JOURNAL OF CANADIAN HEALTHCARE ENGINEERING SOCIETY
45 Issue 2

45 Issue 2
Preparing for next disease outbreak requires harnessing emerging technologies, strategies for infection control
Update to nationally recognized standard Mighty metal helps prevent HAI outbreaks Hospital garden grows veggies and camaraderie




From patient positioning devices to instrument case carts, STERIS Instrument Repair Services provide extensive repair offerings to your facility every step of the way.
• Our repair technicians ensure your positioning devices function effectively.
• Repair services for surgical retractor systems enhance visualization and accessibility to organs during operations, ensuring optimal outcomes.

• Comprehensive repair services for surgical instruments utilized in patient procedures, from general maintenance to complex repairs.
• Regular maintenance of case carts and OR equipment ensures smooth transport of instruments to and from the operating room.

EDITOR/RÉDACTRICE Clare Tattersall claret@mediaedge.ca
PUBLISHER/ Jake Blanchard ÉDITEUR DU GROUPE jakeb@mediaedge.ca
PRESIDENT/PRÉSIDENT Kevin Brown kevinb@mediaedge.ca
SENIOR DESIGNER/ Annette Carlucci CONCEPTEUR annettec@mediaedge.ca GRAPHIQUE SENIOR
GRAPHIC DESIGNER/ Thuy Huynh-Guinane GRAPHISTE roxyh@mediaedge.ca
PRODUCTION Ines Louis COORDINATOR/ inesl@mediaedge.ca COORDINATEUR DE DE PRODUCTION
CIRCULATION MANAGER/ Adrian Holland DIRECTEUR DE LA circulation@mediaedge.ca DIFFUSION
CANADIAN HEALTHCARE FACILITIES IS PUBLISHED BY UNDER THE PATRONAGE OF THE CANADIAN HEALTHCARE ENGINEERING SOCIETY.
SCISS JOURNAL TRIMESTRIEL PUBLIE PAR SOUS LE PATRONAGE DE LA SOCIETE CANADIENNE D'INGENIERIE DES SERVICES DE SANTE.
CHES SCISS
PRESIDENT Jim McArthur
VICE-PRESIDENT Kate Butler
PAST PRESIDENT Craig B. Doerksen
TREASURER Reynold J. Peters
SECRETARY Paul Perschon
20 Microbe-slaying Copper
High-touch surfaces with chemical element selfsanitize, reduce incidence of HAIs
Building on a Legacy CSA Z8000:24 charts new course in infection control
Cultivating Health and Teamwork Nova Scotia hospital’s maintenance department builds unity, community with vegetable garden
Reproduction or adoption of articles appearing in Canadian Healthcare Facilities is authorized subject to acknowledgement of the source. Opinions expressed in articles are those of the authors and are not necessarily those of the Canadian Healthcare Engineering Society. For information or permission to quote, reprint or translate articles contained in this publication, please write or contact the editor.
Canadian Healthcare Facilities Magazine Rate
Extra Copies (members only)
Canadian Healthcare Facilities (non members)
Canadian Healthcare Facilities (non members)
$25 per issue
$30 per issue
$80 for 4 issues
A subscription to Canadian Healthcare Facilities is included in yearly CHES membership fees.
EXECUTIVE DIRECTOR Tanya Hutchison
CHAPTER CHAIRS
Newfoundland & Labrador: Colin Marsh
Maritime: Steve Smith
Ontario: John Marshman
Quebec: Mohamed Merheb
Manitoba: Stephen R. Cumpsty
Saskatchewan: Melodie Young
Alberta: James Prince British Columbia: Mitch Weimer
FOUNDING MEMBERS
H. Callan, G.S.
J. Cyr, S.T. Morawski CHES
4 Cataraqui St., Suite 310, Kingston, Ont. K7K 1Z7 Telephone: (613) 531-2661 Fax: (866) 303-0626 E-mail: info@ches.org www.ches.org Canada
No. 40063056 ISSN # 1486-2530
La reproduction ou l’adaptation d’articles parus dans le Journal trimestriel de la Société canadienne d’ingénierie des services de santé est autorisée à la condition que la source soit indiquée. Les opinions exprimées dans les articles sont celles des auteurs, qui ne sont pas nécessairement celles de la Société canadienne d’ingénierie des services de santé. Pour information ou permission de citer, réimprimer ou traduire des articles contenus dans la présente publication, veuillez vous adresser à la rédactrice.
Prix d’achat du Journal trimestriel
Exemplaires additionnels (membres seulement)
Journal trimestriel (non-membres)
$25 par numéro
$30 par numéro
Journal trimestriel (non-membres) $80 pour quatre numéros
L’abonnement au Journal trimestriel est inclus dans la cotisation annuelle de la SCISS.

IT’S HARD TO believe it has been five years now since the World Health Organization (WHO) declared the COVID-19 outbreak a global pandemic. Government-mandated lockdowns almost immediately followed to prevent the spread of the virus that had already infected more than 118,000 in 114 countries and resulted in nearly 4,300 deaths. These numbers, of course, only reflected reported cases; the reality is many more had contracted the disease and died by this point in time. Since that fateful day in March 2020, Canada’s healthcare systems have adapted and evolved at an unprecedented rate. But there’s always more work to be done.
While the pandemic is now in the rearview mirror, it has not been forgotten as another worldwide health emergency is very likely to occur. Some experts predict it could happen within the next 30 years given the rise in infectious diseases. Preparedness is therefore key.
This brings me to this issue’s lead article, penned by members of Canada’s engineering and design communities who the International Federation of Healthcare Engineering can call upon to assist the WHO with delivering urgent response healthcare design services. Its focus is the WHO and World Food Programme’s Initiate2 project to develop a treatment module that will be the first response globally for infectious diseases in their earliest stages.
Infection prevention and control is a core theme of the spring edition. Other articles explore the efficacy of copper in killing bacteria and viruses, such as healthcare-acquired infections, and advancements in the metal’s use; mechanical, electrical and plumbing strategies for infection control; innovations in infection prevention during construction; and the long-awaited third edition of CSA Z8000, Canadian Health Care Facilities, which was released just last year and has a new safety-first focus on infection control.
Rounding out this jam-packed first issue of 2025, Ontario’s Oak Valley Health walks through a project at Markham Stouffville Hospital that has improved power systems to ensure the healthcare facility continues to run smoothly in the event of power outage. Keeping with the topic of health and safety, Toxic Grime explores the complex challenges posed to air quality by wildfire smoke, the limitations of conventional air filters and a novel solution for improving air filtration. Finally, we close with a feel-good story from Nova Scotia Health about a vegetable garden planted and tended by the maintenance and operations team at St. Martha’s Regional Hospital.
Clare Tattersall claret@mediaedge.ca
The 2025 CHES National Conference will be held in Calgary, Alberta, at the BMO Centre-Stampede Park, September 14-16, 2025. BMO Centre-Stampede Park is conveniently located in the downtown core and close to local amenities.
The theme of the 2025 conference is “Transforming Healthcare Together: Empowering Teams, Inspiring Creativity, Unleashing Knowledge”
The CHES 2025 Education Program is well underway and will once again feature dual tracks with talks on relevant industry topics from high-profile experts in the field.
We are excited to announce our keynote speaker is Ross Bernstein He's a best-selling author of nearly 50 sports books, a peak-performance business speaker and proud member of the Speaker Hall of Fame who will get us all thinking differently about how we can raise our game to the next level
There are plenty of social activities to network! The Great CHES Golf Tournament is tentatively scheduled to take place at the Kananaskis Country Golf Course on Sunday, September 14, 2025.
Join us for the CHES President’s Reception and Gala Banquet again in 2025 at BMO CentreStampede Park The banquet will celebrate the accomplishments of our peers with the 2025 Awards presentations, while enjoying great food and entertainment with friends.
A block of rooms has been reserved at the Calgary Marriott Downtown and there is a conference rate of $245 single/double, plus applicable taxes.


ALONG WITH THE regular challenges of operating our healthcare facilities, economic uncertainty looms with respect to trade tariffs. On March 4, tariffs were issued on Canada. Two days later, the U.S. President temporarily waived the levies on some products. Then, on March 7, he threatened other tariffs on top of those announced for aluminum and steel to take effect mid-March.
How do tariffs affect procurement of equipment and systems for current projects already underway, or planning for future projects? How will the healthcare supply chain be impacted? How will our governments mitigate the impact on healthcare and other industries?
There could be very trying times ahead.
On a personal note, January was a milestone month for me. First, I turned 65 and attained the status of senior citizen. Second, after more than 46 years in the workforce, the last 35 of which were spent in healthcare, I retired from my position as director of facilities at Albright Manor. This is a position that I held for 33 years. As with many things in healthcare, changes occur for different reasons and it was time to hang up the skates. CHES is near and dear to my heart and being part way through my tenure as CHES president, I plan to fulfill my commitment and serve my entire term and then that as past president.
With the arrival of spring, I look forward to attending CHES chapter conferences in Manitoba, the Maritimes, Quebec, Ontario and British Columbia. Planning is in full swing for the 2025 CHES National Conference in Calgary, Sept. 14-16, led by conference chair Paul Perschon and his amazing team of volunteers.
I am also eagerly awaiting to attend the International Federation of Healthcare Engineering Congress in Antwerp, Belgium, in May, and the ASHE Healthcare Facilities Innovation Conference in Columbus, Ohio, in July. We have developed an excellent reciprocal relationship with the American Society of Healthcare Engineering. A few of its executive members will be attending our national conference in Calgary.
Thank you to all CHES members for your continued support and everything you do to make our healthcare facilities operational, safe and comfortable for those who enter.
Jim McArthur CHES National president
Members of the Canadian Healthcare Engineering Society can earn free continuing education units (CEU) by reading the Spring 2025 issue of Canadian Healthcare Facilities and passing a quiz based on articles in the issue. Once you’ve read the issue from cover to cover, simply go online to https://www.surveymonkey.com/r/73PY3G7 to take the quiz. CHES members who pass the quiz will be able to claim one contact hour (0.1 CEU) on their CanHCC or CCHFM certificate renewals.








