Queenwood School Science Extension Journal Volume 1
SCIENCE EXTENSION JOURNAL
Queenwood acknowledges the Cammeraigal people who are the traditional custodians of the land on which the School is built and we pay respect to Elders past, present and emerging.
All information contained in this document is correct at time of printing. Visit QUEENWOOD.NSW.EDU.AU for up-to-date information.
DR CAMILLA HOYOS Q1998
B.APPSC (CONSUMER SCIENCE), B.SC (HONS), MPH, PHD
What I love about being a scientist is that I get to ask and answer questions that will potentially go on to help people. Science is all about discovery and the great thing is that there are so many areas that still need investigating. New discoveries can affect our lives in so many ways. This includes advancing new scientific knowledge that allows us to create new technology, address societal issues, solve everyday problems, and help to inform the decision makers of our community.
What drew me to Science was the critical thinking and problem solving it involved. I liked having a question to answer and learning how to answer it. My journey into Science would have not happened without the amazing experience I had at Queenwood and the teachers that made lessons very enjoyable. I was also interested in
Queenwood Alumnus and CSIRO STEM Collaborator in schools Dr Camilla Hoyos reflects on the value of studying Science in society.
research from a young age, which grew during my university degree. Even though I had done a Science degree, I had focused more on health and had not completed labbased courses. I decided I wanted to do an honours project where I worked researchers and benefitted greatly from my experiences in a public health unit. After graduating I started looking for jobs in clinical research and my first job involved working with people living with asthma. I loved my job and where I worked, so much so I still work at the same medical research institute 21 years later. I learned new techniques such as lung function testing and met new people every day. Very quickly, however, I found that I wanted to learn more so I could identify the questions that needed to be answered and then design the studies to answer them. I chose to do a Master of Public Health and then a few years later a PhD in sleep medicine, the area in which I still work today.
One of the great things about being a researcher is new opportunities, some of them rather unexpected. A few years ago, I decided to volunteer for the CSIRO STEM professionals in schools’ program which matches scientists of all kinds with different schools. To my delight an opportunity to partner with Queenwood arose. In 2018/19 I was involved in the Researchers Initiative where the students were able to develop their own research question and study. We also had a visit to the Woolcock Institute where students visited the sleep lab and did activities such as driving simulation and learning how we measure sleep. It is these experiences that become prominent highlights of my work. Engaging with the community and particularly young people who will go on to be the next generation of researchers, answering difficult questions and making amazing, life-changing discoveries is one of the most enjoyable elements of my job! •
DR MICHELLE GLEESON HEAD OF SCIENCE
B.SC (BIOTECH), B.SC (HONS), PHD, GRAD DIP ED
I am delighted to introduce the Queenwood Journal of Science Extension, Volume 1, 2023.
Science Extension is a multidisciplinary one-unit course studied by Year 12 students in addition to one or more of the Biology, Chemistry and Physics courses in Stage 6.
Science Extension was first taught in NSW in 2019 and is unique in being the only course to culminate in a 2 hour online examination. In addition to the exam, students design and conduct an individual research project and prepare a Scientific Research Report. A selection of these reports, somewhat like an Honours thesis in miniature, are showcased here to demonstrate the depth of their talent, initiative and perseverance.
So, why should students study Science Extension? It is a unique opportunity for students
Our Head of Science, Dr Michelle Gleeson introduces the Science Extension program at Queenwood.
to branch out into an area of passion or interest beyond the constraints of the curriculum. The course is less about content and knowledge, than the processes of working scientifically. Via the course, students move from studying science to experiencing what it means to becoming a scientist themselves. The tangible benefits include substantial gains in critical thinking and analytical skills, which are transferrable to their other courses and onwards into their future studies. The next generation of scientists have a massive job on their hands. They will need to devise innovative solutions for problems we do not even know about yet, to support a growing world population existing in a dynamic and deteriorating environment. There is a reason why Science Extension students are being courted by top universities through their mentoring programs, as they are ready to hit the ground running and thrive in the tertiary Science environment.
2023 marked the fifth year of running Science Extension at Queenwood and our largest cohort to date, with twelve students completing the course in a vibrant and richly collaborative environment facilitated by two teachers. The cohesive nature of the class environment is key to its success. Thrill and disappointment, resilience and determination each come to the fore when students work on their individual projects during this course and we would like to congratulate them on their outstanding performances. These Scientific Research Reports are a fitting tribute to the tenacity, tears, and ultimately the triumph of accomplishment. We particularly congratulate Jessica Mulcahy who was awarded the highly coveted First In State Course Award.
We hope you enjoy exploring their work, and we are sure you will agree that our future is in great hands. We look forward to seeing where this experience leads them. •
MS MERRILYN LEAN SCIENCE EXTENSION TEACHER B.SC DIP ED
Science is a unique process that involves asking questions, making observations, thinking creatively and critically, and testing hypotheses based on the scientific method. This is the core of the practice of Science. Science Extension is a course that I love to teach as it allows students to deeply explore a research question of their choosing in a way that is not possible in other subjects. I have been teaching for a long time, both the HSC and IB, in more than one state in Australia, and this course is unique as it provides students with the opportunity to think like a scientist, and not think just about Science. Analysing evidence-based research increases the ability of the students to identify the intent and thus validity of the vast amounts of information that they encounter in mass media, generating more discerning viewpoints through
Science Extension Teacher
Ms Merrilyn Lean, discusses the unique process involved in the subject.
their questioning.
Science Extension is a course unlike any other in the HSC. Discussions, exploration of scientific papers, and model development and analysis provide opportunities for students to learn from each other and explore their varying opinions to identify what makes them reason differently and ultimately make the decisions that they do. It is a joy to be a part of learning experiences that open the eyes of students as they progress through the course, starting with content that they are very familiar with like bias, and ending with ideas that are highly complex and that are fundamental to the history of philosophy and thus science, such as rationalism and empiricism. I love the passion and confidence that the students demonstrate as their ability to explore their own ideas scientifically grows, and when they recognise that they are now experts in whatever subject they have chosen to investigate. I love
being a part of the development of the critical thinking and problemsolving skills of the students, as they gain more experience in manipulating technological equipment and data bases, confidently taking the lead on their own projects. It is highly rewarding seeing the students give so much of themselves, gaining insights into their own strengths and weaknesses. This course prepares students for the experiences that they will encounter in their future studies at University.
There is a great sense of achievement and pride amongst the students when they finally submit their work and it is a great pleasure to present these Scientific Research Reports. •
JESSICA MULCAHY Q2023 FIRST IN STATE SCIENCE EXTENSION
Little did I know when I first started the Science Extension course the significant impact it would have on me and the skills and knowledge I would gain throughout the course. From the early morning classes to the afternoons spent collecting data for my major work project, there wasn’t one moment when I wasn’t learning something new, which is what I particularly loved about the Science Extension course. The course was particularly interesting as it simultaneously contained very broad and specific topics, which allowed me to apply what I was learning in other areas of Science to add more detail and specificities within my written answers. The course allowed me to learn about aspects of Science that I had never considered before, where I gained further insights into the nuances within Science and in particular in research throughout the scientific research report.
Jessica Mulcahy reflects on her Science Extension experience as a student at Queenwood.
One of my favourite aspects of the Science Extension course was the scientific research report, which allowed me to research further into type 2 diabetes. I was initially influenced by learning about the regulation of blood glucose in Biology, where my interest in this area inspired me to find out more. The nature of Science Extension allowed me to connect with other professionals to gain further information, in particular an endocrinologist who provided me with new insights and knowledge within the area. I loved how the Science Extension course allowed me to take one particular interest and develop it into a scientific research question, where through the assistance of my teachers I was able to conduct experiments and write a scientific research report to do with my findings.
By doing a subject like Science Extension it made a large difference in developing my skills both within the course and in my
other subjects. Not only did the course build my knowledge to do with the background of Science, but also helped me to develop crucial problem-solving skills where I discovered there is often more than one way to solve a problem. I learnt this lesson in my Science Extension project where I faced many challenges as my Science major work experiment was not going to plan. However, through the guidance of Ms Lean and Dr Gleeson I was encouraged to keep persisting whilst we tried many different methods. I believe the Science Extension course is like no other in the HSC as I learnt about topics I previously thought were beyond the scope of high school, which was invaluable in developing my skills within Science. •
To investigate an alternative method to determine the glucose content and therefore glycaemic index of different types of rice.
JESSICA MULCAHY Q2023
Abstract
The purpose of this study is to determine an alternate method to investigate differences in the glucose concentration of different types of rice. Globally, rice provides 35-60% of the caloric intake of over 3 billion people’s diet; however, there is a lack of knowledge about the glucose content of the varieties. A spectrophotometric analysis measured the glucose content of brown, white, brown basmati, white basmati, jasmine and risotto rice at a wavelength of 740λ . An ANOVA found a significant difference (p = 3.4688 × 10 -6) between the glucose concentrations of the 6 types of rice. The Tukey HSD test found the differences between the following types of rice to be significantly different: jasmine and brown basmati, jasmine and white, jasmine and risotto, jasmine and brown, white basmati and white, white basmati and brown, brown basmati and brown, white and brown. Brown rice had the lowest average glucose concentration, followed by risotto rice, both brown basmati and white rice, white basmati rice and jasmine rice. The results from this study can inform decisions about the type of rice eaten to prevent and manage type 2 diabetes, as there is a causal link between the Glycaemic Index (GI) of foods and type 2 diabetes. Diets with high GI foods predispose people to higher blood glucose levels, increasing their risk of developing the disease.
1. Literature review
Glucose is a monosaccharide that is critical to essential metabolic processes including respiration. When glucose enters the bloodstream, it serves as the primary source of energy for the body, and excess glucose is stored in the liver and muscles as glycogen (Goyal, 2022).
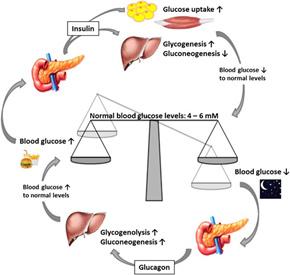
As seen in Figure 1, to maintain stable blood glucose levels, the body relies on the coordination of two hormones: insulin and glucagon. Insulin is produced by beta cells in the pancreas and increases in response to elevated blood glucose levels. Its main function is to promote glucose uptake by liver and muscle cells, converting it into glycogen for storage, while also facilitating the uptake of glucose by other body cells. Conversely, if the blood glucose level is too low, the alpha cells in the pancreas are stimulated to produce glucagon which breaks glycogen in the liver into glucose to release it into the blood (Miller et al, 1997). Simultaneously, a drop in glucose will cause a decrease in insulin and inhibitive signalling to alpha cells, thereby producing more glucagon and triggering the efflux of glucose from cells via breakdown of glycogen. This action helps regulate blood glucose levels and maintain homeostasis (Goyal, 2022).
Glucose is a component of complex carbohydrates including polysaccharides and glucosides, and consequently, holds significant importance in food products (Roder, 2016). The determination of glucose content as well as other nutrients such as vitamins enables a precise evaluation of the nutritional composition, and thus potential health impacts of food. The monitoring of sugar intake is particularly pertinent to type 2 diabetes as it is necessary for people to control the levels of glucose substantially via diet in their blood. Diabetes is a non-infectious disease that occurs when glucose level is constantly too high in the bloodstream, above tolerance levels of 3.5-8mmol/L (Omar, 2018). The disease affects 9.3% of the global adult population aged between 20 to 79 years (World Health Organisation, 2023). There are two types of diabetes, which differ based on their disease mechanism.
Type 1 diabetes is an autoimmune condition where the body’s immune system destroys the beta cells in the pancreas that are responsible for the production of insulin (Smith, 2023). The cause of this autoimmune disease is not comprehensively understood, although many believe that it is linked to a Coxsackie virus B infection in which shared antigens contribute to the development of an autoimmune response (Zafer, 2019). There is currently no cure for type 1 diabetes, but it can be managed through monitoring of glucose levels and use of insulin injections (Smith, 2023).
In type 2 diabetes the body becomes resistant to the effects of insulin. In early stages of the disease, insulin levels are very high as the beta cells increase production of the hormone to attempt to overcome the high amount of resistance. Subsequently beta cells become overworked and damaged, losing the capacity to produce enough insulin. The disease can result from an unhealthy diet, weight gain and a lack of exercise, and many people need oral medications and insulin injections to manage the disease (Goyal, 2022). Type 2 diabetes accounts for approximately 8590% of all diabetes cases and is growing in prevalence (World Health Organisation, 2023). Over time, type 2 diabetes can lead to heart, blood vessel, kidney, nerve, and eye damage due to the high glucose levels leading to advanced glycation end-products where there is an interference with the blood supply to tissues, resulting
Jessica Mulcahy Q2023
FIGURE 1: Glucose homeostasis (Roder, 2016)
in systemic inflammation. This inflammation reduces the elasticity of blood vessels as it interferes with the production of nitric oxide (NO) in the endothelial cells of the blood vessel walls, leaving people prone to atherosclerosis (Smith, 2023).
The Glycaemic Index (GI) of individual foods is one way of classifying types of food. It grades food on a scale from 0 to 100 based on the rate at which the food is digested and the resultant increase in the blood glucose levels, usually over a period of two hours (LeWine, 2021). Glucose has a GI value of 100, and other foods are then compared against this rate, where a low GI value is between 1-55 and includes foods such as green vegetables and eggs. A medium GI value is between 56-69 and includes foods such as raisins and multigrain bread and a high GI value is 70+ and includes foods such as white rice and potatoes (LeWine, 2021). The GI of foods is impacted by many different factors such as the type of starch and sugar present, acidity, and the ripeness of the food (Ellis, 2019).
The Glycaemic Index is directly related to type 2 diabetes, as foods with higher GI will increase the blood glucose levels at a faster rate (Ellis, 2019). Higher GI foods can make it harder to control type 2 diabetes as they are rapidly digested which results in larger spikes in blood glucose. Beta cells will have to work particularly hard with a constant large intake of high GI foods, which can result in insulin resistance. For people who have been diagnosed with type 2 diabetes, lowering their intake of high glycaemic index foods can help control and maintain a stable blood glucose level (Endocrine Society, 2022). This information is also important for people without types 2 diabetes as it can assist in weight loss, and as a preventative measure for the disease.
Rice is a food staple for over 3 million people throughout the world and knowledge of the differences in the types of rice is extremely important in planning meals, to reduce glucose intake (World Health Organisation, 2023). Rice with lower GI include brown rice (GI 55), risotto rice (GI 58) and brown basmati rice (58). Rice with higher GI include jasmine rice (GI 68), white basmati rice (GI 65), white rice (GI 72) (Sydney University, 2020). The glycaemic index of a food is determined by measuring the incremental
area underneath a blood glucose curve of a person over the duration of two hours after a meal. This is a complex method to determine a singular number, and this study will aim to investigate an alternate method to determine the glucose concentration in rice. In addition, there is a lack of conclusive evidence from the limited studies within this area and hence further research is required to be undertaken to directly compare these six different types of rice. This information is essential as it can assist governments and organisations develop education programs and campaigns to educate the public about the differences in glucose within types of rice, with the aim of preventing type 2 diabetes.
This study will seek to fill the gaps in this area to determine whether this alternate method is an appropriate measure of glucose concentration within different types of rice which correlates with the glycaemic index. Due to the effects from type 2 diabetes, it is necessary for further research to be conducted into an alternate method to the current complex method of determining the glycaemic index to determine the availability of glucose levels in different foods, to make people aware of how they could alter their diet to reduce the risk of developing the disease.
2. Scientific research question
To evaluate an alternate method of determining the glycaemic index of different types of rice.
3. Scientific hypothesis
The glucose concentration of rice varieties, as measured by the spectrophotometric analysis, will correlate with the glycaemic index scale.
Jessica Mulcahy
4. Methodology
4.1 Risk/ethical assessment
Risk
Glass beakers dropping on the floor and smashing, where glass could cut a person’s skin causing lacerations.
If water is spilt on the ground, a person could slip on it and fall over, causing bruising or head injuries.
Getting a finger caught or stuck in the centrifuge whilst it is spinning the supernatant.
Amelioration
Ensure to keep the beakers away from the edge of the desk, and immediately clean up any broken glass.
Keep beakers with water away from the edge of the desk and if any water is spilt, immediately clean it up.
Keep hands far away from the centrifuge whilst it is operating and ensure it has been completely turned off before retrieving the supernatant solutions.
Ethical considerations: Within this investigation, there is no use of animals or humans within the testing of glucose concentrations which meant there were minimal ethical considerations. However, a reduction of resources for the food materials used was considered to ensure that excess materials were not wasted during the investigation.
4.2 Justification of equipment
Within the experiment a centrifuge will be utilised, to ensure the solution will be spun at a sufficient rate to separate the heterogenous mixture into the supernatant and solid components. The spectrophotometer is able to read absorbance to three decimal places, ensuring accurate readings, which is also the case for the mass balance. The micropipette has 0.5 µL increments, with an uncertainty of ±0.25 µL, further ensuring accurate data is collected.
4.3 Complications of experimental process
Within this investigation, data was successfully collected for the standard curve, measuring the absorbance of different concentrations of glucose. When determining the absorbance of the six different types of rice, the first method as stated below in section 4.4 was attempted to be followed; however, in addition the supernatant solution of rice, starch, amylase and Benedict’s solution was heated prior to the solution being spun in the centrifuge which was not successful after over a month of manipulating the method and trialling different equipment. The method was then revised to what is described in section 4.5, however, after numerous trials this method was also unsuccessful. Therefore, by using the standard curve as well as published information about the Glycaemic Index levels of different types of rice (Sydney University, 2020), data was extrapolated to create an estimated data set for the research project, suitable for further analysis in the absence of experimentally derived data.
4.4 Method for creating the standard curve
1. 1mL of Benedicts solution and 0.5mL of water were collected using a micropipette and added into a 1.5mL Eppendorf tube and mixed well to ensure sufficient integration.
2. Step 1 was repeated 7 times but the 0.5mL of water was replaced with 0.5mL of 5%, 10%, 15%, 20%, 25%, 30% and 35% glucose solutions.
3. The eight Eppendorf tubes were spun down for 5 minutes in the centrifuge.
4. After 5 minutes, for each concentration of glucose, 0.5mL of the supernatant was placed in a cuvette using a micropipette.
5. 2.5mL of water was added to each of the 8 cuvettes and mixed well.
6. The first cuvette with distilled water was placed into the spectrometer, where the absorbance value was read at the wavelength at 740λ from the computer which is suitable due to the reagent of Benedicts solution being used.
