C.R.U. Malawi crisis response unit

Addressing the Road Traffic Fatality Rate in Malawi
by Hardi Shah
project Title: crisis response unit - c.r.u. malawi
by hardi shah
Project presented to the Faculty of the Department of Architecture College of Architecture and the Built Environment, Thomas Jefferson University
In partial fulfillment of the requirements for the degree of BACHELOR OF ARCHITECTURE
Arch-508 / Design 10: Research and Design Faculty
Associate Professor Chris Harnish
Philadelphia, Pennsylvania
May 2019
table of contents
abstract & research question thesis statement & intentions research & design methods research findings & conclusions design proposal : crisis response unit : c.r.u. design findings & conclusions design proposal development reflection assessment works cited bibliography 06 08 12 20 22 26 48 76 78 80
abstract & research question
Could a deployable, pre-fabricated mobile emergency response unit help reduce the on-site road traffic accident mortality rate?
“Every second counts in a road traffic emergency. Reducing the time it takes for medical services, firefighters and rescuers to arrive on the scene can save lives and limit the severity of the consequences of road accidents for survivors .”
-“New UN Regulation on Automatic Emergency Call System for Road Traffic Accidents Will Reduce Response Times, Save Lives.” Targeted News Service, Nov 23, 2017.
Road traffic injuries are a common cause of hospital visits in Malawi, and they are also the leading cause of adult injuryrelated deaths at 30%. In Malawi, death at the scene of crash may be related with either critical and maximum injury severity or poor post-collision care. Factors such as delay in emergency services, lack of ambulance services, and shortage of prehospital teams contribute greatly to the victims survival till they can access medical attention at a healthcare facility. The
emergency response system and trauma services in Malawi are quite disorganized and at many times non existent. If the goal is to reduce the number of road fatalities on scene, providing adequate post-collision care is imperative.
Even a 10 minutes reduction of the medical response time can be statistically associated with an average decrease of the probability of death by one third, both on motorways and conventional roads. By enabling the first responders at the crash site to conduct efficient triage, the medical staff can quickly recognize which victims need to be taken to a healthcare facility and which can be treated on-site. If the critical victims are identified as early as possible, they can be transported in the emergency vehicle to the nearest healthcare facility while the other victims can be attended to on-site by the paramedics.
thesis statement
“Emergency and trauma services within the country are at best disorganized and often non-existent.” 14
“Adequate post-collision care is key to reducing road fatalities on scene.” 14
“Primary intervention is widely believed to be the most appropriate strategy to prevent traffic collisions” 14
“even a 10 minutes reduction of the medical response time can be statistically associated with an average decrease of the probability of death by one third” 14
Providing a quickly deployable emergency tent structure to conduct on-site triage will improve efficiency of healthcare given at the crash-site.
literature review topics
Urgency of the issue of road traffic accident mortality
Global statistics on RTI mortality rates
National (Malawi) statistics on RTI mortality rates
Types of RTIs & respective fatality rates
Current sequence & encountered issues
The usual RTI timeline: <4 victims
The mass casualty RTI timeline: 20+ victims
Presence (or lack) of post-collision care
Current transportation and ambulance system
Current challenges with medical supplies
Various Mass Casualty Systems currently in place
ASAP Rapid Shelter Systems
Ambubus & FirstLine Technology
Structural Typology
Benefits vs challenges of deformable and mechanical structure in a Malawi context
Deployment criteria for mechanical structure
Types of mechanical deployable structure systems
Telescoping Structure
Tensile Structure
Programmatic Criteria
Contents and functions of an ambulance
START triage system & protocol
Triage category adjacencies & on-site program flow
On-site medical services and utilities respective to program
Case Study Analysis
Various deployable structures
HTS Clearspan Structures
Shelterpod Advanced Shelter
HDT Global 12 bed EMMTS
HDT Global 25 bed EMMTS
Various ambulance, trailer, tent organization strategies
Various program adjacency organizations
Manufacturing Criteria
Shipping container size & proportion availabilities
Shipping container structural details
Trailer form and types
Two axle - hitch symmetrical
Two axle - hitch asymmetrical
One axle - hitch asymmetrical
post collision care: triage
By enabling the first responders at the crash site to conduct efficient triage, the medical staff can quickly recognize which victims need to be taken to a healthcare facility and which can be treated on-site. 5
This can reduce the amount of time that it takes for a critical victim to be recognized and be taken to a healthcare facility.3
This effectively reduces burden on the emergency vehicle and reduces overcrowding at the healthcare facility.3
12 intentions
a mass casualty road traffic accident collision occurs (20-24 people injured) ambulance arrives on scene call to emergency services is placed prelim care is given on site victim(s) are treated in the 2-4 person surgery theater victim(s) transported to nearest healthcare facility staff is not trained to handle victims of such a large crash; improper handling can lead to more injury a significant period of time is lost due to the magnitude of the crash & the lack of efficiency and size of the responding EMTs a significant period of time is lost due to the magnitude of the crash & the small size of the emergency vehicles there is a shortage of staff available to handle the accident there may only be one ambulance available more victims than needed are transported to the hospital there is immense overcrowding & victims are placed on the sidewalk the long wait for medical attention could result in worsened injuries or fatalities on -site triage must be performed but is not the victims do not all fit into the ambulance this call may or may not be placed if that is the case, victims will be taken to healthcare facility via the roadways are difficult to navigate with a large vehicle the victim in critical condition worsens enroute the trip is too long and the critical victim dies the nearest healthcare facility is 20 minutes away the district hospital is 20 minutes away while a central hospital could be 2 hours away the staff is unable to detect a critical patient due to lack of effective triage system and equipment the ED at the facility might not have the services needed to save a victim TRIAGE on-site treatment healthcare facility collision ambulance arrives criticalvictims lesscrowdingin vehicle&hospital quickerhealthcare forcriticalvictims medicalsuppliesarenow reservedforcriticalvictims othervictims Lynn, Mauricio. “Hospital Planning and Response to Sudden Mass Casualty Incidents.” Mass Casualty Incidents, 2016, 25-55. doi:10.1007/978-1-4939-3496-6_3. Harrison, Hooi-Ling, Nigel Raghunath, and Michele Twomey. 2012. Emergency triage, assessment and treatment at a district hospital in malawi. Emergency Medicine Journal : EMJ 29 (11): 924-5. “Road Traffic Deaths.” World Health Organization. March 11, 2016. Accessed February 12, 2019. https://www.who.int/gho/road_safety/mortality/en/.
the roadways are difficult to navigate with a large vehicle
there is a shortage of staff available to handle the accident
staff is not trained to handle victims of such a large crash; improper handling can lead to more injury
benefits of on-site triage
a significant period of time is lost due to the magnitude of the crash & the lack of efficiency and size of the responding EMTs
a significant period of time is lost due to the volume of victims, lack of efficient on-site triage, and few first respondants
prelim care is given on site
The objective is to be able to train medical professionals to be able to identify on-site, the proportion of patients who do not need immediate emergency medical care.A large issue even in developed countries is the wastage of resources on patients who did not need to be taken to the hospital and could have just been treated minimally on site.
a significant time is lost due magnitude of & the small size emergency
the victim in critical condition worsens enroute
This does however require that there be a staff of well trained human resources who can accurately decide how to triage victims on site and decipher whether they need emergency medical attention or not.
intentions 13 Prehospital
on-site triaging. Robert B. Dunne, Scott Compton, Robert D. Welch, Robert J. Zalenski, Brooks F. Bock, Prehosp Emerg Care. 2003 Jan-Mar; 7(1): 85–88.
ambulance arrives on scene
of
effective triage system and equipment
methods methods of research
A.LITERATUREREVIEW
USINGTHE PAULGGUTMANLIBRARY’S DATABASES
BACKGROUNDRESEARCH
-URGENCYOFISSUE
This research on mass casualties and road traffic accidents in Malawi was majorly based on literature review conducted on the Jefferson Library databases and various internet sources. Reliable information was found on PubMed, the United Nations, and the World Health Organization databases as well.
