PBM REFORM CONGRESS STATE LEGISLATION FTC IOWA INSURANCE DIVISION CMS LEGAL ACTION PAYER INITIATIVES MEDIA MARKET DISRUPTORS A Peer-Reviewed Journal | Vol. LXXIX, No. 1 | JAN.FEB.MAR.APR. 2024 INSIDE: Final Words From the Deans 2024 IPA Board Election IPA Headquarters Sale

2570 106th Street, Unit D, Urbandale, IA 50322
Phone: 515.270.0713
Fax: 515.270.2979
Email: ipa@iarx.org | www.iarx.org

PUBLICATION STAFF
Allison Hale, Managing Editor
Kate Gainer, PharmD
Emmeline Paintsil, PharmD, MSLD, BCPS
Mikayla Tice-Harris, PharmD
Seth Brown, JD
Kellie Staiert, MPA
Laura Miller
OFFICERS
CHAIRMAN
Cheri Schmit, RPh – Ames
PRESIDENT
John Hamiel, PharmD – Evansdale
PRESIDENT-ELECT
Jim Hoehns, PharmD, BCPS, FCCP – Cedar Falls
TREASURER
Kristin Meyer, PharmD, BCGP, CACP, FASCP – Marshalltown
SPEAKER OF THE HOUSE
Wes Pilkington, PharmD – Waterloo
VICE SPEAKER OF THE HOUSE
Laura Knockel, PharmD, BCACP – North Liberty
TRUSTEES
REGION



The Journal of the Iowa Pharmacy Association is a peer-reviewed publication. Authors are encouraged to submit manuscripts to be considered for publication in the Journal. For author guidelines, see www.iarx.org/journal
“The Journal of the Iowa Pharmacy Association” (ISSN 1525-7894) publishes 3 issues per year: January/February/March/April issue; May/June/July/August issue; and September/October/November/ December issue by the Iowa Pharmacy Association, 2570 106th Street, Unit D, Urbandale, IA 50322. Periodicals postage paid at Des Moines, Iowa and additional mailing offices.
POSTMASTER: Send address changes to: The Journal of the Iowa Pharmacy Association, 2570 106th Street, Unit D, Urbandale, IA 50322. Published tri-annually, The Journal is distributed to members as a regular membership service paid for through allocation of membership dues. Subscription rates are $80 per year, single copies are $30. Printed by Mittera; Graphic design done by the Iowa Pharmacy Association.
#1 Robert Nichols, PharmD, BCPS – Waterloo REGION #2 Natalie Hunter, PharmD – Cedar Falls REGION #3 John L'Estrange, PharmD, RPh, BCACP – Des Moines REGION #4 Wendy Kinne, PharmD – Boone AT LARGE Micaela Maeyaert, PharmD, BCPS, DPLA – Spirit Lake Morgan Herring, PharmD, BCPS, FAPhA – West Des Moines Brett Faine, PharmD, MS – Iowa City Cory Garvin, PharmD – Wilton HONORARY PRESIDENT Marilyn Osterhaus, RPh – Maquoketa PHARMACY TECHNICIAN Connie Bentrott, CPhT – Ames STUDENT PHARMACISTS Kayla Batdorf – Drake University Rebecca Scribano – University of Iowa Combatting PBM Abuses: From Every Angle pg. 8 FEATURES IPA Headquarters Sale: A New Era for Iowa Pharmacy...... 16 New IPA Podcasts ..................................... 19 Efficacy of Angiotensin II Receptor Blockers .............. 24 2024 Iowa Legislative Session Preview .................... 30 CMS Final Rule & DIR Cliff............................. 33 LIRC Membership Add-on 34 Thank You IPA Supporters 36 2023 IPA Executive Intern Reflections 38 IN EVERY ISSUE President’s Page 4 CEO’s Column 6 IPA in Action ......................................... 16 Practice Advancement ................................. 22 Public Affairs ......................................... 30 Technician Corner ..................................... 35 IPA Foundation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37 Members Section ...................................... 40 Calendar of Events .................................... 42 Time Capsule 43 Mission Statement The Iowa Pharmacy Association empowers the pharmacy profession to improve the health of our communities. Final Words: The Deans pg. 12 2024 IPA Board Election pg. 14 TABLE OF CONTENTS JAN.FEB.MAR.APR. | 3 COVER STORY
IPA, A RECIPE FOR INVOLVEMENT

With all the competing priorities for time and money in our busy lives, it becomes difficult justifying the additional expense to become involved in professional organizations like the Iowa Pharmacy Association. Paying down mortgage, student loans, spending time with family, or donating both time and money to another organization—been there, done that myself.
As I have gotten further along in my career, I see what a mistake that was for my professional wellbeing. IPA has provided close friends, mentors, learning opportunities and support. Now, I do not know what I would do without my IPA Phamily.
The burnout and professional frustration I felt during the COVID pandemic nearly caused me to quit a career that has meant so much to me. Without the ability to share my concerns and feelings with other pharmacists in a non-work setting, I would not be writing this column. The support expressed to me from IPA members got me through tears. I know that IPA can be as meaningful to you. Now is the perfect time to start.
IPA’s membership and elected leadership have all faced the same time, money, and work challenges that all new pharmacists face. Thankfully, IPA has introduced opportunities to participate at your own commitment level. Let me give you some examples.
Try out what IPA offers for free! The INFORMED membership level is a free, no commitment level that lets you become knowledgeable about upcoming activities, events, and what is going on in pharmacy news across the country. This keeps you in the loop and allows you to become more involved when ready.
Got a free couple of hours? Attend an IPA Goes Local event, join a 2/2/2 webinar or Member Forum, or listen to IPA’s What, Why & How or Trailblazers podcast. These allow you to see who is involved, meet IPA Board members and staff, and get updates on future opportunities. These are also great learning opportunities on innovative topics.
Got a couple of days to contribute? Apply to serve on an IPA committee or attend a meeting like Pharmacy Day on the Hill or IPA’s Annual Meeting—one of the best ways to get to know about IPA, have fun and learn something. There are no “vanilla” sessions at IPA events; you see high-quality, national level presenters


and content with the opportunity to claim continuous professional development (CPD) credit for board-certified pharmacists.
The most professionally satisfying conference I have ever attended is an exclusive opportunity for IPA young practitioners, the Decker-Temple Leadership Pharmacy Conference. If you read the tribute to Tom Temple in the previous IPA Journal, you learned about the founding of this opportunity. You do not, however, get to feel the excitement, fun and growth that occurs at this retreat. Mix twenty inspirational young pharmacists from Iowa and Wisconsin, add IPA and PSW staff, and Executive Committees. Add one-part educational sessions, twoparts networking, and two-parts fun. Cook this explosive group in a retreat atmosphere, and out comes the most excited, motivated, and charged up future leaders that I have experienced.
Do not make the same mistake that I made. Get involved in IPA early and often. Stay involved and you will experience friendship and professional fulfillment at a level you will not believe.
See you all at the Annual Meeting! ■
PRESIDENT’S PAGE
IPA President
John Hamiel, PharmD
4 | The Journal of the Iowa Pharmacy Association
Regional Director of Pharmacy, MercyOne Northeast Iowa
Brainstorming at 2023 Board Retreat
2023 Presidential Address
Refer & Earn $1,000 Bonus! Invite other independents to join IPC and earn $1000 for each referral!
Refer a pharmacy They join IPC You earn $1,000! REFER & EARN offer.ipcrx.com/referral www.ipcrx.com For 40 years, IPC has been committed to community pharmacy. By committing to the Cooperative, you’re investing in yourself. • Nation’s Largest GPO • 100% Profit & Rebates Return • Advocate for Community Pharmacy
How it Works
CHANGE IS CHALLENGING. CHANGE IS INEVITABLE. CHANGE IS PROGRESS.
 Kate Gainer, PharmD
Executive Vice President & CEO, Iowa Pharmacy Association
Kate Gainer, PharmD
Executive Vice President & CEO, Iowa Pharmacy Association
The start of 2024 has been a historic time for the Iowa Pharmacy Association. For the first time in over 45 years, IPA moved its headquarters. As the 8515 Douglas Ave, Suite 16 era ended, I’ve had time to reflect on the importance of this move. For the staff, for the members, and for the organization.
Moving the IPA headquarters, and 45+ years of memories within its walls, was a significant undertaking for the IPA staff. It was also an increased time commitment for the PNI Board over the past three years. This board deliberated the best path forward for the Association and met numerous times to evaluate and guide decisions throughout the process.
As news was announced that IPA would be moving its headquarters and selling the previously owned office space, many reflections were shared. History, nostalgia, and many memories made by past staff. Life lessons, influential conversations, and professional milestones by members and leaders of IPA.
It was fun to host a ‘Going Away’ reception (see Page 17) in the final weeks at the old headquarters. Over 40 guests attended and reminisced, sharing stories ‘if these walls could talk’—the stories they would tell.
Most of these stories took place in the IPA boardroom. The boardroom could hold 40 people: 20 around the table and additional seats along the side walls. While a great space for large gatherings, the boardrooms of the future look much different.
In IPA’s new office space, the conference room will seat 12 people, and full IPA Board of Trustees meetings will be hosted off-site. This presents the opportunity to be nimble and move to various locations. Day to day, the IPA staff works from these headquarters. Inevitably, the way we work continues to evolve. Hybrid. Flexible. Asynchronous. The benefit of having a smaller office footprint will serve IPA well financially, and it will create a collaborative environment for the IPA staff for daily work.
Looking forward, the connection IPA members feel to IPA may no longer be to a physical location, or the table, chairs, or artwork in a boardroom. Rather, the inclusive opportunity to feel connected will be for ALL members: to the people next to you, at an IPA event or board meeting; with a committee that meets 100% virtually; or online with colleagues that engage through The Bridge, LinkedIn, or other social platforms. IPA will continue to create meaningful connections—through shared
purpose—every time our members engage and gather (both in real life and the digital world).
In the coming weeks, IPA will host a ‘Welcome’ reception (see Page 42) at the new office. Board members have already been to IPA’s new home, and their feedback is overwhelmingly positive (even with boxes stacked and not unpacked, blank walls, and dust still settling). We are excited for more members to visit and feel proud of the new office as a place for Association members to work and meet.
IPA is evolving to serve the profession of pharmacy as the profession of pharmacy evolves.
While change can be challenging and is inevitable, change is also progress. ■



