Correspondence: Please send all correspondence to The Editor at PO Box 782, Kent Town, SA 5071, or email editor@hepatitissa.asn.au . Editor: James Morrison
Regular Contributors: Cecilia Lim, Joy Sims
Some photos in this publication may have been altered to disguise identifying details of members of the public.
This resource was prepared and printed on Kaurna Country.
Disclaimer: Views expressed in this newsletter are not necessarily those of Hepatitis SA. Information contained in this newsletter is not intended to take the place of medical advice given by your doctor or specialist.
We welcome contributions from Hepatitis SA members and the general public.
SA Health has contributed funds towards this program.
ISSN 2651-9011 (Online)
About
Reducing BBV Risks in the Permanent Make-up Industry
The permanent make up (PMU) industry in Australia is largely unregulated and while sad stories of botched eyebrows and misshapen lips gain media attention every now and then, less has been said about the other risk of unregulated minor cosmetic surgery: infection.
The risk of infection from contaminated equipment, unhygienic settings and carelessness is real, especially infection from blood borne viruses (BBV) such as viral hepatitis. This was recently highlighted in a NSW Health call to customers of a Sydney-based cosmetic clinic to get tested for BBVs.
Adelaide PMU artist, Sara Mac, believes passionately that this aspect of the industry can be changed and is working hard to achieve it from the inside. Sara runs a salon – OHMYBROW (OMB) – that provides cosmetic tattooing services, as well as an academy that trains make-up artists. She has recently joined the Board of the South Australian Hair & Beauty Association (SAHBA) and believes that in the absence
of government regulation and licensing, education and self-regulation by the industry itself becomes all the more important.
OMB Academy offers a full, free-to-access course on blood borne pathogens, and health and safety practices in permanent makeup. A quick check of PMU training organisations in South Australia revealed another three organisations which list health and safety content as part of their course units but none responded to our request for more information.
“As a SAHBA Board member, I believe one of our key goals is to formally collaborate with industry members and promote a unified approach to safety standards,” Hepatitis SA Community News.
She said while it’s great to see other training programs beginning to address health and safety, the Association is unable to ensure the quality of those trainings. She said establishing a standardised document, such as that available for the industry in the US, is crucial for the Australian industry.
Sara Mac (photo supplied)
“SAHBA is currently working on initiatives to support industry self-regulation through consistent safety practices and accessible resources like our Bloodborne Pathogen course, which we hope will serve as a benchmark,” she said.
Sara’s passion for elevating health and blood safety standards in the cosmetic tattoo industry stems from a series of troubling experiences and observations she encountered in her early days in the industry, both as a client and a trainer.
“When I had my eyebrows tattooed, it was a traumatising experience,” she recalled. “What really scared me was the huge gap in professional conduct and health standard. There were numerous red flags. There was no consultation, no service forms, and no treatment guidance.
“I was lying on a fold-out massage table in the dining room of a family home, with the sound of children screaming and pets interacting with me. The lady treating me sat on a faux fur stool, and I never saw her wash her hands between clients. Asking questions felt like an inconvenience to her, and the entire service lasted a mere 20 minutes. For a $700 treatment that involved skin breakage, the level of unprofessionalism was shocking.
“My second experience was no better, raising even more red flags and making me wonder why society, including the long line of women waiting their turn, were okay with such low operational standards.
“When I decided to start my career as a permanent makeup artist, I was appalled by the lack of regulation and the difficulty in finding clear legal compliance or service guidelines. There were no mandatory qualifications, no infection control requirements, and no need to notify the Council. The training I eventually found was only two days long, leaving me more confused than ever. This was when I realised the issue at hand was much more prevalent.”
Sara set out on a journey to develop her own training program while learning the craft herself.
“My goal was to create materials that answered all the questions I had during my quest for competency. There were significant gaps to fill, particularly in clinical etiquette.”
Her determination to advocate for higher industry standards, especially in health and blood safety, was solidified when she began teaching at her academy. Despite including
Blood Borne Pathogens and Infection Control training in her workshops, she still witnessed alarming behaviour.
“One student, ready to treat her first real model, had set up her station with a microblading tool she had used on pig skin during practice. She didn’t see an issue with this until I explained the risks, after which she replaced the tool but didn’t think to change the entire station,” Sara recalled.
“In addition, I’ve seen students drop items on the floor and continue using them, touch other students’ contaminated trolleys, and neglect the essential protective coverings for
reusable items. It was incredibly challenging to instil even the most basic hygiene practices into the artists. If they did this in front of me, a trainer, imagine what they might do behind closed doors.”
Lead by Example
To other PMU artists looking to enhance health and safety in their businesses, Sara’s tips are:
Educate Yourself Thoroughly: Ensure you have a solid understanding of bloodborne pathogens (BBP), infection control, and proper sanitation practices. Continuous education is key; make sure you and your staff complete BBP training annually. Stay connected to local organisations and associations to keep updated with the latest standards and guidelines.
Create and Follow Strict Protocols: Develop comprehensive health and safety protocols for your studio. This includes proper sterilisation of tools, use of disposable materials when possible, and strict hand hygiene. Ensure these protocols are non-negotiable and consistently followed. Additionally, develop an exposure control plan and educate yourself and workers on their obligations around protecting themselves and others.