7. Step 6 was repeated 7 more times with the remaining concentrations of glucose, where all absorbance values were recorded.
8. Data was graphed for the standard curve.
4.5 Method for measuring the absorbance of rice solutions
1. 2g of brown rice was measured using a mass balance and blended in a blender until in the form of a powder.
2. The rice was further ground into smaller fragments with minimal grains present using a mortar and pestle.
3. 100mg of brown rice was poured into a 1.5mL Eppendorf tube using a small funnel.
4. 5mL of a 1% starch solution was measured using a micropipette and poured into the 1.5mL Eppendorf tube with the rice and mixed well.
5. 0.5mL of a 1% amylase solution was collected using a micropipette and added into the same Eppendorf tube.
6. The Eppendorf tube was left upright for 10 minutes.
7. 0.5mL of the supernatant from the Eppendorf tube and 1mL of Benedicts solution were collected, added into a small Eppendorf tube and mixed together.
8. The Eppendorf was placed in the centrifuge and spun for 5 minutes.
9. 0.5mL of this supernatant and 2.5mL of water was measured and placed into a clean cuvette.
10. The cuvette was placed into the spectrometer, and the absorbance value was read at the wavelength of 740λ from the computer.
11. Steps 3-11 were repeated 4 more times for brown rice.
12. Steps 1-12 were repeated with the different rice types of risotto, white, brown basmati, white basmati and jasmine rice.
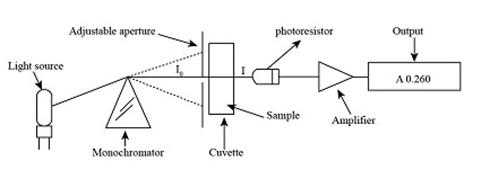
FIGURE 2: The functioning of a spectrophotometer (Trumbo et al., 2013)
5. Results
5.1 Graph and table of standard curve:
Absorbance readings at 740λ based on percentage glucose
glucose (%)
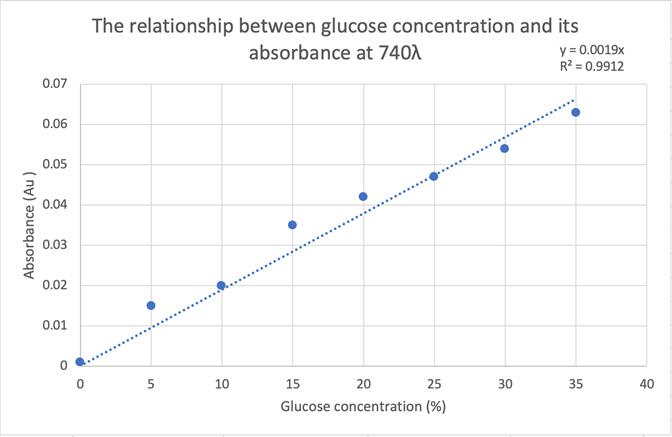
The overall trend in Table 2 and Figure 3 is that as the glucose concentration of a solution increases, the absorbance also increases, highlighted by the very high correlation as the R2 value is 0.9912. The R2 value indicates a positive relationship and a very high correlation between the glucose concentration and absorbance. The equation of the line is y = 0.0019x, which will then be used to determine the glucose concentration of solutions of rice.
TABLE 1: Spectrophotometer readings at 740 λ based on percentage glucose
FIGURE 3: Standard Curve of spectrophotometer readings based on percentage glucose.
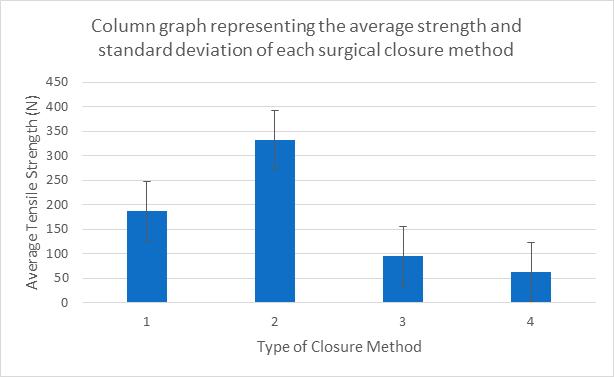
5.2 Graph of difference in the glucose concentration of rice
*Refer to the appendix for the raw data.
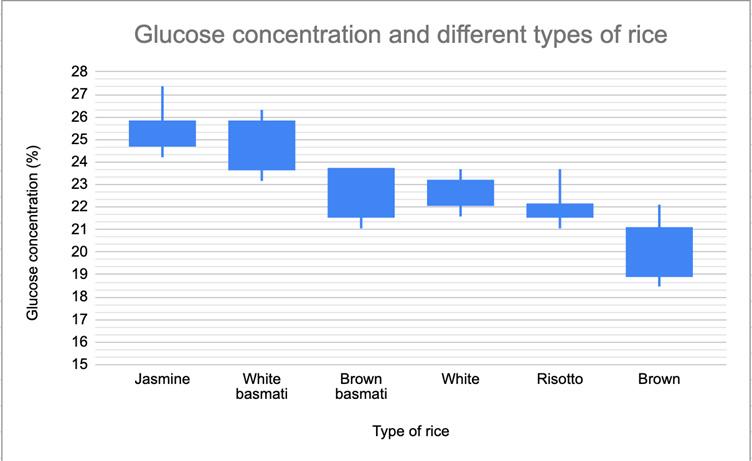
Figure 4 shows the variation in glucose concentration in different types of rice, where brown rice has the lowest concentration and jasmine rice has the highest. The glucose concentration was calculated using the equation of the standard curve y = 0.0019x where each absorbance value was substituted into the y value. The equation was then rearranged to get x as the subject to determine the glucose concentration for each rice.
Sample calculation:
Jasmine rice absorbance = 0.047 Au y = 0.0019x where y = 0.047 Au x = 0.047/0.0019 x 100 x = 24.737%
The types of rice with the highest absorbance were jasmine rice which had an average absorbance of 0.048 and white basmati rice which had an average absorbance of 0.046 and their glucose concentrations were 25.474% and 24.737% respectively when digested with enzyme. Both brown basmati rice and white rice had an average absorbance of 0.043 and average glucose concentration of 22.632%. Risotto rice had an average absorbance of 0.041 and average glucose concentration of 22.061%, and brown rice had the lowest average absorbance of 0.038 and average glucose concentration of 20.116%.
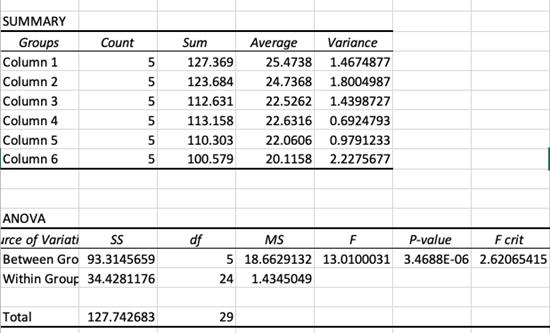
FIGURE 4: Glucose concentration of different types of rice (p = 3.4688 x 10 -6).
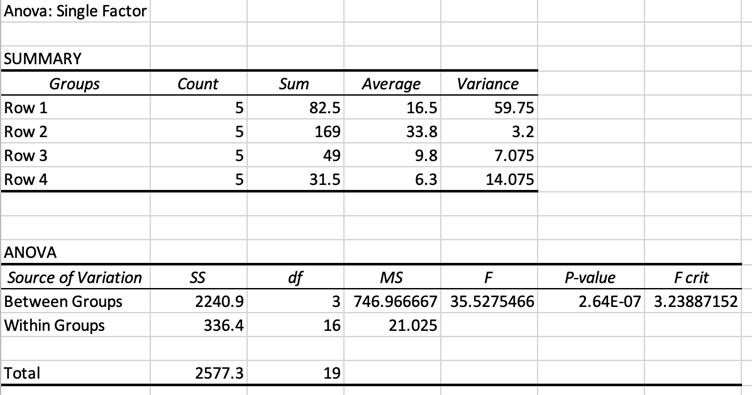
5.3 Statistical analysis
An ANOVA test was conducted as there was one independent variable where the means of more than 2 groups was being compared. The assumptions for an ANOVA test were met including data is quantitative, randomly sampled, data has normal distribution, the variation in each group is similar, means for more than two groups, replicates and not repeats and the investigation is falsifiable. The ANOVA test was conducted on Excel and the p value was determined to be 3.4688 × 10 -6 , which is less than 0.05 meaning there is a statistical difference between the glucose concentration in the six groups and therefore the alternate hypothesis is to be accepted. All the assumptions for an ANOVA test were satisfied such as a large sample size, the data is quantitative, randomly sampled, the variances in each group was similar as shown in Figure 5, means for more than two groups were calculated and the investigation was falsifiable.
Jasmine and Brown basmati
0.0080463
Jasmine and White 0.0111964
Jasmine and Risotto
Jasmine and Brown
White basmati and White
0.0018067
0.0010053
0.0186683
White basmati and Brown 0.0010053
Brown basmati and Brown 0.0411424
White and Brown 0.0302201
FIGURE 5: ANOVA test table which shows the level of statistical significance between the means of the different types of rice.
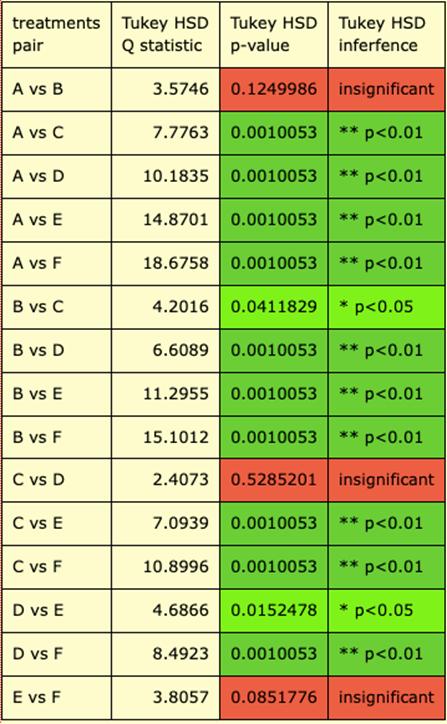
TABLE 2: Tukey HSD test which shows what types of rice are significantly different to one another.
Tukey HSD test results- Results where p<0.05
Types of rice
Tukey HSD p-value
6. Discussion
6.1
Comparison of types of rice and errors in results
The data recorded supported the hypothesis and identified jasmine and white basmati rice with the highest average glucose concentrations of 25.474% and 24.737%, which also directly correlate with the fact that both these types of rice are high glycaemic (GI) foods with GI indexes of 68 and 65. In the middle of the range, brown basmati rice and white rice had slightly lower average glucose concentrations of 22.632%. Brown basmati rice has a GI of 58, which is lower than jasmine and white basmati rice, corresponding with the decrease in glucose concentration. Risotto and brown rice had the lowest average glucose concentrations of 22.061% and 20.116% respectively. Risotto rice has a GI of around 58 and brown rice has a GI of 55, which both correlate with the decrease in absorbance and glucose concentration.
However, white rice is a rice with a GI of 72 and is considered a high glycaemic index food with higher levels of glucose in comparison to the other rices tested (Sydney University, 2020). The results recorded the glucose concentration as 22.632%, which is a possible inconsistency in the results, and further repeats would need to be conducted to determine whether this is the pattern for other repeats, or other finding are recorded.
6.2 Recommendations of types of rice
The type of rice that should be recommended to prevent type 2 diabetes are those with a lower glucose concentration, which based on the results from this study are brown and risotto rice. This is because the sugar within these foods will be absorbed into the bloodstream at a slower rate, resulting in a smaller rise in blood glucose (Zafer, 2019). Additionally, brown rice and risotto rice would be beneficial for people with type 2 diabetes as it will help them maintain a steady blood glucose level and reduce the effect of postprandial hyperglycaemia. People who have been diagnosed with type 2 diabetes or at a greater risk of developing the disease due to genetic or family history should seek to avoid consuming jasmine rice and white basmati rice due to their high glucose concentrations
which if consumed too often or in high portions will result in sudden increases in the blood glucose levels, where the beta cells will have to work at high rates to produce insulin in order to counteract the effects (Omar, 2018). Therefore, an understanding of the glucose concentrations of different types of rice can assist people in finding alternates to higher GI rice types such as jasmine rice and replace it with lower GI rice for example brown rice.
6.3 Suitability of alternate method
The method that was conducted throughout the investigation proved to be a simpler variation to how the Glycaemic Index of foods is usually determined which involves measuring the incremental area underneath a blood sugar curve of an individual person over two hours after a meal, which is a very complex process. With more time and additional resources, this simpler and less time-consuming method could be effectively implemented within laboratories to determine the glucose concentrations of different foods which correlate with their known GI. The method discussed in sections 4.4 and 4.5 was used in a study looking into ‘Quantification of Reducing Sugars Based on the Qualitative Technique of Benedict’ (Hernández-López et al., 2020), however this method focussed on looking into the differences in carbohydrates in different types of sugars. The method in sections 4.4 and 4.5 is essential in determining whether the process would be successful when analysing rice, as rice is a staple food throughout the world, where minimal changes in someone’s diet can lead to a reduction in the incidence of cases of type 2 diabetes. The method discussed was more effective than the other techniques attempted such as using a glucose meter, glucose strips, and heating the Benedict’s reagent as quantitative data is able to be collected allowing for a statistical test to be conducted. Although further experimentation needs to be conducted into the specificities and equipment requirements for this method, the outcomes of this investigation were ultimately able to answer the scientific research question and identified the potential effectiveness of this technique.
Jessica Mulcahy Q2023
6.4 Other studies investigating the Glycaemic Index
Studies have been undertaken to determine the link between the glycaemic index (GI) and the risk of developing type 2 diabetes in both women and men. The Nurses’ Health study uses epidemiology to analyse a variety of factors including hormones, nutrition and disease development. A 61-item food frequency questionnaire was completed by 84 360 women in 1980 to assess the link between nutrient intake and the risk of diabetes. This was followed by an evaluation of each woman’s glycaemic load which linked 915 type 2 diabetes diagnosis with their diet (Liu et al., 2002). The results from this study showed that women in the highest quartile of glycaemic load had a 40% increased risk of developing type 2 diabetes in comparison to women in the lowest quartile. In addition, the study found that cereal fiber was inversely related to the disease risk, where women with a low cereal fibre intake and high glycaemic load had a 2.5-fold higher risk of developing type 2 diabetes. The study found that women in the top quartile of whole-grain consumption had a 27% lower risk of developing diabetes, with a relative risk of 0.73 (p < 0.0001) (Liu et al., 2002).
The Health Professional’s Follow-Up Study is another Harvard based study which evaluates aspects of men’s health and the incidence of diseases. The results were similar for men who were studied as part of this study where it was found that the relative risk for developing type 2 diabetes was 2.17 for men in the highest quartile of glycaemic index and low cereal fibre intake (Liu et al., 2002). These two respective studies highlight the link between the glycaemic index and a person’s risk of developing type 2 diabetes.
6.5
Validity, reliability and accuracy of data
Repeats were conducted for this study, which allowed for an average to be calculated, minimising the chance of random errors; however, other factors such as time and equipment constraints meant consistent data was not able to be collected. Due to technical and time issues, the data for the standard curve was only able to be measured for one repeat, meaning this data recorded was not reliable as more repeats were needed to ensure the results are similar and there are no outliers.
The experiment was accurate as all the measuring equipment used had small increment values, ensuring precise data was gathered. For example, to measure the volume of various liquids, a micropipette was used which accurately measures 0.5 µL, with an uncertainty of ±0.25 µL, and the spectrophotometer read absorbance values to 3 decimal places. However, although the mass balance measured values to 3 decimal places, it was often hard to measure the exact mass on the mass balance of the rice as it was a small value of 2g, which could have resulted in some measurements having slightly different values in comparison to the true value. The apparatus used within the experiment was effective in measuring specific masses and volumes, although, with each of these equipment pieces, there were uncertainties that doing more repeats cannot eliminate.
The investigation was valid as only the independent variable was changed which was the type of rice, whilst the dependent variable was measured which was the absorbance of the rice, and variables such as the same centrifuge and same volume of supernatant were controlled throughout the process. However, there were other variables that were harder to control, for example in Method 2 for Step 6 when needing to leave the Eppendorf tube upright for exactly 5 minutes for all rice types, it was hard to leave them for exactly 5 minutes as all the timers were started at different times. This resulted in some Eppendorf tube solutions being left for slightly longer than others, which could have impacted the separation of the mixtures and the overall glucose concentration of the rice solution. However, during the investigation, it was difficult to make the method work as the centrifuge was not able to spin the solution of rice, starch, amylase and Benedict’s solution at a fast enough rate to separate the heterogenous mixture into two components. Ultimately, this resulted in inconsistent results in the absorbance values between different types of rice.
6.6 Limitations and improvements of study
A key limitation of the investigation is that due to the availability of equipment in the school laboratory, the method was not able to yield consistent results. Throughout the experimental process, numerous
variations of the method were trialled such as using a glucose meter, glucose strips, and heating the Benedict’s reagent before attempting to determine its absorbance. The limitations to do with the equipment available meant no method was able to yield consistent and meaningful results. Accessing the required equipment such as a larger centrifuge that is able to spin the Eppendorf tubes at a faster rate, would determine whether this is a suitable alternate method to measure the glucose concentration within foods. The results were extrapolated by utilising the limited results collected, research on the different GI indexes of rice as well as Excel to create a suitable data set to be analysed.
6.7 Future directions of scientific research
Currently, there has been minimal large-scale investigations into determining the differences in the glucose concentration of different types of rice and how this directly links to type 2 diabetes. Therefore, a future direction of scientific research could be to investigate further the significance of this link with the aim of informing governments and agencies to promote healthy eating. Education programmes and campaigns could be developed by governments to spread information about the type that should be incorporating into the diet of those at risk of type 2 diabetes. In the long term this would have numerous benefits on society as it can act as a prevention method to aim to reduce the incidence of type 2 diabetes.
