Management: Grade 2B, or not 2B, that is the question!
Adam Johnson
Energy Stacking
David Clancy
Maximising Bone Adaptation & Reducing Risk of BSI in Youth Development Footballers via Exercise & Nutrition
Jack Phillips
Back in the Game: Navigating Football after Pregnancy
Jenna Schulz
Integrating Force Plate Technology into Elite Football: Performance
Optimisation and Rehabilitation
Jermaine McCubbine
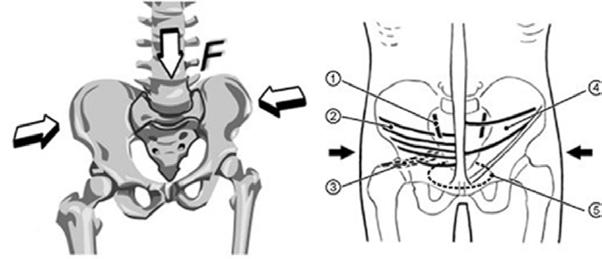
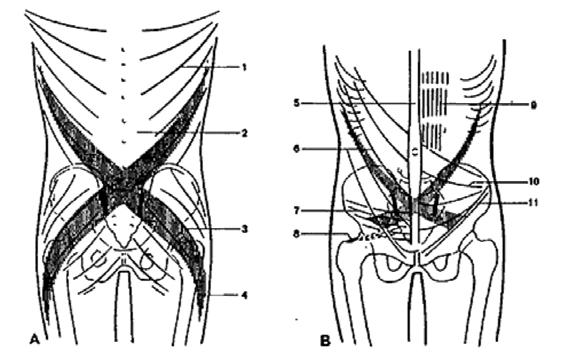
Hamstring Injuries: What Role does the Lumbar Spine and Pelvis Play?
Nick Metcalfe
“Check Engine Light”
Optimising Individualised High-Speed Running Zones in Football. Are we Measuring what we think?
Ronan Kavanagh, Dr. Ryland Morgans, Dr. Jill Alexander
Play Ball (or Don’t): Towards a More Valid Measure of Physical Intensity During Match Play
Benjamin W.C. Jerome,
Jonathan P. Folland, Michael Stoeckl, Ben Mackriell, Thomas Seidl
Enigma Legal provides legal services and advice to managers, coaches and professionals working within the sports industry, its unique structure utilising a panel of expert barristers all with extensive experience of the sports industry, most notably their work with the League Managers Association.
Enigma Legal lawyers are tried and trusted to work in a flexible, agile and responsive way, demonstrating their understanding of the unique demands of the sports industry. A creative and pragmatic approach will ensure that Enigma Legal offers real value to the FMPA Membership.
www.enigmalegal.com
admin@fmpa.co.uk
CEO MESSAGE
Welcome to this extended edition of our magazine publication.
There is an enormous amount of work involved in putting this together and my thanks go to the editorial board and the education team who work so hard to ensure we maintain the high standard and quality of articles our members have come to expect.
When I think how we started with a mere leaflet many years ago and see what we have in production today it never ceases to amaze me how far we have come. The magazine is testimony to the endeavours of members who have contributed, supported, and directed the pathway towards a publication that is not only outstanding within the football arena but is now considered a must read amongst practitioners in the professional game both at home and internationally.
Another area that is developing is Club membership. While this is not something we have precipitated there has certainly been an increase in interest of late since the concept is ultimately beneficial for both staff AND their clubs. Indeed, the FMPA/ Member/Club/Staff assemblage is one that interconnects without fanfare on a daily basis but always with the underlying aim of ameliorating all parties.
In short, many of the benefits we provide as an organisation support the Clubs in their endeavours to provide best practice outcomes for their staff.
This ‘collaboration’ is now being recognised as a win-win for everyone given the ratio of high value (benefits)to low cost (membership).
I am more than happy to discuss the process of Club membership with department leads and can be contacted directly at admin@fmpa.co.uk
Salmon Eamonn Chief Executive Officer
Football Medicine & Performance Association
ONLINE COURSE MPA DIPLOMA
PREPARATION FOR WORK IN PROFESSIONAL FOOTBALL
✓ Health and safety
✓ Safeguarding
✓ Equality/Diversity
✓ Mental Health/wellbeing
✓ Confidentiality
✓ Record keeping
✓ Media TV
✓ Social Media
✓ Expectations of behaviour/general professionalism
✓ Integration within the MDT environment
✓ Insight into the working week
✓ Awareness of un-clinical skills
✓ From `Theory to Practice’
✓ How the science sits in the working environment
✓ What an employer is looking for – Employability, CPD, Reflective Practice, CV
✓ Portfolio design
Includes FREE FMPA membership access for 6 months:
As the 2024/2025 season kicks off, medical and performance practitioners want to ensure that their athletes are in peak condition. This last edition for 2024 focuses on key topics to help ensure that medical and performance practitioners make use of evidence based practice.
In this edition, David Clancy discusses the principles and tools around energisers, detractors, energy mapping, building an energy calendar-and micro-interventions for energy, in the chaotic and hectic football environment.
Adam Johnson, physiotherapist at Everton FC, continues his interesting series on Ankle Syndesmosis injuries, this time focusing on the management of such injuries. Jack Philips from Liverpool FC explains the importance of maximising bone adaptation via exercise/nutrition, to help minimise skeletal damage accumulation. Another interesting topic in this edition is navigating football after pregnancy as Jenna Schulz discusses return to activity through to return to football in the postpartum athlete. Meanwhile, consultant chiropractor Nick Metcalfe details the role the lumbar spine and pelvis play in hamstring injuries.
From a football performance point of view, Benjamin Jerome and colleagues discuss how Ball in Play (BIP) time influences the physical metrics and the physical intensity of match play. On the other hand, Jermaine McCubbine, a strength and conditioning coach working with PSV Eindhoven first team explains the importance of introducing force plate technology in elite football. High speed running is another interesting topic discussed by Ronan Kavanagh and colleagues as a method to enhance performance and prevent injuries.
This will also mark the last edition for 2024. We are delighted to inform you that from 2025, the editorial will be moving to two editions a year which will both be available as hard copy and in digital format. This aims to ensure ongoing high quality editions whilst listening to the membership by bringing back the hard copy of the Football Medicine and Performance Editorial.
We hope that you have found this editorial useful and we would like to take this opportunity to thank you for your unwavering support and to wish you the best of luck for the season ahead.
Dr. Fadi Hassan Editor, FMP Magazine
Dr. Andrew Shafik Editor, FMP Magazine
Dr. Daniela Mifsud Editor, FMP Magazine
ASSOCIATE EDITORS
Ian Horsley Lead Physiotherapist
Dr. Jon Power Director of Sport & Exercise Medicine
REVIEWERS
Matthew Brown Academy Sports Scientist
Lisa Edwards Sports Therapist
Dr. Danyaal Khan Academy Doctor
Mike Brown Head of Physical Performance
Jake Heath Elite Sports Specialist Podiatrist
Dr. Dáire Rooney Doctor
Dr. Manroy Sahni Medical Doctor
Dr. Andrew Butterworth Senior Lecturer
Frankie Hunter Lead Sports Scientist
Dr. Jose Padilla MD Sports Medicine Specialist
Dr. Eleanor Trezise Doctor
Dr. Avinash Chandran Director
Callum Innes Medical Doctor
Kevin Paxton Strength & Conditioning Coach
Medicine And Performance Association t/a Football Medicine & Performance Association Office 5, Bank House, King St, Clitheroe, Lancs, BB7 2EL T: 0333 4567 897 E: info@fmpa.co.uk W: www.fmpa.co.uk
FMPA_Official Officialfmpa fmpa_official LinkedIn: Football Medicine & Performance Association
Cover Image England Goalkeeper Mary Earps receives treatment during the UEFA Women European Championship Qualifiers League match between England Women and France at St. James’s Park on 31st May 2024. Photo: Alamy
The views and opinions of contributors expressed in Football Medicine & Performance are their own and not necessarily of the FMPA Members, FMPA employees or of the association. No part of this publication may be reproduced or transmitted in any form or by any means, or stored in a retrieval system without prior permission except as permitted under the Copyright Designs Patents Act 1988. Application for permission for use of copyright material shall be made to FMPA. For permissions contact admin@fmpa.co.uk
12 Ankle Syndesmosis Management: Grade 2b, or not 2b, that is the Question!
Adam Johnson
17 Energy Stacking
David Clancy
23 Maximising Bone Adaptation & Reducing Risk of BSI in Youth Development Footballers via Exercise & Nutrition
Jack Phillips
30 Back in the Game: Navigating Football after Pregnancy
Jenna Schulz
35 Integrating Force Plate Technology into Elite Football: Performance Optimisation and Rehabilitation
Jermaine McCubbine
40 Hamstring Injuries: What Role does the Lumbar Spine and Pelvis Play?
Part 1: Force Closure of the Pelvis and Anterior Pelvic Tilt
Nick Metcalfe
45 “Check Engine Light” Optimising Individualised High-Speed Running Zones in Football. Are we Measuring what we think?
Ronan Kavanagh, Dr. Ryland Morgans, Dr. Jill Alexander
50 Play Ball (or Don’t): Towards a More Valid Measure of Physical Intensity During Match Play
Benjamin W.C. Jerome, Jonathan P. Folland, Michael Stoeckl, Ben Mackriell, Thomas Seidl
SWIMEX CONTINUES THEIR SUPPORT AS FMPA BUSINESS PARTNER FOR A SIXTH SEASON!
The FMPA is absolutely delighted to continue working with Richard Bishop and the team at SwimEx in the 2024/25 Season.
Eamonn Salmon, FMPA CEO commented “We have thoroughly enjoyed working with Richard over the years and look forward to another successful season ahead.”
SwimEx Sports Fitness, Hydrotherapy Pools and Ice Baths have delivered Sports Wellbeing since 1986.
Richard Bishop, Technical Director, has been in the industry for 36 years and composed the award winning technical paper for the Institute of Swimming Pool Engineers and recently gave a talk on sports hydrotherapy to the Institute.
We recently installed two SwimEx pools at Queens Park Rangers FC including a recovery deep water cold plunge pool with an energy efficient heat pump chilling system. We also worked with the UK Sports Institute updating their water treatment and filtration system on their recovery pool at Bisham Abbey to support Team GB in the build up to the 2024 Paris Olympics.
You can contact Richard Bishop MISPE direct if you would like to discuss a health check on your existing facilities or considering a future hydrotherapy project.
Sporting Edge is a UK based manufacturing company with an expanding global reputation as the leader in the design and provision of Altitude & Environmental Facilities.
Sporting Edge systems deliver measurable fitness and performance improvements in as little as three weeks, with the added benefit of allowing fitness levels to be retained during injury repair – speeding up return to play.
Since 2005, Sporting Edge has consistently set the benchmark for performance, safety, reliability and control for Simulated Altitude, Temperature & Relative Humidity, supported by a number of patents and innovations. Endorsed by the UK Sports Institute (EIS) and with a client list including many UK Universities, Olympic facilities, Professional Sports Teams and Commercial Physical Performance Centres, Sporting Edge have more installations, delivering completely unmatched performance and control, than any other sector company.
Contact info@sportingedgeuk.com for a free, consultation and quote for your altitude/environmental chamber today.
KOMFI CONTINUE AS FMPA BUSINESS
SUPPLIER FOR 2024/25 SEASON
The company behind the Komfi brand Komfi is a division of the GNG Group, an international brand leader and supplier of performance medical, consumer and sports products.
GNG supplies to a number of key industries requiring a wide range of foam-based solutions. As a valued and trusted manufacturer, the company has also been awarded the prestigious ‘Approved Supplier’ status by the NHS.
Our Mattresses - The bedroom should be your sanctuary, and your bed the ultimate place to unwind and drift off to sleep. We offer a range of mattresses to suit your personal comfort choice, whether that be a soft or firm feel, or somewhere in between.
The KomfiMed Collection
An industry first, KomfiMed combines the benefits of the two unique products: medically-proven foam and exclusive TrueGel technology.
Find out more: https://komfi.com
REDUCE TIME OUT THROUGH INJURY
ON THE PITCH
using The best HEAT & ALTITUDE system, running proven training protocols
Reduce Rehab time by up to 20%
Faster recovery More repeat sprints
Up to 35% increase in time to exhaustion
S & C FACT: Running Sporting Edge training protocols in a properly designed Heat & Altitude Chamber will have a greater impact on the fitness and performance of your players than anything else that you may choose to do.
“The potential performance gains of a properly planned hypoxic strategy will outweigh all other forms of modern sport science interventions”
Dr Ben Hollis, Performance Scientist. EIS
REHAB FACT: Time taken to return to full fitness following injury will be reduced significantly when players incorporate gentle altitude sessions into the repair and recovery period.
“Because altitude produces an effective physiological stimulus at low workloads, injured players can retain their fitness and are able to return to play sooner, once their injury has healed.”
Rebecca Toone, PhD Intensive Rehab Physiologist, EIS
FINANCIAL FACT: You can get a world class Heat & Altitude Training Facility that is available 365 days a year for the next 15 years for less than the cost of one 10 day training camp.
Outright Purchase or Finance Options
Ongoing Training Support included
www.sportingedgeuk.com info@sportingedgeuk.com
ANKLE SYNDESMOSIS MANAGEMENT:
GRADE 2B, OR NOT 2B, THAT IS THE QUESTION!
FEATURE / ADAM JOHNSON
Recap and Introduction
This article, regarding the management of ankle syndesmosis injuries, follows on from a prior edition of the FMP magazine which addressed the anatomy and diagnosis of these complicated injuries. Before moving on to the management it is worth briefly recapping on these areas covered in the previous article.
The ankle syndesmosis is predominantly comprised of three different ligamentous structures- Anterior Inferior Tibiofibular Ligament (AITFL), Posterior Inferior Tibiofibular Ligament (PITFL), Tibiofibular Interosseous Ligament (TFIL). The superficial and deep aspects of the Deltoid Ligament also provide key contributions to the stability of the syndesmosis.
Objective assessment is limited within the assessment of these injuries, and so clinicians must look to utilise a number of objective tests as well as imaging modalities to truly categorise the extent of the injury. This article will therefore predominantly reference back to the Modified West Point Criteria1 (Table One) which grades syndesmosis injury into four different gradings, with a distinction made between “stable” or “unstable” injuries which influences management decisions. For this reason, the remainder of the discussion in this article will solely reference this grading system in relation to management decisions.
Management Decisions
Within the literature there is a relatively
clear distinction made between the management strategies for Grade I and Grade III injuries, but with Grade II injuries there is more room for discussion;
• Grade One - The least severe of the ankle syndesmosis injuries. These are injuries that are isolated to the AITFL structure only and are widely accepted as being successfully managed through conservative management.
• Grade Two - As acknowledged within the work of Calder2 Grade two ankle injuries provide debate around appropriate management decisions. Within the article by Calder a proposed algorithm (Figure One) was devised which combined both MRI finding with clinical findings. It is proposed that all grade two injuries will have a positive external rotation test, however if this is in combination with a positive squeeze test and/or Deltoid ligament involvement then it is likely that surgical management will be required to provide a successful rehabilitation outcome. Absence of a positive squeeze test with no Deltoid ligament involvement provides confidence that conservative management is likely to be appropriate.
• Grade Three - As with grade one injuries there is little debate around the management of this grading of injury. All components of the syndesmosis anatomy are involved and without surgical intervention the athlete will not make a successful return to sport and would likely be left with long term disability as a result
of chronic syndesmosis instability.
Conservative Management
As referenced above, non-surgical management appears to be appropriate in grade I and grade IIa injuries. There is however a lack of clarity and consensus as to the optimal management of these injuries3. This section will look to summarise the key components of conservative management;
• Immobilisation - This forms a key component of the management of all grades of syndesmosis injury, as we know from the anatomy that these structures are different to “simple” lateral ankle ligament injuries in the fact that they are tasked with resisting the diastasis of the distal tibiofibular joint during weight bearing. This means that immobilisation is an essential part of management in order to provide the injured structures with an environment in which they are not being continually stressed and irritated. Immobilisation is predominantly achieved through utilisation of a walking boot which ensures that the foot avoids any form of dorsiflexion.
It is proposed that there should be a relatively short period (1-2 weeks) of non-weight bearing status depending on the severity of the injury4, before gradually progressing from partial to full weight-bearing in the boot. As there is a lack of consensus and all injuries will present differently depending on the individual’s anatomy, it is recommended that decisions for removal of the immobilisation boot are made not just on time, but also objective assessment.
Grade IIa injury stable
• Normal Deltoid ligament
• -ve squeeze test
• (ATFL injury?)
Grade II syndesmosis injury
• AITFL rupture +/- IOL injury
• +ve external rotation test
Grade IIb injury “dynamic” instability
• Deltoid injury and/or
• +ve squeeze test
• (+/- PITFL injury)
Conservative management and progressive rehabilitation
Figure 1: Algorithm of proposed management for Grade II syndesmosis injuries. Taken from Calder et al. (2016)
Potential recommendations for key objective markers are seen in Table 2.
