


After years of paying premiums… Why is it So Hard to Collect On My Disability Policy? No matter where you are in the disability claims process, our firm is here to help. Please visit our website, www.disabilitycounsel.net, to view our dentist resource page. If you would like to speak with an attorney about your disability claim, please feel free to call or e-mail Mr. Funk directly. Derek R. Funk, Esq. Direct: 480.685.3638 dfunk@cobelaw.com Scottsdale | Scottsdale Spectrum | 6720 N. Scottsdale Rd., Ste. 150 | Scottsdale, AZ 85253 Salt Lake | Wells Fargo Center | 299 S. Main Street, Ste. 1380 | Salt Lake City, UT 84111 (by appointment)
OFFICIAL PUBLICATION OF THE UTAH DENTAL ASSOCIATION
CONTRIBUTING WRITERS
Dr Kay Christensen
Richard C. Engar, DDS
Dr. Gregory Gatrell
Heidi Nickisch Duggan, MA, MS
Kelly K. O’Brien, MLIS
Myriah Shimatsu
Dr Mark Taylor
Dr Rodney Thornell
Tracy Thorup, B.S.
COVER PHOTO
PUBLISHER: Mills Publishing, Inc.

OFFICE ADMINISTRATOR Cynthia Bell Snow
GRAPHIC DESIGNERS
Ken Magleby
Patrick Witmer
PRESIDENT'
Navigating New Rules and Regulations ASSOCIATION
We're All in This Together
Creating a Legacy
The ADA Library & Archives: The Right Information Anytime, Anywhere
PRACTICE 6
Utah Professional Health Program (UPHP): Providing Support for Healthcare Professionals with Substance Use Disorders
12
ART DIRECTOR Jackie Medina
Paula Bell
The Utah Dental Association holds itself wholly free from responsibility for the opinions, theories or criticisms herein expressed, except as otherwise declared by formal resolution adopted by the association. The UDA reserves the right to decline, withdraw or edit copy at its discretion.

UDA Action is published bi-monthly. Annual subscriptions rates are complimentary to all UDA members as a direct benefit of membership. Non-members $30.
Utah Dental Association, 801-261-5315 1568 500 W Ste. 102, Woods Cross, Utah 84010 uda@uda.org.
UDA Action is published by Mills Publishing, Inc. 801-467-9419; 772 East 3300 South, Suite 200, Salt Lake City, Utah 84106.
Inquiries concerning advertising should be directed to Mills Publishing, Inc. Copyright 2021.
CONTENTS
PRESIDENT Dan Miller
ADVERTISING REPRESENTATIVES
Paul Nicholas
Dr Bryan Trump S MESSAGE
4
5
7
Life is Too Short
Bundling and the New Utah Law
16
8
Oral Pathology Puzzler: Do You See What I See?
9
Prepare Now for Retirement!
Department of Commerce Division of Occupational and Professional Licensing Letter
Research: Dental Procedures Are Safe in Pandemic
What's Your Leadership Style? Dentists are Leaders in their Practices and their Communities
Can I Sell Merchandise From My Dental Office, Such as Vitamins and Minerals, or Electric Toothbrushes?
Warning: Low Battery
Utah Office of Tourism
10
14
17
18
20
22
Goblin Valley State Park Angie Payne for
NAVIGATING NEW RULES AND REGULATIONS
Years ago my family and I had the opportunity to run the Middle Fork of the Salmon River in Idaho. For many river runners this is one of the premier multi day trips in the country and we were excited to have the opportunity. As the trip approached the river level continued to drop below the ideal flow and on the day of our launch the flow was at 2.25 feet which is considered low water. At flows below 2.5 feet the river can be hard to navigate and can also be very hard on equipment. Although all members of the trip were experienced boaters, most had limited experience boating low, technical rivers and some of our group had a very difficult time navigating the river making the days very long and difficult.
I have had numerous other trips to the Middle Fork since and none have been as grueling as that trip. However, it seem I always get invited on low water trips. This year I got invited on to float with another group of friends. I was excited as this trip would be during what is usually the perfect flow, 3.5-4.0 ft. However, this year there was the drought. As we watched the
flows drop to historic lows my hopes of big water and easy navigating were dashed. The flows were going to be well below 2.0 ft. A level known to be extremely difficult.
Fortunately this year we went with a group of seasoned low water Middle Fork boaters. The trip was great and with little difficulty we navigated the challenging river.
This fall at the Utah Dental Association we are gearing up to bring another addition of the Continuous Quality Improvement (CQI) seminar to all dentists in the state. Visiting all of the districts in the state takes a lot of time and effort. I was initially concerned about the time required to travel across the state but it turns out this is one of my favorite.
During the CQI seminar we work to bring the most up to date and important information affecting dentists in the state. Unfortunately, not all of the information is exciting but it is information dentists need to know to successfully navigate the changing rules and regulations.

Last year the change of license classification confused a lot of dentists, and many dentists were improperly licensed in the state, an error that could have profound consequences if left uncorrected.
This year we are bringing new topics and information that dentists in the state need to know.
Make it a priority to attend one of the meetings so you don’t get left behind.
Legislatively in the state the Utah Dental Association has made much progress. We have currently completed the majority of the American Dental Associations insurance intrusion initiatives and we are far ahead of most states.
Individually we would have very little political influence and a difficult time navigating the ever changing rules and regulations. Fortunately for all dentists in the state the staff at the UDA sits quietly in the background working to help make practicing in the state easier for both dentists and patients.
Membership in the UDA has many privileges and like our last low water trip on the Middle Fork of the Salmon River who you team up with makes all the difference.
Dr. Gregory Gatrell UDA President

