The Oxford Handbook of Acceptance and Commitment Therapy
Edited by Michael P. Twohig, Michael E. Levin, and Julie M. Petersen
Oxford University Press is a department of the University of Oxford. It furthers the University’s objective of excellence in research, scholarship, and education by publishing worldwide. Oxford is a registered trade mark of Oxford University Press in the UK and certain other countries.
Published in the United States of America by Oxford University Press 198 Madison Avenue, New York, NY 10016, United States of America.
© Oxford University Press 2023
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, without the prior permission in writing of Oxford University Press, or as expressly permitted by law, by license, or under terms agreed with the appropriate reproduction rights organization. Inquiries concerning reproduction outside the scope of the above should be sent to the Rights Department, Oxford University Press, at the address above.
You must not circulate this work in any other form and you must impose this same condition on any acquirer.
CIP data is on file at the Library of Congress
ISBN 978–0–19–755007–6
DOI: 10.1093/oxfordhb/9780197550076.001.0001
Printed by Sheridan Books, Inc., United States of America
CONTENTS
Contributors ix
Section 1 • Conceptual Foundation
1. Progression of ACT 3
Robert D. Zettle and Kelly G. Wilson
2. Implementing ACT as Contextual Behavioral Science 25
Emily K. Sandoz and Caleb Fogle
3. Primer on Basic Behavioral Principles 42
Thomas J. Waltz and Claudia Drossel
4. A Primer on Relational Frame Theory 77
Colin Harte and Dermot Barnes-Holmes
5. Clinical Behavior Analysis and RFT: Conceptualizing Psychopathology and Its Treatment 109
Carmen Luciano, Niklas Törneke, and Francisco J. Ruiz
Section 2 • General ACT Methods
6. An ACT Approach to Assessment, Case Conceptualization, and Treatment 145
Katrina M. Daigle, Mikala A. Grimaldi, Rebecca Schneider, and Lisa W. Coyne
7. Psychological Flexibility 169
Clarissa W. Ong and Elizabeth H. Eustis
8. Acceptance 182
Rhonda M. Merwin, Ashley A. Moskovich, Angela Pisoni, Sara Freeman, and Carly Onnink
9. Cognitive Defusion 206
Francisco J. Ruiz, Bárbara Gil-Luciano, and Miguel A. Segura-Vargas
10. Present Moment Awareness 230
Matthew S. Herbert and Niloofar Afari
11. Self-as-Context 249
Louise McHugh and Alison Stapleton
12. Values in Acceptance and Commitment Therapy 271
Jenna LeJeune and Jason Luoma
13. Committed Action 295
Lance M. McCracken
Section 3 • Specific Applications of ACT
14. Depression 311
Jacqueline A-Tjak and Louise Hayes
15. ACT for Anxiety and Trauma-Related Disorders 333
Brooke M. Smith, Gregory S. Smith, and Ellen J. Bluett
16. Obsessive Compulsive and Related Disorders 353
Eric B. Lee, Myles Arendtson, and Andy Wall
17. ACT for Eating Disorders 372
Adrienne Juarascio, Paakhi Srivastava, Christina R. Felonis, and Olivia B. Wons
18. Health Promotion and Weight Management for Obesity 391
Jason Lillis and Dayna Lee-Baggley
19. Acceptance and Commitment Training in the Workplace 407
Paul E. Flaxman, Arianna Prudenzi, and Lucie Zernerova
20. Acceptance and Commitment Therapy for Chronic Pain 432
Karlyn A. Edwards and Kevin E. Vowles
21. ACT for Chronic Health Conditions 455
Lilian Dindo, Julia R. Van Liew, and Joanna J. Arch
22. Acceptance and Commitment Therapy for Substance Use 483
Maria Stavrinaki, Megan Kelly, and Maria Karekla
23. Acceptance and Commitment Therapy for Smoking Cessation 501
Jonathan B. Bricker
24. ACT for the Treatment of Psychosis and Schizophrenia-Spectrum Disorders 513
Brandon A. Gaudiano and Stacy Ellenberg
Section 4 • Implementation of ACT
25. Effective Training and Delivery of ACT: The Dissemination and Implementation Issues 537
Robyn D. Walser and Emily Rachel Wharton
26. ACT in Schools: A Public Health Approach 564
Tyler L. Renshaw, Sean N. Weeks, Anthony J. Roberson, and Stephanie Vinal
27. ACT for Children and Adolescents 584
Julie M. Petersen, Louise Hayes, Duncan Gillard, and Joseph Ciarrochi
28. Technology 605
Raimo Lappalainen, Katariina Keinonen, and Päivi Lappalainen
29. ACT in Groups 641
Joanna J. Arch, Lauren B. Finkelstein, and Lilian Dindo
30. Cultural Adaptations of Acceptance and Commitment Therapy 662
Akihiko Masuda, Lucas Morgan, Samuel D. Spencer, Joanne Qinaʻ au, and Duckhyun Jo
31. Acceptance and Commitment Therapy Inside Behavior Analysis 680
Jonathan Tarbox, Amanda N. Chastain, and Thomas G. Szabo
Conclusion
32. Future Directions of Contextual Behavioral Science 711
Rikard K. Wicksell, Niklas Törneke, Lance M. McCracken, Jonathan B. Bricker, Amy R. Murrell, Akihiko Masuda, and Anthony Biglan
33. Creating Progress in Contextual Behavioral Science: Overcoming the Hurdles of the Past—Facing the Challenges of the Future 733
Neal Falletta-Cowden, Steven C. Hayes, and Michelle Forman
Index 755
CONTRIBUTORS
Niloofar Afari, PhD
Professor, Department of Psychiatry, University of California, San Diego
Joanna J. Arch, PhD
Associate Professor, Psychology and Neuroscience, University of Colorado, Boulder
Myles Arendtson, BA
Graduate Student, School of Psychological and Behavioral Sciences, Southern Illinois University, Carbondale
Jacqueline A-Tjak, PhD
Clinical Psychologist, A-Tjak Cursussen, Emmer-Compascuum
Anthony Biglan, PhD
Senior Scientist, Oregon Research Institute, Eugene
Ellen J. Bluett, PhD
Clinical Associate Professor of Behavioral Science, Family Medicine Residency of Western Montana, University of Montana, Missoula
Jonathan B. Bricker, PhD
Professor, Division of Public Health Sciences, Fred Hutchinson Cancer Center and University of Washington, Seattle
Amanda N. Chastain, MA, BCBA
Senior Research Associate, University of Southern California, Los Angeles
Joseph Ciarrochi, PhD
Professor, Institute of Positive Psychology and Education, Australian Catholic University, Austinmer
Lisa W. Coyne, PhD
Assistant Professor, Psychiatry Department, Harvard Medical School, Boston
Katrina M. Daigle, MA, MS, PhD Candidate Psychology Department, Suffolk University, Boston
Lilian Dindo, PhD
Associate Professor, Medicine, Baylor College of Medicine, Houston
Claudia Drossel, PhD
Associate Professor, Psychology, Eastern Michigan University, Ypsilanti
Karlyn A. Edwards, PhD
Postdoctoral Fellow, Department of Anesthesiology, Perioperative, and Pain Medicine, Stanford University, Palo Alto
Stacy Ellenberg, PhD
Clinical Psychology, Postdoctoral Fellow, MindWell Center, Ithaca
Elizabeth H. Eustis, PhD
Research Assistant Professor, Department of Psychological and Brain Sciences Boston University, Boston
Neal Falletta-Cowden, MA
Psychology, Behavior Analysis, University of Nevada, Reno
