PREMIUM HYDROPHOBIC IOL with PUre Refractive Optics (PRO) TEchnology

For your daily range of vision
INDUSTRY DELIVERS DOWN UNDER Melbourne didn't disappoint when the global optometry fraternity came to town 17
DEBUNKING MYTHS AND MISCONCEPTIONS Podcast to shed new light on what it's really like practising as a regional ophthalmologist 37
THE CENTREPIECE OF A DRY EYE CLINIC IPL systems are becoming more commonplace, but how can you get the best out of your device?

03
OCT 2023
AUSTRALIA’S LEADING OPHTHALMIC MAGAZINE SINCE 1975
You’d look good in Specsavers
Ranked as one of Australia’s Best Workplaces for 2023.


NATIONAL OPTICAL INDUSTRY DELIVERS ON WORLD STAGE; OSHOW24 DETAILS REVEALED

Organisers of the combined O=MEGA23 and 4th World Congress of Optometry are hailing the success of the three-day event featuring more than 3,500 attendees, various product launches and a thought-provoking clinical program with some of the latest insights on myopia and other conditions.
The collaboration with Optometry Victoria South Australia and the World Council of Optometry (WCO) meant this year’s event had a distinct international flavour – and the industry responded with around 200 international delegates, and WCO president Professor Peter Hendicott – an Australian –delivering an important update on global efforts to lift eyecare quality and accessibility.
Several high-ranking figures
flew into Melbourne from 8-10 September, signifying the importance of the national market to their global businesses. Tokai Optical, who welcomed president Mr Hirokazu Furuzawa from Okazaki in Japan, Eyetelligence with new US-based CEO Mr Jeff Dunkel, and two key figures from Rodenstock HQ in Germany were just some examples.
Off the back of the event, the Optical Distributors and Manufacturers Association (ODMA) announced details for OSHOW24 returning in Sydney at the Hordern Pavilion 17-18 May 2024.
At O=MEGA23, myopia generated some of the liveliest discussions in the clinical conference program and masterclass sessions.
Most notably, a presentation
from Mr Jim Papas on the new TGA-approved repeated low-level red light (RLRL) therapy from Australian firm Eyerising International received numerous questions from myopia authorities such as Drs Kate and Paul Gifford, while details of a new “breakthrough” soft contact lens
for myopia control by Johnson & Johnson Vision, presented by Dr Noel Brennan, almost filled the Goldfields Theatre. In addition, Specsavers ANZ head of professional services Dr Joe Paul delivered the latest update on myopia prevalence in Australia and New Zealand, estimated at 19.7%.
“This is exactly what these sessions are about. It’s a forum to hear directly from researchers and industry, and drill down into topics with back-and-forth discussions,” ODMA CEO Ms Amanda Trotman said.
“And for anyone who is launching a product, it’s an opportunity for them to hear feedback or what the concerns may be, so they can work
continued page 8
EYE DOCTOR PETITIONS QUEENSLAND POLICYMAKERS
Toowoomba’s Dr Andrew McAllister is behind a new petition calling for funding so that public ophthalmology patients in his local area can avoid the burden of travelling to Brisbane’s Princess Alexandra Hospital for treatment.


The petition was lodged on 8 August 2023 and calls on the Queensland Parliament to address the lack of medical and surgical treatment options for patients in the Darling Downs Health Service area for acute ophthalmology presentations via the private rooms of ophthalmologists in Toowoomba.
McAllister, of Toowoomba Retina & Eye Specialists, said currently there was no public hospital access
for patients in Toowoomba and the Darling Downs, with patients transferred via ambulance or private transport to the closest tertiary hospital with ophthalmology registrars, Princess Alexandra Hospital, 1.5 hours way.
This is despite there being six ophthalmologists in Toowoomba that have private practices. They have offered to see public patients, but McAllister said the hospital has repeatedly said that there is no funding to provide an ophthalmology service.
“We understand the cost pressures that the health service is under, which is why I would like to petition the state parliament for
funding so patients who cannot afford treatment do not have to travel to Brisbane,” he told Insight
“There is a travel and accommodation subsidy available for patients and their carers who may need to spend days to weeks in Brisbane for emergency care and follow up. But why not put this funding towards patients staying within their local health district? Currently patients who cannot afford treatment are traveling out of the Darling Downs district for all ophthalmology treatment. What I am proposing is that funding be provided for patients that need acute medical care, which would include a consultation and surgery
continued page 8
COLLABORATIVE CARE
The best cataract surgery outcomes occur when the optometrist and ophthalmologist are united in their approach. Dr John Hogden and optometrist Jason Holland discuss the importance of a strong two-way communication channel (0.5 CPD). page 31
OCT 2023
AUSTRALIA’S LEADING OPHTHALMIC MAGAZINE SINCE 1975
The trade floor occupied 9,000sqm at the Melbourne Convention and Exhibition Centre.
ZEISS at RANZCO 2023.
Join us at RANZCO 2023 Perth to experience first-hand our latest innovations and digital technologies for advancing your ophthalmic workflow - connecting devices, data and applications.
Meet the Experts
Quick dive sessions at the ZEISS booth collaboration zone by renowned experts sharing their experiences using the latest ZEISS ophthalmic solutions. Q&A opportunity if time permits. Scan QR code for speakers, topics and times.
Decision Making in Retinal Disease Symposium

Join us at the ZEISS Hosted Dinner Symposium, an evening dedicated to the hot topic of Decision Making in Retinal Disease - Stay up to date in one of ophthalmology’s fastest changing spaces with our esteemed panel of experts Prof. Paul Mitchell AO, Dr Jane Khan and Prof. Pearse Keane.
VISUMAX 800 Hands-on Demo

Book a hands-on demonstration of the ZEISS VISUMAX 800 in our dedicated ZEISS Corneal Refractive room and experience lenticule extraction with ZEISS SMILE pro option for faster cut speeds1 and easier tissue separation2
Scan QR code for more info.
Scan QR code for invitation.
Book a demo!
1 Data on file, myopia with optical zone 6.5 mm 2 Data on file, verification report
Carl Zeiss Pty Ltd, NSW 2113 AUSTRALIA. Carl Zeiss (NZ) Ltd, AUCKLAND 1026 NZ.
IN THIS ISSUE
EDITORIAL
NEW DIRECTIONS IN DRY EYE
It’s difficult to imagine the despair of dry eye sufferers years ago when sent home from the optometrist with few options. Notwithstanding the persistent discomfort, the lack of validation would have caused many to lose hope.
Thankfully, the industry has come a long way with pivotal moments like the DEWS II report in 2017, the ophthalmic commercialisation of intense pulsed light systems (IPL), an expanding suite of eye lubricants and anti-inflammatories and a greater emphasis on diet, plus more.

20 64
TESTING GROUND
How crucial are clinical placements for trainee optometrists in Australia?
CONGRESS COUNTDOWN
Everything RANZCO 2023 delegates need to know before jet-setting to Perth.
37 83
DRY EYE DUTY
Melbourne optometrist Dr Nicholas Young details his IPL protocols for dry eye disease.


TAXING TIMES
The implications of recent precedent-setting payroll tax court rulings for eye clinics.

Reaching this point hasn’t been easy. Just ask US ophthalmologist Dr Rolando Toyos who recently told Insight about his years-long journey to convince the market IPL had applications in dry eye. Today, the technology has become commonplace and a key differentiator, especially for independent optometry practices in Australia. In general, high quality dry eye care like this is laying the foundation for practices wanting to build their business through clinical reputation.
Most of these practices can be found in the Insight Dry Eye Directory (page 46), Australia’s most comprehensive dry eye guide that has returned in 2023. A key feature of this year’s listings is the number of practices offering more sophisticated treatment options, ensuring a more personalised level of care. There’s also more practices solely devoted to the disease.
Much of this wouldn’t be possible without the access Australia enjoys to innovative products. Many of these are listed in this year’s directory too, with some notable additions being new IPL platforms, preservative-free eye drops and screening devices.

But to make dry eye a worthwhile venture, practices need the clinical nous. This issue includes discussions with Australian eyecare professionals like Dr Nicholas Young, Mr Raj Maiti and Dr Gayatri Banerjee about how they use IPL in their practices, in different ways. Two Melbourne optometrists also discuss their twist on dry eye care by beautifying the customer journey in a similar vein to the skincare industry.
Dry eye remains a major industry challenge, but there’s probably never been a better time to be a dry eye sufferer, with more engaged optometrists, technology and products than ever before.
INSIGHT October 2023 5
FEATURES OCTOBER 2023 07 UPFRONT 09 NEWS THIS MONTH 81 OPTICAL DISPENSING 82 ORTHOPTICS AUSTRALIA 83 MANAGEMENT 84 SOAPBOX 85 CLASSIFIEDS/CALENDAR 86 PEOPLE ON THE MOVE EVERY ISSUE
MYLES HUME Editor






DV1404-0923 Get in touch 1800 225 307 enquiries@dfv.com.au dfv.com.au Achieve the outcomes that you expect and patients deserve. See us at Booth 1 – 4, RANZCO 54th Annual Scientific Congress 20 – 23 OCT 2023, Perth Convention and Exhibition Centre TOMEY CASIA2 SOPHI Phaco HOYA Vivinex™ IOLs LEICA Proveo 8 OCULUS Pentacam® AXL Wave
Just as Insight went to print, PROF GRAHAM BARRETT, a renowned cataract and refractive surgery expert in WA, has been inducted into the inaugural Ophthalmologist Power List Hall of Fame. Launched by The Ophthalmologist publication in August, he was among 10 “irrefutable giants of ophthalmology” included. The list will be an annual event and each subsequent
UPFRONT STAT
year will see five new figures inducted. IN OTHER NEWS, the Royal Victorian Eye and Ear Hospital is inviting Victorian optometrists to participate in its Glaucoma Community Collaborative Care Program (G3CP). Since 2019, the program has provided greater community-based eyecare for patients with mild to moderate glaucoma in a shared-care arrangement. Participating optometrists gain experience in glaucoma co-management and access
to interactive accredited CPD training. FINALLY, a new study comparing eye health advice from an AI chatbot and ophthalmologists found the quality of their answers were not significantly different. “These results suggest ophthalmologists and a large language model may provide comparable quality of ophthalmic advice for a range of patient questions, regardless of their complexity,” the Stanford researchers stated in JAMA Ophthalmology
WEIRD
Authors of systematic review have suggest installing ultraviolet-C light phone sanitisers near hand-washing stations. The study examined mobile phones in hospital settings from 2019- 2023 across 10 countries and revealed almost half of devices were contaminated with SARS-CoV-2. UV-C lights can kill the germs in five to 10 seconds, and would ensure handwashing would not be undone by picking up a mobile device, the study authors said.
WONDERFUL
Blind and low vision passengers will be able to better navigate Melbourne's tram network with a new app. NaviLens codes, with the appearance of brightly coloured QR codes, will be rolled out. When these are scanned, the associated app audibly provides passengers with information on their current location, routes serving the location, as well as live tram arrival information.
WACKY
University of Southern California researchers are developing a stem cell patch for patients with geographic atrophy (GA). Research so far has indicated that it could restore the structure and function of the retina to improve vision. An upcoming Phase 2b clinical trial will evaluate the efficacy of the implant in 24 patients who have suffered vision loss from GA.
DEVELOPING MYOPIA LEADERS
Reducing a patient’s final level of myopia by one diopter reduces the risk of myopic maculopathy by 40%, regardless of the level of myopia. Page 26

WHAT'S ON
THIS
MONTH
Registration is now open for the 54th RANZCO Congress, taking place at Perth Convention and Exhibition Centre. ranzco.edu/events
Complete calendar page 85
NEXT MONTH SILMO ISTANBUL 23 – 26 NOVEMBER
insightnews.com.au
Published by: 379 Docklands Drive, Docklands VIC 3008 T: 03 9690 8766 www.primecreative.com.au
Chief Operating Officer Christine Clancy christine.clancy@primecreative.com.au
Group Managing Editor Sarah Baker sarah.baker@primecreative.com.au
Editor Myles Hume myles.hume@primecreative.com.au
Journalist Rhiannon Bowman rhiannon.bowman@primecreative.com.au
Commissioning Editor, Healthcare Education Jeff Megahan Business Development Manager Luke Ronca luke.ronca@primecreative.com.au
Client Success Manager Salma Kennedy salma.kennedy@primecreative.com.au
Design Production Manager Michelle Weston michelle.weston@primecreative.com.au
Head of Design Blake Storey Graphic Designer Michelle Weston Subscriptions T: 03 9690 8766 subscriptions@primecreative.com.au
The Publisher reserves the right to alter or omit any article or advertisement submitted and requires indemnity from the advertisers and contributors against damages or liabilities that arise from material published. © Copyright – No part of this publication can be reproduced, stored in a retrieval system or transmitted in any means electronic, mechanical, photocopying, recording or otherwise without the permission of the publisher.

INSIGHT October 2023 7
The SILMO show is heading to Turkey, described as a reliable alternative to China in the optical supply chain since the pandemic. silmoistanbul.com RANZCO SCIENTIFIC CONGRESS
20 – 23 OCTOBER
'BOUTIQUE' OSHOW24 MAKING SYDNEY RETURN
continued from page 3
to address them on the spot and through their marketing.”
On the Friday, there were around 2,500 people on site, comprising 900 delegates, 1,200 trade fair attendees and around 400 industry figures. Saturday saw around 800 visitors, and on Sunday approximately 600.
“When you add that up, that’s well over 3,500 over the three days,” Trotman said.
“We have had around 200 international visitors, with around 70 from our friends in New Zealand, and the conference had around 1,100 attendees, which is what we targeted, especially given the amount of CPD that is available online and through other channels today.”
On the trade fair, Trotman said the quality of the exhibits across the 9,000sqm trade floor “blew her away”.

“There has been a buzz in the hall throughout … and there has been nothing but positive feedback,” she said. “Every exhibitor comes for a different reason; some to sell, some for band awareness and others to catch up with existing clients.”
Companies like EssilorLuxottica, OptiMed, HOYA and Wymond-owned Eyes Right Optical, Modstyle and Sunglass Collective were dominant forces on the trade floor, but some of the smaller stands were innovative in their approach.
New technology on the combined Eyetelligence and Eyerising International stand was a hive of activity. The Australian companies have a common link through Professor Mingguang He and have developed, respectively, an AI system that screens for eye diseases, and the new RLRL therapy just approved for myopia management in Australia.
“Our booth has been packed with visitors from small practices, giant practices, peers and societies. There is a genuine curiosity which I interpret to be really important and means we are in a good place to move towards our long-term goal of adoption to benefit patients and clinicians,” Dunkel, Eyetelligence’s CEO, said.
Mr Mark Wymond, CEO and managing director of Eyes Right Optical, Modstyle and Sunglass Collective, was a major exhibitor and happy with the conversations he had. Eyewear supplied by his companies picked up three categories in the ODMA Awards for Excellence program.
“I’ve been able to connect with so many businesses that would usually take me a month to get around and see, so it’s been very valuable,” he said.
“We have spoken to a lot of key decision makers and buying groups, and when you’re releasing so much new product, it is great to get it out to so many people this quickly. It’s been a great show and we are happy to support it in a large way – it’s
always been good to us.”
O=MEGA23 also marked the official launch of Cylite’s Australian-made HP-OCT, and the company’s CEO Ms Kylee Hall was encouraged by the level of interest. This includes a strong delegation of optometrists operating in the specialty contact lens space, but also larger practice owners, as well as new practice owners, seeking a multi-functional instrument.
“People have been following us for a long time and it’s now nice to say the device is ready for orders and delivery at end of the year. It’s also been an opportunity for us to talk about the uniqueness of our technology, and when people sit down and look at images, they start to realise why it’s so different,” she said.
OSHOW24 DETAILS
ODMA's next event is OSHOW24. Trotman said it made sense to hold it at Sydney's Hordern Pavilion again.
"It provides an intimate boutique feel, the venue rental price means the event is financially viable for both the association and the all-important exhibitors. The public transport links and affordable parking are much appreciated by the trade fair visitors, plus there is so much to enjoy within the Moore Park precinct,” she said.
OSHOW24 is being timed near the end of the financial year and to support the planned ONSW/ACT Super Sunday event on Sunday 19 May in Sydney.
REDIRECTED FUNDING WOULD ALLEVIATE PRESSURE
continued from page 3
if needed. This, in turn, will take pressure off the local health service, reduce emergency presentations to the Princess Alexandra Hospital, the ambulance service, and reduce the time for patients and their carers to travel and stay away from their home and support networks. If funding can be provided for acute treatment, I would like to see chronic conditions ... to be managed within our health district as well.”
McAllister said the common referrals that would normally require an urgent review would be medical and surgical causes of acute vision loss, trauma, and other conditions that are at risk of causing loss of vision, loss of the eye or death. If a patient

is unable to afford medical and surgical management via the private rooms, they need to be referred to the tertiary hospital.
“This is where funding is crucial so patients are able to have treatment locally, and we can offer the best possible care for our patients,” he said.
“The out-of-pocket costs for surgical and hospital admission can be several thousands of dollars if you are not privately insured, which is not rebatable through Medicare, and it is a difficult conversation about this cost when patients are at their most vulnerable. If there is a funding stream available, patients then have the freedom of choice on where and when they have treatment locally.”
McAllister said there was no funding available to establish an ophthalmology department at the local hospital.
“I'd like to see funding available from the local hospital to have an urgent assessment and treatment in Toowoomba," he said.
"Other specialties have this arrangement, but this is because they have a presence at the public hospital already and so are funded. It would be great if the patient can be referred to and assessed by a local ophthalmologist rather than transport the patient to Brisbane. There is the ability for ophthalmologists to see patients with immediate access to care within the district, why not utilise it?”
8 INSIGHT October 2023
Dr Andrew McAllister, Toowoomba Retina & Eye Specialists.
NEWS
AROUND 70 FROM OUR FRIENDS IN NEW ZEALAND, AND THE CONFERENCE HAD AROUND 1,100 ATTENDEES.”
AMANDA TROTMAN, ODMA
Quantify brain waves associated with human sensitivity to provide effective visual clarity and comfort


IN BRIEF
OPHTHALMIC AI
Prominent UK ophthalmologist Professor Pearse Keane – considered a global leader in ophthalmic artificial intelligence (AI) advances – will headline AI in Eye Care (including Indigenous perspectives), a two-day conference in Broome, WA, immediately after the 2023 RANZCO Congress. The event will run Tuesday 24 and Wednesday 25 October 2023 at the Cable Beach Resort and feature experts presenting from the UK, US, India and Australia. The conference is organised by Lions Outback Vision founder and director Professor Angus Turner who said attendees can expect engaging discussion with Aboriginal healthcare leaders regarding the ethics of AI research.
INDEPENDENT CAMPAIGN
Eyecare Plus will produce a new series of videos featuring optometrists being interviewed about what they love most about practising independent optometry. The video series will be shot in Sydney to coincide with the Eyecare Plus member boot camp in October this year. Chairman Mr Martin Gregory said the planned video shoot will provide powerful content for digital marketing into the future.“The Eyecare Plus brand is synonymous with independence and clinical excellence in optometry, so featuring our optometrists in video is the most authentic and powerful way of communicating those values and our point of difference,” he said. Eyecare Plus has recorded similar videos successfully in the past.
LEGAL WIN
In the first 'wage theft' case of its kind in Australian legal history, a Federal Court judge ruled that Peninsula Health breached the Fair Work Act when it did not pay class action lead applicant, Dr Gaby Bolton, for work she was authorised to do while working at Frankston Hospital in 2019 and 2020. It is a major development for junior doctors across Victoria, with seven other class actions lodged against 12 of Victoria’s largest health services. "Payment of our hours will hopefully force hospitals to make a change. This isn't a safe environment for junior doctors, and it certainly wasn't a safe environment for the patients we work so hard to care for," Bolton said. Other health services subject to class actions over unpaid overtime to junior doctors are Monash Health, Latrobe Regional Hospital and Bairnsdale Regional, Western Health, Eastern Health and the Royal Womens', Alfred Health and St Vincent's Hospital, Northern Health, Bendigo Health and Melbourne Health and Northeast Health Wangaratta, the ABC reported.
UNSW SOUNDS ALARM AFTER ACANTHAMOEBA DETECTED IN NSW
Sydney researchers are warning swimmers to remove contact lenses before entering the water to avoid the risk of infection, after identifying Acanthamoeba in seawater at four NSW coastal sites.

The new research, published in Science of The Total Environment, is a collaboration between UNSW Sydney, University of Technology Sydney (UTS) and the University of the West of Scotland.

Acanthamoeba keratitis (AK) occurs when Acanthamoeba infects the cornea, leading to inflammation and damage. According to the current literature, infection is difficult to eradicate due to the absence of drugs that can kill Acanthamoeba in both its cyst and trophozoite life stages. This can lead to vision loss, with around one quarter of AK patients ending up with less than 25% of vision or becoming blind.
Levels of Acanthamoeba in Australian aquatic environments have not been studied until now. During the study, the researchers collected samples from the fours site from August 2019 to July 2020. Acanthamoeba was present in samples
from all four locations, with 38% testing positive. For the most highly urbanised site, more than 50% of the samples tested positive. In contrast, for the least urbanised site, 32% of the samples contained Acanthamoeba
The study found a positive correlation between the presence of Acanthamoeba and elevated levels of the intl1 gene in the water samples. The intl1 gene serves as an indicator of contamination in aquatic habitats due to human activity.
Taken together, this suggests urbanised coastal sites could be impacted by contaminants like sewage, animal faeces and stormwater.
“The contaminated water allows the Acanthamoeba to flourish, as it feeds on the nutrients and a wide range of bacteria,” said first author Mr Binod Rayamajhee.
The researchers also found Acanthamoeba was more prevalent during the summer months. In January, 65% of samples tested positive (the highest rate), compared to 5% in September (the lowest rate).
SPECS FOR BABIES WITH CONGENITAL CATARACTS
The OneSight EssilorLuxottica Foundation recently held a clinic at The Westmead Royal Children’s Hospital in Sydney to provide aphakic spectacles for babies born with congenital cataracts. Eyecare professionals representing the charitable arm of EssilorLuxottica provided the eyewear for 15 babies and their families free-of-charge in July 2023.
Families attending ophthalmology outpatient appointments or surgery are bulk billed under Medciare, and therefore do not face any out-of-pocket costs. But optical aids, medications and other consumables are not covered by Medicare. Further, many children with congenital cataracts have multiple disabilities and/or require extra care, with some parents forgoing gainful employment to become full time carers.
Patients Ailish – both born with congenital cataract – was involved in the recent clinic and was prescribed aphakic glasses as part of visual rehabilitation since cataract surgery at a few weeks of age.

In infants, aphakic contact lenses and/ or aphakic glasses are used initially and a few years later, if surgically appropriate for the patient, then secondary intraocular lens implantation occurs once the eye has reached adult size.
Eye Clinic – Ophthalmology and Orthoptic Departments at The Children's Hospital at Westmead treats on average 12 new babies each year.
10 INSIGHT October 2023
NEWS
Ailish received a pair of aphakic spectacles at the clinic at The Westmead Royal Children’s Hospital.
Acanthamoeba keratitis affects 10-40 Australians per year.
For
For more information please contact your Bausch + Lomb Territory Manager, Customer Service at Customer.Service@bausch.com or scan the code to receive a call back.
PREMIUM HYDROPHOBIC IOL
PUre Refractive Optics
TEchnology
with
(PRO)
of
your daily range
vision
DCIVA: Distance-corrected intermediate visual acuity. UIVA: Uncorrected intermediate visual acuity. UCDVA: Uncorrected distance visual acuity. CDVA: Corrected distance visual acuity. References: 1. V. Tahmaz et. al. Evaluation of a Novel Non-Diffractive Extended Depth of Focus Intraocular Lens – First Results from a Prospective Study. Current Eye Research. 2022. Vol 47, p1149-1155. https://doi.org/10.1080/02713683.2022.2074046 2. Campos, et. al. Preliminary Clinical Outcomes of a New Enhanced Depth of Focus Intraocular Lens. Clinical Ophthalmology 2021:15 4801–4807. © 2023 Bausch & Lomb Incorporated.®/TM denote trademarks of Bausch & Lomb Incorporated and its affiliates. Bausch & Lomb (Australia) Pty Ltd. ABN 88 000 222 408. Level 2, 12 Help Street, Chatswood NSW 2067 Australia. (Ph 1800 251 150) New Zealand Distributor: Toomac Ophthalmic. 32D Poland Road, Glenfield 0627 Auckland New Zealand (Ph 0508 443 5347) LUX.0016.AU.23
comparison to conventional monofocal IOLs:1,2 Superior DCIVA† and UIVA ‡ Comparable high levels of UCDVA § and CDVA §§ Similar dysphotopsia profile with lower incidence of optical side effects
degree of
daily life
In
High
patient satisfaction for
activities Enhanced spectacle independence from far to intermediate distances
MELBOURNE TEAM DELIVER BLUE LIGHT VERDICT
Spectacles marketed to filter out blue light probably make no difference to eye strain caused by computer use or to sleep quality, according to a Melbourne-led review of several randomised controlled trials of the best available evidence so far.

Nor did the study find any evidence that blue-light filtering lenses protect against damage to the retina. Blue-light filtering lenses, also known as blue-light blocking spectacles, have been increasingly prescribed or recommended, often by optometrists, since the early 2000s.
The latest review, published in the Cochrane Database of Systematic Reviews, was led by researchers at The University of Melbourne in collaboration with colleagues at City, University of London and Monash University.
They assessed the effects of blue-light filtering lenses compared with non-blue-light filtering lenses for improving visual performance, providing protection to the retina and improving sleep quality. They analysed data from randomised controlled trials they could find on the topic: 17 trials from six countries.
“We found there may be no short-term advantages with using blue-light filtering spectacle lenses to reduce visual fatigue associated with computer use, compared to non-blue-light filtering lenses,” lead author Associate Professor Laura Downie said.
“It is also currently unclear whether these lenses affect vision quality or sleep-related outcomes, and no conclusions could be drawn about any potential effects on retinal health in the longer term. People should be aware of these findings when deciding whether to purchase these spectacles.”
However, the quality and duration of the studies also needs to be considered.
“We performed the systematic review to Cochrane methodological standards to ensure the findings are robust. However, our certainty in the reported findings should
in the context of the quality of the available evidence. follow-up period consider potential longer-term outcomes.”
SPECSAVERS RANKED AMONG AUSTRALIA’S BEST WORKPLACES
Specsavers has been named as one of Australia’s Best Workplaces for 2023 by Great Place To Work, the global authority on workplace culture. It ranked 8th in the large (1,000 plus employees) category.
The company said the recognition not only acknowledges its delivery of eye and hearing care to all Australians, but also highlights its work to foster a positive, inclusive, and vibrant work environment for employees.
Australia’s Best Workplaces List is determined using The Great Place To Work For All methodology. The Great Place to Work Trust Index Survey enables employees to share confidential quantitative and qualitative feedback about their organisation’s culture by responding to 60 statements on a five-point scale and answering two open-ended questions.
Collectively, these statements describe a great employee experience, defined by high levels of trust, respect, credibility, fairness, pride, and camaraderie.
It is the first time Specsavers has been listed among Australia's Best Workplaces, though it has been an accredited Great Place to Work organisation for the past three years.
ANZ managing director Mr Paul Bott said Specsavers was thrilled to be recognised.
“Our people – our store partners and team members in-store and support office, are the heartbeat of our organisation, and this achievement is a reflection of their dedication and passion for what they do,” he said.
“Specsavers is, and has always been, a company built on great people. Our vision is to change lives through better sight and hearing, and it is our people who help make the difference to the lives of Australians every day.”
The Top 10 Best Workplaces: Cisco, Hilton, Atlassian Inc, DHL Express, REA Group, Marriott International Australia, DHL Supply Chain, Specsavers, Capgemini Australia, Story House Early Learning.

OPTOMETRIST DEVELOPS OWN CHILDREN’S READING CHART
A UK-trained optometrist now practising in New Zealand has developed the new Beardsworth Reading Chart designed to simplify children’s eye tests and address the shortcomings of current testing resources.
Ms Natalie Beardsworth, an optometrist with a special interest in children’s vision, launched her reading chart in New Zealand earlier this year and is now making it available to Australian eyecare professionals.


Previously, she said the only reading charts available were for adults. There was also a ‘Thomas the Tank’ engine reading chart that she said is commonly used with children but is designed for a parent to read to a child, with the vocabulary deemed difficult for small children. Beardsworth set out to develop her own children’s reading chart that needed to be engaging for small children.
“The chart is designed to detect when small children have difficulty reading small font,” she said.
“It is a really useful tool to ascertain whether giving children a little bit of magnification in reading glasses will be helpful. You get the child to read the smallest font they can and put up +0.50DS in front of both eyes. If it is helpful, you will hear the child start to read more fluently or they may comment that it is easier to see. If they do not notice any difference, then reading glasses probably are not going to help.”
12 INSIGHT October 2023 NEWS
The lenses have been recommended since the early 2000s.
Optometrist Natalie Beardsworth using her reading chart with a young patient.
Specsavers ANZ's (from left) Dominic Savill, Stephanie Park, Karen Clancy and Paul Bott.
1800 637 654 @eyesrightoptical ECO FRIENDLY EYEWEAR FOR A GREENER FUTURE Proj ect Gree n ey ew ea r
POSITIVE DRY EYE FINDINGS FOR INMODE PLATFORM
A recent paper investigating transcutaneous radiofrequency (RF)-assisted meibomian gland expression using the InMode Envision platform and Forma-I handpiece in dry eye patients has found the technology is effective, lasting at least six months in most patients.
The multicentre prospective cohort study was published in The Open Ophthalmology Journal by a team of North American ophthalmic professionals and involved 47 patients across three sites from October 2019 to June 2022.
The findings may be useful to Australian practitioners who have recently gained access to the Envision platform, described as a non-surgical, non-drug alternative by InMode for dry eye comprising three distinct technologies. Forma-I is the primary treatment on the Envision platform and features bipolar RF to address the symptoms of dry eye disease caused by meibomian gland dysfunction (MGD) using controlled dermal heating to aid gland expression.
In the recent study, the research team noted a significant improvement in SPEED score from baseline, 15.7 versus 11.4 at one month, 9.1 at three months, and 9.6 at six months. There was also a statistically significant improvement for OSDI at all time points measured.
Similarly, CFS was significantly reduced in each eye at all time points following treatment, with 80% of eyes responding. And TBUT improved after treatment in each eye with an average of 6.3 seconds at one month, 7.1 seconds at three months, and 7.1 seconds after treatment at six months versus 2.8 seconds at baseline.
Marked improvements were also noted in MGS across all time points and patients noted subjective improvement, with a lack of pain and discomfort. “This pilot study … supports the conclusion that the Forma-I treatment was efficacious in treating dry eye symptoms.
Patients believed the treatment significantly improved from their baseline and reported high satisfaction,” the study concluded.
FDA APPROVES IVERIC BIO’S IZERVAY FOR GEOGRAPHIC ATROPHY
The US Food and Drug Administration (FDA) has approved a second therapy for geographic atrophy (GA), with IZERVAY (avacincaptad pegol intravitreal solution) by Iveric Bio given clearance with its new complement C5 inhibitor.
The 4 August announcement follows the American drug regulator’s approval of SYFOVRE (pegcetacoplan injection), which targets complement C3 and has been developed by Apellis Pharmaceuticals. This became the first and only FDA-approved treatment for GA in February 2023.
In a statement, Iveric Bio’s parent company, Astellas Pharma, said IZERVAY was approved for GA secondary to age-related macular degeneration (AMD). The drug is a complement C5 inhibitor and is said to be the only approved GA treatment with a statistically significant reduction (p<0.01) in the rate of GA progression at the 12-month primary endpoint across two Phase 3 clinical trials.
The FDA approval was based on the

GATHER1 and GATHER2 Phase 3 clinical trials, which evaluated the safety and efficacy of monthly 2 mg intravitreal administration of IZERVAY in patients with GA secondary to AMD.
The rate of GA growth was evaluated at baseline, six months, and 12 months. In each registrational trial, over a 12-month period, the primary analysis showed a statistically significant reduction in the rate of GA growth in patients treated with IZERVAY compared to sham.
Slowing of disease progression was observed as early as six months with up to a 35% reduction in the first year of treatment.
Dr Arshad Khanani, director of clinical research at Sierra Eye Associates, in Nevada, said as a C5 inhibitor, IZERVAY has shown to slow GA progression by targeting the source of retinal cell death and may preserve the upstream benefits of the complement system.
GLAUKOS VENTURES INTO NEW TERRITORY IN RADIUS XR DEAL
Glaukos has entered into a collaboration and marketing agreement with Radius XR for the latter’s wearable patient engagement and diagnostic system within the US.
The deal centres on the Radius XR platform, described as a novel portable vision diagnostic and patient engagement system for more efficient detection of eye disease and better management and treatment of sight-threatening conditions.

It combines medical-grade diagnostics, business management tools and patient education resources within a wearable spatial computing device. The hardware and software system is designed to allow medical professionals to diagnose patients accurately, enhance patient engagement and reduce staff workload.
The system also enables patients to perform self-guided vision tests with minimal supervision, aiding in eyecare practices' flow, efficiency and patient experience.

“Today marks a notable milestone for Radius and more importantly, for patients suffering from chronic eye diseases,” said Radius CEO Mr Ammad Khan.
“Glaukos is highly trusted and respected by vision care providers, and this collaboration will provide us with the necessary resources to expedite product development, optimise benefits for eyecare providers and enhance the overall quality of care and access for patients.
14 INSIGHT October 2023 NEWS
Envision is a non-surgical, non-drug alternative for dry eye.
Glaukos is developing therapies for glaucoma, corneal disorders and retinal diseases.
Approval was based on the GATHER1 and GATHER2 trials.

