Dr. Sarah Balaster discusses solutions that support patients' oral health and quality of life
Requisites for success in dental implantology — not just slinging titanium
Dr. Sean Lan
Timing, precision, and success: technique choices for implant placement
Dr. Jaclyn A. Tomsic
Sepsis is serious — recognize the signs
Dr. Stuart L. Segelnick
Winter 2024 n Volume 17 Number 4
Editorial Advisors
Jeffrey Ganeles, DMD, FACD
Gregori M. Kurtzman, DDS
Jonathan Lack, DDS, CertPerio, FCDS
Samuel Lee, DDS, DMSc
David Little, DDS
Brian McGue, DDS
Ara Nazarian, DDS
Jay B. Reznick, DMD, MD
Steven Vorholt, DDS, FAAID, DABOI
Brian T. Young, DDS, MS
CE Quality Assurance Board
Bradford N. Edgren, DDS, MS, FACD
Fred Stewart Feld, DMD
Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, FADI, DICOI, DADIA
Justin D. Moody, DDS, DABOI, DICOI
Lisa Moler (Publisher)
Mali Schantz-Feld, MA, CDE (Managing Editor)
Differentiate your practice
The dental implant market has exploded across the United States, and many dentists want to jump on this trend due to its ability to quickly improve patients’ lives, the relative ease of the procedure, and the potential for significant profit. However, this rise in popularity has also created what many refer to as “the race to the bottom.” Dental offices and DSOs are drastically cutting the price of this procedure to attract patients, while larger offices with high marketing budgets are overshadowing smaller practices. As dentists, we believe the quality of care should shine through all the marketing. Unfortunately, many patients are price shopping because they don’t understand the difference between a provider who has placed 100 implants and one who has placed 10,000. So, how do smaller private practices survive and compete in this climate?
I have worked in over 15 practices that place a large number of dental implants. The practices that struggle to get by tend to lower their prices to rock-bottom levels, lack the right team members, and have poor office culture. On the other hand, successful offices have strong cultures and amazing teams, which translate to exceptional patient experiences.
including but not limited to: print and digital distribution by mail, email, and website for industry tradeshows, educational events, including nonpaid bulk copies and/or digital access provided to events, clients and educational institutions.
ISSN number 2372-6245
The patient experience plays a pivotal role in case acceptance, internal referrals, and overall patient satisfaction. This experience begins with the very first staff member to contact the implant lead through the customer relationship management (CRM) software. Often overlooked, the appointment setter is the first point of connection with the patient and, in my opinion, the most important. Saying the wrong thing or coming across as rude or uneducated, can cause the patient to look elsewhere. With marketing for dental implants becoming increasingly expensive, every mistake at the start of the process becomes even more costly further down the funnel.
Once the patients arrive at the office, the treatment coordinator takes over their care. Many offices fail to recognize the importance of this role. The treatment coordinator needs to be a true salesperson. While we, as dentists, know the best treatment for the patient, someone needs to communicate the value of the treatment and “sell” it effectively. The ideal candidate for this position has a background in sales, the ability to connect with patients, and genuine empathy. Trust in the treatment coordinator, the office, and the dentist makes patients feel comfortable and confident in their decision to move forward with treatment. Full-arch dentistry is expensive, with treatment plans ranging from $20,000 to $50,000. The treatment coordinator also assists patients in financing their treatment, if necessary.
There are many ways to differentiate your office in the competitive implant market. Many patients shop around, searching for the lowest price. By starting with the right appointment setter, you can ensure that your marketing dollars are working to deliver the best return on investment. A skilled treatment coordinator who can connect with patients and close sales will keep your schedule full, allowing you to create new smiles and happy patients.
Drew Phillips, DMD, grew up outside of Atlanta, Georgia, and chose to attend Rollins College in Florida. He graduated with a bachelor’s degree in health communications, and was twice elected captain of their nationally ranked water ski team and recognized as student athlete of the year. He then entered the Dental College of Georgia where he obtained his Doctor of Dental Medicine and graduated as valedictorian. Dr. Phillips completed a General Practice Residency at the Salt Lake City Veterans Affairs Hospital in order to advance his knowledge of complex treatment plans, implants, and sedation dentistry. Dr. Phillips has completed more than 1,000 full arch cases. He is currently licensed in five states and often travels to California and Oregon to assist, perform, and teach other dentists in these advanced procedures.
Disrupting dental care
Dr. Sarah Balaster discusses solutions that support patients’ oral health and quality of life
Cover image of Dr. Sarah Balaster courtesy of Millenium Dental and K Pharmaceuticals.
Dr. Stuart L. Segelnick describes
5
Matt
Gary
How to submit an article to Implant Practice US
Implant Practice US is a peer-reviewed, quarterly publication containing articles by leading authors from around the world. Implant Practice US is designed to be read by specialists in Periodontics, Oral Surgery, and Prosthodontics.
Submitting articles
Implant Practice US requires original, unpublished article submissions on implant topics, multidisciplinary dentistry, clinical cases, practice management, technology, clinical updates, literature reviews, and continuing education.
Typically, clinical articles and case studies range between 1,500 and 2,400 words. Authors can include up to 15 illustrations. Manuscripts should be double-spaced, and all pages should be numbered. Implant Practice US reserves the right to edit articles for clarity and style as well as for the limitations of space available.
Articles are classified as either clinical, continuing education, technology, or research reports. Clinical articles and continuing education articles typically include case presentations, technique reports, or literature reviews on a clinical topic. Research reports state the problem and the objective, describe the materials and methods (so they can be duplicated and their validity judged), report the results accurately and concisely, provide discussion of the findings, and offer conclusions that can be drawn from the research. Under a separate heading, research reports provide a statement of the research’s clinical implications and relevance to implant dentistry. Continuing education articles also include three to four educational aims and objectives, a short “expected outcomes” paragraph, and a 10-question, multiple-choice quiz with the correct answers indicated. Questions and answers should be in the order of appearance in the text, and verbatim. Product trade names cited in the text must be accompanied by a generic term and include the manufacturer, city, and country in parentheses.
Additional items to include:
• Include full name, academic degrees, and institutional affiliations and locations
• If presented as part of a meeting, please state the name, date, and location of the meeting
• Sources of support in the form of grants, equipment, products, or drugs must be disclosed
• Full contact details for the corresponding author must be included
• Short author bio
• Author headshot
Pictures/images/tables
Illustrations should be clearly identified, numbered in sequential order, and accompanied by a caption. Digital images must be high resolution, 300 dpi minimum, and at least 90 mm wide. We can accept digital images in all image formats (preferring .tif or jpeg).
Ensure that each table is cited in the text. Number tables consecutively, and provide a brief title and caption (if appropriate) for each.
Disclosure of AI use
Authors must disclose any AI used in researching, writing, or creating their articles. This includes a language model, machine learning, or similar technologies to create or assist with this submission. If AI was used, please provide a description of the AI-generated content and the name, model or tool used, and manufacturer. If AI was used, please confirm that you take responsibility for the integrity of the content that you are submitting.
References
References must appear in the text as numbered superscripts (not footnotes) and should be listed at the end of the article in their order of appearance in the text. The majority of references should be less than 10 years old. Provide inclusive page numbers, volume and issue numbers, date of publication, and all authors’ names. References should be submitted in American Medical Association style. For example:
Journals: (Print)
White LW. Pearls from Dr. Larry White. Int J Orthod Milwaukee. 2016;27(1):7-8. (Online)
Or in the case of a book: Pedetta F. New Straight Wire. Quintessence Publishing; 2017.
Website:
Author or name of organization if no author is listed. Title or name of the organization if no title is provided. Name of website. URL. Accessed Month Day, Year. Example of Date: Accessed June 12, 2011.
Author’s name: (Single) (Multiple) Doe JF Doe JF, Roe JP
Permissions
Written permission must be obtained by the author for material that has been published in copyrighted material; this includes tables, figures, pictures, and quoted text that exceeds 150 words. Signed release forms are required for photographs of identifiable persons.
Disclosure of financial interest
Authors must disclose any financial interest they (or family members) have in products mentioned in their articles. They must also disclose any developmental or research relationships with companies that manufacture products by signing a “Conflict of Interest Declaration” form after their article is accepted. Any commercial or financial interest will be acknowledged in the article.
Manuscript review and extra issues
All clinical and continuing education manuscripts are peer-reviewed and accepted, accepted with modification, or rejected at the discretion of the editorial review board. Authors are responsible for meeting review board requirements for final approval and publication of manuscripts. If additional issues are desired, they must be ordered from the publisher when the page proofs are reviewed by the authors. The publisher does not stock back issues. Reprints can be purchased after the issue is published.
Proofing
Page proofs will be supplied to authors for corrections and/or final sign off. Changes should be limited to those that are essential for correctness and clarity.
Articles should be submitted to:
Mali Schantz-Feld, managing editor, at mali@medmarkmedia.com
Weathering the storms
Droughts, heat waves, rain, hurricanes, blizzards, tornadoes, wildfires, and earthquakes, or beautiful sunshine — no matter where you live in the U.S., the weather can bring you the bliss of sitting by the pool or bring you scurrying into the safest windowless room for cover. It’s not just the weather’s fluctuations that we need to prepare for — hoping for the best while preparing for the worst is the best way to avoid storms in all aspects of life. Our focus at MedMark publications is to help you be prepared to face all of the issues that may pop up in your practice, to give you better control over your business and clinical decisions, less stress, and more success.
Here are three tips on keeping your head above water, when you feel that flood of anxiety from practice stress.
Lisa Moler Founder/Publisher, MedMark Media
• Pinpoint your stressors: Define what in your practice is keeping you awake at night, and maybe even keep a journal of what is causing you stress at the end of each work day. Are you afraid that your computer systems aren’t secure from cyberattacks? Are you unsure that your equipment is providing the specific information you need to get the best diagnostics? Are you frustrated that you cannot offer the latest treatment opportunities? Before you can fix a problem, you have to be sure of what the problem actually is.
• Establish a practice culture: Make sure that your practice handbook specifically outlines what behaviors and attitudes are acceptable and which will not be tolerated. Have weekly or monthly team meetings to make sure everyone is on the same page. To head off problems before they grow, learn about conflict resolution skills or hiring-and-firing protocols. If you have an office manager, remember to include him/her in these learning opportunities, and make sure your team knows that you are available for the more complicated situations.
• Give yourself the edge over the competition: It is stressful to watch potential patients filling up other dentists’ appointment calendars. In this day of the Internet and technology, you need to reassess your equipment to improve efficiency, accuracy, and increase patient care and options. Especially in this age of social media, you want your patients to see that you, rather than the clinician across the street, have the most up-to-date imaging, more painless protocols, or faster treatment options.
MedMark publications can help you discover what innovations have been developed and how they pertain to your specialty. In our “double feature” Cover Story, Dr. Sarah Balaster talks about addressing complications of implants with the PerioLase® MVP-7™ laser, as well as how to deliver relief of xerostomia with Aquoral lipid-based dry mouth solution. Our CE by Dr. Sean Lan offers information to mitigate difficult implant situations. In her CE, Dr. Jaclyn A. Tomsic writes about the staging protocols of implant surgery as well as the pros and cons of free-hand versus guided implant surgery. Dr. Stuart L. Segelnick describes the warning signs of sepsis and how a timely response may save lives.
In this last issue of 2024, we give you our “umbrella wish” for fair weather, a dedicated and efficient team, a growing loyal patient list, less stress, and more fulfillment of your goals in the coming year.
Remember, every storm passes, and you need to be prepared to make intentional, positive decisions for a stronger and more profitable future.
To your best success, Lisa Moler
Published by
Publisher Lisa Moler lmoler@medmarkmedia.com
Managing Editor
Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com Tel: (727) 515-5118
National Account Manager Adrienne Good agood@medmarkmedia.com Tel: (623) 340-4373
–Dr. Joseph Baptist Oral and Maxillofacial Surgeon Cameo Dental Specialists, Chicago, IL while the doctor partner community provides invaluable resources and camaraderie.”
Empower Your Practice. Elevate Your Care.
We’re proud to champion Dr. Baptist and the 300+ elite dental specialists who have partnered with us to strengthen and enhance their practices. Since 2018, our business experts have been providing customized solutions to help our partners build a robust financial legacy and deliver exceptional patient care. Find out how our powerhouse team of oral and maxillofacial surgeons, endodontists, and periodontists work together to champion your long-term prosperity. specializeddental.com
Disrupting dental care
Dr. Sarah Balaster discusses solutions that support patients’ oral health and quality of life
As the prevalence of dental implants continues to rise, so too does the occurrence of complications such as peri-implant mucositis and peri-implantitis. Addressing these challenges requires patient-focused, innovative solutions. Laser-assisted protocols, such as LANAP® (Laser-Assisted New Attachment Procedure) and LAPIP™ (Laser-Assisted Peri-Implantitis Protocol), provide minimally invasive, effective treatments to reverse peri-implant disease and periodontal conditions. By integrating these advanced techniques, dental professionals can not only treat ailing and failing implants but also differentiate their practices in a competitive market by offering high-quality care that supports long-term implant success.
Laser precision: elevating implantology with minimally invasive technology
More than 3 million Americans currently have dental implants, and that number is growing by approximately 500,000 each year.1 However, this growth is accompanied by a corresponding increase in complications, such as peri-implant mucositis and peri-implantitis. Notably, 80% of patients and 50% of implants will develop peri-implant mucositis, while up to 56% of patients and 43% of implants will experience peri-implantitis.2 This growing issue underscores the urgent need for patient-focused solutions and advanced protocols that not only address these complications but also establish a foundation for long-term success in dental implant cases.
