18 minute read
Understanding the Rectus Femoris Anatomy, Diagnosis & Types of Injuries


UNDERSTANDING THE RECTUS
FEMORIS ANATOMY, DIAGNOSIS & TYPES OF INJURIES
Advertisement
FEATURE / CARLES PEDRET1, IÑIGO IRIARTE2, SANDRA MECHÓ3
1. Sports Medicine and Imaging department. Clínica Diagonal. Barcelona 2. Physical Medicine and Rehabilitation department. Clínicas Ars Médica. Bilbao 3. Radiology department Hospital de Barcelona-SCIAS. Barcelona
Rectus Femoris anatomy
The rectus femoris is a long and fusiform muscle that is part of the femoral quadriceps group. It is located at the most superficial and anterior position. It is the only one that crosses two joints (hip and knee) and has a high proportion of type II muscle fibers, being both circumstances related to a greater tendency to injure1. The distribution of the muscular and connective components of the rectus femoris is key to understand its injuries and will be reviewed here.
The rectus femoris has a proximal and a distal myoconnective junction. At the proximal one, which is the most commonly injured, the rectus femoris originates from 2 tendons mainly. A direct (straight) tendon that originates from the anteroinferior iliac spine (AIIS) and an indirect (reflected) tendon that originates from the acetabular margin and hip capsule. Recently Mechó et al reported a third component, a connective membrane originating from the anterosuperior iliac spine reaching the conjoint tendon2. Both tendons merge a few centimetres distal to its origin, forming the conjoint tendon with the direct tendon located anterior and superficial and the indirect deep and posterior3. The muscular component initiates at this level below the direct tendon and lateral to the indirect tendon (Figure 1).
Most of the fibers of the direct tendon will continue superficial to the muscle, conforming an aponeurotic expansion that becomes broader and thinner covering the proximal third of the muscle´s length, and eventually fusing with the anterior fascia.
On the other side, the indirect tendon, is located medially to the muscular component. Its oval shape progressively changes as it goes distal, getting thinner and longer in a sagittal plane adopting a coma shape at first and flat at the end. It also changes its relative muscular position from medial to the centre forming the called intramuscular central tendon. Finally, it ends at the distal third of the muscle.
The distal myotendinous junction arises in the proximal third of the rectus femoris on Figure 1. Illustration of a lateral overview of a right thigh showing the tendinous origin of the rectus femoris. AIIS: Antero inferior iliac spine; ASIS: Antero superior iliac spine
its posterior face. The connective tissue thickens as it advances distally forming the posterior aponeurosis. The muscular component ends quite proximally, about 15 cm from the superior border of the patella, leaving a free tendon that forms the superficial layer of the quadricipital tendon, the intermediate layer being formed by the vastus medialis and lateralis, and the deep layer being formed by the vastus intermedius. They all insert on the superior border of the patella.
Introduction and epidemiology
Muscle injuries are the most common injuries in sports, accounting for more than 30% of injuries in football players. The hamstring muscle group injuries are the most frequent non-contact injuries according to epidemiologic studies4–7 with an increasing incidence and a really high reinjury risk. Rectus femoris (RF) injuries are approximately 4.6% of all football injuries and have a reinjury incidence of about 15,6%
8–10 .
An early and accurate diagnosis is essential to determine the most appropriate course of treatment. For that purpose imaging tests are gold standard, specifically magnetic resonance imaging (MRI) which can accurately identify the exact anatomical location of the injuries, the presence or absence of oedema, its type and its extension and the amount of connective tissue involved (intramuscular tendon injuries)11–15. It is known that tendon involvement (as a free tendon or as a intramuscular tendon/aponeurosis) is associated with a longer return to play (RTP) and with a higher reinjury risk16–18 .
As we have seen, the anatomy of the RF is highly complex and given this complexity of its anatomy and its connective tissue distribution, different types of injuries can occur. Classification of such injuries is challenging as many injuries cannot be classified with the traditional muscle strain classification systems19 .
