Dr. Claudia Pinter discusses an essential tool in her orthodontic practice
Orthodontic records as evidence
Dr. Laurance Jerrold
The art of hiring and firing for your dental practice
Kristin Tauras, JD
The intersection of airway health in orthodontics
Dr. William E. Harrell, Jr.
When contacting the same tooth, Spark Aligners have better contact surface area than the leading aligner brand. The difference is statistically significant.2
Winter 2024 n Volume 15 Number 4
Editorial Advisors
Lisa Alvetro, DDS, MSD
Daniel Bills, DMD, MS
Robert E. Binder, DMD
S. Jay Bowman, DMD, MSD
Stanley Braun, DDS, MME, FACD
Gary P. Brigham, DDS, MSD
George J. Cisneros, DMD, MMSc
Jason B. Cope, DDS, PhD
Bradford N. Edgren, DDS, MS, FACD
Eric R. Gheewalla, DMD, BS
Dan Grauer, DDS, Morth, MS
Mark G. Hans, DDS, MSD
William (Bill) Harrell, Jr, DMD
John L. Hayes, DMD, MBA
Laurence Jerrold, DDS, JD, ABO
Marc S. Lemchen, DDS
Edward Y. Lin, DDS, MS
Thomas J. Marcel, DDS
Mark W. McDonough, DMD
Randall C. Moles, DDS, MS
Elliott M. Moskowitz, DDS, MSd, CDE
Rohit C.L. Sachdeva, BDS, M.dentSc
Gerald S. Samson, DDS
Margherita Santoro, DDS
Shalin R. Shah, DMD
Lou Shuman, DMD, CAGS
Scott A. Soderquist, DDS, MS
John Voudouris (Hon) DDS, DOrth, MScD
Neil M. Warshawsky, DDS, MS, PC
John White, DDS, MSD
Larry W. White, DDS, MSD, FACD
CE Quality Assurance Board
Bradford N. Edgren, DDS, MS, FACD
Fred Stewart Feld, DMD
Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, FADI, DICOI, DADIA
Circulation Disclosure: Total Circulation May Vary. Publisher retains the right to adjust circulation based on a number of factors including but not limited to: print and digital distribution by mail, email, and website for industry tradeshows, educational events, including nonpaid bulk copies and/or digital access provided to events, clients and educational institutions. ISSN number 2372-8396
A bold decision in practice
“Iwant to improve my smile, but braces are not an option.” I hear this so often from adult patients. Many have simply given up on achieving the smile they’ve always wanted because they can’t imagine enduring the discomfort and visibility of traditional braces. Often, they’ve already been told that their malocclusion is too severe to be corrected without fixed brackets and wires.
We might default to fixed appliances, especially for challenging cases. However, the landscape of orthodontics is evolving, and with advancements in clear aligner technology, we now have new options that better align with what adult patients seek — effective, comfortable, and nearly invisible treatment.
My breakthrough in treating complex cases came when I stopped relying on the tooth movement staging provided by aligner software and instead planned the movements based on the mechanics I intended to apply. The key to success with aligners isn’t just in the plastic trays themselves — it lies in applying the fundamental principles of orthodontics, such as anchorage and reciprocal movements.
Recognizing the potential of this evolving technique, I made a bold decision a few years ago — I went all-in with aligners. I stopped offering braces altogether, aiming to achieve the same level of precision that we expect from fixed appliances. This journey led me to utilize TAD-borne appliances such as the Beneslider1 for full Class II corrections, the Mesialslider1 for molar space closure, and bone-borne expanders to correct a skeletally deficient maxilla, all in combination with aligners.
From my experience with various aligner brands, I’ve found that Spark™ Clear Aligners stand out in a unique way. In my opinion, the most valuable feature is the visualization of simulated roots. Without a clear view of the roots, how can we truly know what crown and root movement is involved to reach the desired outcome? How can we accurately determine whether lower incisor crowding is being corrected through protrusion or simply proclination? This is especially crucial for patients at risk of gum recession. In these cases, focusing on crown proclination rather than bodily movement of the roots is often the best approach to protect periodontal health. The ability to visualize the roots allows clinicians to better understand which tooth movements are involved to reach the desired position and plan the mechanics accordingly.
Moreover, one particularly useful feature of leading aligner brands is the integration with CBCT imaging for treatment planning. This has proven invaluable when planning the placement of interradicular Temporary Anchorage Devices (TADs). By visualizing both the roots and surrounding bone structures in 3D, clinicians can precisely identify optimal sites for TAD insertion, minimizing the risk of root damage and ensuring more stable anchorage.
The evolution of aligner technology has expanded our toolkit as orthodontists, enabling us to offer patients treatment options that align with their lifestyle and esthetic preferences. By investing the time to master aligner techniques and fully embrace this paradigm shift, we can help more adults achieve the smiles they’ve always wanted — without sacrificing comfort or confidence along the way.
Claudia Pinter, DMD, is an orthodontist in private practice in Vienna and Wels, Austria, specializing in esthetic orthodontic treatments with aligners. She is also an Affiliate Professor at Nova Southeastern University in Florida. Her passion for education led her to become the Course Director for the Fellowship in Aligner Orthodontics at RipeGlobal. In 2024, she received the Award for Best Aligner Case at the European Aligner Society Congress.
Disclaimer: Dr. Pinter is a paid consultant of Ormco. Ormco is a medical device manufacturer and does not dispense medical advice. Clinicians should use their own professional judgment in treating their patients.
1. Beneslider and Mesialslider are products of TADMAN GmbH.
Precision with Spark™ Aligners
Dr. Claudia Pinter discusses an essential tool in her orthodontic practice
Cover image of Dr. Pinter courtesy of Ormco.
ORTHO PERSPECTIVE
breathing-smile connection: the intersection of airway health in orthodontics
Dr. William E. Harrell, Jr. offers some insights into the history, growth, and importance of airway health
PUBLISHER’S PERSPECTIVE Weathering the storms Lisa Moler, Founder/CEO, MedMark Media............................... 6
ORTHO PERSPECTIVE
Occlusal harmony: the final frontier in orthodontic excellence (Part 2)
Dr. Gregori M. Kurtzman offers ways to preserve orthodontic outcomes ..........................................16 EDUCATION SPOTLIGHT Orthopreneurs Summit At Sea A floating orthodontic think tank 20
Discover the Power of Data-driven Decisions with Gaidge Analytics
Monitoring efficiency and profitability used to mean juggling a practice management system and clunky spreadsheets. But over 2,000 orthodontic practices found an easier way!
80 + Growth Metrics
Access 80+ metrics on your mission-critical key performance indicators for a complete picture of your practice’s health.
PMS Integration
Gaidge connects to leading orthodontic software for the most accurate analysis of performance.
Competitive Comparisons
Compare your performance to industry data from 1,500+ practices and benchmarking across 11 regions.
Benchmark Notifications
Receive notifications for critical business metrics when you fall below orthodontic industry benchmarks.
art of hiring and firing for your dental practice
Kristin Tauras, JD, discusses how to establish a detailed hiring process and how to fire staff that are detrimental to your practice
Dr.
Dr. Kyle Fagala and Kayla Hallen
Dr. Michael Bicknell discusses an educational opportunity for building practice strategies
Weathering the storms
Droughts, heat waves, rain, hurricanes, blizzards, tornadoes, wildfires, and earthquakes, or beautiful sunshine — no matter where you live in the U.S., the weather can bring you the bliss of sitting by the pool or bring you scurrying into the safest windowless room for cover. It’s not just the weather’s fluctuations that we need to prepare for — hoping for the best while preparing for the worst is the best way to avoid storms in all aspects of life. Our focus at MedMark publications is to help you be prepared to face all of the issues that may pop up in your practice, to give you better control over your business and clinical decisions, less stress, and more success.
Here are three tips on keeping your head above water, when you feel that flood of anxiety from practice stress.
Lisa Moler Founder/Publisher, MedMark Media
• Pinpoint your stressors: Define what in your practice is keeping you awake at night, and maybe even keep a journal of what is causing you stress at the end of each work day. Are you afraid that your computer systems aren’t secure from cyberattacks? Are you unsure that your equipment is providing the specific information you need to get the best diagnostics? Are you frustrated that you cannot offer the latest treatment opportunities? Before you can fix a problem, you have to be sure of what the problem actually is.
• Establish a practice culture: Make sure that your practice handbook specifically outlines what behaviors and attitudes are acceptable and which will not be tolerated. Have weekly or monthly team meetings to make sure everyone is on the same page. To head off problems before they grow, learn about conflict resolution skills or hiring-and-firing protocols. If you have an office manager, remember to include him/her in these learning opportunities, and make sure your team knows that you are available for the more complicated situations.
• Give yourself the edge over the competition: It is stressful to watch potential patients filling up other dentists’ appointment calendars. In this day of the Internet and technology, you need to reassess your equipment to improve efficiency, accuracy, and increase patient care and options. Especially in this age of social media, you want your patients to see that you, rather than the clinician across the street, have the most up-to-date imaging, more painless protocols, or faster treatment options.
MedMark publications can help you discover new innovations and information that can help your practice to thrive. In our Cover Story, Dr. Claudia Pinter talks about how advanced technologies like Spark™ Clear Aligners, Approver Software, and the visualization of simulated roots, are changing the face of orthodontic treatment planning. Our CE by Dr. Laurance Jerrold points out common mistakes in recordkeeping and offers guidance on how orthodontists should maintain records for legal defense. Our second CE, by Kristin Tauras, JD, outlines a detailed hiring and firing process that can save practitioners time and stress. Dr. William E. Harrell, Jr. offers insights into the breathing-smile connection and the importance of airway health.
In this last issue of 2024, we give you our “umbrella wish” for fair weather, a dedicated and efficient team, a growing loyal patient list, less stress, and more fulfillment of your goals in the coming year.
Remember, every storm passes, and you need to be prepared to make intentional, positive decisions for a stronger and more profitable future.
To your best success, Lisa Moler
Published by
Publisher Lisa Moler lmoler@medmarkmedia.com
Managing Editor Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com Tel: (727) 515-5118
National Account Manager Adrienne Good agood@medmarkmedia.com Tel: (623) 340-4373
Social Media Manager Felicia Vaughn felicia@medmarkmedia.com
Digital Marketing & Sales Administrator Sharif Rod sharif@medmarkmedia.com
Website Support Eileen Kane webmaster@medmarkmedia.com
MedMark, LLC 15720 N. Greenway-Hayden Loop #9 Scottsdale, AZ 85260 Tel: (480) 621-8955
Toll-free: (866) 579-9496 www.medmarkmedia.com
www.orthopracticeus.com
Subscription Rate 1 year (4 issues) $149 https://orthopracticeus.com/subscribe/
Precision with Spark™ Aligners
Dr. Claudia Pinter discusses an essential tool in her orthodontic practice
Dr. Claudia Pinter in her practice
As a young orthodontist starting my career in Vienna, Austria — a city with many well-established colleagues — my dream was to serve patients with high esthetic demands. At that time, aligners were considered suitable only for mild malocclusions. However, after attending courses on Spark™ Clear Aligners, I realized that by incorporating the principles of orthodontic biomechanics into aligner treatment plans, the possibilities of what we can achieve with “a piece of plastic” seemed limitless.
The Spark Approver Software became an essential tool in my practice, offering a wide range of features for designing predict-
Claudia Pinter, DMD, is an orthodontist in private practice in Vienna and Wels, Austria, specializing in esthetic orthodontic treatments with aligners. She is also an Affiliate Professor at Nova Southeastern University in Florida. Her passion for education led her to become the Course Director for the Fellowship in Aligner Orthodontics at RipeGlobal. In 2024, she received the Award for Best Aligner Case at the European Aligner Society Congress. A published author in peer-reviewed journals, Dr. Pinter regularly lectures at international dental and orthodontic conferences.
Disclaimer: Dr. Pinter is a paid consultant of Ormco. Ormco is a medical device manufacturer and does not dispense medical advice. Clinicians should use their own professional judgment in treating their patients.
able treatment outcomes. The ability to visualize simulated root positions proved invaluable for planning the biomechanics to achieve the desired tooth movement.
Having previously used other aligner brands, I was pleasantly surprised when patients reported greater comfort and less staining with Spark Aligners. This improved patient experience likely contributed to more compliance with wear time, which, in turn, led to better clinical results.
My plan to create a niche offering of esthetic orthodontic treatments with aligners that achieve the same level of excellence as traditional braces was a success.
Focusing on adult treatments, it was deeply rewarding to see my patients’ newfound smiles and confidence.
In this article, we will explore how advanced technologies like Spark Clear Aligners and Approver Software, as well as the visualization of simulated roots, have revolutionized orthodontic treatment planning.
Case 1
A 17-year-old female patient presented for a second opinion on achieving a more harmonious smile. A previous dentist had suggested veneers for teeth 3-3 in the upper arch, but the patient was uncomfortable with this invasive approach. The intraoral
examination revealed crowding, a deep bite, and a dental Class I relationship on the right side, with a full Class II on the left. The panoramic X-ray indicated the absence of a third molar in the second quadrant.
The treatment objectives were to improve smile harmony, align teeth, and establish functional occlusion.
The treatment plan included sequential distalization in the second quadrant to achieve a Class I dental relationship and a symmetrical upper arch. Spaces of 0.5 mm were planned mesially and distally to the upper laterals for composite buildups, further enhancing tooth proportions. Heavy Class II elastics (full-time wear) were employed to reinforce anchorage during sequential distalization.
An additional 10° of lingual root torque was prescribed for the upper incisors to counteract the retroclination of upper incisors, a potential side effect of Class II elastics.
Technician instructions: Sequential distalization of 50% in the second quadrant, with 10° additional lingual root torque for upper incisors (2-2).
The additional lingual root torque was essential to prevent retroclined incisors, which could lead to anterior pre-contacts and potentially result in a posterior open bite.
Results
A dental Class I relationship was achieved on the right side, with maintained torque in the upper incisors, and the patient expressed satisfaction with her improved smile harmony.
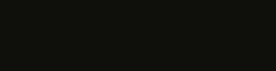
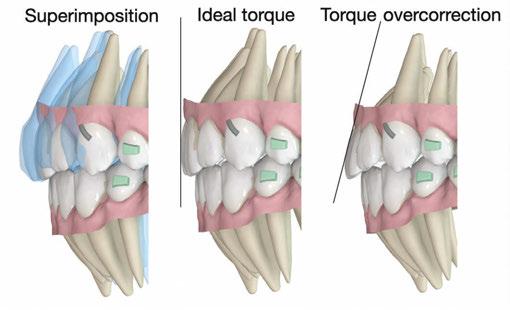
5: The visualization of simulated roots makes it easy for the clinician to see the retraction and lingual root torque that are planned to achieve “ideal torque” and plan 10° of torque overcorrection to compensate for the torque that will be lost during retraction and retroclination that is caused by Class II elastics
Figures 1-3: Case 1. Chief complaint: Enhance the smile esthetics. Intraorally, teeth present with crowding and a dental Class II relation on the left side
Figure 4: Without the visualization of simulated roots, it is difficult to consider the root movement.