• Strengthening - If we think about the mechanism of injury, we will generally have seen an external rotation stress placed upon the ankle. This is likely to have influenced the medial ankle musculature such as tibialis posterior and flexor hallucis longus through excessive lengthening, or pain inhibition. It is therefore suggested that early isometric loading of these structures is important. This should be done in an inner range position initially to avoid stressing the injured syndesmosis structures, before progressing to outer range positions and ultimately eccentric loading in order to assist the ankle in resisting the injury mechanism upon return
to sport. Ankle plantar flexor musculature must also be loaded, this can begin almost immediately as long as performed in a plantar flexed position, again thinking that dorsiflexion will stress the injury site.
• Taping & Bracing - As the athlete progresses out of the immobilisation boot it is important to utilise either braces or strapping. In relation to strapping the main aim is to provide compression of the distal tibiofibular joint and support the injury site so that the athlete does not go from full immobilisation to no support, as this is likely to provide irritation and a delay in successful rehabilitation outcome.
• Return to Running - Anti-Gravity treadmill access is very important within
the rehabilitation of this form of injury in particular. The ability to gradually increase the loading placed upon the ankle is much more likely to provide a successful outcome as it allows for normalisation of gait patterns early on in the process at a time when full bodyweight might still be provocative to the ankle. Also of consideration is that unlike with muscular rehabilitation, this specific injury is likely to find quicker running speeds less provocative. This is because the athlete is likely to go through greater ranges of ankle dorsiflexion at lower speeds, whereas high speed running will promote a stiffer ankle and therefore avoid the ankle dorsiflexion position which will bring the wider anterior talus into the mortise.
Objective Test
External Rotation Test
Squeeze Test
Palpable Tenderness over AITFL
Single Leg Calf Raise from Floor
Criteria For Removal of walking boot
2/10 or less on VAS
2/10 or less on VAS
2/10 or less on VAS
Symptom Free
Table 2: Proposed criteria for removal of an walking boot in the management of ankle syndesmosis injury
Surgical Management
Surgery appears to be the appropriate management decision of unstable grade IIb and grade III injuries. There are two common surgical procedures for these injuries which are explained below;
• Screw Fixation - This is the traditional surgical management strategy for patients with syndesmosis disruption. This procedure utilises a syndesmotic screw which aims to restore the congruent mortise within which the talus sits. One of the well recorded issues with screw fixation is the potential need for removal of the screw either prior to weight-bearing, or when a lack of dorsiflexion range is identified later in the rehabilitation process5. Although the removal of the screw does not add a prolonged period to the rehabilitation, it is still not the ideal scenario in a professional athlete who is looking to minimise time loss to return to sport.
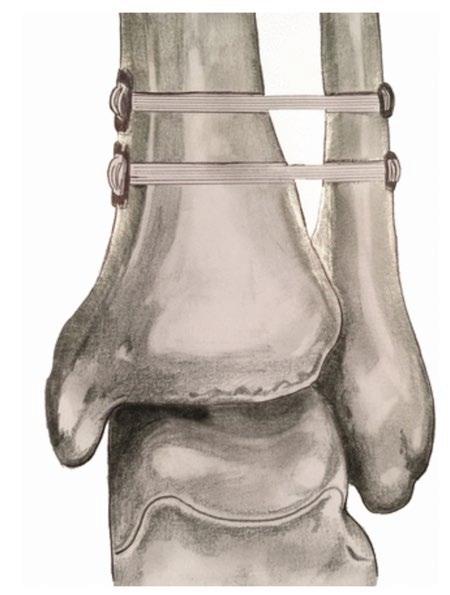
• Suture-Button Fixation - This procedure involves the insertion of a structure known as a “tightrope” which is a non-absorbable and semi-rigid suture, is passed through predrilled holes within the tibia and fibula (Figure Two). This tightrope is then tightened with the lateral suture-button to reduce the syndesmosis to its natural position. The apparent advantages of this form of repair is that weight-bearing is that it allows for a small amount of normal biomechanical movement, an earlier return to weight-bearing and a decreased chance of second surgical procedure to remove the device6. This is still required in some cases though as the suture button can irritate the overlying soft tissues7
Expected Time Loss
As with all injuries sustained within elite sport the first question from the athlete and management will revolve around the time loss expected from these injuries.
As specifically discussed within the work of Wever et al.1 there is a lack of standardisation of terms used within the literature which makes direct comparisons difficult. Table 3 collated below looks
to summarise the expected time losses for all different grades of syndesmosis injuries taken from the relevant published literature, with the terminology used for calculated time loss listed alongside.
Latham et al. (2017) (6)
“Return to sport”
Wever et al. (2022) (1)
“Return
Calder et al. (2016) (2)
“Return
D’Hooghe et al. (2020) (8)
“Return to training”
± 17.2 days (38-108)
days (28-91)
± 22 days (56-161)
Figure 2: Illustration of a syndesmosis tightrope repair. Taken From Latham et al. (2017)
Table 3: Mean time loss following different grades of ankle syndesmosis injuries
References
Summary
• The management of ankle syndesmosis injuries in elite sport is currently predominantly based upon the Modified West Point classification criteria.
• This allows for distinction between “stable” and “unstable” injuries when making management decisions, specifically within grade II injuries.
• For grade I and IIa injuries there is an agreement that conservative management should be undertaken with initial immobilisation and protection of the injury site. There is however a lack of published literature around rehabilitation practices and time loss expectations, particularly in the less severe grade I injuries.
• There is a greater volume of literature surrounding surgical management cases of grade IIb and III injuries within minimum expected time loss for surgical cases being at over nine weeks, even on an accelerated program for rehabilitation.
• Suture button fixation is the preferred surgical intervention of choice for elite athletes as it reduces the risk of secondary surgery, and subsequently greater time loss.
Adam Johnson is a Physiotherapist with 13 years of full time experience working within professional football. Throughout this time he has been heavily involved within short, to mediumterm rehabilitation cases which has driven an interest in the literature surrounding muscle and ligamentous injuries. Alongside his day-to-day work Adam has also been able to get three articles published in peerreview journals.
1. Wever, S., Schellinkhout, S., Workman, M. & McCollum, G.A. (2022). Syndesmosis injuries in professional rugby players: associated injuries and complications can lead to an unpredictable time to return to play. Journal of ISAKOS, 7(4), 66-71.
2. Calder, J.D., Bamford, R., Petrie, A. & McCollum, G.A. (2016). Stable Versus Unstable Grade II High Ankle Sprains: A Prospective Study Predicting the Need for Surgical Stabilization and Time to Return to Sports. Arthroscopy, 32(4), 634-642.
3. Mulligan, E.P. (2011). Evaluation and management of ankle syndesmosis injuries. Physical Therapy in Sport, 12, 57-69.
4. Porter, D.A., Jaggers, R.R., Barnes, A.F. & Rund, A.M. (2014). Optimal management of ankle syndesmosis injuries. Open Access Journal of Sports Medicine, 5, 173-182.
5. Tourne, Y., Molinier, F., Andrieu, M., Porta, J. & Barbier, G. (2019). Diagnosis and treatment of tibiofibular syndesmosis lesions. Orthopaedics & Traumatology: Surgery & Research, 105, S275-S286.
6. Latham, A.J., Goodwin, P.C., Stirling, B. & Budgen, A. (2017). Ankle syndesmosis repair and rehabilitation in professional rugby league players: A case series report. BMJ Open Sport & Exercise Medicine, 3(1), e000175.
7. Willmott, H.J., Singh, B. & David, L.A. (2009). Outcome and complications of treatment of ankle diastasis with tightrope fixation. Injury, 40(11), 1204-1206.
8. D’Hooghe, P., Grassi, A., Alkhelaifi, K., Calder, J., Baltes, T.P.A., Zaffagnini, S., & Ekstrand, J. (2020). Return to play after surgery for isolated unstable syndesmotic ankle injuries (West Point Grade IIB and III) in 110 male professional football players: a retrospective cohort study. British Journal of Sports Medicine, 54(19), 1168-1173.
ENERGY STACKING
FEATURE / DAVID CLANCY
A new way to work in elite football medicine and performance.
No matter what job we have in sport, what work needs our attention, or what we are focusing on at home, having our mind and body focused and in alignment will mean better performance.
Think for a second... if the wheels of a car are worn yet there is a strong engine under the hood, it is only a matter of time before the car will crash or break down. Sometimes we use our engines, our minds, to handle most of our tasks while neglecting our bodies, our wheels in life. The rise of the productivity revolution, and efficiency being a hot topic has perhaps led to an overemphasis on getting things done!
We need to be asking at what cost can we sustain this as part of the team behind the team? A burnout endemic, a worldwide pandemic, and ‘the great resignation’ are signs that we are beginning to understand that there is more to work than getting through a to-do list and being ‘busy’.
Naval Ravikant, investor and entrepreneur has said that to get ahead we need to work more like a lion - sprint when hunting (or doing
inspired work in our case) …then rest, recover and repeat. Elizabeth Grace Saunders, time management coach noted ‘the key to success at work and in life isn’t really starting strong - it’s staying strong.’ How can we stay strong and manage our cognitive load as part of the backroom for a football team? Not easy but worth thinking about, to sustain high levels of care for our athletes.
One needs to know how to maximise and replenish energy. We often hear people say that the difference in people is energy so it’s worth understanding ours more. This article will unpack principles and tools around energisers, detractors, energy mapping, building an energy calendar - and micro-interventions for energy, in a chaotic and hectic football environment.
We are consumed with busyness. Should we consider shifting our attention away from being more time-efficient and productive and to focus on our energy? What about...are you adequately fuelled every day to be your best for your players/ athletes? To keep up in the evolving way of working in football, sometimes we must wear many hats in a day, from head of department at the club, to husband/wife/ father/mother... to coach of the under-8 local
Energisers
List them below (examples below)
• Outdoor walk
• Tidy desk
• Having a glass of water
• Reading fiction
• One minute meditation
football team! We juggle many things and plan around these most of the time. But - do we consider our energy?
So much of what we do now is planned. We take out our to-do lists, spreadsheets or Google calendars and try to follow them. Every 30 minutes we have time-blocked and planned for meetings, rehab sessions…. you name it.
Can we strive to plan our day around what will drain energy and what will replenish it - so that when we must perform highly, we have taken the optimal steps to get there? This does not mean that we only wait until we are ready to do something. As best-selling author Brad Stulberg has said, “mood follows action”. Showing up can be the first best step in getting rid of feelings of tiredness and apathy! Here’s the gold. What would work be like if we could show up as our best version - energised and ready to perform...at the highest level!
Reflection time. For you.
List 5 Energisers and 5 Detractors - what gives you energy, and what depletes your energy. That’s a foundational self-awareness piece to start.
Detractors
List them below (examples below)
• Late night TV
• Scrolling aimlessly on phone
• Messy environments
• Complaining or negative people
• Skipping breakfast
CEO The Nxt Level Group, Sports Medicine & Performance Specialist
We don’t blame our car for running out of diesel. We know that it needs time to refuel or recharge. We seek out stations for petrol or electricity ahead of time. When we are alerted by a simple dashboard signal, we know that there is no option to just plod on. We need to stop.
Energisers are our fuel. They are the actions, behaviours, and habits that fill up our human tank…from actively leaning on our accelerator all day we may burn through our reserves! What is different about how we treat our cars and our bodies? Is it that we do not feel bad about stopping to take the time to refuel the car? When it comes to taking time for us, for self-care and wellbeing…we could be better. We could help ourselves more from a fuelling perspective. There is a way. Energy stacking. It is a game changer for us physios, sports med doctors, S&C coaches, sports scientists, etc.
This roadmap below will outline a simple and clear planning system to stay energised through the day. We need to rid ourselves of the hustle and grind culture to be deeply effective for our team, in flow - and focus on getting things done whilst preserving our health and wellbeing.
Here is a list of some of the most scientifically proven actions to best manage your neurochemistry and hormone release across a day, and in turn maximise your effort by refuelling your energy tank!
�� Morning
• Go outside and get natural sunlight (20 min. within 90 min. of waking) - even if it is cloudy, there is ambient natural light which is good for our circadian rhythm.
• Turn the shower to cold for 1-3 minutes to boost our immune and nervous systems.
• Delaying caffeine intake until 90 min. to use our own system to get us going internally.
• Exercise within 60 min. of waking to charge our metabolism and elevate our mood. 7 min. counts!
☀ Afternoon
• Walk outside, ideally in an environment that has a water or grass feature. This is called blue and green space exposure and is calming and restorative.
• Mindful movement at the desk. Mindfulness can improve attention and focus during the day.
• Hydration. We are made up mostly of water. This is an easy win to stay fresh and engaged!
• One-minute breath-work (e.g. such as a physiological sigh) to nourish our respiratory system.
�� Night
• Quick jot down of plan and primary actions for tomorrow. Win the next day before it starts. This reduces cognitive load, primes us for the next day plus stops our brain from overthinking when it should be resting.
• Enjoy a warm shower 30 min. before bed to alter our body temperature and physiological state in preparation for bed.
Detractors take energy from us. Rushing around. Being under too much pressure. Feeling overwhelmed. Not enough support, etc. This happens but we need to be cognisant of it.
Phones have become our lifelong companions. We are glued to our smartphones, sometimes even whilst driving or crossing the road - which is scary, never mind very dangerous! When we reach an acceptable age to dive into the smartphone world, we never quite look back! You will now have a phone almost always on you - for over 95% of your remaining life. This may be an energy drainer if you do not use it right - and that’s the key. It can help in many ways, but it can be harmful - it impacts our relationships, focus, emotions… our connections with players.
Technology is advancing far faster than we can adapt to it. Evolution is a slow deliberate process for humans, yet in the past 10 years we have seen advancements that give us the ability to connect instantly with almost anyone anywhere in the world. Working in a team has become easier and we can talk with loved ones with the press of a button. However, we are now facing information overload and dwindling attention spans because of this new ease of information access. This is a type of detractor - an action or item that demands cognitive attention with only short-term contentment or health benefits. A culprit that can impact our performance negatively.
Detractors are like ninjas; you don’t really know they’ve struck until you are defeated. Sometimes they bring immense pleasure
now, but deep down we know we will pay for it! Think about that extra bit of ice cream or chocolate cake... satisfying in the moment, but a killer in the aftermath due to sugary spikes in the body. Phones are the primary detractors in the modern world of elite football medicine, performance and beyond. But there are many other culprits such as comparing, complaining, criticising others, high sugary foods, and negative self-talk.
If we do not plan and make time to recharge if depleted due to detractors of energy, we will not function at our best. In the short term, when we operate on autopilot our pre-frontal cortex, the area of the brain associated with higher orders of thinking suffers. As we persist with ‘getting by’ and grinding or hustling the structure and wiring of the brain changes leading to progressively detrimental long-term, sub-par performance. We must balance energisers and detractors.
Do any of these common detractors resonate with you?
�� Morning
• Reaching and scrolling your phone first thing upon waking
•Drifting in and out of sleep on the tube/ bus
• Consuming high-carb or sugary foods
• Not planning for the day ahead at the club properly
☀ Afternoon
• Sitting at a desk for hours with little to no breaks
•Ruminating on past events regarding players, other staff members
• Having one glass of water for the day
• Sticking to work when your family is present for bonding, play and interaction (or glued to your phone!)
�� Evening
• Watching TV or scrolling on a phone until the point of sleep
• Sleeping with your mouth open
• Skipping any form or light-moderate exercise, especially on away/ travel days
• Several nightcaps
• Going all day on little or no food - our fuel
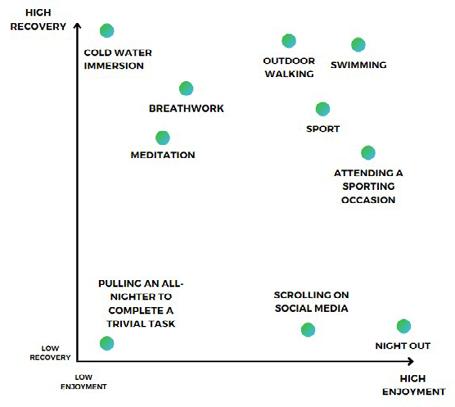
To understand how energisers work for us, we must map them against enjoyment (our instant pleasure and hedonic pursuit) and recovery (how much delayed gratification or health and wellbeing benefit will come because of the action).
Create your own energy ranking map to understand high enjoyment and high recovery practices you can employ, and what could take energy from you - see example figure right to illustrate this.
Another practical tool to help us understand our energy dynamics better is looking at our weekly calendar.
So now it’s time to create your own energy calendar. This won’t be always possible to adhere to. Things happen in football all the time. Schedules change. The manager will want to see you. A player will get injured. An agent will arrive. There will be demands made of you outside your sphere of control. But this will give you a frame to think about to try to control the controllables as best possible.
We can create opportunities, which may create success as we ourselves define it. We know time is always a critical component of a day... how we use it, our most precious resource, especially in relation to player care and performance. Something that can help us with time management is harnessing energy, making it work for us, not against us!