Advanced techniques such as laser-assisted protocols like LANAP®, a patented method for treating periodontal disease (Figure 1) and LAPIP™, which adapts LANAP techniques to address peri-implantitis (Figure 2), offer minimally invasive solutions to reverse these conditions and improve patient outcomes. By integrating these innovative protocols, dental professionals can
Sarah Balaster, DMD, received her Doctor of Dental Medicine from Rutgers School of Dental Medicine and earned her certificate in Periodontics from the New York University College of Dentistry. Prior to that, she attained a Bachelor’s of Arts with honors in Fine Arts from Wesleyan University in Connecticut. Her background in both the visual arts and sciences enables her to work with patients to achieve both an esthetic and healthy smile. She strives to treat patients with minimally invasive surgical therapies, such as LANAP (laser periodontal therapy), minimally invasive gum grafting, and laser-assisted dental implant placement. She has advanced training in and is an instructor of laser dentistry. She has also worked on the development and application of soft tissue (gum) grafting techniques to improve esthetics, function, and patient comfort. She is a member of the American Academy of Periodontics, Northeast Society of Periodontics, Southern Academy of Periodontics, American Dental Association, and the Institute for Advanced Laser Dentistry.
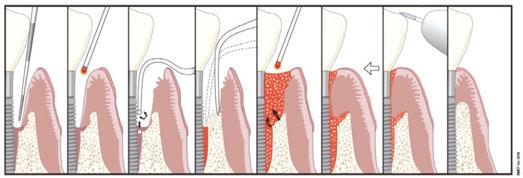
Figure 1: With the LAPIP protocol, laser energy vaporizes bacteria, diseased tissue, and contaminants in soft tissue. A stable fibrin blood clot containing stem cells and growth factors is formed, and new bone is regenerated. Reproduced with permission of Millennium Dental Technologies. Inc., Cerritos, California
effectively treat ailing and failing implants, reverse periodontal disease, and advance the standard of care with patient-friendly and minimally invasive surgery.
The power of protocols
The patented LANAP and LAPIP protocols were developed to provide effective treatment options for periodontal disease and peri-implant disease, respectively. To optimize these innovative techniques, the PerioLase® MVP-7™ laser (Millennium Dental Technologies, Inc., Cerritos, California) was specifically designed
Dr. Sarah Balaster with her three PerioLase lasers and Aquoral spray
to execute these protocols. A 1064-nm Nd:YAG free-running pulse laser, the PerioLase MVP-7 incorporates unique parameters, features, and safety measures for dental professionals to take control over debilitating diseases in their practices.
The LANAP protocol is FDA-cleared for true regeneration of bone, cementum, and periodontal ligament (PDL) on previously diseased root surfaces. Human histology studies have demonstrated remarkable regeneration of these critical structures, showcasing the protocol’s effectiveness in restoring oral health,3,4 even around multi-rooted teeth.
While selectively targeting diseased tissue and preserving healthy structures, the LANAP protocol regenerates bone without the use of additional biologics such as bone grafts or membranes. It is also capable of significantly reducing bacterial load; one study demonstrated 85% of LANAP-treatment patients were culture-negative for orange and red complex bacterial species immediately posttreatment, compared with 83.3% positivity in patients subjected to traditional ultrasonic root debridement only.5
Much like how the LANAP procedure is tailored to treat periodontal disease, the LAPIP protocol is specifically designed for reversing peri-implantitis. Both protocols utilize the same advanced laser technology, allowing for effective decontamination of the implant surface and targeted treatment of infections while minimizing patient discomfort. In a retrospective study involving 249 implants in 138 patients diagnosed with peri-implantitis, the LAPIP protocol demonstrated an impressive 94% survival rate at a median follow-up time of 13.1 months, offering a minimally invasive solution for common complications associated with dental implants.6
Why address periodontal disease in implant patients?
Treating periodontal disease prior to implant placement is crucial for achieving comprehensive oral care. A healthy periodontal foundation is vital for successful implant outcomes,7 and laser technology plays a key role in addressing this often-overlooked aspect of treatment. By incorporating the concepts of LANAP and LAPIP into practice, we can enhance disease management, improve patient satisfaction, and foster better overall oral health. Additionally, LAPIP treatment provides a minimally invasive solution for reversing the ever growing number of ailing and failing implants. The versatility of the PerioLase MVP-7 extends beyond periodontal treatment and peri-implantitis. With adjustable presets, this laser can address a variety of clinical needs, from extractions and hemostasis to implant surface decontamination and maintenance. For instance, laser pocket disinfection post-implant placement can reduce bacterial presence and be incorporated into implant maintenance routines. The BLAST™ protocol, another application of the PerioLase MVP-7, targets foreign body reactions and decontaminates implants and extraction sites, optimizing conditions for osseointegration. By utilizing laser technologies throughout the implant process — from extraction to maintenance — dental practices can reduce the need for biologics, control overhead costs, and improve clinical outcomes.
is scientifically and clinically proven to save ailing and failing implants.
Leading the future of implantology
Integrating laser-assisted protocols like LANAP, LAPIP, and BLAST not only improves patient care but can also position a practice at the forefront of dental implantology. These innovative approaches lead to satisfactory clinical outcomes and can transform patient experiences, resulting in higher acceptance rates. A recent survey of LANAP clinicians revealed that 90.7%
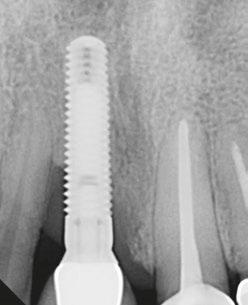
Figures 2A and 2B: 2A. Preoperative X-ray. 2B. Postoperative X-ray at 12 months. The LAPIP protocol is a tissue-sparing, non-destructive treatment that
Case courtesy of Larry Finkbeiner, DDS. Reproduced with permission
2A.
2B.
Figure 3: The PerioLase MVP-7 is a free-running pulsed Nd:YAG laser with exclusive protocols to treat periodontal disease, peri-implantitis, and other conditions
Figures 4 and 5: LANAP procedure
of patients are more willing to accept LANAP treatment than traditional osseous/GTR/GBR surgery.8 By embracing these minimally invasive, laser-assisted techniques, dental professionals have a unique opportunity to provide value-added dental care and deliver personalized treatment. In today’s competitive landscape, distinguishing one’s practice relies on providing advanced, patient-centered care, and laser-assisted protocols are essential for achieving implant success and overall oral health management.
Aquoral at the forefront: breaking the mold of dental commodification with value-based care
In the rapidly evolving landscape of dentistry, commodification presents a formidable challenge for dental implant practitioners. As we witness an increasing focus on affordability and transactional models, many providers find themselves caught in a race to the bottom. Patients are often led to view their care solely through the lens of cost — measuring services based on the price of an implant rather than recognizing the profound impact of regaining a healthy smile and the ability to chew. This mindset diminishes the quality of care, reducing complex treatments to mere transactions and neglecting the holistic aspects of patient health.
So, how do we rise above this trend as providers? By embracing value-based care. This approach prioritizes patient-centric care and health outcomes over the mere provision of services. It’s about addressing the whole patient — identifying unmet
needs and enhancing outcomes that truly matter. By advocating for holistic care, we can transcend the commoditized nature of today’s dental marketplace and empower our patients to see the true value in their oral health journey.
Delivering long-lasting relief while transforming the dry mouth treatment landscape
Addressing dry mouth, or xerostomia, is crucial for enhancing patient care and outcomes. This often-overlooked condition profoundly affects overall health and can lead to significant complications if left untreated. Patients suffering from severe dry mouth are not merely uncomfortable; they face increased risks of choking, oral sores, and even life-threatening conditions in severe cases. Moderate xerostomia can escalate the likelihood of tooth decay, gum disease, cavities, and altered taste, while also contributing to tooth sensitivity and the demineralization of enamel.9 The implications go beyond oral health, as xerostomia can impact nutrition and lead to a reduced quality of life. Patients often report dissatisfaction with removable dentures, experience tissue friction and sticking with full-arch or large fixed implant-supported restorations, and suffer from increased soreness in denture-bearing tissues.10-12
Understanding the multifaceted nature of dry mouth is essential for dental professionals. It can arise from a range of factors, including medications, underlying health issues, and stress. As we strive to offer holistic care, addressing dry mouth is not just an add-on to our treatments; it’s a vital component of patient-centered care. By proactively identifying and managing xerostomia, we can improve patient satisfaction, enhance treatment outcomes, and ultimately restore the quality of life that our patients deserve. This commitment to comprehensive care underscores our role as advocates for our patients’ health and well-being, moving beyond the transactional model to a more integrated approach that truly values the patient experience.
While head and neck cancer patients and those with Sjögren’s syndrome are commonly recognized as affected demographics, they are not the only individuals struggling with dry mouth. Xerostomia is a widespread condition, impacting nearly one in four adults in the United States, yet it often goes undiagnosed or untreated in our practices.
Certain groups are particularly affected, including patients on polypharmacy and those using CPAP machines for sleep apnea. Common causes of dry mouth include medication side effects, autoimmune disorders, radiation therapy, recreational marijuana use, and CPAP usage. It is estimated that xerostomia affects approximately 22% of adults in the U.S., with higher rates among older populations and CPAP users.13 The prevalence of dry mouth increases significantly with the number of medications taken; only 17% of individuals not on medication report experiencing dry mouth, while this rises to 33.5% for those on three medications and reaches 67% for individuals taking seven or more.14 With about 60% of U.S. adults taking at least one prescription medication and roughly a quarter on four or more, the likelihood of xerostomia increases, particularly among those managing chronic conditions like hypertension and diabetes.15
Approximately 33 million adults in the U.S. use CPAP machines16, and studies found 45% of these users experience dry
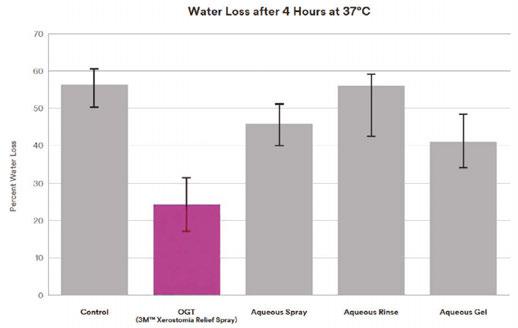
Figure 6: Water loss. Note: *Aquoral was previously released under the name 3M Xerostomia Relief Spray
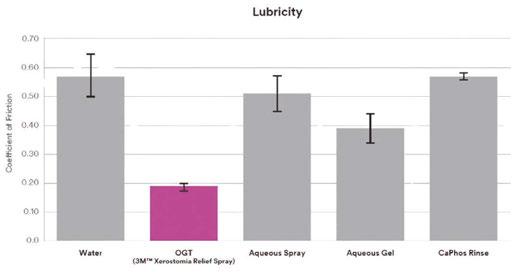
Figure 7: Lubricity
mouth17, often leading to appliance discontinuation due to discomfort. By recognizing the significant impact of xerostomia and addressing it with comprehensive care, we can provide immense value to our patients and differentiate ourselves as healthcare providers.
Despite the high prevalence of dry mouth, both patients and providers often believe that limited treatment options are available. Many practitioners rely on over-the-counter (OTC) waterbased solutions, which provide only temporary relief and require frequent reapplication, especially after eating or drinking. Conversely, prescription medications like pilocarpine offer a more potent solution but come with systemic side effects, limiting their use for many patients. This gap in effective treatment options has left both providers and patients frustrated, with few solutions that can deliver long-lasting relief without complications.
Enter Aquoral, a groundbreaking lipid-based dry mouth solution that addresses the shortcomings of traditional treatments. Unlike water-based solutions that can wash away upon eating or drinking, Aquoral creates a protective lipid layer that provides sustained moisture for up to 6 hours (Figure 6). This innovative prescription-based lipid solution is designed to deliver lasting relief with its advanced Oxidized Glycerol Triester (OGT) technology, making it 4 times as effective in hydrating the tissues and 2 times as effective in maintaining the moisture as many overthe-counter alternatives. This compact and effective solution not only enhances patient comfort but also improves overall quality of life, particularly for CPAP users who suffer from dry mouth during sleep.
Integrating technologies like Aquoral into practice not only demonstrates a commitment to comprehensive patient care but also addresses a critical aspect of oral health that often goes unrecognized. For patients undergoing full-arch implant treatments, managing dry mouth is essential, as it directly impacts the comfort and success of their prostheses. Many mistakenly believe that discomfort from prosthetics sticking to dry tissues is just part of the experience; however, by screening for and bundling Aquoral with full-arch cases, we can enhance the overall patient experience, leading to greater comfort and fewer complaints — note Aquoral’s ability to reduce the coefficient of friction in Figure 7. Ultimately, Aquoral is more than a solution for dry mouth; it exemplifies how we, as dental professionals, can embrace value-based care. By recognizing and addressing hidden patient needs like xerostomia, we can transcend commoditization and provide meaningful, transformative care. Aquoral’s lipid-based technology elevates our treatment protocols, offering effective, long-lasting relief where traditional methods fall short.