1


Inside the world
OF OPHTHALMOLOGISTS IN REGIONAL AUSTRALIA
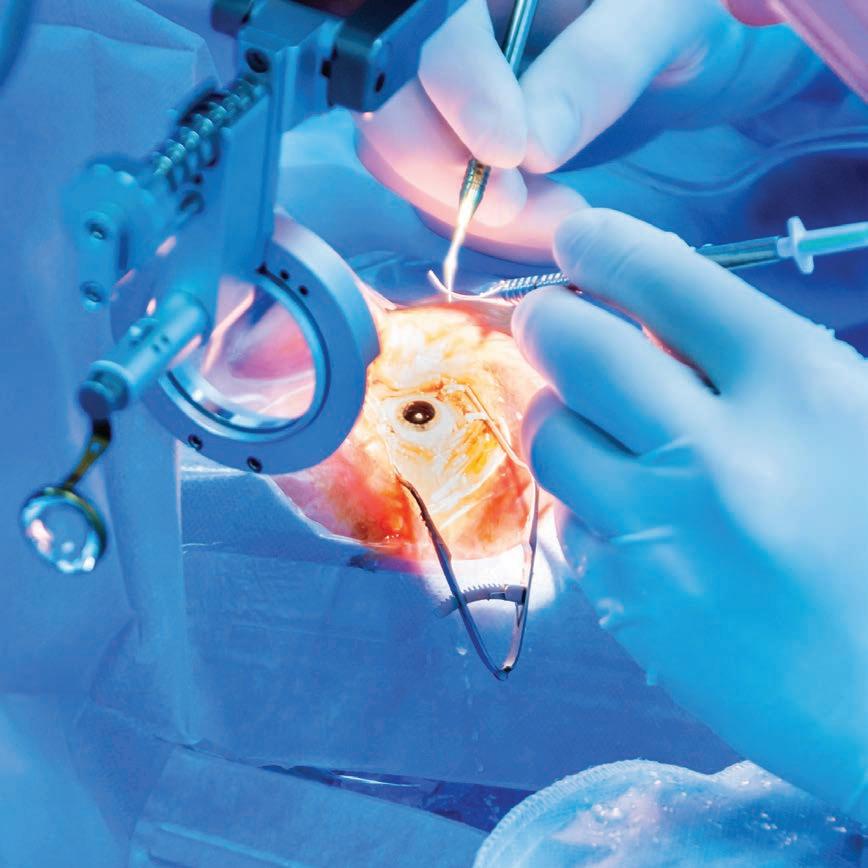
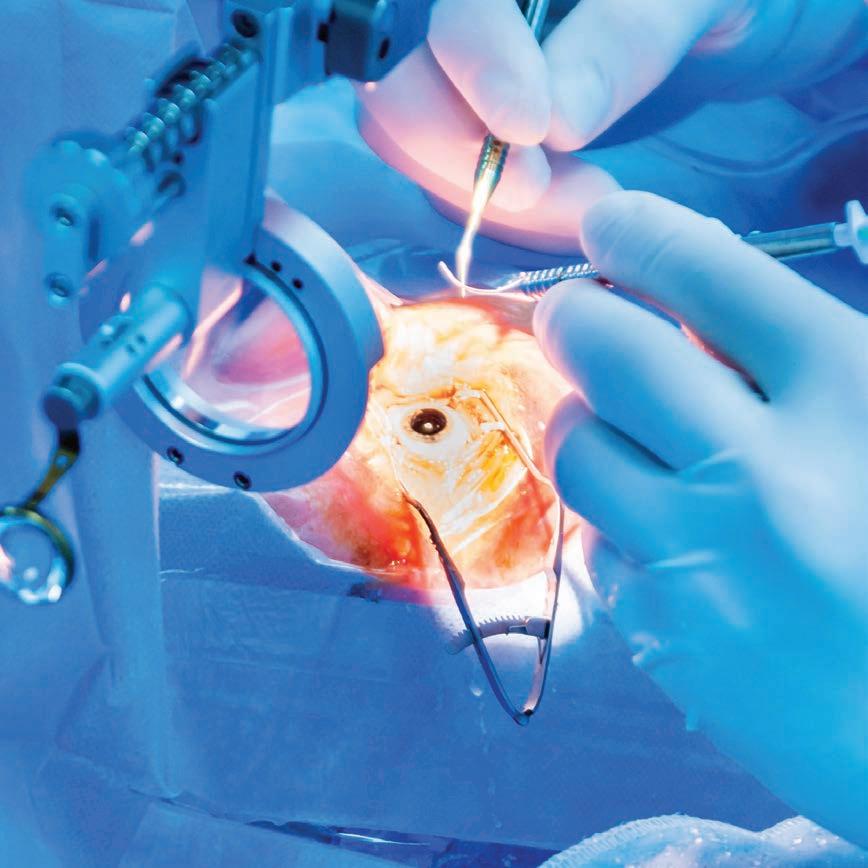
Regional towns are home to some of the top ophthalmologists in Australia and New Zealand, yet they don't often get the recognition they deserve. In a new podcast series, DR SONIA MOORTHY will interview seven guests to gain real-world insights into the delivery of specialist eyecare outside the city lights.
When it comes to the regional ophthalmology workforce in Australia, the conversation is often focused on data, high-level analytics and jargon-filled programs that seek to identify and overcome this longstanding industry issue. But what about the stories behind the specialists delivering eyecare to these communities each day?
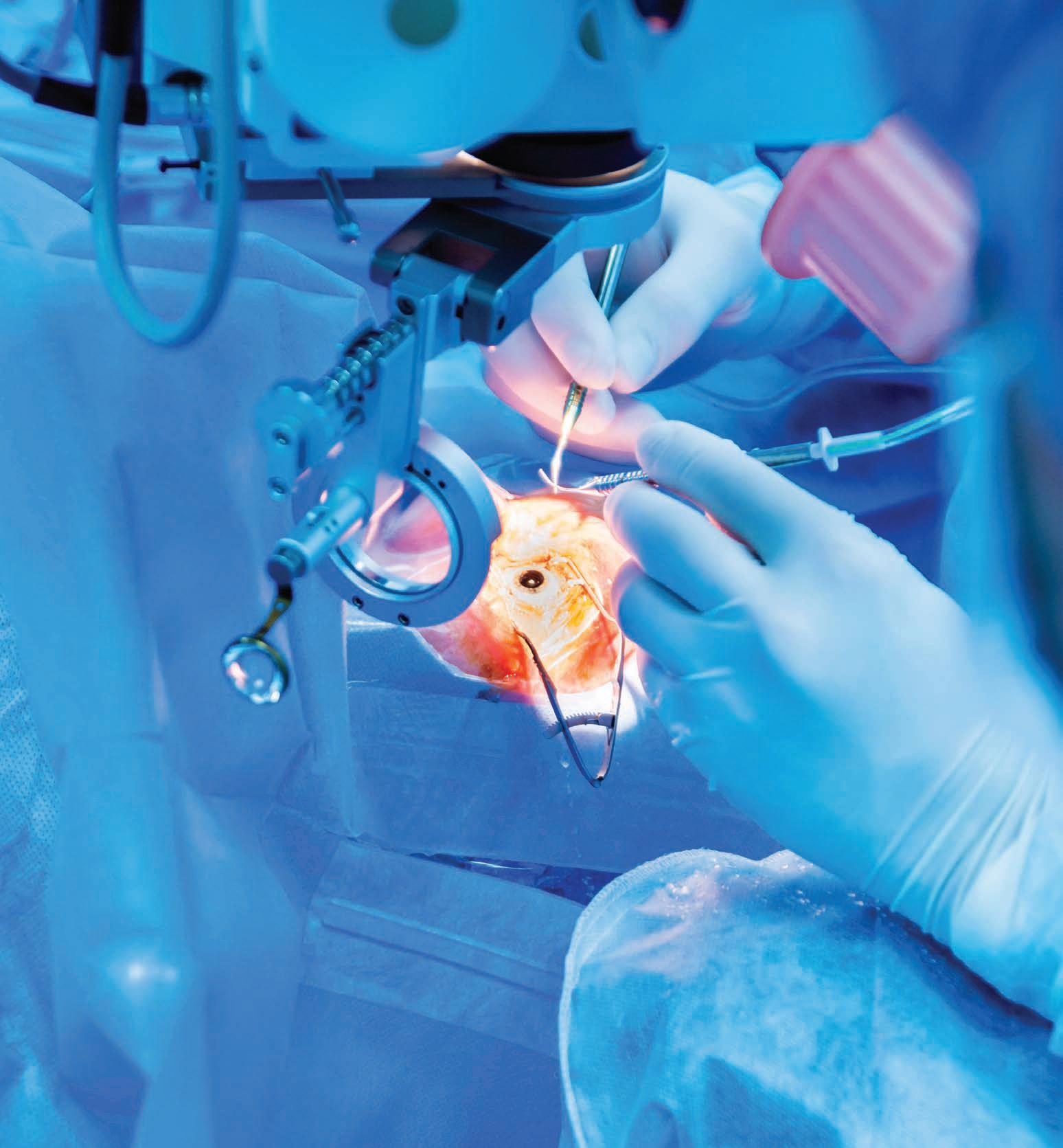
Anecdotes about what it means to be a regional ophthalmologist in Australia and New Zealand will be the focus of a new podcast by Queensland’s Dr Sonia Moorthy.
The first series, supported by Bausch + Lomb (B+L), will interview seven regional ophthalmologists from Australia and New Zealand, covering a range of topics including eyecare delivery challenges, timely and equitable access to eyecare, harnessing a sustainable workforce, gender equality through to the role of industry in region.
“The focus of this podcast is regional services with different perspectives. I want the guests to tell their story. I want to explore how they landed here. What are the things close to their heart? What has kept them going and the beauty of being in region? But also, what are the most challenging aspects?” she says.
"We want to deliver this message to up-and-coming ophthalmologists; but beyond that too, if we're going to tackle the workforce issue, we've got to start at the grassroots level and adopt a collaborative approach."
THE GUESTS
Regional eyecare is a personal passion for Moorthy. As a child in Malaysia, her family moved to multiple remote areas, taking her to the jungles of Bornea where her father managed oil palm and rubber plantations. Upon completing fellowships in paediatric ophthalmology and strabismus at the Singapore National Eye Centre and Moorfields Eye Hospital, London, she returned to Australia and landed in Far North Queensland in 2018.
She practised publicly and privately in Cairns where she attended satellite clinics, providing eyecare to regional and remote communities in the Atherton Tablelands and up to Cape York. Today, she has a primary practice, EyeHub, on the Sunshine Coast and in April 2023 established a satellite clinic an hour away in Gympie.

She’s familiar with the multi-dimensional challenges of regional ophthalmology and, thus, has secured a line-up of regional ophthalmologists with complementary backgrounds, including:
• Dr Andrew Thompson, RANZCO censor-in-chief, ophthalmologist and medical retinal specialist, based in Tauranga in the Bay of Plenty region in New Zealand's North Island
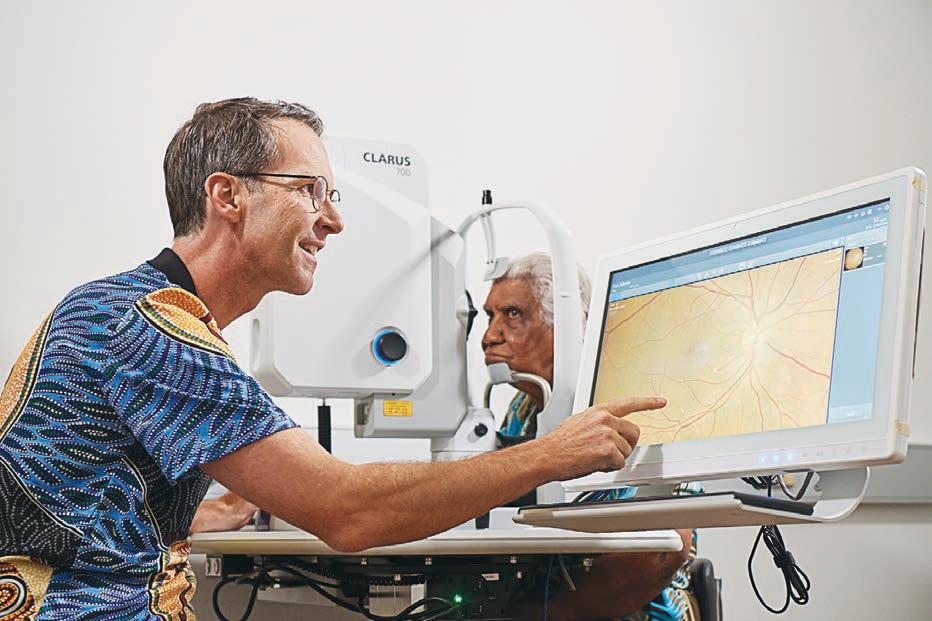
• Prof Angus Turner, ophthalmologist and Lions Outback Vision founder and director, based in Broome in Western Australia
• Dr Neil Sinclair, paediatric ophthalmologist and oculoplastic surgeon, based in Bunbury, Western Australia
• Dr Eline Whist, ophthalmologist, medical retina and uveitis specialist, based in Darwin, Northern Territory
• Dr Brent Skippen, ophthalmologist and oculoplastic surgeon, based in Wagga Wagga, New South Wales
INSIGHT October 2023 17
WORKFORCE
Queensland ophthalmologist and podcast host Dr Sonia Moorthy.
Regional NSW centre Wagga Wagga is home to four opthalmologists, one whom will appear in the podcast.
• Dr Phoebe Moore, ophthalmologist medical retina and uveitis specialist, based in Tamworth, New South Wales
• Dr Andrew McAllister, ophthalmologist and vitreoretinal surgeon, based in Toowomba, Queensland.
On Thompson, Moorthy is excited to provide a New Zealand perspective as she chats to one of the key ophthalmologists in Bay of Plenty and the exemplary public and private eyecare he provides, while simultaneously training the future generation of young ophthalmologists
With Turner,Moorthy will explore his work with Lions Outback Vision that adopts a ‘hub and spoke’ model delivering outreach services to dispersed populations over Western Australia. Recently, he opened The Kimberley Hub in Broome offering a multi-disciplinary base for eyecare services to the Kimberley and Pilbara, with resident ophthalmologists and optometrists working together within a shared-care model.
“This is someone who is potentially harnessing the power of 10 ophthalmologists,” Moorthy says, noting she practised alongside Turner as an unaccredited registrar at The Royal Victorian Eye and Ear Hospital 15 years ago.
“It’s an example of how it really does take a village to make a change and he has certainly achieved that. I think it’s inspirational the ingenuity he has shown to reach this point. It’s an amazing model and worth highlighting.”
Moorthy also has a connection to Skippen who she went through ophthalmology training with. In the early stages of his career, Skippen was a junior doctor at St Vincent’s Hospital and went to Wagga for rural secondment on several occasions. He’s also worked for Médecins
Sans Frontieres (MSF) in Armenia, and in regional areas like Goulburn
REGIONAL WORKFORCE AND ACCESSIBILITY
The imbalance of urban versus regional/ rural eye doctors was laid bare in a 2018 Department of Health ophthalmology workforce report confirming 84% work in big cities. That means some 16% of ophthalmologists work in regional areas, which is insufficient for the 29% of the Australian population that lives regionally.
In highlighting the maldistribution of ophthalmologists, this report, based on 2015 data, highlighted a higher-thanaverage reliance on international medical graduates, an impending critical shortage of paediatric ophthalmologists and a lack of funded training positions in the public sector. RANZCO’s own analysis has also shown that of the ophthalmologists who trained and graduated between 2013 and 2016, 90% reside in urban areas.
The college also has repeatable data from workforce surveys showing people from regional backgrounds proved to be 2.7 times more likely to end up practising regionally, either living regionally or doing outreach regionally. In 2017, 9.3% of RANZCO fellows had a regional background.
As a result, there is a higher priority on people from regional areas and now more than 40% of ophthalmology trainees during the past two to three years have a regional background.
RANZCO has also launched the Regionally Enhanced Training Network. The first rotation commenced in February 2023 and will see selected trainees spend about two-thirds of their time in regional Australia and one-third in urban centres, in the hope they practise regionally when they become full-fledged ophthalmologists.

(student) and Armidale, Wagga and Lismore (doctor). After completing his oculoplastic fellowship, he met his wife in Sydney, before deciding regional NSW was the best place to raise a family.
“His wife’s links to Wagga created that connection. It goes to show when selecting candidates for training positions, it’s true that if you've got someone with regional links they’re more likely to return to the regions,” Moorthy says.
“With Dr Skippen practising in a private group practice, and providing general oculoplastic services alongside training registrars in that part of NSW, he may offer a different lens on the issue. He is also the director of the Regional Medical Specialist Association.”
Moorthy is also excited to interview Moore, one of few female ophthalmologists in regional Australia. After undertaking further training at Bristol Eye Hospital in 2020, subspecialising in retinal diseases and uveitis, she returned to her Tamworth hometown in 2021 to work alongside her father, Dr David Moore at North West Eyes.
“She’s someone I consider ‘under the radar’ who needs to tell their story. She’s a high achiever and seems to have won every top prize you can think of,” Moorthy says.
"On top of her obvious tenacity and intellect, she demonstrates a high EQ. Being the proud mother of two young children, she is following her heart and gone back to Tamworth to do what feels right. She could have easily ended up in a prime teaching institute in Melbourne or Sydney and pursued an academic career alongside her clinical career, but that's not what she's chosen to do – and I want to hear why.”
Whist, another guest, is originally from Norway but moved to Australia to study medicine at the University of Newcastle in 1999. Today, in addition to being a part of Darwin Eye Surgeons, she is a staff specialist at the Royal Darwin Hospital, participating in outreach services to Katherine, Gove and remote communities.
“She also has experience with MSF and volunteered a lot before pursuing ophthalmology. She's a gutsy character, very outdoorsy, and completed broad subspecialty including a fellowship with the Fred Hollows Foundation combined with the Professorial Fellowship in complex uveitis under Prof Peter McCluskey at Sydney Eye Hospital,” Moorthy says.
“Imagine the benefit she is providing to patients in the NT who would not have the opportunity to receive exceptional care from a specialist of this calibre had she not gone up there.”
DISPELLING THE REGIONAL OPHTHALMOLOGIST MYTH
An advantage of the podcast is the ability to have an earnest and honest conversation. Moorthy intends to go deep with her guests, addressing some misconceptions and challenges head on.
“The number one question is: what does it mean to be a regional ophthalmologist in Australia and New Zealand? I’d like that answered because there's an impression in regional areas that we are disconnected and occupy our own universe, lacking skillsets and evidence-based knowledge compared to our colleagues in metropolitan areas. That's a myth I'd like to dispel and the podcast guests will exemplify this,” she says.
“In the regions, you need to get comfortable with being uncomfortable. A lot of the time you’re practising solo, but need to also work hard to surround yourself with a network of specialists in related subspecialty fields like vitreoretinal, cornea and ocular oncology that you can call up should the occasion arise. You need to scale up – and do so broadly – and challenge yourself.”
In her own career, Moorthy has come up against gender inequality. Discrimination has often come from hospital administrators and older specialists, reflecting a generational gap, rather than patients – and matters have been made worse due to a lower-than-desired number of female ophthalmologists working in region, she says.
“Social inequality is a theme that's continued and the more regional you get, the worse it is – and the worse the access to health care is,” she says.
As a visiting medical officer in the Queensland public health system in
18 INSIGHT October 2023 WORKFORCE
Workforce – Ophthalmology July 2018 Department of Health Australia’s Future Health Workforce –Ophthalmology
Cairns, Moorthy says it was a frustrating experience at times.
“Because you can see so many opportunities to do things better. If we could translate the things we do in our private rooms regionally into the public system, many of these challenges would start becoming less insurmountable. Since coming to Sunshine Coast, I’ve offered my services as a general and paediatric ophthalmologist to the public hospital but this hasn’t been taken up. This is beyond me, because I know the wait time for children to see an ophthalmologist is two years, and it’s the same for cataract surgery,” she says.
“That's how the Gympie clinic emerged, and hopefully other regional satellite clinics in future. Is there a cost? Yes, of course, it’s taking time out of an already busy schedule and I've got young kids too, but it's worth it when you see how appreciative the patients are. I came into medicine to make a difference; whilst I did not have this exact vision in mind, I am here now and it feels pretty good to be able to do that.”
EMBRACING THE ROLE OF INDUSTRY
When it comes to providing highly effective ophthalmology services in regional areas, Moorthy says it is important not to overlook the role of industry – a topic she will touch on in the podcast series.
During her early training, especially in the UK, she recalls being advised to tread cautiously with industry interaction to minimise biased clinical decisions.. However, during her RANZCO training, Moorthy believes she would have benefitted from exposure to industry, especially when it came to understanding the constant evolution of technology in ophthalmology.
In terms of regional surgical lists, Moorthy can recall many moments where industry representatives have been instrumental in ensuring the smooth and running of a complex cataract surgery list.
“Bausch + Lomb is an example of this. I was first supported by them during my first public list in Emerald Hospital. Being in Central Queensland miles away from everyone else, it is crucial all the ducks line up to minimise unwanted intra-operative surgical events and maximise list efficiency,” she says.
“In this instance, the staff had not done an ophthalmic list for some time so they were not familiar with the lenses and phaco machine – and something as simple as an incomplete prime can be absolutely disastrous if not recognised. I don’t know what we would have done without those representatives present to guide safe and complete set up, whilst troubleshooting on their feet – it was extremely helpful and gave me the confidence I needed for a successful list.”
 Dr Angus Turner, the founder of Lions Outback Vision, will discuss the work he has done to improve eyecare accessibility in WA.
Dr Angus Turner, the founder of Lions Outback Vision, will discuss the work he has done to improve eyecare accessibility in WA.
Budding optometrists AND THE ROLE OF CLINICAL PLACEMENTS
learn from it. He gave me the ultimate 'hype up' and said that I couldn’t allow myself to feel down or second guess myself after just one experience.
One of the most effective ways to bridge the gap between theoretical knowledge and practical skills is through hosting students for clinical placements in optometry practices. These placements not only provide students with invaluable hands-on experience but also enrich the profession by fostering collaboration and knowledge sharing.
As the largest employer of optometrists in Australia, Specsavers has played a leading role by developing a unique strategy for supporting optometry students in this crucial time of their development.
In 2023 alone, its practices will host more than 450 clinical placements across the Australia and New Zealand store network, with 259 already completed in the 2023/24 student cycle. Of the 259 final year students who have completed their clinical placements, the network has already signed employment contracts with 136 of them, with many more conversations under way.
“In previous years, more than 70% of students found their clinical experience so rewarding that they elected to join Specsavers as a part of its graduate program,” the company’s graduate recruitment manager Ms Sarah Yearsley says.
THE CLINICAL PLACEMENT EXPERIENCE
Not long ago, Deakin University graduate Ms Joanne Cho was one of those students who completed her clinical placement at Specsavers. She did this at the Erina store and said the experience was integral to her becoming the confident and agile optometrist she is today.
Her first impressions were that the practice was big and busy with lots of people to meet, but that became a benefit because with encouragement and support, her abilities quickly grew and she thrived in the environment. The placement tested her and prepared her for the highs and lows of an optometry career.
“I’ll always remember my first pediatric appointment. It was for a four-year-old boy who needed eye drops. He was quite upset and crying and I wanted to limit the stress he was experiencing by undertaking the consult as quickly as possible. As he left, I felt so disappointed in myself, it was a really low moment for me,” she explains.
“The Erina store partner Nathan Ko saw me and straight away. He was so encouraging and talked me through the experience including what I could
“Then Nikesh Tanna, the other optometrist store partner, had finished an appointment and cleared his next one so he could have mentoring time with me straight away. He took me out of the store for a walk to clear my head. I feel like he truly understood what I was going through. Never once did he treat me like I was inexperienced or naive. He was so knowledgeable and generous with his time.”
Between them, and the rest of Specsavers Erina staff, Cho was taught to understand the value of optometry. “We are making more of an impact than we think. My clinical placement set me up with long-lasting relationships, authentic mentoring and learning opportunities that I never would have received in a lecture hall at university,” she says.
From Specsavers Erina’s perspective, hosting clinical placements like this are crucial for training future generations of optometrists. It’s a responsibility the practice takes seriously. Tanna says it's important practices host clinical placements to give the students a chance to receive real-world experience and support before they finish their studies.
“It also gives us a chance to showcase the care, expertise and value provided by our store which can assist in the student’s longer-term career decisions,” he says.
“In her clinical placement, Joanne was given exposure to all areas of the business and gradually introduced to clinical examinations when she was comfortable to move forward. Providing reassurance there was no time restriction, always support to hand and timely feedback. Joanne was extremely helpful in all areas of the practice and willing to help wherever she could.”
A PIONEERING CLINICAL PLACEMENT PROGRAM
Yearsley, the graduate recruitment manager at Specsavers, says many students choose to have their clinical placement at Specsavers because of the company’s accessible locations and the sheer quantity of opportunities available. The network also has locations to meet the preferences of students – whether they wish to be placed in a local metropolitan clinic or experience a regional practice.
“On top of that, Specsavers is a great place to work. In August 2023, we were named one of Australia’s best workplaces. We pair our patient-focused vision and values with high levels of trust, respect, credibility, fairness, pride, and camaraderie,” she says.
“Our investment in clinical equipment and technology, our close working

20 INSIGHT October 2023
Meaningful practical experience and real-world exposure is helping future generations start their optometry career on the right foot in Australia.
relationships with key eye health stakeholders, and our major investments into professional development all contribute to our mission of changing lives through better sight for all Australians and New Zealanders.”
From a clinical placement perspective, Yearsley says Specsavers practices have large patient bases that expose students to a broad range of presentations and provide relevant experience to prepare them for professional practice. “We also use the latest technology, including OCT as standard, to provide comprehensive eyecare services and improve patient outcomes,” she explains.
A CLINICAL PLACEMENT PROCESS
To understand how Specsavers clinical placements work, the recruitment department works with store partners to develop encouraging and supportive environments for students and all team members.
“We have a unique clinical placement process that varies depending on the university and placement schedule which could range from one day to six months in length,” Yearsley says.
Clinical placement orientation is provided for all students and may be in person, virtually or via a pre-recorded video, depending on the placement duration. Each participating practice also has a supervising optometrist specially trained in collaboration with their partnering university and Specsavers to support students and graduates.”
She says supervising optometrists aren’t necessarily store partners, instead it is often an ideal development opportunity for other senior optometrists in the practice. Supervisors volunteer to host student placements because they are committed to helping train the next generation of optometrists. Each university has different requirements, with some more observational and others more hands-on.

“While it isn’t always necessary for practices to have a spare test room
VF2000 NEOPORTABLE VISUAL FIELD ANALYZER
The New Standard in Visual Field Testing
V irtual Reality Visual Field device - incorporates complete Visual Field analysis.
Detailed progression analysis and the most versatile & efficient vision screening technology.
Latest technology provides the same reliability and reports as the “gold standard”.
Supplied complete with a Tablet PC –BlueTooth interface with the VF2000 NEO.
Compact/Space-saving/Portable - can be used anywhere, no need for a darkened room.
when hosting clinical placement students, we do all we can to ensure students have appropriate space to learn,” Yearsley says.
THE BENEFITS OF CLINICAL PLACEMENTS
With hundreds of students graduating each year, Yearsley says optometry practices play a crucial role in providing on-site training and support for students and the benefits extend beyond the placement period alone.
“Hosting students encourages practising optometrists to stay updated with the latest advancements in the field. The inquisitiveness of students often prompts practitioners to revisit their knowledge, sparking a cycle of continuous learning and growth,” Yearsley says.
Active eye tracking –enhances reliability.


Full and Fast Thresholds VF Testing plus Neuro, Kinetic, Ptosis and Estermann tests
FDT Testing
Stereopsis
Visual Acuity and Contrast
Sensitivity
Colour Testing (Ishihara, D15 and Advanced Colour Tests)
Eye Mobility and Strabismus
“THE INQUISITIVENESS OF STUDENTS OFTEN PROMPTS PRACTITIONERS TO REVISIT THEIR KNOWLEDGE, SPARKING A CYCLE OF CONTINUOUS LEARNING AND GROWTH.”
SARAH YEARSLEY SPECSAVERS
Ph: 1800804331 Email: sales@bocinstruments.com.au

GROW YOUR CAREER WITH US www.georgeandmatilda.com.au Email Sam at opportunities@georgeandmatilda.com.au or scan the QR code further study leadership partnership specialty interests
WHEN A TELLS 1,000 WORDS
photo
“CHILDREN HAVE SHORT ATTENTION SPANS, SO I NEED A CAMERA WHICH IS QUICK IN CAPTURING IMAGES BUT ALSO EASY TO POSITION A CHILD'S HEAD.”
DR DEEPA TARANATH ADELAIDE OPHTHALMOLOGIST


IMAGING
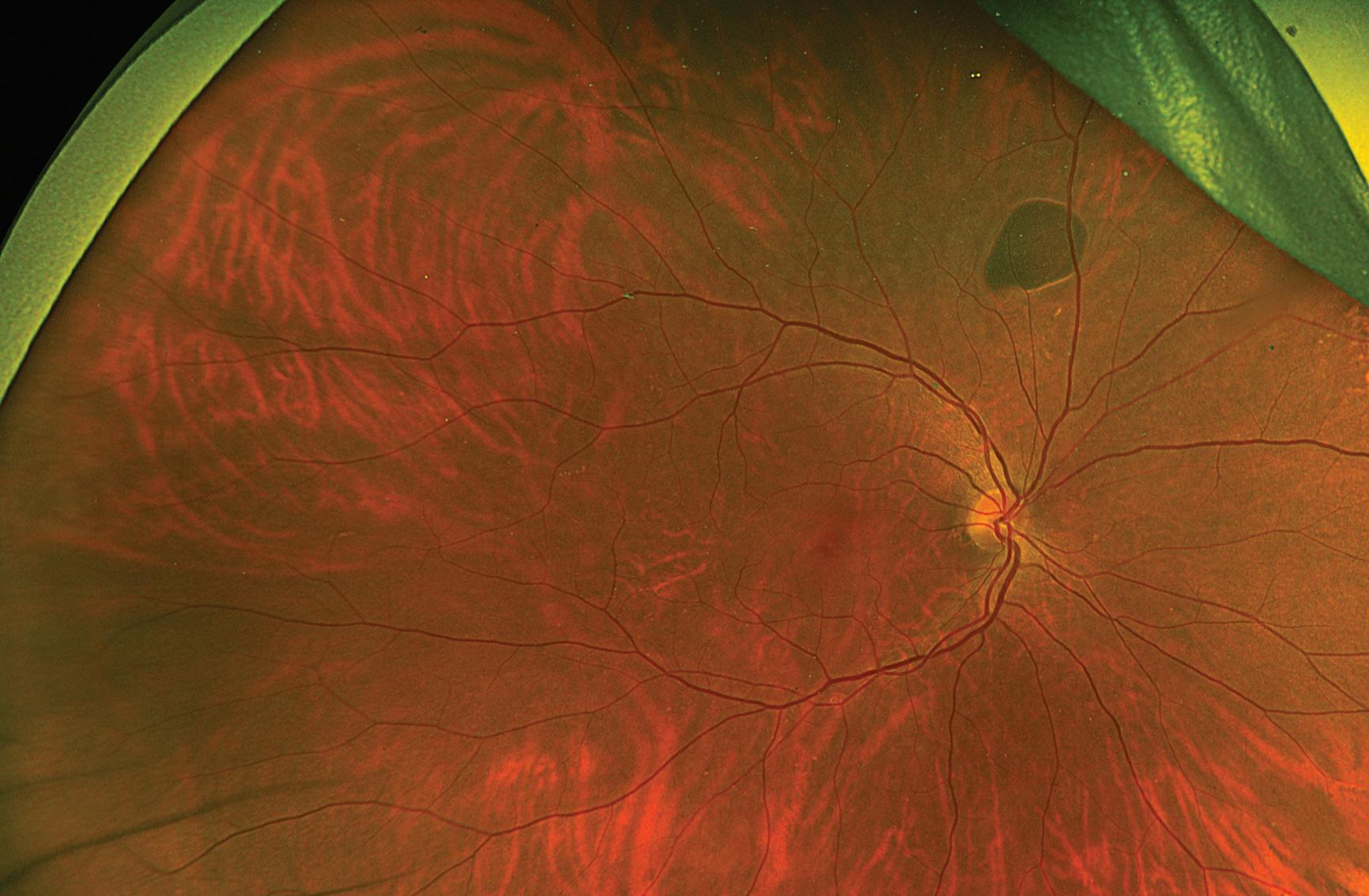
“OPTOS SILVERSTONE IS GOOD FOR GETTING A CROSS SECTIONAL IMAGE OF LESIONS OR TUMOURS, WHICH ALLOWS US TO BETTER CHARACTERISE WHETHER IT MIGHT BE BENIGN OR NOT BENIGN.”
Yet another benefit Taranath has found with Optos UWF is its ability to render a 2D retinal photograph in 3D – a powerful visual communication tool.
“Optos California FA has a 3D module where you can see a three-dimensional eye and how the retina looks inside, so you can show parents where a haemorrhage or lesion is, and I think people have a better understanding and coping mechanism once they know what it is. I think it's a very good educational tool because people believe what they see, more than what they hear,” she says.
“I like to show the 3D image and explain, ‘This is what I've seen. This is why I'm worried, or this is why I'm not concerned because the lesion is not in the sight threatening area, it's not in the macula, it's not near the optic nerve, but it's at the periphery’. That is another advantage of Optos UWF.”

Although only a matter of weeks into using Optos California FA in her clinical practice, Taranath says it’s improving her treatment decision making, including early and more definitive diagnosis.

24 INSIGHT October 2023
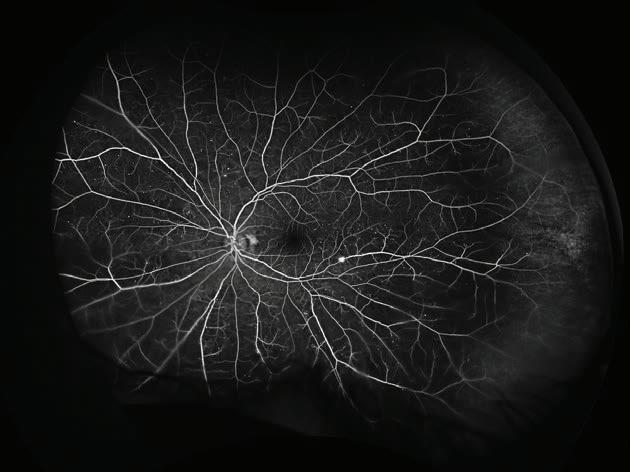
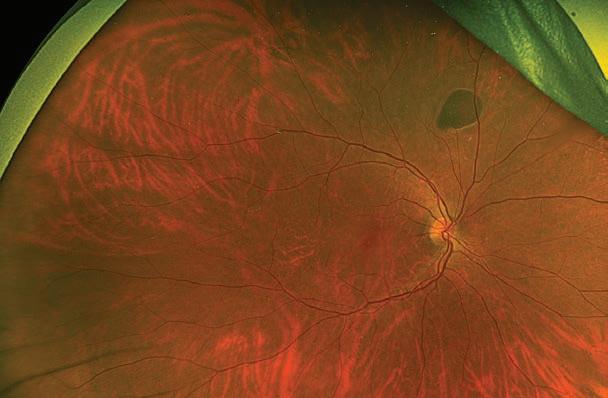
Case 2: A 65-year-old patient with known polypoidal choroidal vasculopathy in the left eye is found incidentally to have a lesion in the right superior retina (Figure 3). Optos Silverstone allows the acquisition of OCT of peripheral regions of the retina, demonstrating this lesion to be a haemorrhagic pigment epithelial detachment (Figure 4), consistent with polypoidal choroidal vasculopathy. Image: Dr Rajeev Chalasani
Case 2: Figure 3
Figure 4
DR RAJEEV CHALASANI SYDNEY RETINAL SPECIALIST
a good view of the overall circulation, and whether there's a new vessel will decide whether you need to treat them with laser or you can just observe them,” Chalasani says.
Experience has also proven Optos UWF is particularly useful for monitoring tumours or lesions around the edge of the retina, Chalasani says, and informing treatment decisions.
“It’s very helpful when you're seeing someone every year to monitor a mole in the eye or something similar. A photo really tells 1,000 words. You can see in an instant whether it has changed in appearance when you've got a high quality image,” he says.
“With lesions in the periphery, seeing if they're changed in size, and if there's a change on the OCT through that lesion, that may well prompt you to be comfortable to continue to monitor them with conservative treatment or may prompt a referral to an ocular oncologist for further assessment. It helps alter your management, or conversely, it gives you reassurance that you can keep doing what you’re doing.”
Chalasani reserves his highest praise for the Optos Silverstone, the only ultra-widefield (UWF) retinal imaging device with integrated, UWF-guided swept-source OCT.

