Guidance on The Management of Mpox Infections for Sexual Health Services
Version: V1
Ratified by:

Infection Prevention and Control Group
Date ratified: 27/09/2024
Job Title of author:
Reviewed by Committee or Expert Group
Related procedural documents
Sexual Health System Lead
Infection Prevention and Control Lead
Infection Prevention and Control Group
IPPOL21 Standard Precautions for Infection Prevention & Control including TBPs and Isolation Precautions
MMSOP32 Ordering, Storage, Transport and Disposal of Vaccines & Medicines Requiring Refrigerated Storage SOP (Cold Chain)
IPPOL03 Infection Prevention and Control Hand hygiene policy
Review date: 27 Sept 2027 (Or sooner if guidance is updated)
It is the responsibility of users to ensure that you are using the most up to date document template – ie obtained via the intranet.
In developing/reviewing these guidelines Provide Community has had regard to the principles of the NHS Constitution.
Version Control Sheet
Version Date
V1 31st May 2022
V2 1st June 2022
Author
Chris Quinn: Clinical Nurse Specialist HIV/AIDS / Acting Service Lead for Essex & Thurrock Sexual Health
Chris Quinn Clinical Nurse Specialist HIV/AIDS / Acting Service Lead for Essex & Thurrock Sexual Health
V3 16th August 2024 Essex and Suffolk Sexual Healthservices
Status
Comment
Updated comments and flowcharts
New Guidance
V1 21st August 2024 Essex and Suffolk Sexual Healthservices
Updated guidance for management of Clade 1 Mpox in line with UKHSA notification for Outbreak of Clade 1 Mpox
Updated comments and guidance – Dr Malaki
1. Background Information on Mpox virus (MPXV)
• There are two known clades of Mpox: Clade I and Clade II
• Transmission of Mpox to humans can be due to zoonotic transmission or personto-person spread
• Clade I Mpox was associated with zoonotic transmission and known to circulate in 5 African countries; Cameroon, Central African Republic, the DRC, Gabon and the Republic of Congo
• Clade I mpox virus (MPXV) is a high consequence infectious disease (HCID) which may be more severe and transmissible than the clade II mpox, which has been present in the UK since 2022
• Infection with Clade I Mpox has been reported to cause more severe mpox disease with a higher case fatality rate
• Clade I mpox virus (MPXV) has historically only been reported in five countries in Central Africa. There is now increasing transmission of clade I mpox in the Democratic Republic of Congo (DRC), and cases are also being reported from other surrounding countries in Central and East Africa
• Between 25 July and 5 August 2024, confirmed Clade I MPXV cases have been reported from Burundi, Kenya, Rwanda and Uganda for the first time, which has expanded the geographical footprint of Clade I MPXV in the African Region.
• Clade II cases have been reported from Benin, Cameroon, Cote D’Ivoire, Ghana, Liberia, Nigeria and South Africa in 2024
• There is evidence of sustained sexual transmission of clade I MPXV in the DRC.
• Sexual transmission should not be used to infer whether an mpox case is likely to be clade I or II
2. Mpox: Case Definition
This guidance has been developed to support Provide Sexual Health Services in the event of a suspected case of Mpox being identified within the sexual health clinic The guidance provides definitions for non-high consequence infectious disease (HCID) monkeypox virus.
When assessing patients for mpox, always take a travel history. Be alert to the possibility of HCID Mpox (Clade I) in all patients with suspected mpox if there is a travel history to the Democratic Republic of the Congo or other specified countries in the African region
Possible Case
A possible case is defined as anyone who fits one or more of the following criteria:
• A febrile prodrome (fever >38 degrees C, chills, headache, exhaustion, muscle ache, joint pain, backache and swollen lymph nodes) compatible with mpox infection, where there is a known prior contact with a confirmed case in the 21 days before symptom onset
• An illness, where the clinician had a suspicion of mpox, such as unexplained lesions, including but not limited to
➢ Genital, ano-genital or oral lesion(s)- e.g. ulcers, nodules
➢ Proctitis- e.g. anorectal pain, bleeding
Probable Case
A probable case is defined as anyone with an unexplained rash or lesion(s) on any part of the body (including genital/perianal, oral) or protitis (anorectal pain, bleeding) who:
• Has an epidemiological case to a confirmed, probable or highly probable case of mpox in the 21 days before symptom onset OR
• Identifies as gay, bisexual or other man who has sex with men OR
• Has had one or more sexual partners in the 21 days before symptom onset
Actions for a possible or probable case:
• Have a low threshold for testing for mpox in patients with clinically compatible presentations with a travel history irrespective of sexual history, using designated testing pathways
• Undertake additional contemporaneous tests to rule out alternative diagnoses if clinically appropriate and if not already done
• Be alert to the possibility of clade I mpox in all patients with suspected mpox if there is a link to the specified countries in the African region (as listed above). Patients with a travel or exposure history indicating possible HCID mpox should be discussed with the Rare and Imported Pathogens Laboratory (RIPL) on 01980 612348 (available 9am to 5pm, Monday to Friday) and the clinical team as soon as possible via the 24/7 Imported Fever Service helpline (0844 778 8990)
• Isolate patients meeting the following criteria as a high consequence infectious disease and contact the Imported Fever Service to discuss urgent testing and typing:
➢ Confirmed or clinically suspected mpox cases but clade not yet known
➢ travel history to the DRC or specified countries where there may be a risk of clade I exposure
➢ link to a suspected case from those countries (listed above), within 21 days of symptom onset and/or there is an epidemiological link to a case of Clade I mpox within 21 days of symptom onset.