Christina R. Felonis, BA
Doctoral Student in Clinical Psychology, Department of Psychology, Drexel University, Philadelphia
Lauren B. Finkelstein, MA
Doctoral Student in Clinical Psychology, Department of Psychology and Neuroscience, University of Colorado, Boulder
Paul E. Flaxman, PhD
Reader in Organizational Psychology, Department of Psychology, City University of London, London
Caleb Fogle, MS
Student in Clinical Psychology, Southern Illinois University, Carbondale
Michelle Forman, MS
University of Nevada, Reno
Sara Freeman, MS
LCMHC Therapist, Mood Treatment Center, Greensboro
Brandon A. Gaudiano, PhD
Professor Psychiatry and Human Behavior, Brown University, Providence
Duncan Gillard, DEdPsy
Senior Psychologist and Creative Director, Connect Wellbeing in Education LLP, Bristol
Bárbara Gil-Luciano, PhD
Associate Professor, Cofounder of Universidad de Nebrija, Madrid Institute of Contextual Psychology (MICPSY), Madrid
Mikala A. Grimaldi, BS
OCD and Anxiety Behavior Specialist, Clinical Research Coordinator, New England Center for OCD and Anxiety, Boston
Colin Harte, PhD
Postdoctoral Researcher, Federal University of São Carlos, Brazil and Paradigma – Centro de Ciências e Technologia do Comportamento, Brazil
Louise Hayes, PhD
Licensed Clinical Psychologist, Director, DNA-V International, University of Almería, Melbourne
Steven C. Hayes, PhD
Foundation Professor of Psychology, Psychology, University of Nevada, Reno
Matthew S. Herbert, PhD
Research Psychologist and Assistant Professor, Research Development Service and Department of Psychiatry, Veterans Affairs San Diego Healthcare System and University of California, San Diego
Dermot Barnes-Holmes, PhD
Professor, Department of Psychology, Ghent University, Belgium
Duckhyun Jo, MA
Doctoral Student, Department of Psychology, University of Hawaii, Honolulu
Adrienne Juarascio, PhD
Assistant Professor, Department of Psychological and Brain Sciences, Drexel University, Philadelphia
Maria Karekla, PhD
Assistant Professor, Department of Psychology, University of Cyprus, Cyprus
Katariina Keinonen, PhD
Senior Lecturer, Department of Psychology, University of Jyväskylä, Jyväskylä
Megan Kelly, PhD
Professor, Department of Psychiatry, University of Massachusetts Chan Medical School, Worcester
Päivi Lappalainen, PhD
Postdoctoral Researcher, Department of Psychology, University of Jyväskylä, Jyväskylä
Raimo Lappalainen, PhD
Professor, Department of Psychology, University of Jyväskylä, Jyväskylä
Eric B. Lee, PhD
Assistant Professor, School of Psychological and Behavioral Sciences, Southern Illinois University, Carbondale
Dayna Lee-Baggley, PhD
Registered Psychologist, Assistant Professor, Family Medicine, Dalhousie University, Halifax
Jenna LeJeune, PhD
Licensed Psychologist, President Portland Psychotherapy Clinic, Training, and Research Center, Portland
Michael E. Levin, PhD
Professor, Department of Psychology, Utah State University, Logan
Jason Lillis, PhD
Associate Professor (Research), Alpert Brown Medical School, The Miriam Hospital and College of Psychology, Providence
Carmen Luciano, PhD
Professor, Department of Psychology, University of Almería, Almería
Jason Luoma, PhD
CEO, Portland Psychotherapy Clinic, Research and Training Center, Portland
Akihiko Masuda, PhD
Professor, Department of Psychology, University of Hawaii at Manoa, Honolulu
Lance M. McCracken
Professor, Clinical Psychology, Department of Psychology, Uppsala University, Uppsala
Louise McHugh, PhD
Professor, School of Psychology, University College Dublin, Dublin
Rhonda M. Merwin, PhD
Associate Professor, Department of Psychiatry and Behavioral Sciences, Duke University Medical Center, Durham
Lucas Morgan, PhD
Clinical Supervisor, Ola Lāhui Behavioral Health, Honolulu
Ashley A. Moskovich, PhD
Assistant Professor, Department of Psychiatry and Behavioral Sciences, Duke University Medical Center, Durham
Amy R. Murrell, PhD
Licensed Psychologist and Affiliate Faculty, Private Practice and Department of Psychology, Murrell Psychological Services, LLC and University of Memphis, Memphis
Clarissa W. Ong, PhD
Research Scientist, Department of Psychological and Brain Sciences, Boston University, Boston
Carly Onnink, BS
Research Assistant, Department of Psychiatry and Behavioral Sciences, Duke University Medical Center, Durham
Julie M. Petersen, MS
Doctoral Student, Department of Psychology, Utah State University, Logan
Angela Pisoni, MA, PhD Candidate
Department of Psychiatry and Behavioral Sciences, Duke University Medical Center, Durham
Arianna Prudenzi, PhD
MSc, BSc Research Fellow, School of Psychology, Institute for Mental Health, University of Birmingham, Birmingham
Joanne Qinaʻau, MA
Doctoral Student, Department of Psychology, University of Hawaii at Manoa, Honolulu
Tyler L. Renshaw, PhD
Associate Professor, Psychology Department, Utah State University, Logan
Anthony J. Roberson, PhD
Assistant Professor, Department of Clinical, Health, and Applied Sciences, University of Houston-Clear Lake, Houston
Francisco J. Ruiz, PhD
Associate Professor, Faculty of Psychology, Fundación Universitaria Konrad Lorenz, Bogotá
Emily K. Sandoz, PhD
BCBA, Emma Louise LeBlanc Burguieres/BORSF Endowed Professor of Social Sciences, Psychology Department, University of Louisiana at Lafayette, Lafayette
Rebecca Schneider, PhD
Assistant Professor, Department of Psychiatry and Behavioral Sciences, Emory University School of Medicine, Atlanta
Miguel A. Segura-Vargas
Graduate Student, Master’s in Psychology, Theory and Research, Faculty of Psychology and Educational Sciences KU Leuven, Leuven
Brooke M. Smith, PhD
Assistant Professor, Department of Psychology, Western Michigan University, Kalamazoo
Gregory S. Smith, PhD, BCBA-D
Assistant Clinical Professor, Department of Applied Behavior Analysis, University of Dayton, Dayton, OH
Samuel D. Spencer, MA
Doctoral Candidate, Department of Psychology, University of Hawaii at Manoa, Honolulu
Paakhi Srivastava, PhD
Assistant Research Professor and Clinic Director, Center for Weight, Eating and Lifestyle, Drexel University, Philadelphia
Alison Stapleton, BA, PhD Candidate School of Psychology, University College Dublin, Dublin
Maria Stavrinaki, PhD
Clinical Psychologist, Department of Psychology, University of Cyprus, Nicosia
Thomas G. Szabo, PhD, BCBA-D, LBA
Assistant Professor, Department of Psychology, Capella University, Minneapolis
Jonathan Tarbox, PhD, BCBA
Associate Professor of Teaching and Program Director, Department of Psychology, University of Southern California, Los Angeles
Niklas Törneke, MD
Psychiatrist, NT Psykiatri AB, Köpingsvik
Michael P. Twohig, PhD
Professor, Department of Psychology, Utah State University, Logan