Figure
Figures 6-8: Case 1 results — patient expressed satisfaction
Case 2
A 32-year-old female patient presented with a desire to enhance her smile. She exhibited large buccal corridors and crowding in the incisors. Intraorally, a deep bite and retroclined upper and lower incisors contributed to a steep interincisal angle.
The treatment goals included achieving parallelism of posterior tooth torque, broadening the smile, creating a smile arc with a gradual front-to-back transition, and centering the midline through distalization of the second quadrant, supported by Class II elastics.
A specific challenge was posed by the retroclined incisors, which required correction of torque while achieving retraction.
Instructions to the Spark Approver Designer: Sequential distalization of 50%, with an additional 10° root torque for upper 2-2. Place a cut in UR4 and a button cutout on LL7.
Removing the upper left wisdom tooth could have facilitated distalization; however, the patient preferred to proceed without its removal.
Final results
A dental Class I relationship was achieved, with adequate overbite and overjet. Smile evaluation demonstrated a broad smile with gradual front-to-back transition, parallelism of posterior tooth torque, and proper posterior occlusion.
Discussion
Aligners are widely recognized for their efficiency in tipping crowns but are often regarded as less effective in achieving root torque. These cases illustrate that Spark Aligners can successfully deliver lingual root torque in the upper incisors. Root torque is critical for an optimal interincisal angle, proper anterior guidance, and improved esthetics. Unlike tipping movements, cli-
nicians are advised to plan an overcorrection of approximately 10° for cases requiring lingual root torque to prevent retroclined incisors at treatment end.
Without root visualization, achieving accurate lingual root torque can be challenging. Spark Approver Software provides root visualization capabilities, allowing clinicians to accurately assess root movements required to meet desired outcomes. This feature enables simulated root visualization even without a CBCT submission. OP
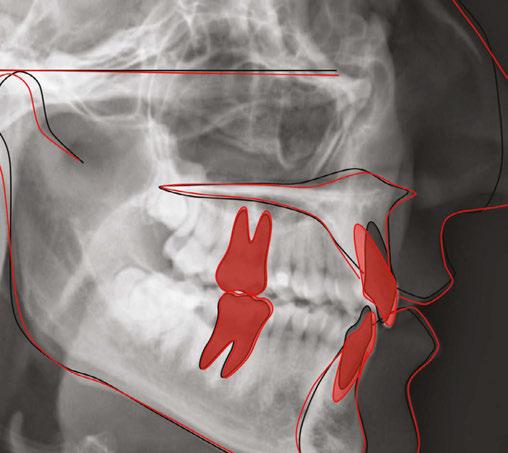
Figure 15: Superimposition of cephalometric tracing. Significant lingual root torque was achieved in the upper incisors
Figures 9-11: Case 2. Chief complaint: Enhance her smile. Intraorally, a deep bite and retroclined upper and lower incisors contributed to a steep interincisal angle
Figures 12-14: Case 2 results
DISCOVER SPARK ™ ON-DEMAND PROGRAM
A new ordering solution for your patients’ needs.
Order any number of Spark Aligners and Prezurv™ Plus Retainers* in a simple, economical, no subscription pricing structure.
INCREASED FLEXIBILITY
Order any number of aligners or retainers directly from the Spark DTX portal.
COST-EFFICIENT
An affordable option for orthodontic treatments, retention, and combo treatments.
MORE CONVENIENT
Reduces the need for in-office printing or dedicated lab space.
The breathing-smile connection: the intersection of airway health in orthodontics
Dr. William E. Harrell, Jr. offers some insights into the history, growth, and importance of airway health
There is a controversy looming in dentistry as it relates to the role of orthodontics in airway health.
• Should orthodontics only be concerned with smile esthetics, facial balance, periodontal health, occlusion, and stability?
• Should orthodontics, including dentofacial orthopedics, be concerned with airway/breathing disorders?
Orthodontic treatment has focused on smile esthetics, facial esthetics, and dental occlusion since its inception,1 and “smile design” has become an important aspect of esthetic dentistry and orthodontics.2 The human airway, especially as it relates to mouth breathing versus nasal breathing affecting health and craniofacial growth, has been an important topic in orthodontics for well over 100 years.3 Unfortunately, with the passage of time, this knowledge has been overlooked, misunderstood, criticized, and forgotten.
This article presents the connection of airway, breathing, smile esthetics, occlusion, and TMJ disorders and how these should be considered as integral parts of the education, training, and integration of a new orthodontic paradigm, as research in medicine and dentistry are confirming that early screening for breathing disorders at age of 3 years old and improving craniofacial growth early (before 6), improves not only dental and facial esthetics, periodontal health, and occlusion, but more importantly, overall breathing and airway dynamics for improvement of long-term health.4 Furthermore, Welkoborsky, et al. (2022),5 found that reproducible rhinomanometric measurements were possible in children aged 3 years and older prompting endorsements from
William (Bill) Harrell, Jr., DMD, ABO, C.DSM, graduated from the University of Alabama School of Dentistry in Birmingham in 1975 and completed his orthodontic residency at the University of Pennsylvania School of Dental Medicine in 1977. He is a Board-Certified Orthodontist (ABO) in private practice in Alexander City, Alabama and Auburn/Opelika, Alabama. Dr. Harrell is also Certified in Dental Sleep Medicine. Dr. Harrell has served as VP and President of the Alabama Association of Orthodontists as the SecretaryTreasurer, VP, and President of the 9th District Dental Society of Alabama; and served on The Board of Trustees and in the House of Delegates of the Alabama Dental Association. He has also served on various committees of the American Association of Orthodontists. Dr. Harrell is the first orthodontic private practice in Alabama to have ConeBeam CT (CBCT) and the first in the US to combine both CBCT and 3D facial imaging (3dMD) in early 2005. Dr. Harrell’s practice focuses on airway-centered orthodontic diagnosis and treatment and TMJ Disorders. Dr. Harrell is the Chairperson of the RadSite ConeBeam CT Standards Committee for setting standards for the insurance industry of reimbursement.
academia healthcare system and providers known as “We Can See at 3.” This new finding prompts screening and rhinomanometry testing with patient cooperation as soon as 3. Sleep-Disordered Breathing (SDB) in children and its long-term negative effects were first described by the late Christian Guilleminault, MD (CG), one of the “fathers of sleep medicine” at Stanford University in 1976.6,7 Early intervention and growth guidance were advocated by CG, and researchers presently at Stanford University6-10 and other experts at other prestigious universities and clinics around the world.6,11-13 This is now known as “Fix Before 6” by the Children’s Airway First Foundation (www.childrensairwayfirst.org) which was founded by Brad and Candy Sparks.
As stated by CG,6,12,14 establishing proper nasal breathing is critical for improving health and decreasing the effects or possibly even eliminating potential co-morbidities later in life. These problems have been associated with obstructive breathing disorders, both during the day and asleep. Additional benefits include creating esthetic and functional results as part of the complete orthodontic and dentofacial orthopedic treatment of our patients. Orthodontics/Dentistry/Dentofacial Orthopedics, which includes airway health, will bring medicine and dentistry closer together. An interdisciplinary team with other allied healthcare professionals and a coordinated approach with a common goal of airway and breathing health is the key to successful treatment of our mutual patients. Diverse opinions are shared and filtered with objective clinical and academic research, leading to diagnosis which then evolves into evidence-based and experience-based therapies. The success or failures of these therapies will vary from patient to patient and doctor to doctor for many reasons. These experiences circle back to confirm or refine the diagnosis and add to clinical knowledge when shared. Patients win when professionals, who may not totally agree with each other, openly share true experiences. Remember, at one time surgeons never washed their hands, put on gloves, or used masks.
Arthur Perry Gordy, DDS, an orthodontist from Columbus, Georgia, is quoted in his article of 1929:15 “In 1836, Charles Dickens, [in the “The Posthumous Papers of the Pickwick Club”16], pointed out the relationship between open mouth, backwardness, and delinquency, that would have saved millions of lives and would have averted millions of life failures had the civilized world realized the true importance of his [Dickens] words.” Dr. C.E. Kells of New Orleans (the father of dental radiography) sent this quote as part of his letter congratulating Dr. Gordy: “You have given the profession and the world something worthwhile; don’t be discouraged — remember Jenner, Pasteur, Roentgen, and Wells.”15,17
Increased nasal resistance, from allergies, habits, or genetics, during growth years affects the craniofacial growth pattern by the alteration of functional nasal airflow and an increased effort to nasal breathe.6,12 This increased effort and strain on the system affects the development of the heart, brain, and other organ systems of the body.18,19 Intraluminal pressure changes from respiratory effort cause structural effects such as narrowed naso-maxillary complex, enlarged turbinates, deviated septum, and altered posture of the mandible, tongue, and head. A conversion to mouth breathing leads to changes in brain function,19 cardiovascular effects, a long facial growth pattern with an obtuse mandibular plane angle and TMJ degenerative changes, resulting in more clockwise rotation of the mandible and encroachment on the airway. This backward growth, along with a lower tongue posture and hyoid position, may lead to a more collapsed airway in the pharyngeal area and naso-maxillary complex in all three planes of space. This results in further increase in nasal resistance.20,21
Health professionals are concerned with long-term implications of this poor growth pattern. CG said, “Pediatric OSA in nonobese children is a disorder of oral-facial growth.”6 Because of the many signs, symptoms, and etiologies involved, evaluation and therapy by Allergist/Sleep Physician/Pediatrician/Dentist/Speech Pathologist/Myofunctional Therapists/ENT is critical for success. What is necessary is expertise in the growth of the craniofacial respiratory complex, more common in pediatric and orthodontic residencies than in many other parts of medical and dental training. Any or all of these disciplines may be required to meet the needs of the individual child at risk.
Imaging
Static 2D imaging such as lateral cephalometric x-rays and advanced 3D volumes, like CBCT, are being used to evaluate the airway. No static imaging can provide dynamic functional information of airway resistance or air flow especially in the nasal region. Computational Fluid Dynamics (CFD), a computer modelling of airflow, and functional MRI (fMRI) of nasal versus mouth breathing are promising new technologies that might be helpful but are just beginning to be researched. Changes to the pharyngeal airway between upright, supine, awake, and sleep states cannot be predicted by static imaging due to variable responses of airway dilator muscle activity and mucosal tissues.
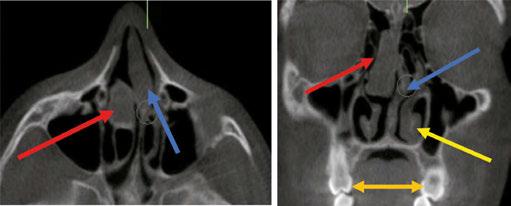
When considering pressure changes and their effects on growth, principles of physics aid in the understanding of how an increase in nasal resistance creates an upstream problem for the craniofacial respiratory complex with a down-stream effect. A deviated septum (Figures 1A and 1B) can cause a 38%-55% increase in nasal resistance versus the open side and results in a pressure drop of 60%-120%.22 In a growing child, this distorts the
shape of airway structures, but is often not discovered until much later in life. Notice the deviated septum (blue arrow) to the left and swollen right middle turbinate (red arrow) and swollen left inferior turbinate (yellow arrow). This is the same patient shown in Figures 3A-4C using 4-Phase Rhinomanometry and Acoustic Rhinometry.
The objective nasal resistance measurements correlate to the structural alterations. Also note the skeletal constriction of the naso-maxillary complex and the dentoalveolar maxillary constriction shown by the lingual inclinations of the maxillary first molars and the narrow maxillary intermolar width (orange arrow 28.2 mm, normal ranges from 36-49 mm4,12,23) contributing to the low tongue posture.
Esthetics
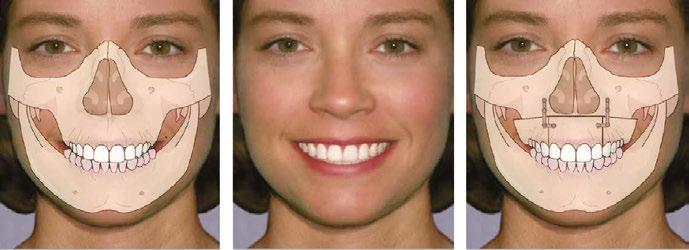
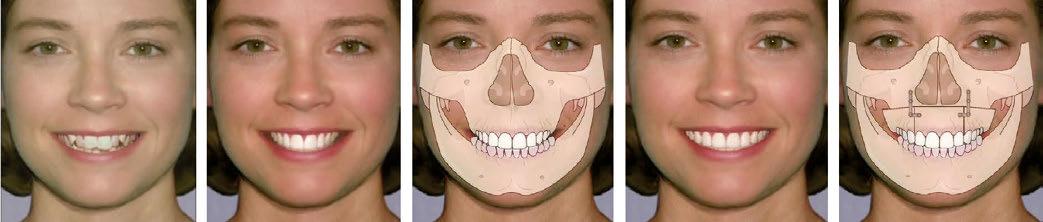
Smile esthetics has always been the mainstay of traditional orthodontic therapy. The esthetic quality of the smile is improved with a wider smile, improved buccal corridors, and a consonant smile arc, etc. Expansion of the maxillae and uprighting the teeth over basal bone while optimizing their AP location accomplishes these goals. Matching mandibular arch dimensions within the more limited boundary conditions available also improves tongue space and airway dimension in the naso-maxillary-mandibular complex (Figures 2A-2C). Figures 2D and 2E show after skeletal expansion either with surgery or skeletal/dentoalveolar enlargement using some form of palatal transverse expansion and/or uprighting and AP development when needed. This results in not only good smile and facial esthetics with broad arches and no dark buccal corridors, but also positively affecting airway dimensions with decreased resistance and increased airflow.
An article by Eric Thuler, MD, PhD (Division of Sleep Surgery, Dept of Otorhinolaryngology, University of Pennsylvania — Perelman School of Medicine, Philadelphia, Pennsylvania), entitled “Transverse Maxillary Deficiency Predicts Upper Airway Collapsibility during Drug-Induced Sleep Endoscopy”24,25 stated, “Our results further the concept that skeletal restriction in the transverse
Figures 1A and 1B: CBCT images of a deviated septum
Figure 2A-2E: Images used with permission and courtesy of Dr. Tom Griffin, DMD - InterActive Communication and Training (IACT), Birmingham, Alabama
dimension and hyoid descent are associated with elevations in pharyngeal collapsibility during sleep, suggesting a role of transverse deficiency in the pathogenesis of airway obstruction.”