Our primary goal in dental implantology has always been to restore function and esthetics with precision and care, but achieving excellence in patient outcomes requires us to consider the entire person and their overall well-being. By focusing on holistic care and addressing every facet of our patients’ needs, we enhance their quality of life. In conclusion, Aquoral presents an opportunity to elevate patient care and break free from the commoditized nature of dental services. By prioritizing valuebased care, we can meet unmet needs like dry mouth, provide innovative solutions that truly improve patient outcomes, and distinguish ourselves in a crowded marketplace. The future of
Learn more about integrating Aquoral into your practice.
aquoralspray.com
dental care is not just about delivering a service — it’s about enhancing lives, and by embracing this approach, we can ensure that our care is as impactful as it is effective.
REFERENCES
1. American Academy of Implant Dentistry. What are Dental Implants? https://aaid-implant.org/what-are-dental-implants/. Accessed October 16, 2014.
2. Zitzmann NU, Berglundh T. Definition and prevalence of peri-implant diseases. J Clin Periodontol. 2008 Sep;35(8 Suppl):286-291.
3. Nevins ML, Camelo M, Schupbach P, Kim SW, Kim DM, Nevins M. Human clinical and histologic evaluation of laser-assisted new attachment procedure. Int J Periodontics Restorative Dent. 2012 Oct;32(5):497-507.
4. Yukna RA, Carr RL, Evans GH. Histologic evaluation of an Nd:YAG laser-assisted new attachment procedure in humans. Int J Periodontics Restorative Dent. 2007 Dec;27(6):577-587.
5. McCawley TK, McCawley MN, Rams TE. Immediate Effects of Laser-Assisted New Attachment Procedure (LANAP) on Human Periodontitis Microbiota. J Int Acad Periodontol. 2018 Oct 1;20(4):163-171.
6. Schwarz GM, Harris DM. Laser-assisted treatment of peri-implantitis: a retrospective cohort study. Gen Dent. 2020 May-Jun;68(3):18-25.
7. Casado PL, Pereira MC, Duarte ME, Granjeiro JM. History of chronic periodontitis is a high risk indicator for peri-implant disease. Braz Dent J. 2013;24(2):136-141.
8. Richman C, Levine RA, Sullivan A, Jiang S, Farber A, Zalewsky J. Perceptions of the LANAP protocol. Decis Dent. 2020 Nov;6(10):18:21-23.
9. American Dental Association. Xerostomia (Dry Mouth. https://www.ada.org/resources/ ada-library/oral-health-topics/xerostomia. Updated April 24, 2023.
10. Chrcanovic, B. R., & Albrektsson, T. (2016). Patient-reported outcomes of implant-supported fixed prostheses: A systematic review. The International Journal of Oral & Maxillofacial Implants, 31(4), 1003-1014.
11. Zitzmann NU, Marinello CP. Patientenzufriedenheit mit abnehmbaren ImplantatRekonstruktionen im zahnlosen Unterkiefer [Patient satisfaction with removable implant-supported prostheses in the edentulous mandible]. Schweiz Monatsschr Zahnmed. 2006;116(3):237-244.
12. Schimmel, M., et al. (2013). The impact of oral health on quality of life in edentulous older adults: a systematic review. Gerodontology, 30(1), 33-40.
13. Fornari CB, Bergonci D, Stein CB, Agostini BA, Rigo L. Prevalence of xerostomia and its association with systemic diseases and medications in the elderly: a cross-sectional study. Sao Paulo Med J. 2021 Jul-Aug;139(4):380-387.
14. Dental, Oral and Craniofacial Data Resource Center. Oral Health U.S., Bethesda, Maryland. 2002 September:115-117 http://drc.hhs.gov/report/pdfs/section14-xerostomia.pdf.
15. Nederfors T, Isaksson R, Mörnstad H, Dahlöf C. Prevalence of perceived symptoms of dry mouth in an adult Swedish population--relation to age, sex and pharmacotherapy. Community Dent Oral Epidemiol. 1997 Jun;25(3):211-216.
16. Liu Y, Carlson SA, Wheaton AG, Greenlund KJ, Croft JB. Sleep Disorder Symptoms Among Adults in 8 States and the District of Columbia, 2017. Preventing Chronic Disease. Published Dec. 30, 2021. Available at https://www.cdc.gov/pcd/ issues/2021/21_0305.htm. Accessed October 23, 2024.
17. Pico-Orozco J, Carrasco-Llatas M, Silvestre FJ, Silvestre-Rangil J. Xerostomia in patients with sleep apnea-hypopnea syndrome: A prospective case-control study. J Clin Exp Dent. 2020 Aug 1;12(8):e708-e712.
Sepsis is serious — recognize the signs
Dr. Stuart L. Segelnick describes lifesaving
warning signs
Acall comes in from an emergency patient soon after you remove a hopelessly infected tooth. Her major concern is having a fever, chills, and feeling downright terrible. She has no difficulty breathing or swallowing, though her mouth still feels swollen. Grace is a middle-aged woman who suffers from diabetes and recently finished chemotherapy for breast cancer. She doesn’t smoke or drink alcohol. Also, she relates getting home too late to pick up the antibiotics that were prescribed. What should she do?
Grace was fortunate to have gone directly to the hospital emergency room and had a CT scan, which didn’t show anything unusual. However, sepsis was suspected, and IV antibiotics were administered. Feeling much better after a night of observation, Grace went home the very next day with a prescription for oral antibiotics.
Untreated or poorly managed periodontal disease, caries, and endodontic and dental alveolar lesions can lead to sepsis. Case reports have been published in dental literature highlighting the morbidity and mortality of dental disease complications. Although rarely reported, post tooth extractions have also been linked to sepsis.1 According to the Centers for Disease Control and Prevention (CDC)2 and the Mayo Clinic,3 bacterial infections are the leading cause of sepsis (viral and fungal infections have also been implicated). When these microbes overwhelm your immune system, your body fights back, causing overt damage to your organs, which may progress to septic shock with the accompanying free fall in blood pressure, organ dysfunction, and ultimate death.
The World Health Organization (WHO) realizes the severity of sepsis and reported that in 2017, sepsis accounted for 20% of all deaths globally. In America, the CDC reports that almost 2 million adults develop sepsis, and 350,000 “die during their hospitalization or are discharged to hospice.” A third of the peo-
Stuart L. Segelnick, DDS, MS, CDE, currently serves as editor of the New York State Dental Journal and the Northeastern Society of Periodontists Bulletin. He is a Diplomate of the American Board of Periodontology and International Congress of Oral Implantologists and President of the Northeastern Society of Periodontists. Dr. Segelnick is an adjunct clinical professor at NYU College of Dentistry Department of Periodontology and Implant Dentistry. He is a Certified Dental Editor (CDE), designated by the American Association of Dental Editors & Journalists. Dr. Segelnick has been recognized multiple times by the International College of Dentists and the American Dental Education Association Gies Foundation for his newsletter production and editorials. He has co-edited five books on dentistry and authored/co-authored multiple scientific articles. He is a fellow of the Pierre Fauchard Academy, the International College of Dentists, and the American College of Dentists. Dr. Segelnick has a private periodontal practice in Brooklyn, New York.
ple who died at the hospital had sepsis during their stay. Even more frightening is that “among adult sepsis survivors, one in three died within a year, and one in six experienced significant, long-term morbidity.”4
Higher risks of acquiring sepsis are found in older people (over 65 years) and children who are under a year old, as well as those inflicted with chronic medical problems, immunocompromised individuals, sepsis survivors, and people recently hospitalized and with severe sickness. Some of the signs and symptoms of sepsis include fever, chills, shivering, sweating, severe pain, fast heart rate, fatigue, hypotension, confusion, and altered mental state.
Tests that your patient’s physician or the hospital will perform if they are suspected of having sepsis include a physical exam, blood cultures, full blood work-up, X-rays, CT scans, and ultrasounds to aid in making a sepsis diagnosis.5 High temperature, elevated heart and respiratory rate, and high white blood cell counts are red flags for sepsis.
Sepsis is considered a medical emergency, and the most important thing you can do is recognize and treat it quickly. Treatment usually includes broad spectrum IV antibiotics, IV fluids, and vasopressors. Monitoring serial lactate measurements is also important. Hospitals must report cases of sepsis to the federal and state government.
According to Mannan, et al., “Early antimicrobial intervention is associated with surviving severe sepsis, making it critical for dentists to understand local factors leading to the crisis and the signs and symptoms of the sepsis-septic shock continuum.”6
In a paper by Sato, et al., the authors stated that “When an oral infection is suspected in an elderly patient, antibiotics should be quickly administered, the patient’s local and systemic state should be confirmed. ... If no improvement is observed, medical attention should be quickly sought.”7
Organizations such as END SEPSIS, the Legacy of Rory Staunton (endsepsis.org) and the Sepsis Alliance (sepsis.org) have accomplished amazing work in bringing awareness to the seriousness of
sepsis. END SEPSIS has been very successful in advocating for guidelines, regulations, and increasing awareness of sepsis.8 A recent New York Times article by Emily Baumgaertner9 tells how the CDC has developed new guidelines in helping recognize and reduce sepsis in hospitals. The article also highlights that, “In 2013, New York became the first state to mandate that all hospitals adopt sepsis protocols, known as “Rory’s regulations.” Rory Staunton was only 12 years old when he died from undiagnosed sepsis, and his parents started a foundation and the END SEPSIS organization. With these wonderful organizations helping to eradicate sepsis, the future looks promising, so much so that even AIs are now being used to detect sepsis!10
A month after my own gall bladder removal surgery, I had already returned to my office on a lighter schedule when I started feeling very fatigued and had pain in my right back flank. After 3 days of decline and pushing myself through the day, I noticed that my hands had started shaking at the end of a patient examination. At that point, I knew I couldn’t continue and had my receptionist cancel the rest of my appointments.
heart for delivery of IV antibiotics
Almost falling asleep at the wheel, I barely managed to drive home. Once home, I made my way to bed and fell right to sleep. At 1 a.m., I awoke bathed in sweat, simultaneously yet uncontrollably shivering and feeling downright awful. I knew something was dangerously wrong. I woke up my wife, and we headed to the hospital ER, where they immediately took my vitals. My blood pressure was extremely low, my heart rate was racing out of control, and my temperature was burning up at 103.3 F. The diagnosis was sepsis! After a CT scan of the abdomen and blood work, I was placed on IV antibiotics. I won’t go into the horrible details of 8 miserable days in the hospital and 4 weeks of IV antibiotics, which were delivered through a picc line (Figure 1) inserted into my arm. I thank G-d every day that I’m alive and able to go back to caring for my family, friends, staff, colleagues,
and patients and cherishing every moment I’m still in this beautiful world. It makes me wonder if I, as a healthcare professional, couldn’t make a timely diagnosis of my own sepsis setting in, how could the average person? Sepsis is a major life-threatening event that dentists must be aware of. Be prepared to advise your patients when sepsis is suspected to head to the hospital ER, because that timely response just might save their lives.
REFERENCES
1. Lee JJ, Hahn LJ, Kao TP, Liu CH, Cheng SJ, Cheng SL, Chang HH, Jeng JH, Kok SH. Post-tooth extraction sepsis without locoregional infection--a population-based study in Taiwan. Oral Dis. 2009 Nov;15(8):602-607.
2. Centers for Disease Control. What is Sepsis? https://www cdc.gov/sepsis/what-is-sepsis.html. Updated August 24, 2023, Accessed February 28, 2024.
3. Mayo Clinic. Sepsis. https://www.mayoclinic.org/diseasesconditions/sepsis/symptoms-causes/syc-20351214 Published February 20, 2023, Accessed February 28, 2024.
4. World Health Organization. Global Report on the Epidemiology and Burden of Sepsis. https://iris.who.int/bitstream/ handle/10665/334216/9789240010789-eng.pdf?sequence=1. Accessed February 28, 2024.
5. WebMD. Sepsis (Blood Infection): Symptoms and Treatment. https://www.webmd. com/a-to-z-guides/sepsis-septicemia-blood-infection. Reviewed February 1, 2024.
6. Mannan S, Tordik PA, Martinho FC, Chivian N, Hirschberg CS. Dental Abscess to Septic Shock: A Case Report and Literature Review. J Endod. 2021 Apr;47(4):663-670.
7. Sato H, Tamanoi T, Suzuki T, Moriyama H, Abe S, Yoshida K, Kawaai H, Yamazaki S. Risk Perception of Septic Shock with Multiple Organ Failure Due to Acute Exacerbation of an Infectious Dental Disease. Ther Clin Risk Manag. 2021 Apr 22;17:365-369.
8. End Sepsis. About End Sepsis. https://www. endsepsis.org/about/. Accessed February 28, 2024.
9. Baumgaertner E. C.D.C. Sets New Standards for Hospitals to Combat Sepsis. https:// www.nytimes. com/2023/08/24/health/sepsis-hospitals-cdc.html. Updated September 22, 2023.
10. Moor M, Bennett N, Plečko D, Horn M, Rieck B, Meinshausen N, Bühlmann P, Borgwardt K. Predicting sepsis using deep learning across international sites: a retrospective development and validation study. eClinicalMedicine Part of The Lancet. August 2023;62(102124) https://www.thelancet.com/journals/eclinm/article/ PIIS2589-5370(23)00301-2/fulltext. Accessed February 28, 2024.
This article was reprinted with permission from the Second District Dental Society of New York (SDDSNY) Bulletin.