Julia R. Van Liew, PhD
Assistant Professor, Behavioral Medicine, Medical Humanities, and Bioethics, Des Moines University, Des Moines
Stephanie Vinal, MS
Doctoral Student, Department of Psychology, Utah State University, Logan
Kevin E. Vowles, PhD
Professor, School of Psychology, Queen’s University of Belfast, Belfast
Andy Wall, BS
Graduate Student, School of Psychological and Behavioral Sciences, Southern Illinois University, Carbondale
Robyn D. Walser, PhD
Assistant Professor, Staff Psychologist, Director, Department of Psychology University of California, Berkeley, National Center for PTSD, TL Consultation Services, Berkeley
Thomas J. Waltz, PhD, LP
Associate Professor, Department of Psychology, Eastern Michigan University, Ypsilanti
Sean N. Weeks, MS
Doctoral Candidate, Department of Psychology, Utah State University, Logan
Emily Rachel Wharton, PsyD Psychologist, Palo Alto Veterans Affairs, Redwood City
Rikard K. Wicksell, PhD
Associate Professor, Department of Clinical Neuroscience, Division of Psychology, Karolinska Institutet, Stockholm
Kelly G. Wilson, PhD
Professor Emeritus of Psychology, Department of Psychology, University of Mississippi, Oxford, Mississippi
Olivia B. Wons, MS, PhD Student Department of Psychological and Brain Sciences, Drexel University, Philadelphia
Lucie Zernerova, PhD
Research Associate, Department of Psychology, City, University of London, London
Robert D. Zettle, PhD
Professor and Director of Clinical Training, Department of Psychology, Wichita State University, Wichita
Progression of ACT
Robert D. Zettle and Kelly G. Wilson
Abstract
Acceptance and commitment therapy (ACT) in the context of its historical and progressive development unfolded within three phases over the past 40 years. Events and influences in an initial phase that culminated in the development of comprehensive distancing as a precursor to ACT in the early 1980s preceded philosophical, theoretical, and conceptual refinements that took place during the next phase of ACT’s progression. These advancements, including the further explication of functional contextualism, rule governance, and relational responding, contributed to the emergence of ACT as a coherent transdiagnostic intervention by the turn of this century. Ever increasing outcome and process research within the last two decades during ACT’s third and most recent stage of progression have been instrumental in solidifying its current empirical status and expanding globalization.
Key Words: history, comprehensive distancing, ACT, functional contextualism, rule governance, relational frame theory
Progression of ACT
As reflected by its title, this article provides an overview of the current status of acceptance and commitment therapy (ACT; S. C. Hayes, Strosahl, & Wilson, 2012) situated within an historical account of the events that have led up to it. In short, we seek to show where ACT is at the moment and the paths that it took to arrive there. We particularly offer an update of the progression of ACT that has occurred since the initial publications concerning its development 10–15 years ago (Cullen, 2008; Zettle, 2005) and a more recent historical overview (Hooper & Larsson, 2015, Ch. 3).
ACT is often presented most simply as the application of a psychological flexibility model of human functioning comprising six interrelated processes: (1) acceptance, (2) defusion, (3) flexible present moment awareness, (4) self-as-context, (5) chosen values, and (6) committed action (S. C. Hayes et al., 2012). For our purposes here, we prefer to define ACT as (1) a psychological approach to the alleviation of human suffering and the promotion of human well-being, (2) based on functional contextualism, and (3) informed by relational frame theory (RFT; S. C. Hayes, Barnes-Holmes, & Roche, 2001) as an associated account of human language and cognition. We will accordingly refer to the progression over time in what might be regarded as technical/methodological, philosophical, and theoretical dimensions or strands within ACT, and how all three became integrated and interwoven with each other in forging its identity and determining its current status. As will be seen, ACT as we know it today, developed from a psychological approach known as comprehensive distancing (Zettle,
2005) that was philosophically based on radical behaviorism (Skinner, 1974) and informed theoretically by Skinner’s (1969) conceptualization of rule-governed behavior.
Disclaimers
Before embarking on our journey, we would like to offer two disclaimers that are applicable to any historical account such as ours. First, key events within such narratives are in hindsight often presented in a more linear and coherent fashion (see Table 1.1) than how they actually
Table 1.1 Timeline of Key Events in the Progression of ACT
Date Event
1982 Rule-governed behavior is extended as a behavior-analytic conceptual model for cognitive-behavioral interventions (Zettle & Hayes, 1982).
First laboratory analogue study of comprehensive distancing’s impact on pain tolerance is conducted and presented (S. C. Hayes, Korn, Zettle, Rosenfarb, & Cooper, 1982).
1984 Results of first randomized clinical trial of comprehensive distancing compared to cognitive therapy for depression are presented (Zettle & Hayes, 1984).
“Making Sense of Spirituality” paper is published describing deictic framing and process of establishing transcendent perspective taking (S. C. Hayes, 1984).
1985 Introductory presentation of RFT (S. C. Hayes & Brownstein, 1985).
Observer exercise added to the comprehensive distancing protocol.
1986 Parameters of contextualism as a broader world view within which radical behaviorism may be subsumed are presented (S. C. Hayes & Brownstein, 1986).
1987 First chapter-length presentation of comprehensive distancing (S. C. Hayes, 1987).
1989 Rule governance is fully reconceptualized within RFT (S. C. Hayes, 1989: S. C. Hayes & Hayes, 1989).
1991 First uses of “acceptance and commitment therapy” (Wilson, Khorakiwala, & Hayes, 1991) and ACT (Wilson & Taylor, 1991) in paper presentation titles.
1993 Functional contextualism is proposed as the philosophical foundation for ACT (S. C. Hayes, 1993).
First use of acceptance and commitment therapy in a publication title (S. C. Hayes & Wilson, 1993).
1999 First book-length presentation of ACT published (S. C. Hayes, Strosahl, & Wilson, 1999).
2001 First-book length presentation of RFT published (S. C. Hayes et al., 2001).
2003 ACT and RFT list serves are started.
First World Conference on ACT, RFT, & The New Behavioral Psychology is held in Linkoping, Sweden.