CHES B.C. continues to work through the process of incorporation. We are finalizing the bylaw revision to meet the needs of the chapter, national organization and province’s Societies Act. Our bylaw committee has been delayed slightly but we continue to strive for incorporation this year.
Planning for our spring conference in Penticton, June 1-3, is well underway. The theme is Healthcare Facilities Beyond Bricks and Mortar. As demands on our facilities grow increasingly complex, the conference looks to explore a vital evolution in healthcare infrastructure. The event will delve into how healthcare environments extend beyond physical structures to embody comprehensive systems of care, innovation and resilience. The education program saw a record number of submissions. Designed to help chapter members excel in their work life, it brings together leaders in healthcare engineering, sustainability, construction, facility management and other disciplines to discuss the holistic role modern healthcare facilities play. Speakers will cover pressing issues like energy efficiency, carbon reduction, digital integration, patient-centred design and pandemic preparedness. Participants will explore emerging technologies, best practices and advanced energy solutions that drive operational efficiencies while fostering healthier, more sustainable spaces for patients and staff alike. The trade show is sold-out with a wait list. I’d like to thank the conference planning committee for their hard work to make the event a success.
CHES B.C. will once again host the Canadian Healthcare Construction Course in November.
The chapter offers a wide array of beneficial opportunities. Members receive complimentary CHES webinar program access, as well as educational sponsorship to help with professional development. Every year we receive some applications but we rarely reach the maximum limit, so please check the B.C. chapter page on the CHES website and reach out if looking for educational funding. Education assistance bursaries are up to $1,000 for CHES B.C. members. The chapter also has a number of perpetual educational bursaries at various provincial post-secondary institutions to help the next generation.
—Mitch
Planning is well in hand for the chapter’s spring education day April 15, at the Victoria Inn in Winnipeg. The theme is Navigating Aging Infrastructure. Registration opened Feb. 21. Most sponsorships have been secured and the schedule is posted on the CHES website. Sessions are as follows:
1. Provincial Healthcare Infrastructure Deficit. Speaker: Ken Klassen, chief executive operations officer, Shared Health.
2. CSA Z8004:22: Long-term Care Home Operations and Infection Prevention and Control. Speaker: Craig Doerksen, executive director, capital and facilities management, Shared Health.
3. Clinical Engineering and Equipment Management/Replacement. Speakers: Agustina Krivoy, director, provincial clinical engineering, Shared Health; Sarah Kelso, regional clinical engineer, Shared Health; and Chris Bzovey, regional clinical engineer, Shared Health.
4. Sustainability and Energy Savings. Speaker: Myles Boonstra, director, environmental sustainability and energy, Shared Health.
5. Carbon Reduction and Commissioning. Speakers: Phil Dompierre, principal, Crosier Kilgour; Matt Froese, associate, Crosier Kilgour.
6. Retrofit Operating Room Opportunities. Speakers: Corey Nation, manager, engineering division, EH Price; David Enns, sales engineer, EH Price; Jordan Enns, product manager, critical environments, EH Price.
7. Roundtable discussion. Host: Craig Doerksen, executive director, capital and facilities management, Shared Health. Panelists: Chet Mohabir, director, Grace Hospital; Brennan Yanchycki, facility manager, Northern Regional Health Authority; Kevin Shmon, director, Interlake-Eastern Regional Health Authority; Brennan Laidlaw, manager, Mikkelsen Coward; Steven McMillan, associate, mechanical, MCW Group of Companies.
Nominations for the Manitoba chapter awards have closed. There are two awards: Excellence in Project Management and Excellence in Facilities Management.
CHES Manitoba will host the Canadian Healthcare Construction Course in conjunction with the Winnipeg Construction Association Nov. 4-5.
The Manitoba chapter will have a stable executive this year and is not expecting any changes.
—Stephen R. Cumpsty, Manitoba chapter chair

As we move forward into 2025, CHES Quebec continues to strengthen partnerships and expand training opportunities. The first quarter has been focused on key initiatives, including collaboration with Santé Québec, preparations for our chapter conference on May 7, and expansion of the Canadian Healthcare Construction Course (CanHCC).
With the creation of Santé Québec, all healthcare authorities are now under one employer. CHES is working to establish relationships with this new entity to ensure continued support for healthcare facility professionals. We have initiated discussions to explore collaboration opportunities.
Planning for the spring chapter conference in Montreal is well underway. We have secured expert speakers, finalized key topics and launched marketing efforts to drive engagement. Sponsorship outreach is ongoing to enhance the event’s reach and impact.
The CanHCC is expanding in 2025, with two scheduled sessions — one in April, the other in December — both in partnership with the Association de la Construction du Québec. Additionally, CHES is committed to translating and adapting the CanHCC into French to be ready for delivery in 2026.
—Mohamed Merheb, Quebec chapter chair
Alors que nous avançons en 2025, la SCISS Québec continue de renforcer ses partenariats et d’élargir ses opportunités de formation. Le premier trimestre a été axé sur des initiatives clés, notamment la collaboration avec Santé Québec, la préparation de notre conférence de chapitre du 7 mai, et l’expansion du Canadian Healthcare Construction Course (CanHCC).
Avec la création de Santé Québec, toutes les autorités de santé sont désormais regroupées sous un seul employeur. La SCISS travaille à établir des relations avec cette nouvelle entité afin d’assurer un soutien continu aux professionnels des infrastructures de santé. Des discussions seront faites pour explorer des opportunités de collaboration.
La planification de la conférence SCISS Québec à Montréal progresse bien. Nous avons sécurisé des conférenciers experts, défini les sujets clés et lancé des efforts marketing pour maximiser l’engagement. La recherche de commandites se poursuit afin d’accroître la portée et l’impact de l’événement.
Le CanHCC prend de l’ampleur en 2025 avec deux sessions prévues: l’une en avril et l’autre en décembre, toutes deux en partenariat avec l’Association de la Construction du Québec (ACQ). De plus, la SCISS s’engage à traduire et adapter le cours en français afin qu’il soit prêt pour une prem-ière session en 2026.
—Mohamed Merheb, chef du conseil d’administration du Québec
Planning is underway for the spring Maritime conference. It will be held May 4-6, at the Delta Beausejour in Moncton, N.B. The theme is Healthcare Infrastructure for a Resilient and Safe Environment. Speaker sessions have been confirmed. We continue to recruit exhibitors and sponsors.
The Maritime chapter is planning to host the Canadian Healthcare Construction Course in Halifax, Oct. 22-23.
Although CHES Maritime has a strong membership base in Nova Scotia and New Brunswick (approximately 280 members), we notably lack membership and leadership from P.E.I. The chapter is actively seeking members and executive representation from this province.
The Maritime chapter worked with IWK Health to submit an article about accessibility improvements in healthcare to CHES’s quarterly journal. It will be published in the summer edition.
An announcement about the 2025 Per Paasche educational bursary has been prepared and will be posted shortly on CHES’s website. All chapter members who are in good standing as well as their immediate family members (children, grandchildren, nieces, nephews and spouses) are eligible to apply for this $1,000 educational bursary.
CHES Maritime continues to offer several financial incentives to members, such as the Per Paasche bursary, contribution to Canadian Certified Healthcare Facility Manager exam fees, spring and fall education days, and other benefits.
—Steve Smith, Maritime chapter chair
The Alberta chapter is excited to provide an update on preparations for the 2025 CHES National Conference, which will be hosted in Calgary. The large planning committee is enthusiastic about the progress made so far and is confident the conference will be a resounding success. We have secured several venues that will cater to the diverse needs of our attendees. The venues are equipped with state-of-the-art facilities to enhance the conference experience. A roster of speakers who are leaders in their fields is lined up. Their insights and expertise will undoubtedly enrich the event. A variety of engaging companion program choices have been curated to ensure all participants, including accompanying guests, have a fulfilling experience. These programs include wellness activities and local excursions. Attendees will have the opportunity to participate in one of two informative and enjoyable tours. These tours are designed to showcase the best of Calgary’s healthcare environment and provide valuable insights into healthcare engineering advancements. A superb golf location has been secured, adding a recreational dimension to the conference that golfers around the world would envy.
CHES Alberta will soon be sending information about chapter elections. Please keep an eye out for this important communication.
Alberta chapter executive members are planning to attend other provincial conferences, including those in Saskatchewan, British Columbia and Ontario. This will allow us to support our colleagues and learn from the great ideas being implemented across the country.
—James Prince, Alberta chapter chair


