How Curiosity Shaped Dr. Pamela Plant’s Career Remedy or Enemy? Personalizing the Prevention, Treatment, and Management of Hereditary Breast and Ovarian Cancer From Biochemistry Research to Professional Development: Mobile Health Apps:
IN THIS ISSUE
Jeah
EDITORS-IN-CHIEF:
Kristen Ashworth
Suraiya Mangra
Kyla Trkulja
EXECUTIVE EDITORS:
Kevan Clifford
Kiko Huang
Alyona Ivanova
Nayaab Punjani
Lizabeth Teshler
SOCIAL MEDIA TEAM:
Lizabeth Teshler (Director)
Lielle Ronen
Abigail Wolfensohn
DESIGN EDITORS:
Stefanie Jinyin Wang (Co-Director)
Nichole Zhou (Co-Director)
Emily Huang
Yu-Wen Jan
Lauren Jones
Jeah Kim
Anaiah Reyes
PHOTOGRAPHERS:
Katherine Guo
Nancy Kim
JOURNALISTS & EDITORS:
Beatrice Acheson
Aria Afsharian
Tesam Ahmed
Jasmine Amini
Gabriela Blaszczyk
Yalda Champiri
Sara Corvinelli
Anthaea-Grace Patricia Dennis
Mia Feldman
Sreemoyee Ghosh
Grace Gibson
Katherine Guo
Kanak Gupta
Rachel Lebovic
Josephine Machado
Mahmudul Mannan
Caroline Marr
Anna Mouzenian
Gharaza Nasir
Karan Patel
Ana Piric
Selina Tang
Kowsar Teymouri
Priya van Oosterhout
Emily Wiljer
Saleena Zedan
By Jeah Kim, MScBMC Candidate (2T5)
www.imsmagazine.com
@IMSMagazine @IMSMagazine
Letter from the EDITORS
Hello Everyone,
As we welcome in the new year—and celebrate 25 years of 21st-century medicine—we have aptly chosen Precision Medicine as our Winter issue theme. Over the last few decades, our healthcare and medical research systems have been revolutionized by this new method to patient care, which moves beyond the traditional “one-size- ts-all” approach. e advancement of precision medicine has been instigated by key scienti c breakthroughs, such as the completion of the Human Genome Project, the discovery of CRISPR-based gene-editing technology, and the expanding use of arti cial intelligence to signi cantly enhance the individualized analysis of patient data.
In this issue, we feature four IMS faculty members that are making signi cant inroads in the eld of precision medicine research: Dr. Daniel Felsky, in the application of precision medicine for mental health; Dr. Carmela Tartaglia, for neurodegenerative diseases; Dr. Joanne Kotsopolous, for breast and ovarian cancer; and Dr. Sun-Ho Lee, for in ammatory bowel disease. In addition, our Viewpoint articles explore the evolving challenges of precision medicine that we face currently, in the context of advancing technology, patient privacy, and the ethical uses of AI. ese articles discuss pressing topics such as genome bank inequities, data and patient con dentiality, integration of patient data in healthcare apps, the current landscape of electronic medical records, and the use of wearable devices in personalized care.
We have also spotlighted three outstanding members of the IMS community in this issue—Dr. Pamela Plant, Dr. Sandy Lee, and Sajee Sujanthan—who have made signi cant and valuable contributions to the institute and beyond.
A big thank you to our amazing team of journalists, editors, and designers for their hard work on this issue. It was wonderful to celebrate with all of you and the rest of the IMS community last year during our inaugural launch party for the Fall 2024 issue. We are looking forward to all of what the future brings for our team in 2025!
Stay warm this winter and happy reading!
Kyla Trkulja
Kyla is a PhD student studying the mechanism of action of novel therapies for lymphoma under the supervision of Dr. Armand Keating, Dr. John Kuruvilla, and Dr. Rob Laister.
@kylatrkulja
Suraiya Mangra
Suraiya is a 2nd year MSc student investigating the effects of neuromodulation interventions on brain morphology in patients with neurodegenerative disorders at the Krembil Research Institute under the supervision of Dr. Andres Lozano.
Kristen Ashworth
Kristen is a PhD student studying the use of a human-based retinal organoid model to investigate cell therapies for genetic eye disease under the supervision of Dr. Brian Ballios at the Krembil Research Institute.
@K_Ashworth01
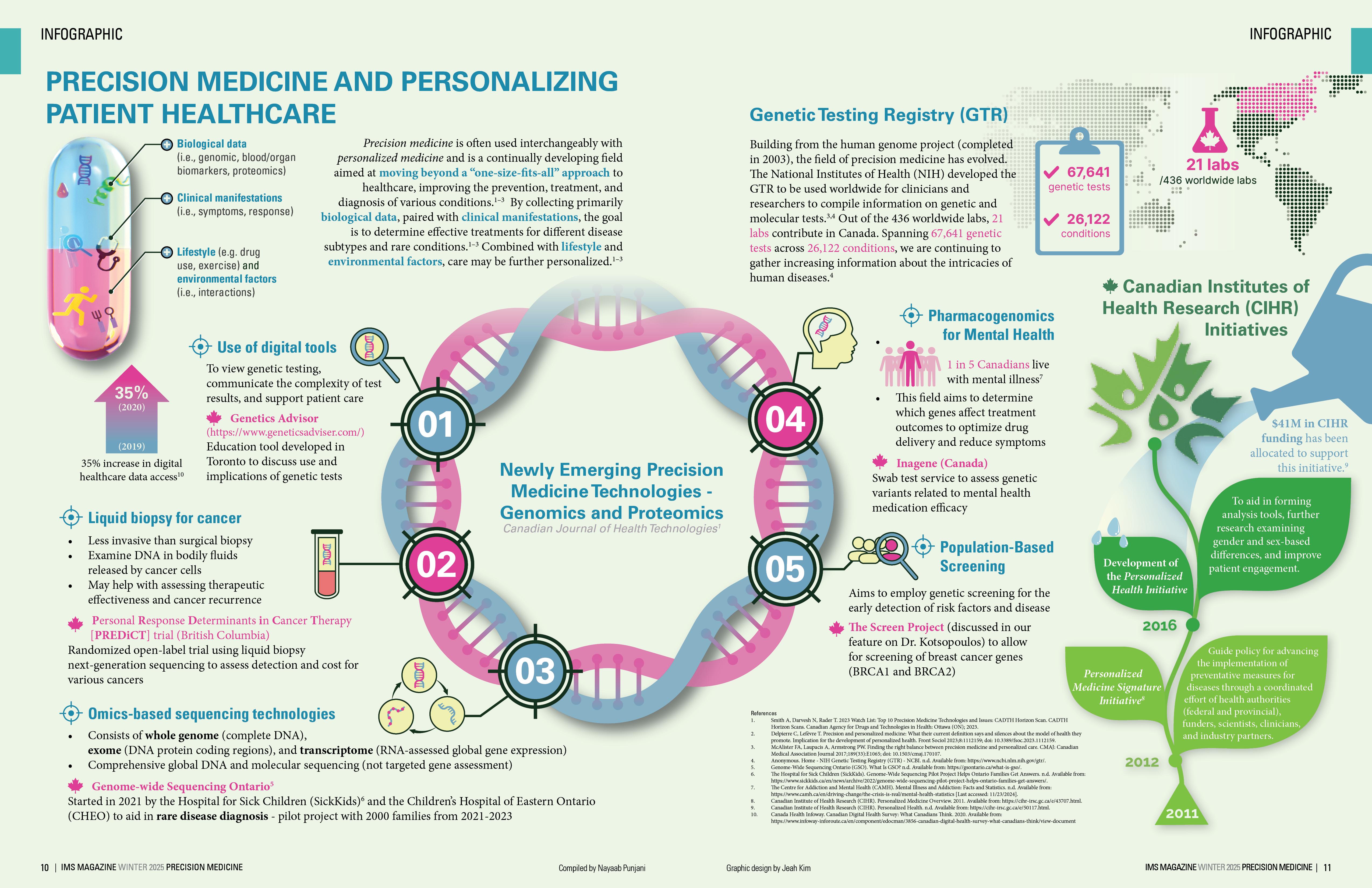
PRECISION MEDICINE AND PERSONALIZING PATIENT HEALTHCARE
Biological data (i.e., genomic, blood/organ biomarkers, proteomics)
(e.g. drug use, exercise) and environmental factors (i.e., interactions)
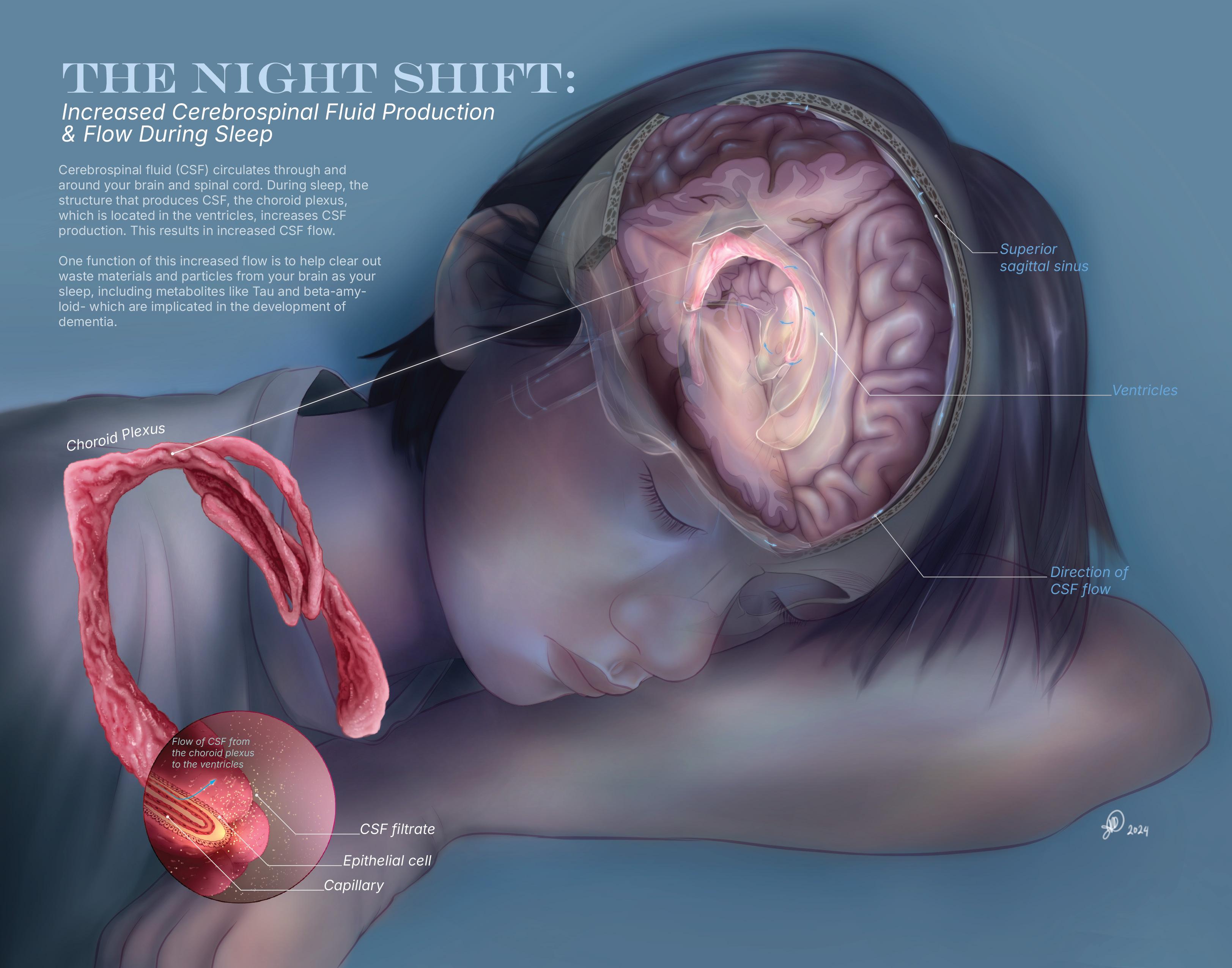
Precision medicine is o en used interchangeably with personalized medicine and is a continually developing eld aimed at moving beyond a “one-size- ts-all” approach to healthcare, improving the prevention, treatment, and diagnosis of various conditions.1–3 By collecting primarily biological data, paired with clinical manifestations, the goal is to determine e ective treatments for di erent disease subtypes and rare conditions.1–3 Combined with lifestyle and environmental factors, care may be further personalized.1–3
Use of digital tools
To view genetic testing, communicate the complexity of test results, and support patient care
Education tool developed in Toronto to discuss use and implications of genetic tests
• Liquid biopsy for cancer
• Less invasive than surgical biopsy
• Examine DNA in bodily uids released by cancer cells
• May help with assessing therapeutic e ectiveness and cancer recurrence
Personal Response Determinants in Cancer Therapy [PREDiCT] trial (British Columbia)
Randomized open-label trial using liquid biopsy next-generation sequencing to assess detection and cost for various cancers
• Omics-based sequencing technologies
01
02
Newly Emerging Precision Medicine Technologies
Genomics and Proteomics
Canadian Journal of Health Technologies
03
• Consists of whole genome (complete DNA), exome (DNA protein coding regions), and transcriptome (RNA-assessed global gene expression)
• Comprehensive global DNA and molecular sequencing (not targeted gene assessment)
Genome-wide Sequencing Ontario5
Started in 2021 by the Hospital for Sick Children (SickKids)6 and the Children’s Hospital of Eastern Ontario (CHEO) to aid in rare disease diagnosis - pilot project with 2000 families from 2021-2023
Precision TechnologiesProteomics Technologies1
Genetic Testing Registry (GTR)
Building from the human genome project (completed in 2003), the eld of precision medicine has evolved. e National Institutes of Health (NIH) developed the GTR to be used worldwide for clinicians and researchers to compile information on genetic and molecular tests.3,4 Out of the 436 worldwide labs, 21 labs contribute in Canada. Spanning 67,641 genetic tests across 26,122 conditions, we are continuing to gather increasing information about the intricacies of human diseases.4
References
67,641 26,122 genetic tests conditions
21 labs /436 worldwide labs
• Pharmacogenomics for Mental Health
•
• is eld aims to determine which genes a ect treatment outcomes to optimize drug delivery and reduce symptoms 1 in 5 Canadians live with mental illness7
Inagene (Canada)
Swab test service to assess genetic variants related to mental health medication e cacy
• Population-Based Screening
Aims to employ genetic screening for the early detection of risk factors and disease e Screen Project (discussed in our feature on Dr. Kotsopoulos) to allow for screening of breast cancer genes (BRCA1 and BRCA2)
1. Smith A, Darvesh N, Rader T. 2023 Watch List: Top 10 Precision Medicine Technologies and Issues: CADTH Horizon Scan. CADTH Horizon Scans. Canadian Agency for Drugs and Technologies in Health: Ottawa (ON); 2023.
Canadian Institutes of Health Research (CIHR)
Personalized Medicine Signature Initiative8
2. Delpierre C, Lefèvre T. Precision and personalized medicine: What their current de nition says and silences about the model of health they promote. Implication for the development of personalized health. Front Sociol 2023;8:1112159; doi: 10.3389/fsoc.2023.1112159.
3. McAlister FA, Laupacis A, Armstrong PW. Finding the right balance between precision medicine and personalized care. CMAJ: Canadian Medical Association Journal 2017;189(33):E1065; doi: 10.1503/cmaj.170107.
4. Anonymous. Home - NIH Genetic Testing Registry (GTR) - NCBI. n.d. Available from: https://www.ncbi.nlm.nih.gov/gtr/.
5. Genome-Wide Sequencing Ontario (GSO). What Is GSO? n.d. Available from: https://gsontario.ca/what-is-gso/.
6. e Hospital for Sick Children (SickKids). Genome-Wide Sequencing Pilot Project Helps Ontario Families Get Answers. n.d. Available from: https://www.sickkids.ca/en/news/archive/2022/genome-wide-sequencing-pilot-project-helps-ontario-families-get-answers/.
7. e Centre for Addiction and Mental Health (CAMH). Mental Illness and Addiction: Facts and Statistics. n.d. Available from: https://www.camh.ca/en/driving-change/the-crisis-is-real/mental-health-statistics [Last accessed: 11/23/2024].
8. Canadian Institute of Health Research (CIHR). Personalized Medicine Overview. 2011. Available from: https://cihr-irsc.gc.ca/e/43707.html.
9. Canadian Institute of Health Research (CIHR). Personalized Health. n.d. Available from: https://cihr-irsc.gc.ca/e/50117.html.
10. Canada Health Infoway. Canadian Digital Health Survey: What Canadians ink. 2020. Available from: https://www.infoway-inforoute.ca/en/component/edocman/3856-canadian-digital-health-survey-what-canadians-think/view-document
Development of the Personalized Health Initiative 2016 2012 2011 04 05
To aid in forming analysis tools, further research examining gender and sex-based di erences, and improve patient engagement.
Guide policy for advancing the implementation of preventative measures for diseases through a coordinated e ort of health authorities (federal and provincial), funders, scientists, clinicians, and industry partners.
DR. MINGYAO LIU Director, Institute of Medical Science Professor, Department of Surgery Senior Scientist, Toronto General Hospital Research
Institute, University Health Network
DIRECTOR’S MESSAGE
Welcome back to our IMS community from another festive holiday season. On behalf of the IMS leadership team, we hope you all had a joyous break filled with companionship, happiness, and relaxation. Between the food, celebrations, and decor, the holidays are a magical way to bring some light into an otherwise long and dark Canadian winter, providing a feeling of warmth and optimism for the months ahead. Therefore, it’s only fitting for the Winter 2025 issue of the IMS Magazine to focus on Precision Medicine, as its advancements in patient care have brought light and hope to many people around the world facing otherwise challenging health conditions.
This issue features faculty that are exploring personalized therapies for patients with a wide range of diseases to improve both their duration and quality of life. Dr. Daniel Felsky is investigating how to create personalized mental health treatment regimens using Whole Person Modeling, while Dr. Carmela Tartaglia is studying precision medicine’s role in the diagnosis of neurodegenerative diseases. Dr. Joanne Kotsopoulos is researching both the screening and treatment of BRCA-mutated cancers so both those at risk of and living with cancer have the best options available to them. Lastly, Dr. Sun-Ho Lee is pioneering how to design personalized approaches to treat irritable bowel disease (IBD), which is currently quite difficult to manage with existing treatments. These IMS faculty members are conducting complex and meaningful research into a wide range of conditions, and it is an honour to be featuring them in the Winter 2025 issue of the IMS Magazine.
