


Digitally
PDAC Approved
2 Year Warranty

Digitally
PDAC Approved
2 Year Warranty
In the past few months, we’ve seen approval of a drug for sleep apnea that was originally intended for diabetics, then became a weight-loss magic bullet, now this. A sleep doctor I work with wondered “Am I going to have to learn how to prescribe tirzepatide now?”
As we continue to address the undiagnosed, a simple (appearing) ring has been FDA cleared to provide diagnostic data. Under-mattress mats, watches, stick-on ‘wearables’ and bedside ‘nearables’ have been added. Every week our news feed provides technological approaches to screening, diagnosing, treating, and following patients in airway management.
Learning how physiology is impacted by poor sleep and individual therapy choices is becoming easier, faster, cheaper and better (because of multiple-night measurement) than ever before.
Treatment, with PAP or oral devices, is not changing so rapidly, but we get new ideas from time to time. Surgery, orthodontics, and nerve stimulation are still on the table for those whose suffering from breathing problems overcomes the barriers to invasive strategies.
With James Nestor’s book Breath kicking it off in 2020, and a pandemic focusing many on breathing health, popular awareness of respiration and its contribution to health and wellness is stronger than ever. People are asking questions of their healthcare team, including dentists, wondering “how is [this] going to improve my breathing?” and, “how can I sleep better?”
Learning about a new device, mask, technique, or colleague is not going to keep any provider ahead of their well-informed patients. Yes, most dentists can learn more
about how a PAP works, physicians can improve their vocabulary about mandibular advancement devices. All of us understanding the plusses and minuses (the real ones, not the myths, like “TMJ” or “Hate CPAP”) of treatment choices will benefit our patients and collegiality. What is necessary is to participate with our patients in discovering what ideas are most likely to work for them. As many have said, ‘you can’t sell what you don’t have on the shelf.’ When our well-informed patients ask us about a new medication, strategy, or positional device, we may not need to understand every detail, but if that moment makes you realize that they’ve heard of something you have not, it’s time to dig in and see what’s been happening while you’ve been practicing good medicine with what you learned ‘back then.’
The future is physiologic assessment over time, and individualized, precision care aimed as close to the root cause as possible, then ongoing monitoring for successful management of chronic disease. Including not resting on our laurels when signs and symptoms are normalized – people change, so do their responses. Embracing new technology and the commitment to ongoing interactions with your patients means change for their healthcare team, too. It’s easier, faster, better, and cheaper than ever. Better medicine.
Do you like what you are reading in DSP? Do you have ideas you want to share about what works in your practice? As Chief Dental Editor, I am happy to consider essays from any reader! Contact me at stevec@medmarkmedia.com.

Steve Carstensen, DDS Diplomate, American Board of Dental Sleep Medicine
8
Cover Story
LuxCreo Helps Unlock Same-Day Sleep Apnea Treatment with EMA 3D
Avoid frustrating delays and build practice value.


Continuing Education
The Trigeminal Nerve: A Key Player in Facial Growth and Nasal Function by Karen Parker Davidson, DHA, MSA, MEd, MSN, APRN, and Donald R. Moeller, DDS, MA, MD, Lieutenant Colonel US Army (retired) Even more to learn about the nerve dentists know best. 26
2 CE CREDITS

14
Future Spotlight Empowering Dentists to Lead in Overall Health Care by Dr. Brett Kessler Message from ADA President.


Medical Insight Review of REM Sleep: Part One – Physiology by Amalia A. Geller, MD
18
Gain a better understanding of what occurs during REM sleep.

22
Medical Insight Hypoglossal Nerve Stimulation: A New Paradigm in Surgical Management of Obstructive Sleep Apnea by Ian Lalich, MD
Read insights about this novel surgical therapy for OSA patients with PAP intolerance.




Feb 28-Mar 1,2025 Pinpoint the Pain: TMD Orofacial Pain and Sleep Apnea
Feb 28-Mar 1,2025
Apr 25-26, 2025
Apr 25-26, 2025
Jun 6-7, 2025
Jun 6-7, 2025
Jun 27-28, 2025
Jun 27-28, 2025
Aug 1, 2025
Oct 3-4, 2025
Medical Billing in Dentistry: The Secrets to Success
2025 Dental Sleep Medicine Mini-Residency (Session 1 of 2)
Medical Billing in Dentistry: The Secrets to Success
2025 Dental Sleep Medicine Mini-Residency (Session 2 of 2)
Dental Sleep Coordinator Course
TMJ & Airway Cadaver Workshop
Medical Billing in Dentistry: The Secrets to Success
Medical Billing in Dentistry (1-Day Course)
2025 Dental Sleep Medicine Symposium







6 Publisher’s Perspective Making the World a Better Place by Lisa Moler, Founder/CEO, MedMark Media
36 Clinical Focus Empowering Dentistry Through Myofunctional Therapy: A Path to Success by Melissa Mugno, OMT, RDH
Working with a therapist benefits the practice, too.


12 Bigger Picture The Lamberg Questionnaire: A Valuable Tool Simplifying Complex Sleep Health Conversations in the Dental Practice by Brittny Murphy, RDH, BS, COM, QOM
Linking medicine and dentistry builds value for treatment.
16 Cardio-Sleep Corner Sleep Inertia: Causes, Symptoms, and Diagnosis by Lee A. Surkin, MD, FACC, FCCP, FASNC, FAASM
Find out what causes sleep inertia, its symptoms, and how it is diagnosed.
34 Inside the Lab Lessons from the Bench Segment 2: Appliance Selection, Designs and Retention Challenges by Laura Sheppard, BS, CDT, TE Choosing devices easier, with more confidence.
38 Networking Spotlight Unreasonable Dip and Bounce by Steve Lamberg, DDS
You can build a coalition in your community.
39 Product Spotlight BioMatch™: Making Oral Appliance Therapy Easy, Fast, Accurate, and Reliable Quality improvement is a constant.
40 Seek and Sleep DSP Strands
Spring 2025
Publisher | Lisa Moler lmoler@medmarkmedia.com
Chief Dental Editor
Steve Carstensen, DDS, D.ABDSM stevec@medmarkmedia.com
Chief Medical Editor
Lee A. Surkin, MD, FACC, FCCP, FASNC drsurkin@n3sleep.com
Associate Editor | Lou Shuman, DMD, CAGS lou@medmarkmedia.com
Editorial Advisors
Jamila Battle, MD (Family/Sleep/Addiction)
Steven Bender, DDS
Jagdeep Bijwadia, MD (Pulmonary, Sleep)
Kevin Boyd, DDS
Saim Choudhry, DO (Internal Medicine, Sleep)
Alison Kole, MD, MPH, FCCP, FAASM (Sleep, Pulmonary, Critical Care)
Karen Parker Davidson, DHA, MSA, M.Ed., MSN, RN
Bertrand de Silva, MD, FCCP, D.ABSM
Daniel Gartenberg, PhD (Behavioral Sleep)
Kristie Gatto, MA, CCC-SLP, COM
Amalia Geller, MD (Neurology, Sleep)
William Hang, DDS, MSD
Steve Lamberg, DDS, D.ABDSM
Ian Lalich, MD (ENT, Sleep)
Christopher Lettieri, MD (Pulmonary, Critical Care, Sleep)
Pat McBride, PhD, CCSH
Jyotsna Sahni, MD (Internal Medicine, Sleep)
Ed Sall, MD (ENT, Sleep)
Alan D. Steljes, MD (Cardiology, Sleep)
Laura Sheppard, CDT, TE
DeWitt Wilkerson, DMD
Scott Williams, MD (Psychiatry, Sleep)
Gy Yatros, DMD

National Account Manager
Adrienne Good | agood@medmarkmedia.com
Sales Assistant & Client Services
Melissa Minnick | melissa@medmarkmedia.com
Creative Director/Production Manager
Amanda Culver | amanda@medmarkmedia.com
Marketing & Digital Strategy
Amzi Koury | amzi@medmarkmedia.com
eMedia Coordinator
Michelle Britzius | emedia@medmarkmedia.com
Social Media
Felicia Vaughn | felicia@medmarkmedia.com
Website Support
Eileen Kane | webmaster@medmarkmedia.com
MedMark, LLC 15720 N. Greenway-Hayden Loop #9 Scottsdale, AZ 85260
Tel: (480) 621-8955 | Toll-free: (866) 579-9496
www.DentalSleepPractice.com
Subscription Rate: 1
Extensive
Medicare
60+





Scan

Lisa Moler Founder/CEO, MedMark Media
Every day, in newspapers, on TV, and social media we see humanitarian efforts across the world. Whether it’s for saving endangered animals, survivors of natural disasters, cures for diseases, or other causes closer to home, we all try as much as possible to open our hearts and wallets for those who could use a boost in life. Dental practices’ own little corners of the world can have their own distinctive ways to create a better place.
It’s easy being green: One of the most popular ways dental offices can show environmental responsibility is by employing “green” programs. The ADA has a page on its website titled “80 ways to make your practice green” (https://bit.ly/4gbMrra) –with suggestions like investing in energy efficient technologies, purchasing furniture made from recycled products, or something as small as using biodegradable cups. Replacing high-energy consuming office lights with energy-efficient lighting will conserve energy and also probably help lower some of the electric bill as well.
One patient at a time: MedMark publications always feature new equipment, technology, and materials. Researchers and inventors of these new dental solutions spend hours of their time, effort, and money improving the dental experience and creating new options for better and more individualized patient care. Whether it’s taking the pain out of root canal treatment, bringing new treatments to those with sleep-breathing issues, inventing implant solutions for those who need special care, creating new aligner and bracket and wire systems to help patients smile again after years of low self-esteem, or taking the fear out of the office for even the youngest dental patients, our articles can help improve patients’ quality of life, while also improving your business. Pay it forward: Some of the most famous key opinion leaders in the dental industry were mentored and encouraged by their peers.
Implementing any new protocol or procedure from the simple to the complex is less stressful when there is someone to call on for advice. We’ve all been there – in any occupation, moving to a higher level means being educated not only from text books or lectures, but hands-on, chairside guidance from someone who has “been there and done that.” Articles in our publications also feature authors who want to share their expertise, and who are often happy to follow up with constructive pointers on how to add their protocols to your practice options.
Love thy neighbor: Dental offices can be a productive part of any community. From contributing to local schools, to visiting classes to talk about better oral care, to participating in veteran’s events, clinicians and their teams can expand their reputation, referrals, and hearts by showing the surrounding areas that their community is important to you too. It isn’t hard to find these activities. Check with your local Chamber of Commerce, community newspaper, school volunteer event staff, or even ask your patients what organizations they may be involved in. Your practice name will stay in potential patients’ minds long after the event is over.
The spring issue is ready to share concepts that will help to build your world. We hope you enjoy this issue’s well thought out/interesting articles, and make some ideas into realities.
It is a small world – and by making it better, your potential patients will be happy you are a part of it.
• Advanced Education with Mini MBA Program and Other Advanced Certificates in Business Management and Leadership
• Retention Strategies
• Operational Support
• Technology Implementation
• Patient Trends & Analytics
• Efficiency Audit
• Competitive Fee Survey
• Production Analysis





More than 30 years ago, orthodontist Dr. Don Frantz invented the EMA device to treat his own obstructive sleep apnea (OSA) – a serious medical condition impacting more than 40 million Americans. EMA works by opening the bite and gently advancing the mandible (or jaw) with elastic straps to increase airway space.



