Anyone who wonders why there is such a huge fuss about measles is well justified.
After all, the recent outbreak in West Texas amounts to only about 300 cases (a number that keeps rising as we have prepared this story) among some 340 million Americans. That is way less than a drop in the bucket. If the US population was only 100 million instead of more than three times that much, the Texas measles cases would represent 0.0003% of the population (that’s three hundred-thousandths). Take that number and make it almost three and a half times smaller and you would have a truly minuscule number, like the weight of a single speck of dust on a scale.
So is the news coverage of the measles outbreak an example of the news media whipping up hysteria for higher ratings, or is there a valid reason for public health experts to be concerned?
Maybe it’s a little of both. News organizations will have to answer for themselves, but in this publi-
cation, let’s examine why measles is of great concern within the medical community. And how, yes, we can easily make measles great again.
What’s the big deal?
Here is a startling fact to begin our examination: measles stands alone among viruses; it is the single most contagious virus known to man. Every discussion of measles automatically contains words like “highly” and “extremely” to describe its potential for transmission. It is so contagious that if someone has it, 90% of the non-immune people they come into contact with will become infected. (People who have never had measles or the measles vaccine are considered non-immune.)
Epidemiologists use a formula resulting in what is called a basic reproductive number, expressed as Ro, to measure how transmissible a given infection would be in which a single case surfaces in a population where all individuals are susceptible. For instance, the Ro number for
the common cold is 2 to 3, meaning that a person with a cold will on average pass it on to 2 or 3 others. For comparison, COVID-19’s Ro number in various estimates ranges from 2.9 to a high of 9.5. Ebola comes in at 1.8. SARS is in the 2 to 4 range. For measles, the generally given range is already very high at 12 to 18, but a 2017 study put its Ro number as high as 203. Measles is the undisputed King Kong of communicable disease.
Between about 1855 and 2005, measles is estimated to have killed about 200 million people worldwide.
To this day, about 1 in 4 individuals who get measles will be hospitalized, and 1 or 2 in every thousand will die. Most deaths occur in children 5 and under, and the majority of deaths are the result of pneumonia caused by measles.
There is no cure for measles, nor any effective treatment. Barring complications, staying hydrated and addressing pain with ibuprofen or acetaminophen is the sole course of treatment.
• Review your
• Call to see if there is
• All services provided at no
Isn’t it old news? It should be. Measles was declared to be eradicated in the United States as of 2000. Across the Americas (North and South), reported measles cases went from 257,790 in 1980 to just 1,754 cases in 2000, then a measly 247 cases in 2010. (Note: “eradicated” doesn’t necessarily mean zero incidents; in the case of measles, it meant that every known case was either imported by a traveler from another country or related to an imported case.)
How was the elimination of such a highly contagious disease accomplished? Simply put, the MMR vaccine
(measles, mumps, rubella). More than a billion people worldwide have been inoculated against measles. Serious adverse reactions occur in less than one MMR vaccination per million administered (<0.0001%).
The measles eradication effort is so successful, at least in the United States, that people have forgotten how dangerous measles can be. As a result, vaccination rates are steadily dropping and measles cases are steadily rising. Remember the 247 cases in all of the Americas in 2010? By 2020 that num-
PARENTHOOD
by Dr. Warren Umansky, PhD
Your child has struggled in school since pre-K. He would have meltdowns where he would turn over furniture, throw things, tear up toys and papers, run out of the room, and be disruptive in every way. A few times every week the school would call you to come pick up your child. Behavior at home was a little better but still full of tantrums and disobedience. The behaviors continued in kindergarten, but the teacher was more willing to work with you and try to keep your child in school. Now, in the fourth grade, your child is delayed academically and still has behavior issues. You talked with your pediatrician last year and she referred you to a mental health professional. She diagnosed your child with Autism Spectrum Disorder and Attention Deficit Hyperactivity Disorder. This is the same diagnosis given a few years ago by a child psychiatrist who recommended a trial on medication. Your spouse refused this option. Over the course of months of seeing the current mental health professional and trying recommended behavior management strategies at home and the school applying many different good interventions in that setting, your child appears to be getting even more aggressive and disruptive. This mental health professional is also urging you to consider a trial on medication. However, your spouse still is resistant to the idea. What do you do?
A. Consult another mental health professional who might offer different options.
B. Consider home schooling to protect your child from schools that won’t meet your child’s needs.
C. Tell your spouse something has to be done, so you will take your child to the pediatrician to start a medication trial.
D. For now, do nothing different. Your child will outgrow the problems.
If you answered:
A. Parents who deny or don’t want to take responsibility for their child’s problem often do “doctor shopping,” hoping to find someone who will tell them what they want to hear. In this case, it is difficult to know what they want to hear; perhaps choice D.
B. Homeschooling fails for most children unless it is done proactively with a good curriculum and includes plans for group activities. This was apparent from COVID experiences. Children who are homeschooled due to their inability to succeed in a classroom setting are deprived of opportunities to learn from trained teachers and real life situations.
C. It is important for your child to feel and be successful. After years of failure to achieve this goal using non-medical approaches, and given the recommendation of at least two healthcare professionals who have seen your child, it might be time for a careful and well-monitored medication trial. Decades of good research and clinical experience support the safety and potential benefits of medication for the types of behavior the child has been exhibiting.
D. It is unlikely that the child will benefit from a wait and see approach. He will fall further behind academically, will have continued damage to self-worth, and will be on the road to more severe consequences in the future.
Dr. Umansky has a child behavioral health practice in Augusta. THE FIRST 40 YEARS ARE
THOUGHTS ABOUT THOUGHTS THOUGHTS
SEPARATION ANXIETY
Editor’s note: Written by local mental healthcare professionals, this series shares thoughts on how people think and act when affected by common and not-so-common mental health conditions.
Carole is 35 years old and married. She and her husband had their first child three years ago. She has always been very protective of their young son, but her husband has noticed that she has become more anxious recently. She refuses to use a sitter and regularly wakes up at night to check on their son while he’s sleeping. She becomes angry if she thinks her husband is playing too roughly, even though their son is laughing and happy. They’ve talked about putting the little boy in preschool, but Carole is reluctant. The other night, the husband woke up to find that Carole was having a panic attack, worried that their son might be kidnapped or hurt while he’s away from her.
Until recently, separation anxiety was considered a disorder only found in children.
A young child who becomes upset at the thought of being away from a parent or guardian or who can’t sleep unless that attachment figure is nearby is a common example of separation anxiety in children.
But the 5th edition of the Diagnostic and Statistical Manual of Mental Disorders has revised the clinical requirements for separation anxiety, acknowledging that adults can be diagnosed with this disorder. In adults, it is usually anxiety about being separated from a child or a romantic partner.
An adult (or child) may be diagnosed with separation anxiety disorder if they meet at least three of the following criteria within at least a sixmonth time period:
• Excessive distress when anticipating or experiencing
ed attacks that can have physical symptoms, like an overwhelming sense of dread, rapid heart rate, chest tightness and difficulty breathing, dizziness, and other symptoms.
Who’s at Risk?
