◼ Non atypical (CCC, columnar cell hyperplasia): B2excision not required.
◼ Atypical: FEA/atypical intraductal proliferation:B3 further tissue examination, submit all tissue, look for ADH, DCIS, invasion.
◼ High grade cytological atypia: DCIS (flat type), B5a
New B3 Management guidelines
◼ Second line VAB (VAE =Vacuum Assisted Excision) is the method of choice for further sampling of B3 lesions.
◼ This applies to all B3 lesions except: papilloma with atypia, cellular fibroepithelial lesions and other rare B3 lesions (spindle cell lesions, vascular lesions…etc).
Third International Consensus
◼ Swiss Minimal-Invasive Breast Biopsy (MIBB) Working Group
◼ Voting by experts: 11 pathologists, 12 radiologists, and 10 specialist gynecologists/specialist medical oncologists/breast surgeons from seven European countries.
◼ If a core-needle biopsy (CNB) returned as B3 lesion on histology, should the lesion be excised?
◼ If so, should it be excised using vacuum-assisted biopsy (VAB) or open surgical excision (OE)?
◼ If the VAB returned a B3 lesion on histology and if the lesion was completely removed on imaging, is surveillance acceptable or should a repeat VAB or OE be performed?
Elfgen et al Virchows Archives 2023 483, pages5–20 (2023)
Summary of atypia follow up
◼ Current UK guidelines, a yearly mammographic follow up for 5 yrs, still apply.
◼ Consult with colleagues and audit your B3 rate.
◼ ? Effect of digital reporting on atypia diagnosis.
◼ Ongoing work to refine follow up strategies.
◼ Various guidelines available for management
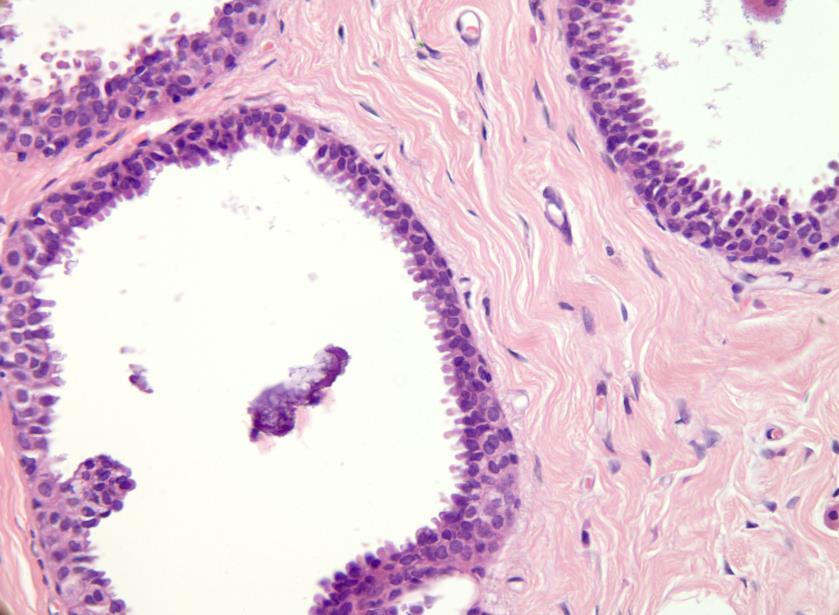
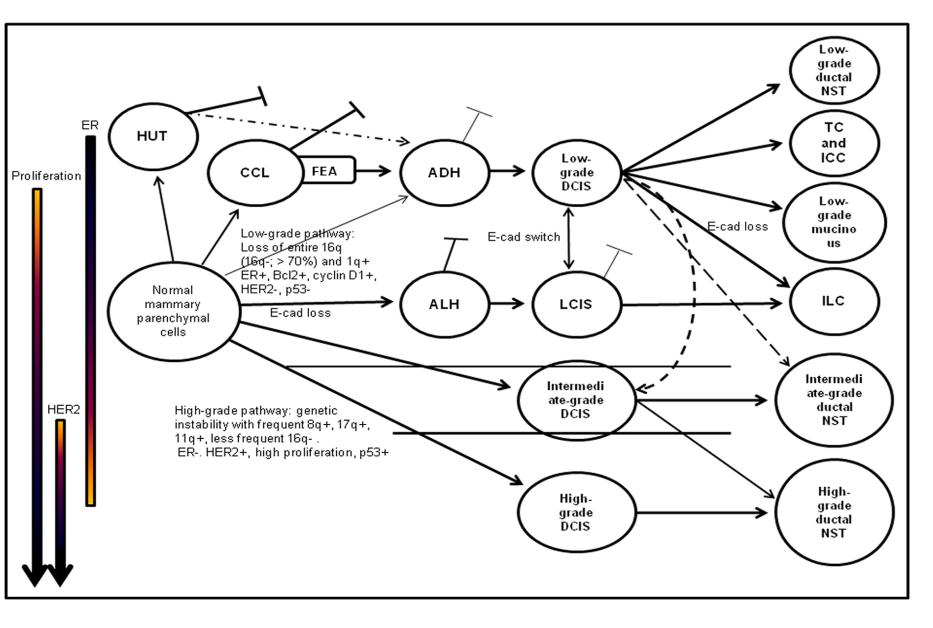
Columnar cell lesions in surgical excision
◼ With atypia: good sampling to exclude more advanced lesions.
◼ Part of low nuclear grade neoplasia lesions.
◼ Associated lesions
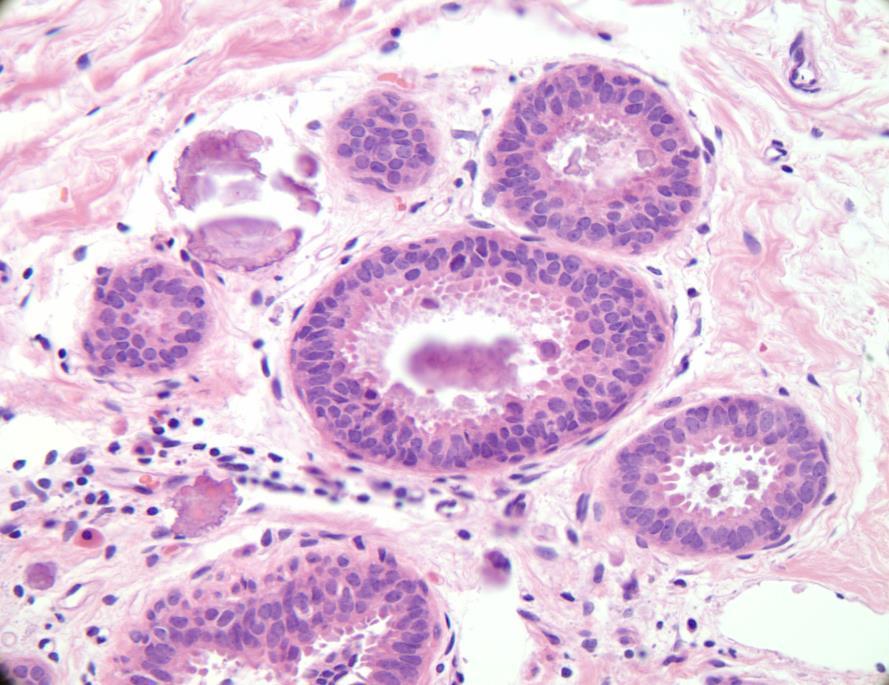
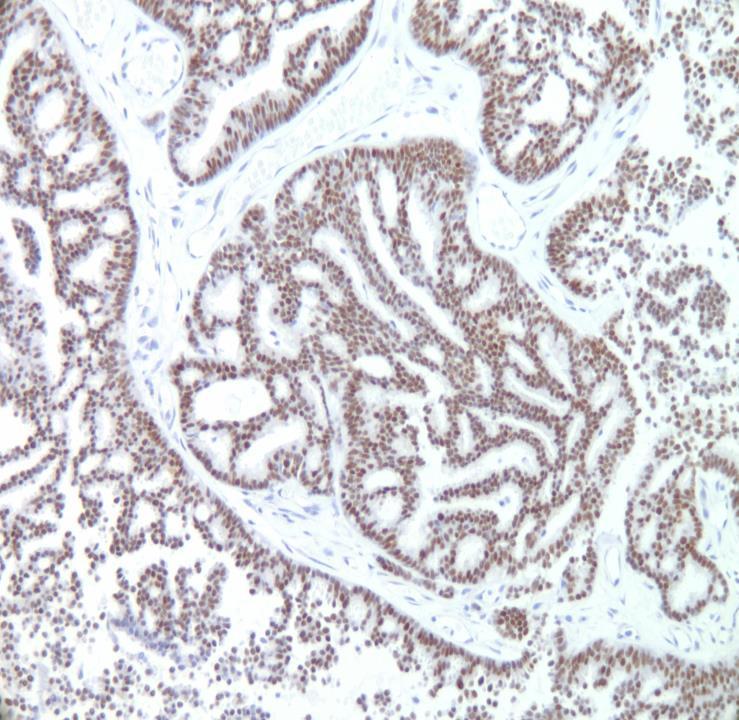
FEA and Lobular insitu neoplasia
Key diagnostic points
◼ FEA with relevant calcifications.
◼ No ADH, DCIS or invasive carcinoma.