“That's their top end device that we have at our Strathfield Retina Clinic. Previously, we were never able to get good OCTs through lesions or areas at the edge of the retina. Whereas the Optos Silverstone takes a photo of the whole retina and allows you to then select an area and perform an OCT through an area right at the edge. It's good for getting a cross sectional image of lesions or tumours, which allows us to better characterise whether it might be benign or not,” he says.
Chalasani also lists the ability to acquire an image quickly, in a comfortable position for the patient, as additional attributes of the device. It’s also
user-friendly, so doesn't take a lot of effort to train staff to use it.
“It's very patient and operator friendly, it gets you the furthest to the retinal periphery compared to other imaging options, and having OCT capability for peripheral areas is really helpful,” he says.
A paediatric patient at Dr Deepa Taranath’s recently opened private clinic, iSight Specialists, with the Optos California FA.
THE MYOPIA OF TOMORROW Leaders
A spectacle-based myopia control intervention has closed the loop on treatment options available in OPSM and Laubman & Pank stores. Now, optometrists in the network can access a range of myopia control options for children and share best practice, driven by a newly established Myopia Leaders advisory panel.
Early in her career, Ms Tegan Matheson upskilled in orthokeratology (orthok) that set her up for one of her more memorable moments as an optometrist. One day, a -20.00D mother brought her myopic six-year-old son to an OPSM practice where – over a three-year period –the orthok Matheson prescribed limited his progression to just -0.50D.
“I remember the moment I told the mother that we have options to combat myopia progression, she broke down. It’s moments like these where our expertise can make a meaningful difference for children with myopia that sparked my passion in this field,” she says.
“It’s great we now have the tools to slow myopia progression. Progressive myopia can impact a child's learning and social development, while increasing their lifetime risk of pathologies including retinal tears, glaucoma, myopic maculopathy and more. For every increase of -1.00D, this increases the lifetime risk of myopia maculopathy by 40% – a staggering statistic that highlights the importance of being proactive with myopia management.”
Another alarming figure is that 50% of the world’s population will be
myopic by 2050 – if current trends continue – and that 10% will have high myopia (-5.00D or more). With this in mind, EssilorLuxottica has made myopia management a priority across its global business.
At the local level, this has taken shape in the form of a new Myopia Leaders group, a panel of 22 optometrists across Australia and New Zealand leading the way with myopia management practice across the OPSM and Laubman & Pank network.

Matheson heads the group, in addition to her role as the country eyecare manager for OPSM in New Zealand.
Six years ago, when she started her optometry career with the business, Matheson noticed opportunities in the myopia management space. This became evident when, as an adopter of orthok early in her career, she soon became the go-to optometrist when another practitioner went on leave. Receiving referrals from other optometrists, she sought to train as many colleagues as possible. But what if all optometrists in the network could prescribe an effective myopia management intervention?
This was the premise of the Myopia Leaders group that launched in July 2023. A partnership with CooperVision is supporting the committee that has already held its first meeting in Sydney, featuring global myopia authority and Australian Dr Kate Gifford.
A key domino that needed to fall was the introduction of the Essilor Stellest spectacle lens in October 2022. Prior to this, optometrists in the network could prescribe CooperVision’s MiSight 1 day soft contact lens, orthok (if skilled in this area), atropine eye drops, bifocal or multifocal spectacles for myopia control.
“Now with Stellest, every patient has a myopia control option, and every optometrist can prescribe myopia control. Across the ANZ network, we have therapeutic and non-therapeutic optometrists, as well as varying levels of experience with different treatment modalities, but
OPTOMETRY
Myopia authority Dr Kate Gifford with EssilorLuxottica’s new Myopia Leaders group at the company’s ANZ head office in July 2023.
“ALL OUR OPTOMETRISTS HAVE ACCESS TO A COMPREHENSIVE RANGE OF MYOPIA CONTROL SOLUTIONS.”
TEGAN MATHESON ESSILORLUXOTTICA RETAIL ANZ MYOPIA LEAD
every optometrist is able to prescribe a pair of spectacles that serves as the traditional optical correction while at the same time controlling for myopia progression.” she says.
“The great thing about Stellest is that it’s very easy to adapt to.”
A top priority for the Myopia Leaders group has been to develop a new framework for best practice myopia management based on the latest evidence. These have been converted into resources to support optometrists in-store, including patient facing educational content and consent forms. These resources have been made available in different languages and will also support a more consistent approach to myopia control across the network.
“The Myopia Leaders group consists of highly engaged optometrists across the EssilorLuxottica network with a strong passion for myopia control. We are also expanding the capability to measure axial length across our network to support our optometrists in monitoring treatment efficacy.”
The greater emphasis on myopia management will allow EssilorLuxottica Retail ANZ to identify knowledge gaps across its network through Stellest prescribing data.
WORKING ALONGSIDE ‘MYOPIA CELEBRITIES’
Mr Brian Mr Brian Peng only graduated from the UNSW optometry school in 2020 but has already built an impressive resume in the field of myopia.

Peng, who practises primarily at Erina OPSM on the NSW Central Coast and was selected for the Myopia Leaders group, was awarded his university’s prize for a thesis on myopia published in a scientific journal. Upon graduating, he continued this work investigating the relationship between the prevalence of myopia and the amount of green space across different regions globally. He was then invited to the Association for Research in Vision and Ophthalmology (ARVO) conference to present his findings.
As he was signing the contract to begin working at OPSM, he found himself accepting a dual role as a content writer for Dr Kate Gifford’s Myopia Profile platform.
Working alongside Gifford – as well as former International Myopia Institute executive director Dr Monica Jong for his research paper – have fuelled his myopia interest, making him an ideal candidate as a Myopia Leader.
“For me, the Myopia Leaders group is an avenue to collaborate with my peers and share knowledge with optometrists who might not be so confident in the myopia management space, but it’s also a chance to bounce ideas off people more knowledgeable than I am,” he says.
“This communication channel allows us to spread awareness and upskill our network. Often optometrists can find themselves spending a lot of time within their consult room, so being able to explore what lies beyond and connect with other like-minded people has been a great opportunity.”
Peng currently prescribes MiSight 1 day, atropine and the most popular option among his patients, Essilor Stellest.
"The familiarity, dual benefit of vision correction and myopia control, and flexible prescription range makes Essilor Stellest an ideal myopia control option that patients understand, and is easy-to-prescribe,” he says.
“From the perspective of a practitioner and researcher, it’s great to see how the evidence is quickly being translated into innovative myopia control options for patients. I love that I can now explain to patients that this is a product designed specifically for myopia control that has been shown to be effective through research. And when there's more confidence from us as practitioners, that transfers to parents and patients.”
A VESTED INTEREST
OPSM Castle Towers optometrist Mr Daniel Wong has skin in the game when it comes to myopia. Short-sighted himself (-1.50D and -1.75D), his wife is -10.00D myopia – and they have two children aged two and five.

When starting out in 2011, he discovered many in the industry were prescribing single vision lenses and advising against persistent up-close work. But he took his first step towards myopia management in an orthok workshop in 2013, and since then has been gradually building his practice to offer the full suite of interventions.
As a Myopia Leader member, he’s part of an orthok focus group and is excited to see myopia becoming a key focus for EssilorLuxottica.
“In the past, there might have been an optometrist here-or-there invited to an orthok workshop who would be left on their own to start building this within their practice, leading to different approaches,” he says.
“It’s important that we continue to lift the standard of care for myopic children. The introduction of effective myopia management options that don’t require a great deal of specialised training such as the Essilor Stellest has democratised myopia management. As research in this
INSIGHT October 2023 27
““I LOVE THAT I CAN NOW EXPLAIN TO PATIENTS THAT THIS IS A PRODUCT DESIGNED SPECIFICALLY FOR MYOPIA CONTROL THAT HAS BEEN SHOWN TO BE EFFECTIVE THROUGH RESEARCH.”
BRIAN PENG ESSILORLUXOTTICA RETAIL ANZ MYOPIA LEADER
OPSM Castle Towers optometrist Daniel Wong took his first step towards myopia management in an orthok workshop in 2013.
Tapping into
OPHTHALMIC OPPORTUNITIES
AFT Pharmaceuticals is highly selective about the products it brings to the Australasian market –and its eyecare portfolio exemplifies this. CEO Dr HARTLEY ATKINSON discusses the company’s dual role as a distributor and innovator on the local ophthalmic scene.

Dr Hartley Atkinson knows just how difficult it can be to bring a drug to market in 2023. As the founder of AFT Pharmaceuticals – a New Zealand-based pharma company punching above its weight – he’s seen the list of requirements expand over the decades whether it be greater demands for approvals and pharmacovigilance, through to accurate marketing, and transparency around carbon emissions and other ESG policies.
In some markets, it has also become challenging for clinical-stage biopharmaceutical to raise the required funds to progress their therapies through vital testing phases.
In Australasia – and increasingly in other markets – AFT has positioned itself as a go-to licensee of pharmaceutical products. This includes an eyecare portfolio built on a preservative-free approach and spearheaded by brands like NovaTears, Opti-Soothe and Hylo, which includes Hylo-Forte – ranked the number one eye lubricant in the Australian market in terms of dollars and units sold.
The diversity within AFT’s business is one of its strengths and eyecare is among a host of therapeutic areas it focuses on. But the company does much more than in-licence products – it has a significant R&D pipeline with 15 investigational products, including an ophthalmic therapy.
In the early days, Atkinson says AFT would typically scour overseas markets for therapies that could fill a distinct gap locally. This was the case with German ophthalmic manufacturers Ursapharm (Hylo range) and Novaliq (NovaTears range). But nowadays the shoe is on the other foot. A major reason for this is the 360-degree service AFT can provide for overseas manufacturers seeking a share in the ANZ market.
The company has experts that take care of regulatory approvals with bodies such as the Therapeutic Goods Administration (TGA) and Pharmaceutical Benefits Scheme (PBS), through to business development activities like marketing, sales and distribution directly to its network of optometrists, ophthalmologists and other healthcare professionals.
Recently, it reached an agreement with San Diego firm Latitude Pharmaceuticals for intellectual property for an anti-bacterial eye drop and, as part of this, AFT will run the full development of this product including a large scale, multisite trial to bring the therapy to market (more details on this below).
“I think these companies choose to work with us due to the breadth of what we can cover – we’re well-placed in areas like drug registration, clinical development, quality assurance, pharmacovigilance and a promotional programme that is compliant with a sophisticated market like Australia,” he says.
“Today, we have the number one selling eye lubricant on the Australian market, so people have worked that out and want to work with us. Over the years we have been offered a number of products. On the bottom of our business cards it says, ‘working to improve your health’ and we have turned down products we think don’t have this aim in mind.”
NOVATEARS BACKED BY PIVOTAL STUDY
AFT, a NZX and ASX-listed firm, has continued its annual trend of posting a record operating revenue, with its latest FY23 figures reaching NZ$156 million (AU$144 m), up 20% on the previous year. Australia continues to be its largest market, accounting for 61% of sales, growing by 23% to NZ$94 million (AU$86 m).
Atkinson says the company’s eyecare portfolio continues to build momentum in Australia, with the latest ophthalmic addition being the glaucoma eye drop Vizo-PF Dorzolatim dorzolamide (as hydrochloride) 20 mg/mL and timolol (as maleate) 5 mg/mL, available in a preservative-free multidose bottle.
He believes there are more opportunities like this. But for now, the company is placing an emphasis on growing the NovaTears range that caters for a large chunk of the dry eye market where more than 85% have the evaporative form of the disease.
The company has been somewhat surprised with the performance of NovaTears + Omega-3. It’s a line extension of the NovaTears eye drop introduced only a few years ago that combines perfluorohexyloctane and concentrated Omega-3 fatty acids of algae origin. However, there is more untapped potential for NovaTears, Atkinson believes.
“There’s a large market in Australia where people take fish oil tablets for their cardiovascular health, but if you’re doing it to promote good eye health via this method then it makes a lot of sense to deliver it topically to the eye. That’s why we're seeing NovaTears + Omega-3 perform better than we thought,” he says.
AFT already has a six-strong team of representatives visiting eyecare practices and an optometry network distribution agreement with Good Optical Services, but has recently appointed 10 salespeople to target the GP setting where NovaTears is a top priority.
“NovaTears has done well, but with the quality of this product, we think it has even greater potential. The range has performed not dissimilar to Hylo at the same point in time; in fact, NovaTears sales are slightly higher comparatively –but then Hylo took off,” he says.
“We saw the GP setting as an important one to drive greater education
28 INSIGHT October 2023
AFT Pharmaceuticals founder and CEO Dr Hartley Atkinson.
BUSINESS
and awareness of the brand. Doctors have a more holistic view of the patient and, as part of ageing, people often have dry eye and are recommended eye drops.”
Atkinson hopes NovaTears can ride the wave of recent US Food and Drug Administration (FDA) approval in May 2023. In America, the therapy is marketed as MIEBO and became the first and only FDA-approved treatment for dry eye that directly targets tear evaporation.
Key to this approval was the GOBI study, a Phase 3, multicentre, randomised, double-masked, saline controlled trial with 26 investigational sites and 597 patients. The work was published in the American Academy of Ophthalmology journal.
The primary sign and symptom end points were change from baseline in total corneal fluorescein staining (tCFS) and eye dryness score (0-100 visual analog scale [VAS]) at week eight. Key secondary end points were change from baseline in eye dryness score at week two, tCFS at week two, eye burning or stinging score (0-100 VAS) at week eight, and central corneal fluorescein staining (cCFS; 0e3 NEI scale) at week eight.
“Ultimately, it showed that dry eye associated with meibomian gland dysfunction provides statistically significant and, importantly, clinically meaningful evidence of the reduction of signs and symptoms of dry eye during eight weeks of treatment with NovaTears,” Atkinson says.
“But the other pleasing aspect was that we were getting statistically significant improvements as early as week two, so the product is working quickly in patients.”
A greenlight from the FDA is a big deal for any product, Atkinson explains.
“It's the world's largest healthcare market and regulatory approval there creates a lot of noise that tends to spill over to other geographies,” he says.
“It’s positive to have NovaTears reinforced by a large, well-conducted, published clinical study that led to approval by the US FDA. As an agency, they are very particular. We’ve had one approval and another one pending for a pain medication and when the FDA arrives, they stay several days to ensure they are happy with study conduct. They audit study sites and request the full open data files and recalculate everything to make sure it corresponds. They are a very thorough organisation.”
NEW HORIZONS, NEW OPPORTUNITIES
Looking ahead, Atkinson can see more opportunities on the horizon for AFT to introduce more preservative-free, multidose therapies in the ophthalmic space.
“We are working on two projects, but hopefully we'll be able to tell you more
about those in time; there is something good happening in America that I think we can bring down to Australia,” he says.
However, Atkinson could provide more details on the October 2023 deal with Latitude Pharmaceuticals. AFT will license Latitude’s key technology to develop a stable antibiotic eye drop for patients at risk of serious eye infections, with a potential addressable market worth US$1 billion (AU$1.5 b) globally.
The licensed intellectual property (IP) involves a patented aqueous stable formulation for an antibiotic eye drop. The antibiotic is already approved for treating various bacterial infections, including those caused by the antibiotic-resistant MRSA (Methicillin Resistant Staphylococcus Aureus) bacteria. However, no approved ophthalmic solution for this antibiotic exists for serious, potentially sight-threatening infections.
Atkinson warns the market is being served with eye drops by compounding pharmacies that come with the risk of contamination. But extensive off-label use has validated the market potential for the antibiotic for treating a number of important ophthalmic conditions.
The program will be included within AFT’s existing R&D budget, which is forecast to be circa NZ$12 million (AU$11 m) per annum in the FY2023 and FY2024 financial years. It’s another example of AFT’s value proposition in the pharmaceutical market, locally and globally.
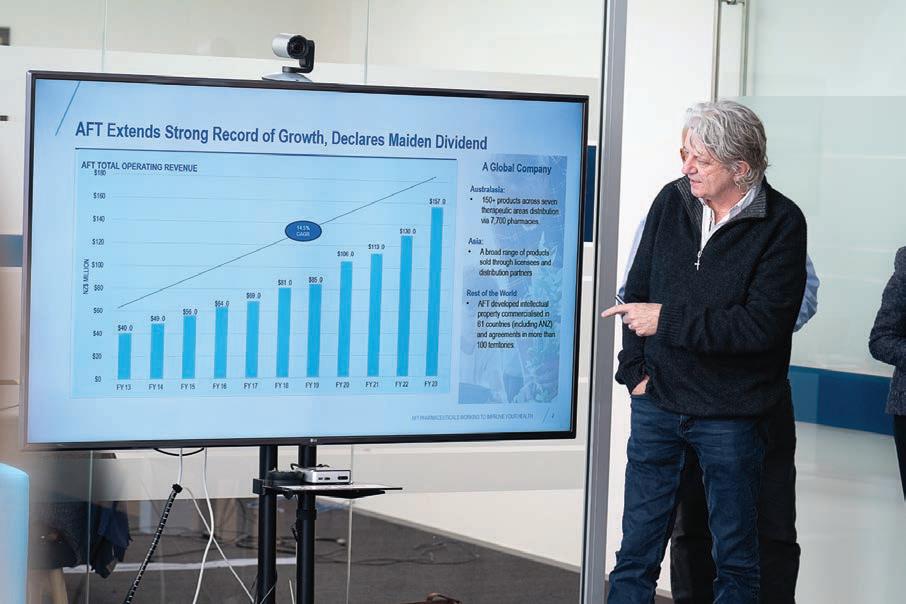
“This is our first R&D project in eyecare. It’s a good opportunity because a lot of these companies in the US, with their economic conditions, are struggling to raise finance, so a company like ours can take it over, conduct the clinical research, studies, formulation, etc, bring it to market and then share in the revenue,” Atkinson says.
“In Latitude, we see a company with strong IP and with the potential to treat eye infections, as well as being used preventatively, it could add up to a sizable market. In saying that, we’ve got three- to-four years of work ahead of us that will involve studies with 300-plus patients, but that’s an area we specialise in, often across multiple sites internationally.”
INSIGHT October 2023 29
AFT is placing a bigger emphasis on educating health professionals on its NovaTears products, a preservative-free eye drop for evaporative dry eye.
AFT continues to post record operating revenue each year, with the FY23 figures 20% up on the previous year.


NOW AVAILABLE Order today and experience the HP-OCT TM difference. info@cyliteoptics.com
At the completion of this article, the reader should be able to improve their management of patients requiring cataract surgery …
Including:
• Review the components of productive post-operative communication
• Understand and manage cataract patient expectations
• Review the elements of a good referral for refractive cataract surgery
• Understand the types of IOLs currently available
CHANGES IN CATARACT SURGERY, PATIENT EXPECTATIONS AND COLLABORATIVE CARE
The best outcomes for patients with cataracts come from strong collaborative relationships between optometrists and ophthalmologists. Each play an important role in the evaluation and management of patients and their expectations. The authors of this article recently held a discussion on the topic, and the following conversation has been edited for clarity and educational content.
W HAT DO PATIENTS EXPECT FROM CATARACT SURGERY?
Jason Holland, optometrist
When I went through university, we did very little on intraocular lenses (IOLs). When a patient developed cataracts, we were told, they had surgery and they got new glasses afterwards. That has changed a lot in recent years.
I think with the way IOL technology is heading, optometrists will have to upskill to develop their understanding of these lenses. Patients are keen to be less reliant on glasses and are starting to ask about their lens options before referral.1
Dr John Hogden, ophthalmologist
A decade ago, the average ophthalmic cataract surgical list consisted predominantly of monofocal IOLs with some surgeons aiming for a monovision refraction. Cataract surgery has improved; it’s relatively quick, highly effective and reliable. We’ve gone from using spherical monofocal lenses, to correcting astigmatism, then on to presbyopia-correction which is the latest advancement.2
Tessa Brushett, Alcon
Recently, Alcon commissioned some market research around patient expectations prior to cataract surgery and found that one in three patients referred for cataract surgery assume that the procedure will mean complete spectacle independence.3 The research challenges the idea that patients are happy with just great distance vision and that they don’t mind wearing glasses for everything else.
Patients were shown an example of vision with the Alcon PanOptix diffractive trifocal IOL, so 6/6
in the distance with some halos and glare and being spectacle independent for intermediate reading; an example of the Alcon Vivity extended range of vision IOL with excellent distance, great intermediate but needing glasses for reading with no glare or halos; and then a monofocal example, great distance but needing glasses for everything else. Ninety per cent said they would be interested in a presbyopia-correcting IOL (PC-IOL).3
Jason Holland
These outcomes really show that we (optometrists) need to initiate discussions about options more – both before referral and at the surgical consultation. Not all patients request trifocal or EDOF IOLs – but it’s obvious they would like to have that chat.
As the trends in patient care go from ‘cataract surgery’ to ‘refractive cataract surgery’, optometrists who want to make informed referrals want to know: how do we define that now, and what’s required?
Tessa Brushett
What we know is: providing information to the patients is almost as important as providing information to the referring ophthalmologist.
If one in three patients assume that they won’t need glasses after surgery, optometrists will need to manage their expectations. Established relationships between optometrists and surgeons allow an open forum for discussion about the IOLs that suit a patient and why they would like it.
Jason Holland
The referral is a big part of getting this process right. With PC-IOLs there is an adaptive process,
MBBS BMedSc RANZCO
The Eye Health Centre, Brisbane
Jason Holland
B.App.Sc i (Hons)(Optom) PGOT, CASA CO
The Eye Health Centre, Brisbane
National Director for Optometry, The Optical Superstore


Tessa Brushett
Surgical Account Manager Alcon Australia

so if the patient has had trouble adapting to multifocal glasses or contact lenses, if they have trouble adjusting to changes in refraction or are very particular personalities, it’s important to let the surgeon know.
Dr John Hogden
Modern cataract surgery is very much a refractive process4 and patients often want certain visual outcomes. The surgeon’s pre-operative process is about pairing the patient to the right lens and then communicating that back to the optometrist.
Jason Holland
In our practice, we use patient lifestyle questionnaires to start conversations about correction options. It prompts them to think about what they might want – often when you ask them, they aren’t sure (and many didn’t even know they have a choice).
THE IMPACT OF DRY EYE
Dr John Hogden
Dry eye is so prevalent in the community, particularly with the aging population. Conditions such as inflammatory eyelid disease, EBMDs (corneal epithelial basement membrane disease) such as map-dot fingerprint dystrophy and visually-significant pterygium often need to be addressed before considering IOL surgery. Optometrists are perfectly placed to identify and address these conditions with a slit lamp examination. These other pathologies might (continues) need to be addressed prior to cataract surgery and the optometrist can prepare the patient by informing them of the
INSIGHT October 2023 31
CLINICAL CPD HOURS This activity meets the OBA registration standards for CPD 0.75
CPD LEARNING OBJECTIVES:
Dr John Hogden
IMPORTANT PATIENT INFORMATION IN A REFERRAL FOR REFRACTIVE CATARACT SURGERY
• Vision history
° How was their vision 10 years ago, and what were their required glasses?
• Lifestyle information
° For example, ‘Patient A loves to garden; she drives a lot picking up the grandchildren, she occasionally uses a pair of readers because she's got a bit of natural monovision that's developed with a cataract.’
• Work situation
° Does the patient use computer screens at work? At what distance?
• Hobbies and sports
• Current correction
° Are they using glasses or contact lenses – single vision, monovision or multifocal?
• Do they have trouble adapting to prescription changes, multifocal glasses or contact lenses?
• Is the patient very particular about their vision?
• Does the patient have a history of dry eye?
• Does the patient have glare sensitivity?
• Have they expressed a motivation for spectacle independence?
need to treat the other issue first to achieve a superior refractive and functional outcome.
Jason Holland
but if you don’t manage the ocular surface and tear film, the patient will still be unhappy. It is one of those issues that requires ongoing care and optometrists need to manage these people long term.
Aggressive management of dry eye by the optometrist will benefit the patient and the ophthalmologist and will facilitate a better patient outcome. A poor tear film delays surgery as we can’t do accurate measurements, topography and biometry. In our clinic, we routinely question the patients about dry eye symptoms, and encourage them to disclose even mild symptoms. We then do an indirect tear break up time and a digital expression of the meibomian glands to examine the quality of the secretions.
By being proactive about dry eye, the patient is more likely to have stable vision and less likely to become a dry eye patient post-operatively.
“ESTABLISHED RELATIONSHIPS BETWEEN OPTOMETRISTS AND SURGEONS ALLOW AN OPEN FORUM FOR DISCUSSION ABOUT WHAT IOLs MIGHT SUIT A PATIENT AND WHETHER THE PATIENT WOULD BE HAPPY WITH THE OUTCOME THAT LENS PROVIDES.”
HOW DO YOU GO ABOUT PATIENT SELECTION?
Jason Holland
Alcon’s Light Intensity Distribution Diagram (figure 2) is a great little visualisation of the differences in the IOLs. Monofocal IOLs, at the top row, are great for distance, but vision drops off quickly when it gets to objects at an intermediate distance.
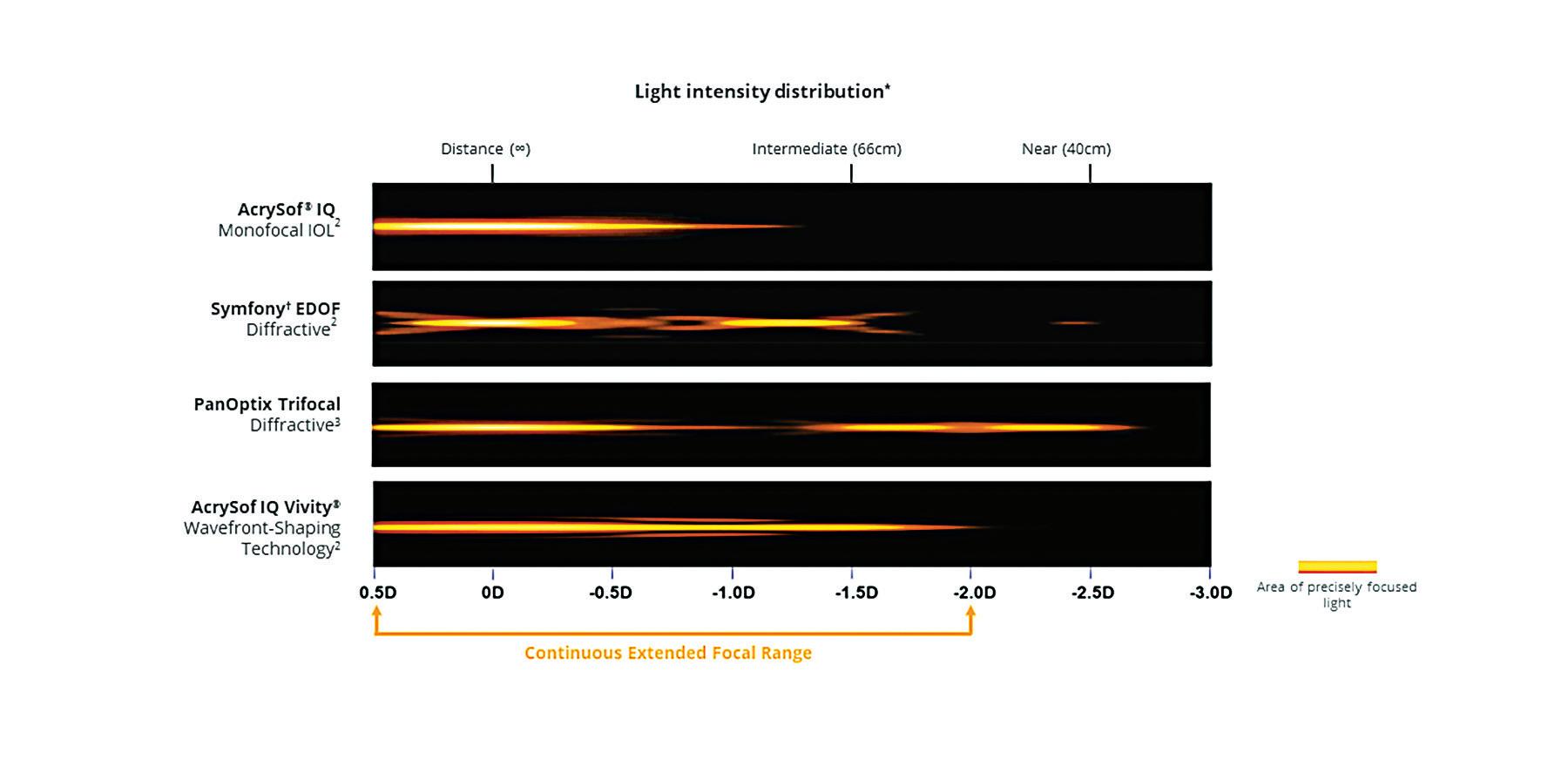
The second row is an earlier diffractive EDOF,
indicate there is not a continuous focus.
The third row is a diffractive trifocal, the PanOptix, where there is a distance focus then a long, clear focus stretch from intermediate to near.
At the bottom is Vivity where the continuous focus stretches from distance all the way through to intermediate.
Dr John Hogden
This graphic is really good as you can see there are pros and cons to every lens; what suits one person may not suit another so you can offer the patient a suite of lenses. In a consultation you try and tailor the offering, the patient may have AMD or severely dry eyes and this may modify what is recommended, but you can educate them and show them what the lenses can do and this works best when it starts with the optometrist.
ASTIGMATISM
Jason Holland
Dr Hogden, with astigmatism and PC-IOLs, do you only correct over 2 diopters, or do you consider half a diopter or more is significant?
Dr John Hogden
At the Eye Health Centre we place incredible importance on the reliable and accurate measurement of astigmatism and to manage any dry eye and other ophthalmic pathology, listening to patients and seeing what their expectations are afterwards to get lens selection and outcomes just right. We can now offer a whole suite of lenses for patients, anything from a monofocal lens, to an EDOF lens or the trifocal, it is about matching the right patient to the right lens.
Astigmatism correction is very important and critical in getting good results for patients and PC-IOLs are less forgiving than a monofocal so we always want to address it. At the

32 INSIGHT October 2023
CPD
Figure 2. Light Intensity distribution diagram.5-7
measures, wavefront Placido, anterior segment OCT, checking the referral to see how much astigmatism is in the patient’s glasses and if it has fluctuated over the years to really nail the refractive outcome. Correcting down to 0.75 diopters of astigmatism is now the standard of care for us.
POST-OPERATIVE CARE
Jason Holland
Research suggests several key things optometrists would like to hear back from the surgeon once the patient is discharged and returns to see them. They want to know if there is a complication as invariably they will be managing that with the ophthalmologist and interestingly they also want to know if the patient is satisfied with the surgery; are they going to walk in saying everything’s great or were there some issues and they’re not satisfied?3
Dr John Hogden
The communication needs to go two ways, there's a lot of onus on the ophthalmologist to feed that information back and close the loop. Optometrists want to know if the surgery was routine? What IOL has the patient been given? What are their refractive needs or other optometric needs after surgery? They may need to see their optometrist six monthly to monitor
for glaucoma. I try to put in as much information as I can about whether they need a weak pair of reading glasses or some sunglasses, whatever their needs might be moving forward. I also like to keep the door open so that if six or 12 months down the track there is an issue, then I can look after the patient and address any issues or any pathology that may have arisen.
INTRODUCING COLORMATIC® 3: THE NEW GENERATION OF COLORMATIC®
Rodenstock’s ColorMatic® 3 lenses change from clear to dark and fade back to clear again 30% faster than the previous generation – making them our fastest photochromic lenses ever.
For more information, speak to your Rodenstock Account Manager.
We need to give all that information in the letter back to the optometrist and try to be really vigilant about it. It’s hard as a clinician when you don’t have all the information, so the more information we can provide the easier the job is afterwards for the patient’s optometrist.
There is a need to hand back to the optometrist at the end of the treatment process. Complex
Available with Biometric Intelligent Glasses
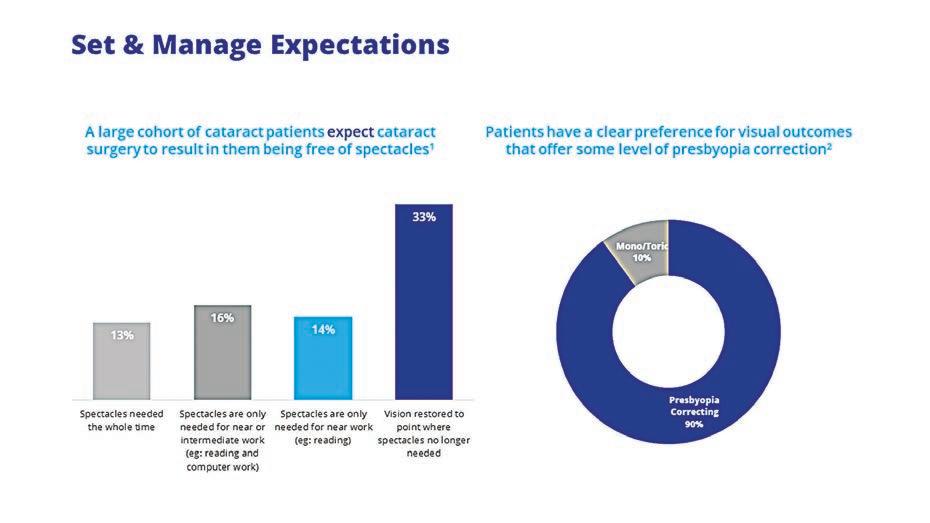 Figure 1. Adapted from Kantar Consumer cataract research.3
Figure 1. Adapted from Kantar Consumer cataract research.3
Frame R3338C
UNDERSTANDING IOLs
Before an optometrist can discuss IOL options with their patients, they need to understand them.

1. Monofocal/Single Vision IOLs
As the name suggests, single vision IOLs offer the patient single vision correction, just like single vision spectacle lenses or contact lenses. The patient will have one focal distance only.

