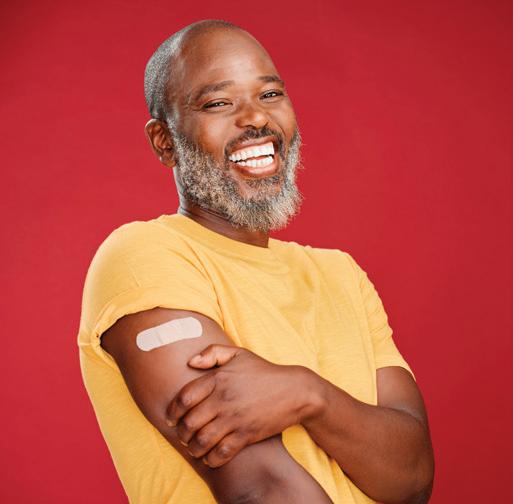
Dinner with a Doctor: Straight talk about the new weight loss drugs | 20
The popularity of new weight management drugs like the semaglutide Wegovy have skyrocketed. How do they work? Are there side effects? Do you have to stay on them for life? Our physician experts answer these questions and more.
The Statesman vs. the Fiery Serpent
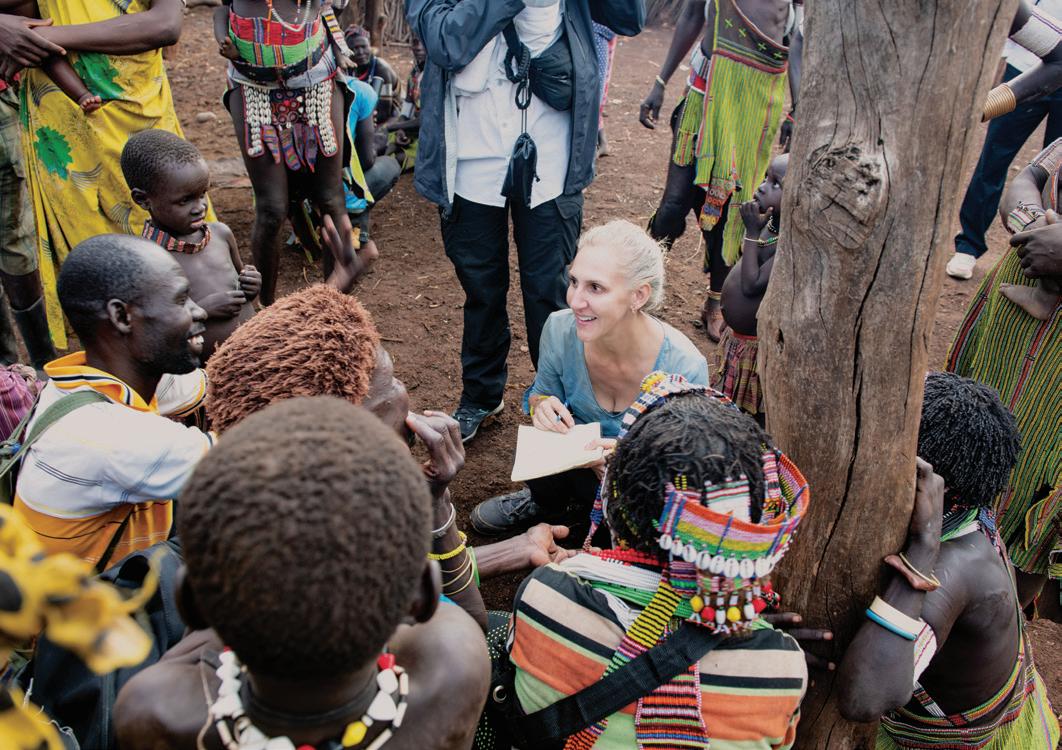
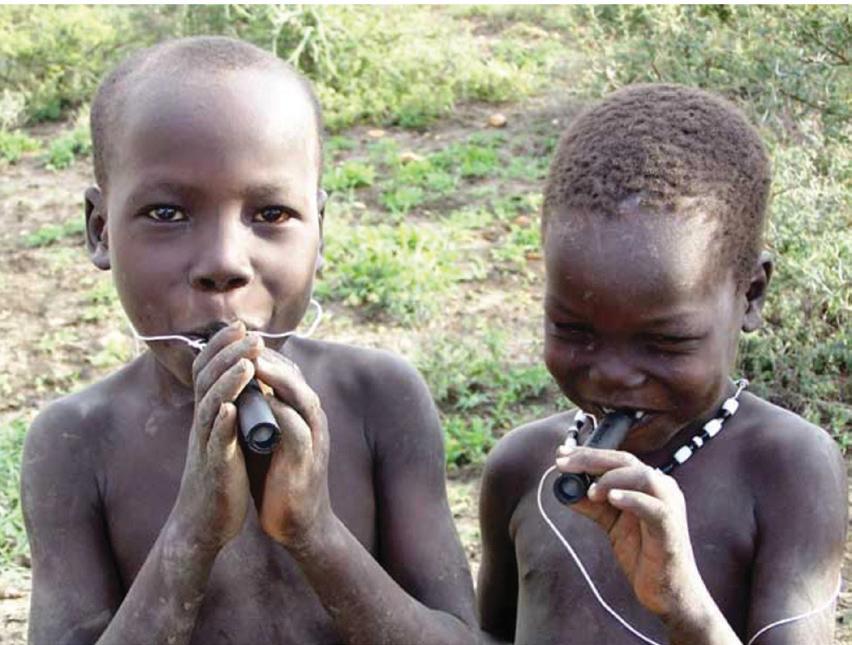
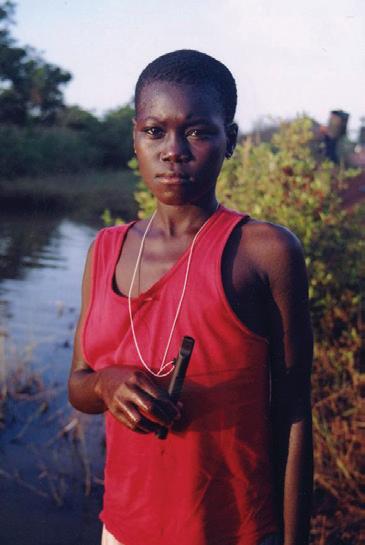
The Carter Center’s fight to eradicate Guinea worm hinges on behavioral change, such as the use of pipe filters.
“It’s a despicable disease. And it was in such remote villages that no one wanted to take on the task. So we decided to take it on.”
Former President Jimmy Carter 1924-2024
No More≠“Wait and See’ | 26
With improved ways to diagnose and treat children with an autism spectrum disorder, researchers are now taking on a larger challenge: getting these tools to all families who need them as soon as possible.
“I am not the fastest, not the best runner, but you put in effort and you learn to enjoy it without the need to come in first.”
Emory Health Digest
Ravi Thadhani, Executive VP for Health Affairs, Executive Director of the Woodruff Health Sciences Center, and Vice Chair of the Emory Healthcare Board
Brian Katzowitz, AVP, Health Sciences Communications
Mary Loftus, Editor
Peta Westmaas, Art Director
Jack Kearse, Photography Director
Martha Nolan, Associate Editor
Plant-based eating 5
Research shows the healthiest diets focus on plant-based, whole, unprocessed foods.
Help for multi-food allergies 7
A new treatment for children with allergies to more than one food shows promise.
the well
To Our Readers 4
A message from Ravi Thadhani, executive VP for health affairs, executive director of WHSC, and vice chair of the Emory Healthcare Board.
The Well 5 Innovative fieldwork. Global health lens. WHSC in the news. Nursing school No. 1. AI and neurology. Deep breathing benefits. Twice yearly injectables for HIV.
4Qs on mold. ALS research. “Health Wanted” podcast. Ferrets and flu spread. Low motivation treatment. Cosmetics risk. Center for New Medicines. Healthcare Test Kitchen. and more
Patient POV 46 Attorneys and parents
Liz and Matt Ames faced a rare cancer together, taking on unexpected roles as patient and caregiver.
Jacob Gniesk, Nicole Golston, Jennifer Johnson, Laura Kahn, Georgia Parmalee, Rob Spahr, Tony Van Witsen, Contributors
Emory University is an equal opportunity/equal access/affirmative action employer fully committed to achieving a diverse workforce, and complies with all applicable federal and Georgia state laws, regulations, and executive orders regarding nondiscrimination and affirmative action in its programs and activities. Emory University does not discriminate on the basis of race, color, religion, ethnic or national origin, gender, genetic information, age, disability, sexual orientation, gender identity, gender expression, or veteran’s status. Inquiries should be directed to the Office of Equity and Inclusion, 201 Dowman Drive, Administration Bldg, Atlanta, GA 30322. Telephone: 404-727-9867 (V) | 404-712-2049 (TDD).
24-Emory Health Digest Fall/Winter
Atlanta Science Gallery’s 'Resilient Earth,' an immersive experience at Northlake Mall, includes exhibits created by Emory researchers and faculty fusing art and science. Exhibit runs through 04.30.2025
Ravi Thadhani, executive vice president for health affairs, executive director of the Woodruff Health Sciences Center, and vice chair of the Emory Healthcare Board
Reimagining Health
I recently gave my annual State of the Woodruff Health Sciences Center (WHSC) address. Our aim remains nothing less than fundamentally reimagining and transforming health and academic medicine.
We are investing in our employees, with thousands receiving substantial raises. Our turnover rates have plummeted almost 50 percent from where they were two years ago.
We’re making investments in patient care across the board and are assisting patients in getting appointments sooner. We have improved access to the point that we see almost 1,000 additional patients a day.
Emory researchers pierced the $1 billion mark in sponsored research for the second year in a row. These dollars employ people as well, bringing almost 11,000 jobs into the system.
We marry the results of this multi-disciplinary research with clinical care, constantly looking for ways to prevent disease and improve health, often through innovative technologies. This magazine’s pages are full of the impact of our research from autism advances (p. 26) to improving food allergies (p. 7), to evaluating combination over-the-
counter tests for COVID-19 and the flu (p. 18).
We are emphasizing outreach that makes us visible in our communities, such as our “One Trained at Every Game” program that holds free CPR and automated external defibrillator (AED) training next to Atlanta’s Mercedes-Benz Stadium on game days.
And we recently celebrated a ribbon cutting for the renovated Emory Autism Center playground, which serves 60 children ages 1 to 5 with and without autism (p. 13), a place where fun lays the foundation for empathy and understanding.
I want to thank each of you for your support, whether you work at Emory University or Emory Healthcare, are a student or trainee, call us your health care home, run the Winship 5K, donate to a specific interest, or look to our experts for accurate health information.
This next year will allow us to continue to build upon our successes, and I look forward to tracking our progress and sharing it with you.
Kind regards,
Ravi Thadhani
PHOTO COURTESY
the well
MAKING A CASE FOR Plant-Based Eating
Excerpt from Plantology: A Cookbook Based on the Science of Plant-Based Eating
ating healthy is not a diet. It’s a way of life. It means choosing to feed your body what it needs to function its best. However, knowing what’s best to eat may not be easy to figure out despite the seemingly infinite amount of available information.
Fortunately, scientific research from around the world shows a common pattern among the healthiest diets—they include plant-based, whole, unprocessed foods. A plant-based diet can prevent chronic diseases, dramatically reverse illnesses like heart disease and diabetes, and help people live longer, more vibrant, and energetic lives.
As a physician and a registered dietitian, we not only recommend a plant-based diet because we know it can lead to remarkable results—we also practice what we preach. We want you to experience the same benefits in your life.
We want to dispel the notion that eating healthy is too difficult, time-consuming, or expensive. [There are] simple, nutritious and delicious meals that are satisfying and don’t require spending a lot of time in the kitchen.
A plant-based diet includes plant foods closest to their natural form: a variety of vegetables, fruits, legumes, whole grains, seeds and nuts. This way of eating avoids or limits meats, dairy products, and eggs. It also limits processed foods, which contain added fat, sugar, and salt.
Many diets such as vegan, vegetarian, Mediterranean, and even omnivore can be considered plant based. A predominantly whole-food, plantbased diet can include animal and processed foods as long as they play a secondary role. Eating plant-based does not mean you have to take an all or nothing approach to plant foods.
A key difference between eating a plant-based diet versus a vegetarian or vegan diet is that plant-based eating is defined by what it includes— high-quality plant food with the maximum amount of nutrients—rather than by what it excludes. Strictly eliminating animal products doesn’t guarantee that your diet is nutritious. Many processed foods, such as pasta, pizza, and desserts, which offer little nutritional value, can be a part of vegetarian diets.
Predominantly whole-food, plant-based eating seeks to minimize food that can harm health by maximiz-
GOOD FATS Natural fats like those found in avocados can help lower cholesterol and blood pressure and reduce inflammation.
ANTIOXIDANTS Herbs and roots can contribute to wellness, such as ginger which can treat nausea and reduce inflammation.
WHOLE GRAINS Whole grains provide fiber, vitamins, minerals and other nutrients.
WHOLE FRUITS Fruits are often high in vitamins and fiber. Kiwis, for example, support heart health, digestive health, and immunity.
PULSES Beans, peas, and lentils are excellent sources of fiber, folate, and potassium.
Jenny Bilko, dietitian for Emory Healthcare
Sharon Horesh Bergquist, Emory internist, associate professor of medicine
ing foods that add to quality of life and longevity.
The main takeaway is that following a plantbased diet does not mean you have to limit yourself to only plant foods. No one food will make or break your diet. However, the more disease-fighting nutrients you consume from plant-based foods, and the less pro-oxidant and pro-inflammatory disease-causing components you get from animal and processed foods, the more you will benefit from what you eat. The higher the dose of plant-based whole foods, the greater the response.
An impressive and growing number of studies support the case that plant-based diets can improve health by preventing, slowing, and even reversing many common diseases.
