• Early/’typical’ lesions: spongiosis and lymphocyte exocytosis
• Overlying parakeratin, acanthosis
• Late lesions: psoriasiform hyperplasia
• Always perform a fungal stain for dermatophyte infection
• Eosinophilic spongiosis (eosinophils in the epidermis with spongiosis)
• Drug reaction
• Allergic/contact dermatitis
• Insect bite reaction
• Pre-bullous bullous pemphigoid
• Langerhan cell vesicles – allergic/contact
• Underlying vascular changes – stasis dermatitis
• Lipping or separation of keratin (‘teapot sign’) – pityriasis rosea
• Hyphae – dermatophyte infection
MCQ 1
33 year old male printer complained of a 3 month history of hand dermatitis. Patch testing was negative. A biopsy showed spongiosis and lymphocyte exocytosis. No Munro’s microabcesses are seen. Identify the most likely diagnosis.
• A. Prebullous pemiphigoid
• B. Psoriasis vulgaris
• C. Irritant/contact eczematous dermatitis
• D. Mycosis fungoides
• E. Drug reaction
Psoriasiform reaction
• Regular elongation and broadening of rete
•Psoriasis
•Lichen simplex chronicus
•Pityriasis rubra pilaris
•Psoriasiform changes in eczematous dermatitis
Psoriasis
• Chronic non-infectious inflammatory dermatosis
• Well demarcated erythematous plaques topped with silvery scales
• Variants: Plaque, Palmoplantar, Scalp, Guttate, Flexural, Nail
• Early
• Vascular proliferation in dermal papillae
• Slight spongiosis
• Established lesions
• Regular acanthosis with regular elongation of rete ridges
• Thinning of supra-papillary epidermal plate
• Parakeratosis
• Increased mitotic activity at the base of epidermis
• Reduced/absent granular cell layer
• Neutrophil pustules – Munro microabscesses
MCQ 2a
• Which statement is false.
• Psoriasis:
a. Can result in alopecia
b. Sacrum affected
c. Pustular form exists
d. Histologically shows spongiform pustule of Kogoj
e. Vascular ectasia is seen with margination of neutrophils
MCQ 2b
• A 34 year old patient presents with multiple silvery skin plaques. A skin biopsy is performed to confirm the diagnosis.
• Identify the finding which would not be consistent with a diagnosis of psoriasis.
a. Can result in alopecia
b. Sacrum affected
c. Pustular form exists
d. Histologically shows spongiform pustule of Kogoj
e. Vascular ectasia is seen with margination of neutrophils
MCQ 2c
• A 34 year old patient presents with multiple silvery skin plaques involving the extensor surface of the limbs, scalp and lower back. The condition is worse after periods of stress and localises to areas of trauma. A skin biopsy is performed to confirm the diagnosis.
• Identify the finding which would not be expected in this condition.
a. Can result in alopecia
b. Sacrum affected
c. Pustular form exists
d. Histologically shows spongiform pustule of Kogoj
e. Vascular ectasia is seen with margination of neutrophils
MCQ 2d
• A 34 year old patient presents with multiple silvery skin plaques involving the extensor surface of the limbs, scalp and lower back. The condition is worse after periods of stress and localises to areas of trauma. A skin biopsy is performed to confirm the diagnosis.
• Identify the finding which would not be expected in this condition.
a. Fibrous replacement of hair follicles
b. Parakeratosis
c. Neutrophilic pustules in the epidermis
d. Vascular ectasia is seen with margination of neutrophils
e. Loss of the granular cell layer
Pityriasis rubrapilaris (PRP)
• Red-orange well demarcated scaling patches
• Islands of sparing
• Can present with erythoderma
• ‘Alternating orthokeratin and parakeratin’ in a checkerboard pattern
• Psoriasiform hyperplasia
Lichen simplex chronicus/nodular prurigo
• Dermatosis related to chronic excoriation without an underlying aetiology
• Common in practice but a difficult exam question to write
• Many biopsies show an element of this with other clues to underlying cause
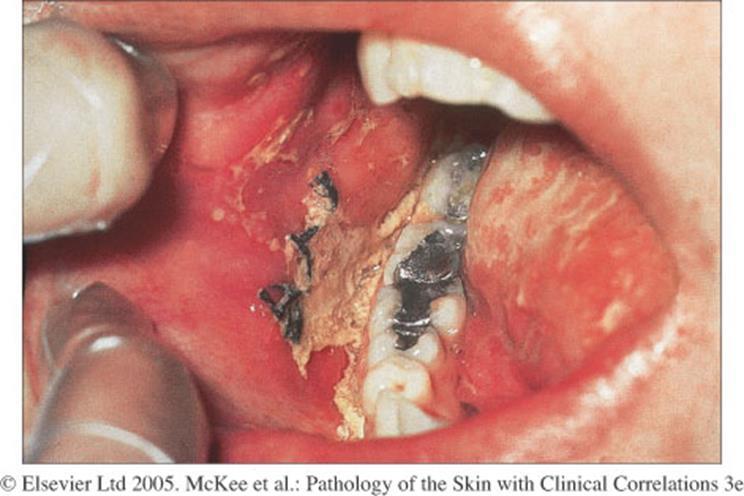
Syphilis
• Secondary syphilis
• Shows a widespread hyperpigmented maculopapular eruption.