2. Presbyopia-correcting IOL (PC-IOL)
There are a few different PC-IOL options now, but the two main categories are: trifocals and extended depth of focus (EDOF) IOLs.
Trifocal IOLs
The Alcon PanOptix trifocal uses diffractive technology which splits the light and gives a focus at distance, intermediate and near. PanOptix has a continuous focus from 40cm to 80cm with an intermediate focal point at 60cm.10,11
Extended depth of focus (EDOF) IOLs
EDOF IOLs generally correct the distance and intermediate vision and functional near vision. Day-to-day, a patient with EDOF IOLs will be generally free of glasses, but will need a weak pair of glasses for reading or iPad use. EDOF IOLs reduce the visual disturbances associated with a full trifocal while still giving some range of vision.12,13
Some ophthalmologists will target a low myopic correction with EDOF IOLs in the non-dominant eye to increase the range of vision but often they still need a weak pair of readers.
Alcon’s Vivity extended range of vision IOL
Alcon’s Vivity IOL uses X-Wave Technology which means the wavefront of light is stretched and shifted, without splitting it, to increase the depth of focus14. It is not a diffractive lens, so you have a much better profile in terms of dysphotopsia, distortion and glare.5,14
The aim of the Vivity IOL is to give patients clear distance and intermediate vision but they are likely to need reading glasses for small print.15,16 The outcomes of a large clinical trial of patients implanted with Vivity IOLs gave a mean unaided binocular vision of 6/6 in the distance, 6/7.5 for intermediate and 6/9 at near.14,17,18
IOLs will require greater collaboration than we have had in the past.
Jason Holland
If you aren’t aware of the type of IOL your refraction can be off so PC-IOLs can catch you off guard. If you haven’t got the letter from the surgeon, it’s important to do unaided vision at distance and at near and you’ll quickly know if the IOL's a monofocal or not, because they will have great distance vision and poor vision up close.
If you have a Vivity lens they will hold the reading card away from them to read it, and with PanOptix or other trifocal IOLs they will be able to read at approximately 60 and 40cm. Routinely we often just do unaided vision at a distance but moving forward, if someone has had cataract surgery, my first step would be to do unaided distance and near vision.
The next step would be retinoscopy to help see what the lens is, you are going to get a droplet like reflection for Vivity, almost like a keratoconic, while for diffractive IOLs you can see the rings clearly. You can also use the slit lamp.
Auto-refraction and duochrome generally don’t work well with PC-IOLs. When I’m refracting an IOL with any sort of multifocality, I’ll use 0.50D steps when refracting or a 0.50D cross-cyl rather than 0.25D.
These IOLs have complicated optics and you’ll find you’ll be less caught out by aberrations or minor idiosyncrasies of the optics if you use a larger step. I also find that you need to be mindful of pushing the plus in the refraction, as you can find that the patient keeps accepting minus and you end up refracting the intermediate part of the IOL.
COMMUNICATIONS IS KEY
Dr
John Hogden
The key message is that communication between ophthalmologists and optometrists is really important. Optometrists know what the best options for patients’ vision corrections are and what works for their patients. They also know what patients expect of surgery and communicating this in your referral helps in the decision process as to what IOL will work best for your patient. Receiving correspondence back from the surgeon helps with understanding what the patient’s needs are moving forward and this should be an open dialogue. There are lots of IOLs out there, we just need to keep talking about it and seeing how we can better serve our patients.
Jason Holland
As Dr Hogden said, the overarching theme is communication. Let’s communicate with our patients better, let’s get more comfortable understanding IOLs and let’s collaborate with surgeons to get better patient outcomes.
REFERENCES
1. Devries D. Preparing patients for cataract surgery. Available at: https://collaborativeeye.com/articles/best-of-aoc/preparing-patients-for-cataract-surgery/ (accessed 24.8.203).
2. Alkharashi M et al. Advances in cataract surgery. Exp Rev Ophthalmol 2013;8(5):447–56.
3. Alcon Data on File: Kantar Consumer Cataract Awareness Research July 2021(Full Report)
4. Raj C Cataract surgery and IOLs: what the doctor ordered? 2018. Available at: https://www.mivision.com.au/2018/07/cataract-surgery-and-iols-what-the-doctor-ordered/ (accessed 24/08/2023).
5. AcrySof IQ Vivity® Extended Vision IOL Directions for Use
6. Alcon Data on File, TDOC-0056392. 18-Jun-2019.
7. Alcon Data on File, TDOC-0056797 *Simulated photopic through-focus point spread function (light intensity [energy]) –polychromatic.
8. AcrySof® IQ Directions For Use
9. AcrySof® IQ PanOptix® Directions for use
10. PanOptix® Diffractive Optical Design. Alcon internal technical report: TDOC- 0018723. Effective date 19 Dec 2014.
11. Kanclerz P et al. Extended Depth-of-Field Intraocular Lenses: An Update. Asia Pac J Ophthalmol (Phila) 2020;9(3):194–202.
12. Kohnen T and Suryakumar R. Extended depth-of-focus technology in intraocular lenses. J Cataract Refract Surg 2020;46(2):298–304.
13. Kohnen T. Nondiffractive wavefront-shaping extended range-of-vision intraocular lens. J Cataract Refract Surg 2020;46(9):1312–13.
14. Leonard C. IOL Review: 2021Newcomers. Rev Ophthalmol April 2021. Available at: https://www.reviewofophthalmology.com/ article/iol-review-2021-newcomers (accessed 15/07/21).
15. Urs ell PG et al. 5 year incidence of YAG capsulotomy and PCO after cataract surgery with single-piece monofocalintraocular lenses: a real-world evidence study of 20,763 eyes. Eye 2020;34(5):960–68.
16. Alcon data on file. 2019. A prospective, randomized, controlled, multicenter clinical study of the AcrySof IQ Extended Depth Of Focus (EDF) IOL:1–1831 (TDOC-0055576).
17. Alcon data on file. 2019. A prospective, randomized, controlled, multi-center clinical study of the AcrySof IQ Extended Depth of Focus (EDF) IOL: 1–2174 (TDOC-0055575).
18. Results from a prospective, randomized, parallel group, subject and assessor masked, multisite trial of 107 subjects bilaterally implanted with AcrySof IQ Vivity® Extended Vision IOL and 113 with AcrySof® IQ IOL with 6 months follow-up. †Snellen VA was converted from logMAR VA. A Snellen notation of 20/20-2 or better indicates a logMAR VA of 0.04 or better, which means 3 or more of the 5 ETDRS chart letters in the line were identified correctly.
NOTE: Insight readers can scan the QR code or visit insightnews.com.au/cpd/ to access a link to this article to include in their own CPD log book.
34 INSIGHT October 2023
CPD - ALCON
Table 1. Alcon IOL designs and features 5,9,10
*Table is intended as a general guide only and is not based on any head-to-head studies

This medicinal product is subject to additional monitoring in Australia. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse events at https://www.tga.gov.au/reporting-problems. Aspen Australia includes Aspen Pharmacare Australia Pty Ltd (ABN 51 096 236 985) and Aspen Pharma Pty Ltd (ABN 88 004 118 594). All sales and marketing requests to: Aspen Pharmacare Pty Ltd, 34-36 Chandos Street, St Leonards NSW 2065. Tel: +61 2 8436 8300 Email: aspen@aspenpharmacare.com.au Web: www.aspenpharma.com.au Trademarks are owned by or licensed to the Aspen group of companies. © 2023 Aspen group of companies or its licensor. All rights reserved. Prepared July 2023. AU-ATR-072023-07585. ASPPH3029. PBS Information: This product is not listed on the PBS. *P-value not available (ATOM 1&2 studies, placebo was a historical control from ATOM 1).ATOM 2 study data available for 5 years with 1 year washout after 24 months.3 EIKANCE 0.01% eye drops (atropine sulfate monohydrate 0.01%) is indicated as a treatment to slow the progression of myopia in children aged from 4 to 14 years. Atropine treatment may be initiated in children when myopia progresses ≥ –1.0 diopter (D) per year.1 Scan to review full Product Information and to order samples, or call 1300 659 646. References: 1. Approved EIKANCE Product Information, 14 March 2023. 2. Chua WH et al. Ophthalmology 2006;113:2285–91. 3. Chia A et al. Ophthalmology 2016;123:391–9. SLOW MYOPIA PROGRESSION BY UP TO 60% WITH ATROPINE 0.01% EYE DROPS AT 2 YEARS COMPARED TO PLACEBO *1-3
THE RESULTS ARE CLEAR
weeks 2
In as little as 2 weeks 1 , NovaTears demonstrated statistically significant and clinically meaningful improvements in the signs and symptoms of Dry Eye Disease associated with Meibomian Gland Dysfunction.
RELIEVES
NovaTears® is a unique preservative-free non-emulsion eye lubricant utilising patented EyeSol® Technology:
Lubricates the surface of the eye, spreading quickly without blurring vision
Preservative, phosphate, water and surfactant free.

NovaTears® acts as a lipid layer stabiliser & evaporative barrier for improved tear film stability & quality:
Stabilises & thickens outer tear film
Allows replenishment of underlying water layer with natural tears.

6 months shelf life after opening Preservativefree
STREAMLINED AUTHORITY CODE 6172
PBS Information:
Authority Required (STREAMLINED): Severe dry eye syndrome in patients who are sensitive to preservatives in multi-dose eye drops.
Reference 1. Tauber J, Berdy GJ, Wirta DL, Krösser S, Vittitow JL, on behalf of the GOBI Study Group, NOVO3 for Dry Eye Disease Associated with Meibomian Gland Dysfunction: Results of the Randomized Phase 3 GOBI Study, Ophthalmology (2023), dol: https://doi.org/10.1016/j.ophtha.2022.12.021.
NovaTears® Eye Drops (Perfluorohexyloctane 100% v/v, 3mL) are for the lubrication and relief of dry and irritated eyes. Do not use NovaTears® with contact lenses. If using any other eye medication, allow at least 15 minutes between using the other product and applying NovaTears®. NovaTears® should not be used in children under 18 years. NovaTears® should not be used while pregnant or breastfeeding. AFT Pharmaceuticals Pty Ltd, Sydney. ABN 29105636413.
Free phone: 1800 238 742 | Email: receptionau@aftpharm.com mydryeyes.com.au
CPD - DRY EYE
PROTECTS
netaP t e d yEeSol®Technology PBS
Listed
At the completion of this article, the reader should be able to improve their management of dry eye disease …
Including:
• Understand the role of IPL treatment in reducing symptoms, improving tear quality and managing inflammation associated with dry eye disease (DED)
• Review the strengths and limitations of established dry eye treatment protocols, including tear supplements, immunosuppressants and thermal heating
• Recognise how IPL treatments, following the 'Toyos Protocol', can improve DED symptoms and signs, reduce inflammation and stimulate meibum liquefaction.
IPL: A PARADIGM SHIFT IN THE TREATMENT OF DRY EYE DISEASE

With dry eye being a multifaceted ocular condition, DR NICHOLAS YOUNG says traditional theories of tear dysfunction are shifting towards inflammation and sensory factors as central causes. Intense pulsed light (IPL) therapy has now emerged as a safe and effective treatment that alleviates symptoms and enhances tear quality.

Objective signs of dry eye include loss of tear film homeostasis, loss of tear stability, hyperosmolarity, as well as ocular surface inflammation and damage. Combining less obvious features such as neurosensory abnormalities, dry eye disease (DED) is a condition of mixed aetiology.1 Subjectively, patients experience a variety of symptoms, ranging from minimal to severe. Dry eye is also the most reported reason for seeking eyecare (other than vision correction)2 and is associated with significant morbidity, and cost to the community.3
PREVALENCE
Prevalence of dry eye is difficult to estimate due to inconsistencies in study design.4 Up to 57% of participants in one Australian study report at least one symptom5 but estimates of about 15%are more common.6 An increased incidence
of disease associated with screen time and comorbidities such as mental health appears to have accompanied the COVID pandemic lockdowns.7
PATHOPHYSIOLOGY
The pathophysiology of DED is multifactorial.8 The dichotomous narratives of ‘aqueous deficiency’ and ‘tear evaporation’, while foundational in their time, are now viewed as simplistic and outdated.
The relentless pursuit of meibomian gland treatments is a soft target with diminished returns and overshadows other pathology, such as tissue inflammation and neurosensory dysfunction.
The strongest clue that tear dysfunction alone is an inadequate target for therapy relies on one simple fact: the signs and symptoms of DED often do not overlap. It is common for patients whose tear metrics are indistinguishable
ABOUT THE AUTHOR:
Dr Nicholas Young BSc(Hons). BOptom PhD(Med)
PGCertOcTher
Optometrist, Clinic Director
Dry Eye Centre, Melbourne, VIC
from each other, to report different types and degrees of symptoms. This view is supported by meta-analysis, where some studies fail to demonstrate any clear association between signs and symptoms at all.9 Tear composition and stability is not a reliable determinant of comfort. Furthermore, no single metric is diagnostic of DED. This is the paradox of DED.
INFLAMMATION AND NEUROSENSORY FUNCTION
The ultimate determinant of comfort is sensation. Uni and polymodal ocular surface trigeminal somatosensory nerve fibres constantly signal information about ocular surface temperature, touch and chemistry to the trigeminal nucleus and spinal cord. Corneal neuropathic pain (allodynia) is said to occur when these nerves respond in the absence of, or to normally non-painful stimuli. Whereas hyperalgesia represents an exaggerated sensation to surface conditions which would normally evoke a response.10
Complex processes involving the immune system
INSIGHT October 2023 37
CLINICAL CPD HOURS This activity meets the OBA registration standards for CPD 0.75
CPD - DRY EYE
LEARNING OBJECTIVES:
Many studies have demonstrated IPL’s positive effects on ocular rosacea and tear function. Pictured: Lumenis OptiLight.
can also affect sensory feedback. Ocular tissue inflammation and nervous system physiology are intricately balanced to provide comfort under normal conditions and physical symptoms when challenged.10 Elevated levels of inflammatory mediators, such as cytokines, MMP’s and reactive oxygen species accompany abnormal sensation in DED. Metanalyses confirm that inflammation, rather than tear dysfunction, is the core of DED.11
ROSACEA
Some of the common types of inflammation found in patients with DED are eyelid inflammation (blepharitis), telangiectasis, conjunctival injection, infection (bacteria, Demodex) and MGD.12 These signs may be accompanied by facial flushing (rosacea).
Rosacea is an inflammatory skin condition characterised by classic patterns of facial erythema and telangiectasias and sometimes cystic or non-cystic acne. There are four primary subtypes: erythrotelangiectatic (vascular), papulopustular (inflammatory), phymatous and ocular. While this classification has recently been updated, ocular rosacea, which bears the clinical features described, can easily be overlooked by the inexperienced observer and is increasingly acknowledged as one of the more significant inflammatory comorbidities of DED.13
CURRENT TREATMENTS
Tear Supplements
Most treatments for DED are tear supplements which promote improvements in one or another, or a combination of tear film components. But short retention times, or retention with blur, inclusion of preservatives and industrial chemicals, overuse, polypharmacy, tachyphylaxis and ineffectiveness or worsening of symptoms, leave many patients requiring alternative or additional care.
osmolarity. However, in my experience, this metric is subject to a high degree of variance;14 making its interpretation difficult in the clinic. Tear supplement efficacy on ocular surface inflammation is unproven and meta-analyses conclude their general effects on DED are clinically indistinguishable from each other.15 Consensus opinion favours tear supplements for transient or mild symptoms. Their use as adjunct therapy following application of more advanced treatments, might also be helpful.
Conversely, next-level immunosuppressants such as cyclosporin, lifitigrast, macrolides and tetracyclines interrupt different cellular processes responsible for upregulation of proinflammatory surface cytokines. While these medications can be very effective, they can also be poorly tolerated and since macrolides and tetracyclines are classed as antibiotics, the latter capable of profound adverse effects on gut health, long-term use is not desirable.
Steroids also have well documented side effects. Findings of iatrogenic facial rosacea following fluorinated steroids use in the 1960s,16 contraindicates these for treating ocular rosacea and has led to the use of non-fluorinated steroids such as hydrocortisone for eyelids.17 However, it has been shown that even this lower-potency steroid can cause contact dermatitis and rebound telangiectasias with prolonged use.18
Thermal Heating: Warm/hot compresses
Heat, externally applied to the eyelid, is often advocated for liquefying meibomian glands. Despite some supportive level two and three data, there remain inconsistencies with this treatment. They include patient compliance, lack of a standardised heating device, and temperature, duration or frequency of treatment.
To ensure a liquid state, meibum’s usual melting temperature is 32°C, which is lower than normal eyelid (33°C) and cornea (37°C) temperatures. However, due to altered chemical composition, gland inspissation can result in phase transition temperatures of around 45°C.19 It would appear then that an external lid temperature of 45°C should be sufficient to melt meibum. However, heat loss occurs between the front and back surface of the eye lid during heating. Indeed, external lid temperatures exceeding 50°C, could be needed to melt stubborn meibum, risking aggravation of conditions such as ocular rosacea. Furthermore, eyelid skin burns have been reported to occur after 35 minutes of continuous exposure to thermal contact of 45°C, as well as from accidental over heating of face masks20 and corneal warpage from excessive heat transfer to the cornea is also a risk.9, 22 Therefore, warming devices should not exceed 5-10 min or 45°C, in order to prevent adverse effects,7,19 but at these temperatures and durations, are most likely ineffective for inspissated glands.
IPL and dermatology
Pulsed dye lasers have been used in dermatology since the early 1980s. They have been used
to treat lesions such as rosacea, port wine stains and haemangiomas. In 1987, studies of rabbit ear veins and human leg veins concluded that a 585nm laser pulsed at 0.45ms could cause thermal coagulation of blood vessels with a diameter less than 0.4mm. However, the treatments caused hyperpigmentation, hypopigmentation, purpura and scarring.21
In 1992, a chance meeting of Drs Mitchel Goldman, Richard Fitzpatrick (dermatologists) with Shimon Eckhouse (engineer), resulted in a prototype flash lamp device designed to improve the flexibility of treatment algorithms around variables such as pulse intensity, duration and frequency. Studies showed that rabbit ear veins could be thermo-coagulated without any significant skin damage , but the first human trials resulted in burning (60%) and scarring (20%). These and similar early findings did nothing to help the development of IPL. Proponents of lasers dismissed IPL as harmful, useless and labelled it the ‘photo burner’. Its further development would see strongly divisive literature published and even defamation litigation pursued in the courts among adversaries of the technology.21
The IPL breakthrough came with the understanding that skin could be protected with the use of a sapphire lightguide, a pause between successive pulses to ‘rest’ the skin, cooling gel to couple the lightguide to the skin and, in the most recent and advanced devices, the use of a refrigerated lightguide.
After its invention in the 1960s as an industrial device for, among other uses, vaporising paint off aircraft, IPL was finally registered by the FDA for skin treatments in August 1995. Its appeal rapidly spread to become arguably the safest and one of the most efficacious aesthetic devices available today.
IPL AND OPTOMETRY
In 2002, a fortuitous discovery by US ophthalmologist Dr Rolando Toyos occurred when it was noticed that patients with both facial rosacea and dry eye disease experienced ocular symptom relief following facial IPL treatment.22 Research continued with the light therapy company Dermamed using a device called the ‘Quadra 4 Diamond Series II’ IPL. This led to the commercialisation of IPL for DED in 2008.
The Dry Eye Centre in Melbourne subsequently acquired this device and became the first clinic in Australia to treat DED with an IPL device developed specifically for dry eye disease.

HOW DOES IPL WORK?
The principle of IPL involves passing a broad spectrum of incoherent light through a sapphire lightguide to the skin via a wavelength cut off filter. The filter excludes ultraviolet light and facilitates wavelength optimisation for targeting chromophores such as red blood cells. IPL devices typically emit light in the wavelength range of 500nm to 1400nm.23
Pulsed light generates multiple instances of light, each being separated by a rest phase. The latter protects the skin epidermis, while the former

38 INSIGHT October 2023 CPD - DRY EYE
With Dermamed’s Quadra 4 Diamond Series II, Dr Nicholas Young's The Dry Eye Centre became the first in Australia to treat DED with an IPL device developed specifically for the condition.
targets the chromophore of interest. The target chromophore for DED is red blood cells, while heat is also absorbed by meibomian glands. Important features of IPL include wavelength optimisation filtering, pulse duration, size, shape and depth for different skin types and treatment effects. In addition, the lightguide should produce a consistent non-degrading flash with integrated cooling.23
If these conditions are met, IPL is a highly standardised, reproducible and measurable procedure. The treatment is performed with calibrated equipment, known and documented metrics, in a controlled space by a suitably qualified practitioner.

THE ‘TOYOS PROTOCOL’
The accepted treatment standard is the ‘Toyos Protocol’.22 It consists of a triple six-millisecond pulse, interspaced with two 50ms rest phases. Treatment takes place directly beneath the lower eyelid lash line, proceeding from tragus to tragus and includes the lateral walls and dorsum of the nose. Depending on face width, up to 17 flashes across the face may be delivered from right to left. Facial contouring imposed by the cheek bone, also necessitates horizontal placement of the sapphire lightguide below the primary treatment zone. Depending on the device in use, direct treatment of the upper eyelids might also be possible.
The Fitzpatrick skin grading scale is used to determine pulse intensity. Treatment may
Anecdotally, spot treatments can be used to treat active chalazia. At the Dry Eye Centre, we receive many referrals for this purpose and have achieved excellent results on both isolated and recurring lesions across the lids.
For DED, approximately four treatments are done usually in three to four-week intervals, depending on the patient and the device. However, this is only a guide and additional treatments might be needed as part of the initial treatment cycle. Improvement should not be promised, as some patients do not respond to IPL. Treatments are
usually also combined with other care routines, the combination of which can remain effective for many months or longer.22 Future maintenance treatments might also be needed depending on the presenting condition.

PATIENT EDUCATION
Treatments are performed with no down time and generally no side effects. However, there are contra-indications for IPL, and practitioners should check with their device supplier for a list of these, and develop a patient informed consent form, before proceeding.
The treatment plan including what to expect before, during and after IPL, as well as success rates and alternatives to IPL, should also be
Earlier in 2023,
pioneer Dr
IPL
Rolando Toyos was in Sydney and provided a demonstration with the Lumenis OptiLight IPL.
discussed with the patient. Practitioners who use devices with degrading flash units, should also inform their patients of this, as treatment efficacy may vary with the lifecycle of the flash cartridge.
Practitioners should also obtain a preceptorship on the use of their device from their device company, education provider or suitably qualified mentor. Injury to patients is possible and IPL should not be used without such training.
MECHANISMS
Thrombosis
Haemoglobin readily absorbs light energy and coagulates red blood cells. Vessel thrombosis follows coagulation.24 Vessel closure is important, not just for cosmesis, but to also reduce tissue damage from an overactive immune system. The concentration of ocular surface inflammatory mediators is reduced following IPL, and it is hypothesised that these reductions interfere with the vicious cycle of inflammation.25
Meibum liquification
Heat from IPL is thought to pass directly into the meibomian gland, facilitating phase transition to a liquid.25 Anecdotally, evidence of this is often seen at the slit lamp immediately following treatment. One of the other characteristics of MGD is the presence of bacteria which contribute to the inspissation of meibum. It is thought that IPL simultaneously eliminates these bacteria.26 The same treatment algorithm also destroys demodex.27
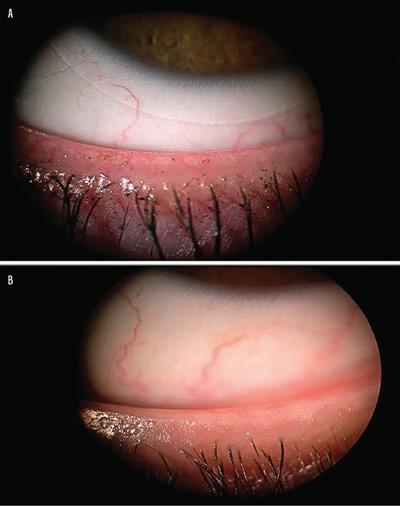
Skin Turnover
Rosacea increases tissue inflammation and epithelial cell turn over. Ocular rosacea affects lid margin and gland duct epithelium. Dead epithelial skin cells create debris which can block meibomian gland orifices. It is hypothesised that IPL reduces tissue inflammation, epithelial cell debris and therefore meibomian gland obstruction.25
Elastin and collagen synthesis
Lid strength is required to pump meibum from their glands to the ocular surface. Age-related extracellular collagen and elastin decline leads to tissue weakening which can affect eyelid apposition reducing the effect of blinking. IPL stimulates collagen and elastin and is thought to play a role in eyelid firming, and blink function, which may help to maintain meibomian gland health. One of the proposed mechanisms of this activity is cellular photo modulation.25
EFFICACY
IPL is both a safe and effective dry eye treatment. Several meta-analyses have now reported positive IPL outcomes. Collectively, they conclude improvements in subjective assessments such as SPEED (symptoms), OSDI (effect on lifestyle) scores and reduction of tear supplement usage.
Objective assessments favour reduced corneal fluorescein staining, improved lipid layer quality and improved tear break up times compared to baseline and in comparison with other conventional therapies.28-32
REFERENCES
1. Craig JP, Nichols KK, Akpek EK, Caffery B, Dua HS, Joo CK, Liu Z, Nelson JD, Nichols JJ, Tsubota K, Stapleton F. TFOS DEWS II definition and classification report. The ocular surface. 2017 Jul 1;15(3):276-83.
2. Doughty MJ, Fonn D, Richter D, Simpson T, Caffery B, Gordon K. A patient questionnaire approach to estimating the prevalence of dry eye symptoms in patients presenting to optometric practices across Canada. Optometry & Vision Science. 1997 Aug 1;74(8):624-31.
3. P flugfelder SC. Prevalence, burden, and pharmacoeconomics of dry eye disease. Am J Manag Care. 2008;14:S102–S106
4. Janine AS. The epidemiology of dry eye disease: report of the epidemiological subcommittee of the international dry eye workshop. Ocul Surf. 2007; 5 (2): 93-107.
5. Chia EM, Mitchell P, Rochtchina E, Lee AJ, Maroun R, Wang JJ. Prevalence and associations of dry eye syndrome in an older population: the Blue Mountains Eye Study. Clinical & experimental ophthalmology. 2003 Jun 1; 31 (3): 229-32.
6. Moss SE Klein R, Klein BE. Prevalence of and risk factors for dry eye syndrome. Archives of ophthalmology. 2000 Sep 1; 118 (9): 1264-8.
7. Neti N, Prabhasawat P, Chirapapaisan C, Ngowyutagon P. Provocation of dry eye disease symptoms during COVID-19 lockdown. Scientific Reports. 2021 Dec 24; 11 (1): 24434.
8. Stern ME, Beuerman RW, Fox RI, Gao J, Mircheff AK, Pflugfelder SC. A unified theory of the role of the ocular surface in dry eye. In Lacrimal Gland, Tear Film, and Dry Eye Syndromes 2 1998 (pp. 643-651). Springer US.
9. Bartlett JD, Keith MS, Sudharshan L, Snedecor SJ. Associations between signs and symptoms of dry eye disease: a systematic review. Clinical Ophthalmology. 2015 Sep 16: 1719-30.
10. B elmonte C, Acosta MC, Gallar J. Neural basis of sensation in intact and injured corneas. Experimental eye research. 2004 Mar 31; 78 (3): 513-25.
11. Wei Y, Asbell PA. The core mechanism of dry eye disease (DED) is inflammation. Eye & contact lens. 2014 Jul; 40 (4): 248.
12. Vis o E, Millan AC, Rodriguez-Ares MT. Rosacea-associated Meibomian Gland Dysfunction – An Epidemiological Perspective. European Ophthalmic Review. 2014; 8 (1): 13–6.
13. Vieira AC, Mannis MJ. Ocular rosacea: common and commonly missed. Journal of the American Academy of Dermatology. 2013 Dec 1; 69 (6): 36-41.
14. Bunya VY, Fuerst NM, Pistilli M, McCabe BE, Salvo R, Macchi I, Ying GS, Massaro-Giordano M. Variability of tear osmolarity in patients with dry eye. JAMA ophthalmology. 2015 Jun 1; 133 (6): 662-7.
15. Pucker AD, Ng SM, Nichols JJ. Over the counter (OTC) artificial tear drops for dry eye syndrome. Cochrane Database of Systematic Reviews. 2016(2).
16. Sneddon I. Adverse effect of topical fluorinated corticosteroids in rosacea. Br Med J. 1969 Mar 15; 1 (5645): 670-3.
17. Bhat YJ, Manzoor S, Qayoom S. Steroid-induced rosacea: a clinical study of 200 patients. Indian journal of dermatology. 2011 Jan; 56 (1): 30.
18. Guin JD Complications of topical hydrocortisone. Journal of the American Academy of Dermatology. 1981 Apr 1; 4 (4): 417-22.
19. Blackie CA, Solomon JD, Greiner JV, Holmes M, Korb DR. Inner eyelid surface temperature as a function of warm compress methodology. Optometry and Vision Science. 2008 Aug 1; 85 (8): 675-83.
20. Eis eman AS, Maus M, Flanagan JC. Second-degree eyelid burn after use of microwave-heated compress. Ophthalmic Plastic & Reconstructive Surgery. 2000 Jul 1; 16 (4): 304.
21. Fodor L, Ullmann Y, Elman M. Aesthetic applications of intense
These analyses include randomised controlled and other study designs with patient numbers ranging from 539 (nine studies)31 to 1,842 (11 studies).28-32 Individual studies report improvements in visible signs of ocular inflammation, such as lid margin telangiectasias.22
CONCLUSION
IPL represents a paradigm shift in the treatment of DED. Many studies have demonstrated its positive effects on ocular rosacea and tear function. However, it is not a first line treatment, is not a cure, and successfully treated patients generally require maintenance treatment. Additionally, practitioners should understand that dry eye is a disease of mixed aetiology.
Duty of care requires a thorough history, knowledge of the presenting condition, investigations and possibly co-management of relevant comorbidities and a sound understanding of the principles and implementation of treatment options. If these conditions are met, the use of IPL in a dry eye clinic can form part of a very rewarding experience for both patient and practitioner.
pulsed light. London: Springer; 2011.
22. Toyos R, McGill W, Briscoe D. Intense pulsed light treatment for dry eye disease due to meibomian gland dysfunction; a 3-year retrospective study. Photomedicine and laser surgery. 2015 Jan 1; 33 (1): 41-6.
23. Toyos R, Desai NR, Toyos M, Dell SJ. Intense pulsed light improves signs and symptoms of dry eye disease due to meibomian gland dysfunction: A randomized controlled study. PLoS One. 2022 Jun 23; 17 (6): e0270268.
24. Meyerstein W. Effect of light on red blood cells. The light sensitivity of blood from different vertebrate species. The Journal of physiology. 1941 Jun 30; 99 (4): 510.
25. Dell, Steven J. "Intense pulsed light for evaporative dry eye disease." Clinical Ophthalmology (2017): 1167-1173.
26. Xue AL, Wang MT, Ormonde SE, Craig JP. Randomised double-masked placebo-controlled trial of the cumulative treatment efficacy profile of intense pulsed light therapy for meibomian gland dysfunction. The Ocular Surface. 2020 Apr 1;18(2):286-97.
27. Fishman HA, Periman LM, Shah AA. Real-time video microscopy of in vitro demodex death by intense pulsed light. Photobiomodulation, Photomedicine, and Laser Surgery. 2020 Aug.
28. Qin G, Chen J, Li L, Zhang Q, Xu L, Yu S, He W, He X, Pazo EE. Efficacy of intense pulsed light therapy on signs and symptoms of dry eye disease: A meta-analysis and systematic review. Indian Journal of Ophthalmology. 2023 Apr; 71 (4): 1316.
29. Demolin L, Es-Safi M, Soyfoo MS, Motulsky E. Intense Pulsed Light Therapy in the Treatment of Dry Eye Diseases: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023 Apr 21; 12 (8): 3039.
30. Miao S, Yan R, Jia Y, Pan Z. Effect of Intense Pulsed Light Therapy in Dry Eye Disease Caused by Meibomian Gland Dysfunction: A Systematic Review and Meta-Analysis. Eye & Contact Lens. 2022 Mar 15:10-97.
31. Leng X, Shi M, Liu X, Cui J, Sun H, Lu X. Intense pulsed light for meibomian gland dysfunction: a systematic review and meta-analysis. Graefe's Archive for Clinical and Experimental Ophthalmology. 2021 Jan; 259: 1-0.
32. Lei Y, Peng J, Liu J, Zhong J. Intense pulsed light (IPL) therapy for meibomian gland dysfunction (MGD)–related dry eye disease (DED): a systematic review and meta-analysis. Lasers in Medical Science. 2022 Dec 19; 38 (1): 1.
NOTE: Insight readers can scan the QR code or visit insightnews.com.au/cpd/ to access a link to this article to include in their own CPD log book.
40 INSIGHT October 2023 CPD - DRY EYE
who received IPL treatment.










































Dry eye care
ON A DIFFERENT WAVELENGTH
More eye clinics are elevating their dry eye service by investing in an intense pulsed light system. An Australian optometrist and ophthalmologist discuss adopting the Thermaeye Plus IPL in their respective practices with some key differences.



Optometrist Mr Raj Maiti has experience running dry eye clinics for anterior segment surgeons in one of New Zealand’s most prestigious private ophthalmology groups, Eye Institute. So, when he embarked on independent practice ownership 18 months ago in Brisbane, he was well-equipped to offer an adjunct dry eye service. But there was a key ingredient missing.
Feeling limited with his current treatment regime of eye drops, lid scrubs, eye masks and eyelid-warmers, he was also concerned about the compliance factor when patients were sent off with home-based therapies. Seeking a longer-lasting approach that could also cater for his most extreme
cases and rosacea, he went in search of an intense pulsed light (IPL) system. Today, there’s an expanding suite of IPL systems designed specifically for dry eye and related ocular conditions. After some trial and error, he landed on the Thermaeye Plus system – becoming the first optometrist in Queensland to install the device at his practice, Eyecare Plus Nundah. Versatility and affordability were key factors in his decision.
“I found the system provided greater control because of the five different filters that offer varying wavelengths allowing me to treat at different depths and skin tones,” he says.
“I can also easily select the duration and energy of each individual pulse, as well as the pulse interval. But I had to be mindful of the budget as well – I found this to be one of the more affordable IPLs available in Australia. For a new optometrist starting out, Thermaeye Plus was giving me all the control I needed, but yet at a more attainable price – and having the longer wavelength to treat meibomian gland dysfunction (MGD) in darker skin types is a useful option.”
Maiti trialled the system with his patients with good results: seeing a 75% improvement in meibomian gland function on average. One of those was a pharmacist, a highly analytical patient who was suffering from recurrent conjunctivitis and irritation for few years.
“She was given a quantifying DEQ-5 questionnaire before we started and then afterwards. After the third session – because we still had one left – I asked how uncomfortable are your eyes in terms of zero to five (five being
42 INSIGHT October 2023
DRY EYE
“IF I HAVE A GOOD OCULAR SURFACE, IT MEANS I CAN ACHIEVE AN IDEAL POSTOPERATIVE RESULT, AVOIDING ISSUES LATER DOWN THE TRACK.”
DR GAYATRI BANERJEE NEPEAN VALLEY EYE SURGEONS
The Thermaeye Plus IPL.
most uncomfortable)? She remarked they were infinitely better. So that was a positive early impression of the instrument,” he says.
“But it’s important to note for me that IPL isn’t a one-hit-fix. I prescribe a combination of anti-inflammatories and lubricants at the beginning of the treatment to take care of the dry eye until the IPL starts working. I squeeze the eyelids and have a good technique of extracting the meibum. Manual expression is crucial to get the most out of the IPL treatment.”
In terms of patient comfort and safety, Maiti has had no complaints. A key feature of the system is an integrated skin cooling system within the handpiece that works to prevent excessive temperature increases to the epidermis, reducing the risk of thermal damage.
Maiti plans to complement his dry eye service with purpose-built diagnostics, investing in a S390L (Firefly) Slit Lamp Microscope, also available through OptiMed. The system offers several dry eye tools, including meibomian gland observation, tear film breakup time, red eye analysis and keratopathy exposure, and tear meniscus height.
“Having the right imaging tools so people can better understand their condition is important. The great benefit with this digital slit lamp is that it has meibography built-in, so there’s no requirement to move the patient to another instrument. They are already sitting against the chinrest, and I can quickly take an infrared photo of the meibomian glands and pull it up on the big screen and show why they might want to consider IPL in future,” he explains.
The introduction of an IPL system has helped differentiate Maiti’s practice compared with corporates located in proximity. He is providing the IPL service for $600 for four sessions as an introductory offer. But he recommends IPL as a second line treatment. Patients are sent home with a home-based treatment as a first line treatment and scheduled for a follow up within four weeks. They are given a blepharitis pamphlet and advised of the IPL clinic-based treatment as a potential next step when symptoms are no better with home-based treatments.

