PH NURSE BUILDS PATIENT SUPPORT Exercise And PH BOOST YOUR HEALTH AND CONFIDENCE
8 WAYS TO MAKE THE MOST OF PHA 2024
The Navigating PAH Pathways program offers free webinars created specifically for patients and caregivers, all led by a PAH Practitioner and sponsored by Janssen.*
Find Answers
Hear an educational presentation from a PAH Practitioner on topics that may be important to you.
Learn Why
Understand more about PAH, the 3 key treatment pathways, and tools to help you track your PAH
Get Talking
Discover how to have more informed conversations about PAH with your care community.
Webinars are available at various dates and times so you can register for one that best fits your schedule.
Your PAH healthcare team should always be your main source of information. This program is not intended to provide medical advice or address specific medical concerns.
All webinars are viewed on a computer; internet access required. PAH=pulmonary arterial hypertension.
* The speaker is a paid consultant presenting on behalf of Janssen Pharmaceuticals, Inc., and must present information in compliance with FDA requirements applicable to Janssen Pharmaceuticals, Inc.
8 Ways To Make the Most of PHA
Get a Sneak Preview of PHA 2024 Scientific Sessions
Going to PHA 2024? Check Out Our Support Groups 18 Exercise and PH: Boost Your Health and Confidence With Activity
Advocacy Brings Hope for a Better Future
Advocacy in Action: PHA Sees Progress on Oxygen Bill, Accumulator Ban
Part D Beneficiaries Starting To See Lower Costs
PH Nurse Creates Support Group To Connect Her Patients
Donor Didn’t Realize She Was Investing in Her Own Future 31 New Bequest Supports Original Conference Scholarship Endowment
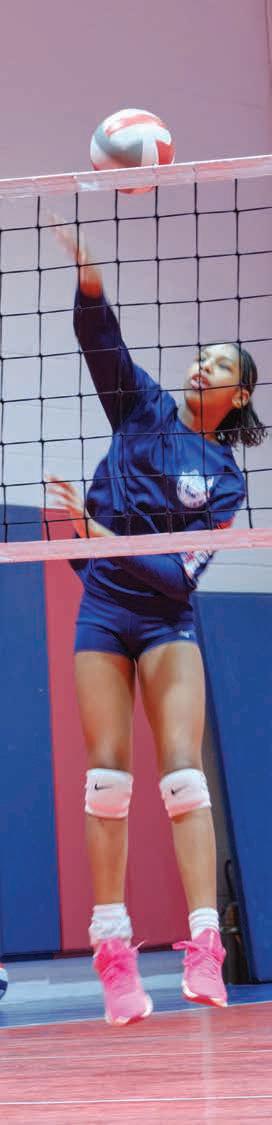
Sydney Lewis plays competitive volleyball, but struggles to breathe after climbing two flights of stairs. In our cover story, Lewis and others discuss the challenges — and importance — of exercising with pulmonary hypertension. Photo by Louis Tinsley.
PUBLISHER
Matt J. Granato (he/him) President & CEO
STAFF
Linda Busche (she/her) Editor-in-Chief
Karen Smaalders (she/her) Vice President, Communications and Marketing
CONTRIBUTORS
Grace Beal, Danielle Clement. Courtney Durham, Jenny Errico, Angela Golden, Kendra Hearon, Haley Johnson, Zan Laughlin, Daniel Layton, Kimberlee Miller, Ayotunde Omitogun, Abby Sickles, Jaeger Spratt, Joanne Szelag, Stanley Szelag Jr., Sara Tyghter, Brittany Watson. Cover story images: Louis Tinsley.
Mary Beth Ramsey (she/her) Graphic Design
CONTACT
301-565-3004
PHAssociation.org
SUPPORT LINE
800-748-7274
We’re here to support anyone with a connection to PH. (Daytime, please.)
Submissions to Pathlight are welcome. Please email your articles, photos and queries to Communications@ PHAssociation.org.
HEADQUARTERS
1629 K St. NW, Suite 300 Washington DC, 20006
BILLING AND MAILING ADDRESS
8401 Colesville Road, Suite 200 Silver Spring, MD 20910
BOARD OF TRUSTEES
Officers
Tony Lahnston, chair
Traci Stewart, RSN, CSN, CHFN, chair elect
Nicole Creech, treasurer
Colleen Connor, secretary
Colleen Brunetti, MEd, CHC, immediate past chair
Matt J. Granato, LLM, MBA, president and CEO, ex officio
Trustees
Todd Bull, MD, Scientific Leadership Council chair elect
Murali Chakinala, MD, FCCP, Scientific Leadership Council immediate past chair
Ramona Doyle, MD, MSc
Anna R. Hemnes, MD, Scientific Leadership Council chair
Kimberly Jackson, RN, BSN, PH Professional Network chair
Mitch Koppelman, PhD
Michelle Ferdinand Liu, MD, MPH, FAAOA
Mike Lentz
Melissa Magness, MSN, APRN, CNP-AC, PH Professional Network chair elect
Mike Naple
Monica M. Penaranda
Diane Ramirez
Doug Taylor
Matt Wall
Delphine Yung, MD, Accreditation and Registry Committee chair
Emeriti ex officio
C. Gregory Elliott, MD, FCCP, MACP
Michael D. McGoon, MD
Edwin Simpson
Judith Simpson, RN, EdS
Honorary
Carl Hicks
PH PROFESSIONAL NETWORK EXECUTIVE COMMITTEE
Kimberly Jackson, RN, BSN, chair
Cheri Abbott, RN, CCRP
April Blakley, RN, BSN
Jessie Dunne, PharmD, BCPS, BCCP
Loida A. Johnson, CRNP
Tisha Kivett, RN, BSN
Melissa Magness, MSN, APRN, CNP-AC, chair-elect
SCIENTIFIC LEADERSHIP COUNCIL
Anna R. Hemnes, MD, chair
Todd M. Bull, MD, chair-elect
Murali M. Chakinala, MD, FCCP, immediate past chair
Eric D. Austin, MD, MSCI
Sonja Bartolome, MD
Vinicio A. de Jesus Perez, MD, FCCP
Teresa De Marco, MD
Ankit A. Desai, MD, FACC, FAHA
Jeffrey Fineman, MD
Robert P. Frantz, MD
Mardi Gomberg-Maitland, MD, MSc
Daniel Grinnan, MD
Gustavo A. Heresi, MD, MSci
Kristin B. Highland, MD, MSCR
Nicholas Kolaitis, MD, MAS
Matthew R. Lammi, MD, MSCR
Peter Leary M.D., PhD
Deborah J. Levine, MD
Wes McConnell, MD
Lana D. Melendres-Groves, MD
Josanna Rodriguez-Lopez, MD
John J. Ryan, MD, MB, BCh, BAO
Sandeep Sahay, MD
Thenappan Thenappan, MD
Anjali Vaidya, MD, FACC, FASE, FACP
Nidhy Varghese, MD
Corey E. Ventetuolo, MD, MS
R. James White, MD, PhD
Distinguished Advisers
David B. Badesch, MD
Erika S. Berman Rosenzweig, MD
Bruce H. Brundage, MD
Richard Channick, MD
C. Gregory Elliott, MD, FCCP, MACP
Karen A. Fagan, MD
Michael D. McGoon, MD
Vallerie V. McLaughlin, MD
Ron Oudiz, MD
CHAIR LETTER from the
Dear PHA Community,
This issue of Pathlight focuses on “Enhancing Quality of Life.” Over the past 16 years, I have seen some amazing developments for the Pulmonary Hypertension Association and its patient community. In particular, I’ve been impressed how pulmonary hypertension treatment has come such a long way.
I distinctly remember when my niece was diagnosed with PH in 2007. The options for treatments were extremely limited and misdiagnosis was common. Seventeen years later, the PH world has made great strides in securing earlier and accurate diagnosis and developing more treatment options.
In March, the Food and Drug Administration approved the 15th and 16th treatments for pulmonary arterial hypertension. Johnson & Johnson’s Opsynvi is the first and only once-daily combination pill of macitentan and tadalafil. Merck’s Winrevair (sotatercept-csrk) is the first PAH drug that works on a new biological pathway that’s different from those targeted by 14 existing FDA approved treatments. [See our story about the two newly approved treatments on pages 10 and 11.]
