• Go through the 22 questions with average of just under 3 minutes to read case and discuss
• We can’t cover all information on the slides and will pick and choose discussion points
• Slides have been made with the intention of serving as notes for you during your revision
• Opportunity to ask questions in the end provided enough time
1. You are a busy consultant pathologist in a post-mortem room currently performing the identification checks with the anatomic pathology technician. The deceased belongs to a Muslim family who are eager to have the postmortem exam completed as soon as possible so they can expedite the burial in keeping with their religious beliefs. You note a discrepancy with the police ID band and the details on the coroner’s permission to examine form. What is the next most appropriate action?
A. Proceed with the post-mortem examination. Submit provisional cause of death and ask the Coroner to correlate the identification.
B. Proceed with the post-mortem examination ensuring toxicology and histology is taken. Submit provisional cause of death and ask the Coroner to clarify the identification.
C. Proceed with the post-mortem examination ensuring toxicology and histology is taken. Submit provisional cause of death and ask the Police to clarify the identification.
D. Refuse to proceed with the post-mortem examination
E. Alert the medical examiner
1. You are a busy consultant pathologist in a post-mortem room currently performing the identification checks with the anatomic pathology technician. The deceased belongs to a Muslim family who are eager to have the postmortem exam completed as soon as possible so they can expedite the burial in keeping with their religious beliefs. You note a discrepancy with the police ID band and the details on the coroner’s permission to examine form. What is the next most appropriate action?
A. Proceed with the post-mortem examination. Submit provisional cause of death and ask the Coroner to correlate the identification.
B. Proceed with the post-mortem examination ensuring toxicology and histology is taken. Submit provisional cause of death and ask the Coroner to clarify the identification.
C. Proceed with the post-mortem examination ensuring toxicology and histology is taken. Submit provisional cause of death and ask the Police to clarify the identification.
D. Refuse to proceed with the post-mortem examination
E. Alert the medical examiner
What happens after someone dies?
Medical Examiner’s Office
Coroner’s Office
Patient dies in community
Ambulance/police attends (ID confirmed by police) Transported to hospital mortuary (or to funeral directors)
Patient dies in hospital Nursing staff contact porters
ID’d in mortuary
Coroner’s request for PM examination.
Also send:
• Circumstances of death (containing police notes)
• Ambulance notes
• GP notes
Await coroner/medical examiner decision
Coroner’s release note:
1. Closed
2. Investigation
3. Inquest or Medical examiner issues Medical Certification of Cause of Death (MCCD)
Release body to funeral directors when permitted
Porters transport body to hospital mortuary
What happens during this period?
• ID band from police, funeral director or hospital checked
• Presence of lines, deterioration, injuries and clothing documented
• Measured (height and width: important for funeral directors and CT scanner)
• Assigned mortuary number and ID band
• Storage place confirmed
• Documentation from the Coroner forwarded to pathologist
Burial/cremation
How we interact with other teams
Coroner’s Officers
Hospital Porters
Transplant team (especially corneas)
Ambulance crew
Mortuary staff
Bereavement Centre/Medical examiner’s Officers
Police officers
Fingerprint team
Funeral directors
Pathologist
2. You have completed a post-mortem examination for the Coroner and submitted the Postmortem Cause of Death form. The cause of death was due to myocardial infarction secondary to coronary artery thrombosis. You receive a call from the Bereavement office who say the wife of the deceased would like to speak about the circumstances of the death. She believes she is responsible for his death as she did not give him his evening meal on time even though he mentioned he was having pangs of hunger. The bereavement staff tell you that she is very distressed and feels that knowing more about the findings may help her cope. Which of the following is the most appropriate response?
A. Invite the patient for a discussion to better elicit her understanding of the situation
B. Tell the bereavement officer to only mention that she is not responsible for the death and disclose no further information
C. Advise the bereavement officer to speak with the Coroner’s Office
D. Refuse to disclose the information and do not elaborate further
2. You have completed a post-mortem examination for the Coroner and submitted the Postmortem Cause of Death form. The cause of death was due to myocardial infarction secondary to coronary artery thrombosis. You receive a call from the Bereavement office who say the wife of the deceased would like to speak about the circumstances of the death. She believes she is responsible for his death as she did not give him his evening meal on time even though he mentioned he was having pangs of hunger. The bereavement staff tell you that she is very distressed and feels that knowing more about the findings may help her cope. Which of the following is the most appropriate response?