“The chair time is currently around 20 minutes, so it's not going to be the primary source of income, but it'll be an additional service that will help address the needs of local community with an ageing population,” he says.
“It's very important, being a small independent, to provide more than what the box retail optical stores do.”
With some optometrists, especially in the US, adding skin rejuvenation to their dry eye service, Maiti anticipates this will be a trend that catches on in Australia – and having the Thermaeye Plus IPL is a way of preparing for this, if the opportunity presents.
IN THE OPHTHALMOLOGY SETTING
Meanwhile, in the ophthalmology setting, the Thermaeye Plus IPL has contrasting objectives.
Dr Gayatri Banerjee, from Nepean Valley Eye Surgeons in Sydney, first had the system installed two years ago. While she does see patients seeking standalone dry eye care, often it’s about treating the ocular surface to optimise cataract surgery outcomes pre- and post-operatively.
There’s also other patients to consider, such as those with a compromised ocular surface due to ongoing use of glaucoma eye drops, or patients receiving intravitreal anti-VEGF injections where the use of disinfectants can strip the ocular surface or highlight underlying issues.
“IPL is not my first line treatment – I would categorise this as one of the later stage therapies, partly because of the fact that it is a procedure and more expensive for patients because they don't receive a Medicare rebate for it,” she says, noting that patients undergo four treatments as part of the initial IPL treatment program.
In a busy private ophthalmology clinic, Banerjee is mindful of the extra chair time IPL can create, but she views it as an investment, avoiding larger issues in future when a patient may return with complaints due to a sub-optimal ocular surface.
“My main objective is a quick, effective treatment that's going to minimise my chair time. If I have a good ocular surface, it means I can achieve an ideal post-operative result, avoiding issues later down the track. I'm not looking to
spend extended amounts of time with the patient repeatedly.”
When first acquiring the Thermaeye Plus IPL, Banerjee thought it principally had a role in rosacea. She was surprised to hear about the applications it potentially had in the dry eye space, so she began attending talks and conducting her own research before expanding its use.
“Patients are equally as mystified by this business of IPL, but it's been through my own observations of their symptoms through OSDI scores and SPEED scores that we are objectively able to say they have improved,” she says.
“Between 50-70% of patients are improved and that’s partly to do with my patient selection and management of their expectations. Over time I have started integrating other functions such as rosacea management. One of the benefits of the Thermaeye Plus is that it has different filters that you can use for various conditions.”
Banerjee continues: “But ultimately cost and comfort were the biggest factors when considering which IPL to purchase. Some of the older generation IPLs could burn and hurt patients, but the newer generation systems don’t, and they can be used on many skin types, including Fitzpatrick type V. I tested it on my own skin, and it has been comfortable for patients. In terms of cost, we analysed what was available, and determined this offered the best value for our practice.”
FILTER APPLICATIONS
520nm – this filter is used to perform treatments involving vascular legions and skin pigmentation defects of patients presenting with Fitzpatrick grade III skin type and below.
650nm – this filter is ideal for treating meibomium gland dysfunction in all skin types, up to Fitzpatrick grade VI skin type.
SA – 800nm – the ultraviolet emission of this filter allows the placement of the handpiece directly on to the eye lid to treat Demodex more efficiently. Additionally, this filter has been shown to stimulate the production of new collagen, improving the tone, texture and luminosity of skin, giving it a ‘lifting effect’ without the need of more invasive treatments.
Source: OptiMed/MDS Medical Technologies
INSIGHT October 2023 43
Optometrist Raj Maiti, owner of Eyecare Plus Nundah, says versatility and affordability influenced his IPL purchase.
FROM LITTLE THINGS
big things grow
In May 2023, two optometrists in the early stages of their careers, Mr Billy Chang and Mr Jeremy Chan, swapped their clinical roles for a seat at a desk in Melbourne Connect, The University of Melbourne’s purpose-built innovation precinct. They represent one of 11 start-ups in the highly coveted Melbourne Accelerator Program (MAP) receiving $20,000 to fast-track their project through an intensive five-month program.
Chang and Chan co-founded their start-up, Aelo, in 2021, but the idea was born earlier than that. It’s an eyecare brand seeking to alleviate the signs and symptoms of dry eye disease, but with a twist. The ultimate aim is to beautify the dry eye customer journey in a similar style to the skincare industry, by creating a self-care experience centred around wellbeing.

“In today's digital age, dry, red, and irritated eyes are becoming increasingly common due to the increased use of digital devices. We're committed to revolutionising the way people think and care for their dry eyes and making it an easy, enjoyable part of their self-care routine,” Chang says.
Avoiding ingredients that are known to be harmful to eyes, Chang and Chan created Aelo’s eyecare package, including an eye mask with USB-C charging cable and eyelid and eyelash cleanser with application brush. Consumers can also purchase Aelo's eyelid and eyelash cleanser separately.
“As optometrists, our patients look to us to solve the cause of their dry eyes, but we are often limited by the products available in the marketplace. Unlike many products on the market, our ingredients won't make eyes feel worse. In fact, we have compiled a list of ingredients consumers should avoid when looking for eyecare products,” he says.
For Chang, the idea behind Aelo started to form once he began working in optometry and was regularly meeting dry eye patients. He completed a Master of Optometry at QUT, graduating in 2018 and immediately moved to Melbourne to begin his first graduate job at OPSM Southland in Cheltenham. A year later, he moved to OPSM Collins St, a boutique store in the city’s CBD.
“I began noticing how dry eye was such a common symptom that patients were reporting. Most people have some form of dry eye, but few know much about it. That's when I decided to investigate it more from a clinical perspective. That motivated me to find a new practice with more exposure to dry eye diagnosis and treatment.”
Chang then joined the Dry Eye Group. Established in 2002 by Mr Jason Teh, the group has three locations in Melbourne – Brighton, Glen Iris, and Surrey Hills – and tailors a dry eye treatment plan to suit each individual’s needs. His increased exposure bolstered his resolve to pursue an idea that had begun brewing.
He saw an opportunity to raise more awareness that eye drops are not the only option – and not the first line of treatment for most cases. He bounced ideas back and forth with his good friend and fellow optometrist, Mr Jeremy
Chan, and together they began building the foundations of Aelo.
Immediately, they realised the need for someone with a research background, so they approached Dr Kwang Cham – a senior lecturer in Optometry and Vision Sciences at The University of Melbourne and director of education research at Melbourne School of Health Sciences – for his advice.
“Given his background, we could go forward with more confidence. Every time we received new information, we ran it by him to check its credibility. He has also played an important role in translating the clinical message we're sending to the general public,” Chang says.
Chang says Aelo – derived from the Latin word ‘eulo’, which means ‘to wash out’ – initially started as a company to build consistency and dry eye knowledge for optometrists and their patients. As an early career optometrist, he struggled to find a platform or database he could easily access that listed all available dry eye treatments.

“That's why we have the Aelo dry eye database now, which optometrists can access online to better understand what dry eye entails and what treatments are out there.”
He also found patients lacked an understanding of how they could better manage their symptoms. He often used a dental hygiene analogy to explain the importance of self-care to his patients undergoing IPL.
“Every six or 12 months you go to the dentist for a deep clean, but if you don't brush your teeth on a daily basis, you're not going to maintain your dental health. It’s the same with dry eyes. If you don't have a good daily self-care routine, over time you develop dry eyes, no matter how often you have IPL treatment.”
44 INSIGHT
Billy Chang presenting Aelo, the company he co-founded, at the MAP launch event. Image: MAP
DRY EYE
Leaving his stable job and patients at Dry Eye Group in Melbourne was a difficult but necessary step optometrist and entrepreneur BILLY CHANG had to take to grow the start-up he co-founded to help dry eye patients.
AELO
“WE WANT TO BUILD A LOCAL AUSTRALIAN BRAND THAT'S REPUTABLE AND EVIDENCE-BASED FOR OPTOMETRISTS TO ENTRUST AND UTILISE AS PART OF THEIR OWN CONSULTATION ROUTINE.”
BILLY CHANG
symptoms and for anyone seeking clear skin and a little pampering with treatments and products that are focused on eye and skin health,” Chang says.
A WINNING SALES PITCH
Before they were accepted into the Melbourne Accelerator Program (MAP) in May 2023, Chang and co-founder Chan had been working on Aelo for the previous 18 months, with assistance from Cham.
In that time, the business was more of a side hustle. They were beginning to gain momentum but were limited in how much they could achieve while both working as full-time optometrists.
They discovered MAP, supported by The University of Melbourne: “Which we really value because the optometry school is there, and they can provide the mentorship and resources we need to help us realise our goals,” he says.
This year, MAP has invested in 11 start-ups, including Aelo, equipping them with $20,000 equity-free funding, inner-city office space and access to Australia’s best business minds to help them accelerate their growth.
Chang and Chan went through a competitive four-stage selection process, which Chang described as similar to a bootcamp, and involved a 1,000-word written application responding to a set list of questions, and a pitch to a panel of private investors.

“I think there were 120 applicants this year; over a series of stages, they [MAP] select 11. This involved pitching our business concept to a panel of 30 investors. It was quite daunting. You can’t see the room before you go in; you walk in to see them waiting with pen and paper for you to deliver your pitch,” Chang says.
The 2023 MAP cohort was announced at a launch event in May, which marked the beginning of a five-month intensive program for Chang and Chan and their MAP peers, who are all co-located at the MAP office in Melbourne Connect, the University of Melbourne’s purpose-built innovation precinct.
Aelo is the only eyecare related start-up in the program.
“One of the conditions of the program is that we have to be in the MAP office working on our start-up full time. As much as I didn't want to, because of the patients I see and the team I worked with, I had to resign from Dry Eye Group,” Chang says.
“I had to carefully manage my finances. Five months can go by fast, but this opportunity is once in a lifetime so I felt I should make the most of that five months and take that leap and see how we go.”
Although it has required an all-in commitment, working in the MAP office in Melbourne Connect where they can share knowledge with other start-ups is paying dividends.
Chang says they are already gaining traction through Aelo’s website from the public wanting to know about dry eye disease. “We want to build a local Australian brand that's reputable and evidence-based for optometrists to entrust and utilise as part of their own consultation routine.”

Multi Award Winning Practices Martin Gregory Chairman, Eyecare Plus Considering your practice ownership options? Looking to buy, sell or join contact Philip Rose 0416 807 546 or philip.rose@eyecareplus.com.au “WE’LL MANAGE YOUR WEBSITE + GENERATE BOOKINGS. SO YOU CAN FOCUS ON YOUR PATIENTS.”
Optometrists Jeremy Chan (left) and Billy Chang co-founded Aelo to improve self-care for dry eye patients. Image: MAP


e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au Banner 470x70.pdf 1 31/8/21 6:07 pm INSIGHT Dry Eye Directory Disclaimer: The Insight Dry Eye Directory is compiled of opt-in participants. If you missed out or need to update your details for next year’s directory, please email myles.hume@primecreative.media.com.au. As one of Australia’s most comprehensive dry eye care resources, the 2023 Insight Dry Eye Directory features a new list of the most current therapies and diagnostics available from leading Australian suppliers. This all-in-one resource also includes a comprehensive list of clinics that have a special interest in dry eye care.
NEW SOUTH WALES / ACT
1001 Optical Shop 1016, Westfield Bondi, Level 1, 500 Oxford St Bondi Junction 2022
Margaret Lam
P (02) 9389 1911
W 1001optical.com.au
Dry eye assessment, Blephasteam therapy, bandage scleral contact lenses, meibomian gland expression, tear film assessment, therapeutic medicines prescribing for dry eye.
Atkins Optometrist EP Gordon
12 St Johns Ave Gordon 2072
Sally Atkins
P (02) 9498 8383
W atkinsoptometrist.com
Comprehensive dry eye assessment and therapies, including OSDI survey, osmolarity check, Medmont meibomography and tear meniscus assessment. Therapy includes heat masks, lipid and aqueous lubricants, lid margin debridement, lid hygiene products and therapeutically qualified optometrists.
Capital Eye
Suite 3B, 3 Sydney Ave Barton 2600
Dr Jack Guan
P (02) 6273 7458
W capitaleye.com.au
Dry eye therapeutic options include IPL, Blephasteam and Blephex.
Domenic Caristo Optometrists
Shop 160 Victoria Rd Gladesville 2111
Domenic Caristo
P (02) 9816 4157
W facebook.com/caristo.optometrists/
We can diagnose dry eye disease and offer a wide range of treatments for patients.
Dry Eye Solution Chatswood
38b Albert Ave Chatswoord 2067
Stephanie Lai
P (02) 91887763
W dryeyesolution.com.au
Comprehensive dry rye assessments, treatment and management, Lumenis OptiLight IPL, meibography - Oculus Keratograph 5M, Toyos Protocols, tailored treatment plans, diet management, optometrists personally trained by Dr Toyos.
Dry Eye Solution Erina
8/2 Ilya Ave Erina 2250
Elizabeth Cubis
P (02) 4312 4273
W dryeyesolution.com.au
Comprehensive dry eye assessments, treatment and management, Lumenis M22 IPL, Toyos Protocols, tailored treatment plans, diet management, optometrists personally trained by Dr Toyos.
Dry Eye Solution Miranda
Suite 8, 46-48 Urunga Pde Miranda 2228
Daniel Poon
P (02) 9188 0850
W dryeyesolution.com.au
Comprehensive dry rye assessments, treatment and management, Lumenis OptiLight IPL, meibography - Oculus Keratograph 5M, Toyos Protocols, tailored treatment plans, diet management, optometrists personally trained by Dr Toyos.
Dry Eye Solution Newcaslte
Westfield, Northcott Dr, Kotara Newcastle 2289
Elizabeth Cubis
P (02) 4088 8886
W dryeyesolution.com.au
Comprehensive dry rye assessments, treatment and management, Lumenis OptiLight IPL, meibography - Oculus Keratograph 5M, Toyos Protocols, tailored treatment plans, diet management, optometrists personally trained by Dr Toyos.
Eastern Suburbs Eye Specialists
Suite 901/3 Waverley St Bondi Junction 2022
Dr Matthew Wells
P (02) 9389 4840
W eseyespecialists.com.au
Dry eye assessments including TBUT, Lipiscan, TearLab osmolarity, comprehensive ocular surface examination. Dry eye treatment includes drops, Blephex and Lipiflow.
Eyecare Kids
Shop 8, 238-262 Bunnerong Rd Hillsdale 2036
SooJin Nam
P (02) 9311 4600
W eyecarekids.com.au
IPL, comprehensive range of dry eye products, and dry eye assessment.
Eyecare Plus Merrylands
3 Memorial Ave Merrylands 2160
Thu Le
P (02) 9637 5047
W eyecareplus.com.au/merrylands/
Comprehensive dry eye assessement with the Oculus Keratograph 5M and management with IPL, Blephasteam and therapeutics eye drops.
Eyewear Youwear
Shop 5, 285A Crown St Surry Hills 2010
Dianne Pyliotis
P (02) 9267 4099
W ewyw.com.au
IDRA dry eye assessment system, Sistemi dry eye treatment, Blephasteam, IPL, meibography.
Marsden Eye Specialists
152 Marsden St Parramatta 2150
Danielle Valencia (orthoptist)
P (02) 9635 7077
W marsdeneye.com.au/
Dry eye assessments using Oculus keratography and tear osmolarity and treatments with heat, massage, lid debridement, meibomian gland expression, lid cleansers and scrubs. Home treatments prescribed customised to each individual.
Morrison's Family Eyecare Centre
81 Wingewarra St Dubbo 2830
Sallyanne Morrison
P (02) 6882 6633
W morrisonseyecare.com.au/
We provide routine eyecare with a therapeuticallyendorsed optometrist. Also assisting dry eye patients with gland expression and Blephadex treament.
Optique Barangaroo
Shop 6, Tower 3 Barangaroo Ave Barangaroo 2000
Chiara D’à Rin
P (02) 9290 3999
W optiquebarangaroo.com.au
Assessment including history of symptoms, medications, general and ocular health with relevance to dry eye, infrared meibography, diagnosis, debridement, heat packs, Blephasteam, expression of glands, Ikervis prescribing if necessary, supplements and appropriate drops.
CLINICS DRY EYE DIRECTORY
...
not a dry eye in sight CLINICS
R&B Optometrist
Shop W1 Banora Shopping Village, 59/71 Darlington Dr Banora Point 2486
Bernhard Kurtz
P (07) 5524 4550
W tweedcityoptical@hotmail.com
Forty-five years of clinical experience treating dry eyes holistically with specific treatments.

Richard Banks Optometrist
7/118 Queen St Woollahra 2025
Richard Banks
P (02) 9328 2842
W rboptom.com.au
Full scope exam, OCT and retinal imaging, punctul plugs, formulated dry eye treatments and solution.
The Eye Practice
Level 3, 50 York St Sydney 2000
Jim Kokkinakis
P (02) 9290 1899
W theeyepractice.com.au
One of Australia’s few tertiary dry eye referral centres. Comprehensive diagnostic and treatment services, which now includes research.
The Eyesite Caringbah
372 Port Hacking Rd Caringbah 2229
Amy Pham
P (02) 8544 0412
W theeyesite.com.au
Comprehensive examination with Medmont topographer (meibography, non-invasive TBUT, anterior eye capture), Blephasteam treatment and manual expression.
Tracton Optometrists
Shop 3/241 Oxford St Bondi Junction 2022
Daniel Tracton
P (02) 9188 9288
W tractonoptometrists.com.au
Tracton Optometrists offers the full range of dry eye treatment services.
UNSW Dry Eye Clinic
Gate 14, Barker St Kensington 2052
Maria Markoulli
P (020 9385 4624
W unsw.edu.au/medicine-health/our-schools/optometry/ optometry-clinic/our-clinics/dry-eye-clinic
The Dry Eye Clinic at UNSW aims to be a state-wide referral centre for the diagnosis, imaging and evidence-based management of dry eye disease. As well as providing a platform for research on dry eyes, this clinic offers dry eye patients a chance to get involved. It also aims to be an advocacy centre for those suffering with dry eye disease.
Westmead Eyes Optometrists
Shop T204A, Westmead Hospital, Hawkesbury Rd
Westmead 2145
Kevin Trac
P (02) 9635 8464
W westmeadeyes.com.au
IPL, Blephasteam, meibomian gland expression, meibomian gland debridement, scleral lenses, punctal plugs, home treatments, Lacritec dry eye supplements, heat masks, Optimel Manuka Honey Gel and Drops, Hylo-Forte, NovaTears eye drops, hypochlorous acid, Nulids.
Woonona Eyecare
391 Princes Hwy Woonona 2517
Emily Langley
P (02) 4284 1344
W woononaeyecare.com.au
Comprehensive dry eye work up complete with meibomian gland imaging. Dry eye managment plan tailored to key issues. IPL treatments performed when appropriate. Confident with ciclosporin prescribing.
VICTORIA / TASMANIA
20/20 Sight'n'Style
161 Main St Mornington 3931
George Sahely
P (03) 5973 5520
W sightandstyle.com.au
Testing including osmolarity measurement, ocular keratograph assessment and Korb meibomian gland expression. Management options including Lipiflow, IPL, Blephex, and therapeutics.
Alfred Nott Optometrists
G14/202 Jells Rd Wheelders Hill 3150
Alan Greenhill
P (03) 9562 1505
W alfrednott.com.au
Assessment of nature and severity of dry eye. Targeted treatment dependent on the outcome of the assessment
and ongoing reviews to adjust treatment to maximise effectiveness.
Altona Optical
63 Pier St Altona 3018
Caroline Burden
P (03) 9398 4279
W altonaoptical.com.au
Antares meibography, E-Eye IPL, Blephasteam, therapeutic treatment of dry eye, Derm dry eye masks.
Australian College of Optometry (ACO)
374 Cardigan St Carlton 3053
Varny Ganesalingam
P (03) 9349 7455
W aco.org.au/dry-eye/
The ACO’s clinic is the only dedicated public health dry eye disease clinic in Victoria. Our clinical treatments include LipiFlow, Blepharo exfoliation, meibomian gland expression, lacrimal lavage, punctal plugs, bandage contact lenses. Referral not required.
Diamond Valley Optical
Shop 15/72 Main Hurstbridge Rd Diamond Creek 3089
Asela Senanayake
P (03) 9438 3286
W diamondvalleyoptical.com.au
We offer Blephasteam, BlephEx, Lumenis IPL, meibomian gland expression, Medmont Meridia dry eye suite and all medical dry eye therapy.
Dry Eye Centre
142 Canterbury Rd Heathmont 3135
Dr Nicholas Young
P (03) 9729 4077
W dryeyecentre.com.au
Comprehensive infra-red diagnostics, osmolarity, aqueous tear testing. Treatments include: tear supplements, immunosuppression, eyelid treatments, Lumenis M22 IPL, Lipiflow, amniotic membranes, autologous serum. Comanaged care of relevant systemic health issues.
Evergreen Optical Carnegie
Shop 2/2-20 Koornang Road Carnegie 3163
Khang Ta
P (03) 9571 3233
W evergreenopitcal.com.au
Meibography, Lipiflow, meibomian gland expression, BlephEx, punctal plugs, cyclosporine.
e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976
1 31/8/21 6:07 pm CLINICS DRY EYE DIRECTORY
www.goodopticalservices.com.au Banner 470x70.pdf
ONCE-DAILY IKERVIS® IN THE PERSPECTIVE STUDY: REAL-WORLD EVIDENCE OF IMPROVEMENT OF SEVERE KERATITIS

IN
DED * 1
*Significant improvements from baseline to Month 12 in mean CFS score (Oxford Grading Scale, P<0.0001).1
Find out more about the PERSPECTIVE study and how Ikervis® can help your patients at eyehealth.com.au
Ikervis® is indicated for the treatment of severe keratitis in adult patients with dry eye disease which has not improved despite treatment with tear substitutes.
PBS Information: Authority Required. Refer to PBS Schedule for full information.
Before prescribing IKERVIS ®, please review the Approved Product Information available from Seqirus Medical Information (1800 642 865) or www.seqirus.com.au/products
This medicinal product is subject to additional monitoring in Australia. This will allow quick identification of the new safety information. Healthcare professionals are asked to report any suspected adverse events www.tga.gov.au/reporting-problems.
MINIMUM PRODUCT INFORMATION: IKERVIS® (ciclosporin 0.1% ophthalmic emulsion). Indication: Treatment of severe keratitis in adult patients with dry eye disease which has not improved despite treatment with tear substitutes. Contraindications: Hypersensitivity to the active substance or any of the excipients; Ocular or peri-ocular malignancies or premalignant conditions; Active or suspected ocular or peri-ocular infection. Precautions: Any reversible underlying conditions, not associated with dry eye disease, should be treated prior to initiating IKERVIS ®; History of ocular herpes; Contact lenses should be removed before instillation of eye drops and re-inserted at wake-up time and careful monitoring of severe keratitis is recommended; Glaucoma – limited experience with IKERVIS®. Exercise caution especially with concomitant betablockers; Co-administration with eye drops containing corticosteroids may potentiate effects of IKERVIS® on the immune system; May affect host defences against local infection and malignancies. Use in Pregnancy (Category C): No data available; Not recommended in pregnancy unless the potential benefit to mother outweighs the potential risk to fetus. Use in Lactation: Insufficient information on breastfed infants; it is unlikely that sufficient amounts are present in breast milk. A decision must be made to discontinue either IKERVIS ® or breastfeeding during treatment. Use in Children: No data available. Interactions with other medicines: No data available. Adverse Effects: Common: erythema of eyelid; lacrimation increased; ocular hyperaemia; vision blurred; eyelid oedema; conjunctival hyperaemia; eye pruritus. Very common: eye pain, eye irritation. Dosage and administration: The recommended dose is one drop of IKERVIS ® once daily to be applied to the affected eye(s) at bedtime.



... not a dry eye in sight
Seqirus (Australia) Pty Ltd. ABN 66 120 398 067. 63 Poplar Road, Parkville Australia 3052. Seqirus Medical Information: 1800 642 865. Seqirus is a trademark of Seqirus UK Limited or its affiliates. Ikervis ® is a registered trademark of Santen S.A.S. and distributed by Seqirus (Australia) Pty Ltd under license from Santen Pharmaceutical Asia Pte Ltd. HSEQ781. Date of preparation: April 2023. AU-Iker-23-0030. Abbreviation: DED: dry eye disease; CFS: corneal fluorescein staining; PBS: Pharmaceutical Benefits Scheme. References: 1. Geerling G, et al. Ophthalmol Ther 2022;11: 1101–1117.
Eyecare Plus Bundoora
Universtity Hill Town Centre, 224 Plenty Rd Bundoora 3083
Jean Walters
P (03) 9467 7580
W eyecareplus.com.au/bundoora/
Diagnosistics, including meibography, NlTBUT, tear osmolality. Treatment options including IPL, Blephasteam, Blephadex, therapeutics.
Eyecare Plus Cheltenham
Suite D 149-151 Centre Dandenong Rd Cheltenham 3192
Dr Flora Luk
P (03) 9583 3596
W eyecareplus.com.au/cheltenham
We provide IPL, low level light therapy mask, meibomian gland assessment, gland expression.

Eyecareplus Springvale
37A Buckingham Ave Springvale 3171
Denise Lee
P (03) 9558 4499
W eyecareplusspringvale.com.au
Meibography, Lipiflow, Eye-light IPL, low level light therapy, Rexon-Eyes, Blephasteam, punctal plugs, Optimel drops and gel, Lacritec, Eyegiene masks, Bruder masks, TranquilEyes, Avenova spray, meibomian gland expression.
Eyescan
467 Toorak Rd Toorak 3142
Dr Harry Unger
P (03) 9826 0740
W eyescan.com.au
We offer a range of treatment options including Oculus Keratograph and IPL.
Leverett & Kindler Optometrists
Shop 3A 35-39 Main St Greensborough 3088
Amelia Na Jiao
P (03) 9435 4866
W leverettandkindler.com.au
In terms of diagnostics, we offer Oculus K5. Treatment: Lumenis IPL, Blephasteam, scleral lenses and a range of dry eye products.
Martin's Eyecare
Shop 1, 359 Main Rd Glenorchy 7010 (Tasmania)
Martin Robinson
P (03) 6272 8423
W martinseyecare.com.au
Detailed dry eye investigation and diagnosis appointments, IPL, lid debridement, meibomian gland expression, mascara, eye drops and eye cleaning.
Peninsula Eye Centre
937 Nepean Hwy Mornington 3931
Justin Sherwin
P (03) 5975 9999
W peninsulaeyecentre.com.au/
We have dedicated ophthalmologists who treat dry eye disease, and a comprehensive dry eye service including all medical therapies (topical and oral), lacrimal interventions (plugs, cautery) and meibomian gland disease therapy (including IPL laser/Tearstim)
Rashelle Cohen Optometrist
263 Glen Eira Rd Caulfield North 3161
Rashelle Cohen
P (03) 9528 1910
W cfmp.com.au/rashelle-cohen-optometry/ Assessment using the Oculus K5 to measure quality and quantity of tears, meibomian gland assessment. Treatment options include Blephasteam, meibomian gland expression, offering treatment options and lifestyle advice.
South West Eye Surgery
174 Koroit St Warrnambool 3280
Dr Vincent Lee
P (03) 5562 4488
W drvincentlee.com.au
Dedicated to accurate diagnostics and therapy of dry eye disease.
The Eye Collective
165 Lonsdale St Dandenong 3175
Adrian Vecchio
P (03) 9792 3077
W eyecollective.com.au
IPL treatment, Blephasteam, Oculus K5 dry eye asssesment, lid debridement and therapeutic interventions.
Visual Q Eyecare
91 Toorak Rd South Yarra 3141
Dr Susana Liou
P (03) 9866 3880
W visualq.com.au
We provide dry eye treatments including Rexon eyes, Meibomask, Blephasteam and an array of dry eye supplements including TheraNutrition and various drops.
Warrnambool Eyecare
152 Liebig St Warrnambool 3280
Matthew Buckis & Jayson Ward
P (03) 5562 2244
W portlandandwarrnambooleyecare.com.au/
Comprehensive dry eye assessment and management, including IPL and meibography.
QUEENSLAND
Aphrodite Livanes Eyecare Plus
71 Cambridge Dr Alexandra Hills 4161
Aphrodite Livanes
P (07) 3824 1878
W livanes.com.au
Antares corneal topographer, Blephasteam, BlephEx treatment, IPL, eye seal masks, eye compress mask and lubricating eye drops.
Best Practice Eyecare
64 Landsborough Pde Golden Beach 4551
Dr Michael Karpa
P (07) 5492 2822
W bestpracticeeyecare.com.au/
Comprehensive evaluation and education with our clinical optometrist with referral to Dr Karpa if required. IPL, heat masks and tea tree foam. Ongoing support.
Buck & Todd Optometrists
103 Alfred St Mackay 4740
Ieuan Rees
P (07) 4957 3066
W bucktodd.com.au/
Comprehensive dry eye assessment including qualitative and quantitative tear film analysis: TBUT, corneal dryness staining, Schirmer's test, Lipiscan and tear film surface quality evaluation. IRPL treatment of meibomian gland dysfunction, demodex blepharitis and Blephasteam. treatment.
Envision Optical
4B, 7 Classic Way Burleigh Waters 4220
Andrew Bowden
P (07) 5593 7844
W envisionoptical.com.au
CLINICS DRY EYE DIRECTORY e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au Banner 470x70.pdf 1 31/8/21 6:07 pm
Viscotears® Gel PF improves the moistening of the ocular surface in the presence of dry eye sensations, burning or tiredness of the eyes, caused for instance:
• by watching television for a long time
• extensive computer work
• dry air from air-conditioning or heating
Preservative free
Moistening and wetting effect1
Viscotears® Eye Gel provides soothing relief for sore, gritty dry eyes. Its long lasting gel formulation is suited for those who:

• need extra protection
• added nighttime support, or
• prefer a heavier gel
Maintains the tear film stability for a period of up to 6 hours2
Viscous gel for nighttime protection
For more information, contact your Bausch + Lomb Territory Manager or Bausch + Lomb Customer Service 1800 251 150
... not a dry eye in sight
Viscotears®
Material was prepared in February 2023 References: 1. Viscotears Gel PF IFU. 2. Viscotears Single Dose Unit 2.0mg/g Eye Gel, EMC, 5.1 pharmacodynamic properties https://www.medicines.org.uk/emc/product/2311/smpc - Accessed Feb 2023 © 2023 Bausch & Lomb Incorporated. ®/TM are trademarks of Bausch & Lomb Incorporated or its affiliates. Bausch & Lomb (Australia) Pty Ltd. ABN 88 000 222 408. Level 2, 12 Help Street, Chatswood NSW 2067 Australia. (Ph 1800 251 150) Vis.0001.AU.23 VISCOTEARS® EYE GEL 10g Tube
Soothing,
eyes
VISCOTEARS® GEL PF 30 × 0.6g Single dose units • Preservative-free • PBS Listed
6
•
long lasting relief for sore, gritty dry
• PBS Listed
H
Digital diagnostic scans including meibography. Treatments including IPL, Lipiflow and therapeutic care.
Eyecare Eyewear
87 Cunningham St Dalby 4405
Tom Roger
P (07) 4669 7072
W ecew.com.au
In addition to prescription eye drops, we provide: Optilight IPL treatment, Medmont Meridia assessment, eyelash and eyelid cleaning, eyelid margin debridement, Blephasteam and meibomian gland expression.
Eyecare Plus Mermaid Beach
Shop 3A, 2431 Gold Coast Hwy Mermaid Beach 4218
Jackson Yip
P (07) 7552 61400
W eyecareplusmermaidbeach.com.au
State-of-the-art dry eye clinic, dry eye assessment and treatment, meibomian gland dysfunction and blepharitis treatment, Rexon-Eye dry eye treatment, IPL, BlephEx blepharitis treatment, and Blephasteam.
Eyecare Plus Nundah
1190 Sandgate Rd Nundah 4215
Raj Maiti
P (07) 3266 6444
W eyecareplus.com.au/nundah
Infrared imaging to diagnose the cause of dry eye, meibography, IPL therapy, lid debridement. Experienced with prescribing topical medications.
Eyes On Edward
57 Edward St Brisbane 4000
Davis Bradley
P (07) 3221 3221
W eyesonedward.com.au
Treatment includes sessions of IPL, BlephEx, Blephasteam, meibomian gland expression, fish oil, Omega-3 and flaxseed tablets, and eye drops, including natural anti-inflammatories and oil supplements.