Measuring nasal resistance
Dynamic airflow through the nose should be objectively measured to aid evidence-based diagnosis and to monitor therapy. The technology is based on the pressure/flow relationship in the awake state in both sitting and supine positions. As a gold standard of care, each level of pressure change dictates the treatment option through interpretation as well as the monitoring of progress pre, mid, and post treatment. The concept of the technology was founded on the physics of “manometry,” the study of pressure measurements and function such as measuring air flow through transnasal pressure differences (Figures 3A-3C). This data is obtained with 4-Phase Rhinomanometry, a technology invented and developed by Dr. Klaus Vogt, MD, DDS, PhD, an ENT, dentist, and PhD since 1966.26
In 1983, The International Standardization Committee on the Objective Assessment of the Nasal Airway (ISCOANA) consisting of experts from Austria, Germany, Greece, Italy, Norway, Latvia, and Ukraine, representing physics, mathematics, statistics, fluid dynamics, biotechnology, and clinical rhinology was formed to write a consensus on the validity of objective measurements of the nasal airway. The committee, chaired and created by Dr. Vogt, last met in Riga, Latvia on the November 2, 2016 to address the existing nasal airway function tests and to take into account physical, mathematical, and technical correctness as a base of international standardization as well as the requirements of the Council Directive 93/42/EEC of 14 June 1993 concerning medical devices. This was necessary because some of the diagnostic procedures currently in use in rhinology, and now dentistry, no longer fulfil the requirements of quality management for medical devices. In addition, recent studies critically evaluating techniques for nasal airway assessment have not addressed technical progress in this field in recent years and the resulting experimental work, which has a great impact on daily practice.
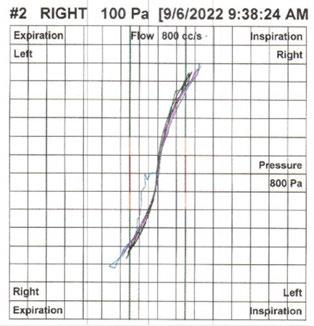
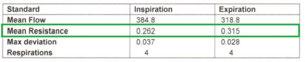
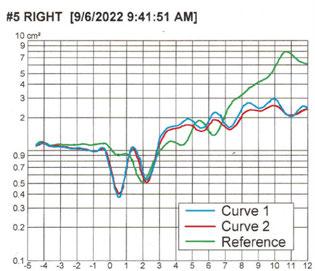
Figure 3A shows the 4 Phase Rhinomanometer unit. Figure 3B shows the Nasal Resistance graph of the right side. The “Tall Lazy
S” represents a normal result. The Mean Resistance of the Right Inspiration is 0.262 and Right Expiration is 0.315, which are close to the normal range less than 0.33 Pa/cm3/sec. Normative values differ based on age, gender, race, and other factors. Women have higher levels of nasal resistance than men, and children even higher, especially neonates. By age five, resistance decreases by 50%. There is continual reduction due to growth of the airway bounding structures until adult resistance is reached. Disease can disrupt this progression at any stage.
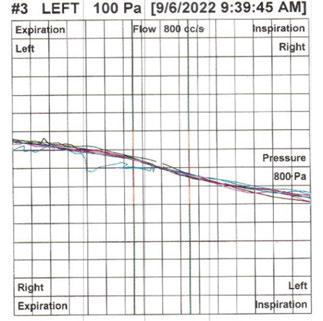
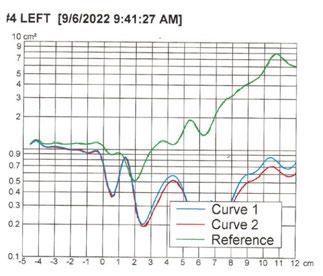
Figure 3C the left side, shows the graph as almost a flat line which shows severely limited nasal flow. Mean Resistance on Inspiration of 3.995 Pa/cm3/sec and on expiration of 12.391 Pa/ cm3/sec. See CBCT in Figures 1A-1B.
To enhance communication of outcomes, an algorithm has been developed by Karen Davidson, RN, PhD,27 called the DAFNE SCORE (www.DAFNESCORE.com), to help clarify the results and give suggestions of common therapies and interprofessional collaboration. The clinician enters data from rhinomanometry; the software provides medically sound guidance.
It is important to understand the differences between rhinomanometry, a measurement of airflow and rhinometry, a structural assessment.
Rhinomanometry measures transnasal pressure differences in the nose — Resistance, Function, Flow (Figures 3A-3C).
Acoustic Rhinometry measures structure/geometry of the nasal cavity using sound waves like sonar (Figures 4A-4C).
Figure 4A shows the acoustic rhinometer being used. The tube sends sound waves (like sonar) through the nose to determine structural integrity.
In Figure 4B, the nasal structure graphs are more closely aligned with the normal curve (green curved line).
In Figure 4C, the measurements of nasal structure in the nasal cavity show that the bottom graphs (red/blue curved lines) are well below the top graph (green curved line) which represents the normal of nasal structure from the nares to the naso-pharynx. These graphs (red/blue curved lines) below the normal curve — (green curved line) represent significant structural abnormality which can be from hard tissues and/or soft tissue being responsible for the obstruction.
Figures 3A-3C: 3A. Patient being tested with a 4 Phase Rhinomanometer unit. 3B. Nasal Resistance graph of the right side. 3C. Nasal Resistance graph of the left side
Figures 4A-4C: 4A. Patient being tested with Acoustic Rhinometer. 4B. Nasal structure graphs for right side. 4C. Nasal structure graphs for left side
When decongested and repeated, if the acoustic waves become closer to the “normal curve” that suggests a soft tissue issue. If there is little to no change, that represents a hard tissue problem. This is extremely important for proper diagnosis of soft tissue issues versus hard tissue issues leading to proper therapy from a MD, ENT, orthodontist, dentist, etc.
A new comprehensive textbook to be published by Springer in mid-to-late 2024 entitled Growing into Breathing Problems: The Quest for Collaborative Lifetime Solutions,11 will discuss pediatric and adult screening and diagnosis, medical and dental therapies, early versus late treatment options, myofunctional therapy, objective measurements of nasal resistance, and surgical solutions. The editors are: William E. Harrell, Jr, DMD, ABO, C.DSM; Pediatric Pulmonologist David Gozal, MD, MBA, PhD; and Pediatric ENT David McIntosh, MBBS, FRACS, PhD, plus 25 other experts in their respective fields.
Mini, micro, and macro smile esthetics, smile projection, smile arc, consonant smile, buccal corridors, etc. are all considered esthetic qualities of a successful and esthetic orthodontic outcome.2 These qualities should be expanded (no pun intended) to the area of improving craniofacial growth, airway, breathing, and TMJ function. Our forefathers in orthodontics were very aware of how obstructed breathing alters craniofacial growth and its effect on the physiology of the body, the occlusion, and dental/ facial esthetics.3 Sometimes, we must go back into history — in order to proceed to the future.
REFERENCES
1. Asbell MB. A brief history of orthodontics. Am J Orthod Dentofacial Orthop. 1990 Sep;98(3):206-213.
2. Sarver D. Smile projection-a new concept in smile design. J Esthet Restor Dent. 2021 Jan;33(1):237-252.
3. Kim KB. How has our interest in the airway changed over 100 years? Am J Orthod Dentofacial Orthop. 2015 Nov;148(5):740-747.
4. Thuler E, Rabelo FAW, Yui M, Tominaga Q, Dos Santos V Jr, Arap SS. Correlation between the transverse dimension of the maxilla, upper airway obstructive site, and OSA severity. J Clin Sleep Med. 2021 Jul 1;17(7):1465-1473
5. Welkoborsky HJ, Rose-Diekmann C, Vor der Holte AP, Ott H. Clinical parameters influencing the results of anterior rhinomanometry in children. Eur Arch Otorhinolaryngol. 2022 Aug;279(8):3963-3972.
6. Huang YS, Guilleminault C. Pediatric obstructive sleep apnea and the critical role of oral-facial growth: evidences. Front Neurol. 2013 Jan 22;3:184.
8. Yoon A, Abdelwahab M, Bockow R, Vakili A, Lovell K, Chang I, Ganguly R, Liu SY, Kushida C, Hong C. Impact of rapid palatal expansion on the size of adenoids and tonsils in children. Sleep Med. 2022 Apr;92:96-102.
9. Guilleminault C, Sullivan SS. Towards restoration of continuous nasal breathing as the ultimate goal in pediatric OSA. Enliven: Pediatr Neonatol Biol. 2014;1(1).
10. Iwasaki T, Yoon A, Guilleminault C, Yamasaki Y, Liu SY. How does distraction osteogenesis maxillary expansion (DOME) reduce severity of obstructive sleep apnea? Sleep Breath. 2020 Mar;24(1):287-296.
11. Harrell W, Gozal D, McIntosh D. Growing into breathing problems: the quest for collaborative lifetime solutions. Springer Publishing in Press 2024.
13. Krishnaswamy NR. Expansion in the absence of crossbite – rationale and protocol. APOS Trends Orthod 2019;9(3):126-137.
14. Marin-Oto M, Vicente EE, Marin JM. Long term management of obstructive sleep apnea and its comorbidities. Multidiscip Respir Med. 2019 Jul 4;14:21.
15. Gordy AP. Mouth breathing and a few facts seldom discussed. The cause, effect & treatment of malocclusion with specific reference to pernicious habits as affecting the physiognomy. Published and presented before the GA State Dental society, 1929.
16. Dickens C. The Posthumous Papers of the Pickwick Club. Chapman & Hall Publishers; 1836.
17. Gordy AP. Nose and throat conditions and allied habits in relation to irregularities of the teeth and development of the jaws. National Health Assoc, 4th District Dental Society of GA; 1929.
18. Zelano C, Jiang H, Zhou G, Arora N, Schuele S, Rosenow J, Gottfried JA. Nasal Respiration Entrains Human Limbic Oscillations and Modulates Cognitive Function. J Neurosci. 2016 Dec 7;36(49):12448-12467.
19. Jung JY, Kang CK. Investigation on the Effect of Oral Breathing on Cognitive Activity Using Functional Brain Imaging. Healthcare (Basel). 2021 May 29;9(6):645.
20. Harvold EP, Tomer BS, Vargervik K, Chierici G. Primate experiments on oral respiration. Am J Orthod. 1981 Apr;79(4):359-372.
21. Linder-Aronson S, Backstrom A. A comparison between mouth and nose breathers with respect to occlusion and facial dimensions. Odont Rev. 1960;2:343-376.
22. Corda JV, Shenoy BS, Lewis L, Prakashini K, Khader SMA, Ahmad KA, Zuber M. Nasal airflow patterns in a patient with septal deviation and comparison with a healthy nasal cavity using computational fluid dynamics. Front. Mech. Eng., Sec. Biomechanical Engineering. 2022;8.
23. Azlan A, Mardiati E, Evangelina IA, A gender-based comparison of intermolar width conducted at Padjajaran University Dental Hospital, Bandung, Indonesia. Dental Journal: Majalah Kedokteran Gigi. 2019;52(4):168-171.
24. Thuler E, Seay EG, Woo J, Lee J, Jafari N, Keenan BT, Dedhia RC, Schwartz AR. Transverse Maxillary Deficiency Predicts Increased Upper Airway Collapsibility during Drug-Induced Sleep Endoscopy. Otolaryngol Head Neck Surg. 2023 Aug;169(2):412-421.
25. Hutz MJ, Thuler E, Cheong C, Phung C, Evans M, Woo J, Keenan BT, Dedhia RC. The Association Between Transverse Maxillary Deficiency and Septal Deviation in Adults with Obstructive Sleep Apnea. Laryngoscope. 2024 May;134(5):2464-2470.
26. Vogt K, Jalowayski AA, Althaus W, Cao C, Han D, Hasse W, Hoffrichter H, Mösges R, Pallanch J, Shah-Hosseini K, Peksis K, Wernecke KD, Zhang L, Zaporoshenko P. 4-Phase-Rhinomanometry (4PR)--basics and practice 2010. Rhinol Suppl. 2010;21: 1-50.
27. Davidson K, Harrell W. Validation of a Novel User Interface and Calculation Method for Determining Nasal Resistance and Patency, in press 2024.
Occlusal harmony: the final frontier in orthodontic excellence (Part 2)
Dr. Gregori M. Kurtzman offers ways to preserve orthodontic outcomes
Occlusion plays a pivotal role in determining the long-term success of orthodontic treatment. Unfortunately, the importance of occlusal refinement post-orthodontics is often overlooked. This article delves into the intricacies of occlusal adjustment, emphasizing its significance in preserving orthodontic outcomes.
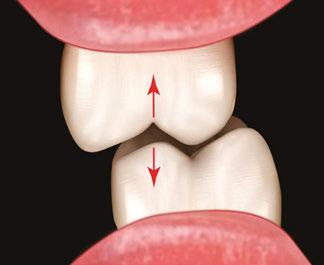
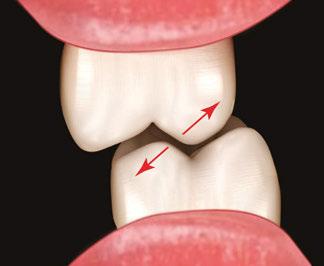
The impact of occlusal forces
Optimal tooth function occurs when occlusal forces are directed along the long axis of the tooth (Figure 1). Contacts between posterior cusp tips and fossa optimally align with this axis. Conversely, contacts on inclined planes exert angular forces, potentially displacing teeth buccally or lingually (Figure 2). These orthodontic-like forces can counteract the achievements of orthodontic treatment. Consequently, meticulous occlusal adjustment is crucial for maintaining the desired esthetic and functional results.