If you have family members with some sort of anxiety disorder, you may have a higher risk of developing separation anxiety. Other risk factors include:
• Early life stresses like the divorce of parents, moving or the loss of a pet or family member
• If you’ve gone through a disaster or other traumatic and unexpected life event
• Having obsessive-compulsive disorder
separation from home or a major attachment figure
• Persistent and excessive worry about losing an attachment figure or of possible harm to them
• Persistent and excessive worry about an incident happening to their attachment figure, like a kidnapping or accident
• Reluctance to go away from home because of fear of separation
• Reluctance to sleep away from home or try to fall asleep without being near an attachment figure
• To have the above not caused by another mental health condition such as autism spectrum disorder or agoraphobia, which is the fear of being in a place where you can’t escape or get help
Separation anxiety can also lead to panic disorder, in which a person experiences frequent, unexpect-
How a person handles stress also makes a difference. Without consistent coping skills, support or self-care to manage anxiety, anyone is at higher risk for an anxiety disorder.
Treatment
Separation anxiety can prevent people from getting an education, earning a living, or developing healthy relationships. People may also brush off separation anxiety in adults as just being “overprotective” or “controlling,” when it is an actual disorder that can be treated.
Cognitive behavioral therapy is often the first-line treatment. In CBT, a therapist will encourage the person to learn what separation anxiety is and normalize the experience so there’s no shame or blame. They work with the person to identify when they are having anxious, negative or unrealistic thoughts. Then they reframe those thoughts by helping them examine evidence for or against what they believe. For example, if a person says, “My son might get kidnapped if he goes to preschool,” the therapist can ask if the preschool has safety measures or secure check-in/ check-out procedures.
24/7, free, confidential mental health hot-line that connects individuals in need of support with counselors across the United States and its territories. People do not have to be suicidal to call. Reasons to call include: substance use disorder, economic worries, relationships, culture and identity, illness, intimate partner violence, depression, mental and physical illness, and loneliness. +
Exposure therapy is another part of CBT. In the example above, Carole might check on her son before she goes to bed and not again until the morning, then work up to hiring a sitter for an hour or two.
Medications can also help. These include anti-anxiety medications like selective
do not require excessive force, as though you’re trying to remove hardened concrete from a construction site.
MEDICAL MYTHOLOGY
TOOTH MYTHS
One myth is that the average person can say our headline ten times — or even five — without messing up. Believe it or not, there are still more tooth myths. Man, that’s even hard to type!
One of the biggest currently is that healthy teeth are white teeth. Blindingly white teeth, in fact. Ask any dentist, and they will tell you that tooth whitening is one of the most commonly requested elective dental procedures.
In truth, tooth truth to be specific, tooth color all by itself can be meaningless as an indicator of dental health. There are various shades of white that are naturally different from person to person depending on things like age and genetics.
In addition, some medications cause tooth discoloration. Needless to say (but we’ll say it anyway), coffee, tea, wine, and tomato-based foods can all stain teeth. If you’re a coffee or tea drinker, you might be amazed by how white your teeth are when you notice the stains inside your coffee or teacup. If ceramic surfaces can become that stained, it’s no wonder that teeth can be too.
Some products designed to whiten teeth actually have a bluish tint that is designed to counteract or cancel any yellow tinge teeth may have. If the teeth have very little yellow, the result can be teeth that are unnaturally
white, like the cold white (almost blue) light that some of the newer car headlights have (see page 10).
Incidentally, if you have not done a whitening treatment lately, whether at your dentist or an at-home OTC option, the myth that such treatments damage enamel and cause extreme tooth sensitivity comes from earlier versions of whitening products. They have gotten much safer over the years.
In summary, the pursuit of white teeth is a personal choice, and certainly a very common choice, but in the same way that white teeth do not signify dental health all by themselves, teeth that are, shall we say, less than white do not mean poor dental hygiene or indicate dental problems. Healthy teeth vary in whiteness.
But still on this general subject, many people pursue whiteness by vigorous brushing. Brushing harder means cleaner teeth, they say. To which dentists will say, not so fast. Scrubbing teeth vigorously with a stiff toothbrush combines two things that are both detrimental to oral health.
Consider for a moment the goal of brushing: it’s to dislodge things like a little sliver of skin from the apple you ate an hour ago, or to make sure no Oreo crumbs have set up camp between your teeth. Such objectives
A soft-bristled brush (why do reputable toothbrush makers even sell the stiff bristles?) and a gentle, circular motion is all that is needed for sparkling clean teeth. It might be a challenge to break the habit of heavy-duty scrubbing, but it’s worth it to avoid damaging enamel over time and causing gums to recede. A soft brush will help; some have a bendy handle which makes exerting a lot of pressure difficult, and some electric toothbrushes (a better option anyway) will automatically shut off if you brush too hard.
Good brushing can lead to another myth: if you brush regularly and well, you don’t need to floss.
Who comes up with these things anyway? False teeth manufacturers?
The tooth truth is that no amount of good brushing can replace what flossing can do. That’s because no toothbrush can go into the crevices and crannies that are no problem for a thin filament of floss. The only topic up for serious debate is if you should brush first and floss second or floss first and brush second. Both strategies have their propenents, although here at Medical Examiner world headquarters we vote for flossing first. But first or second, the key is to do it, and thereby ward off plaque, gum disease, cavities, and bad breath. But as they say, you really only need to floss the teeth you want to keep.
Similarly, there is no substitute to brushing (such as chewing sugar-free gum). It’s better than nothing, but gum can’t take the place of brushing and flossing.
Good oral hygiene will result in something we all want: a toothsome smile.
As everyone was has been diagnosed with cancer knows, the journey can be quite a challenge, both for patients and their loved ones and for doctors.
For doctors, cancer is a formidable opponent. We use the word as though cancer is a single enemy, but there are actually more than 200 types covered by this one umbrella word, and each one has its own unique set of characteristics and behaviors. Additionally, since our DNA is involved each and every case is different from one person to the next, even among patients with the same type of cancer.
Similarly, another complicating factor is that even within a single tumor, cancer cells can vary genetically, meaning that their vulnerability to the attacks oncologists unleash upon them can vary from one cell in a tumor to the next.
Neit her does it help matters that metastasis is a word people in the cancer world must deal with. It describes the development of a secondary malignant growth somewhere else other than the initial site of cancer, turning treatment into something that can sometimes feel a bit like the classic arcade game Whac-A-Mole. Just when you think you’re about to destroy a cancer community, another group of cancerous cells erupts elsewhere. It can be frustrating and anxiety-inducing to be sure. The word metastasis literally means “rapid transition from one point to another.” Nobody wants that, but it happens, and doctors and patients have to deal with it. Cancer is also clever in that it can survive by disguising itself from the immune system or disabling the body’s defense response; and cancer cells can develop resistance to treatments over time, reducing the effectiveness of treatments that worked well in the past.
It all might sound daunting, but there has been tremendous progress in the effective treatment of cancer. As one oncologist told the Medical Examiner not long ago, cancer is gradually being transformed from an acute disease to a chronic disease. In other words, from a killer to a disease we can live with, often for many years with a minimum of adverse effects.
