“The next leap in image quality for cardiac exams is being made possible by refinements in software and through AI.” Philips Healthcare
Page 06
“Living with obesity and/or diabetes can be hard, but know you’re never alone on your journey to
Page 09
BARBARA STREISAND
The acclaimed director, actor, and singer is inspiring women to take charge of their heart health
Advocate for Your Future Health With Cholesterol Testing
High cholesterol can affect anyone, at any age. When it comes to protecting yourself against future health problems, knowledge is power.
We tend to think of high cholesterol and its many negative health impacts as something that afflicts older people. The truth is, anyone, of any age, can have unhealthy levels of low-density lipoprotein (LDL) — otherwise known as “bad” cholesterol.
According to the American Heart Association, between 2017 and 2020, 86.4 million adults in the United States had either high cholesterol (defined as a total cholesterol level over 200 mg/dL) or were on the cusp of the condition. And kids aren’t immune: Between 2009 and 2016, close to 20% of adolescents had higher than healthy cholesterol levels. There is often a genetic component to high cholesterol, so even young people with healthy lifestyles can find themselves dealing with the condition.
A silent threat
Because there are typically no symptoms associated with high cholesterol, blood tests to ascertain cholesterol levels (called lipid panels) are of vital importance. High cholesterol is a progressive condition that worsens over time, silently increasing your risk.
The good news is that getting a lipid panel is faster and easier than you might imagine.
Early and often
Lipid panels are officially not just
for older folks: The Centers for Disease Control and Prevention (CDC) recom mends that children be tested once between the ages of 9 and 11, and again between the ages of 17 and 21. Healthy adults should have their lipids tested every 4-6 years.
There’s one very good reason for these recommendations: Early testing reveals high cholesterol levels sooner, giving patients the chance to advocate for their own health and treat the problem before it progresses into a life-threatening condition. LDL cholesterol can cause a sticky residue called plaque to build up in arteries, shrinking blood flow and potentially leading to cardiovascular health problems like heart disease, stroke, and heart attacks. There is evidence that once cholesterol has caused arteries to clog with plaque, interventions are less effective than if the condition is treated earlier.
Fast and easy
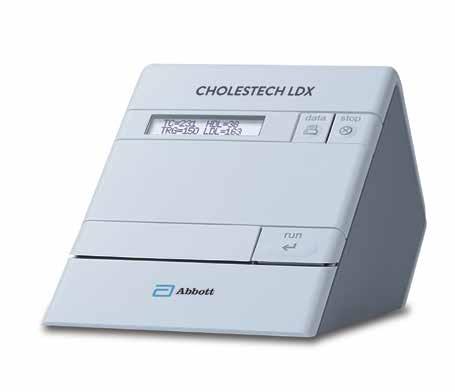
A lipid panel test is a remarkable and easy blood test to conduct. Using a rapid point-of-care testing device like Abbott’s Cholestech LDX™ system, for example, a physician can get accurate cholesterol levels right in their office.
“At Abbott, our focus is empowering people to take control of their health by making healthcare more accessible and convenient,” said Bob
and consumer products businesses.
“One example of this in action is the Cholestech LDX™ point-of-care lipid testing system, which provides patients with lab-accurate cholesterol results in five minutes from one simple fingerstick. This means results are available and treatment decisions can be made during the visit, saving patients the time and expense of a separate trip to the lab, and delayed or even lost follow-up with their care provider.” Because results are immediate with the Cholestech LDX™ System, healthcare providers can work with patients to develop personalized action plans during the same visit. This not only improves access to care, but encourages patients to modify their behaviors and make informed decisions about their health, such as managing cholesterol levels and planning future testing, ultimately empowering them to be proactive about living a longer, healthier life.
Written by Jeff Somers
INTERVIEW WITH Bob Kunkler Vice-President; Toxicology,
Cholestech
Revolutionizing Heart Health: How AI Is Shaping the Future of Cardiac Care
The benefits of AI and machine learning are being realized all across healthcare, and the applications in cardiac care are particularly exciting. David E. Albert, M.D., the founder and chief medical officer of AliveCor, shares his thoughts on how AI is impacting cardiac care currently and what the future may hold.
How can patients be proactive about their heart health?
It’s no secret that heart disease remains the leading killer of Americans, with an estimated 12 million people projected to have one of the most common and potentially dangerous arrhythmias, atrial fibrillation (AFib), by 2030. But the good news is that heart health solutions powered by artificial intelligence (AI) technologies can help patients track and take control of their cardiac health.
In recent years, new and affordable AI-powered cardiac monitoring tools have been introduced that enable individuals to monitor their heart health, no matter where they are, and potentially seek faster care. What’s more, these devices are designed for everyday life, easily fitting into a purse, pocket, or even a wallet.
But the first, most critical step for people concerned about their heart health is to consult with their doctor. In many cases, physicians will recommend an FDA-cleared device that can provide patients with trusted data, even outside of the traditional hospital setting.
How are physicians today able to leverage AI to enhance cardiac care?
AI technology is revolutionizing how and where physicians can administer electrocardiogram (ECG) monitoring. Whereas traditional 12-lead ECG devices are clunky and require extensive resources that are typically available only in hospitals, today, physicians can utilize new AI-powered, FDA-cleared technology, extending opportunities for ECG screenings to remote settings, such as urgent care, primary care, and rural health facilities.
These portable and pocket-sized devices provide outstanding clinical efficiency and performance that is substantially equivalent to state-of-the-art ECG analysis solutions, and can detect 35 abnormalities — including heart attack. Furthermore, the new technology requires just five electrodes (sensors) and has built-in AI-based support to make ECG monitoring far simpler, allowing providers to implement more personalized care for patients.
How do you envision cardiac care evolving in the future?
The future of cardiac care is one where AI and personal health technologies empower and
increasingly connect patients and physicians within a more holistic healthcare ecosystem.
