

Bavchi Seed (Psoralea Corylifonia)
Karanji Chhal (Pongamia Glabra)

Bavchi Seed (Psoralea Corylifonia)
Karanji Chhal (Pongamia Glabra)
Neem Chhal (Azadirachta Indica)
Manjishtha Steamn (Rubia Cordifolia)
Haldi Rhizome (Curcuma Longa)
Raktachandan Heartwood
Amba Haldi Fruit (Curcuma Amada)

Vacha Mool (Acorus Calamus)
Root (Hemidesmus Indicus)



EXECUTIVE EDITOR & PUBLISHER
Dom Daniel CORPORATE OFFICE
22, Shreeji Bhavan, 275-279, Samuel Street, Masjid Bunder (W), Mumbai-4000 03, INDIA.
EMAIL: theaestheticiansjournalindia@gmail.com
Website: theaestheticiansjournal.com
TEL: +91 22 2345 1404 +91 22 2345 5844
Printed, Published, Edited and Owned by Dom Daniel
Printed at Swastik Printer, Gala No.9 & 10, Vishal Industrial Estate, Bhandup (West), Mumbai- 400078. Published at 22 Shreeji Bhavan, 275/279, Samuel Street, Masjid Bunder (West), Mumbai - 400003. India.
“The Aestheticians Journal” takes no responsibility for unsolicited photographs or material ALL PHOTOGRAPHS, UNLESS OTHERWISE INDICATED, ARE USED FOR ILLUSTRATIVE PURPOSE ONLY.
Views expressed in this Journal are those of the contributors and not of the publisher. Reproduction in whole or in parts of texts or photography is prohibited. Manuscripts, Photographs and art are selected at the discretion of the publisher free of charge (advertising excluded). Whether published or not, no material will be returned and remains the property of the publishing house, which may make use of it as seen fit. This may include the withdrawal of publication rights to other publishing houses.
All rights reserved. Reproducing in any manner without prior written permission prohibited.
Published for the period of November -2024
Cover Credit: Alankrita Sahai
Photography: Bani Seth
Make-Up: Charmi Thakral
Welcome to this issue of The Aestheticians Journal, where we delve into the latest advancements and innovations shaping the field of skin care and rejuvenation. Our goal is to provide a comprehensive look at emerging trends, breakthrough technologies, and evidence-based treatments that are redefining beauty standards and patient care.
As the demand for minimally invasive procedures and personalized skincare solutions continues to grow, it's crucial for dermatologists and aesthetic professionals to stay informed about the latest developments. In this edition, we focus on cutting-edge techniques in cosmetic dermatology, including novel injectables, laser treatments, skin-tightening procedures, and regenerative therapies. We also explore the role of new ingredients and formulations in promoting healthy, youthful skin.
Our contributors are leading experts in the field, bringing their clinical experiences, research findings, and insights to the table. Their work not only highlights the efficacy of new treatments but also emphasizes the importance of safety, patient education, and ethical practice in delivering aesthetic results.
As always, we invite our readers to engage with the content, share their experiences, and contribute to the ongoing conversation about the future of aesthetic dermatology. Together, we can continue to push the boundaries of what is possible in this dynamic and ever-evolving field.
In this issue, we have articles on Exosome Therapy for Skin Health Improvement, Treatment for Hair Loss and Nail Surgery and Lasers in Nail Disorders.
HOPE YOU HAVE A GREAT READ
Thanks & Cheers
- Dom Daniel Executive Editor & Publisher





Dr. Farida Modi
MD
Dermatologist and Cosmetologist
Dermacare Skin Clinic & Cosmetic Center, Mumbai
DR. ABHIJIT SHINDE
DR. UDAYKUMAR NESARGI
DR. ABDUL SAMAD
DR. GIRISH H.
DR. RASYA DIXIT
DR. VENKATESH V

Dr. Madhavi Pudi
MBBS (Gold Medallist), DNB, DVD
Dr Madhavi’s Advanced Skin Hair and Laser Clinic, Hyderabad
DR. SATISH K. M.
DR. MANJUNATH HULMANI
DR. SHIKHA TIWARI
DR. SAMIPA MUKHERJEE
DR. SYED SALAHUDDIN
DR. POORNIMA M.
DR. NEELIMA RAVIPATI
DR. PALASHKHA
DR. HARITHA RAVIPATI

Dr. S. Manjula Nagarajan
D.D., M.D., (Dermatology) Consultant Dermatologist, Erode

Dermatologist and Cosmetologist
Dermacare Skin Clinic & Cosmetic Center, Mumbai
SIntroduction mall, extra cellular versicles are particles enclosed by
phospholipid bilayer.
The International Society for extra cellular vesicles has played a pivotal role in shaping extra cellular vesicle research through its guidelines called minimal information for study of extra cellular vesicles. It was introduced in 2014 and updated in 2018.
Depending on their size and biogenesis extra cellular vesicles can be categorised into three main groups.
1) Exosomes - 30 to 150 nm originated from endosomes.
2) Ectosomes - 150 to 1000 nm originated from plasma membrane.
3) Apoptotic bodies- 1000 to 5000 nm formed through blebbing by cells, undergoing apoptosis.
Exosomes, nano-sized extracellular vesicles derived from various cell types, have
garnered significant attention in dermatology for their role in skin regeneration, wound healing, and treating skin disorders. With their ability to facilitate intercellular communication, deliver bioactive molecules, and modulate immune responses, exosomes, particularly those from mesenchymal and adipose stem cells, show great promise in skin repair and hair treatments. Exosomes play a vital role in facilitating communication between skin cells and modulating the skin's microenvironment. Their unique ability to influence skin health and promote regeneration has led to significant therapeutic applications in dermatology.
Exosomes, nano-sized vesicles (30 to 150 nm), contain various biological molecules and have emerged as promising tools for drug delivery due to their biocompatibility and ability
to transport payloads with reduced immunogenicity. Their applications in skin health and rejuvenation have garnered significant interest, especially through topical and transdermal delivery methods. Exosomes facilitate drug penetration through multiple skin routes, including paracellular, transcellular, and trans-appendageal pathways. Exosomes offer a non-surgical treatment option that promotes skin health and enhances appearance. Exosome therapy can address various skin concerns, including wrinkles, uneven skin tone, poor texture, and scars. It also helps to alleviate skin stress signals, dullness, dryness, and sagging, contributing to a more youthful look.

Exosomes function as signalling molecules derived from stem cells, enabling communication between skin cells. When exosomes fuse with target cells, they release crucial information that stimulates skin rejuvenation and regeneration, improving overall skin health. Exosome therapy is generally considered safe.
Exosomes have shown the ability to inhibit melanogenesis, counteracting the production of melanin in skin cells. Traditional tyrosinase inhibitors, such as ascorbic acid and kojic acid, often face stability issues and side effects, limiting their practical use. Hyperpigmentation, characterized by dark spots
due to excessive tyrosinase activity, has been targeted by exosomes derived from adipose stem cells (ASCs). Research indicates that ASCexosomes lower intracellular melanin levels in B16F10 cells without significant cytotoxicity and have been effective in reducing hyperpigmentation in clinical studies. Additionally, combining ASC-derived exosomes with fractional CO2 laser treatment has shown promise in addressing atrophic acne scars.

Skin aging is a major concern, characterized by wrinkles, fine lines, sagging, and pigmentation changes, influenced by intrinsic factors (genetics) and extrinsic factors (environmental stressors like UV exposure). Exosomes have emerged as potential anti-aging agents due to their effects on skin cells. Exosomes derived from bovine milk (MK-Exo) show promise in reducing wrinkles
and enhancing skin moisturization by penetrating the skin barrier. Additionally, adipose-derived stem cell exosomes (ADSC-Exos) mitigate senescence in human dermal fibroblasts (HDFs), promote collagen expression, reduce reactive oxygen species (ROS), and inhibit senescence-associated proteins. Exosomes from Phellinus linteus, a mushroom, exhibit anti-aging effects by delivering miRNAs that inhibit Mical2 expression, which is linked to photoaging. Induced pluripotent stem cell (iPSC)-derived exosomes also inhibit matrix metalloproteinases (MMPs), promoting HDF proliferation and reducing UVB damage. Furthermore, exosomes from apple nanovesicles (ADNV) and bovine colostrum have shown anti-inflammatory properties and improved collagen synthesis, thereby reducing extracellular matrix degradation. Overall, exosomes represent a novel approach in anti-aging treatments by modulating cellular processes, enhancing rejuvenation, reducing inflammation, and promoting tissue repair. As research progresses, exosome therapies may play a pivotal role in anti-aging medicine.

