22, Shreeji Bhavan, 275-279, Samuel Street, Masjid Bunder (W), Mumbai-4000 03, INDIA.
EMAIL: theaestheticiansjournalindia@gmail.com
Website: theaestheticiansjournal.com
TEL: +91 22 2345 1404 +91 22 2345 5844
Printed, Published, Edited and Owned by Dom Daniel
Printed at Swastik Printer, Gala No.9 & 10, Vishal Industrial Estate, Bhandup (West), Mumbai- 400078. Published at 22 Shreeji Bhavan, 275/279, Samuel Street, Masjid Bunder (West), Mumbai - 400003. India.
“The Aestheticians Journal” takes no responsibility for unsolicited photographs or material ALL PHOTOGRAPHS, UNLESS OTHERWISE INDICATED, ARE USED FOR ILLUSTRATIVE PURPOSE ONLY.
Views expressed in this Journal are those of the contributors and not of the publisher. Reproduction in whole or in parts of texts or photography is prohibited. Manuscripts, Photographs and art are selected at the discretion of the publisher free of charge (advertising excluded). Whether published or not, no material will be returned and remains the property of the publishing house, which may make use of it as seen fit. This may include the withdrawal of publication rights to other publishing houses.
All rights reserved. Reproducing in any manner without prior written permission prohibited.
Published for the period of October -2024
Redefining Radiance: Breakthroughs in Aesthetic Dermatology
Aesthetic dermatology continues to evolve rapidly, driven by advances in technology, innovative treatment modalities, and growing patient demand for non-invasive procedures. As the industry strives to meet the expectations of both medical professionals and patients, staying informed about the latest developments is critical for success. This issue delves into emerging trends, such as cutting-edge laser technologies, novel injectables, and personalized skin rejuvenation techniques that push the boundaries of what's possible in enhancing skin health and appearance.
Today, aesthetic dermatology is no longer just about addressing visible signs of aging. It's a holistic approach that combines medical expertise with artistic precision, aiming to create natural-looking results that enhance patients' confidence. Recent advancements have introduced minimally invasive procedures that reduce downtime, promote quicker recovery, and deliver long-lasting results, making cosmetic dermatology more accessible than ever before.
In this ever-changing landscape, dermatologists must balance innovation with patient safety and education. The popularity of social media and patient-driven trends can often lead to unrealistic expectations, making it essential for professionals to provide clear communication, comprehensive consultation, and evidencebased treatments.
This issue’s feature on aesthetic dermatology serves as a comprehensive guide to the latest tools and techniques, offering insights into the science behind these innovations and their clinical applications. As we look ahead, the focus remains on achieving sustainable beauty and wellness, ensuring that each patient’s unique needs are met through safe, effective, and individualized care.
In this issue, we have articles on Microneedling Radiofrequency and Growth Factor Concentrate Combination Treatment for Acne Scars Reduction, Achieve Radiant Skin with Chemical Peels and Growth Factor Concentrate (GFC) for Hair Regrowth.
HOPE YOU HAVE A GREAT READ
Thanks & Cheers
- Dom Daniel Executive Editor & Publisher
Editorial Board Advisory Board
Dr. Preeti Reshamwala
DNB, FCPS, DVD, MBBS (Dermatology)Consultant Dermatologist, Aesthetic Medicine and Hair Transplant
MICRONEEDLING RADIOFREQUENCY and Growth Factor Concentrate Combination
Treatment for Acne Scars Reduction
Dr. Preeti Reshamwala
DNB, FCPS, DVD, MBBS (Dermatology)
Consultant Dermatologist,
Aesthetic Medicine and Hair Transplant Surgeon
Skinoq Healthcare Pvt. Ltd.
Faculty Dermatologist, Baps Hospital
Surat, Gujarat
Introduction
Acne scars.,,are a common . sequela of acne vulgaris,
resulting from altered wound healing in response to inflammation within the pilosebaceous units. Acne scars are primarily categorized into atrophic, hypertrophic, and keloidal types, with atrophic scars being the most prevalent. Atrophic scars are a result of collagen destruction during the healing process, and their classification is based on the depth and size of the tissue loss. Icepick scars, representing 60 to 70 percent of atrophic scars, are characterized by narrow, V-shaped epithelial tracts that extend deeply into the dermis or subcutaneous tissue. Their depth makes them resistant to conventional resurfacing treatments. Boxcar scars account for 20 to 30 percent of atrophic scars. These are wider depressions with
sharply defined vertical edges, ranging from 1.5 to 4.0 mm in diameter. Shallow boxcar scars can be amenable to skin resurfacing treatments, but deeper boxcar scars are more resistant. Rolling scars, which comprise 15 to 25 percent of atrophic scars, are the widest type, potentially reaching up to 5 mm in diameter. They result from fibrous tethering that creates an undulating appearance and require treatment strategies that address the subdermal component. In addition to these atrophic scars, postinflammatory erythema (PIE) and postinflammatory hyperpigmentation (PIH) are common sequelae, with PIE typically observed in individuals with lighter skin and PIH in those with darker skin. These conditions reflect visible inflammation and may be influenced by the persistence of non-viable
treatments, but deeper boxcar scars are more resistant. Rolling scars, which comprise 15 to 25 percent of atrophic scars, are the widest type, potentially reaching up to 5 mm in diameter. They result from fibrous tethering that creates an undulating appearance and require treatment strategies that address the subdermal component. In addition to these atrophic scars, postinflammatory erythema (PIE) and postinflammatory hyperpigmentation (PIH) are common sequelae, with PIE typically observed in individuals with lighter skin and PIH in those with darker skin. These conditions reflect visible inflammation and may be influenced by the persistence of non‐viable Propionibacterium acnes (P. acnes) within the follicle, as well as wound healing processes that involve microvascular changes and epidermal thinning. The presence and severity of acne scars correlate with acne grade and the inflammatory response, which can vary based on the type and extent of immune cell activation and collagen production. 1
Propionibacterium acnes (P. acnes) within the follicle, as well as wound healing processes that involve microvascular changes and epidermal thinning. The presence and severity of acne scars correlate with acne grade and the inflammatory response, which can vary based on the type and extent of immune cell activation and collagen production.1
1: Types of acne scars
global severity rating, and the extent of scar dispersion. Effective scar analysis helps in diagnosing the specific type of scar but also aids in formulating a targeted treatment plan, addressing both aesthetic concerns and functional impacts.1,2
Case 1
Among individuals with acne scars, approximately one‐third exhibit minimal or mild acne, while 40% present with moderate acne. Acne scarring can significantly impair quality of life, imposing a notable psychological and psychosocial burden, including diminished self‐confidence and concerns about body image. Consequently, it is crucial to evaluate the risk of acne scarring in all patients, regardless of acne severity, and to implement early and sustained treatment strategies to mitigate long‐term consequences. Currently, routine assessment of acne scarring risk is not standard practice during consultations. Although the prevalence of scarring is higher among patients with severe acne, a comprehensive evaluation is necessary for all patients, as even those with mild lesions may be susceptible. Key risk factors include a family history of acne scarring and delayed initiation of treatment for acne lesions. Tools such as Tan et al.'s four‐item, self‐administered questionnaire can aid in identifying
Among individuals with acne scars, approximately onethird exhibit minimal or mild acne, while 40% present with moderate acne. Acne scarring can significantly impair quality of life, imposing a notable psychological and psychosocial burden, including diminished self-confidence and concerns about body image. Consequently, it is crucial to evaluate the risk of acne scarring in all patients, regardless of acne severity, and to implement early and sustained treatment strategies to mitigate long-term consequences. Currently, routine assessment of acne scarring risk is not standard practice during consultations. Although the prevalence of scarring is higher among patients with severe acne, a comprehensive evaluation is necessary for all patients, as even those with mild lesions may be susceptible. Key risk factors include a family history of acne scarring and delayed initiation of treatment for acne lesions. Tools such as Tan et al.'s four-item, self-administered questionnaire can aid in identifying individuals at risk for atrophic acne scars, enabling timely and effective intervention. This evidence-based tool evaluates four risk factors: maximum acne severity, duration of acne, family history of atrophic acne scars, and history of lesion manipulation. Additionally, the Facial Acne Scar Evaluation Tool (FASET) offers a practical and reproducible method for assessing existing scars. FASET encompasses three domains: scar counts by size (2–4 mm, >4 mm), overall
A 29-year-old female patient presented to our clinic with a history of acne scars. Upon examination, she was diagnosed with rolling and icepick scars, which developed as a result of grade 3-4 acne she experienced 4-5 years ago. These scars have persisted despite the resolution of her acne. The patient also reported a family history of acne scars on her father's side, but she has no history of hormonal imbalance. She has not been on any oral medications and has been using only topical applications for skin care. Given the current state of her scars, we recommended a treatment plan involving Microneedling RF combined with GFC PRP, to be administered over 4-5 sessions, to help reduce the appearance of her acne scars. The clinical picture of before and after treatment is as shown below after completion of 2 sessions of MNRF with GFC. The iceprick scars have reduced and also the rolling scars showed significant improvement after 2 sessions of the treatment.
