For generations, UPMC Magee-Womens has been advancing women's health care
As one of the largest gynecologic programs in the country, we're delivering more research, innovative therapies, and treatments for women everywhere.
And, of course, we're still delivering more babies.
With more than 160 locations, virtual care options, and online scheduling, access to renowned care has never been more convenient. Visit UPMC.com/DeliveringMore
Dauphin County Medical Society P.O. Box 53 • Robesonia, PA 19551 717-798-9420 • dauphincms.org
2024 DCMS BOARD OF DIRECTORS
Joseph Answine, MD President
Andrew Lutzkanin, III, MD Vice President
Everett C. Hills, MD
Secretary/Treasurer
Shyam Sabat, MD
Immediate Past President
MEMBERS-AT-LARGE
Michael D. Bosak, MD
Robert A. Ettlinger, MD
John Forney, MD
John D. Goldman, MD
Virginia E. Hall, MD, FACOG, FACP
Saketram Komanduri, MD
John C. Mantione, MD
Mukul Parikh, MD
Gwendolyn Poles, DO
Andrew J. Richards, MD, FACS, FASCRS
Jaan Sidorov, MD
Andrew R. Walker, MD
William Wenner, Jr., MD
EDITORIAL BOARD
Gerard Egan, DCMS Executive Director
Joseph F. Answine, MD, Editor in Chief
Robert A. Ettlinger, MD
Gloria Hwang, MD
Puneet Jairath, MD
Mukul L. Parikh, MD
Meghan Robbins
Shyam Sabat, MD
MEDICAL
Denise Ocampo, President
Mariya Starostina
Can You Feel It? UNDER PRESSURE
By JOSEPH F. ANSWINE, MD, FASA
Iwas asked by one of my current anesthesia employers to fill out a survey about my experience working for the company. The multiple-choice answers ranged from 1 (extremely unlikely) to 5 (extremely likely). The first question was whether I liked my immediate supervisor. My answer was 5 (extremely likely).
Not sure exactly who that is, but I really like everyone I work with in the organization. The next was if I am happy with my job. My answer was 5 (extremely likely). I assume they were asking if I like being an anesthesiologist, and I still really do. Then I was asked if I felt supported by my supervisor. My answer was 2 (unlikely). I think all in the organization may want to support me, but they are powerless against the hospital. The last was if I felt I could speak freely at work. My answer was 1 (extremely unlikely). Does anyone out there feel that speaking your mind at work would come without reprisal? We, as physicians, cannot speak out unless it is in absolute agreement with the hospital administration.
This is ALL hospitals, therefore, none should feel special here. Free speech protects you from the United States government, not the institutions. We are heavily scrutinized, whether in how we care for our patients, resources used, our interactions with staff, or our criticisms of the workplace.
We all know a colleague or a few (or maybe you) that have been fired with little or no warning, finding themselves on the street likely with a non-compete in place. If it is “for cause,” it is commonly because someone made a report because they were told by someone who saw the physician do or say something to someone else. That scenario can and does occur. And some of the accusations have little or no validity. But, if the individual is opinionated, questions authority, or has waning productivity, “with cause” becomes easy to achieve.
On the flip side, there may be that one doc who is arrogant, mean, and with questionable ethics. But, with high productivity. Mythical character or not, if he/she exists, do not expect the same institutional wrath as you or your colleague receive. But do not fret. That individual is a fall in productivity away from an escort out the door.
Do not expect your friends and colleagues to come to the rescue, even those with administrative responsibilities, or on hospital staff executive committees. They cannot even if they wanted to. They have families to feed and non-competes as well. When I was a medical student, I was trying to explain to my cardiovascular surgery attending why I did not complete a task he asked me to do. In mid-sentence, he put up his hand and told me: “Your mother is the only one who loves you, she is not here, and I don’t care.” Truthfully, that was the best advice I have ever received. I appreciate my friends having my back, but I do not look for it nor expect it.
My conspiracy theory is that a physician with mediocre skills but quiet and submissive is much more desirable than an exquisite doctor who is outspoken and likely to voice a concern.
I do not anticipate a pizza party at work when I leave (maybe after I leave), but I would rather not be escorted out by security.
I just realized that my name was on the survey. Crap! I have to go find a cardboard box for my stuff.
To my dear friends who have suffered through such events, I love and respect you, your talents, and your friendship.
A MESSAGE FROM THE DCMS EXECUTIVE DIRECTOR, GERARD EGAN
Dear DCMS Members,
I hope you’re enjoying your summer so far! As we dive into these warmer months, I want to remind you about some exciting opportunities and upcoming events with the Dauphin County Medical Society (DCMS).
Firstly, I invite our dedicated members to consider taking on leadership roles within our society. Serving as board members or officers is a chance to leverage your expertise and enthusiasm to shape the future of our medical community. Your leadership will make a significant impact, and we encourage you to explore these opportunities.
Looking ahead, it’s essential to start preparing for the House of Delegates meeting scheduled for October 25 and 26, 2024. This meeting is crucial for discussing and deciding on important matters that affect our profession and the healthcare landscape. Stay connected over the next couple of months by participating in various Pennsylvania Medical Society (PAMED) events leading up to the meeting. Keep an eye out for updates and key dates shared through the PAMED website intended to keep you well-informed.
With our magazine back in full swing, we’re actively seeking articles from members who are passionate about specific healthcare topics and wish to share their insights with colleagues and the community. Your contributions enrich our discussions and strengthen our collective knowledge.
Lastly, I want to thank everyone who has visited our new website and engaged with our Facebook page. Your support is immeasurable so please continue to follow, like, and share our content to spread awareness and stay connected. Look out for additional Dauphin County Coverage emails to keep you informed about upcoming events, opportunities with DCMS and PAMED, or general news and reminders.
Thank you for being part of the Dauphin County Medical Society! We hope you find this next edition informative and engaging. Together, let’s keep connecting, growing, and paving the way for a successful future together. Thank you for being an essential part of our community!
Unplugging Adolescents from Social Media, Naturally
Sby Steph Lee, MD, MPH,
By STEPH LEE, MD, MPH, FAAP
ummer is upon us and it’s the perfect season to incorporate nature time for kids of all ages. Being outdoors is a great way to get fresh air and connect with the environment, which has lots of mental, physical, and emotional benefits for kids.
In the last few years, children and adolescents have experienced increasing rates of depression, anxiety, and feelings of loneliness. In 2019, a longitudinal cohort study of teenagers (12 to 15 years old) found that regardless of baseline mental health status, teenagers who spent more than three hours per day on social media had double the increased relative risk of internalizing problems, exhibiting symptoms of depression and anxiety.[1] Another study found that among 14-year-olds, greater social media use was a predictor for poor sleep, online bullying, poor body image, low self-esteem, and higher symptoms of depression, with girls being affected more than boys.[2] Most recently in 2022, 95% of teenagers (13 to 17 years old) reported using social media, with more than half stating it would be hard to give it up.[3] In 2023, Surgeon General Dr. Vivek Murthy published a Surgeon General’s Advisory on the importance of social connection and the significant consequences when social connection is lacking. [4] Recently, Dr.
Murthy has called for “warning labels” on social media like what has been done for such high-risk products as tobacco and alcohol.