This will allow physicians to create more personalized treatment plans for each patient’s unique needs, while patients themselves can be more engaged in managing their heart health. Here, cardiac care becomes a partnership between technology, patient, and provider, centered on prevention and precision, rather than crisis response.
Organizations like our company, AliveCor, are at the heart of this transformation. Together, we’re combining the power of machine learning, and generative and non-generative AI to bring patients and healthcare providers a portfolio of solutions that aims to democratize access to cardiac care for every patient, everywhere.
Interview with David E. Albert, M.D., Founder and Chief Medical Officer, AliveCor
Photo courtesy of AliveCor
Act ¡Rapido! If You or a Loved One Is Having a Stroke
If you think you or a loved one is having a stroke — face drooping, slurred speech, and arm weakness are all signs of a possible stroke — you have to act quickly and get help right away.
Whenever somebody is having a stroke, they’re losing up to 2 million brain cells every minute,”said Dr. Hugo Aparicio, American Heart Association volunteer expert and associate professor of neurology at Boston University Chobanian and Avedisian School of Medicine. “Every minute counts, and we do have treatments for stroke. Over the last few decades, treatments have been developed that could potentially reverse or even totally cure the symptoms of stroke if you get to the hospital in time.”
A stroke is when a blood vessel carrying oxygen to the brain bursts or is blocked by a clot. It can happen to anyone at any time. Strokes can lead to permanent disability or even death.
Stroke awareness
This is a major health concern, especially in the Hispanic community. While stroke is the fifth-leading cause of death for Americans, it’s the No. 3 cause of death for Hispanic women and the No. 4 cause of death for Hispanic men.
“Forecasts show that stroke will increase by up to 25% in this demographic by the year
2030,” Dr. Aparicio said. “So, there’s a sense of urgency.”
Now, the American Stroke Association, a division of the American Heart Association, has launched a Spanish language website, DerrameCerebral.org. Language barriers can make it hard for people to access proper healthcare. The new website makes it easier for Spanish-speaking people to understand the stroke warning signs and risk factors, helping to reduce gaps in care and improve health for the community.
It’s important to offer health information in Spanish since it’s often the primary or preferred language for many in the Hispanic community.
“Stroke is a potentially very devastating condition,” said Dr. Aparicio, noting patients who seek medical attention sooner will likely have better outcomes.
DerrameCerebral.org provides information on risk factors, stroke prevention, warning signs, treatment, and recovery. On the site users can test their knowledge and skills of the stroke warning signs with the R.Á.P.I.D.O. Experience, a series of games and activities which details what the stroke symptoms look, feel and/or sound like.
The acronym R.Á.P.I.D.O. stands for:
R - Rostro caído (face drooping)
Á - Álteración del equilibrio (loss of balance, or lack of coordination)
P - Pérdida de fuerza en el brazo (arm weakness)
I - Impedimento visual repentino (sudden vision difficulty)
D - Dificultad para hablar (slurred or strange speech)
O - Obtén ayuda, llama al 911 (get help, call 911)
Know your risks
Knowing your family history is essential, since families often share similar risk factors like diabetes or heart disease. Your risk of having a stroke is higher if you have a family member who has had a stroke.
It’s also important to know your blood sugar, blood pressure, and cholesterol numbers; maintain a healthy weight; get regular exercise and adequate sleep; and not smoke.
“It’s better to mitigate and manage what you can well ahead of time,” Dr. Aparicio said.
“And, at the time of a stroke, seek help immediately to have better outcomes.”
Written by Kristen Castillo
Beyond Hardware: How AI Can Make Cardiac Imaging More Accessible
In the past, it’s been common practice to look to advances in computed tomography (CT) imaging system hardware for improvements in cardiac imaging. Innovation in the hardware of the machine itself has helped to make it possible to reach the high scanning speeds necessary to obtain high-quality cardiac images.
WRITTEN BY Ekta Dharaiya Global Clinical Leader, Philips Computed Tomography
One of the advantages of CT scanning is that it is a fast method for creating a 3D image of the heart and coronary arteries. Hardware, though, is rapidly reaching its physical limitations in the ability of CT scanners to provide the additional temporal resolution necessary to increase quality in cardiac exams.
“The next leap in image quality and efficiency for cardiac exams is being made possible by refinements in CT software and through artificial intelligence (AI). Fortunately, these AI advances are now found in the types of CT systems that are more accessible to a wide range of healthcare institutions, which means more patients will have the opportunity to benefit from high-quality cardiac scanning,” said Dr. Atul Gupta, chief medical
officer of diagnosis and treatment at Philips and practicing radiologist.
This is important because coronary computed tomography angiography (coronary CTA) has become the preferred noninvasive imaging exam to help clinicians detect and rule out coronary artery disease (CAD).
Coronary CTA provides a view of the coronary anatomy and helps clinicians visualize atherosclerotic plaque to aid in the detection of lesions that may limit blood flow to the myocardium.
Recently updated guidelines affirm the value of coronary CTA as a first line test for patients with stable or atypical chest pain or other symptoms of angina (a type of chest pain caused by reduced blood flow to the heart), and demand for CTA exams is expected to increase.1
There are multiple challenges in imaging coronary arteries with CT. These arteries are small, about 1 mm or less at their furthest point, and they move rapidly and in multiple directions as the heart beats, which may contribute to blurring during cardiac imaging that can make images less clear. Unpredictable cardiac motion due to irregular and high heart rates can lead to sub-optimal or cardiac exams that can’t be used for diagnosis. The temporal resolution of coronary CTA is insufficient to address motion artifacts from irregular or higher heart rates, resulting in coronary segments that aren’t easy to evaluate, which makes diagnosis harder.
This is why AI solutions, paired with advanced hardware, are so promising.
