Compassion Focussed EMDR in the treatment of shame-based trauma & moral injury”
Prof Derek Farrell MBE
Professor in Trauma Psychology & Veterans Affairs
EMDR Europe Accredited Senior Trainer & BABCP
Accredited CBT Therapist
Trauma Summit - Belfast
June 2024
A Cautionary Note about Today’s Presentation
o This presentation will involve many narratives – some of which are graphic. Their inclusion is purely for the purpose of teaching and knowledge exchange.
o Remember that you are resilient and resourceful individuals please take care of yourself in the best ways you know how.
o As Trauma Therapists, we all subscribe to and invest in the survivor’s journey.
o EMDR therapy has the potential to make the impossible probable. Our experience tells us that this is a frequent occurence.
1. Christopher - Afghanistan veteran
o Ex-Afghanistan veteran, 36-yearold male
o During incursion was ordered to take a shot by his CO
o Victim turned out to be a 9-yearold boy
o Consumed by chaos, selfmedicated with alcohol
o Medically discharged
o Death by suicide
2. Sasha – A survivor of organisational abuse
o Sexual abuse survivor –throughout all her childhood
o Sophisticated paedophile ring
o Highly orchestrated
o @ 7 years of age, was guided through genital mutilation of another girl, similar age
o She found out later, her abuser on this occasion was a Consultant Surgeon
5. Beatrice - A survivor of sexual abuse perpetrated by a Roman Catholic Priest
• Beatrice: “Before my perpetrator dies, what if he seeks forgiveness and repents for his sins. What would God do? If you believe that God is a truly forgiving God, and they believed in the authenticity of the confession, then God would forgive. Upon my perpetrator’s death, he would then be allowed into heaven. If this happens, then heaven is now no longer safe for me. I do not wish to go to a place where my abuser is. So, upon my death, where do I go?”
1. Clients need an explanation to account for their symptoms and their lived experiences
2. This explanation needs to be completely client-centred – specifically tailored to the needs of the individual
3. Collaborative, emotionally charged, empowered working relationship between therapist and client, with the client being ‘heard & valued’, and the therapist ‘bearing witness’ with ‘detached compassion.’
4. Strategy and treatment rationale based on empiricism and realism
5. The client is key to a successful outcome and the ‘final arbiter.’
o EMDR therapy is an empirically supported, experiential, transdiagnostic treatment intervention for pathogenic (trauma) memories
o Involves Bi-focal, dual attention Stimulation (BLS)
o Standard model – faster is better
o EMDR 2.0 – Working Memory Taxation
o Multi-modal intervention
o Involves both spontaneity, intervention, and at times – creativity
o Neuroplasticity: Forging out new connections
o Constellation of the memory network is physically altered creating phenomenological change
o Memory Reconsolidation - shift from reexperience to remembered
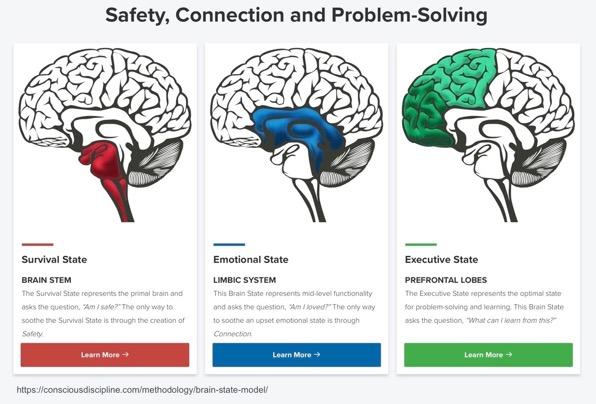
Adaptive Information Processing & The Evolutionary Brain in Compassion Focused Treatment for Moral Injury
• The Adaptive Information Processing Model posits that current life difficulties are informed by past experiences that are inadequately processed and maladaptively encoded, generating symptoms in the client’s life (Laliotis & Shapiro, 2022).
• The brain, from an evolutionary perspective, contains ‘design errors’, which are not the fault of the individual (Gilbert, 2022)
• ‘Moral trauma: the existential, psychological, social, emotional and/or spiritual/ religious damage arising from a violation or betrayal, (by omission or commission), of the core moral framework and manifesting through feelings of shame, guilt, self-condemning and or selfsabotaging behaviours (Jinkerson, 2016)
• ‘a shattering’ of moral beliefs or code(s)
• Ref: Jamieson, N., Maple, M., Ratnarajah, D., & Usher, K. (2020). Military moral injury: A concept analysis. International journal of mental health nursing, 29(6), 1049-1066.
Just as PTSD is a highly politicised medico-legal diagnostic framework, moral injury is also shaped by political and public debate
However, a problem with the current trajectory surrounding moral injury is its focus on the individual and their actions (or inactions), rather than on political, organisational, military, and senior leadership
• ‘our current thinking is increasingly dominated by the left hemisphere's narrowly focussed way of attending to the world……….. nothing short of a paradigm shift will bring about the change needed to counter this dominance.
McGilchrist, I. (2012). The divided brain and the search for meaning: Why we are so unhappy. Yale University Press.
