CLAMPDOWN ON 'SURGEON' TITLE
Ophthalmology groups call for tighter regulation of rogue cosmetic surgery industry.
RANZCO CONGRESS RETURNS FROM HIATUS
Key speakers and product launches planned for Australian ophthalmology's marquee event.
MILESTONE FOR ICONIC OPTOMETRY BRAND
Innovation and differentiation have ensured OPSM's longevity over 90 years.


03
53
63
AUSTRALIA’S LEADING OPHTHALMIC MAGAZINE SINCE 1975 OCT 2022 ENVISTA TORIC IS NOW PRELOADED Focused on Outcomes. Fixated on Stability.


© 2022 Bausch & Lomb Incorporated. ®/TM denote trademarks of Bausch & Lomb Incorporated and its affiliates. Bausch & Lomb (Australia) Pty Ltd. ABN 88 000 222 408. Level 2, 12 Help Street, Chatswood NSW 2067 Australia. (Ph 1800 251 150) New Zealand Distributor: Toomac Ophthalmic. 32D Poland Road, Glenfield 0627 Auckland New Zealand (Ph 0508 443 5347) EVT.0006.AU.22For more information contact your Bausch + Lomb Territory Manager or Customer Service 1800 251 150 ENVISTA TORIC IS NOW PRELOADED enVista Toric calculator now incorporating the EVO 2.0 Formula Scan the code or visit: envista.toriccalculator.com Focused on Outcomes. Fixated on Stability.
AHPRA TO ENFORCE ‘ENDORSEMENT’ MODEL FOR COSMETIC SURGEON TITLE
In a move that has been cautiously welcomed by ophthalmologists and oculoplastic surgeons, medical regulator Ahpra has vowed to clampdown on rogue medical practitioners using the title ‘cosmetic surgeon’ by introducing an endorsement process to establish minimum qualifications.
However, details remain unclear on how the endorsement process will work, with RANZCO and other medical colleges believing the ‘surgeon’ title should be restricted to those who have received full surgical training from an Australian Medical Council-accredited college.
In November 2021, the Australian Health Practitioner Regulation Agency (Ahpra) and the Medical Board of Australia commissioned a review into the cosmetic surgery

industry following media reports and discovered unsafe practices, misleading advertising and substandard marketing across the cosmetic industry.
Within the ophthalmic sector, some oculoplastic/periocular procedures, such as endoscopic brow lift and blepharoplasty, can be cosmetic in nature and are performed by highly trained medical specialists.
Ahpra also found that universal minimum standards for education, training and qualifications are non-existent for cosmetic surgery in Australia, meaning it is possible for any medical practitioner to offer invasive cosmetic procedures without appropriate training or sufficient supervised experience.
In these circumstances, Ahpra said consumers are largely left on their
own when selecting a practitioner to perform cosmetic surgery, having to sift through a plethora of advertising material to make sense of numerous qualifications, to try identify a qualified and competent practitioner.
The inquiry – led by former Queensland Health Ombudsman Mr Andrew Brown and released
OPHTHALMIC SECTOR INCOMES REVEALED
Male ophthalmologists have the largest taxable income out of all occupations in Australia, outranking all other medical specialities and other high-powered careers in law and finance, according to new data from the Australian Tax Office (ATO).
The new data from the 20192020 financial year shows the average taxable income for a male ophthalmologist was $624,500, with the next closest being male neurosurgeons at $599,000.
The national tax department recently released a detailed breakdown of the average taxable income for each job, revealing how much the average optometrist, orthoptist, optical dispenser, optical mechanic and practice manager
takes home each year.
The 2019-2020 data is the latest available, with the average taxable Australian income overall being $63,882. However, the information is limited in nature; for example, it only includes data visible to the tax department and caputres annual incomes of all part-time, casual and fulltime workers. For professions where a greater proportion work part-time, this could skew salaries down. Therefore, when comparing across professions or between men and women, it may not necessarily be a like-for-like comparison.
According to the ATO, the average taxable income of 612 Australian ophthalmologists was $521,000. The average taxable income for
female eye doctors was $285,600 – $338,000 less than their male counterparts.
Meanwhile, the average taxable income across 4,649 Australian optometrists was $92,800. Male optometrists earned $108,900 on average, while females earned $82,300, a difference of $26,600.
For health practice managers the average taxable income was $76,300 (males $97,600 and females $73,300).
The data also shows orthoptists had an average taxable income of $64,600, comprised of 866 females and 130 males. Male orthoptists generated $76,900 on
on 1 September – made 16 recommendations accepted by Ahpra, with the most notable being that the regulator will use the ‘endorsement’ process to establish minimum qualifications for medical practitioners wishing to perform cosmetic surgery. A similar approach is used for therapeutically-endorsed optometrists.
“An ‘endorsement’ recognises that a person has an extended scope-ofpractice in a particular area because they have obtained a specific qualification that has been approved by the Medical Board,” Ahpra stated.
“The training program(s) leading to the qualification also must be accredited by an independent
A COMPREHENSIVE GUIDE FOR DRY EYE CARE IN AUSTRALIA
The Insight Dry Eye Directory has returned in 2022, featuring a new list of the most up-todate therapies and diagnostics available from leading Australian suppliers, and a directory of dry eye clinics.

AUSTRALIA’S LEADING OPHTHALMIC MAGAZINE SINCE 1975 OCT 2022
continued page 8
Some periocular procedures can be cosmetic in nature.
continued page 8
page 34
Secure your future and unleash your potential at Specsavers
As an optometrist, we will help you carve out a solid career path and support you to achieve your professional goals.
And if you’re craving for a meaningful career full of growth, we offer world-class training and development programs from graduate to partnership that will unlock your potential.
We will provide you with a host of professional development opportunities from our ophthalmology-led education programs to our clinical conference and 24/7 access to our MyCPD Portal from the beginning of your time with us.
We also offer market-leading technology and above market salaries, supplemented by additional benefits covering extra annual leave, relocation allowances, and AHPRA fees.
Whether you’re looking for your first job, new opportunities or feel ready to take that next step to partnership, we have a variety of roles and locations to suit your needs.

Be part of the growth and secure your future at Specsavers.
To find out more, contact Marie Stewart on 0408 084 134 or marie.stewart@specsavers.com or visit spectrum-anz.com.
IN THIS ISSUE
DEDICATED TO DRY EYE
Four independents discuss the transformational impact of offering dry eye services.
29 A MULTIFACTORIAL DISEASE
Martin Robinson says optometrists can no longer take a simplistic view of dry eye disease (0.75 CPD).

MAKING DRY EYE WORTHWHILE
It’s a story all too familiar in our industry: a dry eye sufferer seeks help from their eyecare provider, only to be sent home with a lubricating eye drop and without a plan. The result: a disappointed patient whose underlying problem remains unresolved, and a lost business opportunity for the practice.
Over the past decade, high quality dry eye care has presented as a key differentiator for optometry practices wanting to build their business through clinical prowess.
With the rise of work-from-home arrangements –and a wealth of health information at consumers' fingertips – patients are increasingly demanding gold standard care. Thankfully, many Australian optometrists are stepping up by investing in dedicated dry eye clinics, but a major unmet need remains.
For those entertaining a more comprehensive dry eye offering, this issue features 34 pages of coverage to help your journey.
We speak to four independents about how dry eye care has transformed their working day, while reaping commercial benefits thanks to loyal patients who are elated to receive a solution to their suffering.


But to make dry eye work for your business, practitioners need to have the clinical backing. In our CPD content, Tasmanian optometrist Mr Martin Robinson provides real-life examples of how to go beyond symptom management to address the root cause. And UNSW’s A/Prof Maria Markoulli and Ms Zahra Tajbakhsh have authored an article about the Demodex diagnosis and management. Collectively, these articles are worth 1.25 CPD hours.
RANZCO RETURNS
A preview of key speakers and new product launches for this month’s congress in Brisbane.

66 REFRACTION REVOLUTION
Aussie optometrist experiences with a new phoropter, offering refractions in 0.01 D increments.
In many cases, an optometrist is only as good as their tools, so this issue also features Insight’s 2022 Dry Eye Directory where eyecare professionals can find Australia’s most comprehensive resource of treatments and diagnostics, as well a list of dedicated clinics.

Dry eye is a major challenge for the industry, but one brimming with opportunity. With an abundance of cutting-edge equipment, therapies, and highly qualified practitioners, the conditions are ideal to cater for this under-served patient cohort.
MYLES
19 53
EDITORIAL
HUME Editor FEATURES OCTOBER 2022 07 UPFRONT 09 NEWS THIS MONTH 73 OPTICAL DISPENSING 74 ORTHOPTICS AUSTRALIA 75 MANAGEMENT 76 PEOPLE ON THE MOVE 77 CLASSIFIEDS/CALENDAR 78 SOAPBOX EVERY ISSUE INSIGHT October 2022 5
Stunning Clarity, Unparalleled Durability

Our

Designed to protect your lens at every layer, taking everyday protection to the next level. ©2022 Essilor Australia Pty Ltd. September 2022. FR10214.
longest-lasting coating, proven and tested against the harshest of environments nikonlenswear.com/au/
UPFRONT
Just as Insight went to print, SPECSAVERS unveiled its Doug Perkins Medal and Dame Mary Perkins Award winners at its annual SCC event last month. This year’s Doug Perkins Medal winners were Ms Yvonne O’Sullivan, Mr Brian Thio and Ms Claire Curtin from Specsavers Dubbo, NSW, and Mr Lachlan Martin and Ms Hallie McCloy from Specsavers Hornby in Christchurch, recognising their consistently high standards of clinical excellence. Mr Surendran Naidoo from Specsavers Dapto and Ms Jennifer Robinson from Specsavers Dunedin were the Dame Mary Perkins Award recipients,
n WEIRD
Disulfiram, a drug to treat alcoholism, may have ophthalmic applications. It decreases the body’s ability to make retinoic acid, which is linked to vision loss. After administering the drug to nearly blind mice, University of California, Berkeley, researchers found they were more able to detect images on a computer screen compared to mice that weren't given disulfiram.
n WONDERFUL
The operator of Adelaide Metro train services, Keolis Downer Adelaide, has moved to improve accessibility and safety for travellers with low vision by wearing blindfolds to understand the navigational challenges of the visually impaired, while also working in the role as a sighted guide. It has been done in collaboration with Guide Dogs SA/ NT Human Guide Training.
n WACKY
A group of Swedish researchers has tested corneas made from pig skin collagen in 20 people who needed transplants; 14 whom were blind. After two years, they all showed improvement, and those who were blind could see again. The results of this pilot study were published in the Nature Biotechnology journal.


acknowledging an exceptional act of patient care. Both optometrists detected tumours, with Naidoo saving his patient’s life.
IN OTHER NEWS, Queensland Eye Institute vitreoretinal surgeon A/Prof Anthony Kwan performed Queensland’s first surgery for neovascular age-related macular degeneration (AMD) with an anti-VEGF port delivery system that is approved in the US and may have regulatory clearance in Australia soon. Kwan operated on the first patient in Queensland – and 14th in Australia – with the therapy that slowly releases ranibizumab within the eye (over 24 to 36 weeks). It is designed to address the treatment burden of regular anti-VEGF
STAT
LIFE-CHANGING WORK
intravitreal injections, commonly every four to 12 weeks, depending on the disease FINALLY, the Fred Hollows Foundation welcomed the World Health Organization’s confirmation that Vanuatu has eliminated trachoma as a public health problem, making it the first Pacific island nation to do so. “Vanuatu’s validation is encouraging news for several other Pacific nations which are working towards a final push to eliminate trachoma, an ancient disease that should not exist today,” Fred Hollows CEO Mr Ian Wishart said. The Australian NGO Cooperation Program helped fund the initiative. Australia has set a 2025 target to eliminate trachoma.
insightnews.com.au
Published by:
WHAT’S ON
THIS MONTH PROVISION CONFERENCE
21 – 23 OCTOBER
For the first time in its 30-plus-year history, ProVision’s national conference will be open to non-member optometrists and students. optom.provision.com.au/conference
Complete calendar page 77.
NEXT MONTH APVRS 2022
18 – 20 NOVEMBER
The Asia-Pacific Vitreo-retina Society Congress in Taipei attracts leading vitreoretinal specialists from around the world to share their knowledge and experience. 2022.apvrs.org
11-15 Buckhurst Street
South Melbourne VIC 3205
T: 03 9690 8766
www.primecreative.com.au
Chief Operating Officer
Christine Clancy
christine.clancy@primecreative.com.au
Group Managing Editor
Sarah Baker
sarah.baker@primecreative.com.au
Editor
Myles Hume myles.hume@primecreative.com.au
Journalist
Rhiannon Bowman rhiannon.bowman@primecreative.com.au
Commissioning Editor, Healthcare Education
Jeff Megahan
Business Development Manager
Luke Ronca luke.ronca@primecreative.com.au
Client Success Manager
Justine Nardone justine.nardone@primecreative.com.au
Design Production Manager
Michelle Weston michelle.weston@primecreative.com.au
Art Director
Blake Storey
Graphic Design Michelle Weston, Kerry Pert, Louis Romero Subscriptions
T: 03 9690 8766 subscriptions@primecreative.com.au
The Publisher reserves the right to alter or omit any article or advertisement submitted and requires indemnity from the advertisers and contributors against damages or liabilities that arise from material published.
© Copyright – No part of this publication be reproduced, stored in a retrieval system or transmitted in any means electronic, mechanical, photocopying, recording or otherwise without the permission of the publisher.

Since February 2020, 721 cataract surgeries have been performed in rural and remote Indigenous communities under the IRIS program banner. Page 70. INSIGHT October 2022 7
'FIERCELY DIFFERENT OPINIONS' ANTICIPATED
continued
accreditation authority. Once established, it will be easy for consumers to identify whether a practitioner is qualified to perform cosmetic surgery as the endorsement will be listed on the Ahpra public register.”
Australian Society of Ophthalmologists vice-president Dr Peter Sumich said it remained uncertain whether Ahpra and the Medical Board wanted to set the qualification standards itself, or defer to the medical colleges.

“First of all, we need to hammer down what constitutes a cosmetic surgeon, but Ahpra has left that ambiguous because of this endorsement process and who will administer it,” he said.
“I don’t think Ahpra is qualified to determine who is qualified, if that makes sense, especially when there are very few doctors amongst them, most of them are bureaucrats.”
In its submission during the consultation phase, RANZCO said the standards required for surgical procedures should be determined by the body or college whose curriculum most comprehensively covers the anatomy and management of the relevant body part, and by any other college that covers the techniques used most commonly in cosmetic procedures in that region.
“Hence for periocular cosmetic surgery, this would fall into the scope-of-practice of ophthalmologists, oculoplastic surgeons, and plastic surgeons, and for those outside those specialities, practitioners can seek accreditation for certain procedures from the two respective colleges, RANZCO and Royal Australasian College of Surgeons (RACS),” RANZCO stated.
Dr Charles Su is past president of the Australian and New Zealand Society of Ophthalmic Plastic Surgery who has been practising eyelid, lacrimal, and orbit surgery for more than 25 years in the public and private sectors.
He said whoever was performing surgery whether for aesthetic reasons or not, the public would expect someone with complete specialty training in the procedures done on that part of the body, and to have had a full and formal education in the anatomy of that site.
“As ophthalmologists our specialty college is the peak body which confers this for the region of the eye, eyelids, orbit, and lacrimal system. It is clear in the latest report that there is no such safeguard for cosmetic surgery. Any movement toward proper accreditation is good, but I am sure there is still a long way to go,” he said.
In a joint statement, RACS, the Australian Society of Plastic Surgeons (ASPS), Australasian Society of Aesthetic Plastic Surgeons (ASAPS), and the Australian Society of Otolaryngology Head and Neck Surgeons (ASOHNS) said any “grandfathering” of existing cosmetic surgeons would need to be carefully considered under the new endorsement framework as some unscrupulous operators may continue to operate.
“It would also take years to implement. What can be done quickly is to restrict the title of surgeon to those who are registered in a surgical specialty,” they said.
Dr Robert Sheen, president of ASAPS, said that many so-called ‘cosmetic surgeons’ used various training programs as proof of expertise, but some of these required almost no specific surgical training.
“WE WILL USE OUR LEGAL POWERS IN FULL TO BETTER PROTECT CONSUMERS WHO CHOOSE COSMETIC SURGERY. REGISTERED PRACTITIONERS IN THE INDUSTRY CAN EXPECT A RELENTLESS FOCUS”
MARTIN FLETCHER, AHPRA
AHPRA RESPONDS
In other recommendations, Ahpra will establish a targeted Cosmetic Surgery Enforcement Unit – with an immediate injection of $4.5 million.
It also will enforce a ban on testimonials in cosmetic surgery advertising as they are “likely to mislead, deceive and trivialise the risks”.
Medical Board chair Dr Anne Tonkin said it was clear that stronger action was needed now, but she warned setting the standard would be a hotly contested issue.
"There are fiercely different opinions about what qualifications guarantee safe care.
Patient safety will be our core focus as we consult with our stakeholders and develop the endorsement," she said.
"An area of practice endorsement will set standards and make cosmetic surgery training and qualifications clearer. It will empower consumer choice, by identifying who is trained and qualified, and who is not."
Ahpra CEO Mr Martin Fletcher said he was “appalled by the tragic stories of patients who were harmed by doctors taking advantage of them”.
“We want everyone who chooses to have cosmetic surgery to be better informed and protected. We want the doctors who undertake cosmetic surgery to be trained to a safe standard. We want the public to feel confident they are going to be well looked after and, if things go wrong, that they will be supported and that their concerns will be acted on,” he said.
“We will use our legal powers in full to better protect consumers who choose cosmetic surgery. Registered practitioners in the industry can expect a relentless focus.” n
OPTICAL DISPENSER AND MECHANIC INCOMES
$553,600, ophthalmologists $521,000 and otorhinolaryngologist $502,800.
average and females $62,745
Optical mechanics earned $60,666 on average (males $63,000 and females $57,000) and optical dispensers $42,900 (males $49,300 and females $41,200).
When men and women are grouped together, ophthalmology was one of only three medical specialties earning more than half a million dollars, with neurosurgeons topping the list with an average of
An analysis of the data also shows that there was a major gap between the total taxable income of ophthalmologists and their salaries, which is perhaps indicative of a tendency to run small-tomedium sized businesses and invest in other areas.
For example, the average ophthalmology salary was $161,200, which is $359,800 less than the average taxable income for the profession. n
AVERAGE TAXABLE INCOMES
NEWS
from page 3 continued from page 3
8 INSIGHT October 2022
Neurosurgeon – $553,500 Ophthalmologist – $521,000 Otorhinolaryngologist – $502,800 Plastic and reconstructive surgeons – $475,100 Cardiologist – $464,243 Urologist – $442,091 Orthopaedic specialist – $436,400 Anaesthetist – $388,800
IN BRIEF
n EYE TRAUMA IN SPORT
Soccer, AFL and basketball are the most dangerous sports related to emergency eye trauma, a study by The Royal Victorian Eye and Ear Hospital has revealed. The Australian-first study into sports-related eye injuries in people under 18 years of age found that more than 30% of the sample were paediatric patients, suggesting targeted interventions for higher risk sports at school may help to reduce injury and create safer sporting practices. Led by Professor Carmel Crock, Dr Rahul Chakrabarti and Ms Gizem Ashraf, the researchers analysed more than 1,700 Eye and Ear emergency presentations between 2015 and 2020.
n ALCON ACQUISITION
Alcon is set to acquire Aerie Pharmaceuticals, adding the commercial glaucoma products Rocklatan (netarsudil and latanoprost ophthalmic solution) and Rhopressa (netarsudil ophthalmic solution) to its portfolio, as well as AR15512, a Phase 3 product candidate for dry eye disease, and a pipeline of several clinical and preclinical ophthalmic pharmaceutical candidates. According to Alcon, the transaction complements its recent expansion into the ophthalmic pharmaceutical eye drop space, including acquisitions of the exclusive US commercialiation rights to Simbrinza from Novartis in April 2021 and of Eysuvis and Inveltys from Kala Pharmaceuticals in May 2022. The acquisition was valued at US$770 million (AU$1.1 billion).
n ONLINE VISION TEST
Online vision testing pioneer Visibly has received clearance from the US Food and Drug Administration (FDA) for its Visibly Digital Acuity Product (VDAP), making it the first FDA-cleared online visual acuity test on the US market. Visibly’s ondemand, self-administered visual acuity test, which can be completed in about six minutes, enables consumers to renew their spectacle or contact lens prescription online. Consumers can access the test, which is currently available in 40 US states, on the company's website using a combination of a touch screen mobile device and computer connected to the internet. Visibly said completed vision test results are made available to eyecare professionals immediately and securely, helping them evaluate the best course of action for each patient.
OPTHEA SECURES $AU245 MILLION TO BRING MACULAR THERAPY TO MARKET
Australian biopharmaceutical company Opthea has made a major leap towards bringing its macular disease therapy to market after securing AU$245 million in funding from a major global investment firm.
The ASX and Nasdaq-listed company, based in Melbourne, now expects to be fully funded through pivotal Phase 3 trials and pre-commercial activities thanks to the commitment from Carlyle and its life sciences franchise Abingworth, working with their recently formed development company Launch Therapeutics (Launch Tx).

Due to it being a non-dilutive financing transaction – meaning the investment does not include relinquishing ownership – Opthea will retain full worldwide commercial rights to its therapy, OPT-302.
OPT-302 is a VEGF-C/D ‘trap’ inhibitor that Opthea is combining with ranibizumab (Lucentis) or 2.0 mg aflibercept (Eylea) for neovascular age related macular degeneration (nAMD). The Phase 3 trials are then comparing the results to ranibizumab or aflibercept monotherapy.
Under the terms of the agreement, the funds managed by Carlyle and Abingworth will commit US$120 million (AU$173 m) in three instalments and retain an option to commit another US$50 million (AU$72 m).
If OPT-302 is approved in a major market, Carlyle and Abingworth will be eligible to receive fixed success payments and variable success payments of 7% on annual net sales, which terminate after reaching four times the funded amount.
It also comes as the company revealed US$90 million (AU$128 m) equity raising involving a two-tranche placement of new fully paid ordinary shares for institutional investors.
"Opthea is thrilled to enter this strategic arrangement with Launch Tx, and to receive funding from world-leading investors in Carlyle and Abingworth,” Opthea CEO Dr Megan Baldwin said.
“This strategic transaction is expected to fund us through Phase 3 topline
data expected in mid-2024 and strengthens our strategic position to maximise the value of OPT302 … and we are proud to have been selected as Launch Tx’s first partner since its formation.”
Mr Anshul Thakral, CEO of Launch Tx, was excited to partner with Opthea on OPT-302, which he said was a novel drug candidate that has demonstrated superior visual acuity in Phase 2 trials over standard of care anti-VEGF-A therapy in patients with nAMD.
“With this collaboration, we will advance OPT-302 through its ongoing Phase 3 trials and hope to reach regulatory approval in a timely manner, with the intention of bringing this important medicine to patients in need,” he said.
“At Launch Tx, we are committed to working with pharma and biotech partners to expedite late-stage drug development programs. We do this by designing innovative funding models tailored to our partners’ specific needs and leveraging our extensive clinical development, regulatory, and commercialization expertise as needed. This partnership with Opthea is a great example of one such model.”
Intravitreally administered OPT-302 is the subject of two concurrent Phase 3 trials that will each enroll around 990 treatment naïve patients, in combination with the two previously-mentioned, approved anti-VEGF-A treatments.
According to Opthea, OPT-302 has the potential to be positioned as complementary and agnostic with any combined anti–VEGF-A therapy for nAMD, a strategy intended to maximise the commercial opportunity for the therapy.
“In a treatment landscape increasingly crowded with biosimilars and longacting VEGF-A inhibitors, it is exciting to contribute to the advancement of OPT302, the only investigational agent in late stage development with the potential to improve vision outcomes over standard of care for patients with wet AMD,” global retinal disease expert and chief investigator for the Phase 3 COAST study, Dr Charles Wykoff, added. n
NEWS
Dr Megan Baldwin.
INSIGHT October 2022 9
GEORGE & MATILDA EYECARE ATTRACTS TWO WELL-ESTABLISHED INDEPENDENTS IN NSW
Independent optometrists Mr Peter Baker and Mr Dale Rolfe are the latest to bring their practices into the George & Matilda (G&M) Eyecare fold in recent months.
Baker established Peter Baker Optical in Caringbah, New South Wales, in 1987. Rolfe established his first practice in 1989 and continued to grow over the subsequent 30-plus years, and is now principal owner of Rolfe Optometry Group, comprising nine practices located in mid northern NSW.


Rolfe said he had been approached by a number of corporates, but G&M seemed the right choice for him.
“I feel like there is a window of opportunity to get the best value for your business now with competitive tendering increasing sale prices for quality practices, but I don’t believe this will last forever,” Rolfe said.
“I was pleasantly surprised at just how valuable my practice was and this allowed me to make the decision to sell earlier than I had envisaged,” he said.
Better still was the fact G&M is Australian owned and run, Rolfe said.
“I like the idea that G&M are a community of independents and who have all the scale and benefits a corporate would but with an independent heart,” he said.
“G&M ensure that all my practice staff retain their positions, and all the optometrists are given full independence in their clinical decision making. There is no reduction in appointment times and optometrists can continue to follow their passion around their specialties.”
Baker said Peter Baker Optical optometrist Mr Nigel Whittle, along with two support staff, will also be joining G&M.
“Our long-established independent business, Peter Baker Optical, is known for exemplary customer service, outstanding care and product expertise for over 35 years. I was looking to partner with a likeminded and client focused company,” Baker said.
“The opportunity to partner with George & Matilda Eyecare to use their back office and administration systems, together with leveraging their resources, will allow us to provide even greater care and attention to our loyal clientele.”
Baker said the ability to retain the business’ team and maintain high professional service levels was also fundamental in their decision to choose
“The flexibility of G&M’s business model during partner negotiations was extremely important and we got the outcome we were looking for. We certainly are looking forward to the next 35 years,” Baker said.
Whittle said the G&M model presented
“After many years of a career in optometry, I realised I needed an exit strategy – one that works for both myself and is in the best interests of my patients,” he said.
“Having established and grown this practice over 20 years ago, we’re now seeing third and fourth generations of the same family; their future eyecare needs are important to me. At some time, I will move on, so a transition phase was identified; the George & Matilda model ticked most of the right boxes.” n
THE SOUTHERN HEMISPHERE’S BIGGEST OPTICAL EVENT
Biennial event O=MEGA23 is hoping to showcase Australian optometry on the world stage through its partnership with the World Council of Optometry, as registration opened a year out from the event’s launch.
O=MEGA23, in partnership with the 4th World Congress of Optometry (WCO4), will be held in Melbourne from 8-10 September 2023, following a partnership between the Optical Distribution & Manufacturers Association of Australia (ODMA), Optometry Victoria South Australia (OV/SA) and the World Council of Optometry (WCO).
The joint event is expected to attract more than 2,000 global professionals, including optometrists, optical dispensers, ophthalmologists, orthoptists, ophthalmic nurses, practice staff, optical retailers and service providers, technicians and students over three days.
It’s being hailed as the largest optometric clinical conference and trade show in the Southern Hemisphere.
Mr James Wolffsohn, head of both the School of Optometry and Department of Audiology at the UK's Aston University, has been announced as O=MEGA23/ WCO4 keynote speaker.

Having been a Clinical Research Fellow at the University of Melbourne, he has published more than 290 full peer-reviewed papers and presented at numerous international conferences. He is academic chair of the British Contact Lens Association and the International Myopia Institute’s chief scientific officer.
Professor Peter Hendicott, WCO president, said the opening of registrations was an important date for people outside Australia.
“O=MEGA23/WCO4 is an opportunity for optometrists internationally to participate in what will be a high quality
learning and professional development experience, and importantly, allows optometry to highlight its role in the international agenda of securing improved vision and eye health outcomes across the world,” he said.
ODMA acting CEO Ms Amanda Trotman said the trade fair and clinical conference will appeal to an international audience.
“This will be the largest eyewear and eyecare trade fair in Australia, featuring the latest technology, fashion, lenses, frames, equipment, instruments, and accessories.

“The event will also feature an accredited program, with exceptional learning opportunities from clinical speakers from around the world in a multi-stream format including keynote lectures, poster sessions and breakout sessions, along with a networking program," she said.
Early registration discounts will be offered until 30 April 2023. n
10 INSIGHT October 2022 NEWS
James Wolffsohn.
Peter Baker.
Nigel Whittle.

1800 637 654 @eyesrightoptical
TGA APPROVES DRUG TO TREAT TWO PRIMARY CAUSES OF VISION LOSS
Roche Australia has announced the Australian Therapeutic Goods Administration (TGA) registration of Vabysmo (faricimab) for the treatment of neovascular agerelated macular degeneration (nAMD) and diabetic macular oedema (DMO).
Both eye conditions are leading causes of vision loss worldwide and present a growing health issue as populations age and experience increased prevalence of diabetes.
It is estimated that approximately 128,000-192,000 Australians are living with nAMD, and an estimated 40,000 Australians are impacted by DMO, according to Roche.
Vabysmo is the first TGA-registered bispecific antibody approved for the eye in Australia. It specifically recognises and blocks the activity of proteins known as angiopoietin-2 and vascular endothelial growth factor A.
Roche said Vabysmo is administered by four initial four-weekly eye injections.


“Thereafter, the frequency of the ongoing injections will be determined by the treating physician and may be up to 16 weeks apart based on the patient’s anatomic and vision outcomes,” the biotech company said.
Professor Paul Mitchell, director of the Centre for Vision Research at the Westmead Institute for Medical Research, said both nAMD and DMO can have physical, emotional and economic consequences for patients and their families.
“As the conditions progress, people living with nAMD or DMO may become increasingly dependent on their loved ones for everyday activities as well as have their professional and social lives negatively affected,” he said.
Mr Richard Woodfield, country medical director at Roche Australia, said the company is delighted the TGA has
Vabysmo injections may be 16 weeks apart in some cases.
registered Vabysmo for people living with either nAMD or DMO in Australia.
“This registration marks a significant step in our commitment to people living with retinal conditions and we will continue to work collaboratively with the government through the required next steps to ensure eligible Australians are able to access this additional treatment option as soon as possible,” Woodfield said.
Roche’s pharmaceutical division in Australia employs over 300 people. Australian patients have access to around 35 Roche medicines.
Building on its heritage of developing new medicines in oncology, immunology, infectious diseases, and neurology, Roche is now taking on the leading causes of blindness and visual impairment, addressing the critical needs of people living with debilitating eye diseases. The company said its investment in ophthalmology is centred on designing solutions tailored to the biology of the disease. n
POSITIVE RESULTS FOR INVESTIGATIVE GA THERAPY
The Australian macular disease community has welcomed the latest clinical trial results for Apellis Pharmaceuticals’ intravitreal pegcetacoplan, fuelling hope that first potential treatment for geographic atrophy (GA) is on the horizon.
On 24 August, Apellis announced top-line data at 24 months showing increased effects over time with its investigational therapy, targeted C3 therapy, in the Phase 3 DERBY and OAKS studies in GA secondary to agerelated macular degeneration (AMD).
In a pre-specified analysis of GA lesion growth over 24 months, the company reported that both monthly and every-other-month (EOM) pegcetacoplan showed a clinically meaningful reduction in GA lesion growth from baseline compared to sham. Between months 18-24, the pegcetacoplan treatment effect accelerated compared to previous sixmonth periods, with robust reductions
of GA lesion growth versus sham.
The increased effects were driven by a greater slowing of lesion growth by pegcetacoplan and not by an increase in the lesion growth rate in the sham group, which was highly consistent over each of the four six-month intervals (1.0+/-0.05 mm2).
“These trial results give patients hope that the first potential treatment for GA is on the horizon,” said Professor Robyn Guymer, who is a study investigator of the DERBY and OAKS trials, and deputy director of the Centre for Eye Research Australia.