Skin inflammation is a complex response to injury, characterized by redness, swelling, heat, and pain. It can be acute, resolving quickly, or chronic, leading to conditions like psoriasis and atopic dermatitis. Exosomes have emerged as effective regulators of inflammatory responses in these conditions. Overall, exosomes are powerful modulators of inflammation, with potential applications in treating various inflammatory diseases, from autoimmune conditions to
neuroinflammation. As research advances, exosomebased therapies may provide new strategies for managing these complex inflammatory responses.
•
Exosomes play a crucial role in wound healing by influencing angiogenesis, cell proliferation, differentiation, apoptosis, and inflammation. Derived from sources such as mesenchymal stem cells (MSCs), keratinocytes, and immune cells, exosomes regulate the wound healing process by suppressing pro-inflammatory cytokines and promoting tissue regeneration. Exosomes combined with hyaluronic acid (HA) have been studied for their synergistic effects on human dermal fibroblasts (HDFs), enhancing cell proliferation, migration, and gene expression related to wound healing. This combination may lead to improved tissue regeneration and applications in clinical aesthetics. Overall, exosomes are integral to the wound healing process, coordinating intercellular communication and regulating essential biological processes for tissue repair. Their therapeutic potential, particularly for chronic wounds, presents a promising area for future research.

• Scar Formation
Hypertrophic scars and keloids are benign fibroproliferative disorders characterized by abnormal fibroblast proliferation and excessive extracellular matrix (ECM) deposition following skin injury. Exosomes have emerged as key modulators in scar formation, influencing cell activity, reducing inflammation, promoting cell proliferation and migration, and regulating collagen production and degradation.
• Exosomes in Hair Growth
Exosomes are increasingly recognized for their role in promoting hair growth, particularly those derived from dermal papillae. Dermal papilla cells, located at the base of hair follicles, release signals and growth factors that regulate the behavior of adjacent epithelial cells, thereby influencing hair follicle development and the hair growth cycle. Overall, exosomes offer significant potential for hair regeneration by delivering bioactive molecules that stimulate hair follicle cells, promote angiogenesis, reduce inflammation, and activate stem cells. As research progresses, exosome-based treatments may become a pivotal approach for addressing hair loss and enhancing scalp health.
Source of exosomes-
1) Conventional
a) Mesenchymal
b) Adipose tissue
2) Non- conventional
a) Animal product derived exosomes
b) Bacterial, fungal and parasitic derived exosomes
c) Plant derived exosomes
• Topical

Exosomes have gained considerable attention in the cosmetic industry due to their rich composition of proteins, lipids, and other molecules that promote healing, hydration, and skin protection. They enhance collagen production, reduce inflammation, and protect against environmental stressors. Their incorporation into topical products like creams, serums, and masks offers numerous therapeutic benefits. Exosome serums are specifically formulated with exosomes to support skin repair and rejuvenation. Unlike traditional facial serums, which may include other ingredients like antioxidants or hyaluronic acid, exosome serums focus primarily on enhancing cell communication and promoting regenerative processes. Typically, topical applications are used in combination with other treatments, such as microneedling, to enhance
absorption and efficacy. They are commonly employed for overall skin rejuvenation, addressing concerns like fine lines, uneven skin tone, and dryness.

Injectable exosome treatments consist of directly injecting exosome-rich solutions into the skin. This method facilitates deeper penetration and allows for more targeted treatment of specific skin issues, such as deep wrinkles, scars, and areas with significant damage. By delivering exosomes directly to the dermal layer, injectable treatments can yield more noticeable and faster results compared to topical applications. This approach is favoured for its precision and effectiveness in treating localized skin concerns. Furthermore, exosomes can modulate inflammation and promote tissue repair, resulting in enhanced skin texture and overall appearance.

Exosomes are considered safe for use in skincare, as they do not have a live cells and do not have a nucleus, reducing the risk of adverse effects like immune rejection, tumour formation and infection.
Exosome injections are generally well tolerated with minimal side effects. Some individuals may experience temporary redness and swelling and some discomfort at the injection site.
Rarely, multiple foreign body granulomatous reaction at the injection site may be seen.
The therapeutic potential of exosomes in skin applications is vast, offering innovative strategies for enhancing wound healing, minimizing scarring, improving transdermal drug delivery, promoting hair growth, and rejuvenating aging skin. Continued research in this area may lead to novel, effective treatments that integrate exosome-based therapies into clinical practice, providing safer and more effective solutions for various dermatological conditions.

Cosmetic dermatology aims to enhance skin aesthetics while addressing issues such as wrinkles, photodamage, and pigmentation. The subjective nature of success in this field has led to increased interest in artificial intelligence (AI) to improve outcomes. A recent review analyzed 53 studies, revealing several applications of AI: it is increasingly used in medicine, with 38% of physicians employing it for tasks like diagnostics, showing improved accuracy in melanoma classification. AI provides a more objective approach by analyzing images for fine lines and suggesting treatments, reducing human error. It also revolutionizes consultations through rapid, objective evaluations, with tools offering noninvasive assessments of skin quality and hydration. AI can predict treatment sessions needed and optimize patient decisions, while interactive tools engage patients in skincare choices. Despite its promise, AI faces challenges related to data quality, bias, and ethical concerns about privacy. The review emphasizes the need for standardization in data practices and advocates for AI education in medical training to maximize its benefits and address these challenges.
A study involving 1,204 women across four Indian cities revealed that over 80% displayed skin color heterogeneity, with hyperpigmented spots being prevalent. Approximately 40% of the population struggles with pigmentation issues, including hyperpigmentation, melasma, and dark spots, prompting dermatologists to develop safe, innovative solutions. In India, skin pigmentation disorders like melasma and post-inflammatory hyperpigmentation (PIH) are notably common, particularly among women, with melasma affecting 20-30% of women aged 40-65. Factors contributing to these conditions include UV exposure, hormonal changes, and genetics. Recent advancements in laser therapies are yielding unprecedented results in managing pigmentation by targeting melanin accumulation, thereby reducing recovery times. Treatments such as chemical peels and microdermabrasion are gaining popularity for their rejuvenating effects. As awareness of pigmentation disorders increases, ongoing dermatological advancements are providing sustainable solutions that empower patients to achieve clearer skin and restore confidence.


