In this issue
Anterior

Lateral Collateral Ligament Injuries of the Knee - The Precursor to Hamstring Injury
Prevention and rehab of hamstring injuries
Is Your Department
Scoring Goals or Just Hitting the Post?
Nutrition Strategies to Reduce Illness in Football
Neurogenic
football medicine & performance Legal • Education • Recruitment • Wellbeing www.fmpa.co.uk Issue 45 Winter 2023/24 The official magazine of the Football Medicine & Performance Association
Cruciate Ligament (ACL) Surgery: an Interview with surgeon, Andy Williams
Headache & Neck Pain in Athletes
Enigma Legal provides legal services and advice to managers, coaches and professionals working within the sports industry, its unique structure utilising a panel of expert barristers all with extensive experience of the sports industry, most notably their work with the League Managers Association.
Enigma Legal lawyers are tried and trusted to work in a flexible, agile and responsive way, demonstrating their understanding of the unique demands of the sports industry. A creative and pragmatic approach will ensure that Enigma Legal offers real value to the FMPA Membership.

www.enigmalegal.com admin@fmpa.co.uk

CEO MESSAGE
At the beginning of each season, we always look to set in place a project or two that will further the purpose of the association, and this year is no exception.
The MPA Diploma; Preparation for working in Professional Football is the result of several months collaboration with a team of writers and reviewers who have given their time and knowledge in putting together an exceptional on-line course that will benefit practitioners and Clubs alike. A partnership with BASES and other organisations will ensure the course is delivered across all disciplines and we have already had international interest for translation and dissemination of the course in Europe.
The FMPA however is more than an educational facilitator. Our aim has always been to raise standards within our sector; our vision statement is “To create an environment where all facets of player care are delivered to the highest standards”, and this diploma is a step in the right direction. Certainly, no one understands the needs of our members and the nuances of their working environment better than the FMPA, and accordingly it is incumbent of the association to continue to address issues that arise and impact working practices.
Any innovation, of course, needs to be taken in small steps. After all, great things are not done by impulse but by a series of small things brought together.
I am delighted to announce the return of our annual Conference and networking event on May 23rd 2024 at our much-heralded venue, The Radisson Blu Hotel East Midlands. For so many, the Conference brings the curtain down on an arduous season and this is an ideal time to meet colleagues and friends from Clubs within our industry. This year sees a slightly different format being a single day/evening event so you can relax and make the most of the best networking opportunity within our industry.
Salmon Eamonn
Chief Executive Officer Football Medicine & Performance Association
3 www.fmpa.co.uk
FROM THE EDITORS
In this upcoming edition of the Football Medicine and Performance Editorial, we delve deeper into one of the most common injuries seen in football, hamstring injuries. Hamstring Injuries in the first half of the 2023/24 season accounted for 2,319 days lost in the English Premier League. Martin McIntyre discusses the epidemiology of hamstring injuries in his article ‘Unravelling the hamstring quandary’. Further to this Bram Swinnen looks not only at rehabilitating but also reducing the risk of these injuries. Digging further into the aspect of hamstring injury risk, Adam Johnson’s article kindly looks at how lateral collateral ligament (LCL) injuries could predispose athletes to a subsequent hamstring injury. He kindly provides some tips on how to alter rehabilitation based on the increased demands on the biceps femoris following an LCL injury.
With anterior cruciate ligament injuries (ACL) being on the rise in women’s football, the need to understand its management in football medicine and performance is key. In this edition, Dr Eleanor Trezise interviews the renowned Mr Andy Williams discussing the injury mechanism, conservative and surgical treatment options for this injury. The full podcast can be accessed from the FMPA channel on Spotify/Soundcloud/Apple.
This edition also highlights the role of key performance indicators in Elite Performance Settings with Martin Buchheit’s article ‘Is Your MDT Scoring Goals or Just Hitting the Post?’ This article highlights the critical importance of robust communication, transparent decision making structures, progressive personal traits and objective metrics such as player availability.
We hope you enjoy these articles as well as many others in this edition and that they will help improve your evidence-based practice within the world of football to optimise player health and performance.



Sean Carmody Fadi Hassan Andrew Shafik
 Dr.
Dr.
Sean Carmody Editor, FMPA Magazine
Dr.
Fadi Hassan Editor, FMPA Magazine
Dr.
Andrew Shafik Editor, FMPA Magazine
5 www.fmpa.co.uk
FMPA Magazine
Dr. Daniela Mifsud Editor,
Daniela Mifsud
FMPA Business Directory FMPA Business Directory is now available on the FMPA site to give members quick access to products/services. VIEW THE DIRECTORY www.fmpa.co.uk/fmpa-directory
ASSOCIATE EDITORS

Ian Horsley Lead Physiotherapist

Dr. Jon Power Director of Sport & Exercise Medicine
REVIEWERS

Matthew Brown Academy Sports Scientist

Lisa Edwards Sports Therapist


Mike Brown Head of Physical Performance Jake Heath Elite Sports Specialist Podiatrist


Dr. Dáire Rooney Doctor

Dr. Manroy Sahni Medical Doctor
ABOUT
Football Medicine & Performance Association
43a Moor Lane, Clitheroe, Lancs, BB7 1BE

Dr. Andrew Butterworth Senior Lecturer Frankie Hunter Lead Sports Scientist


Dr. Jose Padilla MD Sports Medicine Specialist

Eleanor Trezise Medical Student
T: 0333 456 7897 E: info@fmpa.co.uk W: www.fmpa.co.uk
FMPA_Official Officialfmpa fmpa_official
LinkedIn: Football Medicine & Performance Association
FMPA_Register FMPARegister fmpa_register
Chief Executive Officer Eamonn Salmon eamonn.salmon@fmpa.co.uk
Commercial Manager Angela Walton angela.walton@fmpa.co.uk
Design Oporto Sports www.oportosports.com
Photography Alamy, FMPA, Unsplash
Cover Image
London Stadium, 7th Jan, 2024. FA Cup Third Round - West Ham United versus Bristol City; Lucas Paqueta of West Ham United speaks to Head Physio, Adam Paxton, as he is forced off with an injury.
Photo: Alamy

Dr. Avinash Chandran Director

Callum Innes Medical Doctor

Kevin Paxton Strength & Conditioning Coach
Football Medicine & Performance Association.
All rights reserved.
The views and opinions of contributors expressed in Football Medicine & Performance are their own and not necessarily of the FMPA Members, FMPA employees or of the association. No part of this publication may be reproduced or transmitted in any form or by any means, or stored in a retrieval system without prior permission except as permitted under the Copyright Designs Patents Act 1988. Application for permission for use of copyright material shall be made to FMPA. For permissions contact admin@fmpa.co.uk
7 www.fmpa.co.uk
Dr. Danyaal Khan Academy Doctor
FEATURES
12 Anterior Cruciate Ligament (ACL) Surgery Interview with Andy Williams
16 Lateral Collateral Ligament Injuries of the Knee - The Precursor to Hamstring Injury Adam Johnson
21 Trust Versus Trophies: Manchester City’s Unique Ability to Balance Psychological Safety and Risk-Taking for Optimised Performance
Christian Pszyk
27 Prevention and Rehab of Hamstring Injuries
Bram Swinnen


38 Is Your Department Scoring Goals or Just Hitting the Post?
Martin Buchheit
44 Unravelling the Hamstring Quandary “Elementary my Dear Watson” Injury Risk Assessment – The fundamentals of Specificity!
Dr Martin McIntyre
48 Nutrition Strategies to Reduce Illness in Football
Tom Shaw
52 Neurogenic Headache and Neck Pain in Athletes
Connor Arquette, Catherine Curtin





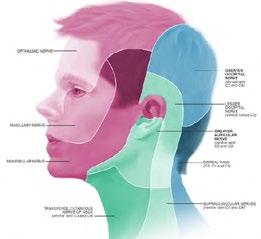 Figure 1.1 Late Swing and Early Stance phases (Kenneally-Dabrowski et al., 2019).
Figure 1.1 Late Swing and Early Stance phases (Kenneally-Dabrowski et al., 2019).
120° 140° 12 27 38
Late swing prior to ground
CONTENTS
9 www.fmpa.co.uk 16 44 21 48
52


TEL: 0333 4567897 EMAIL: CONFERENCE@FMPA.CO.UK TWITTER: @FMPA_OFFICIAL FACEBOOK: @OFFICIALFMPA INSTAGRAM: @FMPA_OFFICIAL RADISSON BLU HOTEL DERBY DE74 2TZ WWW.FMPA.CO.UK #FMPA2024 2024 THURSDAY 23 RD MAY SCAN FOR MORE DETAILS “Contemporary issues in professional sports medicine and performance” & NETWORKING EVENT
The FMPA Conference & Networking Event 2024 will take place on Thursday 23rd May 2024 with the venue at the Radisson Blu East Midlands Hotel.
We are delighted that England Men’s U21 Physiotherapist, Dave Galley will be heading up #fmpa2024 educational content.
As many of you will remember this is a fantastic venue which has hosted all but one of the FMPA Conferences over the last 10 years.
The FMPA Conference is THE medicine and performance event in the professional football calendar, combining excellence in educational content and superb networking opportunities for members and business partners alike.
The Conference this year is aimed at a wide variety of subjects to give practitioners an idea of the medical and performance aspects of our game. We will be looking at the high end performance strategies, through to
Conference Leads

MATT KONOPINSKI
how managerial changes affect us all on the Medicine and Performance side. We aim to encompass the world of the Men’s and Women’s game, Academies and also how external practitioners are currently working alongside medical departments to better serve our players. We will also cover how the world of nutrition works and how this has changed dramatically over the last few years.
We are lucky to have so many highly qualified, experienced and knowledgeable speakers and they will all come together at the end of the day as a round table to answer any of your questions
We are looking forward to, what we are sure, will be an excellent event. Join us by clicking here!

DAVE GALLEY
Education Co-Ordinator FMPA Conference
Conference Speakers
Director of Physiotherapy & Performance
Topic: My Guy

CALLUM WALSH
Elite Performance Management Specialist
Topic: Impacts of managerial change on performance support staff
PROFESSOR DON MACLAREN
Emeritus Professor of Sports Nutrition, Liverpool John Moores University


“The FMPA Conference was, without question, the best conference I have attended in the last 10 years. ”

KEVIN PAXTON High Performance Manager
ALLY BARLOW
Women’s Team Physiotherapist at Chelsea FC
Topic: Why Gender Matters: Disparity between ACL injuries in males and females

Topic: Football and Nutrition: reflections on 25 years working with professional clubs
PHIL HAYWARD
Head of High Performance, Wolverhampton Wanderers
Topic: Lessons learned from the ATP Tour

JOHN LUCAS
Head of Physical Performance, Preston North End FC
Topic: The applied recovery day


DI RYDING
Former Head of Foundation and Youth Development, Manchester United FC
Topic: Tackling Academy Physiotherapy
Sponsorship
We offer fantastic opportunities to exhibit and sponsor FMPA 2024. Full details can be found here. Please feel free to inform companies that you are dealing with at your clubs. Your support is appreciated.
11 conference www.fmpa.co.uk/conferences/fmpa-conference-2024 medicine & performance football
ANTERIOR CRUCIATE LIGAMENT (ACL)
SURGERY: AN INTERVIEW WITH SURGEON,
ANDY WILLIAMS - PART 1
FEATURE
/
ANDY WILLIAMS INTERVIEW BY DR ELLE TREZISE
This is part 1 of 2 of a transcript of the FMPA Podcast episode that was released in March 2024. It has been edited to improve readability.
If you’d prefer to listen, episodes can be found on the FMPA website, Apple Podcasts, SoundCloud and Spotify.
In this podcast episode host Dr Elle Trezise, a medical doctor working in London and a member of the FMPA Education Team, interviews Consultant Orthopaedic Surgeon, Andy Williams.
Dr Elle Trezise
Welcome to this Football Medicine and Performance podcast. I’m Elle Trezise, a member of the FMPA Education Team and your host for this episode. Today, I’m delighted to be joined by Mr Andy Williams.
Mr Williams is a knee surgeon who has worked with many professional athletes, including Premier League football players and Premiership rugby players. He completed his medical training at King’s College Hospital in London before completing orthopaedic training at the Royal National Orthopaedic Hospital in Stanmore, after which he undertook a fellowship in Australia where he gained some of his first experiences in sports related surgery. His expertise now lies in sports related knee injuries and knee ligament issues.
He undertakes approximately 100 anterior cruciate ligament reconstructions every year and 90% of his work is with professional athletes. He is also a prize-winning researcher of knee related issues. Thank you for joining us today.
Andy Williams
A great pleasure. Thank you, and thanks for such a flattering introduction.
Elle
It’s great to have you on board. In this episode, we’re going to discuss anterior cruciate ligament surgery for elite footballers. So already provided a bit of an introduction there, but in your own words, please tell us about your journey to date, and particularly what led to you becoming an orthopaedic surgeon for elite athletes.



Andy
The journey is ever increasing in length. Unfortunately, I’m getting older, but I still love what I do and I think my fascination in surgery and medicine really commenced as a kid. My dad had a member of his staff who was nicknamed surgeon because he kept cutting himself. So, I asked my dad what a surgeon was and when he explained, I found that a really incredible concept. So, from a young age, I was interested, but the assumption at that time was that I was going to inherit the building company and be a builder. But by age 15, it was suggested I might do medicine and my parents and myself thought that was a good thing to do.
As a result, I had my stars lined up in terms of which exams to take, what to study and luckily bit by bit, I achieved those goals. Then, after school went to King’s to study which was a fantastic experience. At that time, I had no idea what I would do. I remember being challenged by a friend of mine who asked me what I was going to do. I said I’d be a GP. He said, “no, you won’t.” I was really insulted by it! I thought, “how do you dare tell me what I’m going to do?” The only doctor I’d ever met at that stage was a GP and I assumed I’d go back home to Devon and be the village GP, if possible. I think that’s what my dad wanted, but it was never going to happen in hindsight.
I fell in love with surgery and I was lucky enough to get a first house [officer] job that involved orthopaedics and I worked for a really lovely man, Michael Mowbray at Croydon. Michael inspired me. He’s a knee surgeon; it’s no surprise I ended up doing what he did. I thought he was great. I did
Andy Williams
feature 12 info@fmpa.co.uk
Dr Elle Trezise
some general surgery there and then came back to King’s.
In fact, I did a professorial medical job because when I was a student, that seemed to be what I was good at, but my heart really wasn’t in it. So, surgery was the way forward and I sort of engineered my own training program as we did in those days. You’d get one job after another, and it was a pretty efficient way of being very well trained. I did a combination of general surgery, orthopaedic surgery, plastics, neurosurgery and cardiothoracics before becoming an orthopaedic registrar at the Royal National [Orthopaedic Hospital]. at Stanmore where I fell under the spell of a number of amazing people who absolutely inspired me to continue and try and excel in that area. Such as George Bentley and Ralph Birch. Just exceptional people amongst a whole number of others. I should mention their names but I won’t for brevity. There are some incredible people that made me full of ambition and drive.
I then went to Australia, which, really, was the most important year of my life. It was the first time I was aware that I was okay, the Australians made me realise I was all right. I wouldn’t say good, but just to be thought of as alright meant the world to me and gave me incredible confidence. When I returned to the UK, I was really tooled up to do the job. That one year of sports surgery experience was truly extraordinary and it really set me up very nicely.
I don’t think I’d have got that experience those 25 years ago in the UK at that time. Things have changed, obviously, but [Australia] was the place to go. I was so grateful for the experience there and also grateful that I was made senior lecturer at Stanmore at the Royal National [Orthopaedic Hospital] on return to the UK, which was like finishing school, if you like, and I always have the backup of Professor George Bentley who would look after me and make sure I made the right decisions.
So that was wonderful before going to Chelsea and Westminster where I was for 15 years. I was an NHS consultant for 18 years, and I was able to really build my knee practice at Chelsea and Westminster. About seven years ago, I think it was, I left the Chelsea and Westminster to concentrate on research at Imperial College [London] and also private practice.
I think things do have to give and if you’re involved in professional sport, as I am and to the level I am (it’s now 90% of my practice), the demand on that service is great and having a NHS practice at the same time is not entirely compatible with
It’s this short little bit of gristle that has dominated my life, certainly my working life, and it turns out it’s really important.
that at this level, so obviously I am very grateful to the NHS for the experience I had. I believe I worked very hard and I hope I delivered a good return on the investment the NHS made in me, but it wasn’t something that could continue. The two weren’t compatible, but I hope I now provide a return in many ways through my academic pursuits and teaching, which I do a lot of, and also my research, which helps guide treatment and management of patients, which I believe in some areas, at least, is to their benefit.
We’ve done some really cool stuff at Imperial College, particularly regarding ACL reconstruction and how to make it more reliable and the risk of re-rupture significantly less. Having done the experimentation, fine-tuned what is actually an old operation, a tenodesis on the lateral side of the knee, I’m delighted to have the data now and publish the data showing that in professional football, for example, where the average re rupture rates in the literature are about 6-8%. If you had a tenodesis in my hands, at least using the patella tendon graft, putting it in the right place and adding a tenodesis, the re-rupture rate is 2%. So that’s been a really gratifying experience.
So, I guess that’s where I am at today. 90% of my clinical work is sports, as I said. My research is clinical in terms of outcome studies on this very special group of people who really test what I do. As a result, we can differentiate treatments. I’m sick and tired of so many papers that say that this treatment is not inferior to another treatment. If you operate on the general public, you often don’t find out what’s better, but if you operate upon athletes, my God, they teach you what works and what doesn’t work. It’s been a joy to do that. Plus, the basic science research at Imperial and on top of that my clinical workload and lecturing, I guess. That’s my life at the moment. I hope that answers your question.
Elle
It’s really interesting to hear about your journey. Now let’s move on to talking a bit about the ACL and then also the surgery for repairing or reconstructing it. To start off, could you tell us a bit about the ACL and what its functions are?
Andy
It’s this short little bit of gristle that has dominated my life, certainly my working life, and it turns out it’s really important. Like all ligaments, it has a structural function in tethering two bones together and helping guide motion of the knee joint.
It’s also important because the nerve endings in it have a very important proprioceptive function. Tension within the ligament is picked up by sensors, which send a message to the brain, and the brain then fine tunes the neuromuscular control of the limb, which is probably the most important stabilizer of a joint, rather than the static function of holding the two bones together.
The static function, due to the orientation of the ligament (it passes from the femur distally in an anterior direction) is that it stops anterior translation of the tibia, but in fact, predominantly stops anterior translation of the lateral tibia, as long as the medial meniscus is intact. Also, with its obliquity in the coronal plane, it controls axial rotation, internal rotation. So, in sports involving a change of direction, it’s really important.
Needless to say, most of the time when we’re walking around, the ligament isn’t that tight. It’s got a little bit of give in it and it’s really a proprioceptive organ, but the only time it takes up the slack is during injury or being in a position of extreme rotation and usually in sport.
The ligament is in the news a lot at the moment because of the increasing awareness of it. It’s an injury that is seen particularly with change of direction sports, so called pivoting
13 medicine & performance football www.fmpa.co.uk
sports, such as football, rugby, et cetera, but also jump land sports.
Netball is almost an ACL disease. The rule that you can take one step after you catch the ball often means the players are off balance. If they were able to take a second or third step, we may see less ruptures in netballers.
Elle
Once injured symptoms can include pain, immediate swelling and a “pop” sound or sensation, as many of our listeners will know, but there’s more than one way to injure the ACL. Could you briefly explain for us the different mechanisms?
Andy
The history is classic in most people and it’s a tragedy that still probably the majority of ACL ruptures don’t have a diagnosis made for some time. They present to A&E, they have an x ray - which usually looks normal, doesn’t always, but usually - and they meet one of the most junior people in the hospital who is is unable to detect the diagnosis. It is a pity because patients sometimes fall through the net and have instability episodes which cause damage to the joint. It really is frustrating that we don’t seem to be able to improve the pickup rates. I know certain studies described that the pickup rate was around 50-50 and it doesn’t seem to have changed 20 years later.
So, the history is absolutely classic. It’s usually a change of direction during sport that goes wrong. Maybe the foot got caught in the ground or they slipped a little bit. Interestingly, that change of direction usually involves some external rotation and a bit of valgus applied to the knee. When we look at MRI scans, there’s a pattern of bone bruising that can only occur with the lateral femur falling off the back of the lateral tibia. In fact, that’s the internal rotation phenomenon. So, I have to say we still haven’t really worked out the mechanism of injury. It occurs during axial rotation, internal or external rotation, most commonly. The other mode of injury is
due to hyperextension, during which the ACL comes up against the anterior surface of the intercondylar notch and it gets guillotined in that way. That’s much less common, but it does occur.
Following the injury, as you said earlier, probably 75 % of patients will feel a pop or a snap in the knee and they’re usually aware of lateral pain. The lateral pain is because there’s effectively a dislocation of the lateral part of the tibiofemoral joint. Truly, it’s a subluxation of the knee, but the lateral femur falls off the back of the lateral tibia. On videos you often see patients grab the lateral side of the knee. Also, with the ligament being vascular, there will be rapid swelling to some degree. Sometimes it’s minor, sometimes not, but there’ll be some swelling in around 90% of cases within 1-2 hours of injury. So, that is the classic story when somebody presents to A&E, for example.
Elle
You’ve talked a little bit about some of the other structures that could be being damaged and what’s happening to them during injury, but typically what do you tend to see in terms of the other structures damaged at the same time as the ACL?
Andy
That’s a really important question. A truly isolated ACL rupture is almost non-existent. For the ACL to rupture, as I mentioned earlier, the femur has to sublux off the back of the lateral tibia. In that motion, the lateral meniscus gets drawn posteriorly and a meniscus tear in the lateral meniscus is significantly more common than in the medial meniscus, but the posterior horn of the medial meniscus, the posterior third, has a very important stabilizing function. It’s almost like a wheel chock under the medial femoral condyle, and we’re increasingly aware of peripheral meniscocapsular separations of the meniscus from the capsule on the medial side as well. So those meniscus injuries are very common.
The posterior root of the lateral meniscus can sometimes avulse, and that’s a classic association with ACL injury. Due to the torsional twist on the knee the medial ligaments and the posterolateral structures are frequently injured as well.
My current research obsession, I think it’d be fair to say, is the deep MCL. The superficial MCL restricts valgus. In early flexion, the most important restraint to external rotation is in fact not the superficial MCL, which was previously thought to be the case, but the deep MCL. We published a study that showed that on about three quarters of MRI scans, there’ll be oedema in the deep MCL associated with ACL rupture and a case that was supposedly an isolated ACL rupture. Increasingly I’m adding MCL surgery to protect my ACL grafts.
Elle
There are both surgical and non-surgical treatment options for ACL injuries. In this episode we’re focusing on the surgical treatment options but when would surgery be recommended over non-surgical management and how soon after injury would you typically do the surgery?
Andy
The first very important statement is not every ACL rupture needs an operation. A bad operation is the worst thing somebody can have, and it unfortunately still occurs, which is depressing. The variability of surgery is one of the biggest challenges in modern medicine.
Obviously, there are some great surgeons out there who do a great job repeatedly. But there are others who seem to be less able to do so and I think to delivering consistency in surgery is something we have to work out as a surgical community to deliver.
The patient has to be educated that they should not put up with anything that is second best.
What I would say is most young active people do best to have a good ACL reconstruction. I’m choosing my words extremely carefully because, as I say, bad surgery or a surgery that has significant complication - which of course does occur even with good surgery - will leave a patient worse off than they would have been without surgery. When it comes to the risk benefit analysis for young active people (obviously I’m biased, I’m a surgeon) but I strongly believe that most young people do well to have a good ACL reconstruction for two reasons. One is to allow them to enjoy life and not have to worry about an unstable knee, and two, because I do genuinely believe it protects the joint.
I know that’s a controversial view and if you look at the literature, you can argue against that, but I think the literature is increasingly showing that a good ACL reconstruction reduces subsequent meniscal pathology and,
feature 14 info@fmpa.co.uk
as night follows day, if you lose meniscal function, you get osteoarthritis.
I think we’re starting to get data that will prove that. On the other hand, I do see patients who come through who’ve had a long period of nonoperative treatment and their knee has deteriorated stepwise whilst some doctor usually or a physio has presided over episodes of instability.
So, non-operative treatment is fine, as long as the patient doesn’t have instability. That can be occult instability, with which the patient’s not aware and that’s the big problem. If a patient falls over, they’ll seek help and I can fix them and everyone’s happy. But if they don’t keep falling over and they think their knee is alright unwittingly they can damage the knee progressively to a pretty bad state and every year I deal with people who really miss the boat and we can help them but they never get a good result because they’ve got osteoarthritis and all I’m doing is putting the brakes on it and they’re in for a series of operations for the rest of their life.
ACL rupture is a very potentially life changing injury in the long term. Most people who have a good ACL reconstruction do very well. I’m now seeing my patients 25 years out. They have a new injury. They’re old and it’s very pleasing to see on their MRI scans, they got little or no osteoarthritis in the majority of cases.
I do strongly believe this is a good operation. I admit it’s hard to prove the protective effect for joint surface, but I think the evidence now for protection of the menisci is overwhelming, actually. The worst thing is a patient having recurrent instability. So, the deal is if you go for non-operative treatment, you need to be really motivated to keep your neuromuscular control up with a maintenance program of rehab exercises, that will be focusing on trunk, pelvis, and balance drills and you’ve got to keep it up for the rest of your life.
The patient has to be educated that they should not put up with anything that is second best. In particular, a feeling of insecurity equals instability and the presence of any swelling is bad news. They should be well advised to get their knees fixed if those things happen.
Elle
Provided a little bit of a spoiler in a bio I was reading for you at the beginning, but do you prefer repair or reconstruction of the ACL? And why?
Andy
Repair of the ACL is something which was dealt with years and years ago, and the results were awful. We were taught that the ACL