How hardware, software, and AI go hand in hand for improved cardiac imaging
The Philips CT 5300 system features NanoPanel Precise, the industry’s first CT detector built from the ground up specifically for AI-based image reconstruction. This detector leverages the full capabilities of Philips Precise Image AI-reconstruction software to deliver high-quality images at much lower radiation dose. Combined with Precise Cardiac motion compensation, Precise Image makes the CT 5300 system particularly suitable for high-quality, motion-free cardiac imaging in patients with high heart rates or heart-rate variability.
Correcting for the motion that happens in cardiac arteries
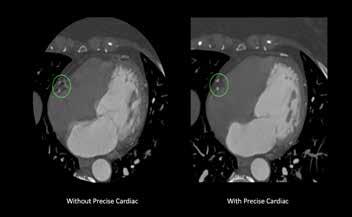
Precise Cardiac is a reconstruction technique that compensates for cardiac motion to improve visualization of the coronary arteries during CT imaging. This enables clinicians to see what’s happening in the coronary arteries.
Precise Cardiac demonstrates significant improvements in image quality of the coronary arteries, compared with standard cardiac CT reconstructions. Applicable for different types of CT exams (retrospectively gated helical exams and prospectively gated axial exams), Precise Cardiac employs efficient filtering techniques in a predefined region around the targeted cardiac phase to identify relevant objects and dynamically track their motion behavior in the localized portion of the cardiac cycle. Motioncorrected images are generated by taking into account the displacement of structures and performing the relevant corrections as part of the reconstruction process.
Smart automation in this advanced CT system
Precise Cardiac is built into the CT workflow, avoiding the need for any manual intervention by the person doing the scanning, the need for data transfer or the need for additional workstations. It improves diagnostic confidence in challenging patients with high or irregular heart rates and can help a clinician salvage some coronary segments previously deemed nondiagnostic using standard cardiac reconstructions, thus increasing diagnostic confidence in coronary CTA exams. Coronary motion correction can potentially reduce the need for a repeat scan.
AI-enabled cardiac scanning at every step
Cardiac imaging is advancing. From scan preparation through reconstruction, the powerful Philips AI-enabled innovations in cardiac imaging matter. Tools like Precise Image AI reconstruction and Precise Cardiac for motion-corrected images help deliver precision in dose, speed and image quality.
As more institutions gain access to AI-enabled CT systems that can offer high-quality cardiac scans at low dose, more patients can benefit. We’d love to have you continue the conversation with your clinician as appropriate.
Talk with your clinician about if cardiac scanning is right for you. Clinicians can reach out to their Philips representative to learn more about AI and cardiac scanning.
REFERENCES
Cardiac imaging is advancing. From scan preparation through reconstruction, the powerful Philips AI-enabled innovations in cardiac imaging matter.
1. Narula J, Chandrashekhar Y, Ahmadi A, et al. SCCT 2021 Expert Consensus Document on Coronary Computed Tomographic Angiography: A Report of the Society of Cardiovascular Computed Tomography. J Cardiovasc Comput Tomogr. 2021 MayJun;15(3):192-217. doi: 10.1016/j.jcct.2020.11.001. Epub 2020 Nov 20. PMID: 33303384; PMCID: PMC8713482 To learn more, scan the QR code.
Precise Cardiac eliminates motion and improves visualization of a right coronary artery (RCA) in a patient with a high heart rate as seen in the image.
Philips CT 5300 computed tomography scanner
How Barbra Streisand Is Advocating for Women’s Heart Health
If Barbra Streisand had her way, all women in America would know that heart disease, known as cardiovascular disease (CVD), is their leading killer. It kills more women than all cancers combined, yet only half of women know that, she says.
Streisand has advocated for gender equity in heart health for more than a decade, though her passion to fight gender inequality dates to her youth. For too long, she says, there was little understanding of women’s CVD in the scientific and medical communities. A large part of the problem stems from gender disparities that span across research, diagnosis, and treatment.
“We all have been culturally exposed to the typical ‘Hollywood heart attack’ through movies and television,” Streisand said. “A man grabs his chest in severe pain and has pain running down his left arm.”
Today, we know that women with CVD often have different symptoms than men. Women’s symptoms can include shortness of breath, nausea, upper body pain, extreme fatigue, indigestion, chest pains, and others. But because these differences were unknown for a long time, sex-related disparities in diagnosis and treatment grew.
Voice for change
In 2007, Streisand read about the gender inequality in medicine that spotlighted the differences in women’s heart healthcare, research, and public awareness compared to men. Her realization that women were not receiving the same quality of care as men
— which explained why women were dying of CVD at disproportionate rates — appalled her and made her decide to use her voice for change.
Streisand started working with Cedars-Sinai Medical Center in Los Angeles and Dr. Noel Bairey Merz, a brilliant researcher and clinician working on female-pattern heart disease. First, Streisand supported a regenerative medicine research fund, then she underwrote the Barbra Streisand Women’s Cardiovascular Research and Education Program in 2008.
Her support, advocacy, and generous philanthropic commitment resulted in the Barbra Streisand Women’s Heart Center, focused on providing leading edge healthcare to women with heart disease, developing research leading to new treatments, and training doctors about women’s CVD.
Streisand soon learned that it wasn’t just doctors and scientists who weren’t talking about women’s heart health. Neither were women themselves.
“Many women don’t want people to know about their heart issues. They do not discuss it,” Streisand said. “They seem ashamed or feel weak because of it.”
Female mice
In 2014, Streisand and Bairey Merz launched the Women’s Heart
Alliance (WHA), a national advocacy and education effort fighting for women’s heart health equity. They were joined by businessman and philanthropist, Ronald Perelman, Dr. Holly Andersen, and NY Presbyterian-Cornell Weill Medical Center.