Actions required by Clinicians:
Isolate patients meeting the following criteria as a high consequence infectious disease
Contact the Imported Fever Service (IFS) (0844 778 8990): - to discuss urgent testing and typing of:-
• Confirmed or clinically suspected mpox cases but clade not yet known and there is a travel history to the DRC or specified countries where there may be a risk of clade I exposure, or a link to a suspected case from those countries (listed above), within 21 days of symptom onset and/or there is an epidemiological link to a case of Clade I mpox within 21 days of symptom onset
• Discuss any patient with suspected mpox and severe or disseminated disease with Imported Fever Service (IFS) (0844 778 8990), even if no travel history is identified.
• Notify the local Health Protection teams on suspicion of Clade I mpox
All confirmed Clade I mpox cases will be managed as HCID through the specialist HCID network
Cases where the clade is unknown, but who have a travel or contact history as above, should be discussed with the Imported Fever Service (0844 778 8990) as soon as possible to ensure appropriate testing and escalation.
All cases meeting the operational definition of an HCID should be discussed with the Imported Fever Service (0844 778 8990)
Operational case definition of Clade I and Clade II
Clade I - manage as HCID cases
(pending confirmation of clade type where appropriate
Confirmed mpox case where clade I has been confirmed
Confirmed or clinically suspected mpox case but clade not yet known
Travel history to the DRC or specified countries where there may be a risk of clade I exposure, or a link to a suspected case from those countries (listed above), within 21 days of symptom onset and/or there is an epidemiological link to a case of Clade I mpox within 21 days of symptom onset
Given the rapid spread of Clade I in the African region, check the UKHSA mpox pages regularly for any updates to the countries included
Clade II - The following patients should be managed using standard mpox precautions, and do not require HCID precautions
Confirmed as Clade II MPXV
Confirmed or clinically suspected mpox but clade not known, and all of the following conditions apply: -
There is no history of travel to the DRC or specified surrounding countries (as above) within 21 days of symptom onset
There is no link to a suspected case from the DRC or specified surrounding countries within 21 days of symptom onset
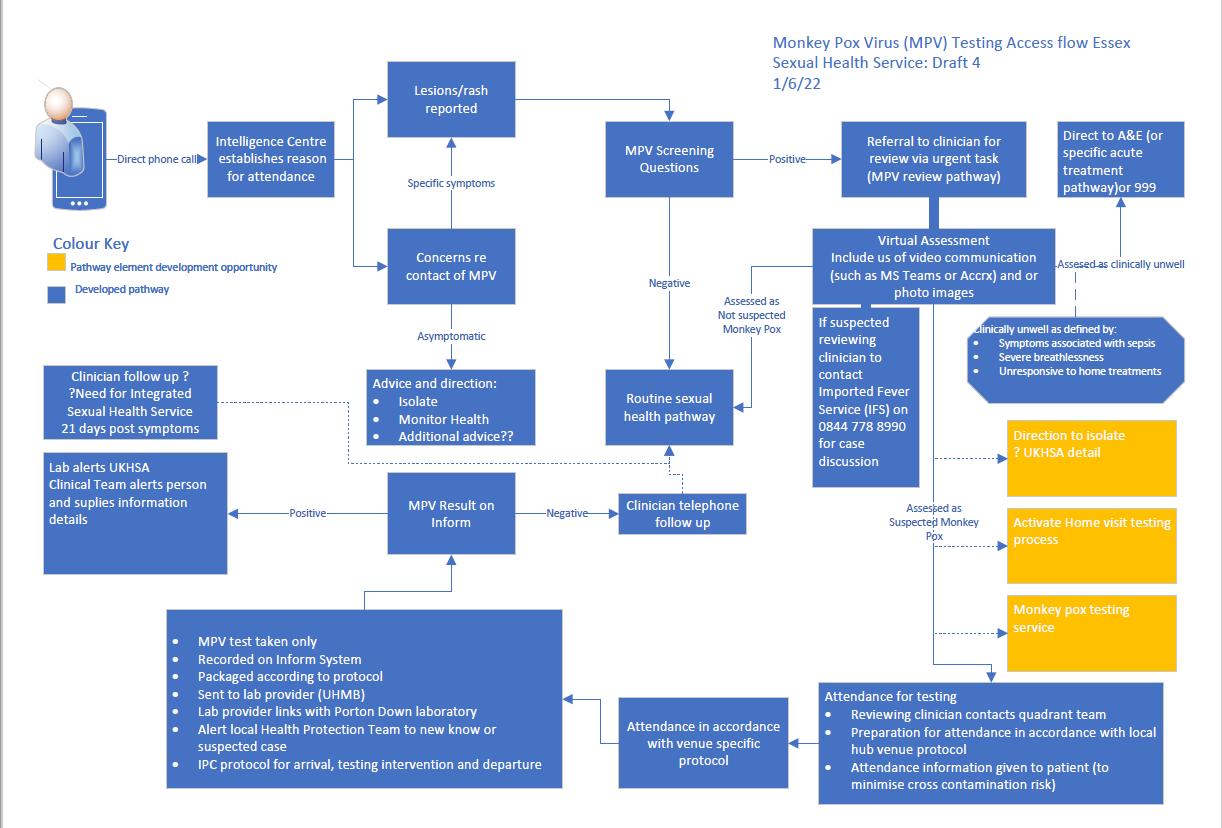
3. Triage by the Navigation Hub