We are also thrilled to be putting the spotlight on some influential members of our IMS community. Dr. Sandy Lee, a recent IMS alum, was an exceptional student leader during her graduate studies with us and is continuing her incredible work at the University of California, Los Angeles (UCLA). Dr. Pamela Plant has tirelessly designed courses and programs focused on professional and career development so students can prepare for success after their time at IMS. Lastly, current student Sajeevan Sujanthan, shares how his numerous research experiences have taught him what’s truly meaningful when figuring out what’s next for a soon-to-be PhD graduate. We also welcomed our new IMS students this Fall at our Orientation, and this issue shares the highlights of the event.
I would like to thank the IMS Magazine’s Editors-in-Chief, Kyla, Kristen, and Suraiya, for their work in directing this issue. As always, I also extend my sincere appreciation to the journalists, editors, photographers, and design team for their contributions to this Winter 2025 issue. I hope you enjoy reading about the exciting advancements in precision medicine, and the optimism for the field brings you a sense of warmth to start the New Year.
Sincerely,
Dr. Mingyao Liu Director, Institute of Medical Science
Photo Credit: Mikaeel Valli
Contributors Winter 2025
Beatrice Acheson is a rst-year MSc student working under the supervision of Dr. Peter St George Hyslop at the Tanz Centre for Research in Neurodegenerative Disease (CRND), where she investigates the genetic and molecular mechanisms underlying microglial dysfunction in Alzheimer’s Disease. When she is not in the lab, Beatrice is likely reading a book, attending a yoga class, or playing beach volleyball.
bea.acheson
Tesam Ahmed is a rst-year MSc student working under the supervision of Dr. Daniel Felsky at the Centre for Addiction and Mental Health. Her research investigates the interaction between structural and functional brain changes and genetic factors to in uence trajectories of psychosis in youth. Outside of the lab, Tesam loves to read, enjoy nature, and spend time with friends.
Jasmine Amini is a rst-year MSc working under the supervision of Dr.Daphne Korczak at the Hospital for Sick Children. Her research interests lie in social media use and family functioning among youth with an acute self-harm or suiciderelated concern. Outside of academia, Jasmine enjoys reading, volunteering, and exploring Toronto.
Gabriela Blaszczyk is a rst year PhD student, working under the supervision of Dr. Raphael Schneider and Dr. Jiwon Oh at St. Michael’s Hospital. She is investigating pre-symptomatic Multiple Sclerosis, with the end goal of understanding early disease and the development of a prognostic test to be used in the clinical setting. In her spare time, Gabriela volunteers as a ski patroller and loves to try new foods around the city.
gabi.blaszczyk
Kevan Cli ord is a PhD student in the IMS program, with a cross-appointment at the Centre for Addiction and Mental Health. Working under the supervision of Dr. Yuliya Nikolova, his research combines bioinformatics and neuroimaging to characterize mechanisms of brain aging at the genetic level, and outcomes on brain structure and function. Outside of the lab, Kevan enjoys trail running, photography, and a good book (preferably while curled up with his cat, Rauru).
Mia Feldman is a rst-year MSc student working under the supervision of Dr. Isabella Caniggia at the Lunenfeld Tanenbaum Research Institute. ey are studying the molecular origins of preeclampsia (high blood pressure in pregnancy) with emphasis on maternalplacental crosstalk in the disease. In their free time, Mia enjoys reading and exploring di erent neighborhoods in Toronto!
Grace Gibson is a rst-year MSc student in the Biomedical Communications program studying to become a medical illustrator. She aims to work in patient-facing media and outreach focused on the LGBTQ community. In her free time, Grace enjoys reading books and painting.
Katherine Guo is a rst-year MSc student working under the supervision of Dr. Shannon Lange at the Centre for Addiction and Mental Health. Her work focuses on patterns of alcohol consumption and its related harms, aiming to better-understand the association between alcohol consumption and suicide mortality. Outside of her academics, Katherine spends her time working on various graphic design projects, taking photos, and exploring the wildlife in and outside of the city. Katherine is also a part of our photography team!
Kanak Gupta is a rst-year MSc student passionate about increasing scienti c knowledge of women’s health issues. She is currently studying sex di erences in the neural circuitry involved in depression at the Centre for Addiction and Mental Health under Dr. Liisa Galea’s supervision. Outside the lab, she loves to write, speed run through artistic hobbies (currently, it’s pottery), and “urban hiking” in Toronto every weekend.
jasmine_amini9
Graphic design by Nichole Zhou
Kiko Huang is a second-year MSc student, currently studying glaucoma through an epidemiological lens under the supervision of Dr. Yaping Jin. Her work aims to investigate various trends in ophthalmology and vision care to gain a better understanding of the health landscape and guide policy. During her free time, she’s likely out exploring all the food that the city has to o er (recommendations appreciated)! kikohuangs
Alyona Ivanova is a PhD student investigating the molecular signature of glioblastoma using spatial -omics technologies at the Hospital for Sick Children under the supervision of Dr. Sunit Das. Alyona is a professional gure skater and a model. Alyona is a creative content manager of Panoramics - A Vision. She enjoys traveling, cooking and reading.
_alyonaivanova_
Rachel Lebovic is a rst-year PhD student at Sunnybrook Health Sciences Centre under the supervision of Dr. Mark Sinyor. She is studying suicide prevention through literature as a tool to teach mental health literacy to youth. She also has an interest in public mental health and the experience of transitional-aged youth in the mental health care system. Outside of research, Rachel enjoys cooking, going for walks, and building Lego. rachel.lebovic
Mahmudul Mannan is a MSc student at IMS investigating the accuracy of di erent baseline serum creatinine
(BSCr) estimation methods to de ne AKI and its stages in hospitalized children under the supervision of Dr. Michael Zappitelli at e Hospital for Sick Children (SickKids), Toronto. Outside of research, Mahmudul provides consultancies and support to newly immigrated physicians in Canada so that they can start their journey in Canada smoothly. Mahmudul loves to spend time with his family and friends, exploring di erent cuisines and new places.
Anna Mouzenian is a rst-year MSc student working under the supervision of Dr. Victor Tang and Dr. Daniel Felsky at the Centre for Addiction and Mental Health. Anna is investigating the use of wearable devices to predict outcomes for substance use disorders. In her free time, she enjoys dancing, hiking and pilates.
anna.violet
Gharaza Nasir is a rst-year MSc student at the Toronto General Hospital Research Institute, where she is investigating the genetic alterations driving Cholangiocarcinoma under the supervision of Dr. Arndt Vogel. Her research focuses on utilizing highthroughput drug screening to identify potential targeted therapies. In her free time, Gharaza enjoys working out, playing video games, and spending time with friends and family.
g.harazanasir
Ana Piric is a rstyear MSc student at the Princess Margaret Cancer Research Tower working under the supervision of Dr. Aaron Schimmer. Her research is focused on the molecular targeting of the mitochondrial protease LONP1 in early development cell models of acute myeloid leukemia (AML). In her free time Ana enjoys yoga, reading, and exploring the food scene in Toronto!
anapiric18
Nayaab Punjani is a h-year PhD student at the Krembil Research Institute in Dr. Michael Fehlings’ Lab. She is studying a neuroprotective peptide drug therapy to treat cervical traumatic spinal cord injury. In her free time she enjoys digital art and nature photography, as well as watching mystery, action, and sci- TV shows and movies. nayaab_punjani
Kowsar Teymouri is a third-year PhD student working under the supervision of Dr. James Kennedy at the Centre for Addiction and Mental Health (CAMH). Kowsar is investigating the role of the immune system genes in schizophrenia and how they are associated with di erent subgroups of schizophrenia. If not at CAMH, you can nd Kowsar running along the lakeshore, creating content for her travel blog, hiking in new trails or painting. kowsar_teymouri
Graphic design by Nichole Zhou
Emily Wiljer is a rst-year MSc student working under the supervision of Dr. Daniel Felsky at the Centre for Addiction and Mental Health (CAMH). Emily is investigating a biopsychosocial approach to cognitive resilience, as well as genetic and epigenetic factors in longevity. In her free time she enjoys reading, going to the gym, and trying new restaurants.
emily.wiljer
Photography Team
Nancy Kim is a rst-year MSc student under the supervision of Dr. Amanda Boyle at the Center of Addiction and Mental Health. Her research focuses on the endocannabinoid system in multiple sclerosis (MS) with the use of PET neuroimaging and histology studies. Outside of her research, she enjoys playing volleyball, exploring restaurants (mostly ramen places) and cafes (for matcha) near the campus.
Copy Editors
Aria Afsharian
Yalda Champiri
Sara Corvinelli
Anthaea-Grace Patricia Dennis
Sreemoyee Ghosh
Josephine Machado
Caroline Marr
Karan Patel
Selina Tang
Priya van Oosterhout
Abigail Wolfensohn
Saleena Zedan
Social Media Team
Lizabeth Teshler (Lead) is a PhD student supervised by Dr. Brian Feldman at e Hospital for Sick Children. Her research investigates how to improve the clinical examination of musculoskeletal health for people with Hemophilia. Outside of research, she loves biking, spending time outdoors and exploring new cities.
Abigail Wolfensohn is a rst-year MSc student in Dr. Mojgan Hodaie’s lab at Toronto Western Hospital. She is researching how the brain’s wasteclearance system functions in people with trigeminal neuralgia, a chronic facial pain condition. In her free time, she enjoys outdoor activities, puzzles, and playing the piano.
abbywolfen
Lielle Ronen is a rst-year MSc student in Dr. Andrew Sage’s Lab at the Latner oracic Surgery Research Labs in PMCRT. Her research investigates smoking damage in donor lungs to improve post-transplant outcomes using Ex-Vivo Lung Perfusion (EVLP). Aside from research, she loves painting, baking, running and trying local restaurants in Toronto.
IMS Design Team
e IMS Design Team is a group of second year MSc students in the Biomedical Communications (BMC) program. Turning scienti c research into compelling and e ective visualisations is their shared passion, and they are thrilled to contribute to the IMS Magazine.
Considering the Whole Person and Population when Applying Precision Medicine to Mental Health
By Tesam Ahmed and Emily Wiljer
Mental health is complex, in uenced by a web of biological, psychological, and environmental factors. Yet, traditional research o en isolates these aspects, overlooking the intricate ways they interact. In the Whole Person and Population Modelling (WPPM) lab at the Centre for Addiction and Mental Health (CAMH), Dr. Dan Felsky and his team are transforming how we understand mental health. Using a data-driven, integrative approach, the lab examines everything from individual genomes to large-scale population data, aiming to unlock new insights into mental health trajectories and outcomes. We sat down with Dr. Felsky to explore how this innovative approach can pave the way for more precise, personalized treatments in mental health care—and what it means for researchers, clinicians, and students alike.
Dr. Dan Felsky began his research journey during his undergraduate degree in biology at the University of Guelph. His interest in genetics earned him a spot in the lab of Dr. Jim Kennedy where he rst investigated genetics and mental illness. Enjoying this experience, he then completed his PhD under the co-supervision of Dr. Aristotle Voineskos and Dr. Jim Kennedy through the Institute of Medical Science at the University of Toronto, integrating neuroimaging with his background in genetics. Upon graduation, Dr. Felsky conducted postdoctoral research under Dr. Philip L. De Jaeger, in a multi-centre
project between Harvard Medical School, the Broad Institute of Massachusetts Institute of Technology and Harvard, and Columbia University. ese collaborations helped him develop his experience in neuroimmunology, neurology, and multiomic data types, which later facilitated the founding of his lab, WPPM, at the Krembil Centre for Neuroinformatics in May 2019.
e excitement around whole-person modeling stems from the breadth of data and approaches used to tackle complex research questions. When asked about past projects exemplifying these possibilities, Dr. Felsky described the ongoing work of a former Master’s student on clustering patients across data types. In collaboration with e Hospital for Sick Children (SickKids), they developed a new machine learning method to identify “unique biopsychosocial pro les across large groups of people in complex data types.” is method was applied to a subsample of the ongoing Toronto Adolescent Youth cohort study, consisting of youth seeking mental health treatment at CAMH. e team integrated brain imaging, cognitive, and demographic data to cluster individual needs and impairments. Dr. Felsky expressed excitement at this new method’s ability to cluster multiple data types reliably, without the usual assumptions, which could account for a broader range of information compared to other clustering algorithms. Future directions include examining whether this cohort responds di erentially to various treatment paradigms, aiding in the development of precision medications.
Another prominent study, conducted in collaboration with new CAMH faculty member Dr. Peter Zhukovsky, was published earlier this year. In the largest study of its kind, they explored how genetic risk pro les interact with modi able risk factors to in uence brain health. ey identi ed speci c genetic loci associated with cortical thickness, white matter hyperintensities (lesions in the brain’s white matter), and cognitive function, and the interaction of these loci with risk factors such as depression and cardiovascular conditions.1 “Critically, we also [looked at] how these genetic in uences on brain structure are modi ed, interacted with, or could be overcome by modi able factors,” says Dr. Felsky. Integrating diverse data types and examining interactions is essential in mental health research, as the same genetic factors can have varied e ects on di erent people. By moving beyond generalized genetic pro les, researchers can better capture the complexity of individual experiences.
Re ecting on challenges in his research, Dr. Felsky highlighted data availability, privacy governance, and transdisciplinary education. In a computational lab, balancing su cient, high-quality data that accurately captures risk features, while maintaining data sovereignty and protection is a constant challenge. “To make something that is impactful, generalizable, and clinically useful, the evidence has to be really strong for people to adopt it, to trust it,” he states. When accessing and collecting data, there is o en
trials, there are very few groups committed to investigating how these emerging tools could exist in our current healthcare system. is presents a roadblock for computational labs, and must be addressed in tandem with the accumulation and analysis of data. Dr. Felsky here points out one of his favourite papers and tells us to read it: “Chaos in the Brickyard”.2
a ne balance to consider with regards to patient risk and population bene ts. In terms of standardizing the whole-person approach, he points out that equipping trainees with the knowledge and skills needed for this type of work is a unique challenge that de es tradition. Despite these challenges, many scientists are working with institutions to assess barriers in data access and analysis.
To ensure maximum impact of this eld of research, Dr. Felsky calls for more collaboration with implementation science—the study of how to integrate research ndings into policy and practice. He highlights a lack of evidence showing that results from predictive modeling in psychiatry can be e ectively applied in clinical practice or population-based screening. Beyond promising clinical
When asked how research can be made more accessible to the public, Dr. Felsky emphasized engaging with the community. He mentions that having patients involved in study design and implementation is essential, as “the best ideas for how to transmit and exchange knowledge come from the people that are using that information.” He adds, “we sometimes forget that scientists are also people, who struggle with the same problems as the rest of society; when it comes to mental health research, we are o en our own ‘customers’.” Dr. Felsky also emphasizes the importance of e ectively communicating ideas to a general audience and fostering conversations among individuals from diverse backgrounds, experiences, and expertise. is approach facilitates knowledge translation and dissemination.
Looking ahead, Dr. Felsky is excited to move beyond classifying mental health and neurological diseases by categories and symptoms, and shi towards framing issues in the context of resilience and risk factors. He describes this approach as “linking the whole lifespan and
understanding how events, even very far in the past, can impact future events [and contribute to] risk and resilience pathways.” is involves examining “time sensitive” windows across the lifespan through diverse biopsychosocial data. An ongoing project aims to identify aspects of physiology, life experience, and behavior that contribute to cognitive resilience and how they interact with non-modi able risk factors such as genetics.
Dr. Felsky underscores the signi cance of thinking broadly and creatively in precision medicine, explaining that strati cation markers in research “could be any reliable measurement,” provided researchers develop and test innovative study designs to group individuals e ectively. O ering guidance to earlycareer scientists, he highlights the importance of embracing new concepts, while maintaining a structured and methodical approach to their work. is balance, he notes, can pave the way for deeper learning, fresh perspectives in research design, and more e ective execution, ultimately driving progress in the eld.
References
1. Zhukovsky, P., Tio, E.S., Coughlan, G. et al. Genetic in uences on brain and cognitive health and their interactions with cardiovascular conditions and depression. Nat Commun 15, 5207 (2024). https://doi.org/10.1038/s41467-024-49430-7
2. Forscher BK. Chaos in the Brickyard. Science. 1963 Oct 18;142(3590):339. DOI: 10.1126/science.142.3590.339
Dr. Daniel Felsky
Photo Credit: Nancy Kim
Head of the Whole Person and Population Modelling lab in the Krembil Centre for Neuroinformatics at CAMH.
Rewriting the Story of Dementia
How Dr. Carmela Tartaglia Is Bringing Precision Medicine to the Fight Against Neurodegenerative Diseases
By Beatrice Acheson
“55 million people worldwide are living with dementia. at is a lot of people. is is too many people to ignore,” Dr. Tartaglia emphasizes. By 2050 this number will increase to 152 million.1 For Dr. Tartaglia, these are not just statistics— they are real patients, each with their own unique story. is perspective drives her work as a Professor in the Institute of Medical Science and a leading ClinicianScientist at the Tanz Centre for Research in Neurodegenerative Diseases and the UHN Memory Clinic at Toronto Western Hospital. Her work aims to transform how we understand, diagnose, and treat the underlying causes of dementia.
Dr. Tartaglia works with a diverse range of neurodegenerative diseases, including Alzheimer’s disease (AD), frontotemporal dementia, progressive supranuclear palsy, and other conditions that a ect behaviour and cognition. Her fascination with these diseases, especially those that alter behaviour such as frontotemporal dementia, stems from her fascination with what de nes an individual’s sense of self. “I’ve always been interested in personality, the way we interact with others, and what de nes us. I’m trying to understand the neural substrate of who we are. One way to do that is by studying brain diseases,” she explains.
e main challenge to overcoming these devastating conditions lies in their heterogeneity. Dr. Tartaglia explains that
“No two patients are alike. Your disease always happens in the landscape of you,” with patients o en having multiple pathologies, as “one brain disease does not protect you against another.” She notes, emphasizing the nuanced nature of neurodegenerative diseases.
e diverse manifestations of neurodegenerative diseases make them an ideal candidate for tailored methods of detection, diagnosis, and treatment. While precision medicine has transformed other elds, such as oncology, similar progress in brain disorders has been slower. Dr. Tartaglia attributes this lag in precision medicine for dementia to two main factors: the di culty of obtaining patient samples and the historical lack of urgency due to the absence of e ective treatments.