Set Up a Clinical Environment: PMU procedures require a clean, professional setting. A home environment isn’t suitable. Your workspace should emulate a clinical space to instil trust and comfort in your clients. Regularly disinfect all surfaces and create a layout that minimises crosscontamination.
Lead by Example: The lack of regulation does not absolve us from the responsibility of setting and upholding high standards. It is imperative to model the behaviour you expect from others and to be the catalyst for positive change in the industry. Always adhere to and demonstrate best practices in hygiene and safety, even if no one is watching
Have a go
The OMB Academy’s Blood Borne Pathogen and Infection Control training is free to access. Anyone interested can enrol at ohmybrow.shop/bloodborne-pathogens. A name and email are required for registration, confirmation of course completion and issue of certificate.
by
Photo
Andrej Lišakov on Unsplash
Introducing SAhrps
Hepatitis SA’s peer-based needle and syringe program, NSP Peer Projects, is now called SA Harm Reduction Peer Services (SAhrps). This rebranding emphasises that the program offers more than just needle and syringe program (NSP) services.
Incorporating Harm Reduction into the name underscores the program’s approach to service delivery and highlights that SAhrps workers and volunteers are Harm Reduction peers. They provide nonjudgmental, friendly, peer support and education, as well as harm reduction services aimed at improving the health and well-being of people who inject drugs.
Harm Reduction
Harm Reduction is an approach to drug use that aims to reduce the negative health, social and legal impacts of drug policy and legislation.
It is a way of promoting health and reducing drug related harm that meets people where they are. Harm reduction focuses on reducing the risks and adverse health consequences associated with drug use without requiring
that people stop using drugs.
SAhrps is a team of people who are able to draw on their lived and living experience to engage with people who inject drugs and provide accurate, relevant harm reduction information and services without stigma or value judgement.
SAhrps Peers at NSPs
By placing peers at NSPs, SAhrps can provide non-judgemental service by people who know the culture and are comfortable and knowledgeable talking about safer injecting.
SAhrps Harm Reduction Peers can provide:
• An extended range of new injecting equipment and disposal options
• Sterile water, wheel filters, Sterifilt filters and tourniquets, available in small amounts at no cost
• Peer education and information to support safer injecting practices
• Harm reduction information on issues relating to injecting drug use and health
• Appropriate referrals to health and social services, including drug treatment services
• Information and education on overdose recognition and response, including accessing and administering naloxone
In addition to peers in primary NSP sites, SAhrps has a Sessional Peer Education Project where peer workers are present on a regular day, or days, each week at NSP sites that engage with priority populations.
This collaboration with other service organisations works effectively to enhance the NSP service at host sites by providing an experienced and knowledgeable peer as a trusted and credible source of information, for both the host site staff and service users.
Workforce Training
SAhrps harm reduction peers can also provide workers with training to support engagement with clients who inject drugs. Training topics include:
• Performance enhancing drugs: an introduction which includes commonly used equipment for injecting
• Overdose awareness
• Viral hepatitis education and prevention of blood borne virus transmission
• Vein care
• Common health issues experienced by people who inject drugs and how to prevent them
• How to engage with people who inject drugs
For training or placement of a peer at your organisation, call SAhrps Coordinator, Carol Holly, on 8362 8443 or email carol@ hepatitissa.asn.au
SAhrps is part of a national network of peer-based harm reduction organisations and programs and is the SA member of the Australian Injecting & Illicit Drug Users
League (AIVL), the Australian national peerled peak organisation representing, and advancing the health and human rights of, people who use and inject drugs.
Along with the new name, SA Harm Reduction Peer Services now also has a logo and an email address (SAhrps@hepsa.asn. au) for general information.
SA Harm Reduction Peer Services will continue to be an integral program of Hepatitis SA, working closely with other teams to support and improve the lives and well-being of people who inject drugs, people affected by viral hepatitis, and the organisation’s broader goal of viral hepatitis elimination by 2030.
Visit bit.ly/sahrps-sites for SAhrps peer worker locations.
