
23 minute read
F- Navi Mumbai



NAVI MUMBAI
Advertisement
Aakanksha Gupte PG190001
B1. About the City
The growth of Mumbai city is constrained by sea towards the south, east and west. As a result, the total land area available for the development of Mumbai is limited. Hence, developmental planners in the late 1960s started exploiting an alternative for dispersal and control of Mumbai’s population. By 1972 the satellite city, Navi Mumbai was developed. (Mumbai: Tourist Attractions: Navi Mumbai) Navi Mumbai formerly known as New Bombay is a twin city of Mumbai, situated between Thane Creek, Sahyadri Mountains and sea coast, which was designed to decongest Mumbai. Eminent architects like Mr. Charles Correa, Mr. Shirish Patel and Mr. Pravin Mehta suggested Navi Mumbai as an alternative to Mumbai. The city was on 17 March 1971, the foundation of the ‘City and Industrial Development Corporation (CIDCO)’ took place which was initiated as per the ‘Companies Act’ of 1956.

Figure F1 Map of MMR with districts and Municipal Corporations Source:https://www.quora.com/Does-Vasai-Virar-Thane-City-Mira-RoadBhayandar-Kalyan-Dombivali-Navi-Mumbai-etc-fall-under-MumbaiMetropolitan-Region-MMR Figure F2 Zones and wards in NMMC Source: https://www.nmmc.gov.in/navimumbai/history1540201195 retrieved, census 2011
Figure F3 Zones and wards in NMMC Source: https://www.nmmc.gov.in/navimumbai/history1540201195 retrieved, census 2011
F1.1. Location
Navi Mumbai is a part of the Mumbai Metropolitan Region. Located in the east of Mumbai, the satellite city is a part of two major districts, namely Thane district and Raigad District as shown in figure F3. The city parallelly has two Municipal Corporations namely, Navi Mumbai Municipal Corporation and Panvel Municipal corporation. The Navi Mumbai Municipal Corporation lies in Thane district whereas Panvel Municipal Corporation lies in Raigad. Other adjacent corporations to the NMMC shown in Figure F1 namely, Ulhasnagar Mahanagar Palika, Bhivandi Municipal Corporation, Thane Municipal Corporation and Bhrihan Mumbai Corporation. (Navi Mumbai Municipal Corporation, n.d.).This report looks at working of NMMC in manageing the pandemic.
F1.2. Demographics
The NMMC is divided into 2 Zones, 8 administrative wards and 111 elective wards as shown in Figure F2. The population under the corporation is 11,20,547 as per the 2011 census. The male population in the city is 6,10,060 whereas the female population is 5,10,487. 8 lakh population is the migrant population settled in Navi Mumbai according to the report by CIDCO in 2017.
F1.3. Administration
Figure F3 shows the organizational structure of the NMMC. Where an Additional Deputy Commissioner was added to tackle the situation. Currently, Mr. Abhijit Bhangar is the Commissioner of the City.


The Deputy Commissioner is helped by an Assistant Medical Officer of Health. The Medical Officer of Health has a ward wise distributed Medical Officers who look after the affairs of the ward. The Medical officer is helped by 10 nurses, 2 Ward boys, 200 ASHA workers and 2 Data Operators. The teachers working in government schools also help. They are responsible for contact tracing. Further, 7 policemen are helping the MO. There are 18 departments in the NMMC which help in the efficient working of the Corporation. 15 Community kitchens set up to help people get food easily. During the phase when migrant workers were to be sent home, 1605 workers were sent to the home town Reva. Meanwhile, Anna Saheb Missal who was the running commissioner ended his tenure and was replaced by Mr. Abhijit Bhanger. After taking over Mr. Bhangar, launched a mission named “Mission Break the Corona Chain”. The
F2. Current COVID19 Scenario in the City
The first case that came in Navi Mumbai was on 19th March 2020. Looking at the COVID cases in the NMMC area, there is a total of 44,521 cases out of which 41,803 people have recovered whereas 901 are deceased. Active cases are 1,817 as of 30th October 2020. The government is conducting rapid antigen tests in huge numbers to track asymptomatic patients and treat them as soon as possible. Till 30th Oct, NMMC has conducted 1,81,368 Rapid Antigen tests and 1,00,499 RTPCR (Navi Mumbai Municipal Corporation, n.d.) As seen in the figure F4, Nerul has highest number of cases, 7,972 with 92.5% recovery rate. Ghansoli is most affected ward with 5,262 total cases, with respect to population (9.40% affected population)
COVID Infrastructure
The NMMC has made provision of three types of facilities to cater to the disease in its different stages. Namely, COVID Care Centers(CCC) that cater to patients with Mild symptoms. The Dedicated COVID-19 Hospitals(DCH) are responsible to take care of the severely affected patients and the Dedicated COVID-19 health Centres(DCHC) are responsible for to care of moderately affected patients. There is a COVID care dashboard on the NMMC website which has updates of all, the vacancies, availability of oxygen and ventilators at the centers. To tackle the situation the NMMC came up with various strategies like for the workers or the citizen who didn’t have access to food, 18 Nivara Kendra were opened wherein people were given food. It was made sure that at least two Nivara Kendra are present in each ward. There were also