Heron Eyecare
147 Russell St Toowoomba 4350
Hugh Bradshaw and Adam Barron
P (07) 4639 2378
W heroneyecare.com.au
We offer tear film analysis, as well as IPL, RexonEye and BlephEx treatments. Bandage and scleral contact lenses. Therapeutically-endorsed prescribing topical steriods, cyclosporin and azithromycin.
Insight Eye Surgery
Suite 203, Level 2, Westside Private Hospital, 32 Morrow St Taringa 4068
Dr Madeleine Adams
P (07) 3154 1515
W insighteyesurgery.com.au/
IPL, Blephasteam, BlephEx, regular reviews and diagnosis. Dry eye report using Sirius machine
iSight Specialists
13-15 Martinez Ave West End 4810
Ophthalmology
P (07) 4775 1633
W isighttownsville.com.au/ We provide initial assessment including meibography and Tearlab as well as slit lamp examination. Treatment includes therapeutic eye dropper and IPL.
Optikus Optometrists
1/3 Chancellor Village Blvd Sippy Downs 4556
Zahn Kidson
P (07) 5456 4300
W optikus.com.au
Resono Rexon dry eye treatment, Blephasteam, meibography, meibomian gland expression, anterior segment imaging, tear layer assessment, lubricants, hot compress, blepharitis treatment.
RA Optometrists
345 Gympie Rd Strathpine 4500
Dom Kelly
P (07) 3205 1593
W raoptometrists.com.au
IPL, Blephasteam and therapuetically-endorsed.
The Eye Health Centre
Level 11, 87 Wickham Tce Brisbane 4000
Jason Holland
P (07) 3831 8606
W theeyehealthcentre.com.au
Offering comprehensive diagnosis of dry eye disease and bespoke treatment options utilising OptiLight IPL, RexonEye, Activa, BlephEx and punctal plugs.
The Eyewear Shop
Shop 15G, 25 Samuel St Camp Hill 4152
Minh Nguyen
P (07) 3395 4105
W theeyewearshop.com.au
We provide comprehensive clinical assessment and therapeutic treatment for all types of dry eye. We offer a range of treatments including Blephasteam, IPL, and tear film slit lamp assessment.
Virginia Henry Optometrists
Shop 13A / 39 Eyre St North Ward 4810
Virginia Henry
P (07) 4724 1700
W virginiahenryoptical.com.au
E-Eye IPL, eye compress packs, lubricants and Lacritec.
Vision Michael Hare Eyecare Plus
17A Nerang St Southport 4215
Michael Hare
P (07) 5532 9566
W visionmichealhare.com.au
Our practice offers Blephasteam.
Vision Michael Hare Optometrists
Stockland Burleigh, 149 West Burleigh Rd Burleigh Waters 4220
Jonathan McCorriston
P (07) 5597 0038
W visionmichaelhare.com.au
Full spectrum optometry services, SBM tear film analysis, Medmont tear film analysis, Schirmer's test, Blephasteam, Blephex, IPL.
Vision Michael Hare Optometrists
Benowa Gardens Shopping Centre, Cnr Ashmore and Benowa Rds Benowa 4217
Jonathan McCorriston
P (07) 5597 0038
W visionmichaelhare.com.au
Full spectrum optometry services, SBM tear film analysis, Medmont tear film analysis, Schirmer's test, Blephasteam, Blephex, IPL.
CLINICS DRY EYE DIRECTORY e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au Banner 470x70.pdf 1 31/8/21 6:07 pm
Preservative-free and phosphate-free

Can be used for 6 months after opening
Compatible with contact lenses



At least 300 measured drops per pack, or 150 treatments (both eyes)
Delivered through the unique COMOD® multi-dose application system

... not a dry eye in sight

PBS Information: Authority Required (STREAMLINED): Severe dry eye syndrome in patients who are sensitive to preservatives in multi-dose eye drops. STREAMLINED AUTHORITY CODE 4105 HYLO®-FRESH, HYLO-FORTE® and COMOD® are registered trademarks of URSAPHARM. AFT Pharmaceuticals Pty Ltd, Sydney. ABN 29105636413. For more information: For product orders: www.aftpharm.com 1800 238 742 1800 814 963 goodoptical.com.au
DRY
IRRITATED EYES lubrication
For severe or chronic dry eye For mild or moderate dry eye
FOR
&
Long-lasting
CLINICS
SOUTH AUSTRALIA
Alleve Eye Clinic
49A Stephen Tce St Peters 5069
Jennifer Rayner
P (08) 7225 9798
W alleveeyeclinic.com.au
Comprehensive diagnosis (using Jenvis Pro software) and management of dry eye including IPL, topical ciclosporin, cold laser therapy, topical steroids, oral tetracyclines and punctal plugs.
Eyre Eye Centre
22 Liverpool St Port Lincoln 5606
Tamra Karolewicz
P (08) 8682 4566
W eyreeyecentre.com.au
OptiLight IPL, Meridia dry eye assessment, Blephasteam, punctal plugs, therapeutics, extensive range of dry eye products.
Gulf and Ranges Optometrists

7 Chapel St Port Augusta 5700
Mitchell Hancock
P (08) 8642 2766
W gulfandranges.com.au/
Diagnostics: TBUT, slit lamp camera, OSDI, vital dye staining. Treatments: IPL, Rexon, punctal plugs, lid debridement, meibomian gland expression, lacrimal lavage. Home treatments: heat masks, lubrication, Lacritec nutritional, supplements and prescription medication. (steroids, ciclosporin, cationorm), blepharitis foam.
Northgate Eye Care
Shop 2 177-195 Fosters Rd Northgate 5085
Dr Jonathan Ucinek
P (08) 7092 2633
W northgateeyecare.com.au
Comprehensive ocular sueface disease assessment. Tailored management plans. In-office heat treatment with expression. Nutritional supplements and slit lamp imaging.
Philip Milford Optometrist
158 The Pde Norwood 5067
Philip Milford
P (08) 8364 3011
W PhilipMilfordOptom.com.au
Banner 470x70.pdf 1 31/8/21 6:07 pm
We concentrate on improving eye tear quality and reducing inflammation with Lipiflow and IPL.
WESTERN AUSTRALIA
Bullseye Optometry clinic - Leederville
217 Oxford St Leederville 6009
Shashi Patel
P (08) 9242 2342
W bullseyeclinic.com.au
Oculus Keratograph 5 assessment, moist heat therapy, meibomian gland expression, IPL, take home packs.
Cooper and Lourie Family Optometrists
Shop 25 Broadway Fair 88 Bdwy Nedlands 6009
Geoff Cooper
P (08) 9386 8581
W cooperandlourie.com.au
Dry eye evaluation, tear film imaging, E-Eye IPL treatment.
Dry Eye WA
Suite 18 135 Riseley St Booragoon 6154
Marilyn Stern
P (08) 6468 5296
W dryeyewa.com.au
Meibography and tear film analysis, IPL, Rexon-Eye, low level light therapy, red light mask for rosacea and scar reduction, BlephEx, swabsticks for blepharitis, Blephasteam, gland expression.
E Eye Place
9/6 Calypso Pde North Coogee 6164
Stephanie Yeo
P (08) 6194 0344
W eeyeplace.com.au
Assessment including Jenvis eye report using Oculus K5. Blephasteam and specialty optometrist only dry eye products.
Ernie Hawes Optometrist
2/52 Davidson Tce Joondalup 6027
Dr Ernie Hawes, optometrist
P (08) 9300 0409
W erniehawes.com.au
Tear film break-up analysis, meibography, lid massage.
Eyecare Plus Glen Forrest
U4 5 Hardey Rd Glen Forrest 6072
Dr Kristin Larson
P (08) 9298 9992
W eyecareplus.com.au/glenforrest
Assessement including meibography, lid debridement, Rexon-Eye, Blephex, Blephasteam, punctal plugs.
Eyes@Optometry
Shop2 Australind Village, 301 Old Coast Rd Australind 6233
Lauren Sears
P (08) 9796 1966
W eyesatoptometry.com.au
Comprehensive dry eye analysis using Tearcheck, IPL (Tearstim) and Blephasteam.
Ezekiel Eyes
69 Hampden Rd Nedlands 6009
Damon J Ezekiel
P (08) 9386 3620
W ezekieleyes.com
We offer a comprehensive dry eye workup and discuss the many options available to our patients.
For Eyes Optometrist
158 High St Fremantle 6160
Adrian Rossiter
P (08) 9335 3433
W foreyes.au
Our dry eye treatment includes IPL and is aimed at key indicator of dry eye including tear film stability, inflammation, and meibomian gland functionality.
I-Vision Optometrists
Shop 13B Leeming Forum, Cnr of Farrington and Findlay Rd Leeming 6149
Adrian Teh
P (08) 6161 5496
W i-visionoptom.com.au
Providing patients with dry eye assessment using non-invasive equipment. IPL therapy, eye drops and prescription eye drops.
WA Opticians
U3/101 Royal St East Perth 6004
P (08) 9221 0577
W waopticians.com.au
Dry eye analysis and management, IPL, Blephasteam.
e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au
DRY EYE DIRECTORY

Are you an analytical person? You’d look good in Specsavers If, like Tasneem, you love the idea of a career where you’ll use the latest technology, like OCT, to help improve people’s lives, you’ll shine at Specsavers. www.spectrum-anz.com Tasneem
Optometrist
EYE DROPS
e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au Banner 470x70.pdf 1 31/8/21 6:07 pm
GRADE OF DRY EYE NAME Company Mild Moderate Severe CELLUFRESH Eye Drops 30 x 0.4mL AbbVie • • • CELLUVISC Eye Drops 30 x 0.4mL AbbVie • • • LIQUIFILM TEARS Eye Drops AbbVie • • • OPTIVE ADVANCED Eye Drops 30 x 0.4mL AbbVie • • • OPTIVE ADVANCED Eye Drops 15mL AbbVie • • • OPTIVE FUSION Eye Drops 30 x 0.4mL AbbVie • • • OPTIVE FUSION Eye Drops 10mL AbbVie • • • OPTIVE Eye Drops 15mL AbbVie • • • OPTIVE Gel Drops 10mL AbbVie • • • OPTIVE Sensitive 30 x 0.4mL AbbVie • • • REFRESH CONTACTS Eye Drops 15mL AbbVie • • • REFRESH LIQUIGEL Eye Drops 15mL AbbVie • • • REFRESH NIGHT TIME Eye Ointment 2 x 3.5g AbbVie • • • REFRESH PLUS Eye Drops 30 x 0.4mL AbbVie • • • REFRESH TEARS PLUS Eye Drops 15mL AbbVie • • • Hylo Forte 10ml AFT Pharmaceuticals/Good Optical Services • • Hylo-Fresh AFT Pharmaceuticals/Good Optical Services • • Nova Tears 3ml AFT Pharmaceuticals/Good Optical Services • Nova Tears Omega-3 3ml AFT Pharmaceuticals/Good Optical Services • • VitaPos Ointment 5gm AFT Pharmaceuticals/Good Optical Services • • Bion Tears UD (28 x 0.4mL) Alcon Laboratories (Australia) Pty Ltd • • Genteal Lubricant Eye Drops 0.3% (10mL) Alcon Laboratories (Australia) Pty Ltd • • Genteal Lubricant Eye Gel 0.3% (10g) Alcon Laboratories (Australia) Pty Ltd • HPMC PAA Gel (10g) Alcon Laboratories (Australia) Pty Ltd • In a Wink Eye Drops 0.3% (10mL) Alcon Laboratories (Australia) Pty Ltd • • Poly Gel UD Lubricant Eye Gel (30 x 0.5g) Alcon Laboratories (Australia) Pty Ltd • Poly Visc (3.5g) Alcon Laboratories (Australia) Pty Ltd • Poly Visc Twin Pack (2 x 3.5g) Alcon Laboratories (Australia) Pty Ltd • Polytears (15mL) Alcon Laboratories (Australia) Pty Ltd • • Systane Balance Lubricant Eye Drops (10mL) Alcon Laboratories (Australia) Pty Ltd • • • Systane Complete Lubricant Eye Drops (10mL) Alcon Laboratories (Australia) Pty Ltd • • Systane Complete Preservative-Free Lubricant Eye Drops (10mL) Alcon Laboratories (Australia) Pty Ltd • • Systane Eye Wash Rinse Solution (120mL) Alcon Laboratories (Australia) Pty Ltd Systane Gel Lubricant Eye Drops (10mL) Alcon Laboratories (Australia) Pty Ltd • Systane Hydration Preservative-Free Lubricant Eye Drops (10mL) Alcon Laboratories (Australia) Pty Ltd • • Systane Hydration UD Lubricant Eye Drops (30 x 0.7mL) Alcon Laboratories (Australia) Pty Ltd • • Systane Lid Wipes Cleansing Wipes (30 pack) Alcon Laboratories
Systane Original Lubricant Eye Drops (15mL) Alcon Laboratories
Pty Ltd • Systane Original UD Lubricant Eye Drops (28 x 0.8mL) Alcon Laboratories (Australia) Pty Ltd • Systane Ultra Preservative-Free Lubricant Eye Drops (10mL) Alcon Laboratories (Australia) Pty Ltd • Systane Ultra UD Lubricant Eye Drops (25 x 0.5mL) Alcon Laboratories
Pty Ltd • Tears Naturale Artificial Tears (15mL) Alcon Laboratories
• • Viscotears Eye Gel Bausch
Viscotears Eye Gel PF Bausch +
BLINK CONTACTS EYE DROPS 10ML Bausch + Lomb (From January 2024) • • BLINK INTENSIVE TEARS PLUS GEL EYE DROPS 10ML Bausch + Lomb (From January 2024) • • BLINK INTENSIVE TEARS PROTECTIVE EYE DROPS 0.4MLX20 Bausch + Lomb (From January 2024) • •
THERAPIES
(Australia) Pty Ltd
(Australia)
(Australia)
(Australia) Pty Ltd
+ Lomb Australia
Lomb Australia
EYE
(HA 0.02%) Glass bottle (NICNAS registered)
DEVICES/EQUIPMENT
e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au Banner 470x70.pdf 1 31/8/21 6:07 pm
GRADE OF DRY EYE NAME Company Mild Moderate Severe BLINK INTENSIVE TEARS PROTECTIVE EYE DROS, 15ML Bausch + Lomb (From January 2024) • • BLINK N CLEAN LENS DROPS 15ML Bausch + Lomb (From January 2024) • • Cationorm Multi Dose 10mL CSL Seqirus • • • Cationorm Single Unit Ampoules x 30 CSL Seqirus • • • Ikervis (1mg/mL ciclosporin) Single Unit Ampoules x30 CSL Seqirus Optimel Manuka + Antibacterial Drops Designs For Vision/Melcare • • Optimel Manuka + Forte Gel Designs For Vision/Melcare • • Optimel Manuka+ Eyelid Cream Designs For Vision/Melcare • • • AUTOLOGOUS Emagin Pty Ltd • • • Hylo Forte 10ml Good Optical Services/AFT Pharmaceuticals • • Hylo-Fresh Good Optical Services/AFT Pharmaceuticals • • Nova Tears 3ml Good Optical Services/AFT Pharmaceuticals • Nova Tears Omega-3 3ml Good Optical Services/AFT Pharmaceuticals • • VitaPos Ointment 5gm Good Optical Services/AFT Pharmaceuticals • • Alcon (including Systane Range) Good Optical Services/Alcon • • Allergan (including Optive Range) Good Optical Services/Allergan • • Cationorm 10ml Good Optical Services/Seqirus (Aust) P/L • • • Cationorm UD 30x0.4ml Good Optical Services/Seqirus (Aust) P/L • • • Johnson & Johnson (including Blink range) Good Optical Services/Johnson & Johnson • • Tears Again (Liposomal Eye Spray) Good Optical Services/Bio Revive • • Optimel Manuka + Forte Gel Good Optical Services/Melcare • • Optimel Manuka + Antibacterial Drops Good Optical Services/Melcare • • Optimel Manuka Cream + Jojoba Oil Good Optical Services/Melcare • • • Optimel Manuka+ Dry Eye drops Jubelee Eyecare Supplies • • • Optimel Manuka+ Eyelid Cream Jubelee Eyecare Supplies • • • Optimel Manuka+ Forte Eye Gel Jubelee Eyecare Supplies • • BlephaDex Liquid NICNAS regitered OptiMed • • • Bruder Hygenic Eyelid solution SPRAY
OptiMed Xalin eye Gel OptiMed • • • Xalin Fresh single dose eye drop OptiMed • • Xalin Hydrate eye drop OptiMed • • Xalin Night Gel OptiMed • • Cequa (ciclosporin 900 microgram/mL) Sun Pharma • • SBM Activa BOC Instruments • • • Debridement equipment, spuds etc Device Technologies/Katena • • • Epilation forceps Device Technologies/Katena • • • Gland expression Forceps Device Technologies/Katena • • • Punctal Plugs - Permanent occlusion Device Technologies/Eagle Vision & Sharpoint • • • Punctal Plugs - Temporary occlusion Device Technologies/ Eagle Vision & Sharpoint • • • Ellis Foreign Body Spub Designs For Vision/Albert Heiss • • • Francis Foreign Body Spud Designs For Vision/Albert Heiss • • • Golf Club Spud Designs For Vision/PRICON • • • Mastrota Forcep Designs For Vision/PRICON • • Mastrota Meibonian Gland Paddle Designs For Vision/PRICON • • Oasis Punctal Plugs Designs For Vision/Oasis • • • C.STIM - I.P.L. (Intense Pulsed Light) System Lumibird Medical • • • Nulids MDG Machine Good Optical Services/NuSight Medical USA • • Ocusoft Compliance Kit 50ml + 100 Pads Good Optical Services/OCuSOFT USA • Ocusoft Hypochlor Gel 59ml Good Optical Services/OCuSOFT USA • Ocusoft Hypochlor Spray 59ml Good Optical Services/OCuSOFT USA • Ocusoft Lid Scrub Bottle 50ml Good Optical Services/OCuSOFT USA • • Ocusoft Oust Demodex Foam 50ml Good Optical Services/OCuSOFT USA • Ocusoft Oust Demodex Sachets 30's Good Optical Services/OCuSOFT USA • Ocusoft Platinum Plus 50ml Good Optical Services/OCuSOFT USA •
DROPS THERAPIES
WIPE/MASK
e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au Banner 470x70.pdf 1 31/8/21 6:07 pm THERAPIES DEVICES/EQUIPMENT GRADE OF DRY EYE NAME Company Mild Moderate Severe Ocusoft Plus Bottle 50ml Good Optical Services/OCuSOFT USA • • Ocusoft Plus Sachets 30s Good Optical Services/OCuSOFT USA • • Ocusoft Sachets 30s Good Optical Services/OCuSOFT USA • • Ocusoft Swab Stix (In Practice Oust & Plus) Box 12 Good Optical Services/OCuSOFT USA • • • Zocular Zest Kit Good Optical Services/Zocular USA • • • Zocular Gel (Syringe) Good Optical Serices/Zocular USA • • • Zocular Eyelid Wipes Good Optical Services/Zocular USA • • • ENVISION InMode • • • Lipiflow - Vector Thermal Pulsation (VTP) Johnson & Johnson Vision • • • Flexx MGE Broad 8mm tips - Titanium OphthalmoPro • Flexx MGE Precision 3mm tips OphthalmoPro • Flexx MGE Roller - Titanium OphthalmoPro • Flexx Spud Debridement OphthalmoPro • MGrx - Dry Eye Treatment System OphthalmoPro • Bleph-Ex OptiMed • • • Blephadex Applicator (in office use only) NICNAS registered OptiMed • Bruder - Collins expressor Forceps OptiMed • • • Bruder - Karpecki punctal plug forceps OptiMed • • • Bruder - Livengood gland expressor paddle OptiMed • • • Bruder - Longnose expressor OptiMed • • • Bruder epilation forceps OptiMed • • • Bruder Karpecki Debrider OptiMed • • Bruder KARPECKI-LINDSTROM Gold Line OSD Instrument Set (contains six instruments). OptiMed • • • Bruder recatangular expressor OptiMed • • • Bruder roller expressor OptiMed • • • Thermaye Plus IPL OptiMed • • Painless Plug (Punctum Plug) Spectrum Surgical • • • Opti-Soothe Preservative-free Eyelid Wipes AFT Pharmaceuticals / Good Optical Services • • • Opti-Soothe Moist Heat Mask Reusable mask AFT Pharmaceuticals/Good Optical Services • • • Avenova Designs For Vision/Avenova • • • Eye Eco Advanced Tea Tree Foaming Facial Cleanser Designs For Vision/Eye Eco • • Eye Eco D.E.R.M. Mask Designs For Vision/Eye Eco • • • Eye Eco Tea Tree Foaming Facial Cleanser Designs For Vision/Eye Eco • • Eye Eco Tranquileyes Advanced XL Kit (moist heat therapy) Designs For Vision/Eye Eco • • • Eye-Eco Eye Seals/Seals 4.0 Designs For Vision/Eye Eco • • • Eye-Eco EyeCloud Designs For Vision/Eye Eco • • • Eye-Eco Onyx Designs For Vision/Eye Eco • • • Eye-Eco Quartz Designs For Vision/Eye Eco • • • I-LID'N'LASH Cleansing Wipes Designs For Vision/I-MED Pharma • • I-LID'N'LASH PLUS Antiseptic Cleansing Wipes Designs For Vision/I-MED Pharma • • Opti-Soothe Preservative-free Eyelid Wipes Good Optical Services/AFT Pharmaceuticals • • • Optisoothe Tea Tree Eyelid Wipes 20's Good Optical Services/AFT Pharmaceuticals • • Opti-Soothe Moist Heat Mask Reusable mask Good Optical Services/AFT Pharmaceuticals • • • Tear Restore Mask + 2 gel inserts Good Optical Services/Tear Restore USA • • The Eye Doctor Allergy Mask Good Optical Services/The Body Doctor UK • • • The Eye Doctor Antibacterial Stye Relief Compress (Single eye patch) Good Optical Services/The Body Doctor UK • • • The Eye Doctor Lid Wipes Sachets 20's Good Optical Services/The Body Doctor UK • • The Eye Doctor Liquid Lid Cleanser (Argon & Coconut Oil/Micellar Water) Good Optical Services/The Body Doctor UK • • The Eye Doctor Sterileyes Antibacterial Click'N'Go Travel Mask Good Optical Services/The Body Doctor UK • • The Eye Doctor Sterileyes Antibacterial Hot/Cold Eye Compress Good Optical Services/The Body Doctor UK • • • The Eye Doctor Tea Tree Lid Wipes 20's Good Optical Services/The Body Doctor UK • • The Eye Doctor Antibacterial Essential Mask Good Optical Services/The Body Doctor UK • • •
WIPE/MASK DIAGNOSTICS
e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au Banner 470x70.pdf 1 31/8/21 6:07 pm
NAME Company DIAGNOSTIC CAPABILITY Meimbography Lipid layer thickness Tear meniscus height Blinking rate/ quality DSLC200 & DEM100/DEM100PLUS BOC Instruments • • • • SBM IDRA BASIC & FULL BOC Instruments • • • • Topcon CA-800 - corneal topography, basic lens fit, Dry eye suite Device Technologies/Topcon • • • • Topcon MYAH - Axial lenth, corneal topography, basic lens fit, Dry eye suiteDevice Technologies/Topcon • • • • Topcon SL-D701 slitlamp w/ DC4 camera for gland imaging Device Technologies/Topcon • • • • Fluoro Touch Designs For Vision/Madhu Instruments I-Pen Designs For Vision/I-MED Pharma OCULUS Keratograph 5M Designs For Vision/OCULUS Optikgerate GmbH • • • • Tear Touch Blue Designs For Vision/Madhu Instruments • • • LipiView Johnson & Johnson Vision medmont meridia Professional Medmont • • Eye-Light OpthalmoPro/Espansione Me-Check OpthalmoPro/Espansione • • MeiboMask OpthalmoPro/Espansione My-Mask OpthalmoPro/Espansione Mediworks D130 (available with S360 slit lamp) OptiMed • • • • Mediworks DEA 520 Dry Eye Diagnostic & Topographer OptiMed • • • • ATLAS 500 ZEISS • • • •
THERAPIES/DIAGNOSTICS
GRADE OF DRY EYE NAME Company Mild Moderate Severe Dry Eye Compress with HydroBlock OphthalmoPro • • • USB Powered Dry Eye Compress with HydroBlock OphthalmoPro • • • BlephaDex Wipe (regular and PRO) NICNAS registered OptiMed BlephaDex Wipe (regular and PRO) NICNAS registered OptiMed • • • Bruder Eye compress OptiMed • • • Bruder Eye compress OptiMed • • • Bruder Eye wipe (NICNAS registered) OptiMed Bruder Eye wipe (NICNAS registered) OptiMed • • • Bruder Eyeleave Eye compress OptiMed • • • Bruder Eyeleave Eye compress OptiMed • • • EyeGiene compress NICNAS registered OptiMed EyeGiene compress NICNAS registered OptiMed • • • OptiMed USB Eye warmer NICNAS registered OptiMed OptiMed USB Eye warmer NICNAS registered OptiMed • • •
THE CONGRESS
Heads West
RANZCO continues to innovate its congress program meaning there’s something for everyone to look forward to at its 54th conference in Perth this month.

RANZCO is always searching for ways to improve the experience at its annual congress. A hybrid online/in-person format has become the norm, and now organisers are shaking it up again with a truncated schedule and no Congress Dinner. The Perth time zone is also expected to cater nicely for the body clocks of eastern seaboard delegates – and there’s plenty of buzz around the Opening Plenary where retired vet Dr Craig Challen will discuss his role in the famous Thai cave rescues in 2018.
This year’s 54th RANZCO Congress is taking place 20-24 October 2023 at the Perth Convention and Exhibition Centre. At the time of writing, there were 732 registrations (577 compared to the same time in 2022 where 2,124 ultimately attended). And 141 booth spaces will be occupied by 66 organisations.
With most delegates traversing Australia’s vast interior, RANZCO is hoping they will capitalise on the opportunities on offer. Perth’s scenery, the desire to see friends and colleagues and attractions such as the ANZEF Cape-to-Cape trek are among the drawcards to entice ophthalmologists to the west.
“The Perth Convention and Exhibition Centre, multitude of social venues and excellent climate present a range of exciting opportunities we will be harnessing. From early morning activities to the Welcome Reception, there will be plenty of opportunities to get some vitamin D,” organisers tell Insight.
“As the majority of delegates come from the east coast, the time difference means they are up at the crack of dawn and we always see high attendance at the hosted breakfast sessions. And this year, for those looking for a bit of health and wellbeing to start the day, this means getting to those activities will be easy. For those attending as virtual delegates, the time zone difference between home and the congress is a factor to consider.”
A feature of more recent congresses has been the hybrid format, brought about by COVID-19 lockdowns. This year, RANZCO is offering a full day’s viewing of live streamed content and it has chosen concurrent courses that will appeal most broadly to the online audience. Video cameras will capture every session – with the content available on-demand shortly after the congress concludes.
“There is a lot of behind the scenes work that goes into making a congress hybrid,” organisers say.
“From the recording, reviewing and hosting, we need to ensure content is secure on our dedicated congress platform. There are a lot of AV, live stream and production technicians scurrying around ensuring that all goes to plan. It includes testing links, feeds, cables and connections multiple times.”
KEY PRESENTATIONS
Delegates can expect the learning and education to roll into the lunch breaks. The Exhibition Hall will host the Education Hub and Senior & Retired Fellows Lounge. Additionally, there will be films and posters, with
the option to view either hardcopy or e-posters.










There’s also an impressive list of keynote speakers this year (detailed on the following page). Challen’s Opening Plenary presentation is highly anticipated, something Scientific Program Committee chair Dr Elsie Chan is excited about.
“I’m looking forward to welcoming Dr Craig Challen, SC OAM and 2019 Australian of the Year to talk about the story of the Tham Luang rescue that highlights the universal nature of leadership skills and risk management strategies,” she says.
Meanwhile, incoming Scientific Program Committee co-chair Dr Clare Fraser believes the neuro-ophthalmology sessions will stir plenty of discussion. “This will feature Professor Neil Miller from John Hopkins Hospital, Wilmer Eye Institute, contributing his wisdom on how to approach the neuro-ophthalmic patient.”
CONGRESS FORMAT CHANGES
A major departure from the traditional congress schedule will be its conclusion on the Monday, instead of the typical Tuesday.
DIAGNOSTIC LASER

Before COVID and then continuing after, organisers noticed a steady decline in the delegate numbers on the Tuesday, and managed to condense this year’s congress without a material effect to the content.
“The proof of the pudding will be in the eating though – so Perth will reveal if this consolidation is here to stay,” the organising committee notes.
The social functions are also being revamped, with the focus on the Welcome Reception (Friday), Graduation and Awards Ceremony and President’s Reception (Saturday) and, notably, no Congress Dinner.
“These changes are again in response to what we’ve been seeing from previous congresses. Previously, the Congress Dinner was the social event … however, we’re seeing a shift away from formal sit-down events to more casual and interactive experiences. So, this year we’ve thrown everything we have at the Welcome Reception,” organisers explain.
ULTRASOUND
“The Graduation and Awards Ceremony and President’s Reception will always be a central part of the congress. It is the culmination of many years of blood, sweat and tears for our trainees and specialist international medical graduates, their colleagues, peers, friends and family. It’s also an opportunity to recognise the outstanding achievements of fellows and trainers.”
SUSTAINABILITY IN FOCUS
Sustainability is increasingly becoming a feature of RANZCO congresses, and the college is marking the next evolution of this with several new initiatives.
“A clear starting point was the RANZCO Congress in 2019 in Sydney with initiatives like ‘Meat-free Monday’. Then, in Brisbane in 2022, we had a sustainability booth, the introduction of a sustainability stream for papers, posters and films and a sustainability prize. For Perth, we’re inviting
64 INSIGHT October 2023 RANZCO PREVIEW
Many delegates are expected to participate in early morning activities due to the Perth time zone.
YDR EEY
industry and delegates to come on the journey with us,” organisers say. The college has invested in new concepts such as:
• Bring your keep cup – with staff washing these for delegates between drinks
• A health and wellbeing space so ophthalmologists can ensure their work set-up is preparing them for career longevity, free of pain and injury.

• Carbon offset of flights and the congress experience, available as an option at registration.

CLOSING REMARKS
For Fraser, the incoming Scientific Program Committee co-chair, other interesting activities to look out for include the introduction of e-posters to ensure virtual delegates are not missing out on any of the action.
“We’re keen to track views on these to see what our delegates’ preferences are for viewing posters. Of course, the Sunday evening ‘Wine and Poster’ viewing will still be a popular event and sees the winners of best papers, posters and films announced,” she says.
Ms Denise Broeren, director of Think Business Events, believes the sustainability focus will be a highlight. She says RANZCO is constantly searching for ways to reduce the congress footprint.

“And to date we’ve reduced the printing aspects and done away with satchels,” she says.
“Building on this, we’re now focussing on raising awareness and encouraging other stakeholders to see where they can cut waste. From reducing waste in the exhibition by considering what is given away and how, to replacing items like paper cups with more sustainable options, everyone can get involved. We’re thrilled that we have close to 15% of delegates contributing to making their attendance sustainable, and hope this percentage continues to climb as the registrations flow in.”
On a lighter note, Ms Alex Arancibia Garcia, head of member services at RANZCO, will be keeping an eye out on the hula hooping session – to be held on the Saturday morning. “I am keen to see who can tap into their inner child and put their serious side aside and get into a novel health and wellbeing activity. "
IMAGING EXCELLENCE A/B/S/UBM Ultrasound Platform RANZCO BOOTH #14-17 • 20MHz annular technology • Image calibration in DICOM format • Standardized A mode for tumar and membrane evaluation • B and UBM probes with integrated motion sensor Contact: salesadmin@ellex.com Call: +61 8 7074 8200
CONGRESS OPENING LECTURE, SAT 21 OCT
DR CRAIG CHALLEN
Dr Craig Challen – an adventurer, cave diver, veterinary surgeon, businessman and pilot – will share an inside account of the 2018 Thai cave rescue. Focusing on the theme of leadership in a challenging environment, he will highlight lessons that can be applied to many contexts, including the medical field. Challenges during the cave rescue will be connected to those faced by medical professionals by exploring critical decision-making processes, emphasising the need for thorough evaluation, quick thinking, and the ability to mitigate risks effectively.

COUNCIL LECTURE, SAT 21 OCT
DR JENNIFER ARNOLD
Arnold, a Sydney based medical retinal specialist and researcher, will illustrate how clinical research can be combined within an everyday ophthalmic practice. She will demonstrate the gradual evolution of knowledge that is incorporated into, and modifies, patient management. Some examples include: reticular pseudodrusen, macular neovascularisation multimodal imaging and classification, photodynamic therapy, refinements in management of nAMD from clinical trials-to-clinical practice through real world evidence.

SIR NORMAN GREGG LECTURE, SAT 21 OCT
DR SHIGERU KINOSHITA

A clinician scientist, Kinoshita is a professor and chair of ophthalmology at Kyoto Prefectural University of Medicine, Japan, with expertise in translational research for severe corneal disease therapies. His presentation will focus on hard-to-treat disorders such as Stevens-Johnson syndrome, chemical injury, Fuchs endothelial corneal dystrophy, and severe corneal endothelial failures. With transplantable cultivated mucosal epithelial sheets developed thanks to corneal regenerative medicine, he hopes more therapies will receive regulatory approvals.
GLAUCOMA LECTURE, SAT 21 OCT
PROF TINA WONG

Wong has many titles, but most pertinent is her position as head of the glaucoma service and senior consultant at the Singapore National Eye Centre. She will highlight the rise in patients undergoing surgery to lower IOP, fuelled by lengthening lifespans and new technology like MIGS. With bleb forming surgeries an important option, unpredictable scarring remain a serious issue, so finding an alternative to Mitomycin C (used in trabeculectomy to prevent scarring) remains elusive. She will examine emerging concepts to deliver safer anti-scarring strategies.
RETINA UPDATE LECTURE, SAT 21OCT
DR FRED CHEN

Presenting on home turf, Chen will delve into many areas, but of interest will be the evolving treatment landscape for both forms of late-stage AMD. With new therapies coming, he will ask whether enough is known about their efficacy and, lacking long term safety data, whether they offer significant gains over current options. As a vitreoretinal surgeon and clinician-researcher in Perth and affiliated with the Lions Eye Institute, he will cover advances in precision medicine, including the Australian-led antisense therapy for Retinitis Pigmentosa type 11.
FRED HOLLOWS LECTURE, SUN 22 OCT

DR ANTHONY BENNETT HALL
Bennett Hall, a vitreoretinal surgeon based in Newcastle who has practised across the world including Africa, will discuss work to prevent blindness from diabetes in low and middle income countries (LMICs). He will highlight the efforts of the Diabetic Retinopathy Network (DR-NET), a program linking eye units in LMICs with eye units in the UK to improve the quality and quantity of eyecare training and service delivery. There are now 28 diabetic retinopathy centres in 20 LMICs including one between RANZCO and Pacific Island programs.
NEURO-OPHTHALMOLOGY UPDATE LECTURE, SUN 22 OCT

DR NEIL MILLER
Miller is a major drawcard for the congress. A global authority on neuro-ophthalmology based at the Johns Hopkins University School of Medicine, he promises several updates that will make ophthalmologists rethink their approach. He says there have been important advances in diagnosis and management of several neuro-ophthalmic disorders, namely optic neuritis, idiopathic intracranial hypertension, visual snow syndrome and management of children with optic pathway gliomas – and ophthalmologists ought to act on them.

66 INSIGHT October 2023 RANZCO PREVIEW KEY
SPEAKERS
DAME IDA MANN MEMORIAL LECTURE, MON 23 OCT
PROF KATHRYN BURDON
An ophthalmic genetics expert based at the Menzies Institute for Medical Research in Tasmania, Burdon will explore the benefits of genetic diagnosis for patients and families, illustrating modern approaches to gene discovery for rare eye disease, as well as important contributions Australia is making to global efforts to understand the clinical impacts of genetic variants.

CATARACT UPDATE LECTURE, MON 23 OCT


DR VINCENZO MAURINO

Maurino is an Italian-British consultant ophthalmologist and director of the cataract service at Moorfields Eye Hospital in London. Delegates will get an insight into his daily cataract practice and the latest changes to his surgical approach. The topics he will cover include complex cataract cases –especially brunescent cataract and those with zonulopathy – high volume cataract surgery and the advent of immediate sequential bilateral surgery, and EDOF IOLs. He will conclude by highlighting the risks of some current IOL designs.
REFRACTIVE UPDATE LECTURE, MON 23 OCT

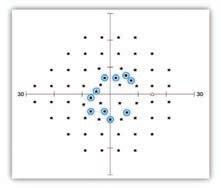
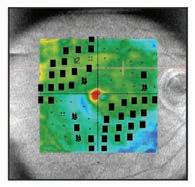

PROF DAN REINSTEIN
Reinstein has devoted his career to the specialty of refractive surgery and has built an impressive career in the field, including writing a definitive textbook on SMILE laser surgery and developing PRESBYOND Laser Blended Vision, now part of the ZEISS platform for presbyopes. He says three major innovations have reached maturity from the forefront of refractive surgery: SMILE, PRESBYOND and ICL sizing – and he will discuss these in detail during his lecture.



See us at Ranzco Booths 18, 19, 20
EXHIBITORS
DFV PROVIDING A GLIMPSE INTO THE FUTURE OF EYECARE
Visitors to the Designs For Vision (DFV) stand can expect to see and experience the latest devices, instruments, and accessories from the distributor’s global network of specialist eyecare manufacturers including HOYA, OCULUS, iCare, DORC, Nidek, D&K Instruments, and others.
DFV is a leading provider of diagnostic and surgical ophthalmic products in Australia and New Zealand and – taking centre stage on its exhibit – will be the new Sophi phaco machine. The system is one DFV says promises to usher in a new era of simplicity, mobility, and safety. This is the first battery driven, wireless phaco device and is equipped with a fast and responsive Triple Pump Fluidics for better control of anterior chamber stability.
Other feaured products will include iCare’s rebound tonometers, considered the market leaders in hand-held tonometry. Delegates can also view the high-resolution TrueColor retinal images produced by the iCare EIDON Ultra-widefield fundus camera. In terms of quality anterior segment tomography, DFV will be exhibiting the OCULUS Pentacam family and its latest member, the OCULUS Pentacam AXL Wave. Stand: 1-4
RAYNER COLLABORATES WITH AUSSIE OPHTHALMIC ROYALTY IN NEW IOL
Rayner’s flagship IOL model, now being adopted by many surgeons in Australia and globally, is the RayOne EMV and EMV Toric.
A feature of the Rayner exhibit, the RayOne EMV is an extending range of vision IOL delivering up to 1.5 D of high-quality vision when used with an emmetropic target. Developed in collaboration with WA’s Professor Graham Barrett, Rayner says RayOne EMV’s truly non-diffractive optic utilises positive spherical aberration to uniquely extend vision whilst avoiding the problems that can arise with diffractive lenses. The IOL’s range of focus can be extended further with a customisable offset for enhanced monovision outcomes.
“For many years I have worked on optimising a lens for monovision, given that it accounts for nearly 30% of all surgeries,” Barrett says. “I collaborated with Rayner on bringing this lens to market as the RayOne EMV, an exciting new product for all surgeons looking to treat presbyopia reliably.”