Figure 1: Types of acne scars
Figure
Before treatment
After treatment
*Figure 2: The iceprick scars have reduced and also the rolling scars showed significant improvement after 2 sessions of MNRF with (GFC) PRP
Case 2
A 32-year-old male patient presented to our clinic with a 4-5 years history of acne scars. Prior to visiting us, he had undergone 4 sessions of fractional CO2 laser and 4 sessions of microneedling. The patient had no other significant medical history and was not on any oral medications for acne, relying solely on topical treatments. Given his condition, we recommended 4 sessions of Microneedling RF (MNRF) combined with Growth Factor Concentrate (GFC) PRP treatment. Upon completion of the 4 sessions, the patient showed visible improvement, with a significant reduction in both rolling scars and icepick scars.
After treatment
*Figure 3 : The significant reduction in both rolling scars and
icepick scars after completion of the 4 sessions of MNRF combined with Growth Factor Concentrate (GFC) PRP treatment
Case 3
A 22-year-old male presented to our clinic with concerns about acne and acne scars that had persisted for 1 year. The patient had discontinued medication 3 months prior, as his acne had cleared, and was now seeking a solution for the remaining scars. He underwent 4 sessions of Microneedling RF (MNRF) combined with Growth Factor Concentrate (GFC) PRP, with each session spaced one month apart. The before and after images demonstrated a significant reduction in acne scars, particularly in fresh scars and rolling scars. This case highlights the effectiveness of the combination treatment of MNRF and GFC PRP in reducing acne scars, especially in cases involving recent scars.
Before treatment
Before treatment
After treatment
*Figure 4 : The significant reduction in acne scars, particularly in fresh scars and rolling scars after 4 sessions of MNRF combined (GFC) PRP
Diagnosis
The diagnosis of acne scars typically involves a combination of clinical evaluation and specialized techniques to assess their type, severity, and characteristics. Clinical examination includes visual inspection by a dermatologist to evaluate the type, distribution, and severity of scars, and palpation to assess the texture and depth of the scars.2
In the evaluation of acne scars, several diagnostic tools and scales are utilized to assess severity and guide treatment. Lesion counting involves recording the number of acne scars through clinical examination and photographic documentation, providing basic quantification. Subjective self-assessment allows patients to rate their scars based on personal criteria like severity and appearance, offering insight into their perception of scar impact but potentially influenced by individual biases. The Acne Scar Rating Scale (ASRS) is a standardized tool that evaluates scars based on type (e.g., icepick, rolling, boxcar) and severity, providing a structured approach for consistent grading.2 Evaluatorbased qualitative and quantitative scarring grading systems involve trained evaluators assessing scars on qualitative aspects (appearance, texture) and quantitative aspects (depth, size), offering detailed and objective assessments using standardized criteria. The Echelle d’Evaluation Clinique des Cicatrices d’acne (ECCA) is a clinical scale designed for a comprehensive evaluation of acne scars, considering texture, color, and overall appearance.2 The Global scale for acne scar severity (SCAR-S) combine clinical and photographic assessments for a broad evaluation of scar severity, often incorporating feedback from multiple evaluators to ensure
accuracy. Imaging techniques such as high-frequency ultrasound measure scar depth and skin structure, three-dimensional imaging creates 3D maps of the skin to quantify scar volume and depth, and dermoscopy uses magnification and illumination to enhance the visualization of scar texture and morphology. Despite the variety of tools available, many do not fully account for all aspects of scar characteristics, such as color changes or the evolution of scars over time.2 High-frequency ultrasound is a valuable diagnostic tool for assessing acne scars by providing detailed images of the skin's layers. This noninvasive technique uses sound waves to measure the depth and structure of scars, offering insights into their severity and the extent of tissue damage. By visualizing the subdermal layers, ultrasound helps evaluate the thickness of scar tissue and its impact on surrounding skin structures.3
Treatment
Treatment of acne scars focuses on enhancing skin texture and appearance through a combination of topical agents and advanced procedures. Retinoids like Adapalene, Tazarotene, and Tretinoin improve skin texture by promoting cell turnover. Glycolic acid exfoliates to reduce superficial scars, while Vitamin C derivatives lighten hyperpigmentation. Tacrolimus helps reduce
redness. Advanced methods such as chemical peels, lasers, cryotherapy, dermal fillers, and surgical techniques like dermabrasion, subcision, and punch excision target different scar types, often in combination therapies to stimulate collagen production and remodel scars effectively. 4,5
Treatment procedure
Microneedling is a popular technique that involves creating micropunctures in the dermis using a mechanical device with small sterilized needles. This process induces microinjuries, triggering the body’s natural healing response and leading to the release of various growth factors (GFs) such as platelet-derived growth factor (PDGF), transforming growth factoralpha (TGF-a), transforming growth factor-beta (TGF-B), fibroblast growth factor (FGF), connective tissueactivating protein (CTAP), and connective tissue growth factor (CTGF). These factors drive neovascularization and neocollagenesis, helping to level atrophic scars and improve skin texture. Microneedling stimulates collagen production, which is beneficial for treating fine lines, wrinkles, and acne scars. The technique, also known as collagen induction therapy (CIT), percutaneous collagen induction (PCI), needle dermabrasion, or intradermabrasion, involves repetitive puncturing of the
skin, with each micropuncture being approximately four cells in diameter and resulting from 250–300 pricks per square centimeter. The targeted intermediate reticular layer of the dermis, rich in stem cells, is key for optimal collagen production. The micro-injuries not only set up a wound healing cascade but also aid in breaking down old, hardened scar tissue. Microneedling can be combined with other modalities such as subcision, platelet-rich plasma (PRP), and chemical peels to enhance overall treatment outcomes.6
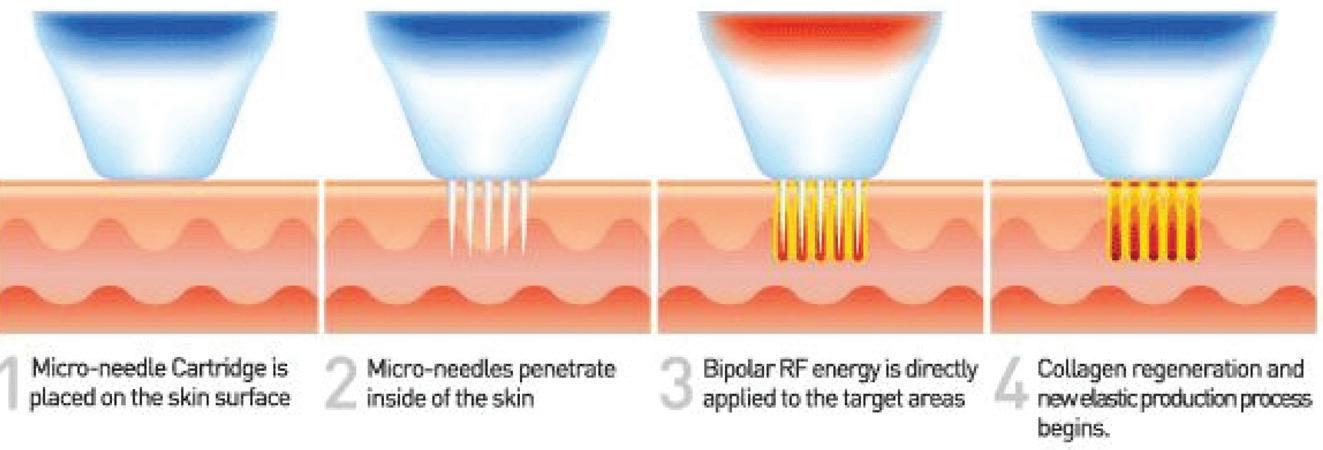
Radiofrequency microneedling is an FDA-cleared, minimally invasive treatment designed to enhance skin texture, tone, and elasticity with minimal downtime. As the latest advancement in radiofrequency microneedling, RF microneedling offers a promising alternative for patients with acne scars. The RF microneedling device utilizes microneedling technology with insulated gold-tipped needles to create microperforations in the epidermal layer. This process induces collagen synthesis and enhances the dermal remodeling response. In combination with radiofrequency energy, which heats the dermal layers to encourage deeper collagen formation, RF microneedling delivers comprehensive skin rejuvenation.6
Radiofrequency microneedling effectively addresses a range of skin concerns, including pore size, acne scars, stretch marks, facial wrinkles, fine lines, hyperpigmentation, and loose skin. Typically, several sessions spaced 4-6 weeks apart are required to achieve optimal results. By replenishing collagen levels, Radiofrequency microneedling helps counteract the effects of aging, such as wrinkles and skin laxity, and improves skin texture and firmness.
Figure 5: Radiofrequency microneedling device
Additionally, Radiofrequency microneedling targets acne scars, which result from inflammation damaging skin tissue and causing insufficient collagen production, as well as stretch marks caused by rapid skin expansion or contraction. Most patients experience significant improvements after a series of 3-6 sessions. The combination of microneedling and radiofrequency offers superior results compared to standalone therapies, enhancing overall skin appearance and providing a more youthful, supple look.7
Radio Frequency (RF) represents an advanced form of microneedling with several distinct differences compared to traditional microneedling. One significant distinction is that RF microneedling employs 36 needles, whereas conventional microneedling typically utilizes between 12-14 needles. The increased number of needles in RF microneedling is crucial because it generates a greater number of micro-injuries within the dermis. This enhanced micro-injury response stimulates a more robust collagen production process, leading to improved skin rejuvenation and enhanced therapeutic outcomes.7 What is RadioFrequency Microneedling?