For years, manufacturing limitations have prevented widespread access to OSA care, which was always a focus for Dr. Frantz. Historically, the FDA-cleared Class II EMA device has been manufactured manually through a traditional thermoforming process. Dr. Frantz’s son, Joe, and his partner from Apex Dental Sleep Lab, Sonnie Bocala, had been searching for years for the right 3D printing solution (resins, hardware, and design software) that truly could allow same-day delivery of EMA to a suffering patient at a reasonable price.
Sonnie has operated dental sleep and TMJ laboratories for decades, including developing various OSA appliances for the industry. Apex Dental Sleep Lab currently manufactures 14 different sleep and snoring appliances, including several variations of the well-known EMA device.
Over the years, processes and materials have improved to allow the traditional thermoformed EMA device to be expanded to include milled and Serena Nylon versions. Each of these digital devices delivers a beneficial EMA device to the patient, but the EMA 3D is more economically priced. And 3D printing an EMA device allows for rapid and scaled delivery to patients, as Sonnie explains: “With a full solution for 3D printing, a doctor can design and
print multiple EMA cases in a two-hour workflow. We needed to find the right partner to make it happen.”
The search ended in November 2023, when Sonnie and Joe visited blustery Chicago to work with LuxCreo in its newly opened headquarters and printing laboratory. They worked with the LuxCreo technology with an eye toward the performance needs for EMA. By the time they left, Sonnie and Joe knew many of their hurdles for EMA 3D could be cleared with LuxCreo’s end-to-end 3D printing system: automated and EMA-specialized design software, four integrated pieces of iLux Pro Dental hardware, and a proprietary FDAcleared resin. Once the FDA issued a new 510(k) clearance for 3D printing of the EMA device (K232735) in May 2024, the pieces were in place to change the course of dental sleep medicine.
While there are many benefits EMA 3D provides to doctors and patients, none may be more important than the immediate relief of a patient’s sleep apnea. For the first time, a doctor can deliver the proven EMA device to an OSA patient within hours of a scan, rather than waiting weeks to receive the appliance from the doctor’s dental laboratory. For a patient suffering multiple apnea events every hour, timeto-treatment matters.
For the doctor, the AI-powered design software allows the EMA 3D appliance to be digitally designed in less than 10 clicks and 10 minutes. Print and processing time with LuxCreo’s integrated solution is under 2 hours.

Ease and speed of manufacturing and delivery of EMA 3D are only the start of the benefits of the product. Other significant benefits to the doctor and patient include:
• Outstanding material durability
• Digitally precise fit and accuracy
• Patient comfort from thinner trays (0.9 mm) than other apnea devices
• Easy to remake or sell in duplicates
• Eliminate costs for lab shipping fees and dental models
Experienced sleep doctors are adopting EMA 3D in their practices and loving the easy workflow, doctor control, and rapid OSA treatment. Dr. Michael Bennett has spent decades treating sleep disorders in Provo, Utah. He explained why the EMA 3D workflow is perfect for his practice and patients: “The process of design is very intuitive and easy to learn. We have happier patients that are getting into treatment sooner than current options. It usually takes 3-4 weeks to get a device in a patient’s mouth, which we can now do in hours. The EMA 3D software gives me a lot of control in my own hands to easily design an FDA-approved apnea device.”
Founded in 2019, LuxCreo set out to change how clear dental appliances are designed and made for dental professionals and patients. LuxCreo engineered from scratch an end-to-end 3D printing system to solve the problems of directly printing clear orthodontic appliances, making the use easy and efficient for dental professionals to adopt in their clinic or laboratory. With a focus on delivering outstanding direct print aligners in just 2 hours from the patient’s scan, Lux-

Creo engineered one-click design and nesting software, four integrated pieces of hardware (taking just 40 inches of counter space), and its proprietary, FDA-cleared, Class II resins.
As a completely integrated system of design software, hardware, and resin, LuxCreo has enabled same-day direct clear aligner service and EMA 3D therapy.

The EMA 3D appliance can be digitally designed in less than 10 clicks and 10 minutes. Print and processing time with LuxCreo’s integrated solution is under 2 hours.

• iLux Pro Dental: A high throughput, small footprint, heated, chairside DLP printer with 50-micron pixel resolution powered by LEAP technology. A single iLux Pro Dental is capable of printing up to 32 EMA 3D appliances in an eight-hour shift.
• LuxDesign Software: Generate tray designs, add bite pads and EMA buttons, and dynamic variable tray thickness for enhancing efficacy and patient comfort.
• iLuxCure Pro: A programmable, multiwavelength, multi-direction, highirradiance post-print cure that can cure six to eight EMA 3D devices within 30 minutes.
• Proprietary Printing Resin: The resin for EMA 3D is a tough, flexible, and accurate clear material with high transparency without manual polishing, enabled by LuxCreo’s Digital Polishing technology. The material has been FDA Class II 510(k) cleared for EMA 3D OSA indications.
For the clinic that adopts the EMA 3D workflow, the financial benefits will be immediate and impactful to the practice. The EMA 3D workflow and resulting device sold to a patient (with medical reimbursement) should yield profits more than 90% of the doctor’s cost to manufacture the device. Indeed, just fifteen EMA 3D cases will pay back the clinic or laboratory’s investment in the required FDAcleared hardware and software.
The clinics and laboratories adopting the EMA 3D workflow will have the protection of being an authorized EMA 3D provider, including the international patents and regulatory clearances covering the workflow and products, and the infrastructure for insurance reimbursements.
LuxCreo’s Chief Revenue Officer, Michael Strohecker, observed, “It has been gratifying being able to leverage some of the special features of the iLux Pro Dental workflow – like digital polishing of devices and 1-click design
and nesting capabilities – to really bring value to what Sonnie, Joe Frantz, and their team are trying to achieve in treating sleep apnea across all patient populations.”
Software Co-Development was the Key
The real engine behind EMA 3D is the co-developed design software: a customized, AI-driven design software that is integrated with a 3D printing solution, allowing an EMA 3D device to be designed in less than 10 clicks and 10 minutes and printed in under 2 hours. EMA Sleep’s expertise in OSA device manufacturing and LuxCreo’s expertise in creating an AI software module to go with its 4D Aligner design platform opened the door for success.
Through the second half of 2024, the two companies worked closely to automate the design of the EMA 3D device for the ease of the end-users. From figuring out how to automate the placement of the patented EMA buttons and bite pads, to understanding the dynamics of fit and jaw movement, to building an easy platform to use, the two companies worked to achieve a unique proposition for the dental professional.
Sonnie Bocala explained the value of the relationship with LuxCreo: “I cannot praise the entire LuxCreo team enough. LuxCreo’s technology allowed for the creation of an EMA-tailored design software solution, solving several key manufacturing challenges around design optimization, automation, and scale. The technical expertise, mechanical/materials experience, and developmental responsiveness of LuxCreo made it possible to create this unique LuxCreo-EMA 3D ecosystem.”
A doctor or laboratory interested in becoming an authorized EMA 3D provider should contact either LuxCreo or EMA Sleep at: www. luxcreo.com/ema or www.ema-sleep.com for more information.
The process for training and software access is easy for everyone:
• Purchase LuxCreo’s iLux Pro Dental hardware and a subscription to the EMA 3D design software.
• Obtain EMA elastic connectors from approved reseller.
• Undergo training and quality assessment in the digital design and 3D print manufacturing of the EMA 3D device.
• Start making and rapidly delivering EMA 3D for patients.




by Brittny Murphy, RDH, BS, COM®, QOM®
In recent years, there has been growing recognition of the interrelationship between oral health, sleep health, and overall health, particularly the role dental professionals can play in identifying and managing sleep-related breathing disorders. Dentists and registered dental hygienists are uniquely positioned to screen for and identify signs and symptoms of sleep related breathing disorders (SRBD).

Dr. Steven Lamberg, DDS, DABDSM, created The Lamberg Questionnaire along with the Lamberg Questionnaire for Pediatric Airway and Sleep (LQ-PAS), both screening tools designed to help dental and medical professionals identify patients who may be at risk for obstructive sleep apnea (OSA) or other sleep related breathing disorders. These questionnaires serve as a practical, user-friendly tool enabling dental professionals to bridge the gap between sleep health and overall health, while also highlighting oral health indications. This article explores the usefulness of the Lamberg Questionnaires, their practical value in a dental setting, and how they aid in simplifying the communication of a complex subject like sleep related breathing disorders to patients. Dr. Lamberg provides the questionnaires free of charge at www.drlamberg.com.
Sleep disorders, especially obstructive sleep apnea, are often underdiagnosed, yet they carry life threatening health risks. Through the Lamberg Questionnaires, you can uncover a patient’s risk for sleep disordered breathing before looking in-
side their oral cavity, through their medical history and direct questioning. Sleep related breathing disorders can be linked to medical conditions including heart disease, obesity, kidney disease, dementia, diabetes, acid reflux, anxiety, stress, autoimmune disorders, and more.
The Lamberg Questionnaire and the Lamberg Questionnaire for Pediatric Airway and Sleep create a streamlined process in the identification of potential sleep related breathing concerns. Rather than relying on a complex set of diagnostic tools, dental professionals can quickly administer these straightforward questionnaires which include traditional sleep screening questions related to sleep quality, snoring and sleep habits, daytime sleepiness, and morning symptoms, along with questions regarding overall health.
The Lamberg Questionnaire is broken down into the categories shown in Table 1.
The Lamberg Questionnaire for Pediatric Airway and Sleep (LQ-PAS) asks relevant questions about symptoms and behavior when a child is sleeping, upon awakening, and throughout the day. There is also a signs and symptoms checklist for airway red flags included for the healthcare professional to fill out.
Incorporating these questionnaires into a routine dental visit is not only an easy task but increases the likelihood of early detection of sleep related breathing disorders, often even before the patient or family is aware. Sleep disordered breathing is a spectrum disorder so early detection can help halt any further progression and potentially alleviate future health issues.
Working collaboratively with other healthcare disciplines ensures timely intervention. The Lamberg Questionnaires only further emphasize the importance of this approach to patient care. Dental offices can begin facilitating communication with sleep specialists and other pertinent healthcare providers ensuring whole body health and comprehensive care. Having such data documented can help streamline the referral process and mitigate unnecessary delays in seeking further treatment.
One of the key challenges in dental practice is explaining the connection between oral health, sleep health, and overall health to patients. Patients are often confused as to why their dentist or dental hygienist is asking about their sleep habits and snoring history. The Lamberg Questionnaires are valuable tools in this regard, as they help break down complex concepts into digestible verbiage. The questionnaires were curated with the patient in mind using clear and direct language. Avoiding medical jargon allows the patients to understand, or at least begin to comprehend, the relevance of the questions being asked and their answers to their sleep health and overall health. When patients begin to check off multiple ‘yes’ answers, curiosity is sparked, and they are more likely to begin engaging in conversation with the provider regarding the results of the questionnaire. At the very least, these questionnaires are building patient awareness. A patient will leave that dental visit with more education than they walked in with and may lead them to evaluate their sleep health and overall health more deeply, returning their next visit ready to take that next step whether it is a sleep study or referral to another clinician. This increased awareness empowers and motivates patients to seek treatment and make changes within their own lives.
The Lamberg Questionnaires provide clinicians with the opportunity to begin discussing potential treatment options whether it is further diagnostic testing, oral appliance therapy, lifestyle changes, or a referral to an airway dentist for further evaluation of the craniofacial respiratory complex.
Dr. Lamberg’s book Treat the Cause…Treat the Airway can be instrumental in helping patients understand the connection between their sleep, airway health, and overall health. Treat the Cause…Treat the Airway delves into the link between sleep related breathing disorders and a range of health problems, clarifying airway’s impact on sleep. Advocating for root cause treatment, the book focuses on underlying causes of airway problems rather than just symptoms. Treat the Cause…Treat the Airway provides a comprehensive understanding of how airway health is deeply intertwined with sleep and general well-being, offering both knowledge and practical strategies for improvement.
To successfully integrate the Lamberg Questionnaires into your dental practice, it is necessary to ensure that your dental team is trained in how to properly administer the questionnaires and interpret the results. If not already done, this may first include office training and education on understanding and identifying the signs and symptoms of sleep related breathing disorders.
When administering the questionnaire, be sure to explain its purpose. At each dental visit, educate your patients about the link between oral health, sleep health, and overall health. Encourage your patients to ask questions if they do not understand the reason this questionnaire is being incorporated. Be sure to have a referral network of sleep specialists and other airway professionals for those who are ready to take the next step. Establishing this network beforehand will provide continuity of care. Be consistent in providing routine screenings for all patients. This will increase early detection and provide continued monitoring and follow up for those at-risk patients.
The Lamberg Questionnaire and The Lamberg Questionnaire for Pediatric Airway and Sleep are valuable assets in a dental practice, offering both a practical screening for sleep related breathing disorders and a simplified way to communicate a complex health concept to patients. By integrating this tool into routine care, dental professionals can enhance their role in the broader healthcare system, ensuring that their patients receive comprehensive care. The ease of use and effectiveness of the Lamberg Questionnaires make them an essential component of modern dental practice, helping to bridge the gap between oral health, sleep health, and overall health.
1.

Dr. Lamberg kindly provides the questionnaires free of charge, scan the QR code for access.