Dr Kathy Chapman, CEO of Macular Disease Foundation Australia, said the loss of central vision through GA results in a significant burden for affected people, families and society, including increased mental health issues, the loss of productivity and job reduction.
"The patient community welcomes these results and any future advances which may help to make a meaningful
difference for patients.”
Studies show that GA lesion growth is correlated with loss of visual function over longer periods of time. The visual function outcomes at 24 months are believed to be due to the limitations of the endpoints when used for GA and the relatively early assessment timeframe. Patients will be treated with pegcetacoplan in the GALE extension study for an additional three years. "These data further reinforce the breakthrough potential of pegcetacoplan, with both monthly and every- other-month treatment demonstrating increased effects across a broad patient population over 24 months,” said Mr Jeffrey Eisele chief development officer at Apellis.
“With a US PDUFA date in November and an EU submission planned later this year, we are committed to bringing pegcetacoplan to patients as quickly as possible." n
NEWS
Prof Robyn Guymer, CERA.
12 INSIGHT October 2022
4. Chamberlain P et al. Myopia Progression in Children wearing Dual-Focus Contact Lenses: 6-year findings. Optom Vis Sci 2020;97(E-abstract):200038. 5. Chamberlain P et al. Myopia progression on cessation of Dual-Focus contact lens wear: MiSight 1 day 7 year findings. Optom Vis Sci 2021;98:E-abstract 210049. 6. Hammond D et al. Myopia Control Treatment Gains are Retained after Termination of Dual-focus Contact Lens Wear with no Evidence of a Rebound Effect. Optom Vis Sci 2021;98:E-abstract 215130. For instructions for use refer to https://coopervision.net.au/patient-instruction. MiSight®, Brilliant Futures™ and CooperVision® are registered



of the Cooper Companies, Inc. and its subsidiaries. EMVCOO0841 ©2022 CooperVision.



children prefer MiSight® 1 day to glasses1,2*† 9/10 Proven by 7 years of clinical data to significantly slow myopic progression with no rebound effect Supported by the Brilliant Futures™ myopia management program Further information at childmyopia.com and coopervision.net.au / coopervision.co.nz *95-100% of children expressed a preference for contact lenses over glasses at each visit over 36 months. †’How much do you like wearing your contact lenses?’ 87/97 (90%) Top box ‘I like contact lenses the best’ Subjective response at 60 months. ‡Compared to a single-vision, 1-day lens over a three-year period; rate of progression maintained out to 6 years. On average, there was no indication that accumulated treatment effect gained following 3 or 6 years of MiSight® 1 day wear was lost during a 12-month cessation study in children aged 8-15 at initiation of treatment. Instead, eye growth reverted to expected, age average myopic progression rates. References: 1. Sulley A et al. Wearer experience and subjective responses with dual focus compared to spherical, single vision soft contact lenses in children during a 3-year clinical trial. AAO 2019 Poster Presentation. 2. CooperVision® data on file, 2019. 3. Chamberlain P et al. A 3-year randomized clinical trial of MiSight® lenses for myopia control. Optom Vis Sci 2019;96:556–567.
trademarks
UP TO -10.00D
VISION EYE INSTITUTE LAUNCHES LASER SURGERY SERVICES IN SOUTH AUSTRALIA
Vision Eye Institute (VEI) is expanding its existing laser service to South Australia, offering refractive surgery options, including LASIK, ASLA/PRK and refractive lens exchange through its partnership with Eye Surgeons SA.

VEI North Adelaide is led by experienced ophthalmic surgeon, Dr Paul Athanasiov, who will perform refractive procedures at the clinic. Athanasiov became VEI’s partner doctor for SA in November 2021, with his two Eye Surgeons SA clinics in North Adelaide and Windsor Gardens now coming under the VEI banner.
He continues to consult at those clinics, as well as VEI’s Kurralta Park facility.
Ophthalmic surgeon Dr Simone Beheregaray will also provide vision correction services at the North Adelaide clinic. She is an experienced ophthalmologist with fellowships in corneal conditions, glaucoma, cataract and refractive surgery and consults at VEI’s Windsor Gardens and North Adelaide clinics.
Mr Greg Brown, VEI’s general manager
said as the largest private provider of ophthalmology in Australia, VEI was well positioned to expand its depth and breadth of service offering.
“Through our recent partnership with Dr Paul Athanasiov and the Eye Surgery SA team, the pathway to launching our refractive surgery services in SA has been seamless,” he said.
“We look forward to welcoming a new cohort of patients though our doors in South Australia as we continue to put our patients, and their eyecare at the forefront
of everything we do.”
Patients seeking laser eye surgery at VEI can access various payment options through its partnership with financial services provider, Latitude. These include interest-free buy now, pay later payment plans covering consultations and surgical procedures up to $10,000, with six to 24-month repayment schedules.
Patients can also book a free, noobligation suitability assessment with one of VEI North Adelaide’s experienced clinical optometrists.
Vision Eye Institute said it had a 30-year history of providing high-quality refractive services to Australians. Its surgeons were among the first to perform laser eye surgery in the country, and two of the original laser groups in Australia later became VEI clinics.


A VEI clinic also recently performed the first SMILE Pro surgery in Australia and New Zealand.
In total, VEI has 20 clinics and 10 day surgeries in New South Wales, Queensland, South Australia and Victoria. n
NOVA EYE LAUNCHES NEW CANALOPLASTY STUDY
Nova Eye Medical has enrolled the first patient in its multicentre study to assess the effectiveness, safety and quality of life outcomes of the canaloplasty procedure using its new iTrack Advance device.
To be conducted across five sites in Germany, the prospective, randomised study, known as CATALYST, will enrol up to 80 patients with mild to moderate, uncontrolled open-angle glaucoma on one to four medications.
Patients will be randomised to treatment with canaloplasty performed in combination with cataract surgery compared to cataract surgery-only.
Key assessment outcomes will include reduction in mean intraocular pressure (IOP) and mean number of glaucoma medications, surgical and postoperative complications, endothelial cell count, and quality of life utilising a patient reported outcome measure.
Professor Norbert Koerber, from Augencentrum Köln-Porz, Köln, Germany, is primary investigator for the CATALYST Study.
An internationally renowned glaucoma surgeon and one of the pioneers of the canaloplasty procedure, Koerber has been performing canaloplasty for nearly two decades.
“I have been a proponent of traditional canaloplasty for many years and continue to offer it to my severe glaucoma patients to push back the need for trabeculotomy or tube shunt surgery. More recently I have adopted canaloplasty via an ab-interno surgical technique in patients with mildmoderate glaucoma,” he said.
“Many of these patients experience unwanted side effects from glaucoma medications or fail to administer their medications as prescribed. For these patients, modern-day canaloplasty, performed via an ab-interno surgical
technique, offers an early surgical intervention that acts in a similar way to angioplasty to flush out the eye’s drainage channel and lower IOP, eliminating or reducing the need for medications.”
Koerber said the major advantage of this new device is that it allows canaloplasty to be a truly single-handed surgical procedure.
“The handpiece features a customdesigned cannula which enables the surgeon to create an opening in the meshwork, before using the injector on the handpiece to guide the microcatheter easily into the canal – all using only one hand," he said.
“We believe this progress in the device design is a crucial step in encouraging more cataract surgeons to perform abinterno canaloplasty in combination with cataract surgery. The combined cataract surgery-canaloplasty procedure offers several benefits to patients." n
NEWS
Dr Simon Ondrejka (right) performs canaloplasty with the iTrack Advance.
"WE LOOK FORWARD TO WELCOMING A NEW COHORT OF PATIENTS THOUGH OUR DOORS IN SOUTH AUSTRALIA"
GREG BROWN, VISION EYE INSTITUTE
Refractice surgery is now available at VEI's North Adelaide clinic.
14 INSIGHT October 2022
GREENFIELD PRACTICE IN BONDI JUNCTION SHORTLISTED IN INTERIOR DESIGN AWARDS
Tracton
Optometrists, an independent practice in the heart of Bondi Junction, which opened last year, has been shortlisted in the Interior Design Excellence Awards (IDEA), Australia's largest independent design awards.
Launched in 2003, the program celebrates the best of Australian interior and product design across 15 categories. Tracton Optometrists is shortlisted in the retail category and is the only optometry practice to be nominated.
Optometrist Mr Daniel Tracton established the business with his wife and operations manager, Ms Michelle Tracton, during the height of COVID-19.
With the street-facing retail space only 50-square metres, they engaged designer Mr Conrad Perry from Perry Design who was able to visualise a bespoke, high-end but functional interior design.
The practice features an extra high glazed shopfront entry flooded with natural light, has product displayed at the front, and two treatment rooms in the rear.
Tracton said it was Perry’s first time designing an optometry practice, and Perry nominated the practice in the IDEA. Award winners will be announced at the IDEA Gala Party in November.
“This is great news for us as we are about to celebrate our one-year anniversary after opening during a tumultuous lockdown time,” Tracton said.
They originally planned to open in early July 2021, but Bondi went into lockdown at the end of June, which resulted in a threemonth delay in opening.
“We opened three weeks before lockdown ended and could only provide critical care. It was a difficult balancing act,” he said.
They also faced further disruption this year when the street was closed off to build a cycle pathway.
“We had no foot traffic for four months during the street’s reconstruction,” he said.
Michelle is currently completing the last module in Certificate IV in optical dispensing at ACOD. n
LIONS EYE INSTITUTE OPENS PERMANENT CLINIC IN PERTH’S EAST
A state-of-the-art Lions Eye Institute clinic has opened in Midland, ensuring people in Perth’s eastern corridor have access to high quality eye health services.
While the Lions Eye Institute (LEI) has operated a clinic in Midland since 2016, under the leadership of Dr Hessom Razavi, it now has a permanent address in the Midland Specialist Centre, located across from the historic Midland Railway Workshops precinct.
“We have been working in the area for more than six years, but this new purposebuilt facility will provide us with the opportunity to expand our service offering and work even more closely with the local community in ensuring they have access to the best possible eyecare,” Razavi said. Razavi will be joined at Lions Eye Institute Midland by fellow LEI doctors Dr Antony Clark, Dr Geoffrey Chan and Dr Jean-Louis de Sousa. All four clinicians are internationally recognised specialists who share the common goal of improving people’s lives.
Together they cover a broad range of eye diseases and disorders, including cataract, pterygium, paediatric ophthalmology, glaucoma, strabismus, oculoplastics, age-related macular degeneration and diabetic eye disease.
In addition to treating patients, all Midland clinicians are involved in teaching,
Lions Eye Institute Midland houses a wide spectrum of ocular sub-specialties.

research and community outreach work.
LEI CEO, Dr Glen Power, said the wide spectrum of ocular sub-specialties, located together in one clinic, had previously only been available in Perth’s western suburbs or CBD.

“We are pleased to be able to offer people to the east of Perth and into the Wheatbelt, access to the highest quality eyecare in a location that is highly accessible,” he said.

The new clinic will also provide a base for student placements from the newly established Doctor of Optometry program at the University of Western Australia (UWA). LEI said it is proud to partner with UWA in developing this course, which was launched in 2021 as Western Australia’s first optometry degree. n
NEW LE SPECS BIO ACETATE EYEWEAR
Sydney-based Sunshades Eyewear is launching new sustainably-focused optical and prescription sunglass collections from Le Specs, adding to the brand’s reptuation as exceptionallydesigned eyewear for Australian lifestyles.

As a market leader in sustainability, the new Le Specs collections are described as “luxuriously crafted” from sustainable bio acetate combining the beauty and qualities of acetate with a plant-based and biodegradable composition.
“The Le Specs bio acetate collection features as part of the new Hollywoodinspired campaign photographed by renowned photographer Georges Antoni in Malabar, Sydney,” Sunshades stated. “Highlight campaign styles
include women's cat-eye silhouette ‘BioLogist’ with gently sweeping curves and unisex frame 'Bio-Nics' designed with European sophistication and Australian refinement. Both styles focus on all-day comfort, and offer a flattering look for all ages and face shapes.”
All Le Specs optical and RX styles are backed with a one-year warranty.
To celebrate the new Le Specs sustainable collections and advertising campaign, Sunshades is offering a suite of marketing material, window displays and promotional items available with all orders.
Contact a local Sunshades Eyewear representative, or email customerservice@sunshadeseyewear. com.au n
NEWS
Sunshades Eyewear is offering a suite of marketing material for the campaign.
Daniel Tracton.
16 INSIGHT October 2022
'RADICAL' NEW APPROACH TO OPTICAL EXTRAS COVER

A radical new ‘extras cover’ health insurance policy launched in August is set to benefit Australian optical patients and optometrists, its founders say.


Mr John Connor and Mr Reece Frazier, former actuaries of the insurance industry, have founded ExtrasJar, based on a new health insurance business model designed to benefit patients and health providers.

Currently 12.5 million Australians pay $12 billion towards ‘extras cover’ and only get $5.6 billion back, according to the pair.
“When you buy health insurance extras, that's exactly what's happening. You're paying extra,” Connor, a senior insurance manager with more than 20 years’ experience, said.
With ExtrasJar, any unused extras money is rolled over to the following year, and it accumulates each year until a policy holder needs to spend it on treatments such as dental, physio or optical.
“It’s the customer’s money to spend on the treatments they want – not what
the health insurance company says they can spend it on. Think of it like a forced savings plan where a nominated amount gets transferred into an account for them to spend on their health when they need it. It’s their money – not the insurance company,” Connor and Frazier said.
The business model, which the pair believe to be a world-first, rewards people who are healthy with a nest egg they can draw upon when they need it.
“If customers have enough money accumulated in their kitty – they can pay for the treatments in full. And it’s easy to pay their dentist, physio or optometrist with the ExtrasJar digital Mastercard,” they said.
ExtrasJar, which has been granted its own Australia Financial Services Licence, launched in August. To help grow the business so more Australians can benefit from the radical approach to health insurance, co-founders Connor and Frazier are offering potential investors the opportunity to buy shares in the company
via a Birchal equity crowdfunding raise.

“On average, Australians are losing more than half of their health insurance extras. That's approximately $514 each per year and more than $10,280 over 20 years. If policyholders choose to leave ExtrasJar, they get all the money they have accumulated in their extras cover nest egg back – no questions asked,” Connor said.
ExtrasJar is also changing the way customers pay for private hospital cover. It does this via a self-deposit feature.
“ExtrasJar hospital cover is just like paying a rental bond to a landlord before you move in,” Frazier said.
“If you damage the house, the repairs will come out of the bond money. It’s the same thing with ExtrasJar, except we call the ‘rental bond’ a self-insurance deposit, which brings down your private hospital cover premium. If you don’t go to hospital that year, you pay less. Any unused deposit is rolled over and used to lower future premiums if there are no claims." n
ExtrasJar co-founders Reece Frazier (left) and John Connor.
DOING WHAT YOU LOVE
At OPSM we invest in our people. Our Optometrists work with state-of-the-art technology, including Optos Daytona, Corneal Topographer, Visual Field, and OCT. As an optometrist, your success is enhanced by a number of great initiatives including financially supported clinical training, mentorship, peer learning communities, leadership programs and commercial development.
At OPSM, your career is limited only by the size of your dreams. We work with you to personalise a role based on your aspirations and support you in making the most of your career. We have amazing opportunities for Optometrists to join our team at OPSM across Australia and New Zealand.

LEARN MORE OPSM.COM.AU/CAREERS VISIT US ON LINKEDIN INTERESTED IN PAVING YOUR OWN PATH? PLEASE CONTACT OPTOMETRY.CAREERS@AU.LUXOTTICA.COM WORKING AT OPSM MEANS YOU’RE PART OF SOMETHING BIGGER. SEE YOURSELF
HOW DRY EYE CAN ELEVATE YOUR PRACTICE
As the prevalence of dry eye continues to rise and new clinical research emerges, more optometrists are taking a special interest in the disease, building distinction into their businesses. Four independent optometrists lend their top tips on setting up a dry eye clinic within their existing practice.
A HAPPY PATIENT IS A LOYAL PATIENT
MS LIZ BARRETT, director of Dry Eye Solution in Erina, NSW, says it is among the first independent dry eye clinics in Australia and New Zealand. The clinic’s sole focus is all aspects of dry eye disease management. Barrett and her team aim to use the best protocols available and treat the root cause of the disease.
Insight (IST): What prompted you to begin offering dry eye diagnosis and treatment?
Liz Barrett (LB): I have worked in the optical industry for over 20 years and saw a huge gap in the treatment available for dry eye patients, yet numbers were increasing. The idea of an independent dry eye clinic brewed for over four years. I read the Osaka study and loved the correlation between dry eye disease and happiness, so every step of building the business had the aim of making the world a happier place. As the business was a new concept, setting up offered many challenges which I enjoyed; designing a new patient management system around the dry eye patient journey, automating all aspects of the business and creating something which can grow easily to more locations.

IST: What were your main considerations when deciding what dry eye diagnostic/treatment technology and equipment to invest in?
LB: For me, Lumenis was the only option. I wanted to provide the best care and protocols to patients and Lumenis makes that possible, combined with direct input from Dr Rolando Toyos (USA), a world leader in the field. The IPL device has the results of his research and knowledge inbuilt and nothing can compare to that. Having the most proven and only TGA and FDA approved IPLs available on the market is important to us.


IST: What methods have you used to advertise or promote your dry eye services?
LB: We had articles published in local media which were beneficial to bringing public awareness, as well as online campaigns. Word-of-mouth has been exceptional. When you successfully treat someone’s lifetime
problem, they shout it from the rooftops. We developed relationships with local GPs, ophthalmologists and optometrists. Being an independent clinic, we are not a threat to eye health professionals, and can assist in providing the best proven care for their dry eye (and rosacea) patients. Educating the public on dry eye disease is important and has been the most effective way to grow the business. It’s becoming more patient-driven and patients want the best treatment available.
IST: How do you stay informed about new dry eye products on the market?
LB: We attend conferences and listen to lots of dry eye podcasts. Dr Toyos is a wealth of information in the latest research, publications, and products. The information in the Lumenis practitioner’s portal is excellent and meeting with reps is always good. We started our own educational Dry Eye Solution YouTube channel to give eye health professionals an opportunity to learn about how to treat dry eye as an inflammatory disease, and to treat the root cause.
IST: What impact has dry eye services had on your business from both a clinical and business perspective?
LB: As we are a dedicated dry eye clinic, the impact that I see is patients’ results. When someone cries with relief and kisses your IPL machine, it makes your heart sing. I feel that you have to be focused on patient results and when you do, your business impacts so many people’s lives. The business is growing because the public is becoming aware of dry eye disease, they want help and we are here to help them.
INSIGHT October 2022 19 DRY EYE - BUSINESS
Liz Barrett with Dr Rolando Toyos at the Dry Eye Summit in Sydney 2022.
OPTOMETRIST AND DRY EYE SUFFERER NOW HELPING OTHERS
MR JASON TEH established In2Eyes Optometry in Surrey Hills, Melbourne in 2002. Aside from full scope eyecare, optometrists Teh and Dr Winter Chan provide contact lens care, including speciality lenses. In2Eyes is also part of the Dry Eye Group, providing comprehensive dry eye assessments and treatments including IPL and Lipiflow.
Insight (IST): What prompted you to begin offering dry eye diagnosis and treatment?
Jason Teh (JT): I am a dry eye sufferer and have been since I was a teenager, so I followed the dry eye landscape closely over the last 12 years looking for options to improve myself and, in turn, others. As soon as diagnostics and treatments were available, I started investing in ways to screen, diagnose and manage the condition.
IST: What were your main considerations when deciding what dry eye diagnostic/treatment technology and equipment to invest in?
JT: I am always looking for the gold standard in eyecare which often involves investing in the best equipment, so as soon as it has become available to the Australian market, I have invested. Sometimes I had no choice as we weren’t spoilt for choice back then.
Other considerations today are treatment times, ability to move technology/ equipment from one location to another, and peer reviews for effectiveness of devices or treatment protocols from colleagues overseas.
IST: What methods have you used to advertise or promote your dry eye services?
JT: Our main methods are clients' word-of-mouth, referrals from other optometrists, ophthalmologists and sometimes GPs and pharmacists. The best way to promote your practice would be to engage the healthcare providers and invite them to view what you have to offer. Another way I have successfully promoted dry eye services is through Google marketing.
IST: How do you stay informed about new products on the market?
JT: Pubmed online search, connect with dry eye key opinion leaders overseas, and connect with dry eye researchers. Every product that comes to Australia will already be available overseas, especially in the US.
IST: What impact has dry eye services had on your business from both a clinical and business perspective?
JT: It’s a point-of-difference from competitors and upskilling always brings more joy and fun to the workday.
Clinically, we are very proud of being able to serve the dry eye community, as it’s a space that is under-represented and there are thousands of sufferers that don’t get the right management. Dry eye patients are super loyal. Being a chronic condition, they will need help for many years to come.
Business wise, it significantly increases the power of word-of-mouth. It’s still the most effective mode of advertising.
It is a big revenue booster for us because it affects all patients at all stages of life. Whether it’s a young patient with contact lenses or an older person on general medications, diabetic or glaucoma patients. It’s easy to start engaging in managing dry eyes as these patients are already coming through the door.
‘WE HAVE INCREASED TURNOVER FOR OUR CLINICAL SERVICES’

JUSTIN GRIBBIN and wife Alayna established Eye Envy Optometrist in Morayfield, Queensland, in 2010. With more than 27 years’ experience, Gribbin’s special interests include treatment and management of dry eye, contact lens fitting, glaucoma and macular degeneration detection, and children’s vision.

Insight (IST): What prompted you to begin offering dry eye diagnosis and treatment?
Justin Gribbin (JG): For me, it was the lack of support for people with dry eye and the fact that so many people are sent out the door with a sample lubricant with not much further thought. Lockdowns also increased the frequency of symptomatic patients.
IST: What were your main considerations when deciding what dry eye diagnostic/treatment technology and equipment to invest in?
JG: I wanted to see proven results. I have spoken to IPL suppliers over the years but have always been happy with the findings and feedback from Lumenis users. I wanted imaging technology for meibography but also wanted this combined with a great topographer for orthokeratology and rigid gas permeable (RGP) fittings.

IST: What methods have you used to advertise or promote your dry eye services?
JG: Social media and local paper advertising as well as in-store banners. I have also contacted local optometrists that do not offer these services but so far referrals from colleagues have been quiet.
IST: How do you stay informed about new dry eye products on the market?

JG: I always look for dry eye conferences and continuing education topics. There are some fantastic Facebook groups for like-minded optometrists as well. I also tend to follow those practitioners at the forefront of dry eye disease treatments on their social media channels.
IST: What impact has dry eye services had on your business from both a clinical and business perspective?
JG: In the last 12 months we have seen a growth in inquiry about dry eye treatments but also increased current patient referrals and word-ofmouth recommendations. These clinics do take extra time to run, however from a business perspective we have increased turnover for our clinical services. As an optometrist, the satisfaction in delivering relief to such a miserable disease is priceless.
20 INSIGHT October 2022 DRY EYE - BUSINESS
KEEP INVESTING IN NEW TECHNOLOGY
Operating since 1989, Heron Eyecare says it is the most clinically progressive and technologically advanced eye health care practice in Toowoomba. Founder Dr Henry Heron practices part-time alongside optometrist and director HUGH BRADSHAW and optometrist Adam Barron.

Insight (IST): What prompted you to begin offering dry eye diagnosis and treatment?

Hugh Bradshaw (HB): Dry eye has been an important part of our practice long before it started ‘booming’ in the last five to 10 years. We live in Toowoomba, which is known as the ‘Garden City’, where allergy and less humidity than coastal areas create the perfect or imperfect climate for dry eye. My former business partner and mentor was an early adopter of therapeutic eyecare and technology. We have therefore evolved as technology developed and have always been one of the first practices in Australia to invest in dry eye management devices.
IST: What were your main considerations when deciding what dry eye diagnostic/treatment technology and equipment to invest in?


HB: When investing in new technology there must be some research evidence supporting the technology. We were one of the first optometry practices in Australia to use an E-Eye IPL after the research evidence supported its efficacy. We did the same for Rexon-Eye. The equipment must also be
economically viable to at least cover the investment costs. We found that IPL and Rexon-Eye met both these requirements, but Lipiflow was too difficult to justify economically.
IST: What methods have you used to advertise or promote your dry eye services?
HB: We currently directly advertise dry eye services in our local newspaper, and through digital media. We have also hosted education events for local GPs, optometrists and pharmacists about dry eye technology and treatments.
IST: What impact has dry eye services had on your business from both a clinical and business perspective?
HB: Dry eye services differentiate us from many of our colleagues as a leader in this field. We have a great relationship with our local optometrists and ophthalmologists and receive referrals from them. We also use scleral contact lenses as a severe dry eye treatment which crosses over with our custom designed contact lens business. These niche areas are only provided by a small percentage of optometrists which reduces competition and protects our business from the highly competitive retail area of optics.
Hugh Bradshaw (from left), former owners Henry and Miriam Heron, and Adam Barron.
BEFORE PRESCRIBING, PLEASE REVIEW APPROVED PRODUCT INFORMATION AVAILABLE ON REQUEST FROM ALLERGAN BY PHONING 1800 252 224 OR FROM www.allergan.com.au/products Allergan Australia Pty Ltd. Level 20, 177 Pacific Highway, North Sydney NSW 2060. ABN 85 000 612 831. ©2022 Allergan. All rights reserved. AU-PRED-220008 V1. Date of preparation: February 2022. ALL2190. PBS Information: PREDNEFRIN FORTE® is listed on the PBS for severe eye inflammation, corneal grafts and uveitis. Reference: 1. Prednefrin Forte Product Information. TAKE ANOTHER LOOK AT PREDNEFRIN FORTE Available now across Australia Indicated for non-infectious ocular inflammation1 and back in stock
At the completion of this CPD activity, optometrists will understand the clinical aspects Demodex infestation.
Including:
• Understand the associated factors behind Demodex infestation
• Identify the clinical signs of Demodex infestation
• Review the clinical management strategies for Demodex
• Review the efficacy of hygiene products and delivery mechanisms currently available against Demodex infestation
DEMODEX INFESTATION: DIAGNOSIS AND MANAGEMENT
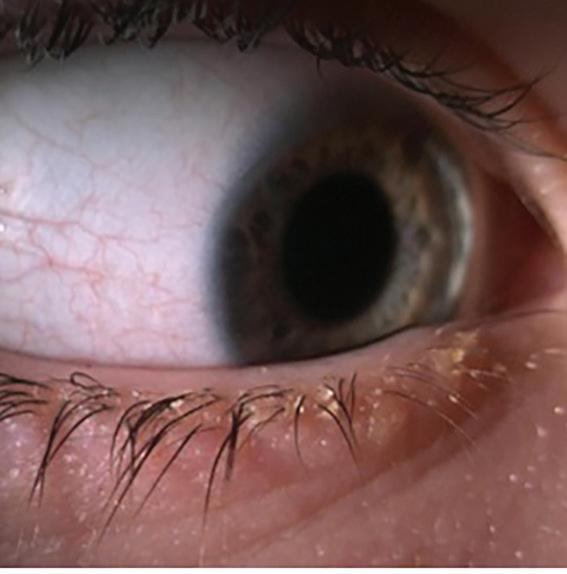
Many patients are surprised to learn their red, uncomfortable eyes could be caused by a species of parasites living on their eyelids. DR MARIA MARKOULLI and ZAHRA TAJBAKHSH explore the clinical implication of Demodex infestation. They provide an overview of the condition, clinical management strategies, and patient education tips to encourage understanding and compliance.
Colourless, hairless and cylindrical-shaped, Demodex mites are the most common ectoparasite in humans. They are extremely small (0.15 mm - 0.4 mm), and, despite their eight legs, they have limited motility.
Two species of Demodex have been identified in humans: Demodex folliculorum (D. folliculorum) and Demodex brevis (D. brevis).
D.folliculorum gather in clusters in the superficial structures of the follicles of the eyelashes – they tend to be larger than D. brevis, which reside alone, anchored deeper in the sebaceous glands.1
Sensitive to light, Demodex mites are more mobile in a dark environment. They are also hostdependent and can survive only a few days ex-vivo. The complete life cycle of each mite is about 15 days, after which the mite bursts and spills its contents into the surrounding tissue.
Demodex can be both commensal and opportunistic. As commensal organisms, they have a symbiotic relationship with humans without causing any harm to their host. However, they have the potential to change their role from ‘commensals’ to ‘parasites’ if the host’s skin environment facilitates their proliferation.2
Once the population of Demodex mites on the skin exceeds a critical level, they can become pathogenic, known as ‘demodicosis’.2 Demodicosis can affect the facial skin as well as eyelids. In a study of participants with Demodex blepharitis, a high density of Demodex mites in the facial skin was also found.3 Demodex can also play a role in pterygium or exacerbate preexisting dry eye.4,5 Daily personal hygiene is not helpful in treating ocular Demodex as it is difficult to reach them because of the deep-set position of eye and eyelid margin.
Interestingly, Demodex mites are not found in the skin of newborn infants; however, they can be found later in childhood – likely due to transmission from family members. Generally,
there is a lower risk of Demodex infestation in children, possibly due to their lower level of sebaceous gland secretions, which result in fewer secretions for the mites.
DEMODEX MITES AND ASSOCIATED FACTORS
The prevalence of ocular Demodex has been reported to range between 14% to 89% in different populations with an increased prevalence with age, dermatological conditions and systemic diseases without any difference between genders.6
Depending on the Demodex infection type (D. folliculorum or D. brevis type), the eyelid appearance and severity can be different. When meibomian gland dysfunction (MGD) and chalazia are present, an overpopulation of D. brevis in the meibomian gland can be observed.
D. folliculorum can be seen in 90% of anterior blepharitis and 60-88% of MGD cases.7,8 This is because of the close proximity of eyelash follicles to the meibomian glands which can affect one another.
There are several associated factors that facilitate the proliferation of Demodex including acne rosacea, leukemia, HIV infection and AIDS, immunosuppression medication, chemotherapy, phototherapy, and chronic dialysis.2,9 Predisposing factors such as contact lens wear, depression, emotional stress, malnutrition, sleep deprivation and skin tumours also have an effect.10,11
Notably, because the concomitance of facial and palpebral Demodex infestation has been reported in patients with Demodex blepharitis,3 a co-management approach between eyecare professionals and dermatologists is important in order to successfully manage both the ocular and facial forms of this condition.
DEMODEX DIAGNOSIS
Cylindrical dandruff at the base of the eyelash is the main clinical presentation of Demodex.12 In
ABOUT THE AUTHORS:
Zahra Tajbakhsh

Optom MSc PhD candidate
School of Optometry and Vision Science, UNSW Sydney A/Prof Maria Markoulli

PhD MOptom GradCertOcTher FBCLA FAAO
Associate Professor | Postgraduate Research Coordinator |
Academic lead
UNSW Dry Eye clinic | School of Optometry and Vision Science Deputy Editor | Clinical and Experimental Optometry Board Member | The Optical Foundation TFOS Ambassador
order to observe an individual mite in the clinical setting using a slit-lamp, the lash can be rotated at its base several times using tweezers, (termed the ‘Mastrota rotation’) until its tail emerges partially from the follicle. Another method is to exert ‘lateral tension’ on the lash to observe the emerging tail from the follicle opening without lash epilation.13
Lash epilation and in-vivo confocal microscopy are two research techniques used to count Demodex. In-vivo confocal microscopy involves applying the probe of the instrument to the eyelid margin. It provides complete observation of the lash contents, without the need to epilate the lash.10 In the lash epilation method, a lash with
CLINICAL CPD HOURS This activity meets the OBA registration standards for CPD
LEARNING OBJECTIVES:
CPD
22 INSIGHT October 2022
cylindrical dandruff is epilated and observed under a microscope for the quantification of the mites attached to it. Both techniques are restricted to the research setting and are influenced by the lash chosen for observation, hence yielding variable results.14
CLINICAL PRESENTATION OF OCULAR DEMODEX
The clinical presentation includes itching, especially along the lid margin, swollen eyelids, and ocular discomfort, symptoms typical of blepharitis. Cylindrical dandruff surrounding the base of the lash are pathognomonic of ocular Demodex. Some patients may present with loose lashes, and misdirected lashes or trichiasis due to Demodex infestation that impact nutrients and follicle structure.6 In more severe cases, Demodex can block the openings of follicles and gland ducts, leading to epithelial hyperplasia and hyperkeratinisation.