Jonathan Haidt, a social psychologist and Professor of Ethical Leadership at the New York University Stern School of Business, recently published a book called The Anxious Generation: How the Great Rewiring of Childhood Is Causing an Epidemic of Mental Illness (Penguin Random House). In his book, he cites statistics showing a significant rise in anxiety, depression, and suicide rates among US adolescents and young adults between 2010 and 2022. While isolation during the pandemic certainly exacerbated these trends, he notes that a significant factor prior to the pandemic was the absence of smartphones and ever-present social media. As these entities have become ubiquitous in the lives of young Americans, so has the rise of psychopathology amidst this demographic. While he advocates for restrictions on smart phones and social media access by schools and parents, especially for younger teens, there are also other readily available remedies to this national dilemma.
Nature can help play a role in enhancing social connections and bolstering mental health resilience in the face of the increasing role social media plays in children’s lives.
continued on next page >
FAAP
Research regarding nature during the pandemic solidified what we’ve known about the benefits of nature as a positive tool for mental health. One study surveyed adolescents (10 to 18 years old) between April and June of 2020, during the initial wave of the pandemic. They found that connection to nature acted as a mediating factor and fueled greater mental wellbeing in those that participated in outdoor activities.[5] Park access has also been shown to help mental health among children and parents, with parents also benefiting by getting in more physical activity.[6]
Being outdoors has been shown to help children with sleep, attention, and mood, and the more in nature, the better. One study has found that green natural settings, versus built outdoor and indoor environments, can reduce ADHD symptoms in children (5 to 18 years old) regardless of age, gender, and income groups.[7] Increased accessibility and increased exposure to nature were both associated with improvement in ADHD symptoms, while actually interacting with nature reduced stress.[8] Even among toddlers and preschoolers (age less than 5 years), physical activity and the great outdoors were associated positively with better sleep outcomes including less evening screen time.[9]
This is all to say that being outdoors and in nature can bolster children’s mental health tremendously and what better time to do that than in summer? Even as little as ten minutes of sitting or walking outdoors can make a positive impact on well-being, as seen with college-age students.[10]
Parents can explore the outdoors together with their children, so that families can bond and unplug from technology and enjoy being in the moment.
Physicians can also play a role in promoting mental health resilience and a
healthy connection to nature by providing prescriptions for outdoor activities. There are programs like Prescribe Outside (https:// prescribeoutside.org/), Philadelphia’s nature prescription program and a partnership between Children’s Hospital of Philadelphia (CHOP), Awbury Arboretum, Let’s Go Outdoors, the USDA Forest Service, and Temple University Center for Sustainable Communities. Research shows these social prescriptions promote connection to nature, strengthen social structures, and improve health on all levels.[11]
When children engage in outdoor play, it fosters a love of nature and the environment which is key for helping children understand the environmental impact we have on our communities and allows adults to raise a healthier, happier generation.
This article was originally published in the Summer 2024 edition of Berks County Medical Record magazine. It has been updated.
[1] Riehm KE, Feder KA, Tormohlen KN, Crum RM, Young AS, Green KM, Pacek LR, La Flair LN, Mojtabai R. Associations Between Time Spent Using Social Media and Internalizing and Externalizing Problems Among US Youth. JAMA Psychiatry. 2019 Dec 1;76(12):1266-1273. doi: 10.1001/jamapsychiatry.2019.2325.
[2] Kelly Y, Zilanawala A, Booker C, Sacker A. Social Media Use and Adolescent Mental Health: Findings From the UK Millennium Cohort Study. EClinicalMedicine. 2019 Jan 4;6:59-68. doi: 10.1016/j.eclinm.2018.12.005.
[3] Vogels E, Gelles-Watnick R, Massarat N. Teens, Social Media and Technology 2022. Pew Research Center.
[4] Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community. Available at: https://www.hhs.gov/sites/default/ files/surgeon-general-social-connection-advisory.pdf (Accessed 15 June 2024).
[5] Jackson SB, Stevenson KT, Larson LR,
Peterson MN, Seekamp E. Connection to Nature Boosts Adolescents’ Mental Well-Being during the COVID-19 Pandemic. Sustainability. 2021; 13(21):12297. https://doi.org/10.3390/ su132112297.
[6] Hazlehurst, M.F., Muqueeth, S., Wolf, K.L. et al. Park access and mental health among parents and children during the COVID-19 pandemic. BMC Public Health 22, 800 (2022). https://doi. org/10.1186/s12889-022-13148-2.
[7] Kuo FE, Taylor AF. A potential natural treatment for attention-deficit/hyperactivity disorder: evidence from a national study. Am J Public Health. 2004 Sep;94(9):1580-6. doi: 10.2105/ajph.94.9.1580.
[8] Tillmann S, Tobin D, Avison W, Gilliland J. Mental health benefits of interactions with nature in children and teenagers: a systematic review. J Epidemiol Community Health. 2018 Oct;72(10):958-966. doi: 10.1136/jech-2018210436. Epub 2018 Jun 27.
[9] Janssen X, Martin A, Hughes AR, Hill CM, Kotronoulas G, Hesketh KR. Associations of screen time, sedentary time and physical activity with sleep in under 5s: A systematic review and metaanalysis. Sleep Med Rev. 2020 Feb;49:101226. doi: 10.1016/j.smrv.2019.101226. Epub 2019 Nov 1.
[10] Meredith GR, Rakow DA, Eldermire ERB, Madsen CG, Shelley SP, Sachs NA. Minimum Time Dose in Nature to Positively Impact the Mental Health of College-Aged Students, and How to Measure It: A Scoping Review. Front Psychol. 2020 Jan 14;10:2942. doi: 10.3389/ fpsyg.2019.02942.
[11] Leavell MA, Leiferman JA, Gascon M, Braddick F, Gonzalez JC, Litt JS. Nature-Based Social Prescribing in Urban Settings to Improve Social Connectedness and Mental Well-being: a Review. Curr Environ Health Rep. 2019 Dec;6(4):297-308. doi: 10.1007/s40572-01900251-7.
Steph Lee, MD, MPH, FAAP, has been a Pediatrician and Public Health physician at Penn State St. Joseph Health Center. She and her family are returning to their home in California this summer. She will be greatly missed by her patients, friends, and colleagues. We wish her and her family the very best.
Nature: An Antidote for the Negative Effects of Social Media on Adolescents and Families
By Douglas Berne, MD, Child and Adolescent Psychiatry, Reading Hospital/Tower Health
In the new Pixar movie “Inside Out 2,” 13-year-old Riley enters puberty, and with it, encounters some new emotions. Most notably, Anxiety takes over control and changes her selfperception. This reflects how anxiety in general becomes a much more important emotion in adolescents, with or without the impact of social media. However, social media is well-documented to have significant negative effects on mood and self-worth in both adults and adolescents. Apps such as TikTok and Instagram provide a never-ending stream of idealized versions of people’s lives that create anxiety in most people, especially in teenage brains that are even less equipped to counter such unfiltered information.
Social media can have potential benefits, for example, helping LGBTQ teens feel connected to a community, especially if they live in a more conservative or isolated area, or helping individuals who live in more isolated areas to feel more connected to others. The ways in which social media is used by teenagers generally creates more anxiety and distress. Most adolescents mindlessly consume social media by passively scrolling or allowing the algorithms to continue pushing videos, creating an echo chamber that worsens moods and fosters feelings of isolation and anxiety. It becomes increasingly difficult to put the device down and walk away, with a self-defeating cycle underway.