4 September / October 2021
PRESIDENT'S MESSAGE What’s your practice worth? Since 1968 Request a FREE MARKET VALUE ANALYSIS www.AFTCO.net | 800.232.3826
WE’RE ALL IN THIS TOGETHER
Sun Tzu in “The Art of War” taught that pitting an enemy off against itself was an extremely effective military tactic. Divide and conquer! Stir them up, separate them into groups, cause them to fight amongst themselves, encourage them to attack one another, and you have severely weakened your enemy. You have compromised their ability to defend themselves, and to wage war against their real enemy.
Never before in my lifetime have I seen more events, more topics, more controversial decisions and directives, more areas of our lives that separate us, as a people, into factions, and foment contention between those factions. Are these organic, or are they carefully orchestrated, and designed by an enemy? Regardless of the cause, the solution is the same. We need to come together and be more unified.
How do we do this? Do we just forget our differences, kiss and make up? Do we disregard our closely held views and acquiesce? Do we compromise our core beliefs, just for the sake of unity?
I would say an emphatic no to all of the above. On the other hand, I would say yes to the following: First, we need to be willing to admit that we might be wrong. Then, we need to turn away from any source of information that promotes division. We need to turn away from any source of information that sows seeds of discord. Discord, divisiveness and contention are much different than a simple difference of opinion. A difference of opinion can be healthy, if it promotes discussion and discovery. But, it can be toxic and damning, if one party simply silences the other.
Most of all, we need to turn away from any source that would claim to have a corner on the truth. Avoid any news outlet or social media platform that claims to be the ultimate fact checker, or a fact checker of any kind, for that matter. Just because an individual or an institution is eminent, prominent or well-known does not automatically make them the ultimate purveyors of truth. Shun any source that would seek to silence their opposition. Unfortunately, the social media giants are some of the worst offenders in this regard. For this reason, they can and should be avoided like the plague. Why do we continue to patronize those that would silence others? The statement, “While I may disagree with what you say, I will defend to the death your right to say it,” has been attributed to both Voltaire and Patrick Henry. Regardless of who said it, it is worth repeating.
Some would argue that it is justifiable to silence others when they are wrong, especially if the claim is that their information is somehow dangerous. But, who determines what is right, and what is wrong? Who really is qualified to make that pronouncement? History is replete with examples of societies
getting it wrong, where commonly held beliefs turned out to be a big mistake.
The sad reality is that many highly respected and eminently qualified experts are being sidelined, de-platformed and silenced. Is truth determined by majority rule, or by those with the biggest microphone? Once again, history would prove otherwise. Free speech is just that “free speech.” Free speech can be uncomfortable. Free speech can even be hurtful. But, to silence anyone or any group, for almost any reason, is antithetical to a truly free society. Does that mean that there should be no consequences for yelling “fire” in a crowded room, when there is no fire? Absolutely not! Nevertheless, we all need to be more tolerant of one another, and more respectful of differing opinions.
People are smart. With open and fair debate, people have always been able to arrive at the truth when a full set of facts is made available to them. As repugnant and reprehensible as censorship is, it has become commonplace. Furthermore, it is probably the most dangerous weapon there is against the discovery of truth, and against a free society.
We will never adequately solve our collective problems, without open discussion and open discourse. No one should ever be silenced, ever. It is the free interchange of ideas that solves problems and benefits society. To use the excuse that “misinformation is dangerous” is not a sufficient reason to silence anyone, especially when there are numerous competent and well-qualified individuals with opinions that differ from the so-called experts. Never has the majority opinion ever determined the truth.
As a society, we are headed down a very dangerous road if we do not get a handle on the discord and division that has grown to take center stage in our lives. Regardless of the source of the discord, we must turn away from it, or it will grow like a cancer and destroy us. Sure, there will always be some differences of opinion, but societies must largely be unified and stand together on the big issues. History teaches those that fail to learn this lesson, eventually disintegrate into chaos.
There is great power in being unified, especially if that unity is based upon the facts. This applies to groups, families, organizations (such as organized dentistry), churches, communities, and societies at all levels. Council together, seek input from all responsible parties, be respectful, look at the information, examine the facts, arrive at a decision together, then move forward in unity. That formula has stood the test of time. It has been successful before, and can be successful again.
Dr Mark Taylor UDA Treasurer

UDA Action 5
ASSOCIATION
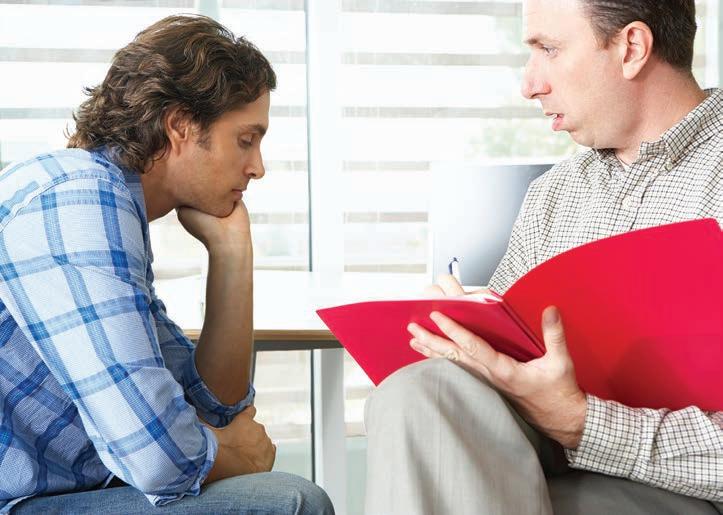
My father-in-law, Jim, started acting weird a few weeks ago, more weird than a fatherin-law usually acts. He put on his clothes backward and got lost in his neighborhood. My mother-in-law assumed a stroke, so she raced him to the emergency room.
The MRI showed a large neoplasm growing on the right temporal lobe of his brain. The attending physician immediately transferred him to Intermountain Medical Center to prep for surgery. Upon arrival, the neurosurgeon looked at the image and decided to hold off surgery for a few days to allow for family and friends to visit Jim. Due to the size and location of the tumor, the surgeon was concerned that Jim would be different after surgery.
Though it is a terminal cancer even with removal of the tumor, the surgeon wanted Jim’s friends and family to have the opportunity to say goodbye to the old Jim because removing brain tumors commonly affects personality, memory and nerve function. Jim enjoyed the next few days very much with friends and family from near and far who came to see him. He was quick to quip that when the surgery was over, he would become a superhero.
The day of the surgery came, and it went better than expected. The surgeon was able to remove a good portion of the tumor, enough to relieve the pressure on the rest of the brain, all while not causing any noticeable damage to brain function. This was wonderful news as Jim could function normally and we could enjoy our remaining time with him.
It has been a couple weeks since the surgery, and Jim’s skull is healing well. Cancer treatment begins today. The diagnosis is Glioblastoma, and treatment is considered successful if it gives him 12-14 months to live. The next few months will be his best, then things will gradually decline and become more difficult.
Our lives can also be like that sometimes. Just when we finally get to a point where we are comfortable (Jim just retired six years ago), unexpected difficulties arise, and we need to reevaluate and refocus. After considering what matters most to us, we should choose what matters most over what matters least. Are we living our best lives? Or are we just hoping for something better to come along eventually?
I am surprised by how many dentists don’t love what they do. Some can’t wait until they retire, others can’t wait to open up enough locations or employ more associates so that they can become more of a business person and less a wet-fingered dentist. They think of hygiene checks as a four-letter word rather than an opportunity to connect with great people. Certain
procedures on the schedule make them cringe, and they hate dealing with insurances.


I know the difficulty of dealing with insurances. Low reimbursement is to blame for much of our dissatisfaction. Yet, very few of us are willing to demand more from the insurances we accept. We are constantly looking to save a few tenths of a percentage point on credit card fees, but don’t think twice about insurance companies discounting our fees by 20 - 50%. Or, we continue to do procedures that we are not great at, nor like very much, because they pay better. Is it worth it? Are you happy, or are you just surviving? Let my father-in-law Jim’s experience be a motivator for you to demand better of your current situation.
As autumn begins and the end of the year approaches, take time to reevaluate how you would like the rest of your life to be, personally and as a dentist. If you are not happy with your current practice, change things to how you want them. For example, if you don’t like your current relationship with insurances, negotiate better fees or go out-of-network. If you are not happy doing some procedures, find good CE to teach you how to have better outcomes, or refer your patients to a colleague that enjoys those procedures.
Life is short and there is no reason to not love what you do. Take advantage of the time you have been given to make a better life for yourself, your family, your employees, and your patients. Not only will you benefit, but so will those nearest to you who care about you the most.
Dr Rodney Thornell ADA Delegate


6 September / October 2021
PRACTICE Text to: 801 -261 -5315 1 I n c l u d e y o u r F i r s t a n d L a s t N a m e 2 Y o u r i n t e r e s t s t o g e t i n v o l v e d : a) House of Delegates - Governance b) UDA Action Committee - Publications c) UDPAC Committee – Legislation d) I know my legislators – Name them & connection e) I’d be willing to be a Collaborative Dentist
LIFE IS TOO SHORT
CREATING A LEGACY ASSOCIATION