It’s full-speed ahead with planning our fall conference to be held Oct. 26-27. This year’s theme is Reimaging Healthcare Facilities, which involves transforming the way we design and use physical spaces to improve patient care and outcomes and create healthcare environments that are more efficient, effective and responsive to the needs of patients and healthcare providers alike. The format for the conference will be similar to that of last year. 2024’s conference was another record-breaking event. The bar continues to be set higher every year. Although we are one of the smaller chapters, we deliver a large conference.
Chapter membership has seen a slight increase and we are actively working on recruitment and retention. Growth in the number of infection prevention and control professionals and people from the province’s capital engineering division is indeed a positive shift. It highlights the evolving nature of CHES and its appeal to a broader range of professionals beyond just those in facilities management. Our efforts to engage vendors, suppliers, consultants and other multidisciplinary team members are commendable. This inclusive approach can foster a richer exchange of ideas and best practices, ultimately benefitting the entire healthcare community. Financially, the chapter is in a solid position. The executive team wishes to invest in the betterment of our members. Whether that is providing education opportunities, sending additional members to the CHES National conference or paying for more webinars, we want to give back to our membership. For this year’s national conference, the chapter will sponsor our full executive team to attend and promote not only St. John’s for the 2026 CHES National Conference, but Newfoundland and Labrador. These initiatives can help foster a supportive and enriching environment for our members.
—Colin Marsh, Newfoundland & Labrador chapter chair
The Ontario chapter executive continues to meet quarterly via virtual means, focused on membership development and member benefits, including bursaries, the Young Professionals Grant and our education events. In late November, we held our first in-person strategy session in Toronto. Thanks to Gary at the Hospital for Sick Children for facilitating a venue.
Planning is well-advanced for our spring conference in my home town of Kitchener. The theme is Engineering Intelligence into Healthcare Facilities. Building on the successes of Blue Mountain and Windsor, we are looking forward to bringing the CHES Ontario family together for more engaging and educative sessions.
The chapter executive continues to engage in networking and advocacy opportunities. I am attending the ASHE Region 6 conference in Rochester, Minn., in early April, to engage with our extended family south of the border.
—John Marshman, Ontario chapter chair
Canadian Healthcare Engineering Society Société canadienne d'ingénierie des services de santé
CHES is seeking both sponsors and candidates for the 2025 Young Professionals Grant. The application forms for Sponsors and Candidates are available on the CHES Website.
Call for Sponsors:
• The YPG sponsorship application form must be completed by the sponsoring organization/company and submitted to the CHES National Office.
• CHES National Office will invoice sponsoring organization/company for $2,500 once candidate applications have been received and approved.
Call for Candidates:
• Young professionals who are or will become architects, engineers (i.e. mechanical, electrical, power, and civil, etc.), technicians or similar technical disciplines are eligible.
• Eligible candidates are those working within a healthcare organization or a company supplying goods or services to healthcare facilities or organizations.
• Eligible candidates must be working in the healthcare field for less than 5 years.
• The YPG application form must be completed by the eligible candidate and submitted to the CHES National Office. In this form, the eligible candidate will be required to provide information on their recent employment and future career aspirations.
• Confirmed candidates will receive complimentary registration for the 2025 National Conference and complimentary membership for the remainder of the 2025-2026 membership year.
For Nomination Forms, Terms of Reference, criteria and past winners www.ches.org / About CHES / Awards
Send nominations to: CHES National Office info@ches.org
By/Par Meagan Webb, Kyle Basilius & Troy Savage
At the beginning of the COVID-19 pandemic, the World Health Organization (WHO) established a help desk to provide design assistance to countries and contacted the International Federation of Healthcare Engineering (IFHE), an official WHO partner, for technical support. The IFHE community responded, identifying a pool of more than 150 potential volunteers, including architects and engineers, across 19 teams, who were tasked with quickly developing plans for COVID-19 facilities and ultimately designed dozens of projects. The WHO subsequently evolved the COVID-19 help desk into the Téchne, the technical science for health network, of which IFHE is a member. IFHE volunteer teams continue to support WHO with assistance beyond COVID-19 support.
AN INNOVATIVE PROJECT
With the rising threat of infectious diseases, ensuring operational readiness and timely response is of paramount importance. To address
L’OMS a créé un service d’assistance au début de la pandémie de COVID-19. Ce service visait à aider les pays dans leurs projets de conception. L’organisation a contacté l’International Federation of Healthcare Engineering (IFHE), son partenaire officiel, pour obtenir un soutien technique.La communauté de l’IFHE a répondu présente. Elle a identifié plus de 150 bénévoles potentiels, comprenant des architectes et des ingénieurs. Ces professionnels ont formé 19 équipes chargées d’élaborer rapidement des plans pour les installations COVID-19. Leurs efforts ont abouti à la conception de dizaines de projets. L’OMS a par la suite réorganisé le service d’assistance COVID-19, qui est devenu le Téchne, c’est-à-dire le Technical science for health network. L’IFHE fait partie de ce réseau. Ses équipes de bénévoles continuent d’apporter leur soutien à l’OMS, dépassant le cadre initial de l’aide liée à la COVID-19.
this, WHO and the World Food Programme (WFP) jointly launched Initiate2 in June 2021 — a five-year initiative aimed at developing technical innovations, such as medical facilities, temporary medical installations or laboratory disease-specific facilities, and providing training and simulations for improved readiness and response capabilities in health emergencies involving infectious diseases. Co-steered by WFP and WHO, and operationally based at the United Nations Humanitarian Response Depot (UNHRD) in Brindisi, Italy, Initiate2 brings together multiple humanitarian actors, non-governmental organizations, United Nations (UN) agencies and member states, as well as research and academic institutions, with a shared mission to forge innovative and standardized solutions for health emergencies’ readiness and response.
Epidemics of infectious diseases are occurring more often and spreading faster and farther than ever before in many regions of the world. The background factors of this threat include biological, environmental and lifestyle changes, among others. A potentially fatal combination of newly discovered diseases and the re-emergence of many long-established ones demands urgent responses in all countries. Planning and preparation for epidemic prevention and control are essential.
The design of infectious diseases treatment centres for health emergency response has improved considerably in recent years. Centres evolved from pure isolation units to patient-focused treatment centres developed to enhance the quality of medical care, infection prevention and control (IPC), patient comfort and community acceptance. However, the construction of such centres may require several weeks, and the first phases of an emergency are still handled with simple infrastructure, which does not allow
Face à la menace croissante des maladies infectieuses, l’OMS et le Programme alimentaire mondial (PAM) ont lancé Initiate2 en juin 2021. Cette initiative quinquennale vise à développer des innovations techniques, telles que des installations médicales temporaires et des laboratoires spécialisés pour certaines maladies. Elle propose également des formations et des simulations pour renforcer les capacités de préparation et de réponse aux urgences sanitaires. Codirigée par le PAM et l’OMS, Initiate2 opère depuis le Dépôt de réponse humanitaire des Nations Unies (UNHRD) à Brindisi, en Italie. L’initiative rassemble divers acteurs humanitaires, des ONG, des agences de l’ONU, des États membres, des institutions de recherche et des établissements universitaires. Leur mission commune: forger des solutions innovantes et standardisées pour affronter les urgences sanitaires impliquant des maladies infectieuses.
Les épidémies de maladies infectieuses surviennent plus fréquemment, se propagent plus vite et plus loin que jamais dans de nombreuses régions du monde. Des changements biologiques, environnementaux et de mode de vie constituent les principaux facteurs de cette menace. Une combinaison redoutable émerge: de nouvelles maladies apparaissent tandis que d’anciennes affections reviennent en force. La préparation à la prévention et au contrôle des épidémies devient donc essentielle pour protéger les populations face à cette réalité sanitaire inquiétante.
La conception des centres de traitement des maladies infectieuses pour les urgences sanitaires s’est nettement améliorée récemment. Ces centres ont évolué des simples unités d’isolement vers des installations centrées sur le patient. Ils visent maintenant à offrir des soins médicaux de qualité, une meilleure prévention des infections, plus de confort pour les malades et une meilleure acceptation communautaire. Toutefois, leur construction nécessite plusieurs semaines. Les premières phases d’urgence s’appuient encore sur des infrastructures basiques qui limitent la qualité des soins et compromettent la sécurité du personnel soignant.
Initiate2 cherche à réduire ces retards en offrant des soins médicaux de haut niveau dès le début d’une épidémie. L’initiative propose un centre de traitement des maladies infectieuses à déploiement rapide, facilement transportable, extensible et autonome. Ce centre peut fonctionner seul ou s’intégrer aux services de santé locaux existants. Cette approche diminue considérablement le temps d’ouverture d’un centre de traitement,