Implant Practice US Webinars
LEARN about the lastest techniques and technology from industry leaders with our free live and archived educational webinars. Our online seminars are a convenient way to access great information and upskill. Check out our most recent webinar:
• Full Arch and Remote Anchorage Implant Complications with hosts Drs. Justin Moody and Dan Holtzclaw
WATCH NOW at https://implantpracticeus.com/webinars/
Figure 1: PICC line removed after 4 weeks, which went from the inner arm through the brachial vein towards the
The psychology of patient decisionmaking in full-arch dentistry
Joanne Villani, RDH,
discusses motivators for case acceptance
In full-arch dentistry, where treatments like implant-retained dentures (AOX) carry significant costs, understanding patient psychology is vital. These treatments represent more than clinical solutions — they’re transformative investments in self-confidence, emotional well-being, and quality of life. Therefore, addressing emotional motivators as well as psychological barriers, particularly through visualization, is essential to gaining case acceptance.
Patients buy smiles, not teeth
Dan Ariely, a behavioral researcher, explains in his book Predictably Irrational that emotions often lead people to overvalue outcomes that meet psychological needs, a concept relevant in healthcare and esthetic treatments, where patients equate procedures with enhanced self-esteem and quality of life.
Overcoming hesitation over cost
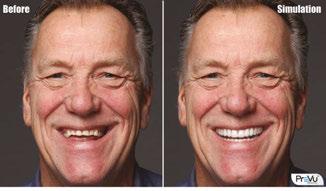
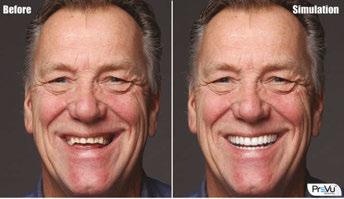
“Patients need to see the transformation before they can believe in it,” explains Dr. Christian Yaste, author of the book A Smile Where There Was None: A Practical Approach to Fixed Full-Arch Implant Dentistry. “Digital tools like PreVu® help patients envision their future. Being able to present a smile preview is an essential part of the consultation process.”
Figures 1A-1B: PreVu digital smile simulation highlighting the esthetic benefits of treatment
Research from Psychology Today underscores the powerful impact of visuals in decision-making, highlighting that imagery capable of evoking strong emotional responses can dramatically increase the likelihood of a positive decision. This is particularly relevant in contexts where individuals struggle to fully envision outcomes, such as transformative dental treatments. Visuals serve as a bridge between abstract possibilities and tangible realities. Visuals not only clarify complex information but also inspire patients to take action with greater confidence and conviction.
Digital smile simulations
In full-arch dentistry, the promise of a functional beautiful smile — and the confidence, freedom, and improved social interactions it brings — can become the driving force behind case acceptance. However, many patients hesitate because they cannot fully imagine how transformative the results will be or how dramatically their appearance could change.
This gap in imagination is where digital smile simulations become invaluable.
Simulations allow patients to visualize their transformation and connect with the life-changing potential of treatment. Visualizing their potential transformation often triggers the “yes” moment.
Joanne Villani, RDH, co-founder of PreVu Software, has over 35 years of dental expertise, including leadership roles in sales and marketing. She is dedicated to helping dental practices grow by increasing case acceptance for cosmetic, restorative, and reconstructive treatments, driven by her belief that everyone deserves a smile they feel confident about. Learn more at prevudental.com.
Simulations help patients shift their focus from cost to the emotional and esthetic benefits, which are often the most compelling factors in their decision. Without this visual aid, patients may struggle to appreciate the life-changing potential of full-arch rehabilitation, leaving them to decline or delay treatment.
A competitive edge
In a competitive market, where patients often seek multiple consultations, practices must differentiate themselves by offering a superior patient experience. Digital smile simulations not only improve case acceptance rates but also demonstrate a patient-centered approach that fosters loyalty and trust.
“High-quality visuals give patients clarity and build trust,” says PJ Jafari, CEO of 10X Dental Partners, a consulting firm specializing in optimizing full-arch dental practices. “When paired with effective communication, treatment simulations help patients feel confident in the practice and in moving forward with treatment.”
What to look for in smile simulation software
Smile simulation software should offer quick, easy-to-use features that can be delegated to the dental team. The simulations must look natural, not overly digitized, to resonate with patients. The software should allow for viewing of simulations on a large screen during consultations, which creates a dramatic “big reveal” moment, and for the ability to print, email, or text those simulations, keeping the benefits of treatment top of mind. This flexibility ensures patients can share the simulations with co-decision makers and receive support from friends or family, increasing confidence in their decision to proceed with treatment.
Conclusion
Patients deciding on full-arch rehabilitation are not merely buying teeth — they’re investing in a life-changing transformation. By tapping into emotional drivers, leveraging digital smile simulations, and fostering trust, dental practices can guide patients toward saying “yes” to treatments that will profoundly improve their lives.
From AOX to AOX²
Multiply Your Success
People Don't Buy Teeth— They
Invest in Life-Changing Transformations.
PreVu is the fastest, easiest software for creating natural-looking treatment simulations to increase case acceptance.
Close More Smile Makeover & Full-Arch Cases With PreVu.
Visualize Transformations: Show patients how treatment will enhance their appearance.
Envision the Future: Help patients understand how they’ll feel and what their life will be like after investing in their smile.
Drive Decisions: Create the emotional connection that motivates high-value purchases.
Maximize Your Marketing Spend.
Boost ROI: Convert marketing leads into high-paying patients by leveraging a proven tool for case acceptance.
Stand Out: Differentiate your practice by showcasing life-changing smile transformations.
Turn Interest Into Action: Inspire patients to take the next step and embrace life-changing treatment.
What Doctors Say About PreVu
"PreVu simulations look incredibly natural and help patients visualize their transformation, making it much easier for them to choose optimal care. It has elevated how we use photography in our practice and has made closing full-mouth reconstruction cases significantly easier. We've integrated PreVu into our office and all our FMR courses—it’s truly a game changer for patients to witness their transformation firsthand. I 100% recommend it to all our doctors."
Dr. Dean Vafiadis Program Director, FMR NYC
“In our practice, we're thrilled with the speed at which we can create simulations by using PreVu. Using Prevu, I've been able to achieve a remarkable 80%-90% closure rate on all my full- arch and All-on-4 cases. It's become an indispensable tool for us! I incorporate it into every consultation and examination because it allows my patients to envision the potential improvements to their smiles and lives.”
Dr. Vanila Choudhry Guru Dentistry, Irvine, CA
Requisites for success in dental implantology — not just slinging titanium
Dr. Sean Lan offers skills that can help clinicians surmount difficult implant situations
Introduction
I’ll never forget the dreaded “pop” of the anterior nasal spine (ANS) as it greenstick fractured while I was placing a nasopalatine implant to finish off a full arch implant rehabilitation of an atrophic maxilla. Actually, there was no audible sound. But in my head, it was loud, clear, and echoing. My thought was, “What do I do now?” This kind of moment (although few and far between) is sure to happen to anyone doing enough volume and pushing their boundaries (responsibly). It’s a matter of when, not if. And when it happens, we are either prepared for it or we are not. “We don’t rise to the level of our expectations; we fall to the level of our training.” Stay tuned until the end to see how I got myself out of this dilemma.
But first I want to present the main goal of this article, which is to discuss important requisite surgical skills as a dental implantologist — the ones that don’t directly involve “dropping screws in.” These skills are not only important for long term success; they build the foundation of our confidence when Sharpey’s fibers hit the fan. Additionally, being able to anticipate complicating factors pre-operatively can guide clinicians in treatment planning and case selection, which ultimately allows us to push our boundaries responsibly while still providing a high quality of care to our patients. Learning these skills very early on in my career was the only reason I was able to mitigate the problem despite never being in that situation before (re: ANS).
Requisites for success
• Hard tissue augmentation
º Varying levels of augmentation
º Fundamental surgical skills
■ Periosteal releasing incision
■ Buccal/lingual flap advancement
º Fundamental suturing/membrane stabilization skills
Sean Lan is a dedicated practitioner based in Stockbridge, Georgia, serving the surrounding areas with a passion for dental implantology and dentoalveolar surgery. After completing his undergraduate and dental degrees at the University of Florida, Dr. Lan embarked on a 1-year AEGD residency, solidifying his interest in dental surgery. He further honed his skills by completing in the AFPDS Implant program with the USAF Department of Prosthodontics and dedicating hundreds of hours reading literature and textbooks. Currently, Dr. Lan works with a nationwide DSO focused on full arch implantology where he serves as a mentor to his peers in and out of the group. You can see more of his work on his Instagram page @DrSeanLan, where his mission is to “Make Reading Sexy Again.”
Disclosure: All cases presented are Dr. Lan’s unless otherwise noted.
Educational aims and objectives
This self-instructional course for dentists discusses important requisite surgical skills for dental implantologists so they can anticipate complicating factors preoperatively and guide treatment planning and case selection appropriately.
Expected outcomes
Implant Practice US subscribers can answer the CE questions by taking the quiz online at implantpracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Identify some needs of hard tissue augmentation. Recognize some methods for bone regeneration.
• Realize some fundamental surgical skills for tissue closure.
• Identify some methods of soft tissue augmentation.
• Realize some reasons to pursue more information on lateral sinus augmentation.
• Soft tissue augmentation
2 CE CREDITS
º Free gingival graft (FGG) with apically positioned flap
• Lateral sinus window (and not necessarily for growing bone)
Like most short-form content, this article is not meant to be a definitive resource. Rather, my goal is to identify key milestones that can help readers accelerate their skills. I hope practitioners of all levels can find something to use in their practices.
Hard tissue augmentation
Hard tissue augmentation can be one of the most daunting new skills to learn. There is so much to consider: patient regenerative potential, biomaterial selection, augmentation techniques, etc. However, it is a valuable skillset to add to your repertoire. A 2008 study by Bornstein, et al., found that 51.7% of implants in the study needed additional hard tissue augmentation.1 I have broken down a general progression in this “skill tree” as well as the fundamental skills that can be applied in other situations.
Hard tissue progression
In general, the less contained or “within the contour” of the native bony architecture the graft is, the more difficult it is to
regenerate bone. Wang and Boyapati described the four major biologic principles for predictable bone regeneration.3 Dubbed the PASS Principles, these are:
• primary wound closure to ensure undisturbed and uninterrupted wound healing
• angiogenesis to provide necessary blood supply and undifferentiated mesenchymal cells
• space maintenance/creation to facilitate adequate space for bone ingrowth
• stability of wound and implant to induce blood clot formation and uneventful healing events
This is why I recommend starting with ridge preservation of a 4-walled socket. Not every 4-walled socket needs ridge preservation (i.e., it can be an option if you can’t place an immediate implant, need to buy time for patient finances, etc.) but it’s a good place to start. There are many ways to approach this.4 In my studies so far, I have broken down the methods into two main categories: techniques that require primary closure (thus moving the mucogingival Junction [MGJ]) and those that do not. The benefit of leaving the MGJ intact reduces the need for soft tissue grafting later on. Allowing the socket to heal by secondary intention can increase the amount of keratinized tissue (KT) (as long as you have attached KT on both flap margins).
After this factor, predictability and relative ease of technique come next in line. The dense polytetrafluoroethylene (dPTFE) ridge preservation technique is one that fulfills all of these preferences. For more information on this, check out Chapter 3 of Dr. Michael Pikos’ book. (Pikos, MA, Miron RJ. Bone Augmentation in Implant
Fundamental Surgical Skills – Hard Tissue Augmentation
Membrane tacking sutures (see “SauFRa” technique)2
Tacks
Fixation screws (e.g. split bone block)
Dentistry: A Step-by-step Guide to Predictable Alveolar Ridge and Sinus Grafting. Quintessence Pub Co.; 2019.) Dr. Pikos has personally taken hundreds of bone cores and found D2 bone at 4 months. dPTFE membrane is more cost effective than a resorbable collagen membrane (RCM). Just pluck it out at 4-6 weeks, and you’ll find complete closure of the site made up of dense connective tissue. Most patients don’t even need topical anesthetic.
Difficulty increases when there are compromises in one or more walls of a socket. There are techniques to deal with these situations, such as the “ice cream cone” technique,6 dPTFE technique for compromised wall sockets (see also, Pikos), and Immediate Dentoalveolar Restoration technique,7 just to name a few. The point is when learning different techniques, there are skills within each technique that we can take and apply to other situations.
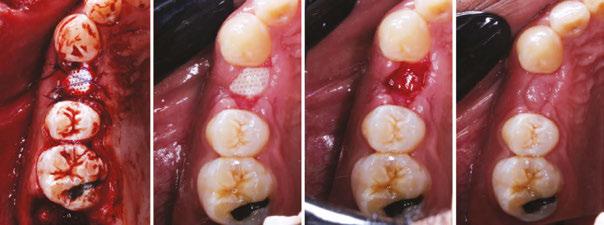
Fundamental surgical skills — hard tissue augmentation (Figure 2)
Buccal/lingual flap advancement is necessary for tension-free closure. This is essential in hard tissue augmentation but is a concept that can be applied any time you try to attain primary closure. You begin to train your eye to see where muscle pull is coming from, thus how/where to relieve it. On full-arch implant rehabilitation or “full-arch” cases, a common mistake I’ve noticed is early incision line opening. This usually occurs when the practitioner is trying to achieve primary closure but did not realize the amount of tension on the flaps beforehand. Just because the practitioner can close a flap on the day of surgery doesn’t mean it will stay closed. In addition, scar tissue from
Figure 1: Suggested hard tissue progression – Increasing degree of difficulty of hard tissue augmentation
Figure 2: Fundamental skills for hard tissue augmentation
previous surgeries can further complicate closure. Prof. Istvan Urban eloquently describes the “periosteo-elastic technique” for flap advancement in Chapter 6 of his landmark textbook (Urban I. Vertical and Horizontal Ridge Augmentation. Quintessence Pub. Co.; 2017). It begins with a gentle periosteal releasing incision (sharp) to open a door past the periosteum into the mucosal layer. Then, it involves semi-sharp and blunt dissection to sever the subperiosteal bundles and stretch the elastic fibers, respectively. This skill transfers well to learning split thickness flap preparation for soft tissue work.