I returned this week from attending the 2021 ADA Presidents-elect conference held at the American Dental Association office in Chicago. This conference is held annually to educate and train next year’s presidents of the societies or associations representing each of the 50 states. For a full day and a half our schedules were filled with presentations from expert business consultants, motivational speakers, and officers and leaders of the ADA. The agenda is also carefully planned and programmed to include ample opportunity to get to know fellow dentists from all over the country and share successes, failures, and issues that are common to the dental communities all across the nation. I felt like I had come to the fountain to get a drink, and was blasted with a firehose! There was so much information to take in!
While there are countless topics and issues that could have been addressed, there was only time to specifically focus on a few select ideas. These ideas included, Remaining Relevant as we Execute Across the Generations; Advancing Health Equity; Leadership and Governance; Reimagining the Future of Membership; and an open discussion on Emerging Issues in the Dental Industry. Fabulous ideas, knowledge, and instruction were presented to help us become better leaders, better dentists, and better resources for the dental professionals we represent and serve. You will, no doubt, in the coming weeks and months, be hearing and reading about a lot of these issues which will also help you to become better leaders, better dentists, and better resources for the health and well-being of the communities you serve. Be prepared and willing to get a drink from the firehose of information to come.
At the conclusion of the conference I was asked what the best part was for me. Attending meetings like this, with all the meeting and greeting and social interacting, usually pushes me a bit out of my comfort zone. But despite all the organization and activities of a great event, the best part for me was the people. I must admit that I have somewhat welcomed and even enjoyed, to an extent, the increased and encouraged isolation that we have experienced as one of the by-products of a global pandemic. But I am also learning that people need each other.
Directly across the street from the ADA office building in Chicago is a landmark building, a fire station, Chicago Engine

98. It is a beautiful old building, well preserved from its 1904 construction, dwarfed by the skyscrapers surrounding it, and still in use today. A block or two away stands an even older edifice, the Chicago Water Tower, built in 1869, standing as another landmark and survivor of the great Chicago fire of 1871 which essentially decimated the rest of this downtown area of the city. I was impressed by the quality of craftsmanship used in these old buildings which has helped them stand through the years. Tools were used by these artisans to bring together bricks, and stones, and mortar to create these great buildings which have stood through time as a legacy long after their creators are gone.

The topics and presentations at the presidents-elect conference were very well planned and created, like the beautiful bricks and stones of the fire station and water tower. But it takes people, a muddy and messy conglomeration of differences coming together in a common cause, to join and blend together to make the mortar that brings things together to create our own legacy.
The best thing was the people. People make the difference. Programs and topics may be the tools, and the tools are there for all to use. The difference comes with how we use them and what we build. The principle asset of an association is community Brochures, plans, and programs can be duplicated. But you can’t duplicate people
As we learn of the many tools that are available for us to use in improving our association, careers, and our lives, let us try to remember that what we do for ourselves is gone when we’re gone, but what we do for others remains forever our legacy.
Dr Kay Christensen UDA President Elect
UDA Action 7
BUNDLING AND THE NEW UTAH LAW
Utah was the first state to pass a law restricting bundling of procedures by dental insurance companies (third-party payers), which was a huge win for Utah dentists and the patients they serve. Front office team members know all too well how “bundling” affects the financial stability and patient relationships of any dental practice. Bundling of dental procedures is defined by the ADA as follows: “claims bundling is the systematic combining of distinct dental procedures by third-party payers that results in a reduced benefit for the patient/beneficiary.” They go on to say, “The ADA considers bundling of procedures to be potentially fraudulent.”
Nothing could lack transparency more than a dentist performing two or three distinct CDT coded procedures that actually define what was performed on a patient, only to have an EOB (estimation of benefits form) “redefine” those services into something completely different, or worse, imply that the dental office billed incorrectly, leaving the patient wondering what actually was completed in their mouth, or worse, if their dental services were needed at all due to misleading verbiage on the above EOB.
The new Utah Law, House Bill 359, took a major step in the right direction, protecting dentists and their patients from the above frequently experienced scenario, and more. However, in this article, we will focus on the “bundling” component with Utah’s new law.
HB359 states, “An insurer may not maintain a dental plan that; uses bundling in a manner where a procedure code is labeled as nonbillable to the patient unless, under generally accepted
practice standards, the procedure code is for a procedure that may be provided in conjunction with another procedure.”

Dental insurance companies can still bundle, but they cannot force you to write off separate services. Examples would be: bundling build-ups with crowns, gingivectomies and crown lengthening with crowns on the same day, diagnostics and treatment procedures with limited exams, and my favorite… bundling bitewings and panoramic x-rays into a full-mouth series. Are there others? Yes, but this is a good start to be aware of.
If a third-party payer becomes non-compliant with our new Utah law, and has verbiage on the EOB that is misleading, and they insist you follow their bundling guidelines, you need to consider filing a complaint with the Utah State Insurance Commission. Do not be afraid to file that complaint. Many think that filing a complaint will get you removed from being a provider to the dental insurance company you have filed against, but nothing could be further from the truth. The more complaints filed just strengthens our position. Having said that, many dental insurance companies understand our plight, and have already made changes to their contracts reflecting the new Utah Dental Law.
During the debates with the major insurance players, I brought up the question, “who determines what ‘generally accepted practice standards’ should be?” As they began to suggest it should be them, we clearly pointed out that it should be licensed dentists in our state, and no one else. The debate ended there. At the bottom of this article you will find a QR Code for “generally accepted practice standards” regarding targeted
Your patients rely on your expertise to evaluate and make recommendations to keep them healthy. Your local independent insurance agent can do the same for you when it comes to suggesting the right combination of coverage to protect the practice you’ve worked hard to build.
Find an independent agent representing The Cincinnati Insurance Company by visiting cinfin.com or by calling Mike Terrell, 800-769-0548. SPEND YOUR
8 September / October 2021
PRACTICE
TIME
EXAMINING YOUR CLIENT’S TEETH, NOT YOUR COVERAGE. © 2019 The Cincinnati Insurance Company. 6200 S. Gilmore Road, Fairfield, OH 45014-5141. Products not available in all states.
procedures by third-party payers. Only dentists are permitted to take the survey that will clearly define generally accepted practice standards. My advice would be to drop your altruistic dental hat, and place on your business hat when answering the questions so you don’t play into the hands of third-party payers. Enough said.
Our new Utah Dental Law regulates plans that are written here in Utah, for Utah companies. If it’s a federally run ERISA plan, or a plan written for a company in a different state, our Utah Law does not apply to those patients. Having said that, the UDA, MPMB, and other entities are working diligently to make those entities follow “state laws.” I can honestly state there has never been a more important time to support our dental associations than now. The fight is on, and we need everyone to support the battle that prevents third-party payers from coming between the doctor/patient relationship.
Let me be very clear on one major point: when dentists perform procedures that have codes and descriptions defined in the ADA CDT Code Book, or even worse, have codes, descriptions, and fees associated with them in their dental insurance contracts, and they do not charge their patient for those legitimate services, they are playing into the hands of those third-party payers to bundle, control, or eliminate those codes from their contracts and CDT Code Books. For those of you who have been practicing since the late 1980’s, you know exactly what I’m talking about. For example, medical charges for such things as local anesthetic and palliative treatment. Need I say more?
Third-Party Payers continually look for “frequency” of procedures, and ways to eliminate, or not pay for them, just to increase their profit margins. Through the years they have been able to eliminate the OSHA code, acid-etch and bonding, and others. In the early 2000’s they attempted to eliminate anesthetic, and more recently have gone after build-ups by “bundling” services until we are trained to no longer charge for them. Do you see the pattern? By eliminating their ability to “bundle” distinct dental procedures, dentists, and their teams, can be paid more fairly for the services they provide instead of doing free dentistry on insured patients.
Tracy Thorup, B.S. CEO, My Practice My Business
801-226-4420
1 The American Dental Association, “Introduction to Dental Benefits” (online). Accessed on 15 August 2021. Available at [https://ebusiness.ada.org/assets/docs/2201.PDF?OrderID=339016].
2 https://ebusiness.ada.org/assets/docs/2201.PDF?OrderID=339016
PRACTICE
ORAL PATHOLOGY PUZZLER: DO YOU SEE WHAT I SEE?
Which of the following represents the best diagnosis for the radioraphic findings in the anterior mandible?
. Periapical cemento-osseous dysplasia