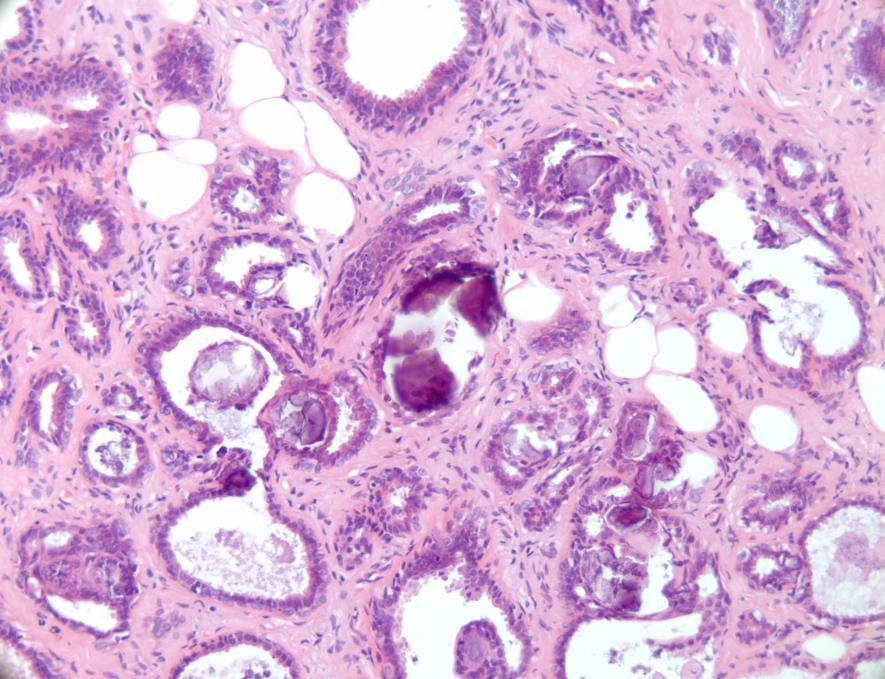
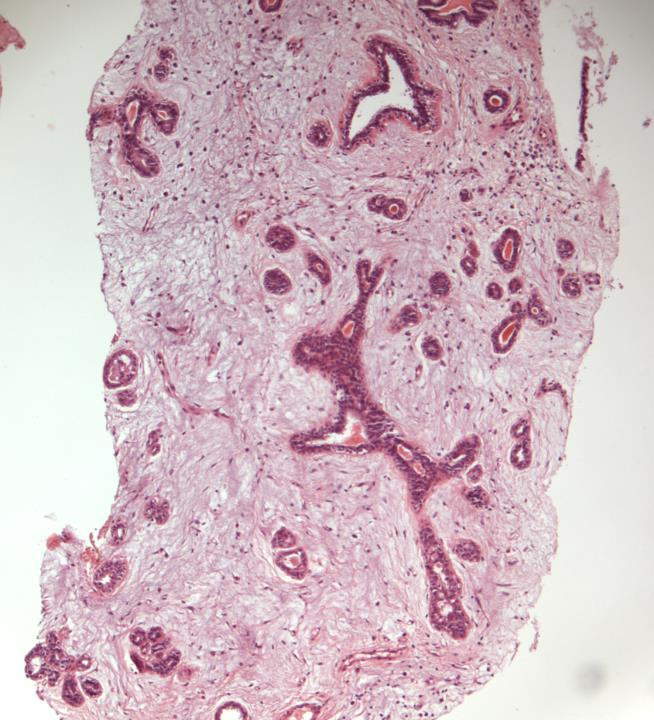
Case 4
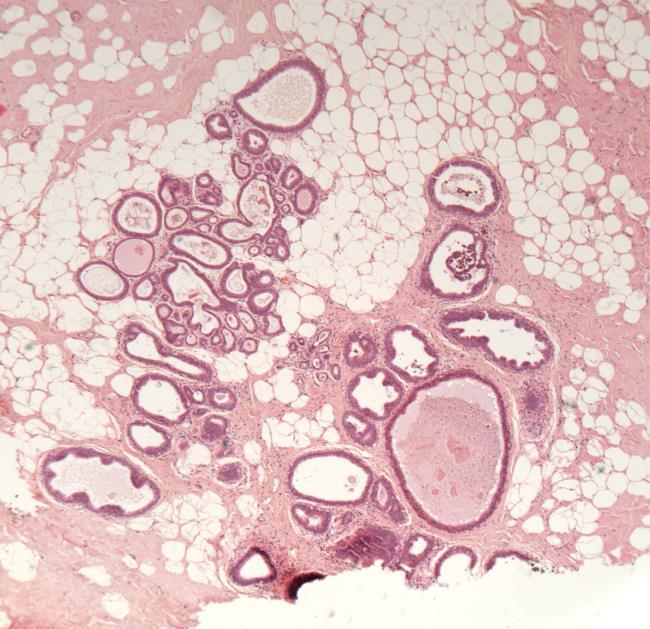
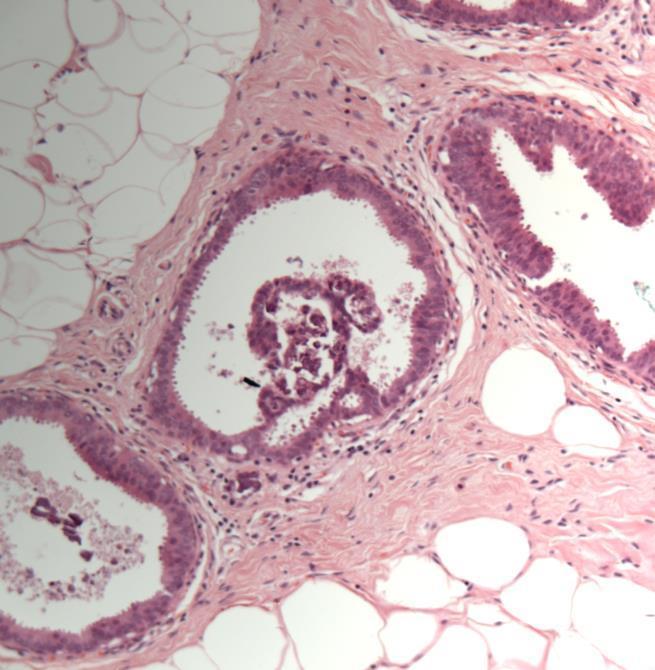
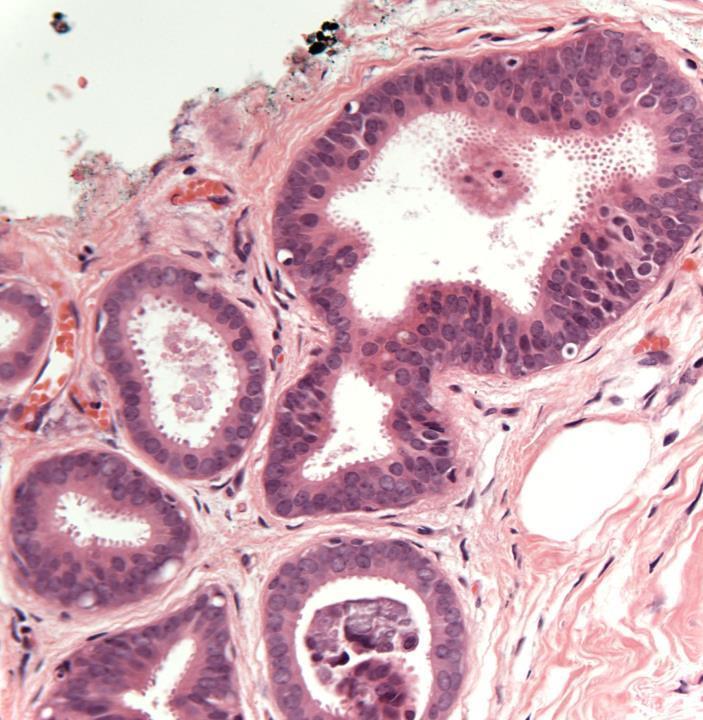
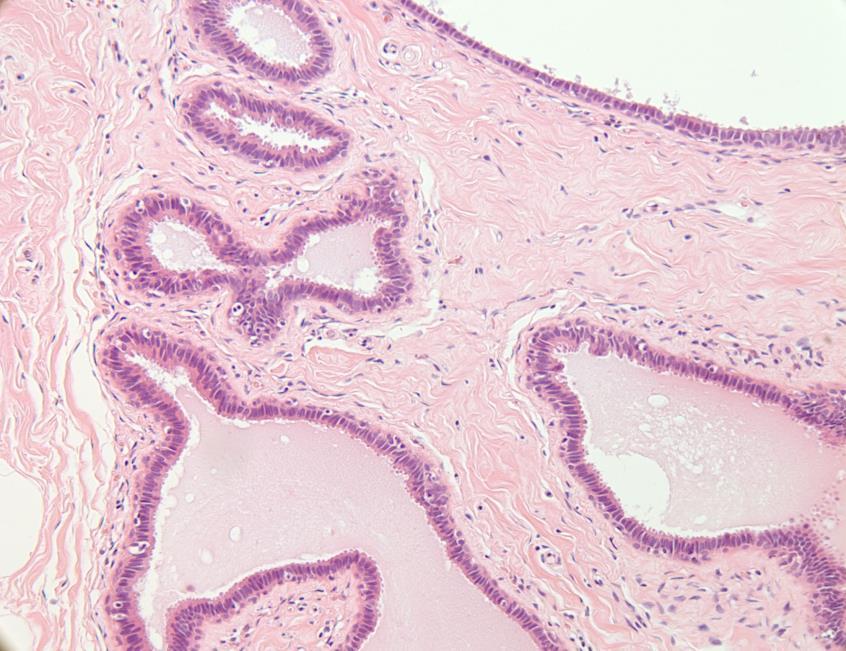
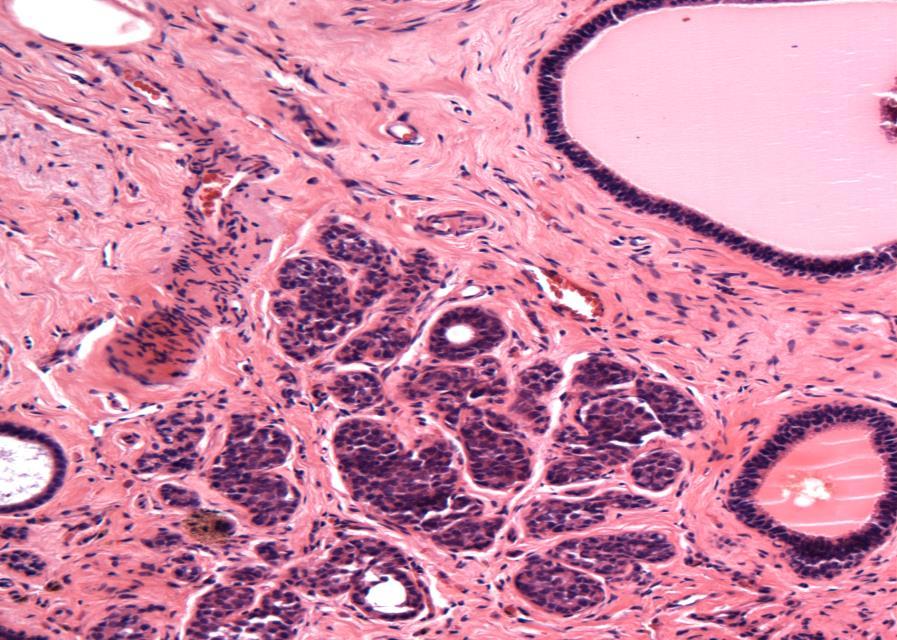
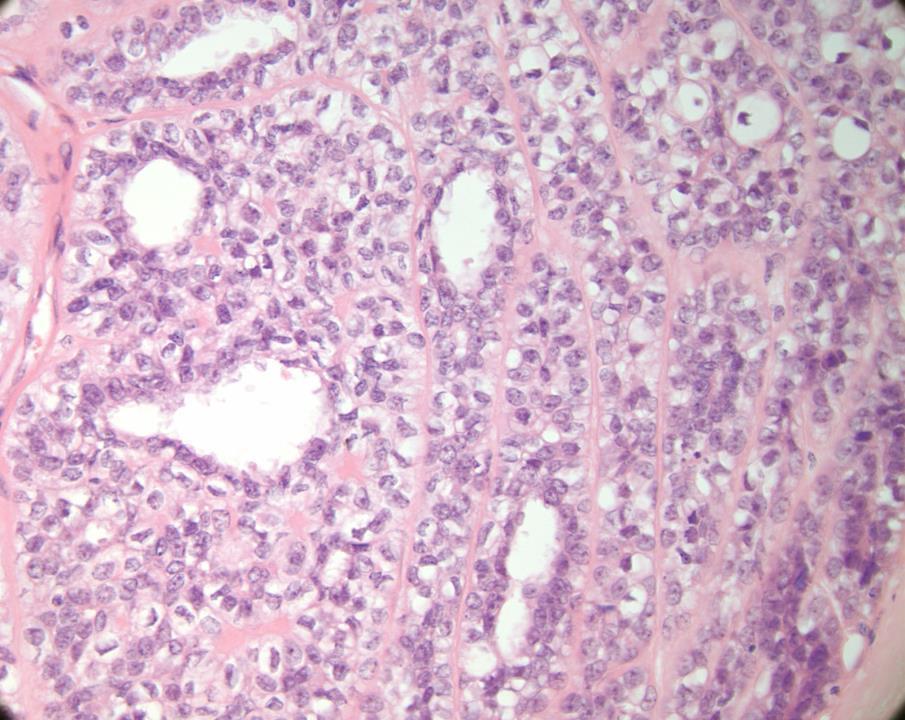
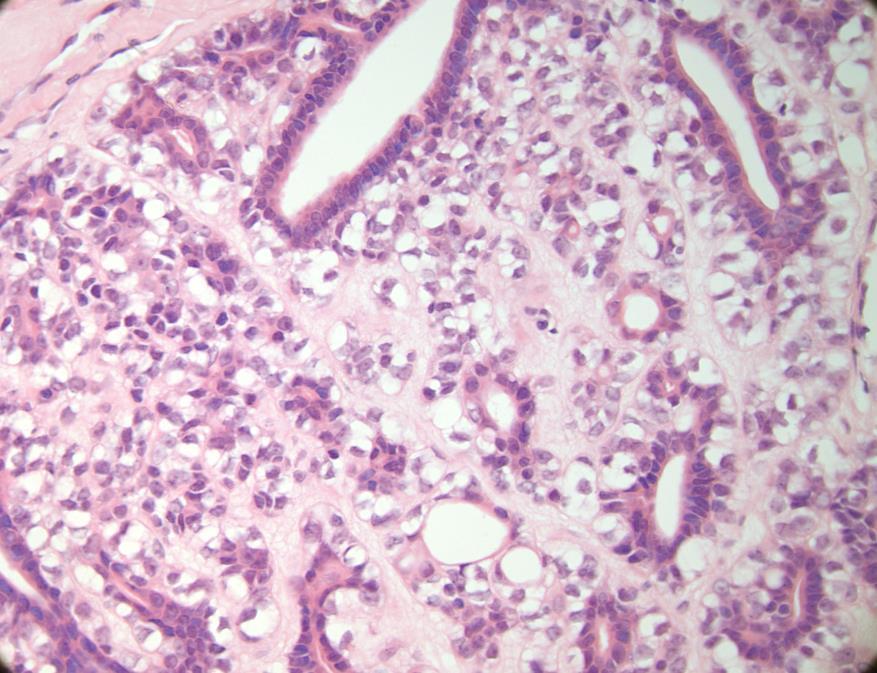
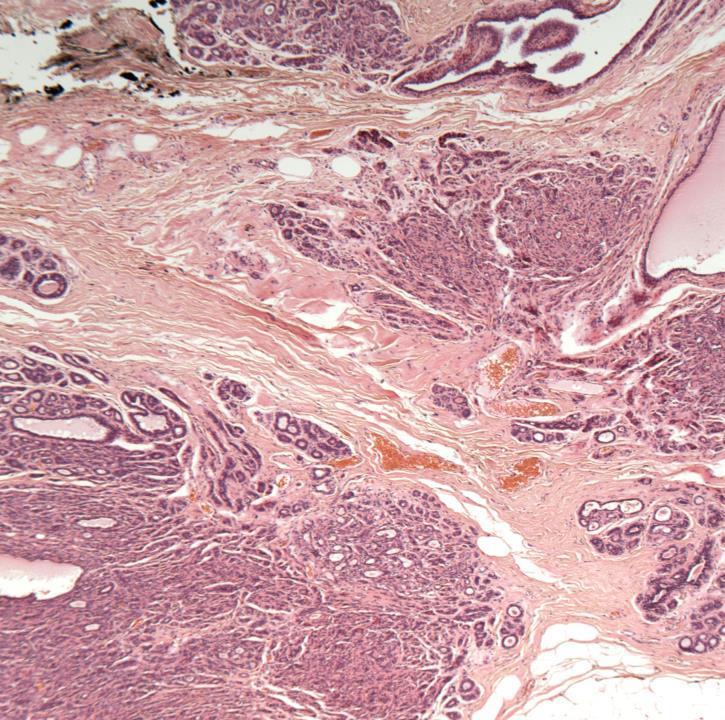
◼ Intraduct papilloma with florid epithelial hyperplasia
and fibrosis
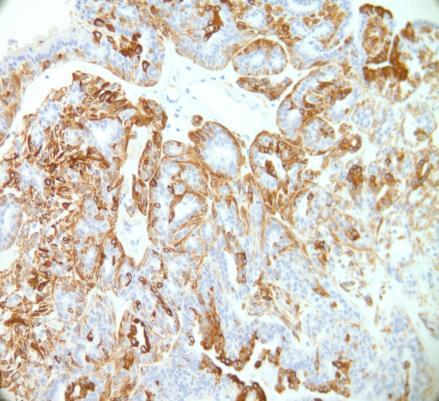
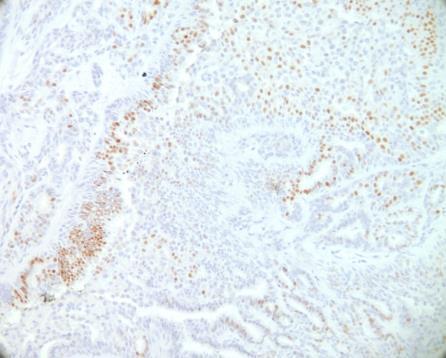
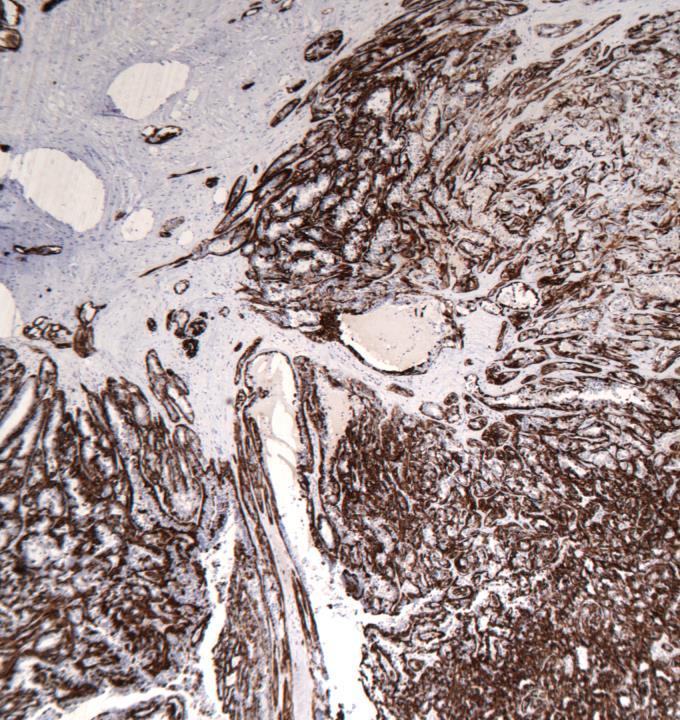
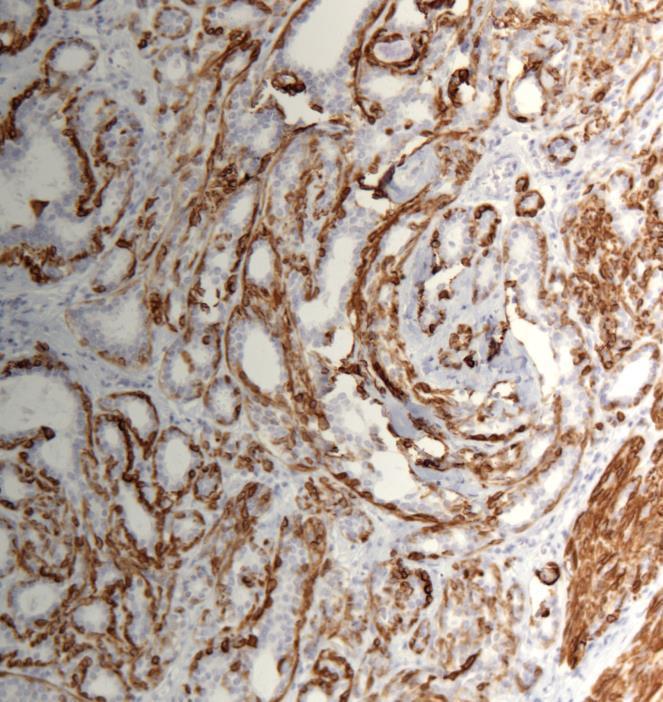
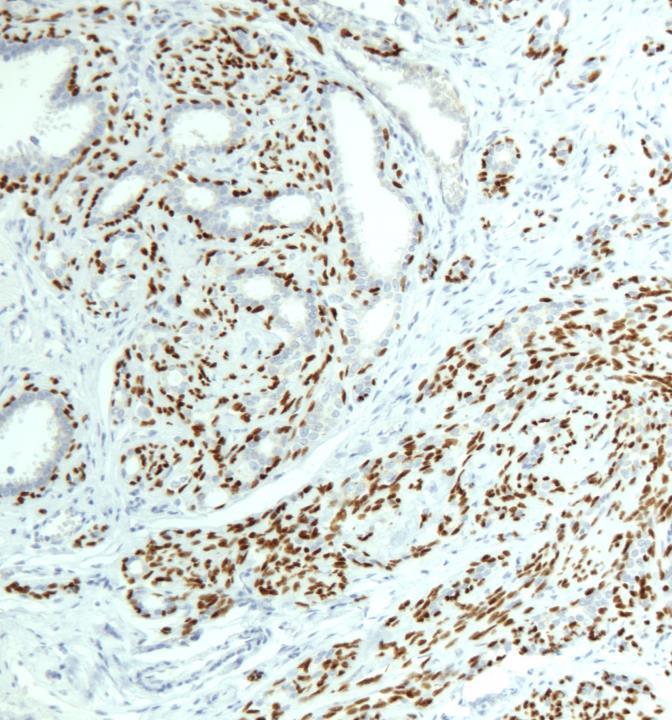
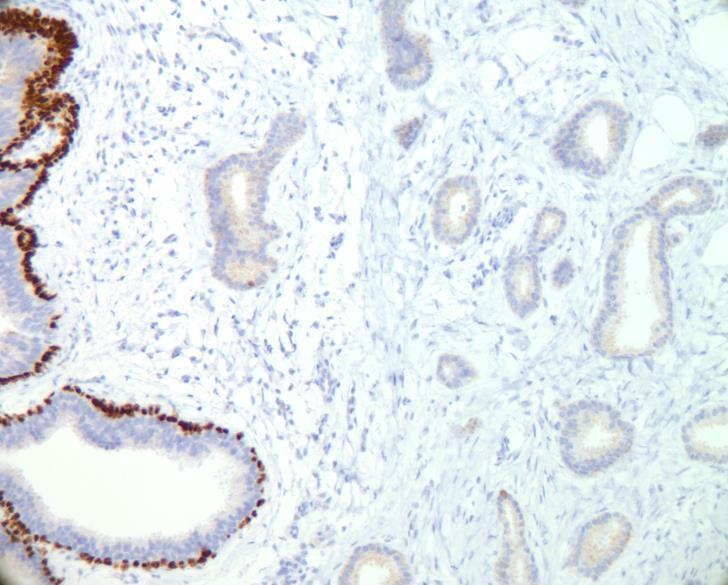
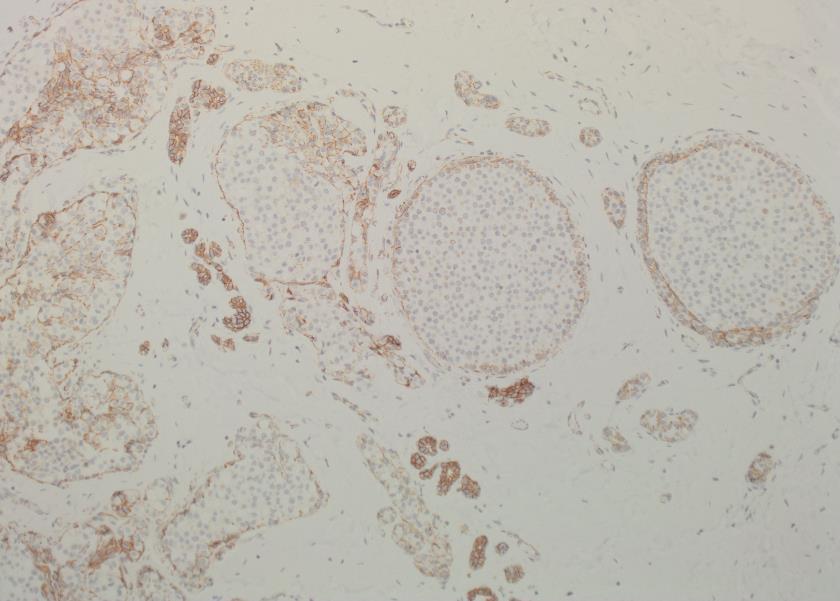
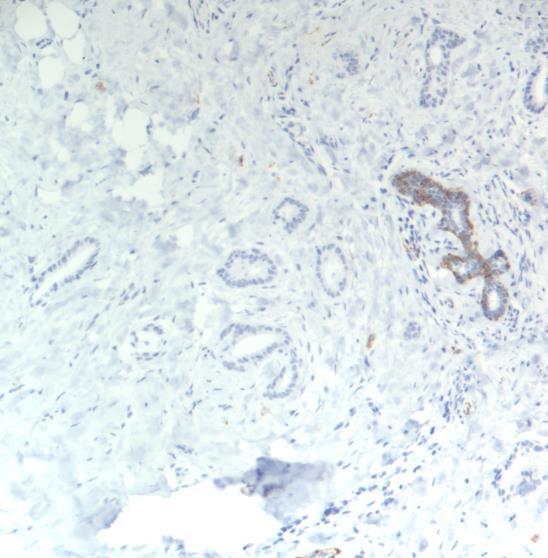
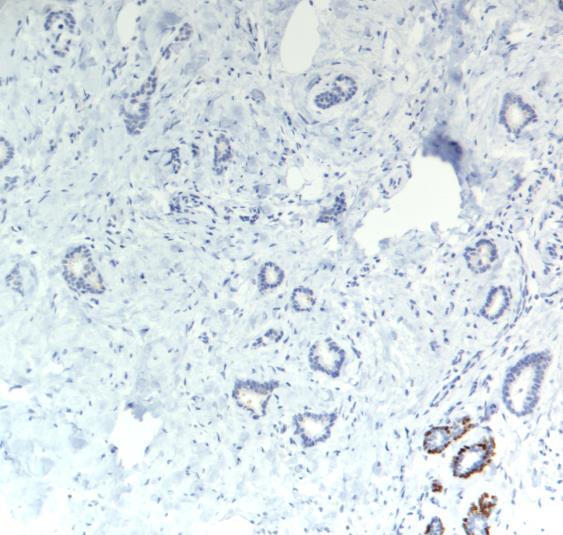
Useful Immunohistochemistry
Papilloma Papillary DCIS CK5
ER Patchy pos