More specifically, by eating a plantbased diet you can:
• Maintain your weight in a healthy range without forfeiting essential nutrients
• Lower your blood sugar and prevent diabetes
• Lower cholesterol and blood pressure levels
• Prevent and reverse heart disease
• Reduce the risk and progression of certain types of cancer
• Reduce the risk of cognitive decline
• Improve your mood, sleep, and energy
• Add healthy years to your life
SLOW COOKER 5-BEAN CHILI
A study of nearly 90,000 people demonstrates the remarkable health benefits from incremental increases in eating plant-based whole foods. The more the participants adhered to eating plant-based food, the lower their rates of having diabetes and hypertension.
Compared to people who ate red meat, poultry, fish, milk, and eggs more than once a week, those who consumed these foods less than once a week had a 28% lower risk of diabetes and a 23% lower risk of hypertension. Those who didn’t eat red meat or poultry at all, but still consumed fish, milk, and eggs, had a 51% lower likelihood of diabetes and a 38% lower risk of hypertension. The group that followed a dietary plan that didn’t include any meat had a 61% lower likelihood of diabetes and a 55% lower probability of high blood pressure. Finally, the group that didn’t consume any animal products at all—no meat, dairy products, or eggs—had a dramatic 78% lower risk of diabetes and a 75% lower chance of hypertension. These results, and those of similar studies, illustrate two main findings:
• Plant-based eating could be even more effective than medication or medical procedures.
• Making small changes in your food choices can remarkably improve your health and well-being. The health advantages of plant-based whole foods take effect within weeks and continue to accumulate with time.
Servings: 6, Per serving: 360 calories, 2.5g total fat, 0g saturated fat, 190mg sodium, 65g total carbs, 24g dietary fiber, 0g added sugar, 22g protein, Food groups: 2 legumes, 1 vegetable, 1 herb
• Five 15 oz cans of beans of choice (black beans, kidney beans, chickpeas, pinto beans, etc.)*
• Two 15 oz cans of diced tomatoes or fire-roasted tomatoes*
• Two 10 oz cans of diced tomatoes with green chiles*
• One 15 oz can of tomato sauce or one 4 oz can of tomato paste*
Place all ingredients into a large 8-quart slow cooker. Stir together. Cook on low for 7–8 hours or high for 3–4 hours.
Innovative Fieldwork
The National Academy of Medicine (NAM) has selected Roxana Chicas, assistant professor at the Nell Hodgson Woodruff School of Nursing, to participate in its American Academy of Nursing Fellowship. Chicas is one of seven health professionals from various disciplines selected for the overall NAM Fellowships program. The fellowship allows early career
Using real-time biomonitoring, Chicas conducted the first field-based intervention study examing ways to reduce core body temperature and improve health among farmworkers in the US.
health science scholars in nursing to participate in evidence-based health care or public health studies that improve patient access and care. Chicas focuses on occupational and environmental health and nephrology. Her research seeks to improve the health of underserved and vulnerable Latinx communities, particularly agricultural workers.–Jacob Gnioski
Help for Multiple Food Allergies
About 8 percent of US children suffer from food allergies, and almost half of those have multiple food allergies. No approved solutions for those allergic to multiple foods existed—until now.
The US Food and Drug Administration recently approved injection of omalizumab (brand name Xolair) for the reduction of allergic reactions, including reducing the risk of anaphylaxis in certain adults and children one year or older with one or more food allergies.
This approval was based on interim findings from a clinical trial that showed a 16-week course of omalizumab, an injectable drug, increased the
amount of milk, peanut, tree nuts, egg, and wheat that some multifood-allergic children could consume without an allergic reaction after exposure.
Emory and Children’s Healthcare of Atlanta were among 10 sites to take part in the first stage of the trial.
“While not a cure, omalizumab is the first medicine available that could help reduce allergic reactions to multiple foods following an accidental exposure, which will provide a great benefit to many of these patients,” says Brian Vickery, Marcus Professor of Pediatric Immunology at Emory’s School of Medicine and chief of the Division of Allergy and Immunology at Children’s.–Rob Spahr
PHOTO KAY HINTON
A Global Health Lens
The Emory Global Health Institute (EGHI) student photography contest showcases compelling and thought-provoking imagery from Emory students. This contest invites participants to share their perspectives on health challenges at home and abroad, fostering cultural sensitivity and awareness.
(People’s Choice Award) 1 2 4 3
1. Colorful Confessions/Chiang Saen, Thailand, by Julia Byrnes, Emory School of Medicine: Baan Kru Nam is home to more than 80 migrant children and Kru Nam, the women who started the home to help end human trafficking in Thailand. (Honorable Mention)
2. Wings of Disease/Jigjiga, Ethiopia, by Jennifer Snyder, Rollins School of Public Health: Close-up of the deadly mosquito species Anopheles stephensi, which is reviving malaria in African urban settings. (Winner)
3. The Heartfelt Smile/Chiang Saen, Thailand, by Emma Constanza, Emory School of Medicine: Emory Health against Human Trafficking provides checkups at Baan Kru Nam Children’s Home.
(Honorable Mention)
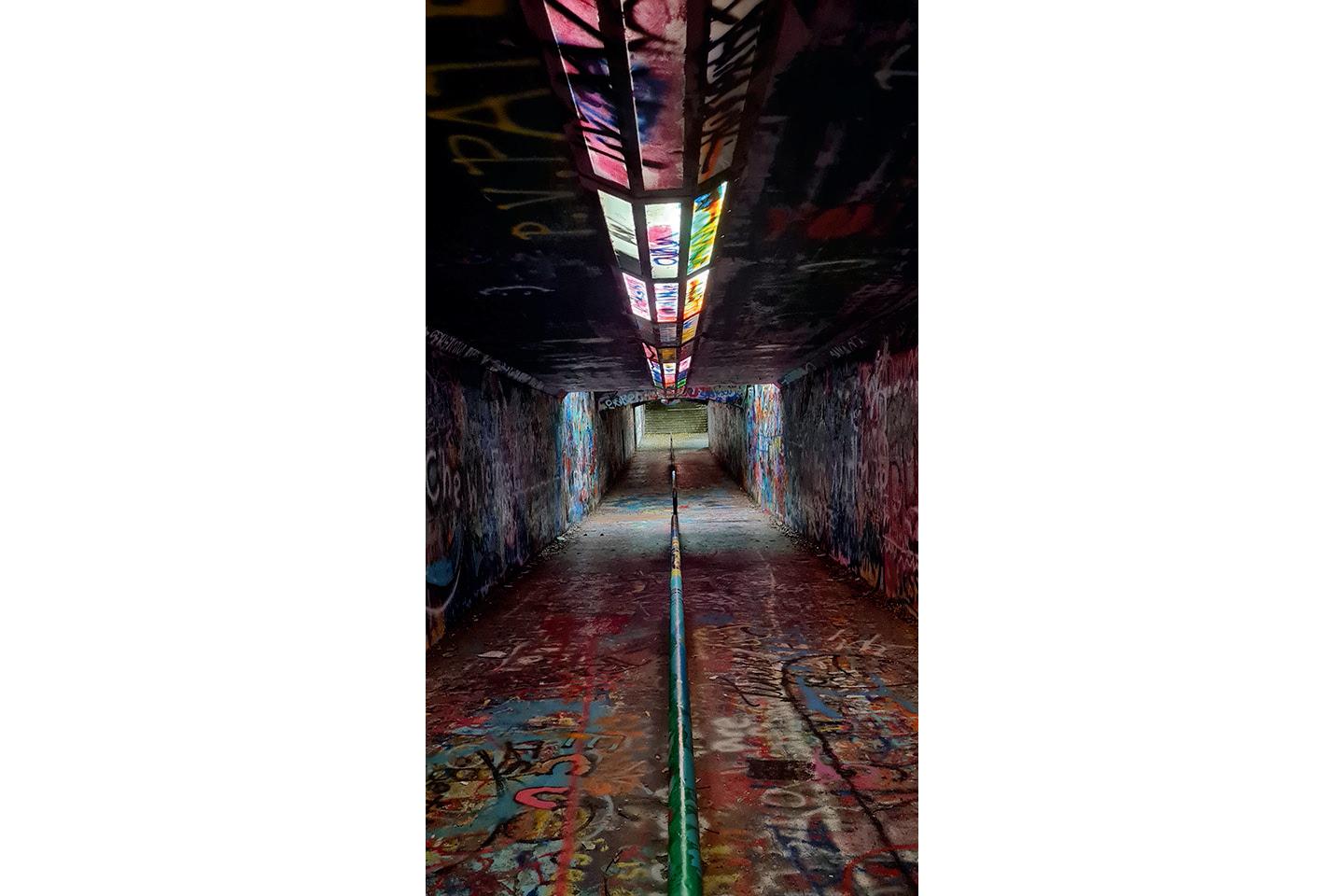
4. The Tunnel of Hope/Raleigh, North Carolina, by Ketki Vinayak Joshi, Rollins School of Public Health: The Free Expression Tunnel is a place anyone can decorate. Participating in the arts can help people cope with mental health conditions.
Nutrition/Caraballo, Dominican Republic, by Audrey Willett, Nell Hodgson Woodruff School of Nursing: Every day across the Dominican Republic, more than 200 children receive a spoonful of peanut butter and vitamins. (Winner)
THE EMORY NELL HODGSON WOODRUFF SCHOOL OF NURSING’S BACHELOR OF SCIENCE (BSN) PROGRAM IS NO. 1 IN THE NATION, according to rankings released by US News & World Report. With this ranking, the school is No. 1 in BSN and master’s degree programs among US nursing schools.
The School of Nursing has been in the top five in the US News' BSN rankings since they began in 2021.
“Having two No. 1 programs is a remarkable achievement,” says Dean Linda McCauley. “It shines a light on our commitment to visionary nurse leadership and our efforts to enhance the profession and health care. I am delighted for our entire school community.”–Best Colleges 2024, US News & World Report.
Deep-Breathing Benefits
Brain scans show slower breathing reduces anxiety and fear, while increasing the ability to reason, so the thinking mind restrains the emotional part of the mind, helping a person evaluate the situation better.
Deeper, slower breathing can also let your body know to come out of fight-or-flight mode, says Anne Bartolucci, clinical psychologist, adjunct assistant professor at Emory School of Medicine and author of Better Sleep for the Overachiever.
“It’s a nice, quick way to calm down, and it’s also a way to signal to yourself that you’re taking care of yourself,” Bartolucci says.–“Six Breathing Exercises to Ease Stress and Anxiety,” Today.com
AI Poised to Transform Neurological Care: “Artificial intelligence will improve care by assisting—not replacing—clinicians and researchers by providing a new perspective that integrates multiple layers and types of data into personalized clinical or preclinical predictions.”–Cassie Mitchell, assistant professor, Coulter Department of Biomedical Engineering at Georgia Tech and Emory, at the American Neurological Association AI Symposium.
“IN THE UNITED STATES, THE STUBBORNLY HIGH RATE OF HIV DIAGNOSES—especially in the US South, and particularly among gay and bisexual men of color and transgender people—demands novel approaches to help people prevent HIV acquisition,” says Colleen Kelley, professor of medicine at Emory and a principal investigator in the Purpose 2 Phase 3 trial. “Because adherence to oral products can be challenging for some people, twice-yearly injectable lenacapavir for PrEP has the potential to be one of the most impactful interventions we could have to drive down new infections and bring us closer to ending the HIV epidemic in the United States.”–“Twice-yearly injectable lenacapavir, an HIV-prevention drug, reduces risk by 96%,” ADVOCATE
ILLUSTRATION YULIA SUTYAGINA
PHOTO EDWARD PIO RODA
HOW TO DEAL WITH 4Qs
Emory pulmonologist
Colin Swenson, an expert in lung disease and asthma, addresses how people can detect and prevent mold in their homes.
How does weather factor into mold risk, such as heavy rains, flooding, water leaks, or high humidity in homes?
Mold’s effects usually aren’t felt until a few days or weeks after a weather event, says Swenson, since it takes a while for mold spores to germinate. Mold spores can blow in through open doors and windows, come in on shoes, clothes, or pets, or with floodwater. First inspect your home for standing water or wet drywall, which create prime conditions for mold growth. The best way to determine if there is mold in your home is your sense of smell. Mold gives off a musty odor, even before you’re able to see any visual signs. There are many different types of mold and not all of them cause disease.
What can be done to prevent mold in a home?
If relative humidity can be kept below 65 percent, spores will not germinate. Turning on the air conditioning, even if you don’t need it, is one way to lower humidity, as well as running dehumidifiers, especially in damp areas like basements. For mold and mildew prevention, you should set the thermostat to 72 degrees in the cooler months and 76 degrees in the warmer months, with the HVAC fan set on auto. Also, run the bathroom fan during and after showers.
What are the health risks from mold exposure?
There are potentially serious health risks, says Swenson, including hypersensitivity reactions, such as allergic bronchopulmonary aspergillosis (ABPA), a condition that can cause severe symptoms, hospitalization, and even death, especially among individuals with preexisting asthma or COPD. Another is hypersensitivity pneumonitis, an immune response that can develop from mold exposure, lead-
ing the body to attack its own lung tissue, creating progressive scarring of the lungs. Some people are at risk of “fungal balls,” which can form in areas of prior lung damage from, for instance, TB or emphysema. These fungal balls, or mycetomas, can cause major bleeding and other respiratory symptoms. Immunocompromised patients and those undergoing chemotherapy are at risk of invasive fungal disease, which is potentially fatal.
Can someone stay in their home after mold has been discovered?
If you already smell or see mold on walls, carpets, or furniture, which often shows up as a discoloration, you will have to take steps to have it cleaned up, Swenson says. He recommends contacting your insurance company, then hiring a professional mold remediation company. If you do decide to tackle a small mold infestation yourself, wear an N95 respirator, protective gloves, and goggles. Swenson recommends getting out of the home until the mold has been remediated or wearing an N95 mask inside the house. EHD
The Emory Autism Center has a new playground designed to promote inclusion and interactive play for children with and without autism.
The center enrolls 65 children with a 1:2 ratio of autistic to neurotypical peers. “It’s more than just a play area, it’s a foundation for building empathy, compassion, and lifelong connections,” says director Mikle South.