Figure F4 COVID cases in various wards Source: https://navimumbai.city/containment-zones-navi-mumbai retrieved
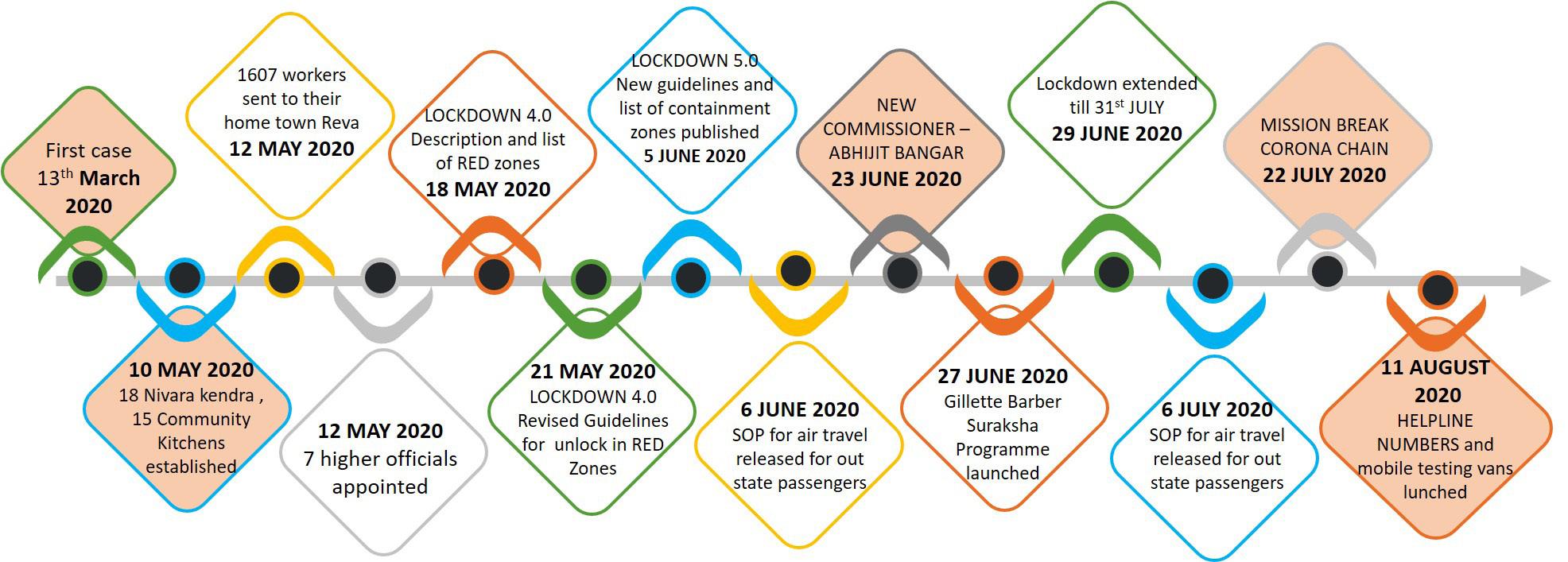
Figure F5 COVID Timeline Source: https://navimumbai.city/containment-zones-navi-mumbai retrieved, Primary mission consists of screening high-risk contacts in the 42 high-risk areas. Further, working on a similar line, Mr. Bhangar, launched a helpline number to make the services accessible for the people. Likewise, he also launched mobile testing vans, responsible for conducting rapid antigen tests in large numbers. (NAVI MUMBAI MUNICIPAL CORPORATION, n.d.) like sickness). If the fever prevails for less than 72 hrs or the doctor gives medicine for Viral/ Influenza.
F3.1 Identification
In identification the processes included are testing, contact tracing and consultation. For identification of the COVID patients, NMMC is adopting following strategies -
F3. Overview Of the COVID19 Management in the City
The C orporation is trying to do its best to contain the spread of the disease. To do that there are various stakeholders performing their jobs diligently. The NMMC is following the policy of 3T’s namely, Test, Treat and Track. The main reason for the spread of the Virus is coming in contact with another corona positive person. The worry starts after the patient starts showing prominent COVID like symptoms, the person is advised to call the COVID call center where the ward counsellor helps the patient with the nearest fever clinic and another necessary query is answered. The doctor is responsible to diagnose the symptoms, check if they are COVID-like or it is ILS (InfluenzaTests Conducted • Rapid Antigen • True NAAT • RT-PCR • CT - SCAN 27 - Urban Public Health Centres converted into fever clinics
MISSION BREAK CORONA CHAIN (22nd July 2020) – conducting rapid testing in 42 containment zones. MOBILE TESTING – dedicated testing vans to ensure early tracing of the COVID patients to target earlier treatment. HELPLINE NUMBER – 8 helpline numbers published on NMMC website
F3.2 Treatment
In treatment process -Home Quarantine, Institutional Quarantine and Hospitalization. Following are the startegies adopted by NMMC for effective implementation of treatment. COVID WAR ROOM (30th JUNE 2020) Tracing the case and allocate quarantine centre or hospital according to the symptoms 80% beds in a hospital to be regulated by NMMC
REAL TIME BED OCCUPANCY DASHBOARD (link on NMMC website)
NODAL OFFICER APPOINTED - to ensure the norms are followed in the hospital.
COVID19 BILL Complaint Centre – to complain if the patient is overcharged.
F3.3 Monitoring and Survilliance
In monitoring and survilliance, contact tracing and sanitization of the area fall in this category, strategies adopted for the implementation are - NUISANCE DETECTION SQUAD A Squad consisting of 100 ex-army personnel to check spitting and other COVID preventive norms.
WHATSAPP GROUP The patient is added to a WhatsApp group in case of home quarantine. The patient is hence supposed to post pictures of the said parameters.
LAST RITES Last rites are conducted for all religions where max 5 family members are allowed.
F4. COVID19 Management Process Analysis F4.1. SWIMLANE Diagram
The diagram shows flow of activities taking place, by various stake holders to provide the service. The diagram here shows the process from the start, when the patient is affected by the virus and is showing the symtopms. After that, the role of the Navi Mumbai Municipal Corporation is described in the whole process.
Patient
Ward Councellor
Doctor
Pathologist
Assist MOH
Teacher
Ward Boys
Police
Timeline
Patient showing COVID like symptoms Contact family consultant
Calling the helpline no.
suggest near by fever clinic
No
Covid like
Yes Medicine for viral
Conduct appropriate test (CT- SCAN/RT - PCR)
No
Result
Send one copy to doctor and other to NMMC head quarter (Asst MOH) Check CoMorbid Conditions
Make a list of daily positive cases Send the list to the ward MO
5 - 14 days 10 min 24 hrs 10 mins Half Day
Inferences:
1. Delay in teachers contacting the patient 2. Delay in MO contacting the patient 3. Delay in sanitisation process.
Mild