. Periapical granulomas
Odontogenic keratocysts
. Lateral Periodontal Cysts
(continued on page 15)
Full Contour Zirconia

✓ Quality Zirconia – Katana
✓ Fast turnaround – as little as three days in lab


✓ Special UDA intro offer
Guided Implant Surgery
✓ Package includes: consultation, surgical guide, custom abutment and restoration
✓ Easy all-in-one price 801.967.0592
Custom Abutment and Crown
✓ Authentic custom abutments


✓ Full contour zirconia restoration included
✓ Easy all-in-one price
UDA Action 9
restorations
a
turnaround time by going digital.
to find out how to get a FIVE
Create more accurate
with
faster
Call
CROWN CREDIT!
digitalcontourlab.com A. B. C. D.
UTAH PROFESSIONAL HEALTH PROGRAM (UPHP):
PROVIDING SUPPORT FOR HEALTHCARE PROFESSIONALS WITH SUBSTANCE USE DISORDERS

Healthcare professionals are widely regarded as heroes. Often this leads people to believe that they are not susceptible to illness themselves. However, we know that health care professionals suffer from substance use disorders at rates that are similar to the general population.
A study funded by the National Institute on Alcohol Abuse and Alcoholism (NIAAA), part of the National Institutes of Health, found that about 10% of Americans will struggle with a substance use disorder at some time in their lives. According to the ADA’s 2003 Dentist Well-Being Survey, dentists may be even more vulnerable to substance use disorders than other populations.
Substance use begins in a variety of ways. It may start with a prescription for an illness or injury, social drinking, or a way to “wind down” after a long day. We know too that there are genetic risk factors that increase the likelihood of people developing a substance use disorder.
In addition to genetic vulnerabilities, we know that healthcare professionals have additional risk factors that may further increase their susceptibility to substance use disorders. These include:
1. High Levels of Stress
2. Exposure to illness trauma and death
3. Access to Prescription Drugs
Stress and trauma are known risk factors for misusing substances as a means of “coping”. Access to prescription drugs and familiarity with their effects often increases the likelihood that healthcare providers will begin to misuse substances. For those who are vulnerable, the consequences are often dire. Tiffanie Brownlee, a Registered Nurse in Utah, shared her experience, “I diverted medications that after I had given my patient their portion, I would take the rest of it for myself. It started out as once or twice and then it just became where I had to.”
When healthcare professionals find themselves struggling with a substance use disorder, they often have no idea where to turn for help. They are afraid to come forward because of concerns that they will lose their livelihood and their community standing. They feel isolated and ashamed. Inevitably, their disease worsens. Eventually, they become hopeless
and depressed. They become impaired and patient care begins to suffer.
Recognizing the need for a program where healthcare professionals can seek help confidentially, the Division of Occupational and Professional Licensing (DOPL) created the Utah Professionals Health Program (UPHP) to assist healthcare professionals who have substance use disorders. Providing a “safe harbor” where healthcare professionals can confidentially self-report provides many benefits to both licensed healthcare professionals and to the public.
Because participation in UPHP is voluntary, the first step is admitting there’s a problem. This is a very difficult step for anyone with a substance use disorder, as their default is denial.
Dr. Elizabeth Howell, MD, MS, an Addiction Psychiatrist & Associate Professor at the University of Utah, said, “The first thing that I think hits most people is that, ‘This can’t be true. I can’t be addicted. I’m too smart. I should know better. I should be able to control this.’. But the truth is, Addiction doesn’t care how smart you are.”
Dr. Jared Hemmert, a Dentist, recounted how he was running out of his prescription and decided to forge one in another person’s name. When it came time to pick up the prescription, Dr. Hemmert said he had an internal struggle, but decided to go through with it. “And all of a sudden, three police cars pull around the building. And they put me in the back of the police car and they took me to jail. I still didn’t think I was a drug addict.”
10 September / October 2021
PRACTICE
Photo: Image licensed by ingram image
While admitting you need help or have a problem is difficult, it is an important step in healing process. The earlier a person can take this step the better. As substance use disorders progress, the persons health and family life deteriorate, legal consequences ensue and careers as well as patients become endangered. There is also strong evidence that substance use disorders are linked to “burn out” and even suicide.
The aim of UPHP is to provide support before these tragic consequences occur. Professions currently eligible to participate in the program include:
-Dentists
-Dental Hygienists
-Physicians
-Physician Assistants
-Nurses
-Pharmacists
-Pharmacy Technicians

-Veterinarians
-Podiatrists
If a healthcare professional with a substance use disorder finds themselves in trouble before reaching out to UPHP, they may have to appear before their professional licensing board. Records of licensing board proceedings are public documents. Public discipline often results in loss of employment, boards of certification, inability to get credentialled with insurers and hospitals and the inability to obtain malpractice insurance. Alternatively, participation in UPHP can avoid many of these issues.
UPHP does not offer treatment; rather it identifies relevant resources, makes appropriate referrals for clinical evaluations and/or treatment, and monitors the ongoing recovery and treatment of professionals. Participation in the program is confidential and takes a non-disciplinary and clinical approach. This approach protects public safety and allows the healthcare professional an opportunity to demonstrate in a non-public, non-disciplinary manner that they can become safe and sober and remain so, while retaining their license.
“The Goal is to help those health professionals who have substance use disorders continue to practice while being monitored confidentially by our division. Of the thousands of cases that I have seen come through…. The vast majority have kept their licenses,” said DOPL Director Mark Steinagel. Those with substance use disorder can feel isolated, lost, and hopeless. UPHP offers resources and a community to turn to. Brownlee, who did not use UPHP services while getting help for substance use disorder, said, “I wish I would have known about it. I wish I would have known that there already was a village of people out there just waiting for someone like me to come forward and say, ‘Please, please, help me.’”
You are not alone. There is hope. To learn more about UPHP, visit UPHP.Utah.gov.
2021-2022
Upcoming University of Utah, School of Dentistry

Continuing Education Lectures:
11/18/21 Oral/Systemic Connection
Scott Summers, PhD – Diabetes Update: hope and help through current research David Okano, DDS, MS – Sugar: It’s not just for caries, too much in your bloodstream can also affect your periodontium and your health
1/13/22 Oral Pathology
Bryan Trump, DDS, MS – “When in Doubt, Cut it Out”Biopsy Principles and Techniques
2/10/22 Enhance Practice Longevity
Lloyd Maye, DPT, OCS – “Oh, My Aching Back”
Nicole Vallieres – Mission Nutrition: How to Choose Wisely
3/11/22 Implant Dentistry
Taylor Manalilli, DDS – FUNdamentals of Implant Planning and Placement
4/21/22 Thriving in Healthcare
Megan Call and Amy Locke – Thriving in Healthcare
Questions: Karin Mishler, Karin.mishler@hsc.utah.edu 801-587-2023
Jerald Boseman, Jerald.Boseman@hsc.utah.edu 801-587-2246