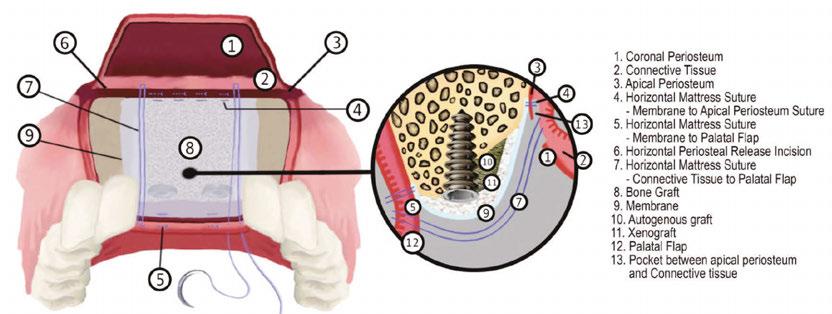
Once tension-free flaps are established, how can they be closed for hard tissue augmentation? The first layer in a double layered closure consists of horizontal/vertical mattress sutures. These tension-relieving sutures reduce/eliminate remaining tension at the margins and evert them. Then, the second layer consists of simple interrupted/continuous sutures to finalize the closure (Figure 4).
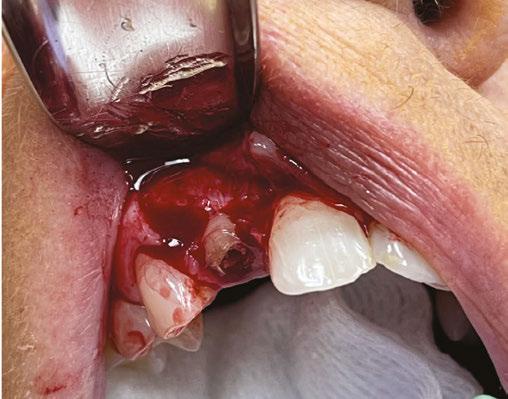
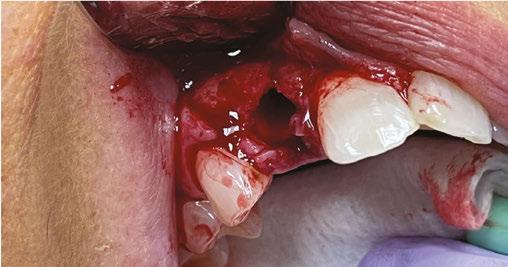
Next, when placing a barrier membrane, how do we stabilize it? This is where the art and creativity come into play. The most approachable techniques to start with are the periosteal vertical mattress,8 poncho technique, and double membrane technique.9 Poncho technique is quite simple and involves cutting a “X” or a small hole in the membrane (or PRF slug) and threading an implant abutment through it (Figure 5). Transosseous sutures involve creating an osteotomy in existing bony architecture with a small diameter bur (e.g., 701 bur) through which a suture can be passed and fixated. An osteotomy can be created through a single cortex, or both. Some use case examples are to apically position flaps for a mandibular overdenture and creating fixation points to suture a resorbable collagen membrane to while repairing a buccal plate fracture (Figure 6).
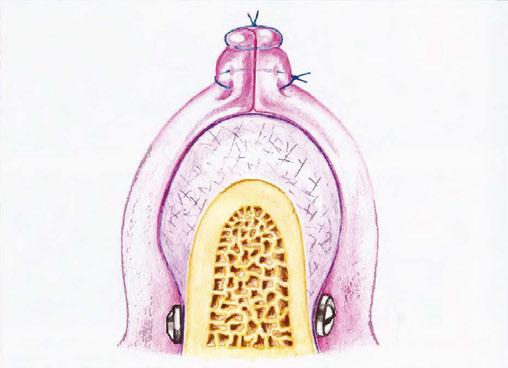
One of my favorite techniques is the membrane-tacking suture which is involved in the “SauFRa Technique” described by Kamat in 2020.10 It is a bit more technique-sensitive, but essentially it is used to stabilize the membrane along the apical and coronal edges. Tacking sutures are placed along the apical membrane edge to the apical periosteum and along the coronal membrane edge to the palatal/lingual flap. It is combined with periosteal vertical mattress sutures on the lateral extent of the membrane to prevent lateral extrusion of graft material. To put it simply, you are making a “Hot Pocket” to contain your graft material (Figure 7). So go on and get creative! There are many techniques to stabilize a membrane such as Ribroast,11 Lasso,12 and using tacks as fixation points for sutures.13
Soft tissue augmentation
This is another daunting topic to tackle; however, it is crucial to have these skills for long term maintenance of dental implants. While the maxilla has an abundance of attached KT, the mandible lacks such supply. Add in loss of vestibular depth, and a seemingly straightforward mandibular overdenture just got harder to manage. In my opinion, the fundamental techniques to start with are the free gingival graft (FGG) and apically positioned
Figure 7: Source: 2020 Kamat “SauFRa Technique.” Note number 4 and 5 for these membrane-tacking sutures
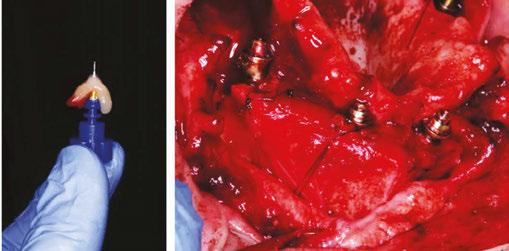
Figure 5 (left): Poncho technique using an implant abutment to secure PRF. Figure 6 (right): Transosseous sutures to fixate resorbable collagen membrane (RCM) for within-the-contour graft of the buccal plate dehiscence defect
flap (APF). These will require the clinician to become proficient in split thickness dissection, which is used for the FGG harvest and preparation of the recipient bed and APF. This will be useful to increase attached KT on the buccal (and sometimes lingual) of the implants. When KT needs to be increased on both sides, this is more often done in a two-stage approach.
The next natural progression is the connective tissue graft (CTG). There are two main types of harvest: the deepithelialized CTG and the sub-epithelialized CTG. De-epithelialized CTG (DFGG) is harvested in a similar fashion as an FGG and followed with subsequent removal of the epithelial layer with a blade. Other methods of de-epithelialization include using a round diamond bur before taking the harvest. Subepithelial CTG (SECTG) involves leaving the epithelial layer intact and harvesting only the connective tissue layer. By nature, DFGG will take a more superficial portion of the CT layer while SECTG will take a deeper portion of the CT layer. There is limited but growing evidence comparing the two methods, but results have shown that there is no significant difference in pain (which is one of the main talking points favoring SECTG). Some studies also show that the deeper the harvest is, the more pain.14-15 In terms of performance, some studies show that DFGG outperforms SECTG in terms of increase in soft tissue thickness. The theory is that the
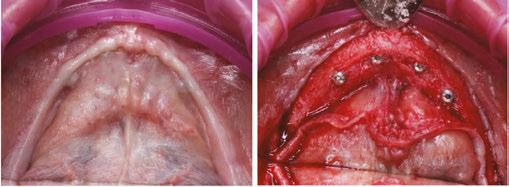
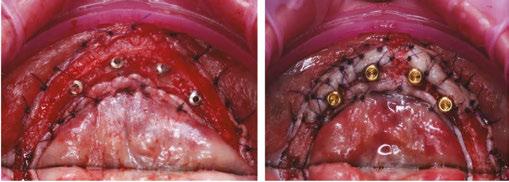
Figures 8A-8E: Vestibuloplasty using FGG and APF. 8A. Pre-op of a Stage II uncovering of mandibular implant overdenture with thin band of KT and limited vestibule. 8B. Buccal and lingual split thickness flaps prepared. Sublingual vasculature preserved. 8C. Buccal and lingual apically positioned flaps. 8D. FGG harvested from edentulous maxilla, closer to crest of edentulous ridge to reduce patient pain. Secured with periosteal suturing and periosteal vertical mattress sutures. The author notes that there are learning points from this case (as there are for every case), but that is not the focus of this discussion. 8E. 4 week post-op
deeper layers of CT have a higher percentage of fatty/glandular tissue instead of dense CT that we are looking for. Clinicians like Dr. Pat Allen and Giovanni Zucchelli advocate for the DFGG whereas Drs. Hurzeler and Zuhr mention that they prefer the SECTG at the time of their textbook was published in 2012. Either way, the DFGG is more approachable technique-wise, so I would recommend to start there.
Finally, we have the rotated pedicle flap in the lineup of highyield fundamental soft tissue skills. This is a useful tool to have to increase tissue thickness around implants and to repair smallto-medium sized oroantral communications (OAC) to spare the buccal fat pad.16 It can be secured in many ways, so use your creativity and the tools you have from your membrane stabilization toolbox! You can suture directly to the flap, periosteum, or even create a transosseous purchase point.
Putting all these fundamental soft tissue skills together, you will be armed with the tools to perform more challenging procedures, like the classic vestibuloplasty via FGG and APF.
Lateral sinus augmentation
While it is important to know how to perform a lateral sinus augmentation, my main goal for pursuing this skill early on was more so to be comfortable working in the sinus. This greatly reduces the stress of displacing a tooth/root/implant into the sinus. The sinus membrane repair technique is also a great tool to have in the toolbox, as it gives you another way of looking at repairing the membrane while minimizing cutting off blood supply from the bony walls.17 In his article, Dr. Michael Pikos describes his modified technique using a slow-resorbing type I collagen membrane for repair of large and complete sinus membrane perforations. The membrane creates space facilitating graft placement. Also, “The biocompatibility and semirigid structural integrity of this membrane, along with external tack fixation, allows for optimal membrane stabilization and maintenance.” As the clinician’s skills advance, these skills can be applied to lifting the sinus membrane for a trans-sinus implant or a pterygoid implant that needs to traverse the sinus.
Putting it all together
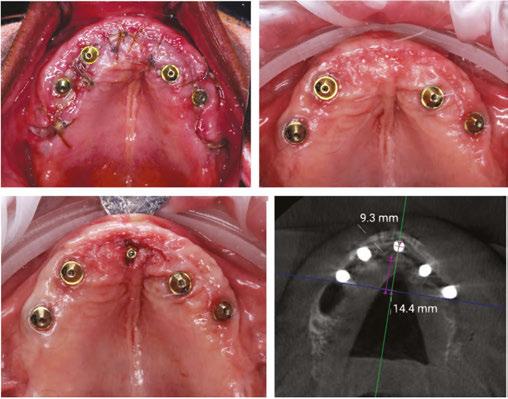
Finally, let’s revisit the opening scenario: how did I end up choosing to manage the greenstick-fractured ANS? My training certainly came in handy that day. This stressful event is evidenced by the fact that I barely managed two clinical photos that day. The patient was planned for a maxillary implant-fixed complete denture. She had an atrophic maxilla with anteriorly and inferiorly pneumatized sinuses. However, with the use of a nasopalatine implant19-20 anteriorly, I was able to achieve adequate AP spread. It was the fifth and last implant I had planned for this case. I fully prepped the osteotomy as the atrophic anterior maxilla lacks sufficient elasticity from trabecular bone. As I placed the implant and was finishing with my torque wrench around 40 Ncm, I felt and saw the ANS greenstick fracture. Since I am not trained on reconstruction plates to reduce bony fractures, I had to think fast. I decided to combine concepts from Urban’s “Sausage” technique as well as membrane tacking sutures from the Kamat’s “SauFRa” technique to stabilize the graft and the ANS. Essentially, this turned into an “unintentional” ridge split.
Conclusion
Learning certain fundamental skills early on in your implant
E.
C.
A.
D.
B.
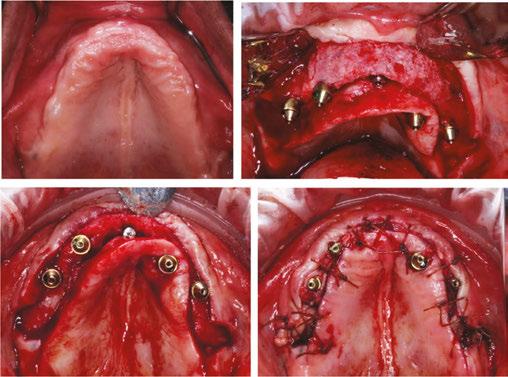
Figures 9A-9I: Management of ANS greenstick fracture via horizontal ridge augmentation. 9A. Pre-op. 9B: Stabilization of ANS greenstick fracture via “sausage”-based technique using two 20x30 RCMs and 4-0 PGCL sutures. Membrane-stabilizing sutures used: periosteal vertical mattress suture (PVMS) at lateral-most extent of the graft area. PVMS at the medial extent of each membrane (another PVMS was added just left of midline after photo was taken). Apical periosteal and palatal membrane tacking sutures. 2.5cc particulate 80/20 FDBA (corticocancellous)/xenograft (porcine) was used. 9C. 6-month post-op. Patient allowed limited wear of denture (shortened flange in anterior) 2 months post-op. 9D. Uncovering with view of the repaired ANS with regenerated bone. Implant placed in NP canal @ 25 Ncm. 9E. Occlusal view. 9F. L-PRF prepared (700 RCF, 8 minutes) and placed all along arch to aid in soft tissue healing. Flaps intentionally sutured to allow healing by secondary intention to increase KT. Conversion prosthesis loaded, patient educated about anterior cantilever. 9G. 1-week follow up. The power of L-PRF. 9H. 3-month follow up. 9I. Uncover at 3 months post placement of NP implant. 9J. CBCT Axial View. AP spread with (14.4 mm) and without (9.3 mm) NP implant
career can improve your treatment planning, manage more complications, and ultimately boost your confidence when pushing your boundaries.