Diagnosis
As in any muscle injury, it is essential to have a diagnosis as early as possible including imaging tests (MRI and/or ultrasound scan) and clinical assessment to accurately prepare for the RTP decision-making process, which allows medical staff to support the athlete’s RTP as soon as possible with a reasonable re-injury risk.
If we understand the injury mechanism and the biomechanics of the RF, and the clinical assessment suspects a RF injury, MRI is required in the first 48-72 hours to confirm the diagnosis. MRI provides details that ultrasound can’t, especially small transversal gaps or longitudinal splits in connective tissue structures (i.e. in the proximal region of the RF where ultrasound is limited due to the different trajectories and disposition of the RF direct tendon, the reflected tendon or the conjoint tendon)20. Once the correct diagnosis has been stablished, the most appropriate treatment is decided, depending on the injury type and specifically on the amount and location of connective tissue affected21–23. Ultrasound scan can also be used in the initial diagnosis and also for follow-up as it provides useful information about the injury, but it is important to note it doesn’t reach the detail level of an MRI.
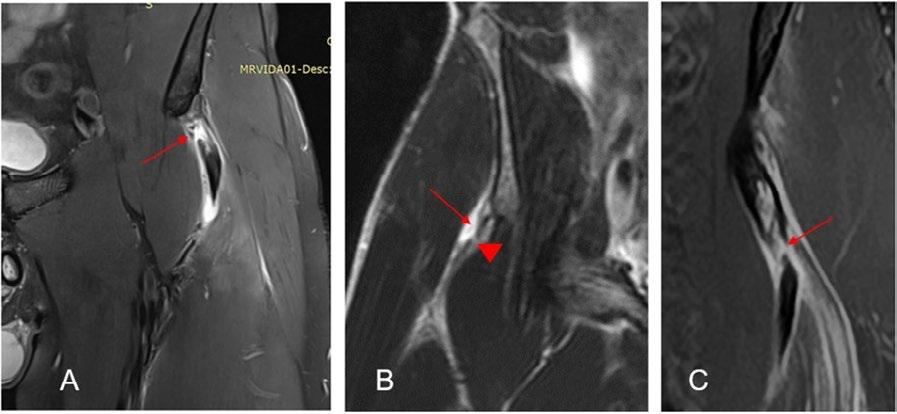
Figure 2. Coronal Proton Density Fat Saturated images of different injuries in the proximal region of the rectus femoris. A) Complete transversal tear of the DT in its preinsertional portion (arrow). B) Partial longitudinal tear of the IT in its insertional portion (arrow). In this case the IT shows as variant of normality an inferior band with a tear (arrowhead). C) Complete transversal tear of the conjoint tendon (arrow) with longitudinal extension to the DT.
Types of injuries in the Rectus femoris
Most injuries affecting the RF muscle can be managed with rehabilitation and physiotherapy treatment normally based in a progressive exercise protocol tailored individually for every case. But for that, we need to define the different types of injuries that could occur in the RF.
Proximal injuries
In this region we can consider injuries affecting the proximal tendons complex. As we have seen in the anatomy section injuries in the proximal part of the RF can be located in the direct tendon (DT), the indirect tendon (IT), the conjoint tendon or any kind of combination.
Due to its particular anatomy, severe injuries affecting the DT and the IT require, normally, surgical treatment especially in professional players22 in order to avoid loss of function and also to decrease the incidence of reinjuries.
