
11 minute read
Protecting Players from the Effects of Concussion: A Knee Jerk Reaction or Better Safe than Sorry?


PROTECTING PLAYERS FROM THE EFFECTS OF CONCUSSION:
A KNEE JERK REACTION OR BETTER SAFE THAN SORRY?
Advertisement
FEATURE / PHILLIP HERITAGE
Introduction
Through the iconic image of Terry Butcher’s bloodied, bandaged head fans and players alike have been aware of the dangers that football can hold when it comes to head injuries. But long-term neurological disease seemed to be the reserve of higher contact sports as chronic traumatic encephalopathy, dementia and Alzheimer’s disease became associated with participation with American Football and more recently, rugby1. However, recent analysis of health data in Scotland has concluded that footballers may similarly face increased risk of developing these diseases , with ex-players three times more likely to be diagnosed with Dementia or Alzheimer’s than their non-playing equivalents2,3. The increased risk, associated with repeated impacts of the head, has been associated with player-to-player, player-to-ground, and playerto-ball contact and led to some proactive initiatives and temporary rule changes aimed at enhancing player protection in the professional game. While concussion injuries are mainly associated with unexpected
Human Performance Lead and Senior Lecturer at AECC University College, Bournemouth
head contact with other surfaces causing greater cranial acceleration5, long-term risks including the development of Dementia and Alzheimer’s have been associated more with sub-concussive effects of heading the ball4 .
How big is the problem?
This is a hard question to answer from outside of the football world. As a former performance analyst in the sport, I know how secretive clubs are about performance and medical data. There are also potential impacts of player data being freely available when transfer dealings and wages may be put at risk through awareness of players’ exposure to repeated head injuries. On an acute level, injury surveillance data is collected by the Football Association but is not published publicly in the way seen by its equivalent governing body for Rugby Union in England (RFU) or the International Olympic and Paralympic Committees.
Relying on published data alone raises a variety of issues with data sets coming from a broad selection of playing levels and environments, with incidence commonly based on collegiate statistics in the United States. Reporting processes and inclusion criteria are also inconsistent between studies, and this means often reporting on head injury incidence generally rather than concussions specifically.
Despite this, some data has been published reporting longitudinal injury surveillance statistics across men’s and women’s international competitions6,7. These studies reflect the research that shows women are at greater risk of concussion than men, with women experiencing one concussion for every 1080 playing minutes versus every 3025 in their male equivalents. However, this only represents the very top of the game and more information is needed on all playing levels. These studies also reported concussions accounted for just 2% of all injuries on average in the competitions covered. Due to variances in assessment between medical staff (e.g. physicians,
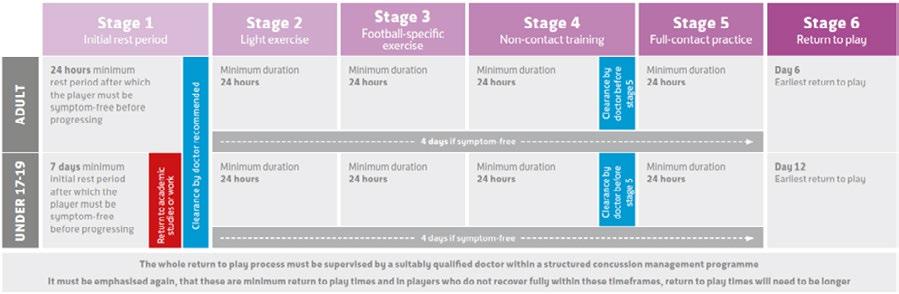
Figure 1. Graphic depicting the timelines for Graduated Return to Play from the FAs Concussion Guidelines (updated 2019) for players after concussion. (a) Standard, (b) Enhanced8 (a) Standard

(b) Enhanced
physiotherapists, sports therapists) and the lack of a definitive diagnostic test it is difficult to draw any conclusions from these numbers .
The greater health concern appears to be in the longer-term impacts of players suffering concussions and sub-concussive injuries 1,2,3. As explained in the introduction, recent research highlights an associated risk with playing football and developing neurodegenerative disease in later life. These studies observed a three-fold increase in the risk for professional footballers developing a neurodegenerative disease compared to the general population2 and that outfield players are at a significantly greater risk than goalkeepers3 .
What has the response been?