for provision of the most advanced medical care available and safety for staff.
Initiate2 looks at how to mitigate these delays by providing the highest level of medical care available at the outset of an outbreak of an infectious disease and a rapid deployable, easily transportable, extendable, self-contained and self-sufficient treatment centre for infectious diseases — one that can be used either as a standalone solution or can integrate sustainably into on-site health services. This reduces the time needed to open an infectious disease treatment centre, thereby enhancing the initial containment phase and reducing the possible spread of outbreaks. It also ensures standardization across emergency actors to offer patients the same quality of care, comfort and IPC standards.
In 2022, the WHO Téchne reached out to IFHE for technical support on the first Initiate2 project: the infectious disease treatment module (IDTM). IFHE volunteers included representatives from Parkin Architects, HH Angus and Associates, Mazzetti and LS3P, who contacted Carleton University in Ottawa for additional expertise. The chosen team has deep experience in the design of healthcare facilities across the globe, as well as in implementing systems design to support infection control procedures in healthcare settings. Given this, the IFHE team’s most recent involvement was well-suited to the healthcare team’s strengths.
The IFHE team was part of a larger design group including WHO and WFP architects and engineers, as well as the WHO Téchne members Politecnico di Torino, Carleton University and University of Toronto. The collective design team designed and supported the
améliorant ainsi le confinement initial et limitant la propagation des épidémies. Elle garantit également une standardisation entre les différents intervenants d’urgence, assurant à tous les patients la même qualité de soins, le même confort et les mêmes normes de prévention des infections.
En 2022, Téchne a demandé l’appui technique de l’IFHE pour son premier projet Initiate2: l’Infectious Disease Treatment Module (IDTM). L’équipe de bénévoles de l’IFHE incluait des membres de Parkin Architects, HH Angus and Associates, Mazzetti et LS3P. Ces experts ont contacté l’Université Carleton pour obtenir des compétences supplémentaires. L’équipe sélectionnée possède une riche expérience dans la conception d’établissements de santé mondiaux et dans l’implémentation de systèmes de contrôle des infections. Cette récente collaboration correspondait parfaitement aux compétences de l’équipe spécialisée en soins de santé.
L’équipe de l’IFHE faisait partie d’un groupe de conception plus vaste. Ce collectif comprenait des architectes et ingénieurs de l’OMS et du PAM, ainsi que des membres de Téchne de l’OMS, du Politecnico di Torino et des universités Carleton et de Toronto. Le groupe a conçu la première version de l’IDTM et supervisé son processus d’appel d’offres et de prototypage. Le module a été livré et testé au centre de formation de l’UNHRD en juin 2023. Cet essai s’est déroulé lors d’une simulation structurée réunissant 75 participants de 25 organisations membres d’Initiate2. L’exercice visait à évaluer le fonctionnement du système dans des conditions de stress, impliquant divers professionnels de l’intervention d’urgence.
tendering and prototyping process of the first iteration of the IDTM. This was delivered and tested at the UNHRD training centre in June 2023, during a structured simulation exercise organized with Initiate2 members — 75 participants from 25 organizations. The objective was to assess the functionality of the system in a stress scenario, involving various professional profiles related to emergency response.
The focus of the IDTM is to allow stakeholders to rapidly deploy and operate treatment modules in emergency situations to safely treat the first patients affected by infectious diseases and protect the healthcare workers who are treating them. However, developing a treatment module that is rapidly deployable with no specialized tools, easily transportable, adaptable to different climates, accepted by the local community, safe for healthcare workers and suitable to respond to an unknown infectious disease outbreak is an extraordinary challenge.
The IDTM was designed to be a solution for all Initiate2 partners, with the aim of creating a human-centred patient care area with a front porch to allow interaction between patients, family and community members without the risk of contamination. A two-sided transfer screen was designed for optimal patient care access from a staff-safe green zone, with articulating gloves on both sides of the patient’s head, allowing for stabilization of the patient before having to don personal protective equipment (PPE) and enter the infected patient’s room for further medical care. It is an in-field innovation.
The inflatable IDTM structure was compartmentalized to separate staff and patient areas while maintaining necessary sightlines and quick response to patients by staff through a transparent screen, without their needing to don full PPE first. In addition to the physical barrier, the separation is also supported by directional airflow. The structure of each module and inserts allows for flexibility and the ability to accommodate more patients if needed.
The design team supported the refinement of the design by addressing opportunities for improvement that were identified during medical and technical testing. These improvements were included in the second prototype tested in Ghana, lastNovember.
Meagan Webb is a principal, senior mechanical engineer and regional leader at HH Angus and Associates. Kyle Basilius is a principal at Parkin Architects and the technical lead architect for the World Health Organization (WHO) and World Food Programme’s Initiate2 project. Troy Savage is a manager of strategic projects and innovation at Mazzetti. Meagan, Kyle and Troy are among the more than 150 engineers and designers who the International Federation of Healthcare Engineering can call on to assist the WHO with delivering urgent response healthcare design services.

L’IDTM vise à permettre aux intervenants de déployer et d’opérer rapidement des modules de traitement en situation d’urgence. Son but est de soigner en toute sécurité les premiers patients atteints de maladies infectieuses et de protéger le personnel soignant. Toutefois, développer un tel module représente un défi considérable. Il doit être rapidement déployable sans outils spécialisés, facilement transportable, adaptable à différents climats, accepté par les communautés locales, sécuritaire pour les professionnels de santé et capable de faire face à une épidémie de maladie infectieuse inconnue.
L’IDTM a été conçu comme une solution collaborative pour tous les partenaires d’Initiate2. Le module crée une zone de soins centrée sur le patient avec un sas d’entrée permettant des interactions sécurisées entre patients, familles et communauté. Les concepteurs ont développé un écran de transfert à double face offrant un accès optimal aux soins depuis une zone verte sécurisée pour le personnel. Des gants articulés placés des deux côtés de la tête du patient permettent de stabiliser celui-ci avant que le personnel n’enfile son équipement de protection et n’entre dans la chambre pour prodiguer des soins supplémentaires. Cette innovation pratique répond aux défis concrets du terrain.
L’IDTM utilise une structure gonflable compartimentée qui sépare les zones du personnel et des patients. Cette conception préserve la visibilité nécessaire et permet une réaction rapide aux besoins des malades grâce à un écran transparent. Le personnel peut ainsi intervenir sans devoir enfiler un équipement de protection complet au préalable. La séparation entre les zones est renforcée par un flux d’air directionnel, complétant la barrière physique. La structure modulaire et ses insertions offrent une grande flexibilité, permettant d’augmenter la capacité d’accueil si la situation l’exige.
L'équipe de conception a contribué à affiner la conception en exploitant les pistes d'amélioration identifiées lors des tests médicaux et techniques. Ces améliorations ont été intégrées au deuxième prototype testé au Ghana en novembre dernier.
Meagan Webb dirige HH Angus and Associates comme ingénieure mécanique principale et responsable régionale. Kyle Basilius travaille comme directeur chez Parkin Architects et supervise le volet technique du projet Initiate2 de l’OMS et du Programme alimentaire mondial. Troy Savage gère les projets stratégiques et l’innovation chez Mazzetti. Ces trois experts font partie des quelque 150 ingénieurs et concepteurs mobilisables par l’International Federation of Healthcare Engineering pour aider l’OMS à développer des services de conception pour les soins de santé d’urgence.
By Andre Saker & Allan Kelly

Oak Valley Health, a community healthcare organization in Ontario, serves patients through Markham Stouffville Hospital, Uxbridge Hospital and the Reactivation Care Centre. In 2022, following a series of severe weather storms in summer, the Markham site, consisting of two buildings — building A, constructed in 1988, and building B, built in 2012 — experienced numerous hydro interruptions. Over three months, there were more than 17 power failures, which affected equipment, staff morale and patient care. In response, Oak Valley Health launched a project to improve its power systems and ensure the hospital could continue to run smoothly in the event of future outages. Implementing a power redundancy project presented a myriad of challenges that had to
be navigated to ensure successful execution. The technical complexity involved in integrating components, such as uninterruptible power supplies (UPS), automatic transfer switches (ATS) and backup generators, demanded meticulous planning and expertise. Substantial upfront costs associated with purchasing and installing specialized equipment posed financial constraints that had to be carefully managed. The impact of pandemic-related backorder timelines exacerbated potential delays in acquiring necessary components. Space limitations within the facilities necessitated innovative solutions for equipment placement. Maintenance of redundant power systems required regular inspections and testing to ensure reliability during emergencies. Adequately training staff to operate and trou-
bleshoot these systems effectively, as well as integrating new systems with existing infrastructure, navigating regulatory compliance and managing associated risks added to the complexity of the project.
In 2011, during the new build, two -225kva UPS were installed that supplied power to the IT critical infrastructure on two different buses. This was very inefficient since the UPS were only operating at 10 per cent capacity at the best of times.
Through redesign of the infrastructure, the UPS are now operating at 30 per cent capacity. The UPS is the main source of power for all critical loads. Should the UPS fail, batteries are the second line of defence. If the batteries reach 80 per cent capacity, the maintenance bypass switches on. In the event the UPS suf-
fers catastrophic failure, it is backed up by a closed transition ATS, bringing seamless power to critical care areas without even a blip in power. To protect these areas if maintenance needs to be done on the ATS, there is a double pole safety switch that transfers power back to the main switchboard.
The project incorporated several critical measures to enhance the hospital’s reliability and efficiency, particularly in key areas. Redundancy was implemented in the operating rooms (ORs) and four emergency trauma and resuscitation rooms to ensure uninterrupted operations during power disruptions. All isolated power receptacles, booms and operating theatre lights are now backed by a UPS, guaranteeing consistent functionality. Vital sign monitors, which previously shutdown even with closed-transition ATS, are now unaffected by power outages or blips. Additionally, OR fan controls have been transitioned to a UPS for continuous operation. The fan system, which consists of two supply motors and two return motors, has also been redesigned. Previously, all motors were on the same bus, meaning a failure of that bus would result in the loss of the fan system. Now, the supply and return fans are connected to separate buses, ensuring no interruption to air changes if one bus fails. These upgrades significantly enhance the hospital’s operational resilience and its ability to provide uninterrupted patient care.
Full UPS and power backup systems were also installed in intensive care units and C-section ORs, crucial areas where uninterrupted power is essential for patient care. All isolated power receptacles, booms, vital sign monitors and red vital receptacles are on UPS.
An ATS has now been installed in the patient care areas of building A. Completed earlier this year, it will further bolster the reliability of the power supply in these critical spaces. During a power interruption, normal power receptacles will automatically switch to emergency power, providing 100 per cent backup power to patient care areas. This setup is particularly important during annual preventive maintenance on the switchgear. Previously, these areas would experience four to six hours without power for normal-powered lights and receptacles during such maintenance. Now, patient care areas will remain
fully operational, ensuring uninterrupted functionality and improved resilience.
A redundant power source was installed for the building automation controls to ensure the continuous operation of critical building systems. This enhancement strengthens the hospital’s ability to provide uninterrupted patient care and significantly improves overall operational efficiency.
Similar to the setup in the new building (building B), where all IT infrastructure is supported by a UPS, the older building (building A) has been upgraded to include the same capability. All critical IT systems are now connected to a central UPS, ensuring uninterrupted functionality. Additionally, security features like door strikes and card readers are backed by a UPS, enhancing reliability and security during power disruptions.
By establishing redundancy in power supply, Oak Valley Health significantly minimized the risk of disruption in case of power failures across Markham Stouffville Hospital.
This multi-tiered approach ensures that even in the event of multiple power feed failures, essential units remain fully operational. This safeguards patient care and also enhances the overall reliability and resilience of emergency infrastructure.
The development of a robust electrical substructure has elevated Markham Stouffville Hospital, delivering substantial improvements for its maintenance team and the hospital as a whole. These upgrades have not only enhanced the efficiency and effectiveness of the department but have also had a far-reaching positive impact across the organization. The strategic enhancement of electrical infrastructure embodies its core values and unwavering commitment to patient care, serving as a source of inspiration for all stakeholders. Collectively, these initiatives strengthen the reliability of hospital infrastructure, minimize downtime and ensure a consistent, dependable power supply to critical systems, further solidifying the organization’s dedication to excellence.