MBBS (Gold Medallist), DNB, DVD
Dr Madhavi’s Advanced Skin Hair and Laser Clinic, Hyderabad
Introduction
Hair loss, also known as alopecia is a prevalent
cosmetic condition that dermatologists frequently encounter. It affects a significant portion of the global population, with estimates suggesting that 60% to 70% of adults worldwide experience some form of hair loss during their lifetime. It is the condition that affects both men and women. In the United States alone, hair loss treatments and associated costs amount to approximately 3.5 billion dollars annually, underscoring the significance of this issue. While hair loss is commonly associated with aging, it can affect individuals of all ages, including children. Around 3% of all paediatrician visits are related to hair loss concerns in children. Identifying and addressing the causes of hair loss in children
is essential to provide appropriate treatment and support for these young patients.1 Dermatologists may also provide guidance and support to individuals dealing with the emotional and psychological impact of hair loss. Hair loss can significantly impact a person's self-esteem, body image and overall quality of life. Dermatologists often work closely with their patients to address these concerns and provide resources and coping strategies.1
Numerous treatments have been developed to resist hair loss, including medications, topical solutions and surgical procedures. Topical minoxidil has been used for many years as treatment for different hair disorders. During the last few years, One treatment that has gained attention in recent years is low-dose oral minoxidil, low-dose
oral minoxidil has proven to be an alternative for patients with alopecia. Minoxidil is a medication originally developed as an oral treatment for hypertension (high blood pressure). However, during clinical trials, it was seen that minoxidil has side effects and one of them was hair growth. This led to the development of topical minoxidil formulations that have been widely used to treat androgenetic alopecia (pattern hair loss). Lowdose oral minoxidil refers to the administration of minoxidil in smaller doses compared to its original use as an antihypertensive medication due to its vasodilatory properties, was found to cause hypertrichosis as a side effect. This led to the development of a topical minoxidil formulation that was marketed in 1986.
The aim is to harness the hair growth benefits of minoxidil while minimizing the potential side effects associated with higher doses. One of the main advantages of lowdose oral minoxidil is its convenience compared to topical formulations. Applying topical minoxidil can be time-consuming and may cause scalp irritation in some individuals. With oral minoxidil, the medication is
taken in pill form, making it easier to incorporate into a daily routine.2 However, it is important to note that like any medication, low-dose oral minoxidil can have potential side effects. These can include dizziness, fluid retention, low blood pressure and increased heart rate. Close monitoring by a healthcare professional is necessary to ensure the treatment is well-tolerated and safe. Even though it is an effective therapy, many patients show poor compliance due to the cosmesis, cost and side-effects.2
Patterned hair loss is indeed the most common cause of alopecia, characterized by progressive thinning, miniaturization and hair loss in specific patterns based on the sex of the patient. Male-patterned hair loss (MPHL) affects up to 50% of males over the age of 50, while female-patterned hair loss (FPHL) is commonly observed in postmenopausal women. Despite its prevalence, treatment options for patterned hair loss have remained relatively unchanged over the years. While newer treatment modalities such as platelet-rich plasma, low-level laser light therapy and microneedling have emerged, their cost and efficacy still need to be further confirmed, this limits their widespread use among most patients.3
Although there have been no clinical trials specifically examining the efficacy of oral minoxidil in the treatment of patterned hair loss, an epidemiological study in Spain revealed that oral minoxidil (OM) is commonly prescribed by dermatologists. The study reported that 50.6% of dermatologists prescribed OM for MPHL and 67.9% and 63% of dermatologists prescribed it for premenopausal and postmenopausal FPHL, respectively.3
While further research, including clinical trials, is needed to establish the efficacy of oral minoxidil for patterned hair loss, its increasing use by dermatologists suggests growing confidence in its potential as a treatment option. It's important for individuals considering oral minoxidil or any other treatment for patterned hair loss to consult with a healthcare professional experienced in hair loss management. They can provide personalized recommendations based on the individual's specific condition and needs, monitor progress and address any concerns or side effects that may arise during treatment.3
The diagnosis of hair loss involves a comprehensive evaluation by a healthcare professional, typically a
dermatologist specializing in hair disorders. It is basically based on appearance and pattern of hair loss. The diagnostic process for hair loss may include the following steps:
Medical History: The healthcare professional will start by taking a detailed medical history, including information about duration of hair loss, any associated symptoms, family history of hair loss, medical conditions, medications, recent illnesses and any significant life events or stressors.4
Physical Examination: A physical examination of the scalp and hair follicles will be performed to assess the pattern and extent of hair loss. The healthcare professional will examine the scalp for signs of inflammation, redness, scaling or other abnormalities. They may also evaluate the hair shafts for signs of breakage or structural abnormalities.4
Pull Test: A pull test may be conducted to assess the strength and stability of the hair follicles. During this test, a gentle tug is applied to a group of hairs to observe the number of hairs that are shed.4
Scalp Biopsy: In some cases, a scalp biopsy may be performed to obtain a small sample of the scalp tissue for further examination under a microscope. This can help especially in cases where the diagnosis is unclear. It can identify the specific cause of hair loss.4
Blood Tests: Blood tests to check for specific medical conditions that can contribute to hair loss, such as thyroid disorders, hormonal imbalances, iron deficiency, autoimmune conditions or nutritional deficiencies.4
Trichoscopy: Trichoscopy involves scalp examination using a specialized device. It examines hair follicles in more detail. It can help identify specific patterns, features or abnormalities that are characteristic of certain types of hair loss.4
Depending on the suspected cause of hair loss, additional diagnostic tests such as hormone levels, autoimmune markers or cultures may be ordered to confirm or rule out specific conditions. The diagnosis of hair loss can vary depending on the underlying cause, which may include conditions such as androgenetic alopecia (male or female pattern hair loss), alopecia areata, telogen effluvium, fungal infections, hormonal imbalances, nutritional deficiencies
or other systemic diseases. A thorough evaluation by a healthcare professional is crucial for an accurate diagnosis and to develop an appropriate treatment plan.4
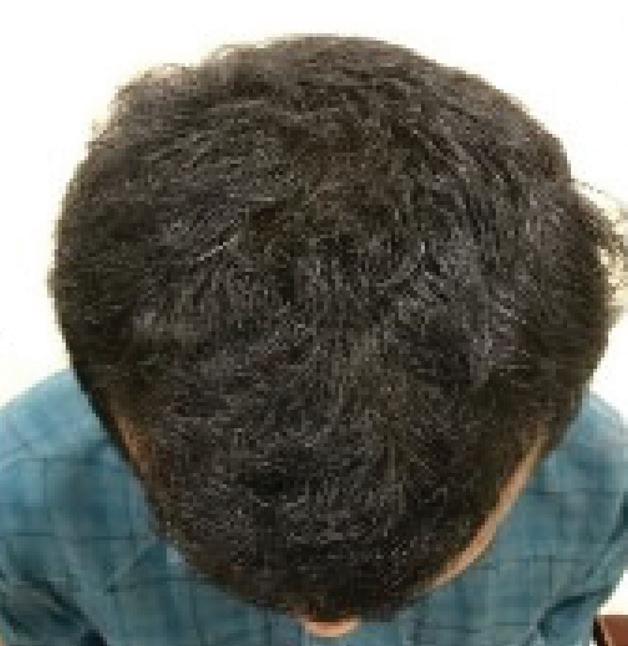
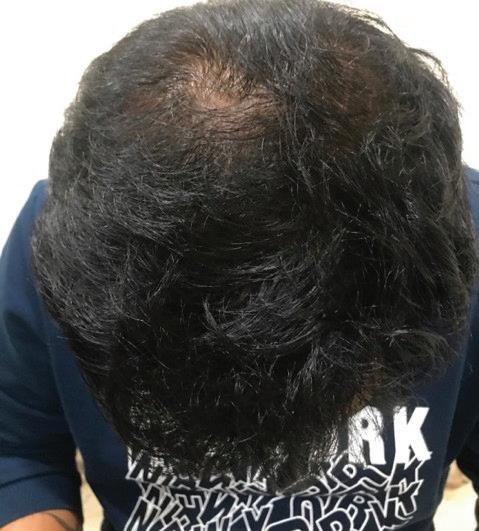
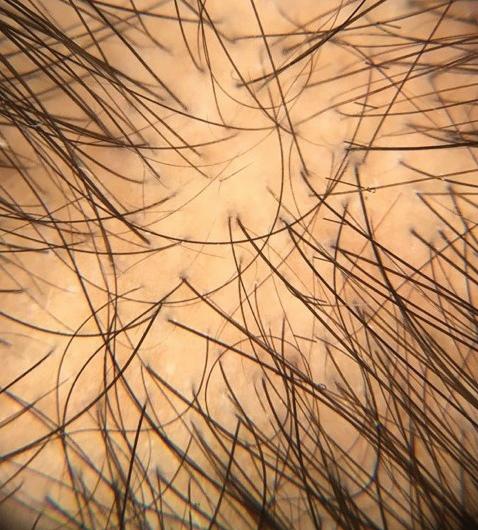
12 patients (Age between 22-30 years) were reporting baldness. The patients were suggested to have routine hair fall investigations such as CBPESR, TSH, RBS, LFT, S.B12, S. Vit. D and serum creatinine at the initial visit. After done the investigations of all patients and they were diagnosed with androgenetic alopecia, Hamilton-Norwood scale III-V pattern. Patient were counselled and advised to oral minoxidil 2.5mg once daily. After four months of taking oral minoxidil 2.5 mg along with topical minoxidil and biotin supplementation, the patient had noticeably thicker hair. Blood pressure was regularly monitored. No other significant positive history was noted and the patient was comfortable taking the oral minoxidil tablets.





