Various medical professionals as well as architectural faculty and alumni provided valuable feedback throughout the process.
-ROADTRAFFICACCIDENTS
-MASSCASUALTYACCIDENTS
LITERATUREREVIEW
USINGTHERESOURCESAVAILABLEONTHE WORLDHEALTHORGANIZATION’SWEBSITES
LITERATUREREVIEW
USINGTHERESOURCESAVAILABLEONTHE UNITEDNATION’SWEBSITES

LITERATUREREVIEW
USINGTHE PUBMEDDATABASEONTHEPAUL GGUTMANLIBRARY’SWEBSITE
14
B.LITERATUREREVIEW
USINGTHE PAULGGUTMANLIBRARY’S DATABASES
CASESTUDIES
-tenttypologies
-ambulancecontents&types
-masscasualtyresponsesystems
-structuralsystems
LITERATUREREVIEW
USINGTHERESOURCESAVAILABLEONTHE WORLDHEALTHORGANIZATION’SWEBSITES
LITERATUREREVIEW
USINGTHERESOURCESAVAILABLEONTHE UNITEDNATION’SWEBSITES
INTERVIEWS
ON&OFFCAMPUSGROUNDS
ELIZABETHKREBS,MDMSC
ASSISTANTPROFESSOR
DEPARTMENTOFEMERGENCYMEDICINE
SIDNEYKIMMELMEDICALCOLLEGE
THOMASJEFFERSONUNIVERSITY
TYCZYNSKA,NICOLEE.
ONLINEINTERVIEWBYHARDISHAH. FEBRUARY06,2019.
PERSONALINTERVIEWBYHARDISHAH APRIL01,2019
15
global statistics on rti fatalities
“Every second counts in a road traffic emergency. Reducing the time it takes for medical services, firefighters and rescuers to arrive on the scene can save lives and limit the severity of the consequences of road accidents for survivors.”10
(“New UN Regulation on Automatic Emergency Call System for Road Traffic Accidents Will Reduce Response Times, Save Lives.” Targeted News Service, Nov 23, 2017.)

Every year, about 1.2 million people die through road traffic crashes worldwide. Majority of these deaths occur in Africa where most of their emergency medical services are underdeveloped.12
MALAWI RANKS 1ST IN AFRICAIN RTI MORTALITY AT 35
FATALITIES PER 100,000 POPULATION.6
THE UNITED NATIONS RECOGNIZES THIS AS A GLOBAL CRISIS AND HAS DEVELOPED A SUSTAINABLE DEVELOPMENT GOAL TO COMBAT THIS.2
BY 2020, HALVE THE NUMBER OF GLOBAL DEATHS AND INJURIES FROM ROAD TRAFFIC ACCIDENTS.2
16
findings
“Goal 3: Good Health and Well-being.” UNDP. Accessed February 10, 2019. http://www.undp.org/content/undp/en/home/sustainable-development-goals/goal-3-good-health-and-well-being.html#targets. “Malawi.” World Health Organization. February 01, 2015. Accessed February 11, 2019. https://www.who.int/gho/countries/mwi/en/. “Road Traffic Deaths.” World Health Organization. March 11, 2016. Accessed February 12, 2019. https://www.who.int/gho/road_safety/mortality/en/.
AT
LEAST
MALAWI, 1/3RD
national statistics on rti fatalities
About 20 road traffic collisions occur every day in Malawi, two of which are fatal and two serious injuries. About 1,000 people are killed in road traffic crashes in Malawi every year. In 2015, 5,700 individuals died in Malawi from a road traffic accident despite there being only one motor vehicle on the road per 40 residents. 6,14
1/3rd Homicide 11% Suicide 15 % Drowning 7% Fires 6% Falls 8% War 3% Poisoning 6% Other 21% Road Traffic Accidents 33% 17 A B i ii iii delay in emergency medical attention lack of ambulance services shortage of pre-hospital teams findings
Death at the scene of crash may be related with either critical and maximum injury severity or poor postcollision care. Delay in emergency services, lack of ambulance services, and shortage of pre-hospital teams certainly contribute to deaths on scene.14 1FATALITY14
POOR POST-COLLISION CARE5,14
ALL INJURY RELATED DEATHSARE DUE TO ROAD TRAFFIC ACCIDENTS.6 Lynn, Mauricio. “Hospital Planning and Response to Sudden Mass Casualty Incidents.” Mass Casualty Incidents, 2016, 25-55. doi:10.1007/978-1-4939-3496-6_3. “Malawi.” World Health Organization. February 01, 2015. Accessed February 11, 2019. https://www.who.int/gho/countries/mwi/en/. Schlottmann, Francisco et al. “Road traffic collisions in Malawi: Trends and patterns of mortality on scene” Malawi medical journal : the journal of Medical Association of Malawi vol. 29,4 (2017): 301-305.
CRITICAL AND MAXIMUM INJURY SEVERITY5,14 IN
OF
road traffic accident types
A road accident refers to any accident involving at least one road vehicle, occurring on a road open to public circulation, and in which at least one person is injured or killed.
A mass casualty incident (MCI), is any number of casualties that exceed the resources normally available from local resources. This is based upon available resources, number of injuries, and severity of injuries.
(“What Is a Mass Casualty Incident?” Classification of Social Media Platforms. Accessed February 27, 2019. https://delvalle.bphc.org/mod/wiki/view. php?pageid=89.)
{MOST COMMON} MOTOR VEHICLE VERSUS PEDESTRIAN COLLISIONS14
FATAL CASES: 44% 14
MOTOR VEHICLE VERSUS BICYCLE COLLISIONS14
FATAL CASES: 41% 14
MOTOR VEHICLE VERSUS MOTORCYCLE COLLISIONS14
FATAL CASES: 41% 14
MASSCASUALTYACCIDENTS,20+VICTIMS
MOTOR VEHICLE VERSUS MOTORVEHICLE COLLISIONS14
TYPICALLY MINIBUS OR TRUCK COLLISIONS14
FATAL CASES: 19% 14
18
“Malawi.” World Health Organization. February 01, 2015. Accessed February 11, 2019. https://www.who.int/gho/countries/mwi/en/. Schlottmann, Francisco et al. “Road traffic collisions in Malawi: Trends and patterns of mortality on scene” Malawi medical journal : the journal of Medical Association of Malawi vol. 29,4 (2017): 301-305. findings
Steps in the sequence from crash site to the healthcare facility
Issues encountered during the process
19 the usual rti timeline: <4 victims
collision occurs (2-4 people injured) ambulance arrives on scene a call to emergency services is placed prelim care is given on site victim(s) are treated in the 2-4 person surgery theater victim(s) transported to nearest healthcare facility a road traffic accident this call may or may not be placed if that is the case, victims will be taken to a healthcare facility via the roadways are difficult to navigate with a large vehicle the victim in critical condition worsens enroute the trip is too long and the critical victim dies all 4 victims are taken in one vehicle but not all 4 need to go the ED at the facility might not have the services needed to save a victim the nearest healthcare facility is 20 minutes away the district hospital is 20 minutes away while a central hospital could be 2 hours away the staff is unable to detect a critical patient due to lack of effective triage system and equipment the 4 victims are fit into a vehicle only designed for 2 Branas, C. C., E. J. MacKenzie, and C. S. ReVelle. 2000. A trauma resource allocation model for ambulances and hospitals. Health Services Research 35 (2): 489-507. Harrison, Hooi-Ling, Nigel Raghunath, and Michele Twomey. 2012. Emergency triage, assessment and treatment at a district hospital in malawi. Emergency Medicine Journal : EMJ 29 (11): 924-5. Schlottmann, Francisco et al. “Road traffic collisions in Malawi: Trends and patterns of mortality on scene” Malawi medical journal : the journal of Medical Association of Malawi vol. 29,4 (2017): 301-305. findings
the mass casualty timeline: 20+
victims
A mass casualty incident (MCI), is any number of casualties that exceed the resources normally available from local resources. This is based upon available resources, number of injuries, and severity of injuries.