7. Conclusion
This alternate method for measuring glucose concentration in different types of rice is a simpler variation to how the glycaemic index of foods is usually determined, which can be further implemented by laboratories. All types of rice had differences in their absorbance which correlated to different glucose concentrations. The order of rices from the highest to lowest glucose concentration was jasmine, white basmati, white, brown basmati, risotto and brown rice. The results recorded using the alternate method showed a correlation between glucose concentrations and the known glycaemic index rating of the different types of rice, highlighting the suitability of this method. The information collected within this investigation is applicable to wider society where people are aiming to decrease or monitor the amount of glucose they are consuming. They should mainly eat brown and risotto rice which have lower glucose concentrations and ultimately have a decreased effect on the blood glucose levels. However, advanced research is required to do with this area to investigate the suitability of the process as an alternate method to determine the glucose concentrations of different types of rice which correlate with their known glycaemic indexes. •
8. References
Ellis, E. (2019). What is glycaemic index. https:// www.eatright.org/health/wellness/diet-trends/ what-is-glycemic-index
Goyal, R. (2022). Type 2 Diabetes. https://www. ncbi.nlm.nih.gov/books/NBK513253/ Hernández-López, A., Felix, D., Sierra, Z., Bravo, I., Dinkova, T., & Avila-Alejandre, A. (2020). Quantification of Reducing Sugars Based on the Qualitative Technique of Benedict. Retrieved from https://www.ncbi.nlm.nih.gov/ pmc/articles/PMC7758970/#!po=28.0488
LeWine, H. (2021). Glycaemic index for 60+ foods. https://www.health.harvard.edu/ diseases-and-conditions/glycemic-indexand-glycemic-load-for-100-foods.
Liu, S., Manson, J., Willett, W. (2002). Glycaemic index, glycaemic load and risk of Type 2 Diabetes. https://www.sciencedirect.com/ science/article/pii/S0002916523058732
Miller, J., Foster-Powell, K., & Colagiuri, S. (1997). The glycaemic index solution. Hodder & Stoughton
Omar, A. (2018). Linear relationship between absorbance and concentration of aqueous sucrose. https://www.researchgate.net/figure/ Linear-relationship-between-absorbanceand-concentration-of-aqueous-sucroseat-k-959_fig2_254364567
Roder, P. (2016). Pancreatic regulation of glucose homeostasis. https:// www.ncbi.nlm.nih.gov/pmc/articles/ PMC4892884/#:~:text=Through%20 its%20various%20hormones%2C%20 particularly,referred%20to%20as%20 glucose%20homeostasis
Smith, H. (2023). What is diabetes? https:// www.niddk.nih.gov/health-information/ diabetes/overview/what-is-diabetes
Sydney University. (2020). Glycaemic Index. https://glycemicindex.com/2020/12/food-forthought-2/
Trumbo, T., Schultz, E., Borland, M., Pugh, M. (2013). Applied spectrophotometry: analysis of a biochemical mixture. https://pubmed.ncbi. nlm.nih.gov/23625877/
World Health Organisation. (2023). Diabetes. https://www.who.int/health-topics/ diabetes#tab=tab_1
Zafer, M. (2019). Low-glycaemic index diets as an intervention for diabetes: a systematic review and meta-analysis. https://pubmed. ncbi.nlm.nih.gov/31374573/
9. Appendix
TABLE 4: Glucose concentration of different types of rice. SPECTROPHOTOMETER
TABLE 3: The relationship between absorbance and different types of rice in a solution.
GLUCOSE CONCENTRATION
The effect of Anabolic Androgenic steroids on Lipoproteins.
PHOEBE CAMPBELL Q2023
Abstract
In recent years, the use of Anabolic Androgenic steroids (AAS) has gained significant attention due to their potential performanceenhancing effects and increased use to gain an athletic advantage. In this, the impact of AAS on lipid metabolism, particularly lipoproteins, triglycerides, and cholesterol, requires further investigation. Administration of AAS is associated with alterations in lipoprotein levels, including an increase in low-density lipoprotein (LDL) cholesterol and triglycerides, while potentially decreasing highdensity lipoprotein (HDL) cholesterol. These changes to lipoprotein profiles can increase the risk of atherosclerosis and cardiovascular disease. However, there is considerable variation in results for studies investigating impacts of AAS usage, potentially due to differences in AAS dosage, duration of use, and individual susceptibility. Further research is needed to elucidate the underlying mechanisms and long-term consequences of AAS-induced alterations in lipoprotein metabolism. Additionally, interventions targeting lipid abnormalities and cardiovascular risk factors should be considered in individuals using AAS to mitigate potential adverse effects on lipid profiles and overall cardiovascular health. This study investigated the effects of AAS on lipoprotein profiles and lipid parameters.
Literature review
Lipoproteins in the blood are intricate round molecular complexes that play a vital role in lipid transport throughout the body (Cleveland Clinic, 2022.) Comprised of lipids and proteins, lipoproteins possess a hydrophobic core that contains triglycerides and cholesteryl esters, while the surface is composed of phospholipids, cholesterol, and apolipoproteins (Feingold, 2000). The phospholipids form a bilayer on the surface, with their hydrophilic heads facing outward and their hydrophobic tails interacting with the core (Feingold, 2000). Apolipoproteins, with their hydrophilic and hydrophobic regions, anchor at the surface, allowing interactions with other lipoproteins and receptors (Liu et al., 2021.) Cholesterol is distributed within the hydrophobic core and surface monolayer, contributing to stability and modulating the fluidity of cell membranes. (Cleveland Clinic, 2022.) This structural arrangement enables lipoproteins to transport hydrophobic lipids in the aqueous environment of bodily fluids, facilitating their delivery to various tissues and organs in the body (Feingold, 2000).
Lipoproteins are classified according to their density, including chylomicrons, very-low-density lipoproteins (VLDL), intermediate-density lipoproteins (IDL), low-density lipoproteins (LDL), and high-density lipoproteins (HDL) (Thompson, 2022). Lipoproteins function as transport vehicles, enabling the absorption, distribution, and utilisation of lipids. Chylomicrons transport dietary lipids, VLDL and IDL deliver endogenous (not attributable to external factors) triglycerides and cholesterol, LDL transports cholesterol to peripheral tissues, and HDL participates in reverse cholesterol transport (Cleveland Clinic, 2022.) The concentration and distribution of lipoproteins in the bloodstream have significant implications for cardiovascular health, with elevated LDL cholesterol and low HDL cholesterol associated with an increased risk of atherosclerosis (Goldberg, 1996.) Lipoprotein abnormalities, such as familial hypercholesterolemia or apolipoprotein deficiencies, can lead to lipoprotein disorders and associated clinical manifestations (Mahmood et al., 2008). Therapeutic interventions, including pharmacological agents and
lifestyle modifications, aim to regulate lipid levels and mitigate cardiovascular risk.
The investigation of low-density lipoprotein (LDL) and high-density lipoprotein (HDL) stands as a pivotal axis in comprehending lipid metabolism and its implications for cardiovascular health. LDL, recognised as the "bad cholesterol," facilitates the transportation of cholesterol to peripheral tissues, thereby contributing significantly to the development of atherosclerosis. Conversely, HDL, often designated as the "good cholesterol," plays a pivotal role in the reverse cholesterol transport process, actively participating in the removal of cholesterol from arterial walls and exerting a protective effect. The intricate interplay and equilibrium between LDL and HDL are fundamental to unravelling the complexities of cardiovascular risk and formulating targeted therapeutic strategies for lipid-related disorders. High-density lipoprotein (HDL) encompasses distinct subfractions, notably HDL-2 and HDL-3, each characterised by varying lipid and protein compositions. HDL-2 exhibits larger particle size and greater cholesterol content than HDL-3. HDL-C represents the total cholesterol carried by HDL particles. These subtypes play pivotal roles in reverse cholesterol transport, mediating the efflux of excess cholesterol from peripheral tissues to the liver for excretion. HDL-2 is associated with enhanced anti-atherogenic properties, while HDL3 may exhibit a less pronounced protective effect. Disparities in HDL subfractions and HDL-C levels contribute to the modulation of cardiovascular risk, with higher levels generally associated with improved cardiovascular outcomes.
Anabolic Androgenic steroids (AAS) are synthetic derivatives of testosterone, a hormone that plays a key role in the development of male reproductive tissues and secondary sexual characteristics (Ganesan et al., 2019.) These steroids have regulated medical purposes that are primarily utilised as a treatment method for hypogonadism. (Cleveland Clinic, 2023.) Hypogonadism is the failure of the gonads to produce the hormones necessary for the effective functioning of the male and female reproductive systems. However, they gained popularity in the 1960s with highperformance athletes and bodybuilders looking for quick and effective gains in muscle strength (National Institute of Drug Abuse, 2023.) AAS upregulates the number of androgen receptors, leading to the potential to increase training intensity, indirectly contributing to increased muscle strength and size (Ganesan et al.,
2019.) They have a stimulatory impact on the brain through their effect on neurotransmitters, antagonism of glucocorticoids and stimulation of growth factors within the central nervous system (Bertozzi et al., 2017). There are a variety of AAS that are used illegally to achieve different physical benefits that are commonly used in conjunction with each other to maximise benefits. Nandrolone phenpropionate and decanoate are slow-acting AAS with the roles of increasing muscle mass through nitrogen retention and providing joint pain relief by promoting collagen synthesis and enhancing bone mineralisation (National Institute of Drug Abuse, 2023.) These slow acting molecules also contribute to an increased production of red blood cells and stimulation of appetite. Dromostanolone is a synthetic AAS that increases the retention of phosphorus, nitrogen and potassium (National Institute of Drug Abuse, 2023.) As a result, increased protein anabolism and a decrease in catabolism of amino acids occur (National Institute of Drug Abuse, 2023.) This is most commonly used by bodybuilders as it increases the density and hardness of muscle. There are limitations in determining the exact number of AAS users, the type of drugs they are using and the severity of their abuse as information about AAS doses and cycle abuse is self-reported and difficult to objectively assess. Additionally, due to the stacking of multiple performance-enhancing drugs, it is difficult to know the true effect caused by AAS (Liu et al., 2021.) It is estimated that the global prevalence of AAS use is between 1% and 5% (AlShareef et al., 2022) currently and is projected to increase in the future. The incidence of AAS misuse has progressively risen in the past two decades (Graham 2014.) A comprehensive synthesis of 187 studies unveiled that engagement in athletic activities and of male gender were linked to the improper use of AAS (Sagoe et al., 2014.) The prevalence of AAS abuse in males is 6.4%, compared with 1.6% in females (Sagoe et al., 2014.) According to the National Institute of Drug Abuse (NIDA) in 2018, the misuse of AAS is primarily observed among male weightlifters in their twenties or thirties. Use of AAS amongst Australian high school students has decreased (National Institute on Drug Abuse, 2021), although levels are still too high according to medical professionals. In a German study, 48.1% of individuals misusing AAS and frequenting fitness centres acquired their supply through interactions with healthcare providers (AlShareef et al., 2022.) According to a 2006 survey involving 500 AAS users, the predominant
route of administration chosen by the majority (99.2%) was through self-administered injections (Sagoe et al., 2014). Approximately 13% of users disclosed involvement in hazardous injection practices like sharing needles, reusing syringes, and vial sharing (AlShareef et al., 2022.)
Much research has been carried out on the impacts of AAS on lipoproteins. The results consistently point to AAS usage causing modifications in lipoprotein profiles. Specifically, AAS use has been associated with an increase in low-density lipoprotein (LDL) levels and triglycerides, while potentially decreasing high-density lipoprotein (HDL) levels (Vanberg & Atar, 2009.) These changes in lipoprotein composition may disrupt the balance of lipoprotein particles, ultimately increasing the risk of atherosclerosis and cardiovascular disease (Jones et al., 2012). However, there is inconsistency of results across research, which can be attributed to differences in AAS dosages, usage durations, and personal vulnerability (Sagoe et al., 2014.) There remains a requirement for additional inquiry to investigate the fundamental mechanisms and enduring repercussions of AAS-triggered shifts in lipoprotein metabolism to develop precise strategies that address potential negative implications on lipid profiles and holistic cardiovascular health (Ferenchick et al., 1995.)
This research is important to educate users of AAS such as athletes and bodybuilders on the longand short-term effects that it may have on their health. Research into the impact of lipoproteins can help users make more informed decisions about the potential risks and benefits of using these substances. This information can guide users in weighing the shortterm gains in muscle mass and performance against the potential long-term health consequences. Research findings can contribute to public health campaigns aimed at educating the general population about the risks associated with AAS use. By highlighting the potential impact of AAS on lipoproteins and cardiovascular health, authorities can discourage the misuse of these substances and promote safer alternatives for achieving fitness goals. It can also inform policies and regulations regarding the use of AAS in sports and recreational settings. Governments and sports organisations can use research findings to implement measures that deter the non-medical use of AAS and protect the health of athletes and the public.
Scientific research question
To investigate the effects of Anabolic Androgenic steroids (AAS) on lipoproteins through a review of published literature and database analysis
Scientific hypothesis
The administration of Anabolic Androgenic steroids (AAS) would have a significant impact on lipoproteins, triglycerides, and cholesterol levels, resulting in alterations in lipid metabolism. It is hypothesised that AAS usage will lead to an increase in low-density lipoprotein (LDL) cholesterol and triglyceride levels, while potentially decreasing high-density lipoprotein (HDL) cholesterol levels.
Methodology
Study Identification
A suitable data set that represented the impact of AAS on lipoproteins was required for this experiment. Thus, it was essential to undertake a comprehensive search to identify relevant studies. This investigation utilised databases such as PubMed, Embase and Scopus using appropriate keywords including ‘Anabolic Androgenic steroids,’ ‘Lipoproteins,’ and ‘cholesterol.’
Inclusion and Exclusion Criteria
Initially, the publication date range was set within 20 years (2003-2023), however, due to the limited reports it was expanded to a 40-year range (1983-2023.) Studies were included if they used human or rodent subjects, reported quantitative data on lipoprotein outcomes and were published in a peer-reviewed journal. Large non-human animal, in-vitro studies and those that did not focus on the effects of AAS on lipoproteins were excluded. Additionally, only research papers with a statistically significant p-value (p<0.05) were included.
Study Selection
In the initial phase, titles and abstracts were assessed to identify studies that could be of potential relevance. Following this, the complete articles of the selected studies were thoroughly examined to determine their eligibility based on the established inclusion and exclusion criteria.
Data Extraction
Data from the selected studies was extracted using a standardised data extraction form. The extracted data included study characteristics (e.g., author, year, sample size), participant demographics (e.g., age, sex), AAS intervention details (e.g., type of AAS, dosage, duration), lipoprotein outcomes (e.g., LDL cholesterol, HDL cholesterol, triglycerides), and relevant statistical data (e.g., means, standard deviations).
Data Analysis
In a professional research environment, a metaanalysis would be conducted to calculate the overall effect of AAS usage on lipoprotein levels. These would be calculated using specialist standardised mean differences (Cohen’s) or other appropriate measures (Haidich, 2010). This would be performed using paid statistical software (e.g. RevMan) that are used for data synthesis. In a secondary schooling context, this is not a feasible method, hence I undertook a report based on study design, participant characteristics and AAS dosage.
Ethical Considerations
As this study involves the analysis of previously published data, ethical approval is not required. However, ethical considerations regarding participant confidentiality and proper citation of the original studies have been upheld.
Safety Considerations
As this study involves gathering data from various sources, external email or video calls involved my teacher to reduce risk of harm. Malware software was utilised to decrease the likelihood of risk from hackers.
Results
This is a summary of the results from all 7 papers included in the report. A full listing of all results, is included in Table 9 in the appendix.
Effects of Androgenic-Anabolic steroids on apolipoproteins and lipoproteinz
(Hartgens, 2004).
Units = mmol/L
Replicates = 35
TABLE 1: Effects of Androgenic-Anabolic steroids on apolipoproteins and lipoprotein.
Conducted across a span of 14 weeks, this study engaged a cohort of 35 participants, composed of 19 AAS users and 16 non-AAS users, all of whom were healthy male strength athletes. The research methodology adhered to a randomised, double-blinded design, wherein blood samples were meticulously collected at baseline, as well as after 8 and 14 weeks. Table 1 shows that after 8 weeks on Anabolic Androgenic steroids (AAS), there were significant changes observed in triglyceride levels, total cholesterol levels, and the various subtypes of high-density lipoprotein cholesterol (HDL-C), with all changes being statistically significant, as shown in the p values, all of which are below 0.05.
Diminished cholesterol efflux mediated by HDL and coronary artery disease in young male anabolic androgenic steroid users
(Souza et al., 2019)
Replicates = 50 AAS user AAS non-user Sedentary control p value
31 (9) 52 53
47 83 86
TABLE 2: Diminished cholesterol efflux mediated by HDL and coronary artery disease in young male anabolic androgenic steroid users.
This study utilised 20 strength-trained AAS users aged 25+-5 years, 20 age-matched strengthtrained non-AAS users and 10 sedentary controls that were enrolled in the cross-sectional study. The methodology included a blood sample being collected in the morning between 8 am and 10 am after 12 hours of fasting and after 30 minutes of resting for lipid assessment. Table 2 shows that individuals using Anabolic Androgenic steroids (AAS) have significantly lower levels of HDL-C and HDL-phospholipids compared with AAS non-users and sedentary controls, while triglyceride levels appear to be higher in AAS users. The results are statistically significant with a p value of 0.04.
Adverse effect of the anabolic–androgenic steroid mesterolone on cardiac remodeling and lipoprotein profile is attenuated by aerobic exercise training
(Fontana et al., 2008)
Units = mg/dL
Replicates = 24
Have three weeks of Control
TABLE 3: Adverse effect of the anabolic–androgenic steroid mesterolone on cardiac remodeling and lipoprotein profile is attenuated by aerobic exercise training
Spanning a 12-week duration, 24 adult mice that were 2 months old were randomly allocated into four groups, each comprising 6 mice. A control was included with no added AAS that involved sedentary and exercised cohorts. During the 6 weeks of their respective training or sedentary periods, the experimental groups – both sedentary and exercised – were administered with the AAS mesterolone. The exercised mice underwent an intensive 6-week regimen of exercise training, systematically implemented across 5 days of every week. Table 3 shows that rats with AAS had significantly higher cholesterol, triglycerides and LDL-C than the control. Rats with AAS who were sedentary had higher cholesterol, triglycerides, LDL-C and lower HDL-C than AAS users who exercised. All results are statistically significant, with p<0.001.
Lipid Profile Changes Induced by Chronic Administration of Anabolic Androgenic Steroids and Taurine
( Rosca et al., 2019)
Replicates = 35
*Classified as an amino acid
4: Lipid Profile Changes Induced by Chronic Administration of Anabolic Androgenic Steroids and Taurine
TABLE
This study spanned the duration of 12 weeks in which 32 healthy Wistar rats were randomly separated into four groups that were administered vehicle, nandrolone decanoate, taurine or a combination of all three. Table 4 shows that the administration of nandrolone decanoate, taurine, or their combination in experimental groups resulted in significantly altered lipid profiles compared to the vehicle group, with changes observed in total cholesterol, triglycerides, HDL-C, and LDL-C levels. The differences in all lipid parameters were statistically significant, p<0.02, indicating the impact of these substances on lipid metabolism.