Minoxidil effects hair growth through various mechanisms. When applied topically or taken orally, minoxidil shortens the telogen (resting) phase of the hair growth cycle and prolongs the anagen (growth) phase. Acts by opening adenosine triphosphate-sensitive potassium channels in vascular smooth muscle cells. This leads to increased hair diameter and length over time. The conversion of minoxidil to its active form (minoxidil sulphate) is a crucial step. This conversion occurs through follicular sulfotransferase activity and this sulfated metabolite is responsible for the pharmacologic action of minoxidil. This suggests that oral minoxidil could have a more direct impact on the hair follicles.5
Minoxidil acts as a vasodilator, which improves blood flow to the hair follicles, supplying them with increased nutrients and oxygen. It also induces the Wnt/ b-Catenin signaling pathway, which plays a role in hair follicle regeneration. Additionally, minoxidil has anti-androgenic properties, meaning it can counteract the effects of androgens that contribute to hair loss. It also possesses anti-inflammatory properties, reducing perifollicular microinflammation and suppressing T lymphocytes and even inhibits the effects of prostacyclin and interleukin1a.5 Minoxidil may stimulate the release of vascular endothelial growth factors, which promote the growth of new blood vessels around the hair follicles, adding in their nourishment and growth. The activation of the a-catenin signaling pathway by minoxidil also contributes to hair follicle regeneration and growth. In the case of scarring alopecias, the use of oral minoxidil can be justified due to its anti-fibrotic properties. It inhibits the enzyme lysyl hydroxylase, which is necessary for collagen cross-linking. By reducing fibrosis, minoxidil may help to improve the condition of the affected scalp in scarring alopecias.6
These various mechanisms of action demonstrate the multifaceted effects of minoxidil on hair growth and highlight its potential as a treatment option for various types of alopecia.6
There are several advantages associated with the use of oral minoxidil for the treatment of hair loss:
• Convenience: Taking oral minoxidil is more convenient than applying topical formulations. Instead of having to apply a solution or foam to the scalp, patients can simply swallow a pill, making it easier to incorporate into their daily routine.7
• Improved Cosmesis : Unlike topical minoxidil, oral minoxidil does not cause changes in hair texture or leave any residue on the scalp. This can result in better cosmesis, particularly for individuals with gray hair or those who prefer not to have
visible product residue on their scalp.7
• Cost-effectiveness: In many cases, oral minoxidil is more cost-effective than topical formulations. Topical minoxidil is often available over the counter, while oral minoxidil typically requires a prescription. However, generic oral minoxidil is generally less expensive than branded topical formulations, offering potential cost savings for patients.7
• Compliance: The convenience and improved cosmesis associated with oral minoxidil can contribute to better patient compliance. Compliance is a crucial factor in the success of any treatment for hair loss, as consistent and long-term use is necessary to maintain the benefits.7
• Potential for Combination Therapy: Oral minoxidil can be used in combination with other topical formulations or treatments for hair loss. This offers the possibility of synergistic effects and a more comprehensive approach to treatment.7
It's important to note that while oral minoxidil has its advantages, it should be prescribed and monitored by a healthcare professional experienced in hair loss management. They can evaluate the individual's specific condition, determine the appropriate dosage and monitor any potential side effects or interactions with
other medications.7
As per the study by Ramos et al comparing the efficacy of 1 mg daily oral minoxidil to topical 5% minoxidil solution, found that oral minoxidil was as effective as the topical solution. The authors also suggested that a lower follicular sulfotransferase activity threshold is required for oral minoxidil to be bioactivated compared to the topical formulation. Topical minoxidil can be associated with certain barriers and side effects, including pruritus, contact dermatitis, changes in hair texture and localized hypertrichosis, which may limit its use in male and female-patterned hair loss.8
It is more convenient for patients to take a pill orally than to apply a topical solution. So oral minoxidil offers practical advantages over its topical counterpart. Additionally, the use of keratin fibers to enhance scalp fullness visually is simpler without the need for topical minoxidil.8
It is important to note that when used as immunotherapy, oral minoxidil may show an initial clinical response after approximately 3 months of treatment. However, individual responses to treatment can vary and it is essential for patients to follow up with their healthcare professionals to monitor progress and adjust treatment plans as needed. These findings
highlight some of the potential advantages and considerations when comparing oral minoxidil to topical minoxidil for the treatment of hair loss. However, it is crucial for individuals to consult with a healthcare professional experienced in hair loss treatment to determine the most suitable approach based on their specific needs and circumstances.9
Oral minoxidil has shown promising results as an effective and safe option for various types of hair loss conditions. Some of these conditions include chronic telogen effluvium, traction alopecia, loose anagen syndrome, alopecia areata, monilethrix, chemotherapy-induced hair loss and even scarring alopecia. While patterned hair loss, specifically female-pattern hair loss, has been the most extensively studied, several authors have reported successful use of low-dose oral minoxidil in men with male-pattern hair loss.8
However, it's important to note that oral minoxidil is still considered an off-label therapy for hair loss i.e the medication is being used for a purpose other than its approved indication. Individualization of treatment is necessary because each patient's condition and response to treatment can vary. Patients who may benefit from oral minoxidil are often young adult patients with moderate patterned hair loss, as well as those who have low compliance with topical minoxidil, experience local intolerance to topical formulations or show no response to topical minoxidil. In these cases, oral minoxidil may be considered as an alternative treatment option. While oral minoxidil has shown outcomes for hair loss conditions, it's important to proceed with caution and ensure proper medical guidance and monitoring to maximize benefits and minimize potential risks. In FPHL, doses ranging from 0.25 to 1.25 mg daily are typically used, while doses ranging from 2.5 to 5 mg/day are employed for MPHL. The low side-effect profile of low-dose oral minoxidil enables long-term adherence to the medication, which, in turn, leads to favourable clinical responses, stabilization and improvement in hair loss.9
While the efficacy of oral minoxidil has been demonstrated in MPHL and FPHL, further studies are needed to explore its effectiveness in other types of alopecia. Additionally, comparative studies comparing oral minoxidil to other commonly used medications for hair loss would provide valuable insights into its relative efficacy and safety. 9
In conclusion, low-dose oral minoxidil shows a safe and effective treatment option for various hair disorders, including MPHL and FPHL. Its practical advantages, such as enhanced cosmesis and cost-savings, make it an appealing
choice for patients who may have difficulties with topical formulations or other systemic treatments. However, additional research is necessary to evaluate its efficacy in other types of alopecia and to compare it with existing treatment options. Oral minoxidil is an off-label medication that has been used as an alternative to topical minoxidil for hair loss treatment. While topical minoxidil is the more commonly prescribed and it is FDA-approved form of minoxidil for hair loss but based on results oral minoxidil has been studied and shown to be effective in various clinical studies for hair loss treatment. The offlabel use of oral minoxidil for hair loss involves prescribing lower doses than those used for its approved indication of hypertension. The specific dosage may vary depending
1. Villasante Fricke AC, Miteva M. Epidemiology and burden of alopecia areata: a systematic review. Clin Cosmet Investig Dermatol. 2015 Jul 24;8:397-403. doi: 10.2147/ CCID.S53985. PMID: 26244028; PMCID: PMC4521674
2. Suchonwanit P, Thammarucha S, Leerunyakul K. Minoxidil and its use in hair disorders: a review. Drug Des Devel Ther. 2019 Aug 9;13:27772786. doi: 10.2147/DDDT.S214907. Erratum in: Drug Des Devel Ther. 2020 Feb 10;14:575. PMID: 31496654; PMCID: PMC6691938.
3. Gupta M, Mysore V. Classifications of Patterned Hair Loss: A Review. J Cutan Aesthet Surg. 2016 Jan-Mar;9(1): 3-12. doi: 10.4103/ 0974-2077. 178536. PMID: 27081243; PMCID: PMC4812885.
on the individual patient and the type of hair loss being treated. It's important to use oral minoxidil under the guidance and supervision of an experienced healthcare professional. They can determine the appropriate dosage, monitor the progress and address any potential side effects or concerns. Even though oral minoxidil gives appropriate results, it's essential to weigh the potential benefits against the individual's specific circumstances and consider other treatment options as well. A discussion with a healthcare professional can help determine the most appropriate approach for addressing hair loss. Physicians experienced in treating hair loss or dermatological conditions are best suited to assess the suitability of low-dose oral minoxidil for an individual
and can closely monitor its effects and potential adverse reactions. It is believed to work by dilating blood vessels, increasing blood flow to the hair follicles, and stimulating hair growth. It is essential to prioritize consumer safety and avoid unattended consumer use of medications without proper medical supervision and minimizing potential risks.
In summary, hair loss is a common cosmetic condition that affects a significant proportion of the population, resulting in substantial healthcare costs. Dermatologists play a crucial role in diagnosing, treating and supporting individuals with hair loss and they help address the associated emotional and psychological effects. By providing comprehensive care, dermatologists contribute to improving the quality of life for those affected by hair loss.
4. Xu, Liwen et al. “A Practical Approach to the Diagnosis and Management of Hair Loss in Children and Adolescents.” Frontiers in medicine vol. 4 112. 24 Jul. 2017, doi:10.3389/ fmed.201 7.00112
5. Patel P, Nessel TA, Kumar D D. Minoxidil. [Updated 2023 Aug 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih. gov / books/ NBK482378/
6. Ramírez-Marín, Hassiel Aurelio, and Antonella Tosti. “Role of Oral Minoxidil in Patterned Hair Loss.” Indian dermatology online journal vol. 13,6 729-733. 12 Oct. 2022, doi:10.4103/idoj. idoj_246_22
7. Ramírez-Marín HA, Tosti A. Role of Oral Minoxidil in Patterned Hair Loss. Indian Dermatol Online J. 2022 Oct 12;13(6):729733. doi: 10.4103/idoj.idoj_246_22. PMID: 36386734; PMCID: PMC9650732.
8. Ramos PM, Sinclair RD, Kasprzak M, Miot HA. Minoxidil 1 mg oral versus minoxidil 5% topical solution for the treatment of femalepattern hair loss: A randomized clinical trial. J Am Acad Dermatol. 2020 Jan;82(1): 252-253. doi: 10.1016/j.jaad. 2019.08.060. Epub 2019 Aug 29. PMID: 31473295.
9. Ramírez-Marín HA, Tosti A. Role of Oral Minoxidil in Patterned Hair Loss. Indian Dermatol Online J. 2022 Oct 12;13(6):729733. doi: 10.4103/idoj.idoj_246_22. PMID: 36386734; PMCID: PMC9650732.