Delegates can visit Rayner staff at their booth to learn more about the excellent patient outcomes this lens can provide, the company says.
Stand: #48-49
LEARN MORE ABOUT LUMIBIRD MEDICAL’S PREMIUM LASERS
The Lumibird Medical (formally Ellex & Quantel Medical)
stand will host demonstrations of its premium range of YAG and retinal laser systems. This includes the new Tango Reflex Neo, featuring Ellex’s secondgeneration Reflex technology to perform PROcap –premium refractive outcome capsulotomy.

Additionally, delegates can speak with the company’s representatives about its comprehensive suite of diagnostic solutions that can benefit their practices today, including ABSolu, Compact Touch and the most recent release, the new generation ultrasound biometer AXIalis.
“As always, the Ellex Lumibird Medical team looks forward to re-connecting and seeing you at this year's event and providing you with a high-quality professional learning and sales experience,” the company says.
Stand: 14-17
FIRST LOCAL OPHTHALMOLOGY SHOWING FOR DRY EYE PLATFORM
The Envision platform, InMode’s non-surgical, non-drug alternative to treat the cause of dry eye, will make its RANZCO Congress debut in Perth.
Recently made available to Australian eyecare professionals, the platform’s complete suite of technologies delivers bipolar radiofrequency (RF) via its Forma-I handpiece, Lumecca-I intense pulsed light (IPL) device, and fractional RF microneedling with the MORPHEUS8, to allow for highly efficacious eyecare procedures, the company says.




A recent paper investigating transcutaneous RF-assisted meibomian gland expression using Forma-I in dry eye patients found the technology is effective, lasting at least six months in most patients. The multicentre prospective cohort study was published in Open Ophthalmology Journal of North American ophthalmic professionals and involved 47 patients across three sites.
Stand: #27
68 INSIGHT October 2023
RANZCO PREVIEW
PM-GL-0077 All rights reserved. ©2021
Innovation is at the core of everything we do. At Glaukos, we push the limits of science and technology to solve unmet needs in chronic eye diseases. Experience a world of firsts in vision care. Learn more at Glaukos.com.
WE’LL GO FIRST
EXHIBITORS
ZEISS TECH ELEVATES EYE CLINICS
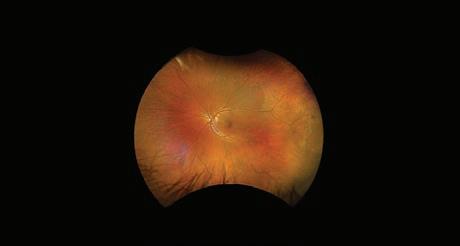

As a Platinum sponsor, ZEISS will be showcasing its innovative range of products and workflows while holding multiple customer events across the three days
Attendees can gain hands on exposure to the ZEISS portfolio and hear firsthand from subject matter experts on how they have incorporated ZEISS technology and workflows into their practice.
The ZEISS Cataract Workflow will take centre stage, highlighting the connected solutions offered by EQ Workplace, IOL Master 700, ARTEVO 800 and QUATERA 700. Attendees can also learn more about the ZEISS IOL portfolio, including the new CT LUCIA 621, a C-Loop hydrophobic IOL which it says is gaining popularity as the monofocal of choice for clinicians across ANZ.

“Our chronic disease management portfolio will focus on ZEISS’s comprehensive retina and glaucoma workplace solutions and diagnostic equipment, including CIRRUS OCT, CLARUS ultra-widefield retinal imaging and the highly anticipated launch of the ATLAS 500 corneal topographer, the latest addition to our portfolio,” ZEISS says.
“Do not forget to register for the VISUMAX 800 wet lab, and experience the femtosecond laser technology that has supported delivery of the SMILE procedure in over 8 million eyes."
Stand: P3
EXPERIENCE OPTOS’ NEW IMAGE MODALITY
A major drawcard of the Optos booth will be its new ultra-widefield colour modality. This new image modality, optomap colour rgb (red/green/blue), is captured simultaneous to the optomap colour rg (red/green). Thus, a single capture delivers two high quality colour ultra-widefield images. As a company, Optos delivers comprehensive retinal imaging devices and evaluation tools to eyecare professionals globally. Most notably, it produces ultra-widefield optomap images of up to 82% or 200-degrees of the retina, something no other device can do in a single capture, the company says.
According to Optos, an optomap image provides a bigger picture and more clinical information, facilitating the early detection, management and effective treatment of disorders and diseases evidenced in the retina.
“More than 2,000 published clinical studies show the long-term value of optomap imaging with OCT in diagnosis, treatment planning, and patient engagement,” the company says.
“Our passion has made optomap the gold standard in eyecare and we are committed to utilising the latest technology, manufacturing new products and software that support optomap to assist eyecare professionals around the world save sight and lives.”
Stand: 136-139
PORTABLE VISUAL FIELD TESTER
BOC Instruments is a well established supplier and service provider for the some of the most reputable ophthalmic equipment, which will be exemplified by its stand at RANACO 2023.
The product range on display will include Frey slit lamps, retinal cameras, Optovue OCTs, autorefractors, chair and stands, and innovative dry eye products.
Delegates are also urged to swing by for demonstrations with the new VF2000 NEO Virtual Reality portable visual field tester with eye tracking. BOC describes this as an evolution in visual field testing, providing “unsurpassed accuracy and efficiency at exceptional value”, which also includes many additional vision testing features.

Stand: 44-45
Alcon is encouraging delegates to visit its booth to hear live presentations from clinical experts, experience live demonstrations and speak with the company about its innovative sustainability solutions and ophthalmic products.
These include the Clareon Autonome PC-IOL family, Centurion, ARGOS, Hydrus and more, that enhance quality of life by helping people see brilliantly, the company says.
Stand: P2
70 INSIGHT October 2023
RANZCO
PREVIEW
ALCON PRODUCT SUITE ON FULL DISPLAY



©2023 Rayner Group, all rights reserved. Rayner and RayOne are proprietary marks of Rayner. All other trademarks are property of their respective owners. Rayner, 10 Dominion Way, Worthing, West Sussex, BN14 8AQ. Registered in England: 615539. EC 2023-30 AU 08/23 MADE IN UK 1. Ferreira TB. Comparison of visual outcomes of a monofocal, two enhanced monofocals and two extended depth of focus intraocular lenses. Presented at ESCRS 2022. 2. RayOne EMV: First Clinical Results, Rayner. Oct 2020. 3. Rayner RayPRO, data on file. 4. Rayner, data on file. 5. Rayner Peer2Peer webinar. May 2022. 6. Royo, M. RayOne EMV and TECNIS Eyhance: A Comparative Clinical Defocus Curve. Data on file. 2021. 7. Bhogal-Bhamra GK, Sheppard AL, Kolli S, Wolffsohn JS. J Refract Surg. 2019;35(1):48-53. For more information call your Rayner representative or 1300RAYNER Extending range without compromise EMV & EMV TORIC “Both the patient satisfaction results and depth of focus curves generated are excellent.” Prof Graham Barrett Join the conversation Search for #Peer2Peer Leading surgeons from around the world share their real-world experience with RayOne EMVwatch engaging webinars, listen to insightful interviews and podcasts, and read interesting case study articles. Visit www.rayner.com/peer2peer to access videos and articles, download resources and join future events and discussions. PeerPeer RayOne EMV – Developing a Lens Perfect for *Almost* Anyone 21
PREVIEW
EXHIBITORS
B+L SHOWCASING PHARMA AND SURGICAL OPTIONS
Since the recent acquisition of AcuFocus, Bausch + Lomb (B+L) is offering the IC-8 IOL and its unique lens technology as part of the company’s comprehensive range of intraocular lenses in Australia and New Zealand. According to B+L, the IC-8 IOL combines the simple, proven principle of small aperture optics to extend depth of focus with the reliable quality of an aspheric monofocal IOL, allowing patients to achieve their best personal vision.

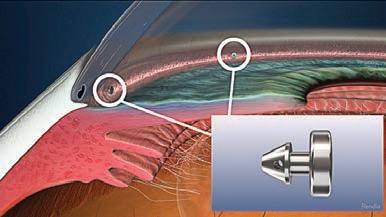
Meanwhile, the company’s pharmaceutical business will be showing two dry eye therapies on the same stand. Namely, these are Viscotears Eye Gel, a translucent, viscous gel containing 0.2% Carbomer that provides soothing longlasting relief for sore, gritty and dry eyes. It will also be exhibiting Viscotears Gel PF, an ophthalmic solution that has a moistening and wetting effect on the eyes. It improves the moistening of the ocular surface in the presence of dry eye sensation, burning or tiredness of the eyes.
They are available in two formulations: Viscotears Eye Gel:10g tube, and Viscotears Gel PF (preservative free): 30 x 0.6g single-dose units – both of which are PBS-listed.
Delegates can visit the B+L booth to find out more about these products, plus more.
Stand: 28-33
GLAUKOS SHOWCASING LATEST MIGS INNOVATION
The iStent inject W will be the focus of the Glaukos exhibit, a therapy described as the gold standard in MIGS. It’s backed by the most robust, diverse, and longest-term body of clinical evidence for any MIGS procedure, Glaukos says, and is also the number one device of its kind in terms of units sold. Optimised outflow is a major feature of the iStent inject W. The stents are multi-directional and together can deliver access to multiple collector channels and arcs of flow that can span five to six clock hours. The stents may also re-establish flow in previously dormant outflow channels.
The iStent inject W supports optimal outcomes after cataract surgery and more, including:
• Micro-invasive and astigmatically-neutral
• Utilises the conventional outflow pathway
• Leaves natural anatomy intact, preserving the potential for future treatment options, including drug delivery devices
• Minimally traumatic to delicate eye tissue and spares conjunctival tissue
• Reduces risk of hypotony by utilising the natural episcleral venous pressure
• Offers postoperative care profile similar to cataract surgery
Stand: 40-41
WHAT WOULD IT BE LIKE TO LIVE WITH GEOGRAPHIC ATROPHY?
At RANZCO, Apellis is inviting delegates to visit “The G.A.llery” at its stand in the exhibition hall. This gallery style setting aims to raise awareness of the significant burden of geographic atrophy (GA) on people with the condition and its impact on daily activities and hobbies.4 As visitors view the exhibits in “The G.A.llery”, the company is encouraging them to reflect on what it would be like to live with vision impairment due to GA.
GA is a leading cause of blindness that affects more than 5 million people globally.1 Approximately 73,000 people are living with GA in Australia.2 GA causes progressive and irreversible vision loss, with GA lesions taking an average 2.5 years from diagnosis to encroach the fovea.3 Vision impairment from GA can lead to reduced independence and quality of life for patents living with the disease.4,5 With no approved treatments available in Australia, this represents a significant unmet medical need in ophthalmology.
Apellis is also hosting a breakfast symposium at 6:30am on Saturday 21 October, featuring local and international GA experts. Note:Referencesavailableuponrequestandintheonlineversion. Stand: 114

LEARN MORE ABOUT CEQUA FOR DRY EYE DISEASE
Sun Pharma is attending RANZCO 2023 and showcasing Cequa (ciclosporin 900 microgram/mL). The therapy is indicated to increase tear production in patients with moderate to severe dry eye where prior use of artificial tears has not been sufficient.1
According to the company, Cequa is available via private prescription and on the PBS from 1 June 2023 for patients with chronic severe dry eye disease with keratitis.2 Cequa comes in a clear, colourless solution, needs to be taken twice daily, and is available in a pack of 60 ampoules containing 0.25 mL of ciclosporin 900 microgram/mL ophthalmic solution – one month supply.

Patient Starter Packs are available to help identify <3% of patients that discontinue use due to instillation site pain3 and a range of resources are available for more information. “Visit the Cequa stand at RANZCO to discuss Cequa and grab a cup of coffee on us,” the company says.
Review Product Information (page 75) before prescribing available from www.ebs.tga.gov.au or Sun Pharma by calling 1800 726 229.
References: 1.CequaApprovedProductInformation.2.Pharmaceutical BenefitsScheme(https://www.pbs.gov.au)3.GoldbergDFetal. Ophthalmology2019;126:1230–7.
Stand: 154-157
72 INSIGHT October 2023
RANZCO
The ONLY single-capture ultra-widefield image takes less than ½ a second.

Enhance diagnostic capabilities, practice efficiency and patient experience.

Better diagnose pathology and preventable eye disease.
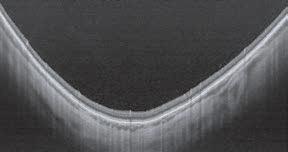

Differentiate your practice and increase revenues.
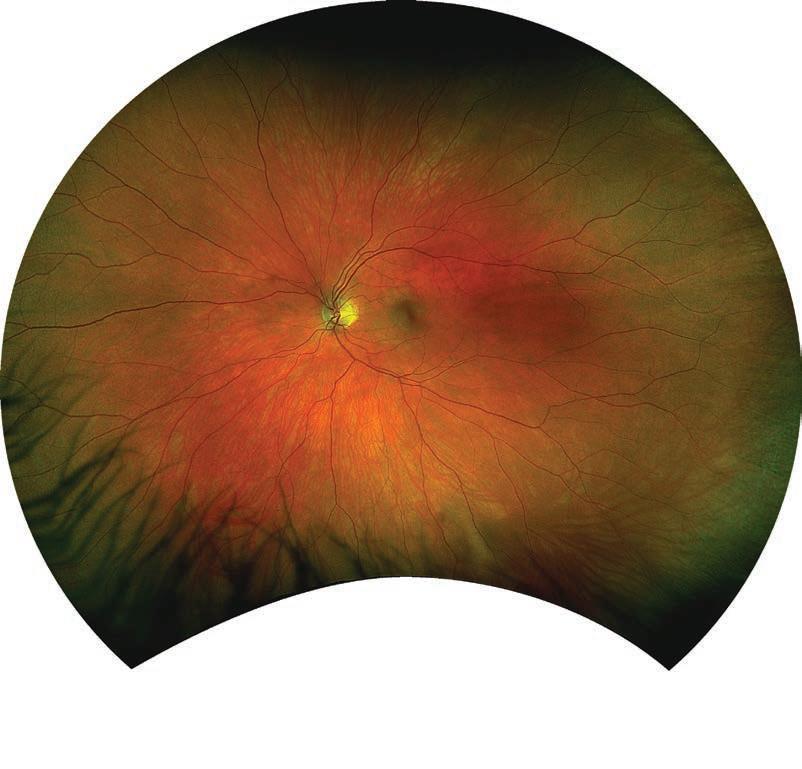
2 3 4 1 2 3 4 1 T: +61 8 8444 6500 | E: auinfo@optos.com | Optos.com Image: SS OCT line and volume scans captured with optomap-guided OCT
patient
and satisfaction.1 Saving
optos’ latest ultra-widefield retinal imaging technology increases
flow
Sight, Saving Lives.
visit duration in a retina
Retina. 2021.
Kehoe. Poster 19. Widefield Patient Care. EAOO 2016
1. Tornambe, The Impact of Ultra-widefield Retinal Imaging on Practice Efficiency, US Ophthalmic Review 2017. 2. Successful interventions to improve efficiency and reduce patient
practice,
3.
EXHIBITORS
NEW DATA REAFFIRMS NOVATEARS’ STRENGTH
NovaTears will be a major focus of the AFT Pharmaceuticals stand at RANZCO 2023 off the back of the pivotal Phase 3 Gobi study reinforcing its effectiveness as a treatment for evaporative dry eye.

NovaTears was first approved in Australia in 2018, and the recent Gobi study laid the foundation for FDA approval in the US earlier this year in May 2023 where it is marketed as MIEBO. From as early as two weeks, the therapy demonstrated statistically significant and clinically meaningful improvements in the signs and symptoms of dry eye disease associated with meibomian gland dysfunction.

In Australia and New Zealand, AFT also supplies NovaTears + Omega-3, a variation of the original NovaTears eye drop that contains concentrated, high quality Omega-3 of plant origin to provide enhanced lubrication and protection for dry and irritated eyes.
AFT has a significant presence in the preservative dry eye space, offering a range of preservative-free options such as HYLO Forte, HYLO Fresh, and Opti-Soothe heat and eyelid wipes.
Stand: 42
DRY EYE FOCUS FOR CSL SEQIRUS
The CSL Seqirus eyecare portfolio includes Cationorm (cationic nanoemulsion) and Ikervis (ciclosporin 0.1% ophthalmic emulsion).
Eighty six percent of people living with dry eye have mixed or evaporative dry eye disease (DED).1,2 Cationorm is a preservative-free, hydrating, and lubricating emulsion targeting all layers of the tear film.3-5 Compatible with all types of contact lenses, Cationorm is designed to be long-lasting, creating a barrier to lock in moisture, giving the eyes the time they need to heal.3-6
Ikervis is a once-daily ciclosporin delivered in a cationic emulsion, 7,8 designed for long-term treatment. 9 Ikervis is indicated for the treatment of severe keratitis in adults with DED that has not improved with artificial tears. 7

For more information including results of recent real world studies visit www.eyehealth.com.au. Contact 1800 642 865 or aunz.medicalinformation@seqirus.com for more information.
PBS INFORMATION: Cationorm Multi Dose (10mL). Authority Required (STREAMLINED) 6172. Refer to PBS Schedule for full authority information. Cationorm (30 x 0.4mL) is not listed on the PBS. See page 49 for the Minimum Product Information, PBS and further information for Ikervis. Please review the Product Information before prescribing.
NOTE: References are available upon request and in the online version of this article.
Stand: 140-143
ATROPINE EYE DROPS TO SLOW MYOPIA PROGRESSION IN CHILDREN
Eikance 0.01%, the first pharmacotherapy registered on the Australian Register of Therapeutic Goods to slow the progression of myopia in Children aged 4 – 14 years1#, may be initiated in children when myopia progresses ≥-1.0 D per year.1
EIKANCE 0.01% single-use ampoules are sealed in foil pouches and are available in packs of 30 x 0.3 mL ampoules. The ophthalmic solution is sterile and preservative-free. EIKANCE 0.01% is a private, prescription only medicine available at community pharmacies across Australia.
To access Product Information and PBS status, turn to page 35.
References:
1.Eikance Approved Product Information
# Australian Register of Therapeutic Goods. Accessed: 15 August 2023.
Aspen Australia, St Leonards NSW 2065. Prepared: August 2023. AU-ATR-082023-06771
Stand: 39
NOTE: Pack image not to scale.
VISIT OPTIMED FOR LATEST IN OCT AND LASERS

On display at the OptiMed exhibit will be the REVO FC fully automated high resolution fundus camera and OCT. This single, high-tech device enables eyecare professionals to capture colour images, and high definition OCT scans with up to 130,000 A scans per second. The advanced optical system ensures high quality imaging at a 45-degree viewing angle. The Structure and Function algorithms of REVO OCT help predict visual field loss and when combined with the new Automated Perimeter PTS, users have a comprehensive analysis suite at their fingertips for glaucoma investigation and treatment resources.

“User friendly with a small footprint, the versatile REVO FC gives you the option of adding further modules like OCT-Angiography, OCT-Biometry, OCTTopography and IOL Calculator at point-of-purchase or in the future. Fully automated, safe and easy-to-use, the REVO FC meets all requirements for modern optical tomographs,” OptiMed says.
Also on display will be the Vision-R 800, Essilor’s phoropter “reinventing prescription to 0.01D”, and the Norlase Leaf and Lion instruments, described as the world’s only fibreless green lasers that minimise maintenance and maximise space.
Stand: 18-20
74 INSIGHT October 2023
RANZCO
PREVIEW
Now
Take control of dry eyes with Cequa2,3†*




† Cequa signicantly reduced corneal staining at 28 days vs vehicle (p<0.01).3* Cequa is indicated to increase tear production in patients with moderate to severe keratoconjunctivitis sicca (dry eye) where prior use of arti cial tears has not been suf cient.2
Please review Product Information before prescribing available from https://sunophthalmology.com.au/pi or Sun Pharma by calling 1800 726 229



tThis medicinal product is subject to additional monitoring in Australia. This will allow quick identi cation of new safety information. Healthcare professionals are asked to report any suspected adverse events at https://www.tga.gov.au/reporting-problems.
CEQUA™ ciclosporin 900 microgram/mL eye drops ampoule. Indications: Increases tear production in patients with moderate to severe keratoconjunctivitis sicca (dry eye) where prior use of arti cial tears has not been suf cient. Contraindications: Hypersensitivity. to the active substance or excipients. Active or suspected ocular or peri-ocular infection, malignancies or premalignant conditions










Precautions: Potential for eye injury and contamination: avoided by not touching the eye or other surfaces with the ampoule tip. Contact



Lenses: remove contact lenses prior and reinsert 15 minutes after administration. Careful monitoring of patients with severe keratitis is recommended. Infections: resolve existing or suspected ocular or peri-ocular infections before initiating treatment and if an infection occurs during treatment, withhold temporarily until infection resolves. Effects on the immune system: may affect host defenses against local infections and malignancies so regular examination of the eye(s) is recommended, e.g. at least every 6 months, when used for long periods. Paediatric use: safety and ef cacy is not established below the age of 18. Pregnancy: Category C. Adverse effects: Very Common and Common: instillation site pain, conjunctival hyperemia and punctate keratitis. Dosage and administration: one drop twice daily (approximately 12 hours apart) into the affected eye(s). Response to treatment should be reassessed at least every 6 months. Can be used concomitantly with articial tears, with a 15-minute interval between products. Storage: Store below 25°C. Do not freeze.

the ampoules in the original foil pouch. Protect from light. Date of
2020.
1. Pharmaceutical Bene ts Scheme. Schedule of Pharmaceutical Bene ts - Effective 1 June 2023. Department of Health, Canberra. www.pbs.gov.au 2. Cequa Approved Product Information. 3. Goldberg DF et al. Ophthalmology 2019; 126:1230–7. Sun Pharma ANZ Pty Ltd ABN 17 110 871 826, Macquarie Park NSW 2113 Ph: 1800 726 229. Fax: +61 2 8008 1613. Med Info: 1800 726 229. Adverse events may be reported to Sun Pharma by either email: adverse.events.aus@sunpharma.com or phone: 1800 726 229. Date of preparation: May 2023. CEQ2023/05ELS PBS Information: Authority Required. Refer to PBS Schedule for full authority information.
Patient Starter Packs help identify <3% of patients that discontinue use due to instillation site pain.3 Patient starter
AVAILABLE Cequa.Samples@sunpharma.com
Store
preparation: February
Reference:
Where artificial tears have not been sufficient.
2*
packs NOW
available on the PBS for patients with chronic severe dry eye disease with keratitis1
VISION IMPAIRMENT FROM GEOGRAPHIC ATROPHY (GA) LEADS TO REDUCED INDEPENDENCE AND QOL1-3

44% of patients with GA required assistance with activities of daily living3*
*A cross-sectional study with a retrospective chart review to examine burden of illness due to GA in patients aged ≥70 years (N=189) with physician-confirmed bilateral symptomatic GA due to AMD, versus patients of a similar age with no ophthalmic condition that in the opinion of the investigator affected visual function. Visit geographicatrophy.com.au to discover more about GA or scan the QR code
©2023 Apellis Australia Pty Ltd. Level 1, 718 High Street, Kew East, Victoria, 3102. ABN 87 600 316 612. August 2023. AU-GA-2300023. APEL0061. AMD: age-related macular degeneration; GA: geographic atrophy; QoL: quality of life. References: 1. Singh RP, et al. Am J Ophthalmic Clin Trials 2019;(1):1-6. 2. Sivaprasad S, et al. Ophthalmol Ther 2019;8(1):115-24. 3. Patel PJ, et al. Clin Ophthalmol 2020;14:15-28.
Ophthalmology Updates!
LOOKS AHEAD OF THE CURVE
Aquestion from a delegate about potential treatment options for a 10-year-old patient with congenital toxoplasmosis who recently presented with a new lesion is the type of interaction Ophthalmology Updates! is known for, and this year’s event was no exception.
Presenter, Professor Justine Smith, was quick to respond, with the session’s chair, Professor Peter McCluskey, also contributing to the discussion about the importance of involving a paediatric specialist in treatment, in this particular case.
The question – and subsequent discussion – was one of many which took place over the two-day conference at The Fullerton Hotel in Sydney 26-27 August. For event convenor Professor Adrian Fung, the opportunity to ask questions is highly valued by delegates, with 200 people attending this year.
“The field of ophthalmology – and the subspecialities within it – changes fast. Treatment options have changed since Ophthalmology Updates! first started in 2016,” Fung said. “This event is an opportunity to learn from each other and share our real-world experiences. There is a lot of discussion on areas where there’s room for debate on the best way to manage patients.”
Fung said the conference model includes revision of a ‘common’ condition across a range of subspecialities, as well as exploration of a ‘frontier’ topic on a topical subject.
“With speakers presenting the newest data in their field, the event provides a yearly concentrated overview from experts on the latest diagnostic techniques and treatments across a range of subspecialties,” Fung said.

An internationally recognised expert in the causes, effects and treatment of uveitis, Smith’s presentation on toxoplasmosis summarised the findings of several papers she has published in the last few years, including one study jointly conducted with the International Ocular Inflammation Society. However, perhaps most telling was an article she co-authored with Associate Professor João Furtado from The University of São Paulo in Brazil, published in Ophthalmology Retina, which “went viral” after being featured in the magazine The Conversation
Across the world, it’s estimated 30-50% of people are infected with Toxoplasma – and infections may be increasing in Australia, Smith warned.
To illustrate, she shared the details of Australian-first research by Flinders University which found more than one-third of lamb mince purchased from supermarkets over a six-month period contained Toxoplasma. Eating undercooked or raw meat is a major risk factor for this disease. About one in 150 people have scars in the back of their eyes consistent with prior infection.
As part of her presentation, Smith also spoke about the changes in medical journal publishing witnessed in her term as editor-in-chief of Clinical and Experimental Ophthalmology, including an increase in research compliance, plagiarism, generative AI, and the need to harness social media. Smith was the first to appoint a social media section editor (Dr Elsie Chan) to the journal.
“AI-generated content, like plagiarism, is a growing problem in publishing. So too is the rise of ‘predatory journals’. These journals have similar names to genuine peer-reviewed journals – therefore causing confusion – and take advantage of authors by asking them to publish for a fee without providing peer-review or editing services. It’s a scam,” Smith said.
Smith, who is the first female editor-in-chief of Clinical and Experimental Ophthalmology and the first to lead a top tier Q1 ophthalmology journal, is stepping down at end of the year after completing a four-year-term.
Professor Dinesh Selva, foundation chair of ophthalmology and visual sciences at the University of Adelaide, delivered a presentation on oculoplastics, bringing attention to a rise in cases of group A Streptococcus, resulting in him seeing more cases of necrotising fasciitis.
Selva also discussed the intricacies of Tenzel flap technique, periocular squamous cell carcinoma (SCC) risk stratification, gene expression profiling, and a new neoadjuvant immunotherapy for advanced SCC, which is showing promise of being a globe-sparing treatment, he said.
HIGHLIGHTS ON DAY 1
Emerging treatments for age-related macular degeneration (AMD) and geographic atrophy (GA) was presented by Professor Robyn Guymer,
INSIGHT October 2023 77 EVENT
About 200 ophthalmologists met in Sydney for the Ophthalmology Updates! conference. Image: David Wilson, Eventphotography.com
and real-world outcomes, which needs to be addressed. To that end, she shared results of the VOYAGER study, an innovative, global, observational study to gain real-world insights into the long-term utilisation of the Port Delivery System (PDS) with ranibizumab and intravitreal faricimab for the treatment of neovascular AMD and diabetic macular oedema.
Guymer highlighted two intravitreal anti-complement therapies which have been recently FDA-approved to treat GA (SYFOVRE from Apellis, and IZERVAY (formerly Zimura) from Iveric Bio) plus others in the pipeline including a gene therapy in development from Gyroscope Therapeutics (acquired by Novartis).
“There are many emerging treatments for GA, but the complement inhibitors pathway is furthest along in clinical studies,” she said.
She warned of an increased risk of nAMD in patients treated for GA and real-world incidences of retinal occlusive vasculitis which were not reported in the clinical studies.
Live polls were held throughout the presentations, with speakers asking delegates multiple choice questions through the event app, shaping discussion.
Associate Professor Michael Lawless polled audience members on their most commonly used IOL during his lecture on the nuances of IOL technologies, discussing Rayner’s new RayOne EMV Toric and comparing EDOF lenses. He also shared 10 tips to improve cataract surgery.
“Use plastic, not metal inside the eye, and press on the primary wound to prevent reflux and toric IOL rotation. Discharge patients at six weeks only after having actively met their expectations. Continue to learn new techniques, and if you start to feel too comfortable, start to worry,” he said.
Lawless also spoke about what factors make a difference in near vision despite the same end points and hinted that the answer would be apparent in the next six months. Looking further ahead, he said chromatic aberration will likely be the next frontier in IOLs, and shared a new IOL concept from Dr Sri Ganesh, known as the swivel haptics IOL prototype.
Following presentations which addressed modifiable risk factors in uveitis (delivered by Associate Professor Anthony Hall) and an overview of MIGS devices (delivered by Dr Nathan Kerr), special guest speaker Dr Norman Swan gave an insider’s view on medicine in the media.
Citing current health issues making headlines in the media, such as The Voice referendum, and the rise and fall of Australian neurosurgeon Dr Charlie Teo, Swan discussed how the media controls the message.
“Media operates on an emotional level. For example, the case against The
Voice – the ‘no vote’ – is framed by what you lose if you vote ‘yes’,” he said.
Swan also highlighted the media coverage of COVID and infectious
“There was a media divide, and the community didn’t know who to trust or believe, made worse by the Federal Government response. There was a crisis of trust. One of the most difficult problems that arose during that time was the clotting problem with the AstraZeneca vaccine, and how that was
“When does myopic traction maculopathy (MTM) require intervention?,” presenter Dr Mali Okada asked the audience on the second day of
Okada, a medical retina and vitreoretinal specialist at the Royal Victorian Eye and Ear Hospital, outlined tips on diagnosing MTM, and discussed macular buckling for myopic macular schisis, with one ophthalmologist in the audience volunteering to share their experience with this surgical procedure.
She also discussed with the audience whether to offer surgery to patients with myopic traction maculopathy and foveal detachment alone.
Speaking on novel drugs, devices and implants in her area of subspeciality, Okada informed the audience on a new drug treatment for proliferative vitreoretinopathy, as tested in the GUARD trial.

The GUARD trial assessed whether postoperative administration of ADX-2191 (intravitreal methotrexate 0.8%, Aldeyra Therapeutics) has an effect on rates of re-detachment due to PVR that requires surgery.
Okada said preliminary results from the trial show promise, with participants given 13 injections over four months, when the risk of PVR is at its highest.
On devices, she highlighted that although the previously mentioned PDS is currently voluntarily recalled due to septum displacement issues, the PAGODA trial has shown that in patients with DMO, implantation of the PDS with ranibizumab with refill/exchanges every six months maintains vision and controls oedema as well as monthly injections of ranibizumab.
She also touched on primary analysis results of the phase 3 PAVILION trial, involving PDS with ranibizumab in the treatment of diabetic retinopathy without centre-involved diabetic macular oedema.
Lastly, Okada summarised a study demonstrating efficacy of intravitreal delivery of ciliary neurotrophic factor (CNTF) using an encapsulated cell implant for the treatment of macular telangiectasia type 2.

Moving from the retina to the cornea, Dr Elsie Chan, a cornea specialist at the Royal Victorian Eye and Ear Hospital, generated discussion on the merits of taking one biopsy or two in cases of suspected cicatrising conjunctivitis.
“Not all cicatrising conjunctivitis is a subtype of Mucous Membrane Pemphigoid (MMP). If in doubt, repeat a biopsy,” Chan said, sharing real-world cases to highlight the importance of repeating a biopsy, even if the first result is negative.
Chan’s presentation also reviewed the ocular surface microbiome and potential treatments manipulating the microbiome. Her discussion on topical antibiotics in ophthalmology and their affect on gut health raised further questions, prompting chair Associate Professor Chameen Samarawickrama to share his experience and views on antibiotics stewardship as editor of the RANZCO therapeutic guidelines.
Paediatric ophthalmologist Dr Craig Donaldson, currently head of the strabismus unit at Sydney Eye Health, updated delegates on Duane Syndrome, a congenital rare type of strabismus which affects females more than males, and left eyes more than right. Donaldson suggested a hearing test for patients with suspected Duane Syndrome, a recommendation that chair Dr Loren Rose also agreed with.
Donaldson also reviewed real-life cases of Brown Syndrome, usually congenital but sometimes the result of trauma such as a dog bite, and Monocular Elevation Deficiency (MED).
Outlining what is new in paediatric ophthalmology, Donaldson spoke about peripheral retinal defocus lenses, including D.I.M.S lenses and H.A.L.T
78 INSIGHT October 2023 EVENT
Dr Norman Swan, special guest speaker.
lenses, with Rose highlighting the importance of emphasising to patients that these only work when they are worn.
He also drew attention to repeated low-level red light therapy (RLRL), with an Australian made device recently receiving TGA approval, and raised the potential of preventatively treating ‘pre-myopes’, those at risk of developing progressive myopia. Finally, he underlined the importance of always checking a child’s pupil function.
Flinders University consultant neuro-ophthalmologist Professor Celia Chen provided a summary of arterial occlusion.
“Follow the roadmap, from carotid arteries to retinal emboli. Where is it from? Find the underlying vascular risk factors. Where will it go? Consider secondary prevention for stroke and heart attack,” she said.
She then turned her attention to the complexities of diagnosing idiopathic intracranial hypertension (IIH), a condition she described as on the rise. The condition was formerly known as Pseudotumor cerebri and benign intracranial hypertension, both of which are now considered inaccurate.
“IIH is not benign – you need a lumbar puncture to confirm diagnosis. Cases of IIH have doubled in the last 10 years and is essentially a diagnosis of exclusion,” she said.
Treatment options include, in order of preference, non-pharmacological (such as weight loss), medical (such as Diamox and Topamax), and surgical (such as venous sinus stenting).“There is no such thing as a quick fix,” Chen said.
Radiologist Dr Geoffrey Parker, who provides diagnostic and interventional radiology support to the Ophthalmology, Head and Neck and ENT Services at Royal Prince Alfred Hospital, used real-life cases to demonstrate where a radiologist can help in diagnosing a range of conditions.
“Imaging is improving. We can see remarkable detail,” he said.





The final speaker, ocular oncologist Dr Li-Anne Lim, zeroed in on uveal melanoma, and a new approach to management of metastatic disease with TGA-approval of Tebentafusp.
“It’s the only drug which makes a meaningful difference to overall survival rates,” she said.