Figure 6: Microneedling in conjunction with platelet-rich plasma (PRP), microneedling radiofrequency (MNRF), or laser treatments are employed for their synergistic effects on skin rejuvenation
Radiofrequency (RF) Microneedling represents the latest advancement in skin rejuvenation technology, designed to stimulate natural collagen production and enhance skin tone and texture across the face, neck, hands, and body. This cutting- edge treatment employs a Three-Fold Approach to achieve comprehensive skin improvement,
combining microneedling (Collagen Induction Therapy), Radiofrequency energy, and LED Light Therapy. Collagen Induction Therapy involves creating precise micro-punctures in the skin to trigger new collagen and cellular renewal. The addition of radiofrequency energy gently heats and tightens the deeper layers of the skin, facilitating electrocoagulation of the dermis and further remodelling of collagen and elastin. The radiofrequency microneedling device features a robotic motor with 36 sterile fine gold-tipped microneedles, providing a comfortable treatment experience with minimal downtime compared to other similar devices.8 (Note: Downtime may range from 6 to 24 hours depending on individual skin type)
Radiofrequency .................
Microneedling is a versatile treatment that effectively targets a range of skin concerns, providing comprehensive improvements in skin quality. By minimizing pore size, it helps achieve a smoother and more refined complexion. The treatment enhances overall skin tone and texture, contributing to a more even and youthful appearance. Its skin-tightening effects reduce laxity, while its ability to diminish fine lines and wrinkles helps restore a more youthful visage. Additionally, Radiofrequency Microneedling addresses
acne scars and stretch marks by stimulating collagen production and promoting skin regeneration, making it an effective solution for various dermatological issues.8
What does the treatment involve?
Before the radiofrequency microneedling treatment, we have to determine the most suitable treatment depth based on patients skin type, sensitivity, and specific concerns. A fullface radiofrequency microneedling treatment typically takes 60-90 minutes. While the procedure can be somewhat uncomfortable, a topical anesthetic is applied 20 minutes prior to minimize discomfort, with many patients describing the sensation as "light pressure” to the face. During the treatment, three passes are made over the entire area at varying depths, creating microscopic channels that remain open for up to 6 hours. To maximize results, it is recommended to wait at least 24 hours before applying makeup; if makeup must be worn, wait at least 6 hours. After the procedure, a hydrating face mask and soothing facial mist are applied to cool the treated area. Daily use of sunscreen with SPF 40 or higher is advised to protect and maintain the results of radiofrequency microneedling treatment.9
What is the difference between radiofrequency microneedling and conventional microneedling?
Conventional microneedling devices operate by gliding across the skin's surface, which may result in uneven delivery of microneedles and potential risk of epidermal abrasion or surface damage. In contrast, the radiofrequency microneedling device uses a robotic motor to gently insert the needles into the skin, providing better precision. The radiofrequency microneedling stands out due to its incorporation of Red and Blue Light Therapy along with Radio Frequency, which traditional microneedling does not include. Red light therapy is a rejuvenation modality that enhances skin tone, texture, and mitigates acne scarring through the stimulation of cellular repair mechanisms. Blue light therapy acts as an antimicrobial intervention, targeting and eliminating
Propionibacterium acnes and thus addressing active acne lesions. Radiofrequency (RF) therapy delivers controlled thermal energy to the dermis, promoting collagen synthesis and skin tightening with minimal to no downtime. The RF energy is transmitted through isolated needles in the device, enabling radiofrequency microneedling to penetrate deeper into the skin by sending energy past the epidermis and directly to the dermis. This technique makes radiofrequency microneedling suitable for darker skin types, as it avoids heat energy that could injure the epidermis and cause pigmentation.
Radiofrequency ............ microneedling stimulates collagen and elastin production in the treatment areas, which can continue for up to six months after the procedure. Radiofrequency microneedling is indicated for fine lines and wrinkles, skin tightening and crepiness, scarring, stretch marks, coarse pores, acne, melasma, and rosacea. Similar to regular microneedling, radiofrequency microneedling is performed in a series of three treatments, spaced four to six weeks apart for optimal results. Patients typically experience accelerated collagen production up to three months after each treatment.10, 11, 12
Why is the Radiofrequency Microneedling treatment
Figure 7: Mechanism of action of radiofrequency microneedling device
so popular?
Radiofrequency...................
Microneedling is a popular skin rejuvenation treatment due to its minimal invasiveness, safety for all skin tones and types, lack of downtime, and consistently stunning results. Many patients experience noticeable skin tightening and a reduction in facial wrinkles within just a few weeks. Additionally, optimal results can often be observed in as few as three treatments, which is fewer than many other skin rejuvenation options might require. Another significant benefit of radiofrequency microneedling treatment is its pain-free nature. The radiofrequency microneedling device uses tiny, insulated microneedles that enter the skin evenly, uniformly, and smoothly ensuring an incredibly comfortable patient experience. There are very few side effects associated with radiofrequency microneedling with the most common being mild facial redness in the treatment area, which typically resolves on its own within 24 hours. Furthermore, radiofrequency microneedling is safe for any skin type and tone, including individuals with darker skin who are more prone to hyperpigmentation. The treatment can also effectively minimize the appearance of stretch marks, acne scars, and pore size on both the face and body. If patients are looking to revitalize
their skin, radiofrequency microneedling is an excellent option that offers extensive benefits.13
Who would be considered an ideal candidate for radiofrequency microneedling?
The radiofrequency microneedling treatment is safe for all skin types and tones, making it a suitable option for nearly anyone interested in skin rejuvenation. This minimally invasive procedure effectively targets sun damage, hyperpigmentation, stretch marks, acne scars, skin laxity, large pores, fine lines, and uneven skin tone. However, individuals with a history of keloid scarring, skin conditions such as eczema and psoriasis, active acne, or cold sore breakouts may not be ideal candidates for radiofrequency microneedling. Furthermore, individuals with a clotting or bleeding disorder or who are on anticoagulant medication may not be appropriate for this treatment. Radiofrequency microneedling may also be unsuitable for patients with eczema, diabetes, active acne breakouts, open infections, or a compromised immune system.13
Is Radiofrequency Microneedling better than traditional Microneedling?
Radiofrequency ....... ......... microneedling treatment represents an advancement over traditional microneedling
by integrating gold-tipped precision microneedling with radiofrequency (RF) energy and LED light therapy. This combination enhances the body's wound healing and collagen production processes, making radiofrequency microneedling a preferred option for many patients compared to conventional microneedling. Several adjunctive treatments can further enhance the benefits of Radiofrequency microneedling, including chemical peels, subcision with dermal fillers, and more. Platelet-rich plasma (PRP) is an excellent complement to Radiofrequency microneedling treatment, as it supports the healing process and enhances collagen induction outcomes.13
Platelet-Rich Plasma (PRP) therapy is an advanced modality in the management of acne scars, leveraging the body’s intrinsic repair mechanisms. PRP is rich in growth factors that stimulate the synthesis of collagen and elastin, crucial extracellular matrix proteins responsible for the skin’s structural integrity and elasticity. The growth factors in PRP facilitate and accelerate the natural wound healing cascade, which, when administered via injection, enhances the reparative processes in damaged tissues, resulting in improved skin texture and a more refined appearance of scars. Additionally, PRP
promotes the regeneration of healthy dermal cells, targeting fibrotic scar tissue and supporting its replacement with newly formed, healthy skin. This regenerative effect optimizes the skin's texture and tone, leading to a more even surface and diminished scar visibility. The minimally invasive nature of PRP therapy entails minimal downtime, making it an advantageous option for patients seeking improvement in acne scars with minimal recovery periods. Given that PRP is autologous, derived from the patient’s own blood, it presents a natural treatment alternative with a reduced risk of adverse reactions or allergic responses, ensuring both safety and compatibility.14
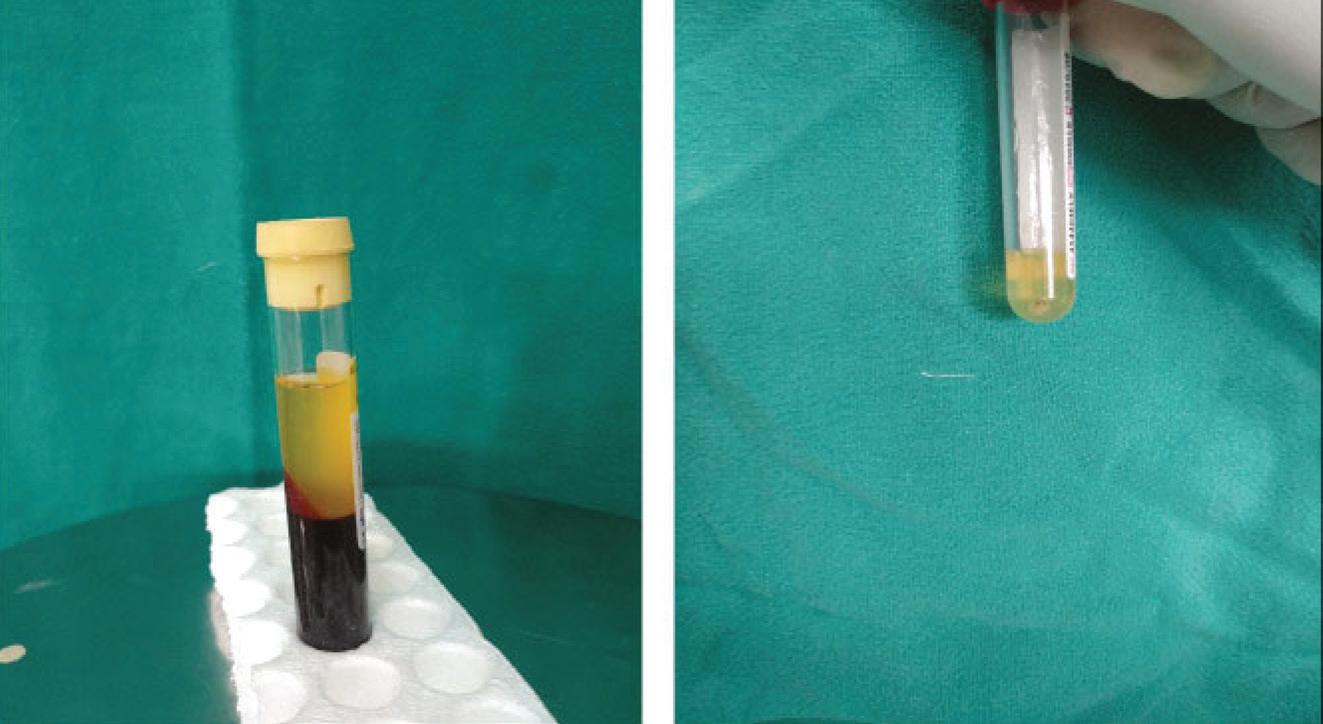
PRP is a portion of plasma obtained from blood, containing four to seven times the concentration of platelets compared to normal plasma.