The response from the Football Association involves a combination of developing educational materials and implementing new rules restricting the volume of heading in training , with a phased increase to the professional level. The publication of the Football Association’s Concussion Guidelines: ‘If in doubt sit them out ’ is aimed at offering guidance on identifying signs and symptoms of concussion, more severe brain injury and the use of graduated return-to-play protocols (Figure 1).
They have also restricted heading for all age groups shown in Figure 2 to reduce the previously reported risk associated with developing neurodegenerative diseases in the future.
Figure 2. The FA Heading Guidance (updated 2020-21)9
Age Group Heading frequency
U7, U8, U9, U10, U11 Heading should not be introduced in training sessions at this age
U12 Heading remains a low priority – 1 session per month & max 5 headers
U13 Heading remains a low priority – 1 session per week & max 5 headers
U14, U15, U16 Heading remains a low priority – 1 session per week & max 10 headers
U18 Heading drills should be reduced as far as possible, taking into consideration the heading exposure in matches
Meanwhile, the Premier League has acted to also restrict the volume of heading exposure in training to “a maximum of 10 higher force headers are carried out in any training week”. This has been based on research conducted by the Premier League, which has observed cranium force exposures due to heading exceeding those seen in activities of daily living, and greater forces observed in youth and female footballers than their adult male counterparts.
The question of heading is one raised regularly with various factors requiring further exploration. Recent criticism has commented that while published data on neurocognitive disease risk in ex-players shows a compelling association, it lacks adequate evidence of causality4:
• Is heading a ball enough to cause a concussion? - This seems unlikely and is unsupported by literature, but research has been restricted by issues with accelerometer accuracy. It is hoped that new gum-shield mounted accelerometers could change this as they provide a solid fixing to the cranium.
However, research on amateur footballers has shown that heading a ball just 15 times causes transient electrophysiological and cognitive impairment, a potential effect of sub-concussive injury10 .
• Does removing heading in children benefit them in older age? - This question is impossible to answer until we see the effects of these recent changes by the Football Association.
• Will the lack of time training at heading reduce the strength of neck musculature which protects the head from the accelerations and decelerations that cause concussive and sub-concussive injury? - This has become a more common part of training in a variety of sports and professions to protect the cranium from high forces in people such as Formula 1 drivers, Rugby Union players and jet pilots. • Should other neck strengthening exercises be included at all levels where heading is limited?
Additionally, a temporary change in the rules was trialled to allow up to two additional permanent substitutions where a player is believed to have suffered a to lessen the competitive impact of removing a player from the field of play. A recent survey of professional football medical professionals highlighted they would like to see the introduction of replacements to allow an assessment, such as the Head Injury Assessment process in Rugby Union to be conducted, the player returned to the pitch upon receiving an all-clear or substituted should they fail11 .
This research also found that 5% and 10% of medical professionals felt under pressure from players and technical staff respectively not to remove a player with a suspected concussion. This highlights to me a lack of awareness of the potential medium- to long-term health repercussions of playing on after suffering a concussion. This is reflected in past research in Italian football , which shows poor knowledge of the signs and symptoms of concussion in football players, and coaches and medical staffs’ reliance on self-reporting to assess players for the injury12. However, more recent research has not been conducted on knowledge and understanding in the English game, or whether playing level affects the quality of care a player is likely to receive.
What more can we do?
The concussion discussion is complicated by timeframes related to mild-traumatic brain injury. The injury presents through a variety of short-term signs and symptoms which can influence player performance and health for days to weeks. Additionally, more sinister health related changes in the brains structure and chemistry that affect quality of life and life expectancy post-career could occur. It is also important to consider medium-term health complications associated with mental health in active and retired players. While this is starting to be researched, current findings have found no greater associated risk so
far13,14 .
To improve our capacity to better understand the scale of the issue and existing practices in place to protect player health, we need to better understand the following:
• How heading affects brain structure and chemistry in the short- to medium-term and how does this influence long-term health? • In the absence of a definitive test for concussion, what assessments are being used most widely and effectively to monitor and protect player neurocognitive health and diagnose concussion? • How the demands of professional sport influence short-term behaviour towards player welfare. • How medical teams design their diagnostic and monitoring protocols for concussion.

Better understanding of these key themes, in my opinion, and the use of longitudinal research to measure how player monitoring, diagnosis and return to play affect neurocognitive health in the short, medium, and long-term is crucial to us gaining a better understanding of the impact of repetitive head injury on player health.