UDA Action 11
The University of Utah School of Dentistry Nationally Approved PACE Program Provider for FAGD/MAGD credit. Approval does not imply acceptance by any regulatory authority or AGD endorsement. 3/1/2020 to 2/28/2024 Provider ID# 363354 University of Utah School of Dentistry is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. University of Utah School of Dentistry designates this activity for 5.5 continuing education credits.
online with this QR code or https://umarket.utah.edu/um2/dentistrycde/ For more course information scan the QR code
Register
PREPARE NOW FOR RETIREMENT!
I retired from the private practice of dentistry on August 1, 1991 as I had no intention of practicing again once I was hired to take the reins at PIE (Professional Insurance Exchange Mutual, Inc.). However, I tried to keep abreast of the latest developments in dentistry and continued to take several CE courses over the years, not only to maintain my dental license to also to stay in tune with the real world of dentistry. After thirty years at the helm, I finally retired from full time work at PIE as of October 16, 2020 and have enjoyed my retirement so far, although I still cover at PIE one day a week when my successor, Dr. David L. Alvord has his County Council meetings since I agreed to do that for him once he won the election last November.
So why have I enjoyed my retirement after almost one year and what words of wisdom to leave with you loyal UDA members? Once reason I was able to retire now instead of waiting until I was 71.5 years old which was the average retirement age for Utah dentists at the end of 2020 is that I had set enough money aside for retirement and also expected some social security income when I turn 70. I have also had the advantage of my wife having a retirement program through her employer as well even though she plans to keep working for a few more years. But one word epitomizes what you have to stick with as a selfemployed dentist and financial security in your future. The word is Discipline.
Over the years I have seen a number of interesting scenarios. I know one dentist who had a goal to retire at age 55, did what he had to do to save financially and was able to retire at that age, only to die five years later at age 60. I have seen others who have set a goal to retire at a certain age, have been careful to set money aside, sold their practices and have enjoyed their retirement keeping busy with travel, church mission service, humanitarian service, and other pursuits they were able to enjoy for several years before they died. Others have lost their spouse but have been able to enter the dating world again, meet a compatible companion and have an enjoyable life anew. Others have not been so lucky, especially those that did not have a good pre-nuptial agreement signed first.
Still other dentists lost what retirement they had worked hard to save by being taken advantage of by people they met at church or other situations that gained their confidence, took their money in the form of an investment, often in real estate or other ventures with an unrealistic promise of a high return only to lose it all. Three of the five medical and dental professionals in the building where I practiced during the 1980s lost money to one of a few well known scams that plagued dentists in the mid-1980s to varying degrees. The scammers did not approach me since I was new in practice and would not have invested with them anyway and the wise physician they approached laughed them out of his office because he could see quickly that their spiel was not legitimate and could not succeed. Unfortunately, many of
the dentists affected had to work a lot longer and pay a big price for their gullibility.
Other dentists I know have done well, but to quote the Beatles, “Their clinging wife doesn’t understand” and spent too much money too fast in their best earning years on expensive cars, jewelry, clothes, homes and the like such that there was not a lot set aside for retirement and selling their practices was not going to bring in enough money to make up what was spent. Now, of course, new graduates are in a large hole when it comes to debt, particularly if they buy a nice home and practice early on, so that is an issue to deal with. But the younger a dentist is when they start setting money aside for retirement, the better. The key is discipline.
One thing I found that I was able to do if I needed some extra money to buy a nice Christmas present for my wife such as a computer, etc. was to work an extra hour one day a week. Then it was easy to be able to buy the present without going into credit card debt, etc. Think of how this would work for you as far as setting that money aside in a retirement account.
Another thing to consider is compounded interest. You are not going to do well with current interest rates well under 1% so you have to find better alternatives. There are several legitimate financial planners who will let you call the shots and pick and manage your own portfolios. You simply have to ask around and talk to colleagues who are given good advice without having to pay exorbitant fees or have their money mismanaged by churning or buying and selling so fast the commissions eat up any profit. If you follow the advice of Warren Buffet, he will tell you that many money managers should not be hired by you at all as they make money no matter how poorly they do mismanaging your investments; instead you should invest wisely and let the value increase through simple compounding.
Following is a table that shows how fast money can grow. This idea has to do with what you can also do for a grandchild as soon as they are born by investing $1,000 in a blue-chip, dividend bearing stock or fund that can gain you 12% per year such that your money doubles every six years, which is not easy these days but still possible with the right one:
Year 1 $1,000
Year 6 $2,000
Year 12 $4,000
Year 18 $8,000
Year 24 $16,000
Year 30 $32,000
Year 36 $64,000
Year 42 $128,000
Year 48 $256,000
Year 54 $512,000
12 September / October 2021 PRACTICE
Year 60 $1,024,000
Year 66 $2,048,000
Year 72 $4,096,000.
Now, in a practical sense, what this means to you young dentists is that you start with $64,000 set aside by the time you are 36 years old. But you are not just letting the money sit but are adding to it every year with at least $1,000 per month if you can. That way you are adding more shares and increasing your compounding. And if you have fears of Social Security not being available when you retire, you have enough set aside anyway. The average dentist in Utah retires at age 70 based on statistics I have kept over the past several years, so you can see how much money you should shoot for having set aside when you are that age.
Dentistry can be a means to an end but for some it is the end as they love dental practice and don’t have a lot of outside interests and don’t want to stop. I have known several dentists that kept practicing well into their 80s because they wanted to! But I have known a few others that did not want to but had no retirement set aside for various reasons and had no choice.
Finally, when you retire you need a plan as far as what you are going to do with your time so you don’t just waste away with no incentive to be productive at anything. For example, I have been building scale models since I was an 8-year old kid and I still build airplanes, cars, spacecraft, etc. and compete in contests, etc. I established a scale model museum in Bountiful with several display cases housing over 300 models so I still have room to grow. In the same suite I have a room I use as a studio to work on water color paintings which I do three days a week. I am also involved in several writing projects and of course play a lot of golf to stay in good physical condition (even though it often ruins a perfectly good walk). I have joined the local Rotary Club in Bountiful and do some fun things to serve my church. I am the public member of two licensing boards with DOPL.
Many of you have similar pursuits and may desire to use your dental skills in humanitarian efforts which is great. The point is, write down a plan of what you want to do when you retire so you can look forward to the day and enjoy being productive and useful, as work should be the means to an end and not the end!
Richard C. Engar, DDS
We have all of the experience, tools, and resources necessary to help you transition your practice into the right hands. We provide expertise on appraisals, practice sales, and everything you might need for a fulfilling practice transition.

UDA Action 13
PASSING A LEGACY IS OUR SPECIALTY. 801.298.4242 | ctc-associates.com Randon Jensen | Larry Chatterley



14 September / October 2021
ORAL PATHOLOGY PUZZLER: DO YOU SEE WHAT I SEE?
(continued from page 9)
Correct answer: (a) Periapical cemento-osseous dysplasia.