Chronic Users of Supraphysiological Doses of Anabolic Androgenic Steroids Develop Hematological and Serum Lipoprotein Profiles That Are Characteristic of High Cardiovascular Risk
(Souto Maior et al., 2011)
Replicates = 44
TABLE 5: Chronic Users of Supraphysiological Doses of Anabolic Androgenic Steroids Develop Hematological and Serum Lipoprotein Profiles That Are Characteristic of High Cardiovascular Risk
This study included 22 adult male subjects that were immersed in a routine of regular engagement encompassing both strength training and low-level aerobic exercises for 12 weeks. The selected cohort was characterised by their status as non-smokers, abstaining from alcohol, and devoid of any illicit drug use. Crucially, every AAS user within the cohort boasted an extensive history of self-administering anabolic-androgenic steroids for a duration surpassing 5 years. Table 5 shows that AAS users have significantly elevated total cholesterol, triglyceride, and low-density lipoprotein cholesterol (LDL-C) levels. In stark contrast, their high-density lipoprotein cholesterol (HDL-C) levels remained notably subdued, both during resting states and subsequent to exercise. This disparity between the AAS user group and their non-AAS-using counterparts exhibits a statistical significance with p <0.001.
Reduced High-Density Lipoprotein-Cholesterol in Power Athletes: Use of Male Sex Hormone Derivates, an Atherogenic Factor
(Alén and Rahkila, 1984)
Units = mmol/L
Replicates = 7 Initial After 8 weeks of AAS use p
TABLE 6: Reduced High-Density Lipoprotein-Cholesterol in Power Athletes: Use of Male Sex Hormone Derivates, an Atherogenic Factor
This study inlcuded a cohort comprising 7 AAS users and 7 non-AAS users, all of whom were categorised as power athletes with a documented absence of AAS usage within the 3 months preceding the investigation. During the 8 weeks of this study the participants self-administered an average dose of 45mg AAS. Blood samples were taken initially and at the completion of the study. Table 6 shows that after 8 weeks of AAS use, there was a significant decrease in high-density lipoprotein cholesterol (HDL-C) levels compared to the initial baseline levels, indicating a negative impact on lipid metabolism. The difference observed in HDL-C levels between the initial and post-AAS use groups was statistically significant with p <0.001.
Serum Lipids in Power Athletes Self-Administering Testosterone and Anabolic Steroids
(Alén and Rahkila, 1985)
Units = mmol/L
Replicates = 32 AAS user Non-AAS user p value
TABLE 7: Serum Lipids in Power Athletes Self-Administering Testosterone and Anabolic Steroids
Spanning a duration of 9 months, this study compared the HDL-C levels of 5 AAS users and 6 nonAAS users, all distinguished as National-level elite athletes across diverse sporting disciplines. The study was carried out during a comprehensive 9 month strength training regimen, during which the AAS users exhibited self-administered an average of 57 ± 24.9mg per day over the initial 6 months of the 9 month study. Table 7 shows that AAS users had significantly lower levels of highdensity lipoprotein cholesterol (HDL-C) compared to non-AAS users, indicating a negative impact of AAS use on HDL-C levels. The difference observed in HDL-C levels between the two groups was statistically significant with a p-value of 0.04.
Summary of Results
*Study conducted on rats Data Triglycerides
Table
TABLE 8: Study of Results
Discussion
The present systematic review examined the effects of AAS on lipoprotein profiles and cholesterol levels based on data from seven selected studies and highlights the impact of AAS on lipid parameters, including total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and triglycerides, in various populations.
Of the selected studies, two were conducted on rodents. The study involving Wistar rats investigated the chronic administration of AAS and its effects on lipid profiles (Rosca et al., 2019). These results demonstrated that AAS users exhibited higher total cholesterol and triglyceride levels in comparison to the control group. Furthermore, HDL-C levels were significantly reduced in the AAS users. In the other rodent study (Fontana et al., 2008), adult male mice aged 2 were used to investigate the adverse effects of the AAS mesterolone (a synthetic derivative of testosterone) on lipid profiles and cardiac remodelling. Sedentary AAS users exhibited higher total cholesterol and triglyceride levels compared to the control group as well as lower HDL-C. The adverse effects of AAS on lipid profiles observed in this study align with the findings from Rosca et al., 2019., further supporting the notion that AAS use can have detrimental effects on lipid profiles. Both of these studies had similar methodologies lasting 12 weeks of drug administration, in which the control and AASadministered rats were randomly placed into groups and blood samples were taken at the beginning and end of the triple-blinded studies. Both studies highlight the potential cardiovascular risks associated with AAS use. Dyslipidaemia, characterised by elevated total cholesterol and triglyceride levels and reduced HDL-C levels, is a known risk factor for cardiovascular disease. The observed lipid profile alterations in rats following AAS administration mirror those reported in human studies, suggesting that these animal models can provide valuable insights into the physiological effects of AAS on lipid metabolism. By being a tripleblinded animal study, the data is more robust and reliable than human studies which rely on users honestly describing their illegal activities. Studies were conducted through animal models, and while they
provide useful information, caution must be exercised when extrapolating findings to human populations. Therefore, further research involving human subjects is necessary to confirm these observations and elucidate the underlying mechanisms.
The earliest study examination of the effects of AAS on HDL-C levels in male power athletes was conducted by Alén & Rahkila (1984). Over an 8-week training period, the study found reduced HDL-C levels in AAS users compared to non-users, suggesting an atherogenic (plaque formation in the arteries of the heart) effect of AAS.
Following that, Alén et al.,(1985) explored serum lipid profiles in national-level top athletes selfadministering testosterone and AAS over a 9-month period. The study revealed significant changes in lipid profiles, including elevated total cholesterol and triglyceride levels, further indicating the adverse effects of AAS use on lipoproteins. It is important to note that both of these studies were conducted at the same research institution by the same researcher.
Advancing to more recent studies, the study Hartgens (2004) examined the effects of AAS on apolipoproteins and lipoprotein in healthy male strength athletes over a 14-week period. This is beneficial as changes can be analysed within lipoproteins, however, if the use is restricted to only 14 weeks, the negative impacts are mostly reversible (Hartgens 2004.) This study employed a randomised, double-blinded design and found significant alterations in lipoprotein profiles among AAS users compared to non-users. These alterations further suggest a negative impact of AAS on lipoprotein metabolism.
The study conducted by Souto Maior et al., (2011) focused on chronic users of supraphysiological (amounts greater than normally typically found in the body) doses of AAS. While this study did not specify the duration, it utilised a questionnaire to assess serum lipoprotein profiles associated with high cardiovascular risk. The findings suggested that chronic users exhibited haematological and serum lipoprotein profiles indicative of increased cardiovascular risk. This highlights the potential long-term consequences of excessive AAS use on cardiovascular health.
Lastly, the study Souza et al., (2019) investigated the impact of AAS use on cholesterol efflux mediated by
HDL and the prevalence of coronary artery disease. This cross-sectional study included strength-trained AAS users and non-users, as well as sedentary controls, exhibiting exercise's effect on the impact of AAS. The results indicated diminished cholesterol efflux and a higher prevalence of coronary artery disease among AAS users. These findings suggest that AAS use may impair the beneficial function of HDL and contribute to the development of coronary artery disease.
Between the studies earliest studies in 1984 and the most recent in 2019, development of analysis techniques has occurred that led to more accurate results due to higher sensitivities. This could explain disparities in results.
In summary, the findings of these studies consistently demonstrate that AAS use is associated with unfavourable alterations in lipoprotein profiles and cholesterol levels. AAS users exhibit dyslipidaemia (imbalance of lipids) characterised by reduced levels of HDL-C, elevated total cholesterol, triglycerides, and lipoprotein levels. These changes collectively contribute to an increased risk of cardiovascular complications in AAS users.
It is important to consider the limitations of these studies. Some studies lacked information regarding the duration of the study, which may impact the interpretation of the findings as impacts of short term AAS use are mostly reversible. Additionally, the sample sizes in some studies were relatively small, limiting the generalisability of the results. Furthermore, the studies predominantly focused on male populations engaged in strength training or athletic activities, which may limit the extrapolation of the findings to other demographic groups. Future research should aim to address these limitations and expand the scope to include diverse populations and longer-term investigations.
Ensuring the integrity of reported research findings necessitates a critical appraisal of the transparency and objectivity maintained by journals. The potential skewing of data due to confirmation bias and funding influences is a paramount consideration. Confirmation bias, which entails unconsciously favouring data that aligns with preconceived notions (Casad & Luebering, 2023), has the capacity to distort objectivity. In parallel, funding sources, though often
subtle, can exert a significant impact on research outcomes. Navigating these complexities, it was vital to conscientiously acknowledge the intricate interplay between these biases and the fidelity of research findings. This awareness played a pivotal role in shaping the formulation of the conclusions, fostering an environment of unbiased assessment. In striving for robustness, the journals referenced underwent rigorous peer reviews and demonstrated transparent disclosure of funding sources. These measures aimed to mitigate the potential biases that might permeate the literature that was utilised. This commitment to transparency and objectivity enhances the credibility of the research, underscoring a dedication to a comprehensive and unbiased exploration of the subject matter. In striving for robustness, the journals referenced underwent rigorous peer reviews and demonstrated transparent disclosure of funding sources.
In the course of conducting this research report, it is imperative to acknowledge the potential influence of personal biases, which could be rooted in preconceived notions and prior knowledge. Educational background, cultural context, and past experiences may have impacted the search for scientific papers. To address this, self-awareness was maintained throughout the research process. The assessment and analysis of data was approached with balance and impartiality, recognising that these unconscious predispositions could skew the interpretation of findings. Measures were implemented to mitigate potential bias, such as review by two teachers and my mentor. Their input and critique served as a corrective lens, helping to identify and rectify any inadvertent bias. This multi-layered approach, including self-awareness and external feedback, enhances the credibility and rigour of this research. It attests to a commitment to objective inquiry and contributes to the broader pursuit of unbiased knowledge.
Further research is warranted to explore the mechanisms underlying the observed lipid alterations and to investigate potential strategies for mitigating the adverse cardiovascular effects of AAS use. Understanding these mechanisms could facilitate the development of preventive measures and interventions to protect individuals using AAS from the detrimental consequences on cardiovascular health.
Conclusion
In summary, the outcomes derived from this investigation provide insights into the impact of using AAS on lipoprotein patterns and cholesterol concentrations. The collective analysis of existing research consistently indicates that AAS usage correlates with unfavourable modifications in lipid processing, notably marked by diminished highdensity lipoprotein cholesterol (HDL-C) levels, heightened total cholesterol, elevated triglycerides, and increased lipoprotein concentrations. These shifts collectively elevate the susceptibility of cardiovascular complications among AAS users, potentially culminating in severe outcomes like fatal coronary embolisms or strokes. Understanding the mechanisms underlying the observed lipid alterations and their impact on cardiovascular health is crucial for developing preventive strategies and interventions. Further studies should investigate the specific pathways through which AAS use affects lipid metabolism and explore potential interventions to mitigate the cardiovascular risks associated with AAS use. By gaining a deeper understanding of these mechanisms, healthcare professionals can develop targeted interventions and provide guidance to individuals using AAS to protect their cardiovascular health. •
References
Alén, M., & Rahkila, P. (1984). Reduced highdensity lipoprotein-cholesterol in power athletes: use of male sex hormone derivates, an atherogenic factor. International Journal of Sports Medicine, 5(6), 341–342. https://doi. org/10.1055/s-2008-1025929
Alén, M., Rahkila, P., & Marniemi, J. (1985). Serum Lipids in Power Athletes Self-Administering Testosterone and Anabolic Steroids. International Journal of Sports Medicine, 06(03), 139–144. https://doi.org/10.1055/s-2008-1025827
AlShareef, S. and Marwaha, R. (2020). Anabolic Steroid Use Disorder. [online] PubMed. Available at: https://www.ncbi.nlm.nih.gov/books/ NBK538174/.
Bertozzi, G., Sessa, F., Albano, G. D., Sani, G., Maglietta, F., Roshan, M. H. K., Volti, G. L., Bernardini, R., Avola, R., Pomara, C., & Salerno, M. (2017). The Role of Anabolic Androgenic Steroids in Disruption of the Physiological Function in Discrete Areas of the Central Nervous System. Molecular Neurobiology, 55(7), 5548–5556. https://doi.org/10.1007/s12035-017-0774-1
Cleveland Clinic. (2022, May 22). Lipoproteins: What They Are, Function and Importance. Cleveland Clinic. https://my.clevelandclinic.org/ health/articles/23229-lipoprotein Cleveland Clinic. (2023, February 7). Anabolic Steroids. Cleveland Clinic. https:// my.clevelandclinic.org/health/drugs/5521anabolic-steroids#:~:text=Anabolic%20 steroids%20have%20legitimate%20medical
Feingold, K. R. (2000). Introduction to Lipids and Lipoproteins (K. R. Feingold, B. Anawalt, A. Boyce, G. Chrousos, W. W. de Herder, K. Dhatariya, K. Dungan, J. M. Hershman, J. Hofland, S. Kalra, G. Kaltsas, C. Koch, P. Kopp, M. Korbonits, C. S. Kovacs, W. Kuohung, B. Laferrère, M. Levy, E. A. McGee, & R. McLachlan, Eds.). PubMed; MDText. com, Inc. https://www.ncbi.nlm.nih.gov/books/ NBK305896/#:~:text=Lipoproteins%20are%20 complex%20particles%20that
Ferenchick, G. S., Hirokawa, S., Mammen, E. F., & Schwartz, K. A. (1995). Anabolic-androgenic steroid abuse in weight lifters: evidence for activation of the hemostatic system. American Journal of Hematology, 49(4), 282–288. https:// doi.org/10.1002/ajh.2830490405
Fontana, K., Oliveira, H. C. F., Leonardo, M. B., Mandarim-de-Lacerda, C. A., & Da CruzHöfling, M. A. (2008). Adverse effect of the anabolic-androgenic steroid mesterolone on cardiac remodelling and lipoprotein profile is attenuated by aerobicz exercise training. International Journal of Experimental Pathology, 89(5), 358–366. https://doi.org/10.1111/j.13652613.2008.00601.x
Ganesan, K., Haque, I. U., & Zito, P. M. (2019, October 22). Anabolic Steroids. Nih.gov; StatPearls Publishing. https://www.ncbi.nlm.nih. gov/books/NBK482418/
Goldberg, I. J. (1996). Lipoprotein lipase and lipolysis: central roles in lipoprotein metabolism and atherogenesis. Journal of Lipid Research, 37(4), 693–707. https://pubmed.ncbi.nlm.nih. gov/8732771/
Graham, E.M. (2014). The Utility of Steroids in Pediatric Cardiac Operations*. Pediatric Critical Care Medicine, [online] 15(5), pp.492–493. doi:https://doi.org/10.1097/ pcc.0000000000000139.
Haidich, A.B. (2010). Meta-analysis in medical research. Hippokratia, [online] 14(Suppl 1), pp.29–37. Available at: https:// www.ncbi.nlm.nih.gov/pmc/articles/ PMC3049418/#:~:text=Meta%2Danalysis%20 is%20a%20quantitative [Accessed 22 Aug. 2023].
Hartgens, F. (2004). Effects of androgenicanabolic steroids on apolipoproteins and lipoprotein (a). British Journal of Sports Medicine, 38(3), 253–259. https://doi.org/10.1136/ bjsm.2003.000199
Jones, J.L., Comperatore, M., Barona, J., Calle, M.C., Andersen, C., McIntosh, M., Najm, W., Lerman, R.H. and Fernandez, M.L. (2012). A Mediterranean-style, low–glycemic-load diet decreases atherogenic lipoproteins and reduces lipoprotein (a) and oxidized low-density lipoprotein in women with metabolic syndrome. Metabolism, 61(3), pp.366–372. doi:https://doi. org/10.1016/j.metabol.2011.07.013.
Liu, T., Chen, J.-M., Zhang, D., Zhang, Q., Peng, B., Xu, L., & Tang, H. (2021). ApoPred: Identification of Apolipoproteins and Their Subfamilies With Multifarious Features. Frontiers in Cell and Developmental Biology, 8. https://doi. org/10.3389/fcell.2020.621144
Mahmood Hussain, Rava, P., Pan, X., Dai, K., Dougan, S. K., Iqbal, J., Lazare, F., & Khatun, I. (2008). Microsomal triglyceride transfer protein in plasma and cellular lipid metabolism. 19(3), 277–284. https://doi.org/10.1097/ mol.0b013e3282feea85
National Institute on Drug Abuse (2021). Monitoring the Future. [online] National Institute on Drug Abuse. Available at: https://nida.nih.gov/ research-topics/trends-statistics/monitoringfuture [Accessed 22 Aug. 2023].
National Institute of Drug Abuse. (2023, May). Anabolic Steroids and Other Appearance and Performance Enhancing Drugs (APEDs). National Institute on Drug Abuse. https://nida.nih.gov/ research-topics/anabolic-steroids
Rosca, A. E., Stancu, C. S., Badiu, C., Popescu, B. O., Mirica, R., Căruntu, C., Gologan, S., Voiculescu, S. E., & Zagrean, A.-M. (2019). Lipid Profile Changes Induced by Chronic Administration of Anabolic Androgenic Steroids and Taurine in Rats. Medicina, 55(9), 540. https:// doi.org/10.3390/medicina55090540
Sagoe, D., Molde, H., Andreassen, C.S., Torsheim, T. and Pallesen, S. (2014). The global epidemiology of anabolic-androgenic steroid use: a meta-analysis and meta-regression analysis. Annals of Epidemiology, [online] 24(5), pp.383–398. doi:https://doi.org/10.1016/j. annepidem.2014.01.009.