A. Invite the patient for a discussion to better elicit her understanding of the situation
B. Tell the bereavement officer to only mention that she is not responsible for the death and disclose no further information
C. Advise the bereavement officer to speak with the Coroner’s Office
D. Refuse to disclose the information and do not elaborate further
Reportable
Reportable deaths
• Doctor unable to issue COD (sudden/unexpected death)
• Death was unnatural or violent (e.g. treatment/medical procedure, related to occupation, drugs/suicide)
• Cause of death unknown
• Death occurred in custody or other state detention
Not reportable
Provisional COD offered by attending doctor
Coroner reviews the circumstances Investigates further PM exam or inquest or both
Coroner refers to NHS medical examiner as feels no further investigation necessary
NHS medical examiner refers to coroner as believes further investigation is necessary
NHS medical examiner reviews
• An experienced medical doctor (ideally a consultant or fully qualified GP) with training in medical examining
• Reviews medical information, interviews relatives/clinicians
• Scrutinises COD offered or provides COD if not offered
Once PM completed and COD form submitted to Coroner body is released (even if COD pending/unascertained)
• An experienced senior doctor (does not have to be a pathologist –many are GPs) employed by the NHS who has undertaken special training
• Act as a safeguard for deaths not reported to the coroner
• Aim is to scrutinise the COD, provide opportunities for the bereaved to raise concerns, provide advice to the Coroner and doctors and have a local overview of patterns in reported deaths
3. Which of the following deaths would not require referral to the Coroner?
A. A 75-year-old gentleman with a long history of interstitial lung disease who used to work as a construction worker
B. Man who dies at home due to disseminated metastatic prostate cancer and his regular GP is away on holiday for the next 3 weeks
C. An 18-year-old gentleman who died shortly after returning home from a night club
D. A 55-year-old man recently diagnosed with chronic lymphocytic leukaemia found dead at home
3. Which of the following deaths would not require referral to the Coroner?
A. A 75-year-old gentleman with a long history of interstitial lung disease who used to work as a construction worker
B. Man who dies at home due to disseminated metastatic prostate cancer and his regular GP is away on holiday for the next 3 weeks
C. An 18-year-old gentleman who died shortly after returning home from a night club
D. A 55-year-old man recently diagnosed with chronic lymphocytic leukaemia found dead at home
Reportable
Reportable deaths
• Doctor unable to issue COD (sudden/unexpected death)
• Death was unnatural or violent (e.g. treatment/medical procedure, related to occupation, drugs/suicide)
• Cause of death unknown
• Death occurred in custody or other state detention
Not reportable
Provisional COD offered by attending doctor
Coroner reviews the circumstances Investigates further PM exam or inquest or both
Coroner refers to NHS medical examiner as feels no further investigation necessary
NHS medical examiner refers to coroner as believes further investigation is necessary
NHS medical examiner reviews
• An experienced medical doctor (ideally a consultant or fully qualified GP) with training in medical examining
• Reviews medical information, interviews relatives/clinicians
• Scrutinises COD offered or provides COD if not offered
Once PM completed and COD form submitted to Coroner body is released (even if COD pending/unascertained)
4. You have performed a post-mortem histology on a 50-year-old gentleman who showed no gross internal examination findings. Histology samples from the heart reveal contraction band necrosis and you list the cause of death as myocardial infarction and submit the cause of death form and the PM report. A few days later you obtain a request from family members for the tissue blocks taken so they can be buried along with the body. Which of the following is the most appropriate responses?
A. Have the blocks ready to collect from the bereavement office at the family’s convenience
B. Do not release the blocks to the family. Ask the family to speak with the Coroner’s Office
C. Do not release the blocks to the family. Instead speak with the funeral director and have them collect the blocks when collecting the body.
D. Do not release the blocks to the family. Inform the family that as the tissue has been processed in a hospital lab consent must be obtained from the laboratory manager
4. You have performed a post-mortem histology on a 50-year-old gentleman who showed no gross internal examination findings. Histology samples from the heart reveal contraction band necrosis and you list the cause of death as myocardial infarction and submit the cause of death form and the PM report. A few days later you obtain a request from family members for the tissue blocks taken so they can be buried along with the body. Which of the following is the most appropriate responses?
A. Have the blocks ready to collect from the bereavement office at the family’s convenience
B. Do not release the blocks to the family. Ask the family to speak with the Coroner’s Office
C. Do not release the blocks to the family. Instead speak with the funeral director and have them collect the blocks when collecting the body.