Brittny Murphy, RDH, BS, COM®, QOM®, is a registered dental hygienist, myofunctional therapist, educator, author, and key opinion leader in sleep and myofunctional therapy. She is the founder of CT Orofacial Myology and cofounder of MyoAir, private myofunctional therapy practices aimed at improving oral and whole-body wellness, through which she has helped hundreds of patients thrive by sleeping and breathing better. Brittny is also the face behind the podcast, “I Spy with My Myo Eye” and has created The Myo Hygienist™ community.

‘Dentistry’s Role in Complete Health’
by Dr. Brett Kessler, President, American Dental Association
In late 2022, I sat in a room of fellow American Dental Association (ADA) Trustees as we sought to answer one question: Why? We were considering why we — as leaders in that moment; as clinicians, researchers, and educators in other moments — did the work that we do every day on behalf of our profession, in service to public health, and in the lives of our patients, students, and the communities where we lived and worked. Amid the many ways and reasons we served, beyond the ADA’s mission and vision, we all arrived at a simple answer: We make people healthy.
The Board adopted this phrase as its strategic why statement, and personally, I was excited about what would come from such a clear declaration of our purpose. Because I’ve always believed that dentistry is essential to a healthy society.
During my general practice residency at a large hospital system in Chicago, I learned firsthand about the integral role oral health plays in overall health. I also saw how the collabo-

An American Dental Association Children’s Airway Event July 24-26, 2025 • Chicago

rative care of medical and dental professionals improved patient outcomes. In my clinical career, I emphasized whole-body health as part of my care philosophy. Though our profession knows that oral health is health, for too long, the two have been treated as separate within the greater health care landscape. Today, as ADA President, I recognize dentistry’s opportunity to elevate and redefine its role in primary care.
A critical element of this is interdisciplinary collaboration, which is the focus of the ADA’s “Dentistry’s Role in Complete Health” symposium, to be held June 13-14 in Chicago. This twoday event is back for its second year, building upon the inaugural symposium’s exploration of dentistry’s role in combatting chronic disease.
Attendees will hear from the foremost experts on such topics as children’s oral health and metabolic syndrome; disease screening and testing; lifestyle-focused medicine and dentistry; periodontal research; and much more. For professionals in sleep medicine, a focus on airway health and its ties to conditions such as hypertension, diabetes, and cardiovascular disease makes this symposium particularly relevant.
The symposium will be a call-to-action for all dentists, physicians, and other professionals to rethink their role in overall care, while examining integrative approaches that strengthen the health care ecosystem and improve patient wellbeing. It will also be a step toward a new era in dentistry — one where all of us are empowered to lead what my mentor and the symposium presenter Dr. DeWitt Wilkerson calls a significant shift from sick care to proactive wellness care.
Dentists should be partners in their patients’ health journeys, especially as patients tend to
see dentists more frequently than their physicians. While caries management will always be part of our work, it’s time for dentistry to move in a direction where providers administer health screenings and manage chronic conditions. (It’s time that our benefit models properly reimburse dentists for these services too.) Additionally, building relationships with patients’ physicians allows for a well-rounded care team that puts patients and their needs at the center.
A lot of this change is already underway. Beyond medical-dental collaborations in federally qualified health centers, dentists are broadening their scope to include airway screening and treatment, tackling issues like obstructive sleep apnea, and offering solutions such as oral appliances and orthognathic surgery.
I believe this is just a hint of what’s to come. The future of healthcare is collaborative, and dentists have a unique opportunity to lead the charge.
“Dentistry’s Role in Complete Health 2025” is designed for every member of the dental team, and I invite you to join us as we engage on fresh
perspectives, make valuable connections, and learn how we can change the trajectory of public health. By working together, we can make people healthy — one patient at a time.
To learn more or to register for Dentistry’s Role in Complete Health: We Make People Healthy, scan the QR code to the right or visit ADA.org/CE. The event offers 15 Continuing Education credits.


Dr. Brett Kessler, a general dentist in Denver, is President of the American Dental Association. He has served in numerous leadership roles, including Colorado Dental Association President (2014-2015) and ADA delegate (2008-2019). Dr. Kessler played a key role in establishing Colorado’s adult Medicaid dental benefit and earned the ADA’s Golden Apple Award for leadership in mentoring. A national speaker on well-being and leadership, he has served on the Council on Dental Wellbeing Advisory Committee and testified before Congress to advance oral health. A graduate of the University of Illinois at Chicago College of Dentistry, he is also an endurance athlete, husband, and father of four.



by Lee A. Surkin, MD, FACC, FCCP, FASNC, FAASM
Have you ever woken up in the morning with an intense urge to go back to sleep even after getting the recommended amount of sleep per night? Do you experience morning grogginess when this happens to you? This phenomenon is what’s known as sleep inertia and although it itself isn’t a bad thing, it can harm cognitive functions and potentially cause other problems if it becomes severe.
Continue reading below to find out what causes sleep inertia, sleep inertia symptoms, and how it is diagnosed.
In short, the feeling of morning grogginess, drowsiness, cognitive impairment, and sleep drunkenness is called sleep inertia. It typically lasts for 15 minutes to an hour, but in more severe cases it can last for up to a
couple of hours upon waking up.
The biological reason why some people experience sleep inertia symptoms hasn’t been determined yet, but experts guess that it helps in maintaining sleep when unwanted wakings occur. So, sleep inertia is thought of as a protective mechanism.
Sleep inertia is most common in people who work long hours or shift work and can negatively affect their safety and well-being.
Due to morning grogginess and sleep drunkenness, these people have a slower reaction time and reduced cognitive alertness.
Generally, the most noticeable sleep inertia symptoms present right after waking up and slowly disappear over time. Now, let’s have a look at the most common symptoms of sleep inertia:
• Morning grogginess
• Sleep drunkenness
• An urge to go back to sleep
• Poor cognitive ability
• Impaired visual attention
• Reduced spatial memory
We already mentioned above that researchers haven’t determined the exact biological cause of sleep inertia. However, according to research, three common theories may explain what causes sleep inertia.
First, it is believed that sleep inertia is caused by increased delta waves in the posterior part of the brain. These waves are also called slow waves and are part of the NREM (non-rapid eye movement) sleep stage and usually increase after periods of lack of sleep or sleep deprivation. So, when the brain hasn’t reduced these waves to prepare for waking up or is awoken during the NREM sleep stage, sleep inertia may occur.
The second potential theory explaining what causes sleep inertia is the adenosine theory. Namely, adenosine is a nucleic acid compound in the brain that is key for sleep and wakefulness. The levels of this compound should be low after waking so if

“Sleep inertia is most common in people who work long hours or shift work and can negatively affect their safety and well-being.”
they remain high it may lead to experiencing sleep inertia symptoms.
Third, based on the stage of sleep, sleep cycles determine the pattern in which blood flows to the brain. One syndrome called CFS (chronic fatigue syndrome) is very similar to sleep inertia and is linked to decreased cerebral blood flow. It is possible that the blood flow reduction after waking leads to sleep inertia symptoms.
If you experience morning grogginess, sleep drunkenness, or other sleep inertia symptoms, ensure you consult your doctor and consider doing a polysomnography sleep study. This will help your doctor see whether or not there’s an underlying sleep disorder affecting your sleep and causing sleep inertia.
Another way to help your doctor diagnose you with sleep inertia is keeping a sleep journal to get an insight into your sleeping patterns. That said, you should take records of the times and the amount you sleep as well as how you feel upon waking and whether or not you experience any symptoms.

Lee A. Surkin, MD, is the Chief Medical Officer of Nexus Dental Systems. A private practitioner in cardiology, sleep medicine, and obesity medicine, he is one of a small group of physicians to be triple board certified in cardiology, sleep medicine, and nuclear cardiology. In 2009, he created Carolina Sleep – the only dedicated sleep medicine practice in eastern NC. Dr. Surkin has created a cardiovascular and sleep healthcare model that includes a multi-faceted diagnostic and treatment approach that is enhanced by a network of relationships with physicians, dentists, respiratory therapists, sleep technologists, and public officials who recognize the important role that sleep medicine has in our daily life. In 2012, Dr. Surkin founded the American Academy of Cardiovascular Sleep Medicine which is a not-for-profit academic organization dedicated to educating healthcare providers, supporting research, and increasing public awareness of the convergence between cardiovascular disease and sleep disorders. In 2014, Dr. Surkin created a new multi-specialty practice called Carolina Clinic for Health and Wellness which combines his specialties with primary care, gynecology, behavioral health and a medical spa. Dr. Surkin is married with three daughters and a golden retriever and resides in Greenville, NC.


by Amalia A. Geller, MD
The reasons we dream and the purpose for Rapid Eye Movement (REM) sleep remain a mystery. We still do not understand why humans need to dream, but we do understand more about the physiology. The purpose of this twopart article is to gain a better understanding of what occurs during REM sleep (part one) and understand the pathological disease states that directly target REM sleep, specifically REM Behavior Disorder (RBD). There are some very interesting hypothetical reasons for the purpose of dreaming which we will touch upon in part two. Part two also will contain several updates on cutting-edge data for diagnosing and managing RBD.
REM sleep occurs about 90 minutes into the sleep cycle in healthy young adults. The first REM episode is the least intense and may only last 5-10 minutes. After this initial episode, REM sleep begins to alternate with Non-Rapid Eye Movement (NREM) at approximately 90-minute intervals. Individuals usually experience 4-5 REM-NREM cycles during sleep. REM sleep cycles increase and become more intense toward the end of sleep with each REM period lasting 30-60 minutes. N3 sleep (the deepest stage of NREM sleep) becomes progressively less frequent during the night, and our final sleep period is made up of N2 NREM and REM.
REM sleep accounts for 20-25% of sleep time in young adults, while only accounting for 17-20% of sleep in the elderly. While REM sleep in infants and children resembles adults, the dominant frequency is slower, and the voltage is higher in younger infants and children. Dominant R frequency increases with age from 3 Hz activity at 7-8 weeks, to 4-5 Hz activity with bursts of saw tooth waves at 5 months, to 4-6 Hz at 9 months, and to prolonged runs/ bursts of notched 5-7 Hz activity by 1-5 years of age. After 5 years of age, REM sleep patterns are similar to adults with the exception of higher amplitude brainwave activity.
REM sleep consists of both sympathetic and parasympathetic activity. The eyes move rapidly behind closed eye lids, heart rate speeds up, and breathing becomes irregular. Respiratory instability — brief pauses with brief episodes of increased respiratory rate — is often seen in children during REM sleep. In contrast to other stages of sleep, in which brain waves slow down, the brain is highly active during REM sleep. REM sleep is known as the stage most associated with vivid dreaming because of heightened brain activity. Most of the cortical regions of the brain are activated. Areas of the brain that control REM are the pedunculopontine tegmentum, pontine lateral dorsal, tegmental, and lateral dorsal nuclei. Cerebral blood flow is increased during REM sleep and decreased during NREM sleep.
Several neurotransmitters are involved in REM sleep. Acetylcholine (ACh) is the main
neurotransmitter during REM sleep produced by the cholinergic neurons in the pedunculopontine tegmental nucleus (PPT) and the lateral-dorsal tegmental nucleus (LDT). ACh is also located in the basal forebrain which projects directly to the cerebral cortex. ACh from the PPT and LDT have an excitatory action on the thalamic relay neurons and inhibit gamma amino butyric acid (GABA) neurons in the thalamus. GABA is located in the ventrolateral preoptic nucleus (VLPO) and other regions throughout the brain. Active during sleep, both GABA and galanin inhibit arousal systems and are inhibited during wakefulness by norepinephrine, 5-HT, ACh, and histamine. The neurotransmitter glycine is responsible for REM muscle atonia.
In addition to the central nervous system activation, there are several important reflexes involved in REM sleep.
• The H reflex is an electrical counterpart of the mono-somatic muscle stretch reflex. During REM sleep, there is a decrease in amplitude of this reflex because motor neurons are hyperpolarized leading to presynaptic inhibition and facilitation of the brain stem neurons. Also, there is facilitation of the lateral hypothalamic and orexinergic neurons.
• The polysynthetic blink reflex is also reduced in amplitude and excitability during NREM but recovered during REM sleep. In fact, the polysynaptic blink reflex is almost the same during REM sleep as it is during wakefulness.
• The flexor reflex is in the lower limbs in humans. This is another synaptic spinal reflex, which has early and late components. It’s mediated by A-delta (δ) and C fibers, which are both types of sensory nerve fibers responsible for transmitting pain signals. During REM sleep, maximum amplitude is seen.
Along with the reflex activity in REM, sympathetic blood flow is decreased to cutaneous and muscular areas of the body but is increased in mesenteric and renal flow. (Note: During all sleep stages, there is decreased GFR, increased renin, increased water reabsorption, and decreased urine production.) Body temperature rises during REM due to an increase in cerebral metabolic activity and cerebral blood flow. However, thermal regulatory mechanisms are essentially inoperative during REM sleep. Thermal regulatory homeostasis is lost thus re-
sponses such as shivering, sweating, and panting should be absent during REM.
There is also autonomic nervous system activity which varies between the two phases of REM sleep – phasic REM sleep and tonic REM sleep.
Phasic REM sleep is a period of REM sleep characterized by bursts of eye movements, muscle twitches, and other physiological changes. There is an increase in sympathetic activity in intermittent bursts during phasic REM. This causes fluctuations in blood pressure, heart rate, cardiac output, coronary artery blood flow, and cardiac metabolic activity as well as causes brady-tachycardia arrhythmias. There is pupil dilation due to cortical inhibition of parasympathetic outflow to the iris. Irregular breathing patterns are exhibited. While diaphragmatic function is maintained, there is intercostal muscle atonia and a decrease in upper airway muscle tone (causes upper airway resistance). Metabolic input for Pa02 and PaC02 through the carotid bodies and central chemoreceptors is blunted. A profound increase in sympathetic activity will be seen in vessels, innervating skin and muscles.
In contrast to Phasic REM sleep, Tonic REM sleep is a period of REM sleep that is characterized by a lack of eye movements, decreased EEG amplitude, and atonia. Increased para-