Platelet-rich plasma (PRP) was prepared using the double-spin centrifugation technique. An initial volume of 8.5 mL of whole blood was drawn from the patient and anticoagulated with 1.5 mL of acid-citrate-dextrose (ACD) solution. The whole blood was centrifuged at 1400 rpm for 10 minutes to separate the buffy coat and plasma from RBC sediments. This supernatant was then centrifuged at 3500 rpm for 10 minutes to obtain PRP, which consists of a plateletrich pellet with the lower one-
fourth of the plasma formed at the bottom of the vial. Calcium gluconate was added as an activator in a ratio of 1:9, i.e., 1 mL of calcium gluconate in 9 mL of PRP. 8 This is higher concentration of platelets.14
A significant reduction in mean boxcar scars count was observed from the second visit onwards, with the maximum improvement noted after three sessions. In the case of icepick scars, the greatest reduction was recorded at the fourth visit. The improvement in rolling scars began from the second visit and continued through the fourth and sixth visits.14
Growth Factor Concentrates (GFC) are vital in treating acne scars due to their regenerative properties that enhance skin repair and remodeling. Rich in growth factors, GFCs stimulate collagen and elastin production, which supports skin structure and elasticity. This process helps remodel scar tissue, smooths skin texture, and reduces scar visibility. GFCs accelerate natural healing, promote healthy skin cell regeneration, and improve skin tone. Often used with other treatments like microneedling or laser therapy, GFCs enhance overall efficacy by addressing scars from multiple angles. The minimally invasive treatment involves little to no downtime and is derived from the patient's own blood, ensuring a natural and safe option with minimal risk of adverse reactions.15
Discussion
Acne scars are a common and distressing result of acne vulgaris, affecting the skin's pilosebaceous units. These scars arise from inflammatory damage and abnormal healing, leading to changes in skin texture and pigmentation. They are primarily classified into atrophic, hypertrophic, and keloidal types, with atrophic scars being the most frequent.1 Post-inflammatory erythema (PIE) and post-inflammatory hyperpigmentation (PIH) also occur as sequelae of acne, with PIE common in lighter skin and PIH in darker skin tones.
Figure 8: Platelet-rich-plasma therapy
Understanding the types of scars and available treatments is essential for effective management. Diagnosing acne scars involves visual inspection, palpation, and specialized tools to assess scar type and severity. Techniques include lesion counting, subjective self-assessment, and scales like the Acne Scar Rating Scale (ASRS) and Echelle d’Evaluation Clinique des Cicatrices d’acne (ECCA). Advanced imaging such as ultrasound and 3D imaging provide detailed views. Treatment requires a multifaceted approach.2 Topical options include retinoids (adapalene, tazarotene), glycolic acid, vitamin C derivatives, tretinoin, and tacrolimus. Combination therapies use silicone gel, Er laser, tranilast, isotretinoin, plasma gel with fractional CO2 laser, and lyophilized growth factors. Advanced treatments involve chemical peels, lasers (fractional and CO2), cryotherapy, dermal fillers, and surgical methods (dermabrasion, subcision, punch excision).3
Microneedling, particularly in its advanced form as radiofrequency microneedling, has significantly advanced the treatment of acne scars by harnessing controlled micro-injuries to stimulate the body's natural healing processes.6 Both traditional microneedling and radiofrequency
microneedling are effective in promoting the production of collagen and elastin— key proteins that maintain skin elasticity and structural integrity.6 Traditional microneedling creates tiny punctures in the skin using a device with small, sterilized needles. These microinjuries trigger the body's natural healing response, which enhances collagen and elastin production. The addition of Platelet-rich plasma (PRP) is derived from a concentration of platelets and growth factors from the patient’s own blood. During microneedling, PRP is injected into the skin, which accelerates the healing process and enhances collagen and elastin production and enhancing skin repair.14 Microneedling Radiofrequency (MNRF) involves penetrating the skin’s surface with tiny needles while simultaneously delivering radiofrequency energy to deeper skin layers. This radiofrequency energy heats the underlying tissue, stimulating the production of collagen and elastin. Laser treatments, such as fractional laser resurfacing, use high-energy light to induce controlled thermal injuries to the epidermis. These thermal injuries can target specific skin issues, such as pigmentation, while also promoting collagen and elastin production. The thermal injuries from laser treatments encourage
the development of fresh, healthy skin cells, improving fine lines, wrinkles, scars, and other skin imperfections. Radiofrequency ................ microneedling integrates these advanced technologies with a sophisticated approach. It employs 36 fine, gold-tipped needles to create precise microchannels in the skin, combined with radiofrequency energy and LED light therapy—red light to stimulate collagen production and blue light to target acne bacteria. This comprehensive approach addresses acne scars and other skin concerns, and the robotic motor used in radiofrequency microneedling ensures precise and comfortable treatment. Growth Factor Concentrates (GFCs) further enhance the treatment of acne scars by providing regenerative properties that support skin repair and remodeling. Rich in growth factors, GFCs stimulate the production of collagen and elastin, helping to remodel scar tissue and improve skin texture. GFCs accelerate natural healing processes and promote the regeneration of healthy dermal cells, which can be particularly beneficial when used in conjunction with microneedling, PRP, or laser treatments.15 Microneedling with PRP, MNRF, or laser operates by creating controlled, microscopic injuries to the epidermis. These micro-injuries trigger the body's natural wound
healing response, promoting the growth of collagen and elastin fibers. Collagen and elastin are essential proteins that provide the epidermis with elasticity and structural support. The combined use of microneedling, PRP, MNRF, laser treatments, and GFCs offers a multifaceted approach to skin rejuvenation. These methods work together to enhance skin appearance, reduce signs of aging, and address various skin concerns through natural healing mechanisms and targeted interventions.6, 14,15 The integration of these technologies represents a significant advancement in dermatological treatments, providing patients with effective, minimally invasive options for improving skin texture and appearance.
Conclusion
The adoption of microneedling and radiofrequency microneedling has significantly impacted dermatological treatments globally by offering effective, minimally invasive options for acne scars and other skin concerns. These technologies democratize access to non-surgical skin rejuvenation, integrating advanced features like
References
1. Fabbrocini G, Annunziata MC, D'Arco V, et al. Acne scars: pathogenesis, classification and treatment. Dermatol Res Pract. 2010; 2010:893080. doi:10.1155/2010/893080.
2. Clark AK, Saric S, Sivamani RK. Acne Scars: How Do We Grade Them? Am J Clin Dermatol. 2018; 19(2):139-144. Doi: 10.1007/s40257017-0321-x
3. Malinowska S, Jagus D, Wozniak W, Mlosek RK. Usefulness of high-frequency ultrasound in the monitoring of laser treatment of acne scars. J Ultrason. 2021;20(83):e279-e283. doi:10.15557/JoU.2020.0049
4. Bikash C, Sarkar R. Topical management of acne scars: The uncharted terrain. J Cosmet Dermatol. 2023; 22(4):1191-1196. doi:10.1111/jocd.15584
5. Basta-Juzbašić A. Current therapeutic approach to acne scars. Acta Dermatovenerol Croat. 2010; 18(3):171-175.
6. Farrukh AK, Ahmad S, Mehrose MY, et al. Efficacy Of Micro-Needling On Post Acne Scars. J Ayub Med Coll Abbottabad. 2019; 31(3):336-339.
7. Kim J, Lee SG, Choi S, et al. Combination of Fractional Microneedling Radiofrequency and Ablative Fractional Laser versus Ablative Fractional Laser Alone for Acne and Acne Scars. Yonsei Med J. 2023; 64(12):721-729. doi:10.3349/ymj.2023.0234.
8. Wootten S, Zawacki ZE, Rheins L, Meschter C, Draelos ZD. An evaluation of electrocoagulation and thermal diffusion following radiofrequency microneedling using an in vivo porcine skin model. J Cosmet Dermatol. 2021; 20(4):1133-1139. doi:10.1111/jocd.13690.