Condition Moderate
Severe Home Quarantine/ COVID care centre admitted to DCHC
admitted to DHC Inform MO
Forward list to the teachers
Conduct basic enquiries by calling patients
Equire about living conditions Make list of high risk contacts Forward the list to the ward boys to conduct test of high risk contacts
10 min 24 hrs 30 mins
WhatApp Valid prescription Get the building
Sanitized
Regular follow up for 10 – 14 days
Inform police
Conduct Rapid Antigen test
-ve
Result
Check co-morbid conditions and oxygen saturation
+ve Inform MO
seal the building and mark containment zone
30 mins 10 mins 15 - 20 mins
Inferences: From the above Swimlane Diagram, the following are the processes identified, namely Identification that includes Symptoms, Diagnosing and Testing. The next stage is the treatment which includes quarantining the patient which might be Home, Institutional, or Hospitalisation. And the last process identified is Monitoring and Surveillance. This includes Contact Tracing and Sanitisation. Key Process Area: COVID19 management services Trigger Event Process Name Symptoms identified for Identification COVID Stage of COVID is Identified Treatment The patient is Monitoring and quarantined/admitted in Survilliance the hospital
Table F1 Process Identification Worksheet
F4.3. Process Profile Worksheets
F4.3.1. Process Identification
Inferences: From the Process Profile worksheet of Identification, the key inputs observed are COVID like symptoms, emergency call center, a ward councilor, doctor, thermometer, PPE kit, Masks, multiple testing kits, fever clinics, testing center, CT Scan and test result is the output. The process unit include transfer of virus, COVID like symptoms, calling at an emergency call center, suggest a fever clinic, going to fever clinic, conducting tests etc. Hence, the patient himself, the pathologist, ward counselor are the important stakeholders of the process. From the worksheet, identifies long waiting for the call and lack of manpower are the two major service risks observed. Hence, the control units are increasing in the number of telephones and recruiting more people. Process Name – Number
Event beginning
Patient coming in contact with COVID positive person
Event ending Additional events
Receive test result Calling emergency call centre, Wearing mask ,Going to doctor, sanitising hands, checking temperature, waiting in que, doctor diagnosing the patient, doctor writing suitable tests, patient going to test centre/hospital to get tested, lab/hospital conducting tests, printing reports Inputs – Items and Sources
COVID like symptoms, emergency call centre, a ward councillor, doctor, thermometer, PPE kit, Masks, multiple testing kits, fever clinics, testing centre, CT Scan.
Test Result Outputs – Items and Customers
Process Units
Transfer of Virus, COVID like symptoms, Calling at emergency call centre, Listen to concerns and suggest a fever clinic, Going to fever clinic. Conducting test Emailing one report to NMMC head quarter and one to the doctor, Diagnosing patient Another COVID positive patient, Patient himself, Patient himself, Ward councillor, Patient himself, Pathologist, Pathologist, Doctor
Service Objective(s)
To identify if the patient is infected by the Virus Patient not showing symptoms (asymptotic), Long waiting for call, Doctor not available, Faulty report, Over queuing of samples, Exchange of samples, Samples of potential patients not taken, Lack of manpower, Infected staff
Key Controls
Increase in number of Rapid Testing, Increasing number of telephone lines, Trained/Certified Doctors, Trained staff, Trained staff, Tracking tested and distributing customers equally, Proactive staff, Frequent Recruitment/staff rotation, Frequent testing of staff Getting tested within 4 days after showing symptoms
Process Unit Owners
Service Risks
Measure of Success
Table F2 Process Profile Worksheet for identification process
Process Name – Number
Event beginning
Knowing the stage of disease (patients with mild symptoms and adequate space at home have choice to home quarantine)
Event ending Additional events