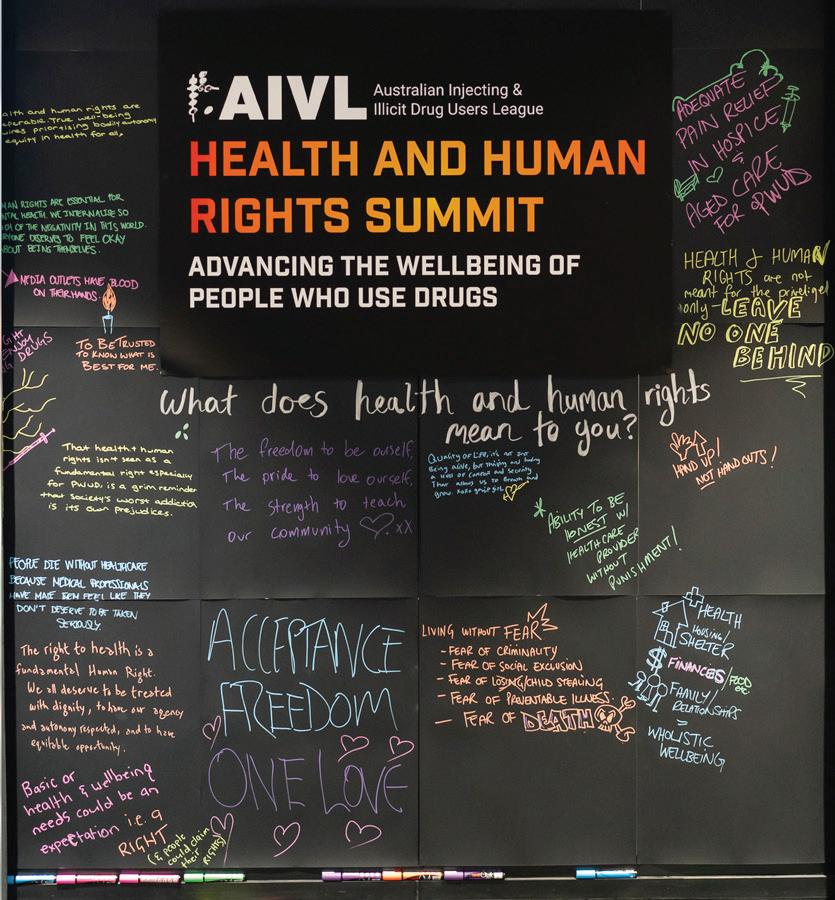
AIVL Health & Human Rights Summit
Held for the first time in Adelaide, the AIVL Health & Human Rights Summit was simultaneously relaxing and inspiring.
What a pleasure it was to have the Australian Injecting and Illicit Drug User League (AIVL) AGM and Summit held in Adelaide (9-11 December 2024). In the past we have gone to Canberra because that’s where the AIVL offices were situated. Much as I like Canberra, we needed somewhere fresh, and Adelaide turned out to be perfect.
When people asked me what to do in their spare time, I said that during the day they should go to the Art Gallery, and in the evening the Botanic Gardens has a glass sculpture exhibition by Dale Chihuly. Everyone was so excited to access these amazing places within a five-minute walk. As you may know, going to these AGMs and summits does not leave a lot of spare time.
I attended the first and third days, because on Tuesday we were filming at Noarlunga, recording peers talking to service users about their experiences at the NSP. We filmed peers talking to me as well, and to be honest that wasn’t great. I wasn’t in a very good mood, and I think that came across loud and clear! But it must have turned out well in the end because the first photo you see on the AIVL website is one of our clients!
“I always enjoy the atmosphere of AIVL AGMs. The lack of judgement, how friendly everybody from all round Australia is, how helpful - leaves a most pleasant feeling. It’s an uplifting environment. My favourite was the talk by the Portuguese delegates from Groups of Activists in Treatment.”
– Penni
On the first day of the summit, the Monday, two members from the Group of Activists in Treatment (GAT) from Portugal, who were
supposed to speak, hadn’t arrived but with some reshuffling of speakers who were present, we were ready to go.
My favourite part of the day was called ‘Setting the Scene: What are our asks for the next 5 years?’, which I liked because we worked with each other to talk about what we want and our expectations. This was done in groups, on butcher’s paper, with many heated discussions about what we want and is it even worth writing it down because it will probably never happen.
“After COVID held us all apart for so long the importance of these events seems even greater – sharing information and knowledge is a core part of how we can improve our services, helping us provide new information and tools for our community.” – Justin Everybody wrote down ‘Respect’: we need to stop discrimination as it physically hurts people and would not be tolerated in any other community. Why is it OK to treat drug users badly? We want the government to stop providing lip service to ideas about harm re-
duction and to actually put more money into real evidence-based harm reduction.
The Australian government formulated harm minimisation as a central part of its national drug policy in 1998, more than a quarter-century ago (the three pillars of the policy are supply reduction, demand reduction, and harm reduction). But harm reduction gets a mere scraping of the available funding. And peer education is one of the most important aspects of harm reduction, yet the government turns its back on us.
‘What are our asks?’ will be made into a document for AIVL and everybody else to work on. Keeping us all connected and on the same page is so very important. We have only ever got anywhere by working in solidarity with each other.
“All attendees got the chance to submit opinions for where AIVL should go from here. The acceptance, equitable input for strategic planning and summaries, combined with the event being in Adelaide, gave me increased feelings of solidarity and keenness to continue to operate with as much positivity as possible in my role.”
– Penni
Hepatitis SA peer Justin did a presentation about getting a drug user organisation off the ground in South Australia. We’ve never had one. We have had peer projects and ser-
vices attached to other organisations, but we have not had one funded by the government to do projects and advocate on its own behalf. What a sterling job Justin did! I was so proud of him because, if it was me, I would be a sweaty, dry-mouthed babbler. It was also interesting to hear from people in other states who didn’t realise SA had never had a drug user organisation.
Tuesday night was the cocktail party—these events are where people relax and introduce themselves to each other. It was also awards night, and it turned out I got the National Peer of the Year award! It was one huge surprise. I did not have a clue.