(“What Is a Mass Casualty Incident?” Classification of Social Media Platforms. Accessed February 27, 2019. https://delvalle.bphc.org/mod/wiki/view. php?pageid=89.)
a mass casualty road traffic accident
on -site triage must be performed but is not
there may only be one ambulance available
a call to emergency services is placed
this call may or may not be placed
the roadways are difficult to navigate with a large vehicle
there is a shortage of staff available to handle the accident
a significant period of time is lost due to the magnitude of the crash & the lack of efficiency and size of the responding EMTs
if that is the case, victims will be taken to a healthcare facility via
staff is not trained to handle victims of such a large crash; improper handling can lead to more injury
20
collision occurs (20-24 people injured) ambulance arrives on scene
findings
the a critical of
more victims than needed are transported to the hospital significant spatial challenges exist at facility causing overflow of patients
RESOURCES
prelim care is given on site
a significant period of time is lost due to the magnitude of the crash & the small size of the emergency vehicles
VICTIMS
casualties >>resources
the ED at the facility might not have the services needed to save a victim
To provide post-collision care with efficiency and reduce the road traffic accident mortality rate, the response time for emergency healthcare must be reduced drastically. By improving upon the efficiency of emergency vehicles with respect to mass casualties, victims of road traffic accidents could obtain medical attention sooner.
When road traffic accidents begin to increase in size, it completely overwhelms the postcollision care system in Malawi which currently struggles to cater to 3-5 person road traffic accidents.3 This particularly challenging category of road traffic accidents is mass casualty road traffic accidents where the number of affected victims is significantly higher.
21
victim(s) are treated in the 2-4 person surgery theater
victim(s) transported to nearest healthcare facility
the long wait for medical attention could result in worsened injuries or fatalities
the victims do not all fit into the ambulance
the victim in critical condition worsens enroute
the trip is too long and the critical victim dies
the nearest healthcare facility is 20 minutes away
the district hospital is 20 minutes away while a central hospital could be 2 hours away
staff is unable to detect critical patient due to lack effective triage system and equipment
Lynn, Mauricio. “Hospital Planning and Response to Sudden Mass Casualty Incidents.” Mass Casualty Incidents, 2016, 25-55. doi:10.1007/978-1-4939-3496-6_3. Harrison, Hooi-Ling, Nigel Raghunath, and Michele Twomey. 2012. Emergency triage, assessment and treatment at a district hospital in malawi. Emergency Medicine Journal : EMJ 29 (11): 924-5. Schlottmann, Francisco et al. “Road traffic collisions in Malawi: Trends and patterns of mortality on scene” Malawi medical journal : the journal of Medical Association of Malawi vol. 29,4 (2017): 301-305.
analyzing the system: current challenges
There are a number of considerations to be able to apply this theory of a deployable tent for on-site triage which is identified here. For example, developing a transportation and ambulance system will need better integration and coordination between the Ministries of Transportation and Health. 14
In terms of triage, developing an efficient triage system specifically for mass casualties will be a challenge as will training and building up the human resources for this position. 14
collision
TRIAGE
developing an efficient triage system specifically for mass casualties
ambulance arrives
developing a transportation and ambulance system will need better integration and coordination between the Ministries of Transportation and Health
training first responders and building up the skilled human resources
providing enough medical supplies in the emergency vehicle
othervictims
on-site treatment
providing enough staff to address all the people in the accident
healthcare facility
healthcare facility
criticalvictims
quickerhealthcare forcriticalvictims
lesscrowdingin vehicle&hospital
medicalsuppliesarenow reservedforcriticalvictims
providing enough space for emergency treatment of the critical patients
22
conclusions
Road Traffic Deaths.” World Health Organization. March 11, 2016. Accessed February 12, 2019. https://www.who.int/gho/road_safety/mortality/en/. Schlottmann, Francisco et al. “Road traffic collisions in Malawi: Trends and patterns of mortality on scene” Malawi medical journal : the journal of Medical Association of Malawi vol. 29,4 (2017): 301-305.
othervictims
analyzing the system: positive impacts
By enabling the first responders at the crash site to conduct efficient triage, the medical staff can quickly recognize which victims need to be taken to a healthcare facility and which can be treated on-site. 5
This can reduce the amount of time that it takes for a critical victim to be recognized and be taken to a healthcare facility.3
This effectively reduces burden on the emergency vehicle and reduces overcrowding at the healthcare facility.3
23 conclusions
accident collision occurs (20-24 people injured) ambulance arrives on scene a call to emergency services is placed prelim care is given on site victim(s) are treated in the 2-4 person surgery theater victim(s) transported to nearest healthcare facility staff is not trained to handle victims of such a large crash; improper handling can lead to more injury a significant period of time is lost due to the magnitude of the crash & the lack of efficiency and size of the responding EMTs a significant period of time is lost due to the magnitude of the crash & the small size of the emergency vehicles there is a shortage of staff available to handle the accident there may only be one ambulance available more victims than needed are transported to the hospital there is immense overcrowding & victims are placed on the sidewalk the long wait for medical attention could result in worsened injuries or fatalities on -site triage must be performed but is not the victims do not all fit into the ambulance this call may or may not be placed if that is the case, victims will be taken to a healthcare facility via the roadways are difficult to navigate with a large vehicle the victim in critical condition worsens enroute the trip is too long and the critical victim dies the nearest healthcare facility is 20 minutes away the district hospital is 20 minutes away while a central hospital could be 2 hours away the staff is unable to detect a critical patient due to lack of effective triage system and equipment the ED at the facility might not have the services needed to save a victim TRIAGE
servedforcriticalvictims
Lynn, Mauricio. “Hospital Planning and Response to Sudden Mass Casualty Incidents.” Mass Casualty Incidents, 2016, 25-55. doi:10.1007/978-1-4939-3496-6_3. Harrison, Hooi-Ling, Nigel Raghunath, and Michele Twomey. 2012. Emergency triage, assessment and treatment at a district hospital in malawi. Emergency Medicine Journal : EMJ 29 (11): 924-5. “Road Traffic Deaths.” World Health Organization. March 11, 2016. Accessed February 12, 2019. https://www.who.int/gho/road_safety/mortality/en/.
on-site treatment healthcare facility ambulance arrives criticalvictims lesscrowdingin vehicle&hospital quickerhealthcare forcriticalvictims medicalsuppliesarenowre-
c.r.u.- crisis response unit
ASSISTING THE HEALTHCARE PROVIDERS ON THE CRASH SITE OF A MASS CASUALTY ROAD TRAFFIC ACCIDENT
Providing a quickly deployable emergency tent structure to conduct on-site triage will improve efficiency of healthcare given at the crash-site.
project goals
Could a deployable, pre-fabricated mobile emergency response unit help reduce the on-site road traffic accident mortality rate?
A deployable, pre-fabricated mobile emergency unit would be able to assist healthcare providers at a crash site and effectively address critical patients as quickly as possible.
This emergency unit strives to be able to provide an effective area for treatment and create some organization on an incredibly chaotic site. By establishing this organization, it is easier for medical staff to be able to triage critical victims quickly and administer emergency stabilization.
