22, Shreeji Bhavan, 275-279, Samuel Street, Masjid Bunder (W), Mumbai-4000 03, INDIA.
EMAIL: theaestheticiansjournalindia@gmail.com
Website: theaestheticiansjournal.com
TEL: +91 22 2345 1404 +91 22 2345 5844
Printed, Published, Edited and Owned by Dom Daniel
Printed at Swastik Printer, Gala No.9 & 10, Vishal Industrial Estate, Bhandup (West), Mumbai- 400078. Published at 22 Shreeji Bhavan, 275/279, Samuel Street, Masjid Bunder (West), Mumbai - 400003. India.
“The Aestheticians Journal” takes no responsibility for unsolicited photographs or material ALL PHOTOGRAPHS, UNLESS OTHERWISE INDICATED, ARE USED FOR ILLUSTRATIVE PURPOSE ONLY.
Views expressed in this Journal are those of the contributors and not of the publisher. Reproduction in whole or in parts of texts or photography is prohibited. Manuscripts, Photographs and art are selected at the discretion of the publisher free of charge (advertising excluded). Whether published or not, no material will be returned and remains the property of the publishing house, which may make use of it as seen fit. This may include the withdrawal of publication rights to other publishing houses.
All rights reserved. Reproducing in any manner without prior written permission prohibited.
Published for the period of September -2024
Genetic Skin Disorders
Genetic skin disorders, such as epidermolysis bullosa, ichthyosis, and neurofibromatosis, represent a significant challenge in dermatology due to their complexity, chronic nature, and profound impact on patients' lives. With the increased ability to diagnose genetic skin disorders accurately, genetic counselling has become an essential component of patient care. Counselling provides patients and their families with crucial information about the nature of the disorder, inheritance patterns, recurrence risks, and available management options. It also supports patients in making informed decisions about family planning, prenatal testing, and early interventions. Genetic counsellors play a vital role in helping patients navigate the emotional and psychological challenges associated with these lifelong conditions.
The integration of advanced genetic testing, personalized medicine, and innovative therapies is reshaping the landscape of care for patients with genetic skin disorders. Continued research is essential to refine these therapies, understand long-term safety and efficacy, and make them accessible to a broader patient population. Collaboration among dermatologists, geneticists, researchers, and patient advocacy groups will be crucial in translating these scientific advancements into real-world clinical practice.
In this issue, we have articles on Thread Lift: A Non-Surgical Solutions for Facial Rejuvenation, hair transplant and Sarcoidosis.
HOPE YOU HAVE A GREAT READ
Thanks & Cheers
- Dom Daniel
Executive Editor & Publisher
Rare Presentations of Sarcoidosis:
A Case Report of 50 Years Male
Dr. Piyali Banerjee, MBBS, DVDL
Dr. Surajit Gorai, MBBS (HONS), MD (Gold Medalist), DNB, MNAMS
Dr. Kinnor Das, MBBS, MD
Successful Hair Restoration: A Case Report on Hair Transplant Part-II
Dr. Avinash Agrawal, MS (General Surgery)
Thread Lift: A Non-Surgical Solutions for Facial Rejuvenation
Dr. Monica Jacob, MBBS, MD, DPB, DAD
Editorial Board
Dr. Piyali Banerjee
MBBS, DVDL [Rims, Ranchi]
Consultant Dermatologist, St Barnabas Hospital and Raj Hospital, Ranchi, India
Consultant Dermatologist, Apollo Clinic, Silchar, Assam
Introduction
Sarcoidosis is a multisystemic granulomatous disease characterized by the presence of non-caseating granulomas. This condition primarily affects young adults and typically presents with reticular opacities in the lungs and bilateral hilar lymphadenopathy. Additionally, it may involve various other sites such as the eyes, skin, joints, and, in some instances, the reticuloendothelial system, musculoskeletal system, exocrine glands,
heart, kidney, and central nervous system.1 Its clinical manifestations ranges a wide spectrum, such as persistent coughing, shortness of breath, cutaneous lesions like papules, nodules, plaques, and infiltrated scars. Due to these overlapping symptoms with other diseases (tuberculosis, certain immune disorder) it is recognized as one of the "Great Imitators" in Dermatology.1 While many individuals’ exhibit symptoms, some may remain asymptomatic. The peak age for the beginning of symptoms
of sarcoidosis is around 40 years of age with a high prevalence among females which is approximately 2 or 3 cases for every one case in males.2
The etiology of sarcoidosis is remains unknown, prompting various hypotheses. These include an aberrant host response to infectious agents like Mycobacterium paratuberculosis, triggering a cell-mediated immune reaction resulting in granuloma formation and subsequent release of cytokines. Genetic predisposition and environmental factors are also implicated. Dysregulation of cell-mediated immunity, particularly involving CD4+ T lymphocytes, leads to cytokine overproduction, notably tumor necrosis factoralpha (TNF-a), interleukin-2 (IL-2), and interferon-gamma (IFN-y), contributing to granuloma formation and sustained inflammation characteristic of sarcoidosis. B lymphocyte hyperactivity and increased immunoglobulin production further exacerbate the condition, with active sarcoidosis often associated with elevated plasmatic immunoglobulin levels. Elevated angiotensinconverting enzyme (ACE) levels, correlating with heightened soluble HLA class I antigen levels in serum, underscore the intricate immunological dysregulation underlying cutaneous sarcoidosis.3
Sarcoidosis presents with a spectrum of manifestations based on the organs involved, warranting vigilant evaluation
by healthcare professionals. Pulmonary involvement stands as the most prevalent manifestation, characterized by symptoms like persistent dry cough, dyspnea, chest pain, wheezing, and night sweats. Lupus Pernio which is a type of cutaneous sarcoidosis that is characterised by the presence of infiltrated erythematoviolaceous plaques affecting mainly head and neck predominantly on the nose, ears, lips and cheeks. It is a marker of chronic sarcoidosis with risk of involvement of other internal organs. Ocular involvement may manifest as uveitis, conjunctivitis, dry eyes, blurred vision, and eye pain. Enlargement of lymph nodes, notably in cervical, axillary, or inguinal regions, signifies lymphatic involvement. Hepatic and splenic manifestations entail hepatomegaly, splenomegaly, and abnormal liver function tests. Cardiac involvement, albeit less common, manifests as cardiomyopathy, arrhythmias, and pericardial effusion. Neurological symptoms, though rare, include cranial nerve palsies, peripheral neuropathy, meningitis, seizures, and cognitive impairment. Given the potential for mimicking other diseases and the presence of asymptomatic cases, a thorough assessment by healthcare professionals is indispensable for accurate diagnosis and management. Symptomatic patients with sarcoidosis often experience a diminished quality of life, frequently accompanied by psychiatric comorbidities
such as depression and anxiety.4
Diagnosing sarcoidosis often involves a combination of clinical evaluation, imaging studies (such as X-rays or CT scans), laboratory tests, and sometimes tissue biopsy to confirm the presence of granulomas. The hallmark histopathological feature is the presence of noncaseating granulomas, characterized by macrophages, multinucleated giant cells, epithelioid cells, lymphocytes, monocytes, mast cells, and fibroblasts.4, 5 Treatment for sarcoidosis aims to manage inflammation, relieve symptoms, and mitigate organ damage. In numerous instances, treatment may not be required as sarcoidosis can spontaneously resolve. However, when treatment is warranted, corticosteroids are commonly prescribed to suppress the immune response and reduce inflammation. Other immunosuppressive agents may be used for individuals who do not respond to or cannot tolerate corticosteroids.6
The advancements in research have improved our understanding of the disease; further studies are needed to unravel its complex pathogenesis and develop more targeted treatment approaches. Early recognition and appropriate management are crucial for optimizing outcomes and improving the quality of life for individuals living with sarcoidosis.
Case Report
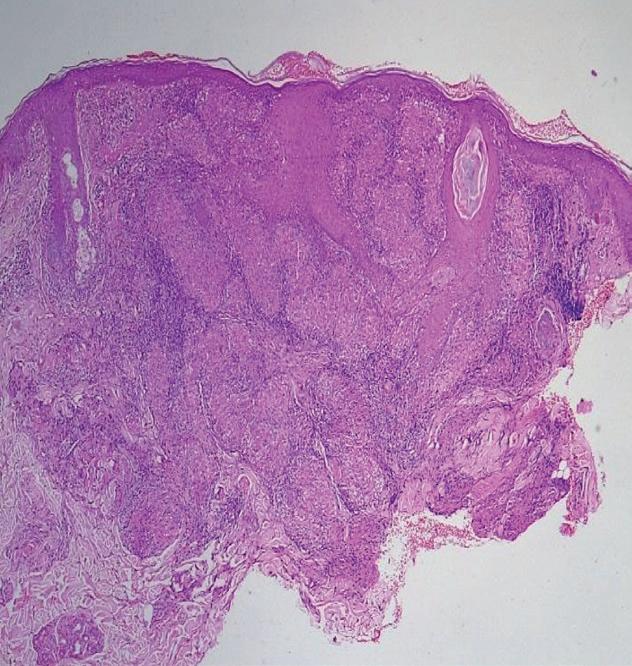
A 50-year-male patient who is on anti-hypertensive and hypoglycemic drugs from last 14 years, presented in outpatient department with a reddish elevated lesion side on both sides of the face with slight itching from last 6 months. He was in Gulf country from last 12 years and returned India on January 2020 following covid outbreak. On March 2020 he noticed a small papule on the right side of the cheek which slowly grow to form a plaque. After application of topical steroids and oral antibiotics usage as prescribed by the general physician he got symptomatically improved. But the lesion reappeared on discontinuation of medicines. From last 6 months he also started developing papule on the left side of the cheek. There is no history of joint pain or any systemic complains, without any mucosal or nail involvement. On examination, right cheek–a 3 cm x 3 cm plaque with induration, mild scaling with erythema is seen [in Figure1]. On the left side of the cheek:- 1cm x 1cm plaque present with slight scaling and erythema near the root of the ear [Figure 2]. His routine blood tests are normal, HIV 1 &2 and VDRL non-reactive, ACE levels are within normal limits {9 u/l}.