Research is currently being conducted to better understand player monitoring, diagnostic and return to play practises in professional football in England. Additionally, it aims to better understand knowledge of concussion and its associated signs and symptoms along with attitudes and behaviours related to player welfare in relation to concussion. You can contribute by scanning this QR code and completing the 10–15-minute survey.
How can we protect our players?
While no definitive test exists to diagnose a concussion, battery tests that measure a variety of physical and cognitive factors do and are widely used and supported by research. As a minimum, clubs must:
• Educate staff and players yearly on the risks of playing with a concussion • Educate staff and players on the signs and symptoms of concussion • Perform baseline assessment of a physical-cognitive test battery (e.g.
SCAT-5) • Regularly re-test physical-cognitive performance to ensure changes in performance are compared to up-to-date results • Implement a Graduate Return to Play protocol that protects their players • Remove any player from training or competition who there is concern has suffered a concussion. If in doubt, sit them out.
Where possible, clubs should also:
• Involve an independent physician/ neurologist in the decision-making process when diagnosing a concussion • Utilising video footage as part of the decision-making process to remove a player from training or competition

1. Lee EB, Kinch K, Johnson VE, Trojanowski JQ, Smith DH, Stewart W. Chronic Traumatic Encephalopathy is a common co-morbidity, but less frequent primary dementia in former soccer and rugby players. Acta Neuropathologica.2019;138: 389-399 2. Russell ER, Mackay DF, Stewart K, MacLean JA, Pell JP, Stewart W. Association of Field Position and Career Length with Risk of Neurodegenerative Disease in Male Former Professional Soccer Players. Journal of the American Medical Association. 2021;78(8):1057-1063 3. Mackay DF, Russell ER, Stewart K, Maclean JA, Pell JP, Stewart W. Neurodegenerative Disease Mortality Among Former Professional Soccer Players. New England Journal of Medicine.2019;381(19): 1801-1808 4. Gouttebarge V. Is the Call to Reduce Heading Exposure in Professional Football to Prevent Dementia Evidence-based? British Medical Journal Open Sport and Exercise Medicine. 2021;7. 5. Mooney J, Self M, ReFaey K. Elsayed G, Chagoya G, Bernstock JD, Johnston JM. Concussion in Soccer: A Comprehensive Review of the Literature. Concussion. 2020;5(3). 6. Junge A, Dvorak J. Injury Surveillance in the World Football Cup Tournaments 1998-2012. British Journal of Sports Medicine. 2013;47: 782-788 7. Junge A, Dvorak J. Football Injuries During the 2014 FIFA World Cup. British Journal of Sports Medicine. 2015;49: 599-602 8. Football Association. The FAs Concussion Guidelines. 2019. https://www.thefa.com/get-involved/ fa-concussion-guidelines-if-in-doubt-sit-them-out [Accessed 3.9.2022] 9. Football Association. English Football Introduces New Guidance for Heading Ahead of 2021-2 Season. 2021. https://www.thefa.com/news/2021/jul/28/20210728-new-heading-guidance-published [Accessed 3.9.2022] 10. Di Virgilio TG, Hunter A, Wilson L, Stewart W, Goodall S, Howatson G, Donaldson DI, Ietswaart, M. Evidence for Acute Electrophysiological and Cognitive Changes Following Routine Soccer Heading. EBioMedicine. 2016;13: 66-71 11. Gouttebarge V, Ahmad I, Iqbal Z, Orhant E, Rosenbloom C, Sas K, Kerkhoffs GMMJ. Concussion in European Professional Football: A view of team physicians. British Medical Journal Open Sport and Exercise Medicine. 2021;7. 12. Broglio SP, Vagnozzi R, Sabin M, Signoretti S, Tavazzi B, Lazzarino G. Concussion occurrence and knowledge in Italian football (soccer). Journal of Sports Science and Medicine. 2010;9: 418-430 13. Taioli E. All Causses Mortality in Male Professional Soccer Players. European Journal of Public Health. 2007;17(6): 600-604 14. Russell ER, McCabe T, Mackay DF, Stewart K, MacLean JA, Pell JP, Stewart W. Mental Health and Suicide in Former Professional Soccer Players. Neuropsychiatry. 2020:91; 1256-1260