To budding implantologists — are you ready to take the next step in elevating your skills? Even if you want to stay with the basics of International Team for Implantology Straightforward Advanced Complex (classification system) (ITI SAC) straightforward cases, thinking about these issues can help you identify and refer cases that can be more complex than it seems on the surface. To my more experienced colleagues — let me know your thoughts! What other high yield skills can one benefit from learning early on?
REFERENCES
1. Bornstein MM, Halbritter S, Harnisch H, Weber HP, Buser D. A retrospective analysis of patients referred for implant placement to a specialty clinic: indications, surgical procedures, and early failures. Int J Oral Maxillofac Implants. 2008 Nov-Dec;23(6):1109-1116.
2. Kamat SM, Khandeparker RV, Akkara F, Dhupar V, Mysore A. SauFRa Technique for the Fixation of Resorbable Membranes in Horizontal Guided Bone Regeneration: A Technical Report. J Oral Implantol. 2020 Dec 1;46(6):609-613.
3. Wang HL, Boyapati L. “PASS” principles for predictable bone regeneration. Implant Dent. 2006 Mar;15(1):8-17.
4. Horowitz R, Holtzclaw D, Rosen PS. A review on alveolar ridge preservation following tooth extraction. J Evid Based Dent Pract. 2012 Sep;12(3 Suppl):149-160.
5. Luongo R, Tallarico M, Canciani E, Graziano D, Dellavia C, Gargari M, Ceruso FM, Melodia D, Canullo L. Histomorphometry of Bone after Intentionally Exposed Non-Resorbable d-PTFE Membrane or Guided Bone Regeneration for the Treatment of Post-Extractive Alveolar Bone Defects with Implant-Supported Restorations: A Pilot Randomized Controlled Trial. Materials (Basel). 2022 Aug 24;15(17):5838.
6. Tan-Chu JH, Tuminelli FJ, Kurtz KS, Tarnow DP. Analysis of buccolingual dimensional changes of the extraction socket using the “ice cream cone” flapless grafting technique. Int J Periodontics Restorative Dent. 2014 May-Jun;34(3):399-403.
7. da Rosa JC, Rosa AC, da Rosa DM, Zardo CM. Immediate Dentoalveolar Restoration of compromised sockets: a novel technique. Eur J Esthet Dent. 2013 Autumn;8(3):432-443.
8. Urban IA, Lozada JL, Wessing B, Suárez-López del Amo F, Wang HL. Vertical Bone Grafting and Periosteal Vertical Mattress Suture for the Fixation of Resorbable Membranes and Stabilization of Particulate Grafts in Horizontal Guided Bone Regeneration to Achieve More Predictable Results: A Technical Report. Int J Periodontics Restorative Dent. 2016 Mar-Apr;36(2):153-159.
9. Bornstein MM, Heynen G, Bosshardt DD, Buser D. Effect of two bioabsorbable barrier membranes on bone regeneration of standardized defects in calvarial bone: a comparative histomorphometric study in pigs. J Periodontol. 2009 Aug;80(8):1289-1299.
10. Kamat SM, Khandeparker RV, Akkara F, Dhupar V, Mysore A. SauFRa Technique for the Fixation of Resorbable Membranes in Horizontal Guided Bone Regeneration: A Technical Report. J Oral Implantol. 2020 Dec 1;46(6):609-613.
11. Fien M, Puterman I, Mesquida J, Bauza G, Ginebreda I. The Ribroast Technique™: An Alternative Method to Stabilize a Resorbable Collagen Membrane for Guided Bone Regeneration. Compend Contin Educ Dent. 2023 Jul-Aug;44(7):408-414.
13. Fien M, Puterman I, Mesquida J, Ginebreda I, Bauza G. Guided Bone Regeneration: Novel Use of Fixation Screws as an Alternative to Using the Buccoapical Periosteum for Membrane Stabilization With Sutures—Two Case Reports. Compendium. Feb. 2024;45(2). https:// www.aegisdentalnetwork.com/cced/2024/02/guided-bone-regeneration-novel-use-of-fixation-screws-as-an-alternative-to-using-the-buccoapical-periosteum-for-membrane-stabilization-with-sutures-two-case-reports. Accessed October 23, 2024.
14. Zucchelli G, Mele M, Stefanini M, Mazzotti C, Marzadori M, Montebugnoli L, de Sanctis M. Patient morbidity and root coverage outcome after subepithelial connective tissue and de-epithelialized grafts: a comparative randomized-controlled clinical trial. J Clin Periodontol. 2010 Aug 1;37(8):728-738.
15. Tavelli L, Ravidà A, Lin GH, Del Amo FS, Tattan M, Wang HL. Comparison between Subepithelial Connective Tissue Graft and De-epithelialized Gingival Graft: A systematic review and a meta-analysis. J Int Acad Periodontol. 2019 Apr 1;21(2):82-96.
16. El Chaar E, Oshman S, Cicero G, Castano A, Dinoi C, Soltani L, Lee YN. Soft Tissue Closure of Grafted Extraction Sockets in the Anterior Maxilla: A Modified Palatal Pedicle Connective Tissue Flap Technique. Int J Periodontics Restorative Dent. 2017 Jan/Feb;37(1):99-107.
17. Pikos MA. Maxillary sinus membrane repair: update on technique for large and complete perforations. Implant Dent. 2008 Mar;17(1):24-31.
18. International Team for Implantology. “SAC Assessment Tool.” ITI, www.iti.org/tools/sac-assessment-tool. Accessed October 1, 2024.
19. Peñarrocha M, Carrillo C, Uribe R, García B. The nasopalatine canal as an anatomic buttress for implant placement in the severely atrophic maxilla: a pilot study. Int J Oral Maxillofac Implants. 2009 Sep-Oct;24(5):936-942.
20. Peñarrocha D, Candel E, Guirado JL, Canullo L, Peñarrocha M. Implants placed in the nasopalatine canal to rehabilitate severely atrophic maxillae: a retrospective study with long follow-up. J Oral Implantol. 2014 Dec;40(6):699-706.
A.
F.
H.
J.
C.
B.
E.
G.
I.
D.
Continuing Education Quiz
Requisites for success in dental implantology — not just slinging titanium LAN
1 A 2008 study by Bornstein, et al., found that ______ of implants in the study needed additional hard tissue augmentation.
a. 25.8%
b. 39.3%
c. 51.7%
d. 65.3%
2. In general, the less contained or “within the contour” of the native bony architecture the graft is, the more difficult it is to
_________.
a. regenerate bone
b. reduce bleeding
c. induce blood clot formation
d. differentiate mesenchymal cells
3. __________ described the four major biologic principles for predictable bone regeneration, dubbed the PASS Principles.
a. Wang and Boyapati
b. Allen and Zucchelli
c. Prof. Istvan Urban
d. Hurzeler and Zuhr
4. The benefit of leaving the mucogingival junction (MGJ) intact reduces the need for soft tissue grafting later on.
a. True
b. False
5. Prof. Istvan Urban eloquently describes the ________ for flap advancement in Chapter 6 of his landmark textbook (Urban I. Vertical and Horizontal Ridge Augmentation. Quintessence Pub. Co.; 2017).
a. “ice-cream cone technique”
b. “periosteo-elastic technique”
c. “dPTFE technique”
d. “immediate dentoalveolar restoration technique”
6. The first layer in a double layered closure consists of _____.
a. simple interrupted/continuous sutures
b. horizontal/vertical mattress sutures
c. the periosteal vertical poncho technique
d. transosseous sutures
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://implantpracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://implantpracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 690
Date Published: December 10, 2024
Expiration Date: December 10, 2027 2 CE CREDITS
7. ______ is quite simple and involves cutting a “X” or a small hole in the membrane (or PRF slug) and threading an implant abutment through it.
a. SauFRa technique
b. Hot pocket technique
c. Poncho technique
d. Simple interrupted suture technique
8. While the maxilla has an abundance of attached KT, the mandible lacks such supply.
a. True
b. False
9. ________ involves leaving the epithelial layer intact and harvesting only the connective tissue layer.
a. Subepithelial CTG (SECTG)
b. Deepithelialized CTG
c. Classic vestibuloplasty
d. Tension-free technique
10. (To secure a rotated pedicle flap) You can suture directly to __________.
a. the flap
b. the periosteum
c. create a transosseous purchase point
d. all of the above
To provide feedback on CE, please email us at education@medmarkmedia.com Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Timing, precision, and success: technique choices for implant placement
Dr. Jaclyn A. Tomsic offers guidance on the timing of implant protocols and methods for more efficient placement
Implant dentistry has evolved immensely since Brånemark initially introduced the concept of osseointegration in the late 1960s. Perhaps one of the most common and intensely debated topics today is the debate between when to pursue the traditional 2-stage protocol versus a 1-stage implant surgery.
In the traditional 2-stage approach, a tooth is extracted and ideally bone grafted for socket preservation. Traditionally, a 3-month waiting period is suggested for soft and hard tissue healing before placing a dental implant.1 At this point, with successful remodeling of the bone graft, a dental implant is placed. The implant is either initially completely submerged under mucosal tissue during the healing process, or more recently, if appropriate primary stability is achieved, a healing abutment is directly connected to the implant fixture at the time of implant surgery. In both situations, an attempt is made to avoid any functional loading during the initial osseointegration process, again typically 12 weeks or 3 months.1 If the implant is buried, it is uncovered in a second minor surgery typically 12 weeks later. If a healing abutment is in place, a final check appointment is still required to check successful osseointegration before sending to the restorative doctor. This 2-stage protocol (of placing an implant in a healed socket and subsequently restoring the implant with a prosthesis) is recognized as a highly predictable treatment modality for partially edentulous patients. This 3-month period has evolved from the original 6-month post extraction healing protocol first introduced by Brånemark.1
As products, knowledge, and experience evolve and improve over time, we have devised alternate ways to accomplish the same goal; thus the one-stage implant placement approach was born. In the 1-stage approach, an implant is placed immediately in a fresh extraction socket, often in combination with bone grafting, guided tissue regeneration, and sometimes immediate restoration. The surgeon extracts a tooth as atraumatically as possible, aiming to preserve as much surrounding bone as possible to be able to attempt immediate implant placement. Over time, this approach has also proven to be successful with no significant differences in treatment outcomes when compared to the 2-stage approach.2
Jaclyn Tomsic MD, DMD, FACS, is an oral and maxillofacial surgeon from Cleveland, Ohio specializing in topics such as: wisdom teeth, dental implants, corrective jaw surgery, facial cosmetic surgery, anesthesia, snoring and sleep apnea, the temporomandibular joint (TMJ), oral cancer, implants, and treating and preventing facial injury.
Educational aims and objectives
This self-instructional course for dentists aims to discuss the benefits and drawbacks of different staging protocols of implant surgery as well as the pros and cons of free-hand versus guided implant surgery.
Expected outcomes
Implant Practice US subscribers can answer the CE questions by taking the quiz online at implantpracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Identify the 2 main types of implant placement. Identify the pros and cons of each method of placement.
• Discuss the advantages and disadvantages of freehand versus guided implant placement.
• Better understand the positive aspects of guided implant surgery.
• Realize how to evaluate and assess an implant case and make an informed decision on plan of surgical treatment.
2 CE CREDITS
Pros and cons of the 2-stage approach
The 2-stage approach has long proven to be a highly predicable and successful method.1 A titanium surface under the appropriate circumstances in the absence of local or systematic disease or infection and without any other determining factors, if left untouched, will osseointegrate and fuse directly with human bone over time. A 3-month osseointegration period has repeatedly shown to be sufficient and reliable, and many longterm studies support this.1 The major drawback of the 2-stage approach is the duration and length of time from start to finish. If starting from the day of extraction, it will take about 6 months before a patient can expect to have a tooth again. For many, this is acceptable. Others want a more efficient timeline. From this, the 1-stage protocol emerged.
Pros and cons of the 1-stage approach
The 1-stage implant placement protocol involves placement of an immediate implant.
Documented pros of immediate implant placement include the following:3
• decreased treatment time
• fewer surgical procedures
• less traumatic surgery
• greater patient satisfaction.
Cons include the following:3
• difficulty in achieving primary stability
• higher risk of failure
• more need for bone grafts
• increased infection risk
This technique has unpredictable soft and hard tissue levels, which in my opinion, can be both a pro and a con. On the one hand, the unpredictability can make it more difficult to present a definitive treatment plan to the patient and increase the need for more regenerative procedures such as bone grafting and guided bone regeneration (GBR). On the other hand, placing an implant in an atraumatic extraction socket where the clinician has been able to preserve the keratinized tissue, gingival structures, and bone can improve implant placement accuracy and lead to better cosmetic outcomes.
Techniques for implant placement
There are essentially three different techniques for implant placement.