Amalia A. Geller, MD, is a board-certified Adult and Pediatric Neurologist with a subspecialty board certification in Sleep Medicine and additional post graduate fellowship training in Epilepsy and neurophysiology. She had a pediatric internship at Arnold Palmer Hospital for women and children and post graduate training in Child Neurology at the University of California at San Diego. Dr. Geller’s Neurophysiology and Epilepsy fellowships were performed at University of California at Irvine and her Sleep Medicine fellowship at the University of Texas Southwestern in Dallas. Dr. Geller splits her practice time between pediatric sleep medicine with a focus on neurologically challenged children (Neuro Developmental Sleep, PLLC) in Boise, Idaho; along with being a Neurohospitalist for NuView Health covering in-patient adult acute stroke and acute neurology tele-medicine; and out-patient Traumatic brain injury (adult and pediatric) with Elevate Clinic in Dallas, Texas. Dr. Geller believes a comprehensive holistic integrative approach is what is imperative to treat children as a whole in order for them to achieve their maximum potential. Dr. Geller is the Nevada medical director for Nexus Dental Systems.

sympathetic and decreased sympathetic activity during tonic REM lead to a decrease in cardiac output, blood pressure, and heart rate as well as pupillary constriction due to parasympathetic drive.
The autonomic instability that occurs during both REM phases of sleep is clinically relevant, particularly when it is tied in with obstructive sleep apnea. During obstructive sleep apnea, there is chronic sympathetic hyperactivity which is linked to hypertension, cardiac ischemia, heart failure, and stroke. Of note, obstructive sleep apnea is now the third leading risk factor for stroke, independent of hypertension, diabetes, and atrial fibrillation.
When measured during sleep, brain waves show clear patterns associated with each sleep stage. In REM sleep, brain activity accelerates, showing markedly different types of brain waves. The EEG will return to a relatively low-voltage mixed frequency pattern. No sleep spindles, K-complexes, or NREM findings will be seen. The chin EMG will also fall to its lowest level. The classic finding will
be seen on EOG channels that will show rapid eye movements. Other sleep architecture we see during REM sleep include Sawtooth EEG waves (7-8 Hz in the posterior dominant region) as well as basic muscle twitches.
As we conclude this review of the physiology of REM sleep, a sleep stage characterized by rapid eye movements, heightened brain activity, and muscle atonia, you can see how REM involves both sympathetic and parasympathetic nervous system activity. The resulting fluctuations in heart rate, breathing, blood pressure, neurotransmitters, and various reflexes highlight the autonomic instability caused during REM. This instability is clinically relevant for sleep conditions like obstructive sleep apnea and REM Behavior Disorder.
Part two of this article, which will be published in the summer issue, will review the fascinating pathophysiology of REM Behavior Disorder. Sleep video links will be available to review actual cases of RBD, and lastly, an update on treatment and management will be provided in detail.

LEARN about the latest techniques and technology from industry leaders with our free live and archived educational webinars. Our online seminars are a convenient way to access great information and upskill. Check out our most recent webinars:
• Mastering Medicare Medical Billing for Oral Medicine and Dentistry with host Dr. Scott S. De Rossi
• Simplifying Sleep Dentistry: Biomatch for easy, fast, accurate and reliable sleep appliances with host Dr. Jonathan Ford
NOW at https://dentalsleeppractice.com/webinars/
• Whole-Team Training
• Ongoing Coaching
• Streamlined Protocols
• Precision Bite Technology
• Patient Education
• In-Network Medical Billing



by Ian Lalich, MD

Hypoglossal nerve stimulation (HGNS) therapy is a relatively new Food and Drug Administration (FDA) approved surgical therapy to treat moderate to severe obstructive sleep apnea in positive airway pressure (PAP) therapy intolerant patients. Inspire Medical Systems manufactures the only FDA approved HGNS device in the United States. The device was approved by the FDA in 2014.1 The now famous Stimulation Therapy for Apnea Reduction (STAR) Trial, apnea-hypopnea index (AHI) reduction did show clinically significant improvements in AHI.2 Over the past decade, multiple studies have documented statistically significant improvements in daytime sleepiness, sleep-related quality of life, improvements in oxygen desaturation index (ODI), and bed partner-reported snoring. Patients have been followed for more than 5 years, and the results have been durable. Patient satisfaction and therapy adherence are impressively high compared to other medical therapies for OSA.2-5
The initial STAR trial data shaped the criteria for implant and the procedure itself and have evolved with additional research since the initial FDA approval.2 To qualify for implantation, the FDA requires a drug-induced sleep endoscopy (DISE) procedure to assess for anatomic characteristics favorable to implant. A DISE procedure is performed in the operating room or procedure suite. Patients are given carefully titrated propofol infusion to induce a sleep state while keeping the patient spontaneously breathing. Airway collapse pattern is assessed at velum, oropharynx, tongue base, and epiglottis. The absence of complete concentric collapse at the velum is favorable for hypoglossal nerve stimulator placement. FDA approval guidelines vary slightly from current Center for Medicare/Medicaid (CMS) Devices guidelines. Currently, patients who qualify for implant must be 18 years old and older, have an AHI between 15-100 (CMS 15-65), a body-mass index (BMI) less than 40 kg/m2 (CMS < 35 kg/m2), must be in-
tolerant to CPAP/BiPAP therapy, and must not show complete concentric collapse (CCC) at the velum on DISE. The apnea and hypopnea events must be primarily obstructive, with less than 25% scoring as central or mixed events. Special consideration for patients with Down Syndrome are approved for patients 13 and older. There have been reports in the literature of patients as young as 4 years old being implanted successfully.6
While seeming straightforward, deciding on PAP intolerance can be quite nuanced. Patients doing well on PAP therapy with good therapeutic outcomes and clinical benefits are not candidates. Patients who like and use PAP therapy but want a surgical option for convenience are not considered appropriate candidates. Patients with poor usage, significant aerophagia, severe leaks despite troubleshooting, dermatologic issues with mask-wearing, recurrent respiratory illness/sinusitis patients, and REM behavior disorder are good candidates. There are patients who are using their therapy but struggle with claustrophobia, insomnia due to PAP therapy, or develop an aversion to therapy. The decision-making for the later group is more difficult and involves careful discussion with the patient. Implementing a multidisciplinary team of sleep providers and otolaryngology providers to discuss patient therapy options is often helpful for decision-making.
The current implant (Inspire IV) is placed with a two-incision approach: a modified submandibular neck utility incision and a sub-clavicular upper chest incision. Placing the device on the right side is preferred, leaving the left side for cardiac devices. Implants can be placed on the left in special situations. Intraoperative electromyography (EMG) mapping of the hypoglossal nerve is performed to select nerve branches that will stiffen/protrude the tongue and exclude branches that will retract and retrude the tongue. The stimulation lead is tunneled to the generator pocket. A breathing sensor is placed between ribs 2 and 3, superficial to the internal intercostals and deep to the external intercostals. The device is tested intraoperatively to assess function. The procedure takes about 1-2 hours and is usually an outpatient procedure. Following implant, the patient must wait a minimum of 4 weeks to allow for healing before activation.
The surgery is well tolerated with much less morbidity than other surgical procedures used to treat obstructive sleep apnea. While
not an exhaustive list, surgical risks include surgical site bleeding/hematoma/seroma, pain at incision/generator site, temporary or permanent injury to the ipsilateral hypoglossal nerve, pneumothorax with respiratory sensor placement, delayed device infection/migration/ extrusion, device/component malfunction, device recall, and risk of general anesthesia. Recent MAUDE database analysis reviewed the overall complication rate of HGNS placement.7 In 2023, there were a total of 414 complications out of 23,743 implants placed (roughly 1.74%). Approximately 75% of complications involved pain, infection, and hematoma/seroma/ edema. Device infection leads to the highest rate of explant (48.6%). The updated complication rate is consistent with the initial complication rates from the STAR trial, which are roughly 2%.2 Overall, HGNS placement is well tolerated and has a low complication rate.
Placement, programming, and follow-up involve a close collaboration between an otolaryngologist and a sleep medicine provider. Following implant and healing, the device is activated by a sleep medicine provider. Initial programming is usually pre-templated, with most patients tolerating traditional programming settings. Functional and presumed therapeutic thresholds are identified during activation/programming. Other programming features allow for delay before therapy initiation, pause duration, and total therapeutic duration. Patients then have an external remote they use to direct their therapy.

Inspire implant, remote, and app

Ian Lalich, MD, is an otolaryngologist based in Minneapolis, MN, who specializes in sleep surgery. He graduated from the University of North Dakota School of Medicine and Health Sciences and completed his residency at the Mayo Clinic College of Medicine and Science, where he also served as a clinical instructor. He currently serves as an attending surgeon at several Minnesota hospitals in the M Health Fairview system. In addition to general otolaryngology, his experience extends to sleep surgery and surgical oncology of the head and neck. He is the recipient of multiple awards including Physician of the Year from M Health Fairview Lakes Medical Center. In 2025, he will assume the role of Medical Director of Otolaryngology-Head and Neck Surgery at M Health Fairview. Dr. Lalich also serves as Vice President of the Minnesota Academy of Otolaryngology.
Following activation, the patient slowly titrates to their therapeutic threshold. Patients are usually advised to advance the voltage one step per week. Device efficacy is assessed once patients are near their threshold voltage setting, sleep well, and wake refreshed without daytime tiredness. Home sleep studies can be useful to check in on a patient’s progress but do not easily allow assessment of the range of therapeutic options. An in-lab HGNS titration polysomnography study is performed in a manner similar to PAP titration. The AHI is evaluated at different voltage thresholds throughout the night, including the presumed therapeutic threshold based on clinical observation during activation/programming and patient feedback. Being mindful of sleep position and sleep stage during titration allows for the most accurate assessment of therapeutic voltage level. Understanding that therapeutic voltage may be lower than expected is also paramount. Over-titration occurs with the continued increase in voltage in anticipation of further reduction in AHI. The additional energy can lead to current spread and activation of antagonistic musculature, resulting in decreased efficacy and patient discomfort. Most patients are therapeutic after the first titration study. If therapeutic voltage was not identified or the therapeutic setting is not well tolerated by the patient, the device can be reprogrammed and the titration process can be repeated. If a therapeutic voltage can not be found or tolerated, complex reprogramming can be performed with combined efforts from the sleep medicine and otolaryngology teams. Performing awake upper airway endoscopy during reprogramming can assist in finding a functional/therapeutic setting that is tolerable. Awake endoscopy may also suggest other changes (head/neck position, body position, mouth posture, et cetera) that would improve the airway.
Hypoglossal nerve stimulation (HGNS) therapy is a novel surgical therapy for OSA patients with PAP intolerance.