2005 Association for Contextual Behavioral Science is established.
Get Out of Your Mind and into Your Life published (S. C. Hayes, 2005).
2008 First meta-analysis of ACT published (Öst, 2008).
2011 Development of the Acceptance and Action Questionnaire-II (AAQ-II; Bond et al., 2011).
2012 The Journal of Contextual Behavioral Science is established.
Second edition of Acceptance and Commitment Therapy published (S. C. Hayes et al., 2012).
unfolded in real time. Accordingly, the development of ACT might be more appropriately viewed as the culmination of a reticulated process that more closely resembles solving a challenging crossword puzzle (S. C. Hayes, Zettle, Barnes-Holmes, & Biglan, 2016) than proving a geometric theorem. In particular, the delineation of functional contextualism did not precede the formulation of RFT, which in turn, then resulted in the creation of ACT (S. C. Hayes et al., 2016). Separate as well as coordinated progress in each of the three dimensions or strands that define ACT contributed to its overall development. Some of these advancements were more obvious and had rather immediate impacts, while others were more subtle with delayed influences.
Second, the history we offer is uniquely our own; indeed, it is difficult to see how it could be otherwise. The contributions and vision of single individuals are often critical in the development of many therapeutic approaches that end up being “branded” [e.g., Freud (1916) in the case of psychoanalysis and Beck (1976) for cognitive therapy], and ACT is no exception. Accordingly, suffice it to say that we would not be writing this article had it not been for our particular relationships with Steve Hayes that began at different junctures during the progression of ACT. Recently, he has reflected on some of his more personal experiences that were instrumental in its origination (S. C. Hayes, 2019).
Our Histories
The relationship between Robert D. Zettle (RDZ) and Steve goes back to the fall of 1976 when both arrived at the University of North Carolina at Greensboro (UNC-G). RDZ was beginning his first year in the clinical psychology program there, and Steve, who at the time had not yet defended his dissertation, had just been hired as a new assistant professor and assigned as RDZ’s faculty advisor. It quickly became obvious that the two shared an interest from a behavior analytic perspective in better understanding the impact of human language and verbal behavior on clinical phenomena. It was an influence that Steve acknowledges had been ignited in him at least three years earlier by Willard Day (S. C. Hayes, 2001). RDZ became Steve’s first doctoral student and for his dissertation completed what is retrospectively commonly regarded as the first randomized clinical trial of what later came to be recognized as ACT (Zettle, 1984). Both left UNC-G not long after its completion to accept academic appointments, RDZ at Wichita State University and Steve at the University of Nevada, Reno (UNR), where his relationship with Kelly G. Wilson (KGW) began.
KGW entered the graduate program in clinical psychology at UNR in the fall of 1989, at which point the Reno lab was well established. Steve had brought several graduate students with him from UNC-G and had attracted several others since his arrival at UNR in 1986. It was a highly productive time on multiple fronts. KGW’s interests mapped well onto the breadth of lab interests at the time. He participated in qualitative clinical research on proto-ACT inspired by Willard Day’s (1969) “behavioral phenomenology,” engaged in basic human operant research on RFT (Wilson & Hayes, 1996), participated in seminars and conferences aimed at fleshing out functional contextualism, published theoretical work on ACT and RFT (S. C. Hayes & Wilson, 1993, 1994), and co-wrote and administered two National Institutes of Drug Abuse (NIDA) funded grants, ultimately co-authoring the first book-length ACT manual just prior to departing for an academic post at the University of Mississippi (S. C. Hayes et al., 1999).
We hope that the account that follows will be sufficiently consistent and coherent to be seen as plausible, while acknowledging that others who have been witnesses to and/or possible contributors to the development of ACT have their own and possibly somewhat different stories to tell. We thus make no claims that our narrative is “true” in the sense of elemental
realism, although we have endeavored to appropriately document events and elements within it whenever possible. Rather, we will defer to readers to determine where between fiction and “history,” as that term is most commonly used, our account falls. Regardless of where it might be placed, it may in our view be deemed as “true” to the extent that it is useful, as suggested by Skinner (1980, p. 308) in his comparison of historical and fictional narratives: “In most of the uses we make of history, fiction will serve as well. We demand consistency and plausibility in lieu of truth and thus preserve what really matters, a bit of vicarious experience.” Like the King advised in Alice’s Adventures in Wonderland, we will “begin at the beginning and go on till [we] come to the end: then stop” (Carroll, 1865).
The Beginning: 1976–1986
In order to present the historical context in which ACT emerged, our story begins just as the first wave of behavior therapy, which had been dominated by interventions based on operant and respondent conditioning principles, was about to be replaced by a second wave featuring cognitive-behavioral approaches (S. C. Hayes, 2004).
Rush et al. (1977) Paper
A key event in this transition, particularly given developments that had preceded it, was the Rush, Beck, Kovacs, and Hollon (1977) randomized clinical trial, which favorably compared cognitive therapy (Beck, Rush, Shaw, & Emery, 1979) to imipramine. This study was particularly noteworthy as it was the first one to report that a psychological approach was superior to medication in treating a psychiatric disorder. By the time of its publication, the need to more effectively address the role of human language and cognition in the initiation, maintenance, and treatment of abnormal behavior had become increasingly apparent to many first-wave behavior therapists, especially those serving adult outpatients. At a theoretical/ conceptual level, however, more visible accounts of verbal-cognitive processes that had been offered by disgruntled behavior therapists (e.g., Mahoney, 1974) were much more mechanistic and mentalistic than behavior analytic in their orientation. At a technical level, related ways of weakening the dysfunctional impact of language and cognition within what by now had come to be regarded as “cognitive-behavior modification” (Meichenbaum, 1977) were largely limited to thought-stopping (e.g., Rimm, 1973) and coping self-statements as part of self-instructional training (Meichenbaum, 1972).
In our view, the Rush et al. (1977) paper transformed how behavior therapy was conceptualized and practiced at the time for at least three reasons. One, any psychotherapeutic approach shown to be more efficacious than pharmacotherapy, especially in treating depression as the most common presenting adult outpatient complaint, understandably received the attention of behavior therapists given their commitment to evidence-based practice. Second, apart from distinctions drawn by Beck (1970) between cognitive and behavior therapy, his treatment package included enough behavioral techniques, such as activity scheduling (Beck et al., 1979, Chapter 7), with which behavior therapists were already familiar, for it to be received as not too different or foreign. However, third and perhaps most importantly, what cognitive therapy offered that was new, namely cognitive restructuring, was a more sophisticated and apparently more efficacious means, relative to thought stopping and self-instructional training, of altering the cognitive control of negative thinking. Not surprisingly, cognitive restructuring as a treatment technique was soon added to existing behavior therapy protocols, thereby giving rise to cognitive-behavior therapy (CBT), even though its relative impact and ostensible mechanisms of action were later called
into question based on component and process analyses of cognitive therapy (Jacobson et al., 1996; Zettle & Hayes, 1986, 1987).