“To achieve heart health equity we needed to expand the research being done and to raise public awareness about heart health issues facing women,” Streisand said.
WHA aims to increase funding dedicated to gender equity in research. For example, the number of women participating in research and clinical trials has increased significantly from less than 10% to one-third.
“I also fought to get female mice in clinical research,” Streisand said. “Why use male mice to study female heart disease?”
WHA’s advocacy has led to greater study of coronary microvascular dysfunction, which affects tiny blood vessels
in women’s hearts with CVD. The Department of Defense is now funding research of heart disease in women and the NIH is requiring research and clinical trials to report results by gender.
Universal screening “Ten years ago, one in three women were dying of heart disease,” Streisand said. “Now, that number is 1 in 4. Women are finally being valued more.”
Looking ahead, Streisand wants universal CVD screening for women, more funding for federally funded women’s health centers of excellence, and an analysis of the effect of sex and gender bias on federal funding for disease research.
She’s grateful for progress but laments that too many women are still dying from CVD. “We have more work to do to reach our goal of equity in the research, prevention, and treatment of women’s CVD,” she said.
Written by Kristen Castillo
Barbra Streisand and Dr. Noel Bairey Merz | Photo courtesy of Cedars-Sinai Medical Center
Managing Cardiovascular Risks With Diabetes and Obesity
Learn about the link between obesity, diabetes, and heart disease — and how to lower your risk.
People who have diabetes and/or obesity are more likely to have heart disease than people without diabetes. In fact, in the United States, a person with diabetes is admitted to the hospital for a major cardiovascular disease (CVD) every 19 seconds. Furthermore, obesity contributes to up to 53% of new type 2 diabetes cases each year and leads to additional CVD diagnoses.
Obesity is a chronic disease in the same league as CVD and diabetes that results from a combination of behavioral, environmental, and genetic factors. Treatment requires a multifaceted approach to achieve better health outcomes and reduce risks for other related conditions/complications.
Unfortunately, stigma, shame, and blame too often keep people who need care for obesity and/or type 2 diabetes from pursuing it. There is no universal approach to obesity care, but rather many treatment options that can be tailored to individual needs, including healthy eating, physical activity, medication, surgery, counseling, and lifestyle changes.
Both obesity and type 2 diabetes can lead to complications that can contribute to conditions such as CVD. These complications include elevated blood glucose (blood sugar), blood pressure, and cholesterol. High blood glucose levels can harm the blood vessels
and nerves needed for heart health. High blood pressure makes this worse by making the blood flow through arteries at a higher pressure. And high LDL cholesterol (sometimes called “bad” cholesterol) causes plaque to build up in the arteries, affecting blood flow. Recognizing these signs early and consulting with a healthcare provider can prevent further complications.
Seeking care
Initiating a conversation with your healthcare provider about your obesity and weight journey is a pivotal step toward improving your overall health and reducing your risk for type 2 diabetes and/or CVD. By sharing your weight-related challenges and experiences, you will help your healthcare provider gain deeper insights into your personal treatment needs.
Regular health visits are also crucial for having your A1C (a picture of your average blood glucose over the past two to three months), blood pressure, and cholesterol levels checked. Assessing these metrics is essential for determining diabetes risk, maintaining heart health, and reducing the risk of CVD. Be sure to discuss the outcomes with your healthcare provider to determine if your current treatment plan is effective or if adjustments are needed to better meet your health goals.
Stay informed
For healthcare providers, staying informed about the latest research and treatment options is essential to their ability to offer the highest quality of care. Knowledgeable and compassionate healthcare providers can create a supportive environment that encourages patients to pursue treatment. Understanding how behavioral, environmental, and genetic factors contribute to obesity also allows healthcare providers to recommend personalized treatment strategies that address specific management needs.
Well-informed healthcare providers are also more likely to help people understand the misconceptions surrounding obesity and/or diabetes, advocate for the people they treat, and ultimately enhance overall care.
Living with obesity and/or diabetes can be hard, but know you’re never alone on your journey to better health. There will always be someone to support you, including those in your network of family, friends, and healthcare providers.
As obesity and type 2 diabetes treatments are unique to each person, remember to work with your healthcare team to develop a treatment plan that fits your needs and helps you reach your goals.
Written by American Diabetes Association®
Seeing Heart Valve Failure From All Sides
A heart surgeon who performed a revolutionary aortic valve replacement therapy on patients with heart valve failure undergoes the procedure himself.
No one was more surprised than Dr. Rick Dearman when he was diagnosed with severe symptomatic aortic stenosis, also known as heart valve failure. As a heart surgeon, he’d treated hundreds of people with the condition. But after noticing that he was more tired and out of breath than usual, his wife — an ICU nurse — laid her head on his chest one night while watching television and told him point-blank: You have a heart murmur.
“I was a typical man, and I said, ‘No, I don’t,’” Dr. Dearman said with a laugh. “But I listened to my chest with my own stethoscope — and there it was.”
In many ways, Dr. Dearman is lucky: Heart valve failure is sometimes referred to as the “silent killer” because the symptoms (primarily shortness of breath, chest pain, and dizziness) can be subtle — or nonexistent. But ignoring those symptoms can be deadly: Up to half of patients diagnosed with symptomatic severe aortic stenosis (sSAS) die within two years unless they undergo treatment.
Effective treatment for heart valve failure exists, including, for many, the less invasive
transcatheter aortic valve replacement (TAVR) procedure. No one knows this better than Dr. Dearman, who has experienced heart valve failure and TAVR as a son, a surgeon — and a patient.
“The TAVR procedure is really pretty amazing,” he said. “I’d say in my career, this would qualify as a medical miracle.”