• Causes: idiopathic, viral, bacterial, fungal, drugs (antibiotics, NSAIDs), other
• Oral, conjunctival, genital lesions not uncommon
• Interface change >lichenoid infammation
• A 44 year old taxi-driver presents with an sudden eruption on the trunk and limbs. Target lesions are present on the hands and feet. His skin biopsy shows basal cell damage with apoptotic keratinocytes.
• Identify the most likely diagnosis.
a. Lichen planus
b. Dermatomyositis
c. Erythema multiforme
d. Chronic graft versus host disease
e. Lichen nitidus
Toxic epidermal necrolysis (TEN)
• Sub-epidermal blisters with necrotic overlying epidermis
• Medical emergency
• Treated as a burns patient
• Main clinical differential – staphylococcal scalded skin
Lupus erythematosus
• Clinically: Sharply demarcated erythematous, scaly patches with follicular plugging.
• Characterised by 1. Interface change +/- lichenoid reaction 2. Superficial and deep perivascular and periadnexal chronic inflammatory cell infiltrate.
3. Hyperkeratosis, follicular plugging and epidermal atrophy.
4. Thickening of basement membrane
5. Increased dermal mucin
Graft versus host disease
• Usually a clinical diagnosis
• Following transplantation the donor's immune cells in the transplant (graft) make antibodies against the patient's tissues (host).
• Organs most often affected include the skin, gastrointestinal (GI) tract and the liver.
• Acute < 100 days
• Chronic > 100 days
Lichen sclerosus
• Pale atrophic patches
• Clinical DD often morphoea
• Lichenoid reaction (often subtle)
• Homogenisation of dermal collagen
• Thickening of basement membrane
• Ectatic vessels
• Underlying inflammatory infiltrate – often contains eosinophils
Vasculopathic conditions
• Vasculopathic just means it involves the blood vessels.
• Conditions include:
• Inflammation of vessels – vasculitis.
• Changes in the walls – porphyria, amyloid.
• Something in the lumen – thrombosis.
• More widespread changes – stasis dermatitis, arteriopathic changes.
Leukocytoclastic vasculitis
• Tissue reaction pattern which can be idiopathic or have underlying associations including drugs, connective tissue disease, infection and systemic vasculitis.
• Intramural neutrophils
• Red blood cell extravasation
• Fibrinoid necrosis
• Leukocytoclasis
Polyarteritis nodosa (PAN)
• Necrotising vasculitis of medium sized vessels
• Uncommon
• Tender nodules
• May develop hypertension, renal failure and neuropathy
• Similar findings to leukocytoclastic vasculitis but involves deeper vessels (into subcutis)
Wegener’s granulomatosis/Granulomatosis with polyangiitis
• Multiple purpuric macules and papules
• Possible to have ulcerating plaques and nodules.
• Histology
• Leukocytoclastic vasculitis.
• May see ill-defined granulomatous infiltrate surrounding vessels.
• c-ANCA positive
• Respiratory tract (nasal and lung) biopsies show necrosis associated with a granulomatous infiltrate
• Which of the following conditions does not show a leukocytoclastic vasculitis?
A. Erythema nodosum
B. Microscopic polyangiitis
C. Wegeners granulomatosis
D. Polyarteritis nodosa
E. Urticarial vasculitis
MCQ 4b
• A 42 year old patient presents with purpuric lesions involving both limbs. Inflammatory markers are raised. A skin biopsy is taken and shows features of a leukocytoclastic vasculitis.
• Identify the condition which does not show this feature.
A. Erythema nodosum
B. Eosinophilic granulomatosis with polyangiitis
C. Granulomatosis with polyangiitis
D. Polyarteritis nodosa
E. Urticarial vasculitis
MCQ 4c
• A 42 year old patient presents with purpuric lesions involving both limbs. Inflammatory markers are raised. A skin biopsy is taken and shows fibrinoid necrosis of vessel walls with leukocytoclasis and red blood cell extravasation.
• Identify the condition which would not show these features.
A. Erythema nodosum
B. Eosinophilic granulomatosis with polyangiitis
C. Granulomatosis with polyangiitis
D. Polyarteritis nodosa
E. Urticarial vasculitis
MCQ 4d
• A 42 year old patient presents with purpuric lesions involving both limbs. Inflammatory markers are raised. A skin biopsy is taken and shows fibrinoid necrosis of vessel walls with leukocytoclasis and red blood cell extravasation.
• Identify the most likely diagnosis.