All patients must be screened for Mpox (MPV) at their point of telephone booking.
Please use this flowchart to triage any questions on Monkeypox.
Patient contacts with suspected MPV
Have you got more one or more or the following symptoms?
Rash / Lesion
Fever
New lump/s in neck, groin or under your arm
YES
Ask below further questions:
Are you gay, bisexual or MSM?
Have you had contact with someone with confirmed MPV in the 21 days prior to the onset of symptoms?
Have you travelled to West or Central Africa in the 21 days prior to the onset of symptoms?
Have you travelled to any of these Countries or had exposure contact with someone who has , TheDRC, RepublicofCongo, CentralAfricanRepublic,Burundi,Rwanda,Uganda, Kenya,Cameroon,Gabon,Angola,SouthSudan, Tanzania,andZambia.
NO
No further action
Offer general advice and to call back if symptoms arise
May consider if appropriate online STI screening
NO to all 3 questions:
Proceed as normal (STI screen)
Offer online testing or Virtual STI risk assessment and appointment for STI screen
General Advice
To follow current UKHSA advice
YES to any of the 3 questions: Assessment via urgent task in local quadrant to clinician as per MPV Pathway. Advise the patient that they will be contacted on the same or next working day
YES: to travel to:
The DRC, Republic of Congo, Central African Republic, Burundi, Rwanda, Uganda, Kenya, Cameroon, Gabon, Angola, South Sudan, Tanzania, and Zambia.
Contact Local HPA team Find your local health protection team in England - GOV.UK (www.gov.uk)
Advise the patient to stay at home and not come to clinic until instructed to do so.
Contact senior Nurse or Dr On duty to discuss case
Email Dr Maliki Ramogi on malaki.ramogi@nhs.net for ESHS or Dr Christy Christy.Kaithampillai@esneft.nhs.uk
Contact list of Doctors/Consultants in Suffolk
Main Email Address telephone number for enquiries provide.suffolksexualhealthservice@nhs.net 0300 303 9982
Dr Julia Elson julia.elson2@nhs.net
Consultant Sinnapah Jebakumar sinnappah.jebakumar@nhs.net
Dr Sujee Munasinghe sujeevani.munasinghe2@nhs.net
Consultant Raouf Moussa raouf.moussa@nhs.net
Dr Katrina Robertson katrina.robertson3@nhs.net
Consultant Evelyn Kerr evelynkerr@nhs.net
Consultant Sarah Edwards sarah.edwards130@nhs.net
Dr Cobus van Dyck cobus.vandyk@nhs.net
With Inform and clinical details to alert them to a potential case
After assessment by a clinician
The patient can be booked into their local quadrant team for attendance for appropriate assessment and testing.