Energy is not wasted or conjured up from thin air. It simply changes form. Energy is stored as potential or is used as kinetic energy. Therefore, we must learn how to manage our energy effectively, and employ the most energy-supporting behaviours in our daily lives. Especially when we are busy at a club or facility. Time blocking (as seen in the below image) shows that to work most effectively we should block out segments of the day, if possible - to complete our job, our focused work. But as we know, this state of output places a heavy burden on our energy stores. This is cognitively demanding, and we pay a high energy price! The players might too.
Looking back over our sample energy map from below, we now are aware of what drives our energy levels high…that potent blend of high enjoyment and high recovery! So, what now? To stack your energy, map out your day in a calendar and employ a policy of for each hour of demanding work, add 5 minutes of a highly energy-replenishing action, such as breathwork or a walk outside the building away from your phone, if you can control it. Spread out throughout a demanding
RANKING ENERGISERS
Energy Calendar
ENERGY MAP
day in this competitive world of professional football, these short, simple behaviours, or micro-interventions are what allow us to continue to produce. They help us stave off brain fog, and general fatigue, while also amplifying our motivation, and most vitally our productivity. We can get more done with less and isn’t it worth preserving the one thing that we cannot truly create…time!
Another reflection piece exercise now.
At the training facility/ ground, do you have any simple and short performance practices to re-charge your energy battery? We need to determine our energy arsenal. That’s where micro-interventions come in. Microinterventions are small things we can do to change our energy, such as a physiological sigh, a 30-second breathing exercise to lower anxiety and stress levels.
The big rocks for energy are the fundamentals: sleep hygiene practices and optimal levels of sleep, nutrient dense
meals, adequate hydration, practicing mindfulness meditation, and moving your body regularly. But sometimes if these are encroached on due to busy training and matchday schedules, deadlines, travel and so forth…that’s when micro-interventions can become very valuable assets for us.
Reflect on small moments you have in your day and how you can affect your energy levels, ramping up or down (sympathetic or parasympathetic), depending on the need.
• Breath work is a game-changer (box breathing an easy win!), ambient light upon rising, cold plunge, sauna (check out Rhonda Patrick, an advocate for heat immersion therapy, who has been on the Joe Rogan Experience podcast), and bite size chunks of mobility exercises all help.
Write down 3 go-to micro-interventions you can start to habit form, short and effective tools that are possible to execute during a busy day at the football club. Be creative.
To maintain high levels of performance, it is important to think about how we are currently investing our energy and how we can re-charge and expand our energy reserves. The ability to change your energy - and know what level you have in your energy battery is worth reflecting on.
Think about where you invest energy, what gives you it, and what takes it away. What recharges your battery and what supercharges it to expand it? This could be anything like tidying your work area and getting rid of clutter. Perhaps it’s about creating a sense of challenge in your work or blocking out time for physical activity, such as a brisk walk. Maybe it’s to re-connect with close friends that you have lost track of. Map your energy and look at your week and patterns over weeks…and you will be on your way to understanding your energy fuel better.
SwimEx Fitness Hydrotherapy and Plunge Pools
SwimEx pools provide sports medicine professionals with the ideal hydrotherapy tool for advanced recovery, training and conditioning. The variable flow water current, power driven underwater treadmills, high performance interiors with therapy protocol work stations and SwimEx EDGE touchscreen fitness monitor create the ultimate aquatic environment for progressive treatment plans and winning training programmes. As used by New England Patriots, Denver Broncos, Jacksonville Jaguars, Baltimore Ravens, Green Bay Packers, Help For Heroes, British MOD, Wolves FC and Strive Sports Academy as used by the British and Irish Lions.
Cold Plunge Pools
The SwimEx chiller system on this Cold Plunge Pool keeps water temperatures at a therapeutic 50oF (10oC).
Hot Plunge Pools
The SwimEx Hot Plunge Pool heating system brings water temperatures up to 104oF (40oC).
1000 T Series
• Accommodates 6-7 people
• Extra Large Treatment Area
• Non-weight Bearing Deep Area
• Multiple Users/Multiple Depths
Custom Plunge Pools
For teams and athletes who require specific treatments, SwimEx can help you create custom plunge pools.
800 T Series
• Multiple Depths
• Non-weight Bearing Deep Area
• Multiple Users
• Flat Floor & Fitness Stations
600 T Series
• Rear Running Pad
• Deep Well up to 2.13m (7ft)
• Multiple Fitness Stations
• Variable Speed Treadmill
MAXIMISING BONE ADAPTATION & REDUCING RISK OF BSI IN YOUTH DEVELOPMENT FOOTBALLERS VIA EXERCISE & NUTRITION
FEATURE / JACK PHILLIPS
Introduction
Youth athletes are prone skeletal physes/ apophyses injuries, traumatic fractures and bone stress injuries (BSI). BSI, occurring due to a mismatch between microdamage formation/removal following repetitive loads, leads to weakness and pain, resulting in significant time loss for athletes.45 It is recommended that all bone overuse injuries are described by the term BSI,45 encompassing stress reactions (altered signal within the marrow, endosteum and/or periosteum) and stress fractures (fracture line evident).4
Football has high osteogenic benefits, demonstrating positive bone adaptations.28 Despite the osteogenic benefits, BSI are common within youth football players. Within football, significant changes in training and matchday demands occur,36 as individuals transition from off-season to pre-season,46 progress in competition level,20 or progress in age groups.36 Such changes can be hazardous, increasing BSI risk.13
Improving the skeletons ability to resist load by inducing mechanoadaptation, and
reducing skeletal damage accumulation, can reduce BSI risk.15,45 This review will discuss a) bone adaptation to loading b) how to improve the skeletons’ ability to resist load by inducing mechanoadaptation, and c) how to manage loads being introduced to the skeleton.
Adaptation to load:
Bone, a highly dynamic tissue,9 adjusts its structure in accordance with the loads placed upon it. Bone is constructed/ reconstructed by bone modelling and remodelling throughout the lifespan.
BSc Sport Science, BSc Physiotherapy, Liverpool Football Club DProf S&C student at St Mary’s University
Bone modelling, a process in skeletal development, involves the construction of bone, via the independent action of osteoblasts and osteoclasts.24 This phase, typically completed by the end of skeletal maturity, involves the process of modifying bone shape and size.24
Bone remodelling, a well-regulated cycle replacing old bone with new bone, continuously repairs skeletal damage. During remodelling, the skeleton relies on constant repair of microdamage to withstand loads placed upon the tissue.24 Up to 10% of the skeletal system is replaced each year, with osteoclast activity initiating bone resorption, prior to being replaced by osteoblasts which aid bone formation. Typically, well regulated, exposure to high impact loading can induce positive bone adaptations. During remodelling osteoclasts are activated, resorbing damaged bone over 10-14 days, increasing tissue porosity and reducing fatigue resistance.15,46 Following this, osteoblasts deposit unmineralised bone matrix replacing the damaged area.32 Re-mineralisation of new bone can take months, resulting in mechanically weaker tissue.15 Whilst high impact loading is
necessary to optimise bone adaptation, excessive loads during early remodelling can lead to increased microdamage and potentially BSI.
Maximising Mechanoadaptation
During adolescence:
Bone adaptations diminish as people age, with the growing skeleton most responsive to exercise and adaptation. Adolescence is a key window for bone mass accumulation with 33-43% of total bone mineral content in adulthood accrued in the years surrounding peak-height-velocity.3 A 10% increase in peak bone mass enhances skeletal growth and reduces fracture risk by 50%.5
Vigorous, high impact, weight bearing exercises promote osteogenesis in adolescents. Participating in football during puberty enhances bone adaptation.11 However, adaptations are often site-specific. Participants in sports such as gymnastics, have greater site specific markers of bone health compared to football players.1 Whilst not backed by evidence, participating in a variety of sports, thus varying site-specific
osteogenic adaptations observed across sports, in theory can mitigate BSI risk.4
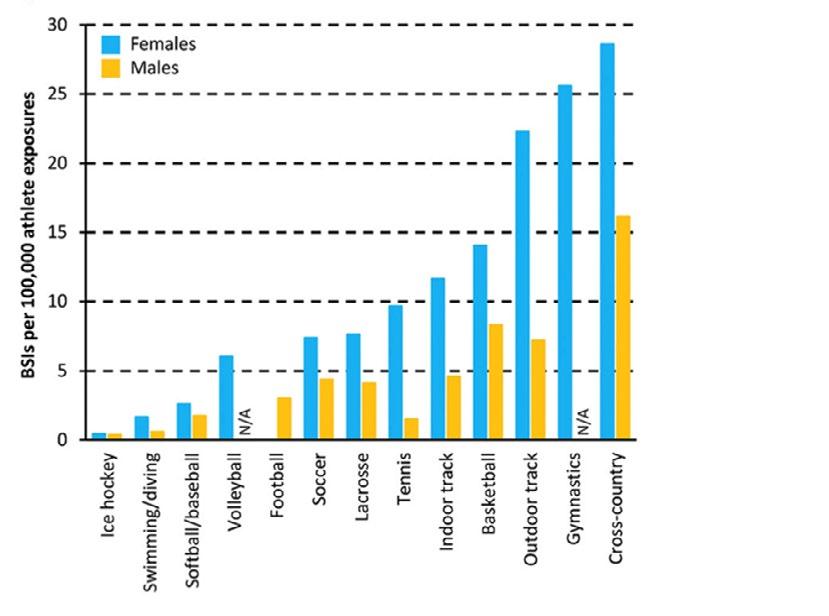
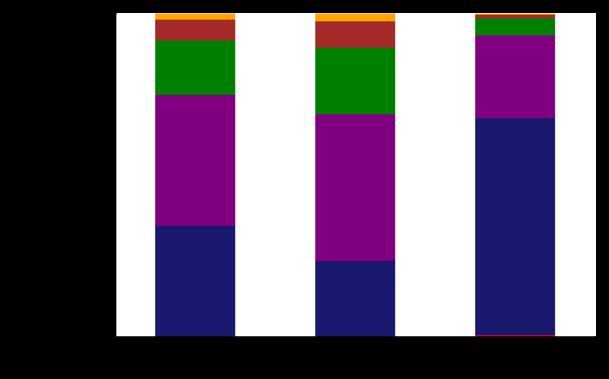
High impact sports induce greater osteogenic potential compared to nonimpact sports.1 However, individuals participating in sports such as basketball, gymnastics and football experience higher BSI rates (see figure 1).46 A clear paradox is evident here, with high impact sport participation protecting and contributing to BSI.15 Whilst the relationship between training volume and BSI is highly dependent on individual characteristics, performing higher training volumes increases injury risk.4 Currently a lack of evidence exists describing the number of training hours linked to BSI,4 yet, delaying early specialisation and limiting yearround participation in the same sport can mitigate risk.4
Via jump-based interventions:
Bone responds best to supraphysiological loads involving high impact, strain and magnitude exercises. Whilst jumping/ plyometrics, a method providing high strain/ impact loading, induces positive skeletal adaptations in adolescents,12 excessive volumes without appropriate rest, reduces the number of loading cycles required to failure.
Strain detection and bone adaptation peaks during early phases of sessions, requiring high impact/strain exercises to be performed during the first part of sessions to maximise adaptive response18 Following 20-40 loading cycles, bones lose up to 95% of mechanosensitivty, limiting Short duration loading should be adopted, with extended durations of loading not leading to proportional increases in bone adaptation.43 Further maximising adaptation, during high impact jumping, bone formation responses increase following longer rest periods between repetitions (10-30s v 1-3s).33 During cyclical loading, fluid flow exhibits an initial peak, reducing each subsequent cycle.37 Rest between repetitions, allowing for fluid flow restoration, stimulates osteocytes to a greater extent increasing osteogenic
Whilst extrapolated from animal studies, bone mass increases more following the take-off phase in comparison to the landing During running, peak tibial ground reaction forces (GRF) typically equate to 2-3 x BW. In contrast, peak tibial Such discrepancies can be attributed to muscle exerting forces on bone above and beyond those It is suggested that during jumping mechanical stress applied
Figure 1: Incidence rates of BSI across different sporting populations47
by muscular contraction is more osteogenic compared to GRF.22 During running, cueing individuals to reduce GRF, increases overall leg loading.2 Similarly, attempting to reduce GRF during landing increases internal loading and bone bending moments.29 With muscular contraction inducing greater bone loading, whilst counter-intuitive, attempting to reduce GRF by cueing softer landings may increase bone loading.
Via periodisation:
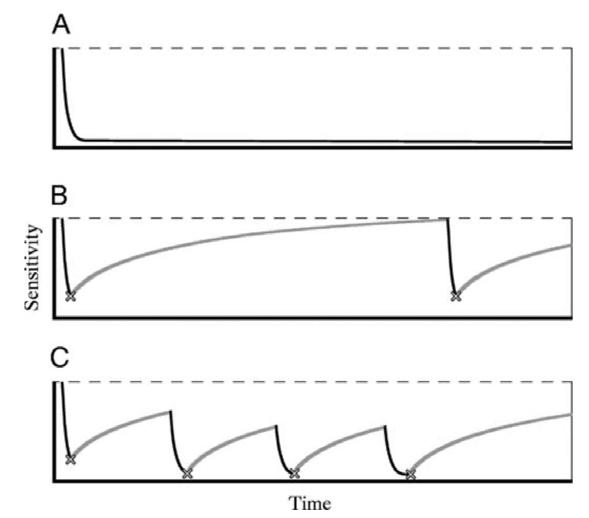
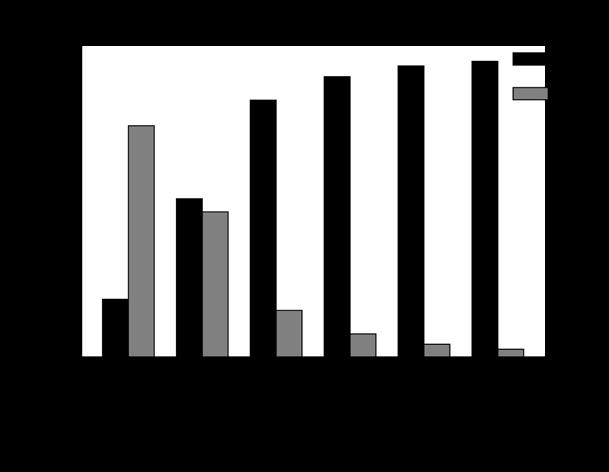
Following adaptations to a new training stimulus, bones lose sensitivity to routine loading.34,43 Periodisation of loading can improve bone cell mechanosensitivty.45 Considering daily periodisation, restoring full mechanosensitivity within bone cells following loading requires 4-8 hours between bouts (see figure 2).6, 33 It is suggested that after a loading bout, the re-organisation process of the actin cytoskeleton reduces the effectiveness of mechanical load detection, taking 8 hours to return to its pre-stimulated state.33
Longer term, plateauing/decreases in bone formation following a new loading stimulus after 15 days43 and 16-18 weeks have been observed.7 As established, with the greatest osteogenic potential being observed during the first part of the day/session, similar findings are observed within training blocks. When sequentially progressing a loading program, earlier phases induce greater adaptations, with osteogenic potential reducing over time. Bone mechanosensitivity can be restored with appropriate de-loading. Within animal studies, a de-load period of 5 weeks following a 5-week loading period, restored mechanosensitivty, increased bone formation and increased fracture resistance.34
Via nutrition:
Nutrition significantly influences bone health. Low energy availability (LEA), a mismatch between dietary energy intake and exercise energy expenditure energy, has a prevalence of 22-58% in athletes,26 reducing markers of bone health and increasing BSI risk.16 Individuals with BSI in anatomical sites with increased trabeculae bone content (pelvis, sacrum, and lumbar spine) display lower BMD values compared to those with cortical BSI.41 Previous BSI within trabeculae rich sites resulted in a 4.6-fold increase in low BMD compared to individuals with cortical BSI.41 Such is the significance of LEA on bone health, specifically within trabeculae rich sites, it is suggested that BSI cannot be managed appropriately without addressing deficiencies.23
As adolescents progress through academy football, significant increases in training energy expenditure (TEE) occur, with some individuals having TEE greater than adult
Figure 2: Reduction in mechanosensitivity following bouts of exercise. A) Mechanosensitivity following no recovery. B) Full restoroation of mechanosensitivity with prolonged recovery. C) Gradual reduction in mechanosensitivity with limited recovery33
players within the EPL.17 Academy players have been observed to have calorie deficits in excess of >1000 calories,17 with some individuals having difficulties matching energy intake with energy expenditure. Increases in energy intake enhance bone formation markers,31 with energy deficient diets increasing bone resorption markers.38 Energy intake recommendations within academy football players suggest 6-8g/kg of CHO, 1.5-2.5g/kg of Fat, and 2g/kg of protein, as an ideal starting point, with key stakeholders being made aware of the energy expenditure demands.17
Reducing Skeletal damage accumulation:
During transitional periods: BSI typically occur 3-4 weeks following major changes in workload.46 Within cancellous bone, bone resorption occurs over a 30–40day period, followed by bone formation over a 150-day period, leading to a 200-day remodelling cycle.10 This process is shorter within cortical bone, with remodelling periods lasting 120 days.10 During the initial period of bone resorption, increased porosity within bone is evident, reducing fatigue resistance.13 With increases in intensity and volume of training when transitioning (off-season to pre-season, post injury, moving up age
groups), early phase remodelling may be stimulated. With reductions in bone structural integrity, appropriately progressing bone loading prior to, or during early transition phases, is important to mitigate BSI risk.45
Within engineering, material fatigue life reflects the number of repetitive loading cycles that can be tolerated prior to failure.8 Stress life plots (S-N curves), utilised to demonstrate this, are expressed as an exponential relationship between applied stress and number of cycles to failure within materials.30 Biological tissues, sharing similar properties, experience considerable changes in the number of cycles to fatigue, following small changes in magnitude.8 Within animals, reducing applied stress by 10% in running, increased the number of cycles to failure by 100%.8 Increases in load magnitude result in exponential increases in bone fatigue, with a one-one relationship existing when considering increases in volume.46 Maintaining distance but reducing running speeds from 3.5 to 2.5m/s, significantly reduced BSI risk within the tibia.9
Whilst progressing volume prior to intensity manages the exponential increase in bone fatigue, bones can become “deaf” to repetitive loading.46 Individuals participating in repetitive sports such as
distance running, have lower markers of bone health compared to participants in multidirectional sports.40 With bone cells failing to respond after just a few minutes of cyclical, unidirectional loading,46 it could be suggested that repetitive, linear based loading, focussed on accumulating volume, may fail to induce optimal bone adaptation.