Fixable, not fatal
Heart valve failure is a condition where the leaflets or flaps in the aortic valve in the heart thicken and narrow, typically due to calcium buildup, allowing less blood to pass through. “These valves are designed like in a machine to regulate flow,” Dr. Dearman explained. “With heart valve failure, the main valve leading out of the heart into the aorta becomes stiff and doesn’t open properly. Pressure builds up and the heart begins to struggle with extra work and can begin to fail.”
Once that failure begins, you can reach a point where the heart is so weakened it cannot recover, so prompt treatment is paramount. But sometimes, these symptoms are so mild they are ignored, turning a fixable condition into
a fatal one. “It happens slowly,” Dr. Dearman noted, “over a period of time. You compensate — you slowly change your level of activity and behavior during the day to accommodate what you feel.”
The impact of heart valve failure will only become more pronounced as the population ages. The disease becomes more severe with age, and it’s estimated that 20% of people over the age of 65 have heart valve failure — a population estimated to more than double in the next four decades. And about 10% of patients diagnosed may die within five weeks without treatment.
The good news is that replacing the affected valve is highly effective: Having the procedure within three months of diagnosis can result in a lower mortality rate and other negative outcomes.
The bad news is that heart valve failure is startlingly undertreated: A 2016 study found that approximately 60% of heart valve failure patients went untreated. Lack of treatment disproportionately affects older generations and other patient subgroups, including women and people in communities of color, who are much
Dr. Richard Dearman, Cardiothoracic Surgeon | Photos by Rob Howard
less likely to undergo valve replacement.
Even when patients diagnosed with heart valve failure eventually undergo a valve replacement procedure, there are usually significant and life-threatening delays: An article published in 2023 found that between 2016 and 2022, nearly 40% of patients still had not been treated up to four years after their diagnosis.
An effective treatment
The reasons so many people with heart valve failure don’t undergo treatment stem in part from outdated attitudes among healthcare professionals. “Historically, heart valve failure was a very high-risk thing to treat,” Dr. Dearman explained. “When the first valves were implanted, the open-heart surgery was only performed when you had absolutely no other options.”
This is beginning to change, partly because of this effective, less invasive treatment option in the form of TAVR. Dr. Dearman’s first experience with TAVR was when it was performed on his 92-year-old father.
“I saw this firsthand with my father — he’s already had previous bypass surgery and a valve replacement — no one was going to do a third heart operation on a 92-year-old man who was in dire straits,” Dr. Dearman explained. “But after TAVR, it was literally a 180-degree turnaround. His heart activity was normal. That was very eye-opening.”
Since then, Dr. Dearman has performed the TAVR procedure about 300 times. The procedure involves placing a replacement valve on a catheter and inserting it through one of the femoral arteries on either side of the groin. The valve is positioned in the heart and expanded, pushing the native leaflets valve aside, and replacing the failing heart valve.
TAVR has been used for decades and can now even be used for patients who are at low risk for surgery. It is a relatively short procedure, often lasting under an hour, and usually results in a short recovery with most patients going home the next day. However, there are risks associated with the TAVR procedure, and the most serious include death, stroke, serious damage to the arteries, or serious bleeding.
Most importantly, TAVR can give people their lives — and quality of life — back. An overwhelming majority of heart valve failure patients who underwent the procedure were alive with improved health and quality of life years later.
Dr. Dearman’s story
Dr. Dearman has always been an active person. He attended college and medical school on an army scholarship, and served 16 years in the U.S. Army Reserve Medical Corps, where he rose to the rank of Lieutenant Colonel and received Meritorious Service Medals in 1985 and 1988.
“The army has very definite physical standards, and I had always been very physically active. I love running, jogging, and aerobic activity,” he said.
But as time passed, he noticed that he became short of breath more easily. “Like everyone, I thought, ‘Well, you’re older. What do you expect?’” he said. “I was putting on weight. And I thought, ‘Well, not only are you older, but you’re fat. What do you expect?’”
After his wife noticed his heart murmur, Dr. Dearman spoke with a fellow cardiologist and determined that the best option was a TAVR. His recovery was relatively fast — he went home the next day and was back at work in the operating room a week later. “When I woke up, I could tell immediately a difference in how I felt,” he said. “It was a dramatic change. The fact that I felt better meant I hadn’t waited until it was too late.”
Unsurprisingly, Dr. Dearman offers words of encouragement for people diagnosed with
Put yourself in the hands of people you trust, think of your family, and think of what life is like now and what you have left to live for.
heart valve failure: “Put yourself in the hands of people you trust, think of your family, and think of what life is like now and what you have left to live for,” he said. “And realize that all that can be extended and improved. Don’t be afraid to face something that can be fixed.”
If you or someone you know has heart valve failure and is experiencing symptoms, don’t wait. Don’t let fixable become fatal. Speak to your doctor right away.
Written by Jeff Somers |
Cardiovascular Health and Anti-Obesity Medications: How to Talk to Your Provider
Dr. Lydia Alexander discusses the importance of treating obesity and cardiovascular disease in women, advocating for informed discussions and personalized care with healthcare providers.
For women, cardiovascular disease (CVD) remains the leading cause of death, with the risk being significantly increased in women with obesity. This makes the need for proper obesity treatment more important than ever.
Proper comprehensive care for obesity treatment can include nutrition therapy, physical activity, behavioral modification, and medical interventions such as medications or surgical procedures. In recent years, there has been a substantial increase in the amount of FDA-approved anti-obesity medications, such as semaglutide (Wegovy) in 2021. These medications effectively manage weight and reduce the risk of CVD, providing enduring options for the comprehensive treatment of obesity and obesity-related complications.
The SELECT trial, conducted from 20182023, was designed to evaluate the effects of semaglutide on weight and cardiovascular health. The results of the study showed that semaglutide significantly reduced the risk of major cardiovascular complications while improving blood pressure and cholesterol levels. The trial highlights the broader health benefits of anti-obesity medications, particularly for cardiovascular health in patients with obesity.