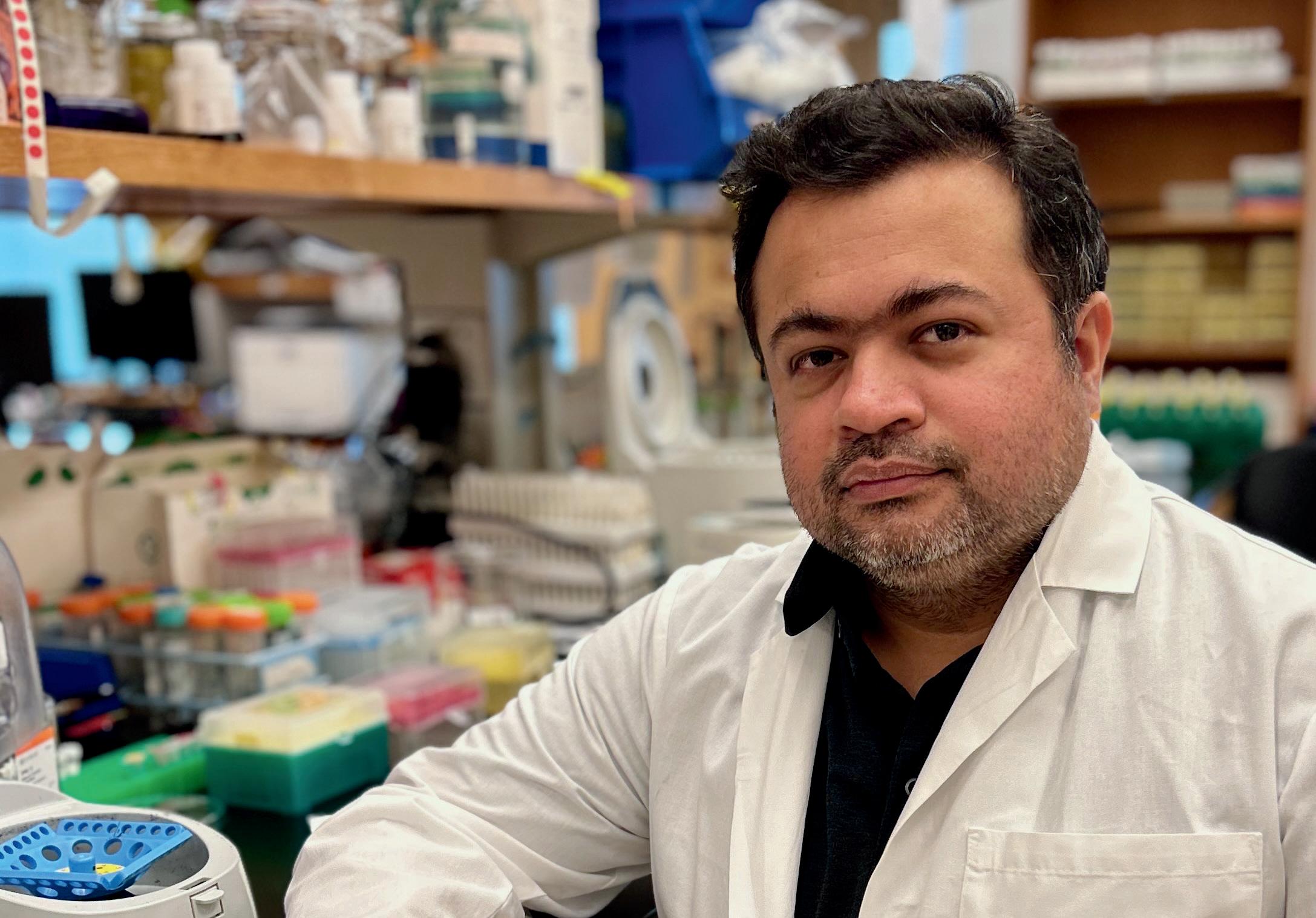
I AM AN EMORY RESEARCHER
Unlocking ALS Mysteries
When Devesh Pant received the 2023 Live Like Lou career development award, he was honored. But even more, he was grateful the grant would support his investigation of amyotrophic lateral sclerosis (ALS).
Pant focuses on neurological and rare neuromuscular diseases in his research. “The key drivers for me to study ALS are the patients affected with this dreadful disease who are striving hard to fight the challenges on a daily basis,” he says.
An instructor in the Department of Cell Biology at Emory’s School of Medicine, Pant has a PhD in biomedicine from Pompeu Fabra University in Barcelona and a master’s in biotechnology from the Indian Institute of Advanced Research in Gandhinagar, Gujarat.
ALS is a disease affecting motor neurons in the brain and spinal cord, which causes progressive weakness and atrophy of muscles. People with ALS gradually lose the ability to walk, talk and, eventually, breathe.
Around the world, ALS is known by different names. “In France, it was called Charcot disease, after French neurologist Jean-Martin Charcot, who first described the symptoms,” Pant says. “In the UK, it’s called motor neuron disease. In the US, it is known as Lou Gehrig’s disease, after the famous baseball player who played for the Yankees and was diagnosed with ALS.”
The foundation, Live Like Lou, is in close connection with Lou Gehrig’s family and provides
resources to ALS families, patients, and researchers.”
Pant’s career path was shaped by international opportunities.
“I received a competitive fellowship from the government of Spain to do my PhD studies in Barcelona. It was a wonderful experience,” he says. “We discovered a novel mutation that causes a rare neurological disease — hypomyelinating leukodystrophy. It’s a childhood neurodegenerative disease that affects the white matter of the central nervous system.”
To study the disease mechanism and determine therapeutic options, Pant developed a zebrafish model in the lab that mimics the disease pathology and tested an FDA-approved drug that lessens symptoms in this model. This work led to a pilot clinical trial at centers worldwide.
Pant joined Emory in late 2020, largely because of the university’s extensive research in neurodegenerative diseases. “There’s a great collaborative ALS research team here, along with core facilities, the Emory ALS Center directed by Dr. Jonathan Glass, and the Center for Neurodegenerative Diseases, with which the lab actively collaborates.”
Pant travels to India annually to visit his family. His interest in biology began at a high school science exhibition.
Because ALS’s progression dramatically diminishes one’s quality of life, “even a small win can make these patients’ lives better,” Pant says. ALS is a heterogeneous disease, with 10% genetic cases and 90% sporadic (meaning the cause is unknown).
“Despite significant research efforts to understand ALS and the influence of various genetic, environmental, and lifestyle factors, the exact pathophysiology of the disease remains unclear,” says Pant, “and no effective treatments are currently available.”
When the Ice Bucket Challenge went viral on social media a decade ago, it inspired more than 17 million people worldwide to dump ice water on their heads and donate to an ALS organization, expanding funding for ALS research and leading to the discovery of several new genes associated with the disease.
Researchers around the world have identified mutations that lead to ALS, but important questions remain.
With the help of collaborators at Emory, Heidelberg, Germany, and the Albert Einstein College of Medicine in the Bronx, Pant set about answering this question: How does a defect in a specific motor protein cause disturbances in the body that can lead to ALS?
Perhaps the most famous case of ALS was seen in physicist and author Stephen Hawking, who was diagnosed when he was 21 and lived with the disease for 55 years—an extremely rare outcome.
“In our lab, we are not discovering any new genes,” Pant says. “All the new ALS-associated genes are identified mainly by clinical geneticists worldwide who see the patients, send patient samples in for genomic sequencing, and identify novel mutations. We get the mutation information and the associated pathological symptoms from these clinical centers. In the lab, we model these genetic mutations using animal models or stem cell cultures to better understand the molecular mechanisms that lead to ALS.”
In the ALS field, therapies are challenging. So far, no treatment can cure, minimize, or even slow the disease progression.
If researchers can develop treatments that block the impact of the genetic mutations, says Pant, they can provide therapeutic hope for patients.
While Pant is primarily a researcher, he’s also been a conduit for families in search of help.
“I’ve met some of the patients, and it provides more motivation to find a solution for them,” he says. “It’s nice to tell them about the research we are doing. I do get emotional when I think about these patients and their families.”–Mary Loftus
Get the full story on Devesh Pant and other Emory researchers
Now Hear This
Emory and WABE present “Health Wanted,” a fun, fresh, and myth-busting alternative to the critical health discussions impacting communities.
Host Laurel Bristow, a research scientist and infectious disease expert at Emory’s Rollins School of Public Health, delivers the week’s essential public health headlines and demystifies the science behind trending topics.
A social media influencer with a following of 381,000 on Instagram, Bristow covers everything from Ozempic to the ozone, interviewing experts and answering listeners’ questions. She has a master's of science from the London School of Hygiene and Tropical Medicine and has worked in infectious disease for a decade.
“In a time filled with misinformation and complex scientific literature, our show aims to provide a wealth of easy-to-digest and scientifically accurate information,” she says. “We aspire to be a beacon of sanity, humor, and vital scientific truth, helping listeners navigate through the noise with clarity and confidence.”
Bristow came to Emory in 2018 as part of the Hope Clinic Vaccine Center, then joined the Emory/Georgia TB Research Advancement Center as associate program director.
Prior episodes of the podcast include the topics of aging, psychedelics, reproductive health, clinical trails, maternal mortality, the opioid crisis, vaccines, microplastics, extreme heat, and mosquitoes.
Listen through Apple, Spotify, RSS, or by visiting wabe.org/healthwanted.
What Ferrets Can Teach Us about Flu Spread
Increasing ventilation in childcare settings may not always be effective at preventing flu virus spread, according to a new study published by a team of researchers at Emory, University of Pittsburgh School of Medicine, and Virginia Tech. The spread of flu viruses is commonly studied in animal models that don’t mimic real-life scenarios of the human experience, making it difficult to evaluate strategies that will be effective in common settings where diseases spread rapidly, such as childcare sites.
As reported in the journal Proceedings of the National Academy of Sciences (PNAS), the team created a play-based model using ferrets to study the spread of flu in a setting that closely mimics a childcare center. In their scenario, one infected ferret interacted with four uninfected animals for a few hours within a playpen area that included toys and other surfaces. “Ferrets are great models for kids because they are playful animals and exhibit many behaviors seen with children in real life, such as close-contact interactions and playing with toys,” says Seema Lakdawala, corresponding author and associate professor at Emory School of Medicine. “They also exhibit key symptoms of influenza that are seen in infected humans.”
Testing high and low ventilation conditions, the researchers examined how many ferrets got sick and the levels of virus in the air and on surfaces. They found that approximately the same number of animals got sick in both venitilation conditions. Although the team did observe slightly less virus in the air with higher ventilation, they measured similar amounts of virus on objects within the playpen.–Georgia Parmalee
See more on Seema Lakdawala and other Emory researchers
Anti-Inflammatory Treatments Show Promise in Treating Low Motivation
People who have depression also can experience low levels of motivation. Researchers have revealed a promising new avenue for treating motivational deficits associated with depression. These motivational impairments have been linked with poor treatment outcomes, diminished quality of life, and heightened suicide risk.
Growing evidence suggests a potential cause of low motivation may be persistent inflammation, which suppresses activity within key circuits in the brain. “These findings build on growing evidence that anti-inflammatory treatments hold promise as a novel approach for addressing motivational deficits in depression,” says senior author Andrew Miller, professor of psychiatry and behavioral sciences at Emory School of Medicine. “By targeting inflammation, we’re not only address-
ing the biological underpinnings of these deficits but also offering new hope for more effective treatment options.”
This study, published in Nature, is the first of its kind to examine the effects of infliximab (a potent anti-inflammatory medication used to treat rheumatoid arthritis) on behavioral and brain markers of motivation in 42 medically stable, unmedicated depressed patients. The study focused on patients who were not only depressed, but also exhibited high inflammation as measured by C-reactive protein (CRP) levels.
Patients who received infliximab demonstrated a greater willingness to exert effort in pursuit of rewards, compared with those who received the placebo. “This is the first study to reveal the impact of an anti-inflammatory drug on brain circuits related to
motivation,” says first author Michael Treadway, Winship Distinguished Research Professor in Psychology. “It’s exciting to see how modulating inflammation can directly influence motivation, one of the most challenging symptoms to treat in depression.”–Jennifer Johnson
Andrew Miller, professor of psychiatry and behavioral sciences at Emory School of Medicine
Common Cosmetics May Pose Health Risk to Pregnant Women, Babies
Products women routinely apply to their skin and hair may be putting them and their babies at risk, according to a new study published in Environmental Health Perspectives. Led by scientists from Emory, Northeastern, and University of Michigan, the study found that chemicals called phenols and parabens may increase the risk of hypertension and high blood pressure during pregnancy and threaten the long-term health of mothers and babies. These chemicals are commonly used as
UV filters in lotions, soaps, shampoos, and sunscreens as well as to prevent the growth of bacteria and mold in cosmetics. “Our findings show these chemicals are associated with really adverse pregnancy outcomes and higher levels of these chemicals can lead to gestational hypertension and to women delivering their babies early and at lower birth weight,” says senior author Stephanie Eick, assistant professor of environmental health and epidemiology at Rollins School of Public Health.–Rob Spahr
Dennis Liotta, co-founder and former executive director, Drug Innovation Ventures at Emory (DRIVE) and the Emory Institute for Drug Development
Haian Fu, professor and chair of the Department of Pharmacology and Chemical Biology, and director, Discovery and Developmental Therapeutics research program, Winship Cancer Institute
Center for New Medicines Is a Hub for Life-Saving Treatments
Emory’s Woodruff Health Sciences Center is developing a drug discovery pipeline for translating fundamental biological discoveries into the next generation of life-saving treatments. The Center for New Medicines will serve as a one-stop hub of advanced technology, infrastructure, and resources, where scientists and physicians will work together to identify unmet medical needs and create solutions to improve health outcomes.
The idea for the center was formulated by co-directors Haian Fu and Dennis Liotta to streamline the process for advancing medical innovation. Em-
ory scientists and clinicians have been at the forefront of discovering treatments for a myriad of diseases of global concern, including HIV, COVID-19, cancer, and hepatitis B. Fu says the new center will focus on some of the most prevalent and confounding diseases, including cancer and neurodegenerative conditions.
“The diverse expertise and robust infrastructure we have at Emory provide a fertile ground for nurturing new transformative treatments,” says Fu.