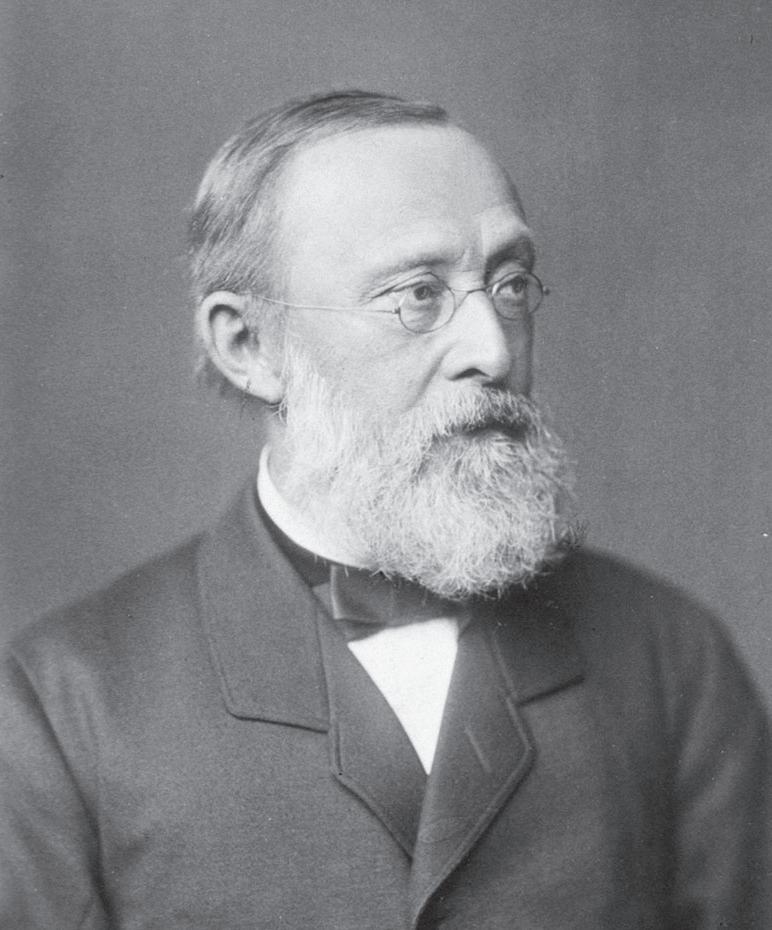
Who is this?
There is a word that appears often in biographies of the medical pioneers we profile in this space issue after issue. That word is polymath. It has nothing to do with mathematics, but instead stems from a Greek word whose literal meaning is “having learned much.”
This man, Rudolf Virchow (1821—1902), is the perfect embodiment of the word. He was a physician, anthropologist, pathologist, prehistorian, biologist, prolific writer and editor, and politician. He is known as “the father of modern pathology,” and to his colleagues, the “Pope of medicine.” He was fluent in German, Latin, Greek, Hebrew, English, Arabic, French, Italian and Dutch.
His doctoral thesis, defended a week after his 22nd birthday, examined corneal manifestations of rheumatic disease. His first scientific paper (published at age 24) contained the earliest known pathological descriptions of leukemia.
He was the first to see the connection between cancer and previously normal cells rather than the then-prevailing wisdom that cancers arose from foreign invaders. Virchow believed that cancer was caused by severe “irritation” of cells. He had observed that certain cancers were associated with white blood cells (macrophages) that produced irritation — what doctors would today call inflammation. His theories were largely ignored, but today doctors realize that mesothelioma, melanoma, and cancers of the lung, prostate, bladder, pancreatic, cervical, esophageal, and head and neck cancers are all strongly associated with long-term inflammation.
Virchow was the first doctor to develop a systematic procedure for conducting autopsies, and the methods he pioneered are still practiced, including retaining important tissue samples for further examination and testing. He was also the first person to analyze hair and recognize its forensic value, meaning that his appearance as an expert witness at a murder trial to testify about hair may also have been a first.
Virchow was among the earliest to recognize that all cells come from cells. In his era, people believed that life could spontaneously spring from non-living matter, the classic example being maggots appearing in decaying meat. The work of Virchow and his contemporaries led to the maxim “Omne vivum ex ovo;” that is, every living thing comes from a living thing (translated literally, “from an egg”).
For that reason, Rudolf Virchow’s scientific mind would not allow him to accept the teaching of evolution. His careful studies and observations over the course of his long career clearly demonstrated to him that life always comes from life. Darwin’s teachings “don’t stand the test of knowledge,” he told a friend. One of Virchow’s former students, Ernst Haeckel, a staunch evolutionist, once said that his one-time professor was “not caring in the least that now almost all experts of good judgment hold the opposite conviction.”
Virchow’s stand had nothing to do with religion, only science: he was a non-believer.
Virchow hopped off a moving streetcar on January 4, 1902, and broke his leg in the process. He never fully recovered, and died that September, a month shy of his 81st birthday. +
Middle Age
BY J.B. COLLUM
I saw him walking in my direction, but he never looked up. My vantage point was proving to be the advantage I hoped it would be. I could even see where one of the other kids was hiding from up here. My little brother Jeremy had mostly covered himself with pine straw in a slight depression behind a tree and some small shrubs, but I could just barely make out a peep of his red shirt from here. We were in the woods behind our house, so the vegetation was fairly dense. I had chosen a very large and tall pine tree to climb as my hiding spot for our elaborate game of tag.
I call it elaborate because in our game that we dubbed “Houdini Chase,” the person who was “It” didn’t cover their eyes and count to some arbitrary number while the others hid. No, that was just a childish game compared to our version, or at least that’s what we thought. Instead, as the name of our game implied, the person who was “It” was tied up and blind-folded and while they were trying to get free, the rest of us hid. The idea was to tie them up just well enough so they would be able to get free, but not until you were safely ensconced in your hiding place.
And there was the rub.
Sometimes, you did too good of a job, and you sat in your perhaps claustrophobic or in my case many times, acrophobic hiding place. But instead of being acrophobic, I was a certified acrophile (if that is even a word). I loved climbing trees or really just about anything higher than its surroundings, even the roof of the house, but that is a story for another day. As I was saying, sometimes you got tired of waiting because you did too good of a job of tying up your adversary. After a while though, with practice, we got so good at getting ourselves untied that this was less of a problem.
Looking back now, I imagined my climbing ability and opportunities would only increase with age. I didn’t know then that tree climbing, like a lot of other wonderful childhood things, was not destined to be a lifetime pursuit. And that indeed, at some point in my life, I wouldn’t be capable of doing it at all anymore.
I thought of this recently as I watched a video on YouTube of a man high up in a tree as he cut off the top with a chainsaw and watched it drop. Whenever I see things like this, in my mind I still think I could do it. But
for some reason, this time was different. I got real with myself and admitted that I couldn’t. It was a sad realization. The last time I climbed a tree, I had no idea it was the last time I would climb a tree.
Life in general is a chain of these types of things. The last time you talk to a loved one, you likely won’t know it is going to be the last time. The last time you pick up your kid and hold them seems ordinary at the time, but eventually, it will be the last time since they will get too big and heavy for you to do it and they probably wouldn’t like it anyway at that point. The last time you drive a car will likely not be special as you won’t know when the keys are going to be taken from you.