D. Do not release the blocks to the family. Inform the family that as the tissue has been processed in a hospital lab consent must be obtained from the laboratory manager
Human Tissue Act
• Not a completely realistic scenario. The coroner would usually have sent instructions regarding blocks as they send the release note.
• HTA website (particularly FAQs section) is a useful resource
5. Examination of the base of the brain shows the following findings. What do these findings indicate?
A. Increased intracranial pressure
B.Haemorrhagic stroke
C.Embolic disease
D.Lacunar infarcts
5. Examination of the base of the brain shows the following findings. What do these findings indicate?
A.Increased intracranial pressure
B.Haemorrhagic stroke
C.Embolic disease
D.Lacunar infarcts
Robbins and Cotran Atlas of Pathology, Fourth Edition
6. You are performing a postmortem examination of a 70-year-old man who was the passenger in a road traffic collision. Resuscitation was attempted but unsuccessful. An image of the patient’s brain is shown below. You are able to displace the material using the blunt side of the blade. What was the likely cause of this finding?
A. Tearing of the bridging veins
B.Rupture of the middle meningeal artery
C.Ruptured berry aneurysm
D.Hypertension
6. You are performing a postmortem examination of a 70-year-old man who was the passenger in a road traffic collision. Resuscitation was attempted but unsuccessful. An image of the patient’s brain is shown below. You are able to displace the material using the blunt side of the blade. What was the likely cause of this finding?
A.Tearing of the bridging veins
B.Rupture of the middle meningeal artery
C.Ruptured berry aneurysm
D.Hypertension
Robbins and Cotran Atlas of Pathology, Fourth Edition
Epidural, subdural and subarachnoid
Epidural haemorrhage: Direct injury to side of the head → rupture of middle meningeal artery
Leptomeninges
• Arachnoid mater (green)
• Pia mater (red)
Becomes infected in meningitis
Subdural haemorrhage: Direct injury to side of the head → rupture of middle meningeal artery
Firm attachment of dura to suture lines: epidural haematoma does not cross suture lines
Subarachnoid haemorrhage: Rupture of aneurysm, head injuries, AVMs
By Mysid - Made by Mysid Inkscape, based on plate 769 from Gray's Anatomy (1918, public domain)., Public Domain, https://commons.wikimedia.org/w/index.php?curid=10493338
Bridging veins at increased risk of tearing with age (brain atrophy)
Middle meningeal artery (epidural haematoma)
Anatomy for Students, Fifth Edition. Copyright
2024 by Elsevier Inc. All rights reserved.
Fractures at this weak point causes a rupture of the anterior branch of the middle meningeal artery. This artery is present between the periosteal lining of the bone and the periosteal layer of the dura
for Students,
Gray's
Gray's
Ability to displace the haematoma
• When brain removed arachnoid mater and pia mater (leptomeninges) are attached
• If there is subdural haematoma → sits on top of the arachnoid → can be scraped off
• If there is subarachnoid haematoma → sits beneath arachnoid → cannot be scraped off
7. You are performing a post-mortem examination on a 40-year-old man who had a history of psychosis, memory deficits and involuntary jerking movements. His father who died at 50 had similar symptoms. Which of the following structures in the normal brain image below would you expect to be abnormal?
7. You are performing a post-mortem examination on a 40-year-old man who had a history of psychosis, memory deficits and involuntary jerking movements. His father who died at 50 had similar symptoms. Which of the following structures in the normal brain image below would you expect to be abnormal?
8. You are reviewing the postmortem histology from the heart. The findings are as depicted in the photomicrograph below. What can be said about the likely age of the infarct?
A.Less than 4 hours old
B.4- 24 hours old
C.1 day to 1 week old
D.>1 week old
E.>4 weeks old
8. You are reviewing the postmortem histology from the heart. The findings are as depicted in the photomicrograph below. What can be said about the likely age of the infarct?
Contraction band necrosis, coagulation necrosis (i.e. loss of nuclei) +/- haemorrhage
(4-24 hours)
Neutrophils + haemorrhage
(>24 hours, most at day 3)
Granulation tissue and macrophages (>1 week) Scar tissue formation
(>2-8 weeks)
9. You are performing a postmortem examination on a 25-year-old athlete who died suddenly. On examination of the heart you see the features below. What is the next appropriate step prior to closing the body?