The response time which could otherwise be wasted attempting to transport each victim to a healthcare facility to then await triage in an overwhelmed facility, is now cut to a fraction by providing an organized space to conduct that triage initially on site. As stated in multiple sources, the quicker the critical victims are addressed on site and taken to a facility of definitive care, the higher the chances of their survival.
two types of deployable structures
Deployable structures can expand and/ or contract due to their geometrical, material and mechanical properties. Such structures may pass from a ‘folded’ to an ‘erect’ state; and in many cases the component parts are connected throughout topologically, but alter their geometry through the process of deployment. In the process of deployment the initial mobility is transformed into a final rigidity. 13
By the application of a force at one or more points, it transforms in a fluid and controlled manner. Despite such ease of transformation, these structures are stable, strong and durable. 13
DEFORMABLE STRUCTURAL
BENEFITS
BENEFITS >> << CHALLENGES CHALLENGES
do not require physical manpower to deploy & assemble
depend upon the elasticity of their members to allow mobility from the deployed to compacted shape
performance dependent on the strain level in the structure and the type of material
limits their applicability to shelter structures, as the stressed structures are not suitable for repeated deployments.13
deployment does not induce any strain in structural elements
robust performance and repeatability of deployment characterise structural mechanisms. They can also compact to a small fraction of their deployed volume.
The deployment process can be controlled or terminated whenever required with the structure assuming any of the intermediate stable configurations.
very difficult to manufacture and more expensive than other conventional structures13
28
Rivas-Adrover, Esther. (2015). Deployable Structures. findings
Spaces must accomodate 3-4 paramedics and provide ‘beds’ for individuals, cabinets for supplies
the ideal deployable tent structure
Volume of the structure must be able to fit into a carry bag and placed in or under a
As the tent is developed, it is critical to set up criteria which can be used to assess the success or failure of the proposed solution.
However, we must also accept that not all of the criteria might be able to be incorporated into a solution. The challenge of this proposal lies in the question of compromise.
29
rate of assembly 2 weight of overall structure 1 square 3 storage & energy capability 4 type of internal space volume of stored structure 6
weight of the structure cannot excede 2530 lbs
The
The time needed to assemble the tent cannot excede 10 minutes
seat
tent should be able to cater to 20 victims and three paramedics
The
each
with
“Rapid Deployment Shelters For Sale | HTS.” Roder HTS USA. Accessed February 11, 2019. https://www.hts-usa.com/products/rapid-deployment-shelters/. Rivas-Adrover, Esther. (2015). Deployable Structures. “SHELTERPOD (RED) Limited Edition.” SHIFTPOD | Advanced Shelter Systems Inc. Accessed February 11, 2019. https://store.advancedsheltersystemsinc.com/responsepod/shelter/shelterpod-r. findings
The tent should be able to hold enough medical supplies & equipment to treat
patient
bed
internal program layout and adjacency
Approximate sq ft of ambulance = 14x7 for one patient
On-site services which need to be provided are:8 sutures
burns fractures
Equipment for these can be provided in go-bags otherwise, beds and water & energy connections are necessary
30
PATIENT URGENCY medical staff crash site victims emergency tent 18’ bed bed bed bed bed bed bed curtain bed bed bed counters & cabinets counters & cabinets bed bed bed bed 36’ 8’ 24’ initial waiting area urgent patient care triage & first aid8 ambulance
Medicine Journal
EMJ 29 (11): 924-5.
of the National Ambulance
BMC Emergency Medicine 18, (2018). doi:http://dx.doi.org/10.1186/s12873-018-0184-3. findings
Harrison, Hooi-Ling, Nigel Raghunath, and Michele Twomey. 2012. Emergency triage, assessment and treatment at a district hospital in malawi. Emergency
:
Mohammed-Najeeb Mahama, Ernest Kenu, Delia Akosua Bandoh, and Nuhu Zakariah Ahmed. “Emergency Response Time and Pre-Hospital Trauma
Survival
Rate
Service, Greater Accra
(January
– December 2014).”
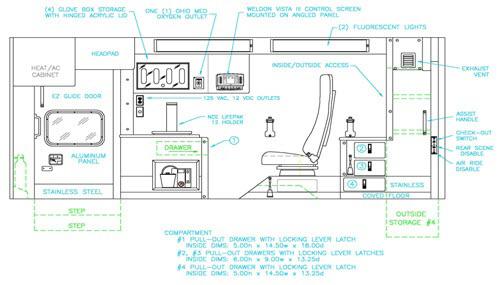
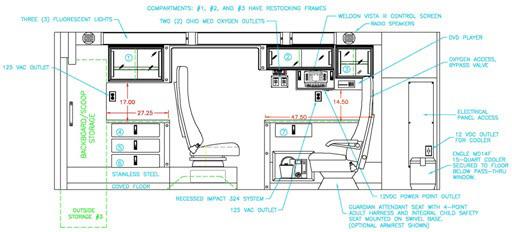
EQUIPMENTINABASICLIFESUPPORTAMBULANCE7
equip. in
EQUIPMENTINAPARAMEDICGO-BAG1
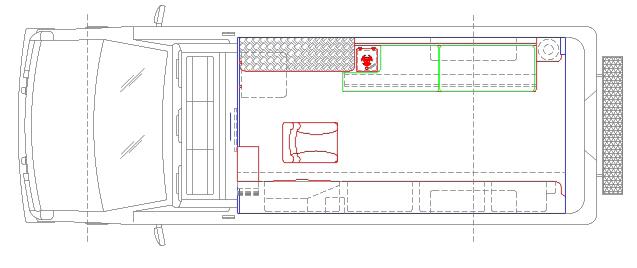
Criteria for the Ambulance:7 size & weight ability to navigate difficult, muddy roads staff accomodation
Criteria for the Paramedic Bags:1 should be battery or solar powered quantity should be sufficient for mass casualty should be able to detach & work independently from ambulance
Branas, C. C., E. J. MacKenzie, and C. S. ReVelle. 2000. A trauma resource allocation model for ambulances and hospitals. Health Services Research 35 (2): 489-507. “Model Comparison Chart.” Demers Ambulances. Accessed February 27, 2019. https://www.demers-ambulances.com/model-comparison-chart/.