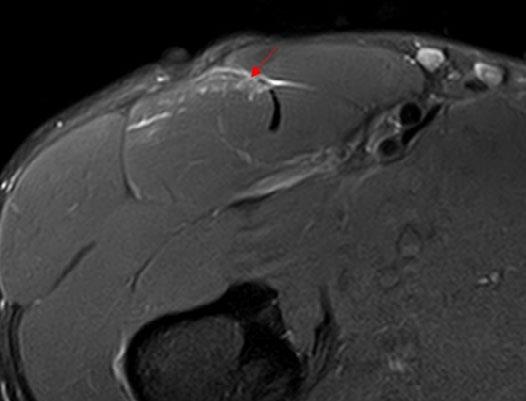
In childhood, avulsion of the anterior inferior iliac spine is not uncommon. The weakest point in the muscle-tendon-bone chain in very young athletes is the unfused physis. Fusion of the secondary ossification centre of AIIS occurs at 16 years of age 23, so children under 16 years of age are at greater risk of suffering a bone avulsion than a tendon injury. In subacute or chronic lesions, the healing process can produce images heterogeneous characteristics that can mimic with some aggressive pathologies and could misinterpreted as a tumour lesion, but the location and the traumatic history help to avoid misinterpretation 17 . Figure 3. Axial Proton Density Fat Saturated image of a tear of the anterior aponeurotic expansion of the DT (arrow). Injury close to the junction with the central tendon.
In case of tendinous injuries, in order to decide the treatment we need to consider if there is a complete transversal rupture of any of these tendons and/or if there is loss of tension or retraction24. It is important to understand that the proximal region of the RF is subjected to high workloads and functional stress, especially in football players.
There is another injury located in the proximal region of the RF which is the rupture of the anterior and superficial aponeurotic expansion (coming from the DT). This concrete injury is well tolerated by players (sometimes is completely underdiagnosed because they don’t complain about it). The treatment is conservative, and the prognosis is good with a fast RTP. But there is an exception; injuries that occur close to the border of the anterior aponeurosis with the central septum (Figure 3) have a high rate of reinjury. It is possible that the divided distribution of the transmission of forces is the cause of the high tendency to reinjury. It is important not to confuse them with conjoint tendon injuries (sometimes similar in terms of imaging).

Injuries affecting the central tendon
The central tendon is the most common site of RF injury in football20, 25. Injuries affecting the intramuscular aponeurosis of the RF are one of the injuries with more peculiarities and controversies that exist in sport.
The central tendon of the RF is one of the most important structures in the quadriceps muscle group and it’s an intramuscular expansion of the IT that conditions completely the function and biomechanics of this muscle. It acts like a whip when kicking, recruiting fibres all along its trajectory and releasing them abruptly to generate more power (also when accelerating, sprinting and decelerating). The presence of the central tendon conditions the bipennate aspect of the inner part of the RF and develops also a myoconnective junction that is significantly overloaded (especially during pre-season in kicking sports, e.g., football).
Injuries at this location are severe, especially in football players. Its treatment is initially with rehabilitation but there are some factors to consider. Injuries affecting the proximal part of the central tendon have worse prognosis than those affecting the distal part23. Also, injuries with extension to the conjoint tendon, with loss of tension or reinjuries, should be considered for surgical treatment21 .
Another important concept is if the injury affects the central tendon itself or if it is a myoconnective (myotendinous) injury. The first group of injuries can be seen as a complete transversal gap (named “bull’s-eye” lesions) or longitudinal splits (Figure 4A, 5A). Myotendinous injuries are those that produce a rupture of the muscle fibres attached to the central tendon but without affection of the latter (Figure 4B, 5B). Usually this type of injury occurs within an overloaded muscle8 . They imply a better prognosis than those affecting the central tendon.
Finally, the degloving injury that involves the indirect myotendinous complex of the RF whereby the inner bipennate muscle belly is separated and dissociated from the superficial unipennate muscle. Such dissociation may lead to retraction of the inner muscle belly25. This injury is the explanation of why, colloquially, we speak about the RF as a muscle within a muscle (Figure 4C, 5C). In those cases where there is no retraction of the inner muscle belly, signs of muscle rupture in the distal portion of the myotendinous junction can be identified by MRI, but the dynamic study by ultrasound ends up being the most optimal diagnostic test at the time of demonstrating a muscle gap26 . Figure 4. Coronal Proton Density Fat Saturated images of different injuries in the central tendon. A) Complete transversal tear of the central tendon in its middle portion (arrow). There is tendon retraction and extensive interstitial oedema. B) Myotendinous injury. Rupture of the muscle fibers attached to the central tendon (arrows) without affection of the central tendon itself. C) Degloving injury. Distal muscular fibers tear, with paraseptal muscle tears that extend cranially. Severe retraction of the central tendon myoconnective junction.