Reduces Acne Outbreaks
Anti-Inflammatory Effect

Microsponge
Microsphere Technology
Promotes Skin Renewal Reduces Pigmentation
Decreases the Visiblity of Wrinkles
Stimulates Collagen Production
Improves Skin Texture
Decreases the Visibility of Pores
Microsphere Technology
The microspheres encapsulate the active ingredients
Microspheres protects active ingredients
The microsphere technology allows for a slower release of active ingredients
Microspheres helps in exfoliation

Tretinoin Cream 0.04% (as Microspheres) In a gel base



Moisturises rough and dry skin
Provides an exfoliating effect for removing dead skin cells Heals cracks and corns present on the feet
Revitalises dry and rough skin

According to a perspective published in Human Genomics, skin pigmentation may act as a "sponge" for certain medications, influencing the rate at which drugs reach their targets. The perspective highlights that many drugs can bind to melanin, resulting in variations in bioavailability and efficacy across different skin tones. The authors note that current FDA toxicity testing guidelines inadequately address the impact of pigmentation on drug interactions, as they primarily focus on white populations. This oversight raises concerns regarding the effectiveness of treatments, such as nicotine patches, for individuals with darker skin tones. To address these issues, the researchers propose the use of 3D skin models with varying pigmentation to better assess drug binding. They also call for a comprehensive examination of FDA guidelines to promote inclusivity in clinical trials. The perspective emphasizes the necessity for systematic evaluations in preclinical research related to skin pigmentation and encourages patients to inquire about the safety of drugs concerning diverse ancestral backgrounds. Overall, recognizing genetic variations in drug metabolism across different populations could enhance trust in the drug development process.

A study in the Journal of Investigative Dermatology confirms significant benzene contamination in benzoyl peroxide (BPO) acne products at room temperature. Testing 111 products, researchers found 34% exceeded the FDA's 2 parts per million (ppm) limit, with some reaching 35.30 ppm. Formulation was identified as the main contributor to benzene levels, with heat and UV exposure increasing its formation. Valisure previously reported levels as high as 1,761 ppm, raising public health concerns. Experts recommend refrigerating BPO products and replacing them regularly to reduce exposure risks.

Researchers have developed the first human skin cell atlas, revealing insights into skin formation before birth and its unique ability to heal without scarring. This groundbreaking study, which also produced a mini organ of skin capable of hair growth, underscores the crucial role of immune cells in scarless repair. The atlas serves as a molecular “recipe” for constructing human skin and understanding hair follicle formation, with significant implications for regenerative medicine, particularly for burn victims and individuals with scarring alopecia. As the body's largest organ, the skin is essential for protection and temperature regulation; however, studying its development has posed challenges due to differences with animal models. This research contributes to the Human Cell Atlas initiative, which aims to map all cell types in the human body, and it is expected to advance the study of congenital skin diseases and enhance regenerative medicine.

A recent meta-analysis suggests that teledermatology may effectively replace traditional in-person dermatology, with high acceptance among patients and clinicians. Analyzing 14 studies from 2004 to 2022, researchers found that telehealth is generally well-accepted and more cost-effective, particularly for conditions like acne, psoriasis, and skin cancer. Store-and-forward (SF) methods, where images are sent for later analysis, received high satisfaction rates (96% for patients), while live interactive (LI) teledermatology via video conferencing saw 89% satisfaction. Despite these advantages, in-person dermatology still provides higher diagnostic accuracy. Patients expressed concerns about privacy and technical issues, while clinicians noted longer consultation times. The review emphasizes the need for more research on teledermatology's accuracy and safety, urging randomized controlled trials and exploration of nonWestern contexts to address existing gaps and promote inclusivity in the field.
In this exclusive interview, we delve into the beauty secrets of a renowned model, Ms. Alankrita who shares her comprehensive skincare and hair care routines. She offers invaluable insights on addressing common concerns such as aging, acne, and sensitivity, emphasizing the importance of personalized

approaches. Alankrita discusses her commitment to using scientifically-backed ingredients and highlights the role of professional guidance in her choices, particularly the advice she receives from her Dermatologist in managing her skin and hair conditions.
1. What is your daily skin care routine and your hair care routine?
My daily skincare routine as suggested by my Dermatologist starts with icing my face and lymphatic drainage to reduce puffiness. I cleanse, apply toner, and use a vitamin C serum, followed by snail mucin moisturizer and sunscreen. In the evening, I cleanse again and use an exfoliating toner twice a week, alternating between hyaluronic acid and retinol serums, then I apply a moisturizer and eye cream. I also incorporate eye patches and face yoga for added relaxation and radiance, keeping my skin healthy and vibrant.
2. How do you adjust your skin care routine for concerns like aging, acne, or sensitivity, and what products do you use for these issues?
To address aging, I use retinol and peptides for their rejuvenating effects. For acne, I rely on salicylic acid and a homemade lemon and aloe pack. For sensitivity, I choose fragrance-free, hypoallergenic products and incorporate calming ingredients like aloevera and chamomile. I always consult my Dermatologist for personalized recommendations, ensuring my skincare routine is effective and tailored to my needs.
3. How do you choose your skin care products? Do you focus on ingredients, brand reputation, or something else?
I totally prefer brands recommended by my Dermatologist they are backed by scientific research and are reputed brands. I always consult my Dermatologist for
professional advice to ensure my skincare choices are effective and tailored to my needs.
4. What do you do to protect your skin and hair from environmental stressors such as UV exposure and pollution?
To protect my face I use broadspectrum sunscreen daily, wear hats for extra protection, and select antioxidant-rich products. For my hair, I apply UV protectant sprays and limit heat styling to minimize damage from pollution and sun exposure. Additionally, I use silk bedcovers to further protect my hair and skin.
5. What are your favourite hair care product, and why do you prefer?
I prefer using a sulfate-free shampoo paired with a hydrating conditioner to ensure my hair stays moisturized. A nourishing
hair oil is essential for achieving shine and controlling frizz. I choose these products based on their effectiveness and the quality of their ingredients.
6. How do you integrate professional treatments, such as facials or hair therapies, into your personal care routine?
I schedule facials or hair therapies every 4 to 6 weeks, depending on the condition of my skin or hair. I always communicate with my Dermatologist about my current routine to ensure the treatments are tailored to my specific needs.
7. What role do you believe lifestyle factors, such as diet and hydration, play in maintaining healthy skin and hair?
A balanced diet rich in vitamins—especially A, C, E, and omega-3 fatty acids—along with staying hydrated, is crucial for maintaining skin elasticity and hair health. Regular workouts and plenty of water intake also play a significant role in my overall wellness.
8. How often do you evaluate and update your skin and hair care products based on changes in your skin condition or seasonal variations?
I assess my products seasonally and after any significant changes in my skin or hair condition. I also stay on the lookout for new products that might better suit my current needs.
9. What specific treatments or products have you found most effective for managing hair concerns
such as dryness or thinning?
For dry hair, I find that deep conditioning masks and leavein conditioners are particularly effective. For thinning hair and as advised by my Dermatologist, I have experienced improvement with topical minoxidil and biotin supplements, as well as exosome and growth factor (GFC) treatments.
10.What recommendations has your Dermatologist given you for maintaining healthy skin and hair care?
My Dermatologist emphasises on the importance of sun protection, consistent use of retinoids for anti-aging and staying hydrated. He also recommends regular check-ups for skin concerns.
11.What advice would you give to someone looking to develop a more effective skin and hair care routine, especially regarding seasonal variations?
I suggest always first to consult a Dermatologist who you feel comfortable with and start with a simple routine and gradually add products based on how your skin and hair responds.

