISQ-12 item score results was remarkable probably indicating the wide efficacy of the magnetic stimulation regardless the age of the patient
S t u d y lim it at io n s
Our long-term objective is to register additional patients to further examine this novel, non-invasive approach to treating complex illnesses such as chronic pelvic pain without sex distinction Moreover, the number of patients enrolled should be increased and a control group should be included for better completeness Lastly, it would be interesting to evaluate the short-term and long-term improvement of the symptoms following the patients after the conclusion of the treatment cycle
CONCLUSIONS
The device we used in this research demonstrated to be a valid tool for the treatment of chronic pelvic pain in female patients Further studies are needed to have a deeper knowledge about the electromagnetic stimulation activity in reducing the hypertonia of the muscles since it could be the right strategy to improve the quality of life of the patients affected
REFERENCES
1 Grimes WR, Stratton M Pelvic Floor Dysfunction’, in StatPearls, Treasure Island (FL): StatPearls Publishing, 2023 Accessed: Dec 14, 2 0 2 3 [ O n l i n e ] Av a
/ NBK559246/
2 World Health Organization (WHO), ICD-11 for Mortality and Morbidity Statistics Accessed: Sept 23, 2023 [Online] Available: https://icd who int/browse11/l-m/en’
3 Dydyk AM, Gupta N Chronic Pelvic Pain in StatPearls, Treasure Island (FL): StatPearls Publishing, 2023 Accessed: Dec 13, 2023 [Online] Available: http://www ncbi nlm nih gov/books/NBK554585/
4 Reavey J, Vincent K Chronic pelvic pain Obstetrics, Gynaecology & Reproductive Medicine 2022; 32:8-13
5 Faubion SS, Shuster LT, Bharucha AE Recognition and management of nonrelaxing pelvic floor dysfunction Mayo Clin Proc 2012; 87:187-193
6 Kadah S, Soh S-E, Morin M, et al Is there a difference in pelvic floor muscle tone between women with and without pelvic pain? A systematic review and meta-analysis J Sex Med 2023; 20:65-96
7 Demetriou L, Krassowski M, Mendes AP, et al Clinical profiling of specific diagnostic subgroups of women with chronic pelvic pain Frontiers in Reproductive Health 2023; 5:1140857
8 Franco JV, Turk T, Jung JH, et al Non-pharmacological interventions for treating chronic prostatitis/chronic pelvic pain syndrome Cochrane Database Syst Rev 2018; 5:CD012551
9 Meister MR, Shivakumar N, Sutcliffe S, et al Physical examination techniques for the assessment of pelvic floor myofascial pain: a systematic review Am J Obstet Gynecol 2018; 219:497 e1-497 e13
10 Spitznagle TM, Robinson CM Myofascial pelvic pain Obstet Gynecol Clin North Am 2014; 41:409-432
11 Kuner R Central mechanisms of pathological pain Nat Med 2010; 16:1258-1266
12 Apte G, Nelson P, Brismée J-M, et al Chronic female pelvic pain-part 1: clinical pathoanatomy and examination of the pelvic region Pain Pract 2012; 12:88-110
13 Bo K, Frawley HC, Haylen BT, et al An Inter national U ro g y n e c o l o g i c a l A s s o c i
Society (ICS) joint report on the terminology for the conservative and nonpharmacological management of female pelvic floor dysfunction Neurourol Urodyn 2017; 36:221-244
14 Pastore EA, Katzman WB Recognizing myofascial pelvic pain in the female patient with chronic pelvic pain J Obstet Gynecol Neonatal Nurs 2012; 41:680-691
15 Dionisi B, Senatori R Effect of transcutaneous electrical nerve stimulation on the postpartum dyspareunia treatment J Obstet Gynaecol Res 2011; 37:750-753
17 Dionisi B, Anglana F, Inghirami P, et al Use of transcutaneous electrical stimulation and biofeedback for the treatment of vulvodynia (vulvar vestibular syndrome): result of 3 years of experience Minerva Ginecol 2008; 60:485-491
18 Meister MR, Sutcliffe S, Badu A Pelvic floor myofascial pain severity and pelvic floor disorder symptom bother: is there a correlation? Am J Obstet Gynecol 2019; 221:235 e1-235 e15
19 Salsi B, Ganassi G, Lopopolo G, et al Approach of Chronic Pelvic Pain with Top Flat Magnetic Stimulation Advances in Urology 2023; 2023:9983301
20 Rogers RG, Coates KW, Kammerer-Doak D, et al A short form o f t h e P e l v i c O rg a n P
Questionnaire (PISQ-12) Int Urogynecol J Pelvic Floor Dysfunct 2003; 14:164-168
21 Rogers RG, Kammerer-Doak D, Villarreal AK, et al A new instrument to measure sexual function in women with urinary incontinence or pelvic organ prolapse Am J Obstet Gynecol 2001; 184:552-558
22 Gilling PJ, Wilson LC, Westenberget AM, et al A double-blind randomized controlled trial of electromagnetic stimulation of the pelvic floor vs sham therapy in the treatment of women with stress urinary incontinence BJU Int 2009; 103:1386-1390
23 Vadalà M, Palmieri B, Malagoli A, Laurino C High-power Magnetotherapy: A New Weapon in Urinary Incontinence? Low Urin Tract Symptoms 2018; 10:266-270
24 González-Isaza P, Sánchez-Borrego R, Lugo Salcedo F, et al Pulsed Magnetic Stimulation for Stress Urinary Incontinence and Its Impact on Sexuality and Health Medicina (Kaunas) 2022; 58:1721
25 Lopopolo G, Salsi B, Banfi A, et al Is It Possible to Improve Urinary Incontinence and Quality of Life in Female Patients? A Clinical Evaluation of the Efficacy of Top Flat Magnetic Stimulation Technology Bioengineering (Basel) 2022; 9:140
26 Isaza PG, Borrego RS, Fusco I A case of stress urinary incontinence after radical prostatectomy successfully treated with an innovative device based on top flat magnetic stimulation World J Urol 2022; 40:1887-1889
27 Dominguez AP, Isaza PG, Pantoja SN, Fusco I Role of top flat magnetic stimulation for urinary incontinence as a debilitating condition of pelvic floor dysfunction: an observational evaluation of Latin American population World J Urol 2023; 41:173-177
28 Filippini M, Biordi N, Curcio A et al A Qualitative and Quantitative Study to Evaluate the Effectiveness and Safety of M a g n e t i c S
Symptoms and Pelvic Floor Disorders Medicina (Kaunas) 2023; 59:879
29 Frigerio M, Barba M, Cola A, et al Flat Magnetic Stimulation for Stress Urinary Incontinence: A Prospective Comparison Study Bioengineering (Basel) 2023; 10:295
30 Biondo A, Isaza PG, Fusco I Efficacy of Top Flat Magnetic S t i m u l a t i o n Te c h n o l o g y f o r F
Incontinence: A Clinical Evaluation World Journal of Nephrology and Urology 2022; 1118-23
31 Biondo A, Murina F, Fusco I Treatment of Pelvic Floor Hypertonic Disorders with top Flat Magnetic Stimulation in Women with Vestibulodynia: A Pilot Study 2023 J Women’s Health Dev 2022; 5:175-184
32 Rosen NO, Dawson SJ, Brooks M, Kellogg-Spadt S Treatment of Vu l v o d y n i a : P h a r m a c
Approaches Drugs, 2019; 79:483-493
33 Li H, Wu RF, Qi F, et al Postpartum pelvic floor function performance after two different modes of delivery Genet Mol Res 2015; 14:2994-3001
34 Özdemır ÖÇ, Bakar Y, Özengın N, Duran B The effect of parity on pelvic floor muscle strength and quality of life in women with urinary incontinence: a cross sectional study J Phys Ther Sci 2015; 27:2133-2137
35 Braekken IH, Majida M, Engh ME, Bø K Are pelvic floor muscle thickness and size of levator hiatus associated with pelvic floor muscle strength, endurance and vaginal resting pressure in women with pelvic organ prolapse stages I-III? A cross sectional 3D ultrasound study Neurourol Urodyn 2014; 33:115-120
36 Nygaard I, Barber MD, Burgio KL, et al Prevalence of symptomatic pelvic floor disorders in US women JAMA 2008; 300:13111316
37 Gümüssoy S, Öztürk R, Kavlak O, et al Investigating Pelvic Floor Muscle Strength in Women of Reproductive Age and Factors Affecting It Clin Nurs Res 2021; 30:1047-1058
38 Overholt TL, Ross C, Evans RJ, Walker SJ Pulsed Electromagnetic Field Therapy as a Complementary Alternative for Chronic Pelvic Pain Management in an Interstitial Cystitis/Bladder Pain Syndrome Patient Case Rep Urol 2019; 2019:5767568
Correspondence
Nicola Mondaini, MD n mondaini@unicz it
Fabio Crocerossa, MD crocerossa@unicz it
Francesco Cantiello, MD cantiello@unicz it
Rocco Damiano, MD damiano@unicz it
Department of Urology, Magna Graecia University of Catanzaro, Catanzaro, Italy
Mauro Gacci, MD maurogacci@gmail com Vincenzo Li Marzi, MD vlimarzi@hotmail com
Department of Minimally Invasive and Robotic Urologic Surgery and Kidney Transplantation, University of Florence, Florence, Italy
Tommaso Cai, MD ktommy@libero it Department of Urology, Santa Chiara Regional Hospital, Trento, Italy
Francesco Lotti, MD francesco lotti@unifi it
Sexual Medicine and Andrology Unit, Department of Experimental and Clinical Biomedical Sciences, University of Florence, Florence, Italy
Sara Tanguenza, MD saratanguenza@gmail com Pelvic Pain Centre, Florence, Italy
Alessandra Comito, MD a comito@elen it
Irene Fusco, MD (Corresponding Author) i fusco@deka it
Beatrice Marina Pennati, MD b pennati@deka it
El En Group, 50041 Calenzano, Italy
Conflict of interest: BMP, IF and AC are employed at El En Group
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest
Institutional Review Board Statement: All the authors declare that the procedures followed were in accordance with the Declaration of Helsinki Informed Consent Statement: Informed consent was obtained from all subjects involved in the study
ORIGINAL PAPER
Utilizing artificial neural network system to predict the residual valve after endoscopic posterior urethral valve ablation
1 Department of Urology, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran;
2 Histomorphometry and Stereology Research Center, Shiraz University of Medical Sciences, Shiraz, Iran;
3 Department of Urology, School of Medicine, Ibb University, Ibb, Yemen;
4 PhD Candidate in Biostatistics, Department of Biostatistics, Shiraz University of Medical Sciences, Shiraz, Iran;
5 Student Research Committee, Shiraz University of Medical Sciences, Shiraz, Iran
Summary
Purpose: To build, train, and assess the artificial neural network (ANN) system in estimating the residual valve rate after endoscopic valve ablation and compare the data obtained with conventional analysis.
Methods: In a retrospective cross-sectional study between June 2010 and December 2020, 144 children with a history of posterior urethral valve (PUV) who underwent endoscopic valve ablation were enrolled in the study MATLAB software was used to design and train the network in a feed-forward backpropagation error adjustment scheme Preoperative and postoperative data from 101 patients (70%) (training set) were utilized to assess the impact and relative significance of the necessity for repeated ablation The validated suitably trained ANN was used to predict repeated ablation in the next 33 patients (22 9%) (test set) whose preoperative data were serially input into the system To assess system accuracy in forecasting the requirement for repeat ablation, projected values were compared to actual outcomes. The likelihood of predicting the residual valve was calculated using a three-layered backpropagating deep ANN using preoperative and postoperative information
Results: Of 144 operated cases, 33 (22.9%) had residual valves and needs to repeated ablation The ANN accuracy, sensitivity, and specificity for predicting the residual valve were 90.75%, 92 73%, and 73 19%, respectively Younger age at surgery, hyperechogenicity of the renal parenchyma, presence of vesicoureteral reflux (VUR), and grade of reflux before surgery were among the most significant characteristics that affected postoperative outcome variables, the need for repeated ablation, and were given the highest relative weight by the ANN system.
Conclusions: The ANN is an integrated data-gathering tool for analyzing and finding relationships among variables as a complex non-linear statistical model The results indicate that ANN is a valuable tool for outcome prediction of the residual valve after endoscopic valve ablation in patients with PUV
Posterior urethral valve (PUV) is the most common cause of congenital bladder outlet obstruction in males, with
various outcomes, from exceedingly severe phenotypes with prenatal death to live-born individuals with acceptable renal function (1) Despite being an uncommon congenital abnormality (prevalence 1-9/100,000), it represents approximately 17% of pediatric end-stage renal disease (ESRD) (1, 2) The current definitive treatment of choice is endoscopic PUV ablation; however, roughly 10% to 30% of patients require a second surgery to achieve adequate valve ablation (3, 4) Any partial outlet obstruction could cause anatomical and functional deterioration in the detrusor muscle of the bladder wall if it is not released quickly enough (5) This indicates the importance of close follow-up after valve ablation (5) It might be challenging to assess the result of endoscopic valve ablation While some investigators suggest that voiding cystourethrogram (VCUG) confirms the adequacy of valve ablation, others offer cystoscopic procedures 6-8 The disadvantages of VCUG are transient dysuria, hematuria, and toilet anxiety On the other hand, the invasive nature and the need for admission and anesthesia are the main disadvantages of the cystoscopic procedure (4, 6) Distinguishing prognostic factors for residual valves after endoscopic valve ablation can aid in developing a better algorithm for managing PUVs and achieving purposeful follow-up for high-risk patients (4)
As a result, new prediction techniques are required to allow for better patient diagnosis and follow-up (9) A study conducted by Shirazi et al to investigate the patients with a higher risk for residual valves after PUV ablation found that younger age at surgery time, hyperechogenicity of renal parenchyma, presence of vesicoureteral reflux, and grade 4 or 5 reflux before surgery were associated with residual valves and need for repeated ablation (4)
The most commonly used form of artificial intelligence (AI) in medicine is artificial neural networks (ANNs) that mimic interconnected brain synapses and networks taught by analyzing input and output databases (10, 11) The system learns to identify variables influencing outcomes, and as more data is incorporated, self-optimization matures, resulting in more accurate predictions and higher accuracy rates for specific outcomes (12)
In the present study, we aimed to investigate the efficacy of ANNs as an intelligible interface to predict the rate of the residual valve after endoscopic valve ablation in children with PUV
MATERIALS AND METHODS
Study design
In a retrospective cross-sectional study, 144 children who were diagnosed with PUV and had undergone endoscopic bladder neck resection and valve ablation between June 2010 and December 2020 in the referral centers (Nemazi Teaching Hospital and Shahid Faghihi Teaching Hospital, Shiraz, southern Iran) were selected to participate in this study The ethics committees of Shiraz University of Medical Sciences approved this project (approval code# IR SUMS MED REC 1399 585), and it was carried out in compliance with the Helsinki Declaration All patient’s parents or legal guardians provided written informed consent before enrolment
Surgical intervention
All primary PUV ablations were performed by a single experienced pediatric urologist (Prof Shirazi) The valves were carefully ablated at the 5, 7, and 12 o'clock positions using an electrical Bugbee, and the visual assessment of the valve destruction ascertained the endpoint of ablation Then, a urethral catheter was left in place and removed 48 hours later Patients were discharged with oral antibiotics
Postoperative follow-up for residual valve assessment
The possible presence of residual valve remnants was assessed by careful clinical, radiological and endoscopic evaluation (13) For that, the patients were assessed with ultrasonography (US) every 3 to 6 months, VCUG 3 months after valve ablation, and a control cystoscopy three to 12 months later, and if a residual valve was found, a second valve ablation was performed (4, 14) Clinically, a persistent symptom of poor stream, nocturnal enuresis in older than 5 years, and persistent or worsened VUR or worsened hydronephrosis in the serial US were also considered
Slight residual valves that did not cause renal impairment or urinary tract infections (UTIs) were excluded (15)
Data collection
Training
set
The network training set accounted for 101 (70%) of the study data The architecture of the education network consists of three layers: input, hidden, and output The number of nodes in the input and output layers corresponds to the number of predictor and response variables The number of hidden layer nodes was determined by trial and error The level criterion below the characteristic performance curve (ROC) was used to find the best network structure Finally, after selecting the best architecture, the network was evaluated and validated in second-stage data that did not play a role in the network training phase
Test set
The network test set accounted for 43 (30%) patients
The final response variable or the final output of the model was a two-state variable with the levels of 0-no residual valve and 1-had residual valve The number of input variables was 24, the same as the independent variables After selecting the input and output variables, a three-layer perceptron network (with an observer) was used, with one neuron in the output layer and 24 neurons in the input layer According to the training data set and independent input variables, 320 combinations were
Variables considered for analysis
Postoperative variables
History of enuresis
Blood pressure (mm Hg)
History of urinary incontinence
Presence of VUR (Grad) in VCUG
Urinary bladder trabeculation (Mild, Moderate, Severe) in US
Bladder diverticula in US
Blood Creatinine level(mg/dL)
Degree of HDN (Mild, Moderate, Severe) in US
Loss of cortico-medullary differentiation
Renal cortical thickness (mm) in US
Size of bladder wall thickness (mm) in US
Preoperative variables
Age (Months)
Birth Weight (Low, Normal)
Time of diagnosis (Prenatal, Postnatal)
Time to PUV ablation (Months)
Grade of VUR in VCUG
Urinary bladder trabeculation (Mild, Moderate, Severe) in US
Bladder diverticula in US
Blood Creatinine level (mg/dL)
Degree of HDN (Mild, Moderate, Severe) in US
Loss of cortico-medullary differentiation in US
Renal cortical thickness (mm) in US
Size of bladder wall thickness (mm) in US
History of recurrent UTI
Proteinuria in urine analysis
Urine culture
Scar in renal DMSA scan
PUV: Posterior urethra va ve; DMSA: Dimercaptosuccin c acid; HDN: hydronephros s; VUR: Vesicoureteral reflux; VCUG: vo ding cystourethrogram; UTI: ur nary tract infect on; US: U trasonography
All the data used in this study, including preoperative and postoperative parameters, are summarized in Table 1
Design, training, and validation of the ANN system
We designed and trained the network with MATLAB software (Mathworks, Natick, MA) using a feed-forward backpropagation error adjustment scheme (16, 17) The data were separated into training and test sets to fit the ANNs (Figure 1)
Figure 1
Schematic design of artificial neural network.
M Shirazi, Z Jahanabadi, F Ahmed, et al
Table 1.
Table 2
Selecting the best neural network model for the recurrent data
0
AUC: Area under the curve
based on 4 to 19 nodes in the hidden layer with a size of 0 8 to 0 95 (0 95, 0 9) to model a three-layer perceptron ANN We evaluated the learning rate of 0 05 to 0 4 (0 4, 0 3, 0 2, 0 1, 0 05) with hyperbolic tangent activity in the hidden layer, sigmoid function activity in the output layer, and post-diffusion learning algorithm After examining all possible models for the structure of the threelayer ANN, the network with 24 input nodes, 10 hidden nodes, one output node, a learning rate of 0 2, and a motion size of 0 9 with an error propagation algorithm as the best ANN to predict the data The number of fitted models for each combination was 20; the best model for each structure is shown in Table 2
Statistical analysis
The mean and standard deviation were used for quantitative variables, and frequency and percentage were used for qualitative variables To evaluate the predictive accuracy of the system for each postoperative variable, the predicted values were compared with the actual outcomes (observed values), and true positive, false positive, accuracy, and precision rates of the system were calculated for the need for repeated ablation All statistical analyses were done using SPSS software (IBM SPSS, version 20, Armonk, New York: IBM Corp), and the significance level was also considered (p < 0 05)
RESULTS
The preoperative characteristics of patients are summarized in Table 3 The mean age at presentation was 8 65 ± 6 12 months Low birth weight was presented in 0 3% of patients The prenatal diagnosis of PUV was performed in 81(56 25%) patients There were 33 (22 91%) patients who required a second valve ablation due to valve remnants Postoperative data of patients are displayed in Table 4
Table 3. Descriptive statistics of preoperative characteristics of the patients
N (%) Variables
8 65 ± 6 12 Age at presentation (years)
5 (0 3) Low Birth Weight 81 (56 25) Prenatally Time to diagnosis
26 80 ± 18 12 Left Differential function in renal DMSA scan
29 63 ± 19 75 Right
AP: anter or-posterior d ameter; PUV: posterior urethra valve, DMSA: dimercaptosuccin c acid; VUR: vesicoureteral reflux; UTI: urinary tract infection
The predictive factor for the residual valve in Regression analysis
In multivariate analysis, the factors below were significantly associated with the residual valve and need for repeated ablation: younger age at operation (odds ratio [OR] 1 142; 95% Confidence interval [CI] 1 006-1 297), high initial serum creatinine (OR: 1 498; 95%CI: 1 0893 257), increased bladder wall thickness (OR: 1 486; 95%CI: 1 014-2 741), higher postoperative serum creatinine (OR: 1 883; 95%CI: 1 181-4 311), presence of renal cortical thickness (OR: 1 185; 95%CI: 1 004-1 721), p
i
n ( O R : 1 5 4 ;
Table 4.
Descriptive statistics of postoperative characteristics of the patients
N (%) Variables
0 617 ± 429 Blood creatinine level (mg/dL)
69 (47 9) No Presence of hydronephrosis
10 (6 95) Right
18 (12 5) Left
47 (32 65) Both
69 (48) No Degree of hydronephrosis
12 (8 3) 1
21 (14 6) 2
24 (16 6) 3
18 (12 5) 4
138 (95 8) Urine analysis
136 (94 4) Urine culture
83 (57 6) Normal Blood pressure (mm Hg)
4 (2 8) Hight
17 (11 8) History of urinary incontinency
15 (10 4) History of enuresis
60 (41 6) 1 Proteinuria in urine analysis
63 (43 7) 2
21 (14 7) 3
33 (22 91) Yes Remnant valve
111 (77 09) No
three (OR: 2 526; 95%CI: 1 208-7 021), presence of reflux grading four (OR: 3 72; 95%CI:1 557-8 899)
ANN model
Three hundred and twenty models were fitted to the 16 structures, as shown in Table 2 We selected model 7 as
2.
The ANN main factors that predict the residual valve
Table 5
Performance of an artificial neural network system in recurrence
AUC Accuracy Negative Positive Tr ue Tr ue predictive Predictive negative positive value value rate rate (specificity) (sensitivity)
Recur rence
AUC: Area under the curve
the best model (green row) among these models The prediction accuracy was 90 73%, and the area under the ROC curve was 0 903 The accuracy, sensitivity, and specificity of the ANN system for predicting the rate of remanent valves were 90 75%, 92 73%, and 73 19%, respectively (Table 5)
The predictive factor for the residual valve in the ANN model
Younger age at surgery, hyperechogenicity of the renal parenchyma, presence of VUR, and grade of reflux before surgery were among the most significant characteristics that affected postoperative outcome variables, the need for repeated ablation, and were given the highest relative weight by the ANN system (Figure 2)
DISCUSSION
In this study, we developed and utilized an ANN system to predict residual valve and ablation needs after endoscopic PUV ablation The accuracy and sensitivity ranged from 90 75% to 92 73%, proving that ANN is a valuable
M Shirazi, Z Jahanabadi, F Ahmed, et al
Figure
tool for the prediction of the residual in PUV patients
Endoscopic primary valve ablation is the ideal initial surgical therapy for PUVs; however determining the absence of remaining valve remains necessitates meticulous examination Some prescribe VCUG for adequacy, while others advise cystoscopy follow-up Both procedures offer advantages and downsides, such as transitory dysuria, enuresis, hematuria, and toileting anxiety, as well as the necessity for general anesthesia for cystoscopy The high incidence rate of remaining leaflets necessitates post-ablation assessment (18)
In this study, to reduce the impact of technical aspects of the first PUV ablation in the presence of remaining valves, all procedures in the research were carried out by the same surgeon with an experienced pediatric urologist with more than 20 years of experience in the pediatric urology field Additionally, as the VCUG alone was insufficient to exclude residual valve tissue (positive and negative predictive values of 56% and 50%, respectively) (7), so cystoscopy was routinely performed on the patients
The reported recurrence rate of residual valves was 10%30% in most studies 13,19 In the same line with previous studies, the recurrence rate in this study was 22 91% A higher recurrence rate was reported in some studies, such as the study carried out by Nawaz et al , who reported 78% residual valves during the follow-up cystoscopy 8
The high rate of residual valves may be attributed to the use of routine follow-up cystoscopy after primary valve ablation
Previous studies have primarily examined the correlation between preoperative factors and postoperative kidney function (20, 21), with limited attention given to the risk of residual remnants valve risk in PUV patients (4) In this study, factors significantly associated with residual valve and need for repeated ablation in regression analysis include younger age at operation, high initial serum creatinine, increased bladder wall thickness, higher postoperative creatinine, renal cortical thickness, severe bladder trabeculation, and advanced reflux grading (three or four) Similarly, Shirazi et al evaluated the relationship between preoperative findings and residual obstructive leaflets after valve ablation The authors found that younger age at PUV ablation, increased renal echogenicity, and the high VUR grade were significantly associated with the presence of residual valves (4) In Nabil et al ’ s study, the authors found that age at presentation and substantial post-void residual volume (PVR) were highly associated with the presence of residual valves (22) Motiwala et al , in their study, recommend using the urethral ratio and bladder wall thickness to assess residual valves (23) Premature birth, prenatal diagnosis, and loss of corticomedullary differentiation unilaterally or bilaterally were all associated with meaningfully higher rates of CKD, ESRD, and the need for many corrective surgeries in PUV patients, according to Bilgutay et al Furthermore, symptomatic presentation, recurrent UTI, and pre-operative and postoperative high VUR were associated with the need for many corrective surgeries but not poor renal outcomes (24) In contrast, some studies mentioned that age of presentation or ablation, urinary diversion, and the bladder neck incision did not significantly affect the outcome of PUV management (24, 25) Nevertheless, assess-
ing the efficacy of the PUV ablation procedure is not uniform and has some drawbacks (4) Additionally, bladder dysfunction after primary valve ablation is caused by the gradual deterioration of bladder contractility due to secondary lower urinary tract obstruction and eventually to myogenic bladder failure (24, 25)
There is a need to develop predictive models to optimize patient selection and patient counseling and to develop further ways to determine the most likely surgical outcomes before surgery is performed In the study, younger age at surgery, hyperechogenicity of the renal parenchyma, presence of VUR, and grade of reflux before surgery were among the most significant characteristics that affected postoperative outcome variables, the need for repeated ablation and were given the highest relative weight by the ANN system The advantage of ANN is that it can simply estimate and notify the relative importance of every variable on PUV outcome without the use of invasive methods The prediction accuracy of the ANN model was 90 73%, and the area under the ROC curve was 0 903 The accuracy, sensitivity, and specificity of the system for predicting the residual valve were 90 75%, 92 73%, and 73 19%, respectively Using a preoperative and postoperative dataset and a readily available cloudbased predictive analytical platform, we indicated that it could precisely train a model that can predict the rate of remnant leaflets valve after endoscopic valve ablation Since predicting patient outcomes based on data sets is not a novel concept, constructing and verifying these predictive models necessitates time-consuming calculations and powerful statistical techniques to be carried out by appropriately qualified professionals (26) Moreover, once these calculations were completed and the result was available and ready for presentation, the statistical data set could become out of date (27) Based on recent clinical data, the ANN system can produce these designs in a reproducible manner a few times, allowing for continuous data entry, real-time constant model retraining, and provision of an output to influence clinical decisionmaking (28) As more input data was fed into the system (24 variables), the system innately augmented the integrated weights between the parameters As a result, the predicted values were very close to the expected value However, no studies have been conducted to date to compare the predictive accuracy of ANN versus regression analysis methods in predicting which patients are at high risk of obstructive remnant leaflets after valve ablation in boys with PUV Previous research on the outcomes of remnant leaflets after valve ablation reported the same predictive accuracy of ANN systems in comparison to statistical models (4, 22, 23) The advantages of the ANN model are that it is the software can be easily used and updated with more preoperative, postoperative, and intraoperative variables in future versions, and the institutes can easily add other features to their software to customize it However, the disadvantages of the ANN model include the absence of underlying causal relationships between data processing algorithms and clinical realities Few published data investigated the role of AI in PUV outcomes For example, Weaver et al used ANNs to predict renal failure in children with PUV using a survival analysis tool They used deep learning imaging features
from US images to predict renal failure accurately They found that the ANNs model could accurately predict which patients will develop renal failure (29) Abdovic et al. utilized ANN to predict the late presentation of PUV in boys with lower urinary tract symptoms The accuracy, sensitivity, specificity, positive predictive value, and negative predictive value of ANNs were 92 7%, 100 0%, 89 7%, 80 0%, and 100 0%, respectively (30)
Study limitation
There are several limitations to the study Firstly, the retrospective nature and low sample size inherently lacked control and randomization This approach is prone to selection bias and attrition due to loss of follow-up, potentially skewing the results However, such surveys can aid in the development of a better methodology for the management of PUVs, as well as the achievement of purposeful follow-up for high-risk patients rather than invasive procedures The assessment of outcomes was also limited, lacking adjustments for critical factors such as depth of incision, surgeon experience, urodynamic evaluation, and needs for anticholinergic therapy Also, we do not include information on the varied outcomes, such as ESRD, dialysis, and renal transplantation, which can influence the outcome This omission could lead to an incomplete understanding of the factors influencing treatment outcomes Therefore, prospective comparative trials will be needed to confirm the predictive value of ANN vs statistical data mining models and validate the system to decide whether or not to proceed with PUV ablation
CONCLUSIONS
In conclusion, the ANN is an integrated data-gathering tool for analyzing and understanding the relationships among variables as a complex non-linear statistical model The accuracy and sensitivity in predicting the rate of the residual valve after the endoscopic valve ablation ranged from 90 75% to 92 73% The results indicate that ANN might be a valuable tool for outcome prediction of the residual valve after endoscopic valve ablation in patients with PUV
ACKNOWLEDGMENTS
The authors would like to thank Shiraz University of Medical Sciences, Shiraz, Iran, and also the Centre for Development of Clinical Research of Nemazee Hospital and Dr Nasrin Shokrpour for editorial assistance
REFERENCES
1 Krishnan A, de Souza A, Konijeti R, Baskin LS The anatomy and embryology of posterior urethral valves J Urol 2006; 175:1214-20
2 Buffin-Meyer B, Tkaczyk M, Stanczyk M, et al A single-center study to evaluate the efficacy of a fetal urine peptide signature predicting postnatal renal outcome in fetuses with posterior urethral valves Pediatr Nephrol 2020; 35:469-75
3 Holmdahl G, Sillen U Boys with posterior urethral valves: outcome concerning renal function, bladder function and paternity at ages 31 to 44 years J Urol 2005; 174:1031-4
4 Shirazi M, Farsiani M, Natami M, et al Which patients are at
higher risk for residual valves after posterior urethral valve ablation? Korean J Urol 2014; 55:64-8
5 Mirone V, Imbimbo C, Longo N, Fusco F The detrusor muscle: an innocent victim of bladder outlet obstruction Eur Urol 2007; 51:57-66
6 Bani Hani O, Prelog K, Smith GH A method to assess posterior urethral valve ablation J Urol 2006; 176:303-5
7 Smeulders N, Makin E, Desai D, et al The predictive value of a repeat micturating cystourethrogram for remnant leaflets after primary endoscopic ablation of posterior urethral valves J Pediatr Urol 2011; 7:203-8
8 Nawaz G, Hussain I, Muhammad S, et al Justification For ReLook Cystoscopy After Posterior Urethral Valve Fulguration J Ayub Med Coll Abbottabad 2017; 29:30-2
9 Lorenzo AJ, Rickard M, Braga LH, et al Predictive Analytics and Modeling Employing Machine Learning Technology: The Next Step in Data Sharing, Analysis, and Individualized Counseling Explored With a Large, Prospective Prenatal Hydronephrosis Database Urology 2019; 123:204-9
10 Rajan P, Tolley DA Artificial neural networks in urolithiasis Curr Opin Urol 2005; 15:133-7
11 Hameed BMZ, AVL SD, Raza SZ, et al Artificial Intelligence and I t s I m p a c t o n U r o l o g i c a l D
: A Comprehensive Review of the Literature J Clin Med 2021; 10
12 Aminsharifi A, Irani D, Pooyesh S, et al Artificial Neural Network System to Predict the Postoperative Outcome of Percutaneous Nephrolithotomy J Endourol 2017; 31:461-7
13 Oktar T, Salabas E, Acar O, et al Residual valve and stricture after posterior urethral valve ablation: how to evaluate? J Pediatr Urol 2013; 9:184-7
14 Wu CQ, Blum ES, Patil D, Smith EA Posterior urethral morphology on initial voiding cystourethrogram correlates to early renal outcomes in infants with posterior urethral valves J Pediatr Urol 2022; 18:813-9
1 5 G a i b i e Z , M a h o m e d N , P e t e r s e n K L , e t a l C a n t h e posterior:anterior urethral ratio on voiding cystourethrogram be used as a reliable predictor of successful posterior urethral valve ablation in male children? SA J Radiol 2020; 24:1820
16 Lawrence J, Luedeking S Introduction to neural networks: design, theory and applications Nevada City, Calif : California Scientific Software; 1994
17 Ertin E Mathematical Methods for Neural Network Analysis and Design: R M Golden, MIT Press, Cambridge, MA, 1996, 419 pp , ISBN 0-262-07174-6 J Neurocomputing 2000; 34:257-8
18 Mo Z, Li M, Xie X, et al Urodynamic changes before and after endoscopic valve ablation in boys diagnosed with the posterior urethral valve without chronic renal failure BMC Urol 2023; 23:5
19 Deshpande AV, Alsaywid BS, Smith GH Setting the speed limit: a pilot study of the rate of serum creatinine decrease after endoscopic valve ablation in neonates J Urol 2011; 185:2497-500
20 Klaus R, Lange-Sperandio B Chronic Kidney Disease in Boys w i t h P o s
Management Biomedicines 2022; 10
21 Long CJ, Bowen DK Predicting and Modifying Risk for Development of Renal Failure in Boys with Posterior Urethral Valves Curr Urol Rep 2018; 19:55
22 Nabil A, Salem A, Salah M, et al The Importance of Second Look Cystoscopy after Posterior Urethral Valve Ablation in Children: Single Center Experience Clin Surg 2019; 4
M Shirazi, Z Jahanabadi, F Ahmed, et al
23 Motiwala T, Sinha A, Rathod KJ, et al Correlation of Urethral Ratio and Bladder Wall Thickness with Cystoscopic Findings in Posterior Urethral Valve Patients to Assess Residual Valves J Indian Assoc Pediatr Surg 2022; 27:53-9
24 Bilgutay AN, Roth DR, Gonzales ET, et al Posterior urethral valves: Risk factors for progression to renal failure J Pediatr Urol 2016; 12:179 e1-7
25 Hennus PM, van der Heijden GJ, Bosch JL, et al A systematic review on renal and bladder dysfunction after endoscopic treatment of infravesical obstruction in boys PLoS One 2012; 7:e44663
26 Popovics P, Penniston KL Current research and future directions in non-malignant urologic research - proceedings of the annual CAIRIBU meeting Am J Clin Exp Urol 2022; 10:449-61
27 Checcucci E, Autorino R, Cacciamani GE, et al Artificial intelligence and neural networks in urology: current clinical applications Minerva Urol Nefrol 2020; 72:49-57
28 Anagnostou T, Remzi M, Lykourinas M, Djavan B Artificial neural networks for decision-making in urologic oncology Eur Urol 2003; 43:596-603
29 Weaver JK, Milford K, Rickard M, et al Deep learning imaging features derived from kidney ultrasounds predict chronic kidney disease progression in children with posterior urethral valves Pediatr Nephrol 2023; 38:839-46
30 Abdovic S, Cuk M, Cekada N, et al Predicting posterior urethral obstruction in boys with lower urinary tract symptoms using deep artificial neural network World J Urol 2019; 37:1973-9
Correspondence
Mehdi Shirazi, MD shirazim@sums ac ir
Zahra Jahanabadi, MD (Corresponding Author) z jahanabadi@yahoo com
Alimohammad Keshtvarz Hesam Abadi, PhD Candidate alimohammad keshtvarz@gmail com
Mohammad Reza Askarpour, MD askarvip2@gmail com
Sania Shirazi, Student saniashirazi046@gmail com
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Single-component artificial urinary sphincter: Outcomes from one centre in Portugal
João Aragão Vital 1 , Miguel Marques Monteiro 1 , Bernardo Lobão Teixeira 1 , Gonçalo Grilo Mendes 1 , Alexandra Rocha 1 , Mariana Madanelo 1 , Sofia Mesquita 1 , Nuno Vinagre 1 , Beatriz Oliveira 1 , Martinha Magalhães 1 , Ana Isabel Lopes 1 , Carlos Ferreira 2 , Paulo Príncipe 1 , Avelino Fraga 1
1 Centro Hospitalar Universitário de Santo António (CHUdSA), Porto, Portugal;
2 Centro Hospitalar Universitário de São João (CHUSJ), Porto, Portugal
Summary
Purpose: Radical prostate cancer treatment is the predominant cause of iatrogenic stress urinary incontinence (SUI) in men, significantly impacting their quality of life (QoL) This prospective single-center study in Portugal aimed to evaluate the outcomes of men with moderateto-severe SUI treated with a single-component artificial urinary sphincter (AUS)
Materials and methods: Male patients with iatrogenic moderateto-severe SUI, determined by a 24-hour pad weight test, were included. The single-component device comprises a cuff linked to a pump unit through a kink-resistant tube The implantation involved perineal incision for cuff placement and an inguinal incision for pump and tank positioning within the scrotum Complications, pad usage, perioperative complications (ClavienDindo classification), and quality of life assessment using the International Consultation on Incontinence Questionnaire-Short Form (ICIQ-SF) questionnaire were documented
Results: Between May 2021 and March 2023, 20 consecutive single-component AUS insertions were conducted at a Portuguese urology department. Follow-up concluded in July 2023, with a mean follow-up duration of 15 months (range: 5-27) Four patients experienced complications necessitating device revision or removal (erosion = 2, infection = 1, mechanical failure = 1) Social continence (0/1 pad/day) was achieved in 70% (14/20 patients), while 30% (6/20 patients) experienced incontinence Perioperatively, one patient was classified as grade 2, while the remaining were grade 0/1 in the ClavienDindo classification The mean ICIQ-SF score reduction was 10 5 points
Conclusions: The single-component AUS shows promising efficacy in managing moderate-to-severe male SUI, offering a good success rate, acceptable complications, improved QoL, and a straightforward surgical procedure.
KEY WORDS: Artificial urinary sphincter; Zephyr Surgical Implants 375; Male stress urinary incontinence; Radical prostatectomy; Quality of life
Submitted 13 May 2024; Accepted 6 June 2024
INTRODUCTION
The prevalence of urinary incontinence (UI) in men can reach up to 39% and tends to rise with advancing age (1) The primary cause of stress urinary incontinence (SUI) among adult men is commonly attributed to iatrogenic
impairment of the external urethral sphincter, predominantly resulting from radical prostate cancer treatment (2) Irrespective of its underlying causes, SUI significantly diminishes the quality of life for those who experience it (3-9) The primary approach for managing male SUI involves pelvic floor muscle training, biofeedback, and electrical stimulation If these conservative methods prove ineffective, surgical interventions are the only available alternative (1-16)
In 1973, the artificial urinary sphincter (AUS) was initially developed to address male moderate-to-severe SUI, eventually establishing itself as the preferred treatment for this pathology (17-19) However, the process of inserting an AUS remains intricate and carries the potential for complications such as erosion, infection, and mechanical failure Introduced in 1983, the last version of American Medical Systems (AMS) 800 device stands as the gold standard of AUS and continues to be utilized to this day (4, 5, 9, 12) While it has demonstrated favorable long-term outcomes, it is important to note that the preparation and execution of the procedure remain intricate, carrying a potential risk of complications In instances of postoperative urethral atrophy, it is not feasible to readjust the cuff, and once activated, there are no available options to modify the pressure of the device (4, 5, 9, 13-16, 20)
The success of the procedure relies heavily on the meticulous preparation of the sphincter, proper connection of its components, and the surgeon's expertise, considering the lengthy learning curve The majority of AUS insertions are performed by surgeons who only conduct a few procedures (between 1 and 3) per year Less than 10% of AUS insertions in the USA are carried out by surgeons who have completed at least 100 procedures, which indicates a lower level of experience (21) As a result, the likelihood of requiring additional surgery increases from 13% to 24% (22)
The purpose of designing Zephyr Surgical Implants (ZSI) 375 is to simplify the process of inserting the AUS The first implantation of ZSI 375 took place in March 2009, making it a relatively recent innovation (23) The cuff is adaptable and placed around the urethra, already connected beforehand Additionally, ZSI 375 eliminates the need for an abdominal reservoir, leading to reduced operating time and avoiding the requirement for abdominal
incision and dissection in previously scarred retroperitoneum By increasing the pressure, it enhances the patient's continence (10, 24)
We conducted an analysis of the outcomes of the AUS ZSI 375 implantation for stress urinary incontinence in 20 male patients, and its influence on the individual's quality of life (QoL)
MATERIALS AND METHODS
Patients
The study employed a prospective, non-randomized design and was conducted at a single urological department in Portugal Between May 2021 and March 2023, 20 consecutive placements of the AUS ZSI 375 were performed in male patients presenting iatrogenic moderate to severe SUI as determined by the 24-hour pad weight test The procedures were carried out by two experienced surgeons Prior to surgery, the pre-operative protocol encompassed patient history assessment, physical examination, urinalysis, cystoscopy to rule out stenosis, a 24hour pad weight test, and urodynamics to exclude overactive bladder All patients had previously undergone pelvic floor muscle training In preparation for the surgical procedures, all patients completed the International C o n
(ICIQ-SF questionnaire)
The study was approved by the Ethical Committee of our center
All study participants provided written informed consent
ZSI 375 Device
The ZSI 375 is a single-component device made up of a cuff linked to a pump unit through a kink-resistant tube The adaptable cuff is designed in a curved shape to prevent creasing It is positioned around the urethra, while the pump unit, which includes a pressure-regulating tank and pump, is situated within the scrotum, specifically in the subdartos pouch It has no abdominal reservoir Once activated, the hydraulic circuit's pressure can be adjusted up or down to enhance the patient's continence (25) The improved hydraulic system of the ZSI 375 PF (pre-filled) has been in use since March 2015, and it is anticipated that the reduced operating time will lead to decreased infection and mechanical failure rates (25)
Surgical procedure
The implantation surgical procedure was carried out under general anesthesia with the patient in the lithotomy position The surgical technique consists in a perineal incision for cuff placement and an inguinal incision for pump and tank placement in the scrotum A 14 Fr Foley urethral catheter is placed for guidance and was removed by routine in the day after surgery The device was activated six weeks later
Follow-up after implantation
The scheduled appointments occurred at intervals of 1, 3, and 6 months following device activation, with subsequent annual appointments Patients documented their daily pad usage in a 7-day diary prior to each visit The fol-
low-up process was concluded in July 2023 Total continence was defined as the absence of any pad usage, while social continence was characterized by the use of 1 pad per day Incontinence was ascribed to individuals who required > 1 pad per day Success was defined as achieving social continence, which encompassed the range of pad usage from 0 to 1 per day Perioperative complications were classified using the Clavien-Dindo classification system The quality of life was evaluated by means of the ICIQ-SF questionnaire, administered both before the surgical procedure and during the follow-up period subsequent to device activation Additionally, a subjective assessment of patient satisfaction was documented
RESULTS
Patient characteristics
A total of 20 patients had the ZSI 375 device implanted, with a mean (range) follow-up of 15 (5-27) months The averaged (range) patient age was 71 5 (62-80) years old The indications were incontinence following radical prostatectomy (RP, n = 11), RP and radiotherapy (n = 8) and transurethral resection of prostate (TURP, n = 1)
Five (25%) patients with a 24h pad weight test between 200-400g and 15 (75%) > 400g The mean (range) ICIQSF score before surgery was 20,8 (17-21) points The mean (range) operative time was 69 (35-100) minutes, and the mean hospital stay was 1 day with catheter removal on the same day The device was activated six weeks later by routine
Complications
Complications leading to a revision or permanent device removal arose in 4 patients: 2 erosions of the urethra with device explantation, 1 infection and 1 mechanical failure both with device re-implantation Perioperatively, one patient was classified as grade 2, while the remaining were classified as grade 0 or 1 in the Clavien-Dindo classification (Table 1)
Pressure adjustment
In 5 (25%) patients, there was a need for device pressure adjustment under radiographic control, in an outpatient setting, to improve continence
Efficacy
Three (15%) patients achieved total continence (0 pads per day), 11 (55%) social continence (1 pad per day), and
Table 1
The aetiology of the incontinence and complications
Aetiolog y Infections Urethral erosions Mechanical complications of incontinence n (%) n (%) n (%)
RP (11 patients) 0 1 (9 1) 1 (9 1)
RP+RT (8 patients) 1 (12 5) 1 (12 5) 0
TURP (1 patients) 000
Total (20 patients) 1 (5) 2 (10) 1 (5)
RP: radica prostatectomy; RT: radiotherapy; TURP: transurethra resection of prostate
J Aragão Vital, M Marques Monteiro, B Lobão Teixeira, et al
Table 2. The efficacy after the implantation of the ZSI 375
Total continence - Social Continence - Incontinence0 pads per day (%) 1 pad per day (%) > 1 pad per day (%)
Moderate SUI (5 patients) 1 (20) 3 (60) 1 (20)
200-400g - 24h
Pad weight test
Severe SUI (15 patients) 2 (13 3) 8 (53 3) 5 (33 3) > 400g - 24h
Pad weight test
Total (20 patients) 3 (15) 11 (55) 6 (30)
Overall success 14 (70)
6 (30%) experienced incontinence (> 1 pad per day), resulting in an overall success rate of 70% (total and social continence) The mean (range) ICIQ-SF score after surgery was 10,5 (0-18) points with a mean reduction of 10,3 points in a scale from 0-21 The grade of satisfaction with the device was 75% (Table 2)
DISCUSSION
In this study, we present our short-term experience with 20 patients who received the ZSI 375 AUS Over a median follow-up period of 15 months, the overall success rate, encompassing total and social continence, reached 70% While the AUS AMS 800 currently stands as the gold standard therapy for moderate to severe SUI in men, c o n c e r n s r e g a r d i n g i t s c o m p l e x i t y , t i m e - c o n s u m i n g nature, inability to adjust device pressure, and the challenge of cuff readjustment in cases of postsurgical urethral atrophy have arisen (4)
The ZSI 375 device represents a relatively recent addition to this field Our study highlighted the simplicity of the surgical procedure, even during the early stages of the learning curve, with notably short surgical times One significant advantage of this device lies in its capacity to adjust internal pressures using the in situ trans-scrotal applicator within an office outpatient setting, offering the potential for improved outcomes post-surgery Enhanced management of pressure escalation following activation is expected to reduce the incidence of urethral erosion (25)
In our study, this procedure was necessary for five patients Regrettably, as of the conclusion date, it has not been possible to assess post-adjustment outcomes
The most frequent complication observed was urethral erosion, which affected 2 (10%) of the patients, a rate comparable to that of AMS 800 (11, 16, 24, 26, 27)
Notably, one of these two patients had undergone previous radiotherapy, a well-recognized adverse factor for sphincter insertion (28) The second patient was catheterized in primary healthcare following a suspected episode of urinary retention, indicating a potential iatrogenic cause
Mechanical failure necessitating device re-implantation occurred in 1 (5%) patient during the early stages of the study, likely attributed to the surgeons' relative inexperience with implanting this new device This rate is also in line with that reported for the AMS 800 (12, 24, 27) Our overall complication rate aligns with that of other report-
ed series involving ZSI 375 implantations (10, 23-25, 29, 30) Assessment of QoL using the ICIQ-SF questionnaire revealed a significant improvement, and a high level of patient satisfaction with the device was noted, possibly attributable to its simplicity Finally, this study has limitations, including a short follow-up duration and a small patient cohort Some patients with prior AMS 800 AUS procedures underwent surgery, and the study was conducted during the early stages of the surgical learning curve Additionally, utilizing the weight pad test after device activation may offer a more accurate measure for assessing real improvements in incontinence
CONCLUSIONS
In this short-term follow-up study, the ZSI 375 AUS demonstrated effectiveness in the management of moderate to severe male SUI, exhibiting a commendable success rate while maintaining a low incidence of complications
The QoL was evaluated using the ICIQ-SF questionnaire, revealing a significant improvement Notably, the surgical procedure proved to be straightforward with a brief learning curve In conclusion, the ZSI 375 AUS emerges as a promising treatment option for moderate to severe SUI in male patients
REFERENCES
1 Bauer RM, Gozzi C, Hübner W, et al Contemporary management of postprostatectomy incontinence Eur Urol 2011; 59:985-996
2 Shamliyan TA, Wyman JF, Ping R, et al Male urinary incontinence: prevalence, risk factors, and preventive interventions Rev Urol 2009; 11:145-165
3 Park HK, Chang S, Palmer MH, et al Assessment of the Impact of Male Urinary Incontinence on Health-Related Quality of Life: A Population Based Study Low Urin Tract Symptoms 2015; 7:22-26
4 Ostrowski I, Sledz E, Ciechan J, et al Current interventional management of male stress urinary incontinence following urological procedures Cent European J Urol 2015; 68:340-347
5 James MH, McCammon KA Artificial urinary sphincter for postprostatectomy incontinence: a review Int J Urol 2014; 21:536-543
6 Sousa-Escandón A, Cabrera J, Mantovani F, et al Adjustable suburethral sling (male remeex system) in the treatment of male stress urinary incontinence: a multicentric European study Eur Urol 2007; 52:1473-1479
7 Leruth J, Waltregny D, de Leval J The inside-out transobturator male sling for the surgical treatment of stress urinary incontinence after radical prostatectomy: midterm results of a single-center prospective study Eur Urol 2012; 61:608-615
8 Kim SW, Walsh R, Berger Y, Kim JH Male Readjustable Sling (MRS) System for Postprostatectomy Incontinence: Experiences of 2 Centers Urology 2016; 88:195-200
9 Van der Aa F, Drake MJ, Kasyan GR, et al Young Academic Urologists Functional Urology Group The artificial urinary sphincter after a quarter of a century: a critical systematic review of its use in male non-neurogenic incontinence Eur Urol 2013; 63:681-689
10 Ostrowski I, Blewniewski M, Neugart F, et al Multicentre experience with ZSI 375 artificial urinary sphincter for the treatment of stress urinary incontinence in men Urologia 2017; 84:148-152
11 Hajivassiliou CA A review of the complications and results of implantation of the AMS artificial urinary sphincter Eur Urol 1999; 35:36-44
12 Herschorn S, Bruschini H, Comiter C, et al Surgical treatment of stress incontinence in men Neurourol Urodyn 2010; 29:179-190
13 Clemens JQ, Schuster TG, Konnak JW, et al Revision rate after artificial urinary sphincter implantation for incontinence after radical prostatectomy: actuarial analysis J Urol 2001; 166:1372-5
15 Elliott DS, Barrett DM Mayo Clinic long-term analysis of the functional durability of the AMS 800 artificial urinary sphincter: a review of 323 cases J Urol 1998; 159:1206-8
16 Lai HH, Hsu EI, Teh BS, et al 13 years of experience with artificial urinary sphincter implantation at Baylor College of Medicine J Urol 2007; 177:1021-1025
17 Scott FB, Bradley WE, Timm GW Treatment of urinary incontinence by an implantable prosthetic urinary sphincter J Urol 1974; 112:75-80
18 Lucas MG, Bosch RJ, Burkhard FC, et al EAU guidelines on surgical treatment of urinary incontinence Eur Urol 2012; 62:11181129
19 Herschorn S The artificial urinary sphincter is the treatment of choice for post-radical prostatectomy incontinence Can Urol Assoc J 2008; 2:536-539
20 Vakalopoulos I, Kampantais S, Laskaridis L, et al New artificial urinary sphincter devices in the treatment of male iatrogenic incontinence Adv Urol 2012; 2012:439372
21 Wilson SK, Aliotta PJ, Salem EA, Mulcahy JJ New enhancements of the scrotal one-incision technique for placement of artificial urinary sphincter allow proximal cuff placement J Sex Med 2010; 7:3510-3515
22 Sandhu JS, Maschino AC, Vickers AJ The surgical learning curve for artificial urinary sphincter procedures compared to typical surgeon experience Eur Urol 2011; 60:1285-1290
23 Ostrowski I, Golabek T, Ciechan J, et al Preliminary outcomes of the European multicentre experience with the ZSI 375 artificial urinary sphincter for treatment of stress urinary incontinence in men Cent European J Urol 2019; 72:263-269
24 Staerman F, G-Llorens C, Leon P, Leclerc Y ZSI 375 artificial urinary sphincter for male urinary incontinence: a preliminary study BJU Int 2013; 111:E202-E206
25 Ostrowski I, Ciechan J, Sledz E, et al Four-year follow-up on a Zephyr Surgical Implants 375 artificial urinary sphincter for male urinary incontinence from one urological centre in Poland Cent European J Urol 2018; 71:320-325
26 Venn SN, Greenwell TJ, Mundy AR The long-term outcome of artificial urinary sphincters J Urol 2000; 164:702-707
27 Kim SP, Sarmast Z, Daignault S, et al Long-term durability and functional outcomes among patients with artificial urinary sphincters: a 10-year retrospective review from the University of Michigan J Urol 2008; 179:1912-1916
28 Queissert F, Huesch T, Kretschmer A, et al Artificial Urinary Sphincter Cuff Size Predicts Outcome in Male Patients Treated for Stress Incontinence: Results of a Large Central European Multicenter Cohort Study Int Neurourol J 2019; 23:219-225
29 Llorens C, Pottek T Urinary artificial sphincter ZSI 375 for
treatment of stress urinary incontinence in men: 5 and 7 years follow-up report Urologia 2017; 84(4):263-266
30 Ostrowski I, Sledz E, Wilamowski J, et al Patients' quality of life after implantation of ZSI 375 artificial urinary sphincter due to stress urinary incontinence Cent European J Urol 2020; 73:178-186
Correspondence
João Aragão Vital, MD joaopvital@gmail com
Miguel Marques Monteiro, MD mmonteiro iam@gmail com Bernardo Lobão Teixeira, MD bernardolat@gmail com
Gonçalo Grilo Mendes, MD goncalo grilomendes@gmail com Alexandra Rocha, MD marialexandrarocha@gmail com Mariana Madanelo, MD marianacmadanelo@gmail com
Sofia Mesquita, MD sofiaoplmesquita@gmail com Nuno Vinagre, MD nunomrvinagre@gmail com
Beatriz Oliveira, MD ana bia 5@hotmail com
Martinha Magalhães, MD martinha a magalhaes@gmail com
Ana Isabel Lopes, BSc analopes urodinamica@chporto min-saude pt
Paulo Príncipe, MD paulo principe@gmail com
Avelino Fraga, MD PhD avfraga@gmail com
Urology Department, Santo António University Hospital Center Largo do Prof Abel Salazar, 4099-001 Porto, Portugal
Carlos Ferreira, MD carlosferreira esr@gmail com
Centro Hospitalar Universitário de São João (CHUSJ)
Conflict of interest: The authors declare no potential conflict of interest
J Aragão Vital, M Marques Monteiro, B Lobão Teixeira, et al
ORIGINAL PAPER
Functional outcome of the one-stage scrotal tunnel + ventral inverted V incision + inverted Y anastomosis technique to treat penile paraffinoma: A single center retrospective study
Muhammad Asykar Palinrungi 1 , Syakri Syahrir 2 , Syarif 1 , Andhini L.R. Palinrungi 3 , Muhammad Faruk 4
1 Department of Urology, Faculty of Medicine, Hasanuddin University - Hasanuddin University Hospital, Makassar, South Sulawesi, Indonesia;
2 Department of Urology, Faculty of Medicine, Hasanuddin University - Dr Wahidin Sudirohusodo Hospital, Makassar, South Sulawesi, Indonesia;
3 Department of Surgery, Akademis Jaury Jusuf Putra Hospital, Makassar, South Sulawesi, Indonesia;
4 Department of Surgery, Faculty of Medicine, Hasanuddin University - Hasanuddin University Hospital, Makassar, South Sulawesi, Indonesia
Summary
Introduction and objective: Penis enlargement through substance injection is common in many countries of Southeast Asia and Eastern Europe. The definitive therapy involves removing the entire skin and the subcutaneous tissue and resurfacing the penile shaft via a singlestage or multi-staged procedure This study aimed to report the functional outcome and esthetics of treating penile paraffinoma patients using the scrotal tunnel + ventral inverted V incision + anastomosis inverted Y technique.