Diagnosing occlusal issues
and 2
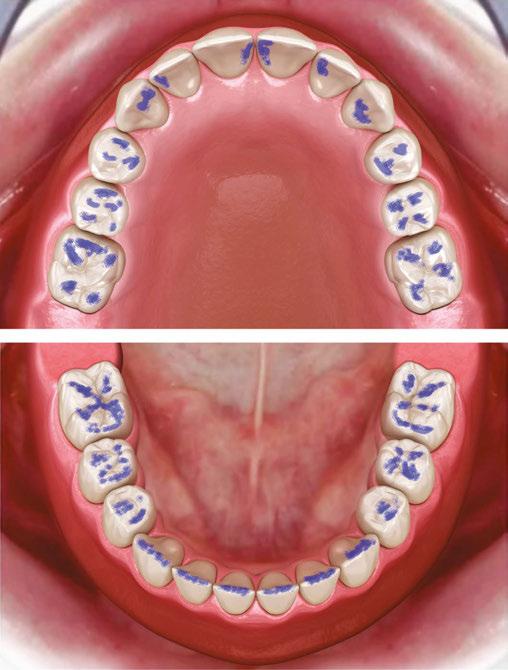
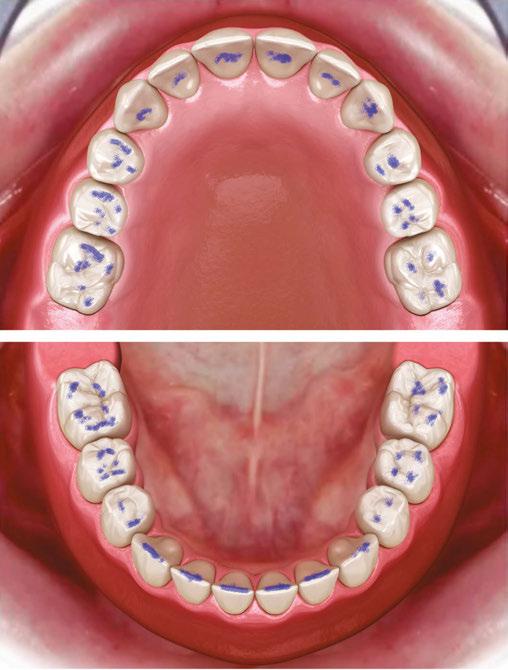
Articulating film is preferred over articulating paper for its thinner profile, which enables more precise identification of contact points. The patient is instructed to bite firmly without grinding, allowing the film to mark the occlusal surfaces. By gently tugging the film, clear contact marks are obtained. Grinding often creates misleading marks, hindering accurate diagnosis.
Occlusal adjustment techniques
The goal of occlusal adjustment is to eliminate contact points on inclined planes, preserving those on proximal marginal ridges which align with the tooth’s long axis. In the anterior maxilla, broad cervical-incisal contacts should be reduced to prevent
Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, FIADFE, DICOI, DADIA, DIDIA, is in private general dental practice in Silver Spring, Maryland. He is a former Assistant Clinical Professor at University of Maryland in the department of Restorative Dentistry and Endodontics and a former AAID Implant Maxi-Course assistant program director at Howard University College of Dentistry. He has lectured internationally on the topics of restorative dentistry, endodontics and implant surgery, removable and fixed prosthetics, and periodontics. He has over 890 published articles, as well as several ebooks and textbook chapters. He can be reached at dr_kurtzman@ maryland-implants.com.
labial tipping. Ideally, anterior contact points should be centered incisally to the cingulum. For the mandibular anterior, contact on canine cusp tips and incisor edges is optimal (Figures 3 and 4).
Figures 1
Figure 3
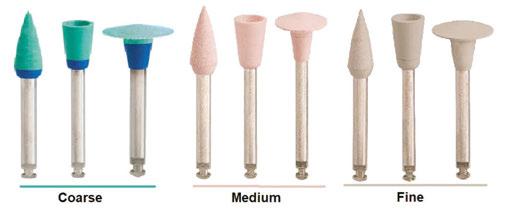
To adjust enamel, composite, or amalgam surfaces, a fine grit football diamond (Figure 5) is effective. For zirconia or ceramic restorations, a zirconia-specific diamond (Great White®Z FOOTBALL 368-023F, SS White) is recommended. When modifying buccal or lingual aspects of posterior cusps or anterior teeth, the previously mentioned diamonds and carbides can be used on enamel, composite, or amalgam. For zirconia or ceramic, a taper fine diamond (Great WhiteZ 850-018F, SS White) is suitable.
Polishing and finishing
Following occlusal adjustment and removal of orthodontic or aligner resin, polishing with Jazz® polishers (SS White) on a slow-speed handpiece is essential (Figure 6). These polishers are available in various grits, shapes (points, cups, disks), and as a comprehensive kit (Reliant Orthodontic Finishing Kit, SS White) for efficient treatment (Figure 7). The occlusal adjustment process can be visualized in four steps: marking with articulating
film (Figure 8A), adjustment with a carbide or diamond (Figure 8B), polishing with a Jazz polisher (Figure 8C), and final occlusion (Figure 8D).
Conclusion
Occlusal harmony is the cornerstone of long-term orthodontic success. Interproximal recontouring, as discussed in Part 1 (Kurtzman GM. The science of stability: tooth modification and occlusal equilibration in orthodontics: a 2-part series. Orthodontic Practice US. Fall 2024;15(3):14-16), often complements occlusal adjustment. Both procedures require precision and attention to detail to achieve optimal esthetic and functional outcomes. By mastering these techniques, clinicians can elevate their orthodontic treatment to new heights.
Acknowledgement: The author would like to thank Robert Wojciechowski for his assistance with creation of the illustrations in the article. This article was provided by SS White.
Figure 7
Figure 4
Figure 6
Figure 5
www.luxcreo.com/industries/4d-aligner/
Orthopreneurs Summit At Sea
A floating orthodontic think tank
This past September, spared by the weather gods, orthodontists met on the high seas for a 4-day fusion of groundbreaking lectures, epic networking, and, yes, an all-youcan-eat buffet.
The Royal Caribbean Serenade of the Seas was transformed into a floating think tank, carrying hundreds of orthodontic practice owners who traded in their scrubs for swim trunks and lanyards. It was like GORP but for practice owners, complete with keynote speeches, AI workshops, and a heck of a lot of sunset selfies.
Anchoring down big ideas: practice-transforming lectures
The event was packed with pivotal insights, but the following were some of the most game-changing lessons from the powerful lectures and keynotes:
John Sileo — Cybersecurity
John Sileo’s story is the stuff of Hollywood (literally) — It was the inspiration behind the blockbuster film Identity Thief, starring Melissa McCarthy and Jason Bateman. After experiencing financial ruin and barely escaping prison, Sileo rose to become one of the world’s most respected cybersecurity advocates. His warning to attendees was urgent: “Over 70% of cyberattacks begin with one simple mistake, like clicking the wrong link.” He didn’t just share stories; he delivered a wake-up call, laying out step-by-step security habits that can make or break a practice.
Stephen Caution — Artificial intelligence
Stephen Caution, AI expert and trailblazing entrepreneur, electrified the room with a bold prediction: “AI is bigger than the internet.” He made it clear that failing to integrate AI into your practice isn’t just a missed opportunity — it’s a strategic mistake. Caution didn’t stop at theory; he presented actionable tools like Runway, Sora, and Trainual that are revolutionizing productivity
today. “If you’re not adopting AI, you’re already falling behind,” he challenged, sparking a sense of urgency among attendees.
Dr. Glenn Krieger — Case acceptance
Dr. Glenn Krieger, Orthopreneurs Founder and CEO, wasn’t pulling any punches when he revealed the secret to boosting case acceptance: “Patients sell themselves when they’re part of the diagnostic process.” By using top-notch clinical photography, Dr. Krieger showed how to empower patients and their advocates, turning them into enthusiastic treatment partners.
Orthodontists set sail Sun, fun, and serious solutions
But let’s not pretend it was all business. The real magic of the Summit was happening off-script. Sushi dinners turned into impromptu brainstorming sessions, and late-night poolside chats felt like group therapy for practitioners trying to navigate the tricky waters of running a practice.
Luis Gutierrez from Las Cruces, New Mexico described:
“There’s a stronger focus on the business side of orthodontics here, which you don’t get anywhere else. You can spend months searching for an answer, and at OP Summit, you can just find it in a casual conversation.”
And then Francesca Pietri from Miami, an OP Summit veteran who has been attending since her residency, added:
“This year was different. It sparked something in me. I left with so much to implement, and the financial investment felt like nothing compared to what I got out of it — professionally and personally.”
Ready for Op Summit 2025?
The buzz from the Summit at Sea hasn’t even had time to fade, but all eyes are already on what’s next: The iconic Caesars Palace in Las Vegas. Orthopreneurs Summit isn’t just an event: it’s an experience, shaking up the way orthodontists think about their practice and their industry.
What’s next? Viva Las Vegas!
To register for this remarkable event, visit OPSummit2025.com/earlybird/.
OP
information was provided by Orthopreneurs.
DR. GLENN KRIEGER´S ORTHOPRENEURS SUMMIT
Free Limo Guarantee
“ATTEND THE FIRST DAY OF THE ORTHOPRENEURS SUMMIT, CHECK OUT ALL THE SPEAKER SESSIONS AND ATTEND THE SOCIAL EVENTS AND IF YOU DON'T CONSIDER IT THE BEST ORTHO MEETING YOU'VE EVER EXPERIENCED, IF IT’S NOT MEETING EVERY EXPECTATION FOR ANY REASON, SIMPLY LET ME KNOW AND I'LL PERSONALLY WRITE YOU A CHECK ON THE SPOT TO REFUND EVERY SINGLE PENNY YOU PAID FOR THE MEETING AND YOUR HOTEL ROOM AND I’LL ARRANGE A PRIVATE LIMOUSINE TO TAKE YOU TO THE AIRPORT AND COVER YOUR FLIGHT BACK HOME. THAT'S HOW CONFIDENT I AM THAT THIS EVENT WILL TRANSFORM YOUR PRACTICE AND YOUR LIFE!”
Orthodontic records as evidence
Dr. Laurance Jerrold explains how proper recordkeeping can make a difference for legal defense
One of the more common mistakes that orthodontists make is not realizing the purpose and extent of a patient’s record. Most of the time, practitioners consider a patient’s orthodontic record to consist of the clinical findings, photos, models, X-rays, and treatment chart. As to the purpose, many believe that we are required by law to keep them, but their primary use is to show what was done on a particular visit. The reality is that they are kept and used for so much more.
Purpose of maintaining records
A patient’s orthodontic record consists of every piece of correspondence of every type as well as the clinical records noted above. The purpose of acquiring and maintaining orthodontic records is the following:
1. To enable and maintain the continuity of care both for the doctor treating the patient as well as for use by any subsequent treating practitioners.
2. To evaluate the patient and adequately diagnose their particular problem.
3. To develop a treatment plan, establish treatment goals, and develop a mechanotherapeutic plan to achieve those goals.
4. To obtain informed consent.
5. To memorialize the treatment rendered on each visit.
6. To document any referrals made and any reports received.
7. To assemble and utilize any and all communications with or regarding the patient such as the following:
a. Intake (personal and employment) data
b. Medical, dental, and social history information
c. Insurance, billing, and accounting records
d. Communications of any type with the patient, relevant third parties, and or other health care providers
e. Laboratory appliance prescriptions
Laurance Jerrold DDS, JD, ABO, FACD, has been the Dean, Chair, and/or Program Director at four ADA CODA-accredited orthodontic programs. He received his DDS as well as his Specialty Certification from New York University. When he became Board Certified in orthodontics, he was recognized as the world’s first third-generation board-certified orthodontist. A firm believer in education, he received his JD from Touro University and his Certificate in Bioethics and the Humanities from Columbia University. His professional background also includes 20+ years in multi-office orthodontic private practice, 30+ years in the practice of law, and over 20 years in full-time orthodontic academia and educational administration. Dr. Jerrold is nationally recognized for his educational contributions to dental risk management and clinical bioethics. He has presented or written over 450 lectures, articles, textbook chapters, and multi-media presentations dealing with orthodontic clinical practice, dental risk management, and clinical chairside bioethics for dental organizations throughout North America.
Educational aims and objectives
This self-instructional course for dentists aims to educate readers on the challenges of dental recordkeeping and how to avoid common legal pitfalls of proper recording and maintenance of patient information.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz online at orthopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can: Identify what constitutes patient clinical records.
• Realize who is responsible for the proper recording of patient information.
• Recognize methods of taking information and maintaining the records properly.
• Realize how to avoid common pitfalls when obtaining, recording, and maintaining patient information.
2 CE CREDITS
8. To document all patient educational and instructional information provided
9. To protect the legal interest of both the doctor and patient
10. To provide data for the following:
a. Quality assurance and outcomes assessments
b. Clinical research endeavors
c. Administrative functions such as scheduling, internal and external marketing endeavors
Not only does orthodontic records acquisition and maintenance enable and provide for the preceding to be accomplished, but arguably its most important role is that of being able to be used as evidence in administrative (State Board of Dentistry) actions, civil (malpractice) suits, as well as in criminal (insurance fraud) cases.
You’ve seen it in countless legal movies and TV programs — some lawyer wants to introduce something into evidence, and the opposing counsel jumps up and says: “Objection your honor, hearsay.” The judge then decides to either sustain the objection thus denying the statements or writings admission into evidence, or he overrules the objection and allows whatever it is to be admitted into evidence. Why is this important? Well, think of it this way. You’ve been sued for malpractice. The cause is irrelevant; you and the patient suing you are in a war of sorts. Some of the many skirmishes that take place during this campaign are: receiving the summons and having to respond to it; both parties having to obtain expert witnesses to testify on their behalf; both parties and their experts having to undergo depositions; pre-trial motion practice; and of course, the trial itself. So far what I have
outlined may seem to be fairly evenly balanced. Ostensibly, both sides have valid arguments, both sides have their experts, and both sides have good attorneys. So, is there anything you can do to give yourself an advantage over the plaintiff? How can you put more bullets in your bandolier than the patient can put into theirs? The answer is that you have your records to help defend you — if you can get them admitted into evidence.
The problem with hearsay
The Legal Information Institute at Cornell Law School defines hearsay1 as …an out-of-court statement offered to prove the truth of whatever it asserts, which is then offered in evidence to prove the truth of the matter. The problem with hearsay is that when the person being quoted is not present, it becomes impossible to establish credibility. As a result, hearsay evidence is generally not admissible in court.
The Federal Rules of Evidence2 notes a number of exceptions to the rule thus allowing for certain types of hearsay evidence to be admitted. Rule 803, Sections 4 and 6 addresses health care practitioners and their “business records.” Rule 803(4) covers statements that are made for the purposes of medical diagnosis or treatment. Subsection 803(4)(A) states that if the statement (the writing) was made for purposes of medical diagnosis or treatment and, as per 803(4)(B), describes a patient’s medical history, their past or present symptoms, their onset, clinical signs or sensations, or belief(s) relating to the cause of their malady, then the statement (writing) may be admitted into evidence.
What constitutes a business record?
Rule 803(6) covers the actual business record itself, in our case, the patient’s chart in its entirety, provided that the writing describes:
A record of an act, event, condition, opinion, or diagnosis if:
A. the record was made at or near the time by — or from information transmitted by — someone with knowledge.
B. the record was kept in the course of a regularly conducted activity of a business, organization, occupation, or calling, whether or not for profit.
C. making the record was a regular practice of that activity.
D. all these conditions are shown by the testimony of the custodian or another qualified witness.
Why are business records considered admissible evidence?