Well done Carol and Fiona on getting me to the cocktail party. I just thought they were being pushy or just weird. I am still shocked by this award, but am very grateful.
There was a photo booth, so after a few drinks that was a popular spot to be. It was a balmy night, and I was happy to be outside, beside the pool, watching as the fruit bats took their nightly flight from the Botanic Gardens. I think everybody had a great night. I know I did.
Wednesday came and, if I am honest, I was feeling a bit exhausted. Listening to people presenting all day can be quite difficult. Fortunately, the two delegates from GAT in Portugal had arrived by then and they injected fresh energy into the day with their presentations.
“It’s a great opportunity to be inspired. From the incredible drug checking systems in Queensland, Victoria, the ACT, and soon NSW, getting up and running despite heavy opposition, to the incredible work done by GAT in Portugal. They show us what is possible when people and organisations come to together to break down the barriers of
stigma and discrimination that impact drug users every day.”
– Justin
João Santa Maria is a peer worker and co-coordinator at GAT, and Malu Salazar is a harm reduction worker and also co-coordinator at GAT. It was interesting to hear from them, as Portugal puts itself forward as a country that treats drug users with some respect and not as criminals. This is unfortunately not the whole truth—they spoke about the high level of homelessness in Portugal, and how this affects the drug using community.
GAT have a drug consumption room, unlike the medical model we have here. Australia could learn a lot from GAT about how to engage with people without making them feel like outcasts. They have a small space that feels welcoming, is brightly painted by the community, and shows no hint of anything medical. In that area people can also smoke, so GAT has access to people who don’t inject. Their ‘injecting area’ is just a room with a couple of desks and everything that is needed, and there are no staff standing over you.
“Highlights for me were: Margie being recognised on a national stadium as ‘Peer Worker of the Year’, unveiling the new SAhrps logo on a national forum and the support/ response from the AIVL membership, and “One Stop Shop’ for People Who Use Drugs: Peer Led Harm Reduction Service in Lisbon Portugal.”
– Fiona
The word ‘treatment’ in the name Group of Activists in Treatment refers to treatment of hepatitis, STIs, HIV, and tuberculosis, not drug treatment. They get people onto treatment, help people with food and emergency assistance, and advocate for people who use drugs. As an NGO, GAT do a huge amount to promote the right for everyone to access health care, no matter who they are. João Santa Maria was a passionate speaker, and even though he was speaking through an interpreter his passion and humour about absurd situations shone through.
The day ended with everybody very tired but happy. It was so good to hear people say Adelaide was the best, the most relaxing AGM/Summit they had been to. Everyone was relaxed—and maybe a little hungover from the cocktail party—but there were smiles all around.
“It was a great conference which covered aspects of discrimination and human rights, a relaxed environment with loads of information sessions and insights into other NSP sites around the country. I found it inspiring and well worth the time and effort.”
– Mark
“It was interesting and informative, really good to meet peers from other orgs and the AIVL team members, hearing about their issues and positive impact. It helped me understand the strong reach we have with community.”
– Andrea
These meetings are the times we get to network and meet people face to face rather than online, or meet people we never would otherwise. Having the glass art in the botanic gardens was a plus. I took a couple of the Western Australia delegates there and they were so surprised how close and easy it was. Go Adelaide!!
As for me, I would love to get our community to enter the AIVL Art project in 2025 or start doing our own workshops, and I am still in a cloud of happiness that two of our SAhrps peers have been awarded for our contributions to the community this year.
Margie Randle SAhrps Peer with contributions from the SAhrps team
Are community pharmacies the answer to boosting hepatitis C testing and cure in under-served groups? A new Burnet Institute study finds introducing a hepatitis C outreach and treatment program in Australian community pharmacies, particularly those already offering methadone or buprenorphine treatment for opioid users, could significantly increase testing, diagnosis, and cure of those living with the virus.
This would be extremely valuable in saving lives and reducing the nation’s health burden, and could be vital if Australia is to reach its target of eliminating viral hepatitis by 2030, which is now just five years away. Even with our current progress, more than 6,000 new hepatitis C infections still occur each year.
The Burnet study, ‘Cost-Effectiveness of Treating Hepatitis C in Clients on Opioid Agonist Therapy in Community Pharmacies Compared to Primary Healthcare in Australia’, was published in the Journal of Viral Hepatitis last month. It demonstrates that providing testing and treatment in more accessible locations, like community pharmacies, can make a real difference.
Despite initial costs, this approach has been proven cost-effective compared to standard care, particularly by reaching under-served populations who might otherwise slip under the radar or actively avoid other healthcare environments.
Study co-author Dr Joshua Ginnane explained how this avoidance actively correlates with increased viral hepatitis risk. “For some people, accessing testing and treatment for hepatitis C through mainstream healthcare services can be difficult due to stigma, limited access, associated costs, and competing priorities,” he said.
“People on opioid replacement therapy often attend their pharmacy multiple times per week and develop good relationships with the health professionals on site.”