Materials and methods: This study was a single-center retrospective descriptive analysis of patients who underwent onestage scrotal tunnel + ventral inverted V incision and inverted Y-shaped anastomosis procedures from January 2013 to December 2023 The following data were collected: chief complaint, reason for the injection, type of fluid injected, duration of surgery, duration of hospitalization, length of follow-up, and results after surgery
Results: Of the 32 patients included in the study, 78% injected liquids in the form of oil and the goal of the majority of patients was penis enlargement (71%). The average age was 36.84 years, and the main complaint was pain in the penis during erection (53%). The average operation time was 130 minutes, hospitalization duration was 2 21 days, primary wound healing was 91%, patient satisfaction level was 97%, and Scale 4 erection hardness was 91%
Conclusions: One-stage surgery for penile paraffinoma produced promising results when the granuloma was limited to the penis and healthy scrotal skin was available to cover the penis.
Penis enlargement through the injection of substances (paraffin, oil, cod liver oil, petroleum jelly, silicone, methacrylates, hyaluronic acid, or collagen patches) is common in Southeast Asian and Eastern European coun-
tries (1, 2) This procedure can be performed by patients, non-professionals, or medical personnel and can present severe consequences in cases of complications (3), including penile deformity, skin necrosis, limited erection due to pressure, and pain during sex (4)
The definitive therapy is to remove the entire skin and subcutaneous tissue and resurface the penile shaft (5)
The technique can be single-staged (simple excision and primary closure, bilateral scrotal flap, one-sheet spiraling full-thickness skin graft, scrotal tunnel + inverted V incision and anastomosis inverted Y technique), or multistaged (6-8)
Erectile function is assessed by measuring erection hardness using the erection hardness score (EHS), which provides specific and readily monitored results (9)
In this study, we report our experience in performing treatment on penile paraffinoma patients using the scrotal tunnel + ventral inverted V incision + anastomosis inverted Y technique, along with the esthetics and functional outcome of the procedure
MATERIALS AND METHODS
We performed a single-center retrospective descriptive study using data collected from January 2013 to December 2023 from patients who underwent single-stage scrotal tunnel + ventral inverted V-incision and anastomosis inverted Y-shape procedures (Figure 1) Figure 2 provides a conceptual illustration of the technique
Data on the chief complaint, reason for the injection, type of fluid injected, duration of surgery, duration of hospitalization, length of follow-up, and results after surgery were collected
The inclusion criteria were as follows: [1] new patient and [2] penile paraffinoma performed in a single stage
Exclusion criteria were [1] penile paraffinoma that affected the skin of the penis and greater than half of the skin of the scrotum, [2] presence of malignancy, and [3] penile paraffinoma coexisting with diabetes mellitus
Figure 2.
Figure 1. Step-by-step representation of the operative stage. Onestage surgical excision steps with scrotal tunnel + ventral inverted V-incision and anastomosis inverted Y-shape A) After the skin of the penis is removed, B) the creation of the tunneling exit hole, C) after the penis is passed under the skin and the glans protrudes from the prepared hole (penile scrotal invagination), D) appearance after suturing, E) inverted V-incision, and F) after suturing into inverted Y-shape
A conceptual illustration of the one-stage surgical excision steps with scrotal tunnel + ventral inverted V-incision and inverted Y-shaped anastomosis A) Paraffinoma in the shaft of the penis, B) excision of the entire paraffinoma in the penile shaft, C) naked penile shaft after the skin is excised, D) measurement of the scrotal tunnel for scrotal flap creation, E) creation of a hole in the scrotum, F) insertion of the penis into the scrotum hole to cover the penis with the skin of the scrotum (penile scrotal invagination), G) inverted V-incision on the ventral penis, and H) inverted Y-shaped suture
M Asykar Palinrungi, S Syahrir, Syarif, et al
This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline Informed consent was obtained from all patients and this study was approved by the Ethics Committee of Hasanuddin University, Makassar, Indonesia (no 304/UN4 6 4 5 31/PP36/2024) with protocol no UH24040277
The five-grade EHS was used to assess erection rigidity [Grade 0 (no enlargement of the penis), Grade 1 (penis enlarges but does not become firm), Grade 2 (penis is hard, but not hard enough to penetrate), Grade 3 (penis is hard enough for penetration but not completely hard), and Grade 4 (penis is completely stiff and firm)] A score of two or less was considered an abnormal EHS (10)
RESULTS
The 32 patients included in this study had an average age of 36 84 years and an average length of hospital stay of 2 21 days Most patients had a history of silicone, oil, or paraffin injections with the main aim of enlarging the penis The characteristics of the data are listed in Table 1
Table 1
Clinical characteristics of patients
EHS:
DISCUSSION
The outcomes we obtained from the 32 patients were positive, whereby 29 patients recovered completely, 2 patients experienced wound infection, and 1 patient presented contractures, which we successfully excised several months later No erection problems were noted according to the EHS, and no sexual activity issues were reported after surgery A one-stage penile paraffinoma excision is faster and easier than a two-stage procedure (requires only one operation, which generally reduces the time for recovery and degree of pain) In addition, this method is more cost-effective (the cost is usually more affordable than a two-stage surgery), has less risk of complications (fewer incisions and tissue manipulations), and allows for a thorough evaluation (the surgeon can perform a comprehensive assessment of the penile tissue during surgery t
addressed) The disadvantages of the one-stage technique are long recovery times (despite only requiring one surgery), swelling and bruising (swelling and bruising are common side effects after surgery), infection (infection is a minor but serious risk after any surgery), nerve damage (nerve damage may occur, which can cause numbness or tingling of the penis), and penile deformity (particularly when the silicone implant is large or has been in place for many years)
Granulomatous reactions resulting from the injection of a foreign body can accumulate in parts of the penis or spread to the entire penile shaft, supra-pubic area, and scrotum (11, 12) When complications occur, the entire foreign object and related skin should be removed to prevent the recurrence or graft loss that can occur if some residue remains (13) Simple excision and primary suturing may be performed in selected cases (14); however, if the penile paraffinoma involves the entire penile shaft without extension to the suprapubic area (84% of the cases in this study) or a small amount of the scrotal area (3% of our cases), then the treatment therapy should involve a radical excision of the fibrotic tissue and the associated skin and the use of scrotal skin to close the open area
The skin of the scrotum has high elasticity, which makes it suitable for covering the penis, despite the presence of hair Most of the surgeries are successful without any complications, and the reconstructed penis has an immediate post-operative tactile sensibility (1, 2, 6, 13)
The two-stage procedure for paraffinoma involves exposing the penis and inserting it into the previously created scrotal tunnel while leaving the glans exposed for urination After a few weeks, the penis is removed from the scrotum (13) In all our cases, we performed a single-stage scrotal tunnel and inverted V incision + inverted Y anastomosis after removing all parts of the penile skin along with the underlying granulomatous tissue (Figure 1) This action is possible because sufficient skin in the scrotum is available to cover the penis The average time required for this procedure is 130 minutes, while the average length of hospital stay is 2 21 days and the average follow-up is 3 4 months
Lumbiganon et al found no significant difference in surgical wound infection, wound dehiscence, or reoperation rate in the one-stage group compared to the two-stage
group; however, the two-stage group had a longer length of stay and lower complication rate Therefore, these two techniques can be considered for reconstruction in penile paraffinoma cases (15) In addition, Dellis et al recommended one-stage surgery after the procedure was performed on 10 patients with safe and effective results (16) This study had several limitations As a retrospective cohort study, it was subject to inherent selection and information biases In addition, the study was conducted at a single center, which may limit the generalizability of the findings Further multicenter, prospective studies are required to validate these results and confirm whether the one-stage scrotal tunnel + ventral inverted V incision + inverted Y anastomosis technique is safe and effective and can provide the appropriate functional and esthetic outcome post-surgery
CONCLUSIONS
Single-stage surgery on penile paraffinoma can be effective when the granuloma is limited to the penis and healthy scrotal skin is available to cover the penis
ACKNOWLEDGMENTS
We acknowledge Ashy Amelia Arista for her help in providing us with the conceptual illustration of the one-stage surgical excision steps for this study
REFERENCES
1 Mahadewa AW, Marinta Y, Nugraha P, Lukman K Candlenut oilinduced sclerosing lipogranuloma of the penis: A case report Int J Surg Case Rep 2023; 110:108673
2 Marín-Martínez FM, Guzmán Martínez-Valls PL, Dekalo S, et al Aesthetic and Functional Results after Single- and Two-Stage Resection and Reconstruction of Penile Paraffinomas - Experience from Two Tertiary Centers and a Surgical Management Algorithm Urology 2023; 171:227-35
3 Dellis AE, Nastos K, Mastorakos D, et al Minimal surgical management of penile paraffinoma after subcutaneous penile paraffin injection Arab J Urol 2017; 15:387-90
4 Shin YS, Zhao C, Park JK New reconstructive surgery for penile paraffinoma to prevent necrosis of ventral penile skin Urology 2013; 81:437-41
5 Kim JS, Shin YS, Park JK Penile skin preservation technique for reconstruction surgery of penile paraffinoma Investig Clin Urol 2019; 60:133-7
6 Dunev VR, Kolev NH, Genov PP Late results of bilateral scrotal flap Urol Case Rep 2019; 27:100920
7 Ismy J, Amirsyah M, Palgunadi IN, et al One-stage Reconstruction of Penile Paraffinoma Using Spiral Stitches FTSG and Evaluation of Sexual Function Plast Reconstr Surg Glob Open 2022; 10:e4048
8 Prasetyono TOH One-sheet spiraling full thickness skin graft for penile resurfacing after paraffinoma excision Medical Journal of Indonesia 2011; 20: 222
9 Mulhall JP, Goldstein I, Bushmakin AG, et al Validation of the erection hardness score J Sex Med 2007; 4:1626-34
10 Silva AC, Silva CM, Morgado A Erection hardness score or penile
Doppler ultrasound: which is a better predictor of failure of nonsurgical treatment of erectile dysfunction? Sex Med 2023; 11:qfad009
11 Downey AP, Osman NI, Mangera A, et al Penile Paraffinoma Eur Urol Focus 2019; 5:894-8
12 Svensøy JN, Travers V, Osther PJS Complications of penile selfinjections: investigation of 680 patients with complications following penile self-injections with mineral oil World J Urol 2018; 36:13543
13 Putra IBOW, Wahyudi I, Rodjani A Penile paraffinoma reconstruction with scrotal flap and surgical outcome: a case report Indonesian Journal of Urology 2019; 26(1)
14 Khairudin MA, Salauddin SA, Ghazali H Scrotal bridge flap reconstructive surgery for extensive penile paraffinoma: steps and outcomes from a single center: a case series African Journal of Urology 2021; 27:113
15 Lumbiganon S, Pachirat K, Sirithanaphol W, et al Surgical treatment of penile foreign body granuloma: Penile shaft reconstruction with single- versus two-stage scrotal flap techniques Int J Urol 2023; 30:681-7
16 Dellis AE, Arkoumanis T, Kyprianou C, Papatsoris AG Paraffinoma, siliconoma and Co: Disastrous consequences of failed penile augmentation-A single-centre successful surgical management of a challenging entity Andrologia 2018; 50:e13109
Correspondence
Muhammad Asykar Palinrungi (Corresponding Author) apalinrungi@yahoo com
Department of Urology, Faculty of Medicine, Hasanuddin University –Hasanuddin University Hospital, Makassar, South Sulawesi, Indonesia Jalan Perintis Kemerdekaan KM 11, Makassar, 90245, South Sulawesi, Indonesia
Syakri Syahrir drsyakrisyahrir@gmail com
Department of Urology, Faculty of Medicine, Hasanuddin University –Dr Wahidin Sudirohusodo Hospital, Makassar, South Sulawesi, Indonesia
Syarif syarifbakri@hotmail com
Department of Urology, Faculty of Medicine, Hasanuddin University –Hasanuddin University Hospital, Makassar, South Sulawesi, Indonesia
Andhini L R Palinrungi dnypalinrungi@gmail com
Department of Surgery, Akademis Jaury Jusuf Putra Hospital, Makassar, South Sulawesi, Indonesia
Muhammad Faruk muhammadfaruk@unhas ac id
Department of Surgery, Faculty of Medicine, Hasanuddin University –Hasanuddin University Hospital, Makassar, South Sulawesi, Indonesia
Conflict of interest: The authors declare no potential conflict of interest
M Asykar Palinrungi, S Syahrir, Syarif, et al
ORIGINAL PAPER
Penoscrotal transposition: Long-term outcome in 29 patients
Dolev Perez 1 , Stanislav Kocherov 2 , Gaudat Jaber 2 , Galiya Raisin 2 , Boris Chertin 1, 2
1 Departments of Urology and 2 Pediatric Urology, Shaare Zedek Medical Center, Jerusalem, Israel
Summary
Objective: Penoscrotal transposition (PST) is a rare anomaly of the external genitalia characterized by malposition of the penis in relation to the scrotum. This transposition may be partial or complete and may be associated with hypospadias, chordee, and other anomalies We have reviewed our experience with the surgical repair of PST utilizing a modified Glenn-Anderson technique
Materials and Methods: Twenty-nine patients with a median age of 5 6 years (8 months-15 years) underwent surgical repair of PST at our institution between 2004-2022 Of those, 20 (69%) had complete PST, while 9 (31%) had partial PST All children were divided into three groups In the first group of 8 (28%) children, repair of PST was an integral part of one-stage male genitoplasty; in the second group of 18 (62%) children, repair of PST was an isolated last stage of the staged hypospadias repair, and the remaining 3 (10%) children underwent PST repair without the presence of hypospadias. All patients underwent modification of the Glenn-Anderson technique involving utilization of bilateral rotational advancement scrotal flap, complete de-tethering of the testis from the internal part of the scrotum when indicated, and relocation of the scrotal compartment in a normal dependent position The follow-up ranged from 6 months to 18 years.
Results: In the first group, five children (62%) underwent Onlay Prepucial Island Pedicle Flap (OIF) hypospadias repair, and three (38%) underwent Long Tubularized Incised Plate Repair (TIP). In the second group, 8 (44%) underwent OIF hypospadias repair, 2 (12%) had Long TIP repair, and the remaining 8 (44%) underwent staged hypospadias repair. Post-operative Clavien Dindo grade III complications presented in three patients in group I and only one patient in group II. In the third group, no postoperative complications were observed
Conclusions: Our data show that penoscrotal transposition correction utilizing the Glenn-Anderson technique is a reliable and durable surgery in the pediatric population These children require careful monitoring till adolescence to ensure that no reoperation is needed
Penoscrotal transposition (PST) is a rare anomaly of the external genitalia, characterized by malposition of the
penis in relation to the scrotum (1) It is categorized as complete or incomplete variants based on the location of the penis In incomplete PST, the more common variant, the penis, lies in the middle of the scrotum, while in complete PST, the penis emerges from the perineum and is covered by the scrotum entirely (2) PST is rarely isolated and frequently occurs with a broad spectrum of malformations, including a strong association with severe hypospadias and chordee (3) Surgery is the gold standard of PST management, with various surgical techniques utilized for PST correction, including reorienting the scrotum inferiorly with limited rotational flaps, inguinal-based groin flaps, or transposing the penis superiorly (4)
This study aimed to evaluate our experience and longterm results with PST correction using a modified GlennAnderson technique
MATERIALS AND METHODS
Study population
Following institutional board approval (Shaare Zedek Medical Center Helsinki Committee approval number 030322-SZMC), we have conducted a retrospective cohort study by collecting data on all patients with PST who underwent surgical repair in our department between 2004 to 2022 A single pediatric urologist (BC) performed all surgeries
Patients were categorized into three groups: in the first group, PST repair was an integral part of one-stage male genitoplasty; in the second group, PST repair was a separate last stage of the staged hypospadias repair; and the third group consisted of patients without hypospadias
Only patients with recent follow-ups entered the study, including patients who attended an office visit or provided a recent photographic image of the operative site and answered questions regarding satisfaction with the surgery, lower urinary function, and curvature status
Additional information included age at the time of surgery, preoperative chordee and hypospadias severity, other genital anomalies and congenital malformations, type of operation, and postoperative complications
The surgical technique
Briefly, all patients were considered for surgery after the age of six months Hormonal supplementation was given
to those with a small phallus, with the utilization of topical testosterone cream twice daily before surgery for one month to accomplish penile lengthening with the avoidance complication of hypothalamus pituitary-testicular axis, as we recently reported (5)
In patients where PST repair was performed as a separate procedure, the first step was to draw lines of an incision around the root of the penis to elevate the transposed scrotum as rotational advancement flaps leaving the dorsal penile skin connected to the skin of mons pubis (Figure 1) Compared to the other surgical techniques, the incision does not meet in the midline as in GlennAnderson Still, it leaves a skin bridge of about 5-10 mm, separating the two incisions and connecting the penile skin to the skin of the mons pubis (Figure 2) The second step included a complete de-tethering of the testis from the internal part of the scrotum when indicated, and the relocation of the scrotal compartment to a typical dependent position (Figure 3) The two scrotal wings were then rotated inferomedially behind the penis (Figure 4) In patients who underwent penoscrotal transposition repair as an integral part of a hypospadias repair, we followed the steps above: full penile degloving and penile curvature correction In these cases, a tunica vaginalis flap was harvested from the testis and spread over the neourethra when indicated as part of the hypospadias repair Figure 5 presents the final result at the end of surgery All patients had one routine follow-up visit six months and one year after surgery Subsequently, those without complications were advised to return to the clinic at age 12 to 13 years and at age 18 years upon the completion of adolescence or before recruitment into the army unless there were urological problems or dissatisfaction with the surgical or functional outcome Figure 6 shows long-term follow-up after Penoscrotal transposition repair
Drawing surgical landmark on external genitalia before surgery, lines of an incision around the root of the penis to elevate the transposed scrotum.
Figure 3. Complete dissection of scrotal flaps.
Figure 4. Scrotal flap rotated inferomedially.
Figure 5
Appearance of the scrotum at the end of surgery
An 18-year-old patient who underwent multiple surgeries with a long-term follow-up for 14 years post-operative
Statistical analysis
Qualitative variables are presented as frequencies and percentages, while quantitative variables are presented as means ± Standard Deviation (SD) All data were analyzed using the Statistical Package for Social Sciences (SPSS) by IBM software version 26 0
D Perez, S Kocherov, G Jaber, G Raisin, B Chertin
Figure 1.
Figure 6.
Figure 2. Designing the scrotal rotational flaps
RESULTS
A total of 29 patients who underwent PST repair using the Glenn-Anderson technique were included Of those, 20 (69%) had complete SPT, while 9 (31%) had incomplete SPT variants Demographic and patient characteristics by group are presented in Table 1
In group I (n = 8), five patients (62%) underwent OIF hypospadias, and 3 (38%) had Long TIP urethroplasty
Two Clavien Dindo grade II complications were observed in this group; both cases developed wound infections which were treated by intravenous antibiotics Three patients (38%) required re-operation for PST due to unsatisfactory cosmetic results at an average of two years after the first operation
In group II (n = 18), eight patients (44%) underwent OIF repair, two (12%) had Long TIP urethroplasty, and the remaining eight (44%) underwent staged hypospadias repair Two patients with Clavien Dindo grade II complications were observed in this group; both have had wound infections treated by intravenous antibiotics Six patients presented with late complications secondary to urethral repair, including a buried penis in two patients (50%), urethercutaneus fistula in three (33%), and meatal stenosis in two patients (17%) Only one patient (5 5%) required secondary PST repair due to unsatisfactory cosmetic results two years following the original procedure
In group III (n = 3), no postoperative complications were observed, and no additional procedures were required (Table 2)
Table 1
Patients characteristics
Group I Group II Group III (n = 8) (n = 18) (n = 3)
Median age at 1s surgery (months) 18 ± 10 79 ± 48 78 ± 51
According to severity of malformation, one (5%) patient with complete penoscrotal transposition had Clavien Dindo grade III following staged hypospadias repair; three (33%) patients with partial penoscrotal transposition had Clavien Dindo grade III following OIF hypospadias repair
During a median follow-up of 13 years, satisfactory a n a t o m i c a l , c o s m e t i c , a n d f u n c
obtained in all patients, excluding a single post-pubertal patient from group II awaiting a re-do PST repair
DISCUSSION
PST describes an improper anatomical relationship between the penis and the scrotum, in which the scrotum is viewed as being improperly positioned in reference to the penis The surgical correction of PST is a very complex one Although one of the most popular surgical techniques for PST repair is the Glenn and Anderson technique, data goes back to the seventies, and the medical literature on its usage and long-term results is scarce (6) In addition, the recent evolution in hypospadias surgical techniques has greatly influenced the approach to penoscrotal hypospadias repair and, as a result, PST surgery
At the beginning of our learning curve, most patients (group I) underwent long TIP hypospadias repair combined with penile curvature repair and simultaneous reconstruction of PST A third of the patients in this group required re-intervention due to unsatisfactory cosmetic results In the second and third groups, patients underwent PST repair as a separate step of hypospadias repair or as an isolated condition, resulting in a better outcome than patients from the first group We have attributed this to the fact that the repair of PST was carried out as a stand-alone procedure, and nowadays, therefore, we do recommend proceeding with PST reconstruction as a separate last stage of male genitoplasty following curvature repair and urethroplasty As we have aforementioned, it is essential to perform a meticulous dissection of the rotational advancement flaps of the scrotum, leaving the dorsal penile skin connected to the skin of the mons pubis
In some cases, complete detachment of the testis on both sides is essential to reach full mobility of the scrotal flaps and to bring them into regular dependent positions below the penile shaft By using this technique as a separate step of male genitoplasty, we preserve the blood supply to the urethra and do not jeopardize the blood supply of the penile shaft skin Being penile edema, one of the most common complications of PST repair (7), we recommend reserving a bridge of the dorsal penile skin during a single and staged repair procedure We believe this maneuver avoids the development of penile edema, speeds overall recovery, and enhances early hospital discharge
We have previously published data on the re-intervention r a t e s i n p
hypospadias repair (8) Approximately 5% of all patients with satisfactory outcomes of hypospadias surgery during childhood required re-intervention after they reached puberty One of the major drawbacks of all studies on PST repair is a lack of long-term data In this study, 21 patients (72%) have reached puberty, and 16 (55%) com-
pleted their puberty period with sufficient post-pubertal follow-up Of those, one patient from group II is waiting for re-intervention due to poor functional results We believe that our modification of the Glenn Anderson technique, allowing an extensive dissection of the scrotal folds without jeopardizing blood supply and preserving skin integrity, as well as the separation of PST surgery from hypospadias and curvature repair, provides the best solution for PST patients with durable long-term results This surgical approach is entirely different from another popular technique for PST repair, proposed by Mark and his colleagues, stating that the penis and not the scrotum were mispositioned (9)
In their technique, after penile straightening, the penis is transferred into a button-hole designed in the skin of the mons-pubis We have had minimal experience with this technique at the beginning of our learning curve and have witnessed tethering of the scrotum to the ventral penile surface in one case and buried penis in the second case Therefore, we have omitted this technique from our surgical armamentarium Since our experience with this technique is very limited, we have not found it appropriate to compare both methods, but only to mention it for the sake of discussion
Our study is not without limitations, which need to be mentioned This a retrospective observation that suffers all the flaws of this kind of study We have reported our outcome only on a single surgical technique and mentioned our dissatisfaction with other techniques in the discussion section However, we do report one of the longest follow-ups on PST repair in the literature with durable post-pubertal data We could not provide any data on the sexual function of our patients following PST repair Still, we do believe that will not be different from our previously published data regarding the sexual and voiding status of the patients who underwent hypospadias repair (10) We did not use any validated questionnaire or objective criteria for cosmetic appearance after surgical correction However, 55% of our patients are capable of expressing their own satisfaction with the appearance of external genitalia, and the success of the operation was defined based on the patients and not the surgeons' or parents’ satisfaction with the surgical outcome Of course, missing data on the sexual and voiding status of these patients will be a subject of our future studies
CONCLUSIONS
PST is a rare genital anomaly with a broad spectrum of presentation, often associated with other anomalies, mainly undescended testis and hypospadias Surgically correcting these anomalies required a complex learning curve with different practice methods
Our data show that penoscrotal transposition correction utilizing the modified Glenn-Anderson technique is a reliable and durable surgery in the pediatric population These children require careful monitoring even in adolescence to ensure that no re-operation is needed The sexual function and voiding status in these patients should be an objective of future studies
REFERENCES
1 Boddepalli Y, Kota M, Banavath A Correction of Penoscrotal Transposition with Hypospadias Single Stage Repair Indian J Surg 2020; 82:1176-1178
2 Fahmy MA, El Shennawy AA, Edress AM Spectrum of penoscrotal positional anomalies in children Int J Surg 2014; 12:983-8
3 Somoza I, Palacios MG, Mednez R, Vela D Complete Penoscrotal Transposition: a three-stage procedure Indian J Surg 2012; 28:450452
4 Pinke LA, Rathbun SR, Husmann DA, Kramer SA Penoscrotal transposition: review of 53 patients J Urol 2001; 166:1865-8
5 Chertin B, Natsheh A, Ben-Zion I, et al Objective and subjective sexual outcomes in adult patients after hypospadias repair performed in childhood J Urol 2013; 190(4 Suppl):1556-60
6 Glenn JF, Anderson EE Surgical correction of incomplete penoscrotal transposition J Urol 1973; 110:603-5
7 Khan M, Majeed A, Hayat W, et al Hypospadias repair: a single centre experience Plast Surg Int 2014; 2014:453039
8 Chertin B, Prat D, Shenfeld OZ Outcome of pediatric hypospadias repair in adulthood Open Access J Urol 2010; 2:57-62
9 Dresner ML Surgical revision of scrotal engulfment Urol Clin North Am 1982; 9:305-10
10 Mureau MA, Slijper FM, van der Meulen JC, et al Psychosexual adjustment of men who underwent hypospadias repair: a norm-related study J Urol 1995; 154:1351-5
Correspondence
Dolev Perez, MD (Corresponding Author) drdolevperez@gmail com
Department of Urology, Shaare Zedek Medical Center Jerusalem, 91031, P o B 3235, Israel Stanislav Kocherov, MD kocherovs@szmc org il Gaudat Jaber, MD jawdat@szmc org il Galiya Raisin, MD rgal@szmc org il
Department of Pediatric Urology, Shaare Zedek Medical Center, Jerusalem, Israel
Boris Chertin, MD Dechertinb@szmc org il
Departments of Urology and Pediatric Urology, Shaare Zedek Medical Center, Jerusalem, Israel
Conflict of interest: The authors declare no potential conflict of interest
D Perez, S Kocherov, G Jaber, G Raisin, B Chertin
ORIGINAL PAPER
Combining ultrasound and elastography for the detection of a
non-palpable, non-sonographically
visualized Peyronie's plaques. Our experience
Gianni Paulis
1 , Giovanni De
Giorgio
2 ,
Andrea Paulis
3
1 Department of Urology and Andrology, Peyronie’s Care Center, Castelfidardo Clinical Analysis Center, Rome, Italy;
2 Section of Ultrasound Diagnostics, Department of Urology and Andrology, Castelfidardo Clinical Analysis Center, Rome, Italy;
Background: B-mode ultrasound (US) medical imaging is very effective in localizing and describing Peyronie's disease (PD) Moreover, elastography is a new technique used to evaluate tissue elasticity to detect penile Peyronie's plaques that are not visible using standard Bmode US
Objective: The main objective of this study was to evaluate the diagnostic efficacy of real-time elastography (RTE) or strain elastography (SE) in PD patients and to determine whether its combined use with standard US improved diagnostic accuracy
Additionally, this study aimed to assess whether RTE was useful for monitoring PD patients undergoing conservative treatment Methods: A group of 37 patients with PD in the active phase was selected based on US examination showing isoechoic or hypo-isoechoic plaques, with or without associated hyperechoic or calcified plaque areas All patients underwent traditional US combined with RTE before starting conservative treatment with antioxidants, during treatment and after treatment After each examination with RTE, a specific “Strain Ratio”(SR) was used to identify the specific elasticity of the tissue
Results: Using B-mode US with RTE, we detected all 13 non-palpable penile plaques present in the 37 PD patients (100% of cases). Using only B-mode US, we detected only 8 of the 13 nonpalpable plaques (61 5% of cases) The Deformation Index (DI) of the plaque decreased during and after treatment in all cases, indicating that RTE is effective for monitoring conservative PD treatment A statistically significant correlation was found between the DI and plaque volume in all patients (p = 0 002)
Conclusions: Our study has shown that the combination of US and RTE methods allowed for a more accurate diagnosis in PD patients
Peyronie's disease (PD) is a pathological condition that affects the tunica albuginea of the penis in males with a genetic predisposition, causing the formation of fibrous plaques (1, 2) The occurrence of PD is more common in Western countries (3 2-13 1%) and less common in
Asian countries (0 6-5 0%) and among populations of black African origin (0 1-3 5%) These differences are probably related to genetic, environmental, and lifestyle factors (3-12) It is hypothesized that the prevalence of PD in men is much higher due to the underreporting of symptoms, as patients may feel embarrassed and choose not to report their embarrassing problem (3) PD can result in penile deformity, penile pain, erectile dysfunction, and psychological distress (anxiety and depression); penile deformities may involve curvature, shortening, torsion, indentations, and hourglass deformity (13-17) The precise cause of PD is not completely understood, but it is generally believed to be initiated by a local injury (1820) Although it can be triggered by traumatic sexual experience or injury, 70% of cases have no specific cause, and patients do not remember a traumatic event (21) When an injury occurs, fibrin is deposited and a small hematoma forms In people without a genetic predisposition to the disease, the hematoma is absorbed back into the penile corpora cavernosa In individuals with a genetic predisposition, the hematoma causes the activation of i n fl
resulting in the formation of chronic inflammatory tissue that progresses to fibrosis over time (22-24) In the last two decades, studies have demonstrated that oxidative stress (OS) is crucial in the development of plaque and the progression of this disease (22-29)
Diagnosing PD involves a medical history, physical examination, penile palpation, photographic documentation of penile curvature, dynamic penile color Doppler US, computed tomography, and Magnetic Resonance Imaging (30-32)
Computed tomography and radiography are excellent at visualizing penile plaque calcifications, while MRI is accurate at identifying plaques in complex locations, such as the corporal septum B-mode US medical imaging is highly useful for localizing and characterizing Peyronie’s plaque Regarding the ultrasound appearance, penile plaques are typically observed as localized areas of hyperechoic thickening of the tunica albuginea, showing strong echogenicity with significant attenuation of the acoustic beam Moreover, elastography is a new and emerging method
that studies the elastic properties of tissue to identify penile plaques that may not be visualized with traditional B-mode US studies Furthermore, elastography is the most suitable imaging modality in PD because it allows for non-invasive highlighting of penile plaques and monitoring of the therapeutic response to various treatments
In addition, elastography has recently been suggested as a diagnostic tool for PD Palpation of the penis is essential in the evaluation of the patient, as most patients with Peyronie's disease have a palpable plaque that is clearly distinguishable from the rest of the penile corpora cavernosa However, documentation with a diagnostic imaging method is often necessary to support the clinical diagnosis B-mode US examination can identify the location, number, size, and echogenicity of the plaques
The main bias and disadvantage of this method is that traditional US can only detect between 40% and 84 2% of palpable plaques (33-36) Elastography is a non-invasive technique that uses an ultrasound probe to measure the mechanical properties of tissue, which can be affected by a disease process, making the tissue more rigid
The different levels of tissue elasticity under the pressure of the ultrasound probe are expressed in a more or less relevant way and evaluated using a color scale
Elastography diagnostic approaches were first developed at the end of the last century and, subsequently, numerous scientific studies have been published (37) Elastography is primarily used to diagnose soft tissue pathologies in the liver, breast, prostate, thyroid, pancreas, nerves, tendons, muscles, and other conditions Furthermore, elastography has also been suggested for studying PD (32-36, 38-44)
The World Federation of Ultrasound Medicine and Biology categorized “elastographic techniques“ as strain elastography (SE), transient elastography, and acoustic radiation force impulse (ARFI) The ARFI techniques can be subcategorized into point shear wave elastography (SWE), 2D SWE, and 3D SWE techniques (45) SE, also known as real-time elastography (RTE), is a qualitative method that assesses the relative stiffness of various tissues and examines how tissues can deform when subjected to external forces and then return to their original shape SE assesses tissue deformation using manual compression or natural motion SE measures the strain caused by "quasi-static" methods, such as manual compression or cardiovascular/respiratory pulsation, and displays the distributions of the strain or normalized strain values within the region of interest (ROI) Tissue deformation can be achieved by manually applying micro-pressure with the ultrasound probe or by using ultrasound pulses of appropriate intensity (44) In the second method of excitation, the ultrasound remains stationary while tissue displacement is induced via internal physiological movements such as cardiac and arterial pulsations and respiratory motion In both cases, the ultrasound images are compared before and after the compression, and the equipment produces a color map that indicates the relative elasticity of the various tissue components, ultimately displaying a specific Strain Ratio (SR) SR is calculated by comparing the strain index of a lesion to that of healthy tissue at the same level SR therefore indicates a measurement of the stiffness of the sampled tissue
SE measures the relative stiffness of tissues within the elastographic region of interest (ROI) overlaid on a B-mode US image; therefore, the ROI must be accurately aligned with the Peyronie’s plaque The color map is shown in real time, overlaid on an ultrasound image of the tissues being examined Usually, the color blue is utilized to indicate low strain (i e , stiff tissue), while red is used to indicate high strain (i e , soft tissue), although the exact color scale may differ depending on the manufacturer of the ultrasound equipment (35) Strain elastography is also used for the diagnostic study of PD In the literature, there are four articles on this topic (33-35, 42) The objective of this study was to evaluate the diagnostic efficacy of RTE in patients with Peyronie's disease and to determine whether its combined use with traditional ultrasound imaging improves diagnostic accuracy This study aimed to determine whether this diagnostic combin
Peyronie's plaques with or without hyperechoic or calcified plaque areas, which cannot be detected with a simple standard US examination This study also aimed to evaluate whether US associated with RTE was effective for monitoring patients with PD undergoing conservative treatment
The secondary objective of this study was to examine the relationship between plaque stiffness and the degree of curvature and plaque volume, as well as to detect the prevalence of anxiety and depression in patients with PD
MATERIALS AND METHODS
The authors conducted this study by collecting and analyzing existing data of 249 patients who visited our Peyronie’s Care Center and underwent US and elastography of the penis from January 1, 2018, to December 31, 2023, and were found to be affected by PD
After applying the inclusion and exclusion criteria, 212 PD patients who were in the stabilized or active phase of the disease and presented exclusively hyperechoic and/or calcified plaques were excluded from the main study
Objectives
The main objective of this retrospective study was to assess the diagnostic efficacy of RTE, also known as SE, in patients with Peyronie's disease (PD) and investigate if its integration with conventional ultrasound (US) imaging enhances diagnostic precision Since this study primarily aimed to determine whether the diagnostic combination of US and RTE could detect non-palpable Peyronie's plaques that cannot be detected via physical examination of the PD patient or via a simple standard US, inclusion criteria were determined for the in-depth study of those PD patients in whom RTE could potentially increase the diagnostic level
Evaluation and diagnosis
The diagnosis of Peyronie's disease was made for all patients after conducting the following assessments: palpation of the penis; photographic documentation of penile deformity (according to Kelâmi) with a goniometric measurement of the angulation; penile US with RTE or penile color Doppler US with RTE (only for patients with
G Paulis, G De Giorgio, A Paulis
associated erectile dysfunction) with plaque measurements (in three dimensions, in mm) and volume calculation (mm3) using the ellipsoid formula (volume = 0 524 × length × width × thickness); and completion of the International Index of Erectile Function (IIEF) questionnaire for measuring erectile function, the visual analog scale (VAS) questionnaire for measuring pain, the Generalized Anxiety Disorder Questionnaire-7 (GAD-7, for anxiety), a n d t h e P a t i e n t H e a l t h Q u e s t i o n n a i r e - 9 ( P H Q - 9 , f o r depression) (46-52) Regarding the last two questionnaires, we decided to also study the psychological condition of these patients, as we believe that psychological distress is a symptom of PD, just like curvature, pain, and erectile dysfunction
To identify and confirm the presence of penile plaque, along with its location and volume, we subjected all 37 patients to combined US and RTE examination of the penis at the time of initial diagnosis and during the planned follow-up assessments during conservative treatment A single andrologist operator performed and evaluated conventional US and SE of the penis on all patients in one session using the same ultrasound device, the Philips Affinity 70 G, and a high-frequency linear array t r a n s d u c e r , t h e P h i l i p s L i n e a r P r o b e L 1 2 - 5 ( P h i l i p s , Washington, United States) The elasticity values were calculated and color-coded to represent tissue elasticity The color scale ranged from red (i e , soft tissue) to blue (i e , stiff tissue), with components showing average strain displayed as green Finally, a calculation indicating a specific SR was displayed on the equipment monitor The areas included in the Strain Ratio calculation are selected by the operator by pointing the probe at the stiffest area and then at the normal tissue (soft)
Inclusion criteria
Patients with Peyronie's disease in the active phase who underwent US examination and presented isoechoic or hypo-isoechoic plaques, with or without associated hyperechoic or calcified plaque areas
Exclusion criteria
Patients with Peyronie's disease in the stabilized or active phase who underwent US examination and presented exclusively hyperechoic and/or calcified plaques
After applying the inclusion and exclusion criteria, 212 PD patients who were in the stabilized or active phase of the disease and presented exclusively hyperechoic and/or calcified plaques were excluded from the main study Finally, a group of 37 patients with Peyronie's disease in the active phase was selected based on US examination and RTE (in the same diagnostic session) showing isoechoic or hypo-isoechoic plaques, with or without associated hyperechoic or calcified plaque areas
Treatment and follow up
As previously indicated, in this study, we specifically focused on the analysis of data relating to US and RTE combination examinations in patients with PD to evaluate whether US associated with RTE is effective for monitoring PD patients undergoing conservative treatment
Therefore, after the first visit of the patients to our andrological center, we performed a combined diagnostic US
and RTE on 37 PD patients before starting conservative treatment with antioxidants Patients underwent US and RTE every six months during and after treatment
Conservative treatments to which these patients were subjected were retrospectively identified from the data in our clinical archive and are not the subject of this article Some of these patients have undergone multiple treatment cycles For completeness, we describe our standard conservative medical treatment: oral L-carnitine 1000 mg + propolis 700 mg + silymarin 400 mg + coenzyme Q-10 100 mg + bilberry 180 mg + ginkgo biloba 240 mg + vitamin E 48 mg + vitamin C 50 mg + superoxide dismutase 11000 IU/g 10 mg/daily and topical diclofenac gel 4%/2 times daily + peri-plaque penile injections (only in the case of plaques with volume ≥ 100 mm3) with pentoxifylline 100 mg (30 G needle) every month for 6 months
Statistical analysis
We utilized CalculatorSoup® software (version of Mar 07, 2023, Ashland, MA,USA) to conduct the statistical analysis involving the calculation of standard deviation and mean, median, and interquartile range (IQR) The Pearson correlation coefficient was calculated using Statistics Kingdom statistical software (version 2017, Melbourne, Australia, http://www statskingdom com) and Excel (version 2011, MS Office, Redmond, WA, USA) In the statistical analyses, a significance level of 5% for alpha error (p-value < 0 05) was considered to demonstrate statistical significance
This study was carried out in accordance with the principles outlined in the Declaration of Helsinki (Fortaleza, 2013) All participants were contacted and gave their informed consent for the study However, sensitive data were anonymized in accordance with privacy regulations as per legislative decree 10 August 2018, n 101 adapted to the General Data Protection Regulation/GDPR (Official Gazette of the Italian Republic, General Series n 205, dated 4 September 2018)
RESULTS
The 37 patients with Peyronie's disease who were selected for this study (with isoechoic or hypo-isoechoic plaques, with or without associated hyperechoic or calcified plaque areas) were aged between 23 and 74 years, with a mean age = 51 3 years (SD ± 14 7)
The plaque volume in the 37 selected patients ranged from 11 5 to 2660 mm3
Table 1 shows the physical and echo-elastographic characteristics of the plaques of the 37 patients
Non-palpable plaques
Using B-mode US with RTE, we detected all 13 non-palpable penile plaques present in the 37 selected PD patients (100% of cases) Using only B-mode US, we detected only 8 of the 13 non-palpable plaques (61 5% of cases)
Soft plaques
When using US examination on 37 PD patients, only one out of seven barely palpable (soft) plaques were detected (14 2%) However, with RTE, all seven soft plaques were detected (100%)
Table 1.
Physical and echo-elastographic characteristics of the plaques of the 37 patients.
Palpator y features of the plaque N cases (out 37) (%) Non-palpable
(35 1)
(18 9)
(16 2)
Ultrasound imaging of the plaque
Hypo-isoechoic 12 (32 4)
Isoechoic 10 (27.0)
Iso-hyperechogenicity (mixed plaque) 1 (2 7)
Iso-hyperechogenicity associated with calcification (mixed plaque) 3 (8 1)
Hypo-isoecogenicity associated with hyperechogenicity (mixed plaque) 2 (5 4)
Hypo-isoecogenicity associated with calcification (mixed plaque) 9 (24 3)
Plaque volume (mm3)
Up to 100 6 (16 2)
From 101 to 300 10 (27 0)
From 301 to 500 5 (13 5)
From 501 to 1000 10 (27 0)
From 1001 to 2000 5 (13 5)
> 2000 1 (2 7)
Strain Ratio of the plaque detected via strain elastography (SE)
> 1 to 2 18 (48 6)
> 2 to 3 16 (43 2)
> 3 to 4.4 3 (8.1)
The Strain Ratio s cons dered patholog ca when it s greater than 1
Isoechoic or hypo-isoechoic plaques
When using US examination, 29 out of 37 isoechoic or hypo-isoechoic plaques, with or without associated hyperechoic or calcified plaque areas, were identified (78 3%), while the remaining 8 plaques (21 6%) were not identified Specifically, the eight plaques that were not identified were completely isoechoic Therefore, using US, entirely isoechoic plaques were found in only 2 out of 10 cases (20%) All 37 plaques were instead identified with RTE (100%)
Ultrasound findings in relation to the volume of PD plaques
Out of 21 plaques with a volume up to 500 mm3, 19
1
plaques (90 4%) were identified, and 2 plaques (9 5%) were not identified using only US, while all 21 plaques were identified with RTE (100%) All 16 remaining larger PD plaques over 500 mm3 were identified with US (100%) and also with RTE
A statistically significant correlation was found between the Deformation Index (Strain Ratio) and plaque volume in the 37 selected patients, p-value = 0 002 (p < 0 05)
Figure 1 shows the graph that highlights this correlation No statistically significant correlation was found between the Strain Ratio and the degree of angulation of the penile curvature of the 37 selected patients: r = 0 2848, r2 = 0 08109, p-value = 0 08759 (p > 0 05)
In Figure 2 below, we present four examples of plaques that were not detected with traditional US but were instead detected with RTE Please note that during each elastography scan, circles (light blue color) were placed by the operator on the stiffer (blue) and normal (soft) areas corresponding to the ROI At the end of this procedure, the elastography software provided the Strain Ratio after the relative calculation
Treatment and follow up
Figure 3 shows the Deformation Index (or Strain Ratio) values of the plaques before, during, and after the treatments The results presented demonstrate that the Strain Ratio decreased during the monitoring at each follow-up assessment
The Strain Ratio value is considered pathological when it is greater than 1 RTE measurements were performed every 6 months during the course of conservative treatment The 37 selected patients underwent multiple treatment cycles, ranging from two to four cycles Some patients underwent a greater number of follow-up assessments because they were observed before the others
Psychological
assessment
The results of the GAD-7 and PHQ-9 questionnaires showed that in the 37 patients with Peyronie's disease, significant anxiety was present in 70 2% of cases and severe anxiety in 18 9% of cases Significant depression was present in 45 9% of cases, with no cases of severe depression
Graph highlighting the relationship between plaque volumes and Deformation Index (or Strain Ratio) values
G Paulis, G De Giorgio, A Paulis
Figure
Figure 2.