Limitations
Hereditary Factors:
Bone health is primarily determined by heritable factors. 60-80% of peak bone mass is genetically pre-determined.19 The genetic influence on bone health is evident
during childhood/puberty, accounting for differences in bone health across population groups.25. Research has suggested a potential genetic pre-disposition to stress fractures.44 Whilst attempting to maximise bone adaptation via physical activity and diet, the importance of genetic/hereditable components cannot be underestimated.
Monitoring:
Commercial wearables attempt to understand/predict overuse injuries by measuring GRF, with increases in GRF assumed to increase bone loading.27 Magnitude of GRF however, fail to reflect the forces experienced by the tissue.27
Despite being unable to capture internal loads placed on bone, surrogate markers such as GPS are utilised to infer bone loading.35 Whilst frequently used, limited research associating GPS metrics with bone load exists.35
Study Heterogeneity:
Bone research advancements have relied upon the utilisation of animalbased research. However, large inherent differences amongst species limit direct translation of interventions.39 A number of recommendations from this review are extrapolated from animal studies22,33,34 becoming a key limitation.
Conclusion
BSI lead to significant periods of time loss for youth athletes. Practitioners should focus on maximising bone adaptation via exercise/nutrition, and aim to reduce skeletal damage accumulation. Practitioners can utilise some of the key take home messages above to help mitigate risk of BSI, and help develop robust skeletons in youth developmental athletes.
Take Homes
• Delaying early specialisation during youth and encouraging athletes to participate in multi-sports can help develop a stronger/ more robust skeleton.
• Providing youth athletes with periods of rest, and limiting year-long participation in one sport, can mitigate risk of BSI.
• Bone responds best to low volume, high impact, high strain exercises (i.e jumping). Bone mechanosensitivity is reduced after just 20-40 loading cycles.
• Performing high impact/strain exercises at the beginning of sessions maximises mechanoadaptation. Providing periods of rest between loading bouts (4-8 hours) can also enhance adaptation.
• Chronic reductions in mechanosensitivity occur. Providing periods of off-loading during meso/macrocycles can restore bone mechanosensitivity.
• Ensuring players are meeting dietary intake requirements is fundamental in reducing risk of BSI in areas with increased trabeculae bone content.
• Magnitude of loading increases bone fatigue exponentially quicker than volume of loading. Progressing training volume prior to intensity during transitional phases could mitigate BSI risk.
References
1. Agostinete, R.R., Vlachopoulos, D., Werneck, A.O., Maillane-Vanegas, S., Lynch, K. R., Naughton, G., and Fernandes, R. A. Bone accrural over 18 months of participation in different loading sports during adolescence. Archives of Osteoporosis, 15: 1-10. 2020
2. Baggaley, M., Willy, R.W., and Meardon, S. A. Primary and secondary effects of real-time feedback to reduce vertical loading rate during running. Scandinavian Journal of Medicine and Sport Science, 27: 501-507. 2016
3. Baxter-Jones, A. D., Faulkner, R. A., Forwood, M. R., Mirwald, R. L., and Bailey, D. A. Bone mineral accrual from 8 to 30 years of age: an estimation of peak bone mass. Journal of bone and mineral research: the official journal of the American Society for Bone and Mineral Research, 26 ,1729–1739. 2011.
4. Beck, B. and Drysdale, L. Risk factors, diagnosis and management of bone stress injuries in adolescent athletes: A narrative review. Sports, 9: 52. 2021
5. Bonjour, J.P., Chevalley, T., Ferrari, S., and Rizzoli, R. (2009) The importance and relevance of peak bone mass in the prevalence of osteoporosis. Salud publica de Mexico, 51: 5-17. 2009.
6. Burr, D.B., Robling, A.G., and Turner, C.H. Effect of biomechanical stress on bones in animals. Bone. 30: 781-786. 2002.
7. Cullen, D.M., Smith, R.T. and Akhter, M.P. Bone-loading response varies with strain magnitude and cycle number. Journal of applied physiology, 91: 1971-1976. 2001
8. Edwards, W. B. Modelling overuse injuries in sport as a mechanical fatigue phenomenon. Exercise and Sport Science Reviews, 46: 224-231. 2018.
9. Edwards, W.B., Taylor, D., Rudolphi, T.J., Gillette, J.C., and Derrick, T.R. Effects of running speed on a probabilistic stress fracture model. Clinical biomechanics, 25: 372–377. 2010.
10. Eriksen E. F. Cellular mechanisms of bone remodelling. Reviews in endocrine & metabolic disorders, 11: 219–227. 2010.
11. Fredericson, M., Chew, K., Ngo, J., Cleek, T., Kiratli, J.M., and Cobb, K. Regional bone mineral density in male athletes: a comparison of soccer players, runners and controls. British journal of sports medicine, 41: 664-668. 2007.
12. Gómez-Bruton, A., Matute-Llorente, Á., González-Agüero, A., Casajús, J.A., & Vicente-Rodríguez, G. Plyometric exercise and bone health in children and adolescents: a systematic review. World journal of pediatrics, 13: 112–121. 2017.
13. Greeves, J.P., Beck, B., Nindl, B.C., and O’Leary, T.J. Current risk factors and emerging biomarkers for bone stress injuries in military personnel. Journal of Science and Medicine in Sport, 26: 14-21. 2023.
14. Gross, T.S., and Srinivasan, S. Building bone mass through exercise: could less be more? British journal of sports medicine, 40: 2-3. 2006.
15. Guerriere, K.L., Castellani, C.M., Popp, K.L., Bouxsein, M.L and Hughes, J.M. Unravelling the physiologic paradoxes that underlie exercise prescription for stress fracture prevention. Experimental Biology and Medicine, 247: 1833-1839. 2022.
16. Hamstra-Wright, K.L., Huxel Bliven, K.C., and Napper, C. Training load capacity, cumulative risk, and bone stress injury: A narrative review of a holistic approach. Frontiers in sports and active living, 3: 665683. 2021.
17. Hannon, M.P., Carney, D.J., Floyd, S., Parker, L.J., McKeown, J., Drust, B., Unnithan, V.B., Close, G.L. and Morton, J.P. Cross-sectional comparison of body composition and resting metabolic rate in Premier League academy soccer players: Implications for growth and maturation. Journal of Sports Sciences, 38: 1326-1334. 2020.
18. Hart, N.H., Nimphius, S., Rantalainen, T., Ireland, A., Siafarikas, A., and Newton, R. U. Mechanical basis of bone strength. Influence of bone material, bone structure and muscle action. Journal of musculoskeletal and neuronal interactions, 17: 114-139. 2017.
19. Heaney, R.P., Abrams, S., Dawson-Hughes, B., Looker, A., Marcus, R., Matkovic, V. and Weaver, C. Peak bone mass. Osteoporosis international, 11: 985. 2000.
21. Ireland, A., Rittweger, J., and Degens, H. The influence of muscular action on bone via strength exercise. Clinical reviews in Bone and Mineral Metabolism, 12: 93-102. 2014.
22. Ju, Y.I., Sone, T., Ohnaru, K., Tanaka, K., Yamaguchi, H. and Fukunaga, M. Effects of different types of jump impact on trabecular bone mass and microarchitecture in growing rats. PLoS One, 9: p.e107953. 2014.
23. Kim, D.R. and Weber, K. Relative Energy Deficiency in Sport (RED-S) and Bone Stress Injuries. Operative Techniques in Sports Medicine, 31: 151025. 2023.
24. Langdahl, B., Ferrari, S., and Dempster, D.W. Bone modelling and remodeling: potential as therapeutic targets for the treatment of osteoporosis. Therapeutic advances in musculoskeletal disease, 8: 225-235. 2016.
25. Levine, M.A. Assessing bone health in children and adolescents. Indian Journal of Endicrinology and Metabolism, 16: 205-212. 2012.
26. Logue, D.M., Madigan, S.M., Melin, A., Delahunt, E., Heinen, M., Donnell, S.M., and Corish, C.A. Low Energy Availability in Athletes 2020: An Updated Narrative Review of Prevalence, Risk, Within-Day Energy Balance, Knowledge, and Impact on Sports Performance. Nutrients, 12: 835. 2020.
27. Matijevich, E.S., Branscombe, L.M., Scott, L.R., & Zelik, K.E. Ground reaction force metrics are not strongly correlated with tibial bone load when running across speeds and slopes: Implications for science, sport and wearable tech. PloS one, 14: e0210000. 2019.
28. Milanovic, Z., Covic, N., Helge, E.W.M., Krustrup, P., and Mohr, M. Recreational football and bone health: A systematic review and metaanalysis. Sports Medicine, 52: 3021-3037. 2022.
29. Mills, C., Pain, M.T,G., and Yeadon, M.R. Reducing ground reaction forces in gymnastics landings may increase internal loading. Journal of Biomechanics, 42: 671-678. 2009.
30. Murakami, Y., Takagi, T., Wada, K. and Matsunaga, H. Essential structure of SN curve: Prediction of fatigue life and fatigue limit of defective materials and nature of scatter. International Journal of Fatigue, 146: 106138. 2021.
31. O’Leary, T.J., Wardle, S.L. and Greeves, J.P. Energy deficiency in soldiers: the risk of the athlete triad and relative energy deficiency in sport syndromes in the military. Frontiers in nutrition, 7: 142. 2020.
32. Raggatt, L.J., and Partridge, N.C. Cellular and molecular mechanisms of bone remodelling. Journal of Biological Chemistry, 285: 2510325108. 2010.
33. Robling, A.G., Burr, D.B., and Turner, C.H. Recovery periods restore mechanosensitivity to dynamically loaded bone. The Journal of experimental biology, 204: 3389–3399. 2001.
34. Saxon, L.K., Robling, A.G., Alam, I., and Turner, C.H. Mechanosensitivity of the rat skeleton decreases after a long period of loading but is improved with time off. Bone, 36: 454–464 (2005).
35. Scott, R., James, R., Barnett, C.T., Sale, C., & Varley, I. Perspectives from research and practice: A survey on external load monitoring and bone in sport. Frontiers in sports and active living, 5: 1150052. 2023.
36. Smalley, B., Bishop. C., and Maloney, S.J. “Small steps or giant leaps?” Comparing game demands of U23, U18, and U16 English academy soccer and their associations with speed and endurance. International Journal of Sports Science & Coaching, 17: 134-142. 2022.
37. Srinivasan, S., Weimer, D.A., Agans, S.C., Bain, S.D., and Gross, T.S. Low-Magnitude Mechanical Loading Becomes Osteogenic When Rest Is Inserted Between Each Load Cycle. Journal of bone and mineral research, 17: 1613-1620. 2002.
38. Taguchi, T., and Lopez, M.J. An overview of de novo bone generation in animal models. Journal of orthopaedic research: official publication of the Orthopaedic Research Society, 39: 7–21. 2021.
39. Taguchi, M., Moto, K., Lee, S., Torii, S., and Hongu, N. Energy Intake Deficiency Promotes Bone Resorption and Energy Metabolism Suppression in Japanese Male Endurance Runners: A Pilot Study, American journal of men’s health, 14: 1557988320905251. 2020.
40. Tenforde, A.S., and Fredericson, M. Influence of Sports Participation on Bone Health in the Young Athlete: A Review of the Literature. PM&R, 3: 861-867. 2011.
41. Tenforde, A.S., Parziale, A.L., Popp, K.L., and Ackerman, K.E. Low bone mineral density in male athletes is associated with bone stress injuries at anatomic sites with greater trabecular composition. The American journal of sports medicine, 46: 30-36. 2018.
42. Turner, C.H., and Pavalko, F.M. Mechanotransduction and functional response of the skeleton to the physical stress: The mechanisms and mechanics of bone adaptation. Journal of Orthopaedic Science, 3: 346-355. 1998b
43. Turner, C.H., Woltman, T.A., and Belongia, D.A. Structural changes in rat bone subjected to long-term, in vivo mechanical loading. Bone, 13: 417–422. 1992.
44. Varley, I., Greeves, J.P., Sale, C., Friedman, E., Moran, D.S., Yanovich, R., Wilson, P.J., Gartland, A., Hughes, D.C., Stellingwerff, T., Ranson, C., Fraser, W.D., and Gallagher, J.A. Functional polymorphisms in the P2X7 receptor gene are associated with stress fracture injury, Purinergic signalling, 12: 103-113. 2016.
45. Warden, S.J., Hoenig, T., Sventeckis, A.M., and Ackerman, K. E. Not all bone overuse injuries are stress fractures: it is time for updated terminology. British Journal of Sports Medicine, 57: 76-77. 2022.
46. Warden, S.J., Edwards, W.B., and Willy, R.W. Optimal load for managing low-risk tibial and metatarsal bone stress injuries in runners. The science behind the clinical reasoning. The Journal of Orthopaedic and Sports Physical Therapy, 51: 322-330. 2021
47. Warden, S.J., Edwards, W.B., and Willy, R.W. Preventing bone stress injuries in runners with optimal workload. Curr Osteoporos Rep. 19(3): 298-307. 2021.
BACK IN THE GAME: NAVIGATING FOOTBALL AFTER PREGNANCY
FEATURE / JENNA SCHULZ, MPT, PHD
Introduction
Alex Morgan (below). Sydney Leroux. Sarah Björk. These women are a few of the growing number of athletes who are returning to elite level of football postpartum. Until recently, it was generally accepted that women had to choose between sport participation and starting a family. While there is an increasing number of athletes returning to sport postpartum, there are many data gaps that still exist, and new evidence is constantly emerging. Furthermore, female athletes have specific biological, sociocultural and environmental considerations that could impact sport and health outcomes.1 While there is limited evidence on return to football postpartum, this article will apply current research, policy and clinical outcomes in return to activity/sport postpartum with a football lens.
Training during pregnancy
The World Health Organization (WHO) recommends 150 minutes of moderatevigorous activity throughout pregnancy, over a span of at least three days, incorporating a variety of resistance and aerobic exercises.2 Physical activity during pregnancy is safe and beneficial for both mom and baby, with many documented mental and physical health benefits.3,4
In 2016, the International Olympic Committee (IOC) published a summary of research in recreational and elite-level athletes. Baring contraindications (e.g. pre-eclampsia, hypertension), women can continue exercise while monitoring for symptoms (e.g. vaginal bleeding, frequent contractions).4 However, sports with contact/collision and sudden deceleration pose a potential risk to the fetus.4 Therefore, football players can still focus
on aerobic and resistance training, as well as football skills (i.e. passing, dribbling, shooting), but should avoid contact situations while pregnant.
In elite athletes specifically, a systematic review demonstrated that engaging in competitive sport before pregnancy resulted in a low reduction in the odds of pregnancy-related low back pain, but no difference between elite athletes and controls in terms of other pregnancyrelated outcomes (low birth weight, incontinence, pelvic girdle pain, maternal depression/anxiety etc.).5 A qualitative study on athlete’s experiences with navigating training during pregnancy highlighted many significant decisions athletes must make.6 For instance, many participants revealed they struggled with the societal norm of choosing between being an athlete or becoming pregnant. Other themes such as pregnancy planning, pregnancy disclosure and discrimination, training pregnant, safety concerns and support/funding were all shared experiences.6 Similarly, coaches and healthcare professionals provided their experiences with working with pregnant and postpartum elite athletes.7 Common themes included lack of female athlete reproductive research, need for evidenceinformed education and training, need to develop evidence-based progression for sport participation, open communication to support athlete-centred care and essential supports and changes required for pregnant/postpartum athletes.7 Therefore, it is essential to improve sport policy, clinician education and athlete resources when navigating training during pregnancy.