A. Erythema nodosum
B. Eczematous dermatitis
C. Epidermolysis bullosa acquista
D. Erythema multiforme
E. Polyarteritis nodosa
Granulomatous inflammation/reaction
Types of granulomatous inflammation
• Sarcoidal
Foreign body
Suppurative
Tuberculoid
Necrobiotic • Interstitial
Differential always includes infection in all patterns of granulomatous inflammation
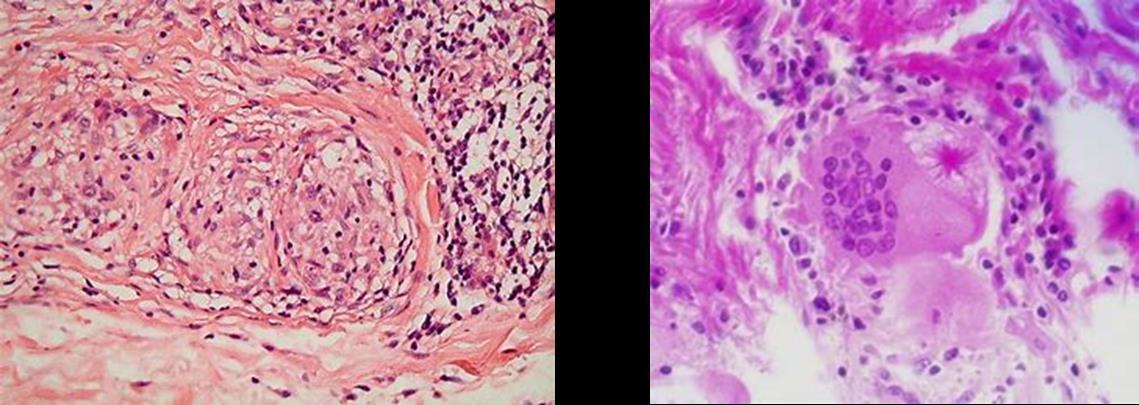
Sarcoidal granulomas
• Sarcoidosis • Reaction to foreign
Secondary Syphilis
Infection • Crohn’s disease
materials
Sarcoidosis
• Multisystem disorder
• Skin, liver, spleen, lung, eyes, lymph nodes
• 10-35% patients with systemic sarcoid have cutaneous lesions
• Sarcoidal granulomas are composed of epithelioid cells and giant cells, some containing asteroid bodies or other inclusions.
Foreign Body Granulomas
• Seen every day
• Scar/re-excision specimens
• Ruptured epidermoid cysts/follicles
Suppurative Granulomas
• Neutrophils within and sometimes surrounding the granuloma. The granulomatous component is not always well defined.
• Infection needs to be excluded – special stains don’t necessarily do this.
• Gram – Bacteria
• PAS and Grocott silver – fungal infection
• Ziehl Neelsen and Wade-Fite –acid fast bacilli
Tuberculosis – Tuberculoid granulomas
• Primary tuberculosis
• Miliary tuberculosis of skin
• Lupus vulgaris
• Scrofuloderma
• Tuberculous gumma
• Tuberculosis cutis orificialis
• Papulonecrotic
Necrobiotic granulomas
• Palisading of histiocytes around degenerate collagen
Necrobiotic granulomatous dermtoses
• Granuloma Annulare – palpable annular lesions on hands, feet or face
• Necrobiosis lipoidica – shiny atrophic yellowish red plaques on shins (62% in diabetics)
• Rheumatoid nodule - a local swelling or tissue lump, over bony prominences which occurs almost exclusively in association with rheumatoid arthritis
• Granuloma annulare
• Superficial/mid dermis
• Often intersitial (‘incomplete’)
• No plasma cells
• Eosinophils
• Mucin stain
• Necrobiosis lipoidica
• Diabetes
• Mid to deep dermis
• Linear pattern
• Plasma cells
• Rheumatoid nodules
• History
• Over joints
• Deep dermis to subcutis
• Palisading of histiocytes around eosinophilic material
• Fibrin/Trichrome stain
MCQ 5a
• Which of the following conditions is not associated with granulomatous inflammation.
A. Sarcoidosis
B. Granuloma annulare
C. Pemphigus vulgaris
D. Fungal infection
E. Tuberculosis
MCQ 5b
• A 58 year year old woman presents with itchy annular skin lesions. She has a history of Crohn’s disease for which she is on systemic therapy. A skin biopsy show aggregates of histiocytes. A Grocott silver stain is positive.
• Identify the most likely diagnosis.
A. Sarcoidosis
B. Granuloma annulare
C. Necrobiosis lipoidica
D. Fungal infection
E. Metastatic Crohn’s disease
MCQ 5c
• A 59 year old lady presents with annular lesions over the dorsal surfaces of both hands. A biopsy shows an interstitial infiltrate of histiocytes with mucin deposition and focal necrobioisis. No plasma cells are seen.