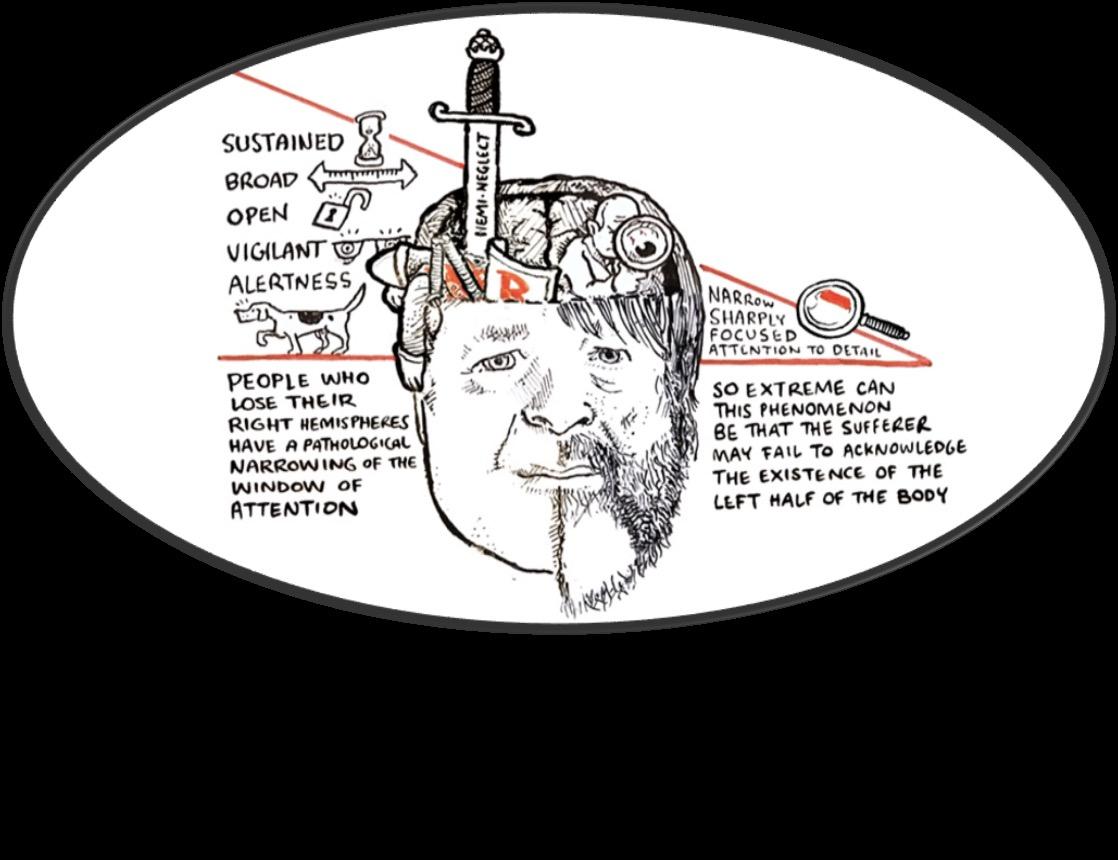
• The left brain pays sharply focused attention to detail and sorts and organizes people and things into neat, orderly categories. The left brain doesn't understand relationships. It's the right brain that understands context and the big picture our relationships with others and how we fit into a complex, non-linear world in which everything is connected.
• Einstein said that the rational mind is a faithful servant, but the intuitive mind is a precious gift, and we live in a world that has honoured the servant but has forgotten the gift.
o “I know I hurt them, but I can allow myself to acknowledge the authenticity of my apology.”
o “What I did was wrong – I will explore an effective way to atone.”
Mantra Orientated Compassionate Body Scan
“As I perform this body scan, I permit myself to experience the warmth of forgiveness and the nurturance of compassion in my journey moving forward. I chose to do this to bring calmness to my present.”
Encouraging the client to imagine (viscerally experience) a wise and compassionate figure (real or imaginary) providing guidance and support during trauma processing can be beneficial.
This figure serves as an internal resource, offering comfort, balance, counternarrative, and perspective.
The Affectionate Breath
Affectionate Breath:
Incorporating mindful breathing, the therapist guides the client to take slow, deep breaths, emphasising a compassionate connection with each inhalation and exhalation. This technique promotes a sense of calmness and safety during the processing.
Inner Child Dialogue: Engaging in a compassionate dialogue with the client's inner child can be powerful. The therapist may guide the client to visualise their younger self and offer words of comfort, understanding, and reassurance.
Compassionate Dialogue with Self-States
• ‘Imagine reaching out to that 6–year old version of you right now:
o How might you read her eyes
o What might they need right at this moment
o How might you meet this need
o What echo would you like to send them
o What echo might you want to receive back
o If you could give them a gift right now, what might that be
o If there were one message you would like to receive from them, what might that message be?
Self-Soothing Touch: Encouraging the client to use self-soothing touch, such as placing a hand over their heart or giving themselves a comforting hug, can enhance the experience of safety and compassion during the reprocessing.