Postpartum return to sport
Often, women are given the “green flag” to return to activity at six weeks postpartum, despite undergoing significant physical, physiological and psychological changes throughout and beyond pregnancy. Some of these changes throughout and post pregnancy include cardiovascular changes, musculoskeletal changes, loss of bone mass and mental health concerns (such as postpartum depression).8 Despite these changes, there is minimal guidance regarding the
management of postpartum concerns that arise in active women. For instance, one study demonstrated that once athletes receive medical clearance to resume training, they report being left without direction for training decisions.9 A recent systematic review also demonstrated that elite athletes return to activity in the early postpartum may have an increased risk of injury.10
A scoping review on guidelines for return to activity/sport postpartum showed that only 11 of 36 studies had specific return to sport guidelines, and only six studies considered the importance of mental health.11 Furthermore, significant factors that influence a successful return to sport postpartum include recovery time, time to manage motherhood and sport demands, sport organisation policies, stereotypes and social support.12 Therefore, there is a need to improve research, clinical practice and policy in order to improve outcomes for athletes looking to return to sport postpartum.
Traditional return to sport frameworks following musculoskeletal injury or surgery involve assessing both physical and mental readiness. Managing postpartum return to sport should be thought of in a similar manner,13 and some frameworks exist to help guide this process.14,15 A whole-systems, biopsychosocial approach beyond the musculoskeletal system (i.e. physical deconditioning, changes to body mass, sleep, breastfeeding, relative energy
deficiency in sport (REDs) postpartum fatigue and thyroid autoimmunity, fear of movement, psychological well-being and socioeconomic considerations) should be considered.16 Furthermore, less of an emphasis should be placed on true timelines, and athletes should progress to the next phase once tolerance, confidence, goals and symptoms indicate.14 Additionally, a multidisciplinary team of all stakeholders involved (athlete, coach, healthcare professionals etc.) should be engaged in this process, to facilitate open communication and support athletecentred care.7
Before beginning any exercise, medical clearance should be sought from a medical professional with expertise in female athletes/women’s health (i.e. pelvic health physiotherapist, gynaecologist, family medicine or sport medicine physician).14 Further, before progressing to the next stage, athletes should be screened for any risk factors such as pelvic floor dysfunction, REDs and postpartum depression.14 Some useful screening tools include the REDs Clinical Assessment Tool-2 (REDs CAT2)17 and the Pelvic Floor Dysfunction-ScrEeNing Tool IN fEmale athLetes (PFD-SENTINEL).18 At any point in the return to sport process, an athlete can return to the previous stage if symptoms (i.e. incontinence, pelvic girdle pain, excessive bleeding, fatigue, poor muscular control etc.) are present.14
We have developed a five-step framework
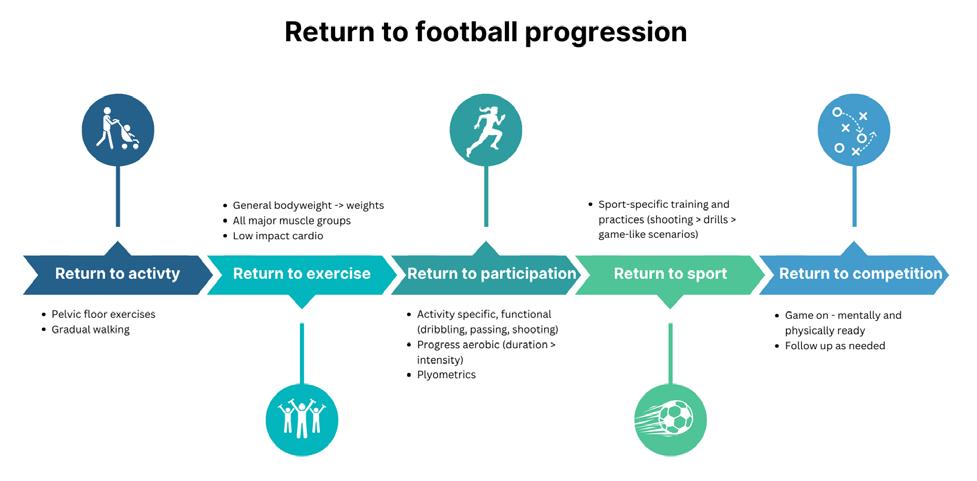
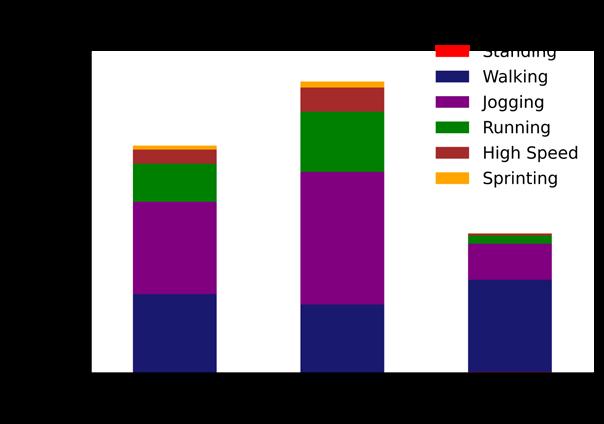
for clinicians and athletes14 based off the results of a scoping review evaluating recommendations for return to activity/ sport postpartum.11 Below we will summarize this framework with specific football-related exercises (Figure 1).
Step 1: Return to activity
Return to activity can begin in the early stages of postpartum. This can begin with pelvic floor muscle training. A gradual return to walking may begin as well, starting with 10 minutes/day and increasing by five minutes/week.
Step 2: Return to exercise
Return to exercise can begin with general bodyweight strength training, and progress to weighted exercises of all major muscle groups. Pertinent muscles for football players would include quads, hamstrings, calves, glutes and core, so exercises such as squats, glute bridges, lunges, hamstring curls etc. can be introduced. Low impact cardio (i.e. cycling, swimming, elliptical) can also be introduced.
Step 3: Return to participation
Activity specific, functional exercises can start being added during this stage (i.e. passing, dribbling and shooting). Aerobic fitness should also be progressed, but duration should always be increased before intensity. For instance, returning to long, easy jogs before adding in sprinting
Figure 1: An example of a return to football progression for postpartum athletes. Adapted from Schulz & Thornton (2024).14
drills. It is important to continue to build strength, and high-intensity exercises such as plyometrics should also be worked into the routine.
Step 4: Return to sport
Return to sport specific training and practices, progressing intensity. For example, starting with just attending shooting practices first, then work into offensive/defensive practices and finally scrimmage-like scenarios. It is important to ensure this is goal specific.
Step 5: Return to competition
This is where the athlete is ready to compete, but make sure they are both mentally and physically ready for competition. The athlete should always follow up with a knowledgeable healthcare professional if they are exhibiting signs and symptoms here, and at any stages.
Conclusion
There are many reported positives and success stories from elite athletes returning to competition after giving
birth. As athletes adjust to their new dual identity, they have reported gaining a sense of pride, motivation, resilience and newfound enjoyment for their sport. Furthermore, their children provide strong motivation to succeed on and off the field of play.12,19,20 Some progress is being made thanks to the advocacy of athletes such as Sarah Björk. FIFA recently announced new protocols to support players during pregnancy and through postpartum, which involves giving players a minimum of 14 weeks paid maternity leave. However, if we truly want to support female athletes, then we all play a crucial role. It is important as clinicians, coaches, researchers and sport organisations that we continue to develop guidelines to aid in this process, and provide a supportive environment for these athletes to excel in. By doing this, we can promote longevity in sport for female athletes, and living in a world where no one should have to chose between becoming a mother or remaining an athlete should be a priority.
Below are some examples of how we can improve the care for postpartum athletes (Figure 2).6,7,11
Clinicians
• Monitor and encourage activity throughout pregnancy and postpartum.
• Provide evidence-based, individualized recommendations and consistent follow up.
• Open communication to support athletecentred care, engage a multidisciplinary team.
• Ensure constant screening and focus on abilities, rather than timelines.
National
and international sport organisations
• Develop clear policies for pregnant and postpartum athletes, including funding.
• Improve training, education and support to athletes, coaches and medical professionals on training during pregnancy/postpartum.
• Increase visibility of athletes who have successfully navigated return to pregnancy and elite sport.
Researchers
• Conduct high-quality primary studies to inform evidence-based recommendations.
• Develop clinical practice guidelines for return to sport with multiple stakeholders (athletes, coaches, clinicians).
Figure 2: Recommendations for clinicians, researchers and sport organizations to improve return to football postpartum.
References
1. Moore IS, Crossley KM, Bo K, et al. Female athlete health domains: a supplement to the International Olympic Committee consensus statement on methods for recording and reporting epidemiological data on injury and illness in sport. Br J Sports Med. 2023;57:1164-1174. doi:10.1136/BJSPORTS-2022-106620
2. World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour.; 2020.
3. Dipietro L, Evenson KR, Bloodgood B, et al. Benefits of Physical Activity during Pregnancy and Postpartum: An Umbrella Review. Med Sci Sports Exerc. 2019;51(6):1292-1302. doi:10.1249/MSS.0000000000001941
4. Bø K, Artal R, Barakat R, et al. Exercise and pregnancy in recreational and elite athletes: 2016 evidence summary from the IOC expert group meeting, Lausanne. Part 1—exercise in women planning pregnancy and those who are pregnant. Br J Sports Med. 2016;50(10):571589. doi:10.1136/BJSPORTS-2016-096218
5. Wowdzia JB, McHugh TL, Thornton J, Sivak A, Mottola MF, Davenport MH. Elite Athletes and Pregnancy Outcomes: A Systematic Review and Meta-analysis. Med Sci Sports Exerc. 2021;53(3):534-542. doi:10.1249/MSS.0000000000002510
6. Davenport MH, Nesdoly A, Ray L, Thornton JS, Khurana R, Mchugh TLF. Pushing for change: a qualitative study of the experiences of elite athletes during pregnancy. Br J Sports Med. 2022;56:452-457. doi:10.1136/bjsports-2021-104755
7. Davenport MH, Ray L, Nesdoly A, Thornton JS, Khurana R, Mchugh TLF. Filling the evidence void: exploration of coach and healthcare provider experiences working with pregnant and postpartum elite athletes-a qualitative study. Br J Sports Med. 2023;0:1-7. doi:10.1136/ bjsports-2023-107100
8. Soma-Pillay P, Nelson-Piercy C, Tolppanen H, Mebazaa A. Physiological changes in pregnancy. Cardiovasc J Afr. 2016;27(2):89-94. doi:10.5830/CVJA-2016-021
9. Davenport MH, Ray L, Nesdoly A, et al. We’re not Superhuman, We’re Human: A Qualitative Description of Elite Athletes’ Experiences of Return to Sport After Childbirth. Sports Medicine. 2022;53(1):269-279. doi:10.1007/s40279-022-01730-y
10. Kimber ML, Meyer S, McHugh TL, et al. Health Outcomes after Pregnancy in Elite Athletes: A Systematic Review and Meta-analysis. Med Sci Sports Exerc. 2021;53(8):1739-1747. doi:10.1249/MSS.0000000000002617
11. Schulz JM, Marmura H, Hewitt CM, Parkinson LJ, Thornton JS. Navigating the ‘new normal’: what guidelines exist for postpartum return to physical activity and sport? A scoping review. Br J Sports Med. 2023;0:1-7. doi:10.1136/bjsports-2023-107166
12. Tighe BJ, Williams SL, Porter C, Hayman M. Barriers and enablers influencing female athlete return-to-sport postpartum: a scoping review. Br J Sports Med. 2023;57:1450-1456. doi:10.1136/bjsports-2023-107189
13. Schulz J, Hewitt C, Thornton J. Back on track: performing on the world stage after pregnancy. Aspetar Sports Medicine Journal. 2024;13(31):212-215. Accessed July 16, 2024. https://journal.aspetar.com/en/archive/volume-13-targeted-topic-sports-medicine-inathletics/back-on-track-performing-on-the-world-stage-after-pregnancy
14. Schulz JM, Thornton JS. Infographic. Return to activity/sport postpartum: a summary of current recommendations. Br J Sports Med. 2024;58(9):511-512. doi:10.1136/bjsports-2023-107856
15. Donnelly G, Moore I, Brockwell E, Rankin A, Cooke R. Reframing return-to-sport postpartum: the 6 Rs framework. Br J Sports Med. 2022;56:241-248. doi:10.1136/bjsports-2021-104461
16. Donnelly GM, Brockwell E, Rankin A, Moore IS. Beyond the Musculoskeletal System: Considering Whole-Systems Readiness for Running Postpartum. J Womens Health Phys Therap. 2022;46(1):48-56. doi:10.1097/jwh.0000000000000218
17. Stellingwerff T, Mountjoy M, McCluskey WT, Ackerman KE, Verhagen E, Heikura IA. Review of the scientific rationale, development and validation of the International Olympic Committee Relative Energy Deficiency in Sport Clinical Assessment Tool: V.2 (IOC REDs CAT2)-by a subgroup of the IOC consensus on REDs. Br J Sports Med. 2023;57:1109-1118. doi:10.1136/bjsports-2023-106914
18. Giagio S, Salvioli S, Innocenti T, et al. PFD-SENTINEL: Development of a screening tool for pelvic floor dysfunction in female athletes through an international Delphi consensus. Br J Sports Med. 2023;57:899-905. doi:10.1136/bjsports-2022-105985
19. Appleby KM, Fisher LA. “Running in and out of Motherhood”: Elite Distance Runners’ Experiences of Returning to Competition after Pregnancy. Women Sport Phys Act J. 2009;18(1):3-17. doi:10.1123/WSPAJ.18.1.3
20. Palmer FR, Leberman SI. Elite athletes as mothers: Managing multiple identities. Sport Management Review. 2009;12(4):241-254. doi:10.1016/j.smr.2009.03.001
INTEGRATING FORCE PLATE TECHNOLOGY INTO ELITE FOOTBALL: PERFORMANCE
OPTIMISATION AND REHABILITATION
Force plates serve as valuable tools for analysing the kinetic characteristics of human movement. They have traditionally been more prevalent and well suited to high-performance environments. However, there has been a shift whereby strength and conditioning coaches, physiotherapists and sports clinicians within the private sector have integrated the technology to greater objectify and provide insights into an individual’s athletic capacities, force generation capabilities and support the overall rehabilitation and return-to-play process.
Despite the increasing use of force plates, the selection of metrics remains a challenge due to the vast array of options available, over 100 metrics, in fact. This abundance can be overwhelming, leaving practitioners unsure of which metrics to choose in order to effectively quantify performance. Not all metrics offer the same level of reliability; some exhibit greater variance and sensitivity than others. Therefore, the primary goal of this article is to transparently outline our approach to integrating force plates into our environment with a primary focus on the metrics I analyse for performance and rehabilitation.
Without data you’re just another person with an opinion
Incorporating force plates into your toolbox can significantly enhance various aspects of performance and rehabilitation. However, if you are only concerned about performance output, for example jump height, then you miss opportunities and insights into the forces involved in bringing about task specific contractions which is crucial information when seeking to make adaptations.
By leveraging force plates, you can:
• Refine performance profiling: Gain a deeper understanding of an athlete’s movement strategies, force production and power outputs. This nuanced data allows for benchmarking and setting training objectives which will address specific strengths and weaknesses.
• Monitoring: Track changes in force production to determine programme effectiveness and inform fatigue and recovery status. Early detection can prompt adjustments to programming, training loads and recovery strategies, leading to optimised “freshness” and decreased risk of injury.
• Rehabilitation: Establish evidencebased criteria to safely progress through rehabilitation phases when clinical milestones have been met. This criteria-based approach ensures that progression does not surpass the functional capacity of the injured structure. Quantifying force output, symmetry, landing mechanics, and dynamic stability to support players getting back to optimal performance in the fastest yet safest possible way.
Theory is great, but until it’s put into practice it’s useless.
Which test(s) you choose to employ must align with the specific context of your environments and most importantly, they must address the questions you seek answers to.
• Is the athlete strong relative to specific joint positions?
• Are they powerful?
• How quickly can they express force?
• What component of the task or contraction mode requires specific attention?
• How elastic are they?
• Do they have loading preferences/ asymmetries?
• What strategies do they employ?
• How does this compare to historical/ normative data?
• How are they adapting/responding to load/imposed stimulus?
• Are they meeting rehab specific entry and exit criteria?
• Are they at increased risk?
These questions are constantly on my mind as I strive to find the answers that will help aid program design and support the multidisciplinary team and players to excel within our environment.
First Team Strength & Conditioning Coach, PSV Eindhoven
In figure 1, you will discover the assessments conducted throughout the 2023/2024 season, aimed at answering some of the aforementioned questions.