“We’re aiming to bridge the gap between scientific discovery and clinical translation.”–Brian Katzowitz
Combination tests for flu, COVID-19 available now
As respiratory virus season arrives in the US, a new tool could be a game changer: over-the-counter combination tests that can detect both flu and COVID-19 with a single sample.
The combination tests offer a convenient way to quickly check for both viruses at home. How reliable are they? Researchers at Emory, Children’s
Healthcare of Atlanta, Georgia Institute of Technology and Grady Health System have played a pivotal role in evaluating these tests.
The Atlanta Center for Microsystems Engineered Point-of-Care Technologies (ACME POCT), led by researchers at Emory, helped test seven of the eight combination tests for flu and COVID-19 now available on store shelves.
More information on combination tests here
PHOTO STEPHEN NOWLAND
‘Healthcare Test Kitchen’ Applies Lessons from Ebola
Ten years ago, as the first patients with Ebola virus to be treated in the US were transported to Emory University Hospital, charge nurse Jill Morgan (below in protective gear) was faced with a pivotal question: How could health care workers be certain of biocontainment? How could the risk be mitigated?
“I never felt like I was exposed to Ebola,” says Morgan. “Our patients who contracted Ebola virus disease were all health care workers themselves traveling in Africa, and none of them knew exactly how they had gotten exposed. They trusted their protocols and processes too. How do we know that we stayed safe because of what we did, instead of being lucky? That’s when I decided that trust is not enough. I want to see the evidence,” adds Mor-
gan, site manager of the Serious Communicable Diseases Unit.
Morgan’s experience caring for highly infectious patients informed her idea for a “Healthcare Test Kitchen” lab, designed to validate bedside materials, procedures, and protocols to ensure pathogen containment and maximum safety for employees, patients, and families. “We want to understand where workers and patients are at risk from infectious pathogens and how we can mitigate those risks,” says Morgan. “Because what doesn’t end up on our clothing or skin doesn't move to the next patient, other staff, or home to our families.”–Lara Moore
Winship Cancer Institute is Georgia’s only National Cancer Institute-designated Comprehensive Cancer Center. Our mission is to discover cures for cancer and inspire hope.
You can help revolutionize the future of cancer care and provide hope.
TODAY’S GIFT TO WINSHIP CANCER INSTITUTE IS TOMORROW’S CANCER CARE.
GIVE TODAY
To make a gift online, visit together.emory.edu/hope1
Get the full story on Emory’s ‘Healthcare Test Kitchen’
PHOTO JACK KEARSE
Straight talk about the new weight loss drugs Taming Hunger
By Mary Loftus • Photos Jack Kearse
Illustrations by Aad Goudappel
It’s a warm evening on General Muir’s outdoor patio, and discussion about new weight management medications such as Ozempic/Wegovy begins among Dinner with a Doctor participants even before the first salmon filet, Reuben sandwich, or lentil plates are served.
Are there side effects? How do I know which drug is right for me? Why won’t my insurance cover it? Is this the miracle drug we’ve been waiting for?
Our physician hosts this evening are Caroline Collins, an internist and specialist in lifestyle medicine, and Meghana Anugu, an internist and obesity medicine specialist. Both are assistant professors in primary care at Emory School of Medicine.
Our panelists included Quinn Eastman, a science and medical writer/editor from Decatur; Margie Roe, an interior designer from Lilburn; Caela Abrams, an attorney in Atlanta; Mike King, a retired journalist/author from Atlanta; Leigh Partington, a marketing and communications manager from Stone Mountain; Ann Cone, a lender in commercial real estate from Peachtree Corners; and Miriam Oyewo, a student at the University of Alabama at Birmingham and Emory intern.
While GLP-1 drugs have been used for years to treat type 2 diabetes, they gained vast popularity after being approved for weight loss in 2021. More than 15 million people in the US are estimated to be taking semaglutides/GLP-1 drugs, or about 6% of the adult population, according to a new health tracking poll from KFF, a Kaiser Family Foundation nonprofit that focuses on health policy in the US.
Semaglutides like Ozempic/Wegovy work in three primary ways. They mimic the natural hormone GLP-1, which helps regulate appetite; slow the rate at which food leaves the stomach; and enhance the secretion of insulin when blood glucose levels are elevated. Tirzepatides like Zepbound/Mounjaro work in a similar manner but mimic two hormones and are associated with greater weight loss.
“Losing weight isn’t just about what you’re doing right now. It’s about your genes, how you grew up, childhood trauma, what stage of life you’re in.”
—Caroline Collins
Meghana Anugu, internist and obesity medicine specialist
Caroline Collins, internist and specialist in lifestyle medicine
In addition to her clinical work, Collins does research on how AI can be used to make medical decisions. “And one of the decisions I’m teaching it to make is who to prescribe GLP-1 medications to,” she says.
Collins was Anugu’s mentor during her medical residency at Emory, and they float ideas back and forth easily throughout the dinner. The first thing they want to make clear is that extra weight is a medical condition.
“Weight management is a personal and professional interest of mine,” says Anugu. “I have struggled with weight throughout my life and, as experts in chronic disease management and as primary care physicians, we know that weight is a crucial part of managing most chronic medical conditions.
“In the same way we recognize and treat medical conditions like high blood pressure, high cholesterol, and diabetes, we should be doing the same for individuals with extra weight. With these individuals, we tend to see higher rates of cardiometabolic conditions such as high blood pressure, high cholesterol, and diabetes, as well as more stress on their joints, which puts them at higher risk for things like arthritis.
“We also know that individuals with extra weight, if it’s the type of fatty tissue that releases more inflammation, have higher rates of neurodegenerative conditions and of different cancers.”
The gut-brain pathway
Although the topic of tonight’s dinner is medication management for weight, says Collins, we should remember that the foundation of any medical condition is understanding one’s health behaviors. What are someone’s eating habits? What is their physical activity?
“Let’s consider how to move our bodies more, how to have restorative sleep, how to avoid risky substances, how to increase social connection and reduce stress,” she says. “All these are a crucial part of therapy.”
“Does taking these medications mean I’m enjoying food less?” asks a panelist.
“Great question,” says Anugu. “Let’s talk about the physiology and pathophysiology. Weight is so complex. It is not just about what you’re eating and how you’re moving your body, it is also about hormones, genetics, dysregulation related to sleep, stress, etc.”
There’s a pathway in your brain that tells you you’re full, and it gets signals from your GI tract and adipose tissue, she says. “But we still eat even when we’re full, right? So that’s more related to the reward-pleasure system. While these drugs increase satiety signals to the brain, they seem to eliminate these emotional or stress cravings as well. People feel like the ‘food noise’ stops and they are less interested in food.”
The next thing the new weight management drugs do are to slow down your GI tract. “When you eat something small, you feel full. This can result in side effects: if things are moving slowly, you’re more likely to get constipated. You’re also more likely, if you overeat, to make yourself nauseous.”
“And how does the drug trigger an insulin response?” continues the panelist.
“GLP-1 agonists like semaglutides do increase insulin secretion in response to glucose in the bloodstream,” says Collins.
Insulin is the hormone that converts sugar inside a person’s cells to energy. If the person doesn’t need the energy, it can be turned into fat cells.
“So if you grew up eating, say, a carbohydrate-heavy diet and have insulin resistance, it’s much harder to lose weight,” Anugu says.
“It’s a cumulative effect,” adds Collins.
Miracle drugs?
“Do we just need to give everyone who is overweight semaglutides and they won’t have a problem anymore?” asks a panelist.
“We see patients who have struggled with weight for a long time and once they start seeing results with medication management, they become more invested in nutrition, physical activity, stress reduction, getting better sleep,” says Anugu. “Those actions are also helping their gut.”
“Why did these medications just burst onto the scene?” asks another panelist.
“I was prescribing similar drugs, like Trulicity, when I was a resident,” says Collins. “We saw
some weight loss with the earlier medications but not nearly to the degree we do with the newer ones. And tirzepatide (Zepbound/Mounjaro) really changed things, because some people are losing weight in ranges similar to those who complete bariatric surgery.”
Anugu says the amount of medication-assisted total body weight loss went from 5-8% with the older FDAapproved drugs to 12-18% with semaglutide, then to 20-28% with tirzepatide. Recent studies have shown even higher weight loss for patients who have been on the drugs for more than a year.
“This is why it’s shaken the landscape of how we treat obesity,” Anugu says. “But here’s the thing: this medication works when you take it, but typically if people stop taking it, they tend to regain a significant amount of weight.”
“Why are they so expensive?” asks a panelist, who says she takes a compounding pharmacy version due to cost.
Indeed, the average retail cost of a 28-day supply of an FDA-approved semaglutide is about $1,000. Some insurance companies cover semaglutides for both
diabetes and weight loss. Medicaid largely covers the drugs when used for type 2 diabetes, but coverage for weight loss is limited.
Semaglutides from compounding pharmacies, which are not FDA-approved, have become popular because they are much less costly. But both physicians say they would strongly recommend not using generic semaglutides from compounding pharmacies because quality, safety, and effectiveness cannot be guaranteed. (Compounding of medications is only allowed when the medication is on
Quinn Eastman science and medical writer/editor
Miriam Oyewo student intern
Ann Cone commercial real estate lender
Mike King retired journalist/ author
Margie Roe interior designer
Caela Abrams attorney Leigh Partington marketing and communications PANELISTS
the FDA short supply drug list.)
“That’s why Emory officially says, we do not recommend you get these from compounding pharmacies,” Collins says. “You don’t know what you’re getting.
“Semaglutides are so expensive to the system,” continues Collins. “We’re trying to figure out how to continue to provide this benefit but not break the system. And that’s a question that every insurance company is trying to answer.
“The problem is, these are not one-time medications,” she says. “These are medicines you would likely need to take for a significant period of time.”
Additional benefits
“But aren’t you then getting a cost savings in diabetes medication and all the other medicines for comorbidities?” asks a panelist.
GLP-1s are clearly beneficial medications, say the doctors. A
host of health benefits have been linked to the drugs beyond treatment for type 2 diabetes and weight loss. “Studies are coming out showing how these medications are helping individuals with kidney disease, sleep apnea, a history of cirrhosis, cardiovascular disease,” says Anugu.
Indeed, multiple studies are also in progress to determine if semaglutides are helpful for Alzheimer’s disease, Parkinson’s, polycystic ovary syndrome (PCOS), alcohol use disorder, and many other ailments.
It appears some of these benefits stem not only from weight loss but from GLP-1 receptor agonists stimulating the body to release insulin appropriately, reducing the impact of sugar.
“If you’re on semaglutides for a while, do you reset your insulin to where it kind of rebounds and does the job better or do we know yet?” asks a panelist.
“Absolutely, you can reset and improve your insulin sensitivity and responsiveness,” says Collins. In fact, we adjust our insulin responsiveness daily, depending on what and when we eat.
“Is there a way to determine my ‘natural weight?’ ” the panelist continues. “To find out if I’m just fighting against where my body wants to be?”
“There’s this concept of your ‘set point’ in the literature, and it theorizes that the weight you’ve been most of your life is your homeostasis, and your hormones
are in balance at this level,” says Anugu. “So if you lose weight below that point, your body will make it harder to maintain that weight loss, and vice versa.
“There are some markers in the labs that endocrinologists or specialists could order, like fasting insulin levels and body composition, or percent of visceral fat (beneath the abdominal wall muscles) vs. subcutaneous fat (just beneath the skin).”
When not to use
Some contraindications exist for GLP-1s: They are not recommended for children under 18, people who are pregnant or nursing or who have type 1 diabetes, diabetic ketoacidosis, a history of pancreatitis, multiple endocrine neoplasia (MEN syndrome), or a specific type of thyroid cancer.
People on semaglutides are often asked to discontinue them for a period of time before surgery, as the slowing of digestion can cause an increased risk of aspiration under anesthesia.
GLP-1s also should not be seen as a golden ticket, but as one tool in the kit of supporting a healthy lifestyle. “It’s still important to look at the underlying factors causing weight gain,” says Collins, “which could be nighttime eating or feelings of depression. If you target these causes, you’re more likely to have weight loss.”
If depression is present, medications like Wellbutrin (which can decrease appetite) and therapy can be game-changers, they say.
“We’re all fixating on these injection medications, but it’s
“It’s always good to maintain a healthy sense of skepticism, but right now the literature on GLP-1 medications looks incredible. And the feedback I’m getting from patients is that it’s changed so many of their lives for the better.”—Meghana Anugu
not just one medicine fits all,” says Collins.
High-fiber foods are “nature’s way of triggering these receptors,” she adds. “That’s why eating plants is really important.”
Taking GLP-1s
“How do you know when you’re on the right level of the medication?” asks a panelist currently taking a semaglutide.
“I think what’s safe is 0.5 to two pounds of weight loss per week and making sure you’re still eating. You shouldn’t feel so full or nauseous that you’re not eating enough. This is crucial,” Anugu says.
Frequent check-ins are important, since some people are “hyperresponders” who lose too much weight too quickly.
“Everyone is different,” says
Collins. “I evaluate how much weight people are losing and how they’re feeling. Are they still eating foods that provide their essential macro- and micronutrients? Based on that, we decide whether to escalate or not.”
“And what about drinking fluids?” asks a panelist.
“Yes, you have to drink water, eat protein—some people supplement with protein shakes— and do weight-bearing exercises/ strength training because you will lose muscle mass, and that affects your metabolism and your risk for osteoporosis,” says Collins.
“How long before people start to plateau?” asks a panelist.
“That is variable. Some people plateau within 10 to 18 months,” Anugu says. “Sometimes that’s a signal to go up on the medication, if they’re still at a weight they’re not
comfortable at and that’s still putting them at risk. As long as they can tolerate a higher dose.”
“When do you move to maintenance levels or wean patients off the medication?” the panelist continues.
“I don’t just look at someone’s weight or BMI. That doesn’t tell you the whole story,” says Collins. “Ideally we would look at lean body mass, how they are feeling, and other indicators.”
“What about switching from one medication to another?” asks a panelist considering transitioning from Ozempic to Mounjaro.
“Mounjaro is more effective for weight loss,” Anugu says. "But in terms of good side effects—meaning decreased rates of chronic disease—we are seeing that across the board.”