How are we to cope with this fact? First, we should live in each and every moment. Don’t be obsessed with the future; not retirement planning, not your next vacation, not the weekend ahead, not tomorrow, not even ten minutes from now. Sometimes, just focus on the moment, especially when that moment is special and fleeting and we never know when a moment will be special. Only the passage of time reveals that to us and it can be a cruel reminder.
So if your parent calls you when you are busy, stop and talk to them for at least a few minutes. Ask yourself, if this was the last conversation you ever had with them, how would you talk to them? If your grandchild is telling you a meandering story that seems like it was designed as a psy-op torture method devised by the KGB, steel yourself for it by remembering that they won’t be young forever. One day it will be the last time they really want to talk to you in that way. Especially if you don’t show them the attention they want at that moment and other moments like it.
As you look at yourself in the mirror and bemoan the additional gray hairs or another wrinkle, remember that in ten years you’d be very happy with your current look, so enjoy it while it lasts. Do the same as you look at your spouse. Take them out on a date night this week. One of those date nights will be the last, and we don’t have the benefit of knowing which one it will be.
J.B. Collum is a local novelist, humorist and columnist who wants to be Mark Twain when he grows up. He may be reached at johnbcollum@gmail.com
THOUGHTS… from page 2
serotonin reuptake inhibitors, or SSRIs. Many psychiatrists like using a combination of CBT and medication.
An in-person or online support group for people struggling with separation anxiety can also be helpful as a safe space where they can express their fears and learn techniques to reduce those fears.
Prognosis
For those with separation anxiety, therapy can result in noticeable improvement after several sessions. Over time, people can learn how to better cope with their fears, challenge their negative thought patterns and feel
James L. Millen, MD
Board Certified, American Board of Internal Medicine
freedom from the limits of anxiety. While this disorder may be more common and accepted in children, for adults with separat ion anxiety, feeling better starts with reaching out for help.
Mia Ulmer, MS, LPC, ATR-BC, CCTP, is a licensed professional counselor at IPS. IPS provides inpatient and outpatient mental health services, with or without a referral, to help patients and their families progress through the care journey. To make an appointment, call 706-204-1366 or visit integratedpsych.care.
Georgia Internal Medicine
Dr. James L. Millen Internal Medicine
and Endocrinology
NOW ACCEPTING NEW PATIENTS
Primary Care • Internal Medicine • Endocrinology
Specializing in expert treatment of: Diabetes • Hypertension • Thyroid Disorders • Preventive Medicine • Endocrine Disorders • General Internal Medicine
706-447-1118
1203 George C. Wilson Dr • Augusta, Georgia 30909
Same or next day appointments available
READ THE EXAMINER ANYWHERE!
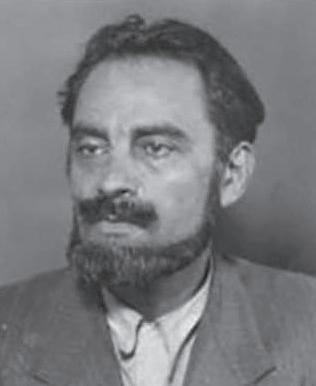
Who is this?
Not everyone in healthcare can be Florence Nightingale, right? Despite the long-running series on page 4, there are clunkers in medicine, and we will examine some of them in this brief series that should be briefer. Unfortunately, there’s enough material to keep this going for a while.
Say what you will about Marcel Petiot, but you have to admit the scheme he cooked up was genius. It was evil and brilliance blended together into one murderous package.
The real mystery is how this man ever came to be a doctor. Born in France in 1897, he was expelled from school multiple times and charged with a string of petty crimes that were dismissed when it became apparent that he had a mental illness. He joined the French Army in World War I, where he exhibited further signs of mental illness and was discharged with a disability pension in late 1918.
Using his veteran’s benefits, he entered an accelerated education program that allowed him to complete medical school in just eight months and be awarded a medical degree.
As a practicing physician, he had access to addictive narcotics which he used liberally and supplied to patients just as generously. He also developed a reputation for performing illegal abortions, for petty theft, and for tax evasion.
His initial foray into murder is only a suspicion: in 1926 he had an affair with the daughter of one of his elderly patients, and she subsequently disappeared. Police investigated but eventually dismissed her case as a runaway.
When World War II erupted, Petiot hatched a clever plot that fit perfectly with the times. With Paris occupied by Nazi troops after Germany defeated France in 1940, Petiot branded himself as a key player in the Resistance movement. He quietly advertised that he could arrange safe passage out of France through Portugal to safety in Argentina or elsewhere in South America for a fee of 25,000 francs per person (about $5,500 today).
When “customers” came to him, they were told to be ready to leave immediately, so they had with them all their money and valuables to take to their new life in South America. As a final step before leaving, Petiot told them that Argentina required all émigrés to be inoculated against disease, so they rolled up their sleeves for Dr. Petiot — and got an injection of cyanide. Petiot then took all their valuables and disposed of the bodies. The system worked so well because everyone who came to him was supposed to disappear, and disappear they did. By the time police discovered the plot, prosecutors estimated the scheme had put as much as 200 million francs in Petiot’s pockets.
His undoing came on March 11, 1944, when his neighbors at 21 Rue le Sueur, near the Arc de Triomphe, complained of a foul stench in the area and dense smoke billowing from the home’s chimney. Police arrived first, summoning firemen who found a coal stove in the basement surrounded by human remains, more of which were discovered in the yard, 27 victims in all (although he was ultimately suspected of more than 60 murders). At his trial on March 26, 1946, Petiot admitted to 19 of the killings, claiming they were German collaborators, but the ju ry was not impressed. On May 25, 1946, the head of Marcel Petiot, riddled with mental illness and malicious schemes, was removed by guillotine.
DINING TABLE CIRCUMCISIONS
By accident or otherwise, we all develop specific holiday traditions. Some have useful rational behind them. Some are far from ordinary. It was Thanksgiving in the flatwoods country of South Georgia a few decades ago. Fall leaves. Cool breezes, but no real cold. Quail hunts. Dove shoots. A family gathering at the old home place down a dirt washboard road. Tobacco barns, chicken houses, hog houses, and grape vines galore on black bottom soil just north of the Okefenokee Swamp. Old timers claimed water rings around their ankles were left over from wet years. Shallow wells 32 feet deep never ran out of water.
Brushy Creek ran through the farm. Men had fished very inch of Brushy Creek for food, not game. They ate what they grew or caught. It was a good life. Given the chance, most would not swap their childhood for the world.
Coy had two boys, Richard
BASED ON A TRUE STORY
(most of the time)
A series by Bad
Billy Laveau
(age 6) and Clyde (age 4).
After Thanksgiving dinner (dinner at noon, supper at dark) of ham (they did not grow turkeys), green beans, sweet potato pie, cornbread, and ambrosia, followed by a brief nap, they got down to business. Uncle had flu shots for all.
Everyone rolled up their sleeves, assembly line style. When Richard got his shot, Clyde figured out he was last. No one had screamed, fainted or acted the fool, but Clyde had seen enough. He was out the door like a scalded house cat, headed toward the pack house. No amount of calling him back worked. Richard ran Clyde down and dragged him back. Clyde was a strong boy and
struggled against restraining hands. Clyde energetically emitted assort grunts, groans, howls and squeals befitting a tied-down, nut-cutting massacre.