9. Alexiades M. Microneedle Radiofrequency. Facial Plast Surg Clin North Am. 2020; 28(1):9-15. doi:10.1016/j.fsc.2019.09.013
10. Connolly D, Vu HL, Mariwalla K, Saedi N. Acne Scarring-Pathogenesis, Evaluation, and Treatment Options. J Clin Aesthet Dermatol. 2017; 10(9):12-2
radiofrequency and LED light therapy to enhance outcomes and patient satisfaction. Reduced downtime and minimal discomfort make these treatments appealing, even to those with busy lifestyles. The shift towards autologous treatments like PRP and Growth Factor Concentrates (GFCs) reflects a trend toward natural, safe options with minimal risk. As these technologies evolve, they continue to provide effective, accessible solutions for healthier, youthful skin worldwide.
11. Singh A, Yadav S. Microneedling: Advances and widening horizons. Indian Dermatol Online J. 2016; 7(4):244-254. doi:10.4103/22295178.185468.
12. Pei S, Inamadar AC, Adya KA, Tsoukas MM. Light-based therapies in acne treatment. Indian Dermatol Online J. 2015; 6(3):145-157. doi:10.4103/2229-5178.156379
14. Dhurat R, Sukesh M. Principles and Methods of Preparation of Platelet-Rich Plasma: A Review and Author's Perspective. J Cutan Aesthet Surg. 2014; 7(4):189-197. doi:10.4103/09742077.150734.
15. Fabbrocini G, Annunziata MC, D'Arco V, et al. Acne scars: pathogenesis, classification and treatment. Dermatol Res Pract. 2010; 2010:893080. doi:10.1155/2010/893080.
*These pictures are a property of the Skinoq Healthcare Pvt. Ltd.. The Aestheticians Journal has obtained special permission from Skinoq to use in the journal. The copyright of this pictures are owned by Skinoq clinic.
What is the link between eczema and prurigo nodularis?
healing like Prurigo nodularis is a chronic skin condition characterized by multiple, intensely itchy bumps that can range from half a centimeter to 2 centimeters in width, with colors varying from flesh-toned to red, brown, or black. It often co-occurs with eczema, particularly atopic dermatitis, which can trigger its development, as scratching can exacerbate symptoms and lead to the formation of raised nodules. Although the exact cause remains unknown, persistent scratching is a key factor, and certain populations—such as African Americans, women, and those aged 51 to 65—are at higher risk. Factors like stress, heat, and tight clothing may worsen the condition. Treatment typically focuses on reducing itchiness and may include corticosteroids, antihistamines, phototherapy, and oral immunosuppressants, alongside recommendations for managing eczema, such as avoiding triggers and adjusting skincare routines. Estimates suggest that up to 72 out of every 100,000 adults in the U.S. are affected each year, highlighting the significance of understanding and managing this condition.
How Managing Comorbidities Can Transform Alopecia Areata Treatment Outcomes
Alopecia areata is an autoimmune condition that leads to patchy hair loss, affecting about 2% of the population, often beginning in early adulthood. It's important for clinicians to recognize and manage comorbidities, as these can impact treatment and overall quality of life. Common comorbidities include thyroid disorders, atopic diseases like eczema, vitiligo, and psoriasis. Patients are significantly more likely to have thyroid issues, making monitoring essential. Alopecia areata is also linked to metabolic conditions such as diabetes and obesity, where lifestyle changes and regular glucose monitoring are crucial. Less common associations include rheumatologic disorders and celiac disease. A multidisciplinary approach that includes regular screening and collaboration between dermatology, endocrinology, and mental health professionals can enhance care. As of September 2024, advancements in treatment include three FDA-approved JAK inhibitors—baricitinib, ritlecitinib, and deuruxolitinib—that block inflammatory pathways and offer new hope for patients with severe alopecia areata. Recognizing and managing these comorbidities not only improves clinical outcomes but also supports the emotional and physical well-being of patients, emphasizing the need for a collaborative, whole-person care approach.
For Maintenance during Post Hair Transplantations
AGA – Androgenetic Alopecia
Areata
Minoxidil stimulates hair follicles via vasodilatation, also slows hair loss.
Finasteride blocks type II 5a reductase inhibitor and inhibits the production of male hormone DHT (dihydrotestosterone), and slows down hair loss.
Topical Finasteride overcomes the systemic effects of oral finasteride
Procapil is a formula that combines vitaminated matrikine with apigenin and oleanolic acid, which reduces the effect of DHT* on hair follicles and increases blood flow circulation in the scalp, promoting healthy, thick hair.
Minoxidil 5.00%
Finasteride 0.10%
Alopecia
Minoxidil 10.00%
Finasteride 0.10%
Procapil
Procapil
Benzyl Nicotinate Vitamin K
Salicylic Acid
Alopecia areata (round hairless patches on the scalp)
Alopecia pityrodes (loss of hair, of the body as well as of the scalp)
Alopecia senilis (loss of hair caused by aging)
Symptomatic hair loss after infectious diseases
Hair damage caused by chemicals
Scalp Energiser
Achieve Radiant Skin with Chemical Peels: A Comprehensive Guide
Dr. Shoma Sarkar
MBBS, MD (Dermatology)
Dermatologist
& Skin Specialist
Mumbai
Aesthetics:
The motivation for aesthetics is basically to achieve the ‘Skin
wound Goals’ which definitely vary for all of us. However, there are some common grounds as well such as everyone wishes to have a ‘Good Skin’ which means a.
• Smooth
• Firm
• Even colored
patients.
Procedures like Chemical peels, Lasers, Lightbased devices, Fillers and neurotoxins, PRP / threads, Mesotherapy are some of the most commonly preferred and performed treatments to attain a balanced, more proportionate and more attractive appearance of the face.
• Free of blemishes
• Free of wrinkles
• No sun damaged skin. Sounds unachievable? It’s not, science makes it easy and yes, possible!
I use all the tools and technology to attain beautiful results, so it’s like a mocktail of therapies prepared and customized according to the need of the patient. In the clinic, I go through a proper counseling and understand the need of the hour and patient and then we reach a conclusion mutually. I apply the scientific approach of aesthetics to my practice and help to treat different problems and concerns of my
Chemical peels: Chemical peels are a popular nonsurgical cosmetic treatment designed to improve the texture and appearance of the skin. By applying a chemical solution to the skin, these peels exfoliate the outermost layers, revealing fresh, new skin beneath. This process helps to reduce the appearance of fine lines, wrinkles, acne scars, uneven skin tone, and other skin imperfections. Chemical peels also stimulate collagen production, promoting a smoother, more youthful complexion over time. They are commonly used on the face, but can also be applied to the neck, hands, and other areas of the body.
Yellow Peel
Yellow peel is a specialized peel with the Retinol being the main component. The concentration of the Retinol being approximately between 1% to 5%. It’s the natural & synthetic derivatives of Vitamin A. Retinol peel is a very good agent and is used for:
1. Skin Rejuvenation
2. Skin Lightening
3. Bridal Glow
4. Body Lightening
5. Skin Resurfacing
6. Toning/Freckles/Melasma
7. Dullness
8. Superficial Lines & Wrinkles
9. Skin Aging & photo aging acne
10. Hyper pigmentation
Retinol works by penetrating deep into the skin and has excellent exfoliating properties because of which the superficial layers of skin is exfoliated and thus gives a beautiful, radiant, new skin which looks more toned, smooth, free of superficial lines & wrinkles. It also makes skin glow, improves and also lifts the skin.
Retinol peels are done every 15 days and repeated every 6 to 8 sessions and can be combined with other products like Mesotherapy, Photo facial & RF treatment to double the results and add up to the longevity of the results of the peel. Yellow peels cannot be done in:
• Hypersensitivity cases
• Atopic skin
• Eczematous & Psoriatic skin
• Pregnancy & Lactation
• During Hepatic infections
thus explaining the steps of the procedure. This peel has a downtime of 7 to 10 days at an average, so the patient has to follow the proper instruction given by us during & after this procedure. Before this peel is done we put the patient on priming cream, it means creams like mild bleaching agent or lightening creams are given so the patient skin gets primed & prepared for the peel. Priming is done 15 to 21 days prior to the peel procedure.
Peel Procedure: The face is properly cleansed & the makeup is removed & the decreasing of the skin is done with an alcohol swab so that the area is completely dry for better absorption. Then occlusion is done with petroleum jelly around the eye, nostrils and around the mouth. Then the first layer of peel is applied and then massaged into the skin and then wait for 15 to 20 minutes and then reapply the second coat after which you tell the patient to keep the peel for 6 hours and then wash it with plain water.
• Photosensitive Skin
Before the peel: The important part is to interview the patient to understand the condition & the expectation
Post Procedure: The first 2 days the patient has mild redness and swelling which subsides by the 3rd day evening & the peeling starts on that particular area, this is the time when the patient has to take care of the skin with the help of prescribed sunscreen & moisturizers, if not taken care one can end up having infection & post inflammatory hyper pigmentation. After the peel, the cleansers should not be
used 6 to 7 hours & then followed by moisturizers & sunscreen. Avoid scrubbing and any other procedure immediately.