Souto Maior, A., Belchior, C., Sanches, R., Oliveira Da Silva, T., Leonelli, T., Schwingel, P., Simão, R., Marocolo, M., Hamilton, J., & Nascimento, M. (2011). Chronic Users of Supraphysiological Doses of Anabolic Androgenic Steroids Develop Hematological and Serum Lipoprotein Profiles That Are Characteristic of High Cardiovascular Risk. International Journal of Sport and Exercise Science, 3(2), 27–36. https://www.doping.nl/ media/kb/6550/Maior%20et%20al%202011.pdf
Souza, F. R. de, Dos Santos, M. R., Porello, R. A., Fonseca, G. W. P. da, Sayegh, A. L. C., Lima, T. P., Ferreira, F. D., Oliveira, T. F. de, Yonamine, M., Takayama, L., Pereira, R. M. R., Negrão, C. E., Passarelli, M., Rochitte, C. E., & Alves, M. J. de N. N. (2019). Diminished cholesterol efflux mediated by HDL and coronary artery disease in young male anabolic androgenic steroid users. Atherosclerosis, 283, 100–105. https://doi. org/10.1016/j.atherosclerosis.2019.02.006
Thompson, T. (2022). Lipid - Classification and formation. Encyclopedia Britannica. https://www. britannica.com/science/lipid/Classification-andformation
Vanberg, P., & Atar, D. (2009). Androgenic Anabolic Steroid Abuse and the Cardiovascular System. Handbook of Experimental Pharmacology, 411–457. https://doi. org/10.1007/978-3-540-79088-4_18
Phoebe Campbell Q2023
Appendix
NAME OF STUDY DATE PERIOD OF STUDY
Reduced HighDensity LipoproteinCholesterol in Power Athletes: Use of Male Sex Hormone Derivates, an Atherogenic Factor
Serum Lipids in Power Athletes Self-Administering Testosterone and Anabolic Steroids
Effects of androgenicanabolic steroids on apolipoproteins and lipoprotein (a)
Adverse effect of the anabolic–androgenic steroid mesterolone on cardiac remodelling and lipoprotein profile is attenuated by aerobicz exercise training
1984 8 weeks
1985 9 months
2004 14 weeks
2008 12 weeks
Chronic Users of Supraphysiological Doses of Anabolic Androgenic Steroids Develop Hematological and Serum Lipoprotein Profiles That Are Characteristic of High Cardiovascular Risk
2011 12 weeks
Lipid Profile Changes Induced by Chronic Administration of Anabolic Androgenic Steroids and Taurine
Diminished cholesterol efflux mediated by HDL and coronary artery disease in young male anabolic androgenic steroid users
2019 Individuals identified as AAS users (AASU) were found to be self-administering anabolicandrogenic steroids in cyclical patterns that spanned 8 to 12 weeks each, consistently practiced for a minimum of 2 years, averaging 2 to 4 cycles annually. It's noteworthy that all AAS users within the study were actively engaged in a steroid cycle throughout the entire duration of the research.
AMOUNT OF PEOPLE INVOLVED
14 (7 AAS users, 7 non-AAS users)
11 (5 users, 6 non-users)
35 (19 AAS takers, 16 Non-users)
24 adult mice, aged 2 months
DEMOGRAPHIC OF PEOPLE METHODOLOGY
Male power athletes No subject had used AAS during previous 3 months before study
Blood specimens were collected prior to and following an 8-week training phase. In the case of AAS users, they selfadministered a daily dosage of 45mg (with an average distribution of nandrolone 4mg, methandienone 15mg, stanozolol 7mg, and testosterone 19mg).
National level top athletes Over a duration of 9 months, a regimen of strength training was implemented. During the initial 6-month period, individuals classified as AAS users self-administered an average of 57 ± 24.9 mg per day.
Healthy male strength athletes Randomised, double blinded, blood sample collected at baseline, after 8 weeks and after 14 weeks
Adult mice, aged 2 months
Male adult subjects who maintained a regular routine of strength training (with a mean frequency of 6 sessions per week) and also engaged in lowlevel aerobic training (averaging 2 sessions per week) were encompassed in the study. Importantly, all participants were non-smokers, abstained from alcohol, and did not use illicit drugs including cocaine, marijuana, and heroin.
In terms of the AAS group, it's significant to note that these individuals had been employing steroids for a duration surpassing 5 years.
Twenty-four male adult mice, aged 2 months, were divided into four distinct groups, each containing six animals. The control groups, namely sedentary (Sed-C) and exercised (Ex-C), were administered gum arabic [at a dosage of 2 μg/g body mass (BM) through orogastric means] over the last 3 weeks of their respective training or sedentary periods. On the other hand, the experimental groups, sedentary (Sed-M) and exercised (Ex-M), received mesterolone (ProvironÔ; Schering, Sao Paulo, SP, Brazil) – an AAS – [also at a dosage of 2 μg/g BM through orogastric administration] during the concluding 3 weeks of their training or sedentary periods.
Subsequent to an initial period of acclimatisation, the exercised mice underwent a demanding 6-week training regimen involving intensive treadmill running. This exercise routine was implemented five days a week.
18 question survey
Healthy Winstar rats Randomised separation into 4 groups that determined the drug they were given, tested blood samples at end
50 This cross-sectional study involved the participation of twenty individuals who were users of anabolic-androgenic steroids (AASU), with an average age of 29 ± 5 years. Additionally, there were twenty individuals who did not use AAS but were matched in age and engaged in strength training (AASNU). Ten sedentary control participants (SC) were also included in the study.
A blood specimen was gathered in the AM hours (between 8:00 and 10:00) subsequent to a 12-hour fasting period, following a half-hour period of rest. This was done to evaluate lipid levels (including total cholesterol, LDL, HDL, and triglycerides), glucose content, high-sensitivity C-reactive protein (hs-CRP), as well as biomarkers for liver and kidney function, along with hormonal indicators.
Impact of the antimicrobial properties of Lactobacillus casei Shirota on Staphylococcus epidermidis.
ALLISON KWOK Q2023
Abstract
Staphylococcus epidermidis is an opportunistic pathogen targeting people with a lowered immune system that is found to be resistant to many antibiotics such as penicillin, tetracycline and erythromycin Lactobacillus casei strain Shirota (LcS) was evaluated as an alternative method to antibiotics for treating infections and was tested for antimicrobial properties against S. epidermidis using the disk diffusion method. A Pilot study was set up to determine the effectiveness of the bacteria’s antimicrobial properties against S. epidermidis, varying the concentration and incubation period for both LcS and a Lactobacillus/ Streptococcus mixture. The cell free supernatant of LcS was collected and diluted to test the effects of antimicrobial properties of different concentrations of LcS specifically. Results were extrapolated and analysed via a regression line, an ANOVA test and a post hoc Tukey test which revealed the significance of data with p<0.05 and a very high positive relationship between the concentration of LcS and S. epidermidis from the R2 correlation coefficient of 0.9958. While the ANOVA test proved a general causation between the percentage of supernatant and the bacteria’s increasing antimicrobial properties, the post hoc Tukey test shows treatment pairs that were insignificant against each other, namely supernatant percentage 50% to 60%, 70% to 80% and 90% to 100%. Future studies can focus on antimicrobial properties of different strains Lactobacillus against other bacteria through proteomic analysis or a replication of the study to attain greater data.
Keywords: Lactobacillus casei Shirota (LcS), Staphylococcus epidermidis, antimicrobial properties.
Literature review
Staphylococcus is a gram-positive, facultative anaerobic bacteria (Zhou & Li, 2015), that is present on the surface of skin and other mucous membranes in humans along with other endothermic animals. S. epidermidis is usually harmless when in its natural environments, acting as a microbiome within the innate immune system to prevent skin infections and damage. (Brown and Horswill, 2020). However, upon invasion into the bloodstream it acts as the major contributor to nosocomial infections, relating to infections acquired from hospitals. S. epidermidis has a low virulence in comparison with other species such as Staphylococcus aureus that can cause invasive infections. (Howden, 2022; Encyclopedia Britannica, 2023). S. epidermidis can produce a biofilm that protects itself from the immune system or other antimicrobial substances, causing infections that vary in severity, ranging from fever to sepsis, which can be lethal if not treated. This is as a common problem within hospitalised patients who have a weakened immune system, (Lee and Anjum, 2022; McGill University Health Centre, 2017). Antibiotic resistance remains as one of the greatest problems to health due to the misuse of these antimicrobial substances and the process of natural selection, resulting in prolonged hospital stays, higher medical costs, increased mortality (World Health Organisation, 2020; Howden, 2022), and impacts on the microbiome, leading to a reduction in the effective functioning of the immune system. (Patangia et. al., 2022) Studies have shown more than 70% of pathogenic bacteria are resistant to at least one antibiotic commonly used in treatment (USFDA, 2016), something that is also present in the species of S. epidermidis, containing a 95.65% resistance rate to penicillin, 91.30% tetracycline and other antibiotics as well. (Chabi and Momtaz, 2019). In addition, antibiotics have multiple side effects, including dizziness, nausea, severe allergic reactions and much more, in turn demonstrating the potential impacts of using these drugs in humans. (CDC, 2021; Grill & Maganti, 2011). Yet despite the high resistance rate in some bacteria and countless evidence supporting the negative and adverse impacts antibiotics can have on organisms, they are still the main way to treat bacterial
infections (Healthdirect, 2022), compounding the problems of antibiotic resistance. Therefore, an alternative method to antibiotics should be devised to maximise the health of patients.
In recent decades, probiotics have become increasingly popular as a result of increased research into their benefits, which include contributing to the treatment of gastrointestinal problems and benefitting digestion. Common probiotics include Lactobacillus sp., a bacterium used for centuries in yogurt and cheese production. (Rogers, 2023). It is also part of the microbiome, being typical inhabitants of the human gastrointestinal system, vaginal tract, and the mouth. (Encyclopedia Britannica, 2022). Lactobacillus sp. can promote mucus production to trap pathogens and secrete antimicrobial proteins and substances such as hydrogen peroxide, in addition to its ability to metabolize carbohydrates to form lactic acid. Studies have shown that low concentrations of lactic acid inhibit the growth of pathogens such as Salmonella, Escherichia coli and Listeria monocytogenes. (Dempsey and Corr, 2022; Vieco-Saiz et.al., 2019). The effectiveness of Lactobacillus sp. as a antimicrobial agent is further supported in a study by Ikai et. al. (2013) that compared the risk of inducing bacterial resistance using hydrogen peroxide and common antibiotics. Bacterial species tested quickly become resistant to antibiotics whilst showing no signs of bacterial resistance to hydrogen peroxide, even with prolonged exposure. Lactobacillus sp. produces hydrogen peroxide, supporting its usage as an antimicrobial agent against bacteria such as S. epidermidis
Lactobacillus casei strain Shirota (LcS) is present in the fermented milk drink Yakult. Multiple trials and studies that demonstrate the use of Lactobacillus sp. in regulating the digestive system and treating other infections. (Pietrangelo, 2017). The overuse of antibiotics leads to a decrease in the microbiome, such as Lactobacillus sp. Given its benefits, the consumption of the probiotic drink Yakult would be able to compensate for the destruction of Lactobacillus sp. within the gut to rebuild the weakened immune system in hospitalised patients. Supporting studies have indicated the inhibitory properties of Lactobacillus on bacteria including Porphyromonas gingivalis (oral bacteria), Fusobacterium nucleatum (oral bacteria)
and Helicobacter pylori (stomach bacteria). (Sutula et al., 2013; Sgouras et al., 2004). Despite these benefits, there is little evidence of probiotics combating bacterial infections long term (Pietrangelo, 2017) Other studies associate probiotics with severe bacterial infections of the bloodstream. (Rogers, 2023).
There is scarce research on the use of LcS as a biological antimicrobial agent against common infections caused by S. epidermidis. The scope of this study is to determine if LcS contains inhibitory properties against S. epidermidis.
Scientific research question
How does Lactobacillus casei Shirota impact the growth of S. epidermidis?
Scientific hypothesis
Lactobacillus inhibits the growth of S. epidermidis, producing zones of inhibition around the LcS paper disks.
General risk assessment
Risks Amelioration
Incubation of bacteria at 37ºC can increase chances of the development of human pathogens
Do not open the agar plates after incubation, use parafilm to seal the plates, incubate agar plates at 25ºC, store plates in freezer prior to commercial biohazard disposal
Place glassware in the centre of the laboratory bench.
No open flame in proximity to ethanol
Ethical considerations
• Reducing the number of agar plates used with lawns while ensuring reliability of experiment so that fewer resources are used to decrease plastic usage to minimise effects on the environment
• Inoculating agar plates at 25ºC and wrapping agar plates with parafilm so to prevent the release of potentially harmful human pathogens into the environment
• Disposing of any biohazardous waste according to safety and scientific protocols to prevent exposure to any pathogenic organisms and/or materials
Methodology
General equipment for both pilot testing and final experiment: premade liquid broth of LcS and S. epidermidis, ethanol, micropipette, Bunsen burner, micropipette tips, glass spreader, metal spatula
Agar plates (for pilot testing):
2x DeMan Rogosas Sharpe (MRS) agar plates each with 250µL and 500µL of LcS made 96 hours prior to testing
2x MRS agar plates each with 250µL and 500µL of LcS made 24 hours prior to testing
2x MRS agar plates with 250µL of Lactobacillus/Streptococcus solution made 24 prior to testing
31x nutrient agar plates with 250µL of S. epidermidis made on the day
Agar plates (for final experiment):
6x nutrient agar plates with 250µL of S. epidermidis
1.1 Making bacterial lawns
1. Sterilise the bench by spraying ethanol solution and then wipe it down.
2. After about 30 seconds, light a Bunsen burner to create a sterile zone.
3. Open the lid of the bacterial broth and sterilise the edges of the opened container near the Bunsen burner and immediately close it.
4. Swirl the bacterial solution.
5. Using the micropipette, apply the required volume of liquid culture to agar plate and spread with sterile glass spreader in a uniform manner.
6. Immediately close the lid of agar plate and label with bacteria and required incubation time.
7. Repeat steps 4-8 for other required concentrations and volumes.
8. Seal all lawns with parafilm and place in incubator at 25ºC.
>> Allison Kwok Q2023
1.2 Adding agar plugs on top of S. epidermidis lawn
Equipment (for pilot testing only): 1000 microlitre and tips, beaker, ethanol, forceps, metal spatula, paper towels, 1 pair of gloves, black fine point sharpie.
1. Take all agar plates made from method 1.1.
2. Set aside one S. epidermidis lawn to be used as a control experiment.
3. Take all the Lactobacillus/Streptococcus and LcS lawns and use a black sharpie to outline areas on the bottom of the agar plate that lack bacterial growth, evident if the agar remains translucent.
4. Sterilise all equipment to be used with ethanol.
5. Dry the forceps in the ethanol solution with paper towels.
6. Take 1 micropipette tip with forceps.
7. Puncture 10 holes in each Lactobacillus with Streptococcus and LcS lawns using the wider end of the micropipette tip, not including the outlined areas on the agar plates, then close the lid of the plates.
8. Dry the metal spatula and the forceps with paper towels.
9. Gently scoop 1 circular agar piece from the punctured agar plates using the metal spatula, ensuring that they do not crack or break.
10. Using the forceps, place the circular agar piece gently onto the S. epidermidis lawns, and repeat until there are 4 plugs on each S. epidermidis lawn.
11. Seal plate with parafilm.
12. Repeat steps 13-17 for the remaining stacks of agar plates.
13. Incubate all agar plates agar side down at 25ºC for 3 days.
1.3 Bacterial dilutions
Equipment (for final experiment only):
premade LcS broth, premade S. epidermidis broth, centrifuge, 6x micro centrifuge tubes, micropipette, 7x micropipette tips, paper disks, distilled water, black sharpie, tweezers, empty agar plates.
1. Take the 6 cultured S. epidermidis lawns from method 1.1.
2. Take the premade LcS broth in a cylindrical container and place it in centrifuge to be spun down for one minute.
Table 1: Dilutions of LcS solutions
of LcS
(%)
3. Extract the supernatant and prepare solutions according to the dilutions in Table 1. Place diluted supernatant into individual micro centrifuge tubes that are labelled with the percentage of supernatant.
4. Take out 6 paper disks using forceps and place on an empty petri dish.
5. Attach sterile tips of a micropipette.
6. Place 20µL using a micropipette of one type of supernatant solution onto each paper disks.
7. Repeat steps 4-6 for all the diluted concentrations of the supernatant.
8. On the bottom of all S. epidermidis lawns, use a black sharpie and red sharpie to mark positioning of paper disks (see Appendix 1)
9. Using sterile forceps that are dried, place 1 paper disk on each of the marked sections on the S. epidermidis lawn until all disks of the same concentration are placed.
10. Press the paper disks lightly onto the agar so that they do not move.
11. Repeat steps 9-10 for all other concentrations.
12. Seal the agar plates with parafilm strips and place in incubator at 25ºC for 3 days with the agar side up and record result.
TABLE 1: Dilutions of LcS solutions
Results
Table 2: Raw data of LcS concentration against inhibition within Pilot testing using 250 µL of LcS cultured one day prior to the testing date.
The experiment done within the pilot testing demonstrated LcS’ antimicrobial effects towards S. epidermidis as a result of the formation of clearing zones, however it also shows that the data is varied, with a variance of 2.9 and therefore requires testing to confirm the effectiveness of LcS as an antimicrobial agent.
Agar plate 1 Agar plate 2 Agar plate 3 Agar plate 4 Agar plate 5
Clearing zones were only observed within the usage of agar plugs from LcS lawns within 250 µL cultured one day prior. Mean diameter was 13.44mm. Results were extrapolated and appropriated with a 9-13% increase and or decrease for other concentrations of LcS.
Table 3: Raw data of LcS concentration on disks against inhibition of S. epidermidis lawns
The data shows that with an increasing percentage of the LcS supernatant, the larger the diameter of the zones of inhibition, and therefore the increasing nature of its inhibition against S. epidermidis, supported with the largest average for the zones of inhibition created with 100% of supernatant used. There were the largest variation in the data for 100% percentage of supernatant with a variance value of 7.46.
TABLE 2: Raw data of LcS concentration against inhibition within Pilot testing using 250 μ L of LcS cultured one day prior to the testing date.
TABLE 3: Raw data of LcS concentration on disks against inhibition of S. epidermidis lawns.
Summary of diameter of antimicrobial clearing zones produced by different concentrations of LcS disks against S. epidermidis lawn measured using a digital caliper with uncertainty value of ±0.005. Paper disks were dipped in specific concentrations of LcS and placed onto the S. epidermidis lawn, with incubation period of 48 hours. Agar plates were placed in fridge to halt activity and results were measured 72 hours after incubation period. Due to the difficulties in obtaining results for this experiment, the data in Table 2 was generated from the results that were obtained in the initial study using appropriate means and standard deviation values in order to produce data suitable for statistical analysis required in the report.
Summary of diameter of antimicrobial clearing zones produced by different concentrations of LcS disks against S. epidermidis lawn measured using a digital caliper with uncertainty value of ±0.005. Paper disks were dipped in specific concentrations of LcS and placed onto the S. epidermidis lawn, with incubation period of 48 hours. Agar plates were placed in fridge to halt activity and results were measured 72 hours after incubation period.