The current version of the device Inspire IV (Model 3028) has a battery rating of 11 years. Patients with the device require generator change following battery depletion. The device is MRI compatible for full body MRI using the appropriate protocol with a 1.5 Tesla magnet. The device is compatible with air travel and should be declared to the TSA to undergo medical device-compatible screening. In August 2024, the FDA approved Inspire V. The device will have a new Bluetooth-enabled patient remote, a new physician programming device. It will not be necessary to place a respiratory sensor. Battery life, MRI conditionality, and air travel compatibility will remain the same. The company expects wide deployment/adoption of the new device in late 2025/early 2026. Current outcomes are measured based on overall AHI reduction, patient usage, and symptom improvement. Patients are classified as Green or Yellow Pathway based on their outcome following titration. Green Pathway patients have an overall AHI of less than 15, patient usage greater than 4 hours per night, and subjective improvement in sleep symptoms. Patients not meeting all Green Pathway criteria are classified as Yellow Pathway and undergo reprogramming and re-titration until they meet Green Pathway criteria.
HGNS therapy is a novel surgical therapy for OSA patients with PAP intolerance. The therapy has excellent outcomes compared to other surgical management options with low complication rates. In appropriately selected patients, HGNS therapy is an excellent surgical option for treating obstructive sleep apnea.
1. Kent DT, Carden KA, Wang L, Lindsell CJ, Ishman SL. Evaluation of Hypoglossal Nerve Stimulation Treatment in Obstructive Sleep Apnea. JAMA Otolaryngol Head Neck Surg. 2019;145(11):10441052. doi:10.1001/jamaoto.2019.2723
2. Strollo PJ Jr, Soose RJ, Maurer JT, et al. Upper-airway stimulation for obstructive sleep apnea. N Engl J Med. 2014;370(2):139-149. doi:10.1056/NEJMoa1308659
3. Woodson BT, Soose RJ, Gillespie MB, et al. Three-Year Outcomes of Cranial Nerve Stimulation for Obstructive Sleep Apnea: The STAR Trial. Otolaryngol Head Neck Surg. 2016;154(1):181-188. doi:10.1177/0194599815616618
4. Woodson BT, Strohl KP, Soose RJ, et al. Upper Airway Stimulation for Obstructive Sleep Apnea: 5-Year Outcomes. Otolaryngol Head Neck Surg. 2018;159(1):194-202. doi:10.1177/0194599818762383
5. Mashaqi S, Patel SI, Combs D, et al. The Hypoglossal Nerve Stimulation as a Novel Therapy for Treating Obstructive Sleep Apnea-A Literature Review Int J Environ Res Public Health. 2021;18(4):1642. Published 2021 Feb 9. doi:10.3390/ijerph18041642
6. Wasserman I, Chieffe DJ, Gipson KS, Skotko BG, Hartnick CJ. Hypoglossal Nerve Stimulation for Obstructive Sleep Apnea in a Young Child With Down Syndrome. Pediatrics. 2024;153(5):e2023063330. doi:10.1542/peds.2023-063330
7. Bentan MA, Nord R. Comprehensive Analysis of Adverse Events Associated With Hypoglossal Nerve Stimulators: Insights From the MAUDE Database. Otolaryngol Head Neck Surg. 2024;171(5):1580-1590. doi:10.1002/ohn.883
• In-Network options with major payors and plans
• Out-of-Network when appropriate
• Reliable, timely, predictable results with best rates
• Access to the Nexus Specialty Physician Network
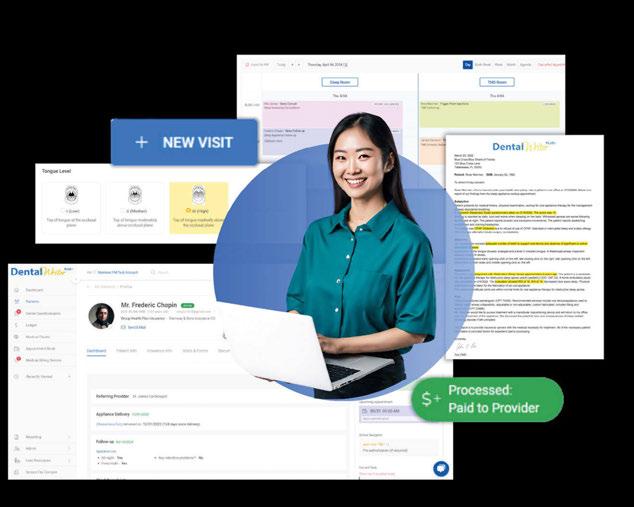
• Nexus billing portal ensures error-free claim submission and tracking
• Personal billing representative
• Complete solution for:
º Sleep Medicine
º Airway Expansion
º TMJ/TMD
º Botox
º CBCT

Getting reimbursement from medical insurance can be a nightmare for dentists. With the Nexus Bill system, you can avoid the common pitfalls of inconsistent payments, endless delays, constantly fighting with insurance companies, and patients refusing care because you are not “In-Network” for medical.

by Karen Parker Davidson, DHA, MSA, MEd, MSN, APRN, and Donald R. Moeller, DDS, MA, MD, Lieutenant Colonel
US Army (retired)

Once the cranial nerves are memorized during anatomy instruction in professional school, day-to-day awareness tends to be limited to nocioception and dysfunction. What may be underappreciated is the role the trigeminal nerve plays in facial growth and development and ongoing function. This self-instructional course for dentists reveals how nasal breathing, sleep-disordered breathing, and functional anomalies are all tied to the fifth cranial nerve, and how comprehensive head-and-neck medicine cannot be practiced without a thorough understanding of it’s contribution.
Dental Sleep Practice subscribers can answer the CE questions online at https:// dentalsleeppractice.com/continuing-education/ to earn 2 hours of CE from reading the article. Correctly answering the questions will demonstrate the reader can:
1. Cite several ways proper growth and development is tied to the functions of the trigeminal nerve.
2. Appreciate the bidirectional influence of the trigeminal and nasal breathing.
3. Consider how diagnosis, evaluation, treatment, and follow-up are intimately involved with the anatomy and function of the fifth cranial nerve.
The trigeminal nerve, the largest and most complex of the cranial nerves, is often seen as the sensory powerhouse of the face. Its vast reach into the oral, nasal, and craniofacial structures makes it central to many physiological processes, from chewing and sensation to breathing and facial growth. Yet, its influence extends beyond simple sensory functions. In the context of facial growth and nasal breathing, the trigeminal nerve plays a crucial role in shaping development and function in ways that affect not only the structure of the face but also overall health, sleep quality, and breathing efficiency.1
This article delves into how the trigeminal nerve contributes to facial growth and development, its impact on nasal breathing, and the implications for dental sleep medicine. By understanding this vital nerve’s role, dental and medical professionals can better address disorders linked to nasal obstruction, sleep-disordered breathing, and developmental anomalies.
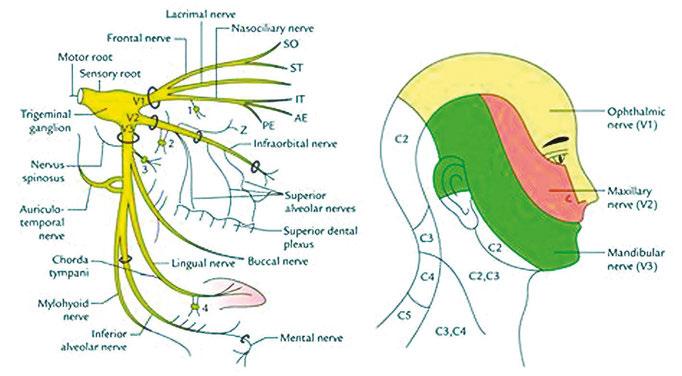
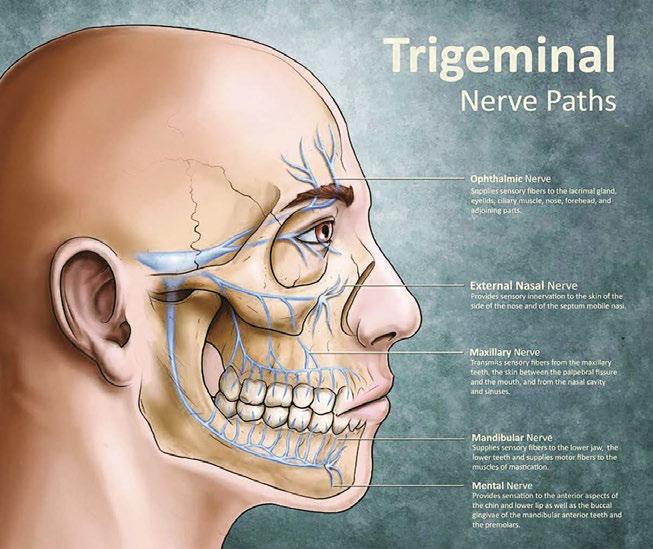
The trigeminal nerve (cranial nerve V) is the largest and most intricate of the cranial nerves, serving essential sensory and motor roles in the face, jaws, and associated structures. It branches into three main divisions: the ophthalmic (V1), maxillary (V2), and mandibular (V3) nerves. Each division is responsible for innervating specific regions of the face. The ophthalmic division (V1) provides sensory input to the forehead, scalp, upper eyelid, and parts of the nose. The maxillary division (V2) carries sensory signals from the midface, including the cheeks, upper lip, upper teeth, and nasal cavity, while the mandibular division (V3) has both sensory and motor functions, innervating the lower lip, jaw, and teeth, and controlling the muscles involved in mastication (chewing).1
The trigeminal nerve’s sensory functions are processed in its nuclei, which are located in the brainstem. These nuclei can be divided into three parts: the mesencephalic nucleus, chief sensory nucleus, and spinal trigeminal nucleus.2 The mesencephalic nucleus, located in the midbrain, is primarily responsible for proprioception, which is the
body’s ability to sense the position of the jaw and muscles during activities like chewing.3 The bite force and pressure is detected in the afferent neural feedback loop from the V3 to the V2, also known as the V2-V3 Bio Feedback Loop, that impacts nasal function discussed later in the article. The chief sensory nucleus, found in the pons, processes sensations such as fine touch and pressure from the face. The spinal trigeminal nucleus, which extends from the pons into the upper spinal cord, processes sensations related to pain and temperature.
The motor functions of the trigeminal nerve stem from its motor nucleus, which is also located in the pons. This motor component controls the muscles of mastication, including the masseter, temporalis, and pterygoid muscles, facilitating essential functions like chewing and biting. In addition, the mandibular branch (V3) supplies motor fibers to other small muscles, such as the tensor tympani, involved in sound dampening, and the tensor veli palatini, which opens the auditory tube during swallowing.
Beyond simple sensory and motor functions, the trigeminal nerve is involved in reflexes that help protect the face and maintain facial integrity. The jaw jerk reflex is a monosynaptic reflex that tests the integrity of the trigeminal nerve, where a tap on the chin causes the jaw to jerk upward. The corneal reflex involves both the trigeminal and facial nerves; when the cornea is stimulated (sensed by V1), the facial nerve triggers a blink response to protect the eye. Similarly, the trigeminal nerve is crucial for the sneeze reflex, where irritation of the nasal mucosa (innervated by V2) leads to a coordinated response involving multiple nerves, causing a sneeze to expel irritants.
The trigeminal nerve interacts with many other cranial and peripheral nerves, forming complex networks that regulate sensory and motor functions in the face, neck, and oral cavity. It works in close association with the facial nerve (cranial nerve VII) in protective reflexes like blinking. It also coordinates with the glossopharyngeal (cranial nerve IX) and vagus nerves (cranial nerve X) in reflexes related to swallowing and the gag reflex, all which I call the hitchhikers of the trigeminal nerve. These interactions are essential for maintaining both voluntary and involuntary facial movements, and play a role in breath-

Dr. Karen Parker Davidson is a graduate of the University of North Carolina at Chapel Hill School of Nursing, attended the University of North Dakota College of Nursing Family Nurse Practitioner program, completed three master’s degree programs at Central Michigan University and University of Phoenix, earned her doctorate in Health Administration with a focus in Health Policy, also from Central Michigan University, and is currently pursuing a PhD in Business Administration with a focus on International Business. With more than three decades of clinical and medical device industry experience in various roles, she also served as a Flight Nurse and Critical Care Nurse in the United States Air Force Reserves with the 315th and 459th Air Wings. She is an adjunct professor, dissertation chair, and health policy SME at Liberty University’s Division of Public & Community Health, School of Health Sciences, and School of Business, and is adjunct faculty at Central Michigan University, School of Health Professions. She is a member of the American College of Healthcare Executives and the National Association of Clinical Nurse Specialists.
As a team member in the development of a medical device for improved manual ventilation in airway emergencies, she received a National Science Foundation award in 2023. Her work as a renowned expert in nasal function, measurements, and patented interpretation algorithms continues. Her most recent research in nasal resistance and rhinomanometry is partnered with Dr. Moeller among the veteran population with mental health disorders and among athletes, and presented as a peer-reviewed poster at the 2024 AAO-HNS meeting and accepted as a poster presentation for the 2025 AAAAI meeting.