Dr. Tartaglia and her team are working to overcome these barriers by introducing new methodologies that leverage individual patient data to address the variability of these diseases. e clinical success of personalized treatments for neurodegenerative diseases will require a sound and robust understanding of the heterogeneity of these pathologies that underlie the symptoms that Dr. Tartaglia witnesses so o en.
e message is clear: it is crucial that we move beyond the “one-size- ts-all” approach to neurodegenerative disease, and this will require more comprehensive
patient data collection, innovative imaging tools, and reliable biomarkers that can capture the complexity of each patient’s condition. Dr. Tartaglia and her team are laying the groundwork for a future in which precision medicine improves patient outcomes and transforms the standard of care. She is optimistic about the direction in which we are headed.
“Until recently, we didn’t have anything. We had MRI, but that isn’t a piece of your brain. Now, in [AD], for example, we have excellent tools. We have cerebral spinal uid analysis, we have positron emission tomography (PET) scans, which allow us to make de nitive diagnoses correctly with 90% certainty,” she says.
Building on such advances, her team is striving for similar breakthroughs for the diagnosis of other neurodegenerative conditions. Recently, Senior Research Associate Ivan Martinez-Valbuena developed an assay to detect 4-RepeatTau to diagnose patients with progressive supranuclear palsy (PSP).2 is assay marks a signi cant step forward, not just for PSP, but as a model for the development of similar diagnostic tools for other neurodegenerative conditions.
Dr. Tartaglia emphasizes the importance of pairing such novel diagnostic tools with better guidelines for the detection of neurodegeneration. “In early stages of disease, there are people with subjective
Dr. Carmela Tartaglia
Clinician-Scientist and Principal Investigator, Tanz Centre for Research in Neurodegenerative Diseases, UHN Memory Clinic at Toronto Western Hospital
cognitive decline. is means they feel like things have changed for them, but when you administer neuropsychological tests, they perform within normal ranges. [One third] of these people have neurodegenerative disease in the brain,” she says. She adds that shi ing diagnostic resources towards this population of patients in early disease stages will open doors to preemptive treatments that target pathology prior to the occurrence of irreversible damage.3
In addition to revolutionizing the diagnosis of neurodegenerative diseases, Dr. Tartaglia hopes to change the way that
we study them. Representative clinical data ensures that personalized strategies are e ective across diverse populations. Ethnic minorities are severely underrepresented in clinical studies, and studies of dementia are no exception.4
To combat underrepresentation in clinical trials, Dr. Tartaglia is integrating her clinical work with her research endeavors. “People of di erent ethnic backgrounds will have di erent propensities for disease. I have promoted embedding research in care approach. I ask patients who have come to the clinic…if they would be willing to contribute [their] data to research. We try to tap into a more diverse population that way,” she explains.
In addition to accessing more diverse patient groups, Dr. Tartaglia is looking to improve clinical trials by minimizing bias in endpoint metrics. Given the nature of cognitive decline, it is di cult to obtain information from the patient themselves. Informants include relatives, spouses, and caregivers who know the patient well enough to comment on their condition.
A 2024 paper by Dr. Tartaglia et al. demonstrated that the Clinical Dementia Rating Sum of Boxes scores, a tool used by researchers to measure the severity of cognitive decline, is heavily in uenced by informant-provided characteristics.5
“If you look at the e ect size from informants, it is almost equal to the
di erence between the treatment arm and the placebo,” she explains. She adds that corrective factors will be crucial to account for such skew. erefore, the implementation of multi-dimensional analyses is necessary to capture the full spectrum of patient experiences.
Despite the challenges of implementing precision medicine for the treatment of neurodegenerative diseases, Dr. Tartaglia is excited for a reality where personalized therapies are the norm, but she believes we will have to embrace the complexity of neurodegeneration to get there. By applying a precision medicine approach, Dr. Tartaglia envisions a future where tailored therapies can not only slow disease progression but also restore a higher quality of life for patients and their families.
References
1. Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. e Lancet [Internet]. 2020 Aug [cited 2024 Nov 13];396(10248):413–
46. Available from: https://linkinghub.elsevier.com/retrieve/pii/ S0140673620303676
2. Martinez-Valbuena I, Tartaglia MC, Fox SH, et al. Four-Repeat Tau Seeding in the Skin of Patients With Progressive Supranuclear Palsy. JAMA Neurology. 2024 Sep 23;
3. Zetterberg H, Schott JM. Objectifying Subjective Cognitive Decline: e Prognostic Role of Alzheimer Biomarkers. Neurology. 2022 Sep 2;10.1212/WNL.0000000000201172.
4. Brijnath B, Croy S, Sabates J, et al. Including ethnic minorities in dementia research: Recommendations from a scoping review. Alzheimer’s & Dementia: Translational Research & Clinical Interventions. 2022 Jan;8(1).
5. Vargas-Gonzalez JC, Chadha AS, Castro-Aldrete L, et al. Informant characteristics are associated with the Clinical Dementia Rating Sum of Boxes scores in the Alzheimer’s Disease patients participating in the National Alzheimer’s Coordinating Center Uniform Data Set. Research square [Internet]. 2024 Autumn;rs.3.rs3982448. Available from: https://pubmed.ncbi.nlm.nih.gov/38559129/
Photo Credit: Dr. Carmela Tartaglia, taken by Sara Yuan
Personalizing the Prevention, Treatment, and Management of Hereditary Breast and Ovarian Cancer
By Rachel Lebovic
One in every 300-400 Canadians, which translates to approximately 100 000-133 000 people, are prone to carrying a mutation in the breast cancer type 1 (BRCA1) or type 2 (BRCA2) gene.1 BRCA1 and BRCA2 are essential genes that function in preventing cancer. Individuals who have a mutation in one of these genes have an increased risk of developing breast, ovarian, and/or prostate cancers, among others.1 With a lifetime risk of up to 80% for breast cancer and up to 20-40% for ovarian cancer,1 there has been signi cant scienti c e orts on evaluating the best way to prevent, treat, and manage these elevated cancer risks.
Dr. Joanne Kotsopoulos, Tier 2 Canada
Research Chair in Hereditary Breast and Ovarian Cancer Prevention, is part of a large Women’s College Hospital (WCH) team studying hereditary breast and ovarian cancer. With faculty appointments at the Temerty Faculty of Medicine and Dalla Lana School of Public Health, Dr. Kotsopoulos integrates her vast skill set to conduct epidemiological studies to further our understanding of cancer risk and prognostic factors to improve upon the management of individuals with mutations in a BRCA gene.
While discussing BRCA-related cancers, the theme of precision and personalized medicine emerged. With regard to prevention, the goal is to understand individual risk factors and their underlying biology to further personalize the screening and prevention regimens to
ensure their maximum e cacy. In terms of treatment, the unique features and interplay of cancer cells, biomarkers, and genetics can inform targeted treatment to best ght each disease. Finally, individualized approaches are being studied post-surgery and in the management of adverse symptoms resulting from cancer treatments to understand which interventions are safe. Dr. Kotsopoulos elaborated on her work in each of these areas.
Personalizing Prevention Tools
In Ontario, the recommendation for female BRCA mutation carriers is to get yearly mammograms with an ultrasound or MRI starting at 30 years of age.2 Unfortunately, there are currently no e ective screening tools for the early detection of ovarian cancer. As a result, it is recommended that carriers undergo preventative removal of their fallopian tubes and ovaries (known as an “oophorectomy”) by the ages of 35-45.3 While these guidelines have been practical, they remain imperfect. Undergoing an oophorectomy at a young age forces premature menopause, accompanied by numerous symptoms that impact quality of life, sometimes with few management options.
A core interest of Dr. Kotsopoulos is prevention through a personalized approach using epidemiological data to assess individual risk among carriers. “We
have the largest cohort of women, over 19 000 women from across the globe,” Dr. Kotsopoulos mentions. ose being followed in this cohort complete a series of questionnaires every two years, answering detailed questions related to oral contraception, breastfeeding, and hormone replacement therapy (HRT) to understand which exogenous factors may further in uence cancer risk. Dr. Kotsopoulos and her team hope that by understanding risk factors and biomarkers (for example, certain proteins in the blood), they may be able to create some sort of algorithm with the help of machine learning to predict an individual’s risk and safely delay preventive ovary removal surgery as long as possible.
“ “
We believe that the more people that are aware of their genetic makeup, the more opportunities there are to prevent.
When it comes to prevention and early detection, one can only act if they are aware of their mutation status. In Canada, individuals must qualify for genetic testing based on various criteria such as a strong family history of cancer or personal cancer diagnosis at a young age (among others). While this remains important for developing a personalized treatment plan, once diagnosed with a BRCA-associated cancer, the window for prevention has passed. e team at WCH, including Dr. Kotsopoulos, are leading
Tier 2 Canada Research Chair in Hereditary Breast and Ovarian Cancer Prevention, Women’s College Hospital
Project will inform recommendations for a nationwide, population-based BRCA screening approach.
Personalizing Treatment and Management
Precision medicine has gained signi cant attention in the cancer community, recognizing that each cancer is unique and should be treated with a targeted approach.4 When it comes to BRCArelated cancers, treatment can be personalized based on gene carrier status. For example, many BRCA-cancers are treated with poly ADP ribose polymerase (PARP) inhibitors. ese inhibitors can speci cally target cancer cells caused by the mutated BRCA gene and subsequently treat the cancer.
To explore this question, Dr. Kotsopoulos is examining her global database of carriers and discovered that, despite existing guidelines, approximately 300 women have chosen to use HRT. With the ability to analyze speci c tumour pathologies, treatment records, and risk factors, the hope is to understand who can safely use HRT. is will o er an opportunity to improve quality of life for young women.
Incredible progress has been made in the management of this unique population over the past 30 years since the BRCA mutations were discovered. When asked about her advice to young women, Dr. Kotsopoulos shared that “knowledge is power.” Know your risk and how to manage it.
e Screen Project,1 an initiative to make BRCA testing available and accessible to all Canadian adults. She highlights, “We believe that the more people that are aware of their genetic makeup, the more opportunities there are to prevent.” By reducing barriers to access genetic testing, e Screen Project has identi ed many individuals who carry the mutation without a family history of cancer. e Screen Project also streamlines and simpli es this process, whereby a saliva collection kit is sent for the individual to complete at home and mail back. Informational pre- and post-test videos are shared, and individualized genetic counselling is o ered based on the results. Longitudinal results from e Screen
An important aspect of personalized care relates to the age discrepancy in cancer diagnosis for BRCA carriers. Dr. Kotsopoulos explained that in BRCA carriers, “it is much more complex. Many female carriers are diagnosed with breast cancer at a young age compared to women without a mutation who are more likely to develop cancer following menopause.” HRT shows promise as a method to help manage menopause symptoms and enhance quality of life post-oophorectomy in BRCA carriers, however, research demonstrates that it may increase the risk of breast cancer. e question then becomes, “Can we safely manage these women with HRT a er a diagnosis?”
References
1. e Screen Project [Internet]. 2024 [cited 2024 Oct 29]. Available from: https://www.womensacademics.ca/active-studies/the-screenproject-study/
2. Breast Cancer Screening for People at High Risk [Internet]. [cited 2024 Oct 29]. Available from: https://www.cancercareontario.ca/ en/guidelines-advice/cancer-continuum/screening/breast-cancerhigh-risk
3. Prevention & Genetic mutations [Internet]. 2024 [cited 2024 Oct 29]. Available from: https://ovariancanada.org/prevention-genetic-mutations
4. Precision medicine [Internet]. 2021 [cited 2024 Oct 30]. Available from: https://cancer.ca/en/research/understanding-cancer-research/ precision-medicine
Dr. Joanne Kotsopoulos
Photo provided by Dr. Kotsopoulos
How Precision Medicine is Outwitting Infammatory Bowel Disease Gut Instincts:
By Mia Feldman
In ammatory bowel disease (IBD) is on the rise worldwide. In Canada, the number of cases is predicted to increase by approximately 1.3-fold by 2035.1 IBD is used to describe two chronic intestinal diseases—Crohn’s disease (CD) and ulcerative colitis. Both are chronic immune mediated disorders of the intestine with a relapsing and remitting course.2 Whereas ulcerative colitis a ects the large intestine, CD can occur in any part of the gastrointestinal tract. Both result in a range of gastrointestinal symptoms, including abdominal pain, diarrhea, and rectal bleeding. In serious cases, individuals may ultimately have surgical resection of the intestine.2 Unfortunately, the cause of the disease remains unknown and there is no cure. is urgent medical mystery is what attracted Dr. Sun-Ho Lee to gastroenterology. Dr. Lee, who is also an IMS alum, practices as a Clinical Scientist at the In ammatory Bowel Disease Centre at Mount Sinai Hospital. He was appointed to Assistant Professor at the University of Toronto in 2023. He focuses on translational IBD research, splitting his time between seeing patients and tackling a new approach to IBD treatment: precision medicine.
Precision Medicine in IBD
IBD is a very heterogenous disease, meaning its causes and clinical manifestations vary greatly from person to person.1 Precision medicine, which predicts disease outcomes based on patient-speci c variables, is conceptually a very useful tool
in the treatment of IBD. For example, does having a parent with IBD increase your risk of having disease? Is there a microbial or genetic factor that predicts your risk of having disease complications? What about having a diet rich in re ned sugars? Dr. Lee describes that ideally, precision medicine would be used for “stratifying a patient to accurately predict the course of disease or the treatment response to a speci c medication,” ensuring the best outcome for each individual. To establish predictive models for IBD based on patient characteristics, signi cant amounts of data must be collected. As a clinicianscientist at the IBD Centre at Mount Sinai Hospital, Dr. Lee has unique access to patient samples, such as intestinal biopsies, as well as stool, urine, and blood samples. Data collected from these samples can be used to extrapolate information about the patient’s genetic susceptibility to IBD and microbiome composition, along with more clinical markers of gut in ammation and gut barrier function, for example. Collecting samples from patients at various time points reveals the chronology of disease progression. Scientists like Dr. Lee can also use this data to classify patients into de ned groups based on their symptoms and how they progress. is process of data collection and classi cation is fundamental in the development of a predictive precision model. e timing of this data collection is crucial. Dr. Lee explained that in most cases, once a patient is diagnosed with IBD a er exhibiting the rst symptoms, they have already undergone a series of treatments such as antibiotic courses, along with other
medications. erefore, studying a cohort of healthy at-risk participants before they become sick is necessary to capture a full and unbiased picture of IBD development and progression.
The GEM Cohort: A New Type of Dataset
Dr. Lee is a lead researcher in the Genetic Environment and Microbial (GEM) Project. e GEM Project was founded in 2008 by Dr. Kenneth Croitoru—a leading physician in the Zane Cohen Centre for Digestive Diseases, and faculty member at the IMS. is international study follows the healthy rst-degree relatives (such as siblings and children) of CD patients, collecting data (like blood and urine samples) from them until they themselves develop CD. Researchers compare baseline biomarkers of those that later develop CD to those that remain healthy, o ering the opportunity to understand the pre-clinical phase of CD. is helps identify early markers and create predictive tools for development of CD. One of Dr. Lee’s earlier projects with GEM assessed participant intestinal barrier function. Dr. Lee and his colleagues used markers in participant urine to characterize the state of the intestinal barrier.3 ey found that those who eventually developed Crohn’s showed signs of abnormal barrier function years before exhibiting symptoms or being diagnosed. is was the rst study to prove abnormal barrier function is a predictor of developing CD. Without the baseline data from patients, collected long before any diagnosis, this nding wouldn’t
Next Steps
have been possible. More recently, Dr. Lee and his colleagues published their ndings on the gut microbiome and its implications in CD.4 By comparing the composition of each participant’s gut microbiome (pre-clinical versus post-diagnosis), they concluded that an altered microbiome could predict CD. us, Dr. Lee’s work provides the IBD world with two potential predictive methods for CD–assessing patient barrier function through the urine and examining their gut microbiomes. Notably, all participants in the GEM project undergo genetic testing. Dr. Lee explained how researchers found little evidence that genetics predicted the likelihood of developing Crohn’s within the GEM cohort. erefore, environmental factors, including diet and gut microbiome, likely contribute to elevated disease risk. Evidently, there is a seemingly endless number of variables that can contribute to, and markers that indicate, the development of IBD.
Taking all patient variables into account is not an easy task. To integrate high dimensional data, Dr. Lee looks to new technology including machine learning (ML). ML algorithms draw conclusions from mass amounts of data. Dr. Lee and his colleagues have recently developed a ML model that integrates data derived from individual rst-degree relatives of those with CD to predict their risk of developing the disease.5 For example, participant pro les can be created via data from urine samples, microbiota characteristics from stool samples, demographic traits, information about diet, and any other relevant information. Inputting these pro les into a ML model, then training and testing them in datasets, serves as a predictive tool for individual patient risk for CD. Dr. Lee’s current model is 80% accurate—showing promise for the future of this technology in clinical settings. But Dr. Lee isn’t satis ed with 80% accuracy, he wants 100%. He believes there is a lot more work to be done. Dr. Lee is inspired by the researchers who have worked on type 1 diabetes (T1D) and rheumatoid arthritis. eir decades of work have resulted in a nuanced understanding of subtypes of disease and the diversity of pre-clinical phases before diagnosis. A thorough understanding of pre-clinical phases of T1D has enhanced disease screening and created avenues for early interventions to improve patient outcomes and to prevent or delay the development of disease. Dr. Lee hopes similar work will be done for IBD, especially with growing evidence that
there is a prolonged pre-clinical phase in the disease. Additionally, with his newly approved grant from the National Institute of Diabetes, Digestive and Kidney Diseases IBD Genetic Consortium, he plans to further develop ML models integrating multi-omics to better stratify the risk of CD recurrence a er surgical resection of the intestine. Dr. Lee’s work exempli es the promise of precision medicine. e heterogeneous nature of the disease means there is no “one size ts all” solution for patients. Accounting for individual patient variables is therefore fundamental in optimizing treatment courses, ensuring the best outcomes and the most e cient healthcare systems. ough current predictive models are insu cient for clinical use, Dr. Lee and his colleagues are working to close the gap in knowledge with innovative solutions. His e orts bring us closer to a future where personalized care is the standard for IBD treatment.