For the most part, they are deemed to be trustworthy. In Timberlake v U.S. Fidelity,3 the court cited a number of different cases and noted:
…The rule cautions, however, that business records will not be admissible where ‘the source of information or the method of circumstances of preparation indicate lack of trustworthiness.’
The rationale behind the business records exception is that such documents have a high degree of reliability because businesses have incentives to keep accurate records. The business records exception is based on a presumption of accuracy, accorded because the information is part of a regularly conducted activity, kept by those trained in the habits of precision, and customarily checked for correctness, and because of the accuracy demanded in the conduct of the nation’s businesses.
If any person in the process is not acting in the regular course of business, then an essential link in the trustworthiness chain fails. It is well established that one who prepares a document in anticipation of litigation is not acting in the regular course of business. (Cits. Omit.)
Further, the court in Monotype v Int’l Typeface4 stated that the elements necessary for a business record to be admitted into evidence are:
A business record is admissible when (1) it is made or based on information transmitted by a person with knowledge at or near the time of the transaction; (2) in the ordinary course of business; and (3) is trustworthy, with neither the source of the information nor method or circumstances of preparation indicating a lack of trustworthiness.
The details of recordkeeping
Let’s go over these elements. New York’s Civil Practice Law and Rules 4518,5 Section 8.08 notes that the writing, the record, must be made by either the person who recorded the event, act, or information or by someone who had personal knowledge of and a duty to record the information accurately. If an orthodontist personally writes his or her entry into the patient’s chart, then he or she is the one with knowledge. If the assistant who performed the procedure is the one who makes the chart entry, then he or she is the one with knowledge. If the doctor performs the treatment but recites what he did to the assistant who then makes the entry into the patient’s record, then they both have knowledge. This is why the clinical notes MUST reflect who actually made the chart entry as it is that person who would have to verify that the information contained in the chart is accurate, which could occur at the deposition phase or at trial.
The “recording” (written entry) of the “transaction” (describing the treatment that was rendered) must be done at or near the time of the transaction. People v Kennedy6 defined this temporal component by noting that when one makes the chart entry, it must be performed at or reasonably close to the time treatment was rendered thus assuring that the recollection of the specifics of the transaction are fairly accurate. It is well accepted that because time blurs memory, to whatever degree, the closer the chart entry is to the point in time that the act occurred makes contemporaneous entries more reliable than temporally remote entries. Requiring this temporal component helps to ensure accuracy and reliability of the recording.
Aspects of “ordinary course of business”
“In the ordinary course of business” has two prongs to it. The first prong requires that the business record was kept in the course of a regularly conducted business activity. Business was defined in Hargett v National Westminster Bank7 as “…any business, institution, association, profession, occupation, and calling of every kind…” Orthodontics, like every other discipline of medicine or dentistry, routinely keeps a record of what diagnostic procedures were performed or data obtained, the diagnosis made, the treatment rendered, the patient’s response to the treatment rendered, a posttreatment evaluation relative to the type and duration of retention required, and the need for appropriate followup if indicated.
Keeping accurate records of the patient’s treatment is uni-
versally done to ensure continuity of care as well as reflecting what was done and the patient’s response to the intervention rendered. It’s what makes the patient’s chart, the business record, reliable since those involved in clinical practice have a legal duty to be accurate in observing and recording the treatment rendered thereby conforming to basic standard of care requirements as well as regulatory requisites.
The second prong is that making the chart entry is a “regular practice” of the business of orthodontics. We routinely keep a record of a patient’s treatment as it would be impractical if not impossible to commit to memory every diagnostic nuance of every case, every aspect of treatment rendered regarding any given case, and every discussion had or instruction given to every patient. In other words, the purpose of the business record is to allow the business in question to function properly. It is precisely because every patient’s record is kept in the manner it is, that it becomes a matter of “a necessary routine practice” resulting in the fact that the record itself becomes reliable and trustworthy.
In summary, the Kennedy opinion6 cited above noted that the business records exception to the hearsay rule …was based upon the recognition that “records systematically made for the conduct of a business as a business are inherently highly trustworthy because they are routine reflections of day-to-day operations and because the entrant’s obligation is to have them truthful and accurate for purposes of the conduct of the enterprise.”
How to take and keep orthodontic records
Now that we know the how and why relating to a patient’s record being admitted into evidence, we now need to turn to how to take and keep orthodontic records of a patient.
Manner of record: In days of yore, the advice was simple — whatever notation you make in the patient’s chart should be done in ink, not pencil. The reason behind this was that penciled entries could be erased and changed, but forensic science could easily detect the year a certain ink was produced.8 Therefore, if one wanted to rewrite their chart years later because now they were getting sued for something, it would be hard for that person to defend a 2014 chart entry made with 2018 ink. Today however most records are computerized, thus, the only admonition is that one is “locked out” after “x” period of time or at the end of the day thus precluding the ability to alter a chart’s entry in any way after that entry was made. It all comes down to trustworthiness and reliability. The legal system must be able to rely on the authenticity and integrity of the entry if it is going to be entered into evidence.
Entering chart notes: The treatment chart needs to reflect who provided the treatment; the doctor, the assistant, the hygienist, etc. It also needs to show who made the chart entry. Remember, the one who made the entry is technically the one who will verify its validity and veracity. Along with this, the record must be sufficiently detailed so that it accurately reflects the treatment that was rendered. Too many chart entries merely state “ortho adj” or something equally uninformative. No one is advocating that the person making the entry write the great American novel — the key phrase is that the entry must accurately reflect whatever procedure was performed or the discussion that was had. In addition, it is advised to keep abbreviations to a minimum, or
in the alternative, to only use those that are universal in nature. One simple example is “L”. Does that mean lower or left? In context, it can be figured out, but no one will know what “SLML” means — shift lower midline to the left.
Altered or missing records: NEVER alter or re-write the patient’s chart. If you are still keeping paper charts, that means no white outs, no black outs, no erasures of any kind. If you make an error, draw a simple line through it so it can still be read, write the words “entry made in error” and then make the correct entry. Any necessary additions or addendums made after the original entry was made, whether using paper or digital charts, should be made in chronological order referencing the date that the addition or addendum refers back to. If it is discovered that you have altered the patient’s record in any way, it reduces your credibility to the jury to about zero. It is an excellent way to lose a lawsuit. Along these lines, if a patient’s chart just happens to disappear due to a convenient fire, flood, or other mishap, most states recognize this as an example of “Spoilation of Records,” and the court will give an instruction to the jury that they may consider that the records are missing because they may have “hurt” the defendant doctor in some way. Thus they are entitled to draw a negative inference from their being missing as by law practitioners are required to obtain, keep, and safeguard the patient’s record.
Non-compliant patients: Document ALL instances of non-compliance such as broken, missed or cancelled appointments, non-cooperation with treatment instructions, poor oral hygiene, not following recommended referrals, etc. All of this goes towards showing various degrees of contributory or comparative negligence on the part of the patient. Think of it this way — your records are there to help you win the case, but if you happen to lose, then hopefully all of this conspicuously noted patient non-compliance may result in the dismissal of the case or, the patient receiving a much smaller award than they would otherwise receive. In addition, make sure all conversations with the patient/parents are documented in sufficient detail and note all unusual questions or responses. Ideally, all instances of non-compliance should “standout” from regular entries, so if your software allows, type those entries in RED, bold, or CAPITALIZED typeface. Still using paper charts? Use a Bic 4-colored pen — black or blue for regular entries, red for non-compliance, and green for next visit.
Timing: Don’t wait until day’s end to write up the patient’s chart. Learn to do it at or near the time the treatment was rendered. If you wait several hours to make your entries, it is not hard to imagine confusing some of Jane’s treatment with that of Joan’s.
Objective versus subjective: Don’t place subjective comments or impressions in the body of the chart — only notate objective data. If you need to write something subjective, like “the patient presented for treatment in an inebriated state” or “appeared unreasonable and distraught,” create a separate page in the file for all subjective entries, keeping those entries in chronological order so they can be incorporated by reference if needed.
Long-term records handling: NEVER part with your original records. You own the records; the patient owns the information contained in the records. You must keep dental records for at least as long as your state’s Statue of Limitations requires. However, be
aware that your state’s Dental Practice Act, Public Health Laws, and other administrative agency’s rules and regulations may have different temporal requirements for retention of medical records; and, often these time periods are much longer than the Statute of Limitations; particularly when minors are involved. You are the custodian of the records. If you die, your estate becomes the custodian. Make sure to discuss this matter with whomever will handle your legal affairs after your passing.
Privacy of records: Don’t leave the chart out or the computer on when the patient is alone with them. They are not made for pleasure reading. Yes, the patient/parent can always request a copy, which you must legally provide9,10 even if they have an outstanding balance.
Access to records: Don’t interfere with a patient’s access to their records. If they complete the required privacy forms and request a copy for themselves or they want them transferred to another doctor, do it. Don’t drag it out or not comply for whatever reason. Whatever your reason is for not complying with a valid records request, it can’t be worth jeopardizing your license as doing so is both illegal and constitutes unprofessional conduct.
Referrals: Be sure to document all referrals made, and if you gave the patient a referral, be sure to follow up and document a) whether the patient cooperated with the referral and b) if they did, make sure you have both read the response from the referred to doctor and filed the response in the patient’s record. It’s very hard to defend doctors who are astute enough to recognize a referral was necessary, which is then followed up by not following up.
Keeping extensive records: Retain copies of ALL correspondence of any and every type that concerns the patient, and make sure that they are appropriately filed in the patient’s record. You don’t want to have to explain why x, y, or z is missing from the patient’s record. When records are missing, the jury does not view you in the best of light.
Re-scheduling: Go over all no-shows at the end of the day. Some patients require an immediate re-appointment, others can wait awhile, but only the doctor knows which is which. You must have some review mechanism in place to track patients who missed appointments and to be able to get them back into the office in a reasonable period of time. To not follow up on missed appointments in a timely manner can actually cause or worsen an injury. You want to be able to prove via written documentation that you made every effort to reschedule uncooperative or non-compliant patients.
Recall appointments: You also want to document missed recall appointments. Recall visits for patients who may not be developmentally, psychologically, or financially ready for treatment are in actuality treatment visits, and missing them can result in a missed opportunity for timely intervention; think ectopically erupting canines. Documenting these appointment failures goes a long way toward proving an affirmative defense that the patient was contributorily negligent.
Filling out forms: Sending out medical history forms in advance or having patients complete these forms on-line prior to their visit can be seen as a mistake waiting to happen. First, it presumes people can read; some can’t. Second, it presumes they understand what is being asked; some don’t. Third, very often, the forms themselves are responsible for limited or inaccurate responses as in many cases there is only a yes or no box that can
be checked, when in reality, if the medical history was obtained in person, one might receive a response of “no, not really” which begs for further exploration or explanation. Learn to obtain them orally. If done properly, it takes a minimal amount of time and enhances the doctor-patient relationship.
Mentioning other doctors: Never tell a patient or write in the chart that a previous doctor did substandard work, overcharged the patient, was experimenting or using an experimental technique, was unethical, dishonest, didn’t know what he was doing, or, that he committed malpractice.
Commenting on products: Don’t attack a product, manufacturer, or vendor unless you can prove whatever your contention or position happens to be as you may be liable for damages to their commercial reputation.
Conclusion
All risk managers, attorneys, consultants, fellow practitioners, and expert witnesses see inadequate or poor quality records much too frequently. Examples are medical history forms not filled out, sections of a clinical exam form left blank, inadequate photographs, and most importantly, poor quality radiographs. If physician’s offices, imaging centers, and hospitals order a test or take an X-ray, and it doesn’t show what they need it to show or is of unreadable quality, they will redo a test, retake a film, or obtain whatever is necessary. We need to operate the same way. If the patient refuses, learn to say goodbye; you do not have to continue treating a patient who refuses to follow direction, instructions, or recommendations.11
Good record taking and record keeping is a skill every doctor needs to develop and incorporate it into their daily practice. If an orthodontist truly wants to practice at the highest level, it won’t happen because he or she uses the newest widget or gizmo. It will be because the doctor wishes to both protect and serve his or her patient while at the same time protecting and serving his or her best interests.
REFERENCES
1. Cornell Law School. Hearsay. https://www.law.cornell.edu/wex/hearsay. Accessed September 29, 2024.
2. Federal Rules of Evidence. U.S. Government Publishing Office, Washington D.C., 2024. https://www.rulesofevidence.org/. Accessed October 21, 2024.
3. Timberlake Construction Co. v Fidelity and Guaranty Co. (US Ct. App. 10th Cir.; No. 94-6080, 94-6149. Nov. 22, 1995). https://caselaw.findlaw.com/court/us-10th-circuit/1463629.html. Accessed October 21, 2024.
4. The Monotype Corporation PLC v. Int’l Typeface Corp. 43 F3d 443 (9th Cir., 1994). https:// casetext.com/case/monotype-corp-plc-v-intl-typeface-corp. Accessed October 21, 2024.
5. New York Consolidated Laws, Civil Practice Law and Rules - CVP Rule 4518. Business records. Findlaw. https://codes.findlaw.com/ny/civil-practice-law-and-rules/cvpny-cplrrule-4518/. Accessed September 29, 2024.
6. People v Kennedy. 68 N.Y.2d 569 (NY Ct. App.) 1986. https://casetext.com/case/people-v-kennedy-30. Accessed October 21, 2024.
7. Hargett v National Westminster Bank. 78 F3d 836 (U.S. Ct. App., 2d Cir.) 1996. https:// casetext.com/case/hargett-v-national-westminster-bank. Accessed October 21, 2024.
8. Speckin Forensic Laboratories. Ink Dating Expert Witness. https://4n6.com/ink-dating-expert-witness/#:~:text=Ink%20dating%20%E2%80%93%20chemical%20tag%3A%20 The,ink%20being%20examined%20was%20manufactured. Accessed September 30, 2024.
9. Social Security. 21st Century Cures Act. 42 USC 201, Public Law 114-255, 130 Stat. 1033 (114th Cong. 2016) https://www.ssa.gov/OP_Home/comp2/F114-255.html. Accessed October 21, 2024.
10. Jerrold L. RRR. Am J Orthod Dentofacial Orthop. 2023 Nov;164(5):750-753.
11. Urrutia v Patino. 297 SW 512, App 10 SW2d 582 (Tex. 1927). https://casetext.com/case/ urrutia-v-patino. Accessed October 21, 2024.