Clyde survived, but did not forget Uncle was the culprit responsible for his discomforts, real and imaginary. From then on, he saw Uncle as a doctor, not a relative. Uncles don’t hurt nephews, he reasoned.
At Christmas, they gathered again, but with prior assurance flu shots only happen once a year.
requiring a small amount of temporary restraint. The pain must be intense, but temporary. Most babies fall asleep quickly afterwards.
As Richard came off the table, Clyde was out the door in a flash. Without urging, and despite his delicate condition, Richard chased Clyde down again and dragged him back.
mas dinner. Christmas and Thanksgiving menus are mirror images.
Clyde had definitely not been informed that his mother had decided both boys should be circumcised — on the dining room table — before dinner. A Jewish doctor who viewed circumcision as a religious event, not a medical hygiene procedure, had delivered the boys.
Richard, being the older, was first. A Plastibell device ensured no post-op bleeding. Richard was stoic and cooperated fairly well, only
The second procedure involved a lot more struggling and verbalizing at high-pitched tones. But in retrospect, both boys did exceedingly well in this unconventional circumcision event.
However, Coy became woozy and unceremoniously laid himself on the floor. No one took much note.
The boy’s foreskins were discarded in the trashcan under the sink. No path reports. No op paperwork. Simple circumcision. Done deal.
The women promptly placed food on the table for the most unusual Christ-
These series of events made an indelible impression upon the boys. Coy recalls this as one of his two fainting spells. The other was when he mashed his finger in the fourth grade was taken to see the doctor. The doctor looked at his finger, stuck it in a bottle of Merthiolate (alcohol solution of Mercury) and inverted the bottle. Coy fainted. Doctor said, “When it burns, it’s fighting germs.” Apparently, it worked. Coy had no finger infection in the following six decades.
To this very day at Thanksgiving and Christmas, they cannot begin a meal without some minor discussion of circumcisions at Christmas. The general populace does not share this family tradition. Nor are they likely to.
But how did this uniquely traumatic Christmas event
TRYTHISDISH
by Kim Beavers, MS, RDN, CDCES
Dietitian Nutritionist, Chef Coach, Author
SUNFLOWER SEED PATÉ
This recipe that a friend gave to me long ago is so good it actually makes me happy. I have tweaked it slightly over the years and it is always a hit!
Ingredients
• 3 cups sunflower seeds (unsalted if available)
• ¾ cup lemon juice
• ¼ cup almond butter
• 3 garlic cloves
• 1-2 teaspoons grated fresh ginger
• 1 teaspoons cumin
• 1 teaspoons sea salt
• ¼ teaspoon dried cayenne pepper or to taste
• 1 cup kale leaves
• 1 red bell pepper, quartered
• 1 cup sweet onion, quartered
• 1 cup fresh parsley stems removed
Directions
Grind sunflower seed in a food processor until they are chopped but not so processed that they turn into sunflower butter (slightly larger than quinoa). Transfer to a large mixing bowl.
Combine the lem on juice, almond butter and the spices (garlic
through pepper) in the food processor and process until mixed. Add all of the vegetables and pulse. There should be little pieces and color of all the vegetables but not big chunks.
Combine the vegetable mixture with the ground sunflower seeds in the mixing bowl. This is great with cut up fresh vegetables or as a sandwich
spread. Serve with veggies (cucumbers, carrots, and red bell pepper), or whole grain crackers of choice.
Yield: 32 servings or 4 cups (serving size: 2 tablespoons)
The boy’s mother died not long after. Coy remarried: Jane, a hospice RN. Jane testifies Coy has not fainted for any reason in recent years. Jane forbids all circumcisions on her dining room table, Christmas or otherwise.
Richard is Senior Vice President of a regional bank. Richard developed the best hand-to-eye coordination known to man and is an expert quail hunter. He passed it on to his daughter Samantha, an All-American collegiate golfer.
Clyde is a tall, muscular businessman who founded a pest control company with over 3,000 commercial and residential clients. Bugs retreat in horror at the very mention of his name.
If you have hankering for a new family tradition, Uncle is open to dinner table circumcisions and flu shots. Cash only. In advance. This has been learned through trial and error. After circumcision, without anesthesia, people don’t tend to be happy nor in the mood to pay up.
Coy won’t faint. Richard will help chase down yous intended victim ... or at least give you directions on how to run with a Plastibell tied on your freshly circumcised penis. Clyde refuses to attend. Claims two foreskin cuttings are all he wants to know about. Jane says to get your own dining room-circumcision table. Her dining table is not for rent. And me? Well, I am a part time Funny Doctor and country author who always tells the truth ... except when I lie.
FYI: No lies herein. You can’t make up stuff this wild and crazy.
Diabetes Exchanges: ½ Vegetable, ½ Lean Meat, 1 Fat
Kim’s comment: This is a great make-ahead appetizer. It is nutrient rich and savory, perfect for a any time of year.
DOWNTOWN 990 Telfair St 706-724-0900
AUGUSTA W. AUGUSTA 3954 Wrightsboro Rd 706-863-9318
MARTINEZ MARTINEZ 4014 Washington Rd 762-685-5555
WARRENVILLE 2355 Jefferson Davis Hwy 803-593-8473
COLUMBIA THOMSON 1213 Washington Rd 706-986-5427 AIKEN AIKEN 536 East Pine Log Rd 803-649-1341
by Anonymous Augusta, Georgia
It was a hot spring or summer day in Dallas, Texas. I was about four years old, the second of six kids. I had an older sister, a younger sister, and most likely another brother in diapers. Mom was pregnant with what would turn out to be paternal twins.
My older sister and I would often visit our friend and neighbor Brooksie to see her small flock of pullets. She had a fenced backyard and a chihuahua that never even pretended to like us. We were barely tolerated only if Brooksie was there with us.
One day I went by on my own, no sister and no Brooksie. But the dog was there. It was inside the fence eating and ignoring my presence. I misinterpreted this for friendship and acceptance at last, so I entered the yard, knelt down, and put my arm around the dog to hug its neck.
I was immediately bitten on the face just to the side of my nose. Running home crying, I tripped in saw grass and was further bloodied on my arms and legs. I arrived at my house unable to tell any details, so mom loaded us all into the car and drove to a doctors office. I ended up receiving most of the rabies series of shots, some of which were in the stomach. Later, sitting around nursing my wounds, I find out that everyone got a sucker except me. Editor’s
WE’RE BEGGING YOU
We’re never too proud to beg. What we’re begging for is “Everyone Has a Story” articles. With your help, this could be (should be) in every issue of the Medical Examiner. After all, everybody has a story of something health- or medicine-related, and lots of people have many stories. See the No Rules Rules below, then send your interesting (or even semi-interesting) stories via e-mail to Dan@ AugustaRx.com or by mail to the Medical Examiner, PO Box 397, Augusta, GA 30903. Thanks!
“And that’s when I fell.”
“He doesn’t remember a thing.”
“I was a battlefield medic.”
“It was a terrible tragedy.”
“I retired from medicine seven years ago.”
“She saved my life.”
“I thought, ‘Well, this is it’.”
“They took me to the hospital by helicopter.”
“Now THAT hurt!”