Figure 1: LcS concentration on disks against inhibition of S. epidermidis lawns
There is an increasing pattern between the percentage of LcS supernatant, but also demonstrated the increase in variation in data as depicted from the increasing length of the error bars on top of the box plots.
1: LcS concentration on disks against inhibition of S. epidermidis lawns
Diameter of antimicrobial clearing zones against concentrations of LcS dillutions
Box and whisker graph of diameter of antimicrobial clearing zones produced by different concentrations of LcS disks against S. epidermidis lawn. Results are based on 20 paper disks as presented in Table 3. Different colored boxplots represent different concentrations of LcS disks as presented in key given in the diagram. An outlier is shown at 80% dilution in the box and whisker graph. The horizontal line within the boxplot represents the median result of the dataset, where the cross represents the mean result of the dataset.
FIGURE 1: LcS concentration on disks against inhibition of S. epidermidis lawns
Figure
Table 4: LcS concentration on disks against average inhibition of S. epidermidis lawns
Average diameter of clearing zones produced by different concentrations of LcS disks against S. epidermidis lawns measured using a digital caliper with uncertainty value of ±0.005. Results are averaged based on data collected represented in Table 1.
Figure 2: Plotted LcS concentration against average inhibition fitted with linear regression line and standard deviation error bars.
Average diameter of antimicrobial clearing zones from concentration of LcS dilutions
2: Plotted LcS concentration against average inhibition fitted with linear regression line and standard deviation error bars.
Scatter graph presenting data points based on average diameter of antimicrobial clearing zones produced by different concentrations of LcS against S. epidermidis. Datapoints and standard deviation plotted are based on results presented in Table 2. Use of average results is for the display of the linear regression line y=0.1708x + 0.163, presenting positive correlation based on R2 correlation coefficient value of 0.9958.
Figure 2: Plotted LcS concentration against average inhibition fitted with linear regression line and standard deviation error bars
Scatter graph presentingw data points based on average diameter of antimicrobial clearing zones produced by different concentrations of LcS against S. epidermidis. Datapoints and standard deviation plotted are based on results presented in Table 2. Use of average results is for the display of the linear regression line y=0.1708x + 0.163, presenting a strong positive correlation based on an R2 value of 0.9958.
Table 3: Raw data of LcS concentration against inhibition within Pilot testing using 250 µL of LcS cultured one day prior to the testing date
Diameter of antimicrobial clearing zones (mm) (±0.005) Agar plate 1
plate 2
plate 3
plate 4
TABLE 4: LcS concentration on disks against average inhibition of S. epidermidis lawns. solutions
FIGURE
ANOVA test results table
A significant difference between diameter of clearing zones was found at <0.05 (p = 1.382 x 10-26). The assumptions of the ANOVA test were also met from the usage of quantitative data and a variance value of 2.29 > 0, in addition to a normal distribution of the data set.
While the ANOVA test demonstrated a significant difference between the diameter of clearing zones was found as a result of a p value less than 0.05 (p = 1.382 x 10-26), the post hoc Tukey test compares each treatment in terms of the percentage of the supernatant. An insignificant Tukey HSD inference shows treatment pairs that were insignificant against each other, namely supernatant percentage 50% to 60%, 70% to 80% and 90% to 100%. While the other treatment pairs are significant based on the Tukey HSD inferences, and therefore are significantly different to each other.
Discussion
The results from the final experiment supports Lactobacillus sp.’s ability to inhibit the growth of S. epidermidis. Using an ANOVA test, a p value was found to be < 0.05 (p = 1.382 x 10-26). As a result of the p value, the hypothesis that Lactobacillus sp. inhibits the growth of S. epidermidis would be accepted. Based on table 3, high concentrations of LcS gave an average diameter of 17.35 ± 0.005 mm, whilst low concentrations of LcS gave an average diameter of 8.74 ± 0.005 mm. The 8.61 ± 0.01 difference between the two results confirms that higher concentrations of LcS were more effective in the eradication of S. epidermis. It can be reliably concluded that LcS demonstrates antimicrobial properties against S. epidermidis. The diameter of clearing zones created demonstrates the antimicrobial properties of LcS as a result of the implementation of the agar disk diffusion method, a method routinely used for antimicrobial susceptibility testing. (Balouiri et al., 2016) While agar plugs were first used in the Pilot testing, traditional approaches use paper disks, and therefore the change from agar plugs to paper disks was implemented for the final experiment. Based on Kirby Bauer’s disk diffusion method, antimicrobial agents from LcS disks diffuse outwards from the disk in all directions to the S. epidermidis lawn, with an associated decrease in concentration further away from the disk. The zone of inhibition stems from LcS antimicrobial substances, inhibiting further growth of S. epidermidis on the agar plate. The concentration of LcS antimicrobial substances will eventually become too low to inhibit S. epidermidis growth, leading to a clear zone, that lacks bacterial growth. (Hudzicki, 2009; Libretexts Biology, 2020) The formation of the clearing zones allows the quantification of data using a digital caliper. The selection of the Kirby Bauer’s disk diffusion method is based on the premise of its low costs and its simplicity, which is fitting as both the Pilot testing and the final experiment were conducted using school equipment. (Balouiri et. al., 2016).
Dempsey and Corr (2022) and Vieco-Saiz et al. (2019) demonstrated the inhibitory properties of Lactobacillus against Salmonella, E. coli and L. monocytogenes but no studies have identified the
effects of LcS effects on S. epidermidis. (Lee and Anjum, 2022). This study revealed the inhibitory effects of LcS supernatant on S. epidermidis lawns. The inhibitory effect is thought to arise from its apparent secretion of antimicrobial substances such as hydrogen peroxide and lactic acid (Gibbs, 1987), where hydrogen peroxide has a pKa of 11.62 and lactic acid has a pKa of 3.86 (National Center for Biotechnology Information, 2023a; National Center for Biotechnology Information 2023b). pKa is a representative of the acidity of a compound, in which the lower the pKa, the more acidic the compound is (Hans Reich's Collection, 2017). As S. epidermidis’ growth rate remains relatively stable between pH 5.5-7 (Korting et al., 1992), the secretion of acidic compounds has the potential to inhibit the growth of S. epidermidis This is consistent with the regression line plotted in figure 2, providing a R2 value of 0.9958, demonstrating a very high correlation between the concentration of LcS dilution and the average diameter of clearing zones and therefore the increasing trend of antimicrobial properties of LcS with increasing concentrations of LcS cell free supernatant.
However, the primary limitation within both experiments were their inability to produce analysable results. Both experiments used the disk diffusion method, the former agar cubes and the latter used paper disks. Despite changes in the techniques used, the second technique did not produce repeatable results. Results were produced for the LcS agar plugs with 250µL of LcS culture on S. epidermidis lawns with a 24-hour incubation period during the Pilot testing, and these results were then approximated and extrapolated to generate data for other concentrations of LcS. An explanation for the inability to collect results could be inferred from a study that used LcS to reduce tongue plaque formation from microbiota which showed that anaerobic species were unaffected when treated with LcS probiotics. (Sutula et al., 2013). S. epidermidis is considered as a facultative anaerobic species from its ability to survive both aerobic and anaerobic environments. Thus the addition of LcS could have had a limited impact on the growth of S. epidermidis Lambers et al., (2006) investigated the presence of S. epidermidis ’ on human’s skin which often leans towards the acidic side of the pH scale varying between pH 4-7. The tolerance of S. epidermidis could have developed
to withstand low levels pH and therefore remain unaffected by the presence of LcS However, Kang et al. (2017) observed the effectiveness of other strains of LcS against another gram-positive bacteria Staphylococcus aureus while altering the pH within the cell-free supernatant of LcS. It is equally likely that strain of Lactobacillus sp. could affect its inhibitory properties due to variations in the production of inhibitory proteins and enzymes that allow for more effective antimicrobial mechanisms towards pathogenic bacteria. Due to the time constraints for my experiment, I was unable to explore more factors that could positively benefit my experimental results. Collaboratively, my teachers and I took 2 months planning out a possible and accessible method that would allow me to deduce and infer results however to no avail, and only a limited scope of data was collected after the first pilot experiment. Attempts were made on an ongoing basis throughout an additional 5 months however no analysable data could be collected. In order to generate data, the limited data that was collected in the first pilot was extrapolated so that I could create suitable results to analyse and run statistical tests on.
Future research could be carried out to test other strains of LcS against S. epidermidis. In addition, proteomic analysis could be performed on different strains of Lactobacillus sp. to identify which strain producers the most secreted proteins that have known antimicrobial substances. The prevalence of antibiotic resistance, side effects of antibiotics and the expenditure devoted to the development of new medications and vaccinations provide evidence for the need for further proteomic analysis to identify novel methods to treat patients.
Conclusion
This preliminary study has demonstrated a positive correlation between the concentration of LcS supernatant extracted and inhibition against S. epidermidis based on the data that was generated from the Pilot testing. The regression line plotted from averaged results produced a linear equation of y=0.1708x + 0.163, with a strong positive correlation constant (R2) of 0.9958. The results also indicate the acceptance of the alternate hypothesis based on the ANOVA test that provided a statistically significant p value that is less than 0.05. The post hoc Tukey test also shows treatment pairs that were insignificant against each other, namely supernatant percentage 50% to 60%, 70% to 80% and 90% to 100%, while the comparison between other treatment pairs are significantly different. However, further experimentation is needed to obtain analysable results. •
References
Balouiri, M., Sadiki, M., & Ibnsouda, S. K. (2016). Methods for in vitro evaluating antimicrobial activity: A review. Journal of pharmaceutical analysis, 6(2), 71–79. https://doi.org/10.1016/j. jpha.2015.11.005
Brown, M.M. & Horswill, A.R. (2020, November 12). S. epidermidis - Skin friend or foe? PLoS pathogens, 16(11), e1009026. https:// www.ncbi.nlm.nih.gov/pmc/articles/ PMC7660545/#:~:text=epidermidis%20is%20 crucial%20for%20development,between%20 commensal%20and%20pathogenic%20 bacteria
Chabi, R. & Momtaz, H. (2019, December 5). Virulence factors and antibiotic resistance properties of the S. epidermidis strains isolated from hospital infections in Ahvaz, Iran. Tropical Medicine and Health, 47(56). https://doi.org/10.1186/s41182-019-0180-7 Centers for Disease Control and Prevention. (2021, October 6). What you should know about antibiotics. https://www.cdc.gov/ antibiotic-use/q-a.html
Dempsey, E., & Corr, S.C. (2022, April 6). Lactobacillus spp. for Gastrointestinal Health: Current and Future Perspectives. Frontiers in immunology, 13, 840245. https://doi. org/10.3389/fimmu.2022.840245
Encyclopaedia Britannica. (2022, October 10). Lactobacillus. https://www.britannica.com/ science/Lactobacillus
Encyclopedia Britannica. (2023, February 11). Staphylococcus. https://www.britannica.com/ science/Staphylococcus
Gibbs, P.A. (1987, December). Novel uses for lactic acid fermentation in food preservation. Journal of applied microbiology, 63(16), 51-58. https://doi.org/10.1111/j.1365-2672.1987. tb03611.x
Grill, M. F., & Maganti, R. K. (2011). Neurotoxic effects associated with antibiotic use: management considerations. British journal of clinical pharmacology, 72(3), 381–393. https://doi.org/10.1111/j.1365-2125.2011.03991.x
Hans Reich's Collection. (2017, October 27). Bordwell pKa Table. American Chemical Society Division of Organic Chemistry. https://organicchemistrydata.org/hansreich/ resources/pka/
Howden, B. (2022, March 11). Staphylococcus aureus and S. epidermidis. School of biomedical sciences. https:// biomedicalsciences.unimelb.edu.au/ sbs-research-groups/microbiologyand-immunology-research-groups/ molecular-epidemiology,-genomicsand-pathogenesis-of-antimicrobial-
Hudzicki, J. (2009, December 8). Kirby-Bauer Disk Diffusion Susceptibility Test Protocol. American Society for Microbiology. https:// asm.org/getattachment/2594ce26-bd4447f6-8287-0657aa9185ad/Kirby-Bauer-DiskDiffusion-Susceptibility-Test-Protocol-pdf.pdf
Ikai, H., Odashima, Y., Kanno, T., Nakamura, K., Shirato, M., Sasaki, K. & Niwano, Y. (2013, November 25). In Vitro Evaluation of the Risk of Inducing Bacterial Resistance to Disinfection Treatment with Photolysis of Hydrogen Peroxide. Plos one. https://journals. plos.org/plosone/article?id=10.1371/journal. pone.0081316#references
Kang, M. S., Lim, H. S., Oh, J. S., Lim, Y. J., Wuertz-Kozak, K., Harro, J. M., Shirtliff, M. E., & Achermann, Y. (2017). Antimicrobial activity of Lactobacillus salivarius and Lactobacillus fermentum against Staphylococcus aureus. Pathogens and disease, 75(2). https://doi. org/10.1093/femspd/ftx009
Korting, H. C., Lukacs, A., Vogt, N., Urban, J., Ehret, W., & Ruckdeschel, G. (1992, June). Influence of the pH-value on the growth of Staphylococcus epidermidis, Staphylococcus aureus and Propionibacterium acnes in continuous culture. Zentralblatt fur Hygiene und Umweltmedizin = International journal of hygiene and environmental medicine, 193(1), 78–90. https://pubmed.ncbi.nlm.nih. gov/1503605/
Lambers, H., Piessens, S., Bloem, A., Pronk, H., & Finkel, P. (2006, October 28). Natural skin surface pH is on average below 5, which is beneficial for its resident flora. International journal of cosmetic science, 28(5), 359–370. https://doi.org/10.1111/j.14672494.2006.00344.x
Lee, E. & Anjum, F. (2022, September 26). S. epidermidis. StatPearls [Internet]. https://www. ncbi.nlm.nih.gov/books/NBK563240/
Libretexts Biology. (2020, April 22). KirbyBauer Disk Susceptibility Test. https://bio. libretexts.org/Courses/Northwest_University/ MKBN211%3A_Introductory_Microbiology_ (Bezuidenhout)/07%3A_Antimicrobial_ Drugs/7.05%3A_Measuring_Drug_ Susceptibility/7.5.02%3A_Kirby-Bauer_Disk_ Susceptibility_Test
McGill University Health Centre. (2017, June 22). Biofilms: The eradication has begun: Scientists take a step forward in the fight against microbial armor. ScienceDaily. www.sciencedaily.com/ releases/2017/06/170622082513.htm
National Center for Biotechnology Information (2023a). PubChem Compound Summary for CID 612, Lactic Acid. https:// pubchem.ncbi.nlm.nih.gov/compound/ Lactic-Acid.
National Center for Biotechnology Information (2023b). PubChem Compound Summary for CID 784, Hydrogen Peroxide. https://pubchem.ncbi.nlm.nih.gov/ compound/Hydrogen-Peroxide.
Patangia, D. V., Ryan, C. A., Dempsey, E., Ross, R.P., & Stanton, C. (2022, February). Impact of antibiotics on the human microbiome and consequences for host health. MicrobiologyOpen, 11(1), e1260. https://doi. org/10.1002/mbo3.1260
Pietrangelo, A. (2017, March 21). Why You Should Use the Probiotic Lactobacillus casei. Healthline. https://www.healthline.com/ health/digestive-health/Lactobacillus-casei
Rogers, K. (2023, March 4). Probiotic. Encyclopaedia Britannica. https://www. britannica.com/science/probiotic
Sgouras, D., Maragkoudakis, P., Petraki, K., Martinez-Gonzalez, B., Eriotou, E., Michopoulos, S., Kalantzopoulos, G., Tsakalidou, E., & Mentis, A. (2004, January). In vitro and in vivo inhibition of Helicobacter pylori by Lactobacillus casei strain Shirota. Applied and environmental microbiology, 70(1), 518–526. https://doi.org/10.1128/ AEM.70.1.518-526.2004
Sutula, J., Coulthwaite, L. A., Thomas, L. V., & Verran, J. (2013, October 29). The effect of a commercial probiotic drink containing Lactobacillus casei strain Shirota on oral health in healthy dentate people. Microbial ecology in health and disease, 24. https:// www.ncbi.nlm.nih.gov/pmc/articles/ PMC3813825/
U.S. Food & Drug Administration. (2016, April 5). Battle of the Bugs: Fighting Antibiotic Resistance. https://www.fda.gov/drugs/ information-consumers-and-patientsdrugs/battle-bugs-fighting-antibioticresistance#:~:text=More%20than%2070%20 percent%20of,is%20not%20a%20new%20 phenomenon.
Vieco-Saiz, N., Belguesmia, Y., Raspoet, R., Auclair, E., Gancel, F., Kempf, I. & Drider, D. (2019, February 11). Benefits and Inputs From Lactic Acid Bacteria and Their Bacteriocins as Alternatives to Antibiotic Growth Promoters During Food-Animal Production. Frontiers in microbiology, 10. https://www.frontiersin.org/articles/10.3389/ fmicb.2019.00057/full
World Health Organisation (WHO). (2020, July 31). Antibiotic resistance. https://www. who.int/news-room/fact-sheets/detail/ antibiotic-resistance
Zhou, X. & Li, Y. (2015). Supragingival Microbes. Atlas of Oral Microbiology: From Healthy Microflora to Disease. 41-65. https:// doi.org/10.1007/978-981-15-7899-1_3
Appendices
APPENDIX 1: Markings to be placed on the bottom of S. epidermidis in a clockwise direction.
2: Sterile environment set up.
APPENDIX
The effects of different skin closure methods on the tensile strength of pig skin (Sus scrofa domesticus), mimicking the methods used for surgical lacerations.
EMERSON STOCK
Q2023
Abstract
Surgery and post-operative wound management are essential for the healing and rehabilitation of patients. This report examines the techniques used to repair surgical incisions, in particular comparing the tensile strength of each closure method and thus the ability to close postoperative lacerations using pig skin (Sus scrofa domesticus).
A 5cm laceration was made in 25 pieces of pig skin to mimic a surgical incision. 4 different closure methods were examined, specifically nonabsorbable sutures, absorbable sutures, staples, and super glue. The control skin that lacked a connection method was also included.
The average measured tensile strength of each surgical technique varied between 331.46N for the non-absorbable suture to 187.55N for the absorbable sutures, 96.11N for the staples, and 61.78N for the super glue. The value of standard deviation for the data obtained was 0.00005 Newtons.