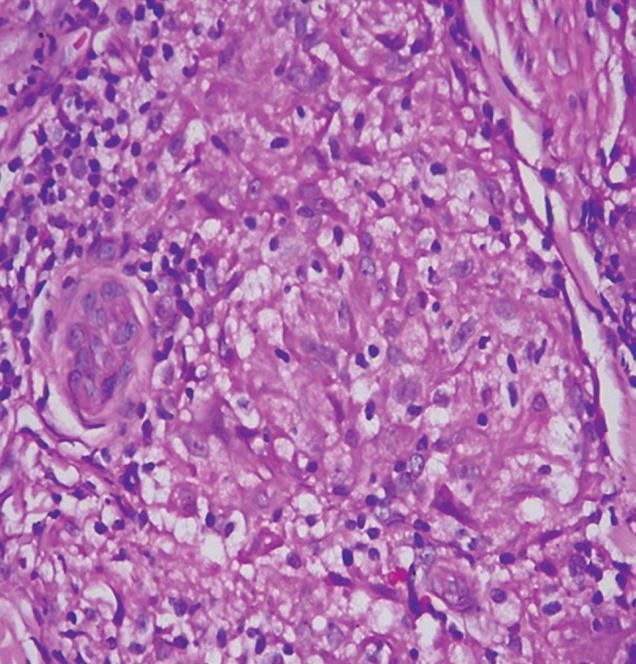
Histopathological examination (HPE) shows epidermis of variable thickness with focal areas of acanthosis and atrophy [Figure 3]. The entire width of dermis shows well delineated granuloma, some of which shows presence of lymphocytes at the periphery
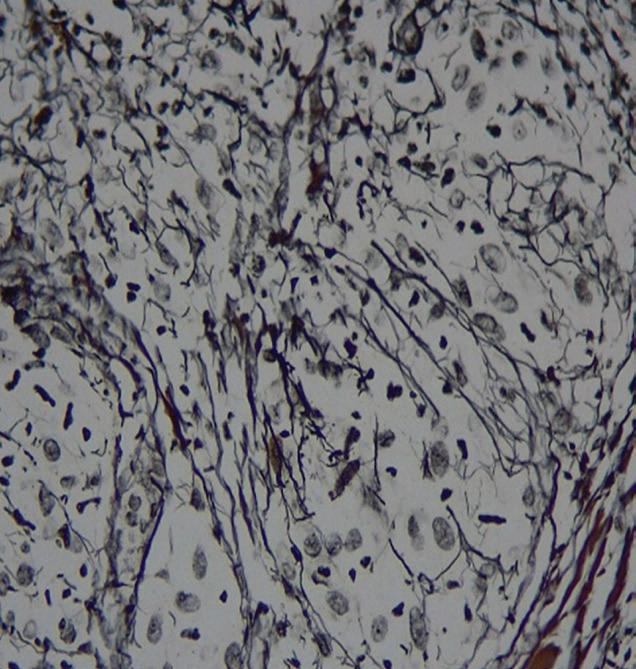
[Figure 4]. Reticulin stain shows reticulin fibres traversing inside the granulomas [Figure 5]. Fite Faraco stain is noncontributory. On the basis of above findings a final diagnosis of Lupus Pernio was made. The patient was started on oral corticosteroids at dosage of 40 mg /day tapered over 3 weeks.
After 1 month of oral and topical corticosteroids moderate flattening of plaque and also decrease in erythema was seen.
1
Figure 3 : HPE on 40X showing non caseating granuloma
Figure 4 : HPE on 400X showing epithelioid granuloma consisting of langhans giant cell
Diagnosis
The diagnostic approach to sarcoidosis involves symptomatology, physical examination findings, and
Figure
: Showing plaque on the right side of the face
Figure 2 : Showing plaque on the left side of the face
Figure 5 : RETICULIN STAIN – Intact black reticulin fibres
various diagnostic tests aimed at confirming granulomatous pathology and evaluating disease severity. Healthcare providers conduct a thorough medical history, exploring symptoms and potential environmental exposures like insecticides or mold. During the physical examination, assessments include evaluating body temperature for systemic inflammation, palpating lymph nodes, spleen, or liver for signs of enlargement suggestive of organ involvement, auscultating lung fields to detect abnormal sounds indicative of pulmonary sarcoidosis, and inspecting the skin for cutaneous manifestations, particularly focusing on areas prone to rashes or lesions, suggestive of cutaneous sarcoidosis.4, 5
Chest X-rays are pivotal in diagnosing sarcoidosis, identifying pulmonary and cardiac granulomas or scarring. Pulmonary sarcoidosis often presents with bilateral hilar lymphadenopathy and reticulonodular opacities on these images. Lung function tests, using the Siltzbach classification system, categorize the severity of pulmonary sarcoidosis based on chest X-ray findings, ranging from Stage 0 to Stage 4. Stage 0 indicates a lack of pulmonary manifestations, Stage 1 indicates the presence of granulomas solely within the lymph nodes. In Stage 2, granulomas are observed in both the lymph nodes and the lungs. Stage 3 denotes exclusive detection of granulomas within the lungs. While, Stage 4 signifies
pulmonary fibrosis, reflecting permanent lung scarring. These classifications guide treatment and monitoring. Additionally, chest X-rays can detect cardiac involvement such as cardiomegaly or pulmonary hypertension, prompting further investigations.4, 5
Tissue biopsy procedures such as bronchoscopy, skin biopsy, or lymph node biopsy play a pivotal role in confirming the presence of granulomas, which is essential for establishing a precise diagnosis of sarcoidosis. During bronchoscopy, a flexible tube equipped with a camera is inserted through the mouth or nose into the airways, allowing visualization and sampling of tissue from the lungs or nearby lymph nodes. Skin biopsies involve the removal of a small piece of skin tissue for examination under a microscope, typically from skin lesions suggestive of cutaneous sarcoidosis. Lymph node biopsies, obtained through surgical excision or needle aspiration, provide samples from enlarged lymph nodes for histological analysis. Analysis of biopsy specimens reveals the characteristic non-caseation granulomas, consisting of aggregates of immune cells, including macrophages, lymphocytes, and epithelioid cells, surrounded by fibrous tissue.4, 5
Blood tests provide valuable insights into blood counts, hormone levels, and kidney function, offering additional information about the body's response to sarcoidosis. Imaging modalities such as MRI or ultrasound allow
visualization of granulomas or inflammation in various organs, including the heart, eyes, or lymph nodes. Specialized tests, like neurological evaluations and eye examinations, are employed to assess potential nervous system or ocular involvement.4, 5 Additionally, cardiac evaluations through tests like ECG, echocardiography, or cardiac MRI are crucial for detecting potentially life-threatening cardiac sarcoidosis.4, 5
The comprehensive diagnostic approach enables accurate analysis of sarcoidosis, facilitates determination of disease extent and severity, and tailors treatment plans to individual patient needs.