Both treatments represent major research breakthroughs for the PH community. Their development and approval show increased understanding of PAH and promise for the future.
The last time the FDA approved a new PAH treatment was in 2015 when Uptravi (selexipag) became available. More recently, the FDA approved Tyvaso (treprostinil) Inhalation Solution for people whose PH is related to interstitial lung disease.
We welcome the new treatments and the development of other new therapies on the horizon, including seralutinib by Gossamer Bio and imatinib by Aerovate. Seralutinib and imatinib are similar to Winrevair in that they target new pathways.
The diagnosis for people with PH and their families is life-changing because of the serious, chronic, progressive
nature of the disease. Every positive step forward we take provides hope for patients and their families. Having joined this wonderful organization with a goal to provide hope to patients and families, it makes me very proud to be part of these accomplishments.
Although we now have 16 PAH treatments in the US, it’s important to remember that we still need medication for other forms of PH. We also need better accessibility to treatment in other parts of the world, as we hear first-hand from Ayotunde Omitogun, a patient from Nigeria, on pages 6 through 9.
PHA supports PH research through grants and professional development opportunities for researchers, scientists and health care professionals. If you’re a PH professional, we encourage you to attend PHA 2024 International PH conference and Scientific Sessions, where you’ll hear from international PH experts, learn about research advancements, and most importantly, meet the people affected by pulmonary hypertension.
I hope to meet many people with PH and caregivers at the Aug. 15-18 conference in Indianapolis. Whether you’re a first timer as I was in 2008, eager to learn about the disease and meet others affected by PH, or a longtime thriver, please stop by and say hello.
I am excited to meet you and honored to work on your behalf.
Tony Lahnston Chair, Pulmonary Hypertension Association Board of Trustees
Shedding Light on ‘Invisible Disease’ Fashion Designer Crusades for PH Awareness
In Nigeria
This page: Ayotunde Omitogun (left) with Jide Owolabi, her partner, caregiver and cofounder of Yo Sabi PH.
Opposite page: Omitogun and Owolabi with her niece and niece’s husband.
Ayotunde Omitogun had no choice but to advocate for her health.
Diagnosed with pulmonary hypertension at 26, Omitogun educated herself on her condition, how to set boundaries and advocate for proper care. Living in Lagos, Nigeria, Omitogun faced a lack of resources, medication and knowledge about PH.
“Everybody here knows about malaria or about cancer, but PH is an invisible disease,” the now 36-yearold said. “I don’t use oxygen outside, so everyone assumes I’m fine. But whenever I cough, people assume I have tuberculosis. PH is not well-known here, so I feel a responsibility to raise awareness.”
Through her participation in “Yo Sabi PH,” an organization she and her partner founded to raise PH awareness and educate doctors and patients about PH research, Omitogun is getting the word out about PH. Omitogun shared her story with the Pulmonary Hypertension Association for World PH Day on May 5. She sheds light on the differences between PH understanding, treatment and resources throughout the world.
ROAD TO DIAGNOSIS
Omitogun was born with an atrial septal defect, which caused a hole in the wall between the heart’s upper chambers. The heart defect was discovered three months after her birth in Hong Kong. Her doctors at the time didn’t think she needed surgery and told her family to monitor her condition.
She and her family moved back to Nigeria when she was 2 years old.
There, doctors also recommended no further treatment. When her family moved to Kenya in the early 1990s, doctors there recommended surgery to close the holes. But Omitogun’s parents didn’t have enough information about the complications of congenital heart defects, so they decided against the surgery.
Omitogun lived a relatively normal life, although she was small for her age. She couldn’t participate in physical activities at school because they triggered her shortness of breath. She experienced minor heart palpitations and chest pain, but not often enough to disrupt her life.
After graduating from high school, she studied to become a fashion designer. Omitogun designed trendy Nigerian outfits called asoebi, which are worn at big parties. She worked
with various lace fabrics, ankara (printed colorful cotton), damask and adire (tie-dye).
She also made contemporary women’s clothes for everyday life until her health started to affect her work.
“I couldn’t perform my job duties, and clients were complaining that I was taking too much time and making a lot of mistakes on the clothes,” Omitogun said. “I was just so fatigued.”
She assumed her heart condition was recurring, so in 2013, she went to different cardiologists and underwent an echocardiogram. She expected to need surgery, but the doctors diagnosed her with pulmonary hypertension and said her heart no longer could be repaired.
“I was shocked. I thought, ‘This is rubbish,’” Omitogun said. “I didn’t know what to say.” She saw several
doctors afterward to confirm the original diagnosis. All said she had PH.
LACK OF ACCESS
Doctors recommended she receive a right heart catheterization for a final diagnosis, but the procedure wasn’t widely available at the time.
In 2016, Omitogun received a right heart catheterization when the procedure became more widely available. The test confirmed her PH, but no one provided answers on how to treat her condition. No one gave her dietary, drug or therapy advice. She learned that mostly through her research.
“I was stubborn,” Omitogun said. “So, I went to India in December 2016 and had doctors there run all the same tests because I just needed true answers — not just a diagnosis, but a plan.”
Her doctors in India confirmed she had pulmonary arterial hypertension and prescribed sildenafil, ambrisentan and diuretics. Until 2023, Omitogun received her prescriptions from India because they weren’t available in Nigeria. Other Nigerian patients who regularly received treatment in the same hospital in India brought Omitogun’s drugs back to her in Lagos.
“This was difficult because my wellbeing relied on whether I received my medications on time or not,” Omitogun said. “Sometimes I’d go months without taking my medications, so I just had to suffer.”
Last year, she became so sick she switched to available medications in Lagos. Her doctors prescribed bosentan and tadalafil for PAH
Omitogun and volunteers at Lagos State University Teaching Hospital plan a PH awareness campaign.
‘Whenever I see an improvement elsewhere, I think ‘How do we get those? I do see the potential for Africa because it’s happening across the world, but I know we won’t get there without advocating for access, for advocating for our care.’
and the diuretics furosemide and Aldactone for water retention. They also prescribed Xarelto to prevent blood clots, and carvedilol, a beta blocker used to treat systemic high blood pressure. Every month she goes to cardiac and pulmonary clinics for checkups and buys her new prescriptions.
Omitogun’s most common symptoms are shortness of breath, fatigue and chest pain. When she feels her oxygen levels drop, she must go to a hospital to receive oxygen treatment.
“It’s my quality of life, so I have to take action,” Omitogun said. “I researched what to drink, what to eat, what treatments are best for alleviating what symptoms and when I go to the hospital to not ask for oxygen but demand it.”
CULTURAL STIGMAS
Women in Nigeria face a lot of pressure to have kids, Omitogun said. She knows that being pregnant with PH is dangerous for the mother and the child, so she decided not to have children.
“People think if you can’t have kids, what is the purpose of your existence,” Omitogun said. “I feel bad and guilty at times, but I’m also very open about
my pulmonary hypertension and have accepted that this is me.”
Nigeria also is a religious country, where many people believe that it’s your fault if you have a disease. Some think that God is punishing you or that you did something bad. After she was diagnosed, people expected Omitogun to devote her life to church and ask for forgiveness.
Instead, she spends her time raising PH awareness. Through Yo Sabi PH, Omitogun plans fundraising walks, educational sessions with medical students about signs and symptoms of PH, and collaborates with pulmonologists and cardiologists on spreading awareness about the latest PH treatments and care. She also shows others how to advocate for themselves.
MOVING FORWARD
Once in a while Omitogun works with tailors to continue her passion for fashion design, but most of her time is spent spreading PH awareness. She is always excited for the next campaign, the next walk or the next education event that will improve the world for those living with PH.
“I live with this every day, so it’s a big passion of mine,” Omitogun said.
“I like to read the latest information and learn new things that could help manage my condition.”
When it comes to advocacy and treatment, Omitogun says Africa is behind compared to other parts of the world, such as Europe, India or the U.S. She said it’s hard to see all these improvements across the globe, but not have access to them.
“Whenever I see an improvement elsewhere, I think ‘How do we get those?” Omitogun said. “I do see the potential for Africa because it’s happening across the world, but I know we won’t get there without advocating for access for our care.”