References
1. Coward S, Benchimol E, Bernstein CN, et al. Forecasting the Incidence and Prevalence of In ammatory Bowel Disease: A Canadian Nationwide Analysis. Am J Gastroenterol. 2024;119(8):1563-1570.
2. John Hopkins Medicine. In ammatory Bowel Disease (IBD); 2024 [cited 2024 November 15]. Available from: https://www. hopkinsmedicine.org/health/conditions-and-diseases/in ammatory-bowel-disease
3. Turpin W, Lee SH, Garay JAR, et al. Increased Intestinal Permeability Is Associated With Later Development of Crohn’s Disease. J. Gastroenterol. 2020;159(6):1995-2250.
4. Garay JAR, Turpin W, Lee SH, et al. Gut Microbiome Composition Is Associated With Future Onset of Crohn’s Disease in Healthy First-Degree Relatives. J Gastroenterol. 2023;165(3):670-681
5. Lee SH, Turpin W, Espin-Garcia O, et al. Development and Validation of an Integrative Risk Score for Future Risk of Crohn’s Disease in Healthy First-Degree Relatives: A Multicenter Prospective Cohort Study. J Gastroenterol. 2024;S0016-5085(24):5401-5405
Dr. Sun-Ho Lee MD, PhD Clinician-scientist at Mount Sinai Hospital
Photo provided by: Dr. Sun-Ho Lee
Master of Science in Biomedical Communications
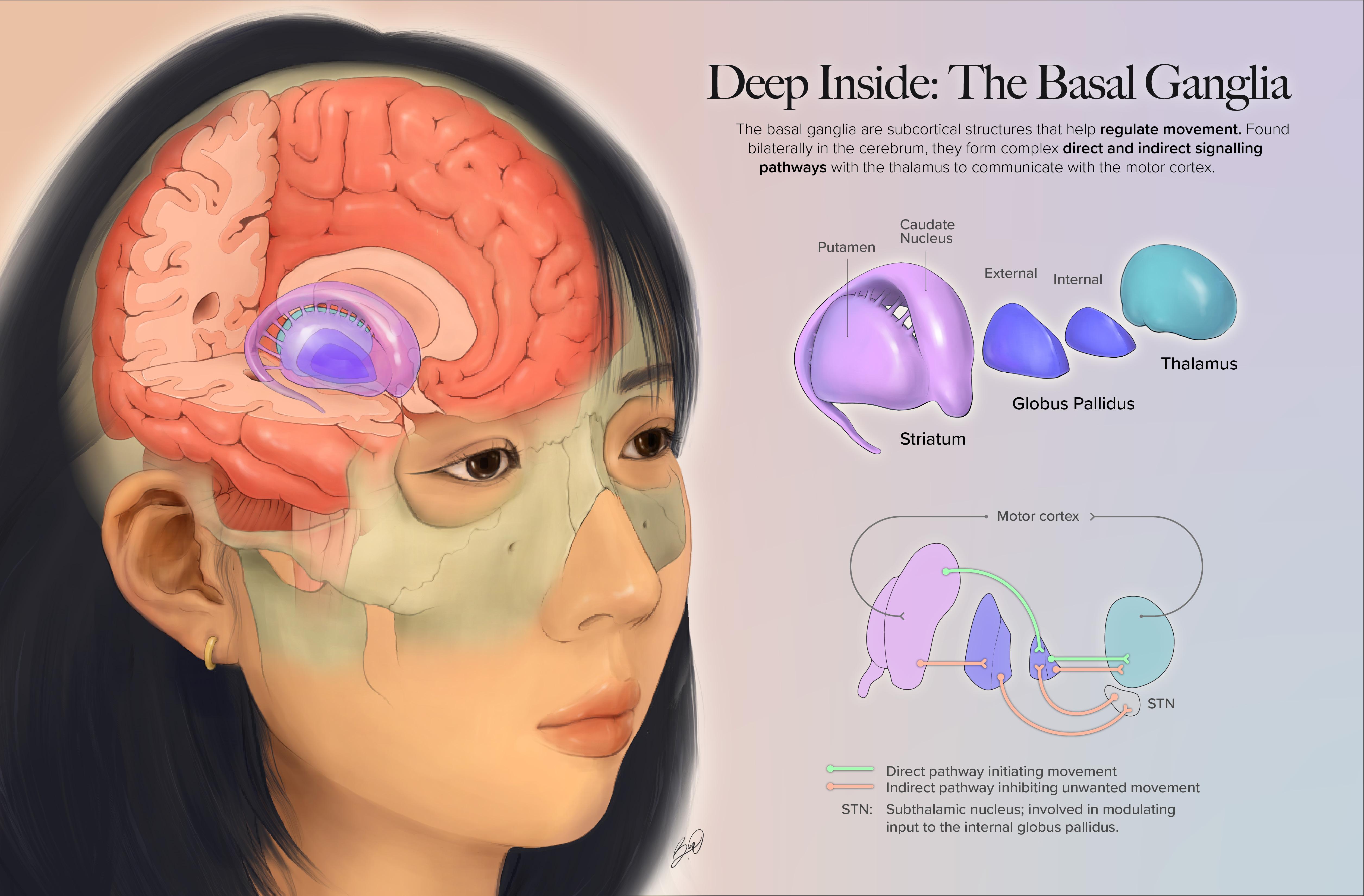
Deep Inside: The Basal Ganglia
Bonnie Wang
roughout my time in the MScBMC program, I have learned new storytelling techniques, design strategies, and ways to visualize scienti c concepts. is neuroanatomy self-portrait feels like a culmination of these e orts, and it’s been wonderful to re ect on my growth since entering the program a year and a half ago. While it’s hard to believe this chapter is nearing its end, I’m excited to see what the last semester has in store!
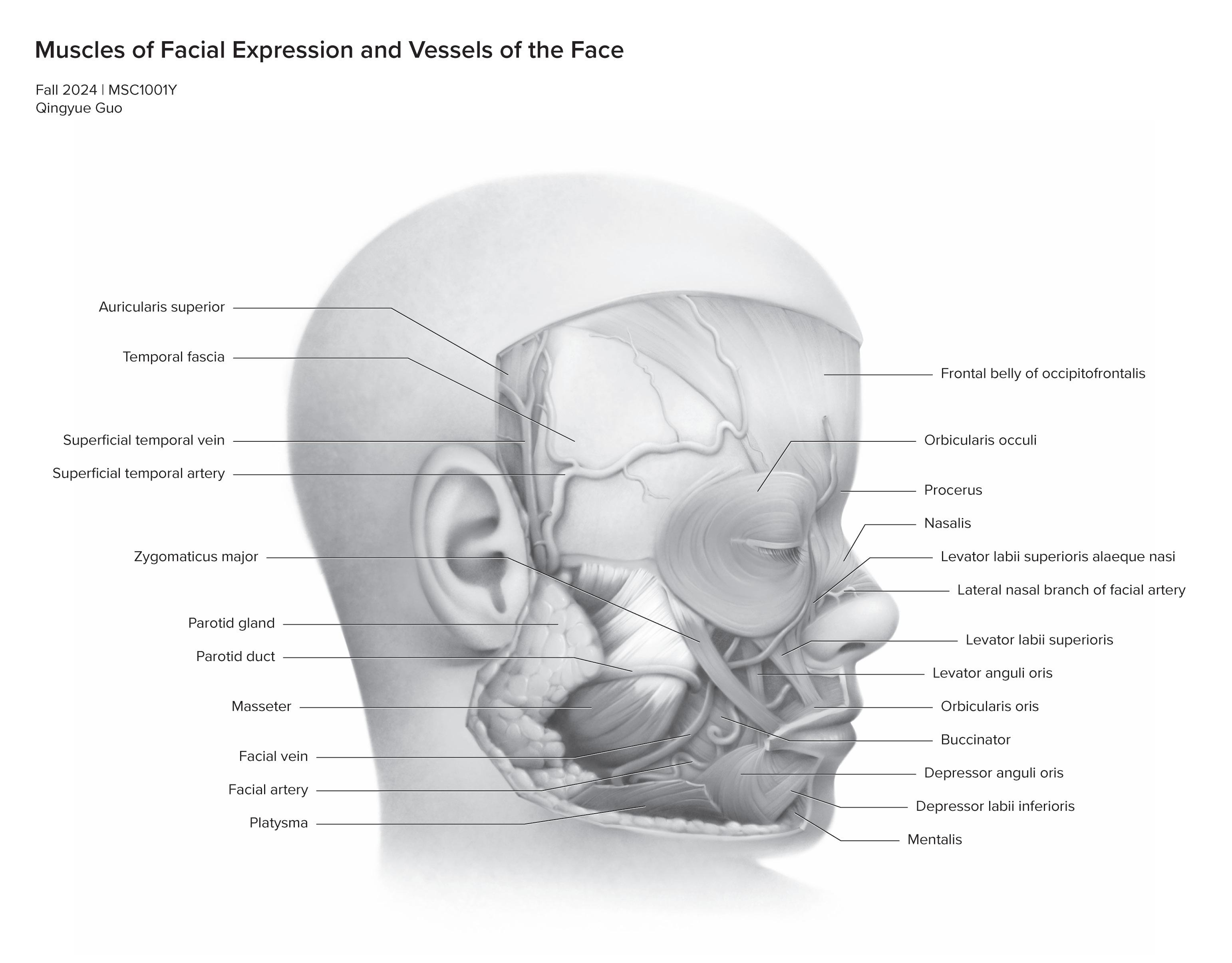
Muscles of Facial Expression and Vessels of the Face
Qingyue Guo
I am Qingyue, a rst-year student in the Master of Science in Biomedical Communications program with a background in Microbiology and Immunology. My passion lies in making science accessible through visual storytelling, and my previous works include creating infographics, illustrations, and graphical abstracts. In the future, I aspire to create engaging visuals that connect professionals and global audiences, fostering understanding of biomedical topics.
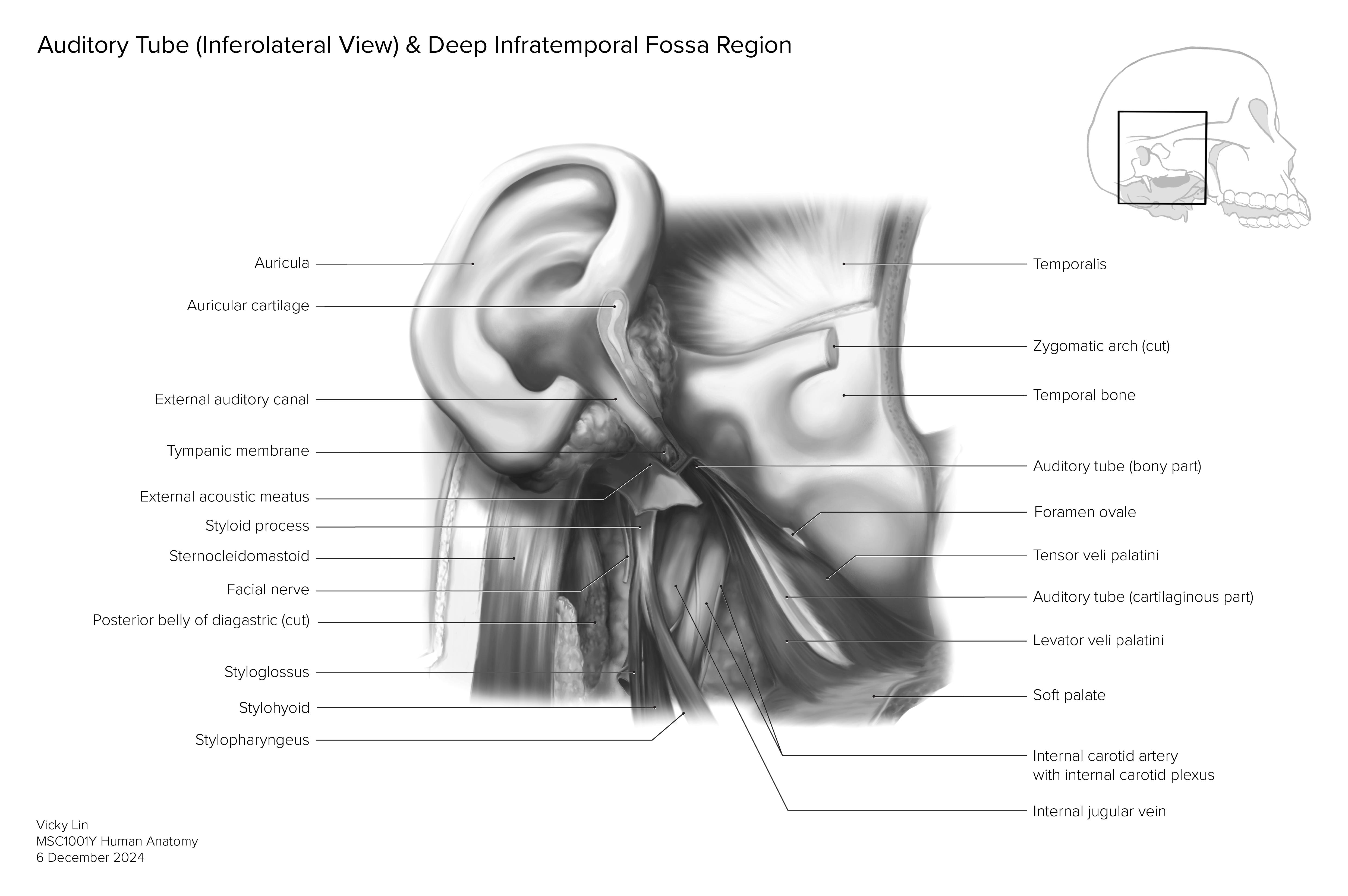
Inferolateral
View of the Auditory Tube
Vicky Lin is a rst-year Master’s student in the Biomedical Communications program at the University of Toronto with a background in Biology from McMaster University. She has worked extensively in multimedia design and print publishing in her previous work experience and is eager to use her passion for science visualization to make tools that help make science accessible for wider audiences.
Vicky Lin
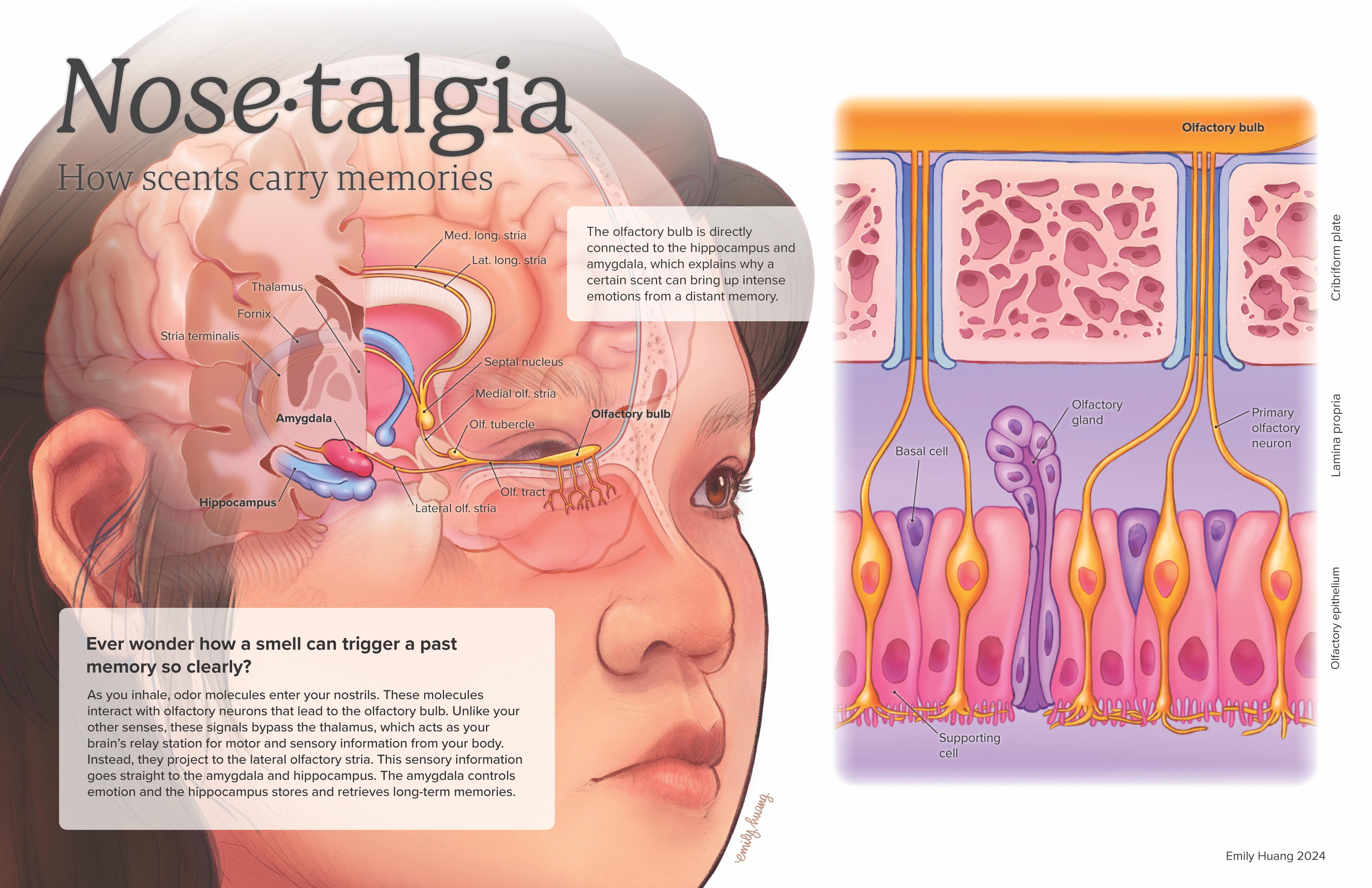
Nose•talgia: How scents carry memories
Emily is a medical and scienti c illustrator committed to creating empathetic, accurate, and accessible visuals. With a strong interest in graphic medicine, she uses storytelling to communicate complex medical concepts with compassion and clarity for a wide range of audiences.