“Remember that it’s important to work with a provider who knows about weight and nutrition and can help you take steps toward creating a healthy lifestyle beyond just taking a specific medication,” Collins says. “The practice of medicine is still an art, not only a science.” EHD
Much has been discovered about autism spectrum disorders in the past decade, from earlier diagnostics to better treatments. Why, then, are so many families still waiting for help?
No More ‘Wait and See’
By Nicole Golston
Depending on who you are, where you live, and your insurance company or health care provider, the journey for children to receive a diagnosis of autism spectrum disorder (ASD) can take a while.
In the US, children with signs of autism experience, on average, two years of delay before diagnosis and even longer if the children are from racially, ethnically, or economically disadvantaged backgrounds.
Valuable years, lost.
This despite decades of research showing that earlier interventions produce better outcomes and the advent of advanced technologies that can assist with diagnoses.
“Most parents of children with autism report having had concerns before the second birthday, yet the median age of a US autism diagnosis is 4 to 5 years,” says Emory neuroscientist Warren Jones, the Norman Nien Distinguished Chair in Autism and director of research at Marcus Autism Center, a subsidiary of Children’s Healthcare of Atlanta.
Objective biomarker tests could help reduce diagnostic delays and connect children with services earlier, says Jones.
Jones and Ami Klin, director, Marcus Autism Center and division chief of
Autism and Developmental Disabilities at Emory School of Medicine, are co-creators of EarliPoint™ Evaluation, the first biomarker-based, eye-tracking diagnostic technology tool.
This FDA-approved tool is authorized for use in children between 16 months and 30 months of age to aid in the diagnosis and assessment of autism.
“We measure the way children look and learn about the world at a rate of 120 times per second using eye-tracking technology,” Klin says. “This behavior, social visual engagement, is a foundational skill for the acquisition of speech, language and communication, and reciprocal social interactions.” Typically developing children take advantage of these “hot spots” of socialization— salient aspects of the social scenes they are watching. “But the way children with autism experience the videos is remarkably different: they look elsewhere, often to objects rather than people, and miss thousands of opportunities for social learning,” he says.
Warren Jones, director of research at Marcus Autism Center
Ami Klin, director, Marcus Autism Center
Researchers at Marcus Autism Center and the School of Medicine identified signs of autism present in the first months of life by following babies from birth to 3 using eye-tracking technology (above) to measure the way they responded to social cues. Infants later diagnosed with autism showed declining attention to the eyes of other people.
Indeed, studies have shown eye tracking of social-visual engagement to be a highly sensitive diagnostic tool, successfully identifying children who were diagnosed with autism by clinical assessment in 80 percent of cases.
While this technology is a major move forward in detecting autism, obstacles remain. The issue: getting health care professionals to use the device and make a clinical diagnosis, says Klin, who has been researching autism for more than 30 years.
“In the past couple of years, we have seen a tremendous uptick of screening for autism. It’s quite high nowadays, but then there are families whose children have screened positive for autism and still they cannot get access to a diagnosis,” says Klin.
Despite a federal mandate in the US that children who show developmental delays before age 3 should be provided with services, he adds, the emphasis on early intervention “rings hollow when parents can’t get a diagnosis. And without a diagnosis, families can’t get access to appropriate treatment.”
The barriers to access, he says, include a paucity of expert clinicians, limited knowledge of the importance
of a diagnosis to families, and an unwillingness by many clinicians to make a diagnosis and/or to adopt newer technologies, among others. “Autism can be diagnosed by any physician or any clinical psychologist with experience in the field. So, primary care pediatricians could potentially make a diagnosis of autism, but they are typically not trained, prepared, or willing to do so,” says Klin. “Many also do not believe that a diagnosis will result in services.”
Emory autism researchers are building on Klin and Jones’s groundwork and other discoveries in the field to create innovative therapies that improve outcomes for those on the spectrum.
Understanding obstacles
Celine Saulnier, a clinical psychologist, adjunct professor at Emory School of Medicine, and owner of Neurodevelopmental Assessment and Consulting Services in Decatur, and Cheryl Klaiman, a professor of pediatrics at Emory School of Medicine and program director for diagnostic services at Marcus Autism Center, met at Yale and worked at the Marcus Autism Center together for a time.
PHOTO: KAY HINTON
They have collaborated on numerous clinical trials, regularly evaluating individuals for ASD, and have written a bevy of research studies and a book on adaptive behavior assessments, a measure of how individuals apply their skills in their everyday routines.
In typical development, a person’s cognitive capacity and skill set are usually one and the same.
“If I have the capacity to perform a skill, whether toothbrushing, dressing, social interaction, conversation—then I do those things within my capacity,” says Saulnier. “In autism that doesn’t happen. For whatever reason, individuals don’t intuitively know how to apply their skills functionally. So, they could have a huge repertoire of language and a high IQ, but they don’t functionally interact with anybody, they don’t know how to navigate the social world. These are adaptive deficits.”
The two researchers focus on diagnostic profiles in general: “What does the autism symptom presentation look like in a 6-month-old vs. a 16-yearold vs. a 60-year-old, and what is the individual’s symptom expression?” asks Saulnier, who works directly with families by providing autism diagnoses to help reduce the backlog.
“We also examine profiles across races and ethnicities,” says Klaiman. Another joint project explored ways to help families gain traction despite delays in diagnosis.
“As soon as parents are concerned, can we find a way to help? Is there anything we can do to address concerns? And even if there are wait lists for diagnosis, are there things they can do as they wait so they don’t feel helpless and worried?” asks Klaiman.
In a collaborative study funded by an Autism Centers of Excellence (ACE) genetics grant through the NIH, the two researchers spoke to families using an interview called the Diagnostic Odyssey. “We did lengthy interviews to try and
understand barriers and formulate potential solutions,” says Klaiman. “Is it educating physicians, so you don’t get a wait-and-see answer? Is it providing more service support at younger ages? Or is it giving parents more information, so you don’t just get a pamphlet? What can be helpful to families?”
Recently, Klaiman was funded by the SPARK Research Match, part of Simons Powering Autism, to transform the Diagnostic Odyssey interview into a questionnaire that will be available to more than 1,000 families who participated in the SPARK genetics study. “We can get a bit broader representation of the barriers across different races and ethnicities as well as ages and geographic spread,” says Klaiman, who oversees the research activities of the clinical research fellows at Marcus Autism Center.
Klaiman’s research also focuses on diagnosing autism in children at earlier ages, and she is excited about extending the eye-tracking biomarker technique in ongoing studies.
“My specific portion is thinking about the characterization and the phenotype (outward presentation) of the babies, from really young ages up until the possible time of diagnosis,” Klaiman says. “Are there underlying differences in their behavior as they develop through time that can help distinguish those who are ultimately diagnosed with autism and those who are not?”
No more ‘wait-and-see’
For Susan Brasher, tenure track assistant professor at the Nell Hodgson Woodruff School of Nursing, there is nothing more frustrating than a delayed diagnosis.
“It’s hard to believe there are still medical professionals who are taking a ‘wait-and-see’ approach,” says Brasher. “I started doing this work in 2013 and I thought if we educate enough, I won’t hear those words ever again.
PREVALENCE OF ASD
About 1 in 36 children has been identified with autism spectrum disorder (ASD).
ASD occurs in all racial, ethnic, and socioeconomic groups
ASD is nearly 4 times more common in boys than girls.
Cheryl Klaiman, professor of pediatrics at Emory School of Medicine
Celine Saulnier, adjunct professor at Emory School of Medicine
“I believe the person closest to a situation is the person who knows the most. For me, that is going to be caregivers, clinicians, and the adolescent or adult with autism. They are going to be the ones telling us what research needs to be done.”–Susan Brasher
Susan Brasher, assistant professor at the Nell Hodgson Woodruff School of Nursing
Vince Calhoun, director of the Center for Translational Research in Neuroimaging and Data Science
Instead, I hear them all the time. Nurse practitioners or pediatricians will say, ‘I’m just not sure. I’m going to wait and see.’ And when a child has a well visit just once a year, that’s an entire year that’s wasted.”
This hesitation to diagnose a child was part of what spurred Brasher, who has a background in pediatric nursing, to pursue a doctorate. Her passion is in training and educating providers on gaps in care and amplifying the voices of parents and families, particularly those who are underserved.
“My research is more participatory. I believe the person closest to a situation is the person who knows the most,” Brasher says. “For me, that is going to be caregivers, clinicians, and the adolescent or adult with autism. They are going to be the ones telling us what research needs to be done, how it should be done, and what outcomes we should look at.”
“I spend a lot of time in the community talking with people, doing focus
groups and listening sessions,” she says. Brasher has written a range of articles on topics such as racial and ethnic disparities in ASD, parent-mediated interventions for ASD and moderate feeding problems, and caring for adults with autism in emergency departments.
“A lot of work I do is training for nurses and nurse practitioner students on autism, especially how social skills, communication, repetitive behaviors, anxiety, aggression, and injury to themselves or other people can impact health and health outcomes,” she says.
Brasher works closely with colleagues at Children’s, the Emory Autism Center, Marcus Autism Center, and the CDC. She also hosts an autistic women’s support group, which started with a grant and developed to be much more. Brasher was meeting with a group of individuals with autism to discuss the transition to adulthood when the only female in the group declared she would like to continue
PHOTO ANGELAFOTO
the discussion with other females on the spectrum, because “it’s just different for women.”
“To her point, women are underrepresented, they’re overlooked, and they often experience things differently than men do,” says Brasher, explaining that females on the spectrum tend to mask or camouflage their feelings to follow societal norms. “This group creates a space where they can build their social interactions and feel connected with other women on the spectrum.”
When Brasher learned from colleague Beth Malow, professor of neurology and pediatrics at Vanderbilt University and director of the Vanderbilt Sleep division, that 80 percent of children on the spectrum have sleep disorders, she wondered about its impact on the child’s behavior and as a cause of stress for parents. With a grant from the American Academy of Sleep Medicine, Brasher will work with Marlow as co-investigators to create community-based education programs to improve sleep in children with ASD.
tional core (PNCC). The team is working on developing advanced analytic and AI-based approaches for analyzing neonate neuroimaging data from at-risk families.
Calhoun and TReNDS researchers from a variety of disciplines aim to use advanced technologies and brain imaging to create biomarkers that can help address relevant areas of brain health and disease.
One of the group’s challenges is taking big data sets and looking for commonalities across mental disorders to find connections that are clinically relevant.
“Nurse practitioners or pediatricians will say, ‘I’m just not sure. I’m going to wait and see.’ And when a child has a well visit just once a year, that’s an entire year that’s wasted.”
–Susan Brasher
Brasher was also involved in a multisite study with colleagues from UCLA compiling interviews with siblings to learn more from their lived experiences. “We had siblings of autistic adults who were in their 20s and 30s and a wide range of levels of autism,” she says. “We heard loud and clear from siblings that yes, there was stress, or yes, we couldn’t go to Disney World because that was too sensory stimulating, but I love my brother, I love my sister. I wouldn’t change [them] for the world. A lot of these siblings go into professions that involve caring for people, teaching, etc.”
Using Big Data and AI
Vince Calhoun, an expert in brain imaging and analysis, is the founding director of the Center for Translational Research in Neuroimaging and Data Science (TReNDS), a collaboration between Georgia State University, Georgia Tech, and Emory.
“We have a center that is focused on neuroimaging and data science with applications to study brain development, brain aging, and clinical brain disorders,” says Calhoun, who has a background in electrical and biomedical engineering.
TReNDS has collaborated with Marcus Autism Center to create a pediatric neuroimaging computa-
“But how do we do something useful with these commonalities without ignoring individuality?” asks Calhoun.
Case in point: In a study published in the April issue of Biological Psychiatry, Calhoun and colleagues compared a large brain imaging dataset of 5,231 individuals diagnosed with schizophrenia, ASD, major depressive disorder, or bipolar disorder and a corresponding control group of almost 9,000 adolescent brain scans from cognitive study participants who did not have a diagnosis.
“We wanted to see if there was any evidence that the brain patterns that are signatures of the chronic disorders would show up in the control group,” says Calhoun.
The researchers did find 100 young adults from the undiagnosed control group whose brain patterns matched those of the diagnosed subjects. Further, “these brain patterns also correlated with early symptoms and genomic risk, suggesting the potential of brain function as an early risk indicator,” notes Calhoun, adding that researchers will explore the relationship further.
Joanna Lomas Mevers, associate professor of pediatrics at Emory School of Medicine, Division of Autism and Related Disorders, and director of clinical operations at Marcus Autism Center, provides interventions for children and parents to resolve issues around urine and bowel training.
Mevers works with children with severe to challenging behaviors, which represents a large population of ASD patients, many of whom are not toilet trained.
“I know (Marcus has) great behavioral solutions when it comes to urine training, so we developed clinical services focusing on urine training and then demonstrated through large outcome studies that these are effective and don’t require any negative procedures.
We can do this mainly by providing positive reinforcers to kids, putting them on a schedule, and it can be done in a relatively short amount of time,” she says.
They also developed a caregiver model that takes a bit longer but empowers parents.
After initial promising results, about half of their clients began returning to the clinic. “Parents were saying, ‘Okay, it’s great my kid pees in the toilet; that’s awesome, but they are not having a bowel movement in the toilet.’ And then you see regression because the mom or caregiver must put them back in Pull-Ups because they might have an accident.”
As the issue persisted, Mevers heard from parents about the difficulty of taking older children out to stores and trying to find changing tables, which were not the appropriate size or weight needed, not to mention the costs of adult diapers.
“I knew we had to solve this problem of bowel movements, as there were not good solutions out there,” says Mevers.
Mevers and team began working with Barbara McElhanon, a pediatric gastroenterologist at Children’s, assistant professor of pediatrics at Emory, and medical director at Marcus Autism Center, where she has a weekly GI Clinic dedicated to patients with autism and cares for patients in the multidisciplinary feeding program.
she says. “Potentially, this is something they can do within the home environment.”
Increasing access
In the past 25 years, John Constantino, a child psychiatrist and expert on neurodevelopmental disorders, especially autism spectrum disorders, and professor of psychiatry and behavioral sciences at Emory, has witnessed the field of children’s mental health mature. But success in the lab didn’t necessarily mean adoption into daily life or the health care system.