Treatment
Corticosteroids: :::
Corticosteroids are the main treatment for sarcoidosis, suppressing cytokine production and granuloma formation. It suppresses cytokine production, including TNF-a and IFN-y, which contribute to granuloma formation. A typical starting dose is 20–40 mg/day, adjusted for severity. Higher doses may be needed for severe cases, but longterm use above 40 mg/day poses toxicity risks without added benefit. Lower doses, especially in pulmonary sarcoidosis, are effective and safer for maintenance therapy.6, 7
Corticosteroid- Sparing Medication:
• Methotrexate, ,,,,,,,,,,, azathioprine, leflunomide, and mycophenolate are frequently used as steroid-
sparing medications in the treatment of sarcoidosis. These drugs are employed when patients require prolonged therapy, have severe disease, or experience significant adverse effects from corticosteroids.6, 7
• Methotrexate: A folic acid antagonist, inhibits purine and pyrimidine metabolism, reducing cytokine production and inflammatory responses. It has demonstrated efficacy in improving symptoms and reducing corticosteroid requirements in pulmonary and extrapulmonary sarcoidosis.6, 7
• Azathioprine: An inhibitor of purine metabolism, decreases T and B cell production and promotes lymphocyte apoptosis, offering similar benefits to methotrexate in reducing corticosteroid dependency.6, 7
• Leflunomide: Leflunomide a dihydroorotase inhibitor, is often used as an alternative or adjunct to methotrexate. It inhibits dividing lymphocytes, leading to a steroid-sparing effect and symptom improvement, particularly in patients with progressive or refractory sarcoidosis.6, 7
• Mycophenolate mofetil (MMF): It inhibits purine nucleotide synthesis in lymphocytes, reducing autoantibody production and inflammatory responses. MMF has shown effectiveness in improving lung function and reducing corticosteroid use in sarcoidosis, especially in cases of neurosarcoidosis.6, 7
Anti-malarial : Chloroquine and hydroxychloroquine are commonly employed in the
treatment of sarcoidosis, with hydroxychloroquine being the preferred choice due to its improved safety profile. Hydroxychloroquine exerts its therapeutic effects through various mechanisms, including interference with antigen presentation, inhibition of T cell activation, modulation of toll-like receptor signaling, and reduction of inflammatory cytokines by T and B cells. This medication has demonstrated efficacy, particularly in managing cutaneous manifestations, hypercalcemia, and certain cases of neurosarcoidosis.6, 7
Tumor Necrosis Factor
(TNF) Antagonists: TNF-a inhibitors, such as infliximab and adalimumab, are utilized in sarcoidosis treatment due to their ability to target specific inflammatory pathways, thereby reducing inflammation and alleviating symptoms in affected organs. These biologic agents offer an effective therapeutic approach for managing sarcoidosis, particularly in cases where conventional treatments like corticosteroids are ineffective or poorly tolerated. Additionally, rituximab, another biologic agent, presents a viable alternative to TNF-y inhibitors, especially in the context of cardiac sarcoidosis. By targeting B cells involved in the immune response, rituximab helps mitigate inflammation and prevent further organ damage, demonstrating its utility in addressing the complexities of sarcoidosis pathology.6, 7
Cyclophosphamide: :::::::::
Cyclophosphamide (CYC) has been successfully used for both refractory or
severe cardiac and CNS sarcoidosis in retrospective series. Cyclophosphamide is typically given intravenously in pulses ranging from 500 to 1200 mg every 3 to 4 weeks. Cyclophosphamide should be reserved for severe and refractory sarcoidosis when no other acceptable therapeutic alternative is available, including tumor necrosis factor inhibitors (TNFi), are available or effective.6, 7
Intravenous immunoglobulin (IVIG) therapy represents a potential treatment option for sarcoidosis-associated small fiber neuropathy, a rare neurological complication arising from sarcoidosis. IVIG therapy involves the administration of concentrated antibodies obtained from pooled plasma of thousands of donors. These antibodies contain a diverse array of immunoglobulins, including IgG, which play a crucial role in modulating the immune response and reducing inflammation within the nervous system. By delivering a high concentration of immunoglobulins, Intravenous immunoglobulin therapy aims to regulate aberrant immune activity and alleviate the inflammatory processes implicated in sarcoidosisassociated small fiber neuropathy.6, 7
Adrenocorticotropic ........ hormone (ACTH) : This medication operates by stimulating multiple melanocortin receptors and inducing endogenous glucocorticoid secretion. Through this mechanism, corticotropic effectively
suppresses the immune response and reduces inflammation, contributing to its potential efficacy in managing sarcoidosis symptoms.6, 7
Implantable CardioverterDefibrillator (ICD) : For individuals diagnosed with cardiac sarcoidosis, where the risk of sudden cardiac death due to arrhythmias is significant, the implantation of an Implantable CardioverterDefibrillator is a crucial intervention. This device serves a dual purpose: monitoring heart rhythms continuously and delivering therapeutic shocks when lifethreatening arrhythmias occur. By constantly monitoring the heart's electrical activity, the implantable cardioverterdefibrillator can promptly detect abnormal rhythms such as ventricular tachycardia or ventricular fibrillation. When such arrhythmias are detected, the device delivers an electrical shock to restore normal heart rhythm, thereby preventing sudden cardiac death.6, 7
Standard Cardiological Care:
Heart Failure Medications:
Patients diagnosed with cardiac sarcoidosis and accompanying ventricular dysfunction often require a combination of medications to manage their condition effectively. Standard heart failure medications such as diuretics, B-blockers, and angiotensin-converting enzyme (ACE) inhibitors are commonly prescribed. Diuretics help alleviate fluid retention by increasing urine production, thereby reducing the workload on the heart.
Beta -blockers work by blocking the effects of stress hormones like adrenaline, which can help slow the heart rate and improve its efficiency. Angiotensin-converting enzyme inhibitors help relax blood vessels and lower blood pressure, reducing the strain on the heart and improving its function.6, 7
Antiarrhythmic ............
Medications and Catheter
Ablation:
Antiarrhythmic medications are prescribed to help stabilize the heart's rhythm and prevent the occurrence of abnormal heartbeats. In some cases, catheter ablation procedures may be recommended. During catheter ablation, a thin, flexible tube is inserted into the heart through a blood vessel, and targeted areas of abnormal electrical activity are destroyed to restore normal heart rhythm. These interventions aim to reduce the risk of sudden cardiac death and improve the overall prognosis for patients with cardiac sarcoidosis.6, 7
Determining the optimal treatment plan for a patient with sarcoidosis involves considering various factors, including disease severity, clinician familiarity with available therapies, potential side effects, and patient preferences. Age, alcohol consumption, pregnancy likelihood, current medications, and coexisting conditions such as diabetes, liver disease, or kidney dysfunction can influence treatment decisions. Due to the likelihood of multiple medications being part of the patient's regimen, it's essential to assess potential
drug interactions when selecting medications.
Discussion
Sarcoidosis is a systemic disease of unknown origin which is characterized by a T-helper cell response involving CD-4 lymphocytes and activated macrophages that aggregate in affected organs.1 In sarcodoisis approximately 10% of cases have a familial component. Mortality, primarily attributed to pulmonary complications, ranges from 2% to 5%, with substantial morbidity due to chronic sarcoidosis-related complications. Sarcoidosis presents with varying onset and manifestations depending on the involved organ system, necessitating a high index of suspicion for diagnosis.8 Sarcoidosis typically exhibits a higher incidence among females, with a majority of cases affecting women. However, the presented case is unique in its own as it is present in a male with bilateral erythematous plaque over the cheek with normal ACE levels, without any pulmonary involvement. As the patient is a known case of diabetes and hypertension, hence immunity dysregulation can be a causative factor along with environmental triggers as the person was in Gulf countries for such a unique presentation.
Diagnosis relies on three primary criteria: Consistent clinical presentation, histopathological evidence of non-caseating granulomas, and exclusion of alternative granulomatous diseases. Tuberculosis and other granulomatous diseases were ruled out through
negative tuberculin skin testing and sputum acid-fast bacilli stain.4 Chest X-ray abnormalities are present in over 90% of patients, but Computed Tomography is commonly used for further evaluation due to increased sensitivity in detecting parenchymal abnormalities and lymphadenopathy. Symmetric involvement on imaging can help differentiate sarcoidosis from other conditions. In our patient, CT findings indicated symmetric involvement, supporting the diagnosis of sarcoidosis.5
Sarcoidosis treatment is tailored to the patient's symptomatic status and disease severity. Asymptomatic Stage I patients typically require no treatment but necessitate annual follow-up to monitor disease progression. For symptomatic individuals in Stages II or III, systemic corticosteroids represent first-line therapy, with close monitoring every three months to assess response and adjust treatment as needed. Methotrexate is commonly employed as a second-line option for pulmonary sarcoidosis, while azathioprine, leflunomide, and TNF-alpha inhibitors like infliximab are reserved for patients intolerant to corticosteroids or experiencing refractory symptoms. Severe pulmonary involvement or progression to pulmonary fibrosis warrants prompt evaluation for lung transplantation. Despite treatment efforts, a significant proportion of sarcoidosis patients experience spontaneous remission;
however, approximately 1020% develop a chronic form of the disease, with a mortality rate ranging from 1-5%.6, 7
An interprofessional healthcare team comprising various specialists is essential for comprehensive disease management, emphasizing patient education, close monitoring, and proactive intervention to optimize outcomes and mitigate potential complications. Regular follow-up, multidisciplinary collaboration, and vigilant monitoring of disease progression and treatment response are integral components of sarcoidosis management strategies.
Conclusion
In conclusion, sarcoidosis presents a diagnostic challenge, especially in elderly patients, and requires a high degree of suspicion and familiarity with imaging features for accurate diagnosis and evaluation. While emergency clinicians must remain vigilant for deadly causes of chest pain, they should also recognize the significance of diagnosing sarcoidosis early, given its potential for longterm morbidity. Emergency department management should involve proper specialty consultation and follow-up for symptomatic patients, ensuring comprehensive care. Treatment of sarcoidosis remains complex and nonstandardized, highlighting the need for further research to inform clinical guidelines and develop more effective treatment regimens. Advancements in understanding the etiology and pathophysiology of
sarcoidosis may lead to preventive or curative interventions in the future, potentially involving personalized medicine approaches based on pharmacogenomics and disease phenotype. Overall, ongoing research efforts are crucial for improving outcomes and quality of life for patients with sarcoidosis.