“OUCH!” NOTHING SEEMED TO HELP, UNTIL...
“The cause was a mystery for a long time.”
“The nearest hospital was 30 miles away.”
“He was just two when he died.”
“I sure learned my lesson.”
“It seemed like a miracle.”
“We had triplets.”
“It was my first year of medical school.”
“It took 48 stitches.”
“The ambulance crashed.”
“I’m not supposed to be alive.”
“This was on my third day in Afghanistan.”
“I lost 23 pounds.”
“My leg was broken in three places.”
“Turned out it was just indigestion.”
“The smoke detector woke me up.”
EVERYONE HAS A STORY
The Cyberknife
Medical specialists (pulmonologists, radiologists, and oncologists) order scans and tests periodically to monitor the growth of cancer in my upper left lung. Two nodules were treated with radiation last April, daily M-F for 6 weeks.
At present, I am having five more radiation sessions with a cyberknife, a precise treatment which is centered on the tumor. According to medlineplus.gov, “Cyberknife is a form of radiation therapy that focuses high-power energy on a small area of the body.” In my case, the machine is focused on the tumor in my lower left lung. A robotic arm, controlled by a computer, positions the cyberknife.
The radiation therapist positions me on the table, which will slide me into the machine. Beforehand, my head is placed into a moldable head cushion; my ankles are tied together by a large rubber band, and my arms are secured with straps. I must remain still during treatment, which lasts 19 minutes. The whole therapy treatment time is about 45 minutes. I like to ask for a warm blanket and a support under my knees. I feel comfortable. I am moved into the machine and treatment begins. The robotic arm moves around me to administer radiation precisely on the tumor.
A scan in the cyberknife has advantages: there is no pre-appointment restriction on food or drink; no needle for an IV and wait time; no contrast dye; breathe normally instead of “breathe, hold your breath, breathe.” (What if the machine forgets to say the second breathe?)
There are side effects to radiation. The ones I experience are the following: extreme fatigue, minor hair loss, loose bowels, weight loss (5-10 percent of former weight. I lost more), frequent coughing, sometimes coughing up sputum
The journey has not been easy. It began in March, 2024 when I was diagnosed with lung cancer. The irony is I have never smoked.
In 2011, I was diagnosed with insidious pancreatic cancer. The survival rate after 5 years was 5-6 percent. I am a survivor. The percentage of survivors now is about 12 percent due to robotic surgery. I will survive lung cancer.
May each of us be a survivor and live a healthy life.
by Dolores Eckles Evans, Georgia
ber had jumped up to 9,996.
And it isn’t just measles amnesia fueling lower vaccination rates. More and more people fall into the “vaccine-hesitant” category, not utilizing the protection vaccines provide by choice for reasons that are usually not science-based.
The specific danger of falling immunization rates when it comes to this disease is that measles is considered endemic. That means it is always present. The world could have zero cases for 10 years, but if immunization completely stopped, measles would come roaring back. As has been demonstrated numerous times in recent years. Prior to the current outbreak there have been localized outbreaks, like the 700 or so cases in 2019 in Brooklyn and Queens, almost half of them infants and children 4 years old or younger.
It’s no big deal for kids, right?
Many older people who had measles as kids view the experience as just a normal part of growing up back then. Well, that was then, this is now.
Although measles can be relatively minor, as mentioned on page 1, it has killed millions, and still has the potential to be deadly. Remember, there is no cure or treatment. And even when measles isn’t fatal, one of its main side effects is immunosuppression. That is why pneumonia is a common and sometimes result of measles. In addition, clinical research has shown that it can take children and adults who get the measles two to three years for their immune systems to fully recover. During that time they are at higher risk for other viruses, bacterial infections, and even death at much higher rates than people who did not get the measles.
But we can make measles great again
In fact, we’re well on our way. Those who remember the measles as just a natural part of growing up in the 50s and 60s had no other option. But in 1963 the measles vaccine was introduced, and cases immediately went from more than half a million cases annually to near zero. The World Health Organization estimates the vaccine prevented 57 million deaths globally between 2000 and 2022. Despite all the past progress, we can still easily reverse the downward trend. The formula to make measles great again is very simple: don’t get vaccinated. Don’t allow your kids to be vaccinated. Tell everyone you know to avoid the measles vaccine. If we all pull together, we can do it. We can make measles great again.
Measles should be this old school, but it is making a comeback thanks to lax attitudes and misinformation.
CRASH COURSE
More Americans have died on US roads since 2009 than in World Wars I & II combined
t’s certainly no secret that headlights are getting brighter. They’re practically blinding sometimes, so it can be hard to say whether brighter lights are a good thing or a bad thing.
On the plus side, old-style headlights did not offer enough visibility to provide sufficient stopping distance for an obstruction in the road ahead. If a car is going 50 mph (73 feet per second) and the headlights only illuminate 50 feet ahead, they are practically worthless for collision avoidance. New bright white headlights cut through the darkness enough to actually do the job they are designed for.
However (we all know what’s coming), you can have the best headlights in the world, but if an oncoming vehicle’s lights are so bright that you’re blinded, the lights are going to cause a collision, not prevent one. And it can be equally distracting and dangerous when the vehicle with the 100,000 watt headlights is behind you.
Standard headlights are often so bright now that drivers will sometimes flick their brights to remind an oncoming driver that he forgot to dim his brights, only to have the oncoming driver respond with, “You thought those were my brights? These are my brights.”
Temporary blindness ensues.
What’s a driver to do?
Well, you could go car shopping. As of 2022, the National Highway Traffic Safety Administration amended its rules to permit headlight technologies that go back over a decade in Europe.
One of the simplest and most basic things newer cars offer, a feature that has been around for a number of years, is automatic dimming. If you’re driving down a dark road with your brights on, they will automatically dim for an oncoming car. That is a handy feature, but it is just the tip of the new headlight iceberg.
So called Adaptive Driving Beam (ADB) headlights offer some significant advantages. The simplest among them incorporate direc-
tional capabilities, so if you’re making a turn or rounding a curve, the headlights turn in that direction instead of beaming straight forward. That can be very useful.
Beyond that are some dramatic new technologies that give new meaning to ADB, redefining the word adaptive.
A number of car makers already offer adaptive headlights which selectively dim high beams for oncoming traffic. For these lights (sometimes called matrix headlights), the passenger-side headlight continues to shine brightly, illuminating the dark country road you’re on, but your driver’s side headlight, the one that could otherwise blind the oncoming motorist, will dim, either through reduced brightness or via small louvers that block or redirect the beam.
It sounds a little space-agey, but matrix headlights have already been available in some European cars for about a decade. Their debut here had to await changes to the federal safety rules for car makers. The adaptive beams are already available as standard equipment on some BMW, Audi, Tesla, and Mercedes-Benz vehicles, and as optional equipment on some moderately-priced Mazda, Toyota, and Hyundai models (and possibly others).
Undoubtedly, more and more cars will offer these lights as standard or optional equipment as time goes by. In the meantime, they can be found as after-market equipment for anyone who has the money ($500-$600+, plus installation).