“I was increasingly concerned that discoveries and advances in knowing what worked with children, what could help them have better lives and better outcomes, were not being applied within the health care system,” he says.
“I was increasingly concerned that discoveries and advances in knowing what worked with children, what could help them have better lives and better outcomes, were not being applied within the health care system.”–John Constantino
“We came up with a combined medical-behavioral model of treating kids with fecal incontinence that has now been through two clinical trials,” Mevers says. “We just finished our last large clinical trial with over 117 kids, randomized between our treatment or treatment as usual, and we are in the process of analyzing those results.” Early results are showing that about 80 percent of patients improve.
“I get emails regularly from people who say, ‘I looked up this study and tried this at home and it worked for my kid; now my kid is bowel trained.’”
The researchers are writing a new grant that if funded will follow the entire toileting process and enable parents to implement some of the procedures, rather than clinicians.
“This is the next step of moving (the toileting methodology) into the real world, so that parents don’t have to find a clinician in their community,”
When he became chief of behavioral and mental health at Children’s Healthcare of Atlanta, he was determined to “model what it would look like if mental health care looked like medical care for a completely representative population of children, including children in the Medicaid program who are governmentally insured.”
Constantino’s new endeavor tackles inequities, delays in diagnoses, and gaps in care.
He anticipates being able to help 7,000–10,000 children per year that “we can enroll in a different level of care: no waiting and high quality. When we develop a treatment plan, no stone is left unturned. The entire evidence base of the field will be delivered by the team at Children’s in collaboration with our partners in the community.”
By the end of June, the first 1,500 children had been seen at Children’s. Now that the foundational system is in place, his next move is to build the research framework. “We are engaging policy analysts, and longitudinal studies experts, and are building a scientific team that will comprise an informatics and policy core associated with the Center for Behavior and Mental Health.”
Additionally, Constantino is concerned about the disparities that Black children with autism experience that white children with autism often don’t.
“Children who are Black and born with autism versus children who are white and born
“Children who are Black and are born with autism versus children who are white and born with autism get diagnosed later, get misdiagnosed more frequently, have much lower access to necessary developmental therapy and educational interventions, and have twice the rate of associated intellectual disability.”–John Constantino
with autism get diagnosed later, get misdiagnosed more frequently, have much lower access to necessary developmental therapy and educational interventions, and have twice the rate of associated intellectual disability,” he says. “It’s enough to have autism, but you combine that with intellectual disability, and it is just an overwhelming one-two combination for development.”
However, preliminary studies Constantino worked on with colleagues at Washington University in St. Louis have shown that Black children who receive developmental therapy gain “essentially seven IQ points for every nine months of developmental therapy,” he says.
Constantino and members of his Children’s team went to the primary care practice at Children’s Hughes Spalding Hospital and found there were around 100 children, 3 years old
and under, whose pediatricians suspected they had autism.
“They were on a waiting list for a diagnosis but there no options for evaluation in the foreseeable future for them,” he says. “We were determined to eliminate this wait list.” Through joint efforts of the Behavioral and Mental Health team and the Marcus Autism Center, the wait list has now been eliminated, and enhanced capacity sustained to ensure that it does not reaccumulate. “If you diagnose children on time and give them the right kind of developmental and educational supports, there is opportunity to spare many of them a lifetime of intellectual disability, which is a serious facet of the disparity.” EHD
Nicole Golston is a freelance writer who lives in Tucker, Ga., with her two young adult children, including a son on the autism spectrum.
Joanna Lomas Mevers, assistant professor of pediatrics at Emory School of Medicine
John Constantino, professor of psychiatry and behavioral sciences at Emory
PHOTO MAMIGIBBS
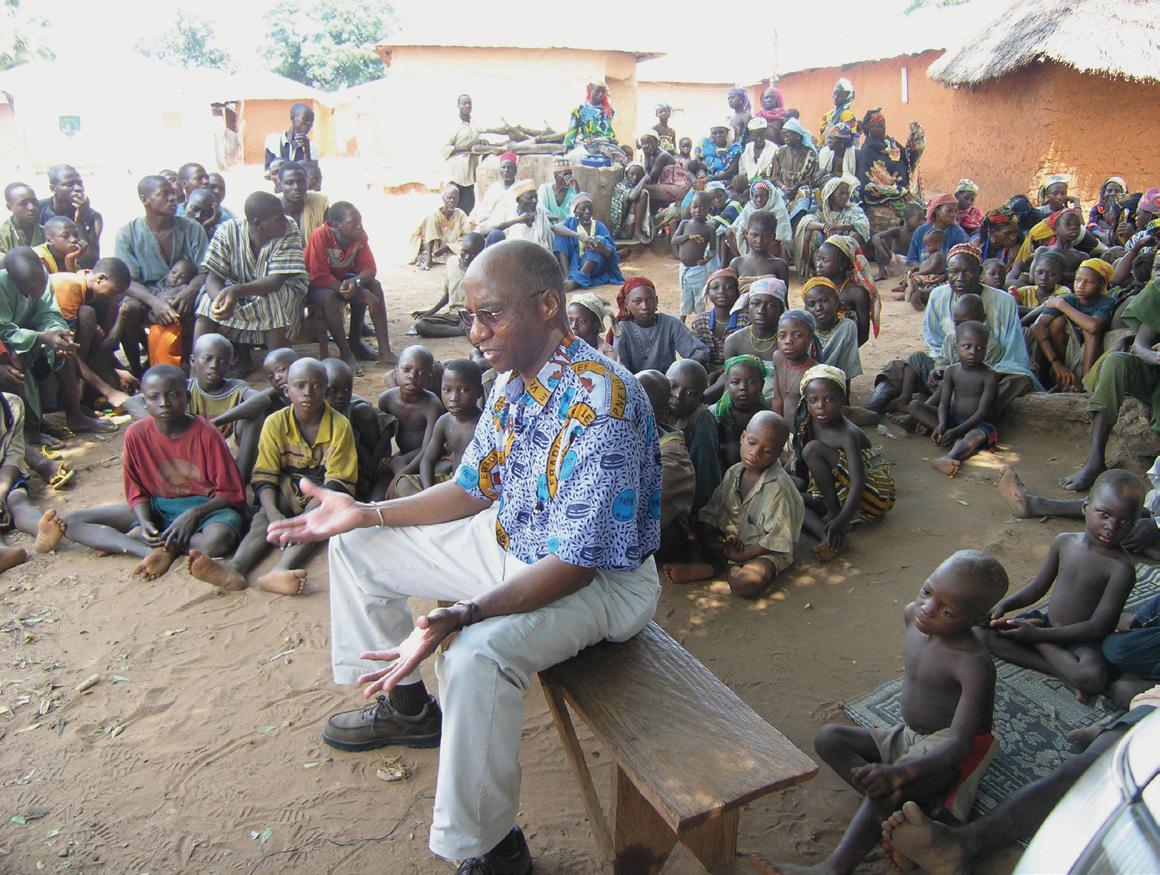
The Statesman vs. the Fiery Serpent
Nearly four decades ago, former President and University Distinguished Professor Jimmy Carter set out to eliminate Guinea worm disease from the globe. He very nearly succeeded.
By Martha Nolan
PHOTO: THE CARTER CENTER/L. GRUBB
“Eradicating Guinea worm disease and the suffering it causes has long been a dream of my grandparents, and they have worked incredibly hard to make it a reality.”–J ason C arter
Former US President Jimmy Carter, who died at 100 on Dec. 29, said on several occasions that he fervently hoped the last Guinea worm would die before him. For centuries, this parasitic plague was endemic in countries around the globe.
Acquired by drinking Guinea worm–contaminated water, the female worm grows inside the human body for up to a year before it emerges—excruciatingly—through a blister. Development, sanitation, and access to clean water eliminated the pest for about 70 percent of the global population, leaving only the most neglected people in the poorest nations vulnerable.
Those were the very people the former president was determined to help.
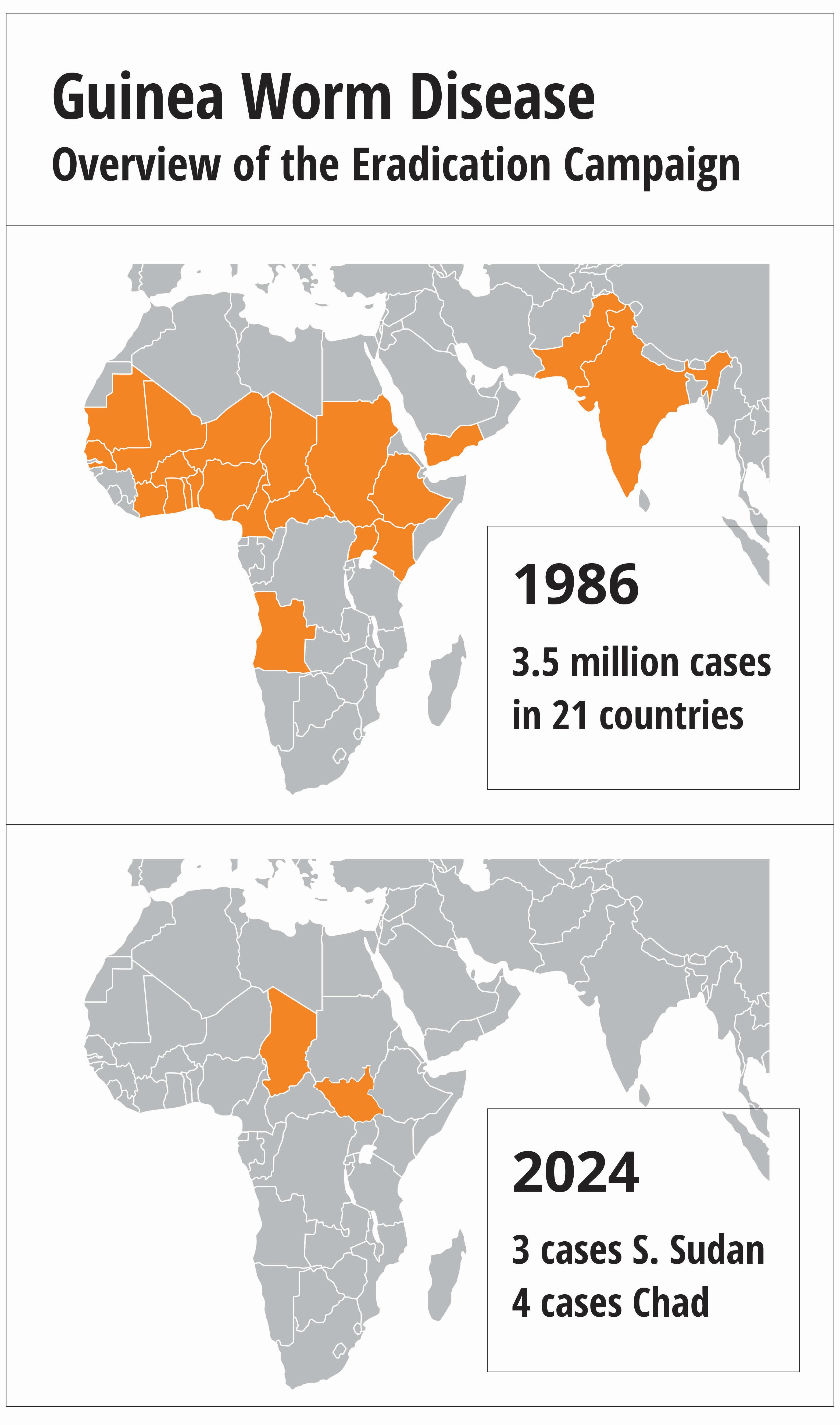
Carter, a University Distinguished Professor at Emory, made it a primary mission to wipe Guinea worm disease from every country in the world. He worked largely through the powerful health arm of his presidential center in Atlanta, the Carter Center. When the Carter Center took up the fight in 1986, there were an estimated 3.5 million cases per year in 21 African and Asian countries. So far this year, just seven human cases have been reported.
Guinea worm is poised to become the second human disease in history to be eradicated, following smallpox.
To achieve this staggering reduction, Carter leveraged the influence, connections, and knowledge gained during his presidency. He supported and supplied a unique coalition of “Guinea worm warriors” made up of endemic countries’ ministries of health, global experts, and community-based health workers. These warriors overcame rainy seasons that left entire communities inaccessible, dispelled long-held beliefs about the cause of Guinea worm disease, and, in some cases, informed country leaders about the existence of the disease in their populations.
Carter even negotiated a cease-fire in a brutal civil war in Sudan so health workers could access the country.
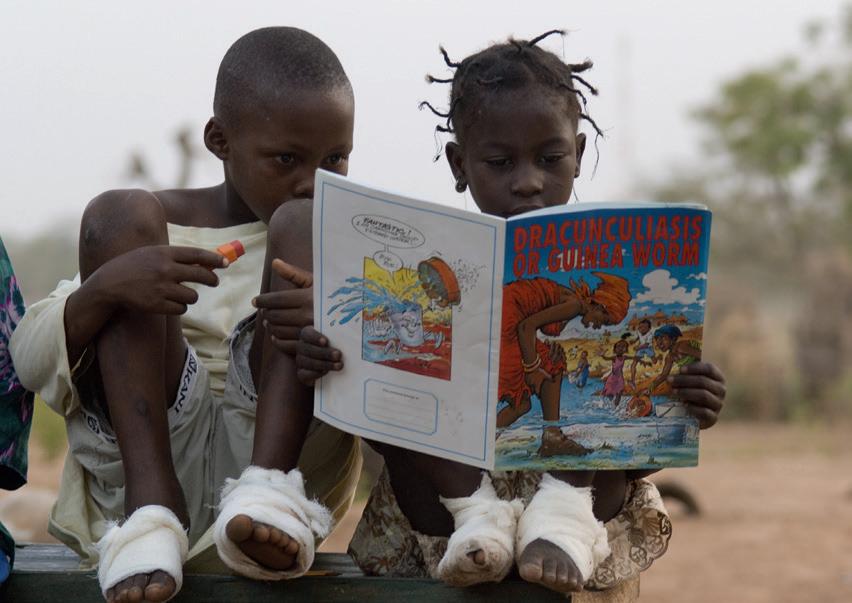
Eradication will be even more extraordinary because it will have been accomplished with no treatment, no vaccine, no acquired immunity, and no cure. The only tool: convincing people in remote regions of the world to change the way they have collected and consumed water for generations.