Patient quarantined/ admitted in the favoured facility. Inform MO, arrival of ambulance, asking affordability of the patient, enquiring about the availability of Mediclaim, helping the person inside the ambulance, checking necessary parameters, dropping the patient in the said facility, Disinfecting the ambulance. Inputs – Items and Sources
Ambulance, necessary equipment in the ambulance, quarantine centre, adequate number of beds and ventilators, Disinfectant in the ambulance (NMMC)
Patient getting required treatment Process Units Outputs – Items and Customers
Process Unit Owners
Knowing the stage of the disease, Informing Medical Officer, Sending the prescription in case of home quarantine, Sending the ambulance, enquiring for affordability/preference of quarantine centre, dropping the patient in the said facility, Disinfecting the ambulance, Providing food Maintaining Hygiene, Update data regarding availability of bed, ventilator. Service Objective(s)
To quarantine/admit the person as soon as possible
Key Controls
Shortening the calling process, Tie ups with NGOs, Additional Housekeeping staff for 24 hrs, Procure more ventilators, Protocol in place for ambulance attendant Keeping up with forecast of possible requirement and making management plan accordingly, Planned alternative for such situation. Doctor, Patient, Medical Officer, Ambulance attendant, Hospital Staff
Service Risks
Delay in sending the prescription in home quarantine, Poor quality food given, Hygiene not maintained in the Quarantine centre/ Hospital, Lack of beds with ventilators, Ambulance not disinfected after last use, Unavailability of ambulance at the said time, Unavailability of bed in the centre at the said time Measure of Success
Patient happy with the Quarantine service
F4.3.2. Process Profile Worksheet - Treatment
Inferences: The process of treatment includes, Quarantine and treatment of the patient. If the patient has mild symptoms, the patient is home quarantined and the prescription is sent to them as soon as the medical officer gets the positive tested result. The medical officer is responsible for following up with the patient for the 14 days quarantine period. If not home quarantined, the patient can be institutional quarantined if the conditions like room size or availability of toilets at home are not fulfilled. Also, if the patient has moderate or severe symptoms they are admitted to the respective hospital. From the process profile worksheet, it is observed that the key processes are, knowing the stage of the infection, informing Medical Officer, sending the prescription in case of home quarantine, regular follow up for 10 – 14 days, sending the ambulance enquiring for affordability/preference of quarantine center, checking necessary parameters, dropping the patient in the said facility, disinfecting the ambulance, admitting the patient in the hospital / quarantine facility, providing food and maintaining hygiene, update data regarding availability of a bed, ventilator, oxygen, etc and the stakeholders being Doctor, Patient, Medical Officer, ambulance attendant, Hospital Staff. Hence, the service risks observed in this case are delay in sending the prescription in case of home quarantine, poor quality food given, hygiene not maintained in the quarantine center/ hospital, lack of beds with ventilators which can be tackled by shortening the calling process, tie-ups with NGOs, additional housekeeping staff for 24 hrs, procure more ventilators. Hence, the measure of success in this would be the patient happy with the quarantine service with the objective of quarantine/admit the person as soon as possible.
F4.3.3. Process Profile Worksheet - Monitoring and Survilliance