6 | The Journal of the Iowa Pharmacy Association
CEO’S COLUMN





RENEW TODAY Live and Virtual Events • CPE through CEimpact • Online Community • IPA Member Forums Advocacy for the Profession • IPA Journal • Leadership Opportunities • Monthly 2/2/2 Webinars PBM/Payer Resources • Weekly Communications • Podcasts • Burnout Resources • LIRC Add-on Legislative Resources • Partner Discounts • Grant Funding • Statewide Protocols • Staff Support www.iarx.org/JOIN_RENEW COLLABORATION | ENGAGEMENT | EXCELLENCE INCLUSION | INNOVATION | INTEGRITY | LEADERSHIP
COMBATTING PBM ABUSES: FROM EVERY ANGLE
The state of Iowa first passed PBM (pharmacy benefits manager) legislation in 2007. Since that time, PBM legislative priorities have been a consistent part of IPA’s advocacy agenda. While states across the country work to address PBM reform through legislative efforts (297 active bills in 2024), there are additional strategies whereby advocacy and action can impact the practices of PBMs. This article highlights several of these strategies and current progress to address PBM reform through: federal legislation (Congress); state legislation; federal regulation (FTC and CMS); state regulation (Iowa Insurance Division); litigation and legal action; payer-led initiatives; media and public relations; and market disrupters.
CONGRESS
Lower Costs, More Transparency Act (H.R. 5378)
Prohibits spread pricing and requires full pass-through in all Medicaid managed care programs; requires state Medicaid pharmacy reimbursement be at a pharmacy’s AAC plus the state’s Medicaid FFS dispensing fee; and limits payments to PBMs to solely administrative fees. This package combines provisions from bills in the House Energy and Commerce, Ways and Means, and Education and the Workforce committees, including the Drug Price Transparency in Medicaid Act (previously H.R. 1613). The bill passed the House of Representatives on December 11, 2023.
Protecting Patients Against PBM Abuses Act (H.R. 2880)
De-links PBM compensation from the cost of medications, prohibits spread pricing, prohibits PBMs from compensating a network pharmacy less than affiliated pharmacies, and includes transparency provisions related to the PBM rebates and administrative fees. Passed subcommittee, moving the bill to a full vote by the House Energy and Commerce Committee.
Medicare PBM Accountability Act (H.R. 5385)
Enhances PBM reporting and conflict of interest disclosure requirements to the Secretary of HHS, stipulates audit and enforcement process. Passed subcommittee, moving the bill to a full vote by the House Energy and Commerce Committee.
Delinking Revenue from Unfair Gouging (DRUG) Act (H.R. 6283)
Requires PBMs to charge a flat fee for drug placement, bans spread pricing, prohibits PBMs from paying affiliated pharmacies more than non-affiliated pharmacies for the same services, and bans patient steering. Introduced by Representative Miller-Meeks [R-IA-1].
Better Mental Health Care, Lower-Cost Drugs, and Extenders Act (S. 3430)
Requires pharmacy reimbursements include professional dispensing fees, expands the definition of ‘essential independent pharmacies’ eligible for enhanced protections, increases the number of reasonable and relevant contract term violations that pharmacists can report to CMS, ensures pharmacies are made whole for certain discount-eligible drugs dispensed under net prices. Combines provisions from other Senate proposals, including Senator Grassley’s PBM Transparency Act.
DIR Cliff Amendment to the Better Mental Health Care, Lower-Cost Drugs, and Extenders Act
In addition to multiple PBM-specific provisions, the Senate Finance Committee adopted Senator Chuck Grassley’s amendment, requiring HHS to report to Congress the impacts of the ‘DIR Cliff’ caused by PBMs responding to the Medicare Part D final rule scheduled to take effect on January 1.
Modernizing and Ensuring PBM Accountability (MEPA) Act (S. 2973)
De-links PBM compensation from Medicare Part D drug prices and increases PBM transparency; requires PBMs to provide pharmacies information on all components to price a Medicare Part D claim; requires HHS to establish standardized pharmacy quality and performance measures under Medicare Part D; prohibits spread pricing in Medicaid and Medicaid managed care plans; includes National Average Drug Acquisition Cost as a floor for future Medicaid payments. This bill passed the SFC July 2023.
The Better Mental Health Care, Lower-Cost Drugs, and Extenders and MEPA Act are expected to be combined during a full vote by the Senate.
FEDERAL TRADE COMMISSION (FTC)
PBM Study Under Section 6(b) (June 2022)
Scrutinizes the impact of vertical integration on access and affordability by shedding light on several practices, including: fees and clawbacks charged to unaffiliated pharmacies; methods to steer patients towards pharmacy benefit manager-owned pharmacies; potentially unfair audits of independent pharmacies; complicated and opaque methods to determine pharmacy reimbursement; the prevalence of prior authorizations and other administrative restrictions; the use of specialty drug lists and surrounding specialty drug policies; the impact of rebates and fees from drug manufacturers on formulary design and the costs of prescription drugs to payers and patients.
FTC Votes to Withdraw Prior PBM Advocacy (July 2023)
FTC warns against reliance on prior conclusions from the Commission and PBM advocacy statements. FTC states, “prior advocacy statements and studies no longer reflect current market realities.”
FTC
Releases Merger Guidelines to Address Healthcare Consolidation (Dec. 2023)
Brings increased attention to healthcare consolidation of insurance plans and PBMs in response to pharmacy groups’ urge to promote competition.
8 | The Journal of the Iowa Pharmacy Association COMBATTING PBMS
CENTERS FOR MEDICARE AND MEDICAID SERVICES (CMS)
CMS Administrator Responds to Grassley’s Request for Information (Oct. 2023)
The letter from CMS Administrator, Chiquita Brooks-LaSure states, “Our meeting with the Iowa Pharmacy Association was informative, and I understand the concerns regarding pharmacy cash flow for rural pharmacies and contracting challenges ahead of the 2024 effective date.” The letter also reiterates past actions taken by CMS regarding the DIR Cliff and PBM response.
CMS Public Memo to PBMs/Plan Sponsors in Response to IPA Advocacy Efforts (Nov. 2023)
In a memo titled, “Application of Pharmacy Price Concessions to the Negotiated Price at the Point of Sale Beginning January 1, 2024,” CMS acknowledges pharmacies' concerns; commits to adopt some proposed solutions such as increased monitoring and enforcement of CMS regulations requiring ‘reasonable and relevant' contract terms, access standards, and prompt payment; and strongly encourages Part D plan sponsors to provide payment plans or alternate payment arrangements to pharmacies ahead of Q1 of 2024.
White House Roundtable (March 2024)
The Biden Administration hosted a roundtable with interested stakeholders, including community pharmacists, Mark Cuban, founder of Mark Cuban Cost Plus Drug Company, and Lina Khan, Chairwoman of the FTC. The roundtable addressed PBMs’ role in the prescription drug supply chain.
STATE LEGISLATION
2024 PBM Legislation (HF 2401)
PA championed PBM legislation during the 2022 Iowa Legislative Session increasing data collection authority and transparency. IPA collaborated with legislators to address inadequate reimbursement, patient choice constraints, and other abusive PBM practices left unaddressed in previous bills. The 2024 bill passed the House (93-3) and Senate Commerce Committee unanimously.
Iowa Insurance Division PBM Legislation (HF 2099/ SF 2357)
After collecting complaints since 2022, IID proposed this bill for the 2024 Iowa Legislative Session, preventing PBM retaliation against pharmacies submitting complaints to regulators. The bill passed the House unanimously and awaits a Senate vote.
STATE REGULATION (IOWA INSURANCE DIVISION)
Iowa Insurance Division Adopts Administrative Rules
Iowa Insurance Division (IID) passes administrative rules implementing HF 2384, passed during the 2022 Iowa Legislative Session. These rules prohibit direct or indirect clawbacks and transactions fees through adjustment, reconciliation, or any other means; specify rebate reporting requirements; prevent any rules or laws from being waived or modified by contract; and make other changes.
Iowa Insurance Division Collects Complaints, Investigates PBMs
Under HF 2384, IID gained enforcement authority over PBMs. After submitting PBM complaints to IID for negative reconciliation, a prohibited practice, an Iowa pharmacy received $137,000 in backpay.
JUDICIAL/LEGAL ACTION
Maquoketa’s Osterhaus Pharmacy Files Class Actions Against PBMs
Osterhaus Pharmacy, Inc. filed two class action lawsuits against major PBMs. The first suit is against CVS Health, Caremark, and Aetna, claiming federal antitrust violations and breach of state contract law relating to DIR fees. The second class action is against UnitedHealth Group and its PBM, OptumRx. The lawsuit claims the defendants assessed pharmacy DIR fees in violation of federal antitrust laws and state laws governing contracts.
PUNCH LLC Lawsuit Continues
Pharmacists United to Necessitate Change (PUNCH) is an LLC formed to pursue a class action lawsuit against OptumRX for their onerous business practices toward independent pharmacies.
Arbitration Wins
• Arizona Pharmacy Claims $3.7 Million Arbitration Win Against CVS Caremark
• Court Upholds $23 Million Judgement Against CVS Caremark for Unfair Pharmacy Reimbursement
NCPA Launches TRUST, LLC
According to NCPA, the entity “will investigate and, when appropriate, litigate or arbitrate on behalf of community pharmacies to recover coerced price concessions, otherwise known as pharmacy direct and indirect remuneration fees.”
PAYER INITIATIVES (IOWA)
Iowa Medicaid Pharmacist Provider Type
In 2019, Iowa Medicaid Enterprises added a new provider type for pharmacists, specifically an authorized pharmacist as defined in Iowa Administrative Code (IAC) 657 – Chapter 391. The addition of provider type 82 allows pharmacists to enroll as a Medicaid provider. Enrollment will permit a pharmacist, pursuant to Statewide Protocols2, to order and dispense naloxone and nicotine replacement therapy tobacco cessation products, as well as to order and administer vaccines to Medicaid members. As part of the administrative rule changes allowing pharmacist enrollment with Medicaid, all vaccine billing and reimbursement is required to process through the Healthcare Common Procedure Coding System (HCPCS) or medical claims billing.
Iowa Medicaid Approves Codes for Flu and Strep A POCT Reimbursement
On October 10, 2023, Iowa Medicaid approved 13 codes, including time based E/M codes, that will allow Iowa pharmacies to bill and receive payment for point-of-care testing for influenza and streptococcus A. Claims for test services should be submitted to the medical benefit. The claim(s) for the prescribed medication(s) resulting from the point-ofcare test in pursuant with the respective protocol will be submitted through the pharmacy benefit. Implementation of the point-of-care
JAN.FEB.MAR.APR. | 9 COMBATTING PBMS
testing and treatment only applies to members who are currently enrolled with a MC Plan. Fee-for-Service (FFS) Members will be added to reimbursement processes in the future.
PAYER INITIATIVES (OTHER STATES)
OH – On January 4th, 2019, the Governor of Ohio signed into law SB 265, which gave pharmacists provider status in the state and allowed Ohio pharmacists to perform services and receive payment after successful credentialing. Ohio Pharmacists affiliated with the Ohio Medicaid program are able to enroll to manage medication therapy in collaboration with a prescribing medical professional; administer a wider range of immunizations, including childhood immunizations; and administer certain injectable medications as permitted by state law.
KY – On March 18, 2021, HB48 required Kentucky health plans to reimburse pharmacists for services within a pharmacist's scope of practice and are otherwise covered by the plan if provided by another healthcare provider. In addition, the reimbursement is to be at a rate not less than that provided to other nonphysician practitioners.
TN - Through legislation that took effect July 1 2017, pharmacists in Tennessee are formally recognized as providers through managed health insurance issuers. “Pharmacists as Providers” (HB 405/SB 461) also includes pharmacists in reimbursement and inclusion in medical networks.
CA – On October 1, 2013, SB 493 was signed into law and recognizes pharmacists as health care providers. It also developed a new classification known as the advanced practice pharmacist (APh). The bill authorizes pharmacists to provide basic care services in collaboration with physicians, medical homes and other systems of care where patients receive treatments. SB 493 expands the range of settings in which pharmacists can practice these services, while also allowing them to independently administer certain vaccines, selected nicotine replacement drugs and hormonal contraceptives.
WA - Washington was the first state in the country to require that commercial health insurance plans include pharmacists in their provider networks. As of January 1, 2017, pharmacists in all practice settings can enroll in commercial health plan provider networks and bill for covered patient care services within the pharmacist’s scope of practice. This legislation applies to commercial health plans providing individual, family, small group and large group coverage. With the passage of this legislation, pharmacists in Washington have been billing for patient care, and increasing access to care.
AR – The Arkansas Medicaid Program will allow pharmacists to enroll individually as atypical providers to prescribe and administer specified drugs and test and screen for certain health conditions, per current allowable protocols. Pharmacists are not billing providers, but they may be rendering providers on medical claims. Pharmacists will be allowed as prescribing providers on pharmacy claims for drugs identified in current protocol.
MEDIA
IPA, Members Engage Media on Pharmacy Closures, PBM Abuses
• “Rx is needed for rural pharmacies” – Iowa Capital Dispatch
• “Iowa has lost more than 10% of pharmacies since 2008, Drake professor finds” – Iowa Capital Dispatch
• “Research shows number of pharmacies down in Iowa” – Des Moines Register
• “Iowa is losing pharmacies. Lawmakers, pharmacists and policy experts say benefit managers to blame” – The Gazette
• “Pharmacy deserts in Iowa: At least 87 pharmacies have closed since 2008” – KCCI
• “Iowa pharmacies closing at alarming rates, new study finds” –WHO 13
• “Pharmacy Closures in Iowa Raise Concerns for Access to Medications” – Express Healthcare Management
• Op-Ed by IPA CEO Kate Gainer – Des Moines Register
• “Legislation moving forward to help Iowa pharmacists facing unprecedented financial woes” – KCCI
Business Groups Sound Alarm on PBM Impacts
• National Association of Manufacturers (NAM) Launches Six-Figure Ad Campaign, Letter to Congress for PBM Reform
• American Free Enterprise Chamber of Commerce Prioritizes PBM Accountability
Iowa Leaders Form Coalition to Address PBMs
• PBM Accountability Project of Iowa
• “Iowa leaders form coalition to advocate for lower prescription drug costs” – Business Record
MARKET DISRUPTORS
Blue Shield of California Unveils Mark Cuban Cost Plus Drug Company Partnership
Blue Shield of California will no longer use CVS-Caremark as its PBM and instead will partner with Amazon Pharmacy and Mark Cuban Cost Plus Drug Company. The insurer expects to save up to $500 million in annual drug costs.
AZ Blue Credentials Pharmacists as Providers
Contracted pharmacists may offer covered services (within the scope of the pharmacy license) in a provider group setting, including MTM, chronic disease management, preventive services, POCT, and patient education.
Arkansas BCBS Credentials Pharmacists for Medical Billing; Medicaid Recognizes Pharmacists as Providers
Arkansas BCBS releases medical billing codes that pharmacists can submit for reimbursement related to clinical services as of February 2023.
Express Scripts Introduces New ‘Cost-plus’ Option
Uses lowest benchmark of Predictive Acquisition Cost, National Average Drug Acquisition Cost, or Wholesale Acquisition Cost to estimate the acquisition cost for an individual drug. ESI will charge a flat pharmacy fee and a second administrative fee of 15%.
CVS Health Announces Plan to Adopt ‘Cost-plus’ Model
Under the new “CostVantage” model, CVS retail pharmacies will be reimbursed based on the cost of the drug plus a set markup and a dispensing fee. In the press release, NCPA has raised questions on what this means for pharmacies not affiliated with CVS.
COMBATTING PBMS
10 | The Journal of the Iowa Pharmacy Association
Y o u N e e d a C Q I P r o g r a m
Mistakes happen. Risky processes become normalized and your operations can shift slightly with staffing changes, new products, and new procedures.
The APMS Patient Safety Organization (PSO) provides Pharmacy Quality Commitment+ (PQC+) Compounding, a confidential, highly secure, continuous quality improvement program. Track and analyze how, when, and where the risk in your workflow occurs so you can reduce Rx corrections and operational costs.
Our program includes:
A web-based reporting portal to collect patient safety events
Tools to chart, graph, and analyze data
Expert advice, tips, and safe practices
Resources to help you meet accreditation and quality improvement requirements
Support to build a just culture of safety
QA Continuing Education and training opportunities
Patient Safety Organizations (PSOs) provide a safe space for members to conduct patient safety work. When you partner with our PSO for your Quality Improvement activities, the collection of quality assurance data and patient safety work is in a protected environment.
We are passionate about medication safety in community pharmacy and are here to walk you through the entire process.

Our customer service team has years of experience in pharmacy and is excited to help.
3
C u s t o m e r S e r v i c e
A P M S P S O S e r v i c e s
2
1 P h a r m a c y Q u a l i t y C o m m i t m e n t + Let's chat! (866)365-7472 info@medicationsafety org
w w w . m e d i c a t i o n s a f e t y . o r g
EMBRACING THE SUNSET
 Renae
Renae
“As the sun sets, it leaves behind a canvas of colors, reminding us that endings can be beautiful preludes to new beginnings.” (Unknown Author)
As I bid farewell as the Dean of the Drake University College of Pharmacy & Health Sciences, the setting sun becomes an appropriate metaphor for the conclusion of my tenure. Much like the warm hues that color the horizon during a sunset, I feel a warmhearted appreciation for the unwavering support and camaraderie that have been integral to my journey as Dean over the past several years, not to mention my three decades as a faculty member and proud IPA member.
The commitment exhibited by the association and its members towards advancing the pharmacy profession and upholding the highest standards of care is nothing short of remarkable. The pride I have always and continue to feel for our Iowa pharmacy family is tremendous, especially when I have attended national Deans’ meetings and shared how we operate in Iowa, which has always garnered admiration from my colleagues. The collaborations with the University of Iowa and the Iowa Pharmacy Association are not just admirable but have significantly contributed to the enhancement of our Drake program.

The support of the pharmacists in this state has helped the College obtain several achievements as

we proudly cultivate future pharmacy professionals by upholding a commitment to excellence in pharmacy education, deliver impactful community service, and implement innovative healthcare professional programs into our academic offerings.
Our curriculum, continuously improving to meet future trends and centered around patient care, equips our graduates with the skills needed to navigate the challenges and seize the opportunities in today's dynamic healthcare landscape.
Our engagement with the community has flourished, embodying the core values of service and collaboration. From health screenings to vaccination clinics and partnerships with local healthcare organizations, the College remains steadfast in making a positive impact on the health and well-being of our community.
The triumphs of the College are a testament to the collective spirit and dedication of our faculty, staff, students, along with the broader pharmacy community who serve as mentors, supporters, role models, and preceptors.
My tenure as Dean has been an extraordinary journey, and I am profoundly grateful for the trust and support I have received from IPA members. I extend my heartfelt appreciation to the Iowa Pharmacy Association for being a pillar of support, fostering advocacy, mentorship, and a commitment to excellence that has played a pivotal role in the growth and success of the Drake College of Pharmacy & Health Sciences.
As the sun sets on my time as Dean, it not only signifies an ending but also marks the beginning of a new chapter. I am confident that under new leadership, the College will not only survive but thrive, making substantial contributions to the pharmacy profession. The dawn of a fresh era promises new perspectives, challenges, and triumphs for the College, and I eagerly anticipate witnessing its continued success, impact, and partnership with the Iowa Pharmacy Association.

In the spirit of embracing new beginnings and endless possibilities, I extend my best wishes to you all, confident that the future holds bright prospects for the college, the profession, and our association. ■
Dean (2016-2024), Drake University College of Pharmacy & Health Sciences
FINAL WORDS: THE DEANS 12 | The Journal of the
Chesnut, EdD, MBA, RPh
Iowa Pharmacy Association
2024 Pharmacy Stakeholder Meeting
BORN OF THE EASTERN SHORE BUT ROOTED IN THE MIDLANDS
The thought of ever living in Iowa let alone becoming a dean never once entered my mind during the early years of my professional journey. Yet, here I am in my 17th year as Dean of the UI College of Pharmacy enmeshed in a culture, both personal and professional, that aligns perfectly with the virtues espoused during my youth.
At the age of 12 ½, I had two paper routes and worked weekends as a dishwasher at a local café in the small town of Acushnet, Massachusetts, my birth home. A solid work ethic runs deep in my family. As the eldest of eight children and observing my parents and grandparents, I simply knew it was important for me to contribute to family needs. Enter the Pharmacist in our town.
Without any hint whatsoever, I learned he had been ‘observing’ me...or more accurately took note of my youthful industriousness. In the summer of '65, he asked if I would like to become a clerk in his Pharmacy. Little did I realize at the time that his offer of employment would result in what is now almost 60 years of meaningful engagement with the profession I love, Pharmacy.
Between my parents, grandparents, and the Pharmacist who hired me and became my life-long mentor (he is in his 90s and still lives in the town in which I was reared), I learned a value system that embraced hard work, honesty, integrity, respect, and a strong desire to serve others
I never set out to be a dean. Frankly, when the opportunity first arose, I declined the invitation to apply, believing that responsibility for managing faculty would be like herding cats. Now in my 24th year of ‘deaning’ (prior to Iowa, I served as Dean at the University of Rhode Island), I have come to appreciate the immeasurable contributions faculty make in educating our professional progeny as well as have the opportunity to share in their joy of witnessing the realization of the hopes and dreams of those students who have graced our halls. The years I have served as Dean have nurtured my soul and brought profound joy in myriad ways that are difficult to articulate. That has been especially so here in Iowa.
In 2007, I arrived in the state, knowing well the high regard and avant-garde reputation of Iowa Pharmacy practitioners and educators. Turning ordinary into extraordinary is routine in Iowa. Always at the vanguard.
Of course, what contributes greatly to this success is the level of collaboration that exists within our Profession. IPA, the State Board of Pharmacy, and the two educational institutions have forged a bond like no other state. I am proud to now be included among the ranks of such highly dedicated professionals.
My formative years on the eastern shore instilled in me a set of values that I lay witness to every day here in Iowa. Indeed, hard work, honesty, integrity, respect, and a strong desire to serve others is engrained in the very fabric of what Pharmacists do in meeting the needs of those served. Their actions trumpet professionalism and servant leadership and underscore why a kid from Massachusetts has embraced fully his new home here in the Midlands. ■
 Donald E. Letendre, BSPh, PharmD, FASHP
Donald E. Letendre, BSPh, PharmD, FASHP


FINAL WORDS: THE DEANS
Dean (2007-2024), The University of Iowa College of Pharmacy
JAN.FEB.MAR.APR. | 13
2019 Pharmacy Stakeholder Dinner
IPA BOARD OF TRUSTEES: 2024 CANDIDATES
The 2024-2025 IPA Board Election is underway. Trustees are elected to serve a two-year term, helping to advance the goals and objectives of the association and connect the needs of members to the daily work of IPA. The following positions are up for election this year.
Voting will take place via electronic ballot, closing on Sunday, March 31 at 11:59 PM. Elected candidates will be installed during IPA’s 2024 Annual Meeting, June 20-21 in Coralville.
FOR THE OFFICE OF PRESIDENT-ELECT:


Steven Martens, PharmD, has been a part of the NuCara family since he first got an antibiotic as a young child. TJ Johnsrud, owner of the company since its beginning over 50 years ago in Conrad, Iowa, was his pharmacist growing up and hired him right after graduation from the University of Iowa in 2002. After managing the Nevada community pharmacy location for his first 6 years, he was then asked to serve as Director of Retail Operations and later as Vice President of Professional Affairs for the company, which is still the position he thoroughly enjoys to this day. Steven has been married to his junior high sweetheart, Patti, for almost 26 years, and they have 4 children, Ashton (20), Preston (17), Weston (13) and Morgan (13), along with their Shih Tzu, Teddy.
Wes Pilkington, PharmD, is the pharmacist and owner at Evans Crossing Pharmacy in Evansdale, Iowa. He is currently serving as the IPA Speaker of the House of Delegates. Wes’ previous involvement in IPA includes the Board of Trustees, the Behavioral Health Ad Hoc Committee, the Iowa Medicaid/PBM Committee, and the Chair of the Policy Committee on Professional Affairs. His association involvement also includes participation in a pilot project involving the health information exchange in the pharmacy, the Operation Impact Immunization project, and the HIV Testing Project. Wes was a participant in the 2014 Leadership Pharmacy Conference, and he received the IPA Distinguished Young Pharmacist of the Year Award in 2019. Wes serves as a preceptor for the University of Iowa College of Pharmacy and Drake University College of Pharmacy. He is currently serving as Chair of the Black Hawk County Board of Health and is serving his second term on the Black Hawk Grundy Mental Health Center Board of Directors. Wes and his wife, Sarah, live in Cedar Falls with their three children.
FOR TRUSTEE REGION 3:


Adam Boon, PharmD, MBA, BCPS, is currently employed by Cardinal Health Innovative Delivery Solutions where he serves as a project manager supporting IU Health, the largest health system in the state of Indiana. Adam has multiple responsibilities centering around pharmacy operations, automation, inventory management, and drug cost control. Prior to his current role, Adam was the Pharmacy Operations Manager at Unity Point Lutheran Hospital in Des Moines. Adam received his PharmD and MBA from Drake University. He became a BCPS in 2011. Adam was recently appointed to the Drake University College of Pharmacy and Health Sciences National Advisory Council. Adam lives in Des Moines with his wife and two children. He enjoys naps and reading comic books from his reasonably sized collection.
Helen Eddy, RPh, MBA, received her B.S. in Pharmacy from the University of Iowa College of Pharmacy and her MBA from Drake University. She has served as the Director of Public Health for Polk County, Iowa since 2018. Her responsibilities include planning, organizing and directing Polk County’s long-term community health strategy. Additional duties include the enforcement of health laws and regulations, community leadership responsibilities, disease control and prevention, emergency preparedness planning, health planning and education, and clinical and laboratory services. Prior to joining the Polk County Health Department, Helen was an executive at Hy-Vee and enjoyed a 30-year career leading pharmacy and health and wellness initiatives. During her tenure at Hy-Vee, she implemented pharmacy education and training initiatives, including immunization, asthma, and diabetes education. Helen also served as the Executive Director of the Healthiest State Initiative.
14 | The Journal of the Iowa Pharmacy Association 2024 BOARD ELECTION
FOR TRUSTEE AT LARGE:

Andrew Stessman, PharmD, currently serves as Broadlawns Medical Center’s Senior Manager of Pharmacy Operations and Community Pharmacy. He received his Bachelor of Science and Engineering from the University of Iowa in 2009. In 2011, he became a certified pharmacy technician, joined the Iowa Pharmacy Association, and worked in a retail pharmacy setting in preparation for pursuit of a career in pharmacy. Andrew received his PharmD from Drake University in 2016, serving in multiple pharmacy organizations including DRxUGS, APhA-ASP and Phi Delta Chi.
Andrew has built his pharmacy career through experience in retail, hospital, and specialty settings with a focus on leadership, leading to his current role. Along with his involvement with the Iowa Pharmacy Association, he also serves his profession through involvement in APhA and ASHP. Andrew is passionate about the pharmacy profession and the continued evolution of the profession of pharmacy as it relates to patient care.
FOR TRUSTEE AT LARGE:


Betsie Frey, PharmD, BCPS, has been a hospital pharmacist for over 22 years and has seen much change in the world of pharmacy. Caring for patients via a team approach is her passion. She loves working with all members of the health care team to create the best care for patients. In the hospital, she has been involved in a variety of committees including P&T, Safety, and Environment of Care. She has been the organizer of the Black Hawk/Bremer County Pharmacy Association for 12 years and is currently on the IPA Education Advisory Committee. In the community, she is a member of the Junior League of Waterloo-Cedar Falls, sits on the membership/communications committee for the Rooted Carrot Co-op, and is a member of St Patrick Catholic Church. Betsie has a strong work ethic and feels she would make a positive impact as a member of the Board of Trustees.
Nick Vogel, PharmD, has been an integral part of Ringgold County Hospital for the past 8 years serving as the Director of Pharmacy. He has previously worked in retail, long-term care and long-term acute care settings. He serves on several hospital-based committees and has been active in the Iowa Pharmacy Association and American Society of Health-System Pharmacists. He currently is on IPA’s Legislative Committee. Nick attended Cardinal’s Leadership Conference in 2001. Nick graduated from University of Missouri-Kansas City School of Pharmacy, where he was awarded the Roche Pharmacy Communications Award as well as a leadership award.
FOR PHARMACY TECHNICIAN:


Kelly Andersen, CPhT, was raised in the heartland, developing a strong sense of community and a passion for healthcare. She laid the foundation for her career by earning her Associate of Arts and Associate of Science degree from Des Moines Area Community College. Kelly became a pharmacy technician in 2000 and pursued national certification as a pharmacy technician (CPhT) in 2006. Kelly has provided exceptional care to her community. Her commitment to accuracy, attention to detail, and genuine compassion for patients have earned her the trust and respect of both colleagues and customers. Currently, Kelly is pursuing a BS in Healthcare Administration at Mercy College to further expand her knowledge and skills to contribute meaningfully to the healthcare industry. Outside of work, she enjoys spending time with her family and in the great outdoors. Whether it’s camping or volunteering at local community events, Kelly values giving back to her community and making a positive impact.
Lori Foster, CPhT, of Springville, has been a pharmacy technician since 1988. Recently retired, she has both hospital and community experience. She has contributed several articles to the IPA Journal and was presented IPA's Pharmacy Technician of the Year Award in 2006. She is also a member of the American Society of Health-System Pharmacists (ASHP). Lori has been interested in serving on the Board of Trustees since the creation of the pharmacy technician seat, and she is a firm believer that membership in the association is an important component of professionalism.
ABOUT THE BOARD: The IPA Board of Trustees is the governing body responsible for advancing the goals and objectives of the association. The Board ensures clear communication between IPA and its members and maintains a strong awareness of members’ needs, desires and attitudes. With that understanding, the Board shapes the association’s personality, defines its goals, sets its budget, and charts its future.
JAN.FEB.MAR.APR. | 15
2024 BOARD ELECTION
IPA HEADQUARTERS SALE
A New Era for Iowa Pharmacy
A significant change is underway for the Iowa Pharmacy Association: the sale of IPA headquarters at 8515 Douglas Ave in Urbandale. For nearly all IPA members, this is the only ‘home’ for IPA that you’ve known. The IPA headquarters has hosted countless Board meetings, committee meetings, receptions, fundraisers, and significant milestones. This space was the backdrop to not only countless events but even more emotions—from joy and laughter; to frustration and anger; to excitement and collegiality—all to benefit the pharmacy profession in our state.
WHY DID IPA SELL ITS HEADQUARTERS?
1. Finances. The proceeds from the sale will be invested for the betterment of the profession. A new lease has been signed for office space that is 50% smaller with lower annual costs to IPA than current ownership costs (property taxes, insurance, condo dues, utilities, maintenance).
2. Modernizing. An update to IPA’s office space will benefit both staff that work in the space daily, as well as members that visit IPA’s headquarters. Space that is new-to-us will have updated technology and a contemporary feel that matches the innovative work of IPA.
3. Flexibility. The way IPA staff work continues to evolve. Recruiting and retaining talented staff is important to ensure IPA can carry out the mission and goals of the organization.
The IPA headquarters at 8515 Douglas Ave, Suite 16, was five owned condo units (6,250 sq ft). IPA owned office space in that location since 1977, with additional space added in 1997. You may remember (or be surprised to learn) we hosted a mortgage-burning ceremony in 1984 when the mortgage papers were burned in a mortar and pestle.
The headquarters was owned by PNI, Inc—IPA’s wholly-owned for-profit subsidiary. The only function of PNI, Inc was ownership of the headquarters. The PNI Board is comprised of IPA Executive Committee members.

Over the years, IPA staff size has fluctuated. During the 1980s, there were 20+ staff members! In 2014, when IPA’s education partner vacated to become a fully remote team, only seven IPA staff members were working from IPA’s headquarters.
In 2015, the PNI Board considered a sale of the headquarters, but ultimately voted to retain ownership and lease 2,000 sq ft. This 5-year lease ended in January 2020. During that time, IPA’s staff grew from seven to ten employees, and at the conclusion of the lease, it was best to have the IPA staff regain use of the full 6,250 square feet. Early discussions regarding updates to the space to meet staff needs were had, though nothing happened immediately.
Then—COVID—March of 2020. The staff transitioned to remote work, evolving over the next two years to the current hybrid work environment. The full staff team of nine all work from the office Tuesday-Wednesday, and the remaining days are flexible. All staff have the capability to work remotely at any time.
As the staff returned to a stable hybrid working environment, the plans to renovate resumed. At this time, the PNI Board evaluated the options of: stay and remodel or sell and relocate.
Due diligence during this process included:
1. Staff and IPA Board of Trustees survey
2. CPA review and analysis
3. Commercial real estate analysis
The PNI Board decided to list the headquarters for sale with two ‘for sale’ options. Option 1: sell all five condo units (leading to relocation). Option 2: sell 2 condo units (leading to a remodel of the remaining 3,750 sq ft). The strongest theme from the Board’s due diligence process was the importance of IPA having an office location. While the staff can work remotely, it was important to both the IPA Board and current staff to maintain an office location.

IPA IN ACTION 16 | The Journal of the Iowa Pharmacy Association


Timeline of Headquarters Sale and Relocation:
1977 – Purchased original condo units in Omega Place location
1997 – Purchased additional condo Unit 18, adding the board room
2014 – CEimpact team moves to a fully remote staff, vacating 4 offices in IPA headquarters
2015 – PNI subleases 2,000 sq ft to a tenant for a 5-year lease term
2020 – Tenant vacates; PNI Board evaluates options
2021 – IPA staff survey re: office
2022 – IPA Board of Trustees survey re: office
2023 – March: PNI Board votes to list property for sale
June: Property listed with CBRE
September: First showing with buyer
October: PNI Board votes to execute sale agreement
November/December: Inspections
2024 – January: 5-year lease signed for new headquarters at: 2570 106th Street, Unit D, Urbandale, Iowa
February: Closing and move into new headquarters space
HOW WAS THE NEW SPACE SELECTED?
IPA toured numerous vacant office spaces and focused on these criteria:
1. Between 3,000-4,000 sq ft
2. West suburbs; with proximity to the Interstate
3. Shared amenities, such as a board/conference room or training room to use as needed
4. Net rent cost at/below IPA’s current headquarters operating expenses
HOW WILL THIS IMPACT MEMBERS AND STAFF?
In a way, selling the IPA headquarters feels like selling a property that has been in your family for generations. There is history and nostalgia. The feelings are different for everyone. It’s important to reflect on these memories, and the emotions with them, and share them.
There is also a lot of work in moving an office. IPA staff was prepared for this, and there was minimal interruption to our typical work. Lastly, for the staff, there is excitement. As an organization, IPA is excited to continue serving our members and the profession from the ‘next home’ for IPA!

IPA IN ACTION JAN.FEB.MAR.APR. | 17
Farewell Open House at 8515 Douglas Ave
2023 BILL BURKE STUDENT PHARMACIST LEADERSHIP CONFERENCE
Led by IPA’s Director of Professional Affairs, Emmeline Paintsil, and IPA’s Executive Fellow, Mikayla Harris, twenty-two student pharmacists from Drake University and the University of Iowa participated in a three-day leadership retreat October 13-15. Participants engaged in discussion and activities on leading pharmacy culture, professional identity formation, change-management models, and navigating pharmacy practice issues. Thank you to all panelists and workshop leaders, including Lynn Kassel, Dalton Fabian, Sarah FitzPatrick, Aaron McDonough, Casey Villhauer, and Sarah Ennis, for contributing to this transformative and successful event. Congratulations to the 2023 Bill Burke Student Pharmacist Leadership Class!
UNIVERSITY OF IOWA
Savannah Anderson
Kylie Juenger
Zach Nunemaker
Stephen Presti
Samson Bishop
Samantha Whitcomb
Abigail Crowner
Sara Hou
Emily Weyenberg
Ruth Black
Kisara Thompson
Emma Smith


DRAKE UNIVERSITY
Rachel Turin
Jillian Hood
Ryanne Trpkosh
Claire Beyhmer
Kaitlyn Thomas
Kayla Batdorf
Ayla Danabasoglu
Lexie Bennett
Deena Alsabbah
Stacia Humphrey
2023 IPA RESIDENTS MEETING
BOB O.’S PORCH MEETING
In September, IPA planned and hosted a meeting on Bob Osterhaus’ porch. Many meetings on Bob O.’s porch have led to historical changes in the profession of pharmacy. As IPA continues to advocate for the modernization of Iowa’s Pharmacy Practice Act, it was important to bring together thought leaders in the state. This meeting served as a mechanism to collect input, identify opportunities, and determine a need for resources framing Iowa as a national leader in implementing a standard of care model.

DRAKE SCHOLARSHIP LUNCHEON
In November, Kate Gainer, Executive Vice President & CEO, and Emmeline Paintsil, Director of Professional Affairs, attended the Drake 14th Annual Scholarship Luncheon to support and recognize student pharmacist scholarship recipients from the Drake University College of Pharmacy and Health Sciences. Each year, the IPA Foundation provides scholarships to ensure that the next generation of pharmacists are well-educated, engaged in their profession, and prepared to become its future leaders.
IPA ON DISPLAY




In October, IPA held its annual Residents Meeting, the first in person meeting since the COVID-19 pandemic. The event was held at Drake University College of Pharmacy and Health Sciences, giving residents the opportunity to meet one another, build connections, and participate in a variety of leadership discussions. The event included conversations on discovering your leadership voice and the importance of being engaged in professional organizations. A highlight of the event was the round table discussion topics, including developing an entrepreneurial mindset, staying on top of your clinical skills, self-care and wellbeing, and transitioning from student to new practitioner. Speakers included IPA President John Hamiel, IPA Chairman Cheri Schmit, IPA Trustee At-Large Morgan Herring, CoraLynn Trewet, Omobola Thompson and Jessica Nesheim. Thank you to the residency program directors for your support of your residents’ personal and professional development!
Exhibiting at events provides unique opportunities to connect with other professionals in the state and share what pharmacists across Iowa are doing in their communities. Recently, IPA attended the University of Iowa Open House, the Iowa Rural Healthcare Association Annual Conference, and the Community Colleges Conference & Tradeshow with Your Life Iowa. The University of Iowa Open House provided IPA staff the chance to meet with student pharmacists to discuss ways to get involved in the profession and IPA. At the Iowa Rural Healthcare Association Annual Conference, IPA staff heard updates on critical access hospitals and community health centers and shared healthcare services that pharmacists can provide to increase accessibility for patients.
IPA MEMBER FORUMS
IPA’s virtual Member Forums are tailored to specific areas of pharmacy practice, serving as platforms to foster connections with pharmacy professionals across the state and stay up-to-date on emerging topics in pharmacy. During September’s Industry & Managed Care Forum, attendees learned about the connections between pharmaceutical industry, policy and advocacy. In November, attendees of the Pharmacy Technician Forum reviewed key information on diabetes care with insights pertinent for pharmacy technicians. To wrap up 2023, the Community & Independent Pharmacy Practice Forum featured General Council from NCPA and attorney John Roberti with an update on the fight against PBMs and ongoing class-action lawsuits. IPA looks forward to continuing to provide these opportunities in 2024! Visit www.iarx.org/forums to register for our upcoming forums.
18 | The Journal of the Iowa Pharmacy Association IPA IN ACTION
NEW IPA PODCASTS
IPA is excited to announce the launch of two new podcasts (one brand new and one reimagined) in 2024. Subscribe today so you don’t miss an episode of either show!
The Trailblazers Podcast, hosted by IPA CEO Kate Gainer and current IPA President John Hamiel, dives into the personal stories of pharmacy leaders and innovators who are redefining the healthcare landscape. Each month, we’ll sit down to hear what ignited these leaders’ passion for pharmacy, as well as discuss challenges, triumphs and lessons learned along the way. Whether you’re just beginning your career path or nearing the end, get ready to embark on an inspiring, thought-provoking, and trailblazing adventure!


HOW TO LISTEN: Tune in on the first Friday of the month wherever you get your podcasts. Available on Spotify and Podbean.
IPA’s What, Why & How podcast, hosted by Seth Brown, Director of Public Affairs, unravels the intricacies of pharmacy and healthcare law and regulation, from Congress to the Board of Pharmacy. Each month, we’ll explore WHAT changes occurred, WHY action was taken, and HOW these changes will impact pharmacy practice. In knowing the What, Why & How, we can navigate the legal landscape together!


HOW TO LISTEN: Tune in on the third Friday of the month wherever you get your podcasts. Available on Spotify, Apple Podcasts, iHeartRadio and Podbean.