By Aldrin Or

On a May afternoon in 2024, the sky above Edmonton turned orange as smoke from distant wildfires blanketed the city — a scene that is becoming disturbingly common across North America. Once a rare event, these smoke incursions are now a recurring threat, and researchers are finding they carry serious health risks. Wildfire smoke’s fine particulate matter (PM2.5) can travel deep into the lungs and even enter the bloodstream. In fact, a National Institutes of Health funded study in medical journal Jama Neurology found that chronic exposure to wildfire PM2.5 was associated with about 18 per
cent higher odds of developing dementia per unit of exposure, far greater than the one per cent increase in risk from other sources of PM2.5.
Breathing smoky air also strains the respiratory and cardiovascular systems. Emergency rooms see spikes in asthma attacks and heart problems on heavy smoke days. During major California wildfires, out-of-hospital cardiac arrests jumped by up to 70 per cent, according to the American Heart Association. When Canadian wildfire smoke blanketed U.S. cities in 2023, hospital visits for heart and lung issues rose nearly 20 per cent, reports the University of Maryland Institute
for Health Computing. Over time, repeated smoke exposure adds up. One study estimated long-term wildfire smoke inhalation contributes to roughly 11,000 premature deaths in the U.S. each year. Children, the elderly, pregnant women, people with chronic lung or heart diseases and outdoor workers are especially vulnerable. Children’s lungs are still developing (and they inhale more air relative to their size), while older adults often have underlying conditions that smoke exacerbates.
Canada’s 2024 wildfire season was among the worst on record, with more than 5.3 million hectares burned. This came on the heels of 2023’s unprecedented 17 million hectares scorched. Fires raged across nearly every province, blanketing large swaths of the country in smoke for weeks. The haze did not respect borders: cities in the U.S. Midwest and Northeast repeatedly choked on drifting Canadian smoke, prompting air quality alerts and health warnings far from the flames. In Toronto, for instance, the air quality health index hit the highest level of 10+ (“very high risk”) during the June 2023 smoke wave.
Scientists link these extreme seasons to climate change. Hotter temperatures and prolonged drought are fuelling bigger, more intense fires across the globe. Climate experts warn average temperatures will rise in Canada as the world warms, leading to longer and more destructive wildfire seasons. Indeed, heading into summer 2025, officials caution tinder-dry forests and record heat could spark another ‘catastrophic’ fire season. In effect, climate change is turning what used to be occasional bad fire years into the new normal, exposing millions of people to hazardous smoke more frequently.
Staying inside offers some protection from wildfire smoke, but fine smoke particles still infiltrate the majority of buildings. The U.S. Environmental Protection Agency notes these
particulates can easily penetrate homes and buildings, raising indoor pollution levels. Moreover, the average particle size in wildfire smoke (about 0.3 microns) is the toughest size for filters to capture effectively. Keeping indoor air clean during a prolonged smoke event is difficult. Wildfire smoke can rapidly clog air filters — during severe smoke, filters might need replacement daily to remain effective.
Few buildings are prepared for that. As filters become loaded with smoke debris, airflow through HVAC systems drops and more particles seep indoors. For this reason, officials advise upgrading to high-efficiency (MERV 13 or higher) filters during wildfire season, if the HVAC system can accommodate them.
Smoke exposure can also weaken filters’ performance. Studies have found smoke particles can reduce the electrostatic charge on high-efficiency filter fibres, making them less able to trap fine particles. Replacing filters promptly after heavy smoke events is critical to maintain air quality. The reality is most homes and offices were not designed to completely keep out smoke. During the worst
smoke waves of 2024, even well-sealed buildings saw indoor air quality decline, underscoring how challenging it is to shield indoor environments from sustained outdoor pollution.
The air filtration industry is racing to adapt. Standards are being updated so that filters are tested under more demanding, smoke-filled conditions. For example, ASHRAE’s latest standard, Method of Testing General Ventilation Air-Cleaning Devices for Removal Efficiency by Particle Size, includes an appendix that intentionally loads filters with fine particles to measure any efficiency loss.
This kind of real-world stress test helps pinpoint filters that won’t quickly degrade in smoky conditions. At the same time, companies are developing tougher filtration technologies to handle wildfire smoke. Some new filters use special coatings or materials to better capture ultrafine particles. One such innovation applies a nano flashing technology to filter media. In an independent study, the treated filter maintained exceptional filtration efficiency after heavy
discharging conditions that simulate wildfire smoke. Advancements like this aim to make filters more effective and more resistant to smoke’s onslaught.
As wildfires worsen, experts emphasize the need for ‘smoke-ready’ buildings and habits. Public agencies now issue alerts and guidelines for smoky days, but ultimately making homes, buildings and cities more resilient to heavy smoke will be crucial in the years ahead. In short, the fight for clean indoor air has become a vital part of living with wildfire smoke. What was once a sporadic nuisance has evolved into a persistent public health challenge — one that governments, businesses and residents are urgently trying to meet with better technology and preparedness.
Aldrin Or is co-chief innovation officer at C-Polar Technologies, which creates pathogen, allergen, fungi and wildfire particulate resilience in air, water, textiles and medical devices. This article was penned with collaborative input from Sam Chung, the company’s vice-president of business development. He can be reached at 604-561-4151 or schung@cpolartechnologies.com.

By Terrance Frank

In Canada, healthcare acquired infections (HAIs) are a perpetual and significant onus on the healthcare system and an economic burden to society. Currently, about one in nine patients contract a HAI during their hospital stay, reports Infection Prevention and Control Canada. Facility managers and operators are tasked with limiting these infections under very challenging conditions that include overcrowding and lack of financial and human resources as budgets are a primary focus. During the COVID-19 pandemic, infection prevention and control (IPAC) staff ratios were at or below recommended limits due to staff illnesses and numerous early retirements, often attributed to mental health stress.
Post-pandemic, what is being done to prevent the spread of future emerging human pathogens in healthcare facilities?
Architects, engineers and healthcare professionals have been working together to create best practices for two major areas of concern: disease transmission by air and hightouch surfaces. In Canada, CSA standards are being updated to identify and incorporate new innovations and best practices for air handling (HVAC) and high-touch surfaces in building designs. Whole building and partitioned duty air ultraviolet-C sterilizing HVAC systems are being utilized to ensure any airborne infectious diseases released can be eradicated before being recirculated. Portable individual air purification units are being placed inside intensive care unit rooms where patients are known to be contaminated, allowing the air to be purified and recirculated only locally. Building waste, vent and drain plumbing systems, laundry facilities and other building utilities are being designed to
prevent the generation of pathogen droplet release from normal utilization.
Air handling system upgrades are relatively easy to define and manage, but pathogens that are spread by surface-to-human transmission present a more challenging problem. A healthcare facility is a miniature city, with staff, patients, visitors and third-party material or service suppliers constantly moving in and out of the building. Mandatory face masking and screening visitors for signs of infection (cough or elevated body temperature) are good practices to prevent the spread of airborne droplet emissions; however, in the case of transmission by high-touch surfaces, this is more difficult to manage.
Every facility has high-touch ‘pinch points,’ defined as common points where two objects come together, posing a health hazard. On an average visit to hospital, a person will
push a button for a parking ticket, press an elevator button, hold the handrail inside the elevator, pull the door handle to a public washroom, touch the patient bed rail and so on.
Beyond these few examples of items a person may come in contact, there are multiple high-touch surfaces in areas where employees and suppliers are permitted. Cleaning all touchpoints in a healthcare facility 24 hours a day is an impossible task. Shortly after cleaning, most surfaces will become re-contaminated before the next cleaning cycle. Also, economics, IPAC staff resources and other priorities ultimately determine what is cleaned and how often, as the manual cleaning process is intensive and expensive.
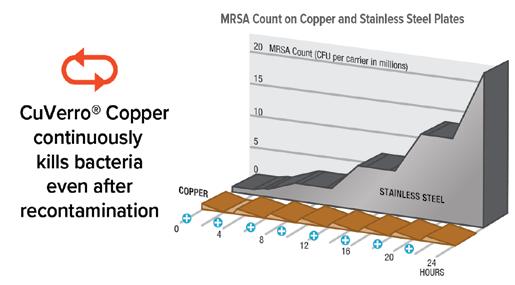
Copper industry professionals and university professors have long studied the efficacy of copper on human pathogens. In 2008, the Copper Development Association convinced the U.S. Environmental Protection Agency (EPA) to categorize and register antimicrobial copper alloys (AMC) as antimicrobial surfaces, with permanent efficacy against six common bacteria typically found in healthcare facilities. A few years later, Health Canada and its Pest Management Regulatory Agency followed suit and approved the claim that copper is effective in killing 99.9 per cent of all gram-negative and gram-positive bacteria within two hours. It also labelled this technology as a supplemental solid sanitizer. In doing so, copper is not just considered antimicrobial; it is bactericidal — the material does not just prohibit growth but kills bacteria.
With this approval, high-touch surfaces could be made from registered AMC alloys to provide perpetual, self-sanitizing function. By deploying this supplemental sanitizing technology, it provides efficacy similar to cleaning surfaces every two hours. This means in-between regular IPAC cleaning protocols, patients’ exposure to any bacterial contamination is reduced. Additionally, in situations where IPAC staffing levels are stretched and IPAC protocols are either missed or poorly executed, the baseline of the supplemental self-sanitizing surfaces provides perpetual efficacy to reduce human exposure to harmful pathogens.
After the EPA and PMRA registrations were granted, the task was to get AMC technology into a multitude of products used in healthcare facilities. In the early years,