Continuing Education Quiz
Orthodontic records as evidence
JERROLD
1. Not only does orthodontic records acquisition and maintenance enable and provide for the preceding to be accomplished, but arguably its most important role is that of being able to be used as evidence in __________.
a. administrative (State Board of Dentistry) actions
b. civil (malpractice) suits
c. criminal (insurance fraud) cases
d. all of the above
2. The Legal Information Institute at Cornell Law School defines _______ as “…an out-of-court statement offered to prove the truth of whatever it asserts, which is then offered in evidence to prove the truth of the matter.”
a. hearsay
b. voir dire
c. mens rea
d. regular course of business
3. The business records exception is based on a presumption of accuracy, accorded because ____________, and because of the accuracy demanded in the conduct of the nation’s businesses.
a. the information is part of a regularly conducted activity
b. the information is kept by those trained in the habits of precision
c. the information is customarily checked for correctness
d. all of the above
4. The clinical notes MUST reflect who actually made the chart entry as it is that person who would have to verify that the information contained in the chart is accurate, which could occur at the deposition phase or at trial.
a. True
b. False
5. The “recording” (written entry) of the “transaction” (describing the treatment that was rendered) must be done __________.
a. right before the transaction
b. up to 3 weeks after the transaction
c. at or near the time of the transaction
d. none of the above
6. The second prong (of the ordinary course of business) is that _______ is a “regular practice” of the business of orthodontics.
a. committing to memory the details of each patient’s treatment
b. making the chart entry
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://orthopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://orthopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 550
Date Published: December 10, 2024
Expiration Date: December 10, 2027
c. remembering the discussions with the patient
d. discussing the patient’s treatment with the assistant
7. ___________ the patient’s chart.
a. NEVER alter or re-write
b. It is acceptable to erase any notes made in pencil in
c. Only the doctor is allowed to erase entries made in pencil in
d. In digital dentistry, it is allowable at any time after treatment to alter
8. The dentist owns the records; the patient owns the information contained in the records.
a. True
b. False
9. If the clinician dies, ___________.
a. the records can be destroyed by the landlord of the office
b. the assistants are in charge of keeping the information private
c. his/her estate becomes the custodian
d. his/her estate is not involved in the custody of the records
10. You want to be able to prove _______ that you made every effort to reschedule uncooperative or non-compliant patients.
a. via verbal consent with the patient
b. via written documentation
c. via verbal communication with the scheduler at the front desk
d. through phone records
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
The art of hiring and firing for your dental practice
Kristin Tauras, JD, discusses how to establish a detailed hiring process and how to fire staff that are detrimental to your practice
There is a common saying in employment law: hire slowly, fire quickly. While in a perfect world, the employer would have the luxury of slowly sorting through a dozen applications, there is a shortage of workers capable and willing to work in a dental practice. The tendency is to hire quickly before the candidate gets away and a hesitation to terminate a poorly performing employee, which is the opposite of the spirit of the legal employment practices.
Despite the seemingly limited job market, the rule of hire slowly and fire quickly is vitally important, especially for private dental providers. The decision goes beyond dental capabilities to who you want to work with you, who you trust to greet and treat your patients, who will be a good fit for your practice, and who will be around in the future.
Hire slowly
You want to make sure the candidate has the qualifications (licenses or skills) that you need, fits well into your dental office environment, and will be around long enough to be of value to you. A rushed decision could mean hiring someone who has the desired technical expertise, but lacks the interpersonal skills needed to work in a small office environment or engage with patients. Or, a rushed decision could mean hiring someone that has fantastic people skills, but is unable to remain focused on the job, lacks the needed skills, cuts corners, and does not work well in stressful situations or confined spaces.
The hiring slowly principle does not mean to spend weeks or months before deciding to hire a candidate. It means to be both intentional and thorough in your hiring practices.
Posting
The hiring slowly process begins with recruiting talent. Whether you are posting an opening or responding to inquiries regarding hiring, make sure that you understand what you are
Kristin Tauras, JD, is a partner in the law firm of McKenna Storer in Chicago, Illinois. She has a litigation practice in the areas of employment law, insurance coverage, and professional malpractice. McKenna Storer is a full-service law firm providing legal services to individuals and small-to-midsize companies, including defending professional malpractice negligence lawsuits and Illinois Department of Professional Regulation investigation, as well as advising dental and medical professionals regarding business and employment matters.
Educational aims and objectives
This self-instructional course for dentists aims to educate readers on the risks and complications of hiring and firing staff or associates in the dental practice.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz online at orthopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Identify key details that should be included in a job post.
• Realize what details applications legally should or should not contain.
Identify red flags that may come up in an interview, regarding demeanor or prior experience.
• Realize the legal aspects and employer’s responsibilities for a “working interview.”
• Identify background checks that should be a part of the hiring process.
• Define reasons for firing quickly and how to avoid the legal ramifications of firing an employee who is not a good fit for your office.
2 CE CREDITS
looking for in a candidate and clearly convey that message. If you do not have a job description of the role you are attempting fill, now is a good time to create a written description. You should post every license and skill that individual must have along with other job requirements and consider posting every desired quality the individual should have. Obviously, you
want your dental professionals to have the license or certification required in your state, and your office personnel to have basic computer knowledge, but also consider what other qualifications you want the individual to have. Some examples include, prior experience, ability to work with children, experience working with the elderly and disabled, experience in a medical or dental office, ability to work in small confined spaces, ability to take direction, experience with charting, and experience with submitting insurance documents.
Applications
You should check with an attorney in your state to verify that your application process complies with your state laws. Do not assume that the application you used for the last several years complies with today’s employment laws. The laws are continuously evolving.
At a minimum, your application should include a place for providing information regarding the following:
1. name and contact information
2. the position the applicant is seeking
3. prior employment history
4. work-related experience
5. education
6. licenses
7. computer/charting proficiency
Your application should also provide a signature line for a verification, stating that the applicant attests that the information they are providing is true and accurate. This will make it easier to withdraw an offer or terminate a person if the information is found to be false.
What you should not ask is more complicated.
More than half the states now have a “ban the box” law, which are laws that prohibit requesting information on an application regarding criminal arrests and convictions.1 Many states also have laws regarding salary history as a means to remediate discrimination in wages.2 The Equal Pay Act (EPA) is another federal employment law giving employees a private right to action for discriminatory pay.
You should also avoid questions that may reveal whether an applicant is a member of a protected class under federal and state equal employment opportunity laws. Many states have laws against disclosing a disability, race, or other historically discriminating categories on a job application. Even in states that do not specifically prohibit this inquiry on the job application, the inquiry into protected classifications may be used as evidence of discrimination. See for example, Title VII of the Civil Rights Act of 1964 (Title VII) (a federal law that prohibits employment discrimination based on race, color, religion, sex, or national origin); The Americans with Disabilities Act (ADA) (a federal law prohibiting discrimination on the basis of actual or perceived disability), and Age Discrimination in Employment Act (ADEA) (a federal law prohibiting discrimination against people over the age of 40).
Use the interview as a time to observe the person’s demeanor, interest level, interactions with others, and how they fit within your office dynamics.”
Interviewing
The interviewing process is vitally important. The inclination is to leave hiring to the office manager, but you should be involved in the interview. Today, most initial screening interviews are done over the phone or through Zoom to determine if the person meets the initial criteria for the job. At this point, you should know enough about the candidates: their educational level, whether they are credentialed, years of experience, and whether they have an interest to work in the location for the hours/days required and the salary range.
Use the interview as a time to observe the person’s demeanor, interest level, interactions with others, and how they fit within your office dynamics.
If the applicants are for a dental professional, ask about the history of their license, whether they have had any disciplinary actions and the status of the actions, lawsuits and claims, whether they currently have insurance and who their current provider is, and whether there is any reason they would not be insurable. Pay close attention to someone who has had several jobs over a short time period or someone who was until recently practicing in a different state. There may be legitimate reasons for the changes, but this could be a red flag that the person is no longer licensed in another state, has had issues in that state, or has a history of job jumping.
If the applicant is an office professional, ask about their experience working in a dental or medical office. You will also want to gauge their understanding of HIPAA and the need to maintain medical and financial privacy. Asking open-ended questions such as, “what was the least pleasant dental experience you have had” and watching the person’s reactions as well as words will disclose information about the person who you are hiring. The same details are important to find out about your office staff as well. Your receptionist may be the first and last contact any patient has with your office; you want it to a positive one.
During the interview, you should make it known if an offer of employment is conditioned on drug screening, criminal background check, or financial background check. This will give the applicant the opportunity to front any issues and decide whether they want to move forward in the hiring process, which may save you from the time and cost associated with background checks.
Working interview versus skills assessment
The working interview is tricky, but may be necessary. You can ask a dental professional to demonstrate their technique, but if you receive compensation for their work, or if they spend time
doing actual work, then you may be required to compensate them for their work.3 (Some dentists find working interviews beneficial because they offer the opportunity to assess the candidate’s technical and interpersonal skills.) Negotiate this in advance if you are asking them to work. You should also check with your malpractice provider and workers compensation provider to verify that the “working interview” is covered by insurance.
References
You should ask for references, but recognize that most people will only provide references from individuals who they know will give a positive reference. Pay attention to what references are not there — especially if none of the references are from recent employers. You should contact the references listed. You should also verify that the references are true references.
Background checks/drug testing
If you use background checks and drug testing, make sure that the candidate knows up front that any job offer will be provisional on a background check and drug test.
Criminal background check: Many states require a written authorization prior to doing a background check. You should follow your state laws before conducting any criminal background check and in determining how to use the information. It is a violation of civil rights to request a background check because of someone’s race.4
Financial background check: Under the Federal Fair Credit Reporting Act (FCRA), the applicant must sign an authorization, and the FCRA notice must be provided on a stand-alone document (not part of the employment application). There are several nuances to this law that should be discussed with an attorney before deciding whether you need this information.
Licensing check: Most states have websites where the public can find information related to licensing renewals and disciplinary actions, such as suspensions and revocation of license. You should never forgo reviewing the licensing information available. If anything is flagged during the search, you should make an inquiry regarding the issues prior to offering employment. You should also inquire about whether there have been any pending investigations, findings, and suspensions of the professional’s Drug Enforcement Administration (DEA) license.
Drug screening: States have different laws related to drug screening. It is vitally important to check with your state’s laws prior to requesting that the applicant submit to a drug screening. This is especially true in states that have legalized the use of cannabis. Where drug screening is permitted, you should use the state-specific drug screening authorization form and follow the state-specific protocol for responses if the drug screening it positive.
Internet and social media: A Google search should not be your only review of an applicant, but it may provide useful information. You may see red flags, such as the sharing of offensive comments or conduct. You may see that there were employers the applicant left off. It may also disclose a person’s tendency to post negative reviews of employers. Or, it may show a person that has a professional footprint.
Decision
When you have all the information, you still need to make the decision whether to hire the applicant. Be thorough in the reasons you want that person to be your employee or not.
Your considerations should include considering both the individual and your needs.
First, does the candidate have the skills and level of experience you need? If the employee has the skills, but lacks the experience, will you be in a position to train the employee while still maintaining office efficiency while the employee gains the experience? Do you have the time and patience to train a newer professional? Be realistic. A recent graduate from a prestigious university may seem appealing, but a person from an established practice may be a better fit for your office. Then again, even a person with years of experience would not be a good fit if you do not agree with their approach to patients or treatment.
Second, does the candidate have a personality that fits well with the office? Does the person interact well with others? Does the person seem like someone you and your patients can communicate with? Most dental and medical offices strive to have a calm environment, beginning with the person who greets the patients, to the professionals who perform the work, to the person who ultimately schedules the follow-up visits and billing. You do not want the environment to be disrupted by having someone join who is caustic, negative, or standoffish. Assume
You should ask for references, but recognize that most people will only provide references from individuals who they know will give a positive reference.”
that the person who came to the interview is that person on the best day. Try to imagine how that person will fit in with your vision for the office.
Third, will the candidate stay? If you follow the hire-slowly principle, you will have already invested time in this candidate. Is there anything in their work history or personality that would lead you to believe that the individual is viewing this position as a stepping stone? You will want to have an employee whom you believe will be around in the long run to make your time and efforts pay off.
Fire quickly
Firing quickly means to take swift action when it is apparent that the employment relationship is not working. For most, it is a difficult decision to fire someone. You have invested time into hiring and training the employee. It is hard to admit that you made a mistake or that it is not working out, especially if you have grown fond of the employee. It is not an easy decision, but if you are considering it, it is probably a necessary decision.
Do not delay in terminating once the reason is apparent. There are several reasons why this should be done swiftly.
Productivity
If an employee is not performing up to your standard, it will negatively impact productivity for both that employee as well as those around the office. It may be that the individual did not have the level of training or experience you believed they had, or needs more training and guidance than you have the time to give. Mistakes can be costly for you and your patients.
Office Culture
It is often said that one bad apple can ruin the bunch. The same is true of one toxic employee. Most dental practices are small enough that one employee can adversely affect office culture. If an employee is not fitting in well to the office culture or is unintentionally or intentionally sabotaging the office dynamics, it makes sense to act swiftly. Similarly, although more subtle, a person who is not pulling their own weight, arriving late, and making errors, will also negatively affect the office dynamics.
Cost
It is expensive to hire, train, and retain good employees. But, it is expensive to have a non-performing or disruptive person in the office. You should not spend time and money on further training someone who is not a good fit for your practice. The money, time, and energy spent trying to train and develop an underperforming employee diverts resources and attention from those who are, and may cause you to lose valuable employees and patients.
Reputation
Most dental offices rely upon repeat business and referrals. Most people do not take the time to research their dental practitioner, but will rely upon their dentist or neighbor in determining
who to see. You cannot afford to have your reputation tainted by one poor employee.
Malpractice
Most obviously, you should terminate someone who is not meeting the appropriate standard of care. This could cause you both financial and reputation harm. But you should also terminate someone who does not meet the standard of decency in their interactions with patients. Someone who is unhappy with the dental procedure performed may sue, but someone who was also treated poorly by the person performing that service is more likely to sue.5 Anyone can make a mistake, but not everyone will know when a mistake was made, how to correct the mistake, and how to treat others.
Other liability
Employers may be held liable for the sexual harassment, discriminatory acts and, in some cases, the criminal acts of its employee. See Title VII, 42 U.S.C. 2000e, employer liability. This liability may extend to liability for acts against co-employees, venders, and patients. Terminating the offending employee may avoid or lessen civil liability.6,7,8
One caveat to the fire quickly rule: If you have a contract or the employee is a member of a union, you need to make sure you follow the steps set forth in the contract prior to termination (such as notice requirements or termination for cause provisions). In those situations, you should contact your attorney for guidance for how to best terminate.
Best practice
Hire with intention people who meet the criteria and fit within the office’s needs and culture. Do not be afraid to fire if the employee is unable to meet the standards or does not work well within your office. Making good choices and following the guidance as discussed above can avoid possible legal risks and lead to a more positive office environment and a stronger practice team.
OP
REFERENCES
1. Ban the Box: U.S. Cities, Counties, and States Adopt Fair Hiring Policies, https:// www.nelp.org/insights-research/ban-the-box-fair-chance-hiring-state-and-local-guide. Accessed October 21, 2024.