Dr. Steph Lee’s article (see page 7) summarizes nicely both the negative impact that social media can have on adolescents and a potential solution in the form of unplugging from devices and going into nature. In addition to having their teens put away the phone, parents would be well-advised to recognize that they are role models. The mother or father staring at a phone on the playground while sending a child out to play is not modeling active engagement.
In addition, spending time “unplugged” allows for both children and adults to spend time feeling more connected to the world around
From the Editor...
Here in Dauphin County, PA, we are fortunate to have several resources for spending time in nature. Boyd Big Tree Preserve and Wildwood Park are well-known for their trails and woods. Fort Hunter Park and the Capital Area Greenbelt offer walking trails along the Susquehanna River and often host outdoor events. We have parts of the Appalachian Trail, as well as trails in the nearby Stony Valley and Peter’s Mountain areas. The county also boasts scenic routes along the Susquehanna River and numerous parks, such as Susquehanna Riverfront Park and Memorial Lake State Park, plus much more.
them rather than the virtual world, and to feel a stronger sense of control of themselves. By going for walks with their children and adolescents, parents can help guide their children to pay attention to the world around them and to facilitate bonding within the family.
As health care providers in our community, we can help families connect to one another as well as to nature by exploring the resources most readily available to them and opportune times to take advantage of our natural environment. This might be as simple as recommending a regular time for the family to walk to one of their local parks or to explore some of our great resources within the county. If parents can prioritize a little family time each week doing this, they will not only help improve connections by spending time together, but also reap benefits of reduced anxiety and harmful behaviors on the part of their children (and themselves).
This article was originally published in the Summer 2024 edition of Berks County Medical Record magazine. It has been updated.
Play, LEARN, HEAL: The Power of Understanding
By DIANA ORABUEZE and MANVITA MAREBOINA
“Hide and seek!” “Jump rope!” “Freeze tag!” The children excitedly exclaimed their favorite games when asked what they enjoyed doing outside. I was at the Centre Hall Library, leading our monthly health literacy event with this month’s event themed ‘Jump into Spring.’ The room buzzed with energy as kids and parents eagerly listened to us share tips on staying active during the warmer months. Our goal was simple: to encourage families to embrace outdoor activities and foster a lifelong love for physical fitness.
But health literacy isn’t just about outdoor games and warm weather. Sometimes, it’s the key to understanding and resolving health concerns. I was reminded of this by my own family’s journey, starting when we immigrated from India to Vandalia, Ohio, with nothing but our bags and each other. When my family moved from India to Strongsville, Ohio, we hoped for a fresh start. But our transition was overshadowed by my younger brother’s health issues. At just 2 years old, he had suffered multiple fractures, despite being a lively child. We were at a loss and felt a growing sense of anxiety as we struggled to communicate with doctors due to the language barrier. As we navigated the medical system, the results of my brother’s numerous tests revealed that he had severe Vitamin D deficiency, which led to weak bones and frequent fractures. It was a surprise for us because we came from a place with plenty of sunshine, yet we never really understood how Vitamin D and calcium are
essential for bone health. The doctors helped us bridge this knowledge gap, guiding us through a plan focused on adequate supplementation and nutrition.
This personal experience – and many more to follow – was a driving force behind our health literacy events. My colleague and I had been hosting these events, with mobile clinic presence, for over a year, and we had already seen the difference that a better understanding of health can make. Our audience grew from a small group to a lively gathering as more families participated. The events became a place for shared stories and laughter. With each session, more parents joined and noticed their children’s behaviors changing for the better. We were on the right track, fostering a new generation that values health, community, and the simple joys of outdoor play.
As a medical student working primarily with rural, Amish, and Mennonite communities, I have observed how limited access to care within these groups has contributed to poor health outcomes. These experiences have influenced my journey as a future pediatrician and have strengthened my commitment to promoting health literacy for children and families. Looking back, there are multiple stories that highlight the importance of continuous health literacy among families, spanning from childhood to adulthood.
In one instance, a week after giving birth, a young Amish woman with type 1 diabetes came to the emergency department showing signs of altered mental status. We learned that she had stopped taking her diabetes medication because auditory hallucinations told her to do so. Concerned about her newborn’s safety, we admitted her for monitoring and initiated antipsychotic treatment, explaining to her family that it was due to postpartum psychosis rather than diabetes complications. This revelation surprised them, as they were not aware that such an event could happen. Despite our explanations about the risks of untreated postpartum psychosis, which can include infanticide, the family remained uncertain about the treatment plan and why she couldn’t be home with her baby.[1] To ensure her continued care, we tailored a follow-up plan that respected her cultural background, finding an inpatient program designed for Amish communities. The patient and her family
gradually came to understand the necessity of our approach, thanks to consistent communication and education from our psychiatric, pediatric, and internal medicine teams.
This lesson carried over into another instance that made clear the impact of communication on patient health. A foster child was brought into the clinic by her foster parents after experiencing shortness of breath while playing outside. Her medical records were scattered across different states, making it complicated to gather a comprehensive history. After several tests, the child was diagnosed with asthma and prescribed an inhaler. However, when the child had another asthma attack at a park a couple of months later, the inhaler seemed to be ineffective. It wasn’t until the foster parents and the child demonstrated how they used the inhaler that we uncovered the problem. While the parents knew how to use it, the child didn’t know the correct technique. She had never practiced using the spacer and struggled to coordinate her breaths to get the full dose of the medication, leading to insufficient treatment during her asthma attack. This simple gap in health literacy led to a serious medical emergency. In all these stories, I saw how communication, understanding, and education are vital in healthcare.
I have come to realize the importance of beginning health education as early as possible and continuing it throughout a person’s lifetime. What if the young boy’s family never understood the role that sunlight, diet, and Vitamin D had on their son’s growth? What if the mother stopped the antipsychotic medications due to fear that the medications would affect breastfeeding? What if the little girl never learned how to properly use her inhaler and suffered a more severe asthma attack?
This is why health literacy is important and why I collaborated with my medical school and community centers to initiate a health curriculum for children. Research indicates that establishing health education in childhood is crucial, as this developmental stage is when children acquire foundational health-related behaviors.[2,3] In recent months, our health literacy program has addressed topics for children’s well-being, including mental health, relationships, personal hygiene, and germ prevention. Our approach was designed to equip children with the knowledge they needed to make informed choices
about their health, while also emphasizing the role parents play in supporting and guiding them. Through our mobile clinic unit and community partnerships with libraries, we have created a safe and non-judgmental space where parents can freely ask questions and seek clarification on health-related matters. This open dialogue is essential for promoting understanding and addressing concerns effectively. By tracking students’ progress through pre- and post-surveys, we are able to continue to grow and make changes to the program to better cater to the community. Through this initiative, I have witnessed firsthand the power of education in enabling families to make healthier choices and advocate for their own well-being.
As healthcare workers, we must remain dedicated to the continued education of our patient population and avoid assuming that medical knowledge is obvious or intuitive. By actively addressing gaps in health literacy, we can empower patients and families with the information they need to make informed decisions about their health. Whether it’s the critical role of Vitamin D in bone health or the correct technique for using an inhaler, providing clear, accessible information can be a lifesaver. By embracing this approach, we have created a space where community members can manage their health effectively and improve patient outcomes – a place where children can play, learn, and heal.
REFERENCES
1. Friedman, S. H., Reed, E., & Ross, N. E. Postpartum Psychosis, 2023. Current psychiatry reports, 25(2), 65–72. doi.org/10.1007/ s11920-022-01406-4.