many manufacturers produced bed rails, IV poles, handrails, sinks, faucet levers, visitor chair arm rests, door hardware and bathroom stall grab bars, among other products. Unfortunately, copper alloys were initially not well-received. The red/orange colour of copper was not seen as attractive by architects and hospital administrators. Copper oxidation with green patina was also viewed as unattractive or even unclean. What’s more, when designing parts for mechanical loading, product design engineers had to develop products with thicker wall copper than regular thin wall stainless tube could handle; copper was too soft and mechanically weak. Ultimately, the cost, aesthetics and mechanical limitations of copper forced many companies to stop offering AMC product options and revert back to regular stainless steel products.
In recent years, an innovative thermal processing technology, used in conjunction with AMC registered with the EPA and Health Canada, has allowed the application of a solid layer of copper to structurally strong substrate materials. These substrate parts can be made from stainless steel, aluminum, some rigid plastics, hardwood and ceramics to meet whatever the end-product design requires.
The new encapsulating AMC provides an attractive white gold, nickel tone finish
that does not tarnish green like pure copper. The thermal AMC fabrication surfaces have a unique microtopography that generates large surface area and therefore higher copper ion availability per unit of surface area. High surface microtopography on copper alloys has been shown to resist the formation of biofilms, which makes copper surfaces easier to clean. All manufactured parts previously made of heavy wall AMC tube, sheet, cast or plate can now be produced more economically with this thermal fabrication/encapsulation process. These new parts have the permanent efficacy of solid copper, with a reduced cost and improved aesthetics.
Since 2019, multiple original equipment manufacturers (OEMs) have provided products with the option of a self-sanitizing surface. Among them are medical devices, patient stretchers, plumbing fixtures, door hardware, IV poles, stethoscopes, handrails, grab bars and a ceramic tile that can be utilized in an operating room (OR) in place of standard wall tile. A study by the University of Waterloo illustrated copper ions have a sanitizer ‘halo’ effect for a gap up to an eighth of an inch wide between copper surfaces. This halo effect allows for grout lines in-between treated ceramic wall tiles and a modified version for floor tiles as
HIGH SURFACE MICROTOPOGRAPHY ON COPPER ALLOYS HAS BEEN SHOWN TO RESIST THE FORMATION OF BIOFILMS, WHICH MAKES COPPER SURFACES EASIER TO CLEAN.
an anti-slip surface. Health Canada recognizes AMC self-sanitizing surfaces as permanent for the life of the item, when cleaned and maintained following standard cleaning protocols — a one-time investment with perpetual efficacy and life cycle. This thermal fabrication technology allows for healthcare facility retrofits of existing surfaces or incorporation in new construction, with multiple OEMs providing the technology as a standard option. In tandem with the advancement in AMC solid surfaces, other manufacturers have made copper oxides that are promoted as an antimicrobial additive to polymer substrates, forming antimicrobial polymeric slabs. These slabs can be used to make countertops for nursing stations and laboratories and patient overbed trays. Some of these AMC technologies have achieved virucidal efficacy registrations
with U.S. and Canadian authorities. Testing by a major west coast Canadian health network for a public transit study has further validated AMC surfaces for both bactericidal and virucidal results.
For large surfaces where it is not practical to fabricate from AMC, such as a wall in a patient room, a major U.S. manufacturer currently produces an EPA-registered paint that contains copper ion, which can be applied on interior surfaces (any colour) with efficacy life of six years in non-commercial applications. (The paint has bactericidal and virucidal claims.) Even if the life span is reduced by 50 per cent in
healthcare applications, walls in an ICU could still have this self-sanitizing advantage.
Architects, engineers and IPAC teams have CSA standards and guidelines for new healthcare and long-term care facility designs: Z8000:24, Canadian Health Care Facilities, and Z8004:22, Long-term Care Home Operations and Infection Prevention and Control. These standards include specific references to the recommended use of self-sanitizing/bactericidal surfaces by way of CSA Z317.12:20, Cleaning and Disinfecting of Healthcare Facilities. Retrofit and new building opportunities for everything from door hardware to elevator touchpoints, public or patient shared washrooms and medical stretchers are now possible. Patient room walls and overbed trays, nursing stations, ICUs and ORs all have a possibility to include AMC self-sanitizing surface technologies in the philosophy of their design.
24_014628_Canadian_Healthcare_Facilities_Spring_CN Mod: January 21, 2025 9:08 AM Print: 01/27/25 page 1 v2.5


Terrance (Terry) Frank has been a technical sales specialist for 43 years. He retired as vice-president of sales from Aereus Technologies Ltd. in December 2023, and now provides technical consulting for Aereus by way of his company Terry Frank Consulting Inc. Terrance’s areas of expertise are related to health and safety as well as environmental science for infection prevention and control with bactericidal copper technologies. He can be reached at 705-890-7517 or terryfrankconsulting@gmail.com.



By Andrew Pratt & Cliff Long

Hospital-acquired infections (HAIs) remain a persistent challenge, affecting approximately one in 31 patients on any given day, according to the U.S. Centers for Disease Control and Prevention. Infection control has always been a high-stakes balancing act but recent global health crises have pushed healthcare engineers and facility managers to rethink their strategies. The interconnected nature of airborne pathogens, waterborne bacteria and touch-based transmission means no single system can work in isolation — effective solutions must be holistic.
Fortunately, advancements in mechanical, electrical and plumbing (MEP) systems are
equipping hospitals with new tools to enhance infection control. From ultraviolet-C (UVC) lighting and HEPA filtration to touchless controls and telemedicine infrastructure, engineering-driven innovations are playing a critical role in creating safer healthcare environments.
While technologies like UV-C lighting, HEPA filtration and touchless controls are not new, their use and adoption in hospitals have radically increased since the pandemic.
UV-C lighting is most effective when utilized in targeted situations, such as air
handling units where it’s applied to cooling coils. These coils, which accumulate condensation in a wet environment, can be prone to microbial growth. UV-C lighting effectively prevents this growth, improving air quality at its source. UV-C lighting can also be used to disinfect critical care spaces like operating rooms (ORs) intensive care units (ICUs) by activating during cleaning cycles when the rooms are unoccupied. Filters are essential for maintaining air quality and infection control in healthcare facilities. By removing particulate matter, microorganisms and other airborne contaminants, filters help create a safer environment for patients and staff. Higher risk