Inspired by this story? Share yours at PHAssociation.org/ the-right-heart.
Are you interested in learning about pulmonary hypertension in other parts of the world? Visit PHAssociation.org/ WorldPHDay.
FDA Approves New Treatment Options
BY MELANIE PADGETT POWERS
MELANIE PADGETT POWERS is a freelance health care writer and editor in the Washington, D.C., area.
The promise of new pulmonary hypertension drugs is starting to come to fruition. The Food and Drug Administration recently approved two new PH drugs: Opsynvi from Johnson & Johnson and Winrevair from Merck.
There are now 16 FDA-approved treatments for pulmonary arterial hypertension.
“We are always very pleased to see industry research that demonstrates a better understanding of PAH,” says Matt Granato, CEO of the Pulmonary Hypertension Association. “The development of a medicine that targets a novel treatment pathway and a onetablet combination pill of two existing drugs expands treatment options for people with pulmonary arterial hypertension.”
Opsynvi, specifically for people with functional class II and III PAH, became available in mid-April. Opsynvi combines two PAH drugs into one tablet that can be taken once a day. The tablet contains macitentan (brand name Opsumit), an endothelin receptor antagonist, and tadalafil (generic), a phosphodiesterase 5 inhibitor.
Clinical guidelines say newly diagnosed patients with low or intermediate risk Group 1 PAH can start on a combination of an ERA and a phosphodiesterase 5 inhibitor. Opsynvi now allows those patients to fulfill those guidelines with just one pill a day.
“Opsynvi can potentially help patients avoid the complexity of two
separate prescriptions, taking multiple pills a day … and potential multiple prior authorizations,” says former PHtreating physician Sean Studer, vice president of medical affairs at Johnson & Johnson. “Anything that one can do to simplify their regimen is often a welcome option to have.”
The prescriptions would mirror the doses patients now take with those two drugs. A patient would start on an Opsynvi pill that has 10 mg of macitentan and 20 mg of tadalafil. If they tolerate it well, they could switch to the Opsynvi pill with 10 mg of macitentan and 40 mg of tadalafil after about one week, Studer says.
So, there could be that change in the pill as the dose increases, especially at the beginning or for the patient that’s new to therapy, Studer says. “Over time, they wouldn’t have to take more than one pill a day to get these treatments.”
Because macitentan can cause serious birth defects, Opsynvi has a boxed warning, as does Opsumit. A boxed warning is the FDA’s strictest safety warning for drugs with serious side effects. The FDA requires female patients to enroll in the MacitentanContaining Products Risk Evaluation and Mitigation Strategy program. This REMS program provides ongoing education and monitoring and requires monthly pregnancy tests.
Beyond that, Studer points out, “It’s important for us that there was no new safety or tolerability signals that came out studying the combination versus the individual components.”
‘Opsynvi can potentially help patients avoid the complexity of two separate prescriptions, taking multiple pills a day … and potential multiple prior authorizations. Anything that one can do to simplify their regimen is often a welcome option to have.’
SEAN STUDER, MD
‘The drug has had a very significant impact on our patients, with marked improvement in functional class and hemodynamics (how blood flows through vessels).’
AARON WAXMAN, MD, PHD
FIRST TREATMENT FOR NEW PATHWAY
Winrevair, the brand name for sotatercept-csrk, is the first FDAapproved activin-signaling inhibitor therapy for PAH. It became available through select specialty pharmacies in April. An activin signaling inhibitor works differently from other PAH drugs. Other PAH drugs are vasodilators that relax the blood vessels and help the blood flow better.
Winrevair acts on structural changes in the blood vessels. The structural changes make the blood vessels thicker, harder and narrower, causing pulmonary pressure to rise. The structural changes occur primarily because of an increase (proliferation) in the number of cells in the vascular wall.
Winrevair is given as a subcutaneous injection every three weeks. It was approved in 45 mg and 60 mg doses. Patients will still take other PAH medications. The Phase 3 STELLAR trial showed that Winrevair significantly improved exercise capacity, increasing six-minute walk distance by about 45 yards, almost half a football field.
The drug “has had a very significant impact on our patients, with marked improvement in functional class and hemodynamics (how blood flows through vessels),” says physician Aaron Waxman, executive director of the Center for Pulmonary Heart Diseases at Brigham and Women’s Hospital in Boston, a PHA-accredited pulmonary hypertension care center. Waxman was an investigator on the Phase 3 STELLAR study, meaning he was in charge of the trial at his center.
Physicians will need to monitor patients when they first start the drug
to make sure they have no dangerous side effects, according to Merck. Patients who take Winrevair will need to have their hemoglobin and platelets monitored before each dose, for at least the first five doses, to see whether dose adjustments are required.
The blood tests are necessary for two primary reasons: The drug could lead to erythrocytosis, an increase in red blood cells that causes blood to move sluggishly through vessels and organs. In addition, the drug could decrease platelet count. Platelets help form blood clots to stop bleeding.
A low platelet count could increase risk for bleeding. In the clinical trials, increased bleeding occurred more often in those who were also receiving prostacyclin infusions.
Winrevair also can cause harm to a fetus, so patients should use contraception while on Winrevair and for at least four months after their final dose, according to Merck. The company also recommends pregnancy testing before starting Winrevair. Based on studies in animals, Winrevair could also impair female and male fertility.
The last time the FDA approved a PAH treatment was in 2015 when Uptravi (selexipag) became available. More recently, the FDA approved Tyvaso (treprostinil) Inhalation Solution for people whose PH is related to interstitial lung disease. Tyvaso helps relieve shortness of breath so people can exercise more easily.
VENTIPSFROM PASTATTEN D E SE » 8 WAYS To Make The Most of PHA 2024
«
PHA 2024 International PH Conference and Scientific Sessions is Aug. 15-18 in Indianapolis. Discover tips to make to meet new friends, connect with familiar faces, navigate the conference space, learn the latest pulmonary hypertension advancements, and maximize your PHA 2024 experience.
When Michelle Liu took her then 2-year-old daughter Esther to her first PH appointment, the pediatric cardiologist gave them some nonmedical advice. Brian Hanna at Children’s Hospital of Philadelphia advised them to attend a PHA International PH Conference and Scientific Sessions because it would change their outlook on pulmonary hypertension.
Since then, the mother and daughter have attended three conferences and gained new experiences each time.
“We met folks at each conference whom we have kept in touch with over the years,” says Liu, a physician and member of the Pulmonary Hypertension Association Board of Trustees. “Although some have passed away, we carry their memories with us and continue to have hope.”
Liu, her daughter Esther and their whole family plan to attend PHA 2024 to celebrate the 10-year anniversary of Esther’s lung transplant. Her donor’s family lives in Indianapolis and will join Liu’s family in the festivities, which will make the occasion extra special.
Liu is among the previous conference attendees who offer advice for navigating the PHA 2024 conference, Aug. 15-18 in Indianapolis. Here are their suggestions:
1
APPLY FOR A SCHOLARSHIP. Helina Ofori and her mother applied for stipends to attend PHA 2022. Ofori cares for her mother who has PH, and the pair co-lead PHA’s Cleveland Support Group. Ofori said she felt blessed to receive the stipend as it helped her enjoy precious time with her mom.
There are three scholarship options: U.S. adult, U.S. pediatric and international, plus a stipend for PHA support group leaders and/or volunteer peer mentors). Scholarships help cover travel and hotel expenses for people with PH and a caregiver and are administered on a first-come, first-served basis. Apply early. Although the scholarship deadline is May 15, the slots fill up quickly.
2
MAKE SURE YOUR MEMBERSHIP IS UP TO DATE. PHA members receive conference discounts, and some are eligible for scholarships or stipends. To be eligible for a scholarship, you need to be a PHA member, demonstrate financial need and meet other criteria.
3
EXPLORE BREAKOUT SESSIONS. PHA volunteer Stephen Carter-Hicks recommends looking at the schedule beforehand and picking a few sessions and activities to attend. By planning your sessions in advance, you can see which are close by to minimize stress and fatigue, he says.
Above: Volunteer support networking event at PHA 2022.