2. Bröder, J., Okan, O., Bauer, U., et al. Health literacy in childhood and youth: a systematic review of definitions and models, 2017. BMC public health, 17(1), 361. doi.org/10.1186/ s12889-017-4267-y.
3. Rowlands G. Health literacy, 2014. Human vaccines & immunotherapeutics, 10(7), 2130–2135. doi.org/10.4161/hv.29603 2014;123(1):e75-e82.
Staying healthy includes
IMMUNIZAT ONS!
BY MADALYN SCHAEFGEN, MD, FAAFP, LEHIGH VALLEY PHYSICIAN GROUP AMBULATORY IMMUNIZATION CLINICAL LEAD AND VICE CHAIR OF PENNSYLVANIA IMMUNIZATION COALITION
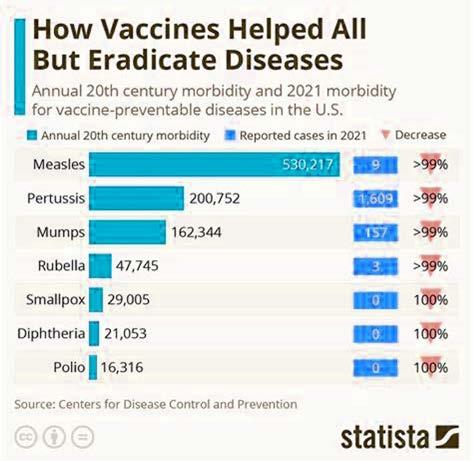
VACCINE-PREVENTABLE DISEASES ARE ON THE RISE.
As we recover from the COVID-19 pandemic, let us not forget that we still have more people dying from COVID than from influenza, and that most of these deaths can be prevented through vaccination. (COVID-19 illness, although declining, resulted in 132 deaths the week of June 8th.) Cases of pertussis, measles, Neisseria meningitidis, and hepatitis A illness are rising, resulting in outbreaks.
THERE IS A DECLINE IN ROUTINE VACCINATIONS SINCE THE PANDEMIC, WHICH HAS SPREAD FROM COVID-19 VACCINES TO ALL VACCINES.
The prior 3 school years (2019–20, 2021–22 and 202223), national coverage with state-required vaccines among kindergartners declined from 95% to approximately 93%. 2023-2024 school year was the first time that MMR vaccine coverage for PA kindergarteners went below 95%. Maintaining community immunity greater than 95% is necessary to reduce risk for vaccine-preventable disease and to protect those whose immune systems are not as robust. Immunization is the most effective means of prevention.
VACCINES WORK.
VACCINE REFUSAL PUTS PEOPLE AT RISK.
Immunize.org has evidence-based references regarding decline in vaccination rates and rising rates of vaccine preventable diseases that you can find at https://www.immunize. org/wp-content/uploads/catg.d/p2069.pdf.
VACCINE EXEMPTIONS ARE ON THE RISE.
Vaccine exemption rates among kindergarteners has increased in 41 states, including Pennsylvania. Childhood immunization coverage levels are lower when non-medical exemptions to requirements are available, especially if they are easy to get. PA allows medical, religious and moral/ethical exemptions to vaccines. PA law requires certain immunizations, but does not require HPV nor MenB. HPV vaccine is extremely effective in preventing HPV-related cancers. Outbreaks of other vaccine-preventable diseases, such as measles, pertussis, and varicella, have been traced to pockets of unvaccinated children. And no one wants to lose a child to meningitis which can be prevented.
VACCINES HAVE BEEN AROUND SINCE THE 1700S , AND THEY CONTINUALLY CHANGE AS TECHNOLOGY AND VIRUSES CHANGE.
Vaccine changes are improvements. U.S. governmental reviews, approvals and monitoring of vaccines is robust. The vaccines go through rigorous testing prior to FDA approval, then have continued monitoring after approval through agencies including The Vaccine Adverse Event Reporting System (VAERS), The Vaccine Safety Datalink (VSD), V-safe, and The Clinical Immunization Safety Assessment (CISA) Project. The newer vaccines are more effective with no more associated risk.
ACIP is meeting on June 26-28 to review and vote on vaccines for RSV, DTaP/Hib/HepB (Vaxelis), COVID-19, influenza (including Avian influenza A H5N1), and pneumococcal (PCV21) vaccines. They will also review Chinkungunya, Dengue (both of which may become more important as travel and global temperatures increase) and MenABCWY. Look for the immunization schedule and schedule changes with guidance at https://www.cdc.gov/vaccines/ schedules/index.html and https://www.cdc.gov/ vaccines/schedules/hcp/schedule-changes.html.
1. THINK ABOUT DRIVERS FOR HESITANCY.
Health care information is found increasingly outside of the physician/clinician-patient relationship.
Misinformation/Disinformation has accelerated exponentially with social media.
Distrust/lack of confidence in vaccines has increased with the COVID-19 pandemic, vaccines.
Polarization regarding vaccines has occurred similar to polarization of the country.
Number of vaccines in the schedule has increased and changed.
Misperceptions and myths occur regarding
a. Low level of risk to disease (invulnerability)
b. Higher risk of adverse events than exists with the vaccine
c. Vaccine ingredients and harm (lack of knowledge)
Vulnerability (pandemic, pregnancy, mental illness, etc.) to be persuaded by “fake news.”
2. REMEMBER THAT PEOPLE WANT WHAT’S BEST FOR THEMSELVES, THEIR CHILDREN, THEIR FAMILIES.
Treat all with empathy and compassion.
Avoid labeling patients or increasing their fears.
Listen and ask questions.
Provide choices. Offering options can reduce vaccine hesitancy.
Remind that a choice to not vaccinate is not a risk-free choice.
3. STRATEGIES TO USE FOR ALL YOUR PATIENTS.
Give a strong recommendation which is personalized to your patient.
a. Providers are a patient’s most trusted source of information on vaccines.
b. Research shows a patient who receives a strong recommendation from a provider is 4–5 times more likely to be vaccinated.
Presume they are interested in getting the vaccine.
Continued on page 14
Increase your vaccine knowledge. If patients have questions about the vaccines, be sure that you AND YOUR STAFF have evidence-based answers! To prepare, see https:// www.cdc.gov/vaccines/hcp/conversations/ preparing-for-parent-vaccine-questions.html.
Have the vaccines available in the office (or refer out if needed).
4. FOR THOSE WHO ARE HESITANT, USE MOTIVATIONAL INTERVIEWING TECHNIQUES.
Ask where they lie on the number continuum to accept a vaccine. (On a scale of 1 to 10, 10 being they are ready to get a vaccine, where are they? Look for the positive – have them express why they did not pick a lower number.)
Ask open-ended questions as to why they do not want to get a vaccine.
Actively listen to the concerns.
REFERENCES
Affirm you hear what they are saying.
Request permission to share what you think. Know your patient. Highlight social norms. Use stories. Present facts.
If they are still unwilling, be patient and be sure to maintain the relationship to discuss another day.
CHANGE
IS HARD BUT INEVITABLE.
Change increases emotions like anxiety. There are 2 ways to cope with change: escape (avoidance, feeling like a victim) and control (managing the change).
VACCINE HESITANCY IS NOT NEW.