A. Obtain blood for toxicology
B. Obtain vitreous humour
C. Obtain a sample of spleen
D. Obtain a sample of lung
9. You are performing a postmortem examination on a 25-year-old athlete who died suddenly. On examination of the heart you see the features below. What is the next appropriate step prior to closing the body?
You are performing the post-mortem examination on a 65-year-old gentleman with a history of myocardial infarction. Examination of the lungs shows pulmonary oedema. Examination of the bowel shows findings as depicted in the photograph below. What gross findings would be expected on examination of the heart?
You are performing the post-mortem examination on a 65-year-old gentleman with a history of myocardial infarction. Examination of the lungs shows pulmonary oedema. Examination of the bowel shows findings as depicted in the photograph below. What gross findings would be expected on examination of the heart?
Contraction band necrosis, coagulation necrosis (i.e. loss of nuclei) +/- haemorrhage
(4-24 hours)
Neutrophils + haemorrhage
• Mural thrombus
(>24 hours, most at day 3)
• Dressler’s pericarditis (autoimmune)
Granulation tissue and macrophages (>1 week)
• Arrythmias
• CCF
Scar tissue formation
(>2-8 weeks)
11. You are performing a post-mortem examination on a 65-year-old female. On examining the heart, you notice the heart appears noticeably large and exhibits a deep blue-purple colour as depicted in the image below. On opening of the pericardium, you see a large haematoma encasing the heart and an area of ventricular perforation. What histological findings would be expected from the heart adjacent to the perforation?
A. Normal heart histology
B. Contraction band necrosis and coagulation necrosis
C. Neutrophilic infiltration of myocardium
D. Early fibrosis
E. Well-established fibrosis
11. You are performing a post-mortem examination on a 65-year-old female. On examining the heart, you notice the heart appears noticeably large and exhibits a deep blue-purple colour as depicted in the image below. On opening of the pericardium, you see a large haematoma encasing the heart and an area of ventricular perforation. What histological findings would be expected from the heart adjacent to the perforation?
A. Normal heart histology
B. Contraction band necrosis and coagulation necrosis
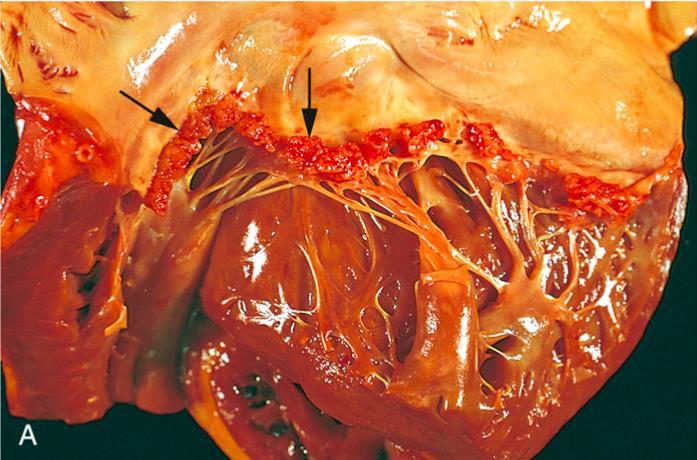
12. You are performing the post-mortem examination of a 75-year-old gentleman who was a lifelong smoker. He died suddenly at home. External examination shows cachexia and tar staining of the nails. You discover a large tumour in the lung with multiple enlarged hilar lymph nodes and similar nodules in the brain. Examination of the heart reveals findings as depicted in the photograph below. The vegetations are present on one side of the valve. How would you best classify this disease process?
A. Infective endocarditis
B. Marantic endocarditis
C. Libman-Sacks endocarditis
D. Rheumatic heart disease
12. You are performing the post-mortem examination of a 75-year-old gentleman who was a lifelong smoker. He died suddenly at home. External examination shows cachexia and tar staining of the nails. You discover a large tumour in the lung with multiple enlarged hilar lymph nodes and similar nodules in the brain. Examination of the heart reveals findings as depicted in the photograph below. The vegetations are present on one side of the valve. How would you best classify this disease process?