Examples of four non-palpable and isoechoic Peyronie's plaques that were not detectable with traditional ultrasound (US) but identified with real-time elastography (RTE)
DISCUSSION
The authors specify that, for the elastography study, they preferred to use SE, also known as RTE SE is preferable for studying superficial pathologies such as plaques that develop in Peyronie’s disease because it has high spatial resolution In fact, in this pathology, SE, owing to its high sensitivity, is important for visualizing the area of fibrosis associated with it, even in the a b s e n c e o f d e t e c t a b l e B - m o d e i m a g e s W e should also add that in order to use SE correctly, it is essential for the procedure to be conducted by an experienced operator and to use the latest technology to achieve the correct visualization of Peyronie’s plaque
Using B-mode US with RTE, we detected all 13 non-palpable penile plaques present in the 37 selected PD patients (100% of cases) Using only B-mode US, we detected only 8 of the 13 nonpalpable plaques (61 5% of cases) In 11 out of these 13 cases, a penile curvature was present Furthermore, in two of these patients with nonpalpable penile plaque who did not report penile pain or erectile dysfunction problems, there was a penile deformity, including both penile curvature and shortening In these two cases the ultrasound diagnosis would have been completely negative without performing RTE We believe that the penile plaques could not be palpated, mainly due to their small size, which in most cases never exceeded a volume of 300 mm3
In a study by Dell’Atti et al , using only B-mode
Figure 3. Deformation Index (Strain Ratio) values of penile plaques in 37 patients with Peyronie's disease, before and after treatment
US to detect non-palpable Peyronie’s plaques, small plaque volumes and fairly similar ultrasound features were found; however, they found 41 non-palpable penile plaques in 386 patients with PD (10 6% of cases) (53) In our study, using only B-mode US, we detected non-palpable plaques in 8 out of 37 cases (21 6% of cases)
Regarding the incidence of non-palpable plaques in patients with Peyronie’s disease, other authors using only B-mode US studies, although with different ultrasound machines, have reported detection rates of 6 0%, 22 5%, and 32 4% in PD cases (33, 54, 55)
Referring to the ultrasound appearance of the plaques (isoechoic or hypo-isoechoic, with associated hyperechogenicity or calcification) using only B-mode US, we detected penile plaques in 29 out of 37 cases (78 3% of cases) However, when using B-mode US with RTE, we detected all 37 penile plaques (100% of cases) in the respective 37 patients
Penile plaques appear as localized areas of thickening in the tunica albuginea on ultrasound, showing strong echogenicity and significant attenuation of the acoustic beam However, in our study, almost all noncalcified penile plaques were found to be isoechoic or slightly hyperechoic compared to the surrounding cavernous tissue The peculiarity of our results is due to the selection of patients due to the inclusion criteria of our study
Nevertheless, there are few articles in the literature that specifically discuss the possibility of the existence of isoechoic plaques (56-58)
In our study, the isoechoic penile plaques detected using only B-mode US were only 2 out of 10 (20% of cases)
Instead, using B-mode US with RTE, we detected all 10 isoechoic penile plaques (100% of cases) in the respective 10 patients However, when the penile plaques were not isoechoic, B-mode US was consistently able to detect all the penile plaques This demonstrates that when B-mode US is combined with RTE, the diagnostic accuracy is significantly improved
Similar results were obtained by other authors who used elastography associated with conventional B-mode US (33-36, 42) Our study has shown a strong statistical correlation between the Strain Ratio values of the plaque and its volume (p-value = 0 002) Of course, it seems logical that increasing the size of the plaque also increases its rigidity; however, this correlation had never been demonstrated in Peyronie’s disease
Otherwise, we did not find any statistically significant correlation between the Strain Ratio and the degree of angulation of the penile curvature angle (p > 0 05) It should be noted that, in our case series, 3 out of 37 patients did not have penile curvature due to the central location of the plaque (between the two corpora cavernosa), and this may have resulted in the absence of this correlation However, other authors, using a different method of elastography (shear wave elastography, SWE), have shown a relationship between the stiffness of the selected plaque area (expressed in kPa) and the curvature angle of the penis (41)
Our study has shown that RTE combined with traditiona l U S i s v e r y u s e f u l f o r m o n i t o r i n g p a t i e n t s w i t h Peyronie's disease during conservative treatment with antioxidants and antifibrotics In this way, in addition to
the reduction in plaque volume, which we could have demonstrated using traditional US alone, we were also able to observe the progressive reduction in the stiffness of the affected area A very similar observation has been made by other authors who, using another elastography method (SWE), have analyzed the changes in elastography after administering a compound made up of Ecklonia bicyclis, Tribulus terrestris, and water-soluble Chitosan (Biovis) (39)
After researching the prevalence of anxiety in patients with PD, we found that 70 2% of cases had significant anxiety, and 18 9% of cases had severe anxiety There are no precise data in the literature regarding the incidence of anxiety symptoms during PD; however, a study by Smith and colleagues found that 81% of PD patients reported "emotional difficulties" (59) After researching the prevalence of depression in PD patients, we found that significant depression was present in 45 9% of cases, with no cases of severe depression Nelson and colleagues found that 48% of PD patients exhibited clinically significant depression (14, 60) We believe that depressive and anxiety symptoms, if not investigated in PD patients using specific questionnaires, may remain unknown or at least be underestimated in terms of severity and prevalence
Our data on the prevalence of anxiety in patients with PD confirm that the anxious and depressive states represent important symptoms of PD, as well as penile pain, penile curvature/deformation, and erectile dysfunction In uroandrological clinical practice, psychologists should be involved in providing supportive treatment to patients with PD In this way, we could reduce the psychological impact of PD, which has been described by some important authors as a psychologically and physically devastating disease (61-65) Although our findings are quite interesting, the limitation of our study is that the sample size was not very large However, our limited sample was determined by very selective inclusion criteria
CONCLUSIONS
RTE is a modern non-invasive technique that can accurately identify penile plaques in patients with Peyronie's disease, complementing B-mode US Furthermore, RTE is very useful for diagnosing the disease at an earlier stage (isoechoic plaque) than B-mode US alone Additionally, RTE is especially valuable when palpation and B-mode US are unable to identify a plaque RTE can also accurately assess plaque stiffness, size, and volume RTE offers an additional method for uro-andrologists to monitor conservative treatment in patients with Peyronie's disease More extensive prospective studies are needed to determine the diagnostic accuracy and clinical utility of this imaging technique
REFERENCES
1 Herati AS, Pastuszak AW The Genetic Basis of Peyronie Disease: A Review Sex Med Rev 2016; 4:85-94
2 Bias WB, Nyberg LM Jr, Hochberg MC, Walsh PC Peyronie's disease: a newly recognized autosomal-dominant trait Am J Med Genet 1982; 12:227-235
4 Rhoden EL, Teloken C, Ting HY, et al Prevalence of Peyronie's disease in men over 50-y-old from Southern Brazil Int J Impot Res 2001; 13:291-293
5 La Pera G, Pescatori ES, Calabrese M, et al Peyronie's disease: prevalence and association with cigarette smoking A multicenter population-based study in men aged 50-69 years Eur Urol 2001; 40:525-530
6 Schwarzer U, Sommer F, Klotz T, et al The prevalence of Peyronie's disease: results of a large survey BJU Int 2001; 88:727-730
7 Johnson HM, Weerakoon P, Stricker PD The incidence, aetiology, and presentation of Peyronie’s disease in Sydney, Australia J Sex Disabil 2002; 20:109-116
8 DiBenedetti DB, Nguyen D, Zografos L, et al A Population-Based Study of Peyronie’s Disease: Prevalence and Treatment Patterns in the United States Adv Urol 2011; 2011:282503
9 Shiraishi K, Shimabukuro T, Matsuyama H The prevalence of Peyronie’s disease in Japan: A study in men undergoing maintenance hemodialysis and routine health checks J Sex Med 2012; 9:2716-2723
10 Stuntz M, Perlaky A, des Vignes F, et al The Prevalence of Peyronie’s Disease in the United States: A Population-Based Study PLoS ONE 2016; 11:e0150157
11 Kyei MY, Mensah JE, Asante E, et al Peyronie’s Disease in People of African Origin: A Mini Review J Ger Ag Res 2017; 1:104
12 Bella AJ, Lee JC, Grober ED, et al 2018 Canadian Urological Association guideline for Peyronie’s disease and congenital penile curvature Can Urol Assoc J 2018; 12:E197-E209
13 Weidner W, Schroeder-Printzen I, Weiske WH, et al Sexual dysfunction in Peyronie’s disease: An analysis of 222 patients without previous local plaque therapy J Urol 1997; 157:325-328
14 Nelson CJ, Diblasio C, Kendirci M, et al The Chronology of Depression and Distress in Men with Peyronie’s Disease J Sex Med 2008; 5:1985-1990
15 Paulis G, Romano G, Paulis A Prevalence, psychological impact, and risk factors of erectile dysfunction in patients with Peyronie’s disease: A retrospective analysis of 309 cases Res Rep Urol 2016; 8:95103
16 Wong A, Tsang SS, O RY, et al Mp33-12 Prevalence of Peyronie’s disease and its psychosexual impact in the chinese population: A large cohort population-based cross-sectional study J Urol 2020; 203:e499
17 Kuja-Halkola R, Henningsohn L, D’Onofrio BM, et al Mental Disorders in Peyronie’s Disease: A Swedish Cohort Study of 3 5 Million Men J Urol 2021; 205:864-870
18 Devine CJ Jr, Somers KD, Ladaga LE Peyronie’s disease: Pathophysiology Prog Clin Biol Res 1991; 370:355-358
19 Devine CJJ, Somers KD, Jordan GH, et al Proposal: Trauma as a cause of Peyronie’s lesion J Urol 1997; 157:285-290
20 Jarow JP, Lowe FC Penile trauma: An etiologic factor in Peyronie’s disease and erectile dysfunction J Urol 1997; 158:1388-1390
21 Segal RL, Burnett AL Surgical Management for Peyronie's Disease World J Mens Health 2013; 31:1-11
22 El-Sakka AI, Salabas E, Dinc ̧ er M, et al The pathophysiology of Peyronie’s disease Arab J Urol 2013; 11:272-277
23 Paulis G, Romano G, Paulis L, et al Recent Pathophysiological
Aspects of Peyronie’s Disease: Role of Free Radicals, Rationale, and Therapeutic Implications for Antioxidant Treatment-Literature Review Adv Urol 2017; 2017:4653512
24 Paulis G, De Giorgio G, Paulis L Role of Oxidative Stress in P e y r o n i e ’ s D i s
Treatment with Antioxidants Int J Mol Sci 2022; 23:15969
25 Sikka SC, Hellstrom WJ Role of oxidative stress and antioxidants in Peyronie’s disease Int J Impot Res 2002; 14:353-360
26 Paulis G, Brancato T Inflammatory mechanisms and oxidative stress in Peyronie’s disease: Therapeutic “rationale” and related emerging treatment strategies Inflamm Allergy Drug Targets 2012; 11:48-57
27 Davila HH, Magee TR, Vernet D, et al Gene transfer of inducible nitric oxide synthase complementary DNA regresses the fibrotic plaque in an animal model of Peyronie’s disease Biol Reprod 2004; 71:1568-1577
28 Bivalacqua TJ, Champion HC, Hellstrom WJ Implications of nitric oxide synthase isoforms in the pathophysiology of Peyronie’s disease Int J Impot Res 2002; 14:345-352
29 Gonzalez-Cadavid NF, Magee TR, et al Gene expression in Peyronie’s disease Int J Impot Res 2002; 14:361-374
30 McCauley JF, Dean RC Diagnostic utility of penile ultrasound in Peyronie's disease World J Urol 2020; 38:263-268
31 Kelâmi A Autophotography in evaluation of functional penile disorders Urology 1983; 21:628-629
32 Parmar M, Masterson JM, Masterson TA, 3rd The role of imaging in the diagnosis and management of Peyronie's disease Curr Opin Urol 2020; 30:283-289
3 3 L a h m e S , Z i m m e r m a n n s V , L i s k e P , e t a l R e a l - T i m e Elastography (RTE) in Patients with Peyronie’s Disease: First Results of a New Imaging Technique for the Detection and Mesurement of Plaques J Urol 2009; 181:280
34 Morana C, Loiero G, Sangiorgio A, et al Elastosonography in the Peyronie's disease: our preliminary experience Arch Ital Urol Androl 2010; 82:269-270
35 Riversi V, Tallis V, Trovatelli S, et al Realtime-elastosonography of the penis in patients with Peyronie's disease Arch Ital Urol Androl 2012; 84:174-177
36 Zhao S, Wu X, Zhang,Y, et al Role of Shear Wave Elastography in the Diagnosis of Peyronie Disease J Ultrason Med 2024; 43:397403
37 Ophir J, Céspedes I, Ponnekanti H, et al Elastography: a quantitative method for imaging the elasticity of biological tissues Ultrason Imaging 1991; 13:111-134
38 Zhang X, Zhou B, Miranda AF, et al A Novel Noninvasive Ultrasound Vibro-elastography Technique for Assessing Patients With Erectile Dysfunction and Peyronie Disease Urology 2018; 116:99-105
39 Trama F, Riccardo F, Ruffo A, et al Elastosonographic Changes in Patients with Peyronie's Disease, before and after Treatment with a Compound Based on Ecklonia bicyclis, Tribulus terrestris, and Water-Soluble Chitosan OJU Journal 2018; 8:77-87
40 Tyloch JF, Tyloch DJ, Adamowicz J, et al Application of threedimensional ultrasonography (3D ultrasound) to pretreatment evaluation of plastic induration of the penis (Peyronie's disease) Med Ultrason 2020; 22:159-163
41 Trama F, Illiano E, Iacono F, et al Use of penile shear wave elas-
tosonography for the diagnosis of Peyronie's Disease: a prospective case-control study Basic Clin Androl 2022; 32:15
42 Richards G, Goldenberg E, Pek H, et al Penile sonoelastography for the localization of a non-palpable, non-sonographically visualized lesion in a patient with penile curvature from Peyronie's disease J Sex Med 2014; 11:516-520
43 Dhawan S, Dhok A, Phatak S, et al Peyronie's Disease Presenting as Curvature of the Penis: A Case Report Cureus 2022; 14:e32055
44 Simon V, Dudea SM, Crisan N, et al Elastography in the Urological Practice: Urinary and Male Genital Tract, Prostate Excluded-Review Diagnostics (Basel) 2022; 12:1727
45 Shiina T, Nightingale KR, Palmeri ML, et al WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 1: basic principles and terminology Ultrasound Med Biol 2015; 41:1126-1147
46 Kelâmi A Autophotography in evaluation of functional penile disorders Urology 1983; 21:628-629
47 Eri LM, Thomassen H, Brennhovd B, et al Accuracy and repeatability of prostate volume measurements by transrectal ultrasound Prostate Cancer Prostatic Dis 2002; 5:273-278
48 Lee JS, Chung BH Transrectal ultrasound versus magnetic resonance imaging in the estimation of prostate volume as compared with radical prostatectomy specimens Urol Int 2007; 78:323-327
49 Rosen RC, Riley A, Wagner G, et al The international index of erectile function (IIEF): A multidimensional scale for assessment of erectile dysfunction Urology 1997; 49:822-830
50 Kahl C, Cleland JA Visual analogue scale, numeric pain rating scale and the McGill pain Questionnaire: An overview of psychometric properties Phys Ther Rev 2005; 10:123-128
51 Spitzer RL, Kroenke, K, Williams, JB, et al A brief measure for assessing generalized anxiety disorder: The GAD-7 Arch Intern Med 2006; 166:1092-1097
52 Kroenke K, Spitzer RL, Williams JB The PHQ-9: Validity of a brief depression severity measure J Gen Intern Med 2001; 16:606-613
53 Dell'Atti L, Galosi AB Sonographic patterns of Peyronie's disease in patients with absence of palpable plaques Int Braz J Urol 2018; 44:362-369
54 Lopez JA, Jarow JP Duplex ultrasound findings in men with Peyronie's disease Urol Radiol 1991; 12:199-202
55 Odiase VO, Whitaker RH Peyronie's disease in a district general hospital Postgrad Med J 1980; 56, 773-776
56 Prando D New sonographic aspects of peyronie disease J Ultrasound Med 2009; 28:217-232
57 Kalokairinou K, Konstantinidis C, Domazou M, et al US Imaging in Peyronie's Disease J Clin Imaging Sci 2012; 2:63
58 Liu Y, Zheng D, Liu X, et al Ultrasound on Erect Penis Improves Plaque Identification in Patients With Peyronie's Disease Front Pharmacol 2019; 10:312
59 Smith JF, Walsh TJ, Conti SL, et al Risk factors for emotional and relationship problems in Peyronie's disease J Sex Med 2008; 5:2179-2184
60 Nelson CJ, Mulhall JP Psychological impact of Peyronie's disease: a review J Sex Med 2013; 10:653-660
61 Taylor FL, Levine A Peyronie's Disease Urol Clin North Am 2007; 34:517-534
62 Bella AJ, Perelman MA, Brant WO, et al Peyronie's disease (CME) J Sex Med 2007; 4:1527-1538
63 Jordan GH, Carson CC, Lipshultz LI Minimally invasive treatment of Peyronie's disease: evidence-based progress BJU Int 2014; 114:16-24
64 Porst H, Burri A, European Society for Sexual Medicine (ESSM) Educational Committee Current Strategies in the Management of Peyronie's Disease (PD)-Results of a Survey of 401 Sexual Medicine Experts Across Europe J Sex Med 2019; 16:901-908
65 El-Sakka AI Medical, non-invasive, and minimally invasive treatment for Peyronie's disease: A systematic review Andrology 2021; 9:511-528
Correspondence
Gianni Paulis, MD (Corresponding Author) paulisg@libero it
Department of Urology and Andrology, Peyronie’s Care Center, Castelfidardo Clinical Analysis Center, 00185 Rome, Italy
Giovanni De Giorgio, MD g degiorgio@analisiclinichecastelfidardo it
Section of Ultrasound Diagnostics, Department of Urology and Andrology, Castelfidardo Clinical Analysis Center, 00185 Rome, Italy
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Can
serum 17-hydroxy progesterone predict an improvement in semen parameters following micro-varicocelectomy?:
A
prospective study
Mohamed Wael Ragab 1 , Mohamed Abbas 1 , Tarek Ramzy 2 , Sameh Fayek GamalEl Din 1 , Mohamed Yousry Elamir 1 , Mohammad H. Alkandari 3 , Abdullah Salem Alshammari 4 , Mohamed Ragab Shehata 1 , Ashraf Zeidan 1
1 Department of Andrology & STDs, Kasr Alainy Faculty of Medicine, Cairo University, Egypt;
2 Department of Chemical Pathology, Kasr Alainy Faculty of Medicine, Cairo University, Egypt;
3 Mubarak Al-Kabeer teaching Hospital, Kuwait;
4 Farwaniyah Hospital, Kuwait
Summary
Background & objectives: Notably, 17-hydroxy progesterone (17-OHP) (17-OHP) is a precursor for testosterone (T) synthesis, and intratesticular testosterone (ITT) is essential for spermatogenesis Varicocele (Vx) has an estimated prevalence of 15% in the general population and 35% in those with primary infertility
We aimed to evaluate the correlation between changes of serum 17-OHP after sub-inguinal micro-varicocelectomy and improvement of semen parameters.
Patients and methods: The current prospective study included 45 infertile men attending the andrology clinic form February 2021 to August 2021 Two semen analyses and hormonal profile were evaluated. Colored duplex ultasonography (CDUS) was done in standing and supine position for accurate measurements of testicular volumes and confirmation of Vx. Patients underwent subinguinal micro-varicocelectomy using a surgical microscope HB Surgitech. We followed them prospectively up for three months following micro-varicocelectomy with serum TT and 17-OHP
Results: Sperm concentration improved significantly from 8.36 ± 5 04 million/ml to 12 52 ± 8 42 million/ml after 3 months following sub-inguinal micro-varicocelectomy (p = 0.001), with normalization of concentration in 15/45 (33%) patients Total motility did not improve significantly but progressive motility improved significantly from 8 62 ± 8 74% to 16 24 ± 14 45% (p = 0 001)
Abnormal forms significantly declined from 96.67 ± 2.03% to 95 75 ± 2 47% (p = 0 009)
Serum 17 OHP and 17 OHP/total testosterone (TT) improved significantly from 1 21 ± 0 45 ng/ml and 0 26 ± 0 09 to 1 42 ± 0 76 ng/ml and 0 3 ± 0 16 (p = 0 013, p = 0 004), respectively, while serum TT did not improve significantly A significant correlation was found between improvement in sperm concentration and both serum 17 OHP and 17 OHP/TT ratio (p = 0 001, p = 004)
Furthermore, change in abnormal sperm forms showed significant correlations with changes in both 17-OHP and 17-OHP/TT
Conclusions: 17 OHP and 17OHP/ TT ratio can be used as biomarkers to detect improvement in semen parameters following sub-inguinal micro-varicocelectomy
KEY WORDS: Sub-inguinal micro-varicocelectomy; 17 hydroxy progesterone; Total testosterone; Sperm count; Progressive sperm motility; Abnormal sperm forms
Submitted 5 April 2024; Accepted 7 May 2024
INTRODUCTION
According to the World Health Organization (WHO), infertility is defined as the inability to achieve pregnancy after one year of unprotected intercourse (1) In mammals, spermatogenesis is totally dependent upon testosterone (T) (2) Androgens are essential for male fertility and maintenance of spermatogenesis and T is the androgen in the testis that is responsible for supporting spermatogenesis (2) In absence of T or functional androgen receptors (AR), males become infertile because spermatogenesis rarely progresses beyond meiosis (Sharpe & Cooper, 1984) T is produced by Leydig cells and acts upon Sertoli and peritubular cells of the seminiferous tubules and drives spermatogenesis (2) It is believed that intratesticular testosterone (ITT) directly stimulates spermatogenesis in men However, the amount of ITT required to initiate spermatogenesis has yet to be determined It is important to note that ITT concentration in healthy men is approximately 100 times greater than T concentration in serum, which suggests that serum T may not be an accurate marker for ITT (3) Additionally, serum T is affected by several factors such as obesity, social environment, age, time of day and infections such as Covid-19 (4) According to Kelly and Jones (2015), low serum T levels are associated with increased fat mass particularly central obesity (5) Intratesticular steroids consist of approximately 70% T, 20% 17-OHP, and smaller percentages of other hormones (6) Amory et al (2008) found that serum 17-OHP strongly reflects ITT concentrations in men with normal gonadotropic function receiving gonadotropin suppression and human chorionic gonadotropin (HCG) (6) 17-OHP was found to correlate with ITT in the presence of normal or near normal HCG stimulation (7) About 70% of 17-OHP is thought to be of testicular origin, the remainder of 17OHP production is thought to be of adrenal origin (7) Notably, 17-OHP is a precursor for T synthesis, and ITT is essential for spermatogenesis but can only be reliably measured with invasive testicular sampling (8) Furthermore, 17-OHP would be useful in conjunction with serum T measurements to assess the ideal dosage of HCG required to treat males with infertility (8) Varicocele (Vx) is significantly associated with primary and secondary infertility due
to the multifactorial way in which they affect fertility (910) Vx is one of the reversible causes and has an estimated prevalence of 15% in the general population and 35% in those with primary infertility (9-10) One of the mechanisms by which Vx can affect the testicles is inducing disturbance of Leydig cell function, resulting in decreased ITT biosynthesis In a meta-analysis, it was found that surgical repair significantly increased testosterone (T) levels in men with Vx (11-14) The negative effect of Vx on male fertility is well studied However, the relationship between clinical Vx and impaired hormonal production is still vague and requires further analysis (15) Thus, we based our current study on two hypotheses The first hypothesis assumes that 17-OHP is a reliable serum biomarker that correlates with ITT levels The second one speculates that Vx is associated with impairment of androgen synthesis Therefore, we analyzed the correlation between Vx repair and semen parameters, using serum TT and 17-OHP preoperative and postoperative measurements
PATIENTS AND METHODS
The current prospective study included 45 infertile men attending the andrology clinic form February 2021 to August 2021 The institutional review board approved the current work that conforms to Helsinki declaration 2013 (16) An informed consent was signed by the patients prior to joining the study and after explaining the possible outcomes of sub-inguinal micro-varicocelectomy
Inclusion criteria
Males suffering from infertility for more than one year (age ranges between 20-51 years old) with at least one abnormal semen parameter (oligoasthnospermia, asthenozoospermia, or teratozoospermia) and a palpable Vx were included
Exclusion criteria
History of intake of medications that affect androgen synthesis, azoospermia, elevated follicle stimulating hormone (FSH), hypogonadotropic hypogonadism, history of previous testicular disease (torsion, trauma and infection), history of Covid-19 infection, history of previous testicular surgery and patients who received chemotherapy or radiotherapy within the last six months were excluded
Age and duration of infertility were reported Sexual history including frequency of intercourse as well as any ejaculation disorder, any past history of testicular disease or previous operation, and any special habits affecting semen parameters including smoking were also reported
Evaluation of testicular size, spermatic cord, vas deferens and grading of Vx were determined Laboratory evaluation included: two semen analyses (one before the operation and another one three months following the subinguinal micro-varicocelectomy) according to the fifth edition of WHO guidelines (2010) (17) and hormonal profile including FSH, luteinizing hormone (LH), total testosterone, estradiol, ACTH and blood sampling for assay of 17-OHP by ELISA commercial kits (preoperative and three months postoperative)
Colored duplex ultasonography (CDUS) (Mindray DP-30 portable ultrasound) in standing and supine position for
accurate measurements of testicular volumes and confirmation of Vx by detection of venous regurge and measurement of maximum venous diameters was conducted Patients underwent sub-inguinal micro-varicocelectomy using a surgical microscope HB Surgitech [5 Step Magnifications (4x, 6x, 10x, 16x & 25x) 45 degree Inclined Binocular Tubes, 12 5x Wide Field Eye Pieces, F=200 mm Objective Lens, Aadesh Complex, Court Road, Near CJM Court, Ambala134003, Haryana, India] We followed patients prospectively up for three months following sub-inguinal microvaricocelectomy with serum TT and 17-OHP
Statistical analysis
Results are expressed as mean, standard deviation, minimum and maximum, or number (%) The KolmogorovSmirnov test for normality was used to measure the distribution of data measured before and after surgery Accordingly, in normally distributed variables, comparison of data from before and after surgery was performed using paired t-tests In abnormally distributed data, comparison between before and after operation data was performed using the Wilcoxon Signed Rank test To perform correlation between change in both 17-OHP and 17OHP/TT ratio and different motility parameters, firstly, we calculated the change that occurred between before and after operation from the equation: after operation minus before operation Secondly, a test of normality was done for these variables Thirdly, Spearman's rho correlation coefficient was used to correlate between variables Statistical Package for Social Sciences (SPSS) computer program (Version 19 Windows) was used for data analysis P-value ≤ 0 05 was considered significant
RESULTS
The history and demographic characteristics of the studied men are shown in Table 1 A significant improvement in sperm count was detected three months following sub-inguinal micro-varicocelectomy (Table 2) A significant improvement of progressive sperm motility three months after sub-inguinal micro-varicocelectomy was o b s e r v e d ( T a b l e 2 ) A b n o r m a l f o r m s s i g n i fi c a n t l y declined from 96 67 ± 2 03% to 95 75 ± 2 47% (Table 2) Preoperative mean TT was 4 86 ng/dl and postoperative mean TT was 4 77ng/dl with no significant improvement three months following sub-inguinal micro-varico-
Table 1.
Descriptive statistics of age, special habits, spouse’s age and menses and duration of infertility
= 45)
M Wael Ragab, M Abbas, T Ramzy, et al
Table
Ranks
Table 3.
Correlations between change in both 17-OHP and 17-OHP/TT ratio and different semen parameters
r- Spearman's rho corre at on coefficient p > 0 05 not significant; *p ≤ 0 05 s gn ficant
celectomy detected (Table 2) On the other hand, preoperative mean 17-OHP was 1 21 ng/ml and it increased significantly to 1 42 ng/ml at 3 months after sub-inguinal micro-varicocelectomy (Table 2)
Consistently, the preoperative 17-OHP/TT ratio had a mean value of 0 26 and significantly increased postoperatively to 0 30 (Table 2) The preoperative means of ACTH, E2, LH and FSH were 33 80 ± 12 73 pg/ml, 18 31 ± 5 73 pg/ml, 4 98 ± 1 81 mIU/ml, 4 42 ± 2 30 mIU/ml, respectively Preoperative scrotal duplex studies showed that left venous diameter ranged from 2 6 mm to 5 5 mm (mean value = 3 58 ± 0 67 mm), while right venous diameter ranged from 1 4mm to 3 7 mm (mean value = 2 5 ± 0 48 mm) with reflux on the left side in 45 patients (100% of the cases) and reflux on the right side in 32 patients (71 1% of the cases) Right testicular volume ranged from 8 25 ml to 20 28 ml (mean = 12 91 ± 2 85 ml), while left testicular volume ranged from 7 23 ml to 19 15 ml (mean = 11 77 ± 2 78 ml) A positive correlation between changes in 17-OHP and changes in the 17-OHP/ TT ratio was found (Table 3) A significant correlation between postoperative sperm count improvement and a postoperative change in serum 17OHP was also shown (Table 3) Moreover, a significant correlation between postoperative sperm count improvement and a postoperative change in 17-OHP/TT ratio was detected (Table 3) Furthermore, change in abnormal sperm forms showed significant correlations with changes in 17-OHP and 17OHP/TT (Table 3) Twenty-nine patients had sperm count improvement after sub-inguinal micro-varicocelectomy (mean change = 4 15 mil/ml) and 27 patients had semen progressive motility improvement (mean change = 7 62%) Twenty-three patients had an elevation in serum 17-OHP level following sub-inguinal microvaricocelectomy (mean change = 0 20 ng/ml) and 28 patients had an elevation in serum 17- OHP/TT ratio (mean change = 0 04)
Figure 1. Mean values of sperm count measured before and
DISCUSSION
The current study documented significant improvements of sperm count and progressive motility and sperm normal forms following sub-inguinal micro-varicocelectomy
Out of 45 patients, 29 (64%) had improvement in sperm count and 14 of those had a normal sperm count following Vx repair However, one patient dropped from severe oligoasthenozoospermia to azoospermia following the operation Our findings of count improvement after surgery were consistent with other studies (18) Twentyseven patients (60%) had improvement in sperm progressive motility three months following the operation
Of those twenty-seven patients, only six patients had normal progressive motility following the operation Before the operation, mean sperm progressive motility was 8 62 % which significantly improved three months following the operation to become 16 24% Also, abnormal forms significantly improved after sub-inguinal micro-varicocelectomy Out of 45 patients, 23 (51 1%) had a significant elevation of serum 17-OHP post-operatively
Twenty-eight patients (62 2%) had a significant elevation of 17 OHP/TT ratio in the follow-up after sub-inguinal micro-varicocelectomy This came in contrast to another study which found that microsurgical varicocele repair resulted in improvements in all evaluated semen parameters, but not in ITT/17-OHP or serum T levels and percentage of normal sperm forms (14) Conversely, mean preoperative total motile count (TMC) was 31 86 %, while 3-month post-varicocelectomy it was 31 78%, with no significant improvement This could be seen contradictory to Lima et al (2020) who suggested a significant improvement of TMC following varicocelectomy (14)
Furthermore, we did not find a significant improvement in serum TT three months following varicocelectomy This
was consistent with previous studies which showed that men with normal serum T were less likely to improve postoperatively (14, 19) Noteworthy, a positive correlation between changes in 17-OHP and improvement in semen concentration were noticed Such results came in alignment with those of one study which suggested that serum 17-OHP strongly reflects ITT concentrations (6) as well as another study which suggested that 17-OHP could be a useful biomarker for ITT (9) Additionally, change in abnormal sperm forms showed significant correlations with changes in 17-OHP and 17-OHP/TT The positive outcome of the semen parameters following the sub inguinal micro-varicocelectomy comes in the same line of a recent study conducted by Kalantan et al (2023) (20) The strengths of this study include the novelty of associating sperm count and progressive motility improvement and sperm abnormal forms after sub-inguinal micro-varicocelectomy with 17-OHP and 17-OHP/TT ratio We tried to control variability in this study by performing all serum measurements between 8 and 10 am Scrotal duplex scans were performed for all patients to guarantee accurate diagnosis of Vx by venous diameter m e a s u r e m e n t , a s s e s s m e n t o f t e s t i c u l a r v o l u m e a n d detection of venous reflux with Valsalva maneuver
Furthermore, we performed multiple follow-up assessments In addition, we potentially identified a serum biomarker that had the ability to characterize men who were deficient in ITT as well as follow up by monitoring these patients for changes in semen parameters This could be seen in alignment with B r i d g e s e t a l (2015) (21)
Hypothetically, we succeeded in presenting 17-OHP and 1 7 - O H P / T T a s p o t e n t i a l b i o m a r k e r s f o r p r e d i c t i n g i m p r o v e m e n t i n s e m e n p a r a m e t e r s f o l l o w i n g s u binguinal micro-varicocelectomy On the other hand, there
M Wael Ragab, M Abbas, T Ramzy, et al
Figure
are several limitations of the current study that must be mentioned Firstly, the small sample size is a major limitation Secondly, we did not follow up the effect of improvement of semen parameters on pregnancy rates Finally, we were unable to measure ITT However, it should be noted that we based the correlation of 17-OHP with ITT on a study conducted by Patel et al (2019) (8)
CONCLUSIONS
According to the current study, sub-inguinal micro-varicocelectomy resulted in significant improvements in sperm count and progressive motility that significantly correlated with changes in 17-OHP and 17-OHP/ TT ratio
ACKNOWLEDGEMENTS
We would to thank the surgeons who did subinguinal micro-varicocelectomy
REFERENCES
1 Jungwirth A, Giwercman A, Tournaye H, et al & European Association of Urology Working Group on Male Infertility European Association of Urology guidelines on Male Infertility: the 2012 update Eur Urol 2012; 62:324-332
2 Sharpe RM, Cooper, I Intratesticular secretion of a factor (s) with major stimulatory effects on Leydig cell testosterone secretion in vitro Mol Cell Endocrinol 1984; 37:159-168
3 Roth M, Page S, Lin K, et al Dose-dependent increase in intratesticular testosterone by very low-dose human chorionic gonadotropin in normal men with experimental gonadotropin deficiency J Clin Endocrinol Metab 2010; 95:3806-3813
4 Duarte-Neto AN, Teixeira TA, Caldini EG, et al Testicular p a t h o l o g y i n f a t a l C O V I D - 1 9 : A d e s c r i p t i v e a
p s y s t u d y Andrology 2022; 10:13-23
5 Kelly D, Jones T Testosterone and obesity Obes Rev 2015; 16:581606
6 Amory JK, Coviello AD, Page ST, et al Serum 17-hydroxyp-rogest e r o n e s t r o n g l y c o r r e l a t e s w i t h i n t
t e r o n
n gonadotropin-suppressed normal men receiving various dosages of human chorionic gonadotropin Fertil Steril 2008; 89:380-386
7 Roth MY, Lin K, Bay K, et al Serum insulin-like factor 3 is highly correlated with intratesticular testosterone in normal men with acute, experimental gonadotropin deficiency stimulated with lowdose human chorionic gonadotropin: a randomized, controlled trial Fertil Steril 2013; 99:132-139
8 Patel A, Patel P, Bitran J, Ramasamy R Can serum 17-hydroxyprogesterone and insulin-like factor 3 be used as a marker for evaluation of intratesticular testosterone? Transl Androl Urol 2019; 8 (Suppl 1):S58-S63
9 Alharbi M, Zini A Epidemiology of Varicocele in Pediatric, Adolescent, and Adult Populations In Sandro C Esteves, Chak-Lam Cho, Ahmad Majzoub, Ashok Agarwal (Eds) Varicocele and Male Infertility Springer 2019 pp 97-106
10 Alsaikhan B, Alrabeeah K, Delouya G, Zini A Epidemiology of varicocele Asian J Androl 2016; 18:179-181
11 Zohdy W, Ghazi S, Arafa M Impact of varicocelectomy on gonadal and erectile functions in men with hypogonadism and infertility J Sex Med 2011; 8:885-893
12 Li F, Yue H, Yamaguchi K, et al Effect of surgical repair on testosterone production in infertile men with varicocele: A metaanalysis Int J Urol 2012; 19:149-154
13 Hsiao W, Rosoff JS, Pale JR, et al Varicocelectomy is associated with increases in serum testosterone independent of clinical grade Urology 2013; 81:1213-1217
14 Lima TFN, Frech FS, Patel P, et al Effect of microsurgical varicocelectomy on semen parameters, serum, and intratesticular testosterone levels BJUI compass 2020; 1:93
15 Bellastella G, Carotenuto R, Caiazzo F, et al Varicocele: An Endocrinological Perspective Front Reprod Health 2022; 4:863695
1 6 W o r l d M e d i c a l A s s
Declaration of Helsinki: Ethical principles for medical research involving human subjects JAMA 2013; 310:2191-2194
17 World Health Organization (WHO) WHO laboratory manual for the examination and processing of human semen 5th ed Geneva: WHO:2010, p 271
18 Schauer I, Madersbacher S, Jost R, et al The impact of varicocelectomy on sperm parameters: a meta-analysis J Urol 2012; 187:1540-1547
19 Rodriguez Peña M, Alescio L, Russell A, et al Predictors of improved seminal parameters and fertility after varicocele repair in young adults Andrologia 2009; 41:277-281
20 Kalantan M, Vienney N, Guillot Tantay C, et al Résultats des cures de varicocèles microchirurgicales sous-inguinales (Results of subinguinal microsurgical varicocelectomy) Prog Urol 2023; 33:481-487
21 Bridges N, Trofimenko V, Fields S, et al Male factor infertility and clomiphene citrate: A meta-analysis the effect of clomiphene citrate on oligospermia Urol Pract 2015; 2:199-205
Correspondence
Mohamed Wael Ragab, MD m w ragab@kasralainy edu eg
Mohamed Abbas, MD mhmdabbas71@yahoo com
Mohamed Yousry Elamir, MD yousr82@kasralainy edu eg
Mohamed Ragab Shehata, M Sc ragabmohamed260491@gmail com
Ashraf Zeidan, MD zeidana2000@gmail com
Department of Andrology & STDs, Kasr Alainy Faculty of Medicine, Cairo University, Egypt
Tarek Ramzy, MD drtarekramzy@yahoo com
Department of Chemical Pathology, Kasr Alainy Faculty of Medicine, Cairo University, Egypt
Sameh Fayek GamalEl Din, MD (Corresponding Author) samehfayek@kasralainy edu eg
Department of Andrology & STDs, Kasr Alainy Faculty of Medicine, Cairo University, Egypt Al-Saray Street, El Manial, Cairo, 11956, Egypt
Mohammad H Alkandari, MD al kandarim@hotmail com
Mubarak Al-Kabeer Teaching Hospital, Kuwait
Abdullah Salem Alshammari, MB BCH astsh51@gmail com Farwaniyah Hospital, Kuwait
Conflict of interest: The authors declare no potential conflict of interest
The present study has been presented as a poster in the 12th European Congress of Andrology Abstract Book
ORIGINAL PAPER
Effect of radiofrequency electromagnetic waves of mobile phone stations on male fertility
4 Urology Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt
Summary
Purpose: To determine the effect of electromagnetic waves of mobile phone stations on several sperm parameters and the male reproductive system.
Methods: This observational study was performed on 216 subjects, aged 18-60 years. Two equal groups of subjects were assigned to group A (study group) if they were living close to cell phone tower stations for at least 6 months and group B (control group) formed from individuals living 100 meters away from cell phone tower stations Every subject underwent a comprehensive history taking, a clinical assessment, and laboratory testing
Results: Regarding morphology index in the studied groups, the exposed group exhibited a trend of reduced percentage of normal morphology compared to the non-exposed group, with no statistical difference between the two groups Regarding the total sperm motility (A+B+C) and progressive sperm motility (A+B) in the studied groups, the exposed group showed a trend of decreased total sperm motility and of progressive sperm motility in contrast to the non-exposed group, with no statistical difference between the two groups.
Conclusions: Personal wrong lifestyles with exposure to electromagnetic waves have shown a trend towards a reduced percentage of normal morphology and reduced motility although nonstatistically significant compared with non-exposed populations.
KEY WORDS: Electromagnetic waves; Mobile phone stations; Male infertility
Submitted 22 April 2024; Accepted 22 June 2024
INTRODUCTION
In recent decades, the estimated prevalence of infertility among couples of reproductive age has risen to 15% (1)
A decline in sperm count, a mobility issue, or a structural issue can all be signs of male infertility disorders that may be brought on by ionizing radiation, electromagnetic waves, stress, and other biochemical variables (2)
With an average of thirty minutes a day spent chatting on mobile phones, people are consequently exposed to a significant amount of radiofrequency electromagnetic radiation (RF-EMR) from these devices (3) Although the effects of RF-EMR from cell phones on semen quality have received
attention recently, the conclusions are still debated The public now believes that mobile phone RF-EMR is a significant risk factor for the deterioration in sperm quality Using a mobile phone is one of the main ways to be exposed to RF-EMR (4)
La Vignera et al (5) showed that RF-EMR hurts seminal tubules, testicular stromal cells, and particularly sperm When it comes to harm, tissues near mobile devices are more vulnerable than those farther away from cellular antennae Furthermore, long-term cell phone use may negatively impact sperm motility (6)
Sperm malfunction, which results in male infertility and DNA damage in the male germ line, is mostly caused by oxidative stress (7) This oxidative stress condition affects spermatozoa primarily because of an increase in reactive oxygen species (ROS) generated by the mitochondria, with complex III of the electron transport chain (ETC) serving as the primary target of this radiation (8) Previous research demonstrated that men's testicular and germ cell function may be negatively impacted by a range of harmful effects from EMWs (9)
In this study, our goal was to determine the effect of electromagnetic waves from mobile phone stations on several sperm parameters and the male reproductive system
MATERIALS AND METHODS
This observational study involving 216 subjects aged 18 to 60 years, was conducted at the Urology Clinic of University Hospitals from December 2022 to July 2023
All procedures performed in this study were in accordance with the ethical standards of the Institution and/or National Research Committee and the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards It received approval from ethical committee of the Faculty of Medicine of Benha University, Faculty of Medicine (cod number:RC 40-11-2022) on November 04, 2022 All subjects provided written informed consent The establishment of portable mobile phone towers in villages raised the concerns of many people neighboring the towers about the harmful effects of these towers and their negative impact on health On this basis, many of
1.
t h e n o r m a l p e o p l e n e i g h b o r i n g these towers volunteered to participate in the study
Subjects with hydrocele, varicocele, orchitis, testicular or epididymal trauma, or any other condition potentially affecting semen quality, as well as those unable to complete sperm extraction through masturbation and individuals with diabetes mellitus, hypertension, cardiac, neurological, liver, renal diseases, or other serious systemic chronic diseases, and smokers were excluded
Participants were divided into two e q u a l g r o u p s : G r o u p A ( s t u d y group) included subjects who by history taking resulted residing close to or within 100 meters from cell phone tower stations for at least 6 months of daily exposure of at least 12 hours per day, and Group B (control group) was composed of individuals living 100 meters away from cell phone tower stations, matched with the study group in terms of age and sex Each subject underwent a thorough history-taking, clinical assessment, and laboratory testing
Semen collection
Regarding age of the studied groups, mean age was lower in the exposed group compared to the non-exposed group, with no statistically significant difference between both groups (Table 1)
Semen was collected in a wide-mouth container Semen appearance and liquid condition was primarly assessed by visual evaluation A pre-weighed container determined semen volume, and microcell slides with 10 μL semen samples were used to examine six fields or a minimum of 200 spermatozoa Technicians, using computeraided semen analysis (CASA), verified results for semen concentration, total sperm count (TSC), vitality (%), pH, motility, and morphology
Statistical analysis
Statistical analysis was performed utilizing SPSS v28 (IBM Inc , Armonk, NY, USA) Unpaired Student's t-test was utilized to compare the two groups based on quantitative data that were reported as mean and standard deviation (SD) Both the chi-square test and, when applicable, Fisher's exact test was utilized to analyse the frequency and percentage (%) of the qualitative variables For statistical significance, a two-tailed P value less than 0 05 was utilized
RESULTS
In this study, 259 subjects were assessed for eligibility, 27 subjects did not meet the criteria and 16 subjects refused to participate in the study The remaining 216 subjects were divided into two groups (108 subjects in each) All subjects were followed up and analyzed statistically (Figure 1)
Regarding seminal volume, sperm count, sperm vitality, and pH, the exposed group had higher mean seminal volume and higher pH compared to the non-exposed group, with no statistical difference between both groups; the exposed group had also lower sperm count and sperm vitality compared to the non-exposed group, with no statistically significant variation between the two groups (Table 2)
Table 1.
Age of the studied groups.
Group A Group B P value (Exposed) (Non-exposed) (n =
Table 2.
Seminal fluid characters of the studied groups. Group A Group B P value
T Mohamed Gharib, K Almekaty, A Mohamed Abdel Aal, et al
Figure
Algorithm of the enrolled patients.
Table 3.