IPA IN ACTION
JAN.FEB.MAR.APR. | 19 Council Bluffs – April 11, 2024 Quad Cities – May 14, 2024 Dubuque – Aug. 29, 2024 IPA GOES LOCAL: Providing Whole-Person Care for People Living with Dementia A Virtual Reality Simulation Black Hawk/Bremer – Sept. 12, 2024 Spencer – Oct. 10, 2024 Iowa City – Nov. 7, 2024
HEALTHCARE HOT TOPICS
PHARMACY WALKOUTS
Working conditions and the well-being of pharmacy professionals in the community setting have been at the forefront of conversations over the last few months. In October, IPA made a public statement of support for pharmacists participating in walkouts. Numerous state and national associations spoke out in support for pharmacy professionals’ right to work in environments that allow for the safe provision of patient care.
IPA Stands with Pharmacists
Across the country this week, pharmacists have been courageous in shining a light on the unsafe working conditions that jeopardize patient care. IPA proudly stands in support of the pharmacists who are protesting to prioritize patient safety.
The latest Pharmacy Workplace and Well-being Report (PWWR) highlights that inadequate staffing, unreasonable metrics, and harassment by patients continue to impact pharmacists and pharmacy staff across the country. Patient safety is at the core of the pharmacy profession, but that is compromised without adequate support. When patient safety is compromised, pharmacists must speak up and act.
In 1999, the IPA House of Delegates adopted policy: IPA supports the rights of pharmacists to negotiate with their respective employers for working conditions that will foster compliance with state and federal law and the standards of pharmaceutical care as established by the profession.
As pharmacists, we take an Oath and are trusted by the public to protect their safety and well-being. Pharmacists should not be subject to work conditions that comprise the best interests of the health and well-being of their patients or their status as a healthcare professional.
340B PROGRAM
The 340B Drug Pricing Program enables covered entities to stretch scarce federal resources and reach more eligible patients. The program has long provided benefits to contract pharmacies since it was first established in 1992. In recent years, however, drug manufacturers participating in the 340B program have imposed restrictions on covered entities by limiting the number of contract pharmacies a covered entity can contract with. Some states, including Louisiana and Arkansas, have passed legislation prohibiting these manufacturer restrictions. These laws were quickly met with legal challenges by manufacturers. Most recently, the Eighth Circuit Court of Appeals upheld an Arkansas law (Act 1103) that prevents manufacturers from restricting the delivery of 340B drugs to contract pharmacies. The Court determined Act 1103 is not preempted by the federal 340B statute, setting up the opportunity for other states to protect the integrity of the 340B program.
PBM VARIATIONS OF COST PLUS MODEL
As PBM reform legislation gains traction in Congress, PBMs attempt to outmaneuver regulators by adopting their own versions of a common pharmacy-backed payment solution—‘cost-plus.’ This model, which accounts for the cost of the drug product, a professional pharmacist dispensing fee, and a flat PBM administrative fee, has been adopted in different forms by two of the ‘Big Three’ PBMs. Express Scripts announced their “ClearNetwork” model in November, followed by CVS Health’s “CostVantage” model in December. Initial reactions from IPA members and the pharmacy profession include skepticism.
CONDITIONS BETTER WORKING FOR PHARMACY
HEALTHCARE HOT TOPICS 20 | The Journal of the Iowa Pharmacy Association