Hurdles remain on the path to eradication, including the recent emergence of Guinea worm in domestic dogs, mainly in Chad. Together with the World Health Organization (WHO), the Centers for Disease Control and Prevention (CDC), and many other partners including Emory, the Carter Center is
A woman uses a Carter Center–donated fine mesh cloth fitted over a clay pot to filter water, the most effective way to prevent Guinea worm disease.
PHOTO: THE CARTER CENTER/E. STAUB
Known cases as of October 2024
staying focused on its founder’s goal.
“Eradicating Guinea worm disease and the suffering it causes has long been a dream of my grandparents, and they have worked incredibly hard to make it a reality,” said Jason Carter, Carter Center board chair and eldest grandson of former President Carter and the late First Lady Rosalynn Carter. “They witnessed firsthand how this work improves the lives of millions of people, and the Carter Center will keep working with our partners until there are zero cases.”
The
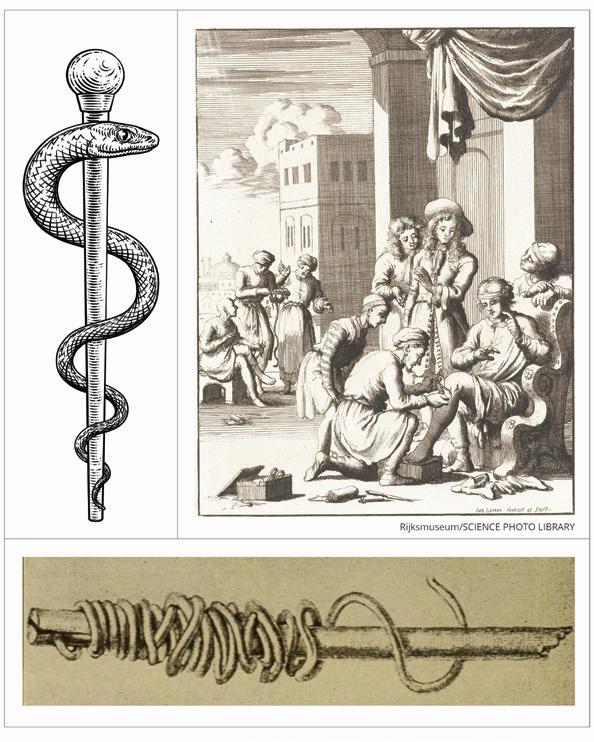
fiery serpent Parasitologists believe the biblical “fiery serpents” that attacked the Israelites who had escaped Egypt might have been
Some contend the snake that coils around a staff in the medical symbol (above) is a Guinea worm, which has plagued humans for thousands of years. These parasites (below) can grow up to three feet long.
Guinea worms. And some contend the snake that coils around a staff in the medical symbol is actually a Guinea worm.
A person contracts Guinea worm from drinking stagnant water contaminated with tiny Cyclops fleas, which eat and then carry parasitic Guinea worm larvae. Once inside a person’s stomach, the flea breaks down and releases the male and female larvae, which mature and roam inside the abdomen until they find a mate. The male dies and the female continues to grow—reaching lengths of up to three feet. Nine to 12 months later, the worm, which resembles a thin strand of spaghetti, finally emerges through a burning blister, usually in the lower limbs. The disease is also known as dracunculiasis, or “affliction with little dragons,” because the worm feels like tiny, hot daggers poking through skin.
Immersing the wound in water can soothe the burn but also causes the worm to release hundreds of thousands of larvae. The cycle may then begin anew.
The treatment is the same as it has been for thousands of years. The worm must be pulled gently from the wound, centimeter by centimeter, and wound around a twig or piece of gauze. The process is agonizingly slow, requiring anywhere from a few days to months to steadily tug the worm free.
Women have described the pain as worse than childbirth. Men have said it is more painful than a gunshot wound. The blister where the worm emerges often becomes infected, and if the worm happens to emerge from a joint, the person can be left crippled. Breaking an emerging worm will cause it to pull back into the body where it will die, calcify, and possibly cause deformities.
Emily Staub, associate director and press liaison to Health Programs for the Carter Center, talks with a local program leader in South Sudan in 2019.
PHOTO:
PHOTO:
‘Public enemy No. 1’
Compounding the disease’s heavy toll, the worms often emerge during the harvest season, devastating not only people’s bodies but their livelihoods. Crops cannot be harvested. Water cannot be collected. Children cannot attend school.
Emily Staub, an alumna of Oxford and Emory College, is associate director and press liaison to Health Programs for the Carter Center. She has seen firsthand the devastation the worm inflicts on its victims. A fierce-faced, massively muscled man, normally stoic like most villagers, lay in the dirt and moaned as a worm was pulled from his leg. A young mother of several children, all of whom had emerging worms, sobbed out her anguish and shame, believing she had brought on a hex that afflicted her children. A six-year-old girl screamed at the top of her lungs outside a dark hut, begging others not to touch the worm coming out of her foot and swatting away their hands.
Another child missed so much school because of Guinea worm that her parents decided not to send her back. “Her life was forever changed by a slim, threefoot-long worm,” says Staub. “Neglected tropical diseases like Guinea worm don’t kill you, but they can take away your opportunities and your dignity.”
Stories such as these explain the names given to Guinea worm through the decades. Roughly translated, these include “the empty granary,” “public enemy No. 1,” “the crippler,” and “the impoverishment.”
As devastating as the worm is, it can easily be stopped by filtering the tiny fleas out of contaminated water and keeping infected people out of water sources. This disease strikes mostly marginalized and isolated people in the poorest of countries, however— places where nothing is particularly easy.
A champion
Donald Hopkins and colleagues at CDC began trying to drum up interest in fighting Guinea worm in the early 1980s. However, the former deputy director and then acting director of the CDC had little success generating support or funding to wage a campaign against a disease most people had never heard of, which occurred in the most desolate of places.
“We started looking around for a celebrity who could bring attention to the cause,” says Hopkins, former director of health programs at the Carter Center and current special adviser for the Guinea Worm Eradication Program. “We were thinking about trying to get Harry Belafonte. But then President Carter got involved, and it was a game changer.”
For his part, Carter adopted the cause shortly after he and his wife, Rosalynn, in partnership with Emory, established the Carter Center, a nongovernmental, nonprofit dedicated to “Waging Peace. Fighting Disease. Building Hope.” Carter wanted his center to focus on areas others were ignoring, and when a friend and former member of his presidential administration told Carter about Guinea worm, he was interested. When he traveled to a small village in Ghana where many of the residents were incapacitated due to Guinea worm, he grew indignant. Among the afflicted villagers was a young
Donald Hopkins, special adviser for the Guinea Worm Eradication Program, talks with villagers in Nigeria about prevention in 2009.
PHOTO: THE CARTER CENTER/E. STAUB
Global politics
woman whom Carter thought was holding her infant. However, when he went to greet the baby, he realized she was holding not her infant but her hugely swollen breast, from which a thin, white worm was emerging.
Carter took up Guinea worm eradication as a personal mission and made it a flagship program of the center. Today, the center’s Guinea Worm Eradication Program, which includes a large number of Emory alumni, is but one of the center’s programs targeting neglected tropical diseases.
“Guinea worm was a disease no one else was willing to tackle—it was ignored by governments and NGOs alike because it was too obscure and afflicted only the world’s most forgotten people,” says Kelly Callahan, an alumna of the Rollins School of Public Health and director of the center’s Trachoma Control Program, who previously worked in the Guinea worm program. “That’s precisely why President Carter decided to take it on.”
That said, Callahan and other Carter Center officials are quick to point out that each country’s Guinea worm program is run by its ministers of health. The Carter Center works closely with government officials to provide technical guidance and logistical and financial support. The Carter Center team knew getting safe water to far-flung, isolated villages was going to be too expensive, too political, and take too long. Instead, the center embraced the option of teaching people in vulnerable areas to filter their water, giving them the low-cost tools to do so.
The challenge was accelerated by Carter’s astute understanding of global politics, connections, and access to leaders across the world as well as personal strength of character. Carter used his international clout to arrange meetings with the leaders of countries where Guinea worm was endemic and often had to educate them about the problem. When he visited Pakistan in the early days of the campaign, the president and the minister of health had never heard of Guinea worm and didn’t know it existed in their country. (Pakistan became the first of the remaining countries with endemic Guinea worm to eradicate it in 1997.)
Not content to only meet with presidents and ministers of health in capital cities, Carter ventured into the most remote villages to see the work firsthand. He convinced some leaders to accompany him to areas they had never visited. And he used his influence to convince countries and corporations to take up the charge. Carter persuaded large companies to create, manufacture, and donate the specialized cloth needed to filter water, portable filter pipes (Guinea worm “straws”) that could be worn around the neck, and larvicide for targeted bodies of stagnant water.
“It’s not possible to overstate President Carter’s impact on Guinea worm eradication,” says Adam Weiss, alumnus of Emory’s Rollins School of Public Health and director of the Carter Center Guinea Worm Eradication Program. “He made inroads with foreign leaders through his diplomacy. The fact that he actually traveled to the more remote villages made such an impact, not only on the villagers but on the health workers and leaders. They knew he meant business, and he was able to get donations to a cause no one had supported before.”
As critical and influential as Carter has been to the eradication efforts, Weiss and others on the eradication team acknowledge that the real work happens on the community level. Health workers from the national program and often the Carter Center worked to train hundreds of thousands of local health workers and
Kelly Callahan, director of the Carter Center’s Trachoma Control Program, shows her digital camera to village children in Ghana in 2010.
PHOTO: THE CARTER CENTER
village-appointed volunteers in their communities. Since the start, health education and training has taken place in more than 23,000 villages across in 21 countries in Africa and Asia.
The volunteers go from dwelling to dwelling or visit farming plots or moving groups, using picture books, skits, stories, and songs to educate their neighbors about how Guinea worm is contracted and how to prevent it.
They demonstrate the ways to properly filter all drinking water, such as using a pipe filter or fitting the cloth filters snugly over a bucket or large clay drum used for household water storage. They explain why people who have a Guinea worm need to stay out of any water sources, and if someone has already gone in the water, they make sure larvicide is swiftly added to that source to prevent transmission. They report anyone who shows signs of an imminent or emergent worm so the individual can be monitored and taken care of at a containment center if they prefer.
The containment centers can offer faster, more
sanitary worm extractions, along with meals, a sleeping mat, access to safe water, and space for dependents. Once the worm is extracted, the person can depart with the bed mat and sheet, and perhaps a bag of sorghum to compensate for the time they missed out on working. “[Carter Center staff] provide the tools and the support, but the village coordinators and volunteers are the ones who were eradicating Guinea worm,” says Sarah Yerian, an alumna of Emory’s Rollins School of Public Health and senior associate director of the Guinea Worm Eradication program. She worked in South Sudan first as a technical adviser, then as a regional coordinator, and later as the Carter Center country lead. “I’d do whatever I could. When I was checking in on one of the villages in my territory, I’d hike out into the fields and gardens if it was planting season. I’d pick up a hoe and do some planting so the woman could sit and talk to the volunteer, who did all the education about Guinea worm and its prevention.”
In places where larger household water filters weren’t feasible, such as populations displaced by con-
flict, the Carter Center borrowed an idea from the Tuareg, a nomadic tribe in West Africa. These tribesmen cut up the larger household filters into smaller bits and tied them to the end of hollow reeds, using them as straws to suck water through. The Carter Center created a more durable prototype patterned after these hand-made devices and added a string so it could be worn around the neck. In 2001, more than 9 million pipe filters were distributed in southern Sudan, which was the largest public health intervention at the time. The design was further refined and manufactured with help from the Danish company Vestergaard. The portable pipe filters have since been distributed in all endemic countries.
his diplomatic ability—including the threat to publicly shame the country’s leaders in a CNN press conference he called for that reason—to help negotiate a six-month-long ceasefire in Sudan between opposing sides that had been engaged in a brutal civil war. The ceasefire, the longest humanitarian ceasefire in history at the time, allowed health workers to access previously inaccessible areas to distribute medicine and preventative health measures going beyond just Guinea worm. In addition to distributing more than 200,000 cloth filters to about 2,000 endemic villages, health workers delivered treatment and education to prevent river blindness, another neglected tropical disease. They also immunized an estimated 100,000 children against measles and polio.
Overcoming obstacles
The path to eradication has been anything but smooth. Ghana had been making significant progress when a new president who did not prioritize Guinea worm prevention efforts came to power. For about 10 years, the number of cases remained stagnant, and local leaders became complacent. Then a big outbreak sent the numbers soaring, erasing years of progress. Carter visited afflicted villages and was so frustrated by the reversal that he threatened to rename the plague Ghana worm. His visit reenergized the program, and Ghana was declared Guinea worm free in 2015.
War posed another roadblock. In 1995, Carter used
Today, conflict and insecurity in places like Mali, South Sudan, and Ethiopia mean people can be displaced and delivery of supplies interrupted. “The benefit of being community based and having nearly 100 percent of your local staff and volunteers native to that country is that, even if people are displaced or put on lockdown temporarily, the staff and volunteers are among them, continuing to teach and monitor,” says Weiss. “That makes the system very resilient.”
The final hurdle: dogs
The current number of Guinea worm cases would be a blinding victory light at the end of an arduous tunnel
Sarah Yerian (far left), senior associate director of the Guinea Worm Eradication Program, demonstrates procedures for treating water sources with larvicide in South Sudan in 2019.
Adam Weiss, director of the Carter Center Guinea Worm Eradication Program, gently pulls a Guinea worm from a young boy’s ankle in Ghana.
A woman in Ghana wears a pipe filter.
PHOTO: THE CARTER CENTER
PHOTO CREDIT: THE CARTER CENTER/E. STAUB
if not for a relatively recent development—the emergence of Guinea worm in domestic dogs in Chad. Though a challenging setback to be sure, those fighting the disease have deployed interventions and are searching for new tools to deal with the canine disease reservoir.