Uniformly pos
SMM present absent
Tips
◼ Assess the overall architecture of the lesion
◼ Look for myoepithelium
◼ Examine solid areas in detail
◼ Look for involvement of adjacent lobules (DCIS)
◼ IHC can be helpful to support your morphological diagnosis
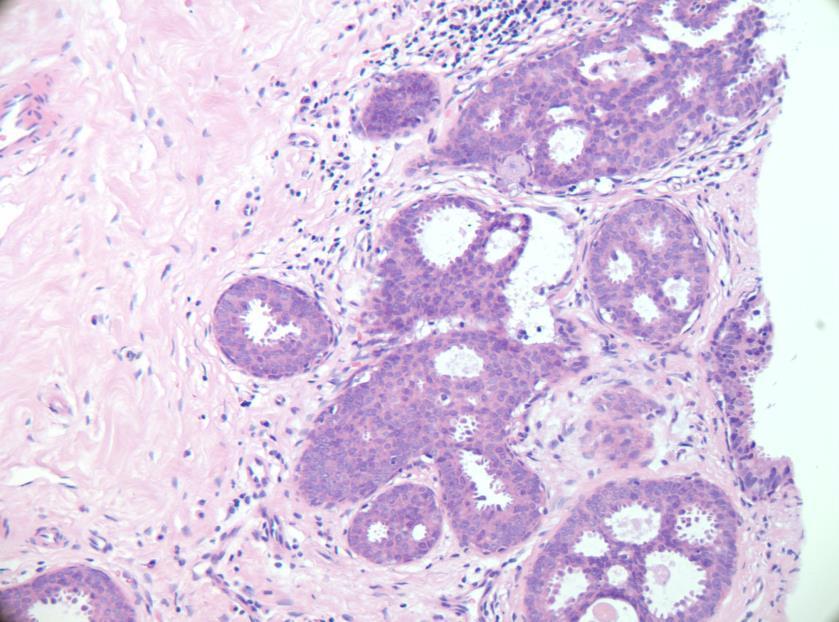
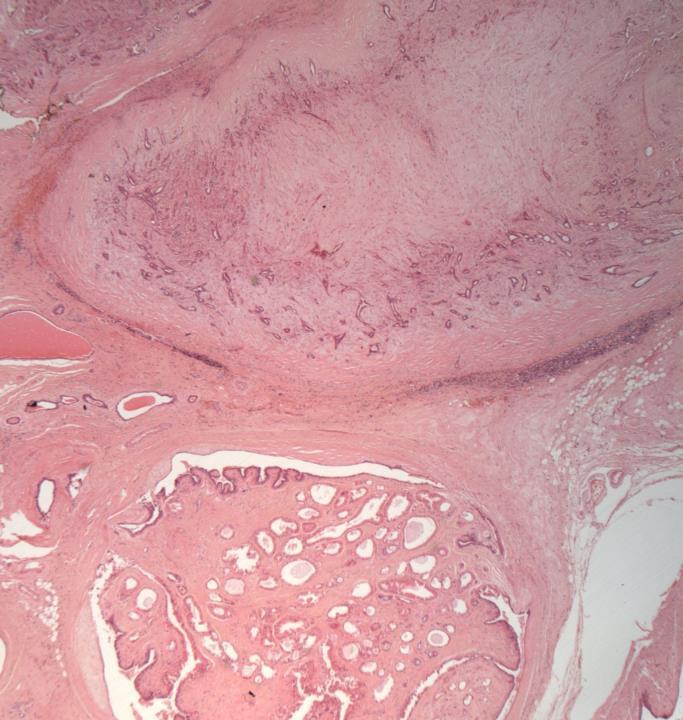
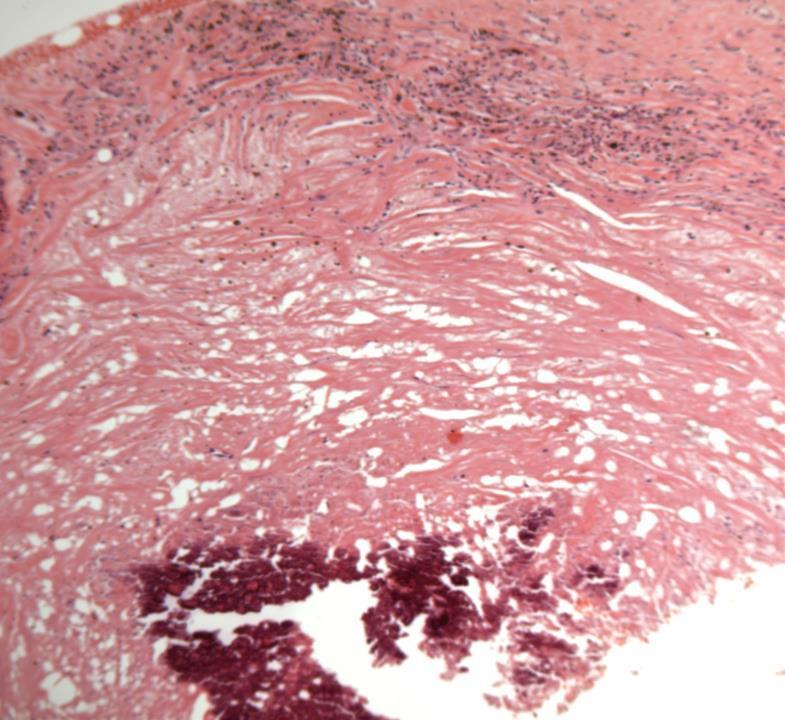
Case 9
◼ sclerosed papilloma/Duct adenoma
◼ Papillomas may undergo sclerosis leading to distortion and pseudo infiltrative growth pattern DD carcinoma.
◼ Duct adenoma: solid occlusive adenosis growth pattern within a duct. Focal papillary architecture may be seen.
◼ Look for focal papillary pattern
◼ Look for myoepithelium
◼ IHC for myoepithelium: SMM, p63
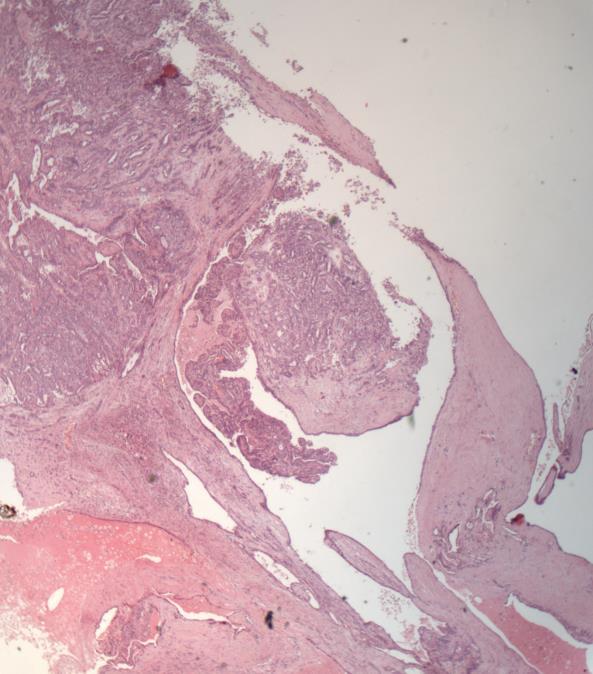
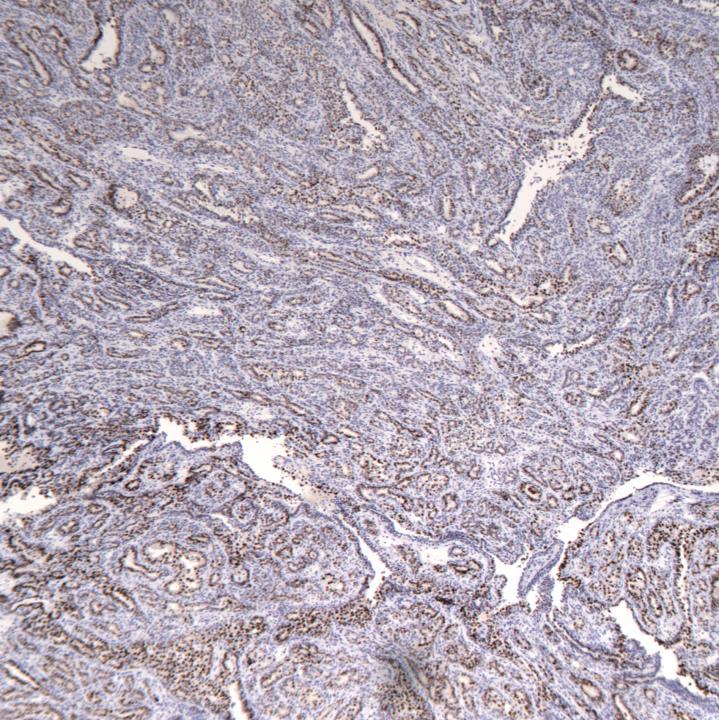
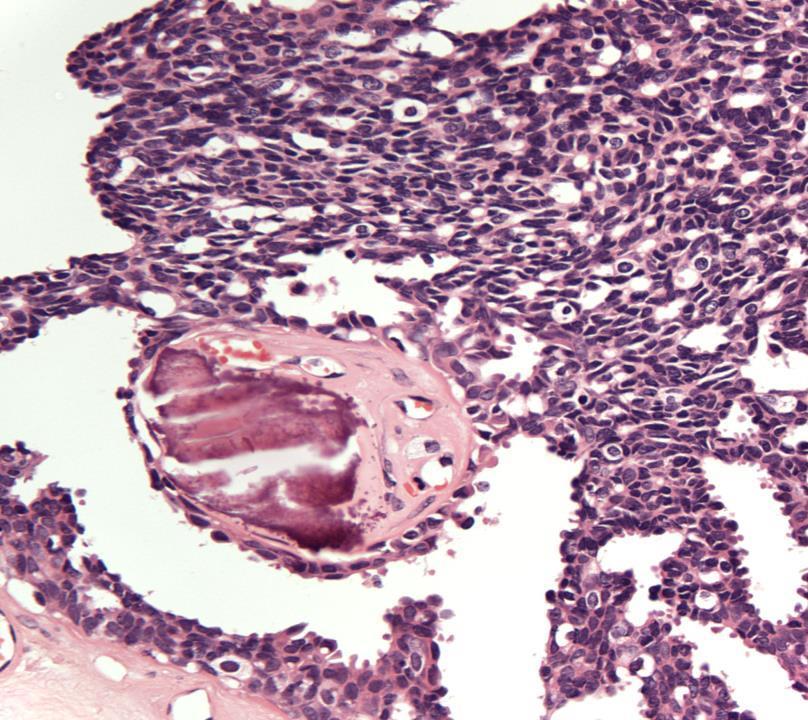
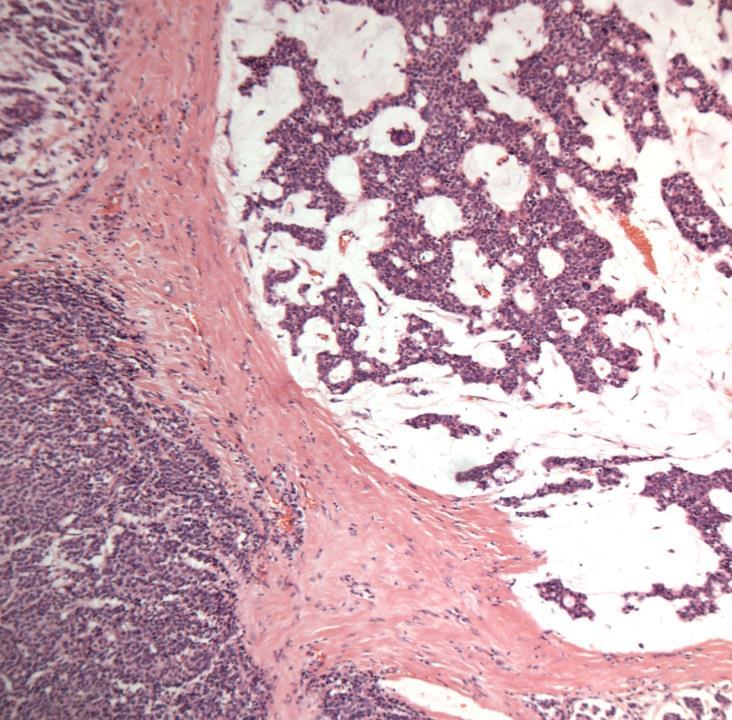
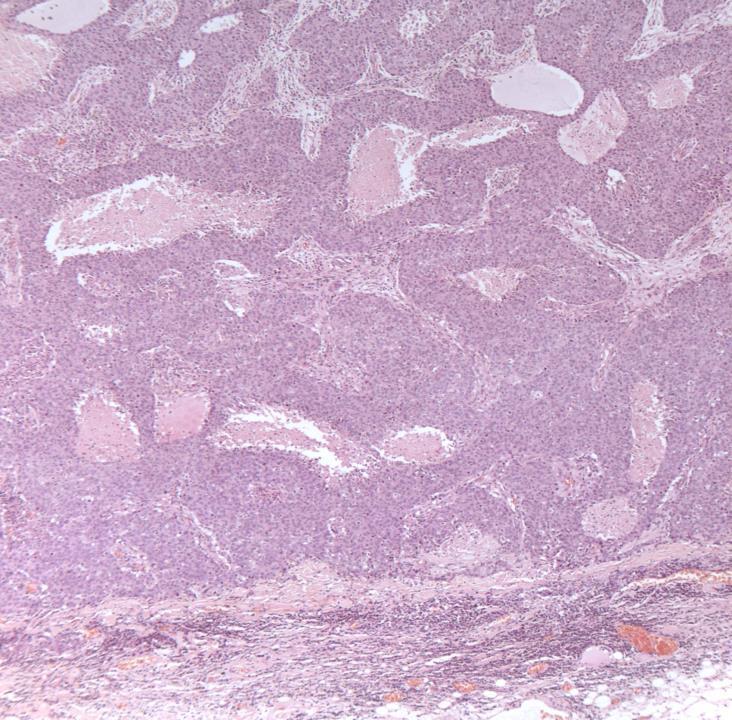