It is important to manage Demodex to prevent contact lens discomfort and dropout. There has been a positive correlation between the presence of Demodex and intolerance to contact lens wear.15 Contact lenses may encourage microorganism accumulation, which provides a more favourable environment for Demodex proliferation.
CLINICAL MANAGEMENT STRATEGIES
The aim of management of Demodex is not to eradicate the mites, but rather to reduce their population in order to restore normal ocular surface ecology. There are several management options for Demodex infestation:

1. Lid scrubs containing tea tree oil (TTO)
2. Combined therapy of both high concentration TTO in-office and exfoliation, and at-home therapy
3. Manuka honey
4. Intense pulsed light (IPL)
The recommended duration of treatment
is for at least two Demodex mite lifecycles. Considering each mite lifecycle is approximately 15 days, a duration of 4-6 weeks of treatment is recommended.
Tee tree oil (TTO) is an essential oil derived from the leaves of a small tree known as Australian Melaleuca alternifolia. It is used topically, applied directly to the eyelid and lash follicles, and it is highly toxic if ingested. Terpinene-4-ol (T40) is the most active TTO molecular compound against Demodex mites (an ingredient found in many lid wipes).
The full mechanism of TTO against Demodex remains largely unknown, however, it is thought that TTO encourages the Demodex mites to migrate out of the follicle, enabling better access for lid wipes and other forms of therapy.
HYGIENE PRODUCTS AND DELIVERY MECHANISMS
We have a range of products available to us now for the management of eyelid disease. Despite the range, they have certain key ingredients in common: most contain mild cleansing surfactants and antimicrobial ingredients. Many also contain TTO. A variety of delivery mechanisms of these products are available, including wipes, pumps, gels and sprays. It is not clear which of these mechanisms is superior and there are no studies on the optimal regimen (once versus twice a day), technique and duration of the procedure (5, 10 or 15 minutes) for eyelid hygiene.
Each delivery mechanism has its own pros and cons.
Wipes – these are single-use and sterile which limits cross-contamination. The application involves gentle pressure along the lash line. Patients need to be trained in-office on how to apply wipes as forceful rubbing may irritate the delicate eyelid skin. In-office education and trial are recommended so that the patient can be warned to expect a cooling or burning sensation.
PATIENT EDUCATION
It’s important for the eyecare practitioners to be proactive rather than reactive in advocating lid hygiene. The following advice should be provided in the counselling process to manage patient expectations and improve patient compliance.
• Inform the patient about the severity of the condition and the consequences of leaving this condition untreated.
• Provide proper instruction on how to use the recommended eyelid cleanser. This is best achieved with written instructions.
• Compliance is greater in symptomatic patients; therefore, it is important to educate both symptomatic and asymptomatic patients about the consequences of not treating.
• Patients should be informed of the lifecycle of the mite and the importance of treating for two lifecycles (four to six weeks) to maintain compliance for the recommended amount of time and return for a follow-up assessment.
• Patients should be informed of potential discomfort with any eyelid cleanser, no matter how minor or how transient, so that patients know what to expect once they return home. Performing an in-office trial with eyelid cleansers, especially those with TTO, may alleviate some of these concerns.
• It is important to consider a co-management approach with dermatologists to manage both ocular and facial form of Demodex blepharitis.
• Be aware of comorbidities such as acne rosacea, dry eye, blepharitis, chalazia that may predispose individuals to Demodex infestation.
Figures 1A-1C. Clinical presentation of Demodex blepharitis.
INSIGHT October 2022 23
(It is reported that a pre-soaked wipe with T40 can cause ‘transient discomfort’).16



In a study that applied a type of T40 wipe twice a day, signs and symptoms of blepharitis
significantly decreased with a reduction of debris along the lash line, and an improvement in meibum quality.17
Pumps – Some patients prefer the pump delivery system. Pumps deliver the product as a foam, cream or liquid which then needs to be rinsed off the eyelid. Foam eyelid cleanser containing TTO and linalool was found to be more effective at alleviating both the signs and symptoms related to ocular surface inflammation over baby shampoo.18 Other studies have shown that this delivery mechanism can improve tear break up time, decrease meibomian gland obstruction and, despite variable compliance, it’s well-tolerated by patients.19,20
Gels – An advantage of gels over other delivery mechanisms is that the gel formulation reduces the degree of friction on the sensitive eyelid skin compared to wipes, and 85% of patients have rated this delivery mechanism as acceptable.21 Gel formulations are applied to the fingertips and, similar to pumps, patients need to be educated regarding proper hand hygiene prior to the use of gel.
Sprays – Relatively new to the market, sprays are either applied directly to the eyelid or to a cotton pad and then rubbed onto the closed eyelids, with no need to rinse. This delivery
mechanism is well tolerated by patients.20 A significant reduction in the overall bacterial load, especially S.epidermidis has been reported, however there is no report about the efficacy of sprays on Demodex as yet.22
Although the majority of the aforementioned products are well-tolerated, each of these products would benefit from demonstration and trial in the clinic. Demonstrations will help set patient expectations regarding any possible transient discomfort that they might experience, and provide clarification as to precisely how the product should be applied to the eyelid, including location, amount of pressure and necessary hand hygiene.
Warm compresses and their effect on ocular Demodex – Eyecare practitioners often recommend lid hygiene along with the use of a warm compress, especially for the management of meibomian gland dysfunction. An obvious question is whether these warm compresses are beneficial or detrimental in the management of Demodex.

Both D. brevis and D. folliculorum prefer lower temperatures, and temperatures above 37°C are damaging, especially for D. folliculorum,9 with the higher temperature eventually paralysing the D. folliculorum’s nervous system.

CPD
Demodex mites
are more mobile in a dark environment.
One study investigated the efficacy of warm compress on Demodex infestation using three devices: a face cloth, the MGDRx eyebag (The EyeBag Company, Halifax, UK) and OPTASE moist heat mask (Scope Ophthalmics Ltd., Dublin, Ireland), over a period of eight weeks. The quantity of Demodex decreased significantly in the group using the OPTASE moist heat mask. While the MGDRx eyebag did not appear to have a significant impact on Demodex quantity, the proportion of Demodex infestation improved significantly by 25 per cent, which suggests that heat may be an important addition to managing Demodex.23
Intense pulsed light (IPL) – Recently, IPL has been recommended as an in-office treatment for Demodex infestation. In a 2019 study, 40 patients were treated with either 5% TTO or IPL over a three-month period.24 Compared with the TTO group, the IPL group had faster improvement. The average number of Demodex decreased significantly after both one and three months of IPL and the overall Demodex eradication rate was 100% compared to 75% for the TTO group.
These results suggest that IPL treatment is efficacious in eradicating Demodex, and patients may accept it more readily since it takes effect more quickly, with minimal effort on their part. A possible mechanism of IPL is that the light produced by the IPL is directed to the skin tissue and absorbed, resulting in the production of heat, which eliminate mites effectively.24
Manuka honey – Topical use of manuka honey has been recently proposed for Demodex treatment. In a clinical trial study, 53 participants with blepharitis were randomly assigned to apply manuka honey microemulsion eye cream to one eye, with the other eye serving as the control eye. After three months of therapy, the eyes treated with manuka honey had a significant decrease in Demodex infestation compared to the control eye. Several factors may attribute to the clinical efficacy of manuka honey, including the established antibacterial, anti-Demodex, and anti-inflammatory properties of manuka honey.25
Micro-blepharoexfoliation – The BlephEx is a device, which consists of a hand-held electromechanical unit and a disposable microsponge that spins rapidly to provide debridement and exfoliation at the lash margin. For the purpose of Demodex blepharitis treatment, the sponge is soaked in a lid-cleaning solution, such as TTO, and then applied to the lid margin for approximately 20-30 seconds. The aim is to remove as much debris as possible, and to debride the lid margin. The eyes are rinsed with saline at the end to remove any debris or solution.
The in-house use of this method has been shown to give a greater improvement in symptoms and has been recommended as a starting point in the management of blepharitis.26 n
1. CASE STUDY
Case history: A 12-year-old male, presented with red and uncomfortable eyes. Vision was unaffected and there was no ocular discharge. In terms of general health, he had recurring tonsillitis.
Ocular examination: On slit-lamp examination, mild bulbar and limbal redness and peripheral corneal infiltrates were observed. Eyelid examination showed transparent matter wrapped around the base of the lashes.
Diagnosis: The diagnosis was Demodex blepharitis contributing to marginal keratitis.
Management: The marginal keratitis was controlled with a 10-day dose of weak corticosteroids. The underlying cause, the Demodex blepharitis, was treated with Demodex wipes used twice a day for six weeks, and in-office Blephex with 50% tea tree oil.
On review six months after his tonsil surgery, his eyelids and cornea were clear. Seven years on to the present day, he continues to be asymptomatic. This is an atypical example of a young child with an underlying health condition that may have contributed to ocular demodex becoming parasitic, and then returning to symbiotic once the underlying systemic condition was managed.
REFERENCES
1. Nicholls SG, Oakley CL, Tan A, Vote BJ. Demodex species in human ocular disease: new clinicopathological aspects. International Ophthalmology 2017; 37: 303-312.
2. Lacey N, Raghallaigh SN, Powell FC. Demodex mitescommensals, parasites or mutualistic organisms? Dermatology 2011; 222: 128.
3. Aumond S, Bitton E . Palpebral and facial skin infestation by Demodex folliculorum. Contact Lens and Anterior Eye 2020; 43: 115-122.
4. Bron AJ, de Paiva CS, Chauhan SK, Bonini S, Gabison EE, Jain S, Knop E, Markoulli M, Ogawa Y, Perez V, Uchino Y, Yokoi N, Zoukhri D, Sullivan DA. TFOS DEWS II pathophysiology report. The Ocular Surface 2017; 15: 438510.
5. Tarkowski W, Moneta-Wielgo J, Młocicki D. Do Demodex mites play a role in pterygium development? Medical Hypotheses 2017; 98: 6-10.
6. Bitton E , Aumond S. Demodex and eye disease. Clinical and Experimental Optometry 2021; 104: 285-294.
7. Tarkowski W, Owczy ska M, Błaszczyk-Tyszka A, Młocicki D. Demodex mites as potential etiological factor in chalazion – a study in Poland. Acta Parasitologica 2015; 60: 777-783.
8. Vipul B, Jagadeesh K R. Blepharitis: always remember demodex. 2014.
9. Zhao YE , Guo N, Wu LP. The effect of temperature on the viability of Demodex folliculorum and Demodex brevis.
Parasitology Research 2009; 105: 1623.

10. Jalbert I, Rejab S. Increased Numbers of Demodex in Contact Lens Wearers. Optometry and Vision Science 2015; 92.
11. Zhao Y-e, Guo N, Xun M, Xu J-r, Wang M, Wang D-l. Sociodemographic characteristics and risk factor analysis of Demodex infestation (Acari: Demodicidae). Journal of Zhejiang University SCIENCE B 2011; 12: 998-1007.
12. Gao Y-Y, Di Pascuale MA, Li W, Liu DT-S, Baradaran-Rafii A, Elizondo A, Kawakita T, Raju VK, Tseng SCG. High Prevalence of Demodex in Eyelashes with Cylindrical Dandruff. Investigative Ophthalmology & Visual Science 2005; 46: 3089-3094.
13. Muntz A , Purslow C, Wolffsohn JS, Craig JP. Improved Demodex diagnosis in the clinical setting using a novel in situ technique. Contact Lens and Anterior Eye 2020; 43: 345-349.
14. Murphy O, O’ Dwyer V, Lloyd-McKernan A. The effect of lid hygiene on the tear film and ocular surface, and the prevalence of Demodex blepharitis in university students. Contact Lens and Anterior Eye 2020; 43: 159-168.
15. Tarkowski W, Moneta-Wielgo J, Młocicki D. <i>Demodex</ i> sp. as a Potential Cause of the Abandonment of Soft Contact Lenses by Their Existing Users. BioMed research international 2015; 2015: 259109.
16. Tighe S, Gao Y-Y, Tseng SCG. Terpinen-4-ol is the Most Active Ingredient of Tea Tree Oil to Kill Demodex Mites. Translational Vision Science & Technology 2013; 2: 2-2.
17. Guillon M, Maissa C, Wong S. Symptomatic Relief Associated With Eyelid Hygiene in Anterior Blepharitis and MGD. Eye & Contact Lens 2012; 38.
18. Sung J, Wang MTM, Lee SH, Cheung IMY, Ismail S, Sherwin T, Craig JP. Randomized double-masked trial of eyelid cleansing treatments for blepharitis. The Ocular Surface 2018; 16: 77-83.
19. Maher TN. The use of tea tree oil in treating blepharitis and meibomian gland dysfunction. Oman journal of ophthalmology 2018; 11: 11-15.
20. Ngo W, Jones L, Bitton E. Short-Term Comfort Responses Associated With the Use of Eyelid Cleansing Products to Manage Demodex folliculorum. Eye & Contact Lens 2018; 44: S87-S92.
21. Doan S. Tolerability and acceptability of Blephagel: a novel eyelid hygiene aqueous gel. Clinical Ophthalmology 2012; 6: 71-77.
22. Stroman DW, Mintun K, Epstein AB, Brimer CM, Patel CR, Branch JD, Najafi-Tagol K. Reduction in bacterial load using hypochlorous acid hygiene solution on ocular skin. Clinical Ophthalmology 2017; 11: 707-714.
23. Murphy O, O’ Dwyer V, Lloyd-Mckernan A. The Efficacy of Warm Compresses in the Treatment of Meibomian Gland Dysfunction and Demodex Folliculorum Blepharitis. Current Eye Research 2020; 45: 563-575.
24. Zhang X , Song N, Gong L. Therapeutic Effect of Intense Pulsed Light on Ocular Demodicosis. Current Eye Research 2019; 44: 250-256.
25. Craig JP, Cruzat A, Cheung IMY, Watters GA, Wang MTM. Randomized masked trial of the clinical efficacy of MGO Manuka Honey microemulsion eye cream for the treatment of blepharitis. The Ocular Surface 2020; 18: 170-177.
26. Murphy O, O’Dwyer V, Lloyd-McKernan A. The efficacy of tea tree face wash, 1, 2-Octanediol and microblepharoexfoliation in treating Demodex folliculorum blepharitis. Contact Lens and Anterior Eye 2018; 41: 77-82.
NOTE: Insight readers can scan the QR code or visit insightnews.com.au/cpd/ to access a link to this article to include in their own CPD log book.
INSIGHT October 2022 25
dry eye care









approach to preservative-free
The PBS LISTED PBS Information, HYLO: Authority Required (STREAMLINED): Severe dry eye syndrome in patients who are sensitive to preservatives in multi-dose eye drops. STREAMLINED AUTHORITY CODE 4105 1. Lemp, M.A., Crews, L.A., Bron, A.J., Foulks, G.N. and Sullivan, B.D., 2012. Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort: a retrospective study. Cornea, 31(5), pp.472-478. AFT Pharmaceuticals Pty Ltd, Sydney | Phone: 1800 238 742 | Email: receptionau@aftpharm.com | ABN 29105636413




aftpharm.com Combine HYLO® + NovaTears® for dual action dry eye relief suffer from a combination of Aqueous Deficient Dry Eye and Evaporative Dry Eye.1 patients Dry Eyein31 More than HYLO®-Fresh + HYLO-Forte® Lubricates the eye NovaTears® Forms a protective layer to reduce tear evaporation HYLO® + NovaTears® Hydration and protection for Dry Eye PBS Information, NovaTears: Authority Required (STREAMLINED): Severe dry eye syndrome in patients who are sensitive to preservatives in multi-dose eye drops. STREAMLINED AUTHORITY CODE 6172 mydryeyes.com.au
Break the eye drought with Viscotears®
When tear fluid production is unstable, the discomfort of dry eye conditions can take hold.1

Viscotears® eye gel can provide relief from this discomfort as it forms a protective film over the surface of the eye for a prolonged time.1
Viscotears® Eye Gel 10g Tube
long lasting relief for Sore, Gritty Dry eyes
Listed
Viscotears® Gel PF 30 × 0.6g single-dose units
a moistening and wetting effect on the eyes2

For more information contact your Bausch + Lomb Territory Manager or Bausch + Lomb Customer Service on 1800 251 150 References: 1. Viscotears Gel IFU. 2. Viscotears Gel PF IFU. © 2022 Bausch & Lomb Incorporated. ®/TM denote trademarks of Bausch & Lomb Incorporated and its affiliates. Bausch & Lomb (Australia) Pty Ltd. ABN 88 000 222 408. Level 2, 12 Help Street, Chatswood NSW 2067 Australia. (Ph 1800 251 150) VIS.0005.AU.22
Soothing,
PBS
Provides
Preservative-free PBS Listed
Including:
•
At the completion of this CPD activity, optometrists will understand the clinical aspects of managing dry eye disease.
Developed a structured approach to dry eye disease
• Appropriately triage the most likely cause of dry eye for each, unique patient
• Understand the value of technology to image the eyes and document many facets of a patient’s eyes and tear film
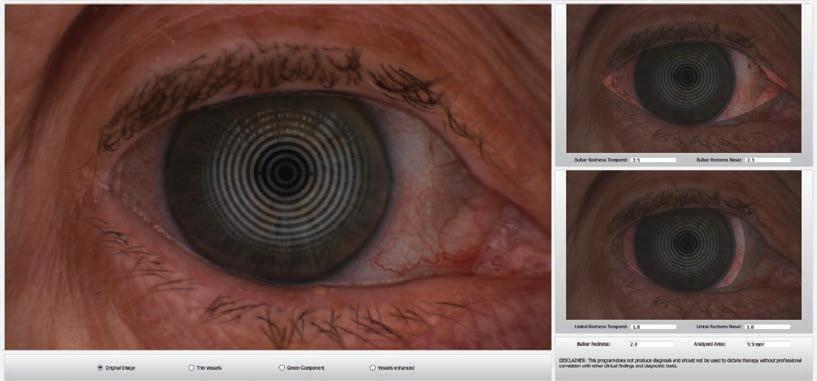
• Recognise the need to implement a combination of therapies to address the multi-factorial causes of each individual case of dry eye disease.
DRY EYE: A MULTIFACTORIAL APPROACH TO A MULTIFACTORIAL DISEASE
The new standard of care for dry eye requires a multifactorial approach – and it's complicated. Tasmanian optometrist MARTIN ROBINSON’s dry eye strategy involves embracing the complexity of the disease and adopting a structured approach so he can go beyond symptom-management to address the underlying causes of each unique presentation.

I
t has been almost five years since the Tear Film and Ocular Surface Society (TFOS) released its Dry Eye Workshop II (DEWS II) report which included an updated internationally-recognised definition of Dry Eye Disease (DED): “Dry eye is a multifactorial disease of the ocular surface characterised by a loss of homeostasis of the tear film, and accompanied by ocular symptoms, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play etiological roles.”1
Clinically, the signs of DED are often poorly correlated with symptoms, and studies have shown more than 40% of subjects showing positive signs of DED are actually asymptomatic.2
BEISTO
The key word in the TFOS’s definition of dry eye disease is “multifactorial”. It’s instructive to
explore some practical cases and see how a structured approach to the multifactorial causes of DED can elicit a diagnosis and treatment path.
In the following examples, we will go through detailed examinations, drawing on ‘BEISTO’, a concept first coined by dry eye pioneer Dr Laura Periman. That is: Bugs/Bacteria, Enzymes, Inflammation, Statis, Temperature and Obstruction. When a sign of any of these BIESTO impediments is found, a different treatment pathway is required.
CASE 1
A 69-year-old post-menopausal Caucasian female presented who had several pairs of spectacles made in the last nine months and was unhappy with all of them. Her case history revealed she was a retired from a long career of clerical paperwork and computer work – 40 hours a week for 40 years in airconditioned offices.
She suffered from Crohn’s, Colitis, reactive airways dysfunction syndrome (RADS) and fibromyalgia. Twelve months before she presented at our clinic, she had a skin cancer removed from her nose bridge which was treated with a topical chemotherapy cream after removal.
In this patient’s case history, there are many areas of possible influence of DED. Among them:
• Inflammatory bowel disease (IBD) including Crohn’s and Colitis. Ocular manifestations for IBD include iritis, episcleritis, optic neuritis, blepharitis and DED. Of these, blepharitis and DED are reported at rates of 24.6% and 57.4%, respectively. Reduced tear volume is the most reported sign.3
CLINICAL CPD HOURS This activity meets the OBA registration standards for CPD
LEARNING OBJECTIVES:
ABOUT THE AUTHOR: Martin Robinson BApp Sc(Optom) Optometrist and Principal Owner, Martin’s Eyecare, Hobart, TAS State President of the Cornea nd Contact Lens Society of Australia TAS (CCLSA) National Vice President CCLSA
DRY EYE - CPD Figure 1 (case 1). OD
redness scan
shows
injected lid margins and capped meibomian glands.
INSIGHT October 2022 29
• R ADS is associated with increased incidence of steroid-induced cataract.
• Fibromyalgia can cause dryness of the eyes and mouth, most associated with ocular pain.
• Chemotherapy often causes dry mouth and dry eyes; this is due, in part, to stem cell damage. Fast replicating stem cells like those in salivary glands, meibomian glands and limbal stem cells are often impacted. Meibomian gland shortening, obstruction and complete atrophy are all reported with systemic and topical chemotherapy.
• Changes to estrogen and androgens can cause DED.
• Administration and computer use can lead to poor blink habits, including incomplete blinking and more rapid blinking.

Examining the patient in a structured way can help to appropriately triage the most likely causes. I perform a Full Jenvis Pro dry eye exam using the Oculus Keratograph K5 device. This aides me in my diagnosis pathway.
Detailed photo/video documentation of this nature at initial examination is helpful to set a baseline to document any improvements or adverse events (AEs) after treatment. In
addition, it is invaluable as a teaching tool to show patients DED signs and prove to them that behaviours such as incomplete blinking are present.
LIST OF FINDINGS FROM INITIAL KERATOGRAPHY ASSESSMENT
• Jenvis Pro examinations delivers a total score out of 100, with a lower score being abnormal. This patient’s scores were, OD: 40; OS:37. Ocular surface disease index score: 60 OSDI is scored out of 100 with the higher number being more symptomatic, above 13 is abnormal.
o With the Jenvis Pro report, I find most people are satisfied when they score above 65 so for this patient we need a 40-60% improvement. WRT OSDI a 30% reduction is considered successful intervention, so we would aim for 40.

• Refraction was unstable, with especial trouble determining astigmatism axis and power.
• No symptoms of Posterior Subcapsular Cataract (PSCC), no iritis, no age-related macular degeneration (AMD) and no episcleritis were seen.
• Tear meniscus was normal and no dry mouth symptoms.
• No ocular pain was reported.
• Incomplete blinking was moderate with 2030% of the cornea surface impacted.
• Blink rate was severe at over 20 blinks a minute. Normal for women is 12-14, so almost double.
• Non-invasive tear break up time (NITBUT) was reduced. It was shorter in the left eye than in the right eye (L>R).


• Meibomian gland shortening and drop-out seen worse nasally in both eyes.
• Lid margin uneven with capped MGs and excess lid biofilm present, but lashes were clean.
• Conjunctiva chemosed, injected and with some conjunctival chalasisalisis but very limited staining of the conjunctiva, and nil
seen on the cornea.
• OSDI severe at 60. But areas of effect were all visual and wind/AC intolerant.
From the initial keratography findings, RADS is not a likely contributor. And as there is no ocular pain and tear volume is normal, fibromyalgia is also unlikely.
The patient’s lashes are clear with no collarettes, but she does have meibomian gland dysfunction so IBD could be a cause. However, her symptoms started 12 months ago, and her IBD is long standing. (10% of people that suffer IBD will experience eye problems in their life, so it is a prudent question to ask when you take the patient’s case history).
The patient’s years of working in offices with computers are likely contributors to the abnormal blinking rate and the incomplete blinking. Her MG changes could be agerelated, menopause-induced or computeruse influenced. The nasal drop out could be caused though the topical chemotherapy use. The conjunctival changes are influenced by the abnormal lid margin combined with the increased blink rate. And the answers she provided to the OSDI questionnaire suggest an unstable normal volume tear film and leads us to a primary diagnosis of evaporative dry eye.
TREATMENTS PRESCRIBED
• Manual lid debridement is indicated to remove the biofilm and clear abnormal epithelial overgrowth of the meibomian glands.
• Avenova hypochlorous acid spray once daily. Hypochlorous acid is useful to reduce the bacterial load on the eyelids, a common cause of the biofilm when makeup is not used.
• Blink training, including slow blinking – close, pause, pause, open, relax. Conjunctival chalasis is partly inflammatory and partly friction caused. If the patient can make full, complete blinks, we can reduce the number of blinks a day, reducing the friction. In addition, full closed eye blinks allow the meibomian gland acini to open, releasing oils.
• Lumenis M22 Intense Pulse Light (IPL) treatment. Four sessions to the periorbital region using the Epstein protocol, avoiding the bridge of the nose where the skin cancer was removed.


o IPL reduces the inflammation seen around the eyelids by eliminating pro-inflammatory blood vessels. Additionally, IPL pulses are photo bio-modulators, able to stimulate the stem cells of the meibomian glands and create smaller, healthier and more active acini.
• After the final IPL session, a Blephasteam and Mastrota eyelid expression will be performed. I prefer to clear any obstructions to meibomian glands with heat and expression, but only after the inflammation is reduced, this reduces the amount of pressure needed to clear
DRY EYE - CPD 30 INSIGHT October 2022
Figure 2 (case 1). OS upper lid margin. Visible biofilm scurf (debris on the surface of the lid margin that collects while new epithelium forms beneath).
Figures 3A and 3B (case 1). OD lower lid. Figure 3A (left): prior to treatment. Figure 3B (right): post-treatment, the lid margin thickness is significantly reduced, and there is less injection.
Figures 4A and 4B (case 1). OD InfraRed meibomian gland scans. Figure 4A (left): prior to treatment. Figure 4B (right): post-treatment. Note: limited change nasally, but there is recovery of identifiable glands temporally, specifically the glands are longer, thinner, and more well defined to the temp side of the central ‘half’ gland. I always try to find an easily identifiable point-of-reference visible in both images.
the glands, resulting in a more comfortable procedure. In addition, I prefer to do a lid debridement first before performing Mastrota expression, again to allow more efficient clearance and reduce and discomfort.

RESULTS
The combination of lid debridement, Avenova and blink training worked well. The patient reported an 80% reduction in symptoms in the first week.
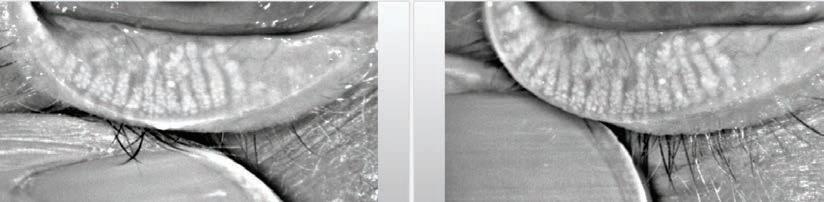

We arranged a repeat refraction and new spectacles, and the patient is very happy. A dry eye success without eye drops. Historically we might have tried artificial tears, and these alone
would have been unlikely to help in this case.
DISCUSSION
I did not prescribe any eyedrops in this case, rather, I followed the signs and symptoms and explored the possible contributors. IBD is possibly a contributor, as are bacteria, her age and sex and her blink habits, but the timeline indicates a specific tipping point where homeostasis was lost. This occurred after the nose skin cancer treatment with topical chemotherapy.
Chemotherapy reduces acini, reduces stem cell activity, and causes meibomian gland atrophy. The significant loss of her nasal






meibomian glands matches this hypothesis. A detailed examination led to a structured treatment plan and an elimination of her symptoms.