2. Chen ES, Moller DR. Etiology of sarcoidosis. Clin Chest Med. 2008;29(3):365-vii. doi:10.1016/ j.ccm. 2008.03.011
3. Hamzeh N, Steckman DA, Sauer WH, Judson MA. Pathophysiology and clinical management of cardiac sarcoidosis. Nat Rev Cardiol. 2015;12(5):278-288. doi:10.1038/ nrcardio. 2015.22
4. Sève P, Pacheco Y, Durupt F, et al. Sarcoidosis: A Clinical Overview from Symptoms to Diagnosis. Cells. 2021;10(4):766. Published 2021 Mar 31. doi:10.3390 / cells10040766
5. Govender P, Berman JS. The Diagnosis of Sarcoidosis. Clin Chest Med. 2015;36(4):585-602. doi:10.1016 / j.ccm.2015.08.003
7. Gerke AK. Treatment of Sarcoidosis: A Multidisciplinary Approach. Front Immunol. 2020;11:545413. Published 2020 Nov 19. doi:10.3389 / fimmu.2020.545413
8. Truong J, Ashurst J. A Case Report of Pulmonary Sarcoidosis: An Uncommon Cause of Chest Pain. Clin Pract Cases Emerg Med. 2020;4(4): 645-648. doi:10.5811 / cpcem.2020.7.48310
Fillers, Hyaluronidase Relieve Orofacial Changes in Patients with Scleroderma
Orofacial changes can refer to a variety of changes that can affect the face and mouth. Recent research has shown that hyaluronidase injections can help improve orofacial changes commonly experienced by patients with scleroderma. In the study researchers asked 303 patients with systemic sclerosis (scleroderma) what bothered them most about their disease from an aesthetic standpoint: Orofacial features, such as thin lips and mouth furrows, or non-facial features, such as fingertip ulceration and waxy changes to the skin. Respondents expressed significant concern about specific orofacial features, including thin lips (73%), mouth furrows (80%), loss of facial lines (68%), and a smaller, tighter mouth (77%).
Researchers reported the case of a 53-year-old woman treated with hyaluronidase for scleroderma-induced microstomia. After four visits over 7 months and a total hyaluronidase dose of 470 IU, the patient reported an improved Mouth Handicap in Systemic Sclerosis (MHISS) score (38 of 48); subjective improvement of symptoms, including greater ease in eating and undergoing dental treatment; and improved mouth closure. Researchers published a cohort study of four women between the ages of 43 and 61 with autoimmune sclerosing conditions that resulted in oral microstomia. Following hyaluronidase injections, all improved in mouth opening capacity and MHISS, with change stabilizing between three and five treatments. In general, patients needed three to four treatments to reach peak effect, and then they reached a plateau. It wasn’t that the treatment wasn’t working anymore, but it was because their oral aperture had gotten to a size of around 5 cm, which is clinically normal. Interestingly, we found that if the patient’s disease flared and their microstomia started to return, when you rechallenged them, they continued to respond. So, patients can continue to use this treatment over time.
In a separate case series of seven patients, researcher prospectively evaluated the effect of HA soft tissue filler for lip augmentation. Study participants experienced statistically significant increases in the difference between pre- and postinjection fullness in both upper and lower lips. Also, the mean posttreatment score fell between “much improved” (2) and “improved” (3) on both the Investigator Global Aesthetic Improvement Scale and the Subject Global Aesthetic Improvement Scale.
Support for Laser Treatment to Reduce NMSC Risk is Increasing
Laser technology has become increasingly important in various medical fields. The idea of using nonablative fractional lasers to reduce the risk of nonmelanoma skin cancer (NMSC) has gained support in recent years, and a key 2017 publication laid the groundwork for current approaches, according to researcher. Researcher demonstrated that geriatric skin responds to ultraviolet B (UVB) differently than young skin because of differences in insulin-like growth factor 1 (IGF-1) levels produced by dermal fibroblasts. As we age, our fibroblasts become senescent, inactive. “They don’t make as many growth factors, particularly IGF-1, and therefore we don’t stimulate the responses. We need more of our growth factors.
In later, separate work, of researcher and colleagues found that using dermabrasion or fractionated laser resurfacing to wound the skin can result in increased dermal IGF-1 levels and normalization of the abnormal pro-carcinogenic UV response associated with geriatric skin — a treatment that has the potential to prevent NMSC. That study “was the epiphany” for fostering interest among researchers in the field of lasers and medicine. In a retrospective cohort study, researcher and colleagues reviewed patients with a history of facial keratinocyte carcinoma (KC). The study population included 43 patients treated with either the 1927- or the 1550-nm nonablative fractional laser (NAFL) and 52 matched controls. The rate of subsequent facial KC development was 20.9% in NAFL-treated patients and 40.4% in controls (relative risk, 0.52, P = .049).
In an ongoing study, researcher and colleagues enrolled 15 patients aged ≥ 55 years to evaluate the restoration of physiologic features and biomarkers in skin treated with 25% trichloroacetic acid (TCA), plus the 1550-nm or 1927-nm NAFL. Four sites on the back were treated and biopsies were taken at baseline and at 3 months post treatment. The protocol involved TCA 25% to speckled frost, with the 1550-nm device set to level 6 at 70 mJ and the 1927-nm device set to level 8 at 20 mJ. Immunohistochemical stains are still pending; however, physiologic changes were noted. Three months after a single treatment, the 1927-nm treated areas showed statistically significant elongation of fibroblasts (consistent with younger fibroblasts) on histology. “Although not a large study, it supports the growing body of research that demonstrates we are improving the health of our patients’ skin with certain types of laser treatments, not just beautifying it,” researcher said.
A Light Face Moisturizer
Laminaria Digitata Extract
Prunus Amygdalus Dulcis
Lecithin
Ceramide-1
Ceramide-2
Ceramide-3
Ceramide-4
Ceramide-6II
Tocopheryl Acetate- Vitamin E
Prevent Dryness
Soothe Sensitive Skin
Help Fight Acne
Regulates skin barrier function
Reduces Trans-epidermal water loss
24 hrs Moisturization
For Products Enquires
feedback@amwillhealthcare.com
Atopic dermatitis
Xerosis
Ichthyosis
Suitable for sensitive skin
Anti-inflammatory effect
Strengthens the skin barrier
Hydagen- aquaporion offers 24 hrs moisturization
Hydagen Aquaporin
Sodium Huyaluronate
Ceramide Complex
Healianthus Annuus Sunflower Oil
Dimethicone
Tocopheryl Acetate
Successful Hair Restoration: A Case Report on Hair Transplant Part-II
Dr.
Avinash Agrawal
MS (General Surgery)
Hair Transplant Surgeon
Director, Acube Aesthetics Clinic, Mumbai
Treatment
The goal of therapeutic interventions is to safely and effectively utilize the mechanisms described above to enhance anagen phase, prolong catagen phase, and ultimately prevent or reverse miniaturization in alopecia to restore or maintain visible hair density. Finasteride and topical minoxidil are the most widely acknowledged treatments for hair loss. Other treatments that stimulate hair regrowth and target specific regulators involved in hair growth will be further elaborated below.