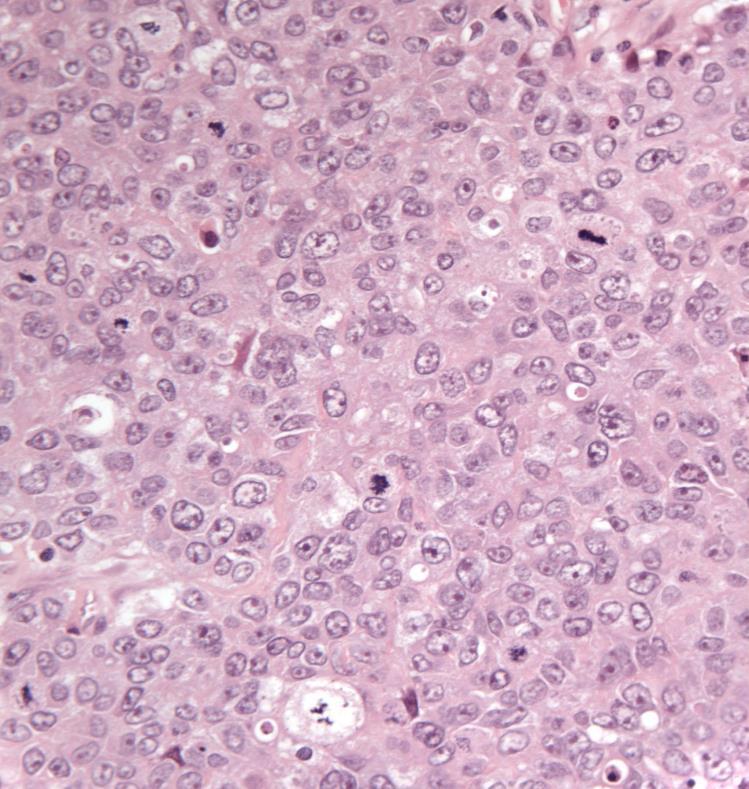
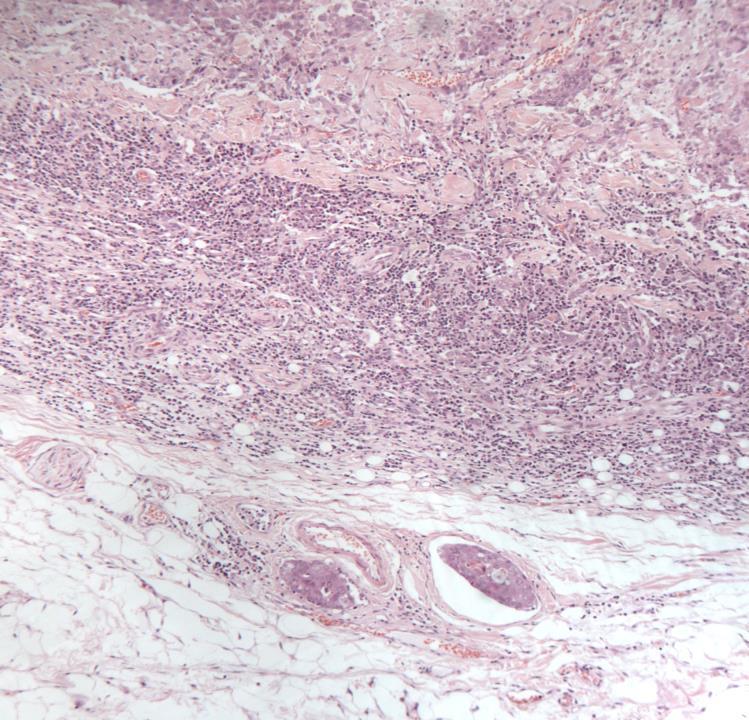
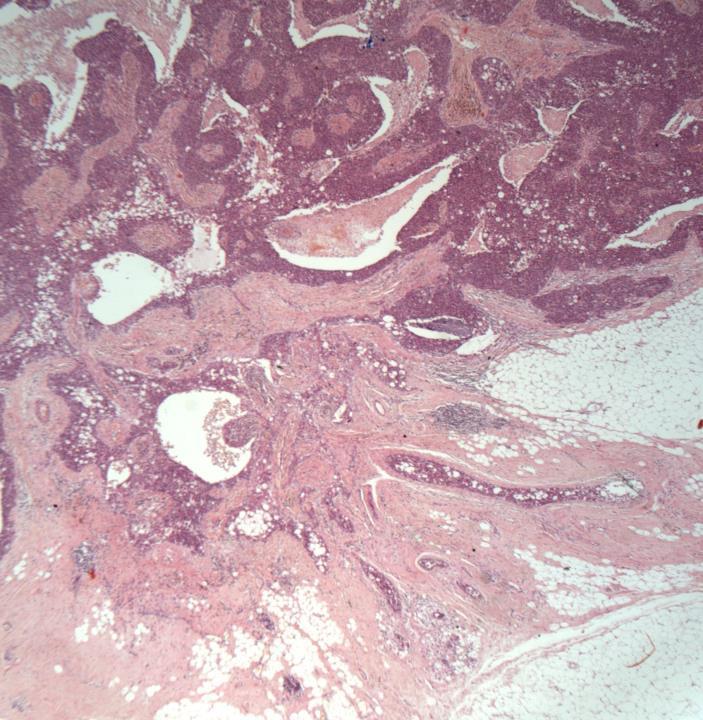
Case 13
◼ DCIS in a papilloma/papillary DCIS, with post surgical changes
◼ Fibrous septa with central hyalinization/infarction : common in lobulated lesions.
◼ Cells: clear, eosinophilic, plasmacytoid.
◼ Satellite nodules can be seen.
◼ Mitotic activity 2 or less/10hpf.
◼ Both epithelial and myoepithelial components can undergo malignancy.
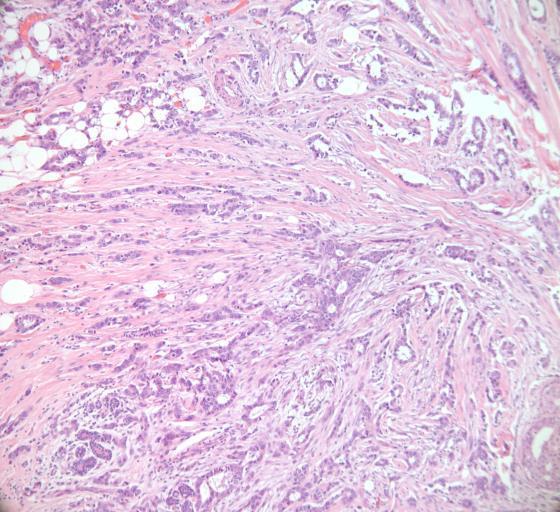
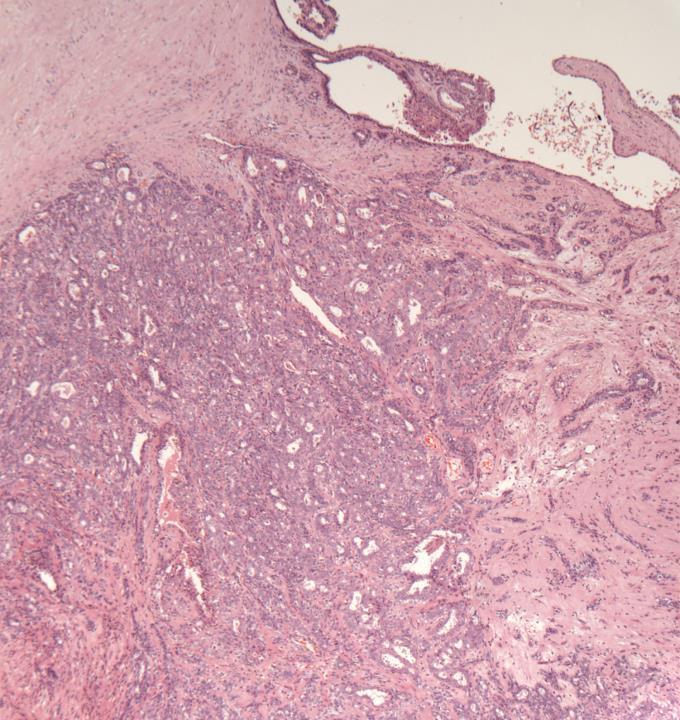
Case 7
◼ Invasive ductal NST carcinoma, grade 1
◼ Sclerosing adenosis
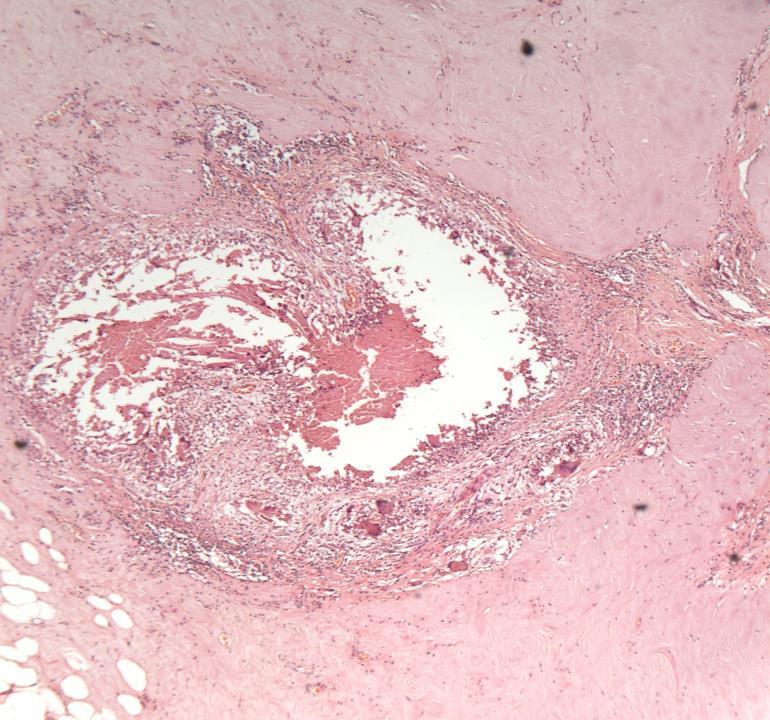
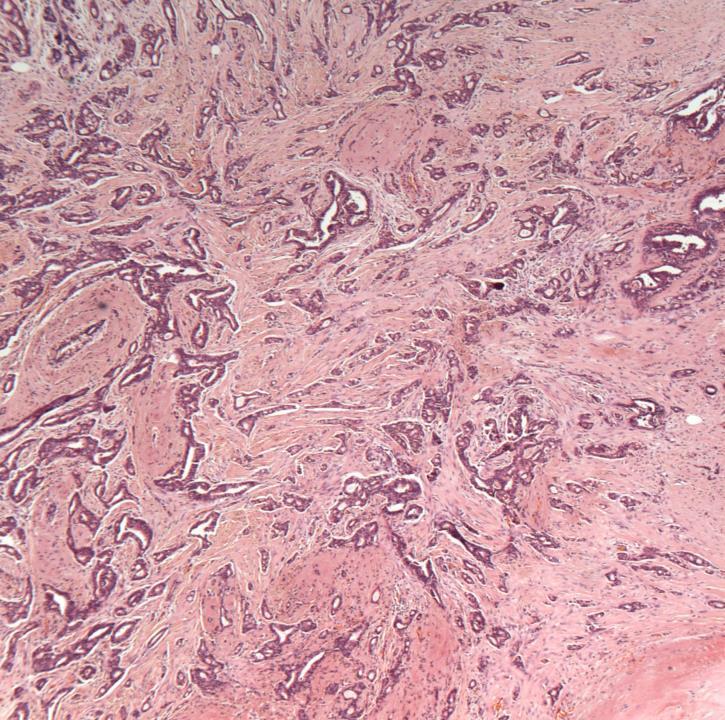
Case 11
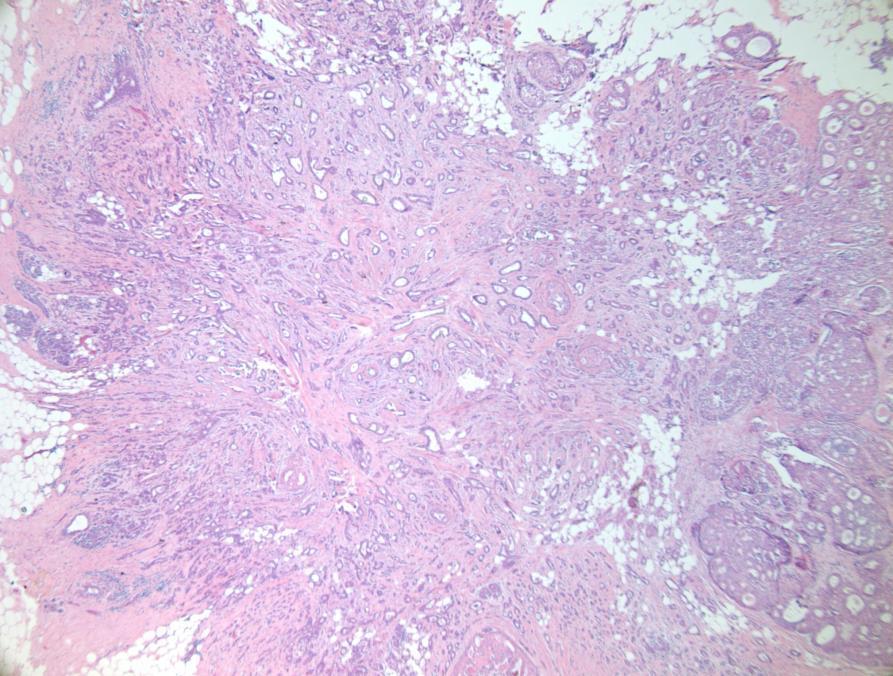
◼ Radial scar.
◼ No atypia or malignancy.
◼ Radial scar/complex sclerosing lesion:
Architecture
Fibroelastotic stroma preserved myoepithelium
No epithelial atypia
DD