In the model, adding the outreach program pathway to pharmacies increased the number of tests from 4178 to 8737 (more than double), the number of diagnoses from 615 to 1285 (also more than double), and the number of cures from 223 to 777 (more than triple) among people on OAT over a 12-month period.
This research forms the foundation of the new EXPAND-C initiative, led by deputy program director of Disease Elimination Professor Joe Doyle, which aims to expand access to hepatitis C testing and treatment through community pharmacies, beginning in Victoria. In the next 24 months, it hopes to conduct more than 1,800 tests, identify up to 600 individuals with hepatitis C and cure hundreds of people living with hepatitis C in that state.
EXPAND-C will also establish a sustainable model for pharmacies to offer testing and treatment for other communicable diseases, thereby strengthening the link between community pharmacies and primary healthcare services. This can then be expanded to cover the whole of Australia, with suitable funding.
READ MORE:
onlinelibrary.wiley.com/doi/10.1111/ jvh.14015
Professor Joseph Doyle, left, leads the EXPAND-C project
First Hepatitis B Rapid Testing in SA
Site Principal Investigator, Lisa Carter testing one the first participants while educators at the far table discuss consent with participants and help them complete a survey
After a long wait, hepatitis B point-ofcare testing finally made its appearance at a community testing event in Adelaide. Hepatitis SA launched the first hepatitis B rapid testing clinic in SA, aptly run on the first day of the first-ever World Hepatitis Testing Week, with the support of Chinese Welfare Services of SA (CWS), a community service organisation that has been operating in the heart of Adelaide city since 1991.
The new hepatitis B rapid test was deployed in a testing clinic that is part of a pilot study to enhance assessment of liver disease and viral hepatitis among migrant and multicultural communities.
The pilot, a sub-study of National Australian Hepatitis C Point-of-Care Testing Program, will conduct hepatitis testing and liver health testing with adult members of multi-cultural migrant communities, to assess the rate of hepatitis C and hepatitis B infection among those tested. All participants receive a $30 shopping voucher.
Due to traffic congestion from Adelaide 500 road closures, the morning started later than planned and participant numbers built up quickly as a result. We were really glad our site Principal Investigator, Lisa, decided at the last minute to invite REDCap data entry veteran, Deborah, to come along to lend a hand. The appearance of our intrepid Chinese-speaking volunteer Vivien, who had battled her way through a 10-minute-turned40-minute journey, made us even happier, as all hands were needed to answer questions, direct participants, provide distraction to alleviate anxieties, and interpret instructions.
Participants are given a diagnostic test for hepatitis B and a screening test for hepatitis C. The hepatitis B diagnostic test looks for the hepatitis B surface antigen, which is a marker of current infection. The hepatitis C test used in this pilot study is the newly approved test that looks for hepatitis C antibodies, which are indicative of either prior or current hepatitis C infection. Both
Results for HCV antibody test delivered in 60 seconds in the ‘membrane unit’ (a single dot means no hepatitis C antibody detected)
tests are carried out with tiny amounts of blood extracted via finger pricks. The hepatitis B test returns results in 15 minutes, and the hepatitis C antibody test in an incredible 60 seconds.
Participants who return positive for hepatitis C antibodies will receive the hepatitis C RNA test using GeneXpert rapid testing technology, and those who return positive for hepatitis B antigen will have a larger blood sample taken, which is sent to the laboratory for the standard panel of hepatitis B tests. Those who return positive for hepatitis C antibody or have had previous hepatitis C infection, will also be given a rapid HIV test.
At the end of the testing-run, participants are given a fibroscan and consultation with a healthcare provider. In this case, it was viral hepatitis nurse, Jeffrey Stewart.
The Liver Care pilot is currently being run in New South Wales and South Australia. The simplicity of the testing process meant it was possible for it to be done by trained community workers and can easily be taken into communities.
This first clinic proved a useful experience. We learnt which arrangements improved workflow, identified potential pitfalls and roadblocks, saw firsthand the importance of cultural peers in fostering community receptiveness and the potential for running more testing clinics.
A total of 21 participants were tested and given fibroscans. Hepatitis SA educator, Jesse Chen, the key liaison between Hepatitis SA and CWS, extended his heartfelt thanks to the CWS team for their invaluable support. “Everything went smoothly. The CWS team’s professionalism and warm hospitality made a significant difference,” he said. This sentiment was strongly endorsed by the rest of the Hepatitis SA team, and gratitude was also extended to Viven without whom there would have been a lot less laughs and, more seriously, some participants left waiting for language support.
The Hepatitis SA team is looking forward to reaching out to other communities, and in time returning to the Chinese community. CWS has invited the Hepatitis SA team back, anytime.
REDCap data entry veteran, Deborah, getting the data in while educators Jesse (left) and Yingbin go through the preliminaries of consent and survey with the next participants. Mirror reflection shows Education Coordinator, Jen, preparing for the next test
World Hepatitis Testing Week
The first ever World Hepatitis Testing Week started on 18 November 2024. Inspired by the European Testing Week campaign, which had been running twice a year since 2013, World Hepatitis Testing Week is a part of a global effort to encourage people to get tested for hepatitis B and hepatitis C. Testing is the first step to getting life-saving care for these two diseases that are the leading causes of liver cancer.