wouldn’t heal. The reason it wouldn’t heal is because synovial fluid doesn’t let the blood clot, whereas if you have an extra articular ligament injury, the blood between the ends of the broken fibres will set and glue - fibrin is nature’s glue - but the reality is ACLs do heal and can heal.
Sometimes we’ll examine a patient acutely and they’ve got a loose knee and a month or two later when they come for surgery, they’ve actually tightened up. But if they’ve still got a positive pivot shift that means that even though the ACL may have healed, it’s not functioning. So, we’ve got to be very careful and differentiate healing.
There’s a lot of interest in non-operative treatment and also repair at the moment. There was a recent British Journal of Sports Medicine publication on a bracing technique from Sydney, Australia. The so called “cross technique” and the MRI scans show healing. I think it’s genuine, but the problem with a MRI scan that looks favourable is that it doesn’t equal a stable knee. So, first of all, you have to be very careful that all that glitters isn’t gold. Just because the ACL looks like it’s joined up doesn’t mean to say it’s actually working unless it’s joined up to the femur in the right position.
The problem with repair is, first of all, we don’t have enough data to know whether it works or not. In elite sports, you’re going to tend to do an operation that works and that’s a reconstruction. What I wouldn’t be prepared to do is effectively an experiment without data. If the data is there and proves to me that an ACL repair is reliable, then I would do it.
Truth is I probably do between 5-8 ACL repairs a year and they’re usually a clean avulsion off the tibia. Whereas in youngsters you often get a bone fragment, though you don’t always.
Those do extremely well. The popularity of ACL repair is really in cases of ACL injury that are close to the bone on the femur and there are now arthroscopic techniques. It means the surgery is less invasive and it’s suddenly become very attractive. The problem is that with the techniques concerned, often there’s a crimping of the ACL which shortens it and therefore you can’t actually get the ACL back up deep into the intercondylar notch where it should be. I suspect that quite a few of the repairs are non-anatomic and so their function is compromised.
Some of the repair enthusiasts - that sounds like an insulting term - but those who are popularizing [repair], use the phrase “it burns no bridges.” Well, I think it’s a really irresponsible phrase because if a poor patient has had an ACL repair, they may be unaware that the ACL is not functioning, and they can actually end up having a lot of damage before the penny drops and they get a reconstruction.
So, I’m sorry to say to the surgeons who promote ACL repair that, like any operation, you can never say it doesn’t burn bridges. It’s a lovely concept, but it just isn’t true. Whatever we do should fix the knee and we should have a high degree of success with it, and at the moment, we just don’t have the data on repair and I don’t believe it’s as reliable as reconstruction.
For my athletes, I would stick with reconstruction.
Part 2 will be released in a future edition of the FMPA editorial. In part 2, Mr Williams discusses considerations when choosing a graft source for reconstructions, how soon after injury surgery should be done, how he works with club staff to optimise outcomes, the importance of psychology and good communication, and his approach to reruptures post-surgery.
15 medicine & performance football www.fmpa.co.uk

LATERAL COLLATERAL LIGAMENT INJURIES OF THE KNEE - THE PRECURSOR TO HAMSTRING INJURY
FEATURE / ADAM JOHNSON
Introduction
Hamstring injuries are now recognised as the most prevalent injury within elite male soccer. This huge burden of time, economic and performance loss has led to a wealth of literature being published to try and better understand the risk factors associated with these injuries. Following a small cohort of players who have sustained hamstring injuries shortly after returning to play from lateral collateral ligament (LCL) knee injuries, this article aims to discuss the potential mechanisms and clinical reasoning by which the LCL injury could predispose an athlete to subsequent hamstring injury.
Instability
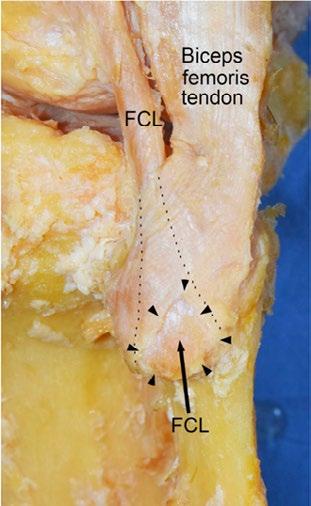
The primary role of the LCL is to provide passive varus stability to the knee, with the biceps femoris muscle providing secondary dynamic stability 1 Anatomically, the LCL is reported to intersect between the medial and lateral heads of the biceps femoris distal insertion and onto the lateral aspect of the fibular head (Figure One). It is proposed that this anatomy means that contraction of the biceps femoris muscle results in compression and subsequent tautness of the LCL 3, which therefore assists in passively stabilises the posterolateral corner (PLC) of the knee.
In the case of a previously injured, and subsequently lax LCL, it could be hypothesised that any contraction of the biceps femoris would not result in the same levels of passive stability being brought about through compression of the LCL. Therefore, the dynamic stabilisers, which include the biceps femoris, are required to work harder to achieve the required levels of stability in the posterolateral corner. This finding of increased biceps femoris activity to function as a dynamic compensatory mechanism is something that has been acknowledged by Limbird et al4within the anterior cruciate ligament (ACL)-deficient knee. The findings of this study suggested that there would be greater activation of
Team Physiotherapist Everton Football Club
First
feature 16 info@fmpa.co.uk
the biceps femoris when transitioning from swing to stance phase of gait. By increasing the secondary demands on the biceps femoris, theoretically the risk of injury would increase if this pattern seen in ACL-deficient patients transfers into the LCL-injured patient.
Another consideration following LCL injury is that there is likely to be increased tibial external rotation as demonstrated via a positive dial test 1. Of specific interest is if increased tibial external rotation is present at 30 degrees of knee flexion, as it has been demonstrated that this is the point at which subjects produced levels of lateral hamstring activation greater than 150% of maximal voluntary contraction5. Again, it could be theorised that if LCL injury results in greater tibial external rotation then demands would be shifted even further onto the lateral hamstrings, potentially contributing to subsequent injury.
Neural Irritation
The biceps femoris has a unique innervation pattern with the long head and short head being innervated by the tibial and peroneal components of the sciatic nerve respectively. This has been proposed as a causative factor to hamstring injury, with either an imbalance in stimulation intensity, or a lack of coordination in the timing of stimulation between the two heads resulting in muscle injury6
Within the research it has been acknowledged that athletes with a history of hamstring injury can present with neural sensitivity on a slump test7. Given that the LCL runs in such close proximity to the common peroneal nerve around the fibula head, it is proposed by this article that extra-neural pathology could drive increased neural sensitivity. It seems appropriate to hypothesise that the initial trauma to the LCL has the potential to produce similar alterations in neural dynamics as can be seen in some athletes with a history of recurrent hamstring injury, therefore increasing the risk of hamstring injury.
Rehabilitation Alterations
• Due to the increased demands on the biceps femoris following LCL injury, it is proposed that simply delivering symmetry or pre-injury strength scores within hamstring testing on return to training will not be sufficient. Rehabilitation should look to provide overloading of the affected hamstring to ensure that the posterior thigh musculature is suitably conditioned to cope with the new demands that will be placed upon it in a sporting environment.
• It is also suggested that when performing rehabilitation work following LCL injury, the potentially
done immediately, prolonged symptoms which were not present prior to knee injury should be addressed for the reasons stated earlier in this article.
Conclusion
• This article hopes to drive discussion and further research surrounding the potential links between initial LCL injury and subsequent hamstring injury.
• As therapists managing LCL injuries, we must look to recognise the biomechanical impacts that laxity resulting from the injury will have, whether that is providing greater stability demands on the musculature around the knee or shifting the demands laterally due to increased external rotation.
• Further interventions such as injection therapy may be required to address instability in those injuries which fall just short of the threshold for surgical reconstruction.
References
1. Chahla, J., Moatshe, G., Dean, C.S. et al. Posterolateral Corner of the Knee: Current Concepts. The Archives of Bone and Joint Surgery 2016;4(2):97-103.
2. Takahashi, H., Tajima, G., Kikuchi, S., et al. Morphology of the fibular insertion of the posterolateral corner and biceps femoris tendon. Knee Surg Sports Traumatol Arthrosc 2017;25:184-191.
new ranges of tibial external rotation must be considered. Therapists must look to work their players in externally rotated positions rather than trying to avoid them, so that the players learn how to tolerate these conditions in a competitive environment.
Further Interventions
• In cases where there is significant varus knee laxity seen on clinical assessment but which does not meet the threshold for surgical repair, it is suggested that injection therapy such as dextrose prolotherapy could form part of the management strategy. These injections aim to promote further stimulation to healing and in turn a reduction in the potentially excessive levels of varus knee laxity.
• It is also recommended that therapists monitor the outcome of the slump test of players following LCL injury. If there is significantly increased neural sensitivity seen on the affected side versus the uninjured side, then there may be a clinical discussion surrounding the efficacy of providing an epidural injection aimed at reducing these symptoms. Although this would not be
3. Tubbs, R.S., Caycedo, F.J., Oakes, W.J. et al. Descriptive Anatomy of the Insertion of the Biceps Femoris Muscle. Clinical Anatomy 2006;19:517-521.
4. Limbird, T.J., Shiavi, R., Frazer, M. et al. EMG profiles of knee joint musculature during walking: Changes induced by anterior cruciate ligament deficiency. Journal of Orthopaedic Research 1988;6(5):630-638.
5. Beyer, E.B., Lunden, J.B. & Giveans, R. Medial and Lateral Hamstrings response and force production at varying degrees of knee flexion and tibial rotation in healthy individuals. International Journal of Sports Physical Therapy 2019;14(3):376-383.
6. Burkett, L.N. Investigation into hamstring strains: The case of the hybrid muscle. Journal of Sports Medicine 1975;3(5):228-231.
7. Kornberg, C. & Lew.P. The Effect of Stretching Neural Structures on Grade One Hamstring Injuries. The Journal of Orthopaedic and Sports Physical Therapy 1989;10(12):481-487.
8. Macdonald, B., McAleer, S., Kelly, S. et al. Hamstring rehabilitation in elite track and field athletes: applying the British Athletics Muscle Injury Classification in clinical practice. British Journal of Sports Medicine 2019;53:1464-1473
Figure 1: A lateral view of the left knee demonstrating the attachments of the Fibular Collateral Ligament and the Biceps Femoris tendon into the lateral aspect of the Fibular head. Taken From - Takahashi et al., 20172
17 medicine & performance football www.fmpa.co.uk

CARE

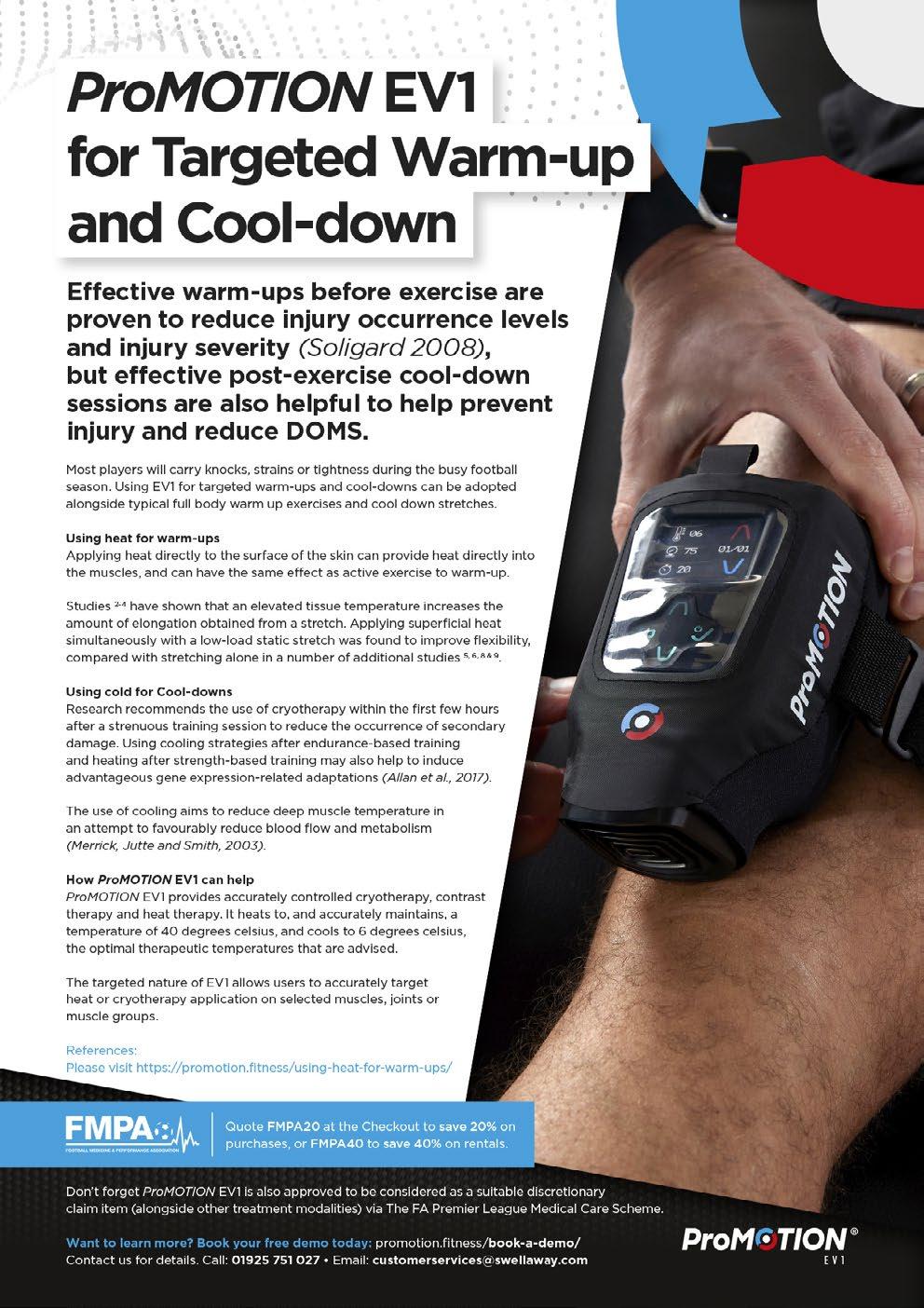
ProMOTION EV1
A versatile device, designed to tackle the key challenges faced with soft tissue injury recovery and rehabilitation. It can also be used for handheld massage, pre-rehab and for targeted warm up/ cool down applications.
FMPA Members can save 20% when purchasing the Elite Package (pictured) and 40% on rentals. Get in touch to find out about other packages available.
ProMOTION EV1 Elite Package
Price: £2,800+vat (including 20% Discount for FMPA Members Use code FMPA20 at the checkout to claim your discount) promotion.fitness/exclusive-fmpa-members-offers/ customerservices@swellaway.com
Tel: 01925 751027