Opposite page, clockwise from top left: Michelle Liu and daughter Ester; PHA 2022 attendees; Nicole Creech and Riley Wiegele; PHA 2022 attendees; Helina and Pat Ofori; Deborah Hines-Bruce and Gary Bruce.
NETWORK WITH PATIENTS AND HEALTH CARE PROFESSIONALS. Ofori recommends sitting at a new table for meals every day to meet new people. She said everyone is super friendly and eager to engage with each other. Through networking, Ofori learned that a lot of health care professionals get into the medical field because of family and friends with rare diseases, which she found interesting and humanizing.
KEEP AN OPEN MIND. Sometimes a spontaneous activity or meeting a new friend may be the most memorable part, Carter-Hicks says. “Embracing opportunities and invitations is a great way to get the full conference experience,” Carter-Hicks says. That’s especially true for Dallas support group leader Gary Bruce, who met his wife and fellow support group leader Deborah HinesBruce at a PHA conference.
EXPLORE A NEW CITY. Conference can be overstimulating with so many fun activities to participate in, but Ofori recommends taking some time to enjoy a new city. Indianapolis has a lot to offer with interesting excursions for the whole family, as we reported in the March issue of Pathlight.
5 6 7 8 4
SHARE YOUR PERSPECTIVE. Think of ways your experience can help others learn something new at conference, Liu says. Whether you have oxygen tips or you’re a long-time thriver ready to help new patients, share your ideas with PHA staff to maximize the conference experience.
DON’T MISS THE FASHION SHOW. One featured session Liu wishes she attended sooner is the fashion show, where patients model stylish ways to wear their oxygen. “We didn’t attend until our third conference, and it truly is a must-see,” Liu says.
There are four categories to model in: formal wear, PHA pride (zebra and purple), sports and superheroes. All models must be people with PH. Fill out the application at surveymonkey.com/r/PHA2024FashionShow to describe your outfit and let us know which category you’ll be modeling in.
Register today at PHAssociation.org/PHA2024.
Get a Sneak Preview of PHA 2024 Scientific Sessions
Health professionals: Mark your calendar for PHA 2024 International PH Conference and Scientific Sessions, August 15-18, in Indianapolis.
This year’s Scientific Sessions, “United Toward a Cure,” will focus on empowering health care professionals through the shared resources of the international pulmonary hypertension community. By leveraging those resources, health care professionals can improve their knowledge and skills to deliver quality, patient-centered care.
One of the highlights of the Scientific Sessions this year is the joint session from the Pulmonary Vascular Research Institute and the
Pulmonary Hypertension Association. The session, “Real-World Evidence in PAH,” will build on the PHA/PVRI session that took place at the PVRI Annual Congress in London earlier this year. Sandeep Sahay, co-director of the pulmonary hypertension and CTEPH programs at Houston Methodist Hospital, will lead the PHA 2024 session.
The session will feature leaders from the PVRI Real World-Evidence and Real-World Data Task Force, who will discuss how real-world evidence can complement knowledge gained through randomized clinical trials. Randomized clinical trials are considered the gold standard for developing scientific evidence about new drugs and therapies. However the results can be difficult
One of the many activities you should add to your PHA 2024 itinerary is a support group. In addition to education sessions, social events and the exhibit hall, PHA 2024 International PH Conference and Scientific Sessions offers 12 on-site support groups for people with PH, families and caregivers.
Experienced patient and caregiver leaders will guide the discussions, where participants can meet others in similar situations, gain support and share knowledge. Join a discussion for tips to address challenges and manage pulmonary hypertension from others who live with the disease. Find your PH community by participating in one of these groups at PHA 2024: Beginning your PH journey: For those recently diagnosed with PH or are trying to find your new normal.
Sandeep Sahay, MD
Yuri Matusov, MD
to generalize for broader, more diverse populations seen in everyday life.
Presenters will cover how RWE/ RWD is relevant to PH, regulatory review and pragmatic clinical trial designs. They will discuss RWE/RWD in relation to PAH as well as regulatory requirements for therapy approval.
Sahay is an associate professor at Houston Methodist with extensive clinical and research interest in pulmonary vascular diseases. He is chair of the American College of Chest Physicians PVD section and associate editor of Pulmonary Circulation, JHLT Open and Respiratory Medicine journals.
Another highlight from the Scientific Sessions will be on changing the paradigm in treating patients with pulmonary hypertension and parenchymal lung disease. The session, led by Yuri Matusov, assistant professor of medicine at Cedars-Sinai Medical Center, will explore interstitial lung
disease, chronic obstructive pulmonary disease and pediatric lung diseaseassociated PH. Presenters will discuss how some people with ILD and COPD respond to systemic pulmonary vasodilators.
Matusov is co-director of the pulmonary hypertension program at Cedars-Sinai, as well as director of research for the pulmonary and critical care fellowship. He is an active researcher in pulmonary vascular disease and intensive care and participates in the Pulmonary Circulation Assembly for the American Thoracic Society.
Other session topics that will be featured during the Scientific Sessions include:
• Translating the ESC/ERS Guidelines and seventh World Symposium recommendations into real world clinical practice.
• Emerging therapies in PH.
• The role of registries and databases in PH.
PH with an associated condition: If you have a condition related to pulmonary hypertension, such as COPD, HHT, HIV, lupus, sarcoidosis, scleroderma and sleep apnea, consider participating in this group.
Chronic thromboembolic pulmonary hypertension: For anyone affected by CTEPH.
Continuing your PH journey: For those who’ve lived with PH for at least eight years.
Young adults: For people with PH between 18 and 35 who want to connect with people in their age group.
Parents: Connect with others raising a child with PH.
Caring for someone with PH: For caregivers or people close to someone with PH (e.g., spouses, partners, friends, children).
PHA conferences attract hundreds of health care professionals, patients and caregivers every two years. Join more than 500 health care professionals for opportunities to network with your peers, earn continuing education credit and engage in need-to-know topics led by renowned PH experts. All PHtreating health care professionals are encouraged to attend.
Learn more about the Scientific Sessions at PHAassociation.org/ PHA2024.
Pump therapy for pulmonary arterial hypertension (Group 1 PH): For those with PAH who use or are considering pump therapy.
Oxygen therapy: For anyone with PH who uses or is considering oxygen therapy.
Men with PH.
Coping with grief: For anyone grieving the loss of a loved one to PH.
Grupo de Hispanohablantes: Para cualquier persona que viva con hipertensión pulmonar y hable español.
Look for the support group schedule at PHAassociation.org/2024.
Exercise And PH
Boost Your Health and Confidence With Activity
Sydney Lewis plays volleyball nearly every day. She competes on a travel team from November through June and on her school team from August through October. She practices three times a week and competes in tournaments most weekends. But she needs an elevator pass at school because of her pulmonary arterial hypertension.
“I can go down the stairs with no problems,” says Lewis, 13, of Leesburg, Virginia. “But a whole two hours of volleyball practice is easier than going up two flights of stairs.”
That’s because steps are by far the hardest thing for anyone to do, whether or not they have PH, says Jim White, a PH specialist and researcher at the University of Rochester Medical Center in New York. When going up stairs, people use their hearts to lift themselves straight up at least 12 feet for every floor.
“If you weigh 100 pounds, you’re moving 100 pounds up 25 feet for two flights,” says White, who worked with the Pulmonary Hypertension Association to create its exercise video series. “If you weigh 200 pounds, that’s even more of a challenge.”
For people with PH, stairs — and other aerobic activity — are even
harder than they are for the general population. But aerobic exercise — with the approval of a patient’s care team — can offer similar benefits to people with PH as it does for those without PH.
Endurance or aerobic activities like walking, stationary bike riding, water walking and swimming increase your heart rate in a sustained way, White says.
EXERCISING WITH PH
Lewis is among the many people who balance physical activity with the challenges of pulmonary hypertension. She plays basketball with her friends or brother, rides her bike or scooter and likes to dance in addition to playing competitive volleyball.
Joanne Szelag, 52, of Suffield, Connecticut, also makes time to exercise, with accommodations for her PH and other health issues. Since she added modified exercise classes to her pulmonary rehab in 2022, her PH and endurance have improved, she feels stronger, and she has less shortness of breath. During a check-up in March, she walked 1,200 feet in six minutes, compared to 900 feet in October 2023. Her echocardiogram showed decreased pulmonary pressure.