Different types of sperm motility of the studied groups
Group A Group B P value (Exposed) (Non-exposed) (n = 108) (n = 108)
Regarding the morphology index, the exposed group had a lower percentage of normal morphology compared to the non-exposed group, with no statistical difference between the two groups (Table 2)
Concerning non-progressive motility, immotility, slow progressive motility, and rapid progressive motility in the groups under study, the exposed group had a reduced rapid progressive motility and slow progressive motility in contrast to the non-exposed group, with no statistical difference between the two groups; the exposed group had higher percentage of non-progressive motility and immotility compared to the non-exposed group, with no statistical difference between the two groups (Table 3)
Regarding the total sperm motility (A+B+C) and progressive sperm motility (A+B) in the studied groups, the exposed group possessed a decreased total sperm motility and progressive sperm motility in contrast to the nonexposed group, with no statistical difference between the two groups (Table 3)
DISCUSSION
Recent years have seen a rise in the number of individuals who own cell phones which use electromagnetic waves As a result, it is now easier to analyse how phone use affects semen quality (11)
In the present study, sperm count, sperm vitality, and pH in the exposed group had a trend of lower seminal volume along with lower pH comared with the non-exposed group; the exposed group had a trend of lower sperm count and sperm vitality, a lower percentage of normal morphology, reduced rapid progressive motility and slow progressive motility, in contrast to the non-exposed group, with no statistical difference between the two groups
Male fertility depends on sperm motility, which has been the subject of earlier studies on the impact of RF-EMR from mobile phones on the quality of male semen (12)
Mobile phones emit radiofrequency-electromagnetic waves (RF-EMWs), which consist of a range of frequencies between 800 and 2200 MHz These waves possess the capacity to penetrate different parts of the human body
and could pose risks to several physiological systems (13) Previous research has investigated a notable reduction in the quantities, viability, and mobility of sperms due to being subjected to RF-EMWs released by cellular devices (14) It can be concluded that cigarette smoking and exposure to electromagnetic waves significantly reduced sperm count, motility, morphology, fertilization rate, and embryo quality (15)
Semen samples exposed to a mobile device for only 10 minutes showed a significant decrease in sperm motility, suggesting that subfertile males may be especially susceptible to RF-EMR (16) Regarding the type of motility impairment, RF-EMR seems to mostly affect spermatozoa's ability to maintain forward progressive motility A study conducted by Erogul and coworkers (17) proved that after an extremely short five minutes exposure to RFEMR, human spermatozoa lost their capacity to maintain both rapid and slow progressive motility Reduced progressive motility seems to be a common side effect of RFEMR exposure, in contrary to other researchers who have shown that larger exposure durations (hours or days) are necessary to produce significant reductions in sperm motility (18, 19) A l - Q u z w i n
h
p between environmental risks and male fertility as indicated by seminal fluid analysis (SFA) that showed that lower semen parameters could result from environmental risks like those found in the home or place of employment They discovered that there is a notable difference in the exposition to environmental risks of subfertile and fertile groups For example, the subfertile group is exposed to mobile phone towers at a larger proportion (29%) than the fertile group (12%) (p = 0 003) It was concluded that an increased risk of SFA anomalies (teratozoospermia) was linked to exposure to environmental hazards These results are consistent with those published by Makker et al (21) who stated that the parameters of semen analysis can be impacted by the electromagnetic radiation (EMR) released by mobile phones and their base station It is now known that the pathophysiological basis for the detrimental effects on spermatozoa is caused by increased m i t o c h o n d r i a l r e a c t i v e o x y g e n s p e c i e s g e n e r a t i o n brought on by EMR, which lowers sperm vitality while promoting the DNA base adduct formation, which ultimately leads to DNA fragmentation and more abnormalities in sperm shape (22)
In Zhang et al (11) study, they discovered a negative correlation between the average daily duration of mobile phone use and the rates of gradually motile spermatozoa, quick increasingly motile spermatozoa, and total motile spermatozoa Fejes et al (23) discovered that there was a positive correlation between the amount of time spent on mobile phones and the slow increasingly motile spermatozoa rate, and an inverse correlation between the two Mobile phone use was linked to the overall motile spermatozoa rate but not to other semen characteristics, according to two prior meta-analyses (24)
Zhang et al (11) found that the primary reason for the decrease in sperm motility could be cell phone RF-EMR Given the expanding tendency of the male reproductive system's degradation, these findings imply that current worries about long-term exposure to RF-EMR from mobile
phones should be treated more seriously Therefore, it is recommended that people cut down on their daily use of mobile phones to prevent additional decreases in sperm motility, which could impact fertility, particularly in men who are of reproductive age and have asthenospermia
Additionally, a study using 358 semen samples from men who were representative of the general male population revealed that sperm motility was the most important factor in determining the likelihood of a natural conception (25) Further investigation found that carrying mobile phones in back pant pockets or using them for more than four hours per day led to a marginal elevation in the DNA fragmentation index (DFI) (26) However, Zhang et al (10) found no variation in the DFI based on the amount of time spent using a mobile phone
Similarly to our findings, Zhang et al (10) discovered no statistically significant variations in the proportion of normal forms and also volume, sperm concentration, or total quantity of sperm in relation to the length of time spent using a mobile phone A cross-sectional study revealed that as daily mobile phone talking time increased, there was a modest drop in the mean semen volume, sperm concentration, and total sperm quantity (10)
Darvish et al (27) outcomes demonstrated that RF negatively affects semen parameters Other systematic review studies have shown that exposure to RF is a risk factor for sperm motility and viability and that exposure to mobile phones was linked to decreased sperm motility and viability but not to decreased sperm concentration (24)
Limitations of our study included the limited sample size and the brief follow-up period In particular the insufficient sample size may explain statistically insignificant results
CONCLUSIONS
Personal wrong lifestyles as exposure to electromagnetic waves have been associated to a trend towards a reduced percentage of normal morphology and reduced motility of sperm cells although differences with normal population were non-statistically significant
REFERENCES
1 Zhu C, Yan L, He C, et al Incidence and risk factors of infertility among couples who desire a first and second child in Shanghai, China: a facility-based prospective cohort study Reprod Health 2022; 19:155-65
2 Babakhanzadeh E, Nazari M, Ghasemifar S, et al Some of the factors involved in male infertility: A prospective review Int J Gen Med 2020; 13:29-41
3 Hasan I, Rubayet Jahan M, Nabiul Islam M, et al Effect of 2400 MHz mobile phone radiation exposure on the behavior and hippocampus morphology in Swiss mouse model Saudi J Biol Sci 2022; 29:102-110
4 Chu KY, Khodamoradi K, Blachman-Braun R, et al Effect of radiofrequency electromagnetic radiation emitted by modern cellphones on sperm motility and viability: An in vitro study Eur Urol Focus 2023; 9:69-74
5 La Vignera S, Condorelli RA, Vicari E, et al Effects of the expo-
sure to mobile phones on male reproduction: a review of the literature J Androl 2012; 33:350-6
6 Okechukwu CE Does the use of mobile phone affect male fertility? A mini-review J Hum Reprod Sci 2020; 13:174-183
7 Mannucci A, Argento FR, Fini E, et al The impact of oxidative stress in male infertility Front Mol Biosci 2021; 8:799-813
8 Houston BJ, Nixon B, Martin JH, et al Heat exposure induces oxidative stress and DNA damage in the male germ line Biol Reprod 2018; 98:593-606
9 Dasdag S, Ketani MA, Akdag Z, et al Whole-body microwave exposure emitted by cellular phones and testicular function of rats Urol Res 1999; 27:219-23
10 Zhang S, Mo F, Chang Y, et al Corrigendum to: Effects of mobile phone use on semen parameters: a cross-sectional study of 1634 men in China Reprod Fertil Dev 2022; 34:1145
11 Hatch EE, Willis SK, Wesselink AK, et al Male cellular telephone exposure, fecundability, and semen quality: results from two preconception cohort studies Hum Reprod 2021; 36:1395-1404
12 Kesari KK, Agarwal A, Henkel R Radiations and male fertility Reprod Biol Endocrinol 2018; 16:118-34
13 Al-Bayyari N The effect of cell phone usage on semen quality and fertility among Jordanian males Middle East Fertil Soc J 2017; 22:178-182
14 Ding SS, Sun P, Zhang Z, et al Moderate dose of trolox preventing the deleterious effects of wi-fi radiation on spermatozoa in vitro through reduction of oxidative stress damage Chin Med J (Engl) 2018; 131:402-412
15 Hamada AE, Bakri S, Belal A, et al The effect of some lifestyle behaviours on male fertility and their effect on sperm quality and linking its quality to fertilization during intracytoplasmic sperm injection (ICSI) EAJBSZ 2023; 15:103-109
16 Zalata A, El-Samanoudy AZ, Shaalan D, et al In vitro effect of cell phone radiation on motility, DNA fragmentation and clusterin gene expression in human sperm Int J Fertil Steril 2015; 9:129-36
17 Erogul O, Oztas E, Yildirim I, et al Effects of electromagnetic radiation from a cellular phone on human sperm motility: an in vitro study Arch Med Res 2006; 37:840-3
18 Gorpinchenko I, Nikitin O, Banyra O, et al The influence of direct mobile phone radiation on sperm quality Cent European J Urol 2014; 67:65-71
19 Rahban R, Senn A, Nef S, et al Association between self-reported mobile phone use and the semen quality of young men Fertil Steril 2023; 120:1181-1192
20 Al-Quzwini OF, Al-Taee HA, Al-Shaikh SF Male fertility and its association with occupational and mobile phone towers hazards: An analytic study Middle East Fertility Society Journal 2016 2016; 21:236-240
21 Makker K, Varghese A, Desai NR, et al Cell phones: modern man's nemesis? Reprod Biomed Online 2009; 18:148-57
22 Mortimer D, Barratt CL, Björndahl L, et al What should it take to describe a substance or product as 'sperm-safe' Hum Reprod Update 2013; 19:1-45
23 Fejes I, Závaczki Z, Szöllosi J, et al Is there a relationship between cell phone use and semen quality? Arch Androl 2005; 51:385-93
24 Adams JA, Galloway TS, Mondal D, et al Effect of mobile tele-
T Mohamed Gharib, K Almekaty, A Mohamed Abdel Aal, et al
phones on sperm quality: a systematic review and meta-analysis Environ Int 2014; 70:106-12
25 Larsen L, Scheike T, Jensen TK, et al Computer-assisted semen analysis parameters as predictors for fertility of men from the general population The Danish First Pregnancy Planner Study Team Hum Reprod 2000; 15:1562-7
26 Rago R, Salacone P, Caponecchia L, et al The semen quality of the mobile phone users J Endocrinol Invest 2013; 36:970-4
27 Darvish L, Amraee A, Akhavan Amjadi M, et al The impact of radiofrequency waves on male infertility: A systematic review (Systematic Review) Shiraz E-Med J 2020; 22:101-9
Correspondence
Tarek Mohamed Gharib, MD tarekgh78@yahoo com
Ashraf Mohamed Abdel Aal, MD Ashrafm1970@gmail com
Mohamed Abdelrahman Alhefnawy, MD Dr mohamedalhefnawy@gmail com Benha University, Faculty of Medicine, Urology Department, Benha, Egypt
Khaled Almekaty, MD Dr khaledhafez@yahoo com
Tanta University, Faculty of Medicine, Urology Department, Tanta, Egypt
Ibrahim Abdel-Al, MD (Corresponding Author) dribrahemuro2011@yahoo com
Urology Department, Faculty of Medicine, Al-Azhar University, Assiut Branch, Egypt Assuit, postal code 71511
Ahmed Haty, MD drahmeduro@yahoo com
Ahmed Shafiea, MD Shafieaahmed2018@yahoo com
Mohamed Elsayed Metwally, MD Mohaelsayed575@yahoo com
Elsayed Elawadey, MD Drsayedawadey@gmail com
Urology Department, Al-Azhar University, Faculty of Medicine, Cairo, Egypt
Hazem Deif, MD hazemdeif@yahoo com
Gamal M Hassan, MD Gamalshrf@yahoo com
Urology Department, Faculty of Medicine, Al-Azhar University, Assiut Branch, Egypt
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
Vasectomy histology: Is it still useful?
Anthony Sim 1 , Panagiotis Nikolinakos 2 , Konstantinos Charitopoulos 2 , Ivo Donkov 2 , Samuel Bishara 2
1 Imperial College London, UK;
2 Department of Surgery West Middlesex Hospital, Twickenham Road, Isleworth, London TW7 6AF
Summary
Objectives: To determine if histological evaluation of the vasa is useful when post-vasectomy semen analysis (PVSA) compliance is low and to determine whether compliance could be predicted.
Methods: A retrospective evaluation of patients undergoing vasectomy between 2018 and 2022 was undertaken. A comparison of the PVSA between three vasa histological categorisations was made: complete divisions, incomplete division(s), absent vas(a) A multivariate model was constructed to predict PVSA compliance.
Results: From 388 patients, 191 (49 2%) undertook PVSA Four patients had a revision of vasectomy. On 3 occasions this was due to the histology findings and once from semen analysis with normal histology There was no significant difference in the number of azoospermic samples (95 4% vs 91 2%, ns), of samples with presence of Rare Non-Motile Sperm (RNMS) (2 6% vs 8 8%, ns) and those with sperm present (2 0 vs 0%, ns), between patients with complete division of the vasa on both sides and those with incomplete division on one side respectively There was no difference in patient characteristics between those who complied with PVSA and those who did not
Conclusions: This paper suggests that there is a role for histological evaluation of the vasa when PVSA compliance is poor. Incompletely divided vasa on histology are not associated with an adverse PVSA.
Vasectomy is a commonly undertaken and effective form of contraception 8 531 vasectomies were performed in the UK in 2021/22, which is 30% below the last pre-pandemic total for 2019/20 (12 157) (1) It is estimated that it is the primary form of contraception for 42 million couples worldwide (2)
Updated vasectomy guidelines for the UK were introduced in 2016, advocating the use of a single post vasectomy semen analysis (PVSA) at 3 months to determine clearance (3) This represents a welcome change in reducing the number of necessary semen analyses However, the need for two PVSAs to determine special clearance has been challenged (4) There is likely to be variation in the management of patients with low numbers of nonmotile sperm present in PVSA, as demonstrated by a recent inter national survey which highlighted a range of
approaches being adopted by clinicians (5) Histological examination of the vasa is not commented upon by the UK guidelines The AUA guidelines state that although histological evaluation is unlikely to cause harm it is not recommended as PVSA is preferred (6) The Faculty of Sexual & Reproductive Healthcare guidelines are more categorically against histology evaluation stating that “Routine histology on vasectomy specimens represents an unacceptable burden on both laboratory staff and time and is expensive” (7) However, there is likely variation in practice here too (8), perhaps out of caution or fear of litigation PVSA makes the pathological examination of the vasa redundant, as the identification of two vasa specimens does not preclude the possibility of vasa duplications or division of the vas on the same side twice (9-12)
It has been our own practice to submit the vasa specimens for pathological evaluation Perhaps the greatest pitfall of vasectomy evaluation is the low compliance with PVSA which has generally been documented to be between 30% and 80% (8, 13-17) Addressing this realworld problem has a greater potential to strengthen vasectomy evaluation, than any further refinement of guidance on the timing and interpretation of the semen analysis Poor compliance presents a real challenge; on the one hand there is increased risk of an unwanted pregnancy, litigation, and unclear appropriation of responsibility; on the other hand, unnecessary resources may be squandered chasing up men who will ultimately never carry out a PVSA
The aim of this study was to evaluate the utility of the vasectomy histology in determining the need for revision vasectomy, in a retrospective cohort of patients who underwent vasectomy between 2018 and 2022 inclusive Material and Methods
An NHS Health Research Authority evaluation questionnaire was completed which determined that ethical approval was not required for the study as only routine health data was evaluated in a retrospective manner
The coding department provided a list of all vasectomies undertaken between 2018 and 2022, including patient age and anaesthetic modality The histology, PVSA and f/u appointment records were extracted from contemporaneous electronic records
Procedures were carried out after written consent and appropriate counselling, under local anaesthetic, general anaesthetic, spinal anaesthetic or sedation In all cases the vasa were excised diathermised and ligated The excised vasa were placed in formalin in sperate pots, labelled
according to side, and sent to the pathology laboratory for evaluation
Semen analysis was requested, and patients were provided with written instructions on how to organise a PVSA at 3 months after the surgery
The histology outcome of the vasectomy was classified as either 2 vasa present and divided, 2 vasa present and one or more incompletely divided, or one or more vasa absent from each side
The semen analysis was conducted a c c o rd i n g t o t h e 2 0 1 6 B r i t i s h
Association of Urology guidelines
Table 1.
Semen analysis according to histological report.
Histolog y Number Semen Azoosper mia RNMS Sper matozoa Revision
vasa present but possible incomplete division
Absent vas on one side
No histology
†: Not significant d fference by Fisher test
The semen analysis outcome, as per guidelines were classified, as present (any motile sperm or > 100,000 immotile sperm), rare non-motile sperm (< 100,000 immotile sperm) or azoospermia (no sperm detected)
Rare non-motile sperm is believed to carry no greater risk of pater nity than absent sperm, and its persistence may be reflective of sperm that’s had previously refluxed in the seminal vesicles or the ampulla of the vas (4, 18)
When more than one semen analysis was carried out the final semen analysis was regarded as definitive and utilised in this analysis
The demographic details of the patient and procedure were recorded including age, ASA and anaesthetic type A comparison of these demographics was made between those who did and did not undertake a PVSA Differences between these two groups were assessed by an unpaired t-test for age, the Mann Whitney U test for ASA grade, and by the Chi Squared test for anaesthetic type
A binary logistic regression was carried out to ascertain whether a predictive model using the patient and operative demographics could determine whether PVSA compliance could be predicted
The proportion of semen analysis outcomes between the different histological categories were compared and evaluated using the Fisher test
Statistical significance was taken as p < 0 05 (two tailed)
Statistical analyses were carried out using Minitab statistical software
RESULTS
388 vasectomies were carried out between 2018 to 2022 and were include in this study For 385 vasectomies, histological evaluation of the vasa took place and in 3 cases this was absent 191 patients (49 2%) undertook semen analysis at 12 weeks or later, 6 patients repeated PVSA once (1 5%) and 197 (50 8%) did not carry out a follow up PVSA
The outcome of PVSA according to the histological classification of the vasa is shown in Table 1
Four patients (1 0%) underwent revision vasectomy Three of these patients were identified through the histology, as they had an absent vas on one side One was identified through the PVSA, which demonstrated sperm though they had 2 vasa histologically confirmed as divided 2 of these 3 patients identified from histology proceeded
1 (100%) 3 (0%) (0%) (75%)
(50%) (50%) (0%) (0%)
to revision vasectomy without PVSA One of these 3 patients had a PVSA prior to revision which demonstrated the presence of sperm All the patients who had a revision vasectomy were histologically confirmed to have had 2 vasa present after the revision procedure
One of the 4 patients who had an absent vas on histology, had only one vas identified at the time of an open procedure and was therefore likely to have ipsilateral absence of the vas, however they did not undertake a follow up PVSA
The semen parameters when two completely identified vasa were compared to when the pathologist flagged one of the sides, though present as being incompletely divided There is no significant difference in the number of azoospermia samples (95 4% vs 91 2%, ns), those with Rare Non-Motile Sperm (RNMS) (2 6% vs 8 8%, ns) and those with sperm present (2 0 vs 0%, ns) between these two groups respectively Incomplete division of the vasa demonstrated a 0% positive predictive power for determining the presence of spermatozoa on PVSA
The demographic details for the study patients are shown in Table 2 There is some incomplete data ASA Class was electronically recorded in 360 patients and the anaesthetic modality in 366 patients GA was the most common anaesthetic (218 patients), followed by LA (141 cases), Sedation (6 cases) and Spinal anaesthetic (1 case) There
Table 2.
Characteristic of vasectomy patients according to PVSA compliance
Age 41 4 40 9 NS α (5 6, n = 191) (6 3, n = 197)
(n = 183) (n = 183)
α: unpaired t-test, b: Mann-Whitney U test, †: Ch Square test
A Sim, P Nikolinakos, K Charitopoulos, et al
Table 3.
Binary logistic regression of variables hypothesised to predict compliance with PVSA Area under ROC curve 0 54
Ter m Coefficient SE Coefficient Z-value P-value
Constant -0 570 0 755 -0 75 0 451
Age 0 0186 0 0175 1 07 0 287
ASA
is no significant difference in age, ASA, or anaesthetic modality between the two groups
Theses variables were used to generate a multivariate model to determine if PVSA could be predicted None of these parameters achieved statistical significance The area under the ROC curve was 0 54 for the prediction of PVSA compliance
DISCUSSION
This paper accords with many others, highlighting the low follow up rate for PVSA that is typical across many practices, with just under 50% of patients complying with follow up Several have investigated the reasons for this, with men citing travel and time constraints (14) and embarrassment (15) as reasons for this Others have looked at strategies for improving follow up including home test kits (19-21), which have yielded variable results and postal notification strategies (22), which improved PVSA compliance
Revision of the BAUS guidelines, to reduce the number of PVSA mandated form two to one is a step in the right direction, and one likely to facilitate compliance, however it seems that we will always be a long way from 100% compliance with PVSA Whilst PVSA will always remain the gold standard, the question remains how we best manage non-compliance and does PVSA alone remain the optimal strategy when there is poor compliance and limited healthcare resources?
If there is 100 percent compliance with PVSA then clearly histology would be completely unnecessary, however, in this study more patients underwent redo vasectomy because of the histopathological findings than from the PVSA Only one patient underwent redo vasectomy through the PVSA alone and three underwent redo vasectomy from the pathology findings
The pathological findings are pertinent to the PVSA if no evidence of vasal tissue can be identified on one or more side From this study, incomplete division of the vasa on one or both sides does not seem to have any impact on the PVSA, and largely reflects the difficulty in obtaining thin perpendicular sections through the vasa for pathological analysis
The paper suggests that there may still be a role for vasa histology when the compliance rate is low as it picked up 75% of the known failures
Lack of compliance and inefficiency of follow up remain a problem, one option would be to shift the responsibility for follow up to the patient by requesting a patient initiated follow up appointment (PIFU), so that a follow up appointment is generated if and when the patient carries
out a semen analysis Patients should be informed clearly, whilst a system is in place to make PVSA possible, they are responsible for making sure this takes place and if they do not undertake PVSA, then they take responsibility for a having a lower level of certainty, for the success of their procedure, at 99 0% (form the histology alone) rather than 99 95% (through PVSA) It may be some men feel that the 1 0% risk is not worth the hassle of a further semen analysis, or by having already undergone a vasectomy, they have already gone above and beyond to provide contraception for themselves and their partner Histology is relatively expensive and costs £95 per case in our institution The cost effectiveness of histology is dependent on the compliance rate and the failure rate of vasectomy Excluding consultation cost, the estimated
£95/(Failure rate x Compliance rate) E g , if the failure rate is 1% and the PVSA compliance rate is 50%, then histological cost per additional failed vasectomy detected is £95/(0 01 x 0 5) = £19000 In this study the actual cost was £12192 per failed vasectomy detection Exploration of alter natives to histology which may provide similar diagnostic information is worthy of further evaluation
The statistical risk of litigation from patients as a result vasectomy is low A review found 67 cases over 28 years from the Westlaw database of US cases (23), though not all US cases may have been captured in this study The simplest approach would be to follow the Faculty of Sexual & Reproductive Healthcare guidelines and abandon the histology, however we feel that under the circumstances of low PVSA compliance retaining the histology facilitates greater stewardship of our patients albeit at a financial cost
There was no significant difference in the demographic factors between those who undertook a PVSA and those who did not Likewise, a predictive model utilising binary logistic regression did not achieve statistical significance for any of the parameters and was only of low predictive power
The number of children that patients had previously was not universally recorded and therefore not utilised in this study Some studies have demonstrated that fatherhood is associated with increased compliance with PVSA (14)
Previous studies have demonstrated that increased age was associated with better PVSA compliance, but we did not find that to be the case in this study (13)
CONCLUSIONS
This paper suggests that there is a role for histological evaluation of the vasa when PVSA compliance is poor, which is likely to be the case in many centres
REFERENCES
1 NHS England Part 4: Sterilisations and vasectomies Available from: https://digital nhs uk/data-and-information/publications/statistical/sexual-and-reproductive-health-services/2021-22/sterilisationsand-vasectomies
2 Haldar N, Cranston D, Turner E, et al How reliable is a vasectomy? Long-term follow-up of vasectomised men Lancet 2000; 356:43-4
3 Hancock P, Woodward BJ, Muneer A, Brown JCK Laboratory g u i d e l i n e s f o r p o s t v a s e c t o m y s e m e n a n a
s i s : A
i o n o f Biomedical Andrologists, the British Andrology Society and the British Association of Urological Surgeons J Clin Pathol 2016; 69:655-60
4 Beder D, Chitale S The clinical impact of British guidelines on post-vasectomy semen analysis Cent European J Urol 2020; 73:558-562
5 Agarwal A, Gupta S, Sharma RK, et al Post-Vasectomy semen analysis: optimizing laboratory procedures and test interpretation through a clinical audit and global survey of practices World J Mens Health 2022; 40:425-41
6 Sharlip ID, Belker AM, Honig S, et al Vasectomy: AUA guideline J Urol 2012; 188:2482
7 F S R H C l i n i c a l G u i d e l i n e : M a l e a n d F e m a
(September 2014) Available from: https://www fsrh org/standardsa n d
2014/
8 Katsoulis IE, Walker SR Vasectomy management in Morecambe Bay NHS Trust Ann R Coll Surg Engl 2005; 87:131
9 Miller S, Couture S, James G, et al Unilateral absence of vas deferens: prevalence among 23,013 men seeking vasectomy Int Braz J Urol 2016; 42:1010-7
10 Carr R Apparent bilateral duplication of the vas deferens Br J Urol 1993; 71:354
11 Erdemir F, Parlaktas BS, Yasar A, Uluocak N Duplicated vas deferens: A rare congenital abnormality Kaohsiung J Med Sci 2008; 24:210-1
12 Karaisli S, Ezer M Duplicated vas deferens: A case report and comprehensive review of the literature Andrologia 2021; 53:e13896
13 Christensen RE, Maples DC Postvasectomy semen analysis: are men following up? J Am Board Fam Pract 2005; 18:44-7
14 Bradshaw A, Owusu R, Ballon-Landa E, et al Poor compliance with post-vasectomy semen analysis: analysis of factors and barriers J Urol 2019; 201:e685
15 Diederichs J, McMahon P, Tomas J, Muller AJ Reasons for not c o m p l e
: https://www cfp ca/content/cfp/65/9/e391 full pdf
16 Maatman TJ, Aldrin L, George BGS, Car-Others G Patient noncompliance after vasectomy Fertil Steril 1997; 68:552-5
17 Derosa R, Lustik MB, Stackhouse DA, McMann LP Impact of the 2012 American urological association vasectomy guidelines on postvasectomy outcomes in a military population Urology 2015; 85:505-10
18 Philp T, Guillebaud J, Budd D Late failure of vasectomy after two documented analyses showing azoospermic semen Br Med J 1984; 289:77
19 Kiessling RJ, Hauser A, Eyre RC, Kiessling AA A new approach to postvasectomy semen analyses eliminates the need to evaluate a fresh specimen Andrology 2023; 11:464-70
20 Welliver C, Zipkin J, Lin B, et al Factors affecting post-vasectomy semen analysis compliance in home- and lab-based testing Can Urol Assoc J 2023; 17:E189-92
21 Trussler J, Browne B, Merino M, et al Post-vasectomy semen analysis compliance with use of a home-based test Can J Urol 2020; 27:10388-93
22 Atkinson M, James G, Bond K, et al Comparison of postal and non-postal post-vasectomy semen sample submission strategies on compliance and failures: an 11-year analysis of the audit database of the Association of Surgeons in Primary Care of the UK BMJ Sex Reprod Health 2022; 48:54-9
23 Blazek AJ, Belle JD, Deibert MP, Deibert CM Legal review of vasectomy litigation and the variables impacting trial outcomes Urology 2019; 131:120-4
Correspondence
Anthony Sim, MD anthony sim21@imperial ac uk Imperial College London, UK
Panagiotis Nikolinakos, MD panagiotis nikolinakos@nhs net
Konstantinos Charitopoulos, MD k charitopoulos@nhs net Ivo Donkov, MD i donkov@nhs net
Department of Surgery West Middlesex Hospital, Twickenham Road, Isleworth, London TW7 6AF
Samuel Bishara, MD (Corresponding Author) samuel bishara2@nhs net
Department of Urology, West Middlesex University Hospital, Chelsea & Westminster Hospital NHS Foundation Trust, London, United Kingdom
Conflict of interest: The authors declare no potential conflict of interest
ORIGINAL PAPER
CFTR Exon 10 deleterious mutations in patients with congenital bilateral absence of vas deferens in a cohort of Pakistani patients
Khush Bakhat 1 , Irsa Mateen 2 , Hina Saif 3 , Kanwal Anwar 1 , Sadaf Sarfraz 1 , Sheza Javaid 1 , Khaleeq-ur-Rehman 4 , Adnan Arshad 1 , Muhammad Mustafa 1
1 KAM School of Life Science, Forman Christian College, (A Chartered University), Lahore, Pakistan;
2 School of Biochemistry, Minhaj University Lahore, Lahore, Pakistan;
3 Department of Emerging Allied Health Technologies, University of Lahore, Pakistan;
4 Department of Urology, Fatima Memorial Hospital College of Medicine & Dentistry, Lahore, Pakistan
Summary
Congenital bilateral absence of vas deferens (CBAVD) is a urological syndrome of Wolffian ducts and is responsible for male infertility and obstructive azoospermia. This study is designed to explore the integrity of exon 10 of CFTR and its role in male infertility in a cohort of CBVAD patients in Pakistan. Genomic DNA was extracted from 17 male patients with CBAVD having clinical symptoms, and 10 healthy controls via phenol-chloroform method Exon 10 of the CFTR gene was amplified, using PCR with specific primers and DNA screening was done by Sanger sequencing Sequencing results were analyzed using freeware Serial Cloner, SnapGene, BioEdit and FinchTV Furthermore, bioinformatics tools were used to analyze the mutations and their impact on the protein function and stability We have identified 4 mutations on exon 10 of CFTR in 6 out of 17 patients Two of the mutations were missense variants V456A, K464E, and the other two were silent mutations G437G, S431S. The identified variant V456A was present in 4 of the studied patients. Whereas, the presence of K464E in our patients further weighs on the crucial importance for its strategic location to influence the gene function at post-transcriptional and protein level Furthermore, Polyphen-2 and SIFT analyze the mutations as harmful and deleterious. The recurrence of V456A and tactically conserved locality of K464E are evidence of their potential role in CBAVD patients and in male infertility. The data can contribute in developing genetic testing and treatment of CBAVD.
Congenital absence of vas deferens (CAVD) is a urological syndrome presumably resulting in abnormalities of the Wolffian ducts It is also a contributing factor to obstructive azoospermia It is categorized into three types: unilateral (CUAVD), bilateral (CBAVD), and congenital bilateral partial aplasia (CPAVD) (1)
CBAVD is the most prevalent subtype that follows an autosomal recessive pattern and accounts for 1-2 % of
sterile but healthy men and up to 25% of obstructive azoospermia cases (2)
To date, two perspectives have been presented regarding the etiology of the CBAVD: vas deferens atresia and vas d
pathological mechanism is required to be further studied and validated, these pathological mechanisms are widely known to be triggered by gene alterations (3)
Mainly CBAVD is diagnosed at adulthood during a medical examination for the exploration of infertility Therefore, it is of prime importance to properly assess infertile men with appropriate clinical work-up, to correctly address the suitable genetic tests in an exclusive way (4) Initially, clinical diagnosis was made on the palpation of the vas deferens (VD), that is, on their intrascrotal portion: the diagnosis was negative if this portion was present and positive if it was absent But in recent times, besides palpation, ultrasound imaging (transrectal and scrotal) is essential for accurate diagnosis (5) The biological alarming signal is a nonpathognomonic trio: hypospermia (semen volume < 1 5 ml), the value of seminal plasma lesser than the reference level (fructose < 13 μmol/ejaculate; Glycerophosphocholine (GPC) < 2 µmol/ejaculate), and acid pH (< 7 0) (6) Hence, on the basis of clinical symptoms, two clinical categories of CBAVD have been reported: CBAVD showing symptoms of cystic fibrosis referred as CF-CBAVD and CBAVD without clinical symptoms of CF referred as isolated CBAVD (iCBAVD) (7) Furthermore, apart from CF associated symptoms, other congenital genitourinary defects, primarily including dysplasia or the absence of seminal vesicles and kidney-related issues contributes towards CBAVD (8, 9) The anatomical anomalies related to CBAVD occur at the embryonic stage Cystic fibrosis transmembrane conductance regulator gene (CFTR) or CFTR mediated anions are essential for normal growth of the male reproductive tract (10) Mutations in the CFTR gene have a crucial impact on the vas deferens development in fetuses aged 12-18 weeks (11) These mutations lead to obstructions and denaturation of the vas deferens due to mucus accumulation, particularly pronounced during embryonic growth Studies showed that proper fluid secretion is crucial for the mesonephric duct to develop correctly (12,
13) When fluid secretion is disrupted, it can lead to underdevelopment and deterioration of the mesonephric duct in the early stages of embryo growth (14)
Until now, over 2000 mutations in the CFTR have been detected, however, not all of them are pathogenic in nature A relatively low number of mutations are causing CFTR associated abnormalities while the rest are not linked with any clinical syndromes Around 370 CFTR mutations are listed in the clinical and functional translation of the CFTR project (CFTR2) (15) These pathogenic variants are classified as mild and severe mutations on the basis of their phenotypic and functional effect Two severe mutations on both alleles of the CFTR causes cystic fibrosis (CF) while one severe and one mild or both mild mutations resulted in CBAVD Moreover, all CF patients have CBAVD (16)
CFTR mutations have been classified into six classes where class I to III variants present severe manifestations and complete loss of CFTR function However, class IV to VI variants present mild phenotypes with reduced CFTR function (2)
CFTR exhibits a great deal of heterogeneity due to the modifications in the base sequence of DNA which leads to altered protein expression Diverse migratory patterns and settlement have led to heterogeneity in mutations worldwide The relationship between CBAVD and CFTR is well established but it is least studied and documented in the Asian population That was the reason of our study aiming to the analysis of the genetic integrity of promoter region and exon 10 of CFTR to identify mutations in individuals with CBAVD in a Pakistani population
MATERIALS AND METHODS
Ethics statement
This study was approved by the Ethical Review Committee of Forman Christian College (A Chartered University) Lahore, Pakistan (ERC-81-2017 Dated: 11, September 2017) All the experiments were performed according to the approved guidelines
Blood sampling and DNA extraction
The term subjects has been used for both patients and healthy controls taking part in our study Archived blood samples from 31 patients with CBAVD and azoospermia together with those of 10 healthy controls were gifted by Fatima Memorial Hospital (FMH), Lahore Pakistan Blood samples were collected for research after the approval of the Institutional Review Board of Fatima Memorial Hospital, Lahore Pakistan (FMH-102018-IRB-520-F Dated: 23, October 2023) and archived for further research Extracted DNAs from 17 patients and 10 healthy controls were selected for further processing The authors had no access to information that could identify individual participants during or after data collection All the patients were examined by the same physi-
cian CBAVD was primarily diagnosed by impalpable scrotal vas on physical examination, followed by ultrasonography Eventually, diagnosis was confirmed by cytobiochemical characteristics: decreased concentration of fructose and carnitine, azoospermia with low pH < 7 and normal hormone concentration (9) All participants had no classical symptoms of CF Written informed consent was taken from the participants for the study Genomic DNA was isolated from whole blood cells by using standard phenol chloroform method (17)
PCR conditions and identification of variants
For screening purposes, the promoter region (PR-CFTR) and exon 10 (EX10-CFTR) were amplified by polymerase chain reaction (PCR) using specific sets of primers (Table 1 - Supplementary Materials) (Figure 1)
PCR conditions for the amplification of selected regions were: initial denaturation at 94°C for 5 minutes followed by 35 cycles of 1 min at 94°C, annealing for 48s at 61 6°C for EX10-CFTR and at 58 8°C for PR-CFTR, elongation carried out at 72°C for 1 minute and final elongation at 72°C for 5 min PCR products of the 17 patients and 10 c
P u r i fi c a t i o n K i t , ( Q i a g e n , V a l e n c i a , C A ) a n d t h e n sequenced by Macrogen (Inc Company, South Korea) DNA sequencing was performed using forward primers of both exon 10 and promoter region labeled as EX10CFTR-FWD and PR-CFTR-FWD respectively; afterwards, sequencing results were analyzed and confirmed using Serial Cloner, SnapGene, BioEdit and FinchTV
K Bakhat, I Mateen, H Saif, et al
Figure 1.
For mutation confirmation, sequencing data with quality chromatogram peaks were selected (Figures 2, 3)
In-silico analysis of CFTR protein with respect to missense mutations (V456A and K464E)
Analysis of conserved amino acid residues
The evolutionary conserved amino acid sequences of CFTR protein were checked by ConSurf By using multiple sequence alignment (MSA) of homologous protein sequences as pri-
Figure 1. (a) Sequence Alignment of Exon10-control, HWP3, HWP4, HWP12 and HWP14: Rectangular box indicates the region expanded to visualize DNA sequence quality (b) Comparison of control and sample DNA sequence with their corresponding in-frame amino acid sequences C and S represent control and sample sequence
Figure 2. (a) Sequence analysis of HWP6, (*) indicate the last base pair of exon 10 and protein sequence comparison with control (b & c) DNA and protein sequence comparison of missense mutations C and S indicate control and sample sequence respectively.
mary input, Consurf calculates a conservation score (1-9) for each amino acid position in the protein sequence where 7-9 score indicates conserved amino acid (18)
Probing of structural and functional effects of mutations HOPE (Have (y) Our Protein Explained) (https://www3 cmbi umcn nl/hope/) was used for analysis of the potential impact of amino acid substitutions on protein function and stability Amino acid sequence of the protein along with information about the mutation was provided as input and
HOPE provided insights into the potential consequences of mutations via integration of various computational approaches (19)
Analysis of missense mutations on protein stability and functional outcomes
To understand the potential out-turn of mutations on protein stability and functions, five different in silico tools were used Polyphen-2 (20) and SIFT (21) were used to find out the harmful effect of variants whereas MuPRO (22, 23), CUPSAT (24) and mCSM (25) were used to anticipate the effects of mutagenesis on protein stability (Table 2)
RESULTS
DNA sequencing and analysis
After a quality control with rigorous selection criteria, sequencing data of 8 patients revealed that 4 mutations in 6 individuals accounted for 35% of total 17 CBAVD patients in our experiment All these mutations were present on exon 10 while we didn’t find any significant mutation in the promoter region of CFTR in the above cohort Of these four identified mutations, two were missense mutations (V456A, K464E) whereas the other two were silent mutations (G437G, S431S)
V456A is an important missense variant identified in four patients (HWP3, HWP4, HWP12 and HWP14) of our study cohort (Figure 1a) Nucleotide sequences of these patients contain base substitution at position 158 of exon 10 where T is replaced by C resulting in change in amino acid valine to alanine (Figure 1b) Previously, V456A was reported in the South Asian population as a CF causing variant Furthermore, its association with male infertility of CBAVD individuals has been established However, other identified mutations were novel and found only in one patient each
Another important point mutation K464E has been identified in one patient (HWP6) We observed base substitution A to G mutation at position 181 of exon 10 which changed amino acid lysine (K) to glutamic acid (E) (Figure 2a) It is important to note that the total length of exon 10 is 183 base pairs and the integrity of DNA sequence near the splice site is critical for RNA splicing machinery to function normally Therefore, in addition to its impact due to change in amino acid, K464E can interrupt spliceosome activity at post-transcriptional level leading to excessive loss of function V456A and K464E are present on the NBD1 domain of CFTR (26) which is crucial for ATP hydrolysis for normal channel function (27)
Interestingly, in addition to V456A, patient HWP14 contains a silent mutation S431S (Figure 2b) This addition-
al mutation does not affect the nature of the amino acid
Another silent mutation G437G has been detected at position 102 of exon 10 in HWP13 (Figure 2c) These two silent mutations are irrelevant in the perspective of protein function but can influence single nucleotide polymorphism (SNP)
Frequency and mutation spectrum of CFTR is variable and known to be confined within different ethnic groups
In this study, we have found genetic mutations on critically functional locations of CFTR in CBAVD patients (Table S2 - Supplementary Materials) The recurrence of V456A mutation in four CBAVD patients highlights its potential role in disease and diagnosis Mutation K464E is crucial due to its location and is capable of affecting CFTR function drastically
Structural visualization of CFTR protein and in silico analysis of identified mutations in exon 10
We visualize the structure of the CFTR protein (PDB ID: 6O1V), using PyMol software (https://pymol org/2/) to explore critical regions and mutations within exon 10 (Figure S4 - Supplementary Materials) The orthoscopic view of CFTR provides an overall structure, while the functional site in exon 10 is highlighted in cyan (Figure S4 - Supplementary Materials) Within this selected region of exon 10, we pinpoint three specific mutations
V456A, K464E, and G437G represented as sticks Each mutation is labeled with its corresponding amino acid change, providing insight into the spatial arrangement of these vital regions within the protein (Figure S4, D-FSupplementary Materials)
ConSurf identified V456 (score: 7) and K464 (score: 9) as conserved and highly conserved residues respectively (Figure S5 - Supplementary Materials) Both Polyphen-2 and SIFT analyze the mutations as harmful and deleterious In case of Polyphen-2, score 0-0 5 means benign effect and above 0 5 is considered damaging whereas for SIFT score 0-0 5 is considered non tolerant and close to 1 00 is allowed (Table 1) Mutational effects of MuPRO, CUPSAT and mCSM suggested the overall mutations resulted in decreased stability, these tools predict ∆∆G (kcal/mol) where negative value indicative of destabilizing mutation (Table 2)
HOPE software revealed structural alterations caused by
Table 1.
In silico checking for the pathogenicity of
Table 2.
Computational analysis of
K Bakhat, I Mateen, H Saif, et al
the V456A (Figure 3A) and K464E (Figre 3B) mutations
T h e s e v i s
impact local protein structure, providing insights into their functional consequences
DISCUSSION
Prior research has documented Cystic fibrosis (CF) as a major autosomal recessive disease in ethnic groups Moreover, there are up to 2000 CFTR mutations that have been reported, with variable frequencies depending on ethnic and geographic backgrounds It is imperative to highlight the various variables of CFTR mutations that are prevalent in a given population to help focus on the diagnostic test It’s a prerequisite for setting up efficient molecular diagnostics and for furthering the genetic treatment to help its prevention (1)
Since the last two decades, growing evidence has revealed a multifaceted function of CFTR in controlling a number of physiological processes associated with male infertility Besides its familiar role of regulating electrolytes and fluid concentration of the male reproductive duct, recent investigations have indicated its participation in previously uncertain processes, such as sperm capacitation and spermatogenesis (26, 27), unfolding further potential reasons associated with male infertility, and strengthening the relation of CFTR mutations with CBVAD
As new forms of infertility in men are identified and linked with CFTR defects and polymorphisms, it wouldn’t be entirely illogical to consider CFTR as the molecular marker of male infertility Based on strong correlation between the quality of sperm and CFTR mutations, a screening of CFTR gene for mutations in obstructive, azoospermia and non-obstructive individuals is suggested before they opt for intracytoplasmic sperm injection due to strong link-up between sperm quality and CFTR mutations (18)
Common mutation panels used for mutation analysis of males with obstructive azoospermia and CBAVD are unable to identify CFTR mutation variants in a given population Initially, the mutation panel was designed to detect the most frequent CF causing mutations in the affected individuals of North European Caucasians (19) On the contrary, the genetic spectrum of South Asian people reported increased prevalence of novel mutation such as F508 which comprises 40-50% of cases as compared to 66% reported CF cases worldwide Moreover, in South Asians frequency of mutation detection is lower than the Caucasians i e ,
Figure 3.
Structural change
V456A (A) and K464E (B) instanced by project HOPE. The protein is colored grey, the side chains of both the wild-type and the mutant residues are indicated as green and red respectively, ligand represented as grey ball structure (B).
50% and 77% respectively Also, in several cases of CF, mutations remained undetected (23)
In our study, screening of CFTR promoter region and exon 10 was achieved by the DNA sequence method in CBAVD patients We have identified one or two mutations in 35% of our sample patients Discovering the presence of V456A in 4 of 17 patients further adds evidence for its pathogenic nature and supports its inclusion in the genetic diagnostic of CBAVD, especially in the South Asian population V456A was initially described as polymorphism (28), but with further investigation the mutation was labeled as a mild disease-causing mutation particularly in adults with Bronchiectasis, while it also paired up with more prominent mutations (F508) (29) Previously, it has been linked with CBAVD as well (28) Regardless, it is a rare mutation occurring only in 2 4% of 78 south Asian patients (30) Danziger et al , and clinical evidence from Uppaluri et al., suggested that V456A holds importance as a disease-causing mutation and is not merely a mild polymorphism (31)
Exon 10 of the CFTR gene codes a portion of the nucleotide-binding domain (NBD I and II) in CFTR protein NBD plays a crucial role in the regulation of CFTR function It is involved in ATP (adenosine triphosphate) binding and hydrolysis, which is necessary for the opening and closing of the chloride channel formed by CFTR ATP binding to NBD triggers conformational changes that enable the channel to transport chloride ions across the cell membrane Mutations in exon 10 can disrupt the structure and function of NBD (I or II); impairing ATP binding, hydrolysis, and overall CFTR channel activity
The impaired ATP binding reduces the ability of CFTR to properly respond to cellular signals and regulate chloride ion transport, contributing to the dysfunction observed in cystic fibrosis Mutations can also affect ATP hydrolysis, which is necessary for channel gating The specific impact of mutations in exon 10 can vary depending on the nature and location of the mutation within the exon (1)
Based on literature, the overlapping function of NBD1 and NBD2 domain and the relation of exon 10 in the proper functioning of NBD domain (32, 33) hints towards a relation between the NBD domains of CFTR protein and the mutations observed in our study group; K464E, a missense variant which is formed as a result of base substitution of A by G at nucleotide position 181 of exon 10 of CFTR
It can be assumed that this mutation could potentially affect the NBD domains, impacting its ability to bind and hydrolyze ATP, as proved, and described by the literature
for other exon 10 mutations The K464E mutation also implicates to be defective for translational protein insertions on the membrane gated channels and ribosome binding (34), whereas the V456A mutation found in four of our CBAVD patients (HWP3, HWP4, HWP12 and HWP14) has been previously linked with its adverse effects on the Nucleotide-binding Domain 1 (NBD1) of the CFTR protein The V456A mutation refers to the substitution of the amino acid valine (V) with alanine (A) at position 456 within NBD1
HOPE server illustrated that mutation driven physicochemical changes in protein might be deleterious In case of V456A, mutated residue is smaller in contrast to wild type and mutation is located within a domain (ABC transporter 1 as annotated in UniProt) important for binding of other molecules and in contact with residues in a domain that is important for the activity of the protein The mutation might affect this interaction and thereby disturb signal transfer from the binding domain to the activity domain (Figure 3A)
Regarding K464E, the size difference of mutated residue (smaller) disturbs the interaction with Mg2+ and might result in destabilization of the domain as divalent cations enhance ATP binding (35) K464 interacts with ligand ATP which might be disturbed by mutation and there is also change in charge of mutated residue (negative) as compared to wild type (positive) where changes in size and charge can cause loss of interaction with ligand (Figure 3B)
Mutations within NBD1, such as the V456A mutation, can disrupt these processes, leading to a dysfunctional CFTR protein and ultimately contributing to the development of cystic fibrosis Therefore, its presence in CBAVD patients emphasize the significance of the mutation in the prevalence of the disease The specific effects of the V456A and K464E mutations on the CFTR protein domain may vary, and further research may be required to fully understand its impact on the progression of CBAVD disease
The new silent mutations S431S and G437G found in two of the patients do not seem to disrupt the coding sequencing as the resultant protein remains the same but further analysis is needed for a more concrete ruling as their influence as single nucleotide polymorphism cannot be ignored based on our study, which involves small number of CBAVD patients and lacks the inclusion of multiple ethnicities in the region On the basis of these promising results, further research needs to be planned on a larger sample size Furthermore, whole genome sequencing and protein analysis are required to be performed for more sensitive and consistent results Hence, there is an extreme need for further investigations in genetics and epigenetics to provide deep understanding of male infertility, especially gene-environmental interaction, not just to provide detailed information about its etiology but also to help in proper genetic counseling Also, further studies will be beneficial to develop preventive measures and therapies
Acknowledgments
We acknowledge the contribution of Rana Salman Anjum for his valuable insight about protein structure analysis and Dr Iahtisham ul Haq for his guidance
Funding disclosure
This study was funded by the Kauser Abdulla Malik School of Life Sciences, Forman Christian College (A Chartered University) Lahore, Pakistan
REFERENCES
1 Cai H, Qing X, Niringiyumukiza JD, et al CFTR variants and renal abnormalities in males with congenital unilateral absence of the vas deferens (CUAVD): a systematic review and meta-analysis of observational studies Genet Med 2019; 21:826-36
2 Halder A, Pandey D CFTR gene variants in Indian congenital bilateral absence of vas deferens & its relevance in genetic counselling Indian J Med Res 2020; 152:535-7
3 Cai Z, Li H Congenital bilateral absence of the vas deferens Front Genet 2022; 13:775123
4 Ferlin A, Dipresa S, Delbarba A, et al Contemporary geneticsbased diagnostics of male infertility Expert Rev Mol Diagn 2019; 19:623-33
5 Daudin M, Bieth E, Bujan L, et al Congenital bilateral absence of the vas deferens: clinical characteristics, biological parameters, cystic fibrosis transmembrane conductance regulator gene mutations, and implications for genetic counseling Fertil Steril 2000; 74:1164-74
6 Mieusset R, Bieth E, Daudin M, et al Male partners of infertile couples with congenital unilateral absence of the vas deferens are mainly non-azoospermic Andrology 2020; 8:645-53
7 Bieth E, Hamdi SM, Mieusset R Genetics of the congenital absence of the vas deferens Hum Genet 2021; 140:59-76
8 Casals T, Bassas L, Egozcue S, et al Heterogeneity for mutations in the CFTR gene and clinical correlations in patients with congenital absence of the vas deferens Hum Reprod 2000; 15:1476-83
9 Akinsal EC, Baydilli N, Dogan ME, Ekmekcioglu O Comorbidity of the congenital absence of the vas deferens Andrologia 2018; 50:e12994
10 Li C-Y, Jiang L-Y, Chen W-Y, et al CFTR is essential for sperm fertilizing capacity and is correlated with sperm quality in humans Human reproduction 2010; 25:317-27
11 Gaillard DA, Carre-Pigeon F, Lallemand A Normal vas deferens in fetuses with cystic fibrosis J Urol 1997; 158:1549-52
12 Hwang TC, Yeh JT, Zhang J, et al Structural mechanisms of CFTR function and dysfunction J Gen Physiol 2018; 150:539-70
13 Shishido H, Yoon JS, Yang Z, Skach WR CFTR trafficking mutations disrupt cotranslational protein folding by targeting biosynthetic intermediates Nat Commun 2020; 11:4258
14 Morris-Rosendahl DJ, Edwards M, McDonnell MJ, et al Wholegene sequencing of CFTR reveals a high prevalence of the intronic variant c 3874-4522A>G in cystic fibrosis Am J Respir Crit Care Med 2020; 201:1438-41
15 Indika NLR, Vidanapathirana DM, Dilanthi HW, et al Phenotypic spectrum and genetic heterogeneity of cystic fibrosis in Sri Lanka BMC Med Genet 2019; 20:89
16 Ferlin A, Stuppia L Diagnostics of CFTR-negative patients with congenital bilateral absence of vas deferens: which mutations are of most interest? Expert Rev Mol Diagn 2020; 20:265-7
17 Gupta N, Sarkar S, Mehta P, et al Polymorphisms in the HSF2, LRRC6, MEIG1 and PTIP genes correlate with sperm motility in idiopathic infertility Andrologia 2022; 54:e14517
18 Ashkenazy H, Abadi S, Martz E, et al ConSurf 2016: an
K Bakhat, I Mateen, H Saif, et al
improved methodology to estimate and visualize evolutionary conservation in macromolecules Nucleic Acids Res 2016; 44:W344-50
19 Venselaar H, Te Beek TA, Kuipers RK, et al Protein structure analysis of mutations causing inheritable diseases An e-Science approach with life scientist friendly interfaces BMC Bioinformatics 2010; 11:548
20 Giordano SH Breast Cancer in Men N Engl J Med 2018; 378:2311-20
21 Flanagan SE, Patch AM, Ellard S Using SIFT and PolyPhen to predict loss-of-function and gain-of-function mutations Genet Test Mol Biomarkers 2010; 14:533-7
22 Soegaard M, Kjaer SK, Cox M, et al BRCA1 and BRCA2 mutation prevalence and clinical characteristics of a population-based series of ovarian cancer cases from Denmark Clin Cancer Res 2008; 14:3761-7
23 Adzhubei I, Jordan DM, Sunyaev SR Predicting functional effect of human missense mutations using PolyPhen-2 Curr Protoc Hum Genet 2013; Chapter 7:Unit7 20
24 Pulumati A, Pulumati A, Dwarakanath BS, et al Technological advancements in cancer diagnostics: Improvements and limitations Cancer Rep (Hoboken) 2023; 6:e1764
25 Pires DE, Ascher DB, Blundell TL mCSM: predicting the effects of mutations in proteins using graph-based signatures Bioinformatics 2014; 30:335-42
26 Lewis HA, Zhao X, Wang C, et al Impact of the deltaF508 mutation in first nucleotide-binding domain of human cystic fibrosis transmembrane conductance regulator on domain folding and structure J Biol Chem 2005; 280:1346-53
Correspondence
Khush Bakhat khushbkht@gmail com
Kanwal Anwar kanwalanwar14@gmail com
Sadaf Sarfraz sadafsarfraz 40@gmail com
Sheza Javaid shezajavaid930@gmail com
Adnan Arshad adnanarshad@fccollege edu pk
KAM School of Life Science, Forman Christian College, (A Chartered University), Lahore, Pakistan
Muhammad Mustafa (Corresponding Author) muhammadmustafa@fccollege edu pk
KAM School of Life Science, S346 Armacost Science Building, Ferozepur Road, Lahore 54600, Pakistan
Irsa Mateen irsamateen biochem@mul edu pk School of Biochemistry, Minhaj University Lahore, Lahore, Pakistan
Hina Saif
hina saif@deaht uol edu pk
Department of Emerging Allied Health Technologies, University of Lahore, Pakistan
Khaleeq-ur-Rehman khaleeqr@hotmail com
Department of Urology, Fatima Memorial Hospital College of Medicine & Dentistry, Lahore, Pakistan
Conflict of interest: The authors declare no potential conflict of interest
27 Ehrhardt A, Chung WJ, Pyle LC, et al Channel gating regulation by the cystic fibrosis transmembrane conductance regulator (CFTR) first cytosolic loop J Biol Chem 2016; 291:1854-65
28 Uppaluri L, England S, Scanlin T Clinical evidence that V456A is a cystic fibrosis causing mutation in South Asians Journal of Cystic Fibrosis 2012; 11:312-5
29 Ziedalski TM, Kao PN, Henig NR, et al Prospective analysis of cystic fibrosis transmembrane regulator mutations in adults with bronchiectasis or pulmonary nontuberculous mycobacterial infection Chest 2006; 130:995-1002
30 McCormick J, Green MW, Mehta G, et al Demographics of the UK cystic fibrosis population: implications for neonatal screening Eur J Hum Genet 2002; 10:583-90
31 Tsui LC, Dorfman R The cystic fibrosis gene: a molecular genetic perspective Cold Spring Harb Perspect Med 2013; 3:a009472
32 Lukacs GL, Verkman AS CFTR: folding, misfolding and correcting the DeltaF508 conformational defect Trends Mol Med 2012; 18:81-91
33 Veit G, Avramescu RG, Chiang AN, et al From CFTR biology toward combinatorial pharmacotherapy: expanded classification of cystic fibrosis mutations Mol Biol Cell 2016; 27:424-33
34 Lakshminarayan R, Phillips BP, Binnian IL, et al Pre-emptive quality control of a misfolded membrane protein by ribosome-driven effects Curr Biol 2020; 30:854-64 e5
35 Ikuma M, Welsh MJ Regulation of CFTR Cl- channel gating by ATP binding and hydrolysis Proc Natl Acad Sci USA 2000; 97:8675-80
CFTR Exon 10 deleterious mutations in patients with congenital bilateral absence of vas deferens in a cohort of Pakistani patients
Khush Bakhat 1 , Irsa Mateen 2 , Hina Saif 3 , Kanwal Anwar 1 , Sadaf Sarfraz 1 , Sheza Javaid 1 , Khaleeq-ur-Rehman 4 , Adnan Arshad 1 , Muhammad Mustafa 1
1 KAM School of Life Science, Forman Christian College, (A Chartered University), Lahore, Pakistan;
2 School of Biochemistry, Minhaj University Lahore, Lahore, Pakistan;
3 Department of Emerging Allied Health Technologies, University of Lahore, Pakistan;
4 Department of Urology, Fatima Memorial Hospital College of Medicine & Dentistry, Lahore, Pakistan
Table S1.