areas require higher efficiency filters, with many inpatient areas requiring MERV 14 final filters. Critical spaces, such as ORs or protective environment rooms, often require HEPA filters. The application of HEPA filters at the terminal diffusers provides the best protection by eliminating any possible contaminant source downstream of the filter before air enters the room. Regular maintenance and timely replacement of filters are essential to ensure optimal performance and compliance with healthcare standards.
Bipolar ionization and electromagnetic field manipulation are promising innovations for air quality improvement. While still not widely implemented, this technology releases charged ions into the air that bind to airborne particles like viruses, bacteria and allergens. The process neutralizes pathogens and causes particles to cluster, making them easier to filter out, and complements approaches like filtration and UV-C lighting.
Touchless technology has been widely adopted in isolation rooms and high-traffic areas like ICUs and neonatal ICUs. The integration of sensor-activated sinks and fixtures is a simple but impactful measure to reduce the risk of cross-contamination.
A pandemic-inspired move that significantly cuts cross-contamination risks is the
expansion of telemedicine. However, it often requires upgrades to low voltage infrastructure to accommodate more telehealth devices, remote monitoring tools and advanced communication systems for patient care. Increased bandwidth added capacity for power distribution and improved HVAC configurations to support telehealth equipment are playing a pivotal role in enabling this transformation.
New strategies in mechanical and electrical systems can address airborne and touchbased transmission but incorporating plumbing system design is essential for a comprehensive approach to infection control. One of the most significant threats in hospital water systems is legionella, a bacterium that thrives in stagnant water and can cause severe respiratory infections.
To mitigate this risk, hospitals employ recirculating systems to keep water moving and prevent stagnation. In Canada, water is typically heated to 160 F for storage in tanks and then mixed to 140 F for distribution, ensuring bacteria are effectively neutralized. Wherever possible, facilities minimize the use of tanktype storage to further reduce the potential for microbial growth. At the point of use, water is tempered to safe distribution temperatures,
balancing disinfection efficacy with user safety.
A well-established method for waterborne pathogen control is copper-silver ionization, which uses electrolysis to disrupt biofilms and neutralize bacteria. In the post-pandemic era, hospitals are shifting toward a zoned approach, applying copper-silver ionization selectively to high-risk water systems, such as those serving patient care areas, while optimizing energy and resource use in lower-risk zones. However, in Canada, best practices typically dictate that copper-silver ionization be applied to the entire water system, ensuring comprehensive protection against waterborne infections.
Negative pressure zones (outbreak control zones) are areas where air pressure is intentionally kept lower than surrounding areas. Mechanical engineers design these zones to direct airflow from ‘clean to contaminated’ spaces, preventing air from moving in the opposite direction and carrying contaminants into clean areas.
Initial response during COVID-19 often involved retrofitting existing spaces into temporary negative pressure zones by installing HEPA filters or adding exhaust fans to create isolation areas, but today hospitals are taking
a more proactive approach.
Many new facilities are incorporating pandemic-ready wings designed to quickly convert zones on patient floors to negative pressure at the flip of a switch. These spaces are outfitted with either pre-installed exhaust fans or by utilizing the base building return/ exhaust fans with the system switched to 100 per cent outside air mode of operation, differential pressure sensors, programmable controls and digital monitoring systems, allowing for seamless transitions to ‘pandemic mode’ without disrupting normal operations.
One challenge with negative pressure zones is their effectiveness depends on wellbuilt walls that are airtight as well as maintenance. Even minor gaps, such as poorly sealed doors or leaky walls, can compromise the entire system, allowing contaminated air to escape.
Exhaust discharge locations are another critical consideration. ASHRAE 170, Ventilation of Health Care Facilities, requires certain exhaust fans, including in airborne infectious isolation rooms, to discharge air at least 10 feet above the roof surface to prevent contaminants from re-entering the building’s breathing zones. Where the
HOSPITALS ARE SHIFTING TOWARD A ZONED APPROACH, APPLYING COPPER-SILVER IONIZATION SELECTIVELY TO HIGH-RISK WATER SYSTEMS, SUCH AS THOSE SERVING PATIENT CARE AREAS, WHILE OPTIMIZING ENERGY AND RESOURCE USE IN LOWERRISK ZONES.
exhaust cannot be discharged in a safe location, bag-in/bag-out HEPA filters can be provided to clean the exhaust air prior to discharging air to the exterior of the building.
MEP systems in hospitals aren’t standalone components; they’re interdependent pieces of a larger infection control puzzle. Success
depends on collaboration across disciplines, from architects and engineers to healthcare providers and facility managers. To get alignment between design intent and operational reality requires expert oversight during construction and commissioning to identify and resolve potential issues.
Andrew Pratt and Cliff Long are principals at Salas O’Brien. Andrew is an expert in mechanical systems design and is responsible for quality control, building information modelling development and resource allocation for a large team of mechanical engineers serving healthcare, the arts, pharmaceuticals and education clients in Canada. Cliff is a prominent mechanical engineer specializing in hospital design across the United States. As a recognized subject matter expert, Cliff excels in the design of HVAC systems, central energy plants, mechanical rooms, piping systems, instrumentation and controls, and energy management solutions. Andrew and Cliff can be reached at andrew.pratt@salasobrien.com and clifton.long@salasobrien.com, respectively.
2025
Hans Burgers Award for Outstanding Contribution to Healthcare Engineering DEADLINE: April 30, 2025
To nominate: Please use the nomination form posted on the CHES website and refer to the Terms of Reference.
Purpose: The award shall be presented to a resident of Canada as a mark of recognition of outstanding achievement in the field of healthcare engineering.
Award sponsored by
2025
Wayne McLellan Award of Excellence in Healthcare Facilities Management DEADLINE: April 30, 2025
To nominate: Please use the nomination form posted on the CHES website and refer to the Terms of Reference.
Purpose: To recognize hospitals or long-term care facilities that have demonstrated outstanding success in completion of a major capital project, energy efficiency program, environmental stewardship program or team building exercise.
Award sponsored by
For Nomination Forms, Terms of Reference, criteria and past winners www.ches.org / About CHES / Awards Send nominations to: CHES National Office info@ches.org
By Stephanie Cini

Infection prevention and control (IPAC) plays a critical role in safeguarding patients and staff during construction at an existing healthcare facility. Embracing technology is essential to addressing the challenges posed by these projects. Advanced tools, materials and strategies are reshaping how healthcare facilities mitigate risks and maintain compliance with stringent standards like CSA Z317.13-22, Infection Control During Construction, Renovation and Maintenance of Health Care Facilities.
Healthcare construction projects present dual narratives: one of progress and modernization, the other of hidden risks. Dust, debris and disruptions to airflow have the potential to carry pathogens into sterile environments,
turning construction zones into hotspots for infection. These risks underscore the importance of proactive strategies to mitigate contamination and maintain safety throughout the construction process.
While regulatory standards provide a framework for infection prevention, challenges often arise in applying these guidelines to real-world scenarios. Innovative technologies, advanced materials and process improvements are helping bridge the gap between planning and practical implementation. These advancements are redefining IPAC strategies in healthcare construction, offering solutions that enhance safety and efficiency while safeguarding vulnerable populations.
Maintaining air quality during healthcare
construction is critical to reducing infection risks. Advanced air filtration systems, such as HEPA filtration combined with ultraviolet-C disinfection, play a pivotal role in achieving this. These systems significantly reduce airborne particulate contamination, protecting patients and staff in nearby areas. In Canadian hospitals, portable HEPA units have been widely adopted to mitigate infection risks during renovations. This approach not only enhances safety but also ensures alignment with the CSA Z317.13-22 standard, which mandates robust air filtration controls in healthcare construction.
Another vital innovation in healthcare construction is the integration of antimicrobial surfaces, which are designed to inhibit micro-
bial growth. These materials have become a cornerstone in healthcare renovations, particularly for high-touch areas, such as door handles, countertops and railings, where contamination risks are highest. In Canada, hospitals and long-term care facilities are increasingly incorporating copper alloy surfaces. These surfaces have been shown to kill more than 99.9 per cent of bacteria within two hours of contact, providing a proactive layer of defence. By reducing contamination at the source, antimicrobial materials complement broader infection prevention measures, including improved hand hygiene practices among staff. Additionally, these materials are valued by construction teams for their durability and practicality, making them an ideal choice for high-traffic healthcare environments.
Finally, digital infection control risk assessment (ICRA) tools are transforming how risks are managed during healthcare construction. These types of tools streamline the process by providing a user-friendly platform for risk identification and mitigation planning. By reducing errors caused by manual coordination, they improve efficiency and enable multidisciplinary teams to apply best practices consistently, even when IPAC expertise is limited. These tools also enhance collaboration, minimizing delays, and ensure compliance with regulatory standards like CSA Z317.13-22.
By implementing all of these advanced IPAC technologies early in the construction process, teams can avoid costly disruptions and delays, as the technologies protect both project timelines and budgets while maintaining the safety of patients and staff.
To maximize the impact of these innovations, healthcare leaders must adopt a thoughtful and strategic approach. Practical steps for construction teams include consulting with IPAC professionals during the design phase, using portable HEPA filtration units to manage air quality, incorporating antimicrobial materials into high-touch areas, and training teams on compliance standards and infection control protocols. It begins by aligning chosen technologies with IPAC goals, ensuring each solution addresses the specific infection risks within their facility. Leaders must also assess the long-term viability of these tools by considering maintenance requirements, cost-effectiveness and compatibility with existing systems. Ongoing investment in staff training is essential,
as even the most advanced technologies rely on knowledgeable and engaged users to be effective. A culture of accountability and collaboration, driven by education, ensures tools are used to their fullest potential.
Additionally, collaboration between IPAC professionals, construction teams and healthcare leaders is key to successful project outcomes. By fostering open communication and ensuring all stakeholders are aligned on infection prevention goals, facilities can create safer environments without compromising construction progress. For example, integrating regular risk assessment meetings into the project timeline helps identify potential issues early and ensures timely implementation of mitigation strategies. This proactive approach not only minimizes risks but also enhances trust and coordination among teams.
Further, the adoption of portable containment units during high-risk construction phases provides an added layer of safety. These units can isolate work zones, preventing the spread of dust and airborne contaminants to adjacent patient areas. Combined with proper air filtration systems, containment
units have proven effective in maintaining sterile environments during renovations, particularly in high-risk areas like operating rooms and intensive care units. Such measures highlight how a comprehensive IPAC strategy can ensure both patient safety and construction efficiency.
Infection prevention in healthcare construction is more than a regulatory obligation — it’s a moral imperative and professional responsibility. By integrating cutting-edge technologies, materials and practices, healthcare facilities can minimize infection risks, protect patients and staff, and ensure operational efficiency during renovations and upgrades.
Stephanie Cini is director of operations at IPAC Consulting, which offers infection control expertise to various sectors, including travel, film productions, dental, long-term care and the construction of healthcare facilities. Stephanie brings more than a decade of management experience specialized consulting expertise in construction and film to her leadership role at IPAC Consulting.
For over 60 years, Crossey Engineering has delivered engineering excellence, shaping iconic projects across Canada and beyond.
Now, we take the next step forward as part of Salas O’Brien — together, we bring deeper expertise, expanded resources, and an unwavering commitment to innovation, sustainability, and client success.
Crossey Engineering is now Salas O’Brien
salasobrien.com/crossey