“This is a great improvement for me,” says Szelag, who was diagnosed in 2016 with Group 2 PH caused by left-
‘I like that my heart is pumping and that I am building strength in my arms.’
JOANNE SZELAG
heart disease. She also has sleep apnea, which can worsen PH symptoms.
HEALTH BENEFITS
Physical activity has been shown to improve symptoms and quality of life for adults with PH. Some small studies have shown similar improvement in children, says Catherine Avitabile, cardiologist at Children’s Hospital of Philadelphia and assistant professor of pediatrics at the University of Pennsylvania School of Medicine. Exercise helps muscles become more efficient at using oxygen. As a result, people with PH can perform regular activities with less fatigue and less shortness of breath for longer periods of time, says Aimee Layton, associate professor of applied physiology in pediatrics at Columbia University Irving Medical Center.
However, people with PH sometimes are less active if their symptoms make them less functional, Avitabile says. Others might be less functional because they aren’t regularly active.
That wasn’t the case for Lewis, who found a way to adapt. She began playing basketball in second grade but switched to volleyball two years later. She discovered that volleyball was much less tiring because of the smaller court. After practice, she’s usually more sore than fatigued.
“The PH doesn’t really affect me,” says Lewis, who was 2 when she was diagnosed with PH. “When playing sports, I stop or slow down if I don’t feel well. Then I speed back when I recover.”
Volleyball isn’t a high heart-rate sport like basketball, White says, which also can explain why Lewis finds her
two-hour practice easier than climbing stairs. “The ‘intensity’ is about mental acuity mainly (knowing where the ball is going) and moving your body into the correct position. Yes, there’s some short sprinting to do that, but it’s not about a mad dash 70 feet down the court for a layup, White says.”
Lewis says her PH isn’t that severe, and she has a high symptom tolerance, her mom says. “She just keeps going,” says Genie Lewis, an emergency room physician at Inova Loudon Hospital in Virginia. “She’s been through a lot more pain than other kids.”
‘I can go down the stairs with no problems, but a whole two hours of volleyball practice is easier than going up two flights of stairs.’
SYDNEY LEWIS
Lewis’ exercise likely contributes to how well she feels. “She can do more than the average person because she does an above average amount of exercise,” Genie Lewis says.
BUILDING STRENGTH AND CONFIDENCE
In addition to improving overall musculoskeletal health, quality of life and symptoms, exercise can improve mental health.
“I feel great after exercise class,” Szelag says. “It builds your confidence. I always had some fear it would make my PH or my legs worse. It has been the opposite. I feel better physically and mentally.”
Szelag was in physical therapy for osteoarthritis in both knees, but her pulmonologist and primary care physician wanted her to add more activity to her routine. A social worker encouraged her to try a seated exercise class for people with mobility challenges at her senior center.
When that class ended in fall 2023, Szelag joined an active and fit class, which includes sitting and standing exercises. All exercises can be modified according to ability. She built up to standing exercises after she received an injection in her knees. “I started slow, and now I can stand up for many exercises (not all) as long as I hold on to a chair.”
Szelag’s class also includes aerobics and lifting light weights while seated. “I like that my heart is pumping and that I am building strength in my arms.”
CONFRONTING CHALLENGES
Despite the benefits of exercise, many patients face barriers to staying physically active. Some people fear harm or injury, breathlessness or inability to keep up. Others don’t want to be bogged down by oxygen tanks or other treatment accessories.
“Oxygen can be heavy, it can run out, people may look at you funny,” Layton acknowledges. But patients often find exercise freeing after they find methods to carry their oxygen, such as biking with saddle bags or using a stroller to hold the tank while walking. They “feel like they have some of their life back despite the disease.”
For Lewis, the hardest thing about having PH and playing sports is a feeling of being different. Most of her teammates don’t know about her PH,
and her coaches don’t really know what it is.
“Last year, the coach wanted me to play better,” Lewis said. “When I slowed down, she would yell at me. I didn’t tell anyone I had PH. They just thought I was lazy.”
Genie Lewis respects her daughter’s decision, so she doesn’t make a big deal, even when the team had to run 108 extra sprints for missing serves. However, she thinks it would be helpful for the coach to know more about PH.
“A lot of kids in this age want to be treated like everyone else,” Genie Lewis says. “But I feel like if I talked to her coach, she would have a different perception.”
Avitabile says it’s normal for her pediatric patients to worry about being singled out for different abilities. While many people like to be active with friends, being compared to friends with different abilities can have a negative effect, especially for
youth. “Children (like adults) usually do best with some form of extrinsic motivation,” she says. “It’s hard to stay active just because it is good for you.”
Those most successful at incorporating exercise into their lives have found an activity that interests them, brings them joy and helps them feel good about themselves, Avitabile says. That could be walking the dog, dancing, biking or playing basketball in the driveway.
‘JUST RIGHT’
Before Layton’s patients start a new physical activity, they undergo a cardiopulmonary exercise test to confirm exercise is safe for them. The test also provides target heart rate zones they can aim for while being active.
“We call it the ‘Goldilocks principle’ — not too hard that you are putting your heart under undue stress but not so easy that you won’t see any improvements in fitness from your exercise,” Layton says.
Joanne Szelag (second from right) and family at her nephew’s wedding. From left: newlyweds Casey and Anthony Szelag and Joanne’s husband Stanley,
Get Motivated WITH THESE 7 TIPS
Talk with your care team about a safe exercise program tailored for you, says patient Joanne Szelag. Or research exercise programs on your own and get approval from your care team. Ask your care team what steps to take to keep you safe. For example, Szelag learned in pulmonary rehab to use her inhaler right before exercise.
Don’t be afraid to try to exercise. It will be difficult at the beginning, and you might feel more short of breath than usual, Szelag says. “However, taking on the challenge of exercise can gradually improve your PH, as it did for me.”
Commit to a routine and start right away, says James White, a pulmonologist and researcher at University of Rochester Medical Center, a Pulmonary Hypertension Association-accredited PH Care Center. Set aside 30 minutes a day a few days a week, even if you can only do two or three minutes before you
have to rest for 30 to 90 seconds. After resting, start again: Exercise and rest until you finish the 30 minutes.
Eventually, you’ll notice that you don’t need to rest as much, and soon you will be exercising for 30 minutes at a time, he says.
Slow down if you get breathless so you don’t pass out. It gets easier the more you get in shape, says Sydney Lewis, who used to need oxygen while sleeping or on flights. “I used to not be able to walk up the street or go up one flight of stairs without fainting,” Lewis says. “Now I can jog up the street. Exercise sure helps with your breathing.”
Work with your care team to get the most from your medication. When Lewis was diagnosed, there were only five FDA-approved medications for PAH. None were for 2-yearolds. Today, Lewis takes selexipag, ambrisentan and tadalafil — each for a different pathway to relax blood vessels and improve blood flow so it’s easier to exercise. When selexipag became
Aimee Layton, MD
Catherine Avitabile, MD
more available for children with PH, Lewis wanted to transition from oral treprostinil so she didn’t have to take a dose in the middle of the school day, her parents let her be part of the decision. Lewis says she was sicker during the transition but now is better than before.
Similarly, Szelag believes her medication regimen has contributed to her improvement: sildenafil to relax her blood vessels; furosemide to eliminate excess fluid that puts pressure on the heart, and an albuterol inhaler. She also watches her fluid intake, follows a low-sodium diet and works closely with her care team.
Consider these words of wisdom from cardiologist Catherine Avitabile. “When patients are having difficulty
‘What are you waiting for? A stronger, more confident and capable you is less than three months away when you start today.’
JAMES WHITE, MD, PHD
getting or staying active, I like to give them the following pep talk:
• You are amazing!
• Stay positive.
• Focus on your strengths.
• Be proud of yourself.
• Tell your family and friends about your activity. They will be proud of you too.
• Remember that even small change is great change.
• Call your care team if you need a virtual high five.
Check out PHA’s exercise video series, White recommends. The videos describe the benefits of exercise, two of which will emerge relatively early on. The first is increased stamina to do the necessities and enjoy the moments of life. The second is increased sense of control and capability. “You CAN do at least some of the things you need and want to do,” White says.