Please reassess PPE needs on attendance.
4. Management of suspected MPV cases in the Sexual Health Department
The clinical assessing the patient for possible MPV should contact UKHSA East of England Health Protection Team on 0300 303 8537 option 1 for advice. For advice out of hours for health professionals only: 01603 481 221. All patients that require testing will also need discussion with the Imported Fever Service on 0844 7788990
Mpox is currently classified as having airborne high consequence infectious disease (HCID). When treating any patient with suspected MPV, all staff should ensure they are wearing appropriate PPE and as a minimum FFP3 mask, gown, gloves and eye protection. They should be isolated in a separate clinic room and appropriate decontamination should take place once the room is vacated. Please see the section Decontamination for further advice.
In the event of identification of suspected case in clinic, either rash or symptoms or informed as a contact.
➢ Arrange attendance at end of clinic
➢ Ensure suspected case is isolated in room (Closed door)or removed from waiting/communal area.
➢ Exposed staff worker removes themselves and must isolate away from other staff in a designated room and contact local health protection team.
➢ Any staff that have contact with case must wear full PPE- FFP3 mask, single use visor/eye protection, full sleeve gown, gloves, (All staff wearing FFP3 masks MUST be fit tested).
➢ For staff who have failed Fit Testing they should use supplied Respirator hoods or exempt from attending to client.
➢ Exclude pregnant staff/ clinically vulnerable staff from contact with patient and exposed staff.
➢ Contact and liaise with the local health protection team and inform infection prevention in working hours via mobile contact or Quality and Safety team 0300 303 2642 Out of hours contact the manager on call 0300 003 0683
➢ For all patients that require testing, discuss with the imported Fever Service 08447788990
➢ Once case transferred to other facility or hospital or area vacated, ensure area closed until instruction from health protection team for cleaning and waste removal
5. MPV Testing with Sexual Health Services
Please remember appropriate PPE when dealing with any suspected MPV case
Frequently Asked Questions (FAQ’s): What sample types are suitable for Monkey Pox PCR testing?
➢ Viral swab in viral culture medium or Viral Transport Medium from an open sore or from the surface of a vesicle. These can be sourced from Pathology Stores as per normal ordering process.
➢ If all the lesions are crusted, scrape scab material into a dry plain universal container and label as above.
It is advised that no other samples are taken from the patient if they are being tested for MPV. The patient should be followed up by a clinician at least 21 days after exposure and offered appropriate assessment, testing and treatment of their symptoms.
N.B Any screening for other STIs at clinician discretion, must be considered on the availability and turnaround times for Mpox results. Screening for other STI’s must be only as soon as clinically feasible or as soon as negative result received with the consideration that this could be done by home testing methods. Further advice should be sought from the local health protection or imported fever service.
6. How do we request MPV PCR testing
➢ Currently no Electronic requesting available; this is under development.
➢ Temporarily all service users are asked to complete the request form using the hyperlink below, and send with the sample:
➢ Please save and add to the patient notes in the attachments section.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment _data/file/721847/P1_Rare_and_Imported_Pathogens.pdf
Please DO NOT complete the SENDERS INFORMATION SECTION but include Clinic/surgery details within the PATIENT/SOURCE INFORMATION section
7. What specific packaging and transport is required?
➢ All MPV PCR samples should be labelled with a biohazard sticker.
➢ All MPV PCR samples MUST be double bagged at source.
➢ All MPV PCR samples MUST be packaged independently of routine samples
➢ All MPV PCR samples must be sent using UN3373 transport packaging.
➢ Please ensure transport boxes are clearly labelled with biohazard sticker.
It is advised that no other samples are taken from the patient if they are being test for MPV. The patient should be followed up by a clinician at least 21 days after exposure and offered appropriate assessment, testing and treatment of their symptoms.
Swabs, sample bags and biohazard stickers are available in the clinics. Please contact the team lead for any queries with sample labelling and packing
8. Coding of MPV cases
Each suspected or confirmed case should be coded within Inform. This can be found on the current sexual health codes. A snapshot of the codes can be seen below.

9. Decontamination
Please follow guidance for cleaning and decontamination of the room as per terminal clean within National standards of healthcare cleanliness in healthcare facilities. This request should be made via Estates and facilities.