• Identify the most likely diagnosis
• Necrobiosis lipoidica
• Sarcoidosis
• Granuloma annulare
• Fungal infection
• Rheumatoid nodules
Blistering conditions
1. Anatomical level of split
2. Mechanism responsible
3. Nature of inflammatory cell infiltrate
Anatomical Level of Split
•Intracorneal/ subcorneal
•Intraepidermal (within stratum spinosum)
•Suprabasal
•Sub-epidermal
•Correlates with clinical type of blister
Mechanism responsible
•Cytopathic
•Spongiotic
•Autoimmune - immunobullous
•Vasculitic
•Trauma
Intracorneal/ Subcorneal
• Impetigo
• Dermatophytosis
• Staphylococcal scalded skin
• Superficial variants of pemphigus
Intraepidermal
• Herpes Infection
• Spongiotic vesicles - blisters
• Friction blister
• Acantholytic disorders
Suprabasal
• Acantholytic
Acantholytic disorders
• Loss of cell-to-cell adhesion in epidermis
• Immune mediated
• Blisters tend to be fragile as suprabasal or above
• Immunofluoresence helps distinguish the pemphigus variants from other conditions
• Multiple tissue reaction patterns now recognised
• Epidermal dysplasia
• Paraneoplastic pemphigus
• Blistering
• Acantholytic
• Both intercellular and linear (BMZ) IgG and C3c on IMF
Subepidermal
• Immunobullous
• Bullous pemphigoid
• Dermatitis herpetiformis
• Epidermolysis bullosa
• Linear IgA ( = Chronic bullous disease of childhood)
• Traumatic
• Vasculitis
• Lichenoid/interface dermatoses
• Bullous diabeticorum
• Bullous amyloidosis
Bullous pemphigoid
• Large often tense blisters with a predilection for trunk and flexural extremities
• Subepidermal blister with eosinophils
• ‘Eosinophilic spongiosis’
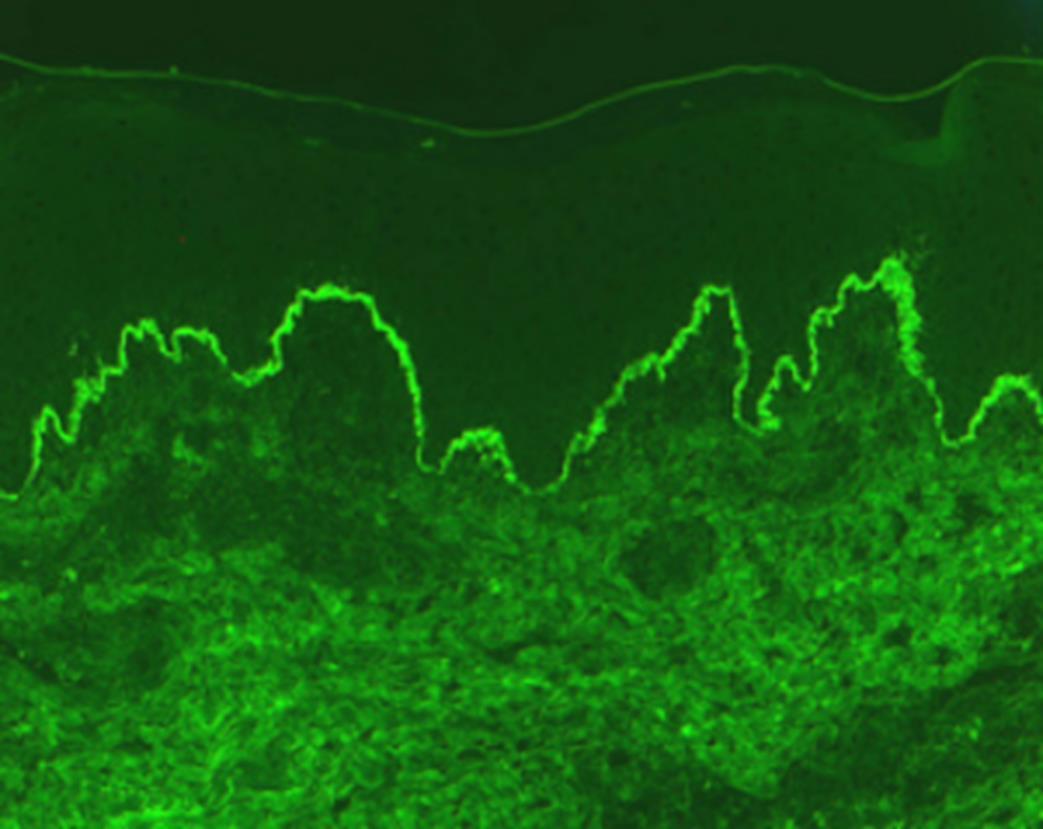
• Direct IMF - linear IgG and C3c at BMZ
• Linear IgG and C3c along BMZ
• Bullous pemphigoid
• Epidermolysis bullosa acquista
• Pemphigoid gestationalis
• Paraneoplastic pemphigus (+chicken wire pattern of intercellular deposition)
Dermatitis herpetiformis
• Young adults
• Intense pruritic vesicles with excoriation
• Predilection for extensor surfaces
• Invariably associated with gluten enteropathy although often subclinical
• Sub-epidermal neutrophilrich blister
• Dermal neutrophil-rich infiltrate with leukocytoclasis
• Neutrophil micro-abscess in adjacent dermal papillae
• Granular IgA in the tips of the dermal papillae on direct immunofluorescence.