Inferences: The process of monitoring and surveillance includes monitoring implementation of said strategies, contact tracing (identification of high-risk contacts), and sanitization of building/ area. After the patient is tested positive in the building, the sanitization team is sent to the building consisting of ward boys and teachers asking about the basic information i.e. prevalence of co-morbid symptoms. If the symptoms prevail then a Rapid Antigen test is done and RT - PCR confirmatory test is suggested. In the worksheet, there is a risk observed as there is always a delay in the sanitization team to reach the residence, after being tested. It is observed that this is the case due to a lack of manpower to execute this task. As shown in the Process Profile Worksheet the process units are inform police about the detected case in the building, sanitised and sealed building/residence of the patient, update the records on the website, mark the area as a containment zone, make a list of highrisk contact, conduct rapid antigen test notify the traced people to get tested, perform a test where Medical Officer, Data Operator, Police Officer, Ward Boys, Pathologist are responsible. Priority service risks observed to be are delay in sanitisation of the building, unavailability of police, police not informed in time where the key controls could be appointing a dedicated sanitization team, asking the building/ residence owners to self sanitize the building wearing proper safety gears helping them with necessary instructions, ensure police staff rotation, NMMC officials crosschecking the people tested, regular check-ups of police officials maintaining proper staff circulation. The data is updated on the dashboard by the NMMC control room. The police have their Twitter page where they update daily numbers. Process Name – Number
Process Owner Monitoring and Survilliance Navi Mumbai Municipal Corporation Description The process of Monitoring and Survilliance to prevent the spread of virus. Triggers
Event beginning
Patient admitted to the Quarantine centre
Event ending
People tested who all came into contact with the patient in last 14 days
Additional events
Inform police about the detected case in the building, update the records on the website, seal the building, mark the area as containment zone, forward the list of contacts to the Police, Trace listed people, Inform pathology of the traced details, notify the traced people to get tested, perform test, Inform the police and NMMC officials about the result. Inputs – Items and Sources
Trained police, trained NMMC officials, protocols in places, SOP for various activities in place, data of citizens, notification infrastructure (message)
Safe citizens Outputs – Items and Customers
Process Units
Inform police about the detected case in the building, Sanitised and sealed building/residence of the patient, update the records on the website, mark the area as containment zone, Make list of high risk contact, Conduct Rapid Antigen test notify the traced people to get tested, perform test Service Objective(s)
To prevent spread of Virus as much possible Delay in Sanitisation of the building, Unavailability of Police, Police not informed in time, All contacts in the list not traced, Notified people didn’t get themselves tested, Infected police officials, Ward boys unavailable
Key Controls
Recruit more staff Ensure police staff rotation Ratio of NMMC officials to be maintained Updated city data NMMC officials crosschecking the people tested Regular check ups of police officials Maintaining proper staff circulation Minimum Number of new cases from the area
Process Unit Owners
Medical Officer, Data Operator, Police Officer,Ward Boys, Pathologist
Service Risks
Measure of Success
Process Name Patient Ward Councellor Doctor Hospital / Quarantine Centre Pathologist Assit MoH
Medical Officer Teacher Ambulance staff Police Official Ward boy
Identification R C R R Treatment R,C Monitoring and Surveillance C R A I
I A R I A R R I R R
Table F5 RACI Chart
F4.5 ServQual Analysis
An analysis was carried out to know about the expection and perception of the citizens. A sample size of 31 people taken from the NMMC area. Questions were framed on the basis of RATER i.e. Reliability, Assurance, Tangibility, Empathy and Responsiveness. The difference between Perception and expectation has helped in determining the issues and good points in the service. In the following graph it is seen that it takes more than 12 hrs for NMMC to contact the patient, once the patient is tested positive. Hence, it leads to delay in processes taking place. Also it may worsen the health situation of the patient.