Behavior Analysis and CBT
With the advent of this second wave of cognitive-behavioral approaches, any presence and influence that behavior analysis had in the development and practice of operant-based interventions within the first wave were diluted even further. It should be noted that Ferster (1967, 1972) had offered a behavior- analytic perspective on verbal psychotherapy that has since been cited as contributing to the development of functional analytic psychotherapy (R. J. Kohlenberg & Tsai, 1991). However, this work, did not readily point to any innovative changes to behavioral therapeutic practice at the time and by the mid- to late 1970s had clearly been overshadowed by a number of the developments already discussed. As a result, turning to the writings of Skinner (1957, 1969) appeared to be the most fruitful approach to take by those wishing to mount a radical behavioral counter-response to the conceptual challenges and practical changes presented by the “cognitive revolution” taking place within behavior therapy.
Even though Skinner considered Verbal Behavior (1957) his most important work (Salzinger, 1990), it became apparent that this work was of limited utility due to its focus on the behavior of speakers while relatively neglecting that of listeners. In short, Skinner’s conceptual analyses of speaking, for example, might help explain why a depressed client’s thinking exemplifies Beck’s (1967, 1987) negative cognitive triad, but not why or how such thinking then influences the emotional reactions and overt behavior of that same client as a listener. Even more importantly, such a limited account had no substantive clinical value in guiding effective ways to weaken such pernicious cognitive control.
By comparison, Skinner’s (1969) formulation of rule-governed behavior, especially when modified and expanded, initially proved to be more useful in several respects in suggesting a radical behavioral framework in which to conceptualize cognitive therapy and related approaches (Zettle & Hayes, 1982). For one, it shifted more focus to the behavior of listeners, including instances in which rule-followers and rule-givers share the same skin. A problematic issue, however, quickly became apparent and was not completely resolved until later when it was extensively addressed by RFT (see Barnes-Holmes et al., 2001, as well as Article 4 this volume). This problem concerned Skinner’s (1966, 1969) topographical definition of rules as “contingency-specifying stimuli.” When this issue was at least temporarily addressed by recasting rules as verbal discriminative stimuli, rule-governed behavior more broadly could be meaningfully reconceptualized as comprising three different functional units (pliance, tracking, and augmenting) under the control of two distinct sets of contingencies, one naturalistic and the other arbitrary and socially mediated.
An expansive conceptual framework that pointed to multiple controlling variables for rule-following, and to a lesser degree for rule formulation, had some rather important practical and theoretical implications. For one, it suggested that coping self-statements may function as plys, or rules whose following is mediated by a verbal-social community, and thus have limited efficacy unless delivered and followed in a public context. This finding had already been reported (Zettle & Hayes, 1979) and subsequently replicated by other related studies (e.g., S. C. Hayes & Wolf, 1984; Rosenfarb & Hayes, 1984).
Comprehensive Distancing
More importantly for the development of ACT, examining cognitive therapy through the lens of rule governance also suggested a new therapeutic approach. This approach, referred to as comprehensive distancing (CD), was further influenced by the personal struggles of S. C. Hayes (2019) with panic attacks at the time. This forerunner of ACT sought to expand the process of distancing from cognitions as the “first critical step” within cognitive therapy (Hollon & Beck, 1979, p. 189) in which clients are encouraged to respond to their depressing thoughts as mere psychological events rather than as immutable facts prior to restructuring them. Many readers will recognize the similarities to emphases on acceptance, defusion, and even mindfulness within ACT, and to what is more often referred to as “decentering” (Bernstein et al., 2015; Safran & Segal, 1996) within mindfulness-based cognitive therapy (Segal, Williams, & Teasdale, 2002).
Formulating rules, thinking, reason-giving (Zettle & Hayes, 1986), and similar verbal activities from a behavior-analytic perspective cannot function as causes for other actions insofar as they cannot be directly manipulated (S. C. Hayes & Brownstein, 1986). Nonetheless, they may participate in controlling relationships with other behavior when sufficiently supported by verbal-social contingencies. For example, a range of destructive and dysfunctional actions may be socially acceptable when justified by a narrative of plausible reasons (S. C. Hayes, 1987). This analysis further suggested the viability of creating a special verbal-social community within the context of therapy in which deleterious cognitive control could be systematically weakened, for example, through acceptance and defusion, without resorting necessarily to change in cognitive content.
Initial empirical support for CD was provided by a laboratory experiment increasing cold pressor-induced pain tolerance (S. C. Hayes et al., 1982) that was published 17 years later (S. C. Hayes, Bissett, et al., 1999), a randomized clinical trial comparing it favorably to cognitive therapy for depression (Zettle & Hayes, 1984), and a series of unsystematic case studies (S. C. Hayes, 1987). While CD included many of the treatment components and techniques that are commonly part of the contemporary practice of ACT, there were also at least two noteworthy omissions. Behavioral homework was included in CD, but because it was not linked to values, it ostensibly functioned more like mood-enhancing behavioral activation (e.g., Martell, Addis, & Jacobson, 2001) than valued action. In short, relatively speaking, CD was more of an acceptance and willingness therapy than an acceptance and commitment to valued action therapy.
Also missing from CD was the Observer exercise (S. C. Hayes et al., 2012, pp. 233–237) that is often used to complement the Chessboard metaphor (which was included) in fostering self-as-context within ACT. This exercise was not added until at least two years later at the suggestion of a graduate student in the Hayes lab (S. C. Hayes, personal communication, March 28, 2005), not coincidentally around the same time of the “Making Sense of Spirituality” paper (S. C. Hayes, 1984). This publication is understandably included in a collection of Hayes’s (2015) canonical papers and merits special mention as beginning the link that would later be solidified between RFT and ACT. It makes no explicit mention of deictic framing, but it elucidates the processes from which the “behavior of seeing seeing from a perspective” (S. C. Hayes, 1984, p. 103) results in a transcending sense of self.
An even bigger boost in retrospect to the relationship being fostered between CD and RFT occurred near the end of what might be regarded as ACT’s decade-long, initial developmental stage with the unveiling of RFT by S. C. Hayes and Brownstein (1985). Sidman’s (1971) report of untrained equivalence classes that emerged between printed words and pictures, as well as between spoken and printed words, in teaching reading to a teen with a severe
intellectual disability, was recognized as a prototype for how a more expansive repertoire of arbitrary applicable relational responding could be acquired as operant behavior. The S. C. Hayes and Brownstein paper also positioned RFT to ultimately subsume rule governance by reconceptualizing rules as verbal stimuli that serve a discriminative function because of their “participation in relational frames established by the verbal community for the purpose of producing such effects” (1985, p. 19).