• Vesiculo-bullous eruption of hepatobiliary disease may also present with dermatitis herpetiformis-like features
• Linear IgA disease (and chronic bullous disease of childhood) show similar morphology
• Older individuals – present with blisters
• Distinguish by immunofluoresence
MCQ 6
• A 68 year old female has a 1/52 history of tense large blisters arising on erythematous skin. A skin biopsy shows a subepidermal blister containing eosinophils.
• Identify the most likely diagnosis.
A.Pemphigus vulgaris
B.Pemphigus foliaceus
C.Darier’s disease
D.Bullous pemphigoid
E.Grover’s disease
Cell poor subepidermal blisters
• Bullous pemphigoid
• Porphyria cutea tarda
• Burns
• Toxic epidermal necrolysis
• Suction blister
• Drugs
• Bullous amyloid
• Bullous diabeticorum
Porphyria cutea tarda
• Increasingly fragile skin hands and feet
• Fluid filled blisters (vesicles and bullae)
• Tiny cysts (milia) arising as the blisters heal
• Increased sensitivity to the sun
• Cell poor sub-epidermal blister
• Deposition of basement membrane material in epidermis – ‘caterpillar bodies’
• Thickening and increased eosinophilic in dermal vessels
• PAS and DPAS
• A. Tissue reaction patterns
• Spongiotic
• Psoriasiform
• Lichenoid
• Vasculopathic
• Granulomatous
• Vesiculobullous
• B. Patterns of inflammation
TUMOURS OF THE SKIN
Skin tumour origin (=normal skin histology)
• Epidermis
• Keratinocytes
• Melanocytes
• Dermis
• Supporting connective tissues – collagen and elastin
• Dermal, ectatic vessels, increased spindled cell/fibroblasts, some are stellate
• Acrichordon
• Increased colon and renal cancer (15%), spontaneous pneumothorax, pulmonary cysts
Question EMQ 1
Options
A.Trichoepithelioma
B.Basal cell carcinoma
C.Halo naevus
D.Compound melanocytic naevus
E.Intradermal melanocytic naevus
F.Blue naevus
G.Keratoacanthoma
H.Lichen planus
I. Malignant melanoma
J. Trichilemmoma
K.Seborrhoeic keratosis
L.Simple lentigo
M.Squamous cell carcinoma
Question 1 A 55 year old female present with a pigmented lesion on the hand. Histology shows naevus cells in the dermis with pigmented dendritic processes with overlying normal epidermis.
• Each of these subjects has a skin biopsy. For each one, select the most likely condition form the list of options. Each may be use once, more than once, or not at all.
Question EMQ 1
Options
A.Trichoepithelioma
B.Basal cell carcinoma
C.Halo naevus
D.Compound melanocytic naevus
E.Intradermal melanocytic naevus
F.Blue naevus
G.Keratoacanthoma
H.Lichen planus
I. Malignant melanoma
J. Trichilemmoma
K.Seborrhoeic keratosis
L.Simple lentigo
M.Squamous cell carcinoma
Question 2
A 35 year old man present with a pigmented lesion on the arm with an outer hypo-pigmented area. Biopsy shows a band of inflammatory cells at the dermo-epidermal junction with scattered bland nests of naevus cells.
• Each of these subjects has a skin biopsy. For each one, select the most likely condition form the list of options. Each may be use once, more than once, or not at all.
Question EMQ 1
Options
A.Trichoepithelioma
B.Basal cell carcinoma
C.Halo naevus
D.Compound melanocytic naevus
E.Intradermal melanocytic naevus
F.Blue naevus
G.Keratoacanthoma
H.Lichen planus
I. Malignant melanoma
J. Trichilemmoma
K.Seborrhoeic keratosis
L.Simple lentigo
M.Squamous cell carcinoma
Question 3
A 28 year old female with a papule on the nose. Histology shows islands of basaloid cells with occasional mitotic activity and papillary mesenchymal bodies.
• Each of these subjects has a skin biopsy. For each one, select the most likely condition form the list of options. Each may be use once, more than once, or not at all.
Question EMQ 1
Options
A.Trichoepithelioma
B.Basal cell carcinoma
C.Halo naevus
D.Compound melanocytic naevus
E.Intradermal melanocytic naevus
F.Blue naevus
G.Keratoacanthoma
H.Lichen planus
I. Malignant melanoma
J. Trichillemmoma
K.Seborrhoeic keratosis
L.Simple lentigo
M.Squamous cell carcinoma
Question 4
A 70 year old man presents with a ulcerated lesion on the face. Skin biopsy shows squamous islands in the dermis with atypia and dyskeratosis.