Dr. Donald R. Moeller graduated from San Jose State University with a bachelor’s degree in Biological Science, entered dental school at the University of California San Francisco, and graduated with a Doctor of Dental Surgery degree and then joined the US Army Dental Corps. He completed his Residency in Oral and Maxillofacial Surgery (OMS) at the Walter Reed Army Medical Center during which time he was also involved in PhD Mentored Research at the Walter Reed Army Institute of Dental Research. This early experience in Surgical Trauma Research motivated him to obtain a graduate degree in Biological Sciences with a Cellular Biology emphasis. After retiring as Chief of Oral and Maxillofacial Surgery at Martin Army Hospital Fort Moore Georgia, Dr. Moeller entered the University of Alabama Medical School at Birmingham where he received a Doctor of Medicine degree. Dr. Moeller completed his Transitional Medical Residency at the Columbus Medical Center and then briefly served as an Assistant Professor of OMS at Augusta University.
Following retirement from a full-time practice in OMS, he re-entered his career as a Neuroscience Researcher in PTSD associated sleep disorders and Traumatic Brain Injuries. He has published several research papers which reported the ability of an Intraoral Neuromodulator™ to reduce PTSD associated nightmares, sleep disruptions, headaches, and Disturbing Nocturnal Behaviors™. His research received a Letter of Commendation from the Department of Defense Center for Psychological Trauma. He is Board Certified in Oral and Maxillofacial Surgery, past Fellow of the American College of Oral and Maxillofacial Surgeons, past member of the American Association of Oral Medicine, and a current member of the American Association of Oral and Maxillofacial Surgeons.
ing and sleep patterns. In essence, the vagus nerve is not stimulated, but feeding off of neural pathway of the trigeminal nerve in the nasobronchial reflexes.3 Breathing exercises are an example; the sympathetic charge in the nasal mucosa is withdrawn allowing the parasympathetic nervous system to become dominant and initiate a vagus response .
In addition to these reflexes, the trigeminal nerve is part of both ascending and descending neural pathways.4 Sensory information collected by the trigeminal nerve is sent through these pathways to the thalamus and the primary sensory cortex, allowing the brain to process sensations such as pain, temperature, and touch. Motor signals originating in the brain are sent down to the trigeminal nerve’s motor nucleus, enabling voluntary movements like chewing and jaw opening.
Understanding the intricate anatomy and physiology of the trigeminal nerve is clinically significant. Trigeminal neuralgia, for example, is a condition characterized by intense facial pain due to dysfunction of the trigeminal nerve, often triggered by simple sensory stimuli. Similarly, the nerve’s involvement in temporomandibular joint (TMJ) disorders shows how dysfunction in the mandibular division can contribute to jaw misalignment and pain. Additionally, sleep-disordered breathing conditions, such as obstructive sleep apnea, may be exacerbated by trigeminal nerve dysfunction, particularly if nasal airflow is compromised.5
Given these vast sensory and motor responsibilities, the trigeminal nerve is vital
for integrating sensory feedback with motor control, allowing for critical functions like chewing, speaking, and breathing to operate harmoniously. But beyond these immediate functions, the trigeminal nerve is intimately connected to the processes of growth, development, and airway management.
Facial growth is a complex interplay of genetic programming, environmental influences, and functional forces. One of the most significant drivers of facial development is the functional stimulus provided by the muscles and bones of the face. The trigeminal nerve plays a crucial role in this process through both its sensory and motor functions.6
The mandibular branch of the trigeminal nerve innervates the muscles responsible for chewing (mastication), including the masseter, temporalis, and pterygoid muscles. The forces generated during mastication create mechanical stresses on the bones of the face, especially the maxilla, mandible, and zygomatic bones.7 These stresses stimulate bone growth and remodeling through a process known as mechanotransduction, in which physical forces are translated into cellular responses that drive bone formation and adaptation. New studies found the trigeminal nerve and the cerebellum stabilize the jaw while running, walking, and jogging, since the muscles change in each activity, meaning the head and neck position is naturally monitored.
Proper chewing in childhood and adolescence is essential for the healthy development of the jaws and facial structure.8 A diet that requires vigorous chewing (such as fibrous, unprocessed foods) stimulates muscle and bone development, while a soft diet can lead to underdeveloped jaws, malocclusion, and even airway constriction.9 Since the trigeminal nerve controls the muscles of mastication, it is a key player in this developmental process.
The sensory branches of the trigeminal nerve, particularly the maxillary and mandibular branches, provide feedback from the
teeth, gums, and surrounding tissues.10 This sensory feedback is essential for coordinating the growth and adaptation of the craniofacial skeleton. Sensory nerve fibers interact with bone cells (osteocytes) and signaling pathways that regulate bone remodeling, ensuring that the bones of the face grow in harmony with functional demands.1
In addition, sensory inputs from the teeth and temporomandibular joint (TMJ) influence the growth of the mandible and maxilla. Orthodontic and dentofacial orthopedic treatments often rely on manipulating these forces to guide facial growth, and understanding the trigeminal nerve’s role can improve the precision and efficacy of such interventions that affect patients who make up the 60% of the population with high nasal resistance and TMJ issues. As stated in the past regrading an increased pressure within the sinus cavities, it is not the heightened pressure disrupting the balance of forces in and around the jaw joint, potentially leading to TMJ symptoms, but the V2-V3 biofeedback loop.
Nasal function plays a vital role in overall health, influencing everything from oxygenation and cardiovascular function to sleep quality and cognitive performance. The trigeminal nerve is deeply involved in regulating nasal airflow and ensuring proper nasal function in the specialty of Functional Rhinology.12,13
The ophthalmic (V1) and maxillary (V2) branches of the trigeminal nerve provide sensory innervation to the nasal cavity. This sensory input allows the body to detect changes in airflow, temperature, and humidity, which helps regulate breathing patterns. For example, when cold air enters the nasal passages, the trigeminal nerve senses the temperature change and signals the body to warm and humidify the air before it reaches the lungs. This process is essential for maintaining optimal respiratory function.
Moreover, the trigeminal nerve’s sensory feedback helps protect the nasal passages from harmful irritants. When the nerve detects irritants like dust or allergens, it triggers reflex actions such as sneezing or nasal congestion to prevent these particles from en-
tering the lungs. This protective mechanism is crucial for maintaining airway health and function.
The trigeminal nerve also plays a role in regulating the tone of the nasal mucosa and blood vessels. Through autonomic reflex pathways, the trigeminal nerve influences vasoconstriction and vasodilation in the nasal passages, helping to control the resistance of the nasal airway. This regulation is particularly important during sleep, when nasal congestion can exacerbate conditions such as obstructive sleep apnea (OSA) in the prone and supine positions, especially in REM sleep where nasal resistance is at its highest point. Sleep-disordered breathing, especially in children, can have long-term effects on facial growth and development. Chronic mouth breathing, often caused by nasal obstruction, alters the normal growth patterns of the face and jaws, leading to a long, narrow face, an underdeveloped maxilla, and a retrusive mandible. These structural changes can further impair breathing, creating a vicious cycle. The trigeminal nerve’s role in maintaining nasal patency is therefore crucial for preventing these developmental issues.
A deep understanding of trigeminal nerve function offers new avenues for diagnosis, treatment, and intervention.
Proper nasal breathing is essential for overall health. The nose filters, warms, and humidifies the air before it reaches the lungs. Any disruption in nasal function can lead to breathing difficulties and associated health issues. The trigeminal nerve’s role in maintaining nasal sensation is thus vital for ensuring effective nasal breathing. The trigeminal nerve’s sensory input plays a crucial role in regulating breathing. Mechanoreceptors and chemoreceptors in the nasal cavity and sinuses, innervated by the maxillary branch (V2), detect changes in airflow, pressure, and the presence of irritants. This sensory information is essential for maintaining effective nasal breathing and triggering reflexes that protect the respiratory system. Malocclusions and other orthodontic issues can impact nasal breathing. For example, a high-arched palate can reduce the nasal airway space, leading to breathing difficulties however, volume, or a bigger nose does not correlate to better nasal function. Orthodontic interventions can help expand the palate, thereby improving nasal airflow. Understanding the interplay between dental structures and nasal function, mediated by the trigeminal nerve, is crucial for comprehensive orthodontic care.
Understanding the role of the trigeminal nerve in facial growth and nasal breathing has significant implications for dental sleep medicine. Here are several key takeaways:
Children with nasal obstruction or chronic mouth breathing are at risk for developing malocclusions, skeletal disharmony, and sleep-disordered breathing conditions such as OSA. Early intervention aimed at restoring nasal breathing and encouraging proper jaw growth is essential. Dental appliances, myofunctional therapy, and orthodontic treatments can guide facial growth and support proper airway development. These interventions often rely on stimulating the muscles and bones innervated by the trigeminal nerve to promote healthy development.
Disorders of the trigeminal nerve, such as trigeminal neuralgia, can cause chronic facial pain and disrupt sleep. While trigeminal neuralgia is primarily characterized by episodes of intense facial pain, the associated discomfort and stress can interfere with sleep quality. Addressing these issues through medical or surgical interventions can significantly improve patients’ sleep and overall well-being.
A biofeedback loop in the context of breathing involves continuous monitoring and regulation of respiratory parameters and nasal function to maintain homeostasis. The trigeminal nerve’s sensory input is a critical component of this loop, providing real-time feedback to the brain about the state of the nasal passages and airflow. When sensory receptors detect a change, such as an obstruction or irritant in the nasal cavity or changes in bite force and pressure, signals are sent via the trigeminal afferent neural pathway to the brainstem. This is more noticeable when using a specialized oral neuromodulating device. The brainstem integrates this information and initiates appropriate responses, such as adjusting the rate and depth of breathing. Increasing nasal resistance, or triggering a sneeze to expel the irritant. Observation and first identified during my time in Dr. Moeller’s clinic, the V2-V3 afferent biofeedback loop in rhinomanometry tracings during active breathing further emphasizes the role of CN5 and vertical height; this novel discovery showed it wasn’t the volume changes and titration that improved the airway in a veteran with PTSD, but the quantifiable variations in transnasal pressure change as a biomarker.
Rhinomanometry, a diagnostic tool that measures nasal airflow and resistance, can provide valuable insights into the function of the nasal passages and the role of the trigeminal nerve in regulating airflow, especially with the involvement of the oral cavity. In cases where nasal obstruction is suspected, rhinomanometry can help identify whether the obstruction is due to structural issues, inflammation, or autonomic dysfunction influenced by the trigeminal nerve.
In orthodontics, treatments such as rapid maxillary expansion (RME) are designed to stimulate the maxilla’s growth and improve nasal airflow. These treatments may also influence the trigeminal nerve’s sensory feedback mechanisms, helping guide bone remodeling and improve facial symmetry, as well as nasal function as a response to treatment to avoid overexpansion and alterations in the pneumatization of the maxillary sinuses. As understanding of the trigeminal nerve’s role in growth and function expands, orthodontic and orthopedic approaches may become more refined, offering targeted interventions for facial growth and airway management.
The trigeminal nerve’s role in facial growth and nasal breathing is both profound and multifaceted. From guiding the development of the craniofacial skeleton to regulating nasal airflow and reflexes, this nerve is essential to many processes that influence overall health, sleep quality, and breathing efficiency. For dental sleep medicine professionals, a deep understanding of trigeminal nerve function offers new avenues for diagnosis, treatment, and intervention in cases of sleep-disordered breathing, malocclusion, and developmental anomalies. By addressing the root causes of these issues, clinicians can help patients achieve better health outcomes, both in their facial structure and their
breathing function. The trigeminal nerve is integral not only in sensory and motor functions but also in regulating various physiological processes, including breathing. This paper extends the exploration of the trigeminal nerve’s role by delving into the afferent neural pathway and the biofeedback loop involved in active breathing. Understanding how these processes are measured is crucial for developing advanced diagnostic and therapeutic strategies in fields such as dentistry, orthodontics, and respiratory medicine..
Future research should focus on further elucidating the intricate connections between the trigeminal nerve and various dental and orthodontic conditions. Advances in imaging techniques and neurophysiological studies will enhance our understanding of these relationships, leading to improved diagnostic and therapeutic strategies. Additionally, interdisciplinary approaches combining dentistry, orthodontics, and otolaryngology will foster a more comprehensive understanding of the trigeminal nerve’s role in craniofacial health. This should also focus on incorporating 4-phase rhinomanometry to further elucidate the role of the trigeminal nerve in the dental practice. Interdisciplinary collaboration between neuroscientists, otolaryngologists, and respiratory specialists will be essential in advancing our understanding of these complex neural mechanisms and improving patient care.
1. Huff T, Weisbrod LJ, Daly DT. Neuroanatomy, Cranial Nerve 5 (Trigeminal). In: StatPearls. Treasure Island (FL): StatPearls Publishing; April 20, 2024.
2. Price S, Daly DT. Neuroanatomy, Trigeminal Nucleus. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539823/
3. Koc D, Dogan A, Bek B. Bite force and influential factors on bite force measurements: a literature review. Eur J Dent. 2010;4(2):223-232.
4. Baraniuk JN, Merck SJ. Nasal reflexes: implications for exercise, breathing, and sex. Curr Allergy Asthma Rep. 2008;8(2):147-153. doi:10.1007/s11882-008-0025-7
5. Bindu B, Singh GP, Chowdhury T, Schaller B. Rhinitis and sleep disorders: The trigeminocardiac reflex link?. Med Hypotheses. 2017;103:96-99. doi:10.1016/j.mehy.2017.04.019
6. Cobo, J.L. et al. Connections between the facial and trigeminal nerves: Anatomical basis for facial muscle proprioception JPRAS Open. 2017;12: 9 – 18.
7. Moss ML, Salentijn L. The primary role of functional matrices in facial growth. Am J Orthod. 1969;55(6):566-577. doi:10.1016/00029416(69)90034-7
8. Oral Health in America: Advances and Challenges [Internet]. Bethesda (MD): National Institute of Dental and Craniofacial Research(US); 2021 Dec. Section 2A, Oral Health Across the Lifespan: Children. Available from: https://www.ncbi.nlm.nih.gov/books/NBK578299/
9. Ramirez-Yañez, G.O. (2019). Craniofacial Growth and Development. In: Liem, E. (eds) Sleep Disorders in Pediatric Dentistry . Springer, Cham. https://doi.org/10.1007/978-3-030-13269-9_3
10. Carlson, D. S. (2005). Growth and Development of the Jaws: Influence of Muscle Function. American Journal of Orthodontics and Dentofacial Orthopedics, 128(5), 533-540.
11. Wu Y, Lan Y, Mao J, Shen J, Kang T, Xie Z. The interaction between the nervous system and the stomatognathic system: from development to diseases [published correction appears in Int J Oral Sci. 2023 Sep 11;15(1):39. doi: 10.1038/s41368-023-00250-3]. Int J Oral Sci. 2023;15(1):34. Published 2023 Aug 15. doi:10.1038/s41368-023-00241-4
12. Vogt K, Parker-Davidson K. Measurement of Nasal Obstruction: Rhinomanometry as basic method in functional rhinology. Facial Plast Surg. 2024;40(3):314-322. doi:10.1055/a-2218-5883
13. Parker Davidson, K. Breathe Through Your Nose, Don’t Pay Through It: The Impact the Healthcare Industry Has on Nasal Function and How We Breathe. PeeDee Publishing; 2022.
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 8 CE credits for only $149 by visiting https://dentalsleeppractice.com/subscribe/.
AGD Code: 730
Date Published: January 31, 2025 Course Expires: January 31, 2028
Legal disclaimer: Course expires 3 years after publication date. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
n To receive credit: Go online to dentalsleeppractice.com/continuing-education/, click on the article, then click on the take quiz button, and enter your test answers
To provide feedback on this article and CE, email us at education@medmarkmedia.com.
by Karen Parker Davidson, DHA, MSA, MEd, MSN, APRN, and Donald R. Moeller, DDS, MA, MD
1. A biofeedback loop is involved with breathing functions to _______.
a. Ensure enough air is moved to fill the lungs
b. Maintain homeostasis between respiratory parameters and nasal function
c. Protect the body from allowing too-cold air into the delicate nasal system
d. Create a sympathetic response to avoid unpleasant or dangerous smells
2. The trigeminal nerve affects nasal resistance by _______.
a. Contracting the nasalis muscle to restrict the nares opening
b. Lifting the palate to partially close the nasopharynx
c. Monitoring diaphragm movement and increasing force to draw more air in
d. Regulating vasoconstriction and vasodilation in nasal passages
3. Forces generated during chewing create stress on facial bones and _______.
a. Are primarily generated by trigeminally-innervated masticatory muscles
b. Are limited by pain receptors transmitting signals through the trigeminal
c. Result in smaller bones with less airway support
d. Must be resisted by inhibitory signals from the trigeminal nerve
4. The special area of interest in nasal function and trigeminal innervation is called _______.
a. Nasal geekdom
b. Nothing special, because the nose operates independently of the trigeminal nerve
c. Functional Rhinology
d. Advanced Rhinoplasty
5. Healthy development of the craniofacial respiratory complex results from _______.
a. Functional Rhinology
b. Stimulation of muscles and bones innervated by the trigeminal nerve
c. Proper assessment after puberty, when growth is mostly complete
d. Guidance by one healthcare provider
6. Future developments and capabilities of providers to affect homeostasis must _______.
a. Develop in innovator’s clinics, as they have the clinical expertise
b. Maintain a proper focus on developing reimbursable codes for procedures
c. Involve many disciplines and technologies to assess structure and function
d. Be rooted in what’s worked so far, to not get too far away from traditional care
7. The trigeminal’s role in physiology includes _______.
a. Sensory afferent pathways
b. Motor control efferent signals
c. Physiologic regulatory biofeedback pathways
d. All of them
8. Nasal resistance inversely affects growth and development of the craniofacial respiratory complex by _______.
a. By increasing the diaphragm pressure needed to overcome a small airway
b. Changing the intraluminal pressure in the developing paranasal sinuses
c. Degrading tissue health in the temporomandibular joint complex
d. Requiring treatment medications that inhibit bone growth
9. Voluntary and Involuntary facial movements are a result of _______.
a. Cervical reflexes such as blinking
b. Conscious effort at developing proper habits
c. Early life development
d. Coordination between various cranial nerves such as V, VII, IX and X
10. The Trigeminal nerve consists of three, (of course), divisions named _______.
a. Larry, Moe, and Curly
b. Maxillary, Mandibular, and Cervical
c. Opthalmic, Mandibular, and Maxillary
d. Maxillary, Opthalmic, and Inferior