Think your employer will cover you in the event of an error or patient lawsuit?
Unfortunately, your employer’s coverage likely has gaps that could leave you stuck paying expensive insurance claims and legal fees out of your own pocket. Luckily, Pharmacists Mutual has your back.
Professional liability insurance coverage for whatever tomorrow brings.
Who we cover. Over 110 years of experience protecting all pharmacists: retail, compounding, hospital, student, volunteer, self-employed, and more
What we cover. Immunizations and other drug administration, research, medication consultation, Good Samaritan acts, defendant expense benefits, and various legal defenses
Not covered?
See policy for full description of coverages. For a free proposal: 800.247.5930 phmic.com/pharmacists
Not on my shift.
PUBLIC HEALTH ENGAGEMENT
IPA continues to engage with the Iowa Department of Health and Human Services (HHS) on a number of public health matters in the state, including RSV, tuberculosis (TB), syphilis, and HIV. This past fall, IPA submitted comments to HHS and the Department of Inspection Appeals and Licensing (DIAL) for reconsideration of their interpretation of pharmacists’ ability to order and administer RSV vaccines under the Immunization Statewide Protocol. Following updates from the CDC, the state level interpretation was updated, and IPA requested HHS to publish an official interpretation which was distributed via their digital distribution channels.
IPA is participating in conversations with local public health associations, Iowa HHS, the Iowa Primary Care Association, and Iowa Medical Society to discuss strategies to address tuberculosis (TB) trends across the state. IPA plans to engage community pharmacies in counties where there is an uptick of active and latent TB infection. IPA has also been invited by Robert Kruse, State Medical Director, to participate in an adhoc workgroup to address barriers Iowans face when accessing post-exposure prophylaxis (PEP) for HIV prevention in response to non-occupational exposures to HIV. This work aligns with IPA’s current grant initiatives around HIV and HCV screening in community pharmacies.
Additionally, IPA has focused on attending monthly ASHP state affiliate calls, White House Briefings, and other pertinent regulatory meetings to provide members with up-to-date public health information. This information continues to be shared via IPA’s website, online community, social media, and weekly TOP 5 communications.
COMMUNITY HEALTH WORKER (CHW) ALLIANCE
In October, IPA was invited to join the Community Health Worker (CHW) Alliance, which is organized by Iowa Health and Human Services, the Iowa Chronic Care Consortium, and DMACC. The alliance includes representatives from local departments of public health, universities and colleges, managed care organizations, health systems, and community-based organizations. The purpose of the alliance is to help create a CHW infrastructure in Iowa to help improve health outcomes and achieve health equity through utilization of CHWs. CHWs are recognized as frontline public health workers who are trusted members of their community and/or have a thorough understanding of the community being served. IPA continues to provide the pharmacy perspective in discussions and promotes the impact pharmacy technicians can have in this space in helping reduce disparities.
CALL FOR GRANT RECCOMENDATIONS
Throughout the year, IPA staff seek out funding to support pharmacy professionals in providing high-quality care, developing innovative services, and transforming practice. Areas that IPA has been engaged in include chronic disease state management, education and promotion of health literacy, provision of screenings and lifestyle interventions such as tobacco cessation, medication disposal programs, and handson trainings, to name a few. Are you currently engaged in projects that you would like to see amplified? Are there areas of practice or issues that IPA should be participating in? Provide your recommendations to IPA staff as well as engage on The Bridge to have your ideas heard. If you have recommendations for projects or grants, contact Emmeline Paintsil at epaintsil@iarx.org
PAI 2030
Supporting health-system pharmacy remains a top priority for IPA, notably as we work to expand pharmacy technician roles, address the rural healthcare workforce shortage, and increase the number of ambulatory care pharmacists embedded in clinics. In February of 2023, IPA’s Board of Trustees voted for the creation of a task force to support the American Society of Health-System Pharmacists’ nationwide campaign, Practice Advancement Initiative (PAI) 2030, to advance pharmacy practice in hospitals and health systems. Objectives of the task force include:
• Identify high-priority, feasible, and impactful focus areas (e.g., pharmacy-driven medication reconciliation, residency program expansion) that help drive pharmacy practice change across the state.
• Help health-system leadership identify where the PAI 2030 recommendations may have the largest impact on their setting and create a customized list of priorities for implementing change.
• Support practice and patient care advancement over the next three years through alignment with PAI 2030 recommendations and implementation of practice-focused and organization-focused initiatives.
• Assist in achieving 100% completion of the PAI 2030 Self-Assessment Tool in every hospital and health system across Iowa by 2024.
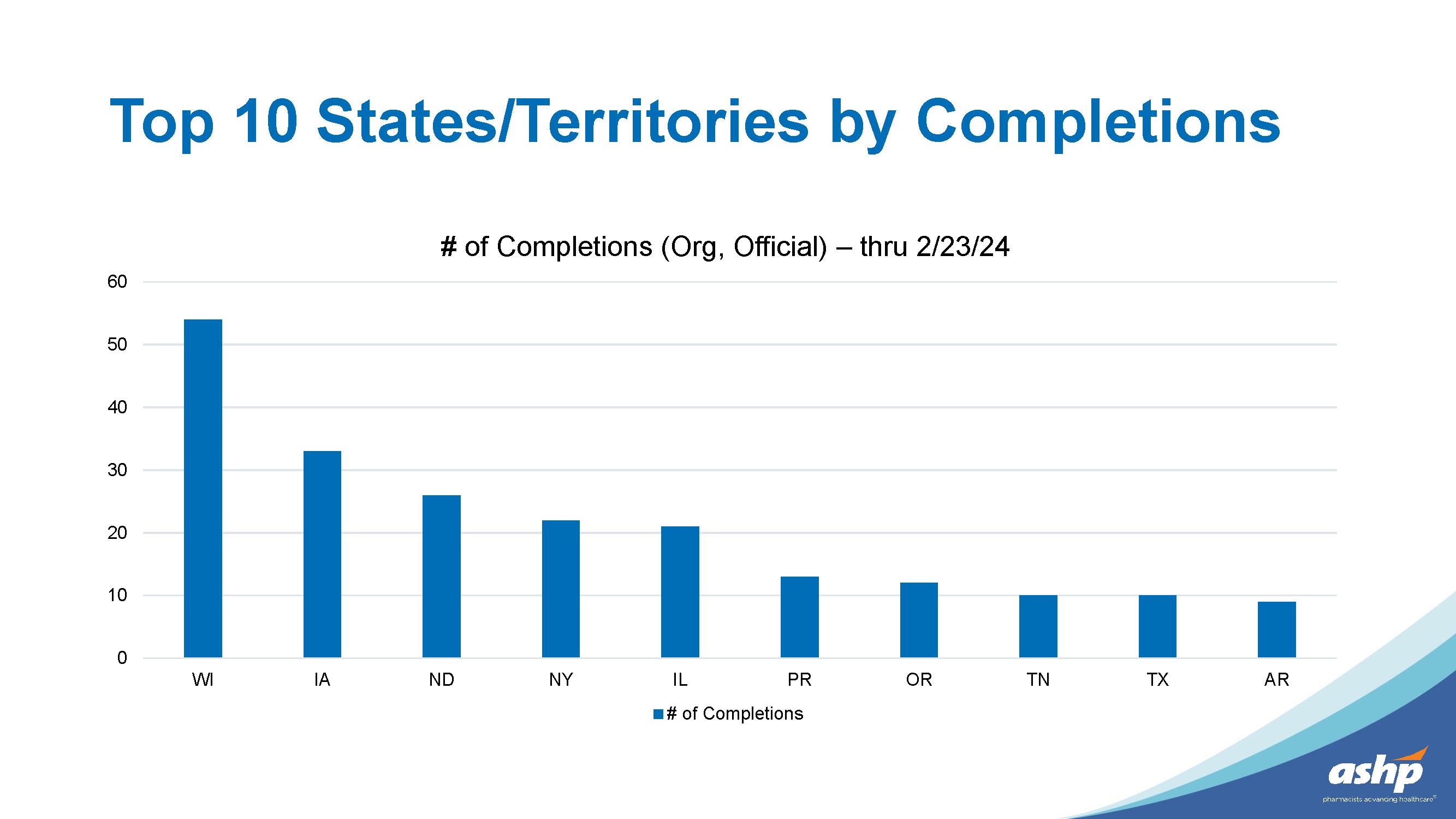
The PAI 2030 Task Force continues to meet regularly, reviews and develops materials, and aids in achieving 100% completion of the PAI 2030 Self-Assessment Tool. To date, Iowa is second in the nation for completion of the organizational assessments. Iowa and New York continue to be recognized by ASHP for efforts and progress in completions of the organization self-assessment tool.
~25% of hospitals have completed the assessment. It’s not too late! Visit https://pai2030tool.ashp.org to complete the assessment for your organization.
Questions? Contact Emmeline Paintsil at epaintsil@iarx.org. See assessment completion rankings by state on Page 23.
IOWA MEDICAID APPROVES CODES FOR FLU AND STREP A POINT-OF-CARE TESTING REIMBURSEMENT
Since 2021, IPA has advocated to Iowa Medicaid for the creation of payable codes under the pharmacist provider type for point-of-care testing (POCT), long-acting injectable administration, and other services that pharmacists provide. In October of 2023, Iowa Medicaid approved 13 codes, including time-based E/M (evaluation and management) codes, that allow Iowa pharmacies to bill and receive payment for point-of-care testing for influenza and streptococcus A. Iowa Medicaid reimburses at 100% of the physician fee schedule rate. Claims for test services should be submitted to the medical benefit. The claim(s) for the prescribed medication(s) resulting from the point-of-care test in pursuant with the respective protocol will be submitted through the pharmacy benefit. Implementation of the point-of-care testing and treatment only applies to members who are currently enrolled with a managed care plan. Fee-for-Service (FFS) members will be added to reimbursement processes in the future. For pharmacists to provide point-of-care-testing and receive payment, you must be enrolled as a provider with Iowa Medicaid and credentialed with each managed care plan. See the full list of approved codes on Page 29.
22 | The Journal of the Iowa Pharmacy Association PRACTICE ADVANCEMENT
DURABLE MEDICAL EQUIPMENT AND VACCINE BILLING TROUBLESHOOTING
The most pressing issue facing IPA members related to Medicaid is medical billing, primarily durable medical equipment (DME) services and access. Every week, IPA receives questions from members, which we escalate to Iowa Medicaid Enterprises (IME) and the Managed Care Organizations (MCOs) during our regular meetings. To pinpoint the barriers and problems to solve, IPA developed a survey to assess successes and challenges in enrolling and credentialing as a pharmacist/ pharmacy provider type and DME enrollment and contracting. A survey was conducted from July 2023 to September 2023 to identify trends in successes and challenges Iowa pharmacies are experiencing in enrolling and contracting as a DME provider, billing, receiving payment, and providing vaccination services. IPA continues to work with IME and the MCOs to find solutions, create resources, and host provider trainings to support pharmacies and pharmacists through this process.
HIV & HCV TESTING PROJECT
January 2024 marked the start of a new grant cycle for the HIV and HCV testing project in community pharmacies. Since 2018, IPA has been collaborating with the Iowa HHS Bureau of HIV, STI and Hepatitis in offering free testing in select community pharmacies across the state. Applying lessons learned from the previous years, the focus of the project in 2024 is to increase testing numbers within the participating pharmacies. In March, IPA held a Project Forum for participating pharmacies, offering opportunities to engage in facilitated discussions on
reducing stigma and to explore innovative strategies to promote point of care testing and increase community engagement. IPA is excited to be partnering with Iowa HHS again in this current grant cycle that will run through 2026.
ACADEMIC DETAILING AND HARM REDUCTION IN COMMUNITY PHARMACIES
In November of 2023, IPA was awarded funding from the National Association of City and County Health Officials (NACCHO) to provide academic detailing around harm reduction in community pharmacies. IPA has developed evolving key messages that will be the most important takeaways from these academic detailing sessions for pharmacy professionals to remember. Through partnerships with the Iowa Health and Human Services Bureau of HIV, STI, and Hepatitis, IPA continues to meet with persons with living experience to gather feedback and refine the key messages. As part of the academic detailing sessions, action kits will be shared with participants that include resources for healthcare professionals and patients, including non-stigmatizing language, state laws regarding harm reduction, testing and treatment services, and training materials. IPA is excited to partner with members to reduce barriers to harm reduction care.
JAN.FEB.MAR.APR. | 23 PRACTICE ADVANCEMENT
Efficacy of angiotensin II receptor blockers to decrease low-density lipoprotein: a systematic literature review
Nirjan Bhattarai, BAL, PharmD Candidate, MS(HIA) Candidate College of Pharmacy and Health Sciences, Drake University, Des Moines, IA, USA
Caesar Yeaman, MS(HIA), EBHC, PharmD Candidate
College of Pharmacy and Health Sciences, Drake University, Des Moines, IA, USA
Braden Weiser, BS, PharmD Candidate
College of Pharmacy and Health Sciences, Drake University, Des Moines, IA, USA
Charles R. Phillips, PharmD, PhD
College of Pharmacy and Health Sciences, Drake University, Des Moines, IA, USA
Address correspondence to Nirjan Bhattarai. Email: nirjanbhattarai@yahoo.com
There are no conflicts of interest to report.
ABSTRACT
Background: Hyperlipidemia is a common condition that compounds the risk for heart disease and stroke, the first and fifth leading causes of death in the United States, respectively. This systematic review aims to identify and synthesize evidence from randomized controlled trials (RCTs) that investigated the effects of angiotensin II receptor blockers (ARBs) on serum low-density lipoprotein (LDL) levels.
Methods: This literature review looked at PubMed, WordCat and Google Scholar to identify and synthesize evidence from RCTs that investigated the effects of ARBs on LDL cholesterol levels. After filtering and excluding, seven studies were left for authors to review.
Results: Results from studies seem to suggest that telmisartan and valsartan may have an effect on lowering LDL concentrations. The effects of ARBs on LDL levels seem to be more pronounced in patients with coronary artery disease (CAD).
Conclusion: The results suggest that telmisartan and valsartan may have an effect on lowering LDL concentrations. Based on current evidence, eprosartan does not have a significant reduction in LDL concentrations; however, more research is needed to make a definite conclusion for the effects of olmesartan and irbesartan. Results support the use of telmisartan and valsartan in conjunction with effective statins for patients with concurrent hypertension and dyslipidemia, especially if comorbidities such as diabetes and CAD are present.
Introduction
Hyperlipidemia is an extraordinarily common condition that includes various disorders originating from genetic and/or acquired means.1
Hyperlipidemia by itself is not serious, however, can be a confounding variable within overarching cardiovascular health, morbidity, and mortality. Hyperlipidemia compounds the risk for heart disease and stroke, the first and fifth leading causes of death in the United States, respectively.2
Low density lipoproteins (LDLs) are widely recognized as a major contributor to atherosclerotic cardiovascular disease, including heart attacks, strokes, and peripheral vascular issues.3 Diabetes and hypertension (HTN) are also significant factors in these conditions, with approximately 15.9% of adults in the United States having diabetes and 48.1% having HTN.4,5
With such a substantial prevalence of metabolic disorders, adherence is a glaring problem country-wide. The Center for Disease Control reports only 54.5% of individuals that could benefit from pharmacotherapy management of hyperlipidemia are actually taking medication.6
In addition to prevalence, cardiovascular disease is responsible for an exorbitant cost of healthcare dollars in the United States, approximately $330 billion annually.6 Angiotensin II receptor blockers (ARBs) could be a helpful additional therapy for these patients. If ARBs are found to significantly lower LDLs, concomitant use in individuals with both HTN and hyperlipidemia could mitigate the aforementioned cost burden.
Other benefits to using ARBs for both HTN and hyperlipidemia would include reducing the burden of polypharmacy–a true risk factor for older patients that is linked to a multitude of adverse outcomes including adverse drug reactions, hospitalizations, falls, and mortality.7-9 The threat of harm from medications is compounded by polypharmacy.10
Metabolic Syndrome and Angiotensin II
Metabolic syndrome (MetS) is a condition characterized by HTN, insulin resistance, and atherogenic dyslipidemia.11 In particular, visceral fat deposits are known to contribute to insulin resistance more than subcutaneous fat, as visceral lipolysis leads to an increased supply of free fatty acids (FFAs) to the liver through the splanchnic circulation.12 This increase in FFAs leads to increased triglyceride synthesis and the production of apolipoprotein B, containing triglyceride-rich very low-density lipoprotein in the liver.12 Additionally, activation of the renin-angiotensin system serves as an important neurohumoral pathway contributing to the development of MetS.12 Angiotensin II (Ang II), formed as a result of angiotensin-converting enzyme activation, is also produced by adipose tissue.12 Obesity and insulin resistance are associated with increased production of Ang II,13 which activates nicotinamide adenine dinucleotide phosphate oxidase and leads to the generation of reactive oxygen species and the oxidation of LDL, which may lead to cardiovascular events or kidney damage.11
24 | The Journal of the Iowa Pharmacy Association LITERATURE REVIEW
Effects of ARBs
ARBs are a class of medications that are used to treat HTN by blocking the action of Ang II at Ang II type 1 (AT1) receptor sites.14 In addition to their use in treating HTN, ARBs have been found to have the following potential benefits in the management of MetS: Improve insulin sensitivity and reduce insulin resistance, reduce the production of inflammatory cytokines, and reduce the accumulation of fat in the liver.14,15 These effects are thought to be mediated via agonism of Ang II type 2 (AT2) receptors by their endogenous ligand since ARBs, particularly newer ones, are selective toward AT1 15 Fatima et al found AT2 expression to be greater in patients with MetS, meaning ARBs may exhibit stronger LDL reduction in these patient populations.
Overall, ARBs have shown promise in the treatment of MetS by improving insulin sensitivity, reducing inflammation, and reducing the accumulation of fat in the liver.15 However, further research is needed to determine the long-term benefits of ARBs in the management of MetS. Particularly, more research is needed to understand how effective ARBs are at lowering LDL levels in various patient populations, especially those with MetS. This review aims to assess any antihyperlipidemic effects of ARBs alone or in combination with HMG-CoA reductase inhibitors. If ARBs are effective at lowering LDLs, it would provide a compelling indication to use ARBs in patients with HTN–a common comorbidity seen in patients with MetS. This review aims to make a recommendation according to its findings.
Methods
The objective of this systematic review is to identify and synthesize evidence from RCTs that investigated the effects of ARBs on LDL cholesterol levels. To be included in this review, studies must have met all the following criteria: (1) be RCTs with either parallel or crossover design, (2) compare an ARB to a placebo or another ARB, or compare HMG-CoA reductase inhibitor monotherapy to its combination with an ARB, and (3) measure LDL cholesterol levels at baseline and after intervention. Studies that did not meet these inclusion criteria were excluded from the review. Furthermore, studies that employed other study designs, studies that only examined ARBs combined with other drugs, studies that were not available in English language, and studies that did not involve human participants were excluded from this systematic review.
PubMed was searched for published literature on 2/13/2023 with the following: ("Angiotensin Receptor Antagonists"[Mesh] OR "Angiotensin II Type 1 Receptor Blockers"[Mesh]) AND "Cholesterol, LDL"[Mesh], applying the filter for randomized controlled trials. Abstracts were then manually screened for inclusion, excluding studies per criteria. Citations and similar articles, suggested by PubMed, to included trials were also considered.
In order to mitigate publication bias, ResearchGate’s WordCat was searched for unpublished literature on 2/20/2023 with the following: ("ARB" or "AT1 receptor blocker" or "AT1 receptor antagonist" or "angiotensin receptor antagonist" or "angiotensin receptor blocker" or "angiotensin II receptor antagonist" or "angiotensin II receptor blocker") and ("LDL" or "low density lipoprotein" or hypercholesterol*). Google Scholar was similarly searched at the same time. Abstracts were then manually screened for inclusion, excluding studies per criteria. Duplications were not recounted.
Two reviewers appraised each full study using a data extraction form and Cochrane’s Risk of Bias 2 (RoB 2) tools for parallel and crossover
RCTs. The data extraction form was modified from Margaret J. Foster, MS, MPH, AHIP, Systematic Reviews Coordinator, Associate Professor, Medical Sciences Library, Texas A&M University. The parallel RoB 2 was last updated on 8/22/2019 while the crossover RoB 2 was last updated on 3/18/2021 as of this review. Differences were broken by a third reviewer.
Substantial clinical and contextual heterogeneity among the included studies precluded a meta-analysis. Instead, a prespecified qualitative analysis was conducted. Each study was categorized as supporting or refuting ARBs lowering LDL, based on the authors’ findings. The reviewers who appraised those studies then intersubjectively factored in the strength of evidence and risk of bias to assign low, middle, or high weight for consideration. Studies that were found to have a high risk of bias per RoB 2 were automatically assigned low weight. Evidence was considered to be stronger if the study was methodologically sound and adequately powered primary analysis, defined as at least 80% power or a p-value at most 0.05, or had at least a three-month follow-up period.
Results
After the literature search from all sources, 17 studies met inclusion criteria. After applying the exclusion criteria, seven studies were ultimately included in this review. Five studies were dropped since they compared an ARB with another blood pressure medication (e.g. dihydropyridine) and failed to compare the ARB to a placebo or another ARB. Four were dropped as they had inconsistent methodologies (i.e. not reporting baseline characteristics and no clear indication of being a RCT). Finally, one duplicate study was dropped.
The final seven studies were internationally published between 2001 to 2016, with 60 to 162 participants and various population parameters. The studies also looked at various ARBs through different durations, yielding mixed results. For all but one study, the authors did not claim to conceal the allocation sequence which was mainly the only concern of bias.
Hanefeld and Abletshauser performed a 12-week, multicentre, double-blind, intention-to-treat, parallel RCT in 2001 with white, hypertensive, German patients, aged 35 to 78 years.16 The study’s experimental arms, each following a three-week dietary intervention, were placebo (n=52) and valsartan 80 mg/day (n=60). No baseline differences were found. Prior to starting treatment, patients went through a stable diet and lifestyle program for 4 weeks followed by a 3 week dietary run-in phase on placebo. Additionally, patients had to have LDL’s less than 160 mg/dL to qualify for the study. Valsartan, compared to placebo, was found to lower LDLs between baseline and termination. Valsartan was found to decrease LDL concentration by 6.3 mg/dl (p = 0.03).
Like Hanefeld and Abletshauser, Derosa et al also performed a 12-month, double-blind, intention-to-treat, parallel RCT. This trial was conducted with Italian patients, an average of 54 years old, with HTN and type 2 diabetes mellitus (T2DM) in 2004.17 Derosa et al evaluated potential changes in LDL when comparing placebo (n=40), telmisartan 40mg/day (n=40), and eprosartan 600 mg/day (n=39). No baseline differences were found. Researchers also stipulated that the study participants must adhere to a strict diet throughout the experiment and perform 30 minutes of daily exercise. A difference in LDL between baseline and termination was only found in the telmisartan group (-11 mg/dl; p < 0.01), which was sustained beyond six months.
JAN.FEB.MAR.APR. | 25
LITERATURE REVIEW
Morawietz et al performed a four-week, multicentre, open-label, blind-endpoint, per-protocol, parallel RCT with German patients, 61 to 68 years old, with stable CAD receiving elective coronary artery bypass grafting in 2006.18 The study’s experimental arms were placebo (n=13), pravastatin 40 mg/day (n=11), irbesartan 150 mg/day (n=14), or pravastatin 40mg/day plus irbesartan 150 mg/day (n=11). Patients were not required to have hypercholesterolemia to qualify for the study. No baseline differences were found. A difference in LDL between baseline and termination was only found in the lone pravastatin group (-0.4 mg/ dl; p < 0.05).
Hong et al performed an eight-month, single-blinded, intention-to-treat, parallel follow up study at Korea University Anam Hospital from March 2005 through September 2006. The patients involved were between 30 to 80 years old and had HTN and significant coronary artery stenosis.19 The study’s experimental arms were telmisartan 40 mg/ day (n = 79) or valsartan 80 mg/day (n = 80). No baseline differences were found, other than the fact that the study contained almost twice as many males as females (107 and 52, respectively). Patients were not required to have hypercholesterolemia to qualify for the study. Concentrations of total cholesterol (TC) and LDLs decreased significantly in both groups. However, changes from baseline were significantly greater in the telmisartan group than the valsartan group. The telmisartan group lowered the LDL concentration by 45.8 mg/dl and valsartan lowered it by 31.5 mg/dl (p < 0.05 for both). The study also found that late lumen loss was reduced significantly in the telmisartan group compared with the valsartan group at an eight-month follow-up. Additionally, the study found that inflammatory markers decreased significantly only in the telmisartan group. It is worth noting that baseline cholesterol may have deceased in all groups because atorvastatin was administered in all patients regardless of baseline cholesterol concentrations.
Kintscher et al performed a four-month, intention-to-treat, double-blind, placebo-controlled, multicenter parallel RCT from 2004 to 2006 in hypertensive German patients with T2DM, stratified by diagnosis of CAD.20 Similarly to Hanefeld and Abletshauser, Kintscher et al had an inclusion/exclusion criteria related to hypercholesterolemia; TC >7.8 mmol/l was a criteria for exclusion in this study. The study’s experimental arms were placebo (n=54) and valsartan 160 mg/day for four weeks followed by valsartan 320 mg/day (n=55) for the remainder of the study duration. There were 53 patients with CAD and 56 without. No significant differences were found between placebo and valsartan groups at baseline, including HMG-CoA reductase use. Despite lower baseline LDL in both CAD groups, a post-intervention difference in LDL between valsartan and placebo was found to lower LDL concentrations by 13.5 mg/dL (p < 0.05). The authors did not note allocation sequence nor concealment, but had an appropriate power analysis with no reported drop-outs.
Rizos et al performed a six-month, randomized, open-label, prospective study in the outpatient Lipid Clinic at the University Hospital of Ioannina from January 2008 to April 2009.21 Enrolled patients had impaired fasting glucose, mixed dyslipidemia (LDL > 160 mg/dL), and primary HTN also, all patients had to undergo a 12-week dietary intervention, prior to being randomly allocated. The study’s three experimental arms were rosuvastatin 10 mg/day plus telmisartan 80 mg/day (n = 52), irbesartan 300 mg/d (n = 48), or olmesartan 20 mg/d (n = 51). No significant differences were found in the baseline characteristics of the three groups. No significant difference was noted between the three groups regarding their effect on LDL concentrations throughout the study period.
Unlike Rizos et al’s open label trial, Park et al performed a two-month, per-protocol, double-blind, double-dummy, multicenter, factorial-design RCT. The study took place in Korea between 2012 and 2013 with Korean patients, ages 20 and older, with moderate essential HTN and dyslipidemia.22 After meeting the inclusion criteria, participants were subjected to 4 weeks of lifestyle change before being randomly allocated to four groups. Importantly, the participants were allocated through a stratified block randomization method using their LDL levels and diastolic blood pressure. The three groups of LDL levels were: (a) 100-130 mg/dL, (b) 130-160 mg/dL and (c) ≥160 mg/dL. The study’s experimental arms were rosuvastatin 20 mg with olmesartan 40 mg (n=61), olmesartan 40 mg (n=36), rosuvastatin 20 mg (n=36), and placebo (n=29). There were no significant baseline differences found between each of the four treatment groups, barring family history of early CHD. There was no statistical significance found regarding the efficacy of olmesartan on LDLs. The authors did note allocation sequence concealment.
Discussion
Each study’s parameters, findings, and assessments by this review are summarized in Table 1. Morawietz et al was the only study assigned low weight, due to its mere one-month duration and concerns about its power. Park et al was assigned middle weight because its duration was only two months, but it had adequate power and strong methodology. All other studies lasted at least three months and had strong methodologies including RCT design. Thus, they were assigned high weight. With the exception of Park et al, however, no study claimed to conceal the allocation sequence, putting these studies at risk of exaggerating their treatment effects.22 Different ARBs and patient populations were examined, as detailed below.
Effective ARBs
Two high-quality studies found valsartan to significantly decrease LDL.16,19 Between them, this effect was observed at doses of 80 to 320 mg/day for three to four months. No study refuted this finding. Hanefeld and Abletshauser, along with Kintscher et al, only found valsartan to reduce LDL by 6.0 to 7.0 mg/dL more than placebo. Larger doses of valsartan appear not to produce clinically significant differences in LDL, suggesting a time-dependent relationship.
Two high-quality studies examined the effect of telmisartan on LDL.17,19 Compared to placebo, telmisartan 40 mg/day significantly lowered LDL after six months. No study refuted these findings. Derosa et al only found this daily dose of telmisartan to reduce LDL by 11 mg/dL after 12 months. Notably, Hong et al found the same daily dose of telmisartan decreased LDL significantly more than valsartan 80 mg/day, a difference of 14.3mg/dL after eight months.
Rizos et al found telmisartan 80mg/day, irbesartan 300 mg/day, and olmesartan 20 mg/day to equivalently lower LDL after six months when combined with rosuvastatin 10 mg/day, but the study was not placebo- or positive-controlled.21 Another study failed to find a difference in LDL reduction between olmesartan 40mg/day and placebo, or rosuvastatin 20 mg/day with and without olmesartan 40 mg/day, but endpoint measurement was merely two months post-baseline.22 It is possible a difference could have been observed had the study’s duration been longer. Similarly, irbesartan 150 mg/day did not decrease LDL more than placebo, and pravastatin 40 mg/day did not benefit from the addition of irbesartan 150 mg/day, after only one month in a study found to have a high risk of bias toward the null.18 However, since olmesartan and
26 | The Journal of the Iowa Pharmacy Association LITERATURE REVIEW
irbesartan appear comparable to telmisartan, which seems to effectively reduce LDL compared to placebo, olmesartan and telmisartan could yield similar results to telmisartan.
No study found eprosartan to lower LDL any more than placebo. One high-quality study found eprosartan 600 mg/day to decrease LDL no more than placebo after one year.17 Thus, evidence is lacking to recommend eprosartan as an adjunctive antihyperlipidemic treatment.
At doses indicated for HTN, valsartan and telmisartan are the only ARBs which seem to decrease LDL, with eprosartan shown ineffective. The literature is weaker regarding olmesartan and irbesartan, but they may be reasonable alternatives, depending on the patient’s insurance.
Current evidence is insufficient to support the use of other ARBs for hypercholesterolemia. Telmisartan appears to decrease LDL more than valsartan, but the effect of both is too modest to treat hyperlipidemia alone. Instead, it is reasonable to preferentially consider valsartan or telmisartan for another indication like HTN in patients with hypercholesterolemia, in addition to a standard of care like HMG-CoA reductase inhibitors. No study evaluated the additive effect of valsartan or telmisartan to HMG-CoA reductase inhibitors, regarding LDL reduction, but it would be reasonable to expect a result similar to that between these ARBs and placebo since they have independent mechanisms of action.
Patient Populations
Most studies looked at patients 30 to 80 years old who had HTN and/ or T2DM, so adequate AT2 receptor expression was likely. To curb dropouts, common exclusion criteria consisted of severe HTN, uncontrolled diabetes, and later stages of heart failure. Additionally, most studies made participants go through a dietary intervention and counseling period before treatments were given, which should have mitigated any regression to the mean that may have occurred otherwise.
Kintscher et al,20 who compared valsartan to placebo in patients with HTN and T2DM, stratified participants into those with and without CAD at randomization. Despite lower baseline LDL in both CAD groups, likely due to prior treatment which would have been washed out during the four weeks before intervention, a post-intervention difference in LDL between valsartan and placebo was only found in those with CAD. Thus, patients with CAD may respond better to the LDL-lowering effects of ARBs than those with only HTN and/or T2DM. This may be due to increased expression of AT2 receptors in these patients. Hanefeld and Abletshauser,16 however, found significantly different LDL reduction between valsartan and placebo in hypertensive patients with or without T2DM or CAD.
All studies of telmisartan included hypertensive patients and most excluded patients without T2DM, including Rizos et al,21 which compared combinations of rosuvastatin with telmisartan, olmesartan, or irbesartan. CAD but not T2DM was among the inclusion criteria of Hong et al,19 though, which compared telmisartan to valsartan. While some evidence suggests a metabolic or cardiovascular comorbidity other than HTN and hyperlipidemia is not essential for newer ARBs like telmisartan to reduce LDL, there are more data from patients with T2DM. In addition to increased expression of AT2,15 these ARBs are believed to increase insulin sensitivity by agonizing peroxisome proliferator-activated receptor-gamma,24 which could explain any improved response among patients with T2DM relative to the general population.
Strengths and Limitations
This review used a comprehensive search strategy that included multiple electronic databases, including gray literature sources, which may reduce publication bias and increase the comprehensiveness of the findings. Additionally, the review included a thorough assessment of study quality using a validated tool, which helped ensure the included studies are of high quality, and reduced the risk of bias in this review. However, the review did not include a meta-analysis, which may have provided a more precise estimate of the effect of ARBs on LDL levels. Furthermore, the review included a relatively small number of studies, all of which were conducted outside the United States, which may limit the generalizability of the findings. This may be due to this review’s exclusion criteria limiting the amount of available evidence.
Conclusion
This systematic review suggests telmisartan and valsartan are modestly effective at lowering LDL concentrations in people with diabetes and HTN. The effects of these agents seem to be more pronounced in people with CAD and the duration required to see a significant difference seems to be at least three months, if not longer. Data from this systematic review add support for the use of telmisartan and valsartan in conjunction with effective statins for patients with concurrent HTN and dyslipidemia, especially further comorbidities such as diabetes and CAD is present. More research is needed to test the effectiveness of ARBs in this disease for a better understanding of effectiveness, especially in the United States.
References
1. Hill M, Bordoni B. Hyperlipidemia. StatPearls Publishing. Published online 2022. Accessed April 10, 2023. https://www.ncbi.nlm.nih.gov/books/NBK559182/
2. “High Cholesterol Facts.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 24 Oct. 2022, https://www.cdc.gov/cholesterol/facts.htm.
3. Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38(32):2459-2472. doi:10.1093/eurheartj/ehx144
4. Health, United States, Annual Perspective, 2020-2021. Published online 2022. doi:https://doi.org/10.15620/cdc:122044
5. Bryan S, Afful J, Carroll M, et al. NHSR 158. National Health and Nutrition Examination Survey 2017–March 2020 Pre-pandemic Data Files. National Health Statistics Reports. 2021;158. doi:https://doi.org/10.15620/cdc:106273
6. Wall HK, Ritchey MD, Gillespie C, Omura JD, Jamal A, George MG. Vital Signs: Prevalence of Key Cardiovascular Disease Risk Factors for Million Hearts 2022 — United States, 2011–2016. MMWR Morbidity and Mortality Weekly Report. 2018;67(35):983991. doi:https://doi.org/10.15585/mmwr.mm6735a4
7. Milton JC, Hill-Smith I, Jackson SH. Prescribing for older people. BMJ. 2008;336(7644):606-609. doi:10.1136/bmj.39503.424653.80
8. Caughey GE, Roughead EE, Pratt N, Shakib S, Vitry AI, Gilbert AL. Increased risk of hip fracture in the elderly associated with prochlorperazine: is a prescribing cascade contributing?. Pharmacoepidemiol Drug Saf. 2010;19(9):977-982. doi:10.1002/pds.2009
9. Caughey GE, Roughead EE, Vitry AI, McDermott RA, Shakib S, Gilbert AL. Comorbidity in the elderly with diabetes: Identification of areas of potential treatment conflicts. Diabetes Res Clin Pract. 2010;87(3):385-393. doi:10.1016/j.diabres.2009.10.019
10. Maher RL, Hanlon J, Hajjar ER. Clinical consequences of polypharmacy in elderly. Expert Opin Drug Saf. 2014;13(1):57-65. doi:10.1517/14740338.2013.827660
11. Rochlani Y, Pothineni NV, Kovelamudi S, Mehta JL. Metabolic syndrome: pathophysiology, management, and modulation by natural compounds. Therapeutic Advances in Cardiovascular Disease. 2017;11(8):215-225. doi:https://doi. org/10.1177/1753944717711379
12. Vaněčková I, Maletínská L, Behuliak M, Nagelová V, Zicha J, Kuneš J. Obesity-related hypertension: possible pathophysiological mechanisms. Journal of Endocrinology. 2014;223(3):R63-R78. doi:https://doi.org/10.1530/joe-14-0368
13. Sinha AD, Agarwal R. Clinical Pharmacology of Antihypertensive Therapy for the Treatment of Hypertension in CKD. Clinical Journal of the American Society of Nephrology. 2018;14(5):757-764. doi:https://doi.org/10.2215/cjn.04330418
14. Barreras A, Gurk-Turner C. Angiotensin Ii Receptor Blockers. Baylor University Medical Center Proceedings. 2003;16(1):123-126. doi:https://doi.org/10.1080/0899828
LITERATURE REVIEW JAN.FEB.MAR.APR. | 27
LITERATURE REVIEW
0.2003.11927893
15. Fatima N, Patel SN, Hussain T. Angiotensin II Type 2 Receptor: A Target for Protection Against Hypertension, Metabolic Dysfunction, and Organ Remodeling. Hypertension. 2021;77(6):1845-1856. doi:10.1161/HYPERTENSIONAHA.120.11941
16. Hanefeld M, Abletshauser C. Effect of the angiotensin II receptor antagonist valsartan on lipid profile and glucose metabolism in patients with hypertension. J Int Med Res. 2001;29(4):270-279. doi:10.1177/147323000102900402
17. DEROSA G, RAGONESI PD, MUGELLINI A, CICCARELLI L, FOGARI R. Effects of Telmisartan Compared with Eprosartan on Blood Pressure Control, Glucose Metabolism and Lipid Profile in Hypertensive, Type 2 Diabetic Patients: a Randomized, Double-Blind, Placebo-Controlled 12-Month Study. Hypertension Research. 2004;27(7):457-464. doi:https://doi.org/10.1291/hypres.27.457
18. Morawietz H, Erbs S, HoltzJ, et al. Endothelial Protection, AT 1 Blockade and Cholesterol-Dependent Oxidative Stress. Circulation. 2006;114(1_supplement). doi:https://doi. org/10.1161/circulationaha.105.001313
19. Hong SJ, Shim WJ, Choi JI, et al. Comparison of effects of telmisartan and valsartan on late lumen loss and inflammatory markers after sirolimus-eluting stent implantation in hypertensive patients. Am J Cardiol. 2007;100(11):1625-1629. doi:10.1016/j. amjcard.2007.06.068
20. Kintscher U, Marx N, Martus P, et al. Effect of high-dose valsartan on inflammatory and lipid parameters in patients with Type 2 diabetes and hypertension. Diabetes Res Clin
Pract. 2010;89(3):209-215. doi:10.1016/j.diabres.2010.04.018
21. Rizos CV, Milionis HJ, Kostapanos MS, et al. Effects of rosuvastatin combined with olmesartan, irbesartan, or telmisartan on indices of glucose metabolism in Greek adults with impaired fasting glucose, hypertension, and mixed hyperlipidemia: a 24-week, randomized, open-label, prospective study. Clin Ther. 2010;32(3):492-505. doi:10.1016/j. clinthera.2010.03.018
22. Park JS, Shin JH, Hong TJ, et al. Efficacy and safety of fixed-dose combination therapy with olmesartan medoxomil and rosuvastatin in Korean patients with mild to moderate hypertension and dyslipidemia: an 8-week, multicenter, randomized, double-blind, factorial-design study (OLSTA-D RCT: OLmesartan rosuvaSTAtin from Daewoong). Drug Design, Development and Therapy. 2016;Volume 10:2599-2609. doi:https://doi. org/10.2147/dddt.s112873
23. Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of bias. Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA. 1995;273(5):408-412. doi:10.1001/jama.273.5.408
24. Suksomboon N, Poolsup N, Prasit T. Systematic review of the effect of telmisartan on insulin sensitivity in hypertensive patients with insulin resistance or diabetes. J Clin Pharm Ther. 2012;37(3):319-327. doi:10.1111/j.1365-2710.2011.01295.
Telmisartan significantly decreased LDL after six months. Placebo and eprosartan did not significantly decrease LDL. Not reported. Some Concerns High
Irbesartan did not significantly lower LDL, alone or with pravastatin, compared to control.
The changes from baseline LDL were significantly greater in the telmisartan group compared to the valsartan group.
Valsartan significantly reduced LDLs compared to placebo only in those with CAD.
ARB did not perform any better than another.
The combination of rosuvastatin and olmesartan did not significantly lower LDLs when compared to rosuvastatin alone. Olmesartan alone did not significantly lower LDLs compared to placebo.
28 | The Journal of the Iowa Pharmacy Association
Study Sample Size (n) Groups Duration (months) Findings Power RoB 2 Weight Hanefeld and Abletshauser 2001 123 Placebo Valsartan 80 mg/day 3 Valsartan significantly decreased LDL compared to placebo. Not
Some Concerns High Derosa et al. 2004 119 Placebo Telmisartan 40 mg/day Eprosartan 600 mg/day 12
reported.
Morawietz et al. 2006 60 Control Pravastatin 40 mg/day Irbesartan 150 mg/day Combination 1
Not
Low Hong et al. 2007 159 Telmisartan 40 mg Valsartan 80 mg 8
reported. High
80% Some Concerns High Kintscher et al. 2010 109 Placebo Valsartan 160 mg/d → 320 mg/d 4
80% Some Concerns High Rizos et al. 2011 151 Rosuvastatin 10 mg/d plus telmisartan 80 mg/d Irbesartan 300 mg/d Olmesartan 20 mg/d 6 One
90% Some Concerns High Park et al. 2016 162 Placebo Olmesartan Medoxomil 40 mg Rosuvastatin 20 mg Combination 2
80% Low Middle
Table 1: A summary of the patients, groups, durations, and findings of each study, along with the calculated risk of bias and recommended weight for consideration.
Appendix
Iowa Medicaid POCT Codes – Continued from Page 22
JAN.FEB.MAR.APR. | 29 IOWA MEDICAID
2024 IOWA LEGISLATIVE SESSION PRIORITIES
The second session of the 2024 Iowa General Assembly commenced on Monday, January 8 with the return of legislators to the Iowa State Capitol. Pharmacy issues continue to take center stage as IPA champions an ambitious slate of legislative priorities.
IPA’s Pharmacy Practice Act modernization bill (HF 555) is still in consideration after passing the House of Representatives and the Senate Health and Human Services Committee last session and the full Senate this session. The House must now consider an amendment to the bill for a final time. The bill aligns pharmacy practice with the current level of pharmacy education. IPA also seeks a $2.4 million appropriation to fund the Medicaid pharmacy reimbursement. Under the last state-sponsored survey conducted in 2021, the cost to dispense a prescription drug increased $0.59/ prescription. Rounding out our top three priorities, IPA will again advocate for PBM reform. IPA collaborated with legislators to introduce HF 2401 which prohibits spread pricing, ensures pharmacists are not discriminated against in relation to payment for services, and ensures pharmacies receive payment for the full cost of the drug product. This bill passed the House 93-3 and awaits a full Senate vote.
Within the first week of session, the Iowa Insurance Commissioner presented data to legislators in the House Commerce Committee on PBM complaints submitted by Iowa pharmacies and patients. In total, over 72,000 PBM complaints were received by the Iowa Insurance Division (IID) since implementation of HF 2384, IPA’s 2022 PBM bill. The Commissioner described this number of complaints as “unacceptable” and encouraged work this session. In this effort, IID introduced PBM legislation (HF 2099/SF 2357) ensuring they have adequate authority to regulate PBM practices.
These priorities, along with a slate of other legislative proposals impacting the profession, will be considered throughout the session. IPA expects to monitor the Governor’s comprehensive Boards and Commissions reform bill for its impact on the Board of Pharmacy. Legislation impacting pharmacist’s professional autonomy is also expected following a July 2023 Special Session on reproductive rights.