Ultimately, as so-called self-driving cars have amply proven, safety technology can only go so far. The #1 safety feature available in any car, new or used, imported or domestic, big or small, sporty or sedate, gleaming or rusty, is an alert, cautious, conscientious driver. No amount of technology can ever replace that primary safety component. +
The blog spot
posted by
Katie Fortenberry, Ph.D.
on May 17, 2018
I believe there’s no such thing as work-life balance. I think this every morning when I leave for work, watching my twoyear-old son press his face against the front window and wave at me as I back down the driveway. It comes up again at work, as I guiltily feel relieved when a patient cancels and I have an unexpected half hour to work on a behavioral science presentation for residents. There is always somewhere else that I should be, and something else that I should be working on.
As a working mother who has been a chronic perfectionist and overachiever, the pressure is always there. If I’m not careful, this pressure turns into guilt. I miss my son’s doctors appointment, and I can’t translate his toddler-speak as easily as I think I should be able to. At work, I fall hopelessly behind in answering emails while wondering when I’ll have time to submit that paper for publication. It’s easy to start berating myself for not being more efficient, for not accomplishing more at work, and then not getting home in time to start dinner.
As the behavioral science educator in our family medicine residency program, I teach work-life balance. Residents vent in support groups about the endless patient demands, of long nights, of stress in their marriages, of their own emotional struggles. So I encourage them to focus on their goals, to reflect on the things they’re grateful for, and put their energy toward what they value most. Take steps to change what stressors can be controlled, and learn to release the ones that cannot.
I hear these words as I say them to our residents, and I resolve yet again to start taking my own advice. And sometimes I can successfully do this. Yet other times, I compose emails in my head as I rock my son to sleep. Or a patient’s struggles sparks one of my own worries, and I find my mind drifting off into my own troubles. Then my work life and my personal life collide into each other again, and I wonder what kind of hypocrite I am that I presume to tell our residents how to live their lives better.
Perhaps I should admit to myself that I can’t achieve balance. Maybe part of me will always want to be in the other part of my life, somehow both working more and spending more time with my family. It hurts to think that I may never be able to spend all the time I want with my son. But I know fighting this guilt won’t help. Instead, I focus on changing my relationship with it and remind myself that even if there isn’t enough time, wishing to be in the other part of my life only takes me away from where I am now. So I close my eyes, and I focus on the feel of my son’s soft hair against my cheek. I focus on the pain in my patient’s voice. I slowly take a deep breath. This is my only moment.
Katie Fortenberry is a psychologist
by Dan Pearson
When bees are exposed to pollen, they always develop hives. How is that possible? They’re bees. Pollen is all they do! What are you reading? Do tell. This article about bees. It’s fascinating.
ACROSS
1. Taylor, famous Augusta actor
4. Follower of The British
9. Stay at Mistletoe
13. Winter rarity here
15. Georgia, for one
16. A of CSRA
17. Fermented grape juice
18. Defective car
19. Quick!
20. Will
22. _____ of Man
23. Sunbathes
24. Electrically charged atom
26. A policeman’s badge
29. Capital of South Africa
34. Specially trained people at the center of a group
35. Create a picture
36. Globe
37. Against, in the back woods
38. _______-deep
39. Indian nursemaid
40. Natal start
41. One-third; made up of three parts
42. Muse of lyric poetry
43. Go before
45. Lumpkin Road school
46. CHOG, previously
47. “Around” prefix
48. Word with tear or tape
51. Horny skin growth
56. Capital of Norway
57. Stop a NASA mission
58. Streetcar (British)
60. Line of stitches
61. Blue _________
62. Trigonometric function
63. Sports award
64. Invitation on a door
65. Male child
DOWN
1. Wash. Rd shoestore
2. Burn ______
3. Marrow location
4. Beech partner word
5. Stalks
6. Type of duck?
7. English private school
8. Conscious; able to perceive
9. Julian Smith building
10. _____ in the Heart
11. Repast
12. ____ de foie gras
14. John Wayne movie
21. Story
25. Giants’ Mel
26. SC utility
27. Golf great Walter (1892-1969)
28. Moron
29. Augusta College
30. Ascend
31. Port _______
32. Angry
33. Loathe
35. Discharged a debt
38. Aftermath of a crash
39. ___________ Row
41. Ted Turner’s movie station
42. Money of Belgium, Austria, Luxembourg, etc.
44. Surgical removal suffix
45. Superior; of higher quality
47. Analyze a sentence
48. Quantity of medicine
49. Employs
50. Applaud
52. Black, to a poet
53. Type of beer
54. Source of eye color
55. Monte _____ Ave.
59. Word on many doors
The Mystery Word for this issue: CAENVCTIA
Simply unscramble the letters, then begin exploring our ads When you find the correctly spelled word HIDDEN in one of our ads — enter at AugustaRx.com
We’ll announce the winner in our next issue!
E X A M I N E R S U D O K U
DIRECTIONS: Every line, vertical and horizontal, and all nine 9-square boxes must each contain the numbers 1 though 9. Solution on page 14.
DIRECTIONS: Recreate a timeless nugget of wisdom by using the letters in each vertical column to fill the boxes above them. Once any letter is used, cross it out in the lower half of the puzzle. Letters may be used only once. Black squares indicate spaces between words, and words may extend onto a second line. Solution on page 14.
Use the letters provided at bottom to create words to solve the puzzle above. All the listed letters following #1 are the first letters of the various words; the letters following #2 are the second letters of each word, and so on. Try solving words with letter clues or numbers with minimal choices listed. A sample is shown. Solution on page 14.
THEBESTMEDICINE
ha... ha...
Adrunk is led into court and up to the bench. “You’ve been brought here for drinking,” said the judge sternly.
“Great,” said the drunk. “Let’s get started!”
Moe: My doctor told me I’m obese.
Joe: Ouch. So then what?
Moe: I got all defensive and told him, “Ok, maybe I am obese. But so is my sister. My mother is obese. My father is obese. My kids are obese. My brother is obese. Obesity runs in my family.”
Joe: Yikes. So then what?
Moe: He said, “Actually, it sounds like nobody runs in your family.”
Moe: Why can’t chickens fly?
Joe: Because of their boneless wings.
Moe: Are you ready to go to the nudist colony with me?
Joe: Are you kidding? I was born ready.
Moe: You know what would be a funny joke if you were a paleontologist?
Joe: I can’t imagine.
Moe: Ok, you’re on a dig and you discover a skeleton. The first thing you uncover is the ulna, so you yell out, “Hey, I think I’ve got something here!” And then after a pause you say, “Never mind. Fossil arm.”
Moe: Why did the fox cross the road? Joe: To get to the chickens.
Moe: They’re laying off all the park rangers. Joe: Yeah. Buffalo petting season is gonna be wild this year.
Moe: What has 4 letters, sometimes 9 letters, but never has 5 letters.
Joe: True.
Moe: What do you get if you rearrange the letters of MAILMAN?
Joe: You’d probably get him VERY ANGRY.
Moe: Did you know piranhas can devour a small child in 30 seconds?
Joe: Wow. I had no idea.
Moe: Well anyway, I lost my job at the Georgia Aquarium today.
Dude: What’s your wifi password?
Bartender: You need to buy a drink first.
Dude: No problem. I’ll have a Coke.
Bartender: Is Pepsi okay?
Dude: Sure. How much is that?