Metrics that matter
It is beyond the scope of this article to dive into great detail on every single test or metric. However, my aim is to provide sufficient context specific information to offer a thorough understanding of the thought processes and rationale for including specific metrics for analysis during the key phases of the countermovement jump (CMJ).
Eccentric peak velocity
A key metric that sets the tone for the rest of the jump. Increased peak velocity results in greater ground reaction forces and elastic energy storage which help better potentiate the concentric phase of the jump. Cohen et al2. refer to a threshold of >1.2ms being acceptable with o.6ms for unilateral CMJs. Thus, assessing how fast and how hard an athlete unloads can determine intent, movement strategy and athlete readiness.
Eccentric braking impulse and force at zero velocity
Eccentric braking impulse and force at zero velocity allows us to gauge how much force is generated up to the lowest portion of the squat. Greater deceleration ability is desirable, as it establishes a foundation for better performance during the concentric phase. Additionally, evaluating athletes’ preferences for loading and asymmetry analysis. Movement strategies, particularly during rehabilitation, can provide insights into confidence/ability to effectively load the injured area.
Eccentric duration
Used simultaneously with peak velocity but assessing time in relation to movement to determine movement strategy. Is the athlete unloading fast or slow? If slow, what are the implications?
Countermovement depth
This is a very good metric to include that can help determine changes within an athlete’s movement strategy and to determine the presence of any neuromuscular
fatigue. What range of motion (ROM) is an athlete working through? Are they shallow or are they deep? How does this affect output? Is this range different from “normal”? Larger ROM is typically associated with longer contraction times as athletes tend to want to muscle through the movement in order to create more time to develop higher concentric impulse to facilitate or maintain their jump height.
Concentric impulse & duration
Evaluating concentric force production involves assessing the force from zero velocity until take-off. The goal is to measure how much impulse an athlete can generate in a brief timeframe. Greater force application leads to increased power and speed. While a larger impulse is advantageous, it is crucial to minimise the time required to create said impulse. Speed of movement is the aim of the game.
Within this metric, it is also good to consider P1 and P2 to assess athlete
Figure 1: Benchmarking athlete assessment process
capabilities further. How much impulse can a player generate within the first 50% of the concentric phase in comparison to the second 50%? Can athletes essentially keep their foot on the gas and continually accelerate or do they start well and just maintain speed until take off?
Time to take off
Total time taken from the start of movement until take off. In football, the ability of players to execute highintensity actions in the shortest amount of time is advantageous and can significantly enhance the chances of sporting success. Assessing contraction times as a whole allows me to effectively determine and compare performance against strategy. Fantastic outputs are not effective if the efficiency is poor and athletes require extended periods of time to produce the same force.
Jump height (impulse-momentum)
This method, grounded in Newton’s laws, offers a dependable and reliable means of quantifying jump height. Considered the gold standard of measurement with intraclass correlation coefficient (ICC) of 0.88-0.97, it calculates the distance from the centre of mass at take-off to the apex of the jump, equating the potential energy at the jump’s peak with the kinetic energy at take-off. This approach circumvents numerous confounding variables encountered with the flight time method, such as uneven take-off and landing positions.1
Reactive strength index (RSI mod impmom)
RSI mod stands out as one of the most comprehensive metrics for evaluating jump performance, offering a concise snapshot of overall performance. It is closely linked to the flight time to contraction time ratio, measuring both the height and speed components of the jump. Since RSI is a ratio metric, made up of two parts and it is crucial to dissect its two components to understand performance changes. Deviations in either direction can result in similar performance outputs, emphasising the need for careful analysis.
Landing phase
In the final phase of the CMJ sequence, we observe the forces exerted on the system upon landing. When analysing the data, I do not assess the landing phase in isolation. Instead, I use it in combination with the eccentric phase to identify any key relationships that may be present. Landing is highly dependent on ability and strategy. High peak landing forces may suggest a stiff landing, which
Figure 2: Specific force plate strength and power assessments commonly utilised within performance and rehabilitation (adapted)3
Posterior chain assessments, *dependent on graft type
DL/ SL Countermovement jump
Squat jump
DL/SL 10-5 hop, drop jump RSI
Hop+hold dynamic stability *time to stabalisation
Fractures (injury mechanism specific, ie. stress or trauma)
Iso squat/mid-thigh pull/knee iso push
Iso soleus/ankle iso push
Iso posterior chain
DL/SL Countermovement jump
Squat jump
DL/SL 10-5, drop jump RSI
Hop+hold dynamic stability *time to stabalisation
could be a compensation strategy for inadequate eccentric strength, limiting the ability to load eccentrically with intensity and speed. This information can then help guide decisions relating to injury risk mitigation as well as setting adequate performance goals.
Rehabilitation
Rehabilitation presents unique contextual considerations where injury specific tests for strength, power and symmetry diagnostics play a crucial role in determining phase progression during
return to sport. While performance testing often works towards achieving aspirational standards, rehabilitation testing adopts a more process orientated approach. It prioritises readiness to progress and a return to baseline prior to transitioning the focus towards performance and aspirational benchmarks.
Figure 2, presents specific force plate assessments which can be utilised to support both rehabilitation and performance3
Typically, following a soft tissue injury the initial focus is on specific isolated work, often involving submaximal isometric contractions. Collaborating with our medical professionals, the force plates can then be utilised to assess a player’s current physical capacity and strength levels. For instance, in the case of returning to play after a hamstring injury, force plates may be employed to conduct the McCall test8 or various other run-specific isometric tests (see Figure 3) to measure peak force, rate of force development (RFD) at particular time points and limb symmetry. Despite isometric training primarily serving as an introduction to loading when other contraction measures are unsuitable, I continue to integrate isometrics as a training modality due to the numerous unique advantages. Plus there is evidence suggesting that there is an isometric component that is relevant during high speed running4 with rate of force development also being linked to sprint performance.6
To provide another example, Kotsifaki et al recently authored an insightful article in the British Journal of Sports Medicine5 regarding optimal tests for assessing knee function post anterior cruciate ligament (ACL) reconstruction. Authors found that at the time of return to sport, athletes who tested on the force plate still present with whole body biomechanical asymmetries, despite passing discharge criteria from common clinical assessments. ACL reconstruction athletes achieved 97% symmetry within horizontal performance tests (hop distance) but only 83% and 77% symmetry in vertical performance tests (jump height and RSI). These findings suggest that vertical performance metrics such as jump height and contraction times are more effective at detecting interlimb asymmetries than commonly used clinical tests and represent a compelling rationale for inclusion in return-toplay assessments.
Summary
Player availability and physical robustness, defined as keeping players injury-free and ready to participate in competition, is extremely important to elite sport teams. Fewer injuries are associated with overall success7, yet no matter how good your coaches’ eyes, we are unable to identify and
quantify specific physical qualities that may need improving to help support this cause. Integrating force plates technology can enable us to better profile, monitor, program and enhance our rehabilitation process, aligning with the company’s mission of achieving success.
Readers should note that I am not exclusively proposing these metrics as the only ones to be monitored. The main intention throughout this article was to illustrate some of my thought processes and how aforementioned metrics can complement each other and provide insights to help us answer the questions we have, in turn optimising player health, performance and physical robustness.
Key take home message
Force plates provide critical and instantaneous data to help us understand the kinematics and kinetics of human movement. They play a crucial role in objectifying and removing any guesswork within our performance or rehabilitation programs, making them indispensable tools. In order to best answer the questions, we have, different metrics may need to be utilised. Having an understanding of key metrics we utilise, how they can be used interchangeably in an elite football environment, may provide some additional clarity and support within your own environments when profiling, monitoring neuromuscular fatigue, or within the rehabilitation and return to play setting.
References
1. Xu, J., Turner, A., Comfort, P. et al. A Systematic Review of the Different Calculation Methods for Measuring Jump Height During the Countermovement and Drop Jump Tests. Sports Med 53, 1055–1072 (2023).
2. Cohen, Daniel & Burton, Adam & Wells, Carl & Taberner, Matt & Díaz, María & Graham-Smith, Philip. (2020). Single vs Double Leg Countermovement Jump Tests: Not half an Apple!
3. Taberner, Matt & Allen, Tom & Cohen, Daniel. (2019). Progressing rehabilitation after injury: Consider the ‘ control-chaos continuum’. British Journal of Sports Medicine. 53. bjsports-2018. 10.1136/ bjsports-2018-100157.
4. Hooren, Bas & Bosch, Frans. (2018). Preventing hamstring injuries - Part 2: There is possibly an isometric action of the hamstrings in high-speed running and it does matter. Sport Performance & Science Reports.
5. Kotsifaki A, Van Rossom S, Whiteley R, Korakakis V, Bahr R, Sideris V, Jonkers I. Single leg vertical jump performance identifies knee function deficits at return to sport after ACL reconstruction in male athletes. Br J Sports Med. 2022 May;56(9):490-498. doi: 10.1136/bjsports-2021-104692. Epub 2022 Feb 8.
6. Slawinski J, Bonnefoy A, Levêque JM, Ontanon G, Riquet A, Dumas R, Chèze L. Kinematic and kinetic comparisons of elite and well-trained sprinters during sprint start. J Strength Cond Res. 2010 Apr;24(4):896-905.
Jermaine is an accredited strength and conditioning coach and is currently working with the first team at PSV Eindhoven, where he brings a wealth of expertise. His educational background includes a BSc in Sports Rehabilitation and an MSc in Strength and Conditioning. Prior to his current position, Jermaine worked within the PSV Youth Programme as the lead academy and U23’s S&C coach and has gained valuable experience at Brentford F.C. and Arsenal Women F.C. This diverse professional background has equipped him with a comprehensive understanding of the distinct needs and demands of athletes from various demographics. Jermaine’s passion lies in maximising the physical and physiological potential of individuals and harnessing the adaptations that augment performance and rehabilitation.
7. Calleja-González J, Mallo J, Cos F, Sampaio J, Jones MT, Marqués-Jiménez D, Mielgo-Ayuso J, Freitas TT, Alcaraz PE, Vilamitjana J, Ibañez SJ, Cuzzolin F, Terrados N, Bird SP, Zubillaga A, Huyghe T, Jukic I, Lorenzo A, Loturco I, Delextrat A, Schelling X, Gómez-Ruano M, López-Laval I, Vazquez J, Conte D, Velarde-Sotres Á, Bores A, Ferioli D, García F, Peirau X, Martin-Acero R, Lago-Peñas C. A commentary of factors related to player availability and its influence on performance in elite team sports. Front Sports Act Living. 2023 Jan
8. McCall A, Nedelec M, Carling C, Le Gall F, Berthoin S, Dupont G. Reliability and sensitivity of a simple isometric posterior lower limb muscle test in professional football players. J Sports Sci. 2015;33(12):1298-304.
Figure 3: Alex Natera Run specific isometric assessments.
FMPA MEMBERSHIP
Expert legal support and representation across employment medico legal and regulatory law
All the benefits of Union membership through the FMPA
Priority member only access to job listings and email alerts 24/7 support from the FMPA and much more…
“I believe FMPA membership is now essential and should be a pre-requisite for any member of staff within our sector.”
Head of Sport Science & Medicine, Premier League
HAMSTRING INJURIES: WHAT ROLE DOES THE LUMBAR SPINE AND PELVIS PLAY?
PART 1: FORCE CLOSURE OF THE PELVIS AND ANTERIOR PELVIC TILT
FEATURE / NICK METCALFE
Introduction
Last year’s London International Consensus and Delphi Study on hamstring injuries (Paton et al, 2023) involving over 112 physicians, physiotherapists, surgeons, scientists, researchers and trainers reached a level of agreement on aspects of managing hamstring injuries. As part of their study 91% of the experts agreed it was “important to assess, treat and prescribe exercises addressing the whole kinetic chain”. The authors go further and discuss a number of lumbopelvic considerations in hamstring injuries such as pelvis biomechanics, sacroiliac joint mobility, force closure, pelvic control, gluteal activation, iliac asymmetry, neuromuscular inhibition and neural mobility.
In this series of articles, I will be looking into these lumbopelvic contributions to hamstring injuries and trying to distil the current research into a handful of simple clinical take-homes for the assessment of your athletes. In today’s article I will be looking at force closure of the pelvis and anterior pelvic tilt.
1. Force closure of the pelvis during the swing phase of running
Dense connective tissue connects the biceps femoris and the sacrotuberous ligament. Tension across both tissues combine to contribute to stability of the sacroiliac joint (Vleeming et al, 1989; Sato et al. 2012; Kim et al, 2023). Other muscles such as the lumbar multifidus, piriformis and gluteus maximus also have direct connections to the sacrotuberous ligament (Soames et al, 1995). During the late swing phase of running, an important point in the gait cycle for hamstring injuries, not only do we have tensioning of the hamstrings onto the sacrotuberous ligament but we also have posterior innominate rotation (and relative nutation of the sacrum) which also creates sacrotuberous ligament tensioning (Vleeming et al, 2012). It’s this combination of muscle activity plus posterior innominate rotation that creates stability at the SIJ and prepares the pelvis for foot strike and weight bearing. This is “force closure” of the pelvis.
So, what if we were to lack adequate posterior rotation of the innominate during this swing phase of gait? Might the muscular components, including the biceps femoris, have to work harder to create the necessary pelvic stability? If the hamstrings are now required to contribute
The long head of biceps has direct connections with the sacrotuberous ligament. Tensioning of both structures contributes to force closure of the pelvis during the swing phase of gait. Picture taken from Sasaki et al, 2021.
more to pelvic stabilisation then won’t it affect their knee flexion or hip extension output? Could this hamstring fatigue or weakness increase the risk of hamstring injury?
In a 2021 systematic review and meta analysis of professional and semi-professional footballers, core stability exercises and hamstring strength exercises (nordics) were two of the four strategies found to have a preventative effect on hamstring injury (Biz et al, 2021). As we’ve just seen above, some of these core muscles and the hamstrings contribute to force closure. Might it be that it’s not just the strength of these muscles that’s protective against hamstring injury but the effect of increased force closure of the pelvis?
To emphasise this point further, if you artificially create force closure (by use of an external pelvic compression belt) it has been shown to alter the recruitment of the pelvic stabilising muscles and increase the terminal range eccentric strength of injured hamstring by 10% and uninjured hamstring strength by 5% with isokinetic testing (Arumugam et al, 2012; Arumugam et al, 2015). It seems that by increasing force closure it frees up the hamstrings to better contribute to terminal knee extension force.
The sacrotuberous ligament is also tensioned with posterior innominate rotation (and relative sacral nutation) contributing to force closure of the pelvis. Picture taken from Sasaki et al, 2021.
Increasing force closure seems to reduce the need for the hamstrings to contribute to force closure. This then increases the strength output of the hamstrings with knee extension. Picture taken from Arumugam et al, 2015.
So how can we ensure maximal force closure during the swing phase of running? Improve the strength in the muscles which contribute to force closure of the pelvis. But it might also be wise to check for adequate posterior innominate rotation, another important contributor to force closure.
Should we find limited posterior rotation we might choose to address it with manual therapy. The fact that the test shows moderate to good intra-examiner reliability means we can attempt to re-check the movement over time for signs of improvement.
Posterior longitudinal sling: Consists of the deep multifidus attaching to the sacrum with the deep layer of the thoracolumbar fascia, blending with the long dorsal sacroiliac joint ligament and continuing on into the sacrotuberous ligament and into the biceps femoris. Picture from Raja et al. (2022)
Muscles contributing to force closure of the pelvis. Transversely oriented muscles press the sacrum between the hip bones. Sacroiliac joint (1) Transverse abdominal (2), piriformis (3), internal oblique (4), and pelvic floor (5). Pictures from Pool-Goudzwaard et al.(1998)
Muscles contributing to force closure of the pelvis. Posterior and anterior oblique sling consists of: Latissiumus dorsi (1), thoracolumbar fascia (2), gluteus maximus (3), iliotibial tract (4). Linea alba (5), external oblique (6), transverse abdominals (7), piriformis (8), rectus abdominis (9), internal oblique (10), ilioinguinal ligament (11). Pictures from Pool-Goudzwaard et al. (1998)
The Gillet test (AKA step test, stork test) has fair to substantial reliability when used as a stand alone test for assessing SIJ motion (Arab et al, 2009) and moderate to good intra-examiner reliability (Ribiero et al, 2021). One thumb on S2, the other thumb on PSIS. You’re looking for the PSIS to rotate medially and caudally as they step up and for the thumb to approximate the other. Expect only a small movement (max 4mm).
2. Anterior Pelvic Tilt:
Anterior pelvic tilt is commonplace in footballers but observing this in a static position is likely to have limited clinical value (Suits, 2021). Instead, it’s an increase in pelvic tilt during movement, specifically the swing phase in gait, that is predictive of hamstring injury in footballers (Scheurman’s et al, 2017). The pelvis plays a fundamental role as a strain regulator of the hamstrings and anterior pelvic tilt produces a significant increase in tissue elongation of all 3 hamstring muscles which is greater proximally compared to distally (Paton et al, 2023; Mendiguchia et al 2024).