MODERNIZE THE IOWA PHARMACY PRACTICE ACT PRIORITY #1
IPA supports modernizing the Iowa Pharmacy Practice Act to cut red tape, align with other healthcare practitioners in the state, increase professional autonomy, and match the evolving practice of pharmacists to improve patient access and outcomes.
PROTECT IOWA MEDICAID REIMBURSEMENT PRIORITY #2
IPA supports laws, regulations and policies that ensure sustainable, accurate, and transparent prescription drug reimbursement under Medicaid. This includes maintaining patient access by paying pharmacies at average acquisition cost, plus a cost of dispensing fee.
IPA supports Medicaid appropriations which fund prescription drug reimbursement, in alignment with the most recent state managed survey ($10.97 per prescription, $2.4 million total).
PREVENT PHARMACY BENEFIT MANAGER (PBM) ABUSES PRIORITY #3
IPA supports continued collaboration with the Iowa Insurance Division and Iowa Legislature to protect patients against PBM abuses and ensure pharmacy viability.
30 | The Journal of the Iowa Pharmacy Association PUBLIC AFFAIRS
Help Advance IPA’s Legislative Agenda...Become a Champion Advocate!
Are you interested in becoming an important partner in helping IPA advance its legislative and regulatory agenda throughout the year? IPA is looking for Champion Advocates across the state of Iowa to build relationships with their elected officials. Help us designate a Champion Advocate in every House and Senate district!
WHAT DO CHAMPION ADVOCATES DO?
• Build relationships outside of the legislative session by hosting pharmacy visits with legislators and delivering PAC contributions when needed.
• Contact legislators during session to explain how pending legislation would affect their pharmacy practice.
• Relay personal experiences to help legislators understand the important roles that today’s pharmacists and pharmacy technicians play in enhancing the healthcare of Iowans.
• Stay informed with bill tracking/IPA’s legislative priorities and participate in biweekly update calls.

By Volunteering as a Champion Advocate: You would be kept up-to-date on the latest information relating to IPA’s advocacy agenda and would be ready to answer the call when IPA needs to make a grassroots push. Contact Seth Brown, Director of Public Affairs, at sbrown@iarx.org or 515-270-0713. He will help you identify your State Senator and Representative and get started with setting up a pharmacy visit.



For more information, visit www.iarx.org/ChampAdvocate
INTERESTED?
STATE GOVERNMENT REALIGNMENT
During the 2023 Iowa Legislative Session, Governor Kim Reynolds proposed a 1,300-page legislative package realigning Iowa’s state government. Following its passage, SF 514 decreased the number of cabinet-level agencies from 37 to 16 and changed oversight of several boards. As part of this move, the Iowa Board of Pharmacy moved from the department of Health and Human Services (DHHS) to the Department of Inspections, Appeals, and Licensing (DIAL).
The bill also created the Iowa Boards and Commissions Review Committee, which is tasked with reviewing Iowa’s current Boards and Commission and providing recommendations on their efficiency. In September, the Committee released its final recommendations to reform Iowa’s boards and commissions, including the Board of Pharmacy.
The Committee’s recommendations relating to the Board of Pharmacy include:
• Establish uniform continuing education requirements set by the Iowa legislature;
• Remove specific professional background requirements for fulltime staff or executive directors of licensing boards under DIAL;
• Remove the “big four” health board’s (Pharmacy, Medicine, Nursing, and Dentistry) independent lobbying authority, and allow DIAL to assume this authority;
• Reduce board membership (Board of Pharmacy reduced to 5 members, Board of Medicine to 7); and
• Establish the Prescription Monitoring Program Advisory Council as a standing subcommittee of the Board of Pharmacy and decrease to no more than five members.
These recommendations are not final and require legislation to become binding.
IPA submitted public comments to the Committee, urging any recommendations to retain historical strengths of the Board. Requests include:
• Ensure the Board’s Executive Director and Compliance Officers are licensed pharmacists to maintain subject matter expertise;
• Avoid consolidation and retain a pharmacy-focused regulatory board to ensure the public health and safety; and
• Provide adequate tools and independence for continued exemplary oversight.
Following release of the recommendations, IPA hosted a webinar with Larry Johnson, Director of the Department of Inspections, Appeals, and Licensing (DIAL), which now houses the Board of Pharmacy. Director Johnson spoke to the current structure of the Board and expected changes and fielded questions and concerns from members.

Scan the QR code to visit IPA’s State Government Realignment FAQ resource!
IPPAC DELIVERIES & PHARMACY TOURS
In 2023, IPA conducted the largest Iowa Pharmacy Political Action Committee (IPPAC) fundraising campaign in recent history. Over $24,000 was raised to support pharmacy proponents in the Iowa State Capitol. These funds were distributed by the IPA Advocacy Team, and assisted by Iowa pharmacies, throughout the interim leading up to the 2024 Iowa Legislative Session. In total, twenty-three (23) candidates from both political parties received IPPAC contributions, many hand-delivered by Iowa pharmacists during tours of their pharmacies.