Despite the availability of effective vaccines and treatments, the World Health Organization’s consolidated global report on viral hepatitis reported that there are over 3,500 hepatitis-related deaths each day worldwide and the data shows these deaths are increasing.
In Australia, close to 300,000 people live with hepatitis B or hepatitis C and liver related deaths are estimated at around over 1,000 each year. One in four Australians living with hepatitis B, and one in five living with hepatitis C, don’t know they have it. This puts them at risk of liver cancer, serious liver disease and premature death.
For individuals, early detection is key to reducing the risk of serious liver disease and testing is an essential part of that process. Hepatitis C testing is now simple and accessible, with rapid point-of-care testing available at community venues. These rapid tests return results in an hour, or the same day, depending on the length of the queue.
In addition, a 60-second hepatitis C antibody test has recently been approved. When
used as a screening process to filter out those with no previous exposure to the virus, the rapid antibody test will reduce the queue for confirmatory RNA tests where results take 60 minutes instead of 60 seconds.
Rapid tests for hepatitis B are also expected to be available soon with a sub-study being run as part of the national Hepatitis C Pointof-Care Testing Program, which is coordinating community-based testing clinics around the country.
At a broader level, the viral hepatitis elimination campaign in Australia has slowed after the initial surge in treatment uptake from cases whom healthcare providers had heldin-wait for the introduction of new hepatitis C treatments. Restrictions during the COVID-19 lockdowns had also reduced testing and diagnosis rates.
Increasing access to testing is crucial to Australia meeting the target of viral hepatitis elimination by 2030. Providing testing services at the community will facilitate diagnosis, but more awareness among community workers and the wider community is needed to encourage people to come forward for testing. World Hepatitis Testing Week is part of that awareness raising process.
To find out more about viral hepatitis testing and how you can get tested, call Hepatitis SA on 1800 437 222. For testing clinics in South Australia, check out the Testing Clinics Calendar at bit.ly/heptestcalendar.
In Memory of William Donohue
Hepatitis SA staff were saddened to hear of the passing of Dr William Donohue. Not all of us have met him personally, but we were all aware of his significant contributions to the hepatitis- and HIV-affected communities. He typified the energy and commitment of the early days of the hepatitis C community movement—commitment he carried through his career.
Hepatitis SA was fortunate to have Dr William Donohue work as a Rural Educator back in 2000 and 2001 when we were the Hepatitis C Council SA. He took to the role with passion, running group and individual education sessions and developing support groups.
Practice, at Adelaide University. The program focused on supporting people to maintain and improve their health and wellbeing as well improve prevention support to people at risk.
He had a particular interest in promoting hepatitis C awareness in prisons and Indigenous communities, travelling extensively during this period to rural and remote locations. He carried out activities with prisoners, prison health staff and officers, and worked closely with the Aboriginal Drug and Alcohol Council to raise awareness about hepatitis C-related issues.
Colleagues from those days recall that William had the knack of making complex medical information accessible for people, something extremely valuable at a time of high stigma and discrimination for people living with hepatic C.
In 2001, William went on to work with the ‘C-Clearly’ program in the Health and Human Diversity Unit of the Department of General
The Commonwealth-funded program aimed to reduce hepatitis C transmission in South Australia, provide holistic services (including dietitians and psychologists) to people living with or at risk of hepatitis C, and increase the pool of health workers with the knowledge and skills to care for people living with or at risk of hepatitis C.
In later years, William was known as the key driver behind the O’Brien Street Practice, which works in partnership with SA Health to provide comprehensive primary health care with a focus on HIV and sexual health. The O’Brien Street Practice is well known as a friendly, supportive GP clinic in Adelaide. To Hepatitis SA workers, it was always that open, friendly clinic where the hep-friendly GP, William Donohue, worked, and to whom we could safely refer clients.
Although William was with Hepatitis C Council SA for only 18 months, his impact lasted far beyond that. To many, he was not only a colleague but a treasured friend. Everyone who knew him remembers William as someone with a lovely smile, a great sense of humour and a laugh which they will always recall.
William Donohue will be greatly missed.
Is hepatitis sexually transmitted? What is ‘safe’? Who is at risk? These are some fundamental questions affecting almost everyone who lives with viral hepatitis.
These resources will help you find out what you need to know, even if you were afraid to ask!