Fibro-osseous lesions are a diverse group of processes characterized by replacement of normal bone by fibrous tissue containing mineralized product. Microscopic lesions are very similar amongst different types of fibro-osseous lesions, which makes clinical and radiographic correlation necessary to establish the diagnosis. Cemento-osseous dysplasia occurs in the tooth-bearing areas of the jaws. It represents the most common fibro-osseous lesion encountered in clinical practice. There are three types: focal, periapical and florid. It is unusual for these lesions to cause bony expansion. Focal cemento-osseous dysplasia exhibits a single site of involvement, 90% occur in females, most commonly encountered in the posterior mandible. Lesions are asymptomatic and are usually smaller than 1.5 cm. Radiographically, lesions vary from completely radiolucent to densely radiopaque. Lesions will have a radiolucent rim with differentiates this from idiopathic osteosclerosis and condensing osteitis. Most commonly, there is a mixed radiolucent-radiopaque pattern and lesions are well defined (see image 2).
Periapical cemento-osseous dysplasia involves the periapical region of the anterior mandible. Multiple lesions are usually present. Ninety percent occur in females with 70% of those occurring in African Americans. Teeth are vital! The lesions are asymptomatic and usually discovered when radiographs are taken for other reasons. Early lesions are areas of radiolucency involving the apex of a tooth, which can appear identical to that of a periapical granuloma or cyst. Tooth vitality testing and the presence of multiple lesions is key. Florid cemento-osseous
dysplasia usually involves a combination of focal and periapical lesions (see image 3).
The other more common fibro-osseous lesions seen in the jaw bones are: fibrous dysplasia and ossifying fibroma. Fibrous dysplasia is a tumorlike condition characterized by replacement of normal bone by fibrous connective tissue intermixed with bone. The chief radiographic feature is a fine “ground-glass” opacification (unless you have seen or worked with ground glass before, a “etched glass” or “frosted glass” may make more sense). This radiographic feature results from superimposition of poorly calcified bone in a disorganized fashion. An ossifying fibroma is a true neoplasm with significant growth potential. The neoplasm is composed of fibrous tissue that contains a variable mixture of bone and cementum. The lesion occurs in a wide age range with lesions resulting in a painless swelling. Root divergence or resorption can occur. Large ossifying fibromas of the mandible demonstrate a characteristic downward bowing of the inferior cortex of the mandible.
Works Cited
Neville, Damm, Allen, Chi (2016). Oral and Maxillofacial Pathology, 4th Ed. St. Louis: Elsevier.
UDA Action 15 PRACTICE
Dr Bryan Trump
image 2
LIKE US ON FACEBOOK! Utah Dental Association
image 3
ASSOCIATION
THE ADA LIBRARY & ARCHIVES: THE RIGHT INFORMATION ANYTIME, ANYWHERE
Take a moment to reflect on the health sciences library you used in dental school. It was perhaps where you went to read all the books you needed for class or to check out the latest research in the dental journals. You likely used it as a study space, spending more than one late night at the group study tables or in a quiet carrel cramming for an important exam. In recent years, you probably used the library’s website to access journals and e-books from your dorm room or a coffee shop off campus. Once you entered practice, you may have found yourself at an institution that provided continued access to dental journals and textbooks, but for many of you, free access to evidence-based, up-to-date information ended the day you graduated.
One of the benefits of American Dental Association (ADA) membership is 24/7 online access to the ADA Library & Archives – thousands of full-text journals and e-books, clinical information resources, clinical calculators and drug information, systematic reviews and clinical guidelines, health care management resources and patient information. You can answer your clinical questions using DynaMed, Cochrane Library, MEDLINE and more, directly from you home or office, and you’ll enjoy direct full-text article linking from PubMed. gov. The ADA Library and Archives provide extensive expert search assistance and education, reference services, data and information referrals, electronic document delivery, all as part of ADA membership and at no additional cost to you.

DynaMed, mentioned earlier, is a clinician-focused tool designed to facilitate efficient and evidence-based patient care. Initially built for medicine, its rigorous and daily review of medical literature provides timely and objective analysis and synthesis frequently of use to dentists and other members of the clinical care team. DynaMed includes drug information, drug interaction notes, dosing and conversion calculators, and more. Notably, ADA members can now generate AMA PRA Category 1 Credit when using DynaMed to answer clinical questions. This process is accomplished entirely on the DynaMed site once the ADA member authenticates through the ADA.org/ library website and creates a personal account on the DynaMed site. Contact the professional staff at the ADA Library for more information.
The ADA Archives, a division of the ADA Library & Archives, provides quality reference and research assistance to ADA staff, members and other dental organizations and institutions searching for information on ADA history, the history of dentistry and biographical information about individuals involved in the profession. Interested in the history of toothbrushes and toothbrush design? Want to know more about pioneering women in dentistry? Interested in the links between golf and dentistry (yes, pun intended)? Want to know the history of the ADA’s involvement in water fluoridation science
and advocacy? Want to identify the outcomes of a House of Delegates resolution? The ADA Archives is a treasure trove of information and the certified archivist on staff is a historical detective extraordinaire.
We invite you to tour the ADA headquarters and visit the physical library at the ADA headquarters the next time you’re in Chicago. While we have converted most of our collection to electronic resources, visiting members can still enjoy the monograph and journal stacks, impressive rare book collections, ADA archives and exhibits on dental history. Members also benefit from the library staff’s expert knowledge of information sources and research. Whether you are visiting the ADA, or calling or emailing from your office, reference and research consultations are part of the perk. We help members with a wide variety of needs from finding guidelines for a specific case or high-level evidence about materials, tools or conditions. We also help members with more in-depth research needs. You might need assistance formulating a research questions for a manuscript, locating citation metrics or deciding which type of publication to pursue for your project. Whatever your need, we are here to help.
You can access all these resources at ADA.org/library and by logging into the website with your ADA credentials. Prefer to interact with a human being? Email us at library@ada.org or call us at 800-621-8099.
While libraries constantly evolve to leverage new technologies, the mission remains to support their users’ information and research needs. We hope the ADA Library & Archives will become your source for lifelong learning, and we look forward to serving you soon.
Heidi Nickisch Duggan, MA, MS Kelly K. O’Brien, MLIS
16 September / October 2021
RESEARCH: DENTAL PROCEDURES ARE SAFE IN PANDEMIC
A new study from The Ohio State University dispels the misconception that patients and providers are at high risk of catching COVID-19 at the dentist’s office. The study was published in May in the Journal of Dental Research.

Because SARS-CoV-2 spreads mainly through respiratory droplets, and dental procedures are known to produce an abundance of aerosols, fears were that flying saliva during a cleaning or a restorative procedure could make the dentist’s chair a high- transmission location.
The Ohio State University researchers set out to determine whether saliva is the main source of the spray, collecting samples from personnel, equipment and other surfaces reached by aerosols during a range of dental procedures.
By analyzing the genetic makeup of the organisms detected in those samples, the researchers determined that watery solution from irrigation tools, not saliva, was the main source of any bacteria or viruses present in the spatter and spurts from patients’ mouths.
Even when low levels of the SARS-CoV-2 virus were detected in the saliva of asymptomatic patients, the aerosols generated during their procedures showed no signs of the coronavirus. In essence, from a microbial standpoint, the contents of the spray mirrored what was in the office environment.
For the study, the team enrolled 28 patients receiving dental implants and restorations using high-speed drills or ultrasonic
scaling procedures in The Ohio State College of Dentistry between May 4 and July 10, 2020. Researchers collected samples of saliva and irrigants before each procedure; 30 minutes after the procedure, they collected condensate from providers’ face shields, the patient’s bib and an area 6 feet away from the chair.
Genome sequencing technology allowed the researchers to first characterize the microbial mix in preprocedure saliva and irrigants, which they could then compare to organisms in the aerosol samples collected later. With the analytical method they used, the researchers did not need to characterize the microbes — they instead looked for variations in sequences that provided enough information to identify the family of bacteria or viruses to which they belonged.
No matter the procedure or where the condensate had landed, microbes from irrigants contributed to about 78% of the organisms in aerosols, while saliva, if present, accounted for 0.1% to 1.2% of the microbes distributed around the room.
Salivary bacteria were detected in condensate from only eight cases. Of those cases, five patients had not used a preprocedural mouth rinse. The SARS-CoV-2 virus was identified in the saliva of 19 patients but was undetectable in aerosols in any of the cases.
Learn more about this study in the Journal of Dental Research (2021); doi.org/10.1177%2F00220345211015948. n
UDA Action 17 PRACTICE
Photo: Image licensed by ingram image
WHAT’S YOUR LEADERSHIP STYLE?
DENTISTS ARE LEADERS IN THEIR PRACTICES AND THEIR COMMUNITIES
While a certain leadership style may be impactful in a specific job, the best leadership is using a blend of these styles. Knowing what style to enforce in workplace situations comes with time, practice and emotional intelligence. Most leaders borrow from a variety of styles to achieve various goals at different times in their careers. By understanding each of these leadership styles and the outcomes they’re designed to achieve, you can select the right leadership style for any given situation.