Figure F6 Response time of NMMC after being tested positive Source: Primary Figure F7 RATER analysis for Reliability Source: Primary Reliability of the govt service, few questions on all the processes were framed and people were asked to rate the conditions on the basis their expectations and perceptions. The gap between P-E shows issues in the process. The difference between perception and expectation has helped in determining the issues and good points in the service. AREAS OF IMPROVEMENT• Prompt availability of bed • Availability of hygenic food • Availability of sanitization facility


Figure F8 RATER analysis for Assurance Source: Primary Assurance The gap between P-E shows issues in the process. The difference between perception and expectation has helped in determining the issues and good points in the service. AREAS OF IMPROVEMENT• NMMC Officials not contacting the relatives of the positive tested patient GOOD POINTS - • The government institutions are abiding by the approved rates. • The testing Labs are following the SOP by informing the NMMC officials about the positive tested patient.

Figure F9 RATER for tangibility of the service Source: Primary
Figure F10 RATER for Empathy of the service Source: Primary Figure F11 RATER for responsiveness of the service Source: Primary
Tangibility of the govt service are found on the basis of the gap between P-E shows issues in the process. The difference between perception and expectation has helped in determining the issues and good points in the service. AREAS OF IMPROVEMENT• Hygiene maintained in the quarantine centers, hospitals and Ambulance. • Bigger room wrt to capacity of the patients. Detailed prescription in case of home quarantine is the service meeting the expectations. Empathy of the govt service are found on the basis of the gap between P-E shows issues in the process. The difference between perception and expectation has helped in determining the issues and good points in the service. AREAS OF IMPROVEMENT• Staff assuring comfort level at every point of the treatment procedure.