CASE 2
A 24-year-old Caucasian male presented on the advice of his dermatologist for a dry eye examination. He had been prescribed Roaccutane for bad acne nine months prior, and his dry eye symptoms started within the first few weeks. The symptoms steadily worsened, and he had seen another optometrist who
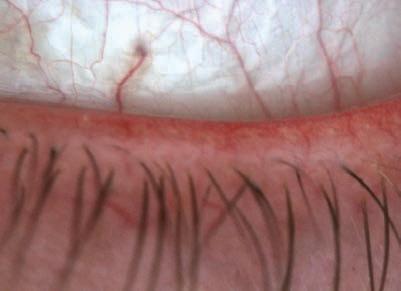





Figure 5 (case 2). OS Lower lid. Significant telangiectatic vessels on the lid margin, a typical presentation of isotretinoin users.

Join Eyecare Plus and benefit from the support and knowledge of experienced members. Looking to buy, sell or join contact Philip Rose 0416 807 546 or philip.rose@eyecareplus.com.au Multi Award Winning Practices
prescribed Optimel 16% eye drops which he was using a few times a day, but they caused significant pain and did not seem to help much.
He described significant light sensitivity most of the time, but worst at night. Air conditioning was unbearable. Psychologically, he was stressed and frightened. A recent graduate from university, he was about to start his first job in a week, and he was frightened that he would not cope.
The areas of preliminary diagnosis in his case are as follows:
• Optimel 16% eye drops are a recognised, effective treatment for signs and symptoms of DED.4 In studies the adverse events are listed as sting and increased injection after instillation, for a short time. This patient reports significant pain and no reduction in his signs or symptoms over some time.
• Acne vulgaris, the condition diagnosed and treated by his dermatologist is a possible cause of the DED. Both acne vulgaris and meibomian glands are influenced by androgenic hormone and strongly correlate with ocular dryness.
• Roaccutane – active ingredient isotretinoin is well documented in being the cause of significantly higher risk of ocular adverse events (AEs), even in the year after treatment cessation. These AEs include blepharoconjunctivitis, keratoconjunctivitis sicca, cutaneous photosensitivity and contact lens intolerance. In fact, Isotretinoin seems to inhibit the ability of the meibomian acinar cells to differentiate, while simultaneously stimulating the epithelial lining the ducts and acini to proliferate. 5
• Certain medications are known to cause photosensitivity.
The Jenvis Pro dry eye report and full eye examination revealed the following:
• OD 65 score OS 44, score OSDI 31.
• Patient and his girlfriend both deny any redness or irritation prior to starting Roaccutane, making acne vulgaris an unlikely cause.
• E xcessive froth seen on his lid margins, and floating in the tear film indicating excess bacterial flora.
• Lid margin telangiectasia, meibomian glands capped and obstructed with no expression seen.
• Meibomian gland scan showed no shortening of glands but very pale ‘ghost like’ appearance
• Incomplete blinking severe >33% of eye not covered.
• OSDI 31 with light sensitivity, soreness and pain, and wind/AC intolerance worst results.
• NITBUT above average, no breakup seen in first test. Test repeated with a fan blowing in the room, NITBUT reduced to seven to eight seconds.
• Inferior staining on conjunctiva, nil staining on cornea
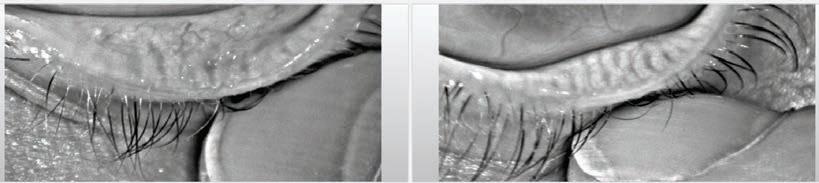

DIAGNOSIS
From the findings we can safely eliminate simple pre-existing MGD from acne vulgaris, no evidence of any prior signs or symptoms. The level of reported pain from Optimel made me uncomfortable, combined with no apparent changes in signs or symptoms and inferior staining, I advised him to cease using it. He reported no other medications
apart from the Roaccutane.
The most likely hypothesis is the isotretinoin has caused his current conditions and the appearance of the eyelids, meibomian gland scans, and other tests indicate a reduction in function and obstruction of at least the outer ducts of the meibomian glands. Isotretinoin has been demonstrated to cause a significant time and dose dependent effect on both the morphology and the proliferation of meibomian glands.
TREATMENT
• Cease Optimel, start Systane Hydration, a better lubricant for the rough lid margins and should help with the inferior staining.
• Blink training, slow blinking as in case 1 to develop improved blink behaviour.
• Ocusoft Hypochlor spray 1/day after a shower to reduce bacterial flora.
• Lumenis M22 IPL for four sessions to periorbital region using the Epstein protocol for 1st session, to reduce the inflammation
• Lid debridement after 1st IPL to remove the biofilm scurf.
COSMETICS AS A CONTRIBUTING CAUSE OF DED
The presence of DED strongly correlates to our patient’s levels of stress, their mental health, and self-esteem; it also affects females more than males. In the past we have been quick to blame hormones for this sex-linked discrepancy, but recent studies have started looking at beauty products, make-up, cosmetics, lotions and wipes, their ingredients, and their impact on the ocular surface.
Cosmetics all contain preservatives; this is essential to limit the growth of bacteria and funguses in cosmetics. However, many preservatives used like benzalkonium chloride, and formaldehyde (FA)-releasing preservatives are toxic to the ocular surface. FA releasing chemicals are also present in many adhesives used to apply the ever more popular eyelash extensions. Studies have shown the dose-dependent effects of these chemicals on MGs, corneal and conjunctival cells, and there is concern about longer term cumulative dose impacts.7
If a patient is using make-up, or lash extensions or skin care products in general, this may add several layers of complexity to a DED assessment.
DRY EYE - CPD 32 INSIGHT October 2022
Figures 5A and 5B (case 2). 5A (left): OS at initial presentation (redness scan). Note significant injection, more nasal, more inferior, some limbal injection. 5B (right): OS as seen after completing treatment. Significant reduction in eye injection and lid injection.
Figures 6A and 6B (case 2). 6A (left): OS meibomian gland at initial presentation. Note ghost like meibomian glands, very faded, poorly defined. 6B (right): OS as seen after completing treatment. More visible glands, improved structure.
• At second IPL, add additional Eyelid IPL using Cox2 metal shields and following the Periman Protocol for eyelids. This is done at lowest fluence and for three pulses per eyelid using a small crystal, for a double pass. This was due to the severe lid inflammation which I felt required more intense treatment.

RESULTS
Systane Hydration gave immediate improvement over Optimel with improved comfort and longer lasting relief, in addition there was no staining. The Hypochlor spray eliminated all froth, his blinking was slower and more complete. His eye redness was greatly reduced, the lid margins were also less injected and less thickened. The meibomian glands have regained structure, definition and their production of meibum was restored, now easy to express with gentle pressure. He was no longer light sensitive, day or night, his stress levels were reported as significantly reduced, and he displayed what I would describe as a return to a self-confident young man. His use of Systane Hydration continued but only on random days where he had put in long hours on the computer.
TAKE HOME MESSAGE
DED is a nuanced condition, multifactorial and complex. We can no longer take a simplistic view of DED, either in its diagnosis or treatment. Its inherent complexity requires multifactorial solutions. We all can do more when it comes to case histories, examinations, and diagnoses.
Our evolving understanding of DED has precipitated an escalation of the use of technology to treat the condition. I feel that technology is not only helpful, but essential to correctly document many facets of a patient’s eyes and tear film. And in many cases, only technology can offer the solutions needed to address the patient’s symptoms of DED.’
I urge all practising eyecare providers to rethink their approach to DED. It will help their practice, improve their bottom line and most importantly, provide the best outcomes for their patients. n
7.
Chen, David A
Volume
Pages
R.
REFERENCES 1. Jennifer P Craig 1, Kelly K Nichols 2, Esen K Akpek et al. TFOS DEWS II Definition and Classification Report. Ocul Surf. 2017 Jul;15(3):276-283. doi: 10.1016/j.jtos.2017.05.008. Epub 2017 Jul 20. 2. Bron AJ, Tomlinson A, Foulks GN, Pepose JS, Baudouin C, Geerling G, Nichols KK, Lemp MA. Rethinking dry eye disease: a perspective on clinical implications. Ocul Surf. 2014 Apr;12(2 Suppl):S1-31. doi: 10.1016/j.jtos.2014.02.002. Epub 2014 Feb 13. PMID: 24725379. 3. Lee HJ, Song HJ, Jeong JH, Kim HU, Boo SJ, Na SY. Ophthalmologic manifestations in patients with inflammatory bowel disease. Intest Res. 2017;15(3):380-387. doi:10.5217/ir.2017.15.3.380 4. Li AL , Li SL, Kam KW, et al Randomised assessor-masked trial evaluating topical manuka honey (Optimel) in treatment of meibomian gland dysfunction. British Journal of Ophthalmology Published Online First: 08 January 2021. doi: 10.1136/bjophthalmol-2020-317506 5. Neudorfer M, Goldshtein I, Shamai-Lubovitz O, Chodick G, Dadon Y, Shalev V. Ocular Adverse Effects of Systemic Treatment With Isotretinoin. Arch Dermatol. 2012; 148 (7): 803–808. doi:10.1001/archdermatol.2012.352 6. Juan Ding, Wendy Kam, David Sullivan; Influence of Isotretinoin on Human Meibomian Gland Epithelial Cells. Invest. Ophthalmol. Vis. Sci. 2012; 53 (14): 598.
Xiaomin
. Sullivan, Amy Gallant Sullivan, Wendy
Kam, Yang Liu. Toxicity of cosmetic preservatives on human ocular surface and adnexal cells, Experimental Eye Research,
170, 2018,
188-197, ISSN 0014-4835, https://doi.org/10.1016/j. exer.2018.02.020. NOTE: Insight readers can scan the QR code or visit insightnews.com.au/cpd/ to access a link to this article to include in their own CPD log book.







The Insight Dry Eye Directory has returned in 2022, featuring a comprehensive list of clinics that have a special interest in dry eye care. This all-in-one resource includes the most up-to-date therapies and diagnostics tools available from leading Australian suppliers. INSIGHT Dry Eye Directory e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au Banner 470x70.pdf 1 31/8/21 6:07 pm Disclaimer: The Insight Dry Eye Directory is compiled of opt-in participants. To update your details for next year’s directory, please email myles.hume@primecreative.com.au
NEW SOUTH WALES / ACT
ATKINS OPTOMETRIST EYECARE PLUS
12 St Johns Ave, Gordon, NSW 2072
Sally Atkins
P (02) 9498 8383
W atkinsoptometrist.com




Ocular lubricants, Omega-3 supplements, lid hygiene, heat compresses and masks, Blephex, dry eye survey and assessment, meibomographer, access to ciclosporin.
CAPITAL EYE
Suite 3B 3 Sydney Ave, Barton, ACT 2600
Dr Jack Guan
P (02) 6273 7458
W capitaleye.com.au
IPL, Ocular 5M Keratograph, Blephasteam, BlephEx, MGD expression.
CUSTOM EYECARE
158 Darby St, Cooks Hill, NSW 2300
Wesley Butler, Rishmie Logendran, Heidi Hunter
P (02) 4927 0500
W customeyecare.com.au
Advanced dry eye diagnosis, management and treatment using latest clinical evidence including eyelid hygiene, steam treatments and gland expression. Monitor for improvements in both signs and symptoms of dry eye disease.
DOUG GRIMSON VISIONWORKS OPTOMETRIST
101 Caldarra Ave, Engadine, NSW 2233
Optometrist
P (02) 8294 3235
W visionworksoptometrists.com.au

Dry eye diagnosis into subtypes. In office therapeutic treatments e.g. debridement, expression and blephasteam.
DRY EYE SOLUTION (OPENING
SPRING 2022)
Albert St, Chatswoord, NSW 2067
Dr Daniel Poon (optometrist)
P (02) 9188 7763
W dryeyesolution.com.au
Dedicated dry eye Clinic, using Toyos Protocols
– Lumenis Optilight IPL, expression, diet, lifestyle, supplements. Complete holistic approach.
Treating DED, MGD, blepharitis, chalazion, styes, ocular rosacea, rosacea.
DRY EYE SOLUTION
8/2 Ilya Ave, Erina, NSW 2250
Dr Anna Spicer (optometrist)
P (02) 4312 4273
W dryeyesolution.com.au
Dedicated dry eye Clinic, using Toyos Protocols
– Lumenis Optilight IPL, expression, diet, lifestyle, supplements. Complete holistic approach.
Treating DED, MGD, blepharitis, chalazion, styes, ocular rosacea, rosacea.
Dedicated dry eye clinic, using Toyos Protocols –
Lumenis Optilight IPL, expression, diet, lifestyle, supplements. Complete holistic approach.
Treating DED, MGD, blepharitis, chalazion, styes, ocular rosacea, rosacea.
EASTERN SUBURBS EYE
SPECIALISTS
Suite 901/ 3, Waverlery St, Bondi Junction, NSW 2022
Dr Matthew Wells
P (02) 9389 4840
W eseyespecialists.com.au
Offer a comprehensive dry eye assessment, and a range of treatments from drops to Lipiflow.
EYECARE PLUS BROADWAY
Shop M110, Level 1, Broadway S/Centre, 1 Bay St, Broadway, NSW 2007
Dr Janice Xue, Dr Soojin Nam
P (02) 9211 6635
W ecplus.com.au
IPL, Blephasteam, Blephex, lid debridement, eye lubricants, supplements.
EYECARE PLUS CHULLORA
Shop 26, Chullora Marketplace, 355 Waterloo Rd, Chullora, NSW 2190
Dr Ali Khalife
P (02) 9642 7799
W ecplus.com.au/dry-eyes/
DOMENIC CARISTO OPTOMETRISTS
Shop 160 Victoria Rd, Gladesville, NSW 2111
Domenic Caristo
P (02) 9816 4157
W facebook.com/caristo.optometrists
Comprehensive dry eye assessment and treatment.



DRY EYE SOLUTION (OPENING 2022)
Cooks Hill, Newcastle, NSW 2200
Ms Liz Cubis
P (02) 4088 8886
W dryeyesolution.com.au
IPL, Blephasteam, Blephex, lid debridement, eye lubricants, supplements.
EYECARE PLUS KAREELA
Shop T2, 1-13 Freya St, Kareela, NSW 2232
Alexander Du
P (02) 9528 2041
W ecplus.com.au
... not a dry eye in sight
DRY EYE DIRECTORYCLINICS
Dry eye assessment, Blephasteam and lid debridement, therapeutic management, Nulids, dry eye products (lubricants, lid wipes, eyelid foams, Lacritec).
EYECARE PLUS MOSS VALE
4/1 Kirkham St, Moss Vale, NSW 2577
Lara Foster

P (02) 4868 2233
W mossvale@eyecareplus.com.au
IPL, Blephasteam, meibomianography, eye drops, neutraceuticals, punctal plugs, tear film assessment.
EYERYS I CARE
Suite 3/142 Argent St, Broken Hill, NSW 2880
Dr Siri Tang
P (08) 8087 8099
W eyerysicare.com.au
MGD expressions, topography, punctal plugs, tear duct irrigation, Optimel products, Blephadex products, lid wipes, Omega-3 capsules and lubricants, NovaTears with Omega. Eye compress wheat bags. In office lid cleansing.
EYERYS I CARE
107 Morgan St, Broken Hill, NSW 2880
Dr Siri Tang
P (08) 8087 8099
W eyerysicare.com.au
MGD expression, punctal plugs, tear duct irrigation, Blephadex wipes, foams. Lid scrubs, Manuka honey products, Evolve, NovaTears, Novatears with Omega. Fish oil and Omega products, Lacritec.
EYEWEAR YOUWEAR
Shop 5, 285A Crown St, Surry Hills, NSW 2010
Dianne Pyliotis
P (02) 9267 4099
W ewyw.com.au
IDRA dry eye assessor, Blephasteam, meibography cameras, biomicroscopy cameras, Sistemi Activa heat and massage treatment, Lumenis IPL, therapeutics.
HANSEN EYECARE PLUS
170 Summer St, Orange, NSW 2800
Jake Hansen
P (02) 6362 2222
W HansenOptom.com.au
Therapeutically endorsed, initial dry eye assessment, meibomian gland expression, IPL, BlephEx/lid margin debridement, offer wide range of dry eye drops and heat masks etc.
ICON
28/2a Cross St, Hurstville, NSW 2220
Michael Mihailidis
P (02) 9580 5766
W iconeyewear.com.au
IPL, Rexon, Lipiflow, Lumenis, keratograph assess, MGD expression.
MARSDEN EYE SPECIALISTS
152 Marsden St, Sydney, NSW 2150
P (02) 9635 7077
W marsdeneye.com.au/
Keratograph to assesses multiple parameters associated with dry eyes and quantify and monitor improvement in patients. A machine that assesses tear osmolarity and use the OSDI questionnaire.
CLINICS
e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au Banner 470x70.pdf 1 31/8/21 6:07 pm




OPTIQUE BARANGAROO
Shop 6, Tower 3 Barangaroo Ave, Barangaroo, NSW 2000
Chiara Da Rin
P (02) 9290 3999
W Info@optiquebarabgaroo.com.au
Meibography, BUT, warm compress, Blephasteam
expression, drop selection, diagnosis and supplements.
R AND B OPTOMETRIST BANORA
POINT
Darlington Dr, Banora Point, NSW 2486
Bernhard Kurtz
P (07) 5524 4550
W facebook.com/rbsoptomertristbanoravillage/
Comprehensive investigation of underlying issues and tailor-made strategies to reduce symptoms.
RJK OPTOMETRY
14 Arthur St, Coffs Harbour, NSW 2450
Michael Jones
P (02) 6651 1139
W rjkoptometry.com.au
Full suite of dry eye services, including IPL.
THE EYE PRACTICE
Level 3, 50 York Street, Sydney, NSW 2000
Jim Kokkinakis
P (02) 9290 1899
W theeyepractice.com.au
Lipiview, meibography, NITBUT, tear volume, infrared tear film analysis, LipiFlow, Lumenis IPL, Miboflo, Rexon-Eye.
TRACTON OPTOMETRISTS
Shop 3/241 Oxford St, Bondi Junction, NSW 2022
Daniel Tracton
P (02) 9188 9288
W tractonoptometrists.com
Full dry eye assessment with a full range of dry eye products. Therapeutically endorsed.
UNSW OPTOMETRY CLINIC
Gate 14 Barker St, UNSW, NSW 2052
Maria Markoulli
P (02) 9384 4624
W optometry.unsw.edu.au/optometry-clinic/dryeye-clinic
A state-wide referral centre for the diagnosis, imaging and evidence-based management of dry eye disease.
WESTMEAD EYES OPTOMETRISTS
Shop T204a, Westmead Hospital, 166
Hawkesbury Rd, Westmead, NSW 2145
Kevin Trac
P (02) 9635 8464
W westmeadeyes.com.au
Blephasteam treatment, meibomian gland expression, fish oil, Omega-3 and Flaxseed tablets, eye drops, therapeutic medications and scleral lenses.
WISE EYES OPTICAL
Shop 4, 2-4 Kenny Street, Wollongong, NSW 2500
Andrew Reveley
P (02) 4227 3330
W wiseeyes.com.au
Comprehensive dry eye assessment, including meibography, Blephasteam, expressions and E-Eye IPL treatments.
VICTORIA
ACUITY EYECARE
200 High St, Lower Templestowe, VIC, 3107
Steve Dinh
P (03) 8850 0400
W acuityeyecare.com.au
We offer meibography, drops, tablets, IPL, blepharitis manangement.
ALTONA OPTICAL
63 Pier St, Altona, VIC 3018
Caroline Burden
P (03) 9398 4279
W visionadvantage.com.au
E-Eye IPL, Blephasteam, at home dry eye treatments, including heat masks.
DRY EYE CENTRE
142 Canterbury Rd, Heathmont, VIC 3135
Dr Nicholas Young
P (03) 9729 4077
W dryeyecentre.com.au
Extensive evaluation of ocular surface disease with Oculus K5 imaging and osmolarity testing. Treatments available include amniotic membranes, Lumenis M22 IPL, Lipiflow, BlephEx, compounded eye drops, Lotemax, Xiidra and Ikervis.
DRY EYE DISEASE CLINIC |
AUSTRALIAN COLLEGE OF OPTOMETRY
374 Cardigan St, Carlton, VIC 3053
Varny Ganesalingam
P (03) 9349 7455
W aco.org.au/dry-eye
The only dedicated public health dry eye disease clinic. Clinical treatments include: LipiFlow, Blepharo exfoliation, meibomian gland expression, Lacrimal lavage, punctal plugs, bandage contact lenses.
e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au Banner 470x70.pdf 1 31/8/21 6:07 pm
MG
CLINICS
EVERGREEN OPTICAL CARNEGIE
Shop 2/2-20 Koornang Rd, Carnegie, VIC 3163
Khang Ta
P (03) 9571 3233
W evergreenoptical.com.au
LipiFlow, BlephEx, Demodex assessment and treatment, Forcep expression, nutritional supplements, punctal plugs.
EYECARE CONCEPTS OPTOMETRY
Suite 14, 828 High St, Kew East, VIC 3102
Dr Philip Cheng
P (03) 9819 7695
W eyecareconcepts.com.au
Comprehensive dry eye assessment, meibography
and anterior eye imaging with Oculus K5 and Medmont Meridia, eye spa treatment with heat masks, Blephasteam, and IPL treatment.
EYECARE PLUS SPRINGVALE
37a Buckingham Ave, Springvale, VIC 3171
Denise Lee
P (03) 9558 4499
W eyecareplusSpringvale.com.au
Comprehensive dry eye work-up using the K5 keratograph, I-Pen, inflammadry and staining. A range of advance treatments such as Lipiflow, IPL, Rexon-Eye and Blephasteam, as well as BlephEx to manage blepharitis.
GRAHAM HILL EYECARE
98 Maude St, Shepparton, VIC 3630
Mark DePaola
P 427212811
W hilleyecare.com.au
K5 dry eye assessment, IPL, blephasteam, therapeutic management, sale of over the counter eyedrops and heat bags.
KOSMAC & CLEMENS
Shop 48C, 134 Condon St, Bendigo, VIC 3550
Ian Clemens
P (03) 5441 8841
W kosmacandclemens.com.au
Dry eye evaluation using latest equipment such as meibography, tear break-up evaluation, fluorescein and lissamine green evaluations, lid expression, prescriptions for tear supplements, cyclosporin etc, and IPL treatment.
KOSMAC & CLEMENS OPTOMETRISTS
Shop 48C Strath Village Shopping Centre, Kennington, VIC 3550
Caleb Van Cooten
P (03) 5441 8841
W kosmacandclemens.com.au
Oculus K5, IPL, Blephasteam, Schirmer test, fluorescein, lissamine green, meibomian gland expression.
LEVERETT & KINDLER
OPTOMETRISTS
Shop 3A & 3C 35-39 Main St, Greensborough, VIC 3088
Amelia Na Jiao
P (03) 9435 4866
W leverettandkindler.com.au
Dry eye test, meibography, Lumenis IPL, Blephsteam, BlephEx, lid margin debridement, meibomian gland expression and range of dry eye products.
SANCTUARY LAKES EYECARE
Shop 18, Sanctuary Lakes Shopping Cent, 300 Point Cook Rd, Point Cook, VIC 3030
Jenkin Yau
P (03) 9395 7530
W eyecarepoint.com.au
Lumenis M22 IPL, Blephex, Blephasteam,
meibomian gland expression, Demodex management, dry eye assessment, including meibography.
SOUTH WEST EYE SURGERY
174 Koroit St, Warrnambool, VIC 3280
Dr Vincent Lee
P (03) 55624488
W drvincentlee.com.au
Diagnosis and treatment of dry eye disease.
VISIONPRO OPTOMETRISTS
288 Main Rd East, St Albans, VIC 3021
Minh Van Tran
P (03) 9364 5509
W visionpros.com.au
Comprehensive dry eye diagnosis and treatment with a range of tear supplements and prescription drops.
QUEENSLAND
ABOUT SPECS OPTOMETRISTS
Shop 35/1 Main St, Springfield Central, QLD, 4300
Sophie Formby
P (07) 3470 0888
W aboutspecs.com.au
MYAH tear and dry eye assessment, dry eye products, including masks, blepharitis treatments and lubricants.
ENVISION OPTICAL
Shop 19, 7 Classic Way, Burleigh Waters, QLD 4220
Andrew Bowden
P (07) 5593 7844
W envisionoptical.com.au
Comprehensive digital diagnostic scanning, with tailored treatment programs including advanced treatment technology such as IPL therapy, Lipiflow thermal pulsation, amniotic membranes and more.
... not a dry eye in sight
DRY EYE DIRECTORY
EYE & LASER CENTRE GOLD COAST
Level 4/2 Short St, Southport, QLD 4215
Dr Frank Howes
P (07) 5555 0800
W eyeandlasercentre.com.au
Rexon, IPL, steam goggles.
EYE ENVY OPTOMETRIST
Shop 56a Morayfield Shopping Centre, Morayfield, QLD 4506
Justin Gribbin
P (07) 5432 3077
W eyeenvyoptometrist.com.au/
Dry eye assessment, Lumenis M22 IPL treatments for dry eye and rosacea, Blephasteam. Meibography and tear film analysis.
EYECARE EYEWEAR
87 Cunningham St, Dalby, QLD 4405
Tom Roger
P (07) 4669 7072
W ecew.com.au

Therapeutic endorsement and prescribing, eyelash and eyelid cleaning, eyelid margin debridement, Blephasteam and meibomian gland expression.
EYECARE PLUS ALEXANDRA HILLS APHRODITE LIVANES OPTOMETRIST
Alexandra Hills Shopping Centre, 71 Cambridge Dr, Alexandra Hills, QLD 4161
Aphrodite Livanes
P (07) 3824 1878
W livanes.com.au
BlephEx and IPL therapy and dry eye solutions (drops, gels or ointments), Eyeseals sleep masks, medicated wipes, and foams such as Blephadex.
EYECARE PLUS ASHGROVE
260 Waterworks Rd, Ashgrove, QLD 4060
Dr Julie Albietz
P (07) 3463 0349
W eyecareplusashgrove.com.au
Dr Albietz’s PhD has equipped her with an extensive clinical research and publication record in the dry eye, tear film and the ocular surface field. Optilight IPL machine, tear film testing, slit lamp imaging, plug insertion.
EYECARE PLUS MERMAID BEACH
Shop 3A, 2431 Gold Coast Highway, Mermaid Beach, QLD 4218
Jackson Yip
P (07) 5526 1400
W eyecareplusmermaidbeach.com.au
Leading dry eye solutions on the Gold Coast. Rexon-Eye, IPL, Blephasteam, meibomian gland expression, dry eye home therapies, OptimelManuka honey eye drops.
H2 VISION CENTRES
Shop 7/ 11-19 Chancellor Village Blvd, Sippy Downs, QLD 4556
Clodagh Sinnott
P (07) 5353 5080
W h2visioncentres.com.au
Dry eye diagnosis, treatments include heat packs, expression and lid scrubs. Initial reviews are fortnightly.
HERON EYECARE
147 Russell St, Toowoomba, QLD 4350
Hugh Bradshaw, Adam Barron
P (07) 4639 2378
W heroneyecare.com.au
IPL, RexonEye, BlephEx, scleral contact lenses, Rx eye drops.
LEES & HENSCHELL OPTOMETRISTS