Performance Climate Control Chamber
Temperature 12 to 40°C; Humidity 30 to 80%; Altitude 0 to 5,750m. 10% discount to all FMPA members, when ordering before 31st March 2024. www.sportingedgeuk.com info@sportingedgeuk.com
Tel: +44 7879 494 279

Komfi Med True Air Hybrid Comfort Mattress
Wake up feeling refreshed and rejuvenated with the KomfiMed True Air Hybrid Comfort Mattress. Buy now

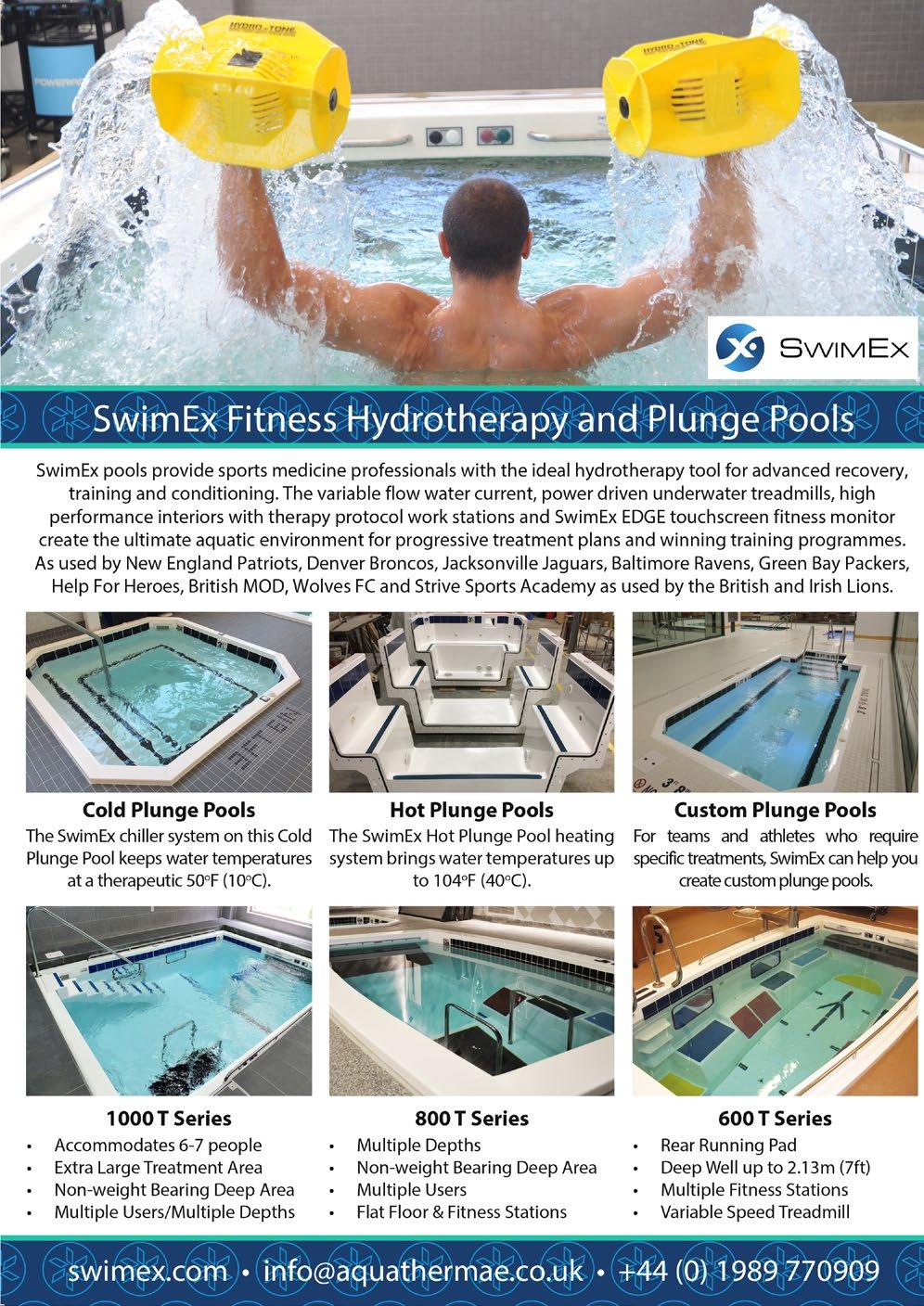
Custom Plunge Pools
For teams and athletes who require specific treatments, SwimEx can help you create custom plunge pools. richard@aquathermae.co.uk 07484 070765 aquathermae.co.uk

ScribePro Team
Our game-changing medical records are designed with clinical integrity and improved player care in mind. The result is a versatile system, enjoyed by sports teams around the world and across sports.
For more information click here
Contact: hello@scribepro.co

Compex SP 8.0
Recover faster, enhance performance, strength/ endurance, help to avoid injury and manage pain with the Compex SP 8.0. Our top of the range wireless stimulator is designed for athletes who train and compete on a regular basis. It combines wireless technology to allow freedom of movement, with the maximum range of programmes and a range of MI-technology to enhance your muscle stimulation experience. For more information on this unit and our full recovery range, please contact helen.cartwright@enovis.com
PLAYER
commercial@fmpa.co.uk www.fmpa.co.uk/commercial-partners/

TRUST VERSUS TROPHIES: MANCHESTER CITY’S UNIQUE ABILITY TO BALANCE PSYCHOLOGICAL SAFETY AND RISKTAKING FOR OPTIMISED PERFORMANCE
FEATURE / CHRISTIAN PSZYK
Manchester City, treble winners, 2022/2023. Now officially the best team in England and across Europe for the past season, Pep Guardiola and his team have created an unique and oft insurmountable machine of success and optimised performances. There have been numerous reasons cited for their imperious form, most notably the managerial genius of Guardiola, and the statistically incredible performances of Erling Haaland, now holding the record for most goals in a 38 game season in the Premier League, and Kevin De Bruyne, often viewed as the best playmaker in world football. However, how has this team of perceived superstars, including the then most expensive Premier League player of all time Jack Grealish and 2022
World Cup winner Julian Alvarez, adapted so well to an idea of the team’s success taking priority over individual plaudits, and what can football learn from their example? While exploring this question, this article will focus on one, but by no means the only element: balance, firstly represented by the compromise between control and creativity, and secondly the balance between psychological safety and pressure (Salcinovic et al., 2022).
From a statistical perspective, over the course of the 2022-2023 season Manchester City were the team with the highest completed passes at 23,263, but only played 51 offside passes, the second lowest total and by far the lowest Premier League average of 1.34
per game and 0.22% of their completed passes, according to FBRef (n.d.). By comparison, however, Liverpool played a Premier League highest 84 passes offside in the 2022/23 season, from their total pass completion being second highest at 20,043, resulting in a 0.42% and an average of 2.21 offside passes per 90 minutes. So why the considerable difference between the two top passing teams? Does Manchester City’s squad simply contain the better judges of space and timing or is it something more intentional in the way Pep Guardiola has set this team up?
By contrast, Brighton and Chelsea, the next two teams in terms of top completed passes metric, both score considerably
21 feature www.fmpa.co.uk medicine & performance football
CPsychol, AFBPsS, EuroPsy
Increased psychological safety in a high performance environment is not a guarantee of sustained success, or success at all
higher than Manchester City, at 0.36% and 0.39%, highlighting that there is a level of consistent overperformance considering the remaining top passers in the league. The observational perspective suggests that the teams in and around Manchester City have equally as impressive plaudits, with players like Trent Alexander-Arnold, Moises Caicedo and Thiago Silva all lauded for their individual passing abilities.
Possession versus Progression
One interpretation of this trend could be the style of play that Manchester City have adopted and perfected over the past few seasons, dominating time on the ball, and favouring recycling and continuously probing the opposition’s defense with
possession, rather than looking to force openings at increased speed, and therefore risk. Generally, the individual statistics underpin this, with pass completion and distance heavily favouring short passes, and the two top passers in terms of frequency, Rodri with 2723 and Ruben Dias with 1928, only producing one offside pass between them, a remarkable 0.02%. This is further supported by the hybrid role debuted by John Stones, as he regularly stepped into midfield and distributed the ball effectively and helped to establish greater control and influence throughout the course of a game.
However, their greatest playmaking threat, responsible for a team high 16

assists, is Kevin De Bruyne and his underlying statistics are in complete contrast to the rest of his team mates. In fact, KDB has played 12 offside passes this Premier League season, third highest overall, and only topped by two players. These were Kieran Trippier on 13, who had made over 800 passes more, and Morgan Gibbs-White with 16, who was by far the most creative player for Nottingham Forest, recording 5 assists more than the next player, who were also the team with the highest percentage of offside passes at 0.7%, a staggering 218% higher than Manchester City’s season average. Therefore, looking at the underlying numbers, how does Kevin De Bruyne continue to play so outwardly carefree with such a high level of risk, when the rest of his team is seemingly the safest team in possession, and directly facilitating Guardiola’s instruction to provide him with the optimal platform for aggressive forward momentum?
The City Mentality
The key factor that stands out is the manner in which KDB is able to attack this very unique and challenging situation with confidence and complete trust in his own ability, knowing that there is no fear of punishment or judgement from his coaches or teammates, and that they will instead continue to support and facilitate his efforts, regardless of immediate results. In a system of strict positional ideals and fixed principles that bring Pep Guardiola’s incredible tactical vision to life, De Bruyne is the player who stands out, perpetually in motion, and was described by his manager as “a guy who has to move, move, move” after Manchester City’s thumping 7-0 win over RB Leipzig in the Champions League Round of 16 in March.
De Bruyne had the second lowest pass completion rate for Manchester City in the Premier League, after only Haaland. The evidence therefore suggests that Kevin De Bruyne is possibly a less impressive, or at least less efficient, passer of the ball than his colleagues. However, the fact that he also has 7.4 Expected Assists more than any of his teammates, and nearly double the number of Key Passes, indicate that it is not that simple. Instead, he is the player who is free to take risks during a game, while still being protected from the potential repercussions of making mistakes and losing the ball in a way that many of his teammates seem to avoid (Wagstaff et al., 2012).
This aligns closely with the new definition of psychological safety proposed by Vella et al. (2022), who summarised
feature 22 info@fmpa.co.uk

psychological safety as “the perception that one is protected from, or unlikely to be at risk of, psychological harm (including fear, threat, and insecurity) in sport” However, increased psychological safety in a high performance environment is not a guarantee of sustained success, or success at all, as recent research has highlighted that making athletes in these highpressured situations too comfortable could result in a negative impact on performance (Taylor et al., 2022). This possibility is heightened by the increased schedule Manchester City faced in the 2022-2023 season, playing 65 games, their highest total in the Premier League era besides the 2020-2021 season, which was interrupted by COVID-19 and presented a different challenge (Rowell et al., 2018).
“Shut up”
The media has occasionally depicted De Bruyne as the rogue maverick, rebelling against the rigidity of Pep Guardiola’s control, seen especially in the coverage around the perceived argument the pair had during the game against Real Madrid in the semi-final of the Champions League. De Bruyne was deemed to have told his manager to ‘shut up’, and soon reports emerged of concerns around the dressing room and a potential clash of personalities and ideas. However, after the game Manchester City players and the manager explained that it was a healthy exchange, and a part of football as it is such a highly intense and often emotional game. Furthermore, within a
psychologically safe team environment, the most beneficial state is labelled by Clark (2020) as Challenger Safety, where team members are provided the space to question and challenge each other, and their superiors.
Within the context of the game, that was exactly what seemed to occur between De Bruyne and his manager, challenging his feedback and sharing his perception of events, and enabling the team to be more productive and progressive as a result. This incident, alongside previous in-game exclamations from De Bruyne, such as the now infamous “let me talk” clip from his side’s game against Napoli in 2017, reinforce that this is a trait that Guardiola has decided is not detrimental to his team. This is highlighted by Jowett et al. (2023), who identified that coaches who give their athletes a voice, and the freedom to express it, inherently create psychological safety and therefore open the door to increased performance with the appropriate implementation.
By comparison, Guardiola has shown that he has no issue challenging and removing the biggest names in his squad if they do not fit his ideals, with examples ranging from Barcelona favourites like Ronaldinho and Deco in his first season, through to Joe Hart and Joao Cancelo more recently at Manchester City. This again reiterates that Kevin De Bruyne’s risk taking and proverbial aggression and drive to progress the ball is a key principle of this
new iteration of Guardiola’s tactical and psychological evolution, and a component that Guardiola, his staff and the club, have actively encouraged, or come to recognise as ultimately being beneficial to the playmaker and the team’s performances.
In a different respect, this can also be seen in the style adopted by players like Jack Grealish, Phil Foden and Riyad Mahrez, all creative mavericks in their own right, but comfortable to be system players that provide a basis for control. The fact that players who are seen as creative and in-game threats are not concerned about their statistical output but are happy to contribute meaningfully in several areas, shows that this is a squad wide mentality that has been specifically trained and entrenched to great benefit, as the need to prove themselves is reduced and they know that they can show their worth without having to be the player who scores or assists relentlessly, and sometimes selfishly. Therefore, for Manchester City’s squad, it is evident that success is not only measured in an individual’s goals and assists metrics, but instead how they are able to contribute to the team’s unified efforts. This is in stark contrast to how other players are viewed by the media, pundits and even some coaching staff, with Grealish often deemed not productive enough despite continued praise from his manager.
Therefore, looking at the system demands that Guardiola has placed upon this
23
www.fmpa.co.uk
medicine & performance football
Manchester City team, it is clear that a culture has been established that gives Kevin De Bruyne the freedom to be his spectacular and devastating self on the football pitch without the fear of direct judgement or retribution. This is despite the fact that he has been benched, injured and rotated throughout the season, highlighting that the team environment is one conducive to being supportive, working as a unit and striving towards the common goal of sustained long-term success, in line with the key elements of maintaining a performance culture for success (Lochbaum et al., 2022 & Salcinovic et al., 2022).
England and Europe, again?
Having already conquered the Premier League, the FA Cup and the elusive Champions League, what next for this footballing juggernaut? Their summer recruitment brought a new dimension of footballing ability into their squad, with several of Europe’s elite ball carriers now present in one team and contributing to this system. These new signings included Matheus Nunes and Mateo Kovacic, where the former is in the 97th percentile for successful take-ons per 90 minutes, and the latter is in the 88th percentile for progressive passes per 90 minutes in the Premier League. Furthermore, Jeremy Doku will play a huge role in this new skillset, as he is well documented as being one of the best one to one players in
European football, which is demonstrated by his progressive carries, successful takeons, touches in the opposition penalty box and progressive passes received all ranked in the 99th percentile for midfielders in European football (FBRef, n.d.).
In conclusion, it could be argued that Pep Guardiola and his staff have created potentially the optimal blend of psychological safety and a clinical edge with players like Erling Haaland and Kevin De Bruyne fully freed to be devastating and truly creative risk-takers. This has been achieved while managing the sociocultural pressures of elite sport and the strain of individual and team relations to promote optimal performance, an interesting anecdotal demonstration of psychological safety and performance working collaboration (Gosai et al., 2023). Therefore all credit has to go to the team’s united effort to maintain this culture and psychological setup, which could have influenced decisions like letting Joao Cancelo go, and ultimately prompting the switch for John Stones into a supporting midfield role (Izquierdo & Anguera, 2021). Moving forward in 2023/2024 it will be exciting to watch the continued development of this treble winning squad, and how this new dimension of ball progression will drive Manchester City to potentially stay ahead of the chasing pack and celebrate further success in England and beyond.
Summary
• Manchester City have combined excellence throughout their team with an ability to look beyond individual outputs, measuring their success in performances and creating an environment that thrives as a unit.
• Psychologically, the players feel safe to be patient and simultaneously recognise which risks are worth taking, and which are counterintuitive to their gameplan.
• Foden, De Bruyne and Haaland and the rest of the squad are embracing a culture of “Challenger Safety”, and are able to adapt and execute their roles accordingly.
Christian Pszyk CPsychol, AFBPsS, EuroPsy
Chartered Sport and Exercise Psychologist, having worked with Premier League academies, British Judo, elite athletes, teams and coaches

References
Clark, T. R. (2020). The 4 stages of psychological safety: Defining the path to inclusion and innovation. Berrett-Koehler Publi shers.
“2022-2023 Premier League Stats.” FB Ref, https://fbref.com/en/comps/9/Premier-League-Stats. Accessed 14 Sept. 2023.
“2022-2023 Jeremy Doku Stats.” FB Ref, https://fbref.com/en/players/fffea3e5/Jeremy-Doku. Accessed 14 Sept. 2023.
Gosai, J., Jowett, S., & Nascimento-Júnior, J. R. A. D. (2023). When leadership, relationships and psychological safety promote flourishing in sport and life. Sports Coaching Review, 12(2), 145-165.
Izquierdo, C., & Anguera, M. T. (2021). The analysis of interpersonal communication in sport from mixed methods strategy: The integration of qualitative-quantitative elements using systematic observation. Frontiers in psychology, 12, 637304.
Jowett, S., Do Nascimento-Júnior, J. R. A., Zhao, C., & Gosai, J. (2023). Creating the conditions for psychological safety and its impact on quality coach-athlete relationships. Psychology of Sport and Exercise, 65, 102363.
Lochbaum, M., Stoner, E., Hefner, T., Cooper, S., Lane, A. M., & Terry, P. C. (2022). Sport psychology and performance meta-ana lyses: A systematic review of the literature. PloS one, 17(2), e0263408.
Rowell, A. E., Aughey, R. J., Hopkins, W. G., Esmaeili, A., Lazarus, B. H., & Cormack, S. J. (2018). Effects of training and co mpetition load on neuromuscular recovery, testosterone, cortisol, and match performance during a season of professional football. Frontie rs in physiology, 9, 668.
Salcinovic, B., Drew, M., Dijkstra, P., Waddington, G., & Serpell, B. G. (2022). Factors influencing team performance: What can support teams in high-performance sport learn from other industries? A systematic scoping review. Sports Medicine-Open, 8(1), 1-18.
Taylor, J., Collins, D., & Ashford, M. (2022). Psychological safety in high-performance sport: Contextually applicable?. Fronti ers in Sports and Active Living, 4, 169.
Vella, S. A., Mayland, E., Schweickle, M. J., Sutcliffe, J. T., McEwan, D., & Swann, C. (2022). Psychological safety in sport: a systematic review and concept analysis. International Review of Sport and Exercise Psychology, 1-24.
Wagstaff, C., Fletcher, D., & Hanton, S. (2012). Positive organizational psychology in sport: An ethnography of organizational functioning in a national sport organization. Journal of applied sport psychology, 24(1), 26-47.
24 info@fmpa.co.uk medicine & performance football feature