by Laura Sheppard, BS, CDT, TE
Many practitioners make it a standard procedure to try out all types of devices on themselves, so they can assess fit, comfort, ease of insertion, removal, and adjustment. This is commendable. However, it can also be a slippery slope. Your patient is not you. I often hear doctors say they did not like one aspect or another of a device when they tried it, so they would not recommend it for their patients. This often leads to prescribing only one or two types of appliances to serve their patients’ needs. This may be a mistake. For best results, select an appliance based on the consult considerations listed below.
If you are using the wrong tools or if you are using the correct tools in the wrong way, the results are the same.
Appliance selection requires an understanding of the appliance designs AND a careful analysis of your patient to select the best option. If in doubt, contact your lab for some insight. Lab consultations are especially helpful when you are not sure which appliance is best. A lab discussion should include the patient’s dental condition, stability, bruxer or clencher, missing teeth or any extreme dental contours. Is the patient an oral or nasal breather? What is the amount of tongue space (tongue scalloping, tongue biter) and character of facial musculature (cheek biter, tight or loose facial musculature, difficulty getting a
Tight Labial Musculature – Lip Seal Difficulty
Lingual, or Inter-occlusal Hardware Mechanism or Buccal Mechanism with Minimal Profile
Labial Thickness Appliance Limited Range of Motion
Orthodontic Tx Repositioning forces are counter to stable tooth positions. In some cases, an invisible retainer may be worn in conjunction with a sleep appliance, but unwanted changes may still occur.
Cosmetic Restorations, Veneers, Isolated Mobile Teeth
Missing Teeth
Edentulous or Partly Edentulous
Notify lab to block out (providing non-contact internal spacing)
Notify lab to block out for draw and fill space with acrylic for adjacent tooth stability, or place a pontic tooth
1. Sleep appliance can be made over current denture prosthetics
2. Duplicate denture technique and directly add bite planes and mechanisms
3. Appliance can be made direct to ridges: Need full prostho impressions and use BP/ORs to establish therapeutic bite registration
Bruxer / Claustrophobic / Restraint Issues
Coverage Appliance - Notify lab to reduce tissue coverage where possible, esp. in posterior
Appliance and/or 1- or 2-Piece Insertion Appliance (allows for optional insertion methods)
Appliance that Allows Opening in Use, More Lateral Freedom, 2-Piece Insertion Appliance
Arthritic Hands Smaller Appliance, 1-Piece Insertion Appliance (allows for optional insertion methods), Easy adjustment Mechanism
Poor Dexterity or Visual Acuity 1-Piece Insertion Appliance (allows for optional insertion methods), Easy Adjustment Mechanism
Metal or Acrylic Allergies
CPAP Dependent
Material Testing Samples from Lab
CPAP Combo Therapy: Appliance can be fitted with attachment to connect to Nasal PAP


lip seal, etc.)? Are they currently or formerly a sleep appliance wearer? Or are they currently or recently an orthodontic patient?
With this information, your lab should be able to help you understand the common pitfalls and determine the best type of appliance for your patient. (See Table 1 for a quick guide for appliance selection.)
The Quad Challenge x 4! The most critical element of any oral appliance is fit and retention. Let’s just start by looking at a single arch device. As you know, depending on the dental anatomy, any type of single-arch, full-coverage appliance like a splint or a retainer can be challenging to passively insert, remove, fit comfortably and be retentive. This is known as the ‘quad challenge’. Now, let’s take an oral sleep appliance involving both arches. With a sleep appliance this singular-arch quad challenge has just multiplied its complications by yet another 4 challenges!
1. Obtaining fit, retention and comfort on two arches.
2. Facilitating insertion, connection, and removal as 2 pieces (or in some cases, 1 piece) while being influenced by the arc of closure in protrusive.
3. Insuring U/L retention during wear & stress, factoring in the confinement of muscular movements and the constant downward forces of the mandible (if U/L appliances are connected).
4. Managing the voluntary or involuntary expression of muscular actions during sleep, causing dislodgement and/or fractures.
Too much retention is infinitely more common in natural dentition than cases lacking it. The cases where teeth are very curvaceous, triangular, tipped or crowded, missing, or perio-involved with root exposure require careful survey of the path of insertion, blocking out of severe undercuts in advance of manufacture, or relieving the appliance
material during seating. Of course, the risk lies in removing too much undercut and rendering a loose fit. Labs today can survey the case with scan & digital design technology, or they can use a manual surveyor.
Not enough retention presents even more challenges. How to create retention where none exists? On cases with short crowns or minimal height of contour, it may be necessary to have buccal undercuts added. Usually, 4 points of retention on the arch is sufficient. Points of retention are commonly placed at the first bicuspids and first molars. You can do this free-hand by building up composite ledges to replicate buccal bulges at the mid-cervical of the teeth.
Another option is to bond a pre-form wedge like the wedges used with invisible aligners. Note: Figure 1 shows wedges placed for alignment. To use this concept for retention, the locking ledge is placed cervically on posteriors to allow for the appliance to snap over. You may decide to soften the severity of the edges based on trial fitting.
My preferred product has always been bondable Crown Contour Attachments from TruTain (Figure 2). These are clear, pre-formed buccal bulges that you can bond in place via light cure. They have a small handle on them that once bonded in place can be twisted off and discarded. Super easy and fast.