31
stored emergency
proposal Suction Catheter Yankauer 18ch x1 Yankauer Mini x1 Black 10fg x1 Orange 16fg x1 Clinical Waste Bag x1 Endotracheal Tube ET Size 9.0 x1 ET Size 8.0 x1 ET Size 7.0 x1 ET Size 6.0 x1 ET Size 5.5 x1 ET Size 5.0 x1 ET Size 4.5 x1 ET Size 4.0 x1 ET Size 3.5 x1 Gel Size 1 x1 Size 1.5 x1 Size 2 x1 Size 2.5 x1 Size 3 x1 Size 4 x1 Size 5 x1 Securing Tape x1 Cook I/O Needle x1 3 Way Tap x2 Sterets x4 Lubrication Sachets x2 K bandage Small x2 500 ml Saline x1 Giving Set x1 GTN Tablets Ipratropium Nebules Ibuprofen Tablets Ibuprofen Sachets Paracetamol Tablets Paracetamol Sachets Salbutamol 5mg Salbutamol 2.5mg Oral Medication Syringe 5ml Diagnostic Equipment (Red Pouch) Sphygmomanometer Stethoscope Blood glucose monitor equipment Thermometer Torch Pen (optional) Mobile Saturations Monitor External Pouch FFP3 Mask x 2 Safety Glasses x 2 Laryngoscopes Combination Blade & Handle Laryngoscope Mil 1 x1 Combination Blade & Handle Laryngoscope Mac 2 x1 Combination Blade & Handle Laryngoscope Mac 3 x1 Combination Blade & Handle Laryngoscope Mac 4 x1 Magills Forceps Adult x1 Magills Forceps Paediatric x1 Thomas Tube Holder Adult x1 Thomas Tube Holder Paediatric x1 CO2 Detector Adult x1 CO2 Detector Paediatric x1 Catheter Mount x1 20ml Syringe x1 Bougie x1 20ml Syringe 2 Drawing up Needle x 5 Saline Flush 10ml x 4 Melonin Small x 5 Vecafix x 4 Sterets 4 Tourniquet x 2 21g Hypodermic Needle (IM use) x 5 23g Hypodermic Needle (IM use) x 5 Miscellaneous Items Clinical Waste Bag x 1 Dressings – Wound Management (Blue Pouch) Dressing Ambulance Small x 2 Dressing Ambulance Medium x 2 Dressing Ambulance Large x 1 Dressing Ambulance X Large x 1 Bandage K Small 1 Bandage K Medium x 1 Bandage K Large 1 Melolin Small x 2 Melolin Medium x 2 Melolin Large x 2 Tape Micropore/Transpore x 1 Bandage triangular 2 Chest Seal Russell x 1 Plasters x 3 Tough Cut Shears 1 Celox Dressing x 1 CAT Tourniquet x 2 Internal End Pouch Sharps Bin x 1 Medicines – Quantities variable (Green or Black Pouch) Aspirin Glucagon Glucose Gel Airway Management MGS Oxygen cylinder 3L x 1 Bag Valve Mask Adult 1L x 1 Bag Valve Mask Paediatric 500ml x 1 Mask O2 100% Adult x 1 Mask O2 100% Paediatric x 1 Mask O2 Medium Concentration Adult x 1 Mask Nebuliser Adult x 1 Mask Nebuliser Paediatric x 1 Nebuliser T Piece x 1 Nasal Cannula x 1 Peak Flow Meter Adult x 1 Peak Flow Meter Paediatric x 1 Peak Flow Tube Adult x 1 Peak Flow Tube Paediatric 1 Fenton Easy Manual Suction Pump 1 Airway Oropharyngeal Size 4 x 1 Size 3 x 1 Size 2 x 1 Size 1 x 1 Size 0 x 1 Size 00 1 Size 000 x 1 Tongue Depressor x 1 Airway Nasopharyngeal Size 32 2 Size 28 2 Size 24 2 Lubricant sachets x 2 Cannulation Equipment 24G Venflon x 2 22G Venflon x 2 20G Venflon x 2 18G Venflon x 2 16G Venflon x 2 14G Venflon x 2 5ml Syringe x 2 10ml Syringe x 4
findings
case studies
Conducting precedent studies has helped establish criteria for the tent and understand how the criteria are balanced, achieved, and compromised in existing situations.
It also serves as an exercise to analyze the existing models and rate their effectiveness in a situation such as a mass casualty road traffic accident. When proposals are created for on-site triage later in the semester, this type of analysis will be utilized to determine the possible failures or successes.
Studying existing emergency tent structures available for commercial, military, & medical use and their successes & drawbacks.
case studies
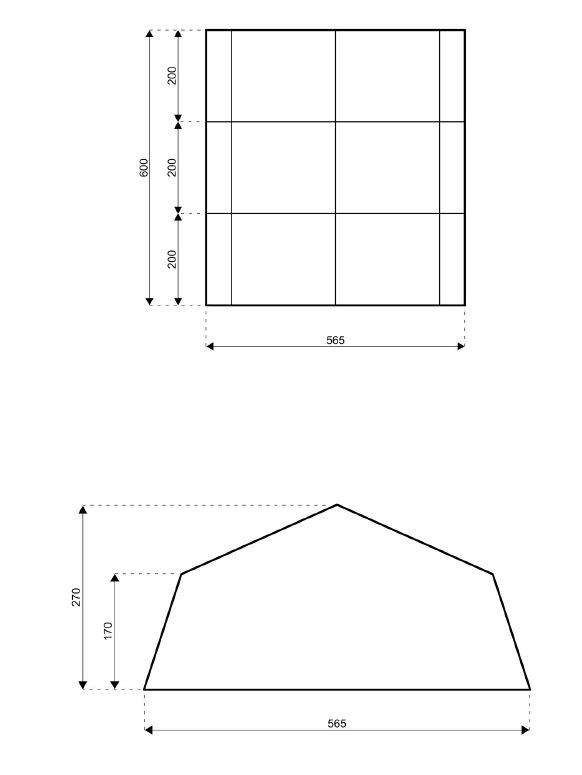
precedent: HTS
Clearspan
Structures
Rapid Deployment Shelters - Emergency Shelters
Tents for humanitarian response and emergency relief

Eave height: 1.70m
Span width: 5.65m
Peak height: 2.70m
Longest component: 2.44m
Maximum length: 6.00m
PRECEDENTANALYSIS
TOTAL COVERED AREA: Tallest height: Height at corner: set-up time: less than 30 minutes
Max allowed wind speed: 60 km/h
Aluminium type: Anodized aluminium profiles
Connecting components: Aluminium couplings
Roof covering type: Robust industrial grade
PVC, Flame retardant
34
00 rate of assembly square footage weight of overall structure type of internal space volume of stored structure storage & energy capability flexibility of vehicles 20’ x 19’ 380 sqft 8.85 ft 5.58 ft
“Rapid Deployment Shelters For Sale | HTS.” Roder HTS USA. Accessed February 11, 2019. https://www.hts-usa.com/products/rapid-deployment-shelters/.
PRECEDENTANALYSIS
135 sqft
Total covered area: set-up time: less than 22 seconds
With practice one person can set up these shelters very quickly. Setting stakes, lines and zipping in the floor will take another couple of minutes.
precedent: shelterpod advanced shelter



Width: 11.5’
Height: 6’ 4”at center 5’10” at Shoulder
Stowed Size: 12” x 12” x 74”
Weight: 65LBS
6-layer super-composite reflective fabric with a fiberglass frame and metal hubs. Reflective, Insulated, and Wind resistant
35 case
studies
00 rate of assembly square footage weight of overall structure type of internal space volume of stored structure storage & energy capability flexibility of vehicles
“SHELTERPOD (RED) Limited Edition.” SHIFTPOD | Advanced Shelter Systems Inc. Accessed February 11, 2019. https://store.advancedsheltersystemsinc.com/responsepod/shelter/shelterpod-r.
precedent: HDT Global 12 Bed EMMTS
A trailer based system complete with power generation, heating and cooling, and water distribution including showers and sinks.
This system provides treatment space for 6 beds with surge capability to 12 beds.
Also has capability to provide negative pressure isolation for 2 to 4 beds. Multiple systems complex together to provide larger multi-bed systems in increments of 25, 50, 100 or more.
Medical equipment included can be tailored to meet your specific requirements, Beds included

PRECEDENTANALYSIS

set-up time: almost one hour
To be operational, system needs: power source water source oxygen connection
12 BED EMERGENCY MEDICAL TREATMENT AND TRIAGE SYSTEM (EMTTS)

36
00 rate of assembly square footage weight of overall structure type of internal space volume of stored structure storage & energy capability flexibility of vehicles
SYSTEM CAN BE USED AS: • Stand off triage and remote treatment capability from your Emergency Department • Augment emergency services for disaster and large scale public events
This 6 – 12 bed rapid deployable infrastructure system provides an on site Emergency Treatment & Triage System (E-MTTS). A trailer based system complete with power generation, heating and cooling, and water distribution. Free standing and designed to be setup in 1 hour. System only needs fuel, water source and oxygen to be operational. This system provides treatment space for 6 beds with surge capability to 12 beds. Also has capability to provide negative pressure isolation for 2 to 4 beds. Multiple systems complex together to provide larger multi-bed systems in increments of 25, 50, 100 or more.
HDT Global. Accessed February 27, 2019. http://www.hdtglobal.com/series/medical-mergency-operations/.
case studies
precedent:
Rapid deployable infrastructure system provides support for 25 patients complete with power generation, heating and cooling, and water distribution. The system is free-standing and designed to be set up in 2 hours. It only needs fuel, a water source and oxygen to be operational. System can be augmented with medical equipment and supply sets to provide for a total turnkey solution to surge hospital capacity. Design promotes efficient traffic flow and improved utilization of staffing resources.