So, what if we observe an increased anterior pelvic tilt during swing phase and poor hip flexor flexibility on the modified Thomas test? Improving the hip flexibility in isolation does not lead to carryover in functional tasks (Mettler et al, 2019); it seems that to affect the tilt it must be combined with strength and motor control exercises (Oh et al, 2017). In terms of frequency and dosage, Mendichugia et al (2024) found improvements in anterior pelvic tilt in active males with three 45-minute sessions per week for six weeks. Each session consisted of about 20% manual therapy (including soft tissue release and post-anterior innominate mobilisation) and 80% active corrective exercise (including hip flexor flexibility, hip extensor strength, neuromuscular control exercises focussing on lumbopelvic control and posterior pelvic tilt) and suggested this multimodal approach could be helpful in the management of hamstring injuries. Anecdotally, as a chiropractor in professional football, players might commonly spend 20-40 minutes with me addressing lumbopelvic mechanics with manual therapy and activation exercises, followed by a session in the gym with the physio or S&C coach working on strength, stability and neuromuscular control. With this combination we see good improvements in lumbopelvic function, hopefully going some way to reducing hamstring injury risk.
Conclusion
• Experts appear in agreement that the kinetic chain and lumbopelvic area should be a consideration in hamstring injuries.
• We’ve seen that posterior innominate rotation and strength of the core and pelvic muscles are important for force closure of the pelvis during the swing phase of running. By maximizing this force closure we may allow the
Observing for an increase in anterior pelvic tilt during a step test or during the swing phase of functional running drills is likely to be more predictive of hamstring injury than observing an anterior pelvic tilt in a static position.
Restricted hip flexor length might lead to an increased anterior pelvic tilt (Zeba et al, 2023). The modified Thomas test has high intra and inter-rater reliability if lumbopelvic movement is controlled (Cady et al, 2022) and is one way of gauging hip flexor length.
hamstring to better contribute to knee flexion and/or hip extension.
• Observing an increase in anterior pelvic tilt during a step test or during the swing phase of running might also be a risk factor for hamstring injury. A multimodal approach of manual therapy, strength
exercises and motor control exercises over a number of weeks can help improve this.
In future articles we will discuss other lumbopelvic considerations in hamstring injuries, including pelvic asymmetry, gluteus maximus strength, neural mobility and neuromuscular inhibition.
Nick Metcalfe is a chiropractor with 16 years experience working with a range of athletes and seven years experience working in professional football (Fulham FC and Brentford FC). He currently consults with Brentford FC and owns two multidisciplinary clinics in south-west London. Nick has a special interest in lumbopelvic function and its influence on lower limb injuries. In a multidisciplinary sports medical team he will assess spine, pelvis and hip function and co-manage both fit and injured athletes alongside the physios and soft tissue therapists.
References
Paton BM, Read P, van Dyk N, Wilson MG, Pollock N, Court N, Giakoumis M, Head P, Kayani B, Kelly S, Kerkhoffs GMMJ, Moore J, Moriarty P, Murphy S, Plastow R, Stirling B, Tulloch L, Wood D, Haddad F. London International Consensus and Delphi study on hamstring injuries part 3: rehabilitation, running and return to sport. Br J Sports Med. 2023 Mar;57(5):278-291.
Arumugam A, Milosavljevic S, Woodley S, Sole G. Effects of external pelvic compression on form closure, force closure, and neuromotor control of the lumbopelvic spine--a systematic review. Man Ther. 2012 Aug;17(4):275-84.
Arumugam A, Milosavljevic S, Woodley S, Sole G. THE EFFECT OF A PELVIC COMPRESSION BELT ON FUNCTIONAL HAMSTRING MUSCLE ACTIVITY IN SPORTSMEN WITH AND WITHOUT PREVIOUS HAMSTRING INJURY. Int J Sports Phys Ther. 2015 Jun;10(3):291-302.
Biz, C.; Nicoletti, P.; Baldin, G.; Bragazzi, N.L.; Crimì, A.; Ruggieri, P. Hamstring Strain Injury (HSI) Prevention in Professional and SemiProfessional Football Teams: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8272.
A. Vleeming, J.P. Van Wingerden, C.J. Snijders, R. Stoeckart, T. Stijnen,Load application to the sacrotuberous ligament; influences on sacroiliac joint mechanics. Clinical Biomechanics Volume 4, Issue 4, November 1989, Pages 204-209.
Sasaki, Takeshi & Kurosawa, Daisuke & Murakami, Eiichi & Watanabe, Takashi. (2021). Physical therapeutic options for residual sacrotuberous ligament pain after treatment of sacroiliac joint dysfunction. Journal of Physical Therapy Science. 33. 646-652. 10.1589/ jpts.33.646.
Sato K, Nimura A, Yamaguchi K, Akita K. Anatomical study of the proximal origin of hamstring muscles. J Orthop Sci. 2012 Sep;17(5):614-8. doi: 10.1007/s00776-012-0243-7. Epub 2012 Jun 6. PMID: 22669443.
Kim M, Yang HM, Yeo IS. Anatomical study of the sacrotuberous ligament and the hamstring muscles: A histomorphological analysis. Clin Anat. 2024 May;37(4):383-389. doi: 10.1002/ca.24082. Epub 2023 Jun 16. PMID: 37329174. Soames, R. (1995) Skeletal system. In: Williams, P.L., Bannister, L.H., Berry, M.M., et al., Eds., Gray’s Anat- omy, 38th Edition, Churchill Livingstone, New York, 425-736.
A. Pool-Goudzwaard, A. Vleeming, C. Stoeckart, C.J. Snijders and M.A. Mens, Insufficient lumbopelvic stability: a clinical, anatomical and biomechanical approach to “a-specific” low back pain. Manual Therapy 3 (1998), pp. 12–20.
Raja, Prabu & Bhat, Shyamasunder & Cruz, Antony & Prabhu, Anupama & Fernandes, Shifra & .S, Nabeela Naaz. (2022). The anatomical myofascial continuum between the neck and eyes. Clinical Anatomy. 35. 10.1002/ca.23835.
Arab AM, Abdollahi I, Joghataei MT, Golafshani Z, Kazemnejad A. Inter- and intra-examiner reliability of single and composites of selected motion palpation and pain provocation tests for sacroiliac joint. Man Ther. 2009 Apr;14(2):213-21. doi: 10.1016/j.math.2008.02.004. Epub 2008 Mar 25. PMID: 18373938.
Vleeming A, Schuenke MD, Masi AT, Carreiro JE, Danneels L, Willard FH. The sacroiliac joint: an overview of its anatomy, function and potential clinical implications. J Anat. 2012 Dec;221(6):537-67. doi: 10.1111/j.1469-7580.2012.01564.x. Epub 2012 Sep 19. PMID: 22994881; PMCID: PMC3512279.
Ribeiro RP, Guerrero FG, Camargo EN, Beraldo LM, Candotti CT. Validity and Reliability of Palpatory Clinical Tests of Sacroiliac Joint Mobility: A Systematic Review and Meta-analysis. Journal of Manipulative and Physiological Therapeutics, 2021; 44(4):307-318. https:// doi.org/10.1016/j.jmpt.2021.01.001.
Mendiguchia J, Garrues MA, Schilders E, Myer, GD, Dalmau-Pastor M. Anterior pelvic tilt increases hamstring strain and is a key factor to target for injury prevention and rehabilitation. Knee Surg Sports Traumatol Arthrosc. 2024; 32: 573–582.
Schuermans J, Van Tiggelen D, Palmans T, Danneels L, Witvrouw E. Deviating running kinematics and hamstring injury susceptibility in male soccer players: Cause or consequence? Gait Posture. 2017 Sep;57:270-277. doi: 10.1016/j.gaitpost.2017.06.268. Epub 2017 Jun 27. PMID: 28683419.
Oh JS, Cynn HS, Won JH, Kwon OY, Yi CH. Effects of performing an abdominal drawing-in maneuver during prone hip extension exercises on hip and back extensor muscle activity and amount of anterior pelvic tilt. J Orthop Sports Phys Ther. 2007;37(6):320-324. doi:10.2519/ jospt.2007.2435
Suits WH. Clinical Measures of Pelvic Tilt in Physical Therapy. Int J Sports Phys Ther. 2021 Oct 1;16(5):1366-1375. doi: 10.26603/001c.27978. PMID: 34631258; PMCID: PMC8486407.
Zeba Z, Hussain ME, Singla D, Tanwar T, Irshad N, Alam MD. Correlation between lumbopelvic stability and hamstring strain recurrence in sprinters. Physiotherapy Quarterly. 2023;31(3):80-85. doi:10.5114/pq.2023.125753.
Cady K, Powis M, Hopgood K. Intrarater and interrater reliability of the modified Thomas Test. J Bodyw Mov Ther. 2022 Jan;29:86-91. doi: 10.1016/j.jbmt.2021.09.014. Epub 2021 Oct 12. PMID: 35248293.
Mettler JH, Shapiro R, Pohl MB. Effects of a Hip Flexor Stretching Program on Running Kinematics in Individuals With Limited Passive Hip Extension. J Strength Cond Res. 2019 Dec;33(12):3338-3344. doi: 10.1519/JSC.0000000000002586. PMID: 29927892.
“CHECK ENGINE LIGHT”
OPTIMISING INDIVIDUALISED HIGH-SPEED RUNNING ZONES IN FOOTBALL. ARE WE MEASURING WHAT WE THINK?
FEATURE / RONAN KAVANAGH, DR. RYLAND MORGANS, DR. JILL ALEXANDER
Introduction
In professional football, the management of high-speed running (HSR) is crucial for enhancing performance and preventing injuries (Buchheit, 2019). Traditionally, HSR and sprint distance (SD) were defined by fixed speed thresholds of 5.5 metres per second (m/s) and 7 m/s respectively (Akenhead & Nassis, 2016). The quantification of high-velocity metrics, however, has long been debated, leading to a recent shift from absolute to relative thresholds to better reflect individual player capabilities (Abt & Lovell, 2009; Harper et al., 2020). Varying methodological approaches employed to individualise high-speed thresholds such as anaerobic threshold have been reported. This can be difficult to implement in team environments with large squads (Baker
& Heaney, 2015). Thus, another marker, namely percentage of maximal sprinting speed (MSS) has been employed to further individualise high-intensity distance in team athletes (Gabbett, 2015). Hunter et al. (2015) found that utilising a single physical marker to determine multiple speed zones can lead to erroneous interpretations of players activities. Thus, maximal aerobic speed (MAS) has recently gained significant interest and has been defined as a practical and time efficient method to assess aerobic capacity in team sport athletes (Baker et al., 2015). Time spent above MAS has been shown to correlate with improvements in aerobic fitness (Fitzpatrick et al., 2018).
Recently, several authors have applied this method to youth athletes, using
field tests to assess athlete’s MAS and MSS (Hunter et al., 2015; MendezVillanueva et al., 2013). This approach allows for the estimation of an individual’s anaerobic speed reserve (ASR) and supports the transition to sprint distance exposures (Hunter et al., 2015). With this information practitioners can also identify the locomotor profile of each player. This in turn helps to identify potential conditioning strategies based on the individual. This individualised approach provides a more accurate representation of a player’s output, which is often underestimated when using absolute thresholds (Abt et al., 2009). Consequently, current research has focused on these metrics to optimise training and potentially minimise injury risk (Colby et al., 2018; Malone et al., 2018).
Current research
A recent study by Kavanagh et al. (2024) demonstrated that the high-intensity distances covered by English Premier League (EPL) players during official match-play differ when employing, individualised rather than absolute thresholds. This discrepancy is particularly evident when a player reaches or exceeds speeds >85% of MSS compared to speeds over the standardised threshold of 7 m/s. Although there is a near-perfect correlation (r = 0.98) between generic and relative speed thresholds, the variations in HSR distance, and distance above MAS suggest that players perform more high-intensity activity when using relative thresholds. Without using individualised HSR thresholds practitioners may be underestimating the strain imposed on players during match-play. This may therefore influence recovery and training periodisation. Knowledge of individualised HSR capabilities enables practitioners to prescribe more precise training loads and potentially reduce injury risks while enhancing aerobic performance (Fitzpatrick et al., 2018).
Similarly, when analysing the most demanding phases of play in the EPL, metrics such as total distance (TD), HSR and SD display significant positional differences (Kavanagh et al., 2023b).
Central defenders (CD) cover the least TD, wide midfielders (WM) cover the greatest TD, regardless of the time
periods analysed. That said, this pattern is not always evident when considering distances covered above MAS. Failing to account for the relative intensity for individual athletes can lead to a substantial underestimation of the intensity during the most demanding phases of match-play. To address this real-world problem, practitioners should develop and monitor short-duration, high-intensity match-based training activities based on positional demands, using distances covered above MAS and ASR as benchmarks. As highlighted by Martín-García et al. (2018), significant differences in high-intensity periods exist between positions even when quantified using a single variable. This stresses the importance of understanding that highintensity periods vary significantly based on the duration of the period, the metric used and playing position. As a result, isolated conditioning may not be the most effective method for preparing players for high-intensity phases.
A comparison of individualised HSR thresholds between senior and U23 players at an EPL club have recently been examined and illustrated significant differences in match-play physical outputs, which arguably would not be identified employing traditional absolute thresholds (Kavanagh et al., 2023a). By exposing U23 players to similar 1st team relative physical demands, practitioners may be able to ensure a smooth transition for the
developing athlete (Houtmeyers et al., 2021). Having a similar level of physical fitness and being accustomed to covering similar weekly loads may allow U23 players to focus on other developmental areas such as technical, tactical, or psychological.
Future directions
Although much progress has been made in determining individualised HSR thresholds through contemporary research, a key factor for practitioners to consider is how these thresholds may influence practice. By incorporating locomotor player profiling through MAS and MSS into assessments, coaches and practitioners can obtain a comprehensive understanding of each players physical capabilities (Figure 1). This dual profiling allows for the creation of individualised training programs that cater to the specific demands placed on players during training and competition. Such precision ensures that training loads are optimised, reducing the potential risk of overtraining and injury while maximising performance. Furthermore, this approach can identify strengths and weaknesses in a player’s fitness profile, enabling targeted interventions that enhance overall athletic development. As football continues to evolve with increasing physical demands, the use of MAS and MSS in locomotor profiling may be essential in maintaining player health, enhancing performance, and gaining a competitive edge. Finally, future research should aim to explore the impact of other contextual variables, namely match location, level of opposition, team formation and possession (Morgans et al., 2024a; Morgans et al., 2024b) on individualised HSR and SD thresholds.
Conclusion
The evolving management of HSR in professional football underscores the importance of individualised HSR thresholds. Evidence of the benefits of individualising HSR thresholds continues to grow. Shifting from absolute to individualised thresholds for HSR and SD has proven to provide a more accurate reflection of each player’s unique capabilities and may assist practitioners in optimising training purpose and outcome. This approach facilitates more precise training prescriptions and can enhance both performance and overall athletic development. As football continues to increase in terms of physical and mental demands on the professional player, integrating locomotor profiling using MAS and MSS will be essential for performance departments to successfully maintain player health and performance in the contemporary game.
Figure 1: Example of locomotor profiling within an elite professional football squad
Authors
Ronan Kavanagh BSc
Parma Calcio 1913
Football Association of Wales
References
Dr. Ryland Morgans
School of Sport and Health Sciences
Cardiff Metropolitan University
Dr Jill Alexander
Football Performance Hub
University of Central Lancashire
Abt, G., & Lovell, R. (2009). The use of individualized speed and intensity thresholds for determining the distance run at high-intensity in professional soccer. J Sports Sci, 27(9), 893-898. https://doi.org/10.1080/02640410902998239
Akenhead, R., & Nassis, G. P. (2016). Training Load and Player Monitoring in High-Level Football: Current Practice and Perceptions. Int J Sports Physiol Perform, 11(5), 587-593. https://doi.org/10.1123/ijspp.2015-0331
Baker, D., & Heaney, N. (2015). Review of the literature normative data for maximal aerobic speed for field sport athletes: a brief review. J. Aust. Strength Cond., 23(7), 60-67.
Buchheit, M. (2019). Programming high-speed running and mechanical work in relation to technical contents and match schedule in professional soccer. Sport Perf & Sci Reports, 64, v1.
Colby, M. J., Dawson, B., Peeling, P., Heasman, J., Rogalski, B., Drew, M. K., & Stares, J. (2018). Improvement of Prediction of Noncontact Injury in Elite Australian Footballers With Repeated Exposure to Established High-Risk Workload Scenarios. Int J Sports Physiol Perform, 13(9), 1130-1135. https://doi.org/10.1123/ijspp.2017-0696
Fitzpatrick, J. F., Hicks, K. M., & Hayes, P. R. (2018). Dose-Response Relationship Between Training Load and Changes in Aerobic Fitness in Professional Youth Soccer Players. Int J Sports Physiol Perform, 1-6. https://doi.org/10.1123/ijspp.2017-0843
Gabbett, T. J. (2015). Use of Relative Speed Zones Increases the High-Speed Running Performed in Team Sport Match Play. J Strength Cond Res, 29(12), 3353-3359. https://doi.org/10.1519/JSC.0000000000001016
Harper, D. J., Morin, J.-B., Carling, C., & Kiely, J. (2020). Measuring maximal horizontal deceleration ability using radar technology: reliability and sensitivity of kinematic and kinetic variables. Sports Biomechanics, 1-17.