Bartender: $3.
Dude: There you go. So what’s the wifi password?
Bartender: You need to buy a drink first. No spaces, all lowercase.
Staring at my phone all day has certainly had no Effect on ME!
By popular demand we’re making at-cost subscriptions available for the convenience of our readers. If you live beyond the Aiken-Augusta area, or miss issues between doctor’s appointments — don’t you hate it when that happens? — we’ll command your mail carrier to bring every issue to your house!
NAME ADDRESS
CITY STATE ZIP
Choose six months for $24 or one year for $42 . Mail this completed form with payment to Augusta Medical Examiner, PO Box 397, Augusta GA 30903- 0397
Thank you for writing in to bring up this important topic. I hope the answers that follow will be informative to you as well as others in your situation.
There is actually a medical term for what you describe: jaundice. If you know French, you’ll recognize the word’s origin and meaning. The French word for yellow is jaune, and it fits: when someone has jaundice their skin and the whites of their eyes can have a yellow cast. Here’s why:
The body is continuously performing maintenance on itself. As one example, something like 200 billion new red blood cells (RBCs) are manufactured every day (give or take several billion). That many also die every day. As RBCs break down, they produce a yellow substance called bilirubin. Rather than simply going to waste, the liver processes bilirubin into bile, which it then releases into the digestive system to help us process the food we eat.
All is well until something disrupts the balance. Maybe the liver isn’t processing bilirubin fast enough, or more RBCs are dying than normal and the liver can’t keep up. For whatever reason, when there is too much bilirubin in the bloodstream it starts to leak into tissues near blood vessels, which means essentially everywhere.
This is no reason to feel embarrassed or ashamed, Yellow Streak. It happens to a lot of people. In fact, you wouldn’t remember it, but you may have started out like this: newborn jaundice is very common, affecting most newborns to some degree, usually resolving itself within a few days. Regular old adults sometimes get jaundice as the result of hepatitis (hepa- brings to mind hepatic, “of or relating to the liver” ). And jaundice can affect as many as 40%of patients in intensive care units. So relax. You’ve got plenty of company.
Ever since I was a kid I wanted to be a firefighter. Most of my friends had childish dreams too, like being cowboys or astronauts when they grew up. They outgrew theirs, but not me. A few months ago my dream finally came true when I was hired as a trainee. The big surprise has been that I am terrified of the situations I’ll be facing every day. I didn’t realize I was such a scaredy cat, but I am a total coward. What do you think I should do? — Got A Yellow Streak a Mile Long +
I hope this answers your question.
Do you have a question for The Advice Doctor about life, love, personal relationships, career, raising children, or any other important topic? Send it to News@AugustaRx.com. Replies will be provided only in the Examiner.
Why read the Medical Examiner: Reason #230 BEFORE READING AFTER READING
THE MYSTERY SOLVED
The Celebrated MYSTERY WORD CONTEST
...wherein we hide (with fiendish cleverness) a simple word. All you have to do is unscramble the word (found on page 12), then find it concealed within one of our ads. Click in to the contest link at www.AugustaRx.com and enter. If we pick you in our random drawing of correct entries, you’ll score our goodie package!
SEVEN SIMPLE RULES: 1. Unscramble and find the designated word hidden within one of the ads in this issue. 2. Visit the Reader Contests page at www.AugustaRx.com. 3. Tell us what you found and where you found it. 4. If you’re right and you’re the one we pick at random, you win. (Winners within the past six months are ineligible.) 5. Prizes awarded to winners may vary from issue to issue. Limited sizes are available for shirt prize. 6. A photo ID may be required to claim some prizes. 7. Other entrants may win a lesser prize at the sole discretion of the publisher. 8. Deadline to enter is shown on page 12.
PROFESSIONAL DIRECTORY
ACUPUNCTURE
Dr. Eric Sherrell, DACM, LAC Augusta Acupuncture Clinic 4141 Columbia Road
706-888-0707 www.AcuClinicGA.com 3633 Wheeler Rd, Suite 365 Augusta 30909 706-432-6866 www.visitrcp.com
L. Carter, MD 1303 D’Antignac St, Suite 2100 Augusta 30901 706-396-0600 www.augustadevelopmentalspecialists.com
Davis Road
Augusta 30907
706-860-4048 Floss ‘em or lose ‘em!
I WAS THINKING
by Pat Tante
IT HAPPENS EVERY YEAR
It happens every year about this time, as the winter cold slips away and the warm promise of spring becomes more of a reality. Spring cleaning of a sort – the day you move your houseplants outside to strengthen and begin a period of growth. They have become dusty during the winter as the motes blew through the heat vents. They have not been fertilized and only watered sporadically so that the catch bowls would not overflow and wet the carpet. What a sorry sight they are.
Spath (short for spathiphyllum, of course) was the first to be put outside. He had gotten quite large over the last few years and had enjoyed a place of plant prominence in the front window. His broad leaves and long stems span the window from side to side, causing me to have to spread the branches to see who has pulled into the front driveway. I lifted him out of the plant stand and struggled through the kitchen to the back door. His long branches caught at the walls and he even brushed half of the magnets off of my refrigerator. I could almost hear him saying, “No, I don’t want to go outside.”
I know that he must have enjoyed the long winter evenings watching the fire glow and listening to the murmur of conversation as we lounged around the living room. I sometimes felt his leaves brush my shoulder as I sat in the chair near the window.
If I missed his regular watering, he would lie down in the pot – that pitiful visual speaking more loudly than words. I was determined that he should go outside this year. It would make him stronger and better able to withstand another winter inside. Besides, a summer outdoors was much like the climate of his native country. I am always surprised when I travel to tropical countries and see the plants that I know as indoor sit-abouts growing into giant viney tangles and trees too big to reach around.
There we were, struggling through the back door, with me trying to assure him that spending the summer in the backyard was the natural thing, not getting long and spindly trying to catch the weak winter sun rays through the window. At last we were outside. I set him near the sliding glass doors so that he would at least have some small vantage point to the inside. He could watch us having dinner, enjoy the candles and not have to feel abandoned to the unaccustomed vicissitudes of nature.
I came back inside and returned to cleaning and vacuuming while Spath watched through the glass door. Later that evening when the wind blew, I could hear him scratching the window trying to get my attention. I could almost hear a soft whining sound coming from the patio.
I knew that he would settle down soon and begin to com-
mune with the new annuals that I had planted in pots. He should find them very interesting – double white impatiens that look like tiny roses, purple-faced petunias, frilly coleus that ripple in the breeze, and a wonderful smelling basil that, at this early point, did not know what was in store when it grew larger.
I kept an eye on Spath for the next few days, being careful that he sat in shade until he became acclimated to the sun. He looked a little droopy at first, but I knew that it was just a matter of time until he began to embrace the sights and sounds of the outdoors and to watch the birds and squirrels.
Then, with lots of water and sunshine, large white blooms that look like a cupped hand would shoot up and the wonderful yellow stamens would drop golden powder onto the leaves. Spath, you are beautiful!
This burst of blossoms will make me think ahead to winter and The Day the Houseplants Come Inside. Spath will complain and spread his newly strong branches to keep from coming indoors. Once inside, he will pout and drop some brown leaves. It happens every year.