PRECEDENTANALYSIS
The hub and spoke version of the 25 bed system features a center core that acts as a control point when joined with open end boot connectors.
Key Features
• Rapid deploying shelters for Mass Casualty Event Response


• 25 bed, isolation capacity
• Boot connectors
• Lighting
• Complete with heating, 3.5 ton ECU, and water distribution system including showers and sinks
• System only needs power source, water source, and oxygen to be operational
• Chairs, tables, desks
• Waste containers
Medical 25 Bed systeMs Square and Hub and Spoke Configurations
• Fire extinguishers
• Cargo trailer
• Center core that acts as a control point when joined with open end boots
• Free standing and designed to be set up in two (2) hours
• Medical equipment included can be tailored to meet your specific requirements
• Beds included with this system
HDT Global 25 Bed EMMTS
A trailer based system complete with power generation, heating and cooling, and water distribution including showers and sinks.
This system provides treatment space for 25 beds with isolation capacity.
Also has capability to provide negative pressure isolation for 2 to 4 beds.
Medical equipment included can be tailored to meet your specific requirements, Beds included
Rapid deployable infrastructure system provides support for 25 patients complete with power generation, heating and cooling, and water distribution. The system is free-standing and designed to be set up in 2 hours. It only needs fuel, a water source and oxygen to be operational. System can be augmented with medical equipment and supply sets to provide for a total turnkey solution to surge hospital capacity. Design promotes efficient traffic flow and improved utilization of staffing resources.
The hub and spoke version of the 25 bed system features a center core that acts as a control point when joined with open end boot connectors.
Key Features
37
00 rate of assembly square footage weight of overall structure type of internal space volume of stored structure storage & energy capability flexibility of vehicles
hdtglobal.com MILITARY INDUSTRIAL COMMERCIAL CONTINGENCY OPERATIONS HOMELAND SECURITY © 2013 HDT Global
To be operational, system needs: power source water source oxygen connection Stand off triage and remote treatment capability from your Emergency Department
set-up time: almost two hours
HDT Global. Accessed February 27, 2019.
case studies
http://www.hdtglobal.com/series/medical-mergency-operations/.
the three component typologies
On-site services which need to be provided are:8
sutures burns fractures
Equipment for these can be provided in go-bags otherwise, beds and water & energy connections are necessary
severe/critical patients
emergency transport access to water, oxygen, and energy
allow for larger sqft easily deployed multiple patients, two EMTs light equipment
AMBULANCE TRAILER CARETENT
typical size= 7’x14’ one patient, two EMTs, driver
ONSITE TRIAGE
allotheron-site facilities
allotheron-site services contains equipment and square footage not available in ambulance
38
findings
39
AMBULANCE TRAILER CARETENT THETRAILERISITSOWNENTITY THECARETENT&AMBULANCEARE
THEAMBULANCEISITSOWNENTITY THECARETENT&TRAILERAREONE ENTITY 1. 2. 3. 4. AMBULANCE AMBULANCE AMBULANCE TRAILER TRAILER TRAILER CARETENT CARETENT CARETENT ALLTHREECOMPONENTSARE INDEPENDENTENTITIES ALLTHREECOMPONENTSAREONE ENTITY-ALLCONNECTED findings
component relationships & strategies
ONEENTITY
successes & drawbacks study 1
TENTPLACEDONROOFOF
INDEPENDENTTRAILERCONTAININGMEDICAL EQUIPMENT(150SQFT)
PROS
FLEXIBILITYOFVEHICLES
VOLUMEOFSTOREDSTRUCTURE
WEIGHTOFOVERALLSTRUCTURE
CONS
RATEOFASSEMBLY
SQUAREFOOTAGE
STORAGE&ENERGY
TYPEOFINTERNALSPACE
ACCORDIANSTYLEMECHANICALLY DEPLOYEDTENT(302SQFT)
*THISSCHEMEALLOWSTHEAMBULANCETOLEAVEWITHACRITICAL PATIENTWHILETHEEMTSHANDLEOTHERVICTIMSWITHMINORINJURIES
40
AMBULANCE TRAILER CARETENT AMBULANCE TRAILER CARETENT AMBULANCE TRAILER CARETENT AMBULANCE TRAILER CARETENT 4. 3.
1. SCHEME1SCOREBOARD 00 rate of assembly square footage weight of overall structure type of internal space volume of stored structure storage & energy capability 5 2 5 2 5 2 5 4 21/35 5 5 5 2 flexibility of vehicles 5 4
2.
AMBULANCE
studies
case
PROS
41 successes & drawbacks study 2 AMBULANCE TRAILER CARETENT AMBULANCE TRAILER CARETENT AMBULANCE TRAILER CARETENT AMBULANCE TRAILER CARETENT 4. 3. 2. 1. SCHEME2SCOREBOARD 00 rate of assembly square footage weight of overall structure type of internal space volume of stored structure storage & energy capability 5 2 5 5 5 5 5 4 22/35 5 2 5 4 flexibility of vehicles 5 0 TENTPLACEDONROOFOF AMBULANCE&TRAILER FLEXIBLESEATINGLOWERED FROMAMBULANCE TRAILERDOORSOPENTOCREATEEXTENSION OFAMBULANCEEQUIPMENT TENTOPENSASAWNINGSTOINCREASESQUARE FOOTAGEONEITHERSIDE(1377SQFT)
ALLOWSMEDICALSTAFFTOACCESSEQUIPMENT& RESOURCESFROMACENTRALCORE
SQUAREFOOTAGE STORAGE&ENERGY VOLUMEOFSTOREDSTRUCTURE TYPEOFINTERNALSPACE CONS RATEOFASSEMBLY FLEXIBILITYOFVEHICLES WEIGHTOFOVERALLSTRUCTURE case studies
case studies
successes & drawbacks study 3
PROS
SQUAREFOOTAGE STORAGE&ENERGY
VOLUMEOFSTOREDSTRUCTURE
RATEOFASSEMBLY
WEIGHTOFOVERALLSTRUCTURE
CONS
FLEXIBILITYOFVEHICLES
TYPEOFINTERNALSPACE
TRAILERISCONNECTEDTOTENT
TRAILERISASSEMBLEDAND POSITIONEDADJACENTTO AMBULANCE
TENTSTRUCTUREISPULLEDDOWN& AROUNDTOCREATEACANOPY
RELEASEFABRICROLLSFROMTOPOF CANOPYTOCREATEA‘CLOSED’TENT
42
AMBULANCE TRAILER CARETENT AMBULANCE TRAILER CARETENT AMBULANCE TRAILER CARETENT AMBULANCE TRAILER CARETENT 4.
TENTPLACEDONROOFOF AMBULANCE(996SQFT)
3. 2. 1.
SCHEME3SCOREBOARD 25/35 00 rate of assembly flexibility of vehicles square footage weight of overall structure type of internal space volume of stored structure storage & energy capability 5 5 4 0 5 5 5 4 5 5 5 4 5 3
AMBULANCEISASSEMBLED ANDPOSITIONEDADJACENTTO TRAILER
PROS
SQUAREFOOTAGE
STORAGE&ENERGY
VOLUMEOFSTOREDSTRUCTURE
RATEOFASSEMBLY
WEIGHTOFOVERALLSTRUCTURE
FLEXIBILITYOFVEHICLES
CONS
TYPEOFINTERNALSPACE
RELEASEFABRICROLLSFROMTOPOF CANOPYTOCREATEA‘CLOSED’TENT
*THISSCHEMEALLOWSTHEAMBULANCETOLEAVEWITHACRITICAL PATIENTWHILETHEEMTSHANDLEOTHERVICTIMSWITHMINORINJURIES
43 successes & drawbacks study 4 AMBULANCE TRAILER CARETENT AMBULANCE TRAILER CARETENT AMBULANCE TRAILER CARETENT AMBULANCE TRAILER CARETENT 4. 3. 2. 1. SCHEME4SCOREBOARD 30/35 00 rate of assembly flexibility of vehicles square footage weight of overall structure type of internal space volume of stored structure storage & energy capability 5 5 4 5 5 5 5 4 5 5 5 4 5 3 CANOPYSTYLEMECHANICALLYDEPLOYEDTENT PLACEDONROOFOFTRAILER(996SQFT) TENTSTRUCTUREISPULLEDDOWN& AROUNDTOCREATEACANOPY AMBULANCEISCONNECTEDTOTENT
case studies
works cited
Branas, C. C., E. J. MacKenzie, and C. S. ReVelle. 2000. A trauma resource allocation model for ambulances and hospitals. Health Services Research 35 (2): 489-507.