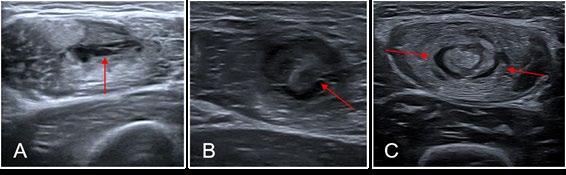

Figure 5. Ultrasound transverse images of different injuries in the central tendon. A) Partial central tendon tear in the posterior portion with interstitial oedema of the myotendinous junction (arrow). B) Myotendinous injury. There is a muscular fibre tear (arrow) and muscular oedema related to overload status. The central tendon is normal. C) Degloving injury. Paraseptal tears surrounding the myotendinous junction of the central tendon.
If we try to classify injuries affecting the central tendon of the RF in terms of prognosis, we can say that the worst prognosis is for those affecting the central tendon itself followed by the myotendinous injuries with central tendon retraction and finally the degloving injuries. This is in general, as always there is the need to individualise and contextualise every injury.
Myofascial injuries of the RF
Myofascial or fascial injuries affecting the RF are the clearest example to understand what exactly a myofascial injury is. They are normally located in the proximal, posterior and lateral region of the RF and are very well tolerated clinically and have a good prognosis20. The treatment is with progressive rehabilitation protocols depending on player subjective feedback, clinical tests and strength tests. The RTP time will vary depending if the injury is myofascial (without affecting the fascia itself) or fascial (with a rupture of the fascia). In case of fascia rupture, bleeding is in the intermuscular space and large haemorrhages can occur, whereas in case of no rupture, bleeding is contained in the intramuscular compartment12. In both cases, the RTP time is normally less than 3 weeks (Figure 6).

Distal injuries. Posterior aponeurosis of the RF
In the distal part of the RF we can find injuries that affect the posterior aponeurosis of the RF which can mimic the injuries affecting the distal myotendinous junction (MTJ) of the medial gastrocnemius (MG)27 . This injury produces a rupture in the posterior aponeurosis of the RF. It is very close to the quadriceps tendon (in fact there is a continuity between the RF posterior aponeurosis and the quadriceps tendon). Depending on how much the posterior aponeurosis is affected, a variable amount of intermuscular haematoma between RF and vastus intermedius can be found. If there is a complete rupture of the posterior aponeurosis, a proximal retraction of the RF muscle could be seen (the clinical image is a stump in the middle of the anterior thigh with a RF contraction). As in the MG this injury can have an extension to the fibres of the quadriceps tendon corresponding to the RF component. All of these factors influence the injury prognosis. Initially this injury is considered to have a rehabilitation protocol as the main treatment (ultrasound guided drainage of the intermuscular haematoma could be necessary) but, in cases where there is a severe retraction or after some reinjuries where the tissue is completely degenerated, surgical treatment can be also considered (Figure 7).
Conclusions
There is a wide range of injuries that can affect RF and they have a great variation in terms of prognosis and treatment options depending on the exact structure affected.
The main objective when suspecting a musculotendinous RF injury is to plan the RTP process in the most correct and individualized way. For that purpose, it is essential to have a diagnosis as early and accurate as possible to know which exact injury we are facing.
Once the diagnosis is confirmed, the treatment options are much clearer and planning the RTP process becomes “easier” (you can’t treat what you don’t know). The decision between rehabilitation or surgical treatment should be made depending on the injury type and the affected structure.