PREVENTION AND REHAB OF HAMSTRING INJURIES
FEATURE / BRAM SWINNEN
Introduction
Hamstring injuries are a major problem in sports, especially those involving intensive sprints, jumps, and kicks, such as football, rugby, track and field, and basketball (Kujala et al. 1997, Woods et al. 2004, Orchard et al. 2002). These injuries are highly prone to recurrence; approximately one-third of them recur, particularly within the first two weeks after an athlete returns to sport (Orchard et al. 2002). The risk of re-injury remains high for at least a year, and often the subsequent injury is more severe than the original strain (Warren et al. 2010). The high recurrence rate shortly after athletes return to sport indicates that many rehabilitation plans may be inadequate (Swinnen 2016). To develop effective rehabilitation programs, it is crucial to address several questions: What are the risk factors that elevate the rate of hamstring injuries and how can training or rehabilitation plans mitigate these risks? Considering a previous hamstring strain is a significant risk factor for
future injuries, it’s important to understand the changes in muscle properties following a strain and why these changes increase the risk of recurrence upon returning to play (Brockett et al. 2004). Identifying the most effective exercises and training parameters is essential for preventing injuries or aiding in rehabilitation to prevent re-injury.
Risk factors
Strength and Fatigue:
During sprinting, the hamstrings need to constantly brake the knee extension generated by the quadriceps muscles (Chumanov et al. 2012). Because the quadriceps are stronger than the hamstrings, the hamstrings will fatigue faster. A significant asymmetry between these muscle groups results in a quicker decline of the eccentric strength of the hamstrings and increases the risk of a hamstring injury (Croisier et al. 2008).
Fatigue: Hamstring injuries occur more frequently in the latter stages of a match (Ekstrand et al. 2011, Woods 2004). Hamstring strength progressively decreases with playtime. The fatigue effect also depends on sprint speed. Higher sprint speeds lead to a greater reduction in eccentric hamstring strength. The diminished ability of the hamstrings to generate force reduces their capacity for energy absorption and increases the risk of hamstring ruptures.
Core instability: The force and stretch of the iliopsoas during the late stance phase and the beginning of the swing phase induce an increased anterior tilt of the pelvis. This anterior pelvic tilt results in greater stretching of the hamstrings of the contralateral leg, which is simultaneously in the late swing phase. The increased pelvic tilting during sprinting, due to core instability and limited pelvic control,

27 feature www.fmpa.co.uk medicine & performance football
High Performance Coach Author of Strength Training for Soccer
results in greater stretch and strain of the hamstrings during the terminal swing phase (Chumanov et al. 2007).
Weak or inhibited gluteal muscles: Shirley Sahrmann said, “Whenever you see a muscle injury, you need to look for a weak synergist.” A synergist is a muscle that performs the same movement or function. Delayed activation of the gluteus maximus can lead to hamstring dominance during hip extension, resulting in a higher load on the hamstring muscles. The gluteal muscle and the long head of the biceps femoris play an important role in stabilizing the pelvis. It has been shown that weakened or delayed activation of the gluteal muscle results in an unstable sacroiliac joint and compensatory activation pattern of the biceps femoris (Nelson-Wong et al. 2012).
Function of the hamstring muscles during sprinting
Most of the hamstring injuries occur during the terminal swing phase and predominantly affect the long head of the biceps femoris (Koulouris et al. 2003; Chumanov et al. 2007). During this phase, as the knee extends and the hip flexes, the bi-articular hamstrings elongate across both joints. The muscles lengthen and contract eccentrically to control knee extension (Chumanov et al. 2012). Just before foot-strike, they reach peak force and length (Thelen et al. 2005a; Thelen et al. 2005b; Schache et al. 2009). At high speeds, EMG activity
in the hamstring muscles during the terminal swing phase surpasses that of maximal voluntary contraction (Kyrolainen et al. 1999). Due to differences in hip extension and knee flexion moment arms, the long head of the biceps femoris experiences significantly larger peak lengths than the semitendinosus and semimembranosus (Thelen et al. 2005a). This increased musculotendon stretch in the biceps femoris may contribute to its higher susceptibility to injury compared to the other hamstring muscles (Thelen et al. 2005a). While peak lengths do not significantly increase with faster sprinting speeds, hamstring muscle force and power do increase steadily with speed (Chumanov et al. 2007; Chumanov et al. 2011; Thelen et al. 2005a; Schache et al. 2010).
Altered muscle properties and higher risk for recurrence
A history of hamstring injury has been linked to a shift in the length-tension curve towards shorter muscle lengths and reduced eccentric strength near full knee extension (Brockett et al. 2004). This suggests that post-strain, the hamstring muscles generate their greatest force at shorter muscle lengths than before the injury, leading to decreased end-range strength. The presence of scar tissue at the injury site, being less compliant than contractile tissue, may be responsible for this shift towards shorter muscle lengths (Kaariainen et al. 2000; Butler et al. 2004). Since peak force during sprinting occurs
at longer muscle lengths, a muscle that produces maximal force at shorter lengths is at a higher risk of re-injury (Brockett et al. 2004). This might be a key reason for the high recurrence rate in the first month after returning to play. Extensive scarring, which makes the muscle less compliant, necessitates that the muscle fibers near the scar tissue elongate more to achieve the same overall muscle length (Butler et al. 2004). Therefore, re-injuries often occur near the site of the prior injury.
Another factor contributing to reduced end-range eccentric hamstring strength is decreased activation of the biceps femoris towards full knee extension (Sole et al. 2011). Many athletes return to sport with inhibition and selective atrophy of the long head of the biceps (Silder et al. 2008; Croisier et al. 2002). The strength abnormalities and scar tissue remodeling can maintain an elevated risk of re-injury for more than six months after the initial muscle strain (Silder et al. 2008; Croisier et al. 2002), highlighting the importance of functional loading and progressive rehabilitation programs.
Eccentric hamstring strengthening Eccentric strengthening of the hamstring muscles in an elongated range of motion forms a critical component of rehabilitation or training (Brockett et al. 2004; Arnason et al. 2008; Askling et al. 2003; Gabbe et al. 2006; Petersen et al. 2011). This training modality has been shown to shift

feature 28 info@fmpa.co.uk
the force-length curve to longer muscle lengths, thereby gradually shifting the optimal muscle length to the zone in which the hamstrings primarily operate (Schmitt et al. 2012; Brockett et al. 2001; Brughelli et al. 2010; Brughelli et al. 2009; Kilgallon et al. 2007). An eccentric training program has been shown to significantly reduce the incidence of both new (60%) and recurrent (85%) hamstring injuries in soccer players (Thorborg 2012). After just 10 days of eccentric hamstring training, a shift in peak torque towards greater muscle lengths has been detected (Brockett et al. 2004; Brockett et al. 2001; Brughelli et al. 2010; Brughelli et al. 2009; Seynnes et al. 2007).
Also regular strength training, using exercises that are more challenging at lengthened ranges of motion, can shift peak torque towards greater muscle lengths (Goldspink et al. 1999, Seynnes et al. 2007).In contrast, static flexibility programs have proven ineffective in influencing the length-tension relationship, and therefore, are not effective in preventing hamstring strains (Arnason et al. 2008).
Re-activating the long head of the biceps femoris
Rehabilitation programs must focus on re-activating the long head of the biceps femoris muscle to counteract the inhibition and atrophy associated with hamstring injury. The long head of the biceps femoris is a thick muscle with a large crosssectional area and short, pennate fibers, making it especially suited for high-force contractions over shorter distances (Kellis et al. 2012; Makihara et al. 2006). During the stance phase of running the hamstring muscles have to contract forcefully while there is less change in muscle length because of the simultaneous hip and knee extension. This is in accordance with research that revealed the forward lunge, which involves simultaneous knee and hip extension, especially loads the long head of the biceps femoris (Mendiguchia et al. 2013). Therefore, exercises that simulate the leg action during the stance phase of running, such as resisted slide-board back lunges, step-ups, or walking lunges, are recommended for countering the inhibition and atrophy associated with hamstring injury. Integrating hip-dominant exercises, like lunges where the length of the hamstrings remains relatively constant, is advised for every athlete’s rehabilitation and training schedule.
Horizontal force production
Acceleration speed is a critical performance characteristic in team sports. Recent research emphasizes that generating large amounts of horizontal force is more
crucial for acceleration than vertical force production (Rabita 2015). Athletes returning to sport post-hamstring injury often show reduced horizontal force and power outputs during sprinting (Mendiguchia et al. 2014). This diminished ability to produce high levels of horizontal force may be linked to the inhibition of the long head of the biceps femoris, highlighting the need for hamstring exercises that replicate muscle actions during a stance phase of sprinting. Decreased horizontal force production capacity during sprint acceleration has been observed following hamstring injuries in football players (Roksund 2017). Additionally, a reduced ability to generate horizontal force during the acceleration phase of sprinting is indicative of an increased risk of hamstring injuries (Edouard 2021). Athletes should incorporate exercises that train horizontal force production for both performance enhancement and injury prevention. However, many traditional lower body strength exercises, like squats, Olympic lifts, and deadlifts, primarily focus on vertical force production.
Re-activating the gluteus maximus and enhancing intermuscular coordination
The gluteus maximus is a very powerful hip extensor and also plays an important role in the stabilization of the lumbo-pelvic region. Pelvic instability, back pain or other lower body injuries can alter the muscle activation timing (Leinonen et al. 2000, Nelson-Wong et al. 2012, Janda 1985). The hamstring muscles then become dominant during hip extension as a result of gluteal inhibition or weakness (Sahrmann 2002). Hip extension is initiated by the hamstrings and erector spinae while the activation of the gluteus maximus is delayed (Leinonen et al. 2000, Nelson-Wong et al. 2012, Janda 1985). The gluteus maximus should be the primary hip extensor. Diminished gluteal function will place a higher load on the hamstrings and increases the risk of hamstring injury. Training the hamstrings in isolation only increases the load on the (in many cases already tired) hamstrings without promoting the correct coordination patterns between glutes and hamstrings. Rehabilitation programs for hamstring injury should focus on restoring proper coordination patterns, consist of exercises that (re-)activate the glutes and enhance the intermuscular coordination between the glutes and hamstrings. An example of such an exercise is the Resisted back lunge (fig. 9). The gluteus maximus is especially active during activities that involve a vigorous hip extension such as sprinting or climbing stairs (Zimmermann et al. 1994). Stabilizing the trunk and pelvis against gravity also requires a strong glute contraction (Marzke et al. 1988). The pull of the cable during
the Resisted back lunge (fig. 9) creates a hip flexion force against which the gluteus maximus has to stabilize. The movement also mimics the hip action during running. As in sprinting, the body should be pulled over the foot through a powerful hip extension. The one-legged stance also enhances the activation of the gluteus medius and maximus.
Explosive posterior pelvic tilt
The pelvis is an essential segment in the proximal-to-distal sequencing of explosive movements (Shan 2005). An explosive backward tilt of the pelvis allows greater force production at the hip level and facilitates an efficient power transfer during sprinting (Sado 2019). The inability to maintain a stable posterior pelvic tilt during sprinting causes premature hamstring fatigue, increases injury susceptibility, and impairs sprint biomechanics (Small 2009).
The differences in efficiency between a neutral and anterior pelvic tilt are related to sprinting technique. An anterior pelvic tilt during sprinting results in too high a heel lift, a foot contact too far in front of the body’s center of gravity at the end of the swing phase, and longer contact times. This is also referred to as back side running mechanics. When the pelvis is in a more neutral position, the high knee action results in more active ground contact, closer to the body’s center of gravity, resulting in shorter contact times and higher ground reaction forces; the so-called front side running mechanics.
The final stage of hamstring rehabilitation
The last phase of hamstring rehabilitation determines the success and the chance of recurrence. Plyometric and ballistic exercises with a horizontal force vector, resisted sprinting and stair sprints are essential to make the transition to full sprint speed.
Resisted sprinting and horizontal-vector plyometrics, such as the alternate leg bound and speed hop, approximate the joint angular velocity of sprinting, but with less hamstring extension (Osterwald 2021). These movements train correct intersegmental control, proximal-to-distal sequencing of rapid movements, and intermuscular coordination. The biceps femoris consists of a higher percentage of fast fibers that are preferentially recruited during explosive movements (Evangelidis 2017). Plyometric and ballistic exercises with a horizontal force vector, resisted sprinting and stair sprints maximally activate the biceps femoris and develop horizontal force and sprint speed. These exercises, together with a progressive partial integration in sports training, will facilitate a successful return-to-play.
29 medicine
performance football www.fmpa.co.uk
&
Selection of most efficient hamstring exercises from a biomechanical perspective
The single-leg RDL (fig.1), Roman chair hamstring curl (fig.2) and the Nordics (fig.3) are the best exercises to improve
eccentric hamstring strength at an elongated ROM (McAllister 2014). These exercises change the optimal length of the hamstrings so that they can produce greater forces with longer muscle lengths (Opar et al. 2012). This is important because



the hamstrings function at greater muscle lengths during sprinting (Chumanov et al. 2007).


 Figure 1: Single-leg RDL
Figure 2: Roman chair hamstring curl
Figure 3: Nordics
Figure 1: Single-leg RDL
Figure 2: Roman chair hamstring curl
Figure 3: Nordics
feature 30 info@fmpa.co.uk
The single-leg RDL & high pull (fig. 4), the Roman chair hamstring curl (fig. 2), the Keiser acceleration (fig. 5) and Horizontal step-up (fig. 6) require an explosive posterior pelvic tilt or the ability to maintain a stable posterior pelvic tilt.
An explosive posterior tilt allows large joint forces at the hip and facilitates an efficient power transfer during sprinting (Sado 2019).
The Horizontal step-up (fig.6) and Keiser acceleration (fig.5) will help improve



horizontal force production. An improved ability to produce horizontal force increases acceleration speed and reduces the risk of hamstring injuries (Rabita et al. 2015, Roksund et al. 2017).


 Figure 4: Single-leg RDL and high pull
Figure 5: Keiser acceleration
Figure 6: Horizontal step-up
Figure 4: Single-leg RDL and high pull
Figure 5: Keiser acceleration
Figure 6: Horizontal step-up
31 medicine & performance football www.fmpa.co.uk
The eccentric RDL slam (fig.7) and hip extension plyos (fig.8) are plyometric exercises specifically targeting the hamstrings. A hamstring injury is a high speed injury. The hamstrings function at high contraction rates during sprinting (Chumanov et al. 2007).
the hamstrings and gluteal muscles. This exercise improves horizontal force production and inter-muscular coordination between the glutes and hamstrings. feature
Plyometric hamstring exercises improve the energy-absorbing capacity of the hamstrings at the speed-end of the spectrum (Swinnen 2016).
The Resisted slideboard back lunge (fig.9) is a very effective exercise to strengthen





 Figure 7: Eccentric RDL slam
Figure 8: Hip extension plyos
Figure 9: Resisted slideboard back lunge
Figure 7: Eccentric RDL slam
Figure 8: Hip extension plyos
Figure 9: Resisted slideboard back lunge
32 info@fmpa.co.uk
Conclusion
In summary, hamstring injuries are a significant concern in sports, and their high recurrence rate necessitates comprehensive prevention and rehabilitation strategies. Addressing risk factors such as strength imbalances, fatigue, core instability, and inhibited gluteal muscles is essential.
Understanding the biomechanics of hamstring function during sprinting and the impact of altered muscle properties post-injury is crucial for effective rehabilitation. Incorporating eccentric hamstring strengthening,
References
re-activating the biceps femoris and gluteus maximus, enhancing intermuscular coordination, and focusing on horizontal force production are key components of successful rehabilitation. The final stage involves plyometric and ballistic exercises to transition athletes back to full sprint speed, ultimately promoting a successful return to play. By addressing these factors, athletes can reduce the risk of hamstring injuries, enhance their overall performance, and extend their careers in sports.
Bram Swinnen earned master’s degrees in both Kinesiology and Physiotherapy. He is the author of ‘Strength Training for Soccer’ (2016) and has trained eight Olympic medalists and various world champions. Bram served as the performance coach and physiotherapist for several Euroleague basketball teams and also worked with the football team FC Anzhi. Currently, he works as a high-performance coach at KRC Genk, is the expert coach for the ASICS Tennis Academy, consults for various federations and teams, and teaches his methodology in two-day courses.