Molly Wells is a biomedical illustrator focused in marine science visualization. She is passionate about branching the worlds of academia, policy, and public outreach. She is currently based in Toronto, ON and completing the MSc Biomedical Communications program at the University of Toronto.
Emily Huang
Molly Wells
Metacarcinus magister 3D sculpt
Graphic design by Nichole Zhou
The Night Shift: Increased Cerebrospinal Fluid Production & Flow During Sleep
Emily
Mao
I am a biomedical communicator based in Toronto, Ontario. rough my time at Biomedical Communications, I hope to hone my communication, research, and art skills in service of creating impactful patient education, outreach, and other pedagogical materials.
Are people of colour being left behind in the advancing feld of genomics?
By Kanak Gupta
Genome Wide Association Studies (GWAS) have been at the frontier of biomedical research’s shi towards precision medicine. Tens of thousands of genetic disease risk factors and trait-associated gene variants have been discovered since the rst GWAS in the early 2000s.1 Moreover, with the availability of data from large-scale genetic biobanks, study sample sizes frequently surpass one million, helping us detect even subtle genetic e ects.2 However, this perfect picture of scienti c advancement is marred by the fact that 95% of participants in all GWAS to date are of European descent.3,4 Are we investigating the mysteries of the human genome, or only the European one? Could precision medicine based on such limited diversity actually be dangerous?
Could precision medicine based on such limited diversity actually be dangerous? “ “
e GWAS Catalog, run collaboratively by the National Human Genome Research Institute and the European Bioinformatics Institute, is a catalogue of all publications utilising GWAS to nd genetic associations for di erent diseases and traits. ese studies source genomic data from private companies such as 23andMe and AncestryDNA, as well as national institutional genomic databases and initiatives, including biobanks in the UK, the US, Canada, Iceland, and China.2 A 2020 report estimated that 38 million individuals worldwide have had their genome sequenced in some capacity; it estimated that this gure may reach 52 million by 2025.5
However, 72% of all subjects within global biobanks come only from three countries: the United States, United Kingdom, and Iceland. In 2023, 90% of participants in discovery stage genomic studies were of European descent (83% in replication-stage GWAS). Genomic data initiatives in China, Japan, South Korea, and India contributed to the majority of the non-European participants. However, African, Latin American, Hispanic, and Indigenous populations only accounted for 1.5% of all participants in discovery stage GWAS and 9% of replication studies.3 Even when geneticists do have access to more diverse samples, they show a preference for European cohorts, citing that controlling for ancestry will
simplify data analysis. Furthermore, new research builds upon existing research, and repeated sampling from older, biased studies to perform new analyses only exacerbates the Eurocentric sampling bias.6
Clearly, the genomic research landscape has a blind spot when it comes to ancestral diversity, leading to a large gap in genetic diversity. Despite all humans sharing the same genetic ancestry, GWAS studies o en lack cross-population transferability due to unaddressed genetic, geographic, and cultural di erences that a ect risk scores for di erent diseases in clinical applications of genetic research.2 A 2019 meta-review indicated that polygenic risk scores are 2 to 4.5 times more accurate in European populations than in East Asian and African populations.7
is oversight can have dangerous consequences. People of colour are more likely than Europeans to receive ambiguous genetic test results, or even erroneous results, indicating they are carriers of genes that increase their risk of certain diseases.6 For example, based on conclusions drawn from European populations, gene variants linked to glycated haemoglobin (HbA1C) are used as diagnostic markers of diabetes. However, a study in rural Uganda revealed that 22% of their participant population had this gene and it was not correlated with diabetes; rather, it was protective
against severe malaria. is study also found several novel genes of interest that were not detected in existing data.3,8 In fact, numerous small studies in non-European populations have revealed useful genetic links that were missed in large sample GWAS because those alleles occur less o en in Europeans.6,9
While the diversity gap in our genomic data is tremendous, it is not insurmountable. Many academics have made calls to increase the diversity of our biobanks, and tools like the GWAS Diversity Monitor can increase awareness and track progress. More recent projects, such as the Trans-Omics for Precision whole-genome sequencing project in the US, have made e orts to recruit a diverse range of participants. Large-scale genome biobanks in Asia have played a signi cant role in increasing non-European genomic data, although 93% of this data remains locally used.2,6
Furthermore, many institutions are funding initiatives to increase geographic and ethnic representation. In South Asia, projects such as IndiGen and Pakistan Alliance on genetic RisK factors for Health (PARKH) have fostered sustainable research collaborations between South Asian and Western institutions.9,10 In Africa, initiatives such as the Human, Heredity, and Health in Africa Consortium, the Uganda Genome Resource, and the Nigerian 100K Genome
“ “
While the diversity gap in our genomic data is tremendous, it is not insurmountable
Project, aim to increase equity and help build genomic research infrastructure.2,6,9 ese projects have already yielded key insights; however, African scientists warn that this increase in data should not only bene t the Western institutions funding the initiatives, but also serve the local populations from whom the data is being collected.11 Globally, e orts are being made to build ethical relationships with Indigenous peoples to encourage their participation in genomic research.12
Increasing the diversity of our genetic biobanks is crucial to decreasing inequity in genomic research. However, cultural and practical shi s in academia are required to increase both the recruitment and utilisation of non-European genomic data. e knowledge we have acquired from our genomic libraries has grown
exponentially since the rst human genome was mapped, but the longer we ignore the gap in our ancestral diversity, the wider the chasm of ignorance becomes. Without prompt action, the very foundations of precision medicine will be built on unequal grounds.
References
1. U elmann E, Huang QQ, Munung NS et al. Genome-wide association studies. Nat Rev Methods Primer. 2021 Aug 26;1(1):1–21.
2. Abdellaoui A, Yengo L, Verweij KJH, et al. 15 years of GWAS discovery: Realizing the promise. Am J Hum Genet. 2023 Feb 2;110(2):179–94.
3. Mills MC, Rahal C. e GWAS Diversity Monitor tracks diversity by disease in real time. Nat Genet. 2020 Mar;52(3):242–3.
4. Mills MC, Rahal C. A scientometric review of genome-wide association studies. Commun Biol. 2019 Jan 7;2(1):1–11.
5. Understanding the Global Landscape of Genomic InitiativesIQVIA [Internet]. [cited 2024 Nov 4]. Available from: https:// www.iqvia.com/insights/the-iqvia-institute/reports-and-publications/reports/understanding-the-global-landscape-of-genomic-initiatives
6. Popejoy AB, Fullerton SM. Genomics is failing on diversity. Nature. 2016 Oct;538(7624):161–4.
7. Martin AR, Kanai M, Kamatani Y et al. Clinical use of current polygenic risk scores may exacerbate health disparities. Nat Genet. 2019 Apr;51(4):584–91.
8. Gurdasani D, Carstensen T, Fatumo S et al. Uganda Genome Resource Enables Insights into Population History and Genomic Discovery in Africa. Cell. 2019 Oct 31;179(4):984-1002.e36.
9. Fatumo S, Chikowore T, Choudhury A, et al. A roadmap to increase diversity in genomic studies. Nat Med. 2022 Feb;28(2):243–50.
10. Divakar MK, Jain A, Bhoyar RC, et al. Whole-genome sequencing of 1029 Indian individuals reveals unique and rare structural variants. J Hum Genet. 2023 Jun;68(6):409–17.
11. Nordling L. African scientists call for more control of their continent’s genomic data. Nature [Internet]. 2018 Apr 18 [cited 2024 Nov 4]; Available from: https://www.nature.com/articles/ d41586-018-04685-1
12. Claw KG, Anderson MZ, Begay RL, et al. A framework for enhancing ethical genomic research with Indigenous communities. Nat Commun. 2018 Jul 27;9(1):2957.
Data Privacy and Security in Healthcare - A Perspective
By Gharaza Nasir
In an age when medicine is becoming as personalized as the technology people use daily, its potential to transform healthcare is undeniable. However, behind every individualized treatment lies a network of data that is powerful, yet vulnerable. A data breach can cause unimaginable damage to millions, thus it is only natural to expect patients to demand the highest standards of privacy and security of their medical data.
Data is essential to modern medicine; being highly valuable to clinicians in creating personalized treatments for patients. Medical data encompasses various types of patient information that will improve individual care, advance research, and drive innovations in treatment. is data is widely used and collected in healthcare to understand patient health and develop disease interventions. One example is genomic data, which includes a patient’s genetic makeup and can pinpoint genetic predispositions for diseases.1 Another example is imaging data, which comes from X-rays, MRIs, ultrasounds, and CT scans, and is crucial for diagnosing and monitoring patient conditions. Imaging data is increasingly being used in AI-based diagnostic tools to detect trends and anomalies in diseases.1 Blood tests, biopsies, and other laboratory tests further provide critical information on various disease markers, which can assist in diagnosing and monitoring patient health.1
In the United States (U.S.), several data leaks have been recorded over the years.2 Two notable events are the cyber attacks on Anthem in 2015 and Change Healthcare this past year.2,3 e attack on Change Healthcare a ected almost 100 million individuals.2 is data breach broke records, surpassing Anthem as the largest known breach of protected health information at a Health Insurance Portability and Accountability Act (HIPAA) regulated entity.3
It is undeniable that entities like Anthem and Change Healthcare handle vast amounts of personal patient data; however, contrary to public misconceptions, they are tightly regulated under stringent laws such as HIPAA.3 While public concern over data privacy with third-party organizations is valid, it is essential to recognize that precautions exist to protect patient data. For example, a er Anthem’s data leak, the organization faced a $16 million penalty, the largest HIPAA settlement to date.3 HIPAA, enforced by the O ce for Civil Rights (OCR), mandates frequent risk assessments and imposes strict access controls to prevent such incidents.3 rough these regulations and penalties, entities like Anthem are held accountable, underscoring that strong systems are in place to protect data privacy even in a landscape of evolving security risks.
While American laws like HIPAA and OCR enforce strict data privacy regulations, these measures do not directly translate beyond U.S. borders. ough Canadian healthcare is not reliant on third-party organizations, patient privacy still remains a high priority, with the Canadian healthcare system enforcing rigorous protocols on the collection, use, and protection of patient information.4 e Personal Information and Electronic Documents Act (PIPEDA), is a federal law that protects all personal information.4 Additionally, provinces and territories have their own legislation that addresses data privacy and protection in healthcare. In Ontario, the Personal Health Information Protection Act (PHIPA) includes several provisions to protect patient data and respond to breaches through actions like reporting abnormalities to the Information and Privacy Commissioner of Ontario (IPC), risk assessment, training programs, and, most importantly, public awareness.5,6
ese protections highlight important ethical questions surrounding data sharing in healthcare. With increasing reliance on digital information systems and datadriven treatments, there is a growing need to balance the bene ts of shared patient data with the ethical duty to respect privacy and autonomy. Key considerations include ensuring patients fully understand how their data will be used, obtaining informed consent, and safeguarding their rights to control personal information.7
Medical data is essential for advancing patient care, yet in recent years there has been a growing concern over how it is protected.
Navigating these ethical dimensions is crucial to building trust and maintaining the integrity of patient-centered care across healthcare systems globally. For instance, what are the implications of the opt-in and opt-out models?7 How do these models di er in patient control over personal data or their trust in the healthcare system? Opt-in requires patients to actively agree to share their data; ensuring they make conscious choices about data use.7 Comparatively, the opt-out model assumes consent of the patient by default, meaning their data can be shared automatically unless they say otherwise.7
Consent models like opt-in and opt-out provide autonomy to patients over how their data is shared, but it is only part of the whole picture. As data sharing needs grow, especially in research and public health, safeguarding privacy becomes more complex. is is where data anonymization comes in. By removing identi able information, like a patient’s name, address and nancial information, healthcare providers can share valuable insights while protecting individual privacy.8 However, the e ectiveness of traditional anonymization methods is increasingly challenged by advancements in AI, which occasionally re-identi es individuals from these seemingly anonymised datasets.8 Newer techniques are being explored to combat these challenges and are essential in building a robust privacy framework.
e journey forward in data security is ongoing. As we look to the future, protecting patient data requires technological solutions and a dedicated commitment from healthcare professionals. Beyond implementing secure data practices, healthcare workers hold the responsibility of educating patients and the public on their rights, thereby empowering them to make informed decisions. Particularly in the age of AI and its integration within the healthcare system, full transparency with patients will not only enhance patient trust, but will also encourage
wider participation in research, as individuals feel more con dent sharing information when they understand how it will be protected and used. By fostering a culture of openness and communication, healthcare providers can build lasting trust and ensure that patient privacy remains a priority as data-driven, AI-enhancing medicine continues to evolve.
References
1. Gupta V, Sachdeva S, Dohare N. Deep similarity learning for disease progression. Trends in Deep Learning Methodologies; 2021. https://doi.org/10.1016/B978-0-12-8222263.00008-8.
2. e HIPPA Journal. Healthcare Data Breach Statistics [Internet]; 2024 [cited 2024 Nov 8]. Available from https://www. hipaajournal.com/healthcare-data-breach-statistics/
3. US Department of Health and Human Services. Anthem pays OCR $16 Million in record HIPAA settlement following largest health data breach in history [Internet]; 2018 [cited 2024 Nov 8]. Available from https://www.hhs.gov/ hipaa/for-professionals/compliance-enforcement/agreements/anthem/index.html
4. Government of Canada. Personal Information Protection and Electronic Documents Act [Internet]. Government of Canada: Justice Laws Website; 2024 [cited 2024 Nov 8]. Available from: https://laws-lois.justice.gc.ca/eng/acts/p-8.6/ page-1.html#h-416888
5. Information and Privacy Commissioner of Ontario. [Internet]. IPC; 2024 [cited 2024 Nov 8]. Available from https:// www.ipc.on.ca/en
6. Aziz S. Cyberattacks on Canadian health care are increasingly common. What can be done? [Internet]. Global News; 2023 [cited 2024 Nov 8]. Available from: https://globalnews. ca/news/10103261/health-care-cyberattacks-canada/
7. De Man Y, Wieland-Jorna Y, Torensma B, et al. Opt-In and Opt-Out Consent Procedures for the Resuse of Routinely Recorded Health Data in Scienti c Research and eir Consequences for Consent Rate and Consent Bias: Systematic Review. J Med Internet Res. 2023;25;e42131. PMID: 36853745; PMCID: PMC10015347.
8. Olatunji IE, Rauch J, Katzensteiner M, et al. A Review of Anonymization for Healthcare Data. Big Data. 2022 March 10. doi: 10.1089/big.2021.0169.
Mobile Health Apps: Remedy or Enemy?
By Grace Gibson
As ever-developing technological advancements transform every part of our lives, the medical eld must also contend with new healthcare technologies alongside their accompanying bene ts and challenges. One area that has seen huge growth in the past decade is mobile healthcare applications (MHAs). As a tool for personal health management, MHAs have great potential for improving healthcare access, empowering patients in their own health management, and reducing inequality in medical care. However, the e ectiveness of current MHAs in improving accessibility and quality of care is questionable. If healthcare apps are to transform the world of medicine, they must rst undergo signi cant transformations themselves.
MHAs have the potential to improve healthcare outcomes for those experiencing healthcare inaccessibility by providing them with personalized health management tools.1 Patients living in a “medical desert,” de ned as a rural area with a low density of healthcare institutions, can utilize apps to attend telemedicine appointments without traveling long distances.2 In the United States, where cost is a detrimental barrier for those without health insurance, an app can help patients triage and use over-the-counter treatments for mild illnesses without a costly doctor’s visit.1 Chronically ill patients who nd it di cult to attend frequent appointments can utilize apps to track their symptoms.3 While these cases remain understudied,
evidence suggests that MHAs can improve some health outcomes, like increasing physical activity and decreasing anxiety symptoms. 4,5
However, the majority of current MHA users are not members of underserved communities.6 MHAs appear to be more e ective for younger, wealthier, more educated, and more technology literate users—demographics with greater overall health access.7,8,9 While results vary, some studies also suggest that MHA users are more likely to report good health, simply utilizing their apps to continue their healthy behaviors.6,8,10 Despite this being an area of potential for MHAs, many people do not engage with health apps for various reasons, including smartphone inaccessibility, technology illiteracy, age, and cost.6,9 If these apps are most e ective among populations already less likely to experience healthcare inequity, MHA use may simply mirror existing inequities.11
Additionally, members of marginalized communities who experience barriers to healthcare need more than personal health tools; they deserve transformative policies to improve healthcare access, including improvements to healthcare infrastructure and specialized training for physicians.2 MHAs o er an opportunity for personalized care, but individual improvements cannot replace community-based change, and personal health management is not a substitute for public health.
Of course, using MHAs as a transformative healthcare solution assumes that the apps themselves are safe, medically accurate, and evidence-based—requirements that many existing MHAs do not achieve.6,12 Anyone can create an app and make it publicly available, o en without oversight or regulation, leading to the proliferation of substandard apps.6 Very few of the currently available apps were created with the involvement of medical professionals, with even fewer evaluated in randomized controlled trials before release.13,14 Additionally, many MHAs fail to implement adequate security measures to protect users’ data, which frequently includes private information about their health. Users are therefore not only vulnerable to typical data sharing practices (i.e. their address or location), they also risk third-party collection of sensitive health information, such as medications they take or diagnoses they receive.6,15
As most MHAs are designed for individual use by the general public, potential negative consequences are alarming. Many app users may not have the health literacy to evaluate medical content, and they may inadvertently absorb false information, leading to inaccurate self-diagnosis or misguided actions in future health management.13 Moreover, many apps are limited in scope and lack the functionality to build truly personalized healthcare solutions.16 While MHAs can help patients take a more active role in their health, most currently available apps are either insu cient to meet users’ needs or even detrimental to their health outcomes.6,13
In such cases, even if the logistics of widespread use are not a factor, MHAs must undergo overall improvements to quality and functionality before they can be considered as transformative healthcare tools.