12 Wongabel St, Kenmore, QLD 4069
Dr Beata Sander
P (07) 3378 7899
W lhvision.com.au
Rexon, heat masks, solutions, prescriptions for pharmacy only medication, dry eye assessment using K5.
LOOKING SMART OPTOMETRISTS
2/44 Pelican Waters Blvd, Pelican Waters, QLD 4551
David O’Neill
P (07) 5439 7844
W LookingSmartOptometrists.com.au
Three full time optometrists that are therapeutically qualified to prescribe a manner of different treatments on PBS. Also offer services such as punctal plugs and Blephasteam.
OPTICAL SUPERSTORE BUNDABERG
Shop 2/149 Bourbong St, Bundaberg, QLD 4670
Andrew Christiansen
P (07) 4152 2506
W facebook.com/
TheOpticalSuperstoreBundaberg/
Comprehensive assessments of dry eye signs including using K5 Keratograph dry eye and meibomian gland analysis. Numerous dry eye products and Blephasteam treatment.
OPTIKUS OPTOMETRISTS
3/1 Chancellor Village Blvd, Sippy Downs, QLD 4556
Zahn Kidson
P (07) 5456 4300
W optikus.com.au
Rexon Eye, Blephasteam, meibography, tear film analysis, gland expression, hot compresses, lubrication.
e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au Banner 470x70.pdf 1 31/8/21 6:07 pm DRY EYE DIRECTORYCLINICS
a dry eye in sight
REFRESH® Eye Drops (Polyvinyl Alcohol and Povidone) are leaving shelves. REFRESH Plus® is formulated with lubricating carmellose sodium (CMC) and is available to relieve dry eyes and discomfort associated with contact lens wear. WHEN PATIENTS WANT TO SEE THE WORLD WITH FRESH EYES, RECOMMEND REFRESH PLUS ® • Contains electrolytes found in natural tears4,5 • Suitable for use after LASIK surgery6 • CMC is an ocular lubricant supported by over 30 years of research7,8 • Fast-acting, long-lasting formula1,2 • Relief from contact lens discomfort6 • Preservative-free relief for eyes sensitive to preservatives3 REFRESH ® HAS RETIRED HELLO REFRESH PLUS® ©2022 Allergan. All rights reserved. ™®Trademark and registered trademark of Allergan, Inc. Allergan Australia Pty Ltd. 177 Pacific Highway, North Sydney, NSW 2060. ABN 85 000 612 831. AU-RFS-220014. ALL-003027-00. Date of preparation: August 2022. References: 1. Bruix A, et al. Arch Soc Esp Oftalmol 2006;81(2):85–92. 2. Noecker RJ. Eye Contact Lens 2006;32(3):148–52. (Funded by an unrestricted educational grant from Allergan, Inc., Irvine, CA.) 3. REFRESH PLUS® Product Information. 4. Alanazi SA et al. Clin Ophthalmol 2019;13:1011–7. 5. Tiffany JM. Eye (Lond) 2003;17(8):923–6. 6. Garrett Q et al. Invest Ophthalmol Vis Sci 2007;48(4):1559–67. 7. Grene RB et al. Cornea 1992;11(4):294–301. (sponsored by Allergan). 8. Adams J et al. Cornea 1992;11(3):134–241. (sponsored by Allergan). PBS Information: Refresh Plus (30 x 0.4ml) is not listed on the PBS.... not
OPTIONS EYECARE PEREGIAN BEACH
Shop 4/220 David Low Way, Peregian Beach, QLD 4573
Helen Kim
P (07) 5471 2399
W Optionseyecareperegian.com
Blephex cleaning tool, hot compress. Digital meibomian gland expression.
SOMERVILLE AND MERRIN OPTOMETRISTS
Shop 10, 11 James St, Toowoomba, QLD 4350
John Merrin
P (07) 4659 9599
W smnoptometrists.com.au
Offer Oculus K5 Analysis, IPL, Blephasteam and therapeutic solutions.
STUART MACFARLANE
OPTOMETRIST
Shop 78, Logan City Centre, Cnr Kingston and Wembley Rds, Logan Central, QLD 4114
Stuart Macfarlane
P (07) 3299 3699
W macfarlaneoptometrist.com.au
Comprehensive dry eye assessment, Blephasteam, punctal plugs, lacrimal lavage.
THE EYE HEALTH CENTRE
Level 11, 87 Wickham Tce, Brisbane, QLD 4000
Jason Holland
P (07) 3831 8606
W theeyehealthcentre.com.au
Comprehensive diagnostic and treatment options, including Optima IPL, Rexon-Eye, BlephEX, Blephasteam, punctal plugs, amniotic membranes and debridement.
THE EYE HEALTH CENTRE
44 South Station Rd, Booval, QLD 4304
Phuc Q. Ngo
P (07) 3282 4396
W theeyehealthcentre.com.au
Diagnostics, KG5, IPL, Blephasteam, serum tears, plus cyclosporin.
THE EYEWEAR SHOP
Shop 15G, 25 Samuel St, Camp Hill, QLD 4152
Minh Nguyen
P (07) 3395 4105
W theeyewearshop.com.au
Blephasteam, tear film slit lamp assessment, Schirmer testing, lacrimal lavage, punctal plugs.
VIRGINIA HENRY OPTOMETRISTS
13A/39 Eyre St, Northward, QLD 4810
Virginia Henry
P (07) 4724 1700
W vmoptical.com.au
E-Eye IPL, ocular lubricants, thermal masks, sleep masks, Antares.
SOUTH AUSTRALIA
FIRE STATION OPTOMETRISTS
40A Sturt St,Mount Gambier, SA, 5290
Hayley Greenfield
P (08) 8725 1303
W firestationoptometrists.com.au
Ocular therapeutics and IPL
GULF AND RANGES OPTOMETRISTS
7 Chapel St, Port Augusta, SA 5700
Mitch Hancock
P (08) 8642 2766
W gulfandranges.com.au
We offer three levels of care icluding theraputics, IPL and Rexon.
ALLEVE EYE CLINIC
49a Stephen Tce, St Peters, SA 5069
Jennifer Rayner
P (08) 7225 9798
W alleveeyeclinic.com.au
Diagnosis and treatment of dry eye with a holistic approach using all evidence-based tools available including IPL, topical ciclosporin, punctal plugs and Manuka honey.
EYRE EYE CENTRE
22 Liverpool St, Port Lincoln, SA 5606
Tamra Karolewicz, Elise Pocknee, Phil Clem, Craig Farmer
P (08) 8682 4566
W eyreeyecentre.com.au
OptiLight IPL, Blephasteam, NuLids, Medmont
Meridia dry eye work-up software, including meibography, punctal plugs, Omega-3 supplements, extensive range of lubricants and lid care, therapeutically endorsed optometrists.
PHILIP MILFORD OPTOMETRIST
158 The Pde, Norwood, SA 5067
Philip Milford
P (08) 8364 3011
W PhilipMilfordoptom.com.au
Comprehensive dry eye analysis with IDRA analyser and treatment including Lumenis IPL and Lipiflow.
WESTERN AUSTRALIA
DRY EYE WA
135 Riseley St, Booragoon, WA, 6154
Marilyn Stern
P (08) 6468 5296
W dryeyewa.com.au
e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au Banner 470x70.pdf 1 31/8/21 6:07 pm CLINICS
Analysis services: Meibography, tear break up time, tear osmolarity. Treatments: manual gland expres sion, BlephEx, IPL, Rexon-Eye, LED light, eye lash and lid cleaning, Blephasteam. Take home treat ments for blepharitis and improved eye comfort.
EYECARE PLUS GLEN FORREST
U4 5 Hardey Rd, Glen Forrest, WA, 6071
Kristin Larson, OD
P (08) 9298 9992
W eyecareplus.com.au/glenforrest
Tear film evaluation, Rexon-Eye resonance treatment, blepharitis treatment, stockist of lid cleansers, eye lubricants and supplements.
EZEKIEL EYES
69 Hampden Rd, Nedland, WA, 6009
Damon J Ezekiel
P (08) 8938 63620
W ezekieleyes.com
IPL , scleral lenses, meibomain gland scanning.
FOR EYES OPTOMETRIST
158 High St, Fremantle, WA, 6160
Adrian Rossiter
P (08) 9335 3433
W foreyes.com.au
Full dry eye assessment, including aqueous deficiency and MGD screening with non-invasive tear break up time and osmolarity. IPL treatment with Lumenis M22 and gland expression performed by qualified ophthalmic medicines prescribing optometrists.
LAUBMAN AND PANK BOORAGOON
Shop 20, Westfield Booragoon, 125 Riseley St
Booragoon, WA, 6154
Perry Yeow
P (08) 9364 7144
W laubmanandpank.com.au/ Dry eye assessment, IPL , BlephEx.
OPSM MIDLAND GATE
Midland Gate Shopping Center, 274 Great Eastern Highway, Midland, WA, 6056
Peter Gardner
P (08) 9274 3565
W OPSM.com.au
Dry eye assessment and management , IPL therapy, Blephasteam heat therapy for meibomian gland dysfunction, Blephex blepharitis treatment.
WA OPTICIANS
101 Royal St, East Perth, WA, 6004
Anna Lim
P (08) 9221 0577
W waopticians.com.au
Comprehensive dry eye analysis, management and treatment, including IPL
TASMANIA
TOTAL EYECARE
9 Magnet Ct, Sandy Ba, TAS, 7005
Andrew Koch
P (03) 6223 5940
W totaleyecare.com.au
Assessment of dry eye, best dry eye products recommended, Rexon-Eye dry eye treatment available.
Eye drops formulated with Carmellose Sodium to provide lubrication and moisture for dry eyes and discomfort associated with contact lens wear.





Refresh
Ointment formulated with paraffin to provide overnight relief for dry eyes.
not a dry eye in sight
...
©2022 Allergan. All rights reserved. ™® Trademark and registered trademark of Allergan, Inc. Allergan Australia Pty Ltd. 177 Pacific Highway, North Sydney, NSW 2060. ABN 85 000 612 831. AU-RFS-220045. Date of preparation: August 2022. PBS Information: Refresh Liquigel (15ml) and Refresh Plus (15ml): Restricted benefit. Refer to PBS Schedule for full restricted benefit information. Refresh Night Time (2 x 3.5g) is listed on the PBS.
Plus (30 x 0.4ml) and Refresh Contacts (15ml): These products are not listed on the PBS
THE REFRESH® FAMILY IS STILL HERE TO RELIEVE AND COMFORT YOUR PATIENTS’ EYES
DRY EYE DIRECTORY
Hylo
Hylo-Fresh
NovaTears Omega-3 3ml
VitaPos Ointment 5gm
Bion Tears UD (28 x 0.4mL)
Genteal Lubricant Eye Drops 0.3% (10mL)
Genteal Lubricant Eye Gel 0.3% (10g)
HPMC PAA Gel (10g)
In a Wink Eye Drops 0.3% (10mL)
Poly Gel UD Lubricant Eye Gel (30 x 0.5g)
Poly Visc (3.5g)
Poly Visc Twin Pack (2 x 3.5g)
Polytears (15mL)
Systane Balance Lubricant Eye Drops (10mL)
Systane Complete Lubricant Eye Drops (10mL)
Systane Complete Preservative-Free Lubricant Eye Drops (10mL)
Systane Eye Wash Rinse Solution (120mL)
Systane Gel Lubricant Eye Drops (10mL)
Systane Hydration UD Lubricant Eye Drops (30 x 0.7mL)
Systane Lid Wipes Cleansing Wipes (30 pack)
Systane Original Lubricant Eye Drops (15mL)
Systane Original UD Lubricant Eye Drops (28 x 0.8mL)
Systane Ultra Preservative-Free Lubricant Eye Drops (10mL)
Systane Ultra UD Lubricant Eye Drops (25 x 0.5mL)
Tears Naturale Artificial Tears (15mL)
CELLUVISC Eye Drops
IRCAL Eye Ointment
Alcon Laboratories (Australia)
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Alcon Laboratories (Australia) Pty Ltd
Allergan
Allergan
LIQUIFILM TEARS Eye Drops Allergan
OPTIVE ADVANCED Lubricant Eye Drops
OPTIVE ADVANCED Preservative-Free Lubricant Eye Drops
OPTIVE FUSION Lubricant Eye Drops
OPTIVE FUSION Preservative-Free Lubricant
OPTIVE GEL DROPS Lubricant
OPTIVE Lubricant
Sensitive Eye
TEARS
Allergan
Allergan
Allergan
Allergan
Allergan
Allergan
Allergan
Allergan
Allergan
Allergan
EYE DROPS THERAPIES EYE DROPS GRADE OF DRY EYE NAME Company Mild Moderate Severe
Forte 10ml AFT Pharmaceuticals / Good Optical Services • •
AFT Pharmaceuticals / Good Optical Services • • NovaTears 3ml AFT Pharmaceuticals / Good Optical Services •
AFT Pharmaceuticals / Good Optical Services • •
AFT Pharmaceuticals / Good Optical Services • •
Pty Ltd • •
• •
•
•
• •
•
•
•
• •
• • •
• •
• •
•
• •
•
•
•
•
• •
• • •
• • •
• •
• •
• •
• •
Eye Drops
• •
Eye Drops
• • •
Eye Drops
• • • OPTIVE
Drops
• • PVA
Eye Drops
• • REFRESH LIQUIGEL
• • • REFRESH NIGHT TIME
• • • Viscotears Eye Gel Bausch + Lomb Australia Viscotears Eye Gel PF Bausch + Lomb Australia Avenova Designs For Vision / Avenova Optimel Manuka + Antibacterial Drops Designs For Vision / Melcare • • Optimel Manuka + Forte Gel Designs For Vision / Melcare • • THERAPIES e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au Banner 470x70.pdf 1 31/8/21 6:07 pm
services.com.au
services.com.au
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
visioncareorders.anz@Alcon.com
australiaenquiries@allergan.com
australiaenquiries@allergan.com
australiaenquiries@allergan.com
australiaenquiries@allergan.com
australiaenquiries@allergan.com
australiaenquiries@allergan.com
australiaenquiries@allergan.com
australiaenquiries@allergan.com
australiaenquiries@allergan.com
australiaenquiries@allergan.com
australiaenquiries@allergan.com
australiaenquiries@allergan.com
australiaenquiries@allergan.com
ausorders@bausch.com
ausorders@bausch.com
info@dfv.com.au
info@dfv.com.au
DRY EYE DIRECTORY TREATMENT TYPE PARTICULARS EmailTear insufficiency/ Aqeuous deficiency Evaporative/ Meibomian gland dysfunction Anti- inflammatory Eye lid Preservative- free Contact lens friendly Prescription Over the counter PBS-listed • • • • • orders@goodoptical services.com.au • • • • • orders@goodoptical services.com.au • • • • orders@goodoptical services.com.au • • • orders@goodoptical
• • • • • orders@goodoptical
• • • • •
• • •
• • • •
• • • •
• • •
• • • •
• • • •
• • • •
• • • •
• •
• • •
• • • •
•
• • • •
•
• •
• • •
• • • •
• • • •
• • • •
• • • •
• • • •
• • •
• •
• • •
• • •
• • • •
• •
• • •
• • •
• • •
• • • •
• • • •
• • •
• • • •
•
• • • • •
• • • • • info@dfv.com.au DRY EYE DIRECTORY ... not a dry eye in sight
Optimel Manuka+
Optimel Manuka+
Optimel Manuka+
BlephaDex
Bruder Hygenic
Xalin eye
Xalin Fresh
Xalin Hydrate
Xalin Night Gel
Cationorm Multi
GRADE OF DRY EYE NAME Company Mild Moderate Severe Optimel Manuka+ Eyelid Cream Designs For Vision / Melcare Fluorescein strips Device Technologies / Clement Clarke • • • AUTOLOGOUS Emagin Pty Ltd • • • Alcon (including Systane Range) Good Optical Services / Alcon Allergan (including Optive Range) Good Optical Services / Allergan • • Cationorm 10ml Good Optical Services / Seqirus (Aust) P/L • • • Cationorm UD 30x0.4ml Good Optical Services / Seqirus (Aust) P/L Johnson & Johnson (including Blink range) Good Optical Services / Johnson & Johnson • • Tears Again (Liposomal Eye Spray) Good Optical Services / Bio Revive • • BLINK CONTACTS EYE DROPS 10ML Johnson & Johnson Vision (AMO) BLINK INTENSIVE TEARS PLUS GEL EYE DROPS 10ML Johnson & Johnson Vision (AMO) • • BLINK INTENSIVE TEARS PROTECTIVE EYE DROPS 0.4MLX20 Johnson & Johnson Vision (AMO) • • BLINK INTENSIVE TEARS PROTECTIVE EYE DROS, 15ML Johnson & Johnson Vision (AMO) BLINK N CLEAN LENS DROPS 15ML Johnson & Johnson Vision (AMO) • •
Dry Eye drops Jubelee Eyecare Supplies • • •
Eyelid Cream Jubelee Eyecare Supplies
Forte Eye Gel Jubelee Eyecare Supplies • • Xiidra (lifitegrast) Novartis Pharmaceuticals Australia Pty Limited • •
Foam NICNAS regitered OptiMed
Eyelid solution SPRAY (HA 0.02%) Glass bottle (NICNAS registered) OptiMed
Gel OptiMed • • •
single dose eye drop OptiMed
eye drop OptiMed • •
OptiMed • •
Dose 10mL Seqirus Cationorm Single Unit Ampoules x30 Seqirus • • • Ikervis (1mg/mL ciclosporin) Single Unit Ampoules x30 Seqirus SBM Activa BOC Instruments • • • Epicon LC Capricornia • • Katt Miniscleral Capricornia • • ARITA MEIBOMIAN GLAND COMPRESSING FORCEPS Designs For Vision / Albert Heiss • • Mastrota Forcep Designs For Vision / PRICON • • Mastrota Meibonian Gland Paddle Designs For Vision / PRICON • • Oasis Punctal Plugs Designs For Vision / Oasis • • • Debridement equipment, spuds etc Device Technologies / Katena • • • Epilation forceps Device Technologies / Katena • • • Gland expression Forceps Device Technologies / Katena • • • Punctal Plugs - Permanent occlusion Device Technologies / Eagle Vision • • • Punctal Plugs - Temporary occlusion Device Technologies / Eagle Vision • • • Nulids MDG Machine Good Optical Services / NuSight Medical USA • • Ocusoft Compliance Kit 50ml + 100 Pads Good Optical Services / OCuSOFT USA • Ocusoft Hypochlor Gel 59ml Good Optical Services / OCuSOFT USA • Ocusoft Hypochlor Spray 59ml Good Optical Services / OCuSOFT USA • Ocusoft Lid Scrub Bottle 50ml Good Optical Services / OCuSOFT USA • • e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au Banner 470x70.pdf 1 31/8/21 6:07 pm THERAPIES DEVICES / EQUIPMENT
info@dfv.com.au
customers@device.com.au
enquiries@emagin.com.au orders@goodoptical services.com.au
orders@goodoptical services.com.au
orders@goodoptical services.com.au orders@goodoptical services.com.au
orders@goodoptical services.com.au
orders@goodoptical services.com.au Mkayrouz@ITS.JNJ.COM
Mkayrouz@ITS.JNJ.COM
Mkayrouz@ITS.JNJ.COM Mkayrouz@ITS.JNJ.COM
Mkayrouz@ITS.JNJ.COM
manager@jubelee.com manager@jubelee.com
manager@jubelee.com
medinfo.phauno@novartis.com sales@optimed.com.au
sales@optimed.com.au
sales@optimed.com.au sales@optimed.com.au
sales@optimed.com.au
sales@optimed.com.au aunz.medicalinformation@seqirus.com
aunz.medicalinformation@seqirus.com
aunz.medicalinformation@seqirus.com
sales@bocinstruments.com.au
info@capcl.com.au
info@capcl.com.au
info@dfv.com.au
info@dfv.com.au
info@dfv.com.au
info@dfv.com.au
customers@device.com.au
customers@device.com.au
customers@device.com.au
customers@device.com.au
customers@device.com.au
orders@goodoptical services.com.au
orders@goodoptical services.com.au
orders@goodoptical services.com.au
orders@goodoptical services.com.au
orders@goodoptical services.com.au
not a dry eye in sight
TREATMENT TYPE PARTICULARS EmailTear insufficiency/ Aqeuous deficiency Evaporative/ Meibomian gland dysfunction Anti- inflammatory Eye lid Preservative- free Contact lens friendly Prescription Over the counter PBS-listed
• • • •
• • • • • • •
• • •
• • • • • • • •
• • •
• • • • •
•
• •
•
• • • • • •
• • • • • • •
• • • •
• • •
• • • •
• • • •
• • • •
• • • • •
• • •
•
•
• •
•
•
•
•
• •
• •
• •
• •
• •
• • •
• •
• •
• •
•
...
DRY EYE DIRECTORY
Bleph-Ex
Blephadex
Bruder
Bruder
Bruder
Bruder
Bruder
Bruder Karpecki
Bruder
Bruder
Bruder
Opti-Soothe Preservative-free Eyelid
Optisoothe Tea Tree Eyelid Wipes
Opti-Soothe Moist Heat Mask Reusable mask
Eye Eco Advanced Tea Tree Foaming Facial Cleanser
Eye Eco D.E.R.M. Mask
Eye Eco Tea Tree Foaming Facial Cleanser
Eye Eco Tranquileyes Advanced XL Kit (moist heat therapy)
Eye-Eco Eye Seals
Eye-Eco EyeCloud
Eye-Eco Quartz & Onyx for lagophthalmos
I-LID'N'LASH Cleansing Wipes
I-LID'N'LASH PLUS Antiseptic Cleansing Wipes
Tear Restore Mask + 2 gel inserts
The Eye Doctor Allergy Mask
The Eye Doctor Antibacterial Stye Relief Compress (Single eye patch)
Optical
Vision
Vision
Eye
Optical Services
Optical Services
Tear
The Body Doctor
The Body
GRADE OF DRY EYE NAME Company Mild Moderate Severe Ocusoft Oust Demodex Foam 50ml Good Optical Services / OCuSOFT USA • Ocusoft Oust Demodex Sachets 30s Good Optical Services / OCuSOFT USA • Ocusoft Platinum Plus 50ml Good Optical Services / OCuSOFT USA • Ocusoft Plus Bottle 50ml Good Optical Services / OCuSOFT USA • • Ocusoft Plus Sachets 30s Good Optical Services / OCuSOFT USA • • Ocusoft Sachets 30s Good Optical Services / OCuSOFT USA • • Ocusoft Swab Stix (In Practice Oust & Plus) Box 12 Good Optical Services / OCuSOFT USA • • • LipiFlow Thermal Pulsation System Johnson & Johnson Vision • • • C.STIM - I.P.L. (Intense Pulsed Light) System Lumibird Medical • • •
OptiMed • • •
Applicator (in office use only) NICNAS registered OptiMed •
- Collins expressor Forceps OptiMed • • •
- Karpecki punctal plug forceps OptiMed • • •
- Livengood gland expressor paddle OptiMed • • •
- Longnose expressor OptiMed • • •
epilation forceps OptiMed • • •
Debrider OptiMed • •
KARPECKI-LINDSTROM Gold Line OSD Instrument Set (contains six instruments). OptiMed • • •
recatangular expressor OptiMed • • •
roller expressor OptiMed • • • Thermaye Plus IPL (DEVICE) OptiMed
Wipes AFT Pharmaceuticals / Good Optical Services • • •
20s AFT Pharmaceuticals / Good Optical Services • •
AFT Pharmaceuticals / Good Optical Services • • •
Designs For Vision / Eye Eco • •
Designs For Vision / Eye Eco • •
Designs For Vision / Eye Eco •
Designs For Vision / Eye Eco • •
Designs For Vision / Eye Eco • •
Designs For Vision / Eye Eco • • •
Designs For
/
Eco • • •
Designs For
/ I-MED Pharma •
Designs For Vision / I-MED Pharma • •
Good
Services /
Restore USA • •
Good
/
UK • • •
Good
/
Doctor UK • • • The Eye Doctor Lid Wipes Sachets 20's Good Optical Services / The Body Doctor UK • • The Eye Doctor Liquid Lid Cleanser (Argon & Coconut Oil/Micellar Water) Good Optical Services / The Body Doctor UK • • The Eye Doctor Sterileyes Antibacterial Click'N'Go Travel Mask Good Optical Services / The Body Doctor UK • • The Eye Doctor Sterileyes Antibacterial Hot/Cold Eye Compress Good Optical Services / The Body Doctor UK • • • The Eye Doctor Tea Tree Lid Wipes 20's Good Optical Services / The Body Doctor UK • • BlephaDex Wipe (regular and PRO) NICNAS registered OptiMed • • • Bruder Eye compress OptiMed • • • Bruder Eye wipe (NICNAS registered) OptiMed • • • Bruder Eyeleave Eye compress OptiMed • • • Eye Gienie compress NICNAS registered OptiMed • • • OptiMed USB Eye warmer NICNAS registered OptiMed • • • e: goodopt@ozemail.com.au p: +61 3 9645 1066 / f: +61 3 9681 7976 www.goodopticalservices.com.au Banner 470x70.pdf 1 31/8/21 6:07 pm THERAPIES WIPES / MASK
orders@goodoptical services.com.au
orders@goodoptical services.com.au
orders@goodoptical services.com.au
orders@goodoptical services.com.au
orders@goodoptical services.com.au
orders@goodoptical services.com.au
orders@goodoptical services.com.au
dyates7@its.jnj.com
salesadmin@ellex.com
sales@optimed.com.au sales@optimed.com.au
sales@optimed.com.au
sales@optimed.com.au
sales@optimed.com.au
sales@optimed.com.au
sales@optimed.com.au
sales@optimed.com.au
sales@optimed.com.au
sales@optimed.com.au
sales@optimed.com.au
sales@optimed.com.au
orders@goodopticalservices.com.au
orders@goodopticalservices.com.au
orders@goodopticalservices.com.au
info@dfv.com.au
info@dfv.com.au
info@dfv.com.au
info@dfv.com.au info@dfv.com.au info@dfv.com.au info@dfv.com.au
info@dfv.com.au
info@dfv.com.au
orders@goodopticalservices.com.au
orders@goodopticalservices.com.au
orders@goodopticalservices.com.au
orders@goodopticalservices.com.au
orders@goodopticalservices.com.au
orders@goodopticalservices.com.au
orders@goodopticalservices.com.au
orders@goodopticalservices.com.au
sales@optimed.com.au
sales@optimed.com.au
sales@optimed.com.au
sales@optimed.com.au
sales@optimed.com.au
sales@optimed.com.au
a dry eye in sight
TREATMENT TYPE PARTICULARS EmailTear insufficiency/ Aqeuous deficiency Evaporative/ Meibomian gland dysfunction Anti- inflammatory Eye lid Preservative- free Contact lens friendly Prescription Over the counter PBS-listed • •
• •
• •
• •
• •
• •
•
• • • •
• • • • •
• • •
• • •
• •
• • •
• • •
• •
• • •
• • •
• • •
• • •
• • • •
• • •
• •
• • • • •
• •
• • • • •
• •
• • • •
• • •
• • • •
• • • •
• • •
• • •
• •
• • •
• • •
•
• •
• • • •
• • • •
• • • • •
• • • • •
• • •
• • •
... not
DRY EYE DIRECTORY

BIOMETRIC INTELLIGENT GLASSES BUILT ON AI TECHNOLOGY B.I.G. NORM™ Rodenstock’s new AI technology and data from over 500,000 biometric eye scans deliver sharper vision to more progressive lens users. By using Artificial Intelligence, Rodenstock brings a new level of biometric precision into lens calculation that will help users achieve sharper vision. Go to: rodenstock.com/bigvisionforall Follow: #BIGVISIONFORALL DIAGNOSTIC CAPABILITY NAME Company Meimbography Lipid layer thickness Tear meniscus height Blinking rate/ quality DSLC200 & DEM100/DEM100PLUS BOC Instruments • • • • SBM IDRA BASIC & FULL BOC Instruments • • • • I-Pen Designs For Vision / I-MED Pharma OCULUS Keratograph 5M Designs For Vision / OCULUS • • • Topcon CA-800 - corneal topography, basic lens fit, Dry eye suite Device Technologies / Topcon • • • • Topcon MYAH - Axial lenth, corneal topography, basic lens fit, Dry eye suite Device Technologies / Topcon • • • • Topcon SL-D701 slitlamp w/ DC4 camera for gland imaging Device Technologies / Topcon • • • • TearLab - Tear Film Osmolarity Diagnostic System IQ Medical Pty Ltd LipiScan Johnson & Johnson Vision • LipiView II Johnson & Johnson Vision • • • MGE (Meibomian Gland Evaluator) Johnson & Johnson Vision medmont meridia Professional Medmont • • Mediworks D130 (available with S360 slit lamp) OptiMed • • • • DIAGNOSTICS
dyates7@its.jnj.com
dyates7@its.jnj.com


info@medmont.com
sales@optimed.com.au






Everyone is invited For the first time in our 30+ year history, we’re giving Members, Non-Member Optometrists and Optometry Students alike the opportunity to experience this not-to-be missed biennial event showcasing the very best that independent optometry has to offer. KEYNOTE SPEAKERS KEITH ABRAHAM KATRINA MCCARTER DYLAN ALCOTT AO AMANDA GORE STEVE SAMMARTINO Register at optom.provision.com.au/conference LOOK FORWARD ProVision National Conference Melbourne 21-23 October 2022 Bulbar redness Tear break up time Interferometry Schirmer test Tear osmolarity Ocular surface staining Meibomian Gland performance/ functionality/ expression tool Measuring/ tracking symptoms Blepharitis examination Email • • • • • • • sales@bocinstruments.com.au • • • • • • • sales@bocinstruments.com.au • info@dfv.com.au • • • • info@dfv.com.au • • • customers@device.com.au • • • customers@device.com.au • • • • customers@device.com.au • dayne.geber@iqmedical.com.au dyates7@its.jnj.com •
•
• • • • •
• • • • • •
DRY EYE DIRECTORY





RANZCO WELCOMES END TO ‘LONG AND ARDUOUS HIATUS’ OF ANNUAL SCIENTIFIC CONGRESS
The long and weary return to an in-person RANZCO Scientific Congress will come to an end this month, as the college puts three years of disruption behind it to deliver the premier Australian ophthalmology event at the Brisbane Exhibition and Events Centre.

When the 53rd congress takes place 28 October – 1 November, it will come as a relief for Dr Elsie Chan, Scientific Program Committee chair, Ms Alex Arancibia, head of RANZCO Member Support and Ms Denise Broeren, director of Think Business Events, who have been tasked with rescheduling the event multiple times since the last in-person congress in November 2019.
“We need to look at this with a lens of humour as it’s been a long road to October 2022. The conference centre, venues, speakers and presenters have been extremely accommodating with so many postponements,” organisers told Insight
At the time of writing, RANZCO had accepted almost 700 registrations, but there is now a trend of delegates booking at the last minute to avoid flight and accommodation cancellation costs in the event of catching COVID-19.
“These registration numbers are a little lower than usual than where we’re
usually at with two months to go, but we expect them to reach well over 1,000 by the time of the congress,” organisers said.
There are more than 70 exhibitors and over 100 booth spaces confirmed, along with six hosted sessions. While online conferences have served their purpose, RANZCO believes the return of face-to-face conferences is paramount so members can meet in a format that best meets their learning and networking needs.
“We have seen the wonders of technology at play with the 52nd congress being virtual. There were high levels of interaction and involvement. However, the congress was missing the corridor chats, interactions in the trade and social functions. We know many members value these, hence the demand for an in-person event. For those that can’t make it for any reason, the congress is hybrid,” organisers stated.
The hybrid format will mean plenaries are live-streamed, and concurrent sessions will be recorded and available a week after the presentations. All content will be available to registered delegates for 90 days, and then housed on RANZCO Learning for members.
“Hybrid can mean any number of things – striking a balance between
having accessible content, managing a complex budget, being sustainable and delivering a great experience is tricky. It is also a juggling act between live, prerecorded and virtual presenters, digital cameras, streaming technology, and all the logistics that go along with it,” organisers said.
“We’re not game to predict what 2023 might look like, but we’re working hard to stay on the cutting edge of conferencing.”
The congress is also set to host new innovative sessions, including concurrent presentations on the Business of Eyes, Sustainability and Health and Wellbeing – which move away from the science of ophthalmology.
There will also be the Named and Update lectures. On the day prior to the congress, there will be a hybrid workshop on Ocular Trauma in Low Resource Settings. And on Saturday 29 October, Dr Lynn Gordon will be addressing the Women in Ophthalmology-hosted luncheon.
The Congress Dinner on Sunday 30 October will feature a procession of handovers, with Past-President Dr Heather Mack AM handing to current President Prof Nitin Verma AM and then on to incoming President Dr Grant Raymond. n
"IT IS A JUGGLING ACT BETWEEN LIVE, PRE-RECORDED AND VIRTUAL PRESENTERS, DIGITAL CAMERAS, STREAMING TECHNOLOGY, AND ALL THE LOGISTICS" CONGRESS ORGANISERS
INSIGHT October 2022 53 RANZCO PREVIEW
ONCOLOGY UPDATE LECTURE, SAT 29 OCT
PROF SARAH COUPLAND
Considered to be a trailblazer in ophthalmic pathology, haematopathology, molecular pathology, and biobanking, the UK-based Australian will host a session called ‘Update on Ocular Lymphomas: what’s new in the WHO’. She will present an overview of the upcoming 5th edition of the World Health Organization Classification (WHO) of Haematolymphoid Tumours focussing on lymphoid neoplasms, and how it relates to the two divisions of ocular lymphomas – ocular adnexal lymphomas and intraocular lymphomas.