Dr. S. Manjula Nagarajan D.D., M.D., (Dermatology) Consultant Dermatologist, Erode

To view the article discussion, scan the QR code
Introduction
The nail serves as an essential aesthetic and functional structure of
the fingertip, characterized by its strength, relative inflexibility, and hardness due to its keratinous composition. As a protective covering for the fingertip, nails shield the delicate tissues underneath from external trauma and damage. Beyond their protective role, nails enable precision and delicacy in tasks such as picking up small objects, facilitated by their firm and resilient structure. This dual function underscores the integral role of nails not only in hand aesthetics but also in enhancing dexterity and tactile sensitivity, essential for various daily activities and tasks requiring fine motor skills.1
Structure and Function:
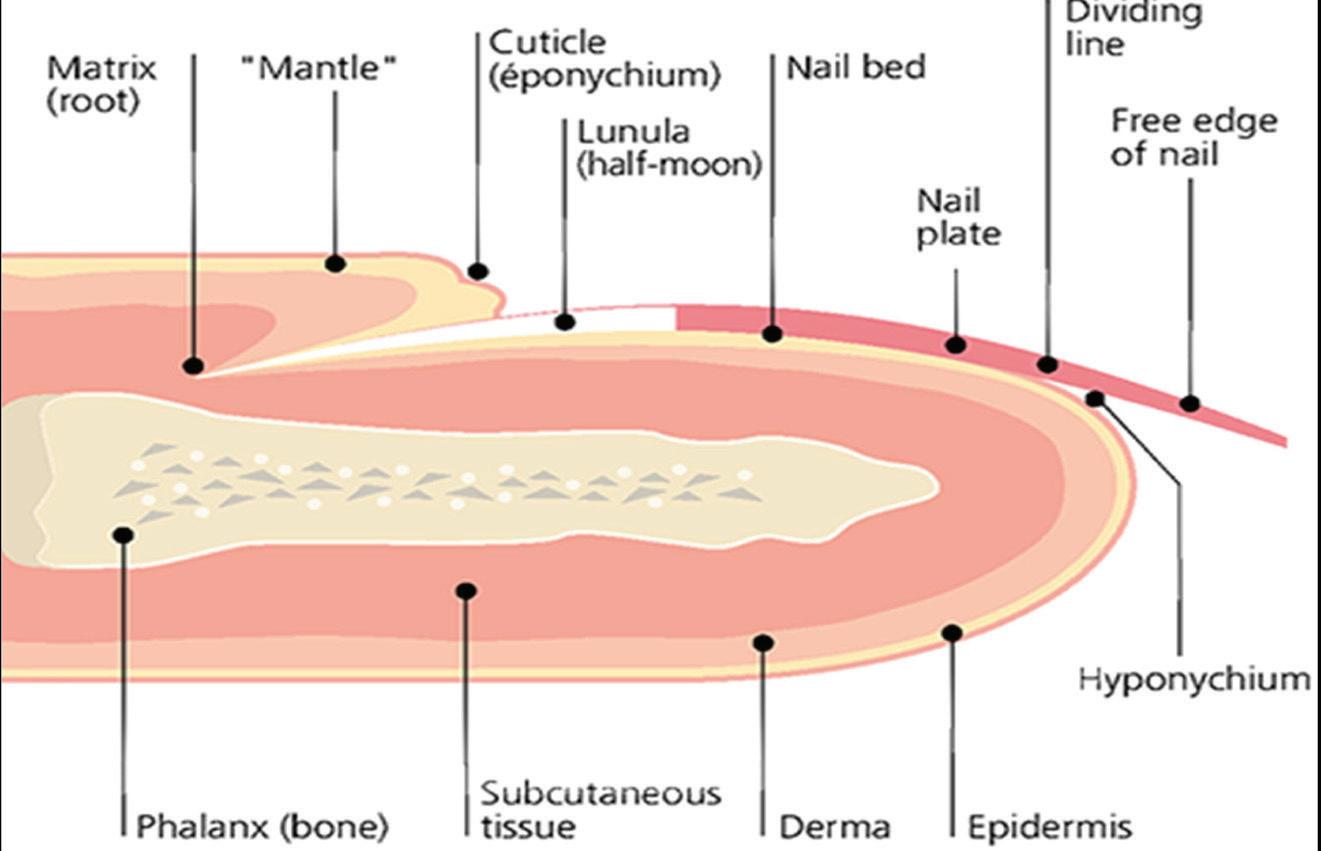
The nail is a complex structure composed of several soft tissue components that surround and support the hard outer nail plate. These
essential structures include the nail folds, mantle, cuticle, nail matrix, nail plate, nail bed, hyponychium, and onychodermal band.2 The nail folds encompass soft tissues that safeguard the edges of the nail plate, offering protection from external trauma. The mantle, covering the nail matrix and base of the nail plate, acts as a protective barrier and aids in the formation and maintenance of the nail. The cuticle, or eponychium, extends from the proximal nail bed to adhere to the nail plate, forming a protective seal that defends against irritants and pathogens, thereby preserving nail health. The nail matrix is responsible for generating onychocytes, the cells that constitute the nail plate, ensuring its strength and durability. The nail plate itself is the visible, keratinized structure that provides flexibility and protection to the underlying nail bed and
matrix. Supported by the nail bed, which nourishes the nail plate, these structures collectively maintain the integrity and functionality of the nail. The hyponychium, positioned beneath the free edge of the nail plate, acts as a barrier against debris and pathogens, promoting hygiene and health. Together, these components contribute to the intricate anatomy and essential functions of the nail, facilitating both aesthetic appeal and practical utility in daily activities.1, 2
Nail disorders encompass a spectrum of conditions that can range from benign to severe, often leading to visible changes or significant deformities. Familiarity with common pathologies such as spongiosis, acantholysis, and hyperkeratosis is crucial for accurate diagnosis and appropriate management. Clinical evaluation integrates patient history, physical examination, and diagnostic tools such as onychoscopy, laboratory tests, imaging modalities, and biopsy for definitive diagnosis.3 Treatment strategies are tailored to the specific underlying pathology and may involve conservative approaches such as topical therapies or more invasive interventions like nail avulsion or matrixectomy. Laser therapy has emerged as a promising therapeutic option for select conditions, offering targeted treatment with minimal adverse effects, thereby enhancing clinical outcomes and patient satisfaction in the management of nail disorders.4
A thorough understanding of nail anatomy is important for clinicians in evaluating and managing nail disorders effectively. By elucidating the complex interplay between nail structures and their pathological manifestations, clinicians can provide comprehensive care, ultimately enhancing patient outcomes and quality of life.
The diagnosis of nail disorders initiates with a comprehensive clinical history, during which healthcare providers gather pertinent details from patients regarding their medical background, symptoms related to nail concerns, prior treatments, and familial history of nail disorders. This thorough approach aids in establishing a chronological sequence of symptoms and identifying potential triggers or underlying conditions contributing to nail abnormalities. Subsequent to the clinical history, a meticulous physical examination of the nail complex is conducted. This includes detailed observation of nail characteristics such as color, shape, texture, and integrity, while also assessing for indications of inflammation, infection, or trauma. Concurrently, a systemic examination is undertaken to screen for systemic conditions or diseases associated with nail irregularities, such as psoriasis, fungal infections, or autoimmune disorders. This systematic evaluation aims to uncover pertinent clinical findings that guide further diagnostic investigations and inform personalized management strategies for patients presenting with diverse nail disorders.3
1. Onychoscopy: ................ Onychoscopy, using a
dermatoscope, provides detailed visualization of the nail plate and surrounding structures. It helps assess texture, color, thickness, and signs of trauma, such as thickening or discoloration, indicating conditions like fungal infections. Examination includes nail folds and cuticles for inflammation or infection clues, and visualizes capillaries for systemic diseases like lupus or vasculitis. It identifies specific features like pitting, onycholysis, and hyperkeratosis, seen in psoriasis or autoimmune disorders. Assessing the hyponychium reveals integrity, aiding in accurate diagnosis and treatment planning for various nail abnormalities.3
2. Laboratory testing:
Laboratory testing in nail disorders assesses overall health and identifies systemic conditions linked to nail changes. Tests include CBC, liver and renal function tests, lipid profile, peripheral smear, and X-rays, revealing insights into inflammation, metabolic disorders, or infections impacting nail health.3
3. Pus Culture and Sensitivity: Pus culture and sensitivity testing of nails is essential for diagnosing and managing bacterial or fungal nail infections. It identifies the specific pathogens and determines antibiotic or antifungal sensitivity, guiding targeted
treatment to minimize resistance and improve therapeutic outcomes. For fungal infections like onychomycosis, it identifies the exact fungus species, crucial for selecting the right antifungal medication.3
Reaction (PCR): Polymerase Chain Reaction (PCR) diagnose the nail disorders by detecting specific DNA or RNA from pathogens directly in nail samples. It enhances accuracy, especially for challengingto-culture organisms, and distinguishes between different microorganism species, guiding precise treatments. PCR's sensitivity in detecting viral DNA or RNA aids in early diagnosis of viral nail infections like HPV. It also monitors treatment response by tracking pathogen levels post-therapy, allowing timely adjustments for better outcomes.3