A. Infective endocarditis
B. Marantic endocarditis (Nonbacterial thrombotic endocarditis)
Immune complex deposition during acute phase (rheumatic fever): autoimmune reaction that occurs 10 days to 6 weeks after GAS infection of throat (in childhood) causes → NES symptoms. Mitral valve prolapse initially, mitral valve stenosis eventually
Extends on to chordae
Infective proliferation on preexisting damaged valves
Thrombus formation due to hypercoagulable state (e.g. malignancy, thrombophilia) on non-damaged valves (or marantic endocarditis)
Immune complex deposition in SLE or antiphospholipid syndrome (autoantibodies against anticoagulant proteins C and S)
Right heart
• IVDU (the injection of drugs causes damage to right sided valves)
• Embolic to lungs
• Staph aureus, Viridans Strep (e.g. S. Sanguinis), Enterococcus
Left heart
• Most common (left sided valves show more wear and tear than right sided)
• Qs may mention history of dental procedures (but there are other causes including IVDU)
13. You are performing a post-mortem examination of an 25-year-old man who collapsed during a friend’s birthday party. His friends report that before his death he seemed to have a lot of energy and seemed jittery. External examination reveals a collapsed nasal bridge. Which of the following are expected on post-mortem examination?
A. Saddle embolism
B. Splitting of the aortic media
C.Lobar pneumonia
D. Twisted bowel
E. Splenic rupture
13. You are performing a post-mortem examination of an 25-year-old man who collapsed during a friend’s birthday party. His friends report that before his death he seemed to have a lot of energy and seemed jittery. External examination reveals a collapsed nasal bridge. Which of the following are expected on post-mortem examination?
Adrenaline, noradrenaline, serotonin and dopamine (monoamines) are closely related neurotransmitters. This particular neurone shows a NE neurone but the same thing will happen with neurones using dopamine and serotonin.
Toxicology tests
Blood/urine
• Ketones
• Ethanol
• Drugs and their metabolites
Vitreous humour
• Mainly glucose (high means something, low means nothing –bacterial consumption)
Hair
• Presence in hair correlates with regular intake of substances
• Can detect multiple substances
• Assess potential drug-facilitated sexual abuse prior to death i.e.
“date rape” with Rohypnol (flunitrazepam)
14. You are performing a post-mortem examination of an otherwise fit and healthy young man who suddenly became ill and died at home. Examination of the lung shows changes as depicted in the photograph below. These changes are most likely caused by which of the following organisms?
A. Staphylococcus aureus
B. Haemophilus influenza
C. Streptococcus pneumoniae
D. Klebsiella pneumonia
E. Pseudomonas aeruginosa
14. You are performing a post-mortem examination of an otherwise fit and healthy young man who suddenly became ill and died at home. Examination of the lung shows changes as depicted in the photograph below. These changes are most likely caused by which of the following organisms?
Polymicrobial (anaerobic organisms of oral cavity e.g. Bacteroides, Fusobacterium)
Aspiration
Community
Strep pneumo
Haemophilus
Moraxella
MS Staph Aureus
Most lobar pneumonias are community acquired Strep pneumo infections
MS Staph Aureus
MR Staph Aureus
Pseudomonas
Strep pneumo
MR Staph Aureus
Gram –ve rods:
• Pseudomonas
• Klebsiella
• Serratia
• E.coli
Enterobacteriaceae
15. You are performing a post-mortem examination on a 65-year-old gentleman who used to work as a mason. He has a history of ischemic heart disease for which he took regular medications. Examination of the lungs shows nodularities in the upper lobes. Histology shows nodules of whirled collagen and fibroblasts as shown in the photomicrograph below. Which of the following is the most likely explanation?
A. Silicosis
B. Asbestosis
C. Rheumatoid nodules
D. Medication induced fibrosis
15. You are performing a post-mortem examination on a 65-year-old gentleman who used to work as a mason. He has a history of ischemic heart disease for which he took regular medications. Examination of the lungs shows nodularities in the upper lobes. Histology shows nodules of whirled collagen and fibroblasts as shown in the photomicrograph below. Which of the following is the most likely explanation?