Finasteride
Finasteride is frequently employed post-hair transplant surgery to enhance and sustain the outcomes of the procedure. By inhibiting 5-alpha-reductase type 2 enzyme activity, finasteride impedes the conversion of testosterone to dihydrotestosterone (DHT). This mechanism is crucial because DHT is implicated in hair follicle miniaturization and subsequent hair loss in androgenetic alopecia (AGA). By reducing DHT
levels, finasteride helps maintain the viability and longevity of transplanted hair follicles, thereby promoting improved hair density and aesthetic results following transplantation.5
Minoxidil
Minoxidil is often utilized as a complementary treatment following hair transplantation to promote hair growth and enhance the overall outcomes of the procedure. It works by stimulating hair follicles, potentially extending the anagen (growth) phase of hair, and increasing blood flow to the scalp. This enhanced blood flow can support the nourishment of transplanted follicles, aiding their survival and promoting quicker healing post-surgery. It is generally recommended to start using minoxidil a few weeks after hair transplantation, once the scalp has sufficiently healed. Regular application as directed can help to accelerate the growth of transplanted hair and improve overall hair density in both the transplanted area and surrounding regions affected by hair loss.5
Prostaglandins
Prostaglandins are utilized in hair treatments primarily for their ability to influence hair growth cycles and promote hair regrowth. They are believed to extend the anagen (growth) phase of hair follicles, which can result in increased hair density and thickness over time. Additionally, prostaglandins are thought to stimulate hair follicle stem cells, enhance blood flow to the scalp, and create a favorable environment for hair growth. In clinical practice, prostaglandins are commonly used in topical formulations applied directly to the scalp. These treatments aim to rejuvenate miniaturized hair follicles, particularly in conditions like androgenetic alopecia (AGA) where hair loss is progressive. Prostaglandins may also complement other hair loss treatments, such as minoxidil or finasteride, to enhance overall efficacy in promoting hair regrowth and improving hair density.5
Cetirizine
Topical cetirizine has been explored for its potential in treating hair-related conditions, particularly its anti-inflammatory properties that could benefit conditions like alopecia areata. While cetirizine is primarily known as an oral antihistamine for allergies, its topical application aims to reduce scalp inflammation, which is often associated with hair loss. Cetirizine inhibit the release of histamine and other inflammatory mediators locally when applied to the scalp. This action could potentially help in
calming the immune response implicated in conditions like alopecia areata, thereby supporting hair follicle health and promoting regrowth.5
Redensyl
Redensyl is an ingredient known for its dual action on hair follicle stem cells, aiming to stimulate hair growth and reduce hair loss. It works by activating the hair follicle stem cells' division (proliferation) and by promoting the production of dermal papilla cells, which play a crucial role in hair follicle formation and growth. Redensyl is often included in topical formulations such as serums and shampoos designed to support hair growth and combat hair thinning.6
Capixyl
Capixyl is another active complex that combines biomimetic peptides with red clover extract. It works by targeting both the hair follicle and scalp environment to enhance hair anchorage, improve hair density, and reduce inflammation that can contribute to hair loss. Capixyl helps strengthen hair follicles, thereby reducing hair shedding and promoting thicker, healthier hair growth. It is commonly found in hair care products aimed at improving scalp health and combating hair loss.6
Procapil
Procapil is a combination of biotinoyl tripeptide-1, apigenin (a flavonoid derived from citrus fruits), and oleanolic acid (extracted from olive leaves). It targets the main causes of hair loss by increasing
blood flow to the scalp, reducing the production of DHT (dihydrotestosterone, a hormone linked to hair loss), and strengthening hair follicles. Procapil helps to prolong the hair growth phase (anagen phase), leading to thicker and stronger hair strands. It is often included in topical solutions and treatments for its beneficial effects on hair follicle health and hair growth promotion.6
Natural ingredients
Hair analysis highlights the importance of minerals (iron, oxygen, hydrogen, nitrogen, sulfur) for hair growth during the anagen phase, which involves increased skin blood vessel activity and angiogenesis. Vitamins, minerals, and herbal supplements regulate angiogenesis, potentially preventing alopecia. Iron supplementation supports hair growth. Niacin (vitamin B3), vitamin B complex, vitamin C, vitamin E, grape seed extract, rosemary oil, sage, nettles, and hibiscus rosasinensis enhance scalp blood flow. Biotin, antioxidants, zinc with grape seed extract support metabolic pathways. Green tea, ginkgo biloba, emu oil inhibit 5-alpha reductase, managing hair loss. Essential fatty acids (evening primrose oil, salmon oil) and amino acids (L-cysteine, L-methionine) improve hair texture and prevent dryness.5
Microneedling
Microneedling has emerged as a promising treatment for hair restoration by stimulating hair growth through multiple mechanisms. During
microneedling, small needles create micro-injuries in the scalp, triggering the release of growth factors and promoting the production of collagen and elastin. This process improves blood circulation to the scalp, enhancing nutrient delivery to hair follicles. Furthermore, the micro-injuries induced by microneedling activate the wound healing response, leading to the release of cytokines and growth factors that support hair follicle regeneration and proliferation. Microneedling also enhances the absorption and effectiveness of topical medications like minoxidil or growth factors when applied immediately after treatment.5
Low- level laser therapy
Low-level laser therapy (LLLT) is utilized in the treatment of hair loss and hair thinning. It works by using low-energy laser light to stimulate hair follicles on the scalp. This stimulation helps to improve cellular metabolism and increase the production of adenosine triphosphate (ATP), which provides energy for cellular processes. The specific wavelengths of light used in LLLT penetrate the scalp and are absorbed by the hair follicles. This absorption stimulates follicles to prolong the anagen (growth) phase of the hair cycle, increase blood flow to the scalp, and enhance nutrient delivery to the follicles. These effects collectively promote hair regrowth, improve hair thickness, and increase hair density over time. LLLT is typically administered using devices such as laser combs,
helmets, or caps that emit controlled amounts of light. LLLT is considered safe, painless, and non-invasive, making it a popular option for both men and women seeking to address various forms of hair loss, including androgenetic alopecia.5
Platelet-rich plasma (PRP)
therapy
Platelet-rich plasma (PRP) therapy is employed in the treatment of hair loss and hair thinning. This procedure entails obtaining a small sample of the patient's venous blood, which undergoes centrifugation to concentrate platelets. These platelets contain various growth factors and cytokines that are believed to stimulate hair follicles, promote hair growth, and improve hair thickness and density. During the PRP treatment procedure, the concentrated platelets are injected into the scalp at the level of the hair follicles. This direct application of growth factors and other bioactive proteins helps to nourish the follicles, prolong the anagen (growth) phase of the hair cycle, and reverse miniaturization of hair follicles. It is considered safe, as it utilizes the patient's own blood, reducing the risk of allergic reactions or adverse effects.5
Fractional lasers therapy
Fractional laser therapy has emerged as a noninvasive treatment option for addressing hair loss and thinning. This technology utilizes fractional laser devices to emit light energy
that creates thousands of microscopic treatment zones (MTZs) in the skin. These zones induce controlled microinjuries, triggering the body's natural healing process and stimulating the production of new collagen and elastin fibers (collagenesis). By enhancing blood circulation in the treated area, fractional laser treatment improves the delivery of oxygen and nutrients to hair follicles, which can promote healthier hair growth. The stimulation of hair follicles through this process potentially increases hair thickness and may extend the anagen (growth) phase of the hair cycle, contributing to stronger and healthier follicles.5
Hair stimulating complex
Hair Stimulating Complex (HSC) is a specialized treatment designed to combat hair loss and foster hair regrowth through a comprehensive approach. By harnessing a synergistic blend of active ingredients, HSC targets various aspects of hair health and growth. It stimulates hair follicles, enhancing their activity and potentially prolonging the growth phase of hair. Moreover, Hair stimulating complex improves blood circulation to the scalp, ensuring optimal delivery of nutrients and oxygen to hair follicles, which promotes stronger and thicker hair growth. Some formulations also include ingredients that inhibit dihydrotestosterone (DHT), a hormone linked to genetic hair loss, and possess anti-inflammatory properties
beneficial for conditions like alopecia areata.5
Cellular therapy
Cellular therapy for hair involves advanced techniques such as platelet-rich plasma (PRP) therapy and stem cell therapy, both aimed at stimulating hair growth and enhancing hair health. PRP therapy harnesses the healing properties of platelets found in the patient's own blood, concentrating growth factors that stimulate hair follicles, extend the growth phase (anagen), and improve hair thickness and density when injected into the scalp. Stem cell therapy, on the other hand, utilizes the regenerative potential of stem cells to promote hair follicle regeneration and support hair growth by injecting stem cells directly into the scalp. These therapies not only stimulate dormant hair follicles to enter the active growth phase but also enhance blood circulation and deliver beneficial growth factors or stem cells, fostering healthier hair follicles and stronger strands. Cellular therapy is customizable based on individual needs and the severity of hair loss, offering a natural and safe treatment option with minimal risk of adverse reactions or rejection since it utilizes the patient's own cells (autologous).5
Wingless- related integration site activators
Wingless-related integration site (Wnt) activators play a crucial role in the treatment of hair loss, particularly in addressing conditions such
as androgenic alopecia (male pattern baldness) and other forms of hair thinning. Wnt signaling pathways are involved in regulating various aspects of hair follicle development, growth, and cycling. By activating Wnt pathways, these activators can stimulate hair follicle regeneration, prolong the anagen (growth) phase of the hair cycle, and promote the differentiation of hair follicle stem cells into hairproducing cells. One of the key mechanisms of Wnt activators involves promoting the proliferation of dermal papilla cells and enhancing their interactions with epithelial cells in the hair follicle. This interaction is essential for maintaining the hair follicle's structural integrity and function. Additionally, Wnt activators can contribute to improving scalp conditions by reducing inflammation and oxidative stress, which are known contributors to hair follicle miniaturization and hair loss.5
Hair Transplantation
Hair transplantation has become one of the most rapidly evolving procedures in aesthetic surgery, continually benefiting from regular advancements in techniques. Recent technological developments and the use of follicular unit grafts have significantly elevated the effectiveness and outcomes of this procedure. These innovations have enabled the creation of extremely naturallooking results, encouraging a growing number of men and women experiencing hair
loss to consider this surgical option. The blend of artistry and scientific precision in harvesting and implanting hair follicles highlights the exciting and innovative nature of modern hair restoration surgery. While age does not restrict hair transplantation, careful evaluation of the pros and cons is necessary, especially for younger patients. Candidates between 20 and 30 years old should have stabilized hair loss before undergoing the procedure. A thorough family history helps assess hair loss patterns and plan the new hairline. Several factors impact the result, including the color, quality, and density of the donor hair and the contrast between hair and skin color. A lower contrast typically yields better results. Additionally, frizzy, curly, or wavy hair characteristics are advantageous for transplantation. Single hair grafts are essential for creating a natural hairline, a critical aspect of hair transplantation. The hairline, being the most visible landmark, often serves as a measure of a surgeon's skill. As suggested by Michelangelo, the ideal hairline in a bald patient can be located by dividing the face into three equal segments. The hairline starts at least 8 cm from the glabella in the midline, curving around the lateral forehead. The lateral hairlines should align parallel to this curve when viewed straight on, typically 9.5–11.5 cm above the lateral canthus of the eyes. Men usually have sharper temporal angles, while women’s angles are more rounded. The shape of the
hairline should also consider the face shape (round, oval, or triangular) and the patient's preferences.Creating a new hairline typically requires 250–300 single hair (micro) grafts. These grafts should be placed in an irregular, saw-toothed pattern to achieve a natural look. Behind the hairline, twohair follicular unit grafts (FUGs) provide coverage, followed by three or four-hair FUGs further back. The less ideal the hair and skin characteristics, the smaller the grafts should be. For density in bald areas, some surgeons use punch grafts (1, 1.25, and 1.5 mm in diameter), which are not recommended where existing hair is present to avoid counterproductive results. Complications are rare, with infections in the recipient areas infrequent. Donor area infections around sutures usually resolve easily. Epidermal cysts may occur and require drainage. Harvesting too large a donor area can cause tension on the suture line, leading to dehiscence and a wide scar.7
Follicular Unit Excision (FUE) and Follicular Unit Transplantation (FUT), often referred to as the strip method, are two popular techniques used in hair transplantation for hair regrowth. Both methods can be used separately or in combination for larger sessions, such as up to 7000 follicular units (FUs). Both techniques aim to achieve natural-looking hair regrowth, but they differ in their approach to harvesting hair follicles from the donor area.8
Follicular Unit Excision (FUE)8
• Method:
o Individual hair follicles are extracted directly from the donor area using manual or motorized punches.