Tubular Carcinoma/grade 1 carcinoma
◼ Absent myoepithelium
◼ Desmoplastic stroma
◼ Epithelial atypia
Radial scar
◼ On core biopsy: B3
◼ Comment on presence/absence of atypia
◼ Second line VAB (VAE)
Case 1
◼ Mixed ductal NST and lobular carcinoma with DCIS and LCIS/PLCIS
◼ E-cadherin can be helpful.
❑ Note: e-cadherin can show heterogeneous/aberrant expression.
❑ Beta catenin and p120 can help in difficult cases.
Beta catenin
Case 8
◼ Invasive mixed lobular and mucinous carcinoma with DCIS
Case 10
◼ Invasive no special type (NST) carcinoma with basal like features.
◼ Lymphovascular invasion
Morphological features of basal tumours
◼ Pushing margin
◼ Central scarring/necrosis
◼ Syncytial growth pattern
◼ Prominent lymphocytic infiltrate
Basal cytokeratins
◼ CK5 (or CK5/6)
◼ CK14
◼ Others : p63, EGFR
Medullary carcinoma
◼ This terminology was dropped in the Blue WHO Book (published Dec 2019).
◼ Invasive ductal carcinoma with medullary like features to be used.
◼ UK guidelines being updated.
◼ Metaplastic carcinoma, grade 3
DCIS
Current WHO Classification for Metaplastic ca
◼ Squamous cell carcinoma
◼ Spindle cell carcinoma
◼ Carcinoma with mesenchymal differentiation
◼ Low grade adenosquamous ca
◼ Fibromatosis like ca
◼ Mixed
All have a basal phenotype
Case 6
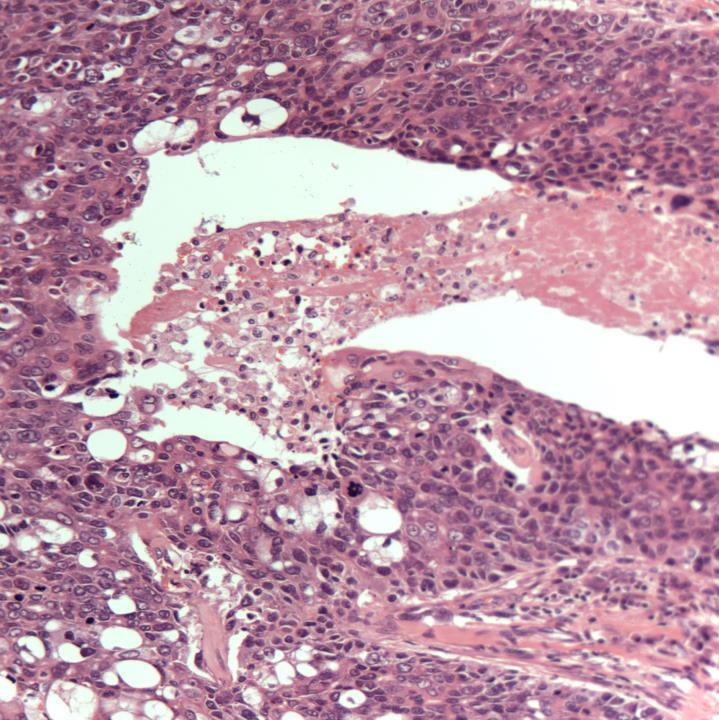
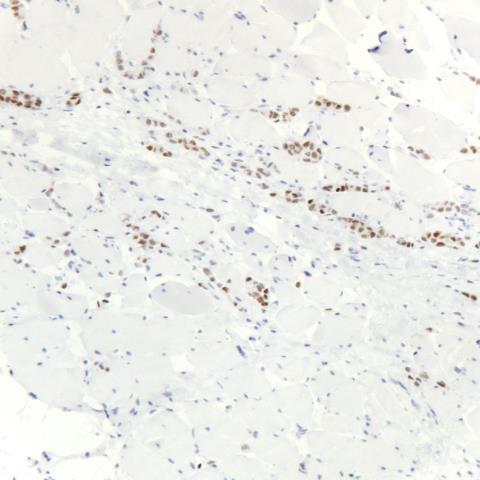
◼ Invasive lobular carcinoma invading muscle
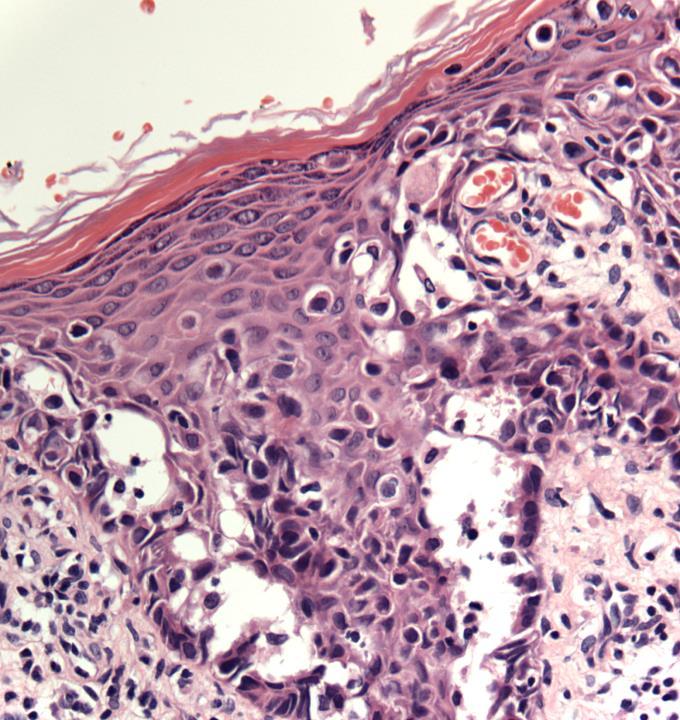
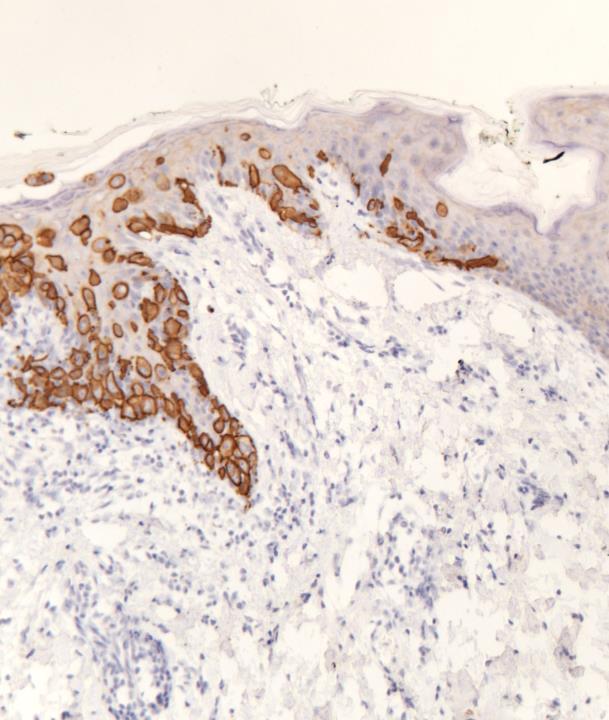
Case 2
◼ Melanoma
◼ Squamous cell carcinoma in situ
◼ Clear cell change/Toker cell hyperplasia
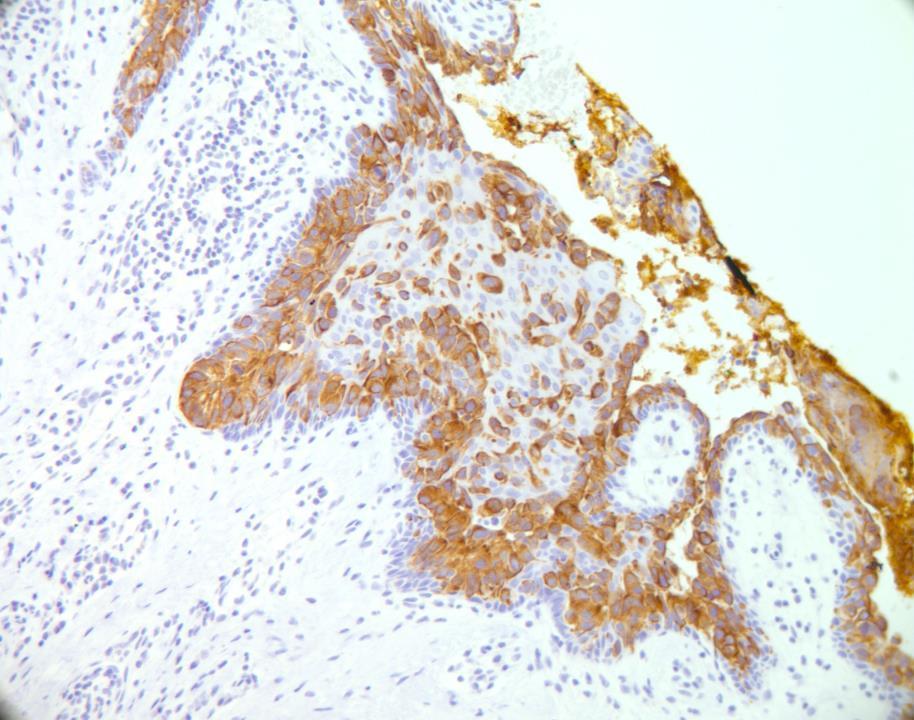
◼ Paget’s disease of nipple with DCIS
Paget’s cells
◼ Positive for EMA, low molec wt cytokeratin
◼ Majority Her2 positive
◼ May express ER, PR
◼ Negative for HMB45, Melan A (and also S100)
Clues
◼ Look for underlying DCIS/invasion.