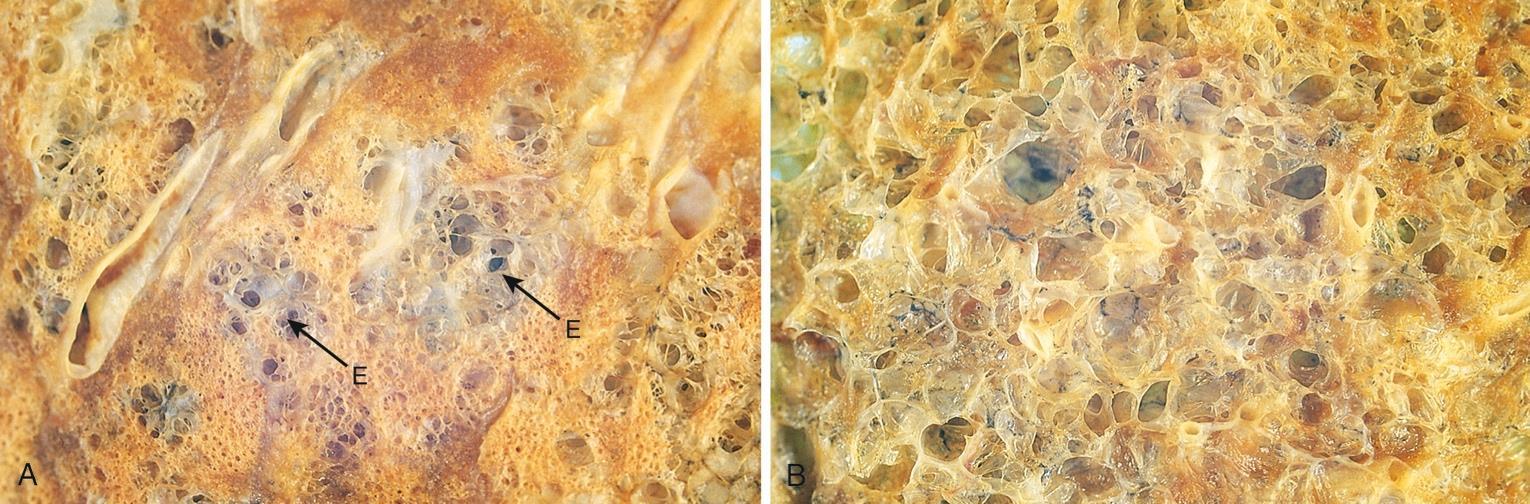
16. You are performing the post-mortem examination on an 85 year old gentleman. Internal examination of the lungs shows findings as depicted in the image below. What can be deduced about the deceased relating to this pathological finding?
A. He was a smoker
B. He was immunocompromised
C. He was a roofer
D. He was taking antibiotics
16. You are performing the post-mortem examination on an 85 year old gentleman. Internal examination of the lungs shows findings as depicted in the image below. What can be deduced about the deceased relating to this pathological finding?
• Asbestos exposure more often causes adenocarcinoma than mesothelioma, but asbestos exposure is the only cause of mesothelioma
17. You are performing a post-mortem examination of a 55-year-old gentleman. You see enlarged airspaces diffusely involving the upper, middle and lower zones of both lungs as depicted in the image below. What other findings would you expect to find elsewhere in the postmortem examination?
B. Hepatic nodularity
C. Red and swollen calf
D. Tricuspid valve vegetations
E. Dissection of the aortic media
A. Splenic infarcts
17. You are performing a post-mortem examination of a 55-year-old gentleman. You see enlarged airspaces diffusely involving the upper, middle and lower zones of both lungs as depicted in the image below. What other findings would you expect to find elsewhere in the postmortem examination?
Mutated alpha-1 antitrypsin A1AT accumulates in hepatocyte
Trypsin (a serine protease) is inhibited by A1AT
Trypsin is not inhibited and continues to damage the alveolar walls
Autosomal codominance:
• PiMM: 100% normal serum A1AT
• PiMS: 80% serum A1AT levels
• PiMZ: ~50%
• PiSS: ~50%
• PiSZ: ~50%
• PiZZ: 10%
Liver cirrhosis
Panacinar emphysema
18. You have been requested by the Coroner to perform an external examination on a 22year-old female who committed suicide via hanging. She was found by her mother who says she had been home alone all day. The police attended the scene and reported no suspicious circumstances. Which of the following findings would be unexpected in this scenario?
A. Posterior lividity
B. Oblique ligature mark
C.Protrusion of the tongue
D. Facial petechiae
18. You have been requested by the Coroner to perform an external examination on a 22year-old female who committed suicide via hanging. She was found by her mother who says she had been home alone all day. The police attended the scene and reported no suspicious circumstances. Which of the following findings would be unexpected in this scenario?