Vaccine opposition/hesitancy has been around ever since the first vaccine was introduced by Jenner in 1796. Why is hesitancy increasing? Big changes over which we have no control (pandemic, climate change), changes in how we view the world (internet, social media), and the decline
16. 2007 National Survey of Children’s Health. Factors associated with human papillomavirus vaccine-series initiation and health care provider recommendation in U.S. adolescent females. Vaccine 2012;30(20):3112-3118
in prevalence of vaccine-preventable diseases (due to prior vaccines and better health care).
ADDRESSING VACCINE HESITANCY.
Intention to vaccinate was consistently correlated with concerns about the disease, trust in health institutions, and previous vaccinations. How do we move from hesitancy to accepting vaccination?
EVERYONE DESERVES A SECOND CHANCE! BE AWARE OF THE VACCINE CATCH UP SCHEDULE. You can find it at https://www.cdc.gov/ vaccines/schedules/hcp/imz/catchup.html.
TRAVELING THIS SUMMER?
Don’t forget vaccines at least 2 weeks prior to the trip. See https://wwwnc.cdc.gov/travel.
Vaccinate! You can save a life!
This article was originally published in the Summer 2024 edition of Lehigh Health magazine. It has been updated.
Medical Management
of the Ge r iatric Patient
By ALEXANDER A. ANSWINE, MD and JOSEPH F. ANSWINE, MD, FASA
This article is written from the perspectives of an internist and anesthesiologist, different backgrounds but not surprisingly, similar concerns. Most importantly, preserving function and quality of life.
If you look up the definition of Geriatric Medicine, it states that it is a medical specialty focused on providing care for the unique health needs of the elderly. The specialty benefits individuals who are managing multiple chronic conditions or experiencing significant age-related complications that threaten quality of daily life. The care is driven by patient goals and preferences, which can vary from preserving function and improving quality of life to prolonging years of life.
By 2050, 1 in 6 individuals throughout the world will be over 65 years of age, therefore, keeping the elderly healthy and productive will be important for our society to continue to progress and flourish.
We have peak organ function at 30, then we lose organ activity at about 1%/year. Therefore, treating an 80-year-old with diminished liver, kidney, and other organ function as if he/she were a 30-year-old would not be reasonable.
The age to start seeing a geriatrician has been arbitrarily set at 65 years old since that is when we in the United States could traditionally retire. However, a younger individual with severe chronic disease and fragility could and should be considered for geriatric care.
The 5 components to geriatric care are: 1) major illnesses 2) mobility 3) presence or absence of mental illness 4) medications taken and 5) what matters to the patient.
Because the 5th component, “what matters most to the patient,” requires more individualized care, protocol-driven medicine is less effective in the elderly. For example: Hypertension is a blood pressure greater than 140/90 mmHg. An A1C should be less than 7% in a diabetic patient. But what if an 85-year-old lady lives alone or is taking care of an ailing husband? Should the blood pressure be lowered, or tighter glucose control be attempted, which would increase the risk of orthostatic hypotension or symptomatic hypoglycemia? Is the risk of passing out or falling greater than the long-term cardiovascular risk of the above diseases if they are “less controlled”? If you see one elderly woman, you have seen just one elderly woman and not them all.
Major Chronic Illness
Eighty percent of the elderly have at least one chronic condition and 77% have at least two. Common chronic illnesses in the elderly are:
• Lungs: COPD, asthma, scarring with restrictive lung disease.
• Activity limiting arthritis.
• Hypertension.
• Type 2 Diabetes.
• Kidney disease/dialysis.
• Parkinson’s Disease.
• Cognitive dysfunction/Dementia.
• Other endocrine diseases such as hypothyroidism.
• Cancer.
Mobility
Mobility may be the most important function (and assessment) in any elderly individual, allowing for independent living. The more mobile an individual is, the less dependent on others for achieving the activities required for daily living (ADLs). Mobility includes decreasing risk of falls and the likely hospitalizations that follow. Therefore, assessing and improving mobility is vital to the elderly for maintenance of independence and quality of life. Improved mobility reduces healthcare utilization and costs as well.
There are many mobility assessment scales. All, however, have similar metrics.
The Elderly Mobility Score (EMS) is one of those assessment tools. It is composed of:
• Going from a lying to sitting position.
• Going from sitting to lying.
• Going from a sitting to standing position.
• Time and assistance needed to go from sitting to standing.
• The ability to stand without support.
• Balance while standing and walking.
• Functional reach (ability to reach for something while standing).
Scoring is as follows:
• Lying to sitting without help: 2 pts, with one person’s help: 1 pt, with the help of 2 or more people: 0 pts.
• Sitting to lying with no help: 2 pts, with one person’s help: 1 pt, with 2 or more people’s help: 0 pts.
• Sitting to standing independently within 3 seconds: 3 pts, sitting to standing independently in longer than 3 seconds: 2 pts, needs the help of one person: 1 pt, needs the help of 2 or more people: 0 pts.
• Standing without help and able to reach without help: 3 pts, can stand but needs help to reach: 2 pts, can stand with support to stay standing: 1 pt, can stand only with assistance: 0 pts.
• Walking with no help: 3 pts, can walk with the help of a frame such as a walker: 2 pts, can walk with aid but unstable: 1 pt, requires another person to walk: 0 pts.
• Can walk 6 meters in under 15 seconds: 3 pts, can walk 6 meters in 16-30 seconds: 2 pts, can walk 6 meters in more than 30 seconds: 1 pt, not able to walk 6 meters: 0 pts.
• Can reach 20 cm: 4 pts, can reach 10-20 cm: 2 pts, reach under 10 cm: 0 pts.
What do the scores mean?
• 14-20 pts: good mobility, therefore, work to maintain and improve overall fitness. Should be able to handle most ADLs. Diet, weight management, yoga, hobbies.
• 10-13 pts: borderline independent/can do some ADLs. Physiotherapy.
• Under 10 pts: needs help with most or all ADLs. Needs significant assistance. Assisted living environment may be needed. Home care with a frequent or constant care giver.
The risk of falling is a major part of mobility assessment. Based on CDC data, 1 in 4 or 14 million adults over 65 report a fall each year. Thirty-seven percent of the elderly report an injury severe enough to be significantly limiting at least for a day. Florida is one of the states with a lower rate of reported falls in 2021, and Wisconsin is one of the highest. Snow and ice possibly? The number of fall deaths in the elderly has increased over the years (78 per
100,000 older adults in the United States in 2021). Fall risk increases with weakness and balance issues, medications (such as sedatives, blood pressure medications, diabetes medications), vitamin deficiencies, foot and leg pain, and environmental risks (such as throw rugs, uneven surfaces, clutter). Healthcare workers can prevent falls by assessing individual fall risk (motility and frailty assessment, asking about environmental risk factors, medication benefit versus risk assessment, etc.).
Assessing “Frailty” is a large part of geriatric care, and mobility is a major component. Frailty is best defined as a state of increased vulnerability across multiple health domains that leads to adverse health outcomes.
Multiple domains are assessed:
• Physical – ADLs (activities of daily living), mobility, falls, self-identified exhaustion, co-morbidities.
• Nutritional – unintentional weight loss, laboratory studies such as albumin.
Many frailty scales have been developed and studied to determine risk of morbidity in the elderly population. There may be sixty or more scales/indexes. Patients’ goals and preferences are taken into consideration (longevity versus functionality) along with the level of frailty when determining care. Elderly, frail patients commonly overestimate the benefits and underestimate the risks of intervention.