o The harvested follicles are then transplanted into the recipient area.
• Advantages:
o Minimal Scarring: Leaves tiny, round scars that are less noticeable and can be hidden by surrounding hair.
o Recovery: Faster recovery time and less post-operative discomfort.
o Flexibility: Ideal for patients who prefer to wear their hair short or have a tighter scalp that makes strip removal difficult.
• Disadvantages:
o Time-Consuming:...........: Generally more timeconsuming than FUT, especially for larger sessions.
o Higher Cost: Typically more expensive per graft due to the labor-intensive nature of the procedure.
o Graft Quality: Risk of higher transection rates (damage to follicles during extraction) if not performed by an experienced surgeon.
Follicular Unit Transplantation (FUT)8
• Method:
o A strip of skin containing hair follicles is excised from the donor area (usually the back or sides of the scalp).
o The strip is then dissected
into individual follicular units under a microscope.
o The individual follicular units are transplanted into the recipient area.
• Advantages:
o Efficiency: Can harvest a larger number of grafts in a single session, which is beneficial for patients needing extensive coverage.
o Quality of Grafts: Follicular units are often of higher quality due to the precision of dissection under a microscope.
o Cost: Generally less expensive per graft compared to FUE.
• Disadvantages:
o Scarring: Leaves a linear scar at the donor site, which can be noticeable if the hair is worn very short.
o Recovery: Longer recovery time and more post-operative discomfort compared to FUE.
o Invasiveness: More invasive than FUE, involving suturing of the donor area.
Combination of FUT and FUE8
• Method:
o Using both FUT and FUE techniques in a single session to maximize the number of grafts harvested.
• Advantages:
o High Graft Yield: Allows for harvesting a large number of grafts, which is beneficial for extensive hair loss.
o Optimized Scarring: Balances the large graft yield of FUT with the minimal
scarring of FUE.
o Versatility: Provides flexibility in donor site utilization and achieves a higher density in the recipient area.
• Disadvantages:
o Complexity: Requires a highly skilled and experienced surgical team.
o Cost and Recovery: Can be more expensive and involve a longer recovery period compared to using a single method.
Discussion
Alopecia, characterized by the loss or absence of hair where it normally grows, presents in various forms—localized or diffuse, temporary or permanent—across all ages and genders. It is broadly categorized into nonscarring and scarring types. Nonscarring alopecias such as androgenetic alopecia, alopecia areata, and telogen effluvium preserve hair follicles, allowing potential regrowth. Androgenetic alopecia is the most prevalent at 37.7%, followed by alopecia areata (18.2%) and telogen effluvium (11.3%). Scarring alopecias like frontal fibrosing alopecia and lichen planopilaris irreversibly destroy follicles. Vellus hair is short and thin, found widely across the body, while terminal hair is long and thick, present on areas like the scalp, eyebrows, eyelashes, beard, axillae, and pubic regions. Hair follicles undergo cycles of growth (anagen, 85%-90%), involution (catagen, <5%), and resting (telogen, 5%-10%), where the anagen phase duration (2-7 years) determines hair length.7
Androgenetic alopecia is influenced by genetic variants of the androgen receptor gene, converting terminal hair to vellus hair postpuberty, while genetic factors in females may involve the X-chromosomal locus AR/ EDA2R. Alopecia areata shortens the anagen phase during immune-mediated acute flares, potentially disrupting hair follicle immune privilege. Genome-wide studies identify susceptibility loci on chromosomes 6, 10, 16, and 18. Telogen effluvium results from stress triggers, causing premature hair follicle entry into the telogen phase and subsequent shedding. Scarring alopecias such as frontal fibrosing alopecia (FFA) and lichen planopilaris (LPP) involve irreversible hair follicle damage and scarring due to inflammation affecting epithelial stem cells in the hair follicle bulge. Several myths surround the causes and implications of hair loss. Contrary to popular belief, weight training and physical activity do not directly cause hair loss; genetics, hormonal factors like dihydrotestosterone (DHT), and aging are primary contributors. Emotional stress and sleep deprivation can exacerbate hair loss temporarily, but they are not direct causes of baldness. Additionally, the notion that bald men are more sexually active or virile lacks scientific basis, as does the myth that frequent ejaculation leads to hair loss. Understanding the true causes of alopecia involves recognizing genetic predispositions, hormonal
influences, and other factors affecting follicle health over time.9
Accurately diagnosing different subtypes of alopecia is crucial for effective management, relying on methods like dermoscopy and biopsy to assess hair loss patterns and confirm diagnoses. Conditions such as androgenetic alopecia can mimic alopecia areata, telogen effluvium, traction alopecia, trichotillomania, frontal fibrosing alopecia (FFA), lichen planopilaris (LPP), and central centrifugal cicatricial alopecia. Alopecia areata's patchy hair loss can resemble tinea capitis or trichotillomania, while diffuse forms may be mistaken for telogen effluvium or drug-induced alopecia. Telogen effluvium shares similarities with androgenetic alopecia and diffuse alopecia areata. Scarring alopecias like FFA and LPP can be confused with conditions such as chronic cutaneous lupus erythematosus, central centrifugal cicatricial alopecia, or folliculitis decalvans due to their inflammatory nature and irreversible follicle damage. A thorough clinical examination, dermoscopy, and possibly a scalp biopsy is essential for accurate differentiation and classification into nonscarring or scarring types, guiding tailored treatment strategies based on the identified cause.4, 9
Managing hair loss involves a multifaceted approach tailored to the specific type and cause of alopecia. For nonscarring alopecia like androgenetic alopecia,
minoxidil and finasteride are commonly prescribed medications that promote hair regrowth by extending the anagen phase and inhibiting DHT production, respectively. In cases of alopecia areata, corticosteroids, topical immunotherapy, or systemic immunosuppressive agents may be used to modulate immune responses and encourage hair regrowth. Telogen effluvium often resolves on its own once the underlying trigger is addressed; managing stress and ensuring adequate nutrition are crucial.5, 9
Home care plays a supportive role in managing hair loss. Gentle handling during washing and brushing, avoiding harsh treatments or styling practices, and maintaining a balanced diet rich in vitamins and minerals are beneficial. Scalp massages with essential oils like rosemary or peppermint oil may promote circulation and support follicle health. Additionally, protecting the scalp from excessive sun exposure and using mild, pH-balanced shampoos can help maintain scalp health. Incorporating these strategies into a comprehensive care plan can effectively manage various types of hair loss, promoting healthier hair growth and enhancing overall well-being. Remember, consistency and patience are key as you work towards restoring your hair's natural vitality and strength.9
Conclusion
In the face of challenges posed by hair loss treatment,
perseverance and endurance are essential. Each individual's journey with hair loss is unique, requiring a personalized approach that seamlessly integrates medical expertise with compassionate care. By embracing advanced therapies, advocating for a balanced lifestyle, and employing diagnostic tools for ongoing evaluation, patients are empowered to take proactive steps in managing their condition. Through steadfast commitment to research and comprehensive support, our aim is to enhance both the physical outcomes and emotional well-being of those affected by hair loss.
References
1. Qi J, Garza LA. An overview of alopecias. Cold Spring Harb Perspect Med. 2014;4(3):a013615. Published 2014 Mar 1. doi:10.1101/ cshperspect.a013615.