A. Posterior lividity
B. Oblique ligature mark
C.Protrusion of the tongue
D. Facial petechiae
Hangings
By goga312 at Russian Wikipedia, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?cur id=9749090
Face
• Petechiae (more common in incomplete hangings)
• Protrustion of tongue (upward pressure from ligature)
• Dried saliva contralateral to point of suspension
Injuries
• Self harm scars
• Bruising: Struggle may occur in response to hanging e.g. regret, pain, hypoxic seizure perimortem
• Fingertip bruising/fingernail abrasions
Lividity or “livor mortis” (blood pooling – fixed after approximately 8 hours)
• Circumferential petechial lividity to the lower legs
• Unexpected findings
• Lividity in a different distribution such as along posterior aspect of body
Hangings
Neck
• Ligature mark
• Dimensions including breadth and depth
• Course around the neck (oblique) and point of suspension
• Bleeding into skin between two loops (i.e. gone around the neck twice)
• Decapitation (partial or complete) –associated with long drop
• Unexpected findings
• Surface injuries inconsistent with suspension
• Horizontal ligature mark
Any suspicion of foul play should be communicated with Coroner’s officers – do not proceed with examination if in doubt
Other things to check
Documentation
• Review police documentation confirming death is not suspicious
• If this information is not present do not proceed
Rope
• Mention material and dimensions
• Number of loops around neck
• Type of knot (running or fixed), position of the knot
Further reading: https://www.rcpath.org/static/7b8672cc-e074-4c32-86e1e18f4d65296e/G179-Deaths-following-known-or-suspected-hanging.pdf
19. A 45-year-old man was recovered from a local river after being spotted by passersby on the adjacent footpath. An ambulance crew was called, and CPR was attempted but unsuccessful. He had a history of alcohol dependence and dilated cardiomyopathy. He had no other medical history. Internal examination reveals moderate atheroma of the left anterior descending and right coronary arteries. There are mild fatty liver changes. The stomach is free of contents and shows appearances as shown in the photograph below. The remainder of the examination including the lungs showed no significant findings. What is the likely cause of death?
A. Submersion
B. Immersion
C. Haemorrhagic shock
D. Septic shock
19. A 45-year-old man was recovered from a local river after being spotted by passersby on the adjacent footpath. An ambulance crew was called, and CPR was attempted but unsuccessful. He had a history of alcohol dependence and dilated cardiomyopathy. He had no other medical history. Internal examination reveals moderate atheroma of the left anterior descending and right coronary arteries. There are mild fatty liver changes. The stomach is free of contents and shows appearances as shown in the photograph below. The remainder of the examination including the lungs showed no significant findings. What is the likely cause of death?
• Froth around mouth and nose (Champignon de mousse)
• Extrinsic material in upper airway e.g. sand, silt or weeds
Lungs
• Lung weight >1000g (may be affected by resuscitation) +/- lung overlapping (latter also seen in deaths secondary to asthma)
• Paultauf spots (bruises on anterior lungs secondary to alveolar haemorrhages secondary to high pressures)
Stomach
• Fluid and debris content (may suggest submersion, but a soft sign)
Notes
• Review police documentation to understand context of the death
• Length of time: water can eventually seep into lungs with time even in immersion death
Drowning
Immersion
Death caused by autonomic response illiciting ischemia/arrythmia. Diagnosis of exclusion
Stomach
• Wischnewsky spots due to cold stress (hypothermia)
Extensor surfaces
• Reddish/brown discoluration (hypothermia)
https://doi.org/10.1007/s12024-012-9342-1
Other things to check
Internal examination
• Heart: evidence of underlying cardiac pathology
• Brain: consideration of neuropathology e.g. epilepsy
Histology and Toxicology
• Lungs: intraalveolar oedema, ruptured alveolar septae (overexpansion i.e. emphysema aquosum), aspirated material
• Wischnewsky spots: gastric mucosal necrosis, hemorrhage and neutrophilic infiltration
• Toxicology: blood, urine and vitreous humour (low threshold to speak with toxicologists as results can be diluted)
• “Analysis of liver, lungs, bone marrow and kidneys for diatoms is of limited utility”
Further reading: https://www.rcpath.org/static/a0eab7db-454b-4556-b9961ecfd8356307/06f19d98-8ca1-40c3-ab3d757e7c258281/Guidelines-on-autopsy-practice-Autopsy-for-bodies-recovered-from-water.pdf
Further reading: https://www.rcpath.org/static/a0eab7db-454b-4556-b9961ecfd8356307/06f19d98-8ca1-40c3-ab3d757e7c258281/Guidelines-on-autopsy-practice-Autopsy-for-bodies-recovered-from-water.pdf By Vader1941 - Own work, CC BY 4.0, https://commons.wikimedia.org/w/ind ex.php?curid=141068485
Diatom – unicellular microalgae
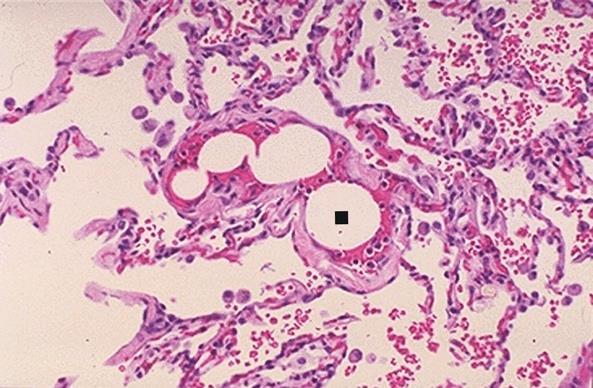
20. You obtained histology and toxicology from the lungs of a 30-year-old deceased man who died after he fell off a ladder at work. Polarisable material is seen with focal foreign body giant cell reaction as per the photomicrograph below. What conclusion can be deduced about the patient from these findings?