Free-hand placement
First is free-hand placement — when surgeons combine the clinical exam with imaging to plan and place an implant. The alveolar bone width is assessed with periapical, panoramic, and three-dimensional cone beam computed tomography (CBCT) to help evaluate and profile the surrounding structures. Periodontal probes, gauges, and calipers are used to sound the bone and measure tissue to get an idea of the height and thickness of the ridge and tissue.
Adjacent and opposing teeth help determine the correct position. Tissue flaps are reflected for direct visualization. Position pins may be used during osteotomy preparation and intraoral imaging to check distances and angulations before final implant placement, and the implant and bone grafts with PRF (platelet rich fibrin) and GBR can be easily performed.
Fully guided placement
In fully guided, A CBCT is taken and converted into a DICOM file; this is accompanied by a digital intraoral impression. This information is merged into the implant-planning software, and the surgeon and often an implant planner, such as a laboratory technician from an outside dental laboratory, place the implant virtually in the best location. Based on this design, a surgical guide is made and sent to the surgeon for use during surgery. In truly fully guided surgery, the entire osteotomy is prepped through the guide, and the implant is placed through the guide.
Half-guided surgery
Lastly there is half-guided surgery. Half guided splits the difference; it is template-based surgically guided osteotomy preparation and free-handed manual implant insertion. This is essentially a guide with a pilot-hole guide.
Aspects of guided surgery
I will now focus on guided surgery. The two most important factors in successful implant placement are angulation and positioning. Is poor angulation and positioning really that bad? Only the clinician can be the judge of that, but what we do know are
More evidence is pointing toward the use of surgical guides as providing better implant placement accuracy and addressing these two factors of angulation and position.”
the potential risks of taking that path. Perforations of the lingual plate or IAN can occur. The prosthetic can be compromised causing poor esthetics or unfavorable occlusal forces to be transmitted to the implants. Inaccurate or non-ideal inter-implant or implant-tooth distance can lead to loss of crestal bone and papilla contour.
More evidence is pointing toward the use of surgical guides as providing better implant placement accuracy and addressing these two factors of angulation and position.
There are obviously cases in which I choose to use free-hand surgery; however, the treating clinician should always make the individual decision as to whether free-hand or a surgical guide would be best for each case.
Case presentation
This 65-year-old female presented for implant consultation due to a failed root canal No. 7, whose crown was hanging on by a thread.
Things that were considered during my exam and planning process:
• The site to be implanted was tooth borne.
• The patient had adequate inter-occlusal distance and good overjet.
• Her clinical and radiographic exam showed a robust buccal plate and adequate palatal bone.
With this information, I proposed extraction and immediate implant placement using a fully guided surgical approach for placement of a Straumann® BLX implant.
Figure 2: On the day of surgery, I reflected a FTMPF and (using gentle elevation and rotational force on the tooth) was able to atraumatically extract tooth No. 7, keeping the buccal plate intact
Figure 5: I placed a BLX 3.75 mm x 14 mm implant through the surgical guide using the implant driver to the 4 hatch-mark at 25RPM and achieved 35N-cm2 primary stability. Given the ideal placement, only a small amount of particulate bone graft was necessary to fill the small gap between the implant and the robust buccal plate
Figures 3 and 4: I placed my surgical guide, and following the virtual plan used the appropriate surgical spoons (also called a curette) created my osteotomy, in this case using the 1+ handle, long drills, and the medium bone-drilling protocol
I felt the immediate placement would give me the best M-D and B-P accuracy, and the use of a surgical guide would counteract the tendency of the drill to be driven off course during placement. Her atraumatic flipper was already fabricated by her general dentist and ready for placement postoperatively.
I was very happy with the outcome of this case. Takeaways from the case include:
• Position and angulation accuracy were maintained as planned.
• Drill and implant did not drive off course.
• Treatment time was efficient – surgery in <1 hour.
• Patient (and surgeon) left happy.
In conclusion, my decision to perform a fully guided surgical plan and technique in this case improved the accuracy, efficiency, and success of the surgery. I feel the outcome of this case will be better with the aid of a virtually planned case and surgical guide, especially in the setting of an immediate extraction site where the osteotomy position, shape, and angulation are harder to control than a well-healed alveolar ridge.
REFERENCES
1. Bassir SH, El Kholy K, Chen CY, Lee KH, Intini G. Outcome of early dental implant placement versus other dental implant placement protocols: A systematic review and meta-analysis. J Periodontol. 2019 May;90(5):493-506. doi: 10.1002/JPER.18-0338. Epub 2018 Dec 5. PMID: 30395355; PMCID: PMC6500770.
2. Byrne G. Outcomes of one-stage versus two-stage implant placement. J Am Dent Assoc. 2010; 141(10):1257-1258.
3. Meng HW, Chien EY, Chien HH. Immediate Implant Placement and Provisionalization in the Esthetic Zone: A 6.5-Year Follow-Up and Literature Review. Case Rep Dent. 2021 Sep 15;2021:4290193. doi: 10.1155/2021/4290193. PMID: 34567810; PMCID: PMC8457954.
Figure 6: Flap was re-approximated, and primary closure obtained
Figure 7: Postoperative panorex image
Continuing Education Quiz
Timing, precision, and success: technique choices for implant placement TOMSIC
1. Traditionally, a _______ waiting period is suggested for soft and hard tissue healing before placing a dental implant.
a. 6-week
b. 3-month
c. 6-month
d. year
2. If the implant is buried, it is uncovered in a second minor surgery typically ________ later.
a. 3 weeks
b. 6 weeks
c. 12 weeks
d. 16 weeks
3. In the 1-stage approach, an implant is placed immediately in a fresh extraction socket, often in combination with _______.
a. bone grafting
b. guided tissue regeneration
c. immediate restoration (sometimes)
d. all of the above
4. A titanium surface under the appropriate circumstances in the absence of local or systematic disease or infection and without any other determining factors, if left untouched, will osseointegrate and fuse directly with human bone over time.
a. True
b False
5. One of the documented pros of immediate implant placement includes _______.
a. decreased treatment time
b. no surgical procedures
c. guaranteed primary stability
d. no need for bone grafts
6. (For the 1-stage approach) Placing an implant in an atraumatic extraction socket where the clinician has been able to preserve the keratinized tissue, gingival structures, and bone can _______ and lead to better cosmetic outcomes.
a. make it more difficult to present a definitive treatment plan
b. improve implant placement accuracy
c. completely eliminate infection risk
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://implantpracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://implantpracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 690
Date Published: December 10, 2024
Expiration Date: December 10, 2027
d. totally eliminate the need for bone grafts
2 CE CREDITS
7. (In freehand placement) The alveolar bone width is assessed with to help evaluate and profile the surrounding structures.
a. periapical, panoramic, and three-dimensional cone beam computed tomography (CBCT)
b. periodontal probes and gauges
c. calipers
d. a digital intraoral impression
8. _______ are used to sound the bone and measure tissue to get an idea of the height and thickness of the ridge and tissue.
a. Periodontal probes
b. Gauges
c. Calipers
d. all of the above
9. In truly fully guided surgery, the entire osteotomy is prepped through the guide, and the implant is placed through the guide.
a. True
b. False
10. Half-guided surgery uses ________.
a. template-based surgically guided osteotomy preparation
b. free-handed manual implant insertion
c. no pilot hole
d. both a and b
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
5 ways to help your practice reduce credit card processing fees
Matt Rej offers tips on how to mitigate the costs of accepting credit cards
Credit cards are convenient for patients and medical practices alike. It’s easy for dentists and specialists to collect payments immediately following an appointment in a way that their patients prefer. This helps keep accounts receivables low and simplifies the medical billing process.
Matt Rej is the managing partner of Merchant Cost Consulting and has been since 2017. Located in Boston, Massachusetts, MCC has been exposing the payments industry since 2016 to help bring transparency to business to ensure they are on the most competitive pricing applicable to their needs. The typical cost savings MCC achieves its clients ranges from 20%-60% on the total fees they currently pay, often without the hassle of making any changes to their current setup. Matt is proficient in Interchange Optimization, Pin Debit Card Routing, Payment Processor Service Markup analysis, and MCC Interchange categorization.
While there’s no debating the convenience of card payments, many practices overlook the credit card processing fees eating into their bottom lines. Dental and specialty practices pay upwards of $7,500 to $12,000 or more on processing fees alone. These costs are often accepted at face value and typically rise over time.
The vast majority of medical practices can save money on credit card processing without switching processors or changing anything. There are five proven ways to reduce processing fees that can potentially save dentists and specialists tens of thousands each year.
1. Audit your statements
Take a look at your last three credit card statements. Credit card processors are notorious for adding extra fees and inflating bills in the hopes that these charges go overlooked. Line items
for terminal fees, AVS fees, PCI compliance fees, IRS reporting fees, terminal fees, and gateway fees are all examples of inflated markups that don’t need to be included on the bill. Identifying and removing these unnecessary charges can instantly save you $2,500 to $4,000 annually.
Beyond the extra charges, look for any inconsistencies from one statement to the next. If the statements are confusing and deceptive, there’s a chance your processor is trying to bury other hidden markups on your statements. It’s suspicious if the fees aren’t presented in a way that’s clear, logical, and easy to understand.
2. Assess your contract
Review the merchant agreement that you signed to start accepting credit cards. It’s a little bit easier to negotiate fees if the contract is nearing its expiration date. Processors don’t want to lose your business. They make money every single time a card is swiped, dipped, or tapped at your practice. Leveraging your contract expiration is a highly effective way to lower your fees.
It’s also worth comparing your contract terms against the statements you’ve audited. Some processors breach contracts by increasing rates or adding fees that weren’t part of the initial agreement. If your processor breached those terms, you’re entitled to compensation in the form of a refund for those overages.
3. Negotiate and push back
There are three components of credit card processing: interchange, assessments, and markups. Interchange fees and assessments are imposed at the card network level by Visa, Mastercard, Discover, and American Express. These are non-negotiable rates that must be paid to the card brand each time one of those cards gets used as a payment. Markups are charged by the processor, and those rates are completely negotiable.
It’s easier to negotiate these rates if you’re on an “interchange plus” pricing plan. This means that you pay the card network’s interchange “plus” the markups imposed by your processor.
Everything other than the interchange fees and assessments can be negotiated. While processors are entitled to some fees for their role in facilitating the transaction, some of these markups are egregious and can often be cut in half.
4. Don’t switch processors
It’s a common misconception that switching processors will help save money on credit card processing. In reality, it’s usually more expensive. New processors will often ask to see what you’re currently paying and then undercut those rates to make their services seem more appealing. But then they inflate the processing rates by adding other markups to your statements. After a year or two, they’ll increase your rates, and you’ll end up paying more than you were with your old processor.
You’re much better off sticking with your current processor and just negotiating directly with them. If you aren’t getting anywhere in your negotiations, you can work directly with a merchant consultant to handle those conversations on your behalf. There’s no risk in going this route, as cost reduction firms aren’t compensated unless you save money.
5. Continue monitoring each statement
Even after you’ve successfully negotiated a reduction, you still need to make sure your statements have been adjusted appropriately. Unfortunately, many processors use deceptive tactics when dealing with merchants. So you can’t always take the word of a sales rep or customer service agent who promised a lower fee. Get everything in writing, and make sure those new rates are reflected on your next statement.
Furthermore, make sure that new hidden fees haven’t been added in place of the ones that were removed. Monthly monitoring is really the way to ensure that your negotiations have paid off, and it should be obvious that your total costs to process payments are lower. Rather than looking at just the fees, it’s often easier to calculate your “effective rate” as a more accurate representation of your average processing fees.1 This is a simple formula. Just divide the total amount that was deducted each month for processing by your total monthly sales. If this rate is higher or remains unchanged after your negotiations, then your processor is still doing something deceptive behind the scenes, and there’s more room to save money.
While there’s no debating the convenience of card payments, many practices overlook the credit card processing fees eating into their bottom lines. IP
REFERENCE
1. O’Keefe C. Average Credit Card Processing Fees (2024). Merchant Cost Consulting. https://merchantcostconsulting.com/lower-credit-card-processing-fees/average-creditcard-merchant-fees/ (accessed January 16, 2024).
Integrating AI in dental practices
Gary Salman explains how to reap the benefits of AI more safely
As artificial intelligence (AI) continues to permeate various healthcare sectors, dental specialty practices such as orthodontics, endodontics, implants, and pediatric dentistry stand to benefit significantly from its integration. AI offers vast potential to enhance diagnostics, streamline patient management, and boost operational efficiency. However, with these advancements come critical considerations around patient data protection and regulatory compliance as well as the need to maintain compliance with the Health Insurance Portability and Accountability Act (HIPAA) security and privacy rules.
The
benefits of artificial intelligence
1. Enhanced diagnostics and patient care
AI has revolutionized diagnostic processes by leveraging machine-learning algorithms to analyze complex datasets, such as radiographic images. This technology can assist in predicting tooth movement and treatment outcomes, enhancing the diagnostic accuracy of decay and anomalies in x-rays, and monitoring patient treatment progress.
2. Streamlined patient management
The automation of routine administrative tasks that AI can handle, from appointment scheduling to patient follow-ups, frees up valuable time for dental professionals to focus on patient care. It also facilitates better patient communication through personalized reminders and post-treatment care instructions, enhancing patient satisfaction and engagement.
3. Operational efficiency
AI tools can optimize inventory management and predict patient flow, leading to better resource allocation and reduced operational costs. Predictive analytics can also take multiple data inputs from systems such as practice management, financial reporting, and insurance claims to identify areas where your practice could improve for growth.