Coach – Described as: motivational
You may be a coaching leader if you:
• are supportive
• offer guidance instead of giving commands
• value learning as a way of growing
• ask guiding questions
• balance relaying knowledge and helping others find it themselves
• are self-aware
Benefits: Coaching leadership is positive nature. It promotes the development of new skills, free-thinking and empowerment;
it revisits company objectives and fosters a confident company culture. Leaders who coach often are seen as valuable mentors.
Challenges: While this style has many advantages, it is more time consuming as it requires one-on-one time with employees. This may be difficult to obtain in a fast-paced environment with time-sensitive priorities.
Visionary – Described as: progress-focused and inspirational
You may be a visionary leader if you are:
• persistent and bold
• strategic
• willing to take risks
• inspirational
• optimistic
• innovative
• magnetic
Benefits: Visionary leadership can help companies grow, unite teams and the overall company, and improve outdated technologies or practices.
18 September / October 2021
PRACTICE
Challenges: Visionary leaders may miss important details or other opportunities because they’re so focused on the big picture. They also may sacrifice the resolution of present-day issues because they are so future-oriented, which could leave their teams feeling unheard.
Servant – Described as: humble and protective
You may be a servant leader if you:
• motivate your team
• have excellent communication skills
• personally care about your team
• encourage collaboration and engagement
• commit to growing your team professionally
Benefits: Servant leaders have the capacity to boost employee loyalty and productivity, improve employee development and decision-making, cultivate trust and create future leaders.
Challenges: Servant leaders can become burnt out as they may put the needs of their team above their own. They may have a hard time being authoritative when they need to be and the organization’s goals may be at risk if the servant leader is only focused on the needs of his or her immediate team.
Autocratic – Described as: authoritarian and results-focused
You may be autocratic leader if you:
• have self confidence
• are self-motivated
• communicate clearly and consistently
• follow the rules
• are dependable
• value highly structured environments
• believe in supervised work environments
Benefits: Autocratic leaders can promote productivity through delegation, provide clear and direct communication, and reduce employee stress by making decisions quickly on their own.
Challenges: This style of leadership can cause stress to the leader by bearing all the weight of the decision-making. The lack of flexibility and rigidness, as well as lack of interest in hearing the ideas from others, can cause resentment on the team.
Laissez-faire – Described as: autocratic and delegatory
You may be a laissez-faire leader if you:
• delegate effectively
• believe in freedom of choice
• provide sufficient resources and tools
• take control if needed
• offer constructive criticism
• foster leadership qualities in your team
• promote an autonomous work environment
Benefits: This style encourages accountability, creativity and a relaxed work environment. Because of this, it also can increase employee retention.
Challenges: This style does not work well for new employees,
as they need guidance and hands-on support in their early days. This method also can lead to a lack of structure, leadership confusion and employees feeling a lack of support.
Democratic – Described as: supportive and innovative
You may be a democratic leader if you:
• value group discussions
• provide all information to your team when making decisions
• promote a work environment where everyone shares their ideas
• are rational
• are flexible
• are good at mediation
Benefits: Under this leadership style, employees can feel empowered, valued and unified. It has the power to boost retention and morale. It also requires less managerial oversight, as employees are typically part of decision-making processes and know what they need to do.
Challenges: This leadership style has the potential to be inefficient and costly as it takes a long time to organize big group discussions, obtain ideas and feedback, discuss possible outcomes and communicate a decision. It also can add social pressure to members of the team who don’t like sharing ideas in group settings.
Pacesetter – Described as: helpful and motivational
You may be a pacesetter leader if you:
• set a high bar
• focus on goals
• are slow to praise
• will jump in to hit goals if needed
• are highly competent
• value performance over soft skills
Benefits: Pacesetting leadership pushes employees to hit goals and accomplish business objectives. It promotes high-energy and dynamic work environments.
Challenges: Pacesetting leadership also can lead to stressed-out employees as they are always pursing toward a goal or deadline. The fast-paced work environment fostered under this style can create miscommunications or a lack of clear instructions.
Transformational – Described as: challenging and communicative
You may be a transformational leader if you:
• have mutual respect with your team
• provide encouragement
• inspire others to achieve their goals
• think of the big picture
• place value on intellectually challenging your team
• are creative
• have a good understanding of organizational needs
Benefits: Transformational leadership values personal (continued on next page)
UDA Action 19
Leadership
connection with their team, which can boost company morale and retention. It also values the ethics of the company and team instead of being overly focused on achieving goals.
Challenges: Since transformational leaders look at individuals, it can cause team or company wins to go unnoticed. These leaders also can overlook details as they are big picture thinkers.
Transactional – Described as: performance-focused
You may be a transactional leader if you:
• value corporate structure
• micromanage
• don’t question authority
• are practical and pragmatic
• value goal-hitting
• are reactionary
Benefits: Transactional leaders facilitate the achievement of accomplishments through short-term goals and a clearly defined structure.
Challenges: Being overly focused on short-term goals and not having long-term goals can cause a company to struggle with
PRACTICE
adversity. This style stifles creativity and is unmotivating to employees who aren’t incentivized by monetary rewards.
Bureaucratic – Described as: hierarchical and duty-focused
You may be a bureaucratic leader if you:
• are detail-oriented and task focused
• value rules and structure
• have a great work ethic
• are strong willed
• have a commitment to your organization
• are self-disciplined
Benefits: This leadership style can be efficient in organizations that need to follow strict rules and regulations. Each person in the team/company has a clearly defined role, which leads to efficiency. These leaders separate work from relationships to avoid clouding the team’s ability to hit goals.
CAN I SELL MERCHANDISE FROM MY DENTAL OFFICE, SUCH AS VITAMINS AND MINERALS, OR ELECTRIC TOOTHBRUSHES?
There are several legal issues to consider when deciding whether to sell merchandise from the dental office. Starting with the contractual issues, it is important to carefully review the terms of all sales contracts and documents with the manufacturer or supplier. Consult a qualified attorney about any terms that make you uncomfortable or that you don’t understand. Having an attorney review a sales agreement, especially one that involves a long-term commitment or a large dollar amount, can be an excellent investment if it saves you time, money, and stress in the long run.
If you sell a product that the purchaser believes to be defective, you may be named in a products liability lawsuit. Investigate the products you choose to sell and their manufacturer to make sure the products are of the highest quality and the manufacturer is a responsible company, and check with your insurance advisor to make sure your business liability policy would protect you and your practice if such a claim arises from any merchandise you sell.
Check with your accountant to determine whether you are responsible for collecting sales tax when you sell the products. If so, you will be required to obtain a resale tax number from the state and submit periodic reports and remittances.
If you lease your practice facility, check the terms of your lease to make sure there is no restriction on selling merchandise or certain categories of products. A shopping center landlord will sometimes restrict tenants from competing with the other tenants by restricting the scope of their businesses. For example, if the anchor tenant is a pharmacy, other tenants may be restricted from selling health and beauty aids.
If you sell products such as dietary supplements or dental products, make sure the products you sell are over the counter and not prescription. The sale of prescription products is highly regulated under state and federal laws.
Be careful not to violate HIPAA, as amended by HITECH, in connection with product sales, particularly if you are considering sending marketing information to patients or allowing another entity to send information to your patients. HIPAA restricts the sale of patient contact information for marketing communications and imposes restrictions on marketing communications to patients without their prior authorization.
A Dentist’s Guide to the Law
246 Things Every Dentist Should Know
20 September / October 2021
Challenges: This style does not promote creativity, which can feel restricting to some employees. This leadership style also is slow to change and doesn’t thrive in an environment that needs to be dynamic. Style (continued)
Save These Dates in 2022
Friday, February 11, 2022
Courtyard Marriott