2. Phillips TG, Slomiany WP, Allison R. Hair Loss: Common Causes and Treatment. Am Fam Physician. 2017;96(6):371-378.
3. Ho CH, Sood T, Zito PM. Androgenetic Alopecia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; January 7, 2024.
4. Kaliyadan F, Nambiar A, Vijayaraghavan S. Androgenetic alopecia: an update. Indian J Dermatol Venereol Leprol. 2013;79(5):613-625. doi:10.4103/0378-6323.116730
5. Wall D, Meah N, Fagan N, York K, Sinclair R. Advances in hair growth. Fac Rev. 2022;11:1. Published 2022 Jan 12. doi:10.12703/r/11-1.
6. Tr P, Ts R, K SK, Prasanna H. A Comparative Study of Topical Procapil With Platelet-Rich Plasma
Therapy Versus Topical Redensyl, Saw Palmetto, and Biotin With Platelet-Rich Plasma Therapy in the Treatment of Androgenetic Alopecia. Cureus. 2023;15(5):e38696. Published 2023 May 8. doi:10.7759/ cureus.38696.
7. Khanna M. Hair transplantation surgery. Indian J Plast Surg. 2008 Oct;41(Suppl):S56-63. PMID: 20174544; PMCID: PMC2825128.
6. Epub 2019 May 28. PMID: 31624428; PMCID: PMC6795649.
9. Al Aboud AM, Syed HA, Zito PM. Alopecia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; February 26, 2024.
LC-OCT Demonstrates Non-Invasive Evaluation Capabilities of Dermal Fillers
Fillers are commonly used to revolumize the midface, cheeks and nasolabial folds. Line-field optical coherence tomography (LC-OCT) may be a useful tool in non-invasively evaluating the capabilities of hyaluronic acid dermal fillers, according to a study published recently. When assessing dermal fillers utilizing LC-OCT, researchers were able to observe distinct characteristics and visualizations immediately after injection and at a later follow-up date. Researchers behind the present study identified several recent investigations of non-invasive evaluation methods for fillers, such as assessment with high-frequency ultrasound and magnetic resonance, for example. A 2018 study published in the same scientific publication outlined the capability of high-frequency ultrasound to distinguish between granulomas, nodules, and dermal filler deposits. In order to assess the efficacy of LC-OCT in applications related to dermal fillers, 6 patients received injectable facial hyaluronic acid fillers and underwent LC-OCT imaging at 3 stages: before, immediately after, and 6-8 weeks post-injection. A dermatopathologist assessed clinical images to identify morphological or reflectivity changes.
Patients included in the study ranged in age between 30 to 59 years. Each patient received dermal filler treatments in various facial locations. At the initial assessment (T0), conducted before the application of dermal fillers, LC-OCT scans revealed the normal characteristics of the skin. The epidermis was clearly distinguishable from the dermis, and vascular structures were visible within the dermis. Notably, researchers observed that the epidermis at the lip area was thicker compared to other sites, such as the tear trough and nasolabial folds.
Scans taken at T1 — immediately after the procedure — showed the fillers as homogenous, hyporeflective areas within the dermis. These areas were clearly differentiated from the surrounding tissues, including blood vessels and other dermal structures. The imaging demonstrated that the filler deposits were distinct and well-defined, with 1 observed deposit measuring approximately 188 micrometers in diameter. At the 6-8 week follow-up visit (T2), LC-OCT imaging illustrated a reduction in the size of the filler deposits compared to their size immediately after application. The filler appeared as smaller hyporeflective areas within the dermis. Additionally, researchers observed significant changes in the dermal collagen fibers. By T2, these fibers had become thicker and more uniformly organized, displaying increased hyperreflectivity.
When comparing the LC-OCT images from T0 and T2, researchers observed notable improvements in dermal collagen. At T2, collagen bundles were thicker and more regularly organized, showing greater hyperreflectivity than at baseline. This suggests that the skin undergoes positive structural changes following filler application, possibly due to the natural remodeling processes and the fillers’ interaction with the dermal tissue. Immediate and follow-up imaging provided researchers with insights into the spatial distribution of fillers and the subsequent changes in skin structure. These observations can guide practitioners in predicting filler behavior over time and in making informed decisions about treatment strategies.
Tailoring Aesthetic Treatments for Patients With Skin of Color
In a recent study, reviewed important considerations for clinicians providing aesthetic care to patients with skin of color. Study reviewed findings evaluating facial aesthetic concerns across genders, ethnicities, and generations; postinflammatory hyperpigmentation; laser settings, specific devices safe for use on patients with skin of color, non-device aesthetic treatments, and how to improve inclusivity and education surrounding treatments for patients with skin of color. Aesthetics ideals and treatments have often focused on the needs and concerns of white female patients. As aesthetic ideals differ among diverse populations, it is important to understand how aesthetic concerns and desires may vary across demographic groups. Importantly, the research findings suggest that aesthetic concerns vary among demographic groups and differ from what current aesthetic paradigms may suggest.
Although laser treatments are popular, all types of dark spots and skin types aren’t suited for them. Melanin-rich skin requires specific laser wavelengths and techniques to avoid targeting the pigment and causing further damage, and alternative approaches or specific wavelengths should be considered. Patients with active acne breakouts, very sensitive skin, or flare-ups of skin conditions could also see more harm than good with certain lasers. However, if a patient’s skin is suited for it, broadband light therapy uses high-intensity light that's gentler than a laser and can be more affordable than traditional lasers.
According to research, uneven skin color and hyperpigmentation were ranked as top facial concerns across a wide array of racial demographics, but most prevalent for Black and Asian women. This illustrates that addressing hyperpigmentation concerns is something healthcare practitioners need to be mindful of when having consultations with diverse patients and ensuring their specific needs are prioritized and met—but they need to take a customized approach to avoid further damage to diverse skin tones. Most importantly, patients need to consult a dermatologist who has experience treating patients with darker skin and who understands the impact lasers will have on melanin-rich skin.
FDA Clears A New Dimension of Radiofrequency (RF) Microneedling Platform for Treatment of Facial Wrinkles
US Food and Drug Administration (FDA) has cleared a multi-application of radiofrequency skin platform for a new indication. The expanded indication, for use in patients with facial wrinkles and Fitzpatrick Skin Types I-IV, adds to the Matrix platform's existing portfolio of FDA clearances for use in dermatological procedures involving hemostasis and electrocoagulation. In this indication, treatment of facial wrinkles is performed through the use of the Matrix Pro RF microneedling applicator.
Clearance for the treatment modality was supported by a retrospective study involving 32 participants. The study, which assessed full-face treatments with the new dimension of radiofrequency (RF) microneedling, demonstrated significant clinical improvements in wrinkle appearance. Key findings include clinically meaningful results, patient satisfaction. The blinded evaluation of treatment photos indicated substantial improvements in facial wrinkle reduction. 94% of participants rated their outcomes as 'much improved' or 'very much improved.
The advanced technology of the new dimension of radiofrequency (RF) microneedling ensures minimal discomfort and downtime, making it a preferred choice for patients seeking quick and visible improvements.
In addition to serving as a skin tightening solution for aging patients, RF microneedling has promise in the expanding GLP-1 receptor agonist market. The Matrix system's ability to regenerate collagen has promise with addressing the loss of facial volume associated with rapid weight loss induced by these highly sought-after injectable medications. The Matrix system incorporates 3 modalities designed to address various aspects of skin aging. The Sublime modality uses infrared light and bipolar RF energy to stimulate dermal collagen production, improving skin tone and texture.
The Sublative modality utilizes fractionated RF energy to target deeper layers of the skin, enhancing texture and reducing the appearance of fine lines. The latest innovation, new dimension of radiofrequency (RF) microneedling, employs short pulse RF microneedling to directly address facial wrinkles by stimulating collagen and elastin production. The Matrix system also incorporates real-time impedance monitoring, ensuring that RF energy is precisely delivered at the appropriate depth. This feature minimizes the risk of complications, such as unintended fat loss.
"Achieving FDA clearance using the new dimension of radiofrequency (RF) microneedling for wrinkle reduction is a testament to our rigorous testing, clinical validation processes, and dedication to advancing outcomes through proven science and technology. This clearance provides healthcare providers and their patients with a reliable, clinically validated treatment option for facial wrinkles.
Several Skin Conditions More Likely in Children with Obesity
With rates of childhood obesity increasing to the point of becoming a public health concern, related skin conditions are also on the rise in the pediatric population, results of new research show. The retrospective cohort study found markedly higher rates of skin infections, atopic dermatitis (AD), and acanthosis nigricans among children with overweight, compared with children with average weight. Many conditions associated with obesity are strong predictors of cardiovascular mortality as these children age, so doctors can play a key role in advocating for weight loss strategies in this population. Previous research has linked obesity, a chronic inflammatory condition, to psoriasis, AD, hidradenitis suppurativa (HS), acne vulgaris, infections, and rosacea in adults. However, there’s scant research exploring the connection between obesity and cutaneous conditions in children.