The End of the Beginning
In summary, by 1986, CD as a precursor to ACT had been developed as (1) a psychological approach to the alleviation of human suffering, (2) based on radical behaviorism and (3) informed by a theoretical model of rule governance. At this juncture, Hayes would relocate to UNR to focus more during the next decade and a half on delineating functional contextualism as a broader philosophical foundation for ACT and RFT as a related conceptual framework in further informing its development. Unfortunately, on a sad and more personal note, especially for RDZ, these advancements would occur without any further contributions from Aaron Brownstein who suddenly passed away far too early in the spring of 1986 (Shull, 1986). Aaron was an astute experimental behavior analyst, but one just as, if not even more interested, in understanding complex human behavior, including clinical phenomena (e.g., Greenspoon & Brownstein, 1967a, 1967b), as he was with the actions of rats and pigeons in Skinner boxes. Although the present article cites only two references in which Aaron was Steve’s co-author, with one of them (Hayes & Brownstein, 1986) published posthumously, both were foundational to the development of functional contextualism (Hayes & Brownstein, 1986) and RFT (Hayes & Brownstein, 1985), and thus, albeit less directly, major influences in the progression of ACT as well. If there is an “unsung hero” in our story, he’s Aaron Brownstein.
Laying the Groundwork: 1986–2000
Grasping the progression of ACT during this period would be difficult without some understanding of the extraordinary social network in which the development occurred. Hayes came to Reno in 1986 in a leadership position as the Director of Training of the Clinical PhD program, later transitioning to Department Chair. Under his leadership, the behavioral presence in the department grew with the addition of Bill and Victoria Follette to the faculty in 1989, the founding of the Behavior Analysis Program by Linda Hayes in 1990, and the subsequent hiring of behavior analysis faculty (L. J. Hayes et al., 2016). The department embodied an extraordinary unity of purpose in the development of behavior analysis theoretically, philosophically, and in various applications. Although there was considerable interest in ACT and CD proto-ACT, which certainly drew the attention of incoming clinical students, that work was very much a product of the behavioral thinking aimed at broadening and deepening the behavioral tradition.
Steve and Linda Hayes were running a lab in tandem when KGW arrived, and the lab meetings became as much a debate society as they were a place to organize the business of a research lab. Assorted elements of the behavioral tradition were poured together there. Willard Day, who had been a faculty member at UNR—had died in the spring of 1989, but his entirely unique view of a behavior theory and philosophy was very much alive (Day, 1969). As referenced earlier, Day had inspired Hayes to examine the behavior analysis of language deeply, but he was also a serious student of the philosophy of science. Indeed, he had taken a sabbatical year to travel to Oxford and read philosophy during the period in which Gilbert Ryle was Waynflete Professor of Metaphysics.
Hayes’s move to Reno was not random. He joined the faculty there while Willard was still alive and active, recognizing it as an historically appropriate place for developing a broad and rich behavioral tradition. The examination of contextualism and a deeper look at pragmatism were natural activities in that environment. That seriousness in the study of behavior theory and philosophy was ever present in a series of seminars, one of which, co-taught by Steve and Linda Hayes, focused solely on Steven Pepper’s (1942) work. The seminar contained five students, Steve and Linda, as well as Jim Owen, a radical behaviorist faculty member from the UNR Speech and Language Department. It was not so much a university course as it was an ongoing debate as we examined psychology through the lens of Pepper’s work. There was no unanimity of view. Table pounding, shouted arguments, and sometimes preposterous thought experiments were common. Linda Hayes launched a series of small seminars throughout the 1990s with a distinctive Kantorian flavor on behavioral philosophy and verbal behavior. These conversations were not confined to the lab and classroom. Rather, they spilled over into the hallways, at lunch, evenings at the Hayes’s residence, as well as through social gatherings at various homes of students and faculty organized under a series of names, including “Food and Philosophy” and “Beer and Behaviorism,” that involved readings and discussions of wildly varying topics relevant to psychology and philosophy.
It was in this context that the groundwork for ACT clinical innovation developed. The broader fleshing out of clinical behavior analysis occurred in a context centered in basic behavior analysis as well as in other perspectives on the use of behavioral thinking to applied problems. Notably, both Bill and Victoria Follette brought with them considerable exposure to the work of Bob Kohlenberg and a functional-analytic psychotherapy perspective (R. J. Kohlenberg & Tsai, 1991). And of course, Barbara Kohlenberg was among the graduate students who had come to Reno from UNC-G with Steve.
The Debut of ACT
By the early 1990s, the philosophical and theoretical systems in which CD had been situated had been supplanted; radical behaviorism had been superseded by functional contextualism; and a Skinnerian model of rule governance had been replaced with RFT. The stage was accordingly set to transform CD into ACT. Comprehensive distancing was always something of a troubling name. Insiders knew that the “distancing” in CD was not initiated to “get away from” troubling thoughts or to get enough separation to see them more objectively and rationally. Instead, its purpose was to create sufficient psychological space within which clients could make contact more broadly with difficult emotional content. Such expanded contact might include recognition of content patterning, contexts that provoked such content, connection of difficult content within personal history, and critically, the functional role such content played in organizing behavior.
A name that requires an explanation is by its nature troublesome. The acronym ACT emerged in the Hayes lab at Reno when a several week-long brainstorming session produced a variety of acronyms, including CAT (contextual analytic therapy) and RAP (radical acceptance psychotherapy). Our best recollection is that the acronym came first, perhaps as a scramble of CAT. ACT had the right flavor as a therapy that was all about getting into action. The acronym lent itself to the spirit of the work, but also as short-hand for the treatment: Accept, Choose, and Take action. ACT also had the advantage that it could be spoken as a word consistent with the treatment—act, not A-C-T. And ultimately as a therapy name, acceptance and commitment therapy was intuitively understandable and consistent with the developing work.
Who actually came up with the ACT acronym and name is lost to KGW, who was there, as well as to Steve Hayes, who was consulted. As best as we can document in official conference programs, the first reference to acceptance and commitment therapy appeared in
the title of a paper presented at the Association for Behavior Analysis (ABA) conference in May 1991 (Wilson et al., 1991). This would place the date of the name change to the fall of 1990, as this was the deadline for the ABA conference paper proposals. A few papers appeared in the vitas at the November 1990 Association for the Advancement of Behavior Therapy Conference; however, those were certainly title changes that happened at or right before their presentations. It took another three years for the name “acceptance and commitment therapy” to first appear in the title of a publication (S. C. Hayes & Wilson, 1994) rather than conference presentations.
Apart from a mere alteration in name, some strategic and technical changes were made to CD that resulted in ACT as we know it today. Probably the most prominent of these changes was the addition of values to the protocols and the explicit linking of committed action to values. Hayes’s personal struggle with panic was his entry point to ACT. KGW came to the work while he was recovering from severe substance dependence; acceptance was important, but purpose and meaning as described by Victor Frankl (1965) were central. Behavior therapists are always interested in selecting the most potent available reinforcers. Understanding them for verbally competent individuals necessarily required a behavioral examination of verbally constructed values and interventions suited to that analysis. At the end of the 1990 academic year, KGW proposed a comprehensive examination on a behavioral analysis of Frankl’s noogenic neuroses and constructed the first values protocols for a NIDA treatment development grant in 1993. Values first appeared in published form in two articles appearing in The Behavior Analyst (S. C. Hayes & Wilson, 1993; 1994).