It is also important to consider other key points during the RTP process that are not only clinical tests, strength test or imaging tests. These include individual internal risk factors (genetics, age, previous injuries etc), external risk factors (overload or overtraining during the RTP process, training or technical mistakes, fatigue…), lumbo-pelvic stability control or other factors such as recovery, sleep and nutrition. Figure 6. Axial proton density fat saturated image (A) and transversal ultrasound corresponding image(B) of a myofascial injury. Myofascial injury with rupture of the fascia, there is interstitial oedema and intermuscular fluid (arrowhead)

Figure 7. Sagittal STIR (short tau inversion recovery) image (A) and longitudinal ultrasound (B) of distal portion of the RF. Complete rupture of the posterior aponeurosis with proximal retraction of the RF and moderate intermuscular haematoma (arrow). Usually these injuries go with an extensive interstitial oedema in the distal myoaponeurotic junction (arrowhead).
1. Johnson MA, Polgar J, Weightman D, Appleton D. Data on the distribution of fibre types in thirty-six human muscles. An autopsy study. J Neurol Sci. 1973 Jan;18(1):111–29. 2. Mechó S, Iriarte I, Pruna R, Pérez-Andrés R, Rodríguez-Baeza A. A newly discovered membrane at the origin of the proximal tendinous complex of the rectus femoris. Surg Radiol Anat. 2022 Jun;44(6):835–43. 3. Hasselman CT, Best TM, Hughes C, Martinez S, Garrett WE. An Explanation for Various Rectus Femoris Strain Injuries Using Previously Undescribed Muscle Architecture. Am J Sports Med. 1995;23(4):493–9. 4. Ekstrand J, Hägglund M, Waldén M. Epidemiology of muscle injuries in professional football (soccer). Am J Sports Med. 2011;39(6):1226–32. 5. Ekstrand J, Hägglund M, Waldén M. Injury incidence and injury patterns in professional football: The UEFA injury study. Br J Sports Med. 2011;45(7):553–8. 6. Hägglund M, Waldén M, Ekstrand J. UEFA injury study - An injury audit of European Championships 2006 to 2008. Br J Sports Med. 2009;43(7):483–9. 7. Ekstrand J, Waldén M, Hägglund M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: A 13-year longitudinal analysis of the UEFA Elite Club injury study. Br J Sports Med. 2016;50(12):731–7. 8. de Visser HM, Reijman M, Heijboer MP, Bos PK. Risk factors of recurrent hamstring injuries: a systematic review. Br J Sports Med [Internet]. 2012 Feb 1;46(2):124 LP – 130. Available from: http://bjsm.bmj.com/content/46/2/124.abstract 9. Ekstrand J, Healy JC, Waldén M, Lee JC, English B, Hägglund M. Hamstring muscle injuries in professional football: The correlation of MRI findings with return to play. Br J Sports Med. 2012;46(2):112–7. 10. Rudisill SS, Kucharik MP, Varady NH, Martin SD. Evidence-Based Management and Factors Associated With Return to Play After Acute Hamstring Injury in Athletes: A Systematic Review. Orthop J Sport Med. 2021;9(11):1–14. 11. Isern-Kebschull J, Mechó S, Pruna R, Kassarjian A, Valle X, Yanguas X, et al. Sports-related lower limb muscle injuries: pattern recognition approach and MRI review. Insights Imaging. 2020;11(1). 12. Patel A, Chakraverty J, Pollock N, Chakraverty R, Suokas AK, James SL. British athletics muscle injury classification: A reliability study for a new grading system. Clin Radiol [Internet]. 2015;70(12):1414–20. Available from: http://dx.doi.org/10.1016/j.crad.2015.08.009 13. Valle X, Mechó S, Pruna R, Pedret C, Isern J, Monllau JC, et al. The MLG-R muscle injury classification for hamstrings. Examples and guidelines for its use. Apunt Med l’Esport [Internet]. 