“Goal 3: Good Health and Well-being.” UNDP. Accessed February 10, 2019. http://www.undp.org/content/undp/en/home/sustainabledevelopment-goals/goal-3-good-health-and-well-being.html#targets.
Harrison, Hooi-Ling, Nigel Raghunath, and Michele Twomey. 2012. Emergency triage, assessment and treatment at a district hospital in malawi. Emergency Medicine Journal : EMJ 29 (11): 924-5.
HDT Global. Accessed February 27, 2019. http://www.hdtglobal. com/series/medical-mergency-operations/.
Lynn, Mauricio. “Hospital Planning and Response to Sudden Mass Casualty Incidents.” Mass Casualty Incidents, 2016, 25-55. doi:10.1007/978-1-4939-3496-6_3.
“Malawi.” World Health Organization. February 01, 2015. Accessed February 11, 2019. https://www.who.int/gho/countries/mwi/en/.
“Model Comparison Chart.” Demers Ambulances. Accessed February 27, 2019. https://www.demers-ambulances.com/model-comparisonchart/.
Mohammed-Najeeb Mahama, Ernest Kenu, Delia Akosua Bandoh, and Nuhu Zakariah Ahmed. “Emergency Response Time and Pre-Hospital Trauma Survival Rate of the National Ambulance Service, Greater Accra (January – December 2014).” BMC
Emergency Medicine 18, (2018). doi:http://dx.doi.org/10.1186/ s12873-018-0184-3.
“New UN Regulation on Automatic Emergency Call System for Road Traffic Accidents Will Reduce Response Times, Save Lives.” Targeted News Service, Nov 23, 2017.
“Rapid Deployment Shelters For Sale | HTS.” Roder HTS USA. Accessed February 11, 2019. https://www.hts-usa.com/products/rapiddeployment-shelters/.
Rivas-Adrover, Esther. (2015). Deployable Structures.
“Road Traffic Deaths.” World Health Organization. March 11, 2016. Accessed February 12, 2019. https://www.who.int/gho/road_safety/ mortality/en/.
Schlottmann, Francisco et al. “Road traffic collisions in Malawi: Trends and patterns of mortality on scene” Malawi medical journal : the journal of Medical Association of Malawi vol. 29,4 (2017): 301-305.
“SHELTERPOD (RED) Limited Edition.” SHIFTPOD | Advanced Shelter Systems Inc. Accessed February 11, 2019. https://store. advancedsheltersystemsinc.com/responsepod/shelter/shelterpod-r.
Sion, Melanie, MD, and Anthony Charles, MD, MPH, FACS. Central Malawi District Hospital Surgical Capacity Assessment. Report. Department of Surgery, Thomas Jefferson University Hospital.
Tyczynska, Nicole E. Online interview by Hardi Shah. February 06, 2019.
“What Is a Mass Casualty Incident?” Classification of Social Media Platforms. Accessed February 27, 2019. https://delvalle.bphc.org/ mod/wiki/view.php?pageid=89.
https://www.who.int/bulletin/archives/80(11)900.pdf
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
final presentation script
The goal of this project was to analyze and combat the high road traffic accident mortality rate in Malawi with a special focus on mass casualty incidents.
To express the weight of this issue, malawi ranks 1st in Africa in road traffic accident mortality rate at 35 fatalities per 100,00 people. The United Nations recognized this as a global issue and set a sustainable development goal which has not been met.
1/3rd of all injury related deaths are caused due to road traffic accidents and 30% of all accidents result in at least 1 fatality. The cause for this has been identified to be the delay in emergency medical attention, lack of ambulance services, and a shortage of pre-hospital teams. This identifies the main issue to lie in the response system for road traffic accidents.
I first looked at the timeline for a typical road traffic accidents and identified the issues in the process in red.
I then looked at the timeline for a mass casualty road traffic accident. A mass casualty is defined as an accident which results in more patients than the local resources are able to handle. In red, I have identified issues that are faced in addition to the ones identified for a typical accident.
As stated before, the main issue lies in the response system for road traffic accidents. This includes the initial triage and urgent care, which is the area of intervention.
This brings me to my thesis question:
Could a deployable prefabricated mobile emergency response unit help reduce the on-site road traffic accident fatality rate?
By enabling the first responders to conduct efficient triage, the medical staff is able to quickly recognize victims in critical condition. These victims could then be transported to a healthcare facility where they will have access to definitive care, while other victims may be treated on site. This will reduce the amount of time that it takes for a critical patient to be recognized and taken to a hospital.
To assist healthcare providers on a chaotic crash site, the crisis response unit, or CRU, will be a deployable emergency unit which will provide a space for the responders to recognize and treat patients.
I studied the three main components of the system: the ambulance, trailer, and tent and established their uses and relationships on the site.
I also established a set of deployment, structural, and programmatic criteria to assess the success or failure of the proposed solution within the context of Malawi.
A goal for this project especially within the context of Malawi, was to be able to design the CRU to be a prefab and efficiently shippable design. A 2-unit set would aim to be fit into a 45 long shipping container.
The timeline of the crash was then reanalyzed as the response system was recreated. After a crash occurs, the police is contacted. As the police race to arrive at the crash-site and deploy the Crisis Response Unit, the ambulance makes it’s way to the crash site. This way, the medical staff is not wasting precious time deploying the tent when they could be triaging
the victims. Once the critical victims are identified, they are stabilized and taken to the healthcare facility while the rest of the patients are addressed on site.
The unit is divided into two sections: the primary treatment zone and the secondary storage zone. The primary zone is home to the emergency supplies, and the connection to oxygen, electricity, and water. The secondary zone contains the larger units needed on site such as the foldable stretchers, go bags, portable batteries, portable oxygen, and extra supplies.
When dealing with a mobile unit, there had to be a flexibility in the features to be able to exist in different conditions. Things such as a PVC fabric for durability, the choice to make a mechanically deployable tent to ensure multiple deployments without causing strain on the physical material, and a structural frame which is modeled from the structure of a durable shipping container were all considered. There also had to be features included to increase the ease in use such as a lever to crank the fabric back into the roll, the walking space within the unit between the supplies, and the footing to assist with the circulation within the site.
The floor plan further clarifies the organization of the components within the unit.
The elevation expresses the location of the utilities with respect to the hitch. To ensure more stability during transport for the utilities, it is located directly above the hitch. The flag is placed to signify the triage category which is being addressed at that time.
The sections express the relationship between the treatment areas and the supplies. Creating the walkway within the unit allows the treatment areas to connect and bleed into each other.
The loads affecting the unit were addressed when the structure was being created. The tension cables at the ends of the telescopic structures are
incorporated to offset the wind uplift.
The overall system can be created using multiple units.
CRU is designed to be able to be walked through and create a continuous circulation within the site for the staff. The circulation flows through the supply corridor of one unit into a covered treatment area in front of the storage space with portable utilities.
The CRU system could also be utilized in case of a larger mass casualty situation such as a flood or fire. A makeshift clinic can be created using these units.