In 2012, some 50 dogs were found to have Guinea worm in Chad, and the numbers climbed each year. The new development confounded Weiss and colleagues. “I’ve been in this program for more than 20 years, and I was taught that this is a human disease, period,” says Weiss. “When it turned up in dogs, we didn’t know if this was a game stopper or a game changer.”
Field staff concluded the dogs were contracting the disease by eating raw fish guts and other aquatic waste discarded when villagers were preparing food. Another intervention was launched—convincing people to bury fish waste and tether dogs, especially if they have emerging worms.
“We estimate some 80 percent, or over 30,000 dogs, at the household level are being tethered,” says Weiss. “As a result, we had a 40 percent decrease in
animal infections in 2024 from 2023.”
Members of the Carter Center Guinea Worm Eradication Program remain convinced eradication can and will be achieved. “We are in one of the best positions we’ve ever been in as far as the momentum and will to get it done,” says Weiss. “Everyone understands the risk. If you let up on the gas pedal at this point, even a little, you risk losing all the ground you’ve made.”
A powerful legacy
When the last Guinea worm dies, untold millions will be spared needless suffering, and not only their health but their opportunities will improve. “In the early years, we found that eliminating Guinea worm from a community had a 29 percent economic rate of return,” says Staub. “In Ghana, one area increased its yam production 50 percent within a year of eradicating Guinea worm. By eliminating Guinea worm from a region, you are eliminating a source of poverty.”
The Guinea Worm Eradication Program also leaves behind reinforced health and surveillance systems in areas that previously lacked them. And the
people who have been involved in the efforts have more opportunities and trained skills. Greg Vaughn, an Emory alumnus and a partner with Spencer Stuart, who sits on the board of trustees at Emory as well as the Carter Center, visited a village in South Sudan that was free of Guinea worm. “I was struck by how being trained and educated as part of the Guinea worm eradication effort opened doors for many,” he says. “Some had gone on to become teachers. Others were working within the county health department. They were able to have better lives as a result of working in the Guinea worm program.”
Perhaps the most powerful legacy of Guinea worm eradication, though, will be hope.
“I think it will change the mindsets of people in the villages as well as people in the ministries of health,” says Hopkins. “They can attack other problems that have lingered through generations, and they can alleviate more suffering.”And, at long last, Jimmy Carter’s most fervent wish will be realized. EHD
“That mental toughness and calmness is helpful in our lives as scientists.”
E ric S undb E rg
Extreme Sports
Can they make you a better scientist?
BY TONY VAN WITSEN • RUNNERS ILLUSTRATION BY FRANK STOCKTON
As a biochemist, Eric Sundberg has always loved structures, especially the three-dimensional structures of protein molecules. “The first time I saw a molecule spin in three dimensions on a computer screen, I was just taken with that,” he says. “What would I do if I were this molecule?”
Given that level of interest in granular details, it isn’t surprising that Sundberg, chair of biochemistry in Emory’s School of Medicine, is also a dedicated rock climber who’s explored a range of cracks, crags and rock faces around the world. “There’s obvious parallels,” he says. “How you assess a structure and how you view a protein. If you were to interact with that protein, what kind of strategy would you have for engaging it? Just like if you look up and there’s a giant crack, what’s my strategy for getting up?”
Eric Sundberg, rock climber and professor of biochemistry, Emory School of Medicine
Ken Carter, Charles Howard Candler Professor of Psychology at Oxford College of Emory, is author of “Buzz!: Inside the Minds of Thrill-Seekers, Daredevils, and Adrenaline Junkies.”
In Their Natural Element LEFT TO RIGHT: Marly van Assen (center), professor of radiology and imaging sciences, on an urban run; Hannah Cebull (left), biomedical engineer, moutain bikes a trail; David Reiter, professor of radiology and imaging sciences, faces down a rock face.
Marly van Assen, long-distance runner and co-director of Emory’s Translational Laboratory for Cardiothoracic Imaging and Artificial Intelligence
Hannah Cebull, mountain biker and postdoctoral biomedical engineer, Emory School of Medicine
David Reiter, rock climber and assistant professor of radiology and imaging sciences
Working hard and playing hard is a way of life for many Emory researchers. Extreme sports provide an almost mystical connection between the two.
“Rock climbing has been the one sport I just can’t quit,” says David Reiter, assistant professor of radiology and imaging sciences, even though he played soccer in college. “I’ve gone off and done other things that are more endurance-sport related, but I always end up coming back to rock climbing. It’s got so many dimensions between the physical and the intellectual and the emotional. For me, it’s a big distraction from the things that create stress in my life.”
Sundberg finds the challenges of climbing less a distraction than a lesson in the appropriate mental state to approach research. “That mental toughness and calmness is helpful in our lives as scientists,” he says. “It’s especially helpful when you’re way past your gear, but also in the way you approach the ups and downs and the progress of your career.”
Kenneth Carter has studied that pattern. The Charles Howard Candler Professor of Psychology at Oxford College of Emory, Carter follows extreme risk seekers and even wrote a book about them: Buzz: Inside the Minds of Thrill-Seekers,
Daredevils, and Adrenaline Junkies.
“It’s easy to think the high-sensation seekers are outgoing extroverts, but that’s not necessarily the case,” Carter says. “Risk is really the price of admission to the kinds of activities or experiences they want to be able to have. It helps connect them with themselves. A lot of the research suggests the emotional regulation they experience from those endeavors is fulfilling as well.”
Mountain biker Hannah Cebull found her rides to be a rewarding break from the pressures of long hours in the lab. A postdoctoral biomedical engineer in the School of Medicine, she loves riding through natural areas during the changing seasons as well as the challenge of keeping her balance on a narrow trail. “If I’m encountering a tough problem and I get really tired,” she says, “I can’t push my body the same way that I can with biking. So having the physical challenge is a nice contrast to the mental challenge that research brings.”
Marly van Assen agrees. “Research is already super competitive,” says van Assen, co-director of Emory’s Translational Laboratory for Cardiothoracic Imaging and Artificial Intelligence and a long-distance runner. “I’m competitive by nature, and this helps me deal with
that because I am not the fastest, not the best runner, but you put in effort and you learn to enjoy it without the need to come in first.”
Last summer, van Assen joined a team of 12 Atlantans competing in an annual relay race from near the peak of Oregon’s Mt. Hood to the beach along the Pacific coast, a total of 197 miles. “I’m from the Netherlands,” van Assen says. “The Netherlands is as flat as you can get. So for me, mountains are super challenging to run, but also really pretty.”
Van Assen climbed Mt. Hood the day before the race. “People were like, ‘You’re gonna run tomorrow,’ ” she says. “‘Do you want to climb up this mountain to touch snow?’ And I was like, ‘Yes!’ So I dragged a few people along and we climbed up, touched snow, then went back.”
Competitors in the Hood-to-Coast race travel in vans when they’re not running. “You don’t really sleep,” van Assen says. “You just do three runs spread out. I had two runs at night. One was at 3 a.m. to downtown Portland. One was at 5 or 6 in the morning through a nature reserve. It is definitely an experience. The finish line is on the beach, and I jumped in the ocean.”
“If I’m encountering a tough problem and I get really tired, I can’t push my body the same way that I can with biking. So having the physical challenge is a nice contrast to the mental challenge that research brings.”
something in a beautiful location with friends. Cebull is part of a women’s mountain bike group that rides together regularly. She recently biked through Vail, Colorado, with a colleague. “We all have very different jobs,” says van Assen about her running group. “It is nice that nobody talks about their work that much. We stayed a day afterward to go hiking.”
That camaraderie is part of the pattern Carter observes. “When you look at it in a broader sense,” he says, “it’s that connection with ourselves, the connection with other people, the sort of unusual experiences that we’re all after.”
Sundberg’s most memorable moment happened when he took a break from a scientific conference in Rio de Janeiro and met a friend to climb a mountain near Rio’s famous beaches.
H anna H C ebull
Besides the intensity of the sport itself, Emory researchers talked about the simple fun of doing
“We get up there,” Sundberg says. “And the protection was kind of dodgy, but it wasn’t super hard climbing. The sun’s going down, the lights of the city are coming up and reflecting on the lagoon, and you can see a sight line to Ipanema, a sight line to Copacabana. We stayed up there, I don’t know, half an hour because we’re going to rappel down in the dark anyways. If you’re not a rock climber, you don’t do that. So the combination of the two has been really spectacular.” EHD
Finding Hope and Inspiration
TAKING ON UNEXPECTED ROLES AS PATIENT AND CAREGIVER
By Laura Kahn
As attorneys and the parents of two active young boys, Matt and Liz Ames didn’t think their hectic yet fulfilling lives could get any busier.
But just before their 10th wedding anniversary, Liz was diagnosed with a rare and aggressive appendiceal cancer. “I was a very healthy person, always very skinny, and I started to feel distended,” says Liz. She went to a hospital where the doctor thought nothing was wrong. “But because I was an advocate for myself, which I’ve learned you absolutely have to be, I demanded a CT scan.” The CT scan results showed appendiceal cancer, which affects just one or two people out of a million each year in the US. After extensive research, the couple
found Charles Staley, chief of the division of surgical oncology at Emory’s Winship Cancer Institute and Holland M. Ware Professor of Surgery at Emory School of Medicine. A specialist in gastrointestinal cancers (GI), Staley’s clinical practice focuses on the surgical treatment of stomach, esophageal, appendiceal, colorectal, and peritoneal surface malignancies. His research focuses on translational studies and novel clinical trials in GI cancers. “He did a masterful job of making us feel as comfortable as possible,” Matt says. “His confidence was inspiring.”
to work out, talk with his rabbi, or connect with his parents.
Find support. Matt’s rabbi introduced him to a young dad in a similar situation. “This connection has become deeply meaningful to me,” Matt says. “He has shared insights and encouragement that only someone in the shoes of a caregiver could provide.”
I realized that if I was going to be any good to Liz and the boys, I needed to focus on myself.
By the end of the first appointment, Liz had a treatment plan that included chemotherapy and extensive surgery to remove diseased tissue in her abdomen. With a clear strategy and resources to help her through, Liz knew what she had to do.
–Matt, Liz’s husband and caregiver
Matt’s role as caregiver, however, was less clear. One day, Liz turned to her husband and said, “I wouldn’t want to be in your shoes.”
Sharing the caregiver journey
Matt decided to share his family’s cancer journey in Through the Impossible: Lessons in Caregiving from a Husband Who’s Been There. A few of his suggestions: Take care of yourself. Work, doctors’ appointments, and being present for his family took a toll on Matt— physically, mentally, and emotionally. One day he received a note from a friend reminding him to take care of himself. He began finding time for himself every day, even just 15 minutes,
WINSHIP FAMILY RESOURCES
Practice gratitude. The couple remained hopeful throughout their difficult experience. The family sets aside time every Friday to reflect and be grateful. In times of crisis, it may be difficult to find gratitude, but Matt urges caregivers to take time to be thankful for even the small things that once seemed unimportant.
Liz is now five years post-cancer diagnosis, and her disease remains in remission. “I’m soaking up every minute,” says Liz.
The family is grateful for the support of friends, family, and Winship. Their physician and nurses remain at the top of their gratitude list.
Staley recognizes the importance of his role as both a surgeon and supporter. “At Winship, we understand that cancer is a family disease,” he says. EHD
Liz’s Story
Winship offers resources to support cancer patients and caregivers throughout diagnosis, treatment, and recovery.
Wendy Baer, director of psychiatric oncology, and a team of social workers provide resources and a chance for families to focus on their mental and emotional well-being.
Patients and caregivers also can access support from Winship’s spiritual health group. The team works across Emory Healthcare to bring spiritual comfort and compassionate support. “It is important for caregivers to have their own resources so that they can tend to their spiritual and emotional needs,” says Caroline Peacock, director of spiritual health at Winship.
Winship Cancer Institute offers a caregiver support group that meets virtually on the third Wednesday of each month from noon to 1:30 p.m. RSVP to hilary.cohen@emoryhealthcare.org, or 404.778.4627.
Watch as Liz Ames tells about her experience from rare cancer diagnosis to remission.
Healing People Depends on THE BUSINESS OF HEALTHCARE
Join the ranks of healthcare leaders making a difference with Emory Executive Education. Our world-class programs are designed to equip you with the skills needed to lead in today’s complex healthcare environment.
Transform your healthcare career with our specialized certificates:
• Business of Healthcare Certificate
• Chief Medical Officer Certificate
• Chief Nursing Executive Certificate
• Healthcare Leadership Program
“Both of my parents died from cancer. More recently, my brother survived kidney cancer. I wanted to do something to honor their strength, and that’s why I made a planned gift to Winship. I would like my bequest to make a difference. The ultimate goal is to fund the research that leads to groundbreaking treatments for cancer. Can you imagine stopping cancer? Wouldn’t that be wonderful?”
—Ouida Hayes Lanier 65G
For the past 11 years, Ouida Lanier has volunteered at Winship, where she greets incoming patients and their loved ones. Her bequest will fund cancer research. If you are similarly moved by the mission of Winship, allow Ouida’s planned gift to serve as an example of how you can make a difference.
The Clifton Corridor
5. Emory National Primate Research Center
6. Emory School of Medicine (education and research buildings) 7. Woodruff Health Sciences Center Administration Building
Emory
2. Emory Clinic (multiple buildings) 3. Winship Cancer Institute
Emory Rehabilitation Hospital
8. Rollins School of Public Health (multiple buildings) 9. Nell Hodgson Woodruff School of Nursing
Emory University Hospital Midtown (multiple buildings)
Across the State and Around the Corner
Emory Healthcare in Georgia
Emory Healthcare is the most comprehensive health system in the state, with locations all over Georgia, including 11 hospitals, 135 outpatient locations in 28 counties, and 13 regional affiliate hospitals in 20 counties. Winship Cancer Network has three locations.
SCIENCE GALLERY ATLANTA
“A World Wrapped in Plastic” explores how Emory health researchers are working to find alternatives to burning plastic for basic household needs in rural Guatemala. 3
Emory University
Alumni Records Office
1762
To support the work of the Woodruff Health Sciences Center, use this QR code to donate directly.