Arnason A, Andersen TE, Holme I, Engebretsen L, Bahr R. Prevention of hamstring strains in elite soccer: an intervention study. Scand J Med Sci Sports. 2008 Feb;18(1):40-8.
Askling C, Karlsson J, Thorstensson A. A hamstring injury occurence in elite soccer players after preseason training with eccentric overload. Scand J Med Sci. 2003 Aug;13(4):244-50.
Brockett CL, Morgan DL, Porske U. Predicting hamstring strain injury in elite athletes. Med Sci Sports Exerc. 2004 Mar;36(3):379-87.
Brockett CL, Morgan DL, Proske U. Human hamstring muscles adapt to eccentric exercise by changing optimum length. Med Sci Sports Exerc. 2001 May;33(5):783-90.
Brughelli M, Cronin J, Mendiguchia J, Kinsella D, Nosaka K. Contralateral leg deficits in kinetic and kinematic variables during running in Australian rules football players with previous hamstring injuries. J Strength Cond Res. 2010 Sep;24(9):2539-44.
Brughelli M, Nosaka K, Cronin J. Application of eccentric exercise on an Australian rules football player with recurrent hamstring injuries. Phys Ther Sport. 2009 May;10(2):75-80.
Butler DL, Juncosa N, Dressler MR. Functional efficacy of tendon repair processes. Annu Rev Biomed Eng. 2004;6:303-29.
Chumanov ES, Schache AG, Heiderscheit BC, Thelen DG. Hamstrings are most susceptible to injury during the late swing phase of sprinting. Br J Sports Med. 2012 Feb;46(2):90.
Chumanov ES, Heiderscheit BC, Thelen DG. The effect of speed and influence of individual muscles on hamstring mechanics during the swing phase of sprinting. J Biomech. 2007;40(16):3555-62.
Croisier JL, Ganteaume S, Binet J, Genty M, Ferret JM. Strength imbalances and prevention of hamstring injury in professional soccer players: a prospective study. Am J Sports Med. 2008 Aug;36(8):1469-75.
Edouard P, Lahti J, Nagahara R, Samozino P, Navarro L, Guex K, Rossi J, Brughelli M, Mendiguchia J, Morin JB. Low Horizontal Force Production Capacity during Sprinting as a Potential Risk Factor of Hamstring Injury in Football. Int J Environ Res Public Health. 2021 Jul 23;18(15):7827.
Ekstrand J, Hagglund M, Walden M. Injury incidence and injury patterns in professional football: the UEFA injury study. Br J Sports Med 2011a;45:5538.
Evangelidis PE, Massey GJ, Ferguson RA, Wheeler PC, Pain MTG, Folland JP. The functional significance of hamstrings composition: is it really a “fast” muscle group? Scand J Med Sci Sports. 2017 Nov;27(11):1181-1189.
Gabbe BL, Branson R, Bennel KL. A pilot randomised controlled trial of eccentric exercise to prevent hamstring injuries in community-level Australian football. J Sci Med Sport. 2006 May;9(1-2):103-9.
Goldspink G. Changes in muscle mass and phenotype and the expression of autocrine and systemic growth factors by muscle in response to stretch and overload. J Anat. 1999 Apr;194(Pt 3):323-34.
Janda V. Pain in the locomotor system - a broad approach. In: Glasgow EF, Twomey LT, Scull ER, Kleynhans AM, Idczak RM, editors. Aspects of manipulative therapy. Edinburgh: Churchill Livingstone; 1985. p. 148-51.
Kaariainen M, Jarvinen T, Jarvinen M, Rantanen J, Kalimo H. Relation between myofibers and connective tissue during muscle injury repair. Scand J Med Sci Sports. 2000 Dec;10(6):332-7.
Kellis E, Galanis N, Kapetanos G, Natsis K. Architectural differences between the hamstring muscles. J Electromyogr Kinesiol. 2012 Aug;22(4):520-6.
Kilgallon M, Donnelly AE, Shafat A. Progressive resistance training temporarily alters hamstring torque-angle relationship. Scand J Med Sci Sports. 2007 Feb;17(1):18-24.
Koulouris G, Connell D. Evaluation of the hamstring muscle complex following acute injury. Skeletal Radiol. 2003 Oct;32(10):582-9.
Kujala UM, Orava S, Järvinen M. Hamstring injuries. Current trends in treatment and prevention. Sports Med. 1997 Jun;23(6):397-404.
33
www.fmpa.co.uk
medicine & performance football
Kyrolainen H, Komi PV, Belli A. Changes in muscle activity patterns and kinetics with increasing running speed. J Strength Cond Res. 1999 Nov;13(4):400-6.
Leinonen V, Kankaanpää M, Airaksinen O, Hänninen O. Back and hip extensor activities during trunk flexion/extension: effects of low back pain and rehabilitation. Arch Phys Med Rehabil. 2000 Jan;81(1):32-7.
Makihara Y, Nishino A, Fukubayashi T, Kanamori A. Decrease of knee flexion torque in patients with ACL reconstruction: combined analysis of the architecture and function of the knee flexor muscles. Knee Surg Sports Traumatol Arthrosc. 2006 Apr;14(4):310-7.
Marzke MW, Longhill JM, Rasmussen SA. Gluteus maximus muscle function and the origin of hominid bipedality. Am J Phys Anthropol. 1988 Dec;77(4):519-28.
McAllister MJ, Hammond KG, Schilling BK, Ferreria LC, Reed JP, Weiss LW. Muscle activation during various hamstring exercises. J Strength Cond Res. 2014 Jun;28(6):1573-80.
Mendiguchia J, Garrues MA, Cronin JB, Contreras B, Los Arcos A, Malliaropoulos N, Maffulli N, Idoate F. Nonuniform changes in MRI measurements of the thigh muscles after two hamstring strengthening exercises. J Strength Cond Res. 2013 Mar;27(3):574-81.
Nelson-Wong E, Alex B, Csepe D, Lancaster D, Callaghan JP. Altered muscle recruitment during extension from trunk flexion in low back pain developers. Clin Biomech. 2012 Dec;27(10):994-8.
Opar DA, Williams MD, Shield AJ. Hamstring strain injuries: factors that lead to injury and re-injury. Sports Med. 2012 Mar;42(3):209-26.
Orchard J, Seward H. Epidemiology of injuries in the Australian Football League, seasons 1997–2000. Br J Sports Med. 2002 Feb;36(1):39-44.
Osterwald KM, Kelly DT, Comyns TM, Catháin CÓ. Resisted Sled Sprint Kinematics: The Acute Effect of Load and Sporting Population. Sports (Basel). 2021 Sep 30;9(10):137.
Petersen J, Thorborg K, Nielsen MB, Budtz-Jørgensen E, Hölmich P. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: a cluster-randomized controlled trial. Am J Sports Med. 2011 Nov;39(11):2296-303.
Rabita G, Dorel S, Slawinski J, Sàez-de-Villarreal E, Couturier A, Samozino P, Morin JB. Sprint mechanics in world-class athletes: a new insight into the limits of human locomotion. Scand J Med Sci Sports. 2015 Oct;25(5):583-94.
Røksund OD, Kristoffersen M, Bogen BE, Wisnes A, Engeseth MS, Nilsen AK, Iversen VV, Mæland S, Gundersen H. Higher Drop in Speed during a Repeated Sprint Test in Soccer Players Reporting Former Hamstring Strain Injury. Front Physiol. 2017 Jan 27;8:25.
Sado N, Yoshioka S, Fukashiro S. A biomechanical study of the relationship between running velocity and three-dimensional lumbosacral kinetics. J Biomech. 2019 Sep 20;94:158-164
Schache AG, Wrigley TV, Baker R, Pandy MG. Biomechanical response to hamstring muscle strain injury. Gait Posture. 2009 Feb;29(2):332-8. Schache AG, Kim HJ, Morgan DL, Pandy MG. Hamstring muscle forces prior to and immediately following an acute sprinting-related muscle strain injury. Gait Posture 2010 May;32(1):136-40.
Schmitt B, Tim T, McHugh M. Hamstring injury rehabilitation and prevention of reinjury using lengthened state eccentric training: a new concept. Int J Sports Phys Ther. 2012 Jun;7(3):333-41.
Shan G, Westerhoff P. Full-body kinematic characteristics of the maximal instep soccer kick by male soccer players and parameters related to kick quality. Sports Biomech. 2005 Jan;4(1):59-72.
Silder A, Heiderscheit BC, Thelen DG, Enright T, Tuite MJ. MR observations of long-term musculotendon remodeling following a hamstring strain injury. Skeletal Radiol. 2008 Dec;37(12):1101-9.
Small K, McNaughton LR, Greig M, Lohkamp M, Lovell R. Soccer fatigue, sprinting and hamstring injury risk. Int J Sports Med. 2009 Aug;30(8):573-8.
Sole G, Milosavljevic S, Nicholson HD, Sullivan SJ. Selective strength loss and decreased muscle activity in hamstring injury. J Orthop Sports Phys Ther. 2011 May;41(5):354-63.
Swinnen B. Strength training for soccer. Routledge. 2016.
Thelen DG, Chumanov ES, Best TM, Swanson SC, Heiderscheit BC. Simulation of biceps femoris musculotendon mechanics during the swing phase of sprinting. Med Sci Sports Exerc. 2005b; 37(11):1911–8.
Thelen DG, Chumanov ES, Hoerth DM, Best TM, Swanson SC, Li L, Young M, Heiderscheit BC. Hamstring muscle kinematics during treadmill sprinting. Med Sci Sports Exerc. 2005a Jan;37(1):108-14.
Thorborg K. Why hamstring eccentrics are hamstring essentials. Br J Sports Med. 2012;46:463–5.
Warren P, Gabbe BJ, Schneider-Kolsky M, Bennell KL. Clinical predictors of time to return to competition and of recurrence following hamstring strain in elite Australian footballers. Br J Sports Med. 2010 May;44(6):415-9.
Woods C, Hawkins RD, Maltby S, Hulse M, Thomas A, Hodson A; Football Association Medical Research Programme. The Football Association Medical Research Programme: an audit of injuries in professional football--analysis of hamstring injuries. Br J Sports Med. 2004 Feb;38(1):36-41.
Zimmermann CL, Cook TM, Bravard MS, Hansen MM, Honomichl RT, Karns ST, Lammers MA, Steele SA, Yunker LK, Zebrowski RM. Effects of stair-stepping exercise direction and cadence on EMG activity of selected lower extremity muscle groups. J Orthop Sports Phys Ther. 1994 Mar;19(3):173-80.
34 info@fmpa.co.uk medicine & performance football feature
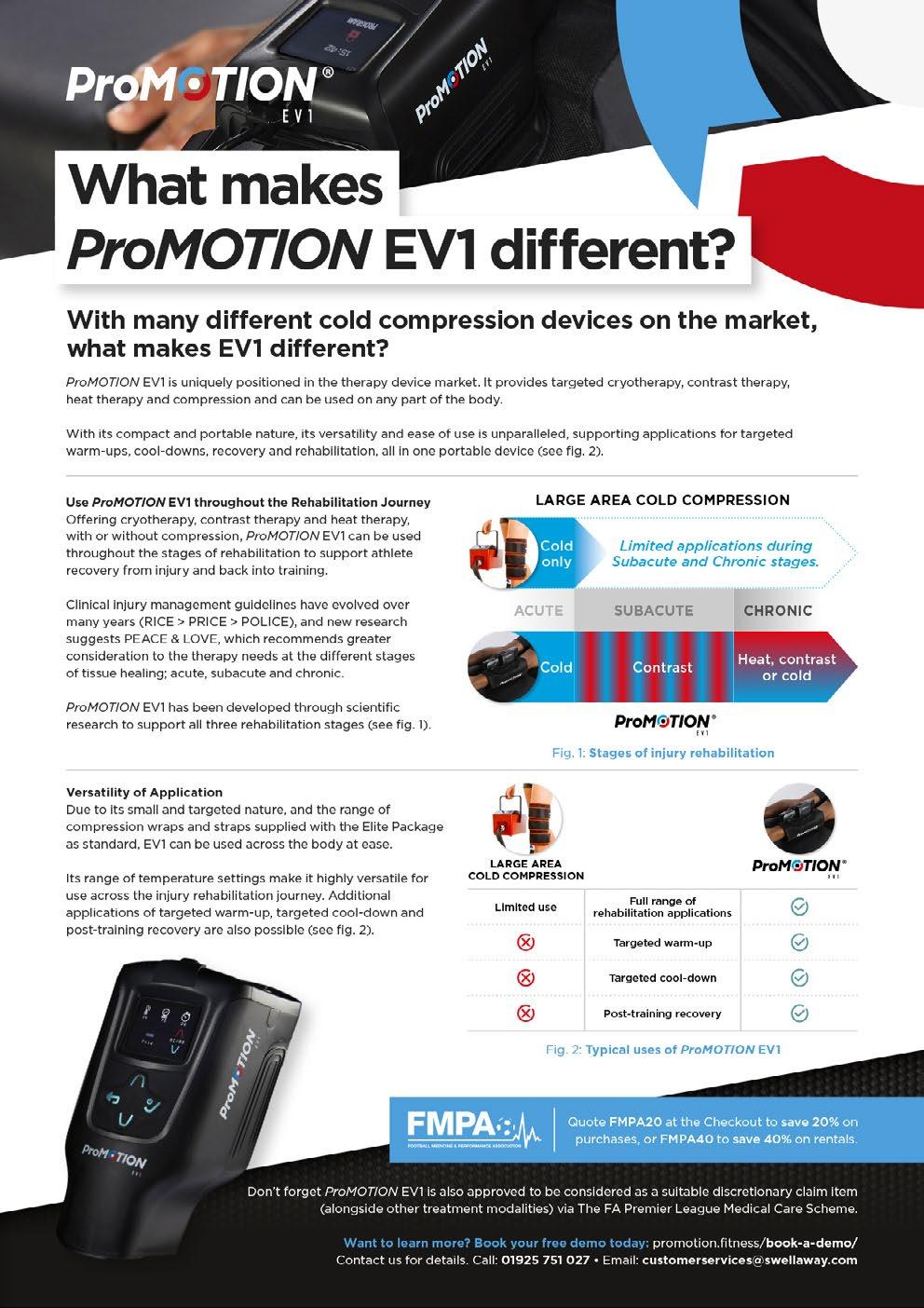



IS YOUR DEPARTMENT SCORING GOALS OR JUST HITTING THE POST?
FEATURE / MARTIN BUCHHEIT
The Role of Key Performance Indicators in Elite Performance Settings
In high-performance corporate environments, Key Performance Indicators (KPIs) are essential tools for evaluating employee performance. KPIs serve as critical metrics that reflect the overall health and progress of an organisation5. These indicators offer a transparent measure of efficiency and output, providing valuable insights into the success of a business at various levels, from the overall company to individual departments and employees. KPIs facilitate goal setting and performance evaluation, enabling organizations to recognize high achievers and identify areas needing improvement. The adaptability of KPIs to emerging trends further enhances their utility, motivating employees through clear and achievable goals. Moreover, KPIs are integral to aligning the efforts of individuals, teams, and departments, fostering a cohesive working environment that drives the organization toward its critical outcomes.
The Risks of Operating Without Adequate KPIs
Navigating elite sports without clear KPIs is like driving without a dashboard: you are in motion but lack insight into your speed, direction, or potential hazards. Without KPIs, assessing progress or performance in sports becomes guesswork, like estimating remaining fuel without a gauge. This issue is stark in football. When a team is on a losing streak, the immediate, often simplistic reaction is to blame the most visible factors: “The players aren’t running enough,” or “The fitness coach isn’t doing their job,” or “We’re losing because of injuries, so the medical staff must be inadequate.” Yet, this is like blaming a car’s empty tank while overlooking the engine or brakes. Without KPIs, diagnosing problems becomes superficial, leading to misplaced blame and overlooked improvement opportunities. KPIs provide a holistic view, essential for making informed decisions and nurturing a culture of continuous enhancement in the fast-paced realm of elite sports5
The Predicament of Staff Evaluation in Elite Football
In elite sports, staff performance evaluations are often overly reliant on team outcomes, which may not accurately reflect the staff’s contributions or the effectiveness of their interventions. This approach often underestimates the specific roles and impacts of various practitioners, resulting in evaluations that are inconsistent and, at times, unduly influenced by likeability and interpersonal skills rather than technical expertise. In such scenarios, being a “nice guy or woman” and one’s charm can overshadow the actual performance and contributions of the staff.4 Such an approach not only fails to recognize the individual merits of the support staff but also overlooks the interconnectedness and interdependencies within performance support teams.
Challenges of Implementing KPIs in Elite Football
The application of KPIs in elite sports, particularly in the context of professional football, presents unique challenges that
Type 3.2 Performance, Montvalezan, France High-Performance Consultant (including City Football Group). Former Head of Performance at PSG, Lille OSC and Olympique de Lyon
feature 38 info@fmpa.co.uk
set it apart from the corporate sector. Unlike the structured environment of corporate entities, the sports realm often lacks clearly defined objectives for staff assessment, making the establishment of KPIs a complex undertaking5. This complexity is further intensified by the nature of team sports, where quantifying support staff’s influence on team success and individual player well-being becomes increasingly challenging. This difficulty arises from a myriad of variables involved, encompassing not only genetic and physiological factors but also many tactical and contextual factors that are beyond the control of club staff, such as luck and unforeseen events in gameplay. These elements collectively contribute to the unpredictable nature of sports performance, adding layers of complexity to staff evaluation5. This complexity deepens when contrasting athlete specific KPIs, like fitness benchmarks6,7, with those for staff evaluation. The significant gap in applying and understanding KPIs for staff, as opposed to athletes, and the weak correlation between traditional sports science metrics and team success (2) call for a nuanced approach to defining and applying KPIs in sports.
Characteristics of Effective KPIs
As shown in the infographics, effective KPIs should:
1. Reflect Contribution to Organisational Success: Clearly show how the staff or department is advancing the organization’s goals.
2. Inform Decision-Making and Performance: Serve as a basis for making informed decisions and driving performance improvements.
3. Prioritise Key Indicators: Focus on the 3-6 most vital indicators that truly reflect key aspects of performance.
4. Be Quantifiable: Be expressed in a clear metric, enabling objective measurement and comparison.
5. Have Defined Frequency: Include a set frequency for assessment to ensure regular monitoring and timely responses to changes.
Multi-Level KPI Implementation
Implementing KPIs in an elite sports organization requires a multi-level approach, considering the different layers within the organization. In our recent investigation5, we particularly emphasize the importance of departmental and staff-level KPIs. This focus is crucial because it highlights how each position or job within a department contributes to the department’s overall success and, consequently, to the success of the entire organization.
medicine & performance football
• Organisation/Club Level: KPIs at this level reflect the overall success and strategic direction of the club or organization.
• Department Level: These KPIs focus on how each department contributes to the broader goals of the organization, ensuring departmental activities align with the overarching objectives.
• Individual Staff Level: Individual KPIs measure the contribution of each staff member, focusing on their specific roles and responsibilities.
Discovering Key Performance Indicators in Elite Sports
Our recent research, “Beyond the Scoreboard: Redefining Performance Staff Assessment in Elite Sports Organisations” published in November 2023 in Sports Performance & Science Reports5, ventured beyond the established understanding of how KPIs function, focusing instead on identifying the most pertinent metrics for monitoring and evaluating staff performance in elite sports settings. Recognizing that the effective use of KPIs hinges on their relevance and specificity to the sports context, we surveyed 51 practitioners from elite sports organizations5. The survey, developed with expert input, aimed to distill a set of practical, applicable KPI suggestions.
Detailed Findings and Examples from the Study
Overall findings
• Among the 51 practitioners surveyed, 87% set objectives for their teams or departments.

• The primary motivation for using KPIs was to gauge the impact of practitioners and departments, notably the MultiDisciplinary Team (MDT).
• Most KPIs were tailored to specific departments and staff.
• The main challenges in implementing KPIs included difficulty in definition (60%) and lack of support from higherups and key stakeholders (26%).
• In terms of staff performance evaluation, a significant 85% of practitioners favored a more process-oriented approach, with a preferred rating of 70-80% for processdriven evaluations.
Communication and Collaboration (Department KPI)
• The KPIs with the highest preference among practitioners about communication were “The overall collaboration process with the coaching staff for player reintegration after injury” (rated as of very high relevance by 75% of the practitioners surveyed) and “Clearly established communication lines and responsibilities between all the staff” (71%)
• Ownership: This KPI is co-owned by the MDT and the technical staff, necessitating collaboration and alignment between both parties.
• Metrics: This can include the existence or not of certain processes, qualitative assessments of communication lines and their effectiveness, feedback from staff and players, and the frequency of successful collaborative projects.
• Frequency of Evaluation: Regular evaluations, such as bi-monthly or quarterly, are recommended to ensure ongoing effective communication and collaboration.
Player Availability and Return to Play (Department KPI)
• Practitioners held the second highest preference for MDT overall KPIs related to “Overall player availability” with 66% very high relevance.
• Ownership: Shared among the MDT, coaching staff, and players. Each group plays a vital role in ensuring player availability and effective return to play (RTP). Indeed, practitioners tended to favor a collective responsibility approach, with the preferred option being a “50% MDT/50% coaching staff” split (43%).
• Metrics: Include player availability rates for training and matches, duration, and success rate of RTP protocols, and player feedback on the RTP process.
• Frequency of Evaluation: Ongoing monitoring with detailed reviews at key milestones in the RTP process and at the end of each playing season.
39
www.fmpa.co.uk
Holistic Player Management, Individual Development, and Prevention Plans (Department KPI)
• The paper also stressed the relevance of “Creating individual player profiles with practical information” (60%), “Offering individual injury prevention routines following screenings” (58%)
• Ownership: Primarily owned by the MDT, in collaboration with players who provide personal insights and feedback.
• Metrics: This could involve progress tracking in individual development plans, adherence to prevention and nutrition protocols, and assessments of physical, mental, and nutritional health.
• Frequency of Evaluation: Regular checkins, such as monthly or quarterly, and as needed based on the individual player’s circumstances.
Personal Growth and Interpersonal Communication (Staff KPI)
• The personal traits KPIs with the highest preferences were “Willingness to progress and grow personally” (75%), “Ability to provide and receive critical and productive feedback to/ from co-workers in the department” (73%), “Strong inter-personal skillsbuild and maintain relationships” (71%) and “Quality of global communication with colleagues in the same discipline” (69%).
• Ownership: Primarily owned by individual staff members, with support
and monitoring from departmental heads.
• Metrics: This could involve selfassessment tools, feedback from peers and supervisors, and professional development milestones achieved.
• Frequency of Evaluation: Annually or semi-annually, aligned with personal development plans.
Table 1 represents the initial phase in developing a detailed KPI matrix for a Multidisciplinary Team (MDT) in elite football, blending insights from our research5 with my extensive 20-year experience in the field, both as a fulltime staff member and a consultant. Crafting this matrix and generating consistent reports is a substantial endeavor, encompassing the formulation of intricate metrics, statistics, and comprehensive data aggregation and reporting mechanisms. While this paper focuses on collective KPIs, it is crucial to acknowledge the significance of individual KPIs as well. Though not discussed here, individual KPIs are equally vital and should be implemented to ensure a holistic and nuanced approach to performance evaluation and enhancement.
Implementing Effective KPIs in Elite Sports Clubs: Coordination and Action
The adage “It’s impossible to read the
label from the inside of the bottle” suggests that internal staff may lack the objectivity to assess and set KPIs effectively. Hence, hiring an external consultant to coordinate KPIs is often preferred. Nonetheless, a well-trained internal staff member, possibly mentored by an external consultant, can also fulfill this role proficiently, especially when confidentiality, like medical data privacy, restricts the sharing of sensitive information externally. This coordinator, whether internal or external, would be responsible for:
1. Maintain Objectivity: Ensure an unbiased approach in setting and assessing KPIs.
2. Possess KPI Expertise: Have the necessary skills to develop KPIs that are relevant, measurable, and aligned with the club’s strategic goals.
3. Handle Data Collection and Monitoring: This involves gathering and analyzing data, including specific metrics like player injury rates, distributing questionnaires for feedback, and tracking KPI effectiveness to reflect real-time performance.
4. Ensure Regular Reporting: Provide consistent updates to the club’s management, ensuring transparency and enabling continuous evaluation of the KPIs.