Sequences of primers used for the PCR amplification, amplicon size along with its position on human genome
Sr. # Primer
Table S2
Identified mutations in CFTR-Exon10
Figure S1
Agarose gel electrophoresis of DNA products: (a) Extracted genomic DNA from selected patients resolved using 1% agarose (b) Validation of 469bp PCR products amplified from promoter region of CFTR (PR-CFTR). (c) Validation of 393bp PCR products amplified from Exon 10 of CFTR (EX10-CFTR)
Figure S2. Sequence alignment using BioEdit of all the processed samples. Red arrows indicate position of V456A mutation.
Archivio Italiano di Urologia e Andrologia 2024; 96(3):12464
K Bakhat, I Mateen, H Saif, et al
Figure S3
Sequence alignment using BioEdit of all the selected samples Red arrows indicate position of V456A mutation
Figure S4
Structure of the CFTR protein (PDB ID-6O1V) is displayed a) The orthoscopic view of CFTR protein b) The functional site in Exon 10 is shown in cyan c) The selected region of Exon 10 and identified mutations (V456A, K464E, and G437G) are represented as sticks d) Mutation V456A e) Mutation K464E f) Mutation G437G Each mutation is labeled with the corresponding amino acid change and highlights the spatial arrangement of critical regions in the protein using PyMol software.
Archivio Italiano di Urologia e Andrologia 2024; 96(3):12464
K Bakhat, I Mateen, H Saif, et al
Figure S5. ConSurf analysis
Archivio Italiano di Urologia e Andrologia 2024; 96(3):12464
ORIGINAL PAPER
Kidney transplantation
restores sex hormone profile and improves sexual function in ESRD patients with erectile dysfunction
Hany M El Hennawy 1 , Omar Safar 2 , Abdullah S Al Faifi 1 , Osama Shalkamy 2, 3 , Mahmoud Z. El Madawie 2 , Saad Thamer 2 , Muath Almurayyi 2 , Abdullah Mohammed Alqarni 4 , Sami Saleh Amri 4 , Ali Abdullah Hawan 4 , Adel Elatreisy 3, 5
1 Surgery Department, Section of Transplantation, Armed Forces Hospitals Southern Region, Khamis Mushayte, 101, Saudi Arabia;
5 Urology Department, King Fahd Armed Forces Hospital, Jeddah, Saudi Arabia
Summary
Background: Erectile dysfunction (ED) and sex hormone profile disturbances are common in ESRD patients Objective: To assess the effect of kidney transplant (KT) and Hemodialysis/peritoneal dialysis (HD/PD) on the serum sex hormone profile and sexual functions in ESRD patients with ED Patients and methods: A single-center, nonconcurrent cohort study included a hundred ESRD patients with ED, on regular HD/PD (group A, n = 50) and after KT (group B, n = 50) at Armed Forces Hospitals Southern Region, KSA
Results: the mean age of patients was 47 3 ± 7 01 and 56 8 ± 9 6 years in groups A and B, respectively The cohorts were comparable regarding patient demographics, apart from a higher incidence of comorbidities in group B After KT the mean testosterone level was higher in Group B (13 64 ± 3 21 nmol/L Vs 10.26 ± 3.26 nmol/L, p < 0.001). Similarly, LH and prolactin levels were lower in group B than in group A (p < 0 05)
As regards sexual function, ED was reported in 92% of patients in group A compared to 42% in group B (p < 0 001) In groups A and B, mild ED was found in 48% and 14% of patients, while moderate ED was found in 16% and 8%, respectively The mean total IIEF-15 score was 36.42 ± 9.33 and 43.87 ± 9.146 in groups A and B, respectively (p = 0 0001) Sexual desire and orgasm were significantly better in Group B.
Conclusions: Our study showed that kidney transplantation could improve erectile function and restore normal sex hormone levels in ESRD male patients with ED, with better outcomes compared to HD/PD.
KEY WORDS: Sex hormones profile; Erectile dysfunction; Kidney transplantation
Submitted 27 April 2024; Accepted 13 June 2024
INTRODUCTION
Hormonal disturbances such as luteinizing hormone (LH), follicle-stimulating hormone (FSH), and prolactin increase, and decreased testosterone levels are associated with Endstage renal disease (ESRD) (1-3) These hormonal changes may lead to sexual dysfunction, especially disorder in sexual arousal (4) In addition, low testosterone levels
have been associated with an increased risk of morbidity and mortality in males with ESRD (5, 6)
Kidney transplantation (KT) has been reported to improve s
However, there are few studies concerning serum pituitary-gonadal hormones and sexual dysfunction during dialysis and post-KT in Saudi populations
This study aimed to evaluate sex hormonal profile and sexual function status in patients with erectile dysfunction (ED) after two treatment modalities for ESRD, including KT and peritoneal/hemodialysis (PD/HD) in Southern Saudi Arabia
PATIENTS AND METHODS
A non-concurrent cohort study included ESRD patients associated with ED after two treatment modalities, including KT and peritoneal/hemodialysis (PD/HD) The study was conducted at the Armed Forces Hospitals Southern Region, KSA, from September 2017 to January 2023 The local institutional ethical committee approved the protocol, and all enrolled patients signed an informed consent form
Inclusion criteria
The study included all married male patients with ED associated with ESRD aged 18-60; in group A, 40 and 10 patients were on HD and PD, respectively In group B, all patients underwent KT between September 2017 and September 2023 and had stable graft function
Exclusion criteria
Primary hypogonadism, hemochromatosis, history of cancer treatment (chemotherapy and radiotherapy), pituitary tumors, hypopituitarism of any etiology, and inflammatory diseases such as tuberculosis and sarcoidosis
Moreover, patients having second KT, rejection within three months after transplantation, unstable postoperative graft function with serum creatinine over 20 mg/L, and sirolimus as part of the immunosuppressive regimen
In addition, patients receiving medication or herbal compounds to restore erectile function or underwent testosterone replacement therapy
During the pre-kidney transplant (KT) evaluation, 50 patients presenting with ED were selected from the urology clinic (Group A) In comparison, an additional 50 patients with ED were chosen from the dialysis unit (Group B) based on predefined inclusion and exclusion criteria
In all transplanted patients, the kidney graft was placed extraperitoneal in the right/left iliac fossa, the renal artery was anastomosed to the common or external iliac artery, and the vein was anastomosed to the common or external iliac vein The ureter was anastomosed to the recipient’s bladder using the Lich-Gregoire technique over a doubleJ ureteric stent We usually remove the ureteric stent after six weeks Immunosuppression for all patients consisted of a triple regimen including tacrolimus, mycophenolate mofetil or mycophenolic acid, and prednisolone
All patients were subjected to a complete medical history through medical examination and routine laboratory investigation In addition, gonadal hormone levels (LH, F S H , f r e e T e s t o s t e r o n e , p r o l a c t i n [ P R L ] ) a n
International Index of Erectile Function (IIEF5-15) questionnaire were assessed pretransplant and 6 months after renal transplantation Major drugs causing ED, such as beta-blockers, alpha-blockers, spironolactone, and thiazide diuretics, were withdrawn six months before starting the study
Measurements
Serum pituitary-gonadal hormones were measured as follows: All blood samples were drawn in the morning (7 00-9 00 a m ) after an overnight fast (12 h) Venous blood samples of the patients with ED were collected during dialysis and 1-2 and 3-4 months postoperatively, respectively Serum prolactin (PRL), follicle-stimulating hormone (FSH), LH, and testosterone levels were measured immediately b y e l e c t r o c h e m i l u m i n e s c e n c e i m m u n o a s s a y (Elecsys System, Roche Diagnostics GmbH, Mannheim, Germany) according to the manufacturer’s instructions All blood samples were measured in duplicate (11)
Moreover, we reported sexual activity after transplantation, sexual desire, degree of erection, satisfaction with sexual activities, frequency of sexual activities, and IIEF5-15 score for all patients
Comparison between the study groups included patient demographics, sex hormone levels, and sexual function status
Statistical analysis
We analyzed the data using the Statistical Package for Social Science (SPSS) software, version 29 (SPSS Inc , Chicago, IL) We presented the numeric variables as a mean and standard deviation, while categorical variables were presented as a frequency and percentage We tested the association between nominal variables using the chi-square test At the same time, the Student’s t-test was applied to define the difference between the means of contin-
uous variables for different groups We used the MannWhitney U test to compare the ordinal variables in two groups A paired-sample t-test was used to detect the significance level between pre-transplant and post-transplant values
RESULTS
Group A included 50 patients with ED on HD/PD, and Group B included 50 patients with ED who underwent living-related donor KT
The cohorts were comparable in terms of patient demographics, including smoking history, duration of peritoneal/hemodialysis, and body mass index Nevertheless, the prevalence of comorbidities, including diabetes mellitus, hypertension, ischemic heart disease, and dyslipidemia, was significantly higher in group B, as shown in Table 1
T h e m e d i a n d u r a t i o n o f p e r i t o n e a l / h e
Group A was 4 years, while the median duration of hemodialysis before KT in Group B was 2 years, with an average of (4 and 3 years), in Groups A and B, respectively Table 1
Table 2 displays the serum sex hormone levels for the study groups at 6-month follow up after KT In group A, FSH, Prolactin, and LH levels were significantly higher, and serum testosterone levels were significantly lower than average range values The mean testosterone level was 13 64 ± 3 21 nmol/L in group B compared to 10 26 ± 3 26 nmol/L in group A with a statistically significant difference (p = 0 0001) Similarly, LH and prolactin lev-
Table 1
Demographic data of the study groups
Parameter
(N)
H M El Hennawy, O Safar, A S Al Faifi, O Shalkamy, et al
Table 2. Comparison in Sex Hormones serum levels between the study groups.
Ser um levels of sex hor mones
Group A Group B p-value
Mean ± SD (Dialysis patients = 50) (KT patients, n = 50)
Before Kidney transplant
6 months After Kidney transplant
Table 3. Degree of erectile dysfunction in the study groups
Ser um
No
Mild
Mild
Moderate
Table 4. The IIEF-15 score in transplant group before & after transplant. The
IIEF 6-8 (intercourse satisfaction)
els were lower in group B than in group A (p < 0 05)
There was no significant difference in the FSH levels, as shown in Table 2
As regards sexual function, ED was reported in 92 % of patients in group A compared to 42% in group B (p < 0 001) In groups A and B, mild ED was found in 48% and 14% of patients, while moderate ED was found in 16% and 8%, respectively, as detailed in Table 3
In group A, the mean IIEF5-15 score was 18 4/30 ± 5 4 (range, 7-30), and the mean total IIEF-15 score was 46 8/75 ± 12 7 (range, 19-75) In group B, one year after successful KT, the mean IIEF5-15 score was significantly higher than group A; it was 22 3 ± 5 7 (p < 001) Similarly, the mean total IIEF-15 score was 55 5 ±13 (p < 001), as depicted in Table 4
Sexual desire and orgasm were significantly better in Group B compared to Group A; similarly, sexual intercourse satisfaction and overall patient sexual satisfaction were significantly higher in Group B, as demonstrated in Table 4
In group B, patients who had improved erectile function post-transplant (n = 34), mean serum testosterone level increased by 48% compared with an 18% increase in patients who reported no change in erectile function (n = 16) (p = 0 001)
DISCUSSION
Erectile dysfunction is defined as the persistent incapability to attain or maintain a penile erection sufficient for satisfactory sexual activity In endstage renal disease, incidence is 50-70% (2) Significant hormonal changes, such as LH, FSH, and prolactin elevation, as well as declines of testosterone and anti-Müllerian hormone (AMH) levels, are the most prominent effects of a decrease in kidney function levels (3, 8) Likewise, our study found similar changes in sex hormone levels in dialysis patients (Table 3)
Total testosterone was inversely associated with ED after adjusting for SHBG Men with both low free testosterone and high SHBG had the highest ED risk (12-14) In addition, high testosterone levels independently predicted a decreased risk of ED in young men (12)
Moreover, the duration of dialysis was more than fifty months, and the FSH level was higher in subjects with longer period of dialysis than that in those dialyzed for a shorter period or not dialyzed (15)
Hyperprolactinemia commonly occurs in CKD, with a prevalence of 30-65% (16) due to declines in excretion and to increased synthesis (17) Clinical features may include ED, decreased libido, infertility, gynecomastia, and reduced skeletal mass (18) cardiovascular events in men with ED are associated with elevated plasma prolactin levels (17, 18)
In addition, the impairment of testicular function seen in advanced uremia is not reversible by maintenance hemodialysis (19) Several studies have demonstrated restoration of pituitary-gonadal axis dysfunction and improved hormonal profile, clinical sexual profile, and fertility after KT (11, 20, 21) It was found that pituitary-gonadal function was nearly restored to the normal range in most recipients about four months postKT (3, 12) Similarly, in our study, normal sex hormone levels were restored within six months post-KT Our study reported that serum testosterone levels were higher in the post-KT group in association with lower plasma prolactin and LH levels There was no noticeable difference in plasma FSH levels between the two groups These results are comparable to the findings of Rahman et al (22) In agreement with several studies (23), during the serial baseline and follow-up assessments, we discovered a significant increase in testosterone levels in the post-KT (p < 0 008) Furthermore, serum testosterone levels were restored to the normal range 3-4 months post-KT in male recipients Consequently, sexual activities and IIEF-15 scores improved markedly post-KT (11, 22) Similarly, our study restored total testosterone levels within six months after KT In our study, we found that patients
with an increase in the IIEF score post-KT showed a rise in mean testosterone levels by 48% compared with an 18% increase in patients with a decrease in the IIEF score post-KT (P = 0 366) This corresponds to an increase in potency During the serial baseline and follow-up assessments, we discovered a significant decrease in prolactin levels in the post-KT group (p 0 006) compared with the other group Similarly, in a study by Reinhardt et al , they reported that prolactin levels fell immediately post-KT and were constant until the end of follow-up (10) Our findings contradicted those of Sikora-Grabka et al (24), who found that both LH and FSH levels decreased significantly during the observation period Successful KT could improve gonadal function, but immunosuppressive medications could also impair it It remains controversial whether KT could improve gonadal, sexual, and reproductive functions, especially in the long follow-up (11) Glucocorticoids affect gonadal function at several levels in the hypothalamic-pituitary-gonadal axis: 1) decreasing the release and synthesis of GnRH by the hypothalamus; 2) decreasing the release and synthesis of LH and FSH by the pituitary gland; 3) modulating of steroidogenesis and/or gametogenesis directly by the testis/ovary (25)
Furthermore, several studies found that plasma testosterone levels were lower in FSH and LH in sirolimustreated recipients than in non-sirolimus-treated controls, although the two groups showed no significant difference in serum prolactin levels in another study (21, 26, 27) Several studies show post-KT recipients’ improvement in the IIEF score (28-30) The impact of KT on ED is controversial Many studies show successful KT may play an essential role in ED improvement (23), (22), which aligns with the current study's findings In our study, ED was reported in 42 % of patients after KT compared to 92 % in patients on regular HD/PD Sexual desire and orgasm were significantly better in post-KT patients
Furthermore, the mean total IIEF-15 score was significantly higher in the post-KT group (p < 001)
Nevertheless, other studies have suggested that ED may persist in 20%-50% of patients (31, 32) Alternatively, it may worsen in patients younger than 45 years post-KT but is unaffected in patients older than 45 years (33) The study has limitations due to its small sample size, singlecenter nature, and retrospective design with data recall bias Future research could consider a prospective randomized trial
CONCLUSIONS
Our study showed that kidney transplantation could improve erectile function and restore normal sex hormone levels in ESRD male patients with ED We demonstrated a significantly higher serum testosterone level and lower levels of luteinizing hormone and prolactin after renal transplantation compared to regular HD/PD
REFERENCES
1 Anantharaman P, Schmidt RJ Sexual function in chronic kidney disease Adv Chronic Kidney Dis 2007; 14:119-25
2 Bailie GR, Elder SJ, Mason NA, et al Sexual dysfunction in dialysis patients treated with antihypertensive or antidepressive medica-
tions: results from the DOPPS Nephrol Dial Transplant 2007; 22:1163-70
3 Eckersten D, Giwercman A, Pihlsgård M, et al Impact of Kidney Transplantation on Reproductive Hormone Levels in Males: A Longitudinal Study Nephron 2018; 138:192-201
4 Anastasiadis AG, Davis AR, Salomon L, et al Hormonal factors in female sexual dysfunction Curr Opin Urol 2002; 12:503-7
5 E l s a f t y M E , H a s a n F H , R a s h e d A M E f f e c t o f R e n a l Transplantation on Gonadal Hormones in Male Patients with End Stage Renal Disease Al-Azhar International Medical Journal 2022; 3:82-6
6 Bello AK, Stenvinkel P, Lin M, et al Serum testosterone levels and clinical outcomes in male hemodialysis patients Am J Kidney Dis 2014; 63:268-75
7 Procci WR, Goldstein DA, Adelstein J, Massry SG Sexual dysfunction in the male patient with uremia: a reappraisal Kidney Int 1981; 19:317-23
8 Eckersten D, Giwercman A, Christensson A Male patients with terminal renal failure exhibit low serum levels of antimüllerian hormone Asian J Androl 2015; 17:149-53
9 Akbari F, Alavi M, Esteghamati A, et al Effect of renal transplantation on sperm quality and sex hormone levels BJU Int 2003; 92:281-3
10 Reinhardt W, Kübber H, Dolff S, et al Rapid recovery of hypogonadism in male patients with end stage renal disease after renal transplantation Endocrine 2018; 60:159-66
11 Wang G chun, Zheng J hua, Xu L gen, et al Measurements of Serum Pituitary-Gonadal Hormones and Investigation of Sexual and Reproductive Functions in Kidney Transplant Recipients Int J Nephrol 2010; 2010:1-6
12 Luo Y, Zhang H, Liao M, et al Sex Hormones Predict the I n c i d e n c e o f E r e c t i l e D y s f u n c t i o n : F r o m a P o p u l a t i o n - B a s e d Prospective Cohort Study (FAMHES) J Sex Med 2015; 12:1165-74
13 Liao M, Huang X, Gao Y, et al Testosterone is associated with erectile dysfunction: a cross-sectional study in Chinese men PLoS One 2012; 7:e39234
14 Antonucci M, Palermo G, Recupero SM, et al Male sexual dysfunction in patients with chronic end-stage renal insufficiency and in renal transplant recipients Arch Ital Urol Androl 2016; 87:299
15 Starzyk J, Grzeszczak W, Kowalski D Effect of many years of hemodialysis therapy on FSH secretion induced by luliberin in men with chronic renal failure Wiad Lek 1993; 46:286-91
16 Yavuz D, Topçu G, Özener Ç, et al Macroprolactin does not contribute to elevated levels of prolactin in patients on renal replacement therapy Clin Endocrinol (Oxf) 2005; 63:520-4
17 Carrero JJ, Kyriazis J, Sonmez A, et al Prolactin Levels, Endothelial Dysfunction, and the Risk of Cardiovascular Events and Mortality in Patients with CKD Clinical Journal of the American Society of Nephrology 2012; 7:207-15
18 Corona G, Rastrelli G, Boddi V, et al Prolactin levels independently predict major cardiovascular events in patients with erectile dysfunction Int J Androl 2011; 34:217-24
19 Prem AR, Punekar SV, Kalpana M, et al Male reproductive function in uraemia: efficacy of haemodialysis and renal transplantation Br J Urol 1996; 78:635-8
20 Pietrzak B, Cyganek A, Jabiry-Zieniewicz Z, et al Function of the ovaries in female kidney transplant recipients Transplant Proc 2006; 38:180-3
H M El Hennawy, O Safar, A S Al Faifi, O Shalkamy, et al
21 Fritsche L, Budde K, Dragun D, et al Testosterone concentrations and sirolimus in male renal transplant patients Am J Transplant 2004; 4:130-1
22 Rahman IA, Rasyid N, Birowo P, Atmoko W Effects of renal transplantation on erectile dysfunction: a systematic review and meta-analysis Int J Impot Res 2022; 34:456-66
23 Kang J, Tian J, Lu Y, et al Erectile function after kidney transplantation: a meta-analysis Transl Androl Urol 2020; 9:1967-79
24 Sikora-Grabka E, Adamczak M, Kuczera P, Wiecek A Serum sex hormones concentrations in young women in the early period after successful kidney transplantation Endokrynol Pol 2018; 69:150-5
25 Whirledge S, Cidlowski JA Glucocorticoids, stress, and fertility Minerva Endocrinol 2010; 35:109-25
26 Huyghe E, Zairi A, Nohra J, et al Gonadal impact of target of rapamycin inhibitors (sirolimus and everolimus) in male patients: an overview Transpl Int 2007; 20:305-11
27 Tondolo V, Citterio F, Panocchia N, et al Gonadal function and immunosuppressive therapy after renal transplantation Transplant Proc 2005; 37:1915-7
28 Teng LC, Wang CX, Chen L Improved erectile function and sex hormone profiles in male Chinese recipients of kidney transplantation Clin Transplant 2011; 25:265-9
29 Nassir A Sexual Function in Male Patients Undergoing Treatment for Renal Failure: A Prospective View J Sex Med 2009; 6:3407-14
30 Pourmand G, Emamzadeh A, Moosavi S, et al Does Renal Transplantation Improve Erectile Dysfunction in Hemodialysed Patients? What is the Role of Associated Factors? Transplant Proc 2007; 39:1029-32
31 Rebollo P, Ortega F, Valdés C, et al Factors associated with erectile dysfunction in male kidney transplant recipients Int J Impot Res 2003; 15:433-8
32 Malavaud B, Rostaing L, Rischmann P, et al High prevalence of erectile dysfunction after renal transplantation Transplantation 2000; 69:2121-4
33 Mirone V, Longo N, Fusco F, et al Renal transplantation does not improve erectile function in hemodialysed patients Eur Urol 2009; 56:1047-53
Correspondence
Hany M El Hennawy, MD
hennawyhany@hotmail com
Abdullah S Al Faifi, MD
Surgery Department, Section of Transplantation, Armed Forces Hospitals Southern Region
1 Andrology Study Program, Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia;
2 Department of Biomedical Sciences, Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia;
3 Ferina Mother and Child Hospital, Surabaya, Indonesia;
4 Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia;
5 Department of Biomedical Sciences, Faculty of Medicine, Universitas Padjadjaran, Sumedang, Indonesia
Summary
Background: Modifying the maternal immune system is necessary to facilitate embryo implantation Modifying the immune system can occur in several ways, including maternal exposure to the partner’s seminal plasma Seminal plasma exposure can occur through sexual intercourse To prove this theory, we investigate the effect of sexual intercourse on the chances of successful in vitro fertilization (IVF) in both fresh and frozen embryo transfer (ET) groups in terms of biochemical and clinical pregnancy.
Methods: This is an observational analytical study with a retrospective cohort study design. This study compared biochemical and clinical pregnancy in patient groups who had sexual intercourse with those who did not have sexual intercourse during the IVF process This study involved 132 participants Results: The results of this study reported that there was no significant difference in pregnancy rates between patients who had sex before ET and those who did not have sex before ET. However, patients who experience orgasm during sex show significant rates of biochemical (p = 0.009) and clinical pregnancy (p = 0 027) rates
Conclusions: Sexual intercourse did not show a significant difference between the groups who had sex before ET and those who did not have sex, but the experience of orgasm every time they had sex recently had a positive impact on reproductive health, especially pregnancy.
One of the most commonly used methods to help infertile couples is in vitro fertilization (IVF) IVF is reported to succeed in only 30-40% of cases (1) Several factors influence the success rate of IVF According to Crawford et al, one of the most critical processes for the success of IVF is embryo implantation; even if the quality of the embryo is excellent, implantation will fail if the endometrial receptivity is insufficient (2) Research reports that endometrial receptivity is closely
linked to the maternal immune response The embryo that will implant in the endometrial wall is likened to an allograft in the maternal body This requires a balance of immune responses in the process so as to avoid any form of attack on the embryo (3) The immune response that plays a dominant role in this process is T-reg; the number of dominant T-reg will produce interleukin-10 (IL-10) and tumor growth factor-beta (TGF-ß) and suppress Th-1 so that the levels of interferon-gamma (IFN-γ), interleukin-12 (IL12), interleukin (IL-2), and tumor necrosis factor-beta (TNFα) would become low (3, 4) T-cell regulation and the involved cytokines contribute to the implantation process T-reg cells also suppress the proliferation and function of leukocyte subsets such as CD4 T cells, CD8 T cells, B cells, and natural killer (NK) cells T-reg cells influence the function of dendritic cells (DCs) and macrophages (4, 5) If this does not occur, implantation will become difficult or, in some cases, hemorrhage will occur, leading to embryonic failure (4, 6, 7) Experts argue that modifying the maternal immune system is necessary to facilitate embryo implantation Modifying the immune system can occur in several ways, including maternal exposure to the partner’s seminal plasma Exposure to seminal plasma, such as during intercourse, has been reported to improve embryo implantation (8, 9) This is because seminal plasma contains many biomolecules, such as TGF-ß, that influence the immune system in the endometrium Several studies have investigated the relationship between seminal plasma exposure and pregnancy success rates However, because they used different methods, the embryo transfer (ET) time group (fresh or frozen) was also not uniform, leading to different results (2, 10) In light of the above, we conducted a study to investigate the effect of sexual intercourse on the chances of successful IVF in both fresh and frozen ET groups in terms of biochemical and clinical pregnancy in Indonesia
MATERIALS AND METHODS
Design of the study
This is an observational analytical study with a retrospective
cohort study design This study compared biochemical and clinical pregnancy in patient groups who had sexual intercourse with those who did not have sexual intercourse during the IVF process The study was conducted at Ferina Mother and Child Hospital, Surabaya, from September to November 2022 The study was approved by the ethic committee with approval number: 193/EC/KEPK/FKUA/2022
Sample size and criteria
This study's participants were RSIA Ferina patients who participated in the assisted reproductive technology program as couples who followed the procedure of both fresh ET and frozen ET with blastocyst embryos We excluded patients with the following criteria: 1) high D-dimer, 2) experienced pain (cough, runny nose, fever) during and after the procedure (observation period), 3) non-compliant according to the ovarian stimulation procedure, 4) husband with obstructive azoospermia, and 5) husband with leukospermia semen analysis examination results Participants were included consecutively according to the research selection criteria until the required number of participants was met This study used a test for a difference between two population proportions (11), therefore, by using reference values from previous studies (12), the minimum number of participants in each group was estimated in 45
Procedure
Patients had initially undergone menstrual examination and stimulation until it was declared that the follicles were developing and prepared for ovum pick-up The collected oocytes were then fertilized to obtain embryo(s) The researcher explained the patients who fit the inclusion and exclusion criteria regarding the research procedure Before the patient underwent the embryo transfer procedure, the patients were told they can have sexual intercourse 1-5 days before the ET procedure However, it was the patients’ choice to have sexual intercourse or not The determination of 1-5 days interval before ET was based on previous studies that conducted exposure to seminal plasma after ovum pick-up (OPU), where the distance from OPU to ET procedures was 3-5 days in fresh embryo transfer procedures (13, 14)
After receiving ET, the patients were placed in the oneday care unit The researcher then conducted an interview on the patient regarding the patient's sexual history during 1-5 days before ET, including the frequency and whether she had an orgasm or not We only interviewed the patients who received blastocyte embryo After that, the patients were observed until 11-14 days after ET, and then the beta-hCG test was carried out using the VIDAS® HCG kit using the ELFA (Enzyme Linked Fluorescent Assay) principle Thus, the patient would be declared pregnant if the beta-hCG level is 25 mIU/mL Then 5-6 weeks later, ultrasound monitoring was conducted on patients who had biochemical pregnancy to detect the gestational sac The patient was declared clinically pregnant if gestational sac was positive
Data analysis
The first analysis was univariate; it was conducted to assess the demographic data and the characteristics of the study participants The second analysis was a bivariate
analysis to analyze the association of sexual intercourse and other sexual intercourse parameters with biochemical (beta-hCG) and clinical (gestational sac) pregnancy; the test used was chi-square or Fisher's exact test
RESULTS
The couples interviewed in this study were primary or secondary infertile couples who were undergoing IVF at Ferina Mother and Child Hospital The participants were 132 couples The participants were divided into two groups The first group included 45 couples who had sexual intercourse 1-5 days prior ET, while the second group included the remaining 87 couples who did not have sexual intercourse The characteristics of the participants can be seen in Table 1
Based on Table 2, 9 85% of the participants had sexual intercourse and were declared pregnant, 24 24% had sexual intercourse and were not declared pregnant, 23 48% did not have sexual intercourse and were declared pregnant, and 42 42% did not have sexual intercourse and were not declared pregnant The results of the chi-square test showed p = 0 436, with RR = 0 81 (95% CI 0 46-1 35), which means that there is no significant relationship between intercourse before ET and the success rate of biochemical pregnancy
Table 1.
Characteristics of the participants
Table 2.
Analysis of pregnancy in relation to sexual intercourse before ET
C Pakpahan, A Agustinus, A Sa’adi, et al
In the group who had sexual intercourse 6 82% were d e c l a r e d c l i n i c a l l y p r e g n a n t a n d 2 7 2 7 % w e r e n o t declared pregnant In the group that did not have sexual intercourse 15 91% were declared pregnant and 50% were not declared pregnant The chi-square test obtained a value of p = 0 59, with RR = 0 83 (CI 95% 0 41-1 60) These results indicate that there is no significant relationship between these two variables
In the group who regularly had sexual intercourse (23x/week) and 15 91% were declared pregnant, whereas those who were not declared pregnant were 34 09% In the group who rarely had sexual intercourse (0-1x/week) 17 42% were declared pregnant whereas those who were not declared pregnant were 32 58% The chi-square test results obtained a value of p = 0 59, with RR = 0 91 (CI 95% 0 56-1 48) In the group that regularly had sexual intercourse 12 88% were declared clinically pregnant, and those who were not declared pregnant were 37 12% In comparison, in the group that rarely had sexual intercourse 9 85% was declared pregnant and those who were not declared pregnant were 40 15% The chi-square test results obtained a value of p = 0 406, with RR = 1 30 (CI 95% 0 70-2 46) (Table 2)
In addition, in the group who stated that they always orgasmed every time they had sexual intercourse 22 73% were declared biochemically pregnant and 29 55% were not declared pregnant were 29 55% In comparison, in the group who did not orgasm every time they had sexual intercourse or orgasmed only sometimes, 10 61% were declared biochemically pregnant and 37 12% were not declared biochemically pregnant The chi-square test results obtained a value of p = 0 009, with RR = 1 96 (CI 95% 1 17-3 37) Regarding clinical pregnancy, in the group who stated that they always orgasmed every time they had sexual intercourse 15 91% were declared clinically pregnant and 36 36% were not declared pregnant In the group who did not orgasm every time they had sexual intercourse or orgasmed only sometimes, 6 82% were declared clinically pregnant and 40 91% were not declared pregnant The chi-square test results obtained a value of p = 0 027, with RR = 2 13 (CI 95% 1 09-4 29) (Table 3) We assumed that there is a correlation between orgasm and the probability of pregnancy However, we agree that it could not be explicitly concluded that orgasm is a positive factor for enhancing pregnancy We can only simply argue that orgasm is a condition that indicates that both psychological and social conditions are favourable
DISCUSSION
Our study aimed to compare the effect of sexual intercourse as seminal plasma exposure to the female reproductive system on the success rate of pregnancy, both biochemical and clinical, in women undergoing assisted reproductive technology (ART) programs This recent study divided the participants into two groups The first group was the group who had sexual intercourse 1-5 days before the ET procedure, and the second group was the group who did not have sexual intercourse 1-5 days before ET
In addition, our study also analyzed the frequency/habit of sexual intercourse outside the ART program, the quality of sexual intercourse in the form of achieving orgasm, the type of infertility, and the ET method (fresh or frozen) on pregnancy success (biochemical and clinical)
Our study reported 45 (34 09%) patients had sexual intercourse before ET Some of the reasons patients did not have sex before ET were the fear and anxiety about sexual intercourse that it might be causing IVF program failure The similar phenomenon was also reported by Courbiere et al , which states that 47% of the patients had difficulty having sex during the IVF program, and 44% experienced a decreasing desire to have sex with their partner (15) Marci et al also reported the same finding, stating that couples had experienced sexual disorders even at the beginning of infertility treatment (16)
Another finding in our study is that there was no association between sexual intercourse before ET and both biochemical and clinical pregnancy rate We reported RR = 0 81 (95% CI 0 46-1 35) in biochemical pregnancy and RR = 0 83 (95% CI 0 41-1 60) in clinical pregnancy Similar results were also reported in a study by von Wolff et al (2013) who reported RR = 0 92 (CI 95% 0 63-1 34) in clinical pregnancy (17)
However, a study in China by Sun et al reported different results Sun et al found that sexual intercourse significantly affected pregnancy success in the ART program (p = 0 005 in biochemical pregnancy and p = 0 045 in clinical pregnancy) (18)
So far, the theory that explains how sexual intercourse can affect the chance of pregnancy is the induction of the immune system of the reproductive organs (uterus) in the process of pregnancy (19) Seminal plasma contains immune substances such as TGF-β which is indispensable in the implantation process, as well as other molecules such as PGE2 and DC (4) In addition, sexual intercourse also increases uterine activity such as contractions that have an impact on embryo implantation (20)
However, the different results in our study might be due to the variation of the length of the interval between sexual intercourse and ET, which is not homogeneous Our study established an interval between sexual intercourse and ET of 1-5 days Most participants in this study had sexual intercourse more than 24 hours before ET In fact some studies supporting a significant role of sexual intercourse, reported the most effective interval between sexual intercourse and ET to be 12-24 hours As reported by Sun et al, Aflatoonian et al and Tremellen et al, there were very few patients who consciously had sex 12-24 hours before ET because many patients were worried that sex within this period would cause failure of ET (18, 21, 22) Another possible reason for the non-significant results is
Table 3. Analysis of orgasmic phase in intercourse before ET with pregnancy
the type of ET performed in our patients The results of the study by Sun et al were significant in the group of patients who performed frozen embryo transfer procedures, while in our participants, both frozen and fresh embryo transfer groups were analyzed simultaneously (18)
Furthermore, the study by Sun et al compared couples who had sex and used contraception with couples who did not have sex before ET So, this study was biased regarding whether pregnancy success was due to seminal plasma exposure or other factors
Our study attempted to adjust the effect of the variable of sexual intercourse evaluating both biochemical and clinical pregnancy, although the small sample size could not have maximized this adjustment (18)
In addition, another possible cause of bias is the difficulty to control the factors beforehand, such as the stimulation protocol used in patients, especially in the fresh ET group
Some studies, such as Lan et al , Ou et al , and Youseff et al , reported that long protocol significantly increased IVF success compared to short protocol (23-25)
Psychological aspects may also contribute to the successful outcomes of IVF programs Matthiesen et al reported that there is a significant relationship between stress and the chances of IVF success (26) The same finding was also reported by Saleem et al in the Tunisian population following an IVF program Stress and anxiety were negatively correlated with success rates (27) At the same time, Courbiere et al stated that patients who follow IVF programs are vulnerable to psychosocial burdens that can affect their daily life (15)
Another contributing factor that may affect IVF success is BMI Bashiri, Halper, and Orvieto stated that uncontrolled BMI affects IVF success (28)
In our study, we did not evaluate length of protocol, psychological factors and BMI that could be factors causing the difference in results with other studies
It has been hypothesized that embryo implantation is s t r o n g l y i n fl u e n c e d b y e n d o m e t r i a l r e c e p t i v i t y
Endometrial receptivity depends on immune factors
Also, the balance of immune factors in the endometrial wall itself is influenced by various factors (3) One of the components of immune system, called T-reg cells, is known to be a key factor to successful implantation T-reg cells play a role in regulating equilibrium in the major histocompatibility complex (MHC) mechanism (3)
Exposure to seminal plasma allows the activation of T-reg cells in the female reproductive organs (uterus), thus supporting embryo implantation Another theory states that sexual intercourse is associated with cervicovaginal immune mediators in young female populations (29) Frequent sexual intercourse also causes a decrease in IgA at ovulation compared to infrequent or no intercourse It also affects the expression of Th-2-like cytokine ratios (IFN-γ < IL-4), P-E2 ratios in the luteal phase compared to other phases (30)
Based on this hypothesis, regular or continuous exposure to a partner's seminal plasma might alter the regulation of T-reg cells in the female reproductive organs Thus, the frequency of sexual intercourse might affect the immune status/condition in the uterus There are still very few studies that report about these findings, especially in the ART population group The study of Konishi et al report-
ed that there was a significant relationship between coitus frequency and increased chances of pregnancy However, these results were tested in populations with natural cycles or without the ART program (31) However, the relationship between the two variables seems to be insignificant in this present study This may be due to lack of information related to the frequency of sexual intercourse The information explored in this study was the history of intercourse in the past before the study participant started ART measures
The association of sexual activity up to orgasm with the success rate of the ART program has not been widely studied Our study reported that orgasm had a significant assoc i a t i o n w i
Frequent/always orgasmic partner sexual activity is associated with a healthy and supportive quality of partner life (32), while a healthy and supportive quality of partner life is needed to maintain the mental state of the study patients in undergoing the ART program Levin also states that semen deposition and uterine contractions during orgasm cause mood changes in women (33) In addition, some theories state that orgasm also facilitates the release of hormones, such as oxytocin, that affect emotions in women
Women with a history of orgasm are reported to be happier and avoid stress (34) The result of the study still need further investigation despite it is significant Also, we argue that orgasm is simply a condition that indicates that psychological and social conditions are favorable
The Fertility Society of Australia notes that the mental quality of couples undergoing ART affects pregnancy outcomes (35) This may be the reason why orgasm can affect ART outcomes In addition, several hypotheses state that orgasm can also affect the human immune system Orgasm increases the number of absolute leukocyte sources and natural killer cells in blood vessels However, the levels and changes in the immune system of female reproductive organs have not been reported (36)
We still realized that there are limitations in our study which is an observational study designed with a retrospective cohort The selection of participants to be included in the groups who were sexually active and non-sexually active groups before IVF was voluntary rather than randomized being a disadvantage when compared to similar studies In addition, information about sexual intercourse is often considered private for patients living in Indonesia Consequently, the information shared about sexual life could be biased because patients are not honest about the information provided Beside this, information about their sexual life is still based on recall memory Finally, a result of the study that should be transferred to the patients is that they should not be afraid to have sexual intercourse before embryo transfer, as was previously reported (37), because even if sexual intercourse does not have an apparent positive effect on pregnancy, it is not proven to have a harmful effect and may even have a positive effect on the psychological and relationship welfare of the couple
CONCLUSIONS
The results of our study did show no significant difference between having sex before ET in terms of chemical and
C Pakpahan, A Agustinus, A Sa’adi, et al
clinical pregnancy chances However, reaching orgasm during intercourse in recent sexual life has a positive impact on the couple's life and could also favourably impact on pregnancy probabilities although the significance of this finding still needs further investigation Exposure to seminal plasma through sexual intercourse is not utterly uncorrelated with pregnancy, therefore also this still needs further investigation Nevertheless, from a positive point of view, couples do not need to be afraid of having sex before ET because it does not have a negative effect but provide a better quality of life for couples
ACKNOWLEDGEMENTS
A big thank you to all the doctors (Eva Setijowati, Hamdani Lunardi, Mona Mariana, Sony Iwan Santoso, Reza Mahendra Putra, I Dewa Ayu Agung Shinta Kamaya, Januar Wijaya, Dwimantoro Iman Prilistiyo, Heri Priyanto, Wendy Hudyarisandi) and nurses at the Ferina Hospital who helped a lot during the research process
REFERENCES
1 Nieschlag E, Behre HM, Kliesch S, Nieschlag S Andrology - Male Reproductive Health and Dysfunction, 3rd ed Munster (DE): Springer Cham; 2010
2 Crawford G, Ray A, Gudi A, et al The role of seminal plasma for improved outcomes during in vitro fertilization treatment: review of the literature and meta-analysis Hum Reprod Update 2015; 21:275-84
3 Hyde KJ, Schust DJ Immunologic challenges of human reproduction: an evolving story Fertil Steril 2016; 106:499-510
4 Guerin LR, Prins JR, Robertson SA Regulatory T-cells and immune tolerance in pregnancy: a new target for infertility treatment? Hum Reprod Update 2009; 15:517
5 Shevach EM CD4+ CD25+ suppressor T cells: more questions than answers Nat Rev Immunol 2002; 2:389-400
6 Aluvihare VR, Kallikourdis M, Betz AG Regulatory T cells mediate maternal tolerance to the fetus Nat Immunol 2004; 5:266-71
7 Shima T, Sasaki Y, Itoh M, et al Regulatory T cells are necessary for implantation and maintenance of early pregnancy but not late pregnancy in allogeneic mice J Reprod Immunol 2010; 85:121-9
8 Pandya IJ, Cohen J The leukocytic reaction of the human uterine cervix to spermatozoa Fertil Steril 1985; 43:417-21
9 Sharkey DJ, Tremellen KP, Jasper MJ, et al Seminal fluid induces leukocyte recruitment and cytokine and chemokine mRNA expression in the human cervix after coitus J Immunol 2012; 188:2445-54
10 Saccone G, Di Spiezio Sardo A, Ciardulli A, et al Effectiveness of seminal plasma in in vitro fertilisation treatment: a systematic review and meta-analysis BJOG 2019; 126:220-225
11 Levy PS & Lemeshow S Sampling of Populations: Methods and Applicatons, 4th ed New Jersey (US): John Wiley & Sons; 2018
12 Bellinge BS, Copeland CM, Thomas TD, et al The influence of patient insemination on the implantation rate in an in vitro fertilization and embryo transfer program Fertil Steril 1986; 46:252-6
13 Chicea R, Ispasoiu F, Focsa M Seminal plasma insemination during ovum-pickup--a method to increase pregnancy rate in IVF/ICSI procedure A pilot randomized trial J Assist Reprod Genet 2013; 30:569-74
14 Friedler S, Ben-Ami I, Gidoni Y, et al Effect of seminal plasma application to the vaginal vault in in vitro fertilization or intracytoplasmic sperm injection treatment cycles-a double-blind, placebo-controlled, randomized study J Assist Reprod Genet 2013; 30:907-11
15 Courbiere B, Lacan A, Grynberg M, et al Psychosocial and professional burden of Medically Assisted Reproduction (MAR): Results from a French survey PLoS One 2020; 15:e0238945
16 Marci R, Graziano A, Piva I, et al Procreative sex in infertile couples: the decay of pleasure? Health Qual Life Outcomes 2012; 10:140
17 von Wolff M, Rösner S, Germeyer A, et al Intrauterine instillation of diluted seminal plasma at oocyte pick-up does not increase the IVF pregnancy rate: a double-blind, placebo controlled, randomized study Hum Reprod 2013; 28:3247-52
18 Sun ZG, Hua Yuan L, Ling Cao X Can the act of sexual intercourse before embryo transfer improve IVF treatment outcome? A Randomized Clinical Trial 2020
19 Robertson SA, Sharkey DJ Seminal fluid and fertility in women Fertil Steril 2016; 106:511-9
20 Fanchin R, Righini C, Olivennes F, et al Uterine contractions at the time of embryo transfer alter pregnancy rates after in-vitro fertilization Hum Reprod 1998; 13:1968-74
21 Aflatoonian A, Ghandi S, Tabibnejad N The Effect of Intercourse a r o u n d E m b r y
Reproductive Technology Cycles Int J Fertil Steril 2009; 2:169-72
22 Tremellen KP, Valbuena D, Landeras J, et al The effect of intercourse on pregnancy rates during assisted human reproduction Hum Reprod 2000; 15:2653-8
23 Lan J, Wu Y, Wu Z, et al Ultra-Long GnRH Agonist Protocol During IVF/ICSI Improves Pregnancy Outcomes in Women With Adenomyosis: A Retrospective Cohort Study Front Endocrinol 2021; 12:609771
24 Ou J, Xing W, Li Y, et al Short versus Long GonadotropinReleasing Hormone Analogue Suppression Protocols in IVF/ICSI Cycles in Patients of Various Age Ranges PLoS One 2015; 10:e0133887
25 Youssef H, El Deeb W, Shawky O, et al GnRH agonist long protocol versus short protocol in women 40 years or more undergoing ICSI: a multicenter study Middle East Fertility Society Journal 2008; 13:63-6
26 Matthiesen SMS, Frederiksen Y, Ingerslev HJ, Zachariae R Stress, distress and outcome of assisted reproductive technology (ART): a meta-analysis Hum Reprod [Internet] 2011; 26:2763-76
27 Sallem A, Essoussi H, Mustapha HB, et al Impact of psychological stress on the outcomes of assisted reproduction in Tunisian infertile women Pan Afr Med J 2021; 40:250
28 Bashiri A, Halper KI, Orvieto R Recurrent Implantation Failureupdate overview on etiology, diagnosis, treatment and future directions Reprod Biol Endocrinol 2018; 16:121
29 Hughes SM, Levy CN, Calienes FL, et al Starting to have sexual intercourse is associated with increases in cervicovaginal immune mediators in young women: a prospective study and meta-analysis Elife 2022; 11:e78565
30 Lorenz TK, Demas GE, Heiman JR Interaction of menstrual cycle phase and sexual activity predicts mucosal and systemic humoral immunity in healthy women Physiol Behav 2015; 152:92-8
31 Konishi S, Saotome TT, Shimizu K, et al Coital Frequency and the Probability of Pregnancy in Couples Trying to Conceive Their
C Pakpahan, A Agustinus, A Sa’adi, et al
First Child: A Prospective Cohort Study in Japan Int J Environ Res Public Health 2020; 17:1-11
32 Costa RM, Brody S Women’s relationship quality is associated with specifically penile-vaginal intercourse orgasm and frequency J Sex Marital Ther; 33:319-27
33 Levin RJ The physiology of sexual arousal in the human female: a recreational and procreational synthesis Arch Sex Behav 2002; 31:405-11
34 Magon N, Kalra S The orgasmic history of oxytocin: Love, lust, and labor Indian J Endocrinol Metab 2011; 15 Suppl 3(Suppl3):S156-61
35 Pre-Conception Health Special Interest Group [cited 2024 Feb 7]; Available from: http://yourfertility org au/resource/effects-of-caffeine-alcohol-and-smoking-on-fertility/
36 Haake P, Krueger TH, Goebel MU, et al Effects of sexual arousal on lymphocyte subset circulation and cytokine production in man Neuroimmunomodulation 2004; 11:293-8
37 Pakpahan C, Agustinus A, Sa'adi A, et al Lay understanding and experience of sexual intercourse among couples with infertility undergoing an assisted reproduction technology program: A qualitative study Heliyon 2024; 10:e26879
Correspondence
Cennikon Pakpahan (Corresponding Author) cennikon pakpahan@fk unair ac id
Andrology Study Program, Department of Biomedical Sciences, Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia
Agustinus Agustinus agustinus27@fk unair ac id
Christian Melka Parmanto c melka88@gmail com
Andrology Study Program, Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia
Ashon Sa’adi ashontanti@gmail com
Auvky Hinting auckyh@gmail com
Lia Hinting lia hinting@gmail com
Ferina Mother and Child Hospital, Surabaya, Indonesia
Andri Rezano
andri rezano@unpad ac id
Department of Biomedical Sciences, Faculty of Medicine, Universitas Padjadjaran, Sumedang, Indonesia
Conflict of interest: The authors declare no potential conflict of interest
Surgical management of obstructing ureteral stones during pregnancy: A systematic review of different techniques
Catarina Laranjo-Tinoco 1 , Maria João Oliveira 2 , Ana Sofia Araújo 1 , Andreia Cardoso 1 , Carlos Oliveira 1, 2 , Paulo Mota 1, 2 , João Pimentel Torres 1, 2
1 Hospital de Braga, Urology Department, Braga, Portugal; 2 University of Minho, School of Medicine, Braga, Portugal
Summary
Introduction: Renal colic is the most common non-obstetric cause of abdominal pain during pregnancy and is associated with a higher risk of complications in these women When invasive treatment is required, options are temporary drainage with ureteral stent (JJ) or percutaneous nephrostomy (PCN), or immediate definitive treatment with ureteroscopy (URS) Our goal was to review the safety and efficacy of these procedures in treating urolithiasis during pregnancy
Methods: Adhering to the PRISMA checklist guidelines, we searched PubMed, Embase, and Scopus databases for articles on the efficacy and complications of the three procedures in pregnant women The quality of evidence and risk of bias were evaluated using the Critical Appraisal Skills Programme and the Institute of Health Economics tools
Results: We included 45 articles, totaling 3424 interventions in pregnant women - 2188 URS, 719 JJ, and 517 PCN URS was the most assessed procedure, with stone-free rates comparable to the non-pregnant patients The most frequent complications were lower urinary symptoms and infections independently of the intervention Obstetric complications for all interventions included 167 cases of preterm labor, resulting in 24 premature births No statistically significant differences in post-operative complications were reported between the procedures in the few comparative studies
Conclusions: Despite the absence of high-quality studies, current evidence suggests that URS, JJ, and PCN are all safe and effective during pregnancy As most patients submitted to temporary drainage require a second procedure post-delivery, primary URS appears more efficient Therefore, it is the preferred option unless there are indications for temporary drainage.