2019 Apr 1 [cited 2020 Sep 14];54(202):73–9. Available from: https://linkinghub.elsevier. com/retrieve/pii/S1886658118300422 14. Baldock J, Wright S, Mcnally E, Wedatilake T. Intratendinous hamstring injuries: Sequential MRIs as a tool to reduce the risk of reinjury in elite sport. BMJ Case Rep. 2021;14(11):1–5. 15. Traumatology SG of the M and TS from the SS of S, Balius R, Blasi M, Pedret C, Alomar X, Peña-Amaro J, et al. A Histoarchitectural Approach to Skeletal Muscle Injury: Searching for a Common Nomenclature. Orthop J Sport Med [Internet]. 2020 Mar 20;8(3):2325967120909090–2325967120909090. Available from: https://pubmed.ncbi.nlm.nih.gov/32232071 16. Pollock N, Patel A, Chakraverty J, Suokas A, James SLJ, Chakraverty R. Time to return to full training is delayed and recurrence rate is higher in intratendinous (‘c’) acute hamstring injury in elite track and field athletes: Clinical application of the British Athletics Muscle Injury Classification. Br J Sports Med. 2016;50(5):305–10. 17. Macdonald B, Mcaleer S, Kelly S, Chakraverty R, Johnston M, Pollock N. Hamstring rehabilitation in elite track and field athletes: applying the British Athletics Muscle Injury Classification in clinical practice. Br J Sports Med [Internet]. 2019;bjsports-2017-098971. Available from: http:// bjsm.bmj.com/lookup/doi/10.1136/bjsports-2017-098971 18. Shamji R, James SLJ, Botchu R, Khurniawan KA, Bhogal G, Rushton A. Association of the British Athletic Muscle Injury Classification and anatomic location with return to full training and reinjury following hamstring injury in elite football. BMJ Open Sport Exerc Med. 2021;7(2). 19. Balius R, Pedret C, Kassarjian A. Muscle Madness and Making a Case for Muscle-Specific Classification Systems: A Leap from Tissue Injury to Organ Injury and System Dysfunction. Sport Med [Internet]. 2021;51(2):193–7. Available from: https://doi.org/10.1007/s40279-020-01387-5 20. Kassarjian A, Rodrigo RM, Santisteban JM. Current concepts in MRI of rectus femoris musculotendinous (myotendinous) and myofascial injuries in elite athletes. Eur J Radiol. 2012 Dec;81(12):3763–71. 21. Lempainen L, Kosola J, Valle X, Puigdellivol J, Ranne J, Orava S, et al. Chronic and Recurrent Rectus Femoris Central Tendon Ruptures in Athletes: Clinical Picture, MRI Findings, and Results of Surgical Treatment. Orthop J Sport Med. 2021;9(2). 22. Lempainen L, Kosola J, Pruna R, Puigdellivol J, Ranne J, Orava S. Operative Treatment of Proximal Rectus Femoris Injuries in Professional Soccer Players: A Series of 19 Cases. Orthop J Sport Med. 2018 Oct;6(10):2325967118798827. 23. Balius R, Maestro A, Pedret C, Estruch A, Mota J, Rodríguez L, et al. Central aponeurosis tears of the rectus femoris: Practical sonographic prognosis. Br J Sports Med. 2009; 24. Lempainen L, Mechó S, Valle X, Mazzoni S, Villalon J, Freschi M, et al. Management of anterior thigh injuries in soccer players: practical guide. BMC Sports Sci Med Rehabil [Internet]. 2022;14(1):1–9. Available from: https://doi.org/10.1186/s13102-022-00428-y 25. Kassarjian A, Rodrigo RM, Santisteban JM. Intramuscular degloving injuries to the rectus femoris: Findings at MRI. Am J Roentgenol. 2014;202(5):475–80. 26. Iriarte I, Pedret C, Balius R CL. Ultrasound of the Musculoskeletal System Anatomical exploration and pathology [Internet]. 2021. 570 p. Available from: https://mskroom.com/books.php 27. Pedret C, Balius R, Blasi M, Dávila F, Aramendi JF, Masci L, et al. Ultrasound classification of medial gastrocnemious injuries. Scand J Med Sci Sport. 2020;30(12):2456–65.