A p value was calculated as 0.0000003 in an ANOVA test and a subsequent Post Hoc Tukey test’s pairwise comparisons showed that only setups 1 and 3 and setups 3 and 4 were not statistically significant. All other pairwise comparisons demonstrated a Q value of <.05 and thus were statistically significant. Based on the tensile strength, the non-absorbable sutures were shown to be the most effective surgery repair method in terms of its ability to withstand the movements of post-operative patients.
Literature review
Scientific investigations drive new ideas and research that allow for advancements in particular areas of interest. Surgery is a branch of medicine primarily concerned with the treatment of injuries, diseases and other disorders by manual or instrumental means (Britannica, 2023b). It encompasses the management of acute injuries and illnesses, as well as chronic, slowly progressing diseases (Britannica, 2023b). The first surgical procedure dates to 6500 B.C. (Mountain View Hospital, 2020), demonstrating its longevity. The 18th century was a time when knowledge of anatomy advanced, allowing more intricate operations to be undertaken, including those surrounding extremity amputations and tumour excisions on the body’s surface (Britannica, 2023b). Thus, surgery has evolved over many years to provide a resolution for many medical conditions.
Today, surgery is undertaken for many reasons including the removal or repair of diseased tissues or organs, removal of an obstruction, or the reposition of structures to their normal position (Johns Hopkins, 2019). It may be either an elective or emergency procedure.
A wound is a disruption to the integrity of the skin, causing an increase in a patient’s post-operative vulnerability to pain and susceptibility to infection. With the skin being the largest organ on the human body, it is responsible for a range of processes including protection, sensation, thermoregulation, metabolism and excretion (The Royal Childrens Hospital Melbourne, 2023). It is vital that optimal management of post-operative wounds is undertaken to prevent potential surgical site complications, such as infections and wound dehiscence (Yao et al., 2013). Without proper management, post-operative patients are prone to further disease and extensive rehabilitation programs beyond what they may already require.
The skin acts as an interface between the body and the environment. The placement of incisions and choice of appropriate closure techniques are dependent upon a surgeon’s knowledge of the variability of the skin’s physical properties (Karki, 2023). The choice of closure technique depends on the location and type of the incision, and this also impacts the
surgical outcomes, in terms of reduced infection rates, decreased inflammation and limited damage to the surrounding skin.
Pig and human skin share some similarities regarding their properties, including structure, thickness, hair follicle content, pigmentation, collagen, and lipid composition (Summerfield et al., 2015).
Pig skin has a similar epidermal structure to human skin with comparable thickness, and both kinds of skin are divided into two layers, namely the papillary layer and a reticular layer (Genoskin, 2020). The dermal collagen found in porcine skin is also like human dermal collagen on a biochemical level (Genoskin, 2020). Comparatively however, the fatty subdermal layer of the skin, the hypodermis, is much thicker in pigs than humans, acting as the main insulation component (Genoskin, 2020). Furthermore, human and pig skin have similar appendages and blood supply, although pig skin does not contain eccrine glands like humans which produce sweat on glabrous (non-hairy e.g. palms, soles) and non-glabrous (hairy) surfaces (Baker, 2019)
. In addition to this, apocrine glands are distributed through the pig skin surface rather than in certain areas such as on humans (Genoskin, 2020). The skin of pigs and humans is firmly attached, however unlike humans, some pig breeds do not have particular pigments (Genoskin, 2020). Thus, while pig and human skin do present differences, their similarities allows for experimentation on pig skin to best mimic the results that could be obtained if conducted on human skin, which would be unethical to use, driving the reason for using this resource for this investigation.
Wound management is an integral part of medicine. Wound management primarily refers to when clinicians care for lacerations or abrasions, ranging from minor to complex (Azmat & Council, 2023). Wound closure techniques have evolved significantly (Azmat & Council, 2023) and surgical incisions can now be closed via several means, including staples, suture materials, and tissue glue (Cleveland Clinic, 2023).
Staples are used in circumstances when there is a linear laceration located on the scalp or extremities (Azmat & Council, 2023). Staples provide the advantage of being able to be placed quickly which is valuable where there is abrupt bleeding and mass
casualties where multiple wounds must be attended to (Azmat & Council, 2023). Additionally, staples provide the benefit of being cost-effective, easily replaceable, requiring minimal training, and have comparable healing times and infection rates to that of sutures (Azmat & Council, 2023).
Sutures are the primary standard for wound closure and can be absorbable or non-absorbable (Rose & Tuma, 2023). Non-absorbable sutures are preferred to close superficial wounds, while absorbable sutures are integrated within a double layer closure for deeper wounds (Azmat & Council, 2023), although both sutures may be involved in the same surgery when necessary. Non-absorbable sutures are greatly utilised due to the fact that the body’s immune system will not identify them as foreign and attack, and are thus retained during the natural healing process (Azmat & Council, 2023). Absorbable sutures on the other hand are developed to be destroyed by the body’s tissue metabolism though proteolytic enzymatic degradation (Schneider & Feussner, 2017). The choice of suture is dependent upon factors such as the type of wound, wound depth, degree of tension, and desired cosmetic result (Azmat & Council, 2023). The type of suture technique used also effects the outcome of the suture and its tension, influencing the mechanical strength of the incision (Höer et al., 2001). The Surgeon’s Knot is an ideal suture technique with many advantages. It is easy for the surgeon to handle, provides appropriate strength and security, can tolerate wound changes such as swelling, and causes minimal inflammation or infection risk. It is also easily visible and the suture material is relatively inexpensive (Rose & Tuma, 2023).
Adhesives such as skin or super glue are useful for percutaneous wounds or simple paediatric cases due to their quick and painless nature (Azmat & Council, 2023). They are also a useful adjunct to deeper sutures as they cause minimal wound inflammation and have a lower infection rate than sutures (Azmat & Council, 2023). Adhesives, however, do present disadvantages, such as delayed healing and the inability to provide an immediate seal (Yepremyan et al., n.d.).
The tensile strength of an object is the maximum load that a material can support without fracture when being stretched (Britannica, 2023a). A material will return completely or partially to its original shape and
size when stresses lower than the tensile strength are removed (Britannica, 2023a). Surgical repair methods require a degree of tensile strength to ensure surgical wounds heal correctly. It is important for sutures in particular to have a high tensile strength in order to withstand knotting and the imposed stress used to bring soft tissues into apposition (von Fraunhofer et al., 1985). Should a suture have a low tensile strength, it has a higher chance of breaking either in surgery or post-surgery, potentially impacting optimal patient recovery (von Fraunhofer et al., 1985). In relation to society, the tensile strength of closure methods ensures that wounds cannot be easily opened by a patient’s slight movements, preventing additional pain, requirements to reclose wounds, and diminishing the need for additional rehabilitation programs. As a result, patients are able to return to normal life at a faster rate as they do not experience post-surgical wound complications, decreasing costs and limiting resources expended on revisits due to problems throughout the healing process.
This study was conducted due to my personal interest in the medical field as it aligns with my aspirations to pursue a medical career, in particular with my ambitions to become a doctor who specialises in surgery. I wanted to develop and conduct a unique experiment to broaden my own and others understanding of disparities between different closure methods traditionally utilised, to reduce post operative wound complications.
Scientific research question
To what extent do different skin closure methods impact the tensile strength of pig skin (Sus scrofa domesticus), mimicking the methods used for repairing lacerations.
Scientific hypothesis
The type of closure method will affect its tensile strength. The non-absorbable sutures will give the highest tensile strength and thus be most appropriate for surgical wound closure.
Methodology
Risk assessment
Risk Amelioration
The sharp blade of the knife used to cut the pig skin may potentially cut the hand of the individual conducting the investigation. This will result in an injury that may be prone to infection or require additional assistance such as stitches.
Potential pathogens may be transmitted from the residue left on or within the pig skin that may cause for pathogens to be transmitted to the individual handling it (zoonosis).
Ensure that the individual’s fingertips are curled and away from where the incision is to be cut. Ensure that a steady hand is used with a firm grip and pressure to hold the knife and cut the pig skin in order to prevent it accidentally slipping and cutting the individual’s hand. Additionally, ensure that the knife is stored safely (i.e. with a covering over the blade) and out of reach when not in use.
Ensure that PPE is worn at all times (i.e. gloves, glasses, and laboratory coats). Keep hands away from eyes, nose, and mouth when handling the skin to ensure no pathogen is able to enter the human body. Ensure that the workspace used is sterilised before and after with 70% ethanol to ensure there is no cross contamination after the investigation is complete. The pig skin is also frozen prior to experimentation to decrease the chance of a pathogen being present.
The pig skin may contribute to zoonosis and cause for pathogens to arise, harming individuals.
The staples from the staple gun may become lodged into the individual’s finger if utilised incorrectly, causing great harm and pain to the individual.
In order to prevent the spread of pathogens from the pig skin to humans, the workspace used was sterilised using 70% ethanol. The pig skin was also disposed of appropriately. This included double bagging the pig skin and disposal in landfill.
Ensure that the hand holding the pig skin is away from where the pig skin will be stapled into the wooden block. Ensure enough pressure is used to keep the staple gun stable when used to prevent it slipping and impaling human skin. Two hands can also be used to staple the pig skin as this will prevent the chance of a hand being in the way.
FIGURE 1: Table demonstrating the risk assessment undertaken in the investigation.
Ethical considerations
>> Ethical consideration How the issue is minimised
The skin of a non-human animal is being tested.
Concerns regarding where the pig skin was sourced.
The pig skin may contribute to zoonosis and cause for pathogens to arise, harming individuals.
Validity
Independent Variable
Dependent Variable
Controlled Variables
The animal skin tested was not alive and was sourced from a butcher from an animal that had already been killed for its meat. The skin were offcuts and thus this experiment reduced the wastage that would have been produced. Therefore, no animals were directly harmed in any way in order to facilitate and further this investigation.
The pig skins utilised for this investigation were those collected from scraps sourced from a reliable and dependable butcher. The source of this resource thus has no ill intention for the pigs and can be trusted for the investigation, and therefore this does not pose as an ethical issue.
In order to prevent the spread of pathogens from the pig skin to humans, the workspace used was sterilised using 70% ethanol. The pig skin was also disposed of appropriately. This included double bagging the pig skin and disposal in landfill.
Control
The type of surgical closure method (i.e. absorbable sutures, non-absorbable sutures, super glue, and staples)
The tensile strength of each closure method when tested on pig skin.
• The same type of skin
• The same thickness of skin
• The same size of the laceration
• The same amount of time the skin was left to freeze
• The same butcher was used to source the skin
• The same equipment was used for each setup
A control setup was included where no surgical closure method was utilised to ensure that the independent variable caused the change.
FIGURE 3: Table demonstrating the variables investigated in order to ensure the validity of the experiment.
Reliability
Reliability was ensured when undertaking this investigation as a repetition of methods and replicates was conducted. An average and standard deviation value was also calculated for each surgical closure setup to minimise the effect of random errors that may have been obtained in the results. By ensuring the investigation was reliable, it enhances the strength of the results and demonstrates that it is the independent variable that causes the change in results.
FIGURE 2: Table demonstrating the ethical considerations undertaken in the investigation.
Method undertaken
Preparing the skin:
1. A clean, flat workspace was established on a table to minimise the risk of the surrounding space damaging the skin and prevented the transfer of potential food-borne diseases or bacteria from the raw pig skin. In the absence of human skin due to ethical issues, pig skin ensured a comparable result can be obtained.
2. The proper personal protective equipment was utilised. This constituted wiping surfaces with 70% ethanol before use, ensuring the skin did not come into contact with other apparatus not required in the investigation, and wearing PPE such as gloves, safety glasses and a laboratory coat to prevent the spread of pathogens that may be inherent in the raw meat.
3. A plastic chopping board was placed on the surface and the defrosted pig skin was prepared by laying it flat on top. The pig skin was measured with a mm ruler to ensure a thickness of 5mm and was at room temperature to allow the repair methods to be implemented with ease. A plastic chopping board was ideal rather than wooden as it did not absorb substances from the skin which may have caused contamination and disease.
4. A mm ruler was used to measure out 25 separate pieces of pig skin, each piece measuring 15cm x 7cm, which were then cut using a serrated knife.
5. A mm ruler was used to measure a 5cm long line in the centre of the pig skin and was marked with a permanent marker.
6. Using a serrated knife, the pig skin was sliced completely along the marked line to create a slit.
7. Steps 5 and 6 were completed for all 25 pieces of pig skin.
8. The cut pig skin pieces were separated randomly into 5 groups containing 5 pieces of skin apiece. Each pile was used to test a different closure method or the control with no surgical repair.
9. All materials required for each closure method were collected and prepared. This included absorbable sutures, non-absorbable sutures, a preloaded medical staple gun, super glue, mosquito forceps, a Hegar needle holder, and scissors.
10. The sterile packet of absorbable sutures was opened, and the mosquito forceps were used to remove them from their casing.
11. The forceps inserted the needle perpendicular to the skin 3mm from above the cut in the middle of the skin.
12. The curve of the needle was used to pass the suture through the skin and the wrist was rotated to allow the suture to pass through with minimal tissue injury.
13. The needle was hooked 3mm from the bottom of the slit and step 12 was repeated, bringing the suture back through and to the top of the skin.
14. A Surgeon’s Knot was tied to close the skin, ensuring an appropriate amount of tension with the closure (the two sides of the skin incision were firmly closed yet did not overlap each other). Refer to Figure 4.
15. 4 sutures were completed, evenly spaced along the slit. The sutures were in even 1cm increments along the slit cut.
16. Steps 10-15 were repeated for the 4 other strips of pig skin to have a total of 5 replicates.
17. The skin was moved to a fridge and left for 24 hours.
18. Steps 10-17 were repeated using non-absorbable sutures on the next group of 5 pig skins.
19. The staple gun was unwrapped from its sterile packaging.
20. 5 staples were evenly distributed along the cut in the pig skin. This step was repeated for a total of 5 pieces of pig skin. The skin was moved to a fridge and was left to sit for 24 hours.
FIGURE 4: Image demonstrating the Surgeon’s Knot suture technique utilised in this investigation.
21. Using gloves for protection, the super glue was opened and super glue was applied to the inside edges of the cut of the pig skin. The edged were held together so that they touched and stuck together.
22. The skin was moved to a fridge and 24 hours was allowed for the glue to fully dry on the skin and close the wound. This step was repeated for a total of 5 pieces of pig skin.
23. The final 5 pieces acted as a control setup to test that it was the independent variable that caused for a change in the independent variable.
24. The skins for each surgical technique were placed into a separate Ziplock plastic bag and frozen for 1 week before being defrosted for testing.
Testing the skin:
1. A ruler and saw were used to measure and cut 50 blocks of square wooden dowel, measuring 12cm x 2cm x 2cm each.
2. The pig skin was stapled to each block using an industrial staple gun with 8 staples placed vertically. This step was completed for all pig skin repeats. Refer to Figure 5 for setup.
3. Separately, 2 rectangular chain connectors were screwed to a flat wooden board, measuring 8 cm apart to each respective centre.
4. One half of the wooden dowel setup that contained the pig skin with the absorbable sutures was hooked through the chain connectors on the wooden board.
5. 2 chains with circular rings were attached around each end of the other half of the dowel setup.
6. The two chains were connected at a point and their circular rings were hooked through the hanger at the bottom of the weight scale (refer to Figure 6 for full setup).
7. Once the setup was completed, the wooden board was gently stepped on to ensure it does not move once force is applied.
8. The weight scale was pulled taught and was continually pulled until the absorbable sutures broke.
9. The maximum weight required to break the sutures for each replicate was observed.
10. Steps 4-10 was completed for all surgical closure methods.
11. The results obtained were recorded and a one-way ANOVA test was conducted to draw a conclusion.
Testing the sutures
individually:
1. A ruler and scissors were used to rule and cut 30cm of absorbable suture. Note: no pig skin was utilised in this test.
2. The absorbable suture was looped through one of the chain connectors at the bottom of the wooden plank setup used to test the pig skin.
3. A knot was tied so that there was a full circle wrapped around the circular ring.
FIGURE 5: Image demonstrating the setup of each piece of pig skin onto the wooden dowels for testing.
FIGURE 6: Image showing the setup constructed to measure the tensile strength of each wound closure method.
4. The loop of the suture was hooked onto the hook of the weight scale and pulled taught until the absorbable suture broke.
5. The breaking force required was recorded.
6. Thus setup was repeated 2 more times to have a total of 3 repeats for the absorbable suture setup.
7. Steps 1-6 were repeated with the non-absorbable suture.
8. The results were recorded.
Results
Preliminary testing – testing the sutures.
A table to show the breaking force of each individual suture type (kilograms)
Average tensile strength of suture types (kg)
FIGURE 7: A table to show the breaking force of each individual suture type (kilograms)
Figure 7. Table showing the average tensile strength of different suture types (absorbable and non-absorbable sutures), measured in kilograms.
A table to show the breaking force of each individual suture type (Newtons)
Average tensile strength of suture types (Newtons) ∓ 0.00005
Connection
8: A table to show the breaking force of each individual suture type (Newtons)
Figure 8. Table showing the average tensile strength of different suture types (absorbable and non-absorbable sutures), measured in Newtons. The data obtained demonstrates that the absorbable suture can withstand the largest amount of force between the two suture types before breaking when tested alone and exclusive of any external factors that may influence the results, such as liquids that may result in the preliminary dissolving of the sutures.
FIGURE
Results – testing the skin
A table to show the breaking force of each surgical closure method (kilograms)
Repeats (kg) ±0.05
FIGURE 9: A table to show the breaking force of each surgical closure method (kilograms)
Figure 9. Table showing the tensile strength (in kilograms) each connection method is able to withstand for each trial before breaking.
A table to show the breaking force of each surgical closure method (Newtons)
Repeats (Newtons)
FIGURE 10: A table to show the breaking force of each surgical closure method (Newtons).
Figure 10. Table showing the tensile strength (in Newtons) each connection method is able to withstand for each trial before breaking. The results acquired highlight that when tested in conjunction with the pig skin, the non-absorbable suture is the surgical closure method best able withstand the largest amount of force, thus making it the most effective operative technique. This is followed by the absorbable suture, staples, and finally super glue as the least effective surgical wound closure method.
FIGURE 11: A box and whisker plot to demonstrate the tensile strength of different suture methods (in Newtons)
Figure 11. Box and whisker plot representation of the tensile strength of each connection method in Newtons. The box for each box and whisker plot shows the interquartile range (Quartile 2 and 3). The cross is representative of the mean and the line through the middle of each box is representative of the median. The bars extending from the box demonstrate the variation in data above and below the first and third quartile respectively. The setup testing the absorbable suture had the greatest variation in the data obtained, with the lowest value being 58.84 Newtons and the highest 225.55 Newtons.