Despite these existing challenges, the potential bene ts of MHAs remain strong, and the future of healthcare technology will likely include further improvements in app development. With our knowledge on necessary changes to MHAs, we can hope to see the creation of a mobile health app landscape that truly does have the power of transforming healthcare for the better.
If healthcare apps are to transform the world of medicine, they must rst undergo signi cant transformations themselves. “ “
References
1. Steinhubl SR, Muse ED, & Topol, EJ. Can Mobile Health Technologies Transform Health Care? JAMA. 2013 11 Dec; 310(22): 2395-96.
2. Flinterman LE, González-González AI, Seils L, et al. Characteristics of medical deserts and approaches to mitigate their health workforce issues: a scoping review of empirical studies in western countries. Int J Health Policy Manag. 2023 15 Aug; 12:7454.
3. Ancker JS, Witteman HO, Hafeez B, et al. “You get reminded you’re a sick person”: personal data tracking and patients with multiple chronic conditions. J Med Internet Res. 2015 Aug 19;17(8):e202.
4. Direito A, Carraça E, Rawstorn J, et al. mHealth Technologies to Inuence Physical Activity and Sedentary Behaviors: Behavior Change Techniques, Systematic Review and Meta-Analysis of Randomized Controlled Trials. Ann Behav Med. 2017 Apr;51(2):226-239.
5. Firth J, Torous J, Nicholas J, et al. Can smartphone mental health interventions reduce symptoms of anxiety? A meta-analysis of randomized controlled trials. J A ect Disord. 2017 Aug 15;218:15-22.
6. Grundy Q. A Review of the Quality and Impact of Mobile Health Apps. Annu Rev Public Health. 2022 Apr 5;43:117-134.
7. Ernsting C, Dombrowski SU, Oedekoven M, et al. Using smartphones and health apps to change and manage health behaviors: a population-based survey. J Med Internet Res. 2017 Apr 5;19(4):e101.
8. Carroll JK, Moorhead A, Bond R, et al. Who Uses Mobile Phone Health Apps and Does Use Matter? A Secondary Data Analytics Approach. J Med Internet Res. 2017 Apr 19;19(4):e125.
9. Krebs P, Duncan DT. Health app use among US mobile phone owners: a national survey. JMIR Mhealth Uhealth. 2015 Nov 4;3(4):e101.
10. Robbins R, Krebs P, Jagannathan R, et al. Health App Use Among US Mobile Phone Users: Analysis of Trends by Chronic Disease Status. JMIR Mhealth Uhealth. 2017 Dec 19;5(12):e197.
11. Singh K, Drouin K, Newmark LP, et al. Many Mobile Health Apps Target High-Need, High-Cost Populations, but Gaps Remain. Health A (Millwood). 2016 Dec 1;35(12):2310-2318.
12. Huang Z, Soljak M, Boehm BO, et al. Clinical relevance of smartphone apps for diabetes management: A global overview. Diabetes Metab Res Rev. 2018 Feb 12;34:e2990.
13. Portenhauser AA, Terhorst Y, Schultchen D, et al. Mobile Apps for Older Adults: Systematic Search and Evaluation Within Online Stores. JMIR Aging. 2021 Feb 19;4(1):e23313
14. Sander LB, Schorndanner J, Terhorst Y, et al. ‘Help for trauma from the app stores?’ A systematic review and standardised rating of apps for Post-Traumatic Stress Disorder (PTSD). Eur J Psychotraumatol. 2020 Jan 9;11(1):1701788.
15. Tangari G, Ikram M, Sentana IWB, et al. Analyzing security issues of android mobile health and medical applications. J Am Med Inform Assoc. 2021 Sep 18;28(10):2074-2084
16. Grossman MR, Zak DK, Zelinski EM. Mobile Apps for Caregivers of Older Adults: Quantitative Content Analysis. JMIR Mhealth Uhealth. 2018 Jul 30;6(7):e162.
Beyond Data:
How precision medicine is revolutionizing EMRs and patient care
By Mahmudul Mannan
On a chilly morning in November 2020, 12-year-old Erica’s parents arrived at the pediatric intensive care unit at Toronto’s SickKids Hospital. Erica carries a CYP2C9 gene variant and was diagnosed with arrhythmia 5 years prior, taking Warfarin to reduce blood clot risk. However, a er taking penicillin for an ear infection, the interaction between the medications and this gene resulted in Erica being hospitalized with an acute subarachnoid hemorrhage. Erica’s su ering could have been avoided if her genomic information from her hometown in Calgary was integrated into her electronic medical record (EMR) at SickKids.
is case highlights a limitation of precision medicine in Canada’s EMRs, as electronic patient records in Ontario are not interlinked with other provinces. Precision medicine, a popular topic nowadays, is also known as “personalized medicine,” “targeted therapy,” or “evidence-based medicine.” It is derived from patients’ health, genomic, lifestyle, and environmental data.2-5 Precision medicine is innovative to healthcare, transforming the traditional “one-size- ts-all” paradigm of treatments to one based on patients’ unique data.2,3 is shi aims to improve care using focused treatments for complex illnesses like diabetes, cancer, and cardiovascular disease. Successfully integrating these various types of patient-speci c data into EMRs is crucial for precision medicine to reach its full potential.
Precision medicine and EMRs o er more than just data integration, they have the potential to enhance preventive care,
optimize treatment e cacy, and improve patient outcomes. Government funders, healthcare systems, and industry partners have been collaborating to support the growth of EMR-linked biobanks for personalized medicine research and implementation. For example, the US-based National Human Genome Research Institute (NHGRI) established a program called the “Electronic Medical Records and Genomics (eMERGE)” network in 2007. Its purpose was to link biobanks to EMRs at multiple sites, perform genomic research embedded in health systems, and establish best practices replicable across health systems.6 In 2015, “2bPrecise” was created as a cloud-based platform to leverage genomic data .7 Additionally, in 2016, Mount Sinai Health System and Regeneron Pharmaceuticals Inc. linked clinical information stored within the EMR to whole exome sequencing on 33,000 DNA and plasma samples, housed in Mount Sinai’s Biobank.8 In Canada, there are multiple EMRs and databases available, including EPIC, Cerner, and AdminData.2,3 In October 2022, Precision Health’s “Health Implementation” group, from the University of Michigan launched “ e Epic Genomics Indicator Module (EGIM)” electronic health record (HER) “MiChart.”9 ese are just some examples of successful integration of precision medicine in di erent EMRs.
Precision data consists of four domains: patient health, omics (genomics, metabolomics), lifestyle, and environmental data.3 In a recent interview, personalized medicine expert, Dr. Abbas
Zavar, stresses that social determinants of health (SODH) should also be added as a domain, such as aboriginal status and education history.3 Among these domains, patient health and omics data are most widely available in Ontario EMRs. In Ontario, health data are stored in electronic health information systems and come from various sources, such as hospitals, community clinics, and medical laboratories. Hospital data systems were revolutionized when the “EPIC” platform launched in June 2018. Before that, genomic data was available in ChartMaxx, an electronic repository of clinical, nancial, and administrative information10, but its reliance on clinical and lab records limited its ability to store genetic data. Genetic, or “Omics” data, is generated from several areas of patients’ biology, including genetic (genomics), protein (proteomics), and metabolic levels (metabolomics). 2 is data comes from community-level labs such as LifeLabs and Dynacare, as well as hospital and private laboratories, and can be used for diagnostic, treatment, or research purposes. However, lifestyle, environmental and SODH data are not commonly available in EMRs yet.
Precision medicine through EMRs enhances patient care in di erent ways. By utilizing patient-speci c data, precision medicine enables the development of personalized treatment plans tailored to each patient’s unique pro le. For example, the e cacy of breast cancer treatment can depend on whether patients have
BRCA1 or BRCA2 genetic variants. Oncologists can customize treatment plans by integrating genetic information into an EMR, improving patient outcomes. Pharmacogenomic data in EMRs enables tailoring prescriptions based on genetic factors that impact drug metabolism, potentially reducing adverse e ects.11 Furthermore, with precision medicine predictive analytics, EMRs can generate recommendations for patients at risk of developing certain diseases, such as diabetes, hypertension, and nephrotic syndrome.2,11
Despite the progress of precision medicine integration into EMRs, several challenges remain. Data standardization and interoperability, complexity in interpretation, data privacy and security, data sharing, and data storage pose complications in implementing precision
secure cloud-based storage systems. Genomic data is also highly sensitive and integrating it into EMRs raises privacy and security concerns. In Ontario, the Personal Health Information Act (PHIPA), and in Saskatchewan, the Health Information Protection Act (HIPA) laws, mandate strict regulations to protect patient data and ensure data privacy. Therefore, most identifiable data are unavailable in EMRs, and data accessed for research purposes must follow rigorous privacy procedures.
A paradigm shift in healthcare is being brought about by the integration of precision medicine into EMRs, which go beyond conventional models to adopt individualized and data-driven treatment strategies. These changes will empower healthcare professionals
References from generalized treatment toward embracing the unique health journey of each individual.
1. Limdi NA, McGwin G, Goldstein JA, et al. In uence of CYP2C9 and VKORC1 1173C/T genotype on the risk of hemorrhagic complications in African-American and European-American patients on warfarin. Clin Pharmacol er. 2008;83(2):312-21.
2. Zavar A, Keshavjee K, Ling S, et al. Preparing for Precision Medicine in Ontario: A Current State Assessment. 2022.
3. Zavar A. Personalized medicine in electronic medical recods (EMRs). In: Mannan M, editor. 2024.
4. König IR, Fuchs O, Hansen G, et al. What is precision medicine? European Respiratory Journal. 2017;50(4):1700391.
5. Sitapati A, Kim H, Berkovich B, et al. Integrated precision medicine: the role of electronic health records in delivering personalized treatment. WIREs Systems Biology and Medicine. 2017;9(3):e1378.
6. Gottesman O, Kuivaniemi H, Tromp G, et al. e Electronic Medical Records and Genomics (eMERGE) Network: past, present, and future. Genetics in Medicine. 2013;15(10):761-71.
7. 2bPrecise. Who is 2bPrecise 2021 [Available from: https://www.2bprecise.com/about2bprecise/.
8. Mount Sinai Health System Launches Collaboration with the Regeneron Genetics Center [press release]. 2016.
9. Michigan Uo. Epic Genomic Indicators Module makes genetic
The Future of Wearable Devices in Standard Healthcare Practices
By Ana Piric
From tness trackers, to smart watches, to fertility rings, to blood glucose monitors, the wearable device industry is ever-expanding, with a projected value of approximately $260 billion by 2030.1 While some devices have already been implemented in the medical eld, such as blood glucose and electrocardiogram monitors,2 technological advancements have ushered in a new era of novel wearable devices in healthcare. However, the implementation of wearable devices in standard healthcare pose inherent challenges that must be addressed.
Wearable devices are typically worn in direct contact with a person’s skin to collect health and tness metrics.2 Depending on the device, they can track parameters such as steps, calories, heart rate, stress levels, menstrual cycles, and sleep quality.2 e monitoring, screening, detection, and predictive capabilities of these devices can inform and empower individuals to play an active role in improving their health.2,3 Ultimately, wearables o er promise of a “more digital, personalised, and preventative medicine.”3
In addition to being used for personal health outcomes, wearables allow for improved clinical care and advancements in biomedical research.3 However, wearable devices also come with their own set of challenges that must be addressed before being integrated into standard healthcare practices.3 One of these challenges is ensuring the quality
of data they produce.3 Unlike traditional medical devices, wearable devices use non-standardized methods and sensors to collect the same parameters.3 For example, oxygen saturation can be measured using watches, rings, or earphones. ese varied data collection methods make it challenging to establish common standards to assess data quality.
ese concerns are compounded by poor data availability across wearable devices.3 O en, researchers cannot download data directly from the device and have to search proprietary archives, which leads to a lack of information about how the data was collected, classi ed, and interpreted.3 A potential solution is the creation of partnerships between healthcare systems and wearable device companies to facilitate high data quality in select devices and the easy transfer of data.3
Beyond data complications, wearable devices are a double-edged sword in terms of health equity.3 e U.S. Centers for Disease Control de nes health equity as the “state in which everyone has a fair and just opportunity to attain their highest level of health.”5 Wearable devices may deepen health inequities through the barriers in who can access and bene t from them, such as those with poor digital literacy and low socioeconomic status.4 As stated by Canali et al., “wearable technology seems to exclude the users that arguably would bene t the most from the use of wearables” such as the elderly and children.3 is not only exacerbates
health disparities, but also leads to misrepresentation in data collection for clinical research.6 For example, in the Apple Heart Study, which aimed to detect irregular heart rhythms (atrial brillation) in users who opted to have their data collected, the selection bias was high, as the 400,000 participant cohort was comprised of young (more than 80% under 55 years) and white (more than 70%) participants.6 e non-representativeness of the sample led researchers to conclude that most users have a low risk of atrial brillation, which may not have been the case in a more diverse study.6,7 Ultimately, the rigour of Apple’s study has come into question despite being one of the largest heart studies detecting atrial brillation through wearable technology.7 is example highlights that to successfully adopt wearable devices in the healthcare system, a major challenge is ensuring their equitable use.
Another way wearable devices can deepen health inequities is through underdeveloped measurement methods.4 An example is the measurement of heart rate and oxygen levels in smartwatches and tness trackers using a technology called photoplethysmography (PPG).4,8 PPG relies on green light signalling, which is known to be inaccurate in patients with darker skin, therefore preventing researchers from obtaining accurate health data from multiple demographics.4 If these devices were to be employed by healthcare providers, their design would
Wearable devices such as smartwatches can be employed to enhance personal health as well as promote better care outcomes in the healthcare setting.3
Photo Credit: Choate C. The impact of Wearable Technology in Healthcare [Internet]. 2024 [cited 2024 Oct 30].
Available from: https://blog.pepid.com/2024/06/07/impact-of-wearable-technology-on-patient-monitoring-inthe-medical-feld/
need to account for diverse populations prior to integration into standard healthcare practice.4
Despite the challenges of implementing specialised medical wearable devices, many are integrated into worldwide healthcare systems, such as blood glucose and electrocardiogram monitors, and more recently, wireless wearable sensor systems for vital sign monitoring in infants and pregnant individuals.4,9 Given the innate higher risk of health complications in these populations, the implementation of wearable devices will particularly bene t
this vulnerable demographic.4 In the case of wireless wearable sensor systems for vital sign monitoring in infants, the injury, scarring, and disruption of skin-to-skin contact associated with wired devices is eliminated, improving neonatal recovery.4 Similarly, wireless vital sign monitoring for pregnant patients allows for remote monitoring, facilitating earlier detection of fetal health complications and quicker interventions by physicians, especially when considering geographic health inequities.4
While the advent of wearable devices, such as smartwatches and tness trackers,
conveniently inform users of their health and tness metrics, there are issues that must be addressed to implement them as part of standard health care practices.3 ese include data quality, accessibility issues, as well as navigating health equity issues arising from demographic di erences and measurement methods.3 ese challenges are surmountable, but necessitate e ective collaboration between wearable device companies and government healthcare systems to integrate these innovative tools into our healthcare system.3
References
1. Philpott J. How are wearable patches revolutionising women’s health? [Internet]. 2024 [cited 2024 Oct 29]. Available from: https://www.medicaldevice-network.com/features/how-are-wearable-patches-revolutionising-womens-health/
2. Schroer A. 15 Examples of Wearable Technology in Healthcare and Wearable Medical Devices [Internet]. 2024 [cited 2024 Oct 29]. Available from: https://builtin.com/articles/wearable-technology-in-healthcare
3. Canali S, Schia onati V, Aliverti A. Challenges and recommendations for wearable devices in Digital Health: Data Quality, interoperability, health equity, fairness. PLOS Digital Health. 2022 Oct 13;1(10). doi:10.1371/journal.pdig.0000104
4. Walter JR, Xu S, Rogers JA. From lab to life: How wearable devices can improve health equity. Nature Commun. 2024 Jan 2;15(1). doi:10.1038/s41467-023-44634-9
5. What is health equity? [Internet]. 2024 [cited 2024 Oct 29]. Available from: https://www.cdc.gov/health-equity/what-is/index.html
6. Lawrence H. Was the Apple Heart Study Virtually Useless? [Internet]. 2019 [cited 2024 Oct 29]. Available from: https:// practicingclinicians.com/the-exchange/was-the-apple-heart-studyvirtually-useless-
7. Koetsier J. Apple Heart Study: What Stanford Medicine learned from 400,000 Apple Watch owners [Internet]. Forbes Magazine; 2019 [cited 2024 Oct 29]. Available from: https://www.forbes.com/ sites/johnkoetsier/2019/03/18/apple-heart-study-what-stanfordmedicine-learned-from-400000-apple-watch-owners/
8. Charlton PH, Marozas V. Wearable photoplethysmography devices. Photoplethysmography. 2023 Nov 29;44(11):401–39. doi:10.1016/ b978-0-12-823374-0.00011-6
9. Kang HS, Exworthy M. Wearing the future—wearables to empower users to take greater responsibility for their health and care: Scoping review. JMIR mHealth and uHealth. 2022 Jul 13;10(7). doi:10.2196/35684
The Road to Discovery: Exploring Sajeevan Sujanthan’s Path to IMS
Se Adventures of Jimmy Neutron, Boy Genius on T.V. as a child, hearing Jimmy punctuate epiphanies with his classic catchphrase—“brain blast!”
Now, years later, Sajeevan Sujanthan nds himself preoccupied with matters of the brain as a PhD candidate at the Institute of Medical Science (IMS). He is currently supervised by Dr. Richard Swartz and is studying cognitive outcomes in patients who have experienced a stroke. While Sajeevan is deeply fascinated with matters related to the brain, he remembers a time when his academic path was not so clear.
Sajeevan entered the University of Toronto in 2015 as an undergraduate student specializing in neuroscience. Despite the label, he didn’t pigeon-hole himself into research one might typically associate with the eld, and instead spent the following summer as a research student working with black widow spiders. While working closely with these creatures is something he’d rather not repeat, Sajeevan describes it as his “ rst foot into research.”
e following year, the professor Sajeevan was working with suggested that he take a second-year research course under her supervision. ere, he ventured into the data collection, analysis, and writing aspects of research. It was an important experience for him, as it was the one that began to spark his interest in this type of work. Sajeevan describes the independence and con dence-building associated with
“I could make my own questions, I could analyze my own results, and actually do things on my own.”