Other benefits like weight loss and a return to more “normal” levels of physical activity could
take months and years, but increased stamina and capability should come within a few weeks or at most two to three months, White says.
Alternate endurance activities with strength training , such as two or three days a week for each type. Strength training is equally important to build upper body muscles that help you feel capable and in control, so you can do the things you need to do every day and the things you want to do on special days. Light weights, stretchy bands, or yoga positions can build your arm, shoulder and chest strength.
“What are you waiting for?” White says. “A stronger, more confident and capable you is less than three months away when you start today.
Get started on your exercise routine with our video series. Visit PHAssociation.org/ classroom/ living-with-ph.
Advocacy Brings Hope For a Better Future
In summer 2022, Kendra Hearon noticed her son Cash was getting tired more often, sleeping a lot even during his classes, moving slower and losing weight. She chalked it up to working hard at football practice and being a normal, busy teenager.
That July, Hearon took her eldest son to the hospital, thinking severe dehydration was making him so sick. After two week-long stays at different hospitals, Cash received his idiopathic pulmonary arterial hypertension diagnosis.
“Cash was extremely sick,” Hearon says. “He was within days of dying. We had no idea.”
Cash’s experience prompted Hearon to get involved with the Pulmonary Hypertension Association community. Hearon, who works in human resources and stays busy as a single parent raising her two boys, is now a committed PH advocate.
PICTURE OF HEALTH
Cash was the last person you’d expect to be sick. Standing at 6' 3" and weighing 250 pounds, his athletic build made him well-suited to play
Left: Cash, Kendra and Reily Hearon.
center position on his high school football team.
He’s always been active: playing football since age 6, playing trumpet in marching band, fishing and riding on his four-wheeler.
He’s usually the life of the party and loves to make people laugh, his mom says. He’s extremely close with his younger brother, Reily, who was born with a congenital heart defect and needed two surgeries as an infant.
But two years ago, Cash was the son with a medical emergency. It was a whirlwind time of life-changing, frightening moments for Cash, his family and friends. At times, Hearon wasn’t sure her son would make it.
In the hospital, Cash’s medical team acted quickly. He was put on supplemental oxygen 24/7 and went from one to two oral medications. The next month, he received his Remunity pump at Monroe Carell Jr. Children’s Hospital at Vanderbilt University Medical Center.
Through it all, Cash had an amazing support system of friends and family. His best friend has been by his side through it all, bringing bottles of Gatorade on that July afternoon when everyone thought Cash was just dehydrated. On a recent night when Cash wasn’t feeling well, they hung out at home, listening to old-school country music singers like George Jones and Conway Twitty.
A MOM’S QUEST
Adjusting to the abrupt change in her eldest son’s life has been challenging. Hearon has sometimes struggled with lonely, scary, dark feelings that stemmed from the reality of his diagnosis.
Last year, she turned to the internet to search for answers and find others in situations similar to her family’s. She found the Pulmonary Hypertension Association and joined PHA’s World PH Day advocacy campaign in May 2023.
“Reaching out to PHA has helped me cope with Cash’s diagnosis,” says Hearon, who is learning about legislation to help people with PH and their families.
A big concern for Hearon is what will happen to Cash as he gets older. His insurance under TennCare Kids through his home state fully covers the expensive triple therapy that is keeping Cash stable, but that coverage will end when he turns 21.
Cash, now 18, works full-time at a boat dock-building company and wants to keep working. He has some good days and some bad, but he manages the physical demands of the job.
Cash has big dreams to one day own a construction business and buy a piece of land to build a house. But Hearon worries he may need to apply for disability to get insurance that would cover his PH treatments. She also realizes he might need to go back to using supplemental oxygen.
Those concerns motivated Hearon to start advocating with PHA. She is working now to ensure a better quality of life for her son’s future.
In the past year, Hearon has met with staff from all three of her legislators’ offices, Republican Sens. Marsha Blackburn and Bill Hagerty and Rep. Chuck Fleischmann. She has asked for the Tennessee legislators’ support of the Safe Step Act and H.E.L.P. Copays Act. She
has described the importance of Cash quickly accessing the lifesaving medication his doctor prescribed without going through the slow process of step therapy.
Hearon also has shared her concerns about the affordability of her son’s expensive medications, and how copay accumulator policies might affect him when he has his own insurance plan. She knows Cash likely will need daily supplemental oxygen as his disease progresses, so she also advocates for easier access to medically appropriate forms of supplemental oxygen.
“I have tried to turn some of my pain into something good,” Hearon says. “My hope is one day for a cure for this terrible disease and for my son to live a long, prosperous, happy, healthy life. I will do everything within my power to see this happen.”
If the Hearon family’s story inspires you, consider getting involved with PHA’s advocacy program. Email us at Advocacy@ PHAssociation.org or call 301-565-3004, ext. 758. Visit PHAssociation.org/ advocate.
ADVOCACY IN ACTION
PHA Sees Progress on Oxygen Bill, Accumulator Ban
Thanks to PHA advocates and other patient organizations, a bill to improve oxygen access has been introduced in Congress.
The bill seeks to remove supplemental oxygen from Medicare’s competitive bidding process, making oxygen and related equipment more affordable and accessible.
The legislation also would improve access to specialist care by requiring insurance to pay for respiratory therapy services. The Supplemental Oxygen Access Reform bill also would spell out patient rights.
The Pulmonary Hypertension Association has advocated for years to improve access to supplemental oxygen. For the past year, PHA has worked with a coalition that includes the American Lung Association, American Thoracic Society and other patient organizations to bring forward oxygen-access legislation.
“The bill’s introduction in the Senate is just the first step,” said Katie Kroner, PHA’s vice president of advocacy and patient engagement. “Advocate voices are essential to drive the new bill through the legislative process.”
PHA also has fought copay accumulators for years. In January, PHA hailed a federal agency’s decision to no longer appeal a 2020 federal court ruling on patient cost-sharing. The ruling prevents insurance companies from shifting health care costs on patients through a burdensome practice known as copay accumulators.
Insurance companies must now count copay assistance from third parties toward deductibles and out-of-pocket costs, as a result of a recent move by the Department of Health and Human Services.
Katie Kroner, PHA’s vice president of advocacy (left), with Colleen Brunetti, immediate past president of the PHA Board of Trustees, and PHA CEO Matt Granato on Capitol Hill.
“This is good news for people with pulmonary hypertension and others who rely on copay assistance to pay for expensive, life-saving medication,” Kroner said. “Copay accumulators allowed insurance companies to profit from copay assistance meant to help patients without reducing patients’ financial burdens.”
Some pharmaceutical companies and charitable organizations offer financial assistance to help patients pay for expensive drugs, such as pulmonary hypertension treatments. However, in 2017, some health insurers began implementing copay accumulator adjustment policies.
The practice allowed beneficiaries to use third-party copay assistance but prevented those payments from counting toward annual deductibles or out-of-pocket maximums. As a result, many people couldn’t reach their deductibles. When their copay assistance grants ran out, many people had to meet their full deductibles for the year. That made it nearly impossible for people with chronic health conditions like PH to afford their life-saving medications.
Patient advocacy groups sued HHS for permitting copay accumulator policies. In September 2023, a federal court in Washington, D.C., called the policies arbitrary and capricious and said they contradicted the intent of the law.
As part of the All Copays Count Coalition, PHA and 85 other patient organizations urge the Health and Human Services Department to quickly enforce the rule and instruct insurers on how to comply.
At least 20 states require insurers to apply payment assistance toward patient deductibles and out-of-pocket limits. PHA will work with the All Copays Count Coalition to distribute information to patients and health care providers on how to combat these now-illegal policies.
Learn more about legislative and regulatory issues that affect the PH community and get involved. Visit PHAssociation.org/advocate.
Considering a Gift to PHA?
Explore These Easy Ways to Increase Your Impact
Questions? Email us at giving@PHAssociation.org Call: 301-565-3004, ext. 755 Online: PHAssociation.org/ donate/information
IRA: If you’re 70½ or older, you can make a gift through your IRA. If you’re over 72, you can make a gift from your required minimum distribution.