State Representative John Wills and State Senator Dave Rowley visited Hughes Healthmart Pharmacy in Emmetsburg on October 19. Credit: Emmetsburg Reporter Democrat


Make a donation to the IPPAC to augment IPA’s efforts at the capitol!
32 | The Journal of the Iowa Pharmacy Association PUBLIC AFFAIRS
U.S. Senator Chuck Grassley and State Senator Mark Costello visited Penn Drug in Sidney on June 28.
L to R: Rep. John Wills, Joel Hoyman, Ed Maier, and Sen. Dave Rowley
L to R: Seth Brown, Stephen Presti, Mikayla Tice-Harris, Sen. Chuck Grassley, Kaitlyn Thomas, and Sen. Mark Costello
CMS FINAL RULE: IPA ACTION TO LESSEN DIR HANGOVER
Direct and indirect remuneration (DIR) fees have long drawn the ire of pharmacies attempting to accurately forecast expenses to run a competitive business. In May of 2022, the Centers for Medicare and Medicaid Services (CMS) proposed rules (CMS-4192-F) to move these ‘pharmacy price concessions’ to the point of sale.
While calls were answered, members soon communicated to IPA that PBM DIR fees for the prior year would be due when pharmacies expect to receive lower reimbursements at the point-of-sale under the new provision. IPA heard members’ concerns and sounded the alarm on the “DIR cliff” to lawmakers, regulators, and other stakeholders.
IPA found an ally in Senator Chuck Grassley [R-IA], as he placed public pressure on CMS to hear from Iowa pharmacies and enact financial safeguards. As a result, IPA members and staff met with CMS to present data on Iowa pharmacy access and urged CMS to take action.

The data included the Pharmacy Access in Iowa Study by Michael Andreski, RPh, PhD, faculty member at Drake University College of Pharmacy and Health Sciences, in collaboration with the Health Professions Tracking Center at the University of Iowa Carver College of Medicine. IPA also conducted the Iowa Pharmacy Association State of Community Pharmacy – 2024 Expectations Survey to illustrate the expectations of community pharmacies in Iowa in light of the upcoming 2024 DIR rule changes. Of note, the data indicated a 38% decrease in independent pharmacies in Iowa and a 19% decrease in rural pharmacies of all types since 2008. Although alarming enough, IPA communicated expectations for the upcoming year were particularly bad, as over 40% of community pharmacies that responded indicated they expect to close or sell within the year.
CMS responded to this data, and calls from other state pharmacy associations at IPA’s request, with a series of public letters to PBMs and Part D plan sponsors promising closer monitoring of PBM activity; stricter enforcement of current CMS regulations relating to ‘reasonable and relevant contract terms,’ prompt payment, and pharmacy access standards; as well as encouraging PBMs to adopt payment plans for pharmacies throughout the cliff. The swift action also led to increased oversight of CMS throughout the DIR cliff, as Senator Grassley filed an amendment in a broader PBM bill by the Senate Finance Committee.
As January 1 has passed and the CMS final rule has taken effect, Iowa pharmacies continue to feel the cash constraints. IPA continues to advocate to Congress and CMS. The ultimate impact will not be known for some time, but it is vital for CMS to understand the impact on pharmacy access from members. Pharmacies can submit concerns and complaints to CMS at partd_monitoring@cms.hhs.gov. These examples enable swift action.
See a full timeline of IPA’s DIR cliff efforts below:
APRIL 24, 2023: Medical Associates Pharmacy in Boone hosts Senator Grassley and conveys concerns of expected cash flow issues as a result of PBMs responding to CMS rulemaking effective January 1, 2024.
JULY 25, 2023: Following further outreach from pharmacies, Senator Grassley seeks information on the agency’s oversight strategy ahead of its rulemaking going into effect in a letter to CMS.
JULY 26, 2023: At a Senate Finance Committee hearing, Grassley amplifies concerns about the challenges the regulatory changes will pose for rural Iowa pharmacies.
SEPTEMBER 28, 2023: Following a September 22 phone conversation with CMS Administrator Brooks-LaSure, Grassley urges the agency to coordinate with PBMs on payment plans for rural pharmacies that are facing financial burdens connected to upcoming regulatory changes.
OCTOBER 12, 2023: At Grassley's request, CMS meets with the Iowa Pharmacy Association.
OCTOBER 19, 2023: IPA calls on Iowa pharmacists to educate on expected pharmacy closures. IPA also encourages other state pharmacy associations to engage their Senators on the Finance Committee to urge CMS to take preventative action.
OCTOBER 26, 2023: Senator Grassley and Iowa pharmacists call on CMS to uphold its commitments to rural pharmacies amid upcoming regulatory changes.
NOVEMBER 6, 2023: CMS publishes a public memo titled, “Application of Pharmacy Price Concessions to the Negotiated Price at the Point of Sale Beginning January 1, 2024.”
NOVEMBER 7, 2023: Grassley proposes an amendment and speaks to IPA’s efforts with CMS during the Senate Finance Committee markup of the Better Mental Health Care, Lower-Cost Drugs, and Extenders Act
DECEMBER 14, 2023: CMS issues another public letter to PBMs and plan sponsors about an increasing number of concerns about certain practices by PBMs that threaten the sustainability of pharmacies. CMS commits to closer monitoring, stricter enforcement of current regulations, and encourages PBMs to adopt payment plans.
DECEMBER 14, 2023: CMS responds to Senator Grassley’s letters calling for insight and action ahead of January 1 rule implementation. The letter refences CMS’ meeting with IPA and acknowledges concerns shared.
JANUARY 1, 2024: CMS’ final DIR rule goes into effect.
PUBLIC AFFAIRS
JAN.FEB.MAR.APR. | 33
NEW! Law Resource Available as Membership Add-on
THE LIRC INCLUDES:
• Monthly email updates
Featuring recent updates, opportunities for public comment, newly adopted rules, sign-on letters, and more!
• Detailed regulatory tracker
• In-depth FAQ page
• What, Why & How Podcast
Available on Spotify and Apple Podcasts
The Iowa Pharmacy Law & Information Resource Center (LIRC) (previously the Law Manual), now completely digital, provides access to an online database containing Iowa Code, Board of Pharmacy rules, Controlled Substance laws, Medicaid and other Healthcare Provider rules, as well as updates and analysis of recent changes, frequently asked questions, and additional resources.


Seeking an educational and accessible law resource? ENGAGED and CONNECTED Pharmacist members can now add a LIRC subscription to their current IPA membership at a discounted rate!
WWW.IARX.ORG/LAWMANUAL EXPLORE LIRC >> PURCHASE LIRC >>
NEWLY CERTIFIED IOWA PHARMACY TECHNICIANS
SEPTEMBER 1-DECEMBER 31, 2023
Katherine Aitken
Haneen Alhatimi
Brett Anderson
Angela Ballard
Savannah Boyle
Morgan Brennecke
Taylor Canavan
Hamna Choudhry
Allysha Clark
Catherine Collison
Benjamin Cooper
Kelsey Creten
Trista Deshaw
Travis Dibbet
Nicole Dvorak
Stephanie Eggers
Fadwa Elkarar
Leah Elliott
Skylar Etten
Abigail Fichter
Amy Finley
Leah Fitch
Gema Franco
Katie Frey
Katie Fritcher
Justin Frye
Sara Fuller
Katherine Gardner
Rhonda Hall
Hugo Hanselman
Taylor Hatfield
Kelly Hayward
Melissa Hazen
Leighla Hebeler
Samantha Hendrix
Emily Herum
Jennifer Ho
Abby Hulten
Sawyer Hunt
Sara Irish
Calea Jones
Sarah Karaman
Bryan Kendall
Amie Kielty
Congratulations to the following technicians!
Jillian Kniep
Kylie Krauss
Kasey Kropp
Michelle Lawton
Carrie Lear
Alyssa Leavens
Hannah Lohman
Leslie Mariette
Crystal Mcfadden
Delaney Mcmullen
Alaina Mendralla
Julia Meska
Mikayla Meyers
Kennady Meyers
Rachael Miller
Kierinn Mobley
Abigail Monk
Tyler Moores
Lejla Mustafic
Irionne Neealy
Daniel Niedert
Jessica Noehl
Rileigh Norton
Towanou Noukonme
Travis Novotny
Brodi Oakley
Jacob Paulsen
Ella Peterson
Abigail Piearson
Heather Plathe
Seth Powers
Ethan Reinier
Geralyn Reising
Ashley Ricketts
Katelyn Rodriguez
Amber Roerden
Sharon Safley
Sydney Sanchez
Ajla Sarajlija
Allison Schliske
Veronica Schlue
Riddhi Shaha Sunil
Kalyani Shimpi Rajendra
Tracey Snodgrass
Debra Stein
Sheldon Steinford
Darian Stevens
Jazzmine Stodden
Jennifer Stroeder
Zakaria Tagba
Jordyn Thole
Katie Thorpe
Bryanne Valletta
Sasha Vancleve
Hanna Wallace
Jordan Webster
Ryan Wenzel
Richelle Werner
Wendy Whitlock
Summer Wiggley
Lisa Woods
Sydney Zeutenhorst
Huijie Zhu


JAN.FEB.MAR.APR. | 35
TECHNICIAN CORNER Patient safety. Professional practice. Community impact. BILLING AND REIMBURSEMENT CONTROLLED SUBSTANCES DIVERSION PREVENTION HAZARDOUS DRUG MANAGEMENT IMMUNIZATION ADMINISTRATION MEDICATION HISTORY MEDICATION THERAPY MANAGEMENT POINT-OF-CARE TESTING REGULATORY COMPLIANCE SUPPLY CHAIN AND INVENTORY MANAGEMENT TECHNICIAN PRODUCT VERIFICATION (TPV) Assessment-Based Certificates Compounded Sterile Preparation Technician® (CSPT®) Certification Certified Pharmacy Technician (CPhT) Advanced Certified Pharmacy Technician (CPhT-Adv) Certification Certifications Build your team with confidence. View PTCB’s full suite at ptcb.org/credentials
THANK YOU IPA SUPPORTERS
IPA sincerely thanks the following individuals who supported our IPPAC and IPA Foundation initiatives in 2023.
IPPAC CONTRIBUTORS
Michael Andreski
Ashleigh Arndorfer
Seth Brown
Sharon Cashman
Gary Christensen
Chris Clayton
Connie Connolly
Kyra Corbett
Jay Currie
Kristina Dotzler
William Drilling
Michele Evink
Dalton Fabian
Steve Firman
Ryan Frerichs
Emily Gajda
Levi Gates
Naomi Graves
Joseph Greenwood
Robert Greenwood
Betty Grinde
John Hamiel
Nathan Harold
Morgan Herring
Elise Houselog
Thomas Johnsrud
Wendy Kinne
Laura Krogh
Micaela Maeyaert
Edward Maier
Erik Maki
Deanna McDanel
Randy McDonough
James Mennen
Kristin Meyer
Robert Nichols
Marilyn Osterhaus
Matt Osterhaus
Robert Osterhaus
Heather Ourth
Wesley Pilkington
Jamie Pitlick
Lisa Ploehn
Diane Reist
Anne Roth
Cheri Schmit
Chelsea Schott
Susan Shields
Nora Stelter
Robert Stessman
Mikayla Tice-Harris
CoraLynn Trewet
Stevie Veach
Nickolas Vogel
Andrew Wagner
IPA FOUNDATION CONTRIBUTORS
PLATINUM LEVEL ($1000+)
Bruce Alexander
Carl Chalstrom
Renae & Eddie Chesnut
Gene Chrischilles
Connie & Chris Connolly
Jay & Ann Currie
Bill Drilling
Michele & Michael Evink
Marla Franck
Mike Ficke (posthumously)
Kate & Bob Gainer
Bob & Cheri Greenwood
Tom Halterman
John Hamiel
Morgan Herring
GOLD LEVEL ($500-$999)
Bill Baer
Cheryl Clarke
Ryan Frerichs
Ben Jagow
June Johnson
Jim Hoehns
Greg Hoyman
TJ Johnsrud
Rick Knudson
Patty & Tod Kumbera
Ed Maier
Randy McDonough
Wendy Mobley-Bukstein
Stephen Mullenix
Wes Pilkington
Lisa Ploehn
Al Shepley
Tom (posth.) & Cathy Temple
JP Webb
Susan Winckler
Allan Zaenger
Julie Kuhle
John L’Estrange
Lindsey Ludwig
Gene & Susan Lutz
Gary & Mary Milavetz
Bob & Ann Osterhaus
Matt & Marilyn Osterhaus
Rachel Otting
Chuck Phillips
Matt & Jamie Pitlick
Anthony Pudlo
Diane & Jeff Reist
Emily Rogers
SILVER LEVEL ($250-$499)
Sharon Cashman
Helen Eddy
John Forbes
Kyle Hilsabeck
Dennis Jorgensen
Steve Firman
Donald E. Letendre
Craig Logemann
Beverly Martin
BRONZE LEVEL ($100-$249)
Vicki Agan
Brian Benson
Michael Bilden
Tammy Bullock
Gary Christensen
Chris & Jen Clayton
Michele Cooper
Melissa Corrigan
John Daniel III
Sarah Derr
Carmen Dunphy
Sarah Grady
Erika Ernst
Peter Fay
Steve Firman
Scott Flores
Susan Frey
Phil Greazel
Tom Greene
Nathan Harold
Dick Hartig
Kirk & Julia Hayes
Grant & Elise Houselog
Sandra Johnson
Jessica Johnson
Susan & Tim Kramer
Robert Schroeder
Susan Shields
Bob Stessman
CoraLynn Trewet
Dave Weetman
Jennifer Williams
Pamela Wiltfang
Deanna McDanel
Jessica Nesheim
Doug Schara
Cheri Schmit
Sarah Sorensen
Nora Stelter
Joan Stover
John & Susan Sutter
Tom Vilsack
Nic Lehman
Nick Lund
Jeri Mace
Erik Maki
Steven Martens
Dana McDougall
Ben & Jessica Meisner
Karen Merrill
Kristin Meyer
Phyllis Olson
Leman Olson
Kelly Percival
Nathan Peterson
Mark Pilkington
Justin Rash
Tim Rice
Mark Richards
Jenna Rose
Michael & Patricia Seifert
Louis Sesti
Matthew Shivers
Scott Sitzman
Jann Skelton
Andy Steichen
Hailey Steuber
John & Sarah Swegle
Mark Swerdlik
IPA SUPPORTERS
36 | The Journal of the Iowa Pharmacy Association
Omobola Thompson
Mikayla Tice-Harris
Louise Trudeau
Jenny Tuttle
Stevie Veach
Sara & Terry Wiedenfeld
John Willmore
Dennis & Patricia Worthen
BUSINESS PARTNER CONTRIBUTORS
Bral Neidert
Carroll Apothecary
Daniel Pharmacy
Drake University College of Pharmacy & Health Sciences
Eide Walton
Greenwood Pharmacy & Compounding Center
Infocus Pharmacy Services
Jacobsen & Company LLP
Main at Locust Pharmacy
Maquoketa Pharmacy, Inc. dba Osterhaus Pharmacy
McKesson
MercyOne Des Moines MHCS
North Iowa Pharmacy Inc
NuCara Pharmacies
Onnen Company
Quad City Area Pharmacy Association
SafeNetRx
Towncrest Pharmacy
University of Iowa College of Pharmacy
Chris Connolly, Wells Fargo Advisors
SILENT AUCTION: CALL FOR DONATIONS
We need your help in hosting a successful silent auction to support student pharmacists, leadership development, and practice advancement!
The 2024 IPA Foundation Silent Auction will take place Thursday, June 20 in Coralville as part of IPA’s 2024 Annual Meeting. Bidding for auction items will open online and via mobile app on Tuesday, June 4 with the first session of the IPA House of Delegates to be held virtually. You can bid against your IPA colleagues no matter where you are!
If you or your pharmacy would like to donate to the silent auction, please contact Laura Miller at lmiller@iarx.org and provide a short description and approximate value of the item(s) you plan to donate. While items will be accepted through the week of Annual Meeting, please notify IPA prior to June 1st in order to have your item(s) listed in the silent auction catalog and event app.
IPA is also accepting monetary donations to purchase items to create auction baskets. Donations can be made in the amounts of $100, $250 or $500, and all donors will be recognized. Scan the QR code below to make a monetary donation to the silent auction today.


2023 OUTCOMES GRANTS
The Outcomes Innovative Pharmacy Grant Program provides financial support for research, education and promotion of innovative pharmacy practice initiatives in the state of Iowa. The following projects were awarded in 2023. Visit www.iarx.org/outcomesgrant
Alice
Maya
Megan
Matthew Witry, PharmD, PhD, Associate Professor, University of Iowa College of Pharmacy
IPA FOUNDATION JAN.FEB.MAR.APR. | 37
Evaluation and Intervention of Vitamin D Supplementation in a Supermarket Community
Pharmacy ($1,000)
Vaccine Screening and Administration in
Chang, PharmD, University of Iowa PGY1 Community-based Pharmacy Resident, Hy-Vee Implementing
Appointment-Based Medication Synchronization Program ($1,200)
Christy Nguyen, PharmD, University of Iowa PGY1 Community-based Pharmacy Resident, MercyOne Pharmacy
and Patient Experience with
Implementation of
a Test-and-Treat Service in a Community Pharmacy ($1,100)
Boguslawski, PharmD, University of Iowa PGY1 Community-based Pharmacy Resident, Greenwood Pharmacy
Implementation and Evaluation of a Long Term Care At-Home Service in a Rural Community Pharmacy Setting ($2,000)
Ditzman, PharmD, University of Iowa PGY1 Community-based Pharmacy Resident, Osterhaus Pharmacy
A Habit-based Intervention to Support Medication Adherence in Primary Care ($10,000)
AN ENRICHING EXPERIENCE

The IPA Max W. Eggleston Executive Internship was a unique experience that allowed me to immerse myself into diverse aspects of pharmacy by gaining hands-on association management experience and further contributing to the advancement of the profession. Every day was different at the association, but interns were typically assigned small tasks and longitudinal projects. These projects were related to policy, social media analytics, strategic planning, and pharmacology.
Throughout the summer, I had the opportunity to delve into various aspects of pharmacy association research and development. One of the most enjoyable projects was developing a Hepatitis C Resource Guide for pharmacists in Iowa because it allowed me to use both my pharmacology knowledge as well as practical skills.
During this internship, I had the privilege of expanding my professional network and developing a more diverse set of hard and soft skills. One of the internship requirements was to engage with pharmacists from various sectors, including industry, public health, policy, and more.