From there, Sajeevan parted ways with the spiders, and spent the next year in psychology research, helping PhD students with patient recruitment. Still, he remembers feeling as though there was something that wasn’t clicking—he missed being able to talk to the participants himself and making that connection.
When looking back on his undergraduate research experience, Sajeevan describes it as being “all over the place,” but he also describes how each opportunity helped him gain perspective and see what research was really like. As he went on, he became more interested in the research aspect of the work—the writing, the methodology, the problem-solving—with the subject matter being a bonus.
At this point, it is perhaps unsurprising that Sajeevan’s path took another turn. A er he moved on from his position assisting PhD students, he went on to do cell-based work at Sunnybrook Hospital. It was during a summer seminar at Sunnybrook that Sajeevan was rst introduced to the idea of becoming a clinician-scientist, which combined his two interests of research and patient interaction.
He started reaching out to clinicianscientists and eventually emailed Dr.
Sunnybrook Health Sciences Centre who was studying outcomes in stroke patients. Sajeevan was particularly interested in stroke, as he has distant family members who have had personal experiences with the condition.
Dr. Swartz recruited Sajeevan to work with him during the summer before the nal year of his undergraduate degree. He enjoyed the work so much that he continued with it part-time throughout the school year. It was through his initial work with Dr. Swartz that Sajeevan nally had the opportunity to experience the face-to-face interaction he’d been missing with patients. ese connections cemented his commitment and passion for clinical research.
“I liked talking to people and hearing their stories—and then I thought, maybe, this is what I wanted to do.”
Sajeevan also describes the mentorship he’s received from Dr. Swartz as being particularly impactful. He recalls how during lab meetings, surrounded by senior lab members, Dr. Swartz would o en stop midway, look at Sajeevan, and explain what was happening. Sajeevan never felt out of place or that he wasn’t being respected “the same way a postdoc or resident was.”
is experience shaped both the kind of mentorship he values and the kind he hopes to provide to others someday.
I liked talking to people and hearing their stories—and then I thought, maybe, this is what I wanted to do “ “
So, as the COVID-19 pandemic hit and Sajeevan’s time as an undergraduate student was coming to a close, he decided to apply to IMS under the same supervisor he had spent the past year and a half with. Nothing was set in stone, but Sajeevan knew the kind of work he liked and knew he wanted to do something tangible that would contribute to society at large and the communities he was a part of.
Sajeevan was accepted into IMS and entered the master’s program in September 2020. His thesis extends the work of a clinical study that was completed two years ago—a randomized trial comparing stroke outcomes in patients who received one of two variations of a tissue plasminogen activating drug that helps dissolve blood clots. Sajeevan notes how, for stroke outcomes, the assessment o en focuses on
di cult. His thesis involves assessing cognitive outcomes through detailed testing to both understand the long-term e ects and improve current cognitive assessment methods for stroke patients in clinical trials.
Halfway through his master’s, Sajeevan decided to take the transfer exam to do a PhD—he liked the work too much to leave it un nished.
One key factor in uencing his choice to pursue a PhD was his experience with his trial participants. He described himself as being fortunate to be able to personally interact with and have conversations with them.
“I heard their story, what they’re missing, and what I can do to help. Each story had an impact on my life.”
Sajeevan also notes the student-led initiatives in IMS as a particular draw of the program. He recalls his seminal work for Youth-of-T Talks with fondness. It was a chance for him to delve into his
Outside of his studies, Sajeevan works as a co-student ambassador with his close friend and colleague Alex Boshart for IMS and spends his spare time mentoring other students through his social media platform @sciencewithsajee, hoping to “pay forward” the mentorship he’s received throughout his own academic career. Not too long ago, he was also in the position of navigating the maze that is the graduate school application process. He remembers how confusing it was and hopes that, through his e orts, he can help students who are going through similar experiences.
Similar to when he rst applied to IMS in 2020, Sajeevan’s plans for the future aren’t set in stone. However, he is aspiring to eventually become a clinician-scientist and plans to apply to medical school once he completes his PhD. Regardless of where his journey takes him, Sajeevan remains committed to making an impact on communities like his own and working to better the lives of those around him through his research and mentorship.
Photo Credit: Katherine Guo
Sajeevan Sujanthan PhD Candidate at IMS
Tumours, Tenacity, and Everything in Between
An Alumni Spotlight on Dr. Sandy Lee
By Jasmine Amini
Graduate studies, at any level, are a period of intense learning and self-discovery. Although developing core skills, such as those of research design and scienti c writing, are essential to growing as an academic, so are skills in leadership and communication. For many individuals, including Dr. Sandy Lee, a 2023 IMS PhD graduate, leadership experiences are, in themselves, essential to becoming a better scientist and conducting more impactful research. Sandy recently sat down with the IMS Magazine to discuss her path to and through graduate school, as well as her future as a scientist in cancer metabolism.
Sandy was always naturally drawn to science. Feeling unsated by her middle school science fairs, Sandy approached her school’s science director to learn about opportunities to explore her interests. It was through this interaction that Sandy rst learned about research and her rst research opportunity. e Sano Biogenius Competition sponsors young Canadians pursuing health science research with a principal investigator (PI). e only caveat? Students had to nd their own PI. Determined, Sandy, at the age of 14, contacted 500 principal investigators before one, Dr. Yvonne Myal, agreed to supervise her. us began Sandy’s journey into cancer research, a journey that has carried her from Winnipeg to Toronto to Los Angeles.
Despite her passion and experience, Sandy’s path to graduate school was
circuitous. A er facing personal and familial health issues that strained her GPA in the rst two years of her undergraduate degree, Sandy, undeterred, began rebuilding her academic record, taking and acing six to seven courses per semester in her nal undergraduate years. Following periods of research in evolutionary biology, epigenetics, and plant biology, Sandy realized she wanted to return to cancer research for her PhD studies. Among the programs Sandy applied to, IMS stood out.
On applying to IMS with a lower cumulative GPA than what was usually considered competitive, Sandy re ected:
“IMS is actually the one department that looked at that [ nal two-year GPA]. ey brought me in for an interview and they asked me what happened because they could see I was capable.”
Sandy acknowledges her supervisor, Dr. Marianne Koritzinsky, for “[taking] a huge risk … I will always be grateful to IMS for giving me a chance because it allowed me to ourish.”
IMS’ wager on Sandy proved fruitful. During her PhD studies, Sandy distinguished herself as an unparalleled student leader, serving as the president of the IMS Student Association (IMSSA), co-founder of the U of T chapter of Love146, an anti-child-tra cking awareness group, and most recently, as a co-founder of Let’s Talk Grad Wellness (LTGW). ese opportunities, Sandy
noted, not only in uenced her as a leader, but also made her a stronger researcher.
“[Being a student leader] shaped me in many ways. I learned that students can’t reach their full potential if they’re not supported. And to be [in] that supportive role changed me immensely as a friend, family member, and scientist.”
e legacy of Sandy’s tireless work with LTGW is enduring. LTGW was founded by IMS students in 2020, shortly a er the onset of the pandemic. Speaking on LTGW’s beginnings: “ is was an initiative that was constantly talked about during my IMSSA co-presidency with Rachel [Dadouch]… en COVID happened. We were like, what if we use this as an excuse to work together again? And that’s how it started… we were trying to nd light in the pandemic.”
LTGW blossomed out of Sandy’s and Rachel’s shared observation that IMS students were struggling and weren’t getting the support they needed from their program. During IMSSA o ce hours, or “mini-therapy sessions,” as Sandy called them, students o en shared their anxieties around expectations with their PIs. When could students take vacation and for how long? How much is too much extra-curricular involvement? How could students bring up di culties with burnout or poor mental health? ese expectations, Sandy articulated, were o en hidden or unspoken.
“ ere’s that big generational gap between PIs and students that we really needed to identify. [LTGW] was about learning how to smooth that gap and facilitate those types of conversations.”
Sandy’s and Rachel’s re ections were the catalyst for the ELEFANT agreement, which was recently rati ed as a program requirement for all IMS graduate students beginning January 2024. With the aim of increased transparency, the ELEFANT agreement was designed to manage PI and student expectations throughout the course of a graduate degree.
Developing LGTW and its initiatives was a formative learning experience for Sandy. Despite its obvious merits, LTGW was not met with acceptance by all faculty members. With recent cultural shi s in
Cancer research is exciting, everything moves so fast and whatever you do, it’s a discovery that makes a di erence to the patient and their families.
“ “
the importance of mental wellness and graduate student wellbeing, some faculty members struggled to recognize the value of the ELEFANT agreement. Learning how to communicate new ideas to a diverse group of leaders and manage emerging con icts were two key skills Sandy developed during this time.
“LTGW helped me get out of my comfort zone and ask the top questions to the higher ups… And those were huge lessons, learning how to frame certain questions, pitch my ideas in a way [so that faculty can] understand I’m not here for short term, but [for] long-term improvements.”
Beyond her countless leadership roles, Sandy was also an extraordinary scholar and teacher. Sandy worked under the supervision of Dr. Marianne Koritzinksy studying the hypoxic microenvironment of tumours through protein folding and metabolism. It was for this work that Sandy received one of only 45 prestigious NSERC Vanier scholarships o ered by U of T’s School of Graduate Studies in 2020. In addition, Sandy developed her mentorship skills as a teaching assistant (TA) and course instructor in the Human Biology Department, quickly becoming a student favourite as demonstrated by her near-pristine “Rate-My-Prof” record.
Currently, Sandy is a post-doctoral researcher in the Shackelford Lab at the University of California, Los Angeles (UCLA) where she continues to study cancer metabolism, combining her PhD
expertise with novel approaches, such as imaging and immunotherapy. Sandy’s passion for her research is palpable, even during a short conversation.
“I just love [cancer research] so much. I love that it makes me feel so speechless and completely lost at times, it’s so humbling. Cancer research is exciting, everything moves so fast and whatever you do, it’s a discovery that makes a di erence to the patient and their families. At the end of the day, that’s what keeps me moving.”
Looking to the future, Sandy aims to further carve out her own niche in cancer research and begin a lab of her own. Her research foci remain steadfast in tumour metabolism and the immune microenvironment in cancer, due to their potential for translational impact. Reflecting on her experiences as a mentor and the kind of lab culture she would like to foster, Sandy emphasized that “I want my group to answer questions in a bold and risky way, without being afraid of failure… I always say there are no stupid questions.”
Sandy’s accomplishments to date are a testament to her resilience, zeal for cancer research, and courage to step outside her comfort zone as a student leader. Despite numerous obstacles, Sandy persisted and spearheaded systemic change to improve the IMS student experience. Her nal piece of advice for current students? “Don’t be afraid to try big things, because you never know until you start.”
Dr. Sandy Lee PhD, postdoctoral fellow at Shackelford Lab, University of California, Los Angeles (UCLA)
Photo Credit: Sandy Lee
From Biochemistry Research to Professional Development: How Curiosity Shaped Dr. Pamela Plant’s Career
By Anna Mouzenian
Dr. Pamela Plant’s professional journey has been fueled by a natural curiosity, a desire to nd creative solutions, and a passion for helping others. ese motivations have shaped her career and now guide her work as the Director of Graduate Professional Development (GPD) at the Institute of Medical Science (IMS). Re ecting on her path, Dr. Plant acknowledges that it wasn’t always straightforward, but each stage brought insights and honed her “tools” for growth, which she now shares with her students.
Her journey at the University of Toronto (U of T) began during her undergraduate studies in Human Biology, where she rst harnessed her curiosity through an undergraduate research project which sparked her love for asking questions and delving into scienti c inquiry. Dr. Plant then completed her Master’s in Cell and Systems Biology, which she describes as an ideal way to “dip her toes in the water” of research rather than directly pursuing a PhD. is experience allowed her to understand the demands and rigours of research, preparing her for the possibility of a future in academia. Dr. Plant ultimately decided to pursue a PhD in Biochemistry at U of T, having a growing interest in translational research and a wanting to focus on projects with a human-centred impact. Dr. Plant emphasized that her “learning” in graduate school was not limited to technical expertise; she gained invaluable skills like problem-solving, analytical thinking, and communication, which she hopes her
students recognize for themselves, as transferable beyond academia.
Outside of the lab, Dr. Plant’s university years were shaped by her commitment to competitive sports. She was a varsity rower, and triathlete, o en training up to six hours a day. is demanding training schedule taught her invaluable life lessons in resilience, goal-setting, and self-management—skills that would later prove bene cial in balancing her academic and professional pursuits. Dr. Plant notes that dedicating oneself to an interest outside academics, (be it competitive sports, music, or community service, for example), fosters valuable tools for selfdiscovery and builds transferable skills applicable to any career. “Plus” she says, “it’s just fun.”
A er over a decade at U of T, Dr. Plant ventured to the University of Lausanne, Switzerland, for her postdoctoral training. is move pushed her far out of her comfort zone, both culturally and professionally, as she navigated a new language and research environment. Conducting research abroad taught her problem-solving in everyday life and underscored the importance of adaptation—a valuable parallel to the independence required in PhD research. Dr. Plant encourages students to consider opportunities abroad, noting that these experiences allow them to develop unique perspectives, skills, and expertise they can bring back to their home institutions/jobs.
Upon returning, Dr. Plant completed another postdoc at the Lunenfeld Institute of Mount Sinai Hospital, where she began contemplating her next steps in academia. Unsure of her exact direction, a er a few years, she welcomed an opportunity at the new Keenan Research Center for Biomedical Science (KRCBS) at St. Michael’s Hospital as a Genomics Specialist and Adjunct Scientist, where she was a core resource supporting labs and their graduate students with their research projects. e KRCBS was still being established at the time and this allowed Dr. Plant the exibility to shape her role and create new programs (such as courses and workshops on various “wet bench” techniques and methodologies) for the students. is illustrated how younger institutions/companies can o en be environments where there is greater freedom in growing one’s role for those who establish their work ethos, intuit the organization’s needs, and pitch new ideas. As she says, “to create your own job.”
Dr. Plant’s enthusiasm for teaching continued to grow during this time, and eventually led to an opportunity to teach the GPD courses at IMS, established by Dr. Reinhart Reithmeier, while he was on sabbatical. With guidance from Dr. Reithmeier and mentors like Dr. Nana Lee, she ran these courses for 3 years until the IMS prioritised professional development for their graduate students and created a new role for Director of the program. ough it was a signi cant shi from
bench science/research to developing professional development programming, Dr. Plant felt the position aligned well with her values of helping students and “creating new things.” It provided an opportunity for her to enable students to integrate practices that were instrumental during her time as a graduate student, such as conducting informational interviews, understanding one’s own values and motivations, and the importance of being involved in meaningful engagements outside of the lab. Dr. Plant’s teaching philosophy centres on hands-on, practical, interactive learning, empowering students for academic success and building
“true success lies in nding joy, meaning, and purpose”
the agency/skills needed for lifelong professional success.
In her role at IMS, Dr. Plant’s focus has been to establish a fulsome program that encourages students to discover the many opportunities outside of academia and medicine, to see “what career ts them.” She encourages students to understand that graduate school is not just a pathway for careers in academia or medicine, that there are “hundreds of ful lling, challenging and lucrative careers” for graduate students in biomedical sciences. In addition to the foundational GPD course, inspired by Dr. Lee and Dr. Reithmeier’s book, Success in Graduate School and Beyond, she is creating a series of career-based courses, to help students gain the necessary skills to leverage into public and private sector jobs. In doing so, she hopes to help students transition into ful lling vocations in diverse elds, not just academia and medicine. If you’re interested in learning more about GPD and want to enroll in their programs, you can visit their website (https://ims.utoronto.ca/graduateprofessional-development) for resources and course o erings.
Beyond academics, Dr. Plant believes deeply in the importance of community engagement. Her curiosity and passion for science extend to outreach, where she has partnered with local libraries to create programs promoting scienti c literacy. She recalls organising a science day at
a local school, where students could be “germ hunters” and explore the “dirtiest” areas of the school by growing swabs (of bacteria) on agar plates—a testament to how educators can bring science to life for younger generations. ese e orts, she notes, are a way to ful l a social responsibility to facilitate scienti c literacy and engage people in the joy of discovery. To this end, she encourages her GPD students to share their work in accessible ways to lay audiences.
Re ecting on her journey, Dr. Plant advises students to remain open to opportunities, change, embrace selfre ection, and pursue roles that align with their values. She emphasises that no job is perfect, but nding one that aligns with your values and lls you with meaning and purpose, can provide long-term ful lment. In the end, Dr. Plant’s story is a reminder that career paths are not o en linear; they require a blend of self-trust and adaptability. is mindset has guided her to a ful lling role where she can channel her passion for teaching and, as she puts it, “share that excitement of learning with others.” For Dr. Plant, true success lies in nding joy, meaning, and purpose, a lesson she strives to impart to the next generation of scientists.
Dr. Pamela Plant Director of Graduate Professional Development at the Institute of Medical Science
Photo Credit: Katherine Guo
Sample ID Unknown: A History of Misuse and Distrust in Genetic Studies of Indigenous Communities
By Emily Wiljer
Who gets to be included in genetics research? Who is willing to have their genome be read like a book? When you read an article claiming the APOE4 gene is linked to Alzheimer’s, what population does that apply to? As of June 2021, 86.3% of all published genetics association studies have been done on White European populations.1 But why is this the case? Is it a research protocol? Or does this stem from a long history of distrust and misuse of data? In reality, it is a complicated blend of both that can be exempli ed by the ways genomics has failed Indigenous communities across the globe.
Genomics is the study of how genes interact with each other and the environment to predict phenotypic variation and disease.2 is approach has been imperative for the development of precision medicine. However, it does not a ect all populations equally: there is an underlying aw in genomics when it comes to equality and representation. Many genetic association studies must be done with a common “genetic ancestry” in participants to limit di erences in genetic variability that occur across di erent populations due to gene ow and global dispersion (the movement of genetic variants across populations and geographic locations).3 However, population substructure is o en strati ed by self-reported race as a proxy for genetic ancestry. is creates a divide amongst subgroups and fails to account for mixed raced (termed admixture) levels of
population that are more representative of society.3 Because of this assumption, research will o en focus on groups of “White” European ancestry, as this population constitutes the largest available data pool.