Although these medications are more accessible, discussing them with your provider is critical, and such conversations are not always easy. Transparent conversations with your provider on such matters can cover sensitive topics such as weight, health issues related to one’s weight, and personal issues, all while potentially introducing bias.
It is essential for women to approach these conversations with confidence and a clear understanding of how anti-obesity medications, as part of a comprehensive obesity treatment plan, can benefit overall health.
How to prepare for your visit
• Know your health history and your lifestyle, and be ready to articulate what has/ has not worked for you in the past.
• Create a list of questions or concerns that address the benefits and risks of the
medications and how they align with your overall health goals.
• Articulate your health goals. (Have an idea of what you are looking for from a medication, know what tests to ask for, what you want to measure, etc.)
• If you face bias and/or resistance from your provider, advocate for yourself and your health goals. Seek a second opinion if the treatment plan isn’t a good fit for you.
How to discuss obesity treatment with your patients
• Avoid assumptions about the patient, their lifestyle choices, and their health history.
• Stay up-to-date on the best options to build comprehensive obesity treatment plans, including up-to-date, FDA-approved anti-obesity medication options.
• Focus on overall health goals for your patient (beyond weight loss) and how you can provide them with the proper knowledge and support.
• Approach treatment with a compassionate, non-judgmental attitude while using person-first language.
Once you have determined the best direction for you to take with medications, it is crucial to have ongoing care and follow up with your provider. Regular and ongoing surveillance
by your provider will allow them to monitor the effectiveness of the medication, help you manage side effects, provide support and guidance, and adjust treatment to align with your health goals.
Addressing obesity and cardiovascular health is vital for women’s well-being. Antiobesity medications, when paired with healthful nutrition, physical activity, and behavioral modification, offer an opportunity to treat obesity and lower cardiovascular risks.
Open, compassionate, and informed discussions with your provider are key to creating a personalized treatment plan. By approaching these conversations with preparation and confidence, you can work collaboratively with your provider to develop a treatment plan that works specifically for you. When you advocate for your health with your provider, you not only enhance your well-being, but you can also serve to inspire others to approach their health journey with improved confidence and determination.
Written by Lydia Alexander, M.D., DABOM, DACLM, MFOMA, President, Obesity Medicine Association
REFERENCES
1. Lincoff AM, Brown-Frandsen K, Colhoun HM, Deanfield J, Emerson SS, Esbjerg S, Hardt-Lindberg S, et al. “Semaglutide and cardiovascular outcomes in obesity without diabetes.” NEJM, https://doi.org/10.1056/NEJMoa2307563.
Obesity Experts’ Go-to Oral Medication — That Your Primary Doctor May Not Know About
Sometimes diet and exercise are not enough to help the 100 million Americans with obesity lose weight and prevent health conditions, including heart disease.
That’s why doctors are encouraging adults and adolescents with obesity to consider taking prescription medicine in combination with making lifestyle changes, including a reduced-calorie diet and more physical activity.
Maria knows the struggle to lose weight. “I have tried all types of diets through my adult life, workouts, everything known to man,” she said. “I eat very healthy and always have.”
It wasn’t until her doctor prescribed a weight loss drug, Qsymia®, that she was able to lose 60 pounds. She’s been taking the oral, non-injectable medicine for 22 months and has kept the weight off. She says she hasn’t experienced side effects.
“This is the only thing I have been able to maintain weight loss on,” she said, explaining she’s “satisfied and happy” with her weight loss. “My blood work has been excellent, and I look and feel great.”
Obesity
The CDC reports 2 in 5 adults are obese, which means they have a body mass index (BMI) of 30 or higher. The chronic disease costs $173B a year in added medical expenses.1
“Obesity is a chronic inflammatory state,” said Vivus LLC consultant Dr. Pamela R. Rama, a cardiologist at Baptist Heart Specialists in Jacksonville Beach, Florida.
People with obesity are at greater risk for health challenges like coronary artery disease, which is a buildup of plaque in the arteries, as well as diabetes, high blood pressure, cancer, stroke, and more.2
Obesity is also a health challenge for young Americans. The CDC says 22% of youth ages 12-19 are obese.3 Experts predict that 80% of obese adolescents will continue to be obese in adulthood.4
“Seek evaluation for the child as
early as you think you see an issue,” said Dr. Suzanne Cuda, a pediatric obesity specialist in San Antonio. “Really be proactive for your child, because this is a disease.”
Dr. Cuda, a consultant for Vivus LLC, says managing chronic weight loss can help youth in all aspects of their lives, including improving their self-esteem. It may also help reduce their risk of chronic metabolic diseases like diabetes and heart disease.
Lifestyle changes and weight loss drugs
Losing weight can lower a person with obesity’s risk of heart disease and other chronic conditions. Typically, the first treatment for people with obesity is reducing caloric intake and increasing activity. But if that doesn’t work or doesn’t work well enough, doctors can prescribe weight loss drugs to their patients. Combining medicine with lifestyle changes can be an effective and sustainable approach to weight loss and
chronic weight management.
Qsymia, phentermine and topiramate extended-release capsules, marketed and sold by VIVUS LLC, has been FDA approved for over a decade for use in patients with obesity who have a BMI of 27 or higher and have at least one weight-related medical condition, such as high blood pressure.
Qsymia, pronounced Kyoo-simee-uh, is informally known as obesity medicine experts’ best-kept weight loss secret. Studies support the non-injection weight loss drug’s efficacy. A twoyear study found adults receiving the top dose lost 10.5% of their body weight, while those receiving the mid-dose lost 9.3%, compared to the placebo group, which lost 1.8%.5 Another study shows it reduced systolic blood pressure, a cardiovascular disease risk factor, in patients who were overweight or obese.6
Since 2022, Qsymia has been FDA-approved for treating obesity in adolescents ages 12-17 who have a (BMI) in the 95th percentile or greater.