Theoretical Developments
Following the publication of an entire book dedicated to Aaron Brownstein and rule-governed behavior (S. C. Hayes, 1989), the reconceptualization that had begun with the Hayes and Brownstein (1985) paper and expanded by Hayes (1987) moved even further away from a traditional Skinnerian perspective to one that was more clearly based within RFT. Especially noteworthy in this volume was a chapter written by Hayes and Hayes (1989) whose stated purpose was “to apply a relational perspective to the issue of rule-governance. Behavior controlled by verbal stimuli is a different kind of behavior because it involves different psychological processes” (p. 177). In this endeavor, several basic elements of RFT were referenced that predated the expanded coverage they would later receive within the S. C. Hayes et al. (2001) text; aka “the purple book.” In particular, mutual entailment, combinatorial entailment, transfer of stimulus functions, and contextual control over relational responding (i.e., Crel and Cfunc) were all explicated in accounting for “the verbal action of the listener as a basis for rule-governance” (p. 153).
This emergent thinking in rule governance and RFT was a hot topic within the lab at Reno and spawned a variety of basic experimental laboratory research, including an experimental analysis of the development of relational responding in infants (Lipkens, 1992). There were also studies examining relational responding in complex human behavior, including network structure (e.g., B. S. Kohlenberg, 1994; Wilson & Hayes, 1996), transformation of motivational functions (Ju, 2000), and propagation and durability of networks among pathology-relevant stimuli (Wilson, 1998). These studies represented a quite organic followup from the dissertations that had been completed in Hayes’s lab at UNC-G on language development, stimulus equivalence, and rule-governed behavior, including those by Devaney (1985), Rosenfarb (1986), Wulfert (1987), and, importantly, the publication of David Steele’s
dissertation, which was arguably the first clearly relational frame theory-oriented experimental analysis, (though it was not called RFT at the time; Steele & Hayes, 1991).
Philosophical Developments
Expanding beyond a strict Skinnerian conceptualization of rule-governed behavior quite understandably led to a closer critical examination of radical behaviorism itself as the philosophical framework within which it was embedded. The building out of a behavioral community at Reno provided a fertile environment for launching a theoretical and philosophical discussion with similarly interested individuals from around the world, resulting in a series of books and conferences, including Dialogues on Verbal Behavior (L. J. Hayes & Chase, 1991), Understanding Verbal Relations (S. C. Hayes & Hayes, 1992), Varieties of Scientific Contextualism (S. C. Hayes, Hayes, Reese, & Sarbin, 1993), Behavior Analysis of Language and Cognition (L. J. Hayes, Hayes, Ono, & Sato, 1994), and Investigations in Behavioral Epistemology (L. J. Hayes & Ghezzi, 1997). In an edited volume focused on elucidating scientific contextualism (S. C. Hayes et al., 1993), Hayes argued that contextualism as one of Pepper’s (1942) four world views could be meaningfully divided into descriptive and functional variants. While Skinner’s (1974) radical behaviorism clearly can be regarded as contextualistic, Hayes regarded it as dogmatic in that it reflected the purposes of science to predict and control behavior rather than Skinner’s own selection of that particular goal. Functional contextualism in which goals are explicitly linked to the clearly articulated preanalytic values of predicting and influencing behavior was instead recommended as a philosophical foundation for psychological interventions, thus allowing for a functional contextualism with goals other than prediction and influence.
Clinical Developments
During the 1990s, mainstream CBT was highly focused on treatment outcome studies. CBT treatment protocols were devised for psychiatric diagnoses, with outcomes studied in randomized clinical trials (RCTs) funded by the National Institutes of Health (NIH). The workgroup at Reno had taken a very different turn, as reflected in the intensive work on theory, philosophy, and basic empirical work discussed previously. Although grant-funded RCTs were not the focus, three NIH studies were funded during this time period that were all developmental and exploratory in nature. The first study was a protocol development grant from NIDA funded in 1993 examining the application of ACT to poly-substance abuse, in which the first values protocols were formalized. That grant was followed by a subsequent RCT extending that protocol development, funded in 1997. Both of these grants were directed by KGW. Finally, a study involving the treatment of nicotine dependent participants was funded in 2000, spearheaded by Elizabeth Gifford, that explored an integration of ACT and functional-analytic psychotherapy principles. Finally, Steve Hayes served as a consultant to a training project at a large Seattle-based health maintenance organization. The result was an innovative field effectiveness study in which the treatment was not studied per se, but rather the focus was the exposure of a cohort of therapists to ACT training over an intensive year of training and supervision. The study importantly involved a diverse mental health population being seen in primary care and a community mental health clinic with neither fixed diagnoses nor protocol length (Strosahl, Hayes, Bergan, & Romano, 1998).
In addition to these grant-funded efforts, small, unfunded dissertation studies examined a broad array of presenting concerns in a variety of clinical settings. Bach (2000) tested a brief protocol with patients presenting with psychotic symptoms at a regional psychiatric hospital. Geiser (1992) treated chronic pain patients at a Reno pain clinic. This period also produced a
series of analogue studies examining components thought to be central to ACT, such as acceptance, thought suppression, and metaphor (Afari, 1996; McCurry, 1991; Pistorello, 1998; Walser, 1998). Khorakiwala’s (1991) dissertation used a variant of Willard Day’s behavioral phenomenology in a qualitative analysis of processes of change in proto-ACT.
From the start, the development of ACT was an iterative and reticulated process. ACT development was never merely a therapy development project. Rather ACT began and continues to be a component of a much broader effort. The focus was on careful theory and philosophy, enriched by experimental analyses, and qualitative research on therapy processes, stretching from the lab to the clinic and back again. All this was with an eye toward laying a foundation for a broadly applicable theory of human suffering, struggle, and its remediation. This work did not go unnoticed. During the 1990s, Dermot Barnes-Holmes, soon joined by Yvonne Barnes-Holmes, launched what would become the most productive human operant lab in the world, beginning in Cork, Ireland. Frank Bond applied ACT principles to workplace environments and published the first organizational behavior management application of ACT, giving rise to a stream of related research (Bond & Bunce, 2000). Carmen Luciano produced an active lab in Almeria, Spain, with research stretching from basic research to clinical applications. All of these interactions, stretching from basic theory and philosophy, from the lab to the clinic, culminated in the publication of the first book-length description of ACT (S. C. Hayes et al., 1999) and set the foundation for a global treatment development effort.
Making a Mark on the World: 2000–Present
By this juncture in our story, the first book-length presentation of ACT had been published (S. C. Hayes et al., 1999) and a comparable one covering RFT (S. C. Hayes et al., 2001) was about to appear, leading to the international dissemination of ACT and a rather rapid proliferation in several types of research related to it. In retrospect, such sudden growth and visibility, as will be seen, perhaps quite understandably eventually led to considerable pushback by ACT’s critics and skeptics.