A. Patient was a cocaine user
B. Patient was a heroin user
C. Patient was a sandblaster
D. Patient worked with aluminium
20. You obtained histology and toxicology from the lungs of a 30-year-old deceased man who died after he fell off a ladder at work. Polarisable material is seen with focal foreign body giant cell reaction as per the photomicrograph below. What conclusion can be deduced about the patient from these findings?
These are perivascular talc granulomas. The polarisable material is talc, which is used to dilute the heroin. It is present in and around blood vessels of the lung (first organ to receive the injected blood). There may be associated MNGC reaction.
21. You perform the postmortem examination on a 63-year-old female with a history of alcohol dependence. She had no history of any other medical conditions. Blood tests from a recent over 60s health check at her GPs office were normal including cholesterol and HbA1c. Her relatives are sure that the death was related to alcohol consumption. Identification of which of the following substances would confirm the relatives suspicions?
A. Lactate
B. Beta-hydroxybutyrate
C. Thiamine
D. Glucose
21. You perform the postmortem examination on a 63-year-old female with a history of alcohol dependence. She had no history of any other medical conditions. Blood tests from a recent over 60s health check at her GPs office were normal including cholesterol and HbA1c. Her relatives are sure that the death was related to alcohol consumption. Identification of which of the following substances would confirm the relatives suspicions?
A. Lactate
B. Beta-hydroxybutyrate
C. Thiamine
D. Glucose
Ketoacidosis
• Ketones – usually low level compounds that serve as alternate energy source.
• Main ketones: Acetoacetate and beta-hydroxybutyrate
• Problem: at high levels are toxic and cause acidosis
• Due to any reason that glucose cannot be utilised
• Two main causes
• Diabetic ketoacidosis (in type 1 diabetes; type 2 have just enough insulin response to avoid acidosis, but instead “allowed time” to develop high sugar levels and hyperosmolar state)
• Vitreous: raised glucose
• Alcohol dependence (indirectly halts TCA cycle)
• Vitreous: not raised glucose
Glucose
Type 1 diabetes
Autoimmune destruction of Beta cells in Islet of Langerhans (Pancreas)
Taken to other cells (brain is particularly reliant if no glucose available) and converted back to Acetyl CoA to enter TCA cycle. Only issue is ketones are acidic and can make you very sick and potentially fatal in high concentrations.
Alcohol dependence
NAD+ not NADH needed to allow TCA cycle to continue. Overconsumption of NAD causes halt of TCA cycle and then body completely reliant on ketones
Acetoacetate
Acetone
3-Hydroxybutyrate
22. You are a trainee who has just joined the consultant pathologist in reporting postmortem lung histology on a 40-year-old female patient. The consultant asks you based on the finding observed in the photomicrograph below what can be deduced about the deceased?
A. She was an IV drug user
B. She has vegetations on the tricuspid valve
C. She had a swollen and painful calf
D. She was pregnant
E. She was immunocompromised
22. You are a trainee who has just joined the consultant pathologist in reporting postmortem lung histology on a 40-year-old female patient. The consultant asks you based on the finding observed in the photomicrograph below what can be deduced about the deceased?