• Each of these subjects has a skin biopsy. For each one, select the most likely condition form the list of options. Each may be use once, more than once, or not at all.
Question EMQ 1
Options
A.Trichoepithelioma
B.Basal cell carcinoma
C.Halo naevus
D.Compound melanocytic naevus
E.Intradermal melanocytic naevus
F.Blue naevus
G.Keratoacanthoma
H.Lichen planus
I. Malignant melanoma
J. Trichilemmoma
K.Seborrhoeic keratosis
L.Simple lentigo
M.Squamous cell carcinoma
Question 5
A 68 year old man with multiple papules on the face. Histology shows epidermal proliferation with glycogenated keratinocytes, peripheral palisade and thickened basement membrane. No atypia or mitoses are seen.
• Each of these subjects has a skin biopsy. For each one, select the most likely condition form the list of options. Each may be use once, more than once, or not at all.
Non-melanoma skin cancers
Non-melanoma skin cancers
• Squamous cell carcinoma
• Basal cell carcinoma
• Cumulative genetic abnormalities
• Chromosomal aberrations can be
• Structural rearrangements
• Copy number variations
• Often associated with
• Age
• UV exposure
TNM – T stage NMSC
MCQ 7a
• Predisposing factors for squamous cell carcinoma are all the following except:
a. UVB exposure
b. HPV Infection
c. Immunosuppression
d. Scarring
e. HHV-8 Infection
MCQ 7b
• A 35 year old presents with an invasive poorly differentiated squamous cell carcinoma of the scalp.
• Identify the most likely aetiological factor.
a. Solar damage/sun exposure
b. Immunosuppression
c. HHV8 infection
d. Previous radiotherapy
e. Idiopathic
• A 72 year old presents with a squamous cell carcinoma of the scalp. An excision biopsy is performed and reported as per the RCPath dataset.
• Identify which feature would upstage the tumour to pT3.
a. Perineural invasion –subcutis nerves
b. Location in head and neck
c. Depth of invasion 5.5mm
d. Clinical diameter >20mm
e. Lymphovascular invasion
MCQ 9
• A 72 year old presents with an ulcerating tumour of the scalp. He has had androgenetic alopecia for many years. A biopsy shows basaloid nests of atypical cells infiltrating the dermis.
• Identify the most likely predisposing factor in this case.
a. Solar damage
b. Immunosuppression
c. Gorlins syndrome
d. Xeroderma pigmentosum
e. Underlying lichen planopilaris
Keratoacanthoma
• Classic History – rapidly increasing in size then may regress
• Crateriform squamoproliferative lesion
• Epithelial Collarette
• Bulbous nested downgrowths with well defined borders
• Neutrophil microabscesses
• Abundant glassy cytoplasm
Merkel cell carcinoma
• Primary cutaneous neuroendocrine carcinoma
• UV radiation
• Clonal integration of Merkel cell polyomavirus (MCPyV)
• x10 in HIV +ve
• x5-10 in solid organ recipients
• x40 in patients with chronic lymphocytic lymphoma
• Cell of origin unknown – possibly not a Merkel cell
• MCPyV positive and negative tumours
• Negative group
• More mutations in TP53 and RB1 genes
• UV mutation signature
• Higher mutation burden
• Positive for neuroendocrine markers
– chromogranin, synaptophysin and CD56
• Main clinical difficulty:
• Is it primary skin tumour or metastasis?
• Panel of immunohistochemistry
• CK7 –ve, CK20 +ve, TTF1 -ve
• MCPyVm IHC
Benign epithelial entities
Inverted Follicular Keratosis
• ? Variant of seborrhoeic keratosis
• Numerous whorls/ eddies – eosinophilic flattened squamous cells arranged in an onion-peel fashion
• No cytological atypia
Clear Cell Acanthoma
• Arise on the shin of elderly females
• Distinctive tumour
• Collarette often seen at periphery
• Pale cells
• Intraepidermal neutrophils
• PAS and EMA positive
Cutaneous Horn
• Viral Wart
• Seborrhoeic keratosis
• Actinic keratosis
• Lichenoid keratosis
• Squamous cell carcinoma
Melanocytic neoplams
Tumours: Melanocytic neoplasms
Common blue naevus
• Dorsum of hands and feet
• Slate blue nodule
• Melanocytes are of the same appearance as naevus of Ito/Ota but show much greater density
• Epidermis normal
• Melanocytes contain fine granules of melanin
Tumours: Melanocytic neoplasms
Cellular blue naevus
• Usually larger than a common blue naevus (1-3 cms)
• 50% over the buttocks
• Histopathology
• Areas similar to blue naevus admixed with more cellular islands composed of closely aggregated, rather larger spindle shaped cells with ovoid nuclei and abundant pale cytoplasm.