Trichloroacetic acid
(TCA): The TCA Peel is a highly-advanced treatment that helps the skin look younger and makes it glow. It is a medium-depth facial chemical peel procedure that when applied and peeled from your skin’s surface, will remove all the acne and marks. It keeps the skin out of unusual protuberances. It rejuvenates the skin regardless of age, skin color or type. It accelerates your transformation and offers healthier skin. TCA peel works on the principle of removing dead and damaged skin cells from the layers in depth of skin and replace them with living and healthier skin cells. It is based on the application of mixing Trichloroacetic acid with a blue solution. The removal of the dead skin cells exfoliate
the skin and help achieve tighter, clearer and healthier skin. TCA peel is preferred over a full-skin layer laser resurfacing because it takes considerably lesser time to recover.
The treatment can be performed on the face as well as arms, legs, and neck. It reduces or completely removes wrinkles, unusual skin pigmentations, sun damage or even unhealthy skin. After a successful TCA peel treatment, one can expect a total rejuvenation of your skin. The peel automatically removes damaged skin layers, improves the skin tone, reduces the number of scars, unusual pigmentations and helps maintain healthier skin. If the skin is youthful, one will instantly see the glow on the skin. TCA peel treatment can be performed as many times as you desire until the results are achieved. It is usually performed at a four-week interval if multiple treatments are required. TCA peel treatment if performed annually guarantees long-term maintenance of healthy and happy skin.The treatment procedure will require a minimum of 30 to 45 minutes for a particular condition. The TCA peel usually requires a minimum of two treatments or more. Both the treatments are spaced out over weeks or even months, to help the skin heal and reveal its initial glow. Some patients with relatively dark or poor skin conditions may also need three to four treatments. Overall, the TCA peel has helped all kinds of patients with different ages and skin types to achieve healthier and happier skin.
10% Arginine.... + Hyaluronic acid Peel: In this procedure, we use a peel which is a concentration of lactic acid, Vitamin E, Citric Acid, and Arginine. This peel instantly gives a glow and without any downtime.
The peel is very mild and has agents which help in neutralizing the free oxygen radicals, thus giving the skin a refreshed look.
The skin looks more radiant and this peel is also combined with hydrameso therapy, where Vitamins like Vitamin C & Vitamin E, HA are penetrated into the skin which adds up to the glow and also
revitalizes the skin from within. This peels also hydrates the skin simultaneously as it contains lactic acid. Followed by which we use a nourishing pack which consists of natural mineral & salts. This peel can be done once in every week for 8 to 10 sessions. Also, can be taken any time before any function. This peel can be done in all the age groups and both sexes. This peel can also be done on the body like hands, neck, and back.
Glycolic peel: In this procedure the skin is cleansed, followed by microdermabrasion, then glycolic peel is used to exfoliate the superficial skin, so as to remove the dead and damaged skin.
Then bio light treatment is given which helps in reducing any bacterial load, superficial lines and pigmentation.
Thus, the detoxification takes place and the skin looks younger & refreshed, Vitamin infusion with help of electroporation is done. This entire procedure gives a very healthy-looking skin.
This procedure is done once in 15 days and 6 to 8 sessions are recommended for optimum results.
Detox peel is done for the patient who have dehydrated & dull Skin, smokers, photodamaged skin, stubborn tanning post vacation, post hangovers. This peel can be done on both the sexes and age group between 20 to 60 years of age. It is highly recommended to do this treatment from one of the best skin doctor.
Azelaic acid, Kojic acid, Arbutine, Phytic acid, Ascorbic acid Peel: There are various types of chemical peels available today. These peels are designed according to different skin types. These peel is a chemical treatment that has multiple ingredients. Benefits of these Peel:
• Mainly designed to decrease areas of skin discoloration and hyperpigmentation. It reduces excess melanin production by impeding explicit enzymes.
• It provides a fair complexion.
• It can be used to enhance the look of facial skin, abdomen, and legs.
• These peel can help in reducing acne scars, dull skin, dry skin, and blemishes.
• Chloasma can be decreased with this peel.
• It also maintains the skin’s oil production that helps to improve acne and blackheads.
Azelaic acid, Kojic acid, Arbutine, Phytic acid, Ascorbic acid peel is one of the leading depigmentation methods. This process has two steps:-
1. In the first step, a thick mud mask is applied to the affected area. It contains Kojic acid, Phytic acid, Ascorbic acid, and Titanium Dioxide. The mask must be kept on the face for 6 to 10 hours. The total time of application varies as per the skin type and pigmentation conditions. Then after, wash with the cleanser.
2. In the second step, you need to apply topical antispot cream. This cream will help to sustain the results obtained with the these peel. It also protects the area of pigmentation. The cream must be used up to one year with these peel.
Azelaic acid, Kojic acid, Arbutine, Phytic acid, Ascorbic acid peel works to emend hyperpigmentation while controlling the excessive production of melanin in the melanocytes. It hinders tyrosinase activation within the melanosome. It also reduces the oxidation stress and creation of excess
melanin. These peel works as a preventive and corrective mechanism. It provides long-lasting and instant results. It is best for all skin types. It delivers results in one or two weeks. These peel is mainly used on the face. It can also be used on other parts of the body like abdomen, back and legs. It can be used as a post-peel home care regiment.
If you are using Azelaic acid, Kojic acid, Arbutine, Phytic acid, Ascorbic acid peel then glycolic peels and other lighting agents will not be used. Some pinkness can be anticipated on the skin after using the peel. You should not have any pain. The patches of excess melanin will reduce after two weeks of treatment. The results will enhance with time. You need to apply sunscreen daily.
The effect of the result depends on your skin type. Some factors that affect the longevity of cosmelan treatment are as follows:-
• Hormonal imbalances
• Exposure to sun (UV radiation)
• Use of the cosmelan cream
Patient need to visit 15 days after starting the treatment or visit a good skin clinic for this peel. There is follow up treatment after one month.
Black Peel: Black peel is a natural organic peel used to treat pimples, marks & oily skin. Black peel is developed for clearing up oily blemishes, the key ingredient is Acetic Acid obtained through the fermentation of black rice and it has been well known in Asia for traditional healthy vinegar. It has long been used for health benefits due to the high content of organic materials, minerals essential amino acids. Black peel is added with salicylic acid and Jasmonic acid to improve oily problem skin. It also contains potassium iodide to relieve skin irritation and Bio sulphur to dry to sebum.
Black peel is done on all stages of Acne. Multiple sessions are required depending upon the severity of Acne. Black peel is very effective and has a mild downtime like scaling for few days. It is repeated once in 21 days. The results can be appreciated right from the 1st session.
The skin is cleansed, toned and then extraction is done (blackheads & whiteheads). Then black peel is applied. 2 to 3 coats of peel are applied over the oozing or bleeding acne, lesions opened by extraction then it is left for 5 to 10 minutes and removed with a wet sponge. Post-procedure Bio light and Sebohydra infused mask is applied to the face to calm down and hydrate the irritated skin. Black peel is also very effective in treating body acne.
Summary
Chemical peels are a versatile and effective solution for those seeking to improve their skin's appearance without undergoing surgery. By selecting the appropriate type of peel, individuals can achieve smoother, more youthful skin tailored to their specific needs and concerns. As with any cosmetic treatment, it's important to consult with a qualified skincare professional to determine the best approach for individual skin types and goals.
Aesthetic market to triple by 2029, driven by non-surgical procedures
The aesthetic market is experiencing significant growth, primarily driven by increased public awareness and understanding of aesthetic procedures, which has led to a rising demand for devices and techniques that facilitate these interventions.
India is emerging as a key player in this global market, with projections indicating a threefold expansion to approximately USD 3.02 billion by 2029. This growth is attributable to factors such as a preference for noninvasive treatments like botulinum toxin injections and dermal fillers, rising disposable incomes, and a health-
conscious population. Additionally, societal perceptions are shifting, with aesthetic procedures increasingly recognized for their positive effects on self-esteem and overall well-being. Nonsurgical treatments now outnumber surgical options globally, with botulinum toxin remaining the most prevalent, as reported by the International Society of Aesthetic Plastic Surgery, which notes over 9 million procedures performed, reflecting a 26.1% increase. Hyaluronic acid treatments follow closely, with 4.3 million procedures recorded. The demographic landscape is also evolving, as women represent 85.7% of consumers, but there is growing acceptance among men and millennials, reshaping the industry's dynamics. Currently valued at around USD 1.62 billion, India’s aesthetic medicine market is expected to grow at a compound annual growth rate (CAGR) of 13.2%, highlighting the increasing demand for these treatments and India’s potential to become a global leader in the aesthetic medicine sector.
What Medical Dialogues: Permanent Makeup Pigments Increase Risk of Allergic Contact Dermatitis, finds research.
The A recent study indicates that permanent makeup pigments can heighten the risk of allergic contact dermatitis, particularly from inorganic compounds like iron oxides and titanium dioxide. Symptoms such as redness, itching, and swelling may develop months or even years post-procedure. The findings underscore the need for better regulation and thorough pre-procedure testing to minimize risks.