Lim is a clinical senior lecturer at the University of Sydney and involved in the ocular oncology multidis ciplinary team at The Kinghorn Cancer Centre at St Vincent’s Hospital in Sydney.
At this year’s conference, she also reported on a promising neoadjuvant therapy being trialled at St Vincent's Hospital in Sydney. The drug, Darovasertib, and the corresponding NADOM trial, shows it has the potential to save eyes with uveal melanoma from enucleation.
Channel Nine news aired a report, ‘Cancer drug trial saves Queensland man's eye from massive melanoma’, in June this year.
“It’s changing the paradigm,” Lim said.
PBS Information:
2.5 mL) is listed on the PBS as antiglaucoma preparations and miotics.

Before prescribing please review Product Information available via www.aspenpharma.com.au/products or call 1300 659 646.






Minimum Product Information: XALATAN® (Latanoprost 50 µg/mL) Eye Drops. Indication: Reduction of intraocular pressure (IOP) in patients with open-angle glaucoma or ocular hypertension. Contraindications: Hypersensitivity to ingredients. Precautions: Change in eye colour due to increased iris pigmentation; heterochromia; eyelid skin darkening; reversible eyelash and vellus hair changes; macular oedema often associated with aphakia / pseudoaphakia; other types of glaucoma; contact lenses; severe or brittle asthma; herpetic keratitis; driving or using machines – transient blurry vision; elderly: no data; children: do not use, no data; lactation- metabolites present in breast milk, risk / benefit. Pregnancy: Category (B3) Interactions: other prostaglandins, thiomersal. See PI for details. Adverse Effects: Eye Disorders: blurred vision, burning, conjunctivitis, excessive tearing, eye pain, foreign body sensation, hyperaemia, iris hyperpigmentation, itching, punctate epithelial erosions, grittiness, stinging, eyelash and vellus hair changes, punctate keratitis, blepharitis, eyelid oedema, localised skin reaction on eyelids; Systemic: bronchitis, upper respiratory tract infection, eczema, rash, urinary tract disorder, abnormal liver function, myalgia, arthralgia, dizziness, headache, rash, chest pain, asthma, dyspnoea . See PI for details and other AEs. Dosage and Administration: One eye drop in the affected eye(s) once daily. Other eye drops should be administered at least 5 minutes apart.



References: 1. Clinical Practice Guide for the Diagnosis and Management of Open Angle Glaucoma. Optometry Australia 2020 2. Australian Commission on Safety and Quality in Healthcare Active Ingredient Prescribing Guide - list of medicines for brand consideration December 2022
Aspen Australia includes Aspen Pharmacare Australia Pty Ltd (ABN 51 096 236 985) and Aspen Pharma Pty Ltd (ABN 88 004 118 594). All sales and marketing requests to: Aspen Pharmacare Pty Ltd, 34-36 Chandos Street, St Leonards NSW 2065. Tel: +61 2 8436 8300 Email: aspen@aspenpharmacare.com.au Web: www.aspenpharma.com.au Trademarks are owned by or licensed to the Aspen group of companies. © 2023 Aspen group of companies or its licensor. All rights reserved. Prepared: July 2023 AU-LAT-072023-07653

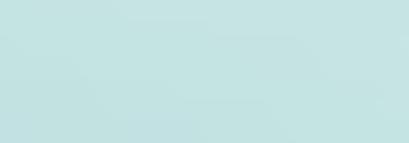



✔
If clinically necessary for the treatment of your patient, prescribe by brand and disallow brand substitution2
A first choice for glaucoma management1
A/Prof Michael Lawless.
BEING A 'PEOPLE-PERSON' IS HELPING THIS DISPENSER MAKE A DIFFERENCE
DISPENSER DETAILS
Name: Joshua OronceSimpson
1. What initially attracted you to a career in optical dispensing, and how did you enter the profession?


I was 19-years-old and had spent my first couple of years out of school working in luxury retail. I decided to leave without a job to go to. With spare time up my sleeve, I walked in to my local optometrist for an eye test. We began discussing my interests, hobbies and the fact that a week earlier I had resigned from my job. They encouraged me to apply for a position in the practice as they thought I would be a great fit. The following week, I started as an assistant and the rest is history.


2. What are your main career highlights?
Attaining my Cert IV in Optical Dispensing in 2015, followed by working at a well-established behavioural optometrist and leading their dispensing team. They have a special interest in paediatric and neurological care which helped cement my understanding of what I had learnt in my Cert IV, but it also allowed me to hone my skills and expose me to things I may not always see in day-to-day practice.
I now work with another pre-eminent practice who’s passion is in eyewear and in my spare time, I started my own side business, Spex in the City, where I offer a mobile optical dispensing service and provide one-on-one dispensing to people in their own home or workplace. This was spawned from COVID when people were reluctant to leave home as it allows a hybrid of online and face-to-face dispensing. While still in its infancy, it is gaining traction and has benefitted many people. My clients include those that are less-mobile, struggle to find the time to organise spectacles during traditional hours, or those that enjoy dedicated one-on-one time.
3. What are your strengths as an optical dispenser and what excites you about your job?
I believe that my strengths come from being a people-person; being adaptable to the
person in front of me and managing their expectations. While being technically-minded is essential, being a people-person can make the difference between a good dispenser and a great dispenser. I love to build a strong and genuine rapport and tend to do this by not only getting to know them, but their family members and care givers and I will often give up anecdotes of myself to help strengthen that rapport. Adapting to their personality, and mirroring their body language, tone of voice and enthusiasm also makes it much easier to align with them if any conflict comes up in future. It also helps make you more credible when giving recommendations. Managing expectations is another important skill, especially with lifestyle dispensing and dispensing progressives. I find using metaphors helps (i.e. progressives are like a Swiss army knife, it can do lots of things, but not necessarily lots of things well).
What excites me is using all my skills to make a tangible difference and adding value in p eoples lives.
4. If you could go back and provide advice to yourself at the beginning of your optical dispensing career, what would you say?
Take your time, it’s OK if you get it wrong –and if you can make an engineer happy with their spectacles, you can pretty much make a nyone happy.
5. What do you see as the key opportunities and challenges facing the future of optical dispensing in Australia?
Changing the public’s perception of what a dispenser is and what they do. I would be rich if I had a dollar for every time a patient realises that we are much more than a ‘sales person’. Organisations such as ODA and ACOD are playing such an important role in helping us regain our credibility and changing public perceptions.
6. How do you ensure your skills and knowledge stay current in such a fast-moving industry?
I try and stay up-to-date with our industry by attending events; most recently SILMO in Singapore, watching webinars (thanks ODA), YouTube videos (Laramy-K offer some great videos), keeping in touch with all reps and customer service teams – they are a wealth of knowledge.
7. Why did you become a member of ODA, and what value do you see in the organisation?
It is wonderful to have a united voice that represents the dispensing community. They have so many resources at their fingertips that makes them indispensable.
8. What would you say to others thinking of joining Optical Dispensers Australia?
If you are looking for a supportive community with a wealth of knowledge, join!

80 INSIGHT October 2023
Joshua Oronce-Simpson has started a side business offering a mobile optical dispensing service to people in their own home or workplace.
Founded in 2022, OPTICAL DISPENSERS AUSTRALIA’S mission is to transform the optical dispensing industry by creating a community where optical dispensers and their associates can feel supported and inspired through education, events, networking, and employment advice, plus more. Visit: www.odamembers.com.au
Position: Owner/optical dispenser Location: Perth Years in industry: 11
FLIPPING THE SCRIPT ON SAFETY EYEWEAR
RECOMMENDING PRESCRIPTION SAFETY EYEWEAR TO THE RIGHT PATIENT COULD BE THE DIFFERENCE BETWEEN A MINOR AND MAJOR MISHAP. WAYNE PUXTY PROVIDES AN OVERVIEW OF THIS AT-TIMES OVERLOOKED EYEWEAR CATEGORY.


As qualified optical dispensers, our remit is to offer the most appropriate eyewear options. A significant part of our day involves collecting information and synthesising that into a product recommendation. Prescription safety eyewear is one of those. With Bolle Safety Australia stating that “9/10 eye injuries can be prevented with proper protection” and that of all head injuries, 45% are eye injuries, prescription safety eyewear has an important role to play.
This eyewear is the combination of a safety frame and prescription lenses tested to comply with the requirements of Australian Standards (AS/NZS1337.6:2012
Personal Eye Protection, Part 6: Prescription eye protectors against low and medium impact).
This means the frame has been tested by a third-party certifier like SAI Global to ensure they meet the minimum requirements for protection and durability. The lens material has also been tested in various prescription combinations when fitted to a specific frame. This provides the manufacturer with a range of prescriptions for a specific frame option. The certified prescription range can vary from frame-to-frame and supplier-to-supplier.
Certified prescription safety eyewear can only be supplied by a licensed manufacturer. There are several in Australia, including some of the larger lens suppliers as well as other companies dedicated to prescription safety eyewear. When a prescription falls outside the certified range, a compliant product can be manufactured.
Hoya Safety Eyewear states that “in this instance the manufacturer is declaring that their product is compliant and must be able
The third-party certification is not provided in this instance. Simply edging lenses into a safety frame will not provide the certification or guarantee of eye protection and should be avoided.
FRAMES
Gone are the days when practices held their obligatory six safety frames. Manufacturers are continually adding new frames style options, so hiding them away should no longer be the ‘norm’. With expanding options, suppliers have made finding the most appropriate option easy.
LENSES
Lens options and designs vary among suppliers. Single vision, bifocal, progressives, occupational progressives and anti-fatigue are all available with different treatment options.
Clear, photosensitive and sunglasses are all available. Sunglasses are typically supplied in a polarised version however some manufacturers can also offer a dye tint version for those who prefer or require non-polarising. Photosentive options are readily available along with anti-reflection and anti-fog coatings.
The lens range options in prescription safety eyewear are smaller than those available in conventional eyewear, but there are options to suit most applications.
LENS MATERIALS
Lens materials are based on the tested protection that each provides. Typically, for medium impact protection, Trivex (1.53n) or Polycarbonate (1.59n) are used. These lens materials provide protection from an object travelling at 40 meters per second (medium impact). Trivex offers
Abbe number (less birefringence and chromatic aberration). Some suppliers offer a low impact alternative which provides protection from an impact travelling less than 12 meters per second. The main material for this is CR39 1.5n.
IS THE EYEWEAR CERTIFIED?
Safety frames are marked with the standard they comply with and the license number of the manufacturer. This way you can confirm they have been tested and will provide the appropriate protection. Lenses are marked as well. Usually in the upper temporal area out of the general line of vision. These markings are a combination of letters that denote particular characteristics of the eyewear. A logo or defining symbol defines who the manufacturer is. The letter ‘R’ denotes the lenses are corrective/prescription. An ‘I’ or ‘F’ indicates the lenses are compliant to provide medium impact protection. And the letter ‘O’ relates to the lens colour, outdoor and untinted. Some lenses may have a number (1-3) which shows their tint density as per the sunglass standards.
WHO SHOULD WE RECOMMEND TO?
Discussing the customer's workplace and job tasks is the best way to uncover the information for a recommendation.
PSG suggests that “working with metal is one of the most common sources of work-related eye injuries”.
WHEN SHOULD IT BE REPLACED?
Trent from RxSafety suggests prescription safety eyewear should be replaced in the following instances:
• If it’s received an impact, as it may not withstand a subsequent impact.
• If the prescription requirements have changed or expired
• If the eyewear is two years or more in age. Most of us understand what a potential risk might be to our customers’ eyes and vision of our customers. Don’t ignore it, discuss it and recommend prescription safety eyewear.
ABOUT THE AUTHOR: Wayne Puxty has 34 years’ optical industry experience, including roles as an optical dispenser, laboratory technician, practice manager and trainer and assessor for other employees. He has been a practice owner for the past 17 years, with his two locations specialising in prescription safety eyewear. He is also an Advisory Board Member for Optical Dispensers Australia.
DISPENSING INSIGHT October 2023 81
WAYNE
PUXTY
“MANUFACTURERS ARE CONTINUALLY ADDING NEW SAFETY FRAMES STYLE OPTIONS, SO HIDING THEM AWAY SHOULD NO LONGER BE THE ‘NORM’.”
Prescription safety eyewear should ideally be replaced after two years or more.
RE-WRITING THE RULES OF DRY EYE MANAGEMENT
AN ORTHOPTIST-LED DRY EYE CLINIC ESTABLISHED IN SYDNEY IS PROVING ORTHOPTISTS HAVE THE SKILLS AND KNOWLEDGE TO IMPROVE PATIENT EDUCATION AND ACHIEVE BETTER OUTCOMES FOR PATIENTS WITH DRY EYES.

Dry eye disease (DED) is a complicated and pervasive ophthalmic condition that, while frequently diagnosed, is poorly categorised, understood and managed by both patients and professionals.
This frequently stems from the fact that for many years DED has been an oversimplified diagnosis. Many patients have been left sifting through the shelves of drops at their local chemist, feeling overwhelmed and frustrated.
In a large ophthalmic practice, many of these patients present to us highly symptomatic. Despite potentially possessing more visually debilitating ocular co-morbidities, their main concern is the constant burning, pain and other symptoms of DED.
The case history is often long and complicated with the patient having seen multiple health practitioners and trialling many different eye drops, yet the resounding conclusion is ‘but nothing works’.
At Marsden Eye Specialists in Castle Hill, Penrith and Parramatta in NSW, we came to the realisation that better avenues for the assessment, education and treatment of dry eyes were necessary for our patients and our practice.
Patients have high expectations when being seen in a private ophthalmology
Fortunately, DED has seen a recent resurgence of interest. Work by the Tear Film & Ocular Surface Society (TFOS) Dry Eye Workshop II has helped improve our understanding of the pathophysiology of DED and provide evidence-based management guidelines.
In March 2020 we established an orthoptist led dry eye clinic at Marsden Eye Specialists. Importantly, this means the burden of DED management is shared in our practice with excellent use of orthoptic skills.
Orthoptists have the skills and knowledge base to improve patient education and achieve better outcomes for patients with dry eyes thereby increasing satisfaction within their work environment.
Our orthoptic led dry eye clinic was established as a service to existing patients that aims to:
• improve patient education
• enable comprehensive assessment and accurate diagnosis
• provide an avenue for in-clinic dry eye treatments
• alloc ate a large amount of time to each patient
• ensure patients feel their concerns are heard.
The benefits of the dry eye clinic include improved patient understanding of their condition, improved compliance and more customised treatments.
The Marsden Eye Specialists dry eye clinic runs fortnightly and new patients are given one hour appointments. We use Ocular Surface Disease Index (OSDI), keratography and tear osmolality for our diagnostics.
The orthoptist then explains the results to the patient and spends time educating the patient on their type of DED and associated diagnoses such as meibomian gland dysfunction (MGD) and blepharitis. This includes providing a tailored home treatment regime.
We have created our own Marsden Eye Specialists education and treatment handouts based on the outputs from the TFOS Dry Eye Workshop II reports including which products relevant to the diagnosis are easily available for patients to source.
Finally, the orthoptist performs any
necessary treatments including warm compress and massage, lid hygiene, eyelid debridement and meibomian gland expression.
Despite the impacts of the COVID pandemic, patients continued to present to the dry eye clinic. In the two years since its inception, we had 110 new patients attend, resulting in 170 treatments being performed by the orthoptists.
On presentation, 6% of our patients had aqueous deficiency DED, 30% had evaporative DED and 64% had combination DED. Of great significance was the fact that 94% of patients had MGD and therefore required in-clinic treatments.
After initial assessment in the dry eye clinic, patients return to the care of their referring ophthalmologist or are requested to return to the dry eye clinic if further management is required. Patients who have an inadequate response to dry eye clinic interventions are referred back to their ophthalmologist for more specific treatments or further investigations of underlying systemic disease.
At Marsden Eye Specialists we have found the orthoptic led dry eye clinic to be a valuable service that fills what was a niche gap in the services we provide. This internal collaborative approach to DED management has reduced the DED burden on often time poor ophthalmologists and increased the skills and autonomy of our orthoptic team.
Our patients are also happier with 80% of patients experiencing an improvement in symptoms on their OSDI after only one visit to the dry eye clinic. If our patients, orthoptists and ophthalmologists are happy then it is clear that there is a need for more ophthalmology practices to offer this type of DED management.
ABOUT THE AUTHOR: Mitchell Bagley is Orthoptic Team Leader at Marsden Eye Specialists and Research Centre Parramatta, Castle Hill and Penrith. He completed a Master of Clinical Vision Sciences at University of Technology.

82
MITCHELL BAGLEY
“WE HAVE FOUND THE ORTHOPTIC LED DRY EYE CLINIC TO BE A VALUABLE SERVICE THAT FILLS WHAT WAS A NICHE GAP IN THE SERVICES WE PROVIDE.”
Orthoptist Mitchell Bagley discussing a dry eye diagnosis with a patient.
ORTHOPTICS AUSTRALIA strives for excellence in eye health care by promoting and advancing the discipline of orthoptics and by improving eye health care for patients in public hospitals, ophthalmology practices, and the wider community. Visit: orthoptics.org.au
WHAT NEW TAX RULINGS MEAN FOR EYE CLINICS
THEIR OWN BUSINESSES.
The NSW tribunal decision from Thomas v Naaz, September 2021, and the subsequently rejected appeal in March 2023, has put medical practice operators on notice.
At the crux of this case: the medical practice in question entered into contracts with doctors and provided rooms and shared services. The practice billed patients on behalf of the doctors, and then paid the doctors, keeping a portion as a management fee. It was ruled these payments to doctors were indeed wages and subject to payroll tax, rather than an invoiced management fee.
Now, other practitioners are pondering whether they should be classified as medical practice employees working under ‘relevant contracts’, with respect to state payroll tax legislation. It’s not the first time such a ruling has caused uncertainty, with the Victorian legal system making similar rulings against optometry network The Optical Superstore in 2019/20.

The payroll tax harmonisation agreement means that medical practices in all states (except Western Australia) may be liable for additional payroll tax expenses. The WA Government has stated it does not intend to change its laws based on tribunal decisions in other states.

In South Australia and Queensland, amnesties have been issued for GPs. Recently, the NSW Government announced a 12 month “pause” on payroll tax audits, penalties and interest for GPs and their practices, but Victoria hasn’t made any such announcement.
Following the recent Thomas v Naaz appeal dismissal in March, state revenue office rulings have recently been released online. These aim to provide clarity on the application of contractor provisions regarding payroll tax liability for medical centre businesses that contract medical and health practitioners. It’s important to note there is no change to the provisions; the law has not changed, but is additional information about their interpretation.
So, what does this mean for medical practices?
Ultimately, steps should be in place to ensure that the service contracts between practitioners and the practice entity do not qualify as ‘relevant contracts’ under the guidelines.
Further, practices should ensure doctors are collecting their own fees directly, rather than through any facility of the practice. This is because funds being collected and paid through the practice may be construed as evidence of wages as part of an employment relationship.
Practices should ensure the agreements accurately reflect the legal relationship between the practitioner and practice. They should also ensure the communications and actions of the facility do not represent the practitioners as if they are employees, or that their relationship with the facility has features of an employer-employee relationship. This includes things like specifying when leave can be taken, controlling rosters etc.
If the State Revenue Office is convinced there are no ‘relevant contracts’ in place
at the practice, then there is a lower risk it could be the target of an audit. But if the State Revenue Office is not convinced the practitioners have engaged the practice as service providers – and instead can be seen as employees – the practice should look to the exemptions for ‘relevant contracts’ stated in the rulings.
This may also mean if the agreement is a sub-lease arrangement that the details and leases are accurate and appropriate. The exemptions are:
1. Issuing s ervices to the public – a practitioner facility requires a decision from the State Commissioner regarding this exemption that is required every financial year.
2. 90-day rule – this is a matter of law and does not require private ruling or a determination from the chief commissioner. This will purely exempt practitioners who have performed services at the facility less than 90 days within a financial year. Important to note that a day may be an hour or a full day.
3. Patients having care delivered by more than one person – in an ophthalmology clinic this can be relevant to orthoptists/ technicians that screen or perform diagnostic testing. Notably, these people must be employed directly by that practitioner and not the facility.
It’s important all practices consider their governance structures, financial structures and give consideration to the rulings. Plus, practices might want to thinking about other services, other than doctors, that may fall under this ruling.
It’s vital all practitioners also consider this issue. Should an audit be conducted and financial liabilities repaid, it does not necessarily relate only to the practice/ facility, but may extend to the practitioner. Remember, the rulings have dated the conditions from 2018 and audits can be retrospective for a period of five years. It is recommended business owners and managers get their own advice from advisors that understand the relevant legislation, and recent legal cases.
MANAGEMENT INSIGHT October 2023 83
RECENT COURT AND STATE TAX RULINGS OVER PAYROLL TAX AND THE RELATIONSHIP BETWEEN MEDICAL PRACTICES AND PRACTITIONERS HAVE PROMPTED EYE CLINICS TO CONSIDER THE IMPLICATIONS FOR
“SHOULD AN AUDIT BE CONDUCTED AND FINANCIAL LIABILITIES REPAID, IT DOES NOT NECESSARILY RELATE ONLY TO THE PRACTICE/ FACILITY, BUT MAY EXTEND TO THE PRACTITIONER.”
ABOUT THE AUTHOR: Donna Glenn has been the business manager at Gordon Eye Surgery in Sydney for over 16 years. She is also an advisory member of the RANZCO Practice Managers Committee, chairs the RANZCO Professional Standards committee and is a NSW representative for the AAPM committee.
Practices may now need to ensure the service contracts between practitioners and the practice entity do not qualify as ‘relevant contracts’.
AI, FUNDUS IMAGING AND LIFE-THREATENING HEADACHES
physicians to screen patients for these life-threatening conditions as soon as they present.
However, due to the limited time and resources in EDs, managing for all these potential conditions can be a challenging and time-consuming endeavor.3
This is the problem we’re working to solve. Artificial intelligence (AI) systems have huge potential to help healthcare practitioners make more informed decisions and improve the treatment they provide to patients. The eye can be quickly and easily imaged, making it a good target for AI systems that could be used in busy environments like EDs.
The retina is also a window to the central nervous system, and changes in it can be signs of issues throughout the rest of the body.4
Our AI system has shown great potential to accurately detect papilledema from retinal images, but it has not yet been tested in real-world settings.
We collaborated with Monash Medical AI Group and an industry partner to integrate the AI system into a retinal camera. Our Smart Camera is designed to automatically take retinal images and detect the presence of papilledema with high accuracy.

Physicians just need to ask the patients to get into position, and the Smart Camera completes the scan and provides a diagnosis report in about two minutes.
once in their life. It is the fourth-most common reason people present at ED –in 2018 more than 4.9 million Australians visited ED for a headache.1
Although the vast majority of headaches are not serious, a small percentage will be a symptom of a life-threatening condition – such as a brain tumor or an intracranial hemorrhage.2 These patients require urgent treatment and it is critical for
Papilledema – a swelling of optic disc – is a consequence of intracranial hypertension.5 It is one of the most important red flags for a potentially life-threatening headache.6 Although many emergency departments have the tools needed to examine the fundus, it can be difficult for physicians to use this equipment in a busy setting.7
Because of this, examination of the optic disc is not always well-performed in ED.8 To solve this, my team at CERA and I have developed a Smart Camera powered by AI to screen for these red flags.
It is designed to help physicians screen for these life-threatening headaches more smoothly. Furthermore, it is fully automatic and portable, making it easy to use in emergency settings.
Our next steps are to refine the AI algorithm with more diverse clinical data to further improve its accuracy, and also undertake clinical validation trials to assess its feasibility and performance in the real-world setting of an emergency department.
If successful, it could prove to be a reliable, rapid, and cost-effective screening solution for headache management.
We also foresee that we could potentially expand the use of the Smart Camera to other neurological and eye conditions.
Our system is one of several projects at CERA using AI to spot conditions through the eye, ranging from heart disease to Alzheimer’s.
All have a great potential to assist doctors treat their patients.
NOTE: References will appear in the online version of this article. version of this article.
Name: Dr Lisa Zhuoting Zhu

Qualifications: MD, PhD
Organisations: Centre for Eye Research
Position: Primary Investigator, Ophthalmic Epidemiology
Location: Melbourne
Years in profession: 4
THE EYE CAN BE QUICKLY AND EASILY IMAGED, MAKING IT A GOOD TARGET FOR AI SYSTEMS THAT COULD BE USED IN BUSY ENVIRONMENTS.
84 INSIGHT October 2023
SOAPBOX
The AI research team (from left) Dr Lisa Zhuoting Zhu, PhD student Zhen Yu and Dr Alice Chen with the Smart Camera.
2023 CALENDAR
OCTOBER
RANZCO SCIENTIFIC CONGRESS
Perth, Australia
20 – 23 October ranzco.edu/events
ORTHOPTICS AUSTRALIA ANNUAL CONFERENCE
Perth, Australia
21 – 24 October orthoptics.org.au
EYECARE PLUS BOOTCAMP AND AGM
Sydney, Australia
27 – 28 October y.safier@eyecareplus.com.au
SPECSAVERS CLINICAL CONFERENCE
Sydney, Australia
28 – 29 October specsaversclinicalconference. com.au
NOVEMBER
HONG KONG INTERNATIONAL OPTIC FAIR
Hong Kong
8 – 10 November hktdc.com/event/hkopticalfair/en
SILMO INSTANBUL
Istanbul, Turkey
23 – 26 November silmoistanbul.com/en
DECEMBER
ASIA PACIFIC TELEOPHTHALMOLOGY SOCIETY CONGRESS
Pattaya, Thailand
2 – 3 December 2023.asiateleophth.org
THE 16TH CONGRESS OF THE ASIA-PACIFIC VITREO-RETINA SOCIETY (APVRS) 2023
Hong Kong
8 – 10 December 2023.apvrs.org
JANUARY 2024
SKI CONFERENCES FOR EYECARE PRACTITIONERS
San Vigilio, Italy
13 – 20 January skiconf.com
FEBRUARY 2024
MIDO EYEWEAR SHOW
Milan, Italy
3 – 5 February mido.com
ANZGS CONGRESS 23
Hobart, Australia
16 – 19 February anzgsconference.com
ASIA-PACIFIC ACADEMY OF OPHTHALMOLOGY (APAO) CONGRESS
Bali, Indonesia. 22 – 25 February 2024.apaophth.org
To list an event in our calendar email: myles.hume@primecreative.com.au
MARCH 2024
SKI CONFERENCES FOR EYECARE PRACTITIONERS
Furano, Japan
3 – 10 March skiconf.com
APRIL 2024
AUSTRALIAN VISION CONVENTION (AVC)
Gold Coast, Australia
6 – 7 April optometryqldnt.org.au
MAY 2024
OSHOW24
Sydney, Australia 17 – 18 May o-show.com.au
$40k Sign-on bonus
Optometrist opportunities in Regional Australia
Although 2023 has been a challenging year across the world, Specsavers continues to show steady growth, with 11 new stores already opened this year and more to come. This growth is creating more opportunities for patient focused optometrists to join us. We offer flexible rosters to support work/life balance, access to the latest technology (including OCT in every store free for every patient) and extremely attractive salaries – with $40k sign-on bonuses in selected locations. We will provide you with excellent opportunities for career development – including Pathway to Partnership, outreach opportunities and the chance to mentor new graduates. Join us now!
$50k sign-on bonus – Designate Partnership in Emerald, QLD Specsavers Emerald has an exciting opportunity for an experienced Optometrist to join the store on a 2-year Designate Partner program - No upfront cost and opportunity to try partnership before committing long term. Specsavers Emerald is
a 3 test room store with a varied patient demographic and an extremely welcoming, supportive and social team. You will be supported with a relocation package tailored to your needs, be partnered with an experienced Specsavers Retail Partner and have access to our Pathway and Partnership development program for duration of time in role.
Optometrist opportunity –Specsavers New Plymouth, NZ
Seeking a talented optometrist to join our extraordinary team at Specsavers New Plymouth. We offer cutting-edge technology, a friendly environment, and a commitment to professional growth. Embrace the breathtaking beauty of the region and enjoy a perfect work-life balance. Explore stunning coastal views and immerse yourself in a vibrant arts scene. Don’t miss this incredible opportunity to be part of Specsavers New Plymouth. Apply now and unlock a rewarding journey in one of New Zealand’s most spectacular locations.
Graduate Opportunities
The Specsavers Graduate Recruitment Team have a number of exciting graduate opportunities available across Australia and New
Zealand. With continued growth in providing eyecare to patients across ANZ, now is an exciting time to join and be part of the company bringing Optometry to the forefront of the healthcare industry. At Specsavers, you will have access to cutting edge technology and be part of leading the way in changing lives through better sight.
Fly In, Fly out Locum Opportunities across Australia
Are you an experienced Optometrist looking to combine work and travel? If so, we are offering unbeatable opportunities across our Australia store network.
Working as a locum with Specsavers means you will receive great rates, have access to market leading technology and work with excellent Optometrists and retail staff. We will organise and cover the cost of your travel including car hire, flights and accommodation. If you’re passionate on delivering professional and outstanding eye care, and you would like to explore Specsavers fly in fly out opportunities around Australia, get in touch now.
LET’S TALK!
In a few short years, Specsavers has achieved market leadership in Australia and New Zealand with more people choosing to have their eyes tested and buy their prescription eyewear from Specsavers than any other optometrist. To learn more about these roles, or to put your hand up for other roles as they emerge, please contact us today:
Joint Venture Partnership opportunities enquiries: Kimberley Forbes on +61 (0) 429 566 846 or E kimberley.forbes@specsavers.com
Australia Optometrist employment enquiries: Marie Stewart – Recruitment Consultant marie.stewart@specsavers.com or 0408 084 134
Locum employment enquiries: Matthew Cooney matthew.cooney@specsavers.com or 0447 276 483
New Zealand employment enquiries: Chris Rickard –Recruitment Consultant chris.rickard@specsavers.com or 0275 795 499
Graduate employment enquiries: apac.graduateteam@specsavers.com
Specsavers YOUR CAREER, NO LIMITS Visit spectrum-anz.com
All Specsavers stores now with OCT
ON THE MOVE
Asgari as its New Director of Business development for

OPTOMETRY AUSTRALIA WELCOMES ADDITION TO COMMUNICATIONS TEAM



With over a decade of experience in public relations, strategic communications and media relations, Ms Katie Quirk joins Optometry Australia in the role of Communications Coordinator. During her years spent agency-side, she worked with dozens of clients in the B2B and B2C space as well as managed the PR retainer for ODMA in 2016. A major part of her role at Optometry Australia will be driving communication and public relations activity around the organisation’s consumer facing initiative, Good vision for life.
Eyerising International, which recently received TGA approval for its repeated low-level red light therapy for myopia control, has appointed Mr Manny Pascual as its Head of Operations. He comes to the role after three years as a Marketing Director at CooperVision. At Eyerising, he will be responsible for marketing and will be present at several upcoming conferences, as well as overseeing logistics and other functions now that the device can be used in Australia and other markets.

CENTRE FOR OCULAR RESEARCH & EDUCATION
ANNOUNCES KEY
PROMOTION
Ms Deborah Jones, who presented at O=MEGA23/ WCO4 in Melbourne, has been promoted to Lead Clinical Scientist at the Centre for Ocular Research & Education (CORE). She is also clinical professor at the School of Optometry and Vision Science, University of Waterloo. Her primary clinical focus is on pediatric optometry and her main area of research is in myopia control.
ACUFOCUS CEO TAKES PROMINENT ROLE AT B+L AS PART OF MERGER


Following the acquisition of AcuFocus and its small aperture intraocular technology, Bausch + Lomb has appointed Mr Al Waterhouse as its Executive Vice President and Chief Supply Chain and Operations Officer. Waterhouse most recently served as President and CEO of AcuFocus and has held leadership positions at healthcare and medical device companies, including Abbott Medical Optics, Advanced Medical Optics and PCI Pharma Services.

SENIOR MEDICAL ADVISOR ROLE
With the resignation of Dr Joel Naor as Chief Medical Officer in July, Dr Kenneth Sall been appointed as Senior Medical Advisor at Opthea, a Melbourne and ASX-listed clinical stage biopharmaceutical company. Sall will assume responsibility for safety oversight of the Opthea’s Phase 3 clinical trials investigating OPT-302, a novel VEGF-C/D ‘trap’ inhibitor, for the treatment of neovascular age-related macular degeneration.
DO YOU HAVE CAREER NEWS TO SHARE? EMAIL EDITOR MYLES HUME AT MYLES.HUME@PRIMECREATIVE.COM.AU TO BE FEATURED.
CAREER
86 INSIGHT October 2023
Insight's monthly bulletin keeps the Australian ophthalmic sector updated on new appointments and personnel changes, nationally and globally.
People
ARGOS Biometer. Measures up better than the rest.1-6
Connected surgical planning starts with the ARGOS ® Biometer. Experience faster, †1-4 easier ‡2 and better §1-2,5-6 optical biometry, even for cataracts. Combine with one touch planning and VERION TM image guidance for integrated workfl ow from the clinic to the operating suite. 7,8 Ask Alcon for a demonstration today.





†Based on acquisition rates compared to IOLMaster* 700 (n=622; p<0.0001),1,4 IOLMaster* 500 (n=107-188; p-value not reported),2,3 LENSTAR* LS900 (n=107; p-value not reported).2 ‡Based on a higher success rate of acquiring the axial length measurement in eyes with dense cataract (96% of cases for ARGOS® compared with 77% for the IOLMaster* 500 and 79% with LENSTAR* LS900; p-value not reported).2 ARGOS® Biometer has shown better acquisition rates in dense cataract compared to IOLMaster* 700 (n=622; p<0.0001),1 IOLMaster* 500 (n=107; p-value not reported)2 and LENSTAR* LS900 (n=107; p-value not reported).2 ARGOS® Biometer has shown better predictive accuracy in medium-long eyes (n=23; p<0.001)5
and precise measurement (n=318;p-value not reported)6 than IOLMaster* 500. *Trademarks are the propertyof their respective owners. References:



1. Tamaoki A et al. Ophthal Res 2019;19:1–13. 2. Shammas HJ et al. J Cataract Refract Surg 2016;42:50–61. 3. Hussaindeen JR et al. PLoS ONE 2018;13(12):e0209356. 4. ZEISS* IOLMaster*700 510k Submission 2015. 5. Whang W et al. Sci Rep 2018;8(1):13732.
6. Shammas HJ. Accuracy of IOL power formulas with true axial length versus simulated axial length measurement in 318 eyes using an OCT biometer. 2019 ASCRS ASOA Annual Meeting. May 2019. 7. VERIONTM Reference Unit User Manual 2019. 8. ARGOS® Biometer User Manual 2019.
©2023 Alcon Inc. Alcon Laboratories (Australia) Pty. Ltd. ABN 88 000 740 830. Phone: 1800 224 153. Auckland New Zealand NZBN 9429047030480 Phone: 0800 809 189. ALC-003345-00 ANZ-ARB-2300013
EFFICIENT INTEGRATED DIAGNOSTICS

Join the home of some of the best optometrists in the business. With our experience and support, we offer the freedom to practice full-scope optometry or choose a specific area of interest. Accelerate your career aspirations with OPSM. Visit opsm.com.au/careers today.
CHOOSE TO SPECIALISE IN THE FIELD YOU LOVE