The facts
Hep C factsheets: sex and transmission
Hepatitis NSW. Sydney, 2023. 3p. factsheet
In Our Library Sexual transmission: the facts
Information about the general methods of hepatitis C transmission; whether it’s possible that it can be transmitted during sex; how it might affect relationships; safe sex and sexually transmitted diseases; and safe sex info for men who have sex with men. bit.ly/hcvsex
Hepatitis B and relationships
Hepatitis Australia, Canberra, 2020. 1p. article
Although most people get hepatitis B at birth, it can be transmitted in other ways including sex. This article contains information about how it is spreads, how to
communicate your diagnosis to those who may be affected, and how you can keep your partner safe. With reference links to further information. bit.ly/hbvrelation
How to stay safe
True or Gammon - STIs with Janty and Jecinta
Aust Dept of Health and Aged Care, Canberra, 2024. Video 6 minutes
Deadly comedian Janty Blair yarns with Aboriginal Health Practitioner, Jecinta from Darwin, NT. In a relaxed and humorous way they shed light on some myths about STIs. Primarily aimed at a female audience. bit.ly/truthorgammon
True or Gammon - STIs with Aaron and Tawhio
Aust Dept of Health and Aged Care, Canberra, 2024. Video 5:30 minutes
Aaron Fa’aoso sits down with deadly Aboriginal Health Practitioner, Tawhio from Tennant Creek, NT. to answer all your ‘burning questions’ about STI’s. This one is aimed primarily at men. bit.ly/truthorgammon2
Beforeplay
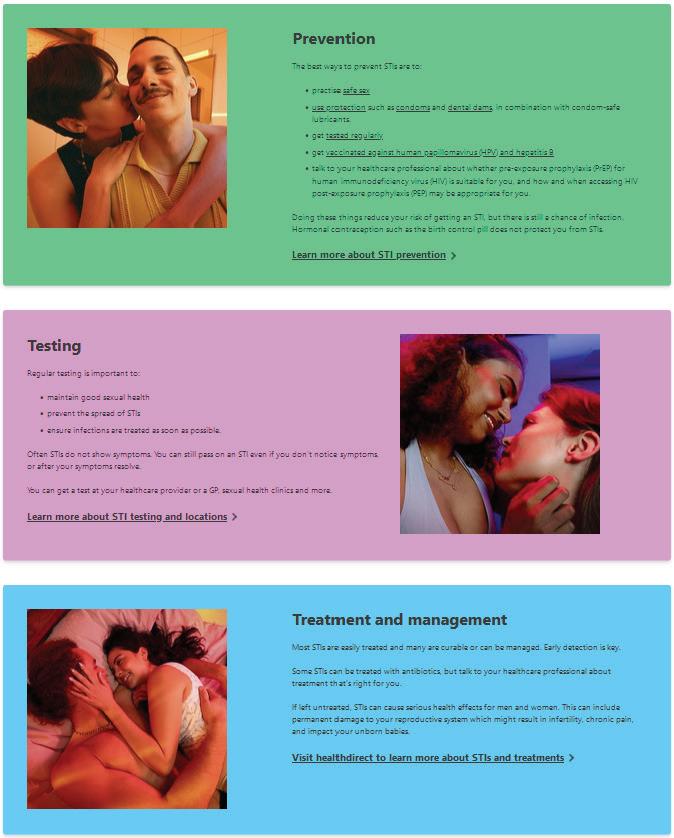
Aust Govt Dept of Health and Aged Care, Canberra, 2024. Website
Comprehensive information about sexual health for young people in the form of videos, posters, fact sheets and FAQs. The site covers prevention,
testing and listings of local services and resources – with a section specifically for First Nations peoples and one with translated materials. health.gov.au/sti
Get tested: Better to know
Aust Federation of AIDS Organisations Anwernekenhe National HIV Alliance, Sydney 2022. Website
Sexual health resource for Aboriginal and Torres Strait Islander people with information about common STIs, what to do and where to get tested. bettertoknow.org.au
Dating in Australia - sexual health
Family Planning Victoria, 2020. Video 3:12 minutes
How do international students in Australia feel about accessing sexual health services? Family Planning Victoria speaks to young people about how to navigate the health system. Part of a series of 7 videos. bit.ly/datingoz
Find a service
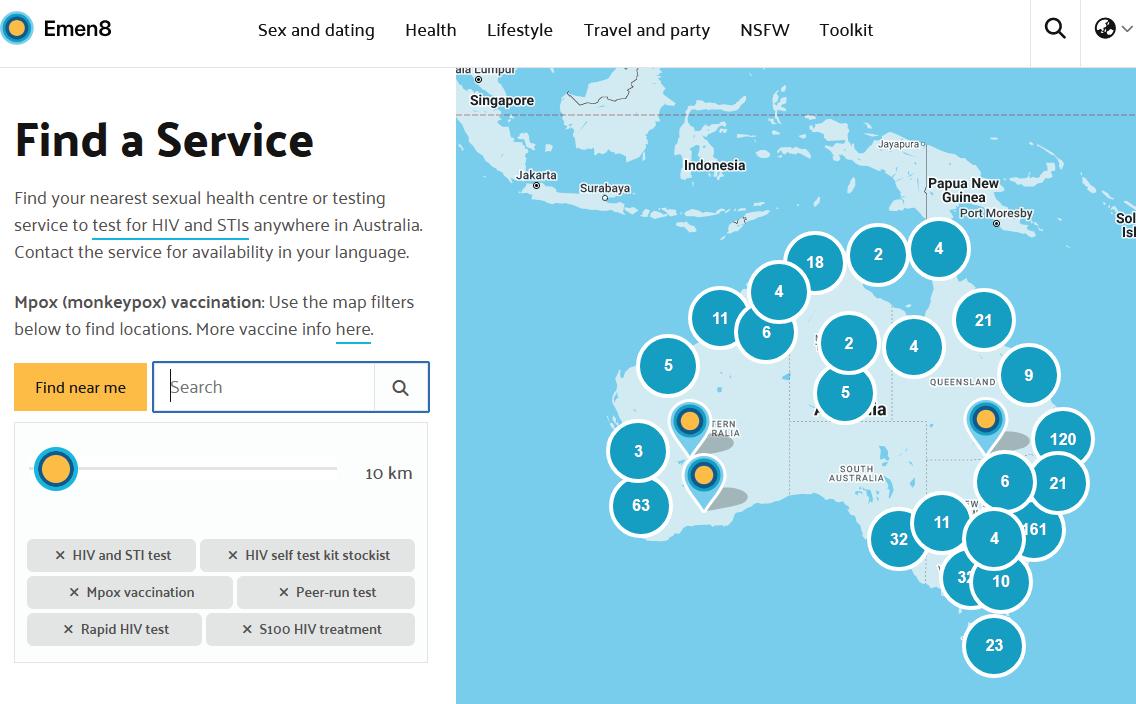
Emen8, Australia
Sexual health and wellbeing initiative for gay, bisexual and other men who have sex with men: link goes to the search engine for STI testing sites including those run by peers. emen8.com.au/find-a-service
Play safe (safe sex)
NSW Health, Sydney, 2021. Website.