Laura Sheppard BS, CDT, TE, is a practicing 40 year board-certified dental laboratory technician with her AAS in Dental Technology and BS in Education for Allied Health. Named to the ‘Top 25 Women in Dentistry’ roster by Dental Products Report, Laura has been nationally recognized and published as an expert and educator in the development and implementation of Dental Sleep Medicine and Quality Systems since 1993. As the design collaborator for DSG APM Positioner™ and DSG Remed-eze™, inventor for DSG Relaxer™, and co-inventor of MicrO2™ aka ProSomnus® AI, Laura’s expertise and contributions in dental sleep device invention, design, manufacturing, and regulatory compliance has been utilized to the success of many of today’s advanced sleep devices.
by Melissa Mugno, OMT, RDH
In the ever-evolving landscape of dentistry, particularly within the realm of sleep dentistry, the integration of myofunctional therapy (MFT) stands out as a transformative approach. As a passionate myofunctional therapist, my mission is to simplify the complexities of treatment planning for dental professionals while enhancing patient outcomes. The essence of my work lies in addressing critical aspects of oral health, such as breathing patterns, tongue posture, and oral habits – elements that profoundly impact the efficacy of dental treatments.
While many dental professionals are familiar with the fundamental principles of MFT, it is vital to remember its profound implications on overall dental health. At its core, MFT focuses on correcting improper oral and facial muscle function. This involves not only recognizing but addressing soft tissue dysfunction, which can significantly affect a patient’s ability to breathe and adapt to dental appliances.
Breathing is a foundational aspect of life, yet many patients struggle with dysfunctional breathing patterns. This struggle can lead to inadequate oxygenation during dental procedures, discomfort with appliances, and even long-term health complications. By incorporating myofunctional therapy into treatment

plans, we can help patients breathe easier, tolerate appliances more comfortably, and improve overall compliance.
One of the most powerful tools in my toolkit is the ability to identify and address hidden pain points – those “unseen rocks” that can disrupt progress for both dentists and patients. Early in my career, I realized that effective problem-solving begins with understanding these challenges.
For Dentists: These pain points might include managing patient anxiety, appliance intolerance, or inefficient treatment processes. For example, I worked with a dentist who struggled with high cancellation rates due to anxious patients. By introducing nasal breathing techniques, we were able to create a more calming experience.
Contrary to popular belief, just because someone is alive doesn’t mean they’re breathing well. Many patients needing large restorative treatment plans suffer from myofunctional disorders and poor breathing habits. Overbreathing (hyperventilation) can exacerbate feelings of anxiety and racing thoughts. Through Myofunctional Therapy (MFT), we can teach simple, effective techniques that patients can use to experience immediate results. These techniques not only help patients feel calmer during appointments but also lead to improved attendance and a more positive experience for both the dentist and the patient.
For Patients: Pain points often center on discomfort, frustration with lengthy treatment timelines, or confusion about their oral health needs. One patient I worked with experienced fatigue and jaw pain during orthodontic treatment, which led to frustration and a lack of compliance. Through MFT exercises focused on tongue posture and swallowing patterns,
we addressed the root causes of their discomfort. Over time, these exercises reduced their pain, increased their energy levels, and re-engaged them in the treatment process.
Patient X, a 64-year-old woman, presented to her dentist with significant clenching and grinding issues. Her dentist recommended an appliance to address these concerns, but she struggled to tolerate it. Frustrated and convinced that the appliance was a profit-driven suggestion, she almost left the practice. This is a common scenario where patients, seeking someone to blame, often direct their frustration at the provider.
The dentist, who I was working to onboard with MFT, mentioned this case to me. I suggested that I try some therapy with her to help her become more comfortable with the appliance and, more importantly, to build her awareness of why and how she had developed these habits in the first place.
Step
I spent time getting to know her and understanding her frustrations. This trust-building phase is something many busy practices simply don’t have the time to offer, but it’s a critical step in creating buy-in for treatment.
We started slowly with a soft chewing device called the Myo Munchee. This served two purposes:
1. It helped her grow more comfortable with the sensation of having something in her mouth.
2. The bristles on the appliance desensitized the soft tissue around her cheeks and began the process of acclimating her to chewing and swallowing with the appliance.
Breathing, chewing, and swallowing might seem automatic, but for many patients, they are surprisingly challenging and need to be retrained.
After a few weeks, we incorporated exercises to engage her tongue and soft palate, like humming while chewing. These exercises gave her a sense of control and started building strength in her soft palate.

Six weeks into therapy, she began asking questions and noticing things about her own anatomy – such as her tight frenum and how much she relied on her neck muscles to compensate for her tongue’s limited mobility. This growing awareness helped her connect the dots and engage more fully in her treatment journey.
After successfully tolerating her appliance, Patient X decided to continue treatment and took further steps by opting for a tongue-tie release. Recognizing the benefits of a more functional approach, she also began adult expansion therapy to address her airway and overall oral structure.
This case highlights how MFT can serve as a powerful ally for both dentists and patients. I like to think of us as AIRWAY Traffic Controllers – we aim to ensure clear communication and help navigate tough obstacles, making the path to better oral and overall health as smooth as possible. By addressing the root causes, fostering trust, and empowering patients, we create outcomes that benefit everyone involved.

Melissa Mugno is a pioneer within the modern Myofunctional Movement. Since becoming an Orofacial Myofunctional Therapist in 2014, she has improved the lives of hundreds of patients, lectured around the country, and raised the standards of the profession. Her background as a Dental Hygienist and experience in the fields of Orthodontics and Pedodontics contributes to her success. Melissa treats patients of all ages suffering from wide range of conditions stemming from adverse myofunctional habits. She now resides in Las Vegas where she enjoys being with her family, cooking and being involved in her community. Melissa is part of the Smart Mouth team and is also a Breathe Associate at the Breathe Institute in Los Angeles with Dr. Zaghi, MD ENT.
by Steve Lamberg, DDS
“Beyond frustrated” is a common refrain from dentists beginning their journey into sleep medicine. The importance of building dental sleep medicine into their practices appears yoked to a host of insurmountable obstacles that include: where to get quality education, how to train the staff, how to market the addition of wellness to existing and new patients, how to manage medical insurance and billing, and how to get accepted into the medical community in your area to achieve a necessary team of specialists. Many become discouraged quickly and abandon this path forward to provide these most important services. Creating solutions to the many obstacles led to the creation of the Pediatric and Adult Airway Network of New York, affectionately known as PAANNY.
What is PAANNY and how does it respond to the problems at hand? First and foremost, it is an educational forum and recognizes that we cannot advance our patient care without sharing information across the many silos of healthcare. Bringing together speakers from every field of medicine and dentistry and allied health fields that relate to airway and sleep issues provides a solid foundation for building teams of like-minded individuals. We all share the recognition that networking leads to optimal patient care – an idea proven to be sustainable. This May will mark our 9th annual event in New York. We quickly realized that networking should be geographically oriented. There’s no point in connecting with specialists in faraway states

Dr. Steve Lamberg has been practicing comprehensive restorative dentistry in Northport, NY for 40 years. Always passionate about sleep and wellness, he became a Diplomate of the American Board of Dental Sleep Medicine in 2011 and has served on their board review faculty. He holds several patents, and is the inventor of the Lamberg SleepWell Appliance, which is FDA-cleared for the treatment of OSA. Dr. Lamberg also launched and serves as the director of the Pediatric and Adult Airway Network of New York (PAANNY), to provide a local platform where dentists, physicians, orofacial myologists, and other related professionals learn and collaborate on treatment patients of all ages. Additionally, Dr. Lamberg serves as a Scientific Advisor at the Kois Center in Seattle and teaches a course there titled Restorative Dentistry for the Airway Compromised Patient. His recently published book for the general public, “Treat the Cause…Treat the Airway” correlates many common medical conditions to airway and sleep and is available on Amazon.

you cannot share patient care with. The best way to overcome the initiating problems of dental sleep medicine in any practice is to have a PAAN(NY) in your practical referring distance area.
This year the title of the program is Unreasonable Dip and Bounce. This headline draws from three popular books. The first being Unreasonable Hospitality, written by Will Guidara of Eleven Madison Park fame, and expresses the pressing energy to give people more than they expect. The Dip is from Seth Godin’s book by the same name and refers to overcoming the normal setbacks to achieve your goals. Finally Bounce, by Mathew Syed, refers to finding confidence and provoking the positive to become a champion at anything. These three words embody the qualities of our membership.
Perhaps getting this type of organization going in your area seems daunting. A Brazilian friend taught me long ago that you can either “Learn through your head or learn through your feet”. We learned through our feet, and it was lots of hard work to figure out how to keep everyone satisfied with the annual symposium. There’s no need for you to employ the trial and error we went through, as you can learn through your head. We can help you get started with a proven formula that will bring everyone together. Consider joining us on May 1 and May 2 to see what we have created and copy and paste our recipe in your neighborhood. It’s hard to imagine dental sleep medicine success without a group like PAANNY in your area. It literally checks all the boxes to help you overcome the most common obstacles.
As the politics of medicine and insurance companies have created a Dip to overcome, now is our time to Bounce. Going beyond patients’ expectations creates good energy and everyone benefits. For more information on the program this Spring, please visit PAANNY.org.
Delivering successful oral appliance therapy (OAT) for obstructive sleep apnea (OSA) starts with a diagnosis and a referral from a sleep physician. Yet, many dentists report that their patients are steered toward CPAP therapy or even referred to another local dentist for OAT.
Often, this happens because sleep physicians are unsure about the reliability of oral appliance therapy or question the dentist’s ability to deliver appliances that meet the patient’s needs.
But what if there was a solution that could simplify the process, build trust with sleep physicians, and deliver unmatched patient experience?
BioMatch by Panthera Dental is changing that narrative. With its streamlined Single-Step ordering and design process, patient records are easily submitted directly from the intraoral scanner. Then, without any additional steps required, Panthera Dental’s design team using purpose-built design software and 4.0 Smart manufacturing, engineer an appliance that is specifically matched to the patient’s unique anatomy.
The appliance is designed to mitigate the risk of known OAT side effects such as occlusal changes like overjet, overbite, diastema and open contacts. Panthera Dental’s proprietary design software suggests to the technician a vast range of over 350 design combinations, allowing the delivery of a fully optimized patient matched drop-in fit appliance in just 10 days.
BioMatch ensures every appliance is delivered on time, is perfectly matched to the patient’s unique anatomy, and fits with minimal chairside adjustments. This builds confidence, for patients, sleep physicians, and your dental team. Backed by its 360 Device Warranty, which ensures Panthera Dental will replace any device free of charge, no questions asked for 36 months, your peace of mind is guaranteed.
Is BioMatch Reliable?
Reliability is the cornerstone of BioMatch. Panthera Dental’s 4.0 Smart Manufacturing integrates automation, robotics, M2M communication*, 3D printing and purpose-built design software into its proprietary tech stack. This

streamlines processes and delivers a drop-in fit appliance that fits with a minimum of adjustments.
Each appliance is manufactured using biocompatible PA2200 nylon, a durable medical-grade material that ensures patient safety and long-term usability.
The automated and interconnected processes allow Panthera Dental to mass customize appliances with unmatched consistency and quality.
Our 8-day design and manufacturing commitment ensures that appliances are in your office in just 10 days from scan to delivery, so you can treat your patients without delay and with total confidence.
Panthera Dental understands the challenges dentists face when incorporating sleep treatments into their practice. BioMatch is a comprehensive, dentist-friendly solution designed to:
• Streamline Your Workflow: With just a Single-Step, BioMatch eliminates complexities, making the ordering and design process easy and intuitive.
• Save Chair Time: Deliver appliances matched to your patient’s unique anatomy, with a drop-in fit that requires minimal adjustments, letting you focus on patient care.
• Build Referrals: Strengthen your relationships with local sleep physicians by providing them with reliable, effective OAT solutions that maximize patient experience.
• Enhance Patient Experience: BioMatch appliances are designed for comfort and mitigating risk of side effects, improving patient outcomes.
To learn more, contact Panthera Dental at www.pantheradental.com or info@panthera dental.com.
*Youssef Abdelmajied, F. (2022). Industry 4.0 and Its Implications: Concept, Opportunities, and Future Directions. IntechOpen. doi: 10.5772/intechopen.10252

For the solution, visit www.dentalsleeppractice.com. Theme: This Issue 0 of 6 theme words found. E H T A R B A I A N P E I N E T M E R A P E L R A N E R E E M S I C T A A T N E L P P L A R O T