INTERVIEW WITH Dr. Pamela Rama Cardiologist, Baptist Heart Specialists (Jacksonville, Fla.)
INTERVIEW WITH Dr. Suzanne Cuda Pediatric Obesity Specialist (San Antonio, Texas)
A study published in the New England Journal of Medicine reported that in a 56-week, randomized, double-blind trial, adolescents with obesity who received mid and top doses of Qsymia had a statistically significant reduction in BMI and improved cholesterol levels.7
“The great majority of kids do great; they tolerate the medications,” Dr. Cuda said. “Their families are good about modifying the diet and helping to increase activity.”
Effectiveness
Qsymia is safe, effective, and less expensive than injectable weight loss medications. In a report in The Institute for Clinical and Economic Review (ICER), Qsymia has the lowest annual net price of $1,465, a big savings compared to the price of semaglutide, which has an annual net price of $13,618.8
It’s also one of the most effective
weight-loss medications. The same report found “greater weight loss was seen with semaglutide and with phentermine/ topiramate” than other weight-loss drugs.
Patient perspectives
Patients who’ve taken Qsymia praise the pill for helping them control their weight. For example, Michele, who gained 40 pounds during menopause, says she couldn’t lose weight even though she was eating healthy. “I’ve already lost 35 pounds since being on it,” she said, calling the weight loss medicine “wonderful.”
Other patients say the drug helps them manage their weight while they’re also managing chronic health conditions. Pamela, who has a thyroid condition, has been taking Qsymia for a year and has lost 20 pounds. “I finally feel better and in control of my weight.”
Another patient, Stephanie, has struggled with her weight for most of her
QSYMIA is a combination of phentermine, a sympathomimetic amine anorectic, and topiramate, indicated as an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in:
• Adults with an initial body mass index (BMI) of:
• 30 kg/m2 or greater (obese) or
• 27 kg/m2 or greater (overweight) in the presence of at least one weight-related comorbidity such as hypertension, type 2 diabetes mellitus, or dyslipidemia
• Pediatric patients aged 12 years and older with BMI in the 95th percentile or greater standardized for age and sex.
Limitations of Use:
• The effect of QSYMIA on cardiovascular morbidity and mortality has not been established
• The safety and effectiveness of QSYMIA in combination with other products intended for weight loss, including prescription and over-the-counter drugs, and herbal preparations, have not been established
IMPORTANT SAFETY INFORMATION
Qsymia can cause serious side effects, including:
• Birth defects (cleft lip/cleft palate). Patients who are pregnant must not take Qsymia. If you become pregnant while taking Qsymia, stop taking Qsymia immediately, and tell your healthcare provider right away.
• Qsymia may slow the increase in height in children 12 years and older, when used for a long time.
• Increases in heart rate.
• Suicidal thoughts or actions. Call your healthcare provider right away if you have any of these symptoms, especially if they are new, worse, or worry you: thoughts about suicide or dying; attempts to commit suicide; new or worse depression; new or worse anxiety; feeling agitated or restless; panic attacks; trouble sleeping (insomnia); new or worse irritability; acting aggressive, being angry, or violent; acting on dangerous impulses; an extreme increase in activity and talking (mania); other unusual changes in behavior or mood.
• Serious eye problems, which include any sudden decrease in vision, with or without eye pain and redness, or a blockage of fluid in the eye causing increased pressure in the eye (secondary angle closure glaucoma). These problems can lead to permanent vision loss if not treated.
Do not get pregnant while taking Qsymia. Do not drink alcohol while taking Qsymia. Do not drive a car or operate heavy machinery, or do other dangerous activities until you know how Qsymia affects you.
Qsymia is a federally controlled substance (CIV) because it contains phentermine and can be abused or lead to drug dependence. Keep Qsymia in a safe place to protect it from theft. Never give your Qsymia to anyone else as it may cause death or harm them.
QSYMIA may cause a severe rash with blisters and peeling skin, especially around the mouth, nose, eyes, and genitals (Stevens-Johnson Syndrome). Qsymia may also cause
life, especially after she was diagnosed with an autoimmune disease. She’s been taking Qsymia on and off for four years and credits it with helping her manage her cravings. “I wasn’t always hungry, and lost weight and maintained it,” she said. “This journey is not as easy as some people think. It’s a battle each and every day.”
Promising therapies
With obesity on the rise — researchers project that nearly half of all Americans will have obesity by 2030 — it’s more important than ever to have effective treatments.9
“It looks like there’s a light at the end of the tunnel that we’re finally being able to treat these patients and reverse this disease,” said Dr. Rama, who has been treating patients with obesity for over 20 years.
Written by Kristen Castillo
To learn more, visit QSYMIA.com
a rash with blisters and peeling skin over much of the body that may be life-threatening (Toxic Epidermal Necrolysis). Call your healthcare provider right away if you develop a skin rash or blisters.
Common side effects of Qsymia in adults include numbness or tingling in the hands, arms, feet, or face (paraesthesia); dizziness; change in the way foods taste or loss of taste (dysgeusia); trouble sleeping (insomnia); constipation; and dry mouth. Common side effects in pediatric patients aged 12 years and older include depression, dizziness, joint pain, fever, flu, and ankle sprain.
These are not all of the possible side effects of Qsymia.
Call your doctor for medical advice about side effects. You may report side effects to VIVUS at 1-888-998-4887 or FDA at 1-800-FDA-1088.
References
1. “Adult Obesity Facts.” Centers for Disease Control and Prevention, www.cdc.gov/ obesity/php/data-research/adult-obesity-facts.html.
2. “About Coronary Artery Disease (CAD).” Centers for Disease Control and Prevention, https://www.cdc.gov/heart-disease/about/coronary-artery-disease.html.