feature 40 info@fmpa.co.uk
KPIs Sub KPIs Ownership Metrics Frequency of assessment
Communication within MDT
Communication
Player availability
Communication outside MDT
100% MDT
Channels in place Processes
Organisation
Feedback from staff and players
Ratings by an independent person
Shared with Technical staff Channels in place Processes
Organisation
Feedback from staff and players
Ratings by an independent person
Overall Player Availability (simple metrics)
Overall Player Availability (advanced metrics)
Lay-off times and RTP durations
Re-injury rate
Shared with Technical staff and players
Shared with Technical staff and players
% available for training
% available for match
Number of players unavailable per match
Injury rate and burden /1000hrs of training and match exposures
Ratings by an independent person
Shared with players Days lost per injury, per context and mechanism of injury, per muscle group
Shared with Technical staff and players
RTP approach & content 100% (at least first phases)
Individualised performance training plans
Individualised prevention program
100% (up to what coaches permit)
100% (up to what coaches permit)
Rate per injury, per context and mechanism of injury, per muscle group
Evidenced-informed
Structured documents for sharing and collaboration
Clear benchmarks and milestones
Ratings by an independent person
Player feedback on their experience
Evidenced-informed
Structured documents
Liker scale rated by an independent person
Evidenced-informed
Structured documents
Ratings by an independent person
Adherence to programs
Player feedback on their experience
Bi-monthly or quarterly
Bi-monthly or quarterly
Weekly
Annually
Annually
Annually
Annually
Bi-monthly or quarterly
Bi-monthly or quarterly
Nutrition and overall hygiene education plans & interventions
100% MDT
Evidenced-informed
Structured documents
Ratings by an independent person
Adherence to programs
Player feedback on their experience
literature
Bi-monthly or quarterly
custom-made databases
Table 1: Example of department KPIs. Benchmarks for these KPIs can be found in existing
or are derived from
created by external consultant experts.
Holistic Player Management
41 medicine
www.fmpa.co.uk
& performance football
Utilization of KPIs by Decision Makers
The second key aspect is how club decision-makers utilize KPI insights. These individuals or teams must leverage the data and analysis from the coordinator to make informed choices. Essential factors include:
1. Actionable Insights: KPIs should offer practical recommendations, not just data, enabling tangible performance enhancements.
2. Feedback Loop: Establishing a continuous dialogue between decision-makers and the KPI coordinator ensures KPIs adapt to the club’s changing needs and challenges.
3. Informed Adjustments and Strategic Decisions: Decision-makers must be ready to make informed changes in areas like staff training, resource distribution, or strategic direction, guided by a deep understanding of KPI implications for club performance.
Conclusion: Elevating Performance Evaluation in Elite Sports
This editorial underscores the pivotal role of Key Performance Indicators (KPIs) in revolutionizing evaluations of departments and staff within elite football. Our research highlights the critical importance of robust communication, transparent decision-making structures, progressive personal traits, and objective metrics such as player availability. By incorporating these elements with external guidance into a well-structured KPI framework, clubs can achieve a system of evaluation that is not only more objective and comprehensive but also inherently fair.
References
1. Buchheit M & Carolan D. The Noble Ranks of Performance Roles – Who’s a king – who’s a duke? Sport Performance & Science Reports, 2019, May, #60, V1
2. Buchheit M, Gormley S, Hader K and McHugh D. The Performance Science Index: relationships with estimated market value and relative overall sporting performance of a selection of elite football (soccer) teams. Sport Perf & Science Reports, Nov 22, 177, v1.
3. Buchheit M, King R, Stokes A, Lemaire B, Grainger A, Brennan D, Norman D, Mäkinen A, Ruggiero H, Shelton A, Sammons G, Bridges M, McHugh D, Delaval B, and Hader K. Return to play following injuries in pro football: insights into the real-life practices of 85 elite practitioners around diagnostics, progression strategies, and reintegration processes. Sport Perf & Sci Reports, #180, Jan 2023
4. Buchheit M & Perry GM. EGOals. Exercising your EGO in high-performance environments. Amazon printing, October 4, 2021.
5. Buchheit M, Schuster L and King R. Beyond the Scoreboard: Redefining Performance Staff Assessment in Elite Sports Organisations. Sport Performance & Science Reports, 2023, November, #210, V1
6. Cardinale M. Key performance indicators. In: NSCA’s Essentials of Sport Science. Champaign, IL: Human Kinetics, Inc, 2022.
7. Clubb J, Allen S, Yung K. Selection of Key Performance Indicators for Your Sport and Program: Proposing a Complementary Process-Driven Approach. Strength and Conditioning Journal ():10.1519/SSC.0000000000000813, October 30, 2023. | DOI: 10.1519/SSC.0000000000000813

42 info@fmpa.co.uk medicine & performance football feature
UNRAVELLING THE HAMSTRING QUANDARY “ELEMENTARY MY DEAR WATSON” INJURY
RISK ASSESSMENT – THE FUNDAMENTALS OF SPECIFICITY!
FEATURE / DR MARTIN McINTYRE, M.MED.SCI., BSC., H.DIP
Hamstring Injuries in the first half of the 23/24 season accounted for 2,319 days lost in the Premier League, the greatest of all injuries (Sky Sports 2023) with 13% of all players reported to experience a hamstring issue (Maniar et al., 2023). The research indicates incidence is increasing with hamstring injury occurrence doubling from 12% to 24% over a 20 year period (Ekstrand et al., 2022). It is widely debated that increases in sprinting speeds and match exposure are contributing factors. With the great advances in performance and conditioning, in propelling our players to record speeds, how can we improve from a performance context that is predisposing our players to hamstring risk? Advances in screening, technology and sports science have led to the introduction of pre-session screening, monitoring fatigue and
recovery, but what are we missing ? We know that there are a large number of risk factors associated with hamstring injury however, previous injury is still the strongest risk factor and with a relatively high reoccurrence rate which may indicate that our sensitivity to identifying underlying deficits needs to improve. Subsequently, with this is mind, one would think we need to re-examine our approach and in the spirit of one great English detective, examine the “Elementary”, “Basic” and “Fundamental” clues to solving these issues.
The Clues!
Mechanism of injury
Hamstring injury in field sports are either sprint or stretch based. Sprint related injuries occur during linear acceleration or
in high speed running, whereas stretch related injuries are seen in deceleration, lunging, landing, jumping or kicking (Gronwald et al., 2022). Running is the main mechanism of injury at high speed and accounts for 48%- 81% of all hamstring injuries (Roe et al.,2018; Wilson et al., 2007; Askling et al., 2013) (Table 1.1). The biomechanics of the gait cycle have also been widely researched.
Time of injury
It is difficult to correctly identify the specific time of injury in running, due to the neural delays or latencies in reporting the injury (KenneallyDabrowski et al., 2019, Schache et al., 2010). Particularly, as deceleration during the late swing phase of highspeed running usually occurs in less than 250 milliseconds (Rodríguez-Rosell et al., 2018).
Australian Rules American Football Gaelic Football Soccer Rugby Sprint Type 81% 74.4% 73% 48% 47% Stretch Type Kicking/ Pick up the ball 19% - Kicking (4.4%) Turning (3.5%) Landing (1.9%) 52% Decel (18%) Kicking (6%) Tackling (6%) Rucking (6%)
Table 1.1 Mechanism of Hamstring strain injury in field sports (Hagel et al., 2005 ; Elliott et al., 2011; Roe et al., 2016; Gronwald et al., 2022; Kerrin et al., 2022).
feature 44 info@fmpa.co.uk
Table 1.1 : Mechanism of Hamstring strain injury in field sports (Hagel et al., 2005 ; Elliott et al., 2011; Roe et al., 2016; Gronwald et al., 2022; Kerrin et al., 2022).
Late swing prior to ground

There is a wide consensus however, that HSI is likely to occur in either late swing phase or early stance (Chumanov et al., 2011, Chumanov et al., 2012, Orchard et al., 2012, Schache et al., 2010, Yu et al., 2008, Heiderscheit et al., 2005, Schache et al., 2009), or possibly even in the transition from late swing to early stance (Liu et al., 2017) (Figure 1.1).
Forces and moments
The most commonly injured portion is the biceps femoris long head (BFlh). In late swing it is required to tolerate between 10.5-26.4 N.Kg-1(KenneallyDabrowski et al., 2019). It also reaches 110% of its maximum resting length and
has the greatest excitation levels at this point (Thelen et al., 2005).
It is clear from the research that when we piece together this puzzle the hamstring becomes injured in running in late swing or early stance. The large moments and forces at this point in the gait cycle being responsible, now let’s explore our current strategies in the mitigation of injury.
Observation of the scene
- The current strategy ! Our current strategy includes a number of modes of testing and devices to evaluate concentric, eccentric and isometric strength. This is summarised below
Early stance phase with ground reaction
Isokinetic dynamometry
Used to assess concentric, eccentric and isometric strength at speeds of 300/sec to 3000/sec. Peak torque, angle of peak torque, rate of torque development, ratios which include opposite, conventional, functional, mixed ratios have been proposed with various degrees of success (Lee et al., 2009; Croiser et al., 2002; Baroni et al., 2020). The main considerations in relation to IKD are 1) to reduce the measurement error by testing in isolation 2) aligning the centre of the knee in midrange and 3) testing at 600/sec in order to increase the accuracy of the device (McIntyre et al., 2022; Baltzopoulos et al., 2012).
80kg Athlete
Figure 1.1 Late Swing and Early Stance phases (Kenneally-Dabrowski et al., 2019).
120° 140° 140° 150°
Figure 1.1: Late Swing and Early Stance phase (Kenneally-Dabrowski et al., 2019).
f Flexion moment; e Extension moment
Table 2.3 :Hip and Knee kinetics with associated muscle tendon force (means) of the BFlh (adapted from Schache et al. (2012), Kenneally-Dabrowski et al. (2019), Chumanov et al. (2007).
Early Swing Late Swing Stance Early Swing Late Swing Stance Hip Moment 4.3fNm.kg-1 4.2fNm.kg-1 4.1e Nm.kg-1 344 Nm 336 Nm 328 Nm Knee moment 1.0eNm.kg-1 1.8fNm.kg-1 3.6eNm.kg-1 80 Nm 144 Nm 288 Nm Muscle-tendon force - 36.4 N.kg-1 28 N.kg-1 - 2912 N 2240 N
Table 2.3: Hip and Knee kinetics with associated muscle tendon force (means) of the BFlh (adapted from Schache et al., (2013), Kenneally-Dabrowski et al., (2019), Chumanov et al., 2007)).
45 medicine & performance football www.fmpa.co.uk
Nordic fall assessment
Nordic falls are widely accepted as an exercise modality to reduce hamstring injury and have also been implemented as a testing modality. However using this exercise as a clinical modality does not identify future injury risk due to variability in the break point, EMG activity and the relationship between the force hook and the force at the hamstrings (Opar et al., 2021; Van Dyk et al. 2017, McIntyre et al., 2020 ; Delahunt et al., 2016; Ruan et al., 2021).
Prone and supine isometric testing
More recently isometric and prone isometric testing has been adopted in many clubs using force plates (Supine) or load cells (Prone). Generally this has been administered as it is quick easy to perform and players are at low risk of injury, prior to and following training. This provides an indication of muscle performance in a lengthened position at 30 0 of knee flexion. Intra, Inter-rater reliability, repeatability are the main considerations. It is also worth considering these positions (in comparison to an upright posture when running) and the effect of gravity on the musculoskeletal and motor system (9.8 m/s) given these are performed in supine and prone positions.
Hypothesis
With the hamstring been at its most vulnerable in late swing/early stance can we replicate this point in time with a methodology which is quick, efficient, reliable and repeatable. Our research based at Liverpool John Moores University over a four year period investigated this
hypothesis under the guidance of Dr Martin McIntyre, Dr Mark Lake, Professor Bill Baltzopoulos, Dr Rob Erskrine and Dr Mark Robinson.
Examination – The Research Thesis
Nordic eccentric strength was not predictive of previous nor future HSI whereas a new methodology examining isometric bilateral and unilateral strength (isometric torque) better identifies those with residual strength deficits following injury (Mc Intyre et al., 2022b). These tests had high reliability and were developed specific to the mechanism of injury in late swing/early stance with 30 0 of knee flexion in the tested limb and 20 0 of hip extension in the contralateral limb.
The Final Goal
Following this research thesis, a design group at Sheffield Hallam University led by Dr Martin McIntyre and consisting of Dr Ben Heller, Dr John Kelley and Dr Nick Hamilton produced the HRIG (Hamstring Rig). This novel device for the testing of isometric hamstring strength specific to the mechanism of injury in sprinting. Further research and development of the testing methodology showed high Interrater reliability ICC (CI 95%) of 0.86 (CI 0.74-0.92) with the typical error of 19N (14-27N). Unilateral isometric testing showed high Interrater reliability ICC (CI 95%) of 0.92 (CI 0.85-0.96) with the typical error of 23N (18-34N).Intra-rater reliability was also high, ICC (CI 95%) of 0.93 (CI 0.89-0.97) with the typical error of 20N (16-27N). Unilateral isometric testing showed high Intra-rater reliability ICC (CI 95%) of 0.93 (CI 0.89-0.96) with

the typical error of 22N (18-30N). The methodology is safe and quick to administer with three maximum repetitions of 3-5 seconds (Figure 1.2).
Subsequently the development of normative data (N, N.kg -1, Nm, Nm.kg -1) has revealed the device to be sensitive and accurate for injury association. It is recommended that players possess 3.3 Nm.kg -1 to protect them from injury. The HRIG is sensitive to detecting residual deficits following hamstring injury. Screening, to monitor fatigue and recovery is also undertaken efficiently pre-training to determine an athlete’s performance status. Further research has also allowed the device to assist in the diagnosis and prognosis, following injury. The specificity of the test position produces results which are both sensitive and meaningful to prospective injury. In our next article we will explore both the specificity of this position and the use of isometrics to create a more robust athlete, thereby protecting players and increasing player availability.
Conclusions
• Be specific – mimic the mechanism of injury when undertaking hamstring assessment to maximise sensitivity.
• Ensure the methodologies have a high intra and inter rate reliability.
• Isometric assessment is quick and safe to perform both pre/post training and games. Particularly important with the time sensitivity of the modern day player and performance teams. Subsequently the development of normative data has revealed the device to be sensitive and accurate to injury association. It is recommended that players possess 3.3 Nm.kg-1 to protect them from injury. Screening to monitor fatigue and recovery is undertaken efficiently pre training to determine an athlete performance status. Further research has also allowed the device to assist in the diagnosis and prognosis following injury. The specificity of the test position is producing results which are both sensitive and meaningful to prospective injury.

In our next article we will explore both the specificity of this position and the use of
feature 46 info@fmpa.co.uk
Figure 1.2: HRIG - Isometric unilateral testing position similar to late swing/early stance with isometric force assessment.
References
Askling, C., Tengvar, M.,Thorstensson, A. 2013. Acute hamstring injuries in Swedish elite football: a prospective randomised controlled clinical trial comparing two rehabilitation protocols. British Journal of Sports Medicine Medicine, 47(15):953-9
Baltzopoulos, B., King, M., Gleeson, N., De Ste Croix, M. 2012. The Bases expert statement on measurement of muscle strength with isokinetic dynamometry. Sport and Exercise Science, 31, 12-13.
Baroni, B, Ruas, C, Ribeiro-Alvares, J., Pinto, R. 2020. Hamstring-to-quadriceps torque ratios of professional male soccer players: A systematic review. Journal of Strength and Conditioning Research, 34, 281-293
Chumanov, E., Heiderscheit, B., Thelen, D. 2007. The effect of speed and influence of individual muscles on hamstring mechanics during the swing phase of sprinting. Journal of Biomechanics, 40, 3555-62.
Chumanov, E., Heiderscheit, B., Thelen, D. 2011. Hamstring musculotendon dynamics during stance and swing phases Of high-speed running. Medicine and Science in Sports and Exercise, 43, 525-32.
Chumanov, E., Schache, A., Heiderscheit, B., Thelen, D. 2012. Hamstrings are most susceptible to injury during the late swing phase of sprinting. British Journal of Sports Medicine, 46, 90.
Croisier, J., Forthomme, B., Namurois, M., Vanderthommen, M., Crielaard, J. 2002. Hamstring muscle strain recurrence and strength performance disorders. American Journal of Sports Medicine, 30, 199-203.
Ekstrand, J., Bengtsson, H., Waldén, M., Davison, M., Khan, K., Hägglund, M. 2022. Hamstring injury rates have increased during recent seasons and now constitute 24% of all injuries in men’s professional football: the UEFA Elite Club Injury Study from 2001/02 to 2021/22. British Journal of Sports Medicine.
Elliott, M., Zarins, B., Powell, J., Kenyon, C. 2011. Hamstring muscle strains in professional football players: A 10-year review. American Journal of Sports Medicine, 39, 843-50.
Gronwald, T., Klein, C., Hoenig, T., Pietzonka, M., Bloch, H., Edouard, P., Hollander, K. 2022. Hamstring injury patterns in professional male football (soccer): a systematic video analysis of 52 cases. British Journal of Sports Medicine, 56(3), 165-171.
Hagel, B. 2005. Hamstring injuries in Australian football. Clinical Journal of Sport Medicine, 15(5), p.400.
Heiderscheit, B., Hoerth, D., Chumanov, E., Swanson, S., Thelen, B., Thelen, D. 2005. Identifying the time of occurrence of a hamstring strain injury during treadmill running: A case study. Clinical Biomechanics, 20, 1072-8.
Kenneally-Dabrowski, C., Brown, N., Lai, A., Perriman, D., Spratford, W., Serpell, B. 2019. Late swing or early stance? A narrative review of hamstring injury. Scandinavain Journal of Medicine and Science in Sports, 29(8):1083-1091
Kerrin, F., Farrell, G., Tierney, P., Persson, U., De Vito, G., Delahunt, E., 2022. Its not all about sprinting: mechanisms of acute hamstring strain injuries in professional male rugby union—a systematic visual video analysis. British Journal of Sports Medicine, 56(11), pp.608-615.
Lee, M., Reid, S., Elliott, B., Lloyd, D. 2009. Running biomechanics and lower limb strength associated with prior hamstring injury. Medicine and Science in Sports and Exercise, 41, 1942-51
Liu, Y., Sun, Y., Zhu, W. and Yu, J., 2017. The late swing and early stance of sprinting are most hazardous for hamstring injuries. Journal of Sport and Health Science, 6 (2), p.133.
Maniar, N., Carmichael, D., Hickey, J., Timmins, R., San Jose, A., Dickson, J., Opar, D. 2023. Incidence and prevalence of hamstring injuries in field-based team sports: a systematic review and meta-analysis of 5952 injuries from over 7 million exposure hours. British journal of sports medicine, 57(2), 109-116. McIntyre, M., 2022. Hamstring muscle strength assessment and the association of injury with injury risk in Gaelic football. Doctoral thesis, Liverpool John Moores University.
Mc Intyre, M. 2020. Eccentric hamstring strength in club Gaelic football. International Society for Biomechanics in Sport Proceedings Archive: Vol. 38 (1), Article 241.
Mc Intyre, M., Lake, M., Baltzopoulos, B., Reilly, C. 2022b. Reliability and bilateral strength imbalances of a new isometric test to identify previous hamstring strain compared to eccentric strength. “ International Society for Biomechanics in Sport Proceedings Archive: Vol 40 (1), Article 101.
Opar, D., Timmins, R., Behan, F., Hickey, J., van Dyk, N., Price, K., Maniar, N. 2021. Is pre-season eccentric strength testing during the nordic hamstring exercise associated with future hamstring strain injury? A systematic review and meta-analysis. Sports Medicine, 51(9), pp.1935-1945.
Orchard, J., Driscoll, T., Seward, H., Orchard, J. 2012. Relationship between interchange usage and risk of hamstring injuries in the australian football league. Journal of Science and Medicine in Sport, 15, 2016.
Rodríguez-Rosell, D., Pareja-Blanco, F., Aagaard, P., González-Badillo, J. 2018. Physiological and methodological aspects of rate of force development assessment in human skeletal muscle. Clinical Physiology and Functional Imaging, 38, 743-762
Roe, M., Blake, C., Gissane, C., Collins, K. 2016. Injury scheme claims in gaelic games: A Review of 2007-2014. Journal of Athletic Training, 51, 303-8.
Roe, M., Malone, S., Delahunt, E., Collins, K., Gissane, C., Persson, U., Murphy, J., Blake. C. 2018. Eccentric knee flexor profiles of 341 elite male academy and senior gaelic football players: Do body mass and previous hamstring injury impact performance. Physical Therapy in Sport, 31, 68-74.
Ruan, M., Li, L., Zhu, W., Huang, T. & Wu, X. 2021. The relationship between the contact force at the ankle hook and the hamstring muscle force during the nordic hamstring exercise. Frontiers In Physiology, 12, 210.
Schache, A., Dorn, T., Wrigley, T., Brown, N., Pandy, M. 2013. Stretch and activation of the human biarticular hamstrings across a range of running speeds. European Journal of Applied Physiology, 113, pp.2813-2828.
Schache, A., Kim, H., Morgan, D., Pandy, M. 2010. Hamstring muscle forces prior to and immediately following an acute sprinting-related muscle strain injury. Gait Posture, 32, 136-40.
Schache, A., Wrigley, T., Baker, R., Pandy, M. G. 2009. Biomechanical response to hamstring muscle strain injury. Gait Posture, 29, 332-8 Sky Sports 2023. Premier League injuries. Available at www.skysports.com/football/news/11095/13033280/premier-league-injuries-brentfordnewcastle-and-sheffield-united-suffered-most-man-utd-suffered-most-individual-injuriess
Thelen, D., Chumanov E., Best, T, Swanson, S., Heiderscheit, B. 2005. Simulation of biceps femoris musculotendon mechanics during the swing phase of sprinting. Medicine and Science in Sports and Exercise, 37, 1931-8
Van Dyk N., Bahr, R., Burnett, A., Whiteley, R., Bakken, A., Mosler, A., Farooq, A., Witvrouw, E. 2017. A comprehensive strength testing protocol offers no clinical value in predicting hamstring injury: a prospective cohort study of 413 professional football players. Bristih Journal of Sports Medicine 51(23):1695-1702 Wilson, F., Caffrey, S., King, E., Casey, K., Gissane, C. 2007. A 6-Month prospective study of injury in Gaelic Football. British Journal of Sports Medicine, 41, 317-21 Yu, B., Queen, R. M., Abbey, A. N., Liu, Y., Moorman, C. T., Garrett, W. E. 2008. Hamstring muscle kinematics and activation during overground sprinting. Journal of Biomechanics, 41, 3121-6
47 medicine & performance football www.fmpa.co.uk