Houtmeyers, K. C., Jaspers, A., Brink, M. S., Vanrenterghem, J., Varley, M. C., & Helsen, W. F. (2021). External load differences between elite youth and professional football players: ready for take-off? Sci Med Footb, 5(1), 1-5. https://doi.org/10.1080/24733938.2020.178 9201
Hunter, F., Bray, J., Towlson, C., Smith, M., Barrett, S., Madden, J., Abt, G., & Lovell, R. (2015). Individualisation of time-motion analysis: a method comparison and case report series. Int J Sports Med, 36(1), 41-48. https://doi.org/10.1055/s-0034-1384547
Kavanagh, R., Carling, C., Malone, S., Di Michele, R., Morgans, R., & Rhodes, D. (2023a). ‘Bridging the gap’: Differences in training and match physical load in 1st team and U23 players from the English Premier League. Int J Sports Sci Coach.
Kavanagh, R., Di Michele, R., Oliveira, R., McDaid, K., Rhodes, D., & Morgans, R. (2024). The relationships between distances covered above generic and relative speed thresholds by male soccer players in English Premier League matches across two competitive seasons. The effects of positional demands and possession. Biology of Sport, 41(4), 77-86.
Kavanagh, R., McDaid, K., Rhodes, D., McDonnell, J., Oliveira, R., & Morgans, R. (2023b). An Analysis of Positional Generic and Individualized Speed Thresholds Within the Most Demanding Phases of Match Play in the English Premier League. Int J Sports Physiol Perform, 1(aop), 1-11.
Malone, S., Owen, A., Mendes, B., Hughes, B., Collins, K., & Gabbett, T. J. (2018). High-speed running and sprinting as an injury risk factor in soccer: Can well-developed physical qualities reduce the risk? J Sci Med Sport, 21(3), 257-262.
Martín-García, A., Casamichana, D., Díaz, A. G., Cos, F., & Gabbett, T. J. (2018). Positional differences in the most demanding passages of play in football competition. J Sports Sci Med, 17(4), 563.
Mendez-Villanueva, A., Buchheit, M., Simpson, B., & Bourdon, P. C. (2013). Match play intensity distribution in youth soccer. Int J Sports Med, 34(2), 101-110. https://doi.org/10.1055/s-0032-1306323
Morgans, R., Di Michele, R., Ceylan, I. H., Ryan, B., Haslam, C., King, M., Zmijewski, P., & Oliveira, R. (2024a). Physical match performance of elite soccer players from the English Championship League and the English Premier League: The effects of opponent ranking and positional differences. Biology of Sport, 42(1), 29-38.
Morgans, R., Radnor, J., Fonseca, J., Haslam, C., King, M., Rhodes, D., Żmijewski, P., & Oliveira, R. (2024b). Match running performance is influenced by possession and team formation in an English Premier League team. Biology of Sport, 41(3), 275-286.
PLAY BALL (OR DON’T): TOWARDS A MORE VALID MEASURE OF PHYSICAL INTENSITY DURING MATCH PLAY
FEATURE / BENJAMIN W.C. JEROME1, MICHAEL STOECKL2, BEN MACKRIELL2, THOMAS SEIDL2, JONATHAN P. FOLLAND1
One of the major talking points in professional football over the last few years has been the amount of time the ball is actually in play, commonly referred to as ball-in-play (BIP) time. In fact, significant rule changes were implemented for the Premier League 2023-24 season, whereby match officials have been instructed to add on any time accrued due to intentional timewasting and specific events (e.g. injuries, substitutions, celebrations) at the end of matches. These rule changes have seen an increase in BIP time during the 2023-24 season of around 3 minutes compared to the 2022-23 campaign. But how does BIP time influence the physical metrics, and more specifically, the physical intensity of match play? This report summarises an aspect of our paper published in the European Journal of Sports Sciences (Jerome et al., 2023).
The ‘traditional’ approach
For over 40 years the traditional approach of quantifying the physical demands during
match play has simply involved reporting the total distance covered, as well as the distances covered within specific speed categories, during the whole match (i.e. over 90+ minutes; Bradley & Ade, 2018). However, a football match consists of alternating ball in play (BIP) and ball out of play (BOP) periods, due to an average 108 stoppages/ BOP periods per match (Siegle and Lames, 2012). Previous studies have reported that total BIP time throughout a match is in fact only ~54 minutes on average (Riboli et al., 2021), with ~40 minutes of BOP. This may have consequences for measuring the physical demands of football as BOP is thought to involve markedly lower physical intensity (resting and minor repositioning in preparation for set piece etc.) compared to when the ball is actually in play.
So, why does BIP time matter?
Quantifying match play physical demands during whole match time, which includes this substantial proportion of low-intensity BOP time, likely underestimates the intensity when the ball is actually in play (Gabbett,
2015). Also considering the known variability in the number and duration of stoppages per match (Siegle & Lames, 2012), there may also be substantial variability in the amount of BOP and BIP time between matches, which may influence and potentially confound comparisons of whole match distances between matches. In other words, differences in player physical data could be due to the underlying structure of a match (i.e. more or less BIP time), rather than purely a reflection of the physical demands when the ball is in play. Therefore, whole match distances may lack validity compared to quantifying intensity as the rates of distance covered during BIP.
Data sample and physical metrics
1,083 matches from four seasons of a major European league were analysed. On-ball event data and optical tracking data were collected and provided by Stats Perform. The duration of each match was divided into periods of BIP and BOP, in order to quantify physical metrics during these specific periods. Whole match time was 95:36 ± 2:12 min:s which consisted
1 School of Sport, Exercise and Health Sciences, Loughborough University, UK;
Stats Perform, Chicago, USA
Figure 1: (A) Absolute distance covered within different speed categories and in total (height of the column) during whole match time, ball-in-play (BIP) and ball-out-play (BOP) time, (B) Distance covered within different speed categories as a percentage of total distance covered during whole match time, ball-inplay and ball-out-play time, and (C) Within each speed category, the percentage of whole match distance covered during either ball-inplay or ball-out-play time. Data is expressed as the average per outfield player (adapted from Jerome et al., 2023).
of BIP time of 57:18 ± 4:12 min:s or 59.9 ± 4.8% of whole match time, as well as BOP time of 38:30 ± 5:00 min:s or 40.1 ± 4.8% of whole match time.
Stats Perform tracking data were used to derive the distances (m) and rates of distance (m•min-1) covered: standing (<0.16 m•s-1), walking (0.16-1.97 m•s-1), jogging (1.97-3.97 m•s-1), running (3.97-5.47 m•s-1), high-speed (5.47-7.0 m•s-1), sprinting (> 7.0 m•s-1) and total distance.
Distance covered during whole match, ball-in-play and ball-out-play time
Players on average covered a total distance of 10,960 ± 371 m during whole match time, with 8,292 ± 558 m (76% of whole match distance) covered during BIP time and 2,669 ± 367 m (24% of whole match distance) covered during BOP time (Fig.1a). During BOP a high proportion of the distance covered was walking (67.2 ± 3.1%; Fig.1b) and this was greater than during either BIP (23.6 ± 1.8%) or whole match time (34.2 ± 2.0%). Whereas during BIP the proportion of distance covered within all speed categories above walking was significantly greater than either BOP or whole match time (Fig. 1b).
Rate of distance covered during whole match, ball-in-play and ball-out-play time
There were profound differences in the rate of distance covered between periods of BIP vs BOP, being 2-fold higher overall and 8- to 33-fold higher for the rates of distance covered within running, high-speed and sprinting categories. More specifically, commonly used whole match metrics that aggregate BIP and BOP had a rate of total distance covered that was 22% lower than during BIP and therefore gave a substantial underestimate compared to BIP. Moreover, there were even larger differences between whole match time and BIP for the rates of distance covered running (-52%), high-speed (-62%) and sprinting (-65%). Therefore, traditional methods of quantifying the physical intensity during match play as distances, and even rates of distance covered, during the whole match (i.e. over 90 minutes) do not accurately reflect the physical intensity of match play (during BIP).
Figure 2: (A) Rate of distance covered within different speed categories and in total (height of the column) during whole match time, ball-in-play and ball-out-play time, (B) Rate of distance covered during the whole match within different speed categories, percentage difference compared to the rate of distance covered during ball-in-play (whole match rates>ball-in-play rates, positive values; whole match rates<ballin-play rates, negative values). Data is expressed as the average per outfield player (reproduced from Jerome et al., 2023).
Summary
It’s recommended that applied practitioners and researchers adopt a more valid and direct approach to quantifying the physical intensity during match play as rates of distance covered during BIP. This does not mean that whole match metrics (e.g. total distance covered) do not provide some useful information pertaining to the overall volume of physical work completed, but importantly, they don’t accurately reflect the physical intensity of match play. Whilst BIP is not a new concept, its use for determining physical metrics (i.e. specific to BIP) is a relatively novel development. However, some global positioning system companies (e.g. STATSports) have started to integrate features into their products which allow coaches and practitioners to record BIP time during a match or training sessions, which could be used to quantify physical metrics as rates of distance covered during BIP.
Practical applications:
• The present findings demonstrate greater rates of distance covered in total (+22%), and especially at higher speeds (running +52%; high-speed +62%; sprinting +65) when accounting for stoppages (i.e. BOP time). Prescribing programs based on whole match average demands is likely to result in players being underprepared for the higher intensity demands which occur during BIP.
• Therefore, quantifying match physical demands as a rate during BIP provides an accurate index of physical intensity. Such information can be used to inform appropriate training load prescription; ensuring that players are conditioned to cope with the actual match physical demands, return-to-play protocols (e.g. incremental increase in session intensity) and optimal recovery, according to the intensity of match play.
• Overall, these findings suggest that practitioners utilising GPS analysis for training and workload monitoring should consider BIP time when designing training activities, to accurately replicate the demands of competitive match play in professional football.
References
Bradley, P.S., & Ade, J. D. (2018) Are current physical match performance metrics in elite soccer fit for purpose or is the adoption of an integrated approach needed?. International Journal of Sports Physiology and Performance, 13(5), 656-664.
Gabbett, T.J. (2015) Influence of ball-in-play time on the activity profiles of rugby league matchplay. The Journal of Strength & Conditioning Research, 29(3), 716-721
Siegle, M., & Lames, M. (2012). Game interruptions in elite soccer. Journal of Sports Sciences, 30(7), 619-624.
Jerome, B. W., Stoeckl, M., Mackriell, B., Seidl, T., Dawson, C. W., Fong, D. T., & Folland, J. P. (2023). The influence of ball in/out of play and possession in elite soccer: Towards a more valid measure of physical intensity during competitive match-play. European Journal of Sport Science, 23(9), 1892-1902.
Riboli, A., Semeria, M., Coratella, G., & Esposito, F. (2021). Effect of formation, ball in play and ball possession on peak demands in elite soccer. Biology of Sport, 38(2), 195-205.
Adjustable Cold Therapy
Intermittent Compression
One Easy Application
Monthly Rental*
£250 ex VAT / £300 inc VAT
Accelerate Recovery from Injury or Surgery
Used by surgeons, healthcare professionals, athletes and rehabilitation units around the world, Game Ready now offers monthly Rental Systems to allow everyone the opportunity to recover like an elite athlete.
Rental Systems include:
࢚ Control unit, AC adapter, connector hose, carry bag & one fully assembled anatomical wrap from range available.
࢚ UK delivery within 24-48 hours & Return Shipping*
࢚ Information pack with easy-to-follow instructions & treatment guidelines.
࢚ Equipment cleaned to hospital infection control standards.
࢚ New fabric sleeve applied to every wrap.
For further information: Email ukrental@gameready.co.uk or call 01344 379797
SWIMEX REFURBISH THE FILTRATION SYSTEM AT BISHAM ABBEY TO HELP TEAM GB’S
BUILD-UP TO THE PARIS OLYMPICS
Aqua Thermae are specialists in professional sports and medical hydrotherapy, delivering considered solutions for our clients. We proudly distribute the world class SwimEx pool range across the UK, Ireland and the rest of Europe, whilst also managing projects further afield in the Middle East.
Our clients include The UK Sports Institute, Team GB, British Ministry of Defence Special Forces, University research pools, specialist medical clinics and hospitals. Recent projects include Queens Park Rangers’ training ground, installing a SwimEx 600T performance and recovery pool, a deep water ice bath and plunge cold recovery pool with energy efficient heat pump chiller. We also installed the SwimEx 600T at the Strive elite sports academy in Jersey which will be hosting the South Africa squad, the Rugby World champions, for pre-Autumn international training. They have previously hosted the British & Irish Lions, England Rugby, Leicester Tigers, Sale and Bath Rugby.
The success and delivery of elite sports performance and recovery aquatic-based solutions is founded on experienced design specification and selection of premium quality equipment designed to exceed the industry guidance. Richard Bishop M.P.W.T.A.G, Technical Design Director, has 37 years industry experience and composed the award winning technical paper for the Institute of Swimming Pool Engineers, and presented talks on Sports Hydrotherapy Design to the Institute.
This spring, we refurbished the filtration system at Bisham Abbey to help Team GB’s build-up to the Paris Olympics. We were honoured to work with The UK Sports Institute and Team GB, and proud in receiving wonderful first-hand feedback from the athletes and the medical team.
Whether you are looking for a brand new hydrotherapy suite from ice bath to sauna, or seeking to upgrade your existing filtration and water treatment facilities to enhance and look after your existing pool equipment, Aqua Thermae are available to support your project across the UK and Europe. We can provide a simple health check with guidance on your existing facilities, design consultation and supply of a new project through to professional planned maintenance services, to the ultimate peace of mind after-care.
Well maintained hydrotherapy resources will protect your athletes and, in many cases, help
deliver accelerated recovery outcomes, ensuring the players return to the field sooner with more resilience, to help prevent repeat injuries.
As we proudly say “Aqua Thermae Services aim to design well and deliver far more”
Performance and Physiotherapy Pools
SwimEx Pools are handcrafted, custom-built marine grade pools, similar to an ocean racing yacht. They are custom built to order for each client and can be emblazoned to reflect the sports teams’ colours and branding.
SwimEx was designed over 40 years ago to deliver a unique laminar flow resistance experience from its patented paddlewheel water flow drive, which can be enhanced with custom deep wells, physiotherapy stations and underwater motorised treadmills
Recovery Pools
We also install SwimEx hot and cold deep water recovery pools for accelerated recovery and prevention of D.O.M.S. post-training and between matches. We can supply selfcontained individual ice baths through to full team recovery pools.
Filtration
We minimise chemical inputs into the pool water for a better bathing experience and lower running costs by hyper filtration screening the water more efficiently with advanced filter medias and deep bed filters. By removing the particulate matter more effectively we reduce the amount of traditional chlorine required to keep the pool water safe. Energy saving control on the water flow further enhances the operation of the system.
Water Treatment
Our water treatment systems are specified for each pool and include advanced UV systems and accurate pH, chlorine monitoring and control, all linked to the internet so we can provide monitoring which allow for rapid remote technical support, 24/7.
Climate Control
One of the largest cost factors operating an indoor hydrotherapy suite will be the heating energy costs. We can help design and enhance your heating system to ensure the pool water, air temperature and humidity are maintained in harmony and balance. This will lead to substantial savings in operational costs.
Training
We offer a comprehensive planned maintenance service schedule along with professional training of on-site staff to ensure the pools are operated efficiently and deliver safe bathing water.
MEMBERSHIP OFFER
We are pleased to offer a free initial pool plant health check and guidance report for existing pools to all UK and Ireland FMPA members. Contact Richard Bishop direct to discuss: Email richard@aquathermae.co.uk Tel 07484 070765 www.aquathermae.co.uk www.swimex.com
LEGAL Compromise agreement
“...I took your advice and have been working with the FMPA lawyer on the conclusion of my contract. Martin from his swift response on day one has been a real rock on my side and he has stayed in contact with me at regular intervals. His professionalism and knowledge of the football contract has helped me to be both realistic and hopeful regarding my case. We are now at the final stages of discussions with the club and the financial and emotional support I have has come through my contact with Martin. I am also immensely grateful to the FMPA for your help and support at this difficult time. At a low point in my life both the FMPA and Martin have helped me get the contractual situation sorted with as little fuss as possible and that’s been important to me and my family.”
Head of Medicine, League Two
Contract review
“...I just wanted to drop you an email to let you know how helpful Martin has been this last week. Although away, and with poor signal, he consistently made the effort to respond quickly to my questions when the club came back with updated terms. I believe his guidance has been fundamental to my negotiations.”
Head Physiotherapist, Premier League
“...Thank you so much. Really appreciate your help with this, it’s brilliant that the FMPA offer this service to its members. This stuff can be a minefield.”