It is clear that research protocols themselves call for racial strati cation, but the question persists of how we can expand the data availability to include a more diverse and representative population. Indigenous data in genetic research is vastly underrepresented, included in only 0.02% of genetic association studies published globally in 2019.4 Consequently, there is a lack of reference for genetic variants in Indigenous populations, which is needed to draw clinically relevant conclusions. Although researchers are starting to acknowledge a need for an expansion in data, the barrier goes both ways. Harm and misuse of Indigenous biological samples in research is rampant globally and throughout history. A lack of applicable results, informed consent, community involvement, and a perpetuation of stereotypes has created a pattern of distrust and has made Indigenous communities less compelled to participate in genetic research.4
One of the most famous examples concerns the Havasupai Tribe in Arizona, USA. In 1989, Arizona State Researcher, erese Markow, was recruited to perform a genetic study with the promise of community engagement and education on the prevalence of diabetes. What the
study participants didn’t know was that the researchers, without approval, went on to use the samples given by the tribe in studies on schizophrenia, migration, alcoholism, and inbreeding. When these studies came out, a lawsuit was led by the Havasupai Tribe for misuse and lack of informed consent. ey felt that such studies, on topics taboo to their community, performed harm both culturally and dignitary to the group.4,5 is clear undermining of informed consent created a decades long legal battle for the Havasupai and a foundation of distrust and skepticism when consenting to research.
In British Columbia, Canada, the Nuu-chah-nulth people had a similar experience. Dr. Ryk Ward from the University of British Columbia (UBC) was recruited to test DNA samples to potentially identify why rheumatoid arthritis was so frequent and severe in this community. Dr. Ward never completed the study on rheumatoid arthritis, but brought the samples with him when he moved around the world for academic appointments. In total, over 100 papers were published that included the Nuuchah-nulth people’s DNA, including studies on human migration and retroviruses4. However, it was not until the release of a documentary inspired by Dr. Ward’s genetic studies that the Nuu-chahnulth were aware of this secondary use of their samples. e community worked with UBC to recover their samples and formed their own research ethics committee to
ensure that their consent would not be violated again in such a manner.4
Beyond lack of consent, an egregious ethics violation in itself, Indigenous DNA data has also been used to propagate negative and harmful stereotypes of their communities. In New Zealand, the Māori community was part of a study concerned with high and low-nicotine metabolism. e researchers made claims of a “warrior gene” that linked Polynesian migration routes, aggressive behavior in monkeys, and Māori smoking cessation rates, despite the fact that the genetic variation being studied was present in all populations globally4. is blatant and inaccurate insult led to a publicly understood reluctance from the Māori community to participate in further genetics research, and increased their distrust in the scienti c community.4
ese stories are not isolated incidents. As we enter the age of precision medicine and genomics, we must strive to learn from these events. To scientists, biological samples may be a means to an end, but to some cultures, including some Indigenous populations, they mean much more. Dr. Frank Dukepoo, a Hopi geneticist, described this relationship: “To us, any part of ourselves is sacred. Scientists say it’s just DNA. For an Indian, it is not just DNA, it is part of a person, it is sacred, with deep religious signi cance. It is part of the essence of a person.”6
Going forward, we must analyze how we approach genomics, not only by
questioning our own practices but by considering why some people may be more reluctant to share their DNA, especially minority populations who have been targeted historically. Recognition of sovereignty, community-engaged research, and e ective guidelines built in partnership with Indigenous, or other minority communities should lay a clear and constructive path forward for diversity in genomics.4
References
1. Fatumo S, Chikowore T, Choudhury A, Ayub M, Martin AR, Kuchenbaecker K. A roadmap to increase diversity in genomic studies. Nat Med. 2022;28(2):243-250. doi: 10.1038/s41591-021-01672-4.
2. Gwynne K, Jiang S, Venema R, Christie V, Boughtwood T, Ritha M, et al. Genomics and inclusion of indigenous peoples in high income countries. Hum Genet. 2023 Sep;142(9):1407-1416. doi: 10.1007/ s00439-023-02587-5.
3. Race, Ethnicity, and Genetics Working Group. e use of racial, ethnic, and ancestral categories in human genetics research. Am J Hum Genet. 2005 Oct;77(4):519-32. doi: 10.1086/491747.
4. Garrison NA, Hudson M, Ballantyne LL, Garba I, Martinez A, Taualii M, et al. Genomic research through an indigenous lens: Understanding the expectations. Annual Reviews; 2019(20):495-517. https://doi.org/10.1146/annurev-genom-083118-015434
5. Sterling RL. Genetic research among the havasupai: A cautionary tale. Virtual Mentor. 2011;13(2):113-117. doi: 10.1001/virtualmentor.2011.13.2.hlaw1-1102
6. Petit C. Trying to study tribes while respecting their cultures / hopi Indian geneticist can see both sides . 1998. Available from: https://
Humanity and the Price of Progress
In Klara and the Sun
By Beatrice Acheson
The age of precision medicine is upon us. With the rapid rise of arti cial intelligence and the accessibility of tools like whole genome sequencing, scientists are achieving feats that once seemed impossible. While these developments will no doubt revolutionize medicine, we must confront the unfortunate paradox that arises when we advance medical technology: we will cure people in ways that we did not know were possible, but we may also worsen existing inequities in ways that we cannot yet fully grasp.
Kazuo Ishiguro’s Klara and the Sun explores a ctional future that explores these ethical dilemmas and o ers insight into the potential consequences of advancement made at the expense of humanity.1
In his rst novel since winning the Nobel Prize in Literature in 2017, Ishiguro depicts an eerily plausible dystopia in which children have Arti cial Friends–humanoid robots powered by arti cial intelligence and programmed as companions. Some children in Ishiguro’s futuristic landscape are “li ed,” having undergone genetic editing to enhance inherent attributes such as intelligence and disease susceptibility, while others have not. “Substitutions” have replaced entire job sectors with genetically enhanced individuals. Ishiguro presents a reality where the line between human and machine is blurred, compelling the reader to confront the complex relationships we have with one another, ourselves, and technology in a world in which technology is rapidly evolving.
e narrative unfolds through the perspective of Klara, an Arti cial Friend waiting to be bought. Unlike other Arti cial Friends, Klara is a keen observer. She is uniquely attentive to human emotion. To her delight, Klara is selected by Josie, a li ed child who is overcoming the side e ects of genetic editing. Upon entering Josie’s life, Klara is confronted with the harsh realities of a society where genetic editing has become the norm; Josie’s friend, Rick, is unable to go to university because of his status as “unli ed,” and Josie’s father, a former engineer, is “substituted” despite his ability and skill. rough Klara’s perspective, Ishiguro provides a lens for readers to examine human relationships and societal dynamics. Her observations illuminate a future where precision medicine serves those with privilege but hurts those without, raising pressing ethical questions for Klara’s ctional society as well as our own.
Klara pieces together bits of information about the people around her, gradually building her understanding of the world. Klara is a nonhuman and defamiliarized narrator with a viewpoint entirely di erent than our own, and her perspective allows Ishiguro to emphasize the thin line that exists between human and machine, and to caution us of the implications of crossing it. In Ishiguro’s ctional world, existing class disparities are exacerbated. rough Klara’s perspective, Ishiguro challenges the reader to re ect on the social
consequences of unchecked technological advances in a world in which humanity itself is rede ned.
Importantly, Klara and the Sun is as hopeful as it is unsettling. As Klara works to ful ll her programmed purpose—to know and befriend Josie—Ishiguro reminds us of what makes humanity unique and why technology can never replace that. rough her experience, Klara learns that “there was something special, but it wasn’t inside Josie. It was inside of those that loved [Josie].” Klara’s insight reminds us that humanity is rooted in our ability to love, empathize, and connect. As we embrace the era of precision medicine and develop novel, individualized treatments, it is essential that we prioritize the preservation of our humanity just as stringently as we pursue technological advancements. Precision medicine will only be equitable when we commit as deeply to what unites us as we do to understanding what makes us di erent.
References
1. Ishiguro K. Klara and the Sun. Toronto: Vintage Canada; 2021.
Book Cover Design: Peter Adlington
Learning About the Roots of Multiple Sclerosis Research in Beautiful København
By Gabriela Blaszczyk
At the start of my PhD in September 2024, I had the special opportunity to attend the meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS) in beautiful København (Copenhagen), Denmark. As someone who has been involved in multiple sclerosis (MS) research for the past three years, I was excited to partake in the 40th anniversary of the world’s largest MS meeting, making it particularly inspiring to present my research and learn from groundbreaking leaders in the eld. e conference opened with a ceremony that was attended by Her Majesty Queen Margarethe of Denmark, a patron of MS research in her country for over 60 years.
ECTRIMS welcomes both clinicians and researchers, making it a meaningful experience for a basic life sciences researcher such as myself. Session and scienti c poster presentation topics ranged from novel clinical approaches to new disease mechanisms, emphasizing how crucial communication between these two elds is for driving development of novel MS treatments.
An exciting presentation at ECTRIMS 2024 addressed the revision of the MS diagnostic criteria. is year, along with the increased number of novel approaches for diagnosis, the criteria was broadened to encompass the earliest forms of MS. is change will provide these individuals earlier access to MS-approved treatments rather than
waiting for full MS symptoms to develop, improving both disease prognosis and quality of life.
As a graduate student, the highlight of travelling to conferences is the opportunity to discover the host city. I found the best method of getting around København was by bike. Unlike most North American cities, the bicycle lanes felt safe and provided convenience when making my way to the conference and exploring the city.
I was told that København is best experienced from the water, so I took a canal tour and was not disappointed! e city itself is surrounded by water on all sides with a series of canals running through it. e views of the city were captivating, beginning with the famous Nyhavn canal lined with colourful homes from the 17th and 18th centuries, reminiscent of the Canadian Maritime Provinces. e tour explored the spiral church tower in Christianshavn, an addition to the Christ Saviour Church
from 1752, and a boat house community in the Indre By borough.
What really struck me about København was the pace of life that locals had. Although I was visiting during the week, I admired the locals out on restaurant patios, parks, and bridges. e people there delight in time with friends and the rare glimmer of sunshine this Nordic country experiences throughout the year.
Travelling to and attending the 40th ECTRIMS meeting in beautiful København set the scene for my PhD journey ahead. What I will take forward with me are the lessons from the Danish people: to live life at a slower pace and to savour sunlight while we have it, all while being fueled by the excitement of new scienti c ndings and connections made at the largest meeting for MS research in the world!
17th and 18th century homes in Nyhavn
Photo Credit: Gabriela Blaszczyk
Bicycle parking outside of a market in downtown København
Photo Credit: Gabriela Blaszczyk
The IMS Magazine’s Fall Issue Launch Party
Celebrating the Accomplishments of Our IMS Community Members
By Suraiya Mangra, Kyla Trkulja, & Kristen Ashworth
Since its founding in 2011, the IMS Magazine has focused on the publication of quarterly issues that highlight the achievements of IMS students, faculty, and alumni. Upon publication, the articles are shared in print and online—but an in-person element to celebrate the individuals highlighted in the issue was missing. is year, the IMS Magazine leadership team had a vision to change that with the rst-ever launch party, which brought the Hart House Music Room to life on November 21st, 2024, as students and faculty gathered to meet the IMS Magazine team members, designers, and those featured in the Fall 2024 issue of the magazine focused on Cardiovascular Health. e party marked a massive milestone in our team’s journey by bringing the IMS community to showcase the combined e orts that brought this recent issue together.
While the aim of the IMS Magazine has always been to bring research within IMS to a wider audience, the magazine’s goal going into this academic year was to also be recognized as a student group outside of the seasonal issues we produce by getting directly involved in the IMS community. e launch party provided a pivotal opportunity to do this, especially in the midst of the largest team growth the magazine has ever experienced.
e evening began with some opening remarks from IMS Director Dr. Mingyao Liu, an enthusiastic supporter of the magazine since its founding. Dr. Liu
emphasized the signi cance of this event, bringing people together in-person to showcase the work being done both by the IMS Magazine team and those highlighted in the most recent issue. A er a warm re ection on how far the magazine has come over the last 13 years, Dr. Liu expressed his gratitude towards the community at IMS, and how events that bring everyone together are what make the program stand out among others.
Following his statement, us editorsin-chief gave a brief overview on the founding, evolution, and goals of the magazine before introducing the members of this year’s executive and design teams. Despite many of the members of both teams stepping into their roles in September, they have worked tirelessly
to ensure the successful release of this Fall 2024 issue. e editors then gave an overview of the articles and IMS students, faculty, and alumni featured in this most recent issue—which was also signi cant due to it revisiting Cardiovascular Health, a topic covered 10 years ago in 2014. It was inspiring to see the changes in perspective and new developments in the eld since then.
Of course, this evolution from the previous edition to now would not have been possible if not for the hard work of our faculty, student, and alumni contributors, some of which kindly agreed to join us for a panel discussion to share their insights and perspectives. Dr. Osami Honjo and Dr. Paaladinesh avendiranathan, two IMS faculty members whose research
Hart House
The front of the Hart House Music Room was organized to create a warm and welcoming space for introductory remarks and the panel discussion.
Dr. Mingyao Liu
Dr. Mingyao Liu providing the opening remarks for the launch party
Photo Credit: Suraiya Mangra
Photo Credit: Emily Yeung
was featured, as well as our alumni and faculty spotlights, Dr. Aadil Ali and Dr. Tony George, engaged in an insightful discussion about the challenges to research and scienti c careers, future directions in the eld, and provided their advice to budding scientists and trainees in the IMS community. e discussions were lled with interesting topics such as the strategic use (and cautionary tales) of arti cial intelligence (AI) in research, planning the next steps in our careers a er graduating from IMS and whether students should consider remaining in Canada or relocating elsewhere, and the importance of having dedicated mentors that will allow us to achieve our potential. Attendees were lled with hope and optimism in the end, enthused by a conversation that was educational and stimulating, which set the tone for the rest of the evening.
A er the panel discussion, microphones were turned o , music was turned on, and the room was buzzing with people networking and socializing with the panelists and other IMS community members over hors d’oeuvres. Conversation and laughter lled the room as attendees got to know the IMS Magazine journalists, designers, and executives, as well as those featured in the Fall 2024 issue and others involved in IMS leadership. Connections were made between many members of the IMS community, making the event a huge success, and one that will be continued every Fall in the years to come.
The 2024/2025 IMS Magazine leadership team: Lizabeth Teshler, Nayaab Punjani, Kyla Trkulja, Suraiya Mangra, Kristen Ashworth, Kevan Clifford, and Kiko Huang
IMS Director and Associate Director, Dr. Mingyao Liu and Dr. Lucy Osborne, with the IMS Magazine editors-in-chief and panelists featured in the Fall 2024 issue, Dr. Osami Honjo, Dr. Paaladinesh Thavendiranathan, Dr. Aadil Ali, and Dr. Tony George
IMS Magazine team members Nayaab Punjani, Kevan Clifford, Kiko Huang, Lizabeth Teshler, and Sara Corvinelli at the registration desk for the event. Leadership Team
IMS Leadership Team and Launch Party Panelists Registration Desk
Photo Credit: Emily Yeung
Photo Credit: Kristen Ashworth
Photo Credit: Kristen Ashworth
IMS Orientation 2024: A Warm Welcome for the New Cohort of Scientists
By Kowsar Teymouri
On the bright, lively morning of September 12th 2024, Toronto buzzed with its usual energy, but something extra exciting was happening at the iconic Faculty Club: the Institute of Medical Science (IMS) was rolling out the red carpet (metaphorically, of course) to welcome its newest cohort of graduate students! e IMS student association (IMSSA) executive team and the ever-organized and resourceful Emilie DesRosiers—our amazing IMS Admissions and Recruitment Administrator—had poured their hearts into planning an orientation to remember.
e day kicked o with a cozy breakfast in the stunning Faculty Club dining room, where new students were strategically seated with upper-year students to spark networking and conversation. No awkward silences here—just the buzz of future scientists connecting over co ee and pastries. At the registration table, enthusiastic volunteers greeted students with warm smiles, snazzy name tags, tote bags stu ed with IMS swag (hello, free merch!) and essential info to jumpstart their academic adventure. en came the dynamic duo of IMSSA presidents, Hamzah Khan and Stefan Aguiar, whose energy as MCs could rival a double shot of espresso.
e program o cially began with opening remarks from the IMS director, Dr. Mingyao Liu, who emphasized the vital role of the community at the IMS. From there, the stage was packed with
resourceful introductions—students got the inside scoop on everything from the Centre for International Experience to IMS-speci c programs like the Professional Development Initiative, the Equity, Diversity, and Inclusion (EDI) committee, and the always-popular IMS Research Rounds. To keep things fun, the IMS core team even shared their favourite snacks while explaining their roles.
As any seasoned graduate student will tell you, orientations are an information marathon, so a well-deserved break followed. Enter the IMS Passport activity: students collected stamps from various student group booths, turning a break into a fun scavenger hunt and starting conversations that led to instant sign-ups.
Dr. Mingyao Liu set the tone with inspiring opening remarks, highlighting the importance of student experience and community values at IMS
A er the break, Nayaab Punjani, the teaching assistant (TA) for the MSC1010/1011 seminar series in translational research, gave a quick and helpful rundown of the course
expectations. en, everyone’s favourite graduate coordinators, Dr. John Vincent and Dr. Isabella Caniggia, wrapped things up with a treasure trove of tips to help students navigate their degrees.
Just like that, another IMS orientation was in the books. We’re le with fantastic photos, cherished memories, and a vibrant new class of 2024 IMS researchers. Welcome to the family, new students—we can’t wait to see the incredible things you’ll achieve!
The new IMS cohort kick-started their journey by networking with peers over a delicious breakfast
IMSSA Presidents Hamzah Khan and Stefan Aguiar delivered an engaging overview of resources and student groups available for IMS students
The iconic IMS Orientation selfe wasn’t quite a selfe this year, but just as memorable!
Photo provided by the IMS Students’ Association (IMSSA)
Photo provided by the IMS Students’ Association (IMSSA)
Photo provided by the IMS Students’ Association (IMSSA)
Photo provided by the IMS Students’ Association (IMSSA)