Donor-advised fund: If you have a donor-advised fund, you’ve already set aside money for charitable donations, so giving from this fund won’t cost you anything extra.
Stock: You can give appreciated securities to PHA rather than sell them and donate their proceeds. This option comes with tax benefits and helps diversify your assets.
Employer matching gift programs: Check with your employer to see if they match charitable contributions from employees. You can double or triple the impact of your donation, depending on your employer’s program.
Use the FreeWill online tool to explore giving options: freewill.com/smartgiving/phassociation.
Part D Beneficiaries Starting To See Lower Costs
Kim Everett of Manitowoc, Wisconsin, was surprised in March when she went to refill a pulmonary hypertension medication. Her pharmacist said her next medication would be free because she had reached the catastrophic coverage threshold.
Although Everett was aware of changes to Medicare Part D because of the Inflation Reduction Act, she hadn’t realized how much they would benefit her.
The Inflation Reduction Act, enacted in 2022, reduces out-of-pocket prescription costs for Medicare Part D beneficiaries. The legislation is significant for the PH community because of the high cost of treatments for complex pulmonary conditions.
OUT-OF-POCKET SPENDING CAP
One of the most significant changes this year is an out-of-pocket spending cap on some prescription drugs. When patient spending reaches $8,000, known as the catastrophic coverage phase, they no longer have to pay a 5% copay for prescriptions covered under Part D.
The payments that count toward the threshold include out-of-pocket costs, plus the value of certain payments made on behalf of the beneficiary, including Medicare’s Extra Help program and manufacturer discounts.
Everett didn’t realize the change applied to all her Part D-covered drugs, not just the ones for PH.
“This is going to change how I ask my doctors to manage my scripts,” says Everett, who is no stranger to the cost of treatments.
Diagnosed in 1983 with lupus, Everett has struggled with blood clotting and bleeding issues. In 2003, she was diagnosed with pulmonary arterial hypertension related to her lupus. She typically takes at least six medications, many of
which are costly. Sometimes she has to combat her autoimmune symptoms with over-the-counter allergy medications because the prescription allergy drug is too expensive.
“I’m looking forward to next year when it will be even easier to deal with the copay costs,” Everett says.
OTHER CHANGES
In 2025, Medicare will cap Part D beneficiaries’ out-of-pocket costs at $2,000 and give them the option to spread that expense over 12 months.
Previously, beneficiaries paid a 5% copay when their drug spending reached the catastrophic phase. There was no limit on how much beneficiaries paid for coinsurance, which made many high-cost medications unaffordable.
Another key change this year is that all Part D beneficiaries who qualify for Medicare Extra Help (low income subsidy) will be eligible for full subsidies. That means they will have no premiums, no deductibles and lower coinsurance for brand and generic drugs.
The change applies to Part D beneficiaries who earn less than 150% of the federal poverty level. The income threshold previously was 135%. The change will make medications more affordable and accessible for eligible Medicare beneficiaries.
Watch PHA’s five-minute video with details about the 2024 policy changes. Find out which payments will count toward the catastrophic threshold: shorturl.at/dCPQS.
Questions? Contact PHA’s Treatment Access program at Inflation@ PHAssociation.org or call 240-485-0758.
PH Nurse Creates Support Group To Connect Her Patients
BRITTANY WATSON is the pulmonary arterial hypertension nurse coordinator for The Oregon Clinic, a Pulmonary Hypertension Association-accredited PH Care Center. She also leads the Northeast Portland PHA support group. Watson, who has spent most of her 11-year nursing career in pulmonary and critical care, lives in West Linn, Oregon, with her 18-month-old daughter Norah, husband Charlie and their needy dachshund Rodney.
BY BRITTANY WATSON
Before working in pulmonary care, I knew little about PH. In nursing school, I learned only that pulmonary hypertension exists and that it’s rare. On the job, I learned that PH is a complex disease that requires a lot of support and guidance from the health care system.
Change to: I’m truly blessed to have had the opportunity to learn in-depth about PH, which has enabled me to better support the PH community.
SUPPORT AND CONNECTION
I started a PHA support group in 2023 because I was finding that a lot of my patients needed more support and connection from others who understood their disease. As a support group leader, I can extend my care for our PAH community. We meet every three months via Zoom.
The most rewarding part of leading a PHA support group is serving the PAH community. If I can create even the smallest amount of support for the community, that is enough reward for me.
I’m proud that our community is so welcoming and gracious to one another. It’s truly heartwarming to see
how people living with PAH support each other.
The people who inspire me most are PAH doctors Grant Farr, Lianne Lin, Wayne Strauss and Rhett Cummings, as well as physician assistant Caitlin Fields. Their dedication to patient care and the PAH community is phenomenal.
I also find our PAH patients inspiring. They have so much courage, strength and motivation to tackle the daily burdens of PAH.
If you are considering starting a PHA support group, my advice would
be to do it. It can be a little time consuming, but it is well worth the effort.
Start a support group. Apply to become a PHA support group leader: PHAssociation.org/get-involved/ volunteer. PHA will provide you with training and resources every step of the way.
Find a support group: PHAssociation.org supportgroups.
Donor Didn’t Realize She Was Investing in Her Own Future
Kimberlee Miller had never heard of pulmonary hypertension before her mother’s 2007 diagnosis. Little did she know, the diagnosis not only redefined her mother’s future but also her own.
In the early days of her mother’s diagnosis, when information was scarce and support even scarcer, the Pulmonary Hypertension Association emerged as a beacon of hope. Amid uncertainty, Miller found solace in PHA. Its online community became a lifeline, offering not just answers but an abundance of understanding and empathy. Sadly, Miller’s mother Brenda lived only another 18 months after her diagnosis.
Fifteen years later, Miller was experiencing shortness of breath and went to a cardiologist to determine the cause. History seemed to repeat itself as she underwent a right heart catheterization, confirming she had pulmonary arterial hypertension.
“The diagnosis had an eerie familiarity, reminiscent of my mother’s diagnosis years ago,” Miller recalls.
In the past 16 years, Miller has seen firsthand how understanding and awareness of PH has evolved in the medical community. She appreciates the awareness PHA has brought to the disease and advancements in treatment options.
When her mom was diagnosed, Miller had to explain to health care
providers that Brenda had PH, but the provider often didn’t know what it was. When Miller gave doctors her mom’s medication list, which included high doses of sildenafil, they looked at her quizzically, since that medication was known as Viagra. Today, when Miller tells a health care professional that she has PH, they generally recognize her condition.
“When my mom was diagnosed, there were only two medications approved to treat PH. There are now 15, with more on the way.”
SUPPORTING PH RESEARCH
Miller started contributing to PHA soon after her mother’s diagnosis.
“By giving to PHA, I knew that my donations would help bring awareness and make a positive impact on the lives of those dealing with the disease,” she says. “I never imagined that I would see
the seeds I had sown come to harvest in my own life. I didn’t know I was investing in my own future.”
To those considering giving to PHA, Miller’s message is unequivocal: Donate. It’s a tangible expression of support that fuels groundbreaking research and lifesaving initiatives, she says. PHA’s work to support researchers and educate the medical community is made possible by people like Miller.
Support PHA by making a gift of any amount meaningful to you. Your generosity fuels our mission to improve and extend the lives of those affected by PH and supports valuable programs and research. Visit PHAssociation.org/ donate.
Kimberly Miller (right) and her mother Brenda (left).
New Bequest Supports Original Conference Scholarship Endowment
’The Smiths have left an indelible mark on PHA through their commitments both in life and after.’
- COURTNEY DURHAM, PHA
Barbara Smith had difficulty finding hope when she was diagnosed with pulmonary hypertension in 1995, just months after losing her daughter Angela Smith-Kline and a sister to PH.
When Smith attended PHA 1996 International PH Conference and Scientific Sessions, her outlook changed. She and her husband Vern found comfort in the conference, where they learned the latest information about PH and found a support network of others facing the same challenges.
At the time, she said, “I met some of the bravest, most compassionate and energetic people I've ever known, who were not only managing their disease, but living with it.”