◼ Paget’s cells may lie singly in all layers of epidermis or as basal clusters
◼ Look for melanin, junctional activity, full thickness dysplasia
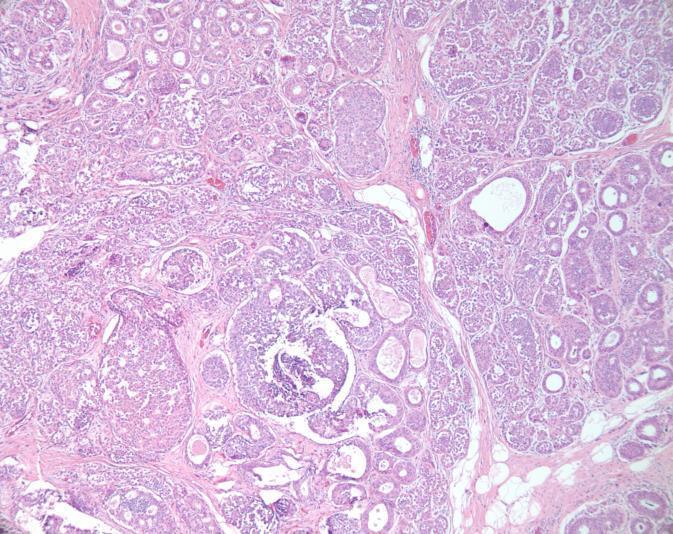
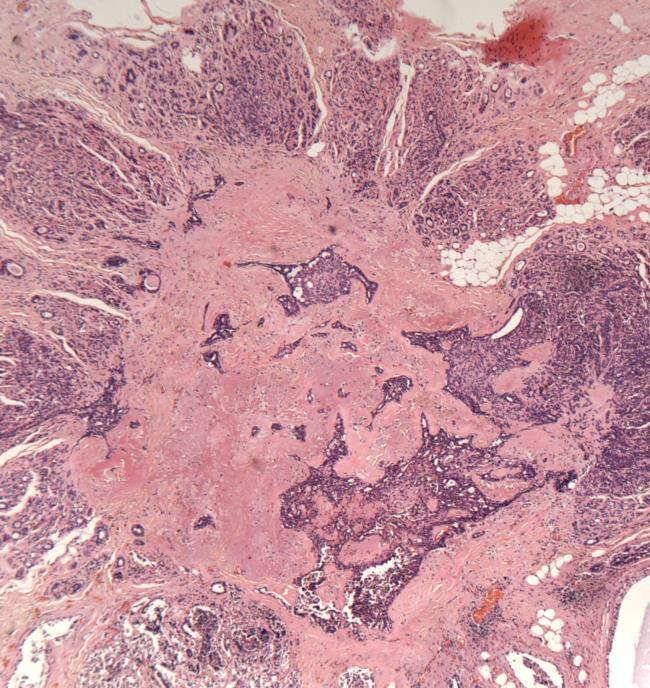
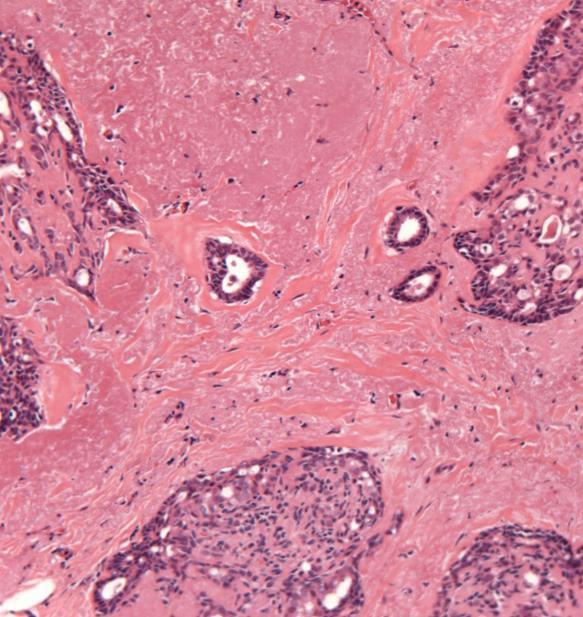
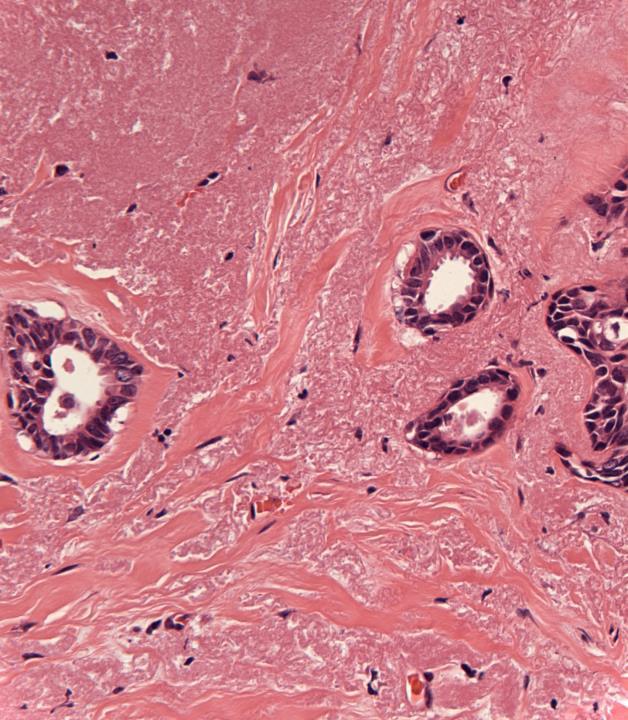
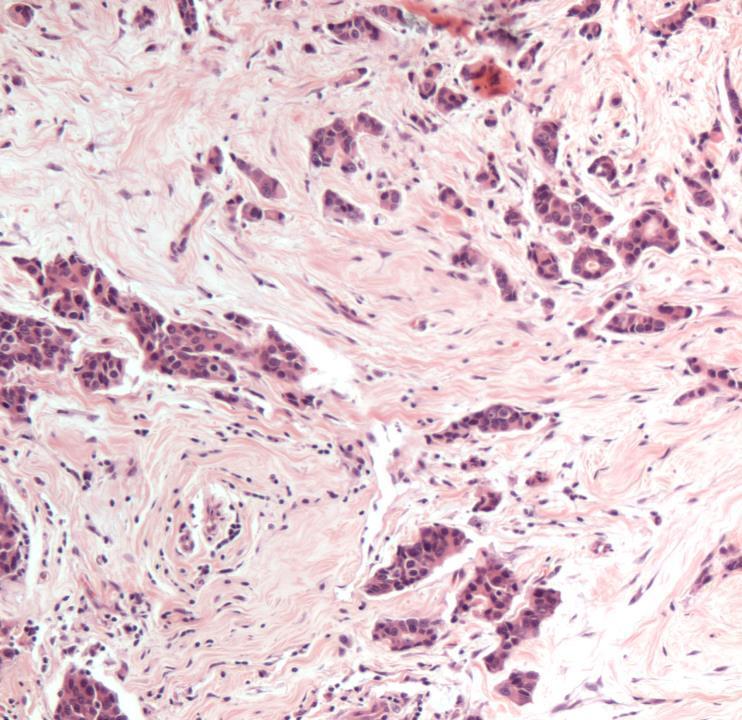
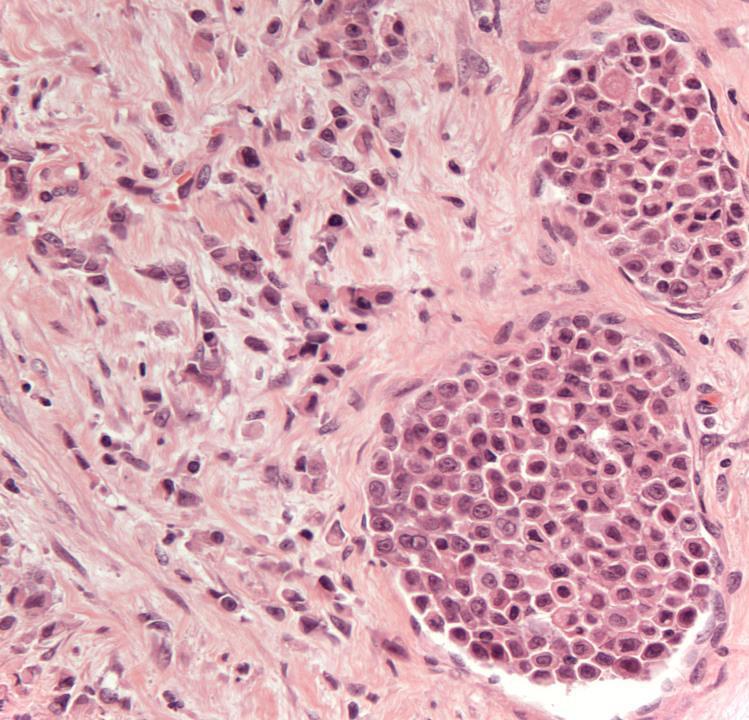
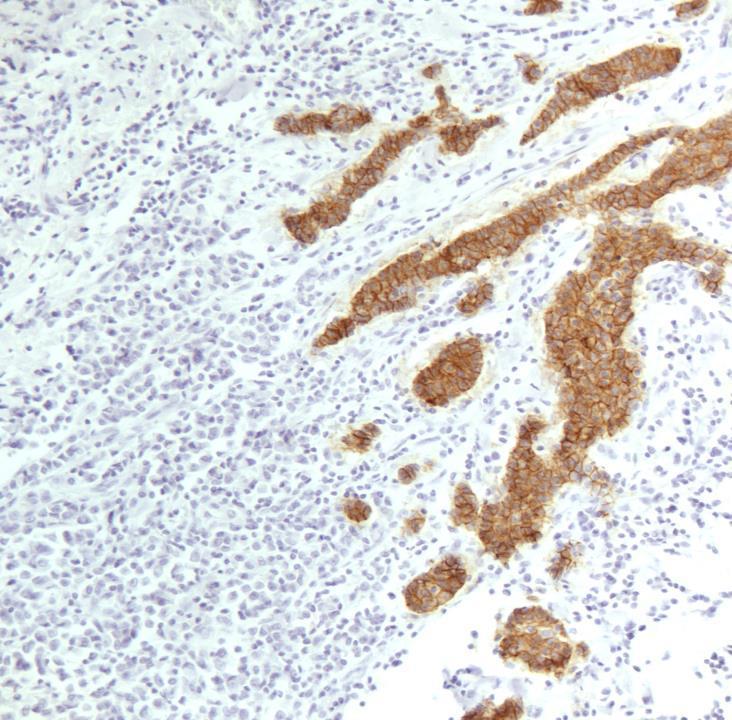
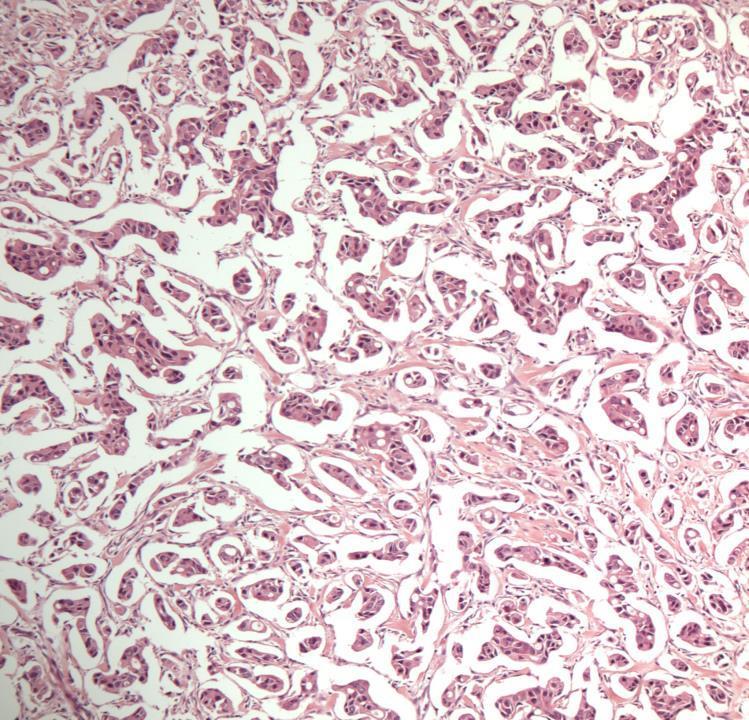
Case 5
◼ Invasive micropapillary carcinoma
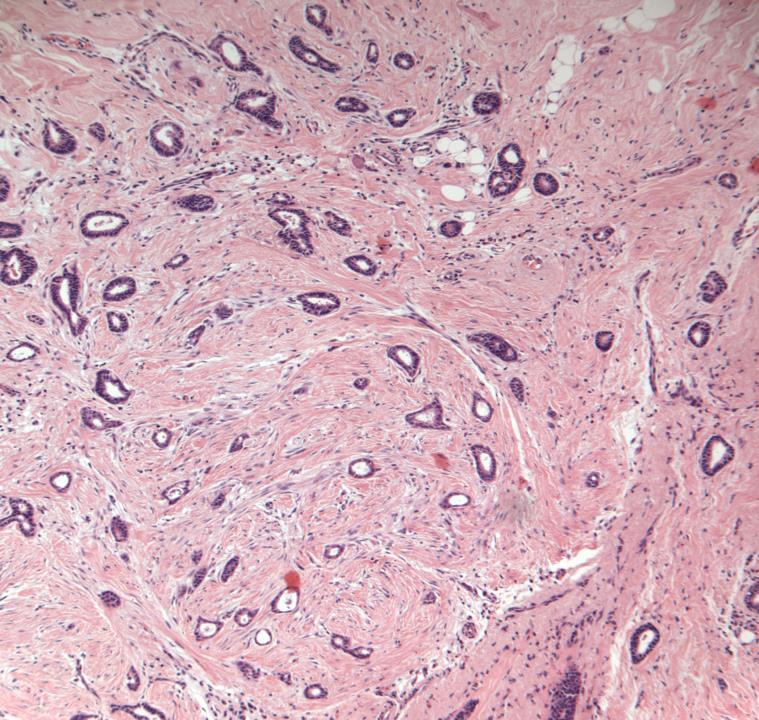
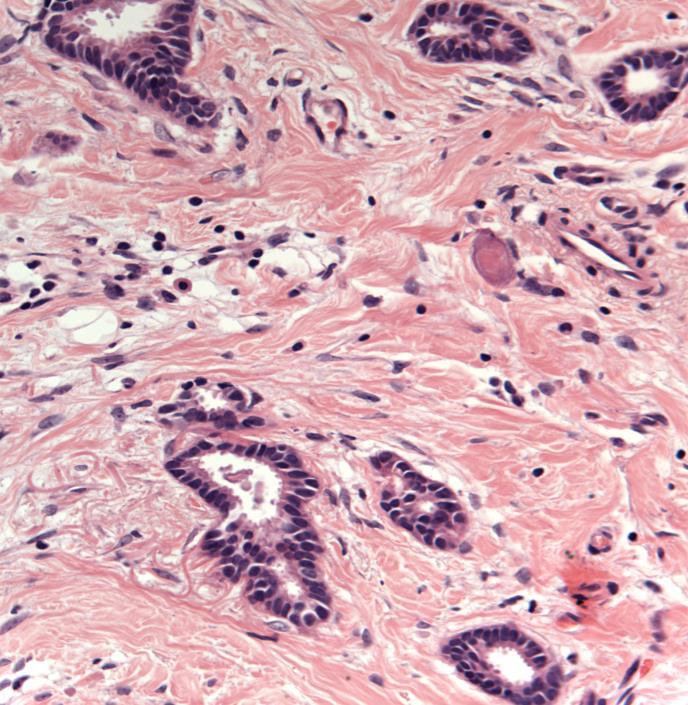
Case 16
◼ Mammotome core biopsy for calcs, R3
◼ Invasive tubular carcinoma (B5b).
◼ Look for calcification and comment on its presence/absence
◼ Angulated tubules without conspicuous myoepithelium: suspect invasion, do myoepithelial markers to confirm.
Case 17
◼ Increasing calcifications from previous screen, history of WLE for DCIS
◼ Fat necrosis, haemosiderin deposition, scarring
◼ Calcification of appropriate size
◼ No DCIS or invasive carcinoma
◼ Dystrophic calcification- B2
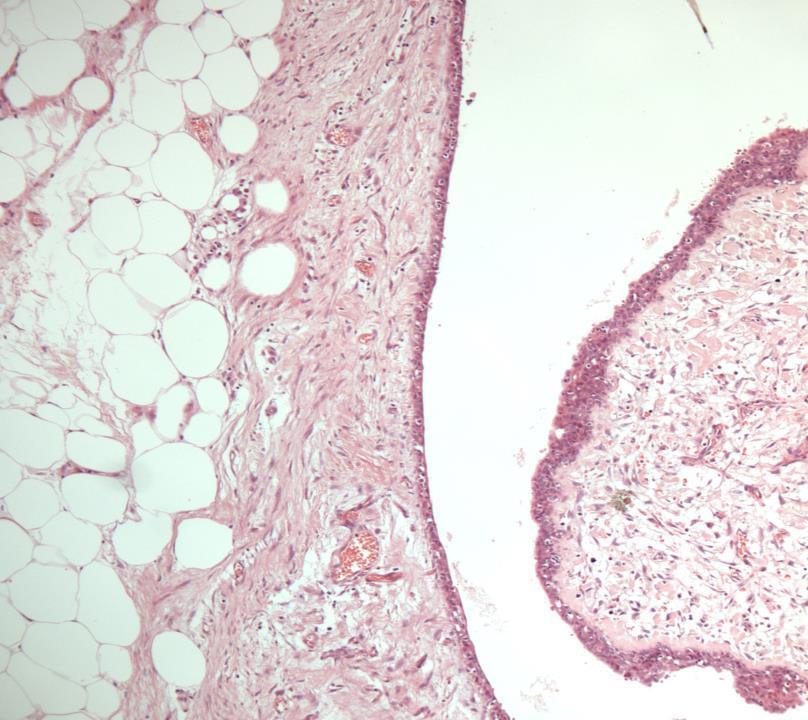
Case 18
◼ U/S guided core biopsy of a solid mass
◼ Myxoid fibroadenoma
– B2