The Globalization of ACT
The Association for Contextual Behavioral Science (ACBS) was established in 2005 as the primary organizational home for researchers as well as practitioners of ACT and RFT. Very quickly, however, it also attracted an increasingly broader array of contextually minded clinicians and scientists. ACBS currently has over 9000 members (n.d.-h) representing a diverse range of interests within contextual behavioral science; including evolution science, comparative psychology, climate change, the use of psychedelics, and psychodynamic psychotherapy.
ACBS provides access to a wide array of materials and resources about ACT, including notices of training opportunities, as well as postings of publications and assessment instruments, in addition to treatment manuals and protocols. Even prior to the formal founding of ACBS, a concerted effort had already been underway to disseminate ACT beyond its origination in the United States. Although ACBS was not incorporated until 2005, it was born in tragedy. Steve Hayes was preparing to fly to Sweden to do a workshop for Psykolog Partners, a Swedish company that provided a variety of mental health services. The day Dr. Hayes was to fly, he got a call canceling his flight. In fact, every flight in the United States was canceled that day—Tuesday, September 11, 2001. Undaunted, Psykolog Partners went beyond rescheduling the workshop and organized the first proto-ACBS conference, held in Linköping, Sweden, in August 2003. Since 2006, when ACBS assumed responsibility for organizing world
conferences, over half of them by design have been held outside the United States—in the United Kingdom, the Netherlands, Italy, Australia, Germany, Spain, Canada, and Ireland—in an effort to make ACT research and practice more accessible to the rest of the world (n.d.-g). While U.S. residents still constitute the largest membership subgroup within ACBS (17%), as of this writing, another 92 nations, or roughly 47% of the world’s countries, from every continent save Antarctica, are now represented.
ACBS has worked hard at inclusion. Membership dues are values-based. The member gets to choose their dues, with individuals from wealthier countries being encouraged to pay higher dues. The ACBS website is wiki, allowing all members to access and share treatment and educational materials. ACBS has resisted certification of therapists. It does recognize ACT trainers through a peer review process, but this is not a profit-making effort.
Evidence of the strategy’s success in establishing an international community is provided by the current composition of 40 affiliated ACBS chapters worldwide (n.d.-f). The majority of them (i.e., 26, or 65%) are outside the United States and have been variously organized nationally (e.g., Argentina and Finland), regionally (e.g., Australia and New Zealand), and, in some instances, by linguistic communities (e.g., Dutch speakers in Belgium and the Netherlands and French speakers in Belgium and France). ACT has grown by resisting exclusivity, instead promoting an organization of contextual therapies. Many of these chapters have already hosted successful conferences of their own or have plans to do so, thus further increasing ACT’s local and regional presence and influence. ACT’s international visibility has also been increased, albeit to perhaps not the same degree, by the creation of organizational affiliates of ACBS (n.d.-e), as, for example, in Africa, India, the United Arab Emirates, and Western Balkans; where chapters have not yet been firmly established. ACT’s increased globalization and worldwide reach is reflected not only by the diversity of the ACBS membership list, but over the past 5 years by 11 related intervention projects that have been conducted in countries that appear on lists of low- to middle-income countries (ACBS, n.d.-c). One of the most recent examples of this outreach was the implementation and evaluation of an ACT-based, self-help intervention for South Sudanese refugees (Tol et al., 2020).
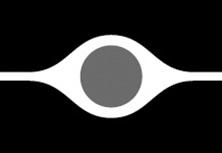
Figure 1.1 Cumulative Number of ACT Outcome Publications
Note. The figure includes “in press” publications listed as of May 2022 at https://contextualscience.org/ACT_Rando mized_Controlled Trials
Research Progression of ACT
The increasing number of projects conducted in impoverished regions of the world has been part of a broader exponential growth of ACT-related research within several domains occurring over the last two decades. (see Figure 1.1)
OutcOme research
For ease of discussion, we will provide separate overviews of research that has evaluated the efficacy and effectiveness of ACT during this most recent stage of its progression.
efficacy research
As seen in the accompanying figure, the number of publications from 1985 to 2000 (i.e., four) that compared the efficacy of ACT to other interventions and/or various control conditions increased by nearly 300% during the next 5 years. The growth has increased exponentially over the last two decades to where there are as of this writing over 900 efficacy studies that have either been published or are “in press.” Although measures of symptomatic relief have been the primary outcome variables in such investigations, researchers increasingly have also examined improvements in quality of life (S. C. Hayes, Luoma, Bond, Mausda, & Lillis, 2006) and, even more recently, increases in flourishing as additional dependent measures in evaluating ACT’s impact (Bohlmeijer, Lamers, & Fledderus, 2015).
By 2010, enough randomized trials of ACT had been accumulated that systematic reviews and meta-analyses of its efficacy began appearing. Most of these initial evaluations, unlike later and more recent ones (ACBS, n.d.-k), focused on ACT more broadly rather than on its treatment of specific presenting problems (e.g., Veehof, Oskam, Schreurs, & Bohlmeijer, [2011] for chronic pain, Bluett, Homan, Morrison, Levin, & Twohig, [2014] for anxiety disorders and OCD, and Howell and Passmore [2019] for depression). Two meta-analyses that received more attention and reaction within the ACT community than most were critical ones by Öst (2008, 2014). In his first publication, Öst (2008) concluded that ACT trials did not merit recognition as an empirically supported treatment, despite significant and moderate effect sizes, because of a relative lack of methodological rigor compared to traditional CBT studies. In response to a subsequent rejoinder to his criticisms (Gaudiano, 2009), Öst (2009) conceded that ACT research was not funded at levels comparable to CBT trials, but maintained that the American Psychological Association’s recognition of ACT as having “moderately strong” empirical support for treatment of depression was unjustified.
A second and updated meta-analysis by Öst (2014) 6 years later was even more critical of ACT. In this work, Öst concluded that there had been no methodological improvements in outcome research over that period of time. Moreover, he noted a deterioration in overall effect size, resulting in no basis for regarding ACT as a “well-established” treatment for any disorder. A robust response from a team of ACT researchers (Atkins et al., 2017) that catalogued a plethora of factual and interpretational errors that likely biased Öst’s conclusions was followed by an equally spirited rebuttal (Öst, 2017) that to date has effectively ended the back-andforth sparring.
Perhaps both motivated by and despite Öst’s criticisms, ACT researchers have become increasingly successful in obtaining external funding (ACBS, n.d.-i). Moreover, efficacy research on ACT has progressed to the point that the Society of Clinical Psychology (SCP) has recognized the therapy as an evidence-based treatment approach for multiple psychiatric disorders. More specifically, SCP (Division 12 of the American Psychological Association) has affirmed ACT’s transdiagnostic status by concluding that it enjoys strong empirical support in the treatment of chronic pain (n.d.-a), and modest support in addressing depression