Isotretinoin Induced Xerosis
Chelitis, Photodermatitis of Lips
Benzophenone-3
Kokum Butter
Shea Butter
Squalene
O.M.C
Vitamin E
Lip Lick Dermatitis
Growth Factor Concentrate (GFC) for Hair Regrowth: A Case Presentation
Dr. Parul Khot
DNB (Dermatology & Venereology) DVD, MBBS
Dermatologist & Cosmetologist
Skiin Ace Clinic, Mumbai
HIntroduction air loss, a distressing condition affecting millions globally, has
spurred advancements in dermatological treatments aimed at restoring hair growth and improving scalp health. Among these innovations, Growth Factor Concentrate (GFC) has emerged as a promising therapeutic option, leveraging the regenerative potential of natural growth factors to rejuvenate hair follicles and promote hair regrowth. This introduction explores the role of GFC in hair restoration, highlighting its mechanisms, clinical applications, and potential benefits in addressing various forms of hair loss. Growth factor concentrate is derived from the patient's own blood plasma, similar to PlateletRich Plasma (PRP), but further refined to concentrate specific growth factors essential for tissue repair and regeneration. These growth factors include fibroblast growth factor (FGF), vascular endothelial growth factor (VEGF), and platelet-derived
growth factor (PDGF), among others, which play crucial roles in stimulating cellular proliferation, angiogenesis, and collagen synthesis— key processes in hair follicle maintenance and growth.1
Growth factor concentrate (GFC) offers a promising approach to hair restoration by leveraging its multifaceted mechanisms to rejuvenate hair follicles and stimulate optimal hair growth. GFC activates key signaling pathways to transition follicles from the resting (telogen) to the growth phase (anagen), leading to thicker, denser hair. It enhances blood circulation through angiogenesis, ensuring follicles receive essential nutrients and oxygen while its anti-inflammatory properties create a healthier scalp environment. Clinical studies and anecdotal evidence support GFC's efficacy in improving hair density and quality, particularly for conditions like androgenetic alopecia and alopecia areata.
Using the patient's own biological materials, GFC minimizes risks and offers a non-invasive alternative to surgical options. Ongoing research into combining GFC with therapies like PRP and mesotherapy promises further advancements in hair restoration, reinforcing its role as a significant and innovative solution for various hair loss conditions.1
Case report
A 40- Years - old male presented with hair thinning since 2 years. He observed gradual hair fall due to his long hours in the sun while shooting. There is no history of diabetes or any other medical issue and no other family members has early hair loss history. On examination patient had thinning of the scalp on frontal area, parietal area and vertex. His hair had become thin and rough. The treatment was initiated with 4 GFC’S and mesotherapy 6 sessions spaced at 15 days interval each. Concurrently, the patient received oral supplementation with finasteride and topical application of minoxidil for a duration of 4 months. By the end of the treatment period the patient was very happy in the end of 4 months and continuing for maintenance.
Before treatment
After treatment
Figure 1 : After 4 months of treatment: GFC along with mesotherapy
Diagnosis
Diagnosing hair disorders involves a thorough assessment integrating clinical history, physical examination, and specialized diagnostic techniques. Dermatologists use methods like trichoscopy to examine the scalp and hair follicles, assessing density, diameter, growth patterns, and scalp condition to identify conditions such as alopecia areata, androgenetic alopecia, telogen effluvium, or scalp infections. Additional tests, such as pull tests or scalp biopsies, confirm diagnoses or rule out underlying causes. The card test distinguishes between newly growing, broken, and miniaturized hairs, while the hair pull test and tug test assess hair shaft integrity and resilience. Trichoscopy provides detailed visualization of hair follicles,
and scalp biopsy offers histopathological confirmation of conditions like androgenetic alopecia. Laboratory investigations and genetic testing reveal underlying causes, such as hormonal imbalances or genetic predispositions, guiding personalized treatments. This comprehensive diagnostic approach ensures accurate identification of hair disorders, promoting effective management and hair regrowth.2
Treatment
The treatment landscape for hair loss has evolved significantly, with growth factor concentration (GFC) emerging as a promising therapeutic approach. GFC therapy involves harnessing the regenerative properties of growth factors derived from the patient's own blood to potentially slow down hair loss progression. By injecting concentrated growth factors directly into the scalp, GFC therapy aims to nourish follicular cells, prolong the anagen (growth) phase of hair, and promote thicker, healthier hair growth.
i) Platelet-rich plasma therapy: Platelet-rich plasma (PRP) therapy is a promising treatment for hair loss, including androgenetic alopecia and alopecia areata, by promoting hair follicle rejuvenation and growth through multiple mechanisms. Rich in growth factors like PDGF, TGF-a, VEGF, and IGF, PRP stimulates the proliferation and differentiation of dermal papilla and other follicular cells, enhancing hair
growth and shaft diameter. It extends the anagen phase and reduces the telogen phase, improving hair density and thickness. PRP also promotes angiogenesis, enhancing blood circulation and nutrient delivery to the scalp, while its anti-inflammatory properties mitigate scalp inflammation, creating a favorable environment for hair growth. Additionally, PRP stimulates the production of extracellular matrix components, supporting follicle structure and hair shaft anchorage, contributing to overall follicular health and longevity.3
ii) Epidermal growth factor (EGF): Platelet-rich plasma (PRP) combined with epidermal growth factor (EGF) is increasingly used to treat hair loss, including androgenetic alopecia. PRP, derived from the patient's own blood, contains growth factors that stimulate hair follicle activity and promote growth. EGF enhances hair regeneration by activating the Wnt/b-catenin signaling pathway and promoting proliferation of mesenchymal stem cells through the ERK and AKT pathways. While continuous EGF expression can potentially disrupt follicular growth and morphology, PRP-EGF therapy is effective in rejuvenating dormant hair follicles, extending the growth phase of existing hair, and encouraging thicker, healthier hair growth.4
iii) Fibroblast growth factors: Fibroblast growth factors (FGFs), such as FGF-7 (KGF) and FGF-10, are crucial for hair follicle growth and
maintenance. They stimulate hair follicle stem cells by interacting with FGFR2b and FGFR1b receptors, promoting proliferation and differentiation to generate and support follicles. FGFs regulate the hair growth cycle by inducing follicles to enter the anagen phase, enhancing hair shaft production and extending growth periods. They also promote angiogenesis, ensuring a steady blood supply for follicle health, and support cell proliferation, survival, and matrix functions necessary for hair shaft formation and structural integrity. Overall, FGFs play a key role in fostering robust hair growth and maintaining healthy follicles.5
iv) Insulin-like growth factor-1: Insulin-like growth factor-1 (IGF-1) is a promising treatment for various types of hair loss, including androgenetic alopecia. It promotes hair growth by interacting with IGF-1 receptors on dermal papilla cells, stimulating their proliferation and differentiation, and extending the anagen phase for longer, denser hair. IGF-1 also has antiapoptotic effects, prolonging follicular cell lifespan and functionality. It enhances scalp blood circulation through angiogenesis, ensuring optimal nutrient and oxygen delivery to hair follicles. Additionally, IGF-1 supports follicular health by promoting cell proliferation and tissue repair, maintaining the structural integrity of hair follicles and fostering robust hair growth.6
v) Transforming growth factor-beta: Transforming growth factor-beta (TGF-B) is crucial in regulating hair follicle biology by influencing the transitions between the growth (anagen), regression (catagen), and resting (telogen) phases of hair follicles. TGF-B can induce the shift from anagen to telogen, potentially leading to hair thinning if dysregulated. It also plays a role in tissue remodeling and wound healing by managing extracellular matrix production, which maintains follicular structure. Additionally, TGF-B modulates inflammatory responses in the scalp, impacting immune regulation and inflammatory pathways, which can influence conditions like alopecia areata.7
vi) Vascular endothelial growth factor: Vascular endothelial growth factor (VEGF) is essential for angiogenesis, the formation of new blood vessels, and plays a crucial role in hair loss and androgenic alopecia. VEGF promotes blood vessel growth in the scalp, increasing blood flow to hair follicles and ensuring they receive vital oxygen, nutrients, and growth factors. By enhancing scalp microcirculation, VEGF supports hair follicle regeneration and maintenance. Therapies that leverage VEGF or stimulate its production aim to improve nutrient supply to follicles, promoting natural hair growth and effectively addressing hair loss issues.8
vii) Platelet-derived growth factor: Platelet-derived growth factor (PDGF) is vital
for hair follicle health and regeneration. Found in platelet granules, PDGF stimulates the proliferation of dermal papilla cells and fibroblasts, which are crucial for maintaining robust hair follicles. It also has antiinflammatory effects, helping to reduce scalp inflammation linked to conditions like androgenic alopecia. In clinical settings, PDGF is used in therapies such as plateletrich plasma (PRP) treatments to enhance hair follicle activity, stimulate growth, and improve hair quality, highlighting its potential in combating hair loss and promoting healthier hair growth.9
Apart from Growth Factor
Concentrate (GFC), various treatments are available for addressing hair loss and promoting regrowth. Finasteride, an oral medication, treats androgenic alopecia by inhibiting 5-alpha reductase, reducing the conversion of testosterone to dihydrotestosterone (DHT). Minoxidil, a topical treatment, enhances blood flow to hair follicles by dilating scalp blood vessels. Spironolactone, particularly effective for women with androgenic alopecia, blocks androgen receptors and inhibits DHT production in the adrenal glands and ovaries. Low-level laser therapy (LLLT) and Lightemitting diode (LED) therapy are non-invasive options that use specific wavelengths of light to stimulate cellular metabolism and blood circulation, promoting hair regrowth. Mesotherapy involves injecting a blend of vitamins, minerals,
and amino acids into the scalp, nourishing follicles and enhancing circulation. Exosomes, released by stem cells, contain proteins, lipids, and nucleic acids that stimulate hair follicle cells, promoting cellular activity and proliferation. Microneedling creates microscopic punctures in the scalp, enhancing blood flow and nutrient delivery to follicles, and triggering the release of growth factors like PDGF and VEGF, which support hair growth. Hair transplantation, through techniques like Follicular Unit Transplantation (FUT) and Follicular Unit Extraction (FUE), relocates hair follicles from donor areas to thinning or balding areas, restoring density and natural growth. Lastly, fibroblast growth factors (FGFs) stimulate dermal papilla cells and keratinocytes, essential for maintaining healthy follicles and promoting hair growth.10, 11,12,13
Discussion
Hair loss disorders, while not life-threatening, significantly impact the quality of life for affected individuals. The global market for hair growth-promoting agents is substantial, driven by the demand for effective treatments like minoxidil, which promotes hair follicle transition from telogen to anagen stages but can cause adverse dermatological effects such as dryness and irritation. Finasteride is effective for androgenic alopecia in males but not recommended for females due to potential side effects.