St. George, Utah 2022
March 31 – April 1, 2022
Salt Palace Convention Center Salt Lake City, Utah
 2022 UDA Spring Seminar
UDA Convention
2022 UDA Spring Seminar
UDA Convention
WARNING: LOW BATTERY
stress on their bodies. This could be as simple as posting a positive quote and picture in the breakroom or writing a genuine note of appreciation for your team in a common area. Make sure to be a positive example yourself first, and then figure out how to make the positive energy contagious. Having a positive environment creates relationships and a team is stronger when they care about each other and enjoy working together. Don’t allow negativity to affect the whole office.
3. Host a fun team event to boost morale and light the mood in the office. With trying time from the pandemic nearly in the rearview mirror, lifting up your team’s burned-out spirits can keep your retention rates where you need them. Host a fancy coffee bar on Mondays in the break room. Turn Thursday into Thankful Thursdays and show your gratitude. This can be in the form of an email shout-out, verbal praise during a meeting, or even a handwritten thank you card. You can even go all out and offer a pool or bowling night and invite the whole family to show appreciation for the team’s resilience and hard work.
How are you feeling over a year after COVID-19 took over nearly every aspect of our lives? Are you relieved to have the hardest days behind you or are you still exhausted and in need of a recharge? Do you wonder if your dental practice and team are still being impacted? How do you perceive your team members well being vs. how they’re actually feeling?
Dental teams have been working under new conditions for what seems far longer than a year and a half. The extra PPE, obsessive cleaning, heightened protocols and longer hours have impacted them. Your team may also be navigating patient anxiety, financial instability and health concerns. Many small businesses, just like your dental practice, may be struggling to hire a full team. This can also affect the positivity and morale of the office, and all of this combined can cause stress and burnout for you and your team. This level of mental overload and exhaustion isn’t overcome by an extra day off or donuts at the next huddle. Empathy and a plan for recovery are the answers.
Here are a few tips on how you can help your employees and you bounce back and recharge.
1. Check in with each of your employees individually. Ask them how they’re doing, how they’re feeling and what they need to recharge. You might be surprised by their answers. And those answers might give you some great ideas that aren’t hard to implement in your workplace culture.
2. Start a positivity campaign in the office. Optimistic and positive employees are better at coping with and recovering from stressful situations, reducing the harmful effects of

4. Now with travel more accessible, make sure to allow (and encourage) your staff to take time off. Encourage each person to take a long weekend or full week off to do something fun. If someone takes time off, make it clear to everyone that they should respect their personal time and not contact that individual. The mental shift and reboot will benefit both the individual as well as your dental practice.
5. Respect boundaries! If a team member says “No” to covering an extra shift assume it is for a good reason. Most people struggle with setting boundaries for themselves and in the end suffer from the stress it causes in their personal life.
6. Create your own boundaries. Lead by example and create healthy boundaries for yourself. Separate work from home. While we all need to catch-up on work, make it a goal that you only work on a work da and set a firm quitting time each day. Don’t check work voicemails or emails off hours. So long as you have an emergency contact on your office voicemail, there isn’t a need to constantly check messages for non-urgent matter. Give yourself a break!
Covid-19 may not quite be a thing of the past, but we can move forward with stronger, more resilient teams by taking a muchneeded break to prioritize resting, recharging, and resetting.
Myriah Shimatsu Colorado Dental Association 2021
22 September / October 2021
PRACTICE
Photo: Image licensed by ingram image






One Company...Many Solutions LIVE SURGERY PLACING MINI-IMPLANTS with DR. TODD SHATKIN THURSDAY, MARCH 31st & FRIDAY, APRIL 1st 2022 Learn Minimally Invasion Implant Procedures from Dr. Todd E. Shatkin! 1.888.4.SHATKIN or register online at www.shatkinfirst.com Authorized Distributor of Shatkin FIRST is designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing education programs of this program provider are accepted by the AGD for Fellowship/Mastership and membership maintenance credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. The current term of approval extends from (April/18/2018) to (April/18/2019). Provider ID# (217959) Before F.I.R.S.T.® Stent & Pilot Hole Implant Placed After F.I.R.S.T.® A SOLUTION FOR FIXED, FULL ARCH RESTORATIONS, SINGLE TEETH REPLACEMENT & UPPER & LOWER DENTURE STABLIZATION SAVE $200 ON ANY OF OUR 2 DAY COURSE MINI DENTAL IMPLANTS, A MINIMALLY INVASIVE TREATMENT OPTION for STABILIZING DENTURES & REPLACING MISSING TEETH Register Online at uda.org VISIT OUR REGISTERBOOTH TO WIN: FREE Admission to any Shatkin TrainingF.I.R.S.T. Course offered in Buffalo, NY VISIT US @ the UTAH DENTAL CONVENTION OUR 2022 TRAINING COURSE SCHEDULE Buffalo, NY ................................................................. FEBRUARY 4 & 5 Buffalo, NY ............................... (ADVANCED) MARCH 10 & 11 & 12 Buffalo, NY APRIL 7 & 8 Buffalo, NY MAY 12 & 13 Buffalo, NY ........................................ (ADVANCED) JUNE 9, 10 & 11 Orlando, FL Disney ................................................... AUGUST 5 & 6 Buffalo, NY ........................................................... SEPTEMBER 16 & 17 Buffalo, NY OCTOBER 28 & 29 Buffalo, NY ............................ (ADVANCED) NOVEMBER 17, 18 & 19

To learn how easy it is to begin prescribing electronically, contact a Henry Schein One specialist (833) 907-1747 or visit HenryScheinOne.com/ePrescribe/UT With ePrescribe from Henry Schein One, you can easily enable contactless prescriptions for your patients while meeting your state mandate on prescribing controlled substances, plus: • Send prescriptions to major retail pharmacies that require electronic prescription submission • View patient prescription history through the Prescription Drug Monitoring Program (PDMP) • Check for adverse drug-to-drug interactions and inappropriate dosing ePrescribe Helps You Check Requirements O Your List Contactless Prescriptions Meet Your State Mandate