2. HR Dive. Salary History Bans. https://www.hrdive.com/news/salary-history-ban-stateslist/516662. Updated May 8, 2024.
3. American Dental Association. Recruiting: Working Interviews vs. Skills Assessments, https://www.ada.org/resources/practice/practice-management/10_recruiting_working_interviews. Accessed October 21, 2024.
4. Federal Trade Commission Consumer Advice. Employer Background Checks and Your Rights. https://consumer.ftc.gov/articles/employer-background-checks-your-rights. Published August 2023.
5. Pour H, Subramani K, Stevens R, Sinha P. An overview of orthodontic malpractice liability based on a survey and case assessment review. J Clin Exp Dent. 2022 Sep 1;14(9):e694-e704.
6. Cornell Law School Legal Information Institute. 42 U.S. Code § 2000e – Definitions. https://www.law.cornell.edu/uscode/text/42/2000e. Accessed October 21, 2024.
7. Society for Human Resource Management (SHRM).Employment Law 101. Employer Liability for Sexual Harassment. https://www.shrm.org/topics-tools/news/employmentlaw-101-employer-liability-sexual-harassment. Accessed October 21, 2024.
8. U.S. Equal Employment Opportunity Commission. Enforcement Guidance on Harassment in the Workplace. https://www.eeoc.gov/laws/guidance/enforcement-guidanceharassment-workplace. EEOC issued a new guidance on April 29, 2024.
Continuing Education Quiz
The art of hiring and firing for your dental practice TAURAS
1. Despite the seemingly limited job market, the rule of _________ is vitally important, especially for private dental providers.
a. hire quickly and fire slowly
b. hire slowly and fire quickly
c. hire infrequently and fire infrequently
d. hire additional employees so you don’t have to worry about replacing them
2. You want to make sure _________.
a. the candidate has the qualifications (licenses or skills) that you need
b. fits well into your dental office environment
c. will be around long enough to be of value to you
d. all of the above
3. (When creating a job description) You should post every license and skill that individual must have along with other job requirements and consider posting every desired quality the individual should have.
a. True
b. False
4. More than half the states now have a “ban the box” law, which are laws that prohibit requesting information on an application regarding __________.
a. criminal arrests and convictions
b. recent real estate transactions
c. retail debt
d. former employers
5. The is another federal employment law giving employees a private right to action for discriminatory pay.
a. Health Insurance Portability and Accountability Act (HIPAA)
b. Equal Pay Act (EPA)
c. Working Interview Act (WIA)
d. Federal Fair Credit Reporting Act (FCRA)
6. (When hiring) If the applicants are for a dental professional, ask about the history of their license, _______, and whether there is any reason they would not be insurable.
a. whether they have had any disciplinary actions and the status of the actions
b. lawsuits and claims
c. whether they currently have insurance and who their current provider is
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://orthopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://orthopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 550
Date Published: December 10, 2024
Expiration Date: December 10, 2027
d. all of the above
7. During the interview, drug screening, criminal background check, or financial background check.
a. you should not mention the upcoming
b. you should make it known if an offer of employment is conditioned on
c. you should let another member of the staff bring up the possible
d. you should surprise the candidate with the
8. (For a working interview) You can ask a dental professional to demonstrate their technique, but if you receive compensation for their work, or if they spend time doing actual work, _________.
a. then you may be required to compensate them for their work
b. you definitely are not required to compensate them for their work
c. you should not tell them that you are being compensated for your work
d. you should not negotiate possible compensation with them in advance
9. You should who is not a good fit for your practice.
a. spend more time and money to provide extra training for someone
b. not spend time and money on further training someone
c. have an office meeting to discuss the employee
d. give at least 6 months’ probation to an employee
10. Employers may be held liable for the sexual harassment, discriminatory acts and, in some cases, the criminal acts of its employee.
a. True
b. False
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
The custom approach to digital IDB
(And how it saves time and money)
When Dr. Paul Trotter took over his father’s practice, he faced a big decision. The business had expanded rapidly, and there was a lot of work for one doctor. Should he hire another associate? Or should he figure out how to optimize his time and manage the practice himself?
Dr. Trotter opted for the second path. The only associate he’d ever worked with was his father — and he wanted to keep it that way.
Before his father’s retirement, the practice relied on conventional braces — a timeline that stretched an average of 18 appointments over 21 months.
But now, Dr. Trotter has cut those appointments from 18 to 11 — and increased revenue per appointment from $388 to $670 without hiring another associate.
Getting there took some trial and error.
In 2020, Dr. Trotter dabbled with KLOwen, a fully customized orthodontic solution. The KLOwen Software and their U.S.based digital lab team help doctors create custom prescriptions for every tooth and every patient.
Unlike other custom solutions, KLOwen offers a full portfolio of custom brackets, including metal and clear twin, and metal self-ligating — all at a reasonable price point.
At the same time, Dr. Trotter also experimented with digital Indirect Digital Bonding (IDB) utilizing conventional brackets. Both solutions provided a customized tray that helped guarantee optimal bracket placement at the beginning of the patient’s journey.
But from there, the two solutions couldn’t be more different.
As a patient progressed, the work required with digital IDB cases became less efficient — and more tedious. Dr. Trotter still had to spend additional appointments handling wire bends and repositionings.
Meanwhile, patients with the KLOwen custom prescription were coming back for fewer appointments and showing superior outcomes. The KLOwen appointments could also be managed by the staff with fewer doctor-intensive detailing appointments.
“KLOwen was obviously a better solution,” Dr. Trotter said. “We dove all in.”
As many doctors can relate, switching to a new clinical workflow can be a big lift for the team. Dr. Trotter has worked with his team for years. It was important they understood the “why” behind the transition to KLOwen.
He explained he wanted to keep the family business in the family. He also acknowledged the change would require some initial extra effort from his team. But once they fully adopted KLOwen, he promised it would save everyone time and stress and enhance the patient experience, without compromising outcomes.
And in the end, Dr. Trotter’s Gaidge data proved he was right.
“Going from conventional to digital IDB reduced appointments from 18 to 15,” Dr. Trotter said. “But going from digital IDB to KLOwen knocked off four additional appointments. We also increased our revenue per appointment from $388 with conventional to $475 with digital IDB to $670 with KLOwen an almost 73% increase from conventional to custom.”
Even better, the KLOwen appointments are less stressful, more streamlined, and less physically demanding. Dr. Trotter can have real conversations with patients (or their parents). He no longer feels like he’s “running on a hamster wheel” to make it through his schedule.
Since the custom prescriptions generated by KLOwen Software reduce the number of doctor-intensive appointments, Dr. Trotter’s team can also better predict the practice’s workflow. They worked hard to learn the new solution — and feel “empowered” by the results they’ve helped create.
Dr. Trotter says his team jokes that they’ll quit if he ever goes back to conventional braces or digital IDB.
“Digital IDB alone wasn’t customized enough. With KLOwen, we’ve maintained the quality of our practice without hiring an additional associate,” said Dr. Trotter.
“Whatever your ‘why’ is — whether it’s cutting back hours or finding time to take on new patients — KLOwen will empower it. This is custom done right.”
This information was provided by KLOwen. OP
Study methodology: Sample size (n= 450) reflects consecutively debonded cases (July 2020 – December 2022) across three treatment modalities: 1) MBT direct bond, 2) MBT delivered with digital IDB, and 3) custom braces delivered with digital IDB. Study data originally presented at Gaidge 360 in February 2023 (selected less complicated cases while getting started).
Practice management in orthodontics
Dr. Michael Bicknell discusses an educational opportunity for building practice strategies
In today’s evolving orthodontic field, effective practice management is critical for delivering high-quality care while improving operational efficiency. At Ultimate Orthodontic Academy (UOA), we guide orthodontists in integrating innovative strategies into their practices, enabling them to achieve predictable outcomes, streamline workflows, and elevate patient satisfaction.
Managing outcomes for efficiency
Managing the outcome — the end result — throughout treatment minimizes overall complexity. Efficiency at every stage of the patient journey reduces treatment times, improves predictability, and ensures deliverables are met with fewer errors. By focusing on outcomes, practices can reduce workdays, staffing needs, and opportunities for mistakes, all while maintaining exceptional care.
Traditional practice management often overlooks this outcome-focused approach. However, I have seen its transformative impact in my own practices and believe it is a game-changer for the orthodontic community. This insight has driven my passion to share knowledge globally through UOA’s programs, designed to help orthodontists optimize their practices and better serve their patients.
Insights from Dr. Michael Bicknell
At UOA, we emphasize patient-centered, efficient, and high-quality care. Tailoring treatment plans to individual patients improves outcomes while reducing inefficiencies. As a key contributor to UOA’s educational programs, I aim to empower orthodontists with proven strategies that enhance their practices and elevate the standard of care.
Training and education
UOA provides comprehensive training in orthodontic techniques and practice management. Our programs teach systems and methodologies that empower orthodontists to streamline operations and enhance patient care. By prioritizing efficiency, we help practices achieve better results with less effort.
Michael Bicknell, DDS, MS, a board-certified orthodontist and Diplomate of the American Board of Orthodontics, owns Advanced Orthodontic Specialists in Elmhurst, Illinois and founded the Ultimate Orthodontic Academy. A graduate of the University of Illinois at Chicago, he is dedicated to advancing orthodontic care through efficient, esthetic-focused treatment. With thousands of educational hours delivered globally, Dr. Bicknell’s lectures inspire orthodontists to optimize their practices, improve patient outcomes, and adopt innovative approaches that elevate the standard of care.
Disclosure: Dr. Bicknell co-founded Ultimate Orthodontic Academy.
UOA’s educational offerings
Online courses
UOA’s online courses accommodate busy orthodontists, providing flexible learning options that cover essential topics in practice management and clinical techniques. These courses feature expert insights, interactive modules, and video demonstrations that allow participants to learn at their own pace while implementing actionable strategies in their practices.
In-person courses
For those who prefer hands-on learning, UOA’s in-person courses offer immersive sessions with direct access to instructors and peers. These courses include live demonstrations and collaborative discussions, enabling participants to gain practical skills while networking within the orthodontic community.
Leveraging technology
Incorporating digital tools is vital for modern orthodontic practices. UOA emphasizes the use of advanced imaging and treatment planning software, which improves precision and reduces errors. Additionally, our training includes practice management software to simplify appointment scheduling, billing, and patient progress tracking.
Building a cohesive team
A cohesive team is essential for effective practice management. UOA provides guidance on team dynamics, fostering communication and collaboration among staff. A well-trained team improves patient experiences, supports innovation, and drives continuous improvement.
Conclusion
By focusing on managing outcomes, leveraging technology, and building strong teams, orthodontic practices can achieve greater efficiency and deliver exceptional care. UOA is committed to providing orthodontists with the tools and knowledge they need to optimize operations, enhance patient outcomes, and thrive in an ever-changing field. In today’s ever-changing market of shrinking margins, improving efficiency is one of the simplest and most effective ways to boost profitability. OP
4 ways to factor marketing into your practice management
Dr.
Kyle Fagala
and
Kayla
Hallen offer strategies to attract new patients
When you think of practice management, what comes to mind? Is it team building? Billing? Marketing? If digital marketing isn’t at the top of your list, you’re falling behind. Every practice should center its practice management strategy around these 4 digital marketing tips to boost your new patient acquisition.
Budget for growth
Getting more new patients doesn’t come free. While you might be able to maintain your current new patient rates with a 3%-5% gross revenue budget, you’ll need to spend 7%-10% to start seeing growth.
Your budget makes the rest of your digital marketing strategy possible. The higher investment allows you to create a more robust plan including advanced SEO strategies, ads that help you compete for higher cost-per-click keywords, content creation, and more — all of which bring more patients through your doors.
Build a targeted paid ad strategy
Google and Meta (Facebook) ads are the standard for generating brand awareness and immediate lead generation across search and social media platforms. Both work differently for different purposes. Google search ads, for example, target users in the middle of an active search for orthodontic services, while Meta lead ads can help you get in front of a larger audience while capturing their information for future marketing purposes.
Dr. Kyle Fagala is a trusted authority and highly sought-after speaker in Orthodontics. As the owner of Saddle Creek Orthodontics and co-founder of Neon Canvas, a digital marketing agency, Dr. Fagala delivers exceptional patient care and offers invaluable strategies for practice growth. He hosts “The Digital Orthodontist: Live!” podcast, authored two children’s books, and is a Key Opinion Leader for 3M Oral Care. Dr. Fagala graduated from UT Memphis in 2013 with a master’s degree in Dental Science and teaches Development of Occlusion at the University of Tennessee Health Science Center. He lives in Germantown with his wife Anna, their four children, an Aussiedoodle named Sammie, and three peacocks: Jim, Pam, and Dwight.
Kayla Hallen has been a dedicated presence in the orthodontic industry since 2010, working in diverse settings from start-ups to multi-location practices. Her journey from scheduling and marketing to treatment coordination and office management gave her an insider’s understanding of the industry. Joining Neon Canvas in 2023 as Director of Client Development, she combines years of hands-on expertise with an empathetic approach, truly connecting with her clients and their teams. Kayla resides outside of Chicago in Lake Bluff, Illinois, with her husband Graham and their five young children.
Google and Meta alike offer detailed targeting opportunities. Google allows you to target users by location, relevant keywords, user behavior, etc. Meta allows you to target specific demographics like age, area, and even interests. Using a mixed strategy of both Google and Meta ads can give you the highest chances of gathering leads at different points throughout their buying journey.
Prioritizing local SEO
Traditional search engine optimization strategies won’t work for local orthodontic practices. You don’t need to rank No. 1 in the country for “braces for teens,” and frankly, you never will. Instead, you need to turn your focus to Google’s local aspects, like the Google Maps Pack or your Google Business Profile.
Local SEO works to pair searchers’ service queries with responses that are nearest their physical location. You’re not competing with the entire internet, you’re competing with other local orthodontists in your area. So, to do that, you need to generate reviews, update your Google Business Profile regularly, and ensure that your name, address, and phone number are consistent across all online directories. You’ll also want to develop a local keyword strategy that reflects on all features of your website, including your blog, treatment pages, and more.
Engage patients on social media
When potential new patients (or their moms) research orthodontic practices in the modern era, they’re not just looking at your website; they’re looking at your entire digital footprint, and that usually means deep diving into your social media account. That means your social media presence works very similarly to the home page on your website. Its job is to offer a snapshot of what you’re known for and what patients can expect when they visit your practice. Not having an account at all often seems fishy in this day and age. Having a well-curated presence can set you apart from your competition.
Post educational, informative, and engaging content that potential new patients will genuinely find helpful. Highlight your practice amenities and team members to show familiar faces and build rapport before they even step foot in your office.