NUTRITION STRATEGIES TO REDUCE ILLNESS IN FOOTBALL
FEATURE / TOM SHAW
Introduction
Professional football teams with high player availability are more successful.1 Therefore, maintaining high player availability is a top priority for sports science and medical practitioners. Compared with injury, illness incidence appears to be relatively small among professional football teams (8 per 1000 player hours vs 1.5 per 1000 player days).2,3 Nevertheless, illness can cause significant time loss which negatively impact team performance and success, particularly in congested fixture schedules. Fortunately, nutritional interventions can help prevent and treat illness and therefore increase player availability. Here I present a case study describing the nutritional interventions we are using to reduce illness at AC Sparta Praha.
Our illness problem
Upper respiratory tract infections (URTI) and gastrointestinal complaints are the most common illnesses experienced by footballers.2 Such illnesses resulted in 28 days lost per season among first team players at a French Ligue 1 club.3 But in the 2022-23 season we recorded 109 and 39 sick days in first team
players and support staff, respectively. Many of these occurred during intensive periods where many important matches were played, so a repeat of 148 sick days was unthinkable as we aim to win another league title and make progress in Europe. So, we resolved to find nutritional interventions which could help to reduce the illness burden.
Solving with food first…
Players should follow a balanced diet to avoid deficiency in nutrients required for proper immune function. However, they often undereat carbohydrate, fibre, omega-3 fatty acids and key micronutrients4 needed for optimal immunity due to factors such as poor dietary variety, limited cooking skills and routine. Since players eat most of their meals at the training centre and take extras home, we sought to find ways to enrich them with these important nutrients.
We continued to reinforce the importance of fuelling adequately with carbohydrates to support performance and health and therefore provided plenty of carbohydrate options at mealtimes. In addition, we introduced fruit pots
to eat in the changing room after training (Figure 1). These replaced traditional fruit platters, a change which alone likely reduced the spread of infection. The contents of the fruit pots vary according to the demands of the day, where they are themed as ‘immunity’ on lighter training days and as fuelling’ on heavier training days or around matches. The immunity pots contain fruits rich in vitamin C and phytonutrients such as berries, orange, and kiwi, whereas the fuelling pots contain more carbohydrate-rich fruits including mango, pineapple, grapes, and apple. The fruit pots have proved very popular and provided the added benefits of increased dietary fibre and variety.
We found ways to integrate more fruits and vegetables at the buffet, too. For example, we hide more herbs and vegetables in sauces, curries, soups and often stuff them in lean meats and fish. We also leaned into traditional Czech staples such as lentils, cabbage, vegetable purees and pickles to increase fibre and micronutrient intake. And when availability allowed, we included more exotic fruits to further increase variety and provide an interesting talking point.
Performance Nutritionist, AC Sparta Praha
feature 48 info@fmpa.co.uk

makes sense since staff also get sick and may pass it onto players. Besides, staff are important members of the team and their absence denies us valuable skills, knowledge, and personality needed to win football matches.
An excellent review on nutrition and athlete immune health by Prof. Neil Walsh is foundational to our supplement approach.5 In it he offers a new theoretical perspective which considers immune resistance (our ability to destroy pathogens) and immune tolerance (our ability to contain pathogens at a non-damaging level). It seems athletes typically have normal immune resistance and supplements offer little benefit in strengthening it to reduce infections. However, some supplements can help reduce infections by improving our immune tolerance.
Probiotics are live microorganisms which, when taken over several weeks, increase the numbers of beneficial gut bacteria that support immune function. Consequently, URTI incidence and duration are decreased by ~50% and 2 days, respectively.6 Vitamin C is an essential antioxidant which similarly decreases URTI incidence by ~50% when supplementing with 0.25-1.0 g per day.7 Vitamin D is an essential fatsoluble vitamin involved in numerous aspects of immunity. Since we obtain it primarily from sunlight exposure, deficiency is common in the winter months and URTI risk increases as a result. Fortunately, daily supplementation
micronutrients to prevent deficiency without risking over-supplementation. Within 24 hours of someone showing URTI symptoms, we provide a daily dose of 75 mg zinc lozenges for the duration of the illness. In doing so, we can reduce URTI duration by ~3 days through zinc’s ability to quench viral activity.9, 10
Conclusion
Having applied these strategies, we currently stand at 65 sick days. This is 56% lower than last season’s total with less than half the season to play. This is an impressive return, particularly when considering our match and travel schedules are more intense this season. Of course, we cannot discount other factors which may have influenced this such as better stress management, sleep habits, and hygiene practices away from the club. However, little else has changed which gives us confidence our interventions are working. One reflection is that we could have tracked days where individuals showed symptoms but were not absent, which may have provided richer insights.
In conclusion, illness can be a significant contributor to time loss for some football teams and particularly those playing congested fixtures during the winter months. However, our club case study suggests that following the nutritional interventions outlined in Table 1 can help to decrease the illness burden and increase player availability:
Tom Shaw is the current Performance Nutritionist at AC Sparta Praha. He has worked at the club for over a year and oversees the performance nutrition strategies of the first, second, and academy teams. In his first year, Tom helped the club win its first league championship in nine years and qualify for the knockout stages of the UEFA Europa League. His approach is playerdriven and performance-focused, and he is particularly passionate about the application of behaviour change science to optimise player development. Tom obtained his bachelor’s degree in Sport and Exercise Science and master’s degree in Sports Nutrition from Liverpool John Moores University.

Questions or comments? Email to shaw@sparta.cz or follow Tom on LinkedIn where he regularly shares football nutrition strategies and insights.
References
1. Hägglund, M. et al (2013). Injuries affect team performance negatively in professional football: an 11-year follow-up of the UEFA Champions League injury study. British Journal of Sports Medicine, 47, 738-732.
2. Ekstrand, J. et al (2011). Injury incidence and injury patterns in professional football: the UEFA injury study. British Journal of Sports Medicine, 45, 553-558.
3. Bjorneboe, J. et al. (2016). Role of illness in male professional football: not a major contributor to time loss. British Journal of Sports Medicine, 50, 699-702.
4. Orhant, E. et al. (2010). A three-year prospective study of illness in professional soccer players. Research in Sports Medicine, 18, 199-204.
5. Macuh, M. et al. (2022). Dietary Intake, Body composition and Performance of Professional Football Athletes in Slovenia. Nutrients, 15, 82.
6. Walsh, N. (2019). Nutrition and Athlete Immune Health: New Perspectives on an Old Paradigm. Sports Medicine, 49, 153-168.
7. Hao Q., Dong B.R., Wu, T. (2015). Probiotics for preventing acute upper respiratory tract infections. Cochrane Database Systematic Reviews.
8. Hemilä, H. & Chalker, E. (2013). Vitamin C for preventing and treating the common cold. Cochrane Database Systematic Reviews.
9. Martineau, A. R. et al. (2017). Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and metaanalysis of individual participant data. British Medical Journal, 356:i6583.
10. Hemilä, H. (2017). Zinc lozenges and the common cold: a recent meta-analysis comparing zinc acetate and zinc gluconate, and the role of zinc dosage. Journal of the Royal Society of Medicine Open, 8, 1-7.
11. Eby G. A.. (2010). Zinc lozenges as a cure for the common cold: a review and hypothesis. Medical Hypotheses, 74, 482-492.
Supplement Proposed mechanism of action Dose Timing Vitamin C Antioxidant. 250 -500 mg Daily Vitamin D Anti-inflammatory. 2000 iu Daily Probiotic Mutual symbiont. Reinforces the gut barrier against pathogens. 1010 live bacteria Daily Zinc lozenges Antiviral agent with antioxidant and anti-inflammatory properties. 75 mg Within 24 h of symptom onset until cessation
Table 1: Nutritional supplements to improve immune tolerance in athletes (adapted from Walsh, 20195)
49 medicine
football www.fmpa.co.uk
Fig 1: Post-training fruit pots as a more hygienic alternative to traditional platters. The fruits and nutritional content vary according to the nutritional theme for the day (i.e. immunity vs fuelling).
& performance
ONLINE COURSE MPA DIPLOMA
PREPARATION FOR WORK IN PROFESSIONAL FOOTBALL
✓ Health and safety
✓ Safeguarding
✓ Equality/Diversity
✓ Mental Health/wellbeing
✓ Confidentiality
✓ Record keeping
✓ Media TV
✓ Social Media
✓ Expectations of behaviour/general professionalism
✓ Integration within the MDT environment
✓ Insight into the working week
✓ Awareness of un-clinical skills
✓ From `Theory to Practice’
✓ How the science sits in the working environment
✓ What an employer is looking for – Employability, CPD, Reflective Practice, CV
✓ Portfolio design
Includes FREE FMPA membership access for 6 months:
• FMPA resources
• FMPA publication
• Free access to BJSM
• FMPA podcasts
• FMPA education
• Latest Jobs


• Sports Scientists • Physiotherapists • Doctors • Analysts • Sports Therapists • S & C Coaches • Fitness Coaches • Soft Tissue Therapists • Sports Rehabilitators • Sports Psychologists • Nutritionists • Podiatrists
Contact us at: admin@fmpa.co.uk 0333 4567897 www.fmpa.co.uk/courses/mpa-diploma Scan for more info:
“Any practitioner wanting to enter the volatile, uncertain, complex and ambiguous world of professional football at any level; senior ladies, men’s or Academy would greatly benefit from undertaking this course. I would suggest any Head of Performance in bigger organisations may “enrol” new practitioners on this course and ask for their written learning outcomes… A start of formal reflective practice, CPD & an annual review.”
Grant Downie OBE, Consultant in Medicine & Performance Solutions
This unique course is designed for new graduates and those entering into a professional sports arena for the first time. The course is designed to prepare prospective employees in those areas that are specific to a Club environment.

ONLINE COURSE
MPA DIPLOMA
“The MPA diploma is an excellent resource and qualification to help newly graduated practitioners with the transition into professional sport. Bridging the gap between formal education and the practicalities of the industry.”
Russ Wrigley, Head of Academy Sports Science & Medicine, Blackburn Rovers FC
PREPARATION FOR WORK IN PROFESSIONAL FOOTBALL
50 hours of learning over 6 months
©2024
Completing the Medicine and Performance Association (MPA) Diploma demonstrates a real commitment to engage with and fully understand the role of practitioners working in the unique environment of an MDT within professional football.
Contact us at:
admin@fmpa.co.uk
0333 4567897
www.fmpa.co.uk/courses/mpa-diploma
Ltd.
MPA
All rights reserved.
Scan for more info:
NEUROGENIC HEADACHE AND NECK PAIN IN ATHLETES
FEATURE / CONNOR ARQUETTE M.D., CATHERINE CURTIN M.D.
This article is kindly shared from the Aspetar Sports Medicine Journal Volume 13. Thank you to our colleagues at Aspetar for kindly allowing us to share this article
Introduction
Head/neck pain is common in elite athletes but the diagnosis and treatments are often not clear. Nerve injury/compression represents a head/neck pain pathology that has historically been underrecognised and requires a specific treatment plan1. Athletes commonly suffer head and neck trauma and these injuries can result in swollen, painful nerves. Identifying nerve compression is critical as effective treatments are available. Unfortunately, too often, nerve compression is missed leading to persistent suffering and inability to return to play.
The recognition of the morbidity caused by painful compressed nerves in the head and neck has blossomed over the last twenty years. Dr. Guyuron serendipitously noticed the role of compressed nerves in pain in his plastic surgery
practice. He then proceeded to study in detail the pathology and demonstrate the efficacy of surgical decompression2. Since his 2000 paper, his work has provided a guide to the nerves at risk of compression and others have built upon this foundational knowledge improving our care of these patients3. Now physicians are better equipped to diagnose and treat these painful nerves.
Athletes represent a population with unique risks for nerve injury and compression. In many sports, play puts the head and neck at risk for blunt forces or whiplash. Whiplash is a sudden forceful flexion and extension of the neck and occurs in many high-impact sports4. Concussions and traumatic brain injury also occur frequently in sports and there are international efforts to minimize their impacts5. After whiplash or concussion, many athletes experience posttraumatic headaches with the prevalence of acute post-traumatic headache as high as 90%. At 6 months post-injury, 30–50% of patients still experience headaches. It is now clear that a
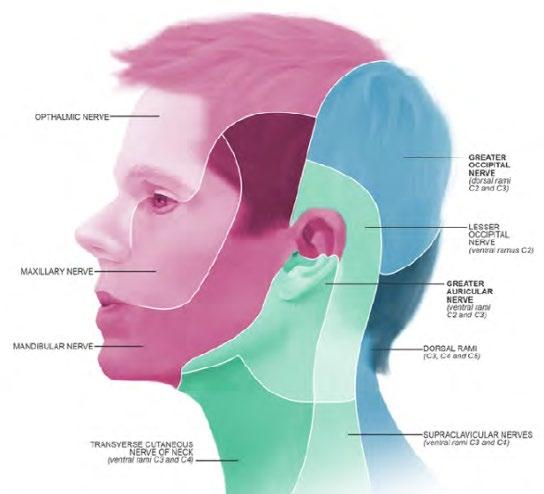
portion of post-traumatic head pain is caused by peripheral nerves that become swollen and subsequently compressed6. This article will provide information regarding relevant nerve anatomy and clinical presentations to aid in recognition, treatment, and return to play.
Diagnosis
The diagnosis is made by gathering many pieces of information to localize the pain generator. First, a full history is required. If symptoms occur after a trauma this points to a posttraumatic process. If a patient states that the head pain is orthostatic, improved when lying flat, or associated with ringing in their ears, this can suggest a cerebral spinal fluid (CSF) leak leading the provider down a different treatment pathway. CSF leaks should be considered in patients with head pain after skull fractures and have been described in many different athletes7
Immediately following a detailed history comes the physical exam. Palpation along the anatomical course of the affected nerve paying particular attention to common compression points is crucial. Tenderness at known points of compression is an important finding. Additionally, in the case of the brachial plexus and dorsal scapular nerves, provocatory actions, like head rotation and cervical flexion may reproduce or intensify symptoms. Sensory examination can show dysesthesia or decreased sensation in the distribution of the compressed nerve. Thus, a strong understanding of the nerve sensory distributions is critical (Figure 1).
If a diagnosis of nerve compression is suspected, the next diagnostic step is a focal injection with local anaesthetic with or without steroids. The diagnostic block is considered positive if the patient has at least 70% reduction of pain and symptoms following injection. It is important for patients to understand that the relief from the block only lasts for a short time. The patient should record the results of their block and alert their provider the next day. Otherwise, as time passes the patient can forget the impact of the block on their pain.
Imaging, especially ultrasound, can be a valuable tool in diagnosis. Recent advances in ultrasound technology along with the increased use of point-of-care ultrasound have allowed for bedside examination of nerve and musculoskeletal anatomy. These exams can show increased diameter of the nerve suggesting swelling and compression. Ultrasound can also be used to guide diagnostic and therapeutic nerve injections improving test accuracy and symptom relief.
Division of Plastic and Reconstructive Surgery Department of Surgery Stanford University School of Medicine, Palo Alto, CA, USA
feature 52 info@fmpa.co.uk
Figure 1: “Dundee - Drawing Dermatome map of head” at AnatomyTOOL.org by Annie Campbell, ©University of Dundee School of Medicine, license: Creative Commons AttributionNonCommercialNoDerivs. Reviewed by: Dr. Penny Lockwood, Dr. David Stewart, Dr. Patrick Spielmann.