Responsiveness of the govt service are found on the basis of the gap between P-E shows issues in the process. The difference between perception and expectation has helped in determining the issues and good points in the service. AREAS OF IMPROVEMENT• Time taken by sanitization team to reach the residence after being tested positive • Effective recommendations for the issues mentioned. GOOD POINTS • Time taken to receive prescription in case of home quarantine.
From the above analysis and a composite RATER analysis we can see that assurance is the parameter performing well where as reliability is the factor to be considered to be worked on.


Figure F12 Composite RATER ANALYSIS. Source: Primary

Figure F13 Vector image showing COVID treatment team Source: www.pngtree.com
F4.6 . FMEA
Inferences: With the help of pointing system, the FMEA analysis was done on the issues listed dow in ServQual Analysis. The points were rated on the basis of severity, occurance and detectatbility on the scale of 1 - 10. The points having Risk Priority number more than 480 was marked as service risk.

FUNCTION POTENTIAL FAILURE MODE POTENTIAL CAUSE OF FAILURE RPN RPN Differenc e
%age Improved
TESTING
NMMC takes >12hrs to contact the patient after being tested positive Delay in sending test report from the lab
Lack of manpower to make the number of calls 441 36 405 91.8
504 24 480 95.2
TREATMENT
Unhygenic food treatment given more importance over provision of good food lack of manpower in the organization structure 448 18 430 89.5
378 24 354 93.6
Lack of budget 120 48 72 60.0
Monitoring and survilliance
Unhygienic Quarantine centres
Unavailability of Bed Beds fully occupied 336 36 300 89.2 No beds kept as stand by for emergency situations 448 24 424 94.6 Emotional concerns for relatives 252 24 228 90.4
Lack of manpower to maintain the quarantine centers 576 24 552 95.8
Availability of sanitising facility whenever called for. Lack of manpower
Delay in sanitisation process Lack of manpower to cater to the demand 343 36 307 89.5
504 18 468 92.8
Table F6 FMEA - Difference in new RPN
F4.6 . FMEA
Inferences: Frome the FMEA, recommendations are given on the basis of the service risks found • Service Risk - Prompt availability of bed. Possible Recommendation - Keeping a spare beds in the hospital for thet extremely severe cases. • Service Risk - Availability of hygenic food
Possible Recommendation - Giving contract to the NGOs. • Service Risk - Unhygenic Quarantine facility
Possible Recommendation - This risk is arising due to lack of manpower. Hence, if the workers are motivated to work by giving them a increment in the salary, mediclaim policy and a bed booking in the quarantine center. • Service Risk - Availability of sanitization facility whenever called for. • Possible Recommendation - This risk is arising due to lack of manpower in NMMC. Hence, dedicated sanitization team or integrating other department in order to fullfill the need would help cater to the situation better. Further, on the basis of the recommendations, new RPN was found. The new RPN tells the level of improvement that is possible after the new recommendations are inculcated. Further, the difference between original RPN nad new RPN was found. And the percentage of improvement was noted. On the basis of the percentage, points are marked on the Service Audit Profile.
F5. Service Concept
Service Concept: INCREASE IN EFFICIENCY AND FOCUS ON PUBLIC HEALTH Organising Idea: A service aiming to increase the efficiency of the health department and focusing on the PUBLIC HEALTH for tackling the COVID by identification of the disease, consulting, isolating, treating and preventing the spread as much possible.
Service Provided:
Awareness, screening, health guidelines and SOPs medications, quarantine facility, mobile testing facility, helpline facility, help line number, ambulance service, trained and qualified staff, containment zones, sanitization, food in quarantine centers, listing down of NGO’s for providing food to the poor, COVID mitigation plan
Service Reveived:
Awareness, guidance and ways to tackle COVID, medications, isolation COVID testing, testing facility at the door step, solution of the queries, containment, transportation to the hospital with care, trained assistance, Food facility during isolation
F6. Service Audit Profile
The figure F14 shows the service audit profile of the COVID management service provided by NMMC. The firm line on the left shows the existing situation of the service on the basis of the perception of the people taken in the ServQual analysis above. The average P-E of the responses show the position on the profile where they are percieved. The dashed line on the profile, shows the level of improvement possible after the recommendations are implemented. Inference: The servise risk can be mitigated to approx. 90% if the recommendations are taken into consideration.
Figure F14 Service Audit Profile Source: Primary

F7. Conclusion
From the study of the city and the analysis done using various tools. It is observed that NMMC need improvement in following aspects : Identification : It takes more than 12 hours by NMMC to get in touch with the patient after being tested as positive Treatment: Hygiene in quarantine centres, ambulance and food. Monitoring and Survilliance: Time taken by sanitization team to reach the residence after a positive case. According the recommendations it is likely to improve the Service Quality in Managing the Pandemic

Figure F15 Vector image showing health sector fighting COVID19 Source: www.pngtree