Make marketing the focal point of your practice management
If you’re missing any of these key orthodontic marketing techniques, you could be missing out on qualified leads, consultation bookings, and new patients across the board. Start with your budget, and then build out a strategy from there. And if you need help, you know who to call.
Real-world experiences
As the popularity of digital bonding using DIBS AI from OrthoSelect continues to grow, we thought readers would appreciate hearing how the system has made a change for doctors who have adopted it in their practice. Dr. David Lowe has been using DIBS AI for about 18 months. Here are some highlights from his own experience:
Tell us a little bit about yourself.
I’m an orthodontist in Port Orange, Florida. I’ve been in practice for 28 years and have been using DIBS AI since May of 2023.
How has using DIBS AI changed your practice?
It has improved my practice and really changed my world. I have bonded 256 cases now with DIBS AI. I rarely, if ever, do direct bond anymore. My staff dread it if we’re ever going to do a direct-bond case, and so do I because DIBS AI really has made things so much easier. With my direct-bond cases, I would be there 35-40 minutes. Now I can do my bondings in about 8 minutes. I still do them myself, even though technically speaking, the staff can do it. I still want to add that value that the doctor is actually doing something because they don’t see me treatment planning on the screen. We’ve noticed that my cases are getting done faster, and it was really shocking to me that we have fewer broken brackets since I started doing it.
What evidence have you seen to support using DIBS AI?
Let me show you the numbers and how much better it has made my practice. I’ve now finished 20 of the cases I’ve started. I had my treatment coordinator go through the charts and look at some numbers of the 20 DIBS AI cases and the previous 20 direct-bond cases. We looked at actual treatment months, the number of appointments, and the number of repositions (see Table 1). How much I immediately saw an improvement really shocked me. So, the average treatment months of the last 20 DIBS AI cases is 10.89, whereas my last 20 direct cases 19.85.
The number of appointments are 7.4 on average as opposed to 12.8 for my direct bond cases.
What
do your patients think of using DIBS AI?
Most of the patients don’t know any better because they haven’t had braces done directly. But I have had cases where they have siblings who I’ve treated. And it’s been a noticeable difference that the parents have been able to see.
Have
you run into any issues with using DIBS AI?
There is one problem that we’re having — because we’re getting done faster, I need to adjust my payment plans to reflect that. And that’s the other issue is that insurance is only paying quarterly, and if I’m getting them done that quickly, well, that’s been a little bit of an issue. As I get more confident in being able to determine exactly how long the case is going to go, I’m sure we will figure that out.
To see the full interview with Dr. Lowe, or to learn more about how DIBS AI can transform your practice, scan the QR code.
This information was provided by OrthoSelect.
Table 1: Treatment comparisons
Dr. David Lowe
Integrating AI in dental practices
Gary Salman explains how to reap the benefits of AI more safely
As artificial intelligence (AI) continues to permeate various healthcare sectors, dental specialty practices such as orthodontics, endodontics, implants, and pediatric dentistry stand to benefit significantly from its integration. AI offers vast potential to enhance diagnostics, streamline patient management, and boost operational efficiency. However, with these advancements come critical considerations around patient data protection and regulatory compliance as well as the need to maintain compliance with the Health Insurance Portability and Accountability Act (HIPAA) security and privacy rules.
The benefits of artificial intelligence
1. Enhanced diagnostics and patient care
AI has revolutionized diagnostic processes by leveraging machine-learning algorithms to analyze complex datasets, such as radiographic images. This technology can assist in predicting tooth movement and treatment outcomes, enhancing the diagnostic accuracy of decay and anomalies in x-rays, and monitoring patient treatment progress.
2. Streamlined patient management
The automation of routine administrative tasks that AI can handle, from appointment scheduling to patient follow-ups, frees up valuable time for dental professionals to focus on patient care. It also facilitates better patient communication through personalized reminders and post-treatment care instructions, enhancing patient satisfaction and engagement.
3. Operational efficiency
AI tools can optimize inventory management and predict patient flow, leading to better resource allocation and reduced operational costs. Predictive analytics can also take multiple data inputs from systems such as practice management, financial reporting, and insurance claims to identify areas where your practice could improve for growth.
Gary Salman is CEO and co-founder of Black Talon Security (www.blacktalonsecurity.com). A leader in the cybersecurity field, Gary has a 25+ year background in law enforcement and healthcare technology. His firm monitors and secures approximately 50K computers and networks worldwide and has trained tens of thousands of dental and other healthcare professionals.
Protecting patient records and ensuring HIPAA compliance
With the integration of AI, safeguarding patient information becomes paramount. Dental practices must adhere to HIPAA regulations, which mandate the protection of individual health information. Here are key considerations:
• Data storage and flow: Encrypt all stored and transmitted patient data to prevent unauthorized access. This ensures that even if data is intercepted, it remains unreadable to unauthorized individuals. AI often requires your data to be analyzed and stored in many places at a given time. This creates additional risk for your practice, because the bigger your digital footprint, the bigger the risk. Some AI applications can store your data on 3-4 different server networks at a given time.
• Data access controls: Implement strict access controls, ensuring that only authorized personnel have access to sensitive information. Use multi-factor authentication to add an extra layer of security. Many AI companies either purposely or inadvertently share your patient data, with or without your permission. Ask the AI company for their policies for data sharing and retention.
• Regular internal and external audits: Conduct regular security audits to identify vulnerabilities and ensure compliance with HIPAA standards. Internal audits help maintain the integrity of the data protection mechanisms put in place within your practice — but don’t neglect third-party risk. Unfortunately, many AI companies are still in “start-up” mode. Often hiding behind a “HIPAA Compliant” badge, they may fail to have anything more than basic security precautions in place to protect your patient data, putting you at a tremendous risk in the event of a breach.
How to submit an article to Orthodontic Practice US
Orthodontic Practice US is a peer-reviewed, quarterly publication containing articles by leading authors from around the world. Orthodontic Practice US is designed to be read by specialists in Orthodontics, Periodontics, Oral Surgery, and Prosthodontics.
Submitting articles
Orthodontic Practice US requires original, unpublished article submissions on orthodontic topics, multidisciplinary dentistry, clinical cases, practice management, technology, clinical updates, literature reviews, and continuing education.
Typically, clinical articles and case studies range between 1,500 and 2,400 words. Authors can include up to 15 illustrations. Manuscripts should be double-spaced, and all pages should be numbered. Orthodontic Practice US reserves the right to edit articles for clarity and style as well as for the limitations of space available.
Articles are classified as either clinical, continuing education, technology, or research reports. Clinical articles and continuing education articles typically include case presentations, technique reports, or literature reviews on a clinical topic. Research reports state the problem and the objective, describe the materials and methods (so they can be duplicated and their validity judged), report the results accurately and concisely, provide discussion of the findings, and offer conclusions that can be drawn from the research. Under a separate heading, research reports provide a statement of the research’s clinical implications and relevance to orthodontics. Continuing education articles also include three to four educational aims and objectives, a short “expected outcomes” paragraph, and a 10-question, multiple-choice quiz with the correct answers indicated. Questions and answers should be in the order of appearance in the text, and verbatim. Product trade names cited in the text must be accompanied by a generic term and include the manufacturer, city, and country in parentheses.
Additional items to include:
• Include full name, academic degrees, and institutional affiliations and locations
• If presented as part of a meeting, please state the name, date, and location of the meeting
• Sources of support in the form of grants, equipment, products, or drugs must be disclosed
• Full contact details for the corresponding author must be included
• Short author bio
• Author headshot
Pictures/images/tables
Illustrations should be clearly identified, numbered in sequential order, and accompanied by a caption. Digital images must be high resolution, 300 dpi minimum, and at least 90 mm wide. We can accept digital images in all image formats (preferring .tif or jpeg).
Ensure that each table is cited in the text. Number tables consecutively, and provide a brief title and caption (if appropriate) for each.
Disclosure of AI use
Authors must disclose any AI used in researching, writing, or creating their articles. This includes a language model, machine learning, or similar technologies to create or assist with this submission. If AI was used, please provide a description of the AI-generated content and the name, model or tool used, and manufacturer. If AI was used, please confirm that you take responsibility for the integrity of the content that you are submitting.
References
References must appear in the text as numbered superscripts (not footnotes) and should be listed at the end of the article in their order of appearance in the text. The majority of references should be less than 10 years old. Provide inclusive page numbers, volume and issue numbers, date of publication, and all authors’ names. References should be submitted in American Medical Association style. For example:
Journals: (Print)
White LW. Pearls from Dr. Larry White. Int J Orthod Milwaukee. 2016;27(1):7-8. (Online)
Or in the case of a book: Pedetta F. New Straight Wire. Quintessence Publishing; 2017.
Website:
Author or name of organization if no author is listed. Title or name of the organization if no title is provided. Name of website. URL. Accessed Month Day, Year. Example of Date: Accessed June 12, 2011.
Author’s name: (Single) (Multiple)
Doe JF Doe JF, Roe JP
Permissions
Written permission must be obtained by the author for material that has been published in copyrighted material; this includes tables, figures, pictures, and quoted text that exceeds 150 words. Signed release forms are required for photographs of identifiable persons.
Disclosure of financial interest
Authors must disclose any financial interest they (or family members) have in products mentioned in their articles. They must also disclose any developmental or research relationships with companies that manufacture products by signing a “Conflict of Interest Declaration” form after their article is accepted. Any commercial or financial interest will be acknowledged in the article.
Manuscript review and extra issues
All clinical and continuing education manuscripts are peer-reviewed and accepted, accepted with modification, or rejected at the discretion of the editorial review board. Authors are responsible for meeting review board requirements for final approval and publication of manuscripts. If additional issues are desired, they must be ordered from the publisher when the page proofs are reviewed by the authors. The publisher does not stock back issues. Reprints can be purchased after the issue is published.
Proofing
Page proofs will be supplied to authors for corrections and/or final sign off. Changes should be limited to those that are essential for correctness and clarity.
Articles should be submitted to: Mali Schantz-Feld, managing editor, at mali@medmarkmedia.com
Best practices for cybersecurity
To protect against cyber threats, dental practices should adopt comprehensive cybersecurity measures so they can identify and mitigate cyber risk. The “Cybersecurity Standard of Care for Dental Practices” includes the following:
• Vulnerability identification and remediation: Hackers use sophisticated tools to identify vulnerabilities on your firewall and computers and leverage these weaknesses to break in and exploit your network. Cybersecurity companies offer sophisticated tools that scan your computers and firewalls daily looking for these exploitable vulnerabilities. The more sophisticated scanners not only identify the vulnerabilities on the computers but can autonomously remediate them.
• Staff cyber training: Educate staff on cybersecurity best practices, including recognizing phishing attempts and safe internet usage. Regular training sessions will help maintain a security-conscious culture within the practice. To be HIPAA compliant, this must be an ongoing, documented process, not a quick “over lunch” conversation. Seek out cybersecurity companies that offer comprehensive training and understand the unique vulnerabilities in workflows of dental practices.
• Penetration testing: An ethical hacker should be attempting to break into your network at least twice per year to test the defensive measures of your network. This test should not be performed by your IT company, but an independent cybersecurity company.
• Incident response plan: Develop a written response plan for potential cyberattacks or any emergency that could disrupt your practice. This plan should outline the steps for containment, investigation, and communication to minimize the impact of the emergency. Rehearse the plan annually to ensure all team members know their role when responding, and to evaluate for any needed improvements to the plan.
• AI-based anti-virus: Utilize more advanced anti-virus software that leverages AI to detect and fight back against more sophisticated attacks. This software must be managed and watched 24/7 by security engineers to be most effective.
Practical steps for successful AI integration
1. Choosing the right AI tools
Select AI solutions that meet the specific needs of your practice. Evaluate various tools based on their functionality, ease of integration, and compliance features. Consider solutions that offer seamless integration with existing systems and have a proven track record in the dental industry. Ask to review their third-party cybersecurity evaluation and HIPAA risk assessment. You don’t want their breach to become your breach.
2. Staff adoption
Ensure that your team is well-prepared to work with AI technologies. Comprehensive training and documented processes will facilitate a smoother transition in their workflows and help staff understand the benefits, risks, and limitations of AI tools. Staff should always use caution when uploading any data that contains confidential information such as employee or patient data into these systems. You may be violating State and Federal laws without realizing it.
3. Ask for a proof of concept
The best way to assess if adding AI to your practice will provide value is to ask for a 90-day proof of concept period to fully understand how it will function. However, you’ll want to be sure you have reviewed their data handling and security protocols prior to giving the tool access to your data.
Balancing advanced technologies with data security
Integrating AI offers transformative benefits, from improved diagnostics to enhanced operational efficiency. However, this technological advancement requires a balanced approach that prioritizes patient data protection and regulatory compliance. By implementing robust cybersecurity measures and choosing the right AI tools, dental specialty practices can harness the power of AI successfully. As AI continues to evolve, embracing these technologies while maintaining vigilance over data security will ensure that your practice remains both innovative and compliant in its operations. OP
Integrating AI offers transformative benefits, from improved diagnostics to enhanced operational efficiency. However, this technological advancement requires a balanced approach that prioritizes patient data protection and regulatory compliance.”
Use
MY NEW STANDARD OF CARE.
Dr. Ed Davis
“Since integrating DentalMonitoring, my patient starts have increased by 30%, yet it did not increase my workload. The convenience it offers patients has been a key factor in growing my practice.”
BUY 100 CASES GET 80 CASES FREE (only 67¢ ea.)
+200 FREE MOLAR TUBES +1 FREE CURING LIGHT!
BUY 300 CASES GET 300 CASES FREE (only 60¢ ea.)
+400 FREE MOLAR TUBES +2 FREE CURING LIGHTS!
- Available in .018 or .022, Roth or MBT * & your choice of hooks
- Available loose or individual patient packs of 5-5, 6-6, or 7-7
- Offset bicuspids & vertical slot also available
*Allure Ortho does not imply endorsement by Dr. Roth or by Doctors
"I've been using the Allure Ortho Mini twin in my office for the better part of the last decade and I love it. I'm able to keep a low overhead without sacrificing quality. This is all wrapped up in Allure Ortho's exceptional customer service. You get great quality, great prices and service that is the best around. I highly recommend using this bracket."
--- Dr. David Harmon, Jr. | President of Middle Atlantic Society of Orthodontists (MASO) | Mitchellville, MD
Introducing the
REPO GUN
bracket repositioning gun
Repositioning Brackets Has Never Been Easier!
ONLY $69 ea.
-E asily remove brackets so that you can reposition them without distorting the base or crimping the slot
- Autoclavable to 270°
“We love our repo guns. It allows us to predictably remove metal braces without bending the base or wings so they can be reused for our reposition appointments. It’s a huge money saver for our practice.”