The above domains are relatively consistent between the multiple frailty scales. One example of a frailty scale is the “Frailty Phenotype” which looks at weakness, slow movement, low energy, weight loss, and falling. Others like the “Accumulating Deficits” scale include depression, cognitive decline, physical decline, nutrition, and social stressors. Regardless of the scale used, assessing frailty is a key component of the geriatric workup.
Mental Illness
Common mental illnesses in the elderly are depression, cognitive impairment, and delirium.
Depression diagnoses include:
• Mild Depression.
• Major Depression (with or without psychosis).
• Persistent Depressive Disorder (fewer symptoms but of longer duration).
• Bipolar Disorder.
• Depression due to a medical condition (e.g. hypothyroidism, post-CVA, post-MI).
• Adjustment Disorder with Depression (related to a life stressor/bereavement).
Depression symptoms include:
• Alteration in sleep.
• Loss of interest/apathy.
• Guilty or worthless feelings.
• Fatigue.
• Inability to concentrate.
• Loss of appetite.
• Psychomotor agitation or retardation (common).
• Suicidal thoughts.
• Cognitive Impairment (depression must be ruled out in a dementia work-up).
As for treatment, the elderly are notoriously undertreated for fear of treatment side effects. Common treatment regimens include SSRIs (usual first line therapy), and SNRIs. If these classes of drugs are used, following lab work for hyponatremia due to SIADH, and QT prolongation is important. Tricyclics (more anti-cholinergic effects so less commonly used) can be considered, as well as other anti-depressants with different modes of action. Electroshock Therapy (ECT) can be considered especially in patients with psychosis. Psychotherapy may be the best choice before medications for mild depression.
Neurocognitive disorders in the elderly include:
• Alzheimer’s Disease.
• Frontotemporal Dementia.
• Lewy Body Disease.
• Vascular/CVA Induced.
• Trauma Induced.
• Substance Abuse Induced.
• Inherited Disease (e.g. Huntington’s Disease).
• Parkinson’s Induced.
• Infection Induced (e.g. HIV).
• Major Illness Induced.
• Unknown/Unspecified/Multiple Etiologies.
Symptoms include:
• Memory impairment.
• Language difficulties.
• Difficulty with orientation.
• Executive function difficulties (ability to do daily tasks and adapting to changes).
Behavior disturbances can be the first sign of dementia. The presence of neuropsychiatric symptoms leads to greater impairment and faster decline. More than 50% of dementia patients have neuropsychiatric symptoms.
Treatment modalities for neurocognitive disorders require ruling out or treating physical causes (e.g. thyroid disease, sleep apnea, etc.). Non-pharmacologic therapy is more difficult based on physician training but a good first line due to lack of medication side effects. It should start with working with patients and caregivers to develop structure.
Pharmacologic therapy may include anti-psychotics (some efficacy but higher mortality with these meds/used but most not FDA approved in this patient population), anti-depressants (conflicting evidence of improvement), benzodiazepines (only for emergency agitation use), and cholinesterase inhibitors (increases available acetylcholine).
Delirium is much more common in the elderly as compared to younger individuals.
Symptoms involve rapidly developing cognitive impairment, confusion, disorientation, hallucinations, sleep/wake disturbance, and depression. There is commonly a fluctuating course.
Delerium could be medication induced, substance withdrawal induced, or secondary to
Continued on page 18
medical illness. Symptoms could last weeks to months. Based on a study from 2011 (Delirium in the Elderly), 20%-79% of hospitalized elderly patients experience delirium during their stay. Delerium patients are more likely to have prolonged hospital stays and less likely to be discharged to home. Furthermore, they have higher overall mortality.
The treatment is to fix the underlying cause.
Common causes in hospitalized patients include:
• Infection
• Withdrawal
• Metabolic (electrolytes, glucose, etc.)
• Trauma
• Brain pathology
• Hypoxia
• Acute vascular abnormalities such as stroke
• Arrhythmias
• Toxins/Heavy Metals
The etiology of delirium is obviously in the brain. It originates in the Reticular Activation System (RAS) which is a collection of neurons in the medulla, pons, and thalamus. It is important for changing states of consciousness / sleep-wake cycle. It also is involved with focus / directing our attention. The RAS atrophies as we age which may be why we become prone to delirium as we get older. Many neurotransmitters are present in the RAS, but the 2 main ones are acetylcholine and norepinephrine. Altered levels of neurotransmitters especially a decrease in acetylcholine can lead to delirium. Therefore, just about anything that alters neurotransmitter and neuronal activity will lead to delirium in susceptible patients: medications (e.g., anticholinergics) , bladder infections stimulating the Vagus Nerve (cranial nerve 10), any other infections, inflammation, electrolyte or glucose abnormalities altering neuronal activity, alterations in the sleep-wake cycle, withdrawal or abuse of any psychoactive medications (alcohol, pills), vitamin deficiencies, and so on.
Medications
Polypharmacy is the use of multiple drugs
to treat a disease or multiple diseases.
It is much more common in the elderly. The elderly occasionally have multiple physicians each prescribing medications which are unknown to the other providers. Studies show that many elderly patients are on 5 or more prescription drugs. Greater than 5 medications lead to at least a 25% risk of adverse drug reactions. One common adverse drug reaction is a change in cognition, mimicking dementia. The geriatrician will frequently evaluate a patient’s drug list for redundancies and potential negative interactions. Over-the-counter medications such as “pain medications,” “antacids,” and “vitamins” are included since they can interact with prescription drugs. Geriatricians commonly will “de-prescribe” medications (take away some of the medications) as we age. Common diseases in the elderly leading to polypharmacy are hypertension, heart failure, high cholesterol, diabetes, arthritis or other pain syndromes, and dementia.
The American Geriatric Society (AGS) developed the Beers Criteria for medications in the elderly. It is used to identify potential harmful drugs and drug interactions in the elderly. It is frequently revised/drugs added/ removed/reclassified.
The categories of drugs are:
• Medications considered to potentially be inappropriate. (Hospice care excluded.) Example: Aspirin.
• Medications potentially inappropriate in patients with certain diseases. (Hospice care excluded.) Example: Opioids.
• Medications to be used with caution. Example: SGLT2 inhibitors.
• Potentially inappropriate drug-drug interactions. Example: ARBs and Lithium.
• Medications requiring dosage readjustments based on renal function. Example: Rivaroxaban.
The current Beers Criteria list can be downloaded from multiple sites. What questions would a geriatrician ask about medications?
• Do the drug and diagnosis match?
• Is this a high-risk medication?
• Are there duplicate medications on the list?
• Are there potential drug-drug interactions with the meds on the list?
• Are there drug-disease interactions?
• Are there over-the-counter drugs that should be removed?
• Are there drugs on the list that need frequent laboratory monitoring?
• Is there a problem with drug adherence?
• Is the drug truly needed?
• Can I simplify the regimen?
What Matters
Aligning medical decisions and care with a patient’s goals is an important part of geriatric care. The “what matters” conversation could and should occur yearly, after major life events, changes in health status, whenever the patient wants to talk about it. Patient wishes must be coordinated with and consistent among all care teams (geriatrician, specialists, surgeons). Older patients have a higher rate of healthcare-related complications, delay in care, and dis-coordination of care. Caregivers must be involved as cognition changes. Cultural / Religious beliefs MUST be considered and even emphasized.
Common WHAT MATTERS questions a geriatrician may ask are:
• What is important to you today?