THE FRED HOLLOWS LECTURE, SAT 29 OCT PROF CLARE GILBERT

Prof Gilbert is trained in surgical retina and worked as a clinical ophthalmologist in the UK for 10 years. She has worked at the International Centre for Eye Health at the London School of Hygiene & Tropical Medicine, UK since 1990, with her main research interest being blindness in children in low and middle income countries. Her lecture will focus on ‘Inequity in Eye Health’, defining the issue before presenting data from national surveys and other studies in Africa and Asia, highlighting inequity in access to eyecare services.
RETINA UPDATE LECTURE, SUN 30 OCT
PROF JAMES BAINBRIDGE
Prof Bainbridge – consultant retinal surgeon at Moorfields Eye Hospital and chair of retinal studies at University College London – will outline key challenges facing retinal gene therapies. For example, the supplementation of large genes will depend on new vector systems, while optimal safety and efficacy will demand improved control of dosing and inflammatory responses. Gene editing advances offer the potential for permanent correction, but trials for novel approaches must have appropriate quality of life outcome measures.
UVEITIS UPDATE LECTURE, SUN 30 OCT
PROF DEBRA ANNE GOLDSTEIN

Prof Goldstein received her medical degree from McGill University, Canada, where she completed an ophthalmology residency and pursued a fellowship in uveitis and ocular immunology followed by a second uveitis fellowship at University of Illinois. She has published over 250 peer-reviewed papers and book chapters, and has lectured globally. Goldstein is the Magerstadt Professor of Ophthalmology and the director of the Uveitis Service at Northwestern University’s Feinberg School of Medicine.
THE DAME IDA MANN MEMORIAL LECTURE, SUN 30 OCT
PROF HELEN DANESH-MEYER

Prof Danesh-Meyer is the first female Professor of Ophthalmology in New Zealand and holds the Sir William and Lady Stevenson chair in ophthalmology and head of academic neuro-ophthalmology and glaucoma. She was the youngest appointed professor at the University of Auckland Faculty of Medical and Health Sciences and one of the few women who is professor in a surgical speciality. She is a clinicianscientist, publishing around 200 papers in glaucoma and neuro-ophthalmology and has raised over $15 million in grant funding.
CATARACT UPDATE LECTURE, MON 31 OCT

PROF GRAHAM BARRETT


The WA ophthalmologist behind the Barrett IOL formulae will provide an update on the different type of extended depth of focus (EDOF) or ‘monofocal-plus’ IOLs that are likely to challenge the multifocal IOL category as a preferred lens for cataract surgery. EDOF IOLs can be used in conjunction with modest levels of monovision for additional spectacle independence, but an understanding of the optical principles is important, as well as familiarity with clinical data, patient outcomes and even an element of philosophy in selecting the right lens.
THE SIR NORMAN GREGG LECTURE, MON 31 OCT
PROF IAN MCALLISTER
In his lecture ‘Retinal vein occlusion: Where are we and where are we going?’, Prof McAllister – a Professor of Ophthalmology at UWA, and a consultant ophthalmologist and board director of LEI – will ask why the industry is no closer to developing a lasting cure for this condition, despite it being described in literature 168 years ago. He will examine progress to address obstruction to venous outflow and understanding of the sequence of cytokine upregulation that occurs to more appropriately target the induced dysregulation.
INVITED SPEAKERS 54 INSIGHT October 2022 RANZCO PREVIEW
CORNEA UPDATE LECTURE, MON 31 OCT
PROF DONALD TAN

Descemets membrane endothelial keratoplasty (DMEK) has come of age for corneal endothelial replacement, but Prof Tan (DukeNational University of Singapore) says it's fraught with technical challenges in complex cases with anterior segment co-morbidities. He will present a staged approach involving reconstruction of the anterior chamber (AC) with iris removal and placement of an artificial iris, followed by DMEK.
GLAUCOMA UPDATE LECTURE, TUE 1 NOV
DR JANEY WIGGS
Dr Wiggs (Harvard Medical School, the Ocular Genomics Institute and Mass. Eye and Ear) will review known glaucoma genes and genetic risk variants as well as the clinical utility of genetic testing patients. She will say that genetic testing using early-onset glaucoma genes can identify pre-symptomatic mutation carriers as well as inform risk assessment and genetic counseling. More recently, polygenic risk scores (PRS) derived from genome-wide association studies are useful for risk stratification in adult populations.

THE COUNCIL LECTURE, TUE 1 NOV PROF FRANK MARTIN
Prof Martin, a prominent Sydney-based paediatric ophthalmologist, will discuss the current status of preschooler vision screening in Australia, which varies from state-to-state. Vision 2020 established an early intervention committee in 2021 to develop a national framework for 3.5 to 5-year-olds based on the NSW StEPS protocol. RANZCO has included early detection in childhood as one of the two pillars of its Vision 2030 plan and will play a leadership role in implementing a National Preschooler Vision Screening Program.

Perform Premium Capsulotomy with Tango ReflexTM by



Posterior Capsular Opacification (PCO) is a common consequence following cataract surgery. With newer generation of IOLs, higher precision is required to perform posterior capsulotomy.
The Tango ReflexTM offers leading-edge YAG laser technology, delivering a four nanosecond Ultra Gaussian pulse at high peak power - achieving the industry’s lowest optical breakdown energy at 1.5 mJ. Performing capsulotomy at lower more efficient energy levels, the Tango ReflexTM enables a perfectly, centered, and precise capsulotomy - a safe and highly effective treatment option for all types of IOL’s whilst achieving successful patient outcomes.

Contact: salesadmin@ellex.com Call +61 8 7074 8200 | ellex.com
Ellex®
Capsulotomy, Ellex – Step 1: multifocal lens Capsulotomy, Ellex – Step 2: multifocal lens Images courtesy of Karl Brasse, MD, MRCOphth RANZCO Exhibit #45
AFT PHARMACEUTICALS EXPANDS INTO GLAUCOMA ARENA
AFT Pharmaceuticals is set to launch glaucoma therapy Vizo-PF Dorzolatim dorzolamide (as hydrochloride) 20 mg/mL and timolol (as maleate) 5 mg/mL eye drop solution multi-dose in December 2022.
Therapeutic Goods Administration has approved the therapy for elevated intraocular pressure (IOP) in patients with ocular hypertension or open-angle glaucoma when concomitant therapy is appropriate.
It is the first therapy AFT is bringing to market under its new Vizo-PF umbrella brand, focusing on preservative-free options in multidose bottles for glaucoma patients.
The Pharmaceutical Benefits Advisory Committee has recommended it for listing on the PBS.
Before prescribing, review the full Product Information. Approved PI is available online at www.ebs. tga.gov.au or on request from AFT Pharmaceuticals.
AFT has a significant presence in the dry eye space, offering a range of preservative-free options such as HYLO Forte, HYLO Fresh, NovaTears, NovaTears + Omega-3 and OptiSoothe heat and eyelid wipes.
Booth: #42
HIVE OF ACTIVITY AT THE ELLEXLUMIBIRD MEDICAL BOOTH
The combined Ellex and Quantel Medical product portfolios offer a suite of advanced treatment solutions to drive greater value to ophthalmologists.


On its booth at RANZCO 2022, eyecare professioanls can discover more on how Lumibird Medical is helping shift the paradigm towards proactive glaucoma care with G.L.A.S.S. (Glaucoma Laser Assisted SolutionS). The approach is said to offer a complete laser therapy solution for every stage of glaucoma disease; including SLT with Ellex’s Tango Reflex multi-modality YAG/SLT laser and SubCyclo with Quantel Medical’s Vitra 810 SubLiminal laser.
In addition, attendees can view the company’s suite of ultrasound diagnostic solutions including the new next-generation ultrasound, AXIalis, Quantel Medical’s integrated and compact biometer and pachymeter.
RANZCO 2022 will also be a key opportunity to present C. STIM – the new intense pulsed light (IPL) device to treat dry eye disease.

Booth: #45
Bausch + Lomb (B+L) will continue to focus its efforts on developing innovative products that meet the growing patient demand for premium cataract options by previewing the new LuxSmart Intraocular Lens (IOL) during RANZCO Brisbane.
LuxSmart IOLs utilise Pure Refractive Optics (PRO) technology, a design that is based only on refractive profiles and has no diffraction areas, so patients are less likely to experience dysphotopsia, B+L stated.

With the launch of this new platform, the company now offers a complete range of innovative IOLs in Australia and New Zealand.
B+L is encouraging delegates to visit its team at RANZCO to find out more about the new LuxSmart and full suite of surgical products.
Booth: #27
BAUSCH + LOMB INTRODUCES A NEW IOL RAYNER OFFERS GLIMPSE OF NEW PREMIUM SOLUTIONS
Rayner is urging congress delegates to visit its exhibit at RANZCO Brisbane and speak to its experienced team to learn about its latest premium solutions – including:
• RayOne EMV – described as a highly versatile non-diffractive premium lens developed in collaboration with Australia’s Professor Graham Barrett. RayOne EMV offers >1.5 D increased range of focus (emmetropic targeting), monofocal levels of contrast sensitivity, dysphotopsia as well as high levels of patient satisfaction. Its positive spherical aberration design provides a more natural range of vision with a smoother transition between distance and near eyes. A toric version is coming soon to Australia.
• Sulcoflex – Rayner says these are elegant pseudophakic supplementary IOLs for treating refractive surprise. Celebrating its 15-year anniversary in 2022, the Sulcoflex platform is said to be safe, predictable and effective, and designed to avoid the potential problems of ‘piggy-back’ IOLs. Sulcoflex is available with an aspheric, toric or trifocal optic.
• HASA Optix – premium single use recyclable instruments with quality standards as high as reusable, designed to support sustainability within ophthalmology. These are coming soon to Australia.
Booth:
EXHIBITORSRANZCO PREVIEW
#39
56 INSIGHT October 2022








OCULUS PENTACAM® CELEBRATING D.O.R.C. EVA NEXUS HOYA VIVINEX™ LEICA PROVEO 8 DUCKWORTH TITANIUM INSTRUMENTS VR / PHACO SYSTEM NEW! Designs For Vision Technology Showcase at RANZCO 2022 1800 225 307 dfv.com.au Designs For Vision is a brand of ParagonCare Group Australia Pty Ltd SEE, SHARE, TRIAL & CELEBRATE. ICARE UWF IMAGING
LUXTURNA (VORETIGENE
NEPARVOVEC): DON’T DELAY GENETIC TESTING

LUXTURNA is an approved gene therapy for the treatment of adult and paediatric patients with inherited retinal dystrophy caused by pathological biallelic RPE65 mutations and who have sufficient viable retinal cells.1
Irreversible retinal degeneration occurs well before a patient’s vision deteriorates, so genetic testing should be performed as soon as possible before a patient’s viable retinal cells have disappeared.1–3
LUXTURNA is reimbursed. Funding criteria apply at approved Luxturna treatment centres. Before prescribing, please review Product Information available on page 61.
References: 1. LUXTURNA® Australian Approved Product Information 2. Menghini M, et al. Exp Opin Orphan Drugs. 2020; 8(2–3): 67–78. 3. Jacobson SG, et al. Investig Ophthal Visual Sci. 2008; 49(10): 4573–4577.
Novartis Pharmaceuticals Australia Pty Limited. ABN 18 004 244 160. 54 Waterloo Road, Macquarie Park, NSW 2113. AU-21831. Sept 2022. Booth: #16
DFV OFFERING DEMOS ON BROAD EQUIPMENT RANGE

Designs For Vision (DFV) will unveil the new D.O.R.C. EVA Nexus (pictured) at RANZCO 2022, described as a highly intelligent cataract and vitreo-retinal system that promises a big step forward with the new Smart IOP feature. The VacuFlow VTi (Valve Timing intelligence) and trocar cannula system are designed to optimise the entire surgical experience.
Via DFV, Hoya Surgical Optics will showcase its standard-setting IOLs for cataract surgery and congress delegates can feel the excellence of titanium surgical instruments from Duckworth & Kent.
The DFV booth will also provide an experience to learn about the latest OCULUS Pentacam biometry and wavefront refraction systems. Practitioners can experience the benefits of two decades of continuous development and innovation that changed the way ophthalmology is practised.
“Also, don’t miss out on the exceptional True-Colour, UltraWidefield retinal imaging of ICARE’s EIDON retinal cameras, with FAF and FA options. DFV & ICARE are also celebrating the 20th anniversary of their ground-breaking rebound tonometer which has revolutionised ophthalmic practice,” DFV stated.
“Come by the DFV booth for a personal demonstration and some exceptional offers.”
Booth:
LATEST OPHTHALMIC TECH FROM ZEISS TO BE UNVEILED
ZEISS will be showcasing numerous exciting product launches, as well as hosting interactive face-to-face events at the upcoming RANZCO Congress. On the stand ZEISS Cataract Workflow will take centre stage, showcasing the latest in connected devices, implants and data management.
A core element of this connected workflow is ZEISS QUATERA 700; something the company describes as a whole new experience in phacoemulsification. QUATERA uses the ZEISS-patented QUATTRO Pump to offer chamber stability independent of IOP and flow. The system brings together all elements of ZEISS Cataract Workflow, rendering it the single sterile OR cockpit for a more effective and efficient cataract procedure.
Visitors to the ZEISS booth can also experience the latest addition to the ZEISS IOL product portfolio, CT LUCIA 621. This monofocal

hydrophobic C-loop platform offers unique ZEISS optics and leverages the ZEISSpatented asphericity concept to mitigate against potential decentration challenges and confidently deliver impressive visual outcomes.
Elsewhere on the stand, the ZEISS VISULAS green laser with new SLT option is said to offer a safe and effective treatment for patients with primary open-angle glaucoma. With optional image and video capture to improve digital documentation and ability to view historical diagnostic data within FORUM Glaucoma Workplace, clinicians can now check and document the patient condition on the VISULAS workstation before/after treatment.

The connectivity theme will continue with the new FORUM Cloud Viewer. This cloud-based solution facilitates collaboration with fellow eyecare professionals in a secure platform designed to access, store and share diagnostic data from any location.
“Simply select data from a particular case, compose a message and send it to both FORUM and non-FORUM users using a realtime chat function whilst email notifications keep everyone up to date,” ZEISS stated.
Booth: #17
EXHIBITORSRANZCO PREVIEW
#36 and #36B
ZEISS VISULAS. ZEISS QUATERA 700 58 INSIGHT October 2022

An enhanced monofocal IOL delivering >1.5D of high quality natural vision1,2 TORIC COMING SOON TO AUS* NEW ©2022 Rayner, all rights reserved. Rayner, RayOne and Sulcoflex are proprietary marks of Rayner. All other trademarks are property of their respective owners. Rayner, 10 Dominion Way, Worthing, West Sussex, BN14 8AQ. Registered in England: 615539. EC 2022-206 09/22 MADE IN UK Learn more about our latest premium solutions at RANZCO (Booth #39) 1.Ferreira T. et al. Presented at Winter ESCRS 2022. 2.Rayner, data on file. 3.Venter et al. J Refract Surg; 2014. 4.Amon MI. Cataract Refract Surg Today Europe; 2009. 5.Kahraman G, Amon M, Vienna, Austria. J Cataract Refract Surg; 2010. 6.Manzouri B et al. Asia-Pacific Journal of Ophthalmology; 2017. • An elegant solution for treating refractive surprise. • Safe, predictable and effective.3 • Designed to avoid the potential problems of ‘piggy-back’ IOLs.4,5,6 • Available with an aspheric, toric or trifocal optic. Sulcoflex pseudophakic supplementary IOLs HASA Optix premium single use recyclable instruments* • Constant quality: Quality standards as high as reusable. • Sustainable organisational solution: One instrument set paper pouch per surgery. • Cost controlling: Integrated solutions to allow the calculation of a fixed cost per surgery. *Currently undergoing TGA review.
PREVIEW
DEVICE TECHNOLOGIES TO UNVEIL LASER AND DIAGNOSTIC TECH
At RANZCO Brisbane, Device Technologies Australia will be exhibiting the Eyestar.



Since introducing the system to the Australian market in late 2021, it continues to advance with the recent launch of two new modular upgrades.
The extended topogrpahy and anterior segment modules, now available on the Eyestar, are said to offer cataract and refractive surgeons a “one-stop-shop” for their surgical planning.
“These new modules enable extended anterior and posterior topography measurement areas, as well as 18mm anterior segment OCT imaging.
Combined with the existing C-Suite, surgeons can now evaluate all relevant ocular properties in a single instrument to promote improved refractive outcomes,” the company said. Booth: #34
OPTIMED – ‘GIVE YOUR PATIENTS THE BEST OF VISION’
Optimed will be exhibiting a range of its market leading Takagi, FISO and Optopol products and will launch what is described as the “game changing” Essilor Vision S-700 Auto Phoropter station and Vision R-800 Refraction System.
“These innovative, space saving systems make refraction fast, precise and simple, providing a unique immersive experience that opens up exciting possibilities to boost business,” the company stated.
“They make Refraction comfortable for the patient and create a fascinating user experience with results presented in simulated real-life experiences to enhance the patients confidence. The Vision R-800 delivers for the first time ever Refracting to 0.01 dioptre and the Vision S-700 enables Refraction that doesn’t require an equivalent of six meters as both systems utilize a patented liquid crystal optical module as opposed to individual lenses.”
According to OptiMed, both systems make refraction more precise, easier to perform for the practitioner and more comfortable for the patient.
Booth: #40
PREDNEFRIN FORTE AVAILABLE AGAIN IN AUSTRALIA
Prednefrin Forte (prednisolone acetate/phenylephrine hydrochloride) is back in stock and available across Australia via Allergan, an AbbVie company.
The therapy is indicated for patients with non-infectious severe ocular inflammation,1 such as acute iritis; iridocyclitis; scleritis; episcleritis; uveitis; resistant ocular allergy and inflammation following surgery.
Prednefrin Forte has supported patients with non-infectious ocular inflammation for over three decades.*1 after it was first approved for use in Australia on 14 October 1991.1
PBS Information: Prednefrin Forte is listed on the PBS for severe eye inflammation, corneal grafts and uveitis.

Before prescribing, please review approved product information available on request. More information is also available on Page 21.
Reference
1. Prednefrin Forte Product Information.
Booth: #35
UWF RETINAL IMAGING WITH GUIDED, SWEPT SOURCE OCT
Optos says it is the pioneer in ultrawidefield (UWF) retinal imaging that enables eyecare professionals to discover, diagnose, document and treat ocular pathology. The company’s latest technologies combine UWF retinal imaging with integrated optical coherence tomography (OCT).


“Silverstone is the most powerful tool yet for examining the retina. The only ultra-widefield retinal imaging device with integrated, UWF-guided swept source OCT, Silverstone produces a 200° single-capture optomap in less than ½ second and enables guided OCT scanning across the retina and into the far periphery,” the company stated.
Silverstone also allows non-mydriatic, non-contact imaging through most cataracts and small (2mm) pupils.
According to the company, routine optomap has been shown to enhance pathology detection and disease management, and to improve clinic flow.
Now with integrated swept source OCT, Silverstone facilitates examination of the retina from vitreous through the choroidal-scleral interface.
Booth: #28
60 INSIGHT October 2022 EXHIBITORSRANZCO
Essilor Vision S-700.
Essilor
Vision R-800.
IRDs: DON’T LEAVE GENETIC TESTING UNTIL

IT’S TOO LATE
YOUR PATIENT A GENETIC DIAGNOSIS TODAY.

Scan the QR code to visit MedHub for eligibility criteria and providers. OFFER
Irreversible retinal degeneration occurs well before a patient’s vision deteriorates.1,2 An early genetic diagnosis may unlock the possibility of therapy before viable retinal cells have disappeared.1–3 For healthcare professionals only. Please review full Product Information before prescribing. Scan QR code for full LUXTURNA Product Information. Alternatively, please contact med info at 1800 671 203 or visit www.novartis.com.au/products/healthcare-professionals/products to access the full Product Information. References: 1. Menghini M, et al. Exp Opin Orphan Drugs. 2020; 8(2-3): 67–78. 2. Jacobson SG, et al. Investig Ophthal Visual Sci. 2008;49(10): 4573–4577. 3. LUXTURNA Australian approved Product Information. Novartis Pharmaceuticals Australia Pty Limited. ABN 18 004 244 160. 54 Waterloo Road, Macquarie Park,NSW 2113. AU-19355. McCann Health NOLX23709M. January 2022. LUXTURNA is reimbursed. Funding criteria apply at approved treatment centres. This medicinal product is subject to additional monitoring in Australia. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse events at www.tga.gov.au/reporting-problems
































See more, know more with more Insight Subscribe FREE and receive the latest news Insight is mobile and tablet friendlyFind jobs and advance your career with Insight’s Classifieds Get to know the newest products from suppliers across Australia Insight’s new website keeps you updated on the latest industry news and information. With a world-class responsive design, Insight is now accessible seamlessly on any device, 24/7. Sign-up FREE to our eNewsletters and industry reports delivered weekly straight to your inbox. www.insightnews.com.au
THE SECRETS BEHIND
OPSM’s longevity
Marking its 90-year anniversary in October 2022, today’s leaders of EssilorLuxottica-owned OPSM reflect on the attributes that have made it an iconic Australian optometry brand and how innovation and differentiation will ensure its future.
Macquarie Street, Sydney, was home to the first OPSM store. Spelt in full at the time (Optical Prescription Spectacle Makers), it opened with five staff and added a sixth the following year – a 17-year-old trainee optical dispenser – with all frames and lenses on consignment.

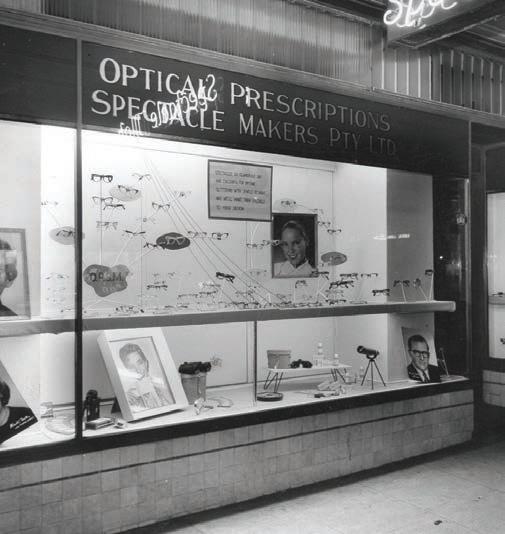
Today, 90 years on, the brand is one of the most-recognised in Australian and New Zealand optics, morphing into a vertically-integrated eyecare business with the backing of its parent company Luxottica (now EssilorLuxottica) since 2003.
Along its journey, OPSM has recorded countless highlights, including evolution of a new customer in-store experience using walk up frames displays (1962), a trend that caught on industry-wide. Its history also involves contact lens manufacturing (1939 and 1970) and expansion into New Zealand (1995).
And, as this issue goes to print, one of the most significant changes is taking place as the EssilorLuxottica merger takes shape at the local level, seeing the businesses come under one roof in North Sydney. For OPSM, this has opened new possibilities for advanced lens technology and equipment from Essilor, helping elevate the customer experience in almost every way and allowing OPSM to stamp its mark on areas like myopia management.
Mr Matteo Accornero, who heads up EssilorLuxottica’s retail operations in Australia and New Zealand, says globally there are few optical retail chains that can claim to possess an archive of black-and-white photos from such a distant past. He says it’s proof of a precious legacy that has withstood the test of time with its original values intact, while setting modern-day optical business trends.

“OPSM has a rich and strong heritage in the Australian market. As we celebrate the 90th anniversary since its foundation, it is the perfect time to acknowledge the evolution that has made OPSM a brand synonymous with optical care and assistance for Australian consumers,” he says.
“The brand story clearly shows how OPSM has been championing evolution since its foundation in the 1930s, pioneering important changes in the eyecare industry. Most of the business results achieved are attributable to the implementation of some important strategic choices that go from
improved store design to the evolution of optometrist consultancy room to always making the customer experience central during the entire process, with increased support from digital instruments.”
Today, with a network of approximately 440 stores and 3,100 employees in the OPSM and Laubman & Pank network in Australia and New Zealand, Accornero says the brand is looking to the future with new confidence.

Central to this approach is OPSM’s Clarifye digital eye exam experience, a new patient journey based on the latest technology developed by EssilorLuxottica. It incorporates advanced instruments like a sevenin-one eye health screening assessment and a high precision eye test measurement of 0.01D, aiming to offer faster and more accurate prescriptions.
“We have invested not just in the retail space but also in the optometry consulting rooms. We are dedicating more space to the professional area and investing more in cutting edge instruments,” Accornero explains.
“All things going to plan, we will have close to 150 stores with Clarifye by the end of 2022 – we are currently sitting at about 100. The Clarifye journey is being enhanced with a new dispending tool, Visioffice 3, which allows us to open up further top tier lenses owing to more advanced and personalised patient measurements.”
INSIGHT October 2022 63 OPTOMETRY
“LATER THIS YEAR, WE’RE PLANNING ON INTRODUCING … OUR HUGELY DESIRED STELLEST LENS, WHICH WILL ROLL INTO AN ALL-ENCOMPASSING MYOPIA PROGRAM”
MATTEO ACCORNERO RETAIL ANZ GENERAL MANAGER
In the past 12 months, OPSM has welcomed about 100 new graduates and 80 experienced optometrists and has refurbished approximately 100 stores since the beginning of the year.
“Later this year, we’re planning on introducing Eyezen Kids and our hugely desired Stellest lens, which will roll into an all-encompassing myopia program, to provide better support for our younger patients,” Accornero says.
“We strongly believe that this myopia program will positively impact lives by enabling children everywhere to learn, express themselves and fulfill their potential.”
In addition, the company is investing further in digitalising the patient journey. This involves collecting more information from patients prior to consultation, with this visible in the optometrist’s consultation room. Consultation results will also be digitised, saving time and reducing paper consumption.
Patient contact processes will be upgraded, allowing patients to confirm, reschedule or cancel their appointments at the touch of a button. The process of contacting no-show or cancelled patients will be automated.
On the dispensing/retail front, OPSM is investing in its digital platform, Leonardo, that can be accessed on demand, whether it’s on a computer before a patient arrives or on a store iPad between appointments.
“With a focus on eyewear, eyecare, lenses, optics, brand storytelling, customer experience and personal development, Leonardo brings together category experts to share their knowledge with the goal of developing leaders in our industry to give our patients a premium service,” Accornero says.
OPSM HISTORY
1932 The first OPSM store opened in Macquarie Street, Sydney
1934 Purchased and installed the first automatic bevel edging machines to be used in Australia.
1939 Started a contact lens manufacturing service in Sydney with English optometrist Ken Ireland, who became the first person to make contact lenses in Australia with equipment ordered from overseas.
1950 Began stocking surgical instruments after requests from eye surgeons who were experiencing difficulty sourcing equipment.
1962 Publicly listed on the Australian Stock Exchange (ASX).
1962 Evolution of the customer in-store experience through the creation of the first walk-up displays, so customers could select frames. Prior to this, frames were hidden away. This display method spread across OPSM and throughout the world.
1970 The company acquired the license to manufacture soft contact lenses in Australia.
ELIZABETH KODARI ANZ EYECARE OPERATIONS DIRECTOR

“Innovation is at the heart of our business, especially when we talk about lenses. We have embarked on a plan to transform our lens portfolio by offering world renowned brands such as Varilux, Eyezen, Crizal and even more from Transitions. These new lenses bring to life our latest in digital design and personalisation which are among our greatest differentiators.”
Accornero says OPSM is also expanding its branded lens assortment to offer greater customisation and a continued ‘perfect fit’.
“We are providing Ray-Ban, Oakley and Costa branded lenses in wider designs, amping up our frame and lens perfect fit, together with the authenticity credentials which our patients have come to expect,” he explains.
In recent years OPSM has also invested in SmartShopper, an intuitive tool that allows customers to interact digitally with the entire catalogue of
1970 Over 100 stores established for the group.
1977 After 20 years of lobbying, OPSM played a leading role in changing government regulations around optometry (except in SA , QLD and Tasmania).
1990 The number of OPSM stores jumped to 268.
1991 OPSM Bagot House opened in Adelaide, SA , becoming the largest optical retailer in the Southern Hemisphere.
1991 OPSM chaired the National Optometric Panel, developing a relationship between OPSM and optometric professionals; between 1991 and 1996. As government legislation changed from state-to state, OPSM started employing optometrists for its stores.
1995 Established the first OPSM store in New Zealand.
2001 Acquired Australian optical brand Laubman & Pank.
2003 OPSM group acquired by Italian eyewear conglomerate Luxottica.
2005 Luxottica delisted OPSM Group shares from ASX
2010 OPSM opened the Eye Hub concept store in Hawthorn, Victoria, unveiling a new brand image. It offers customers everything in one place, including optometry expertise, advanced scanning technology, friendly informed service, on site labs, innovative interactive testing environments and a dedicated eye health learning zone.
2013
2011 OPSM rolls out Optos ultra-wide digital retinal scans across its network, an exclusive leading-edge technology at the time.