Gary Salman is CEO and co-founder of Black Talon Security (www.blacktalonsecurity.com). A leader in the cybersecurity field, Salman has a 25+ year background in law enforcement and healthcare technology. His firm monitors and secures approximately 50K computers and networks worldwide and has trained tens of thousands of dental and other healthcare professionals.
Protecting patient records and ensuring HIPAA compliance
With the integration of AI, safeguarding patient information becomes paramount. Dental practices must adhere to HIPAA regulations, which mandate the protection of individual health information. Here are key considerations:
• Data storage and flow: Encrypt all stored and transmitted patient data to prevent unauthorized access. This ensures that even if data is intercepted, it remains unreadable to unauthorized individuals. AI often requires your data to be analyzed and stored in many places at a given time. This creates additional risk for your practice, because the bigger your digital footprint, the bigger the risk. Some AI applications can store your data on 3-4 different server networks at a given time.
• Data access controls: Implement strict access controls, ensuring that only authorized personnel have access to sensitive information. Use multi-factor authentication to add an extra layer of security. Many AI companies either purposely or inadvertently share your patient data, with or without your permission. Ask the AI company for their policies for data sharing and retention.
• Regular internal and external audits: Conduct regular security audits to identify vulnerabilities and ensure compliance with HIPAA standards. Internal audits help maintain the integrity of the data protection mechanisms put in place within your practice — but don’t neglect third-party risk. Unfortunately, many AI companies are still in “start-up” mode. Often hiding behind a “HIPAA Compliant” badge, they may fail to have anything more than basic security precautions in place to protect your patient data, putting you at a tremendous risk in the event of a breach.
Best practices for cybersecurity
To protect against cyber threats, dental practices should adopt comprehensive cybersecurity measures so they can identify and mitigate cyber risk. The “Cybersecurity Standard of Care for Dental Practices” includes the following:
• Vulnerability identification and remediation: Hackers use sophisticated tools to identify vulnerabilities on your firewall and computers and leverage these weaknesses to break in and exploit your network. Cybersecurity companies offer sophisticated tools that scan your computers and firewalls daily looking for these exploitable vulnerabilities. The more sophisticated scanners not only identify the vulnerabilities on the computers but can autonomously remediate them.
• Staff cyber training: Educate staff on cybersecurity best practices, including recognizing phishing attempts and safe internet usage. Regular training sessions will help maintain a security-conscious culture within the practice. To be HIPAA compliant, this must be an ongoing, documented process, not a quick “over lunch” conversation. Seek out cybersecurity companies that offer comprehensive training and understand the unique vulnerabilities in workflows of dental practices.
• Penetration testing: An ethical hacker should be attempting to break into your network at least twice per year to test the defensive measures of your network. This test should not be performed by your IT company, but an independent cybersecurity company.
• Incident response plan: Develop a written response plan for potential cyberattacks or any emergency that could disrupt your practice. This plan should outline the steps for containment, investigation, and communication to minimize the impact of the emergency. Rehearse the plan annually to ensure all team members know their role when responding, and to evaluate for any needed improvements to the plan.
• AI-based anti-virus: Utilize more advanced anti-virus software that leverages AI to detect and fight back against more sophisticated attacks. This software must be managed and watched 24/7 by security engineers to be most effective.
Practical steps for successful AI integration
1. Choosing the right AI tools
Select AI solutions that meet the specific needs of your practice. Evaluate various tools based on their functionality, ease of integration, and compliance features. Consider solutions that offer seamless integration with existing systems and have a proven track record in the dental industry. Ask to review their third-party cybersecurity evaluation and HIPAA risk assessment. You don’t want their breach to become your breach.
2. Staff adoption
Ensure that your team is well-prepared to work with AI technologies. Comprehensive training and documented processes will facilitate a smoother transition in their workflows and help staff understand the benefits, risks, and limitations of AI tools. Staff should always use caution when uploading any data that contains confidential information such as employee or patient data into these systems. You may be violating State and Federal laws without realizing it.
3. Ask for a proof of concept
The best way to assess if adding AI to your practice will provide value is to ask for a 90-day proof of concept period to fully understand how it will function. However, you’ll want to be sure you have reviewed their data handling and security protocols prior to giving the tool access to your data.
Balancing advanced technologies with data security
Integrating AI offers transformative benefits, from improved diagnostics to enhanced operational efficiency. However, this technological advancement requires a balanced approach that prioritizes patient data protection and regulatory compliance. By implementing robust cybersecurity measures and choosing the right AI tools, dental specialty practices can harness the power of AI successfully. As AI continues to evolve, embracing these technologies while maintaining vigilance over data security will ensure that your practice remains both innovative and compliant in its operations. IP
Integrating AI offers transformative benefits, from improved diagnostics to enhanced operational efficiency. However, this technological advancement requires a balanced approach that prioritizes patient data protection and regulatory compliance.”
Specialty1 Partners
Better care. Better business. Better oral health.
“Our primary focus has always been patient and partner satisfaction, and we have found that this approach truly resonates with the specialists we bring on board.” – Dr. Daryl Dudum, Founding Partner and Co-CEO
Specialist founded — Specialist led — Specialist supported
We are proud to be the only Specialty Partnership Organization founded, led, and supported by dental specialists. Specialty1 Partners (S1P) is your best choice for taking your specialty dental practice to the next level of success and patient care.
With over 225 partner practices spanning 28 states, S1P is the leader in enabling its partners to focus on patient care while benefiting from the support of a network of seasoned professionals dedicated to the success of their practices. S1P provides operational, financial, and administrative support services to fuel clinical excellence, growth, and financial security. Ensuring your ability to focus on your patients and your future is what we do best.
225+ practices — 350+ specialists — 28 states
Practice owners — Your focus, Our support
Joining Specialty1 Partners is the starting point for a more fulfilling career and a path to a more secure future. You’ll have
a professional team behind you to manage the administrative tasks currently consuming time and energy better spent caring for your patients.
Realize your vision
We enable our Partner practices to maintain clinical autonomy in caring for their patients without also having to manage the back-office aspects of their business.
Focus on patient care — Your specialty practice will no longer need to manage back-office complexities, enabling you to spend more time and energy keeping patients healthy.
Secure your future — As a member of our growing family of practices, you’ll have the potential to realize financial upside from our continued successful growth.
Do more of what you love — By no longer having to manage all the complexities of running a practice, you’ll have the time and energy to pursue other personal and professional interests.
Level up your practice — Elevate your ability to focus on patient care while a team of professionals manages the complexities associated with running a specialty practice.
If you would like more information about Specialty1 Partners and to see how we can work together, please visit https://www. specialty1partners.com/.
This information was provided by Specialty1 Partners.
DEXIS digital ecosystem expands with three new innovations to streamline and connect dental workflows
DEXIS has announced upgrades to aid clinicians in important workflow. A new X-ray platform is now available. Developed and produced in Tuusula, Finland, the ORTHOPANTOMOGRAPH™ OP 3D™ EX captures consistently accurate images through a straightforward, easy-to-learn workflow. The unit has a wide range of field-of-view sizes for implant placement, endodontics, periodontics, and analysis for airway and TMJ. Also, a new software release will provide advanced tools to plan and execute same-day, prosthetically driven implants.
Serving as the unifying software and central hub of the ecosystem, DTX Studio™ Clinic stores and manages all patient data as well as helps clinicians execute each step of the implant process from diagnostics to delivery. Its functionality allows practitioners to plan an implant treatment and generate a surgical guide chairside in less than 3 minutes. Clinicians can virtually extract teeth, adjust photorealistic abutments and crowns, and create an automated surgical guide that can be sent to a lab or produced in-house for same-day delivery. In addition, an intraoral scanning software update offers scan quality and usability improvements as well as clear visualizations of progressive dental issues over time, through a new tool called Oral Compare. Additionally, the software’s new integration with SmileFy allows for the ability to simulate treatment outcomes chairside, giving patients further confidence in proposed treatment plans.
To learn more, visit https://www.dexis.com.
Integral, a biotechnology company, enters the dental market
Integral Dental has announced the launch of its first product, OraclePI, the only early diagnostic test for peri-implant disease, according to the company. The test delivers a disease diagnosis and personalized care plan recommendations based on patient-specific data. While implant success rates are high, the greatest risk of failure is peri-implantitis. OraclePI enables clinicians to gain insight into 100% of the bacteria present at the implant site, diagnoses the state of infection, and makes recommendations on most effective antibiotics and other treatments. By combining cutting-edge genomic sequencing and AI, OraclePI empowers dentists with actionable insights to improve patient outcomes through personalized care.
OraclePI is available for purchase and being offered in 10 kit packs for a limited time. To learn more, visit IntegralDental.bio.
Established hands-on clinical training curriculum through Institute for Advanced Laser Dentistry (IALD) sets the standard for laser manufacturers that may be “lase-y”
Millennium Dental Technologies, Inc., focused on dental laser-assisted regeneration (LAR) technology and innovative procedures, announced the adoption of its mandatory hands-on laser training for dentists to help ensure patient safety and successful clinical outcomes using its PerioLase® MVP-7™ Nd:YAG free-running pulsed laser. Millennium Dental Technologies is the developer of the LANAP protocol for the treatment of moderate to severe periodontal disease, the only FDA-cleared protocol with scientific proof for true bone regeneration, resulting in new cementum, periodontal ligament, and alveolar bone on a previously diseased root surface.
The IALD is a non-profit educational and research organization dedicated to offering the highest level of laser training and proficiency. The institute’s training program includes 5 days of didactic and hands-on, live-patient treatment using the PerioLase MVP-7. The program is an intensive clinical training curriculum that guides dentists through step-by-step treatment protocols.
For more information, visit http://www.lanap.com or http:// www.theiald.com.
Cellerant and Dental Innovation Alliance (DIA) announce strategic partnership to advance innovation in dentistry
Cellerant Consulting Group and Dental Innovation Alliance (DIA) announced a strategic partnership uniting two forward-thinking organizations in the dental industry, reflecting a shared vision to improve patients’ quality of life through cutting-edge innovation. Together, they will foster new opportunities for collaboration, driving efficiency, enhancing patient care, and empowering dental professionals to stay at the forefront of technological progress. By bringing together Cellerant’s experience in growing early-stage companies with DIA’s innovative model where dental leaders invest in and coach entrepreneurs, this partnership will enable more dental professionals to access transformative tools and resources that elevate patient care across the board.
To learn more about partnering to make an impact in the dental industry, please visit www.dialliance.com. To learn more about Cellerant’s role in bringing new technology into dentistry, please visit www.cellerantconsulting.com.
Cool Jaw ® — a new generation of hot/cold therapy
In the early 90s, Medico International Inc. partnered with leading oral and maxillofacial surgeons to develop a new generation of hot/cold therapy. Cool Jaw® has paved the way to postoperative hot/cold therapy through the creation of our exclusive, hands-free wraps’ patented design. The hands-free Cool Jaw system reduces postoperative swelling and discomfort and allows patients to recover in a convenient manner. Choose from multiple styles of Cool Jaw facial wraps in several colors and varying compression levels. Combine with our extensive variety of hot/cold gel packs to create a post-op recovery solution that best suits your patients.
Our most popular wrap (T-800C) utilizes a unique, patented pocket design that allows patients to fulfill their postoperative care instructions easily without compromising compression. The wraps are fully adjustable ensuring a perfect fit for your patients. Simply slip your frozen or heated gel packs into the patented pocket design, and they remain in place over the recovery area. They also feature a built-in chin cup that helps maintain proper positioning and reduce slippage. All of our wraps are washable and feature Velcro® on top of the head for a fully adjustable fit. Cool Jaw’s hands-free hot/cold therapy system helps promote patient compliance and reduce post-op complications.
implants and cosmetic injections such as Botox. These packs come in a variety of color options to match your office or simply add an element of FUN to any procedure. Choose from bright solid colors as well as eye-catching glitters. These reusable gel packs are 4" in diameter and remain flexible when frozen, allowing for uniform cold therapy. They feature one soft-sided surface that shields the skin from direct contact with the frozen pack.
Our Clear Cold Gel Packs (T-400) are ideal for a variety of cold therapy applications. These sturdy reusable gel packs freeze solid and remain cold for extended periods of time — up to an hour!
All 3x6 Hot/Cold Gel Packs (T-420 & T-425) remain pliable when frozen, contour to the face, and provide patients with more post-op therapy options, including heat. These reusable gel packs shape to the patient’s face, allowing for comfortable, continuous hot/cold therapy.
Cool Jaw’s reusable hands-free system arrives ready to hand out to your patients, including preprinted, patient-friendly instructions for added convenience. Each Cool Jaw system is packaged with your choice of either two or four gel packs. Ordering a wrap with four gel packs allows patients to alternate gel packs between freezings/heatings and ensures a seamless recovery period.
Our Soft-Sided Round Gel packs are a convenient, post-op cold therapy option for after numerous procedures including
Customization is a subtle, yet effective way to promote your practice and enhance your professional image. Cool Jaw helps you to continue promoting your practice long after the surgery date. Cool Jaw’s designers work seamlessly with your staff to help you choose the best colors and layout to ensure your brand shines. Since our products are reusable, patients tend to save them “just in case.” As result, your information is easy to find, and referrals increase. All of our products can be customized with your practice logo and information for long lasting promotion. Let your practice speak for itself! For more information, visit https://cooljaw.com.