• What makes you happy?
• What makes life worth living?
• What do you worry about?
• What are some goals you hope to achieve in the next six months or before your next birthday?
• What would make tomorrow a really great day for you?
• What else would you like us to know about you?
• How do you learn best (listening, reading, watching videos)?
A Quick Introduction into Palliative Care
The World Health Organization (WHO) describes the field of palliative care as a form of specialized medical care that aims to optimize
the quality of life and alleviate the suffering of patients with serious illnesses. Through palliative care, the focus is placed on ensuring the person is best equipped to continue enjoying their life to the fullest while remaining as independent as possible. Palliative care can include things like managing symptoms and providing whatever support is needed to overcome or control these symptoms (pain, nausea, shortness of breath, etc.). Palliative care can occur along with curative and life-extending care. Hospice care, on the other hand, is a specific form of palliative care designed for individuals with a life-limiting illness who are no longer pursuing curative treatment.
Procedures/Anesthesia in the Geriatric Population
Avoiding stress within any population, especially the elderly, is important to maintain stability and functionality. However, stress finds them in the form of needed surgical intervention requiring anesthesia.
Studies show that nearly 40% of all surgeries are done on individuals over 65, a group that represents only 16% of the population.
Based on an article published in JAMA in 2022 (Gill TM, Vander Wyk B, Leo-Summers L, Murphy TE, Becher RD. Population-Based Estimates of 1-Year Mortality After Major Surgery Among Community-Living Older US Adults. JAMA Surg. 2022;157(12)), nearly 1 in 7 or 13.4% of older adults die within a year after major surgery. Major surgery being defined as any procedure in an operating room requiring the use of general anesthesia for a non-percutaneous non-endoscopic invasive operation. Of the individuals in the study, more than 1 in 4 categorized as frail and nearly 1 in 3 categorized as having dementia died during or after major surgery.
So, can you be too old to have surgery? That is not the right question. The right question is whether the surgery will benefit the elderly patient based on health and “what matters” to the individual.
From an article entitled “Frailty: Evaluation and Management” (Am Fam Physician. 2021;103(4):219-226.): “Do not recommend aggressive or hospital-level care for a frail older person without a clear understanding of the patient’s goals of care and the possible benefits and harms.”
Input from a geriatrician and possibly a palliative care specialist including an assessment of frailty should be part of the pre-operative evaluation. Surgeons and anesthesiologists struggle with looking past the acute problem and incorporating “what matters” into the conversation. Experience has demonstrated that if patients and caregivers are not given non-operative or conservative options, many assume that none exist, or they may be doing “the wrong thing” by considering a non-surgical care path.
The most common peri-operative complications in the elderly are neurologic with delirium being most frequent, pulmonary including ventilator support, and cardiac including myocardial infarction. (Preventing Postoperative Complications in the Elderly. Anesthesiol Clin. 2011 March; 29(1): 83–97.) All will prolong hospital stay
and reduce the chance for discharge to home.
Therefore, we must educate our anesthesia and surgical colleagues to include frailty and patient wishes into their thoughts, discussions, and peri-operative plans when caring for the geriatric patient.
Summary
A common saying is that a child is not a small adult. Another one should be that an elderly person is not just an adult with greying hair. Oedipus realized this when answering the sphinx’s riddle thereby saving his life and freeing the Thebans. Maybe we as physicians should realize it too.
The geriatric specialist or geriatrician is and will continue to be quite busy and a very important part of the lives of millions of people. The elderly population is growing rapidly. We must keep them active and productive.
Accepted for publication in Anesthesiology News 2024.
PAMED members are encouraged to meet with and develop relationships with their local state representatives and state senators. Building these relationships helps PAMED achieve the legislative goals for physicians and patient care.
In February, a group of ten Pennsylvania Medical Society (PAMED) members attended the AMA’s National Advocacy Conference in Washington, D.C. This year, the PAMED physicians had meetings with legislators or staff from 14 offices of the PA congressional delegation, including Congressman Dan Meuser and Congressman Glenn Thompson. Among the issues and legislation discussed was the critical need to reverse the Medicare physician payment cuts that took effect on Jan. 1, 2024, and the importance of increasing the number of graduate medical education training slots.
As part of the National Advocacy Conference, PAMED Board Member Michael Suk, MD, led a panel discussion about the impact of Medicare cuts to rural health care. As part of the panel, Dr. Suk was joined by PAMED Board Vice Chair Lorraine Rosamilia, MD, who demonstrated the need for Medicare reform to ensure that those in rural settings can continue to receive important care in their communities.
In Pennsylvania, PAMED participated in a hearing on challenges surrounding rural health care for the Senate Majority Policy Committee and a joint hearing with the House Professional Licensure Committee and the House Health Committee on improving access to health care. Former PAMED Board of Trustee David Csikos, MD, was among the panel to testify on challenges to rural health care.
With the legislature quiet the beginning of this year, the PAMED Government
LEGISLATIVE UPDATES
Relations team was on the move, visiting different districts in Pennsylvania. They were recently part of a legislative forum held by the Lycoming County Medical Society with Senator Yaw, Rep. Jamie Flick and Rep. Joe Hamm. There they discussed legislation on noncompete agreements and POLST.
PAMED has seen notable movement on three key issues:
Amending Medical Practice Act (Senate Bill 559 & Senate Bill 560) – On March 18, the PA Senate passed Senate Bill 559 and Senate Bill 560 to amend the Medical Practice Act and the Osteopathic Medical Practice Act regarding athletic trainers. The legislation would allow athletic trainers to perform certain specified procedures with the direction of a licensed physician and pursuant to a written protocol.
The bills would also amend the definition of a “physically active person” to include anyone that participates in an individual or team sport, an athletic competition, a performing art, a recreational activity, or a military exercise. The bills have now been referred to the House Professional Licensure Committee for consideration in the House.
Telemedicine Service Insurance Coverage (House Bill 1512) – On March 25, the PA House Insurance Committee considered House Bill 1512, legislation which would require health insurers to cover and pay for health care services provided via telemedicine. Unfortunately, the legislation does not address the issue in a comprehensive manner and only covers the insurance question.
PAMED has been engaged in negotiations over several legislative sessions regarding telemedicine and fully supports Senate Bill 739, a more comprehensive telemedicine bill currently waiting consideration in the
Senate Appropriations Committee.
PAMED informed the House Insurance Committee that it supports moving House Bill 1512 forward in the legislative process to continue momentum on this issue, but we continue to press for an amendment encompassing the already-negotiated comprehensive provisions contained in Senate Bill 739.
Prohibit Non-compete Agreements (House Bill 1633) – On March 27, the PA House Health Committee overwhelmingly approved House Bill 1633, legislation which would prohibit all non-compete agreements in employment contracts for health care practitioners. PAMED supports significantly restricting the geographic reach and duration of a hospital or health system’s non-compete agreements, but we also believe legislation on this issue needs to recognize the needs and concerns of small independent physician practices that require protection against predatory poaching of established community physicians.
PAMED is working with the prime sponsor and Committee Chairman to develop an acceptable amendment that balances these concerns. We have communicated to the Committee we support moving House Bill 1633 forward in the legislative process as we continue our negotiations on final language.
In addition to these issues, PAMED has also seen some movement on the following issues:
PAMED Supports Call to Action with PCCJR – PAMED joined the Pennsylvania Coalition for Civil Justice Reform in urging legislators to establish an Interbranch Commission on Venue. This commission is needed to resolve the problems associated with the recession of the medical liability venue rule.