• Extends into the superficial subcutis
• May have atypical features
Special variants of melanocytic naevi
• Halo Naevus
• Spitz naevus
• Pigmented spindle cell naevus of Reed
• BAP1 inactivated naevus/melanocytoma
• Deep penetrating naevus/melanocytoma
• Dysplastic naevus
Tumours: Melanocytic neoplasms
Halo Naevus
• Clinical appearance
• Nest of naevus cells in the papillary dermis associated with a lympho-histiocytic inflammatory cell infiltrate
• Prominent vertical orientation of cells are noted.
• Heavily pigmented + melanophages.
• Junctional clefting is noted in some cases.
Tumours: Melanocytic neoplasms
Deep penetrating naevus/melanocytoma
• First described by Helwig et al and 1989
• Dermal based melanocytic lesion composed of pigmented spindled and/or epithelioid cells with deep architecture
• Melanocytes maintain size and pigmentation throughout the dermis (i.e. don’t mature)
• Morphological overlap with conventional, blue and Spitz naevi
• Rarely progress to melanoma
• WNT activated deep penetrating/plexiform melanocytoma
• Caused by combined activation of MAP-kinase and WNT signalling pathways
• Beta catenin – nuclear positive
• Usually BRAF positive
Tumours: Melanocytic neoplasms
Tumours: Melanocytic neoplasms
Dysplastic Naevus
• Clinically and histologically form a continuum extending from common naevus to a superficial spreading melanoma
• Histopathology
• Architectural atypia
• Lentiginous proliferation of melanocytes
• Bridging between adjacent rete ridges
• Lamellar fibroplasia
• Cytological atypia
• Shouldering of dermal component
Tumours: Melanocytic neoplasms
Malignant melanoma
• Useful pointers to malignant melanoma
• Ulceration
• Asymmetrical Lesion
• Architectural Atypia
• Pagetoid Spread
• Diffuse cytological atypia with prominent eosinophilic nucleolus
• Dermal Mitoses
• Lack of Maturation
• Regression
• Factor in age!
Tumours: Melanocytic neoplasms
Tumours: Melanocytic neoplasms
• Melanoma associated with CSD
• Superficial spreading melanoma
• Lentigo maligna melanoma
• Desmoplastic melanoma
• Melanoma not associated with CSD
• Spitzoid
• Acral
• Mucosal
• Uveal
• Melanoma arising in congenital naevi
• Melanoma arising within blue naevi
• Nodular melanoma
Tumours: Melanocytic neoplasms
Tumours: Melanocytic neoplasms
Superficial spreading melanoma
• May develop in any part of the body and at any age. It is commonly noted on the trunk and lower extremities.
• Episodic skin damage – episodes of sun burn
• Histologically , the lesion is characterized by proliferation of atypical melanocytes at all levels in the epidermis.
• The tumour cells are present singly and in nests.
• Pagetoid spread in the epidermis.
Lentigo Maligna
• In 1969, Clark and Mihm described LM
• Most frequently occurs on the sun-exposed face and upper extremities of elderly people (chronic sun exposure)
• Histologically, there is proliferation of atypical melanocytes singly and in nests along the basal layer of the epidermis.
Tumours: Melanocytic neoplasms
Nodular melanoma
• 2nd most common subtype of melanoma. It represents 15% of all melanomas.
• The most common sites for nodular melanoma are the trunk, head, and neck.
• Macroscopically, the lesion presents as a nodular, polypoid or pedunculated dark brown or blue black lesion. May also present as an amelanotic nodule.
• Often ulcerated
• Often no junctional component – dd. metastasis
Tumours: Melanocytic neoplasms
MCQ 10
• All the following lesions are benign except
A. Spitz naevus
B. Lentigo maligna
C. Cellular blue naevus
D. Naevus of ota
E. Freckles
Acral lentiginous melanoma
• The most common type of malignant melanoma in skin type
3+
• Peak incidence in the seventh decade for males and in the sixth decade for females.
• These lesions are usually located on palmar, plantar and subungual skin.
• Lentiginous and some nesting proliferation of atypical melanocytes.
• Perineural invasion not uncommon
• Genetic mutation in cKIT most common Tumours:
• A 23 year old woman presents with a changing melanocytic lesion on the sole of the foot. An excision biopsy shows malignant melanoma.
• Identify the most likely genetic mutation.
c. ALK
d. k-RAS
e. Tyrosine kinase
a. cKIT
b. BRAF
• Breslow thickness
• Most important prognostic factor
• Only for invasive lesions
• Measure from Granular cell layer
• If Ulcerated; base of ulcer Tumours: Melanocytic
• A 27 year old man presents with a pigmented lesion on the upper arm. An excision biopsy is performed. The lesion is compound in nature with prominent Pagetoid ascent in the epidermis and multiple dermal mitoses (3 per mm2).