2019 OPSM re-opens its flagship store in George Street, Sydney
2019 Introduced audiences to its Life.Focused platform through an advertising campaign starring actor Liam Hemsworth.
2020 OPSM offers tele optometry for its customers due to COVID-19 restrictions.
2021 OPSM introduces the Clarifye patient experience to selected stores.
2022 OPSM’s parent company Luxottica opens its first joint office with its partner Essilor in North Sydney as EssilorLuxottica.
64 INSIGHT October 2022 OPTOMETRY
-
“OVER THE PAST FIVE YEARS WE HAVE INVESTED OVER $500,000 IN SCHOLARSHIPS TO SUPPORT OUR OPTOMETRIST’S PROFESSIONAL DEVELOPMENT”
Luxottica beyond what is in stock in-store. It includes a virtual try-on feature thanks to augmented reality and advanced proprietary virtual mirroring technologies.
ENDLESS CAREER OPPORTUNITIES
Eyecare operations director at Luxottica ANZ, Ms Elizabeth Kodari, joined the company in 2015. A former optometrist at OPSM George St, Sydney, she believes OPSM’s longevity is a combination of its investment in its people and technology.
“Optometry as a profession has changed. Now more than ever, optometrists and graduates are looking for employers that listen and are adaptive to change. We offer our optometrists a diverse range of experiences to ensure their continued professional success. Whether they want to be a clinical optometrist or business leader, the opportunities are endless.”
Kodari says more opportunities, choice and time to practise full scope optometry are just some of the reasons optometrists accelerate their career with OPSM.
“Over the past five years we have invested over $500,000 in Luxottica Eyecare Development Award (LEDA) scholarships to support our optometrist’s professional development. We continually invest in the latest technologies to ensure our optometrists can detect more pathology than a standard eye examination,” she adds.
“One of the competitive advantages underpinning OPSM’s past and future success is our vertically integrated business model. Our 360-degree view of everything from design to construction provides unique insights into patient behaviour, trends and encourages innovation.”
She says OPSM has remained at the leading edge. Its optometrists use
start-of-the-art technologies, and at the height of the pandemic implemented tele optometry consultations so non-urgent patients could still seek care.
“Our investment in technology also translates to our premium eyecare products. EssilorLuxottica recently partnered with Meta to create smart glasses in our iconic Ray-Ban frame. We have a strong commitment to myopia management and through our partnership with Essilor, have expanded our portfolio with the inclusion of the highly anticipated Stellest lens,” she says.
Beyond technology, Kodari says OPSM has worked with Diabetes Australia and the KeepSight diabetes eye check initiative, with over 20,000 patients registered through its optometrists in less than 12 months.
But Kodari is most proud of OneSight EssilorLuxottica Foundation, a charitable organisation providing access to quality vision care and glasses in underserved communities worldwide. OPSM optometrists can volunteer with OneSight and impact the lives of the one in seven people who lack access to proper vision care.
“During my time with OPSM, I have had the privilege of being part of numerous OneSight clinics and giving back to our local communities,” she says.
“Our OneSight EssilorLuxottica Foundation and the group’s ambitious implementation of corporate social responsibility programs – such as ‘Eyes on the Planet’ that includes our company’s commitment on climate change and is the first major step to becoming carbon neutral in our direct operations by 2025 – is something we are extremely proud of.
“Innovation and differentiation will continue to be key pillars in the future of the OPSM brand. Our adaptability and 90 years of heritage expertise will ensure OPSM’s continued success in an ever-evolving optometry landscape.” n
RE-THINKING REFRACTION WITH liquid optics
The Vision-R 800 auto phoropter allows optometrists to perform refraction with 0.01 D increments.
Four years of R&D have been invested in Essilor’s latest phoropter technology, supplied by OptiMed, that Australian optometrists say is transforming the refraction experience for practitioners and patients.

First developed in the early 1900s, the phoropter has been synonymous with vision care, becoming a central tool in the optometrist’s technological armamentarium. While many optical instruments have been eventually superseded, this iconic instrument has withstood the test of time and remains fundamentally similar to original models developed more than 100 years ago.
One of the largest advances in phoropter technology has been the introduction of digitalisation and automatic functions. But ophthalmic lens and equipment manufacturer Essilor has been exploring ways to optimise the phoropter even further for a better patient and practitioner experience. Thus, in 2020, it introduced the Vision-R 800 auto phoropter to the Australian market.
Supplied by Sydney-based ophthalmic device distributor OptiMed, which formed a joint-venture with Essilor in 2019, the Vision-R 800 is said to offer continuous power changes and makes refraction more precise, easier to perform and more comfortable.
For example, in the traditional refraction procedure, values are rounded to 0.25 D at each stage where inaccuracies accumulate. Whereas the Digital Infinite Refraction procedure on the Vision-R 800 means the refraction is conducted with 0.01 D increments and the final value is rounded to the nearest 0.25 D, with four solutions presented for the optometrist. The final prescription can be offered to the patient as a precise refraction for Essilor Advanced Vision Accuracy (AVA) lenses or conventional for standard type lenses.
It achieves this with a revolutionary optical module Essilor has developed
containing a precisely adjustable novel liquid lens, in addition to a smart refraction program using unique algorithms.
Further, optometrists are reporting that the smooth power changes and a wider field of vision make refraction comfortable for the patient. The eye test is shorter and along the refraction procedure, variation steps are adjusted to patient sensitivity, making differences easier to perceive. At the end of the test, the Vision-R 800 phoropter also offers patients the experience of comparing refractions in simulated real-life conditions, a key tool for practices to demonstrate the value of their products and service.
Optometrist Ms Alison Steer operates the first Western Australian practice to have the Vision-R 800 installed. This occurred in 2020 amid a major upgrade of her namesake independent practice in Albany – located 400km south of Perth – just as Essilor’s latest phoropter was being released. Since then, it has reaped major clinical benefits while also increasing her business’ profit margin.
Before the installation, the practice’s existing phoropter was manually operated and had no links to her Sunix practice management system, so she was keen to upgrade to an automated phoropter, both for ongoing ergonomics and patient experience.
Steer ultimately invested in a complete integrated system that also incorporated Essilor’s new WAM (Wave Analyzer Medica) 800 auto refractor.
“It has been an excellent patient experience and we have got a lot of positive comments regarding the ‘new equipment’. Apart from the clinical benefits, the Vision-R 800 promotes a progressive, clinically up-to-date image and experience for my patients,” she says.
66 INSIGHT October 2022
VISION CARE
“Clinically it gives a streamlined examination process and the ability to refine the prescription to a greater degree than other phoropters on the market. We can offer a greater degree of vision accuracy for those clients who prioritise high precision for their eyewear solutions. In one simple step we can demonstrate the difference between the standard ‘0.25’ step refraction result and the high precision option.”
Commercially, she’s also now able to demonstrate the benefits of a new prescription easily and efficiently which has enabled increased sales.
“We are now able to offer the high precision lenses which is a great pointof-difference and increased profit margin.”
In terms of which features she has found most impressive, Steer describes the ease of comparing the old spectacle prescription with the new high precision subjective prescription as an excellent function.
She has also found useful the ability to customise the testing programs to her own protocols and system. The instant data transfer into Sunix also means less manual transfer and less opportunity for transcription errors.
As a medium-sized independent in a regional centre, Steer says it is vital optical businesses like hers continue to invest in leading-edge technology so she can continue to support two fulltime optometrists and five additional staff to service the community of Albany, in the WA’s Great Southern Region.
“I have had a strong relationship with OptiMed for many years as they provide excellent equipment, advice and backup service. Mark Stapleton and Brad Miller, our local team, provide advice, backup and servicing as required and excellent installation,” she explains.
“Independents need to have access to all the latest technology to be able to offer the high-end examination experience and diagnostic capabilities to their patients. Our point-of-difference is to offer patients a premium, customised experience throughout the visit and the Vision-R 800 is part of that process.”
A SIGNIFICANT INVESTMENT THAT WAS WORTH IT
Around 400km west of Albany, patients at Margaret River Optical are also benefiting from the precision of the Vision-R 800, which adds to the practice’s other Essilor instruments including a Visioffice digital dispensing system and ALM 700 vertometer.

After deliberating for several months, principal optometrist Ms Allyson McIvor decided to invest in the technology to replace her manual phoropter and has been impressed with the visual outcomes of her scripts and the subsequent increased foot traffic brought about by word-of-mouth recommendations.
In particular, introducing the Vision-R 800 – and its 0.01 D increments – has allowed her to elevate her lens offering with premium-level Essilor lenses incorporating its AVA technology, offering prescription accuracy within 1/100th of a diopter.
Although some practices charge extra for this level of service, McIvor has decided not to, and has applied it for distance, multifocal and occupational lens prescriptions on a routine basis – which has been beneficial for those patients who might be more sensitive to small changes.
“It was a significant investment and we did consider it for a few months beforehand, but I don’t regret it at all. It did take a while to adapt and fine tune until I was comfortable with it, but as an independent practice it’s important to have a point-of-difference through the ability to order the most up-to-date lenses. There is no one in the surrounding area who has anything like this,” she explains.
“People are loving their vision and glasses; there’s definitely a ‘wow factor’ that comes with it and we have people visiting the store saying they have come for the technology. We’ve also had great success in terms of accuracy, I can’t remember our last remake.”
Like Steer, McIvor has found the script comparison feature easy for patients to follow.
KEY FEATURES
• Patented automated optical module powered by digitally controlled motors
• Simultaneous and instantaneous changes or sphere, cylinder and axis
• Sphere range -20.00 D to +20.00 D in 0.01 D increments
• Cylinder range 8.00 D in 0.01 D increments
• Axis range from 0° to 180° in 1° steps
• All changes in a continuous and smooth way
The phoropter contains an optical module Essilor has developed containing a precisely adjustable novel liquid lens.
“Also, instead of images on a chart, the Vision-R 800 has the ability to display real life images that can incorporate visual cues such as depth and shading so patients can get a real-life idea about how the prescription will impact their distance vision for driving, for example. There’s also a setting that can change to night time vision that you can prescribe for, a lot of binocular vision functions are easy to use and, I will add, in this climate, it’s COVID-friendly because you’re not standing over the patient adjusting the dials.”

SETTING YOUR PRACTICE APART
Specialeyes is a four-practice optometry business also located in WA, with stores in Perth, Subiaco, Cottesloe and the University of WA. Its Cottesloe site is well established with two optometrists and five front-of-house staff, catering to an upmarket demographic.
Principal optometrist Mr Simon Hogan, who took over the practice from his father after practising in the UK for several years, says the practice’s old refractor head looked dated. But after a practice renovation, the new Vision-R 800 offered the possibility of more precise refraction, while still being easy-to-use and good for retinoscopy.
“I have been surprised how much difference the precision Rx makes with some patients,” he explains.
“Being one of the first with the new technology it also helps separate our services from the competition. Our patients are seeking a different offering to the one’s being so well marketed by the corporates, so everything we can do to stay ahead and at the very worst, level with them, is important.
“OptiMed’s support has been fantastic with their implementation.” n
INSIGHT October 2022 67
WA optometrist Alison Steer says with the Vision-R 800 she can now offer high precision lenses, creating a point-of-difference and increased profit margin for her independent practice.
DRY EYE, GLAUCOMA AND BEYOND
Glaucoma treatment marks the next horizon for AFT Pharmaceuticals, as it seeks to solidify its position as a leader in the ophthalmic eye drop market with preservative-free-only products, CEO HARTLEY ATKINSON says.
preservatives so we saw an opportunity with preservative-free, because when you've got an eye infection, you wouldn't want to be putting anything else extra that might cause irritation,” Atkinson adds.
“Overall, we are seeing good growth in our eyecare portfolio. We’re in seven therapeutic areas in Australia, and ophthalmology is our largest chunk of revenue. We want to keep growing it, which is why we are expanding in glaucoma therapies.”
GLAUCOMA THERAPY TO BE PBS-LISTED
While much of the focus has been on AFT’s dry eye and chloramphenicol range, the company is set to make its well-documented foray into glaucoma later this year.
The company currently has three approved preservative-free versions of well-established glaucoma therapies licenced from Europe, which it will market under the umbrella brand Vizo PF.

The first to launch this December will be Vizo-PF Dorzolatim dorzolamide (as hydrochloride) 20 mg/mL and timolol (as maleate) 5 mg/mL eye drop solution multi-dose. Its main comparator is currently Cosopt.
The Australian ophthalmic market continues to be a happy hunting ground for New Zealand-based AFT Pharmaceuticals, with the company poised to build on its rapid success in the dry eye space with an expansion in prescription glaucoma therapies later in 2022.

The NZX and ASX-listed firm has continued its annual trend of posting a record operating revenue, with its latest FY22 figures reaching $130 million, up 15% on the previous year. Australia continues to be its largest market, accounting for around 60% of sales, growing by 12.3% to $76.7 million.
Founder and CEO Dr Hartley Atkinson says the company’s eyecare portfolio has gone from strength-to-strength in Australia, with AFT enjoying a niche in offering licensed preservative-free ophthalmics. Well-established dry eye products, including the HYLO range, NovaTears, and Opti-Soothe heat and eyelid wipes have continued their growth trajectory and, as such, AFT has retained the number two position in the lubricating eyecare category in Australia and the number one selling product (HYLO-Forte).
AFT’s overall Australia FY22 revenue growth has largely been driven by new launches, with the most notable eyecare products being its preservative-free treatment for eye infections, Ocuzo, and a new Opti-Soothe 3-in-1 eyecare treatment kit for dry eye.
Atkinson says the company has also been “pleasantly surprised” with the performance of NovaTears + Omega-3, a line extension of the popular NovaTears eye drop introduced only two years ago that combines perfluorohexyloctane and concentrated Omega-3 fatty acids of algae origin.
“That product has done better than we expected and quite a few of our customers have seen the benefit and point-of-difference created by having Omega-3 included in the formulation, as opposed to a strategy of taking fish oil supplements,” he says.
“One of the advantages of the NovaTears base (EyeSol) is that you can dissolve compounds that are not water soluble, where most eye drops are relying on something like an emulsion, which can cause blurring. So it’s a unique formulation in that respect.”
Ocuzo, AFT’s chloramphenicol 5mg/mL pharmacist-only 10mL eye drop launched in the first quarter of 2022, is also making in-roads as the only preservative-free option in its category, with an addressable market of 600,000 units per year.
“That’s a significant market; chloramphenicol eyedrops traditionally contain
The company is currently evaluating the launch date for a Vizo-PF Bimatoprost 300 microgram/mL (comparator Lumigan PF), which has been recommended for PBS listing. AFT also has approval for Vizo-PF Bimatotim 0.3/5 bimatoprost 300 microgram/mL and timolol (as maleate) 5 mg/mL.
With respect to Vizo-PF Dorzolatim, the Therapeutic Goods Administration has approved this for elevated intraocular pressure (IOP) in patients with ocular hypertension or open-angle glaucoma when concomitant therapy is appropriate.
“This is a classic glaucoma product that's been approved in the Australian market. We've applied for a PBS listing, and we're looking to launch that on 1 December. The opportunity we saw is that although there are some glaucoma products that are preservative-free, they're generally in single dose ampoules, which are fiddly to use and cause environmental waste, so we saw this as a better option,” Atkinson says.
“Like dry eye, glaucoma is a long-term condition that unfortunately doesn’t suddenly resolve overnight. So having a preservative-free product that avoids irritation and that is easy to use in a multidose container seems to be a useful angle for patients and the Australian market.”
The Pharmaceutical Benefits Advisory Committee (PBAC) recommended Vizo-PF Dorzolatim for PBS-listing at its March 2022 meeting. In its submission, AFT estimated it would substitute for 5% market share in the first year of listing (5,000 to < 10,000 prescriptions), increasing to approximately 25% by year six (30,000 to < 40,000 prescriptions).
ON THE HORIZON
Hartley says AFT’s Australian operations – which has increased to 40 people – are expanding, as the company sets a goal to crack $100 million in revenue in the country.
He anticipates that will happen in 2023/24, largely thanks to the fact AFT did not let the pandemic slow the growth of expanding its licensed portfolio, which currently account for 75-80% of its entire range.
“We continue to see considerable opportunities to accelerate growth and have significantly increased both our in-licensing and product R&D pipeline activities where we are also now looking into eyecare. We also believe the gradual move worldwide to living with COVID and our ability to now travel across borders to meet with both existing and new customers will allow a gradual return to a more normal trading environment,” Atkinson says.
68 INSIGHT October 2022
PHARMACEUTICALS
AFT Pharmaceuticals founder Hartley Atkinson (right) says the company is building its R&D pipeline, which may include eyecare products in future.
“Our pure drug development business develops products for global markets. We're selling into about 58 countries around the world at the moment, and we are trying to build that over the next couple of years to around 100.”
While he can’t comment at length, Atkinson is also watching with interest as German ophthalmic product manufacturer Novaliq applies to the US Food and Drug Administration for a new cyclosporin ophthalmic solution for
dry eye disease. Novaliq is the producer of the NovaTears range, supplied by AFT in Australia and New Zealand, and the cyclosporine product, called CyclASol, uses the same pioneering water-free technology EyeSol.


CyclASol has reportedly demonstrated in two independent adequate and well-controlled, multicentre studies (ESSENCE-1 and ESSENCE-2) clinically meaningful and statistically significant improvements in the indication.

Effects on the ocular surface include a statistically significant reduction in total corneal fluorescein staining (tCFS) score favouring CyclASol in both studies at days 15 and 29. Up to 71.6% of patients responded within four weeks with a clinically meaningful improvement of ≥3 grades in total corneal staining. This proportion of responders was significantly higher compared to vehicle-treated patients in both studies.
Results from a 12-month long-term study confirmed that the effects are maintained, and even improved for most sign and symptom endpoints.
Head-to-head data versus Restasis (cyclosporin) from a phase 2 study suggest that CyclASol has a stronger and faster therapeutic effect on the ocular surface, Novaliq reported.
“This is the first submission of a novel product category of water-free topical drug therapies utilising EyeSol as a drug carrier,” Novaliq CEO Mr Christian Roesky says.
“CyclASol is a first-of-a-kind drug therapy and aims to expand treatment success for patients with dry eye disease and their eyecare professionals. If approved by the FDA, CyclASol addresses important unmet medical needs in dry eye disease through its ocular surface healing effect combined with high comfort of administration.” n
Australia continues to be the largest market for AFT Pharmaceuticals, with its ophthalmic eye drop portfolio a key driver of this. George & Matilda Eyecare is currently recruiting Optometrist to join our team in Airlie Beach, Innisfail & Atherton. Reach out to our HR Team at opportunities@georgeandmatilda.com.au to find out more. Is the warm weather and luxurious beaches of Far North Queensland calling you?
In 2019, Dr Tim Henderson operated on Marie Briscoe, from Tijikarla – about two hours from Alice Springs. He could see Marie was anxious but after a hug and reassuring words she was happy to proceed with cataract surgery in her left eye. At post-operative assessment, Marie was 6/12 vs 6/60 prior to surgery.

THE OPHTHALMOLOGIST BEHIND the IRIS program
DR TIM HENDERSON talks with Insight about the realities of providing tertiary eyecare in the vast Northern Territory via the outreach program which IRIS helps support, the necessity of portable equipment, and challenges securing staffing and funding.
Igrew up in central Africa, so it feels more like home to me than any urban setting ever would,” a voice echoes down the line from Alice Springs.
It’s Dr Tim Henderson, director of ophthalmology at Alice Springs Hospital who also visits dozens of remote communities each year with support from the Indigenous and Remote Eye Health Service (IRIS), which delivers eyecare and eye surgery directly to communities in remote and rural Australia to help address preventable vision loss.
The regional eye service, using equipment secured and placed through the IRIS Taskforce, undertakes regular outreach visits to Indigenous and remote communities to provide access to world-class eye health services.

The service, funded through a grant from the Australian Government and coordinated by Vanguard Health, ensures patients receive eyecare and eye surgery closer to home, in their community, and in a timely way. This reduces the impact on the local community and greatly improves the overall patient experience.
Since July 2021, IRIS has supported 199 cataract surgeries; 81 have been completed this year.
“If you were to include the last program where 522 cataract surgeries were performed, the total number would be 721 since February 2020, to date,” Henderson says.
After originally intending to stay for three years, he has now been living in Alice Springs for 22 – 11 of those involved with the IRIS program.
“I trained in the UK , I did my subspecialty training in Adelaide, in cornea and anterior segment. I had brilliant general ophthalmology surgical skills training as well, which is specifically what you need here,”
70 INSIGHT October 2022 PROFILE
Dr Tiger Zhou (registrar) assesses Benny’s eyes post operatively, in 2019. Benny only saw hand movements in his right eye prior to his cataract surgery. He worked at Woolworths stacking shelves and found that he was pushing his trolley into shelves due to his deteriorating eyesight. After the surgery, Benny said he went home and thought: ‘What amazing people they are … I can look through two eyes again’.
"
Henderson says.
“And I worked in the UK in the public hospital service, so it didn't faze me taking on a salaried position, which many Australian-trained ophthalmologists wouldn't normally consider for a fulltime role.”
He was invited to join the IRIS Taskforce in 2011. In those early days, it was about talking to people on the ground, finding ways to channel the Commonwealth funding to the areas that most needed it, initially focusing on equipment to set the foundations for the service.
“The funding allowed us to ensure all the remote communities got the same basic equipment to make it much easier to provide outreach services. It resulted in 32 different communities getting the basics of a slit lamp table base and two stools.”
Commonwealth funding allowed IRIS to purchase and place 50 slit lamp tables; 32 were located in the NT and the remaining were placed in other areas of need.
For Henderson, having the same platform setup everywhere has meant he only needs to transport the more expensive part of the slit lamp, the optical and illumination system. He can perform laser treatment in remote communities and rely on the stability of the platform for safe portable laser treatment in each location.
“The standard base set-up also allows the visiting optometry services to use the same base set-up and recent extra funding through the Brien Holden Vision Institute has upgraded the slit lamp tops which will continue to work with the IRIS Taskforce supplied tables, hopefully for another 15 years,” he says.
Henderson says spending funding on portable equipment has been incredibly cost-effective. It has allowed the service to achieve the aim of establishing a reliable setup to perform eye specialist outreach effectively.
“A long time ago, I got asked by somebody involved in outreach, ‘Why can't you just take a small plane and take less equipment?’. To which I responded, ‘You want me to half do my job?’,” Henderson says.
Having portable equipment negates the need for many patients to travel. Henderson isn’t exaggerating when he says patients in remote areas often require a week away from home to travel to and from Alice Springs for a hospital appointment.
“We are quite portable, but we're also dependent on some high-tech equipment and if you can get small enough portable versions of it, there's a lot we can do out there,” he says.
“Until people understand logistics, they don't understand why outreach is such a cost-effective way of providing care. The reality is that most of these patients won't otherwise get care because there's so many other competing demands on their time.”
He continues: “Intraocular surgery requires meticulous care and a sterile hospital environment but providing this in central Australia saves hundreds of patients from having to travel interstate or going without the care they deserve.”
When he first arrived in Alice Springs, Henderson recalls feeling privileged to have the opportunity to introduce up-to-date cataract surgery by phacoemulsification.

He says the technical difficulty of some of the surgery has repeatedly reinforced his opinion that the public service should be equipped with the best and most effective equipment to give the greatest chance of an optimal outcome for every patient. This has resulted in timely updates allowing regular surgery and supporting intensive eye surgery weeks prior to COVID.
TREATMENT IN AN AREA THE SIZE OF SPAIN
The IRIS Taskforce support has enabled regular visits to 32 different communities annually over the past 11 years, but the introduction of a regular bus service to some communities has reduced that number to
26 for the last few years.
The outreach service goes as far north as Elliott, 760km north of Alice, as far west as Kintore, 450km from Alice Springs or eight hours-plus driving; and to Docker River in the southwest. It also visits Mutitjulu, the community next to Uluru and Finke, which is as far south as it goes; and in northeast it extends to Lake Nash (Alpurrurulam), which is only a twohour drive from Mount Isa.
“Basically, the regional outreach service that the IRIS Taskforce funding helps support covers a catchment area the size of Spain; one million square kilometres,” Henderson explains.
“It's lots of discrete communities of 200-400 people, and they all deserve decent eyecare, from youth through to elderly, many of whom have significant problems with managing diabetes and multiple co-morbidities. Trachoma is still a health issue, giving impetus to encouraging children and adults to adopt good hygiene and health care practices.”
Henderson is supported by Aboriginal liaison officer Ms Veronica Stafford, whose position is funded by the Fred Hollows Foundation, orthoptists, eye nurses and a receptionist and outreach co-ordinator when visiting outreach communities. Ophthalmology training registrars also participate on rotation. There are also an increasing number of colleagues who visit for locum weeks to support the service, many are previous registrars or fellows who are established consultants around the country but set time aside to return and share the work.
He does not provide any routine vision screening, if possible. This is performed by a comprehensive optometry outreach program supported by Commonwealth funding through the Visiting Optometry Scheme (VOS) and mainly run through the Brien Holden Vision Institute (BHVI) which means that all remote communities get an optometrist visiting up to three times a year for routine screening.
“They know that they can refer urgent cases to me, so it's a good dynamic partnership. And that's why I can afford to say I don't want to see any ‘normal eyes’ because it's a waste of my specialist expertise,” Henderson says, adding that he will still see patients who have missed screening when there is time to do so.
“I want to spend more time with less people so that I can perform laser treatment, administer intravitreal injections, and obtain sufficiently
INSIGHT October 2022 71
Ophthalmologist Dr Tim Henderson has worked in Alice Springs for 22 years.
informed consent in preparation for surgery. Having an Aboriginal liaison officer makes a massive difference for people to have somebody who can provide cultural brokerage. We also involve family members, and clinic members if they're available, but having somebody who is familiar with what the discussions are around is really helpful.”
Henderson’s time is predominantly spent performing cataract surgery and treating diabetic retinopathy – but not necessarily always with intravitreal injections.
He says there's an important role for laser in populations that haven't got access to regular clinics. Henderson is continually encouraging trainees about how valuable laser is if it's done at the correct time, in the correct place, and often means people don't need to keep returning for frequent recurrent injections.
“It can be quicker to administer an injection to treat diabetic retinopathy but if you have patients who aren't going to be able to keep turning up regularly, you could be setting them up for poorer outcomes. Combining laser and an injection when you first see the patient can work extremely well, the injection produces the prompt response to treatment. By the time it's wearing off, the laser is starting to cut in and stabilise things further, so you may not need to see them for up to four months, which is much more manageable for people who feel like their vision is fine.
“It's an important lesson for our training doctors. We have had a number of young patients present this year for the first time with blind level vision due to very advanced end stage diabetic retinopathy."
He continues: “The complexity of the environment where patients are, means they can't necessarily make their diabetic eyecare a higher priority. It ends up getting left to become so advanced, it becomes really difficult to try and undo and at least rescue some sight. It's sad particularly because it's largely avoidable.”
Henderson performs both focal and pan-retinal photocoagulation for diabetic retinopathy, as well as anti-VEGF injections, but doesn’t have a portable OCT at his disposal.
“I wouldn't mind one but I'm old enough to know that before OCT, you could diagnose clinically significant macular oedema by examining the patient carefully. Some clinicians can forget that. They ask, ‘Where's the OCT? Where's the machine technology?’.”
For Henderson, frequently operating on “unpredictable and technically difficult” complex cataracts has sharpened his surgical skills. If they've got a red reflex, it's a bonus.
“These are patients who've resisted surgery for years. And it's not unusual to have patients on the list with light perception or hand movements vision due to a dense white cataract. Patients can be difficult to track down, often present late and are reticent to proceed with surgery," he says.
"Several of my colleagues who have helped with surgery weeks have commented on how rarely they see such advanced cataracts despite busy practices.
“Unless you're used to dealing with complex cataracts, it's very easy to get caught out, drop the lens and then have to send patients interstate for vitreoretinal rescue. There isn't a vitreoretinal surgeon next door in the adjoining theatre.
“The stakes are much higher, because if a patient gets a poor outcome, that community will probably not want cataract surgery for another five, 10, 15 years.”
Despite the risks, Henderson says cataract surgery is incredibly rewarding.
“It's also good to teach registrars about more complicated cases. I quite often say to them, ‘I may not be able to let you do a lot of completely independent surgery, but I hope you'll see an awful lot of difficult cataract surgery and complications that can occur and hopefully how to get out of most of them’.”
FUNDING AND STAFFING
Adequate funding and staffing are constant challenges for Henderson in his capacity at Alice Springs Hospital and with the IRIS Taskforce.
It’s a case of supplementing the limited resources that exist through the public hospital system. But public services are already under-resourced and often don't have the capacity to deal with the workload.
“One of the difficult things is there is no alternative whatsoever for patients to receive eyecare here unless they travel interstate or to a private hospital in Darwin. Everything we do is in the public hospital and clinical status determines priority,” Henderson says.
When it comes to funding, Henderson says politicians typically focus on short-term quantity outcomes, which doesn’t factor in the nuances of providing eyecare to the whole of central Australia.
“Politicians like numbers. They want to know how many cataract operations have been performed, rather than looking at the background. I don't want to do a cataract surgery blitz then sit on our laurels and say, ‘We can't do any more operations’.
“I need the baseline level of throughput to be adequate all the time. That needs a stable team of staff to be able to run the service all the time, so that once you've got a patient who's finally ready for surgery, you don't say, ‘Sorry, we can't operate until we do the next surgery week’. You have to have the capacity, which means you've got to have staff with experience and sufficient staff for backup,” he says.
“That's been a problem with sufficiently skilled scrub staff but also staff rotating and moving to other roles, because that was the only way they could get promoted. But they take with them all their specialist expertise. It's been a significant problem in the last year or two. Hopefully we'll find ways to address that. But having funding for a position which is intended to support specialist skills is really valuable.”
Henderson says the University of Melbourne’s Indigenous Eye Health Unit led by Professor Hugh Taylor has built a solid foundation of statistics and information on the cost-effectiveness of surgical intervention and healthcare in the Indigenous population.
“What is needed is long-term guaranteed IRIS funding for a comprehensive IRIS eye surgery team for the Alice," he says.
“One huge encouragement in 2022 is the presence of second specialist and colleague Dr Katarina Creese who has been able to make time away from her role in Melbourne to spend a year in Alice Springs as a longterm locum. It is great to be able to share the workload and challenges with an experienced general ophthalmologist.” n
72 INSIGHT October 2022 PROFILE
The slit lamp and stools setup is replicated in remote communities.
COMPENSATED POWERS
LABS WILL OFTEN SUPPLY LENSES WITH COMPENSATIONS INCORPORATED, EVEN WHEN THE PRACTITIONER HASN’T SPECIFIED ANY ANGULAR PARAMETERS. GRANT HANNAFORD EXPLAINS WHY – AND HOW DISPENSERS CAN PROVIDE OPTIMAL OUTCOMES USING COMPENSATED POWERS.