PAMED is a founding member of the PCCJR and continues to lead the way on venue rule review. Want to learn more about Venue? Visit www.pamedsoc.org/venuerule.
PAMED Opposes House Bill 2037 –PAMED has come out to oppose House Bill 2037, which amends the Pharmacy Act to allow pharmacists and pharmacy techs to administer all injectable medications, biologicals, and immunizations to patients 3 years of age and older. This bill passed the House Children and Youth Committee this week. PAMED will continue to monitor its movement and oppose HB 2037.
Additional Legislation – Moving out of committee is Senate Bill 739, legislation that will require health insurers to cover telemedicine services, and House Bill 1754, which would mandate that health insurers cover the costs associated with diagnostic testing to determine patients’ biomarkers
on specific health issues. PAMED is hoping both these issues will be taken up by the full House this summer.
PAMED opposes SB 25 which would Expand the Scope of Practice for Certified Nurse Practitioners by eliminating their current requirement for a collaborative agreement with a physician.
PAMED Meets with Pennsylvania Stakeholders to Address ED Overcrowding
– PAMED leaders Kristen Sandel, MD, and Andrew Lutzkanin, III, MD, along with PAMED CEO Martin Raniowski, were thrilled to participate in a solution-focused stakeholder meeting addressing ED Overcrowding hosted by the Pennsylvania Department of Health. This meeting comes after PAMED’s Task Force on ED Overcrowding sought support from Governor Josh Shapiro for governmental assistance in tackling this enormous challenge within the healthcare community.
Pennsylvania’s Acting Secretary of Health, Dr. Debra Bogen, said, “Overcrowding in emergency departments impacts quality of care, patient safety, and patient and family satisfaction as well as staff burnout. At this first meeting, we heard different perspectives on the reasons for overcrowding, how it impacts or is impacted by other areas of the healthcare system, and some innovative potential solutions. I truly appreciated the eagerness I heard from all involved to work together toward solutions.”
For additional information, members can go to www.knowledgecenter@ pamedsociety.org to log in.
This year is an election year! To see a full list of important dates for the 2024 Pennsylvania elections, visit vote.pa.gov/About-Elections/Pages/ Upcoming-Elections.aspx.
RESTAURANT REVIEW
Close your eyes sometime and picture an early Saturday evening at a rustic restaurant with the aroma of firewood, a window view of a peaceful country creek, and soft jazz. It would make your blood pressure drop 10 points. You’ll find that feeling once you step in The Barn Restaurant at Allenberry.
Set among the limestone buildings whose origins were from the construction by relatives of Davy Crockett in the late 1700s, The Barn underwent renovations a few years ago, and now serves New American cuisine with farm-to-table sourcing. Chef Jeremy Kimple oversees the seasonally changing menu, and a dinner can be enjoyable before walking over to the nearby Playhouse.
Start the relaxation with a glass from the beer and wine selections, or with craft cocktails like the C.E.O. (blood orange, orange vodka, Solerno blood orange liqueur, and citrus soda). Or go with the Old Crockett, with Makers 46 Bourbon, house bitters and smoked cherries.
Salads include a Caesar, baby spinach, and Asian chicken. Small plates, for an appetizer or a light dinner, include the popular truffle fries and Brussels sprouts. Korean char-grilled octopus came plated with sweet sautéed vegetables, in just the right amount of glaze.
For entrees, the medium-sized scallops were pan-seared and attractively presented, and both the lobster ravioli and the salmon were highly recommended by the friendly staff. To enjoy with a Cabernet, try the Short Rib Wellington (with cremini
THE BARN RESTAURANT AT ALLENBERRY
mushrooms and buttermilk blue cheese), or the tender New York Strip, also topped with blue cheese crumbles.
Finish the evening with a treat from the dessert menu, including a cheesecake assortment or their popular cinnamon sticky buns, also available at the Breeches Bakery next door.
Now you can close your eyes...
THE BARN RESTAURANT AT ALLENBERRY
1559 Boiling Springs Road Boiling Springs, PA 17007
717-258-3211
With the arrival of Italian immigrants to America, their cuisine slowly spread from the port cities of the Atlantic westward into the mainstream. Like so many other ethnic foods, it took a left turn along the way, dissimilar to that of its native land. The real deal can be found at Luna, presented by Chef Donato Bologna and the many staff raised and trained in Italy. In my high school yearbook profile, it states that I “love Italian food,” so trust me that it was a pleasure to drive to this new trattoria just south of downtown Mechanicsburg for a first visit.
Most restaurant quality dishes from European nations got their starts from top chefs (think French cuisine), whereas the first cookbooks in Italy from the last two centuries stemmed from the common folk, enjoying the farm and seaside choices of their sun-soaked Mediterranean peninsula. Good Italian food is based on simplicity. Many popular dishes have only a few ingredients, relying on quality rather than complexity of preparation. On their fertile soil, they had access to livestock, vegetables, and aromatic herbs, plus the fruits of their seas along the abundant coastlines. Freshness takes priority; only lower quality food is mass produced, not to be found at any good New Jersey Italian deli. The separation of flavors takes precedence over the blending of ingredients...think of how your tongue would feel tasting the components of Short Rib Ravioli Primavera. And, of course, there is the eminence of the tastes and aromas of wine, from the world’s largest producer of it.
LUNA ITALIAN CUISINE
Speaking of which, wine selections are made under the direction of the owner, Vito Serradella, following his extensive culinary experiences in Europe. Cocktails include the Peach Bellini Martini (vodka, peach schnapps and peach nectar, topped with prosecco), and a Spicy Blood Orange Margarita (with a jalapeno and a rim of an interesting and pleasant spice, tajin).
After being seated in a dining room reminiscent of an Italian villa with swirling marble floors, start the meal with one of a dozen antipasti, including bruschetta, arancini (rice balls), or fresh calamari or octopus. I usually roll my eyes when friends post their meal photos on social media, but the popular Mamma Buffala would be an exception for its artistry. A large mound of imported mozzarella is filled inside with oozing cream and soft tiny mozz balls, colorfully drizzled with green pesto, tomatoes, and a balsamic glaze.
House-made al dente pastas and risottos include Southern Italian dishes like Linguini Fruiti Di Mare, and a pitch-black Luna Nera squid ink linguini with mushrooms in a light tomato sauce. From the dairy- and meat-rich North around Milan, try the Pappardelle Alla Bolognese, or the Mushroom and Truffled Risotto.
For secondo, a glass display of carne (including Tomahawk Steak and Lollipop Lamb Chops) and pesce (starring branzino and swordfish) greets you at the host station. Or, try the Luna Special, Tagliata di Carne, thinly sliced ribeye with arugula, cherry tomatoes, and shaved parmesan.
If you still have room, dinner can last long afterward with dolce, roasted Italian coffee, and after dinner liqueurs. Bon appetit, knowing that this was no Six Brothers Macaroni Garden Pizzeria.
LUNA ITALIAN CUISINE
100 Legacy Park Mechanicsburg, PA 17050
717-620-8683
Improve health care for you, your family and your community.
Find out what you can learn from your DNA through WellSpan’s community health research program.
Sign up for no-cost genetic screening at wellspan.org/GeneHealthProject.
Questions? Call 717-356-5395 or email us at GeneHealthProject@wellspan.org.