Pregnancy induces anatomic, metabolic, and chemical changes in the urinary tract that would predispose pregnant women to stone formation: both uterine extrinsic compression and progesterone’s relaxing effect on ureteral smooth muscle cause physiologic hydronephrosis in 90% of pregnant women, especially on the right side, exacerbat-
ed by an increase in the glomerular filtration rate, which leads to higher urinary calcium and uric acid concentrations However, urolithiasis prevalence is similar in pregnant and non-pregnant women, mostly due to the simultaneous increase in inhibitory factors (such as citrate, magnesium, and glycoproteins) (1) One large cohort study demonstrated an incidence of 0 2% of symptomatic urolithiasis in pregnancy (2)
Nevertheless, renal colic is the most common non-obstetric cause of abdominal pain and subsequent hospitalization during pregnancy, especially in the second and third trimesters (1), and it is associated with a higher risk of complications, such as premature rupture of membranes, spontaneous abortion, preterm labor, and preterm birth (2) Most cases of symptomatic urolithiasis are non-complicated and can be managed conservatively with vigilance, hydration, and analgesia This is successful in 70-80% of cases with spontaneous stone passage (2, 3) Invasive treatment should be considered within a multidisciplinary discussion in cases of persistent pain or vomiting, signs of infection, decline in renal function, obstructive stones in solitary kidney, bilateral obstruction, or obstetric complications (4) The different available procedures are temporary drainage with a percutaneous nephrostomy (PCN) or a double-J stent insertion (JJ), or definite treatment with ureteroscopy (URS) (4)
I f f e v e r o r o t h e r s i g n s o f i n f e c t i o n a r e p r e s e n t , ureteroscopy is contraindicated and urgent temporary drainage is required Temporary drainage is also usually preferred in cases of large stone burden, complex anatomy, bilateral stone disease, obstetric complications, or presentation in the first trimester or near full term Ureteral stenting or percutaneous nephrostomy placement are usually fast procedures, require minimal anesthesia, and can be radiation-free, but they require a second definitive intervention postpartum to treat the stone, often need multiple catheter exchanges during pregnancy, and are poorly tolerated (4) Consequently, definitive treatment with ureteroscopy started becoming the firstline procedure, when possible
Our main objective with this systematic review is to evaluate the safety and efficacy of ureteroscopy, double-J stent insertion, and percutaneous nephrostomy in the treatment of renal colic during pregnancy
Laranjo-Tinoco, M J Oliveira, A S Araújo, et al
METHODS
We elaborated the present review according to the Preferred Reporting Items for Systematic Reviews and Metaanalyses (PRISMA) 2020 checklist (5)
Search strategy
The primary search was conducted using the PubMed, EMBASE, and Scopus databases, for articles published before November 2021 Our query was “(pregnancy OR pregnant) AND (renal colic OR urolithiasis) AND (nephrostomy) AND (ureteral stent OR JJ) AND (ureteroscopy) AND (drainage OR urinary diversion OR urinary catheterization)” Additionally, we used the “snowball” method, tracking references and citations of found articles to identify additional relevant studies The search results were organized using EndNote with identification and removal of duplicates Two independent researchers (CLT and MJO) screened the titles and abstracts of the search results against the inclusion criteria Subsequently, the same two researchers analyzed full-text reports for eligibility Any disagreement was solved through discussion and consensus A third reviewer (JPT) resolved any disagreement during report selection and did the final review
Eligibility criteria
Our PICOS definition was: Participants: Pregnant women with urolithiasis; Intervention: Ureteroscopy (or double-J stent insertion or percutaneous nephrostomy placement
when no ureteroscopy was performed); Comparators: Double-J stent insertion or percutaneous nephrostomy placement or conservative treatment; Outcomes: Procedure efficacy or intervention success, perioperative and postoperative complications, and obstetric complications; Study design: This systematic review included randomized controlled trials, cohort studies (prospective or retrospective), case-control studies, and case series
The articles were considered when they fulfilled the following inclusion criteria: pregnant women; treatment, including ureteroscopy, ureteral stent insertion, and/or nephrostomy; English language
The exclusion criteria were: non-pregnant; other types of treatment; other languages; grey literature; full text not available; reviews and case reports; animal studies
Data extraction and management
The following data was collected from each study: author’s names; country and year of publication; study duration, design, and objective; sample characteristics (sample number, mean age, mean gestational age or trimester); inclusion and exclusion criteria; type of treatment; intervention success; perioperative, postoperative, and obstetric complications; imaging considerations; relevant conclusion and limitations
Critical appraisal of included studies
The quality assessment and risk of bias were carried out by
Figure 1. PRISMA methodology flowchart for article selection.
C
Figure 3
Institute of health economics quality appraisal checklist for case series studies.
Figure 2
Critical appraisal skills programme checklist for cohort studies.
1) Did the study address a clearly focused issue?
2) Was the cohort recruited in an acceptable way?
3) Was the exposure accurately measured to minimize bias? 4) Was the outcome accurately measured to minimize bias? 5a) Have the authors identified allimportant confounding factors?
5b) Have they taken account of the confounding factors in the design and/or analysis?
6a) Was the follow-up of subjects complete enough?
6b) Was the follow-up of subjects long enough?
7) What are the results of this study? 8) How precise are the results? 9) Do you believe the results?
10) Can the results be applied to the local population?
11) Do the results of this study fit with other available evidence? 12) What are the implications of this study for practice?
Green circles (+) represent low risk of bias, red circles (-) represent high risk of bias; yellow circles (?) indicate unclear risk of bias
two independent reviewers using the Critical Appraisal Skills Programme (CASP) checklist (6) for cohort studies and the Institute of Health Economics checklist (7) for case series studies Any disagreement was solved by discussion and consensus or by the involvement of the third reviewer
EVIDENCE SYNTHESIS
Study selection
The flowchart in Figure 1 describes in detail the implemented search method
Critical appraisal
The quality assessment of the studies included in this review is presented in Figure 2 and Figure 3
Within the cohort studies, the most failed criteria were related to the recruitment of the cohort in an acceptable way, since some articles did not mention the exclusion criteria (3, 8-33) and to the identification and the consideration of confounding factors in the design Within the case series, all articles failed to meet the follow-
1) Was the hypothesis/aim/objective of the study clearly stated? 2) Was the study conducted prospectively? 3) Were the cases collected in more than one center? 4) Were patients recruited consecutively? 5) Were the characteristics of the patients included in the study described? 6) Were the eligibility criteria for entry the study clearly stated? 7) Did patients enter the study at a similar point in the disease? 8) Was the intervention of interest clearly described? 9) Were additional interventions (co-intervention) clearly described? 10) Were relevant outcome measures established a priori? 11) Were outcomes assessors blinded to the intervention that patients received? 12) Were the relevant outcomes measured using appropriate objective/subjective methods? 13) Were the relevant outcome measures made before and after the intervention? 14) Were the statistical tests used to assess the relevant outcomes appropriate? 15) Was follow-up long enough for important events and outcomes to occur? Green circles (+) represent low risk of bias, red circles (-) represent high risk of bias; yellow circles (?) indicate unclear risk of bias
C Laranjo-Tinoco, M J Oliveira, A S Araújo, et al
ing criteria: cases collected in more than one center, presentation of eligibility criteria for entering the study since none of them presented exclusion criteria, and use of statistical tests to assess the relevant outcomes
Characterization of the studies
A summary of the main characteristics and conclusions of each article included in our systematic review is presented in Table 1
Abdel-kader et al. (2013) 34
et al. (2014) 9
et al. (2006) 20
Pre-term uterine contractions (n=1). All patients delivered at term without adverse fetal outcomes
(n=2) All patients delivered at term without adverse fetal outcomes Atar et al. (2012) 35
All patients delivered at term without adverse fetal outcomes
All patients delivered at term without adverse fetal outcomes
Bozkurt
Butticè et al. (2017)
Choi et al. (2016) 39 Korea
Cocuzza et al. (2010) 29
Denstedt et al. (1992) 49 Canad a
Drescher et al. (2019) 3
Dumitrache et al (2013) 30
Elgamasy et al. (2009) 50
Fathelbab et al. (2016) 40 Egypt
Georgescu et al. (2014) 31 Roma nia
Semirigid URS successful in 87.5%, improving to 93.75% with flexible URS.
Haghpanah et al. (2018) 32 Iran Prospective cohort study 23 1st T: 69.5% 0 11 12 Not specified
Bladder irritability (n=8)
Haller et al. (1993) 33 Croati a
Hoscan et al. (2012) 10
Isen et al. (2012) 11 Turkey
Dysuria and urgency (n=12), hematuria (n=5)
Ureteric edema, minor laceration or bleeding (n=5); stone migration (n=2), stone not reached (n=2) UTI (n=4), renal colic (n=2), prolonged hematuria (n=1), bladder irritability (n=4)
JJ: UTI (n=1), stent-related symptoms (n=4) PCN: UTI (n=2) No statistically significant differences
1 PCN placement after failure of JJ insertion. 1 nephrectomy due to chronic pyelonephritis in an excluded kidney.
Ureteric edema, minor ureteric laceration or bleeding (n=5); stone migration (n=3), stone not reached (n=2) UTI (n=3); Bladder irritability (n=3)
Pre-term labor after PCN (n=1); all other patients delivered at term without adverse fetal outcomes
JJ: Ureteral double-J stent; PCN: Percutaneous nephrostomy; URS: Ureteroscopy; USA: United States of America; UTI: Urinary Tract Infection
Regarding the study design, we included 41 cohort studies (2, 3, 9-47) and 4 cases series (48-51) Five (11 1%) of the cohort studies analyzed had a prospective design (17, 32, 35, 40, 44) There were no randomized controlled trials
A total of 3424 interventions in pregnant patients were evaluated The studies reported a mean age varying from 22 to 30, with a total age range between 16 and 42 The second trimester was the most common timing of presentation and treatment of renal colic Gestational age range varied from 8 to 38 weeks (8, 10,11, 15, 18, 19, 21, 24, 25, 27, 31, 34, 36, 38, 43, 44, 50, 51), and 24 studies reported treatment in the three trimesters (2, 3, 9, 11-13, 16, 17, 20, 22, 23, 25-27, 31, 32, 36, 40-42, 44, 46, 47, 51)
RESULTS OF INCLUDED STUDIES
Type of treatment
Ureteroscopy was performed in all studies when there were indications for interventional treatment and no indications for temporary drainage (fever, large stone burden, complex anatomy, bilateral stone disease, obstetric complications, presentation in the first trimester or near fullterm) were present
A total of 2188 ureteroscopies were performed Most studies included only semirigid ureteroscopies, but flexible ureteroscopy was also used in 9 studies (12, 16, 20, 26, 27, 29, 31, 44, 45)
Stone management was either with lithotripsy (pneumatic or laser) (10, 11, 18, 20, 22, 25, 27, 28, 36, 42-44, 47,52), with stone extraction with baskets or forceps (16, 24, 45, 49) or using both approaches in different patients (9, 14, 15, 19, 21, 23, 29, 31, 34, 35, 37, 38, 40, 46) Five studies, with a total of 1233 ureteroscopies, did not specify the
URS: premature uterine contractions with threatened abortion (n=1)
All patients delivered at term without adverse fetal outcomes
All patients delivered at term without adverse fetal outcomes
Unconfirmed abortion suspicion (n=12)
All patients delivered at term without adverse fetal outcomes
stone management technique used during the procedure (2, 3, 12, 13, 30)
Seventeen studies reported double-J stenting at the end of the procedure when needed (9, 11, 19-23, 25, 27-29, 31, 35, 37, 38, 40, 47)
Temporary drainage was reported in every study when the indications mentioned before were present, fever being the most common trigger A total of 719 double-J stents were inserted and 517 percutaneous nephrostomy tubes were placed
Concerning ureteroscopies, Bozkurt et al found no statistically significant differences between pregnant and nonpregnant women (38) The other articles reported the complications without comparing groups Most studies reported minor ureteral injuries including edema, small lacerations or perforations, or bleeding, in a total of 33 events (10, 25, 31, 35-37, 44) Only Rashid et al used the Satava Classification (52) and reported 5 intraoperative G1 ureteral injuries in semirigid ureteroscopy (44) Stone migration during ureteroscopy happened 64 times (18, 22, 25, 27, 28, 30, 31, 36, 40, 46, 47) and the stone could not be reached in 9 cases (10, 25, 31, 36)
Specific perioperative complications for JJ and PCN were not reported Among 19 articles with 138 double-J stent insertions (2, 3, 11, 13, 14, 16, 17, 24, 26, 29, 30, 32-34, 39, 42, 45, 49, 50), and 11 articles with 344 PCN (3, 11, 26, 30-33, 39, 48, 49, 51), no perioperative complications were reported
Perioperative complications were not specified at all in 2 articles (2, 15)
C Laranjo-Tinoco, M J Oliveira, A S Araújo, et al
Postoperative complications
Postoperative complications were compared between the different procedures in 4 studies (3, 32, 36, 47) Song et al reported that the double-J stent group had the highest rate of complications (52 9%) compared to the ureteroscopy and percutaneous nephrostomy groups but without a statistically significant difference (47) One retrospective cohort revealed no significant difference in complications between primary ureteroscopy and ureteral stent placement; while moderate or severe lower urinary tract symptoms (LUTS) were significantly lower in the ureteroscopy group, flank pain was not (36) No difference between ureteral stent and percutaneous nephrostomy complications was also noted in a prospective study (32) Regarding urinary tract infections (UTIs), Drescher et al presented an infection rate of 8 7% in patients treated with ureteroscopy and/or ureteral stent placement and 19 6% in patients who received percutaneous nephrostomies (3)
In a retrospective cohort, ureteroscopy complications were compared between 41 pregnant patients with 62 non-pregnant women who also underwent surgery, revealing no higher complication rate in the pregnant population (38) Concerning complications related to each procedure type, in patients submitted to URS, 97 UTIs were reported in 12 articles (3, 9, 10, 21-23, 25, 31, 35, 36, 38), and urosepsis was diagnosed 13 times (15, 36, 37) Irritative lower urinary tract symptoms such as dysuria, pain, bladder irritability, and urgency were observed 45 times in 6 studies (29, 31, 35, 38, 40, 49) Colicky pain was reported in 5 patients (20, 31, 45), and hematuria was observed 10 times (23, 31, 40, 47) Eleven studies did not observe any ureteroscopy postoperative complications (11, 12, 14, 16, 19, 24, 26, 30, 34, 42, 46)
The most frequently reported postoperative complication associated with ureteral stents was bladder irritability This complication was observed 28 times (8, 10, 22, 25, 47, 49), and Rivera et al reported one case of multiple hospitalizations for pain control (45) Other complications related to ureteral stents were stent encrustation or migration, documented 16 times (17, 22, 25, 47, 50, 53) Rivera et al reported that 6 patients required multiple stent exchanges (45) 7 urinary tract infections were reported in 3 studies (22, 25, 32) and LUTS and hematuria were observed 13 times (17, 25, 29) No postoperative complications associated with ureteral stent insertion were reported in 10 studies (11, 14, 16, 24, 26, 30, 33, 34, 39, 42)
In reference to PCN complications, 10 nephrostomy tube obstructions were described,47,48,51 some requiring tube exchanges There were 2 cases of localized skin infections (47), 61 cases of UTI,3 and 1 case of sepsis after PCN placement (48) Persistent pain was reported in 2 articles (47, 51) No complications were observed after PCN on 6 articles (11, 26, 30, 33, 39, 42)
Obstetric complications
All studies followed the pregnancies until term Obstetric outcomes were evaluated and managed by obstetricians Twenty-three articles did not mention any adverse obstetric outcome (8, 10, 11, 14, 16, 18, 20, 23, 24, 26, 29-34, 37-40, 42, 44, 51) and all patients from these studies d e l i v e r e d a t t e r m w i t h o u t a d v e r s e f e t a l o u t c o m e s Furthermore, Shirvan et al followed the children up to
the age of 5 with no evidence of mental or physical development alterations (46)
The most frequent obstetric complications reported were preterm uterine contractions and preterm labor Premature uterine contractions were reported 52 times in 6 studies: 50/288 (17 4%) ureteroscopies and 2/62 (3 2%) double-J insertion (9, 10, 15, 25, 31, 36) One retrospective study focused specifically on this topic, and while reporting the largest frequency of uterine contractions during the first 12 hours after ureteroscopy (45 54%), there were no severe maternal or fetal complications or premature deliveries
The authors propose some measures to reduce the odds of uterine contractions: shorten the surgical time, use phloroglucinol after the procedure, treat pain and infection, and monitor the multiparas more closely, as they seem to have a higher risk of contractions (15)
The selected articles reported a total of 167 cases of preterm labor and 24 premature deliveries (3, 12, 28, 36, 47-50) A population-based retrospective cohort observed that when compared to conservative management, ureteral stent/ureteroscopy patients had higher rates (n = 90, 11 2%) of preterm labor while percutaneous nephrostomy patients had the highest rate (n = 61, 19-5%) Urologic intervention with ureteral stent and/or ureteroscopy, and PCN each independently increased the risk of preterm delivery (3) Ordon et al further concluded that stone disease during pregnancy significantly increased the risk of an adverse birth outcome The risk was higher if the stones required intervention, compared with conservative treatment, and temporary drainage (nephrostomy tubes or stents) had the largest magnitude of risk for an adverse birth outcome (2) Another cohort study documented 7 cases of induction of labor before term due to stent intolerability, concluding that patients who were treated with temporary stents were significantly more likely to be induced before spontaneous labor when compared with ureteroscopy patients (45) Contradicting this evidence, Bayar et al compared the number of preterm births between ureteroscopy (n = 15, 36%) and double-J stent insertion (n = 7, 24%), reporting no significant differences between them (36)
There was only one case of in-utero fetal mortality one week after a double-j stent was placed but it was not due to urological reasons (36)
Obstetric outcomes were not mentioned in 2 articles (17, 43)
Procedure efficacy
Stone-free rate of URS was between 73% and 100% (9, 10, 12, 18, 23, 26, 29, 31, 34, 36, 40, 43, 44, 46) One study that compared URS stone-free rates between pregnant and non-pregnant women showed no statistically significant differences (38) However successful, a study with 101 ureteroscopies performed reported that 26 patients showed incomplete pain relief immediately after URS, but improved with painkillers in the following 12h (15) Only 3 studies reported unsuccessful ureteroscopies, mainly due to ureteral stenosis or stone migration, in 13-19% of the cases (22, 25, 47)
Most temporary drainage procedures were successful There were no reported failures in nephrostomy tube placement In regard to ureteral stents, placement failure
Laranjo-Tinoco, M J Oliveira, A S Araújo, et al
occurred at varying rates (12-75%), requiring drainage with PCN or ureteroscopy (11, 25, 33, 42, 47) In one study with 30 double-J stents successfully placed, 67% of the patients had a clinical improvement in pain relief immediately and soon after surgery, but 10% reported no difference and 23% had a worsening of symptoms, with either an increased analgesic requirement or the development of new symptoms related to stent placement (17) Procedure efficacy was not mentioned in 17 studies (2, 3, 13, 16, 19-21, 24, 27, 28, 30, 32, 35, 37, 48, 50, 51)
Radiation exposure
Pre-operative imaging was mainly acquired with ultrasound MRI was used in selected cases with questionable ultrasound (12, 14, 25, 34, 47) Plain x-ray, intravenous urography and computed tomography was rarely used (12, 16, 18, 26, 33, 41, 51) Most surgical procedures were performed under direct vision and ultrasound guidance; intra-operative fluoroscopy was reported in 8 studies (12, 14, 16, 26, 29, 45, 48, 49) Radiation doses were inconsistently reported
DISCUSSION
Ureteroscopy was the most reported procedure, totaling 2188 interventions Temporary drainage procedures amounted to 1236 interventions Procedures were not specified by trimester, but most were performed in the second and third trimesters URS was performed in all trimesters, and 2 studies used flexible ureteroscopes only in the third trimester (27, 31) Song et al suggested that double-J stents should be preferentially placed in third trimester pregnant patients, due to the frequent need for replacement after 4-6 weeks (47) Densted et al recommended PCN placement before 22 weeks of gestation, and JJ subsequently (49) Conversely, there are descriptions of JJ placement in the first trimester without adverse outcomes (17, 32, 36, 41) Most procedures did not cause any type of perioperative or postoperative complications
When perioperative complications occurred, they were minor, like minimal ureteral injuries during ureteroscopy
A total of 106 perioperative complications were documented out of 2188 ureteroscopies performed (overall rate of 4 84%); the most common were stone migration, ureteral injury, and bleeding The only comparative study between ureteroscopy in pregnant and non-pregnant women did not report significant differences (38) It is noteworthy that only one article used the Satava Classification for ureteral injury (44) This classification enables the classification of ureteral injuries and could be an important tool for standardizing such complications Standardization is important when comparing the results of different studies, which would have been of value to this review Specific perioperative complications for JJ and PCN were not reported Postoperative complications were also mostly minor
There were few comparative studies: two did not report statistically significant differences in postoperative complications between procedures (32, 47), but Bayar et al described a lower rate of moderate or severe LUTS in URS (with double-J stent insertion when needed) than in those treated only with JJ insertion (36), and one study revealed a higher rate of UTI with nephrostomies (3)
Studies have described that the most common postoper-
ative complications after ureteroscopy are fever, UTI, and bleeding, after double-J stent insertion are stent-related discomfort, infection, and encrustation and after percutaneous nephrostomy are sepsis, local bleeding, and tube obstruction (53) The same conclusions could be assessed by this review
The overall documented complication rate for URS was 7 7% The most frequent complications were lower urinary symptoms and urinary infections, with 13 cases of urosepsis (0 5%) According to a worldwide multicenter study that analyzed peri and postoperative complications associated with ureteroscopy, the most common perioperative complications were bleeding, perforation, and failed access and it happened in 4 2% of cases (53) This study represented a non-pregnant population, so the evidence presented in our systematic review shows a marginally higher rate of complications in pregnant patients Ureteral stenting complications were bladder irritability in most patients, encrustation, and stent migration, in a total of 8 2% complications PCN had the highest rate of complications (14 8%), and they were fever, bacteriuria, tube obstruction, and hematuria
Regarding obstetric complications, premature contractions were mostly reported for ureteroscopies The rate of reported preterm labor was 4 8%, with 0 7% premature births considering all procedures A comparative study showed no statistically significant differences in preterm labors between URS and JJ patients (36), while another reported a higher rate of preterm induction of labor in JJ patients due to catheter intolerability (45) Two studies reported that percutaneous nephrostomy had the highest rate of adverse birth outcomes (2, 3)
In terms of procedure efficacy, the mentioned stone-free rate varied from 73% to 100%, with no differences between pregnant and no pregnant women (38) Ureteral dilation in pregnancy helps the insertion of the ureteroscopes, enhancing the success of this procedure (47) Besides primary URS decision, URS was also the procedure of choice when temporary drainage failed Radiation exposure is a concern during pregnancy Consequently, ultrasound was the most used pre-operative and intra-operative imaging modality However, fluoroscopy was still used in some studies (12, 14, 16, 26, 29, 45, 48, 49) with descriptions of low dose settings, protection equipment and pulsed imaging to reduce exposure
The validity of this systematic review depends largely on the quality of the available evidence
We included predominantly retrospective case series and cohort studies, typically conducted in single-center settings without a comparative design, which results in an absence of high-quality study designs The lack of explicitly defined exclusion criteria in several studies raises the possibility of selection bias Additionally, samples were chosen by convenience, which compromises the external validity of the results
Noteworthy limitations within this review encompass heterogeneity in both sample characteristics and outcome measurement Variability in sample sizes across studies introduces a notable source of potential bias, influencing the generalizability of conclusions Furthermore, the absence of standardization in outcome measurement, with divergent approaches to measuring the same outcome
C
across studies, hinders the comparability and correlation of reported results
In conclusion, there is a lack of well-designed high-quality studies on the effect of stone surgical treatments in the pregnant population Future studies should consider the inclusion of larger sample sizes, multiple centers, and randomized patient assignment to ensure homogeneous sample characteristics Despite these limitations, this systematic review summarizes the available evidence on a challenging topic, hence its value
CONCLUSIONS
Invasive treatment may be required for the treatment of urolithiasis during pregnancy, so it is important to assess which procedures are suitable for this population Based on the findings of this systematic review, ureteroscopy, double-J stent insertion, and percutaneous nephrostomy are safe and effective treatment options in this setting, with minor complications and no severe adverse obstetric or fetal outcomes Since all three procedures are considered safe, primary ureteroscopy should be considered as the first-line procedure whenever feasible, minimizing the need for subsequent interventions, as opposed to temporary drainage However, individual patient assessment in a multidisciplinary discussion is crucial to identify cases where temporary drainage remains the appropriate treatment approach In these cases, the trimester of presentation might influence the option used, as early p l a c e m e n t o f d o u b l e - J s t e n t s m i g h t w a r r a n
exchange during pregnancy
REFERENCES
1 Rosenberg E, Sergienko R, Abu-Ghanem S, et al Nephrolithiasis during pregnancy: Characteristics, complications, and pregnancy outcome World J Urol 2011; 29:743-7
2 Ordon M, Dirk J, Slater J, et al Incidence, treatment, and implications of kidney stones during pregnancy: A matched populationbased cohort study J Endourol 2020; 34:215-21
3 Drescher M, Blackwell RH, Patel PM, et al Antepartum nephrolithiasis and the risk of preterm delivery Urolithiasis 2019; 47:441-8
4 Semins MJ, Matlaga BR Management of urolithiasis in pregnancy Int J Womens Health 2013; 5:599-604
5 Page MJ, McKenzie JE, Bossuyt PM, et al The PRISMA 2020 statement: An updated guideline for reporting systematic reviews BMJ 2021; 372:n71
6 Critical Appraisal Skills Programme (CASP) Checklist for Cohort Study [Internet](2018) Accessed: November, 23: http://www caspuk net/casp-tools-checklists
7 Institute of Health Economics (IHE) Quality Appraisal of Case Series Studies Checklist [Internet] (2016) Accessed: November, 23: https://www ihe ca/publications/ihe-quality-appraisal-checklist-forcase-series-studies
8 Loughlin KR Management of acute ureteral obstruction in pregnancy utilizing ultrasound-guided placement of ureteral stents Urology 1994; 43:412
9 Adanur S, Ziypak T, Bedir F, et al Ureteroscopy and holmium laser lithotripsy: Is this procedure safe in pregnant women with
ureteral stones at different locations? Arch Ital Urol Androl 2014; 86:86-9
10 Hoscan MB, Ekinci M, Tunçkıran A, et al Management of symptomatic ureteral calculi complicating pregnancy Urology 2012; 80:1011-4
11 Isen K, Hatipoglu NK, Dedeoglu S, et al Experience with the diagnosis and management of symptomatic ureteric stones during pregnancy Urology 2012; 79:508-12
12 Johnson EB, Krambeck AE, White WM, et al Obstetric complications of ureteroscopy during pregnancy J Urol 2012; 188:151-4
13 Lee SJ, Rho SK, Lee CH, et al Management of urinary calculi in pregnant women J Korean Med Sci 1997; 12:40-3
14 Lemos GC, El Hayek OR, Apezzato M Rigid ureteroscopy for diagnosis and treatment of ureteral calculi during pregnancy Int Braz J Urol [Internet] 2002; 28:311-5
15 Li C, Guo L, Luo M, et al Risk factors of uterine contraction after ureteroscopy in pregnant women with renal colic Int Urol Nephrol 2021; 53:1987-93
16 Lifshitz DA, Lingeman JE Ureteroscopy as a first-line intervention for ureteral calculi in pregnancy J Endourol 2002; 16:19-22
17 Ngai HY, Salih HQ, Albeer A, et al Double-j ureteric stenting in pregnancy: A single-centre experience from iraq Arab J Urol 2013; 11:148-51
18 Rana AM, Aquil S, Khawaja AM Semirigid ureteroscopy and pneumatic lithotripsy as definitive management of obstructive ureteral calculi during pregnancy Urology 2009; 73:964-7
19 Scarpa RM, De Lisa A, Usai E Diagnosis and treatment of ureteral calculi during pregnancy with rigid ureteroscopes J Urol 1996; 155:875-7
20 Akpinar H, Tüfek I, Alici B, Kural AR Ureteroscopy and holmium laser lithotripsy in pregnancy: Stents must be used postoperatively J Endourol 2006; 20:107-10
21 Shokeir AA, Mutabagani H Rigid ureteroscopy in pregnant women Br J Urol 1998; 81:678-81
22 Tan S-T, Chen X, Sun M, Wu B The comparation of effects and security of double-j stent retention and ureteroscopy lithotripsy in the treatment of symptomatic ureteral calculi during pregnancy Eur J Obstet Gynecol Reprod Biol 2018; 227:32-4
23 Tawfiek ER Ureteroscopy during pregnancy with follow-the-wire technique Afr J Urol 2009; 15:245-9
24 Travassos M, Amselem I, Filho NS, et al Ureteroscopy in pregnant women for ureteral stone J Endourol 2009; 23:405-7
25 Wang Z, Xu L, Su Z, et al Invasive management of proximal ureteral calculi during pregnancy Urology 2014; 83:745-9
26 Watterson JD, Girvan AR, Beiko DT, et al Ureteroscopy and holmium:Yag laser lithotripsy: An emerging definitive management strategy for symptomatic ureteral calculi in pregnancy Urology 2002; 60:383-7
27 Zhang S, Liu G, Duo Y, et al Application of ureteroscope in emergency treatment with persistent renal colic patients during pregnancy PLoS One 2016; 11:e0146597
28 Butticè S, Laganà AS, Vitale SG, et al Ureteroscopy in pregnant women with complicated colic pain: Is there any risk of premature labor? Arch Ital Urol Androl 2017; 89:287-92
29 Cocuzza M, Colombo JR, Jr , Lopes RI, et al Use of inverted fluoroscope's c-arm during endoscopic treatment of urinary tract
obstruction in pregnancy: A practicable solution to cut radiation Urology 2010; 75:1505-8
30 Dumitrache M, Merticariu M, Rascu S, et al C139 our clinic's experience with the management of renal colic in pregnancy Eur Urol Suppl 2013; 12:e1247, C139
31 Georgescu D, Mulţescu R, Geavlete B, et al Ureteroscopy -first-line treatment alternative in ureteral calculi during pregnancy? Chirurgia (Bucur) [Internet] 2014; 109:229-32 Available from: h t t p s : / / w w w r e v i s t
alternative-in-ureteral-calculi-during-pregnancy/
32 Haghpanah A, Irani D, Dehghani A Complications of temporary urinary diversion using nephrostomy tube or jj ureteric stent in pregnant women with symptomatic urolithiasis Arab J Urol 2018; 16:S20-S
33 Haller H, Mozetić V, Topljak-Polić D, et al Management and complications of urolithiasis during pregnancy Int J Gynaecol Obstet 1993; 40:135-9
34 Abdel-Kader MS, Tamam AA, Elderwy AA, et al Management of symptomatic ureteral calculi during pregnancy: Experience of 23 cases Urol Ann 2013; 5:241-4
35 Atar M, Bozkurt Y, Soylemez H, et al Use of renal resistive index and semi-rigid ureteroscopy for managing symptomatic persistent hydronephrosis during pregnancy Int J Surg 2012; 10:629-33
36 Bayar G, Bozkurt Y, Acinikli H, et al Which treatment method should be used in pregnant patients with ureteral calculi? Two center comparative study Arch Esp Urol [Internet] 2015; 68:43540 Available from: https://www aeurologia com/EN/Y2015/V68/I4/ 435#2
37 Bozkurt Y, Penbegul N, Soylemez H, et al The efficacy and safety of ureteroscopy for ureteral calculi in pregnancy: Our experience in 32 patients Urol Res 2012; 40:531-5
38 Bozkurt Y, Soylemez H, Atar M, et al Effectiveness and safety of ureteroscopy in pregnant women: A comparative study Urolithiasis 2013; 41:37-42
39 Choi CI, Yu YD, Park DS Ureteral stent insertion in the management of renal colic during pregnancy Chonnam Med J 2016; 52:123-7
40 Fathelbab TK, Hamid AMA, Galal EM Ureteroscopy for treatment of obstructing ureteral calculi in pregnant women: Single center experience Afr J Urol 2016; 22:106-9
41 Jarrard DJ, Gerber GS, Lyon ES Management of acute ureteral obstruction in pregnancy utilizing ultrasound-guided placement of ureteral stents Urology 1993; 42:263-7; discussion 7-8
42 Juan YS, Wu WJ, Chuang SM, et al Management of symptomatic urolithiasis during pregnancy Kaohsiung J Med Sci 2007; 23:241-6
43 Polat F, Yeşil S, Kıraç M, Biri H Treatment outcomes of semirigid ureterorenoscopy and intracorporeal lithotripsy in pregnant women with obstructive ureteral calculi Urol Res 2011; 39:487-90
44 Rashid AO, Abdala RY Safety and efficacy of flexible and semirigid ureteroscopy with laser lithotripsy for the management of ureteral calculi in pregnancy Afr J Urol 2021; 27:46
45 Rivera ME, McAlvany KL, Brinton TS, et al Anesthetic exposure in the treatment of symptomatic urinary calculi in pregnant women Urology 2014; 84:1275-8
46 Keshvari Shirvan M, Darabi Mahboub MR, Rahimi HR, Seyedi A The evaluation of ureteroscopy and pneumatic lithotripsy results in pregnant women with urethral calculi Nephrourol Mon 2013; 5:874-8
47 Song Y, Fei X, Song Y Diagnosis and operative intervention for problematic ureteral calculi during pregnancy Int J Gynaecol Obstet 2013; 121:115-8
48 Khoo L, Anson K, Patel U Success and short-term complication rates of percutaneous nephrostomy during pregnancy J Vasc Interv Radiol 2004; 15:1469-73
49 Denstedt JD, Razvi H Management of urinary calculi during pregnancy J Urol 1992; 148:1072-4
50 Elgamasy A, Elsherif A Use of doppler ultrasonography and rigid ureteroscopy for managing symptomatic ureteric stones during pregnancy BJU Int 2010; 106:262-6
51 Kavoussi LR, Albala DM, Basler JW, et al Percutaneous management of urolithiasis during pregnancy J Urol 1992; 148:106971
52 Tepeler A, Resorlu B, Sahin T, et al Categorization of intraoperative ureteroscopy complications using modified satava classification system World J Urol 2014; 32:131-6
53 Somani BK, Giusti G, Sun Y, et al Complications associated with ureterorenoscopy (urs) related to treatment of urolithiasis: The clinical research office of endourological society urs global study World J Urol 2017; 35:675-81
Correspondence
Catarina Sousa Laranjo Tinoco (Corresponding Author) cat tinoco@gmail com Sete Fontes - São Victor, 4710-243 Braga, Portugal
Maria João Oliveira mariajboliveira3110@gmail com
Ana Sofia Araújo anasofiaparaujo94@gmail com
Andreia Cardoso afds cardoso@gmail com
Carlos Oliveira carlos oliveira81@gmail com
Paulo Mota damota paulo@gmail com
João Pimentel Torres joaonunobpt@gmail com
Conflict of interest: The authors declare no potential conflict of interest This article was previously presented as a meeting abstract at the 40th World Congress of Endourology on September 27, 2023
C Laranjo-Tinoco, M J Oliveira, A S Araújo, et al
A
systematic review and meta-analysis of short- and long-term complications of early versus delayed penile prosthesis implantation in patients with ischemic priapism
Agustin J Nanda De Niro 1 , Gede Wirya Kusuma Duarsa 2 , Marshal Harvy Wicaksono 1 , Pande Made Wisnu Tirtayasa 2 , Kadek Budi Santosa 2 , I Wayan Yudiana 2 , Nyoman Gede Prayudi 2
1 Intern Doctor of Urology Surgery Department Prof dr I G N G Ngoerah General Hospital, Bali, Indonesia;
2 Urology staff of Urology Surgery Department Prof dr I G N G Ngoerah General Hospital, Bali, Indonesia
Summary
Background: This study determined pooled estimates of short- and long-term complications of early versus delayed implantation of penile prosthesis in patients with ischemic priapism.
Methods: We searched Pubmed, ProQuest, Scopus, EBSCOHost, and other sources from January 1, 2013, to March 2023. All study designs were included except animal studies, review articles, and consensus documents. Of the 214 articles, four studies were included in the systematic review, and further meta-analysis included three studies (PROSPERO CRD42023411005).
Results: The short-term complication rate was lower with early implantation than with later implantation (β= -2.08; 95%
Confidence Interval [CI] = -3 54, -0 6; p = < 0 05) A similar value was also found in the pooled analysis for long-term outcomes, defined as overall satisfaction rate, which is better with early implantation than later (β = 2 18; 95% CI = 1 35, 3 02; p = < 0 05)
Conclusions: The results of the pooled analysis confirmed that short-term complications were significantly lower with early implantation than with delayed implantation Overall satisfaction rates were higher in early implantation than in delayed implantation of penile prostheses
"Priapism" describes a pathological condition characterized by a prolonged erection of more than four hours without sexual stimulation This condition can be divided into subtypes of low, high, and intermittent flow (1) Ischemic priapism is the most common form of priapism and accounts for 90-95% of all cases Although a common form, ischemic priapism is rare, with an overall incidence of 1 5 cases per 100 000 person-years (1, 2) Most cases of priapism have an idiopathic etiology; others may be related to hematologic abnormalities, intracavernosal injection of vasoactive drugs, illicit drug use, or malignancy (3, 4) Ischemic priapism is considered a form of compartment syndrome caused by hypoxia, hypercapnia, acidosis, and glucopenia in the erectile tissue In the first 12 hours after
an episode of priapism, O2 partial pressure decreases as the closed compartment prevents the supply of fresh, oxygenated blood, resulting in initial thickening and interstitial edema without smooth muscle necrosis (3, 5) Necrosis of the corpus cavernosum muscle was seen after 24 hours After 24 hours, the risk of irreversible comprehensive smooth muscle changes leading to refractory erectile dysfunction is over 90%, and after 72 hours, there is no hope for recovery of erectile function (2, 3, 6) Failure to respond to aspiration and instillation of a-agonists suggests that irreversible changes have occurred in the smooth muscle of the corpus cavernosum At this stage, shunt surgery may successfully induce decongestion but will not reverse the ischemic damage, and refractory erectile dysfunction will persist in the long term (1, 4, 7) Refractory erectile dysfunction cannot be treated conservatively, and penile prosthesis implantation is the only way to achieve the stiffness required for penetrative intercourse Penile prosthesis implantation at this stage can be very difficult due to diffuse corporal fibrosis, which complicates corporal dilation and is associated with an increased risk of distal/proximal cross-over complications and urethral perforation or injury (4, 8-10) In addition, the duration of the procedure significantly increases the risk of postoperative infection In addition, fibrosis results in some shortening of the penis After implantation, most patients still complain of penile shortening, which is one of the reasons for men's dissatisfaction with penile prostheses (11, 12)
Immediate implantation of a penile prosthesis is usually simple, reduces pain, and allows an earlier return to sexual activity Despite the above advantages, immediate implantation of penile prostheses is associated with penile edema, increased risk of infection, and distal perforation, especially in patients with a history of shunt surgery (7, 13, 14) Delayed implantation of penile prostheses is now considered a surgical challenge with a high complication rate Delayed implantation is also associated with suboptimal satisfaction Several studies suggest that penile prostheses should be implanted in patients with refractory ischemic priapism at the acute stage when irreversible erectile smooth muscle damage has occurred (11, 15) Currently, there is no general agreement on the timing of
penile prosthesis implantation in patients with ischemic priapism, as outcomes are variable This review examines the current literature on priapism, with a focus on evaluating short-term and long-term outcomes in adult men undergoing direct implantation of a penile prosthesis for the treatment of acute ischemic priapism unresponsive to medical therapy or shunt surgery
METHODS
Search strategy and selection criteria
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) for conducting meta-analyses (http://www prisma-statement org/), two independent reviewers performed data extraction (AJ, GW) Disagreements were resolved in a discussion among all investigators, and if necessary, they were analyzed and clarified by IW For the literature search, we used the PubMed, EbscoHost, Scopus, and ProQuest databases from January 1, 2023, to March 2023 We also reviewed and manually searched the references and identified the possible dates from the conferences The systematic search for terms and combinations used the following terms: "penile prosthesis"; "priapism"; "early"; "delayed"; "graft"; "satisfaction"; "complications"
Original research articles were included if they met the following criteria: (a) diagnosis of acute priapism, (b) comparison of penile prosthesis implantation: early vs delayed, and (c) if the study provided information on clinical characteristics and outcomes of the two techniques We excluded animal studies, review articles, and consensus documents The exclusion criteria were as follows: (a) the study was a review article, letter to the editor, animal study, commentary, or consensus document; (b) the study did not focus on priapism patients or the diagnosis was unclear If the patients were from the same hospital and the cases overlapped, we selected only the publication with the largest number of cases The protocol was registered with the international prospective register of systematic reviews (PROSPERO), in accordance with PRISMA-P guidelines (PROSPERO CRD42023411005) (16) The protocol for this systematic review has been previously described (17) All identified studies are included in this review
Quality assessment and Risk of Bias
The five authors of the review classified each of the included studies as 'risk of bias’ Risk of bias in Randomized Controlled Trial (RCT) was assessed using the tools recommended in the Cochrane Handbook for Systematic Review of Interventions Additional items were included to determine the risk that confounding factors may explain the results ROBINS-1 quality ratings for non-randomized studies were used to assess the quality of observational studies For each study, a pragmatic approach was used to assess the risk of confounding
Statistical analysis
The primary outcomes of interest in the study were shortand long-term complications of penile prostheses at early and late implantation Short-term complications included pain, palpable nodules, residual curvature, infection, and erosion of the prosthesis, while long-term complications included quality of life, overall satisfaction, sexual satisfaction, penetration ability, erectile dysfunction, and increased curvature I2 was used to assess heterogeneity between studies A fixed-effects model was used when I2 was < 50%, and when I2 was > 50%, a random-effects model was chosen In the fixed-effects model, population effect sizes were assumed to be the same for all studies In contrast, the random-effects model attempted to generalize the results beyond the included studies by assuming that the selected studies were random samples from a larger population If there was statistical heterogeneity in the results, a further sensitivity analysis was performed to determine the source of heterogeneity
Sensitivity analyses were performed only for meta-analyses that evaluated primary/main outcomes (including outliers) Sensitivity analyses were performed in three different ways by excluding (1) each study individually, (2) studies identified as outliers, and (3) studies with a moderate and high risk of bias After each analysis, the consistency and significance of the meta-analysis results are reassessed A study is considered an outlier if the 95% Confidence Interval (CI) of the study is outside the 95% CI of the combined effect when the Forest Plot is viewed visually The Forest plot shown refers only to the metaanalysis with outliers After excluding significant clinical heterogeneity, the random-effects model with coefficient estimation (b) was used as the effect size for the meta-
A J Nanda De Niro, G Wirya Kusuma Duarsa, M Harvy Wicaksono, et al
Figure 1.
Flow diagram of study selection.
Table 1. Study characteristics
analysis (ES) When p was < 0 05, the result was considered statistically significant (2-sided) All data were analysed using STATA ver 15 software
Overview of the study selection
The PRISMA diagram for the entire study selection process is shown in Figure 1 An initial search of four databases yielded 212 studies, while additional records identified through references and conferences included two studies Subsequently, 154 studies were excluded because they did not meet the requirements of the automation tool, and 48 duplicate studies were also excluded Of the remaining 12 studies, a total of 6 studies were identified as reviews, and 2 studies did not compare early and delayed penile prostheses Ultimately, four studies were selected and included in this systematic review and three studies were included in the meta-analysis
Studies characteristics
The characteristics of the included studies are summarized in Table 1 All included studies were retrospective studies using medical records The total number of ischemic priapism patients from four studies was 287, with 187 patients undergoing early penile prosthesis implantation and 100 patients undergoing delayed penile prosthesis implantation The operational definition for categorizing
patients as "early" or "delayed" was different in each study The time from onset of priapism to implantation was 31 hours to less than three weeks in the early group In the delayed group, it was 3 weeks to more than 6 months Three studies reported initial treatment before implantation in the form of physical aspiration, irrigation, instillation of a-agonists, and T-shunt surgery (open distal and percutaneous) In patients with early implantation, 178 patients were treated with malleable implants and 9 others with inflatable implants In patients with delayed implantation, 66 patients used malleable implants and 34 others used inflatable implants Most studies stated that deformable implants were preferred because they are less expensive
Risk of Bias
The risk of bias assessment is presented using two summary figures (Figures 2, 3) for each study according to all risk of bias domains Two studies have a low risk of bias, and the other two studies have a potentially moderate risk of bias When assessing the risk of confounding, all studies had a moderate risk of bias, mainly due to the type of penile prostheses that may have influenced study results There is a moderate risk of bias in participant selection, with the exception of one study that did not include complete information on patient selection (published as a conference proceeding at a symposium) All studies have a moderate risk
of bias in the classification of interventions, while the remaining domains have a low risk, except for one study that has a moderate risk of selection bias in outcome reporting This study does not explain exactly how many patients in each group experienced complications but only reports the frequency of complications present, and more than one complication may occur in each patient
Short-term complications
In the meta-analysis of short-term complications, all studies were included in the analysis Nevertheless, the results of heterogeneity analysis using I2 showed a high heterogeneity of 82 6% Sensitivity analysis using Forest plots
Figure 2
Risk of bias summary: review authors' assessment of each risk of bias for each included study
Figure 3. Risk of bias chart: review authors' assessment of each risk of bias item, presented as a percentage of all included studies.