Includes comprehensive information about who should get tested, what testing involves, and how much it might cost. Includes searchable list of where to get tested in all states and territories. playsafe.health.nsw.gov.au
For complete listings of resources available online for this topic go to Hepatitis SA Library
Catalogue at bit.ly/ hepsasex
Hepatitis SA provides free information and education on viral hepatitis, and support to people living with viral hepatitis.
Postal Address:
Kaurna Country PO Box 782
Kent Town 5071
(08) 8362 8443 1800 437 222
www.hepsa.asn.au
Community News: hepsa.asn.au/ communitynews
Library: hepsa.asn.au/library
@HepatitisSA
@hep_sa
Resources: issuu.com/hepccsa
Email: admin@hepatitissa.asn.au
Free hepatitis A, B and C information, confidential and non-judgemental support, referrals and printed resources.
We can help. Talk to us. Call or web chat 9am–5pm, Mon–Fri
Information Support
HEPATITIS SA BOARD
Chair
Arieta Papadelos
Vice Chair
Bill Gaston
Secretary
Sharon Eves
Treasurer
Michael Larkin
Ordinary Members
Lindy Brinkworth
Bernie McGinnes
Janice Pope
Memoona Rafique
Lucy Ralton
Tamara Shipley
Kerry Paterson (CEO)
Hepatitis SA has a wide range of hepatitis B and hepatitis C publications which are distributed free of charge to anyone in South Australia.
To browse our collection and place your orders, go to hepsa.asn.au/orders or scan the QR code below:
Viral Hepatitis Community Nurses
Viral Hepatitis Nurses are nurse consultants who work with patients in the community, general practice or hospital setting. They provide a link between public hospital specialist services and general practice, and give specialised support to general practitioners (GPs) to assist in the management of patients with hepatitis B or hepatitis C. With advanced knowledge and skills in testing, management, and treatment of viral hepatitis, they assist with the management of patients on antiviral medications and work in shared care arrangements with GPs who are experienced in prescribing medications for hepatitis C or accredited to prescribe section 100 medications for hepatitis B. They can be contacted directly by patients or their GPs:
CENTRAL ADELAIDE LOCAL HEALTH NETWORK
Queen Elizabeth Hospital
Phone: 0423 782 415, 0466 851 759 or 0401 717 953
Royal Adelaide Hospital
Phone: 0401 125 361 or (08) 7074 2194
Specialist Treatment Clinics
NORTHERN ADELAIDE LOCAL HEALTH NETWORK
Phone: 0401 717 971 or 0413 285 476
SOUTHERN ADELAIDE LOCAL HEALTH NETWORK
Phone: 0466 777 876 or 0466 777 873
Office: (08) 8204 6324
Subsidised treatment for hepatitis B and C are provided by specialists at the major hospitals. You will need a referral from your GP. However, you can call the hospitals and speak to the nurses to get information about treatment and what you need for your referral.
• Flinders Medical Centre Gastroenterology & Hepatology Unit: call 8204 6324
• Queen Elizabeth Hospital: call 8222 6000 and ask to speak a viral hepatitis nurse
• Royal Adelaide Hospital Viral Hepatitis Unit: call Anton on 0401 125 361
• Lyell McEwin Hospital: call Bin on 0401 717 971
Visit hepsa.asn.au - no need to log in, lots of info & pdates
Follo the HepSAY blog - hepsa.asn.a /blog
Order print resources - hepsa.asn.a /orders/ Follo s on T i er @hep_sa or Facebook @Hepa sSA
Full range of syringes and needles. Water and filters also available in limited quantities for free.
Free hepatitis A, B and C information, confidential and non-judgemental support, referrals and printed resources. We can help. Talk to us. Call or web chat 9am–5pm, Mon–Fri