This experience not only broadened my understanding of the pharmacy landscape but also facilitated the development of skills crucial for a well-rounded professional. An impactful facet of this opportunity was the chance to meet Senator Chuck Grassley and visit

two struggling pharmacies in rural Iowa. These visits provided invaluable insights into the challenges faced by these pharmacies, shedding light on topics like DIR fees and Pharmacy Benefit Managers (PBMs)—subjects that are often only briefly touched upon in the curriculum but are highly relevant in real-world practice. Moreover, I had the unique experience of attending an emergency session at the Capitol building, further deepening my understanding of legislative processes and their implications for the pharmacy profession.
The most significant lesson I’ve learned from this internship is the value of effective teamwork and collaboration. I had the opportunity to work on a variety of projects with different teams, but the project that stands out the most was analyzing IPA’s strategic planning data. Initially, I attempted this project independently, but I encountered several roadblocks and progress was slow. It wasn’t until I reached out to the team for input that I was able to make headway.
Additionally, I gained an understanding of how to maintain authenticity within a professional setting. The experience taught me the importance of staying true to myself while navigating the complexities of the professional world. I discovered that authenticity not only enhances personal satisfaction but also fosters genuine connections and contributes to a positive work environment. This lesson in authenticity has become a cornerstone of my approach to professional interactions, allowing me to express my unique perspectives and values while contributing meaningfully to the workplace.
Lastly, I wish to express my sincere gratitude to Kate Gainer and Emmeline Paintsil for their instrumental roles in making this internship an enjoyable and enriching experience. Their commitment to creating a comfortable learning environment, where students can actively participate in discussions, has been invaluable in shaping my professional growth. ■
 2023 Executive Intern, Drake University College of Pharmacy & Health Sciences
2023 Executive Intern, Drake University College of Pharmacy & Health Sciences
INTERN REFLECTIONS
Kaitlyn Thomas, PharmD Candidate
With fellow students at IPA Annual Meeting 2023
Stephen Presti & Kaitlyn Thomas
38 | The Journal of the Iowa Pharmacy Association
Visiting Penn Drug in Sidney, IA
INVESTING IN THE FUTURE
My story with the Iowa Pharmacy Association began by attending Pharmacy Day on the Hill. Leading up to the event, I was excited but considerably nervous to speak with legislators and explain the value of pharmacists. Despite my initial uncertainties, the guidance from IPA and the collective energy of the association’s membership filling the capitol bolstered my confidence to interact with legislators and left me eager to expand my involvement with IPA. In the following weeks, I learned about the Executive Internship in Association Management, which I saw as a unique and challenging opportunity for personal development. Although my understanding of pharmacy associations was limited, I was enthusiastic to learn about the many projects and initiatives of IPA. In particular, I wanted to learn more about advocacy so I could lead advocacy initiatives at the college of pharmacy. These factors led me to apply for the internship, and when I received the offer, I was enthusiastic to accept.
I joined the staff in the lead up to the 2023 IPA Annual Meeting. My role in preparing for the meeting was largely to support the association’s policy committees. The policies written by these committees are debated upon at the House of Delegates, and if adopted, serve as the basis for IPA’s initiatives to support the profession. Knowing the importance of their work, I enjoyed listening to their deliberations and facilitating the process. The IPA policy committees are uniquely comprised of pharmacists, pharmacy technicians and student pharmacists, and this incorporation of voices from a cross section of the profession is a defining characteristic of IPA’s initiatives and is instrumental in addressing and overcoming the issues we face. Contributing to the IPA policy process was a memorable experience, and I will certainly pursue future opportunities to stay engaged in the association’s policy development.
The internship also provided me with firsthand insights into the issues confronting the pharmacy profession and opportunities to advocate for their solutions. One notable instance was our attendance at Senator Grassley’s visits to rural Iowa pharmacies, where I heard personal stories from rural pharmacy owners about the ongoing economic challenges stemming from PBM abuses. This experience reinforced my appreciation for the benefit pharmacies can confer on the health of rural communities. Later in the internship, I was able to discuss these observations when I attended the 2023 Lincoln Dinner in Des Moines and had the unique opportunity to advocate for PBM reform to presidential candidates. Professional advocacy is an ongoing effort that will be at the forefront of my mind throughout my career, and I am committed to taking an active role in raising awareness for its importance.
Although policy and advocacy activities were what drew me to the internship, I also learned a tremendous amount about the profession and IPA’s other initiatives. I got to attend meetings with key stakeholders in the profession, including an Iowa Medicaid Drug Utilization Review, a Board of Pharmacy meeting, the IPA Board of Trustees meeting, and many more. I also really enjoyed the opportunity of traveling through the Des Moines area to meet with pharmacy leaders in distinct corners of the profession. Through completing this internship, I gained a valuable, overall understanding of the profession.
In addition to the many great experiences from the internship, a bonus was working with Kaitlyn, my counterpart from Drake’s College of Pharmacy. For the first time in the internship’s history, IPA welcomed a student from each of the state’s colleges of pharmacy. Kaitlyn and I collaborated on many projects, and our skills complimented each other’s well. I appreciated her artistic and creative contributions to our presentations and the overall positive energy she brought to the experience. This collaboration throughout the internship greatly improved the experience and serves as a reminder of the importance of building strong connections across the state—a lesson I will carry forward in my career.
My internship experience with the Iowa Pharmacy Association was highly memorable and impactful. This truly was a great summer, and I am thankful for IPA’s investment in future leaders. Reflecting on the internship, I am confident that the pharmacy profession will continue to strengthen and overcome challenges through the leadership of the association. My final takeaway is that the work of IPA will lead to a better future for pharmacy, and I highly recommend all pharmacy professionals in Iowa stay engaged with the association and invite their colleagues to do the same. ■


INTERN REFLECTIONS
2023 Executive Intern, The University of Iowa College of Pharmacy
Stephen Presti, PharmD Candidate
JAN.FEB.MAR.APR. | 39
Speaking with presidential candidates about PBMs at the 2023 Lincoln Dinner
MEMBERS SECTION
IOWA PHARMACIST RUNNING FOR STATEHOUSE
Brett Barker, PharmD, Vice President of Operations for NuCara Pharmacy and Senior Policy Advisor for IPA, has announced his candidacy for Iowa House District 51. Current Representative Dave Deyoe is retiring, leaving a vacant seat. In a statement, Brett shared, “I am running for the Iowa House because my depth of experience in economic development, healthcare, rural revitalization, and foster care will help our state enact policies where families can thrive and the next generation is proud to call home.” House District 51 covers parts of Story and Marshall counties, including the communities of Nevada and Huxley. Learn more about Brett’s campaign at www.barkerforiowa.com

NEW CORPORATE PARTNERSHIP OPPORTUNITIES
In November, IPA unveiled a brand-new Corporate Partnership Prospectus for companies interested in building connections with Iowa pharmacy professionals, showcasing their products and services, and being in the know on all-things-pharmacy in the state. IPA now offers four levels of Corporate Partnership—Diamond, Platinum, Gold and Silver—with the ability to reach IPA members year-round. A new offering of note is an invitation extended to IPA Corporate Partners at all levels to join IPA’s weekly Legislative Committee calls. During these calls throughout the Iowa Legislative Session, IPA Partners can listen in and contribute to the discussion on legislative activity impacting pharmacy. Visit www.iarx.org/partners for more information.
MEMBER MILESTONES




Congratulations to Erik Maki, PharmD, BCPS, who has been appointed to his second term as a pharmacist member on the Board of Pharmacy. Thank you, Erik, for your public service!
Congratulations to JP Webb, PharmD, BCACP, BC-ADM, who has been appointed to his first term as a public member on the Board of Physical and Occupational Therapy. Thank you, JP, for your public service!
Congratulations to Patty Kumbera, BSPh, MBA, who was awarded Drake University College of Pharmacy and Health Sciences’ highest honor, the Lawrence C. and Delores M. Weaver Medal of Honor, in 2023!
Congratulations to T.J. Johnsrud, RPh, who was awarded the University of Iowa Center for Advancement’s 2023 Distinguished Alumni Achievement Award!






Congratulations to Susan Winckler, BSPh, JD, who received the 2023 Osterhaus Medal for Lifetime Achievement Award from the University of Iowa College of Pharmacy!

Congratulations to John Daniel II, BSPh, and Steve Firman, BSPh, MBA, who were awarded the University of Iowa College of Pharmacy’s Distinguished Alumni Award!
Congratulations to Gary Milavetz, BS, PharmD, who received the University of Iowa College of Pharmacy’s 2023 Honorary Alumni Award!
Congratulations to Kimerly Metcalf, CPhT-Adv, who was appointed by the Board of Pharmacy to the Iowa Monitoring Program for Pharmacy Professionals Committee!
Happy retirement to Jeff Longstaff, RPh, pharmacist and owner of Medicap Pharmacy in Creston for more than 40 years!
Happy retirement to Dean Renae Chesnut, EdD, MBA, RPh, who has served Drake University College of Pharmacy and Health Sciences for nearly 30 years in various roles and as Dean for the last 8 years. Dean Chesnut is completing an administrative sabbatical through the fall of 2024, after which she will officially retire. Thank you for your leadership, Dean Chesnut!

Best of luck to Dean Donald E. Letendre, BSPh, PharmD, FASHP, who is stepping down after 17 years as Dean of the University of Iowa College of Pharmacy. Dean Letendre plans to remain on faculty as a professor in the Department of Pharmacy Practice and Science to pursue scholarly work. Thank you for your leadership, Dean Letendre!

Happy 60th anniversary to Daniel Pharmacy, serving the Fort Dodge community since 1963! An open house and ribbon cutting with the Greater Fort Dodge Growth Alliance was held in December. Mayor Matt Bemrich proclaimed December 14 as Daniel Pharmacy Day.
IN MEMORIAM
Harold (Hal) Jackson, an integral member of the Winterset community with Jackson Pharmacy, passed away in October of 2023. Hal was a continuous supporter of the University of Iowa, both athletics and the College of Pharmacy. Hal served on the IPA Board of Trustees as Honorary President from 2002-2003 and received the Bowl of Hygeia Award in 2004.
Russel (Russ) Johnson, owner of family business Hammer Pharmacy in Des Moines’ East Village, passed away in December of 2023. Russ started working for his father in the pharmacy at the age of 11 and went on to found Medicap Pharmacy in 1971. Russ gave generously to support Iowa Pharmacy, serving as president of the IPA Foundation and receiving the Bowl of Hygeia Award in 1994.
MEMBERS SECTION 40 | The Journal of the Iowa Pharmacy Association
ENGAGED Pharmacist
Michael Chan
Jennifer Egbert
Brittni Frankel
Steve Frigo
Aaron Johnston
Sarah Reis
Melissa Shatek
Zoey Sjogren
Allison Smith

Kathryn Smith
Nicholas Strickler
CONNECTED Pharmacist
Bryan Schneider
Business Partner
Thorson Drug Inc
MCMH Pharmacy
Associate Member
Bristol Myers Squibb
Pharmacy Technician
Jenifer Carpenter
Sara Dreyer
Jennie Givens
Sara Hedlund
Bonita Meketsy
Patcharapa Tiamwech
Elizabeth Warriner
Alexa Winkel




WELCOME NEW MEMBERS MEMBERS SECTION September 1-December 31, 2023 WWW.IARX.ORG/ACCESSCPE NEW 1-Click Activation! No Code Needed! 1. Go to www.iarx.org/AccessCPE and select Activate My CE Plan 2. Log in to your IPA account 3. Select your CE library (Pharmacist or Technician) 4. Start learning! JAN.FEB.MAR.APR. | 41
IPA EVENTS
Find additional details for these events and more at www.iarx.org. Click on “Calendar of Events” under the Events tab. APRIL
9 2/2/2 Webinar – Seeking Pharmacist Licensure: Best Practices and Updates from the Iowa Board of Pharmacy
11
12
24
26
8
14
14
21
11
20
21
Onnen Company has been serving our customers’ needs since 1964. Fourth generation owned and operated, we offer endless industry knowledge through dedicated sales reps, management and owners with well over 100 years combined experience. We have a knowledgeable, unparalleled, and dedicated customer service staff to help you through the order process. Thank you for trusting us to continue to serve your prescription packaging and pharmacy supply needs.







CALENDAR OF EVENTS
2024
IPA Goes Local: Southwest Iowa Pharmacists Association (Council Bluffs)
Insight
to Advocacy: Pharmacy Practice Act Update
New
Headquarters Welcome Reception (Urbandale)
IPA
IPA Specialty Pharmacy Forum
2024
MAY
IPA Health-System Leadership Forum
2/2/2 Webinar
Prescription
Professionalism: Responding
Patient
–
for
to Inappropriate
Requests
IPA Goes Local: Quad Cities (Davenport)
NAPLEX-MPJE Review Course
2024
JUNE
2/2/2 Webinar – Poison Control Pulse Check: Recent Trends and Emerging Risks
IPA Annual Meeting: Day 1 (Coralville)
IPA Annual Meeting: Day 2 (Coralville)
Events are subject to change. Watch IPA communications for updates. UPCOMING
42 | The Journal of the Iowa Pharmacy Association
Rx Tape • Dosing Supplies • Custom Forms • Checks Envelopes • Padded Mailers • Shipping Supplies Toners • Printer Supplies • Pens • Calendars Magnets • Ad Specialties • and much more! What can Onnen do for you? Phone Toll Free 800.373.7162 Local Phone 515.276.0479 Fax Toll Free 800.373.7163 Local Fax 515.276.8341 www.onnencompany.com email: sales@onnencompany.com Prescription Labels and Forms. Laser and Thermal formats available. Vials in most brands. Save money on Secure brand. Free logo on Secure caps. Wide selection of Prescription Equipment and Compounding supplies. Pill Cards in both Cold Seal and Heat Seal versions. Stock and Custom printed bags for pharmacy.
19
96
Issues & Events That Have Shaped Iowa Pharmacy (Or Are Fun to Remember!)
MARCH:
The American Pharmacists Association (APhA) initiated its first community pharmacy-based demonstration project, Project ImPACT. Four Iowa pharmacies (Lutz Pharmacy, Drug Mart Pharmacy, Travis Pharmacy, and Osterhaus Pharmacy) were part of the nationwide project designed to demonstrate how pharmacists could enhance compliance and play a role in disease management related to hyperlipidemia. The patient care period lasted just over two years, and the study results were published in March of 2000.

APRIL:
APhA premiered its national radio program, The Pharmacist Minute. The program, funded by Pepcid® AC Acid Controller™, aired on over 1000 radio stations nationwide and eventually became international. The educational program was created to show the role of a pharmacist and how pharmacy was changing to impact the consumer. By November, The Pharmacist Minute was reaching more 2.8 million listeners daily.
JULY:
The Iowa Board of Pharmacy Examiners approved a request from the University of Iowa Hospitals and Clinics (UIHC) to conduct a pilot program utilizing electronic signatures for specific prescriptions. The program involved providers in designated ambulatory care clinics associated with the Department of Internal Medicine. The pilot was part of the Computer-Based Patient Record project at UIHC that included generating and printing prescriptions and maintaining online records.
AUGUST:
The Health Insurance Portability and Accountability Act of 1996 (HIPAA) was passed. This federal law protects the privacy and security of health data, referred to as Protected Health Information (PHI). The law was created to make health care more efficient and to increase the number of Americans with health insurance coverage. It was initially introduced in the House in March of 1996 but was not signed by the President until August 21st.
OCTOBER:
The Health Sciences Center of the University of Iowa created the Iowa Pharmacist Database. The database contained biographical, educational, and professional information for active Iowa pharmacists. The database was longitudinal so that trends could be tracked over time.
Data from June 1996 included the following highlights:
• 64.3% of pharmacists worked in community pharmacy
• 19.5% of pharmacists worked in a hospital
• 33.8% of community pharmacists, the largest group, worked in an independent pharmacy
• The largest age category was 40-49 years
• 60% of pharmacists were male
• 95% of pharmacists held a BS Pharm •

The Iowa Pharmacy Association Foundation is committed to the preservation of the rich heritage of pharmacy practice in Iowa. By honoring and remembering the past, we are reminded of the strong tradition we have to build upon for a prosperous future for the profession.
PHARMACY TIME CAPSULE
JAN.FEB.MAR.APR. | 43
Flovent
Remeron
Combivent
Aricept
Lipitor
Diovan • Topamax APPROVED MEDICATIONS www.lilly.com
• Humalog •
• Allegra • Zyprexa •
•
•
•