Figure 4 Forest plot short-term complications
revealed that two studies were outliers In the follow-up analysis, one outlier study was excluded due to the small sample size
The results of a random-effects meta-analysis on shortterm complications showed that complications were significantly lower with early implantation of penile prosthesis than with delayed implantation (b = -2 08 (-3 54, -0 61); p = < 0 05) (Figure 4) Funnel plot results are in Figure 5 shows asymmetric results, highlighting the potential for publication bias
Long-term complications
The meta-analysis of long-term complications showed that
A J Nanda De Niro, G Wirya Kusuma Duarsa, M Harvy Wicaksono, et al
patients were satisfied with the outcome of the prosthesis, including sexual intercourse and overall comfort This analysis included three studies In this case, there was no clear assessment of overall satisfaction in one study The results of the meta-analysis on satisfaction rate showed that early implantation of the penile prosthesis had significantly better satisfaction than delayed implantation (b = 2 18 (1 35, 3 02); p = < 0 05) (Figure 6) The results of the funnel plot show that there is no outliers (Figure 7)
DISCUSSION
The decision about penile prosthesis in an acute episode of ischemic priapism is still based on expert opinion that referred to small or retrospective studies, hence decisionmaking should be discussed between the patient and the urologist (11, 18) This study is the first systematic review and meta-analysis to exclusively include a comparative study of the short- and long-term complications of early and delayed penile prosthesis implantation
A c c o r d i n g t o a r e t r o s p e c t i v e s t u d y c o n d u c t e d b y Palmisano et al , the immediate implantation of a soft penile prosthesis for patients with refractory ischemic priapism leads to instant pain alleviation, preservation of sexual function, and penile size, as well as higher surgical reproducibility in an emergency Furthermore, ischemic priapism's financial and resource burden on the healthcare system may be decreased (19) The previous systematic review by Capece et al showed that all studies found superiority of early versus delayed penile prosthesis implantation in patients with ischemic priapism; however, this superiority was merely speculative because none of the studies were designed to compare the outcome of early versus delayed implantation (20) In this study, however, the pool effect size from a meta-analysis provided better certainty about the outcome of penile prosthesis implantation in the 287 patients with ischemic priapism For both short-term and long-term complications, the pooled analysis showed significantly better outcomes for early implantation (p< 0 05) than for delayed implantation Infection is the most common complication after early implantation of penile prostheses, especially in patients with postoperative aspiration, injection, or shunt (12, 21, 22) It can be caused by the penetration of bacteria through the skin into the sterile compartment and by cavernous edema, which prevents antibiotics from penetrating the cavernous tissue (1, 10, 21) Nevertheless, postoperative infections are generally treatable The most challenging aspect of penile prosthesis implantation in delayed cases is existing corpus cavernosum fibrosis Difficult physical dilatation with Hegars dilators can be replaced with cavernotomes to cover difficult dilatations, called corporal drilling (23, 24) This difficult situation can be complicated by urethral injuries, lateral or distal perforations, or cylindrical branches Extensive corporal fibrosis and difficult dilation have resulted in the penile prosthesis being reduced in size to accommodate the corporal compartment (7, 20) This condition results in decreased penile length and is ultimately associated with lower overall patient satisfaction (7, 24) Indeed, in the study by Salman et al , satisfaction after penile prostheses were found to reach 100% in patients with delayed
Figure 6 Forest Plot long-term complications
Figure 5. Funnel Plot short-term complications
Figure 7. Funnel Plot long-term complications
A J Nanda De Niro, G Wirya Kusuma Duarsa, M Harvy Wicaksono, et al
implantation, although this was also based on the baseline condition of the patient, who had a long history of penile fibrosis, shortening, and impotence (12)
To date, the exact timing of prosthesis insertion when fibrosis has occurred is not known with certainty The timing of complete fibrosis after an acute attack of priapism is also unknown Sedigh et al described mild dilatation after one week of priapism (25), similar to the study performed by Salman et al in which mild dilatation was performed within 5 days of establishing a diagnosis of priapism (12) Conflicting results were presented by Hebert et al , who indicated a greater benefit in reducing the rate of severe complications when penile prosthesis implantation and reimplantation were performed within the first 4 months after the onset of corporal fibrosis (24)
Although the benefits of early penile prosthesis surgery are well documented and continue to be studied, the psychological impact on patients with ischemic priapism who must make an urgent decision to undergo penile prosthesis surgery and then receive the results is an interesting topic In the four studies included in this review, patients undergoing delayed penile prosthesis implantation were mostly unprepared for the surgery to be performed From a psychological perspective, the impact of penile prosthesis implantation on patients' overall quality of life has not been studied Currently, some reports recommend delaying the procedure for up to a week to give patients more time to understand their situation (11, 25) Although delayed treatment increases endogenous fibrosis, a delay may be justified if the psychological benefits of a longer duration outweigh the negative effects Further studies on this topic should be initiated
This study has some limitations Studies comparing early and delayed penile prosthesis implantation are very limited; moreover, all study designs performed are retrospective studies, which have their limitations in influencing confounding factors The relatively large heterogeneity in short-term complications remains a limitation of the study The differences may be due to patient demographic characteristics, surgeon experience, a technique used, type of implant, and timing of prosthesis insertion
CONCLUSIONS
This systematic review and meta-analysis is the first study to include a comparative examination of the short-term and long-term complications of early and delayed penile prosthesis implantation The results of the pooled analysis confirmed that short-term and long-term complications were significantly lower with early implantation than with delayed implantation Studies on the psychological impact of early penile prosthesis implantation are suggested for further investigation to optimize treatment outcomes for patients with ischemic priapism
REFERENCES
1 Mishra K, Loeb A, Bukavina L, et al Management of Priapism: A Contemporary Review Sex Med Rev 2020; 8:131-9
2 Biebel MG, Gross MS, Munarriz R Review of Ischemic and Nonischemic Priapism Curr Urol Rep 2022; 23:143-53
3 Bivalacqua TJ, Allen BK, Brock G, et al Acute Ischemic Priapism: An AUA/SMSNA Guideline J Urol 2021; 206:1114-21
4 Ericson C, Baird B, Broderick GA Management of Priapism: 2021 Update Urol Clin North Am 2021; 48:565-76
5 Yücel ÖB, Pazır Y, Kadıoglu A Penile Prosthesis Implantation in Priapism Sex Med Rev 2018; 6:310-8
6 Reddy A, Finley L, Horrall S Hyperosmolar hyperglycemic syndrome in a young boy Proc (Bayl Univ Med Cent) 2019; 32(4):627
7 Zacharakis E, Garaffa G, Raheem AA, et al Penile prosthesis insertion in patients with refractory ischaemic priapism: early vs delayed implantation BJU Int 2014; 114:576-81
8 Salem EA, El Aasser O Management of ischemic priapism by penile prosthesis insertion: prevention of distal erosion J Urol 2010; 183:2300-3
9 Tausch TJ, Zhao LC, Morey AF, et al Malleable penile prosthesis is a cost-effective treatment for refractory ischemic priapism J Sex Med 2015; 12:824-6
10 Joice GA, Liu JL, Burnett AL Medical treatment of recurrent ischaemic priapism: a review of current molecular therapeutics and a new clinical management paradigm BJU Int 2021; 127:498-506
11 Reddy AG, Alzweri LM, Gabrielson AT, et al Role of Penile Prosthesis in Priapism: A Review World J Mens Health 2018; 36:4
12 Salman B, Elsherif E, Elgharabawy M, Badawy A Early versus delayed penile prosthesis insertion for refractory ischemic priapism Arab J Urol 2022; 21:76-81
13 Rees RW, Kalsi J, Minhas S, et al The management of low-flow priapism with the immediate insertion of a penile prosthesis BJU Int 2002; 90:893-7
14 Muneer A, Ralph DJ Immediate Placement of a Penile Prosthesis as First-line Treatment for the Management of Ischaemic Priapism Eur Urol Focus 2019; 5:529-30
15 Ha AS, Han DS, Wallace BK, et al A population-based analysis of predictors of penile surgical intervention among inpatients with acute priapism Int J Impot Res 2023; 35:107-113
16 Page MJ, McKenzie JE, Bossuyt PM, et al The PRISMA 2020 statement: an updated guideline for reporting systematic reviews Syst Rev 2021; 10:1-11
17 De Niro AJN, Kusuma Duarsa GW, Yudiana IW, et al Penile Prosthesis Implantation in Priapism: is Early Indicating Better Outcomes? PROSPERO 2023 CRD42023411005 [cited 2023 Apr 9] PROSPERO Available from: https://www crd york ac uk/prospero/#myprospero
18 Krzastek SC, Smith R An update on the best approaches to prevent complications in penile prosthesis recipients Ther Adv Urol 2019 [cited 2023 Apr 9]; 11 Available from: /pmc/articles/ PMC6329024/ Krzastek SC, Smith R An update on the best approaches to prevent complications in penile prosthesis recipients Ther Adv Urol 2019; 11:1756287218818076
19 Palmisano F, Vagnoni V, Franceschelli A, et al Immediate insertion of a soft penile prosthesis as a new option for a safe and costeffective treatment of refractory ischemic priapism Arch Ital Urol Androl 2021; 93:356-60
2 0 C a p e c e M , F a l c o n e M , C a i T , e t a l P e n i l e P r o s t h e s i s
Implantation in Refractory Ischaemic Priapism: Patient Selection and Special Considerations Res Rep Urol 2022; 14:1
21 Moore J, Whelan TF, Langille GM The use of penile prostheses in the management of priapism Transl Androl Urol 2017; 6(Suppl 5):S797-803
22 Yafi FA, Hellstrom WJG Immediate Placement of Penile Prosthesis for the Management of Ischemic Priapism as First-line Treatment Eur Urol Focus 2019; 5:531-2
23 Krughoff K, Bearelly P, Apoj M, et al Multicenter surgical outcomes of penile prosthesis placement in patients with corporal fibrosis and review of the literature Int J Impot Res 2022; 34:86-92
24 Hebert KL, Yafi FA, Wilson S Inflatable penile prosthesis implantation into scarred corporal bodies: timing may decrease postoperative problems BJU Int 2020; 125:168-72
25 Sedigh O, Rolle L, Negro CLA, et al Early insertion of inflatable prosthesis for intractable ischemic priapism: our experience and review of the literature Int J Impot Res 2011; 23:158-64
26 Johnson M, Hallerstrom M, Chiriaco G, et al PD44-01 A comparison between early and delayed penile prosthesis insertion in men with refractory ischaemic priapism J Urol 2019; 201(Supplement 4)
27 Elhawy MM, Fawzy AM Outcomes of low-flow priapism and role of integrated penile prosthesis management African Journal of Urology 2021; 27:1-8
Correspondence
Agustin J Nanda De Niro, MD deniro nanda@yahoo co id
Gede Wirya Kusuma Duarsa gwkduarsa@gmail com
Marshal Harvy Wicaksono marshalharvy@gmail com
Pande Made Wisnu Tirtayasa wisnu tirtayasa@gmail com
Kadek Budi Santosa busanbsa@gmail com
I Wayan Yudiana yanyud@yahoo com
Nyoman Gede Prayudi prayudi blonx@yahoo com
Prof I G N G Ngoerah General Hospital
Jl Diponegoro, Dauh Puri Kelod, Denpasar, Bali
Conflict of interest: The authors declare no potential conflict of interest
REVIEW
The potential role of intracavernosal injection of platelet-rich plasma for treating patients with mild to moderate erectile dysfunction: A GRADE-Assessed systematic review and meta-analysis of randomized controlled trials
Niwanda Yogiswara 1, 2 , Fikri Rizaldi 1, 3 , Mohammad
Ayodhia
Soebadi 1, 3
1 Department of Urology, Faculty of Medicine, Universitas Airlangga, Indonesia;
2 Dr Soetomo General-Academic Hospital, Surabaya, East Java, Indonesia;
3 Universitas Airlangga Teaching Hospital, Surabaya, East Java, Indonesia
Summary
Introduction: Platelet-rich plasma (PRP) has shown positive effects on enhancing erectile function in animal studies. Human clinical trials are limited and provide contradictory results This review aims to conduct a meta-analysis of the available Randomized controlled trials (RCT) to assess the efficacy of PRP in males with ED Methods: A systematic review was carried out following the Cochrane Handbook of Intervention and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and registered in PROSPERO (CRD42023441655)
Results: A total of three RCTs were included in the analysis for a total of 221 patients with mild to moderate ED The patients receiving PRP reported significantly better improvement of IIEFEF score during 1,3- and 6-months follow-up compared to the placebo group (mean difference [MD] 2.66, 95% confidence interval [CI] 1 48 to 3 83, p < 0 01; MD 2 11, 95%CI 0 13 to 4.09, p = 0.04; MD 2.99, 95%CI 1.79 to 4.19, p < 0.01). The pooled analysis indicated that attainment of minimally clinical important difference (MCID) was significantly higher in patients receiving PRP compared to the placebo group during one and 6-month follow-up (odds ratio [OR] 5 51, 95%CI 1 2 to 254, p = 0 03; OR 5 64, 95%CI 2 05 to 15 55, p < 0 01; respectively) Encouragingly, no major AEs were reported in all three trials in the PRP and placebo groups (p = 0 99)
Conclusions: This review highlights the potential role of PRP in providing short-term improvement of erectile function parameters for up to 6 months in mild to moderate ED patients Future RCTs with longer-duration follow-ups and more standardized treatment protocols are necessary to gain sufficient details on PRP's long-term effectiveness and safety.
KEY WORDS: Platelet-rich plasma; Erectile dysfunction; Regenerative medicine; Sexual and reproductive health; Reproductive health
Submitted 24 May 2024; Accepted 7 June 2024
INTRODUCTION
Erectile dysfunction (ED) is one of the most common male sexual dysfunctions globally (1) This condition not only impairs the patient's quality of life, but it also has a detri-
mental impact on their partners (2) Treatment of ED is tailored to its underlying etiology, which is highly individualized, ranging from conservative, medicinal, and surgical approaches (3) Conservative approaches, such as lifestyle adjustments and risk factor management, can be advised for individuals with mild ED; however, patients with symptomatic ED may require medical or even surgical therapeutic approaches (4) Several treatments are available to control the symptoms, including PDE5i, topical vasoactive therapy, and a vacuum erection device (5) Nevertheless, studies reveal that the majority of ED patients have poor compliance; data suggest that one out of four patients will discontinue pharmacological therapy, with one of the most common reasons is the unwillingness to depend on pharmacological medicine and the desire for natural, spontaneous erections (6) Therefore, the ability to achieve a natural spontaneous erection is one of utmost importance in patients with ED The main problem with the earlier ED treatment paradigm is that it focuses on alleviating symptoms rather than restoring natural erectile function or halting disease progression Accordingly, researchers worked on discovering alternate treatments that might naturally improve erectile function (7) Recently, a group of treatments known as regenerative medicine aim to restore the structure and function of erectile tissues, such as Low-intensity shockwave therapy (LISWT), stem cell therapy, and platelet-rich plasma (PRP) (7-9) PRP, a novel regenerative therapy with high rejuvenating potential and minimal side effects, contains various platelet growth factors produced from whole blood, such as fibroblast growth factor (FGF), platelet-derived growth factor (PDGF), and vascular endothelial growth factor (VEGF), which can heal injured penile tissue and restore erectile function (10, 11) In animal studies, researchers discovered that PRP can successfully enhance natural erectile function (12-14) Human clinical trials, on the other hand, remain scarce and conflicting (15-17) Therefore, the aim of this study is to conduct a meta-analysis of the available Randomized controlled trials (RCT) to assess the efficacy of PRP in males with ED
MATERIAL AND METHODS
Study protocol and search strategy
The search was carried out with several online databases such as PubMed, Scopus, and ScienceDirect, utilizing Medical Subject Headings (MeSH®) terms relevant to platelet-rich plasma and erectile dysfunction for publications published up to July 2023 following the Cochrane Handbook of Intervention and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (18, 19) The detailed review protocols were available in PROSPERO (CRD42023441655)
Article eligibility criteria
The inclusion criteria were sexually active men diagnosed with erectile dysfunction (ED) according to the International Index of Erectile Function (IIEF) score, receiving the intervention of intracarvernosal injection of PRP, compared to the intervention of placebo, reporting one of the following t h e o
e (MCID), change of International Index of Erectile FunctionErectile Function (IIEF-EF) from baseline, Sexual Encounter Profile question 3 (SEP-3), peak systolic velocity (PSV), enddiastolic velocity (EDV), minor adverse events, and major adverse events All studies without full-text and nonEnglish were excluded
Data collection and quality assessment
To ensure accuracy in collecting baseline characteristics for the study, two independent authors used a piloted data collection sheet Any discrepancies were resolved through discussion involving a third author C o l l e c t e d d a t a i n c l u d e d p
' b a s e l i n e c h a r a c t e r i s
c s , s u c h a s study location, study design, number of participants, age, follow-up period, and the first author's name Data gathering was done using Microsoft Excel® 2021 The Cochrane Risk of Bias (RoB) Tool 2 was utilized to assess the bias risk of the RCTs included in the study (20)
Data synthesis and presentation
The effect size estimates of the metaanalysis were displayed as odds ratio (OR) and mean difference (MD) with 95% confidence interval (95% CI) for binary and continuous outcomes, respectively Where the data from trials were presented as median and range, the mean and standard deviation (SD) were computed using Wan et al 's formula (21) When a study did not provide sufficient information on the change in SD, we calculated data imputation using the formula for imputing SD from the baseline (18) The model used for analysis was
selected based on the heterogeneity of the included study
We used the I² index and heterogeneity 𝝌² test to evaluate heterogeneity between the studies The study being analysed had considerable heterogeneity, as indicated by I² > 50% and heterogeneity p-value < 0 05 Therefore, the random-effects DerSimonian and Laird Model was chosen for the analysis If the heterogeneity was not significant, the fixed-effects model would have been used instead (3) In this study, we considered a p-value < 0 05 statistically significant To evaluate the certainty of evidence, the Grading of Recommendations, Assessment, Development, and E
GRADEpro GDT (22) All statistical analyses were performed using STATA® 16
RESULTS
Baseline characteristics and risk of bias of the included trials
The initial database search revealed 1 050 abstracts related to the use of PRP in ED patients Thirteen studies were extracted for full-text eligibility assessment after screening the abstract using the pre-defined eligibility criteria Finally, three double-blinded RCTs were included in the review as
N Yogiswara, F Rizaldi, M Ayodhia Soebadi, et al
Figure 1. PRISMA flow diagram 2020
Table 1.
displayed in Figure 1 Table 1 represents the baseline characteristics of the participants of the included trials Trials were conducted on several continents with similar ages and nutritional statuses The majority of the participants were classified with mild and mild-moderate ED Figure 2 displays the summary of the risk of bias Assessment by evaluating the five domains There were some concerns regarding bias arising from the randomization process in the Trial by Poulios et al , as there were insufficient details regarding the randomization methods (17) The trial by Masterson et al showed some concerns
2. Risk of bias assessed using RoB2 by Cochrane
in terms of bias due to missing outcome data, as the trial reported a high rate of patients excluded from analysis (16) However, the analysis summary demonstrated an overall low risk of bias among the included trials
Treatment protocols and outcomes of the included trials
Table 2 provides detailed information regarding the trial protocol and outcomes The percentage rate of participants excluded from the final analysis ranged from 3% to 29% due to loss of follow-up or missing outcome data All included trials take the PRP sample from the patient's autologous blood samples, with 2-3 injection sites sepa-
Table 2
Treatment protocols and outcomes of the trials
Sexually active male aged 40-70 yo
Mild- moderate ED
ED treatment cessation - Sexually active male aged 45-60 yo - Mild- moderate ED
et
ED treatment cessation - Sexually active male aged 30-75 yo - Mild- moderate ED - PDE5i treatment continued
Psychogenic ED
Major pelvic surgery
Abnormal testosterone level
Psychogenic ED
Urological surgery
Abnormal testosterone level
Psychogenic ED
Abnormal HbA1c level
Poulios, et al. 2021
Shaher, et al 2023
Masterson,
al 2023
Figure
rated in 2 sessions at 2-week- to 4-week intervals All of the included trials demonstrated higher IIEF change in the PRP group compared to the placebo group, with the most remarkable change of IIEF from baseline reported by Poulios et al with the adjusted mean difference of 3 9 (1 8, 5 9, p < 0 01) (17) In terms of minimally clinical important difference (MCID), earlier trials by Poulious et al. and Shaher et al reported that PRP had a higher attainment of MCID compared to placebo (69% vs 27%, p < 0 01; 70% vs 16%, p < 0 01; respectively), with the exception of an insignificant difference by Masterson et al (60% vs 41 7%, p = 0 226) (16)
After six months of follow-up, trials showed no major or minor adverse effects, except for penile plaque in one of the PRP groups and hematoma in one of the placebo groups in the trial by Masterson et al (16)
Results from pooled analysis
The meta-analyses were conducted from three trials for a total of 221 patients with mild to moderate ED Figure 3 displays the pooled analysis of patients receiving PRP, which demonstrates significantly better improvement of IIEF-EF score during 1,3- and 6-months follow-up com-
Figure 3. Change of IIEF-EF score in (a) 1 month, (b) 3 month, and (c) 6 months between ED patients receiving PRP and placebo
pared to the placebo group (MD2 66, 95% 1 48 to 3 83, p< 0 01; MD 2 11, 95%CI 0 13 to 4 09, p = 0 04; MD 2 99, 95% CI 1 79 to 4 19, p < 0 01, respectively) The pooled analysis indicated that attainment of MCID was significantly higher in patients receiving PRP compared to the placebo group during one and 6-month follow-up [odds ratio (OR) 5 51, 95%CI 1 2 to 254, p = 0 03; OR 5 64, 95%CI 2 05 to 15 55, p < 0 01; respectively], as displayed in Figure 4 Encouragingly, there were no major AEs reported in all 3 trials in the PRP and placebo groups (p = 0 99)
Results from the assessment of certainty of evidence Table 3 provides detailed information regarding the assessment of certainty evidence The evidence certainty indicated that the change in IIEF-EF from one to six months follow-up had a moderate level of certainty, with no serious problems regarding inconsistency, imprecision, or other factors The analysis of MCID change revealed low certainty of evidence due to considerable imprecision concerns arising from the wide range of confidence intervals The rating was downgraded due to significant heterogeneity in the included trials, but upgraded because of its large effects size (23)
N Yogiswara, F Rizaldi, M Ayodhia Soebadi, et al
Table 3.
Outcome
1
6
6 month MCID
a Low risk of bias according to the assessment of RoB 2;
b Downgraded because h gh heterogeneity in the ncluded trials evaluated by I2 ndex;
c Downgraded because the ncluded tr als restr cted to patient with m ld-moderate erect le dysfunct on w th heterogeneous treatment protocols;
d Downgraded because the inc uded tr als demonstrated a w de range of conf dence interva s;
e Upgraded because of the effect s arge
Figure 4
MCID in (a) 1 month, (b) 3 month, and (c) 6 months between ED patients receiving PRP and placebo
DISCUSSION
Recent developments in the field of erectile dysfunction t h e r a p y h a v e u n d e r g o n e a p a r a d i g m s h i f t , m o v i n g beyond the mere treatment of symptoms to address the underlying pathology through regenerative medicine (24) Earlier reviews have previously highlighted the potential benefits of integrating regenerative medicine in improving erectile function, with the majority emphasizing shockwave therapy (25-28) The evidence regarding regenerative medicine is growing and even the EAU guideline is now recommending it as part of treatment for selected ED patients (7, 29, 30)
The findings of our review provided an additional interesting new insight into PRP as a novel regenerative therapy for ED PRP's use in medical therapy has been grown since its inception in the recent decades, with reports of use in orthopedics, neurology, dermatology, cardiothoracic surgery, and now urology (31-34) Although the use of PRP in urology is still in its infancy, several animal trials and observational studies have demonstrated the benefits in patients with bladder dysfunction, bladder pain syndrome, cystitis, Peyronie's disease, and ED (13, 35, 36)
To determine the role of PRP in patients with ED, several outcomes are evaluated One of the most important endpoints to consider is the IIEF-EF score The EF domain included specific questions about erection frequency, erection firmness, penetration ability, maintenance frequency, maintenance ability, and erection confidence that were intended to determine the severity of ED (37) The improvement of IIEF-EF score reflects the benefits of the treatment for ED patients The significance of PRP in improving IIEF-EF score was first demonstrated in a placebo-controlled trial by Poulios et al which found an adjusted mean difference of 3 9 points compared to the placebo group during the six-month follow-up (17) This evidence is further supported by a recent trial by Shaher et al which showed a significantly higher IIEF-EF in the PRP group (15) In contrast, the latest RCT in the American population showed an insignificant difference in IIEF-EF score between the PRP and placebo groups In this review, we discovered that in six month follow-up, PRP significantly improve IIEF-EF score compared to placebo, with a mean difference of 2 99 points When we look solely at the aggregate mean difference on the pooled analysis between PRP and placebo, the difference is relatively minor and it might be clinically irrelevant In order to objectively measure the clinical relevance of PRP for treating ED, we analysed the attainment of MCID, an endpoint to determine the minimum amount of objective change required in the EF domain to be meaningful to patients (38, 39) Prior trials by Poulios et al and Shaher et al found that patients who received PRP obtained a greater MCID at the final follow-up compared to those who received placebos (15, 17) However, the latest trial by Masterson et al observed a slightly higher but statistically insignificant difference in MCID (16) When the evidence was pooled, the analysis revealed a significantly greater attainment of MCID in PRP during the final follow-up, with an OR of 5 64 times compared to placebo
Previous studies have also demonstrated significant improvements in other patient-reported outcome measures, including SEP-2 and SEP-3 in the PRP group
However, due to limited data, a meta-analysis could not be performed
Several trials evaluated objective parameters, including penile vascular parameters In Shaher et al 's trial, notable enhancements were observed in peak systolic velocity and end diastolic velocity (15) However, the most recent trial by Masterson et al found no meaningful differences (16) Insufficient data makes it impossible to conduct a meta-analysis, and a definitive conclusion on alterations in penile vascularity cannot be drawn from the existing evidence
Regarding safety, extant trials have reported minimal to no side effects of PRP in patients with ED during shortterm follow-up Notably, Masterson et al reported a single minor side effect in both treatment groups, with no major side effects observed during the trial (16) Our review of the literature demonstrates that pooled analyses revealed insignificant differences in side effects between PRP and placebo arms It is important to note, however, that available studies only reported a limited period of follow-up, and the long-term safety of PRP in ED patients has yet to be well-established
All trials uniformly applied specified exclusion criteria, which was participants with anatomical, hormonal, and psychogenic causes of erectile dysfunction The observed difference in the included trial might be attributable to the heterogeneity of treatment protocols For example, the trial by Masterson et al used two sessions of a total of 5 ml of PRP concentrated from 120 ml of autologous blood (16) On the other hand, Poulios et al used two sessions with a total of 10 ml of PRP concentrated from 60 mL of autologous blood (17) According to earlier studies, several factors, including overall platelet concentration, leucocyte and hemoglobin concentrations, the technique of activation of PRP, and mean-platelet volume (MPV) level, could affect the bioavailability of growth factors and play a role in determining the success rate of PRP in ED patient (30, 40) Theoretically, the different PRP concentrations in the trials might affect the study's primary endpoints Furthermore, increasing the number of injections or adjusting the period between injections might result in greater improvements in IIEF-EF In this review, we cannot delve further to conduct meta-regression or subgroup analysis according to different treatment protocols due to the unmet required number of available trials (18)
The exact mechanism of how PRP improves erectile function is not yet fully understood However, several theories suggest platelets are crucial in coagulation and promoting wound healing following an injury (41) Platelets also contain various growth factors, such as FGF, PDGF, and VEGF These growth factors, as catalysts of regenerative processes, play a critical role in the recruitment of stem cells, modulation of inflammatory responses, and stimulation of angiogenesis These intricate functions are responsible for the regeneration and repair of tissues (42) In general, our analysis demonstrates a significant shortterm improvement of the erectile function in mild to moderate ED patients receiving intracavernosal PRP compared to placebo with minimal side effects The evidence's overall certainty level ranged from low to moderate, indicating that more research is quite probable to sig-
N Yogiswara, F Rizaldi, M Ayodhia Soebadi, et al
nificantly influence our confidence in the effect estimate and will probably affect the estimate (23, 43) Despite the demonstrated benefit of PRP, careful caution should be taken before implementing this treatment in daily practice, because the available trials had limited sample sizes, short follow-up durations, and heterogenous treatment protocols Currently, the international guideline classify PRP as a novel erectile dysfunction treatment that should only be implemented in clinical trials (29) However, It is possible that in the near future, further clinical trials will shed light on the significance of PRP for ED Longer-term follow-up trials are required to establish the long-term efficacy and safety of PRP, as well as a more detailed analysis of the dose and interval of PRP injection to determine the most optimal treatment protocol Moreover, the benefit of combining PRP with other regenerative medicines might also be explored in future clinical trials
CONCLUSIONS
Our findings highlights potential role of PRP as part of future ED treatment Results from high-level evidence demonstrate a short term improvement of erectile function parameters up to 6 months in mild to moderate ED patients following intracavernosal injection of PRP Future RCTs with longer duration follow-up and more standardized treatment protocols are necessary for gaining sufficient details on long-term effectiveness and safety of PRP
REFERENCES
1 Kessler A, Sollie S, Challacombe B, et al The global prevalence of erectile dysfunction: a review BJU Int 2019; 124:587-99
2 Fisher WA, Eardley I, McCabe M, Sand M Erectile dysfunction (ED) is a shared sexual concern of couples I: couple conceptions of ED J Sex Med 2009; 6:2746-60
3 Salonia A, Bettocchi C, Boeri L, et al European Association of Urology Guidelines on Sexual and Reproductive Health-2021 Update: Male Sexual Dysfunction Eur Urol 2021; 80:333-57
4 Pastuszak AW Current Diagnosis and Management of Erectile Dysfunction Curr Sex Health Rep 2014; 6:164
5 Lowy M, Ramanathan V Erectile dysfunction: causes, assessment and management options Aust Prescr 2022; 45:159
6 Kim SC, Lee YS, Seo KK, et al Reasons and predictive factors for discontinuation of PDE-5 inhibitors despite successful intercourse in erectile dysfunction patients Int J Impot Res 2014; 26:87
7 Chung DY, Ryu JK, Yin GN Regenerative therapies as a potential treatment of erectile dysfunction Investig Clin Urol 2023; 64:312
8 Pérez-Aizpurua X, Garranzo-Ibarrola M, Simón-Rodríguez C, et al Stem Cell Therapy for Erectile Dysfunction: A Step towards a Future Treatment Life (Basel) 2023; 13:502
9 Brunckhorst O, Wells L, Teeling F, et al A systematic review of the long-term efficacy of low-intensity shockwave therapy for vasculogenic erectile dysfunction Int Urol Nephrol 2019; 51:773
10 Pavlovic V, Ciric M, Jovanovic V, Stojanovic P Platelet Rich Plasma: a short overview of certain bioactive components Open Medicine 2016; 11:242
11 Sundman EA, Cole BJ, Fortier LA Growth factor and catabolic
cytokine concentrations are influenced by the cellular composition of platelet-rich plasma American Journal of Sports Medicine 2011; 39:2135-40
12 Liao CH, Lee KH, Chung SD, et al Intracavernous Injection of Platelet-Rich Plasma Therapy Enhances Erectile Function and Decreases the Mortality Rate in Streptozotocin-Induced Diabetic Rats Int J Mol Sci 2022; 23:3017
13 Huang YC, Wu CT, Chen MF, et al Intracavernous Injection of A u t o l
Associated Erectile Dysfunction in a Rat Model Sex Med 2021; 9:100317
14 Tai HC, Tsai WK, Chang ML, et al Intracavernous injection of platelet-rich plasma reverses erectile dysfunction of chronic cavernous nerve degeneration through reduction of prostate hyperplasia evidence from an aging-induced erectile dysfunction rat model FASEB J 2023; 37:e22826
15 Shaher H, Fathi A, Elbashir S, et al Is Platelet Rich Plasma Safe and Effective in Treatment of Erectile Dysfunction? Randomized Controlled Study Urology 2023; 175:114-9
16 Masterson TA, Molina M, Ledesma B, et al Platelet-rich Plasma f o
17 Poulios E, Mykoniatis I, Pyrgidis N, et al Platelet-Rich Plasma (PRP) Improves Erectile Function: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial J Sex Med 2021; 18:926-35
18 Higgins JP, Green S (Eds) Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series 2008 The Cochrane Collaboration
19 Page MJ, McKenzie JE, Bossuyt PM, et al The PRISMA 2020 statement: an updated guideline for reporting systematic reviews BMJ 2021; 372:n71
20 Higgins JPT, Altman DG, Gøtzsche PC, et al The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials BMJ 2011; 343:d5928
21 Wan X, Wang W, Liu J, Tong T Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range BMC Med Res Methodol 2014; 14:135
22 Guyatt GH, Oxman AD, Vist GE, et al Rating Quality of Evidence and Strength of Recommendations: GRADE: an emerging consensus on rating quality of evidence and strength of recommendations BMJ 2008; 336:924
23 Balshem H, Helfand M, Schünemann HJ, et al GRADE guidelines: 3 Rating the quality of evidence J Clin Epidemiol 2011; 64:401-6
24 Raheem OA, Natale C, Dick B, et al Novel Treatments of Erectile Dysfunction: Review of the Current Literature Sex Med Rev 2021; 9:123-32
25 Man L, Li G Low-intensity Extracorporeal Shock Wave Therapy for Erectile Dysfunction: A Systematic Review and Meta-analysis Urology 2018; 119:97-103
26 Zou ZJ, Tang LY, Liu ZH, et al Short-term efficacy and safety of low-intensity extracorporeal shock wave therapy in erectile dysfunction: a systematic review and meta-analysis International Braz j Urol 2017; 43:805-21
27 Yao H, Wang X, Liu H, et al Systematic Review and Meta-Analysis of 16 Randomized Controlled Trials of Clinical Outcomes of LowIntensity Extracorporeal Shock Wave Therapy in Treating Erectile Dysfunction Am J Mens Health 2022; 16:15579883221087532
28 Campbell JD, Trock BJ, Oppenheim AR, et al Meta-analysis of randomized controlled trials that assess the efficacy of low-intensity shockwave therapy for the treatment of erectile dysfunction Ther Adv Urol 2019; 11:1-13
29 Salonia A, Bettocchi C, Carvalho J, et al Sexual and reproductive health EAU Guidelines Edn presented at the EAU Annual Congress Amsterdam, 2021
30 Francomano D, Iuliano S, Dehò F, et al Regenerative treatment with platelet-rich plasma in patients with refractory erectile dysfunction: short-term outcomes and predictive value of mean platelet volume Minerva Endocrinol 2023
31 Collins T, Alexander D, Barkatali B Platelet-rich plasma: a narrative review EFORT Open Rev 2021; 6:225
32 Shen YX, Fan ZH, Zhao JG, Zhang P The application of plateletrich plasma may be a novel treatment for central nervous system diseases Med Hypotheses 2009; 73:1038-40
33 Bava ED, Barber FA Platelet-rich plasma products in sports medicine Phys Sportsmed 2011; 39:94-9
34 White C, Brahs A, Dorton D, Witfill K Platelet-Rich Plasma: A Comprehensive Review of Emerging Applications in Medical and Aesthetic Dermatology J Clin Aesthet Dermatol 2021; 14:44
35 Culha MG, Erkan E, Cay T, et al The Effect of Platelet-Rich Plasma on Peyronie’s Disease in Rat Model Urol Int 2019; 102:218-23
36 Dönmez MI, Inci K, Zeybek ND, et al The Early Histological
Effects of Intravesical Instillation of Platelet-Rich Plasma in Cystitis Models Int Neurourol J 2016; 20:188
37 Cappelleri JC, Rosen RC, Smith MD, et al Diagnostic evaluation of the erectile function domain of the International Index of Erectile Function Urology 1999; 54:346-51
38 Rosen RC, Allen KR, Ni X, Araujo AB Minimal clinically important differences in the erectile function domain of the International Index of Erectile Function scale Eur Urol 2011; 60:1010-6
39 Cook CE Clinimetrics Corner: The Minimal Clinically Important Change Score (MCID): A Necessary Pretense J Man Manip Ther 2008; 16:E82
40 Cavallo C, Roffi A, Grigolo B, et al Platelet-Rich Plasma: The Choice of Activation Method Affects the Release of Bioactive Molecules Biomed Res Int 2016; 2016:6591717
41 Anastasiadis E, Ahmed R, Khoja AK, Yap T Erectile dysfunction: Is platelet-rich plasma the new frontier for treatment in patients with erectile dysfunction? A review of the existing evidence Frontiers in Reproductive Health 2022:4:944765
42 Kakudo N, Morimoto N, Kushida S, et al Platelet-rich plasma releasate promotes angiogenesis in vitro and in vivo Med Mol Morphol 2014; 47:83-9
43 Guyatt G, Oxman AD, Akl EA, et al GRADE guidelines: 1 Introduction-GRADE evidence profiles and summary of findings tables J Clin Epidemiol 2011; 64:383-94
Correspondence
Niwanda Yogiswara niwandayogiswara@gmail com
Dr Soetomo General-Academic Hospital, Surabaya, East Java, Indonesia
Fikri Rizaldi
fikririz@gmail com
Mohammad Ayodhia Soebadi (Corresponding Author) yodisoebadi@gmail com
Universitas Airlangga Teaching Hospital, Surabaya, East Java, Indonesia
Conflict of interest: The authors declare no potential conflict of interest
This article was presented at the 45th Annual Scientific Meeting of Indonesian Urological Association
N Yogiswara, F Rizaldi, M Ayodhia Soebadi, et al
Redefining kidney transplantation procedure among adult Lupus nephritis: Expedient review approach and meta-analysis from
1 Department of Urology, Universitas Sumatera Utara Hospital, Universitas Sumatera Utara, Medan, Indonesia;
2 Division of Urology, Department of Surgery, Faculty of Medicine, Universitas Sumatera Utara - Haji Adam Malik General Hospital, Medan, Indonesia;
3 Division of Rheumatology, Department of Internal Medicine, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia;
4 General Practitioner, Putri Hijau Level II Military Hospital, Medan, Indonesia;
5 General Practitioner, Djasamen Saragih Hospital, Pematang Siantar, Indonesia;
6 General Practitioner, Sipirok Hospital, South Tapanuli Regency, Indonesia;
7 Department of Pediatrics, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia;
8 Department of Parasitology, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia;
9 Department of Nutrition, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia
Summary
Background: The actual prognostic impact of prior lupus nephritis (LN) diagnosis on end-stage kidney disease (ESKD) patients remains questionable, especially in relation to outcomes of kidney transplantation (KTx) We aim to determine the survival of the graft and recipient after the KTx procedure among patients with ESKD due to LN in comparison to non-LN.
Methods: This meta-analysis included retrospective studies from the last two decades, focusing on the KTx’s outcomes among ESKD due to LN in comparison to non-LN We establish the graft/recipient survival rate at different follow-up intervals as the primary outcome, and acute graft rejection and pooled graft failure rate as secondary outcomes All analyses were performed with the random-effect model (REM) and were presented as odd ratio (OR; within 95% confidence interval (CI)) The protocol of this study was registered in PROSPERO: CRD42023394310
Results: A total of 1,299 KTx (368 LN patients) from 10 studies with >10 years of follow-up were thoroughly reviewed All checkpoints (at 1-, 5-, 10, and 15-year post-KTx) on graft survival rate demonstrated comparable outcomes in either LN or non-LN (e.g., at 10-year follow up (OR, 1.08 [0.40, 2.91]; p = 0 88) Similar findings at all checkpoints for recipient survival rate were also observed without statistically significant difference between LN and non-LN arm (e g , at 10-year checkpoint; OR, 0.99 [0.68, 1.46]; p = 0.98). Both of our secondary analyses also presented insignificant differences (p = 0 70 and = 0.16, respectively).
Conclusions: Our findings suggested that prognosis of ESKD due to complicated LN is equal compared to ESKD associated with non-LN etiologies, suggesting the impact of LN as the inducing cause of ESKD on KTx outcome is relatively neglectable
Advancing into 3rd decade of the new millennium, progress of organ replacement care is rapidly evolving due to its promising prospect as the next definitive treatment for degenerative and chronic diseases Kidney transplantation (KTx) is currently the state-of-art procedure to attenuate symptoms of end-stage kidney disease (ESKD), offering nearly “permanent” restoration despite requiring long-term close observation on the recipients (1, 2) The etiologies of ESKD are diverse, often resulted from multisystem damage and longstanding pathologic involvement of the kidney as observed in systemic lupus erythematosus (SLE) (3) Immune-complex deposition plus abnormal interplay of immune cells’ response in SLE may cause persistent kidney damage termed lupus nephritis (LN), which is clinically confirmed by laboratory and biopsy evaluation (4)
The prevalence of SLE among the global population is estimated to be between 48 to 366 6 per 100 000 individuals, with at least 50% of cases developing LN at some point, and 10-30% progressing further into ESKD (5, 6) ESKD is the most aggravating complication of LN, that primarily affects young female population (mean diagnosis age of 31 2 years old) and has a 10-20% probability to progress into ESKD within 15 years from diagnosis (7)
As a kidney replacement therapy, KTx offers major prospects on treatment’s effect longevity, although individuals with SLE/LN might possess higher risk for developing worse prognostic value Although outcomes of KTx h a d b e e n g e n e r a l l y a s s o c i a t e d t o o t h e r f a c t o r s a s ethnic/racial differences, related to the genetical susceptibility and local lifestyle, the apparent influence on KTx outcome of prior LN diagnosis, as the underlying etiology, remains questionable, specifically in the last couple of decades with some remarkable breakthroughs in transplant-molecular science (8, 9)
Regardless its distinctive autoimmune origin and subse-
S Mirsya Warli, A Raga Ginting, N Nandita Firsty, et al
quent requirement of systemic management, should the general transplant care be extended to LN-related KTx? Is the outcome of KTx recipients remarkably worse than general population, hence requiring early robust observation? Should the current research progress be focused on preventing SLE-related flare after KTx?
This review is aimed to define the prognostic aspect of kidney-transplanted individuals after ESKD following complicated LN in comparison with non-LN etiologies, by focusing on the grafts and recipients’ survival plus the overall rejection status
MATERIALS AND METHODS
Registration and protocol
The protocol of this review had been approved and registered in PROSPERO: International Prospective Register of Systematic Reviews under issue ID CRD42022376362
Study design, search strategy, and eligibility criteria
We conducted this study based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) protocol to address our main clinical question on whether the KTx’s outcomes among individuals with LN with ESKD are different to those of ESKD due to other etio l o g i e s O n l i n e e l e c t r o n i c d a t a b a s e s e g , P u b M e d , ScienceDirect, Cochrane Library and ProQuest were thoroughly searched to retrieve all eligible literatures (in English) until November 2022 We employed Boolean method to connect the keywords on abstract/title-based identification i e (“Lupus Nephritis”) AND (“Systemic Lupus Erythematosus”) AND (“Kidney Transplantation”)
Each keywords derivatives or synonyms e g , ‘renal transplantation’ for the ‘kidney transplantation’ phrase was also included through “OR” keywords in between Duplicate
d o c u m e n t s w e r e a u t o m a t i c a l l y i d e n t i fi e d b y u s i n g Mendeley (version 1 19 8) software, and subsequently removed The literatures were initially screened by two authors (S M W and N N F ) through relevant abstractto-full text identification, followed by group discussion with other co-authors for any identified discrepancies
To date, most of the studies investigating KTx were designed as either cohort or case-control analysis, considering that the procedure itself is a “personalized approach” for both donor (either living or deceased) and recipient, therefore assumption to organize a trial-based investigation is impractical in this case Consequently, the reviewed literatures mainly consisted of studies with aforementioned designs (cohort and/or case-control), covering an adequate period of time (≥ 10 years of coverage from either single- or multi-centre records) in a geographical region (or nation), but not restricted to specific continent or race Studies older than a decade are included in this review since we aimed to synthesize reliable evidences from previous years (or the new millennia i e , > year 2000), capturing how the progress had evolved over time However, we also excluded nationwide cohort, which might solely rely on medical records and were often conducted by independent investigators (outside of the KTx-eligible centres) to reduce “gap” in population size and avoid potential statistical bias
Risk of bias assessment and data extraction
The risk-of-bias (RoB) were collectively assessed by three authors (N N F , A J V , and S C S ), using a criteria appraisal tools by Joanna Briggs Institute (JBI), each specifically designed for estimating the bias level of both cohort and case-control studies (10, 11) Discrepancies between each interpretation were resolved through a re-assessment of respective studies in an internal discussion with the first author (S M W ) To systematically summarize our finding, we extracted the following information from each study: its design, region and period, diagnosis of included patients and controls, both arm ’ s characteristics (age, donor status, pretransplant dialysis status, and pretransplant dialysis duration (in months))
In the quantitative analysis, we applied proportional-odds model to compare each group which focused on graft and patient survival analysis as the primary outcomes We also secondarily investigate the acute graft rejection (< 1 month) to represent short-term graft-host interaction and overall graft-failure, accumulated throughout the fullduration of cohort and case-control studies
Effect measures and statistical analysis
Variations might be observed considering both cohort and case-control studies were included in the final analysis (as indicated by I square (I2) value) Therefore, this meta-analysis will be conducted by a random-effect model (REM) to reduce the heterogeneity’s impact on the final estimation The statistical analysis was performed by Review Manager (RevMan) 5 4 to capture our review model on Forest plots whilst estimating odd-ratio (OR) value in 95% confidence interval (CI; P value of < 0 05 was considered to be statistically significant) This review also attempted to conduct sub-group analysis on graftand patient-survival based on time-point of follow-up (e g , 1-year, 5-year, 10-year, and 15-year after KTx ) However, it should be noted that not all studies provide complete reports from the aforementioned checkpoints due to limitations in the observation period and reporting model
We prefer OR over risk ratio (RR) parameter since our review also comprised of case-control study, in which the latter study model is basically tracking the exposure from cases and controls populations (rather than identifying the exposure, then analyzing the subsequent outcomes); thus OR is more preferrable in this situation (12) Inclusion of case-control study in this review is justifiable, considering KTx procedure among LN patients are relatively uncommon requiring an individualized care, hence we prioritize to synthesize as much evidence as possible A meta-epidemiological study by Lanza et al suggested that meta-analysis with both cohort and casecontrol studies included might possess no statistically significant difference in estimating treatment effects, which can be applied as well in our study (13) A set of sensitivity analysis was conducted as well by restricting the analysis to investigations which included only adult age populations (> 18 years old), performed the KTx from living donor source > 50 0% of the total, cohort-only analysis, and applying leave-one-out approach by removing individual studies one at a time to confirm its overall influence in pooled estimation
RESULTS
After thorough identification of studies from literature (Figure 1), we included 10 studies (8 retrospective cohorts) from multiple regions with at least 10 years of investigation period (Table 1)
Uncontrolled studies, nationwide investigations, studies that included general rheumatic diseases other than SLELNs, and those with different aims (e g , focusing on ethnic/race influence, re-transplantation, etc ) were excluded from the final analysis (Figure 1) All patients were diagnosed with ESKD due to LN’s complication following SLE diagnosis, and were compared to a control group (i e , ESKD resulting from any other disease except for LN or SLE’s kidney manifestation) All studies enlisted > 50 individuals in total, though the participant’s distributions were not always in 1:1 ratio and the study population might be compared to a control group twice it size (e g , 25 vs 50 individuals) (14-23)
A total of 368 KTx procedure from LN arm were com-
pared to 931 controls, with majority of studies consisting of females (mostly > 70 0% of the total study size), except for a cohort by Pampa-Saico in 2019 The mean ages (or median) of the populations were relatively homogenous, ranging from 3rd to 5th decade of life Though variability in population’s age occurred, inclusion of all the cohorts is still within our review scope since specific limitation on studied population’s age was not applied The donor status of the transplanted kidney included both living (either related or unrelated donor) and deceased donor Five studies (Ghafari et al , Horta-Baas et al , Lionaki et al , Park et al , Ramirez-Sandoval et al , and Roozbeh et al ) reported living donors to be > 50 0% of organ source Pretransplant dialysis method and duration were also provided on Table 1 though significant difference on baseline characteristics was not observable The RoB assessment results in Table 2 demonstrated the majority of confounding aspects in our studies were completely reported based on the JBI-based quality scoring
Figure 1. Process of identifying the eligible studies by utilizing PRISMA 2020 flow diagram
a L ving-related donor; b Living-unrelated donor; c Both HD-PD; d No pretransplant dia ys s at al ; * Sign f cant base ine difference (p < 0 05)
ESRD: End-stage renal d sease; GN: Glomerulonephr tis; LN: Lupus nephr t s; NA: not avai ab e
Table 2
11)
Graft and recipients’ survival
Our first primary analysis on graft survival demonstrated that there was not any statistically meaningful difference between the two arms based on the modelled proportional-odd estimation (Figure 2) On sub-group analysis at 1-year post-KTx, the estimated OR value was 0 79 [0 38, 1 62] in 95% CI (p > 0 05), slightly favouring LN population though statistical difference was not significant However, analysis at the following checkpoint (5year post-KTx) revealed a lower OR of 0 74 [0 41, 1 32] in 95% CI (p = 0 31)
The latter results represent a lower possibility of longer surviving grafts among non-LN population despite this change does not directly translate into a significant finding upon 95% CI estimation Further analysis on 10- and 15-year post-KTx demonstrated that the long-term follow-up of
graft survival does not show any difference between the two groups Moreover, our analysis also depicted a progressively reduced graft survival rate throughout the observation period (only 46 8% vs 28 2% of the transplanted kidney will survive after 10 years in LN vs non-LN etiology, respectively) Comparison of those rates with those observed at earlier checkpoints (e g , 1st year (89 7% vs 86 9; p = 0 52, and 5th year 62 3% vs 63 5%; p = 0 31) revealed consistent reductions on graft survival, which even lower rates at 15th year with only 42 4% (LN) vs 38 2% (non-LN); p = 0 83 Those percentages were congregated from the Figure 2 by calculating the event-to-total rate in each arm (i e , grafts’ survival rate per total KTx performed) Overall analysis on the recipient survival comparison demonstrated similar outcomes to the corresponding graft status after several years of follow-up (Figure 3) On 1-year
Firsty, et al
Risk of bias assessment by checklists provided by Joanna-Briggs Institute (10,
Graft survival after 1, 5, 10, and 15 years of follow-up post-kidney transplantation
post-KTx, the estimated OR value was 0 94 [0 26, 3 43] in 95% CI (p > 0 05) Conversely to the previous analysis, we observe that after 5 years of KTx the OR value of recipient survival is slightly favouring non-LN population (1 52 [0 72, 3 21] in 95% CI (p = 0 27)) Nevertheless, this finding does not possess any significance in our estimation model though the findings are interesting to be elaborated further Further analysis on 10- and 15-year post-KTx disclosed similar results with those observed for graft, as this analysis failed to show any difference (both p > 0 05) Additionally, we observed a remarkable challenge of trans-
plantation care in relation to the progressively reduced recipient survival rate after years of observation In comparison, the 1st year survival rate was 96 3% vs 95 7% (p = 0 93) in LN and non-LN arm, respectively However, the patients’ survival rate was massively affected throughout the years with reduced values at 5th year (80 8% vs 74 0%; p = 0 27), 10th year (69 3% vs 59 6%; p = 0 98), and 15th year (65 1% vs 61 8%; p = 0 75)
Acute and chronic graft rejection status
Secondary investigation was conducted on the recorded
Figure 2.
S Mirsya Warli, A Raga Ginting, N Nandita Firsty, et al
Figure 3.
Recipient survival after 1, 5, 10, and 15 years of follow-up post-kidney transplantation.
rejection rate within acute graft reaction period (< 1 month) and pooled graft failure during each complete study period (Figure 4)
The estimation of acute rejection demonstrated an OR value of 1 06 [0 77, 1 47] in 95% CI (p = 0 70) The following analysis on pooled graft failure disclosed similar o u t c o m e s w h i c h d e l i n e a t e d i n s i g n i fi c a n t d i f f e r e n c e among both groups, as represented by a OR value of 1 48 [0 86, 2 55]; 95% CI (p = 0 16) For that reason, our results concluded that the etiology of LN hardly influence the grafts’ reaction rate in both short- and long-term observation
Sensitivity analysis
The influence of living-donor graft status was not observed on all analysis, since most of the sub-group estimation remain statistically insignificant However, at 5-year postKTx checkpoint of grafts’ survival analysis, we observe a significant finding (p < 0 05) with the OR value at 0 41 [0 24, 0 69] in 95% CI, favouring the LN arm by only including studies with > 50 0% living-donor percentage Further sensitivity analysis on pooled rejection status also demonstrated similar outcomes to our primary report, with neither LN nor non-LN having better estimation on both acute rejection (OR 1 01 [0 61, 1 68]; p = 0 98) and graft
Archivio Italiano di Urologia e Andrologia 2024; 96(3):12627
Figure 4
Meta-analysis of graft’s reaction on acute- and chronic-phase post-renal transplantation after maximum follow-up period in each study.
failure variable (OR 1 97 [0 84, 4 60]; p = 0 12) in 95% CI Those sensitivity analysis draw a confounding question on LN-etiology influence; how does the population has better grafts’ survival in 5-year post-KTx checkpoint, but also possess similar pooled graft failure risk?