By Barry Hunt

The first edition of CSA Z8000, Canadian Health Care Facilities, was a landmark success when published in 2011. It was the culmination of years of collaboration and thoughtful debate from healthcare experts across the country that literally set the gold standard for hospital design in Canada.
One of Z8000’s crowning achievements was the advent of 100 per cent single patient rooms in new hospitals. Not only did these rooms offer more peace and privacy for patients and their families, but there was the very reasonable prospect of delivering better patient outcomes as well.
The standard paid off, handsomely. A post-occupancy review has since confirmed new healthcare facilities built to Z8000:11 have 50 per cent lower healthcare-acquired infection (HAI) rates.
The long-awaited third edition of Z8000 is now hot off the press. Z8000:24 is another bold step forward for Canada, and the right thing to do for patients, particularly for its welcome new safety-first focus on infection control: “The healthcare facility shall be planned and designed to be safe for all building occupants in terms of both the prevention of healthcare-acquired infections and the control of infectious diseases.”
Going forward, under the standard, planning for new hospitals “shall include participation by representatives of the stakeholders that are involved and have expertise in infection prevention and control issues and practices.”
Z8000:24 breaks new ground by clearly advocating for a prudent approach to infection control.
“The health status of occupants in a healthcare facility is not always known and so every precaution should be taken to prevent the transmission of illness from patient to patient,
from the patient to the healthcare provider and from the building to its occupants,” the standard says.
In 2011, Z8000 specified requirements for hand hygiene sinks, including offset drains, no overflows, no aerators and to be of generous minimum dimensions to reduce splash and aerosolization that may lead to transmission and infection.
What does post-occupancy evaluation show?
A Z8000:11 sink makes a big difference. But in the wake of current global trends, more protection is needed.
There is exponential growth of sink and drain-related pathogens of high consequence like Candida auris and carbapenem-resistant Enterobacter propagating in hospitals around the world. Z8000:24’s approach to address this menacing reality — the new normal that is anything but normal — is objective-based, stating hand hygiene sinks shall be designed to minimize transmission of pathogens.
Leaving no doubt, Z8000:24 goes on to say, “Mandatory: Hand hygiene sinks shall be designed and engineered to prevent the growth of bacteria, mould and biofilm in drains, and to prevent the release of pathogenic bioaerosols.”
The approach and message couldn’t be clearer.
Despite the healthcare industry’s best efforts to employ traditional practices, HAIs have continued to increase for more than a decade. Perhaps, unsurprisingly, with the onset of COVID, HAIs have risen to a level beyond what was projected even a few short years ago.
Just as Z8000:11 was bravely on the forefront when it specified single patient rooms in 2011, Z8000:24 has boldly taken the position that the “planning processes for infection prevention and control should include consideration of new and emerging technologies.” This includes incorporating automated infection prevention technologies like ultraviolet (UV) disinfection and self-sanitizing surfaces that are approved by Health Canada.
Many of these emerging technologies have been in use by early adopters now for up to 15
PEER-REVIEWED STUDIES HAVE FOUND THAT THE 10 TO 15 PER CENT OF PATIENTS WHO ACQUIRE A HAI ARE IN HOSPITAL AN EXTRA WEEK FOR COMMON INFECTIONS AND TWO EXTRA WEEKS FOR MULTIDRUG RESISTANT ORGANISM INFECTIONS.
years, but they are still new to the vast majority of people working in Canadian healthcare. It’s often said about healthcare in Canada that it takes 17 years from innovation to implementation. In 2015, CSA published the express document, Evaluating Emerging Materials and Technologies for Infection Prevention and Control — the very items now included in Z8000:24 — to try to reduce Canada’s implementation lag.
UV is still considered ‘new’ by many. Fortunately, the updated standard includes an informative and comprehensive addendum to facilitate understanding and implementation. Annex E not only details UV technology, types of devices and their applications, but outlines the qualifications necessary for operation, maintenance and commissioning. Guidance for annual preventive maintenance, testing, safety and training is also included.
According to HealthCareCan, Canada renews healthcare infrastructure at a rate of about two cent per year. At that rate, it would take 50 years and several hundred billion dollars to update the country’s hospitals to Z8000:24. Alternatively, existing hospitals could be retrofitted to include the infection control measures included in the standard in relatively short order for much less.
The average length of stay (ALOS) in Canadian hospitals is seven days, reports Statista. Peer-reviewed studies have found that the 10 to 15 per cent of patients who acquire a HAI are in hospital an extra week for common infections and two extra weeks for multi-drug resistant organism infections. Hospitals that are compliant to Z8000:11 are twice as effective at preventing infections as older hospitals.
Simple math suggests the overall improvement in ALOS of Z8000:11 is likely to translate into a productivity gain (bed gain) of five to 10 per cent. It’s quite conceivable the newest version of the standard could lead to a further productivity gain of five to 10 per cent for new hospitals. That could deliver a total 10 to 20 per cent gain for older non-Z8000 facilities.
In today’s overcrowded healthcare facilities, freeing up five to 20 per cent of patient beds would be welcome relief. Canada currently operates on average at 99 per cent of bed capacity across the country’s 95,000 beds with some hospitals now peaking at 200 per cent capacity during respiratory season. Reducing HAIs nationwide has the potential to free up somewhere between 5,000 to 20,000 sorely needed beds — with the same staff and no additional workload.
In 1863, Florence Nightingale wrote, “It may seem a strange principle to enunciate as the very first requirement in a hospital that it should do the sick no harm.” She started the world on a new evidence-informed, systematic, engineered approach to hospital design to reduce infections with concepts like good ventilation, sunshine and fastidiously clean, sanitary conditions.
Today, CSA Z8000:24 picks up where Nightingale left off, charting a new course in infection control with the advent of automated infection control technology and a commitment to the precautionary principle.
Barry Hunt is co-founder of the Coalition for Healthcare Acquired Infection Reduction, retired from an industry career developing solutions for healthcare, and an active volunteer contributor to CSA standards and other organizations.
By Chris Stover

In an inspiring display of teamwork and community spirit, the maintenance and operations team at St. Martha’s Regional Hospital in Antigonish, N.S., has transformed an overgrown flower box into a thriving vegetable garden.
The spring 2024 initiative not only revitalized a neglected space and fostered stronger team bonds, it also provided fresh produce for a local charity, demonstrating how teamwork and generosity can make a meaningful impact both inside and outside the workplace.
Herbs used to grow in the old flower box behind the hospital’s carpentry shop for use in the kitchen. Overlooked for years, it had fallen into disrepair.
“It was just full of weeds and the wooden box was all rotted,” says Darrell Novak, assistant manager of maintenance and operations at St. Martha’s. “Every day I’d walk by and notice just how awful it looked.”
Novak saw an opportunity to create a shared project that would not only improve the hospital grounds but also enhance team cohesion and feed people in the community who could use a hand.
He gathered his eight-member team together, made up of plumbers, carpenters, electricians and maintenance workers, and explained how he’d like to fix it up. The group enthusiastically took up the challenge and built a new 12-foot by four-foot raised bed out of spruce, and then planted vegetables instead of flowers.
For months they worked on the little garden, planting green peppers and tomatoes, surrounded by a border of flowering herbs. The result was a resounding success.
“The green peppers were unbelievable and the tomatoes huge and red,” says Novak. “The garden required minimal upkeep — just some weeding and watering — but it
brought us together in a meaningful way.”
Novak and his team donated their first harvest to the Antigonish Community Fridge, a community-organized and run initiative that operates out of two locations — the local library and the agricultural centre — to improve access to healthy, nutritious food.
“While we weren’t looking for recognition for the donation, I did want the wonderful effort made by the team recognized.”
John Hann, director of maintenance and operations, was impressed by the initiative.
“It’s such a positive thing for this group to have come together like this and also provide such a wonderful gift of fresh produce to community members who may be struggling,” says Hann.
Novak emphasizes the project was not just about growing food for the community fridge but strengthening good working relationships. The garden project proved to be just the right catalyst for team building.
“It brought us together and built trust,” he says. “It helped improve communication between management and non-management employees. Working together in the garden made us work better together on other projects.”
The success of the garden has inspired Novak and his team to expand their efforts in 2025.
“It’s working for the team and it makes everyone feel appreciated,” he says. “When people feel valued, it goes a long way in creating a better work environment and overall team performance.”
Reflecting on his own experiences growing up as one of the youngest of 14 children, Novak understands the importance of appreciation.
“A little bit of recognition from older siblings made a huge difference,” he says. “In the workplace, it’s the same. If you show appreciation, you get better quality work and create a better atmosphere.”
Chris Stover is senior communications advisor for people and culture on the communications and marketing team at Nova Scotia Health.
We are pleased to announce that now monitors 50 plus hospitals Ontario region.
We are pleased to announce that now monitors 100 plus hospitals Ontario region.
Labour Canada has fully “acknowledged” the scope of work provided in the semiannual inspection program. In addition, the written documentation contributes greatly to the hospital accreditation programs.
Labour Canada has “acknowledged” the scope work provided in the semiannual inspection program. In addition, the written documentation contributes greatly to the hospital accreditation programs.
Further we are always pooling the knowledge resources of Infection Control and Engineering Groups like CHES, the ventilation inspection program is in a evolution to meet future healthcare needs for patients and staff.



h l ti and inspection of the hospital building audit this year Some of u have already taken advantage f our new software program which in conjunction with our patented robotics, allows us to minimize ceiling access requirements.

Further we are always pooling the knowledge resources Infection Control and Engineering Groups like CHES, the v inspection program is in evolution to meet future healthcare patients and staff. and inspection of the hospital building audit this year. Some of u have already taken advantage f our new software program which in conjunction with our patented robotics, allows us to minimize ceiling access requirements.
ventilation fire dampers may be part of





Aereus Copper I Bactericidal Copper meets CSA Z317.12:20
Health Canada PMRA as a "Supplemental Self Sanitizing Solid"
Self Cleaning surfaces 24/7 as a baseline of protection. Killing 99.9% of bacteria within 2 hours of contact.