Aregular source of contention between practitioners and lens laboratories is the subject of compensated powers. Many practitioners complain that if they ordered a specific power, let’s say +5.00DS, then why did the lab send them +4.94/-0.16 x 163?
GRANT HANNAFORD
“IF YOU DON’T TELL THE LAB THE FITTING CONDITIONS THEN AVERAGE VALUES MAY BE APPLIED, HENCE THE ARRIVAL OF THE LENSES WITH SOME VARIATION FROM THE ORDER”
The primary source of these changes is the relationship between the refracting, or testing, environment and the ‘as worn’ position of the lenses. The most common setup for phoropter heads, and also most trial frames, is one that is perpendicular to the principal axis of the visual system. This results in tilt and wrap of zero degrees, and vertex distances that typically range from 12 to 18mm. In phoropter heads, depending on the design, the vertex distance can be up to 30mm, however the design of the units tends to have this in place for the lowest powers to minimise the impact on effective power.
If we wish to ensure the patient experiences the same power at the cornea (and in some lens designs at the fovea) between the refraction and their final fitted spectacles, it is necessary to compensate for position of wear.
The first of these compensations is typically vertex distance. The expression should be familiar from our studies and is a simple application of a power modification in the context of the change of the distance from the lens to the eye.
We then consider the effect of tilt on the power. The expression for effective power due to tilt is perhaps not as familiar as that for vertex power, but may be verified by taking a spherical lens and simply observing the effect of tilting the lens on the lens rest. We should see that as the lens is tilted an amount of cylinder is induced, despite there actually being none in the lens.
The most common setup for phoropter heads, and most trial frames, is one that is perpendicular to the principal axis of the visual system.
first then apply those results back in for wrap, using a tilt of 10 degrees, a wrap of three degrees and n=1.498, we get a result of +5.06/-0.02, reversing the order of operations gives +5.23/-0.15, ignoring axis for the time being. Further complication arrives when we consider spherocylindrical prescriptions where we attempt to consider power sequentially in the vertical and horizontal meridians in short, it is not generally possible to reliably perform power compensations using the expression above.
How can we reconcile this? The solution is to not consider the tilt and wrap sequentially, rather we need to define the plane of the spectacles with both tilt and wrap in place simultaneously as described by Keating (1995), Harris (1998, 2002). Doing this we discover an effective tilt of 10.44 degrees, but perhaps more importantly the axis of our new reference plane is 16.79 degrees. We now have an angle in three-dimensional space that defines the relationship between the tilt/wrap of the spectacles and the plane of the phoropter head (or trial frame), and an axis that can be used in calculations.
from the lens laboratories, allowing for variation due to proprietary considerations. In this case we achieve effective powers of +5.14/-0.17 x 163.5 and compensated powers of +4.94/-0.16 x 163.2.
When receiving our lenses from the lab we will often see that some compensations have been applied, even without having specified angular parameters. This is most often due to the lab understanding that, despite no tilt/wrap being specified, there will be tilt/wrap for almost every pair of spectacles. Experience tells us that these will range from eight to 10 degrees for tilt and two to three degrees for wrap. Importantly, if you don’t tell the lab the fitting conditions then average values may be applied, hence the arrival of the lenses with some variation from the order. n
Effective power for wrap is calculated using the same expression, but it is at this point that we encounter a problem. The overwhelming majority of spectacles have both tilt and wrap, so we need to consider the order of operations. If we take a +5.00DS lens and calculate for tilt
This technique is significantly more powerful as it allows inclusion of spherocylindrical power sets without modification to the process. Understandably it is somewhat more involved, however the results are consistently in line with those that we see
ABOUT THE AUTHOR: GRANT HANNAFORD is a qualified lens designer, has completed an MSc (optometry) and is undertaking doctoral research in ocular biometry and emmetropisation. He co-owns a private independent optometry practice in the Southern Highlands of NSW and is the Director of the Academy of Advanced Ophthalmic Optics, is a Fellow of the ABDO and ADOA, and was recently nominated as a finalist in the 2022 International Optician of the Year Award. He is also the past Chairman of the NSW Optical Dispensers Education Trust and past Vice President of ADOA (NSW) and a current appointee to the Australian Standards Committee for Spectacles.
Fsph = F 1+ sin2 θ Fcyl = Fsph tan2 θ
DISPENSING INSIGHT October 2022 73
2n
ORTHOPTIC-LED DIABETIC RETINOPATHY SCREENING IN REMOTE COMMUNITIES

The ophthalmology department at Palmerston Regional Hospital (PRH), a campus of Royal Darwin Hospital (RDH), is the eye hub for the Top End of the Northern Territory (NT), and it caters to a large Aboriginal and Torres Strait Islander demographic.
through the Commonwealth-funded Visiting Optometrist Scheme (VOS).
MADELAINE MOORE
“THE PILOT’S MAIN SUCCESSES INCLUDE
REACHING ASYMPTOMATIC AND PREPRESBYOPIC PATIENTS WHO WOULD NOT SELF-PRESENT TO OPTOMETRY”
Diabetes mellitus affects 12% of Aboriginal and Torres Strait Islander people living in rural and remote locations and is among the leading causes of preventable blindness for this population group.1
Screening plays a critical role in early detection and treatment of diabetic retinopathy (DR) and it is recommended that Indigenous patients with diabetes receive an annual eye check.

The Australian Government funds the Provision of Eye Health Equipment and Training (PEHET) program, with the aim of engaging remote area general practitioners, nurses and Aboriginal Health Practitioners (AHP) to screen for diabetes using a retinal camera. The rollout included installation of retinal cameras across a high number of remote primary healthcare centres.
This program has had varying levels of success across the country, however, due to the NT’s transient workforce and remote health workers’ overburdened workloads, there has been scarce uptake of this initiative in the Top End. The good news is a number of NT communities are equipped with a retinal camera.
The average diabetes screening rates across remote communities in the Top End are 33%, and the majority of these eye checks are being delivered
The VOS program does not have further funding to increase its services, so a pilot study of orthoptic-led diabetes screening clinics was conducted. To maximise diabetic patient attendance, the clinic was delivered at the same time the diabetes educator and remote GP were visiting the clinic.
The aim of the pilot was to deliver a shorter consult and maximise the volume of patients. The work-up solely consisted of visual acuity with pinhole and undilated fundus photo using the Canon Digital Non-Mydriatic Retinal Camera. Working with the diabetes educators, the pilot aimed to recruit pre-presbyopic asymptomatic patients, who likely would not present to optometry.
The pilot included three days of service to three different communities; Palumpa, Wadeye and Nauiyu. The total number of patients who presented was 33, with the findings listed in Table 1.
Two of the three patients with DR were new detected patients. The two patients with no view were awaiting cataract surgery on the public hospital waitlist. The incidental finding was reviewed with the ophthalmologist and referred to RDH for additional investigation.
The pilot encountered similar challenges to any remote Indigenous community clinic, including a low patient attendance day due to sorry business within the community.
Another challenge included clinics without the retinal camera, which required the team to transport the portable camera, which was heavy and awkward to get in and out of the chartered flight.
The orthoptist is an appropriate candidate to deliver DR screening as they are trained to confidently detect and grade DR on fundus images, as well as recognise other abnormalities, which may be intimidating for GPs who are not experienced in eye health.
Additionally, when incidental findings do occur, the close working relationship with ophthalmologists provides an efficient review pathway. The other benefit of the pilot was the opportunity to provide
capacity building to the Aboriginal Health Practitioners. The high volume and repetitive workflow made it easier to consolidate the skill.
The pilot’s main successes include reaching asymptomatic and pre-presbyopic patients who would not self-present to optometry, no need for patients to undergo dilation, capacity building, and the short duration consult with minimal wait times reducing the number of people who ‘do not wait’.
If the program proves to be a success, I believe expanding the Medicare funding item to include orthoptists will be a necessary measure to make it viable. n
REFERENCE
ABOUT THE AUTHOR: MADELAINE MOORE is an orthoptist and Indigenous eye health coordinator working in Royal Darwin Hospital, Northern Territory. She has a Bachelor of Health Sciences/Master of Orthoptics (La Trobe University) and a Postgraduate in Health Service Management (Griffith University).
 1. National Aboriginal and Torres Strait Islander Health Survey, 2018-19 financial year, Australian Bureau of Statistics (abs.gov.au)
ORTHOPTICS AUSTRALIA strives for excellence in eye health care by promoting and advancing the discipline of orthoptics and by improving eye health care for patients in public hospitals, ophthalmology practices, and the wider community Visit: orthoptics.org.au
ORTHOPTIST AND INDIGENOUS EYE HEALTH COORDINATOR IN THE NORTHERN TERRITORY’S TOP END, MADELAINE MOORE, EXPLAINS HOW A LACK OF FUNDING TO EXPAND EXISTING SERVICES HAS LED TO A PILOT FOR ORTHOPTIC-LED DIABETES SCREENING CLINICS.
1. National Aboriginal and Torres Strait Islander Health Survey, 2018-19 financial year, Australian Bureau of Statistics (abs.gov.au)
ORTHOPTICS AUSTRALIA strives for excellence in eye health care by promoting and advancing the discipline of orthoptics and by improving eye health care for patients in public hospitals, ophthalmology practices, and the wider community Visit: orthoptics.org.au
ORTHOPTIST AND INDIGENOUS EYE HEALTH COORDINATOR IN THE NORTHERN TERRITORY’S TOP END, MADELAINE MOORE, EXPLAINS HOW A LACK OF FUNDING TO EXPAND EXISTING SERVICES HAS LED TO A PILOT FOR ORTHOPTIC-LED DIABETES SCREENING CLINICS.
74 INSIGHT October 2022
Upskilling of an Indigenous Allied Health Australia (IAHA) student in the community of Maningrida.
Findings No. No Diabetic Retinopathy 27 Mild Diabetic Retinopathy 1 Moderate Diabetic Retinopathy 2 No view 2 Incidental finding 1 Total 33 Table 1. Results from the diabetic eye disease screening pilot involving three communities.
CAN PRACTICE STAFF REALLY WORK FROM HOME?

HEALTHCARE FRONT-OF-HOUSE STAFF RECRUITMENT, RETENTION AND FLEXIBILITY IN A “POST PANDEMIC” WORLD HAS EMERGED AS A KEY CHALLENGE AND SPURRED A ONCE-UNTHINKABLE NOTION: MEDICAL RECEPTIONISTS WHO WORK FROM HOME, WRITES LUCY PETERS.
LUCY PETERS
"STAFF HAVE SHOWN THEY CAN EFFECTIVELY PERFORM SOME TASKS REMOTELY AND ARE NOW DEMANDING THIS"
With hidden smiles behind masks, more arrival screening procedures and receptionists having to send patients home for telehealth or testing precautions before presentation, the face of medical practices has undergone a seismic shift over the past two years. Add to this increasing patient demands for faster service plus demands to maintain shorter overall waiting time; we need to adapt to the pandemic’s long term impacts. We work in healthcare to help patients, but this is constantly changing; in fact, most teams thrive on these changes (even if they don’t know it!) and welcome new improvements. Some recent changes have led to new opportunities to ensure practices survived and patients received best possible care, but staff have now come to expect them.
This includes flexibility and working from home (WFH) options. While education and staff development are still vital to the practice’s success, we have to think outside the box in today’s market to attract and retain new staff. Good leadership is no longer enough. For years the leading cause for staff turnover was management, now we are hearing that location is becoming number one and flexibility number two. The Conversation recently reported a survey showing almost half of employees would look for a new employer rather than give up the ability to WFH at least part of the time.
Pre-2020 we would have said WFH receptionists was mostly out of the question. However, staff have shown they can effectively perform some tasks remotely and are now demanding this.
Allowing staff to WFH on an ongoing basis could be a good method to:
• Increase staffing where perhaps symptoms or close contact protocols mean they cannot be in the practice, but feel well enough to work;
• ●Recruit university students now studying online, and are available during working hours;
• ●Retain the staff you had WFH during the pandemic who liked it and don’t want to come back;
• ●Include as part of a future Flexible Working Arrangement consideration.
To facilitate this, practices should consider protocols for WFH requests and implement standardised practices.
Firstly, it must be a fair and equitable process. Appropriate tasks should be worked out first then offered to all staff who meet the Award level to perform them. For example, will they be handling importing of records only and creation of tasks based on queries that the on-site team then triage, or will they be receiving practice phone calls or calling patients to confirm appointments. The consideration for moving forward would be based on their ability to perform these tasks independently, practice needs and meeting the rest of the requirements.
Secondly, there are the logistical and legal practicalities:
•
●Is the employee’s security & IT capable to WFH? Are they willing to accept the internet and phone costs (usually less than travel to the workplace) and can they ensure a private space where no patient information will be overheard or printed?
•
●Does their work area meet WHS standards? The AAPM provide an excellent checklist staff can complete and managers sign off, including loaned IT equipment.
•
●Does your practice have a secure remote desktop with VPN or two factor ID (keep a list so these permissions are revoked when team members leave) as well as relevant program licenses and accessibility?
•
●If phone calls are made, is there a soft phone option (i.e. an app or desktop program that dials into your main lines)?
If more basic call forwarding is used, ensure personal mobiles are set to private number when dialing out.
Finally, there are the day-to-day management tools for WFH staff to work independently yet feel part of the team:
•
●Do they have easy-to-access tools such as PDF quick steps/videos?
•
●Do they know how to log their time and report completed duties? Is this measurable for future time in motion studies?
•
●Do they have a daily check-in or
meeting? How are daily concerns and comms maintained (for example a WhatsApp/signal chat group or Teams/ Zoom)
•
●If they are working independently for long periods, are regular all team meetings setup to ensure changes are communicated and practice culture/ practitioner standards are maintained?
The pandemic has provided a new opportunity to rethink workplace practices. Front-of-house employees are the lifeblood of health clinics and flexible working arrangements could be a way to stand out in this competitive recruitment environment. n
Disclaimer: This article is intended to provide commentary and general information. It does not constitute legal or employment advice. You should seek legal or other professional advice before relying on any content, and practise proper employment decision making with regard to the individual circumstances.
ABOUT THE AUTHOR: LUCY PETERS is an AAPM Certified Practice Manager at Gordon Eye Surgery in Sydney. She has more than 16 years’ experience in medical practices both in the UK & Australia and has been Chair of the RANZCO Practice Manager's Advisory Group since 2017.

MANAGEMENT
INSIGHT October 2022 75
Practices should consider protocols for WFH requests and implement standardised practices.
People ON THE MOVE
Insight's monthly bulletin to keep the Australian ophthalmic sector updated on new appointments and personnel changes, nationally and globally.
OPTICAL DISPENSERS AUSTRALIA BOARD UPDATE
Gladys Mak has joined Optical Dispensers Australia (ODA) Advisory Board. Mak is an experienced optical dispenser with diverse industry background both in Australia and internationally. She is one of the instructors delivering the optical dispensing workshop for the Doctor of Optometry program at University of Western Australia. She has extensive experience in frame manufacturing and product development.
SPECSAVERS DISPENSER JOINS OPTICAL DISPENSERS AUSTRALIA BOARD

Linden Sawyers, a retail partner at Specsavers Baldivis in WA, has also been appointed to the Optical Dispensers Australia Advisory Board. Sawyers has worked in the eye health industry for almost 20 years across independent and corporate. With a Cert IV in Optical Dispensing and an FBDO accreditation under way, Sawyers is passionate about the educational opportunities available for dispensers. She is also as a member of the Specsavers ANZ Dispensing Advancement Partner Advisory Group.
B+L TERRITORY MANAGER ARRIVES WITH MEDICAL INDUSTRY EXPERIENCE

Kiyoko Robertson has joined Bausch + Lomb as Surgical Territory Manager and will support the Newcastle area, NSW. Robertson is a trained nurse in both the human and veterinary fields where she spent 25 years of her career. Originally from the US, she has been in Australia for 12 years and spent the last four years as a Territory Manager in Orthopaedic Trauma. Now settled in Newcastle, Robertson is excited to start this new phase of her career in surgical ophthalmology.
NURSING BACKGROUND AND EXTENSIVE EXPERIENCE WITH MEDICAL DEVICES
Bianca Dowman has joined Bausch + Lomb as a Surgical Territory Manager for New South Wales. She has had success within the medical device industry and brings over 20 years of experience across several surgical specialties. Dowman’s nursing background and extensive experience with medical devices, along with her Master’s in Business Administration, have her well-positioned to welcome this new challenge in surgical ophthalmology.
HOYA SALES MANAGER RETURNS TO THE FOLD

Matt Dowd has re-joined HOYA as its Queensland State Sales Manager. His extensive knowledge within the optical wholesale and retail markets, along with his qualifications in optical mechanics and dispensing, have him well-positioned to welcome this new challenge and lead HOYA’s sales team in the Sunshine State, HOYA said.
CONTACT LENS EXPERT JOINS CENTRE FOR OCULAR RESEARCH & EDUCATION




Specialty contact lens innovator Dr Daddi Fadel, DOptom, FSLS, FBCLA, FAAO, FIACLE, joined the Centre for Ocular Research & Education (CORE) in September 2022. Fadel is one of the world’s best-known designers and fitters of scleral lenses for irregular cornea and orthokeratology lenses for myopia control. Her appointment as a clinical scientist will advance CORE’s expanding specialty contact lens initiatives.
Do you have career news to share?
Email editor Myles Hume
to be featured.
CAREER 76 INSIGHT October 2022
at myles.hume@primecreative.com.au
OCTOBER 2022
CCLSA ICCLC 2022
Sydney, Australia
15 – 17 October icclc2022.com.au
PROVISION NATIONAL CONFERENCE
Melbourne, Australia
21 – 23 October eventbrite.com.au
EYECARE PLUS NATIONAL CONFERENCE 2022
Broadbeach, Australia
28 – 30 October web.cvent.com
RANZCO 53RD SCIENTIFIC CONGRESS
Brisbane, Australia
28 October – 1 November ranzco2022.com
ORTHOPTICS AUSTRALIA ANNUAL CONFERENCE
Brisbane, Australia
28 – 31 October orthoptics.org.au
ISMSICS LAUNCH AUSTRALIA & NEW ZEALAND CHAPTER Brisbane, Australia
29 October ranzco2022.com
NOVEMBER 2022
ASIA OPTOMETRIC CONGRESS & AEGEAN OPTOMETRIC CONFERENCE
Kuala Lumpar, Malaysia 15 – 16 November asiaoptometriccongress.com/ 3rd-asia-optometric-congress
ASIA-PACIFIC VITREO-RETINA SOCIETY CONGRESS
Taipei, Taiwan
18 – 20 November 2022.apvrs.org
JANUARY 2023
HONG KONG INTERNATIONAL OPTICAL FAIR
Hong Kong
9 – 11 January event.hktdc.com
FEBRUARY 2023
MIDO
Milan, Italy 4 – 6 February mido.com
ANZGS CONGRESS
Queenstown, New Zealand 16 – 19 February anzgsconference.com
100% OPTICAL
London, UK
25 – 27 February 100percentoptical.com
APRIL 2023
AUSTRALIAN VISION CONVENTION
Gold Coast, Australia
1 – 2 April events@optometryqldnt.org.au
ARVO 2023
New Orleans, US
23 – 27 April arvo.org/annual-meeting
JUNE 2023
WORLD GLAUCOMA CONGRES
Rome, Italy
28 June – 1 July worldglaucomacongress.org
Graduate Recruitment Team are currently looking for new
Looking at starting your career with a
mentor
first
and New Zealand and we have continued to develop our comprehensive two-year Graduate Program providing a support network and structured program to assist you in your development.
are the largest employer of Graduate
All Specsavers stores nowwith OCT
The Graduate Recruitment Team are currently looking for new graduates to join our teams in North QLD, NT, and WA, providing generous regional salary and relocation packages.
Interested in relocating to NZ? Specsavers has a range of opportunities for NZ optometrists looking to return home. From North to South, we have fantastic opportunities for optometrists at all levels.
And as a Specsavers optometrist, you’ll have the chance to advance your skills and become part of a business that is focused on transforming eye health outcomes in New Zealand. Be equipped with the latest ophthalmic equipment (including OCT in every store for use with every patient) and develop your clinical experience across a range of interesting conditions and an ever-growing patient base.
You’ll also have the support of an experienced dispensing and pre-testing team, the mentorship of store partners and access to an exemplary professional development program.
There’s no place like home – so if you’re ready to return, let us help you.
Optometrist Joint Venture Partnership opportunity – Northam, WA
Optometrist partnership opportunity in Northam with a with a 50% shareholding on offer! Northam is situated at the confluence of the Avon and Mortlock Rivers, about an hour drive east of Perth, in the picturesque Avon Valley. The store opened in 2021 and is located in the Northam Boulevard Shopping Centre anchored by retail drawcards Woolworths and Target, the Centre also has ample parking available. The store is 126sqm in size and offers 2 Optical test rooms, a dedicated Audiology room, 6 dispense desks, 1068 frame count and state of the art equipment including OCT.
Up to $150k Optometrist opportunity – Specsavers Northwest Tasmania
Work with an extremely warm, welcoming and experienced Retail team supporting a loyal and varied patient demographic including lots of pathology and neurological workups. Have access to market leading technology – including OCT along with access to excellent opportunities for professional development including the opportunity to focus on a specialty area of interest or pathway to partnership. Flexible roster to support work/life balance and additional annual leave and relocation support if applicable. 2 amazing opportunities available if you want to go with a friend!
Highest package ever! $180,000 for the growing Mobile Optometrist Role Specsavers is growing our community based Mobile Optometry Team Nationally, With home based locations in Newcastle, Perth & Melbourne along with longer term Fly in Fly out roles available. With an amazing $180,000 package on offer. You will experience a wide variety of cases, whilst being able to explore different regions of Australia. We are looking for someone who has the desire and flexibility to travel.
SO LET’S TALK!
In a few short years, Specsavers has achieved market leadership in Australia and New Zealand with more people choosing to have their eyes tested and buy their prescription eyewear from Specsavers than any other optometrist. To learn more about these roles, or to put your hand up for other roles as they emerge, please contact us today:
Joint Venture Partnership opportunities enquiries:
Australia Optometrist employment enquiries: Marie
Recruitment Consultant marie.stewart@specsavers.com
Locum employment enquiries:
New Zealand employment
Graduate employment enquiries:
2022 CALENDAR To list an event in our calendar email: myles.hume@primecreative.com.au SPECSAVERS – YOUR CAREER, NO LIMITS VISIT SPECTRUM-ANZ.COM
Kimberley Forbes on +61 (0) 429 566 846 or E kimberley.forbes@specsavers.com
Stewart –
or 0408 084 134
Cindy Marshall cindy.marshall@specsavers.com or 0450 609 872
enquiries: Chris Rickard –Recruitment Consultant chris.rickard@specsavers.com or 0275 795 499
apac.graduateteam@specsavers.com
graduates
dedicated
and graduate team to support you in your
steps? Specsavers
Optometrists across Australia
NEUROPATHIC PAIN IN THE EYE
in other cases it is a secondary effect of the condition which may only occur in some instances. For example, in patients who have suffered injuries leading to paralysis or are afflicted with diseases of the nerves themselves, such as in multiple sclerosis, damage to the somatosensory system is part of the primary pathophysiology of the disease and the resulting pain is a manifestation of this harm.3
pain from stimuli that are normally not painful (allodynia) or pain that persists after the causative insult has ceased to exist.3 Use of a questionnaires, including the Ocular Pain Assessment Survey (OPAS), is recommended to document the pain.7
BY A/PROF ALEX HUI
The International Association for the Study of Pain recently updated its definition of pain for the first time since 1979 to be “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage”.1 This definition is important for clinicians to understand, as pain is not only confined to tissue damage or injury, but also the experience associated with the stimulus.
Indeed, analgesia, which is commonly used to denote the management of pain, is more specifically defined as the reduction or absence of the sensation of pain in response to a typically painful stimulus.1 Unfortunately, for a subset of patients, it is the system that signals pain through the nerves and gives the perception of pain that can be dysfunctional; this leads to neuropathic pain which can be quite different than pain associated with direct tissue damage.
Neuropathic pain is inherently a disease of the somatosensory system and as such, is referred to colloquially as “nerve pain”.2 There are numerous aetiologies for neuropathic pain. In many instances the link between a disorder of the somatosensory system and the presence of neuropathic pain is apparent, while
For other aetiologies, damage to the nerves and thus pain signalling may not always be present. Examples of this include diabetic neuropathy as well as herpes zoster, where the pathophysiology of the primary condition can lead to nerve dysfunction and cause pain sensation, but is not always a feature of these diseases.3 It is also important to note that “regular” pain caused by the stimulation of our pain receptors due to insults, can also be converted to neuropathic pain if it is not treated promptly and persists for long periods of time.
In the eye, common causes of neuropathic pain include dry eye, post corneal and refractive surgery, and herpetic infection. These neatly represent some of the possible locations along the trigeminal nerve through to the cornea that can be afflicted.2,4,5 Reactivation and replication of herpetic viruses in the nasociliary branch of the trigeminal nerve not only leads to viral shedding and the clinical manifestations of ocular herpes, but may also damage the nerves themselves and disrupt nerve signalling which leads to persistent pain.4 Anterior segment and refractive surgery damage nerves in an iatrogenic manner: corneal nerves can be cut or otherwise suffer trauma due to the procedure.5 Dry eye disease also involves neurosensory abnormalities, as found in the definition for the disease in the TFOS DEWS II report.6 Here, the thought is that there may be some link between the chronic inflammation induced by the disease that affects the health of nerves on the ocular surface.2
For the eyecare practitioner, identifying patients at risk of developing neuropathic pain is crucial to ensure prompt and appropriate management. Clinicians should identify patients who experience pain that is out of proportion to their clinical signs (hyperalgesia),
Management of neurologic pain centres on controlling the primary condition as much as possible. Earlier involvement of the patient’s general practitioner or referral to a pain specialist should be considered, particularly for conditions such as herpes zoster ophthalmicus where post herpetic neuralgia can be severe and has the potential for long term impact on quality of life.4 For the ocular surface, management of neuropathic pain often begins with the use of anti-inflammatory therapy or autologous serum, as decreasing inflammation has been shown to have a positive impact on reducing pain.7 n
REFERENCES
1. International Association for the Study of Pain. Terminology. 2020 [cited 2022 19/07/2022]; Available from: https://www. iasp-pain.org/resources/terminology/.
2. Rosenthal, P. and D. Borsook, Ocular neuropathic pain. British Journal of Ophthalmology, 2016. 100(1): p. 128.
3. Jensen, T.S. and N.B. Finnerup, Allodynia and hyperalgesia in neuropathic pain: clinical manifestations and mechanisms. Lancet Neurol, 2014. 13(9): p. 924-35.
4. Sampathkumar, P., L.A. Drage, and D.P. Martin, Herpes zoster (shingles) and postherpetic neuralgia. Mayo Clin Proc, 2009. 84(3): p. 274-80.
5. Moshirfar, M., et al., Neuropathic Corneal Pain
Following LASIK Surgery: A Retrospective Case Series. Ophthalmology and therapy, 2021. 10(3): p. 677-689.
6. Craig, J.P., et al., TFOS DEWS II Definition and Classification Report. Ocul Surf, 2017. 15(3): p. 276-283.
7. Nortey, J., et al., Topical Therapeutic Options in Corneal Neuropathic Pain. Frontiers in Pharmacology, 2022. 12.
Name: Adjunct A/Prof Alex Hui Qualifications: OD, PhD, GradCertOcTher, FAAO Organisation: School of Optometry and Vision Science, Faculty of Medicine and Health, UNSW Sydney; Centre for Ocular Research and Education, School of Optometry & Vision Science, University of Waterloo Position: Adjunct Associate Professor (UNSW); Head, Biosciences (Waterloo) Location: Toronto, Canada
Years in profession: 12

IN THE EYE, COMMON CAUSES OF NEUROPATHIC PAIN INCLUDE DRY EYE, POST CORNEAL AND REFRACTIVE SURGERY, AND HERPETIC INFECTION.
SOAPBOX
78 INSIGHT October 2022
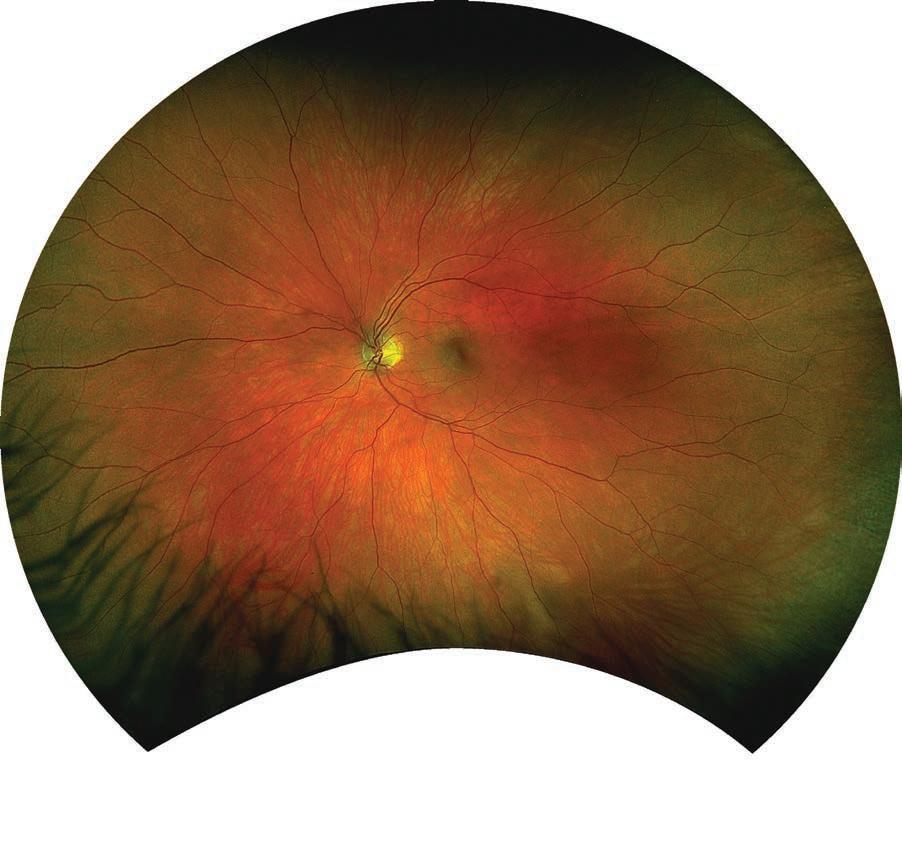

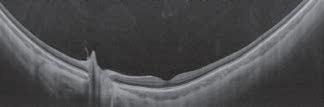
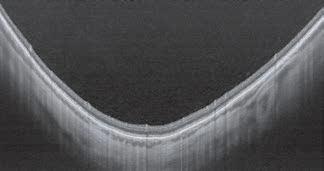

Saving Sight, Saving Lives. Optos’ latest ultra-widefield retinal imaging technology increases patient flow and satisfaction.1 Optos.com T: +61 8 8444 6500 E: auinfo@optos.com Image: SS OCT line and volume scanscaptured with optomap-guided OCT The ONLY single-capture ultra-widefield image in less than ½ a second. Enhances practice efficiency and patient experience.2 Helps diagnose pathology earlier.3 Differentiate your practice and increase revenue.2 1. Tornambe, The Impact of Ultra-widefield Retinal Imaging on Practice Efficiency, US Ophthalmic Review 2017. 2. Successful interventions to improve efficiency and reduce patient visit duration in a retina practice, Retina. 2021. 3. Kehoe. Poster 19. Widefield Patient Care. EAOO 2016 2 2 3 3 4 4 1 1
a new
in


Introducing
experience
phaco. Our answer to your phaco efficiency demands: • Z EISS patented QUATTRO Pump ® • D igitally integrated surgical workflow • A utomated Ultrasound Power on Demand Contact your local ZEISS representative for more information or to book a demonstration. ZEISS QUATERA 700 NEW! ZEISS AU: 1300 365 470 NZ: 0800 334 353 med.au@zeiss.com Carl Zeiss Pty Ltd, NSW 2113 AUSTRALIA. Carl Zeiss (NZ) Ltd, AUCKLAND 1026 NZ.