(The Forest plot outcomes of these sensitivity analysis are available on supplementary data)
DISCUSSION
Current research in transplantation care is focused on improving the prognosis, by avoiding graft rejection or subsequent organ failure The transplant procedure is a demanding task in modern medicine, and issues need to be addressed beforehand, as donor organ shortage and preservation, recipients’ compatibility, technological limitation, and the main issue reviewed in this study that was graft and recipient survival in a special population (2, 24, 25) The role of other renal replacement therapy (RRT) is considered to be pivotal and often deemed to be the only regular ESKD ‘treatment’ option available in remote regions Both haemodialysis and peritoneal dialysis hold much advantages in early-cost effectiveness and are relatively “attainable” in short-term, yet their advantages remain controversial in continuous and long-term run (26) The patient may discontinue the dialysis and proceed to KTx option since its overall outcomes are significantly better than prolonged and routine dialysis, which eventually involves pitfalls on the individuals’ quality of life (1, 27) However, transplantation may involves the
risk of early (< 1 month) or longer-term host-graft reaction, though it is generally accepted that the patient may achieve high survival rate in case of minimal rejection event (28) Moreover, chronic graft rejection will eventually lead into lower graft survival, creating the necessity to identify the outcome-influencing factors
Donor transplantation procedure requires a complex collaboration to establish recipient eligibility and organ availability Eligible recipients are placed on a “waiting list” and selected based on several “qualifications” related to life expectancy (26, 29) The statement “different ESKD’s etiology might manifest unique outcomes” is related to the personalized medicine program, based on the theoretically reasonable idea that a pathology might induce a specific reaction in a specific patient Though the recurrence-related concern is relatively rare among LN, it was presumed to be correlated with high-titers of anti-phospholipid antibodies, therefore the immunosuppressive options of post-KTx care may significantly reduce its impact (30, 31) The 2020 clinical guideline by Kidney Disease Improving Global Outcomes (KDIGO) placed the recommendation “not excluding” for selection of LN patients to KTx but also assessed that minimal disease activity should be achieved prior to the procedure (32) Even though the recommended waiting time to transplant among LN patients is ideally as short as possible, European League Against Rheumatism and European Kidney Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) suggested that the patients should achieve controllable disease for at least 3-6 months prior
S1.
Graft’s survival after 1, 5, 10, and 15 years of follow-up post-renal transplantation limited to studies which included 50 0% living-donor
to be eligible for KTx (33) Considering its autoimmune course, combination of the underlying dysfunctional immune reaction plus expected host-graft’ reaction could theoretically drive the prognostication of much worse outcomes of RTx for LN patients Requirements of standardized induction and maintenance therapy for both LN and transplantation procedures is another issue to be resolved Performing KTx on serologically active SLE might involve an higher risk of subsequent recurrence and lower graft/recipient survival, thus, apart from its complicated LN, the underlying lupus should be quiescent or stable within minimal or no immunosuppressive influence (34, 35)
The main objective of our study was to determine whether LN may significantly influence KTx outcomes, so we solely scoped the survival-related outcomes without describing much of its influencing factors from each study To our knowledge, this is the first systematic review and meta-analysis to compare LN versus non-LN etiology among ESKD patients which received KTx Revisiting the outcomes of this demanding procedure is unquestionably essential to establish the impact of this variable in patients who underwent KTx
This review basically concluded that there are no signifi-
cant differences (p > 0 05) between LN versus non-LN arm, according to proportional-odds estimation at different timing of follow-up (1-, 5-, 10-, and 15-years postKTx) The results are relatively consistent throughout each observation period, though the latter checkpoint only involved 3-4 studies at the most If the analysis was aimed solely to OR values, fluctuations at each checkpoint, were statistically inconsistent Throughout each c h
observe even a slightest suggestion to differentiate the outcomes, excluding the hypothesis that LN might negatively influence the graft/recipient survival This lack of differences might be originated from diverse etiologies included in non-LN population or other factors such race/ethnicity or others, although our simplified conclusion is that LN might, in fact, did not involve a worse prognostic value compared to KTx procedures in general Several controversies around possible factors influencing graft and patients’ survival after KTx had been elaborated, and yet, the most commonly described variables are the absence of induction treatment, multiple immunosuppressant medication, pre-existing comorbidities, higher body mass index, donor/recipient of Afro-American race, non-living donor, longer dialysis time, prior dialysis
S Mirsya Warli, A Raga Ginting, N Nandita Firsty, et al
Figure
Figure S2.
Meta-analysis of recipients’ survival after 1, 5, 10, and 15 years of follow-up post-renal transplantation limited to studies which included 50.0% living-donor.
S3
Meta-analysis of graft’s reaction on acute- and chronic-phase post-renal transplantation after maximum follow-up period in each study; limited to studies which included 50.0% living-donor.
Figure
S Mirsya Warli, A Raga Ginting, N Nandita Firsty, et al
method, lower adherence to treatment or routine control, and delayed graft function (36-38)
It is highly perceivable that the concomitant SLE might theoretically worsen outcome of KTx procedures considering the similarity of risk factors between graft loss and the SLE (37, 39, 40) Specific evaluation on the causes of graft loss was not performed in this study, even though chronic graft nephropathy was the most common etiology, followed by thrombotic events which are related to anti-phospholipid antibody (APA) positivity or pregnancy
The population age was younger in LN arm, raising the hypothesis that this might affect the outcome of the procedure Did it favour the survival or early onset translated into more severe course of disease?
Another issue is the statistical design of the studies which estimated the prognosis by hazard-ratio (HR) value in Kaplan-Meier curve Since not all studies provided those details, we adapted our approach to the proportionalodds model evaluating values corresponding to each checkpoint of follow-up, although this choice is our main limitation in providing more accurate estimation in survival rate, Our review primarily consisted of retrospective studies that lack the advantages of randomization and all the benefits of trial-investigation
We incorporated both case-control and cohorts into the same pooling of analysis because of the scarcity of the included studies that obliged us to perform a meta-analysis of all the studies available at that point Only 3 casecontrol studies (Lionaki et al , Naransjo-Escobar et al , and Roozbeh et al ) were included in the final analysis (16, 18, 22), however it should be underlined that differences in design compared to other retrospective cohorts may act as an important selection bias (originated from case-control studies) in this review (41) Nevertheless, our primary outcome was statistical confirmation of KTx outcome to justify KTx among LNs, since it might offer better quality of life or superior survival rate compared to individuals in routine dialysis schedule
We encourage future original studies on LN-ESKD-KTx subjects to be focused on identifying factors preceding grafts loss and subsequent recipient mortality in order to evaluate not only grafts rejection rate but also the best modality of control of SLE activity and prevention of LN recurrence by managing the most appropriate immunosuppressants
CONCLUSIONS
KTx procedure in ESKD with LN etiology is equally beneficial in short- and long-term outcomes compared to procedure in patients with non-LN etiologies since no s t a t i s t i c a l l y s i g n i fi c a n t d i f f e r e n c e o f o u t c o m e s w e r e observed Hence no special care was practically required on the LN population Recommendation to perform KTx among eligible participants including individuals with SLE should be advocated considering that current transplantation care had progressed into more specific and personalized approach Therefore, this review is expected to assist global transplant community in tailoring better strategies and preventing KTx’s-related pitfall among complicated-LN patients
REFERENCES
1 Wang JH, Skeans MA, Israni AK Current Status of Kidney Transplant Outcomes: Dying to Survive Adv Chronic Kidney Dis 2016; 23:28
2 Chapman JR What are the key challenges we face in kidney transplantation today? Transplant Res 2013; 2:1-7
3 Chan TM, Yung S, Yap DYH A review of advances in the understanding of lupus nephritis pathogenesis as a basis for emerging therapies F1000Res 2020; 9:F1000 Faculty Rev-905
4 Hahn BH, McMahon M, Wilkinson A, et al American College of Rheumatology Guidelines for Screening, Case Definition, Treatment and Management of Lupus Nephritis Arthritis Care Res 2012; 64:797-808
5 Barber MRW, Drenkard C, Falasinnu T, et al Global epidemiology of systemic lupus erythematosus Nat Rev Rheumatol [Internet] 2021; 17:515-32
6 Almaani S, Meara A, Rovin BH Update on Lupus Nephritis Clin J Am Soc Nephrol [Internet] 2017; 12:825-35
7 Tektonidou MG, Dasgupta A, Ward MM Risk of End-Stage Renal Disease in Patients With Lupus Nephritis, 1971-2015: A Systematic Review and Bayesian Meta-Analysis Arthritis Rheumatol 2016; 68:1432-41
8 Newman KL, Fedewa SA, Jacobson MH, et al Racial/Ethnic Differences in the Association between Hospitalization and Kidney Transplantation among Waitlisted End Stage Renal Disease Patients Transplantation 2016; 100:2735-45
9 Rybicka-Kozlowska E, Andreoni K, Kozlowski T Racial differences in renal transplantation: How do we bridge the gap? Surg (United States) [Internet] 2021; 170:333-5
10 Joanna Briggs Institute Checklist for Cohort Studies [Internet] j b i g l o ba l ; 2 02 0 A v a i l a bl e f ro m : h t t
files/2021-10/Checklist for Cohort Studies docx
11 Joanna Briggs Institute Checklist for Case Control Studies [Internet] jbi global; 2020 Available from: https://jbi global/sites/ default/files/2021-10/Checklist for Case Control Studies docx
12 Ranganathan P, Aggarwal R, Pramesh C Common pitfalls in statistical analysis: Odds versus risk Perspect Clin Res 2015; 6:222
13 Lanza A, Ravaud P, Riveros C, Dechartres A Comparison of estimates between cohort and case-control studies in meta-analyses of therapeutic interventions: A meta-epidemiological study PLoS One 2016; 11:1-12
14 Ghafari A, Etemadi J, Ardalan MR Renal Transplantation in P a t i e n t s W i t h L u p u s N e p h r i t i s : A S i n g l e - C e n t e r E x p e r i e n
Transplant Proc 2008; 40:143-4
15 Horta-Baas G, Camargo-Coronel A, Miranda-Hernández DG, et a l R
Comparison of graft survival with other causes of end-stage renal disease Reumatol Clin 2019; 15:140-5
16 Lionaki S, Kapitsinou PP, Iniotaki A, et al Kidney transplantation in lupus patients: A case-control study from a single centre Lupus 2008; 17:670-5
17 Moroni G, Tantardini F, Gallelli B, et al The long-term prognosis of renal transplantation in patients with lupus nephritis Am J Kidney Dis 2005; 45:903-11
18 Naranjo-Escobar J, Manzi E, Posada JG, et al Kidney transplantation for end-stage renal disease in lupus nephritis, a very safe procedure: A single Latin American transplant center experience Lupus 2017; 26:1157-65
19 Pampa-Saico S, Marcén-Letosa R, Fernández-Rodríguez A, et al Kidney transplantation in systemic lupus erythematosus: Outcomes and prognosis Med Clin 2019; 153:460-3
20 Park H, Park WY, Kang SS, et al Clinical Outcomes of Kidney Transplantation in Patients With Biopsy-Proven Glomerulonephritis Transplant Proc 2018; 50:1009-12
21 Ramirez-Sandoval JC, Chavez-Chavez H, Wagner M, et al Long-term survival of kidney grafts in lupus nephritis: a Mexican cohort Lupus 2018; 27:1303-11
22 Roozbeh J, Eshraghian A, Raeesjalali G, et al Outcomes of kidney transplantation in patients with systemic lupus erythematosus Iran J Kidney Dis 2011; 5:53-6
23 Yu TM, Chen YH, Lan JL, et al Renal outcome and evolution of disease activity in Chinese lupus patients after renal transplantation Lupus 2008; 17:687-94
24 Kupiec-Weglinski JW Grand Challenges in Organ Transplantation Front Transplant 2022; 1:1-5
25 Black CK, Termanini KM, Aguirre O, et al Solid organ transplantation in the 21st century Ann Transl Med 2018; 6:409-409
26 Kaballo MA, Canney M, O’Kelly P, et al A comparative analysis of survival of patients on dialysis and after kidney transplantation Clin Kidney J 2018; 11:389-93
27 Yngman-Uhlin P, Fogelberg A, Uhlin F Life in standby: Hemodialysis patients’ experiences of waiting for kidney transplantation J Clin Nurs 2016; 25:92-8
28 Neild GH Life expectancy with chronic kidney disease: an educational review Pediatr Nephrol [Internet] 2017; 32:243-8
29 NHS Blood and Transplant Kidney acceptance criteria Available from: https://www odt nhs uk/transplantation/kidney/kidney-acceptance-criteria/#
30 Pramudya D, Hertanto DM, Pitaloka AT, Tjempakasari A, Pranawa Lupus nephritis and kidney transplantation: past, present and future Bali Med J 2023; 12(2):1802-7
31 Pattanaik D, Green J, Talwar M, Molnar M Relapse and Outcome of Lupus Nephritis After Renal Transplantation in the Modern Immunosuppressive Era Cureus 2022; 14:e20863
32 Chadban SJ, Ahn C, Axelrod DA, et al KDIGO Clinical Practice Guideline on the Evaluation and Management of Candidates for Kidney Transplantation Transplantation 2020; 104(4S1 Suppl 1):S11-S103
33 Fanouriakis A, Kostopoulou M, Cheema K, et al 2019 Update of the Joint European League against Rheumatism and European Renal A s s o c i a t i o n - E u r o p e a n D i a l y s i s a n d T r
n (EULAR/ERA-EDTA) recommendations for the management of lupus nephritis Ann Rheum Dis 2020; 79:S713-23
34 Wilhelmus S, Bajema IM, Bertsias GK, et al Lupus nephritis management guidelines compared Nephrol Dial Transplant 2016; 31:904-13
35 Morales E, Galindo M, Trujillo H, Praga M Update on Lupus Nephritis: Looking for a New Vision Nephron 2021; 145:1-13
36 Rodelo J, González LA, Ustáriz J, et al Kidney transplantation outcomes in lupus nephritis: A 37-year single-center experience from Latin America Lupus 2021; 30:1644-59
37 Legendre C, Canaud G, Martinez F Factors influencing long-term outcome after kidney transplantation Transpl Int 2014; 27:19-27
38 Albuquerque BC, Salles VB, Tajra RDP, Rodrigues CEM Outcome
and Prognosis of Patients With Lupus Nephritis Submitted to Renal Transplantation Sci Rep 2019 Aug 12; 9(1):11611
39 Gergianaki I, Bortoluzzi A, Bertsias G Update on the epidemiology, risk factors, and disease outcomes of systemic lupus erythematosus Best Pract Res Clin Rheumatol 2018; 32:188-205
40 Nee R, Jindal RM, Little D, et al Racial differences and income disparities are associated with poor outcomes in kidney transplant recipients with lupus nephritis Transplantation 2013; 95:1471-8
41 Palumbo SA, Robishaw JD, Krasnoff J, Hennekens CH Different Biases in Meta-Analyses of Case-Control and Cohort Studies: An Example from Genomics and Precision Medicine Ann Epidemiol 2021; 58:38-41
Correspondence
Syah Mirsya Warli, MD, PhD warli@usu ac id
Department of Urology, Universitas Sumatera Utara Hospital, Universitas Sumatera Utara, Medan, Indonesia
Division of Urology, Department of Surgery, Faculty of Medicine, Universitas Sumatera Utara - Haji Adam Malik General Hospital, Medan, Indonesia
Jl Dr Mansyur, No 66, Medan, North Sumatera, 20154, Indonesia
Andi Raga Ginting andi raga@usu ac id
Division of Rheumatology, Department of Internal Medicine, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia
Naufal Nandita Firsty acnaufal06@gmail com
General Practitioner, Putri Hijau Level II Military Hospital, Medan, Indonesia
Adrian Joshua Velaro ajoshuav@gmail com
General Practitioner, Djasamen Saragih Hospital, Pematang Siantar, Indonesia
Stephani Clarissa Sembiring stephaniclarissas@gmail com
General Practitioner, Sipirok Hospital, South Tapanuli Regency, Indonesia Department of Pediatrics, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia
Dewi Masyithah Darlan dewi2@usu ac id
Department of Pediatrics, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia
Zaimah Zulkarnaini Tala zaimah@usu ac id
Department of Nutrition, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia
Conflict of interest: The authors declare no potential conflict of interest
The initial version of this study has been presented as poster presentation session of World Congress of Nephrology (WCN) 2023 by the International Society of Nephrology (ISN) from March 30th to April 2nd, 2023 in Bangkok, Thailand
LETTER TO EDITOR
Comment to “An unusual ‘linitis plastica’ like breast cancer bladder metastasis”
1 Department of Surgical and Diagnostic Integrated Sciences (DISC), University of Genova, Genova, Italy;
2 IRCCS Ospedale Policlinico San Martino, Genova, Italy;
3 Casa di Cura Musumeci GECAS, Gravina di Catania, Italy
KEY WORDS: Breast cancer; Bladder cancer; Metastasis; Linitis plastica; Haematuria
Submitted 4 July 2024; Accepted 6 July 2024
Dear Editor,
We read with interest the recently published article by Farci et al , titled “An unusual ‘linitis plastica’ like breast cancer bladder metastasis” and we congratulate with the authors for the very interesting topic and case presented (1) The authors have correctly reported data from the literature regarding the rate of bladder metastases from breast cancer, which appear to be approximately 2 4% of all bladder metastases However, a recent systematic review of the literature 2 including 45 articles highlighted how in reality this percentage may be underestimated and probably higher As indicated, some studies have reported rates of metastatic bladder involvement in breast cancer patients as high as 7% (2, 3) Most clinical presentations occur with the appearance of hematuria, sometimes even several years after the initial diagnosis of breast cancer In the case presented by colleagues 1 this occurred approximately 5 years after the diagnosis of breast cancer, and also in other cases presented in the literature the presentation of the metastasis can occur even more than 30 years after the diagnosis (2, 4)
This delay in presentation can often make a timely diagnosis of the metastasis itself difficult, as the appearance of hematuria often occurs after the end of the usual oncological follow-up for breast cancer (5) A further difficulty in this sense, during the follow-up, is also a lack of mutual knowledge on the part of the urologist and breast surgeon of the respective pathologies This can lead to a more difficult histopathological and immunohistochemical diagnosis post-TURB (6), given by the failure to communicate the previous history of breast cancer to the pathologist himself
A further focus must be placed on the fact that breast cancer is a pathology which is not only unfortunately relatively frequent in females, but sometimes also in young women in an aggressive and locally advanced form (7, 8)
This draws attention to the importance of a correct medical history of patients, especially young ones, to better understand the appearance of hematuria and better direct the differential diagnosis, even with the aid of biomarkers (8, 9)
Fortunately, bladder metastases from breast cancer remain rare events, although not exceptional It therefore becomes essential, in our opinion, to also take this possibility into consideration in order to carry out a correct and timely diagnosis
REFERENCES
1 Farci R, Tolu S, Trombetta M, et al An unusual "linitis plastica" like breast cancer bladder metastasis Arch Ital Urol Androl 2024; 96:12483
2 Malinaric R, Balzarini F, Granelli G, et al From women to women-hematuria during therapy for metastatic breast cancer, what to suspect and when to be alarmed; Bladder metastasis from breast cancer-our experience and a systematic literature review Front Oncol 2022; 12:976947
3 Hagemeister FB Jr, Buzdar AU, Luna MA, Blumenschein GR Causes of death in breast cancer: a clinicopathologic study Cancer 1980; 46:1627
4 De Rose AF, Balzarini F, Mantica G, et al Late urinary bladder metastasis from breast cancer Arch Ital Urol Androl 2019; 91:60-62
5 Cornacchia C, Dessalvi S, Santori G, et al Breast Edema after Conservative Surgery for Early-Stage Breast Cancer: A Retrospective SingleCenter Assessment of Risk Factors Lymphology 2022; 55:167-177
6 Mantica G, Simonato A, Du Plessis DE, et al The pathologist's role in the detection of rare variants of bladder cancer and analysis of the impact on incidence and type detection Minerva Urol Nefrol 2018; 70:594-597
7 Fregatti P, Gipponi M, Diaz R, et al The Role of Sentinel Lymph Node Biopsy in Patients With B5c Breast Cancer Diagnosis In Vivo 2020; 34:355-359
8 Malinaric R, Mantica G, Lo Monaco L, et al The Role of Novel Bladder Cancer Diagnostic and Surveillance Biomarkers-What Should a Urologist Really Know? Int J Environ Res Public Health 2022; 19:9648
9 Lopez-Gonzalez L, Sanchez Cendra A, Sanchez Cendra C, et al Exploring Biomarkers in Breast Cancer: Hallmarks of Diagnosis, Treatment, and Follow-Up in Clinical Practice Medicina (Kaunas) 2024; 60:168
Correspondence
Raquel Diaz, MD raqueldiaz ge@gmail com
Piero Fregatti, MD piero fregatti@unige it
Carlo Terrone, MD
carlo terrone@med uniupo it
Federica Murelli, MD federica murelli@unige it
Guglielmo Mantica, MD (Corresponding Author) guglielmo mantica@gmail com
IRCCS Policlinico San Martino, Largo Rosanna Benzi 10, 16132, Genova, Italy
Rosario Leonardi, MD urologialeonardi@gmail com
Casa di Cura Musumeci GECAS, Gravina di Catania, Italy
Conflict of interest: The authors declare no potential conflict of interest
LETTER TO EDITOR
How much does mitochondrial dysfunction affect male infertility?
Ernesto Di Mauro 1 , Gianluigi Cacace 1 , Vincenzo Morgera 1 , Roberto La Rocca 1 , Luigi Napolitano 1 , Pietro Saldutto 2 , Vincenzo Maria Altieri 2, 3
1 Department of Neurosciences, Reproductive Sciences and Odontostomatology, University of Naples "Federico II", Naples, Italy;
Nowadays male infertility is considered one of the most important “diseases” worldwide (1) More than 15% of couples are infertile, in half of these cases it is related to male factors, and in approximately 60% of idiopathic male infertility it is closely related to decreased sperm motility (2)
Mitochondria are particularly structurally and functionally organelles in male gametes, involved into adenosine triphosphate (ATP) production through oxidative phosphorylation (OXPHOS) to support sperm mobility, production of steroid hormones in the testis, regulation of cell proliferation, regulation of reactive oxidation species (ROS) signaling, calcium homeostasis, capacitation, acrosome reaction, and metabolism (3, 4) Approximately 80 mitochondria are present in the midpiece of spermatozoa (5) To the best of our knowledge mitochondrial dysfunction is often associated with the aging process and it is related to several diseases, includes male infertility (6) Oxidative stress (OS) due to the overproduction of ROS in mitochondria is one of the major causes of these disorders accounting approximately 30-80% of male infertility (7) Exposure to ROS induces structural and functional damage in proteins, membrane, calcium homeostasis, DNA in spermatozoa, and this affects sperm motility, ability to penetrate oocytes, and embryonic development (7-10) Even though the exact mechanisms of mitochondrial dysfunction in male fertility impairment remains still unclear, it is known that age-dependent alterations of the epididymis can cause alterations in sperm mitochondrial functioning (11, 12) Mitochondrial are involved into all spermatogenesis and fertilization mechanisms: sperm motility, gamete production, steroid hormone production, cell signaling, proliferation, epigenetic regulation, cell differentiation and cell death (6) Steroidogenesis involves the mobilization of cholesterol from lipid droplets and/or the plasma membrane, its transportation into mitochondria under the pulsatile secretion of LH and consequent cAMP production, the formation of pregnenolone within the mitochondria, and the subsequent conversion of pregnenolone into the ultimate steroid products by enzymes located in the smooth endoplasmic reticulum (13) Spermatozoa’s ability to move relies entirely on the functionality of the OXPHOS pathways (14) Given that sperm mitochondrial DNA (mtDNA) contains genes that encode OXPHOS-related proteins, any deviation in mtDNA could potentially affect sperm motility In the last twenty years, research has emphasized the connection between the quality of mtDNA and sperm motility by examining mutations, duplications, and deletions in human sperm mtDNA (15) These investigations have shown that point mutations, single nucleotide polymorphisms (SNPs), and haplogroups within mtDNA can significantly impair semen quality (16) Sperm mitochondrial deletion is a marker of mtDNA integrity and damage Men with suboptimal semen parameters tend to exhibit a higher prevalence of sperm mitochondrial DNA deletions compared to men with normal sperm parameters (17)
The sperm mitochondrial DNA copy number, representing the number of mtDNA copies per nuclear DNA copy, serves as a sensitive biomarker of male fertility Variations in human mtDNA copy numbers are linked to decreased sperm motility and fertility decline (18)
Finally, oxidative stress initiates the spermatozoa's progression along the intrinsic apoptotic pathway, starting from the loss of mitochondrial membrane potential (MMP), which leads to the formation of oxidative DNA adducts, DNA fragmentation, and ultimately culminates in cell death (19)
Several oral supplements have been proposed in male infertility treatments as well as L-carnitine, arginine, alpha-lipoic acid, coenzyme Q10, vitamins, zinc, selenium, and they regulate mitochondrial homeostasis Coenzyme Q10 (CoQ10) is abundant in mitochondria and plays a crucial role in the electron transport chain, facilitating ATP production Additionally, CoQ10 possesses potent antioxidant properties that can potentially surpass those of cellular antioxidants
E Di Mauro, G Cacace, V Morgera, et al
such as tocopherol and resveratrol, making it effective in countering attacks from ROS (20, 21) Carnitine plays an important role in fatty acid metabolism by transporting fatty acids across the mitochondrial membrane (22) Vitamin D prevents protein oxidation, lipid peroxidation, autophagy, mitochondrial dysfunction, inflammation, oxidative stress, epigenetic modifications, DNA abnormalities, and calcium and ROS signaling (23)
Due to the pivotal role of mitochondria in sperm motility and overall fertility, assessing mitochondrial functionality becomes an essential topic in male infertility treatment, aiding in the development of targeted interventions to improve reproductive outcomes Furthermore, several randomized controlled trial, in vitro and in vivo studies research are necessary to better highlighted their involvement in the physiopathology of infertility
ACKNOWLEDGMENTS
This publication was produced with the co-funding European Union - Next Generation EU, in the context of The National Recovery and Resilience Plan, Investment Partenariato Esteso PE8 "Conseguenze e sfide dell'invecchiamento", Project Age-It (Ageing Well in an Ageing Society)
REFERENCES
1 Leslie SW, Soon-Sutton TL, Khan MA Male Infertility In: StatPearls [Internet] Treasure Island (FL): StatPearls Publishing; 2024 [cited 2024 Mar 3] Available from: http://www ncbi nlm nih gov/books/NBK562258/
2 Park YJ, Lee BM, Pang WK, Ryu DY, et al Low Sperm Motility Is Determined by Abnormal Protein Modification during Epididymal Maturation World J Mens Health 2022; 40:526
3 Park YJ, Pang MG Mitochondrial Functionality in Male Fertility: From Spermatogenesis to Fertilization Antioxidants 2021; 10:98
4 Shivaji S, Kota V, Siva AB The role of mitochondrial proteins in sperm capacitation Journal of Reproductive Immunology 2009; 83:14-8
5 Freitas MJ, Vijayaraghavan S, Fardilha M Signaling mechanisms in mammalian sperm motility Biol Reprod 2017; 96:2-12
6 Durairajanayagam D, Singh D, Agarwal A, Henkel R Causes and consequences of sperm mitochondrial dysfunction Andrologia 2021; 53:e13666
7 Agarwal A, Virk G, Ong C, Du Plessis SS Effect of Oxidative Stress on Male Reproduction World J Mens Health 2014; 32:1
8 McLachlan RI, Kretser DM Male infertility: the case for continued research: Even with modern assisted-reproduction technologies, clinical assessment and basic research on male infertility are essential Medical Journal of Australia 2001; 174:116-7
9 Fusco GM, Cirillo L, Abate M, et al Male infertility, what Mobile Health Applications “know”: quality analysis and adherence to European Association of Urology Guidelines Arch Ital Urol Androl 2022; 94:470-5
10 Pereira R, Sá R, Barros A, Sousa M Major regulatory mechanisms involved in sperm motility Asian J Androl 2017; 19:5
11 Wang JJ, Wang SX, Tehmina, et al Age-Related Decline of Male Fertility: Mitochondrial Dysfunction and the Antioxidant Interventions Pharmaceuticals 2022; 15:519
12 Fusco F, Longo N, De Sio M, et al Impact of Circadian Desynchrony on Spermatogenesis: A Mini Review Front Endocrinol (Lausanne) 2021; 12:800693
13 Wang Y, Chen F, Ye L, et al Steroidogenesis in Leydig cells: effects of aging and environmental factors Reproduction 2017; 154:R111-22
14 Ruiz-Pesini E, Lapeña AC, Díez-Sánchez C, et al Human mtDNA Haplogroups Associated with High or Reduced Spermatozoa Motility Am J Hum Genet 2000; 67:682-96
15 Amaral A, Lourenço B, Marques M, Ramalho-Santos J Mitochondria functionality and sperm quality Reproduction 2013; 146:R163-74
16 Kumar P, Sangeetha N Mitochondrial DNA mutations and male infertility Indian J Hum Genet 2009; 15:93
17 Ieremiadou F, Rodakis GC Correlation of the 4977 bp mitochondrial DNA deletion with human sperm dysfunction BMC Res Notes 2009; 2:18
18 Faja S, Nelson Darling L Variation in restricted and repetitive behaviors and interests relates to inhibitory control and shifting in children with autism spectrum disorder Autism 2019; 23:1262-72
19 Aitken ML, Limaye A, Pottinger P, et al Respiratory Outbreak of Mycobacterium abscessus Subspecies massiliense in a Lung Transplant and Cystic Fibrosis Center Am J Respir Crit Care Med 2012; 185:231-2
20 Tiwari S, Mohanty TK, Bhakat M, et al Comparative evidence support better antioxidant efficacy of mitochondrial-targeted (Mitoquinone) than cytosolic (Resveratrol) antioxidant in improving in-vitro sperm functions of cryopreserved buffalo (Bubalus bubalis) semen Cryobiology 2021; 101:125-34
21 El-Sherbiny HR, Abdelnaby EA, El-Shahat KH, et al Coenzyme Q10 Supplementation enhances testicular volume and hemodynamics, reproductive hormones, sperm quality, and seminal antioxidant capacity in goat bucks under summer hot humid conditions Vet Res Commun 2022; 46:1245-57
22 Yang K, Wang N, Guo HT, et al Effect of L-carnitine on sperm quality during liquid storage of boar semen Asian-Australas J Anim Sci 2020; 33:1763-9
23 Matta Reddy A, Iqbal M, Chopra H, et al Pivotal role of vitamin D in mitochondrial health, cardiac function, and human reproduction EXCLI J 2022; 21:967-990
Correspondence
Ernesto Di Mauro, MD
ernesto dimauro@unina it Gianluigi Cacace, MD cacace gianlu@gmail com
Vincenzo Morgera, MD vincemorgera87@gmail com
Roberto La Rocca, MD robertolarocca87@gmail com
Luigi Napolitano (Corresponding Author) dr luiginapolitano@gmail com
Department of Neurosciences, Reproductive Sciences and Odontostomatology, University of Naples "Federico II", Naples, Italy
Pietro Saldutto, MD pietro saldutto@gavazzeni it
Vincenzo Maria Altieri, MD vincenzomaria altieri@gmail com
UO Urologia, Humanitas Gavazzeni, Bergamo, Italy
Conflict of interest: The authors declare no potential conflict of interest
LETTER TO EDITOR
Monkeypox: A new threat for healthcare and urology?
Rosario Leonardi 1 , Angelo Cafarelli 2 , Alessandro Calarco 3 , Renzo Colombo 4 , Ottavio de Cobelli 5 , Ferdinando De Marco 6 , Giovanni Ferrari 7 , Giuseppe Ludovico 8 , Stefano Pecoraro 9 , Domenico Tuzzolo 10 , Guglielmo Mantica 11 on behalf of UrOP (Urologi Ospedalità Gestione Privata)
1 Casa di Cura Musumeci-Gecas, Gravina di Catania, Italy;
2 Urology Unit, Villa Igea, Ancona, Italy;
3 Department of Urology, San Carlo di Nancy Hospital, Rome, Italy
4 Department of Urology, Vita e Salute San Raffaele University, Milan, Italy;
5 Department of Urology, IEO European Institute of Oncology, IRCCS, Milan, Italy;
6 I N I Grottaferrata, Rome, Italy;
7 Hesperia Hospital, Modena, Italy;
8 Miulli Hospital, Acquaviva delle Fonti, Bari, Italy;
Monkeypox is an emerging zoonotic viral disease caused by the Monkeypox virus, traditionally confined to central and west Africa (1, 2), which has recently spread to other regions worldwide, making it a global health concern Monkeypox was first identified in humans in 1970 in the Democratic Republic of the Congo and the transmission is mainly due through direct contact with infected animals or people Sporadic outbreaks have occurred for decades However, as is happening for other infective diseases (3), the globalization, increased international travel and migration has facilitated the spread of the virus to previously unaffected regions, highlighting its growing importance for public health
A first monkeypox international outbreak was recorded in 2022-2023, while in 2024 the number of cases increased significantly, so much so that the World Health Organization (WHO) prudently declared a state of global health emergency (4) Furthermore, in recent days the first case of a patient affected by the Clade I variant Monkeypox, which is more aggressive and virulent, was recorded in Europe
Although monkeypox patients primarily presents with dermatological or systemic symptoms, such as fever, skin rashes and pox-like lesions, it can also lead to urological complications, necessitating specialized attention (5) Among urological manifestations, genital lesions have been described in the literature (6-10) These lesions may be painful and appear as vesicles on the external genitalia In some cases, monkeypox can lead to prostatitis, urethritis and orchitis, making difficult the differential diagnosis from other causes of such diseases (11, 12) For a correct and prompt diagnosis, as well as reporting suspected cases, it is important that the urologist is also aware of the possible urological clinical presentation of Monkeypox Unfortunately, as with COVID-19, Monkeypox could create additional healthcare organization (13) and training issues for urology residents As was per other infectious outbreaks, the potential impact on surgical training and clinical exposure may be significant One of the primary concerns is the potential reduction in clinical opportunities During the previous COVID-19 pandemic, elective surgeries were postponed or canceled (14), limiting residents' hands-on experience in performing and assisting urological procedures This reduction in surgical volume can hinder the development of essential technical skills that are crucial for urologists Furthermore, the need for infection control measures may limit direct patient interaction In some Institutions, residents may be restricted from certain areas of the hospital, which can interfere with their ability to perform delicate procedures and communicate effectively with patients, increasing the use of Telemedicine (15-18) Likewise, a possible epidemic/pandemic could strain the availability of teaching faculty, resulting in reduced mentorship and fewer educational and academic opportunities (19)
A monkeypox pandemic might presents significant risks to the scheduling of urological surgeries and the management of waiting lists As previously happened for COVID-19, during a pandemic, hospitals often reallocate resources, including operating rooms, staff, and supplies, to manage the immediate demands of the infectious outbreak This can lead to the postponement of non-urgent surgeries, which directly impacts patients awaiting urological procedures (13) As a result, the already long waiting lists can grow longer, with patients experiencing increased anxiety, discomfort, or wors-
R Leonardi, A Cafarelli, A Calarco, et al
ening of their conditions while they wait Moreover, the prioritization of emergency and urgent cases may lead to a backlog of elective surgeries that becomes increasingly difficult to manage as the pandemic continues For all these reasons and many more, we should have learned lesson from COVID-19 and be ready if this Monkeypox emerging viral disease will become pandemic As we doctors always say “prevention is better than cure”! In this possible scenario, the role of us urologists also become important both to prevent the possible spread of the virus by promptly recognizing patients with urological symptoms, and by organizing healthcare facilities as best as possible and immediately in the unfortunate case of a new pandemic
REFERENCES
1 Graham F Daily briefing: Raising the alarm about the monkeypox virus Nature 2024 Aug 14 doi: 10 1038/d41586-024-02671-4 Epub ahead of print PMID: 39147816
2 Urban N, Valencak J, Bauer WM, et al Diary of human monkeypox: Illustrations of the clinical course J Eur Acad Dermatol Venereol 2023; 37:e672-e674
3 Mantica G, Van der Merwe A, Terrone C, et al Awareness of European practitioners toward uncommon tropical diseases: are we prepared to deal with mass migration? Results of an international survey World J Urol 2020; 38:1773-1786
4 Eurosurveillance editorial team Note from the editors: WHO declares mpox outbreak a public health emergency of international concern Euro Surveill 2024; 29:240815v
5 Catto JWF Monkeypox and the Urologist: Playing an Important Role in This Emerging Global Outbreak Eur Urol 2022; 82:631-632
6 Moreno-Matson MC, Ocampo MA, Sáenz Rengifo D, Valero HP Penile necrosis due to monkeypox Urol Case Rep 2023; 51:102554
7 Wegrzyn GH, Kilianek M, Yallapragada S, et al Genitourinary Mpox: A case report & primer for urologists Urol Case Rep 2023; 51:102559
8 Hamid TA, Elmekresh A, Parkar AZ, et al Male genital lesions in monkeypox virus infection: a case series Can J Urol 2023; 30:11562-11567
9 Lee J, McLean J, Zucker J, et al Mpox Genital Lesions: A Large Single-center Experience With Intermediate Follow-up J Urol 2023; 210:510-516
10 Milano E, Belati A, De Santis L, et al First Case of Paraphimosis as a Severe Complication of Monkeypox Vaccines (Basel) 2022; 11:63
11 Kranz J, Bartoletti R, Bruyère F, et al European Association of Urology Guidelines on Urological Infections: Summary of the 2024 Guidelines Eur Urol 2024; 86:27-41
12 Bausch K, Mantica G, Smith EJ, et al Genitourinary Tuberculosis: A Brief Manual for Urologists on Diagnosis and Treatment from the European Association of Urology Urological Infections Panel Eur Urol Focus 2024; 10:77-79
13 Leonardi R, Bellinzoni P, Broglia L, et al Hospital care in Departments defined as COVID-free: A proposal for a safe hospitalization protecting healthcare professionals and patients not affected by COVID-19 Arch Ital Urol Androl 2020; 92:67-72
14 Campi R, Amparore D, Checcucci E, et al Exploring the Residents' Perspective on Smart learning Modalities and Contents for Virtual Urology Education: Lesson Learned During the COVID-19 Pandemic Actas Urol Esp (Engl Ed) 2021; 45:39-48
15 Ambrosini F, Di Stasio A, Mantica G, et al COVID-19 pandemic and uro-oncology follow-up: A "virtual" multidisciplinary team strategy and patients' satisfaction assessment Arch Ital Urol Androl 2020; 92:78-79
16 Mirone V, Di Bello F, Morra S, et al Telemedicine and social media: A contemporary analysis of the most shared content by internet users Arch Ital Urol Androl 2024; 96:11206
17 Mirone V, Abate M, Fusco GM, et al Telemedicine and YouTube™: Video quality analysis before and after COVID-19 pandemic Arch Ital Urol Androl 2023; 95:11341
18 Mirone V, Celentano G, Collà, et al Perceptions and attitudes toward the use of telemedicine for the postoperative outpatient urological care during the COVID-19 pandemic in an Academic Hospital in Southern Italy Arch Ital Urol Androl 2022; 94:375-379
19 Carrion DM, Rodríguez-Socarrás ME, Mantica G, et al Interest and involvement of European urology residents in academic and research activities An ESRU-ESU-ESUT collaborative study Minerva Urol Nefrol 2020; 72:384-387
Correspondence
Rosario Leonardi, MD - urologialeonardi@gmail com Casa di Cura Musumeci-Gecas, 95030 Gravina di Catania, Italy
Angelo Cafarelli, MD - angelocafarelli78@gmail com Urology Unit, Villa Igea, Ancona, Italy
Alessandro Calarco, MD - alecalarco@gmail com Department of Urology, San Carlo di Nancy Hospital, Rome, Italy
Renzo Colombo, MD - colombo renzo@hsr it Department of Urology, Vita e Salute San Raffaele University, Milan, Italy
Ottavio De Cobelli, MD - ottavio decobelli@ieo it Department of Urology, IEO European Institute of Oncology, IRCCS, Milan, Italy
Conflict of interest: The authors declare no potential conflict of interest
Ferdinando De Marco, MD - ferdinandodemarco@gmail com
I N I Grottaferrata, Rome, Italy
Giovanni Ferrari, MD - gferrari@hesperia it Hesperia Hospital, Modena, Italy
Giuseppe Ludovico, MD - giuseppeludovico@hotmail com
Miulli Hospital, Acquaviva delle Fonti, Bari, Italy
Stefano Pecoraro, MD - uropec@gmail com NEUROMED, Avellino, Italy
Domenico Tuzzolo, MD - info@casadelsole it; dometuzzolo@alice it
Urologi Ospedalità Gestione Privata (UrOP), Italy
Guglielmo Mantica, MD (Corresponding Author) guglielmo mantica@gmail com
Department of Surgical and Diagnostic Integrated Sciences (DISC), University of Genova, Genova, Italy
INSTRUCTIONS TO AUTHORS – ARCHIVIO ITALIANO
OPEN ACCESS
Open access publishing does have its costs. Information regarding authors’ payment are not made available to editors and reviewers ensuring that they cannot be influenced in their selection of papers for publication by payment conditions or limitations. The Article Processing Charge for publication in this journal is EUR 300,00 (plus VAT, if applicable).
Our fees cover the costs of peer review, copyediting, publication, different format of publication (HTML, PDF), inclusion in many Open Access databases.
All bank charges shall be borne by the payer. Please note that our fees do not include taxes (VAT):
- Private or public ITALIAN customers (individuals, universities, hospitals, other organizations) must ALWAYS add VAT (IVA) at standard rate (4%);
- European Union PRIVATE customers must add the standard rate of their own country VAT tax;
- European Union private/public ORGANIZATIONS (universities, hospitals, others with regular VAT number) should not add any taxes at standard rate, provided that they indicate their VAT number;
- Outside the European Union, individuals and organizations should not add any taxes at standard rate.
Important: Authors are NOT required to pay at the moment of submission. If the paper is accepted, the Managing Editor of Open Access Edition will guide the Authors through the payment procedure. No article will be published before waiver or payment.
According to the United Nations list of Least Developed Countries (LCDs) available from: http://www.un.org/en/development/desa/policy/cdp/ldc2/ldc_countries.shtml Authors coming from those countries are entitled to ask for a discount.
A “Formal Request for discount” has to be forwarded to the Managing Editor of Open Access Edition, after receiving the acceptance letter. The Editorial Committee will then evaluate the merits of each individual case.
Any other informal request (such as comments at the moment of submission, or made in the covering letter of the revised version) will not be taken into consideration.
FAST-TRACK PEER REVIEW
All papers published in Archivio Italiano di Urologia e Andrologia (AIUA) are peer reviewed. Fast-track peer review (4 weeks) can be obtained by supplementary fee of € 488 (VAT included).
METHODS OF PAYMENT Authors can pay their fees by: PayPal is the most recommended and secure payment system. It enables you to pay getting your payment receipt immediately and without sharing your financial information. Other methods of payment are:
Bank transfer
BANK NAME: Banca Popolare di Sondrio, Branch #1, Strada Nuova 75, I-27100 Pavia, Italy
ACCOUNT HOLDER: PAGEPress Srl
BIC/SWIFT: POSOIT22
IBAN: IT85Y0569611301000005086X83
Credit Card The credit card form to be filled and returned either via e-mail or via fax is available for download here.
Check sent by surface mail Checks must be made payable to PAGEPress Srl and must be sent to our full postal address: PAGEPress Publications, via A. Cavagna Sangiuliani 5, 27100 Pavia, Italy.
Note: In any method of payment you choose, kindly specify: 1. journal name; 2. paper ID number; 3. first author.
IMPORTANT TO KNOW
REGISTERED DRUGS, DIET SUPPLEMENTS, NUTRACEUTICALS, MEDICAL DEVICES
Authors of papers that contain references to registered drugs, diet supplements, nutraceuticals and medical devices are requested to buy a minimum amount of 100 reprints at a cost of € 1.500 (1 to 4 pages) or € 2.000 (5 to 8 pages). Prices for the purchase of number of reprints greater than 100 can be negotiated with Edizioni Scripta Manent At present, Edizioni Scripta Manent let everyone to read, print and download papers from website, but retains copyright for republishing and distribution rights for commercial purpose.
TRANSLATION
Translation of manuscripts in Italian language is offered on payment.
Translation and reprints can be requested to Edizioni Scripta Manent by e-mail to info@edizioniscriptamanent.eu
AUTHORS’ RESPONSIBILITIES
Manuscripts are accepted with the understanding that they have not been published or submitted for publication in any other journal.
Authors must submit the results of clinical and experimental studies conducted according to the Helsinki Declaration on clinical research and to the Ethical Code on animal research set forth by WHO (WHO Chronicle 1985; 39:51). The Authors must obtain permission to reproduce figures, tables and text from previously published material. Written permission must be obtained from the original copyright holder (generally the Publisher).
MANUSCRIPT PRESENTATION
Authors must submit their manuscripts (MAC and WINDOWS Microsoft Word are accepted) after registration and login to the link: http://www.aiua.it. Surface or e-mail submission are not accepted.
Manuscripts must be written in English language in accordance with the “Uniform Requirements for Manuscripts submitted to biomedical journals” defined by The International Committee of Medical Journal Editors (http://www.ICMJE.org). Manuscripts
in Italian language can be published after translation (expenses will be charged to the Authors). Manuscripts should be typed double spaced with wide margins. They must be subdivided into the following sections:
TITLE PAGE
It must contain: a) title; b) a short (no more than 40 characters) running head title; c) first, middle and last name of each Author without abbreviations; d) University or Hospital, and Department of each Author; e) last name, address and e-mail of all the Authors; f) corresponding Author; g) acknowledgement of conflict of interest and financial support.
SUMMARY
Authors must submit a summary (300 words, 2000 characters) divided by subheadings as follows: Objective(s), Material and method(s), Result(s), Conclusion(s). After the summary, three to ten key words must appear, taken from the standard Index Medicus terminology.
TEXT
For original articles concerning experimental or clinical studies, the following standard scheme must be followed: Summary - Key Words - Introduction - Material and Methods - Results - Discussion - Conclusions - References - Tables - Legends - Figures.
Case Report should be divided into: Summary - Introduction (optional) - Case report(s) - Conclusions - References
Supplementary Materials can be added for online publication.
SIZE OF MANUSCRIPTS
Literature reviews, Editorials and Original articles should not exceed 3500 words with 3-5 figures or tables, and no more than 30 references.
Case reports, Notes on surgical technique, and Letters to the editors should not exceed 1000 words (summary included) with only one table or figure, and no more than three references. No more than five authors are permitted.
REFERENCES
References must be sorted in order of quotation and numbered with arabic digits between parentheses. Only the references quoted in the text can be listed. Unpublished studies cannot be quoted, however articles “in press” can be listed with the proper indication of the journal title, year and possibly volume. References must be listed as follows.
JOURNAL ARTICLES
All Authors if there are six or fewer, otherwise the first three, followed by “et al.”. Complete names for Work Groups or Committees. Complete title in the original language. Title of the journal following Index Medicus rules. Year of publication; Volume number: First page. Example: Starzl T, Iwatsuki S, Shaw BW, et al. Left hepatic trisegmentectomy Surg Gynecol Obstet. 1982; 155:21.
BOOKS
Authors - Complete title in the original language. Edition number (if later than the first). City of publication: Publisher, Year of publication. Example: Bergel DIA. Cardiovascular dynamics. 2nd ed. London: Aca de mic Press Inc., 1974.
BOOK CHAPTERS
Authors of the chapters - Complete chapter title. In: Book Editor, complete Book Title, Edition number. City of publication: Publisher, Publication year: first page of chapter in the book. Example: Sagawa K. The use of central theory and system analysis. In: Bergel DH (Ed), Cardiovascular dynamics. 2nd ed. London: Aca demic Press Inc., 1964; 115.
TABLES
Tables must be numbered in Arabic digits and referred to in the text by progressive numbers. Every table must be accompanied by a brief title. The meaning of any abbreviations must be explained at the bottom of the table itself.
FIGURES
(Graphics, algorithms, photographs, drawings). Figures must be numbered and quoted in the text by number. The meaning of symbols or abbreviations must be indicated. Histology photograph legends must include the enlargement ratio and the staining method. Legends must be collected in one or more separate pages.
• Do not include any illustrations as part of your text file. • Do not prepare any figures in Word as they are not workable. • Line illustrations must be submitted at 600 DPI.
• Halftones and color photos should be submitted at a minimum of 300 DPI. • Power Point files cannot be uploaded. • If possible please avoid transmitting electronic files in JPEG format or save the JPEG at the highest quality available • PDF files may be uploaded.
MANUSCRIPT REVIEW
Manuscripts are evaluated by the Editorial Board and/or by two referees designated by the Editors. The Authors are informed in a time as short as possible on whether the paper has been accepted, rejected or if a revision is deemed necessary. The Editors reserve the right to make editorial and literary corrections with the goal of making the article clearer or more concise, without altering its contents. Submission of a manuscript implies acceptation of all above rules.
PROOFS
Authors are responsible for ensuring that all manuscripts are accurately typed before final submission. Galley proofs will be sent to the first Author. Proofs should be returned within seven days from receipt.
Salutepertutti.it è un progetto indipendente. Abbonati per i tuoi pazienti in sala d’aspetto.