5. Biopsy: It includes examination of tissue samples from affected nails or surrounding skin. It identifies specific conditions like infections, tumors, or inflammatory disorders through histopathological examination, guiding accurate treatment plans by confirming diagnoses and distinguishing between benign and malignant conditions. Biopsy also detects microbial pathogens for targeted
antimicrobial therapy, assesses inflammatory changes, evaluates nail growth abnormalities, and distinguishes melanocytic lesions, ensuring precise management tailored to patient needs.3
6. Immunofluorescence: Immunofluorescence is essential in diagnosing nail disorders by detecting specific proteins or antibodies in tissue samples from affected nails or surrounding skin. It identifies autoantibodies for autoimmune conditions like lupus erythematosus or pemphigus vulgaris, detects inflammatory markers in conditions such as psoriasis or lichen planus, and helps diagnose fungal or viral infections. This technique distinguishes between nail lesions caused by infections, inflammation, or neoplastic conditions, guiding precise treatment strategies. It also monitors treatment response by tracking changes in protein expression or antibody deposition, improving patient management and outcomes.3
7. Antinuclear Antibody (ANA) Profile: The Antinuclear Antibody (ANA) Profile is essential in diagnosing nail disorders, especially autoimmune diseases affecting connective tissues. It detects autoantibodies against cell nuclei, identifying conditions like systemic
lupus erythematosus (SLE), scleroderma, or Sjögren's syndrome, which can cause distinct nail changes such as pitting or discoloration. Positive ANA results suggest systemic autoimmune involvement, guiding treatment and monitoring disease progression.3
8. Magnetic Resonance
Imaging (MRI): Magnetic Resonance Imaging is essential for assessing nail disorders by providing detailed anatomical information and detecting soft tissue abnormalities like inflammation, edema, or tumors not visible with other imaging methods. It evaluates bone, joint structures, and vascular anatomy around the nails, identifying conditions such as osteomyelitis, arthritis, or vascular issues like vasculitis.
MRI's high sensitivity detects deep-seated infections or abscesses, guides management of traumatic injuries like fractures, and identifies benign or malignant tumors early.3
Findings from.................. histopathological ... .... ..... investigation
• Spongiosis: Intercellular edema within the epidermis.4
• Acantholysis: The loss of intercellular cohesion between epidermal cells which leads to formation of intraepidermal blisters or vesicles, which
are fluid-filled sacs within the epidermis.4
• Parakeratosis
The retention of nuclei within the stratum corneum layer of the epidermis.4
• Hyperkeratosis:
Thickening of the stratum corneum layer, with orthokeratosis specifying thickening without retained nuclei.4
• Hypergranulosis: .........
Thickening of the stratum granulosum layer or the presence of a granular layer where absent normally.4
• Hypogranulosis: Indicates thinning or loss of the stratum granulosum layer.4
• Acanthosis: Thickening of the stratum spinosum layer.4
• Exocytosis: The migration of cells, such as inflammatory or blood cells, into the epidermis.4
• Papillomatosis: Irregular fluctuation of the epithelial surface overlying dermal papillae.4
• Atrophy: Thinning of either the dermis or the epidermis.4
• Pagetoid migration: Abnormal cell spreading upward in the epidermis.4
• Koilocyte: A suprabasal cell with a condensed nucleus and surrounding halo.4
Treatment of fungal nail infections aims to achieve
complete cure, defined as both mycologic (negative KOH microscopy and nail culture) and clinical resolution (a normal-looking nail). It is important for patients to understand that nail growth is slow, and improvements can continue even after treatment ends. Options include oral antifungals like terbinafine and itraconazole, which are preferred due to their accessibility and effectiveness, though fluconazole may also be used off-label. Terbinafine is often preferred in the elderly due to its lower side effect profile. Topical antifungals like ciclopirox, efinaconazole, and tavaborole offer alternatives with minimal systemic risks but require long treatment durations and may be less effective. Physical treatments like surgery for ingrown nails or severe infections, nail debridement can complement antifungal therapy, potentially enhancing outcomes. Devices such as lasers and photodynamic therapies exist and it is effective for fungal infections, promoting nail regrowth and enhancing appearance without harming surrounding tissues. The choice between surgery and laser therapy depends on the condition's severity and individual factors, aiming for optimal nail health and function.3, 5
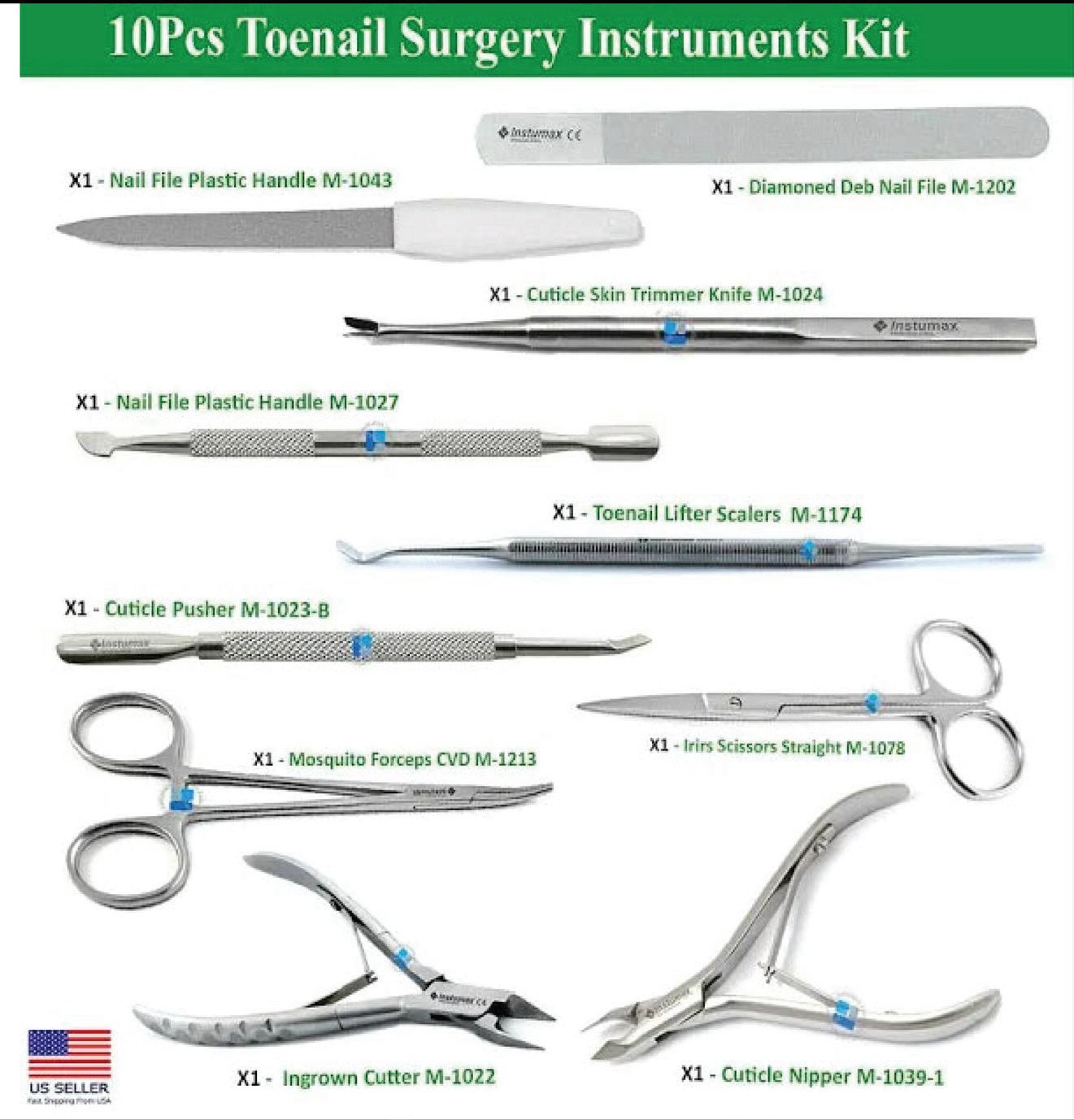
Nail surgery, encompassing procedures like nail avulsion and matrixectomy, addresses various nail disorders from ingrown toenails to fungal infections, providing targeted relief and promoting nail health. Typically performed as outpatient procedures under local anaesthesia, these surgeries minimize disruption to daily life. Advancements in techniques and technology underscore the continued value of nail surgery for longterm relief from troublesome nail conditions.3, 5
Before any surgical procedure, several essential steps must be taken to ensure patient safety and procedural success. Firstly, a consent form outlining the details and risks of the surgery must be carefully reviewed and signed by the patient or their legal guardian. This ensures informed consent and mutual understanding of the procedure. Next, a thorough pre-anaesthetic assessment is conducted to evaluate the patient's fitness for anaesthesia, identifying any potential risks or complications. Following this, appropriate premedication is administered to prepare the patient for the surgery, which may include medications to reduce anxiety or induce relaxation. Lastly, ensuring the
availability and readiness of appropriate surgical instruments and equipment is crucial to facilitate a smooth and efficient operation. These meticulous steps collectively contribute to maintaining high standards of patient care and safety throughout the surgical process.3, 5
There are several types of ingrown toenails, each with distinct characteristics and specific treatment needs:
Pincer nails curve sharply, embedding into the skin, causing pain and inflammation. Licatured nails involve skin folding around the nail, creating a pinching effect often due to congenital factors or chronic trauma. Tile-shaped nails are wide and grow into the nail fold, leading to discomfort and an
increased risk of infection. Spicule nails feature small nail fragments penetrating the skin, triggering inflammation and pain.3,5