The layout of the supply and storage zones determines the types of treatment areas. Critical treatment areas can be created where the supply and utility zone is located adjacent to the storage zone as that area has access to resources available in both zones of the unit. Other treatment areas are adjacent to only the supply & utility zone.
This creates a grid like organization on an otherwise chaotic site. While patients travel along this grid.
The staff can travel along a different grid utilizing the corridors within the unit.
CRU strives to be able to provide an effective area for treatment and create some organization on an incredibly chaotic site.
By establishing this organization, it is easier for medical staff to be able to triage critical victims quickly and administer emergency stabilization.
The response time which could otherwise be wasted attempting to transport each victim to a healthcare facility to then await triage in an overwhelmed facility, is now cut to a fraction by providing an organized space to conduct that triage initially on site.
bibliography
“Rhino RT/R5 Telescopic Bollard.” Rhino Security. Accessed May 06, 2019. http://www.rhinosecurity.co.uk/post-barriers/steel-telescopicposts/137-2/.
“Specification for Rigid Stretchers.” doi:10.3403/00259128. https:// techlemstretchers.com/wp-content/uploads/2018/11/Techlem-Cataloguerev4-webNA.pdf
“Strap Drive | Telescoping Field Mast | 8 to 18 Meters | MIL-STD-810.” The Will-Burt Company. Accessed May 06, 2019. https://www.willburt.com/ products/telescopic-masts/qeam/hdtm/.
“3G Aluminum Alloy Stretcher.” Medical Stretchers - Ambulance Stretchers - Mobi Medical Supply. Accessed May 06, 2019. https://medicalstretchers.com/2-ambulance-stretchers.
“ASAP® RAPID SHELTER SYSTEMS.” Deployed Logix. Accessed May 06, 2019. https://deployedlogix.com/asap-rapid-shelter-systems/#tab-id-1.
“ETFE and PTFE Structures.” Fabric Architect. Accessed March 26, 2019. https://www.fabricarchitect.com/material-choices.html.
“First Aid Product™.” First Aid Product: Wholesale Direct to the Public! Why Pay Retail?™. Accessed March 05, 2019. https://first-aid-product.com/ disaster-survival/triage-supplies-s-t-a-r-t-triage-kits.html.
“Mass Casualty Management Systems.” World Health Organization. April 2007. Accessed March 3, 2019. https://www.who.int/hac/ techguidance/tools/mcm_guidelines_en.pdf?ua=1.
“Mass Casualty Oxygen System (MCOS).” First Line Technology. Accessed May 06, 2019. https://www.firstlinetech.com/product/mcos/.
“Mass Casualty, START Triage and the SMART Tag System.” Lecture, Boston, March 06, 2019. Accessed March 6, 2019. https://www. blessinghealth.org/sites/default/files/users/user15/EMS_START_Triage_ SMART_Tags_2017.pdf.
“Telescoping Mast | Unlimited Deployment | No Maintenance.” The WillBurt Company. Accessed May 06, 2019. https://www.willburt.com/ products/telescopic-masts/pneumatic-locking/non-military/.
“BP Medical Supplies.” Accessed March 05, 2019. https://www. bpmedicalsupplies.com/products/Disaster-Relief-MCI/Triage-Supplies/.
“Goal 3: Good Health and Well-being.” UNDP. Accessed February 10, 2019. http://www.undp.org/content/undp/en/home/sustainabledevelopment-goals/goal-3-good-health-and-well-being.html#targets.
“Malawi.” World Health Organization. February 01, 2015. Accessed February 11, 2019. https://www.who.int/gho/countries/mwi/en/.
“Model Comparison Chart.” Demers Ambulances. Accessed February 27, 2019. https://www.demers-ambulances.com/model-comparison-chart/.
“New UN Regulation on Automatic Emergency Call System for Road Traffic Accidents Will Reduce Response Times, Save Lives.” Targeted News Service, Nov 23, 2017.
“Rapid Deployment Shelters For Sale | HTS.” Roder HTS USA. Accessed February 11, 2019. https://www.hts-usa.com/products/rapiddeployment-shelters/.
“Road Traffic Deaths.” World Health Organization. March 11, 2016. Accessed February 12, 2019. https://www.who.int/gho/road_safety/ mortality/en/.
“SHELTERPOD (RED) Limited Edition.” SHIFTPOD | Advanced Shelter Systems Inc. Accessed February 11, 2019. https://store. advancedsheltersystemsinc.com/responsepod/shelter/shelterpod-r.
“What Is a Mass Casualty Incident?” Classification of Social Media Platforms. Accessed February 27, 2019. https://delvalle.bphc.org/mod/ wiki/view.php?pageid=89.
Branas, C. C., E. J. MacKenzie, and C. S. ReVelle. 2000. A trauma resource allocation model for ambulances and hospitals. Health Services Research 35 (2): 489-507.
Chokotho, Linda, Wakisa Mulwafu, Kathryn H. Jacobsen, Hemant Pandit, and Chris Lavy. 2014. The burden of trauma in four rural district hospitals in malawi: A retrospective review of medical records. Injury 45 (12): 206570.
Haac, Bryce E., Jared R. Gallaher, Charles Mabedi, Andrew J. Geyer, and Anthony G. Charles. 2017. Task shifting: The use of laypersons for acquisition of vital signs data for clinical decision making in the emergency room following traumatic injury. World Journal of Surgery 41 (12): 306673.
Harrison, Hooi-Ling, Nigel Raghunath, and Michele Twomey. 2012. Emergency triage, assessment and treatment at a district hospital in malawi. Emergency Medicine Journal : EMJ 29 (11): 924-5.
HDT Global. Accessed February 27, 2019. http://www.hdtglobal.com/ series/medical-mergency-operations/.
https://www.who.int/bulletin/archives/80(11)900.pdf
Lynn, Mauricio. “Hospital Planning and Response to Sudden Mass Casualty Incidents.” Mass Casualty Incidents, 2016, 25-55. doi:10.1007/978-1-
4939-3496-6_3.
Mohammed-Najeeb Mahama, Ernest Kenu, Delia Akosua Bandoh, and Nuhu Zakariah Ahmed. “Emergency Response Time and Pre-Hospital Trauma Survival Rate of the National Ambulance Service, Greater Accra (January – December 2014).” BMC
Repoussis, Panagiotis P., Dimitris C. Paraskevopoulos, Alkiviadis Vazacopoulos, and Nathaniel Hupert. 2016. Optimizing emergency preparedness and resource utilization in mass-casualty incidents. European Journal of Operational Research 255 (2): 531-44.
Rivas-Adrover, Esther. (2015). Deployable Structures.
Samuel JC, Akinkuotu A, Villaveces A et al. (2009) Epidemiology of injuries at a tertiary care center in Malawi. World Journal of Surgery 33, 1836–1841.
Samuel, J. C., E. L. P. Campbell, A. G. Charles, and B. A. Cairns. 2010. Burn epidemiology and burn care in malawi: Outlining prevention strategies. Injury Prevention 16 (Supplement 1): A61-.
Schlottmann, Francisco et al. “Road traffic collisions in Malawi: Trends and patterns of mortality on scene” Malawi medical journal : the journal of Medical Association of Malawi vol. 29,4 (2017): 301-305.
Sion, Melanie, MD, and Anthony Charles, MD, MPH, FACS. Central Malawi District Hospital Surgical Capacity Assessment. Report. Department of Surgery, Thomas Jefferson University Hospital.
Tyczynska, Nicole E. Online interview by Hardi Shah. February 06, 2019.
Yu, Christopher, Keenan Crane, and Stelian Coros. “Computational Design of Telescoping Structures.” ACM Transactions on Graphics36, no. 4 (2017): 1-9. doi:10.1145/3072959.3073673. https://www.cs.cmu. edu/~christoy/Projects/Telescopes-sig2017.pdf