Sadly, Smith passed away in October 2005. Soon after, Vern created the Pulmonary Hypertension Association’s first endowed fund, the Barbara L. Smith Endowment. The endowment provides scholarships for people with PH and caregivers to attend PHA conferences, which helped Smith to find strength during her most difficult times.
Since his initial endowment, more than 1,500 people with PH and caregivers have received scholarships to help them attend PHA conferences. Vern contributed to the endowment until his death in October 2023, when PHA learned that Vern had made provisions for PHA in his will. The Smiths’ business, S&S Electric, also has generously supported PHA for many years.
When Vern passed away in October of 2023 at 84, he left a substantial planned gift to PHA to support the endowment he created in memory of his wife and daughter.
“Such a giving act is a testament to Vern’s enduring philanthropic nature,” said Courtney Durham, director of individual giving, PHA. “It shows his commitment to uplifting the PH community in memory of Barbara and her passion to find a cure for pulmonary hypertension and help those impacted by the disease. The Smiths have left an indelible mark on PHA through their commitments both in life and after.”
COMMITMENT TO THE COMMUNITY
Before Smith died, she devoted nearly10 years to volunteering with PHA. She served on the PHA Board of Trustees from 2002 to 2005 and was the volunteer coordinator for PHA 2004.
In the association’s early years, Barbara set aside a room in her family’s Florida electrical business and recruited family volunteers to help fill orders for brochures and “Pulmonary Hypertension: A Patient’s Survival Guide.” She covered the postage costs herself.
She once said, “I lost my sister and best friend to this disease. I lost my daughter to this disease. Now, I have this disease. I don’t know why I’m still here if it’s not to help other patients.”
If you’re interested in leaving a lasting legacy through PHA, email us at giving@ phassociation.org, call 240-485-0755 or visit freewill.com/PHAssociation.
QUICK TAKES
HOW TO REACH US TEL 301-565-3004 | FAX 301-565-3994
EMAIL PHA@PHAssociation.org
WEB PHAssociation.org
Papers Show How PHA Supports PH Research
PHA research initiatives have informed two recent research papers that increase understanding of pulmonary hypertension. PHA grant recipient Catherine Simpson of Johns Hopkins University explored the kynurenine pathway’s involvement in systemic sclerosis-associated pulmonary arterial hypertension. Simpson’s study, published in the American Journal of Physiology Lung Cellular and Molecular Physiology, used data from the PVDomics project and was partly funded by the PHA’s Aldrighetti Research Award for Young Investigators.
University of California-SF researchers, led by Jacqueline
DesJardin looked into PHA Registry data to explore why men’s survival rates are worse than women’s, despite having more favorable baseline characteristics. DesJardin’s paper, published in the Journal of Heart and Lung Transplantation, addresses a significant phenomenon in PH research: the sex paradox. Hear from DesJardin at PHA 2024 International PH Conference and Scientific Sessions, Aug. 15-18, in Indianapolis, where DesJardin will be a presenter and moderator.
CALENDAR OF EVENTS
■ PHA Events
■ National O₂breathe Events
■ Community Fundraising Events
JUNE 15
Detroit O₂breathe Walk
JUNE 29
Greater Washington, D.C. O₂breathe Walk
AUG. 15-18
PHA 2024 International PH Conference and Scientific Sessions Indianapolis PHAssociation.org/conference
OCT. 26
PHA Connects: PH Community Workshop Phoenix PHAssociation.org/phworkshop
See our calendar at PHAssociation.org/ events.
VIRTUAL FUNDRAISERS
Visit PHAssociation.org/pha-fundraising-events to find a fundraising event in your area.
QUESTIONS? Contact us at 240-485-0762 or events@PHAssociation.org.
Pictured, top to bottom: Jacqueline DesJardin, MD; Catherine Simpson, MD.
PHA’S LEGACY OF HOPE
To honor those who have included PHA in their estate plans or whose legacies have been realized, PHA created the Legacy of Hope Society. PHA is pleased to recognize the following members:
Laura* and Rino Aldrighetti*
Alice A. Arnott*
Sandra A. Awood*
Dauna L. Bauer*
Sylvia M. Becherer*
Joan F. Bennett-Schenecker*
Kris L. Best
Gloria G. Blodgett*
Dorothy E. Bradley*
Mary M. Brady*
R. J. Braun
Roberta F. Browning* and Lee A. Broadbent
Rita and Bruce Brundage
Colleen Brunetti
John and Mary Ann Butler
Stephen Carter-Hicks
Colleen and Shawn Connor
Jane P.* and Harold P. Cooper
James F. Corbett*
Nicole M. Creech
Laura H. D’Anna
Charles W. DeVier, III*
Linda M. Feibel*
Barbara T. Gamer
Stacey Gausling*
Franklin D. Gillespie*
Jeffery S. Hall*
Tammy A.* and Dean S. Hazen
Carl Hicks, Jr.
Phyllis M. Hill*
Jackie Holt
Richard L. Horrocks
Constance G. Ives*
Terri L. Jakuboski*
Stanley T. Jusinski
Laura J. Kelly*
James Kenney
Jessie Kohler-Wenninger
Terri L. Kopp*
Debbie L. and Mitchell Koppelman
Frank D. Koppelman*
Dee* and Walter Kruger*
Gloria J. Lang*
Marie* and Ronald J. Levendoski
Mary Jo* and Thomas Linnen*
Sally Maddox*
Sherry Mannel
Bonnie and Michael D. McGoon
Kay McMillin
Joseph W. Mihuc*
Linda Miles*
Karen S. Moody
Larry D. Moody
Pamela R. Morris
Marjorie D. Mott*
Joyce L. Mowrer*
Pamela and Timothy O’Connor
Helina Ofori
Dorothy M.* and Harry J. Olson*
Theresa “Terry” E. (Cavanaugh) O’Reilly*
Rita and Guy Orth
Patricia R.* and Gerald D. Paton*
Cynthia and John R. Pickles
Jean D. Pitcher*
Carol L. Powell*
Frances A. Price
Carol J. Posner* and Marc Priore
Susan Tess Rae*
Diane Ramirez
Cyndy D. Reynolds*
Dorothy A. Ryan*
James Ryan*
Louise C.* and Gene P.* Salvucci
Judith and Edwin L. Simpson
Kelley Skumautz
Laverne Smith*
Joanne Sperando
Marcia and Jack Stibbs
Helena M. Strauch*
Douglas R. Taylor
Frank A. Tobac*
Martha and Carlos Torres
Deborah J. and Roger K. Towle
Carol B. Ungar
Reinhold Vogel*
Carol E. Vreim
Daniel R. Walsh*
Sharon K. Wendt
Andrea and Stephen L. White
* deceased
Passages
Since the Pulmonary Hypertension Association began publishing Pathlight, “Passages” has provided a place to memorialize people with pulmonary hypertension who pass away. PHA extends its sympathy to the families and friends of these individuals and rededicates itself to its mission in their memory.
Eliana Alderete
Angela Blake Fields
Carol A. Edwards
Matthew Farhart
Gail W. Fricks
Lee Ann Holstein
Brenda P. Kendrick
Cayla Kim
Mickey Krause
Michael Loe
Joyce A. Lorow
Alverne M. Nyhuis
Vicki Olson
David S. Rogers
David Sasaki
Gregory Smith
Nancy K. Stephens
Joyce Stroup
Linda A. Sullivan
Keith Tropp
Karen R. Verlander
Francine P. Williams
The accuracy of this list is important to us. Please contact the PHA office at 301-565-3004 x746 or Passages@PHAssociation.org to share the name of your recently deceased loved one or report an error or omission.
Your donations in memory of others, in honor of others and in support of our mission mean so much to the entire PH community, and we thank you.
If you sometimes feel overwhelmed when it comes to finding answers to your questions about pulmonary arterial hypertension (PAH), you’re not alone. There are others in the PAH community who’ve been right where you are now.
Life with PAH isn’t meant to be navigated alone. That’s why the PAH Initiative was created.
The PAH Initiative reflects United Therapeutics’ commitment to providing you with knowledge and inspiration based on science and research in PAH today. Whether you’ve just been diagnosed or have been living with PAH for a while, we understand the frustrations and fears you may be experiencing.
Peggy, a PAH patient and PAH Initiative Ambassador, with her family.