surrounding area. This stage is characterized by discomfort and sensitivity at the nail fold. As the condition progresses to the second stage, new granulation tissue forms at the edges of the ingrown toenail, exacerbating pain and inflammation. Early intervention is essential to prevent additional complications. In the third and most severe stage, the skin around the toenail becomes chronically inflamed and keep oozing pus, indicating infection and significant discomfort. Treatment strategies are tailored to the severity of each stage, focusing on relieving pain, reducing inflammation, and addressing any underlying medical conditions that could complicate healing.3, 5

The ingrown toenails, severity is classified into three stages based on the extent of inflammation and tissue involvement. In the initial stage, the nail has grown into the skin on the side, causing localized pain and inflammation of the
Surgical treatment of ingrown toe nail Ingrown toenails commonly known as onychocryptosis, or ungus incartus, is a prevalent and troublesome issue among adolescents and young adults, particularly in their second and third decades of life. Patients typically present with symptoms such as localized nail pain, and in severe cases, serious purulent or bloody discharge, sometimes accompanied by difficulty walking. This condition primarily affects the toes and is often precipitated by factors such as improper nail trimming, wearing tight footwear, or trauma to the nail plate. The pathogenesis involves the nail plate penetrating the adjacent skin, leading to inflammation, discomfort, and potential infection. Prolonged irritation can result in the formation of granulation tissue and hypertrophy of the surrounding skin. Contributing factors include genetic predisposition, variations in nail shape or size, and underlying medical conditions affecting nail growth or skin integrity. Effective management strategies aim to alleviate symptoms, promote healing, and prevent recurrence through tailored interventions based on the severity and specific characteristics of the condition.3, 5
1. de Berker D. Nail anatomy. Clin Dermatol. 2013;31(5):509-515. doi:10.1016/j. clindermatol.2013.06.006
2. McCarthy DJ. Anatomic considerations of the human nail. Clin Podiatr Med Surg. 1995;12(2):163-181.
3. Wollina U, Nenoff P, Haroske G, Haenssle HA. The Diagnosis and Treatment of Nail Disorders. Dtsch Arztebl Int. 2016;113(29-30):509-518. doi:10.3238/arztebl.2016.0509.
4. Dika E, Starace M, Alessandrini A, et al. The Histopathologic Evaluation of Diagnostic
Procedures in Nail Melanoma. Dermatol Pract Concept. Published online April 1, 2023. doi:10.5826/dpc.1302a92
5. Beuscher TL, Kelechi TJ. Onychomycosis: Diagnosis, Treatment, and Prevention. J Wound Ostomy Continence Nurs. 2019;46(4):333-335. doi:10.1097/WON.0000000000000556
Note - Stay tuned for Part II, coming in our December 2024 issue!






The Vitiligo, affecting about 1% of the global population, is more visible in darker skin and often leads to stigma and impaired quality of life. Common triggers include stress and sunburn, with over half of cases appearing before age 20, raising concerns about co-morbid autoimmune disorders. Essential micronutrients like Zinc (Zn), Copper (Cu), and Selenium (Se) are important for immune function and oxidative stress management. A meta-analysis of 41 studies (3,353 vitiligo cases) found significant declines in serum Zn (SMD = -0.86; P < 0.0001) and Cu (SMD = -0.50; P < 0.0001) levels in vitiligo patients, while Se levels were slightly elevated, especially in Asian populations. These findings underscore the potential roles of Zn and Cu in vitiligo management and highlight the need for further research on micronutrient supplementation to improve patient outcomes.


The aesthetic medical devices market is projected to reach approximately £13.73 billion in 2024, with a compound annual growth rate (CAGR) of 3.20%, reaching £18.82 billion by 2034. This growth is driven by social media influence, Western beauty standards, and a preventive care culture, increasing demand for cosmetic procedures. Rising disposable incomes in emerging economies enable more individuals to afford these treatments, while technological advancements support the expansion of aesthetic clinics and medical spas worldwide. Healthcare practitioners, including dermatologists and cosmetic surgeons, are adopting aesthetic devices due to growing consumer awareness. Companies are diversifying their product offerings to include body contouring, skin tightening, and facial rejuvenation, with non-energy-based devices dominating the market at 89.99%.


Market leading LED pioneers Dermalux has launched the Tri-Wave MD, the most powerful phototherapy device in the world, designed to revolutionise aesthetic and medical treatments.
The performance of the new Dermalux Tri-Wave MD is unmatched, with the largest, adjustable four-pod head in the Dermalux range. The Tri-Wave MD treatments over broad skin areas with unparalleled efficiency, capable of delivering up to 240 j/cm² in a single treatment session.
The new device uses multiple wavelengths concurrently from singular wavelength LEDs, ensuring clinicians can target multiple symptoms in a single treatment, whilst reducing treatment time. This guarantees more reliable performance and predictable results, and is unique to Dermalux. Other LED devices on the market require the changing of LED heads for each wavelength, increasing treatment time.
“The Dermalux Tri-Wave enhances everything we do”, continues Kate Monteith-Ross. “From treatment experiences to outcomes. The tide is turning, there is a massive regenerative, biohacking and longevity movement; feeling good is as important as looking good. To get the best results what is inside needs to work for you.”
The device regenerates skin, with indications including:
• Acne: mild, moderate and severe. Inflammatory and noninflammatory
• Dermatitis
• Pain (musculoskeletal)
• Redness/dyschromia
• Wound Healing/acute wound healing
Diamond Flower Peel™ system is Organic, most innovative system in microdermabrasion technology. This improved method first delivers a controlled, yet powerful stream of pure organic flower grains to the skin in order to slough off dead cells, leaving the skin smooth and fresh, while promoting new skin and collagen growth.
















Khellin Extract (as Trachyspermum Ammi)
Pantothenic Acid (as D-Pantothenate, Calcium)
Pantothenic Acid (as D-Pantothenate, Calcium) Picrorhiza Kurroa Extract

Vitamin A (as Retinyl Acetate), Vitamin B1 (as Thiamine Mononitrate), Vitamin B2 (as Riboflavin), Vitamin C (as L-Ascorbic Acid), Vitamin E (as D-Alpha-Tocopheryl Acetate), Folic Acid, Magnesium (as Magnesium Carbonate), Niacin (as Nicotinamide), Zinc (as Zinc Sulphate), Iron (as Ferrous Fumarate), Manganese (as Manganese Chloride), Copper (as Cupric Sulphate), Iodine (as Potassium lodide), Selenium (as Sodium Selenite), Chromium (as Chromium (III) Chloride)

Supports