3. “Childhood Obesity Facts.” Centers for Disease Control and Prevention, https://www. cdc.gov/obesity/php/data-research/childhood-obesity-facts.html.
4. Simmonds M, Llewellyn A, Owen CG, Woolacott N. “Predicting adult obesity from childhood obesity: a systematic review and meta-analysis.” Obes, https://pubmed.ncbi. nlm.nih.gov/26696565/.
5. Garvey WT, Ryan DH, Look M, Gadde KM, Allison DB, Peterson CA, Schwiers M, Day WW, Bowden CH. “Two-year sustained weight loss and metabolic benefits with controlled-release phentermine/topiramate in obese and overweight adults (SEQUEL): a randomized, placebo-controlled, phase 3 extension study” Am J Clin Nutr, https:// pubmed.ncbi.nlm.nih.gov/22158731/.
6. Bays HE, Hsia DS, Nguyen LT, Peterson CA, Varghese ST. “Effects of phentermine / topiramate extended-release, phentermine, and placebo on ambulatory blood pressure monitoring in adults with overweight or obesity: A randomized, multicenter, double-blind study.” Obesity Pillars, https://doi.org/10.1016/j.obpill.2024.100099.
7. Kelly AS, Bensignor MO, Hsia DS, Shoemaker AH, Shih W, Peterson C, Varghese ST. “Phentermine/Topiramate for the Treatment of Adolescent Obesity.” NEJM, https:// evidence.nejm.org/doi/10.1056/EVIDoa2200014.
8. “Report at a Glance: Obesity Management.” Institute for Clinical and Economic Review, https://icer.org/wp-content/uploads/2022/10/Obesity-RAAG_October-2022.pdf.
9. Ward ZJ, Bleich SN, Cradock AL, Barrett JL, Giles CM, Flax C, Long MW, Gortmaker SL. “Projected U.S. State-Level Prevalence of Adult Obesity and Severe Obesity.” NEJM, https://www.nejm.org/doi/full/10.1056/NEJMsa1909301.
Disclosure Statements
Drs. Rama and Cuda are Vivus LLC consultants.
101261.01-USP
What People Don’t Understand About Obesity and Weight Loss
There are countless misconceptions and social stigmas surrounding obesity and weight loss.
Ken Hall, CEO of Medi-Weightloss, is here to break them down.
What are the current stigmas surrounding obesity, and how can we start to shift these?
One of the most prevalent stigmas is the belief that obesity is solely the result of poor self-control or laziness. This oversimplified view ignores the complex interplay of factors such as genetics, metabolism, environment, and mental health.
One of the most effective ways to combat stigma is through education. This involves educating the public, healthcare professionals, and policymakers about the complex factors that contribute to obesity. Highlighting that obesity is a chronic, multifactorial medical condition — rather than a lifestyle choice — can help change perceptions. Using respectful and person-first
language, such as “person with obesity” rather than “obese person,” can make a significant difference in reducing stigma. This approach emphasizes the person rather than defining them by their condition and shifts the focus from blaming individuals to understanding the condition as a medical issue that requires appropriate care.
How can people take a more holistic approach to weight loss to improve their long-term health?
A holistic approach to weight loss involves addressing not just the physical aspects, but also the emotional, mental, and social factors that contribute to well-being. At Medi-Weightloss, our mission is to empower patients in their pursuit of wellness through weight loss.
This means looking beyond just the number on the scale and focusing on overall health improvements. Notably, our clinical outcomes have proven that healthy and meaningful weight loss leads to improved lipid profiles and reduced blood pressure, which in turn has been proven to significantly lower the risk of developing cardiovascular diseases such as heart attack and stroke.
Maintaining weight can be more chal lenging than losing it due to physiolog ical adaptations, psychological factors, and environmental influences. Having a plan in place for maintenance is important. Select a weight loss partner or program that emphasizes education, sustainable habits, ongoing monitoring, and expert support to make long-term weight maintenance achievable.
Sponsored
Combating Obesity With Comprehensive, Patient-Centric Weight Loss Solutions
Obesity is a global health crisis, increasing the risk of chronic conditions like diabetes, heart disease, and metabolic syndrome.
Today’s buzz around solving obesity focuses on new weight loss medications, often hailed as a “wonder shot.” However, when you read the clinical studies, they reference that these injections are most effective when combined with a comprehensive medical weight loss program. Successful programs combine medical supervision with nutritional guidance, behavioral therapy, physical activity, and the appropriate weight loss medications.
For 20 years, Medi-Weightloss has been at the forefront of the fight against the obesity epidemic, offering patient-centered, evidence-based solutions. At the heart of its approach is a commitment to delivering a personalized, multi-faceted program.
Unlike one-size-fits-all weight loss programs, Medi-Weightloss tailors each patient’s program to meet their unique goals, medical history, and clinical needs based on a thorough medical evaluation and lifestyle assessment. This approach ensures patients receive a plan that is safe, effective, and sustainable, making it possible to maintain their weight loss.
The Medi-Weightloss program emphasizes continuous monitoring and support via regular check-ins with healthcare professionals. These appointments allow for ongoing adjustments to their weight loss medications, nutritional plan, and physical activity goals, ensuring continued alignment with the patient’s evolving needs. This
consistent engagement helps patients stay motivated and accountable, which is crucial for success.
Empowering patients through education and behavioral modification equips them with the knowledge to make informed and aware decisions. This fosters lifestyle changes, positively contributing to a patient’s sustained weight loss and overall quality of life.
Medi-Weightloss is leading the way in the fight against obesity. Through personalized, comprehensive care and a supportive approach, combined with the appropriate weight loss medications, the program provides a proven path to achieving wellness through weight loss.
Written by Medi-Weightloss
a Free Assessment and take the first step toward empowering your journey to wellness through weight loss.