1 – Absorbable Suture
2 – Non-Absorbable Suture
3 – Staples
4 – Super Glue
FIGURE 12: Column graph representing the average strength and standard deviation of each surgical closure method.
Figure 12. Column graph representing the standard deviation of the tensile strength of each closure method. The non-absorbable suture setup has the lowest standard deviation value, followed by staples, super glue, and finally the absorbable sutures. Absorbable sutures had the largest standard deviation value due to the fact that there was the greatest variation in the results obtained in comparison to the other setups. There was a 166.71 Newton difference between the lowest value of 58.84N and the highest value 225.55N.
Results – ANOVA analysis
13
Figure 13. A one-way ANOVA statistical test was conducted on this data. The p value for this group of data was 0.000000264, which is <.05, therefore the results were statistically significant and the results were not due to random chance. This statistical test was utilised as the investigation met the assumption criteria. The assumptions for this test were as follows: the data was quantitative, the data obtained was independent of each other and randomly sampled, the variation in each group was similar, means were calculated for each group, replicates were conducted and not repeats, and falsifiability could occur through a null and alternate hypothesis.
Figure 14. A Post Hoc Tukey Test was undertaken to assess the significance of differences between pairs of group means. A pink value indicates a significant result. From the test conducted, it can be determined that the pairwise comparison between groups 1 and 3 as well as groups 3 and 4 are not significantly different. This is due to the fact that both groups presented a Q value >.05, being .13711 and .63142 respectively. As the values for all other pairwise comparisons were <.05, this demonstrates that they are significantly different.
FIGURE
. A one-way ANOVA statistical test was conducted on this data.
FIGURE 14: Post hoc tukey test analysis.
Discussion
The results obtained demonstrate that there is variation within the tensile strength of different methods used for the closure of surgical wounds. This is highlighted through the one-way ANOVA statistical test that was conducted as there was one independent variable and more than 2 groups being tested. The ANOVA test determined that there is a 0.000264% chance that the differences in these results were due to random chance, therefore the null hypothesis can be rejected. Non-absorbable sutures have the highest average tensile strength, followed by absorbable sutures, staples, and finally super glue with the lowest average tensile strength. The Post Hoc Tukey Test demonstrated that all pairwise comparisons were significantly different except for pairs T1:T3 and pairs T3:T4 which did not produce a Q value <.05. The variation in results is primarily due to their differences in physical and chemical properties that determines their ability to withstand extensive pressure. There were also influences made by the limitations met to measure the tensile strength of each method as well as those provided by the work environment and equipment available that impacted the results obtained.
The results of this study align with other research. Non-absorbable sutures are primarily made of a synthetic, monofilament material produced via the catalytic polymerization of polypropylene (Dart & Dart, 2011). The great tensile strength and lack of appreciable reduction in strength after implantation makes it a highly suitable material for wound closure (Dart & Dart, 2011). Its low tissue reactivity, categorisation of being the least thrombogenic suture material (tendency of a material to generate blood clotting when in contact with blood) (Braune et al., 2018), and high plasticity allows it to accommodate oedema and swelling without injuring the skin (Dart & Dart, 2011). Polypropylene non-absorbable sutures and their withstanding tensile strength and low tissue reactivity allow it to perform as a desirable closure method for skin and thus in surgery. However, while polypropylene non-absorbable sutures pose many benefits, they also exemplify limitations. The cut ends of the suture are sharp and can cause irritation and
should multiple be used, it can amplify pain for patients (Suzuki & Resnik, 2018). The high memory of the suture can also decrease knot security as the material attempts to move back into its original shape (Tree, 2023). The effectiveness of non-absorbable sutures as a surgical wound closure method found in this study aligns with the results found by Sofii et al who investigated the effect of differing suturing materials for abdominal fascia wound closure on the collagen I/III expression ratio in rats (2020). Their results demonstrated that a significantly higher collagen I/III ratio was observed with monofilament non-absorbable sutures than multifilament absorbable sutures showing that non-absorbable sutures provided a more beneficial effect on decreasing the occurrence of an incisional hernia post-surgery (Sofii et al., 2020). This supports the findings of this current study that non-absorbable sutures are an effective surgical wound closure method. According to the results obtained, the absorbable suture was the closure method with the second highest tensile strength measured with an average of 187.55 Newtons and a standard deviation value of 75.90N. This is concurrent with previous research, where absorbable sutures are seen to retain their tensile strength for a limited time period as when inserted into the human body they lose most of their tensile strength in 1-3 weeks and are fully absorbed within 3 months (Bregstein et al., 2011). Comparatively, non-absorbable sutures retain their tensile strength for over 2-3 months (Chu, 2013). In the week where the pig skin was frozen and then defrosted, the absorbable sutures began to dissolve and thus its subsequent tensile strength was lower than that of the non-absorbable suture, even though it was higher when tested independently and without liquid present. The pig skin was frozen due to equipment technicalities that forbade testing to be undertaken immediately and thus freezing it ensured that the skin stayed viable to test in the future. Absorbable sutures provide many benefits for surgical wound closure as their material makeup, such as polymers, can easily dissolve into the body and do not need to be removed by a doctor (WebMed Editorial, 2021), making them ideal for surgical sites as the body can break them down over time. They can also be inserted into areas inside the body that surgeons would not be able to reach after the surgery is complete and
the topmost surgical entry point is sealed (WebMed Editorial, 2021). Some individual’s bodies may be extra-sensitive and recognise absorbable sutures as a foreign substance, thus reacting and delaying the healing process, a limitation of this method (WebMed Editorial, 2021). The results obtained in this investigation can be supported by a study undertaken to compare suture strengths for clinical applications (Vasanthan et al., 2009). Polyglactin (PG) and polyglactin-fast absorbing (PG-FA) were two absorbable sutures tested by combining them with sterile human saliva and human serum within this study. The results obtained demonstrated that between days 1 and 3 of testing, the tensile strength of both these absorbable suture types decreased significantly (Vasanthan et al., 2009), aligning with this investigation as the absorbable suture’s tensile strength was higher prior to its contact with and preliminary dissolving of the pig skin. The results obtained from the Post Hoc Tukey Test also support these findings where the pairwise comparison between the absorbable and non-absorbable sutures created the value Q = 8.44 (p = .00011), demonstrating they are statistically significant. By being statistically significant, it exemplifies the difference in the tensile strength of the two setups is not due to random chance.
Staples had the third highest tensile strength of all the methods tested with an average of 96.11 Newtons and a standard deviation of 26.08N. Like sutures, staples close surgical incisions, although they do not dissolve into the skin nor need to be tied manually to be inserted (Jewell, 2019). They do, however, need to be removed by a medical professional. Staples are inserted into the skin via a staple gun, decreasing closure time by 3-4 times compared to traditional sutures (Physician One, 2023), serving as a major advantage when dealing with large openings. Metal staples, however, cause a much greater risk of infection. In a study by Smith et al, the risk of developing a superficial wound infection after orthopaedic surgical procedures was over three times greater after staple closures than suture closures (2010). Surgical staples are commonly made of stainless steel and titanium (Turner, 2022), allowing for its high tensile strength. Plastic staples can also be utilised for patients with metal allergies or scar tissue remnants (Turner, 2022). Surgical staples compress
tissue, connecting two pieces of skin together with staggered rows of B-shaped staples (Turner, 2022). With this mechanism, the staple is not fully inserted through the skin like that of a suture, but rather sits on the skin’s surface, resulting in its reduced comparative tensile strength (Trott, 2012).
Surgical glue, also known as octyl-2-cyanoacrylate adhesives or liquid stitches, are commonly used by doctors to close wounds such as lacerations, incisions made during laparoscopic surgery, and wounds on the face (Ponkshe, 2023). Surgical adhesives provide many benefits, such as decreased infection rates, reduced time required in the operating theatre, minimised scarring, is child-friendly, allows patients to return to everyday life quickly, and no material is needed to be removed (Ponkshe, 2023). However, surgical glue is more expensive than sutures, individuals may have an allergic reaction to the glue, and the glue cannot be used for slow-healing processes (Ponkshe, 2023). As shown in this study, surgical adhesives have a moderate tensile strength as it forms a bond across wound edges (Doctors Express, 2021), but like staples, it does not penetrate all layers like a suture.
With the resources available in a high school setting, there were limitations that arose with experimental design throughout the investigation. The initial method to measure the tensile strength of each connection method was not successful as it was difficult to attach manual weights to the pig skin without compromising its integrity (i.e. tearing the skin to attach the hook would have caused an unfair test). Moreover, the pieces of skin cut to test were initially too large as the skin to connection method ratio was too great, testing the tensile strength of the skin itself rather than the tensile strength of the connection method. The length and width of the skin pieces were both minimised accordingly. Another limitation is that the movement utilised to test the tensile strength may not entirely reflect how a patient moves postsurgery. The investigation conducted only tested the tensile strength in one direction, while a patient would potentially have a much greater range of movements, such as lateral, diagonal, and twisting motions.
Freezing the skin for a week added the additional limitation that particularly targeted the nonabsorbable suture as they began to break down due
to the secretions in the skin and defrosting process, diminishing the ability for this setup to be at its tensile strength. Therefore, the value and data obtained would be lower than the actual tensile strength value for the absorbable suture setup.
In order to improve this investigation, preliminary testing of each surgical closure method in the pig skin could have been conducted prior to the actual experimentation in order to ensure that the apparatus was suitable for the investigation. Additionally, by conducting this experiment in a scientific laboratory, a Universal Testing Machine (UTM) could be accessed to test the tensile strength of each closure method more accurately than the home-made apparatus designed for this experiment.
Continued research into methods of closure may result in an eradication of infection rates, limited irritability to the patient (i.e., due to the ends of suture materials), as well as be able to withstand the multiple multi-directional movements patients undertake post-surgery. This would lead to less post-operative complications derived from wound closure methods and thus decrease additional rehabilitation programs or assistance required for patients, including closing wounds that may reopen due to patient movement.
Validity, accuracy, reliability
Validity
This experiment is valid because the scientific method was followed as all variables are kept constant (such as the size of the pig skin, the length of the incision, the laboratory conditions, and the time taken to test each connection method), except for the independent variable, which is the type of surgical connection method. A control was also included, which was no connection method holding the skin together. The control allows for a comparison with the other setups so that it is determined that it is the independent variable that causes the difference in the results. The method addressed the research question. The validity of this experiment, however, would have been improved through controlling the width of each piece of pig skin. While they were relatively similar at approximately 5mm, they were not the exact size due to them being offcuts which may have influenced the results obtained.
Accuracy
The experiment is accurate because measuring instruments were used that allowed precise data to be gathered. For example, rulers were used which measure in millimetre increments. The weight scale however was more prone to human error as it measured in half-kilogram increments and thus readings could not be done on a smaller and more precise scale. If we had used an electric weight scale which measured to grams and 3 decimal places, it would have made the experiment more accurate.
Reliability
The experiment is reliable due to the replicates undertaken for each closure technique, and an average and standard deviation value was calculated for each setup to minimise the effect of random errors. The repeats were checked to see if they were concurrent for each situation and no values obtained were ignored as no outliers were present within the data. The experimental setup for this investigation, however, would have been more reliable if repeats had been conducted at least 10 times before calculating an average for each setup.
>> Conclusion
When comparing methods for surgical wound closure, the most effective method was found to be non-absorbable sutures followed by absorbable sutures, staples, and finally super glue as the least effective method. All methods provided both advantages and disadvantages that are necessary when considering surgical wound closure, however the tensile strength in particular varies greatly between setups. Non-absorbable sutures are the most effective due to their consistently high tensile strength. Their formation via the catalytic polymerization of polypropylene also allows it to withstand biochemical processes, preventing its breakdown by the body’s own enzymes and immune system. Absorbable sutures are not as effective as non-absorbable sutures due to the fact that its tensile strength decreases as they begin to dissolve. Staples are the third most effective method of wound closure as they are not fully inserted through the skin like a suture but instead sit on the surface. Super glue was observed to be the least effective method of repair, also addresses only the top layer of the skin. Ultimately, while each setup can be utilised for post-operative surgical wound closure, setups such as the nonabsorbable and absorbable sutures are more ideal than staples and super glue as they provide the greatest guarantee of being able to withstand patient movement while simultaneously decreasing a patient’s vulnerability to pain and discomfort. Therefore, this reflects that the material used determines the tensile strength of the closure. •
References
Azmat, C. E., & Council, M. (2023). Wound Closure Techniques. In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/ books/NBK470598/
Baker, L. B. (2019, July 17). Physiology of sweat gland function: The roles of sweating and sweat composition in human health—PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/ PMC6773238/
Braune, S., Lendlein, A., & Jung, F. (2018). Hemocompatability of Biomaterials for Clinical Applications. https://www.sciencedirect. com/topics/medicine-and-dentistry/ thrombogenicity
Bregstein, J., Sonnett, F. M., & Roskind, C. G. (2011). Pediatric Secrets (5th ed.). https:// www.sciencedirect.com/topics/nursing-andhealth-professions/absorbable-suture Britannica. (2023a). Tensile strength | Definition, Unit, & Facts | Britannica. https:// www.britannica.com/science/tensile-strength Britannica. (2023b, June 9). Surgery | Definition, History, Type, & Techniques | Britannica. https://www.britannica.com/science/surgerymedicine
Chu, C. C. (2013). Biotextiles as Medical Implants. Woodhead Publishing. https:// www.sciencedirect.com/topics/engineering/ nonabsorbable-suture
Dart, A. J., & Dart, C. M. (2011). Comprehensive Biomaterials (Vol. 6). https://www. sciencedirect.com/topics/medicine-anddentistry/nonabsorbable-suture-material
Genoskin. (2020, March 4). Top differences between human and animal skin. Genoskin. https://genoskin.com/blog/2020/03/04/ human-vs-animal-skin/
Höer, J., Klinge, U., Schachtrupp, A., Töns, C., & Schumpelick, V. (2001). Influence of suture technique on laparotomy wound healing: An experimental study in the rat. Langenbeck’s Archives of Surgery, 386(3), 218–223. https:// doi.org/10.1007/s004230000196
Jewell. (2019, January 11). Surgical Staples: How They Are Placed, Removed, and Help You Heal. Healthline. https://www.healthline.com/ health/surgical-staples
Johns Hopkins. (2019, November 19). Purpose of Surgery. https://www.hopkinsmedicine. org/health/treatment-tests-and-therapies/ purpose-of-having-surgery
Kaihan Yao, Bae, L., & Yew, W. P. (2013). Postoperative wound management. Australian Family Physician, 42(12). https://www.racgp. org.au/afp/2013/december/post-operativewound-management
Karki, D. (2023). Physical Properties of Skin. https://www.thieme.in/image/catalog/ Agrawal_1_Chapter.pdf
Mountain View Hospital. (2020). The Evolution of Surgery. https://mountainview-hospital. com/about/newsroom/the-evolution-ofsurgery#:~:text=6500%20B.C.%3A%20 Evidence%20of%20trepanation,surgery%20 after%20a%20head%20wound.
Ponkshe. (2023, May 13). Stitches, Staples, or Skin Glue (Liquid Stitches): Which Do You Need? https://www.webmd.com/first-aid/ stitches-staples-glue
Rose, J., & Tuma, F. (2023). Sutures And Needles. In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/ NBK539891/
Schneider, A., & Feussner, H. (2017). Chapter 6—Classical (Open) Surgery. In A. Schneider & H. Feussner (Eds.), Biomedical Engineering in Gastrointestinal Surgery (pp. 221–267). Academic Press. https://doi.org/10.1016/B9780-12-803230-5.00006-3
Smith, T. O., Sexton, D., Mann, C., & Donell, S. (2010). Sutures versus staples for skin closure in orthopaedic surgery: Meta-analysis. The BMJ, 340, c1199. https://doi.org/10.1136/bmj. c1199
Sofii, I., Dipoyono, W., Prima, H., Sari, Y. M., Fauzi, A. R., & Gunadi. (2020). The effect of different suturing materials for abdominal fascia wound closure on the collagen I/III expression ratio in rats. Annals of Medicine and Surgery, 60, 106–109. https://doi. org/10.1016/j.amsu.2020.10.033
Summerfield, A., Meurens, F., & Ricklin, M. E. (2015). The immunology of the porcine skin and its value as a model for human skin. Molecular Immunology, 66(1), 14–21. https://doi. org/10.1016/j.molimm.2014.10.023
Suzuki, J. B., & Resnik, R. R. (2018). Misch’s Avoiding Complications in Oral Implantology. 402–439.
The Royal Childrens Hospital Melbourne. (2023). Clinical Guidelines (Nursing): Wound assessment and management. https:// www.rch.org.au/rchcpg/hospital_clinical_ guideline_index/Wound_assessment_and_ management/
Tree, T. N. (2023). Different Types of Nonabsorbable Sutures. Meril Life. http://www. merillife.com/blog/medtech/different-typesof-non-absorbable-sutures
Trott, A. T. (2012). Chapter 14—Tissue Adhesives and Alternative Wound Closure. In A. T. Trott (Ed.), Wounds and Lacerations (Fourth Edition) (pp. 192–205). W.B. Saunders. https://doi. org/10.1016/B978-0-323-07418-6.00014-9 Turner, T. (2022). Surgical Staplers and Staples – Surgery and Removal. Drugwatch. Com. https://www.drugwatch.com/surgicalstaplers/
Vasanthan, A., Satheesh, K., Hoopes, W., Lucaci, P., Williams, K., & Rapley, J. (2009). Comparing suture strengths for clinical applications: A novel in vitro study. Journal of Periodontology, 80(4), 618–624. https://doi. org/10.1902/jop.2009.080490
von Fraunhofer, J. A., Storey, R. S., Stone, I. K., & Masterson, B. J. (1985). Tensile strength of suture materials. Journal of Biomedical Materials Research, 19(5), 595–600. https://doi. org/10.1002/jbm.820190511
WebMed Editorial. (2021, June 8). What to Know About Absorbable Sutures. WebMD. https://www.webmd.com/a-to-z-guides/whatto-know-absorbable-sutures
Yepremyan, M., Yepremyan, A., & Bugarin, A. (n.d.). Surgical Glue: A Brief Overview. September 02, 2014. https:// austinpublishinggroup.com/biomedicalengineering/fulltext/ajbe-v1-id1020.php#Title
STAY UP TO DATE ON THE LATEST QUEENWOOD NEWS BY FOLLOWING US ON FACEBOOK, X, INSTAGRAM AND LINKEDIN.