Therefore, there is a critical need for new hair growthpromoting drugs. Various growth factors such as FGF1, FGF-2, FGF-7, FGF-10, IGF-1, IGF-2, and EGF have shown promise in promoting hair cell proliferation and regeneration both in laboratory settings and animal models. Studies have demonstrated that EGF and TGF-B stimulate hair cell regeneration in avian utricles, while FGF-2 and IGF-1 have facilitated hair cell regeneration in rat utricular models. KGF has been noted for its protective effects on hair follicles against damage induced by UV irradiation and other agents. Additionally, FGF-1, FGF-2, and EGF have been found to maintain high proliferation and multipotent potential in human hair folliclederived mesenchymal stem cells.14
Injections utilizing Growth Factor Concentrate (GFC) effectively stimulate hair growth by fortifying existing hair, prolonging the anagen phase of hair follicles, and transforming vellus hairs into terminal hairs. This treatment can attenuate further hair loss by delivering essential growth factors directly to the scalp. However, GFC therapy may not suit advanced hair loss, and patient eligibility can be restricted by medical conditions or regulatory factors. Administered by qualified professionals under standardized protocols, GFC therapy is minimally invasive and generally welltolerated, though minor side effects like temporary pain or
swelling may occur. The therapy is particularly suited for early to moderate hair thinning or androgenic alopecia, offering a targeted approach compared to topical treatments. Unlike medications such as minoxidil or finasteride, which require ongoing use, GFC therapy aims to rejuvenate hair follicles and improve overall follicular health, potentially yielding longerlasting outcomes. While individual responses vary and multiple sessions may be necessary, GFC therapy enhances scalp health and hair density with minimal discomfort and rapid recovery, making it a favorable, less invasive alternative to hair transplantation.However, it is essential to recognize that individual responses to this treatment can vary significantly. Optimal outcomes depend on factors such as the selection of appropriate growth factors, the timing of treatment sessions. Therefore, consulting with a practitioner experienced in growth factor treatment for hair loss is crucial to maximize therapeutic benefits.1,10
References
1. Steward EN, Patel H, Pandya H, et al. Efficacy of Platelet-Rich Plasma and Concentrated Growth Factor in Treating Androgenetic Alopecia - A Retrospective Study. Ann Maxillofac Surg. 2020;10(2):409-416. doi:10.4103/ ams. ams_154_19.
2. Singh S, Muthuvel K. Practical Approach to Hair Loss Diagnosis. Indian J Plast Surg. 2021; 54(4):399-403. Published 2021 Dec 27. Doi: 10.1055/ s-0041-1739240
3. Paichitrojjana A, Paichitrojjana A. Platelet Rich Plasma and Its Use in Hair Regrowth: A Review. Drug Des Devel Ther. 2022;16:635-645. Published 2022 Mar 10. doi:10.2147/ DDDT. S356858.
4. Shin SH, Koh YG, Lee WG, Seok J, Park KY. The use of epidermal growth factor in dermatological practice. Int Wound J. 2023;20(6): 2414-2423. doi:10.1111/ iwj.14075.
5. Lin WH, Xiang LJ, Shi HX, et al. Fibroblast growth factors stimulate hair growth through β-catenin and Shh expression in C57BL/6 mice. Biomed Res Int. 2015; 2015:730139. doi:10.1155/ 2015/ 730139.
6. Trüeb RM. Further Clinical Evidence for the Effect of IGF-1 on Hair Growth and Alopecia. Skin Appendage Disord. 2018;4(2):90-95. doi:10.1159 / 000479333.
7. Shin H, Yoo HG, Inui S, et al. Induction of transforming growth factor-beta 1 by androgen is mediated by reactive oxygen species in hair follicle dermal papilla cells. BMB Rep. 2013;46(9): 460-464. doi:10.5483/ bmbrep.2013.46.9.228.
8. Yano K, Brown LF, Detmar M. Control of hair growth and follicle size by VEGF-mediated angiogenesis. J Clin Invest. 2001;107(4) :409417. doi:10.1172/ JCI11317
9. González R, Moffatt G, Hagner A, et al. Plateletderived growth factor signaling modulates adult hair follicle dermal stem cell maintenance and self-renewal. NPJ Regen Med. 2017;2:11. Published 2017 Apr 14. doi:10.1038/ s41536017-0013-4
Conclusion
Growth factor concentrate represents a promising advancement in the field of hair restoration. Its ability to harness the body's natural healing mechanisms offers hope to those experiencing hair loss, providing a potential solution that goes beyond conventional treatments. As research continues to refine this therapy, GFC holds the promise of improving outcomes and restoring confidence for individuals seeking effective hair regrowth solutions.
10. Nestor MS, Ablon G, Gade A, Han H, Fischer DL. Treatment options for androgenetic alopecia: Efficacy, side effects, compliance, financial considerations, and ethics. J Cosmet Dermatol. 2021;20(12):3759-3781. doi:10.1111 / jocd.14537.
11. Woo J, Suh W, Sung JH. Hair Growth Regulation by Fibroblast Growth Factor 12 (FGF12). Int J Mol Sci. 2022;23(16):9467. Published 2022 Aug 22. doi:10.3390/ ijms23169467
12. Yano K, Brown LF, Detmar M. Control of hair growth and follicle size by VEGF-mediated angiogenesis. J Clin Invest. 2001;107(4): 409417. doi:10.1172/ JCI11317
13. González R, Moffatt G, Hagner A, et al. Platelet-derived growth factor signaling modulates adult hair follicle dermal stem cell maintenance and self-renewal. NPJ Regen Med. 2017;2:11. Published 2017 Apr 14. doi:10.1038/ s41536-017-0013-4
14. Lin WH, Xiang LJ, Shi HX, et al. Fibroblast growth factors stimulate hair growth through β-catenin and Shh expression in C57BL/6 mice. Biomed Res Int. 2015;2015: 730139. doi:10.1155/ 2015 / 730139
Fat Transfer for Breasts, Buttocks, Calves and Face: Get Curves in all the Right Places
Fat transfer, or fat grafting, is an increasingly popular aesthetic procedure that redistributes adipose tissue to enhance areas like the breasts, buttocks, calves, and face. This technique allows individuals to use unwanted fat from "problem areas" to achieve naturallooking volume and contour. It effectively reduces deep lines, wrinkles, and acne scars while providing a customizable alternative to implants, especially for enhancing breast symmetry. Key benefits include minimal rejection risk and seamless integration with
surrounding tissues, though candidates must have sufficient fat to harvest. The preparation of fat is critical for long-term success, making the process more time-consuming and potentially more expensive than traditional fillers. While fat grafting carries risks, including inflammatory responses and irregularities, it is essential to consult a board-certified plastic surgeon experienced in this procedure for optimal results.
Enhancing Sexual Health Histories in Dermatology: A Comprehensive Modern Approach for Diverse Populations.
According to the CDC's 2022 STI Surveillance Report, sexually transmitted infections (STIs) have increased by 1.9% over the past five years, highlighting an ongoing public health concern, particularly among LGBTQ+ individuals—especially men who have sex with men—and racial or ethnic minority groups. This heightened incidence may reflect disparities in access to quality sexual health care rather than solely sexual behaviors, as evidenced by data indicating that Black individuals report less frequent oral and anal sex yet have higher STI prevalence compared to Hispanic and White populations. Education regarding STIs, their symptoms, and complications remains insufficient among adolescents and adults, and dermatologists frequently encounter STIs with cutaneous manifestations, such as mpox, syphilis, herpes, and HPV. It is crucial for dermatologists to feel confident in obtaining a comprehensive sexual health history, despite limited training on sexual and gender minority issues in medical education and residency programs. The CDC's 5 P's framework—Partners, Practices, Protection from STIs, Past history of STIs, and Pregnancy plans—provides a structured approach to gather sexual health histories in a trauma-informed manner. Additionally, inclusive language that avoids gender assumptions can facilitate patient communication. Recognizing the diversity of sexual identities and practices is essential, as STI risk varies among different sexual orientations and relationship structures. Research indicates that monogamous individuals do not necessarily report lower STI rates compared to those in consensually non-monogamous relationships, underscoring the importance of thorough sexual health assessments. Furthermore, dermatologists can enhance their evaluations by integrating clinical findings with social history, such as travel or participation in high-risk activities, to better inform STI risk assessments. As STIs continue to rise, it is imperative for dermatologists to adopt comprehensive sexual health histories, employing open-ended, nonjudgmental questions to provide culturally competent care, especially for sexual minorities, while emphasizing the importance of education and prevention strategies, including vaccination and regular screening for STIs.