◼ A minority can be associated with Carney’s syndrome: Familial condition of cutaneous and cardiac myxomas, spotty cutaneous pigmentation, endocrine overactivity and melanotic schwannoma.
◼ Most patients with myxoid fibroadenomas, however, do not have a systemic abnormality: discuss at the MDT meeting
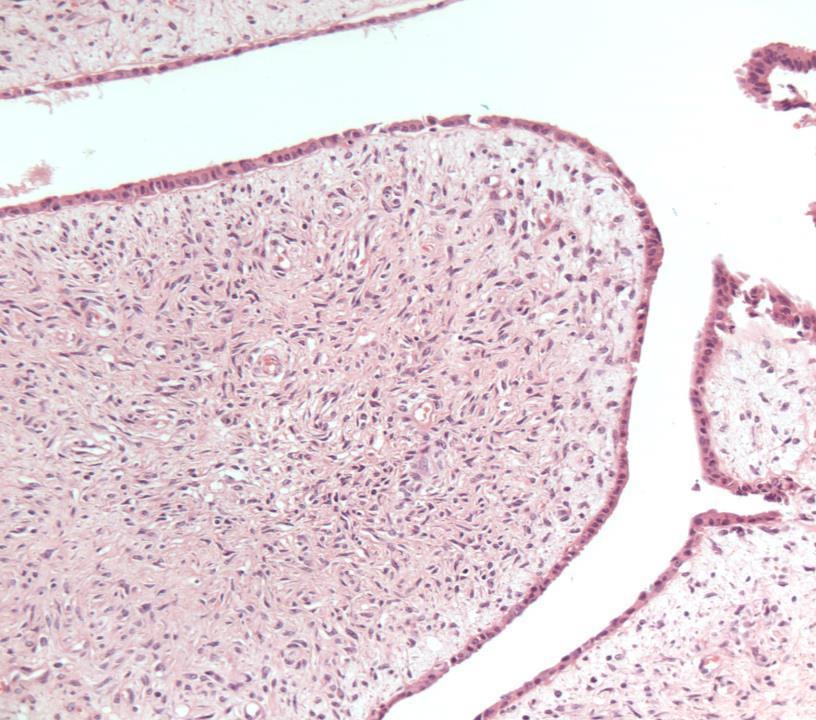
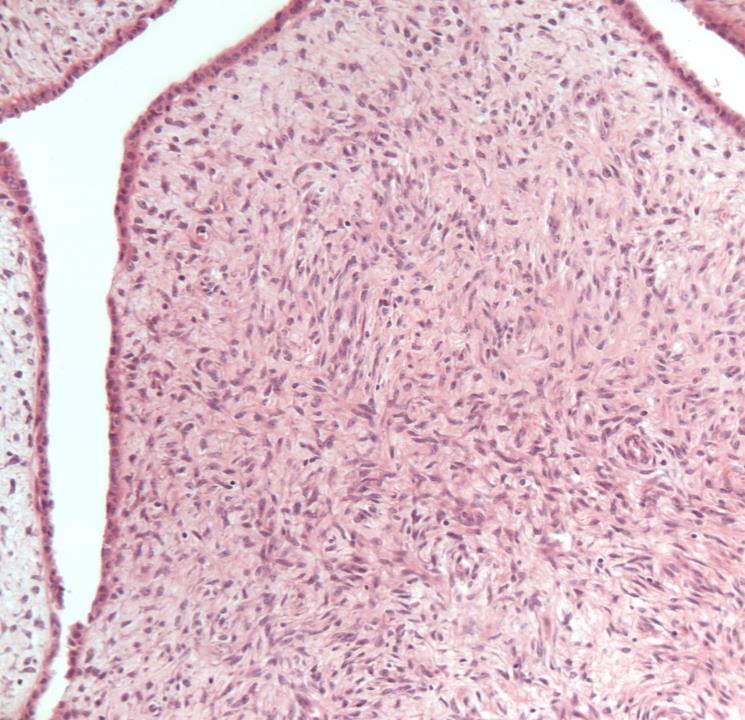
Case 19
◼ Fibroepithelial lesion
◼ Stromal overgrowth
◼ Stromal cellularity
◼ Leaf-like pattern
◼ Stromal atypia
◼ Infiltrative margin
◼ Phyllodes tumour (borderline)
◼ Cellular fibroepithelial lesion and benign phyllodes are managed similarly.
◼ Borderline and malignant phyllodes: excision with margin.
DD: Spindle cell lesion on core biopsy
◼ Look for biphasic pattern
◼ Look for DCIS
◼ A panel of cytokeratins (including basal cytokeratins) to exclude metaplastic carcinoma
Technical considerations
B coding
Benign lesions mimicking malignant
Malignant lesions mimicking benign lesions
Metastases
Non epithelial lesions
Pitfalls in hormone receptors
Birmingham Breast Pathology Update Course
◼ Friday 7 November (first week of November each year)
◼ One day virtual with slide seminar
◼ 7CPD credits
◼ https://birminghambreastpathology.co.uk/ bbpuc-register/ Thank you