• Identify the most important prognostic factor.
a. Depth of invasion
b. Macroscopic diameter
c. Presence of dermal mitoses
d. Pagetoid ascent
e. Absence of tumour infiltrating lymphocytes
• Microsatellite – Foci of metastatic tumour cells in the skin or subcutis adjacent or deep to but discontinuous from the primary tumour detected in microscopic examination of tissue
• Satellite metastasis – Foci of clinically evident cutaneous and/or subcutaneous metastasis occurring within 2cm of but discontinuous from the primary melanoma
• In-transit metastasis – Clinically evident cutaneous and/or subcutaneous metastasis occurring >2cm from the primary melanoma in the region between the primary and the regional lymph node basin
• Any cutaneous metastasis that does not fall into the above categories is considered distant metastasis and staged under the M category
Tumours: Melanocytic neoplasms
Question EMQ 2
Options
A.MelanA
B.SOX10
C.S100
D.HMB45
E.P16
F.BRAF V600E
G.BAP1
H.Ki67
I. Beta-catenin
J. NTRK
K.ROS1
L.ALK
M.PRAME
Question 1
An intradermal melanocytic lesion show spindle cell morphology with fibrillary cytoplasm. A diagnosis of deep penetrating melanocytoma is suspected on H&E sections.
Identify the IHC stain which would be most helpful in confirming this diagnosis.
• Each of these immunohistochemistry stains can be used in diagnosing melanocytic lesion. Identify the more relevant option based on the descriptions above.
Question EMQ 2
Options
A.MelanA
B.SOX10
C.S100
D.HMB45
E.P16
F.BRAF V600E
G.BAP1
H.Ki67
I. Beta-catenin
J. NTRK
K.PRAME
Question 2
A 9 year old child presents with a compound melanocytic lesion demonstrating epithelioid morphology and prominent Kamino bodies. Identify the IHC stain which would be most helpful in confirming this is a Spitzoid lesion.
• Each of these immunohistochemistry stains can be used in diagnosing melanocytic lesion. Identify the more relevant option based on the descriptions above.
Question EMQ 2
Options
A.MelanA
B.SOX10
C.S100
D.HMB45
E.P16
F.BRAF V600E
G.BAP1
H.Ki67
I. Beta-catenin
J. NTRK
K.PRAME
Question 3
A 52 year old patient is diagnosed with malignant melanoma. Complete loss of which IHC stain suggests homozygous deletion of CDKN2a?
• Each of these immunohistochemistry stains can be used in diagnosing melanocytic lesion. Identify the more relevant option based on the descriptions above.
Question EMQ 2
Options
A.MelanA
B.SOX10
C.S100
D.HMB45
E.P16
F.BRAF V600E
G.BAP1
H.Ki67
I. Beta-catenin
J. NTRK
K.PRAME
Question 4
A 72 year old patient presents with an ill defined junctional melanocytic lesion on their face and is diagnosis with lentigo maligna. IHC is performed and one of the markers show strong and diffuse nuclear positive staining throughout the lesion, helping to confirm the diagnosis. Identify the most likely answer.
• Each of these immunohistochemistry stains can be used in diagnosing melanocytic lesion. Identify the more relevant option based on the descriptions above.
Question EMQ 2
Options
A.MelanA
B.SOX10
C.S100
D.HMB45
E.P16
F.BRAF V600E
G.BAP1
H.Ki67
I. Beta-catenin
J. NTRK
K.PRAME
Question 5
A 31 year old patient is diagnosed with stage pT4b invasive malignant melanoma. Which IHC stain should be performed to guide further management.
• Each of these immunohistochemistry stains can be used in diagnosing melanocytic lesion. Identify the more relevant option based on the descriptions above.
Question EMQ 2
Options
A.MelanA
B.SOX10
C.S100
D.HMB45
E.P16
F.BRAF V600E
G.BAP1
H.Ki67
I. Beta-catenin
J. NTRK
K.PRAME
Question 6
A 25 year of patient presents with a melanocytic lesion on their arm. They have a FHx of thyroid and renal cancer and ocular melanoma. The lesion is compound and shows mixed naevoid and epithelioid morphology on H&E sections with an associated lymphocytic infiltrate. Identify the relevant IHC stain to confirm the specific diagnosis in this case.
• Each of these immunohistochemistry stains can be used in diagnosing melanocytic lesion. Identify the more relevant option based on the descriptions above.
Thank you and good luck!
Acknowledgment to Dr Mikheil and Dr Iskander H Chaudhry
Sarcoma and soft tissue tumours involving the skin
• Dermatofibrosarcoma protuberans
• Angiosarcoma
• Clear cell sarcoma (melanoma of soft tissue)
Dermatofibrosarcoma protuberans (DFSP)
• Superficial fibroblastic neoplasm
• Prone to local recurrence
• Characteristic storiform arrangement of monomorphic spindled cells strongly positive for CD34
• t(17;22)(q21.3;q13.1) results in COL1A1-PDGFB fusion
Angiosarcoma
• Malignant neoplasm of blood vessels
• Head and neck of elderly patients
• In areas of lymphoedema
• Post-radiotherapy
• MYC positive in >90% cases related to lymphoedema and radiotherapy
Clear cell sarcoma (melanoma of soft tissue parts)
• Morphologically and immunohistochemistry profile same as a melanoma