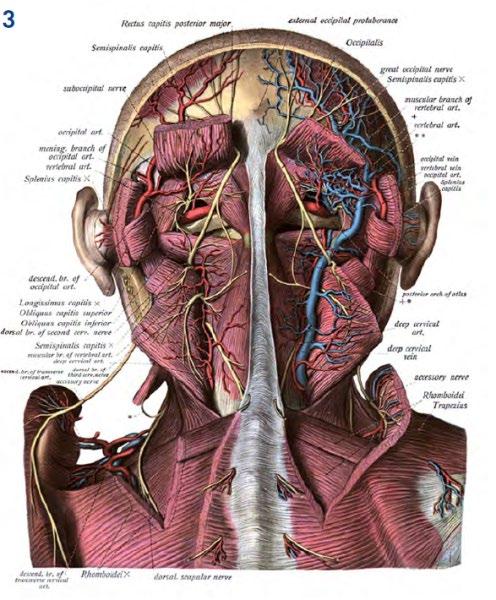
Treatment
Botox
Botox has been used for decades in the treatment of dystonia, seizures, muscle hypertrophy, and rhytids in cosmetic patients. With its controllable dosedependent paralytic effect, it is postulated that the therapeutic effect of this medication lies in its ability to provide muscle relaxation reducing the pressure on the nerve. Recent literature suggests that botulinum toxin also has an analgesic mechanism of action independent of its effect on muscle relaxation8, 9. The PREEMPT protocol is the standard protocol utilizing Botox in the treatment of head pain10
Therapy
Physical therapy by means of stretching, massage, and traction therapies serves as another nonsurgical option to attempt to reduce pain. For patients with nerve compression, the success level of correcting the compression is variable but can be invaluable to address posture compensations that negatively impact return to play.
Surgery
If the physical exam supports nerve compression and the patient has had a positive response to a diagnostic injection, surgical decompression of the nerve serves as an effective treatment. Detailed descriptions of each surgical release technique are beyond the scope of this article, however, there is one central guiding principle for these procedures – surgeons should take care to identify and release all possible sites of compression paying special attention to the anatomical course of the nerves.
Specific Nerves at Risk
Nerves are commonly at risk for compression along transition points: crossing a joint, passing between tissue planes, exiting a bony foramen, et cetera. This next section will review the anatomy of common nerves and known compression locations in the head and neck. This is not an exhaustive list and providers should be aware that any nerve could be at risk of compression. If pain is focal, a review of nerve anatomy can provide insights into possible pain generators.
Anatomy
Greater Occipital Nerve11-14
The greater occipital nerve arises from the lateral dorsal ramus of C2 to innervate the semispinalis capitis muscle and provide cutaneous sensation to the posterior scalp. The nerve runs lateral to midline ascending between the obliquus capitis inferior and the semispinalis before entering the semispinalis muscle medially around 5cm inferior to the occipital protuberance and then travels superolaterally within the muscle before exiting the muscle. This exit point, which is often the point of compression, is typically 1.5 cm lateral of midline, 3.5 cm inferior to the occipital protuberance, and 2 cm deep to the skin (Figure 2 and 3).
There are several well-recognized points of nerve compression. The surgeon should identify the nerve as is travels through the semispinalis and then explore the nerve proximally and distally assessing for other points of compression such as a crossing artery and as the nerve traverses the trapezius muscle insertion at the nuchal line.
Figure 2: The “x” marks the point where the greater occipital nerve transitions superficially through the semispinalis. “OP” represents the occipital protuberance.
53 medicine & performance football www.fmpa.co.uk
Figure 3: Anatomy of the posterior neck “Sobotta 1909 fig.696 - Nerves and vessels of the nuchal region, deep layer - English labels” at AnatomyTOOL.org by Johannes Sobotta is in the Public Domain.
Lesser Occipital Nerve11, 12, 15
The lesser occipital nerve is the ventral ramus of C2 and sometimes C3 supplying sensory innervation to the superior, postauricular skin, and lateral neck. The nerve emerges from beneath the sternocleidomastoid muscle (SCM) about 6-7cm lateral to midline, at the middle portion of the muscle, superior to the emergence of the great auricular nerve. The nerve then runs parallel to the SCM before penetrating the subcutaneous plane at a variable location (Figure 4).
Supraorbital Nerve16-20
The supraorbital nerve is a branch of the frontal nerve, which originates from the ophthalmic branch of the trigeminal nerve supplying sensation to the frontoparietal scalp. The nerve exits the bony skull via the supraorbital notch/foramen along the superior orbital rim around 3 cm lateral to midline, corresponding to the medial limbus of the eye topographically. Beyond the supraorbital foramen, the nerve most commonly forms superficial (medial) and deep (lateral) divisions. The superficial division divides into smaller branches that pass cephalad over the frontalis muscle to innervate the scalp in a fanlike pattern. The deep division typically travels between the periosteum and the galea running superolateral toward the temporal fusion line then running parallel and 0.5cm medial to this fusion line prior to dividing into smaller branches to innervate the scalp.
Supratrochlear Nerve21, 22
The supratrochlear nerve is a terminal branch of the frontal nerve, which is a branch of the trigeminal nerve ophthalmic division (V1) that passes through the superior orbital fissure on its way to supply sensation to the skin and soft tissues of the glabella, lower forehead, and upper eyelid. The nerve runs along the medial roof of the orbit exiting the orbit via the frontal notch around 1.5cm lateral to midline, and always medial to the supraorbital neurovascular bundle. After this, the nerve splits into two branches before entering the corrugator muscle. It then travels intramuscularly before exiting the muscle about 1.5cm superior to the orbital rim and then continuing superficially to supply sensation to the skin.
Dorsal Scapular Nerve23, 24
The dorsal scapular nerve arises from the ventral ramus of C5 within the posterior cervical triangle. It then proceeds deep to the prevertebral fascia and pierces the middle scalene muscle traveling between the posterior scalene muscle and the serratus posterior superior and levator scapulae muscles to innervate the rhomboid muscles. It passes under the
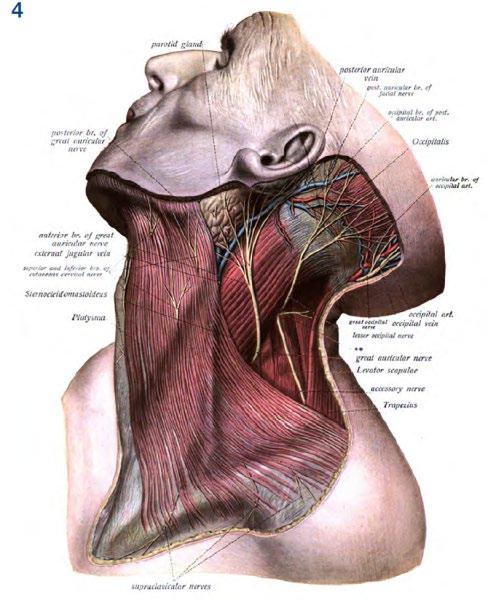
levator scapulae muscle and then becomes superficial between the rhomboid major and minor muscles. It then travels caudally along the medial border of the scapula.
Suprascapular Nerve
The suprascapular nerve originates from the upper trunk of the brachial plexus with contributions from C5 and C6. It travels with the brachial plexus before proceeding posteriorly to the superior border of the scapula and then passes through the suprascapular notch. The nerve courses caudally until it reaches the scapular spine, where it passes through the spinoglenoid notch and under the spinoglenoid ligament. The suprascapular nerve innervates the supra- and infraspinatus (Figure 5).
levator scapulae muscle and then becomes superficial between the rhomboid major and minor muscles. It then travels caudally along the medial border of the scapula.
Clinical Presentation
Greater and lesser occipital nerves1, 25
Greater occipital nerves can be injured from direct blows to the back of the head or be stretched from a whiplash injury. These patients typically present with pain localized to the sub-occipital and occipital areas. Patients typically have tenderness where the nerve transitions superficially (Figure 2). Sometimes, this pain can radiate frontally to trigeminal-innervated areas of the head due to connections between the extracranial occipital nerves and the intracranial trigeminal
Figure 4: Lateral neck nerve anatomy “Sobotta 1909 fig.697 - Nerves and vessels of the neck, first superficial layer - English labels” at AnatomyTOOL.org by Johannes Sobotta is in the Public Domain.
feature 54 info@fmpa.co.uk
nerves. When frontal radiation is present, photophobia and nausea can often accompany the localized posterior pain.
This injury can derail an athlete’s career as was seen in the case of Briana Scurry. She was an elite football goalie and Olympic gold medalist who had a concussion during play and continued to have severe pain in her suboccipital region after her initial trauma. Ultimately, she retired from her sport before she was diagnosed with greater occipital nerve injury and underwent successful nerve decompression surgery (www.brainandlife.org/articles/olympicsoccer-goalie-briana-scurry-brain-injury).
Lesser occipital nerves present with pain just posterior to the sternocleidomastoid and the pain can radiate behind the ear. Palpation is very helpful for this diagnosis with the nerve localized beneath the area. There can be more than one branch of the lesser occipital nerve and surgeons should look systematically in the area to ensure full release.
Supraorbital/supratrochlear nerves26-28
Patients with supraorbital and supratrochlear neuralgia typically present with localized headache or pain in or above the eyebrow with possible extension up into the scalp above the nerve. Pain related to compression of these nerves is often reproducible by compression over the supraorbital notch or the area directly overlying the nerve with associated tenderness. This injury can be associated with compressive
glasses and goggles. It should be considered when treating a patient with “swimmer’s migraine”29
Dorsal scapular nerve30
Patients with compression of the dorsal scapular nerve often report pain just medial to the scapula. Patients can feel tightness and weakness along the levator scapulae, rhomboid major, rhomboid minor, particularly with scapular retraction. Patients may present with winging of the scapula. Interestingly, patients can also have pruritus of the midscapular region along with radiation of pain along the posterolateral shoulder, arm, and forearm. This nerve can be injured in athletes with repetitive overhead movements such as volleyball, tennis, or baseball but has also been seen in other sports such as boxing and following whiplash injuries.
Suprascapular nerve
Patients with suprascapular nerve compression will complain of shoulder pain and often a feeling of weakness. On physical examination, there can be weakness in shoulder abduction and external rotation. There can also be isolated atrophy of the infraspinatus with entrapment at the spinoglenoid notch. The suprascapular is a common nerve compression in athletes. It is frequently seen in overhead athletes such as volleyball, tennis, and baseball pitchers. This entrapment can be amenable to arthroscopic release making for an easy return to play31
Surgery Outcomes
Surgical decompression was once thought to be a placebo treatment. As evidenced by recent studies, this is far from the case. Evans et al32 published a meta-analysis reviewing the outcomes of the surgical treatment of migraines. The 18 studies reviewed demonstrated a reduction in migraine headache severity and intensity. Similarly, ElHawary et al33 published a metaanalysis reviewing nerve decompression for the same indication and found a reduction in severity, intensity, and duration. Furthermore, they were also able to analyze the safety profile of the procedure with the most common complication being transient paresthesia and numbness. Other complications reported included itching, hyposensitivity, hair loss, and seroma. For the patient with the correct diagnosis, surgery to address the compressed nerve is safe, effective, and has low morbidity.
Conclusions
Neuropathic pain is becoming an increasingly recognized etiology for head and neck pain, especially following sports injuries. Furthermore, surgical neurolysis can provide sustained resolution of symptoms when recognized. This article provides a detailed review of relevant anatomy and clinical presentation highlighting treatment options for patients presenting with common nerve compressions as an etiology for head and neck pain. The first step to recovery is recognition.
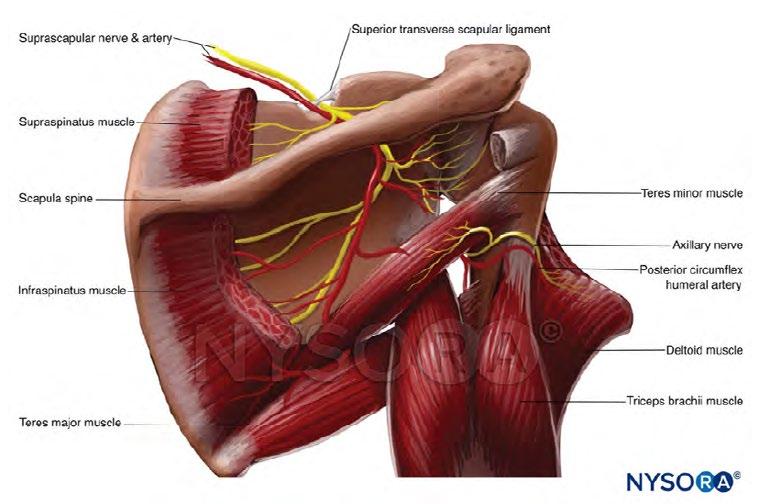
55 medicine & performance football www.fmpa.co.uk
Figure 5: “NYSORA - Drawing Posterior view of shoulder - English labels” at AnatomyTOOL.org by New York School of Regional Anesthesia and VisionExpo.Design, license: Creative Commons Attribution-NonCommercialNoDerivs.
References
1. Blake P, Burstein R. Emerging evidence of occipital nerve compression in unremitting head and neck pain. J Headache Pain. 2019;20(1):76.
2. Guyuron B, Varghai A, Michelow BJ, Thomas T, Davis J. Corrugator supercilii muscle resection and migraine headaches. Plast Reconstr Surg. 2000;106(2):429-34; discussion 35-7.
3. Janis JE, Barker JC, Javadi C, Ducic I, Hagan R, Guyuron B. A review of current evidence in the surgical treatment of migraine headaches. Plast Reconstr Surg. 2014;134(4 Suppl 2):131S-41S.
4. Tsoumpos P, Kafchitsas K, Wilke H-J, Evaνgelou K, Kallivokas A, Habermann B, et al. WHIPLASH INJURIES IN SPORTS ACTIVITIES. CLINICAL OUTCOME AND BIOMECHANICS. British Journal of Sports Medicine. 2013;47(10):e3-e.
5. Patricios JS, Schneider KJ, Dvorak J, Ahmed OH, Blauwet C, Cantu RC, et al. Consensus statement on concussion in sport: the 6th International Conference on Concussion in Sport-Amsterdam, October 2022. Br J Sports Med. 2023;57(11):695-711.
6. Zaremski JL, Herman DC, Clugston JR, Hurley RW, Ahn AH. Occipital neuralgia as a sequela of sports concussion: a case series and review of the literature. Curr Sports Med Rep. 2015;14(1):16-9.
7. Umana GE, Pucci R, Palmisciano P, Cassoni A, Ricciardi L, Tomasi SO, et al. Cerebrospinal Fluid Leaks After Anterior Skull Base Trauma: A Systematic Review of the Literature. World Neurosurg. 2022;157:193-206 e2.
8. Park HJ, Lee Y, Lee J, Park C, Moon DE. The effects of botulinum toxin A on mechanical and cold allodynia in a rat model of neuropathic pain. Can J Anaesth. 2006;53(5):470-7.
9. Park J, Park HJ. Botulinum Toxin for the Treatment of Neuropathic Pain. Toxins (Basel). 2017;9(9).
10. Diener HC, Dodick DW, Aurora SK, Turkel CC, DeGryse RE, Lipton RB, et al. OnabotulinumtoxinA for treatment of chronic migraine: results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia. 2010;30(7):804-14.
11. Dash KS, Janis JE, Guyuron B. The lesser and third occipital nerves and migraine headaches. Plast Reconstr Surg. 2005;115(6):1752-8; discussion 9-60.
12.Becser N, Bovim G, Sjaastad O. Extracranial nerves in the posterior part of the head. Anatomic variations and their possible clinical significance. Spine (Phila Pa 1976). 1998;23(13):1435-41.
13. Israel JS, Kempton SJ, Afifi AM. Prospective Analysis of the Greater Occipital Nerve Location in Patients Undergoing Occipital Nerve Decompression. Ann Plast Surg. 2018;81(1):71-4.
14. Janis JE, Hatef DA, Ducic I, Reece EM, Hamawy AH, Becker S, et al. The anatomy of the greater occipital nerve: Part II. Compression point topography. Plast Reconstr Surg. 2010;126(5):1563-72.
15. Pantaloni M, Sullivan P. Relevance of the lesser occipital nerve in facial rejuvenation surgery. Plast Reconstr Surg. 2000;105(7):2594-9; discussion 600-3.
16. Jeong SM, Park KJ, Kang SH, Shin HW, Kim H, Lee HK, et al. Anatomical consideration of the anterior and lateral cutaneous nerves in the scalp. J Korean Med Sci. 2010;25(4):517-22.
17. Knize DM. A study of the supraorbital nerve. Plast Reconstr Surg. 1995;96(3):564-9.
18. Cuzalina AL, Holmes JD. A simple and reliable landmark for identification of the supraorbital nerve in surgery of the forehead: an in vivo anatomical study. J Oral Maxillofac Surg. 2005;63(1):25-7.
19. Beer GM, Putz R, Mager K, Schumacher M, Keil W. Variations of the frontal exit of the supraorbital nerve: an anatomic study. Plast Reconstr Surg. 1998;102(2):334-41.
20. Janis JE, Ghavami A, Lemmon JA, Leedy JE, Guyuron B. The anatomy of the corrugator supercilii muscle: part II. Supraorbital nerve branching patterns. Plast Reconstr Surg. 2008;121(1):233-40.
21. Janis JE, Hatef DA, Hagan R, Schaub T, Liu JH, Thakar H, et al. Anatomy of the supratrochlear nerve: implications for the surgical treatment of migraine headaches. Plast Reconstr Surg. 2013;131(4):743-50.
22. Miller TA, Rudkin G, Honig M, Elahi M, Adams J. Lateral subcutaneous brow lift and interbrow muscle resection: clinical experience and anatomic studies. Plast Reconstr Surg. 2000;105(3):1120-7; discussion 8.
23. Cho H, Kang S, Won HS, Yang M, Kim YD. New insights into pathways of the dorsal scapular nerve and artery for selective dorsal scapular nerve blockade. Korean J Pain. 2019;32(4):307-12.
24. Tubbs RS, Tyler-Kabara EC, Aikens AC, Martin JP, Weed LL, Salter EG, et al. Surgical anatomy of the dorsal scapular nerve. J Neurosurg. 2005;102(5):910-1.
25. Djavaherian DM, Guthmiller KB. Occipital Neuralgia. StatPearls. Treasure Island (FL)2023.
26. Evans RW, Pareja JA. Expert opinion. Supraorbital neuralgia. Headache. 2009;49(2):278-81.
27. Agrawal SM, Kambalimath DH. Trigeminal neuralgia involving supraorbital and infraorbital nerves. Natl J Maxillofac Surg. 2010;1(2):179-82.
28. Pareja JA, Lopez-Ruiz P, Mayo D, Villar-Quiles RN, Carcamo A, Gutierrez-Viedma A, et al. Supratrochlear Neuralgia: A Prospective Case Series of 15 Patients. Headache. 2017;57(9):1433-42.
29. O’Brien JC, Jr. Swimmer’s headache, or supraorbital neuralgia. Proc (Bayl Univ Med Cent). 2004;17(4):418-9.
30. Muir B. Dorsal scapular nerve neuropathy: a narrative review of the literature. J Can Chiropr Assoc. 2017;61(2):128-44.
31. Garcia Junior JC, Paccola AM, Tonoli C, Zabeu JL, Garcia JP. Arthroscopic Release of the Suprascapular Nerve: Surgical Technique and Evaluation of Clinical Cases. Rev Bras Ortop. 2011;46(4):403-7.
32. Evans AG, Hill DS, Grush AE, Downer MA, Jr., Ibrahim MM, Assi PE, et al. Outcomes of Surgical Treatment of Migraines: A Systematic Review & Meta-Analysis. Plast Surg (Oakv). 2023;31(2):192-205.
33. ElHawary H, Barone N, Baradaran A, Janis JE. Efficacy and Safety of Migraine Surgery: A Systematic Review and Meta-analysis of Outcomes and Complication Rates. Ann Surg. 2022;275(2):e315-e23
56 info@fmpa.co.uk medicine & performance football feature

LEGAL Compromise agreement
“...I took your advice and have been working with the FMPA lawyer on the conclusion of my contract. Martin from his swift response on day one has been a real rock on my side and he has stayed in contact with me at regular intervals. His professionalism and knowledge of the football contract has helped me to be both realistic and hopeful regarding my case. We are now at the final stages of discussions with the club and the financial and emotional support I have has come through my contact with Martin. I am also immensely grateful to the FMPA for your help and support at this difficult time. At a low point in my life both the FMPA and Martin have helped me get the contractual situation sorted with as little fuss as possible and that’s been important to me and my family.”
Head of Medicine, League 2
Contract review
“...I just wanted to drop you an email to let you know how helpful Martin has been this last week. Although away, and with poor signal, he consistently made the effort to respond quickly to my questions when the club came back with updated terms. I believe his guidance has been fundamental to my negotiations.”
Head Physiotherapist, Premier League
“...Thank you so much. Really appreciate your help with this, it’s brilliant that the FMPA offer this service to its members. This stuff can be a minefield.”
Lead Sports Scientist, Premier League
JOIN TODAY www.fmpa.co.uk/legal Tel: 0333 4567897