According to the researcher, childhood obesity is defined as a body mass index, which is weight in kg divided by the square of height in m2, at or above the 95th percentile for age and sex in children aged 2 years or older. They collected data on AD, HS, rosacea, psoriasis, and acanthosis nigricans (a thickened purplish discoloration typically found in body folds around the armpits, groin, and neck). They also gathered information on comorbidities. Acanthosis nigricans, which is linked to metabolic syndrome, type 2 diabetes, and insulin resistance, was more prevalent among children with obesity (20,885 cases in the with-obesity group and 336 in the without-obesity group, for a relative risk [RR] of 62.16 and an odds ratio [OR] of 64.38). Compared with their average-weight counterparts, the children with obesity had higher rates of comorbidities, including type 2 diabetes. Researcher noted that children with diabetes and obesity had increased risks for every skin condition except for infections of the skin and subcutaneous tissue when compared with children without obesity. Such infections were the most common skin conditions among children without obesity. This was expected just due to the fact that children are outside, they’re playing in the grass and the dirt, and they get infected. Still, these infections were three times more common in youngsters with obesity.
Although acanthosis nigricans is “highly correlated” with type 2 diabetes, “not as many children as we would expect in this population have developed type 2 diabetes.” This might make some sense, though, because these children are still quite young. “When dermatologists recognize this skin condition, they can advocate for weight loss management to try to prevent it.” Other conditions seen more often in the overweight children with overweight included: hypertension, hyperlipidemia, obstructive sleep apnea, polycystic ovarian syndrome, attention-deficit/hyperactivity disorder, major depressive disorder, depressive episodes, and anxiety (all P < .001).
Dr. Monica Jacob
MBBS, MD, DPB, DAD
Cosmetologist, Obesity
Consultant and Antiaging PhysicianDirector of Bodyz wellness, India
Diploma in Aesthetic Medicine
(American Academy of Aesthetic Medicine)
Hair transplant,
(American Academy of Aesthetic Medicine)
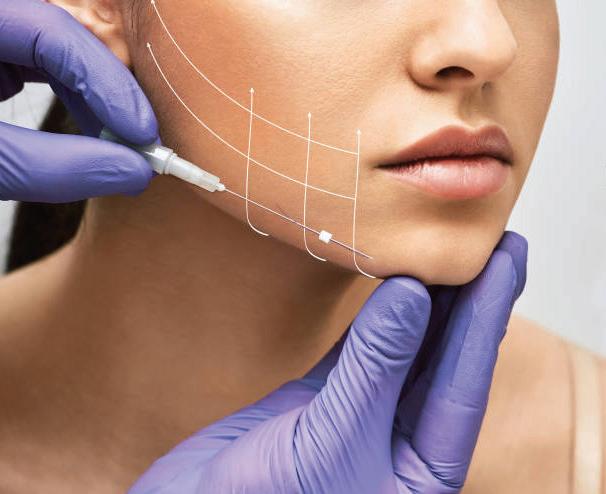
Thread Lift: A Non-Surgical Solutions for Facial Rejuvenation
Thread Lift, a non-surgical face alternative. Thread Lift is a cosmetic procedure aimed at lifting and tightening the skin, providing a rejuvenated and youthful appearance and natural-looking result without the downtime and risk associated with surgery. The threads used in the procedure are typically made up of biodegradable materials like , polydioxanone (PDO) or polycaprotonone (PCL), which dissolves over time and stimulates the body's natural production of collagen. Collagen is a protein that is essential for maintaining the skin's elasticity and firmness and its production decreases with age, leading to sagging and wrinkles by stimulating collagen production. Thread Lift not only provides an immediate lifting effect but also improves skin texture and elasticity over the following months.
Dermal fillers are a popular cosmetic treatment used to restore volume, smooth out wrinkles, and enhance facial contours. These injectable substances are typically composed of hyaluronic acid, a naturally occurring substance in the skin that helps maintain hydration and elasticity. Over time, our skin loses its natural hyaluronic acid, collagen, and elastin, leading to sagging skin, fine lines, and a loss of facial volume. Dermal fillers are designed to address these issues by replenishing lost volume and providing structural support to the skin, resulting in a more youthful and rejuvenated appearance.
Additionally, dermal fillers can be used to enhance facial features such as the lips, cheeks, and chin, dermal fillers are a versatile and effective solution for individuals looking to enhance their appearance, restore facial volume, and reduce the signs of aging.
Botox, the go to treatment for wrinkles and beyond. Botox is a purified form of botulinum toxin.
Botox serves as a potent muscle relaxant. It works by blocking the signals from nerves to muscles. It prevents the release of acetylcholine a neurotransmitter responsible for muscle contraction. This temporary relaxed muscle activity results in reduction of wrinkles and fine lines, particularly in areas prone to dynamic expression, such as forehead, around the eyes, gross fit, and between the brows. This effect of the Botox typically becomes visible within a few days and can last up to 3 to 6 months, depending on individual factors and the area treated.
TYK2 Inhibitor Effective for Psoriasis in Phase 2 Study
Psoriasis is a skin condition that's thought to be caused by an immune system problem that causes skin cells to grow too quickly. The most common type of psoriasis is plaque psoriasis, which results in dry, scaly patches on the skin or scalp. Many people with psoriasis have a family history of the disease, and some external factors that may increase the chances of developing it include infections, certain medications, smoking, and obesity. According to result of current study, zasocitinib, a tyrosine kinase 2 (TYK2) inhibitor, at oral doses of ≥ 5 mg led to greater skin clearance than placebo over a period of 12 weeks, in a phase 2b study.
Researchers performed a phase 2b, randomized, double-blind trial to assess the efficacy, safety, and tolerability of different doses of zasocitinib in adults with moderate to severe psoriasis (mean age, 47 years; 32% women). A total of 287 patients were randomly assigned to receive one of the four oral doses of zasocitinib (2 mg, 5 mg, 15 mg, or 30 mg, once daily) or a matched placebo for 12 weeks, followed by a 4-week safety monitoring period. The primary outcome was the proportion of patients achieving a ≥ 75% improvement in the Psoriasis Area and Severity Index score (PASI 75) from baseline at week 12.
At week 12, PASI 75 was achieved by 18%, 44%, 68%, and 67% of patients receiving zasocitinib at doses of 2 mg, 5 mg, 15 mg, and 30 mg, respectively, vs 6% of patients receiving placebo. PASI 90 was achieved in 8%, 21%, 45%, and 46% of patients receiving zasocitinib at 2 mg, 5 mg, 15 mg, and 30 mg, respectively, and in no patients in the placebo group. At week 12, 10%, 27%, 49%, and 52% of patients receiving zasocitinib at 2 mg, 5 mg, 15 mg, and 30 mg, respectively, had no or mild disease (a score of 0 or 1) according to the Physician Global Assessment tool vs 4% in the placebo group. Zasocitinib, an advanced, potent, and highly selective oral TYK2 inhibitor bioengineered to optimize target coverage and functional selectivity, achieved biologic-level efficacy with complete skin clearance observed after only a 12-week treatment period in up to one third of patients, with a low incidence of known tolerability issues and absence of serious toxic effects that are characteristic of [Janus kinase] 1-3 inhibition.
Study Identifies Oral Antibiotics Linked to Severe Cutaneous Reactions
Potentially life-threatening cutaneous adverse drug reactions (cADRs) are associated with commonly prescribed oral antibiotics, according to a large, population-based, nested case-control study of older adults, spanning two decades.
The findings, published recently, underscore the importance of judicious prescribing, with preferential use of antibiotics associated with a lower risk when clinically appropriate. Researcher said, we hope our study raises awareness about the importance of drug allergy and gains support for future studies to improve drug allergy care. It is important to recognize symptoms and signs of a severe drug rash and promptly stop culprit drugs to prevent worsening reaction. Serious cADRs are “a group of rare but potentially life-threatening drug hypersensitivity reactions involving the skin and, frequently, internal organs. Typically delayed in onset, these reactions include drug reaction with eosinophilia and systemic symptoms, Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN) — the most severe cADR, which has a reported mortality of 20%-40%.”
Although it has been speculated that some oral antibiotics are more likely than others to be associated with serious cADRs, there have been no population-based studies examining this, they added. The study included adults aged 66 years or older and used administrative health databases. A cohort of 21,758 older adults (median age, 75 years; 64.1% women) who had an ED visit or hospitalization for serious cADRs within 60 days of receiving antibiotic therapy was matched by age and sex with 87,025 antibiotic-treated controls who did not have a cutaneous reaction. The median duration of antibiotic prescription was 7 days among cases and controls, and among the cases, the median latency period between antibiotic prescriptions and hospital visits for cADRs was 14 days. Most of the case patients went to the ED only (86.9%), and the rest were hospitalized. The most commonly prescribed antibiotic class was penicillins (28.9%), followed by cephalosporins (18.2%), fluoroquinolones (16.5%), macrolides (14.8%), nitrofurantoin (8.6%), and sulfonamides (6.2%). Less commonly used antibiotics (“other” antibiotics) accounted for 6.9%. Macrolide antibiotics were used as the reference because they are rarely associated with serious cADRs, noted the researcher, and the multivariable analysis, adjusted for risk factors associated with serious cADRs, including malignancy, chronic liver disease, chronic kidney disease, and HIV.
Venue: Hotel Ginger, Near Domestic Airport, Vile Parle (East) Mumbai